
adverse external ocular effects of topical ophthalmic therapy ...
112
ADVERSE EXTERNAL OCULAR EFFECTS OF TOPICAL OPHTHALMIC THERAPY: AN EPIDEMIOLOGIC, LABORATORY, AND CLINICAL STUDY* BY Fred M. Wilson II, MD INTRODUCTION FOR CENTURIES THE ART OF MEDICINE HAS BEEN OF GREAT IMPORTANCE AND VAL- ue to patients and practitioners alike. When specific remedies were few, physicians relied heavily, and often successfully, on physical and envi- ronmental therapy, placebos, prognostication with reassurance and sup- port, and the Hippocratic principle of first doing no harm. More recently, as the science of therapeutics has advanced, we have come to rely progressively more on the seemingly wondrous capabilities of our drugs and less on the art of our profession. As a result, and because no drug is entirely safe, we may sometimes subject our patients to treat- ment which does more harm than good. In general medicine, the importance of adverse reactions to drugs has been the subject of some controversy. The preponderance of evidence and opinion suggests that we live in an overmedicated society and that adverse reactions constitute a problem of considerable magnitude. 1"2 The opposing view is that the problem has been overemphasized and that inappropriate fear of undesirable effects can reduce unacceptably the benefits to be derived from medications.3 Despite this difference of opin- ion, all agree that the problem is not a trivial one; that no drug is com- pletely safe; that drug reactions can be clinically confusing or even serious when they develop; that they are never acceptable when they can be prevented; and that every effort should be made to minimize their occur- rence. *From the Corneal and External Ocular Disease Service, Department of Ophthalmology, Indiana University School of Medicine, Indianapolis. Supported in part by a grant from Research to Prevent Blindness, Inc, New York and by Indiana University Computing Center Grant No 350706. TR. AM. OPHTH. Soc. vol. LXXXI, 1983
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of adverse external ocular effects of topical ophthalmic therapy ...

ADVERSE EXTERNAL OCULAR EFFECTSOF TOPICAL OPHTHALMIC THERAPY: ANEPIDEMIOLOGIC, LABORATORY, AND
CLINICAL STUDY*
BY Fred M. Wilson II, MD
INTRODUCTION
FOR CENTURIES THE ART OF MEDICINE HAS BEEN OF GREAT IMPORTANCE AND VAL-
ue to patients and practitioners alike. When specific remedies were few,physicians relied heavily, and often successfully, on physical and envi-ronmental therapy, placebos, prognostication with reassurance and sup-port, and the Hippocratic principle of first doing no harm.More recently, as the science of therapeutics has advanced, we have
come to rely progressively more on the seemingly wondrous capabilitiesof our drugs and less on the art ofour profession. As a result, and becauseno drug is entirely safe, we may sometimes subject our patients to treat-ment which does more harm than good.
In general medicine, the importance of adverse reactions to drugs hasbeen the subject of some controversy. The preponderance of evidenceand opinion suggests that we live in an overmedicated society and thatadverse reactions constitute a problem of considerable magnitude. 1"2 Theopposing view is that the problem has been overemphasized and thatinappropriate fear of undesirable effects can reduce unacceptably thebenefits to be derived from medications.3 Despite this difference of opin-ion, all agree that the problem is not a trivial one; that no drug is com-pletely safe; that drug reactions can be clinically confusing or even seriouswhen they develop; that they are never acceptable when they can beprevented; and that every effort should be made to minimize their occur-rence.
*From the Corneal and External Ocular Disease Service, Department of Ophthalmology,Indiana University School of Medicine, Indianapolis. Supported in part by a grant fromResearch to Prevent Blindness, Inc, New York and by Indiana University ComputingCenter Grant No 350706.
TR. AM. OPHTH. Soc. vol. LXXXI, 1983

Topical Ophthalmic Therapy
We need to know much more about the overall good and harm thatresult from the drugs that we prescribe and about the circumstances inwhich adverse effects occur.4 Cluff2 wrote that these matters ". . . must beestimated in practical settings that involve many unselected patients withdifferent types of clinical problems, who are treated with many differentdrugs and managed by many different physicians."
In this thesis I attempt to make just such an estimation, in the hope thatit might help us better to respect, anticipate, prevent, recognize, andtreat external ocular diseases that are induced by topical medications. Myspecific purposes are to elucidate: (1) the prevalence and nature of suchdiseases, (2) the variables that are associated with them, and (3) some ofthe clinical and laboratory features that typify them. The investigationalaspect of the study consists of three parts: (1) a computerized epidemio-logic study, (2) laboratory studies, and (3) clinical observations.
REVIEW OF THE LITERATURE
Although topical drugs for the eyes have caused undesired effects sinceantiquity, very little was written on the subject until recent times.One of the earliest reports of an ocular reaction to a topical medication
was von Graefe's6 description in 1864 of dermatoconjunctivitis caused byatropine. He mentioned the problem in passing as early as 1855.7 Theo-dore and Schlossman8 cited evidence that follicular conjunctivitis fromphysostigmine was observed as far back as 1878.
At first, drug reactions were attributed to chemical irritation, contami-nation of solutions by molds, or idiosyncrasy.8 The concept of allergy hadto await further advances in the science of immunology during the earlyyears of the 20th century. Woods9 led the way with his textbook of 1933,which insinuated into ophthalmology the new immunologic principles ofthe time but which gave almost no attention to the effects of drugs.Woods'0 wrote later, in 1937, that three types of allergic conjunctivitis
were recognized by 1933: (1) a transient one, characterized by acuteswelling of the eyelids and conjunctiva; (2) a slowly-developing type withconjunctival follicles and eczema of the eyelids; and (3) a chronic follicularreaction without eczema. Only the second type was attributed to drugs,usually atropine or butyn.An awareness of the importance of drug reactions became evident even
a few years earlier. In 1921, Jackson"l wrote an essay on the dangers of
855

Wilson
overtreatment, especially with silver nitrate, yellow oxide of mercury,atropine, or butyn. He referred specifically to the inadvisability of usingtopical drugs too frequently or for too long a period of time. Hosford andMcKenney12 concluded in 1933 that yellow oxide of mercury was greatlyoverused and that it was more often harmful than beneficial. In 1949,Thygeson'3 re-emphasized the importance of overtreatment, pointing outthat catarrhal conjunctivitis was often treated excessively, especially withsilver nitrate, so that a chemical conjunctivitis became superimposed on abacterial one. Fedukowicz and associates14 wrote in 1955 that the overuseof topical antibiotics often caused the same problem. By 1949, Thygeson13had worked out the essential differences between the presumably toxicfollicular conjunctivitis caused by eserine or pilocarpine and the allergiceczematoid dermatoconjunctivitis caused by atropine.
In their textbook on ocular allergy in 1958, Theodore and Schlossman8compiled most ofwhat was then known about immunology as it applied tothe eye. They devoted entire chapters to drug-induced allergies andirritations and discussed cytologic findings and differential diagnosis. Thiswas the first comprehensive work pertaining to drug-induced problems ofthe external eye, and most of the information remains valid today.
Havener's'5 textbook of 1966 on ocular pharmacology contained thor-ough and analytic descriptions of many of the possible adverse results ofophthalmic therapy and emphasized the importance of philosophic con-siderations in the rational application of treatment. Fraunfelder,16 in1976, published a reference book tabulating drug-induced ocular sideeffects and drug interactions. In this book he also announced the estab-lishment in the United States of a National Registry of Drug-InducedOcular Side Effects, under his direction. In 1979, Wilson17 published areview of adverse drug effects on the external eye.
MATERIALS
COMPUTERIZED EPIDEMIOLOGIC STUDY
I studied 1024 consecutive patients who had external ocular diseases andwho were referred to me between January 1, 1977 and December 31,1980. I accept patients only from ophthalmologists, so there were noreferrals from other kinds of practitioners. I excluded cases of glaucoma,uveitis, cataract, vitreoretinal disease, strabismus, neuro-ophthalmic andorbital disease, and general ophthalmic examinations unless external ocu-lar problems coexisted.
856

Topical Ophthalmic Therapy
LABORATORY STUDIES AND CLINICAL OBSERVATIONS
These studies and observations derived from my overall clinical experi-ence between July 1, 1973 and July 1, 1982, with no restrictions as toprimary diagnosis or source of referral.
METHODS
I interviewed, examined, and diagnosed all patients after preliminaryhistories were taken by ophthalmology residents.
Laboratory studies were performed when indicated and included, invarious cases, scrapings or smears stained by Giemsa, Gram, Ziehl-Neel-son, or fluorescent-antibody techniques; cultures for bacteria, fungi, orviruses; analyses of tear lysozyme; measurements of various serum anti-body titers; cutaneous patch tests; intradermal skin tests; and conjunctivalor cutaneous biopsies. With the exception of the fluorescent-antibodystudies, I evaluated all scrapings and smears myself.
COMPUTERIZED EPIDEMIOLOGIC STUDY
Classification of PatientsEach patient was classified according to one of four general diagnosticcategories: (1) those who had adverse reactions to topical ophthalmicmedications (hereafter referred to as "drug cases"); (2) those who hadinflammatory external diseases without adverse drug reactions ("inflam-matory controls"); (3) those who had external diseases that were notassociated with inflammation or drug reactions ("noninflammatory con-trols"); and (4) those who had adverse reactions that were clearly causedby preservatives in contact-lens solutions ("contact-lens cases").To be categorized as a drug case, a patient had to have a drug reaction
that was, insofar as I could determine, unanticipated, unrecognized, ormisunderstood by the referring ophthalmologist; clinically unacceptablein terms of the patient's underlying diagnosis; and clinically important.The reaction also had to constitute a major reason for the patient's com-plaints, clinical findings, or referral. I excluded even relatively severedrug effects if they were expected or acceptable under the circumstancesof their occurrence. For example, any patient with toxic papillary kerato-conjunctivitis secondary to intensive treatment of a-bacterial corneal ulcerwas classified as an inflammatory control case because this kind of reactionis usually unavoidable and must be tolerated if a cure is to be effected.
I considered only reactions that were caused by topical ophthalmicmedications and that affected the external eye or adnexa. Intraocular
857

Wilson
problems such as glaucoma or cataract from topical corticosteroids wereexcluded, as were systemic reactions to topical drugs and reactions tosystemic medications. I also ignored virtually all of the many complica-tions of topical corticosteroids because their ability to cause problems is asubject ofmuch controversy and because it is often difficult to prove causeand effect. However, I did classify as a drug case any patient who hadsevere rebound inflammation after the abrupt and injudicious cessation ofsteroid.
Contact-lens wearers with papillary reactions were classified as contact-lens cases only ifpreservatives in contact lens solutions were unequivocal-ly at fault. Cases that might have been related to lens deposits or otherfactors were classified as inflammatory controls.
Patients were classified as inflammatory controls if they had any symp-toms or signs (eg, hyperemia, discharge, erosions, or corneal vasculariza-tion) that, by any stretch of the imagination, might have suggested to thereferring ophthalmologist the presence of an inflammatory process. Inother words, cases in this category were ones for which the prescribing ofdrugs by referring doctors was understandable, if not justifiable.
Noninflammatory controls were patients who had conditions with nosigns or symptoms of inflammation and so would not be treated withdrugs by any reasonable practitioner, eg, quiet conjunctival nevus, pin-guecula, corneal arcus, cornea farinata, or cornea guttata without edema.
Recording of Data and Variables StudiedFor all patients, I recorded on NCS Trans-Opticg computer cards dataconcerning all of the variables that are cited in the tables. Drugs, physicalagents, and preservatives were recorded only if they were used within 3weeks of the time of my first examination, so as to exclude medicationsthat probably had little or no effect in causing the drug reactions that wereobserved.
Computerization of DataAfter preliminary scanning and correction of out-of-bounds values, thedata were built into a data base using the Statistical Analysis System (SAS)of the SAS Institute, Inc, Cary, North Carolina. 18 Four sets of data werebuilt-one for each diagnostic category-thus facilitating analysis of eachset by itself or in combination with any of the others.
Analysis of DataFrequency counts were obtained by using SAS procedure FREQ for bothunivariate and cross-tabulation frequencies. 18
858

Topical Ophthalmic Therapy
I subjected frequency tables to chi-square testing to look for significantdifferences between diagnostic categories. In most instances I compareddrug cases with inflammatory controls because other comparisons wereapt to be less meaningful; there was usually no reason to compare drugcases with noninflammatory controls because patients in the latter cate-gory generally had no reason to be treated with drugs. Chi-squares wereobtained by using the library of BASIC statistical programs that werewritten by Janet C. Weber, PhD, of our Department of Ophthalmology.
All 2 x 2 chi-squares were calculated using Yates' correction for con-tinuity.'9 Chi-square tables larger than 2 x 2 were checked to be surethat they obeyed Cochran's rule. 19Homogeneity of variance was evaluated whenever t-tests and one-way
analyses of variance were performed. If the hypothesis of homogeneitycould not be accepted at the 10% level, the approximate statistic wascalculated.20 I used Satterthwaite's21 approximation for degrees of free-dom in cases of unequal variance.When the numbers of cases in two groups being compared were very
different, eg, 4 vs 793 cases, Fisher's19 exact probability method was usedfor the 2 x 2 tables. This method provides a P value, but not a x2 value.Two-tailed probabilities were calculated with this method, as well as withall other statistical analyses in this thesis.Groups of binary or dichotomous variables which were similar, such as
patients' complaints or drugs used, were often evaluated in combinationto see what patterns of variables occurred most or least often. I used the.method of Levine and Byrd22 to convert the binary variables into patternsof zeros and ones.
I considered as statistically significant those results which had probabil-ities (P) of less than 0.05 (5%), after rounding off to two decimal places, ofoccurring by chance alone.
LABORATORY STUDIES
CulturesI took all cultures and inoculated the media in the office prior to sendingthem to the University Microbiology Laboratory. For bacteria and fungi Iused sheep's blood agar, chocolate agar, beef-heart-infusion agar, Sabou-raud's agar without cycloheximide, and para-aminobenzoic acid broth.Epithelial scrapings for viral cultures were put into Hanks' balanced saltsolution medium for transport to the laboratory. I used the Anaswab® andAnaportg systems for anaerobic bacterial cultures.
859

Wilson
Light MicroscopyTissues for routine light microscopy were preserved in 10% neutral buf-fered formalin prior to processing by standard methods.
Electron MicroscopySpecimens for transmission electron microscopy were fixed in 3% phos-phate-buffered glutaraldehyde; rinsed in 0.1 M phosphate buffer; post-fixed in 1% phosphate-buffered osmium tetroxide; rinsed in 0.1 M s-col-lidine buffer; stained with s-collidine-buffered uranyl acetate-oxalate; anddehydrated in ethyl alcohol and propylene oxide. The tissues were em-bedded in Epon 812®. Thick sections were stained with 1% toluidineblue and were examined by light microscopy. Thin sections were stainedon copper grids with 2% uranyl acetate and lead citrate.
RESULTS
COMPUTERIZED EPIDEMIOLOGIC STUDY
Diagnostic CategoryThe number of patients in each of the four diagnostic categories is shownin Table I. Drug reactions occurred in 13.09% of all patients.
Year and Season of ReferralThe numbers of patients in different diagnostic categories did not differsignificantly by year or season of referral.
TABLE I: CLASSIFICATION OF PATIENTS BYDIAGNOSTIC CATEGORY
DIAGNOSTIC CATEGORY NO (%)
Drug cases* 134 (13.09)Inflammatory controlst 793 (77.44)Noninflammatory controlst 93 (9.08)Contact-lens cases§ 4 (0.39)
Total 1024 (100.00)
*Cases with clinically important adverse reac-tions to drugs.
tCases with inflammatory external ocular dis-eases but without adverse reactions to drugs.tCases with noninflammatory external oculardiseases and without adverse reactions todrugs.§Cases with adverse reactions to preserva-tives in contact lens solutions.
860

Topical Ophthalmic Therapy
AgeThe ages of patients in different diagnostic categories are tabulated inTable II. Contact-lens patients tended to be two or three decades young-
er than patients in other categories (contact-lens cases vs drug cases, P =
0.0119). Otherwise, age was not significant.
Sex, Marital Status, and RaceThese demographic features considered singly or in any combinationwere not significant.
Types of Treating PractitionersTable III shows the different kinds of practitioners who treated patientswith topical ophthalmic medications before referral to me.
Compared with inflammatory controls, drug cases were significantlymore likely to have been treated by each type of practitioner exceptnonophthalmic specialists and lay persons (patients themselves and theiracquaintances).The totals of the column percents in Table III show that, overall, drug
cases were treated by a wider variety of types of practitioners than were
patients in other diagnostic groups. The same can be seen better bylooking at Table IV, which shows the most frequent combinations (pat-terns) of kinds of treating practitioners. The variety of individuals whotreated drug cases as compared with inflammatory controls was highlysignificant (P = 6.07 x 10-7) when the five most frequent treating-prac-titioner patterns were considered.One of the patterns was that of no treatment, which admittedly consti-
tutes a bias in favor of showing a greater variety of treating practitionersfor drug cases since there could be no drug cases that were not treated.Nevertheless, the difference between drug cases and inflammatory con-
trols remained highly significant even when the no-treatment pattern wasexcluded (P = 1.30 x 10-4).
TABLE II: AGE
AGE
DIAGNOSTIC CATEGORY RANGE MEAN ± SD* MEDIAN
Drug cases 1-84 49.86 ± 20.37 54Contact-lens cases 15-33 23.75 ± 4.79 23.5Inflammatory controls 2-90 48.01 ± 21.65 50Noninflammatory controls 1-89 42.88 ± 22.13 40
*SD = standard deviation.Contact-lens cases vs drug cases: t = 2.5485, P = 0.0119, df = 136,indicating younger patients in contact-lens category.
861

Wilson
00 -I
E z ool,. .sX~~~~~~~0Cs_
a 8 OC Oq D D AC, E
;; xZ e aooo
C- 3 _
rar mt0 00eq inc O
C; 10C ct 0 0C> )o~ 8 0 a t X t > oo E
CU~iC' ~ci 6 iCU~ ~ ~ ~~ ~ ~ ~ ~ ~ ~ ~ ~~~~~~~r
z0 E m_ ^^ ° ot 3
FZ\e ; ° E | 8 i °
0~U -c
CU
C
CU~~~~~~~~~~~~~0
z~~~~~~~
862

Topical Ophthalmic Therapy
Eel] 0O
C's O6t~- oM
000 O
C 00 00
sOt- 00
- 0o
C O0 -cq1 ell_ t-
O e0O O QU:Ci C1 0_~~~~~~~~~~~
- 0 0 - t
in O't I"0 (0tO _
-
a0o
> 6 0I 0
I.. 0 0
(U 2- ,* U
o bCCd-wU 0 "I
863
c3)C-1
cl1
0,
8 8
o 0
00 OI6 CO
0Q 0
Ku oz z0z
Cu
z
0nU
Cu
Cu
z
0P:P:U
CuCu0
z
p
0
0
Cuz0
p
5
z
0
0
z
o
Lz~x
0
- CDco Ci
0
E'
wa bOo + o +0 a 0 0
;;4.E Xt+O M'-
bC Cu b- C)a.. C
b.a D*,a, S.C.) C.)
oz o
Oz CI

Even treatment merely by one or more ophthalmologists in addition tothe referring one was highly significantly associated with drug reactions(drug cases vs inflammatory controls, P = 1.62 x 10-4).
Number of Treating PractitionersTable V lists the number of practitioners who treated patients prior totheir referral to me. The number of treating practitioners was highlysignificantly related to the development of drug reactions (drug cases vsinflammatory controls, P = 2.20 x 10-7).As was the case with kinds of treating practitioners, there was a great
difference between the number of drug cases and the number of inflam-matory controls who were not treated at all, simply because it is impos-sible for a drug case not to have been treated; but, even after excludingcases that had no treatment, the presence of a larger number of treatingpractitioners remained highly significant for drug cases (drug cases vsinflammatory controls, P = 2.02 x 10-5).
Number of Practitioners ConsultedTable VI concerns the number of practitioners, whether they treated ornot, who were consulted by patients before seeing me. Drug cases con-sulted significantly more practitioners than did inflammatory controls (P= 0.00167).
Number of Practitioners Consulted Who Did Not TreatTable VII shows how often practitioners who were consulted did notprescribe treatment. Significantly fewer practitioners who did not treatwere consulted by drug cases than by inflammatory controls (P = 1.46 x10-4).
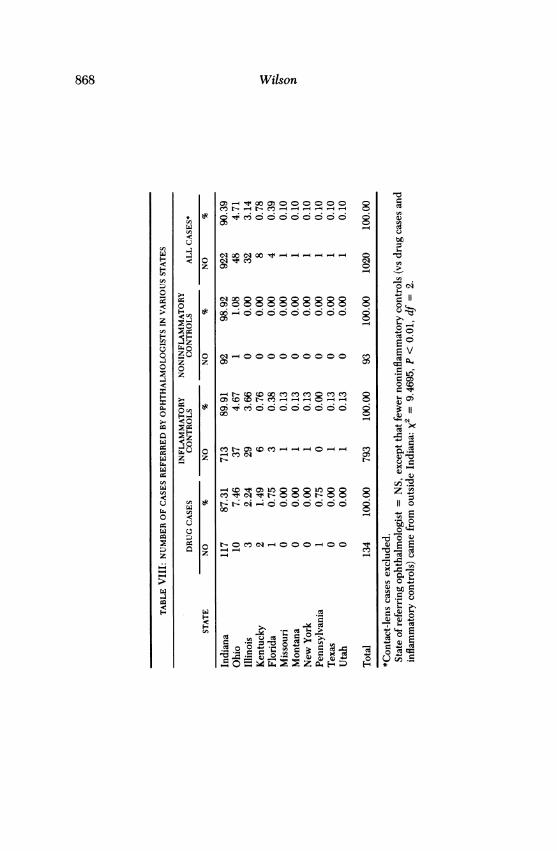
Towns and States of Referring OphthalmologistsTable VIII lists the number of cases that were referred by ophthalmolo-gists in various states. The cities or towns of their practices were alsotabulated and analyzed statistically but are not included in the Table.Altogether, there were 52 towns in 11 states. Thirty (57.69%) of the townswere in Indiana, and 22 (42.31%) were in other states. With two excep-tions, I found no significance either for towns or states of referring oph-thalmologists. There was one town in Indiana from which ophthalmolo-gists referred significantly more drug cases than inflammatory controls (P= 0.012). Significantly fewer noninflammatory controls, compared withdrug cases and inflammatory controls, were referred from outside Indiana(P < 0.01).
864 Wilson

Topical Ophthalmic Therapy
t-cli 5oo 9~
ZQU o oooo_o Cnz Z0
wo _)o c
z CzCn °z
OZ000000I t
tCt C5 C5
C; _z
0
ZOW-N n 0000
Q
00 -30-c
LL z
C)0 +~~~~zP ~ F
865
x
cs
N
et
Cco
clicli
00
P
r-
i1n
U,
unct
CZ
.^ 1'A
_CZ .C
x. C)btb
0;
r-
C)
z
6
4-
wF-
V)
z
0
Uw
0X
z
CF

866 Wilson
o 8>c c880 8
z zo - o
z
000000 8
a)C oo> __q,-scCIX r o ~~~- t- co) o o
o Q1 onckfoof 0
z z
>~~~~~cclo- El6z o6 XiO'c
z t jCOII
z z 1f~~cC3 1,t
0 0~~~~~~~~~~~~~~~~~~~~~~~~~~~I

Topical Ophthalmic Therapy
t- CIO1-
z c
z80
<0-n Z i ;4 <
0x ZU o Es0NOt-o00
no C')no °mo' eo co 8 8nx
z ze
c E
0 C>,f
-1c C)
U
6
0CIIC-1 CD~~~~~~~l
0~~~~~~
-~~~~~t
867
Wilson
o6 ° n° ° °85c5c i i< c
Cto CD00o cooooo 0c
e -- Co --- - - -
M 1-05 CI - - - 0I
00~~~~~~~~~
oz o"e8888 8 =1
w;e qoo oo o o D
t- C) CO C0 >o0 0 o
~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
0 S0 o oi-oooooooooe O 1
oto 0:
0 00
i;i CoQtOe oo
~4-
z ~~~~~~~~~~~~~~~no0 Oo3 ; z E2 |
868

Topical Ophthalmic Therapy
Referring OphthalmologistsAll individual referring ophthalmologists were tabulated using code num-bers instead of names. There were 170 in all. Drug cases were referred by78 individuals, representing 45.88% of referring doctors. Ninety-twoophthalmologists (54.12%) referred no drug cases.
It would not have been meaningful to compare each doctor with allothers because the number of cases referred by any one person was toosmall. Therefore, I looked arbitrarily at those individuals who referredthree or more drug cases and compared them with all other referringophthalmologists (Table IX) in an effort to determine whether drug-casereferrals were distributed evenly throughout the sample of referringdoctors or whether a relatively small proportion ofpractitioners referred adisproportionate number of drug cases.There were 14 ophthalmologists who referred three or more drug
cases; the incidence of drug cases among all referrals by these physiciansranged from 13.04% to 75.00%. The 14 doctors (8.24% of all referringophthalmologists) referred 39.55% of all drug cases and referred a signifi-cantly higher percentage of drug cases, as opposed to inflammatory con-trols, than did the other 156 referring physicans (P = 1.609 x 10-5,Table IX).To compare those physicians who referred three or more drug cases
with others, I looked also at ophthalmologists who referred ten or moreinflammatory controls because these doctors obviously saw, and referred,substantial numbers of patients who might conceivably have requiredtreatment with topical drugs. Only one of these doctors referred a per-centage of drug cases (14.29%) that was within the range of that of the
TABLE IX: COMPARISON OF REFERRAL PA1TERNS OF OPHTHALMOLOGISTSWHO REFERRED THREE OR MORE DRUG CASES WITH THOSE OF ALL OTHER
REFERRING OPHTHALMOLOGISTS
DRUG CASES INFLAMMATORYREFERRED CONTROLS REFERRED
REFERRINGOPHTHALMOLOGISTS NO % NO %
Those who referredthree or more drugcases (n = 14) 53 39.55 153 19.29
All others (n = 156) 81 60.45 640 80.71
Total 134 100.00 793 100.00
The 14 ophthalmologists referred a higher percentage of drug cases, ascompared with inflammatory controls, than did all other ophthalmolo-gists: X2 = 26.0592, P = 1.609 x 10'.
869

doctors who referred three or more drug cases. All of the other physicianswho referred ten or more inflammatory controls referred drug cases witha frequency of only 0.00% to 9.09%, indicating that only some ophthal-mologists who see inflammatory external-ocular diseases get into troublewith drug reactions more than 10% of the time, as judged by theirreferrals.
General Locations of Referring OphthalmologistsThe general locations (northern, central, or southern Indiana or out-of-state) of referring ophthalmologists were not significantly related to thekinds of cases that were referred, except that significantly fewer nonin-flammatory controls were sent from out-of-state (P < 0.01).
General Locations of Patients' ResidencesThe general areas of residence of patients in various diagnostic categorieswere not significant.
Comparison of General Locations of Referring Ophthalmologistsand PatientsI calculated how often referring ophthalmologists and patients in variousdiagnostic categories were from the same or different general locales. Imade this comparison to find out whether "doctor-shopping" (which in-cludes forsaking nearby ophthalmologists for more distant ones) was as-sociated with drug reactions; it was not.Patients' ComplaintsTable X lists the symptomatic complaints that were voiced by, or elicitedfrom, patients in different diagnostic categories. "Other" complaints in-cluded blepharospasm, ectropion, entropion, inturned lashes, loss oflashes, bloody tears, conjunctival hemorrhage, difficulties with contactlenses, and "something my doctor wanted checked."
All complaints except opacity, mass or pigmentation, blepharitis, and"other" were more frequent in the drug-case group than in the inflamma-tory-control category. Five complaints were statistically significant: red-ness, P = 6.6 x 10-7; photophobia, P = 0.019; itching, P = 0.0056;tearing, P = 0.0036; and discharge, P = 1.94 x 10-6.Number of Patients' ComplaintsPatients in various diagnostic categories are classified according to num-bers of symptomatic complaints in Table XI. The number of complaintswas significantly greater for drug cases than for inflammatory controls (P< 0.0001). The prime symbols in the footnote of the Table, eg, t' asopposed to t, indicate that variances were unequal.
870 Wilson

Topical Ophthalmic Therapy
o 0o080"f-84 80888C0
No0 1- oo-o-oI 000ocz z -
sc qo -o xz 0
-U~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
z Zw CO0d Qc oeOU)sObC )F ucq c
0~~~~~~~~~~~z0
8 0 o o- o -cs co c00oci_ _ .z -o~0 cS 0 In -_It-0 000 cq e0
<~~~c -; 4 5 ?-6 cs cs cD C4 4 0U)c's ci C4 C5 t-
0z z 0C'1s - - n b m O _ V e 00 01
U~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~o 11 -,;a
S~~~~~~~~~~~~~~~~~~~~~~fEFX 0e ">t:Og>nII> 0s.o
11CqC
-o~~~~~~~~~~~~~~t, 0 o0 0 C o 0q o o _ 0 0 xU l3O_ 0 cs cs ot- cs4 U" cq_-_ Dbo Ocq0o stcs t. l
v vC C) 0 r- to1
0 5 ° Q D E~~~1 t--- c5i o6;6 c. ,. 6 6 i6 B i .c o6 x ;
z:: m v=v v > Xo Xv o- -0~
871

Wilson
ciCN )II,CClcE; cs
06 L6 C'o 5C 5C
& ci~~~~~~~~~~~~c
<H ~~~~~~~~~~~~~~~~~~~+1C
o o_ Ntt c o o o o o o C CD co °
z z _ -s_az
LO LO x_ LON tooc
-F <0 -e ci b2 _ r c c
CD
,z c, @ o s t e n t x s o o o oci
oUOtc-I) c cs N 3 CO _ LK r
H -
ot
H ZU cNliS<~~~~~~c8lclo9o _o_oo
0
X~~~~~~11
.. C _ _'_CI Lt~~~~~~J co co) o
J -zOc_cinci-c9 2
z~~~~~~~~~~~~t ~~ ~ ~ ~ ~ ~ c G
zw - irS 0
H~~~~~~~~~~~~~~~
z
>1
872

Topical Ophthalmic Therapy
Number of Ophthalmic Preparations Used by Patients for PresentIllnessesTable XII shows the total numbers of topical ophthalmic preparations thatwere used by patients from the onsets of their illnesses to the times theywere seen by me. Each drop or ointment was counted as a single prepara-tion, even though it may have contained more than one pharmacological-ly-active ingredient in addition to preservatives and other additives.Drug cases used a mean of 4.28 + 2.38 preparations (range, 1 to 13).
The patient who used 13 medications was actually exposed to a total of 19pharmacologically active agents and 14 preservatives (33 different chemi-cals, not counting buffers, vehicles, and the like). The mean for inflamma-tory controls was 2.01 + 1.66 (range, 0 to 10). Drug cases used signifi-cantly more preparations than did inflammatory controls (P < 0.0001).Compared with inflammatory controls, drug cases also used multiplepreparations (number uncertain) significantly more often (P = 7.48 x10-5).There were 200 cases that had no treatment. Of the 824 treated cases,
134 were drug cases (Table I), so the incidence of drug reactions amongtreated cases was 16.26% (134/824).
Number of Ophthalmic Preparations Being Used by PatientsWhen Seen by MeThis information is in Table XIII. The mean number ofpreparations beingused by drug cases was 1.69 ± 1.42 (range, 0 to 9), whereas the mean forinflammatory controls was 0.98 + 1.00 (range, 0 to 5). Some drug caseswere using nothing when I saw them because the referring physicians orthe patients stopped treatment in anticipation of the consultation. Never-theless, reactions from previously used medications were often still pres-ent, and drug cases were using significantly more preparations than wereinflammatory controls (P < 0.0001).
Number of Days of Treatment Prior to ReferralTable XIV shows the total number of days patients were treated before Isaw them.The mean for patients who had drug reactions was 246.95 ± 760.545
(range, 5 to 5475) days; for inflammatory controls it was 67.36 ± 213.146(range, 0 to 2190) days. Drug cases were treated significantly longer thanwere inflammatory controls (P = 0.0178).
873

Wilson
rt- cli
0M C) o o co0o0000
- CcI -
M C toi o nO I, cMcM -_ 00010 1- 0 t- M -
_10 N_1
8 8 8
C)
00 0 0)00 0)
r~- 0M CIO
o o0o
t-
o C)
_ _0_400_O000000000 0 0
0t~~-0)-rq- M C-t- C,6 i6C6U) _0 C6Cn 0 0U O ci
MSCM - _ttoM CtLO C O~O O O Cn co
00)00 C -e0 0u0C1 -_ _0 0) C)
C6~
O_CC)'t'10 0t-000_)0 + z o0"0- 000)v
2'
874
V:
z0)Ut
0
z
.-
0.
0
0)
0
0
z9
0.
::
4..0
Lf
Zz Z
60
20uO_ 0
z 8
QZU
U0Z
Zz
0)
00co"Itl6
cq+1
CS
0
-
O_
+1
C)
CS
6
0!
+1in
00co
00C0
10
<,00
^b
|4-1
;e CZ
o *
0
as= Xco
E Mt
bbbt
0C)4.-
0t -t C)
G .5 "0>xt
o Y N,
*-
8
1-
C0+1
00 =

Topical Ophthalmic Therapy
oc 8 GOO 8 8 8 8 8 8 8
-cs _co o o o o
00 _
0 _
05 cq u: in cq_oooo
c c elq
t-wo eq-oooo
-16
co cq CDeq
eq
-D e~ i
Ct ci-
0 cb o- O _
0 eq
0D 0
66~
0
CU
(U t ~~~ -2 +1
== C
875
z
z
CA
z
z
x
z
w
m
zQ ozz0
<0
0
in
816
00,
6
-+1ind
eq
't(M+1
0,
11
6
16ro.o
19CU0
P0
10CU
C
eo
..un
.o
8t,04-
. £CE
Q)
£o6
8 IQ

Wilson
TABLE XIV: NUMBER OF DAYS OF TREATMENT PRIOR TO REFERRAL
DAYS OF CONTACT-LENS INFLAMMATORY NONINFLAMMATORYTREATMENT DRUG CASES CASES CONTROLS CONTROLS
Range 5-5475 0 0-2190 0-2920Mean ± SD 246.95 ± 760.545 0 67.36 ± 213.146 40.44 ± 337.191Unknown 28 (20.90%) 3 (75.00%) 399 (50.32%) 18 (19.35%)
Drug cases vs inflammatory controls (mean days of treatment): t' = - 2.4059, P = 0.0178, df' =109.5.
Number of Nondrug Cases in Which Treatment Was Avoided, Stopped,or Substantially Reduced Three Weeks or More Prior to ConsultationNot infrequently, referring ophthalmologists purposely avoided, stoppedor substantially reduced treatment once they decided to refer patients forconsultation. Patients themselves sometimes did the same, especially ifprior treatments seemed not to help. Table XV shows how often thisoccurred and so gives some indication of how many patients might havehad drug reactions that were not evident at the times ofmy examinations.
I considered reduction of treatment to have been "substantial" if morethan half of a patient's medications had been discontinued. I judgedwhether a drug reaction might previously have been present by consider-ing not only the number of drugs that had been stopped, but the kinds ofdrugs and whether their cessation made the patient better or worse. Ofcourse, these data are based largely on educated guesses; I tabulatedthem not for the sake of speculation, but to estimate as best I could mypossible margin of error in calculating the incidence of drug reactions, ie,how many drug cases I might have missed simply because I did not seethem quite soon enough.
Thirty (3.78%) of the inflammatory controls were thought to have haddrug reactions that disappeared by the time they came to me, so theincidence of drug cases could have been as high as 16.02% (134 definitedrug cases + 30 probable ones = 164 + 1024 total cases) instead of13.09%. Among treated cases (Table XII) this would represent a possibleincidence of 19.90% (164 . 824 treated cases). Ninety-two (11.60%)other inflammatory controls may have had drug reactions, but the evi-dence was weak.
Eye(s) Involved with Primary DiagnosisThere was no significance to the eye(s) involved, except that all of thecontact-lens cases were bilateral.
876

Topical Ophthalmic Therapy
TABLE XV: NUMBER OF NONDRUG CASES IN WHICH TREATMENT WAS AVOIDED, STOPPED, ORSUBSTANTIALLY REDUCED THREE WEEKS OR MORE PRIOR TO CONSULTATION*
CONTACT-LENS INFLAMMATORY NONINFLAMMATORYCASES CONTROLS CONTROLS
AVOIDANCE OR REDUC-TION OF TREATMENT NO % NO % NO %
No 2 50 459 57.88 84 90.32Yes, and drug reaction
probably occurred 0 0 30 3.78 0 0.00Yes, but drug reaction
probably did not occur 1 25 203 25.60 8 8.60Yes, uncertain whether
drug reaction occurred 0 0 92 11.60 0 0.00Unknown 1 25 9 1.13 1 1.08
Total 4 100 793 100.00 93 100.00
*These data indicate that the incidence of drug reactions among all patients might haveranged anywhere from 13.09% (Table I) to 16.02% (see discussion of Table XV in text); andamong treated patients, from 16. 26% (Table XII) to 19.90% (discussion ofTable XV in text).
Drugs Used by Patients with Drug ReactionsTable XVI lists the pharmacologically active agents which were used bypatients who had drug reactions. For comparison, the Table also showsthe frequencies of use of these drugs by patients in the inflammatory-con-trol group and (in the footnotes) the other two diagnostic categories.
Drugs which are available in various concentrations were designated as"weak" or "strong," depending on whether the concentration was above orbelow the mean of the strengths in common use. For example, pilocar-pine is available in concentrations of 0.25% to 10%; but only strengths upto 4% are in general use, so I considered anything less than 2% as weakand more than 2% as strong.
Drugs which are marketed both as drops and ointments were alsotabulated separately according to the form used.The same drug was sometimes present in more than one (although
never in more than two) of the medications used by a patient, and thisinformation was also recorded.Drug cases used a total of 44 different pharmacologically active agents,
not counting different forms and strengths and unspecified drugs. These44 drugs represent 83.02% of the 53 pharmacologically active drugs whichwere used by all patients. Contact-lens cases used none of the drugs, andnoninflammatory controls used only four: bacitracin, cyclopentolate,physostigmine, and prednisolone.
877

Wilson
TABLE XVI: DRUGS USED BY PATIENTS WITH DRUG REACTIONS*
INFLAMMATORYDRUG CASES CONTROLS SIGNIFICANCE
DRUGS USED NO % NO % P
Acetylcysteine, strong(20%)
AmphotericinAntazolineAntipyrineAtropine, dropsAtropine, ointmentAtropine, unspecifiedAtropine, all formsBacitracin, in one medi-
cationBacitracin, in two medi-
cationsBacitracin, totalCarbachol, strong (> 1.5%)Chloramphenicol, dropsChloramphenicol, ointmentChloramphenicol, un-
specifiedChloramphenicol, all formsCromolyn (4%)CyclopentolateDexamethasone, in one
medicationDexamethasone, in two
medicationsDexamethasone, totalDipivefrinEchothiophate, strong (>0.125%)
Epinephrine bitartrate,weak (< 1%)
Epinephrine hydro-chloride, weak (-G 1%)
Epinephryl borate, strong(> 0.5%)
Epinephrine, all forms, in-cluding dipivefrin
ErythromycinFluorometholoneGentamicin, drops, in one
medicationGentamicin, drops in two
medicationsGentamicin, drops, totalGentamicin, ointmentGentamicin, unspecifiedGentamicin, all formsGramicidin
4 2.99 01 0.75 13 2.24 79 6.72 217 5.22 234 2.99 46 4.48 817 12.69 35
12 8.96 34
3 2.24 015 11.19 341 0.75 1
20 14.93 483 2.24 9
2 1.49 125 18.66 581 0.75 24 2.99 3
15 11.19 31
0 0.0015 11.19 t1 0.75
1 0.75
1 0.75
2 1.49
1 0.75
5 3.737 5.228 5.97 '
22 16.42
1 0.7523 17.1611 8.213 2.24
37 27.61 t13 9.70
0.00 17.334 1.465 x 10-40.13 .. NS0.88 ... NS2.65 4.829 0.02642.90 ... NS0.50 5.600 0.01721.01 7.087 0.007854.41 13.296 5.29 x 10-4
4.29 4.35 0.0349
0.00 11.55 0.00114.29 9.58 0.00240.13 ... NS6.05 12.00 8.965 x 10-41.13 NS
0.13 NS7.31 16.73 1.762 x 10-40.25 NS0.38 7.21 0.0074
3.91 11.40 0.0011
1 0.13 NS32 4.04 10.76 0.00151 0.13 NS
0.13 ...
0 0.00 ...
3 0.38 ...
2 0.25 ...
6 0.76 6.3017 2.14 ...2.,8 3.53 ...
17 2.14 54.46
NS
NS
NS
NS
0.012NSNS
2.25 x 10-7
0.00 ... NS2.14 59.05 1.397 x 10-71.26 21.95 4.156 x 10-50.50 ... NS3.91 91.29 1.064 x 10-81.89 21.28 4.928 x 10-5
878

Topical Ophthalmic Therapy
TABLE XVI: DRUGS USED BY PATIENTS WITH DRUG REACTIONS* (CONTINUED)
INFLAMMATORYDRUG CASES CONTROLS SIGNIFICANCE
DRUGS USED NO % NO % x2 p
Homatropine 8Hydrocortisone, in one
medication 4Hydrocortisone, in two
medications 1Hydrocortisone, total 5Idoxuridine, drops 12Idoxuridine, ointment 11Idoxuridine, unspecified 2Idoxuridine, all forms 25Medrysone 1Naphazoline, in one medi-
cation 4Naphazoline, in two medi-
cations 1Naphazoline, total 5Neomycin, drops, in one
medication 23Neomycin, drops, in two
medications 2Neomycin, drops, total 25Neomycin, ointment, inone medication 8
Neomycin, ointment, intwo medications 1
Neomycin, ointment, total 9Neomycin, unspecified 1Neomycin, all forms 35Pheniramine 1Phenylephrine, in one
medication 9Phenylephrine, in two
medications 1Phenylephrine, total 10Physostigmine, in one
medication 1Physostigmine, in two
medications 0Physostigmine, in three
medications 0Physostigmine, total 1Pilocarpine, weak (< 2%) 3Pilocarpine, strong (> 2%) 2Pilocarpine, unknown
strength 3Pilocarpine, any strength 8Polymyxin, drops, in one
medication 22
5.97 31 3.91 ... NS
2.99 3
0.75 03.73 38.96 78.21 91.49 2
18.66 180.75 9
2.99 16
0.75 03.73 16
17.16 28
1.49 118.66 29
5.97 10
0.75 06.72 100.75 0
26.12 390.75 1
6.72 30
0.75 07.46 30
0.75 0
0.00 1
0.38 7.21 0.0074
0.00 ... NS0.38 11.40 0.00110.88 33.29 3.995 x 10-61.13 23.92 2.590 x 10-50.25 ... NS2.27 65.93 7.283 x 10-1.13 ... NS
2.02 ... NS
0.00 ... NS2.02 ... NS
3.53 38.40 1.749 x 10-6
0.13 ... NS3.66 44.32 7.574 x 10-
1.26 10.99 0.0013
0.00 ... NS1.26 14.38 3.77 x 10-40.00 ... NS4.92 67.290 6.456 x 10-80.13 ... NS
3.78 ...
0.003.78 ...
0.00 ...
0.13 ...
NS
NSNS
NS
NS
0.00 2 0.25 ... NS0.75 3 0.38 ... NS2.24 11 1.39 ... NS1.49 7 0.88 ... NS
2.24 2 0.25 5.136 0.02225.97 20 2.52 ... NS
16.42 27 3.40 36.217 2.457 x 10-6
879

Wilson
TABLE XVI: DRUGS USED BY PATIENTS WITH DRUG REACTIONS* (CONTINUED)
INFLAMMATORYDRUG CASES CONTROLS SIGNIFICANCE
DRUGS USED NO % NO % x2 p
Polymyxin, drops, in twomedications
Polymyxin, drops, totalPolymyxin, ointment, inone medication
Polymyxin, ointment, intwo medications
Polymyxin, ointment, totalPolymyxin, all formsPrednisolone, in one medi-
cationPrednisolone, in two medi-
cationsPrednisolone, totalPyrilamineScopolamineSulfacetamide, drops, inone medication
Sulfacetamide, drops, intwo medications
Sulfacetamide, drops, totalSulfacetamide, ointment, inone medication
Sulfacetamide, ointment, intwo medications
Sulfacetamide, ointment,total
Sulfacetamide, all formsSulfisoxazole diolamineTetracaineTetracycline, dropsTetrahydrozolineTimolol, strong (0.5%)TrifluridineTropicamideVidarabineZinc sulfateOne drug, unspecifiedTwo drugs, unspecifiedThree or more (multiple)
drugs, unspecifiedt
2 1.49 124 17.91 28
10 7.46 16
1 0.75 011 8.21 1635 26.12 44
12 8.96 69
0 0.00 112 8.96 701 0.75 03 2.24 2
15 11.19 82
2 1.49 417 12.69 86
9 6.72 13
1 0.75 0
10 7.46 1327 20.15 993 2.24 02 1.49 11 0.75 13 2.24 1110 7.46 105 3.73 41 0.75 3
24 17.91 231 0.75 14 2.99 534 2.99 14
7 5.22 1
0.13 NS3.53 49.09 1.024 x 10-6
2.02 10.55 0.001065
0.00 ... NS2.02 13.426 5.275 x 10-45.55 59.61 1.322 x 10-7
8.70 ... NS
0.13 ... NS8.83 .. NS0.00 ... NS0.25 5.136 0.0222
10.34 ... NS
0.50 ... NS10.84 ... NS
1.64 10.656 0.0015
0.00 ... NS
1.64 13.75 4.702 x 10-412.48 5.100 0.02230.00 11.547 0.00120.13 ... NS0.13 ... NS1.39 ... NS1.26 18.249 1.119 x 10-40.50 9.285 0.002760.38 ... NS2.90 50.586 3.482 x 10-0.13 ... NS6.68 ... NS1.77 ... NS
0.13 29.115 8.605 x 10-6
*Only drugs used by patients within 3 weeks of their being seen by me are included; drugs thatwere not used by any drug cases are excluded from this table.No contact-lens patient used any of the drugs in this table; noninflammatory controls used four(each by one patient only): bacitracin, in one medication; cyclopentolate; physostigmine, in onemedication; and prednisolone, in one medication.
tThis does not specify the total number of cases that used three or more drugs (see Table XII), butonly the number of cases that used three of more unspecified (unknown) drugs.
880

Topical Ophthalmic Therapy
Ten Drugs Used Most Commonly by Patients with Drug ReactionsThese are shown, in order of decreasing frequency, in Table XVII.
Physical Agents Used by PatientsThe type and number of physically active agents (artificial tears, lubricat-ing ointments, hypertonic agents, and contact lens solutions) that wereused by patients are listed in Table XVIII. Unlike pharmacologicallyactive drugs, physical agents were used by patients in all diagnosticcategories; but drug cases used no physical agent significantly more oftenthan did inflammatory controls. Not unexpectedly, patients who hadreactions to contact lens solutions did use such solutions significantlymore often than did inflammatory controls (one or two contact lens solu-tions: P = 2.262 x 10-4; any use of contact lens solutions: P = 8.390 x10-9).
Preservatives in Medications Used by PatientsTable XIX shows the preservatives to which patients were exposed byreason of their use of topical ophthalmic medications, including physicalagents and, in the case of contact-lens patients, contact lens solutionseven if they were not instilled directly onto the eye.Drug cases were exposed to certain preservatives significantly more
often than were inflammatory controls (see Table XIX for statistical val-ues).
TABLE XVII: TEN DRUGS USED MOST COMMONLYBY PATIENTS WITH DRUG REACTIONS*
PATIENTS WITH DRUGREACTIONS
DRUGS USED NO %
Gentamicin 37 27.61Neomycin 35 26.12Polymyxin 35 26.12Sulfacetamide 27 20.15Chloramphenicol 25 18.66Idoxuridine 25 18.66Vidarabine 24 17.91Atropine 17 12.69Dexamethasone 15 11.19Bacitracin 15 11.19
*Despite their inclusion in the "top ten," notall of these drugs are likely to cause drugreactions; see discussion in text.
881

Wilson
> oe g't o o o 't el _ 0 VI 0o0 eq 0oI=Go m co _oZoo n oo ocX
- 1 -0 C0Z .o ocq
00 00
m~~~~~~~~~~~~~N°2u°oX~~~~~~~~~~~0 ItItIgn°°E38°°°°HS A, o x,, w .CU
0~~~1
Z <Z Z O 8 3W t- oU~~~~~~~~~~~UOZeOOO e tOOOO>>OtOqJC.8
0 z o ~~~~~~~~~~~~~~~r Q m
Z
as 8 co 0 08 8 ° o t 3
_~~~~~~~~~~~~~~~~~~~~ X00tce0_o_0o_o s3-c; 8 x1
Wu ) O '08
Sva Q@, = t Q 2 e _ X | _5,0 U
ell -ioeD C- O cq co
,, O _D_ CO)
cu
z~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
0)~~~~~~~0 CU4-
0U 4.
0z O
~~~4
882

Topical Ophthalmic Therapy 883
z > cp-nz rt zzzzz z zzz z x
Q z'z oz
z >e- D- -- - - -
u;O x N S xx xxx x x ul x cn
0 z _~~ 0 roNteo
*~~~~~~~~~~~~~~~~~~~Z >zo - co o° e 8 o 8 0-4 - g g
Pz SzC4 C
m~~~~~~~~~~~~~~0 8zo0 t0 -0 it c-ici 04 5
mo zv 0 0 1,_ 0 0-q1ts C00 eN 0
z z
0z
Niz~~~~~o c6 6 I o 6 6o6 o6e6 ; C
z0
z z o- o 4o N
_ C> C in100c 1_ loin
z 01t olONs N0bs
0 0 0 C) 0 -4ciU b o- 4 CO_ oM- eqinCo 0!0gY
wt- t- t- cq In t- N~eqr r- tC-
'~~~~~ Z ~~~~~~~~~o eq cif e
Q 00000 0~~~~~- M-4 1-4 eq -cq
Q~~~~~~~~~~~~~Q)> Q e r 0i 01-- oo- c<0 c1e.- Cq
0~~~~~~~
o 0 0 bO ~~ 0'R X Z.0~~~~~~~~~~~~~~C

cn cn Cl) cn0 z z m 8$zzzz z z zzz ze-1-o
66
6: 6
000
6 6
00 0 0cl 2 C43 o
-!_ _4
N Ut _ oo)oo oo
666Z 0
8 8
o o)
0C0_ 0
m 91o _4
-4
_- 05oo
-0
oo U) aa
ao Z o
_4 o -4
U113C)eo
t- - ocQ cs
000cn0cnzzzz
eqctU)U cncn v)ctzzz z8zo
6 6
CO O es
C-i O C-i
C')0 C'
C- - C')
1- -""0007) 07)
geo~O O U)Ci Cin Cin
0000 0 0 _0_
C~6C C 6 65 4 5- e eq -- "-
Oc U O U- 0 t- 0 ) 0e eq eq - eq
eq - C')
t- 0 t-
Co O O C",CiOOCi
CO) O- O
oo C0 cO
_ _4
eC 0 009eq eq-
0 0 O 0
O C) 0 0
C 00 0n 0O00t0 0
_ CD NC'e _C
0)v/oJ) _ 0 0 0e_c<SE_C00 09 o"e
Z U. z
0 Z
z =-
Z
UaQ0
.)0z :Q Cz
0Z
0zz
0
z
0
~zUoz z
z
0 eC)Z
U z
w tR
C)
0
aw
zz0W3
zp
ZF
0
Q
U)
z0
Q0
p0Ut
Oi
0
0-
xw.-
co
Z jo0 Ww2u

OQ U) Ct Ct Cn U)O z zz z z6
00 CI
66
o5 o
C's c5 6 6
COOCO
00 00 t -
II oo CV 8 C)
4 -0
(M -4L
I0
cooz; z z z z z z 8
Cl)
t- N0
o o 0o 0
CO cq O cC01
8 8 8888
Cn C5 C56 C;
eqC O Oc)C
- 0 0M CD- 1-n cli ci66c.-
_c to o
- 0 0)OC)C~0_00
1-
cO Q cq
CO 0 CO
-COO CC CO
C011 C'
in _
Ce6 OC] U)
-n0 0 0e C 0 o0c
CO 00 0) O _1
Os C C 4 C-~6
in 01 CIO C COt ~ ~ ~ wstc s c
0 ~ ~ ~ s s - '
b
0>
r >41Od c l -t C0 OC
a,E 4 E Xj c
Cd
v v e
Coto
t-
t-
0C-
cn
Uptz *;
z
z z
0
>U Q
EZI
z8 zz
0u:Z z
U ZO
ziV0.
aW
zZ
0U
zWP
0
z0V)
Oz
0
P
aW7_
0.kX-
..
_
-1go

0
0
6d
IT"
C0cn 0cn V) cIzzzz z
i, 0000
C.-O
C', 0000O
t0C' m10i
to Z Z Z
t- o6~
a;O C5
eq -
t- Ci-C.]C' Oeq
Cnz
Ut
6
in
ci
ineq
CV)
-
0
t-
1-
x
6
0
8
U)
6
0
C43
I,,:i
vCi
b .) .,.
a'C i.CuC
Cu"
CuCuC._Cu
Cu
a.)
G.V)
NG.)
0X
Cu"0C
.2tC0oCu"-
z R8
a. .b-.°CX,, CCu#3>-
Cuo.)>-.D
2 vo
1.. 0*-;CuU
G. b n* ;-,-
886
CX Cl) CnZ Z Z
cn cn cnZ Z Z
_ Ct 0
C;_;C
C. , U.
CiC_ C
zz_
C o C'3
000o
000C
Ut4->
X
o gU.CD_ Z
oL
:
z z
Z Zz
0
z
<0~Cu58 0z z
Utz
z
o 0
if
Ut
C-,
CT.u0 z
z r.0
-*y
aiWZ
zP
z
0
V-)
cn
I-z
co
ifWrA
c-
z0P
13
C-
W2
z
ifW
..
Wif
W
Cu
an
ifCu

Topical Ophthalmic Therapy
Contact-lens cases were exposed to the following preservatives signifi-cantly more often than were inflammatory controls: boric acid; chlorhexi-dine gluconate; edetate, strong (> 0.5%); edetate, any strength; thimero-sal, weak (s- 0.005%); and thimerosal, any strength.
Diagnoses Associated with Drug ReactionsTable XX lists, in order of frequency, all diagnoses that were associatedwith drug reactions. Most of the diagnoses were underlying ones, ie,conditions for which patients were seen and treated by referring oph-thalmologists, but some of them (denoted in the Table by italics) couldhave been the results of drug reactions themselves.
Seventeen patients (12.69% of all drug cases) had no diagnoses otherthan drug reactions. Ofthe remaining diagnoses, 33 (47.14%) representedactive processes, whereas 37 (52.86%) were inactive (22 cases, 31.43%) orresolving (15 cases, 21.43%) problems.
Association of Keratoconjunctivitis Sicca with Specific Drug ReactionsI looked more closely at the diagnosis ofkeratoconjunctivitis sicca becauseit was the most common underlying diagnosis and because I had theclinical impression that it was an important predisposing factor for thedevelopment of drug reactions-at least for toxic papillary ones.
Keratoconjunctivitis sicca was more common, but not significantly so,among drug reactions as a whole (21.64%) than among inflammatorycontrols (15.76%, Table XX); but when I looked individually at specifickinds of drug reactions, I found that keratoconjunctivitis sicca was associ-ated significantly more often with toxic papillary reactions than withinflammatory controls (P = 0.0224, Table XXI). Furthermore, 27 of the29 patients (93.10%) who had keratoconjunctivitis sicca and drug reac-tions had toxic papillary reactions without scarring.
Most Common Diagnoses Among All PatientsThere were 36 diagnoses that had an incidence of more than 1% among allpatients of all diagnostic categories. Seven diagnoses (19.44%) were, ormight have been, drug or preservative reactions. All of the possiblydrug-related problems occurred with a frequency of less than 3%, exceptfor toxic papillary reactions without scarring; this was the third mostcommon diagnosis, occurring in 10.35% of all patients in the study,surpassed only by keratoconjunctivitis sicca and herpetic keratitis.Drug reactions as a whole (excluding reactions to preservatives in
contact lens solutions) numbered 134 (13.09%, Table I) and so constitutedthe second most common diagnosis, exceeded only by the 155 cases(15.14%) of keratoconjunctivitis sicca.
887

Wilson
TABLE XX: DIAGNOSES ASSOCIATED WITH DRUG REACTIONS
DIAGNOSES
INFLAMMATORYDRUG CASES CONTROLS SIGNIFICANCE*
NO % NO % P
Keratoconjunctivitis sicca 29Herpes simplex keratitis, inac-
tive 22Post-herpetic indolent epithe-
lial ulcert 19.No diagnosis.other than drug
reaction 17Glaucoma, active 14Herpes simplex keratitis, re-
solving 10Indolent epithelial ulcer (not
post-herpetic), active 8Herpes simplex keratitis, active 7Lacrimal outflow obstruction 5Chronic atopic keratoconjunc-
tivitis, active 4Adenoviral keratoconjunc-
tivitis, resolving 3Anterior-membrane corneal
dystrophy, active 3Herpes zoster keratitis, inac-
tive 3Infectious eczematoid dermati-
tis 3Neurotrophic keratopathy 3Recurrent corneal erosion syn-drome, inactive 3
Staphylococcal blepharitis, ac-tive 3
Acute catarrhal conjunctivitis,resolving 2
Adenoviral keratoconjunctivi-tis, inactive 2
Chalazion, active 2Corneal ulcer, bacterial or fun-
gal, inactive 2Herpes zoster keratitis, re-
solving 2Pemphigoid 2Recurrent corneal erosion syn-drome, active 2
Salzmann's nodular corneal de-generation 2
Seborrheic blepharitis, active 2Superficial punctate keratitis ofThygeson, resolving 2
Superior limbic keratocon-junctivitis, active 2
Trachoma, inactive 2
21.64 125 15.76 NS
16.42 34 4.29 3.836 x 10-6
14.18 7 0.88 5.313 x 10-8
12.69 0 0.00 8.123 x 10-910.45 39 4.92 0.0272
7.46 18 2.27 0.0074
5.97 11 1.39 0.00585.22 33 4.16 NS3.73 2 0.25 0.00194
2.99 8 1.01 NS
2.24 7 0.88 NS
2.24 37 4.67 NS
2.24 6 0.76 NS
2.24 5 0.63 NS2.24 6 0.76 NS
2.24 10 1.26 NS
2.24 48 6.05 NS
1.49 1 0.13 NS
1.49 0 0.00 0.04161.49 0 0.00 0.0416
1.49 0 0.00 0.0416
1.49 5 0.63 NS1.49 10 1.26 NS
1.49 18 2.27 NS
1.49 4 0.50 NS1.49 34 4.29 NS
1.49 0 0.00 0.0416
1.49 8 1.01 NS1.49 12 1.51 NS
888

Topical Ophthalmic Therapy 889
TABLE XX: DIAGNOSES ASSOCIATED WITH DRUG REACTIONS (CONTINUED)
INFLAMMATORYDRUG CASES CONTROLS SIGNIFICANCE*
NO % NO % P
TrichiasisAcute catarrhal conjunctivitis,
inactiveAnterior-membrane corneal
dystrophy, inactiveAphakiaChemical burn, activeChronic catarrhal conjuncti-
vitis, activeConjunctival telangiectasia
(Osler-Weber-Rendu)ConjunctivochalasisCorneal abrasion, activeCorneal abrasion, inactiveCorneal edema secondary to
iridocyclitisCorneal laceration, inactiveCorneal perforation, inactiveCorneal ulcer, bacterial or fun-
gal, resolvingEntropionErythema multiforme, inactiveErythema multiforme, resolv-
ingGlaucoma, resolvingHerpes zoster keratitis, activeInclusion conjunctivitis, activeIndolent epithelial ulcer (not
post-herpetic), resolvingInterstitial keratitis, inactiveIridocyclitis, activeKeratoprosthesis, infectedMooren's corneal ulcer, inac-
tivePapiUary keratoconjunctivitis,
contact-lens-induced, activefPapillary keratoconjunctivitis,
contact-lens-induced, inac-tive*
Papillary keratoconjunctivitis,contact-lens-induced, resolv-ing*
Phlyctenulosis, inactivePterygium, inactivePurulent conjunctivitis (blen-
norrhea), resolvingRosacea keratoconjunctivitis,
active
2 1.49
1 0.75
1 0.751 0.751 0.75
1 0.75
1 0.751 0.751 0.751 0.75
1 0.751 0.751 0.75
1 0.751 0.751 0.75
1 0.751 0.751 0.751 0.75
1 0.751 0.751 0.751 0.75
1 0.75
1
10 1.26
1 0.13
13 1.641 0.131 0.13
7 0.88
0 0.000 0.000 0.005 0.63
1 0.130 0.000 0.00
7 0.881 0.131 0.13
0 0.000 0.007 0.88
16 2.02
1 0.1333 4.161 0.130 0.00
1 0.13
0.75 5 0.63
0.75 1 0.13
1 0.751 0.751 0.75
1 0.75
1 0.75
7 0.883 0.389 1.13
0 0.00
13 1.64
DIAGNOSES
NS
NS
NSNSNS
NS
NSNSNSNS
NSNSNS
NSNSNS
NSNSNSNS
NSNSNSNS
NS
NS
NS
NSNSNS
NS
NS

Wilson
TABLE XX: DIAGNOSES ASSOCIATED WITH DRUG REACTIONS (CONTINUED)
INFLAMMATORYDRUG CASES CONTROLS SIGNIFICANCE*
DIAGNOSES NO % NO % P
Rosacea keratoconjunctivitis,inactive 1 0.75 1 0.13 NS
Rosacea keratoconjunctivitis,resolving 1 0.75 8 1.01 NS
Rubeola keratitis, resolving 1 0.75 0 0.00 NSScleritis, active 1 0.75 11 1.39 NSScleritis, resolving 1 0.75 0 0.00 NSSeborrheic blepharitis, inactive 1 0.75 0 0.00 NSSeborrheic blepharitis, resolv-
ing 1 0.75 0 0.00 NSStaphylococcal blepharitis, in-
active 1 0.75 4 0.50 NSSuperficial punctate keratitis ofThygeson, inactive 1 0.75 1 0.13 NS
Vernal keratoconjunctivitis, ac-tive 1 0.75 12 1.51 NS
*Significance calculated by Fisher's exact probability method, which does not provide x2.tDiagnoses in italics can, themselves, be reactions to drugs or preservatives.tPossibly caused by preservatives in contact lens solutions; because this was uncertain,these cases were excluded from the contact-lens diagnostic category.
Types of Drug Reactions Among Drug CasesIn Table XXII are the types and numbers of drug reactions (excludingcontact-lens cases) that I saw. Toxic papillary reactions without scarringwere the most common, accounting for 79.10% of drug cases and 10.35%
TABLE XXI: ASSOCIATION OF KERATOCONJUNCTIVITIS SICCA WITH SPECIFICDRUG REACTIONS
SIGNIFICANCE, SICCAPRESENT, SPECIFICDRUG REACTIONS VS
SICCA PRESENT INFLAMMATORYCONTROLS*
SPECIFIC DRUG REACTIONS NO % P
Allergic contact reactions (n= 14) 1 7.14 NS
Toxic papillary reactionswithout scarring (n =106) 27 25.47 0.0224
Toxic calcific band-shapedkeratopathy (n = 3) 1 33.33 NS
All others (n = 11) 0 0.00
*Incidence of sicca among inflammatory controls was 125/793 (15.76%;see Table XX); significance calculated by Fisher's exact probabilitymethod.
890

Topical Ophthalmic Therapy
TABLE XXII: TYPES OF DRUG REACTIONS AMONG DRUG CASES*
% OF DRUGTYPES OF REACTIONS NO REACTIONS % OF ALL CASES
Individual drug reactionstAnaphylactoid reactionsAllergic contact reactionsToxic papillary reactions
without scarringPapillary reactions with
scarring (pseudopem-phigoid)
Toxic follicular reactionswithout scarring
Toxic follicular reactionswith scarring (pseudo-trachoma)
Nonspecific (papillary) ci-catrizing reactions (notpseudopemphigoid orpseudotrachoma)
Toxic calcific band-shaped keratopathy
Pharmacologic or immu-nologic rebound in-flammation
Cumulative deposition ofdrugt
Drug-induced alterationof melanin
Phototoxic reactionsPhotoallergic reactions
Coexisting drug reactionsToxic papillary reactions+ Allergic contact re-actions
+ Toxic follicular reac-tions without scar-ring
+ Pseudotrachoma+ Rebound inflam-mation
Coexisting reactions,total
0 0.0014 10.45
106 79.10
2 1.49
13 9.70
1 0.75
0 0.00
3 2.24
4 2.99
0 0.00
0 0.000 0.000 0.00
1 0.75
4 2.991 0.75
3 2.24
7 5.22
*Contact-lens cases excluded.tTotal number of reactions exceeds total number of drug cases (134)because some patients had more than one type of reaction.4Some examples of cumulative deposition of drug (adrenochrome depos-its) were seen but were excluded because they were of no clinical signifi-cance.
0.001.37
10.35
0.20
1.27
0.10
0.00
0.29
0.39
0.00
0.000.000.00
0.10
0.390.10
0.29
0.68
891

of all cases. Allergic contact reactions constituted 10.45% of drug reac-tions and 1.37% of all cases. Toxic follicular reactions without scarringoccurred in 9.70% of drug cases and in 1.27% of all cases. All otherindividual drug reactions were infrequent, representing less than 3% ofdrug reactions and less than 1% of all cases.
Seven patients (5.22% of drug cases, 0.68% of all cases) had more thanone kind of drug reaction. All of these patients had toxic papillary reac-tions. One had a coexisting allergic contact reaction; four had toxic follicu-lar reactions without scarring; and one had a toxic follicular reaction withscarring (pseudotrachoma).
Ocular Tissues Affected by Various Drug ReactionsThis information is shown in Table XXIII. The eyelids were affected onlyby allergic contact reactions. The conjunctiva was always spared only incases of toxic band-shaped keratopathy. All other drug reactions affectedthe conjunctiva or cornea, or both, with varying frequencies. The likeli-hood and sequences of involvement of different ocular tissues by variouskinds of drug reactions will be dealt with in more detail later.
ACCURACY OF REFERRING OPHTHALMOLOGISTS' DIAGNOSES
Table XXIV shows the frequency with which referring ophthalmologists'diagnoses of patients' underlying ocular diseases (exclusive of drug reac-tions) were correct or incorrect. I counted the diagnosis as correct if theophthalmologist knew the underlying condition, eg, glaucoma, even if heor she did not recognize a superimposed drug reaction, eg, toxic follicularconjunctivitis caused by echothiophate iodide. Looked at in this way, thediagnosis was "correct" in 62 (46.27%) of drug cases, although the drugreaction itself was suspected in only 5 of 134 patients (3.73%). Even withthis liberal definition of correct diagnosis, drug cases had a very signifi-cantly higher incidence of incorrect diagnoses than did inflammatorycontrols (P = 8.30 x 10-7). Noninflammatory controls were diagnosedcorrectly more often (77.42% of cases). The underlying diagnosis wascorrect in two (50.00%) of four contact-lens cases.
DRUGS THOUGHT CLINICALLY TO HAVE BEEN PRIMARILY RESPONSIBLE FOR DRUG
REACTIONS
In Table XXV are the pharmacologically active agents that were thoughtclinically to have caused drug reactions.Neomycin was the drug that was blamed more frequently (16.42% of
drug cases, drops more often than ointments), although multiple drugs
892 Wilson

893
rz- 0 05 05 0 0 0
1U+
u Z~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~CZ~~~~~~~~~~~~~~~~~
'0 10 00 Q 0l
z0+ -co - 0 c05 Z 0
- 0
z
0 ~~~~~~Z Cu0 O 4
uz X~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~C
z
0 0 0) 0) 0 C) 0l
16C (6 6 6; C
0 O0 0 0) c
0 0
~~~~0~ ~ ~ X U
bC 04~~~~~~~~
C.) =0 , r w0:
< 0d o0 o..bo
0W.uC0)0 0 ~0P.buC E. - bc . (U - E- .

Wilson
0 ~ ~ ~
.u 0
0z
0
0
cI0 q
oo
~~~ ~ ~ ~~~~~o
ez. e
b
~~ ~ ~ ~ ~ ~ ~ ~ .
0 ~ ~~Co
~ ~ 0
Qo~~~.6 ir
~~~~~~~~~~~~~i
894

Topical Ophthalmic Therapy
TABLE XXV: DRUGS THOUGHT CLINICALLY TO HAVE BEENPRIMARILY RESPONSIBLE FOR DRUG REACTIONS
PATIENTS WITH DRUGREACTIONS
DRUGS NO %
Acetylcysteine, strong(20%)
AntipyrineAtropine, ointmentCarbachol, strong (> 1.5%)Chloramphenicol, dropsEchothiophate, strong (>0.125%)
Gentamicin, dropsGentamicin, ointmentGentamicin, unspecifiedGentamicin, totalIdoxuridine, dropsIdoxuridine, ointmentIdoxuridine, unspecifiedIdoxuridine, totalNaphazolineNeomycin, dropsNeomycin, ointmentNeomycin, totalPilocarpine, weak (s 2%)Pilocarpine, unspecifiedPilocarpine, totalTetracaineTrifluridineVidarabineZinc sulfateMultiple drugs (three ormore) blamed, cause un-known
Unknown, insufficient in-formation (no blame)
No pharmacologicallyactive agent blamed
3 2.241 0.752 1.491 0.755 3.73
1 0.7515 11.193 2.242 1.4920 14.935 3.738 5.971 0.75
14 10.452 1.4916 11.946 4.48
22 16.421 0.753 2.244 2.992 1.492 1.49
11 8.211 0.75
22 16.42
2 1.49
17 12.69
(three or more), cause unknown, were blamed equally often. Gentamicinwas next most common (14.93%, drops more than ointments). Next was"no pharmacologically active agent blamed" (12.69%), meaning that pre-servatives were thought to have been at fault. Idoxuridine followed(10.45%, ointment more than drops). Vidarabine (available only as anointment) was blamed in 8.21% of cases. All other drugs were blamedwith a frequency of less than 3.00%, with pilocarpine being next in line(2.99%).
895

DRUGS THOUGHT CLINICALLY TO HAVE CONTRIBUTED SECONDARILY TO DRUG
REACTIONS
Most drug reactions were thought to have been caused, or aggravated, bymore than one drug.Unknown or multiple drugs were blamed secondarily most often
(16.42% of drug cases), followed by vidarabine (5.22%). Then came afour-way tie with chloramphenicol (drops more than ointment), gentami-cin (ointment more than drops), idoxuridine (drops more than ointment),and neomycin (drops more than ointment) all being blamed in 4.48% ofcases. All other drugs were blamed less than 2.00% of the time.
RELATIVE RISKS OF DRUGS THAT WERE BLAMED MOST OFTEN FOR CAUSING OR
CONTRIBUTING TO DRUG REACTIONS
By adding together the number of times a drug was blamed primarily(Table XXV) or secondarily (Table XXVI) and then dividing by the num-ber oftimes the drug was used (Table XVI), a risk factor for the drug could
TABLE XXVI: DRUGS THOUGHT CLINICALLY TO HAVE CONTRIBUTEDSECONDARILY TO DRUG REACTIONS
PATIENTS WITH DRUGREACTIONS
DRUGS NO %
AmphotericinAntazolineChloramphenicol, dropsChloramphenicol, ointmentChloramphenicol, unspecifiedChloramphenicol, totalGentamicin, ointmentGentamicin, unspecifiedGentamicin, totalIdoxuridine, dropsIdoxuridine, ointmentIdoxuridine, unspecifiedIdoxuridine, totalNeomycin, dropsNeomycin, ointmentNeomycin, totalPheniraminePilocarpine, weak (s 2%)Pilocarpine, strong (> 2%)Pilocarpine, totalSulfacetamide, drops (30%)Tetracycline, dropsTimolol, strong (0.5%)TrifluridineVidarabineUnknown or multiple drugs blamed
1 0.752 1.494 2.991 0.751 0.756 4.484 2.992 1.496 4.483 2.242 1.491 0.756 4.485 3.731 0.756 4.481 0.751 0.751 0.752 1.491 0.751 0.751 0.751 0.757 5.22
22 16.42
896 Wilson

Topical Ophthalmic Therapy
TABLE XXVII: RELATIVE RISKS OF DRUGS THAT WERE BLAMED MOSTOFTEN FOR CAUSING OR CONTRIBUTING TO DRUG REACTIONS*
RELATIVE RISKS
AMONG ALL CASES AMONG DRUG CASESDRUGS MOST OFTEN BLAMED BLAMED/USED = (%) BLAMED/USED = (%)
Idoxuridine 20/43 (46.51) 20/25 (80.00)Vidarabine 18/47 (38.30) 18/24 (75.00)Gentamicin 26/68 (38.24) 26/37 (70.27)Neomycin 28/74 (37.84) 28/35 (80.00)Pilocarpine 6/28 (21.43) 6/8 (75.00)Chloramphenicol 11/83 (13.25) 11/25 (44.00)Multiple drugs (three or
more) 22/355 (6.20) 22/104 (21.15)
*For drugs blamed see Tables XXV and XXVI; for drugs used see TableXVI; for frequency of multiple-drug use see Table XII.
be calculated (Table XXVII). The risk factors are expressed as percentagesand were calculated for all cases taken as a whole, as well as for drugcases. The factors for all cases indicate how often patients who usedparticular drugs developed drug reactions, whereas the factors for drugcases indicate how often specific drugs that were used were also blamed.
PHYSICAL AGENTS THOUGHT CLINICALLY TO HAVE BEEN PRIMARILY RESPONSIBLE
FOR DRUG REACTIONS
No physically active agent itself was blamed primarily for any drug reac-tion, although preservatives in artificial tears were blamed in 8.96% ofdrug cases (Table XXVIII). Contact-lens cases were excluded from thetabulation because all of them, by definition, were attributed to preserva-tives in contact lens solutions.
TABLE XXVIII: PHYSICAL AGENTS THOUGHT CLINICALLY TOHAVE BEEN PRIMARILY RESPONSIBLE FOR DRUG REACTIONS*
PATIENTS WITHDRUG REACTIONS
PHYSICAL AGENTS NO %
None 115 85.82Artificial tearst 12 8.96Lubricating ointments 0 0.00Hypertonic agents 0 0.00Contact lens solutions 0 0.00Unknown (no blame) 7 5.22
*Contact-lens cases excluded; preservatives in contactlens solutions were obviously blamed in all such cases.
tIn all cases it was the preservatives, and not the artifi-cial tears themselves, that were blamed for the drugreactions.
897

PHYSICAL AGENTS THOUGHT CLINICALLY TO HAVE CONTRIBUTED SECONDARILY TO
DRUG REACTIONS
Preservatives in artificial tears were thought to have contributed second-arily to 4.48% of drug reactions.
PRESERVATIVES THOUGHT CLINICALLY TO HAVE BEEN PRIMARILY RESPONSIBLE FOR
DRUG REACTIONS
Preservatives that were blamed for drug reactions are listed in TableXXIX. Preservatives were thought to have been of primary importance in37.31% of cases, but this does not mean that preservatives alone causeddrug reactions this often. There were many instances in which it wasimpossible to separate the relative roles of pharmacologically activeagents and preservatives, so that it was often necessary (and more mean-ingful) to record both a drug and a preservative as being primarily respon-sible for a drug reaction. I did the same for drugs and preservatives that Ithought contributed secondarily to drug reactions. To have done other-wise would have forced me to exclude from consideration some drugs andpreservatives that were actually important in the evolution of drug reac-tions.
TABLE XXIX: PRESERVATIVES THOUGHTCLINICALLYTO HAVEBEEN PRIMARILY RESPONSIBLE FOR DRUG REACTIONS*
PRESERVATIVES
NoneBenzalkonium chloride,weak (s 0.01%)
Benzalkonium chloride,strong (> 0.01%)
Benzalkonium chloride, un-
specifiedBenzalkonium chloride,
totalEdetate, weak (6 0.5%)Edetate, unspecifiedEdetate, totalPhenylmercuric nitrateMultiple drugs (three or
more), preservatives un-
known (blamed)Unknown, insufficient in-
formation (no blame)
*Contact-lens cases excluded.
PATIENTS WITHDRUG REACTIONS
NO %
84 62.69
15 11.19
2 1.49
3 2.24
20 14.932 1.491 0.753 2.242 1.49
20 14.93
5 3.37
898 Wilson

Topical Ophthalmic Therapy
Preservatives were not blamed in 84 cases (62.69%), meaning thatpharmacologically active agents alone were responsible. The most fre-quently blamed preservatives were benzalkonium chloride (weak moreoften than strong) and multiple (three or more) drugs, preservativesunknown-both in 14.93% of cases. Next was edetate (2.24%, weak moreoften than unspecified strength), followed by phenylmercuric nitrate(1.49%).
Thimerosal, weak, was blamed for all four cases of contact-lens reac-tions.
PRESERVATIVES THOUGHT CLINICALLY TO HAVE CONTRIBUTED SECONDARILY TO
DRUG REACTIONS
Benzalkonium chloride (weak more often than strong) was blamed sec-ondarily in 27.61% of drug cases. Boric acid was thought to have contrib-uted to one case (0.75%).No preservative was blamed secondarily for contact-lens reactions.
RELATIVE RISKS OF PRESERVATIVES THAT WERE BLAMED MOST OFTEN FOR CAUSING
OR CONTRIBUTING TO DRUG REACTIONS
Risk factors for preservatives (Table XXX) were calculated in the sameway as were risk factors for pharmacologically active agents (TableXXVII).
It was not possible to calculate the overall risk factor for thimerosal inthe causation of contact-lens reactions because there were too manycontact-lens wearers in the entire series whose contact lens solutions andpreservatives were unknown.
TABLE XXX: RELATIVE RISKS OF PRESERVATIVES THAT WERE BLAMED MOSTOFTEN FOR CAUSING OR CONTRIBUTING TO DRUG REACTIONS*
RELATIVE RISKS
AMONG ALL CASES AMONG DRUG CASESPRESERVATIVES BLAMED/USED = (%) BLAMED/USED = (%)
Benzalkonium chloride 57/391 (14.58) 57/111 (51.35)Multiple drugs (three or
more), preservatives un-known (blamed) 20/220 (9.09) 20/41 (48.78)
Phenylmercuric nitrate 2/25 (8.00) 2/9 (22.22)Edetate 3/364 (0.82) 3/59 (5.08)
*Contact-lens cases excluded. For preservatives blamed see TableXXIX; and for preservatives used see Table XIX.
899

PRESERVATIVES PRESENT IN MEDICATIONS THOUGHT CLINICALLY TO HAVE CAUSED
DRUG REACTIONS
I looked at preservatives (whether or not they were blamed) that werepresent in medications that were blamed for drug reactions. This providesa more objective analysis of preservatives that might have caused drugreactions, in contrast to the more subjective listings of blamed preserva-tives in Table XXIX.Of course, more preservatives were present than were blamed. Other-
wise, preservatives present and preservatives blamed were loosely, butreasonably, concordant. Benzalkonium chloride was most often present(54.58% of cases) and most often blamed (42.54%). Edetate was next mostoften present (23.88%) and blamed (2.24%). Third in presence was thi-merosal (17.91%), but it was not blamed for any drug reactions. Threepreservatives followed that were present but not blamed, and then camephenylmercuric nitrate; it was seventh in presence (3.73%) and thirdmost often blamed (1.49%). Unknown preservatives were present in14.93% of cases and were blamed with the same frequency.
DRUGS BLAMED CLINICALLY FOR SPECIFIC KINDS OF DRUG REACTIONS
I tabulated the pharmacologically active agents that were blamed (pri-marily, secondarily, and altogether) for specific kinds of drug reactions, incontrast to drugs that were blamed when all drug reactions were consid-ered together.Neomycin (ointment more often than drops) was blamed most fre-
quently (21.43% of cases) for allergic contact reactions. Next was genta-micin (14.29%; drops and ointment equally often, although drops wereblamed primarily more than was ointment). Six other drugs (antipyrine;atropine, ointment; chloramphenicol, drops; pilocarpine, weak; vi-darabine; and zinc sulfate) were blamed once (7.14%), as were multipledrugs (three or more).
Drugs blamed for toxic papillary reactions without scarring were: neo-mycin (24.53%, drops more often than ointment); gentamicin (23.58%,drops more often than ointment); multiple drugs (three or more) blamed(20.75%); vidarabine (15.09%); idoxuridine (13.21%, ointment more oftenthan drops); chloramphenicol (9.43%, drops more often than ointment);pilocarpine (3.77%, weak and strong equally often); trifluridine and acet-ylcysteine, strong (each 2.83%); and antazoline and tetracaine (each1.89%). All other drugs (pheniramine; tetracycline, drops; and timolol,strong) were blamed with a frequency of 0.94%. Idoxuridine and vidara-bine were blamed primarily equally often (8.49%); vidarabine was blamed
900 Wilson

Topical Ophthalmic Therapy
more often overall (15.09%) only because it was blamed secondarily(6.60%) more often than was idoxuridine (4.72%).One (50%) of two cases of papillary reactions with scarring (pseudo-
pemphigoid) was attributed to pilocarpine, unspecified strength. Theother patient used multiple drugs (echothiophate, timolol, sulfacetamide,epinephrine hydrochloride, bacitracin, pilocarpine 4%, medrysone, and apreparation containing pilocarpine 3% and epinephrine bitartrate 1%); sothe cause was unknown, although the sequence of clinical events sug-gested that epinephrine might have been the major offender.
Idoxuridine (drops and ointment equally often) was blamed primarilyor secondarily for 46.15% of toxic follicular reactions without scarring.Then came vidarabine (30.77%). All other drugs were blamed only once(7.69%): atropine, ointment; carbachol, strong; echothiophate, strong;and multiple drugs (three or more) blamed.
Multiple drugs (three or more) were blamed for the single case of toxicfollicular reaction with scarring (pseudotrachoma). Not even a speculativecause could be ascertained because the patient had used nearly all of thedrugs that cause follicular reactions (antiviral agents, miotics, epineph-rine, and atropine).
Preservatives were blamed for the three cases of toxic calcific band-shaped keratopathy. Two (66.67%) of the patients used sulfisoxazole diol-amine drops (one for 2 years and one for 6 years) containing phenylmer-curic nitrate as the preservative; one of these patients (the one who usedsulfisoxazole for 2 years) also used a pilocarpine solution that was pre-served with benzalkonium chloride 0.01% and boric acid. The thirdpatient had previously used a 4% pilocarpine solution for 20 years; thepreservative was unknown but was probably phenylmercuric nitrate.Two (50%) of the pharmacologic or immunologic rebound inflamma-
tions resulted from the unwise and abrupt cessation of topical corticoste-roid preparations (dexamethasone, both drops and ointment in one case;prednisolone in the other case). The other two patients (50%) had re-bound inflammation from excessive use of naphazoline, a topical vasocon-strictor.
Neither drops nor ointments were blamed significantly more often forany specific kind of drug reaction.
Preservatives Blamed Clinically for Specific Kinds of Drug ReactionsEdetate (usually weak) was the preservative that was blamed most often (3of 14 cases, 21.43%) for allergic contact reactions. Multiple drugs (threeor more), preservatives unknown, were blamed in one case (7.14%).
901

Preservatives were blamed as primary causes in only these 4 (28.57%) ofthe 14 cases; they were not blamed at all as secondary causes.
Preservatives were blamed primarily for 20 (18.87%) of the 106 cases oftoxic papillary reactions without scarring; they were blamed secondarilyin 38 cases (35.85%) and so were thought to have played a role in 58 cases(54.72%). Benzalkonium chloride (weak more often than strong) was in-criminated in all of these 58 cases except one; boric acid was blamedsecondarily in one case.
Preservatives were not blamed in either of the two cases of papillaryreactions with scarring (pseudopemphigoid).
Although their identities were unknown, one or more preservatives inmultiple drugs (three or more) were blamed primarily for 1 (7.69%) of the13 cases of toxic follicular reactions without scarring. The other 12 cases(92.31%) were attributed to pharmacologically active agents.The one case of toxic follicular reaction with scarring (pseudotrachoma)
was thought to have been caused by pharmacologically active agentsrather than by preservatives.Two of the three cases (66.67%) of toxic calcific band-shaped keratop-
athy were clearly the result of exposure to a preservative (phenylmercuricnitrate). This was probably true also for the other case, but I had to recordthe etiology as unknown because I could not be sure what preservativewas present in the patient's pilocarpine eyedrops.
I did not blame preservatives in any of the four cases of pharmacologicor immunologic rebound inflammations.
NUMBER OF DAYS REQUIRED FOR DRUG REACTIONS TO IMPROVE OR CLEAR AFTER
CESSATION OF CAUSATIVE AGENTS
This information (Table XXXI) was not always available because somepatients were referred to me for only a single consultation, or for short-term care, and so returned to their referring ophthalmologists for follow-up examinations.
It took about three times longer for drug reactions to clear than toimprove.
CLINICAL FINDINGS AND COMPLICATIONS ASSOCIATED WITH VARIOUS DRUG
REACTIONS AND CONTACT-LENS CASES
Clinical findings, some of which can be considered complications of theuse of drugs, that were associated with specific kinds of drug reactions arelisted in Table XXXII.
Wilson902

Topical Ophthalmic Therapy
TABLE XXX: NUMBER OF DAYS REQUIRED FOR DRUGREACTIONS TO IMPROVE OR CLEAR AFTER CESSATION OF
CAUSATIVE AGENTS
DAYS TO DAYS TOVARIABLE IMPROVE* CLEARt
Range 2-49 7-93Mean + SD 11.58 + 8.60 33.46 ± 21.40Median 9 28.5
*Data available for 52 cases (38.81%), unknown for 82(61.19%).
tData available for 26 cases (19.40%), unknown for 108(80.60%).
Diffuse epithelial keratopathy refers to a generalized swirling, opacifi-cation, and granularity of the corneal epithelium, as opposed to merepunctate staining. Coarse focal epithelial keratopathy refers to focal, gray-white, slightly elevated epithelial lesions that resemble those of Thyge-son's superficial punctate keratitis. Infectious eczematoid dermatitis re-fers to an eczematoid dermatitis (blepharitis) that results from a cell-medi-ated (type-IV) hypersensitivity to bacterial infection of the conjunctiva oreyelids, usually with Staphylococcus aureus or 3-hemolytic Streptococ-cus pyogenes.
LABORATORY STUDIES
CYTOLOGIC FINDINGS IN CONJUNCTIVAL SCRAPINGS FROM DRUG CASES
In general, the cytologic findings in cases of toxic or allergenic reactions totopical ophthalmic medications consisted of activated or degeneratedepithelial cells, or both; small to moderate numbers of inflammatory cells;and mucus.
Activated epithelial cells showed enlargement and pleomorphism (of-ten in the form of elongated, "tadpole" shapes, Fig 1), binucleation ormultinucleation, clumping of nuclear chromatin, and prominent or mul-tiple nucleoli. Despite their pleomorphism, these cells were obviouslybenign and lacked features of malignant atypia such as pronounced angu-lation, mitotic figures, dense basophilia, and increased nucleocytoplasmicratios.
Degenerated epithelial cells were characterized by karyorrhexis (rup-ture of the nucleus), karyolysis (swelling of the nucleus with dissolution ofchromatin), pyknosis (shrinkage of the entire cell), and keratinization(granular cytoplasm first and an amorphous, pale blue cytoplasm later;
903

Wilson
TABLE XXXII: CLINICAL FINDINGS AND COMPLICATIONSASSOCIATED WITH VARIOUS DRUG REACTIONS AND CONTACT-
LENS CASES
DRUG REACTIONS ANDASSOCIATED FINDINGS NO %
Allergic contact reactions (n = 14)Diffuse epithelial keratopathyFilamentary keratopathyInfectious eczematoid dermatitis
Staphylococcus aureus onlyS aureus + 1 Streptococcus,group A
S aureus + 1 streptococci,groups A and B
Infectious eczematoid dermatitis,total
Pseudogeographic epithelial defectPost-herpetic*Not post-herpetic
Pseudogeographic epithelial defect,total
Punctal occlusionPunctal stenosisToxic papillary reactions without scar-
ring (n = 106)ConjunctivochalasistDiffuse epithelial keratopathyWith coarse focal epithelial ker-
atopathyDiffuse epithelial keratopathy, totalFilamentary keratopathytPseudodendrite
Post-herpeticNot post-herpetic
Pseudodendrite, totalPseudogeographic epithelial defect
Post-herpeticNot post-herpetic
Pseudogeographic epithelial defect,total
Punctal stenosisPapiUary reactions with scarring
(pseudopemphigoid; n = 2)Canalicular stenosisChronic dacryocystitisCicatricial entropionConjunctival scarring
PalpebralPerilimbal
Conjunctival scarring, totalCorneal keratinization (inferior)Corneal scarringDiffuse epithelial keratopathy
1 7.141 7.14
1 7.14
1 7.14
1 7.14
3 21.43
2 14.291 7.14
3 21.431 7.141 7.14
1 0.947 6.60
1 0.948 7.555 4.72
2 1.894 3.776 5.66
18 16.988 7.55
26 24.532 1.89
1 50.001 50.002 100.00
1 50.001 50.002 100.001 50.001 50.001 50.00
904

Topical Ophthalmic Therapy
TABLE XXXII: CLINICAL FINDINGS AND COMPLICATIONSASSOCIATED WITH VARIOUS DRUG REACTIONS AND CONTACT-
LENS CASES (CONTINUED)
DRUG REACTIONS ANDASSOCIATED FINDINGS NO %
PannusCircumferential (3600)Inferior and superior
Pannus, totalPunctal stenosisTrichiasisToxic follicular reactions without scar-
ring (n = 13)Follicles
Bulbar conjunctivaCaruncleLower fornixSemilunar foldUpper palpebral conjunctiva
Pseudodendrite (post-herpetic)Pseudogeographic epithelial defect
(post-herpetic)Punctal occlusionPunctal stenosisToxicfollicular reactions with scarring(pseudotrachoma; n = 1)
Conjunctival scarring, upper andlower palpebral
FolliclesLimbusLower fornixUpper palpebral conjunctiva
Pannus (worse superiorly)Punctal stenosisToxic calcific band-shaped keratop-
athy (n = 3)Location
CentralPeripheral
MercurialentisPharmacologic or immunologic re-bound inflammation (n = 4)
Confluent keratic precipitatesFibrin in anterior chamberHyphemaHypopyonIncreased corneal edemaIncreased hyperemiaIncreased painPseudogeographic epithelial defect,
post-herpeticContact-lens cases (n = 4)Gross pannus
1 50.001 50.002 100.001 50.001 50.00
1 7.692 15.3813 100.003 23.082 15.381 7.69
2 15.381 7.693 23.08
1 100.00
1 100.001 100.001 100.001 100.001 100.00
1 33.332 66.672 66.67
2 50.001 25.001 25.001 25.002 50.004 100.002 50.00
2 50.00
1 25.00
905

Wilson
TABLE XXXII: CLINICAL FINDINGS AND COMPLICATIONSASSOCIATED WITH VARIOUS DRUG REACTIONS AND CONTACT-
LENS CASES (CONTINUED)
DRUG REACTIONS ANDASSOCIATED FINDINGS NO %
Micropannus 1 25.00Papillae
Giant, upper palpebral conjunctiva 1 25.00Medium-sized, limbus 1 25.00Small, lower palpebral conjunctiva 4 100.00Small, upper palpebral conjunctiva 4 100.00
Diffuse epithelial keratopathyEntire cornea, worse above 2 50.00Upper cornea only 2 50.00Upper cornea plus limbus 1 25.00
Coarse punctate subepithelial scarring 1 25.00
*Post-herpetic refers to simplex or zoster.tTlhickened, redundant, inferior bulbar conjunctiva, occludinglower punctum.tOne case was manifested by a worsening of pre-existing fila-mentary keratopathy from keratoconjunctivitis sicca.
shrinkage and ultimate disappearance of the nucleus; and angulation ofcell borders; Fig 2A and B).
Inflammatory cells were absent in roughly 20% of cases; when theywere present, neutrophils were more plentiful than were mononuclearcells in about two thirds of cases. In about half of the remaining cases,mononuclears predominated; in the other half the numbers of the twotypes of cells were approximately equal.
PRESENCE OF EOSINOPHILS IN CONJUNCTIVAL SCRAPINGS FROM DRUG AND
CONTACT-LENS CASES
I found eosinophils in 6 of 14 cases (42.86%) of allergic contact reactions(Fig 3), and in 1 of 4 cases (25%) of contact-lens reactions, among patientsin the computerized study (Table XXXIII). I excluded eosinophils thatwere attributable to underlying diagnoses (as opposed to drug reactions)or to scraping-induced conjunctival bleeding (which can bring about theappearance of 1% to 3% eosinophils from the bloodstream). The actualincidence of eosinophils in allergic contact reactions may have been high-er since I did not perform scrapings in five cases (35.71%); the incidencein scrapings taken was 66.67%. The eosinophils were never degranulated.I also found basophils in one case of allergic contact dermatoconjunctiv-itis.
906

Topical Ophthalmic Therapy
FIGURE 1Activated epithelial cell showing enlargement and pleomorphism in form of an elongated,"tadpole" shape. Conjunctival scraping from patient with toxic papillary keratoconjunctivitis
caused by neomycin (Giemsa, x 1000).
Eosinophils were conspicuously absent in all other kinds of drug reac-tions, except that I found them in one case of toxic papillary keratocon-junctivitis without scarring and in one case of toxic follicular conjunctivitiswithout scarring; neither of these cases was included in the computerizedstudy.
RESULTS OF EXTERNAL OCULAR CULTURES FROM DRUG (AND CONTACT-LENS) CASES
The results of cultures, broken down according to types ofdrug reactions,are shown in Table XXXIV. Many different organisms were isolated frompatients who had allergic contact reactions, toxic papillary reactions with-out scarring, and pseudopemphigoid. By contrast, only Staphylococcusepidermidis was found in cases of toxic follicular reactions without scar-ring, pseudotrachoma, toxic calcific band-shaped keratopathy, reboundreactions, and contact-lens cases, although cultures were not taken inmany of these cases because they were thought clinically not to have beenindicated.
907

FIGURE 2A: An activated ("tadpole-shaped") epithelial cell beginning to show degeneration in form ofearly keratinization, as indicated by granular cytoplasm (keratohyalin granules) and angula-tion of cell borders. Conjunctival scraping from patient with toxic papillary keratoconjunc-tivitis caused by neomycin (Giemsa, x 1000). B: Group of epithelial cells showing latekeratinization. Nearly all intracellular structure has been lost, and cells have coalesced intoan amorphous, pale-blue keratin scale. Conjunctival scraping from patient with toxic papil-
lary keratoconjunctivitis caused by gentamicin (Giemsa, x 1000).
....
....

Topical Ophthalmic Therapy
FIGURE 3Eosinophils (arrows) in conjunctival scraping from patient with allergic contact dermatocon-junctivitis caused by atropine. Patient had no other ocular disease to account for presence of
eosinophils (Giemsa, x 1000).
LIGHT MICROSCOPY OF TOXIC PAPILLARY CONJUNCTIVITIS WITHOUT SCARRING
CASE 1
A 68-year-old white male used gentamicin eyedrops four times daily for 1 monthbefore cataract surgery because preoperative cultures revealed Proteus mirabilis.Cultures just before surgery showed no growth. At the time of surgery, thepatient had no ocular disease other than cataract and toxic papillary conjunctivitisfrom gentamicin.With the patient's informed consent I took a biopsy from the inferonasal bulbar
conjunctiva at the time of cataract surgery. It revealed moderate acanthosis, milddisruption of the epithelial surface (separations and protrusions of epithelial cells),formation of pseudoglands of Henle (infoldings of proliferating epithelial andgoblet cells), increased numbers of goblet cells, increased amounts of mucus onthe epithelial surface (Fig 4A), and an intense infiltration of inflammatory cells inthe stroma and epithelium (Fig 4A and B). The inflammatory cells consistedmainly of lymphocytes and monocytes, although occasional plasma cells were alsofound.
909a

Wilson
TABLE XXXII: PRESENCE OF EOSINOPHILS INCONJUNCTIVAL SCRAPINGS FROM DRUG (AND
CONTACT-LENS) CASES*
EOSINOPHILS PRESENT
TYPE OF DRUG REACTION NO %
Allergic contact reactions (n = 14)t 6 42.86Toxic papillary reactions without
scarring (n = 106) 0 0.00Papillary reactions with scarring
(pseudopemphigoid; n = 2) 0 0.00Toxic follicular reactions without
scarring (n = 13) 0 0.00Toxic follicular reactions with scar-
ring (pseudotrachoma; n = 1) 0 0.00Toxic calcific band-shaped keratop-
athy (n = 3) 0 0.00Pharmacologic or immunologic re-bound inflammation (n = 4) 0 0.00
Contact-lens cases (n = 4) 1 25.00
*Eosinophils attributable to underlying diseases such asatopic keratoconjunctivitis or pemphigoid were exclud-ed, as were small numbers (1% to 3%) of eosinophilsthat appeared in scrapings which were associated withconjunctival bleeding.tThe true incidence of eosinophils may be higher sincescrapings were not done in five cases.
CYTOLOGY OF PSEUDOGEOGRAPHIC EPITHELIAL DEFECTS
CASE 2
A 43-year-old white male was being treated by his referring ophthalmologist withtopical dexamethasone phosphate 0.01% twice daily for herpes simplex disciformkeratitis when two sterile pseudogeographic epithelial defects developed (Fig5A). These were misinterpreted as indicating recurrence of active viral prolifera-tion in the epithelium, so the steroid was stopped abruptly and vidarabine wasstarted three times daily, along with atropine 1% four times daily.The epithelial defects worsened. The patient developed intractable pain; fibrin
in the anterior chamber; a small hypopyon; and increased hyperemia, cornealedema, keratic precipitates, and iridocyclitis. The ophthalmologist hospitalizedthe patient and treated him with narcotics and topical, subconjunctival, andintravenous antibiotics in addition to the topical vidarabine and atropine. Therewas no improvement over the course of 2 weeks, so the patient was sent to me forpossible enucleation.My diagnoses were: (1) sterile, post-herpetic, pseudogeographic epithelial de-
fects with toxic papillary keratoconjunctivitis secondary to vidarabine; (2) immu-
910

Topical Ophthalmic Therapy
TABLE XXXIV: RESULTS OF EXTERNAL OCULAR CULTURES FROM DRUG(AND CONTACT-LENS) CASES
RESULTS NO %
AUergic contact reactions (n = 14)Staphylococcus aureus*Staphylococcus epidermidisCultures not donePseudomwnas thomasiitStreptococcus pyogenes, group B*Pseudomonas aeruginosaRhizopus sp.Streptococcus pneumoniaeStreptococcus pyogenes, group A*Viral culture, no growthToxic papillary reactions without scarring
(n = 106)Cultures not doneStaphylococcus epidermidisStreptococcus viridans (not group D)Corynebacteria sp. (diphtheroids)No growthPseudomonas thomasiitStaphylococcus aureusAlternaria sp.Anaerobic culture, no growthCephalosporium sp.Geotrichum sp.Propionibacterium sp. (anaerobic culture)Papillary reactions with scarring (pseudopem-
phigoid; n = 2)Proteus mirabilisPseudomonas thomasiitStaphylococcus aureusStaphylococcus epidermidisToxicfollicular reactions without scarring
(n = 13)Cultures not doneNo growthToxicfollicular reactions with scarring (pseudo-
trachoma; n = 1)Cultures not doneToxic calcific band-shaped keratopathy (n = 3)Cultures not donePharmacologic or immunologic rebound inflam-
mation (n = 4)Cultures not doneStaphylococcus epidermidisContact-lens cases (n = 4)Cultures not doneStaphylococcus epidermidis
5 35.715 35.713 21.432 14.292 14.291 7.141 7.141 7.141 7.141 7.14
73 68.8725 23.586 5.663 2.833 2.833 2.832 1.891 0.941 0.941 0.941 0.941 0.94
1 50.001 50.001 50.001 50.00
11 84.622 15.38
1 100.00
3 100.00
3 75.001 25.00
3 75.001 25.00
*Sometimes associated with infectious eczematoid dermatitis (see Ta-ble XXXII).tFormerly known as lysine-negative Pseudomonas cepacia.
911

Wilson912

Topical Ophthalmic Therapy
CAE2 A: Seile pothreic psuoeorpi epithelia deet (oecnrly an oe
dsfo keras....... :. : . ...N features ct.:: .: .... .. .. ....... ... ... ...... .......*~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. :....'... '..........
8>-, i~~~~~~~~~~~~~~~~~~~~~~~~~~~~.. ............
Epith<R.|.selial deet were miinterpete as iniaigrapaaceoievrsads
li ,~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. ... ... ..t
112~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.. .. .......-E:IF i we9~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~....... ! ; K ...n .:-
FIGURE 5CASE 2. A: Sterile, post-herpetic, pseudogeographic epithelial defects (one centrally and oneat nasal limbus) with toxic papillary keratoconjunctivitis caused by vidarabine; immunologicrebound inflammation from cessation of topical steroid; and underlying herpes simplexdisciform keratouveitis. Note features characteristic of non-viral epithelial defects: smoothlyundulating borders with rolled-under epithelial edges and rose-bengal staining of beds.Epithelial defects were misinterpreted as indicating reappearance of live virus and soresulted in the abrupt cessation of steroid (with subsequent rebound inflammation) and thestarting of antiviral therapy (with subsequent toxic papillary reaction and further inhibitionof epithelial healing). B: Healing of epithelial defects 1 month after restarting topicalcorticosteroid, stopping vidarabine, and patching. Use of corticosteroid is nlot to be con-strued as standard treatment for such epithelial defects; it was used only to counteract therebound inflammation that resulted from its sudden withdrawal. C: Scraping from base ofcentral epithelial defect shown in A. Degenerating and keratinizing epithelial cells and raremononuclear cells (Giemsa, x 200). D: Scraping from base of central epithelial defect shownin A. Degenerating and keratinizing epithelial cells with clumps and strands of mucus
(Giemsa, x 100).
FIGURE 4CASE 1. A: Biopsy of inferonasal conjunctiva from patient with toxic papillary conjunctivitiscaused by gentamicin. Acanthosis, mild disruption of epithelial surface, formation of pseu-dogland of Henle (space designated by asterisk and formed by vertical infolding of proliferat-ing epithelial and goblet cells), increased numbers of goblet cells, and mucus on epithelialsurface (arrow). Note also infiltration of lymphoid cells beneath and within epithelium(hematoxylin and eosin, x 100). B: Lymphoid (mononuclear) cells, including occasionalplasma cells (arrows), infiltrating subepithelial conjunctival stroma (hematoxylin and eosin,
x 400).
913

nologic rebound inflammation from cessation of topical steroid; and (3) underlyingherpes simplex disciform keratouveitis (Fig SA).
After taking scrapings of the central epithelial defect, I restarted the topicalsteroid three times daily; stopped the vidarabine; continued the atropine; andpatched the eye. All symptoms and signs improved, and I was able gradually totaper the medications and eventually to stop them. The epithelial defects healedin 1 month (Fig 5B), and the patient recovered and regained 20/50 uncorrectedvision after 4 months.
Scrapings from the base of the central epithelial defect revealed mucus anddegenerated and keratinizing epithelial cells, the two often enmeshed (Fig 5C andD); rare mononuclear cells were also present.
CASE 3
A 67-year-old white male developed herpes zoster ophthalmicus. One monthlater, after treatment with unknown topical medications, a sterile, post-herpetic,pseudogeographic epithelial defect appeared (Fig 6A). This was treated by thereferring ophthalmologist with tobramycin and atropine twice daily, withoutimprovement, for 20 days prior to referral. Corneal sensation was absent, so theepithelial defect could not be attributed solely to the effects of drugs. Neverthe-less, it did not heal until 1 month after I stopped the tobramycin (substitutingsulfacetamide 10%); started artificial tears preserved with chlorobutanol; andprescribed a therapeutic soft contact lens. The atropine was continued.
Scrapings from the base of the epithelial defect (Fig 6B) revealed degeneratingand keratinizing epithelial cells and mucus. One trinucleated activated epithelialcell was found. Moderate numbers of neutrophils, and a few mononuclear cells,were also present.
Scrapings from the edge of the defect showed large clumps of epithelial cellsand a few inflammatory cells (mainly neutrophils) enmeshed in mucus (Fig 6C).Many of the epithelial cells were degenerated and incompletely keratinized. Raretrinucleated epithelial cells were present.
LIGHT AND ELECTRON MICROSCOPY OF TOXIC FOLLICULAR CONJUNCTIVITIS
CASE 4
A 73-year-old white female had a corneal transplant for aphakic bullous keratop-athy and was treated postoperatively with prednisolone acetate drops 1%, sulfa-cetamide drops 10%, and atropine drops 1%, all twice daily. Approximately 3months after surgery, she developed toxic follicular conjunctivitis without itching,presumably secondary to atropine. The lower palpebral conjunctiva showed scat-tered follicles, tiny papillae, and 2 + hyperemia (Fig 7A). The bulbar conjunctivawas 1+ hyperemic but was otherwise normal except for minimial punctate stain-ing with rose bengal inferonasally. The upper palpebral conjunctiva was normal,and there was no dermatitis.
914 Wilson
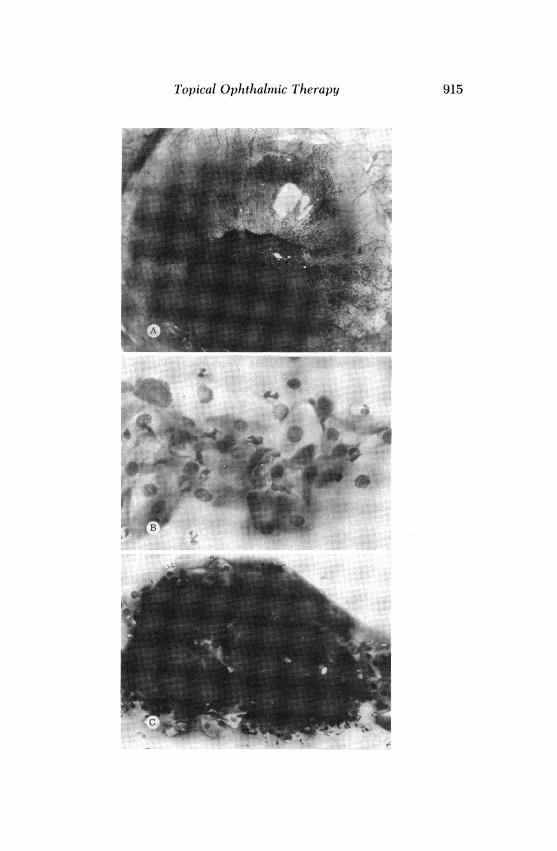
Topical Ophthalmnic Therapy 915

Conjunctival scrapings revealed only scant mucus and occasional mononuclearcells. Cutaneous patch tests with all three of the commercially prepared eyedrops(with their preservatives) were negative.With the patient's informed consent, I excised one of the follicles. All follicles,
and the hyperemia, disappeared approximately 6 weeks after the atropine wasstopped (Fig 7B).
Light microscopy showed mildly acanthotic epithelium; in places its surface wasirregular as the result of vertical elongations of superficial cells (Fig 8A). A fewlymphoid cells were found within the epithelium. The subepithelial stromashowed a focal accumulation of lymphoid cells surrounding what appeared to be agerminal center, ie, a roughly circular zone of relatively large and pale lympho-blasts (Fig 8B).
Electron microscopy revealed epithelial acanthosis with degenerative changesof some of the most superficial epithelial cells and mild activation of some of thedeeper epithelial cells (Fig 9A). Some areas of the epithelium also showed inter-cellular and intracellular edema. Examination of the subepithelial stroma con-firmed the presence of a true lymphoid follicle consisting of lymphoid cells(lymphocytes and monocytes) surrounding lymphoblasts (Fig 9B and C). Rareplasma cells were found beneath the epithelium (Fig 9D).
CASE 5
A 77-year-old white female developed bilateral follicular conjunctivitis after usingdipivefrin for 7 months in both eyes for glaucoma. She had also used timolol 0.5%in both eyes for 8 months. The right eye had been treated additionally withprednisolone acetate 1% one to four times daily and a preparation of prednisoloneacetate 0.25% with sulfacetamide 10% one or two times daily for 8 monthsfollowing a corneal transplant for aphakic bullous keratopathy. None of the pa-tient's bottles of dipivefrin was used for more than 40 days, so it should have beenreasonably fresh.The right eye was 1+ hyperemic with follicles in the lower fornix and lower
palpebral conjunctiva. The left eye, which had not been treated with a steroid,was more severely affected and showed 2+ hyperemia and prominent follicles
FIGURE 6CASE 3. A: Sterile pseudogeographic epithelial defect following ophthalmic zoster. Lesion issufficiently narrow that it might also be called a pseudodendrite. Base of defect stains withrose bengal. Punctate staining is greatest in intensity inferonasally (lower right of photo-graph), where drugs gravitate, and is attributable in large part to the use of tobramycin for20 days. B: Scraping from base of epithelial defect shown in A. Degenerating and keratiniz-ing epithelial cells, moderate numbers of neutrophils, and occasional mononuclear cells.Mucus and occasional activated epithelial cells (including one that was trinucleated) werealso found but are not shown in this field (Giemsa, x 200). C: Scraping of edge of epithelialdefect shown in A. Large clumps of degenerating and keratinizing epithelial cells, andmoderate numbers of neutrophils, enmeshed in mucus. Rare activated epithelial cells and
mononuclear inflammatory cells were also present (Giemsa, x 100).
916 Wilson

Topical Ophthalmic Therapy 917
FIGURE 7CASE 4. A: Toxic follicular conjunctivitis after 3 months' use of atropine drops. Follicle thatwas excised is indicated by arrow. B: Resolution of toxic follicular conjunctivitis 45 days after
stopping atropine.
Me

Wilson
FIGURE 8CASE 4. A: Light microscopy of epithelium overlying lymphoid follicle shown in Fig 7A. Mildacanthosis with surface irregularities secondary to vertical elongations of superficial epithe-lial cells. Infiltration of epithelium by lymphoid cells (arrow; epoxy-embedded 1-,ug section,toluidine blue, x 1000). B: Focal accumulation of subepithelial lymphoid cells surroundingcircular zone of large, pale lymphoblasts, probably representing true lymphoid follicle with
germinal center (epoxy-embedded l-,u section, toluidine blue, x 200).
inferiorly (Fig 10A), on the semilunar fold and caruncle (Fig lOB), at the limbus(Fig lOC), and on the bulbar conjunctiva (Fig lOB and C). Both eyes showed scantmucopurulent discharge and mild punctate staining with rose bengal ofthe infero-nasal bulbar conjunctiva, worse on the left. The corneas were unaffected. Therewas no clinical evidence of conjunctival scarring or dermatitis.
Conjunctival scrapings from the left eye revealed mildly activated and degener-ated epithelial cells (some with early keratinization as evidenced by cytoplasmickeratohyaline granules), moderate numbers of neutrophils, occasional mononu-clear cells and eosinophils, and mucus. Cutaneous patch tests using commerciallyprepared dipivefrin and timolol (with their preservatives) were negative.With the patient's informed consent I excised one of the lower palpebral
follicles. Thinking that the patient had toxic follicular conjunctivitis (with super-imposed early allergic contact conjunctivitis because of the presence of hyper-emia, conjunctival punctate staining, neutrophils, and eosinophils), I stopped thedipivefrin but continued all other topical medications. The hyperemia cleared inthe right eye, and improved in the left eye, in 1 month. After 2 months, both eyeswere white and the follicles were shrinking; they were essentially gone after 4months (Fig lOD).
Light microscopy of the biopsy showed a lymphoid follicle consisting of asubepithelial mass of lymphoid cells in a circular configuration (Fig 11A). Large,pale-staining lymphoblasts were present in the center of the follicle (Fig 11A andB). Among the lymphoblasts were a few large macrophages containing darkclumps of engulfed nuclear material. Such macrophages are referred to as tingiblebodies and are characteristic of fully-developed, mature germinal centers23 (FigliB). As is typical of lymphoblasts, the large, pale cells in the germinal centerwere pyroninophilic, indicating the presence of large amounts of cytoplasmic
918

Topical Ophthalmic Therapy
FIGURE 9CASE 4. A: Electron microscopy of epithelium overlying follicle shown in Fig 7A. Benignatypia (activation) of subsurface epithelial cells and confluence and degeneration (probablyearly keratinization) of superficial epithelial cells. Intercellular and intracellular edema(relatively clear areas between and within epithelial cells). Normal superficial microvilli andmicroplicae (original magnification, x 3000). B: Subepithelial lymphocytes (L) and mono-cytes (M) in periphery of follicle, surrounding lymphoblast (LB) from germinal center.Lymphocytes and monocytes are characterized by relatively compact, indented nuclei andby marginal and paramarginal clumping of chromatin (heterochromatin). Monocytes havemore cytoplasm than do lymphocytes; both have many free particles of ribonucleoprotein,and moderate numbers of mitochondria, in their cytoplasm (original magnification, x 3000).C: Enlarged view of lymphoblast shown in B. Entire cell is enlarged, and nucleus containslarger amount of finely dispersed chromatin (euchromatin) and lesser amount of denselyclumped chromatin (heterochromatin) as compared with lymphocytes and monocytes, ac-counting for pale staining by light microscopy. Nuclear membrane is prominent, as aremitochondria (ovoid bodies containing lamellae) and lysosomes (dark circular bodies). Norough endoplasmic reticulum but many free cytoplasmic ribosomes (original magnification,x 8300). D: Subepithelial plasma cell (left) next to epithelial cell (upper right). Plasma cellhas dense, focal clumping of nuclear chromatin and prominent rough endoplasmic reticulum
and Golgi apparatus (original magnification, x 13,000).
919

Wilson
.R
o..
r
'i
FIGURE 10CASE 5. A: Follicular conjunctivitis after 7 months' use of dipivefrin for glaucoma. B: Follicleson the caruncle, semilunar fold, and bulbar conjunctiva. C: Follicles at the limbus and onbulbar conjunctiva. D: Follicular conjunctivitis essentially cleared 4 months after stopping
dipivefrin.
ribonucleic acid (Fig 11C). Although conjunctival scarring was not evident clini-cally, formation of new collagen was found in the periphery of the follicle and inthe overlying epithelium (Fig liD).
Electron microscopy revealed mild abnormalities of the epithelium much likethose shown in Fig 9A: acanthosis, vertical and horizontal elongations of epithelialcells, and intracellular and intercellular edema. The periphery of the subepithe-lial follicle consisted of lymphoid cells (lymphocytes, monocytes, and occasionalplasma cells; Fig 12A). Fibroblasts producing collagen were also found in a fewareas near the surface of the follicle (Fig 12B). The germinal center of the follicleshowed typical lymphoblasts and tingible bodies (Fig 12C and D).
CLINICAL OBSERVATIONS
This part of the thesis deals with clinical observations that I have madeover the past 11 years-observations that do not lend themselves well tocomputerized or laboratory study but that I consider to be importantresults of my studies of adverse reactions to topical ophthalmic medica-tions.
920

Topical Ophthalmic Therapy
, jhis > s 5 |FIGUE 11 -wE
:.: ..i ....v i w < S _.-NI
CASE 5 A Lih mirscp on on of loe pperl fllce shown in; Fi O'Lmhi
......ll .... .-R 'S, ..2iW.s.
large cells in germinal center i spyroninophilic (red stainingXwith pyronine). . .large
CAmonSE ofr:ibonucmicracid, as isoypcaof lymerpholpbast (mlicethylngren pyoinelOA 1000).iD:llFraionofenpewy(dr cllage (earlyft samng)ypobatinsuefcialteri(phle ofefllstrice;(epoxye-em~~~~~beddedl-,uigsection, toluidineblue,xx200).:Pl-tiigImhbat n w
THE MEIAINITR
Thellprveoper taingil bofdiestrimcohgsofithe enutmost impoertmancen indetecingl
cAendepreelningh erugpoyeabedde lowersctionsItlusdinsufficentmleelshtownas watmeoid
catlsions aeriperbeing uelsed eastoetnyhephbastsinentemaneglectlltomenhtio eones
embedica1getions,anbcumulative ande the may bePaevstidntnlmhband sacondtingforldevsomedorngall bofdtespmate'scromplasints atuetheatmaeriofeainaterion.l
large cells in germinal center is pyroninophilic (red-staining with pyronine), indicating largeamounts of ribonucleic acid, as is typical of lymphoblasts (methyl-geen-pyronine, x 1000).D: Formation of new collagen (early scaring) in superficial periphery of follicle (epoxy-em-
bedded vl-ug section, toluidine blue, x 200).
THE MEDICATION HISTORY
The proper taking of a history is of the utmost importance in detectingand preventing drug reactions. It is insufficient merely to ask what medi-cations are being used, because the patient may neglect to mention onesthat were used but were later stopped. The effects of previously usedmedications can be cumulative, and they may be evident and accountingfor some or all of the patient's complaints at the time of examination.Insofar as is possible, it is important to ascertain all medications that havebeen used (and how often and for how long) since the onset of illness, andwhich ones were associated with improvement or worsening. This knowl-edge helps not only to evaluate the patient's present condition, but todetermine subsequent therapy.
Patients sometimes fail to mention the use of nonprescription drugsand so should be asked ifthey are using anything "just to soothe the eyes. "
These preparations may contain preservatives, vasoconstricting agents, or
921

Wilson
.R~~~~~~~~~~~~~~.
FIGURE 12CASE 5. A: Electron microscopy of periphery of follicle shown in Fig 11 (one of those in Fig10A). Lymphoid cells (L) with indented nuclei, marginal clumping of chromatin, scantcytoplasm, diffusely arrayed particles of cytoplasmic ribonucleoprotein, and moderate num-bers of mitochondria. One plasmablast (P) is also present; it has a prominent rough endo-plasmic reticulum but differs from a mature plasma cell by virtue of its larger nucleus(original magnification, x 3000). B: Production of collagen fibrils (early scarring) by fibro-blasts in subepithelial periphery of follicle (original magnification, x 21,700). C: Germinalcenter of follicle showing typical lymphoblasts with large nuclei that contain mostly euchro-matin, sometimes with nucleoli; prominent nuclear membranes; many free cytoplasmicribosomes; and moderate numbers of mitochondria. Tingible body (macrophage with darkclumps of engulfed nuclear material) is seen at upper right (original magnification, x 3000).D: Enlarged view of tingible body from follicular germinal center (original magnification,
x7000).
heavy metals that can cause problems. Patients also tend not to mentionthe use of"home remedies."
Careful inquiry may be needed to determine whether a medication hashelped. For example, patients with dry eyes often say that artificial tearshave not helped, prompting the physician to turn to more potent, phar-macologically active preparations. It is important to ask if the tears helpedeven for a few minutes or an hour or two, whereupon the patient willoften say something like, "They did make me feel better for a while after Iput them in, but I used them for 3 weeks and I'm still not well." This kind
922

Topical Ophthalmic Therapy
of statement indicates that the treatment was at least partially successfulbut that the patient has an incomplete understanding, and unrealisticexpectations, of what the medications can do. The patient's main concernmay be that the problem is not responding to treatment as it should andthat some more serious consequence, eg, "blindness," may result. Such apatient may be more in need of unhurried explanation and reassurancethan of more drugs, as is true of so many patients who have externalocular diseases.
It is worthwhile to try to find out, in general, whether the patient hasimproved or worsened since onset of the present illness; when correlatedwith the number and types of medications that have been used, thisinformation may provide some clue as to whether too much, or too little,treatment has been given. The time of any turn for the worse can give anindication of which drugs might have been harmful or, at least, nothelpful.
If the patient has recently stopped some medications (let's say 2 weeksearlier), it should be determined whether the problem has since im-proved or worsened; but this should not be done by posing a leadingquestion, eg, "How have you done since you stopped those drops?" It isbetter to ask rather casually, sometime after discussing when the dropswere stopped, "Do you think that you have been getting better or worsein the past couple of weeks?" This kind of approach is more likely to elicitan objective, rather than a subjective and emotional, response from thepatient.A history of allergies to drugs must always be taken, and some thought
must be given to whether those drugs bear similarities to the ones thepatient has been using or to ones which are being considered for use. Forexample, it would be inadvisable to prescribe gentamicin for a patientwho has a history of allergy to neomycin since both drugs are aminogly-cosides.
DIAGNOSIS AND ITS RELATIONSHIP TO THE OVERTREATMENT SYNDROME
Hardly anyone would argue that a correct diagnosis is not more conduciveto proper therapy than is an incorrect one. Unfortunately, the diagnosis ofexternal ocular disease is not always easy.Many red eyes look alike, at least superficially. When the diagnosis is in
doubt, the temptation can be strong to treat any inflammation with atopical corticosteroid and any possible infection with one or more of themost potent broad-spectrum antibiotics (as drug-company representativesand leaflets so often advise), often with an antiviral agent thrown in for
923

good measure. This kind ofapproach is inconsiderate and unscientific andoften leads to iatrogenic harm in the form of the overtreatment syndrome(Fig 13).The overtreatment syndrome begins when a patient's disease or com-
plaint is treated, often without benefit of accurate diagnosis, with one ormore topical medications which eventually produce toxic or allergic reac-tions. The adverse effects obscure any improvement of the underlyingcondition and make it seem to have worsened, thus creating the impres-sion that still more drastic therapy is needed. The medications are then
DISEASE
DRUG
ADVERSE EFFECT
MORE DRUG - WORSE DISEASE
STOP DRUG
CUREFIGURE 13
Overtreatment syndrome. Patient's external ocular disease is treated, often without specificdiagnosis, with one or more topical medications. Drug-induced adverse effects develop andare misinterpreted as worsening of the underlying disease. More medication is prescribed,and problem is perpetuated until treatment is stopped; a "cure" may then result if original
disease has abated, either spontaneously or as result of treatment.
Wilson924

Topical Ophthalmic Therapy
increased in frequency, supplemented, or changed (usually to equally orstill more potent preparations); and the adverse effects are perpetuatedand aggravated. A vicious cycle is established which may not be inter-rupted until treatment is stopped or greatly reduced, whereupon thepatient improves or even recovers fully, the original problem not infre-quently having disappeared.
Imprecise diagnosis leads not only to excessive treatment (in the hopeof covering all diagnostic possibilities), but to prolonged treatment (be-cause prognosis depends on diagnosis). It is not possible to anticipatewhen, and with what treatment, a condition might improve if its progno-sis is not known. One example is adenoviral ("epidemic") keratoconjunc-tivitis, which improves or clears spontaneously 3 or 4 weeks after an oftenexplosive onset which causes much concern (if not diagnosed) for bothpatient and physician. The spontaneous improvement and benign coursecannot be predicted if the problem is not recognized, so treatment whichis excessive, unnecessary, and harmful is apt to be prescribed, especiallywhen the patient fails to respond to therapy after 1 or 2 weeks.
Eyedrops, especially artificial tears, often dry and form flakes on theeyelids and eyelashes and can then be mistaken for the fibrin collarettes ofstaphylococcal blepharitis, with the result that potent antibiotics are pre-scribed unnecessarily for patients who have dry eyes. Eyedrop flakes aregray-white and adhere randomly to the lashes, whereas true collarettesare honey-colored; form at the bases of the lashes; are often pierced bythe lashes; and are associated with inflammation or ulceration of theeyelids and with the well-known conjunctival and corneal features ofstaphylococcal blepharitis.Although inaccurate diagnosis, with reliance instead on "shotgun" or
otherwise erroneous therapy, is a major cause of the overtreatment syn-drome, other factors can be involved and will be discussed below.
SELECTION OF DRUG(S)
Sometimes the primary diagnosis is essentially correct, but an inappro-priate selection of drugs produces adverse reactions and a disappointingclinical result. This situation is so prevalent that I can mention only a fewof the most common examples that I have encountered.
"Doubling up" of drugs, ie, the simultaneous use ofmore than one drugin a pharmacologic class, is hardly ever helpful and is always potentiallyharmful. I have seen patients with drug reactions who were using at anygiven time: more than one antiviral agent, more than one cycloplegic,more than one miotic, more than one antibiotic having essentially the
925

same activity (eg, gentamicin and tobramycin), more than one vasocon-strictor (eg, naphazoline with and without antihistamine), or a combina-tion of artificial tears which exposed the patient to virtually every preser-vative in use today.
Epithelial defects of the cornea are worrisome because they are painfuland can predispose to bacterial or fungal ulcers. As a result, cornealabrasions, recurrent erosions, and epithelial keratopathies of many kindsare likely to be treated with a multiplicity of toxic and allergenic drugswhich inhibit epithelial healing and smoothing. Very often, these prob-lems respond better to less treatment, not more.An antiviral drug can justifiably be used prophylactically (in relatively
small doses) to "cover" steroid therapy of disciform keratouveitis causedby herpes simplex. Evidence that it is worthwhile for zoster is scant, tosay the least; but it has been my experience that antivirals are used almostroutinely (often in large doses and for long periods of time) for both ofthese problems, regardless of whether steroid is also being used. Antivi-rals are also given (or at least are not stopped) for patients who havenothing but inactive "ghost" scars in Bowman's layer as the result ofprevious herpes simplex or zoster epithelial keratitis. As I shall discuss inmore detail later, this kind of error is the result of failure to evaluateproperly the level of activity of disease.The importance of ciliary pain is often overlooked. The aching or
throbbing pain that can result from spasm of the iris and ciliary muscleswhenever uveitis or corneal disease is present can be most distressing tothe patient. If it is not attended to, the patient will continue to complainbitterly and will insist that something more be done; and if it is notrealized that ciliary pain is the problem and that it can be alleviated by theuse ofa cycloplegic agent (and by the application of local heat, elevation ofthe head during sleep, and sometimes by patching or a soft contact lens),the physician may resort to excessive treatment. I have seen this happenwith several external ocular diseases: herpetic disciform keratouveitis,recurrent corneal erosion syndrome, and others, but most often withscleritis. It is surprising how often these patients are found to be usingseveral potent topical and oral medications-sometimes even narcotics-but no cycloplegic agent. Usually, many of the drugs can be stopped ifatropine is prescribed. Other patients, who have mild scleritis, are con-cerned only with the cosmetic problem of redness and need nothing morethan the intermittent use of a topical vasoconstrictor and cold compresses.
Drugs may by selected illogically because their effects and intendedpurposes are misunderstood. This seems to happen most often with rela-tively new preparations. For example, I know of at least two patients with
926 Wilson

Topical Ophthalmic Therapy
corneal edema who were treated with a hypotonic artificial tear in thebelief that it would "dry out" the cornea; both patients developed drugreactions to the benzalkonium preservative. In other cases it is the natureof the disease that is not understood. I have seen many patients (somewith drug reactions) who had staphylococcal blepharitis but who weretreated only with antibiotic drops instilled into the conjunctival sac,rather than with ointments applied to the eyelids.Newly introduced drugs tend to be favored over older ones. Advertise-
ments, which often cite the results of studies that have been supported bydrug companies themselves, lend support to the idea that newer is better,even though most new preparations offer only one or a few limitedadvantages over previously available ones, often at the cost of greatertoxicity or allergenicity. New broad-spectrum topical antibiotics, some-times combined with a steroid, are especially likely to enjoy widespreadand almost indiscriminate use in accordance with the current fashion. Thefirst in my memory was neomycin. Next was chloramphenicol. Then camean interlude during which antibiotics were partially supplanted by idox-uridine as one of the mainstays of external disease treatment. The nextfavorite was gentamicin, although it offers little advantage over other lesstoxic and allergenic drugs except that it is active against Pseudononas.This organism can cause hypopyon corneal ulcers, postoperative endoph-thalmitis, dacryocystitis, and, very rarely, conjunctivitis, but it is other-wise hardly ever involved in external ocular disease. Tobramycin (some-times with the concurrent use of gentamicin) is now beginning to be usedfor practically everything, despite the fact that it should be used mainlyfor those few Pseudomonas infections that are resistant to gentamicin, asdetermined by antibiotic-sensitivity tests. I have encountered almost asmany strains of Pseudomonas that were sensitive to gentamicin and resis-tant to tobramycin.
INTERPRETATION OF CLINICAL SIGNS AND COURSE
Misinterpretation of the clinical signs and course after treatment is begunis a common contributing factor in the development and intensification ofdrug reactions.
Initial Improvement.-Treatment often brings about initial improve-ment, but this does not mean that the treatment will go on helpingindefinitely, especially in the face of a later deteriorating clinical course.Even proper therapy can be continued too long. An antibiotic or antiviralagent may cure a bacterial conjunctivitis or dendritic keratitis, respective-ly, within a few days, but continued use of the drug after it is no longer
927

needed may lead to trouble, especially if more medications are addedfrom time to time.
Another possible source of confusion is the lubricating effect which ispossessed by all topical ophthalmic medications. Any drug, even a toxic orallergenic one, can be of some help for a while simply because it lubri-cates the ocular surface. The resulting improvement, which is especiallylikely to be seen in patients who have dry eyes, can delude both thepatient and physician into thinking that the drug itself is beneficial andthat it should be continued. Conversely, confusion can arise even ifa drugreaction is correctly suspected and all drugs are stopped. The patient mayseem to worsen, at least for a while, because lubrication is no longer beingprovided.
Evaluation of the Activity ofDisease.-It seems obvious that drugs areindicated only so long as disease is active, but the differences betweenactive and inactive diseases are not always readily apparent. Failure torecognize inactivity often leads to unnecessary prolongation of treatment.
Drug-induced eczema, discharge, or punctate staining of the corneaand conjunctiva can mask healing of underlying disease. Pseudodendritesand pseudogeographic epithelial defects can be mistaken for active epi-thelial herpetic keratitis or, sometimes, even for bacterial or fungal cor-neal ulcers, with the result that antiviral or antibiotic agents are started orincreased when they should be stopped or reduced.
Insofar as the corneal stroma is concerned, it is important to differenti-ate inactive scars and vessels from the true signs of active stromal disease,namely, noncoalescent or coalescent cellular infiltrate, edema, stromalnecrosis, or stromal lysis ("melting"). None of these findings is likely to becaused by drugs, except that prolonged use of topical anesthetic can causestromal infiltrate (without necrosis) and topical steroid can enhance lysisof stromal collagen.
MODIFICATION OF THERAPY
When a patient fails to respond satisfactorily to initial therapy, it is unwisemerely to write more prescriptions and to ignore the possibility that thepatient might benefit from discontinuation of drugs that have not helped.Even if a drug reaction is suspected, it is usually thought of loosely as
an "allergy" by both patient and physician. This leads to the notion thatalmost any change in therapy will solve the problem. Actually, most drugreactions are toxicities rather than allergies, so the mere substitution ofone drug for another will accomplish nothing if the new drug (or itspreservative) is as toxic as the old one.
Wilson928

Topical Ophthalmic Therapy
Preservatives are seldom thought of as possible causes of drug reac-tions, so that the preservatives to which patients are exposed often remainthe same despite several changes of drugs.
PHYSICAL FINDINGS AND OTHER OBSERVATIONS RELATING TO SPECIRC KINDS OFDRUG REACTIONS
I discuss here clinical features, many of which have not been previouslydescribed or emphasized, that I have found in association with specifictypes of drug reactions.Anaphylactoid Reactions.-I can attest to the fact that these reactions
are rare. I have seen only four cases: one caused by sulfacetamide; one bybacitracin; and two by proparacaine hydrochloride (Fig 14). All of thesepatients had itching, chemosis, and angioedema of the eyelids within afew minutes after instillation of the offending drug. Redness was mild tomoderate. The discharges were watery and mucoid and contained rare orno eosinophils.
Allergic Contact Reactions.-The allergic contact reaction begins as anapparently nonspecific, papillary keratoconjunctivitis that is characterizedby itching, hyperemia, mild mucopurulent discharge, and punctate stain-ing of the conjunctiva and cornea (more prominent with rose bengal thanwith fluorescein, and worse inferonasally). This phase lasts for a few daysto 2 or 3 weeks, depending on the patient's degree of sensitivity to the
FIGURE 14Acute anaphylactoid dermatoconjunctivitis from instillation of proparacaine hydrochlorideonly minutes before. Mild dermal edema of eyelids (angioedema), moderate chemosis and
conjunctival hyperemia, watery and mucoid discharge, and itching.
929

hapten, its concentration, and how frequently it is used. The character-istic and diagnostic eczematoid dermatitis then appears, first in the skin ofthe nasal aspect of the lower eyelid because this is where drugs andsecretions spill over onto the skin. I have observed that the mucocuta-neous margin of the eyelid often stains with rose bengal just before, orcoincident with, the first appearance of dermatitis (Fig 15A). The derma-titis spreads eventually to affect most or all of the lower eyelid, the malarregion, and the upper eyelid. Frank cutaneous ulceration, or any in-volvement of the forehead, nose, or other parts of the face, usuallyindicates a superimposed allergic contact reaction to secondary infectionwith Staphylococcus aureus or ,-hemolytic Streptococcus (infectious ec-zematoid dermatoconjunctivitis, Fig 15B).The upper eyelid is more severely affected than the lower one only if
the offending drug has been applied directly to the skin of the eyelidsrather than having been instilled into the conjunctival sac. Patients whotreat their eyelids seem to give more attention to the upper eyelid than tothe lower, probably because the former is more prominent (larger, morevisible, and more mobile).
I have never seen a topical ophthalmic medication cause an allergiccontact dermatitis that was not preceded by and associated with a red eyeunless the drug was applied only to the eyelids. If the eye is white, thedermatitis must be attributed to something else such as shampoo, per-fume, or cosmetics, as was pointed out years ago by Theodore andSchlossman. 8The cornea is slightly more resistant than the conjunctiva, in that the
former seems never to be affected before the latter (Table XXIII).Early allergic contact reactions may be mistaken for staphyloccal ble-
pharitis, thus leading to more treatment rather than less, because bothconditions manifest scaling and flaking of the eyelids. The two problemscan be distinguished, although their differences are subtle. Staphylococ-cal blepharitis is usually worse on the upper eyelids, whereas contactreactions are worse below. Staphylococcal blepharitis affects only themargins of the eyelids (unless infectious eczematoid dermatitis is alsopresent), while contact allergy involves also the non-marginal skin of theeyelids. The punctate staining of staphylococcal blepharitis is in the areaof the inferior limbus, but that of contact reactions is worse on theinferonasal cornea and bulbar conjunctiva.
Early allergic contact reactions without dermatitis are almost indistin-guishable from toxic papillary reactions without scarring. Both conditionsshow little more than hyperemia, papillary conjunctivitis, punctate stain-ing of the inferonasal conjunctiva and cornea, and mild mucoid or muco-
Wilson930

FIGURE 15A: Early allergic contact reactions (in this case from atropine) can sometimes be diagnosedby noting rose-bengal staining of mucocutaneous margin of lower eyelid. Finding is oftenseen before, or coincident with, first appearance of eczematoid dermatitis on inferonasaleyelid. B: Frank cutaneous ulceration ("raw skin"; arrows) in allergic contact dermatocon-junctivitis suggests possibility of infectious eczematoid dermatoconjunctivitis, ie, delayedhypersensitivity to secondary infection with Staphylococcus aureus or Streptococcus pyo-
genes (in this case to both).

purulent discharge. Nevertheless, the presence of itching or of eosino-phils in conjunctival scrapings (Table XXXIII) suggests strongly that thereaction is allergic rather than toxic. Punctate staining limited to thecornea is more likely to indicate toxicity (Table XXIII).The concurrent use of topical corticosteroids does not prevent the
development of contact allergy, although it does delay onset and slowprogression. This can be observed easily in any patient who has a bilateralreaction but is using corticosteroid in only one eye. Corticosteroids mayeventually make the problem worse by predisposing to secondary infec-tion.
Toxic Papillary Reactions Without Scarring.-These very commonreactions are most often mistaken for external ocular diseases that are notdrug-induced. The diagnosis depends on a careful analysis of the drughistory and the exclusion of other possibilities. The distribution of thepunctate staining, which is more prominent with rose bengal than withfluorescein in all but the most severe cases (because the epithelium isusually abnormal but not absent), is the most valuable diagnostic sign (Fig16A and B). The staining of both toxic and allergic drug reactions is worseinferonasally, where drugs tend to gravitate, and so can be differentiatedfrom most other external ocular diseases that have other characteristicstaining patterns (Fig 17). However, I have found that conjunctival mucusalso can cause staining of the inferior and inferonasal bulbar conjunctiva,especially in patients who rub their eyes (Fig 17G). I have demonstratedthis to my own satisfaction by rubbing the lower eyelid over strands ofconjunctival mucus.
Although it is not common, toxic or mechanically irritating ointmentsor suspensions (but not solutions) occasionally cause punctate stainingalong the upper limbus (Fig 17A) because they become entrapped be-neath the upper eyelid. This is most likely to occur if the upper palpebralconjunctiva has medium-sized or giant papillae among which the drugscan become enmeshed.
In most cases the inferonasal punctate staining of toxic papillary reac-tions affects both the conjunctiva and cornea (Table XXIII). The conjunc-tiva is usually first and more extensively involved, but the staining canaffect only the cornea, especially if it is already compromised by dryness,exposure, loss of sensation, or other disease.
Several problems in addition to mere punctate staining are possible,including diffuse epithelial keratopathy, coarse focal epithelial keratop-athy, filamentary keratopathy, pseudodendrite, pseudogeographic epi-thelial defect, and punctal stenosis (Table XXXII).
Pseudodendrites are slightly heaped masses of abnormal, opaque epi-
932 Wilson

Topical Ophthalmic Therapy 933
FIGURE 16A: Toxic papillary keratoconjunctivitis of left eye after prolonged use of neomycin. Pseudo-geographic epithelial defect of cornea. Note that fine and coarse punctate staining with rosebengal is worse inferiorly and inferonasally, where drugs gravitate. B: Enlarged view of eye
showing extensive punctate staining of inferonasal bulbar conjunctiva and cornea.
- ... -il m..
!4:,,.XX- .:: ......10"

Wilson
K(;)F@ M(M) N 0
FIGURE 17Staining patterns (usually more prominent with rose bengal than with fluorescein) of toxicand allergic drug reactions and conditions with which they may be confused. A: Drug-in-duced toxicity or allergy. Staining of cornea and conjunctiva is worse inferonasally. Rarely,ointments or suspensions cause upper limbal staining because they become entrappedbeneath the upper eyelid. B: Keratoconjunctivitis sicca. Staining affects the interpalpebralzone of exposure. C: Keratoconjunctivitis sicca with superimposed drug toxicity or allergy.D: Papillary keratoconjunctivitis secondary to wearing of soft contact lenses (usually causedby allergy to thimerosal). Diffuse punctate epithelial keratopathy, worse above, often inswirling, vortex pattern. Also some staining above upper limbus and around entire limbus.E: Normal perilimbal staining in soft contact-lens wearer without papillary keratoconjuncti-val reaction. F: Normal staining in hard contact-lens wearer without papillary keratocon-junctival reaction. G: Staining caused by inferonasal gravitation of increased amounts ofconjunctival mucus, especially in patients who rub their eyes. H: Staining from recentinsertion of Schirmer strip. I: Factitious (self-induced) conjunctivitis from rubbing or scrap-ing of inferior conjunctiva or from instillation of irritating substance into lower cul-de-sac. J:Superior limbic keratoconjunctivitis. Staining usually extends higher on upper bulbar con-junctiva, but less far down on cornea, than that of contact-lens-induced papillary keratocon-junctivitis. K: Inferior staining of staphylococcal blepharokeratoconjunctivitis. L: Neurotro-phic keratopathy (sometimes post-herpetic). M: Fine and coarse punctate epithelial stainingas caused by adenovirus, molluscum contagiosum, rubeola, inclusion conjunctivitis, orsuperficial punctate keratitis of Thygeson. N: Nonspecific fine epithelial staining caused byseborrheic blepharitis or initial stage of adenoviral keratitis. 0: Fine punctate epithelialkeratopathy, worse above, of vernal catarrh, "floppy-lid" syndrome, or early contact-lens-
induced papillary keratoconjunctivitis.
thelial cells in sinuously linear or dendritiform configurations. Theysometimes occur following the healing of a gross epithelial defect becausethe advancing waves of epithelium come together in a dendritiform pat-tern. These pseudodendrites often have the shape of a horizontal "Y" ordouble-ended "Y.," Other pseudodendrites are the result of the physiolog-ic centripetal slide of corneal epithelial cells toward the general area of
934

Topical Ophthalmic Therapy
the Hudson-Stiihli line; the cells normally accumulate, before exfoliating,in this horizontally linear area, but they become visible if they have beenrendered opaque by the toxic effects of drugs. Pseudodendrites stainmore prominently with rose bengal than with fluorescein because most ofthe cells are abnormal rather than absent. Some fluorescein staining doesoccur because loose intercellular junctions allow pooling ofthe dye amongthe cells, as well as its penetration into the underlying and surroundingstroma.
Pseudogeographic "ulcers" (Figs 5, 6, and 16) are sterile, nonhealingepithelial defects that mimic geographic or amoeboid herpetic keratitis.They are often caused, aggravated, or perpetuated by toxic drugs andmust be differentiated from the similar lesions that are caused by activereplication of Herpesvirus in the corneal epithelium. The pseudogeo-graphic defect has a smoothly undulating and rolled-under edge, whereasthe herpetic lesion has a more irregularly geographic and heaped border.The base of the pseudogeographic ulcer stains with rose bengal because ofthe presence of degenerated epithelial cells and mucus, as I have shownin some of my case reports. The epithelium at the edge of the ulcer isloosely adherent to Bowman's layer, so fluorescein seeps into the immedi-ately subjacent and surrounding stroma. The staining pattern of the her-petic geographic ulcer is just the opposite, ie, the base stains with fluores-cein because previously infected epithelial cells have sloughed; the edgestains with rose bengal because the most recently infected cells are swol-len and abnormal, but not yet absent. Unlike the pseudographic defect,which remains essentially stable for days or weeks at a time, herpeticamoeboid ulcers usually expand and change shape relatively rapidly.Finally, pseudogeographic ulcers are common; herpetic dendrites are notuncommon, but their expansion to geographic ulcers that contain livevirus is very rare, partly because of the now widespread use of antiviralagents. As is so often true when the diagnosis is uncertain, less treatmentis more likely to be helpful than is more treatment. Neither pseudogeo-graphic nor truly herpetic defects are likely to be harmed by the cessationof toxic drugs and the use of gentle debridement, artificial tears that donot contain benzalkonium, and patching or the application of a therapeu-tic soft contact lens.
Eosinophils do not appear in conjunctival scrapings from cases of toxicpapillary reactions (Table XXXIII) unless an allergic reaction is also pres-ent.
As is shown by Table XXI, keratoconjunctivitis sicca is a predisposingfactor for the development of toxic papillary reactions but not for otherdrug reactions.
935

Topical corticosteroids may reduce the hyperemia of toxic papillaryreactions, but they have no other beneficial effect.
Except for the characteristic decrease of corneal sensation, the toxicmanifestations of the chronic use of topical anesthetics (Fig 18) are at firstthe same as those of toxic papillary reactions in general: papillary re-sponse, punctate staining, mucoid or mucopurulent discharge, and pseu-dogeographic epithelial defect. Later, findings appear which seem to beunique for anesthetics: coalescent cellular infiltration (without necrosis) ofthe comeal stroma; and iridocyclitis, sometimes with keratic precipitates,hypopyon, or hyphema. Corneal infiltrates resembling Wessely rings canalso develop, suggesting the possibility of a coexisting antibody-mediatedreaction.
Papillary Reactions With Scarring (Pseudopemphigoid).-These reac-tions are essentially the same as toxic papillary reactions without scarringexcept that conjunctival scarring or keratinization (worse below) and cor-neal pannus are also present (Tables XXIII and XXXII).Pseudopemphigoid is rare and develops almost always after years (rare-
ly months) of use of certain antiglaucoma medications: pilocarpine, echo-
FIGURE 18Toxic effects of several months' use of topical anesthetic (proparacaine hydrochloride).Conjunctival hyperemia, nonhealing epithelial defect of cornea, circular stromal infiltratewithout necrosis (small asterisk), confluent keratic precipitates on endothelium (large as-
terisk), and small hypopyon.
Wilso'n936

Topical Ophthalmic Therapy
thiophate, or epinephrine (Fig 19). The preponderance ofevidence is thatthese reactions are toxic rather than allergic, although some workers havefound immunofluorescent evidence of the participation of humoral anti-body.',' In two cases from which I took conjunctival biopsies (oneattributed to pilocarpine and the other to epinephrine), direct and indi-rect immunofluorescent studies were negative.
I suspect from clinical observations (of more than just the two cases inthe computerized study) that pseudopemphigoid is simply the end-resultof longstanding and severe toxic papillary keratoconjunctivitis.
Differentiation from true pemphigoid depends on analysis of the drughistory, age, laterality, conjunctival cytology, and associated systemicfindings. True pemphigoid occurs only rarely in patients under 60 years ofage and is always bilateral. It usually shows at least a few eosinophils inconjunctival scrapings (unlike pseudopemphigoid, Table XXXIII) andmay be associated with vesiculobullous lesions of the skin or mucosae andwith eosinophils in the peripheral blood.
Pseudopemphigoid can develop despite the concurrent use of topicalsteroid.
Toxic Follicular Reactions Without Scarring.-Drug-induced folliclescan appear in any area of the conjunctiva but are most common andprominent in the lower fornix (Table XXXII). I have also seen drugs causelimbal follicles (Fig lOC), although not in cases in the computerizedstudy. The cornea is usually spared (Table XXIII). When it is affected, it isusually found to have a post-herpetic pseudodendrite or pseudogeograph-ic defect, and these problems are probably manifestations of superim-posed toxic papillary effects and are not directly related to toxic follicularreactions.
FIGURE 19A: Pseudopemphigoid following years of use of epinephrine hydrochloride. Inferior con-junctival scarring and keratinization with formation of symblepharon. B: Same patient
showing moderate scarring of upper palpebral conjunctiva.
937

Eyes with drug-induced follicles may be moderately inflamed, but theyare often surprisingly white or show only mild hyperemia and papillaryhypertrophy. Even the inferonasal punctate staining that is so commonwith other kinds of drug reactions is absent unless one of those reactionscoexists.
Punctal stenosis or occlusion sometimes develops despite the absenceof any other signs of conjunctival scarring.
Eosinophils do not appear in conjunctival scrapings unless an allergiccontact reaction is also present (Table XXXIII).
Topical corticosteroid does not prevent toxic follicular conjunctivitis,but it can reduce the associated inflammation and has a moderatelyinhibitory effect on the development of the follicles.The follicle-inducing drugs are atropine (Figs 7 through 9), miotics,
epinephrine and dipivefrin, and antiviral agents. In addition to the caseshown in Figs 10 through 12, I have seen two other cases of follicularconjunctivitis caused by dipivefrin. Only six cases have been previouslyreported.26 None of my cases had dermatitis or positive patch tests, andall but one lacked eosinophils in conjunctival scrapings.
Trifluridine seems to be the least toxic antiviral agent that is nowavailable, but I have twice seen it cause toxic follicular conjunctivitiswithout scarring (Fig 20). I am not aware of this having been specificallyreported, although various authors27,' have alluded to the fact that someof the toxic effects of the various antiviral agents (mainly punctate epithe-liopathy and punctal stenosis) are similar.
Toxic Follicular Reactions With Scarring (Pseudotrachoma).-I haveseen several cases of pseudotrachoma (Fig 21), although only one ap-
FIGURE 20A: Toxic follicular conjunctivitis after use of trifluridine four times daily for 4 months. Limbalfollicles were also present. B: Limbal follicle (arrow) in toxic follicular conjunctivitis causedby use of trifluridine five times daily for 2 months (different case from that shown in A).
938 Wilson

Topical Ophthalmic Therapy
FIGURE 21A: Pseudotrachoma caused by several years' use of pilocarpine. Gross superior pannus. B:Resolving conjunctival follicles (round light reflexes) following cessation of pilocarpine.
Wispy conjunctival scarring (also present on upper palpebral conjunctiva).
peared in the computerized study. I have concluded clinically that theydo not differ essentially from toxic follicular reactions without scarring.The conjunctival scarring, corneal vascularization, and occasional regionallymphadenopathy of pseudotrachoma seem merely to be the ultimateconsequences of longstanding or unusually severe toxic follicular kerato-conjunctivitis.
Toxic Calcific Band-Shaped Keratopathy.-My observations revealedlittle that is new about this entity, except that it still exists and that it canbe caused by phenylmercuric nitrate in sulfisoxazole diolamine (Fig 22A).All previous reports have incriminated phenylmercuric nitrate in pilocar-pine, although mercurialentis has twice been attributed to the samepreservative in sulfisoxazole diolamine. 17'29 Mercurialentis was present inone of my two "sulfisoxazole" cases (Table XXXII). The calcific depositswere paracentral in one case and peripheral in the other. One of thedeposits had "swiss-cheese holes" (round areas of lucency), as are oftenseen in other kinds of calcific band-shaped keratopathy. A third case wascaused by unknown drugs or preservatives and had peripheral depositsand mercurialentis (Fig 22B). My fourth case was caused by the oldpilocarpine with phenylmercuric nitrate (no longer marketed) and alsohad mercurialentis (Fig 22C). All four patients had normal levels of serumcalcium and phosphorus. None of the deposits progressed after the cau-sative drugs (preservatives) were stopped.There was no clinical evidence of conjunctival involvement in any of
the four cases (Table XXIII). Eosinophils were not found in conjunctivalscrapings (Table XXXIII).Pharmacologic or Immunologic Rebound Inflammation.-These reac-
tions are generally considered to be of minor importance because theoveruse of topical vasoconstricting agents usually causes nothing more
939

Wilson940

Topical Ophthalmic Therapy
than a slight worsening of pre-existing hyperemia. Nevertheless, this canlead to the prescribing of still more drugs and, thus, to the developmentof more severe drug reactions.The intense rebound inflammation that can result from the sudden
cessation of topical corticosteroid is less well known and is far moreserious. This problem is especially likely to occur when a patient withherpetic disciform keratouveitis develops a breakdown of the cornealepithelium (Fig 5). The epithelial defect is usually sterile and comes aboutas a result of several factors, including neurotrophic effects, stromal in-flammation and edema, and the use of epitheliotoxic drugs (especiallyantiviral agents); but if it is misinterpreted as a reappearance of live virus,antiviral therapy will be continued or increased and steroid therapy willbe decreased or stopped-just the opposite of what should be done. Thepatient may then develop severe pain, increased hyperemia and cornealedema, confluent keratic precipitates, fibrin in the anterior chamber,hypopyon, and even hyphema (Table XXXII).
Papillary Reactions Caused by Contact Lens Solutions.-It is now wellestablished that preservatives in contact lens solutions can cause giantpapillary conjunctivitis that mimics vernal catarrh (Fig 23A); but I havefound that, even with otherwise severe involvement, the papillae may berelatively small and unimpressive (Table XXXII; Fig 23B). When this isthe case, the reaction can be mistaken easily for superior limbic kerato-conjunctivitis because nearly all of the signs (papillary hypertrophy, hy-peremia, punctate epithelial keratopathy, and superficial corneal vascu-larization) are worse above.
Several clinical features of the contact-lens problem are important forits diagnosis, especially when giant papillae are lacking (Table XXXII).The punctate staining of the cornea may be disseminated but is worseabove and often shows a swirling, vortex pattern (Fig 17D). Perilimbalstaining, with or without limbal swelling, is also usually present. Superiormicropannus, or even gross pannus, is common; the latter may be thickand fleshy (Fig 23C). Superior filamentary keratopathy (Fig 23D) occursrarely but is another source of confusion with superior limbic keratocon-junctivitis.
FIGURE 22A: Peripheral toxic calcific band keratopathy (arrow) caused by several years of exposure tophenylmercuric nitrate in sulfisoxazole diolamine. "Swiss-cheese holes" were present. Mer-curialentis was absent. B: Peripheral toxic calcific band keratopathy (with mercurialentis)caused by unknown drugs or preservatives (but probably caused by several years' use ofpilocarpine containing phenylmercuric nitrate). "Swiss-cheese holes" were not present. C:Central toxic calcific band keratopathy (with mercurialentis) caused by years of use ofpilocarpine preserved with phenylmercuric nitrate. "Swiss-cheese holes" were present.
941

Wilson
E..-
FIGURE 23A: Giant papillary reaction on upper palpebral conjunctiva as occurs with delayed hypersen-sitivity to thimerosal in contact lens solutions or with vernal catarrh. B: Small, rather thangiant or medium-sized, papillae on upper palpebral conjunctiva in papillary keratoconjunc-tivitis caused by delayed hypersensitivity to thimerosal in contact lens solutions. Despitethe rather unimpressive papillae, this patient had an extensive gross pannus. C: Thick,fleshy, gross superior pannus in contact-lens syndrome caused by thimerosal. Same patientas B. D: Superior filamentary keratopathy in contact-lens syndrome caused by thimerosal.
Papillae on upper palpebral conjunctiva were medium-sized.
The punctate staining of superior limbic keratoconjunctivitis is limitedto the upper fifth or sixth of the cornea and usually extends higher on theupper bulbar conjunctiva than does that of the contact-lens syndrome (Fig17J). Corneal vascularization in superior limbic keratoconjunctivitis takesthe form of a micropannus, not a gross pannus.The papillary contact-lens reaction typically appears after several
weeks, months, or years of successful contact-lens wear because it takestime for patients to become sensitized to the causative preservative(s).Once the reaction starts, it worsens steadily if the lenses continue to beworn. The patient experiences a progressively more rapid onset, andincreased severity, of redness, discomfort, itching, and discharge witheach successive reinsertion of the lenses. All of these symptoms improvewhenever the contacts are discontinued, but these patients resist notwearing their lenses because they see so poorly without them once theepithelial keratopathy affects the visual axis. In contrast, the centralcornea is never involved in superior limbic keratoconjunctivitis, so these
942

Topical Ophthalmic Therapy
patients usually give up their contacts voluntarily because of the irritationthat they produce.
Severe contact-lens reactions can take up to 6 months to heal complete-ly, and resuming the contacts even for a few minutes can undo severaldays or more of healing.
Eosinophils, many of which are degranulated, are numerous in vernalcatarrh. They are often absent and are seldom numerous (and not degran-ulated) in the contact-lens reaction (Table XXXIII). Eosinophils do notappear in the superior limbic keratoconjunctivitis.
It seems very likely now from the work ofWilson and co-workers,30 andfrom my own experience, that nearly all of these contact-lens syndromesare caused by delayed hypersensitivity to thimerosal in contact lens solu-tions. I was unsure of this when I began the computerized study, so Ialmost certainly underestimated the prevalence of the problem. I classi-fied these cases as inflammatory controls, or as drug cases if reactions totopical medications were also present, unless I could prove that thimero-sal was at fault. There were 16 such cases that were not classified as"contact-lens cases" (13 in the inflammatory-control category and 3 in thedrug-case category, Table XX). If we assume that all of these cases werecaused by allergy to thimerosal, the incidence of the problem rises from0.39% (Table I) to 1.95% (4 definite cases plus 16 probable ones =20/1024 = 1.95%). Of all of these, 15% (3/20) had superimposed reactionsto topical medications. In support of the idea that most of these reactionsare caused by thimerosal, I can point out that I have seen only twopatients (neither of whom was included in the computerized study) whodid not do well with soft contact lenses when they avoided all preserva-tives and switched to disinfection by heat in saline solution withoutpreservatives. Of course, some of my patients simply stopped wearingcontacts, which is always the ideal solution to this problem, and I cannotknow whether the elimination of thimerosal would have been successfulin these cases.
RECOVERY FROM DRUG REACTIONS
If a change of drugs has been beneficial, it is important to try to under-stand why. The improvement is more often attributed to the starting of anew drug than to the stopping of an old one, yet the new drug mayperpetuate, or eventually cause or contribute to, a drug reaction.
It is not generally known that drug reactions may not improve or clearquickly after the causative drug is stopped. Patients usually expect im-provement within 2 or 3 days. Physicians realize that healing may be
943

Wilson
slower, but they, too, sometimes become impatient and conclude toosoon that a cessation or change of drugs has not helped, at which timethey may yield to the temptation to prescribe more medication.As is shown in Table XXXI, some drug reactions do improve within 2 or
3 days, but 11 or 12 days are needed on the average. Some cases show nosigns of improvement until more than 1 month has passed. A few reac-tions clear in 1 or 2 weeks, but more than 1 month is usually required.Some cases clear only after 2 or 3 months.
Fig 24 illustrates the most common courses of recovery after treatmentis stopped or changed. Of course, some drug reactions, eg, toxic calcific
COURSES OF RECOVERY FROMADVERSE DRUG EFFECTS
ON EXTERNAL EYE
A: 4¢4
1h b
rZ4E-4ou 2
rzl 1
0
0 1 2 3 4 5 6
WEEKSFIGURE 24
Some patients (solid line) with drug-induced ocular inflammation improve almost immedi-ately after drugs are stopped but may require 3 or 4 weeks to recover completely. Others(regularly broken line) show little or no improvement for 2 or 3 weeks and do not clear for atleast 6 weeks. Patients whose medications include topical corticosteroids (irregularly brokenline) may actually suffer temporary rebound worsening when drugs are stopped, because of
the sudden loss of the steroids' anti-inflammatory effects.
944

Topical Ophthalmic Therapy
band-shaped keratopathy or conjunctival scarring, do not clear, althoughtheir progression can be stopped by discontinuing the causative agents.Drug-induced punctal stenosis or occlusion may or may not clear sponta-neously.
DISCUSSION
COMPUTERIZED EPIDEMIOLOGIC STUDY
Incidence of Drug ReactionsApproximately 13% of patients in the computerized study had clinicallyimportant adverse reactions to topical drugs. When I considered the factthat physicians and patients tended to stop or reduce treatment in antici-pation of referral, I found that the incidence of drug reactions might havebeen as high as 16% had I seen some of the patients sooner, before theirdrug reactions disappeared.
In fact, the incidence of adverse reactions was about 16% among pa-tients who were given any treatment at all. Another 3% to 4% probablyhad reactions that cleared shortly before my first examination, making thetrue incidence among treated patients possibly as high as 19% to 20%.These frequencies of ophthalmic drug reactions are similar to the fre-quencies of major drug reactions that have been observed in hospitalizedgeneral medical patients (12.5% to 24.8%). 3My calculations underestimate the magnitude of the ophthalmic drug
problem because I excluded several kinds of adverse effects (includingnearly all of those related to steroids).
Allergic reactions to preservatives in contact lens solutions were pres-ent in at least 0.39% of cases, but there were several cases which I did notclassify as "contact-lens cases" because it was not known at the time thestudy was undertaken that nearly all papillary reactions in contact-lenswearers are caused by allergy to thimerosal. I have shown that the trueincidence of this problem was probably closer to 2% of all external-diseasecases that were referred. The incidence of superimposed reactions totopical drugs (prescribed because the patients were having trouble withtheir contacts) was 15%.
PATIENT-RELATED DEMOGRAPHIC VARIABLES
The patient-related variables of year or season or referral, age, sex, mari-tal status, and race (singly or in any combination) were not statisticallysignificant as risk factors for the development of drug reactions, although
9_45

patients with reactions to contact lens solutions were significantlyyounger by 20 to 30 years than were patients with reactions to drugs.
In general medicine, on the other hand, women, the very old, and (to alesser extent) the very young are more likely to have adverse reactions todrugs.32 Elderly patients and young children over-react to systemic med-ications because they have lower body weights and relatively inefficientenzymatic and physiologic mechanisms for the metabolic breakdown andclearance of drugs. Older patients are also more likely to need medicaltherapy because of their greater susceptibilities to most kinds of diseases.Women may have drug reactions more often only because there are moreelderly women than men.Ophthalmic patients are different. They are usually treated only with
topical medications, so that body weight, hepatic enzymes, and renalclearance become relatively unimportant. Involutional problems of theeye are seldom amenable to medical therapy and are not likely to betreated with drugs, and patients of all ages are almost equally susceptibleto inflammatory external ocular diseases that do require treatment withtopical medications.The general locations of patients' residences (northern, central, or
southern Indiana, or out-of-state) were not significant.
VARIABLES RELATED TO PRACTITIONERS
Except for lay persons (patients themselves and their friends and rela-tives) and nonophthalmic medical specialists, all kinds of practitioners(including optometrists and all types of physicians) contributed to thedrug problem in that they gave treatment to drug cases significantly moreoften than to inflammatory controls. In other words, the risk of develop-ing a drug reaction related not so much to the kind of treating practitioneras to whether or not treatment was prescribed.
Ophthalmologists were associated far more significantly than were oth-er kinds of practitioners with having been involved in the treatment ofdrug cases more than of inflammatory controls, but this does not meanthat ophthalmologists treat less skillfully. We have already seen thatvirtually all types of practitioners were more likely to have treated drugcases than inflammatory controls. Ophthalmologists predominated be-cause the study was designed to include only cases referred from themand because they are the practitioners who are responsible for managingall kinds of cases, including the most difficult and recalcitrant ones. I canassure the reader, without fear of worthy contradiction, that if any non-ophthalmic practitioner were to be so bold as to assume (even partially)such a responsibility, the incidence of adverse drug reactions would
946 Wilson

Topical Ophthalmic Therapy
increase considerably, as would the incidence of improper treatment withor without drug reactions; not only would more patients be harmed, butfewer would be helped.Drug cases were much more likely than were inflammatory controls to
have been treated by several different kinds of practitioners and by alarger number of practitioners, indicating that the development of drugreactions is related to the total amount of treatment given.
Patients with drug reactions consulted significantly more practitioners(whether they treated or not) than did inflammatory controls, althoughthe significance was not nearly so great as was that for treating prac-titioners. The 'relationship of drug reactions to number of practitionersconsulted probably reflects indirectly the importance of the total amountof treatment and suggests that practitioners are more likely to treat thannot to treat. Only 11.94% of practitioners consulted by drug cases, incontrast to 34.30% of those consulted by inflammatory controls, did notprescribe treatment. I suspect that all of this means that more prac-titioners were consulted by drug cases because their problems wererecalcitrant and failed to respond to treatment.
For the most part, the towns and states of referring ophthalmologistswere unimportant. There was only one town (which was in Indiana),among the 52 towns in 11 states, from which local ophthalmologistsreferred significantly more drug cases than inflammatory controls. Signif-icantly fewer noninflammatory controls were referred from outside Indi-ana, probably because only more severe, inflammatory cases are likely tobe referred long distances.
All of the drug cases were referred by slightly less than half of thereferring ophthalmologists. The remainder of the ophthalmologists re-ferred no drug cases. So, in this study, roughly one of every two ophthal-mologists saw patients who had, or eventually developed, adverse drugreactions that were sufficiently severe as to require referral. There were14 ophthalmologists (8.24%) who referred drug cases significantly moreoften than inflammatory controls. These doctors referred almost 40% ofthe drug cases and clearly tended to overtreat their patients. Regardlessof the number of inflammatory external diseases that they saw, only thesefew ophthalmologists were so likely to overtreat as to cause 10% or moreof their referrals to be drug cases.
COMPARISON OF GENERAL LOCATIONS OF REFERRING OPHTHALMOLOGISTS AND
PATIENTS
Patients who resorted to seeking care from relatively distant ophthalmol-ogists (one form of "doctor-shopping") were no more susceptible to drug
947

Wilson
reactions than were patients who sought care closer to home, but patientswho consulted or were treated by more than one practitioner (other formsof "doctor-shopping") were significantly more likely to have drug reac-tions.
PATIENTS' COMPLAINTS
At the time that I saw them, patients with drug reactions had significantlymore symptomatic complaints than did inflammatory controls, probablybecause many drug cases suffered the symptoms of their underlyingdiseases in addition to the adverse effects of treatment. In other cases theunderlying problems had disappeared and had been replaced by drugreactions. Five or more complaints suggested the presence of a reactionto drugs or preservatives (including those in contact lens solutions),whereas three or fewer complaints were usually associated with the ab-sence of such a reaction.The complaints of redness, discharge, tearing, itching, and photo-
phobia, in decreasing order of frequency, were voiced significantly moreoften by drug cases than by inflammatory controls. I was unable to deter-mine the numbers and kinds of complaints that patients had before theirdrug reactions developed.
VARIABLES RELATED TO DRUGS, PHYSICAL AGENTS, AND PRESERVATIVES
Drug cases used significantly more topical ophthalmic preparations thandid inflammatory controls and were doing so when they came to me. Theuse of four or more preparations, all at once or at different times, in-creased considerably the risk of a drug reaction; the use of multiplepreparations (number uncertain) was even more significantly related tothe presence of a drug reaction. Inflammatory controls usually used twoor fewer preparations.Drug cases were treated for significantly longer periods of time. The
figures were highly variable, but patients with drug reactions were treat-ed roughly three to four times longer than were inflammatory controls.
Certain drugs were used significantly more often by drug cases than byinflammatory controls: acetylcysteine, antipyrine, atropine, bacitracin,chloramphenicol, cyclopentolate, dexamethasone, epinephrine and di-pivefrin, gentamicin, gramicidin, hydrocortisone, idoxuridine, neomycin,pilocarpine, polymyxin, scopolamine, sulfacetamide, sulfisoxazole diol-amine, timolol, trifluridine, vidarabine, and three or more unspecifieddrugs. The ten drugs used most often by drug cases were, in order ofdecreasing frequency: gentamicin, neomycin, polymyxin, sulfacetamide,
948

Topical Ophthalmic Therapy
chloramphenicol, idoxuridine, vidarabine, atropine, dexamethasone, andbacitracin; but the computer is not omnipotent. As is true of all statisticalinformation, these data must be interpreted in the light of clinical experi-ence and common sense. Despite their statistical significance and associa-tion with drug cases, not all of these drugs are likely to cause drugreactions.
Acetylcysteine 20% is toxic, whereas the 10% solution is relatively welltolerated; but it, too, can sometimes produce irritation if it is used forlong periods of time by patients who have dry eyes.
Antipyrine is known to be allergenic and was blamed for one of mycases of allergic contact dermatoconjunctivitis.
Despite their more frequent use by patients with drug reactions, I donot think that commercial preparations of bacitracin, cyclopentolate, dex-amethasone, gramicidin, hydrocortisone, polymyxin, sulfacetamide, sulfi-soxazole diolamine, or timolol have any significant allergenicity or toxic-ity. Bacitracin, gramicidin, and polymyxin are statistically guilty only byassociation because they are usually marketed and prescribed in combina-tion with neomycin, which is highly toxic and allergenic. Very rarely,bacitracin can cause an allergic contact or anaphylactoid reaction. "Forti-fied" bacitracin (10,000 U/ml) is highly irritating.
Cyclopentolate, dexamethasone, hydrocortisone, sulfacetamide, andtimolol were used more often by drug cases mainly because their clinicalfindings indicated a need for these kinds of medications and because thesedrugs are in common use. Rarely, cyclopentolate, timolol, or sulfaceta-mide have caused anaphylactoid reactions, and sulfacetamide has beenknown to cause contact allergy.
Chloramphenicol, pilocarpine, and scopolamine are mildly toxic andallergenic and occasionally cause toxic papillary or allergic contact reac-tions. Pilocarpine can also produce follicular conjunctivitis, pseudopem-phigoid, or pseudotrachoma, as can idoxuridine.
Epinephrine, dipivefrin, atropine, vidarabine, and trifluridine are oth-er definite causes of follicular conjunctivitis, and epinephrine can proba-bly cause pseudopemphigoid or pseudotrachoma. My histopathologicstudies revealed conjunctival scarring also in association with follicularconjunctivitis caused by dipivefrin, although no cicatrization was evidentclinically.
Atropine, gentamicin, idoxuridine, and neomycin are common causesof contact allergy, and all but atropine also produce toxic papillary reac-tions. Trifluridine seems to be less allergenic and toxic than is idoxuri-dine, while vidarabine is intermediate between the two.
Sulfisoxazole diolamine was important only because it was preserved
949

with phenylmercuric nitrate and so was associated with the developmentof toxic calcific band keratopathy.The calculation of risk factors revealed that the following drugs were
most likely to cause adverse reactions, in order ofdecreasing risk: idoxuri-dine (which caused trouble in 46.51% of patients for whom it was used),vidarabine, gentamicin, neomycin, pilocarpine, chloramphenicol, andmultiple (three or more) drugs. Tobramycin also probably would haveranked high on the list, but it was not commercially available at the timeof the study.
It is obvious that more highly concentrated drugs are at least as likely tocause adverse effects as are less concentrated ones. Nevertheless, moredrug reactions were caused by relatively weak preparations than bystrong ones, showing that even the weaker concentrations of commercial-ly marketed medications are sufficiently strong as to cause problems.Similarly, no drug had to be present in more than one of a patient'smedications in order to cause a reaction.
Neither drops nor ointments were blamed significantly more often fordrug reactions as a whole or for any specific kind of reaction, despite thefact that all drops contain preservatives but many ointments do not.Ointments that are applied to the skin are thought to predispose tocontact allergy because they enhance the penetrability of drugs throughthe keratin layer'7; but this seems not to be true for the eye, probablybecause its surface is not normally keratinized. Also, ointments are pre-scribed slightly less often for ophthalmic disorders than are drops.
In Table XXXV I have summarized the toxic and allergenic propensitiesof various drugs and preservatives as determined by this study.The use of physical agents was pertinent in that patients with contact-
lens reactions used contact lens solutions significantly more often than didother patients, and preservatives in artificial tears were blamed primarilyfor 8.96%, and secondarily for 4.48%, of drug reactions. Preservatives intears fell between idoxuridine and vidarabine in propensity for causingdrug reactions and were equal to chloramphenicol, gentamicin, idoxuri-dine, and neomycin for contributing to them. In other words, preserva-tives in artificial tears were the second most common cause of adverseeffects in this study.
Certain preservatives were significantly associated with the develop-ment ofdrug reactions: benzalkonium chloride, boric acid, chlorobutanol,edetate, parabens, phenylmercuric nitrate, sodium bisulfite or thiosul-fate, thimerosal, and multiple unknown preservatives. A slightly differentgroup of preservatives was associated with the presence of contact-lensreactions: boric acid, chlorhexidine gluconate, edetate, and thimerosal.
Wilson950

Topical Ophthalmic Therapy
-F--F--0 00 0
ooo o o ooo o o ozzzzzzzzozzz
0 0
4- 4-F-4
o o oo
Z Z Z OZa;Z O ZZ O
+F4-FCu
0 0 0 0 0 0zzzzzz
Cu
._
0 000O 8 < 0Z ZZZOOZ
>1 >
0 0>1 ;Y O >1 O- ;,
uO Z tOa) .QId) 1 4Cu I, 0 .C )
O uUCCd co )z d C e
0z
0 00zz z
0 00zz z
00zz =
0 0r-') r "-> 1
00ed4 00 4) () 2
C g =
0 5- C0 a E-yy0 "a;0 -~ Cu -~ *~ .~ ~ .~ ~ ~ 0 - e
951
OQa
0tCF-
<F-
0u
x-
po
0
0
0u
0
0
1)"

Wilson
000 0 00
zzz z zz
0
coz
COD
._
0 0 o 8
z z zo
0 0 00
z z zz
ECu0
0is020.
D
o0 EjCU5 5
ko
0m3
8 8
Q0 0:Y Q,
_
U) C)U)
E o o0
0CuCu*_
o. .Q
952
00u=so
ga
0zXo
RZXgo
Cu
J0
.-
oUW X
Cu
Cu0t0z0
0
00
z0 3
0 t
(00u
Cu

Topical Ophthalmic Therapy
As was true of the statistics pertaining to drugs, the data concerningpreservatives require some interpretation. Benzalkonium is clearly verytoxic. Boric acid seems to have only mild toxicity, as does chlorobutan-ol. 3' 34
Parabens are definite, but apparently not common, contact sensitizers.Edetate was the preservative that was blamed most often for contactallergy (21.43% of cases). Thimerosal occasionally causes contact reactionsin patients who do not wear contact lenses, but it seems to be responsiblefor almost all papillary keratoconjunctival reactions in patients who dowear contacts.30'33Contact-lens patients typically manifest allergy to thi-merosal only after weeks, months, or years of successful lens wear, sothey may be more susceptible to sensitization mainly because they areexposed to the preservative for long periods of time as they clean, disin-fect, and lubricate their lenses. The fact that patients with contact-lensreactions were also exposed significantly more often than were inflam-matory controls to boric acid, chlorhexidine gluconate, and edetate sug-gests that these preservatives may sometimes contribute to, or cause, theproblem. Boric acid would be expected merely to cause some super-imposed toxic papillary reaction, but chlorhexidine and edetate couldvery well act as contact sensitizers in some cases.32
Phenylmercuric nitrate's only adverse effect was its ability to causecalcific band keratopathy (and mercurialentis).
I found nothing to indicate that sodium bisulfite or thiosulfate is toxic orallergenic. It seemed to be used statistically more often by drug casesonly because of its prevalence in several anti-infective, anti-inflammatory,and vasoconstricting preparations.
Benzalkonium chloride was the preservative that had the highest riskfactor, causing adverse effects in 14.58% of all patients who were exposedto it, followed (in order of decreasing risk) by multiple unknown preserva-tives in three or more medications, edetate, and phenylmercuric nitrate.As was true of drugs, preservatives did not have to be present in high
concentrations or in more than one of a patient's medications to be able tocause trouble.
Overall, 87.31% of drug reactions were attributed primarily to pharma-cologically active agents, and 12.69% to preservatives. Pharmacologicallyactive agents alone were blamed for 62.69% of reactions.
LATERALITY OF DISEASE
Drug reactions did not affect either or both eyes significantly more oftenthan did other external diseases, except that all preservative-inducedcontact-lens reactions were bilateral.
953

RELATIONSHIPS OF DRUG REACTIONS TO OTHER DIAGNOSES
Among all external diseases, drug reactions as a whole were second infrequency only to keratoconjunctivitis sicca. The third most commonindividual diagnosis was drug-induced toxic papillary keratoconjunctivi-tis, occurring in more than 10% of all patients and ranking in frequencyjust below dry eyes and herpes simplex keratitis.
Certain diagnoses were found in conjunction with drug reactions signif-icantly more often than with control cases, suggesting that patients withthese problems are especially likely to be overtreated: herpes simplexkeratitis, inactive or resolving; indolent epithelial ulcer, post-herpetic ornot post-herpetic; glaucoma; lacrimal outflow obstruction; adenoviral ker-atoconjunctivitis, inactive; chalazion, inactive; bacterial or fungal cornealulcer, inactive; and superficial punctate keratitis of Thygeson, resolving.About 13% of all drug cases had no diagnoses other than their drug
reactions, indicating that their original problems had disappeared andcould no longer be identified. Of those drug cases that did have associateddiagnoses, only about 47% had active disorders; the rest had inactive(31%) or resolving (21%) diseases. Therefore, about 44% of patients withdrug reactions (13% with no other diagnoses and 31% with inactive ones)were typical victims of the overtreatment syndome and needed little ornothing more than the cessation of offending drugs in order to be cured.The same could reasonably be said of many, if not most, of the 21% ofpatients who had resolving problems. The 47% of patients who had activediseases usually needed therapy but were treated excessively. So, as wehave seen before, drug reactions are related both to the amount of treat-ment and to the length of time it is given, with the latter probably beingslightly more important. We must be careful not to prescribe more treat-ment than is needed and, especially, not to continue it too long.
Keratoconjunctivitis sicca was a statistically significant predisposingfactor for the development of toxic papillary keratoconjunctivitis, proba-bly because the dry eye has an already abnormal surface and unstable tearfilm and is less able to dilute and carry away drugs and preservatives thatare applied to it. Realizing this, it seems incongruous that so manyartificial tears contain benzalkonium, which is by far the most toxic pre-servative in current use.
Incorrect diagnosis by treating or referring physicians was highly sig-nificantly related to the development of drug reactions. Intensive treat-ment was often prescribed even when no specific diagnosis was at hand.In general, the presence of inflammatory signs and symptoms combinedwith an uncertain diagnosis seemed to result in the prescribing of a larger
954 Wilson
Topical Ophthalmic Therapy
number ofpotent drugs, and their continuation for longer periods of time,than did other clinical circumstances.
TYPES OF DRUG REACTIONS ENCOUNTERED
Contrary to popular belief, most reactions to topical ophthalmic medi-cations are toxicities, not allergies. Nearly 80% of all drug cases had toxicpapillary reactions, and an additional 10% had toxic follicular reactions;only about 10% of the reactions were clearly allergic, and all of these tookthe form of eezematoid contact dermatoconjunctivitis, with or withoutkeratitis. There were no anaphylactoid reactions in the computerizedstudy, and I have encountered only four in the past 13 years. About 5% ofthe drug cases had more than one kind of reaction, one of which wasalways a toxic papillary one.
Unlike patients who did not wear contact lenses, those who did andwho developed drug-related problems nearly always had true allergies (tothimerosal in their contact lens solutions), although I found some evi-dence to suggest that these patients might also have had toxic reactions toboric acid or allergies to chlorhexidine gluconate or edetate.
HEALING OF DRUG REACTIONS
Many drug reactions heal slowly. When they are suspected, the physicianshould make every effort to prohibit the use of all potentially toxic andallergenic drugs and preservatives for at least 6 weeks and should notconclude sooner that the cessation of medications has not helped. Severereactions to thimerosal in contact lens solutions may take as long as 6months to disappear completely-or longer if the patient intermittentlyreinserts the lenses, even for only a few minutes at a time.CLINICAL FINDINGS AND COMPLICATIONS ASSOCIATED WITH DRUG REACTONS
Certain exterual ocular physical findings should always raise the suspicionof a drug-induced etiology, although all of these problems can also haveother causes: eczematoid dermatitis (with or without infection), diffuse orfocal epithelial keratopathy, pseudodendrites, pseudogeographic epithe-lial defects, filamentary keratopathy, pannus, calcific band-keratopathy,papillary or follicular conjunctivitis, conjunctival scarring or ker-atinization, punctal or canalicular stenosis, chronic dacryocystitis, tri-chiasis, and cicatricial entropion.
Patients who have reactions to the chronic use of topical anesthetics canalso have infiltrates in the corneal stroma, including Wessely rings. Thesepatients and those who have rebound inflammations from the abruptcessation of steroid may develop hypopyon, hyphema, or fibrin in theanterior chamber.
9"55

In contrast to previous descriptions of the syndrome of papillary ker-atoconjunctivitis in contact-lens wearers, I found that these patients oftenhave only small, rather than giant, papillae, even though other findingssuch as hyperemia, discharge, pannus, and epithelial keratopathy may befar-advanced.
LABORATORY STUDIES
Conjunctival Cytology of Drug ReactionsThe earliest abnormal cytologic feature of allergic or toxic drug reactionswas the presence of activated epithelial cells. These are cells whosemorphology has been altered, in ways that I have already described, byreason of accelerated rates of mitosis and maturation. Activated epithelialcells are indicative only of subacute or chronic inflammation and so arenot diagnostic of drug reactions.
Epithelial cells normally flatten and elongate as they approach theconjunctival surface; but if their maturation is speeded up sufficiently,they begin to die prematurely and so show signs of degeneration andkeratinization as they reach the surface. These changes, then, naturallyfollow activation.
Cytoplasmic "toxic granules" have been described in the conjunctivalepithelial cells of patients with toxic reactions to topical ophthalmic anti-biotics.'4 I have seen these irregular, deeply basophilic granules but donot consider them to be specific for drug reactions. The granules arefound in the company of degenerating and keratinizing epithelial cells andare probably no different from the keratohyaline granules that routinelyappear during early epithelial keratinization.
Inflammatory cells generally appeared in conjunctival scrapings onlyafter the epithelial abnormalities had begun. This is not surprising in viewof the fact that the inflammatory cells originate from the blood vessels ofthe conjunctival stroma and must work their way to the surface beforethey can be found in scrapings, whereas the epithelial cells are on or nearthe surface from the outset.
Neutrophils predominated in about two thirds of the cases, but thisseemed merely to be a function of the severity of the drug reaction.Mononuclear cells usually appeared first and were more numerous inrelatively mild cases. Neutrophils came later and predominated in themore severe reactions.The finding of eosinophils is usually considered to be indicative of a
type-I immunologic response, and it has been written that these cellsshould not and do not appear in type-IV hypersensitivities such as allergic
956 Wilson

Topical Ophthalmic Therapy
contact dermatoconjunctivitis. 3' - Nevertheless, when I looked for them,I found eosinophils in two thirds of allergic contact reactions and in onefourth of contact-lens cases, both of which are presently classified astype-IV hypersensitivities. These findings are understandable now thatwe know that the lymphocytes that mediate delayed (type-IV) hyper-sensitivity can release one or more eosinophil-chemotactic factors.'7
I also found basophils rarely in cases of contact allergy. Basophils areknown to appear along with eosinophils in some allergic diseases of theeye37 and to be prominent in some kinds of cutaneous contact allergyJones-Mote hypersensitivity).'7
CONJUNCTIVAL CULTURES
Patients with allergic contact reactions, toxic papillary reactions withoutscarring, or pseudopemphigoid had abnormal external ocular flora. Theircultures revealed more true pathogens, opportunistic pathogens, gram-negative organisms, and fungi than are normally found.Some of the organisms may have been related to the patients' underly-
ing diseases. For example, diphtheroids are more common in patientswho have dry eyes, and these patients are also more likely to have toxicpapillary reactions to drugs. However, most of the alterations in florawere typical of, and can be better attributed to, the effects of the long-term use of topical antibiotics and steroids. 17
HISTOPATHOLOGIC STUDIES
Most of the results of the histopathologic studies are self-explanatory, so Ishall mention here only those points that deserve additional discussion.
Toxic Papillary Conjunctivitis Without Scarring.-The histopathologyof the biopsy, along with the previously cited cytologic findings, suggest-ed that the typical punctate staining of toxic papillary and some otherdrug reactions may be related to several factors other than losses ofindividual epithelial cells, including eruptions of increased numbers ofgoblet cells, degeneration and keratinization of epithelial cells, and sur-face irregularities caused by epithelial activation and acanthosis and byformation of pseudoglands of Henle. Abnormal losses of epithelial cellsoccur too, because the normal processes of sloughing and replacement aredisrupted by activation, degeneration, and inflammation.The fact that subepithelial and intraepithelial inflammatory cells were
present in the biopsy does not mean that immunologic mechanisms mustbe incriminated in the pathogenesis of toxic papillary reactions. It is wellknown that purely toxic or irritating substances can produce intense in-flammation.
957

Wilson
Pseudogeographic Epithelial Defects.-The bases of pseudogeographicepithelial defects stain with rose bengal because they contain degenerat-ed and keratinizing epithelial cells with an admixture of mucus. A fewmononuclear or polymorphonuclear inflammatory cells and activated epi-thelial cells may also be found.The edges of pseudogeographic defects show the same findings except
that the abnormal epithelial cells are heaped and curled under them-selves.
Toxic Folliculkr Conjunctivitis.-The histopathologic studies of toxicfollicular conjunctivitis revealed that drugs (at least atropine and dipivef-rin) can induce the development of true lymphoid follicles with lympho-blastic germinal centers. The presence of lymphoblasts defines the struc-tures as true follicles, as opposed to the mere focal accumulations oflymphoid cells that have been found previously (HB Ostler, MD: verbalcommunication, June 1977; written communication, August 1979).The dipivefrin-induced follicle also showed tingible bodies and subclin-
ical conjunctival scarring. The tingible bodies are evidence of follicularmaturity and appear when some of the lymphoblasts exhaust their life-spans and become engulfed by macrophages.The finding that drugs can cause true and mature lymphoid follicles
does not refute previous workers' conclusions that these reactions aretoxic and not allergic. I found almost nothing to indicate that my caseswere of allergic origin, so I suspect that the follicle-inducing drugs mayact much as do nonantigenic mitogens such as phytohemagglutinin, con-canavalin A, and pokeweed mitogen. These substances induce mitosesand lymphoblastic transformations of lymphocytes by nonimmunologicmeans, probably by binding to receptor sites that are distinct from thoseto which antigens attach.38The histopathologic finding of new-collagen formation in the dipivefrin
case suggests that conjunctival scarring would eventually have becomeevident clinically and that any drug-induced follicular reaction mightcicatrize if it were allowed to persist for a sufficiently long period of time.
CLNICAL OBSERVATIONS
As was true of the histopathologic studies, most of the detailed clinicalobservations speak for themselves, so I shall simply summarize now themost important general concepts that I have learned, and that I wish toemphasize, concerning our clinical and philosophic approaches to topicalophthalmic therapy.
Reliance on drugs is nowhere more prevalent in ophthalmology than inthe field of external diseases, and the ocular surface and adnexa fall prey
958

Topical Ophthalmic Therapy
often to the misuse, overuse, or adverse effects of topical medications.The reasons are many and include: (1) the delicacy of the external eye andthe ease with which drugs may be applied to it; (2) the many potentpreparations now available and the multiplicity of their components; (3)misleading advertising campaigns and unrestrained enthusiasm for newdrugs; (4) unrealistic expectations by both patients and clinicians of theefficacies ofdrugs; (5) limited appreciation by patients and practitioners ofthe potentially harmful effects of drugs, and inattention to these effects asthey develop; (6) pressures to take positive therapeutic action rather thanto allow largely untreatable or self-limited disorders to run their naturalcourses; and (7) the usually unfounded belief that "shotgun therapy" cansubstitute for specific therapy based on accurate diagnosis.
Frustrating difficulties with diagnosis are common and probably willcontinue to plague us for generations to come. It is understandable thatwe might hope and search for drugs that are safe "cure-alls," as patientsand practitioners of every variety have done for centuries. Unfortunately,despite all of our progress, any notion that such drugs are now availableremains illusory. Indeed, it seems often that our drugs become potential-ly more harmful as they become more efficacious.
Nevertheless, some practitioners habitually'prescribe one or more ofthe newest and most highly touted drugs, almost irrespective of diagno-sis, in the hope that this might somehow take care of any possible prob-lem. Duke-Elder5 summed it up well when he wrote, "One of the defectsof medicine, as I see it, however, is and always has been the uncriticalenthusiasm with which new drugs or therapeutic techniques tend to beaccepted."When we reach first for the most potent drugs, we usually reach also for
the most harmful ones; and, too often, these drugs are not even likely tobe beneficial. No amount of neomycin, chloramphenicol, idoxuridine,vidarabine, trifluridine, gentamicin, or tobramycin (with or without ste-roid) will help patients who have keratoconjunctivitis sicca, inactive orresolving herpes simplex keratitis, indolent epithelial defects, no diagno-sis other than drug reaction, or glaucoma, which were the underlyingproblems in almost 90% of patients who developed reactions (Table XX).The same drugs are also of little or no value for a surprisingly largenumber of all other external diseases.
I believe that it is better to undertreat than to overtreat when thecorrect diagnosis and treatment are in doubt, except when the eye isimmediately and seriously threatened, as by copiously purulent conjunc-tivitis, hypopyon corneal ulcer, or endophthalmitis. Less glamorous, butrelatively bland and harmless, medications such as sulfacetamide, bacitra-
959

Wilson
cin, erythromycin, polymyxin, artificial tears without toxic or allergenicpreservatives, or lubricating ointments will effect as many, if not more,"cures" as will the previously mentioned, and supposedly better, broad-spectrum antibiotics and antiviral agents. When we are unable to make aquick, specific diagnosis, we may turn to the latter drugs in an effort tosave time and to get on to the next patient in the busy waiting room.Actually, it is more time-saving in the long run to use the milder, butusually equally efficacious, drugs because they are not likely to obscurespontaneous or drug-induced improvement by producing adverse reac-tions.
It is generally accepted, throughout all of medicine, that the physicianshould prescribe the minimal amount of treatment that will achieve thedesired result. The ultimate extension of this concept is that properpractice sometimes calls for the use of no active treatment whatsoever, aswas expressed in the 17th century by Sydenham39 (the "English Hip-pocrates," 1624-1689):
It is a great mistake to suppose that Nature always stands inneed of the assistance of Art . . nor do I think it below meto acknowledge that, when no manifest indication pointed outto me what was to be done, I have consulted the safety of mypatient and my own reputation effectually by doing nothingat all.
Sydenham was not a therapeutic nihilist. In fact, he helped to prevent thedisappearance of many useful drugs that might have fallen into disfavorbecause they did not fit neatly into one theory of medical practice oranother; but he did adhere to the Hippocratic principle of trying to aidnatural healing by any reasonable means while, at the same time, takingcare to do no harm.40Nor do I advocate therapeutic nihilism. All of our drugs, even the most
potentially harmful ones, are useful in some situations; but I do believe,as this study has shown, that we should select drugs on the basis of theirusefulness for specific indications and not because of their newness,popularity, or potency. We should remember that the more potent, toxic,or allergenic the drug, the fewer are its indications. When the indicationsare uncertain, we should prescribe so as to minimize our chances ofcausing the many, and prevalent, problems that have been the subject ofthis study.We should recall the admonishment of Sir William Osler41:
In the fight which we have to wage incessantly againstignorance and quackery among the masses and follies of allsorts among the classes, diagnosis, not drugging, is our chief
960

Topical Ophthalmic Therapy
weapon of offence. Lack of systematic personal training inthe mwthods of the recognition of disease leads to themisapplication of remedies, to long courses of treatment whentreatment is useless, and so directly to that lack of confidencein our methods which is "apt to place us in the eyes of thepublic on a level with empirics and quacks.
Finally, we should be ever mindful of the prayer of Sir Robert Hutchi-son (1871-1960), which is posted in London Hospital42:
From inability to let well alone: from too much zeal for thenew and contempt for what is old: from putting knowledgebefore wisdom, science before art, and clevemess beforecommon sense, from treating patients as cases, and frommaking the cure of the disease more grievous than theendurance of the same, Good Lord, deliver us.
SUMMARY AND CONCLUSIONS
New knowledge of adverse external ocular reactions to topical ophthalmicmedications was obtained by means of a computerized epidemiologicstudy, laboratory studies, and clinical observations. Listed below are themajor findings and conclusions that represent facts or concepts that werepreviously unknown, uncertain, misunderstood, or forgotten:
1. The incidence of clinically important drug reactions among all caseswas at least 13.09% and may have been as high as 16.02%. Among treatedpatients it was at least 16.26% to 19.90%. Taken together, drug reactionswere the second most common external disease diagnosis.
2. The incidence of each kind of drug reaction was determined. Toxicpapillary reactions accounted for 79.10% of drug cases and 10.35% of allcases. Toxic papillary keratoconjunctivitis was the third most commonsingle diagnosis.
3. The following epidemiologic factors were found to be related to thedevelopment or presence of drug reactions: number and variety of treat-ing practitioners, number of practitioners consulted, number of practi-tioners consulted who treated, specific ophthalmologist consulted (8.24%of ophthalmologists referred 39.55% of all drug cases and showed a ten-dency habitually to overtreat), number and kinds of patients' symptomaticcomplaints, number of medications prescribed and used, number of daysof treatment, particular drugs and preservatives used (but not theirstrengths or vehicles), underlying (primary) diagnoses, and inaccuracy ofreferring ophthalmologists' diagnoses. Patients with dry eyes were espe-cially at risk for the development of toxic papillary reactions.
961

4. Among all cases, the incidence of reactions to preservatives (mainlythimerosal) in contact lens solutions was 0.39% to 1.95%, depending onwhether definite or probable cases, respectively, were considered. Theincidence among the 54 patients who used daily-wear lenses (excludingextended-wear therapeutic and optical contacts) was 7.41% for definitereactions and 37.04% for probable ones.
5. Factors relating to the development of papillary contact-lens reac-tions were daily wear, number of days of wear, and, especially, thepreservatives to which the patients were exposed. Reactions occurredmore often with soft lenses than with hard ones.
6. Ofpatients with drug reactions, 5.22% had two different ones simul-taneously. Coexisting reactions to pharmacologically active agents werealso present in 15% of patients who reacted to preservatives in contactlens solutions.
7. The ocular tissues that were affected by each kind of drug reactionwere tabulated, and the relative degrees and sequences of involvementwere discussed.
8. The frequencies with which particular drugs, physical agents, andpreservatives were used and caused or contributed to adverse effectswere determined for drug reactions as a whole and for each specific kindof reaction. Preservatives (mainly benzalkonium) in artificial tears weresecond only to idoxuridine as a cause of trouble. Preservatives were alsoof major importance in the causation of contact-lens reactions and toxiccalcific band keratopathy; otherwise, pharmacologically active agentswere the main offenders. Risk factors were calculated for the most poten-tially harmful drugs and preservatives.
9. The times required for improvement and clearing of drug and con-tact-lens reactions were determined and were found to be considerablylonger than previously thought.
10. The clinical manifestations and complications that were associatedwith drug and contact-lens reactions were studied and described. Severalnew findings emerged, including ways in which early allergic contactreactions (with or without secondary infection) can be differentiated fromtoxic papillary reactions or staphylococcal blepharitis; the detailed clinicalfeatures of toxic follicular reactions without scarring and the fact thattrifluridine can cause such reactions; and the importance of realizing thatpapillary reactions to preservatives in contact lens solutions may manifestsevere hyperemia, discharge, pannus, and punctate or filamentary epi-thelial keratopathy without the concomitant presence of the usual giantpapillae and that some of these cases can be confused with (but can also bedifferentiated from) superior limbic keratoconjunctivitis.
962 Wilson

Topical Ophthalmic Therapy
11. The conjunctival cytology of drug reactions was described andclarified, as was the cytology of pseudogeographic epithelial defects. Thesequential changes in conjunctival scrapings were elucidated, and it wasshown that eosinophils are common in allergic contact reactions. Baso-phils were found for the first time in conjunctival contact allergy. Drug-induced "toxic granules" were thought to be the same as keratohyalinegranules.
12. The external ocular flora associated with drug reactions were tabu-lated, and evidence was presented in support of the idea that the pro-longed use of topical medications may adversely alter the flora.
13. The histopathology of toxic papillary conjunctivitis was studied bylight microscopy. Surface abnormalities, epithelial changes, and mono-nuclear inflammation were found.
14. Atropine and dipivefrin-induced follicles were examined by lightand electron microscopy. Both biopsies revealed true lymphoid follicleswith germinal centers, and the dipivefrin case also showed germinal-cen-ter tingible bodies (indicating follicular maturity) and peripheral follicularscarring.
15. Clinical observations concerning the etiology, pathogenesis, diag-nosis, treatment, healing, and prevention of drug reactions were present-ed. Among other considerations, staining patterns, the effects of steroids,and the possible relationships between noncicatrizing and cicatrizingreactions were discussed.
16. Pleas were made for generally more conservative and reasonedapproaches to topical ophthalmic therapy.
ACKNOWLEDGMENTS
I gratefully acknowledge the help of the following people in the comple-tion of this project: Janet C. Weber, PhD, for computer work; Jack F. vander Vliet for histotechnology; Kenneth G. Julian, Donald A. Ent, andFrank Radaker for photographic processing; Michael P. Goheen andMargaret J. Harger for preparing tissues for electron microscopy and forassisting me at the electron microscope; Nina D. Pick for library research;and Renee L. Rowell for typing the manuscript.My sponsors, G. Richard O'Connor, MD and Merrill Grayson, MD
helped me to design the study. Fred M. Wilson, MD and Robert A.Hyndiuk, MD, helped me in the preparation of the typescript.
This work was inspired by my teachers, who taught me the importanceof the art, as well as the science, of medicine: Doctors Wilson, Grayson,and O'Connor; Phillips Thygeson; and H. Bruce Ostler.
963

Wilson
REFERENCES
1. Lee PR: America is an overmedicated society, in Lasagna L (ed): Controversies inTherapeutics. Philadelphia, WB Saunders Co, 1980, pp 4-15.
2. Cluff LE: Is drug toxicity a problem of great magnitude? Yes!, in Lasagna L (ed):Controversies in Therapeutics. Philadelphia, WB Saunders Co, 1980, pp 44-50.
3. Karch FE: Is drug toxicity a problem of great magnitude? Probably not., in Lasagna L(ed): Controversies in Therapeutics. Philadelphia, WB Saunders Co, 1980, pp 51-57.
4. D'Arcy PF, Griffin JP: Preface to the second edition, in D'Arcy PF, Griffin JP (eds):latrogenic Diseases, ed 2. Oxford, England, Oxford University Press, 1979.
5. Duke-Elder S, Ashton N, Smith RJH, et al: System of Ophthalmology, VII, TheFoundations of Ophthalmology: Heredity, Pathology, Diagnosis, and Therapeutics. StLouis, CV Mosby Co, 1962.
6. von Graefe A: Therapeutische Miscellen. I. Aqua chlori. Arch fur Ophthalmol 1864;10(pt2):191-208.
7. : Ueber die lineare Extraction des Linsenstaars. Arch fur Ophthalmol 1855;l(pt2):219-286.
8. Theodore FH, Schlossman A: OcularAllergy. Baltimore, Williams & Wilkins Co, 1958.9. Woods AC: AUergy and Immunity in Ophthalmology. Baltimore, Johns Hopkins Press,
1933.10. : Clinical problems of allergy in relation to conjunctivitis and iritis. Arch Oph-
thalmol 1937; 17:1-17.11. Jackson E: Over treatment. Am J Ophthalmol 1921; 4:781-783.12. Hosford GN, McKenney JP: Ointment of yellow mercuric oxide (Pagenstecher's oint-
ment): Its use and abuse. JAMA 1933; 100:17-19.13. Thygeson P: Diseases of the conjunctiva, in Berens C (ed): The Eye and Its Diseases, ed
2. Philadelphia, WB Saunders Co, 1949.14. Fedukowicz H, Wise GN, Zaret MM: Toxic conjunctivitis due to antibiotics. Am J
Ophthalmol 1955; 40:849-856.15. Havener WH: Ocular Pharmacology. St Louis, CV Mosby Co, 1966.16. Fraunfelder FT: Drug-Induced Ocular Side Effects and Drug Interactions. Phil-
adelphia, Lea & Febiger, 1976.17. Wilson FM II: Adverse external ocular effects of topical ophthalmic medications. Surv
Ophthalmol 1979; 24:57-88.18. Helwig JT, Council KA (eds): SAS User's Guide, 1979 ed. Cary, North Carolina, SAS
Institute Inc, 1979.19. Siegel S: Nonparametric Statistics for the Behavioral Sciences. New York, McGraw-
Hill Book Co, 1956.20. Welch BL: On the comparison of several mean values: An alternative approach. Biome-
trika 1951; 38:330-336.21. Satterthwaite FE: An approximate distribution of estimates of variance components.
Biometrics (Bulletin) 1946; 2:110-114.22. Levine L, Byrd D: Packing and unpacking with SPSS. Statistical computing bulletin (of
Indiana University Bloomington Academic Computing Services) 1981; 1(pt4):3-5.23. Ehrich WE: Lymphoid tissues: Their morphology and role in the immune response, in
Samter M, Alexander HL (eds): Immunological Diseases. Boston, Little, Brown and Co,1965, p 262.
24. Patten JT, Cavanagh HD, Allansmith MR: Induced ocular pseudopemphigoid. Am JOphthalmol 1976; 82:272-276.
25. Ostler HB, Okumoto M, Daniels T, et al: Drug-induced cicatrization of the conjunctiva,in O'Connor GR (ed): Immunologic Diseases of the Mucous Membranes: Pathology,Diagnosis, and Treatment. New York, Masson Publishing, 1980, pp 149-158.
26. Theodore J, Leibowitz HM: External ocular toxicity of dipivalyl epinephrine. Am JOphthalmol 1979; 88:1013-1016.
964

Topical Ophthalmic Therapy
27. Jones BR: Rational regimen of administration of antivirals. Trans Am Acad OphthalmolOtolaryngol 1975; 79:104-108.
28. Falcon MG, Jones BR, Williams HP, et al: Adverse reactions in the eye from topicaltherapy with idoxuridine, adenine arabinoside, and trifluorothymidine, in SundmacherR (ed): Herpetische Augenerkrankungen. Munich, JF Bergmann, 1981, pp 263-267.
29. Garron LK, Wood IS, Spencer WH, et al: A clinical pathologic study of mercurialentismedicamentosus. Trans Am Ophthalmol Soc 1976; 74:295-320.
30. Wilson LA, McNatt J, Reitschel R: Delayed hypersensitivity to thimerosal in softcontact lens wearers. Ophthalmology 1981; 88:804-809.
31. Martin EW: Hazards of Medication. A Manual on Drug Interactions, Contraindica-tions, and Adverse Reactions with other Prescribing and Drug Information, ed 2.Philadelphia, JB Lippincott Co, 1978, p 1.
32. D'Arcy PF: Epidemiological aspects of iatrogenic disease, in D'Arcy PF, Griffin JP(eds): Jatrogenic Diseases, ed 2. Oxford, England, Oxford University Press, 1979, pp23-28.
33. Mondino BJ, Salamon SM, Zaidman GCV: Allergic and toxic reactions in soft contactlens wearers. Surv Ophthalmol 1982; 26:337-344.
34. Takahashi N: Quantitative cytotoxicity of preservatives evaluated in cell culture withChang's human conjunctival cells -ffect of temperature on cytotoxicity. Jpn J Oph-thalmol 1982; 26:234-238.
35. Allansmith NIR: Allergy of the lids, in Golden B (ed): Ocular Infla?nmnatory Disease.Springfield, Ill, Charles C Thomas Publisher, 1974, pp 251-264.
36. Ocular allergy-diagnosis and management, in Golden B (ed): Ocular Inflam-matory Disease. Springfield, Ill, Charles C Thomas Publisher, 1974, pp 14-27.
37. Thygeson P: The cytology of conjunctival exudates. Amn J Ophthalmol 1946;29: 1499-1512.
38. Lakin JD: The immune respoinse and hypersensitivity reactions, in Patterson R (ed):Allergic Diseases: Diagnosis and Managemnent, ed 2. Philadelphia, JB Lippincott Co,1980, p 14.
39. Sydenham T: quoted by Lasagna L (ed): Controversies in Therapeutics. Philadelphia,WB Saunders Co, 1980, p 2.
40. Sonnedecker G: Kremners and Urdang's History of Pharmacy, ed 4. Philadelphia, JBLippincott Co, 1976.
41. Osler W: Chauvinism in medicinie, in Osler W (ed): Aequanimitas, with Other Ad-dresses to Medical Students, Nurses, and Practitioners of Medicine, ed 3. Philadelphia,P Blakiston's Son and Co, 1932, p 283.
42. Hutchison R: quoted by D'Arec PF, Griffin JP: Preface to the first edition, in D'ArcyPF, Griffin JP (eds): latrogenic Diseases, ed 2. Oxford, England, Oxford UniversityPress, 1979.
965




















