
Morphometric Analysis of Ophthalmic Optical Coherence ...
179
Morphometric Analysis of Ophthalmic Optical Coherence Tomography Images by Sieun Lee B.Sc. (Hons.), Simon Fraser University, 2009 Thesis Submitted in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy in the School of Engineering Science Faculty of Applied Sciences c Sieun Lee 2015 SIMON FRASER UNIVERSITY Spring 2015 All rights reserved. However, in accordance with the Copyright Act of Canada, this work may be reproduced without authorization under the conditions for ”Fair Dealing”. Therefore, limited reproduction of this work for the purposes of private study, research, criticism, review and news reporting is likely to be in accordance with the law, particularly if cited appropriately.
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Morphometric Analysis of Ophthalmic Optical Coherence ...

Morphometric Analysis of Ophthalmic
Optical Coherence Tomography Images
by
Sieun LeeB.Sc. (Hons.), Simon Fraser University, 2009
Thesis Submitted in Partial Fulfillment
of the Requirements for the Degree of
Doctor of Philosophy
in the
School of Engineering Science
Faculty of Applied Sciences
c© Sieun Lee 2015
SIMON FRASER UNIVERSITY
Spring 2015
All rights reserved.
However, in accordance with the Copyright Act of Canada, this work may be
reproduced without authorization under the conditions for ”Fair Dealing”.
Therefore, limited reproduction of this work for the purposes of private study,
research, criticism, review and news reporting is likely to be in accordance
with the law, particularly if cited appropriately.

APPROVAL
Name: Sieun Lee
Degree: Doctor of Philosophy
Title: Morphometric Analysis of Ophthalmic Optical Coherence To-mography Images
Examining Committee: Chair: Dr. Andrew RawiczProfessor, School of Engineering Science
Dr. Mirza Faisal Beg Co-Senior Supervisor
Professor, School of Engineering Science
Dr. Marinko V. Sarunic Co-Senior Supervisor
Associate Professor, School of Engineering Science
Dr. Paul J. Mackenzie Supervisor
Assistant Professor, Department of Ophthalmology
and Visual Sciences, University of British Columbia
Dr. Pierre Lane Internal Examiner
Associate Professor of Professional Practice, School
of Engineering Science
Dr. J. Crawford Downs External Examiner
Professor of Ophthalmology, School of Medicine,
University of Alabama at Birmingham
Date Approved: April 14, 2015
ii
Partial Copyright Licence
iii

Abstract
Optical coherence tomography (OCT) provides in-vivo, high-resolution, cross-sectional
images of the inner structures of the eye. This dissertation outlines the construction and
application of a computational pipeline for morphometric analysis of 3D retinal and peripap-
illary OCT images for extracting clinically meaningful information based on shape features.
The images were acquired by a prototype 1060-nm swept-source OCT system and pro-
cessed to enhance the image quality. Next, retinal layers and structures in the optic nerve
head (ONH) and laminar regions were segmented. A graph-cut based, robust 3D algo-
rithm was implemented for automated segmentation of the retinal layers. The segmented
structures was measured by quantitative shape parameters, such as 3D layer thickness
and Bruch’s membrane opening (BMO) dimension.
A special focus was given to establishing anatomical correspondence across multiple
OCT images, for longitudinal or cross-sectional data, via registration. In the first approach,
retinal surfaces from two OCT images were registered by a mathematical current-based
deformation followed by spherical demons registration. In the second approach, retinal
surfaces and their signal values (ex. layer thickness) from several OCT images were jointly
varied to generate a group mean template serving as the common atlas.
In the clinical application of the pipeline, peripapillary OCT volumes of 52 myopic eyes
from normal and glaucomatous subjects were studied. Retinal layer thicknesses, and
shape features of BMO, Bruch’s membrane, and the anterior laminar region were mea-
sured and statistically analyzed. Significant differences were observed between the nor-
mal and glaucomatous groups, demonstrating glaucomatous deformation, and structural
changes correlated with myopia suggested a possible explanation to the high glaucoma
susceptibility associated with advanced myopia.
Image analysis; Image processing; Shape analysis; Optical coherence tomography;
Ophthalmology
iv

Acknowledgments
The work in this thesis could not have been possible without the constant mentor-
ship, encouragement, and guidance from my co-senior supervisors, Dr. Faisal Beg and
Dr. Marinko Sarunic, who took me on as an undergraduate student seven years ago and
personally saw through my growth as a researcher. I am also very grateful to Dr. Paul
Mackenzie for the supervision and guidance, with sharp insights of a clinician and stimu-
lating discussions. I am very thankful for my examining committee, Dr. Andrew Rawicz, Dr.
Pierre Lane, and Dr. J. Crawford Downs, for taking the time and effort to provide valuable
assessment of my work.
I am indebted to my fellow students at Biomedical Optics Research Group and Medical
Image Analysis Lab for their support and friendship. I am especially thankful to Dr. Evgeniy
Lebed, Ms. Sherry Han, and Ms. Morgan Heisler, with whom I had a chance to work closely
through various projects. I also thank the research collaborators in Canada and France for
the opportunities to benefit from their expertise and dedication.
My friends and family have stood by me throughout my graduate years. Words cannot
express my gratitude to my parents for their unwavering love and support. Lastly, I want to
thank God for giving the joy, gratitude, and deeper meaning in my life.
v

Contents
Approval ii
Partial Copyright License iii
Abstract iv
Acknowledgments v
Contents vi
List of Tables ix
List of Figures xi
1 Introduction 1
2 Background 4
2.1 The human eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
2.1.1 Retina . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
2.1.2 Fovea and optic nerve head . . . . . . . . . . . . . . . . . . . . . . . 6
2.2 Glaucoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.3 Optical coherence tomography . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.4 OCT in ophthalmology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3 Image Acquisition and Preprocessing 11
3.1 Acquisition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
3.2 Quality control and data management . . . . . . . . . . . . . . . . . . . . . 12
3.3 Preprocessing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
vi

3.3.1 Motion correction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
3.3.2 Bounded variation image smoothing . . . . . . . . . . . . . . . . . . 19
3.4 Summary of contributions . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
4 Segmentation 22
4.1 Manual segmentation of ONH structures . . . . . . . . . . . . . . . . . . . . 22
4.2 Automated segmentation of retinal layers . . . . . . . . . . . . . . . . . . . 24
4.3 Choroid segmentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
4.3.1 Comparison of choroid segmentation in in 830 nm and 1060 nm OCT
images . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
4.3.2 Repeatability analysis of choroidal thickness measurements in age-
related macular degeneration . . . . . . . . . . . . . . . . . . . . . . 30
4.4 Summary of contributions . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
5 Retinal Surface Registration 44
5.1 Exact surface-to-surface registration . . . . . . . . . . . . . . . . . . . . . . 46
5.1.1 Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
5.1.2 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
5.1.3 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
5.2 Repeatability Analysis in Longitudinal OCT Images . . . . . . . . . . . . . . 60
5.2.1 Materials and Methods . . . . . . . . . . . . . . . . . . . . . . . . . 60
5.2.2 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
5.3 Atlas-based Shape Variability Analysis and Classification of OCT Images
using the Functional Shape (fshape) Framework . . . . . . . . . . . . . . . 75
5.3.1 Atlas Estimation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
5.3.2 Variability Analysis and Classification . . . . . . . . . . . . . . . . . 86
5.3.3 Experimental Results . . . . . . . . . . . . . . . . . . . . . . . . . . 91
5.3.4 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
5.4 Summary of contributions . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100
6 Optic Nerve Head Morphometrics in Myopic Glaucoma 101
6.1 Participants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102
6.2 Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
vii

6.2.1 Acquisition and processing . . . . . . . . . . . . . . . . . . . . . . . 103
6.2.2 Segmentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
6.2.3 Measurements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
6.2.4 Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
6.3 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 108
6.4 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 110
6.4.1 Nerve Fiber Layer Thickness . . . . . . . . . . . . . . . . . . . . . . 111
6.4.2 Bruch’s Membrane Opening Shape . . . . . . . . . . . . . . . . . . 112
6.4.3 Peripapillary Bruch’s Membrane Shape . . . . . . . . . . . . . . . . 113
6.4.4 Choroidal Thickness . . . . . . . . . . . . . . . . . . . . . . . . . . . 115
6.5 Anterior lamina cribrosa region morphometrics . . . . . . . . . . . . . . . . 115
6.6 Summary of contributions . . . . . . . . . . . . . . . . . . . . . . . . . . . . 116
7 Conclusion 131
7.1 Future directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133
Bibliography 135
viii

List of Tables
4.1 Descriptive Statistics of the Choroidal Thickness Measured by the First Rater
(Rater 1), Second Rater (Rater 2), and the Algorithm (Auto) . . . . . . . . . 35
4.2 Intraclass Correlation and Paired Mean Difference for Choroidal Thickness
Measurement Between the Raters (Rater 1, Rater 2) and the Algorithm (Auto) 35
4.3 Intraclass Correlation and Paired Mean Difference for Choroidal Thickness
Measurement Between the Repeat Scans by the Raters (Rater 1, Rater 2)
and the Algorithm (Auto) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
4.4 Results of Multivariable Regression Analysis Between Drusen Area and
Choroid Thickness Measured by the Rater (Rater 1 and Rater 2) and the
Automated Algorithm (Auto) . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
5.1 BMO area mean, minimum, maximum, standard deviation, and coefficient
of variation for 9 repeat measurements over 3 weeks from 6 healthy subjects. 62
5.2 BMO eccentricity mean, minimum, maximum, standard deviation, and coef-
ficient of variation for 9 repeat measurements over 3 weeks from 6 healthy
subjects. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
5.3 RNFL thickness standard deviation . . . . . . . . . . . . . . . . . . . . . . . 66
5.4 Choroidal thickness standard deviation . . . . . . . . . . . . . . . . . . . . . 71
5.5 Accuracies, sensitivities, and specificities of the classification of healthy,
glaucomatous, and suspect RNFLs . . . . . . . . . . . . . . . . . . . . . . . 95
5.6 Accuracies, sensitivities, and specificities of the classification of healthy and
glaucomatous RNFLs by RNFL thickness only and RNFL posterior surface
geometry only . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
5.7 Accuracies, sensitivities, and specificities of the classification of healthy,
glaucomatous, and suspect RNFLs based on unregistered RNFLs . . . . . 97
ix

6.1 Demographics and Clinical Characteristics of the Study Subjects by Group 103
6.2 Performance of the automated segmentation of peripapillary structures . . 108
6.3 Multiple Regression Analysis of Shape Parameters With Age, Axial Length,
and Mean Deviation (MD): Mean Nerve Fiber Layer Thickness, BMO Area,
BMO Eccentricity, BMO Planarity, BMO Depth, Mean BM Depth, and Mean
Choroidal Thickness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119
6.4 Multiple Regression Analysis of Shape Parameters With Age, Axial Length,
and Mean Deviation (MD): Mean Nerve Fiber Layer Thickness, BMO Area,
BMO Eccentricity, BMO Planarity, BMO Depth, Mean BM Depth, and Mean
Choroidal Thickness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 120
x

List of Figures
1.1 OCT visualization of the optic nerve head. . . . . . . . . . . . . . . . . . . . 2
1.2 Computational pipeline of ophthalmic OCT images. . . . . . . . . . . . . . . 3
2.1 a) Schematic of the human eye. The image is from Wikimedia.org and repro-
duced here under the Creative Commons License. b) Light micrograph of a
vertical section through central human retina. The image is from Webvision
[105] and reproduced here under the Creative Commons License. . . . . . 5
2.2 a) Schematic of the optic nerve head, a reproduction from Gray’s Anatomy.
b) Ganglion cell axonal pattern. The image is from Webvision [105] and
reproduced here under the Creative Commons License. . . . . . . . . . . . 7
2.3 a) Progressive vision loss in glaucoma. Image source: National Eye In-
stitute, National Institutes of Health. b) Glaucomatous deformation in the
laminar region.1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
2.4 A simple Michelson interferometer schematic of optical coherence tomogra-
phy. (BS: beam splitter.) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.5 Ophthalmic OCT imaging of a) macular region and b) peripapillary region. . 10
3.1 Schematic of the swept-source optical coherence tomography system setup.
Source: Axsun SS Module; PC: polarization controller; BD: balanced detec-
tor; fn, focal length of the lens, where n = 1, 2, 3.[194] . . . . . . . . . . . . 12
3.2 Prototype optical coherence tomography system set up at the Eye Care
Centre, Vancouver General Hospital. . . . . . . . . . . . . . . . . . . . . . . 13
3.3 (a) Imaged region and scanning direction displayed on fundus photography.
(b) Volume reconstruction from raw data. (c) Volume visualized in 3D. . . . 14
3.4 A quick-check image of an OCT dataset. . . . . . . . . . . . . . . . . . . . . 15
xi

3.5 The first column shows the sectioning plane of the images in the second
column, and the third column illustrates motion visible in each of these im-
ages. In the first row, a B-scan (fast scan) is shown (b) in the direction of
frame acquisition (a). In the second row, an axial cross section (slow scan)
(e) orthogonal to the B-scan (as shown in (d)) displays wave-like axial mo-
tion artifact (f). In the third row, a sum-voxel en-face image in the plane (e)
displays lateral and elevation motion artifact (i) by the uneven blood vessel
boundaries and discontinuities in the image. . . . . . . . . . . . . . . . . . . 16
3.6 (a) Slow scan with maximum cross-correlation displacement profile. (b)
Same scan corrected by flattening the profile. (c) Same scan corrected by
fitting a smooth curve to the profile. The red arrows in (b) and (c) indicate
the cup depth measured in each image. (d) Volume before motion correc-
tion. The volume has been rotated that the axial axis lies vertically and the
en-face plane lies horizontally. (e) Same volume after smooth-fitting motion
correction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
3.7 Example of BV smoothing . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
4.1 Example of a) automated segmentation of retinal layers and b) manual point
segmentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
4.2 Top: B-scan of a 1060-nm OCT macular volume. Bottom: Automated seg-
mentation of inner limiting membrane (green), Bruch’s membrane equivalent
(cyan), and estimated choroid-sclera boundary (CS-boundary). . . . . . . . 28
4.3 Macular OCT images (Left) and their segmentations (Right). Top: 830-nm
2D averaged EDI-OCT scans acquired with Cirrus SD-OCT. Middle: 830-
nm 3D scans acquired with Cirrus SD-OCT. Bottom: 1060-nm 3D scans
acquired with the prototype 1060-nm SS-OCT. . . . . . . . . . . . . . . . . 29
4.4 Segmentation of a 3D macular scan acquired with 830-nm Cirrus SD-OCT
system. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
4.5 Segmentation of a 3D macular scan acquired with 1060-nm prototype SS-
OCT system. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
4.6 a) Sumvoxel projection of the macular choroid in a 1060-nm scan b) Total
retinal thickness colormap. c) Choroid thickness colormap. . . . . . . . . . 32
xii

4.7 Example of an automated subfoveal choroidal thickness measurement. Top
shows the original image. Bottom shows the segmented image. The ILM
(green), BM (blue), and choroid-sclera (CS) boundary (magenta) were seg-
mented automatically, and the choroidal thickness was measured as the ver-
tical distance between BM and CS boundary at the red dash line indicating
the foveal pit. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
4.8 Bland-Altman plots showing the interrater variability of choroidal thickness
measurements between the two manual raters (left), and between the man-
ual raters (averaged) and the automated algorithm. The dotted lines indicate
the upper and lower 95% confidence interval limits (N = 83). . . . . . . . . 36
4.9 Examples of segmentation by the first rater (red), second rater (yellow), and
the algorithm (magenta). The first and second scans show the three mea-
surements close to each other. In the third scan, the posterior choroidal
boundary is located deep with low edge strength, and the automated mea-
surement is smaller than the manual measurements. In the fourth scan a
large drusen reduces the visibility of the posterior choroidal boundary. . . . 42
4.10 Example of different choroid-sclera boundary measurements by the first
rater (red), second rater (yellow), and the algorithm (magenta). . . . . . . . 43
4.11 Repeat scans of the same fovea with different image quality. . . . . . . . . . 43
5.1 The proposed registration scheme. (a) The subject S is first brought into
close proximity with the template T by the method of surface currents φc
to produce an in-exact matching result. (b) A point-to-point correspondence
between S and T is achieved by registering φc(S) to T via spherical demons.
The end result matches the topology of the template. (c) Registration of the
four anatomical surfaces (ILM, BM, NFL and choroid) to the template by
φs(φc(Si)). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
5.2 3D checkerboard pattern propagation by the computed inverse mappings
Φ−1i . The top row shows the propagated checkerboard patterns of the NFL
surface while the bottom row shows the propagated checkerboard pattern
on the ILM surfaces. The surfaces shown in the first column are the NFL
and ILM surfaces of the template T . . . . . . . . . . . . . . . . . . . . . . . 51
xiii

5.3 Left column: NFL. First image: mean NFL thickness of the control group.
Second image: mean NFL thickness of the glaucomatous group. Third and
fourth images: t and p-values, respectively. Right column: choroid. First
image: mean choroidal thickness, shown in mm, of the control group. Sec-
ond image: mean choroidal thickness of the glaucomatous group. Third and
fourth images: t and p-values, respectively. . . . . . . . . . . . . . . . . . . 57
5.4 Phantom longitudinal data registration and validation. (a) Schematic depict-
ing the presence of a focal damage on the NFL and retinal thinning. Blue and
green lines represent the surfaces at time points 1 and 2, respectively. (b)
3D rendering of the phantom NFL surface at time point 2, showing the mod-
eled focal damage and retinal thinning. Colormap represents the computed
NFL thickness. (c) NFL surface at time point 1. (d) Modified NFL surface at
time point 2. The surface is translated by [0.4, 0.6, 0.2]mm, and rotated by
−10. Red rectangles highlight the modeled changes in morphometry. (e)
Surface from (d) registered to the surface from (c). Colormap represents the
differences in NFL thickness between time point 1 and registered time point
2. (f) The colormap from (e) thresholded by the intrinsic axial resolution
of the OCT system. Red represent decreased NFL thickness while green
represents increased NFL thickness. . . . . . . . . . . . . . . . . . . . . . . 58
5.5 Longitudinal analysis of NFL and choroidal thickness. Top row: Surfaces
and data from Time Point 1. Second row: Surfaces and data from Time
Point 2 (one year later). Third row: Surfaces and data from Time Point 1
registered to surfaces from Time Point 2. Fourth row: Difference in thickness
measurements from the two time points. Last row: thresholded difference in
thickness, in terms of the axial resolution of the OCT system lc (lc = 6µm).
Increased and decreased thicknesses are represented by green and red,
respectively. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
5.6 Diurnal pattern of BMO area. . . . . . . . . . . . . . . . . . . . . . . . . . . 64
5.7 BMO area measurements over three weeks. . . . . . . . . . . . . . . . . . 65
xiv

5.8 Variability analysis of retinal nerve fiber layer (RNFL) thickness over 3 weeks.
Row 1: original RNFL thickness maps measured at 9 different time points
(t0: baseline, t1 – t8: follow-up) in 3 weeks. Row 2: follow-up RNFLs were
registered to the baseline, establishing point-to-point correspondence be-
tween each follow-up RNFL and the baseline RNFL as the common tem-
plate. In Row 2, RNFL thickness values are shown remapped onto the reg-
istered RNFLs. Row 3. Vertex-wise RNFL thickness difference between the
baseline and each follow-up RNFL. Row 4. Difference maps in Row 3 are
shown normalized by the axial coherence length of the system. . . . . . . . 66
5.9 Voxel-wise time-average and standard deviation of RNFL thickness over 3
weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
5.10 Histograms of RNFL thickness standard deviation. . . . . . . . . . . . . . . 68
5.11 Cumulative distribution function plots of RNFL thickness standard deviation. 69
5.12 RNFL thickness standard deviation map overlaid on enface images. . . . . 70
5.13 Variability analysis of choroidal thickness over 3 weeks. Row 1: original
choroidal thickness maps measured at 9 different time points (t0: baseline,
t1 – t8: follow-up) in 3 weeks. Row 2: follow-up choroids were registered
to the baseline, establishing point-to-point correspondence between each
follow-up choroid and the baseline choroid as the common template. In
Row 2, choroid thickness values are shown remapped onto the registered
choroids. Row 3. Vertex-wise choroidal thickness difference between the
baseline and each follow-up choroid. Row 4. Difference maps in Row 3 are
shown normalized by the axial coherence length of the system. . . . . . . . 71
5.14 Voxel-wise time-average and standard deviation of RNFL thickness over 3
weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
5.15 Histograms of RNFL thickness standard deviation. . . . . . . . . . . . . . . 73
5.16 Cumulative distribution function plots of RNFL thickness standard deviation. 74
5.17 Illustration of the algorithm principle : the estimated mean template (
x , f )isagradient−descent−basedupdateofaninitialfshape(x init,f init).
The notation (xt,f t) symbolizes the state of the template at iteration t. . . . 86
xv

5.18 (a) Aligned RNFL surfaces with RNFL thickness mapping, (b) mean tem-
plate of all RNFLs, (c) mean template of normal RNFLs only, and d) mean
template of glaucomatous RNFLs only. Note the low estimated RNFL thick-
ness of the mean glaucomatous template as compared to that of the mean
normal template. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
5.19 Observed RNFLs (top row) and their reconstructions from a common mean
template (bottom row). Note that the reconstruction agrees with the pattern
of the original RNFL thickness with an overall smooth and noise-reduced
profile. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
5.20 Functional convergence with gradient descent optimization. . . . . . . . . . 92
5.21 Left: Voxel-wise t-test significance map of retinal nerve fiber layer (RNFL)
thickness between normal (N = 26) and glaucomatous (N = 27) eyes, with
the red region indicating p < 0.05. Right: The same map with the log of the
p-value. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92
5.22 Leave-one-out cross validation accuracy with varied regularization parame-
ter ε. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
5.23 LDA classifier for Healthy vs. Glaucoma data in A) functional residual, B)
initial momenta in x-direction, C) initial momenta in y-direction, and D) initial
momenta in z-direction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
6.1 Image processing and segmentation. A B-scan is shown (a) in the original
form, (b) smoothed and edge-enhanced, and (c) segmented for inner lim-
iting membrane (ILM, magenta), posterior boundary of retinal nerve fiber
layer (NFL, purple), Bruch’s membrane (BM, green), Bruch’s membrane
opening (BMO, red), and choroid–sclera boundary (CS boundary, blue).
The CS boundary was defined as the outermost boundary of the choroidal
blood vessels, which was consistently visible in all volumes. In (d), the seg-
mented structures are displayed in 3D. Although shown here in a B-scan,
the smoothing and segmentation were performed in 3D, not frame by frame. 103
xvi

6.2 Shape parameters. (a) An example B-scan. (b) Nerve fiber layer thickness
was measured as the closest distance to ILM from each point on the poste-
rior NFL boundary. (c) Bruch’s membrane reference plane was defined as
the best-fit plane to BM points 2 mm away from the BMO center. (d) Bruch’s
membrane opening depth was measured as the normal distance between
the BM reference plane and BMO center. (e) Bruch’s membrane depth was
measured as the normal distance between each point of BM and the BM
reference plane. (f) Choroidal thickness was measured as the closest dis-
tance to BM from each point on the posterior choroid boundary. Although
shown here in a B-scan, all parameters were defined and measured in the
full 3D volume. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
6.3 Sectorization. Elliptical annuli were drawn at 0.25, 0.75, 1.25, and 1.75
mm from Bruch’s membrane opening (BMO). The annuli were divided into
608 angular sectors of superior (S), nasal (N), inferior (I), and temporal (T)
and 308 angular sectors of superior-nasal (SN), inferior-nasal (IN), inferior-
temporal (IT), and superior-temporal (ST). . . . . . . . . . . . . . . . . . . . 106
6.4 Peripapillary retinal nerve fiber layer (NFL) thickness. All thickness colour
maps are in scale and right-eye orientation. The region within 0.25 mm from
Bruch’s membrane opening (BMO) was excluded. The graph plots the NFL
thickness averaged over the region between 0.25 and 1.75 mm from BMO,
with outliers in each group marked by red circles. . . . . . . . . . . . . . . . 118
6.5 Bruch’s membrane opening disc margin correspondence and planarity of
BMO. Bruch’s membrane opening points overlaid on en face images gen-
erated by summing the 3D OCT volumes in the axial direction. Red points
indicate where the BMO is posterior (into the page) to reference plane, and
green points indicate where the BMO is anterior (out of the page) to the
reference plane. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121
6.6 Bruch’s membrane opening shape measurements. (A) Bruch’s membrane
opening area, (B) BMO eccentricity, and (C) mean BMO planarity, distributed
by (i) group and versus (ii) age, (iii) axial length, and (iv) MD. Outliers in each
group are marked by red circles in plots (i). . . . . . . . . . . . . . . . . . . 122
xvii

6.7 Peripapillary BM depth. All depth maps are in scale and right-eye orienta-
tion. The BM depth is measured with respect to the BM reference plane at
each point on BM. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123
6.8 Bruch’s membrane opening and mean BM depth measurements. (A) Bruch’s
membrane opening depth and (B) mean BM depth distributed by (i) group
and versus (ii) age, (iii) axial length, and (iv) MD (C). Intereye differences of
BMO depth and BM depth are also plotted versus intereye MD difference.
Outliers in each group are marked by red circles in plots (i). . . . . . . . . . 124
6.9 Bruch’s membrane depth sectoral analysis. (A) Sectorized group averages
of Bruch’s membrane (BM) surface depth. The colour in each sector in-
dicates the mean absolute magnitude of the normal distance between BM
and its fitted plane. Elliptical annuli are drawn at 0.25, 0.75, 1.25, and 1.75
mm from Bruch’s membrane opening (BMO). The annuli are divided into
60ngular sectors of superior (S), nasal (N), inferior (I), and temporal (T), and
30ngular sectors of superior-nasal (SN), inferior-nasal (IN), inferior-temporal
(IT), and superior-temporal (ST). (B) Average BM depth by angular sector
for the whole BM surface. (C) Average BM depth by angular sector for the
inner annulus only (0–0.25 mm distance from BMO). . . . . . . . . . . . . . 125
6.10 Peripapillary choroidal thickness. All thickness colour maps are in scale and
right-eye orientation. The region inside and within 0.25 mm from Bruch’s
membrane opening (BMO) was excluded. . . . . . . . . . . . . . . . . . . . 126
6.11 Choroidal thickness measurements. Choroidal thickness distributed by (i)
group, and versus (ii) age, (iii) axial length, and (iv) MD. . . . . . . . . . . . 127
6.12 Choroidal thickness sectoral analysis. (A) Sectorized peripapillary choroidal
thickness. Elliptical annuli are drawn at 0.25, 0.75, 1.25, and 1.75 mm
from Bruch’s membrane opening (BMO). The annuli are divided into 60
degrees angular sectors of superior (S), nasal (N), inferior (I), and tem-
poral (T), and 30 degrees angular sectors of superior-nasal (SN), inferior-
nasal (IN), inferior-temporal (IT), and superior-temporal (ST). (B) Average
choroidal thickness by angular sector. . . . . . . . . . . . . . . . . . . . . . 127
xviii

6.13 Graphical description of anterior lamina insertion points (ALIP) to Bruch’s
membrane opening (BMO) distance (left) and anterior lamina cribrosa sur-
face (ALCS) depth (right). . . . . . . . . . . . . . . . . . . . . . . . . . . . . 128
6.14 Enface projection of Bruch’s membrane openings (BMO, red) and anterior
lamina insertion points (ALIP). . . . . . . . . . . . . . . . . . . . . . . . . . 129
6.15 Saddling of the Bruch’s membrane opening (BMO) and anterior lamina in-
sertion points (ALIP). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 130
6.16 Multiple regression of anterior lamina insertion point (ALIP) area and depth
with axial length and mean deviation. . . . . . . . . . . . . . . . . . . . . . . 130
xix

Chapter 1
Introduction
In the past two decades, optical coherence tomography (OCT) (Figure 1.1)in ophthal-
mology and vision science has introduced a whole new level of ocular imaging capacity for
the clinicians and scientists. The noninvasive, in-vivo technology provides volumetric and
cross-sectional images of the anterior and posterior sections of the eye in high resolution.
Ocular anatomy is visualized in 3D in-vivo, complementing the conventional enface view of
the eye with an ophthalmoscope. The state of the internal tissue structures thus visualized
can be correlated with visual functions and presence and progress of diseases, and serve
as a valuable guide in clinical decision making and monitoring treatment effectiveness.
Ophthalmic OCT has also created a new class of medical images, a rich, dense source
of clinically relevant morphological information. Qualitative examination of OCT images
provides fast and intuitive understanding of in-vivo anatomy; however, a full utilization of
the the wealth of information in the highly detailed 3D images requires quantitative mea-
sures and computational techniques capable of processing and analyzing complex shape
information in a large scale. This is especially true in research investigating patterns and
trends in structural mechanisms underlying the eye’s growth, function, and pathology.
This thesis presents a comprehensive computational pipeline for ophthalmic OCT im-
ages, from image acquisition to clinically meaningful statistical inferences. The main moti-
vation for this work was glaucoma, the leading cause of irreversible blindness in the world
[8]. Glaucoma is complex, multi-factorial neuropathy in the retinal nerve fiber layer (RNFL).
The primary risk factor and treatment focus is elevated intraocular pressure (IOP), sug-
gesting pressure-induced structural damage as part of the disease mechanism. However,
the relationship between the IOP and glaucoma is yet far from clear, with large individual
1

Figure 1.1: OCT visualization of the optic nerve head.
variability. OCT can image the optic nerve head (ONH), the major site of glaucomatous
deformation, and the shape information in the images can be extracted and analyzed to
find features significant in the disease progression. Are there common shape characteris-
tics in glaucomatous ONHs, and how do these vary among individuals, and change over
time? What are the possible confounding factors that also affect the ONH anatomy? Is
there any regional pattern in glaucomatous RNFL thinning, and if so, what does it signify
in the pathogenesis? Are there shape features that distinguish eyes that are more suscep-
tible to the disease, or may explain the variability in the effectiveness of treatment? These
are some of the questions that motivated us to develop a series of tools for large-scale,
quantitative shape analysis using ophthalmic OCT images.
The thesis is organized by following chapters which also outline the computational
pipeline visualized in Figure 1.2.
Chapter 3, Acquisition and Preprocessing discusses the setup of the prototype
1060-nm swept-source OCT system used for image acquisition, and preprocessing steps
including motion correction using maximum cross correlation and bounded variation im-
age smoothing. The images were then segmented for relevant anatomical features, as
presented in Chapter 4, Segmentation, with manual segmentation of the ONH structures
and graphcut-based automated segmentation of the retinal layers. Chapter 5, Registra-
tion describes two registration methods that establishes anatomical correspondence in
comparison of retinal surfaces from different time points or subjects: surface-to-surface
exact registration of retinal surfaces based on mathematical currents, and atlas genera-
tion from multiple retinal surfaces using the fshape framework. Lastly, Chapter 6, Optic
2

Figure 1.2: Computational pipeline of ophthalmic OCT images.
Nerve Head Morphometrics in Myopic Glaucoma, presents shape measurements and
statistical analysis in myopic normal and myopic glaucomatous ONHs.
3

Chapter 2
Background
2.1 The human eye
The human visual sensory organ consists of two eyes located in the bony orbits in the
front upper part of the skull. The eye is a slightly asymmetrical globe of approximately 24
millimetres in anterior-posterior diameter among adults [167].
Eighty-five percent of the outermost coat of the eye consists of the sclera - an opaque,
collagenous tissue that protects and maintains the eye’s structural integrity. It attaches to
the surrounding muscles and connective tissues, and provides paths for blood vessels and
nerves to pass in and out of the eye. The front centre of the outer coat is the transparent
cornea, which serves both protective and refractive functions.
The anterior segment of the eye includes the cornea, iris, lens, and ciliary body, as
shown in Figure 2.1 a). The iris is an opaque layer with a hole in the centre called the pupil,
of which the the size is controlled by the muscles in the iris. As a camera’s aperture stop,
the iris regulates the amount of the light that enters the eye and effect of light diffraction
and aberration.
The lens is the eye’s principal refractive element. Its refractive power is varied by a
ring of muscle in the ciliary body. The changing refractive power of the lens allows the
eye to focus in different distances. The ciliary body contains the ciliary processes, which
produces the aqueous humour, a watery fluid filling the space between the cornea and iris
(anterior chamber) and the iris and lens (posterior chamber). Beyond the anterior segment,
majority of the optic globe is occupied by the gel-like vitreous humour.
4

Figure 2.1: a) Schematic of the human eye. The image is from Wikimedia.org and re-produced here under the Creative Commons License. b) Light micrograph of a verticalsection through central human retina. The image is from Webvision [105] and reproducedhere under the Creative Commons License.
The retina is a thin sheet-like tissue that lines the posterior two-thirds of the inner sur-
face of the eye. The light passes through the cornea, lens, and the vitreous humour, and
reaches the retina where 100 million photoreceptors receive and process the light signal.
The visual information is transmitted via the the optic nerve that exists the eye on the
posterior-nasal side and leads to the visual cortex of the brain. Between the retina and
sclera is the choroid, a vasculature layer supporting the retina.
2.1.1 Retina
The retinal layers, shown in Figure 2.1 b), represents the functional and anatomical
hierarchy of the retina, described below from the outermost to the innermost layer.
The outermost layer is the retinal pigment epithelium (RPE) between the photorecep-
tors and Bruch’s membrane of the choroid. The RPE is a single continuous layer containing
melanin pigments and transport sites of materials to and from the retina.
The photoreceptors lie in the next four layers: the outer segment, inner segment, outer
nuclear layer, and outer plexiform layer. The light-detecting photopigments of the photore-
ceptors are located in the outer segment along the posterior border of the retina. Any
5
light, therefore, must pass through the rest of the retinal tissue before it reaches the pho-
topigments. The metabolic activities of the photoreceptors occur in the inner segment
containing mitochondria.
The outer nuclear layer (ONL) contains the nuclei of the photoreceptors, separated from
the inner segment by the external limiting membrane (ELM) or outer limiting membrane
(OLM). The axons and synaptic terminal endings of the photoreceptors are in the outer
plexiform layer (OPL), which subdivides into the Henle’s fibre layer containing the axons,
and the outer synaptic layer containing the terminals.
Between the photoreceptors and the retinal ganglion cells connected to the brain, there
are two intervening pathways: vertical and lateral. In the vertical pathways, photoreceptor
signal is delivered directly to a ganglion cell via a bipolar cell. In the lateral pathways, sig-
nals from multiple photoreceptors are received by a horizontal cell and inputted to bipolar
cells, or amacrine cells connect vertical pathways by receiving inputs from bipolar cells and
other amacrine cells and outputting to bipolar cells, other amacrine cells, or ganglion cells.
The inner nuclear layer (INL) contains the nuclei of these intermediate cells. The bipolar
cell terminals, amacrine cell processes, and ganglion cell dendrites interact in the inner
plexiform layer (IPL). The cell bodies of the ganglion cells and some amacrine cells are
contained in the ganglion cell layer (GCL), and the ganglion cell axons lie in the nerve fiber
layer (NFL). Finally, the retina borders the vitreous at the inner limiting membrane (ILM).
2.1.2 Fovea and optic nerve head
The fovea, shown in Figure 2.1 a), is a depression in the retina and responsible for
the central vision. In the fovea, the inner retinal layers of the intermediate and ganglion
cells are not present, and only the retinal pigment epithelium, outer and inner segments,
outer nuclear layer, some outer plexiform layer, and inner limiting membrane are present.
The centre of the fovea has the highest density of cones, resulting in the highest spatial
resolution in the the central visual field. The fovea is located in the macula, an oval-shaped,
pigmented area.
The optic nerve head, shown in Figure 2.1 a), is where all the retinal ganglion cell axons
converge in bundles and exit the eye. As shown in Figure 2.2 a), the layer structure of
the retina and choroid terminate, and the innermost nerve fiber layer (NFL) containing the
6
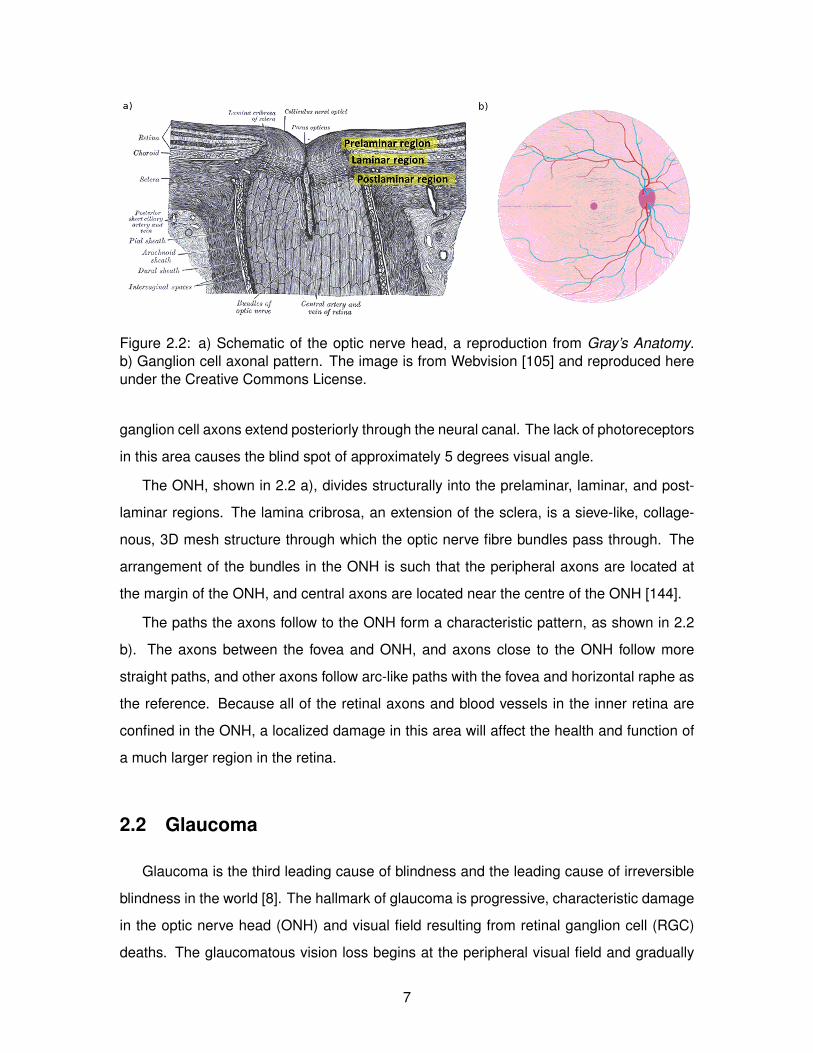
Figure 2.2: a) Schematic of the optic nerve head, a reproduction from Gray’s Anatomy.b) Ganglion cell axonal pattern. The image is from Webvision [105] and reproduced hereunder the Creative Commons License.
ganglion cell axons extend posteriorly through the neural canal. The lack of photoreceptors
in this area causes the blind spot of approximately 5 degrees visual angle.
The ONH, shown in 2.2 a), divides structurally into the prelaminar, laminar, and post-
laminar regions. The lamina cribrosa, an extension of the sclera, is a sieve-like, collage-
nous, 3D mesh structure through which the optic nerve fibre bundles pass through. The
arrangement of the bundles in the ONH is such that the peripheral axons are located at
the margin of the ONH, and central axons are located near the centre of the ONH [144].
The paths the axons follow to the ONH form a characteristic pattern, as shown in 2.2
b). The axons between the fovea and ONH, and axons close to the ONH follow more
straight paths, and other axons follow arc-like paths with the fovea and horizontal raphe as
the reference. Because all of the retinal axons and blood vessels in the inner retina are
confined in the ONH, a localized damage in this area will affect the health and function of
a much larger region in the retina.
2.2 Glaucoma
Glaucoma is the third leading cause of blindness and the leading cause of irreversible
blindness in the world [8]. The hallmark of glaucoma is progressive, characteristic damage
in the optic nerve head (ONH) and visual field resulting from retinal ganglion cell (RGC)
deaths. The glaucomatous vision loss begins at the peripheral visual field and gradually
7

Figure 2.3: a) Progressive vision loss in glaucoma. Image source: National Eye Institute,National Institutes of Health. b) Glaucomatous deformation in the laminar region.1
progresses to the centre, as shown in 2.3 a), often going unnoticed by the patient until the
damage is significant.
The major risk factor in glaucoma is elevated intraocular pressure (IOP), and the treat-
ments is often directed to the control of IOP [173, 74, 13, 66]. The pathophysiology of
glaucoma is complex and multifactorial, and the mechanisms governing the optic neu-
ropathies and their connection to IOP are yet to be fully understood, except the insult to
the RGC axons, especially within the lamina cribrosa, has been identified as one of the
central events of the disease.
A notable expression accompanying glaucomatous neuropathy is profound structural
alteration in the prelaminar, laminar, and postlaminar regions of the ONH, shown in 2.3
b) [11]. There is general posterior deformation of the peripapillary scleral flange and the
lamina cribrosa which contributes to the glaucomatous “cupping.” The prelaminar tissue
and the laminar cribrosa thickens and the neural canal expands posteriorly. In the most
severely affected eyes, the lamina cribrosa migrates out of the sclera toward the pia sheath.
1Reprinted from Experimental Eye Research, Vol. 93, Abbot Clark, David Garway-Heath, Jonathan Crow-ston, Claude F. Burgoyne, A biomechanical paradigm for axonal insult within the optic nerve head in aging andglaucoma, pp. 120-132, Copyright 2011, with permission from Elsevier.
8

Figure 2.4: A simple Michelson interferometer schematic of optical coherence tomography.(BS: beam splitter.)
2.3 Optical coherence tomography
Optical coherence tomography (OCT), first proposed in 1991 [80], is a tomographic
imaging modality based on light interference. Figure 2.4 shows a simplified description
of an OCT system: a low-coherence near-infrared beam from the source is split between
an imaging target and a reference arm with a mirror, and the light that penetrates and
subsequently backscatters from the target is interfered with the reference beam. In the
first generation of OCT systems, or time-domain OCT, the length of the reference arm
was varied, and the interference magnitude over this distance yielded a single line scan
along the depth of the target, called an A-scan. Repeating this axial scan while moving the
incidental beam transversely across the target produced a two-dimensional cross-sectional
image, or a B-scan, as shown in Figure 2.5. A full three-dimensional, volumetric image can
be generated by a series of B-scans.
In Fourier-domain OCT (FD-OCT), implemented in 1995 [46], the length of the ref-
erence arm is kept constant, and the depth and magnitude information of an A-scan is
resolved by a Fourier transformation of the interference fringes, measuring all light echoes
in the axial direction simultaneously. With the increased imaging speed [139, 138] and
greater signal-to-noise ratio [115, 32, 26], FD-OCT has become the standard in applica-
tion and research.
In the first type of FD-OCT, a low-coherence light source is used, and the interference
spectrum is measured with a spectrometer and a high-speed camera. In the second type,
known as swept-source OCT, a narrow-bandwidth light source sweeps the interference
spectrum, and the interferometer output is a function of time [38].
9

Figure 2.5: Ophthalmic OCT imaging of a) macular region and b) peripapillary region.
2.4 OCT in ophthalmology
Since its onset, OCT has been rapidly and widely adopted in ophthalmology and vision
science for several merits. The eye is a biological system designed to focus light with
minimum attenuation and scattering, and the OCT scanning beam reaches and resolves
the inner structures of the eye by the same way any visible light travels in the eye. The
power of the light source is well below the ANSI recommended level of ocular exposure of
a collimated beam [33], providing a noninvasive means of in-vivo, cross-sectional imaging
of the eye. In comparison with other in-vivo ophthalmic imaging modalities, OCT offers
a balance of image resolution, ranging from 1 to 15 µm, and tissue penetration depth of
about 2 mm. OCT is described as “filling the gap” between the ultrasound, which provides
high penetration but low resolution, and microscopy, which provides high resolution but low
penetration [38].
Ophthalmic OCT imaging can be divided into anterior, retinal (macular), and peripapil-
lary imaging, depending on the target image region (Figure 2.5). OCT images serves as a
fast and intuitive visual examination of the state of the anatomy, and as a information-rich
data source for large-scale, quantitative analysis of the shape, texture, and other anatomi-
cal features that are clinically relevant.
10

Chapter 3
Image Acquisition and Preprocessing
3.1 Acquisition
All data presented in this thesis, except when specified, were acquired using a proto-
type swept-source optical coherence tomography (SS-OCT) system with a 1060-nm wave-
length source, developed by Biomedical Optics Research Group (BORG) at Simon Fraser
University [194]. The system schematic is shown in Figure 3.1. The 1060-nm wavelength
of the source provides better penetration of the beam in the optic nerve head (ONH) and
choroidal region than the conventional 800-nm source [194]. The swept-source design al-
lows for the fast A-scan rate of 200kHz. The axial resolution of the system is approximately
6 micrometres, and the lateral resolution ranged from 12 to 20 micrometres, calculated
based on the optics of the system, scan angle, and axial lengths of individual eyes.
The image acquisition was performed at the Eye Care Centre, Vancouver General Hos-
pital, Vancouver, British Columbia, Canada. The OCT system was mounted on a standard
slit-lamp biomicroscope with an aligning stage, as shown in Figure 3.2. The subject was
seated with the head resting against the chin and forehead support to reduce motion, and
asked to focus on a fixation target. The acquisition time lasted approximately 1.6 seconds
per full 3D image volume. The image was acquired using a custom C++ and LabView
software performing a series of real-time signal processing such as dispersion compensa-
tion and fast Fourier transform, and real-time B-scan display to assist the user in image
alignment and checking the image quality.
The scan pattern was raster such that a series of B-scans was acquired to generate a
full 3D volume, as shown in Figure 3.3. A typical physical dimension of the imaged space
11

Figure 3.1: Schematic of the swept-source optical coherence tomography system setup.Source: Axsun SS Module; PC: polarization controller; BD: balanced detector; fn, focallength of the lens, where n = 1, 2, 3.[194]
was 2.8 mm in the axial direction, and 4.5 to 8 mm in the lateral directions, depending on
the lateral resolution based on the eye’s axial length. A typical voxel dimension of an image
volume was 1024 (axial) x 400 (lateral) x 400 (lateral) voxels.
3.2 Quality control and data management
Image quality control and data management are crucial part of working with a prototype
imaging system, especially as a larger number of subjects are imaged, and multiple studies
share the same datasets.
The goal of the image quality control in the data acquisition stage is to reduce, as much
as possible, artefactual variability among the images that can affect subsequent processing
and analysis. Common issues include motion-related artifact, signal-to-noise ratio, image
focus, and the position of the field-of-view relative to a reference anatomical landmark,
such as the fovea or optic nerve head. These are primarily subject-dependent, with the
age and eye condition affecting the subject’s clarity of vision and ability to focus for the
duration of image acquisition.
During the acquisition, the system user aligns the imaging location based on the real-
time B-scan and enface views in the acquisition software, and data with a large eye move-
ment or blinks are discarded. Minimum of 4-5 datasets are acquired for each eye, and after
the imaging session, visually examined through quick-check images, shown in Figure 3.4.
Data with poor quality are discarded, and the remaining data are securely transferred and
stored, in the original raw format, in a file system at Simon Fraser University with multilevel
back ups.
12

Figure 3.2: Prototype optical coherence tomography system set up at the Eye Care Centre,Vancouver General Hospital.
Proper data management, for the raw image data and associated technical and clinical
data, is important for several reasons. First, since the data is acquired from human sub-
jects, security and privacy concerns are critical. Second, a typical raw data size ranges
from 300 - 400 MB and necessitates a careful planning to save storage space. Third, the
image processing pipeline is multi-staged, flexible, and in large part automated, requiring
consistency in file format and naming convention, and directory structure. Lastly, each im-
age dataset is associated with metadata, such as OCT system parameters and subject’s
clinical information, and good organization of the raw data, metadata, and processed data
becomes essential as more than one studies are conducted over time involving the same
datasets.
13

Figure 3.3: (a) Imaged region and scanning direction displayed on fundus photography. (b)Volume reconstruction from raw data. (c) Volume visualized in 3D.
3.3 Preprocessing
The raw data, after fast Fourier transform and dispersion compensation, is built into
a 3D image volume, as shown in 3.3. The subsections below describe the subsequent
preprocessing steps: motion correction and image smoothing.
3.3.1 Motion correction
Motion in OCT images
Although the chin rest, forehead support, and fixation target reduce head and body
motion, involuntary fixational eye movements still occur. Fixational eye movements are
divided into tremor, drift, and microsaccades [125]. These movements have been charac-
terized by their general pattern, amplitude, frequency, duration, and speed, by externally
tracking the rotation angle of the eye.
Tremor is wave-like motion of high frequency (∼90 Hz) and low amplitude (less than 1
arcminute). Assuming a simple model with the centre of the eye rotation at the centre of
the eye and the average human eye diameter of 24 mm, the angular amplitude of tremor
approximately translates to less than 3.5 nm in the ONH, which is smaller than the system
axial resolution of 6 micrometres and unlikely to be detected. Drift is a gradual movement
with relatively low maximum speed of 30 arcminutes per second. This yields the maximum
displacement of 4.4 nm per frame, which would not be noticeable within a single frame.
Drift occurs between fast, twitch-like movements called microsaccades. There is a large
14

Figure 3.4: A quick-check image of an OCT dataset.
variance in characterization of this movement among different studies, and average me-
dian amplitude is 45 µm, with interval frequency between 0.4-2.6 Hz. This indicates that
microsaccades is likely the most visible source of motion artifact across multiple frames in
OCT volumetric images acquired by a raster scan pattern.
Real-time eye tracking in OCT has been implemented in prototypes [122, 150] and
the latest line of commercial systems. This involves instant adjustment of scanning beam
position to compensate for eye motion during acquisition; however, this approach entails
significant hardware modification to the standard OCT setup with additional cost, requires
regular calibration, and detects lateral motion only.
There are two considerations in characterizing the motion artifact in 3D-OCT images.
First, because the fixational eye movements are constantly present and the shape of
the ocular structures and blood vessel patterns vary in each eye, obtaining an accurate,
motion-free 3D image of the human ONH in-vivo is, technically, not possible. Second, the
motion itself has three-dimensional translational and rotational degrees of freedom and
15

Figure 3.5: The first column shows the sectioning plane of the images in the second col-umn, and the third column illustrates motion visible in each of these images. In the firstrow, a B-scan (fast scan) is shown (b) in the direction of frame acquisition (a). In the sec-ond row, an axial cross section (slow scan) (e) orthogonal to the B-scan (as shown in (d))displays wave-like axial motion artifact (f). In the third row, a sum-voxel en-face image inthe plane (e) displays lateral and elevation motion artifact (i) by the uneven blood vesselboundaries and discontinuities in the image.
varies in each eye and imaging session such that exact characterization is difficult. How-
ever, a heuristic approach can be taken based on the clinical knowledge and observation
from a large number of datasets. Based on the fixational eye movement characteristics and
qualitative examination of the images, a single frame (B-scan) acquired in 0.004 second
is approximated as an instantaneous, motion-free snapshot. The subject motion then can
be considered as motion of the frames relative to a stationary target, which is illustrated in
Figure 3.5. In an ideal case, each frame in a volume is motion-free (Figure 3.5(b)) with all
frames aligned in a row in a single orientation (Figure 3.5(c)). This is the assumption made
during the volume reconstruction of the raw data. However, an orthogonal cross -section
of an actual reconstructed volume (slow scan, Figure 3.5(d) and (e)) reveals fluctuating
artefactual peaks due to motion in the axial direction (Figure 3.5(f)) where each column in
16

Figure 3.5(d) represents a single B-scan frame. Motion in the other two directions (Figure
3.5(i)) is visible in Figure 3.5(h), a sum-voxel enface image created by summing all or-
thogonal cross-sections in the enface direction in Figure 3.5(g). Each row in Figure 3.5(h)
represents a single frame and motion in the lateral direction is seen in the small artifactual
ripples in the edges of the blood vessels. In several locations, there are abrupt discontinu-
ities in the image due to motion in the elevation direction, in which a frame either repeats
(jump forward) or skips (jump backward) several frames. This motion is particularly prob-
lematic because it is perpendicular to the frames and there is no information in the acquired
frames to interpolate for such a gap. For example, subject eye motion resulting in a verti-
cal displacement creates a discontinuity in the enface reconstructions, and the size of the
jump cannot be determined by simply observing the neighbouring frames. This problem is
intrinsic to the scanning direction and raster scan pattern.
Post-acquisition motion correction by maximum cross-correlation
Rizzo et al.[165] corrected lateral motion by matching blood vessels in the OCT en-face
sum-voxel image and motionless fundus photography using warping registration, although
this method does not address axial motion. Another widely used approach is to acquire
a small number of “fast scans” in the slow scan direction, and use these as references
for motion correction [152, 201]. However, this may introduce a new source of error if
the reference frames are not acquired at precise locations relative to the volume with the
continuous eye motion and time difference between the reference frames and the other
frames. Hu et al. [78] first automatically segmented several surfaces with strong edges
using graph-cut approach, and translated frames to flatten one of the segmented surfaces.
The automatic flattening may affect the anatomical information in the image. Both of the
latter two methods only address motion in the axial direction.
The correction method used in our pipeline is a modified version of the maximum cross
correlation technique [114], a 3D extension of a method presented in an early seminal
paper on OCT [73], which proposed correcting motion artifact in a 2D OCT image using
maximum cross-correlation of adjacent columns. In 3D OCT, each frame is approximated
as a motionless unit and translated against the next frame. The amount of displacement
which yields the maximum cross-correlation with the neighboring frame is noted. The
17

cross-correlation measures the similarity between two adjacent frames. Briefly, for a vol-
ume of N frames of a size X by Y , for each pair of frames Fn and Fn+1, n = 1 .. N − 1, a
cross-correlation vector Cn of length 2M + 1 was computed. First, Fn+1 was padded by M
pixels in the top and bottom such that the size of the padded Fn+1 was X by Y + 2M . The
mth element of Cn was then
Cn[m] =X∑i=1
Y∑j=1
Fn(i, j)Fn+1(i, j +m− 1), m = 1..M. (3.1)
The equation computes pixel-wise 2D cross-correlation between two adjacent frames as
Fn “slides up and down” relative to Fn+1 over the distance of 2M + 1
Because the frames are densely sampled in space, anatomical difference between two
consecutive frames is minimal and localized, and it does not affect the frame-to-frame
correlation significantly. The displacement of the maximum cross-correlation position, or
the index of the maximum value in C for each frame, thus captures the shift of the entire
frame due to the subject motion and the natural curvature of the eye. In Figure 3.6(a), the
maximum correlation displacement profile in white curve overlaid on a slow scan closely
follows the wave-like motion artifact. After approximating motion artifact by the maximum
correlation displacement profile, a common practice is to translate each frame such that
the profile is flattened, as shown in Figure 3.6(b) [29, 69, 24]. However, this neglects
the gradual curvature in the eye and any rapid change in topology that may contribute to
the displacement estimated by correlation. In Figure 3.6(a), the displacement profile dips
slightly near the optic cup due to its sharp slopes, and the flattening correction (Figure
3.6(b)) raises the cup bottom to compensate for this. In order to reduce such distortion as
a byproduct of correction, we fit the profile to a smooth curve instead of flattening it. This
smooth curve serves to model the natural curvature of the eye which is apparent in a single
motion-free frame. The curve is selected in an interactive setting, where the user is shown
a motion-free frame (ex. Figure 3.5(b)) and an orthogonal slice of all such frames with
the motion profile, such as in Figure 3.6(a). The user can vary a cubic-spline smoothing
parameter and see the resulting correction immediately applied to the profile and the slice,
displayed in real time. By comparing and matching the amount of curvature visible in
the motion-free frame and the slice in the orthogonal direction, the level of smoothness
for correction can be qualitatively determined. Figure 3.6 5(c) displays the result of the
correction by fitting a smooth curve with the selected fitting curve shown in white. The optic
18

cup depth (marked by red double-arrow line) in the flattened correction in Figure 3.6 5(b)
measured 20% less than that of the smooth-fitted correction, indicating flattening can alter
the ONH topology by overcompensation, and the smooth curve fitting better preserves
the variable topology. Figure 3.6 (d) and (e) compare a volume before and after motion
correction by smooth fitting, and there is noticeable improvement in the image quality after
correction.
The maximum cross-correlation technique is a relatively simple, fast, and effective mo-
tion correction method that does not require additional scans or computationally expensive
processing. One of the limitations of the maximum cross-correlation method is that the
motion in lateral direction is less resolvable due to the lack of strong vertical edges in
the frames, except in the optic cup region. In the frames that do not contain dominant
vertical structures, it is possible that the shifting position of the vertical shadows of con-
verging blood vessels is falsely classified as lateral motion. This is similar to the windowing
problem in computer vision, where positional ambiguity arises from the camera frame con-
taining only partial boundary of a continuous object while moving in a direction parallel
to the boundary. Such directionality in correction effectiveness is a common problem in
post-acquisition motion correction methods.
3.3.2 Bounded variation image smoothing
By its light-based nature, OCT images inherently consists of “speckles.” Smoothing
an OCT image can reduce the effect of speckles and image noise, and better resolve
anatomical features. However, conventional image smoothing filters, such as Gaussian,
often do not discriminate between unwanted speckle noise and structural boundaries we
wish to observe.
A variational approach[193] considers the problem as an optimization of a functional
with the antithetical constraints of i) smoothing the original image and ii) preserving certain
desired features in the same image. A minimization expression can be written as
E(I; Io) = Q(I) + λC(I, Io) (3.2)
where the first term measures the quality of the new image I, and the second term penal-
izes the distance between I and original image Io. C(I, Io) can be simply defined as the
19

L2-norm
C(I, Io) =
∫Ω|I(x)− Io(x)|2dx. (3.3)
The Q(I) term should penalize the magnitude of gradient in the image. This can be
achieved by the bounded variation norm
Q(I) =
∫|∇I|dx (3.4)
and the minimization equation 3.2 can be written as
E(I; Io) =
∫|∇I|dx+
∫Ω|I(x)− Io(x)|2dx. (3.5)
The standard gradient descent can be performed in the form of
I(n+1) = I(n) + δt
(div
(∇I(n)
|∇I(n)|
)− 2λ(I(n) − Io)
)(3.6)
The derivatives are discretized and approximated in 3D for numerical computation. Fig-
ure 3.7 shows an example of an image before and after BV smoothing. After the smoothing,
the image appears less noisy, and the anatomical structures are more clearly visible. The
bounded variation smoothing is particularly effective for OCT speckles, since it penalizes
rapidly edges, such as speckles, while preserving larger, more gradual edges, such as a
structural boundary.
3.4 Summary of contributions
The contributions described in this chapter and partially published in [114] are:
• OCT image quality control and data management.
• Axial motion correction using frame-to-frame maximum cross-correlation.
• OCT image smoothing by bounded variation optimization.
The processing steps described in this chapter were applied to all data presented in the
subsequent chapters, except when specified.
20

Figure 3.6: (a) Slow scan with maximum cross-correlation displacement profile. (b) Samescan corrected by flattening the profile. (c) Same scan corrected by fitting a smooth curveto the profile. The red arrows in (b) and (c) indicate the cup depth measured in each image.(d) Volume before motion correction. The volume has been rotated that the axial axis liesvertically and the en-face plane lies horizontally. (e) Same volume after smooth-fittingmotion correction.
Figure 3.7: Example of BV smoothing
21

Chapter 4
Segmentation
After the motion correction and smoothing described in the previous chapter, the im-
age volumes were segmented for anatomical structures. The segmentation targets were
divided into automatically-segmented retinal layer boundaries and manually-segmented
non-layer structures in the optic nerve head (ONH).
Layer boundaries and their segmentation are shown in the Figure 4.1 a). Of the par-
ticular importance are the inner limiting membrane (ILM) (anterior boundary of the retina),
Bruch’s membrane (BM)(posterior boundary of the retina), and the posterior boundary of
the choroid marking also the anterior boundary of the sclera.
In the optic nerve head (ONH) region segmentation in Figure 4.1 b), the anterior-most
retinal nerve fiber layer (NFL) is shown bending posteriorly towards the optical neural canal
to exit the eye, where all other retinal layers discontinue. Non-layer landmarks in this region
include the Bruch’s membrane opening (BMO), scleral canal wall, anterior lamina cribrosa
surface (ALCS), and anterior laminar cribrosa insertion points (ALCIP).
4.1 Manual segmentation of ONH structures
Manual segmentation was done in points, as shown in Figure 4.1 b), in 2D frames.
Amira 5.2 (FEI Company, Hillsboro, OR) was used for interactive visualization and seg-
mentation.
In raster manual segmentation, each of the B-scans from the raster acquisition pattern
is segmented. A custom Amira script displayed the volume in three slaved orthogonal
cross-sections, and on each B-scan the target structures were marked. This segmentation
22

Figure 4.1: Example of a) automated segmentation of retinal layers and b) manual pointsegmentation.
method was validated in our previous study with three different raters and sixteen eyes
[198].
In radial manual segmentation, the rater was first presented with the en-face summed
voxel projection image of the image volume, and selected two points: an approximate
centre of the optic cup and another on the outer boundary of the region of interest. This
produced a predefined number of radial slices orthogonal to the en-face plane with the
centre and width determined by the two user-selected points. The slices were spaced at a
constant angle.
There are three advantages to using radial slices for manual segmentation rather than
the original B-scans [114]. First, the user can specify the region of interest by manually
selecting the centre of the volume. Second, the radial slicing provides dense segmenta-
tion near the centre of the volume at a cost of more sparsely sampled peripheral area,
often of less importance and morphological complexity. This dense sampling at the centre
allows the rater to segment fewer frames per volume. B-scan segmentation is performed
on at least every other frame, whereas in radial segmentation, 40 slices may suffice for
approximating the centrally located optic cup. Lastly, radial slices provide more consis-
tency and control during manual segmentation, as the ONH is generally axially symmetric
23

and radial slices vary less than raster frames. 3D visualization of the result of manual
point-segmentation in radial slices is shown in Figure 4.1 b).
4.2 Automated segmentation of retinal layers
Challenges in automated OCT retinal layer segmentation include discontinuities in the
layer boundaries due to blood vessel shadowing, and lack of contrast and clarity of the
layer boundaries, which is made worse by the speckle nature of the OCT. Several groups
reported on automated segmentation of the retinal layers employing various techniques
[14, 86, 170, 3, 51, 60, 43, 52, 132, 120, 136]. One of the most successful among these
has been the 3D graph-theoretic approach developed and applied extensively by the Sonka
group in University of Iowa [67, 51, 52, 78]. The underlying key work by Li et al. [119], sum-
marized below, optimally segments surfaces in 3D by transforming the segmentation prob-
lem into a minimum s-t cut problem of a multi-dimensional arc-weighted graph. The main
advantages are that the optimality can be controlled by cost functions and built-in geomet-
ric constraints including smoothness and interrelations of multiple surfaces. Garvin et al.
[51, 52] extended this work by including regional constraints for more robust segmentation
of the retinal layers.
The algorithm begins with a multicolumn model: an image volume of the dimension X,
Y , and Z is considered as a 3D matrix I(x, y, z) and the segmented surface is N(x, y) ∈
z = 0, ..., Z − 1, with x = 0, ..., X − 1 and y = 0, ..., Y − 1 such that the surface is defined
to intersect with one voxel of each column parallel to the z-axis.
A node-weighted directed graph G = (V,E) with a node V (x, y, z) ∈ V uniquely as-
signed to each voxel I(x, y, z) ∈ I. The node cost w(x, y, z) is given by:
w(x, y, z) =
c(x, y, z) if z = 0
c(x, y, z)− c(x, y, z − 1) otherwise
The cost function for the retinal layer segmentation was given by vertical gradient of the
intensity value of each pixel.
The arcs are divided into intracolumn, intercolumn, and intersurface arc sets. The
intracolumn arc set Ea is given by
Ea = 〈V (x,y, z), V (x,y, z − 1)〉|z > 0 (4.1)
24

and the intercolumn arc set by
Er =
〈V (x,y, z), V (x+ 1,y,max(0, z −∆x))〉|x ∈ 0, ..., X − 2, z ∈ z∪
〈V (x,y, z), V (x− 1,y,max(0, z −∆x))〉|x ∈ 0, ..., X − 1, z ∈ z∪
〈V (x, y, z), V (x, y + 1,max(0, z −∆y))〉|y ∈ 0, ..., Y − 2, z ∈ z∪
〈V (x, y, z), V (x, y − 1,max(0, z −∆y))〉|y ∈ 0, ..., Y − 1, z ∈ z∪
where ∆x and ∆x are smoothness parameters such that if I(x, y, z) and I(x + 1, y, z′)
are on the surface, |z − z′| ≤ ∆x, and if I(x, y, z) and I(x, y + 1, z′) are on the surface,
|z − z′| ≤ ∆y.
The surfaces are expected not to intersect or overlap, and given surfaces N1 and N2
with graphs G1(V1, E1) and G2(V2, E2), the intersurface arc set is given by
Es =
〈V1(x,y, z), V2(x,y, z − δu)〉|z ≤ δu∪
〈V2(x,y, z), V1(x,y, z + δl)〉|z < Z − δl∪
〈V1(0, 0, δl), V2(0, 0, 0)〉
The construction of the graphs establish the following lemmas.
Lemma 1. Any k feasible surfaces in I correspond to a nonempty closed set in G with the
same total cost.
Lemma 2. Any nonempty closed set in G defines k feasible surfaces in I with the same
total cost.
Lemma 3. A minimum nonempty closed set C∗ in G specifies the optimal k surfaces in I.
C∗ in Lemma 3 can be computed by a minimum s-t cut in a related graph Gst = (V ∪
s, t, E ∪ Est), where s is a source, t is a sink, and Est is a new arc set defined as follows.
The source is connected to v/inV −, with V − denoting all nodes in G with negative costs
and arc costs −w(v). The sink is connected to v/inV +, with V + denoting all nodes in G
with nonnegative costs and arc costs w(v). A finite cost s-t cut (S, T ) of Gst has the total
cost c(S, T )
c(S, T ) = −w(V −) +∑v∈S−s
w(v) (4.2)
where w(V −) is fixed and is the cost sum of all nodes in V −. Since S − s is a closed set,
the cost of a cut (S, T ) in Gst and that of the corresponding closed set in G differ by a
25

constant. Therefore, the source set of a minimum cut in Gst corresponds to a minimum
closed set C∗ in G. The optimal k surfaces correspond to the upper envelope of C∗.
We implemented this algorithm to successfully segment retinal layers (Figure 4.1 a)),
and also the choroid, as expounded in the following subsection.
4.3 Choroid segmentation
The choroid is the layer of vasculature and connective tissue between the retina and
sclera. The critical metabolic role of the choroid in providing nutrients and removing waste
products from the retina makes it an important factor in development of retinal pathol-
ogy. Recently, interest in in-vivo visualization and quantitative analysis of the choroidal
structure has been growing with the advancement in OCT technology. However, imaging
and segmentation of the posterior surface of the choroid – choroid-sclera (CS boundary)
boundary - still remains a challenge as the light signal intensity decreases sharply be-
yond the retina due to light absorption and scattering at the retinal pigment epithelium and
among choroidal vasculature. Reliable automated measurement of the choroid therefore
requires both an acquisition system capable of resolving the CS boundary as well as a
robust segmentation algorithm.
Enhanced depth imaging (EDI) OCT [174] improves the visualization of the choroid by
positioning the spectral domain (SD) OCT closer to the eye. This pushes back the peak
signal location (zero delay) from the conventional vitreo-retinal interface towards the outer
scleral border. Since the choroid is placed closer to the zero delay, the imaging sensitivity
in the region is enhanced. In SD-OCT, the Fourier transform produces two equivalent mir-
ror images. Conventional instruments display only one of the images in which the anterior
portion of the retina is facing up in the screen. In EDI-OCT, the physical displacement of the
instrument results in the inverted mirror image being displayed. EDI-OCT has been used to
measure the choroid in normal eyes [124], high myopia [50], central serous chorioretinopa-
thy [85, 126], and AMD [123]. Additionally, OCT with a longer wavelength source [183], and
polarization-sensitive (PS) OCT [151] showed improved visualization of the choroid.
In the majority of studies, choroidal thickness has been measured manually, although
automated segmentation of the choroid-sclera interface and measurement of the choroidal
thickness have been implemented in three-dimensional 1060 nm OCT using a statistical
26

model [99], in three-dimensional 890 nm OCT using graph-cut [203, 79], and in polarization
sensitive OCT [181].
We used the 3D graph-cut algorithm, described in the previous subsection, for seg-
menting the anterior surface (Bruch’s membrane equivalent, BM) and posterior surface
(CS boundary) of the choroid. First, the inner limiting membrane (ILM) and interface be-
tween the inner and outer segment were segmented for their strong edge contrast. The
latter was smoothed, fitted to a convex hull, and redrawn by piecewise cubic interpolation
to serve as a reference layer to segment BM and limit the search region. Convex hull and
interpolation were required to handle images with retinal pigment epithelial detachments
caused by drusen, which results in reduced intensity at Bruch’s membrane equivalent.
After the BM was found, the choroid-sclera boundary was searched for in the region pos-
terior to the BM as a smooth surface with high intensity gradient. The initial choroid-sclera
boundary segmentation was smoothed and interpolated similarly as in BM, based on the
assumption that the boundary is smoothly varying and encompasses all choroidal capillar-
ies, which creates the dark/bright contrast within the choroid. An annotated B-scan and its
final segmentation result are shown in Figure 4.2.
4.3.1 Comparison of choroid segmentation in in 830 nm and 1060 nm OCT
images
For the commercial OCT system, Cirrus spectral domain OCT (SD-OCT) (software
version 6, Carl Zeiss Meditec, Inc., Dublin, CA) was used to acquire 24 3D macular scans,
all centred at the fovea. For the prototype OCT system, the in-house custom 1060-nm
swept-source OCT (SS-OCT) system described in Section 3.1 was used to acquire 10 3D
macular scans. All human imaging was conducted with ethics approval from Simon Fraser
University or the University of British Columbia, and in accordance with the guidelines
of the Declaration on Helsinki. The images were processed with motion correction and
smoothing as described in Section 3.3, and segmented using the algorithm above.
Representative OCT data and segmentation results are presented in Figure 4.3. An
830-nm 2D EDI-OCT scan with segmentation was included as a reference as it was ac-
quired by the same Cirrus SD-OCT machine used to acquire the 830-nm 3D volumes.
27
Figure 4.2: Top: B-scan of a 1060-nm OCT macular volume. Bottom: Automated seg-mentation of inner limiting membrane (green), Bruch’s membrane equivalent (cyan), andestimated choroid-sclera boundary (CS-boundary).
In the model of Cirrus SD-OCT used in this experiment the EDI function was only avail-
able in 2D. Additionally, the 2D EDI-OCT scan was averaged over 20 lines with proprietary
Selective Pixel Profiling for improved image quality, which is unavailable in 3D.
In Figure 4.3, the 830-nm 3D scan (middle) shows poorer image resolution and more
severe signal attenuation in the choroidal region compared to the 2D averaged EDI-OCT
scan (top) from the same system. We observed in one of our studies [111] that even
with averaging and EDI technique the signal intensity and sensitivity fall-off at the posterior
choroidal region was considerable, and often the CS boundary was not clearly visible.
The automated segmentation and subfoveal choroid thickness measurement for the 2D
EDI scans performed relatively well with intra-class correlation (ICC) of 0.85 with expert
raters and 0.87 between two consecutive repeat scans. For the 3D scans, the repeat scan
ICC was 0.99 for the 24 sample subjects (44 datasets in total). This implies that despite
the poorer image resolution the inherently 3D segmentation algorithm benefited from the
volumetric dataset and the smoothness constraint in the additional dimension for more
28

Figure 4.3: Macular OCT images (Left) and their segmentations (Right). Top: 830-nm2D averaged EDI-OCT scans acquired with Cirrus SD-OCT. Middle: 830-nm 3D scansacquired with Cirrus SD-OCT. Bottom: 1060-nm 3D scans acquired with the prototype1060-nm SS-OCT.
consistent result. However, the automated subfoveal choroid thickness measurement from
the 3D scans was significantly smaller than the manual and automated measurements
from the 2D EDI scans. This shows that although the automated segmentation was highly
repeatable, the 830-nm 3D scan was generally inadequate for visualizing the CS boundary
detected in the 2D EDI scan.
In the bottom row of Figure 4.3, the 1060-nm prototype SS-OCT 3D scan shows
brighter choroid region with greater amount of detail of the choroidal vasculature com-
pared with the 830-nm 3D scan. The CS boundary is also better visible and segmentable
by the automated algorithm.
Figures 4.4 and 4.5 further demonstrate the 3D segmentation of an 830-nm macular
scan (Figure 4.4) and 1060-nm macular scan (Figure 4.5). The inner limiting membrane
(green) and boundaries of the choroidal layer (cyan, magenta) are plotted as 3D surfaces.
As shown in Figure 4.3, the segmentation is consistent throughout in each volumes but
29

Figure 4.4: Segmentation of a 3D macular scan acquired with 830-nm Cirrus SD-OCTsystem.
more detailed choroidal structures and deeper CS boundary are visible in the 1060-nm
scan in comparison with the 830-nm scan.
The segmentation result can be used to flatten the volume and generate a sumvoxel
projection of the choroidal layer as shown in Figure 4.6 a). Figure 4.6 b) and c) display
an example of a total retinal thickness map and choroid thickness map generated from the
segmentation.
4.3.2 Repeatability analysis of choroidal thickness measurements in age-
related macular degeneration
The potential role of the choroid in the development of nonneovascular age-related
macular degeneration (AMD) is yet an underexplored aspect of the disease. Studies have
shown decreased blood volume and abnormal flow in eyes with nonneovascular AMD com-
pared to normal eyes [153, 63]. Berenberg et al. reported a significant association between
increased drusen extent, and decreased choroidal blood volume and flow in patients with
nonneovascular AMD [7]. The critical function of the choroid in providing nutrients to pho-
toreceptors and removing waste products from the RPE suggests any abnormalities in the
layer affecting the metabolic support may contribute to the development of AMD [62, 48].
30

Figure 4.5: Segmentation of a 3D macular scan acquired with 1060-nm prototype SS-OCTsystem.
In this section we present manual and automated measurements of subfoveal choroidal
thickness in EDI-OCT scans from patients with nonneovascular AMD. Measurement re-
peatability and correlation to drusen area were examined. Automated segmentation of
the choroidal boundaries used the graph-cut–based algorithm described in the previous
subsection 4.3.1.
Methods
A total of 88 eyes from 44 patients under the care of the retina service at University
of British Columbia (UBC) was included in the study based on the diagnosis of bilateral
nonneovascular AMD and age of 55 years or older. Participants were enrolled between
February 2012 and May 2012. We recruited patients with the full spectrum of drusen size,
including small drusen, intermediate drusen, large drusen, and drusenoid pigment ep-
ithelial detachments [31, 1]. Patients with other macular pathology, including neovascular
AMD, geographic atrophy, and macular dystrophy, were excluded. Participants with signif-
icant ocular media opacity also were excluded. Each patient underwent a full ophthalmic
examination, including biomicroscopy, best-corrected visual acuity using Snellen charts,
intraocular pressure and dilated fundus examination. For statistical analysis, Snellen acu-
ity was converted to logMAR equivalents. Informed consent was obtained from all patients,
31

Figure 4.6: a) Sumvoxel projection of the macular choroid in a 1060-nm scan b) Total retinalthickness colormap. c) Choroid thickness colormap.
and the study was approved by the Research Ethics Board at the UBC and adhered to the
tenets of the Declaration of Helsinki.
Cirrus SD-OCT (software version 6; Carl Zeiss Meditec, Inc., Dublin, CA) was used
for acquisition of two or more 3D macular cube scans (200 A-scans per B-scan, 200 B-
scans) and 2D EDI raster scans, all centred on the fovea. The wavelength of the Cirrus
machine was 830 nm, and the EDI scans used an average of 20 lines with proprietary
Selective Pixel Profiling. This is different from Heidelberg EDI-OCT, which averages 100
lines with eye tracking. The macular cube scans were acquired over a region of 6 x 6
mm and selected for minimum signal strength of 6 out of 10. For the 3D macular cube
scan, the scans with the highest signal strength were used for further analysis. For the EDI
raster scans, the two scans with the highest signal strength were used. Drusen area and
volume data in macular cube scans were obtained automatically by the Cirrus SD-OCT
software [61]. The software first segments the RPE and determines by interpolation a
virtual RPE free of deformation, referred to as the RPE floor. The drusen area and volume
are computed based on the distance between the real RPE and the virtual RPE at each
measurement data point. The algorithm ignores RPE deformation below a given threshold
to reduce noise.
For manual measurement of subfoveal choroidal thickness, two independent investiga-
tors measured the distance between Bruch’s membrane equivalent and the choroid-sclera
interface at a single point below the fovea using Cirrus SD-OCT software’s built-in caliper
32

function in three separate sessions. One investigator was a fellowship-trained medical reti-
nal specialist, and the other was a biomedical engineer trained on choroidal evaluation
by the medical retinal specialist. The observers met beforehand to agree on the defini-
tion of the choroid-sclera interface as the outermost dark-to- bright boundary. Only the
2D EDI scans were used for the measurement. For each eye two different EDI scans
were measured once each by each investigator, and then the EDI scan with higher signal
strength was measured two more times to assess intrarater variability. In each session
the investigators were blinded to each other’s measurements and also their own previous
measurements of the same scans. Repeated measurements were 2 to 4 weeks apart.
Automated measurements were made on the same EDI scans that were measured by
the investigators. An example of the final segmentation result is shown in Figure 4.7. After
the segmentation was obtained, the centre of the fovea was located as the point on the ILM
segmentation with minimum slope, and the vertical distance between BM and the choroid-
sclera boundary was measured as the subfoveal choroidal thickness. In some scans the
centre of the fovea could not be identified reliably, either due to severe deformation in the
foveal region caused by the disease or failure to centre the scan at the fovea during the
acquisition stage. In such cases choroidal thickness was measured at the centre of the
scan for manual and automated measurements.
The minimum, maximum, mean, SD, and coefficient of variation (CV) were computed
for the manual and automated measurements. Intrarater, interrater, and interscan variabil-
ity of the measurements was assessed with intraclass correlation coefficients (ICC) and
pair-wise t-tests. The choroidal thicknesses measured by the raters and automated algo-
rithm were assessed for correlation with drusen area using linear regression analysis. A
generalized linear model was used to find the age-adjusted association of the subfoveal
choroidal thickness with drusen area. SPSS (Version 19; SPSS, Inc., Chicago, IL) was
used for the statistical analysis.
Results
In the study group of 44 subjects total, 31 were females (70%) and 13 were males
(30%). The average age of the participants was 75.7±8.4, ranging from 60 to 91. Of the
patients 40(91%) were taking age-related eye disease (AREDS) vitamin supplementation.
No patient was a current smoker, and eight patients (18%) were previous smokers who
33
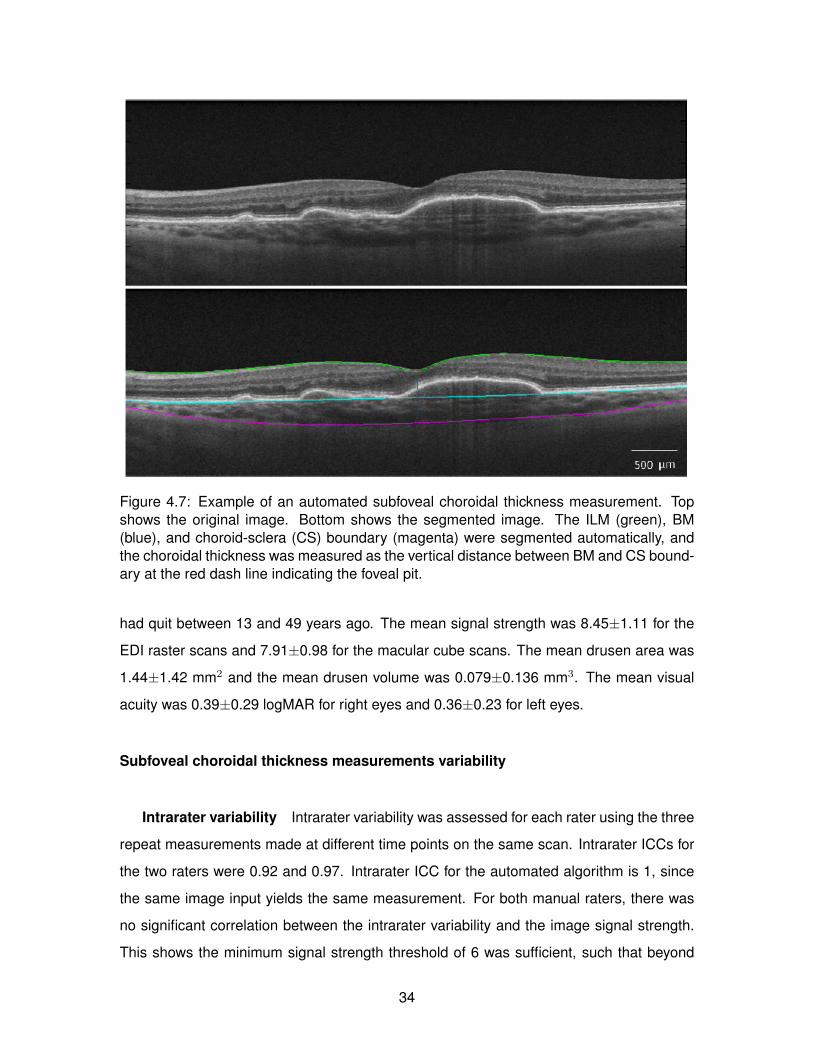
Figure 4.7: Example of an automated subfoveal choroidal thickness measurement. Topshows the original image. Bottom shows the segmented image. The ILM (green), BM(blue), and choroid-sclera (CS) boundary (magenta) were segmented automatically, andthe choroidal thickness was measured as the vertical distance between BM and CS bound-ary at the red dash line indicating the foveal pit.
had quit between 13 and 49 years ago. The mean signal strength was 8.45±1.11 for the
EDI raster scans and 7.91±0.98 for the macular cube scans. The mean drusen area was
1.44±1.42 mm2 and the mean drusen volume was 0.079±0.136 mm3. The mean visual
acuity was 0.39±0.29 logMAR for right eyes and 0.36±0.23 for left eyes.
Subfoveal choroidal thickness measurements variability
Intrarater variability Intrarater variability was assessed for each rater using the three
repeat measurements made at different time points on the same scan. Intrarater ICCs for
the two raters were 0.92 and 0.97. Intrarater ICC for the automated algorithm is 1, since
the same image input yields the same measurement. For both manual raters, there was
no significant correlation between the intrarater variability and the image signal strength.
This shows the minimum signal strength threshold of 6 was sufficient, such that beyond
34

N Minimum, µm Maximum, µm Mean, µm SD, µm CV (%)
Rater 1 83 145 521 246 63 25Rater 2 83 99 526 214 68 32
Auto 83 107 447 203 53 26
Table 4.1: Descriptive Statistics of the Choroidal Thickness Measured by the First Rater(Rater 1), Second Rater (Rater 2), and the Algorithm (Auto)
ICC 95% CI Paired Mean Difference, µm P Value
Rater 1 and rater 2 0.96 0.94− 0.98 30.56 < 0.001Rater 1 and auto 0.85 0.77− 0.90 45.51 < 0.001Rater 2 and auto 0.84 0.75− 0.89 15.39 < 0.016
Table 4.2: Intraclass Correlation and Paired Mean Difference for Choroidal Thickness Mea-surement Between the Raters (Rater 1, Rater 2) and the Algorithm (Auto)
this threshold the signal strength did not affect the measurement repeatability significantly.
The first rater showed a small, but statistically significant positive correlation between the
intrarater variability and average choroidal thickness (r = 0.27, P = 0.01), suggesting that
greater choroidal thickness was associated with greater intrarater variability. The intrarater
variability of the two raters was not correlated significantly (r = 0.16, P = 0.12) which im-
plies that there were no consistent scan features that contributed to the variability between
raters.
Interrater variability Interrater variability was assessed between the raters and the
automated algorithm. The values for the raters were averaged over the three repeated
measures to reduce the effect of intrarater variability. Of total 88 eyes, 5 for which the
difference between the average manual measurement and automated measurement was
greater than 40% were excluded from analysis as unsuccessful. Descriptive statistics, ICC
values, and paired sample t-test results are shown in Tables 4.1 and 4.2.
The ICC between the raters was 0.96, which was higher than the ICC between the
first rater and the automated algorithm (0.85), and the second rater and the automated
algorithm (0.84).
The paired t-test between the two raters indicated a statistically significant mean dif-
ference (mean difference 31 µm, P < 0.001), such that the first rater measured generally
larger choroidal thickness than the second rater. The pair-wise difference between the
raters was not correlated significantly with the choroidal thickness, drusen area, or drusen
35

Figure 4.8: Bland-Altman plots showing the interrater variability of choroidal thickness mea-surements between the two manual raters (left), and between the manual raters (averaged)and the automated algorithm. The dotted lines indicate the upper and lower 95% confi-dence interval limits (N = 83).
volume. This implies that “shadowing” of the underlying choroid by drusen did not con-
tribute significantly to variability. Correlation between the two raters was 0.93 (P < 0.001).
The paired t-test between the raters and the automated algorithm indicated a statisti-
cally significant mean differences (mean difference with the first rater 46 µm, mean differ-
ence with the second rater 15 µm, P < 0.001 for both), such that the automated algorithm
measured generally smaller choroidal thickness than both raters, but closer to the second
rater. The mean difference between the second rater and the automated algorithm was
less than that between the second and first rater. The pair-wise difference between the au-
tomated algorithm and the raters was correlated with the thickness (r = 0.70, P < 0.001),
which implies that larger choroidal thickness measurement by the manual raters has a
higher chance of yielding greater discrepancy with the automated measurement. The dif-
ference was not correlated significantly with drusen area or volume. Correlation of the
automated algorithm was 0.77 (P < 0.001) with the first rater and 0.76 (P < 0.001) with the
second rater.
Bland-Altman plots of the agreement between the raters, and between the manual
(average of the two raters) and the automated algorithm are presented in Figure 4.8.
Interscan Variability Interscan variability was assessed between two repeat scans
measurements of the same eye. Of 88 eyes, 6 eyes were excluded from analysis: 5
with largely different repeat scans, 1 with optic nerve head imaged instead of fovea. The
36

ICC 95% CI Paired Mean Difference, µm P Value
Rater 1 0.91 0.86− 0.94 -10.28 0.049Rater 2 0.96 0.94− 0.97 -10.98 0.002
Auto 0.87 0.80− 0.92 4.76 0.249
Table 4.3: Intraclass Correlation and Paired Mean Difference for Choroidal Thickness Mea-surement Between the Repeat Scans by the Raters (Rater 1, Rater 2) and the Algorithm(Auto)
result is tabulated in Table 4.3. The first rater’s interscan ICC was 0.91, the second rater’s
interscan ICC was 0.96, and the automated algorithms interscan ICC was 0.87.
However, in the paired samples t-test, the mean difference between the first and second
scan measurements was significant for the raters (p-value ¡ 0.05), but not for the algorithm.
A possible explanation is different bias in different measurement sessions by the human
raters. The raters measured the first set of scans first, and after two weeks or more mea-
sured the second set of scans. Since the scans were acquired within a minute each other,
and there was no cause for a consistent and recurring systematic difference between the
first and second scans, the significant mean difference can be attributed to the fact that
in the second session the raters tended to measure larger choroidal thickness. Since the
automated algorithm does not have such intrarater variability, the measurement difference
between the scans was not session-dependent, and the mean difference between the first
and second scans was not significant.
The interscan variability of the raters was not correlated significantly with the interscan
variability of the automated algorithm, and showed that generally there was no certain set
of scans in which the raters and algorithms had small or large interscan variability. The
interscan variability was not correlated with choroidal thickness, drusen area, or drusen
volume for all methods.
Correlation Between Choroidal Thickness and Drusen Area Drusen area was corre-
lated significantly and inversely with choroidal thickness for both raters and the algorithm
(Table 4.4) for multivariate analysis, including age, which was not a statistically significant
predictor of drusen area.
37

Outcome Predictor Beta (SE) P Model R2
Drusen area Age -0.037 (0.042) 0.38 0.12Choroid Thickness, rater 1 -0.006 (0.003) 0.05
Drusen area Age -0.031 (0.041) 0.45 0.16Choroid Thickness, rater 2 -0.007 (0.003) 0.02
Drusen area Age -0.036 (0.018) 0.84 0.26Choroid Thickness, auto -0.005 (0.002) 0.02
Table 4.4: Results of Multivariable Regression Analysis Between Drusen Area and ChoroidThickness Measured by the Rater (Rater 1 and Rater 2) and the Automated Algorithm(Auto)
Discussion
We have compared the subfoveal choroidal thickness measured by two expert raters
and an automated algorithm on EDI-OCT raster scans of nonneovascular AMD patients.
The agreement between the two raters was high, but with a statistically significant mean
difference. The agreement between the raters and the automated algorithm was less than
that between the raters, but acceptable [106]. The raters and the algorithm showed compa-
rably good repeat scan repeatability with slightly higher ICC values for the raters; however,
the raters displayed statistically significant mean difference between the first and second
scan measurements, which was not present for the automated algorithm. This may be
attributed to intrarater, or intersession, variability in manual measurement.
The raters felt it was difficult to identify confidently the choroid-sclera boundary in many
scans. However, the overall result shows high ICCs for intrarater, interrater, and interscan
repeatability among the two raters. The automated algorithm did not have intrarater vari-
ability, and had lower, but fair interrater and interscan repeatability relative to the raters.
A recent article published in IOVS presented a similar comparative analysis of a commer-
cial automated algorithm and manual graders on drusen segmentation [106]. The drusen
volume agreement was comparable between the manual graders (ICC = 0.98), and be-
tween the average of the graders and algorithm (ICC = 0.94); however, the drusen area
agreement was significantly higher between manual graders (ICC = 0.99) than between
the average of the graders and algorithm (ICC = 0.64).
The OCT scan signal strength level beyond the given threshold of 6 did not affect the
measurement. Drusen area and volume also were not correlated with measurement re-
peatability or interrater agreement for the raters and the algorithm. From observation, most
38
drusen in our study did not affect the visibility of the choroid except in a few cases. Even
when a drusen of a substantial size shadowed the choroid, the raters and the algorithm
were capable of some level of interpolation from surrounding regions where the choroid-
sclera boundary was visible.
The discrepancy between the interrater (manual) measurements, and the manual and
automated measurements was influenced by two factors: weak image intensity at the pos-
terior choroidal boundary and different definitions of the posterior choroidal boundary. A
thicker choroid implies a deeper posterior boundary where light penetration may be low,
resulting in decreased image intensity and edge clarity. Of the total 88 eyes, 6 eyes had
the choroidal thickness greater than 330 µm, and the automated segmentation was un-
successful for 4 of them (total 6 scans were categorized as unsuccessful). The value 330
µm was selected to include the cluster of unsuccessful segmentation at large choroidal
thickness. Edge clarity also is dependent on the overall image quality and the peak signal
location, which is determined at acquisition of the EDI-OCT scans. When the peak signal
location is closer to the anterior choroid and the image intensity fall off is large the anterior
blood vessels may have significantly higher contrast than the vessels near the posterior
edge of the choroid. In these cases the algorithm may falsely detect a boundary inside
the choroid resulting in a smaller thickness measurement. Unusually large drusens also
contribute to low edge clarity. Examples are shown in Figure 4.9.
One systematic factor in smaller automated measurements compared to manual mea-
surements was how the posterior choroidal boundary was defined by the raters and al-
gorithm. The algorithm searched for a relatively smooth boundary of strong dark-to-bright
contrast, which ideally corresponds to the posterior edge of the dark, large blood vessels at
the bottom of the choroid. On the other hand, the raters occasionally chose the outermost
(most posterior) edge they could identify as a smooth boundary (Figure 4.10). The thick-
ness difference between the innermost dark-to-bright boundary chosen by the algorithm
and the dark-to-bright boundary chosen by the raters could be explained physiologically by
the presence of the heavily pigmented suprachoroidal layer (lamina fusca). The thickness
of the suprachoroidal space is approximately 30 microns [182], which is close to the mean
thickness difference that we observed between the raters and algorithm.
Interscan repeatability on two consecutive scans of the same fovea was affected by
patient motion and image quality of the scans. Even when the repeat scans are imaged
39

approximately at the same location at the fovea, the amount of light penetration and the
corresponding image intensity at the choroid is low, and the visibility of choroidal structures
can be sensitive to even small changes between repeat scans. A pair of repeat scans
with a large difference in image quality, and a large interscan variability for the raters and
automated algorithm is shown in Figure 4.11.
We note the metric used in the study was the choroidal thickness below the fovea,
where the choroid tends to be the thickest, and accordingly the least visible. Also, the
choroidal thickness measurement was made on a single point and not averaged over a
region. This likely also contributed to the measurement variability and agreement for the
raters and automated algorithm.
The number and size of drusen is an important risk factor for predicting the progression
of AMD [1]. We found that choroidal thickness was correlated with drusen area, suggesting
that this may be an important parameter to follow in clinical practice and in clinical trials.
Manual and automated choroidal thickness measurements were found to correlate with
drusen area, suggesting that either would be adequate for clinical use. While manual mea-
surements tend to be less variable, obtaining these measurements can be time-consuming.
Automated measurement, thus, offers the advantage of being more applicable to a clinical
setting.
This study has presented manual and automated measurements of subfoveal choroidal
thickness in nonneovascular AMD patients using EDI-OCT scans. The manual raters
agreed with each other better than they agreed with the automated algorithm, which still
showed a fair level of agreement with the manual raters (ICC between the raters = 0.96,
ICC between the raters and the algorithm = 0.84, 0.85). All methods performed relatively
well in measurement repeatability in repeat scans. The manual measurements appeared
to be subject to possible biases in different raters and different rating sessions. The auto-
mated algorithm measurement was determined only by the given scan, but showed greater
sensitivity to image quality. As such, the manual and automated measurements of the sub-
foveal choroidal thickness in 2D EDI-OCT scans should be used with consideration. The
performance of the automated algorithm, and to some extent manual raters, is likely to
benefit from 3D or more in-depth imaging modalities, such as polarization sensitive OCT
or 1060 nm OCT.
40
The correlation of the automated choroid measurements with the drusen area was com-
parable to that of the manual measurements, indicating clinical relevance of the automated
measurements in studying the relationship between the drusen and choroid. The auto-
mated measurement showed potential for faster speed and reduced labour cost in clinical
practice and clinical trials.
4.4 Summary of contributions
The contributions described in this chapter and published in [109, 111] are:
• Manual segmentation of the ONH landmarks on radial scans.
• Implementation of automated 3D segmentation of retinal layers using graph-cut.
• Choroid segmentation
– Automated choroid segmentation in 830 nm and 1060 nm OCT images.
– Variability analysis of manual and automated subfoveal choroidal thickness mea-
surement.
The automated retinal layer segmentation tool developed here contributed to studies in
subretinal fluid detection [35], validation of radial optical coherence tomography acquisition
[107], visualization of speckle variance OCT [187], in addition to retinal surface registration
and morphometric analysis studies presented in the following chapters.
41

Figure 4.9: Examples of segmentation by the first rater (red), second rater (yellow), andthe algorithm (magenta). The first and second scans show the three measurements closeto each other. In the third scan, the posterior choroidal boundary is located deep withlow edge strength, and the automated measurement is smaller than the manual measure-ments. In the fourth scan a large drusen reduces the visibility of the posterior choroidalboundary. 42

Figure 4.10: Example of different choroid-sclera boundary measurements by the first rater(red), second rater (yellow), and the algorithm (magenta).
Figure 4.11: Repeat scans of the same fovea with different image quality.
43

Chapter 5
Retinal Surface Registration
The conventional approach to measure the anatomical difference between two OCT im-
ages is to predefine an anatomical parameter, measure it in each image, and compare the
values. Examples of such metrics are optic cup volume, cup-to-disk ratio, Bruch’s mem-
brane opening (BMO) area, retinal layer tilt, and retinal layer thicknesses representative of
the degree of cellular damage in retina due to diseases such as glaucoma [101, 87, 149,
128, 59].
Aside from the pathophysiological relevance of these parameters, there is often poor
anatomical correspondence across images, raising the question whether a particular pa-
rameter yields anatomically comparable measurements for a valid comparison between
multiple eyes. Lack of correspondence may originate from poor parameter definition, such
as in the case of the optic cup-to-disc ratio, where the cup or disk boundary often does
not correspond to a single anatomical structure within an eye or across eyes, resulting
in inconsistency among measurements [178, 160, 162, 21, 199]. Another cause for poor
inter-subject or time point correspondence can be lack of stable landmarks, such as in the
case of retinal layer thickness maps which terminate, not at an anatomical boundary, but
at the image acquisition frame.
In the latter case, in order to make any comparison or create a population or group
mean of multiple OCT images, it becomes necessary to artificially define regional corre-
spondence. This is often done based on a certain orientation and distance with gross
anatomical landmarks. In sectoral or regional retinal layer thickness analysis of macular
or peripapillary OCT scans, sectors are delimited by superior, inferior, temporal, and nasal
orientations (often simply in reference to the image frame), and distance from landmarks
44

such as the foveal pit or optic disc. However, it is unclear how the anatomical similarity
is established by these orientation and landmark distances – one may ask whether the
retinal nerve fiber layer (RNFL) thickness at a specified distance (say two millimetres) from
BMO in one eye is comparable to the RNFL thickness at the same distance from a much
larger BMO in another eye, or the distance should be adjusted according to the BMO size.
Averaging measurements over a region may somewhat mitigate the effect of this unknown
“mismatch,” but at the cost of losing measurement sensitivity and detail.
Recent studies have directly and indirectly addressed this issue in various ways. One is
to define parameters that are more anatomically consistent across multiple subjects. Sev-
eral groups confirmed the high inter-measurement variability of enface image based pa-
rameters such as the cup-to-disk ratio [178, 160, 162, 21, 199], and suggested alternatives
like BMO-based parameters as more reliable structural measurements [21]. Peripapillary
sectors were adjusted to better align to individual BMO dimensions [112], and foveal-BMO
axis has been shown, compared to the conventional superior-inferior-temporal-nasal orien-
tation by the image frame, to be less affected by acquisition factors such as the participant’s
head tilt and to have better anatomical and physiological justification [21, 71].
Registration of OCT images has been performed in 2D enface with stereo disc pho-
tography [166], and a series of repeated OCT scans were registered in both 2D [97] and
in 3D [197] in order to improve the image signal-to-noise ratio by averaging the registered
images. The voxel-wise correspondence in such application is established under the as-
sumption that the images are the same except for the acquisition modality or artifacts;
comparison of the data is not the main objective. Longitudinal OCT images of the same
eye at multiple time points have been rigidly aligned with 3D SIFT registration [140] and
with a combination of blood vessel registration and a graph-cut based A-scan matching
[141]. Many commercially available OCT systems now include techniques to track and
match the eye position in consecutive imaging sessions [53]. These methods are still lim-
ited to general alignment of the images by rigid registration, and do not direct quantify the
morphological difference between the images.
Few studies have specifically examined nonrigid cross-sectional registration of OCT
images of multiple subjects in the context of morphological comparison and group averag-
ing. In Gibson et al. [54], segmented optic cups were registered to a single template optic
45

cup, first by bringing each target into close proximity of the template via rigid and non-
rigid intensity-based volumetric registration and achieving point-to-point correspondence
by mapping the surfaces into a spherical domain and registering by spherical demons al-
gorithm [192]. The process was validated by dice coefficient of the matched cups and a
group average optic cup was created. In Chen et al. [23] registration of macular OCT scans
began first with rigid translation which aligned the foveae and subsequent A-scan affine
transformation to match ILM and Bruch’s membrane, the anterior and posterior bound-
aries of the retina, respectively. The A-scans were further deformed smoothly using radial
basis functions in order to refine the alignment of the retinal layers.
In the following sections, two methods of retinal surface registration are presented - ex-
act one-to-one retinal surface matching, and atlas generation of multiple retinal surfaces.
The segmentation algorithm described in Section 4.2 segmented the retinal layer bound-
aries, or the retinal surfaces in 3D. The segmentation output, in the form of high-density 3D
point clouds, were converted into triangular meshes using Delaunay triangulation. Sub-
sequently, at each vertex of the surfaces, we computed layer thicknesses, defined as the
closest Euclidean distance between the two surfaces corresponding to the posterior and
anterior boundaries of a retinal layer.
5.1 Exact surface-to-surface registration
5.1.1 Methods
Our proposed registration scheme consists of two parts: an in-exact, currents-based
estimation of the deformation φc, which brings the template and subject surfaces into close
proximity of each other, followed by spherical demons registration φs to produce exact
matching between the subject and template. The final deformation, a composition of φc
and φs, will be denoted by Φi = φs(φc(Si)), where Si refers to subject i.
Currents
The surfaces extracted from the segmentation algorithm described above are repre-
sented as currents [184] - objects that reside in a linear space with a computable norm.
Equipping surfaces with a computable norm allows the measurement of how ‘close’ two
surfaces are to each other.
46

Let S and T be two discretized submanifolds of Rn represented in the space of currents
via summation of the surface’s discretized elements (Dirac currents δ). That is, the surface
S is represented as S =∑
f δηfcf where f denotes the face of a triangulated surface, cf its
center, and ηf denotes the face’s normal vector. The optimal registration from S to T is
performed through minimization of the following functional:
J(vt) =
∫ 1
0‖vt‖2V︸ ︷︷ ︸
regularizer
dt+ λ ‖φ]S − T‖2H︸ ︷︷ ︸data attachment
(5.1)
where φ represents a diffeomorphism corresponding to the flow of vector fields vt at time
t = 1, and φ]S is the push-forward of S defined below.
The pull-back φ]ω of a differential 2-form ω by a mapping φ is the 2-form defined by
φ]ω(x)(u1 ∧ u2) = ω(φ(x))(dxφ ·u1 ∧ dxφ ·u2). The push-forward of φ on a current S is the
current φ]S such that for every differential 2-form ω, φ]S(ω) = S(φ]ω). In a finite, discrete
setting the data attachment term of the functional J can be written as
A =∥∥∥∑
f
δηfcf −
∑g
δηgcg
∥∥∥2
H=∑f,f
k(cf , cf )〈ηf , ηf 〉
+∑g,g
k(cg, cg)〈ηg, ηg〉 − 2∑f,g
k(cf , cg)〈ηf , ηg〉 (5.2)
where∑
f δηfcf and
∑g δ
ηgcg represent the discrete versions of φ]S and T , respectively, cf and
ηf represent the centres and normal vectors of the respective faces (triangular elements)
and k is a positive kernel defining a Reproducing Kernel Hilbert Space (RKHS) norm on
Hilbert space H. In the framework of these deformations, it has been shown [184] that the
optimal vector fields to be found from Eq. 5.1 take the form
vt(x) =N∑i=1
G(qi(t), x)αi(t), (5.3)
where qi(t) = φxi(t) are the trajectories of the surface’s vertices xi and the momentum
vectors αi(t) are the solutions to the following system of linear equations
∂
∂tqj(t) =
n∑i=1
G(qi(t), qj(t))αi(t). (5.4)
where G is a positive kernel inducing a RKHS norm on V . It turns out that, from a compu-
tational perspective, it is easier to find the deformation in terms of the momentum vectors
47

Figure 5.1: The proposed registration scheme. (a) The subject S is first brought into closeproximity with the template T by the method of surface currents φc to produce an in-exactmatching result. (b) A point-to-point correspondence between S and T is achieved byregistering φc(S) to T via spherical demons. The end result matches the topology of thetemplate. (c) Registration of the four anatomical surfaces (ILM, BM, NFL and choroid) tothe template by φs(φc(Si)).
αi(t) rather than the trajectories qi(t), which are needed to calculate vt, and thus we re-
place the functional J from Eq. 5.1 by
J(αi(t)) =
∫ 1
0
N∑i,j=1
G(qi(t), qj(t))〈αi(t), 〈αj(t)〉dt+A(qi(1)) (5.5)
For computational details on computing the variation functional J(αi(t)) we refer the
reader to [57].
Spherical Demons Registration
The currents-based registration, achieved by minimization of J , brings the template
T and subject S surfaces into close proximity of each other. However, a point-to-point
correspondence is yet to be achieved (Figure 5.1). Since the goal is to achieve a topology-
preserving and an invertible transformation, a simple projection of vertices from the trans-
formed template to subject surface is insufficient as it does not guarantee that the transfor-
mation will be invertible.
To achieve a point-to-point correspondence between S and T , we project each of the
four anatomical surfaces of S and T onto a hemispherical domain. In mapping the anatom-
ical surfaces to a hemisphere, the surfaces are first transformed to a circle-bounded planar
48

graph [202]. The boundary vertices are assigned a fixed position on the unit circle, non-
boundary (interior) vertices are expressed as a nonnegative weighted sums of their neigh-
bor vertices, and the equations are solved for new positions of the nonboundary vertices
[47]. By this construction, all nonboundary vertices lie within the unit disc. Using an in-
verse stereographic projection from point [0, 0, 1] onto a unit sphere, this disc surface can
be warped to a hemispherical surface. Finally, by mirroring this surface across the equator,
the spherical representation of surfaces are presented to the spherical registration algo-
rithm to form a point-to-point correspondence between the spherical representations of
surfaces.
Registration of the surfaces in the spherical domain is performed by the method known
as spherical demons, detailed in [190]. Briefly, spherical demons based registration of
surfaces involves applying the registration φs to φc(S) (the inexactly matched surface found
by the method of currents), where φs is found by minimizing the following functional:
(γ, φs) = arg minγ,φs‖ζ(T )− ζ(φs(φc(S)))‖2 +
1
σ2x
dist(γ, φs) +1
σ2T
Reg(γ). (5.6)
Here γ refers to a hidden transformation that acts as a prior on φs, and σ2x, σ
2T are the
tradeoff parameters to the last two terms in the objective function. The term dist(γ, φs) in
Eq. 5.6 encourages φs to be close to γ and Reg(γ) penalizes the gradient magnitude of
the displacement filed γ. For details on appropriate choices of dist(γ, φs), Reg(γ) on a
spherical domain, and on minimizing the objective function in Eq. 5.6, we refer the reader
to [191]. The authors of [190] employed cortical thickness as the function ζ to perform
the registration of cortical surfaces in the spherical domain. This method has been altered
in [54] to employ the coordinate function ζ, defined by ζ(·) = (·x, ·y, ·z) on each vertex of
(·), to register spherical representations of the ILM with a high degree of precision. In a
nutshell, maximizing the overlap of the coordinate functions for registration is essentially
akin to finding a regularized straight line correspondence between the two surfaces. The
smoothness constrain ensures that this transformation is invertible. Following the strategy
of [54], we use ζ to perform registration between two spherical representations of surfaces.
Since currents-based surface matching and the spherical demons are guaranteed to be
invertible, the combination of currents-based matching followed by spherical demons reg-
istration also produces a mapping that is smooth and invertible. With this method one can
49

now perform statistics on the vertex-wise measurements of each subject by transforming
any surface-indexed biomarker into template coordinates.
For a typical volumes consisting of approximately 100,000 vertices, the total run time
of our registration algorithm, between a template and target volume, was about 11.5 hours
on a computer with an i7 Intel CPU running at 3.50GHz and 32GB’s of memory.
5.1.2 Results
We imaged a small cohort: 3 healthy subjects and 3 glaucomatous subjects. From each
subject, we acquired volumetric OCT images of both eyes (OD and OS). Ethics review of
this study was approved by Simon Fraser University (SFU).
For each subject, we registered the four extracted surfaces: ILM, NFL, BM, and choroid,
and two different measurements: NFL thickness and choroidal thickness, to a common
template by the registration methodology described above. One of the healthy subjects
was chosen to serve as the template. Each subject was then registered to the template;
this allows us to directly compare measurements at vertices on the registered surfaces. A
schematic illustrating the proposed registration process is shown in Figure 5.1.
As it is commonly done with verification of registration algorithms when ground truth
is unavailable, we relied on a visual assessment (Figure 5.2) to evaluate the fidelity of
our proposed registration method. A 3D coloured checkerboard-texture, plotted on the
template surface T as a colormap, was propagated to the subject surfaces Si by the inverse
of the computed final surface registration Φ−1i , showing the mapping of points between the
surfaces. Fig. 5.2 shows the propagation of the checkerboard pattern to the NFL and ILM
surfaces of several subjects. One can see that the relative anatomical locations of the
different coloured patches closely match those of the template surface.
Group Differences
Since all subjects’ surfaces have been resampled into a common space, the vertices
number, arrangement and location are directly comparable. Hence, if the surface consists
of NT vertices with each having a thickness value (either NFL or choroidal), each subject’s
surface can be represented as a point in RNT dimensional space and standard dimension-
ality reduction and multivariate statistical analysis tests can be applied.
50

Figure 5.2: 3D checkerboard pattern propagation by the computed inverse mappings Φ−1i .
The top row shows the propagated checkerboard patterns of the NFL surface while thebottom row shows the propagated checkerboard pattern on the ILM surfaces. The surfacesshown in the first column are the NFL and ILM surfaces of the template T .
After establishing point-to-point correspondence between the registered surfaces, we
localized significant differences in NFL and choroidal thickness measurements across the
control and glaucomatous subject groups. This localization was carried out using the Surf-
Stat package [27], a collection of routines designed to analyze univariate and multivariate
surface data, based on linear mixed effects models and random field theory [186]. At each
vertex on the NFL and choroid surfaces, a mixed effects model was used to identify vertex-
wise differences in NFL and choroidal thickness. Clusters of vertices where the vertex-wise
differences are above a threshold (p = .001) were identified and a correction for multiple
comparisons was performed. The significance of each cluster is assessed by comparing
the extent of the cluster with an analytic distribution of cluster extents based on T-fields, as
described by [15].
Fig. 5.3 shows the t-values and clusters of p-values that contained significantly differ-
ent measurements in choroidal and NFL thickness between the two subject groups. From
the images shown in the bottom row of Fig. 5.3, we observe that there are significant
(p = .001) differences in the choroidal thickness between healthy and glaucomatous sub-
jects, occurring primarily in inferior regions of the optic nerve head. NFL thinning of the
glaucomatous group is observed to occur predominantly in the superior-temporal region,
concentrated around the blood-vessels flowing to the optic cup.
51

Longitudinal Analysis - phantom data
The surface registration framework presented in this paper allows us to not only analyze
cross-sectional group differences (Section 5.1.2) but also analyze longitudinal changes
(changes over time) for one individual subject.
In a validation of our proposed registration scheme, we generated phantom longitudinal
data by simulating changes in ONH morphometry. Simulated changes were performed
by deforming the NFL surface to model the presence of focal damage on the NFL and
retinal thinning (Figure 5.4(a)). The focal damage was modeled by creating a small circular
depression in the NFL and retinal thinning was modeled by deforming a small region of the
NFL around the BMO towards the ILM (Fig. 5.4(b)). Following these deformations, we
recomputed the new NFL thickness and applied an affine transformation to the surface,
intended to simulate artificial differences between subsequent acquisitions. The entire
surface was translated by [0.4, 0.6, 0.2]mm and rotated by applying the following rotation
matrix
R =
cos(θ) −sin(θ) 0
sin(θ) cos(θ) 0
0 0 1
, (5.7)
where θ = −10, to each vertex of the surface. The original surface, shown in Figure 5.4(c),
is referred to as time point 1, and the new, deformed surface, shown in Figure 5.4(d),
is referred to as time point 2. Using our proposed registration scheme, we registered
the surface from time point 2 to the surface from time point 1. Following the registration
process, the differences between the original and the new, simulated NFL thicknesses
are shown in Figure 5.4(e). As expected, the regions of modeled NFL thickness difference
appear as ’hot spots’ on the difference map. We note that there are other regions that show
slight differences in the registered NFL thickness, primarily in the periphery regions of the
NFL. These errors are due to the fact that the modified surface at time point 2 contains an
affine transformation relative to the surface at time point 1. In registering the two surfaces,
we applied the registration scheme as presented in Section 5.1.1, without pre-registering
with an affine registration. An accurate affine pre-registration step would likely further
improve the registration results. Finally, we thresholded the observed differences in the
NFL thickness in terms of the intrinsic axial resolution of the OCT system. The thresholded
map of the differences is shown in Figure 5.4(f). We observe differences only in the regions
52

that we have manually modified: increased NFL thickness in the region where we modeled
the focal damage, and decreased NFL thickness where we modeled retinal thinning.
Longitudinal Analysis - real data
In this experiment we tracked the changes in NFL thickness and choroidal thickness of
a 36-year-old male subject, imaged at two different time points 1 year apart. The top two
rows of Figure 5.5 show the NFL thickness and choroidal thickness of this single subject,
imaged at two time points (Time Point 1 and Time Point 2), separated by approximately one
year. The surfaces and measurements from Time Point 1 were registered to the surfaces
of Time Point 2 by the method described in Section 5.1.1. The registered surfaces and
measurements are shown in the third row of Figure 5.5. Once the homology between
the surfaces belonging to the two time points has been established, we can visualize and
study the changes in the computed NFL and choroidal thicknesses. The changes in the
computed NFL and choroidal thickness are shown in the fourth row of Figure 5.5. To better
understand the changes in NFL and choroidal thickness, we normalized the difference to
the axial resolution lc of the OCT system. The axial resolution for the system used to image
this particular subject was lc = 6µm. We observed that the NFL thickness predominantly
decreased in the region surrounding the blood vessels by 1 − 3lc. Similarly, choroidal
thickness was also found to be decreased, primarily in the inferior region around the BMO.
Few isolated regions showed an increase in choroidal thickness by 1lc.
5.1.3 Discussion
We have reported on a novel registration method capable of point-to-point comparison
between, not only intra-subject, but also inter-subject retinal OCT data. In this section we
discuss some of the limitations and goals for further improvement of this proof-of-concept
work.
In Figure 5.2, propagation of the template surface is shown for 10 target surfaces.
In each case, the optic disc is shown to serve as a strong morphological landmark that
functions as a major determinant in overall deformation. The optic disc center is commonly
used as a reference structure in rigidly aligning OCT images for retinal layer thickness
analysis by lateral translation. The result in Fig. 5.2 indicates that the proposed nonrigid
registration sufficiently handles the misalignment between the discs within the sample data
53

used in this study, and that disc alignment is an intrinsic part of the registration process
due to the role of the optic disc as a prominent shape feature. However, in the phantom
data experiment in Section 5.1.2, we observed that a global affine transformation to a test
image was not fully restored by the nonrigid registration only, and caused some regions of
slight difference in the result. Although this difference was less than the axial resolution of
the image and the rest of the simulated retinal thinning and deformation were accurately
detected, performing a 3D affine pre-registration before the nonrigid registration will likely
improve the final registration result and reduce the deformation energy for the nonrigid
registration. Further experimentation is needed to investigate how a pre-registration, such
as aligning disc centres by translation and rotation, would affect the registration accuracy.
The phantom data experiment in Section 5.1.2 demonstrated the axial-resolution level
of accuracy of the registration algorithm; however, the final accuracy and vertex-wise cor-
respondence of real data of different eyes would still depend on the accuracy and re-
peatability of the rest of the processing pipeline, in particular the layer segmentation. The
segmentation module in this study has been used in one of our studies [112] where 192
retinal layers from 50 eyes were segmented with 88-92% agreement with a trained man-
ual rater. Similar in the study, the automatically segmented surfaces in this report were
checked and corrected by a manual rater before layer thickness measurement and regis-
tration. This potentially introduces intra-rater variability to the data which may undermine
the overall vertex-wise correspondence. A detailed comparative study of retinal segmen-
tation algorithms and their influence on subsequent registration remains a topic for future
research.
We note that the registration algorithm in this study was implemented in MATLAB and
not optimized for speed. The current run time of 11.5 hours per registration may be sig-
nificantly reduced by using efficient implementations in C++, and also by exploiting the
massively-parallel architecture of a GPU. Including an affine pre-registration may also re-
duce the run time of the nonrigid registration step.
Another important question to be addressed is the effect of template choice on registra-
tion. The current algorithm registers a target set of surfaces to a template set of surfaces,
and when several eyes are thus individually registered to a single template, it establishes
a common spatial correspondence among the eyes based on the anatomy of the template
eye. Thickness at each point can be compared and averaged among the subject eyes
54

and a pseudo-mean anatomy can be also created by computing the average deformation
between the template and targets. In such way, a normative mean topology and thickness
map of healthy eyes can be generated that can serve as a reference to quantify the devi-
ation of a particular eye from the normative model. However, it is not clear whether and
how such a mean template would be affected by the choice of the initial template - more
specifically, how close the initial template is to the true mean of the averaged observations.
This effect will also likely depend on the number of total observations being averaged. We
hope to further investigate these issues in more detail and with a larger cohort, and com-
pare mean retinas generated by the same data but with different initial templates, and by
different numbers of subjects.
We demonstrated that this method can be used to localize the regions where significant
changes in morphometric measurements (NFL and choroidal thicknesses) are occurring
between healthy and glaucomatous subjects on a vertex-to-vertex basis. This offers an
advantage over having to resort to averaging measurements in localized regions, as is
commonly done in analyzing ONH morphometry [137]. The proposed registration scheme
can potentially serve as a powerful tool in computer-aided diagnosis methods that employ
classification algorithms. These classification algorithms [27, 44] typically require accurate
registrations of morphometric measurements to a common template, which our proposed
registration scheme is able to provide.
Our method is also applicable as a precursor to image intensity-based registration and
would help initialize the high-dimensional nonrigid algorithms to better avoid local mini-
mums. In addition to cross-sectional analysis, the proposed registration scheme allows
us to perform longitudinal studies of morphometric measurements, where the goal is to
study disease progression over time, or determine if the subject has converted from being
healthy to diseased between subsequent scans.
The proposed exact surface registration method is not limited to registering surfaces
extracted from OCT, and can be used for registering surfaces extracted from other imaging
modalities, such as MRI and CT. Automated diagnoses of neurodegenerative diseases,
such as Alzheimer’s, commonly rely on registering whole-brain morphometric measure-
ments such as cortical thickness and Gyrification [107] to a common template which could
be potentially achieved with the registration method proposed in this paper.
55

The proposed registration method uses several surfaces to compute deformation from
subject to template over an entire volume. This can potentially aid Tensor-Based Mor-
phometry (TBM) [116] analysis in detecting local volumetric changes that would otherwise
be impossible to detect with standard TBM analysis due to high speckle noise level in OCT
images.
56

Figure 5.3: Left column: NFL. First image: mean NFL thickness of the control group. Sec-ond image: mean NFL thickness of the glaucomatous group. Third and fourth images:t and p-values, respectively. Right column: choroid. First image: mean choroidal thick-ness, shown in mm, of the control group. Second image: mean choroidal thickness of theglaucomatous group. Third and fourth images: t and p-values, respectively.
57

Figure 5.4: Phantom longitudinal data registration and validation. (a) Schematic depictingthe presence of a focal damage on the NFL and retinal thinning. Blue and green linesrepresent the surfaces at time points 1 and 2, respectively. (b) 3D rendering of the phan-tom NFL surface at time point 2, showing the modeled focal damage and retinal thinning.Colormap represents the computed NFL thickness. (c) NFL surface at time point 1. (d)Modified NFL surface at time point 2. The surface is translated by [0.4, 0.6, 0.2]mm, androtated by −10. Red rectangles highlight the modeled changes in morphometry. (e) Sur-face from (d) registered to the surface from (c). Colormap represents the differences inNFL thickness between time point 1 and registered time point 2. (f) The colormap from (e)thresholded by the intrinsic axial resolution of the OCT system. Red represent decreasedNFL thickness while green represents increased NFL thickness.
58

Figure 5.5: Longitudinal analysis of NFL and choroidal thickness. Top row: Surfaces anddata from Time Point 1. Second row: Surfaces and data from Time Point 2 (one yearlater). Third row: Surfaces and data from Time Point 1 registered to surfaces from TimePoint 2. Fourth row: Difference in thickness measurements from the two time points. Lastrow: thresholded difference in thickness, in terms of the axial resolution of the OCT systemlc (lc = 6µm). Increased and decreased thicknesses are represented by green and red,respectively.
59

5.2 Repeatability Analysis in Longitudinal OCT Images
The registration method described in the previous section is particularly applicable for
longitudinal analysis in which images of the same eye taken over time are compared to de-
tect change. In this section, we present registration-based repeatability analysis of Bruch’s
membrane opening area, retinal nerve fibre layer (RNFL) thickness, and choroidal thick-
ness.
5.2.1 Materials and Methods
The study followed the tenets of the Declaration of Helsinki, and informed consent was
obtained from the subjects. Ethics review for the study was approved by Simon Fraser
University (SFU) and University of British Columbia (UBC).
The images were acquired at the Eye Care Centre in June and July 2014 from 6 healthy
female participants (age: 29.5 ± 3.4) without glaucoma or any other clinically significant
conditions. Each of the participants underwent a 10-2 visual field test and obtained a mean
deviation (MD) greater than -1. Both left and right eyes were imaged 9 times over 3 weeks,
with minimum 22 hours and maximum 6 days and 2 hours between consecutive scans.
All images were acquired using the custom swept-source OCT system described in
Section 3. 1.. Each image consisted of 400 B-scans, each with 400 A-scans, and 1024
pixels per A-scan. The axial resolution was 6 µm and the lateral resolution varied from 12
µm to 20 µm depending on the eye’s axial resolution. The images were centered at the
optic cup.
The images were corrected for axial motion using cross-correlation of adjacent frames,
and bounded variation smoothing was applied in 3D to reduce the effect of speckles and
enhance the edges in the image, as described in Chapter 3. Automated layer segmenta-
tion was performed for retinal nerve fiber layer (RNFL) and choroid using the 3D graph-cut
based algorithm in Section 4.2. Bruch’s membrane opening (BMO) was segmented man-
ually on 80 2D radial slices. An ellipse was fitted to the segmented BMO points. All
subsequent reference to BMO refers to this best-fit BMO ellipse. RNFL and choroid were
cropped to 0.25 mm from the BMO ellipse because the layer termination points are am-
biguous near BMO.
60

The parameters measured were BMO area and eccentricity, which are intrinsic anatom-
ical parameters unaffected by regional correspondence, and RNFL and choroid layer thick-
ness, which was measured as the closest 3D Euclidean distance from each vertex of the
posterior surface of the layer to the anterior surface. Layer thickness is an extrinsic param-
eter in that one cannot compare a thickness value from one image to another from another
image without establishing their anatomical correspondence.
Registration was performed surface-to-surface as described in the previous section,
and in this study, between posterior RNFL surfaces and between posterior choroid sur-
faces. Prior to registration, all surfaces were aligned by matching BMO centroids, and
cropped to annuli with the width of 1 mm and inwardly bound at BMO. The cropping was
performed for dimensional consistency across the surfaces, since the OCT images have
different lateral dimensions due to the eyes’ axial length, and in each image the BMO is
only approximately centered relative to the image frame.
5.2.2 Results
For repeatability analysis, the first of the 9 repeat scans for each eye was designated
as the baseline image, and the eight subsequent images were registered to the baseline
image as the common template. The assumption was that in the imaging period of 3-
weeks, for the healthy subjects, there are no clinically significant structural changes, and
any difference between the baseline and a follow-up data are either noise during the image
acquisition or processing, or temporary anatomical changes within the normal range. The
goal of the experiment was to quantify such noise floor.
BMO area
Table 5.1 and Table 5.2 summarizes the BMO area and eccentricity repeat measure-
ments over three weeks from the six healthy subjects.
Subject 2 with larger BMO area measurements showed greater standard deviation and
coefficient of variation. However, excluding Subject 2 as an outlier, the correlation between
BMO area with its standard deviation was only suggestive (p = 0.044, R = 0.65), and
coefficient of variation was not significantly correlated with BMO area (p = 0.394).
Figure 5.6 plots BMO area by the time of acquisition during the day. Each curve repre-
sents a single eye, but the points on the curve are measurements made on different days.
61

Subject Eye Mean Minimum Maximum Standard deviation Coefficient of(mm2) (mm2) (mm2) (mm2) Variance (%)
S1 OD 1.95 1.92 1.99 0.024 1.22OS 2.20 2.16 2.25 0.035 1.61
S2 OD 5.30 4.87 6.03 0.380 7.17OS 5.65 5.22 6.09 0.298 5.27
S3 OD 2.39 2.30 2.47 0.050 2.09OS 2.22 2.14 2.28 0.042 1.87
S4 OD 1.24 1.19 1.29 0.029 2.37OS 1.36 1.31 1.43 0.037 2.71
S5 OD 2.03 2.00 2.10 0.038 1.88OS 2.23 2.18 2.30 0.042 1.87
S6 OD 2.50 2.42 2.59 0.049 1.94OS 2.44 2.38 2.55 0.066 2.68
Table 5.1: BMO area mean, minimum, maximum, standard deviation, and coefficient ofvariation for 9 repeat measurements over 3 weeks from 6 healthy subjects.
The OD-OS pair of the same subject can be distinguished as two curves with the same
time points. The figure indicates there is no consistent diurnal pattern in BMO area across
the eyes, but some intereye similarity can be observed. As it can be expected from 5.1,
S2 OD-OS have much larger BMO area measurements and also much larger fluctuation
of the measurement values.
Figure 5.7 plots BMO area by the number of days from the baseline. As in Figure
5.6, each curve represents a single eye, and the OD-OS pair of the same subject can
be distinguished as two curves of the same time points. In Figure 5.6, there appears no
longitudinal trend in BMO area over three weeks, and in none of the eyes BMO area was
significantly correlated with time from baseline. As in Figure 5.6, S2 OD-OS shows the
greatest change of value over three weeks.
RNFL Thickness
The first row of Figure 5.8 shows RNFL thickness of Subject 1 OS measured over 3
weeks, with t0 as the first measurement and baseline time point, and t1 to t8 follow-up time
points. The follow-up RNFLs were registered to the baseline RNFL, establishing point-
to-point correspondence between each follow-up RNFL and the baseline RNFL, and thus
among all RNFLs with the baseline RNFL as the common template. The second row of
62

Subject Eye Mean Minimum Maximum Standard deviation Coefficient ofVariance (%)
S1 OD 1.08 1.06 1.10 0.012 1.08OS 1.08 1.01 1.12 0.032 2.94
S2 OD 1.26 1.17 1.32 0.042 3.38OS 1.21 1.12 1.25 0.040 3.28
S3 OD 1.10 1.07 1.13 0.025 2.27OS 1.07 1.05 1.10 0.019 1.75
S4 OD 1.14 1.09 1.23 0.041 3.62OS 1.10 1.05 1.14 0.029 2.64
S5 OD 1.09 1.06 1.11 0.018 1.62OS 1.07 1.04 1.09 0.017 1.56
S6 OD 1.17 1.15 1.20 0.015 1.31OS 1.24 1.22 1.27 0.016 1.30
Table 5.2: BMO eccentricity mean, minimum, maximum, standard deviation, and coeffi-cient of variation for 9 repeat measurements over 3 weeks from 6 healthy subjects.
Figure 5.8 shows the RNFL thickness of t1 to t8 mapped onto the registered RNFLs. Point-
to-point difference in RNFL thickness between the baseline and each follow up is visualized
in the third row of the same figure, and the last row shows the difference maps normalized
by the axial coherence length of the OCT system l = 6µm.
The common template registration and resulting spatial correspondence between the
images of the same eye allows for voxel-wise statistics. The left image of Figure 5.9 shows
the time average RNFL thickness of each eye over the 3-week period; even in averaging
9 images, shape details and intereye similarities are clearly preserved. The right image of
Figure 5.9 shows the time standard deviation of RNFL thickness over time. Distribution of
standard deviation values in Figure 5.9 is presented in histograms in Figure 5.10, in which
the y-axis represents the number of voxels, and x-axis voxel-wise standard deviation, and
in cumulative distribution function plots in Figure 5.11, which mark the number of voxels
with a 3-week standard deviation equal or less than the value on the x-axis. These are
summarized in Table 5.3, where the mean standard deviation is less than 10 µm for all
eyes except S4 OS, majority of eyes show 95 percentile standard deviation of less than 3
coherence lengths (18 µm), and more than 90% of the voxels have standard deviation of
less than 2 coherence lengths in most eyes.
Figure 5.12 shows the overlay of Figure 5.9 on enface overlay images. The regions
with high RNFL thickness variability correspond to the regions of intraretinal blood vessels.
63

Figure 5.6: Diurnal pattern of BMO area.
Choroidal Thickness
Similarly to Figure 5.8, the first row of Figure 5.13 shows choroidal thickness of Subject
1 OS measured over 3 weeks, with t0 as the first measurement and baseline time point,
and t1 to t8 follow-up time points. The follow-up choroids were registered to the baseline
choroid, establishing point-to-point correspondence between each follow-up choroid and
the baseline choroid, and thus among all choroids with the baseline choroid as the common
template. The second row of Figure 5.13 shows the choroidal thickness of t1 to t8 mapped
onto the registered choroids. Point-to-point difference in choroidal thickness between the
baseline and each follow up is visualized in the third row of the same figure, and the last row
shows the difference maps normalized by the axial coherence length of the OCT system
l = 6µm.
64

Figure 5.7: BMO area measurements over three weeks.
The left image of Figure 5.14 shows the time average choroidal thickness of each eye
over the 3-week period; The right image of Figure 5.14 shows the time standard deviation
of choroidal thickness over time. Distribution of standard deviation values in Figure 5.14
is presented in histograms in Figure 5.15, and in cumulative distribution function plots in
Figure 5.11. These are summarized in Table 5.4. The mean standard deviation higher for
the choroid than the RNFL data in Table 5.3 because of the layer’s vasculature structure.
65

Figure 5.8: Variability analysis of retinal nerve fiber layer (RNFL) thickness over 3 weeks.Row 1: original RNFL thickness maps measured at 9 different time points (t0: baseline, t1– t8: follow-up) in 3 weeks. Row 2: follow-up RNFLs were registered to the baseline, es-tablishing point-to-point correspondence between each follow-up RNFL and the baselineRNFL as the common template. In Row 2, RNFL thickness values are shown remappedonto the registered RNFLs. Row 3. Vertex-wise RNFL thickness difference between thebaseline and each follow-up RNFL. Row 4. Difference maps in Row 3 are shown normal-ized by the axial coherence length of the system.
Subject Eye Mean SD Medium SD SD at 95 percentile % of voxels withµm µm µm SD < 2l = 12µm
S1 OD 4.45 4.05 8.05 99.1OS 5.69 5.21 10.21 98.4
S2 OD 6.02 4.77 13.47 92.7OS 4.94 4.24 10.96 96.3
S3 OD 8.21 7.33 16.59 84.4OS 6.17 5.10 14.97 90.6
S4 OD 8.49 7.73 18.01 82.7OS 10.26 8.66 22.90 74.3
S5 OD 5.23 4.40 11.06 97.0OS 4.10 3.57 8.14 99.1
S6 OD 3.99 3.57 7.56 99.7OS 4.56 4.06 8.83 99.2
Table 5.3: RNFL thickness standard deviation
66

Figure 5.9: Voxel-wise time-average and standard deviation of RNFL thickness over 3weeks.
67

Figure 5.10: Histograms of RNFL thickness standard deviation.
68

Figure 5.11: Cumulative distribution function plots of RNFL thickness standard deviation.
69

Figure 5.12: RNFL thickness standard deviation map overlaid on enface images.70

Figure 5.13: Variability analysis of choroidal thickness over 3 weeks. Row 1: originalchoroidal thickness maps measured at 9 different time points (t0: baseline, t1 – t8: follow-up) in 3 weeks. Row 2: follow-up choroids were registered to the baseline, establishingpoint-to-point correspondence between each follow-up choroid and the baseline choroidas the common template. In Row 2, choroid thickness values are shown remapped ontothe registered choroids. Row 3. Vertex-wise choroidal thickness difference between thebaseline and each follow-up choroid. Row 4. Difference maps in Row 3 are shown normal-ized by the axial coherence length of the system.
Subject Eye Mean SD Medium SD SD at 95 percentile % of voxels withµm µm µm SD < 2l = 12µm
S1 OD 6.82 5.72 14.44 91.8OS 7.48 6.44 15.23 87.8
S2 OD 9.05 8.40 16.59 79.8OS 7.72 7.15 14.09 89.0
S3 OD 10.24 8.86 21.45 77.2OS 8.26 7.41 15.53 87.6
S4 OD 7.97 7.50 12.96 92.1OS 8.41 7.81 14.52 88.0
S5 OD 11.65 10.09 24.42 64.8OS 7.94 7.10 14.85 88.5
S6 OD 4.38 4.07 7.65 99.7OS 6.03 5.77 9.74 98.6
Table 5.4: Choroidal thickness standard deviation
71

Figure 5.14: Voxel-wise time-average and standard deviation of RNFL thickness over 3weeks.
72

Figure 5.15: Histograms of RNFL thickness standard deviation.
73

Figure 5.16: Cumulative distribution function plots of RNFL thickness standard deviation.
74

5.3 Atlas-based Shape Variability Analysis and Classification
of OCT Images using the Functional Shape (fshape) Frame-
work
The existing registration methods, including the one presented in the previous section,
register one OCT image or surface to another. In order to quantify the shape variability
among a group of OCT images using such a method, it is necessary to choose one as the
template, and the correspondence among the images is established by registering the rest
of the images to the chosen template. The choice of the template image or surface then
becomes a source of bias and influences the overall analysis result, while being often arbi-
trary and lacking in justification. This would be especially concerning in a cross-sectional
comparison where the eyes do not share the same shape features.
In this section, we propose a novel approach to analyzing variability in retinal OCT
images by the fshape framework [17]. The fshape, or functional shape, framework con-
siders a geometrical surface, such as a retinal layer surface, and functions defined on
the surface, such as retinal layer thickness, together as a single object. The “distance,”
i.e. the shape difference between two retinas, is measured by both geometry and one or
more physiological or morphological signals defined on the geometrical surface. This is a
conceptual departure from previous works in which the goal is to first establish anatomi-
cal correspondence between two eyes and then to compare the functional values at the
resulting corresponding locations.
There are several advantages to the fshape approach. First, the mathematical abstrac-
tion allows variability analysis, or comparison, beyond the frame of anatomy; given any
one or more surfaces and functional values, the fshape framework can measure the inter-
subject or inter-time point difference. This allows for combination of any number of features
- for example, ILM topology and total retinal thickness, BM topology with RNFL thickness,
or ILM and BM topology - and to investigate individually and jointly which features are
more (or less) differentiating between a disease and control group. The core of the fshape
framework is generation of a mean template of multiple fshapes. A hyper template is taken
as a simple model of a prototype fshape. This hyper template is evolved through an opti-
mization process that simultaneously minimizes i) geometric-functional distance from the
75

current template to the observations, and ii) dissimilarity between the transformed mean
template and the observations. This approach eliminates the need to choose one of the
existing data as a template, mitigating the issue of template selection and bias. In addition,
the fshape framework registration does not rely on specific anatomical or image features
based on prior knowledge. Given decent segmentation and measurements, the generality
and versatility of the algorithm allows it to be applied broadly and robustly.
5.3.1 Atlas Estimation
The central goal of the fshape framework is to recover the inter-subject variability both
in the geometry of the retina surfaces as well as in their signals (i.e the thickness maps).
This is unlike the more usual approach to image registration in which signals may be com-
pared directly on a common simple geometrical support. Following the standard process
in computational anatomy [98, 40, 121], the primary step is to estimate an atlas from the
population, which serves as a template object with the variation of the subjects in the pop-
ulation. The obvious difficulty in this situation is that both geometrical supports and func-
tional maps on the supports vary concurrently. To tackle this, we propose a methodology
based on the notion of functional shape or fshape introduced in our previous publications
[19, 18], which has the crucial advantage of treating both geometry and function together
while providing important flexibility for the algorithms. In the following sections we summa-
rize the major features of this approach and present the computational algorithms. More
complete mathematical presentations can be found in [19, 18].
Fshape spaces
In the fshape framework, a geometrical structure and its associated scalar field are
considered as a single object called a functional shape, or fshape, and its geometrical and
functional variations are processed jointly. Thus, in general, an fshape consists of a pair
(X, f) where X is the geometrical support, i.e a surface in the 3D ambient space, and f
is a function defined on this surface. In our particular application, the pair of a retinal layer
surface and a retinal layer thickness mapped on the surface is modeled as an fshape.
A particularly simple way to model a population of functional shapes is to consider
the ensemble as a set of surfaces generated by diffeomorphic deformations of a common
source surface X = G.X0 where G is a certain predefined group of deformations, and
76

functions defined on these shapes such that for a given X ∈ X , f is an L2 function on
the surface X (in the sense that the surface integral on X of f2 is finite). This eventually
defines a vector bundle of fshapes denoted F containing all objects of the form (X, f) with
X ∈ X , f ∈ L2(X).
In this frame, geometric-functional transformations of a given fshape (X, f) in the bun-
dle F simply consists in the combination of a deformation φ ∈ G and the addition of a resid-
ual function ζ ∈ L2(X) which gives the new fshape (Y, g).= (φ, ζ).(X, f) with Y = φ(X)
the deformed geometrical support and g = (f + ζ) φ−1 the new modified and transported
function on Y .
The main motivation of this model is that, provided the group of geometrical deforma-
tions is equipped with a certain metric dG, it becomes straightforward to measure now
distances between fshapes in F . One can simply take the minimal length of all paths
between them, which can be written as :
dF ((X, f), (Y, g))2 = inf(φ,ζ)
dG(Id, φ)2 + ‖ζ‖2L2(X)
∣∣φ(X) = Y, (f + ζ) φ−1 = g
(5.8)
Constructing relevant deformation groups and their metrics has been a wide field of study.
In this thesis, our reference model shall be the Large Diffeomorphic Metric Mapping (LD-
DMM) framework [4], where diffeomorphisms are constructed as flows of time-varying
vector fields of the 3D space belonging to a certain Hilbert space V , generally a repro-
ducing kernel Hilbert space. Given such a space V and the corresponding L2 space
of time-varying vector fields modeled on V , namely L2([0, 1], V ), one considers for any
v ∈ L2([0, 1], V ), the flow φv1 at time 1 and GV = φv1 | v ∈ L2([0, 1], V ) the associated
group of diffeomorphisms [193]. The Hilbert metric on vector fields induces in turn a Rie-
mannian metric on the group of deformations GV such that for any φ ∈ GV :
dG(Id, g)2 =
inf
∫ 1
0‖vt‖2V | v ∈ L2([0, 1], V ), φv1 = φ
(5.9)
Thus, in the LDDMM model, the optimization over φ ∈ G in (5.8) can be replaced by the
optimization on the space of time-varying deformation fields v. Combined with functional
variations, this provides fshape bundles spaces with a similar metric structure which has
several interesting properties, which are developed more thoroughly in [19].
77

Atlas formulation
Let us now consider a population of N observations (Xi, f i)i=1,..,N where the Xi’s are
the retinal surfaces and f i the corresponding thickness maps. One can introduce a gener-
ative model where the observations are obtained as geometric-functional transformations
of a common template fshape (X, f) plus some noise terms, such that:
(Xi, f i) = (φi, ζi).(X, f) + εi (5.10)
Above, (φi, ζi) are the hidden variables of transformations from the template to each sub-
ject, and εi are noise variables that must account for the fact that the observations cannot,
and in fact, should not, be obtained exactly as transformations of the template. The rea-
son is that real datasets present inter-subject variability caused by noisy irregularity in the
shape and signals, variations that do not result from the geometric-functional transforma-
tion model presented here. Defining such a noise model for textured surfaces is not trivial,
and it will be discussed further in the next subsection.
Under such a model, the purpose of atlas estimation is to recover from the observa-
tions both the template fshape (X, f) and the transformation variables (φi, ζi) which, as will
be described in a following section, enables to perform statistical analysis on population
variability or classification between different groups, for example. In a perfect noiseless
situation, this is the problem of computing a Karcher mean in the fshape bundle space F
generated from (X, f). With the presence of noise, one needs to relax the exact matching
conditions by introducing dissimilarity measures (also commonly referred as data attach-
ment terms) between two fshapes that do not necessarily belong to a common fshape
bundle. With an assumption that such a dissimilarity measure can be defined (this shall be
discussed in the next subsection) as a certain functional between the fshapes, the problem
of atlas estimation undertakes the following variational form :
(X, f, φi,∗, ζi,∗) =
arginfX,f,φi,ζi
N∑i=1
(dGV (Id, φi)2 + ‖ζi‖2L2(X)
+A((φi, ζi).(X, f), (Xi, f i))
)(5.11)
where GV is the group of geometrical deformations of the template modeled on the Hilbert
space V , and A the dissimilarity measure. The optimization is performed on the shape of
78

the template X, its mean thickness signal f in L2(X), the deformations φi (or equivalently
the deformation fields vi such that φi = φvi
1 ) and the residual signals ζi in L2(X). Each ith
observation contributes the sum of the geometric-functional transformation metric in (5.8)
and the measure of dissimilarity A between the transformed template and the observation.
The formulation above is only partly formal as it has not been specified in what space
the optimization over the template shape occurs. We refer the reader to [19] for a more
precise exposition on this topic as well as for the proof of existence of such variational
problems in a continuous setting. The following sections focus on the discrete equivalent
of the minimization problem and how it can be solved numerically.
Dissimilarity terms between fshapes
We first make a quick digression to define the dissimilarity functional A in (5.11), which
should also give some insight on interpretation of the noise variables in the generative
model of (5.10). Even in purely geometrical cases, establishing a dissimilarity measure for
practical applications is not a simple problem; one needs to establish a criterion of prox-
imity between surfaces without any point-to-point correspondence and of possibly different
topologies. In fshapes, the adjunction of signal functions defined on varying geometrical
supports presents a greater challenge.
For usual curves and surfaces, a widespread idea inherited from geometric measure
theory is to represent shapes as generalized distributions and induce metrics from these
distribution spaces. This has been consistently exploited in several past applications in
computational anatomy as in [57, 58, 40, 39, 41]. In all these examples, authors build upon
the concepts of current or varifold to embed geometrical shapes into common functional
spaces equipped with kernel-based Hilbert metrics.
Such frameworks can be naturally extended to the case of functional shapes, as suc-
cessfully demonstrated in [20] for currents and later in [19] for varifolds. The latter has
the advantage of not requiring any orientation for the shape surfaces and provides greater
robustness. In what follows, we give a brief simplified presentation of the fvarifold setting
detailed in [19].
79

In the fvarifold framework, a surface with signal is represented as a distribution of its
non-oriented normal vectors located at different positions in space and attached with cor-
responding real signal values. More precisely, any fshape (X, f) is considered as a distri-
bution µ(X,f) on the product space R3 × P (R3)×R, with P (R3) being the projective space
of all lines in R3, and is formally the sum of Diracs :
µ(X,f).=
∫Xδ(x,←→n (x),f(x))dH2(x) (5.12)
where←→n (x) denotes the (unoriented) line in P (R3) generated by the unit normal vector to
the surface X at point x, and H2 the usual 2-dimensional volume measure on the surface.
All possible fshapes are thus embedded into this common space of distributions.
As a functional space, distributions on R3×P (R3)×R can be equipped with various pos-
sible metrics or pseudo-metrics that can induce the dissimilarity criteria between fshapes.
Among these, the ones generated by positive kernels constitute a particularly interesting
category. For our purpose, positive kernels can be obtained as the product of three kernels
defined respectively on R3, P (R3) and R. If we denote them kg, kn and kf , it can be shown
we can induce a Hilbert (pseudo-) metric for any two fshapes (X, f) and (Y, g) :
〈µ(X,f), µ(Y,g)〉W ∗ =∫∫X×Y
kg(x, y).kn(←→nX(x),←→nY (y)).
kf (f(x), g(y))dH2(x)dH2(y) (5.13)
and A.= ‖µ(X,f) − µ(Y,g)‖2W ∗ = 〈µ(X,f) − µ(Y,g), µ(X,f) − µ(Y,g)〉W ∗ can be a suitable dis-
similarity term between (X, f) and (Y, g) (see [19] for an extensive presentation of the
properties of such metrics).
Depending on the choice for the kernels, various attachment terms are possible. As
apparent in (5.13), these do not assume any preliminary matching between the points
of X and Y or landmark extraction. Instead, kernel kg provides a spatial smoothness
to compare relative positions of the points on the two surfaces, and kernel kn allows to
compare relative positions of the normal vectors, while kf gives a measure of proximity
between the signal values attached to the fshapes. From now on, we shall take for kg a
Gaussian kernel on R3 of a certain scale σg, i.e.
kg(x, y) = e− |x−y|
2
σ2g .
80

A similar notion of a ’Gaussian kernel’ also exists on the more complex space P (R3) and
can be written as
kn(←→u ,←→v ) = e− 2
σ2n(1−〈−→u ,−→v 〉2)
for any unit vectors −→u and −→v generating the corresponding elements←→u ,←→v . Note that kn
is intrinsically independent of the orientations of the vectors −→u and −→v . The kernel width σn
is to be thought as a scale on the quotient sphere of unoriented unit vectors. Finally, the
last kernel kf can be also taken to be Gaussian
kf (a, b) = e− (a−b)2
σ2f
in which case (5.13) can be explicitly written as
〈µ(X,f), µ(Y,g)〉W ∗ =
∫∫X×Y
e− |x−y|
2
σ2g . e− 2
σ2n(1−〈−→nX(x),−→nY (y)〉2)
.
e− (f(x)−f(y))2
σ2f dH2(x)dH2(y) . (5.14)
The choice of Gaussian kernels is neither unique nor canonical; however, it results in
dissimilarity terms that are parameterized by three scales σg, σn and σf , allowing flexibility
and sensitiveness at various levels. Multiscale optimization can be easily facilitated by
combining different kernel values.
Discrete framework
A discrete representation of the functional surfaces is finite polyhedral surfaces with
signal values attached to each vertex. This can be expressed entirely by three matrices :
a P × 3 matrix x of the coordinates of the P vertices xk in R3, (x = (xk)1≤k≤P ), a P × 1
column vector f of the P values fk.= f(xk) ∈ R of the signal (f = (fk)1≤k≤P ), and
T × 3 connectivity matrix C that contains the list of T faces (assumed to be triangles for
simplicity) such that each row contains 3 integers corresponding to the indices of triangle
vertices.
The geometric-functional transformation on fshapes presented in 5.3.1 can be simply
translated to a discrete setting as follows. Given a discrete fshape (x,f), a diffeomorphism
φ, and a residual discrete signal ζ on the vertices of x, the transformation becomes :
(φ, ζ).(x,f) = ((φ(xk))1≤k≤P , (fk + ζk)1≤k≤P ) (5.15)
81

Note the connectivity matrix remains unchanged through the transformation. In such a
Lagrangian formulation, particles flow and transport their signals to new spatial locations.
The L2 norm of a signal ζ on a surface X in (5.8) may be approximated as
‖ζ‖2L2(X) ≈T∑l=1
f2l .|Tl| (5.16)
where for the lth triangle, |Tl| is the area of the triangle and f l is the average of the three
signal values at its vertices. This provides a Riemann sum approximation of the continuous
case. Higher order finite element approximations could be also used.
Similarly, the fvarifold-norm data attachment terms presented in 5.3.1 has a simple
discrete equivalent. The fvarifold associated with a polyhedral functional surface (x,f ,C)
can be associated with a finite sum of Diracs∑T
l=1 |Tl|.δ(xl,←→nl ,f l)
, where every triangle is
approximated by |Tl|.δ(xl,←→nl ,f l)
, xl being the barycenter, f l the mean signal value from the
three vertices, and ←→nl the unit unoriented normal vector to the triangle, obtained by the
wedge product of the two edge vectors. Now, given two discrete fshapes (x,f ,C1) and
(y, g,C2), the fvarifold data attachment term resulting from (5.14) approximates to :
A =
T1∑k=1
T1∑l=1
|Txk |.|Txl |.e− |xk−xl|
2
σ2g . e− 2
σ2n(1−〈←→nxk ,
←→nxl 〉
2). e− (fk−fl)
2
σ2f
−2
T1∑k=1
T2∑l=1
|Txk |.|Tyl |.e
− |xk−yl|2
σ2g . e− 2
σ2n(1−〈←→nxk ,
←→nyl 〉
2). e− (fk−gl)
2
σ2f
+
T2∑k=1
T2∑l=1
|T yk |.|Tyl |.e
− |yk−yl|2
σ2g . e− 2
σ2n(1−〈
←→nyk ,←→nyl 〉
2). e− (gk−gl)
2
σ2f (5.17)
The dissimilarity terms can be therefore computed based only on kernel evaluations be-
tween point positions, normal vectors, and signal values. However, this is numerically
expensive with the quadratic complexity of the number of triangles T1 and T2 of the two
surfaces. Several numerical methods can be implemented to provide fast computations
(see [18] Section 2.3.3 for a thorough discussion on the topic). For our application of
retinal surfaces, each consisting of approximately 20000 triangles, direct but massively
parallelized computations on GPU was chosen as the best trade-off between efficiency
and precision.
Lastly, we examine the discretization of the diffeomorphic transformations in the group
GV . As mentioned earlier, these can be parameterized by time-varying vector fields in
L2([0, 1], V ). This representation can be further reduced, since we are searching among
82

the optimal vector fields that link one given shape to another, or, in other words, among
geodesics in a certain Riemannian manifold of diffeomorphisms. As highlighted in re-
cent works in connection with optimal control theory, for example in [2], such geodesics
can be entirely described by the initial position and an initial momentum variable p0, and
the dynamics of the deformation is governed by a coupled system of Hamiltonian equa-
tions called the shooting equations. In the case of our discrete surfaces and V a cer-
tain RKHS of vector fields obtained by a vector kernel KV , this initial momentum can
be thought as a set of vectors p0 = (pk,0) attached to every vertex xk of the surface
for which v0(x) =∑P
k=1KV (xk, x)pk,0, and the reduced Hamiltonian undertakes the form
H(x,p) =∑n
k,l=1 pTkKV (xk, xl)pl. The shooting equations are then
x(t) = ∂pH(x(t), p(t))
p(t) = −∂xH(x(t), p(t))(5.18)
given the initial conditions x(0) = x and p(0) = p0. The resulting deformation is obtained
by flowing any initial condition x to time 1 through (5.18). An important consequence of
this is that the optimization of the template deformations φi in (5.11) can be formulated
as a minimization over initial momenta pi, all of which are made of a finite number of
vectors attached to the points of the template shape x. In addition, the energy of such a
deformation (given by the geodesic distance dGV ) can be also expressed based only on
the initial momentum p0 such that
dGV (Id, φv1)2 = H(x,p0) =
P∑k,l=1
pTk,0KV (xk, xl)pl,0. (5.19)
Numerical scheme for atlas estimation
The atlas estimation problem of (5.11) can be now formulated in the discrete setting.
The observations are N discrete fshapes given by xi, f i and the corresponding triangula-
tion matrices. The template is an fshape (x,f) given by a finite number of vertices, faces
and thickness values attached. The geometrical deformations of the template are summed
up by initial momenta variables pi, and the residual signals ζi are considered as vectors of
signal values attached to every template vertex, and thus of the same size as f . The final
83

form of the minimization functional is then as follows :
J(x,f , (pi), (ζi)).= γf .‖f‖L2 +
N∑i=1
(H(x,pi) + γζ‖ζi‖2L2
+γWA((φi, ζi).(x,f), (xi,f i))
)(5.20)
where ‖.‖L2 is given by (5.16),H(., .) by (5.19), and the dissimilarity termsA((φi, ζi).(x,f), (xi,f i))
by (5.14) and (5.15). γf , γζ and γW are strictly positive weighting coefficients leading to
different balance between the terms. Note that the additional presence of ‖f‖L2 (com-
pared to (5.11)) is to provide more regularity to the estimated template signal and it is also
a condition to guarantee the existence of solutions as explained in detail in [19].
Eventually, we are led to the problem of joint minimization with respect to all (finite-
dimensional) variables x,f , (pi), (ζi). This is still a very high-dimensional space since
each variable is roughly of dimension P , the number of template vertices, and the func-
tional J , essentially through the data attachment terms, fails from having any nice convexity
property. A reasonable approach to perform the actual optimization is a standard adaptive
step gradient descent on all variables simultaneously at each step. For this, one needs
to specify an initialization of the template fshape, denoted as xinit,f init, where the shape
given by xinit and its triangulation matrix should give a crude estimation of the observa-
tions, for instance, in global topology. Input initialization for the momenta and residual
signals pi and ζi is also needed, and it is often sufficient to set pi = 0 and ζi = 0. From
the expressions given above, computation of the gradient with respect to the variables
f = (fk)k=1,..,P and ζi = (ζik)k=1,..,P is quite straightforward and detailed in [19]. The gra-
dient with respect to the template position x and the momenta pi is slightly more involved.
‖f‖L2 , ‖ζi‖L2 and H(x,pi) can be easily differentiated with respect to x and pi, but the
dissimilarity metrics A((φi, ζi).(x,f), (xi,f i)) depends a priori on the deformed version
of the template, i. e. xi .= φi(x), f
i .= f + ζi. Each deformation φi is itself obtained
from x and pi by flowing forward in time the Hamiltonian equations (5.18). It has been
demonstrated in [40, 2] that the gradient of A((φi, ζi).(x,f), (xi,f i)) with respect to pi and
x can be computed by flowing backward in time the adjoint Hamiltonian system along the
trajectory of x and p :
Q(t) = −(∂2x,pH(x(t), p(t)))∗Q(t)
+(∂2x,qH(x(t), p(t)))∗P (t)
84

Algorithm 1 Atlas estimation on functional shapes
Require: N functional shapes (xi,f i), initialization of the template fshape (x = xinit,f =f init) and the gradient descent step δ.
1: set pi = 0 and ζi = 0 for all i ∈ 1, .., N.2: while Convergence do3: for i=1,..,N do4: Flow (x,f) by forward integration with pi and store the deformed template at time
1 (xi, fi).
5: Compute the gradients of ‖f‖L2 , H(x,pi), ‖ζi‖2L2 with respect to x, f , pi and ζi.
6: Compute the fvarifold representations of (xi,f i) and (xi, fi).
7: Compute the gradient ∇xiA((xi, fi), (xi,f i)) with respect to the final point config-
uration.8: Apply the backward integration of (5.20) and deduce ∇xA((xi, f
i), (xi,f i)) and
∇piA((xi, fi), (xi,f i)).
9: end for10: Update variables :
x← x+ δ∇xJ
f ← f + δ∇fJ
pi ← pi + δ∇piJ
ζi ← ζi + δ∇ζiJ
11: Compute new functional J(x,f , (pi), (ζi)) and possibly adapt step δ by line search.12: end while13: return template functional shape (x,f), N initial momenta (pi) and functional residu-
als (ζi).
P (t) = −(∂2p,pH(x(t), p(t)))∗Q(t)
+(∂2x,pH(x(t), p(t)))∗P (t) (5.21)
where the adjoint variablesQ and P are set with the end-time conditionsQ(1) = −∇xiA((xi, fi), (xi,f i))
and P (1) = 0. Then the gradients are∇xA((xi, fi), (xi,f i)) = −Q(0) and∇piA((xi, f
i), (xi,f i)) =
−P (0).
85
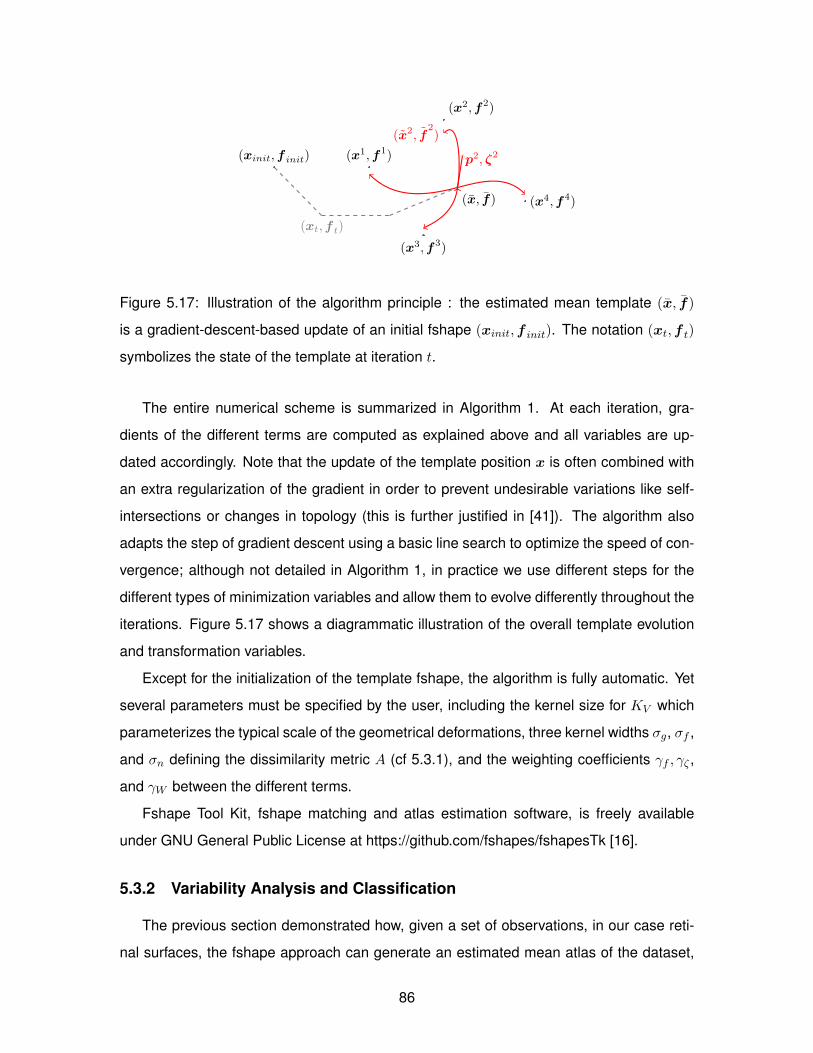
(xinit,f init)
(x, f)
(x1,f1)
(x2,f2)
(x2, f2)
(x3,f3)
(x4,f4)
(xt,f t)
p2, ζ2
Figure 5.17: Illustration of the algorithm principle : the estimated mean template (x, f)
is a gradient-descent-based update of an initial fshape (xinit,f init). The notation (xt,f t)
symbolizes the state of the template at iteration t.
The entire numerical scheme is summarized in Algorithm 1. At each iteration, gra-
dients of the different terms are computed as explained above and all variables are up-
dated accordingly. Note that the update of the template position x is often combined with
an extra regularization of the gradient in order to prevent undesirable variations like self-
intersections or changes in topology (this is further justified in [41]). The algorithm also
adapts the step of gradient descent using a basic line search to optimize the speed of con-
vergence; although not detailed in Algorithm 1, in practice we use different steps for the
different types of minimization variables and allow them to evolve differently throughout the
iterations. Figure 5.17 shows a diagrammatic illustration of the overall template evolution
and transformation variables.
Except for the initialization of the template fshape, the algorithm is fully automatic. Yet
several parameters must be specified by the user, including the kernel size for KV which
parameterizes the typical scale of the geometrical deformations, three kernel widths σg, σf ,
and σn defining the dissimilarity metric A (cf 5.3.1), and the weighting coefficients γf , γζ ,
and γW between the different terms.
Fshape Tool Kit, fshape matching and atlas estimation software, is freely available
under GNU General Public License at https://github.com/fshapes/fshapesTk [16].
5.3.2 Variability Analysis and Classification
The previous section demonstrated how, given a set of observations, in our case reti-
nal surfaces, the fshape approach can generate an estimated mean atlas of the dataset,
86

along with the geometrical and functional distances from the template to each of the ob-
servations. A group average retina in itself is useful for purposes such as qualitative and
quantitative group comparisons. The shape and signal distances of individual observations
can serve as metrics for inter-eye variability.
Augmenting the fshape framework with a classification module is thus a natural ex-
tension with several merits. On experimental data with confirmed diagnosis, automated
classification can demonstrate the mean template-based variability of retinas has indeed
anatomical and clinical relevance. Furthermore, a classification module can determine
whether a particular anatomical feature, thickness or topology of a layer, is significantly
correlated with a disease. This can lead to better understanding of the structural mani-
festation of the disease in terms of cause or effect. Lastly, automated classification is an
example of the fshape framework application that can directly assist in clinical decision
making.
The initial momenta (pi) and functional residuals (ζi) in 5.3.1, representing the retinal
layer surface topology and associated retinal layer thickness respectively, are used for clas-
sification. Two classificaiton methods were tested: a set of Weka 3 software modules [68]
performing feature selection based on information gain followed by a support vector ma-
chine classification (InfoGainSVM), and a tunable variation of linear discriminant analysis
(LDA) classifier. The LDA classifier is described in the following subsections.
Regularized LDA on Hilbert space valued dataset
LDA is a classic linear classification method that may be viewed as a weighted principal
component analysis (see chapter 4 of [70] for an introduction). We discuss hereafter the
particular case in which the data points x1, · · · , xN belong to a separable Hilbert space H
of a possibly infinite dimension. As mentioned, in our particular application, the xi’s will be
functional residuals and/or the geometrical initial momenta.
Within- and between-class scatter operators We assume that the N observations at
hand are divided into K classes C1, · · · , Ck such that 1, · · · , N =⋃Kk=1Ck. The mean of
the k-th class is xk = 1Nk
∑i∈Ck xi where Nk = Card(Ck). Let us define the within-class
scatter operator Sw : H → H
87

Sw(·) =1
N
K∑k=1
∑i∈Ck
〈xi − xk, ·〉H (xi − xk)
and the between-class scatter operator Sb : H → H
Sb(·) =1
N
K∑k=1
Nk〈xk − x, ·〉H (xk − x) .
In the case where H is of finite dimension, the matrix associated to the operator Sw (or Sb)
is the standard within-class (or between-class) scatter matrix.
Finite dimensional representation We denote H0 = Span (xi, . . . , xN ) ⊂ H and q =
dim(H0). In our framework, H is high (or infinite) dimensional, and, in practice, q equals to
N . We then denote fH0 : H0 → H0 the restriction to H0 of any linear mapping f : H → H
such that f(H0) ⊂ H0. In particular, we may consider the restrictions Sw,H0 and Sb,H0 of
the scatter operators Sw and Sb, respectively.
Let us now choose an arbitrary isometric linear mapping L : H0 → Rq in order to get a
finite representation of the data
xi = Lxi ∈ Rq.
By definition we have ‖xi‖Rq = ‖xi‖H . From now on, we will work with this new represen-
tation of the data and we may consider their corresponding scatter operators Sw, Sb : Rq →
Rq defined as,
Sw = LSw,H0L† and Sb = LSb,H0L
†,
where L† : Rq → H0 is given by 〈L†a, x〉H = 〈a, Lx〉Rq for any x ∈ H0 and a ∈ Rq.
When the xi’s form a basis of H0, an effective way to build an isometric mapping L is
to introduce the mapping γ(x) = (〈x, xi〉H)Ni=1 for any x ∈ H0 and the Gram matrix G =
[〈xi, xj〉H ]Ni,j=1 ∈ RN×N . It is then easy to check that the linear mapping Lx = G−12γ(x) is
isometric.
Discriminant axes in the finite dimensional space In our framework, the within-class
scatter operator Sw may not be invertible in general. We consider the following regulariza-
tion of the within-class scatter operator
Sεw = Sw + εIdRq , (5.22)
88

where ε > 0 is a regularization parameter which has to be calibrated by the user as de-
scribed below.
The discriminant spaces of the LDA are given by the eigendecomposition of
Aε = (Sεw)−1Sb.
The number of non-vanishing eigenvalues is limited by the rank of Sb which is less than
K − 1. In general, we have the K − 1 corresponding unit eigenvectors u1, . . . , uK−1 ∈ Rq
that will be used to derive the discriminant axes in H.
Classification with regularized LDA The rationale behind the isometric dimension re-
duction is that the unit vectors
u` = L†u` ∈ H0, ` = 1, . . . ,K − 1
are the eigenvectors corresponding to the non-vanishing eigenvalues of AεH0= (Sw,H0 +
εIdH0)−1Sb,H0 , as in [49]. This classic trick avoids numerical issues as the matrix inversion
is performed in the small dimensional space Rq.
Then, given a new observation y ∈ H we use directly the discriminant axes u1, . . . , uK−1
to define a classification rule. For instance, when K = 2 (a two-class classifier) we have
u1 ∝ (Sεw)−1(x1 − x2) where the ∝ symbol means “collinear to”. The discriminant rule is
then a threshold on y → 〈u1, y − x〉H .
Calibration of the regularization parameter The regularization parameter ε > 0 can be
optimized with a leave-p-out cross-validation (CV) procedure. Note that we do not need
to compute the Gram matrix G appearing in the definition of the isometric mapping L at
each stage of the CV. This is very helpful since the operation may be costly depending on
the magnitude of N . Instead, the N ×N “full” Gram matrix Gf with all the observations is
computed once, and the (N − p)× (N − p) Gram matrices G are obtained by deleting the
p rows and columns of Gf corresponding to the p left-out observations.
In our simulations, surprisingly small values of the regularization parameter ε, ranging
from 0.001 to 1, generally yielded better CV results. We provide below a short analysis on
the LDA behaviour for small values of ε.
Let H1 ⊂ H0 be the linear subspace of H defined by
H1 = Sw(H) = Span xi − xk|1 ≤ k ≤ K, i ∈ Ck
89

Figure 5.18: (a) Aligned RNFL surfaces with RNFL thickness mapping, (b) mean templateof all RNFLs, (c) mean template of normal RNFLs only, and d) mean template of glauco-matous RNFLs only. Note the low estimated RNFL thickness of the mean glaucomatoustemplate as compared to that of the mean normal template.
Figure 5.19: Observed RNFLs (top row) and their reconstructions from a common meantemplate (bottom row). Note that the reconstruction agrees with the pattern of the originalRNFL thickness with an overall smooth and noise-reduced profile.
Denoting pH⊥1 : H → H the linear projection onto the linear space orthogonal to H1, it can
be shown that
limε→0
ε(Sεw)−1Sb = pH⊥1Sb.
The limit is taken here in the sense of the operator norm ‖f‖ = maxx,‖x‖H=1 ‖fx‖H
for any linear f : H → H. This indicates when the chosen ε > 0 is small, discriminant
information is found orthogonal to the within-class variations. In particular, when K = 2
and ε vanishes, the discriminant axis is u1 ∝ pH⊥1 (x1 − x2).
90

5.3.3 Experimental Results
Peripapillary OCT images from 53 eyes with confirmed diagnosis from 10 controls, 10
bilateral glaucoma patients, and 7 unilateral glaucoma patients were included in the exper-
iment. Written consent forms were obtained from all participants and ethics review was
approved by the Office of Research Ethics at Simon Fraser University (SFU) and the Re-
search Ethics Board of the University of British Columbia (UBC). In addition to OCT imag-
ing, all participants were subject to a battery of standard tests, including dilated stereo-
scopic examination of the optic nerve, stereo disc photography analysis and visual field
abnormality check, to ensure there was no other pathology present. The acquired im-
ages were smoothed, segmented, and measured for retinal layer thickness as described
in Chapter 3 and 4.
Mean template generation
The mean templates of retinal nerve fiber layer (RNFL) posterior surfaces and associ-
ated RNFL thickness maps were generated as described in Section 5.3.1. The surfaces
were aligned at the BMO centroid prior to the mean template generation, as shown in in
Fig. 5.18 (a). The physical dimensions of the images vary as the imaging field of view
changes depending on the axial length of the eye. Fig. 5.18 (b), (c), and (d) respec-
tively show the mean templates generated from all eyes (N = 53), bilaterally normal eyes
(N = 20), and glaucomatous eyes (N = 26). Qualitatively, the normal mean template in
Fig. 5.18 (c) displays the characteristic hourglass pattern in RNFL thickness, whereas the
glaucomatous mean template in Fig. 5.18 (d) show much thinner RNFL thickness overall,
with superior peripapillary RNFL slightly more preserved compared to the inferior region.
Fig. 5.19 shows the observed RNFL surfaces (top row) and their approximations (bot-
tom row) from a common mean template of 53 RNFLS in Fig. 5.18 (b). As described in the
previous section, the ith approximation is a deformed version of the template, such that
xi.= φi(x), f
i .= f+ζi. The salient shape features are reproduced, in particular the RNFL
thickness pattern and the BMO location and size. The level of detail in approximation can
be tuned by user specified parameters including kernel sizes for geometric deformation
and dissimilarity metric, and runtime parameters in the gradient descent optimization.
91

Figure 5.20: Functional convergence with gradient descent optimization.
Figure 5.21: Left: Voxel-wise t-test significance map of retinal nerve fiber layer (RNFL)thickness between normal (N = 26) and glaucomatous (N = 27) eyes, with the red regionindicating p < 0.05. Right: The same map with the log of the p-value.
Fig. 5.20 shows the convergence of the minimization functional (5.20) in computing the
mean template of 53 RNFLs in Fig. 5.18 (b) with the adaptive gradient descent optimization
process in Section 5.3.1. In the actual computation, the algorithm was run with three sets of
different kernel sizes for σg, σf , and σn. This allowed refinement of the result by reducing
the kernel sizes at successive runs with each ending at either reaching the predefined
maximum number of iterations per run or minimum change of the functional value with the
given set of parameters.
In Fig. 5.20, the first run begins at Iteration 0 with the functional value at 1.34 × 104
and ends at Iteration 40 with the energy reduced to 2.47 × 103. The second run begins at
Iteration 41 with a new set of kernel sizes and the starting functional evaluated at 1.28 ×
103. This run ends at Iteration 44 because ∆J becomes less than the preset minimum of
10−4. The third run begins at Iteration 45, again with smaller kernel sizes, and the energy
stabilizes around 6.94× 102.
92

T-test between healthy and glaucomatous RNFL thickness residuals
The mean templates of the normal (c) and glaucomatous (d) RNFLs in Fig. 5.18 qual-
itatively show the difference between the two groups. In order to identify the spatial loca-
tions of the thickness difference, a vertex-wise t-test was performed using the functional
(thickness) residual ζi, the vertex-wise thickness offset between the template and its ap-
proximation of the ith observation. The t-test compared the means of the residuals of 26
normal RNFLs and 27 glaucoma RNFLs at each voxel on the mean template of all RNFLs
in Fig. 5.18 (b).
The result is shown in Fig. 5.21. On the left, the voxels with p-values less than 0.05
are marked in red and indicate the regions with statistically significant RNFL thickness dif-
ference between the normal and glaucomatous RNFLs. Most of the peripapillary region
shows significance, except at the image boundaries, where the f-shape correspondence
may be less reliable due to the different imaging field of view size, and in the region immedi-
ately temporal to BMO. More interesting pattern is shown in the right image, which displays
the log of the p-value. Cooler colors indicate smaller p-values and greater statistical sig-
nificance across the multiple RNFLs. The figure shows that glaucomatous thinning occurs
most distinctly in the inferior-temporal region of the RNFL, which agrees with previous stud-
ies [146, 135, 9, 101, 200] that the inferior peripapillary region is the most distinguishing
between normal and glaucomatous eyes, especially in the early stage of the disease. Un-
like the previous studies, however, our analysis shows full spatial detail without averaging
in sectors, and reveals a clear pattern of statistical significance that resembles the charac-
teristic thickness pattern of a healthy RNFL. The result suggests that the most significant
amount of glaucomatous thinning, or the earliest of the thinning, may occur along the RNFL
ridges where the RNFL is naturally the thickest.
Classification
As described in Section 5.3.2, classification experiments were performed using Weka
InfoGainSVM and LDA classifiers, on the momenta pi, which represents the vertex-wise
geometric deformation of the template to the ith observation, and functional residuals
ζi, the vertex-wise thickness offset between the template and the approximation of the
93

Figure 5.22: Leave-one-out cross validation accuracy with varied regularization parameterε.
ith retina. For each experiment, the LDA classifier was trained by leave-one-out cross-
validation, with the best-performing regularization parameter ε chosen from values by test-
ing 0.001 to 1 as shown in Fig. 5.22.
Healthy vs. Glaucoma Age-matched (59.6 ± 6.7) normal (N = 10) and glaucomatous
(N = 18) RNFLs were classified with the result in Table 5.5. Both Weka and LDA mod-
els yielded high classification rates, with the LDA model classifying a test sample drawn
from the data 144 times with no error. The result indicates that the fshape metrics of
the peripapillary RNFL posterior surface and RNFL thickness can be used to predict the
clinical diagnosis of glaucoma with high accuracy, and confirms the connection between
vision loss that bases glaucoma diagnosis, and characteristic morphological changes in
the RNFL.
Healthy vs. Suspect Glaucoma is generally bilateral, affecting both eyes of the patient,
and often asymmetric, such that the affected fellow eyes exhibit different degrees of sever-
ity. In unilateral primary glaucoma in which only one eye is diagnosed with glaucoma, the
healthy fellow eye is at a greater risk of developing glaucoma in the future than healthy
eyes of bilaterally normal subjects [104, 180]. Based on this, we labeled 7 healthy fel-
low eyes from unilateral glaucoma cases as suspect, and attempted to detect these from
healthy eyes of bilaterally nonglaucomatous subjects. The classification result of the bilat-
erally healthy eyes (N = 19, mean age: 43.4± 14.8) and suspect eyes (N = 7, mean age:
57.1± 12.4) are shown in Table 5.5.
94

Method Accuracy (%) Sensitivity (%) Specificity (%)
Healthy vs. GlaucomaWeka 94.23 94 90LDA 100.00 100.00 100.00
Healthy vs. SuspectWeka 83.10 83 76LDA 91.67 88.89 92.59
Table 5.5: Accuracies, sensitivities, and specificities of the classification of healthy, glauco-matous, and suspect RNFLs
Figure 5.23: LDA classifier for Healthy vs. Glaucoma data in A) functional residual, B)initial momenta in x-direction, C) initial momenta in y-direction, and D) initial momenta inz-direction.
That both models appear to distinguish the suspect eyes from the bilaterally healthy
eyes is noteworthy, considering that the suspect eyes are prediagnosis and without func-
tional loss or other conventional clinical features of glaucoma. As expected, the classifi-
cation rates are lower than those between confirmed glaucomatous eyes and bilaterally
healthy eyes in the previous experiment, but still high, particularly with the LDA model
of 88.89% sensitivity and 92.59% specificity. The result suggests the fshape metrics may
capture some subtle morphological changes in the RNFL that precedes vision loss in glau-
coma.
In LDA classification, an intuitive way to understand the result is to visualize the classi-
fier, or the direction that yields the maximum between-class variance. The LDA classifier
for the Healthy vs. Glaucoma dataset is visualized in Fig. 5.23 on the mean template
95

Method Accuracy (%) Sensitivity (%) Specificity (%)
Healthy vs. Glaucoma, RNFL thickness onlyWeka 93.99 94 97LDA 100.00 100.00 100.00
Healthy vs. Glaucoma, RNFL posterior surface geometry onlyWeka 81.43 81 70LDA 81.94 84.04 78.00
Table 5.6: Accuracies, sensitivities, and specificities of the classification of healthy andglaucomatous RNFLs by RNFL thickness only and RNFL posterior surface geometry only
RNFL, in functional residual (RNFL thickness), and x, y, and z coordinates of initial mo-
menta representing the template deformation. The relative magnitude can be interpreted
as the degree of contribution to the classification, and it can be seen that RNFL thickness
was a more decisive factor in the classification of healthy and glaucomatous eyes than
posterior RNFL surface geometry. The map in Fig. 5.23 A, which is the spatial pattern
of classification contribution of RNFL thickness residual, is similar to the right image of
Fig. 5.21, which is the statistical significance map of the group difference between the two
classes. This confirms that the LDA classification was the most influenced by the regions
where there are the most significant difference between the healthy and glaucomatous
eyes.
RNFL thickness vs. RNFL surface geometry In order to compare the discriminating
power of RNFL thickness against RNFL posterior surface geometry, and to confirm what
was shown in Fig. 5.23, we repeated the Healthy vs. Glaucomatous classification with
RNFL functional residual (RNFL thickness) and initial momenta (RNFL posterior surface
geometry) separately. The result is summarized in Table 5.6.
As expected from Fig. 5.23, the classification result with RNFL thickness only is com-
parable to that with both RNFL thickness and geometry, and superior to the result with
RNFL geometry only. However, it is interesting to note that posterior RNFL surface without
the thickness information appears to still discriminate the healthy and glaucomatous eyes
to some degree. This, along with the characteristic pattern in Fig. 5.21, suggests that the
magnitude of RNFL thinning in glaucoma is not uniform across the peripapillary region,
and the surface topology is altered along with the overall reduction in tissue volume.
96

Method Accuracy (%) Sensitivity (%) Specificity (%)
Healthy vs. Glaucoma, unregistered RNFLWeka 84.52 85 79LDA 95.83 98.13 89.19
Healthy vs. Suspect, unregistered RNFLWeka 74.29 74 47LDA 89.58 80.00 74.31
Table 5.7: Accuracies, sensitivities, and specificities of the classification of healthy, glauco-matous, and suspect RNFLs based on unregistered RNFLs
Classification with unregistered RNFLs The above classifications for Healthy vs. Glau-
coma and Healthy vs. Suspect were repeated with the same eyes, but instead of the fshape
metrics of the RNFL thickness residual and initial momenta, the original RNFL thickness
and RNFL posterior surface point coordinates were used. The result in Table 5.7 shows
relatively high classification success rates, but compared to the results in Table 5.5, all
accuracies, sensitivities, and specificities are consistently lower for both Weka and LDA
models. The specificity values are especially lower, indicating that the fshape metrics were
able to reduce the number of false positive classifications with the unregistered original
data.
5.3.4 Discussion
We present a novel application of the powerful fshape framework that can simulta-
neously compute the variability in shape and associated signals in retinal optical coher-
ence tomography (OCT) images. Fshape-based analysis and classification was performed
on healthy and glaucomatous peripapillary retinal nerve fiber layers (RNFL). The fshape
framework enabled creation of a mean atlas RNFL surface and RNFL thickness from mul-
tiple eyes, and quantification of the difference among the observed RNFLs with the mean
template as the reference. This approach is a compelling and complementary improvement
to the conventional sector analysis of the retina, and it has a potential for broad applica-
tion in studying longitudinal changes and cross-sectional differences in both anatomy and
physiological signals. Below we discuss few of the details involved in successfully applying
the algorithm for OCT data.
The fshape framework extracts the shape and signal variability in a given data, but
prior knowledge of the cause of the variability is important in preprocessing the data and
97

interpretation of the result. For example, there were several artifactual shape discrepancies
in the original OCT images used in this thesis. The image field-of-view size varied for
each retina due to the eye’s axial length. Bruch’s membrane opening (BMO) was only
approximately centered relative to the image frame, and the axial position of the RNFL
relative to the image frame varied. Since we were specifically interested in shape variability
due to pathology, the input data was preprocessed prior to the fshape pipeline in order to
reduce such unwanted noise and to minimize its effect in the result. Before the experiment,
it was confirmed that there was no correlation between presence or severity of glaucoma
and the subject’s axial lengths or the relative BMO position. The surfaces were therefore
aligned at the BMO center, as shown in Fig. 5.18 a), to bring them as close as possible
with each other without altering the surface topology. Additionally, RNFL within 0.25 mm
from BMO was excluded, because the exact termination point of the layer in the region
is often ambiguous. The input surfaces were then concentric with respect to BMO and
centrally overlapping, but the outer edges were mismatched due to the differing image
size, which is visible in Fig. 5.18 a). Whereas BMO is a true anatomical structure and a
valid registration landmark, the image boundary is purely artificial except in its relation to
the subject’s axial length. We were therefore wary that a mean template and estimated
momenta at the boundary region would be affected by this mismatch. This may also have
confounded the classification as the momenta and functional residuals at the boundary
have less spatial correspondence across the eyes. However, the regions near the outer
boundary also make the least contribution to the classification of healthy and glaucomatous
eyes, as it can be seen in Fig. 5.21 and 5.23. One way to possibly mitigate the boundary
effect is to crop the images, for example, to the largest commonly overlapping region. The
disadvantage is that this could waste a significant amount of data, and the cropping must
be done in a way that does not introduce artificial bias.
Choosing a good initial hyper template is also important in the computation and quality
of the final mean template. The hyper template must be topologically equivalent to the
observations, and as unbiased as possible. An implicit assumption is that the observations
from which a mean template is generated are topologically similar. Retinal layer surfaces in
OCT images can be modeled in relatively simple shapes; a surface from the macular region
is a 3D planar surface, and a surface from the peripapillary region with optic cup in the
center is a 3D planar surface with a hole in the center. In these cases, a prototype template
98

can be generated without difficulty, and even incorporate simple pre-measurements such
as the average width and length of the observed layers. However, complex structures like
lamina cribrosa can pose a greater challenge in choosing a suitable hyper template.
A potential application of the fshape framework is to create population-based normative
atlases of the retina using large data cohorts. Statistical distribution of the retinal morphol-
ogy in healthy subjects can be computed voxel-wise on the atlas. A test subject’s retina can
then be compared to the atlas to quantify its deviation from the healthy mean, and assess
the disease risk or severity based on the population statistics. Such comparison of a tar-
get subject to an existing atlas would require matching. In matching of a template fshape
(X, f) and a target fshape Xt, f t, the purpose is for the template to approximate the target
as closely as possible, and to obtain the distance between the two by the deformation φt
and functional residual ζt of the approximation. This is written as the minimization of the
functional
(φt, ζt) = arginfφt,ζt
dGV (Id, φt)2 + ‖ζt‖2
L2(X)
+A((φt, ζt).(X, f), (Xt, f t))
and similarly to Eq. 5.11, GV is the the group of geometrical deformations of the template
on the Hilbert space V , and A is the dissimilarity measure between the target and the tem-
plate approximation. Unlike the atlas estimation, the optimization in matching is performed
only on φt and ζt which can be done exactly as explained in Section 5.3.1. Such matching
would also allow one to directly compare one mean template to another.
Future work will include a comprehensive investigation of the optic nerve and macular
morphology in a larger data using the fshape and classification modules presented here.
The goal is to better detect and understand the shape changes or differences correlated to
diseases such as glaucoma. In this report only RNFL was examined, but any other retinal
layer can be similarly analyzed, in any combination of layers, surface topology, thickness,
etc. Shape and signal from multiple eyes will be made comparable by a common atlas, and
significance of a metric, region, or anatomical structure can be tested by statistical analysis
including the classification modules above. In this work the mean template generation
and classification process yielded convincing results despite of the mismatch between the
RNFL sizes and relative BMO locations. Another direction of future research is to apply the
fshape framework to structures like lamina cribrosa, which is not only more topologically
99

complex but also much less consistently visible across eyes than retinal layers. It may be
possible that the combined framework can extract common shape information from multiple
lamina cribrosa images with varying and limited visibility.
5.4 Summary of contributions
The contributions described in this chapter and published in [113] and submitted for
publication in IEEE Transactions on medical Imaging:
• Surface-to-surface registration of retinal surfaces by current-based approximation fol-
lowed by spherical demons registration.
• Repeatability analysis of BMO shape and RNFL and choroidal thickness in healthy
subjects using the surface-to-surface registration.
• Atlas-based shape analysis and classification of retinal surfaces using the fshape
framework
A manuscript is in preparation for publication on the repeatability analysis.
100

Chapter 6
Optic Nerve Head Morphometrics in Myopic
Glaucoma
The pathophysiology of glaucoma, although not fully understood, involves damage to
the retinal ganglion cell axons at the level of the lamina cribrosa [156, 155, 5]. Uncon-
trolled intraocular pressure (IOP) likely triggers several parallel, but interacting, mecha-
nisms including direct axonal damage, disturbances in neuro-metabolism and microvas-
cular supply, glial activation, and extensive remodeling of the connective tissues of the
lamina cribrosa and surrounding tissues throughout the development and progression of
glaucoma [154, 131, 75, 13, 28, 145, 168, 169, 30, 64, 65, 185]. The peripapillary tissues
that surround the optic nerve itself have also been implicated as possible contributors to
glaucomatous changes, both in experimental and modeling studies [36]. Atrophic features
of the peripapillary tissues which appear to be associated with glaucoma can include thin-
ning of the peripapillary scleral tissue [189], and loss of almost all retinal and deeper layers
separating the subarachnoid space from the vitreous cavity [37].
Myopia presents unique challenges for the management of glaucoma. Population-
based studies have indicated a greater prevalence of glaucoma in myopes [133, 188]. The
shallow cupping and pale neuro-retinal rim of high myopia make optic nerve head assess-
ment difficult. Myopic individuals can show abnormal results on structural and functional
testing because normal databases are composed of individuals with low refractive error
[45, 134]. Coexisting pathologies, particularly myopic degeneration, cloud interpretation
of visual field changes in advanced glaucoma. Cup-to-disk ratio and retinal nerve fiber
layer (RNFL) thickness measured by commercial optical coherence tomography (OCT)
101

and confocal scanning laser ophthalmoscopy (CSLO) were shown to be less effective in
discriminating glaucomatous and nonglaucomatous subjects with high myopia [130], with
several studies reporting RNFL thinning associated with myopia [81, 102, 171]. There are
theoretical grounds to suggest that myopic eyes may be more sensitive to a given IOP as
a result of the larger globe size and thinner, more compliant tissues [142, 172, 182].
In studies comparing highly myopic glaucomatous eyes to non-highly myopic glauco-
matous eyes, the former showed significant histological difference in the peripapillary re-
gion including elongation and thinning of the scleral flange [96]. Comparison of colour
stereo optic disc photography showed more pronounced optic nerve damage, larger and
more elongated optic discs, and shallower optic cups in myopic glaucomatous eyes [91,
92, 34].
To further understand the features of the myopic optic nerve in glaucoma, we have
imaged the optic nerve and surrounding peripapillary tissues in myopes, both with and
without glaucoma, and performed quantitative shape measurement and analysis.
6.1 Participants
A total of 27 subjects were recruited for this study: 5 young healthy controls (10 eyes,
mean age = 29.8 ± 3.6), 5 older healthy controls (10 eyes, mean age = 57.0 ± 4.4), 7
patients with unilateral glaucoma (14 eyes, mean age = 57.2 ± 12.4), and 10 patients
with bilateral open-angle glaucoma (19 eyes, mean age = 55.7 ± 12.6). Ethics review for
this study was approved from Simon Fraser University (SFU) and from the University of
British Columbia (UBC). The study was conducted in accordance with the guidelines of the
Declaration of Helsinki, and informed consent form was obtained from each participant.
All participants had axial lengths greater than 24 mm. A diagnosis of open-angle glau-
coma was made clinically by a fellowship-trained glaucoma specialist based on full exam-
ination including dilated stereoscopic examination of the optic nerve, analysis of stereo
disc photography, and typical reproducible Humphrey SITA-Standard white on white visual
field abnormality. No reference to OCT images was made for the purposes of categorizing
subjects for the study. Severity of glaucomatous visual field loss was quantified by Visual
Field Mean Deviation (MD) values. Participant demographics are tabulated in Table 6.1.
102
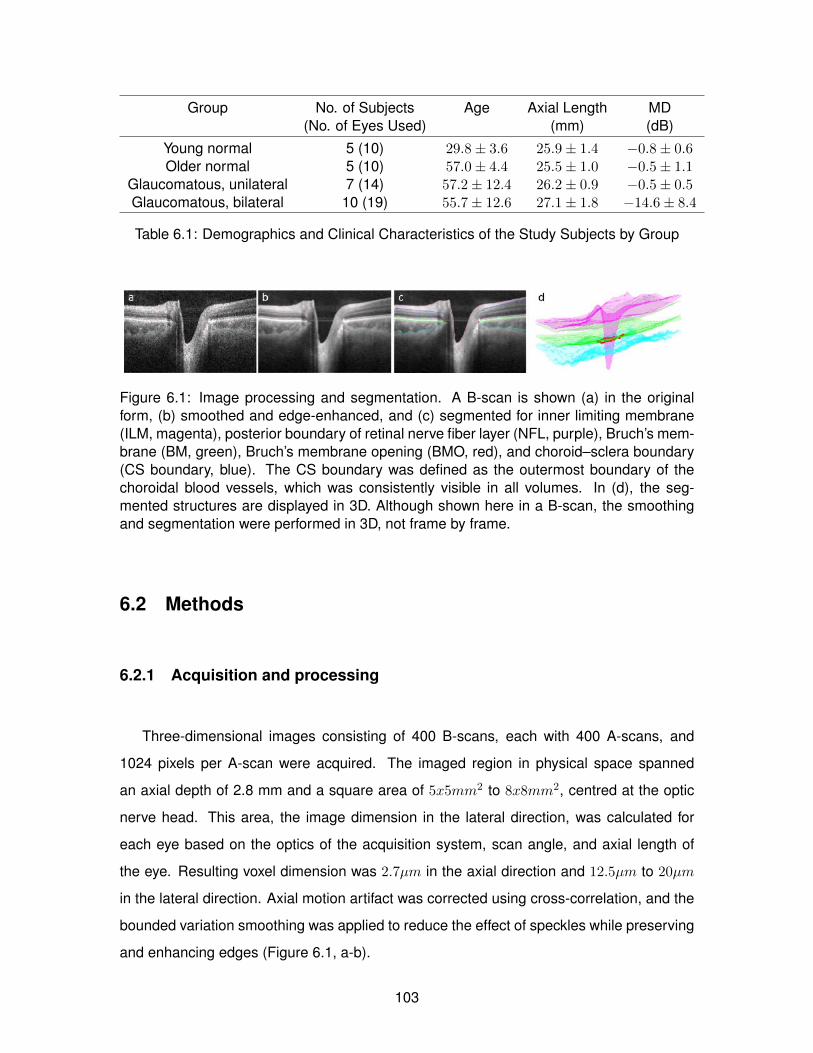
Group No. of Subjects Age Axial Length MD(No. of Eyes Used) (mm) (dB)
Young normal 5 (10) 29.8± 3.6 25.9± 1.4 −0.8± 0.6Older normal 5 (10) 57.0± 4.4 25.5± 1.0 −0.5± 1.1
Glaucomatous, unilateral 7 (14) 57.2± 12.4 26.2± 0.9 −0.5± 0.5Glaucomatous, bilateral 10 (19) 55.7± 12.6 27.1± 1.8 −14.6± 8.4
Table 6.1: Demographics and Clinical Characteristics of the Study Subjects by Group
Figure 6.1: Image processing and segmentation. A B-scan is shown (a) in the originalform, (b) smoothed and edge-enhanced, and (c) segmented for inner limiting membrane(ILM, magenta), posterior boundary of retinal nerve fiber layer (NFL, purple), Bruch’s mem-brane (BM, green), Bruch’s membrane opening (BMO, red), and choroid–sclera boundary(CS boundary, blue). The CS boundary was defined as the outermost boundary of thechoroidal blood vessels, which was consistently visible in all volumes. In (d), the seg-mented structures are displayed in 3D. Although shown here in a B-scan, the smoothingand segmentation were performed in 3D, not frame by frame.
6.2 Methods
6.2.1 Acquisition and processing
Three-dimensional images consisting of 400 B-scans, each with 400 A-scans, and
1024 pixels per A-scan were acquired. The imaged region in physical space spanned
an axial depth of 2.8 mm and a square area of 5x5mm2 to 8x8mm2, centred at the optic
nerve head. This area, the image dimension in the lateral direction, was calculated for
each eye based on the optics of the acquisition system, scan angle, and axial length of
the eye. Resulting voxel dimension was 2.7µm in the axial direction and 12.5µm to 20µm
in the lateral direction. Axial motion artifact was corrected using cross-correlation, and the
bounded variation smoothing was applied to reduce the effect of speckles while preserving
and enhancing edges (Figure 6.1, a-b).
103

6.2.2 Segmentation
Inner limiting membrane (ILM), the posterior boundary of nerve fiber layer (NFL), Bruch’s
membrane (BM), Bruch’s membrane opening (BMO), and the choroid–sclera boundary
(CS boundary) were segmented for this study (Figure 6.1 c). The automated segmenta-
tion result was examined and corrected by a trained research engineer using a custom
script in Amira (version 5.2; Visage Imaging, San Diego, CA, USA). Segmented surfaces
were overlaid on the original grayscale image and viewed simultaneously in three separate
orthogonal planes for better visualization of the structural boundaries obscured by blood
vessel shadows. The rater was able to scroll back and forth through the volume in any one
of the three orientation views while the other two orthogonal views and location pointers
were slaved and updated accordingly.
Bruch’s membrane opening was defined as the termination point of the high-reflectance
BM/retinal pigment epithelium (RPE) complex on the OCT image (Figure 6.1 c). This
corresponds to a pigmented and thus clinically identifiable structure, or a nonpigmented
and thus clinically invisible structure [161, 22]. The BMO was segmented manually by a
trained research engineer on 40 radial slices extracted from the volume, intersecting at the
approximated center of the BMO and spaced at a constant angle of 4.5 degrees.
6.2.3 Measurements
Seven shape characteristics were defined and measured on the segmented ILM, NFL,
BM, BMO, and CS boundary: NFL thickness, BMO area, BMO eccentricity, BMO planarity
[175], BMO depth, BM depth, and choroidal thickness. The parameters are graphically
described in Figure 6.2.
Nerve fiber layer thickness was measured at each pixel of the posterior NFL surface as
the closest distance to the ILM surface. The NFL within 0.25 mm from BMO was excluded
because near and inside BMO, NFL changes into vertical fiber bundles. For statistical
analysis, NFL thickness was averaged over an elliptical annulus, inwardly bounded at 0.25
mm from BMO and outwardly bounded at 1.75 mm from BMO. This provided a level of
anatomical consistency in averaging measurements over multiple eyes with different image
and BMO sizes.
104

Figure 6.2: Shape parameters. (a) An example B-scan. (b) Nerve fiber layer thickness wasmeasured as the closest distance to ILM from each point on the posterior NFL boundary.(c) Bruch’s membrane reference plane was defined as the best-fit plane to BM points 2mm away from the BMO center. (d) Bruch’s membrane opening depth was measuredas the normal distance between the BM reference plane and BMO center. (e) Bruch’smembrane depth was measured as the normal distance between each point of BM andthe BM reference plane. (f) Choroidal thickness was measured as the closest distance toBM from each point on the posterior choroid boundary. Although shown here in a B-scan,all parameters were defined and measured in the full 3D volume.
To quantify the BMO shape, an ellipse was fitted to the segmented BMO points by
first finding the best-fit plane using principal component analysis (PCA) [90] and fitting
an ellipse to the projection of the BMO points on the plane by least-squares criterion.
Bruch’s membrane opening area and BMO eccentricity were calculated from the fitted
ellipse. Bruch’s membrane opening planarity, or how much the BMO deviates from a plane,
was measured as the mean of the normal distance between the segmented BMO points
and its best-fit plane.
For the BM shape parameters, BMO depth and BM depth, a BM reference plane [175]
was first established by selecting points on BM along a circle 2 mm from the center of
the BMO and fitting a plane with PCA. Bruch’s membrane opening depth was measured
as the normal distance from the BMO center to the BM reference plane and reflects the
posterior depth of BMO with respect to the BM reference plane. Bruch’s membrane depth
was defined as the normal distance from each pixel of the BM surface to the BM reference
plane. For statistical analysis, BM depth was averaged over an elliptical annulus, inwardly
bounded at BMO and outwardly bounded at 1.75 mm from BMO. Furthermore, BM depth
105

Figure 6.3: Sectorization. Elliptical annuli were drawn at 0.25, 0.75, 1.25, and 1.75 mmfrom Bruch’s membrane opening (BMO). The annuli were divided into 608 angular sectorsof superior (S), nasal (N), inferior (I), and temporal (T) and 308 angular sectors of superior-nasal (SN), inferior-nasal (IN), inferior-temporal (IT), and superior-temporal (ST).
was averaged in regional sectors as shown in Figure 6.3. Four elliptical annuli, with the
innermost boundary of the BMO ellipse and consecutive boundaries at 0.25, 0.75, 1.25,
and 1.75 mm from the BMO ellipse, were drawn. Elliptical annuli with fixed distances from
the BMO ellipse were chosen over concentric circles centred at the BMO center because
of considerable variability in size and eccentricity of BMO among individuals. The annuli
were also divided into eight angular sectors: nasal, superior, temporal, inferior (60 degrees
each) and superior-nasal, inferior-nasal, inferior-temporal, and superior-temporal (30 de-
grees each). Such sectorization allowed generating comparable group means for different
regions (e.g., superior versus inferior, nasal versus temporal) as well as aggregating mea-
surements of multiple eyes without losing all regional information.
Choroidal thickness was measured at each pixel of the posterior choroid boundary (CS
boundary) as the closest distance to the BM surface. The choroid within 0.25 mm from
BMO was excluded because choroid termination near sclera canal was often unclear and
indistinguishable. Similarly to BM depth, for statistical analysis, choroidal thickness was
averaged in the elliptical annulus and regional sectors as described above.
106

6.2.4 Analysis
Subjects were divided into four groups: young normal (five subjects, 10 eyes, mean age
= 29.8±3.6 years), older normal (five subjects, 10 eyes, mean age = 57.0±4.4), glaucoma
suspect (seven subjects, seven eyes, mean age = 57.2±12.4), and glaucoma (17 subjects,
26 eyes, mean age = 55.7± 12.6). The suspect group consisted of the apparently normal
contralateral eyes of the patients with unilateral glaucoma [103, 179]. For all analysis and
graphical presentation, left eyes were flipped horizontally into right-eye orientation.
Nerve fiber layer thickness, BM depth, and choroidal thickness were mapped on two-
dimensional (2D) en face colour maps. Bruch’s membrane depth and choroidal thickness
were further plotted in the regional sectors described in the previous section. All seven
shape characteristics (NFL thickness, BMO area, BMO eccentricity, BMO planarity, BMO
depth, BM depth, choroidal thickness) were scatter plotted and compared between groups
and against age, axial length, and MD. For BM depth and choroidal thickness, regional
sectors were also compared by averaging measurements in each sector for all eyes in each
group. Multiple linear regression was performed on the shape parameters against age,
axial length, and MD. For the regression, only the right eye of each subject was selected to
avoid artificial reinforcement of a trend due to intereye correlation. Outliers were excluded
from the regression by a threshold of two standard deviations. IBM SPSS Statistics Version
19 (IBM Corp., Armonk, NY, USA) was used to perform multiple linear regression on each
of the seven dependent variables against the three independent variables, as the following
equation:
Shape Parameter (e.g. BMO Area) = α+β1∗Age+β2∗Axial length+β3∗Mean deviation
Regression was performed with all eyes and repeated for two subsets: normal eyes
(young normal and older normal, 10 subjects) and older eyes (all subjects age 50 or older,
18 subjects). Lastly, multiple regression was performed on intereye difference of the shape
parameters with intereye difference of axial length and MD.
107

ILM NFL BM CS Boundary
Corrected region, % 8.0± 12.3 8.6± 10.5 7.8± 8.8 12.2± 15.3Mean correction, pixels 28.6± 31.0 7.6± 12.2 7.4± 13.4 18.6± 12.5Mean correction, mm 0.077± 0.084 0.020± 0.033 0.020± 0.036 0.050± 0.033
Table 6.2: Performance of the automated segmentation of peripapillary structures
6.3 Results
Out of 53 eyes, three eyes from two subjects were excluded from NFL and choroid
analysis because the layer boundaries could not be segmented with confidence, either au-
tomatically or manually. Table 6.2 summarizes the performance of the automated segmen-
tation by (1) percentage of correction, calculated by dividing the number of corrected pixels
by the total number of pixels (400 x 400 pixels), and (2) amount of correction, calculated
by the difference between the automated segmentation and manual correction averaged
over all corrected pixels. Out of 202 automatically segmented surfaces, 10 surfaces (three
ILM, two posterior NFL boundary, two BM, three CS boundary) from six volumes had a
manual correction rate greater than 50% and were categorized as unsuccessful. These
cases were attributed to severe pathological deformation, image artifact, and poor image
contrast.
Figure 6.4 illustrates the NFL thickness mapping for all subjects by group and demon-
strates the characteristic hourglass pattern of thicker NFL in superior and nasal regions
relative to temporal and nasal regions. The accompanying scatter plot shows the distri-
bution of mean NFL thickness, averaged over the region between 0.25 and 1.75 mm from
BMO, between groups. As expected, NFL thickness decreases in the glaucomatous group.
In multiple regression (Table 6.3), NFL thickness was significantly correlated with MD, and
the intereye difference in NFL thickness was significantly correlated with the intereye dif-
ference in MD (Table 6.4).
Figure 6.5 illustrates the delineated BMO points overlaid on the sum-voxel, en face view
of the image volumes for all subjects. Red points indicate where the BMO is positioned
posterior (into the page) to its plane (best-fit plane to all BMO points), and green points
indicate where the BMO is positioned anterior (out of the page) to the plane. The variable
correspondence between the BMO, delineated from 3D OCT image, and clinical disc mar-
gin can be seen. In Figure 6.6, three BMO shape parameters (area, eccentricity, mean
108
planarity) are plotted by group and against age, axial length (AL), and MD. In multiple re-
gression of the same parameters with age, AL, and MD (Table 6.3), all three parameters
of BMO area, eccentricity, and planarity were significantly correlated with AL.
Figure 6.7 illustrates BM depth with respect to the BM reference plane at every point
across the whole BM for each subject. Warm colours, or positive distance values, indicate
that the BM surface is posterior to the reference plane; cool colours, or negative distance
values, indicate that the BM surface is anterior to the reference plane. In Figure 6.8, BMO
depth and mean BM depth are plotted by group and against age, AL, and MD. Bruch’s
membrane opening depth captures the degree of posterior deviation of BM at BMO. A
larger BMO depth reflects a greater degree of steepness between from the BM reference
plane and BMO. Mean BM depth is the mean of the absolute BM depth value, averaged
over the region between BMO and 1.75 mm from BMO, and reflects the degree to which the
overall BM shape deviates from a plane. A larger mean BM depth indicates a less planar
BM, while a smaller mean BM depth indicates a flatter BM. In multiple regression of BMO
depth and mean BM depth with age, AL, and MD (Table 6.3), some correlation existed
between BM depth and AL and MD. More significant correlations were observed between
the intereye difference of BMO depth and intereye MD difference, and also between the
intereye difference in mean BM depth and intereye MD difference.
Figure 6.9 presents the sectoral analysis of BM depth with sectors divided by both radial
distance from BMO and angular sectors. In Figure 6.9A, BM depth is shown averaged in
each sector across each group. A greater overall BM depth, indicating a greater degree of
global deviation from a plane, can be seen in the older normal and glaucomatous groups
compared with the young normal group. In Figures 6.9 B and C, BM depth is plotted by
angular sectors only, starting from temporal and proceeding clockwise to inferior-temporal
region. In Figure 6.9 B, all BM depth points in the same angular sectors were averaged,
each sector extending from BMO to 1.75 mm from BMO. In Figure 6.9 C, only the BM
depth points between BMO and 0.25 mm from BMO were averaged by angular sectors.
In both cases, BM depth is smaller in young normal eyes compared to older normal and
glaucomatous eyes, with a general pattern of smaller BM depth in the nasal region.
109

Figure 6.10 illustrates choroidal thickness at every point across the whole choroid for
each subject. Compared to NFL thickness or BM depth, there is a larger individual variabil-
ity in the magnitude and spatial pattern of choroidal thickness. There is, however, visible
similarity between fellow eyes. The young normal group generally exhibited thicker choroid.
In Figure 6.11, mean choroidal thickness, averaged over the region between 0.25 and
1.75 mm from BMO, is plotted by group and against age, AL, and MD. In multiple regression
with age, AL, and MD (6.3), choroidal thickness was significantly correlated with age, and
within the age-matched group (50+), also with axial length.
Figure 6.12 presents the sectoral analysis of choroidal thickness, similarly to Figure
6.9 for BM depth. In Figure 6.12, all groups display the thickest choroid in the superior or
superiornasal sector and the thinnest choroid in the inferior sector.
6.4 Discussion
In this study we have examined RNFL thickness, BMO shape, BM planarity, and choroidal
thickness in myopic subjects both with and without glaucoma. Most patients had asymmet-
ric glaucoma, which allowed us to also compare the intereye difference in the degree of
glaucoma and axial length with the intereye difference in the shape parameters, thus con-
trolling for large intersubject differences. We found that the dimension and shape of BMO
tended to change with axial length but not with age or degree of glaucoma. Peripapillary
BM position was associated with distance from BMO such that BM was more posterior
closer to BMO. Large variability in BM depth was noted between subjects; but within sub-
jects, our analysis revealed an association between degree of glaucoma and BM depth.
Finally, choroidal thickness appeared to decrease with age but not with the presence of
glaucoma.
In displaying images in en face view and NFL thickness, BM depth, and choroid thick-
ness colour maps, we chose to use the same size scale for all images rather than scaling
the images to the same presentation size. Differences in scan size were due to the axial
length differences between the eyes, and a common scale allowed a truer, in-scale vi-
sual comparison, including that of varying BMO size and level of BM stiffness among the
subjects.
110

In the sectoral analysis, the sectors were divided by angles measured with reference
to the acquired image frame. A more anatomically consistent approach would be using
the axis between the center of the BMO and fovea (foveal–BMO axis), which aligns with
the direction of the nerve fiber bundles[72]. It has been shown that there is intrasubject
and intersubject variability in the correspondence between the acquired image frame and
the foveal–BMO axis [22, 148]; using the foveal–BMO axis in future studies will reduce the
effect of individual variability and result in more anatomically equivalent and comparable
sectors across multiple individuals.
The eyes that were grouped as “suspect” in this study were the normal-appearing fellow
eyes of subjects with glaucoma. No reference to OCT imaging was made during diagnosis.
Outliers in the dataset were included in the scatter plots but excluded from the mul-
tivariate regression analyses. The most extreme example was a glaucomatous eye with
axial length of 31.3 mm, which was also a full millimetre longer than that of its fellow (glau-
comatous) eye. At such extreme axial lengths of pathologic myopia, different mechanisms
may be at play than generally seen in the rest of the dataset. With the exception of this
eye, our axial lengths were between 24 and 30 mm, and the results are applicable only to
this range.
6.4.1 Nerve Fiber Layer Thickness
In nonmyopic eyes, characteristic ONH features are more apparent. In myopic eyes,
however, the myopic tilt, shallow laminar position, decreased contrast of neuroretinal rim
tissues, and peripapillary degenerative changes can make preperimetric glaucoma detec-
tion more difficult. Optical coherence tomograpy imaging of the NFL can be particularly
beneficial in these patients.
As expected, we observed decreasing NFL thickness in subjects with glaucoma and
significant negative correlations between NFL thickness and severity of glaucoma quanti-
fied by MD (Figure 6.4; Table 6.3). These findings agree with a large body of research on
NFL in glaucoma [100, 88, 129, 6] and provided an internal control for imaging, segmen-
tation, and analysis method in our study. Among the studies on NFL thickness of normal
myopic subjects, Bendschneider et al.[6] and Budenz et al.[10] found significant correla-
tions in NFL thickness with both age and axial length, whereas Leung et al. [118] and
Rauscher et al.[159] reported no correlation with age but with axial length. In age-matched
111

studies, several groups [81, 102, 171] reported significant correlation between NFL thick-
ness and axial length, while the last saw large variability in the correlation depending on
the quadrant, with the inferior quadrant showing the highest correlation and the temporal
quadrant showing the weakest correlation. Hoh et al.[77] found no significant correlation
between NFL thickness and axial length among 132 young males. Our measurement of
NFL thickness was not correlated with age or axial length. The varying results of previous
studies possibly indicate that age and axial length, compared to MD, are more subtle and
easily confounded factors; and the small sample size and presence of glaucoma patients
in this study likely made it difficult to detect meaningful influence by age or axial length.
6.4.2 Bruch’s Membrane Opening Shape
We quantified BMO shape by three parameters: area, eccentricity, and planarity. Figure
6.5 illustrates the large variability in BMO shape between myopic patients with and without
glaucoma. The figure also demonstrates the large variability in the correspondence be-
tween the clinical disc margin and BMO between myopic patients, again with and without
glaucoma. This supports an increasing body of evidence that the clinical disc margin is clin-
ically heterogeneous, even within an individual eye [161, 22, 199, 178, 162, 176, 177],and
suggests that similar issues also exist in myopes.
We observed larger BMO area with increasing axial length (Figure 6.6A; Table 6.3).
This finding is not artifactual since the pixel dimension was corrected for axial length, and
it is consistent with previous studies showing increasing disc area with increasing axial
length [93, 117, 143]. We also noted a small but significant (P < 0.05) negative correlation
between age and BMO size. This may represent type I error in our population and needs to
be further investigated. However, if confirmed, we speculate that this could reflect the pre-
sumed greater compliance of younger tissues, resulting in outward expansion of BMO as
seen in nonhuman primate (NHP) experimental glaucoma [5, 55, 175, 56]. Bruch’s mem-
brane opening eccentricity increased with increasing axial length; that is, as axial length
increased, the BMO tended away from a circular to a more elliptical shape (Figure 6.6
B; Table 6.3). Regarding the orientation of the BMO ellipse, or the direction of its major
axis, 61%, or 32 out of a total 52 BMOs, were oriented in the nasal-temporal direction;
23%, or 12 BMOs, were oriented in the superiornasal– inferior-temporal direction. Seven
BMOs were oriented in the superior-temporal–inferior-nasal direction, and only 1 BMO was
112

oriented in the superior-inferior direction. This pattern can be seen in Figure 6.5. Bruch’s
membrane opening planarity (by which we measure how much BMO deviates from a plane)
also appeared to increase slightly with axial length (Figure 6.6 C; Table 6.3). Bruch’s mem-
brane opening planarity can be related to a small but consistent saddle configuration of
BMO we observed (Figure 6.5). In this saddle configuration, BMO tended to be posteriorly
displaced along its long axis and anteriorly displaced along its short axis. Furthermore,
BMO planarity was indeed correlated with BMO eccentricity (Pearson correlation = 0.613,
P = 0.001), such that a more elliptical BMO was correlated to more deviation from a plane.
It should be noted this BMO saddling is small in magnitude ( 0.03 mm on average) relative
to the length of BMO ( 1 mm on average), and BMO is still a relatively planar structure. We
are unsure whether the BMO saddling is a feature unique to myopes, how it reflects under-
lying stresses and strains on BM, or whether it corresponds to local variability in deep ONH
morphology such as the recently reported horizontal laminar ridge [147]. We are currently
analyzing the 3D morphology of BM in more detail in a greater number of subjects and
hope to investigate these questions in future studies.
In summary, BMO appeared to become larger, more elliptical, and less planar with in-
creasing axial length. No relationship was seen between glaucoma severity (as measured
by MD) and BMO shape, which agrees with previous studies [157, 76]. The change in
BMO shape associated with longer axial length in this study may be a ramification of global
structural change in myopia, including elongation of the eye due to growth and remodeling
mechanism driven by visual error signal.
6.4.3 Peripapillary Bruch’s Membrane Shape
All eyes showed increasing posterior deformation of BM with increasing proximity to
BMO (Figures 6.7, 6.9B). Within the same subject, there appeared to be a good inter-
eye correspondence in the degree of posterior deformation. In BMO depth and mean BM
depth, no significant group difference was observed between the nonglaucomatous and
glaucomatous eyes (Figures 6.8A, 6.8A). However, a significant correlation existed be-
tween the intereye differences of BMO depth and mean BM depth with the intereye MD dif-
ference (Figure 6.8C; Table 6.4), suggesting that when intersubject variance is partitioned,
greater BMO depth and BM depth are associated with a greater degree of glaucomatous
113

damage. Similar change was also observed in a longitudinal study of experimental glau-
coma in NHPs [175]. These data are illustrated in a sectoral analysis in Figure 6.9, which
presents, with small but consistent associations with the presence of glaucoma, a visible
BM depth increase with age. The statistical significance of the group mean difference be-
tween the young normal (n = 5) and older normal subjects (n = 5) was 0.084 with the
right eyes and 0.037 with the left eyes, suggesting a relationship that would possibly be
more apparent with a larger dataset. Taken together, the results suggest that in the myopic
subjects under study, despite the large intersubject variability in BM position, there is an
association of BM depth with age and a smaller but consistent association with degree of
glaucoma. Axial length was also correlated with BM depth among the older, age-matched
normal and glaucoma subset of the data. The exact shape and regional pattern of this devi-
ation requires further investigation to analyze the slope, change of slope (bending/bowing),
and differences and similarities in the effect of myopia and effect of glaucoma.
The increase in BM depth may be a direct mechanical result of increased IOP or a
secondary deformation resulting from tissue remodeling of deeper structures, such as the
lamina cribrosa and peripapillary sclera, in a complex interplay of aging, myopia, and glau-
coma. The peripapillary sclera was shown to become posteriorly deformed and displaced
in early glaucomatous monkey ONH [189], and the peripapillary scleral thickness near the
scleral canal and optic nerve meninges was shown to decrease significantly with increas-
ing axial length [163]. Posterior cupping of the lamina cribrosa (LC) and posterior migration
of the laminar insertion in the connective tissue remodeling in response to elevated IOP in
glaucoma [30, 189, 12] may also influence posterior deformation of BM. Ocular elongation
and IOP both influence ONH remodeling, and it is an important challenge to understand
the combined impact and mechanism, particularly in the context of higher glaucoma sus-
ceptibility among people with advanced myopia.
Myopia, especially high myopia, has been a complicating factor in glaucoma in that it
is associated with structural changes in the peripapillary region. Optic disc area and area
of the peripapillary region with chorioretinal atrophy were correlated with degree of myopia
along with disc elongation [143, 93, 83, 25, 158, 94], and the LC was shown to be thinner
in highly myopic eyes than in non-highly myopic eyes [95]. In highly myopic glaucomatous
eyes, compared to non-highly myopic glaucomatous eyes, optic disc area, elongation, cup
length, and peripapillary atrophy were significantly larger [92, 34] LC was thinner [95], and
114

rim loss was greater. In our study of myopic glaucomatous subjects, we aimed to observe,
in relation to myopia and glaucoma, not only the changes in RNFL but also their effect on
Bruch’s membrane and the opening. These are relatively robust structures not directly sub-
ject to glaucomatous atrophy, and thus better indicators of mechanical or pressure-related
deformation associated with both myopia and glaucoma. A recent study by Johnstone et
al. [89] suggests posterior migration of BMO with age in relation to age-related choroidal
thinning. This questions the appropriateness of the BMO as a reference structure in shape
measurement. However, in establishing the reference plane in this study, we used BM
points 2 mm outward from the BMO centroid [175]. A typical model of ONH deformation in
glaucoma, originating from the LC region and including cupping, also suggests that the BM
may be more mechanically stable at its peripheral region than at its opening. In summary,
our study demonstrated large differences between myopic subjects in peripapillary mea-
surements with smaller but consistent peripapillary changes associated with glaucoma.
6.4.4 Choroidal Thickness
Thinner mean choroidal thickness was associated with increased age, and also with
axial length among older, age-matched subjects (Table 6.3). Mean deviation was not a
significant factor in choroidal thickness. These results are in agreement with several stud-
ies that have reported macular choroidal thinning with both age [84] and high myopia [50].
Maul et al. [127] found that peripapillary choroidal thickness was associated with age, axial
length, central corneal thickness, and also diastolic ocular profusion pressure in glaucoma
suspects and patients. In recent studies, choroidal thickness was not correlated with glau-
comatous damage [127, 42, 164]. In our sectoral analysis (Figure 6.12), we observed a
regional pattern of the thickest choroid at superior or superior-nasal region and the thinnest
in inferior region.
6.5 Anterior lamina cribrosa region morphometrics
32 eyes from 17 of the myopic participants (7 normal, 4 unilateral glaucoma, 6 bilateral
glaucoma) were additionally segmented for anterior lamina insertion points (ALIP), and
anterior lamina cribrosa surface (ALCS). Area, eccentricity, and planarity of ALIP were
measured by ellipse-fitting. The height, skew, and length of the anterior scleral canal were
115

characterized by vertical, horizontal, and normal distances between BMO and ALIP. ALCS
depth was measured from a reference plane fit to ALIP. Multiple regression analysis was
performed to assess the effect of age, axial length (AL), and mean deviation (MD). Right
eyes (OD, N = 17, 10 normal, 7 glaucomatous) and left eyes (OS, N = 15, 8 normal, 7
glaucomatous) were analyzed separately, along with intereye difference.
Figure 6.14 shows the enface images and overlaid with BMO (red) and ALIP (blue).
ALIPs are larger than BMOs (OD: p = 0.0007, OS: p = 0.0015) and positioned nasally from
BMO and more centrally relative to the retinal blood vessels. ALIPs were also generally
elongated in the nasal-temporal direction; the canal was consistently skewed toward the
nasal direction. Figure 6.16 display the saddle-like topology of the ALIP found in several
cases.
The ALIP area was positively correlated with AL (OD: p = 0.0007, OS: p = 0.0270).
The vertical, horizontal, and normal distance between BMO and ALIP centroids were not
significantly correlated with any factor. ALCS depth was correlated with MD (OD: p =
0.0001, OS: p = 0.0026), and with AL (OD: p = 0.0012), and in inter-eye difference, with MD
only (p = 0.014). ALCS depth was also correlated with Bruch’s membrane depth measured
in the previous section (OD: p = 0.003, OS: p = 0.043). The intereye difference of ALCS
depth was also correlated with the intereye difference of BM depth (p = 0.001). The results
are plotted in 6.16.
In conclusion, the posterior bowing of the ALCS was more prominent and significant
than overall posterior migration represented by the ALIP position relative to BMO. ALCS
shape may be affected by axial length; this is more apparent among normal subjects.
Lastly, BM ”bowing” or depth (distance of BM surface from a reference plane) was corre-
lated with ALCS depth.
6.6 Summary of contributions
The contributions described in this chapter and published in [196, 195, 108, 112] are:
• ONH morphometrics of myopic glaucoma
– Measurement of RNFL thickness, choroid thickness, BM bowing, BMO dimen-
sion, scleral canal dimension, and ALCS depth
– Group comparison between normal, suspect, and glaucomatous subjects
116

– Multiple regression of the shape parameters with age, axial length, and MD
117

Figure 6.4: Peripapillary retinal nerve fiber layer (NFL) thickness. All thickness colour mapsare in scale and right-eye orientation. The region within 0.25 mm from Bruch’s membraneopening (BMO) was excluded. The graph plots the NFL thickness averaged over the regionbetween 0.25 and 1.75 mm from BMO, with outliers in each group marked by red circles.
118

Part Corr. Coeff. (P-values)
n R F(Sig.) Age AL MD
Mean nerve fiber layer thicknessAll data 25 .92 38.55 (<.001) - - .89 (<.001)Normal, YN, and ON - - - - - -Age-matched, 50+ 16 .86 11.95 (.001) - - .75 (<.001)
BMO areaAll data 25 .71 7.18 (.002) -.34 (.038) .69 (<.001) -Normal, YN, and ON 10 .86 5.47 (.038) - .83 (.008) -Age-matched, 50+ 16 .78 6.13 (.009) -.45 (.030) .59 (.007) -
BMO eccentricityAll data 26 .59 3.94 (.022) - .42 (.025) -Normal, YN, and ON 10 .80 3.54 (.088) - .59 (.053) -Age-matched, 50+ - - - - - -
BMO planarityAll data 25 .69 6.70 (.002) - .40 (.019) -Normal, YN, and ON - - - - - -Age-matched, 50− - - - - - -
BMO depthAll data - - - - - -Normal, YN, and ON - - - - - -Age-matched, 50+ - - - - - -
Mean BM depthAll data - - - - - -Normal, YN, and ON - - - - - -Age-matched, 50+ 16 .67 3.30 (.058) - .62 (.014) -0.49 (.040)
Mean choroidal thicknessAll data 24 .75 8.82 (.001) -.59 (.001) - -Normal, YN, and ON 10 .84 4.92 (.047) -.81 (.010) - -Age-matched, 50+ 16 .76 5.59 (.012) -.56 (.011) -.45 (.034)
Table 6.3: Multiple Regression Analysis of Shape Parameters With Age, Axial Length, andMean Deviation (MD): Mean Nerve Fiber Layer Thickness, BMO Area, BMO Eccentricity,BMO Planarity, BMO Depth, Mean BM Depth, and Mean Choroidal Thickness
119
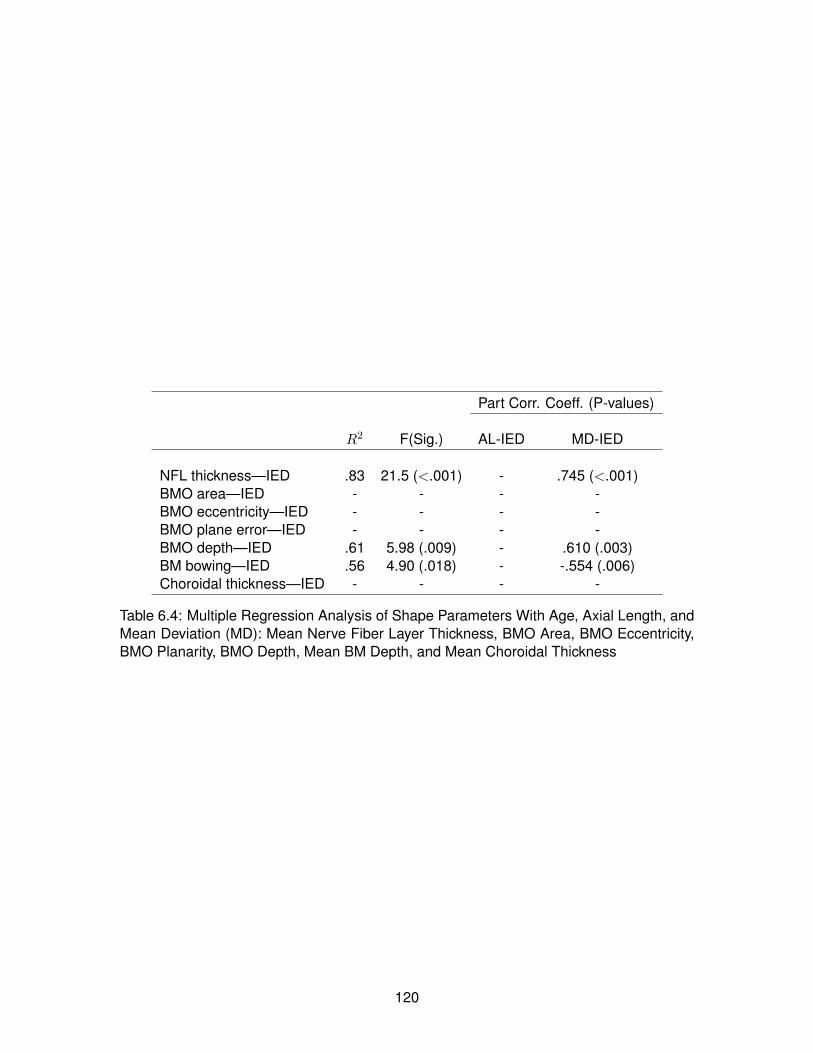
Part Corr. Coeff. (P-values)
R2 F(Sig.) AL-IED MD-IED
NFL thickness—IED .83 21.5 (<.001) - .745 (<.001)BMO area—IED - - - -BMO eccentricity—IED - - - -BMO plane error—IED - - - -BMO depth—IED .61 5.98 (.009) - .610 (.003)BM bowing—IED .56 4.90 (.018) - -.554 (.006)Choroidal thickness—IED - - - -
Table 6.4: Multiple Regression Analysis of Shape Parameters With Age, Axial Length, andMean Deviation (MD): Mean Nerve Fiber Layer Thickness, BMO Area, BMO Eccentricity,BMO Planarity, BMO Depth, Mean BM Depth, and Mean Choroidal Thickness
120

Figure 6.5: Bruch’s membrane opening disc margin correspondence and planarity of BMO.Bruch’s membrane opening points overlaid on en face images generated by summing the3D OCT volumes in the axial direction. Red points indicate where the BMO is posterior(into the page) to reference plane, and green points indicate where the BMO is anterior(out of the page) to the reference plane.
121

Figure 6.6: Bruch’s membrane opening shape measurements. (A) Bruch’s membraneopening area, (B) BMO eccentricity, and (C) mean BMO planarity, distributed by (i) groupand versus (ii) age, (iii) axial length, and (iv) MD. Outliers in each group are marked by redcircles in plots (i).
122

Figure 6.7: Peripapillary BM depth. All depth maps are in scale and right-eye orientation.The BM depth is measured with respect to the BM reference plane at each point on BM.
123

Figure 6.8: Bruch’s membrane opening and mean BM depth measurements. (A) Bruch’smembrane opening depth and (B) mean BM depth distributed by (i) group and versus (ii)age, (iii) axial length, and (iv) MD (C). Intereye differences of BMO depth and BM depthare also plotted versus intereye MD difference. Outliers in each group are marked by redcircles in plots (i).
124

Figure 6.9: Bruch’s membrane depth sectoral analysis. (A) Sectorized group averagesof Bruch’s membrane (BM) surface depth. The colour in each sector indicates the meanabsolute magnitude of the normal distance between BM and its fitted plane. Elliptical annuliare drawn at 0.25, 0.75, 1.25, and 1.75 mm from Bruch’s membrane opening (BMO). Theannuli are divided into 60ngular sectors of superior (S), nasal (N), inferior (I), and temporal(T), and 30ngular sectors of superior-nasal (SN), inferior-nasal (IN), inferior-temporal (IT),and superior-temporal (ST). (B) Average BM depth by angular sector for the whole BMsurface. (C) Average BM depth by angular sector for the inner annulus only (0–0.25 mmdistance from BMO).
125

Figure 6.10: Peripapillary choroidal thickness. All thickness colour maps are in scale andright-eye orientation. The region inside and within 0.25 mm from Bruch’s membrane open-ing (BMO) was excluded.
126

Figure 6.11: Choroidal thickness measurements. Choroidal thickness distributed by (i)group, and versus (ii) age, (iii) axial length, and (iv) MD.
Figure 6.12: Choroidal thickness sectoral analysis. (A) Sectorized peripapillary choroidalthickness. Elliptical annuli are drawn at 0.25, 0.75, 1.25, and 1.75 mm from Bruch’s mem-brane opening (BMO). The annuli are divided into 60 degrees angular sectors of superior(S), nasal (N), inferior (I), and temporal (T), and 30 degrees angular sectors of superior-nasal (SN), inferior-nasal (IN), inferior-temporal (IT), and superior-temporal (ST). (B) Aver-age choroidal thickness by angular sector.
127

Figure 6.13: Graphical description of anterior lamina insertion points (ALIP) to Bruch’smembrane opening (BMO) distance (left) and anterior lamina cribrosa surface (ALCS)depth (right).
128

Figure 6.14: Enface projection of Bruch’s membrane openings (BMO, red) and anteriorlamina insertion points (ALIP).
129
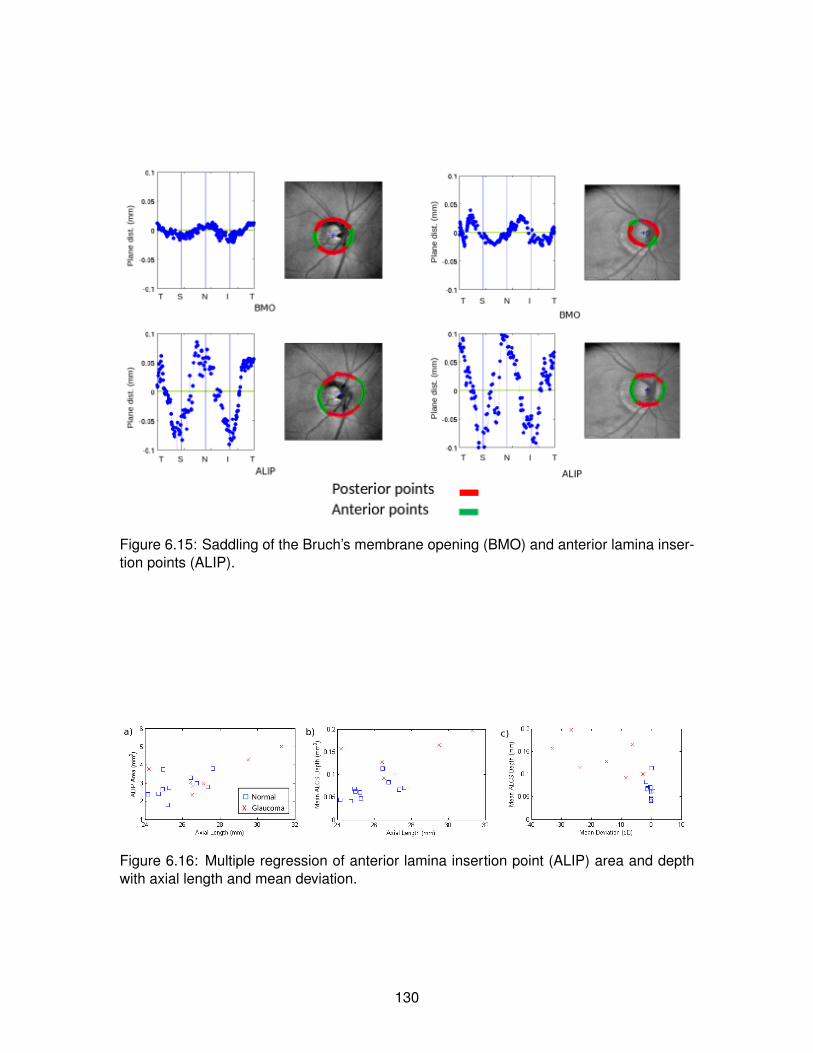
Figure 6.15: Saddling of the Bruch’s membrane opening (BMO) and anterior lamina inser-tion points (ALIP).
Figure 6.16: Multiple regression of anterior lamina insertion point (ALIP) area and depthwith axial length and mean deviation.
130

Chapter 7
Conclusion
In this thesis, we have presented a comprehensive computational pipeline for process-
ing, segmentation, registration, and morphometric analysis of retinal and peripapillary op-
tical coherence tomography.
In Chapter 3, the image acquisition and preprocessing steps were described, with fo-
cus on motion correction and image smoothing. The involutary microsaccadic movement
of the eye creates axial and lateral motion artefacts in OCT images. A simple and effec-
tive method to remove the wave-like axial motion artefact is to first obtain an approximated
motion profile by finding the axial translation of the maximum cross-correlation between
adjacent frames. The profile was smoothed by curve-fitting, and the frame positions were
adjusted according to the smoothing. The image volume was additionally enhanced by
3D bounded variation image smoothing, which optimizes a functional that balances the
smoothness of the image and faithfulness to the original image. This resulted in smooth-
ing the image speckles while preserving and visually enhancing the edges of anatomical
structures.
In Chapter 4, manual and automated segmentation methods were presented. Non-
layer features in the optic nerve head (ONH), such as the Bruch’s membrane opening
(BMO) and anterior laminar insertion points (ALIP), were point-segmented manually on
radial scans extracted from the original 3D volume. Retinal layers were segmented au-
tomatically using a graph-cut based method, which transformed the image volume into a
node-weighted directed graph such that the cut of the associated arc-weighted graph cor-
responded to the optimal 3D surfaces in the volume. A cost function involving the vertical
intensity gradient yielded successful segmentation of the horizontal layer structure of the
131

retina. We applied the automated segmentation to segment the choroid, the vasculature
layer posterior to the retina of which the posterior boundary is often unclear due to light
absorbtion and scattering. Choroid from 830-nm OCT images, 1060-nm OCT images,
and enhanced-depth imaging (EDI) OCT images were segmented. Measurement of the
subfoveal choroidal thickness from automated segmentation was compared with those of
expert human raters, and demonstrated solid performance with potential for clinical appli-
cation.
In Chapter 5, we presented two registration methods of retinal surfaces - surface-to-
surface exact registration, and atlas template generation from multiple surfaces. Reg-
istration establishes anatomical correspondence for comparing multiple retinal surfaces.
The first method brings two surfaces in close proximity by mathematical current measure,
and achieves one-to-one spatial correspondence between the surfaces through spherical
demons registration. We applied this technique to measure repeatability of retinal nerve
fibre layer (RNFL) and choroidal thickness maps, which showed high repeatability relative
to the image axial coherence length; the RNFL thickness was more variable in the regions
of retinal blood vessels, and the choroidal thickness was in average more variable than the
RNFL thickness, suggesting blood flow affects the layer thickness measurement.
The second method uses the fshape framework, in which a geometrical surface in 3D
and signals mapped onto the surface are considered as a single object of fshape. In order
to obtain the mean atlas of multiple fshapes, a simple initial hyper template is chosen, and
its geometrical deformation and signal residuals are varied simultaneously to minimize the
template’s deformation distance to its approximation to each of the observed fshapes, and
the dissimilarity between each of the template’s approximation and the corresponding ob-
servation. The observed fshapes are compared via the distances to the common mean
template (atlas) from their estimated fshapes. Using this framework, we generated mean
RNFL surfaces and thickness maps for normal and glaucomatous eyes and visualized the
discriminative power over the peripapillary region between the normal and glaucomatous
RNFLs. Additionally, automated classification was performed by a linear discriminant anal-
ysis (LDA) method, and info-gain based support vector machine (SVM) method, and both
yielded high automated classification rate between normal and glaucomatous groups and
between normal and glaucoma-suspect groups based on the RNFL fshape measures.
132

In Chapter 6, a comprehensive ONH shape analysis of myopic glaucoma was pre-
sented. We acquired 52 eye images from young normal, older normal, glaucoma-suspect,
and glaucoma groups, which were processed, segmented, and measured for features such
as the RNFL thickness, choroidal thickness, BMO dimension, Bruch’s membrane (BM)
bowing, scleral canal dimension, and anterior lamina cribrosa surface (ALCS) depth. Multi-
ple regression was performed to assess the correlation of the shape parameters to the sub-
jects’ age, degree of myopia measured by the eye’s axial length, and degree of glaucoma
severity measured by the mean deviation (MD), which in turn indicates the amoutn of visual
field loss. From the results, we found that along with the MD value, axial length affected the
ONH morphology significantly and may be a confounding factor in glaucoma development,
which also possibly explain the high susceptibility of glaucoma among those with advanced
myopia. Severe glaucoma (large MD magnitude) was associated with greater BM bowing
and ALCS depth, confirming the posterior deformation of glaucomatous ONH in-vivo.
The contributions of this thesis are published in [196, 114, 195, 111, 109, 112, 113]
and submitted for publication in [110]. A manuscript on the repeatability study in Chapter
5, and the anterior laminar region morphometrics in Chapter 6, are under preparation.
7.1 Future directions
The future directions of the work presented in this thesis are discussed in individual
sections in more detail.
One direction is more extensive application of the tools presented here in clincal stud-
ies. The repeatability study in Section 5.2 can be applied to longitudinal data over longer
periods of time in glaucomatous eyes to track change; in particular, the RNFL and other
retinal layers can be monitored for further tissue loss after treatement. The fshape atlas-
based variability analysis in Section 5.3 can be applied to a larger dataset with various
features, focusing on confirming the regional pattern of RNFL thinning in glaucoma, and
testing other layers, such as the choroid, for changes with glaucoma progression. The
application of the morphometric tools in this thesis is not limited to glaucoma studies, and
can be extended to other eye diseases involving structural changes.
One of the more immediate methodoligcal improvements in the pipeline is including the
retinal blood vessels as a reference structure. We are currently investigating automated
133

segmentation of the retinal blood vessels to perform pre-registration alignment of longitudi-
nal data, and to mark the regions with more variable retinal layer thickness measurements.
Automated segmentation of the Bruch’s membrane opening (BMO) is another potential
future project. Accurate automated BMO segmentation is challenging largely due to the
heavy blood-vessel shadowing near the optic cup surface. However, since our morphome-
tric measurements are largely based on the best-fit ellipse of the BMO, and the manual
segmentation of the BMO is limited in measurement repeatability, it may suffice for the
machine to approximate the BMO than aiming to mark the exact location.
An important physiological parameter not considered in the thesis is the intraocular
pressure (IOP), and it is not clear how much the shape measurements presented in the
thesis would be affected by the change in IOP. Our group is currently revising the image
acquisition protocol such that IOP measurement can be obtained for each imaging subject.
In ONH morphometrics, one of the future projects is improved characterization of the
Bruch’s membrane bowing. Although the BM depth in Chapter 6 quantifies the crude
“flatness” of the BM surface, a more detailed analysis may reveal topological characteristics
that better distinguishes myopia-related, glaucoma-related, or age-related deformations.
Another shape parameter to be considered is the myopic tilt [82] of the optic disk, which
may affect the BM bowing measurement.
134

Bibliography
[1] Age Related Eye Disease Research Group. A randomized, placebo-controlled, clini-
cal trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc
for age-related macular degeneration and vision loss: AREDS report no. 8. Archives
of ophthalmology, 119(10):1417–36, October 2001. 31, 40
[2] S. Arguillere, E. Trelat, A. Trouve, and L. Younes. Shape deformation analysis from
the optimal control viewpoint. arXiv:1401.0661, Jan 2014. 83, 84
[3] Ahmet Murat Bagci, Mahnaz Shahidi, Rashid Ansari, Michael Blair, Norman Paul
Blair, and Ruth Zelkha. Thickness profiles of retinal layers by optical coherence
tomography image segmentation. American journal of ophthalmology, 146(5):679–
87, November 2008. 24
[4] M. F. Beg, M. I. Miller, A. Trouve, and L. Younes. Computing large deformation metric
mappings via geodesic flows of diffeomorphisms. International journal of computer
vision, 61(139-157), 2005. 77
[5] Anthony J Bellezza, Christopher J Rintalan, Hilary W Thompson, J Crawford Downs,
Richard T Hart, and Claude F Burgoyne. Deformation of the lamina cribrosa and an-
terior scleral canal wall in early experimental glaucoma. Investigative ophthalmology
& visual science, 44(2):623–37, February 2003. 101, 112
[6] Delia Bendschneider, Ralf P Tornow, Folkert K Horn, Robert Laemmer, Christo-
pher W Roessler, Anselm G Juenemann, Friedrich E Kruse, and Christian Y Mardin.
Retinal nerve fiber layer thickness in normals measured by spectral domain OCT.
Journal of glaucoma, 19(7):475–82, September 2010. 111
[7] Thomas L Berenberg, Tatyana I Metelitsina, Brian Madow, Yang Dai, Gui-Shuang
Ying, Joan C Dupont, Lili Grunwald, Alexander J Brucker, and Juan E Grunwald. The
135
association between drusen extent and foveolar choroidal blood flow in age-related
macular degeneration. Retina (Philadelphia, Pa.), 32(1):25–31, January 2012. 30
[8] Rupert R A Bourne, Gretchen A Stevens, Richard A White, Jennifer L Smith, Seth R
Flaxman, Holly Price, Jost B Jonas, Jill Keeffe, Janet Leasher, Kovin Naidoo, Konrad
Pesudovs, Serge Resnikoff, and Hugh R Taylor. Causes of vision loss worldwide,
1990-2010: a systematic analysis. The Lancet. Global health, 1(6):e339–49, De-
cember 2013. 1, 7
[9] Christopher Bowd, Linda M Zangwill, Charles C Berry, Eytan Z Blumenthal, Cris-
tiana Vasile, Cesar Sanchez-Galeana, Charles F Bosworth, Pamela A Sample, and
Robert N Weinreb. Detecting early glaucoma by assessment of retinal nerve fiber
layer thickness and visual function. Investigative Ophthalmology & Visual Science,
42(9):1993–2003, 2001. 93
[10] Donald L Budenz, Douglas R Anderson, Rohit Varma, Joel Schuman, Louis Cantor,
Jonathan Savell, David S Greenfield, Vincent Michael Patella, Harry A Quigley, and
James Tielsch. Determinants of normal retinal nerve fiber layer thickness measured
by Stratus OCT. Ophthalmology, 114(6):1046–52, June 2007. 111
[11] Claude F Burgoyne. A biomechanical paradigm for axonal insult within the optic
nerve head in aging and glaucoma. Experimental eye research, 93(2):120–32, Au-
gust 2011. 8
[12] Claude F Burgoyne and J Crawford Downs. Premise and prediction-how optic nerve
head biomechanics underlies the susceptibility and clinical behavior of the aged optic
nerve head. Journal of glaucoma, 17(4):318–28, January. 114
[13] Claude F Burgoyne, J Crawford Downs, Anthony J Bellezza, J-K Francis Suh, and
Richard T Hart. The optic nerve head as a biomechanical structure: a new paradigm
for understanding the role of IOP-related stress and strain in the pathophysiology
of glaucomatous optic nerve head damage. Progress in retinal and eye research,
24(1):39–73, January 2005. 8, 101
136

[14] Delia Cabrera Fernandez, Harry M. Salinas, and Carmen A. Puliafito. Automated
detection of retinal layer structures on optical coherence tomography images. Optics
Express, 13(25):10200, December 2005. 24
[15] J. Cao. The size of the connected components of excursion sets of χ2, t and F fields.
Advances in Applied Probability, 31(3):579–595, September 1999. 51
[16] B Charlier, N Charon, and A Trouve. Fshapes tool kit, December 2014. 86
[17] Benjamin Charlier, Nicolas Charon, and Alain Trouve. The fshape framework for the
variability analysis of functional shapes. April 2014. 75
[18] N. Charon. Analysis of geometric and functional shapes with extensions of currents.
Application to registration and atlas estimation. PhD thesis, ENS Cachan, 2013. 76,
82
[19] N. Charon, B. Charlier, and A. Trouve. The fshape framework for the variability
analysis of functional shapes. ArXiv:1404.6039, Apr 2014. 76, 77, 79, 80, 84
[20] N. Charon and A. Trouve. Functional currents : a new mathematical tool to model
and analyse functional shapes. JMIV, 48(3):413–431, 2013. 79
[21] Balwantray C. Chauhan and Claude F. Burgoyne. From clinical examination of the
optic disc to clinical assessment of the optic nerve head: A paradigm change. Am.
J. Ophthalmol., 156(2):218–227, August 2013. 44, 45
[22] Balwantray C Chauhan and Claude F Burgoyne. From clinical examination of the op-
tic disc to clinical assessment of the optic nerve head: a paradigm change. American
journal of ophthalmology, 156(2):218–227.e2, August 2013. 104, 111, 112
[23] Min Chen, Andrew Lang, Howard S. Ying, Peter A. Calabresi, Jerry L. Prince, and
Aaron Carass. Analysis of macular OCT images using deformable registration.
Biomed. Opt. Express, 5(7):2196–2214, Jul 2014. 46
[24] Yueli Chen, Laurel N. Vuong, Jonathan Liu, Joseph Ho, Vivek J. Srinivasan, Iwona
Gorczynska, Andre J. Witkin, Jay S. Duker, Joel Schuman, and James G. Fuji-
moto. Three-dimensional ultrahigh resolution optical coherence tomography imaging
of age-related macular degeneration. Optics Express, 17(5):4046, March 2009. 18
137

[25] E Chihara and K Chihara. Covariation of optic disc measurements and ocular param-
eters in the healthy eye. Graefe’s archive for clinical and experimental ophthalmol-
ogy = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie,
232(5):265–71, May 1994. 114
[26] Michael Choma, Marinko Sarunic, Changhuei Yang, and Joseph Izatt. Sensitivity ad-
vantage of swept source and Fourier domain optical coherence tomography. Optics
Express, 11(18):2183, September 2003. 9
[27] Moo K Chung, Keith J Worsley, Brendon M Nacewicz, Kim M Dalton, and Richard J
Davidson. General multivariate linear modeling of surface shapes using SurfStat.
NeuroImage, 53(2):491–505, November 2010. 51, 55
[28] George A Cioffi. Ischemic model of optic nerve injury. Transactions of the American
Ophthalmological Society, 103:592–613, January 2005. 101
[29] Rogerio A Costa, Mirian Skaf, Luiz A S Melo, Daniela Calucci, Jose A Cardillo,
Jarbas C Castro, David Huang, and Maciej Wojtkowski. Retinal assessment using
optical coherence tomography. Progress in retinal and eye research, 25(3):325–53,
May 2006. 18
[30] J Crawford Downs, Michael D Roberts, and Ian A Sigal. Glaucomatous cupping of
the lamina cribrosa: a review of the evidence for active progressive remodeling as a
mechanism. Experimental eye research, 93(2):133–40, August 2011. 101, 114
[31] Catherine Cukras, Elvira Agron, Michael L Klein, Frederick L Ferris, Emily Y Chew,
Gary Gensler, and Wai T Wong. Natural history of drusenoid pigment epithelial
detachment in age-related macular degeneration: Age-Related Eye Disease Study
Report No. 28. Ophthalmology, 117(3):489–99, March 2010. 31
[32] Johannes F. de Boer, Barry Cense, B. Hyle Park, Mark C. Pierce, Guillermo J. Tear-
ney, and Brett E. Bouma. Improved signal-to-noise ratio in spectral-domain com-
pared with time-domain optical coherence tomography. Optics Letters, 28(21):2067,
November 2003. 9
[33] Francois C Delori, Robert H Webb, and David H Sliney. Maximum permissible expo-
sures for ocular safety (ANSI 2000), with emphasis on ophthalmic devices. Journal
138

of the Optical Society of America. A, Optics, image science, and vision, 24(5):1250–
65, May 2007. 10
[34] A Dichtl, J B Jonas, and G O Naumann. Histomorphometry of the optic disc in highly
myopic eyes with absolute secondary angle closure glaucoma. The British journal
of ophthalmology, 82(3):286–9, March 1998. 102, 114
[35] Weiguang Ding, Mei Young, Serge Bourgault, Sieun Lee, David A Albiani, Andrew W
Kirker, Farzin Forooghian, Marinko V Sarunic, Andrew B Merkur, and Mirza Faisal
Beg. Automatic detection of subretinal fluid and sub-retinal pigment epithelium fluid
in optical coherence tomography images. Conference proceedings : ... Annual Inter-
national Conference of the IEEE Engineering in Medicine and Biology Society. IEEE
Engineering in Medicine and Biology Society. Annual Conference, 2013:7388–91,
January 2013. 41
[36] J Crawford Downs, J-K Francis Suh, Kevin A Thomas, Anthony J Bellezza, Richard T
Hart, and Claude F Burgoyne. Viscoelastic material properties of the peripapillary
sclera in normal and early-glaucoma monkey eyes. Investigative ophthalmology &
visual science, 46(2):540–6, February 2005. 101
[37] J Crawford Downs, Hongli Yang, Christopher Girkin, Lisandro Sakata, Anthony
Bellezza, Hilary Thompson, and Claude F Burgoyne. Three-dimensional histomor-
phometry of the normal and early glaucomatous monkey optic nerve head: neural
canal and subarachnoid space architecture. Investigative ophthalmology & visual
science, 48(7):3195–208, July 2007. 101
[38] Wolfgang Drexler and James G. Fujimoto, editors. Optical Coherence Tomography.
Biological and Medical Physics, Biomedical Engineering. Springer Berlin Heidelberg,
Berlin, Heidelberg, 2008. 9, 10
[39] S. Durrleman, P. Fillard, X. Pennec, Alain Trouve, and Nicholas Ayache. Registration,
atlas estimation and variability analysis of white matter fiber bundles modeled as
currents. NeuroImage, 55(3):1073–1090, 2010. 79
139

[40] S. Durrleman, X. Pennec, Alain Trouve, and Nicholas Ayache. A forward model to
build unbiased atlases from curves and surfaces. Proc. of the International Work-
shop on the Mathematical Foundations of Computational Anatomy, 2008. 76, 79,
84
[41] S. Durrleman, M. Prastawa, N. Charon, J.R Korenberg, S. Joshi, G. Gerig, and
A. Trouve. Deformetrics : morphometry of shape complexes with space deforma-
tions. Neuroimage, 101:35–49, 2014. 79, 86
[42] Joshua R Ehrlich, Jeffrey Peterson, George Parlitsis, Kristine Y Kay, Szilard Kiss,
and Nathan M Radcliffe. Peripapillary choroidal thickness in glaucoma measured
with optical coherence tomography. Experimental eye research, 92(3):189–94,
March 2011. 115
[43] Tapio Fabritius, Shuichi Makita, Masahiro Miura, Risto Myllyla, and Yoshiaki Yasuno.
Automated segmentation of the macula by optical coherence tomography. Optics
express, 17(18):15659–69, August 2009. 24
[44] Yong Fan, Dinggang Shen, Ruben C Gur, Raquel E Gur, and Christos Davatzikos.
COMPARE: classification of morphological patterns using adaptive regional ele-
ments. IEEE transactions on medical imaging, 26(1):93–105, January 2007. 55
[45] R D Fechtner. Review of normative database construction in available oct models
highlighting differences. In FDA/American Glaucoma Society Workshop on the Va-
lidity, Reliability, and Usability of Glaucoma Imaging Devices, 2012; Silver Spring,
MD. 101
[46] A.F. Fercher, C.K. Hitzenberger, G. Kamp, and S.Y. El-Zaiat. Measurement of in-
traocular distances by backscattering spectral interferometry. Optics Communica-
tions, 117(1-2):43–48, May 1995. 9
[47] Michael S. Floater. Mean value coordinates. Computer Aided Geometric Design,
20(1):19–27, March 2003. 49
[48] E Friedman. A hemodynamic model of the pathogenesis of age-related macular
degeneration. American journal of ophthalmology, 124(5):677–82, November 1997.
30
140

[49] Jerome H. Friedman. Regularized discriminant analysis. Journal of the American
Statistical Association, 84(405):pp. 165–175, 1989. 89
[50] Takamitsu Fujiwara, Yutaka Imamura, Ron Margolis, Jason S Slakter, and Richard F
Spaide. Enhanced depth imaging optical coherence tomography of the choroid in
highly myopic eyes. American journal of ophthalmology, 148(3):445–50, September
2009. 26, 115
[51] Mona K Garvin, Michael D Abramoff, Randy Kardon, Stephen R Russell, Xiaodong
Wu, and Milan Sonka. Intraretinal layer segmentation of macular optical coherence
tomography images using optimal 3-D graph search. IEEE transactions on medical
imaging, 27(10):1495–505, October 2008. 24
[52] Mona Kathryn Garvin, Michael David Abramoff, Xiaodong Wu, Stephen R Russell,
Trudy L Burns, and Milan Sonka. Automated 3-D intraretinal layer segmentation of
macular spectral-domain optical coherence tomography images. IEEE transactions
on medical imaging, 28(9):1436–47, September 2009. 24
[53] Andrea Giani, Marco Pellegrini, Alessandro Invernizzi, Mario Cigada, and Giovanni
Staurenghi. Aligning scan locations from consecutive spectral-domain optical coher-
ence tomography examinations: A comparison among different strategies. Invest.
Ophthalmol. Vis. Sci., 53(12):7637–7643, 2012. 45
[54] E. Gibson, Mei Young, M.V. Sarunic, and M.F. Beg. Optic nerve head registration
via hemispherical surface and volume registration. Biomedical Engineering, IEEE
Transactions on, 57(10):2592–2595, Oct 2010. 45, 49
[55] Michael J A Girard, J-K Francis Suh, Michael Bottlang, Claude F Burgoyne, and
J Crawford Downs. Scleral biomechanics in the aging monkey eye. Investigative
ophthalmology & visual science, 50(11):5226–37, November 2009. 112
[56] Michael J A Girard, J-K Francis Suh, Michael Bottlang, Claude F Burgoyne, and
J Crawford Downs. Biomechanical changes in the sclera of monkey eyes exposed to
chronic IOP elevations. Investigative ophthalmology & visual science, 52(8):5656–
69, July 2011. 112
141
[57] J. Glaunes, A. Trouve, and L. Younes. Diffeomorphic matching of distributions: a
new approach for unlabelled point-sets and sub-manifolds matching. In Proceedings
of the 2004 IEEE Computer Society Conference on Computer Vision and Pattern
Recognition, 2004. CVPR 2004., volume 2, pages 712–718. IEEE, 2004. 48, 79
[58] J. Glaunes and M. Vaillant. Surface matching via currents. Proceedings of Infor-
mation Processing in Medical Imaging (IPMI), Lecture Notes in Computer Science,
3565(381-392), 2006. 79
[59] Alberto O. Gonzalez-Garcıa, Gianmarco Vizzeri, Christopher Bowd, Felipe A.
Medeiros, Linda M. Zangwill, and Robert N. Weinreb. Reproducibility of RTVue
retinal nerve fiber layer thickness and optic disc measurements and agreement
with Stratus optical coherence tomography measurements. Am. J. Ophthalmol.,
147(6):1067–1074, June 2009. 44
[60] Erich Gotzinger, Michael Pircher, Wolfgang Geitzenauer, Christian Ahlers, Bernhard
Baumann, Stephan Michels, Ursula Schmidt-Erfurth, and Christoph K. Hitzenberger.
Retinal pigment epithelium segmentation by polarization sensitive optical coherence
tomography. Optics Express, 16(21):16410, September 2008. 24
[61] Giovanni Gregori, Fenghua Wang, Philip J Rosenfeld, Zohar Yehoshua, Ninel Z Gre-
gori, Brandon J Lujan, Carmen A Puliafito, and William J Feuer. Spectral domain
optical coherence tomography imaging of drusen in nonexudative age-related mac-
ular degeneration. Ophthalmology, 118(7):1373–9, July 2011. 32
[62] J E Grunwald, S M Hariprasad, J DuPont, M G Maguire, S L Fine, A J Brucker,
A M Maguire, and A C Ho. Foveolar choroidal blood flow in age-related macular
degeneration. Investigative ophthalmology & visual science, 39(2):385–90, February
1998. 30
[63] Juan E Grunwald, Tatyana I Metelitsina, Joan C Dupont, Gui-Shuang Ying, and
Maureen G Maguire. Reduced foveolar choroidal blood flow in eyes with increasing
AMD severity. Investigative ophthalmology & visual science, 46(3):1033–8, March
2005. 30
142

[64] Rafael Grytz, Christopher A Girkin, Vincent Libertiaux, and J Crawford Downs. Per-
spectives on biomechanical growth and remodeling mechanisms in glaucoma(). Me-
chanics research communications, 42:92–106, July 2012. 101
[65] Rafael Grytz, Ian A Sigal, Jeffrey W Ruberti, Gunther Meschke, and J Crawford
Downs. Lamina Cribrosa Thickening in Early Glaucoma Predicted by a Microstruc-
ture Motivated Growth and Remodeling Approach. Mechanics of materials : an
international journal, 44:99–109, January 2012. 101
[66] Li Guo, Stephen E Moss, Robert A Alexander, Robin R Ali, Frederick W Fitzke, and
M Francesca Cordeiro. Retinal ganglion cell apoptosis in glaucoma is related to
intraocular pressure and IOP-induced effects on extracellular matrix. Investigative
ophthalmology & visual science, 46(1):175–82, January 2005. 8
[67] Mona Haeker, Xiaodong Wu, Michael Abramoff, Randy Kardon, and Milan Sonka.
Incorporation of regional information in optimal 3-D graph search with application for
intraretinal layer segmentation of optical coherence tomography images. Informa-
tion processing in medical imaging : proceedings of the ... conference, 20:607–18,
January 2007. 24
[68] Mark Hall, Eibe Frank, Geoffrey Holmes, Bernhard Pfahringer, Peter Reutemann,
and Ian H Witten. The WEKA data mining software: an update. ACM SIGKDD
explorations newsletter, 11(1):10–18, 2009. 87
[69] Masanori Hangai, Yumiko Ojima, Norimoto Gotoh, Ryo Inoue, Yoshiaki Yasuno,
Shuichi Makita, Masahiro Yamanari, Toyohiko Yatagai, Mihori Kita, and Nagahisa
Yoshimura. Three-dimensional imaging of macular holes with high-speed optical
coherence tomography. Ophthalmology, 114(4):763–73, April 2007. 18
[70] Trevor Hastie, Robert Tibshirani, and Jerome Friedman. The Elements of Statistical
Learning (2nd edition). Springer Series in Statistics. Springer New York Inc., 2009.
87
[71] Lin He, Ruojin Ren, Hongli Yang, Christy Hardin, Luke Reyes, Juan Reynaud, Stu-
art K. Gardiner, Brad Fortune, Shaban Demirel, and Claude F. Burgoyne. Anatomic
143

vs. acquired image frame discordance in spectral domain optical coherence tomog-
raphy minimum rim measurements. PLoS ONE, 9(3):e92225, March 2014. 45
[72] Lin He, Ruojin Ren, Hongli Yang, Christy Hardin, Luke Reyes, Juan Reynaud, Stu-
art K Gardiner, Brad Fortune, Shaban Demirel, and Claude F Burgoyne. Anatomic
vs. acquired image frame discordance in spectral domain optical coherence tomog-
raphy minimum rim measurements. PloS one, 9(3):e92225, January 2014. 111
[73] M R Hee, J A Izatt, E A Swanson, D Huang, J S Schuman, C P Lin, C A Puliafito,
and J G Fujimoto. Optical coherence tomography of the human retina. Archives of
ophthalmology, 113(3):325–32, March 1995. 17
[74] Anders Heijl. Reduction of Intraocular Pressure and Glaucoma Progression.
Archives of Ophthalmology, 120(10):1268, October 2002. 8
[75] M R Hernandez. The optic nerve head in glaucoma: role of astrocytes in tissue
remodeling. Progress in retinal and eye research, 19(3):297–321, May 2000. 101
[76] Esther M Hoffmann, Linda M Zangwill, Jonathan G Crowston, and Robert N Wein-
reb. Optic disk size and glaucoma. Survey of ophthalmology, 52(1):32–49, January
2007. 113
[77] Sek-Tien Hoh, Marcus C C Lim, Steve K L Seah, Albert T H Lim, Sek-Jin Chew,
Paul J Foster, and Tin Aung. Peripapillary retinal nerve fiber layer thickness varia-
tions with myopia. Ophthalmology, 113(5):773–7, May 2006. 112
[78] Zhihong Hu, Michael D Abramoff, Young H Kwon, Kyungmoo Lee, and Mona K
Garvin. Automated segmentation of neural canal opening and optic cup in 3D spec-
tral optical coherence tomography volumes of the optic nerve head. Investigative
ophthalmology & visual science, 51(11):5708–17, November 2010. 17, 24
[79] Zhihong Hu, Xiaodong Wu, Yanwei Ouyang, Yanling Ouyang, and Srinivas R. Sadda.
Semiautomated segmentation of the choroid in spectral- domain optical coher-
ence tomography volume scans. Investigative Ophthalmology and Visual Science,
54(3):1722–1729, March 2013. 27
144

[80] D Huang, E. Swanson, C. Lin, J. Schuman, W. Stinson, W Chang, M. Hee, T Flotte,
K Gregory, C. Puliafito, and al. Et. Optical coherence tomography. Science,
254(5035):1178–1181, November 1991. 9
[81] Son C Huynh, Xiu Ying Wang, Elena Rochtchina, and Paul Mitchell. Peripapillary
retinal nerve fiber layer thickness in a population of 6-year-old children: findings by
optical coherence tomography. Ophthalmology, 113(9):1583–92, September 2006.
102, 112
[82] Young Hoon Hwang, Chungkwon Yoo, and Yong Yeon Kim. Myopic optic disc tilt and
the characteristics of peripapillary retinal nerve fiber layer thickness measured by
spectral-domain optical coherence tomography. Journal of glaucoma, 21(4):260–5,
January. 134
[83] S M Hyung, D M Kim, C Hong, and D H Youn. Optic disc of the myopic eye: rela-
tionship between refractive errors and morphometric characteristics. Korean journal
of ophthalmology : KJO, 6(1):32–5, June 1992. 114
[84] Yasushi Ikuno, Kana Kawaguchi, Takeyoshi Nouchi, and Yoshiaki Yasuno. Choroidal
thickness in healthy Japanese subjects. Investigative ophthalmology & visual sci-
ence, 51(4):2173–6, April 2010. 115
[85] Yutaka Imamura, Takamitsu Fujiwara, Ron Margolis, and Richard F Spaide. En-
hanced depth imaging optical coherence tomography of the choroid in central serous
chorioretinopathy. Retina (Philadelphia, Pa.), 29(10):1469–73, January. 26
[86] Hiroshi Ishikawa, Daniel M Stein, Gadi Wollstein, Siobahn Beaton, James G Fuji-
moto, and Joel S Schuman. Macular segmentation with optical coherence tomogra-
phy. Investigative ophthalmology & visual science, 46(6):2012–7, June 2005. 24
[87] Glenn J. Jaffe and Joseph Caprioli. Optical coherence tomography to detect and
manage retinal disease and glaucoma. Am. J. Ophthalmol., 137(1):156–169, Jan-
uary 2004. 44
[88] Glenn J Jaffe and Joseph Caprioli. Optical coherence tomography to detect
and manage retinal disease and glaucoma. American journal of ophthalmology,
137(1):156–69, January 2004. 111
145

[89] John Johnstone, Massimo Fazio, Kulawan Rojananuangnit, Brandon Smith, Mark
Clark, Crawford Downs, Cynthia Owsley, Michael J A Girard, Jean Martial Mari, and
Christopher A Girkin. Variation of the axial location of Bruch’s membrane opening
with age, choroidal thickness, and race. Investigative ophthalmology & visual sci-
ence, 55(3):2004–9, March 2014. 115
[90] I.T. Jolliffe. Principal Component Analysis. Springer Science & Business Media,
2002. 105
[91] J B Jonas and W M Budde. Optic nerve damage in highly myopic eyes with chronic
open-angle glaucoma. European journal of ophthalmology, 15(1):41–7, January
2005. 102
[92] J B Jonas and A Dichtl. Optic disc morphology in myopic primary open-angle glau-
coma. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von
Graefes Archiv fur klinische und experimentelle Ophthalmologie, 235(10):627–33,
October 1997. 102, 114
[93] J B Jonas, G C Gusek, and G O Naumann. Optic disc, cup and neuroretinal rim size,
configuration and correlations in normal eyes. Investigative ophthalmology & visual
science, 29(7):1151–8, July 1988. 112, 114
[94] Jost B Jonas. Optic disk size correlated with refractive error. American journal of
ophthalmology, 139(2):346–8, February 2005. 114
[95] Jost B Jonas, Eduard Berenshtein, and Leonard Holbach. Lamina cribrosa thickness
and spatial relationships between intraocular space and cerebrospinal fluid space in
highly myopic eyes. Investigative ophthalmology & visual science, 45(8):2660–5,
August 2004. 114
[96] Jost B Jonas, Shefali B Jonas, Rahul A Jonas, Leonard Holbach, and Songhomitra
Panda-Jonas. Histology of the parapapillary region in high myopia. American journal
of ophthalmology, 152(6):1021–9, December 2011. 102
146

[97] Thomas Martini Jørgensen, Jakob Thomadsen, Ulrik Christensen, Wael Soliman,
and Birgit Sander. Enhancing the signal-to-noise ratio in ophthalmic optical coher-
ence tomography by image registration—method and clinical examples. J. Biomed.
Opt., 12(4):041208, August 2007. 45
[98] S. Joshi, B. Davis, M. Jomier, and G. Gerig. Unbiased diffeomorphic atlas construc-
tion for computational anatomy. NeuroImage, 23:S151–S160, 2004. 76
[99] Vedran Kajic, Marieh Esmaeelpour, Boris Povazay, David Marshall, Paul L Rosin,
and Wolfgang Drexler. Automated choroidal segmentation of 1060 nm OCT in
healthy and pathologic eyes using a statistical model. Biomedical optics express,
3(1):86–103, January 2012. 27
[100] Akiyasu Kanamori, Makoto Nakamura, Michael F T Escano, Ryu Seya, Hidetaka
Maeda, and Akira Negi. Evaluation of the glaucomatous damage on retinal nerve
fiber layer thickness measured by optical coherence tomography. American journal
of ophthalmology, 135(4):513–20, April 2003. 111
[101] Akiyasu Kanamori, Makoto Nakamura, Michael F.T Escano, Ryu Seya, Hidetaka
Maeda, and Akira Negi. Evaluation of the glaucomatous damage on retinal nerve
fiber layer thickness measured by optical coherence tomography. Am. J. Ophthal-
mol., 135(4):513–520, April 2003. 44, 93
[102] Shin Hee Kang, Seung Woo Hong, Seong Kyu Im, Sang Hyup Lee, and Myung Douk
Ahn. Effect of myopia on the thickness of the retinal nerve fiber layer measured
by Cirrus HD optical coherence tomography. Investigative ophthalmology & visual
science, 51(8):4075–83, August 2010. 102, 112
[103] M A Kass, A E Kolker, and B Becker. Prognostic factors in glaucomatous visual field
loss. Archives of ophthalmology, 94(8):1274–6, August 1976. 107
[104] MA Kass, AE Kolker, and B Becker. Prognostic factors in glaucomatous visual field
loss. Archives of Ophthalmology, 94(8):1274–1276, 1976. 94
[105] Helga Kolb. Simple Anatomy of the Retina. University of Utah Health Sciences
Center, January 2012. xi, 5, 7
147

[106] J R Landis and G G Koch. The measurement of observer agreement for categorical
data. Biometrics, 33(1):159–74, March 1977. 38
[107] Evgeniy Lebed, Sieun Lee, Marinko V Sarunic, and Mirza Faisal Beg. Rapid ra-
dial optical coherence tomography image acquisition. Journal of biomedical optics,
18(3):036004, March 2013. 41, 55
[108] S. Lee, S. X. Han, M. Young, P. J. Mackenzie, M. F. Beg, and M. V. Sarunic. Op-
tic nerve head and peripapillary morphometrics in myopic glaucoma. presented at
Association of Research in Vision and Ophthalmology (ARVO), Orlando, FL, May,
2014. 116
[109] Sieun Lee, Mirza F. Beg, and Marinko V. Sarunic. Segmentation of the macular
choroid in OCT images acquired at 830nm and 1060nm. In B. Bouma and R. Leit-
geb, editors, Optical Coherence Tomography and Coherence Techniques VI, volume
8802, page 88020J, Munich, 2013. Optical Society of America. 41, 133
[110] Sieun Lee, Nicolas Charon, Benjamin Charlier, Karteek Popuri, Evgeniy Lebed,
Pradeep Reddy Ramana, Marinko V. Sarunic, Alain Trouve, and Mirza Faisal Beg.
Atlas-based shape analysis and classification of retinal optical coherence tomogra-
phy images using the functional shape (fshape) framework. IEEE TRANSACTIONS
ON MEDICAL IMAGING, 2015. submitted for publication. 133
[111] Sieun Lee, Nader Fallah, Farzin Forooghian, Ashley Ko, Kaivon Pakzad-Vaezi, An-
drew B Merkur, Andrew W Kirker, David A Albiani, Mei Young, Marinko V Sarunic,
and Mirza Faisal Beg. Comparative analysis of repeatability of manual and auto-
mated choroidal thickness measurements in nonneovascular age-related macular
degeneration. Investigative ophthalmology & visual science, 54(4):2864–71, April
2013. 28, 41, 133
[112] Sieun Lee, Sherry X. Han, Mei Young, Mirza Faisal Beg, Marinko V. Sarunic, and
Paul J. Mackenzie. Optic nerve head and peripapillary morphometrics in myopic
glaucoma. Invest. Ophthalmol. Vis. Sci., 55(7):4378–4393, July 2014. 45, 54, 116,
133
148

[113] Sieun Lee, Evgeniy Lebed, Marinko V Sarunic, and Mirza Faisal Beg. Exact surface
registration of retinal surfaces from 3-d optical coherence tomography images. IEEE
transactions on bio-medical engineering, 62(2):609–17, February 2015. 100, 133
[114] Sieun Lee, Mei Young, Marinko V. Sarunic, and Mirza Faisal Beg. End-to-end
Pipeline for Spectral Domain Optical Coherence Tomography and Morphometric
Analysis of Human Optic Nerve Head. Journal of Medical and Biological Engineer-
ing, 31(2):111–119, April 2011. 17, 20, 23, 133
[115] R. Leitgeb, C. Hitzenberger, and Adolf Fercher. Performance of fourier domain vs
time domain optical coherence tomography. Optics Express, 11(8):889, April 2003.
9
[116] Alex D Leow, Igor Yanovsky, Neelroop Parikshak, Xue Hua, Suh Lee, Arthur W Toga,
Clifford R Jack, Matt A Bernstein, Paula J Britson, Jeffrey L Gunter, Chadwick P
Ward, Bret Borowski, Leslie M Shaw, John Q Trojanowski, Adam S Fleisher, Danielle
Harvey, John Kornak, Norbert Schuff, Gene E Alexander, Michael W Weiner, and
Paul M Thompson. Alzheimer’s disease neuroimaging initiative: a one-year follow up
study using tensor-based morphometry correlating degenerative rates, biomarkers
and cognition. NeuroImage, 45(3):645–55, April 2009. 56
[117] Christopher Kai-Shun Leung, Arthur Chak Kwan Cheng, Kelvin Kam Lung Chong,
King Sai Leung, Shaheeda Mohamed, Charles Sing Lok Lau, Carol Yim Lui Cheung,
Geoffrey Chin-Hung Chu, Ricky Yiu Kwong Lai, Calvin Chi Pui Pang, and Dennis
Shun Chiu Lam. Optic disc measurements in myopia with optical coherence tomog-
raphy and confocal scanning laser ophthalmoscopy. Investigative ophthalmology &
visual science, 48(7):3178–83, July 2007. 112
[118] Christopher Kai-Shun Leung, Shaheeda Mohamed, King Sai Leung, Carol Yim-Lui
Cheung, Sylvia Lai-wa Chan, Daphne Ka-yee Cheng, August Ki-cheung Lee, Glo-
ria Yuk-oi Leung, Srinivas Kamalakara Rao, and Dennis Shun Chiu Lam. Retinal
nerve fiber layer measurements in myopia: An optical coherence tomography study.
Investigative ophthalmology & visual science, 47(12):5171–6, December 2006. 111
149

[119] Kang Li, Xiaodong Wu, Danny Z Chen, and Milan Sonka. Optimal surface segmenta-
tion in volumetric images–a graph-theoretic approach. IEEE transactions on pattern
analysis and machine intelligence, 28(1):119–34, January 2006. 24
[120] Shijian Lu, Carol Yim-lui Cheung, Jiang Liu, Joo Hwee Lim, Christopher Kai-shun
Leung, and Tien Yin Wong. Automated layer segmentation of optical coherence
tomography images. IEEE transactions on bio-medical engineering, 57(10):2605–8,
October 2010. 24
[121] J. Ma, M. I. Miller, and L. Younes. A Bayesian generative model for surface template
estimation. Journal of Biomedical Imaging, 2010:16, 2010. 76
[122] Gopi Maguluri, Mircea Mujat, B H Park, K H Kim, Wei Sun, N V Iftimia, R D Fer-
guson, Daniel X Hammer, Teresa C Chen, and Johannes F de Boer. Three dimen-
sional tracking for volumetric spectral-domain optical coherence tomography. Optics
express, 15(25):16808–16817, December 2007. 15
[123] Varsha Manjunath, Jordana Goren, James G Fujimoto, and Jay S Duker. Analysis
of choroidal thickness in age-related macular degeneration using spectral-domain
optical coherence tomography. American journal of ophthalmology, 152(4):663–8,
October 2011. 26
[124] Ron Margolis and Richard F Spaide. A pilot study of enhanced depth imaging optical
coherence tomography of the choroid in normal eyes. American journal of ophthal-
mology, 147(5):811–5, May 2009. 26
[125] Susana Martinez-Conde, Stephen L Macknik, and David H Hubel. The role of fixa-
tional eye movements in visual perception. Nature reviews. Neuroscience, 5(3):229–
240, March 2004. 14
[126] Ichiro Maruko, Tomohiro Iida, Yukinori Sugano, Akira Ojima, Masashi Ogasawara,
and Richard F Spaide. Subfoveal choroidal thickness after treatment of central
serous chorioretinopathy. Ophthalmology, 117(9):1792–9, September 2010. 26
[127] Eugenio A Maul, David S Friedman, Dolly S Chang, Michael V Boland, Pradeep Y
Ramulu, Henry D Jampel, and Harry A Quigley. Choroidal thickness measured by
150

spectral domain optical coherence tomography: factors affecting thickness in glau-
coma patients. Ophthalmology, 118(8):1571–9, August 2011. 115
[128] Felipe A. Medeiros, Linda M. Zangwill, Christopher Bowd, Roberto M. Vessani,
Remo Susanna Jr, and Robert N. Weinreb. Evaluation of retinal nerve fiber layer, op-
tic nerve head, and macular thickness measurements for glaucoma detection using
optical coherence tomography. Am. J. Ophthalmol., 139(1):44–55, January 2005. 44
[129] Felipe A Medeiros, Linda M Zangwill, Christopher Bowd, Roberto M Vessani, Remo
Susanna, and Robert N Weinreb. Evaluation of retinal nerve fiber layer, optic nerve
head, and macular thickness measurements for glaucoma detection using optical
coherence tomography. American journal of ophthalmology, 139(1):44–55, January
2005. 111
[130] Gustavo B Melo, Rodrigo D Libera, Aline S Barbosa, Lia M G Pereira, Larissa M Doi,
and Luiz A S Melo. Comparison of optic disk and retinal nerve fiber layer thickness
in nonglaucomatous and glaucomatous patients with high myopia. American journal
of ophthalmology, 142(5):858–60, November 2006. 102
[131] D S Minckler, A H Bunt, and G W Johanson. Orthograde and retrograde axoplasmic
transport during acute ocular hypertension in the monkey. Investigative ophthalmol-
ogy & visual science, 16(5):426–41, May 1977. 101
[132] Akshaya Mishra, Alexander Wong, Kostadinka Bizheva, and David A Clausi. Intra-
retinal layer segmentation in optical coherence tomography images. Optics express,
17(26):23719–28, December 2009. 24
[133] P Mitchell, F Hourihan, J Sandbach, and J J Wang. The relationship between glau-
coma and myopia: the Blue Mountains Eye Study. Ophthalmology, 106(10):2010–5,
October 1999. 101
[134] G V Moraes. How does construction and statistical modeling within oct nor-
mative databases compare with standard automated perimetry databases? In
FDA/American Glaucoma Society Workshop on the Validity, Reliability, and Usability
of Glaucoma Imaging Devices, 2012; Silver Spring, MD. 101
[135] J.C. Morrison and I.P. Pollack. Glaucoma: Science and Practice. Thieme, 2011. 93
151
[136] Jean-Claude Mwanza, Jonathan D Oakley, Donald L Budenz, Robert T Chang,
O’Rese J Knight, and William J Feuer. Macular ganglion cell-inner plexiform layer:
automated detection and thickness reproducibility with spectral domain-optical co-
herence tomography in glaucoma. Investigative ophthalmology & visual science,
52(11):8323–9, January 2011. 24
[137] Jean-Claude Mwanza, Fouad E Sayyad, and Donald L Budenz. Choroidal thick-
ness in unilateral advanced glaucoma. Investigative ophthalmology & visual science,
53(10):6695–701, January 2012. 55
[138] N. A. Nassif, B. Cense, B. H. Park, M. C. Pierce, S. H. Yun, B. E. Bouma, G. J.
Tearney, T. C. Chen, and J. F. de Boer. In vivo high-resolution video-rate spectral-
domain optical coherence tomography of the human retina and optic nerve. Optics
Express, 12(3):367, 2004. 9
[139] Nader Nassif, Barry Cense, B. Hyle Park, Seok H. Yun, Teresa C. Chen, Brett E.
Bouma, Guillermo J. Tearney, and Johannes F. de Boer. In vivo human retinal imag-
ing by ultrahigh-speed spectral domain optical coherence tomography. Optics Let-
ters, 29(5):480, 2004. 9
[140] Meindert Niemeijer, Mona K Garvin, Kyungmoo Lee, Bram van Ginneken, Michael D
Abramoff, and Milan Sonka. Registration of 3D spectral OCT volumes using 3D
SIFT feature point matching. In SPIE Medical Imaging, pages 72591I–72591I. Inter-
national Society for Optics and Photonics, 2009. 45
[141] Meindert Niemeijer, Kyungmoo Lee, Mona K. Garvin, Michael D. Abramoff, and Milan
Sonka. Registration of 3D spectral OCT volumes combining ICP with a graph-based
approach. volume 8314, pages 83141A–83141A–9, 2012. 45
[142] Hideki Nomura, Fujiko Ando, Naoakira Niino, Hiroshi Shimokata, and Yozo Miyake.
The relationship between intraocular pressure and refractive error adjusting for age
and central corneal thickness. Ophthalmic and Physiological Optics, 24(1):41–45,
January 2004. 102
152

[143] C Oliveira, N Harizman, C A Girkin, A Xie, C Tello, J M Liebmann, and R Ritch.
Axial length and optic disc size in normal eyes. The British journal of ophthalmology,
91(1):37–9, January 2007. 112, 114
[144] Clyde W. Oyster. The Human Eye: Structure and Function. Sinauer Associates,
2006. 7
[145] Mona Pache and Josef Flammer. A sick eye in a sick body? Systemic findings in
patients with primary open-angle glaucoma. Survey of ophthalmology, 51(3):179–
212, January 2006. 101
[146] Rajul S. Parikh, Shefali Parikh, G. Chandra Sekhar, Rajesh S. Kumar, S. Prabakaran,
J. Ganesh Babu, and Ravi Thomas. Diagnostic capability of optical coherence to-
mography (Stratus OCT 3) in early glaucoma. Ophthalmology, 114(12):pp. 2238–
2243, 2007. 93
[147] Sung Chul Park, Saman Kiumehr, Christopher C Teng, Celso Tello, Jeffrey M Lieb-
mann, and Robert Ritch. Horizontal central ridge of the lamina cribrosa and regional
differences in laminar insertion in healthy subjects. Investigative ophthalmology &
visual science, 53(3):1610–6, March 2012. 113
[148] Nimesh B Patel, Joe L Wheat, Aldon Rodriguez, Victoria Tran, and Ronald S Har-
werth. Agreement between retinal nerve fiber layer measures from Spectralis and
Cirrus spectral domain OCT. Optometry and vision science : official publication of
the American Academy of Optometry, 89(5):E652–66, May 2012. 111
[149] Lelia A. Paunescu, Joel S. Schuman, Lori Lyn Price, Paul C. Stark, Siobahn Beaton,
Hiroshi Ishikawa, Gadi Wollstein, and James G. Fujimoto. Reproducibility of nerve
fiber thickness, macular thickness, and optic nerve head measurements using Stra-
tus OCT. Invest. Ophthalmol. Vis. Sci., 45(6):1716–1724, June 2004. 44
[150] Michael Pircher, Bernhard Baumann, Erich Gotzinger, Harald Sattmann, and
Christoph K. Hitzenberger. Simultaneous SLO/OCT imaging of the human retina
with axial eye motion correction. Optics Express, 15(25):16922, 2007. 15
153

[151] Michael Pircher, Erich Gotzinger, Oliver Findl, Stephan Michels, Wolfgang
Geitzenauer, Christina Leydolt, Ursula Schmidt-Erfurth, and Christoph K Hitzen-
berger. Human macula investigated in vivo with polarization-sensitive optical coher-
ence tomography. Investigative ophthalmology & visual science, 47(12):5487–94,
December 2006. 26
[152] Benjamin Potsaid, Iwona Gorczynska, Vivek J. Srinivasan, Yueli Chen, James Jiang,
Alex Cable, and James G. Fujimoto. Ultrahigh speed Spectral / Fourier domain OCT
ophthalmic imaging at 70,000 to 312,500 axial scans per second. Optics Express,
16(19):15149, September 2008. 17
[153] Constantin J Pournaras, Eric Logean, Charles E Riva, Benno L Petrig, Stephane R
Chamot, Gabriel Coscas, and Gisele Soubrane. Regulation of subfoveal choroidal
blood flow in age-related macular degeneration. Investigative ophthalmology & visual
science, 47(4):1581–6, April 2006. 30
[154] H Quigley and D R Anderson. The dynamics and location of axonal transport block-
ade by acute intraocular pressure elevation in primate optic nerve. Investigative
ophthalmology, 15(8):606–16, August 1976. 101
[155] H A Quigley, E M Addicks, W R Green, and A E Maumenee. Optic nerve damage
in human glaucoma. II. The site of injury and susceptibility to damage. Archives of
ophthalmology, 99(4):635–49, April 1981. 101
[156] H A Quigley, R M Hohman, E M Addicks, R W Massof, and W R Green. Morphologic
changes in the lamina cribrosa correlated with neural loss in open-angle glaucoma.
American journal of ophthalmology, 95(5):673–91, May 1983. 101
[157] H A Quigley, R Varma, J M Tielsch, J Katz, A Sommer, and D L Gilbert. The relation-
ship between optic disc area and open-angle glaucoma: the Baltimore Eye Survey.
Journal of glaucoma, 8(6):347–52, December 1999. 113
[158] R S Ramrattan, R C Wolfs, J B Jonas, A Hofman, and P T de Jong. Determinants
of optic disc characteristics in a general population: The Rotterdam Study. Ophthal-
mology, 106(8):1588–96, August 1999. 114
154

[159] Frederick M Rauscher, Navneet Sekhon, William J Feuer, and Donald L Budenz.
Myopia affects retinal nerve fiber layer measurements as determined by optical co-
herence tomography. Journal of glaucoma, 18(7):501–5, September 2009. 111
[160] Alexandre S. C. Reis, Neil O’Leary, Hongli Yang, Glen P. Sharpe, Marcelo T. Nicolela,
Claude F. Burgoyne, and Balwantray C. Chauhan. Influence of clinically invisible, but
optical coherence tomography detected, optic disc margin anatomy on neuroretinal
rim evaluation. Invest. Ophthalmol. Vis. Sci., 53(4):1852–1860, April 2012. 44, 45
[161] Alexandre S C Reis, Neil O’Leary, Hongli Yang, Glen P Sharpe, Marcelo T Nicolela,
Claude F Burgoyne, and Balwantray C Chauhan. Influence of clinically invisible, but
optical coherence tomography detected, optic disc margin anatomy on neuroretinal
rim evaluation. Investigative ophthalmology & visual science, 53(4):1852–60, April
2012. 104, 112
[162] Alexandre S.C. Reis, Glen P. Sharpe, Hongli Yang, Marcelo T. Nicolela, Claude F.
Burgoyne, and Balwantray C. Chauhan. Optic disc margin anatomy in patients with
glaucoma and normal controls with spectral domain optical coherence tomography.
Ophthalmology, 119(4):738–747, April 2012. 44, 45, 112
[163] Ruojin Ren, Ningli Wang, Bin Li, Liaoqing Li, Fei Gao, Xiaolin Xu, and Jost B Jonas.
Lamina cribrosa and peripapillary sclera histomorphometry in normal and advanced
glaucomatous Chinese eyes with various axial length. Investigative ophthalmology
& visual science, 50(5):2175–84, May 2009. 114
[164] Jin Young Rhew, Yun Taek Kim, and Kyu Ryong Choi. Measurement of subfoveal
choroidal thickness in normal-tension glaucoma in Korean patients. Journal of glau-
coma, 23(1):46–9, January 2014. 115
[165] Susanna Ricco, Mei Chen, Hiroshi Ishikawa, Gadi Wollstein, and Joel Schuman.
Correcting motion artifacts in retinal spectral domain optical coherence tomography
via image registration. Medical image computing and computer-assisted intervention
: MICCAI ... International Conference on Medical Image Computing and Computer-
Assisted Intervention, 12(Pt 1):100–7, January 2009. 17
155

[166] Susanna Ricco, Mei Chen, Hiroshi Ishikawa, Gadi Wollstein, and Joel Schuman.
Correcting motion artifacts in retinal spectral domain optical coherence tomography
via image registration. In Med. Image. Comput. Assist. Interv. (MICCAI’09) Part I,
pages 100–107, London, UK, September 2009. 45
[167] Paul Riordan-Eva and Emmett Cunningham. Vaughan & Asbury’s General Ophthal-
mology, 18th Edition. McGraw Hill Professional, 2011. 4
[168] Michael D Roberts, Vicente Grau, Jonathan Grimm, Juan Reynaud, Anthony J
Bellezza, Claude F Burgoyne, and J Crawford Downs. Remodeling of the connec-
tive tissue microarchitecture of the lamina cribrosa in early experimental glaucoma.
Investigative ophthalmology & visual science, 50(2):681–90, February 2009. 101
[169] Michael D Roberts, Ian A Sigal, Yi Liang, Claude F Burgoyne, and J Crawford
Downs. Changes in the biomechanical response of the optic nerve head in early
experimental glaucoma. Investigative ophthalmology & visual science, 51(11):5675–
84, November 2010. 101
[170] Marco Ruggeri, Hassan Wehbe, Shuliang Jiao, Giovanni Gregori, Maria E. Jock-
ovich, Abigail Hackam, Yuanli Duan, and Carmen a. Puliafito. In vivo three-
dimensional high-resolution imaging of rodent retina with spectral-domain optical co-
herence tomography. Investigative Ophthalmology and Visual Science, 48(4):1808–
1814, April 2007. 24
[171] Giacomo Savini, Piero Barboni, Vincenzo Parisi, and Michele Carbonelli. The influ-
ence of axial length on retinal nerve fibre layer thickness and optic-disc size mea-
surements by spectral-domain OCT. The British journal of ophthalmology, 96(1):57–
61, January 2012. 102, 112
[172] Ian A Sigal, John G Flanagan, and C Ross Ethier. Factors influencing optic nerve
head biomechanics. Investigative ophthalmology & visual science, 46(11):4189–99,
November 2005. 102
[173] Alfred Sommer. Relationship Between Intraocular Pressure and Primary Open An-
gle Glaucoma Among White and Black Americans. Archives of Ophthalmology,
109(8):1090, August 1991. 8
156

[174] Richard F Spaide, Hideki Koizumi, Maria C Pozzoni, and Maria C Pozonni. Enhanced
depth imaging spectral-domain optical coherence tomography. American journal of
ophthalmology, 146(4):496–500, October 2008. 26
[175] Nicholas G Strouthidis, Brad Fortune, Hongli Yang, Ian A Sigal, and Claude F Bur-
goyne. Longitudinal change detected by spectral domain optical coherence tomog-
raphy in the optic nerve head and peripapillary retina in experimental glaucoma. In-
vestigative ophthalmology & visual science, 52(3):1206–19, March 2011. 104, 105,
112, 114, 115
[176] Nicholas G Strouthidis, Jonathan Grimm, Galen A Williams, Grant A Cull, David J
Wilson, and Claude F Burgoyne. A comparison of optic nerve head morphology
viewed by spectral domain optical coherence tomography and by serial histology.
Investigative ophthalmology & visual science, 51(3):1464–74, March 2010. 112
[177] Nicholas G Strouthidis, Hongli Yang, J Crawford Downs, and Claude F Burgoyne.
Comparison of clinical and three-dimensional histomorphometric optic disc margin
anatomy. Investigative ophthalmology & visual science, 50(5):2165–74, May 2009.
112
[178] Nicholas G. Strouthidis, Hongli Yang, Juan F. Reynaud, Jonathan L. Grimm, Stu-
art K. Gardiner, Brad Fortune, and Claude F. Burgoyne. Comparison of clinical and
spectral domain optical coherence tomography optic disc margin anatomy. Invest.
Ophthalmol. Vis. Sci., 50(10):4709–4718, October 2009. 44, 45, 112
[179] R Susanna, S M Drance, and G R Douglas. The visual prognosis of the fellow eye
in uniocular chronic open-angle glaucoma. The British journal of ophthalmology,
62(5):327–9, May 1978. 107
[180] R Susanna, SM Drance, and GR Douglas. The visual prognosis of the fellow eye
in uniocular chronic open-angle glaucoma. The British Journal of Ophthalmology,
62(5):327–329, 1978. 94
[181] Teresa Torzicky, Michael Pircher, Stefan Zotter, Marco Bonesi, Erich Gotzinger, and
Christoph K Hitzenberger. Automated measurement of choroidal thickness in the
157

human eye by polarization sensitive optical coherence tomography. Optics express,
20(7):7564–74, March 2012. 27
[182] William B. Trattler, Peter K. Kaiser, and Neil J. Friedman. Review of Ophthalmology:
Expert Consult - Online and Print. Elsevier Health Sciences, 2012. 39, 102
[183] A. Unterhuber, B. Povazay, B. Hermann, H. Sattmann, A. Chavez-Pirson, and
W. Drexler. In vivo retinal optical coherence tomography at 1040 nm - enhanced
penetration into the choroid. Optics Express, 13(9):3252, May 2005. 26
[184] Marc Vaillant and Joan Glaunes. Information Processing in Medical Imaging, volume
3565 of Lecture Notes in Computer Science. Springer Berlin Heidelberg, Berlin,
Heidelberg, July 2005. 46, 47
[185] Bo Wang, Jessica E Nevins, Zach Nadler, Gadi Wollstein, Hiroshi Ishikawa,
Richard A Bilonick, Larry Kagemann, Ian A Sigal, Ireneusz Grulkowski, Jonathan J
Liu, Martin Kraus, Chen D Lu, Joachim Hornegger, James G Fujimoto, and Joel S
Schuman. In vivo lamina cribrosa micro-architecture in healthy and glaucomatous
eyes as assessed by optical coherence tomography. Investigative ophthalmology &
visual science, 54(13):8270–4, December 2013. 101
[186] K J Worsley, J Cao, T Paus, M Petrides, and A C Evans. Applications of random
field theory to functional connectivity. Human brain mapping, 6(5-6):364–7, January
1998. 51
[187] J. Xu, S. Han, S. Lee, M. Cua, M. Young, A. merkur, A. Kirker, D. Albiani,
F. Forooghian, P. Mackenzie, and M. V. Sarunic. Real-time acquisition and display of
flow contrast in macula and onh with speckle variance oct. presented in the annual
meeting of Association of Research in Vision and Ophthalmology (ARVO), Orlando,
FL, May. 41
[188] Liang Xu, Yaxing Wang, Shuang Wang, Yun Wang, and Jost B Jonas. High myopia
and glaucoma susceptibility the Beijing Eye Study. Ophthalmology, 114(2):216–20,
March 2007. 101
[189] Hongli Yang, J Crawford Downs, Christopher Girkin, Lisandro Sakata, Anthony
Bellezza, Hilary Thompson, and Claude F Burgoyne. 3-D histomorphometry of the
158

normal and early glaucomatous monkey optic nerve head: lamina cribrosa and peri-
papillary scleral position and thickness. Investigative ophthalmology & visual sci-
ence, 48(10):4597–607, October 2007. 101, 114
[190] B T Thomas Yeo, Mert Sabuncu, Tom Vercauteren, Nicholas Ayache, Bruce Fischl,
and Polina Golland. Spherical demons: fast surface registration. Medical image
computing and computer-assisted intervention : MICCAI ... International Conference
on Medical Image Computing and Computer-Assisted Intervention, 11(Pt 1):745–53,
January 2008. 49
[191] B T Thomas Yeo, Mert R Sabuncu, Tom Vercauteren, Nicholas Ayache, Bruce Fischl,
and Polina Golland. Spherical demons: fast diffeomorphic landmark-free surface
registration. IEEE transactions on medical imaging, 29(3):650–68, March 2010. 49
[192] B.T.T. Yeo, M.R. Sabuncu, T. Vercauteren, N. Ayache, B. Fischl, and P. Golland.
Spherical demons: Fast diffeomorphic landmark-free surface registration. Medical
Imaging, IEEE Transactions on, 29(3):650–668, March 2010. 46
[193] L. Younes. Shapes and diffeomorphisms. Springer, 2010. 19, 77
[194] Carolyn Mei Young. High-speed volumetric in vivo medical imaging for morphometric
analysis of the human optic nerve head. PhD thesis, November 2011. xi, 11, 12
[195] M. Young, S. Lee, M. F. Beg, P. J. Mackenzie, and M. V. Sarunic. High speed mor-
phometric imaging of the optic nerve head with 1um oct. presented at Association
of Research in Vision and Ophthalmology (ARVO), Fort Lauderdale, FL, May 1-5,
2011. 116, 133
[196] M. Young, S. Lee, E. Gibson, K. Hsu, M. F. Beg, P. J. Mackenzie, and M. V. Sarunic.
Morphometric analysis of the optic nerve head with optical coherence tomography.
In Joseph A. Izatt, James G. Fujimoto, and Valery V. Tuchin, editors, Proceedings of
SPIE - The International Society for Optical Engineering, pages 75542L–75542L–6,
February 2010. 116, 133
[197] Mei Young, Evgeniy Lebed, Yifan Jian, Paul J. Mackenzie, Mirza Faisal Beg, and
Marinko V. Sarunic. Real-time high-speed volumetric imaging using compressive
159

sampling optical coherence tomography. Biomed. Opt. Express, 2(9):2690–2697,
Sep 2011. 45
[198] Mei Young, Sieun Lee, Mahmoud Rateb, Mirza F Beg, Marinko V Sarunic, and Paul J
Mackenzie. Comparison of the clinical disc margin seen in stereo disc photographs
with neural canal opening seen in optical coherence tomography images. Journal of
glaucoma, 23(6):360–7, August 2014. 23
[199] Mei Young, Sieun Lee, Mahmoud Rateb, Mirza F. Beg, Marinko V. Sarunic, and
Paul J. Mackenzie. Comparison of the clinical disc margin seen in stereo disc pho-
tographs with neural canal opening seen in optical coherence tomography images.
J. Glaucoma, 23(6):360–367, August 2014. 44, 45, 112
[200] Linda M Zangwill, Christopher Bowd, Charles C Berry, Julia Williams, Eytan Z Blu-
menthal, Cesar A Sanchez-Galeana, Christiana Vasile, and Robert N Weinreb. Dis-
criminating between normal and glaucomatous eyes using the Heidelberg retina to-
mograph, GDx nerve fiber analyzer, and optical coherence tomograph. Archives of
ophthalmology, 119(7):985–993, 2001. 93
[201] Robert J. Zawadzki, Alfred R. Fuller, Stacey S. Choi, David F. Wiley, Bernd Hamann,
and John S. Werner. Correction of motion artifacts and scanning beam distortions
in 3D ophthalmic optical coherence tomography imaging. In Fabrice Manns, Per G.
Soederberg, Arthur Ho, Bruce E. Stuck, and Michael Belkin, editors, Biomedical
Optics (BiOS) 2007, pages 642607–642607–11. International Society for Optics and
Photonics, February 2007. 17
[202] R. Zayer, C. Rossl, and H.-P. Seidel. Discrete tensorial quasi-harmonic maps. In
International Conference on Shape Modeling and Applications 2005 (SMI’ 05), vol-
ume 0, pages 276–285, Los Alamitos, 2005. IEEE Comput. Soc. 49
[203] Li Zhang, Kyungmoo Lee, Meindert Niemeijer, Robert F Mullins, Milan Sonka, and
Michael D Abramoff. Automated segmentation of the choroid from clinical SD-OCT.
Investigative ophthalmology & visual science, 53(12):7510–9, November 2012. 27
160




















