
Determinants of Left Ventricular Hypertrophy and Systolic Dysfunction in Chronic Renal Failure
8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Determinants of left ventricular hypertrophy in patients with recent diagnosis of essential hypertension Francesco Buono a , Salvatore Crispo a , Gennaro Pagano a , Giuseppe Rengo a , Marta Petitto b , Fabrizia Grieco b , Bruno Trimarco b , and Carmine Morisco b Objective: Development of left ventricular hypertrophy (LVH) is a multifactorial phenomenon. We retrospectively assessed the risk factors for LVH in patients with recent diagnosis of essential hypertension. Methods: We analysed 1518 participants with recent diagnosis of essential hypertension (2 years). The duration of hypertension was established after cross- checking the patients’ history and the records of the general practitioners’. The following cardiovascular (CV) risk factors were considered: age (men >55 years, women >65 years), SBP >140 mmHg, DBP >90 mmHg, obesity, diabetes, hypercholesterolemia, low or high-density lipoprotein (HDL)-cholesterol (men <40 m/dl, women <50 mg/dl), and chronic kidney disease (CKD). Results: Age, prevalence of metabolic diseases, CKD, and the severity of hypertension were higher in patients with LVH. One hundred and twenty-two (8%) patients did not have CV risk factors, whereas 288 (19%), 472 (31.1%), 351 (23.1%) and 285 (18.8%) patients had one, two, three and more than three CV risk factors, respectively. At univariate analysis, CV risk factors for LVH where found to be sex, age, SBP, low HDL-cholesterol, obesity, diabetes, CKD, and metabolic syndrome. In the multivariate analysis, the independent predictors of LVH were found to be sex, age, SBP, obesity and diabetes. A significant correlation was found between indexed left ventricular mass and body mass index (r 2 ¼ 0.167), age (r 2 ¼ 0.077) and SBP (r 2 ¼ 0.055). Conclusion: This study reveals that, in patients with recent diagnosis of essential hypertension obesity represents the most important modifiable CV risk factor for LVH. Keywords: left ventricular mass, obesity Abbreviations: CKD, chronic kidney disease; CV, cardiovascular; GFR, glomerular filtration rate; HDL-c, , high-density lipoprotein-cholesterol; HR, Heart rate; LDL, low-density lipoprotein; LVH, left ventricular hypertrophy; LVM, left ventricular mass; MS, Metabolic syndrome INTRODUCTION L eft ventricular hypertrophy (LVH) is a common feature of target organ damage in hypertension [1] and is an independent risk factor for cardiac [2], and cerebral events [3]. Development of LVH is a biological phenomenon that involves genetic determinants, mech- anical forces, neuro-hormonal stimulation, inflammatory mediators, and metabolic abnormalities, resulting in the activation of complex molecular pathways [4]. Moreover, cardiac growth is also an age-dependent process [5]. This complexity, in clinical practice, is evidenced by the variety of determinants that have been identified as risk factors for LVH in hypertensive patients. Despite, the established link between high blood pressure (BP) and LVH, some studies have documented a weak relationship between BP levels and LVH [6,7]. Moreover, studies have shown that subjects with metabolic risk factors [8] or with metabolic syndrome [9] have elevated left ventricular mass or increased pre- valence of LVH, suggesting that the magnitude of left ventricular mass and LVH is affected by anthropometric parameters, or metabolic abnormalities rather than BP levels. It should be emphasized that these results are influenced by several factors such as the sample size of the study, the criteria used for definition of LVH, the state of antihypertensive therapy, and the heterogeneity of patient clinical characteristics (i.e. age, duration of hypertension, race, sex and comorbidity). These observations underscore the need to more rigorously evaluate LVH risk factors for hypertensive patients in a more homogeneous context. It is reasonable to hypothesize that the determinants of cardiac growth play different roles in the pathogenesis of LVH during the natural history of hypertension. According to this view, the contribution that different risk factors, alone or in combination, have in the genesis of LVH should be assessed by comparing similar phases of hypertensive disease. Assessing LVH risk factors, at the onset of hypertension allows for the evaluation, in a homogeneous context, of the contributions of hemodynamic, metabolic, and anthropometric alterations on the development of LVH. Journal of Hypertension 2013, 31:000–000 a Dipartimento di Scienze Mediche Traslazionalie, Fondazione Salvatore Maugeri, IRCCS, Istituto Scientifico di Telese Terme and b Dipartimento Scienze Biomediche Avanzate, Universita ` FEDERICO II, Napoli, Italy Correspondence to Carmine Morisco, MD, PhD, Dipartimento di Scienze Mediche Traslazionali, Universita ` FEDERICO II, Napoli. Via S. Pansini n. 5, 80131 Napoli, Italy. Tel: +39 081 7462256; e-mail: [email protected] Received 27 February 2013 Revised 10 June 2013 Accepted 13 August 2013 J Hypertens 31:000–000 ß 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. DOI:10.1097/HJH.0b013e328365c87d Journal of Hypertension www.jhypertension.com 1 De Novo Submission
Transcript of Determinants of Left Ventricular Hypertrophy and Systolic Dysfunction in Chronic Renal Failure

CE: Alpana; HJH/203191; Total nos of Pages: 8;
HJH 203191
De Novo Submission
Determinants of left ventricular hypertrophy inpatients with recent diagnosis of essential hypertension
Francesco Buonoa, Salvatore Crispoa, Gennaro Paganoa, Giuseppe Rengoa, Marta Petittob,Fabrizia Griecob, Bruno Trimarcob, and Carmine Moriscob
Journal of Hypertension 2013, 31:000–000aDipartimento di Scienze Mediche Traslazionalie, Fondazione Salvatore Maugeri,
Objective: Development of left ventricular hypertrophy(LVH) is a multifactorial phenomenon. We retrospectivelyassessed the risk factors for LVH in patients with recentdiagnosis of essential hypertension.
Methods: We analysed 1518 participants with recentdiagnosis of essential hypertension (�2 years). Theduration of hypertension was established after cross-checking the patients’ history and the records of thegeneral practitioners’. The following cardiovascular (CV)risk factors were considered: age (men >55 years, women>65 years), SBP >140 mmHg, DBP >90 mmHg, obesity,diabetes, hypercholesterolemia, low or high-densitylipoprotein (HDL)-cholesterol (men <40 m/dl, women<50 mg/dl), and chronic kidney disease (CKD).
Results: Age, prevalence of metabolic diseases, CKD, andthe severity of hypertension were higher in patients withLVH. One hundred and twenty-two (8%) patients did nothave CV risk factors, whereas 288 (19%), 472 (31.1%),351 (23.1%) and 285 (18.8%) patients had one, two,three and more than three CV risk factors, respectively.At univariate analysis, CV risk factors for LVH where foundto be sex, age, SBP, low HDL-cholesterol, obesity, diabetes,CKD, and metabolic syndrome. In the multivariate analysis,the independent predictors of LVH were found to be sex,age, SBP, obesity and diabetes. A significant correlationwas found between indexed left ventricular mass and bodymass index (r2¼0.167), age (r2¼ 0.077) and SBP(r2¼ 0.055).
Conclusion: This study reveals that, in patients with recentdiagnosis of essential hypertension obesity represents themost important modifiable CV risk factor for LVH.
Keywords: left ventricular mass, obesity
Abbreviations: CKD, chronic kidney disease; CV,cardiovascular; GFR, glomerular filtration rate; HDL-c, ,high-density lipoprotein-cholesterol; HR, Heart rate; LDL,low-density lipoprotein; LVH, left ventricular hypertrophy;LVM, left ventricular mass; MS, Metabolic syndrome
IRCCS, Istituto Scientifico di Telese Terme and bDipartimento Scienze BiomedicheAvanzate, Universita FEDERICO II, Napoli, Italy
Correspondence to Carmine Morisco, MD, PhD, Dipartimento di Scienze MedicheTraslazionali, Universita FEDERICO II, Napoli. Via S. Pansini n. 5, 80131 Napoli, Italy.
INTRODUCTION Tel: +39 081 7462256; e-mail: [email protected]Received 27 February 2013 Revised 10 June 2013 Accepted 13 August 2013
J Hypertens 31:000–000 � 2013 Wolters Kluwer Health | Lippincott Williams &Wilkins.
DOI:10.1097/HJH.0b013e328365c87d
Left ventricular hypertrophy (LVH) is a commonfeature of target organ damage in hypertension [1]and is an independent risk factor for cardiac [2], and
cerebral events [3]. Development of LVH is a biological
Copyright © Lippincott Williams & Wilkins. UnauthJournal of Hypertension
phenomenon that involves genetic determinants, mech-anical forces, neuro-hormonal stimulation, inflammatorymediators, and metabolic abnormalities, resulting in theactivation of complex molecular pathways [4]. Moreover,cardiac growth is also an age-dependent process [5]. Thiscomplexity, in clinical practice, is evidenced by the varietyof determinants that have been identified as risk factors forLVH in hypertensive patients. Despite, the established linkbetween high blood pressure (BP) and LVH, some studieshave documented a weak relationship between BP levelsand LVH [6,7]. Moreover, studies have shown that subjectswith metabolic risk factors [8] or with metabolic syndrome[9] have elevated left ventricular mass or increased pre-valence of LVH, suggesting that the magnitude of leftventricular mass and LVH is affected by anthropometricparameters, or metabolic abnormalities rather than BPlevels. It should be emphasized that these results areinfluenced by several factors such as the sample size ofthe study, the criteria used for definition of LVH, the state ofantihypertensive therapy, and the heterogeneity of patientclinical characteristics (i.e. age, duration of hypertension,race, sex and comorbidity). These observations underscorethe need to more rigorously evaluate LVH risk factors forhypertensive patients in a more homogeneous context.
It is reasonable to hypothesize that the determinants ofcardiac growth play different roles in the pathogenesis ofLVH during the natural history of hypertension. Accordingto this view, the contribution that different risk factors,alone or in combination, have in the genesis of LVH shouldbe assessed by comparing similar phases of hypertensivedisease.
Assessing LVH risk factors, at the onset of hypertensionallows for the evaluation, in a homogeneous context,of the contributions of hemodynamic, metabolic, andanthropometric alterations on the development of LVH.
orized reproduction of this article is prohibited.www.jhypertension.com 1

CE: Alpana; HJH/203191; Total nos of Pages: 8;
HJH 203191
Buono et al.
Since 1997, we have formed a network, the CampaniaSalute Network, among the Hypertension Center ofthe Federico II University Hospital (Naples, Italy), 23 com-munity hospital-based hypertension clinics, and 60 generalpractitioners (GPs) from our district area, including morethan 12 000 patients with essential hypertension [10,11].In this context, we retrospectively assessed the risk factorsfor LVH in patients with recent diagnosis of essentialhypertension.
METHODS
Study design and populationWe retrospectively screened for all hypertensive patientswith age at least 18 and 80 years or below, who werereferred from October 1998 to September 2009 to theHypertension Clinic of the ‘Federico II’ University, Naples,Italy, for diagnosis or treatment of hypertension. In ournetwork, the patient’s medical history, demographiccharacteristics, anthropomorphic measures, physicalexamination data, hemodynamic, and laboratory variablesand results of other diagnostic procedures, collected at eachvisit, are routinely stored in a dedicated database [10].Before analysis, all data were screened for missingor contradictory entries and values outside of the normalrange.
The research protocol was approved by the EthicsCommittee of our Institution. On their initial visit, allpatients provided written consent for subsequent analysisof their data.
Patients with recent diagnosis of hypertension (�2 years)were considered eligible for the analysis. The duration ofhypertension was established after cross-checking thepatients’ history and the records of the GPs.
Office BP was measured by a physician using a mercurysphygmomanometer with the patient in a seated positionfor at least 10min; three BP measurements were obtained at5-min intervals. The average of these measurements wasused. Patients were classified as hypertensive if they weretaking antihypertensive drugs or if the average of the threemeasurements was at least 140 mmHg for SBP or at least90mmHg for DBP on two or more separate clinic visits [12].For this study, we used hemodynamic, anthropomorphic,biochemical, and ultrasound variables that were collectedat the first clinic visit in our center.
Serum creatinine, fasting plasma glucose, serum totalcholesterol, high-density lipoprotein (HDL)-cholesterol,and triglycerides were determined by standard methods.Low-density lipoprotein (LDL)-cholesterol was calculatedby means of the Friedewald formula [13]. Glomerularfiltration rate (GFR) was calculated by the MDRD formula[14]. Chronic kidney disease (CKD) was defined as anestimated GFR of 60ml/min per 1.73 m2 or less [15]. Type2 diabetes mellitus was diagnosed if the fasting plasmaglucose was at least 126 mg/dl, confirmed by repeatedmeasurement on a different day, or when patientswere taking insulin or hypoglycemic medications [16].Hypercholesterolemia was defined as a serum level ofLDL-cholesterol of at least 130 mg/dl or the use of lipid-lowering agents [17]. Metabolic syndrome was defined onthe basis of the modified ATP-III criteria [17] as the presence
Copyright © Lippincott Williams & Wilkins. Unaut2 www.jhypertension.com
in addition to hypertension of at least two of the followingabnormalities: serum triglyceride at least 150 mg/dl; serumHDL-cholesterol less than 40 and more than 50mg/dl inmen and women, respectively; fasting plasma glucose atleast 110 mg/dl in nondiabetic patients; and BMI at least30 kg/m2. As reported by different authors [18], BMI waschosen instead of waist circumference because this lattervariable was not routinely measured in our outpatient clinicuntil 2003–2004. Patients were defined as obese if they hada BMI at least 30.0 kg/m2 [19].
Target values of BP were considered less than 140/90and less than 130/80 mmHg in nondiabetic and diabeticpatients, respectively [20].
Patients with evidence of secondary hypertension,congestive heart failure, significant aortic or mitralregurgitation by color-Doppler echocardiography, andCKD requiring dialysis treatment were excluded from theanalysis. History of cerebrovascular disease (transientischemic attack or stroke, and dementia), or coronary arterydisease (myocardial infarction, angina, coronary arterybypass graft, percutaneous transluminal coronary angio-plasty) was considered as exclusion criterion. Patients forwhom a good-quality ultrasound recording was notobtained were also excluded from the analysis, as wellas patients with incomplete medical history or laboratoryevaluation.
EchocardiographyEchocardiograms were performed using ultrasoundmachines (Sonos 1500 Hewlett-Packard, 1998–2005;SONOS 2500 Hewlett-Packard, 2005–2008; SONOS 5500Philips, 2008–2009) with dedicated transducers of 2.5 MHz,with the patients supine in the left lateral position. Two-dimensional guided M-mode left ventricular internaldimension and interventricular septal and posterior wallthicknesses were measured at end diastole according to theAmerican Society of Echocardiography recommendations[21] on three cardiac cycles at or just below the tips of themitral leaflets in parasternal long-axis and short-axisviews. All echocardiograms were performed and analyzedat the Hypertension Clinic of the ‘Federico II’ University byinvestigators who were unaware of patients’ clinical data.Left ventricular mass was calculated from a necropsy-validated formula [22] and normalized for height in metersto the power of 2.7 (LVMi) [23,24]. LVH was defined as LVMiat least 51 g/m2.7, to provide a more stringent allowance forobesity [25]. Left ventricular ejection fraction was calculatedfrom four-chamber and two-chamber views using themodified biplane Simpson method [26]. From mitral inflowDoppler tracings, the following measurements were carriedout: peak velocity of early transmitral inflow wave (E) andpeak flow velocity of late transmitral inflow wave (A).Impaired diastolic function was defined by an E/A ratioof less than 1 [27].
Statistical analysisData were analyzed using SPSS software (version 19, SPSSChicago, Illinois, USA). Data are expressed as means�standard deviation (SD) or as proportions, with com-parisons performed using Student’s t tests, or x2 tests, as
horized reproduction of this article is prohibited.Volume 30 � Number 1 � Month 2013
CE: Alpana; HJH/203191; Total nos of Pages: 8;
HJH 203191
Determinants of left ventricular hypertrophy
appropriate. Correlations between variables were assessedwith Pearson’s correlation coefficient. Odds ratios (OR)with 95% confidence intervals (CI) were used to test differ-ences for categorical variables in 2� 2 tables. Univariateand multivariate regression analyses were performed toidentify independent predictors of LVH. Variables that weresignificant in univariate analysis at a probability level of lessthan 0.05 were entered into a multivariate model. We testeda model using as covariates, sex, and conventional cardio-vascular (CV) risk factors [20]: age (men >55 years, women>65 years), SBP (>140mmHg), DBP (>90mmHg), obesity,diabetes, hypercholesterolemia, low HDL-cholesterol (men<40 mg /dl, women<50mg /dl), metabolic syndrome, andCKD. In a second model, multivariate analysis was adjustedfor the presence of antihypertensive therapy. A probabilitylevel of less than 0.05 was considered significant.
RESULTS
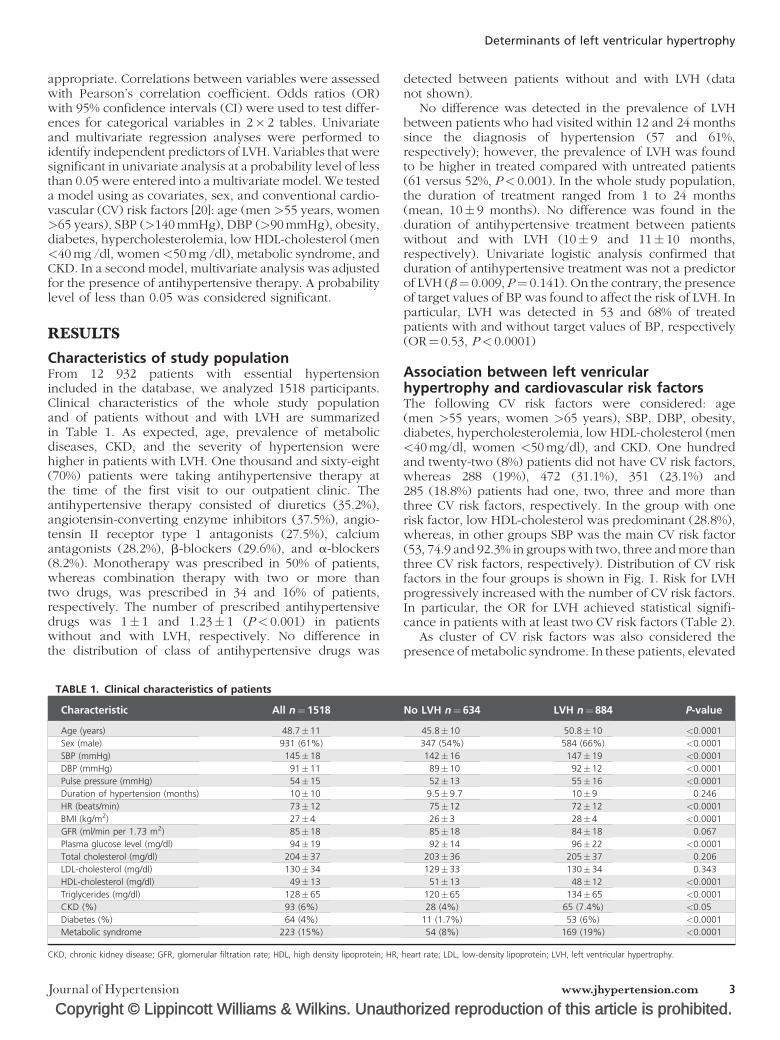
Characteristics of study populationFrom 12 932 patients with essential hypertensionincluded in the database, we analyzed 1518 participants.Clinical characteristics of the whole study populationand of patients without and with LVH are summarizedin Table 1. As expected, age, prevalence of metabolicdiseases, CKD, and the severity of hypertension werehigher in patients with LVH. One thousand and sixty-eight(70%) patients were taking antihypertensive therapy atthe time of the first visit to our outpatient clinic. Theantihypertensive therapy consisted of diuretics (35.2%),angiotensin-converting enzyme inhibitors (37.5%), angio-tensin II receptor type 1 antagonists (27.5%), calciumantagonists (28.2%), b-blockers (29.6%), and a-blockers(8.2%). Monotherapy was prescribed in 50% of patients,whereas combination therapy with two or more thantwo drugs, was prescribed in 34 and 16% of patients,respectively. The number of prescribed antihypertensivedrugs was 1� 1 and 1.23� 1 (P< 0.001) in patientswithout and with LVH, respectively. No difference inthe distribution of class of antihypertensive drugs was
Copyright © Lippincott Williams & Wilkins. Unauth
TABLE 1. Clinical characteristics of patients
Characteristic All n¼1518
Age (years) 48.7�11
Sex (male) 931 (61%)
SBP (mmHg) 145�18
DBP (mmHg) 91�11
Pulse pressure (mmHg) 54�15
Duration of hypertension (months) 10�10
HR (beats/min) 73�12
BMI (kg/m2) 27�4
GFR (ml/min per 1.73 m2) 85�18
Plasma glucose level (mg/dl) 94�19
Total cholesterol (mg/dl) 204�37
LDL-cholesterol (mg/dl) 130�34
HDL-cholesterol (mg/dl) 49�13
Triglycerides (mg/dl) 128�65
CKD (%) 93 (6%)
Diabetes (%) 64 (4%)
Metabolic syndrome 223 (15%)
CKD, chronic kidney disease; GFR, glomerular filtration rate; HDL, high density lipoprotein; HR,
Journal of Hypertension
detected between patients without and with LVH (datanot shown).
No difference was detected in the prevalence of LVHbetween patients who had visited within 12 and 24 monthssince the diagnosis of hypertension (57 and 61%,respectively); however, the prevalence of LVH was foundto be higher in treated compared with untreated patients(61 versus 52%, P< 0.001). In the whole study population,the duration of treatment ranged from 1 to 24 months(mean, 10� 9 months). No difference was found in theduration of antihypertensive treatment between patientswithout and with LVH (10� 9 and 11� 10 months,respectively). Univariate logistic analysis confirmed thatduration of antihypertensive treatment was not a predictorof LVH (b¼ 0.009, P¼ 0.141). On the contrary, the presenceof target values of BP was found to affect the risk of LVH. Inparticular, LVH was detected in 53 and 68% of treatedpatients with and without target values of BP, respectively(OR¼ 0.53, P< 0.0001)
Association between left venricularhypertrophy and cardiovascular risk factorsThe following CV risk factors were considered: age(men >55 years, women >65 years), SBP, DBP, obesity,diabetes, hypercholesterolemia, low HDL-cholesterol (men<40mg/dl, women <50mg/dl), and CKD. One hundredand twenty-two (8%) patients did not have CV risk factors,whereas 288 (19%), 472 (31.1%), 351 (23.1%) and285 (18.8%) patients had one, two, three and more thanthree CV risk factors, respectively. In the group with onerisk factor, low HDL-cholesterol was predominant (28.8%),whereas, in other groups SBP was the main CV risk factor(53, 74.9 and 92.3% in groups with two, three and more thanthree CV risk factors, respectively). Distribution of CV riskfactors in the four groups is shown in Fig. 1. Risk for LVHprogressively increased with the number of CV risk factors.In particular, the OR for LVH achieved statistical signifi-cance in patients with at least two CV risk factors (Table 2).
As cluster of CV risk factors was also considered thepresence of metabolic syndrome. In these patients, elevated
orized reproduction of this article is prohibited.
No LVH n¼634 LVH n¼884 P-value
45.8�10 50.8�10 <0.0001
347 (54%) 584 (66%) <0.0001
142�16 147�19 <0.0001
89�10 92�12 <0.0001
52�13 55�16 <0.0001
9.5�9.7 10�9 0.246
75�12 72�12 <0.0001
26�3 28�4 <0.0001
85�18 84�18 0.067
92�14 96�22 <0.0001
203�36 205�37 0.206
129�33 130�34 0.343
51�13 48�12 <0.0001
120�65 134�65 <0.0001
28 (4%) 65 (7.4%) <0.05
11 (1.7%) 53 (6%) <0.0001
54 (8%) 169 (19%) <0.0001
heart rate; LDL, low-density lipoprotein; LVH, left ventricular hypertrophy.
www.jhypertension.com 3

CE: Alpana; HJH/203191; Total nos of Pages: 8;
HJH 203191
0
20
40
60
80
100 Age
SBP
DBP
Obesity
Diabetes
Hypercholesterolemia
Low HDL-C
CKD
1RF 2RFs 3RFs >3RFs
Pre
vale
nce
(%
)
FIGURE 1 Distribution of different risk factors (RF) in patients categorized for the number of cardiovascular RF. CKD, chronic kidney disease; HDL-C, high densitylipoprotein-cholesterol.
Buono et al.
plasma levels of triglycerides were present in 180 (81%)patients, low levels of HDL-cholesterol were present in185 (83%) patients, elevated fasting plasma glucose levelswere present in 55 (25%) patients, and obesity was presentin 128 (58%) patients. The presence of metabolic syndromesignificantly increased the risk of LVH (OR: 2.539; 95% CI:1.831–3.515; P< 0.0001).
Risk factors for left ventricular hypertrophyRisk of LVH was evaluated in relation to sex and thepresence of conventional CV risk factors. At univariateanalysis, risk factors for LVH were found to be male sex,age, SBP, low HDL-cholesterol, presence of obesity,diabetes, metabolic syndrome, and CKD. In the multivariateanalysis, independent predictors of LVH were found tobe sex, age, SBP, obesity and diabetes (Table 3). Whenthe model was adjusted for the presence of antihyperten-sive treatment, risk factors for LVH remained unchanged:age (b:�0.787, P< 0.0001), sex (b:�0.45, P< 0.0001), SBP(b: �0.41, P< 0.0001), obesity (b: �1.799, P< 0.0001);diabetes (b: �0.768, P¼ 0.029).
In a further analysis, patients were grouped accordingthe number of CV risk factors. The sub-groups consistedof patients with two, three and more than three CV riskfactors. The following covariates were considered sex, age,SBP, obesity and diabetes. Multivariate analysis showed thatin the sub-group of patients with two CV risk factors,age, obesity and male sex were associated with enhancedrisk of LVH, whereas in all other sub-groups, only age andobesity increased the risk for LVH (Table 4).
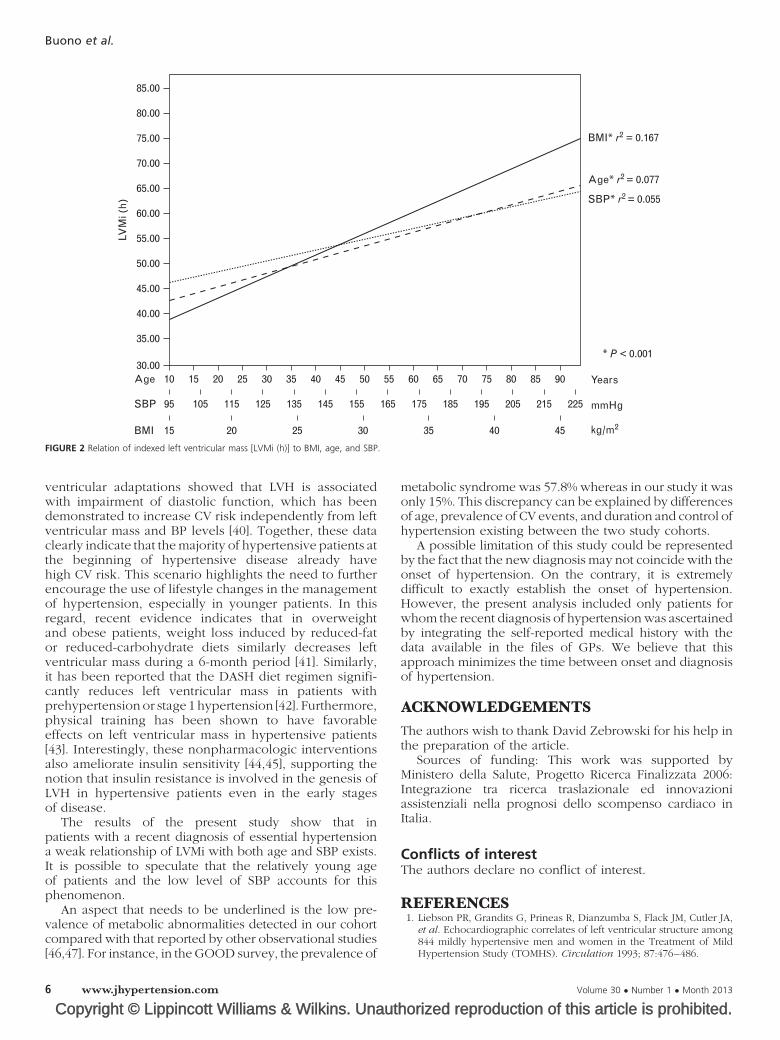
A significant correlation was found between LVMiand BMI, age, and SBP. The highest coefficient correlationwas detected for BMI (r2: 0.167, P< 0.0001). However, ageand SBP also correlated with LVMi, although with a weakercoefficient (r2: 0.077, P< 0.0001; and r2: 0.055, P< 0.0001,respectively Fig. 2).
Copyright © Lippincott Williams & Wilkins. Unaut
TABLE 2. Odds ratio (95% confidence interval) for left ventricular hy
Number of risk factors n (%)
1 288 (19%)
2 472 (31.1%)
3 351 (23.1%)
>3 285 (18.8%)
CI, confidence interval.
4 www.jhypertension.com
Hemodynamic adaptation to pressure overloadPatients with LVH had lower but preserved systolic function(left ventricular ejection fraction: 64� 5%) compared withpatients without LVH (66� 5%, P< 0.0001). Impaired dias-tolic function was more frequent in patients with LVH. Infact, the E/A ratio was 1.1� 0.2 and 0.9� 0.2 (P< 0.0001)in patients without and with LVH, respectively. Moreover,an E/A less than 1 was detected in 209 (33%) and in521(59%; P< 0.0001) patients without and with LVH,respectively.
DISCUSSIONEssential hypertension is a complex disease characterizedby hemodynamic, and metabolic abnormalities, oftenassociated with anthropometric alterations [28]. In this studywe demonstrated that in patients with a new diagnosisof hypertension, age, sex, and obesity are the major riskfactors for development of LVH. Although identification ofsex, age and obesity as major risk factors for LVH [29–31]seems to be merely confirmatory, the present study extendsprevious observations because it was conducted exclu-sively in those patients with a documented recent diagnosisof hypertension, and we simultaneously analyzed hemo-dynamic, metabolic, and anthropomorphic characteristicsof patients. This allowed us to better define the role of thespecific contribution that each CV risk factor has in develop-ment of LVH during the natural history of hypertension.
Identification of obesity as the main modifiable riskfactor for LVH at the onset of hypertension, is not a trivialobservation, as it provides a better definition of the CV riskfactors at the beginning of hypertension, which, in turn,may help us to improve therapeutic strategies in hyper-tensive patients. Several mechanisms can account for therole that obesity plays in the genesis of LVH in hypertensivepatients. For instance, obesity can exert its trophic effect on
horized reproduction of this article is prohibited.
pertrophy in patients with different number of risk factors
Odds ratio 95% CI P-value
1.21 0.79–1.86 0.388
1.61 1.07–2.4 0.025
1.96 1.29–2.97 0.002
4.4 2.8–6.92 0.0001
Volume 30 � Number 1 � Month 2013

CE: Alpana; HJH/203191; Total nos of Pages: 8;
HJH 203191
TABLE 3. Predictors of left ventricular hypertrophy at univariate and multivariate analyses
Risk factor
Univariate analysis Multivariate analysis
b Wald P value b Wald P-value
Age �0.91 43.17 <0.0001 �0.82 30.8 <0.0001
Sex (male) �0.47 19.88 <0.0001 �0.41 12.57 <0.0001
SBP �0.37 12.45 <0.0001 �0.32 7.84 0.005
Obesity �1.24 60.84 <0.0001 �1.19 45.58 <0.0001
Diabetes �1.24 14.65 <0.0001 �0.81 5.34 0.021
HDL-C �0.23 4.28 0.038 �0.17 1.62 0.202
CKD �0.54 5.4 0.020 �0.46 3.38 0.066
MS �0.932 31.5 <0.0001 �0.226 1.13 0.287
DBP �0.18 3.09 0.079
LDL-C �0.03 0.07 0.785
CKD, chronic kidney disease; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; MS, metabolic syndrome.
Determinants of left ventricular hypertrophy
the myocardium by increasing load conditions [25,30],or sympathetic stimulation [32] and by impairing cardiacmitochondrial biogenesis and function [33].
We found that diabetes has only a marginal role as a riskfactor for LVH. This observation appears to be in contrastwith previous observations indicating that diabetes plays apivotal role with regards to an increase in left ventricularmass [34] in hypertensive patients. This discrepancy couldbe attributable to different clinical characteristics of thestudy population. In particular, Palmieri et al. analyzedthe population of the HyperGEN study, which includedpatients with a long history of hypertension, whereaswe included only patients with a recent diagnosis ofhypertension. However, both diabetes and obesity arecharacterized by insulin resistance. It is noteworthy thatthis metabolic abnormality plays a role in the pathogenesisof LVH [8]. Thus, it is reasonable to speculate that the stateof insulin resistance accounts for the increased risk ofLVH related to obesity. In this case, development of LVHcould be the result of two faces of insulin resistance.This speculation is consistent with the concept thatanthropomorphic and metabolic components of the insulinresistance state, independent of BP level, contribute tohypertension-induced target organ damage [35]. Unfortu-nately, the retrospective design of our study did not allowus to establish the role that insulin resistance plays in theobesity-mediated increased risk of LVH at the onsetof hypertension.
In the present study, we found a higher prevalenceof LVH (58%) in comparison to other large-scalepopulation-based Italian studies [36,37]. We believe thatthis discrepancy can be accounted for by the follow-ing reasons. First, to establish the presence of LVH, we
Copyright © Lippincott Williams & Wilkins. Unauth
TABLE 4. Predictors of left ventricular hypertrophy at multivariate afactors
Risk factor
Two risk factors Th
b Wald P-value b
Age 0.631 5.29 0.021 0.486
Sex (male) 0.484 6.01 0.014 0.376
Obesity 1.01 8.84 0.003 1.08
SBP 0.347 2.86 0.090 �0.129
Diabetes 0.687 0.34 0.561 0.634
Journal of Hypertension
normalized left ventricular mass by height, whereas themajority of previous studies normalized left ventricularmass by body surface area. It should be noted that inour hands, left ventricular mass normalized by body surfacearea underestimates the occurrence of LVH (35%). Inaddition, we analyzed patients with a recent diagnosis ofhypertension. In our study, 30% of patients never receivedantihypertensive treatment, and the others were treatedonly for a short time.
Although the purpose of this study was not to evaluatethe effect of antihypertensive treatment on development ofLVH, we found that duration of treatment did not affect therisk of LVH. Similar results were found when we consideredlonger duration of treatment. In fact, in a further cohortof hypertensive patients (n¼ 2044) treated for a periodranging from 3 to 5 years, univariate logistic analysisconfirmed that duration of antihypertensive treatmentwas not a predictor of LVH (b: 0.054, P¼ 0.404).
The high prevalence of LVH revealed in patients witha new diagnosis of hypertension is consistent with theconcept that in some cases the development of LVHprecedes the development of hypertension [38,39], especi-ally in those patients with anthropometric abnormalitiesand metabolic diseases. In these cases, we believe thatLVH is an expression of a BP-independent trophic effecton the myocardium, rather than a subclinical manifestationof pressure overload-induced organ damage. Our view iscorroborated by studies in hypertensive patients withincreased BMI or metabolic syndrome, which shows thatdecrease of LVH is independent of BP reduction [18].
The present study shows that LVH is associated withat least two CV risk factors in almost 75% of ourpatient population. In addition, analysis of functional left
orized reproduction of this article is prohibited.
nalysis in patients categorized for number of cardiovascular risk
ree risk factors >Three risk factors
Wald P-value b Wald P-value
2.96 0.085 1.116 10.26 0.001
2.44 0.118 0.092 0.085 0.771
12.34 <0.0001 1.24 13.42 <0.0001
0.199 0.656 0.374 0.365 0.546
1.06 0.303 0.536 1.116 0.281
www.jhypertension.com 5
CE: Alpana; HJH/203191; Total nos of Pages: 8;
HJH 203191
1030.00
35.00
40.00
45.00
50.00
55.00
60.00
65.00
70.00
75.00
80.00
85.00
Age
LVM
i (h
)
SBP
BMI
Years
* P < 0.001
mmHg
kg/m2
Age* r2 = 0.077
SBP* r2 = 0.055
BMI* r2 = 0.167
95
15 20 25 30 35 40 45
105 115 125 135 145 155 165 175 185 195 205 215 225
15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90
FIGURE 2 Relation of indexed left ventricular mass [LVMi (h)] to BMI, age, and SBP.
Buono et al.
ventricular adaptations showed that LVH is associatedwith impairment of diastolic function, which has beendemonstrated to increase CV risk independently from leftventricular mass and BP levels [40]. Together, these dataclearly indicate that the majority of hypertensive patients atthe beginning of hypertensive disease already havehigh CV risk. This scenario highlights the need to furtherencourage the use of lifestyle changes in the managementof hypertension, especially in younger patients. In thisregard, recent evidence indicates that in overweightand obese patients, weight loss induced by reduced-fator reduced-carbohydrate diets similarly decreases leftventricular mass during a 6-month period [41]. Similarly,it has been reported that the DASH diet regimen signifi-cantly reduces left ventricular mass in patients withprehypertension or stage 1 hypertension [42]. Furthermore,physical training has been shown to have favorableeffects on left ventricular mass in hypertensive patients[43]. Interestingly, these nonpharmacologic interventionsalso ameliorate insulin sensitivity [44,45], supporting thenotion that insulin resistance is involved in the genesis ofLVH in hypertensive patients even in the early stagesof disease.
The results of the present study show that inpatients with a recent diagnosis of essential hypertensiona weak relationship of LVMi with both age and SBP exists.It is possible to speculate that the relatively young ageof patients and the low level of SBP accounts for thisphenomenon.
An aspect that needs to be underlined is the low pre-valence of metabolic abnormalities detected in our cohortcompared with that reported by other observational studies[46,47]. For instance, in the GOOD survey, the prevalence of
Copyright © Lippincott Williams & Wilkins. Unaut6 www.jhypertension.com
metabolic syndrome was 57.8% whereas in our study it wasonly 15%. This discrepancy can be explained by differencesof age, prevalence of CV events, and duration and control ofhypertension existing between the two study cohorts.
A possible limitation of this study could be representedby the fact that the new diagnosis may not coincide with theonset of hypertension. On the contrary, it is extremelydifficult to exactly establish the onset of hypertension.However, the present analysis included only patients forwhom the recent diagnosis of hypertension was ascertainedby integrating the self-reported medical history with thedata available in the files of GPs. We believe that thisapproach minimizes the time between onset and diagnosisof hypertension.
ACKNOWLEDGEMENTSThe authors wish to thank David Zebrowski for his help inthe preparation of the article.
Sources of funding: This work was supported byMinistero della Salute, Progetto Ricerca Finalizzata 2006:Integrazione tra ricerca traslazionale ed innovazioniassistenziali nella prognosi dello scompenso cardiaco inItalia.
Conflicts of interestThe authors declare no conflict of interest.
REFERENCES1. Liebson PR, Grandits G, Prineas R, Dianzumba S, Flack JM, Cutler JA,
et al. Echocardiographic correlates of left ventricular structure among844 mildly hypertensive men and women in the Treatment of MildHypertension Study (TOMHS). Circulation 1993; 87:476–486.
horized reproduction of this article is prohibited.Volume 30 � Number 1 � Month 2013
CE: Alpana; HJH/203191; Total nos of Pages: 8;
HJH 203191
Determinants of left ventricular hypertrophy
2. Koren MJ, Devereux RB, Casale PN, Savage DD, Laragh JH. Relationof left ventricular mass and geometry to morbidity and mortality inuncomplicated essential hypertension. Ann Intern Med 1991; 114:345–352.
3. Verdecchia P, Porcellati C, Reboldi G, Gattobigio R, Borgioni C,Pearson TA, Ambrosio G. Left ventricular hypertrophy as an independ-ent predictor of acute cerebrovascular events in essential hypertension.Circulation 2001; 104:2039–2044.
4. Morisco C, Sadoshima J, Trimarco B, Arora R, Vatner DE, Vatner SF.Is treating cardiac hypertrophy salutary or detrimental: the two facesof Janus. Am J Physiol Heart Circ Physiol 2003; 284:H1043–H1047.
5. Ganau A, Saba PS, Roman MJ, de Simone G, Realdi G, Devereux RB.Ageing induces left ventricular concentric remodelling in normotensivesubjects. J Hypertens 1995; 13:1818–1822.
6. Devereux RB, Savage DD, Sachs I, Laragh JH. Relation of hemo-dynamic load to left ventricular hypertrophy and performance inhypertension. Am J Cardiol 1983; 51:171–176.
7. Ganau A, Devereux RB, Pickering TG, Roman MJ, Schnall PL, SantucciS, et al. Relation of left ventricular hemodynamic load and contractileperformance to left ventricular mass in hypertension. Circulation 1990;81:25–36.
8. Rutter MK, Parise H, Benjamin EJ, Levy D, Larson MG, Meigs JB, et al.Impact of glucose intolerance and insulin resistance on cardiacstructure and function: sex-related differences in the FraminghamHeart Study. Circulation 2003; 107:448–454.
9. Burchfiel CM, Skelton TN, Andrew ME, Garrison RJ, Arnett DK, JonesDW, Taylor HA Jr. Metabolic syndrome and echocardiographic leftventricular mass in blacks: the Atherosclerosis Risk in Communities(ARIC) Study. Circulation 2005; 112:819–827.
10. De Luca N, Izzo R, Iaccarino G, Malini PL, Morisco C, Rozza F, et al.The use of a telematic connection for the follow-up of hypertensivepatients improves the cardiovascular prognosis. J Hypertens 2005;23:1417–1423.
11. Izzo R, de Simone G, Chinali M, Iaccarino G, Trimarco V, Rozza F, et al.Insufficient control of blood pressure and incident diabetes. DiabetesCare 2009; 32:845–850.
12. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JLJr, et al. Joint National Committee on Prevention, Detection, Evalua-tion, and Treatment of High Blood Pressure. National Heart, Lung, andBlood Institute; National High Blood Pressure Education ProgramCoordinating Committee. Seventh report of the Joint National Com-mittee on Prevention, Detection, Evaluation, and Treatment of HighBlood Pressure. Hypertension 2003; 42:1206–1252.
13. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concen-tration of low-density lipoprotein cholesterol in plasma, without use ofthe preparative ultracentrifuge. Clin Chem 1972; 18:499–502.
14. Hallan S, Asberg A, Lindberg M, Johnsen H. Validation of themodification of diet in renal disease formula for estimating GFR withspecial emphasis on calibration of the serum creatinine assay. Am JKidney Dis 2004; 44:84–93.
15. Schiffrin EL, Lipman ML, Mann JF. Chronic kidney disease: effects onthe cardiovascular system. Circulation 2007; 116:85–97.
16. Standards of medical care in diabetes-2006. Diabetes Care 2006; 29(Suppl 1):S4–S42.
17. Executive Summary of The Third Report of The National CholesterolEducation Program (NCEP) Expert Panel on Detection, Evaluation,And Treatment of High Blood Cholesterol In Adults (Adult TreatmentPanel III). JAMA 2001; 285:2486–2497.
18. De Simone G, Okin PM, Gerdts E, Olsen MH, Wachtell K, Hille DA,et al. Clustered metabolic abnormalities blunt regression ofhypertensive left ventricular hypertrophy: the LIFE study. Nutr MetabCardiovasc Dis 2009; 19:634–640.
19. Clinical Guidelines on the Identification, Evaluation, and Treatment ofOverweight and Obesity in Adults-The Evidence Report. NationalInstitutes of Health. Obes Res 1998; 6 (Suppl 2):51S–209S.
20. Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R,Germano G, et al. The Task Force for the Management of ArterialHypertension of the European Society of Hypertension (ESH) and ofthe European Society of Cardiology (ESC). J Hypertens 2007; 25:1105–1187.
21. Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendationsregarding quantitation in M-mode echocardiography: results of asurvey of echocardiographic measurements. Circulation 1978;58:1072–1083.
Copyright © Lippincott Williams & Wilkins. UnauthJournal of Hypertension
22. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I,Reichek N. Echocardiographic assessment of left ventricularhypertrophy: comparison to necropsy findings. Am J Cardiol 1986;57:450–458.
23. De Simone G, Daniels SR, Devereux RB, Meyer RA, Roman MJ, deDivitiis O, Alderman MH. Left ventricular mass and body size innormotensive children and adults: assessment of allometric relationsand impact of overweight. J Am Coll Cardiol 1992; 20:1251–1260.
24. De Simone G, Devereux RB, Daniels SR, Koren MJ, Meyer RA, LaraghJH. Effect of growth on variability of left ventricular mass: assessment ofallometric signals in adults and children and their capacity to predictcardiovascular risk. J Am Coll Cardiol 1995; 25:1056–1062.
25. Cuspidi C, Giudici V, Negri F, Meani S, Sala C, Zanchetti A, Mancia G.Improving cardiovascular risk stratification in essential hypertensivepatients by indexing left ventricular mass to height (2.7). J Hypertens2009; 27:2465–2471.
26. Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigen-baum H, et al. Recommendations for quantitation of the left ventricleby two-dimensional echocardiography. American Society of Echocar-diography Committee on Standards, Subcommittee on Quantitation ofTwo-Dimensional Echocardiograms. J Am Soc Echocardiogr 1989;2:358–367.
27. Poirier P, Bogaty P, Garneau C, Marois L, Dumesnil JG. Diastolicdysfunction in normotensive men with well controlled type 2 diabetes:importance of maneuvers in echocardiographic screening for preclin-ical diabetic cardiomyopathy. Diabetes Care 2001; 24:5–10.
28. Messerli FH, Williams B, Ritz E. Essential hypertension. Lancet 2007;370:591–603.
29. Bella JN, Devereux RB, Roman MJ, O’Grady MJ, Welty TK, Lee ET, et al.Relations of left ventricular mass to fat-free and adipose body mass: thestrong heart study. The Strong Heart Study Investigators. Circulation1998; 98:2538–2544.
30. De Simone G, Devereux RB, Roman MJ, Alderman MH, Laragh JH.Relation of obesity and gender to left ventricular hypertrophy innormotensive and hypertensive adults. Hypertension 1994; 23:600–606.
31. Gardin JM, Wagenknecht LE, Anton-Culver H, Flack J, Gidding S,Kurosaki T, et al. Relationship of cardiovascular risk factors toechocardiographic left ventricular mass in healthy young black andwhite adult men and women. The CARDIA study. Coronary Artery RiskDevelopment in Young Adults. Circulation 1995; 92:380–387.
32. Grassi G, Seravalle G, Cattaneo BM, Bolla GB, Lanfranchi A, ColomboM, et al. Sympathetic activation in obese normotensive subjects.Hypertension 1995; 25:560–563.
33. Niemann B, Chen Y, Teschner M, Li L, Silber RE, Rohrbach S. Obesityinduces signs of premature cardiac aging in younger patients: the roleof mitochondria. J Am Coll Cardiol 2011; 57:577–585.
34. Palmieri V, Bella JN, Arnett DK, Liu JE, Oberman A, Schuck MY, et al.Effect of type 2 diabetes mellitus on left ventricular geometryand systolic function in hypertensive subjects: Hypertension GeneticEpidemiology Network (HyperGEN) study. Circulation 2001; 103:102–107.
35. El-Gharbawy AH, Kotchen JM, Grim CE, Kaldunski M, Hoffmann RG,Pausova Z, et al. Predictors of target organ damage in hypertensiveblacks and whites. Hypertension 2001; 38:761–766.
36. Verdecchia P, Carini G, Circo A, Dovellini E, Giovannini E, LombardoM, et al. Left ventricular mass and cardiovascular morbidity in essentialhypertension: the MAVI study. J Am Coll Cardiol 2001; 38:1829–1835.
37. Mancia G, Carugo S, Grassi G, Lanzarotti A, Schiavina R, Cesana G, SegaR, Pressioni Arteriose Monitorate E Loro Associazioni (PAMELA) Study.Prevalence of left ventricular hypertrophy in hypertensive patientswithout and with blood pressure control: data from the PAMELApopulation. Pressioni Arteriose Monitorate E Loro Associazioni.Hypertension 2002; 39:744–749.
38. Post WS, Larson MG, Levy D. Impact of left ventricular structure on theincidence of hypertension. The Framingham Heart Study. Circulation1994; 90:179–185.
39. De Marco M, de Simone G, Roman MJ, Chinali M, Lee ET, Russell M, etal. Cardiovascular and metabolic predictors of progression of prehy-pertension into hypertension: the Strong Heart Study. Hypertension2009; 54:974–980.
40. Schillaci G, Pasqualini L, Verdecchia P, Vaudo G, Marchesi S, PorcellatiC, et al. Prognostic significance of left ventricular diastolic dysfunctionin essential hypertension. J Am Coll Cardiol 2002; 39:2005–2011.
orized reproduction of this article is prohibited.www.jhypertension.com 7

CE: Alpana; HJH/203191; Total nos of Pages: 8;
HJH 203191
Buono et al.
41. Haufe S, Utz W, Engeli S, Kast P, Bohnke J, Pofahl M, et al. Leftventricular mass and function with reduced-fat or reduced-carbohydrate hypocaloric diets in overweight and obese subjects.Hypertension 2012; 59:70–75.
42. Blumenthal JA, Babyak MA, Hinderliter A, Watkins LL, Craighead L, LinPH, et al. Effects of the DASH diet alone and in combination withexercise and weight loss on blood pressure and cardiovascular bio-markers in men and women with high blood pressure: the ENCOREstudy. Arch Intern Med 2010; 170:126–135.
43. Pitsavos C, Chrysohoou C, Koutroumbi M, Aggeli C, Kourlaba G,Panagiotakos D, et al. The impact of moderate aerobic physical trainingon left ventricular mass, exercise capacity and blood pressure responseduring treadmill testing in borderline and mildly hypertensive males.Hellenic J Cardiol 2011; 52:6–14.
Copyright © Lippincott Williams & Wilkins. Unaut8 www.jhypertension.com
44. Liese AD, Nichols M, Sun X, D’Agostino RB Jr, Haffner SM. Adherenceto the DASH Diet is inversely associated with incidence of type 2diabetes: the insulin resistance atherosclerosis study. Diabetes Care2009; 32:1434–1436.
45. Houmard JA, Tanner CJ, Slentz CA, Duscha BD, McCartney JS, KrausWE. Effect of the volume and intensity of exercise training on insulinsensitivity. J Appl Physiol 2004; 96:101–106.
46. Schillaci G, Pirro M, Vaudo G, Gemelli F, Marchesi S, Porcellati C,Mannarino E, et al. Prognostic value of the metabolic syndrome inessential hypertension. J Am Coll Cardiol 2004; 43:1817–1822.
47. Kjeldsen SE, Naditch-Brule L, Perlini S, Zidek W, Farsang C. Increasedprevalence of metabolic syndrome in uncontrolled hypertensionacross Europe: the Global Cardiometabolic Risk Profile in Patientswith hypertension disease survey. J Hypertens 2008; 26:2064–2070.
Reviewers’ Summary Evaluations
Reviewer 1Pressure-overload is only one among the many other deter-minants of hypertensive left ventricular hypertrophy (LVH)development. In order to comprehensively evaluate thesefactors in patients with recent (� 2 years) diagnosis ofessential hypertension, the authors took advantage of the‘Campania Salute Network’. Age, systolic blood pressure,obesity and diabetes were independent predictors of LVH.These data confirm that metabolic factors play an importantrole in modulating pressure-overload hypertrophy. Unfortu-nately, the retrospective nature of the study did not allow athorough evaluation of the contribution of insulin resistancein determining hypertension-related cardiac organ damage.
Reviewer 2This is a large study assessing the determinants ofleft ventricular hypertrophy (LVH) in patients withrecent diagnosis of essential hypertension. The authorsconfirm that the already established risk factors play asignificant role in the development of LVH andobesity represents the most important risk factor for thedevelopment of LVH in newly diagnosed hypertensivepatients. Obesity represents an epidemic with seriousconsequences that strains economic resources andburdens the healthcare system. Once again, preventionconstitutes the only option in order to decrease totalcardiovascular risk.
horized reproduction of this article is prohibited.Volume 30 � Number 1 � Month 2013




















