detection of herpes simplex virus in dengue negative
130
DETECTION OF HERPES SIMPLEX VIRUS IN DENGUE NEGATIVE PATIENTS WITH SUSPECTED HSVE OR MENINGOENCEPHALITIS BY REAL TIME PCR ASSAY DISSERTATION SUBMITTED TO In partial fulfillment of the requirement for the degree of DOCTOR OF MEDICINE IN MICROBIOLOGY (Branch IV) M. D. (MICROBIOLOGY) Register No.: 201714303 of THE TAMIL NADU DR. M. G. R MEDICAL UNIVERSITY CHENNAI- 600032 DEPARTMENT OF MICROBIOLOGY TIRUNELVELI MEDICAL COLLEGE TIRUNELVELI- 11 MAY 2020
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of detection of herpes simplex virus in dengue negative

DETECTION OF HERPES SIMPLEX VIRUS IN DENGUE NEGATIVE
PATIENTS WITH SUSPECTED HSVE OR MENINGOENCEPHALITIS
BY
REAL TIME PCR ASSAY
DISSERTATION SUBMITTED TO
In partial fulfillment of the requirement for the degree of
DOCTOR OF MEDICINE IN MICROBIOLOGY
(Branch IV) M. D. (MICROBIOLOGY)
Register No.: 201714303
of
THE TAMIL NADU DR. M. G. R MEDICAL UNIVERSITY
CHENNAI- 600032
DEPARTMENT OF MICROBIOLOGY
TIRUNELVELI MEDICAL COLLEGE
TIRUNELVELI- 11
MAY 2020

BONAFIDE CERTIFICATE
This is to certify that the dissertation entitled “DETECTION OF
HERPES SIMPLEX VIRUS IN DENGUE NEGATIVE PATIENTS WITH
SUSPECTED HSVE OR MENINGOENCEPHALITIS BY REAL TIME
PCR ASSAY” submitted by Dr. G. MALATHI to the Tamilnadu Dr. M.G.R
Medical University, Chennai, in partial fulfillment of the requirement for the
award of M.D. Degree Branch – IV (Microbiology) is a bonafide research work
carried out by her under direct supervision and guidance.
Head of the Department,Department of MicrobiologyTirunelveli Medical College,
Tirunelveli.

CERTIFICATE
This is to certify that the Dissertation “DETECTION OF HERPES
SIMPLEX VIRUS IN DENGUE NEGATIVE PATIENTS WITH
SUSPECTED HSVE OR MENINGOENCEPHALITIS BY REAL TIME
PCR ASSAY” presented herein by Dr.G. MALATHI, is an original work done
in the Department of Microbiology, Tirunelveli Medical College Hospital,
Tirunelveli for the award of Degree of M.D. (Branch IV) Microbiology under my
guidance and supervision during the academic period of 2017-2020.
The DEANTirunelveli Medical College,
Tirunelveli - 627011

DECLARATION
I solemnly declare that the dissertation titled “DETECTION OF
HERPES SIMPLEX VIRUS IN DENGUE NEGATIVE PATIENTS WITH
SUSPECTED HSVE OR MENINGOENCEPHALITIS BY REAL TIME
PCR ASSAY” is done by me at Department of Microbiology, Tirunelveli
Medical College Hospital, Tirunelveli. I also declare that this bonafide work or a
part of this work was not submitted by me or any others for any award, degree,
or diploma to any other University, Board, either in India or abroad.
The dissertation is submitted to The Tamilnadu Dr. M.G.R.Medical
University towards the partial fulfilment of requirements for the award of M.D.
Degree (Branch IV) in Microbiology.
Place: Tirunelveli
Date:
Dr.G. MALATHIPostgraduate Student,
Register No. 201714303M.D Microbiology,
Department of Microbiology,Tirunelveli Medical College,
Tirunelveli.

ACKNOWLEDGEMENT
My Research project is made possible with the support of many people. I
take this opportunity to express my gratitude towards them.
I am grateful to The Dean, Dr.S.M. Kannan M.Ch, Tirunelveli Medical
College and Tirunelveli Medical College hospital, Tirunelveli for permitting me
to carry out this study.
It is with great privilege and respect that I express my cordial and humble
thanks to Dr.C.Revathy, M.D., Professor and Head, Department of
Microbiology, Tirunelveli Medical College, whose kindness, guidance and
constant encouragement enabled me to complete this study.
I also thank Dr.P.Gnanaguru,M.D., AssociateProfessor, Department of
Microbiology, Tirunelveli Medical College, for his support for my project.
I am very thankful to Dr.M.AshihaBegum,M.D., Associate Professor,
Department of Microbiology, Tirunelveli Medical College, for the
encouragement throughout the period of study.
I am very grateful to.Dr.V.P.AmudhaM.D. , Associate Professor,
Department of Microbiology, Tirunelveli Medical College, for the constant
support rendered throughout the period of study and encouragement in every
stage of this work.
I sincerely thank my Co-guide Dr.M.Kanagapriya., M.D, Asst.Prof.
Department of Microbiology, Tirunelveli Medical College without whose
encouragement, motivation and guidance this work would not be possible.
I express my sincere gratitude to Dr.I.M.RejithaM.D., Asst.Prof
Department of Microbiology, Tirunelveli Medical College for her
encouragement, support, and corrective comments during the research period.

I am highly obliged to my Assistant Professors Dr.B.Cinthujah M.D., Dr.
G.Velvizhi M.D., M.D., Dr.S.Gowri, M.D, Dr.R.Nagalakshmi M.D.,
Dr.K.Subha M.D., Dr.Suyambu Meenakshi M.D., Department of
Microbiology, Tirunelveli Medical College, for their evincing keen interest,
encouragement, and corrective comments during the research period.
I also thank Dr.Sucila Thangam.G M.D., Associate professor in Madurai
Medical College for her guidance and support during the research period.
Special thanks are due to my co-postgraduate colleagues Dr.A.Sangeetha,
Dr.V.Ashwini, Dr.S.K.Jayaswarya, Dr.Roohee Zubaidha for never hesitating
to lend a helping hand throughout the study. I express my sincere thanks to all
my senior collegues for their helpful and supportive attitude in completing my
project.
I express my sincere thanks to all my senior collegues
Dr.UmaMaheshwari.R, L.Gracia Paul, Dr.M.SaiShruti, Dr.E.Manimala,
Dr.MayaKumar, for their helpful and supportive attitude in completing my
project.
I would also wish to thank my junior post-graduate colleagues,
Dr. R.Priyadharshini, Dr.M.Sri Vidhya, Dr.V.Thanalingam, Dr.S.I.Saheed
Askar, Dr.ReachelReena.D, Dr.Rajasri.A.G, Dr.Aparna.V.S, Dr.Kaviya.C,
Dr.LathaBharathi.C for their help, motivation and support.
Special thanks to Mr.V.Chandran, Mrs Uma ,Miss Karputhamani for
their helpful and supportive role in completing my project.
Thanks are due to the, Messer V.Parthasarathy, S.Pannerselvam,
Murugesan ,S.Santhi, S.ArifalBeevi, S.AbulKalam, Arul Selvi ,T.Jeya,
K.Sindhu, K.Mangai, ArulSelvi, Kutty Raj, Manivannan, K.Umayavel,
Sreelakshmi, Jeyalakshmi and other supporting staffs for their services
rendered.
I am indebted to my husband Dr. E. Elayaraja, my son E. Aryan, my
parents, brothers and in laws and all the family members for not only their

moral support but also for tolerating my dereliction of duty during the period of
my study.
I also thank Dr.Bhavani MD(SPM) for her guidance in the statistical
work.
And of course, I thank the Almighty for His presence throughout my
work. Without the Grace of God nothing would have been possible.


CERTIFICATE – II
This is to certify that this dissertation work titled “DETECTION OF
HERPES SIMPLEX VIRUS IN DENGUE NEGATIVE PATIENTS WITH
SUSPECTED HSVE OR MENINGOENCEPHALITIS BY REAL TIME
PCR ASSAY” of the candidate Dr.G.MALATHI with registration Number
201714303 for the award of M.D. Degree in the branch of MICROBIOLOGY
(IV) . I personally verified the urkund.com website for the purpose of plagiarism
Check. I found that the uploaded thesis file contains from introduction to
conclusion pages and result shows 3 percentage of plagiarism in the dissertation.
Guide & Supervisor sign with seal


CONTENTS
S. No Title Page No
1 INTRODUCTION 1
2 REVIEW OF LITERATURE 4
3 AIMS AND OBJECTIVES 48
4 MATERIALS AND METHODS 49
5 RESULTS 65
6 DISCUSSION 87
7 SUMMARY 94
8 CONCLUSION 96
9 BIBLIOGRAPHY
10 ANNEXUREPROFORMA
CONSENT FORMMASTER CHART

LIST OF ABBREVATIONS
HSV - Herpes Simplex Virus
HSE - Herpes Simplex Encephalitis
CDC - Centre for Disease Control and Prevention
CNS - Central Nervous System
CSF - Cerebrospinal Fluid
CT - Computed Tomography
MRI - Magnetic Resonanace Imaging
PCR - Polymerase Chain Reaction
EEG - Electroencephalogram
DV - Dengue virus
JEV - Japanese Encephalitis virus
EBV - Ebstein Barr Virus
CMV - Cytomegalo virus
VZV - Varicella Zoster Virus
HHV - Human Herpes virus
KSHV - Kaposi sarcoma herpes virus
HIV - Human Immuno Deficiency virus
AIDS - Acquired Immuno Deficiency Syndrome
DNA - Deoxyribonucleic acid
ADEM - acute disseminated encephalomyelitis

AES - Acute encephalitis syndrome
ICTV - International Committee on Taxonomy ofViruses
dsDNA - double stranded DNA
mRNA - messenger Ribodeoxy nucleic acid
VP - virion protein
ICP - Infected cell protein
ORF - Open reading frame
LAT - Latency Associated Transcripts
MTR - morphological transforming region
RR - Ribonucleotide reductase
HVEM - Herpes virus entry mediator
CPE - cytopathic effect
TK - Thymidine kinase
CMI - Cell mediated immunity
TAT -Turnaroundtime
STD - Sexually Transmitted Diseases

LIST OF IMPORTANT TABLES
SLNO
TITLE PAGENO
1. CNS INFECTION CAUSING VIRUSES 5
2. VIRAL CAUSES OF AES/MENINGOENCEPHALITIS 6
3. CLASSIFICATION OF HERPES VIRUSES 10
4. CSF FINDINGS IN VIRAL MENINGOENCEPHALITIS 41
5. DIAGNOSTIC CRITERIA FOR ENCEPHALITIS 52
6. PCR RESULTS 62-63
7. HSV 1 POSITIVE DISTRIBUTION IN STUDY
POPULATION
67
8. MINOR CRITERIA PRESENCE IN THE STUDY
POPULATION
72
9. PROFILE OF ASSOCIATED FACTORS WITH HSV 1
POSITIVE DISTRIBUTION IN STUDY POPULATION
85-86

1
1.INTRODUCTION
Herpes simplex virus belongs to family alphaherpesviridae, a DNA virus is
a widespread human pathogen. Among the Herpes viruses group, the two
serotypes HSV-1 and HSV-2 both infect epithelial cells. HSV-1 is normally
associated with oral infections and lesions above waist and HSV-2 is
associated with genital infections and lesions below waist. Herpes simplex
virus (HSV) play a major role as a cause of meningitis or encephalitis1 . It is
the most common cause of acute sporadic, fatal encephalitis cases world
wide2. HSV is well known to undergo latency and cause various clinical
diseases when it gets activated under conditions like stress, fever,
immunosupression etc. The virus also causes other organ system diseases.
About 30 percent of cases result from the initial infection with the herpes
simplex virus; the majority of cases are caused by reactivation of an earlier
infection.
Most people acquire herpes simplex virus type 1 (the cause of cold sores or
fever blisters) in childhood. Annually it occurs in 10 to 20% of viral
encephalitis cases in the developed world3 and in India too. The Centre for
Disease Control and Prevention (CDC) estimate the incidence of Herpes
Simplex Encephalitis to be approximately 40 to 50 cases per year
worldwide; however, disease occurrence is undoubtedly higher4. More than
half of untreated cases are fatal.

2
HSVE (Herpes Simplex Virus Encephalitis) due to herpes simplex virus type
1 can affect any age group. It is associated with significant mortality and
morbidity, and its outcome is directly correlated with the rapid onset of
antiviral therapy.
Manifestations of HSV encephalitis in the older child and adult are
indicative of the areas of pathology in the brain. The classical presentation
of HSVE- include primarily a focal encephalitis associated with fever,
altered consciousness, bizarre behavior, disordered mentation, and localized
neurologic findings. These clinical signs and symptoms generally are
associated with evidence of localized temporal lobe disease, as demonstrated
by neurodiagnostic procedures5. A CT scan may not reveal abnormalities
until 3-5 days following symptom onset and even contrast enhanced MRI
may be negative.
Clinical diagnosis is often unreliable, as many neurologic syndromes may
mimic HSVE6 . No pathognomonic findings exist for herpes simplex
encephalitis; however, classical presentation in the absence of other causes
should strongly suggest this disease. Even then clinical presentation of
Herpes Simplex Virus Encephalitis (HSVE) is not classically constant, in a
patient. Since the mortality in untreated patients is 70%, and only 2.5% of
all patients returns to normal neurologic function, it is vital to make early
diagnosis9.

3
Historically, diagnosis of CNS infections was accomplished only by brain
biopsy7. The evaluation of CSF specimens from patients with biopsy-proved
HSV encephalitis had more than 95% specificity and 100% sensitivity.
Nowadays PCR assessment of the CSF has become the diagnostic of
choice8.
The experience with PCR shows that it is a useful tool for diagnosis of HSV
encephalitis9. RT-PCR is positive early in the disease and is suitable for a
rapid diagnosis as the turnaround time(TAT) is only a few hours12,13.
Generally the test remains positive during the first week of therapy.
The evaluation of CSF PCR can also be used to follow therapeutic outcome
in patients with HSV encephalitis. Persistence of HSV DNA in the CSF of
newborns with HSV encephalitis at the completion of antiviral therapy
predicts poor neurologic outcome10 . PCR is also being used to detect HSV
DNA in mucocutaneous lesions because it has an improved sensitivity and
specificity.11 Herpes group of viruses have specific antiviral therapy
available (Acyclovir), and early diagnosis can alert the clinician for timely
initiation of specific therapy and prevent the high mortality and morbidiity.
This study was undertaken in Tirunelveli Medical College Hospital,
Tirunelveli to identify the Herpes simplex virus in suspected viral
Meningoencephalitis cases. The present study will help clinicians in early
diagnosis, treatment plan and control strategies in developing diagnostic
algorithm in our Institution.
4
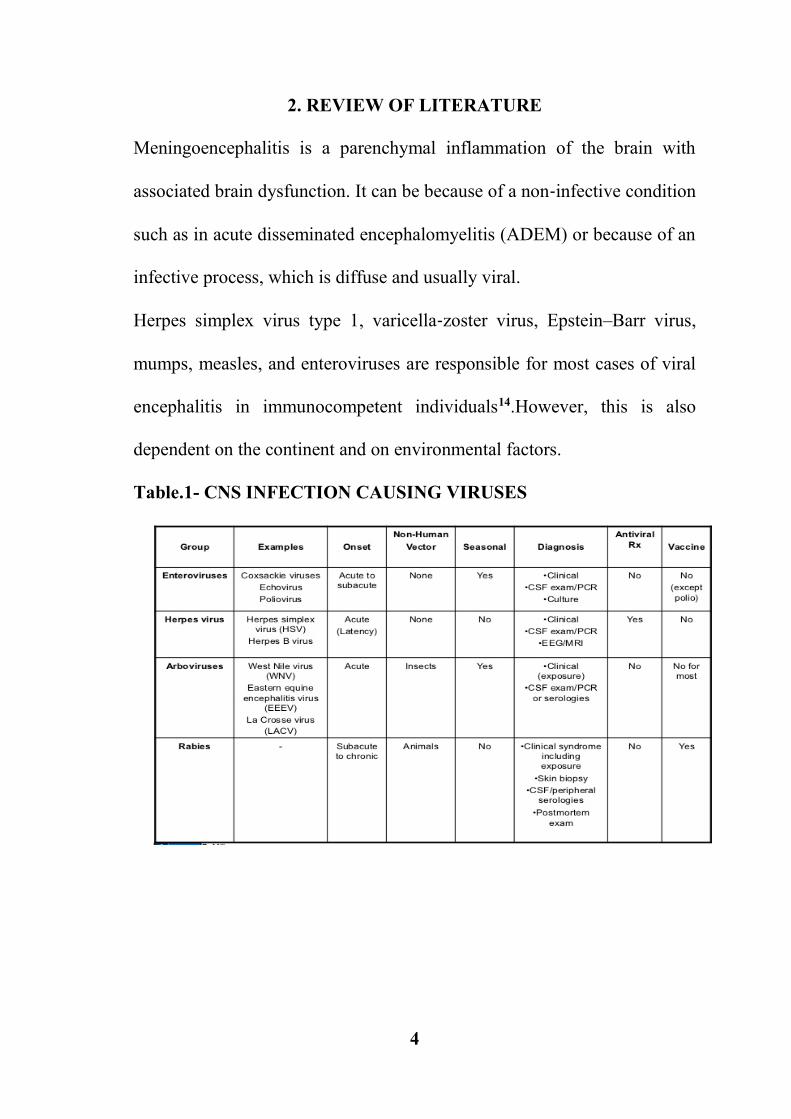
2. REVIEW OF LITERATURE
Meningoencephalitis is a parenchymal inflammation of the brain with
associated brain dysfunction. It can be because of a non‐infective condition
such as in acute disseminated encephalomyelitis (ADEM) or because of an
infective process, which is diffuse and usually viral.
Herpes simplex virus type 1, varicella‐zoster virus, Epstein–Barr virus,
mumps, measles, and enteroviruses are responsible for most cases of viral
encephalitis in immunocompetent individuals14.However, this is also
dependent on the continent and on environmental factors.
Table.1- CNS INFECTION CAUSING VIRUSES

5
ACUTE ENCEPHALITIS SYNDROME
Acute Encephalitis Syndrome (AES) is defined as the fever of acute onset
and a change in mental status and/or new onset of seizures in any age group
and season of the year. AES is an emerging public health problem claiming
thousands of lives and the disease most commonly affects children and
young adults and can lead to considerable morbidity and mortality.
Table-2.Viral Causes Of Aes/Meningoencephalitis
DNA VIRUSES RNA VIRUSESHERPES VIRUSES NON POLIO ENTERO
VIRUSES ARBOVIRUSES
- HSV(Herpes SimplexVirus)
- VZV(Varicella ZosterVirus)
- CMV(Cytomegalo Virus)- EBV(Ebstein-Barr Virus)
- JEV(Japanese EncephalitisVirus)
- Dengue Virus- West Nile Virus
In India, it has been estimated that a population of 375 million people
residing in 171 endemic districts of 17 states are at a risk of acquiring AES15
. High incidence of AES in India include the dengue virus(DV), enterovirus,
herpes simplex virus (HSV), measles virus, and Chandipura virus16,17
[Whitely RJ et al]; however, the etiology of AES remains unknown in 68–
75% of the patients18 [Huppatz C et al].
An accurate identification of the organism causing AES is essential for
surveillance and patient management because some of these infections are
preventable or treatable. Although bacteria viruses and protozoan parasites

6
may cause encephalitis, among these the viruses are the most common and
important cause of encephalitis. Cases of AES have been reported from
many of Indian states, but the aetiological agent has been identified in only
minimal of cases.
Among all viral encepahalitis that is encountered in India, JE appears to be
of greater significance during outbreaks as well as in sporadic cases. Herpes
virus, enterovirus, measles virus, mumps virus and rubella virus also
constitute significant numbers in sporadic and outbreak cases in India19.The
agent profile causing AES is varies from place to place. Clinical and
neurodiagnostic tests can usually establish the presence of encephalitis but
do not necessarily establish the aetiologic cause, which often remains
unknown.
HERPES SIMPLEX ENCEPHALITIS
Viral encephalitis is inflammation of the brain, caused by many number of
viruses.
Herpes simplex virus (HSV-1) encephalitis is the commonest cause of fatal
sporadic encephalitis in the world19. Worldwide, an estimated 66 percent of
the population has herpes simplex virus type 1 (HSV-1) infection15. HSV-1
is typically transmitted from person to person via infected oral secretions
during close contact. After initial infection, HSV-1 establishes chronic
infection in neural ganglia and reactivates on mucosa and skin.

7
Although infections are frequently asymptomatic, they can produce a variety
of signs and symptoms. These include recurrent oral or perioral lesions
("cold sores"), skin and mucous membrane lesions, including genital lesions,
ocular infections (eg, herpetic keratitis), and serious systemic illnesses such
as encephalitis and neonatal disease involving multiple organs.
HSV TYPE 1 AND 2
There were two types of HSV established in few studies HSV 1 and
2[Schneweis; Dowdle, Nahmias et al]. Herpes simplex encephalitis is
almost exclusively caused by HSV-1. HSV-2 is manifested by meningitis.
But, in 4-7% of patients, HSV-2 has been found to be associated with non-
neonatal focal herpetic encephalitis11[Whitely et al.; Aurelius, Johnsson et
al].
Herpes simplex virus encephalitis manifest in different forms:
In children > 3 months and in adults, HSE is usually focal and is caused
by herpes simplex virus type 1 (HSV-1).
In neonates, there is generalized encephalitis, and the cause is herpes
simplex virus type 2 (HSV-2), acquired during delivery.
HSE have to be differentiated from herpes simplex meningitis, which is
more commonly caused by HSV-2 than by HSV-1 and which have a strong
association with a herpetic genital infection.
Herpes simplex encephalitis is either an acute or subacute disease causing
cerebral dysfunction. Brain infection is most often due to direct neuronal

8
transmission of the virus from a peripheral site to the brain via the cranial
nerves19. Antiviral therapy ,may doesn’t help in complete cure in herpes
simplex encephalitis (HSE)and had been associated with risk of morbidity
and death20.
There is no clear pathogenesis factors making a role in HSE infection. The
clinical syndrome is often characterized by the rapid onset of fever,
headache, seizures, focal neurologic signs, and impaired consciousness. The
most important neurologic sequelae of HSV is Encephalitis. It is a
devastating disease with significant morbidity and mortality, despite
available antiviral therapy.
EPIDEMIOLOGY
HSV-1 encephalitis is the most common fatal sporadic encephalitis
worldwide, accounting for approximately 10 to 20 percent of the 20,000
annual viral encephalitis cases3,21 [Levitz RE; Whitley RJ;]. The infection
arises in all age groups, with one-third of all cases occurring in children and
adolescents22 [ Whitely RJ et al;]. HSV is also the most commonly
identified pathogen among hospitalized patients diagnosed with encephalitis
in Australia18 [Huppatz C et al;].
Worldwide, it contributes to 10-20% cases of viral encephalitis3. [Levitz
RE;] The incidence of this disease, Herpes Simplex Encephalitis (HSE) is
very difficult to estimate, because only few patients with severe disease
report to hospital whereas mild and self limiting cases usually go

9
unrecognised. In India, HSE appears to be under diagnosed, probably due to
lack of awareness and diagnostic facilities. Surprisingly, till 1992 only
occasional case reports were available23.[Ravi V;]. In 1993, Satish
Chandra et al reported 9 cases of HSE and later in 1996 compiled data on
51 cases24.
However, clear epidemiological and serological studies for viruses are not
available in many parts of the country, due to lack of virology research
laboratories. Thus, case percentage of viral encephalitis and HSE proportion
are difficult to estimate. Early diagnosis of HSE is essential because early
introduction of antiviral therapy can significantly decrease mortality and
morbidity associated with this disease3.
Table 3: CLASSIFICATION OF HERPES VIRUSES
VIRUS ABBREVIATION GENUS ICTV SPECIESNAME
Herpes simplexvirus type 1 HSV 1 α 1 Human herpes
virus 1Herpes simplex
virus type 2 HSV 2 α 1 Human herpesvirus2
Varicella-zostervirus VZV α 2 Human herpes
virus3Epstein–Barr
virus EBV γ 1 Human herpesvirus4
Humancytomegalovirus HCMV β 1 Human herpes
virus5Human
herpesvirus 6 HHV-6 β 1 Human herpesvirus6
Humanherpesvirus 7 HHV-7 β 2 Human herpes
virus7Kaposi’ssarcoma-associated
herpesvirus
HHV8/KSHV γ 2 Human herpesvirus8

10
VIROLOGY
NOMENCLATURE
Family : Herpesviridiae
Subfamily : alphaherpesvirus
Genus : Simplex virus
Species : Herpes simplex virus-1
Herpes simplex virus-2
Enveloped : yes
Genome : Double stranded DNA
Herpes simplex viruses were the first of the human herpes viruses to be
discovered and are among the most intensively investigated of all viruses.
Their attractions are their biologic properties, particularly their abilities to-
(a) cause a variety of infections,
(b) remain latent in their host for life, and
(c) reactivate to cause lesions at or near the site of initial infection.
They serve as models and tools for the study of translocation of proteins,
synaptic connections in the nervous system, membrane structure, gene
regulation, gene therapy, cancer therapy, and a myriad of other biological
problems, both general to viruses and specific to HSV.

11
MORPHOLOGY
Herpes virus is spherical & enveloped virus containing icosahedral capsid.
The capsid is composed of 162 capsomers & envelope carries surface
glycoprotein spikes.
Size: 100-200 nm in diameter.
Genetic Material:- Linear dsDNA.
STRUCTURE OF VIRION
Figure 1: Structure of Virion
The HSV virion consists of four elements:
(a) an electron-opaque core containing the viral DNA,
(b) an icosahedral capsid surrounding the core,
(c) a largely unstructured proteinacous layer called the tegument that
surrounds the capsid, and (d) an outer lipid bilayer envelope exhibiting

12
spikes on its surface25. Early studies the structure of the HSV virion through
electron microscopy (EM) and biochemical analysis of the virion
components. More recent cryo-EM studies have defined the nucleocapsid
structure to 8.5 Ã… resolution26. The most detailed analysis of the whole
virion used cryo-electron tomography to define its structure to 7 nm
resolution27. The above study defined the virion as a spherical particle with
an average diameter of 186 nm, which extended to 225 nm with spikes
included.
The nucleocapsid was located in an eccentric position with one edge of the
nucleocapsid close to the envelope and the other, the distal pole, 30 to 35
nm from the envelope. The tegument showed a particulate structure with
some 7 nm filaments apposed to the membrane. The tegument cap on the
distal pole was connected to the envelope by 4 nm wide linkers.
Figure 2 : Schematic picture of virion

13
VIRUS PROTEINS
HSV proteins have also been named based on serial numbering of the virion
proteins on a gel (e.g., VP1/2), on the open reading frame (ORF) encoding
them (e.g., UL8) or as infected cell proteins (e.g., ICP5). Probably as a result
of the past thorough analysis of HSV virions by classic biochemical
approaches, no mass spectrometry studies of HSV virions have been
reported.
Early biochemical studies concluded that all of the virion proteins were
made after infection, and in the early studies it was concluded that no host
proteins could be detected in purified virion preparations. More sensitive
techniques are likely to detect host proteins, but the critical issue is to
determine if any host proteins are essential for virion structure. Of the
approximately 30 known and 10 suspected virion proteins, at least 11 are on
the surface of the virion (accessible to antibody) and at least 10 are
glycosylated.
CORE
The core contains the double-stranded DNA (dsDNA) genome wrapped as
a toroid or spool in a liquid crystalline state28. A small fraction of the virion
DNA may be circular29,30 . The viral DNA genome is described in detail
below. The core does not contain highly basic proteins that would neutralize
the negative charges on viral DNA to allow proper folding within the capsid,
but highly purified virions do contain the polyamines spermidine and

14
spermine in a nearly constant ratio of 1.6 ± 0.2:1, or approximately 70,000
molecules of spermidine and 40,000 molecules of spermine per virion31.
TEGUMENT
The space between the undersurface of the envelope and the surface of the
capsid, designated as the tegument , is largely unstructured, except for some
apparent icosahedral structure around the pentons and it is composed of at
least 20 viral proteins.
CAPSID
The capsid is composed of 162 capsomers arranged in icosahedral
symmetry. The outer shell of the capsid is composed of four viral proteins,
VP5 (UL19), VP26 (UL35), VP23 (UL18), and VP19C (UL38). VP5, the
major capsid protein, is present in five copies in each penton capsomere and
six copies in each hexon capsomere in this icosahedral shell. VP26 is present
in six copies as a ring on top of the VP5 subunits on each hexon.
ENVELOPE
The envelope consists of a lipid bilayer with approximately 11 different viral
glycoproteins embedded in it.
LIPIDS
It has been assumed that HSV acquires the envelope lipids from its host. The
hypothesis that the lipid composition of the viral envelope is determined by
the host was supported by the observation that the buoyant density of the
virus was host cell dependent on serial passage of HSV-1 alternately in HEp-

15
2 and chick embryo cells32 . One study suggest that the virion lipids are
similar to those of cytoplasmic membranes and different from those of
nuclear membranes of uninfected cells33.
REGULATION OF GENE EXPRESSION
The transcription of the viral genome during infection occurs in a cascade-
like fashion which results in immediate-early, early, and late viral mRNAs.
No prior viral protein synthesis is required for expression of α (immediate-
early) genes and these α genes are responsible for the expression of the other
genes in a regulated way. β (early) genes expression is totally independent
of viral DNA, encode proteins and enzymes which are directly involved in
DNA synthesis and nucleotide metabolism.
The beta (β) genes are inducers and they activates the last group of genes,
the gamma (γ) or late genes, coding for the many structural proteins in the
HSV virion, including capsid proteins, which are translated in the cytoplasm
and then imported into the nucleus where capsid assembly occurs34.
ENTRY OF HSV INTO HOST CELLS
HSV entry requires binding of virus to cell surface receptors and fusion of
the virion envelope with the cell plasma membrane (Spear et al., 2000; Spear
and Longnecker,2003). The initial attachment is mediated through viral
glycoprotein C (gC) and/or gB to cell surface heparan sulfate
proteoglycans35 This fusion requires gB, gD, gH, and gL36,37,38

16
Three cell surface receptors for HSV have been identified: the first
receptor herpes virus entry mediator A(HveA or HVEM) is a member of the
tumor necrosis factor receptor (TNFR) family. The other two receptors are
HveB and HveC38,39,40,41. It is also reported that HveC allows entry of virus
by directly interacting with gD, as shown for HveA39,42 . Recently both
HveB and HveC were found to be novel cell-cell adhesion system
components, and to belong to the Ig superfamily. They were therefore
renamed as nectin-1 and nectin-2, respectively 38,43
LIFE CYCLE OF HSV
HSV replicates by three rounds of transcription that yields: immediate-early
(α) proteins regulating viral replication; early (β) proteins in DNA
synthesizing and packaging ; and late
(γ) proteins, mostly are of virion proteins.

17
Fig:3 Diagrammatic representation of herpesvirus replication cycle
(Metteinletter;)34.
PATHOGENESIS
NEUROTROPISM
HSV-1 and HSV-2 most often are associated with infection in distinct and
different areas, i.e. they show a hitherto unexplained typespecific
neurotropism. In neonatal children, HSV-1 and HSV-2 can cause
meningoencephalitis. In both manifestations, the brain and the meninges are

18
involved, but the infection is less severe when HSV-1 is diagnosed44.
When causing encephalitis in adults, HSV-1 preferably infects the limbic
system and the temporal lobes. This infection results in severe damage
including necrosis in the affected area45. Memories, language, olfaction,
behaviour and emotions are functions associated with these regions of the
brain, and the affected areas are often linked to neurological sequelae that
can be life-long.
In contrast, the meninges are the main target during HSV-2 infection of the
CNS in adults45. Consisting of three membranes, the meninges surround and
protect the brain and spinal cord, and infection leads to acute symptoms such
as severe headache, neck pain and nuchal rigidity.
Importantly, many of these patients develop recurrent meningitis46. In
addition, focal symptoms such as urinary retention in patients with HSV-2
meningitis may be linked to myelitis in the lumbosacral region47 . Despite
such attacks, adults with primary and recurrent HSV-2 CNS infections of
the CNS rarely display long lasting symptoms or permanent sequelae48.
The human pathogenesis of HSE in is not well understood. The neurons will
suffer a lytic and hemorrhagic process distributed asymmetrically
throughout the medial temporal and inferior frontal lobes. Wasay et al
reported temporal lobe involvement in 60% of patients. 49

19
Half of patients demonstrated temporal and extratemporal abnormalities,
and some demonstrated extratemporal lesion. Cerebellar and brainstem
involvement is uncommon.
The pathogenesis remains unclear, but have both virus-mediated immune-
mediated processes. The ability of HSV-1 to induce apoptosis in neuronal
cells, not a feature of HSV-2, gives the explanation that HSV-1 is
responsible for all cases of herpes simplex encephalitis older children and
adults in a study by Esiri MM et al50.
The temporal tissue destruction is described in an immunohistologic
autopsy study of patients succumbing to HSE within weeks in the pre-
acyclovir period. The rapid progression of spreading viral infection in the
limbic cortex, from one side to other side of brain, in a period of 3 weeks
results in severe necrosis and inflammation in infected areas of the brain51.
Infection of brain parenchyma is mainly due to direct neuronal transmission
of the virus from a peripheral site to the brain via the trigeminal or olfactory
nerve. There is no increase in prevalence in debilitated hosts, but the
presentation may be atypical in these patients. HSV-2 is the prime agent in
HIV-AIDS patients.
In about one third of cases the encephalitis is primary; in the other it occurs
in patients with preexisting HSV infection which is due to reactivation of
a latent peripheral infection in the neurons or to reactivation of a latent
infection in the brain. Even asymptomatic individuals may present with

20
latent HSV infection in the brain. In a postmortem study, HSV was present
in the brains of 35% of patients with no evidence of neurologic disease at
the time of death.31
Neonatal HSE may be a sole CNS infection or disseminated multiorgan
involvement.
HSV INFECTION
HSV is a natural pathogens for humans, with particular affinity for the
nervous tissue. The
virus spread from person to person by infected secretions, classically oral
secretions for HSV-
1 and genital secretions for HSV-2. There are three types of herpetic
infections:
Lytic infection,
Latent infection
Transforming infection.
In a lytic infection, virus multiply inside the nucleus of infected cell. This
is followed by production of infectious virions before lysis of infected cells,
partly due to suppression of host protein synthesis by a structural protein
named virus host shutoff (vhs) protein, encoded by
the UL41 gene52.
In latent infection, viral DNA is maintained in a non-replicative state and
persists in the nucleus as an episome for the entire life of the individual52.

21
Virus may reactivate following a variety of local or systemic stimuli to cause
recurrent disease.53
During latency, the viral lytic genes are extremely repressed and only a
single transcription unit encoding the latency-associated transcripts (LATs),
remain active54,55. The most abundant LAT is a 2.0-kb RNA56,57 which is
also detected during productive infections58 in a study by Ahmed et al..
The other LATs are 1.4- and 1.5-kb(kilobase) long which can only be
detected during latency.59
The molecular mechanisms controlling latency and reactivation remain
poorly understood and is a focus of active investigation.
The possibility that herpes simplex virus has transforming potential has been
a focus of interest. Numerous studies have shown that, both HSV-1 and
HSV-2 are able to transform the morphological phenotype of rodent cells.
In a study by Das et al; it was given that the transformation by HSV-1 does
not require the entire viral genome, but is attributed to a region located
between map units 0.31 and 0.42 designated as morphological transforming
region of HSV-1 (mtr-I)60.
Failure to detect viral DNA in transformed cells led to the hit-and-run
hypothesis of HSV-1 Transformation as noted in a study by McDougall61.
Within the HSV-2 genome there are two unique morphological transforming
regions designated as mtr II and mtr III located between map

22
units 0.585 and 0.63 and 0.42 and 0.58 62. MtrII and mtrIII encompass for
the large subunit of viral ribonucleotide reductase (RR1) which has
transforming potential63,64,65
HUMAN DISEASE
HSV-1 and HSV-2 are common human pathogens that can cause primary
and recurrent infections of mucous membranes. Primary HSV infections are
usually symptomatic but may be sub clinical. Recurrent infections are
generally less severe than the primary infection. The most commonly seen
clinical manifestations include oro-facial and genital lesions. Ocular
infections may include any part of the eye including the retina, conjuctiva,
cornea and eyelids.66,67,68
Meningitis is usually benign, but the HSV encephalitis has been associated
with high mortality [Tyler et al.;]. Neonates are particularly at risk for
serious HSV infections; early treatment appears to be an important
determinant of the outcome69 [Kimberlin et al.,]. In addition,
immunocompromised patients are at risk of developing more severe HSV
infections.
Cutaneous HSV infections are uncommon in healthy persons but may be
seen in a number of skin disorders such as eczema herpeticum and atopic
dermatitis70 [Yoshida and Umene].
Herpetic whitlow is infection of fingers among dentists and other health care
workers71 [Szinnai et al] whereas infection on bodies of wrestlers is called

23
herpes gladiatorum. Erythema multiforme is frequently associated with
HSV infection72,73,74 [Sun et al.; Aurelian et al.; Ono et al].
Before the introduction of antivirals HSE was associated with a 70%
mortality rate, but despite reduced mortality to around 10-20%, morbidity
after antiviral treatment is still high, where the majority of patients are left
with remaining neurological sequelae75.
EPIDEMIOLOGY OF HSV INFECTION
The prevalence of HSV-2 infection among health adult populations is higher
in the USA than in Europe. Furthermore, HSV-2 seroprevalence varies
widely among European countries76
[Malkin et al]. In some, but not all countries, HSV-2 seroprevalence appears
to be increasing. The most recent data available in the United States
demonstrate a 30% increase of HSV-2 seroprevalence over the past two
decades 76,77[Malkin; Bünzli et al].
The higher HSV-2 seroprevalence has been reported among patients
attending sexually transmitted disease (STD) clinics77,78 [Gottlieb et al.;
Weiss]. The situation is not well characterized on African content but
available data suggest that HSV-2 seroprevalence is higher than in the
United States 78,79[Smith and Robinson; Weiss].
In a study by Geiger et al; interferon-gamma–knockout mice was used to
show how interferon-gamma gives protection against HSV-1–mediated cell
death in neurons.81 Those studies suggest a varied presentation and severity

24
of encephalitis. Recent research suggests that an inborn error of interferon-
mediated immunity is a predisposing factor the HSV-1 infected individual
to developing HSE. 82Also supporting research studies research suggests the
signaling pathways of interferon-beta production helps in controlling HSV
replication in the brain.83
HSE can be caused either by primary or recurrent infection84 and can occur
in all age groups, although it is more common in elderly. Recurrent infection
is likely if antibodies against HSV-1 are present at onset of neurological
symptoms. This is the case for at least 2 of 3 HSE patients, both adults
[Nahmias AJ et] and children85 [De Tiege X et al]. However, it is unclear
if the infection is due to reactivation of virus from the site of latency,
activation of virus already in the brain or infection with a new, neurovirulent
strain of the virus.
SOCIO DEMOGRAPHICS FACTORS
HSE has a bimodal age distribution, occurring in peak at age less than 20
years and a second peak in age more than 50 years. In younger patients it
is primary infection, whereas in older persons is a reflection of
reactivation of latent infection. About one in three cases occur in children.
Genital infection is almost equa in both sexes, but more prevalent in the male
because of anatomy. There is no specific racial predilection.

25
PRIMARY INFECTION
Man is the natural host, mode of spread is by contact, through skin or
mucous membrane. Due to acantholysis vesicles are produces. When the
vesicle collapses, ulcer is formed which is called as herpetic ulcer. A period
of short viraemia occurs causing local spread, and also disseminated
throughout the body. The spread of the virus is usually stopped, but can
enter the craniospinal ganglia which is central to the neurological infection.
LATENCY PROPERTY
The virus capacity to escape from the immune reaction results in its
continuous presence in certain tissues as latent ones. Number of techniques
can reveal virus in about half of normal trigeminal ganglia and also in
cervical, sacral and vagal ganglia. The exact mechanism of latency of the
virus is unknown, it is because of ;-
(i) True latency - virus does not multiply but present within the cell in
integration with the cellular chromosome.
(ii) Virus deligence - this is not static, but there is a low grade productive
virus infection which prevents cell destruction.

26
REACTIVATION
The precipitating factors include:
Fever
Infection
Stress
Exposure to radiation/uv light
Physiological(menstruation)
Others
The cause is however indecisive, and craniospinal ganglion is the
source. Many static and dynamic theories are projected.
HERPES INFECTIONS IN CNS
The manifestations of HSV disease in the CNS are as follows:
1. Psychiatric disorder - this is conjectural at present
2. Meningitis - this appears to be a rare complication
3. Mild diffuse encephalitis
4. Severe focal encephalitis
5. Neonatal Herpes Simplex Encephalitis

27
There is no sexual predilection in this infection. Encephalitis can occur
either primarily or in a previous immunized persons as:
(i) primary diseease
(ii) virus reactivation
(iii) exogenous infection in an individual with virus latency
HERPES ENCEPHALITIS
There is a previous history of recurrent mucocutaneous herpes in one third
of the cases. But it is uncertain it is a latent state from reactivation of sensory
ganglion to brain or its primary latency in the brain. HSE is more common
in older age group and neonates where it is caused by HSV-1 and HSV-2
respectively86. Whitley et al, found no characteristic racial, age, sex or
seasonal predilection.87 In this series, disease was more common in patients
of age > 40 years and < 20 years. Male : Female ratio was 2:1 and disease
was more common during summer and rainy season (61%). The term HSE
is usually applied to focal and severe disease (acute necrotising
encephalitis), which may be insidious to violent in onset24.
Prodromal phase of 4-10 days with nonspecific symptoms is common in
HSE88 . Prodrome is characterised by fever and constitutional symptoms.
Common neurological manifestations included altered sensorium, seizures,

28
abnormal behaviour, focal neurological deficit, ataxia, aphasia, visual field
defects and papilloedema87.
Patients with abnormal behaviour had marked cognitive impairment in the
form of disorientation to time, place and person, excitement and purposeless
motor movements, which were not goal directed. Seizures occured within
one week of the onset of neurological symptoms, mostly within three days.
In few patients, seizures were the first symptom of nervous system
involvement. Atypical cases included patients without focal deficit and
slowly progressive course89 .Such cases usually come to specialist at later
stage and create diagnostic confusion.
GLASGOW OUTCOME SCALE(GCS)
Grade 1 : Death within a month.
Grade 2 : Coma
Grade 3 : Severe disability (Conscious, needs assistance).
Grade 4 : Moderate disability (Neurological or intellectual
impairment, but independent).
Grade 5 : Good recovery (independent with or without minimal
neurological impairment).

29
NEONATAL HERPES SIMPLEX ENCEPHALITIS
The predominant pathogen is HSV-2 (75% of cases), which is usually
acquired during delivery. The risk increases to 40% if the mother acquire
genital herpes during pregnancy. Prolonged rupture of the membranes (>6
h) and intrauterine monitoring (eg, attachment of scalp electrodes) are risk
factors. In about 10% of cases, HSV (often type 1) is acquired post partum
by contact with an virus shedding individual91.
EXOGENOUS REINFECTIONS
The primary infection confine to a localized anatomical site. The recurrence
can occur in the same site caused by reactivation and also in a remote site.
Remote infection may be due to a different virus strain i.e; reinfection by
HSV-2 in a person already immune to HSV-1 or a different HSV-1 strain.
CLINICAL FEATURES
HSV is involved in different clinical manifestations which includes :
1. Acute gingivostomatitis
2. Herpes Labialis
3. Ocular Herpes
4. Herpes Genitalis
5. Meningitis/Encephalitis

30
6. Neonatal herpes
1.ACUTE GINGIVOSTOMATITIS
It is the commonest manifestation of primary infection. It manifests as
minor lesion to severe ulcer. More commonly affected is the hard palate
which manifest as pain and bleeding gums with necrotic bases. Other
features like fever, sore throat, dysphagia will be present. Herpetic
dermatitis, herpetic whitlows and genital herpes also co exist. One of the
similar infection is infectious mononucleosis. Rapid relief of symptoms can
occur in this disease.
2. HERPES LABIALIS
This is a recurrent oral infection. Present as oral ulcers by the virus. The
primary signs like pruritis, tingling and warm sensation usually precedes the
infection. This is followed by redness, papules and vesicle formation. When
it ruptures it heals by drying.
3. OCULAR HERPES
HSV causes mild external superficial lesions, to severe visual defects
a. Primary HSV keratitis ;- presents with grittiness, pain, blurred vision
and lacrimation. Initially presents with small predendritic corneal ulcers. In

31
due course they heal and may produce large serpentine dendritic ulcer.
Corneal anaesthesia can occur. It usually heals after few weeks
b. Recurrent HSV keratitis ;- 2 forms occur- dendritic and stromal.
c. HSV conjunctivitis ;- Conjunctivitis, blepharitis, and circumocular
dermatitis commonly present. Diagnosis is difficult if there is no corneal
ulceration.
d. Iridocyclitis, chorioretinitis and cataract ;- Mild reflex iritis is a
complication of viral keratitis leading to severe iridocyclitis. Chorioretinitis
and cataract can occur in newborn infection which can lead to loss of sight.
4. HERPES GENITALIS
These may be primary or recurrent. Secondary bacterial infection are
common in these lesions . It presents with Dysuria and urinary retention in
both primary and recurrent genital infection. Radiculitis and mild meningitis
may occur. Recurrent lesions in the perianal area are more resistant to
healing than oral lesions.
5. HERPES SIMPLEX MENINGITIS/ENCEPHALITIS
Aseptic meningitis which is almost always mild. Both HSV-1 or HSV-2 can
cause this complication due to primary genital infection. More common with
HSV-2 infection. Herpes simplex encephalitis (HSE) is a severe focal

32
hemorrhagic encephalitis. the mortality rate is ~ 70% and in survivors severe
neurological sequelae can occur. HSE can have a sudden or insidious onset.
The prodromal phase presents with fever, malaise , headaches and
personality changes. The parenchymatous involvement is presented with
seizures, speech and visual defects, paralysis, , personality changes and
coma. EEG is always abnormal with delta waves slow rhythms and periodic
discharges and the CSF is usually lymphocytic. Neuroimaging may show
focal lesions and mass effects.
6.NEONATAL HERPES
The prognosis is very grave in case of disseminated infection. In premature
infants, infection is very severe. The prognosis is better if infection occurs
after 1 week. Brain involvement is usually serious. The risk of
developmental abnormalities is more.
The first manifestations of disease like Poor feeding, weight loss, loose
stools and respiratory distress presents with characteristic lesions on the
skin, mouth or the eye. Splenomegaly and jaundice with liver failure may
occur.
DIAGNOSIS OF HSV INFECTION
Efficient laboratory testing is an essential component for management and
development of strategies to prevent transmission of HSV infection. Current

33
laboratory methods used to diagnose HSV infections include: virus
detection, antigen detection, DNA detection and serological tests.
Virus detection methods through culturing and DNA detection, particularly
using polymerase chain reaction (PCR), are applicable during active
infection in patients presenting with lesion. Antigen detection method can
be nearly as sensitive as culture methods92 [Ashley and Wald], and the most
sensitive strategy is to perform both tests.
Serological tests allows identification of silent carriers of HSV infection and
provide useful information in symptomatic patients when virological tests
such as culture, antigen detection and PCR are not helpful93 [Woolley et al.;
Ashley].
The application of HSV type specific serological tests has been difficult due
to strong serological cross-reactivity caused by the extensive antigenic
similarities between the two viruses95,96 [Schmid et al.; Tunbäck et al]. The
identification of type-specific glycoproteins G-1 (gG-1) and gG-2 in the
mid-1980s seemed to resolve this difficult97,98, [Marsden, et al., Roizman,
et al], because it is antigenically distinct for the two viruses. Since the
demonstration of two antigenic types, numerous test formats have been
developed to detect type specific antibodies94 (Ashley).
For diagnostics of alphaherpesvirus CNS infections, Real Time polymerase

34
chain reaction (RT-PCR) on CSF to detect viral DNA is the gold standard.
In RT-PCR, a set of primers and a probe target a conserved sequence of the
genome that will be amplified and quantified.
RT-PCR as a diagnostic procedure can be used in the acute phase of the CNS
infection, where virus usually can be detected in CSF in the initial phase of
CNS disease and up to one-two weeks after onset of disease. However, PCR
cannot be used in later stages of the infection, and in recurrent episodes of
HSM, viral DNA is not always detectable.
Furthermore, at least in HSE, PCR results may be negative for HSV in the
beginning of the infection (days 1-3), but a second CSF sample taken a few
days later might confirm the diagnosis99 . For neonatal HSV infection, PCR
on material from herpetic lesions, serum, CSF and conjunctival swabs are
used. Positive PCR findings are valid for diagnostics in new-borns during
their first month. It has been demonstrated that uninfected new-borns can
present with positive IgG levels from a mother who has experienced HSV
infection during the perinatal period, due to maternal antibodies delivered
across the placenta100.
ANTIVIRAL TREATMENT
CNS infections caused by alphaherpesviruses have, unlike many other viral
CNS infections, a highly recommended antiviral therapy available in the
form of the nucleoside analogue acyclovir. Acyclovir is a structural
analogue of 2-deoxyguanosine, apart from a modification in the cyclic ring

35
where the 3’-positioned carbon has been removed (Figure 21). The 3’ carbon
is normally involved in creating a phosphodiester bridge to the following
nucleotide.
The introduction of acyclovir in HSE therapy markedly reduced the
mortality rate from 70% to the current 10-20%101. The effectiveness and
nontoxicity of acyclovir is explained by the design of the drug. For acyclovir
to be activated, an initial phosphorylation step is needed, which can
effectively be performed by the viral TK, while host cell TK is one million
times less capable to phosphorylate acyclovir102. Therefore, acyclovir is
selectively activated in infected cells and is almost harmless to non-infected
cells, providinga non-toxic profile. After the initial activation, the acyclovir
molecule is further phosphorylated by cellular kinases to its active state.
The activated form of acyclovir can then be incorporated into the viral DNA
chain, where the activity of viral DNA polymerase is selectively inhibited
and further elongation of the chain is blocked due to the blocking in the 3’
carbon position of the molecule.
Acyclovir is very effective when given intravenously, but has a low
bioavailability when given orally103 [Kimberlin DW et al]. However, the
bioavailability is greatly improved when the aa valine is connected to the
molecule, resulting in an L-valylester prodrug of acyclovir known as
valacyclovir (Figure 21). Once inside the systemic circulation, valacyclovir

36
is transformed to acyclovir via esterase, and therefore valacyclovir is
preferred in oral therapy [Kimberlin DW et al ].
For HSE and HSV myelitis, the recommended duration of intravenous (i.v.)
acyclovir is 14 days to 21 days while for HSM and VZV meningitis the
duration of therapy is usually 7 days, where only more severe symptoms or
extensive vomiting results in a recommendation of i.v. acyclovir, otherwise
oral medication is used 104[Studahl M, et al].
Treatment of primary HSM can be performed with antiviral therapy,
although the CNS infection can often heal by itself (one exception is in
immunocompromised patients105 [Mommeja-Marin H, et al]. In recurrent
episodes, antiviral treatment can be beneficial, but the severity of the
symptoms may determine if antiviral therapy is needed.
In neonatal HSV infections, acyclovir is given i.v. for 21 days, and followed
by 6 months oral treatment. Antiviral therapy improves the outcome of
neonatal HSV infection, especially if administered early. Better antiviral
response has been reported in HSV-1 infected neonates than for HSV-2
infected neonates, although studies have demonstrated that neonatal patients
can experience neurological sequelae after antiviral treatment regardless of
virus106 [Engman ML et al ] The effects of long-term follow-up use of
valacyclovir to reduce morbidity in HSE patients was tested in a recent
study107 [Gnann JW et al]. The hypothesis was that reduction of persistent,
low-level HSV replication in CNS after the initial i.v. acyclovir treatment

37
with oral administration of valacyclovir would reduce the neuropsychiatric
sequelae and improve the outcome. However, no significant differences
were found between the intervention group and the control group given
placebo.
DIAGNOSTIC METHODS
1. Imaging
Imaging in patients with encephalitis is useful tool in diagnosis. CT scanning
is useful to rule space-occupying lesions or brain abscess. MRI is sensitive
for detecting demyelinating lesions of central nervous system. However, the
location of abnormal signal can attimes be suggestive of specific etiologies:
I. Temporal lobe involvement is evidence of HSV encephalitis, although
other herpes viruses (e.g., VZV, EBV, human herpesvirus 6) can also
produce this clinical picture.108
FIG-4: HERPES SIMPLEX ENCEPHALITIS

38
II. Involvement of the thalamus or basal ganglia may be observed in the
setting of encephalitis due to respiratory viral infection, Creutzfeld-Jacob
disease & arbovirus,
III. The presence of hydrocephalus may suggest nonviral etiologies, such as
bacteria, fungal, or parasitic agents
Imaging in viral encephalitis reveals brain parenchymatous edema in the
acute phase probably due to cytotoxicity. Depending on the virus
generalized or focal site may be involved such as temporal lobes in HSV
encephalitis. Early diagnosis is important for appropriate management.
Viral encephalitis has a predilection for young and elderly.in developing
countries it is the most common focal viral encephalitis. MRI is the
investigation of choice and diagnosis has to be confirmed by doing PCR for
the virus in the CSF. CT scan is necessiated before attempting lumbar
puncture to look for signs of raised intra cranial pressure.
Fig-5: HERPES ENCEPHALTITIS

39
2. Electroencephalography is most commonly abnormal in encephalitis.
Temporal
Lobe abnormality is suggestive of HSV encephalitis109.
Fig-6: EEG IN HSV
3. Cerebrospinal fluid findings
Cerebrospinal fluid (CSF) findings, usually confirm the presence of
infection in CNS. Increased white blood cell (WBC) count( < 200/mm3),
with a lymphocytic predominance ,elevated protein concentration( usually
<150 mg/dL) and normal glucose concentration are common CSF
abnormalities in patients with viral encephalitis .Red cells and xanthocromia
usually denotes picture of HSV infection; necrotizing encephalitis.

40
Table-4: CSF FINDINGS IN VIRAL MENINGOENCEPHALITIS
WBC count (Cells/mm3) 50-100
Primary cell type Mononuclear
Glucose(mg/dl) > 45
Protein(mg/dl) < 100
CSF analysis is an important step in the diagnosis of Encephalitis. The
opening CSF pressure should be measured and CSF should be tested for cell
count, glucose, and protein. The more Specific diagnostic tests to include:
polymerase chain reaction (PCR) tests for viruses, culture for bacteria, fungi
and mycobacteria and serology for the arboviruses. However, even with use
of polymerase chain reaction testing, the etiology in most cases remains
undefined110 .
HSV, is usually fatal if untreated hence it is crucial to rule out the possibility
of HSV should be considered particularly if there is focal lesion confined
to thte temporal lobe. Identification of HSV in the CSF is a rapid, sensitive,
and specific diagnostic test for HSV encephalitis111.
4. Serologic testing is most important for patients with persistent symptoms
and for whom diagnosis is not established by the routine investigations. Also
it helps in the retrospective evaluation of HSV infection in the affected
individuals for antibody titrating.Convalescent serological testing to be done
only after three weeks from the onset of the clinical illness.

41
5. Brain biopsy — As a last resort, brain biopsy can be considered in the
patient if the etiology of encephalitis is still unknown
VIRAL CULTIVATION
Swabs from lesions, throat washings,CSF and blood(5ml) are inoculated in
cell lines such as human foreskin fibroblasts, MRC-5, A549,
rhabdomyosarcoma, mink lung epithelial cell line, primary rabbit kidney,
CV-1, Vero and HEp-2 cells and show CPE (enlarged, refractile round with
, multinucleated giant cell) after 2 -3 days.The CPE starts focally but spreads
rapidly to affect other parts of the monolayer.112[Ameetha singh et al]
Inoculation in Chorioallantoicmembrane in chick embryo gives larger pocks
resembling Variola.
MOLECULAR METHODS
Molecular methods include Detection of viral DNA by molecular techniques
with high specificity [Ameetha singh et al]. It is a most sensitive and
specific method. Conventional molecular methods include detection of
amplified viral DNA by PCR using type- specific primers, or using common
primers followed by hybridization probes. The real time PCR reduces the
rate of false negative results and is a very rapid and sensitive diagnostic
method.[Ameetha singh et al].
42
REAL TIME PCR
Real time PCR provides a rapid and sensitive method to determine the
presence of target specific amplifiable viral DNA. This assay detects both
the serotypes of HSV and distinguishes between them. It is not a time
consuming assay unlike cultivation method. The results are accurate unlike
serological tests. Real time PCR detects even minimal amount of viral DNA
by using specific Taqman probe or Syber green. This is a reference assay
used in quantitative analysis of viral load which is useful in the evaluation
of neonatal herpes infection and considered as prognosis marker in therapy.
This is not used widely in all laboratories because of expensive probe price
[Wald et al].
Studies reveal that Real-time PCR had a sensitivity of 100% and a specificity
of 99% as compared to nested PCR. In comparisons with conventional PCR,
the main advantages of real-time PCR are speed and quantitativeness.
Furthermore, a real-time PCR assay can reduce the likelihood of
contamination, because of no post-amplification analysis such as agarose gel
electrophoresis [Bhumesh kumar et al].
DIFFERENTIAL DIAGNOSIS
These include primary CNS tumours or metastatic tumors, autoimmune
diseases, paraneoplastic diseases. Other non-viral infectious etiologies to
consider in the patient with suspected CNS infection include brain abscess,

43
syphilis, tuberculous meningitis, and fungal meningitis (e.g., coccidioides),
which can present with similar clinical picture.
MANAGEMENT
A.GENERAL MANAGEMENT
Steriods has minor role in the management of HSV infections. In
immunosuppressive conditions dosage should be adjusted. Hypersensitivity
in any stage of the infections is an indication for steroids. Supportive
management is generally followed in case of secondary bacterial or fungal
infections in mucocutaneous lesions.
B. ANTIVIRAL CHEMOTHERAPY
The indications of antiviral chemotherapy is minimal, bearing high cost
being the main concern. In severe primary infection and brain infection,
antiviral therapy is indicated especially in immunocompromised and
neonates. The indication of treatment depends on the severity of the disease.
Antiviral therapy should be started within 3 days of the onset of symptoms
which makes it more effective than delayed initiation.
1. Acyclovir – Presently the drug of choice. Acyclovir require the presence
of a HSV-encoded The enzyme thymidine kinase helps in its conversion to
its active form. This selectively inhibits HSV DNA polymerase causing

44
premature chain termination for its incorporation into viral DNA. Acyclovir
is available in 4 formulations : oral, iv, cream or ointment.
The side effects are few. Bone marrow depression is the adverse effect of
long term acyclovir therapy but its occurrence is minimal. Drug resistant
strains of the virus are mainly because of- negative enzyme variants,
resistant mutant enzyme (Tk) and pol mutants causing drug resistance, Tk-
variants are more common than mutants which causes reduced
pathogenicity. In drug resistant cases, Foscarnet and ara-A are the drugs of
choice .
2. Famciclovir - It is the prodrug of active form penciclovir, a guanosine
analog. The bioavilability is high and has a long half life in oral form. It has
a higher affinity for HSV thymidine kinase than for HSV DNA polymerase.
Indicated in primary and recurrent genital herpes and has a longer
suppressive effect..
3. Valaciclovir - It is the prodrug of acyclovir but is much more effectively
absorbed in the gut. Indication is same as famciclovir.
4. Idoxuridine and trifluorothymidine – the drug has high systemic
toxicity and has local action. Also trifluorothymidine has the same
indication but its usage is limited.

45
5. Vidarabine (ara-A) – this can be used as iv form in encephalitis and
infection in neonates. Only topical preparation available for ocular
infections. But this is not a licensed product.
HSV VACCINES
Several recombinant subunit vaccines are under trial. Many studies
depicting its effectiveness in reducing the frequency and severity of
recurrent disease had been put, but its preventive infection is
uncertain. Primary viral infection prevention by vaccine have been tested
without success. Continue research in that process is still going on.113
PROGNOSIS
The prognosis of HSE by specific chemotherapy has no clear vision so far.
The outcome in HSE is dependent on various prognostic factors and
treatment quality. With progressive cerebral oedema and damage to
neurological system, even death can occur. The cerebral oedema should be
managed effectively with dexamethasone, osmotics (mannitol), supportive
management and surgical decompression if needed. Encephalitis is often
fatal within weeks. A study by Whitley et al revealed a higher percentage
of mortality in untreated patients and severe neurological sequelae in
patients who survivied114 .
Mortality in patients treated with acyclovir was lower than with vidarabine.
Lower mortality is mainly due to the pre-treatment diagnosis by polymerase

46
chain reaction (PCR) rather than brain biopsy and also identified earlier in
the disease process.
The neurologic status and age of the patients at the time of diagnosis is a
main factor in the development of neurological sequlae. Comatose
individuals have a poor prognosis irrespective of their age. In conscious
patients, the prognosis is better with younger age. Significant morbidity
exists among those treated. Neurologic outcomes in survivors treated with
acyclovir are as follows:
No or mild deficits - 38%
Moderate deficits - 9%
Severe deficits - 53%
Memory loss is often anterograde even with successful treatment of the viral
encephalitis. A study by Utley et al showed that patients who had presented
earlier for treatment had better cognitive outcomes115 .
Elbers and colleagues followed properly treated children for 12 years after
the HSE. They found seizures in 44% of the children and developmental
delay in 25% of the children. They concluded that HSE continues to be
associated with poor long-term neurologic outcomes despite appropriate
therapy116.
Shelley and colleagues reported a case of intracerebral hematoma occurring
in a patient successfully treated with a full course of acyclovir after apparent

47
eradication of the virus. The hematoma occurred in the region of the
encephalitis117 .
PREVENTION
There is no promising preventive measures against herpes simplex virus
infection. The universal presence of virus implies that nothing can be done
to prevent its environmental transmission. No preventive role of HNIG is
there in HSV infections. Prophylactic chemotherapy is useful for frequent
and severe recurrent herpes infections. Caesarean section has been shown
some success in preventing infection in newborn babies. Intravenous
acyclovir treatment in woman in labour had no specific role in the prevention
of virus transmission.

48
3. AIMS AND OBJECTIVES
1. To detect Herpes Simplex virus in cerebrospinal fluid (CSF) samples
in Dengue negative patients with clinically suspected HSE or
Meningo-encephalitis by molecular study-Real Time Polymerase
chain reaction(PCR)
2. To Investigate satisfactory and crucial clinical signs as guide to
perform HSV-PCR in a rapid diagnosis of herpes simplex virus
encephalitis.
3. To assess the need for the ongoing antiviral therapy in HSV PCR
negative encephalitis cases.

49
4. MATERIALS AND METHODS
The present study was undertaken at the Department of Microbiology,
Tirunelveli Medical College for a period of one year from June 2018
– July 2019
This was a prospective cross sectional study.
This study was aimed to detect Herpes simplex virus (HSV) from
cerebrospinal fluid samples of Meningo-encephalitis patients by
molecular method- PCR.
MATERIALS
A total of 50 CSF Samples from suspected Meningo-encephalitis cases,
were taken for the study.
Inclusion criteria:
1. All patients with history of fever and clinical signs and symptoms
suggestive of Viral Encephalitis
2. Age group-children and adults
Exclusion criteria:
1. Patients proven positive for other prevalent circulating virus like
Dengue, JE serologically.
Ethical clearance:
The study was started after getting ethical committee clearance from the
institution.

50
Informed consent:
Informed consent was obtained from all patients/patient attenders included
in this study.
Proforma:
A predesigned structured proforma with information on sociodemographic
variables such as age, education, occupational status, geographic location,
income and clinical and laboratory findings and treatment outcome were
recorded as objective data.
Sample storage:
The CSF samples were stored at -70°C Deep freezer till test run.
Safety precautions:
All the procedures were carried out in biological safety cabinet (type 2) with
universal precautions.
METHODS
SAMPLE
CSF samples from 50 patients with clinically suspected
meningoencephalitis were collected under aseptic precautions by standard
procedures. They were then processed and stored according to the standard
guidelines.

51
Clinical Criteria:
The criteria for cases suspected of meningoencephalitis were
Fever >38°C,
Seizures
Altered mental status and
Other critical manifestations.
Laboratory Criteria :
Blood , CSF biochemical analysis(cell count, protein), Irregularity in brain
CT scan and MRI findings were also obtained from patients case file.
Polymerase chain reaction was performed using primer, which amplified
DNA sequence for HSV(1 &2).
Diagnostic criteria:*
Table-5: DIAGNOSTIC CRITERIA FOR ENCEPHALITIS
Major criteria Minor criteria(2 required for possible encephalitisand >/=3 required for Probable orconfirmed encephalitis)
Altered mental status Fever >38°c(100.4°F) within 72 hrsbefore or after presentationGeneralized or partial seizuresNew onset focal neurologic findingCSF leukocytosisAbnormality in NeuroimagingAbnormality on EEG consistent withencephalitis
*[Adapted from Clinical Infectious Diseases ;Venkatesan et al]126

52
CSF SAMPLE COLLECTION
CSF had been collected by physician from suspected cases of
meningoencephalitis at the very first presentation on admission, under strict
aseptic precaution by lumbar puncture . After collection immediate transport
to the laboratory without delay is recommended. Usually 3 tubes are
collected for biochemistry, microbiology and cytology respectively. In case
of suspected viral meningitis immediate preservation in deep freezer is
necessary.
EXAMINATION OF CSF
An examination of CSF involves the following:
1. Macroscopic examination
2. Biochemical analysis of CSF
3. Cytology
4. Direct Microscopy
5. Culture and sensitivity (for confirmation of bacterial/fungal culture
negativity)
6. Serological methods
7. Molecular method- PCR(method of this study)
MACROSCOPIC EXAMINATION
Macroscopically it should be clear in normal conditions. In case of viral
infections also, CSF is usually clear. Herpes simplex encephalitis (HSE), as
well as other forms of hemorrhagic encephalitis, may be associated with

53
increased red blood cells (RBCs) and xanthochromia in the CSF. The fluid
should be sent for PCR evaluation to detect herpes simplex virus (HSV)
DNA; PCR is highly specific and remains positive for as long as 5 days after
initiation of treatment.
BIOCHEMICAL ANALYSIS OF CSF
CSF examination is critical to establish the diagnosis and reveals, acutely, a
typical viral profile:
Mildly to moderately elevated protein (60-80 mg/dL),
Normal glucose, and
A moderate pleocytosis (up to 1000 leukocytes/µL).
Mononuclear cells usually predominate, though early in
fulminant encephalitis, polymorphonuclear leukocytes
predominate.
Normal CSF protein level is 15-40mg/dl and normal CSF
glucose level is 45-8-mg/dl.
CYTOLOGICAL EXAMINATION
In case of viral infections, lymphocytic predominance is seen.
WBC Count- 50 -100 cells /cumm
Primary cell type- mononuclear
Glucose- >45mg/dl
Protein- <100mg/dl

54
DIRECT MICROSCOPY
It includes Gram staining, India ink and KOH mount. To rule out bacterial,
fungal infection.
CULTURE AND SENSITIVITY
In case of bacterial or fungal meningoencephalitis culture is the gold
standard, but in this study culture plays no role due to its nonavailability.
Bacterial Growth any has been processed and reported. Culture positive
samples were excluded.
SEROLOGICAL METHODS
The detection of antibodies in the serum and CSF can help in the diagnosis
of some viral infections. Dengue IgM, Dengue NS1 and JE IgM ELISA had
been done for detecting IgM ANTIBODIES in fever cases and suspected
meningoencephalitis cases. Positive samples were excluded from the
study.
MOLECULAR METHOD
POLYMERASE CHAIN REACTION
(HELINI HSV-1 & HSV-2 Genotyping Real time PCR)
INTRODUCTION
The HELINI HSV-1 & 2 Real-time PCR Kit contained reagents and
enzymes for the specific amplification of 85bp region of the HSV-1 & HSV-
2 genome, and for the direct detection of the specific amplicon in FAM and
HEX channels.

55
PRINCIPLE
Pathogen detection of the polymerase chain reaction is based on the
amplification of specific regions of the pathogen genome. In Real time PCR
the amplified product was detected via fluorescent dyes. These are usually
linked to Oligonucleotide probes that bind specifically to the amplified
product. Monitoring the fluorescence intensities during the PCR run(i.e., in
real time) allows the detection and quantitation of the accumulating product
without running in agarose gel electrophoresis following by gel
documentation.
PCR ASSAY
DNA EXTRACTION
Table-6: KIT COMPONENTS
No of reactions 50
Carrier RNA 250µl
Proteinase K 1 ml
Lysis buffer 10ml
Elution buffer 5ml
Wash buffer-1 18ml
Wash buffer-2 12ml
Spin columns with collection tube 50

56
EXTRACTION PRINCIPLE
Cells are lysed during a short incubation with chaotropic salt, which
immediately inactivates all nucleases. Cellular nucleic acid bind selectively
to special glass fibres pre-packed in the purification filter tube. Bound
nucleic acids are purified in a series of rapid wash and spin steps to remove
contaminating cellular components. Finally low salt elution releases the
nucleic acids from the glass fibre. This simple method eliminates the need
for organic solvent extractions and nucleic acid precipitation, allowing for
rapid purification of many samples simultaneously.
MATERIALS REQUIRED
Micropipettes
Sterile pipette tips
Disposable powder-free gloves
Vortex mixer/water bath
Centrifuge with rotor for 1.5ml reaction tubes
Ethanol(100%)
All purification steps were carried out at room temperature as per
manufacture guidelines.
PROCEDURE
Add 20µl of Proteinase K to the bottom of a fresh 1.5ml centrifuge
tube,

57
Add 200 µl of whole human blood, plasma or serum or CSF.
Add 200 µl of Lysis Buffer. Mix well by pulse vortexing for 15
seconds.
Add 5 µl of Carrier RNA and 5 µl of Internal control template.
Mix immediately by briefing vortexing and centrifuge few seconds to
bring down drops to the bottom of the tube.
Incubate ate 56°C for 10 min.
Add 220 µl of ethanol and mix well by vortex for 30 seconds. Spin
down few seconds to bring down drops to bottom of the tube.
Transfer entire sample into the Purefast® Spin column. Centrifuge at
8000rpm for 1 min. discard the flow-through and place the column
back into the same collection tube.
Add 500 µl of Wash buffer-1 to the Purefast® Spin column.
Centrifuge at 8000 rpm for 1 min and discard the flow-through. Place
the column back into the same collection tube. Add 500 µl of Wash
buffer-2 to the Purefast® Spin column. Centrifuge at 10000rpm for 1
min and discard the flow-hrough. Place the column back into the same
collection tube.
Repeat Wash buffer-2 wash once.
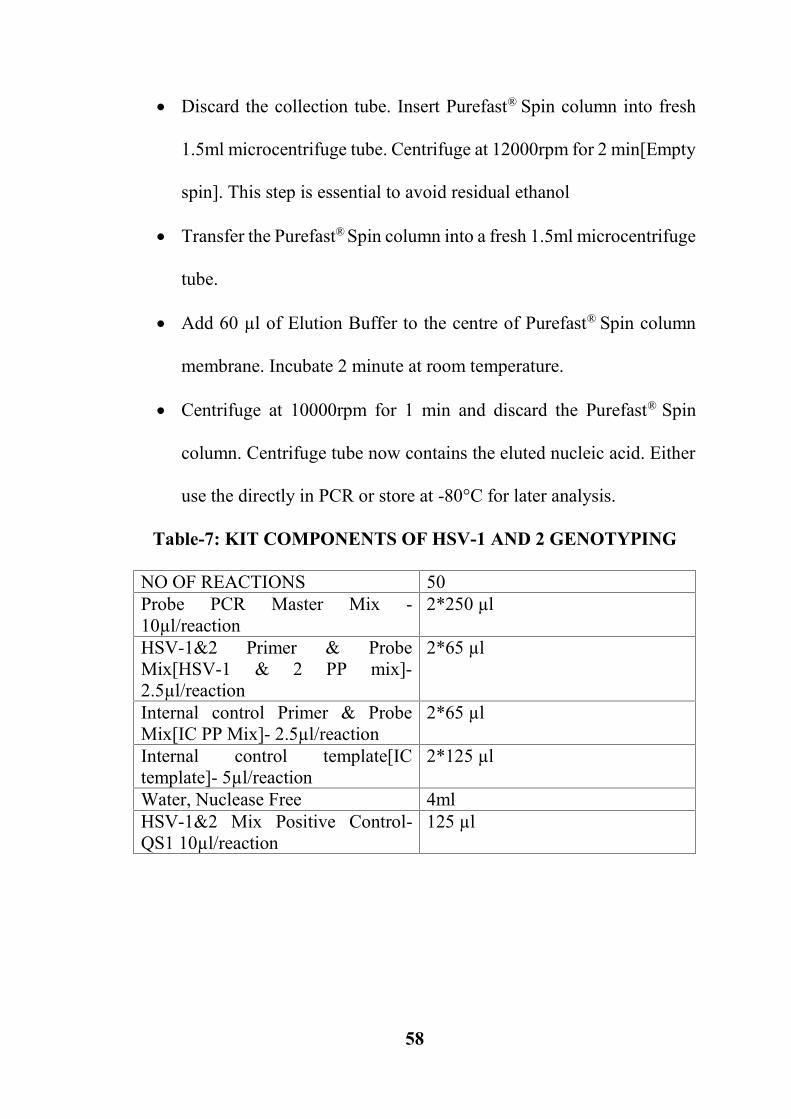
58
Discard the collection tube. Insert Purefast® Spin column into fresh
1.5ml microcentrifuge tube. Centrifuge at 12000rpm for 2 min[Empty
spin]. This step is essential to avoid residual ethanol
Transfer the Purefast® Spin column into a fresh 1.5ml microcentrifuge
tube.
Add 60 µl of Elution Buffer to the centre of Purefast® Spin column
membrane. Incubate 2 minute at room temperature.
Centrifuge at 10000rpm for 1 min and discard the Purefast® Spin
column. Centrifuge tube now contains the eluted nucleic acid. Either
use the directly in PCR or store at -80°C for later analysis.
Table-7: KIT COMPONENTS OF HSV-1 AND 2 GENOTYPING
NO OF REACTIONS 50Probe PCR Master Mix -10µl/reaction
2*250 µl
HSV-1&2 Primer & ProbeMix[HSV-1 & 2 PP mix]-2.5µl/reaction
2*65 µl
Internal control Primer & ProbeMix[IC PP Mix]- 2.5µl/reaction
2*65 µl
Internal control template[ICtemplate]- 5µl/reaction
2*125 µl
Water, Nuclease Free 4mlHSV-1&2 Mix Positive Control-QS1 10µl/reaction
125 µl

59
PCR AMPLIFICATION
Reaction set up as follows:
Table-8: DETECTION MIX
Components HSV-1 & 2
Probe PCR Master Mix 10 µl
HSV-1&2 PP Mix 2.5 µl
IC PP Mix 2.5 µl
Purified DNA Sample 10 µl
Total reaction volume 25 µl
PCR vials were centrifuged briefly before placing into thermal cycler.
Taq enzyme activation – 15 min at 95°C
Denaturation- 20 sec at 95°C
Annealing/Data collection- 20 sec at 95°C 40 cycles
Extension - 20 sec at 72°C
HSV-1 = FAM Channel
HSV-2 = HEX Channel
Internal Control = CY5 Channel

60
INTERPRETATION
Reading the graph
Step-1
Only test sample wells were selected, Cy5 channel selected and graph of
internal control amplification viewed.
NO PCR inhibition in the reaction.
Step-2
NTC or Positive controls[Qualitative] selected, FAM/HEX channel
selected, and the graph of amplification is viewed.
NTC is flat with no Ct value. This suggested there is NO contamination in
the reagent, environment and fine pipetting.
The PC was amplified as per their copy numbers. This justified that the
reagents storage conditions and reaction parameters were found as
prescribed.
Step-3
HSV-1: In FAM channel, NTC well and test sample wells were selected one
by one and the graph/amplification were analyzed.
HSV-2: In HEX channel, NTC well and test sample wells selected one by
one and the graph/amplification were analyzed.

61
TEST RESULTS
Table-9: PCR RESULTS
SampleNo
HSV-1 HSV-2 InternalControl
1 NOT DETECTED NOT DETECTED POSITIVE2 NOT DETECTED NOT DETECTED POSITIVE3 NOT DETECTED NOT DETECTED POSITIVE4 NOT DETECTED NOT DETECTED POSITIVE5 NOT DETECTED NOT DETECTED POSITIVE6 NOT DETECTED NOT DETECTED POSITIVE7 NOT DETECTED NOT DETECTED POSITIVE8 DETECTED NOT DETECTED POSITIVE9 NOT DETECTED NOT DETECTED POSITIVE10 NOT DETECTED NOT DETECTED POSITIVE11 NOT DETECTED NOT DETECTED POSITIVE12 NOT DETECTED NOT DETECTED POSITIVE13 NOT DETECTED NOT DETECTED POSITIVE14 DETECTED NOT DETECTED POSITIVE15 NOT DETECTED NOT DETECTED POSITIVE16 NOT DETECTED NOT DETECTED POSITIVE17 NOT DETECTED NOT DETECTED POSITIVE18 NOT DETECTED NOT DETECTED POSITIVE19 NOT DETECTED NOT DETECTED POSITIVE20 NOT DETECTED NOT DETECTED POSITIVE21 NOT DETECTED NOT DETECTED POSITIVE22 NOT DETECTED NOT DETECTED POSITIVE23 NOT DETECTED NOT DETECTED POSITIVE24 NOT DETECTED NOT DETECTED POSITIVE25 NOT DETECTED NOT DETECTED POSITIVE26 NOT DETECTED NOT DETECTED POSITIVE27 NOT DETECTED NOT DETECTED POSITIVE28 NOT DETECTED NOT DETECTED POSITIVE29 NOT DETECTED NOT DETECTED POSITIVE30 NOT DETECTED NOT DETECTED POSITIVE31 NOT DETECTED NOT DETECTED POSITIVE32 NOT DETECTED NOT DETECTED POSITIVE33 NOT DETECTED NOT DETECTED POSITIVE34 NOT DETECTED NOT DETECTED POSITIVE35 NOT DETECTED NOT DETECTED POSITIVE36 NOT DETECTED NOT DETECTED POSITIVE

62
37 NOT DETECTED NOT DETECTED POSITIVE38 NOT DETECTED NOT DETECTED POSITIVE39 NOT DETECTED NOT DETECTED POSITIVE40 NOT DETECTED NOT DETECTED POSITIVE41 NOT DETECTED NOT DETECTED POSITIVE42 NOT DETECTED NOT DETECTED POSITIVE43 NOT DETECTED NOT DETECTED POSITIVE44 NOT DETECTED NOT DETECTED POSITIVE45 NOT DETECTED NOT DETECTED POSITIVE46 NOT DETECTED NOT DETECTED POSITIVE47 NOT DETECTED NOT DETECTED POSITIVE48 NOT DETECTED NOT DETECTED POSITIVE49 NOT DETECTED NOT DETECTED POSITIVE50 NOT DETECTED NOT DETECTED POSITIVE
TestsampleHSV 1orHSV 2
Negativecontrol
Positivecontrol
Internalcontrol
Interpretation
Positive Negative Positive Positive Detected
Negative Negative Positive Positive Not Detectedor beyonddetection limit
STATISTICAL ANALYSIS
Staistical analysis was done using SPSS (Statistical Package for Social
Sciences). The proportional data of this study were analysed using Pearson’s
Chi Square test.

63
Figure-6: Positive Samples Amplification Curve
Figure-7: Positive Control Graph

64
Figure-8: Heat Map of Part of Test run samples

65
5. RESULTS
The study population include 50 clinically suspected cases of
meningoencephalitis who were admitted in various wards (medicine, IMCU,
PICU and Neurology) of Tirunelveli Medical College Hospital.
CSF samples collected from clinically suspected meningoencephalitis
cases were subjected to macroscopic and microscopic analysis, cytology,
culture, biochemical analysis and Polymerase Chain Reaction. PCR was the
detection method for the identification of Herpes Simplex Virus DNA in the
suspected clinical samples The socio-demographic profile age, sex, and
seasonal distribution of the study population were also analysed.
66
Table-10: HSV 1 Positive distribution in study population:
HSV 1 Positivity Frequency Percentage
Positive 2 4%
Negative 48 96%
Total 50 100%
Chart 1: HSV 1 Positive distribution in study population:
In the present study, HSV DNA was detected in CSF from 2 of the 50
patients. The 2 patients were in the age group of 26 and 35 years and both
were HSV-1 positive. The prevalence rate of HSV positivity in this study
was 4%. [Table -10;Chart -1]
4%
96%
Positive Negative

67
1.SOCIODEMOGRAPHIC PROFILE:
Table -11: Age distribution of study participants:
Age Frequency Percentage< 1 year 17 34%1-18 years 9 18%>18 years 24 48%Total 50 100%Mean age 36.3Standard deviation 21.5Range 2 months – 75 years
Chart 2: Age distribution of study participants:
In this study, 34% patients in the age group <1 year, 18% in 1-18 years
and 48% in the age group > 18 years were commonly affected by
meningoencephalitis .The 2 positive cases fell in the age group >18 years.
The mean age was 36 years and with a Standard deviation 21.5 and a
Range of 2months to 75yrs [Table -11;Chart -2].
0%
10%
20%
30%
40%
50%
< 1 year 1-18 years >18 years
34%
18%
48%

68
Table -12: Gender distribution of study population:
Age Frequency Percentage
Male 27 54%
Female 23 46%
Total 50 100%
Chart 3: Gender distribution of study population:
Male and female were almost equally affected in this study. The male to
female ratio is 1.2:1. Both of the positive cases were male in this study.
[Table -12;Chart -3]
Female46%
Male54%

69
Table -13: Monthly distribution of cases:
Age Frequency Percentage
January – April 11 22%
May – August 26 52%
September - December 13 26%
Total 50 100%
Chart 4: Monthly distribution of cases:
Increased number of cases were observed during the months of May-August
in this study. Although cases were found to occur throughout the year, the
positive cases were reported in the month of May-August. [Table -13;Chart
-4]
0% 10% 20% 30% 40% 50% 60%
January – April
May – August
September - December
22%
52%
26%
70
II.CLINICAL FEATURES:
Table -14: Distribution of disease onset:
Onset of disease Frequency Percentage
Acute 34 68%
Sub-acute 16 32%
Total 50 100%
Chart 5: Distribution of disease onset:
Meningoencephalitis cases with an acute onset were more commonly noted
than sub-acute presentation in this study. In 68% cases onset was acute in
nature, but it has no significant association(p=0.312). [Table -14;Chart -5]
68%
32%
Acute Sub-acute

71
Table-15: Minor criteria presence in the study population:
Minor criteria Descriptives
Fever 1
Seizures 1
Focal Neurologic Deficit(FND) 1
Abnormal EEG 1
Abnormal CSF 1
Abnormal Imaging 1
Mean number of minor criteria
present
2.4
Standard deviation 1.03
Range 1 – 6
Both major and minor diagnostic criteria were analyzed. Major criteria was
satisfied by all cases included in the study. The minor criteria was applied
in calculating CF score in the study. The mean number of minor criteria
present in this study was 2.4 and it had a range of 1-6. The minor diagnostic
criteria helps in identifying the probable and confirmed case of
meningoencephalitis. [Table -15].

72
Table-16: Distribution of Minor diagnostic criteria in study population:
Minordiagnostic
criteria
Present Absent PresentPercentage
Fever 39 11 78%Seizures 34 16 68%Focal NeurologicDeficit
18 32 36%
Abnormal EEG 14 36 28%Abnormal CSF 12 38 24%AbnormalImaging
14 36 28%
Chart.6 Distribution of Minor diagnostic criteria in study population:
In the present study, Fever was the predominant minor criteria which
accounts for 78% followed by seizures 68%, FND 36%, Abnormal Imaging
28%, Abnormal EEG 28%, Abnormal CSF 24%. Based on the minor criteria
CF score was calculated. [Table -16; Chart -6].
0% 20% 40% 60% 80%
Fever
Seizures
Focal Neurologic Deficit
Abnormal EEG
Abnormal CSF
Abnormal Imaging
78%
68%
36%
28%
24%
28%
Present Percentage

73
Table- 17: CF score distribution among study population:
CF score Frequency Percentage
2 28 56%
3 11 22%
>3 5 10%
Chart -7: CF (Clinical Feature )score distribution among study
population:
The CF score of 2 denotes the number of probable Meningoencephalitis
cases and score of =/>3 indicates the number of confirmed cases of
Meningoencephaltis. [Table -17;Chart -7]. Though both PCR positive and
negative cases met the criteria for CF score, it had no significant
association(p=0.122) in this study. [Table -28].
56%
22%
10%
2 3 >3

74
Table-18: Case Definition In Study Population:
Definition Frequency Percentage
Probable case 28 56%
Confirmed case 16 32%
Chart.8 Case Definition In Study Population:
With respect to the diagnostic criteria, the percentage of probable
encephalitis cases was found to be 56%(28 cases) and confirmed
encephalitis cases accounts for 32%(16 cases) in this study. [Table -
18;Chart -8].
56%
32%
Probable case Confirmed case

75
Table-19: Meningeal irritation signs distribution in study population:
Meningeal irritation Frequency Percentage
Present 20 40%
Absent 30 60%
Total 50 100%
Chart 9: Meningeal irritation signs distribution in study population:
In this study, meningeal signs was present in 40% of cases whereas it was
merely present or absent in 60% of cases. [Table -19;Chart -9]. Though there
were similarities in clinical features like Fever, focal neurological deficits,
Meningeal signs, among PCR positive and negative cases, this was not
statistically significant.(p=0.322. p=0.058, p=0.155). [Table -28].
40%
60%
Present Absent

76
Table- 20: Glasgow coma score(GCS) distribution in study population:
GCS Frequency Percentage
<5 2 5.7%
5-10 8 23%
>10 25 71.3%
Chart 10: Glasgow coma score (GCS) distribution in study population:
Among the study population, 71.3% cases had a GCS of <10, 23% in 5-10
and 5.7% in <5. [Table -20;Chart -10]. The PCR positive cases had a GCS
score <5 which is significant.(p=0.021) [Table -28].
<56%
5-1023%
>1071%

77
III. CSF PROFILE:
Table -21: CSF macroscopic profile distribution in study population:
CSF Macroscopic Frequency Percentage
Clear 42 84%
Turbid 4 8%
Blood stained 4 8%
Total 50 100%
Chart 11: CSF macroscopic profile distribution in study population:
In the CSF macroscopic analysis, most of the samples were found to be
Clear which was 84% , and in the remaining samples 8% were Turbid and
Blood stained respectively[Table -21;Chart -11].
84%
8% 8%
Clear Turbid Blood stained

78
Table -22: CSF Cytology profile distribution in study population:
CSF Cytology Frequency Percentage
Acellular 41 82%
Lymphocytic predominance 6 12%
Erythrocytic 2 4%
Lymphocytes in eosinophilic
background
1 2%
Total 50 100%
Chart 12: CSF Cytology profile distribution in study population:
In this study ,acellular pattern was predominant with a frequency of 41,
contributing 82%. Lymphocytic predominance was found in 14% of cases
which has a strong association with viral etiology and in 4% cases it was
erythrocytic. [Table -11;Chart -2]. CSF abnormality was demonstrated
both in PCR positive and negative cases(p=0.01). [Table -22;Chart -12].
Acellular
Lymphocytic predominance
Erythrocytic
Lymphocytes in eosinophilicbackground
82%
12%
4%
2%

79
Table -23: CSF Leukocytes profile distribution in study population:
CSF Leukocytes Frequency Percentage
Nil 36 72%
<100 9 18%
100-200 3 6%
>200 2 4%
Total 50 100%
Chart 13: CSF Leukocytes profile distribution in study population:
Elevated leukocyte count was observed in 10% of cases, of which 4% of
cases had leukocyte count of >200 cells/cumm in this study. [Table -
11;Chart -2]. Leukocyte elevation was found in both PCR positive and
negative cases(p=0.001) [Table -23;Chart -13].
0%10%20%30%40%50%60%70%80%
Nil <100 100-20 >200
72%
18%
6% 4%

80
Table -24: CSF RBC profile distribution in study population:
CSF RBC Frequency Percentage
Nil 41 82%
Present 9 18%
Total 50 100%
Chart 14: CSF RBC profile distribution in study population
In this study, Erythrocytes were seen in CSF in 18% in the study group. In
3 out of the 9 cases it was found to be more than the normal count. [Table -
24;Chart -14].
Nil82%
Present18%

81
Table -25: CSF glucose profile distribution in study population:
CSF glucose Frequency Percentage
Normal 45 90%
Abnormal 5 10%
Total 50 100%
Mean 60.8
Standard deviation 18.9
Range 35 - 147
Chart 15: CSF glucose profile distribution in study population:
In the study, the mean glucose level was calculated as 60.8 and falls within
the range of 35-147. The percentage of patients having normal glucose
level was 90%.[Table -25;Chart -15].
90%
10%
Normal Abnormal

82
Table-26: CSF protein profile distribution in study population:
CSF Protein Frequency Percentage
Normal 30 60%
Abnormal 20 40%
high low 13 7 26 14
Total 50 100%
Mean 35
Standard deviation 24.4
Range 9 – 96
Chart 16: CSF protein profile distribution in study population:
In this study, CSF protein count was elevated in 26% of patients and was
normal in 60% of the cases. [Table -26;Chart -16].
60%
40%
Normal Abnormal

83
Table-27: Neuroimaging profile distribution in study population:
Imaging results Frequency Percentage
Focal lesion 7 14%
Diffuse involvement 8 16%
Normal 35 70%
Chart 17: Neuroimaging profile distribution in study population:
Among the 50 patients , 15 patients had abnormal imaging findings.
Focal lesion was present in 14% of cases and 16% of cases had diffuse
abnormalities. CT scan was found to be normal in 70% of cases. [Table -
27;Chart -17].
14%
16%
70%
Focal lesion
Diffuse involvement
Normal

84
OUTCOME
Almost (91.6%) of the patients either became normal or discharged at
request and a few (8.4%) had neurological impairment after completion of
treatment in PCR negative cases. Out of the 2 positive cases in this study,
one died and the other had neurological sequlae which constitutes 50%
respectively.
Table-28:Profile of associated factors with HSV 1 Positive distribution
in study population:
Variables HSVPOSITIVEN – 2 (%)
HSVNEGATIVEN – 48 (%)
P value
Age<35 years> 35 years
2 (100%)0 (0%)
32 (66.7%)16 (33.33%)
0.322
SexMaleFemale
2 (100%)0 (0%)
25 (52%)23 (48%)
0.183
Onset of diseaseAcuteSub-acute
2 (100%)0 (0%)
32 (66.7%)16 (33.33%)
0.312
CF score>3 criteria present<3criteria present
2 (100%)0 (0%)
3 (6.2%)45 (93.8%)
0.122
FeverPresentAbsent
1 (50%)1 (50%)
38 (79%)10 (21%)
0.329
SeizuresPresentAbsent
2 (100%)0 (0%)
32 (66.7%)16 (33.3%)
0.322
Focal neurologicaldeficitPresentAbsent
2 (100%)0 (0%)
16 (34%)31 (66%)
0.058

85
Abnormal imagingPresentAbsent
2 (100%)0 (0%)
12 (25%)36 (75%)
0.021
Abnormal CSFPresentAbsent
2 (100%)0 (0%)
10 (21%)38 (79%)
0.010
Abnormal EEGPresentAbsent
2 (100%)0 (0%)
12 (29.2%)36 (75.4%)
0.009
Meningeal signsPresentAbsent
2 (100%)0 (0%)
30 (62.5%)18 (37.5%)
0.155
GCS<5>5
2(100%)0 (0%)
0 (0.0%)33 (100%)
0.021
CSF profileMacroscopicClearBlood stainedTurbid
1 (50%)1 (50%)0 (0%)
41 (85.4%)3 (6.2%)4 (8%)
0.297
CSF cytologyLymphocyticpredominanceAcellularErythrocytic
2 (100%)0 (0%)0 (0%)
5 (10.4%)41 (85.4%)2 (4.1%)
0.122
CSF Leukocytes>100<100
2 (100%)0 (0%)
3 (6.2%)45 (93.8%)
0.001
ImagingFocalDiffuseNormal
2 (100%)0(0.0%)0(0.0%)
5 (10.4%)8 (16.6%)35 (73%)
0.004
Antiviral treatmentGivenNot given
2 (100%)0 (0.0%)
17 (35.4%)31 (64.6%) 0.110
Follow upNeurological sequeleDeathDischarged
1 (50%)1 (50%)0 (0%)
4 (8.4%)044 (91.6%)
0.004

86
In this study, HSV-1 DNA was detected in CSF samples from 2 (4%) of 50
patients. HSV-2 DNA was detected in any of the patients. Both the positive
cases had temporal abnormalities in Neuroimaging and was significant.
(p=0.004). MRI results were available for only 4 cases with significant
lesions which contributes minimally in this study. EEG demonstrated
temporal lobe abnormality of 100% in positive cases and 29.2% in PCR
negative cases(p=0.009). GCS score, CSF leukocyte, CSF, EEG and
Neuroimaging had significant association with PCR positivity
(p=0.021,p=0.001,p=0.010,p=0.009,p=0.021). And the mortality due to
HSV Encephalitis in this study was 50% among the positive cases.(Table-
28)
STATISTICAL TESTS USED:
Data was entered into Microsoft Excel (Windows 7; Version 2007) and
analyses were done using the Statistical Package for Social Sciences (SPSS)
for Windows software (trial version 22.0; SPSS Inc, Chicago). Descriptive
statistics such as mean and standard deviation (SD) for continuous variables,
frequencies and percentages were calculated for categorical variables. Bar
and Pie charts were used for visual representation of data. Chi square test
was used for testing association of various factors with HSV positivity. In
case of lesser expected counts Fishers exact test was used. Level of
significance was set at 0.05.

87
6. DISCUSSION
Herpes simplex virus causes both meningitis and encephalitis. The
distinction that HSV-1 is associated with encephalitis and HSV-2 causes
meningitis, is not absolute, and studies have noted crossover of both the
manifestations is noted.114. It is not unusual for encephalitis and meningitis
to coexist in the same patient as meningoencephalitis.
It has been recognized that HSE is a difficult disease to diagnose. The main
findings for HSE patients were altered consciousness, fever, headache,
seizures and personality change Neurodiagnostic studies disclose focal
abnormalities in most patients; however, such findings do not discriminate
between focal encephalitis due to HSV and focal encephalitis due to other
etiologies.115 Similar studies by Aurelius E etal and Klapper PE et al; have
addressed the HSV DNA detection by PCR in CSF samples.
In India, HSE appears to be under diagnosed, probably due to lack of
awareness and diagnostic facilities. HSV was known for its latency with
intermittent reactivations and, therefore, PCR remains the gold standard test
for their detection 116 . Therefore, this method is presently the best one to
detect the spectrum of HSE.
In the present study, the study population were restricted to suspected
meningoencephalitis cases with respect to the above consideration and
among the suspected cases, 50 cases which met the criteria for performing

88
the molecular detection was taken up for the study which was conducted in
Tirunelveli Medical College for a period of 1 year.
6.1 SOCIODEMOGRAPHIC PROFILE
Among the 50 patients included in this study, the mean age of the study
population was 36.5 and distribution of cases were almost equal in all age
group of which age group >18yrs is 48%.
The Male to Female ratio was 1.2:1 and the disease was present through out
the year the maximum cases were reported during the months of May-
August. This is in concordance with a study by Whitley RJ et al where
there was no characteristic racial, age, sex or seasonal predilection.
6.2 CLINICAL FEATURES
In this study, the disease onset in suspected Meningoencephalitis cases were
found to be Acute(68%) and Sub acute(32%) irrespective of the time of
presentation of cases to the institution, a similar finding was mentioned in
a study by Wayne E Anderson.
Among the diagnostic criteria for Meningoencephalitis, all the patients
selected for the study satisfied the major and minor diagnostic criteria which
were calculated based on a adapted reference from a study by Venkatesan
et al.
In this study, the percentage of probable encephalitis cases was found to
be 56%(28 cases) and confirmed encephalitis cases accounts for 32%(16
cases). The remaining cases even though not fully satisfying the diagnostic

89
criteria , a high clinical suspicion of meningoencephalitis was there which
made them to be included in the study.
In the present study, Fever was the predominant minor criteria which
accounts for 78% which was similar to many studies by Whitely et al,
Chatterjee et al; and 68% of patients presented with seizures which is also
consistent with the study by Whiteley et al; where the percentage of seizures
was 67% and focal neurologic deficits were present in 36% of the suspected
patients which is also similar to the study(Whitely et al), in which 33% of
the cases presented with focal neurologic deficits.
A causal or temporal relationship between peripheral lesions (eg, herpes
labialis) and HSE ususally does not exist and hence in this study it was not
taken into account as a significant factor1. Also, many febrile diseases can
precipitate herpes labialis. Therefore, the presence or absence of such lesions
neither confirms nor excludes the diagnosis.
In this study, the most frequent findings on physical examination were fever
and mental status abnormalities which were present in almost all the
cases.Although the presence of fever, headache, behavioral changes,
confusion, focal neurologic findings, and abnormal cerebrospinal fluid
(CSF) findings were suggestive of HSE in this study, no pathognomonic
clinical findings could reliably distinguish HSE from other neurologic

90
disorders with similar presentations which was similar to a study by whitely
RJ et al120
In this study, meningeal signs were present in 40% of cases whereas it was
merely present or absent in 60% of cases. Among the study population, 2
positive cases had a GCS <5 which had a significant association with the
disease.
6.3 CSF PROFILE
In the CSF macroscopic analysis most of the samples were found to be
Clear which accounts for 84% , in the remaining samples 8% were Turbid
and Blood stained respectively. This clearly depicts that the etiology may
be predominantly of Viral origin or due to empirical antibiotic therapy which
was emphasized in a study by Gaurav B Modi ;
In HSV PCR–positive cases, patients had elevated leukocyte and protein
counts in CSF. A study by Jeffry P Simko et al119 shows that pre screening
of CSF specimens had more value in the utility of PCR.
CSF abnormality was found to be present in 24% of the patients which
includes elevated leukocyte count corresponding to 28% patients in this
study. The 2 positive cases had elevated leukocyte count with a lymphocytic
predominance which had a causal association with positivity.

91
Erythrocyte presence in CSF was found to be 18% in this study group, which
was similar to a study by Tyler KL et al121 , in which about 20% of patients
had RBCs in their CSF profile which may be due to a Hemorrhagic HSV
encephalitis following a non-traumatic tap. The percentage of patients
having normal glucose level was 90%.
Even cases with subtle CSF abnormalities presenting with features of
meningoencephalitis should be screened cautiously for HSV infection prior
to PCR amplification. This approach is much important earlier in the disease
which was described in a study by Fodor PA et al122;
CSF parameters were used to screen specimens before PCR analysis for
HSV DNA detection as indicated in a study by Tang et al123. Of the 50
CSF specimens tested, 2 HSV PCR positive cases had an elevated leukocyte
count of >100 cells/mm3 and elevated protein level of >45mg/dl which
showed significant association with the disease.
The identification of patients with suspected viral meningoencephalitis
infection by CSF PCR to detect the Herpes simplex virus DNA, was the
first of a kind in our institution. After the opening of VRDL, it is possible to
identify patients with suspected viral infection and to decide whether
antiviral therapy offers any therapeutic advantage to such patients.
Anecdotal reports by Berger JR had suggested that acyclovir may reduce
the recurrences of symptoms in such patients.124

92
6.4 NEURODIAGNOSTIC STUDIES
In a study by Whitely et al, Neurodiagnostic studies disclose focal
abnormalities in most patients; however, such findings do not discriminate
between focal encephalitis due to HSV and focal encephalitis due to other
etiologies.
In this study, results of at least one neurodiagnostic study was altered in all
PCR-positive cases. The correlation between localizing temporal
abnormalities shown by CT, EEG, or MRI and a positive PCR assay was
high (Table.31). EEG demonstrated abnormality in all the PCR-positive
cases(100%) and 29.2% of PCR-negative cases (P=0.009). A positive PCR
assay was 6.5 times more likely to occur in cases in which temporal
abnormalities were found during EEG. Focal abnormalities were present in
the EEG of two PCR-positive cases.
Forty three patients underwent CT of the brain. Focal Temporal
abnormalities were found in 100% of the PCR-positive cases and 10.4% of
the PCR-negative cases. Temporal abnormalities shown by CT were
significantly associated with a positive PCR assay(P=0.004). The
Abnormalities revealed by imaging were edema, contrast enhancement, low
density lesion and infrequently hemorrhage. Imaging was the most useful
test in this study. Among the PCR positive cases, 1 had Abnormal MRI
finding.

93
The severity of the disease was assessed by the frequency of patients with
altered level of consciousness and the frequency of patients who died were
associated with CNS infection. In this study, reduced conscious level was
present in all the cases which was in concordance with a study by Whiteley
et al; Teba et al 125 in his study evaluated the utility of PCR based assay of
CSF in the management of patients with suspected HSVE and suggested that
empiric therapy with Acyclovir can be widely used without laboratory
confirmation. And, so, in their model, they compared a PCR-based approach
with empiric therapy that corresponds to current practice. In another study
by Whitley et al114; the overall mortality rate associated with HSE in
acyclovir-treated patients was 28%. The mortality associated with Acyclovir
therapy was 50% in this study, which was mainly due to the increased
severity of the disease presented in a late stage.
In this study, HELINI HSV-1 & 2 Real-time PCR Kit was used for the
detection of specific amplification of HSV-1 & HSV-2 in all the
meninogoencephalitis patients. Among the 50 patients 2 were positive for
HSV-1 and HSV-2 was not detected in any of the patients. This was in
concordance with many other studies.4,8,24 The ease of availability of PCR
as a non invasive method with high specificity and sensitivity will be helpful
in improved diagnosis and the prompt usage of antiviral therapy thereby
providing better outcomes in suspected Herpes Simplex
Meningoencephalitis patients.

94
7.SUMMARY
This study included 50 clinically suspected cases of
Meningoencephalitis patients admitted in medical wards of
Tirunelveli Medical College Hospital, who met the criteria for
performing the molecular study- Real Time Polymerase Chain
Reaction for HSV DNA detection.
The study population included patients of all age groups with no
sexual predilection.
HSV DNA detection by Real Time PCR was successful with a
positivity rate of 4% in this study.
PCR was positive for HSV-1 in Two patients with features of
Meningoencephalitis. There was no HSV-2 positive cases detected in
this study.
This study revealed the predominant presence of HSV-1 in this group
of patients.
The most common findings in this study were Fever and altered
mental status.
Fever was the predominant clinical feature in this study which
accounts for 78% and seizure accounts for 68% of the patients,
followed by Focal neurologic deficits which was present in 33% of
the patients.

95
The 2 positive cases had an elevated leukocyte count of >100
cells/mm3 and elevated protein level of >45mg/dl which shows a
significant association with the disease.
No significant association was found between the clinical features of
patients with positive PCR and patients with negative PCR results.
The GCS score of the positive cases had a significant association with
the disease severity.
CT/MRI and EEG findings, CSF white blood cell count were each
independently associated with positive PCR results.
Prescreening of CSF samples is a valid method to improve the utility
of this PCR.
PCR analysis allows the antiviral therapy to be performed efficiently.
To conclude, the results manifested in this study illustrated the worth
of the PCR for the diagnosis.

96
8.CONCLUSION
In suspected Herpes Simplex Encephalitis (HSE), the workup must be
initiated rapidly and treatment should not be delayed. General laboratory
studies will not be helpful in diagnosis but may show evidence of infection.
A high index of suspicion is required in case of immunocompromised
patients. No specific pathognomonic clinical findings will be associated with
HSV Encephalitis. Focal neurologic deficits, cerebrospinal fluid (CSF)
pleocytosis, and abnormalities on computed tomography (CT) scanning may
not be present initially. In such circumstances, the diagnosis can be
confirmed only by means of an early Real time Polymerase Chain Reaction
(PCR) which will have an added advantage of being a non-invasive
diagnostic method. Diagnostic modalities are similar in all age groups
including neonates, children and adults. On first admission, preliminary
findings of at least 2 important clinical features126 along with the abnormal
CSF cytology and differential counts is sufficient to perform HSV-PCR,
which will ultimately result in a rapid diagnosis of Herpes Simplex Virus
Encephalitis. Neurological sequelae among survivors were dependant on
the neurologic status and age of the patient at the time of diagnosis. Patients
who are comatose at the time of diagnosis will have a poor prognosis
irrespective of their age. In this study, we conclude that detection of HSV
DNA by PCR analysis of CSF samples can also reveal a wider spectrum of
clinical manifestations of Herpes simplex Virus Encephalitis.

BIBLIOGRAPHY
1. Whitley RJ. Herpes simplex viruses. In: Fields BN, Knipe DM, eds.Virology, New York: Raven Press; 1990.
2. Olson LC, Buescher EL, Artenstein MS. Herpesvirus infections of thehuman central nervous system. N Engl J Med 1967.
3. Herpes simplex encephalitis: a review. Levitz RE Heart Lung.
1998;27(3):209. Division of Infectious Diseases, Hartford Hospital,
Conn 06102-5037, USA.
4. Prevalence of Herpes Simplex Virus (Types 1 and 2), Varicella-Zosterhttps://www.ncbi.nlm.nih.gov › articles
5. Whitley RJ, Soong SJ, Hirsch MS, et al. 19 Herpes simplexencephalitis: vidarabine therapy and diagnostic problems. N Engl J Med1981
6. Whitley RJ, Barnes DW. CNS disease associated with varicella-zostervirus and herpes simplex virus infections. In: Frank B (ed.), NeurologicClinics. Philadelphia: WB Saunders Company; 1986
7. Lakeman FD, Whitley RJ. Diagnosis of herpes simplex encephalitis:application of polymerase chain reaction to cerebrospinal fluid frombrain-biopsied patients and correlation with disease. National Instituteof Allergy and Infectious Diseases Collaborative Antiviral Study Group[see comments]. J Infect Dis 1995.
8. Epidemiological Studies and Molecular Characterization of HerpesSimplex https://www.omicsonline.org › open-access
9. Criteria for Performing PCR in Cases of Suspected Herpes Encephalitis,JOURNAL OF CLINICAL MICROBIOLOGYFeb. 2000, p. 940 Vol. 38, No. 2
10.Kimura H, Futamura M, Kito H, et al. Detection of viral DNA inneonatal herpes simplex virus infections: frequent and prolonged

presence in serum and cerebrospinal fluid. J Infect Dis1991;164:289–293
11.Whitley RJ, Lakeman AD, Nahmias AJ, et al. DNA restriction-enzymeanalysis of herpes simplex virus isolates obtained from patientswith encephalitis. N Engl J Med 1982;307:1060–1062.
12.Puchhammer-Stockl E, Popow-Kraupp T, Heinz FX, et al.Establishment of PCR for the early diagnosis of herpes simplexencephalitis. J Med Virol 1990;32:77–82.
13.Rowley A, Lakeman F, Whitley R, et al. Rapid detection of herpessimplex virus DNA in cerebrospinal fluid of patients with herpessimplex encephalitis. Lancet 1990;335:440–441.
14.Koskiniemi M, Rantalaiho T, Piiparinen H, et al. Infections of thecentral nervous system of suspected viral origin: a collaborative studyfrom Finland. J Neurovirol 2001; 7: 400–408.
15.Hanley DF, Johnson RT, Whitley RJ Arch Neurol. 1987;44(12):1289.Department of Neurology, Johns Hopkins Hospital, Baltimore, MD21205.
16.Viral encephalitis. Whitley RJ N Engl J Med.1990;323(4):242. Department of Pediatrics, University of Alabama,Birmingham School of Medicine 35294.
17.Herpes simplex encephalitis: children and adolescents. Whitley RJ,Kimberlin DW Semin Pediatr Infect Dis. 2005;16(1):17
18.Etiology of encephalitis in Australia, 1990-2007. Huppatz C, DurrheimDN, Levi C, Dalton C, Williams D, Clements MS, Kelly PM EmergInfect Dis. 2009;15(9):1359
19.WayneEAndersonHerpesSimplexEncephalitis2018,emedicine.medscape.com/article/1165183-overview.
20.Whitley RJ, Herpes simplex encephalitis;adolescents and adults .Antiviral Res 2006 sep.71(2-3): 141-8
21.Whitley RJ. Viral encephalitis. N Engl J Med 1990;323:242–250.

22.Whitley RJ, Kimberlin DW. Herpes simplex: encephalitis children andadolescents. Semin Pediatr Infect Dis 2005;16:17–23
23.Ravi V : Viral infections of the central nervous system. Progress inClinical Neuro Sciences 1992; 8 : 27-35.
24.Satish chandra P, Ravi V, Shankar SK : Herpes simplex encephalitis :Clinicopathological and virological appraisal. Progress in ClinicalNeuro Sciences1996; 11 : 167-186
25.Roizman B, Furlong D. 1974. The replication of herpesviruses, p.229—403. In H. Fraenkel-Conrat and R. R. Wagner (ed.),Comprehensive Virology. Plenum Press, NY.
26.Zhou ZH, Dougherty M, Jakana J, et al. Seeing the herpesvirus capsidat 8.5 A. Science 2000;288:877–880.
27.Grunewald K, Desai P, Winkler DC, et al. Three-dimensional structureof herpes simplex virus from cryo-electron tomography. Science 2003.
28.Booy FP, Newcomb WW, Trus BL, et al. Liquid-crystalline, phage-likepacking of encapsidated DNA in herpes simplex virus. i1991. .
29.Poffenberger KL, Roizman B. Studies on noninverting genome of aviable herpes simplex virus 1: presence of head-to-tail linkages inpackaged genomes and requirements for circularization after infection.J Virol 1985;53:587–595
30.Strang BL, Stow ND. Circularization of the herpes simplex virus type1 genome upon lytic infection. J Virol 2005;79:12487–12494
31.Gibson W, Roizman B. Compartmentalization of spermine andspermidine in the herpes simplex virion. Proc Natl Acad Sci U S A 1971
32.Spear PG, Roizman B. Buoyant density of herpes simplex virus insolutions of caesium chloride. Nature 1967;214:713
33.Van Genderen IL, Brandimarti R, Torrisi MR, et al. The phospholipidcomposition of extracellular herpes simplex virions differs from that ofhost cell nuclei. Virology 1994;200:831–836.
34.Mettenleiter, T.C. (2004). Budding events in herpesvirusmorphogenesis. Virus Research. 106, 167-180.

35.Cheshenko, N., and Herold, B.C. (2002). Glycoprotein B plays apredominant role inmediating herpes simplex virus type 2 attachmentand is required for entry and cell to-cell spread. J Gen Virol. 83, 2247-2255.
36.Muggeridge, M.I. (2000). Characterization of cell-cell fusion mediatedby herpes simplex virus 2 glycoprotein gB, gD, gH and gL intransfected cells. J. Gen. Virol. 81, 2017-2027.
37.Pertel, P.E., Fridberg, A., Parish, M.L., Spear, P.G. (2001). Cell FusionInduced by Herpes Simplex Virus Glycoprotein gB, gD, and gH-gL Requires a gD Receptor but Not Necessarily Heparan Sulfate.Virology. 279, 313-324.
38.Lopez, M., Cocchi, F., Menotti, L., Avitabile, E., Dubreuil, P.,Campadelli-Fiume, G. (2000). Nectin2α (PRR2α or HveB) andNectin2δ Are Low-Efficiency Mediator for Entry of HerpesSimplexVirus Mutanst Carrying the Leu25Pro Substitution in Glycoprotein D.J. Virol. 74,1267-1274.
39.Connolly, S.A., Whitbeck, J.C., Rux, A.H., Krummenacher, C., vanDrunen Little-van denHurk, S., Cohen, G.H., Eisenberg, R.J. (2001).Glycoprotein D Homologs in Herpes Simplex Virus Type 1,Pseudorabies Virus, and Bovine Herpes Virus Type 1 Bind Directly toHuman HveC (Nectin-1) with different affinities. Virology 280, 7-18.
40.Krummenacher, C., Baribaud, F., Ponce de Leon, M., Baribaud, I.,Whitbeck, J.C., Xu, R.,Cohen, G.H., Eisenberg, R.J. (2004).Comparative usage of herpesvirus entry mediator A and nectin-1 bylaboratory strains and clinical isolates of herpes simplex virus. Virology322, 286-299.
41.Jogger, C.R., Montgomery, R.I., Spear, P.G. (2004). Effects of linker-insertion mutations in herpes virus 1 gD on glycoprotein-induced fusionwith cells expressing HVEM or nectin-1.Virology 318, 318-326.
42.Whitbeck, J.C., Connolly, S.A., Willis, S.H., Hou, W., Krummenacher,C., Ponce de Leon., M., Lou, H., Baribaud, I., Eisenberg, R.J., Cohen,

G.H. (2001). Localization of the gDBinding Region of the HumanHerpes Simplex Virus Receptor, HveA. J. Virol. 75, 171-180
43.Satoh-Horikawa, K., Nakanishi, H., Takahashi, K., Miyahara, M.,Nishimura, M., Tachibana, K., Mizoguchi, A., Takai, Y. (2000).Nectin-3, a New Member of Immunoglobulin-like Cell AdhesionMolecules That Shows Homophilic and Heterophilic Cell-CellAdhesion Activities. J. Biol. Chem. 275, 10291-10299.
44.Corey L, Whitley RJ, Stone EF, Mohan K. Difference between herpessimplex virus type 1 and type 2 neonatal encephalitis in neurologicaloutcome. Lancet. 1988;1(8575-6):1-4.].
45.Studahl M, Lindquist L, Eriksson BM, Gunther G, Bengner M,Franzen-Rohl E, et al. Acute viral infections of the central nervoussystem in immunocompetent adults: diagnosis and management. Drugs.2013;73(2):131-58
46.Bergstrom T, Vahlne A, Alestig K, Jeansson S, Forsgren M, Lycke E.Primary and recurrent herpes simplex virus type 2-induced meningitis.J Infect Dis. 1990;162(2):322-30
47.Oates JK, Greenhouse PR. Retention of urine in anogenital herpeticinfection. Lancet. 1978;1(8066):691-2
48.Noska A, Kyrillos R, Hansen G, Hirigoyen D, Williams DN. The roleof antiviral therapy in immunocompromised patients with herpessimplex virus meningitis. Clin Infect Dis.2015;60(2):237-42
49.Wasay M; Mekan SF; Khelaeni B; Saeed Z; Hassan A; Cheema Z;Bakshi R Extra temporal involvement in herpes simplex encephalitis.Eur J Neurol. 2005; 12(6):475-9
50.Esiri MM10.HSV-induced apoptosis in herpes encephalitis.Curr TopMicrobiol Immunol. 2005; 289:79-111
51.J Neurol Sci. 1982; 54(2):209-2612.Herpes simplex encephalitis. Animmunohistological study of the distribution of viral antigen within thebrain.

52.Roizman, B., and Pellett, P.E. (2001). The Family Herpesviridae: ABrief Introduction. In: Knipe, D.M., and Howley, P.M. (Eds.), FieldsVirology. Fourth ed. Lippincott, Williams and Wilkins, Philadelphia,pp. 2381-2396.
53.Sawtell, N.M., and Thompson, R.L. (2004). Comparison of HerpesSimplex Virus Reactivation in Ganglia In Vivo and in ExplantsDemonstrates Quantitative Qualitative Differences. J. Virol. 78, 7784-7794.
54.Stevens, J.G., Wagner, E.K., Devi-Rao, G.B., Cook, M.L., andFeldman, L.T. (1987). RNA complementary to a herpesvirus α genemRNA is prominent in latently infected neurons. Science. 235, 1056-1058.
55.Peng, W., Henderson, G., Inman, M., BenMohamed, L., Perng, G.C.,Wechsler, S.L., Jones, C. (2005). The Locus Encompassing theLatency-Associated Transcript of Herpes Simplex Virus Type 1Interferes with and Delays Interferon Expression in ProductivelyInfected Neuroblastoma Cells and Trigeminal Ganglia of AcutelyInfected Mice. J. Virol. 79, 6162-6171.
56.Rødahl, E., and Haarr, L. (1997). Analysis of the 2-Kilobase Latency-Associated Transcript Expressed in PC12 Cells Productively Infectedwith Herpes Simplex Virus Type 1: Evidence for a stable, NonlinearStructure. J. Virol. 71, 1703-1707.
57.Inman, M., Perng, G.C., Henderson, G., Ghiasi, H., Nesburn, A.B.,Wechsler, S.L., Jones, C.(2001). Region of Herpes Simplex Virus Type1 Latency-Associated Transcript Sufficient for Wild-Type SpontaneousReactivation Promotes Cell Survival in Tissue Culture. J. Virol. 75,3636-3646.
58.Ahmed, M., Lock, M., Miller, C.G. (2002). Regions of the HerpesSimplex Virus Type1Latency-Associated Transcript That Protect Cellsfrom Apoptosis In Vitro and ProtectNeuronal Cells In Vivo. J. Virol.76, 717-729.
59.Kang, W., Mukerjee, R., Frasser, N.W. (2003). Establishment andmaintenance of HSV latent infection is mediated through correctsplicing of the LAT primary transcript. Virology. 312, 233-244.

60.Das, C.M., Zhang, S., Shillitoe E.J. (1994). Expression of the mutagenicpeptide of herpes simplex virus type 1 in virus-infected cells. Virus Res.34, 97-114.
61.McDougall, J.K. (2001). `’Hit and run’’ transformation leading tocarcinogenesis. Dev.Biol.(Basel). 106, 77-83.
62.Jones, C. (1995). Cervical Cancer: Is Herpes Simplex Virus Type 11 acofactor?. Clinical Microbiology Review. 8, 549-556.
63.Aurelian, L. (1998). Herpes simplex virus type 2: Unique biologicalproperties includeneoplastic potential mediated by PK domain of thelarge subunit of ribonucleotide reductase. Frontiers in Bioscience 3,237-249.
64.Aurelian, L., Kokuba, H., Smith, C.C. (1999). Vaccine potential ofherpes simplex virus type 2 mutant deleted in the PK domain of thelarge subunit of ribonucleotide reductase (ICP10). Vaccine.17,1951-1963.
65.Smith, C.C., Yu, Y.X., Kulka, M., Aurelian, L. (2000). A Novel HumanGene Similar to the Protein Kinase (PK) Coding Domain of the LargeSubunit of Herpes Simplex Virus Type 2 Ribonucleotide Reductase(ICP10) Codes for a Serine-Threonine PK and Is Expressed inMelanoma Cells. J. Biol. Chem. 275, 25690-25699.
66.Ganatra, J.B., Chandler, D., Santos, C., Kuppermann, B., Margolis, T.P.(2000). Viral Causes of the Acute Retinal Necrosis Syndrome. Am JOphthalmol 129, 166-172.
67.Liesegang, T.J. (2001). Herpes Simplex Virus Epidemiology andOcular Importance. Cornea. 20, 1-13.
68.Umene, K., and Kawana, T. (2003). Divergence of reiterated sequencesin a series of genital isolates of herpes simplex virus type 1 fromindividual patients. J. Gen. Virol. 84, 917-923
69.Kimberlin, D.W., Lin, C.Y., Jacobs, R.F., Powell, D.A., Frenkel, L.M.,Gruber, W.C., Rathore, M., Bradley, J.S., Diaz, P.S., Kumar, M.,Arvin, A.M., Gutierrez, K., Shelton, M., Weiner, L.B., Sleasman,J.W., Murguia de Sierra, T., Soong, S.J., Kiell, J., Lakeman, F.D.,

Whitley, R.J. (2001). Natural History of Neonatal Herpes SimplexVirus Infections in the Acyclovir Era. Pediatrics. 108, 223-229.
70.Yoshida, M and Umene, K. (2003). Close association of predominantgenotype of herpes simplex virus type 1 with eczema herpeticumanalysed using restriction fragment length polymorphism ofpolymerase chain reaction. J. Virol. Methods. 109, 11-16.
71.Zinnai, G., Schaad, U.B., Heininger, U. (2001). Multiple herpeticwhitlow lesions in a 4-year-old girl: case report and review of theliterature. Eur. J. Pediatr. 160, 528-533.
72.Sun, Y., Chan, R.K.W., Tan, S.H., Ng P.P.L. (2003). Detection andGenotyping of Human Herpes Simplex Viruses in Cutaneous Lesionsof Erythema Multiforme by Nested PCR. J.Med. Virol. 71, 423-428.
73.Aurelian, L., Ono, F., Burnett, J. (2003). Herpes simplex virus (HSV)-associated erythema multiforme (HAEM): A viral disease with anautoimmune component. Dermatol online J. 1, 1-27.
74.Ono, F., Sharma, B.K., Smith, C.C., Burnett, J.W., Aurelian, L. (2005).CD34+ Cells in the Peripheral Blood Transport Herpes Simplex VirusDNA Fragments to the skin of patients with Erythema Multiforme(HAEM). J. Invest. Dermatol. 124, 1215-1224. Hjalmarsson A,Blomqvist P, Skoldenberg B. Herpes simplex encephalitis in Sweden,1990-2001: incidence, morbidity, and mortality. Clin Infect Dis.2007;45(7):875-80].
75.Malkin, J.E. (2004). Epidemiology of Genital Herpes Simplex VirusInfection in Developed Countries. Herpes. (Suppl. 1), 2A-23A
76.Bünzli, D., Wietlisbach, V., Barazzoni, F., Sahli, R., Meylan, P.R.A.(2004).Seroepidemiology of Herpes Simplex virus type 1 and 2 inWestern and Southern Switzerland in adults aged 25-74 in 1992-93: apopulation-based study. BMC Infect. Dis. 4, 10.
77.Gottlieb, S.L., Douglas Jr, J.M., Schmid, D.S., Bolan, G., Iatesta, M.,Mallote, C.K.,Zenilman, J., Foster, M., Baron, A.E., Steiner, J.F.,Peterman, T.A., Kamb, M.L. (2002).Seroprevalence and Correlates ofHerpes Simplex Virus Type 2 Infection in Five Sexually Transmitted-Disease Clinics. J. Infect. Dis. 186, 1381-1389.

78.Weiss, H. (2004). Epidemiology of Herpes Simplex Virus Type 2Infection in the Developing World. Herpes. (Suppl. 1), 24A- 35A.
79.Smith, C.C., Yu, Y.X., Kulka, M., Aurelian, L. (2000). A Novel HumanGene Similar to the Protein Kinase (PK) Coding Domain of the LargeSubunit of Herpes Simplex Virus Type 2 Ribonucleotide Reductase(ICP10) Codes for a Serine-Threonine PK and Is Expressed inMelanoma Cells. J. Biol. Chem. 275, 25690-25699.
80.Mbopi-Keou, F.X., Robinson, N.J., Mayaud, P., Belec, L., Brown,D.W.G. (2003). Herpes simplex virus type 2 and heterosexual spread ofhuman immunodeficiency virus infection in developing countries:hypothesis and research priorities. Clin. Microbiol. Infect. 9, 161-171.
81.Geiger KD; Nash TC; Sawyer S; Krahl T; Patstone G; Reed JC;Krajewski S; Dalton D; Buchmeier MJ; Sarvetnick N Interferon-gamma protects against herpes simplex virus type 1-mediated neuronaldeath.Virology. 1997; 238(2):189-97
82.Zhang SY; Abel L; Casanova JL Mendelian predisposition to herpessimplex encephalitis. Handb Clin Neurol. 2013; 112:1091-7
83.Menasria R; Boivin N; Lebel M; Piret J; Gosselin J; Boivin G BothTRIF and IPS-1 adaptor proteins contribute to the cerebral innateimmune response against herpes simplex virus 1 infection. JVirol. 2013; 87(13):7301-8
84.Nahmias AJ, Whitley RJ, Visintine AN, Takei Y, Alford CA. Herpes-Simplex VirusEncephalitis - Laboratory Evaluations and TheirDiagnostic-Significance. J Infect Dis.1982;145(6):829-36
85.De Tiege X, Heron B, Lebon P, Ponsot G, Rozenberg F. Limits of earlydiagnosis of herpes simplex encephalitis in children: a retrospectivestudy of 38 cases. Clin Infect Dis.2003;36(10):1335-9 Bale JF; Viralencephalitis. Med Clin North Am 1993; 77: 25-42
86.Bale JF; Viral encephalitis. Med Clin North Am 1993; 77: 25-42
87.Whitley RJ, Soong SJ, Linneman C Jr. et al : Herpes simplexencephalitis. Clinical assessment. JAMA 1982; 247 : 317-32021

88.Jhonson KP, Rosenthal MS, Lerner PI : Herpes Simplex encephalitis,its course in five virologically proven cases. Arch Neurol 1972; 27 :103-108
89.Klapper PE, Cleator GM, Longson M : Mild forms of herpesencephalitis, J Neurol Neurosurg Psychiatry 1984; 47 : 1247-1250
90.Whitley RJ, Herpes simplex encephalitis;adolescents and adults .Antiviral Res 2006 sep.71(2-3): 141-8
91.Kimberlin D; Herpes simplex virus, meningitis and encephalitis inneonates. Herpes. 2004; 11 Suppl 2:65A-76A
92.Ashley, R.L., and Wald, A. (1999). Genital Herpes: Review of theEpidemic and Potential Use of Type-Specific Serology. Clin.Microbiol. Rev. 12, 1-8
93.Wooley, P.D., Chandiok, S., Pumphrey, J., Sharratt, S., Shanley, L.,Bennett, S. (2000).Serological prevalence of herpes simplex virus type2 amongst GUM clinic attenders in adistrict general hospital setting. Int.J. STD AIDS 11, 379-382.
94.Ashley, R.L. (2001). Sorting out the new HSV type specific antibodytests. Sex. Transm. Inf. 77, 232-237
95.Schmid, D.S., Brown, D.R., Nisenbaum, R., Burke, R.L., Alexander,D., Ashley, R., Pellett, P.E., Reeves, W.C. (1999). Limits in Reliabilityof Glycoprotein G-Based Type-Specific Serologic Assays for HerpesSimplex Virus Types 1 and 2. J. Clin. Microbiol. 37, 376-379.
96.Tunback, P., Liljeqvist, J.Å., Löwhagen, G.B., Bergström, T. (2000).Glycoprotein G of herpes simplex virus type 1: identification of type-specific epitopes by human antibodies. J. Gen. Virol. 81, 1033-1040.
97.Marsden, H.S., Buckmaster, A., Palfreyman, J.W., Hope, R.G., Minson,A.C. (1984).Characterization of the 92,000-dalton glycoproteininduced by herpes simplex virus type 2. J. Virol. 50, 547-554
98.Roizman, B., Norrild, B., Chan, C., Pereira, L. (1984). Identificationand preliminary mapping with monoclonal antibodies of a herpes

simplex 2 glycoprotein lacking a known type 1 counterpart. Virology133, 242-247
99.Guffond T, Dewilde A, Lobert PE, Caparros-Lefebvre D, Hober D,Wattre P. Significance and clinical relevance of the detection of herpessimplex virus DNA by the polymerase chain reaction in cerebrospinalfluid from patients with presumed encephalitis. Clin Infect Dis.1994;18(5):744-9
100. Sullender WM, Yasukawa LL, Schwartz M, Pereira L, HensleighPA, Prober CG, et al. Typespecific antibodies to herpes simplex virustype 2 (HSV-2) glycoprotein G in pregnant women, infants exposed tomaternal HSV-2 infection at delivery, and infants with neonatal herpes.J Infect Dis. 1988;157(1):164-71.
101. Whitley RJ, Alford CA, Hirsch MS, Schooley RT, Luby JP, AokiFY, et al. Vidarabine versus acyclovir therapy in herpes simplexencephalitis. N Engl J Med. 1986;314(3):144-9.
102. Kimberlin DW, Whitley R. Antiviral therapy of HSV-1 and -2. In:Arvin A, Campadelli-Fiume G, Mocarski E, Moore PS, Roizman B,Whitley R, et al., editors. Human Herpesviruses: Biology, Therapy, andImmunoprophylaxis. Cambridge: Cambridge University Press; 2007.
103. Kimberlin, D.W., Lin, C.Y., Jacobs, R.F., Powell, D.A., Corey, L.,Gruber, W.C., Rathore, M., Bradley, J.S., Diaz, P.S., Kumar, M., Arvin,A.M., Gutierrez, K., Shelton, M., Weiner, L.B., Sleasman, J.W.,Murguia de Sierra, T., Weller, S., Soong, S.J., Kiell, J., Lakeman, F.D.,Whitley, R.J. (2001). Safety and Efficacy of High-Dose IntravenousAcyclovir in the Management of Neonatal Herpes Simplex VirusInfections. Pediatrics. 108, 230-238.
104. Studahl M, Lindquist L, Eriksson BM, Gunther G, Bengner M,Franzen-Rohl E, et al. Acute viral infections of the central nervoussystem in immunocompetent adults: diagnosis and management. Drugs.2013;73(2):131-58.
105. Mommeja-Marin H, Lafaurie M, Scieux C, Galicier L,Oksenhendler E, Molina JM. Herpes simplex virus type 2 as a cause ofsevere meningitis in immunocompromised adults. Clin InfectDis.2003;37(11):1527-33

106. Engman ML, Adolfsson I, Lewensohn-Fuchs I, Forsgren M,Mosskin M, Malm G. Neuropsychologic outcomes in children withneonatal herpes encephalitis. Pediatr Neurol. 2008;38(6):398-405.
107. Gnann JW, Jr., Skoldenberg B, Hart J, Aurelius E, Schliamser S,Studahl M, et al. Herpes Simplex Encephalitis: Lack of Clinical Benefitof Long-term Valacyclovir Therapy. Clin Infect Dis. 2015;61(5):683-91.
108. Wasay M, Mekan SF, Khelaeni B, Saeed Z, Hassan A, Cheema Z,Bakshi R.Extra temporal involvement in herpes simplex encephalitis.Eur J Neurol. 2005;1:475.
109. Misra UK, Kalita J.Neurophysiological studies in herpes simplexencephalitis. Electromyogr Clin Neurophysiol.1998;3:177
110. Kupila L, Vuorinen T, VainionpääR, Hukkanen V, Marttila RJ,Kotilainen P.Etiology of aseptic meningitis and encephalitis in an adultpopulation. Neurology. 2006;66:75
111. Lakeman FD, Whitley RJ.Diagnosis of herpes simplex encephalitis:application of polymerase chain reaction to cerebrospinal fluid frombrain-biopsied patients and correlation with disease. National Instituteof Allergy and Infectious Diseases Collaborative Antiviral StudyGroup.J Infect Dis. 1995;171:857
112. Ameeta Singh, J Preiksaitis, B Romanowski. The laboratorydiagnosis of herpes simplex virus infections. Can J Infect Dis MedMicrobiol 2005;16(2):92-98.
113. Jones, C.A, and Cunningham, A.L. (2004). Vaccination Strategiesto Prevent Genital Herpes and Neonatal Herpes Simplex Virus (HSV)Disease. Herpes 11, 12-17. Review
114. Whitley RJ; Soong SJ; Dolin R; Galasso GJ; Ch'ien LT; Alford CA;Adenine arabinoside therapy of biopsy-proved herpes simplexencephalitis. National Institute of Allergy and Infectious Diseasescollaborative antiviral study. N Engl J Med. 1977; 297(6):289-94
115. Utley TF; Ogden JA; Gibb A; McGrath N; Anderson NE; The long-term neuropsychological outcome of herpes simplex encephalitis in aseries of unselected survivors. Neuropsychiatry Neuropsychol BehavNeurol. 1997; 10(3):180-9

116. Elbers JM; Bitnun A; Richardson SE; Ford-Jones EL; Tellier R;Wald RM; Petric M; Kolski H; Heurter H; MacGregor D; A 12-yearprospective study of childhood herpes simplex encephalitis: is there abroader spectrum of disease? Pediatrics. 2007; 119(2):e399-407
117. Shelley BP; Raniga SB; Al-Khabouri J; Unusual late complicationof intracerebral haematoma in herpes encephalitis after successfulacyclovir treatment. J Neurol Sci. 2007; 252(2):177-80 dateWhitley RJ; Soong SJ; Linneman C; Liu C; Pazin G; Alford CAHerpes simplex encephalitis. Clinical Assessment. JAMA. 1982;247(3):317-20
118. Moumitha Adhikari And Rabindranath Chatterjee LaboratoryEvaluation Of Cases Of Meningitis Attending A Tertiary Care HospitalIn India; An Observational Study; International Journal Of Nutrition,Pharmacology, Neurological Diseases; July-September 2013/Vol3/Issue 3
119. Jeffry P Simko, Angela M Caliendo, Kay Hogle, James VersalovicDifferences in Laboratory Findings for Cerebrospinal Fluid SpecimensObtained from Patients with Meningitis or Encephalitis Due to HerpesSimplex Virus (HSV) Documented by Detection of HSV DNA ClinicalInfectious Diseases, Volume 35, Issue 4, 15 August 2002, Pages 414–419
120. Whitley RJ; Cobbs CG; Alford CA; Soong SJ; Hirsch MS;Connor JD; Corey L; Hanley DF; Levin M; Powell DA; Diseases thatmimic herpes simplex encephalitis. Diagnosis, presentation, andoutcome. NIAD Collaborative Antiviral Study Group JAMA. 1989;262(2):234-9
121. Tyler KL. Herpes simplex virus infections of the central nervoussystem: encephalitis and meningitis, including Mollaret's. Herpes2004;11 Suppl 2:57A–64A.
122. Fodor PA, Levin MJ, Weinberg A, Sandberg E, Sylman J, TylerKL. Atypical herpes simplex virus encephalitis diagnosed by PCRamplification of viral DNA from CSF, Neurology,1998 vol. 51 (pg. 554-9)

123. Tang YW, Hibbs JR, Tau KR, et al. Effective use of polymerasechain reaction for diagnosis of central nervous system infections, ClinInfect Dis,1999, vol. 29(pg. 803-6)
124. Berger JR. Benign aseptic (Mollaret's) meningitis after genitalherpes, Lancet,1991, vol. 337(pg.1360-1)
125. Tebas P, Nease RF, Storch GA. Use of the polymerase chain reactionin thediagnosis of herpes simplex encephalitis: A decision model. AmJ Med 1998;105:287-95.
126. Venkatesan A, Tunkel AR, Bloch KC, et al. Case definitions,diagnostic algorithms, and priorities in encephalitis: consensusstatement of the international encephalitis consortium. Clin InfectDis 2013;57:1114–1128)

ANNEXURE
PROFORMA
DATA SHEET FOR COLLECTION OF SOCIO DEMOGRAPHIC, CLINICAL
AND LABORATORY DATA FOR DETECTION OF HERPES SIMPLEX
VIRUS(HSV) IN ENCEPHALITIS PATIENTS: EVALUATION OF
DIAGNOSTIC UTILITY OF HSV DETECTION BY REAL TIME
POLYMERASE CHAIN REACTION(PCR)
Name: Age/Sex: Date of Admisiion:
H/o Present Illness:
Fever>38°cHeadacheNausea/vomitingAltered mental status
Low level of consciousnessAgitationLethargy
Critical manifestationsFocal weaknessSeizures
Other rashes/ulcers
Past HistoryPrevious history of similar illness
NatureInvestigation and treatment particulars
Clinical examination:PulseBlood Pressure

General examination
CNS Examination:Alteration of consciousnessDysphasiaAtaxiaSeizuresHemiparesisCranial nerve defectsVisual field lossPapilledema
Investigations:Objective Data:
Blood - Complete HaemogramCSF-Cell Count
GlucoseProteinGram StainCultureSerology
CSF CytologyEEGCT SCANMRI
Study Method:
Real Time Polymerase chain reaction(PCR) for HSV DNA
Inference:

PATIENT CONSENT FORM


Diagnostic criteria Antiviral treatment
in yearsin
monthsin days
major-mustrequired
minor(1-6)
2-possible case
>/=3-confirmed case
Macroscopy Glucose Protein CSF Leukocyte/cubicmmCSF RBC/ cumm(Normal
Adult 0-10/cumm)Meningeal signs Acyclovir
1 3 - - Fch 2583 PICU January Acute 2 1,3 clear 61 22 Acellular Nil Nil Present 13 Normal Normal - NO Negative discharged
2 1 6mon - Mch 10001 PICU February Acute 2 1,2 clear 56 45 Acellular Nil Nil Absent 12 Normal Normal - NO Negative discharged
3 4 Mch 10002 PICU February Acute 1 2 clear 55 18 Acellular 2 Nil Present 14 Normal Normal - NO Negative NA
4 7 - - Mch 16005 PICU March Subacute 1 2 clear 60 48 Acellular 1 Nil Absent 13 Abnormal Normal - NO Negative NA
5 10 - - Fch 16121 PICU March Subacute 2 1,5,6 clear 48 25Lymphocytic
predominance>200 few Present 12 Abnormal
Hypodensity in thalamic
area suggestive of
cortical edema
- YES Negative NA
6 46 - - M 18332 Medicine ward March Acute 3 1,5,6 clear 75 10 Acellular Nil Nil Absent 12 Abnormal Hydrocephalus - YES Negative discharged
7 71 - - M 18775 Medicine ward March Subacute 3 1,2,3, clear 51 22 Acellular Nil Nil Absent 8 Normal Normal - NO Negativeneurologica
l sequlae
8 26 - - M 19458 IMCU March Acute 6 1,2,3,4,5,6 clear 40 75Lymphocytic
predominance>300 Nil Present 3 Abnormal
Bilateral fronto temporal
enhancment seen- YES
HSV-1
POSITIVE
neurologica
l sequlae
9 23 - - F 19700 IMCU March Acute 2 1,3 clear 57 18 Acellular Nil Nil Absent 11 Normal Normal - YES Negative NA
10 75 - - M 20191 Medicine ward March Subacute 4 2,4,5,6 clear 105 45 Acellular Nil very few Present 9 AbnormalB/L periventricular&basal
ganglion lesion
Left occipito parietal lobe
infarctYES Negative
neurologica
l sequlae
11 3 9mon - Fch 33557 PICU April Subacute 3 2,5,6 clear 53 17 Acellular Nil Nil Absent - Abnormalleft frontal cerebral
hypoattenuation- YES Negative NA
12 - 9mon - Mch 33683 PICU May Acute 2 1,2 clear 50 17 Acellular Nil Nil Absent - - Normal - NO Negative Recovered
13 - - 27 Mch 35221 PICU May Acute 2 1,2 clear 45 85 Acellular Nil Nil Absent - - - - NO Negative NA
14 35 - - M 37941 IMCU May Acute 5 2,3,4,5,6 Blood stained 55 68
Lymphocytic
predominance with few
erythrocytes
>100 few Present 2 Abnormal -
Hyperintense B/L
temporal lobe
hemorrhagic lesion
YESHSV-1
POSITIVEDeath
15 18 - - M 46883 IMCU June Subacute 2 1,2 clear 41 9 Acellular Nil Nil Absent 10 Normal Normal - NO Negative NA
16 47 - - M 49272 Neurosurgery June Subacute 2 2,3 clear 62 25 Acellular Nil Nil Absent 12 Normal Normal - YES Negative Recovered
17 9 - - Fch 50009 PICU June Subacute 1 2 clear 73 15 Acellular Nil Nil Absent 12 Normal Normal - NO Negative Recovered
18 58 - - F 52400 IMCU June Acute 2 1,2 clear 72 19 Acellular Nil very few Present 13 Normal Normal - NO Negative Recovered
19 45 - - F 52434 Medicine ward June Acute 3 1,4,5 clear 80 20 Acellular Nil Nil Present 12 Abnormal Cerebral edema - YES Negative Recovered
20 55 - - M 52658 Neurology June Acute 4 2,4,5,6 slightly turbid 59 15
Lymphocytic
predominance with few
erythrocytes
>80 15-20 Present 12 AbnormalRight parietal temporal
lesion- YES Negative NA
21 55 - - M 52705 Medicine ward July Acute 1 2 clear 93 38 Acellular Nil Nil Present 13 Normal Normal - NO Negative discharged
22 30 - - F 52711 IMCU July Acute 2 1,3 clear 44 20 Acellular Nil Nil Present 11 Normal Normal - NO Negative NA
23 - 9mon - Fch 53266 PICU July Subacute 1 1 clear 57 11 Acellular Nil Nil Absent - Normal Normal - NO Negative NA
24 1 6mon - Fch 53292 PICU July Subacute 2 1,3 clear 65 32 Acellular Nil Nil Absent - Normal Normal - NO Negative Recovered
25 - - 4 Fch 53338 SNN July Acute 3 2,5,6 Blood stained 40 89 Erythrocytic few 20-25 Absent - - Diffuse cortical lesion - NO Negative NA
26 20 - - F 53423 IMCU July Acute 2 1,3 clear 65 12 Acellular Nil Nil Present 10 Normal Normal - YES Negativedischarged
at request
27 70 - - F 55536 Medicine ward August Subacute 3 1,2,6 Turbid 147 50 Acellular Nil Nil Absent 9 Normal -B/L temporo-occipital
lesion with old infarctsYES Negative
neurologica
l sequlae
28 1 6mon - Mch 56062 PICU August Acute 3 1,2,6 clear 58 12 Acellular Nil Nil Absent - Normal Diffuse cortical lesion - NO Negative sequlae
29 45 - - M 56771 Medicine ward August Subacute 2 2,6 clear 56 23 Acellular Nil few Present 11 NormalDiffuse parenchymal
edema- YES Negative Recovered
30 39 - - F 57014 Labour ward August Acute 2 1,3 clear 42 16 Acellular Nil Nil Absent 13 Normal Normal - NO Negative NA
31 40 - - M 57135 Medicine ward August Acute 2 2,3 clear 59 28 Acellular Nil Nil Absent 12 Normal Normal - YES Negative Recovered
32 1 3mon - Fch 57254 PICU August Acute 2 1,4,6 clear 57 10 Acellular Nil Nil Absent - Abnormal -Hyperintense B/L
cerebral hemisphereYES Negative NA
33 35 - - F 57295 Neurology August Acute 3 1,2,4 clear 73 31 Acellular Nil Nil Present 14 Abnormal Normal - NO Negative NA
34 - 2mon - Mch 57545 PICU August Acute 3 1,3,6 clear 65 85 Acellular Nil few Absent - -Left temporo parietal
hypodensity- YES Negative NA
35 33 - - F 57790 Neurology August Acute 2 1,2 clear 76 22 Acellular Nil Nil Present 14 Normal Normal - NO Negative discharged
36 8 - - Fch 60247 PICU August Acute 2 1,3 clear 41 25 Acellular Nil Nil Present 12 Normal Normal - NO Negative NA
37 9 - - Fch 61430 PICU August Acute 2 1,2 clear 54 19 Acellular Nil Nil Present 12 Normal Normal - NO Negative NA
38 60 - - M 62766 Neurology September Acute 5 1,3,4,5,6 slightly turbid 85 35Lymphocytic
predominance>50 few Present 8 Abnormal Diffuse cerebral edema - YES Negative
Discharge at
request
39 - 11mon - Mch 63113 PICU September Acute 2 1,2 clear 53 14 Acellular 2 Nil Absent - Normal Normal - NO Negative discharged
40 10 - - Fch 63341 PICU September Acute 1 2 clear 50 22 Acellular Nil Nil Absent 12 Normal Normal - NO Negative NA
41 30 - - M 64862 IMCU September Subacute 3 1,3,5 slightly turbid 55 62 Acellular Nil Nil Present 11 Abnormal Normal - YES Negative sequlae
42 56 - - M 65854 Neurology September Acute 2 2,3 clear 60 41 Acellular Nil Nil Absent 13 Normal Normal - NO Negative NA
Sex IP. No. Ward Month
Annexure Line list Data
GCS
ScoreEEG Pattern CT Scan MRI Scan
HSV REAL
TIME PCRFolow-up
Clinical Onset
(Acute/Subacute)
CF Score
(1 to 6)
CSF Findings
CSF Cytopathology
Age
CSF
Sample
No.

Diagnostic criteria Antiviral treatment
in yearsin
monthsin days
major-mustrequired
minor(1-6)
2-possible case
>/=3-confirmed case
Macroscopy Glucose Protein CSF Leukocyte/cubicmmCSF RBC/ cumm(Normal
Adult 0-10/cumm)Meningeal signs Acyclovir
Sex IP. No. Ward MonthGCS
ScoreEEG Pattern CT Scan MRI Scan
HSV REAL
TIME PCRFolow-up
Clinical Onset
(Acute/Subacute)
CF Score
(1 to 6)
CSF Findings
CSF Cytopathology
Age
CSF
Sample
No.
43 64 - - M 66871 Neurology September Acute 3 2,4,5 Blood stained 56 70
Lymphocytic
predominance with few
erythrocytes
>120 10 Absent 10 Abnormal Normal - YES NegativeDischarge at
request
44 - 8mon - Fch 67008 PICU October Acute 2 1,2 clear 75 48 Acellular Nil Nil Absent - Normal Normal - NO Negative NA
45 55 - - M 67078 Neurology October Subacute 2 1,2 clear 68 21 Acellular 4 Nil Absent 14 Normal Normal - NO Negative NA
46 - - 4 Fch 67152 SNN October Acute 2 1,2 Blood stained 35 93 Erythrocytic 30-40 Nil Absent - - - - NO Negative NA
47 - 8mon - Fch 67288 Neurosurgery October Subacute 2 1,2 clear 45 20 Acellular Nil Nil Absent - Normal Normal - NO Negative NA
48 - 6mon - Mch 68112 Neurosurgery November Acute 2 2,3 clear 71 52 Acellular 3 Nil Absent - - Normal - NO Negative NA
49 18 - - M 69473 Medicine ward November Subacute 2 1,3 clear 60 48Scattered lymphocytes in
eosinophilic background2 Nil Absent 6 Normal - - YES Negative
neurologica
l sequlae
50 - - 4 Mch 69801 SNN December Acute 2 1,2 clear 45 96 Acellular Nil Nil Present 0 - - - NO Negative NA