Delay in Neurovenous Flaps: Experimental and Clinical Experience
7
ORIGINAL ARTICLE Delay in Neurovenous Flaps Experimental and Clinical Experience Ahmet Karacalar, MD,* Oytun I ˙ dil, MD,† Ahmet Demir, MD,* Ethem Gu ¨neren, MD,* Tekin S ¸ims ¸ek, MD,* and Mesut O ¨ zcan, MD† Abstract: The objective of this study was to examine the effects of the standard surgical delay in the flaps based on the cutaneous branches of the vascular axis around a superficial sensory nerve. The delay procedure was experimentally tested in rats and subsequently used in patients. In the experimental study, the survival of a delayed inferior epigastric neurovenous flap was compared with that of a nondelayed inferior epigastric neurovenous flap. One type of clinically applica- ble delay pattern (standard bipedicled technique) was employed. A 3 3 cm flap was raised in 20 female Wistar rats assigned randomly to 2 groups. Each group consisted of 20 flaps. The standard bi- pedicled delay pattern increased the percentage survival of the delayed inferior epigastric neurovenous flap. The survival percent- age of the delayed flaps was 59.8 185.0 (P 0.5). The histologic findings of the skin revealed that our delay procedure enhanced the perfusion of the flap by dilating the arterial network. Stimulated by our experimental findings, we used the island bipedicled surgical flap delay or combined strategic-standard delay in the distally pedicled sural flap successfully on 9 cases. Key Words: delay, neurovenous flap, sural flap, tissue defect (Ann Plast Surg 2004;53: 481– 487) T he concept of flaps based on the cutaneous branches of the vascular axis around a superficial sensory nerve has expanded the horizons in reconstructive surgery. The classic example of this concept is the distally pedicled sural flap. This flap appears to be a simple and reliable means of providing good-quality coverage for medium-sized skin de- fects for foot reconstruction. However, partial or total necro- sis of the sural flaps persists as a major source of morbidity for patients with risk factors including diabetes, extensive trauma, and massive soft-tissue injury and for patients with large tissue defects. Based on a thorough analysis of compli- cation rates in patients with high-risk factors, Baumeister et al 1 reported that diabetes, arteriosclerosis, and venous insuf- ficiency were the most important risk factors for the distally pedicled sural flap. In their study, the necrosis rate was 33% in patients with any concomitant disease. A delay procedure as commonly used in random flaps would improve the reli- ability and dimensions of the procedure. Also, it may be valuable if the defect requires an extended reach of the flap. In the experimental part of this article, we studied the effects of standard bipedicled delay procedure in an animal model. Our previous experimental studies have been funda- mental to this study. 1,2 As stated in those studies, we call the flap based on the inferior epigastric nerve “neurovenous” because both the neurocutaneous artery and longitudinal plexus around the inferior epigastric vein are involved in flap survival. Stimulated by our experimental findings, we used the delayed distally pedicled sural flap in 9 cases with risk factor. MATERIALS AND METHODS Part I: Experimental Study Forty female Wistar rats weighing 250 mg were used in the experimental study. The rats were anesthetized by intra- peritoneal pentobarbital (50 mg/kg). The inferior epigastric neurovenous flap (3 3 cm) was used as the flap model. The flaps were elevated on the basis of the inferior epigastric vein, nerve with the loose areolar tissue around the vein, and nerve. The inguinal mammary gland was used as an inferior corner of the medial border of the flap to dissect all flaps in an identical fashion. The limits of the flap were extended beyond the ipsilateral nipple line laterally, to include the distribution of the inferior epigastric nerve in the flap. The flaps contained skin, panniculus carnosus, and the epigastric fat pad. Using sterile technique, bilateral flaps were designed in each rat. Received September 17, 2003 and accepted for publication, after revision, March 9, 2004. From the *Department of Plastic and Reconstructive Surgery, Ondokuz Mayy ´s University, Samsun, Turkey; and †Uludag ˘ University, Bursa, Turkey. Reprints: Dr. Ahmet Karacalar Ondokuz Mayy ´s U ¨ niversitesi, Ty ´p Faku ¨ltesi Plastik ve Rekonstru ¨ktif Cerrahi A.D. Samsun,55139, Turkey; E-mail: [email protected] Copyright © 2004 by Lippincott Williams & Wilkins ISSN: 0148-7043/04/5305-0481 DOI: 10.1097/01.sap.0000137246.76119.79 Annals of Plastic Surgery • Volume 53, Number 5, November 2004 481
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Delay in Neurovenous Flaps: Experimental and Clinical Experience
ORIGINAL ARTICLE
Delay in Neurovenous FlapsExperimental and Clinical Experience
Ahmet Karacalar, MD,* Oytun Idil, MD,† Ahmet Demir, MD,* Ethem Guneren, MD,*Tekin Simsek, MD,* and Mesut Ozcan, MD†
Abstract: The objective of this study was to examine the effects ofthe standard surgical delay in the flaps based on the cutaneousbranches of the vascular axis around a superficial sensory nerve. Thedelay procedure was experimentally tested in rats and subsequentlyused in patients.
In the experimental study, the survival of a delayed inferiorepigastric neurovenous flap was compared with that of a nondelayedinferior epigastric neurovenous flap. One type of clinically applica-ble delay pattern (standard bipedicled technique) was employed. A3 � 3 cm flap was raised in 20 female Wistar rats assigned randomlyto 2 groups. Each group consisted of 20 flaps. The standard bi-pedicled delay pattern increased the percentage survival of thedelayed inferior epigastric neurovenous flap. The survival percent-age of the delayed flaps was 59.8 � 185.0 (P � 0.5). The histologicfindings of the skin revealed that our delay procedure enhanced theperfusion of the flap by dilating the arterial network.
Stimulated by our experimental findings, we used the islandbipedicled surgical flap delay or combined strategic-standard delayin the distally pedicled sural flap successfully on 9 cases.
Key Words: delay, neurovenous flap, sural flap, tissue defect
(Ann Plast Surg 2004;53: 481–487)
The concept of flaps based on the cutaneous branches ofthe vascular axis around a superficial sensory nerve has
expanded the horizons in reconstructive surgery. The classicexample of this concept is the distally pedicled sural flap.This flap appears to be a simple and reliable means ofproviding good-quality coverage for medium-sized skin de-
fects for foot reconstruction. However, partial or total necro-sis of the sural flaps persists as a major source of morbidityfor patients with risk factors including diabetes, extensivetrauma, and massive soft-tissue injury and for patients withlarge tissue defects. Based on a thorough analysis of compli-cation rates in patients with high-risk factors, Baumeister etal1 reported that diabetes, arteriosclerosis, and venous insuf-ficiency were the most important risk factors for the distallypedicled sural flap. In their study, the necrosis rate was 33%in patients with any concomitant disease. A delay procedureas commonly used in random flaps would improve the reli-ability and dimensions of the procedure. Also, it may bevaluable if the defect requires an extended reach of the flap.
In the experimental part of this article, we studied theeffects of standard bipedicled delay procedure in an animalmodel. Our previous experimental studies have been funda-mental to this study.1,2 As stated in those studies, we call theflap based on the inferior epigastric nerve “neurovenous”because both the neurocutaneous artery and longitudinalplexus around the inferior epigastric vein are involved in flapsurvival. Stimulated by our experimental findings, we usedthe delayed distally pedicled sural flap in 9 cases with riskfactor.
MATERIALS AND METHODS
Part I: Experimental StudyForty female Wistar rats weighing 250 mg were used in
the experimental study. The rats were anesthetized by intra-peritoneal pentobarbital (50 mg/kg). The inferior epigastricneurovenous flap (3 � 3 cm) was used as the flap model. Theflaps were elevated on the basis of the inferior epigastric vein,nerve with the loose areolar tissue around the vein, and nerve.The inguinal mammary gland was used as an inferior cornerof the medial border of the flap to dissect all flaps in anidentical fashion. The limits of the flap were extended beyondthe ipsilateral nipple line laterally, to include the distributionof the inferior epigastric nerve in the flap. The flaps containedskin, panniculus carnosus, and the epigastric fat pad. Usingsterile technique, bilateral flaps were designed in each rat.
Received September 17, 2003 and accepted for publication, after revision,March 9, 2004.
From the *Department of Plastic and Reconstructive Surgery, OndokuzMayys University, Samsun, Turkey; and †Uludag University, Bursa,Turkey.
Reprints: Dr. Ahmet Karacalar Ondokuz Mayys Universitesi, Typ FakultesiPlastik ve Rekonstruktif Cerrahi A.D. Samsun,55139, Turkey; E-mail:[email protected]
Copyright © 2004 by Lippincott Williams & WilkinsISSN: 0148-7043/04/5305-0481DOI: 10.1097/01.sap.0000137246.76119.79
Annals of Plastic Surgery • Volume 53, Number 5, November 2004 481
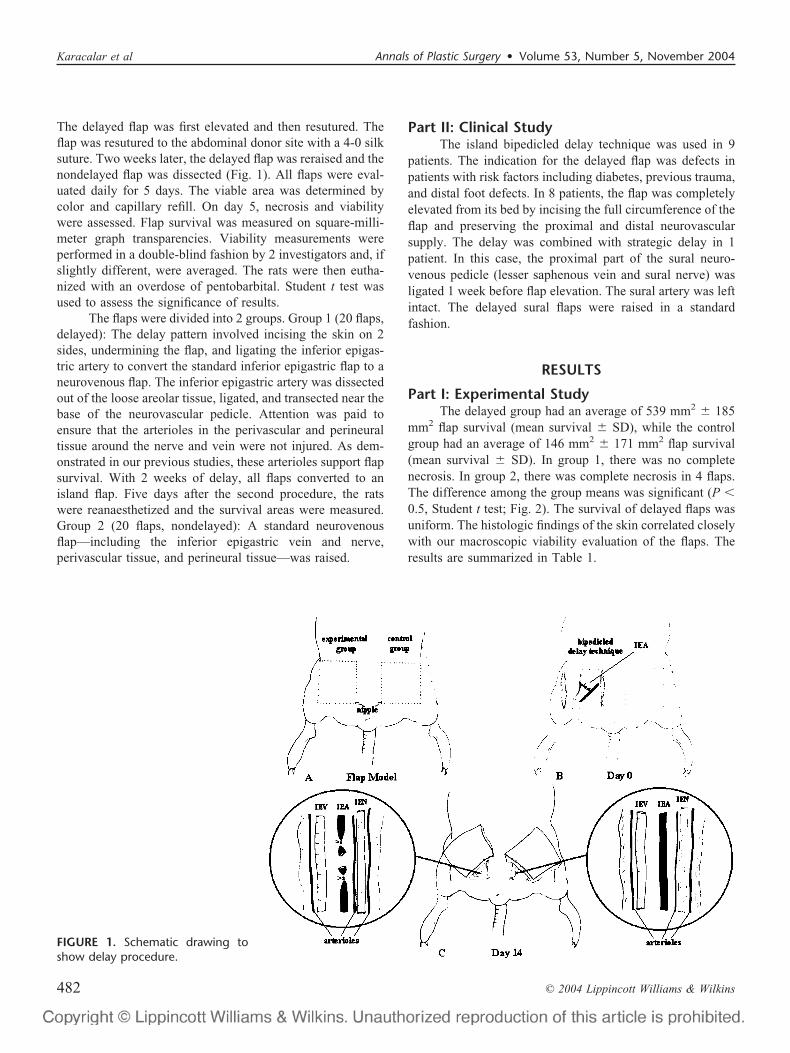
The delayed flap was first elevated and then resutured. Theflap was resutured to the abdominal donor site with a 4-0 silksuture. Two weeks later, the delayed flap was reraised and thenondelayed flap was dissected (Fig. 1). All flaps were eval-uated daily for 5 days. The viable area was determined bycolor and capillary refill. On day 5, necrosis and viabilitywere assessed. Flap survival was measured on square-milli-meter graph transparencies. Viability measurements wereperformed in a double-blind fashion by 2 investigators and, ifslightly different, were averaged. The rats were then eutha-nized with an overdose of pentobarbital. Student t test wasused to assess the significance of results.
The flaps were divided into 2 groups. Group 1 (20 flaps,delayed): The delay pattern involved incising the skin on 2sides, undermining the flap, and ligating the inferior epigas-tric artery to convert the standard inferior epigastric flap to aneurovenous flap. The inferior epigastric artery was dissectedout of the loose areolar tissue, ligated, and transected near thebase of the neurovascular pedicle. Attention was paid toensure that the arterioles in the perivascular and perineuraltissue around the nerve and vein were not injured. As dem-onstrated in our previous studies, these arterioles support flapsurvival. With 2 weeks of delay, all flaps converted to anisland flap. Five days after the second procedure, the ratswere reanaesthetized and the survival areas were measured.Group 2 (20 flaps, nondelayed): A standard neurovenousflap—including the inferior epigastric vein and nerve,perivascular tissue, and perineural tissue—was raised.
Part II: Clinical StudyThe island bipedicled delay technique was used in 9
patients. The indication for the delayed flap was defects inpatients with risk factors including diabetes, previous trauma,and distal foot defects. In 8 patients, the flap was completelyelevated from its bed by incising the full circumference of theflap and preserving the proximal and distal neurovascularsupply. The delay was combined with strategic delay in 1patient. In this case, the proximal part of the sural neuro-venous pedicle (lesser saphenous vein and sural nerve) wasligated 1 week before flap elevation. The sural artery was leftintact. The delayed sural flaps were raised in a standardfashion.
RESULTS
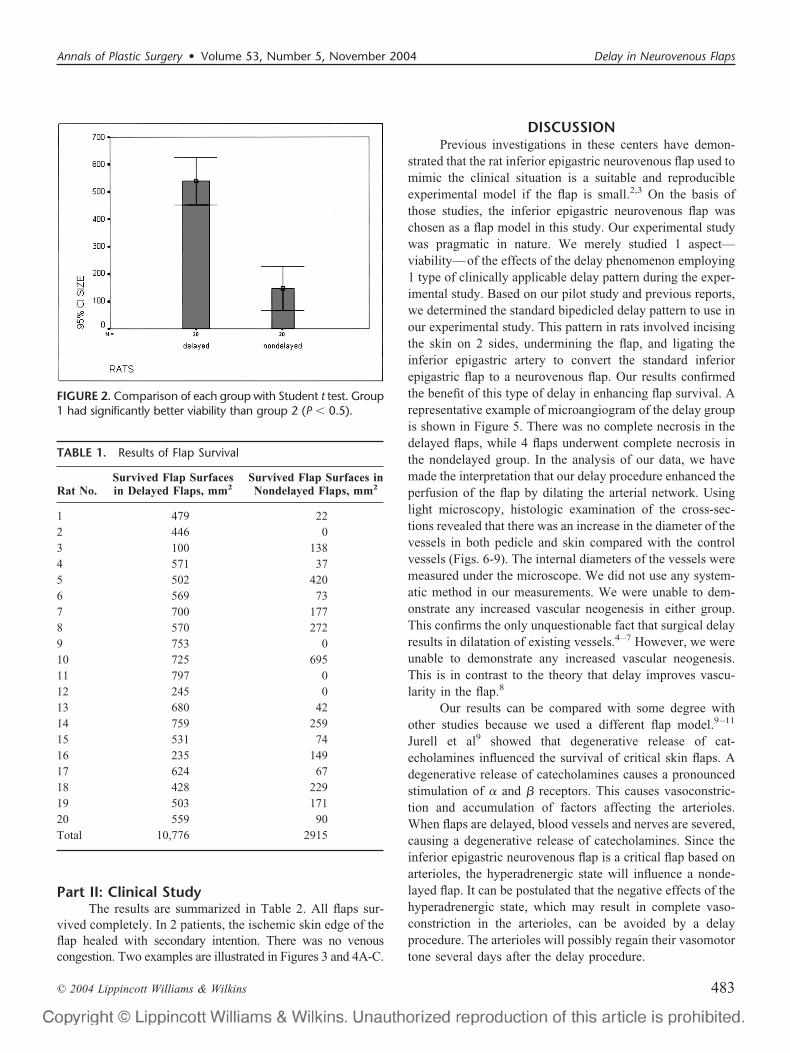
Part I: Experimental StudyThe delayed group had an average of 539 mm2 � 185
mm2 flap survival (mean survival � SD), while the controlgroup had an average of 146 mm2 � 171 mm2 flap survival(mean survival � SD). In group 1, there was no completenecrosis. In group 2, there was complete necrosis in 4 flaps.The difference among the group means was significant (P �0.5, Student t test; Fig. 2). The survival of delayed flaps wasuniform. The histologic findings of the skin correlated closelywith our macroscopic viability evaluation of the flaps. Theresults are summarized in Table 1.
FIGURE 1. Schematic drawing toshow delay procedure.
Karacalar et al Annals of Plastic Surgery • Volume 53, Number 5, November 2004
© 2004 Lippincott Williams & Wilkins482
Part II: Clinical StudyThe results are summarized in Table 2. All flaps sur-
vived completely. In 2 patients, the ischemic skin edge of theflap healed with secondary intention. There was no venouscongestion. Two examples are illustrated in Figures 3 and 4A-C.
DISCUSSIONPrevious investigations in these centers have demon-
strated that the rat inferior epigastric neurovenous flap used tomimic the clinical situation is a suitable and reproducibleexperimental model if the flap is small.2,3 On the basis ofthose studies, the inferior epigastric neurovenous flap waschosen as a flap model in this study. Our experimental studywas pragmatic in nature. We merely studied 1 aspect—viability—of the effects of the delay phenomenon employing1 type of clinically applicable delay pattern during the exper-imental study. Based on our pilot study and previous reports,we determined the standard bipedicled delay pattern to use inour experimental study. This pattern in rats involved incisingthe skin on 2 sides, undermining the flap, and ligating theinferior epigastric artery to convert the standard inferiorepigastric flap to a neurovenous flap. Our results confirmedthe benefit of this type of delay in enhancing flap survival. Arepresentative example of microangiogram of the delay groupis shown in Figure 5. There was no complete necrosis in thedelayed flaps, while 4 flaps underwent complete necrosis inthe nondelayed group. In the analysis of our data, we havemade the interpretation that our delay procedure enhanced theperfusion of the flap by dilating the arterial network. Usinglight microscopy, histologic examination of the cross-sec-tions revealed that there was an increase in the diameter of thevessels in both pedicle and skin compared with the controlvessels (Figs. 6-9). The internal diameters of the vessels weremeasured under the microscope. We did not use any system-atic method in our measurements. We were unable to dem-onstrate any increased vascular neogenesis in either group.This confirms the only unquestionable fact that surgical delayresults in dilatation of existing vessels.4–7 However, we wereunable to demonstrate any increased vascular neogenesis.This is in contrast to the theory that delay improves vascu-larity in the flap.8
Our results can be compared with some degree withother studies because we used a different flap model.9–11
Jurell et al9 showed that degenerative release of cat-echolamines influenced the survival of critical skin flaps. Adegenerative release of catecholamines causes a pronouncedstimulation of � and � receptors. This causes vasoconstric-tion and accumulation of factors affecting the arterioles.When flaps are delayed, blood vessels and nerves are severed,causing a degenerative release of catecholamines. Since theinferior epigastric neurovenous flap is a critical flap based onarterioles, the hyperadrenergic state will influence a nonde-layed flap. It can be postulated that the negative effects of thehyperadrenergic state, which may result in complete vaso-constriction in the arterioles, can be avoided by a delayprocedure. The arterioles will possibly regain their vasomotortone several days after the delay procedure.
TABLE 1. Results of Flap Survival
Rat No.Survived Flap Surfacesin Delayed Flaps, mm2
Survived Flap Surfaces inNondelayed Flaps, mm2
1 479 222 446 03 100 1384 571 375 502 4206 569 737 700 1778 570 2729 753 010 725 69511 797 012 245 013 680 4214 759 25915 531 7416 235 14917 624 6718 428 22919 503 17120 559 90Total 10,776 2915
FIGURE 2. Comparison of each group with Student t test. Group1 had significantly better viability than group 2 (P � 0.5).
Annals of Plastic Surgery • Volume 53, Number 5, November 2004 Delay in Neurovenous Flaps
© 2004 Lippincott Williams & Wilkins 483
Our results in the experimental study were sufficientlyconvincing to encourage us to use the standard delay inclinical cases. However, there are some hemodynamic differ-ences between the distally pedicled sural flap and the animalmodel. In our previous study, we showed that the rat inferiorepigastric flap is based on 5 to 8 arterioles with an externaldiameter of less than 120 �m.3 This flap can be accepted asa low-flow critical flap because the arterioles are fundamen-tally unstable vessels. It is known that beyond the arteries,blood pressure drops rapidly, and the linear flow velocitydecreases. Unlike the inferior epigastric neurovenous flapmodel, the sural flap has hemodynamic vigor. In addition, itsvenous drainage is much more disturbed than that of theinferior epigastric neurovenous flap. The valves of the lessersaphenous vein are capable of blocking the reverse drainage.
It is obvious that these differences do not allow accurateextrapolation to human application. Therefore, we decided touse a modification of the animal model in our clinical cases.In 8 cases, the flap was completely elevated from its bed byincising the full circumference of the flap and preserving theproximal and distal neurovascular structures (Fig. 10). Com-pared with the standard bipedicled delay technique used inthe experimental study, we think this pattern (the islandbipedicled delay technique) initiates the delay phenomenonby decreasing blood flow significantly.
Based on our experience related to the sural flap andprevious reports, we progressed to using a combination ofstandard and strategic delay, believing it to have addedadvantages. We thought that the proximal ligation of thelesser saphenous vein during the delay may decrease flap
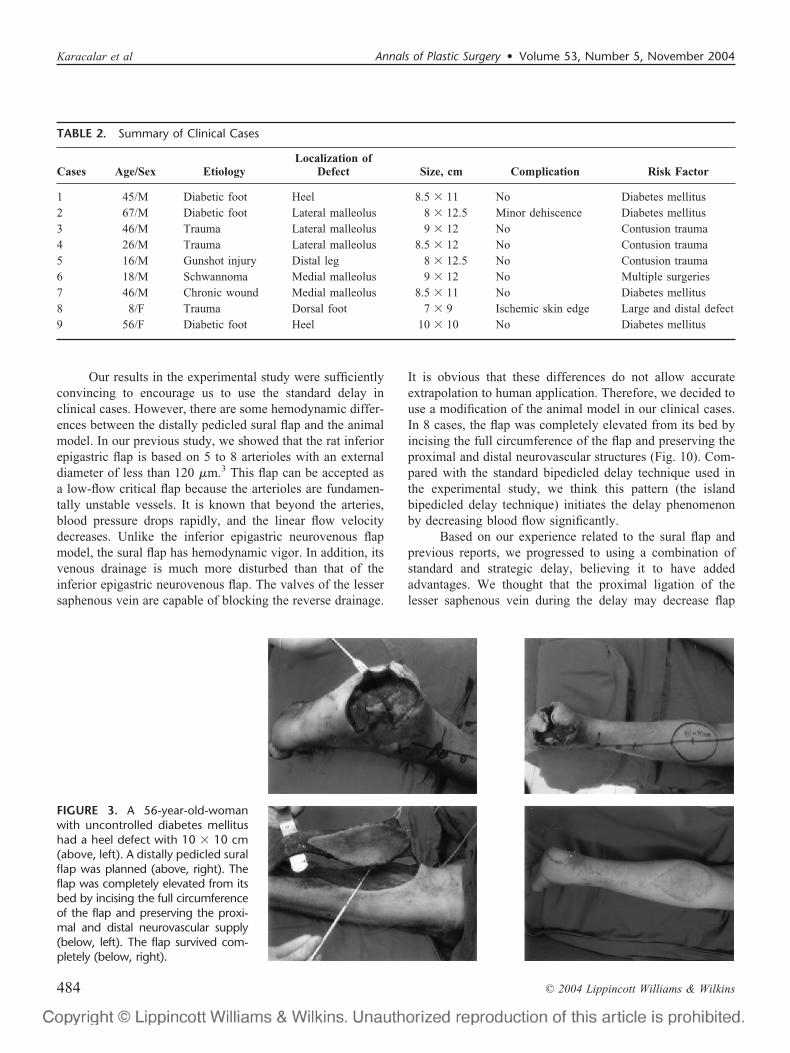
FIGURE 3. A 56-year-old-womanwith uncontrolled diabetes mellitushad a heel defect with 10 � 10 cm(above, left). A distally pedicled suralflap was planned (above, right). Theflap was completely elevated from itsbed by incising the full circumferenceof the flap and preserving the proxi-mal and distal neurovascular supply(below, left). The flap survived com-pletely (below, right).
TABLE 2. Summary of Clinical Cases
Cases Age/Sex EtiologyLocalization of
Defect Size, cm Complication Risk Factor
1 45/M Diabetic foot Heel 8.5 � 11 No Diabetes mellitus2 67/M Diabetic foot Lateral malleolus 8 � 12.5 Minor dehiscence Diabetes mellitus3 46/M Trauma Lateral malleolus 9 � 12 No Contusion trauma4 26/M Trauma Lateral malleolus 8.5 � 12 No Contusion trauma5 16/M Gunshot injury Distal leg 8 � 12.5 No Contusion trauma6 18/M Schwannoma Medial malleolus 9 � 12 No Multiple surgeries7 46/M Chronic wound Medial malleolus 8.5 � 11 No Diabetes mellitus8 8/F Trauma Dorsal foot 7 � 9 Ischemic skin edge Large and distal defect9 56/F Diabetic foot Heel 10 � 10 No Diabetes mellitus
Karacalar et al Annals of Plastic Surgery • Volume 53, Number 5, November 2004
© 2004 Lippincott Williams & Wilkins484
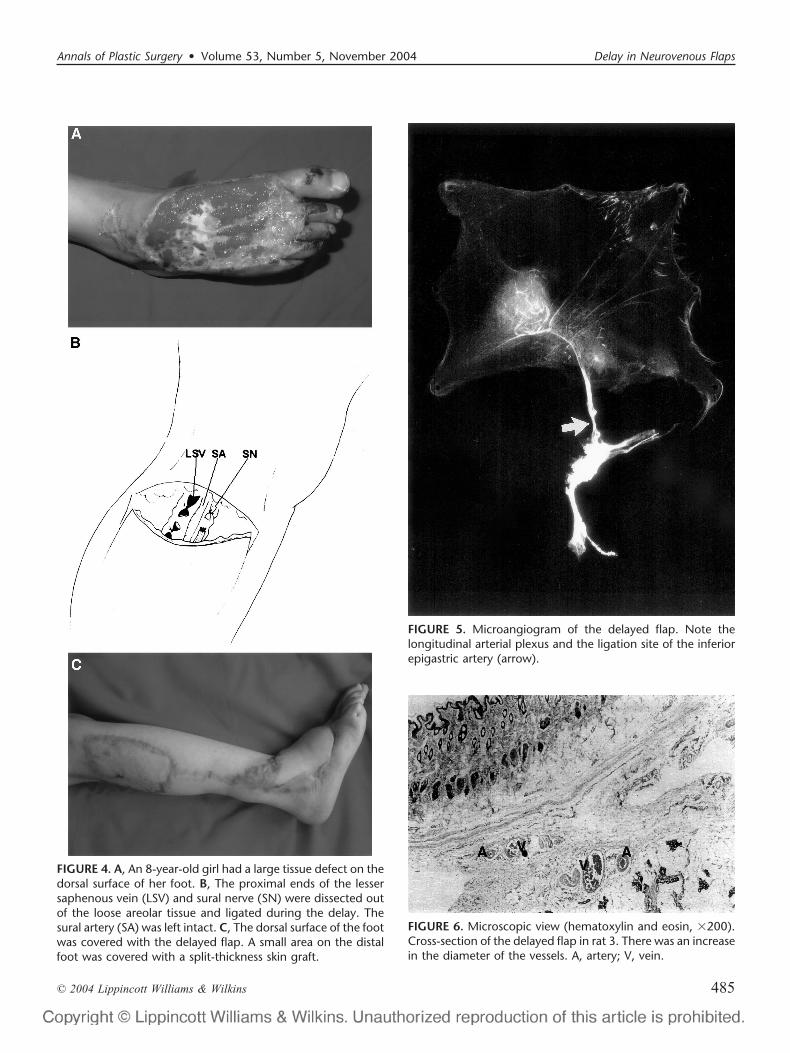
FIGURE 4. A, An 8-year-old girl had a large tissue defect on thedorsal surface of her foot. B, The proximal ends of the lessersaphenous vein (LSV) and sural nerve (SN) were dissected outof the loose areolar tissue and ligated during the delay. Thesural artery (SA) was left intact. C, The dorsal surface of the footwas covered with the delayed flap. A small area on the distalfoot was covered with a split-thickness skin graft.
FIGURE 5. Microangiogram of the delayed flap. Note thelongitudinal arterial plexus and the ligation site of the inferiorepigastric artery (arrow).
FIGURE 6. Microscopic view (hematoxylin and eosin, �200).Cross-section of the delayed flap in rat 3. There was an increasein the diameter of the vessels. A, artery; V, vein.
Annals of Plastic Surgery • Volume 53, Number 5, November 2004 Delay in Neurovenous Flaps
© 2004 Lippincott Williams & Wilkins 485
edema and congestion by reversing the venous flow. In thestudy by Almeida et al,12 the duplex scan showed that venousdrainage through the lesser saphenous vein was slow, stren-uous, and at a continuous pace during the immediate postop-erative period, tending to become phasic and more physio-logical at a later period. They reported that venous congestionwas the main cause of flap necrosis. It is generally acceptedthat the valves of the lesser saphenous vein may block thereverse flow and lead to partial flap necrosis. Tsuzuki et al13
reported that even mild venous inadequacy reduces flapsurvival when arterial inflow is impaired. We did not observeany swelling or venous congestion in our case. This may beattributed to the strategic delay procedure which prevented
flap edema and congestion by reversing the venous flow.There was no remarkable difference of postoperative progressbetween the 2 groups. However, a side-by-side comparison isnot scientific because strategic delay was performed in only 1patient, while standard delay was performed in 8 patients.Further studies in this field are warranted.
Although the use of a distally pedicled flap has beenwell documented in the literature, little attention has beenpaid to the delay procedures of this flap. Yıldırım et al14
ligated the proximal part of the sural neuroarteriovenouspedicle several days before flap elevation in electrical burns.They have claimed that their delay pattern improved flapsurvival. However, Restifo et al15 found that this type ofdelay may not address complete protection of the contralat-eral zones in a TRAM flap.
In conclusion, the rat inferior epigastric neurovenousflap seems to be a readily available model for studying the
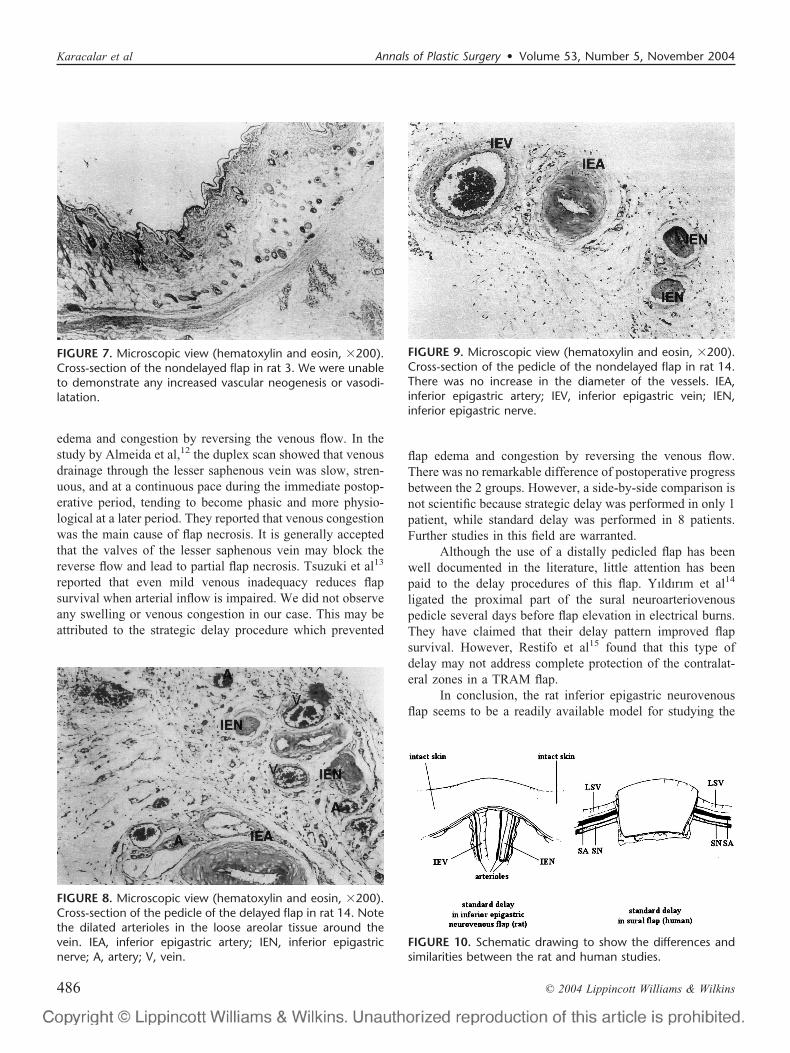
FIGURE 8. Microscopic view (hematoxylin and eosin, �200).Cross-section of the pedicle of the delayed flap in rat 14. Notethe dilated arterioles in the loose areolar tissue around thevein. IEA, inferior epigastric artery; IEN, inferior epigastricnerve; A, artery; V, vein.
FIGURE 10. Schematic drawing to show the differences andsimilarities between the rat and human studies.
FIGURE 7. Microscopic view (hematoxylin and eosin, �200).Cross-section of the nondelayed flap in rat 3. We were unableto demonstrate any increased vascular neogenesis or vasodi-latation.
FIGURE 9. Microscopic view (hematoxylin and eosin, �200).Cross-section of the pedicle of the nondelayed flap in rat 14.There was no increase in the diameter of the vessels. IEA,inferior epigastric artery; IEV, inferior epigastric vein; IEN,inferior epigastric nerve.
Karacalar et al Annals of Plastic Surgery • Volume 53, Number 5, November 2004
© 2004 Lippincott Williams & Wilkins486

effects of delay phenomenon. The standard bipedicled delaytechnique increases the percentage survival of the inferiorepigastric neurovenous flap. While the mechanism of actionis speculative, there is strong evidence to support the conceptthat the delay procedure enhances the perfusion of the flap bydilating the arterial network. The island bipedicled delaytechnique has been successful in our patients with high riskfactors.
REFERENCES1. Baumeister SP, Spierer R, Erdmann D, et al. A realistic complication
analysis of 70 sural artery flaps in a multimorbid patient group. PlastReconstr Surg. 2003;112:129–140.
2. Karacalar A, Idil O, Kahveci Z, et al. The neurovenous (or adiponeu-rovenous) epigastric flap in the rat. Eur J Plast Surg. 2000;23:283–288.
3. Karacalar A, Ozturk H, Ozcan M. Effect of surgical denervation on theviability of inferior epigastric neurovenous flaps in the rat. Ann PlastSurg. 2000;45:298–304.
4. Hendel PM, Lilien DL, Buncke HJ. A study of the pharmacologiccontrol of blood flow to delayed skin flaps using xenon washout, part II.Plast Reconstr Surg. 1983;71:399–407.
5. Pang CY, Forest CR, Neligan PC. Augmentation of blood flow indelayed random skin flaps in the pig: effect of length of delay period andangiogenesis. Plast Reconstr Surg. 1986;78:68–74.
6. Johnson K, Hunt TK, Brennan SS, et al. Tissue oxygen measurements indelayed skin flaps: a reconsideration of the mechanisms of the delayphenomenon. Plast Reconstr Surg. 1988;82:328–336.
7. Callegari PR, Taylor GI, Caddy CM, Minabe T. An anatomic review ofthe delay phenomenon, I: experimental studies. Plast Reconstr Surg.1992;89:397–407.
8. Garcia PB, Nieto CS, Ortega JMR. Morphological changes in thevascularisation of delayed flaps in rabbits. Br J Plast Surg. 1991;44:285–290.
9. Jurell G, Hjemdahl P, Fredholm BB. On the mechanism by whichantiadrenergic drugs increase survival of critical skin flaps. Plast Re-constr Surg. 1993;72:518–523.
10. Palmer B. Sympathetic denervation and reinnervation of cutaneousblood vessels following surgery. Scand J Plast Reconstr Surg. 1970;4:93–99.
11. Pearl RM. A unifying theory of the delay phenomenon: recovery fromthe hyperadrenergic state. Ann Plast Surg. 1981;7:102–112.
12. Almeida MF, Costa PR, Okawa RY. Reverse-flow island sural flap.Plast Reconstr Surg. 2002;109:583–591.
13. Tsuzuki K, Yanai A, Tange I, et al. The influence of congestion andischemia on survival of an experimental vascular pedicle island flap.Plast Reconstr Surg. 1990;84:789–793.
14. Yıldırım S, Akan M, Gideroglu K, et al. Distally-based neurofasciocu-taneous flaps in electrical burns. Burns. 2002;28:379–385.
15. Restifo JR, Ward BA, Scoutt LM, et al. Timing, magnitude, and utilityof surgical delay in the TRAM flap, II: clinical studies. Plast ReconstrSurg. 1997;99:1217–1223.
Annals of Plastic Surgery • Volume 53, Number 5, November 2004 Delay in Neurovenous Flaps
© 2004 Lippincott Williams & Wilkins 487