
December 24, 1881, Vol. 33, No. 861 - FRASER - St. Louis Fed
Upload
khangminh22Category
view
2download
0
December 2020
Volume: 24 Issue: 4
ISSN 1301-2193
JOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND METABOLISM OF TURKEY

COPYRI GHT HOLDER / YAYI N SAHİBİNİN ADI
Society of Endocrinology and Metabolism of Turkey / Türkiye Endokrinoloj i ve Metabolizm a Derneği adına
L. Füsun Saygılı, MD
MANAGI NG CLERI CAL DI RECTOR / SORUMLU YAZI İŞLERİ MÜDÜRÜ
Nilgün Başkal, MD
ADRESS FOR MANAGEMENT / YAYI N İDARE MERKEZİ The Society of Endocrinology and Metabolism of Turkey
Meşrut iyet Caddesi No: 29/ 12 Kızılay, Ankara, TURKEY
Phone / Tel: + 90 312 425 20 72
Fax / Faks: + 90 312 425 20 98
web: www.turkjem .org
E-m ail / E-posta: president@tem d.org.t r
PUBLI CATI ON TYPE AND PERI ODS / YAYI NI N TÜRÜ VE PERİYODU
Turkish Journal of Endocrinology and Metabolism is published 4 ( March, June, Septem ber and Decem ber) t im es a year.
Local perid publicat ion.
Turkish Journal of Endocrinology and Metabolism 3 ayda bir olmak üzere yılda 4 sayı (Mart , Haziran, Eylül ve Aralık) yayınlanır.
Yaygın/ Süreli.
The Turkish Journal of Endocrinology and Metabolism is indexed in Em erging Sources of Citat ion I ndex ( ESCI ) ,
Brit ish Library, CI NAHL, Directory of Open Access Journals ( DOAJ) , EBSCO, EMBASE, I ndex Copernicus, SCOPUS,
ProQuest , TÜBİTAK / ULAKBİM TR I ndex, TürkMedline, Türkiye Citat ion I ndex.
For requests concerning subscript ion inform at ion and advert ising, please contact the Publisher:
Publishing House- Publisher / Basıldığı Yer-Basım cı-Yayım cı
Ortadoğu Reklam Tanıt ım Yayıncılık Turizm Eğit im İnşaat Sanayi ve Ticaret A.Ş. (Türkiye Klinikler i)
Address: Nasuh Akar Mah. Türkocağı Cad. No: 30 Balgat - Ankara Turkey
Phone / Tel: + 90 312 286 56 56
Fax / Faks: + 90 312 220 04 70
E-m ail / E-posta: info@turkiyeklinikler i.com
Web page: www.turkiyeklinikler i.com
The services of “Art icle Tracking ( Autom at ion) ”, “Layout”, “W eb Site Design- Operat ion” and “e- Mailing” are provided
by Türkiye Klinik ler i.
Bu derginin “Makale Takip (Otom asyon) ”, “Mizanpaj ”, “Web Sitesi Tasarım -İlet işim ” ve “Toplu e-Posta” hizm et ler i Türkiye Klinikler i
tarafından sağlanm aktadır.
Publicat ion Date: 10.12.2020
I SSN: 1301-2193
E-I SSN: 1308-9846
December / Aralık 2020 Vol / Cilt: 24 No / Sayı: 4
Türkiye Klinikleri
JOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND METABOLISM OF TURKEY

Ow ner on Behalf of the Society of
Endocrinology and Metabolism of Turkey
L. Füsun Saygılı, Ege University Faculty of Medicine, İzm ir, Türkiye Editor- I n- Chief Nilgün Başkal, Ankara University Faculty of Medicine Retired Lecturer, Ankara, Turkey Deputy Editor
Murat Faik Erdoğan, Ankara University Faculty of Medicine, Ankara, Turkey Associate Editors Hasan Ali Altunbaş, Akdeniz University Faculty of Medicine, Antalya, Turkey Dilek Gogas Yavuz, Marmara University Faculty of Medicine, İstanbul, Turkey Neslihan Başçıl Tütüncü, Başkent University Faculty of Medicine, Ankara, Turkey
Stat ist ical Consultant At illa Halil Elhan, Ankara, Turkey Levent Dönm ez, Antalya, Turkey Derya Öztuna, Ankara, Turkey Can Ateş, Van, Turkey Language Editor Jennifer Gabriel, California, USA
Honorary Board Sem a Akalın, Marm ara University Faculty of Medicine Ret ired Lecturer, İstanbul, Turkey
Met in Arslan, Gazi University Faculty of Medicine Ret ired Lecturer, Ankara, Turkey
Gürbüz Erdoğan, Ufuk University Faculty of Medicine, Ankara, Turkey
Olcay Gedik, Hacet tepe University Faculty of Medicine Ret ired Lecturer, Ankara, Turkey
Sadi Güngoğdu, I stanbul University Cerrahpaşa Faculty of Medicine Ret ired Lecturer, İstanbul, Turkey
Hüsrev Hatem i, İstanbul, Turkey
Şazi İm am oğlu, Uludağ University Faculty of Medicine Ret ired Lecturer, Bursa, Turkey
Senay Molvalılar, İstanbul, Turkey
Candeğer Yılm az, Ege University Faculty of Medicine Ret ired Lecturer, İzm ir, Turkey
Editor ia l Board Ersin Akarsu, Gaziantep University Faculty of Medicine, Gaziantep, Turkey
Müjde Aktürk, Gazi University Faculty of Medicine, Ankara, Turkey
Faruk Alagöl, Koç University Faculty of Medicine, İstanbul, Turkey
Maria Alevizaki, Athens University School of Medicine,Athens, Greece
İnan Anaforoğlu, Medical Park I nternat ional Trabzon Hospital, Trabzon, Turkey
Yalçın Aral, Bozok University I nst itute of Health Sciences, Yozgat , Turkey
Ayşegül Atm aca, Ondokuz Mayıs University Faculty of Medicine, Sam sun, Turkey
Göksun Ayvaz, Liv Hospital, Ankara, Turkey
Öm er Azal, Gulhane Educat ion and Research Hospital, Ankara, Turkey
Mustafa Kem al Balcı, Akdeniz University Faculty of Medicine, Antalya, Turkey
J Paul Banga, University of Duisburg-Essen Faculty of Medicine, Germ any
David Baylink, Lom a Linda University, California, USA
Fahri Bayram , Erciyes University Faculty of Medicine, Kayseri, Turkey
Jens Bollerslev, Oslo University Hospital, Norway
Erol Bolu, Mem orial Atasehir Hospital, İstanbul, Turkey
Steen Joop Bonnem a, Odense University Hospital, Denm ark
Bekir Çakır, Yıldır ım Beyazıt University Faculty of Medicine, Ankara, Turkey
Mehtap Çakır, Kent Hospital, İzm ir, Turkey
Berr in Çet inarslan, Kocaeli University Faculty of Medicine, Kocaeli, Turkey
Ahm et Çorakçı, Ufuk University Faculty of Medicine, Ankara, Turkey
Abdurrahm an Çöm lekci, Dokuz Eylül University Faculty of Medicine, İzm ir, Turkey
Selçuk Dağdelen, Hacet tepe University Faculty of Medicine, Ankara, Turkey
Hatice Sebila Dökmetaş, Istanbul Medipol University Faculty of Medicine, İstanbul, Turkey
Leonidas H Duntas, Evgenideion Hospital, University of Athens, Greece
Belgin Efe, Eskişehir Osm angazi University Faculty of Medicine, Eskişehir, Turkey
Sevinç Eraslan, Dokuz Eylul University Faculty of Medicine, İzm ir, Turkey
Tom ris Erbaş, Hacet tepe University Faculty of Medicine, Ankara, Turkey
Mehm et Erdoğan, Ege University Faculty of Medicine İzm ir, Turkey
Eda Ertörer, Başkent University Adana Dr. Turgut Noyan Hospital, Adana, Turkey
John W. Funder, Monash University, Victor ia, Aust ralia
Hossein Gharib, Mayo Clinic, Minnesota, USA
Sait Gönen, İstanbul University Cerrahpaşa Faculty of Medicine, İstanbul, Turkey
Nilgün Güvener, Okan University Faculty of Medicine, İstanbul, Turkey
Serdar Güler, Liv Hospital, Ankara, Turkey
Sevim Güllü,Ankara University Faculty of Medicine, Ankara, Turkey
Zeliha Hekim soy, Celal Bayar University Faculty of Medicine, Manisa, Turkey
Larry Jameson, Perelman School of Medicine Univ. Of Pennsylvania, Philadelphia, USA
Pınar Kadıoğlu, İstanbul University Cerrahpasa Faculty of Medicine, İstanbul, Turkey
Ahm et Kaya, Selcuk University Meram Faculty of Medicine, Konya, Turkey
Fahret t in Keleşt im ur, Health I nst itutes of Turkey, Ankara, Turkey
Mustafa Kut lu, Gulhane Educat ion and Research Hospital, Ankara, Turkey
Pierre J. Lefebvre, University of Liege Faculty of Medicine, Liege, Belgium
Connie Newm an, NYU School of Medicine, New York, USA
Tae Sun Park,Chonbuk Nat ional University Medical School, Jeonju, Korea
Andreas F. H. Pfeiffer, Charité Universitaetsm edizin Berlin, Germ any
Gilles Russ, Pr Leenhardt La Pit ie Salpet r iere Hospital, France
İlhan Satm an, İstanbul University İstanbul Faculty of Medicine, İstanbul, Turkey
Füsun Saygılı, Ege University Faculty of Medicine, İzm ir, Turkey
Alper Sönm ez, Gulhane Educat ion and Research Hospital, Ankara, Turkey
Tüm ay Sözen, Hacet tepe University Faculty of Medicine, Ankara, Turkey
İbrahim Şahin, İnönü University Faculty of Medicine, Malatya, Turkey
Mustafa Şahin, Ankara University Faculty of Medicine, Ankara, Turkey
Refik Tanakol, İstanbul University İstanbul Faculty of Medicine, İstanbul, Turkey
Ali Rıza Uysal, Ankara University Faculty of Medicine, Ankara, Turkey
Kürşad Ünlühızarcı, Erciyes University Faculty of Medicine, Kayseri, Turkey
Ayşe Kubat Üzüm , İstanbul University İstanbul Faculty of Medicine, İstanbul, Turkey
I r fan Vardarli, Ruhr-University, Bochum , Germ any
Anthony Weetm an, The University of Sheffield, Sheffield, UK
Sem a Yarm an, İstanbul University İstanbul Faculty of Medicine, İstanbul, Turkey
Bülent Okan Yıldız, Hacet tepe University Faculty of Medicine, Ankara, Turkey
JOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND METABOLISM OF TURKEY

AI MS AND SCOPE
Turk ish Journa l of Endocr inology and Metabolism
( Turk J Endocrinol Metab) is the peer- reviewed per iodical
on clinical and exper im ental endocr inology and m etabolism
diseases and related fields. I t is the official j ournal of the So-
ciety of Endocr inology and Metabolism of Turkey and is pub-
lished quarter ly (March, June, Septem ber and Decem ber) as
hardcopy and an elect ronic j ournal at www.turkjem .org. The
m anuscr ipts are published in English.
The journal publishes or iginal research papers, reviews and
case reports which pr im arily focus on clinical endocr inology.
The journal's aim is to be essent ial for both endocr inologists
and clinical pract it ioners. Open Access Policy Turkish Journal of Endocrinology and Metabolism is an open
access journal under the Creat ive Commons 4.0 I nternat ional
Licence (CC BY-NC-SA 4.0) . This journal provides im m ediate
open access to its content on the pr inciple that m aking rese-
arch freely available to the public supports a greater global
exchange of knowledge. The journal does not dem and sub-
m ission and art icle processing charge (APC) from authors.
Open Access Policy is based on rules of Budapest Open Ac-
cess I nit iat ive (BOAI ) [ Link]
I nst ruct ions for online m anuscript subm ission, current issues
and archives of the journal can be found at www.turkjem.org.
Please do not send m anuscr ipts to the editor ial off ice. For
other related issues you m ay contact the editor ial office. Subscript ion inform at ion Turkish Journal of Endocrinology and Metabolism is dist r ibu-
ted free of charge to all endocrinology academ icians and ins-
t ructors serving in our count ry. Access to full- text art icles of
all issues of the j ournal is free at the j ournal’s website www.turkjem .org I nst ruct ions for authors I nst ruct ions for authors are published in the j ournal pages
and can be accessed at t he web sit e of t he j ournal
www.turkjem .org
Materia l Disclaim er Statem ents or opinions expressed in the m anuscripts publis-
hed in Turkish Journal of Endocrinology and Metabolism ref-
lect the views of the author(s) and are not the opinions of the
editors, the editorial board and the publisher. The editors, edi-
tor ial board and the publisher disclaim any responsibilit y or
liabilit y for such m aterials. Advert ising Policy Turk ish Journal of Endocr inology and Metabolism re-ceives advert ising support for its pr int and elect ronic edit ions and m aintains editor ial integrity through policies that define the Editor ial/ Advert iser relat ionship: ■ Pr int and elect ronic advert ising does not influence editor ial decisions, and advert ising is not an endorsem ent by the Pub-lisher, Editor, or the Editor ial Board. ■ Turk J Endocrinol Metab reserves the r ight to refuse any advert ising for any reason preserving the condit ions consis-tent with the journal’s high standards of healthcare editor ial. ■ Editors have full and final authority for approving print and elect-ronic advertisements and for enforcing the advertising policy. ■ Pr int advert isem ents are interspersed throughout the jour-nal but do not interrupt the flow art icles. The journal website contains online banner advert ising. ■ To avoid implied endorsement by the Journal, the art icle, or the authors of the art icle; advert isements are not adjacent to art icles addressing the product or its disease state. ■ The Publisher reserves the right to print the word “Advert ise-ment” on any advert isement where it may not be clear, so rea-ders can dist inguish readily between advert ising and editorial. I t is the responsibilit y of the advert iser and it s agencies to adhere to appropriate legal requirem ents and regulat ions. For all advert ising inform at ion, please contact reklam @turkiyeklinikler i.com The journal is pr inted on acid- free paper.
All r ights are reserved. Rights to the use and reproduct ion, including in the elect ronic m edia, of all com m unicat ions, papers, photographs and illust rat ions appea-
r ing in this journal belong to the Turkish Journal of Endocrinology and Metabolism . Reproduct ion without pr ior writ ten perm ission of part or all of any m aterial is
forbidden. The journal com plies with the Professional Principles of the Press.
The paper used the pr int this journal conform s to I SO 9706: 1994 standard (Requirem ents for Perm anence) . The Nat ional Library of m edicine suggests that bio-
m edical publicat ions be pr inted on acid free paper (alkaline paper) .
Reviewing the art icles’ conform ity to the publishing standards of the Journal, typeset t ing, reviewing and edit ing and edit ing the m anuscripts and abst racts in En-
glish and publishing process are realized by Türkiye Klinikler i.
JOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND METABOLISM OF TURKEY
I N STRUCTI ON S FOR AUTH ORS Turkish Journal of Endocrinology and Metabolism (Turk J Endocrinol Metab) is-sues papers on all aspects of endocr inology. The journal is the scient if ic pub-lishing organ of the Society of Endocr inology and Metabolism of Turkey and has been published quarter ly (March, June, Septem ber and Decem ber) since 1997. I n addit ion to or iginal art icles, case reports, review art icles, let ters to the editor, educat ional art icles, sect ions of quest ion and answers, abst racts from lit erature and announcem ents of congresses/ m eet ings are also pub-lished. Turkish Language I nst itut ion dict ionary and orthography guide should be taken as basic for literary. The idiom s used should be checked.The scien-t if ic and ethical liabilit y of the m anuscr ipts belongs to the authors and the copyr ight of the m anuscr ipts belongs to the Turkish Journal of Endocr inology and Metabolism . The authors should subm it t he signed copyr ight t ransfer form together with their m anuscr ipts. Authors are responsible for the con-tents of the m anuscr ipt and accuracy of the references.The authors should guarantee that their m anuscr ipts has not been published and/ or is not under considerat ion for publicat ion in any other per iodical. This requirem ent does not apply to papers presented in scient if ic m eet ings and whose sum m aries, not exceeding 250 words, are published. I n this case, however, the nam e, date and place of the m eet ing in which the paper was presented should be stated. The signed statem ent of scient if ic cont r ibut ions and responsibilit ies of all authors is required.
Turkish Journal of Endocrinology and Metabolism does not charge any art icle subm ission or processing charges.
Peer- review Editor ial policies of the journal are conducted according to the rules advised by Council of Science Editors and reflected in the Uniform Requirem ents for Manuscripts Submit ted to Biomedical Journals: Writ ing and Edit ing for Biomed-ical Publicat ion (ht tp: / / www.icm je.org/ ) .
Subm it ted m anuscripts are subjected for double-blind peer- review. The sci-ent ific board guiding the select ion of the papers to be published in the Jour-nal consists of elected experts of the Journal and if necessary, selected from nat ional and internat ional experts in the relevant f ield of research. All m anuscripts are reviewed by the editor, sect ion associate editors and at least three internal and external expert referees. All research art icles undergo re-view by stat ist ical editor as well.
Submitted manuscripts are also subjected for the evaluation of plagiarism, dupli-cate publication by automatic software. Authors are obliged to acknowledge if they published study results in full or in part in form of abstracts.
The authors of the accepted m anuscripts should be in consent that the editor and associate editors could m ake correct ions without changing the m ain text of the paper.Manuscr ipt form at should be in accordance with Uniform Re-quirem ents for Manuscr ipts Subm it ted to Biom edical Journals: Writ ing and Edit ing for Biom edical Publicat ion (ht tp: / / www.icm je.org/ ) .
For details: ht tp: / / www.turkjem .org/ pages/ peer- review-ethic-5
General Guidelines Manuscr ipts can only be subm it ted elect ronically through the web site (ht tp: / / www.turkjem.org) after creat ing an account . This system allows online submission and peer- review.The manuscripts are archived according to ICMJE-www.icm je.org, I ndex Medicus (Medline/ PubMed) and Ulakbim -Turkish Medicine I ndex Rules. Rejected manuscripts, except artwork are not returned.
For the experimental, clinical and drug human studies, approval by ethical com-mit tee and statement on the adherence of the study protocol to the internat ional agreements (Helsinki Declarat ion revised 2013 (https: / / www.wma.net/ wp-con-tent/ uploads/ 2016/ 11/ DoH-Oct2013-JAMA.pdf) are required. In experimental an-imal studies, the authors should indicate that the procedures followed were in accordance with animal rights (Guide for the care and use of laboratory animals,
https: / / www.nap.edu/ read/ 12910/ chapter/ 1) and they should obtain animal ethic com m it tee approval. The Ethic Com m it tee approval docum ent should be sub-m it ted to the Turkish Journal of Endocrinology and Metabolism together with the m anuscript .
The approval of the ethic committee, statement on the adherence to international guidelines mentioned above and that the pat ients` informed consent is obtained should be indicated in the ` Material and Method` sect ion and is required for case reports whenever data/ media used could reveal ident ity of the pat ient. The dec-larat ion of the conflict of interest between authors, inst itut ions, acknowledge-ment of any financial or material support, aid is mandatory for authors submitt ing manuscript and the statement should appear at the end of manuscript . Review-ers are required to report if any potent ial conflict of interest exists between re-viewer and authors, inst itut ions.
Original Art icles Clinical research should comprise clinical observat ion, new techniques or labo-ratory studies. Provided that these manuscripts are writ ten with lower-case let-ters, they should include the t it le in Turkish/ English, the background and the key words in Turkish/ English, introduct ion, materials and methods, results ( findings), discussion, references, tables, charts, pictures and they should be writ ten in ac-cordance with Journal Agent rules. They should not exceed sixteen (A4) pages.
I t is recommended to present research art icles and meta-analysis/ systematic re-views art icle according to the guidelines on specific design of the study: random-ized studies (CONSORT), observational studies (STROBE), studies on diagnostic accuracy (STARD), meta- analysis and systematic review (PRISMA, MOOSE) and other study designs (www.equator-network.org).
Author I nform at ion The nam e and the surnam e of the authors should be writ ten without abbrevi-at ion. The academ ic t it les, the affiliat ions and the addresses of these affilia-t ions should be clearly declared. Furtherm ore, the contact inform at ion of the corresponding author should be entered to the system . Since e-m ail will be used prim arily for the contact with the authors, the e-m ail of the correspond-ing author should be indicated. I n addit ion the phone and the fax num bers should be also indicated.
Tit le Page This page should include the t it les of the manuscript , key words and running t i-t les. I n Turkish manuscripts the t it le in English should also take place. Likely, Turkish t it le should be ment ioned for art icles in foreign language. I f the content of the paper has been previously presented or its abstract has been published, an explanat ion should be made in this page about this issue. I f there are any grants and other financial supports by any inst itut ions or firms for the study, in-format ion must be provided by the authors.
Abstract Turkish and English sum m aries of the m anuscript should take place in a m an-ner that it will not exceed 250 words. The keywords should be writ ten at the end of the sum m ary. The references should not be cited in the sum m ary sec-t ion. As far as possible, use of abbreviat ions is to be avoided. I f any abbrevi-at ions are used, they m ust be taken into considerat ion independent ly of the abbreviat ions used in the text . The sum m ary should be writ ten with four run-ning t it les.
Purpose: The goal of the study should be clearly stated.
Materia l and Method: The study should be defined, the standard cr iter ia; it should be also indicated whether the study is random ized or not , whether it is ret rospect ive or prospect ive, the stat ist ical method, if any, should be indicated.
Results ( Findings) : The detailed result of the study should be given and the stat ist ical significance level should be indicated.
JOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND METABOLISM OF TURKEY
I N STRUCTI ON S FOR AUTH ORS Discussion: I t should reflect the results of the study, the favorable and un-favorable aspects should be declared.
Key w ords: At least three and maximum eight key words. ( in English and in Turkish) Do not use abbreviat ions in the key words. Turkish key words will be provided by the editorial office for the authors who are not Turkish speakers. I f you are not a native Turkish speaker, please re-enter your English keywords to the area provided for the Turkish keywords. English key words should be provided from Medical Subject Headings (ht tp: / / www.nlm.nih.gov/ mesh/ ) while Turkish key words should be provided from http: / / www.bilimterim leri.com.
Original researches should have the following sect ions;
I nt roduct ion Brief explanat ion about the topic should be done, the object ive of the study should be indicated and these should be supported by the literature inform a-t ion.
Materia ls and Methods The study design should be described, it should be indicated whether it is intervent ional randomized or observat ional, whether it is ret rospect ive or prospect ive, the number of t r ials, the characterist ics, studied variables and spe-cific methods, the used stat ist ical methods should be indicated. I f any, it should be indicated that the results should be scrut inized.
Results ( Findings) The results should be given, the tables and the pictures should be given in num erical order and, the results should be indicated as % and/ or p-values.
Discussion The obtained values should be discussed with its favorable and unfavorable as-pects and, they should be com pared with literature.
Study Lim itat ions: Study Lim itat ions and st rengths, and direct ions for fur-ther research or im plicat ion m ust be discussed.
Conclusion: The conclusion of the study should be highlighted.
Authors cont r ibut ions, Declarat ion of conflict of interest and Acknowledge-m ents should appear at the end of the m ain text of m anuscript .
References Accuracy of reference data is t he author ’s responsibilit y. References should be num bered according to the consecut ive cit at ion in t he text . References should be indicated by parenthesis in the text . I f t here is Turk ish Reference, at tent ion should be paid to indicate this. Journal t it les should be abbreviated according to the st y le used in the I ndex Medicus. All t he references, books, papers and sim ilar ar t icles should be cit ed as references should be wr it t en according to the rules of t he I nternat ional Com m it tee of Medical Journal Ed-it ors Uniform Requirem ents for Manuscr ipt s Subm it ted to Biom edical Jour-nals ( ht tp: / / www.nlm .nih.gov/ bsd/ uniform _requirem ents.htm l) .
Journal: The surnam es of the authors and the init ial of authors’ nam es, the t it le of the paper, the t it le of the journal ( the original abbreviat ion stated in the journal) , year, volum e and the page num bers.
Exam ple: Collin JR, Rathbun JE. I nvolut ional ent ropion: a review with evalu-at ion of a procedure. Arch Ophthalm ol. 1978; 96: 1058-1064.
Book w it h a Single Aut hor : The surnam e and t he in it ial of t he author, t he t it le, chapt er and sect ion, t he nam e of t he edit or, t it le of t he book , place of publicat ion, nam e of t he pr int ing house, year of pr int , page num -bers.
Exam ple: Herbert L. Conjunct ivit is, kerat it is and infect ions of periorbital st ruc-tures. I n: Arm st rong D, Cohen J, eds. The I nfect ious Diseases (1st ed) . Philadelphia; Mosby Harcourt ; 1999; 11; 1-8.
Book Chapter: The surname and the init ial of the author, chapter and sect ion, nam e of the editor, t it le of the book, place of publicat ion, nam e of the pr int-ing house, year of pr int , page num bers.
Exam ple: O’Brien TP, Green WR. Periocular I nfect ions. I n: Feigin RD, Cherry JD, eds. Textbook of Pediat r ic I nfect ious Diseases (4th ed) . Philadelphia; W.B. Saunders Com pany; 1998: 1273-1278.
Visual Materials ( Tables, Graphics, Figures, and Pictures) : All tables, graphics or figures should be enumerated according to the sequence within the text and a brief descript ive capt ion should be writ ten. The abbreviat ions used should be definitely explained in the figure’s legend. Especially, the text of tables should be easily understandable and should not repeat the data of the main text. I llustrat ions that already published are acceptable if supplied by permission of authors for publicat ion. The details of the pictures should be dist inguishable and they should be recorded in JPEG format and in 500 pixels per inch at least .
Case Reports I t should consist of the t it le, sum m ary, key words, sum m ary in English, key-words, int roduct ion, case report , discussion and references, the case or the cases should be worth to be presented, it should cont r ibute to literature, and all of them should not exceed 5 papers in (A4) sizes.
Review I t should include new topics, the own experiences of the author, if possible, and the references also. I t should consist of the t it le in Turkish, the summary, the key-words, the t it le in English, the summary in English and the keywords in English.
Let ters to the Editor They should be assays in the “ review” m anner in various topics or the assays concerning the art icles published in the Turkish Journal of Endocrinology and Metabolism with the cont r ibut ive content or contents as quest ions that do not exceed 200 words.
Scient ific Let ters The m anuscripts should be error- free in the sum m aries com piled from the ar-t icles in other journals, the author names (surname, name) should be writ ten, the journal t it le should be writ ten with its original abbreviat ion, its year should be indicated and, the nam e and he surnam e of the t ranslator should be indi-cated under the m anuscript . Correspondence
All correspondences can be done to the following postal address or to the fol-lowing e-m ail address, where the journal editor ial resides:
Address: Ankara University Faculty of Medicine, Departm ent of Endocrinology and Metabolism , Ankara, Turkey
Phone: + 90 312 508 21 00
Fax: + 90 312 309 45 05
E-m ail: nilgun.baskal@tem d.org.t r
“This journal licenced under the term s of the Creat ive Com m ons 4.0 I nterna-t ional Licence (CC BY-NC-SA 4.0) ”
JOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND METABOLISM OF TURKEY

CONTENTS
Original Art icles 2 5 3 Demographic and Clinical Features of Medullary Thyroid Carcinoma
Medüller Tiroid Karsinomunun Demografik ve Klinik Özellikleri
Pınar Şişm an, Buket Biçer, Hikm et Öztop, Soner Cander, Özen Öz Gül,
Gökhan Ocakoğlu, Canan Ersoy, Erdinç Ertürk
2 6 1 The Associat ion Between Thyroid Volum e and I nsulin Resistance
in Pat ients with Non-Funct ional Adrenal I ncidentalom a
Non-Fonksiyonel Adrenal İnsidentalom alı Hastalarda İnsülin Direnci ve Tiroid Volüm ü Arasındaki İlişki
Murat Şahin, Ayten Oğuz, Dilek Tüzün, Sem iha Çalkaya, Kam ile Gül
2 7 0 Frequency of Nodular Goiter in Pat ients with Non-Funct ional Adrenal I ncidentalom a
Non-Fonksiyonel Adrenal I nsidentalom alı Hastalarda Nodüler Guat r Sıklığı
Mustafa Can, Melia Karaköse, Muham m et Kocabaş, İlker Çordan, Hat ice Çalışkan Burgucu,
Mustafa Kulaksızoğlu, Feridun Karakurt
2 7 7 A Slight Cont r ibut ion of Ret roperitoneal Fat Accum ulat ion to the Metabolic Com orbidit ies of Pat ients
with Autonom ous Cort isol Product ion
Ret roperitoneal Yağ Bir ik im inin Otonom Kort izol Üret im i Olan Hastaların
Metabolik Kom orbiditeler ine Hafif Derecede Katkısı
Mustafa M. Barış, Ahm et Peker, Ozan Bozkurt , Mustafa Seçil, Öm er Dem ir, Serkan Yener
2 8 4 Knosp and Hardy Grading System s are Useful in Predict ing Persistence of Male Hypogonadism
in Prolact inom as Following Prolact in Norm alizat ion
Knosp ve Hardy Sınıflamaları, Prolakt inoması Olan Erkek Hastalarda Prolakt in Normalizasyonunu Takiben
Hipogonadizminin Kalıcılığını Öngörmede Yararlıdır
Gülay Şimşek Bağır, Aylin Güneşli, Filiz Ekşi Haydardedeoğlu, Okan Sefa Bakıner,
Özlem Alkan, Melek Eda Ertörer
2 9 3 Role of AGR2 Expression in Specim ens from Pituitary Adenom a Tissue on Tum or Behavior
Hipofiz Adenom Doku Örnekler inde AGR2 Ekspresyonunun Tüm ör Davranışı Üzerine Etkisi
Sem a Çiftçi Doğanşen, Öm ür Günaldı, Ayla Solm az Avcıkurt , Barış Çolluoğlu,
İlhan Yılm az, Meral Mert , Osm an Tanrıverdi
3 0 0 The Effects of Psychological Focus Group Therapy on the Quality of Life of Fem ale Pat ients with Acrom egaly
Kadın Akrom egali Hastalarında Psikoloj ik Focus Grup Terapisinin Hayat Kalitesi Üzerine Etkiler i
Özlem Haliloğlu, Sema Sözer, Özge Polat Korkmaz, Serdar Şahin, Emre Durcan, Gökhan Oral, Pınar Kadıoğlu
December / Aralık 2020 Vol / Cilt: 24 No / Sayı: 4
JOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND METABOLISM OF TURKEY

3 0 8 Clinical Profile and Changing Et iological Spectrum of Hyperprolact inemia at a Tert iary Care Endocrine Facility
Üçüncü Basam ak Bir Endokrin Kuruluşunda Hiperprolakt inem inin Klinik Profili ve
Değişen Et iyoloj ik Spekt rum u
Junaid Rashid Dar, Moom in Hussain Bhat , Javaid Ahm ad Bhat , Raiz Ahm ad Misgar,
Shariq Rashid Masoodi, Mir I ft ikhar Bashir, Arshad I qbal Wani
3 1 4 Cardiovascular Morbidity in Diabet ic Non-Alcoholic Fat ty Liver Disease (NAFLD) Using
NAFLD Fibrosis Score as an Early I ndicator
Erken Bir Gösterge Olarak Non-Alkolik Yağlı Karaciğer Hastalığı (NAYKH) Fibrozis Skoru Kullanılarak
Diyabet ik NAYKH'de Kardiyovasküler Morbidite
Prit i Shahapure, Shim pa Sharm a
3 2 1 Serum Levels of 8-OHdG in Pat ients with Hashim oto’s Thyroidit is
Hashim oto Tiroidit i Olan Hastalarda Serum 8-OHdG Düzeyler i
Fatem eh Esfahanian, Seyedeh Mahdieh Fotouk Kiaie, Roghayeh Ghelich, Zohreh Jadali
3 2 7 Pneum ococcal, I nfluenza, Hepat it is B, and Tetanus Vaccinat ion Rate and Vaccine Awareness
in Pat ients with Type 2 Diabetes
Tip 2 Diyabetli Hastalarda Pnömokok, İnfluenza, Hepatit B, Tetanoz Aşılama Oranları ve Aşı Farkındalığı
Arzu Cennet Işık, Seydahm et Akın, Nazire Aladağ, Ersin Engin Şimşek
Review Art icles 3 3 5 Dealing with COVI D-19: Through Endocrinologist ’s Eyes
Endokrinologların Gözüyle COVI D-19 ile Mücadele
Cem Sulu, Pınar Kadıoğlu
3 4 3 Glucagon-Like Polypept ide-1 and Brain
Glukagon Benzeri Polipept id-1 ve Beyin
Okan Sefa Bakıner, Akadlı Kürşad Özşahin
Case Report 3 5 6 Giant Malignant Pheochrom ocytom a: A Unique Case Report from Turkey
Dev Malign Feokrom ositom a Vakası
Dam la Tüfekçi, Yasem in E. Günay, Ahm et Suat Dem ir, İr fan Nuhoğlu, Hülya Coşkun,
Özge Üçüncü, Mustafa Koçak
JOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND METABOLISM OF TURKEY

EDITORIAL
Dear esteemed readers of TurkJEM Family,
In simple terms the role of the immune system is to protect the body against attacks by foreign invaders. To accomplish such a
task, many cells share specific tasks to identify threats, send alarms and fight viruses, bacteria and other foreign or harmful el-
ements. The Immune system after getting unwanted signals from such threats reacts to these invaders. This happens almost
every day in our bodies, beyond our control. One’s immune system is constantly learning and adapting to harmful elements.
Immune system is a dynamic process, it creates new defenses that are stored for next time, too. The thick gel on the inside of
bones are called marrow. It does a lot of work for your immune system that you may never observe. This is why marrows also
contain many secrets of the immune system. To strengthen the immune system enough vitamin D, calcium, magnesium, and
other trace mineral is needed in our diet. These vitamin and minerals improves your immune system and improves our enduring
power by taking care of our bone system. The risk of COVID-19 infection in patients is due not only to the severity of the viral
infection but also to the host's immune response. This is why diabetes, COVID-19 and patient immune system is strongly inter-
related. According to the WHO more than 425 million individuals have diabetes worldwide and projections show this number
rising to 629 million by 2045. Research shows that the incidence of patients in intensive care having diabetes is twofold higher
compared to that of non-intensive care patients with COVID-19. National Health Service England showed that the risk of COVID-
19 mortality in either Type 1 or Type 2 diabetes is independently associated with the level of hyperglycemia. Effect of COVID-
19 infection on the immune system diabetes may be more susceptible to moderate or severe diseases associated with infection
due to the immune system’s altered with the consequences of diabetes.
All this literature review simply shows that a strong action plan is needed to fight diabetes is not a must solely for COVID-19 but
for the coming virus attacks.
For this issue we have some interesting research in: “Demographic and Clinical Features of Medullary Thyroid Carcinoma”, “The
Association Between Thyroid Volume and Insulin Resistance in Patients with Non-Functional Adrenal Incidentaloma”, “Fre-
quency of Nodular Goiter in Patients with Non-Functional Adrenal Incidentaloma”, “A Slight Contribution of Retroperitoneal Fat
Accumulation to the Metabolic Comorbidities of Patients with Autonomous Cortisol Production”, “Knosp and Hardy Grading
Systems are Useful in Predicting Persistence of Male Hypogonadism in Prolactinomas Following Prolactin Normalization”, “Role
of AGR2 Expression in Specimens from Pituitary Adenoma Tissue on Tumor Behavior”, “The Effects of Psychological Focus Group
Therapy on the Quality of Life of Female Patients with Acromegaly”, “Clinical Profile and Changing Etiological Spectrum of
Hyperprolactinemia at a Tertiary Care Endocrine Facility”, “Cardiovascular Morbidity in Diabetic Non-Alcoholic Fatty Liver Disease
(NAFLD) Using NAFLD Fibrosis Score as an Early Indicator”, “Serum Levels of 8-OHdG in Patients with Hashimoto’s Thyroiditis”,
“Pneumococcal, Influenza, Hepatitis B, and Tetanus Vaccination Rate and Vaccine Awareness in Patients with Type 2 Diabe-
tes”, “Dealing with COVID-19: Through Endocrinologist’s Eyes”, “Glucagon-Like Polypeptide-1 and Brain” and “Giant Malignant
Pheochromocytoma: A Unique Case Report from Turkey”.
Wish you a very healthy and pleasant Holiday Season. Please take care of yourselves and your patients.
With my best regards,
Nilgün Başkal MD
Editor-in-Chief
JOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND METABOLISM OF TURKEY
Dem ographic and Clinical Features of Medullary Thyroid Carcinom a
Medüller Tiroid Karsinom unun Dem ografik ve Klinik Özellik ler i
Pınar ŞİŞMAN, Buket BİÇER* , Hikm et ÖZTOP* , Soner CANDER* * , Özen ÖZ GÜL* * ,
Gökhan OCAKOĞLU* * * , Canan ERSOY* * , Erdinç ERTÜRK* *
Clinic of Endocrinology and Metabolism, Medicana Hospital, Bursa, TURKEY * Department of I nternal Medicine, Uludağ University Faculty of Medicine, Bursa, TURKEY
* * Department of Endocrinology and Metabolism, Uludağ University Faculty of Medicine, Bursa, TURKEY * * * Department of Biostat ist ics, Uludağ University Faculty of Medicine, Bursa, TURKEY
Original Art icle Turk J Endocrinol Metab. 2020; 24: 253-260
Object ive: Medullary thyroid carcinom a (MTC) is an agg-ressive neuroendocrine tum or affect ing the parafollicular C cells of the thyroid gland. This study aim edto analyze de-m ographic and clinical factors that m ight affect the progno-sis of MTC andevaluate the long- term outcom es of surgery in MTC pat ients at a single center. Materia l and Methods: A total of 36 pat ients with a confirm ed MTC diagnosis based on histopathological exam inat ion and underwent surgery-during 2000–2015 were exam ined. Archived files of these pat ients were reviewed, and data on clinical, biochem ical, and radiological test results were assessed. Factors affec-t ing disease- free survival were also evaluated. Results: Thedurat ion of the follow-up of the pat ients was 80.3± 76.1 m onths. MEN2A was detected in three pat ients (8.3% ) . Twelve pat ients (33.3% ) had m etastasis at the t im e of di-agnosis. During the follow-up period, local recurrence was observed in 13 (36.1% ) pat ients. Nine pat ients (25% ) pre-sented m etastasis at follow-up. The m ean disease- free sur-vival was high in sporadic MTC compared to hereditary MTC. Conclusion: The study observed asignificant cont r ibut ion tothe hereditary nature of the disease on prognosis. Howe-ver,other prognost ic factors such as gender, nodule charac-ter ist ics, recurrence and m etastasis, and t reatm ent m odalit ies did differsignificant . Pat ients with MTC should be evaluated to know if the disease is sporadic or hereditary. The sm all sam ple size in this study rest r icts the power of stat ist ical analysis; therefore, further prospect ive studies are necessary to reveal the other cont r ibutory prognost ic fac-tors in MTC. Keyw ords: Medullary thyroid cancer; m alignancy;
RET m utat ion; thyroidectomy; follow-up
Am aç: Medüller t iroid karsinom (MTK) , t iroid bezinin para-foliküler C hücreler inin nadir görülen agresif seyir li bir nö-roendokr in tüm örüdür. Çalışm anın am acı, m erkezim izde opere olan MTK’lı hastalarda prognozu etkileyen dem ogra-fik ve klinik faktörleri analiz etmek ve hastalığın uzun dönem sonuçlarını değerlendirm ekt ir. Gereç ve Yöntem ler: Çalış-m am ıza, m erkezim izde 2000-2015 yıllar ı arasında opere olup postoperat if histopatoloj ik değerlendirm ede MTK tanısı alan toplam 36 hasta dâhil edildi. Tüm hastaların arşiv dos-yaları gözden geçir ildi ve klinik, biyokimyasal ve radyoloj ik veriler i incelendi. Hastalıksız sağ kalım ı etkileyen faktör ler analiz edildi. Bulgular: Çalışm am ızda hastaların ortalam a takip süresi 80.3± 76.1 aydı. Üç hastada (% 8,3) MEN2A m evcut tu. On ik i hastada (% 33,3) tanı anında m etastaz vardı. Takip süresince hastaların 13’ünde (% 36,1) lokal nüks gözlendi. Dokuz hastada (% 25) izlem inde m etastaz gelişt iği görüldü. Ortalam a hastalıksız sağ kalım , kalıt sal MTK ile karşılaşt ır ıldığında sporadik MTK'da yüksekt i. Sonuç: Çalışmamızda, kalıtsal hastalığın varlığının prognoza önem li katkısı olduğu saptandı. Bununla bir lik te, cinsiyet , nodül özellikleri, nüks, metastaz varlığı ve tedavi yöntem leri gibi diğer faktör ler in prognoz üzerinde anlam lı bir farka yol açm adığı gözlendi. MTK’lı hastalar, hastalığın sporadik veya kalıtsal olup olm adığı açısından değerlendir ilm elidir. Çalış-m am ızdaki az sayıda hasta istat ist iksel analizin gücünü kı-sıt ladığından, MTK’ya katkıda bulunan prognost ik faktör ler i saptam ak için prospekt if çalışm alara iht iyaç duyulm aktadır. Anahtar kelim eler: Medüller t iroid kanseri; m alignite;
RET m utasyonu; t iroidektom i; izlem
2 5 3
Address for Correspondence: Pınar ŞİŞMAN, Clinic of Endocrinology and Metabolism , Medicana Hospital, Bursa, TURKEY Phone: + 90 532 155 08 11 E- m ail: drpinarsism an@gm ail.com
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 31 Jul 2019 Received in revised form : 02 Sep 2020 Accepted: 04 Sep 2020 Available online: 30 Sep 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
01
9-6
68
18

254
I nt roduct ion Medullary thyroid carcinom a (MTC) is a rare neuroendocrine tumor of the parafollicular C cells of the thyroid gland (1) . The sporadic form of the disease is seen in approxim ately 75% of all cases. The rem aining MTC cases develop as a hereditary disease, occurr ing as a part of type 2 m ult iple endocrine neo-plasia (MEN2) syndrom e (2) . MEN 2A con-st itutes 95% of all MEN 2 cases (3) .
Most frequent ly, sporadic MTC is seen be-tween the fourth and sixth decades. The 10-year survival rates for pat ients with stage I , I I , I I I , and I V MTC are 100, 93, 71, and 21 percent , respect ively. Pat ient ’s age and tum or stage at the t im e of diagnosis are the significant independent factors in prognosis (4) . System ic metastasis is seen in most pa-t ients with regional lym ph node m etastasis; with 90% probabilit y, the residual disease is detected either biochem ically or radiologi-cally after surgery, in case of pre-operat ive regional lym ph node m etastasis (5,6) . Early m etastases of the tum or to cervical lym ph nodesare seen; the m ost com m on areas for distant m etastases include liver, lungs, bones, and less frequent ly,the brain and skin (7) . Germ line rearranged during t ransfect ion (RET) m utat ions are a useful predictor of tum or aggressiveness (4) . These m utat ions are 98, 95, and 88 percent in MEN 2A, MEN 2B, and fam ilial MTC, respect ively (7) . They are also m utated in approxim ately 50% of all sporadic cases of MEN (8) .
The m ainstay of t reatm ent is the com plete resect ion of the thyroid tum or and any re-gional m etastases. However, the m ost appropriate t reatm ent is less evident in pa-t ients with residual or recurrent disease and distant m etastases (4) . The best predict ive factor for recurrence- free survival is postop-erat ive biochem ical rem ission. Serum calci-tonin and, m ore im portant ly, carcinoembryonic ant igen (CEA) are used as tum or m arkers for MTC. I n the presence of norm al serum CEA and undetectable serum calcitonin values, pat ients are considered to be biochem ically cured and have the best prognosis (7,9) . The purpose of this study is to analyze the dem ographic and clinical fac-tors that m ay affect the prognosis and to evaluate the long term outcom es of surgical t reatm ent in MTC pat ients at a single cen-ter.
Materia l and Methods Thirty-six pat ients with MTC who underwent surgery at Uludag Medical University Hospi-tal between 2000 and 2015 were recruited into the study. The study was perform ed in accordance with the Helsinki Declarat ion and approved by the Ethical Com m it tee of Uludag University. Writ ten informed consent was obtained from all study part icipantsbe-fore the init iat ion of the study. The dem ographic data, clinical history, and pre-operat ive biochem ical param eters were evaluated using the pat ients’ file data. Pre-operat ive neck ult rasonography was used to assess the longest diam eter of the nodule. Pathological result s of the thyroidectom y perform ed were reviewed, and character is-t ics of the tum or along with the presence of any lym ph node m etastasis were noted. Surgical and other related therapeut ic data, along with the tum or stage, were assessed. RET proto-oncogene m utat ion analyses were assessed to determ ine if the disease was sporadic or hereditary. Absence of hy-perparathyroidism and pheochrom ocytom a and no fam ily history of MTC was defined as sporadic cases. I n the presence of specific RET proto-oncogene m utat ion, MEN2A was considered if one or m ore fam ily m em bers had hyperparathyroidism or pheochrom ocy-tom a,whereas MEN2B was considered if at least one fam ily m em ber presented m or-phological characterist ics of the disease with pheocrom ocytom a (7) .
During follow-up, the pat ients’ f iles were also evaluated for recurrence and distant m etastasis. Factors affect ing disease- free survival, such as the pat ients’ dem ographic character ist ics, radiological data, and t reat-m ent effects, were also assessed.
Stat ist ical Analysis
The log- rank test was used to determ ine the difference between Kaplan-Meier curves for disease- free survival t im e. Median survival t im e with the related standard error was re-ported. Cox proport ional hazard regression procedure was perform ed after the Kaplan-Meier analysis to determ ine the prognost ic factors that affect disease- free survival t ime. Results were reported as hazard rat ios with 95% confidence intervals (CI ) and re-lated p-values. All analyses were done using SPSS 22( I BM Corp. Released in 2012. I BM
Şişm an et al. Turk J Endocrinol Metab. Medullary Thyroid Carcinom a 2020; 24: 253-260
2 5 4
SPSS Stat ist ics for Windows, Version 21.0. Arm onk, NY: I BM Corp.) . A p-value p< 0.05 was considered to be stat ist ically significant .
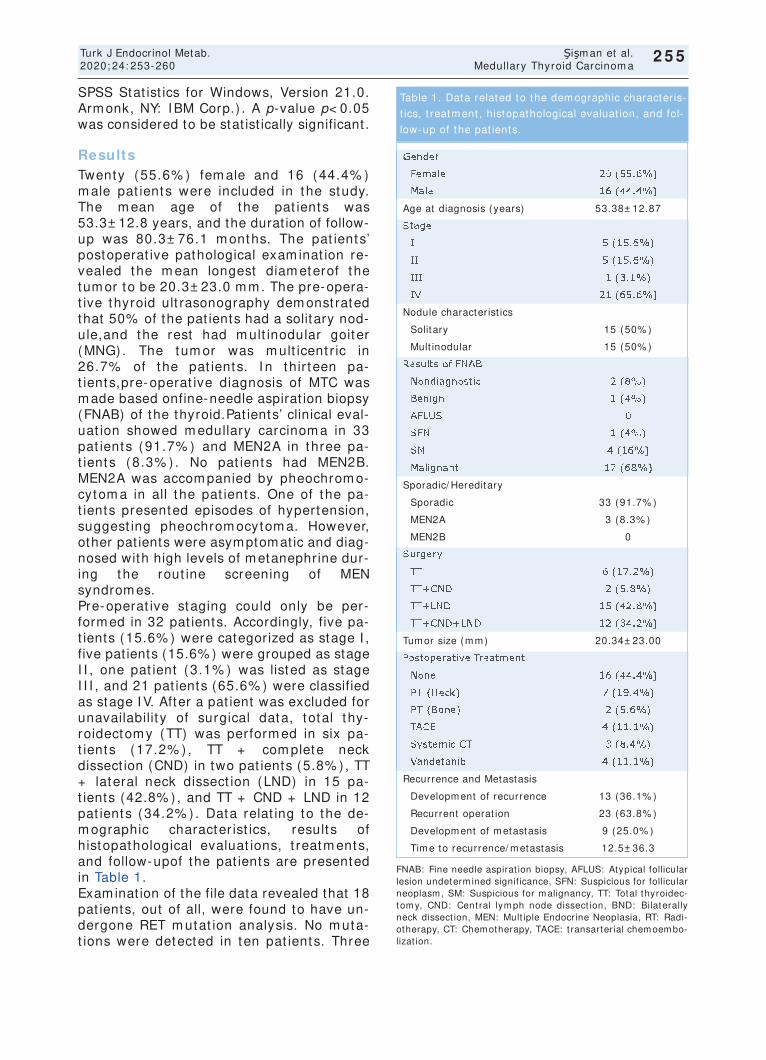
Results Twenty (55.6% ) fem ale and 16 (44.4% ) m ale pat ients were included in the study. The m ean age of the pat ients was 53.3± 12.8 years, and the durat ion of follow-up was 80.3± 76.1 m onths. The pat ients’ postoperat ive pathological exam inat ion re-vealed the m ean longest diam eterof the tum or to be 20.3± 23.0 m m . The pre-opera-t ive thyroid ult rasonography dem onst rated that 50% of the pat ients had a solitary nod-ule,and the rest had m ult inodular goiter (MNG) . The tum or was m ult icent r ic in 26.7% of the pat ients. I n thir teen pa-t ients,pre-operat ive diagnosis of MTC was m ade based onfine-needle aspirat ion biopsy (FNAB) of the thyroid.Pat ients’ clinical eval-uat ion showed m edullary carcinom a in 33 pat ients (91.7% ) and MEN2A in three pa-t ients (8.3% ) . No pat ients had MEN2B. MEN2A was accom panied by pheochrom o-cytom a in all t he pat ients. One of the pa-t ients presented episodes of hypertension, suggest ing pheochrom ocytom a. However, other pat ients were asymptomat ic and diag-nosed with high levels of m etanephrine dur-ing the rout ine screening of MEN syndrom es. Pre-operat ive staging could only be per-form ed in 32 pat ients. Accordingly, five pa-t ients (15.6% ) were categorized as stage I , five pat ients (15.6% ) were grouped as stage I I , one pat ient (3.1% ) was listed as stage I I I , and 21 pat ients (65.6% ) were classified as stage I V. After a pat ient was excluded for unavailabilit y of surgical data, total thy-roidectom y (TT) was perform ed in six pa-t ients (17.2% ) , TT + com plete neck dissect ion (CND) in two pat ients (5.8% ) , TT + lateral neck dissect ion (LND) in 15 pa-t ients (42.8% ) , and TT + CND + LND in 12 pat ients (34.2% ) . Data relat ing to the de-m ographic character ist ics, result s of histopathological evaluat ions, t reatm ents, and follow-upof the pat ients are presented in Table 1. Examinat ion of the file data revealed that 18 pat ients, out of all, were found to have un-dergone RET m utat ion analysis. No m uta-t ions were detected in ten pat ients. Three
255
Turk J Endocrinol Metab. Şişm an et al. 2020; 24: 253-260 Medullary Thyroid Carcinom a
2 5 5
Gender
Fem ale 20 (55.6% )
Male 16 (44.4% )
Age at diagnosis (years) 53.38± 12.87
Stage
I 5 (15.6% )
I I 5 (15.6% )
I I I 1 (3.1% )
I V 21 (65.6% )
Nodule character ist ics
Solitary 15 (50% )
Mult inodular 15 (50% )
Results of FNAB
Nondiagnost ic 2 (8% )
Benign 1 (4% )
AFLUS 0
SFN 1 (4% )
SM 4 (16% )
Malignant 17 (68% )
Sporadic/ Hereditary
Sporadic 33 (91.7% )
MEN2A 3 (8.3% )
MEN2B 0
Surgery
TT 6 (17.2% )
TT+ CND 2 (5.8% )
TT+ LND 15 (42.8% )
TT+ CND+ LND 12 (34.2% )
Tum or size (m m ) 20.34± 23.00
Postoperat ive Treatm ent
None 16 (44.4% )
RT (Neck) 7 (19.4% )
RT (Bone) 2 (5.6% )
TACE 4 (11.1% )
System ic CT 3 (8.4% )
Vandetanib 4 (11.1% )
Recurrence and Metastasis
Developm ent of recurrence 13 (36.1% )
Recurrent operat ion 23 (63.8% )
Developm ent of m etastasis 9 (25.0% )
Tim e to recurrence/ m etastasis 12.5± 36.3
Table 1. Data related to the dem ographic character is-
t ics, t reatm ent , histopathological evaluat ion, and fol-
low-up of the pat ients.
FNAB: Fine needle aspirat ion biopsy, AFLUS: Atypical follicular lesion undeterm ined significance, SFN: Suspicious for follicular neoplasm , SM: Suspicious for m alignancy, TT: Total thyroidec-tom y, CND: Cent ral lym ph node dissect ion, BND: Bilaterally neck dissect ion, MEN: Mult iple Endocrine Neoplasia, RT: Radi-otherapy, CT: Chem otherapy, TACE: t ransarter ial chem oem bo-lizat ion.
256
Şişm an et al. Turk J Endocrinol Metab. Medullary Thyroid Carcinom a 2020; 24: 253-260
2 5 6
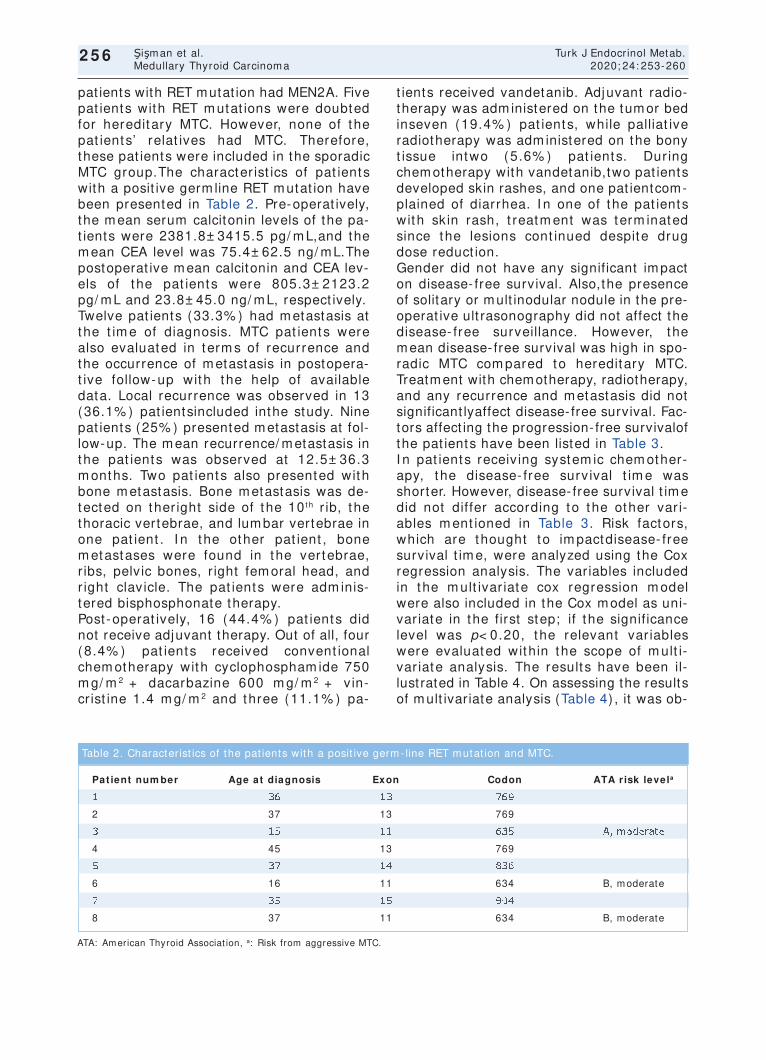
pat ients with RET mutat ion had MEN2A. Five pat ients with RET m utat ions were doubted for hereditary MTC. However, none of the pat ients’ relat ives had MTC. Therefore, these pat ients were included in the sporadic MTC group.The character ist ics of pat ients with a posit ive germ line RET m utat ion have been presented in Table 2. Pre-operat ively, the m ean serum calcitonin levels of the pa-t ients were 2381.8± 3415.5 pg/ m L,and the m ean CEA level was 75.4± 62.5 ng/ m L.The postoperat ive m ean calcitonin and CEA lev-els of the pat ients were 805.3± 2123.2 pg/ m L and 23.8± 45.0 ng/ m L, respect ively. Twelve pat ients (33.3% ) had m etastasis at the t im e of diagnosis. MTC pat ients were also evaluated in term s of recurrence and the occurrence of m etastasis in postopera-t ive follow-up with the help of available data. Local recurrence was observed in 13 (36.1% ) pat ientsincluded inthe study. Nine pat ients (25% ) presented m etastasis at fol-low-up. The m ean recurrence/ m etastasis in the pat ients was observed at 12.5± 36.3 m onths. Two pat ients also presented with bone m etastasis. Bone m etastasis was de-tected on ther ight side of the 10 t h r ib, the thoracic vertebrae, and lum bar vertebrae in one pat ient . I n the other pat ient , bone m etastases were found in the vertebrae, r ibs, pelvic bones, r ight fem oral head, and r ight clavicle. The pat ients were adm inis-tered bisphosphonate therapy. Post-operat ively, 16 (44.4% ) pat ients did not receive adjuvant therapy. Out of all, four (8.4% ) pat ients received convent ional chem otherapy with cyclophospham ide 750 m g/ m 2 + dacarbazine 600 m g/ m 2 + vin-cr ist ine 1.4 m g/ m 2 and three (11.1% ) pa-
t ients received vandetanib. Adjuvant radio-therapy was adm inistered on the tum or bed inseven (19.4% ) pat ients, while palliat ive radiotherapy was adm inistered on the bony t issue intwo (5.6% ) pat ients. Dur ing chem otherapy with vandetanib,two pat ients developed skin rashes, and one pat ientcom-plained of diarrhea. I n one of the pat ients with skin rash, t reatm ent was term inated since the lesions cont inued despite drug dose reduct ion. Gender did not have any significant im pact on disease- free survival. Also,the presence of solitary or mult inodular nodule in the pre-operat ive ult rasonography did not affect the disease- free surveillance. However, the m ean disease- free survival was high in spo-radic MTC com pared to hereditary MTC. Treatment with chemotherapy, radiotherapy, and any recurrence and m etastasis did not significant lyaffect disease- free survival. Fac-tors affect ing the progression- free survivalof the pat ients have been listed in Table 3. I n pat ients receiv ing system ic chem other-apy, the disease- free survival t im e was shorter. However, disease- free survival t im e did not differ according to the other var i-ables m ent ioned in Table 3. Risk factors, which are thought to im pactdisease- free survival t im e, were analyzed using the Cox regression analysis. The var iables included in the m ult ivar iate cox regression m odel were also included in the Cox m odel as uni-var iate in the first step; if the significance level was p< 0.20, the relevant var iables were evaluated within the scope of m ult i-var iate analysis. The result s have been il-lust rated in Table 4. On assessing the results of m ult ivar iate analysis (Table 4) , it was ob-
ATA: Am erican Thyroid Associat ion, a: Risk from aggressive MTC.
Pat ient num ber Age at diagnosis Exon Codon ATA r isk levela
1 36 13 769
2 37 13 769
3 15 11 635 A, m oderate
4 45 13 769
5 37 14 836
6 16 11 634 B, m oderate
7 35 15 904
8 37 11 634 B, m oderate
Table 2. Character ist ics of the pat ients with a posit ive germ - line RET m utat ion and MTC.

served that the r isk factors that m ay have had an im pact on the disease- free survival t ime could not be determ ined. Although fac-tors like system ic chem otherapy, num ber of m etastat ic lym ph nodes, and percentage change in the value of CA m easurem ents were found to be significant when analyzed by univariate analysis, they could not be de-term ined as r isk factors in the m ult ivar iate analysis m odel.
Discussion MTC accounts for approxim ately 3-5% of all thyroid carcinom a. A solitary thyroid nodule is the m ost com m on presentat ion of spo-radic MTC (75-95% ) (4) . Nevertheless, the hereditary t ype usually encom passes both m ult ifocal and bilateral disease (10) . Spo-radic MTC affects indiv idualsbetween the fourth and sixth decades most frequent ly. I n the present study, the pat ients’ m ean age
257
Turk J Endocrinol Metab. Şişm an et al. 2020; 24: 253-260 Medullary Thyroid Carcinom a
2 5 7
H: Hazard Rat io; Mult ivar iate cox regression m odel is significant (p= 0.040) . RT: Radiotherapy, CT: Chem otherapy.
Univariate Model Mult ivariate Model
Risk Factor B H p- value B H p- value
Gender
Fem ale(Ref.Cat .) Reference - Reference -
Male 0.63 1.88 0.197 1.45 4.26 0.956
Nodule character ist ic
Solitary(0) (Ref.Cat .) Reference Reference -
Mult inodular(1) -0.88 0.42 0.164 -0.09 0.92 0.996
System ic CT
None(Ref.Cat .) Reference - Reference -
Yes 1.08 2.95 0.047 -1.10 0.34 0.966
Num ber of Metastat ic LN 0.04 1.04 0.013 0.10 1.10 0.955
% Change of CA 0.05 1.06 0.018 0.11 1.11 0.897
Table 3. Determ inat ion of the factors affect ing the disease- free survival t im e.
DFS: Disease-Free Survival, CT: Chem otherapy, RT: Radiotherapy.
Num ber of pat ients at r isk Num ber of recurrence Durat ion of Mean DFS
Risk Factor ( % ) ( % ) in Months p- value
Gender
Fem ale 20 (55.55% ) 8 (40% ) 143± 23.76 0.186
Male 16 (45.45% ) 9 (56.25% ) 135.73± 43.68
Nodule character ist ic
Solitary(0) 14 (48.28% ) 7 (50% ) 69.69± 16.80 0.150
Mult inodular(1) 15 (51.72% ) 4 (24.67% ) 238.53± 41.21
Sporadic/ Hereditary
Sporadic(0) 10 (27.78) 3 (30) 94.50± 18.60 0.360
Genet ic (1) 26 (72.22) 14 (53.85) 134.38± 33.77
RT (Neck)
Yes 7 (20) 4 (57.14) 37.14± 13.72 0.234
No 28 (80) 12 (42.86) 168.35± 35.66
System ic CT
Yes 7 (19.44) 5 (71.43) 41.43± 21.91 0.035
No 29 (80.56) 12 (41.38) 168.71± 35.66
Table 4. The m ult ivar iate analysis of the relevant variables.

258
was 53.3± 12.8 years, which was in accor-dance with the literature reports. The pre-operat ive thyroid ult rasonography revealed a solitary nodule in 50% of the pat ients and MNG in the rest . The tumor was mult icent r ic in 26.7% of all pat ients, and 2 of 3 (66.6% ) pat ients with MEN2A. The pathological Tum or-Node-Metastasis (pTNM) cr iter ia for clinicopathologic tum or staging is basedon tum or diam eter, pres-ence or absence of ext rathyroidal spread, local or regional lymph node metastases,and distant m etastases (4) . The m ean longest diam eter of the tum or was 20.3± 23.0 m m on postoperat ive pathological exam inat ion of pat ients in the present study. Pre-opera-t ive staging could only be perform ed in 32 pat ients. Accordingly, five pat ients (15.6% ) were categor ized as stage I , f ive pat ients (15.6% ) as stage I I , one pat ient (3.1% ) as stage I I I , and 21 pat ients (65.6% ) as stage I V. Twelve pat ients (33.3% ) presented m etastasis at diagnosis. MTC usually m etastases to the cent ral neck nodes. Pre-operat ive serum calcitonin and CEA levels play a signif icant role in deter-m ining the extent of lym ph node m etas-tases. Machens et al. dem onst rated that the progressive increase in pre-operat ive calci-tonin levels is associated with metastases to lym ph nodes of the ipsilateral cent ral and lateral neck regions, the cont ralateral cen-t ral neck, and the upper m ediast inum , re-spect ively (11) . I n another study, five-year relapse- free survival rates were obtained to be 90% in pat ients with postoperat ive serum calcitonin < 10 pg/ m L, and 61% in pat ients with serum calcitonin levels above 10 pg/ mL (12) . I n the present study, the pa-t ients’ pre-operat ive m ean serum calcitonin levels were 2381.8± 3415.5 pg/ m L, and the m ean CEA level was 75.4± 62.5 ng/ m L. Modigliani et al. found that the five-year re-currence rate was only 5% in pat ients t reated by biochem ical m ethods (13) . The m ean follow-up period in the current study was 80.3± 76.1 m onths.Thir teen pat ients (36.1% ) presented with local recurrence, while nine pat ients (25% ) exhibited m etas-tasis at follow-up. The m ean recurrence/ m etastasis t im e in the pat ients was 12.5± 36.3 m onths. The goals of management of metastat ic MTC include locoregional disease cont rol, allevia-
t ion of sym ptom s of horm onal excess, and cont rol of m etastases. The t reatm ent op-t ions include palliat ive surgery, external beam radiat ion therapy (EBRT) , and sys-tem ic therapy with tyrosine kinase inhibitors (14) . I n this study, 16 (44.4% ) pat ients did not receive adjuvant therapy; adjuvant ra-diotherapy was adm inistered on the tum or bed in 7 (19.4% ) pat ients, while palliat ive radiotherapy was adm inistered on the bony t issuein 2 (5.6% ) pat ients. The authors of one of t he m ost extensive studies on MTC dem onst rated that there is no dif ference in local or regional relapse-free rates between pat ient s t reated wit h and without EBR (15) . Another studyproved thatEBRT did not signif icant ly benefit over-all surv ival in node-posit ive pat ients (16) . Sim ilar result s were observed in the pres-ent st udy establishing t hat radiotherapy had no signif icant effect on disease- free survival. MTC is resistant to cytotoxic chem otherapy. Cytotoxic chem otherapeut ic regim ens used in MTC show a short- term response rate of 15–20% . Today, cytotoxic chem otherapeu-t ic regim ents are not recom m ended be-cause of low response rates and the availabilit y of m ore effect ive t reatm ent op-t ions (4) . RET inhibitors have provided sig-nif icant clinical benefit s. I n a random ized, double-blind phase I I I t r ial, vandetanib showed stat ist ically signif icant advantages in term s of object ive response rate, disease cont rol rate, and biochem ical response (17) . I n the sam e study, 12% pat ients re-ceiv ing vandetanib discont inued t reatm ent because of toxicit y while 35% pat ients re-quired dose reduct ions due to an adverse event (4) . Ret rospect ive exam inat ion of the pat ient f iles in the present revealed that 4 (8.4% ) pat ients had received convent ional-system ic chem otherapy with cyclophos-pham ide 750 m g/ m 2 + dacarbazine 600 m g/ m 2+ vincr ist ine 1.4 m g/ m 2 while 3 (11.1% ) pat ients had received vandetanib t reatm ent . However, t he two t reatm ent m odalit ies did not have any posit ive effect on disease- free survival. The adverse effect of vandetanib was seen in all three pat ients ( two pat ients developed a sk in rash, and one pat ient had diarrhea) . This study also has som e lim itat ions. First , the inclusion of only a sm all num ber of pa-
Şişm an et al. Turk J Endocrinol Metab. Medullary Thyroid Carcinom a 2020; 24: 253-260
2 5 8

t ients lim ited the stat ist ical power of analy-ses. Also, the small sample size did not allow stat ist ical evaluat ion of all param eters, which m ight have affected the prognosis. The ret rospect ive design of this study is the second lim itat ion. The third lim itat ion is that the RET m utat ion status was not known in 50% of the cases. Although the num ber of pat ients included in the study was insufficient , stat ist ically sig-nificant adverse effects of the hereditary na-ture of the disease on disease- free survival have been dem onst rated. Due to these lim -itat ions, this study m ay not be considered suitable to support the suggest ion that the inheritance of the disease has a negat ive ef-fect on disease- free survival. Nonetheless, pat ients with MTC should be evaluated forthe sporadic or hereditary nature of the disease.
Literature repor t s t hat pat ients with high-r isk m ut at ions develop MTC ear lier t han pat ient s w it h m oderat e- r isk m ut at ions ( 18) . A study exploredthe long- term out -com es of MTC in MEN2 pat ients according to the RET m utat ion r isk categor ies, and it was found t hat pat ient s w it h t he highest RET m utat ion r isk were associated with in-fer ior outcom es and surv ival com pared to t hose w it h m oderat e and high r isk ( 19) . Another studyfound no stat ist ically signif i-cant dif ference bet ween pat ient s w it ha high and m oderat e r isk of m ut at ions in t erm s of overall surv ival and dist ant m etastat ic disease after diagnosis. The au-thors suggested that RET m utat ion classif i-cat ion could be perform ed based ondisease onset ( ear ly vs. late) (20) .
Conclusion MTC is aggressive. The stage of the disease at diagnosis and complete surgical resect ion is the m ost im portant prognost ic factor. Ad-juvant t reatments such as radiotherapy, sys-tem ic chem otherapy, and vandetanib are considered when com plete resect ion cannot be achieved or in case of recurrence. This study establishes a significant cont r ibut ion of the hereditary nature of the disease on prognosis. However, other factors did not have anysignificant difference on prognosis. The authors deliberate that further prospec-t ive studies are necessary to revealany ad-
dit ional cont r ibutory prognost ic factors in MTC.
Source of Finance During this study, no financial or spiritual sup-port was received neither from any pharma-ceutical company that has a direct connection with the research subject, nor from a company that provides or produces medical instruments and materials which may negatively affect the evaluation process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions I dea/ Concept: Özen Öz Gül, Pınar Şişman; Design: Buket Biçer, Hikmet Öztop; Control/ Supervision: Soner Cander, Canan Ersoy; Data Collect ion and/ or Processing: Pınar Şişman, Özen Öz Gül; Analysis and/ or Interpretat ion: Gökhan Ocakoğlu; Literature Review: Pınar Şişman; Writ ing the Art icle: Pınar Şişman; Crit ical Review: Soner Cander, Erdinç Ertürk; References and Fundings: Hik-met Öztop; Materials: Buket Biçer.
References 1. Geller G, Laskin J, Cheung WY, Ho C. A ret rospect ive
review of the m ult idisciplinary m anagem ent of m edullary thyroid cancer: eligibilit y for system ic therapy. Thyroid Res. 2017; 10: 6. [ Crossref] [ PubMed] [ PMC]
2. Calvo J, Torrealba G, Sáenz A, Santam aría C, Mor-era E, Alvarado S, Roa Y, González M. Genet ic and clinical features of medullary thyroid carcinoma: the experience of a single center in Costa Rica. J Can-cer Epidem iol. 2016; 2016: 9637173. [ Crossref] [ PubMed] [ PMC]
3. Maciel LMZ, Magalhães PKR. Medullary thyroid car-cinom a - adverse events dur ing system ic t reat-m ent : r isk-benefit rat io. Arch Endocr inol Metab. 2017; 61: 398-402. [ Crossref] [ PubMed]
4. Wells SA Jr, Asa SL, Dralle H, Elisei R, Evans DB, Gagel RF, Lee N, Machens A, Moley JF, Pacini F, Raue F, Frank-Raue K, Robinson B, Rosenthal MS, San-toro M, Schlum berger M, Shah M, Waguespack SG; Am erican Thyroid Associat ion Guidelines Task Force on Medullary Thyroid Carcinom a. Revised Am erican Thyroid Associat ion guidelines for the m anagem ent of m edullary thyroid carcinom a. Thyroid. 2015; 25: 567-610. [ Crossref] [ PubMed] [ PMC]
259
Turk J Endocrinol Metab. Şişm an et al. 2020; 24: 253-260 Medullary Thyroid Carcinom a
2 5 9
5. Pelizzo MR, Boschin I M, Bernante P, Toniato A, Pi-ot to A, Paget ta C, Nibale O, Ram pin L, Muzzio PC, Rubello D. Natural history, diagnosis, t reatment and outcom e of m edullary thyroid cancer: 37 years ex-per ience on 157 pat ients. Eur J Surg Oncol. 2007; 33: 493-497. [ Crossref] [ PubMed]
6. Machens A, Schneyer U, Holzhausen HJ, Dralle H. Prospects of rem ission in m edullary thyroid carci-nom a according to basal calcitonin level. J Clin En-docr inol Metab. 2005; 90: 2029-2034. [ Crossref] [ PubMed]
7. Lee CR, Lee S, Son H, Ban E, Kang SW, Lee J, Jeong JJ, Nam KH, Chung WY, Park CS. Medullary thyroid carcinom a: a 30-year experience at one inst itut ion in Korea. Ann Surg Treat Res. 2016; 91: 278-287. [ Crossref] [ PubMed] [ PMC]
8. Nelkin B. Recent advances in the biology and ther-apy of m edullary thyroid carcinom a. F1000Res. 2017; 6: 2184. [ Crossref] [ PubMed] [ PMC]
9. Kim BH, Kim I J. Recent updates on the m anage-m ent of m edullary thyroid carcinom a. Endocr inol Metab (Seoul) . 2016; 31: 392-399. [ Crossref] [ PubMed] [ PMC]
10. Heshm at i HM, Gharib H, van Heerden JA, Sizem ore GW. Advances and cont roversies in the diagnosis and m anagem ent of m edullary thyroid carcinom a. Am J Med. 1997; 103: 60-69. [ Crossref] [ PubMed]
11. Machens A, Dralle H. Biom arker-based r isk st rat ifi-cat ion for previously unt reated m edullary thyroid cancer. J Clin Endocr inol Metab. 2010; 95: 2655-2663. [ Crossref] [ PubMed]
12. Pellegrit i G, Leboulleux S, Baudin E, Bellon N, Scollo C, Travagli JP, Schlumberger M. Long- term outcome of medullary thyroid carcinoma in pat ients with nor-m al postoperat ive m edical im aging. Br J Cancer. 2003; 88: 1537-1542. [ Crossref] [ PubMed] [ PMC]
13. Modigliani E, Cohen R, Campos JM, Conte-Devolx B, Maes B, Boneu A, Schlum berger M, Bigorgne JC, Dum ont ier P, Leclerc L, Corcuff B, Guilhem I . Prog-nost ic factors for survival and for biochem ical cure
in m edullary thyroid carcinom a: results in 899 pa-t ients. The GETC Study Group. Groupe d'étude des tum eurs à calcitonine. Clin Endocr inol (Oxf ) . 1998; 48: 265-223. [ Crossref] [ PubMed]
14. Raue F, Frank-Raue K. Long- term follow-up in m edullary thyroid carcinom a. Recent Results Can-cer Res. 2015; 204: 207-225. [ Crossref] [ PubMed]
15. Brier ley J, Tsang R, Sim pson WJ, Gospodarowicz M, Sutcliffe S, Panzarella T. Medullary thyroid cancer: analyses of survival and prognost ic factors and the role of radiat ion therapy in local cont rol. Thyroid. 1996; 6: 305-310. [ Crossref] [ PubMed]
16. Mart inez SR, Beal SH, Chen A, Chen SL, Schneider PD. Adjuvant external beam radiat ion for m edullary thyroid carcinom a. J Surg Oncol. 2010; 102: 175-178. [ Crossref] [ PubMed] [ PMC]
17. Wells SA Jr, Robinson BG, Gagel RF, Dralle H, Fagin JA, Santoro M, Baudin E, Elisei R, Jarzab B, Vasselli JR, Read J, Langm uir P, Ryan AJ, Schlum -berger MJ. Vandetanib in pat ients with locally ad-vanced or m etastat ic m edullary thyroid cancer: a random ized, double-blind phase I I I t r ial. J Clin Oncol. 2012; 30: 134-141. [ Crossref] [ PubMed] [ PMC]
18. Frank-Raue K, Rondot S, Raue F. Molecular genet ics and phenom ics of RET m utat ions: I m pact on prog-nosis of MTC. Mol Cell Endocr inol. 2010; 322: 2-7. [ Crossref] [ PubMed]
19. Raue F, Bruckner T, Frank-Raue K. Long- term out-com es and aggressiveness of hereditary m edullary thyroid carcinom a: 40 years of exper ience at one center. J Clin Endocr inol Metab. 2019; 104: 4264-4272. [ Crossref] [ PubMed]
20. Voss RK, Feng L, Lee JE, Perr ier ND, Graham PH, Hyde SM, Nieves-Munoz F, Cabanillas ME, Wagues-pack SG, Cote GJ, Gagel RF, Grubbs EG. Medullary thyroid carcinom a in MEN2A: ATA m oderate- or high- r isk RET m utat ions do not predict disease ag-gressiveness. J Clin Endocr inol Metab. 2017; 102: 2807-2813. [ Crossref] [ PubMed] [ PMC]
260
Şişm an et al. Turk J Endocrinol Metab. Medullary Thyroid Carcinom a 2020; 24: 253-260
2 6 0
The Associat ion Betw een Thyroid Volum e and I nsulin Resistance in Pat ients w ith
Non- Funct ional Adrenal I ncidentalom a Non-Fonksiyonel Adrenal İnsidentalom alı Hastalarda
İnsülin Direnci ve Tiroid Volüm ü Arasındaki İlişki
Murat ŞAHİN, Ayten OĞUZ, Dilek TÜZÜN, Sem iha ÇALKAYA, Kam ile GÜL
Department of Endocrinology and Metabolism, Kahramanmaraş Sütçü İmam University Faculty of Medicine, Kahramanmaraş, TURKEY
Original Art icle Turk J Endocrinol Metab. 2020; 24: 261-269
Object ive: This study aim ed to invest igate the associat ion between insulin resistance ( I R) and thyroid volum e (TV) along with thyroid nodule in pat ients with nonfunct ional ad-renal incidentaloma (NFAI ) . Material and Methods: Forty-five NFAI pat ients with a m ean age of 59.00± 7.00 and 43 healthy cont rols of com parable age and body m ass index (BMI ) were included. Sociodem ographic data, fast ing plasm a glucose (FPG) , alanine am inot ransferase (ALT) , in-sulin, lipid, and hormonal parameters, TV, nodule frequency, and adrenal m ass dim ensions were ret rospect ively recor-ded in all the pat ients. Resuls: Triglycer ide (TG) , insulin, HOMA-I R, basal cort isol, and cort isol levels after dexam et-hasone suppression test (DST) were significant ly higher in the pat ient group (p< 0.05) . Although the frequency of thyroid nodules was higher in the pat ient group than in the cont rol group, this f inding was stat ist ically insignif icant (64.4% and 53.5% , respect ively, p= 0.296) . TV was signifi-cant ly higher in the NFAI group (13.30± 5.95 and 5.99± 3.04, respect ively p< 0.001) . After grouping the par-t icipants according to insulin resistance; BMI , FPG, t r iglyce-r ide, and fast ing insulin levels were significant ly higher in the I R group (p< 0.05) . Though the frequency of thyroid no-dules was higher in those with IR, it was not stat ist ically sig-nificant (62.2% and 56.9% , p= 0.617) .TV was significant ly higher in part icipants with I R (11.23± 7.15cm ) com pared to those without I R (8.64± 4.77) (p= 0.045) . Conclusion: I n-creased insulin resistance was observed in pat ients with NFAI . I t may play a role in increasing the TV and nodule for-m at ion, besides subclinical cort isol secret ion. Keyw ords: Adrenal adenom a; insulin resistance;
thyroid volum e
Am aç: Non- fonksiyone adrenal insidentalom alı (NFAI ) has-talarda insülin direnci ( I R) ile t iroid volüm ü (TV) ve t iroid nodüller i arasındaki ilişkiy i değer lendirm ekt ir. Gereç ve Yöntem ler: Endokrinoloj i ve Metabolizm a Hastalıkları po-lik liniğine başvuran or talam a yaşlar ı 59,00± 7,00 olan 45 NFAI olan hasta ile benzer yaş ve vücut k it le indeksi (VKİ) ’ye sahip 43 sağlık lı kont rolalındı. Çalışm aya alınan bi-reylerinsosyodemografik verileri, açlık plazma glukoz (APG), alaninam inot ransferaz (ALT) , açlık insülinseviyesi, lipid ve horm onal param etreler i, TV, nodül sıklığı, adrenal kit le bo-yut ları ret rospekt if olarak dosyadan kaydedildi. Bulgular: Hasta grubu (n= 45) ve kont rol grubu (n= 43) karşılaşt ır ıldı-ğında hasta grubunda t r igliser id, insülin, HOMA-I R, kort izol ve deksam etazonsupresyon test i (DST) sonrası kort izol se-viyesi anlam lı düzeyde daha yüksek saptandı (p< 0,05) . Ti-roid nodül sık lığı, hasta grubunda kont rol grubuna göre anlam lı olm am akla bir likte daha yüksek (% 64,4 ve % 53,5, p= 0,296) , TV ise hasta grubunda anlam lı seviyede daha yüksekt i (13,30± 5,95 ve 5,99± 3,04, sırasıyla, p< 0,001) . Kat ılım cılar I R’ye göre gruplandır ıldık lar ında I R olanlarda; VKİ, APG, t r igliser id ve açlık insülin seviyeler i anlam lı dü-zeyde daha yüksek saptandı (p< 0,05) .Tiroid nodül sıklığı, IR olanlarda daha yüksek olmakla bir likte istat ist iksel olarak anlam lı değildi (% 62,2 ve % 56,9, p= 0,617) . TV ise, I R olanlarda (11,23± 7,15 cm ) olm ayanlara (8,64± 4,77) göre anlam lı derecede daha yüksekt i (p= 0,045) . Sonuç: NFAI ’lı hastalarda I R artm ışt ır ve TV art ışı ile nodül oluşumunda et-kili olabilir. Ayrıca subklinikkort izolsekresyonu da etkili diğer faktör olarak görünm ektedir. Anahtar kelim eler: Adrenal adenom ; insülin direnci;
t iroid volüm ü
2 6 1
Address for Correspondence: Murat ŞAHİN, Departm ent of Endocrinology and Metabolism , Kahram anm araş Sütçü İm am University Faculty of Medicine, Kahram anm araş, TURKEY
Phone: + 90 344 280 34 03 E- m ail: m uratsahin@m e.com
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 27 Jun 2020 Received in revised form : 03 Aug 2020 Accepted: 25 Aug 2020 Available online: 30 Sep 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
75
02

I nt roduct ion Adrenal incidentalom a (AI ) is a m ass, inci-dentally discoveredduring radiologic imaging for another condit ion. A recent study re-ported the prevalence of AI as approxi-m ately 7% (1) . Only 12% of the adrenal incidentalomasare hormonally act ive; the re-m aining 88% incidentalom asare nonfunc-t ioning (2) . I nsulin resistance ( I R) refers to the insufficient biological response to normal insulin concent rat ions; it form s a significant m etabolic syndrom e com ponent . I R is in-volved in the pathogenesis of diseases like polycyst ic ovary syndrom e, dyslipidem ia, and type 2 diabetes m ellit us. I t has been suggested that I R m ay cause tum or devel-opm ent by hyperinsulinem ia-associated m i-togenic effects. I R is frequent ly observed in pat ients with nonfunct ional adrenal inciden-taloma (NFAI ) , which may be a consequence of either hyper insulinem ia on the adrenal gland or slight ly increased cort isol produc-t ion that is clinically undetectable (3) . I nsulin is a thyroid growth factor that st im -ulates proliferat ion in thyroid cell cultures. Som e studies suggest that I R also exerts goit rogenic effects (4) . A few research type-shave established that overexpression of in-sulin receptors is acrucialrevelat ion in thyroid carcinogenesis (5) . Thyroid disorders have been reported to re-m arkably increasethe frequency of thyroid nodules in NFAI pat ients (6) . However, there is insufficient data to show thyroid volum e (TV) increase. This study aim ed to assess the associat ion between I R and thyroid nodule and TV and other associated factors in NFAI pat ients.
Materia l and Methods This ret rospect ive study was carr ied out be-tween 2016 and 2018. I nst itut ional review board approval was obtained from the local ethics com m it tee (Date of Approval: 20.03.2019; Decree No: 2019/ 05) . The study was conducted in accordance with the Helsinki Declarat ion Principles.
Subjects and Study Protocol
All subjects referred to the author ’s outpa-t ient clinic with adrenal incidentalom a be-tween 2016 and 2018 (n= 95) were recorded. At the f irst v isit , CT or MRI was performed to confirm the diagnosis. Adrenal
masses with benign features including regu-lar m argins, size m easuring less than 4cm , and an at tenuat ion value of less than 10 Hounsfield unit s were defined as adrenal adenoma. Basal hormone and dynamic tests were perform ed to determ ine the funct ion-alit y of incidentalom a. Pat ients with non-funct ional incidentalom a were included in the study. Fift y pat ients, including those who did not com plete their exam inat ions or had a hy-perfunct ioning m ass [ high dehy-droepiandrosterone sulfate (DHEAS) levels, hyperaldosteronism , Cushing syndrom e (CS) , pheochrom ocytom a] , were excluded. While 45 NFAI pat ients with a m ean age of 59.00± 7.00 were included in the study. Pa-t ients with a known history of suprarenal or pituitary surgery, those on steroid therapy, thyroid dysfunct ion, cancer,coronary artery disease, chronic renal failure, or liver failure were not included in the study. Also, pa-t ients with imaging findings of a size greater than 4cm , irregular sharp m argins, invasion to the adjacent st ructures, heterogeneous densit y, and low- fat content that suggests m alignancy were not included in the study. Pat ients adm it ted to the outpat ient clinic were analyzed ret rospect ively, and those-showing the involvem ent of adrenal glands during im aging (abdom inal ult rasound, ab-dom inal tom ography, and abdom inal MRI ) were ident ified. The study also included 43 healthy cont rols with sim ilar dem ographic character ist ics and no adrenal m ass in radi-ological im aging.
Horm onal Evaluat ion
Blood sam ples were obtained at 8: 30am for sodium, potassium, adrenocort icot ropic hor-m one (ACTH) , DHEAS, and plasm a cort isol to determ ine horm one act ivity of the adre-nal m ass. A low dose (1 m g) dexam etha-sone suppression test (DST) was performed. Dexam ethasone was adm inistered at 11.00 pm , and cort isol valuesbelow 1.8 m cg/ dL-were considered normal. Plasmaaldosterone concent rat ion (PAC) / Plasm a renin concen-t rat ion (PRC) in blood sam ples drawn after 15 m in of rest following at least 2 h of up-right posit ion (walking or standing) was con-sideredfor the exclusion of pr im ary aldosteronism . Typical values of PRC and PAC are 5.3-34 pg/ m L and 38-313 pg/ m L,
262
Şahin et al. Turk J Endocrinol Metab. Thyroid Volum e and I nsulin Resistance in Adrenal I ncidentalom a 2020; 24: 261-269
2 6 2

respect ively, and obtained values of ≤38 were considered norm al (7) . To rule out pheochrom ocytom a, m etanephr ine and norm etanephrine were studied in a 24-hour ur ine sam ple collected in 25% hydrochlor ic acid container following a special diet devoid of food and drinks containing phenolic acid for f ive days. The typical values of ur ine m etanephr ine and norm etanephr ine were 52-341 ug/ day and 88-444 ug/ day, respec-t ively, and pat ients exhibit ing high values of up to 1.5 t im es the upper lim it were ex-cluded from the study.
Anthropom etr ic Measures
Height (meter) , weight (kg) , and BMI values of all pat ients were recorded. Body m ass index was calculated using the form ula-BMI = weight / height 2 ( kg/ m 2) . BMI values between 18.5-24.9 kg/ m 2 were evaluated as norm al, those between 25-29.9 kg/ m 2 as overweight , and those ≥30 kg/ m 2 as obese.
Biochem ical Analyses
Blood sam ples were drawn ear ly in the m orning while the pat ients fasted for at least 8 hto assess fast ing insulin (FI ) , fast-ing plasm a glucose (FPG) , horm onal, and lipid param eters. Glucose was analyzed by the glucose hex-okinase method.Total cholesterol, high-den-sit y lipoprotein-cholesterol (HDL-C) , and t r iglyceride (TG) were spect rom et r ically ex-am ined by Advia 1800 (Siemens, Healthcare Diagnost ic I nc, USA) . Chem ilum inescence enzym e im m unoassay kits (ADVI A Centaur XP, Siem ens, Healthcare Diagnost ic I nc,I re-land) were used for DHEAS, ACTH, and cor-t isol m easurem ents. Norm al values were as follows: ACTH (9-52 pg/ mL) , DHEAS (35-560 µg/ dL) , Cort isol (5-23 µg/ dL) , I nsulin (6-27 uI U/ m L) , thyroid st im ulat ing horm one (TSH) (0.4-4.2 µI U/ m L) , and free T4 (0.8-2.7 ng/ dL) . A pat ient having a value of ≥2.5, obtained by the form ula Hom eostasis Model Assess-m ent- I R (HOMA-I R) , was believed to have insulin resistance.
Convent ional Thyroid Ult rasonography
Thyroid ult rasound was performed using the sam e device (GE Logiq P5 PRO) by a single endocr inologist for every study part ici-pant ,and thyroid nodules, parenchym al fea-
tures, and thyroid volum e were recorded. Each lobe volum e was calculated using the form ula volum e (m L)= π/ 6 x width x depth x length (8) . The total volum e was est i-m ated as the sum of both the lobes.
Stat ist ical analysis
Data were presented as ar ithm et ic m ean and standard deviat ion. The dist r ibut ion of the sam ples was evaluated with the Shapiro-Wilk test . The independent t - test was used to com pare the two groups with norm ally dist r ibuted data. The Mann-Whit-ney U, a nonparam et r ic test , was used for data without norm al dist r ibut ion. Mult iple regression analysis was perform ed to deter-m ine the effects of categorical and cont inu-ous var iables on TV and the frequency of thyroid nodules. Enter m ethod was used for regression analysis. A “p” value of less than 0.05 was considered stat ist ically significant . The associat ion between the frequency dis-t r ibut ions of categorical variables was eval-uated using the Chi-Square test . Descript ive stat ist ics were expressed as mean ± SD. Rel-at ive possibilit ies were expressed as odds rat io (OR) and confidence interval (CI ) . I n pat ients with adrenal incidentalom a, factors associated with TV were evaluated using-Pearson’s andSpearm an’s correlat ion tests. The data were analyzed using the 25 th ver-sion of the IBM SPSS (Stat ist ical Package for Social Sciences) package program .
Results Of the 95 AI pat ients, 68.4% (n= 65) had non- funct ional adenom a while 32.6% (n= 30) had funct ional adenoma. Twenty pa-t ients with NFAI were excluded from the study due to m issing data; thus, thestudy was cont inued with the rem aining 45 pa-t ients. Besides, 43 indiv iduals without AI who applied to the Endocrinology outpat ient clinic were taken as a cont rol group. The mean BMI and age of the pat ient and control groups were stat ist ically sim ilar (m ean age, 59.00± 7.00 and 59.45± 17.00, respect ively; p= 0.310) (m ean BMI 32.99± 7.03 and 32.25± 6.04, respect ively; p= 0.601) . The Dem ographic, laboratory, and radiologic findings of both groups are sum m arized in Table 1. Com orbidit ies (hypertension, hy-perlipidem ia, atherosclerot ic heart disease) were significant ly higher in the pat ient group
263
Turk J Endocrinol Metab. Şahin et al. 2020; 24: 261-269 Thyroid Volum e and I nsulin Resistance in Adrenal I ncidentalom a
2 6 3
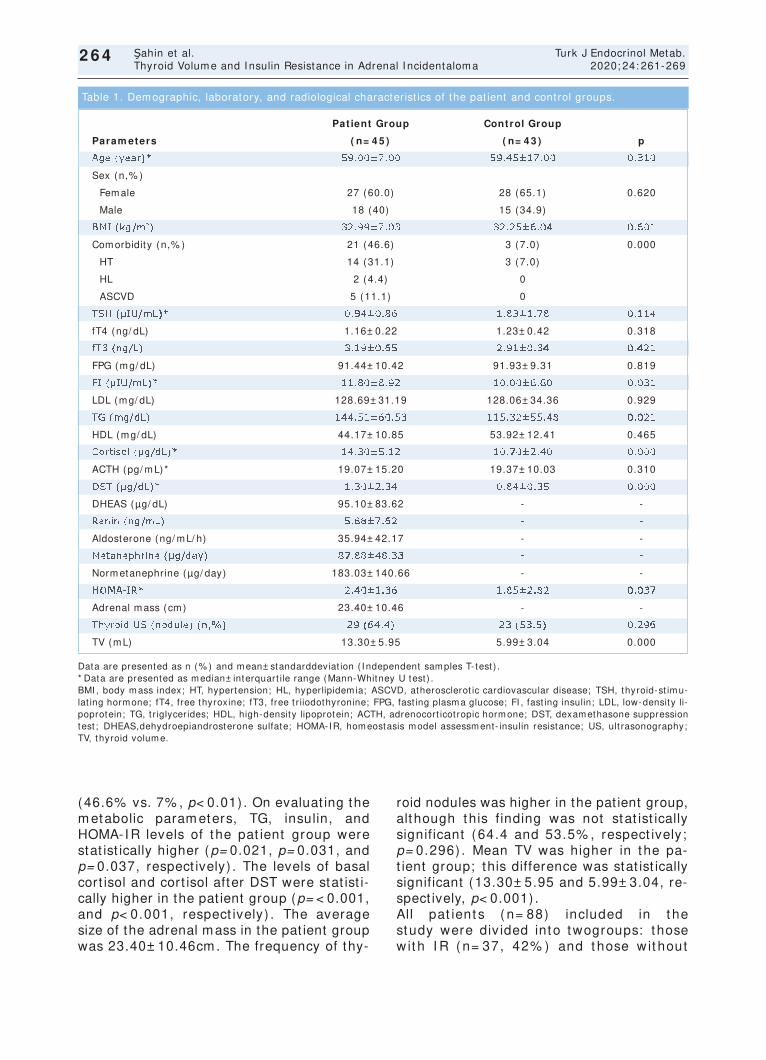
264
(46.6% vs. 7% , p< 0.01) . On evaluat ing the m etabolic param eters, TG, insulin, and HOMA-I R levels of the pat ient group were stat ist ically higher (p= 0.021, p= 0.031, and p= 0.037, respect ively) . The levels of basal cort isol and cort isol after DST were stat ist i-cally higher in the pat ient group (p= < 0.001, and p< 0.001, respect ively) . The average size of the adrenal mass in the pat ient group was 23.40± 10.46cm . The frequency of thy-
roid nodules was higher in the pat ient group, although this f inding was not stat ist ically signif icant (64.4 and 53.5% , respect ively; p= 0.296) . Mean TV was higher in the pa-t ient group; this difference was stat ist ically significant (13.30± 5.95 and 5.99± 3.04, re-spect ively, p< 0.001) . All pat ient s ( n= 88) included in t he study were div ided into twogroups: t hose w it h I R ( n= 37, 42% ) and t hose w it hout
Şahin et al. Turk J Endocrinol Metab. Thyroid Volum e and I nsulin Resistance in Adrenal I ncidentalom a 2020; 24: 261-269
2 6 4
Data are presented as n (% ) and m ean± standarddeviat ion ( I ndependent sam ples T- test ) . * Data are presented as m edian± interquart ile range (Mann-Whitney U test ) . BMI , body m ass index; HT, hypertension; HL, hyperlipidem ia; ASCVD, atherosclerot ic cardiovascular disease; TSH, thyroid-st im u-lat ing horm one; fT4, free thyroxine; fT3, free t r iiodothyronine; FPG, fast ing plasm a glucose; FI , fast ing insulin; LDL, low-density li-poprotein; TG, t r iglycerides; HDL, high-density lipoprotein; ACTH, adrenocort icot ropic horm one; DST, dexam ethasone suppression test ; DHEAS,dehydroepiandrosterone sulfate; HOMA-I R, hom eostasis m odel assessm ent- insulin resistance; US, ult rasonography; TV, thyroid volum e.
Pat ient Group Control Group
Param eters ( n= 4 5 ) ( n= 4 3 ) p
Age (year) * 59.00± 7.00 59.45± 17.00 0.310
Sex (n,% )
Fem ale 27 (60.0) 28 (65.1) 0.620
Male 18 (40) 15 (34.9)
BMI (kg/ m 2) 32.99± 7.03 32.25± 6.04 0.601
Com orbidity (n,% ) 21 (46.6) 3 (7.0) 0.000
HT 14 (31.1) 3 (7.0)
HL 2 (4.4) 0
ASCVD 5 (11.1) 0
TSH (µI U/ m L)* 0.94± 0.86 1.83± 1.78 0.114
fT4 (ng/ dL) 1.16± 0.22 1.23± 0.42 0.318
fT3 (ng/ L) 3.19± 0.65 2.91± 0.34 0.421
FPG (m g/ dL) 91.44± 10.42 91.93± 9.31 0.819
FI (µI U/ m L)* 11.80± 8.92 10.00± 6.60 0.031
LDL (m g/ dL) 128.69± 31.19 128.06± 34.36 0.929
TG (m g/ dL) 144.51± 60.53 115.32± 55.48 0.021
HDL (m g/ dL) 44.17± 10.85 53.92± 12.41 0.465
Cort isol (µg/ dL)* 14.30± 5.12 10.70± 2.40 0.000
ACTH (pg/ m L)* 19.07± 15.20 19.37± 10.03 0.310
DST (µg/ dL)* 1.30± 2.34 0.84± 0.35 0.000
DHEAS (µg/ dL) 95.10± 83.62 - -
Renin (ng/ m L) 5.88± 7.62 - -
Aldosterone (ng/ m L/ h) 35.94± 42.17 - -
Metanephrine (µg/ day) 87.88± 48.33 - -
Norm etanephrine (µg/ day) 183.03± 140.66 - -
HOMA-I R* 2.40± 1.36 1.85± 2.82 0.037
Adrenal m ass (cm ) 23.40± 10.46 - -
Thyroid US (nodule) (n,% ) 29 (64.4) 23 (53.5) 0.296
TV (m L) 13.30± 5.95 5.99± 3.04 0.000
Table 1. Dem ographic, laboratory, and radiological character ist ics of the pat ient and cont rol groups.
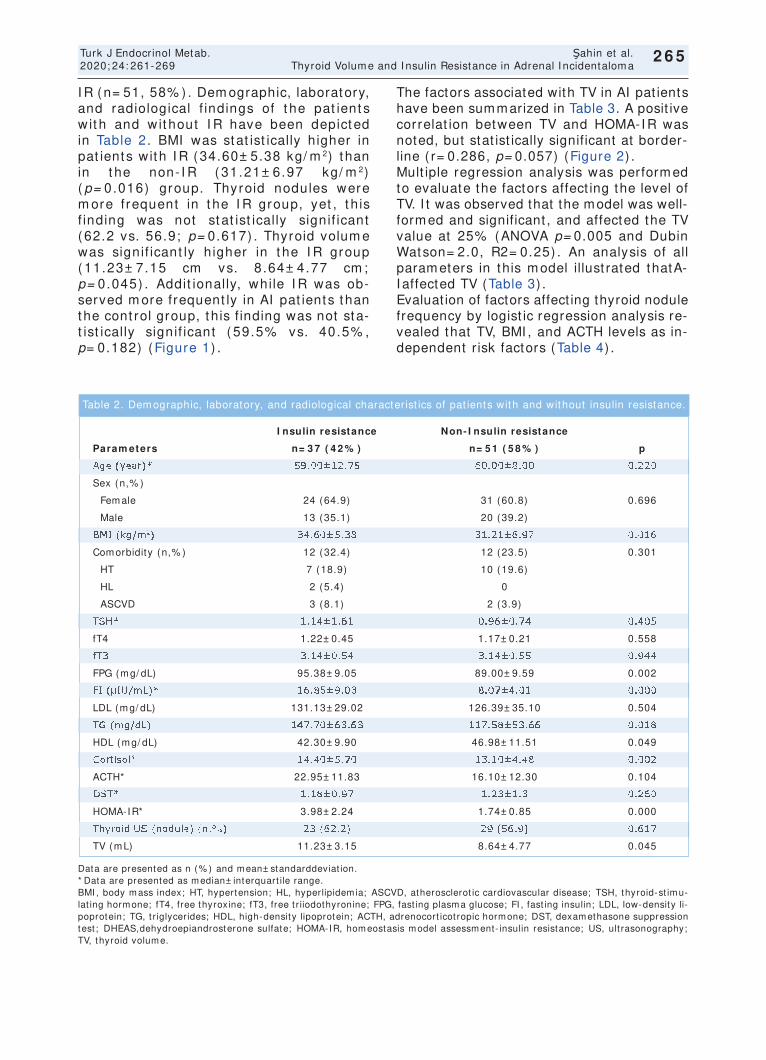
I R (n= 51, 58% ) . Dem ographic, laboratory, and radiological f indings of t he pat ient s w it h and w it hout I R have been depict ed in Table 2. BMI was stat ist ically higher in pat ients with I R (34.60± 5.38 kg/ m 2) t han in t he non- I R ( 31.21± 6.97 kg/ m 2) ( p= 0.016) group. Thyroid nodules were m ore frequent in t he I R group, yet , t h is f inding was not st at ist ically signif icant ( 62.2 vs. 56.9; p= 0.617) . Thyroid volum e was signif icant ly h igher in t he I R group ( 11.23± 7.15 cm vs. 8.64± 4.77 cm ; p= 0.045) . Addit ionally, while I R was ob-served m ore frequent ly in AI pat ients than the cont rol group, t his f inding was not sta-t ist ically signif icant ( 59.5% vs. 40.5% , p= 0.182) (Figure 1) .
The factors associated with TV in AI pat ients have been summarized in Table 3. A posit ive correlat ion between TV and HOMA-I R was noted, but stat ist ically significant at border-line ( r= 0.286, p= 0.057) (Figure 2) . Mult iple regression analysis was perform ed to evaluate the factors affect ing the level of TV. I t was observed that the model was well-form ed and significant , and affected the TV value at 25% (ANOVA p= 0.005 and Dubin Watson= 2.0, R2= 0.25) . An analysis of all param eters in this m odel illust rated thatA-I affected TV (Table 3) . Evaluat ion of factors affect ing thyroid nodule frequency by logist ic regression analysis re-vealed that TV, BMI , and ACTH levels as in-dependent r isk factors (Table 4) .
265
Turk J Endocrinol Metab. Şahin et al. 2020; 24: 261-269 Thyroid Volum e and I nsulin Resistance in Adrenal I ncidentalom a
2 6 5
Data are presented as n (% ) and m ean± standarddeviat ion. * Data are presented as m edian± interquart ile range. BMI , body m ass index; HT, hypertension; HL, hyperlipidem ia; ASCVD, atherosclerot ic cardiovascular disease; TSH, thyroid-st im u-lat ing horm one; fT4, free thyroxine; fT3, free t r iiodothyronine; FPG, fast ing plasm a glucose; FI , fast ing insulin; LDL, low-density li-poprotein; TG, t r iglycerides; HDL, high-density lipoprotein; ACTH, adrenocort icot ropic horm one; DST, dexam ethasone suppression test ; DHEAS,dehydroepiandrosterone sulfate; HOMA-I R, hom eostasis m odel assessm ent- insulin resistance; US, ult rasonography; TV, thyroid volum e.
I nsulin resistance Non- I nsulin resistance
Param eters n= 3 7 ( 4 2 % ) n= 5 1 ( 5 8 % ) p
Age (year) * 59.00± 12.75 60.00± 8.00 0.220
Sex (n,% )
Fem ale 24 (64.9) 31 (60.8) 0.696
Male 13 (35.1) 20 (39.2)
BMI (kg/ m 2) 34.60± 5.38 31.21± 6.97 0.016
Com orbidity (n,% ) 12 (32.4) 12 (23.5) 0.301
HT 7 (18.9) 10 (19.6)
HL 2 (5.4) 0
ASCVD 3 (8.1) 2 (3.9)
TSH* 1.14± 1.61 0.96± 0.74 0.405
fT4 1.22± 0.45 1.17± 0.21 0.558
fT3 3.14± 0.54 3.14± 0.55 0.944
FPG (m g/ dL) 95.38± 9.05 89.00± 9.59 0.002
FI (µI U/ m L)* 16.85± 9.03 8.07± 4.01 0.000
LDL (m g/ dL) 131.13± 29.02 126.39± 35.10 0.504
TG (m g/ dL) 147.70± 63.63 117.58± 53.66 0.018
HDL (m g/ dL) 42.30± 9.90 46.98± 11.51 0.049
Cort isol* 14.40± 5.70 13.10± 4.48 0.002
ACTH* 22.95± 11.83 16.10± 12.30 0.104
DST* 1.18± 0.97 1.23± 1.3 0.260
HOMA-I R* 3.98± 2.24 1.74± 0.85 0.000
Thyroid US (nodule) (n,% ) 23 (62.2) 29 (56.9) 0.617
TV (m L) 11.23± 3.15 8.64± 4.77 0.045
Table 2. Dem ographic, laboratory, and radiological character ist ics of pat ients with and without insulin resistance.
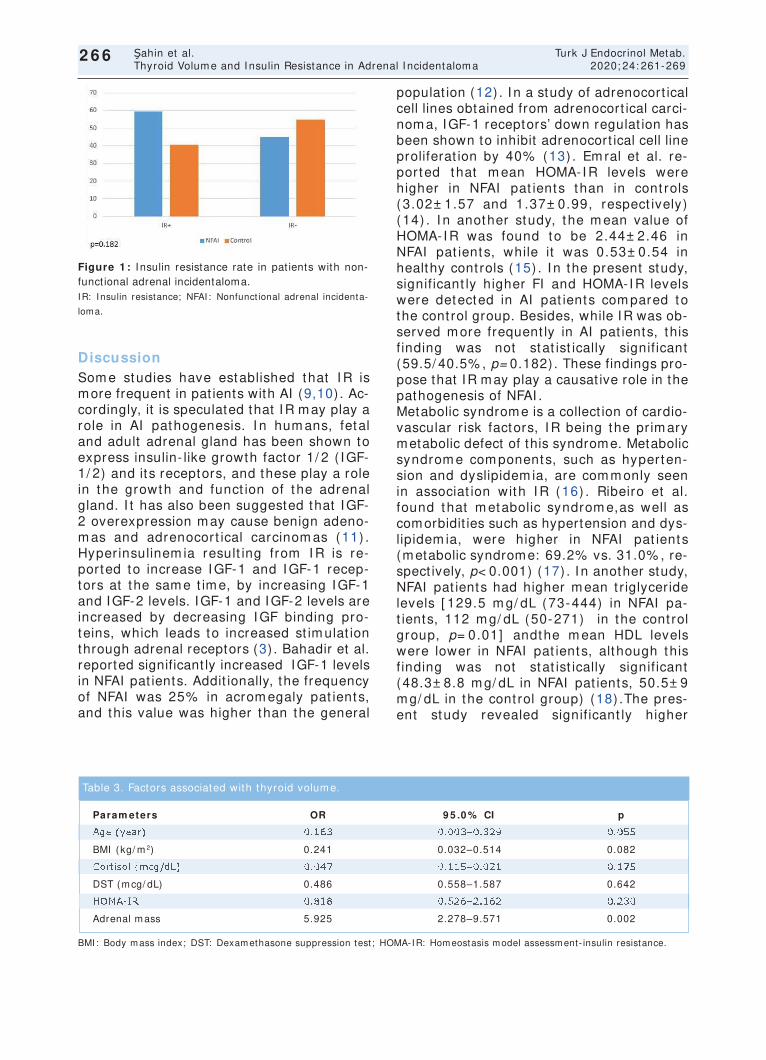
Discussion Som e studies have established that I R is more frequent in pat ients with AI (9,10) . Ac-cordingly, it is speculated that I R may play a role in AI pathogenesis. I n hum ans, fetal and adult adrenal gland has been shown to express insulin- like growth factor 1/ 2 ( I GF-1/ 2) and its receptors, and these play a role in the growth and funct ion of the adrenal gland. I t has also been suggested that I GF-2 overexpression m ay cause benign adeno-m as and adrenocort ical carcinom as (11) . Hyper insulinem ia result ing from I R is re-ported to increase I GF-1 and I GF-1 recep-tors at the sam e t im e, by increasing I GF-1 and I GF-2 levels. I GF-1 and I GF-2 levels are increased by decreasing I GF binding pro-teins, which leads to increased st im ulat ion through adrenal receptors (3) . Bahadir et al. reported significant ly increased IGF-1 levels in NFAI pat ients. Addit ionally, the frequency of NFAI was 25% in acrom egaly pat ients, and this value was higher than the general
populat ion (12) . I n a study of adrenocort ical cell lines obtained from adrenocort ical carci-noma, I GF-1 receptors’ down regulat ion has been shown to inhibit adrenocort ical cell line proliferat ion by 40% (13) . Em ral et al. re-ported that m ean HOMA-I R levels were higher in NFAI pat ients than in cont rols (3.02± 1.57 and 1.37± 0.99, respect ively) (14) . I n another study, the m ean value of HOMA-I R was found to be 2.44± 2.46 in NFAI pat ients, while it was 0.53± 0.54 in healthy cont rols (15) . I n the present study, signif icant ly higher FI and HOMA-I R levels were detected in AI pat ients com pared to the cont rol group. Besides, while I R was ob-served m ore frequent ly in AI pat ients, this f inding was not stat ist ically signif icant (59.5/ 40.5% , p= 0.182) . These findings pro-pose that IR may play a causat ive role in the pathogenesis of NFAI . Metabolic syndrome is a collect ion of cardio-vascular r isk factors, I R being the pr im ary metabolic defect of this syndrome. Metabolic syndrom e com ponents, such as hyperten-sion and dyslipidem ia, are com m only seen in associat ion with I R (16) . Ribeiro et al. found that m etabolic syndrom e,as well as comorbidit ies such as hypertension and dys-lipidem ia, were higher in NFAI pat ients (metabolic syndrome: 69.2% vs. 31.0% , re-spect ively, p< 0.001) (17) . I n another study, NFAI pat ients had higher m ean t r iglyceride levels [ 129.5 m g/ dL (73-444) in NFAI pa-t ients, 112 m g/ dL (50-271) in the cont rol group, p= 0.01] andthe m ean HDL levels were lower in NFAI pat ients, although this f inding was not stat ist ically signif icant (48.3± 8.8 m g/ dL in NFAI pat ients, 50.5± 9 m g/ dL in the cont rol group) (18) .The pres-ent study revealed signif icant ly higher
266
Şahin et al. Turk J Endocrinol Metab. Thyroid Volum e and I nsulin Resistance in Adrenal I ncidentalom a 2020; 24: 261-269
2 6 6
Figure 1 : I nsulin resistance rate in pat ients with non-funct ional adrenal incidentaloma. IR: I nsulin resistance; NFAI : Nonfunct ional adrenal incidenta-
loma.
BMI : Body m ass index; DST: Dexam ethasone suppression test ; HOMA-I R: Hom eostasis m odel assessm ent- insulin resistance.
Param eters OR 9 5 .0 % CI p
Age (year) 0.163 0.003–0.329 0.055
BMI (kg/ m 2) 0.241 0.032–0.514 0.082
Cort isol (m cg/ dL) 0.047 0.115–0.021 0.175
DST (m cg/ dL) 0.486 0.558–1.587 0.642
HOMA-I R 0.818 0.526–2.162 0.230
Adrenal m ass 5.925 2.278–9.571 0.002
Table 3. Factors associated with thyroid volum e.
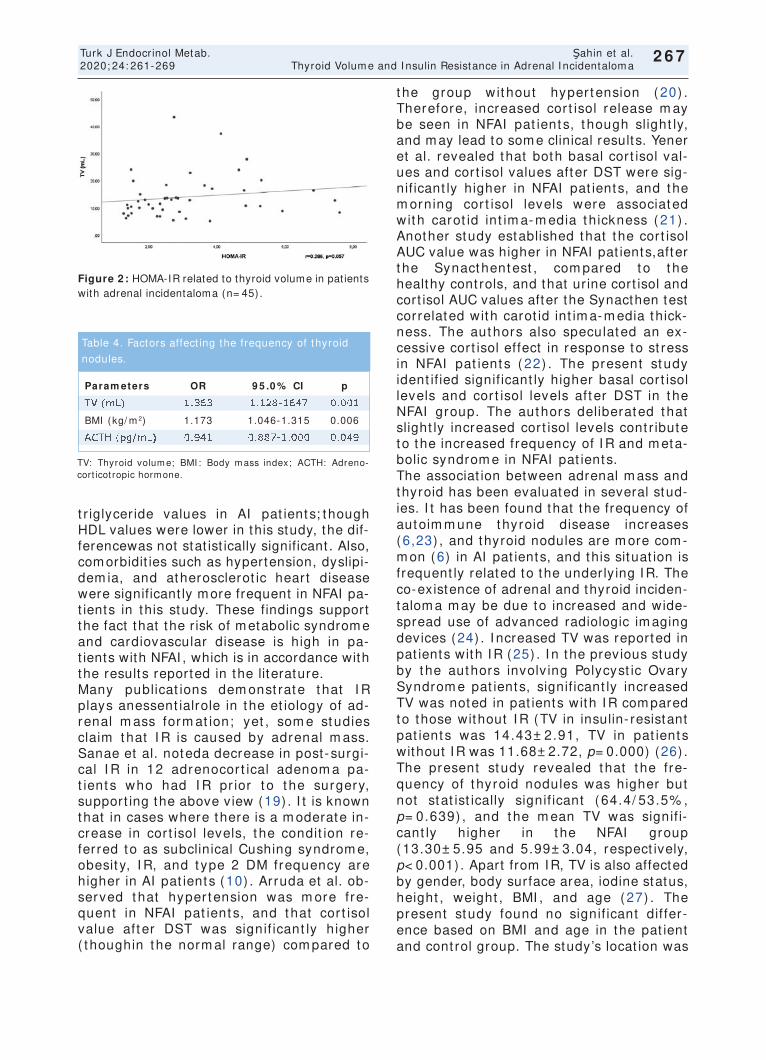
t r iglycer ide values in AI pat ients; though HDL values were lower in this study, the dif-ferencewas not stat ist ically significant . Also, com orbidit ies such as hypertension, dyslipi-dem ia, and atherosclerot ic heart disease were significant ly more frequent in NFAI pa-t ients in this study. These findings support the fact that the r isk of m etabolic syndrom e and cardiovascular disease is high in pa-t ients with NFAI , which is in accordance with the results reported in the literature. Many publicat ions dem onst rate t hat I R plays anessent ialrole in the et iology of ad-renal m ass form at ion; yet , som e studies claim that I R is caused by adrenal m ass. Sanae et al. noteda decrease in post- surgi-cal I R in 12 adrenocor t ical adenom a pa-t ient s who had I R pr ior t o t he surgery, support ing the above view (19) . I t is known that in cases where there is a m oderate in-crease in cor t isol levels, t he condit ion re-ferred to as subclinical Cushing syndrom e, obesit y, I R, and t ype 2 DM frequency are higher in AI pat ients (10) . Arruda et al. ob-served t hat hyper tension was m ore fre-quent in NFAI pat ient s, and t hat cor t isol value aft er DST was signif icant ly higher ( thoughin the norm al range) com pared to
t he group wit hout hyper tension (20) . Therefore, increased cor t isol release m ay be seen in NFAI pat ient s, t hough slight ly, and m ay lead to som e clinical results. Yener et al. revealed that both basal cor t isol val-ues and cort isol values after DST were sig-nif icant ly higher in NFAI pat ients, and the m orning cor t isol levels were associated wit h carot id int im a- m edia t hickness ( 21) . Another study established that the cort isol AUC value was higher in NFAI pat ients,after t he Synacthentest , com pared t o t he healthy cont rols, and that ur ine cort isol and cort isol AUC values after the Synacthen test correlated with carot id int im a-m edia thick-ness. The authors also speculated an ex-cessive cort isol effect in response to st ress in NFAI pat ient s ( 22) . The present st udy ident if ied signif icant ly higher basal cor t isol levels and cor t isol levels aft er DST in t he NFAI group. The authors deliberated t hat slight ly increased cort isol levels cont r ibute to the increased frequency of I R and m eta-bolic syndrom e in NFAI pat ients. The associat ion between adrenal m ass and thyroid has been evaluated in several stud-ies. I t has been found that the frequency of autoim m une thyroid disease increases (6,23) , and thyroid nodules are m ore com -m on (6) in AI pat ients, and this situat ion is frequent ly related to the underly ing I R. The co-existence of adrenal and thyroid inciden-talom a m ay be due to increased and wide-spread use of advanced radiologic im aging devices (24) . I ncreased TV was reported in pat ients with I R (25) . I n the previous study by the authors involv ing Polycyst ic Ovary Syndrom e pat ients, signif icant ly increased TV was noted in pat ients with I R com pared to those without I R (TV in insulin- resistant pat ients was 14.43± 2.91, TV in pat ients without I R was 11.68± 2.72, p= 0.000) (26) . The present study revealed that t he fre-quency of t hyroid nodules was higher but not stat ist ically signif icant ( 64.4/ 53.5% , p= 0.639) , and the m ean TV was signif i-cant ly higher in t he NFAI group (13.30± 5.95 and 5.99± 3.04, respect ively, p< 0.001) . Apart from I R, TV is also affected by gender, body surface area, iodine status, height , weight , BMI , and age (27) . The present study found no signif icant dif fer-ence based on BMI and age in the pat ient and cont rol group. The study’s locat ion was
267
Turk J Endocrinol Metab. Şahin et al. 2020; 24: 261-269 Thyroid Volum e and I nsulin Resistance in Adrenal I ncidentalom a
2 6 7
Figure 2 : HOMA-IR related to thyroid volume in pat ients with adrenal incidentaloma (n= 45).
TV: Thyroid volum e; BMI : Body m ass index; ACTH: Adreno-cort icot ropic horm one.
Param eters OR 9 5 .0 % CI p
TV (m L) 1.363 1.128-1647 0.001
BMI (kg/ m 2) 1.173 1.046-1.315 0.006
ACTH (pg/ m L) 0.941 0.887-1.000 0.049
Table 4. Factors affect ing the frequency of thyroid
nodules.

the Mediterranean region, which is a m ildly iodine-deficient area (28) . Hence,the differ-ence in thyroid volum e difference is consid-erably not due to age, BMI , and iodine status. However, a posit ive border line cor-relat ion between TV and HOMA- I R in pa-t ients with AI was observed (p= 0.057) . I n addit ion, AI was found to be an independent r isk factor for an increase in TV, alt hough this factor does not affect HOMA- I R and thyroid nodules. The authors also noted that an increase in TV, BMI , and ACTH affects the frequency of thyroid nodules. These findings suggest that increased TV may be detected in AI pat ients, and I R may be a significant cont r ibut ing fac-tor. However, HOMA-I R was not found to be effect ive on TV and nodularity,which may be due to the sm all sam ple size of the study. Therefore, the authors deliberate that the slight ly increased cort isol secret ion m ight be responsible for the increased nodular ity. I n conclusion, this study proves that hyper-insulinem ia increases the r isk of goiter in AI . Also, a slight r ise in cort isol secret ion in NFAI pat ients may increase TV by causing IR, and these pat ients m ust be evaluated for nodu-lar goiter.
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions I dea/ Concept : Mustafa Şahin; Design: Mustafa Şahin; Cont rol/ Supervision: Mustafa Şahin, Ayten Oğuz, Dilek Tüzün, Kam ile Gül; Data Collect ion and/ or Process-ing: Mustafa Şahin, Sem iha Çalkaya, Ayten
Oğuz, Dilek Tüzün; Analysis and/ or I nter-pretat ion: Mustafa Şahin, Ayten Oğuz, Dilek Tüzün; Literature Review: Mustafa Şahin; Writ ing the Art icle: Mustafa Şahin; Cr it ical Review: Mustafa Şahin, Ayten Oğuz, Dilek Tüzün; References and Fundings: Mustafa Şahin; Materials: Mustafa Şahin.
References 1. Reim ondo G, Castellano E, Grosso M, Priot to R,
Puglisi S, Pia A, Pellegrino M, Borret ta G, Terzolo M. Adrenal incidentalomas are t ied to increased risk of diabetes: findings from a prospect ive study. J Clin Endocrinol Metab. 2020; 105: dgz284. [ Crossref] [ PubMed]
2. Cawood TJ, Hunt PJ, O'Shea D, Cole D, Soule S. Rec-ommended evaluat ion of adrenal incidentalomas is cost ly, has high false-posit ive rates and confers a risk of fatal cancer that is sim ilar to the risk of the adre-nal lesion becoming malignant ; t ime for a rethink? Eur J Endocrinol. 2009; 161: 513-527. [ Crossref] [ PubMed]
3. Muscogiuri G, De Mart ino MC, Negri M, Pivonello C, Simeoli C, Orio F, Pivonello R, Colao A. Adrenal mass: insight into pathogenesis and a common link with in-sulin resistance. Endocrinology. 2017; 158: 1527-1532. [ Crossref] [ PubMed]
4. Rezzonico J, Rezzonico M, Pusiol E, Pitoia F, Niepom-niszcze H. I nt roducing the thyroid gland as another vict im of the insulin resistance syndrome. Thyroid. 2008; 18: 461-464. [ Crossref] [ PubMed]
5. Vella V, Sciacca L, Pandini G, Mineo R, Squatrito S, Vigneri R, Belfiore A. The IGF system in thyroid can-cer: new concepts. Mol Pathol. 2001; 54: 121-124. [ Crossref] [ PubMed] [ PMC]
6. Arduc A, I sik S, Ozuguz U, Tutuncu YA, Kucukler FK, Ozcan HN, Berker D, Guler S. Relat ionship between thyroid nodules and non- funct ioning adrenal inci-dentalomas and their associat ion with insulin resist-ance. Endocr Res. 2014; 39: 99-104. [ Crossref] [ PubMed]
7. Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, Stowasser M, Young WF Jr. The man-agement of primary aldosteronism: case detect ion, diagnosis, and t reatment: an Endocrine Society Clin-ical Pract ice Guideline. J Clin Endocrinol Metab. 2016; 101: 1889-1916. [ Crossref] [ PubMed]
8. Hegedüs L. Thyroid ult rasound. Endocrinol Metab Clin North Am . 2001; 30: 339-360. [ Crossref] [ PubMed]
9. Akkus G, Evran M, Sert M, Tet iker T. Adipocytokines in non- funct ional adrenal incidentalomas and rela-t ion with insulin resistance param eters. Endocr Metab Immune Disord Drug Targets. 2019; 19: 326-332. [ Crossref] [ PubMed]
10. Sydney GI , Ioakim KJ, Paschou SA. Insulin resistance and adrenal incidentalomas: a bidirect ional relat ion-ship. Maturitas. 2019; 121: 1-6. [ Crossref] [ PubMed]
11. Angelousi A, Kyriakopoulos G, Nasiri-Ansari N, Kara-georgou M, Kassi E. The role of epithelial growth fac-tors and insulin growth factors in the adrenal neoplasms. Ann Transl Med. 2018; 6: 253. [ Crossref] [ PubMed] [ PMC]
268
Şahin et al. Turk J Endocrinol Metab. Thyroid Volum e and I nsulin Resistance in Adrenal I ncidentalom a 2020; 24: 261-269
2 6 8
12. Bahadir CT, Ecemis GC, Atmaca H. Does IGF-1 play a role in the et iopathogenesis of non- funct ioning adrenocort ical adenom a? J Endocrinol I nvest . 2018; 41: 1317-1323. [ Crossref] [ PubMed]
13. Ribeiro TC, Jorge AA, Montenegro LR, Almeida MQ, Ferraz-de-Souza B, Nishi MY, Mendonca BB, Latron-ico AC. Effects of Type 1 insulin- like growth factor re-ceptor silencing in a human adrenocort ical cell line. Horm Metab Res. 2016; 48: 484-488. [ Crossref] [ PubMed]
14. Emral R, Aydoğan Bİ, Köse AD, Demir Ö, Çorapçıoğlu D. Could a nonfunct ional adrenal incidentaloma be a risk factor for increased carot id int ima-media thick-ness and metabolic syndrome. Endocrinol Diabetes Nutr. 2019; 66: 402-409. [ Crossref] [ PubMed]
15. Evran M, Akkuş G, Berk Bozdoğan İ, Gök M, Deniz A, Sert M, Tet iker T. Carot id int ima-media thickness as the cardiom etabolic r isk indicator in pat ients with nonfunct ional adrenal mass and metabolic syndrome screening. Med Sci Monit . 2016; 22: 991-997. [ Cross-ref] [ PubMed] [ PMC]
16. Sasaki N, Ozono R, Higashi Y, Maeda R, Kihara Y. As-sociat ion of insulin resistance, plasma glucose level, and serum insulin level with hypertension in a popu-lat ion with different stages of ımpaired glucose me-tabolism . J Am Heart Assoc. 2020; 9: e015546. [ Crossref] [ PubMed] [ PMC]
17. Ribeiro Cavalari EM, de Paula MP, Arruda M, Carraro N, Mart ins A, de Souza K, Coelho MC, de Oliveira E Silva de Morais NA, Moraes AB, Vieira Neto L. Non-funct ioning adrenal incidentaloma: a novel predict ive factor for metabolic syndrome. Clin Endocrinol (Oxf) . 2018; 89: 586-595. [ Crossref] [ PubMed]
18. Imga NN, Topcuoglu C, Berker D, Turhan T. Serum amyloid A, paraoxonase-1 act ivity, and apolipopro-tein concentrat ions as biomarkers of subclinical ath-erosclerosis r isk in adrenal incidentaloma pat ients. Arch Med Res. 2018; 49: 182-190. [ Crossref] [ PubMed]
19. Midorikawa S, Sanada H, Hashim oto S, Suzuki T, Watanabe T. The improvement of insulin resistance in pat ients with adrenal incidentaloma by surgical re-sect ion. Clin Endocrinol (Oxf ) . 2001; 54: 797-804. [ Crossref] [ PubMed]
20. Arruda M, Mello Ribeiro Cavalari E, Pessoa de Paula M, Fernandes Cordeiro de Morais F, Furtado Bilro G, Alves Coelho MC, de Oliveira E Silva de Morais NA, Choeri D, Moraes A, Vieira Neto L. The presence of nonfunct ioning adrenal incidentalomas increases ar-
terial hypertension frequency and severity, and is as-sociated with cort isol levels after dexam ethasone suppression test . J Hum Hypertens. 2017; 32: 3-11. [ Crossref] [ PubMed]
21. Yener S, Genc S, Akinci B, Secil M, Demir T, Comlekci A, Ert ilav S, Yesil S. Carot id int ima media thickness is increased and associated with morning cort isol in subjects with non-funct ioning adrenal incidentaloma. Endocrine. 2009; 35: 365-370. [ Crossref] [ PubMed]
22. Androulakis I I , Kaltsas GA, Kollias GE, Markou AC, Gouli AK, Thomas DA, Alexandraki KI , Papamichael CM, Hadj idakis DJ, Piadit is GP. Pat ients with appar-ent ly nonfunct ioning adrenal incidentalomas may be at increased cardiovascular risk due to excessive cor-t isol secret ion. J Clin Endocrinol Metab. 2014; 99: 2754-2762. [ Crossref] [ PubMed]
23. Karakose M, Karbek B, Sahin M, Arslan MS, Topaloglu O, Erden G, Demirci T, Calıskan M, Delibasi T. The as-sociat ion of autoim m une thyroidit is and non- func-t ional adrenal incidentalomas with insulin resistance. Arch Endocrinol Metab. 2015; 59: 42-46. [ Crossref] [ PubMed]
24. Vardanian AJ, Hines OJ, Farrell JJ, Yeh MW. Inciden-tally discovered tumors of the endocrine glands. Fu-ture Oncol. 2007; 3: 463-474. [ Crossref] [ PubMed]
25. Kushchayeva YS, Kushchayev SV, Startzell M, Cochran E, Auh S, Dai Y, Lightbourne M, Skarulis M, Brown RJ. Thyroid Abnormalit ies in Pat ients With Ex-t rem e I nsulin Resistance Syndrom es. J Clin En-docrinol Metab. 2019; 104: 2216-2228. [ Crossref] [ PubMed] [ PMC]
26. Sahin M, Demircioglu D, Oguz A, Tuzun D, Sarica MA, I nanc E, Gul K. Does insulin resistance increase thy-roid volum e in pat ients with polycyst ic ovary syn-drome? Arch Endocrinol Metab. 2017; 61: 145-151. [ Crossref] [ PubMed]
27. Suzuki S, Midorikawa S, Fukushim a T, Shim ura H, Ohira T, Ohtsuru A, Abe M, Shibata Y, Yamashita S, Suzuki S; Thyroid Examinat ion Unit of the Radiat ion Medical Science Center for the Fukushim a Health Managem ent Survey. System at ic determ inat ion of thyroid volume by ult rasound examinat ion from in-fancy to adolescence in Japan: the Fukushima Health Managem ent Survey. Endocr J. 2015; 62: 261-268. [ Crossref] [ PubMed]
28. Erdoğan MF, Ağbaht K, Altunsu T, Ozbaş S, Yücesan F, Tezel B, Sargin C, I lbeğ I , Art ik N, Köse R, Erdoğan G. Current iodine status in Turkey. J Endocrinol I n-vest . 2009; 32: 617-622. [ Crossref] [ PubMed]
269
Turk J Endocrinol Metab. Şahin et al. 2020; 24: 261-269 Thyroid Volum e and I nsulin Resistance in Adrenal I ncidentalom a
2 6 9

Original Art icle Turk J Endocrinol Metab. 2020; 24: 270-276
270
Frequency of Nodular Goiter in Pat ients w ith Non- Funct ional Adrenal I ncidentalom a
Non-Fonksiyonel Adrenal I nsidentalom alı Hastalarda Nodüler Guat r Sıklığı
Mustafa CAN, Melia KARAKÖSE, Muham m et KOCABAŞ, İlker ÇORDAN,
Hat ice ÇALIŞKAN BURGUCU, Mustafa KULAKSI ZOĞLU, Feridun KARAKURT
Department of Endocrinology and Metabolism, Necmett in Erbakan University Meram Faculty of Medicine, Konya, TURKEY
Object ive: Thyroid nodules and metabolic disorders such as obesit y, insulin resistance ( I R) , and dyslipidem ia are fre-quent ly reported in pat ients with non- funct ional adrenal in-cidentalom a (NFAI ) . This study aim ed to evaluate the st ructural and funct ional propert ies of the thyroid gland and to elucidate whether there is any relat ionship between these and m etabolic param eters in pat ients with NFAI . Mater ia l and Methods: Fifty- four pat ients diagnosed with NFAI and 54 age, gender, and body mass index (BMI ) matched healthy cont rols were included in the study. Free thyroxine ( fT4) , thyroid-st im ulat ing horm one (TSH) , ant i- thyroperoxidase ant ibody (ant i-TPO) , fast ing blood glucose (FBG) , fast ing in-sulin level, lipid profiles, C- react ive protein (CRP) levels were est im ated in the pat ients and cont rols. Furtherm ore, pat i-ents and cont rols were evaluated by ult rasonography to de-term ine thyroid st ructure, thyroid volum e, and thyroid nodules. Results: The mean total thyroid volume of the NFAI group (13.48± 6.3 m L) was significant ly higher as com pared to that of the cont rol group (13.13± 10 m L) (p< 0.001) . Thyroid nodules were detected in 18 (33.3% ) of 54 subjects in the NFAI group and 16 (29.6% ) of 54 subjects in the con-t rol group, result ing in an insignif icant difference (p = 0.836) . However, the average number of thyroid nodules was significant ly higher in the NFAI group (1.72) compared to the cont rol group (1.06) (p< 0.001) . The thyroid nodule size of the NFAI group (17.83± 9.01 m m ) was also significant ly lar-ger than the cont rol group (11.68± 4.68 m m ) (p= 0.017) . Moreover, a significant associat ion between the thyroid no-dule and TSH (p= 0.026) and between thyroid nodule size and adenom a size (p= 0.046) in the NFAI group was prono-unced. Conclusion: I n our study, we found that certain pa-ram eters related to the thyroid gland, such as thyroid volum es, average num ber of thyroid nodules, and thyroid nodule sizes, were significant ly higher in NFAI pat ients than in healthy cont rols. There was no signif icant difference in term s of thyroid funct ions and thyroid nodule frequency. I n this regard, studies with larger sam ple size, encom passing all factors that m ay affect thyroid st ructure and funct ions, are essent ial. Keyw ords: Adrenal incidentalom a; thyroid nodule; goiter
Am aç: Nonfonksiyonel adrenal insidentalom alı (NFAİ) has-talarda; t iroid nodüller i ve obezite, insülin direnci ve dislipi-dem i gibi m etabolik bozukluklar yaygın olarak görülür. Bu çalışmanın amacı, NFAİ olan hastalarda t iroid bezinin yapısal ve fonksiyonel özellik ler ini ve bu özellik ler le m etabolik para-m et reler arasında bir ilişki olup olm adığını belir lem ekt ir. Gereç ve Yöntem ler: NFAİ tanısı alan 54 hasta ile yaş, cin-siyet ve vücut kit le indeksi (VKİ) uyum lu 54 sağlık lı kont rol çalışmaya dâhil edildi. Hasta ve kontrol gruplarının serbest t i-roksin (sT4) , t iroid st imülan hormon (TSH) , ant i- t iroperoksi-daz ant ikoru (ant i-TPO) , açlık kan şekeri (AKŞ) , açlık insülin seviyesi, lipid profiller i, C- reakt if protein (CRP) düzeyler i öl-çüldü. Ayrıca, hasta ve kont rol grupları t iroid yapısı, t iroid hacm i ve t iroid nodüller inin belir lenm esi için ult rasonografi ile değerlendir ildi. Bulgular: Ortalam a toplam t iroid hacm i NFAİ grubunda (13,48± 6,3 m l) kont rol grubuna göre (13,13± 10 m l) anlam lı olarak yüksekt i (p< 0,001) . NFAI gru-bundaki 54 hastanın 18’inde (% 33,3) , kont rol grubundaki 54 hastanın 16’sında (% 29,6) t iroid nodülleri tespit edildi ve an-lam lı fark saptanm adı (p= 0,836) . Ortalam a t iroid nodül sa-yısı NFAİ grubunda (1,72) kont rol grubuna göre (1,06) anlam lı olarak yüksekt i ( p< 0,001) . Tiroid nodülü boyutu NFAİ grubunda (17,83± 9,01 m m ) kont rol grubuna göre (11,68± 4,68 m m ) anlam lı olarak yüksekt i (p= 0,017) . Ay-rıca, NFAI grubunda t iroid nodülü ile TSH (p= 0,026) düzeyi arasında ve t iroid nodülü boyutu ile adenom boyutu (p= 0,046) arasında anlam lı bir ilişki tespit edildi. Sonuç: Ça-lışm am ızın sonuçlarına göre, NFAI hastalarında t iroid hacim -ler i, or talam a t iroid nodül sayıları ve t iroid nodül boyut ları norm al popülasyona göre daha yüksek, t iroid fonksiyonları ve t iroid nodül sıklığı normal popülasyonla benzer olarak tes-pit edildi. Bu konu ile ilişkili olarak, daha büyük örneklem bo-yutuna sahip olan, t iroid bezinin yapısını ve fonksiyonlarını etkileyebilecek tüm param etreler i içeren çalışm alara iht iyaç vardır. Anahtar kelimeler: Adrenal insidentaloma; tiroid nodülü; guatr
2 7 0
Address for Correspondence: Mustafa CAN, Departm ent of Endocrinology and Metabolism , Necm et t in Erbakan University Meram Faculty of Medicine, Konya, TURKEY
Phone: 90 332 223 60 00 E- m ail: can1120can@gm ail.com
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 09 Apr 2020 Received in revised form : 04 Aug 2020 Accepted: 24 Aug 2020 Available online: 30 Sep 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
54
27

I nt roduct ion The adrenal m asses ident if ied by chance dur ing perform ed radiological im aging m ethods, conducted for reasons other than adrenal disease, are defined as adrenal inci-dentalom a. Studies have revealed the prevalence of this disease is about 3% in the 50s and inreases with age, up to 10% (1) . NFAI accounts for approximately 80% of AI ’s (2) . Thyroid nodules are com m only observed in the populat ion. Nodule incidences are known to increase with age, and the sonographic prevalence is found to reach 50% over 50 years. I n our count ry, the sonographic prevalence of thyroid nodules was est imated to be 23.5% between 18-65 years of age and 37.4% above 65 years of age (3) . Ad-vanced age, fem ale gender, iodine defi-ciency, and radiat ion exposure are predisposing factors that augm ent the inci-dence of thyroid nodules (4) . Recent stud-ies have docum ented a high prevalence of insulin resistance, m etabolic syndrom e, and obesity is associated with an increase in thy-roid volum e and nodule frequency in iodine-sufficient regions (5) . The response of endocrine cells to growth-st im ulat ing factors dictates the process of adrenal and thyroid nodular format ion (6,7) . Adrenocort icot ropic horm one (ACTH) and TSH are the main growth st imulat ing factors that t r igger the growth of adrenal and thy-roid cells. Moreover, the insulin/ insulin- like growth factor system is thought to be re-sponsible for prom ot ing the growth of adre-nal and thyroid cells (8,9) . Metabolic disorders, including obesit y, in-sulin resistance, dyslipidem ia, are also com-m on in pat ients with NFAI (10) . Com pared to the norm al populat ion, insulin resistance is m ore frequent in NFAI pat ients. The hy-perinsulinem ia accom panying insulin resist-ance induces act ivat ion of insulin/ I GF receptors and causes a m itogenic effect on the adrenal cortex. I nsulin resistance is also found to be correlated with adenom a size (11) . The presence of com m on growth factors st im ulat ing the growth of adrenal and thy-roid cells, coupled with the increased fre-quency of thyroid nodules in pat ients with m etabolic disorders such as obesity, insulin resistance, and dyslipidem ia ( com m on in
NFAI pat ients) , indicate that there m ay be a relat ionship between NFAI and thyroid nod-ules. I n our study, we t r ied to evaluate the st ruc-tural and funct ional status of the thyroid gland in NFAI pat ients and to determ ine if there is a relat ionship between them and the m etabolic param eters.
Materia l and Methods This study was conducted between 01.01.2020 and 31.03.2020 at Meram Fac-ulty of Medicine, Departm ent of Endocrinol-ogy, and Metabolism . The study protocol was approved by the Ethics Com m it tee of Meram Medical Faculty on 21/ 02/ 2020 with the decision num bered 2020/ 2325 and was carried out following the Helsinki Declarat ion Pr inciples. I nform ed consent was obtained from all part icipants. The study com prised of 54 pat ients diagnosed with NFAI . The di-agnosis of adenom a was achieved by an un-enhanced CT scan. The adrenal lesion was accepted as an adenom a if at tenuat ion was ≤10 HU on an unenhanced CT scan. Pa-t ients with adrenal lesion at tenuat ion > 10 HU on an unenhanced CT scan were ex-cluded from the study. No specific horm one excess signs and/ or sym ptom s were de-tected in pat ients with NFAI . There were no signs and/ or sym ptom s of act ive endocrine or non-endocr ine disease that could affect screening test results. All NFAI pat ients were diagnosed with Cushing’s syndrom e, sub-clinical Cushing’s syndrom e, and pheochro-m ocytom a, and NFAI pat ients with hypertension and/ or hypokalem ia were also screened for pr im ary hyperaldosteronism . NFAI pat ients were subjected to a 1 m g overnight dexam ethasone suppression test to rule out a diagnosis of Cushing’s syn-drom e. The test was perform ed by adm inis-t rat ion of 1 m g dexam ethasone at 11 pm , and determ inat ion of fasting plasm a cort isol at 8 am the following day. Pat ients without serum cort isol levels < 1.8 µg/ mL were ex-cluded from the study. I n term s of pheochrom ocytom a, pat ients with 24-hour ur inary m etanephr ine or norm etanephr ine levels equal to or higher than two t im es the upper lim it of norm al were excluded from the study. I n term s of pr im ary hyperaldos-teronism , pat ients having a plasm a aldos-terone concent rat ion > 15 ng/ dL or plasm a
271
Turk J Endocrinol Metab. Can et al. 2020; 24: 270-276 Nodular Goiter in Pat ients with Adrenal I ncidentalom a
2 7 1
aldosterone/ plasm a renin act ivity rat io > 20 were excluded from the study. Based on these tests, pat ients whose AI was deter-m ined to be non- funct ional were included in the study. The cont rol group incorporated 54 healthy volunteers. Cont rol subjects were selected from healthy volunteers with norm al adre-nal im aging (abdom en and/ or adrenal CT) who m atched with the pat ients in term s of age, gender, and BMI . Pat ients and healthy cont rols under 18 and over 65 years of age, with known thyroid disease, diabetes m elli-tus, hyperlipidem ia, chronic liver and kidney diseases, atherosclerot ic cardiovascular dis-ease, were excluded from the study. The height (m ) , weight (kg) , hip circum fer-ence (HC) , waist circum ference (WC) of pa-t ients and cont rols were assessed, and WHR (Waist-Hip Rat io) was calculated. After a 10-m inute rest per iod, blood pressure was measured from both arms and was recorded as systolic (SBP) diastolic (DBP) . Biochem ical and horm onal laboratory data of the pat ients were collected from pat ient files. I R was com puted according to the for-m ula below. HOMA-I R (Hom eostat ic Model Assessm ent of I nsulin Resistance) : (FBG (mg/ dL) × fast-ing insulin (m U/ l) / 405) . The lower and upper lim its were as follows: TSH: 0.28-4.5 m U/ L; fT4: 0.94-1.77 ng/ dL; ant i-TPO Ab: 0-35 U/ m L. Ant i-TPO concen-t rat ions exceeding 35 I U/ m L were consid-ered posit ive. The pat ients and cont rols underwent ult ra-sonography at our clinic under the supervi-sion of an experienced endocrinologist using a 12MHz linear probe on a LOGI Q 3 ult ra-sonography (US) device. Lesions larger than 3 m m detected in the US were regarded as nodules. Thyroid volum es were est im ated separately for each lobe using the ellipt ical shape volum e form ula (× width × length × height × 0.479) . Adding up both the thyroid lobe volum es, the total thyroid volum e was obtained. Stat ist ical analysis was com puted using the SPSS 22.0 (Stat ist ical Package for Social Sciences) program . Cont inuous var iables were represented as m ean ± standard devi-at ion for norm al dist r ibut ion and as m edian (m inimum-maximum) if the dist r ibut ion was not norm al. I n the com parison of independ-
ent group differences, the significance test of the difference between the two m eans ( I ndependent sam ples t - test ) was used when the param et r ic test assum pt ions are provided; The Mann-Whitney U test was ap-plied to com pare the independent group dif-ferences when the param et r ic test assum pt ions were not provided. Pearson’s and Spearm an’s tests were adopted for cor-relat ion analysis between num erical var i-ables showing norm al dist r ibut ion. For differences, p < 0.05 value was considered stat ist ically significant .
Results The study involved 108 cases, including 54 NFAI pat ients and 54 healthy cont rol. Of the 54 pat ients, 36 (66.6% ) were fem ale, 18 (33.4% ) were m ale. The m ean age of the NFAI pat ients was 48.89 ± 10.7 years. The cont rol group (54 subjects) com prised of 35 (64.8% ) fem ale and 19 (35.2% ) m ale. The m ean age of the cont rol group was 48.57± 10.5 years (Table 1) . Adenom a was located on the r ight in 17 pat ients (31.5% ) , on the left in 28 pat ients (51.9% ) , and bi-laterally in nine pat ients (16.7% ). The mean adenom a size was 20.7± 7.5 m m . Hypertension (HT) was detected in 22 (40.7% ) of 54 NFAI pat ients and 10 (18.5% ) of 54 cont rols. Stat ist ical analysis revealed the frequency of HT was signif i-cant ly higher in the NFAI group (p= 0.020) . BMI , WHR, SBP, DBP, FBG, plasm a insulin, HOMA-IR, total cholesterol, and LDL-C (Low-Density Lipoprotein-Cholesterol) levels were higher in the NFAI group than the cont rol group, though the difference was stat ist i-cally insignif icant . HDL-C (High-Densit y Lipoprotein-Cholesterol) , TG (Tr iglycer ide) , CRP (C-React ive Protein) , TSH, fT4, ant i-TPO levels were lower in the NFAI group com -pared to the cont rol group, but there was no significant difference (Table 1) . Total thyroid volum e was 13.48± 6.3 m L for the NFAI group and 13.13± 10 m L of the cont rol group. The total thyroid volum e of the NFAI group was significant ly higher than the cont rol group (p< 0.001) . Thyroid nod-ules were observed in 18 (33.3% ) of 54 NFAI pat ients and 16 (29.6% ) of 54 con-t rols. No significant difference was obtained between the NFAI and cont rol groups in term s of the presence of thyroid nodules
272
Can et al. Turk J Endocrinol Metab. Nodular Goiter in Pat ients with Adrenal I ncidentalom a 2020; 24: 270-276
2 7 2
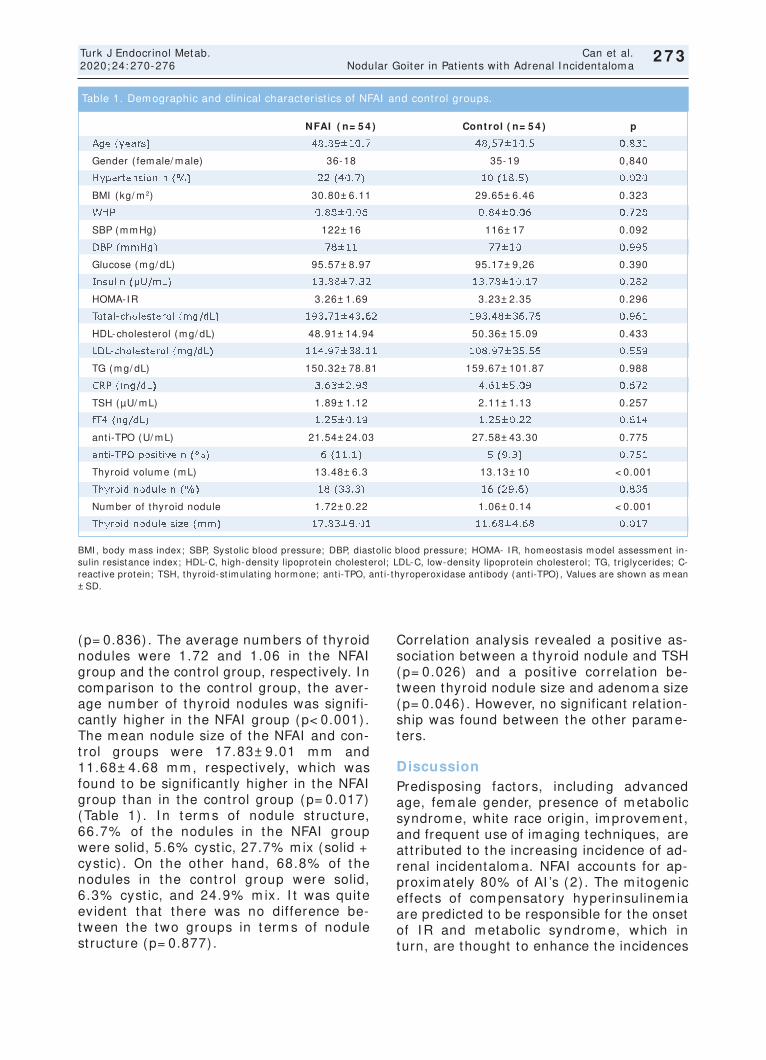
273
Turk J Endocrinol Metab. Can et al. 2020; 24: 270-276 Nodular Goiter in Pat ients with Adrenal I ncidentalom a
2 7 3
(p= 0.836) . The average num bers of thyroid nodules were 1.72 and 1.06 in the NFAI group and the control group, respect ively. I n com parison to the cont rol group, the aver-age num ber of thyroid nodules was signifi-cant ly higher in the NFAI group (p< 0.001) . The m ean nodule size of the NFAI and con-t rol groups were 17.83± 9.01 m m and 11.68± 4.68 m m , respect ively, which was found to be significant ly higher in the NFAI group than in the cont rol group (p= 0.017) (Table 1) . I n term s of nodule st ructure, 66.7% of the nodules in the NFAI group were solid, 5.6% cyst ic, 27.7% m ix (solid + cyst ic) . On the other hand, 68.8% of the nodules in the cont rol group were solid, 6.3% cyst ic, and 24.9% m ix. I t was quite evident that there was no difference be-tween the two groups in term s of nodule st ructure (p= 0.877) .
Correlat ion analysis revealed a posit ive as-sociat ion between a thyroid nodule and TSH (p= 0.026) and a posit ive correlat ion be-tween thyroid nodule size and adenoma size (p= 0.046) . However, no significant relat ion-ship was found between the other param e-ters.
Discussion Predisposing factors, including advanced age, fem ale gender, presence of m etabolic syndrom e, white race origin, im provem ent , and frequent use of imaging techniques, are at t r ibuted to the increasing incidence of ad-renal incidentalom a. NFAI accounts for ap-proxim ately 80% of AI ’s (2) . The m itogenic effects of com pensatory hyper insulinem ia are predicted to be responsible for the onset of I R and m etabolic syndrom e, which in turn, are thought to enhance the incidences
BMI , body m ass index; SBP, Systolic blood pressure; DBP, diastolic blood pressure; HOMA- I R, hom eostasis m odel assessm ent in-sulin resistance index; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, t r iglycerides; C-react ive protein; TSH, thyroid-st imulat ing hormone; ant i-TPO, ant i- thyroperoxidase ant ibody (ant i-TPO) , Values are shown as mean ± SD.
NFAI ( n= 5 4 ) Control ( n= 5 4 ) p
Age (years) 48.89± 10.7 48,57± 10.5 0.831
Gender ( fem ale/ m ale) 36-18 35-19 0,840
Hypertension n (% ) 22 (40.7) 10 (18.5) 0.020
BMI (kg/ m 2) 30.80± 6.11 29.65± 6.46 0.323
WHR 0.88± 0.06 0.84± 0.06 0.728
SBP (m m Hg) 122± 16 116± 17 0.092
DBP (m m Hg) 78± 11 77± 10 0.995
Glucose (m g/ dL) 95.57± 8.97 95.17± 9,26 0.390
I nsulin (µU/ m L) 13.88± 7.32 13.78± 10.17 0.282
HOMA-I R 3.26± 1.69 3.23± 2.35 0.296
Total-cholesterol (m g/ dL) 193.71± 43.62 193.48± 36.76 0.961
HDL-cholesterol (m g/ dL) 48.91± 14.94 50.36± 15.09 0.433
LDL-cholesterol (m g/ dL) 114.97± 38.11 108.97± 35.56 0.559
TG (m g/ dL) 150.32± 78.81 159.67± 101.87 0.988
CRP (m g/ dL) 3.63± 2.98 4.61± 5.09 0.672
TSH (µU/ m L) 1.89± 1.12 2.11± 1.13 0.257
fT4 (ng/ dL) 1.25± 0.19 1.25± 0.22 0.614
ant i-TPO (U/ m L) 21.54± 24.03 27.58± 43.30 0.775
ant i-TPO posit ive n (% ) 6 (11.1) 5 (9.3) 0.751
Thyroid volum e (m L) 13.48± 6.3 13.13± 10 < 0.001
Thyroid nodule n (% ) 18 (33.3) 16 (29.6) 0.836
Num ber of thyroid nodule 1.72± 0.22 1.06± 0.14 < 0.001
Thyroid nodule size (m m ) 17.83± 9.01 11.68± 4.68 0.017
Table 1. Dem ographic and clinical character ist ics of NFAI and cont rol groups.
of both adrenal incidentalom a and thyroid nodule in the iodine-sufficient regions, re-cent ly (12) . Some previous studies have reported that IR and other m etabolic disorders that are com -ponents of m etabolic syndrom e are often seen in NFAI pat ients (13,14) . I t is pre-sumed that the undetectable amount of cor-t isol secreted from AI , leads to the developm ent of these m etabolic disorders (15,16) . Furtherm ore, com plete recovery of metabolic disorders following surgical resec-t ion of adenom a in pat ients with NFAI has also been shown as im portant evidence to substant iate the relat ionship between NFAI and m etabolic disorders (17-19) . On the other hand, with the growth factor- like ef-fect of insulin, com pensatory hyperinsuline-m ia observed in I R m ay lead to the onset of adrenal incidentalom a (5) . Terzolo et al. reported that SBP, DBP, OGTT (Oral Glucose Tolerance Test ) 2nd-hour glu-cose level, insulin sensit iv it y index ( I SI ) level were signif icant ly higher in pat ients with NFAI than cont rols. Terzolo et al. also highlighted enhanced levels of FBG, fast ing insulin, LDL-cholesterol, HDL-C, TG in NFAI pat ients; however, this result failed to por-t ray any stat ist ical significance (20) . Peppa et al. showed that in the NFAI group, SBP, DBP, TG, HOMA-I R, and FBG levels were higher than the cont rol group and HDL-C were lower than the cont rol group (10) . On the cont rary, in our study, no difference be-tween NFAI and cont rol groups was wit -nessed in term s of SBP, DBP, WHR, HOMA-I R, FBG, fast ing insulin, total choles-terol, and LDL-C levels. There are lim ited studies invest igat ing thy-roid st ructure and funct ions in pat ients with NFAI . The ret rospect ive and prospect ive au-topsy studies, explor ing the relat ionship be-tween thyroid nodules and adrenal adenom as, reported no relat ion between them (21) . I n the study conducted by Arduç et al. with NFAI pat ients, they found the number of subjects with thyroid nodules and the num ber of thyroid nodules higher in the NFAI group than in the cont rol group. How-ever, the correlat ion analysis failed to dem onst rate any param eter associated with the num ber of subjects with thyroid nodules and the num ber of thyroid nodules. There was no significant difference between NFAI
and cont rol groups in term s of thyroid vol-um e, TSH, FBG, insulin level, HOMA-I R, and lipid levels (22) . I n the present study, thy-roid volume, the average number of thyroid nodules, and thyroid nodule size were sig-nificant ly higher in the NFAI pat ients. Nonetheless, there was no difference between NFAI and cont rol groups in terms of the number of cases with thyroid nodules. No correlat ion was obtained be-tween other m etabolic param eters and thy-roid param eters. Another study, elucidat ing the relat ionship between thyroid funct ions and m etabolic syndrome components, established a signif-icant relat ionship between lipid levels and fT4 levels and also between fT4 levels and I R (23) . I n a study by Karaköse et al. with NFAI pat ients, they reported that fT4, ant i-thyroglobulin, and ant i-TPO levels were sig-nificant ly higher in the NFAI group compared to the cont rol group, whereas, thyroid vol-um es, TSH, and fT3 levels were com parable in both the groups. Moreover, they deter-m ined a signif icant relat ionship between HOMA-I R levels and thyroid volum e and fT4 levels (24) . The present study failed to ob-tain any difference between NFAI and con-t rol groups in term s of TSH, fT4, and ant i-TPO levels. Owing to the presence of com m on growth factors that st imulate the growth of both ad-renal and thyroid cells, coupled with the in-creased frequency of thyroid nodules in m etabolic disorders such as obesity, insulin resistance, and dyslipidem ia, which are com m on in NFAI pat ients, it was assum ed that thyroid sizes, thyroid nodule frequency, and the num ber of nodules would be higher in NFAI pat ients. The finding from our study clearly indicated signif icant ly higher levels of thyroid vol-um es, the average num ber of thyroid nod-ules, and thyroid nodule size in NFAI pat ients than healthy cont rols. However, there was no difference between the groups in terms of the frequency of thyroid nodules. We believe that the absence of any differ-ence between the groups in terms of the fre-quency of thyroid nodules m ay be just ified by the fact that factors that m ay affect the thyroid st ructure such as iodine deficiency were not est im ated in our study and the sam ple size was sm all.
274
Can et al. Turk J Endocrinol Metab. Nodular Goiter in Pat ients with Adrenal I ncidentalom a 2020; 24: 270-276
2 7 4

Conclusion Our study thus concluded that thyroid vol-um es, the average num ber of thyroid nod-ules, and thyroid nodule sizes in NFAI pat ients were signif icant ly higher than healthy controls. Nevertheless, there was no difference between NFAI pat ients and con-t rols in term s of thyroid funct ions and thy-roid nodule frequency. I n this regard, for further in-depth knowledge, it is essent ial to conduct studies with a larger sam ple size and, including all factors that m ay affect thyroid st ructure and funct ions.
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions I dea/ Concept : Mustafa Can, Melia Karaköse, Fer idun Karakurt ; Design: Mustafa Can, Melia Karaköse, Mustafa Kulaksızoğlu; Con-t rol/ Supervision: Feridun Karakurt , Mustafa Kulaksızoğlu; Data Collect ion and/ or Pro-cessing: Mustafa Can, Muhammet Kocabaş, İlker Çordan; Analysis and/ or I nterpretat ion: Mustafa Can, Melia Karaköse; Literature Re-view: Muham m et Kocabaş, İlker Çordan; Writ ing the Art icle: Mustafa Can, Muhammet Kocabaş; Cr it ical Review: Melia Karaköse, Hat ice Çalışkan Burgucu; References and Fundings: Mustafa Can; Materials: Muham-met Kocabaş, Hat ice Çalışkan Burgucu.
References 1. Barzon L, Sonino N, Fallo F, Palu G, Boscaro M.
Prevalence and natural history of adrenal inciden-talom as. Eur J Endocr inol. 2003; 149: 273-285. [ Crossref] [ PubMed]
2. Young WF Jr. Managem ent approaches to adrenal incidentalom as. A view from Rochester, Minnesota. Endocrinol Metab Clin North Am. 2000; 29: 159-185. [ Crossref] [ PubMed]
3. Turkey Associat ion of Endocrinology and Metabolism Thyroid Diseases Diagnosis and Treatm ent Guide. 2019; 143.
4. Rojeski MT, Gharib H. Nodular thyroid disease. Eval-uat ion and m anagem ent . N Engl J Med. 1985; 313: 428-436. [ Crossref] [ PubMed]
5. Ayturk S, Gursoy A, Kut A, Anil C, Nar A, Tutuncu NB. Metabolic syndrome and its components are as-sociated with increased thyroid volum e and nodule prevalence in a m ild- to-m oderate iodine-deficient area. Eur J Endocrinol. 2009; 161: 599-605. [ Cross-ref] [ PubMed]
6. Studer H, Derwahl M. Mechanism s of nonneoplast ic endocr ine hyperplasia- -a changing concept : a re-v iew focused on the thyroid gland. Endocr Rev. 1995; 16: 411-426. [ Crossref] [ PubMed]
7. Derwahl M. Molecular aspects of the pathogenesis of nodular goiters, thyroid nodules and adenom as. Exp Clin Endocrinol Diabetes. 1996; 104 Suppl 4: 32-35. [ Crossref] [ PubMed]
8. Kim ura T, Van Keym eulen A, Golstein J, Fusco A, Dumont JE, Roger PP. Regulat ion of thyroid cell pro-liferat ion by TSH and other factors: a cr it ical evalu-at ion of in v it ro m odels. Endocr Rev. 2001; 22: 631-656. [ Crossref] [ PubMed]
9. Ribeiro TC, Lat ronico AC. I nsulin- like growth factor system on adrenocort ical tum or igenesis. Mol Cell Endocrinol. 2012; 351: 96-100. [ Crossref] [ PubMed]
10. Peppa M, Boutat i E, Koliaki C, Papaefstathiou N, Garoflos E, Econom opoulos T, Hadj idakis D, Rapt is SA. I nsulin resistance and m etabolic syndrom e in pat ients with nonfunct ioning adrenal incidentalo-m as: a cause-effect relat ionship? Metabolism . 2010; 59: 1435-1441. [ Crossref] [ PubMed]
11. Peppa M, Koliaki C, Rapt is SA. Adrenal incidentalo-m as and cardiom etabolic m orbidit y: an em erging associat ion with ser ious clinical im plicat ions. J I ntern Med. 2010; 268: 555-566. [ Crossref] [ PubMed]
12. Tsatsoulis A. The role of insulin resistance/ hyperin-sulinism on the r ising t rend of thyroid and adrenal nodular disease in the current environm ent . J Clin Med. 2018; 7: 37. [ Crossref] [ PubMed] [ PMC]
13. Grum bach MM, Biller BM, Braunstein GD, Cam pbell KK, Carney JA, Godley PA, Harr is EL, Lee JK, Oertel YC, Posner MC, Schlechte JA, Wieand HS. Manage-m ent of the clinically inapparent adrenal m ass ( " in-cidentaloma") . Ann I ntern Med. 2003; 138: 424-429. [ Crossref] [ PubMed]
14. Terzolo M, Bovio S, Reim ondo G, Pia A, Osella G, Borret ta G, Angeli A. Subclinical Cushing's syn-drom e in adrenal incidentalom as. Endocrinol Metab Clin North Am . 2005; 34: 423-439. [ Crossref] [ PubMed]
15. Terzolo M, Bovio S, Pia A, Conton PA, Reim ondo G, Dall'Asta C, Bem porad D, Angeli A, Opocher G, Mannelli M, Am brosi B, Mantero F. Midnight serum cort isol as a m arker of increased cardiovas-cular r isk in pat ients with a clinically inapparent ad-renal adenom a. Eur J Endocr inol. 2005; 153: 307-315. [ Crossref] [ PubMed]
275
Turk J Endocrinol Metab. Can et al. 2020; 24: 270-276 Nodular Goiter in Pat ients with Adrenal I ncidentalom a
2 7 5

276
Can et al. Turk J Endocrinol Metab. Nodular Goiter in Pat ients with Adrenal I ncidentalom a 2020; 24: 270-276
2 7 6
16. Yener S, Genc S, Akinci B, Secil M, Dem ir T, Com -lekci A, Ert ilav S, Yesil S. Carot id int im a m edia thickness is increased and associated with m orning cort isol in subjects with non- funct ioning adrenal in-cidentalom a. Endocrine. 2009; 35: 365-370. [ Cross-ref] [ PubMed]
17. Midor ikawa S, Sanada H, Hashim oto S, Suzuki T, Watanabe T. The im provem ent of insulin resistance in pat ients with adrenal incidentalom a by surgical resect ion. Clin Endocrinol (Oxf ) . 2001; 54: 797-804. [ Crossref] [ PubMed]
18. Bernini G, Moret t i A, I acconi P, Miccoli P, Nam i R, Lucani B, Salvet t i A. Anthropom et r ic, haem ody-namic, humoral and hormonal evaluat ion in pat ients with incidental adrenocort ical adenomas before and after surgery. Eur J Endocrinol. 2003; 148(2) : 213-219. [ Crossref] [ PubMed]
19. Linos DA, Sty lopoulos N, Rapt is SA. Adrenalom a: a call for m ore aggressive m anagem ent . Wor ld J Surg. 1996; 20: 788-792. [ Crossref] [ PubMed]
20. Terzolo M, Pia A, Alì A, Osella G, Reim ondo G, Bovio S, Daffara F, Procopio M, Paccot t i P, Borret ta G, An-geli A. Adrenal incidentalom a: a new cause of the
m etabolic syndrom e? J Clin Endocr inol Metab. 2002; 87: 998-1003. [ Crossref] [ PubMed]
21. Sington JD, Syn WK, Suvarna SK, Rassl DM, Jenk-ins RC, Weetm an AP, Ross RJ. Lack of associat ion between thyroid and adrenal nodules: a histologi-cal study. J Endocr inol I nvest . 1999; 22: 262-265. [ Crossref] [ PubMed]
22. Arduc A, I sik S, Ozuguz U, Tutuncu YA, Kucukler FK, Ozcan HN, Berker D, Guler S. Relat ionship between thyroid nodules and non- funct ioning adrenal inci-dentalom as and their associat ion with insulin re-sistance. Endocr Res. 2014; 39: 99-104. [ Crossref] [ PubMed]
23. Roos A, Bakker SJ, Links TP, Gans RO, Wolffenbut-tel BH. Thyroid funct ion is associated with com po-nents of the m etabolic syndrom e in euthyroid subjects. J Clin Endocr inol Metab. 2007; 92: 491-496. [ Crossref] [ PubMed]
24. Karakose M, Karbek B, Sahin M, Arslan MS, Topaloglu O, Erden G, Dem irci T, Calıskan M, Delibasi T. The associat ion of autoim m une thyroidi-t is and non- funct ional adrenal incidentalom as with insulin resistance. Arch Endocr inol Metab. 2015; 59: 42-46. [ Crossref] [ PubMed]
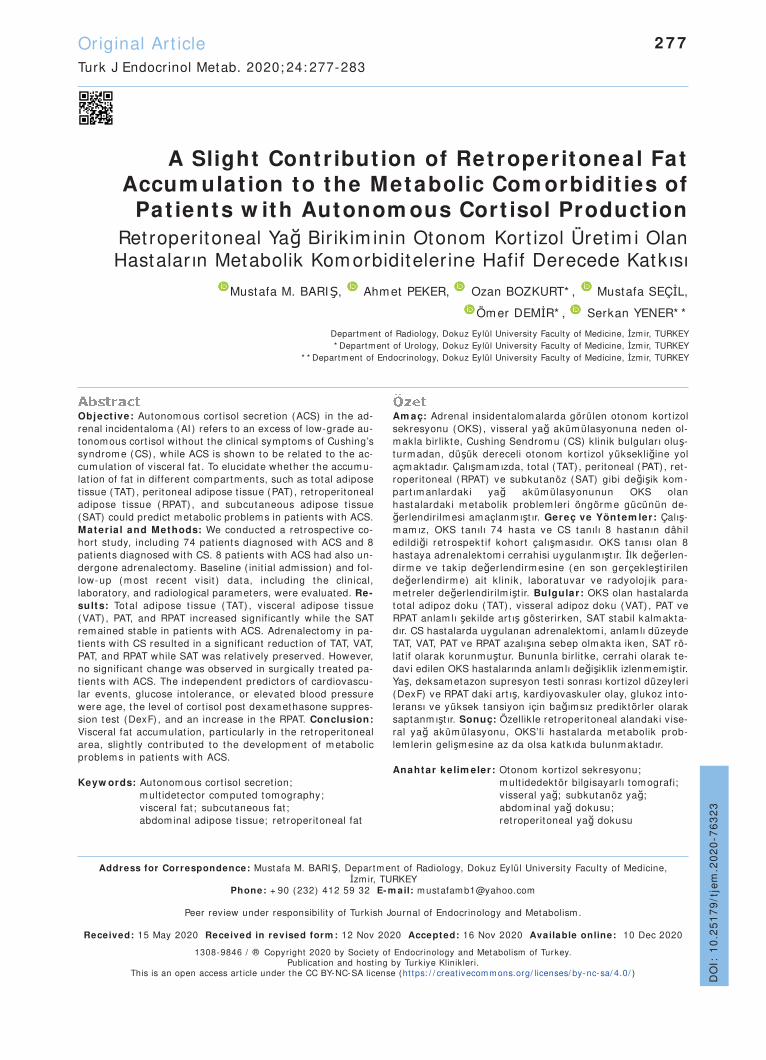
A Slight Contr ibut ion of Retroperitoneal Fat Accum ulat ion to the Metabolic Com orbidit ies of
Pat ients w ith Autonom ous Cort isol Product ion Retroperitoneal Yağ Bir ik im inin Otonom Kort izol Üret im i Olan Hastaların Metabolik Kom orbiditeler ine Hafif Derecede Katkısı
Mustafa M. BARIŞ, Ahm et PEKER, Ozan BOZKURT* , Mustafa SEÇİL,
Öm er DEMİR* , Serkan YENER* *
Department of Radiology, Dokuz Eylül University Faculty of Medicine, İzmir, TURKEY * Department of Urology, Dokuz Eylül University Faculty of Medicine, İzmir, TURKEY
* * Department of Endocrinology, Dokuz Eylül University Faculty of Medicine, İzmir, TURKEY
Original Art icle Turk J Endocrinol Metab. 2020; 24: 277-283
Object ive: Autonom ous cort isol secret ion (ACS) in the ad-renal incidentaloma (AI ) refers to an excess of low-grade au-tonomous cort isol without the clinical symptoms of Cushing’s syndrom e (CS) , while ACS is shown to be related to the ac-cum ulat ion of visceral fat . To elucidate whether the accum u-lat ion of fat in different com partm ents, such as total adipose t issue (TAT) , peritoneal adipose t issue (PAT) , ret roperitoneal adipose t issue (RPAT) , and subcutaneous adipose t issue (SAT) could predict metabolic problems in pat ients with ACS. Materia l and Methods: We conducted a ret rospect ive co-hort study, including 74 pat ients diagnosed with ACS and 8 pat ients diagnosed with CS. 8 pat ients with ACS had also un-dergone adrenalectomy. Baseline ( init ial adm ission) and fol-low-up (m ost recent v isit ) data, including the clinical, laboratory, and radiological parameters, were evaluated. Re-sults: Total adipose t issue (TAT) , v isceral adipose t issue (VAT) , PAT, and RPAT increased significant ly while the SAT rem ained stable in pat ients with ACS. Adrenalectomy in pa-t ients with CS resulted in a significant reduct ion of TAT, VAT, PAT, and RPAT while SAT was relat ively preserved. However, no significant change was observed in surgically t reated pa-t ients with ACS. The independent predictors of cardiovascu-lar events, glucose intolerance, or elevated blood pressure were age, the level of cort isol post dexam ethasone suppres-sion test (DexF) , and an increase in the RPAT. Conclusion: Visceral fat accum ulat ion, part icular ly in the ret roperitoneal area, slight ly cont r ibuted to the developm ent of m etabolic problem s in pat ients with ACS. Keyw ords: Autonom ous cort isol secret ion;
m ult idetector com puted tom ography; v isceral fat ; subcutaneous fat ; abdom inal adipose t issue; ret roperitoneal fat
Am aç: Adrenal insidentalom alarda görülen otonom kort izol sekresyonu (OKS) , visseral yağ aküm ülasyonuna neden ol-m akla bir likte, Cushing Sendrom u (CS) klinik bulguları oluş-turm adan, düşük dereceli otonom kort izol yüksekliğine yol açmaktadır. Çalışmamızda, total (TAT) , peritoneal (PAT) , ret-roperitoneal (RPAT) ve subkutanöz (SAT) gibi değişik kom -part ım anlardaki yağ aküm ülasyonunun OKS olan hastalardaki m etabolik problem ler i öngörm e gücünün de-ğerlendir ilm esi am açlanmışt ır. Gereç ve Yöntem ler: Çalış-m am ız, OKS tanılı 74 hasta ve CS tanılı 8 hastanın dâhil edildiği ret rospekt if kohort çalışm asıdır. OKS tanısı olan 8 hastaya adrenalektom i cerrahisi uygulanmışt ır. İlk değerlen-dirm e ve takip değer lendirm esine (en son gerçekleşt ir ilen değer lendirm e) ait k linik, laboratuvar ve radyoloj ik para-m et reler değerlendir ilm işt ir. Bulgular: OKS olan hastalarda total adipoz doku (TAT) , visseral adipoz doku (VAT) , PAT ve RPAT anlam lı şekilde art ış göster irken, SAT stabil kalm akta-dır. CS hastalarda uygulanan adrenalektomi, anlam lı düzeyde TAT, VAT, PAT ve RPAT azalışına sebep olm akta iken, SAT rö-lat if olarak korunm uştur. Bununla bir lit ke, cerrahi olarak te-davi edilen OKS hastalarında anlam lı değişiklik izlenmemişt ir. Yaş, deksametazon supresyon test i sonrası kort izol düzeyleri (DexF) ve RPAT daki art ış, kardiyovaskuler olay, glukoz into-leransı ve yüksek tansiyon için bağım sız prediktör ler olarak saptanm ışt ır. Sonuç: Özellik le ret roperitoneal alandaki vise-ral yağ aküm ülasyonu, OKS’li hastalarda m etabolik prob-lem lerin gelişm esine az da olsa katkıda bulunm aktadır. Anahtar kelim eler: Otonom kort izol sekresyonu;
m ult idedektör bilgisayarlı tom ografi; v isseral yağ; subkutanöz yağ; abdom inal yağ dokusu; ret roperitoneal yağ dokusu
2 7 7
Address for Correspondence: Mustafa M. BARIŞ, Departm ent of Radiology, Dokuz Eylül University Faculty of Medicine, İzm ir, TURKEY
Phone: + 90 (232) 412 59 32 E- m ail: m ustafam [email protected]
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 15 May 2020 Received in revised form : 12 Nov 2020 Accepted: 16 Nov 2020 Available online: 10 Dec 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ )
DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
63
23

I nt roduct ion The visceral adiposity and ectopic fat accu-m ulat ion pose a cardiom etabolic r isk. Vis-ceral adipose t issue (VAT) , m easured by com puted tom ography (CT) or m agnet ic resonance imaging (MRI ) , is an independent m arker for m etabolic and cardiovascular m orbidity and m ortality (1-3) . Visceral adi-pose t issue has dist inct ive propert ies not shared by subcutaneous adipose t issue (SAT) , such as exacerbat ing hyperinsuline-m ia, increased hepat ic product ion of t r iglyc-er ide- r ich lipoproteins and glucose, as well as increased product ion of inflam m atory cy-tokines. I n physiological condit ions, subcu-taneous adipose t issue serves as a metabolic pool for excess t r iglycerides. Sev-eral observat ions have shown that the accu-m ulat ion of VAT occurs when the expandabilit y and plast icity of SAT fail (3) . Endogenous hypercort isolism results in re-dist r ibut ion of fat t issue that leads to cent ral obesity and metabolic complicat ions such as glucose intolerance, elevated blood pres-sure, and future myocardial infarct ion. Ex-posure to chronic glucocort icoid is associated with the expansion of adipose t is-sue and a posit ive balance of lipid storage, suggest ing an increase in the total body li-pogenesis despite the increased lipolysis (4) . The effects of cort isol on VAT result in different features. The m RNA expression of the glucocort icoid receptor is higher in om ental fat than in the SAT; thus, glucocor-t icoids induce insulin resistance in hum an om ental fat t issue but not in subcutaneous adipocytes (5-7) . Glucocort icoid induces lipolysis that is prom inent in SAT, while the overexpression of lipoprotein lipase induces increased uptake of t r iglyceride by the ab-dom inal adipocytes, result ing in increased deposit ion of om ental fat (4) . Autonom ous cort isol secret ion (ACS) in the adrenal incidentalom a (AI ) refers to an ex-cess of low-grade autonomous cort isol with-out showing any clinical sym ptom s of Cushing’s syndrome (CS) (8) . Previous stud-ies have clearly dem onst rated that pat ients with ACS have an increased rate of m eta-bolic com orbidit ies and cardiovascular m or-talit y com pared to their non- funct ioning counterparts (9,10) . One ret rospect ive cohort study by our group (11) along with one cross-sect ional study
(12) dem onst rated signif icant ly increased VAT at the t im e of adm ission and follow-up of pat ients with ACS. I n this study, we hy-pothesized that the change of fat m ass in different com partm ents of adipose t issue m ight contribute to the increased prevalence of m etabolic and cardiovascular com orbidi-t ies in pat ients with ACS at the t im e of fol-low-up. For this purpose, we evaluated the AI pat ients with ACS, assessed their long-term com orbidit ies, and analyzed whether the alterat ions in different fat com partm ent areas had any im pact on the developm ent of m etabolic and cardiovascular deter iora-t ions.
Materia l and Methods
Data Collect ion
This ret rospect ive study was approved by the ethics com m it tee of Dokuz Eylül Univer-sit y Hospital (Dokuz Eylul Universitesi Girisimsel Olmayan Arast irmalar Et ik Kurulu, file no: 2017/ 19-13, dated 27.07.2017) and was conducted as per the Helsinki Declara-t ion Principles. The need for inform ed con-sent was waived by the ethics com m it tee. We used the data of 74 pat ients diagnosed with ACS and 8 pat ients diagnosed with CS. We used data of all eligible pat ients who at-tended the rout ine follow-up between Janu-ary 2017 and January 2019. We also recruited 8 pat ients having ACTH- indepen-dent overt hypercort isolism (CS) with fol-low-up scans perform ed due to unrelated condit ions. The exclusion cr iter ia were as follows: suppressed levels of DexF dur ing adm ission and follow-up, non-adenom a ap-pearance on com puted tom ography (CT) , pr im ary hyperaldosteronism , pheochrom o-cytoma, adrenalectomy without prior follow-up, act ive m alignancy, and lack of baseline and/ or follow-up evaluat ion.
Horm onal Assessm ent of Part icipants
The horm onal evaluat ion of the part icipants included the m easurem ent of cort icot rophin (ACTH) and dehydroepiandrosteanadione (DHEAS) , overnight 1 m g dexam ethasone suppression test (DST) , ur inary m etanephr ine, norm etanephr ine, and plasm a aldosterone to plasm a renin act ivity rat io. Autonomous cort isol product ion (ACS) was defined in the thresholds of post-DST
Barış et al. Turk J Endocrinol Metab. Ret roperitoneal Fat and the Com orbidit ies 2020; 24: 277-283
2 7 8

cort isol which was recom m ended by the ESE-ENSAT guidelines (8) .
Rout ine Follow - up Protocol
We suggest an annual follow-up to all the AI pat ients for the first three years, and then the durat ion m ay depend on the individual. At each follow-up visit , the physical exam i-nat ion, im aging, horm onal evaluat ion, rou-t ine laboratory tests with invest igat ions on m etabolic com orbidit ies are carr ied out .
Measurem ents and Rout ine Laboratory I nvest igat ions
The Adrenal incidentalom a (AI ) pat ients un-derwent clinical evaluat ion at each v isit , where concom itant type 2 diabetes mellitus, ar ter ial hypertension, and cardiovascular events were tested. Clinical sym ptom s and signs of hypercort isolem ia, along with weight , height , waist circum ference, and blood pressure (Erka, Bad Tölz, Germ any) , were noted. A systolic blood pressure of 140 m m Hg or higher and a diastolic blood pres-sure of 90 m m Hg or higher was used to di-agnose hypertension. Also, the diabetes m ellitus was diagnosed according to the cr i-ter ia of the Am erican Diabetes Associat ion (ADA) at the t im e of assessm ent . The cur-rent sm okers were defined as indiv iduals who were current ly sm oking any type of to-bacco, whereas form er sm okers were peo-ple who had ceased sm oking at least six m onths before the assessm ent , and non-sm okers were pat ients who had never sm oked.
Measurem ent of the Fat Com partm ent Areas
One invest igator who was blinded to the bio-chem ical data m easured the fat com part -m ent areas during the rout ine follow-up CT scans. Unt il 2008, CT im aging in our inst i-tute was perform ed through an Mx8000 Quad scanner (Philips Medical System s) , which was subsequent ly replaced by a Philips Brilliance 64 scanner (Philips Medical System s) . An axial view was used with the subject ly ing in the supine posit ion. The fat compartments were measured on Philips Ex-tended Brilliance Workspace (software ver-sion V3.5.0.22.54) using QCT (quant itat ive com puted tom ography) software. A single slice was evaluated at the level of L1/ 2 disk space, which was ident ified for fat m easure-
m ents because the VAT at the T12-L1 and L1-L2 landm arks had m uch st ronger associ-at ions with m etabolic syndrom e than those at the other sites. The fat area m easure-m ent m ethod was described in our previous study (11) . Addit ionally, we further divided the visceral fat into peritoneal and ret roperi-toneal areas along the boundary, which was com prised of the poster ior surface of sm all bowels, the anterior wall of the aorta, medial border of the spleen, posterom edial border of liver, anter ior border of the vertebral col-um n, and inner-m ost wall m uscles of the poster ior abdom en. The interfascial planes, anterior perirenal fascia (Gerota fascia) , and poster ior perirenal fascia (Zuckerkandl fas-cia) were visible in m ost of the part icipants, which was also used to out line the boundary (Figure 1) . Per itoneal adipose t issue (PAT) was calculated by subt ract ing the ret roperi-toneal adipose t issue (RPAT) from visceral adipose t issue (VAT) . Subcutaneous fat was defined as the adipose t issue area between the skin and the outerm ost abdom inal m us-cle wall. The SAT area was calculated by subt ract ing the VAT area from the TAT area. The rat io of VAT to SAT area (V: S) and VAT to TAT (V: T) area were also calculated to elim inate the possible bias, which was sec-ondary to the differences found in individual body size.
Stat ist ical Analysis
Stat ist ical analyses were perform ed using SPSS version 20.0 (SPSS I nc, I llinois, USA) . The dist r ibut ion of var iables was assessed using The Kolm ogorov Sm irnov test . Var i-ables with asymmetric dist r ibut ion were pre-sented as m edian values and (m in-m ax) values. For cont inuous variables with asym -m etr ic dist r ibut ion, differences between the groups were analyzed using the Mann-Whit-ney U test or the I ndependent sam ples T-
test . Changes in the m easurem ents of the fat area between the baseline and follow-up were analyzed using the Wilcoxon signed-rank test for repeated m easurem ents. Lo-gist ic regression analysis m odels were used to invest igate the im pact of the fat com -partm ent-specific changes on the develop-m ent of m etabolic com orbidit ies. Two- tailed tests were conducted, and the results of all stat ist ical analyses were considered signifi-cant if P< 0.05.
Turk J Endocrinol Metab. Barış et al. 2020; 24: 277-283 Ret roperitoneal Fat and the Com orbidit ies
2 7 9
Results
Baseline Characterist ics of Pat ients
The baseline dem ographic and endocr ine data of pat ients with ACS (n= 74) is de-scr ibed in Table 1. Addit ionally, 8 pat ients with CS were also recruited. Out of the 74 pat ients with ACS, 8 pat ients underwent adrenalectom y because of the tum or size and CT appearance (n= 3) or worsening of the metabolic profile during follow-up (n= 5) .
Changes in the Measurem ent of the Fat Area During Follow - up
Fat area measurements during follow-up are described in Table 2. The total adipose t is-sue, VAT, PAT, and RPAT showed a significant increase while the SAT rem ained stable in pat ients with ACS. Adrenalectomy in CS pa-t ients resulted in a significant reduct ion of TAT, VAT, PAT, and RPAT while SAT was rela-t ively preserved. However, no signif icant change was observed in surgically t reated pat ients with ACS.
Associat ion Betw een Fat Accum ulat ion and Metabolic Com orbidit ies
Fat com partm ent-specific changes and their im pact on the developm ent of m etabolic co-m orbidit ies were invest igated in pat ients with ACS (Table 3) . We conducted several logist ic regression analysis m odels for this purpose, where all the m odels included in-dependent var iables such as age, gender, follow-up DexF, and fat m ass change in dif-ferent com partm ents (deltaRP, deltaP, and deltaSC separately in each m odel) for the developm ent or deter iorat ion of m etabolic com orbidit ies (AHT, DM, CVD) . Age was the sole independent variable that predicted Cardiovascular disease (CVD) with an odds rat io (OR) of 1.18, 1.32, and 1.44 (p< 0.05 in all m odels) . The cont r ibut ion of the DexF, gender, or fat m ass change in dif-ferent com partm ents was not signif icant . Delta RP was the only significant independ-ent predictor of glucose tolerance deteriora-t ion, recording an OR of 1.02 (p= 0.038) . The assessment of factors that predicted the
Barış et al. Turk J Endocrinol Metab. Ret roperitoneal Fat and the Com orbidit ies 2020; 24: 277-283
2 8 0
Figure 1 . Adipose t issue com partm ents are highlighted in blue color. ( a) The highlighted areas of adipose t issue were m easured to calculate TAT, ( b) Blue colored areas show the m easurem ent of the SAT, ( c) and ( d) highlight PAT and RPAT, respect ively. TAT: Total adipose t issue; SAT: Subcutaneous adipose t issue; PAT: Peritoneal adipose t issue; RPAT: Ret roperitoneal adipose t issue.
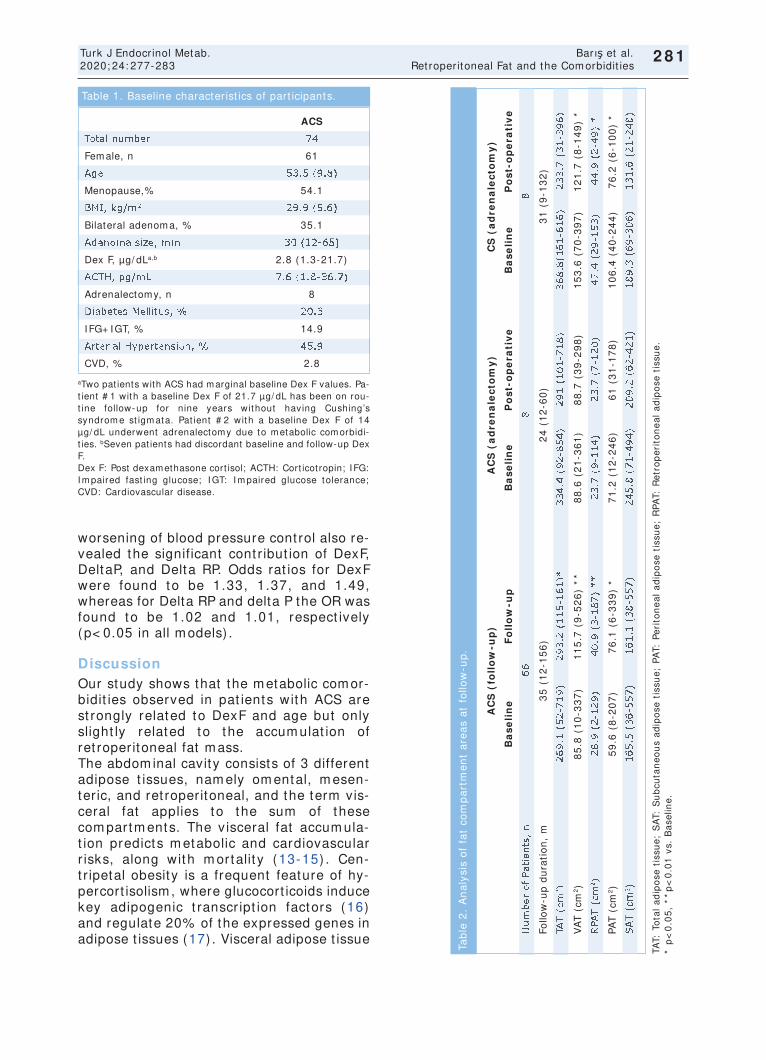
worsening of blood pressure cont rol also re-vealed the significant cont r ibut ion of DexF, DeltaP, and Delta RP. Odds rat ios for DexF were found to be 1.33, 1.37, and 1.49, whereas for Delta RP and delta P the OR was found to be 1.02 and 1.01, respect ively (p< 0.05 in all m odels) .
Discussion Our study shows that the m etabolic com or-bidit ies observed in pat ients with ACS are st rongly related to DexF and age but only slight ly related to the accum ulat ion of ret roperitoneal fat m ass. The abdom inal cavity consists of 3 different adipose t issues, nam ely om ental, m esen-ter ic, and ret roperitoneal, and the term vis-ceral fat applies to the sum of these com partm ents. The v isceral fat accum ula-t ion predicts m etabolic and cardiovascular r isks, along with m ortalit y (13-15) . Cen-t r ipetal obesity is a frequent feature of hy-percort isolism , where glucocort icoids induce key adipogenic t ranscr ipt ion factors (16) and regulate 20% of the expressed genes in adipose t issues (17) . Visceral adipose t issue
Turk J Endocrinol Metab. Barış et al. 2020; 24: 277-283 Ret roperitoneal Fat and the Com orbidit ies
2 8 1
ACS
Total num ber 74
Fem ale, n 61
Age 53.5 (9.8)
Menopause,% 54.1
BMI , kg/ m 2 29.9 (5.6)
Bilateral adenom a, % 35.1
Adenom a size, m m 30 (12-65)
Dex F, µg/ dLa,b 2.8 (1.3-21.7)
ACTH, pg/ m L 7.6 (1.8-36.7)
Adrenalectomy, n 8
Diabetes Mellitus, % 20.3
I FG+ I GT, % 14.9
Arter ial Hypertension, % 45.9
CVD, % 2.8
Table 1. Baseline character ist ics of part icipants.
aTwo pat ients with ACS had marginal baseline Dex F values. Pa-t ient # 1 with a baseline Dex F of 21.7 µg/ dL has been on rou-t ine follow-up for nine years without having Cushing’s syndrom e st igm ata. Pat ient # 2 with a baseline Dex F of 14 µg/ dL underwent adrenalectomy due to m etabolic com orbidi-t ies. bSeven pat ients had discordant baseline and follow-up Dex F. Dex F: Post dexamethasone cort isol; ACTH: Cort icot ropin; I FG: I m paired fast ing glucose; I GT: I m paired glucose tolerance; CVD: Cardiovascular disease.
TAT:
To
tal
ad
ipo
se t
issu
e;
SA
T: S
ub
cuta
ne
ou
s a
dip
ose
tis
sue
; PA
T: P
eri
ton
ea
l a
dip
ose
tis
sue
; R
PAT:
Re
tro
pe
rito
ne
al
ad
ipo
se t
issu
e.
* p
<0
.05
, *
*p
<0
.01
vs.
Ba
selin
e.
AC
S (
foll
ow
-up
)A
CS
(a
dre
na
lec
tom
y)
CS
(a
dre
na
lec
tom
y)
Ba
se
lin
eF
oll
ow
-up
Ba
se
lin
eP
os
t-o
pe
rati
ve
Ba
se
lin
eP
os
t-o
pe
rati
ve
Nu
mb
er
of
Pati
en
ts,
n6
68
8
Follo
w-u
p d
ura
tio
n,
m3
5 (
12
-15
6)
24
(1
2-6
0)
31
(9
-13
2)
TAT
(cm
2)
26
9.1
(5
2-7
19
)2
93
.2 (
11
5-1
61
)*3
34
.4 (
92
-85
4)
29
1 (
10
1-7
18
) 3
68
.8(1
61
-61
6)
23
3.7
(3
1-3
96
)
VA
T (
cm2)
85
.8 (
10
-33
7)
11
5.7
(9
-52
6)
**
88
.6 (
21
-36
1)
88
.7 (
39
-29
8)
15
3.6
(7
0-3
97
)1
21
.7 (
8-1
49
) *
RPA
T (
cm2)
28
.9 (
2-1
29
)4
0.9
(3
-18
7)
**
23
.7 (
9-1
14
) 2
3.7
(7
-12
0)
47
.4 (
29
-15
3)
44
.9 (
2-4
9)
*
PAT
(cm
2)
59
.6 (
8-2
07
)7
6.1
(6
-33
9)
*7
1.2
(1
2-2
46
)6
1 (
31
-17
8)
10
6.4
(4
0-2
44
)7
6.2
(6
-10
0)
*
SA
T (
cm2)
16
5.5
(3
6-5
57
)1
61
.1 (
38
-55
7)
24
5.8
(7
1-4
94
)2
09
.2 (
62
-42
1)
18
9.3
(6
9-3
06
)1
31
.6 (
21
-24
8)
Tab
le 2
. A
na
lysi
s o
f fa
t co
mp
art
me
nt
are
as
at
follo
w-u
p.
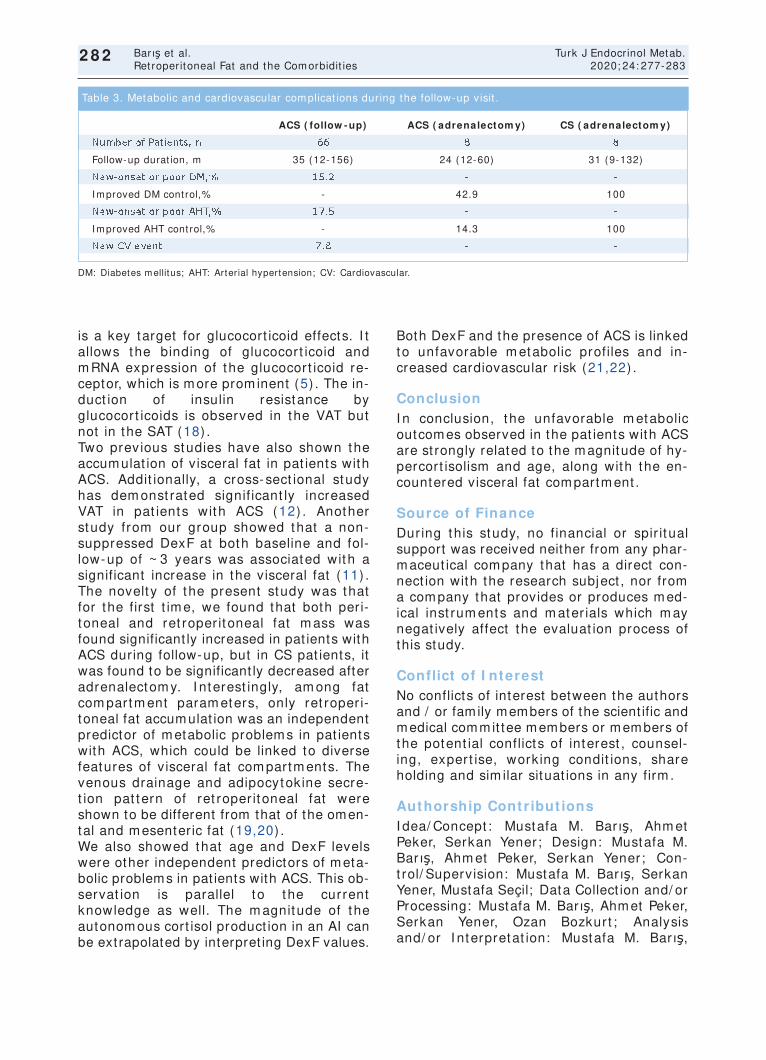
is a key target for glucocort icoid effects. I t allows the binding of glucocort icoid and m RNA expression of the glucocort icoid re-ceptor, which is more prom inent (5) . The in-duct ion of insulin resistance by glucocort icoids is observed in the VAT but not in the SAT (18) . Two previous studies have also shown the accum ulat ion of visceral fat in pat ients with ACS. Addit ionally, a cross-sect ional study has dem onst rated signif icant ly increased VAT in pat ients with ACS (12) . Another study from our group showed that a non-suppressed DexF at both baseline and fol-low-up of ~ 3 years was associated with a significant increase in the visceral fat (11) . The novelt y of the present study was that for the first t im e, we found that both peri-toneal and ret roper itoneal fat m ass was found significant ly increased in pat ients with ACS during follow-up, but in CS pat ients, it was found to be significant ly decreased after adrenalectom y. I nterest ingly, am ong fat com partm ent param eters, only ret roper i-toneal fat accum ulat ion was an independent predictor of m etabolic problem s in pat ients with ACS, which could be linked to diverse features of visceral fat com partm ents. The venous drainage and adipocytokine secre-t ion pat tern of ret roper itoneal fat were shown to be different from that of the omen-tal and m esenteric fat (19,20) . We also showed that age and DexF levels were other independent predictors of m eta-bolic problems in pat ients with ACS. This ob-servat ion is parallel to the current knowledge as well. The m agnitude of the autonom ous cort isol product ion in an AI can be ext rapolated by interpret ing DexF values.
Both DexF and the presence of ACS is linked to unfavorable m etabolic profiles and in-creased cardiovascular r isk (21,22) .
Conclusion I n conclusion, the unfavorable m etabolic outcom es observed in the pat ients with ACS are st rongly related to the m agnitude of hy-percort isolism and age, along with the en-countered visceral fat com partm ent .
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions I dea/ Concept : Mustafa M. Barış, Ahm et Peker, Serkan Yener; Design: Mustafa M. Barış, Ahm et Peker, Serkan Yener; Con-t rol/ Supervision: Mustafa M. Barış, Serkan Yener, Mustafa Seçil; Data Collect ion and/ or Processing: Mustafa M. Barış, Ahm et Peker, Serkan Yener, Ozan Bozkurt ; Analysis and/ or I nterpretat ion: Mustafa M. Barış,
Barış et al. Turk J Endocrinol Metab. Ret roperitoneal Fat and the Com orbidit ies 2020; 24: 277-283
2 8 2
DM: Diabetes m ellitus; AHT: Arter ial hypertension; CV: Cardiovascular.
ACS ( follow - up) ACS ( adrenalectom y) CS ( adrenalectom y)
Num ber of Pat ients, n 66 8 8
Follow-up durat ion, m 35 (12-156) 24 (12-60) 31 (9-132)
New-onset or poor DM,% 15.2 - -
I m proved DM cont rol,% - 42.9 100
New-onset or poor AHT,% 17.5 - -
I m proved AHT cont rol,% - 14.3 100
New CV event 7.8 - -
Table 3. Metabolic and cardiovascular com plicat ions during the follow-up visit .
Serkan Yener, Ozan Bozkurt ; Literature Re-view: Writ ing the Art icle: Ahm et Peker, Serkan Yener, Öm er Dem ir; Crit ical Review: Mustafa Seçil, Öm er Dem ir ; Mater ials: Serkan Yener, Ozan Bozkurt , Öm er Dem ir.
References 1. Fox CS, Massaro JM, Hoffm ann U, Pou KM, Mau-
rovich-Horvat P, Liu CY, Vasan RS, Murabito JM, Meigs JB, Cupples LA, D'Agost ino RB Sr, O'Donnell CJ. Abdom inal v isceral and subcutaneous adipose t issue com partm ents: associat ion with m etabolic r isk factors in the Fram ingham Heart Study. Circu-lat ion. 2007; 116: 39-48. [ Crossref] [ PubMed]
2. Neeland I J, Ayers CR, Rohatgi AK, Turer AT, Berry JD, Das SR, Vega GL, Khera A, McGuire DK, Grundy SM, de Lem os JA. Associat ions of visceral and ab-dom inal subcutaneous adipose t issue with m arkers of cardiac and m etabolic r isk in obese adults. Obe-sity (Silver Spring) . 2013; 21: E439-E447. [ Crossref] [ PubMed] [ PMC]
3. Neeland I J, Ross R, Després JP, Matsuzawa Y, Ya-mashita S, Shai I , Seidell J, Magni P, Santos RD, Ar-senault B, Cuevas A, Hu FB, Griffin B, Zam bon A, Barter P, Fruchart JC, Eckel RH; I nternat ional Ath-erosclerosis Society; I nternat ional Chair on Car-diom etabolic Risk Working Group on Visceral Obesit y. Visceral and ectopic fat , atherosclerosis, and cardiom etabolic disease: a posit ion statem ent . Lancet Diabetes Endocr inol. 2019; 7: 715-725. [ Crossref] [ PubMed]
4. Geer EB, I slam J, Buet tner C. Mechanism s of gluco-cort icoid- induced insulin resistance: focus on adi-pose t issue funct ion and lipid m etabolism . Endocrinol Metab Clin North Am . 2014; 43: 75-102. [ Crossref] [ PubMed] [ PMC]
5. Ferraù F, Korbonit s M. Metabolic com orbidit ies in Cushing's syndrom e. Eur J Endocr inol. 2015; 173: M133-M157. [ Crossref] [ PubMed]
6. Rebuffé-Scrive M, Brönnegard M, Nilsson A, Eldh J, Gustafsson JA, Björntorp P. Steroid horm one recep-tors in hum an adipose t issues. J Clin Endocr inol Metab. 1990; 71: 1215-1219. [ Crossref] [ PubMed]
7. Veilleux A, Laberge PY, Morency J, Noël S, Luu-The V, Tchernof A. Expression of genes related to gluco-cort icoid act ion in hum an subcutaneous and om en-tal adipose t issue. J Steroid Biochem Mol Biol. 2010; 122: 28-34. [ Crossref] [ PubMed]
8. Fassnacht M, Arlt W, Bancos I , Dralle H, Newell-Price J, Sahdev A, Tabar in A, Terzolo M, Tsagarakis S, Dekkers OM. Managem ent of adrenal incidentalo-m as: European Society of Endocr inology Clinical Pract ice Guideline in collaborat ion with the Euro-pean Network for the Study of Adrenal Tum ors. Eur J Endocr inol. 2016; 175: G1-G34. [ Crossref] [ PubMed]
9. Di Dalm azi G, Pasquali R, Beuschlein F, Reincke M. Subclinical hypercort isolism : a state, a syndrom e, or a disease? Eur J Endocrinol. 2015; 173: M61-M71. [ Crossref] [ PubMed]
10. Di Dalm azi G, Vicennat i V, Garelli S, Casadio E, Ri-naldi E, Giam palm a E, Mosconi C, Golfier i R, Pac-capelo A, Pagot to U, Pasquali R. Cardiovascular
events and m ortality in pat ients with adrenal inci-dentalom as that are either non-secret ing or associ-ated with interm ediate phenotype or subclinical Cushing's syndrome: a 15-year ret rospect ive study. Lancet Diabetes Endocr inol. 2014; 2: 396-405. [ Crossref] [ PubMed]
11. Yener S, Baris M, Peker A, Dem ir O, Ozgen B, Secil M. Autonom ous cort isol secret ion in adrenal inci-dentalomas and increased visceral fat accumulat ion dur ing follow-up. Clin Endocr inol (Oxf ) . 2017; 87: 425-432. [ Crossref] [ PubMed]
12. Debono M, Prem a A, Hughes TJ, Bull M, Ross RJ, Newell-Price J. Visceral fat accum ulat ion and post-dexam ethasone serum cort isol levels in pat ients with adrenal incidentaloma. J Clin Endocrinol Metab. 2013; 98: 2383-2391. [ Crossref] [ PubMed]
13. Abraham TM, Pedley A, Massaro JM, Hoffm ann U, Fox CS. Associat ion between visceral and subcuta-neous adipose depots and incident cardiovascular disease r isk factors. Circulat ion. 2015; 132: 1639-1647. [ Crossref] [ PubMed] [ PMC]
14. Kuk JL, Katzm arzyk PT, Nicham an MZ, Church TS, Blair SN, Ross R. Visceral fat is an independent pre-dictor of all- cause m ortality in m en. Obesity (Silver Spring) . 2006; 14: 336-341. [ Crossref] [ PubMed]
15. Nicklas BJ, Penninx BW, Cesari M, Kritchevsky SB, Newm an AB, Kanaya AM, Pahor M, Jingzhong D, Harr is TB; Health, Aging and Body Com posit ion Study. Associat ion of visceral adipose t issue with in-cident m yocardial infarct ion in older m en and wom en: the Health, Aging and Body Com posit ion Study. Am J Epidem iol. 2004; 160: 741-749. [ Cross-ref] [ PubMed]
16. Tom linson JJ, Boudreau A, Wu D, At las E, Haché RJ. Modulat ion of early hum an preadipocyte different i-at ion by glucocort icoids. Endocr inology. 2006; 147: 5284-5293. [ Crossref] [ PubMed]
17. Lee MJ, Gong DW, Burkey BF, Fr ied SK. Pathways regulated by glucocort icoids in om ental and subcu-taneous human adipose t issues: a m icroarray study. Am J Physiol Endocr inol Metab. 2011; 300: E571-E580. [ Crossref] [ PubMed] [ PMC]
18. Hazlehurst JM, Gathercole LL, Nasir i M, Arm st rong MJ, Borrows S, Yu J, Wagenm akers AJ, Stewart PM, Tom linson JW. Glucocort icoids fail to cause insulin resistance in human subcutaneous adipose t issue in vivo. J Clin Endocrinol Metab. 2013; 98: 1631-1640. [ Crossref] [ PubMed]
19. Hung CS, Lee JK, Yang CY, Hsieh HR, Ma WY, Lin MS, Liu PH, Shih SR, Liou JM, Chuang LM, Chen MF, Lin JW, Wei JN, Li HY. Measurem ent of v isceral fat : should we include ret roper itoneal fat? PLoS One. 2014; 9: e112355. [ Crossref] [ PubMed] [ PMC]
20. Tchernof A, Després JP. Pathophysiology of hum an visceral obesit y: an update. Physiol Rev. 2013; 93: 359-404. [ Crossref] [ PubMed]
21. Debono M, Newell-Pr ice J. Subclinical hypercort i-solism in adrenal incidentalom a. Curr Opin En-docr inol Diabetes Obes. 2015; 22: 185-192. [ Crossref] [ PubMed]
22. Di Dalm azi G, Pasquali R. Adrenal adenom as, sub-clinical hypercort isolism , and cardiovascular out-com es. Curr Opin Endocr inol Diabetes Obes. 2015; 22: 163-168. [ Crossref] [ PubMed]
Turk J Endocrinol Metab. Barış et al. 2020; 24: 277-283 Ret roperitoneal Fat and the Com orbidit ies
2 8 3
Original Art icle Turk J Endocrinol Metab. 2020; 24: 284-292
284
Knosp and Hardy Grading System s are Useful in Predict ing Persistence of Male Hypogonadism
in Prolact inom as Follow ing Prolact in Norm alizat ion Knosp ve Hardy Sınıflam aları, Prolakt inom ası Olan
Erkek Hastalarda Prolakt in Norm alizasyonunu Takiben Hipogonadizm inin Kalıcılığını Öngörm ede Yararlıdır
Gülay ŞİMŞEK BAĞI R, Aylin GÜNEŞLİ* , Filiz EKŞİ HAYDARDEDEOĞLU,
Okan Sefa BAKI NER, Özlem ALKAN* , Melek Eda ERTÖRER
Department of Endocrinology and Metabolism, Başkent University Adana Dr. Turgut Noyan Teaching and Medical Research Center, Adana, TURKEY * Department of Radiology, Başkent University Adana Dr. Turgut Noyan Teaching and Medical Research Center, Adana, TURKEY
Object ive: Despite serum prolact in norm alizat ion and tum or shr inkage being obtained using dopam ine agonist t reatm ent , hypogonadism m ay persist in several m en with prolact inom as. I n this study, we evaluated the effects of tum or m agnet ic reso-nance im aging features on the persistence of hypogonadism am ong norm oprolact inem ic m en with prolact inom as object ively using Knosp and Hardy grading system s. Mater ia l and Met -hods: The pat ients with prolact inomas who achieved serum pro-lact in norm alizat ion using cabergoline therapy were evaluated, respect ively. The extent of tum or growth was evaluated on the basis of Knosp and Hardy grading systems both at diagnosis and six m onths of m edical therapy with serum prolact in norm aliza-t ion. Results: A total of 28 cases (18 m acro- and 10 m icropro-lact inom as) were included. After six m onths of t reatm ent with cabergoline, all m icroprolact inom a pat ients with hypogonadism at baseline showed recovery (3, 100% ) . Moreover, nine of 14 m acroprolact inom a pat ients with hypogonadism at inclusion re-covered at the end (group 1) , and five did not (group 2) . Base-line Knosp grades and Hardy num bers did not differ between groups. However, higher Knosp grades and Hardy numbers were observed in pat ients who consistent ly had low serum testoste-rone in the sixth m onth (group 2) (p= 0.01, p= 0.02, respect i-vely) . All pat ients in group 2 had invasive tum ors (Hardy num ber I I I - I V) both at inclusion and the sixth m onth according to this classificat ion. Conclusion: We dem onst rated that m ac-roprolact inom as with persistent hypogonadism despite serum prolact in normalizat ion more commonly showed cavernous sinus invasion and sellar dest ruct ion. We proposed that Knosp and Hardy grading system s are useful in predict ing the persistence of m ale hypogonadism in prolact inom as following prolact in nor-m alizat ion. Keyw ords: Prolact inom a; m ale; hypogonadism ;
m agnet ic resonance im aging
Am aç: Prolakt inom ası olan erkek hastalarda, dopam in agonist-ler i ile tedavi sonrası serum prolakt in norm alizasyonu ve tüm ör küçülm esi sağlanm asına rağm en hipogonadizm devam edebilir. Bu çalışm ada, norm oprolakt inem ik erkek prolakt inom a hastala-rında, Knosp ve Hardy sınıflam alarını kullanarak tüm örün m an-yet ik rezonans görüntülem e özellik ler inin, kalıcı hipogonadizm gelişim i üzer ine etkisini objekt if olarak değerlendir idik. Gereç ve Yöntem ler: Kabergolin tedavisi ile serum prolakt in norm a-lizasyonu sağlanan prolakt inom a hastaları ret rospekt if olarak değer lendir ildi. Hem tanı anında hem de m edikal tedavi ile serum prolakt in norm alizasyonunun sağlandığı alt ıncı ayda tüm ör büyüm esinin derecesi Knosp ve Hardy sınıflam aları kul-lanılarak değerlendir ildi. Bulgular: Yirm i sekiz olgu (18 m akro ve 10 m ikroprolakt inom a) dâhil edildi. Alt ı aylık kabergolin te-davisi ile başlangıçta hipogonadizm i olan bütün m ikroprolakt i-nom a olgularında (3, % 100) hipogonadizm düzeldi. Başlangıçta hipogonadizm i olan 14 makroprolakt inoma olgusunun 9’unda hi-pogonadizm düzelirken (Grup 1) , 5 tanesinde hipogonadizm devem et t i (Grup 2) . Tanı anındaki Knosp ve Hardy skor lar ı gruplar arasında fark lılık gösterm edi. Bununla bir lik te, alt ıncı ayda düşük serum testosteronu olanlarda Knosp ve Hardy skor-lar ı daha yüksek olarak bulundu (Grup 2) ( sırasıy la p= 0,01, p= 0,02) . Bu sınıflam aya göre Grup 2’deki tüm hastaların hem tanı anında hem de alt ıncı ayda invaziv tüm örler i (Hardy I I I - I V) vardı. Sonuç: Serum prolakt in norm alizasyonuna rağm en hipo-gonadizm i düzelm eyen m akroprolakt inom a olgularında, kaver-nöz sinüs invazyonu ve sellar dest rüksiyonun daha sık olduğunu gösterdik. Prolaktnom ası olan hastalarda, prolakt in norm alizas-yonunu takiben erkek hipogonadizm inin kalıcılığını öngörm ede Knosp ve Hardy sınıflam alarının yardım cı olabileceğini düşün-m ekteyiz. Anahtar kelim eler: Prolakt inom a; erkek; hipogonadizm ;
m anyet ik rezonans görüntülem e
2 8 4
Address for Correspondence: Gülay ŞİMŞEK BAĞI R, Departm ent of Endocrinology and Metabolism , Başkent University Adana Dr. Turgut Noyan Teaching and Medical Research Center, Adana, TURKEY
Phone: + 90 322 3272727-2117 E- m ail: gulaysim [email protected]
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 01 Jul 2020 Received in revised form : 16 Sep 2020 Accepted: 16 Oct 2020 Available online: 30 Oct 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ )
DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
76
88

285
Turk J Endocrinol Metab. Şimşek Bağır et al. 2020; 24: 284-292 The Effects of Tum or Magnet ic Resonance I m aging Features Am ong Men with Prolact inom as
2 8 5
I nt roduct ion Prolact inom as are the m ost com m on func-t ional pituitary adenom as, with an annual incidence of 30 per 100,000 people (1) . Several of them are m icroadenom as, and the fem ale to m ale rat io is 20: 1; however, no difference is observed with regard to gender for m acroadenom as (2) . Elevated prolact in level causes sexual dys-funct ion by inhibit ing gonadot ropin- releas-ing hormone pulse frequency and amplitude. Moreover, it causes decreased libido, im po-tence, oligosperm ia, or azosperm ia in m ale pat ients. Men typically harbor larger and m ore invasive prolact inom as and present with m ore severe signs (3-6) . Hypopitu-itar ism result ing from a big tum or size and invasiveness m ay worsen the sym ptom s of hyperprolact inem ia in m acroprolact inom as. Prolact in levels are associated with tum or size and, as expected are typically higher in m ale pat ients (2,3) . Magnet ic resonance im aging (MRI ) is the gold standard m ethod for evaluat ing pitu-
itary adenom as. Pituitary tum or volum e can be m easured using different m ethods, such as perim eter or ellipsoid m ethods. I n addi-t ion, Knosp and Hardy grading system s are object ive tools that provide crucial inform a-t ion about pituitary space-occupying lesions. The Knosp grading system indicates tum or encroachm ent or invasion into the cav-ernous sinuses (CVS) . I t grades the parasel-lar extension of the tum or towards the cavernous sinus in relat ion to the int racav-ernous carot id artery. According to this clas-sif icat ion, grades 3 and 4 tum ors are invasive pituitary tum ors. The Hardy grad-ing system considers both the sella base-m ent disrupt ion denoted by num bers 0- I V and most ly suprasellar extension denoted by let ters A-E. I n the Hardy grading system, in-vasive adenom as can be either grade I I I or grade I V tum ors, and suprasellar extension is not considered a radiological marker of in-vasiveness, as shown in Figure 1 (7-10) . Dopam ine agonist (DA) therapy is recom -m ended for lower ing prolact in levels, de-
Figure 1 . Classificat ion systems characterizing pituitary adenomas. a) Hardy classificat ion system, Sella turcica tumors can be invasive (grade I I I ; localized sellar dest ruct ion, grade I V; diffuse dest ruct ion) . b) Knosp classificat ion system used to quant ify invasion of the cafernous sinus (grade 3; the tum or extends laterally to the internal carot id artery within the cav-ernous sinus, grade 4; total encasm ent of the int racavernous carot id artery) .10

creasing tum or size, and restor ing gonadal funct ions for pat ients with both m icro- and m acroadenom as. Opt im al t reatm ent out-com es for prolact inom a include serum pro-lact in norm alizat ion and tum or shr inkage with the reversal of tum or m ass effects (11-13) . Although serum prolact in norm alizat ion and tum or shrinkage can be obtained using DA t reatment , serum testosterone levels remain under normal levels in several men (14-16) . Furtherm ore, severe hypogonadism m ay even persist . Radiological determ inants of the persistence of hypogonadism in m en with prolact inom a t reated with DA are not clear. I n the literature, several studies have reported the effects of tum or size on the persistence of m ale hypogonadism , al-though no accurate data exist about tum or invasiveness (17-21) . This study aim ed to evaluate the effects of tum or MRI features on the persistence of hypogonadism am ong m en with prolact ino-m as, whose serum prolact in levels were normalized with DA therapy by using the ob-ject ive Knosp and Hardy grading system s.
Materia l and Methods This ret rospect ive study was perform ed at the Outpat ient Endocr inology Clinic of Baskent Universit y Facult y of Medicine, Adana hospital between 2013 and 2017. Male pat ients with prolact inom a who achieved serum prolact in norm alizat ion and whose serum testosterone m easurem ents and pituitary MRI s were perform ed at the sixth m onth of m edical therapy were re-cruited in the study, and their m edical records were collected. A total of 28 out of 175 m ale prolact inom a pat ients were found to be eligible for inclusion. All pat ients were t reated with cabergoline using a dose t it ra-t ion regim en. Pituitary MRI findings of these 28 pat ients were evaluated by the sam e neuroradiolo-gist both at diagnosis and the sixth m onth of cabergoline t reatm ent with prolact in nor-m alizat ion. The MRI s using a 1.5-T scanner were perform ed using MR System Magne-tom Avanto (Siem ens, Erlangen, Germ any) . Adenoma volumes were calculated manually on sagit tal and coronal T1A views using three dim ensions. They were categorized as m icroadenom a (diam eter, < 1 cm ; volum e,
< 0.52 cm 3) and m acroadenom a (diam eter, ≥1 cm ; volum e, ≥0.52 cm 3) depending on the size. The extent of tum or growth was evaluated on the basis of Knosp and Hardy grading system s both at diagnosis and the sixth m onth of m edical therapy with serum prolact in norm alizat ion. All inform at ion about laboratory tests ( folli-cle-st im ulat ing horm one [ FSH] , luteinizing horm one [ LH] , total testosterone, and pro-lact in levels) was recorded. Gonadot ropin deficiency was diagnosed depending on low or “ inappropriately norm al” serum FSH and LH levels combined with serum testosterone below the reference values: FSH norm al range: 1.42-15.4 m I U/ m L, LH norm al range: 1.24-7.8 m I U/ m L, and total testos-terone norm al range: 2.41-8.27 ng/ m L (2) . None of the pat ients received testosterone replacem ent therapy dur ing the study pe-r iod. The Ethics Commit tee of Faculty of Medicine, Baskent University approved the study (Pro-j ect No. KA 18/ 205, approval date: 10/ 07/ 2018) perform ed in accordance with the declarat ion of Helsinki pr inciples.
Stat ist ical analysis
Stat ist ical analysis was perform ed using SPSS software (Version 16.0, SPSS I nc., Chicago, I L, USA) . All num erical data were expressed as m edian values (m inim um -m axim um ) . For each cont inuous var iable, norm alit y was checked using Kolm ogorov-Sm irnov and Shapiro-Wilk tests and his-togram s. Groups were com pared using the Mann-Whitney U test for the data not nor-m ally dist r ibuted. The pre- and post-m ea-surem ent data were analyzed using the Wilcoxon test . The categorical variables be-tween the groups were analyzed using the Chi-squared test or Fisher ’s exact test . A p-value of < 0.05 was considered stat ist ically significant .
Results A total of 28 cases (18 m acro- and 10 m i-croprolact inom as) were included. Table 1 shows the general character ist ics of the pa-t ients with m acro- and m icroadenom as at presentat ion. More num ber of pat ients with m acroprolact inom a had hypogonadism at inclusion: 14 (77.8% ) vs. 3 (30.0% ) (p= 0.019) . More than one deficient hor-
286
Şimşek Bağır et al. Turk J Endocrinol Metab. The Effects of Tum or Magnet ic Resonance I m aging Features Am ong Men with Prolact inom as 2020; 24: 284-292
2 8 6
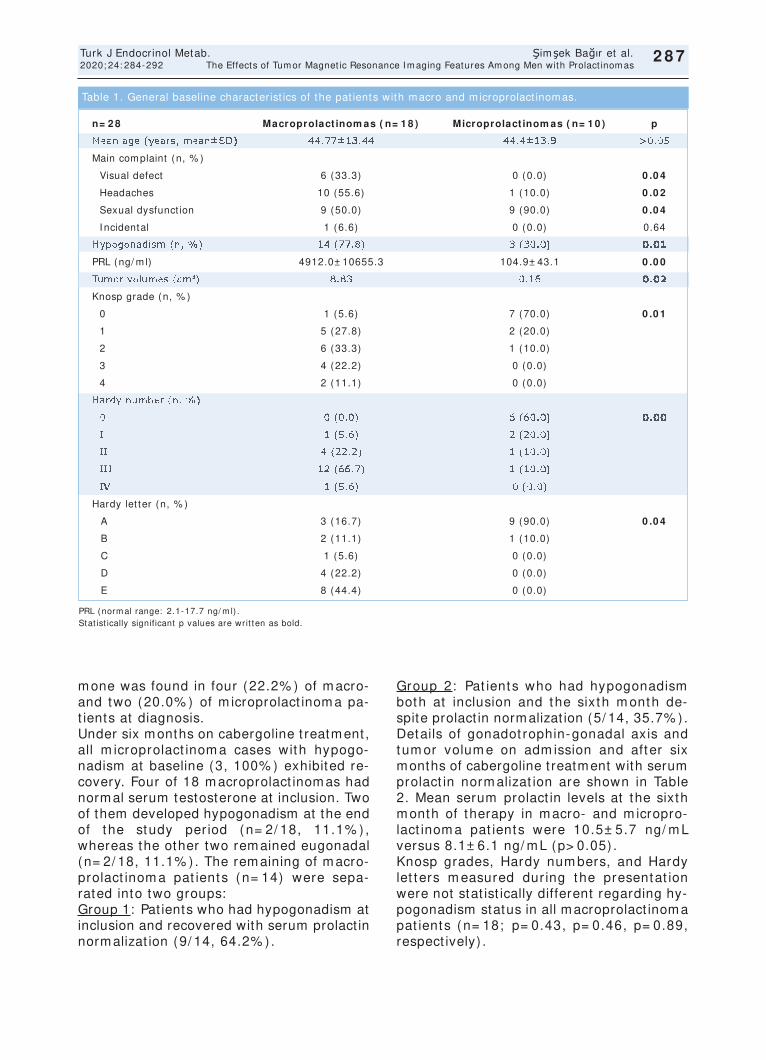
287
Turk J Endocrinol Metab. Şimşek Bağır et al. 2020; 24: 284-292 The Effects of Tum or Magnet ic Resonance I m aging Features Am ong Men with Prolact inom as
2 8 7
m one was found in four (22.2% ) of m acro- and two (20.0% ) of m icroprolact inom a pa-t ients at diagnosis. Under six months on cabergoline t reatment , all m icroprolact inom a cases with hypogo-nadism at baseline (3, 100% ) exhibited re-covery. Four of 18 m acroprolact inom as had normal serum testosterone at inclusion. Two of them developed hypogonadism at the end of the study per iod (n= 2/ 18, 11.1% ) , whereas the other two rem ained eugonadal (n= 2/ 18, 11.1% ) . The rem aining of m acro-prolact inom a pat ients (n= 14) were sepa-rated into two groups: Group 1: Pat ients who had hypogonadism at inclusion and recovered with serum prolact in norm alizat ion (9/ 14, 64.2% ) .
Group 2: Pat ients who had hypogonadism both at inclusion and the sixth m onth de-spite prolact in normalizat ion (5/ 14, 35.7% ). Details of gonadot rophin-gonadal axis and tum or volum e on adm ission and after six months of cabergoline t reatment with serum prolact in norm alizat ion are shown in Table 2. Mean serum prolact in levels at the sixth m onth of therapy in m acro- and m icropro-lact inom a pat ients were 10.5± 5.7 ng/ m L versus 8.1± 6.1 ng/ m L (p> 0.05) . Knosp grades, Hardy num bers, and Hardy let ters m easured dur ing the presentat ion were not stat ist ically different regarding hy-pogonadism status in all macroprolact inoma pat ients (n= 18; p= 0.43, p= 0.46, p= 0.89, respect ively) .
PRL (norm al range: 2.1-17.7 ng/ m l) . Stat ist ically significant p values are writ ten as bold.
n= 2 8 Macroprolact inom as ( n= 1 8 ) Microprolact inom as ( n= 1 0 ) p
Mean age (years, m ean± SD) 44.77± 13.44 44.4± 13.9 > 0.05
Main com plaint (n, % )
Visual defect 6 (33.3) 0 (0.0) 0 .0 4
Headaches 10 (55.6) 1 (10.0) 0 .0 2
Sexual dysfunct ion 9 (50.0) 9 (90.0) 0 .0 4
I ncidental 1 (6.6) 0 (0.0) 0.64
Hypogonadism (n, % ) 14 (77.8) 3 (30.0) 0 .0 1
PRL (ng/ m l) 4912.0± 10655.3 104.9± 43.1 0 .0 0
Tum or volum es (cm 3) 8.83 0.16 0 .0 2
Knosp grade (n, % )
0 1 (5.6) 7 (70.0) 0 .0 1
1 5 (27.8) 2 (20.0)
2 6 (33.3) 1 (10.0)
3 4 (22.2) 0 (0.0)
4 2 (11.1) 0 (0.0)
Hardy num ber (n, % )
0 0 (0.0) 6 (60.0) 0 .0 0
I 1 (5.6) 2 (20.0)
I I 4 (22.2) 1 (10.0)
I I I 12 (66.7) 1 (10.0)
I V 1 (5.6) 0 (0.0)
Hardy let ter (n, % )
A 3 (16.7) 9 (90.0) 0 .0 4
B 2 (11.1) 1 (10.0)
C 1 (5.6) 0 (0.0)
D 4 (22.2) 0 (0.0)
E 8 (44.4) 0 (0.0)
Table 1. General baseline character ist ics of the pat ients with m acro and m icroprolact inom as.
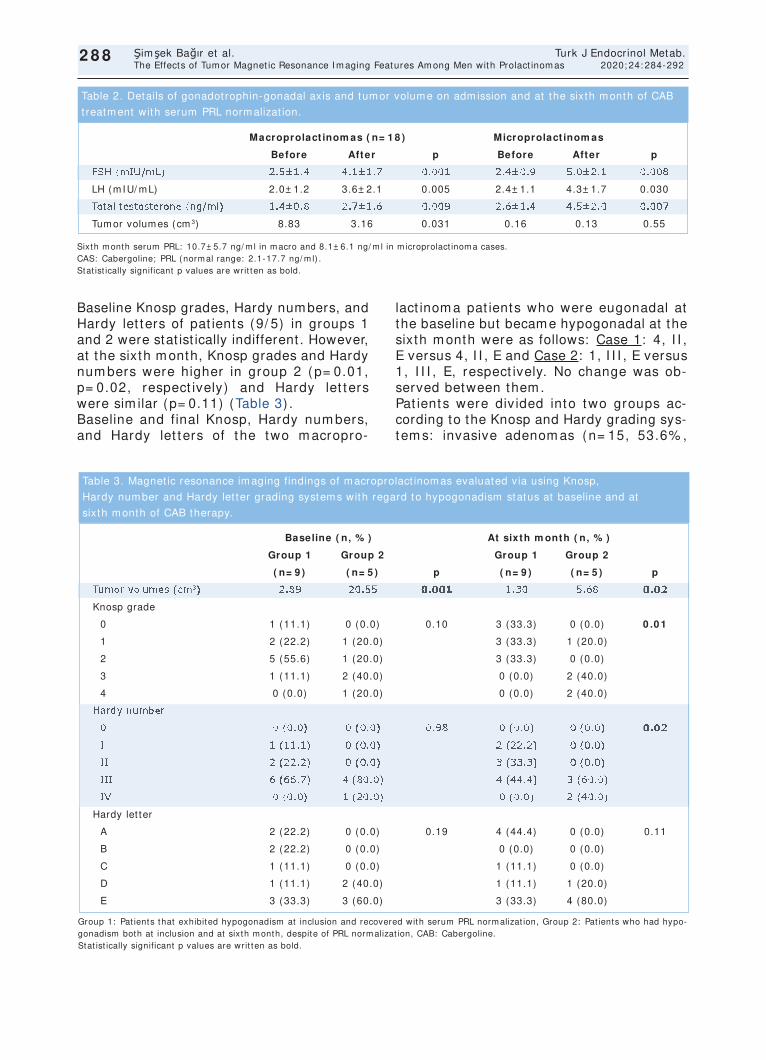
288
Şimşek Bağır et al. Turk J Endocrinol Metab. The Effects of Tum or Magnet ic Resonance I m aging Features Am ong Men with Prolact inom as 2020; 24: 284-292
2 8 8
Baseline Knosp grades, Hardy numbers, and Hardy let ters of pat ients (9/ 5) in groups 1 and 2 were stat ist ically indifferent . However, at the sixth month, Knosp grades and Hardy num bers were higher in group 2 (p= 0.01, p= 0.02, respect ively) and Hardy let ters were sim ilar (p= 0.11) (Table 3) . Baseline and final Knosp, Hardy num bers, and Hardy let ters of the two m acropro-
lact inom a pat ients who were eugonadal at the baseline but became hypogonadal at the sixth m onth were as follows: Case 1: 4, I I , E versus 4, I I , E and Case 2: 1, I I I , E versus 1, I I I , E, respect ively. No change was ob-served between them . Pat ients were div ided into two groups ac-cording to the Knosp and Hardy grading sys-tem s: invasive adenom as (n= 15, 53.6% ,
Sixth m onth serum PRL: 10.7± 5.7 ng/ m l in m acro and 8.1± 6.1 ng/ m l in m icroprolact inom a cases. CAS: Cabergoline; PRL (norm al range: 2.1-17.7 ng/ m l) . Stat ist ically significant p values are writ ten as bold.
Macroprolact inom as ( n= 1 8 ) Microprolact inom as
Before After p Before After p
FSH (m I U/ m L) 2.5± 1.4 4.1± 1.7 0.001 2.4± 0.9 5.0± 2.1 0.008
LH (m I U/ m L) 2.0± 1.2 3.6± 2.1 0.005 2.4± 1.1 4.3± 1.7 0.030
Total testosterone (ng/ m l) 1.4± 0.8 2.7± 1.6 0.009 2.6± 1.4 4.5± 2.0 0.007
Tum or volum es (cm 3) 8.83 3.16 0.031 0.16 0.13 0.55
Table 2. Details of gonadot rophin-gonadal axis and tum or volum e on adm ission and at the sixth m onth of CAB
t reatm ent with serum PRL norm alizat ion.
Group 1: Pat ients that exhibited hypogonadism at inclusion and recovered with serum PRL norm alizat ion, Group 2: Pat ients who had hypo-gonadism both at inclusion and at sixth m onth, despite of PRL norm alizat ion, CAB: Cabergoline. Stat ist ically significant p values are writ ten as bold.
Baseline ( n, % ) At sixth m onth ( n, % )
Group 1 Group 2 Group 1 Group 2
( n= 9 ) ( n= 5 ) p ( n= 9 ) ( n= 5 ) p
Tum or volum es (cm 3) 2.89 20.55 0 .0 0 1 1.30 5.68 0 .0 2
Knosp grade
0 1 (11.1) 0 (0.0) 0.10 3 (33.3) 0 (0.0) 0 .0 1
1 2 (22.2) 1 (20.0) 3 (33.3) 1 (20.0)
2 5 (55.6) 1 (20.0) 3 (33.3) 0 (0.0)
3 1 (11.1) 2 (40.0) 0 (0.0) 2 (40.0)
4 0 (0.0) 1 (20.0) 0 (0.0) 2 (40.0)
Hardy num ber
0 0 (0.0) 0 (0.0) 0.98 0 (0.0) 0 (0.0) 0 .0 2
I 1 (11.1) 0 (0.0) 2 (22.2) 0 (0.0)
I I 2 (22.2) 0 (0.0) 3 (33.3) 0 (0.0)
I I I 6 (66.7) 4 (80.0) 4 (44.4) 3 (60.0)
I V 0 (0.0) 1 (20.0) 0 (0.0) 2 (40.0)
Hardy let ter
A 2 (22.2) 0 (0.0) 0.19 4 (44.4) 0 (0.0) 0.11
B 2 (22.2) 0 (0.0) 0 (0.0) 0 (0.0)
C 1 (11.1) 0 (0.0) 1 (11.1) 0 (0.0)
D 1 (11.1) 2 (40.0) 1 (11.1) 1 (20.0)
E 3 (33.3) 3 (60.0) 3 (33.3) 4 (80.0)
Table 3. Magnet ic resonance im aging findings of m acroprolact inom as evaluated via using Knosp,
Hardy num ber and Hardy let ter grading system s with regard to hypogonadism status at baseline and at
sixth m onth of CAB therapy.
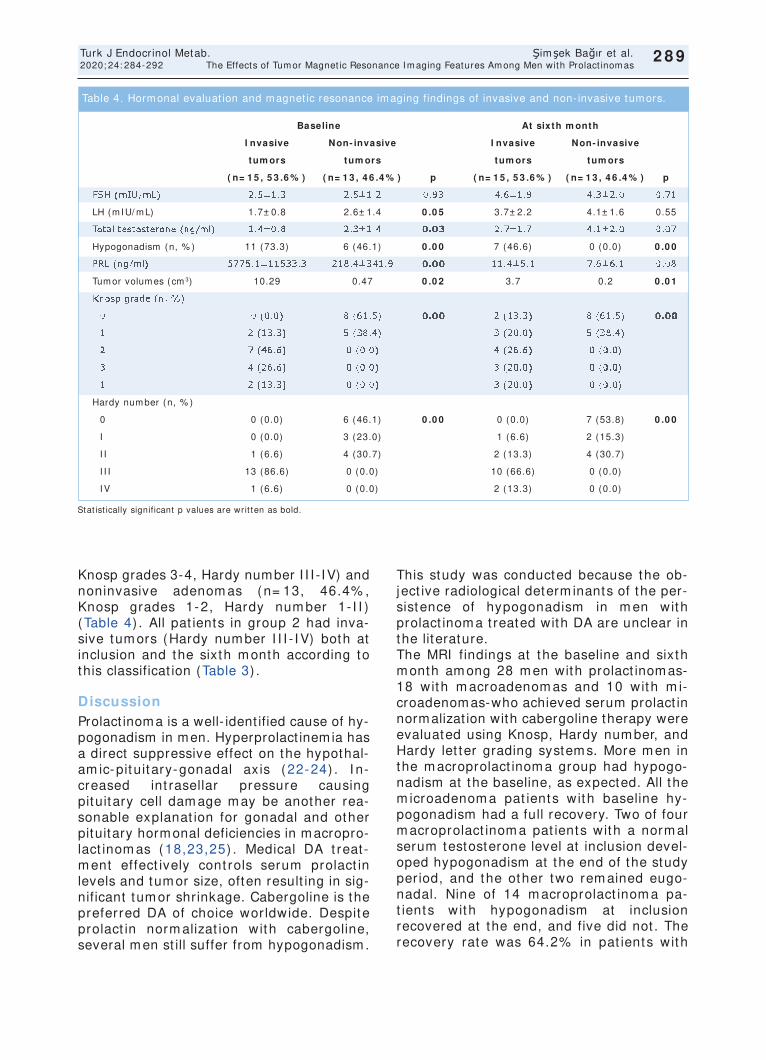
289
Turk J Endocrinol Metab. Şimşek Bağır et al. 2020; 24: 284-292 The Effects of Tum or Magnet ic Resonance I m aging Features Am ong Men with Prolact inom as
2 8 9
Knosp grades 3-4, Hardy number I I I - IV) and noninvasive adenom as (n= 13, 46.4% , Knosp grades 1-2, Hardy num ber 1- I I ) (Table 4) . All pat ients in group 2 had inva-sive tum ors (Hardy num ber I I I - I V) both at inclusion and the sixth m onth according to this classificat ion (Table 3) .
Discussion Prolact inoma is a well- ident ified cause of hy-pogonadism in men. Hyperprolact inemia has a direct suppressive effect on the hypothal-am ic-pituitary-gonadal axis (22-24) . I n-creased int rasellar pressure causing pituitary cell dam age m ay be another rea-sonable explanat ion for gonadal and other pituitary hormonal deficiencies in macropro-lact inom as (18,23,25) . Medical DA t reat-m ent effect ively cont rols serum prolact in levels and tum or size, often result ing in sig-nificant tum or shrinkage. Cabergoline is the preferred DA of choice wor ldwide. Despite prolact in norm alizat ion with cabergoline, several m en st ill suffer from hypogonadism .
This study was conducted because the ob-ject ive radiological determ inants of the per-sistence of hypogonadism in m en with prolact inom a t reated with DA are unclear in the literature. The MRI findings at the baseline and sixth m onth am ong 28 m en with prolact inom as-18 with m acroadenom as and 10 with m i-croadenomas-who achieved serum prolact in normalizat ion with cabergoline therapy were evaluated using Knosp, Hardy num ber, and Hardy let ter grading system s. More m en in the m acroprolact inom a group had hypogo-nadism at the baseline, as expected. All the m icroadenom a pat ients with baseline hy-pogonadism had a full recovery. Two of four m acroprolact inom a pat ients with a norm al serum testosterone level at inclusion devel-oped hypogonadism at the end of the study per iod, and the other two rem ained eugo-nadal. Nine of 14 m acroprolact inom a pa-t ients with hypogonadism at inclusion recovered at the end, and five did not . The recovery rate was 64.2% in pat ients with
Stat ist ically significant p values are writ ten as bold.
Baseline At sixth m onth
I nvasive Non- invasive I nvasive Non- invasive
tum ors tum ors tum ors tum ors
( n= 1 5 , 5 3 .6 % ) ( n= 1 3 , 4 6 .4 % ) p ( n= 1 5 , 5 3 .6 % ) ( n= 1 3 , 4 6 .4 % ) p
FSH (m I U/ m L) 2.5± 1.3 2.5± 1.2 0.93 4.6± 1.9 4.3± 2.0 0.71
LH (m I U/ m L) 1.7± 0.8 2.6± 1.4 0 .0 5 3.7± 2.2 4.1± 1.6 0.55
Total testosterone (ng/ m l) 1.4± 0.8 2.3± 1.4 0 .0 3 2.7± 1.7 4.1± 2.0 0.07
Hypogonadism (n, % ) 11 (73.3) 6 (46.1) 0 .0 0 7 (46.6) 0 (0.0) 0 .0 0
PRL (ng/ m l) 5775.1± 11533.3 218.4± 341.9 0 .0 0 11.4± 5.1 7.6± 6.1 0.08
Tum or volum es (cm 3) 10.29 0.47 0 .0 2 3.7 0.2 0 .0 1
Knosp grade (n, % )
0 0 (0.0) 8 (61.5) 0 .0 0 2 (13.3) 8 (61.5) 0 .0 0
1 2 (13.3) 5 (38.4) 3 (20.0) 5 (38.4)
2 7 (46.6) 0 (0.0) 4 (26.6) 0 (0.0)
3 4 (26.6) 0 (0.0) 3 (20.0) 0 (0.0)
1 2 (13.3) 0 (0.0) 3 (20.0) 0 (0.0)
Hardy num ber (n, % )
0 0 (0.0) 6 (46.1) 0 .0 0 0 (0.0) 7 (53.8) 0 .0 0
I 0 (0.0) 3 (23.0) 1 (6.6) 2 (15.3)
I I 1 (6.6) 4 (30.7) 2 (13.3) 4 (30.7)
I I I 13 (86.6) 0 (0.0) 10 (66.6) 0 (0.0)
I V 1 (6.6) 0 (0.0) 2 (13.3) 0 (0.0)
Table 4. Horm onal evaluat ion and m agnet ic resonance im aging findings of invasive and non- invasive tum ors.

m acroprolact inom as. Knosp, Hardy num ber and Hardy let ter grades at the baseline did not differ am ong the 14 hypogonadal m acroprolact inom a pat ients with regard to the f inal status. However, higher Knosp grades and Hardy num bers, but not Hardy let ters, were observed in pat ients who con-sistent ly had a low serum testosterone level in the sixth m onth (Group 2) . All pat ients in group 2 had invasive tum ors both at inclu-sion and dur ing the sixth m onth according to this classificat ion. A lim ited number of studies exist about male prolact inom a and hypogonadism in the cur-rent m edical literature. The norm alizat ion of serum testosterone levels ranged between 50% and 60% in m ales with the successful t reatm ent of hyperprolact inem ia (3) . Kar-avitaki et al. t reated 12 m acroprolact inom a pat ients with cabergoline, 44% of whom had recovered from hypogonadism (22) . Tirosh et al. t reated 71 m en who had pituitary m acroadenom as with cabergoline. Hypogo-nadism has been observed in 57 of 63 pa-t ients (90.5% ) at presentat ion, whereas only 22 of 65 (33.8% ) have had low testos-terone levels following t reatm ent and pro-lact in suppression (26) . Shim on et al. studied 12 m ales with giant prolact inom as who were t reated with cabergoline. Testos-terone levels, init ially low in all pat ients, were norm alized in eight pat ients (67% ) (27) . Colao et al. studied 41 m ales with m acroprolact inom a who were t reated with cabergoline. Testosterone deficiency was ob-served in 73% of them at presentat ion; after six m onths of cabergoline t reatm ent , 60.9% of pat ients recovered (20) . Tirosh et al. reported that pat ients with an adenom a diam eter of greater than 20 m m m ore fre-quent ly presented with hypogonadism than sm aller adenom as. The prevalence of hy-pogonadism has been found to be 87.6% (64/ 73) at presentat ion and 33.3% (23/ 69) following t reatm ent am ong m acroprolact in-om a pat ients (17) . Keeping in accordance with the literature, 64.2% of our m acropro-lact inom a pat ients with hypogonadism at the baseline gained norm al gonadal func-t ions with prolact in norm alizat ion. I n daily clinical pract ice, the m edical t reat-m ent of m icroprolact inom as alm ost always results in the recovery of gonadal status in m en. However, som e m acroprolact inom a
pat ients recover, but others do not , and it is clear that the current ly used term inat ion, macroprolact inoma, is not sufficient to iden-t ify indiv iduals who would have persistent hypogonadism . This study was the f irst in the m edical lit erature to use the validated grading systems, Knosp and Hardy, in defin-ing tum or MRI propert ies in prolact inom as beyond the t radit ional m icro-m acro term i-nat ion. Higher Knosp grades and Hardy num bers at the sixth m onth in MRI s of the m acropro-lact inom a pat ients with persistent hypogo-nadism under line the negat ive effects of CVS invasion and sella dest ruct ion but not the suprasellar extension. The high grades of the two m acroprolact inom a pat ients who becam e hypogonadal following prolact in normalizat ion also pointed to the importance of CVS invasion and sella basem ent disrup-t ion in the persistence of hypogonadism. We proposed that increased int rasellar pressure m ay be a reasonable explanat ion for our re-sults. Gonadot roph horm one-secret ing cells are known to be located widely throughout the pituitary gland. The int rasellar pressure of m acroprolact inom as that exhibit parasel-lar extension toward the CVS m ay be higher than the ones that grow upward to the suprasellar system because of the barr ier funct ion of CVS bone walls. This m ay result in gonadot roph cell dam age and thus the persistence of hypogonadism . This study had a few lim itat ions. The ret ro-spect ive design and the low num ber of pa-t ients included m ay be cr it icized. However, consider ing the pat ient num bers in sim ilar studies in the literature, we believed it m ight be appreciated.
Conclusion I n this study, we clearly dem onst rated that m acroprolact inom as with persistent hypog-onadism despite serum prolact in norm aliza-t ion m ore com m only showed CVS invasion and sella dest ruct ion using Knosp and Hardy grading system s. This m ay be at t r ibuted to their possibly higher int rasellar pressures than that of the tum ors with suprasellar ex-tension lacking bony barr iers. We concluded that the Knosp and Hardy grading system s are useful in predict ing the persistence of m ale hypogonadism in pro-lact inomas following prolact in normalizat ion.
290
Şimşek Bağır et al. Turk J Endocrinol Metab. The Effects of Tum or Magnet ic Resonance I m aging Features Am ong Men with Prolact inom as 2020; 24: 284-292
2 9 0
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conf lict s of int erest bet ween t he au-thors and / or fam ily m em bers of t he sci-ent if ic and m edical com m it tee m em bers or m em bers of t he potent ial conflict s of inter-est , counseling, exper t ise, work ing condi-t ions, share holding and sim ilar sit uat ions in any f irm .
Authors Contr ibut ions
I dea/ Concept : Melek Eda Ertörer, Gülay Şimşek Bağır; Design; Melek Eda Ertörer, Gülay Şimşek Bağır; Control/ Supervision: Melek Eda Ertörer, Gülay Şimşek Bağır, Okan Sefa Bakıner; Data Collect ion and/ or Process-ing: Gülay Şimşek Bağır, Filiz Ekşi Haydardedeoğlu, Okan Sefa Bakıner; Analy-sis and/ or I ntepretat ion: Melek Eda Ertörer, Gülay Şimşek Bağır, Özlem Alkan, Aylin Güneşli; Literature Review: Melek Eda Ertörer, Gülay Şimşek Bağır, Özlem Alkan, Aylin Güneşli; Writ ing the Art icle: Gülay Şimşek Bağır, Melek Eda Ertörer; Crit ical Reviewing: Melek Eda Ertörer; References and Funding; Gülay Şimşek Bağır, Melek Eda Ertörer; Mate-rials: Gülay Şimşek Bağır, Melek Eda Ertörer.
References 1. Fernandez A, Karavitaki N, Wass JA. Prevalence of
pituitary adenomas: a community-based, cross-sec-t ional study in Banbury (Oxfordshire, UK) . Clin En-docr inol (Oxf ) . 2010; 72: 377-382. [ Crossref] [ PubMed]
2. Melm ed S, Kleinberg D. Pituitary m asses and tu-m ors. I n: Melm ed S, Polonsky KS, Larsen PR, Kro-nenberg HM, eds. William s Textbook of Endocr inology (13th ed) . Philadelphia; Elsevier ; 2016; 260-266. [ Crossref]
3. Gillam MP, Molitch ME. Prolact inom a. I n: Melm ed S, ed. The Pituitary (3rd ed) . San Diego; Elsevier ; 2011; 475-531. [ Crossref]
4. Liu W, Zahr RS, McCartney S, Cetas JS, Dogan A, Fleseriu M. Clinical outcom es in m ale pat ients with lactot roph adenom as who required pituitary sur-gery: a ret rospect ive single center study. Pituitary. 2018; 21: 454-462. [ Crossref] [ PubMed]
5. Andereggen L, Frey J, Andres RH, El-Koussy M, Beck J, Seiler RW, Christ E. Long- term follow-up of pr im ary m edical versus surgical t reatm ent of pro-lact inom as in m en: effects on hyperprolact inem ia, hypogonadism , and bone health. World Neurosurg. 2017; 97: 595-602. [ Crossref] [ PubMed]
6. Nishioka H, I noshita N. New WHO classificat ion of pituitary adenomas (4th edit ion) : assessment of pi-tuitary t ranscript ion factors and the prognost ic his-tological factors. Brain Tum or Pathol. 2018; 35: 57-61. [ Crossref] [ PubMed]
7. Davies BM, Carr E, Soh C, Gnanalingham KK. As-sessing size of pituitary adenomas: a comparison of qualitat ive and quant itat ive m ethods on MR. Acta Neurochir (Wien) . 2016; 158: 677-683. [ Crossref] [ PubMed] [ PMC]
8. Knosp E, Steiner E, Kitz K, Matula C. Pituitary ade-nom as with invasion of the cavernous sinus space: a m agnet ic resonance im aging classificat ion com -pared with surgical f indings. Neurosurgery. 1993; 33: 610-617. [ Crossref] [ PubMed]
9. Hardy J, Som m a M. Surgical t reatm ent by t ranssphenoidal m icrosurgical rem oval of the pitu-itary adenom a. I n: Colins W, Tindall G, eds. Clinical Managem ent of Pituitary Disorders. 1st ed. New York; Raven; 1979; 209-217. [ Crossref]
10. Di I eva A, Rotondo F, Syro LV, Cusim ano MD, Ko-vacs K. Aggressive pituitary adenom as- -diagnosis and em erging t reatm ents. Nat Rev Endocr inol. 2014; 10: 423-435. [ Crossref] [ PubMed]
11. Melm ed S, Casanueva FF, Hoffm an AR, Kleinberg DL, Montori VM, Schlechte JA, Wass JA; Endocrine Society. Diagnosis and t reatm ent of hyperpro-lact inem ia: an Endocr ine Society clinical pract ice guideline. J Clin Endocr inol Metab. 2011; 96: 273-288. [ Crossref] [ PubMed]
12. Beshyah SA, Sher if I H, Chent li F, Ham rahian A, Khalil AB, Raef H, El-Fikki M, Jam bart S. Manage-m ent of prolact inom as: a survey of physicians from the Middle East and North Afr ica. Pituitary. 2017; 20: 231-240. [ Crossref] [ PubMed]
13. Dogansen SC, Selcukbir icik OS, Tanrikulu S, Yarman S. Withdrawal of dopam ine agonist therapy in pro-lact inom as: I n which pat ients and when? Pituitary. 2016; 19: 303-310. [ Crossref] [ PubMed]
14. Pinzone JJ, Katznelson L, Danila DC, Pauler DK, Miller CS, Klibanski A. Pr im ary m edical therapy of m icro- and m acroprolact inom as in m en. J Clin En-docr inol Metab. 2000; 85: 3053-3057. [ Crossref] [ PubMed]
15. Berezin M, Shim on I , Hadani M. Prolact inom a in 53 m en: clinical character ist ics and m odes of t reat-m ent (m ale prolact inom a) . J Endocr inol I nvest . 1995; 18: 436-441. [ Crossref] [ PubMed]
16. Andrysiak-Mam os E, Kaźm ierczyk-Puchalska A, Zo-chowska E, Sowińska-Przepiera E, Sagan L, Kojder I , Syrenicz A. Evaluaton of therapy with cabergoline in m en with m acroprolact inoa. Pom eranian J Life Sci. 2015; 61(3) : 263-9. [ Crossref] [ PubMed]
17. Tirosh A, Benbassat C, Lifshit z A, Shim on I . Hy-popituitar ism pat terns and prevalence am ong m en with m acroprolact inom as. Pituitary. 2015; 18: 108-115. [ Crossref] [ PubMed]
291
Turk J Endocrinol Metab. Şimşek Bağır et al. 2020; 24: 284-292 The Effects of Tum or Magnet ic Resonance I m aging Features Am ong Men with Prolact inom as
2 9 1

292
Şimşek Bağır et al. Turk J Endocrinol Metab. The Effects of Tum or Magnet ic Resonance I m aging Features Am ong Men with Prolact inom as 2020; 24: 284-292
2 9 2
18. I glesias P, Bernal C, Villabona C, Cast ro JC, Arr ieta F, Díez JJ. Prolact inom as in m en: a m ult icent re and ret rospect ive analysis of t reatm ent outcom e. Clin Endocr inol (Oxf ) . 2012; 77: 281-287. [ Crossref] [ PubMed]
19. Sibal L, Ugwu P, Kendall-Taylor P, Ball SG, James RA, Pearce SH, Hall K, Quinton R. Medical therapy of m acroprolact inom as in m ales: I . Prevalence of hy-popituitar ism at diagnosis. I I . Proport ion of cases exhibit ing recovery of pituitary funct ion. Pituitary. 2002; 5: 243-246. [ Crossref] [ PubMed]
20. Colao A, Vitale G, Cappabianca P, Br igant i F, Cic-carelli A, De Rosa M, Zarr illi S, Lom bardi G. Out-com e of cabergoline t reatm ent in m en with prolact inom a: effects of a 24-m onth t reatm ent on prolact in levels, tum or m ass, recovery of pituitary funct ion, and sem en analysis. J Clin Endocr inol Metab. 2004; 89: 1704-1711. [ Crossref] [ PubMed]
21. Shim on I , Benbassat C. Male prolact inom as pre-sent ing with norm al testosterone levels. Pituitary. 2014; 17: 246-250. [ Crossref] [ PubMed]
22. Karavitaki N, Dobrescu R, Byrne JV, Grossm an AB, Wass JA. Does hypopituitar ism recover when m acroprolact inom as are t reated with cabergoline? Clin Endocrinol (Oxf ) . 2013; 79: 217-223. [ Crossref] [ PubMed]
23. Ciccarelli A, Guerra E, De Rosa M, Milone F, Zarr illi S, Lom bardi G, Colao A. PRL secret ing adenom as in m ale pat ients. Pituitary. 2005; 8: 39-42. [ Crossref] [ PubMed]
24. Walia R, Bhansali A, Dut ta P, Khandelwal N, Sialy R, Bhadada S. Recovery pat tern of hypothalam o-pitu-itary- test icular axis in pat ients with macroprolact in-om as after t reatm ent with cabergoline. I ndian J Med Res. 2011; 134: 314-319. [ PubMed] [ PMC]
25. Arafah BM, Prunty D, Ybarra J, Hlavin ML, Selm an WR. The dominant role of increased int rasellar pres-sure in the pathogenesis of hypopituitar ism , hyper-prolact inem ia, and headaches in pat ients with pituitary adenom as. J Clin Endocr inol Metab. 2000; 85: 1789-1793. [ Crossref] [ PubMed]
26. Tirosh A, Benbassat C, Shim on I . Short - term de-cline in prolact in concent rat ions can predict future prolact in norm alizat ion, tum or shrinkage, and t im e to rem ission in m en with m acroprolact inom as. En-docr Pract . 2015; 21: 1240-1247. [ Crossref] [ PubMed]
27. Shim on I , Benbassat C, Hadani M. Effect iveness of long- term cabergoline t reatm ent for giant pro-lact inom a: study of 12 m en. Eur J Endocr inol. 2007; 156: 225-231. [ Crossref] [ PubMed]

Role of AGR2 Expression in Specim ens from Pituitary Adenom a Tissue on Tum or Behavior
Hipofiz Adenom Doku Örnekler inde AGR2 Ekspresyonunun Tüm ör Davranışı Üzerine Etkisi
Sem a ÇİFTÇİ DOĞANŞEN, Öm ür GÜNALDI * , Ayla Solm az AVCI KURT* * ,
Barış ÇOLLUOĞLU* , İlhan YI LMAZ* , Meral MERT, Osm an TANRI VERDİ*Department of Endocrinology and Metabolism,
University of Health Sciences, Bakırköy Dr. Sadi Konuk Training and Research Hospital, İstanbul, TURKEY * Department of Neurosurgery, University of Health Sciences,
Bakırköy Prof. Dr. Mazhar Osman Training and Research Hospital for Neurology, Neurosurgery and Psychiat ry, * * Department of Medical Biology, Balıkesir University Faculty of Medicine, Balıkesir, TURKEY
Original Art icle Turk J Endocrinol Metab. 2020; 24: 293-299
Object ive: To invest igate the anterior gradient 2 (AGR2) mRNA expression, which perform s various cellular funct ions such as cell m igrat ion, different iat ion, and proliferat ion in t issue specim ens from pituitary adenom as. Materia l and Methods: A total of 44 pituitary adenom a specim ens (20 fem ale/ 24 m ale) from pat ients, and ten norm al brain t issues (5 fem ale/ 5 m ale) operated for epi-lepsy surgery (cont rol group) were included in the study. Speci-m ens were stored at -80 ° C throughout the study. Molecular assessm ent of pituitary adenom as and cont rol brain t issues was perform ed to quant ify m RNA expression of AGR2using real- t im e PCR. Dist r ibut ion of AGR2 m RNA expression levels was evaluated according to pituitary adenom a subtypes, tum or aggressiveness, or invasiveness. Results: Expression levels of AGR2 m RNA in cor-t icot roph (n= 5) and som atot roph adenom as (n= 14) were higher com pared to cont rol brain t issues (p= 0.045 and p= 0.005, respec-t ively) ; however, expression levels of AGR2 m RNA in lactot roph (n= 3) , gonadot roph (n= 14) , and non-secretory adenom as (n= 7) were sim ilar to the cont rol brain t issues. The thyrot roph adenom a (n= 1) was not included in the analysis. Expression levels of AGR2 m RNA were sim ilar in fem ale and m ale pat ients. The expression levels of the AGR2 m RNA were higher in non- invasive tum ors (n= 20) than invasive tum ors (n= 24) (p= 0.001) , and in the non-aggressive tum ors (n= 27) than aggressive tum ors (n= 17) (p= 0.018) . A negat ive correlat ion between expression levels of AGR2 m RNA and Ki-67 labeling index ( r= -0.328; p= 0,029) was obtained. However, no correlat ion was found between the expres-sion levels of AGR2 m RNA and age or m axim um tum or diam eter. Conclusion: AGR2 expression is inversely correlated to invasive-ness and aggressiveness, independent ly from age and sex in pi-tuitary adenom as. Keyw ords: Anter ior gradient 2; AGR2; pituitary adenom a;
aggressiveness; invasiveness; somatotroph adenoma
Am aç: Migrasyon, farklılaşm a ve proliferasyon gibi çeşit li hücresel görevler i olan anter ior gradient 2 (AGR2) expresyonunun hipofiz adenom doku örnekler inde değerlendir ilm esi. Gereç ve Yöntem -ler: Bu çalışm aya, 44 hastanın (20 kadın/ 24 erkek) hipofiz ade-nom doku örnekler i ve epilepsi cerrahisi uygulanan 10 hastanın (5 kadın/ 5 erkek) da normal beyin dokusu örnekleri kontrol grubu ola-rak kabul edilerek dâhil edilm işt ir. Tüm doku örnekler i çalışılana kadar -80° C’de saklanmışt ır. Dokularda AGR2 m RNA ekspresyonu real- t ime PCR kullanılarak kullanılarak değerlendir ilm işt ir. Hipofizer adenom unun subt ipi, tüm örün agresif liği ve invaziv liğine göre AGR2 m RNA ekspresyonunun dağılım ına bakılm ışt ır. Bulgular : AGR2 m RNA ekspresyonu kort ikot rop adenom larda (n= 5) ve so-m atot rop adenom larda (n= 14) , kont rol beyin dokusundan daha yüksekt i (sırasıyla, p= 0,045 ve p= 0,005) , bununla bir likte lactot-rop adenomlarda (n= 3) , gonadotrop adenomalarda (n= 14) ve non-sekretuar adenom larda (n= 7) kont rol beyin dokusuna göre benzer idi, t irot rop adenom lar ise (n= 1) hesaplam alara dâhil edilm em işt ir. AGR2 m RNA ekspresyonu kadın ve erkeklerde benzerdir. İnvaziv olm ayanlarda (n= 20) , invasiv tüm örlerden (n= 24) , agresif olm a-yanlarda (n= 27) ise agresif tüm örlerden (n= 17) AGR2 m RNA eks-presyonu anlam lı derecede yüksekt i ( sırasıy la, p= 0,001 ve p= 0,018) . AGR2 m RNA ekspresyonu ile Ki-67 labeling index ara-sında bir negat if korelasyon ( r= -0,328; p= 0,029) saptanırken yaş ve m aksim um tüm ör boyutu arasında bir korelasyon saptanm adı. Sonuç: AGR2 ekspresyonu yaş ve cinsiyet ten bağım sız olarak hi-pofiz adenom larının agresifliği ve invazivliği ile ters orant ılıdır. Anahtar kelim eler: Anterior gradient 2; AGR2; hipofiz adenoma;
agresiflik; invazivlik; som atot rof adenom
2 9 3
Address for Correspondence: Sem a ÇİFTÇİ DOĞANŞEN, Departm ent of Endocrinology and Metabolism , University of Health Sciences, Bakırkoy Dr. Sadi Konuk Training and Research Hospital, İstanbul, TURKEY
Phone: + 90 212 414 71 71/ 1215 E- m ail: drsem aciftci@hotm ail.com
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 10 Jun 2020 Received in revised form : 16 Sep 2020 Accepted: 25 Sep 2020 Available online: 16 Oct 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
66
63
This study only w as presented as a poster presentat ion at 2 1 st European Congress of Endocrinology: ECE 2 0 1 9 w hich w as held in May 1 8 - 2 1 , 2 0 1 9 , Lyon, France.

I nt roduct ion Pituitary adenomas are benign tumors. Al-though they are relat ively rare among all in-t racranial tumors, these tumors have an increased risk of morbidity and mortality (1) . Several complicat ions caused by hyperfunc-t ioning adenomas form one reason for the in-creased risk (2) . Another reason is the compression symptoms caused by the mass effect of adenoma as up to 50% of pituitary adenomas exhibit invasive or aggressive be-havior (3,4). The et iopathogenesis of pituitary adenomas has not been completely eluci-dated, and genetic mutat ions have been iden-t ified in less than 5% of all cases. There is no reliable biological marker to define the ag-gressive behavior of adenoma (5) . Therefore, aggressive pituitary adenomas are rarely rec-ognized in the early stages; this leads to ther-apeut ic challenges in the subsequent period. Anter ior gradient protein 2 (AGR2) is from fam ily of protein disulphide isom erase gene (6) . I t plays a crucial role in providing endo-plasm ic ret iculum hom eostasis and part ici-pates in cellular funct ions, including cell m igrat ion, different iat ion, and proliferat ion (6,7) . I t has been reported that AGR2 over-expression m ay be associated with the de-velopm ent of various m alignancies such as breast , lung, ovary, prostate, colon, and pancreas; however, there are cont roversial data on this topic (8) . There are lim ited studies about the role of AGR2 expression in pituitary adenom as (9,10) . I n this study, the authors aim ed to assess the im portance of AGR2 expression in both ident ifying pituitary adenom a subtypes and tum or aggressiveness in t issue specim ens from pituitary adenom as.
Materia l and Methods The study was performed on adenoma spec-imens obtained from 44 pat ients (20 female, 24 m ale) who underwent pituitary surgery for two years. Pat ients with non-adenom a-tous sellar lesions in the histopathological exam inat ion perform ed after surgery were excluded. Norm al brain t issues obtained from ten pat ients (5 fem ale, 5 m ale) who underwent epilepsy surgery with norm al pi-tuitary im aging were included as a cont rol group. All the t issue sam ples were form alin-fixed and em bedded in paraffin blocks be-fore being stored at -80° C unt il assays.
All procedures in this study com plied with the 1964 Helsinki Declarat ion and were ap-proved by the Ethics Com m it tee of the Bakirkoy Dr. Sadi Konuk Training and Re-search Hospital. Writ ten inform ed consent was obtained from all part icipants. The AGR2 gene expression in t issue samples com prised 3-steps: RNA isolat ion, synthesis of complementary DNA (cDNA) from RNA by reverse t ranscript ion, and dem onst rat ion of gene expression with real- t im e polym erase chain react ion (RT-PCR) .
RNA I solat ion from Tissue Sam ples
RNA was isolated from frozen t issues of ade-nom a or the brain by TRI zol™ reagent . The process followed was: t issue sam ples were hom ogenized by adding 1 m L of TRI SOL ™ reagent to 50-100 m g of the t issue sam ple and incubated for 5 m inutes. The super-natant was separated by cent r ifugat ion and t ransferred to an RNAse- free m icro-cen-t r ifuge tube (1.5 m L) ; 1 m L of GENEzol™ reagent was added to it for homogenizat ion. The m icro-cent r ifuge tube was disturbed, and the sam ple was re-cent r ifuged; the upper liquid phase was then t ransferred into another tube, followed by the RNA precipi-tat ion step. One volum e of isopropanol was added to the liquid phase and m ixed, which was incubated for 10 m inutes and cen-t r ifuged to obtain an RNA pellet . After cen-t r ifugat ion, the supernatant was carefully rem oved and discarded. One m L of ethanol was added to wash the RNA pellet , and the sam ple was vortexed, then re-cent r ifuged, and the supernatant thus obtained was re-m oved. The resultant RNA pellet was dried, and the dry pellet of RNA was re-suspended by RNAse- free water. I t was then incubated at 55-60°C for 15 m inutes. The isolated RNA was stored at -80° C.
cDNA Synthesis from RNA
One µg of t he t otal isolated RNA was ut i-l ized for cDNA synt hesis. One m icrogram of t ot al isolat ed RNA, 1 µL of random pr im er, and dH2O were m ixed to obtain a t ot al volum e of10 µL. The obt ained m ix-ture was incubated for 5 m inutes at 65° C before being placed on ice. Then, 5X reac-t ion buffer, RNase inhibit or ( 0.5 µL) , dNTP m ix ( 2 µL) , and reverse t ranscr ipt ase ( 2 µL) were annexed t o obt ain 20 µL of t he
294
Çiftçi Doğanşen et al. Turk J Endocrinol Metab. AGR2 Expression in Pituitary Adenom as 2020; 24: 293-299
2 9 4

t ot al react ion volum e. I t was placed in a PCR device at 42° C (60 m inutes) and 70° C (5 m inutes) .
AGR2 Gene Expression by RT- PCR
Applied Biosystem s Step One Plus hardware was ut ilized for the RT-PCR analyses (Gene All SYBR Green Master Mix) . Sam ples were assayed in t r iplicate, and react ions were generated using their genes and act in beta (ACTB) genes. The levels of gene expression were quant if ied with Applied Biosystem s 7500 Fast Real-Tim e PCR System Software. AGR2 gene expression levels were described according to the threshold cycle (Ct ) , and ACTBs were ut ilized as reference genes that acted as an internal reference to norm alize the RNA expression and were calculated as 2–∆∆CT.
Assessm ent of Param eters That Could Be Related to AGR2 m RNA Expression in Adenom a Tissues
According to pituitary adenom a subtypes, the dist r ibut ion of AGR2 m RNA expression levels ( cor t icot roph, som atot roph, lac-tot roph, gonadot roph, thyrot roph, and non-secretory adenom as) was com pared. The correlat ions between AGR2 m RNA expres-sion levels and age, m axim um tum or diam -eter, and Ki-67 labeling index were assessed. Ki-67 labeling index was scored with the eye-balling m ethod after the MI B1 ant ibody staining of adenom as t issues. Adenom a size grading and cavernous sinus invasiveness were assessed according to Hardy and Knosp classif icat ions, respec-t ively (11,12) , and the dist r ibut ion of AGR2 m RNA expression levels according to Hardy and Knosp classificat ion grade of adenomas. Pituitary tum or aggressiveness was deter-m ined according to the m anagem ent of ag-gressive pituitary tum ors and carcinom as in the European Society of Endocrinology Clin-ical Pract ice Guideline (4) . According to this guideline, aggressive tum ors were defined as rapidly growing with radiologically inva-sive tum ors and/ or clinically significant tu-m oral enlargem ent , although opt im al standard t reatm ents such as surgery, m ed-ical therapy, and radiotherapy. AGR2 m RNA expression levels were com pared in inva-sive/ noninvasive and aggressive/ non-ag-gressive tum ors.
SPSS 21.0 version was used for the stat ist i-cal analyses. Descript ive stat ist ical m ethods and quant itat ive data were used to assess the data. Frequency and percentage rates were used to define categor ical var iables; m ean± standard deviat ion (SD) was used to descr ibe num erical var iables. The Chi-square test was ut ilized to com pare cate-gorical variables. I nter-variable relat ionships were assessed with Spearm an’s correlat ion analysis. Com parisons between qualitat ive data were m ade with Fisher ’s exact , Pear-son’s Chi-square, and Fisher-Freem an-Hal-ton’s tests. The stat ist ical analyses of m olecular calculat ions were perform ed by the One-way ANOVA and Student ’s T- test . Ap-value< 0.05 was considered stat ist ically significant .
Results
The m ean age of 44 pat ients (20 fem ale, 24 male) was 47± 15 ( range, 20-71) years. Out of 44 pituitary adenom a t issues, there were 5 ACTH-posit ive cort icot roph adenom as, 14 GH-posit ive som atot roph adenom as, 3 PRL-posit ive lactot roph adenomas, 14 LH-and/ or FSH-posit ive gonadot roph adenomas, seven non-secretory adenom as with no im -m unoreact iv it y, and one TSH-posit ive thy-rot roph adenom a according to im m unohistochem ical staining. While cort i-cot roph, som atot roph, thyrot roph, and lac-tot roph adenom as exhibited horm one hyperfunct ion, there was no hyperfunct ion in gonadot roph adenom as. Expression lev-els of AGR2 m RNA in cort icot roph and so-m atot roph adenom as were higher in com par ison to the cont rol brain t issues (p= 0.045 and p= 0.005, respect ively) ; how-ever, expression levels of AGR2 m RNA in lactot roph, gonadot roph, and non-secretory adenom as were sim ilar to those in the con-t rol brain t issues (p> 0.05) (Figure 1) . Thy-rot roph adenom a (n= 1) was not included in the stat ist ical analysis. Expression levels of AGR2 m RNA were sim ilar in fem ale and m ale pat ients. The m ean adenom a diam eter was 28 ± 16 ( range, 4-75) m m . The dist r ibut ion of ade-nomas according to Hardy and Knosp classi-f icat ion is Hardy 0 (n= 3) , Hardy 1 (n= 2) , Hardy 2 (n= 12) , Hardy 3 (n= 9) , Hardy 4 (n= 18) and Knosp 0 (n= 4) , Knosp 1
295
Turk J Endocrinol Metab. Çiftçi Doğanşen et al. 2020; 24: 293-299 AGR2 Expression in Pituitary Adenom as
2 9 5
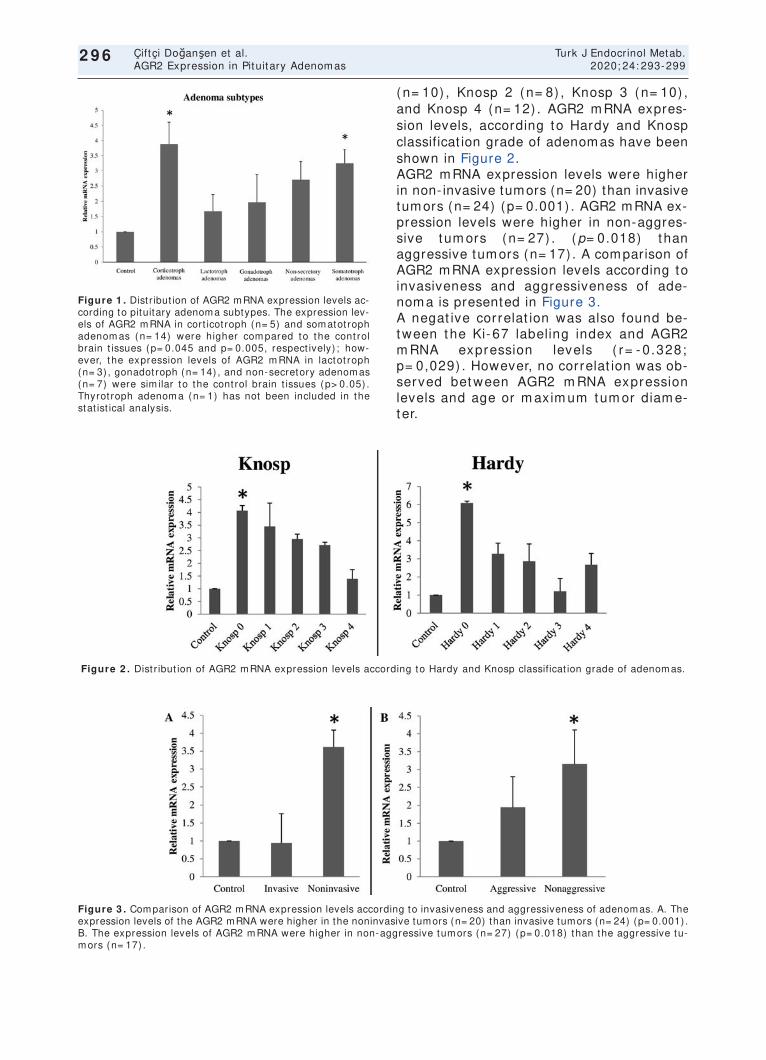
(n= 10) , Knosp 2 (n= 8) , Knosp 3 (n= 10) , and Knosp 4 (n= 12) . AGR2 m RNA expres-sion levels, according to Hardy and Knosp classificat ion grade of adenom as have been shown in Figure 2. AGR2 m RNA expression levels were higher in non- invasive tumors (n= 20) than invasive tum ors (n= 24) (p= 0.001) . AGR2 m RNA ex-pression levels were higher in non-aggres-sive tum ors (n= 27) . (p= 0.018) than aggressive tum ors (n= 17) . A com parison of AGR2 m RNA expression levels according to invasiveness and aggressiveness of ade-nom a is presented in Figure 3. A negat ive correlat ion was also found be-tween t he Ki- 67 labeling index and AGR2 m RNA expression levels ( r= - 0.328; p= 0,029) . However, no correlat ion was ob-served bet ween AGR2 m RNA expression levels and age or m axim um tum or diam e-ter.
296
Çiftçi Doğanşen et al. Turk J Endocrinol Metab. AGR2 Expression in Pituitary Adenom as 2020; 24: 293-299
2 9 6
Figure 1 . Dist r ibut ion of AGR2 mRNA expression levels ac-cording to pituitary adenoma subtypes. The expression lev-els of AGR2 m RNA in cort icot roph (n= 5) and som atot roph adenom as (n= 14) were higher com pared to the cont rol brain t issues (p= 0.045 and p= 0.005, respect ively) ; how-ever, the expression levels of AGR2 m RNA in lactot roph (n= 3) , gonadot roph (n= 14) , and non-secretory adenom as (n= 7) were sim ilar to the cont rol brain t issues (p> 0.05) . Thyrot roph adenom a (n= 1) has not been included in the stat ist ical analysis.
Figure 2 . Dist r ibut ion of AGR2 m RNA expression levels according to Hardy and Knosp classificat ion grade of adenom as.
Figure 3 . Comparison of AGR2 mRNA expression levels according to invasiveness and aggressiveness of adenomas. A. The expression levels of the AGR2 mRNA were higher in the noninvasive tumors (n= 20) than invasive tumors (n= 24) (p= 0.001) . B. The expression levels of AGR2 m RNA were higher in non-aggressive tum ors (n= 27) (p= 0.018) than the aggressive tu-m ors (n= 17) .

Discussion I n this study, we demonst rated the negat ive relat ionship between tum or aggressiveness and AGR2 expression in pituitary adenomas. Previous studies have proved overexpres-sion of AGR2 in var ious m alignancies such as breast , lung, ovary, prostate, colon, and pancreas cancers and suggested that it m ight be associated with poor prognosis and m etastasis or resistance to chem otherapy (8) . The reason is that AGR2 plays an im -portant role in the hom eostasis of the endo-plasm ic ret iculum (6,7) and m ay gain pro-oncogenic funct ion in the m icroenviron-ment of the tumor via secret ion from the ex-t racellular m at r ix (13) . I t m ay also play a role in inflam m at ion, im m unogenicit y, an-giogenesis, and thus rem odeling of the ex-t racellular m at r ix in tum or niche m icroenvironm ent (14) . I n vivo and in vit ro invest igat ions showed that it is involved in the tum or niche signaling or m ay also be present in cancer stem cells niche and chem oresistance niche (14) . For all t hese reasons, AGR2 expression levels were found to be related to poor prognosis in m alignan-cies. However, we found a negat ive associa-t ion between AGR2 expression and aggressiveness in pituitary adenom as but these tum ors are not m alignant . Sim ilar re-sults were reported in two studies assessing AGR2 expression in pituitary adenom as (9,10) . I n the first study, AGR2 expression was assessed in pituitary adenom a t issues by immunohistochemical staining, and AGR2 staining was found to be negat ive in the ma-jor it y of aggressive adenom as (9) . I n the same group’s subsequent study, the authors assessed the use of serum AGR2 levels in the different iat ion between adenom atous and non-adenom atous lesions of the pitu-itary gland. The sam e study showed that serum AGR2 levels were higher in cont rols than in pat ients with non-adenom atous pi-tuitary lesions and that serum AGR2 levels were lower in larger tum ors, although the difference could not reach a stat ist ical sig-nificance (10) . The present study result s, together with those from the above-m ent ioned studies, support the negat ive correlat ion between AGR2 expression and aggressiveness in pi-tuitary adenom as. The present study also direct ly presented AGR2 gene expression in
adenom a t issues; thus, result s regarding gene expression, protein synthesis, and serum levels have been shown consistent ly in pituitary adenom as. I t is current ly challenging to draw definit ive conclusions on the reason for decreased AGR2 expression in pituitary adenomas, un-like other m alignancies. However, literature reports studies stat ing that AGR2 expression was associated with lower tum or grade or proliferat ive index, m ore prolonged overall survival, and bet ter prognosis in colorectal cancers, non-sm all cell lung carcinom a, and breast cancer, which are in agreem ent with the f indings of the present study (15-17) . These cont radictory data m ay be due to dif-ferent m utat ions of AGR2 that affect func-t ions of AGR2 protein (14) . The effects of the underlying m echanism of AGR2 in pituitary adenom a are unclear. The AGR2 expression is induced by several st im -ulat ions such as sex hormones, endoplasm ic ret iculum st ress, and hypoxia (6,18,19) . AGR2 mRNA was significant ly upregulated in response to est radiol t reatment (20) . Zhang et al. (21) have reported that AGR2 mRNA is androgen inducible, depending on dose and t im e. The literature has also shown that es-t rogens and androgens increase AGR2 ex-pression in breast and prostate cancers, respect ively (22,23) . Presum ably, the de-creased AGR2 expression in invasive pitu-itary adenom as m ay be due to hypogonadism , which is m ore likely to be present ; however, this opinion is hypothet i-cal. I t was also shown that AGR expression is regulated in glioblastom a, an int racranial malignant tumor, by hypoxia- induced factor-1 (HI F-1) , which is related to the cont rol of growth angiogenesis in the tumor (24) . HI F-1 alpha expression is shown to be present in pituitary adenom as (25) ; thus, undiscov-ered m echanism s m ay determ ine the rela-t ionship between AGR2 expression and adenom a’s aggressiveness through this pathway. Further studies invest igat ing both HI F-1 alpha and AGR2 expression will clar ify this issue. I n t his study, AGR2 expression was also evaluated according to adenom a subtypes. Although the num ber of pat ients was low in this com par ison, AGR2 expression was higher in cor t icot roph and som atot roph adenom as. However, AGR2 expression was
297
Turk J Endocrinol Metab. Çiftçi Doğanşen et al. 2020; 24: 293-299 AGR2 Expression in Pituitary Adenom as
2 9 7

sim ilar in the other adenom as com pared to brain t issues. A sim ilar result was observed in another study, and AGR2 expression was found m ore frequent ly in cor t icot roph and som atot roph adenom as (9) . I n t he other study by the sam e researchers, the highest serum AGR2 level was observed in som a-tot rophic adenom as. Although the present study results are sim ilar to those on AGR2 expression in som atot roph and cort icot roph adenom as, m ore extensive studies are needed to clar ify the exact m echanism s af-fect ing AGR2 expression in t hese adeno-m as. The study’s m ajor lim itat ion is the low sam -ple size; the study period was rest r icted to two years to prevent t issue sam ples’ relia-bility. The number of pituitary adenoma sur-ger ies was m uch higher dur ing the study period, but som e were lesions with m im ick-ing adenom a or adenom a t issues that could not be obtained in a few m icroadenom as. I n addit ion, som e t issue sam ples were ex-cluded due to technical reasons. However, despite the lim ited num ber of sam ples eval-uated, finding a relat ionship between AGR2 expression and tum or aggressiveness will shed light on further studies. I n part icular, a com parison of horm one secret ion pat terns and AGR2 expression in a larger sam ple will help establish a t reatm ent plan for hyper-funct ioning adenom as. Another lim itat ion was the failure to obtain normal pituitary t is-sues for com parison due to ethical reasons. Future studies with t issues from cadavers will reveal m ore definit ive result s. The st rength of this study lies in the establish-ment of a negat ive correlat ion between ade-noma aggressiveness and AGR2 expression, which was sim ilar to that observed in the two previous studies (9,10) . This would play a significant role in determ ining the progno-sis and individualized t reatm ent in pituitary adenom as. I n conclusion, AGR2 expression is inversely correlated to aggressiveness and invasive-ness in pituitary adenomas. Moreover, AGR2 expression is associated with the adenom a subtype; AGR2 expression is increased, es-pecially in som atot roph adenom as. How-ever, m ore com prehensive and extensive studies are required to understand the exact m echanism or pathway of act ion of AGR2.
Com pliance w ith ethical standards
Ethical Approval
All procedures in this study complied with the 1964 Helsinki Declarat ion and were approved by the Bakırkoy Dr. Sadi Konuk Training and Research Hospital Ethics Commit tee.
I nform ed Consent
I nformed consent was obtained from all par-t icipants included in the study.
Source of Finance During this study, no financial or spiritual sup-port was received neither from any pharma-ceutical company that has a direct connection with the research subject, nor from a company that provides or produces medical instruments and materials which may negatively affect the evaluation process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions I dea/ Concept : Sem a Çiftçi Doğanşen, Ayla Solm az Avcıkurt ; Design: Sem a Çift çi Doğanşen, Öm ür Günaldı; Cont rol/ Supervi-sion: Sem a Çift çi Doğanşen, Meral Mert , Osm an Tanrıverdi; Data Collect ion and/ or Processing: Sem a Çift çi Doğanşen, Barış Çolluoğlu, İlhan Yılm az; Analysis and/ or I n-terpretat ion: Ayla Solm az Avcıkurt , Sem a Çift çi Doğanşen; Literature Review: Sem a Çiftçi Doğanşen; Writ ing the Art icle: Sem a Çiftçi Doğanşen; Crit ical Review: Sema Çiftçi Doğanşen, Meral Mert ; References and Fundings: Meral Mert , Öm ür Günaldı; Mate-r ials: Ayla Solm az Avcıkurt , Öm ür Günaldı.
References 1. Molit ch ME. Diagnosis and t reatm ent of pituitary
adenom as: a review. JAMA. 2017; 317: 516-524. [ Crossref]
2. Cooper O, Melmed S. Subclinical hyperfunct ioning pi-tuitary adenomas: the silent tumors. Best Pract Res Clin Endocrinol Metab. 2012; 26: 447-460. [ Crossref]
3. Di I eva A, Rotondo F, Syro LV, Cusim ano MD, Ko-vacs K. Aggressive pituitary adenom as- -diagnosis and em erging t reatm ents. Nat Rev Endocr inol. 2014; 10: 423-435. [ Crossref] [ PubMed]
298
Çiftçi Doğanşen et al. Turk J Endocrinol Metab. AGR2 Expression in Pituitary Adenom as 2020; 24: 293-299
2 9 8
4. Raverot G, Burm an P, McCorm ack A, Heaney A, Pe-tersenn S, Popovic V, Trouillas J, Dekkers OM; Eu-ropean Society of Endocrinology. European Society of Endocrinology Clinical Pract ice Guidelines for the m anagem ent of aggressive pituitary tum ours and carcinom as. Eur J Endocr inol. 2018; 178: G1-G24. [ Crossref] [ PubMed]
5. Melm ed S. Pathogenesis of pituitary tum ors. Nat Rev Endocr inol. 2011; 7: 257-266. [ Crossref] [ PubMed]
6. Higa A, Mulot A, Delom F, Bouchecareilh M, Nguyên DT, Boism enu D, Wise MJ, Chevet E. Role of pro-oncogenic protein disulfide isomerase (PDI ) fam ily member anterior gradient 2 (AGR2) in the control of endoplasm ic ret iculum hom eostasis. J Biol Chem . 2011; 286: 44855-44868. [ Crossref] [ PubMed] [ PMC]
7. Brychtova V, Voj tesek B, Hrstka R. Anterior gradient 2: a novel player in tum or cell biology. Cancer Let t . 2011; 304: 1-7. [ Crossref] [ PubMed]
8. Tian SB, Tao KX, Hu J, Liu ZB, Ding XL, Chu YN, Cui JY, Shuai XM, Gao JB, Cai KL, Wang JL, Wang GB, Wang L, Wang Z. The prognost ic value of AGR2 ex-pression in solid tum ours: a system at ic review and m eta-analysis. Sci Rep. 2017; 7: 15500. [ Crossref] [ PubMed] [ PMC]
9. Toht i M, Li J, Ma C, Li W, Lu Z, Hu Y. Expression of AGR2 in pituitary adenomas and its associat ion with tum or aggressiveness. Oncol Let t . 2015; 10: 2878-2882. [ Crossref] [ PubMed]
10. Toht i M, Li J, Tang C, Wen G, Abduj ilil A, Yizim P, Ma C. Serum AGR2 as a useful biom arker for pituitary adenom as. Clin Neurol Neurosurg. 2017; 154: 19-22. [ Crossref] [ PubMed]
11. Hardy J, Vezina JL. Transsphenoidal neurosurgery of int racranial neoplasm . Adv Neurol. 1976; 15: 261-273. [ PubMed]
12. Knosp E, Steiner E, Kitz K, Matula C. Pituitary ade-nom as with invasion of the cavernous sinus space: a m agnet ic resonance im aging classificat ion com -pared with surgical f indings. Neurosurgery. 1993; 33: 610-617. [ Crossref] [ PubMed]
13. Fessart D, Dom blides C, Avr il T, Er iksson LA, Be-gueret H, Pineau R, Malr ieux C, Dugot-Senant N, Lucchesi C, Chevet E, Delom F. Secret ion of protein disulphide isom erase AGR2 confers tum or igenic propert ies. Elife. 2016; 5: e13887. [ Crossref] [ PubMed] [ PMC]
14. Delom F, Nazaraliyev A, Fessart D. The role of pro-tein disulphide isom erase AGR2 in the tum our niche. Biol Cell. 2018; 110: 271-282. [ Crossref] [ PubMed]
15. Fr it zsche FR, Dahl E, Pahl S, Burkhardt M, Luo J, Mayordom o E, Gansukh T, Dankof A, Knuechel R,
Denkert C, Winzer KJ, Dietel M, Krist iansen G. Prog-nost ic relevance of AGR2 expression in breast can-cer. Clin Cancer Res. 2006; 12: 1728-1734. [ Crossref] [ PubMed]
16. Fritzsche FR, Dahl E, Dankof A, Burkhardt M, Pahl S, Petersen I , Dietel M, Kr ist iansen G. Expression of AGR2 in non sm all cell lung cancer. Histol Histopathol. 2007; 22: 703-708. [ Crossref] [ PubMed]
17. Riener MO, Thiesler T, Hellerbrand C, Am ann T, Cathom as G, Fr it zsche FR, Dahl E, Bahra M, We-ichert W, Terracciano L, Krist iansen G. Loss of ante-r ior gradient-2 expression is an independent prognost ic factor in colorectal carcinom as. Eur J Cancer. 2014; 50: 1722-1730. [ Crossref] [ PubMed]
18. Lee E, Lee DH. Em erging roles of protein disulfide isom erase in cancer. BMB Rep. 2017; 50: 401-410. [ Crossref] [ PubMed] [ PMC]
19. Chevet E, Fessart D, Delom F, Mulot A, Voj tesek B, Hrstka R, Murray E, Gray T, Hupp T. Em erging roles for the pro-oncogenic anter ior gradient-2 in cancer developm ent . Oncogene. 2013; 32: 2499-2509. [ Crossref] [ PubMed]
20. Wilson CL, Sim s AH, Howell A, Miller CJ, Clarke RB. Effects of oest rogen on gene expression in epithe-lium and st roma of normal human breast t issue. En-docr Relat Cancer. 2006; 13: 617-628. [ Crossref] [ PubMed]
21. Zhang JS, Gong A, Cheville JC, Sm ith DI , Young CY. AGR2, an androgen- inducible secretory protein overexpressed in prostate cancer. Genes Chrom o-som es Cancer. 2005; 43: 249-259. [ Crossref] [ PubMed]
22. Salmans ML, Zhao F, Andersen B. The est rogen-reg-ulated anterior gradient 2 (AGR2) protein in breast cancer: a potent ial drug target and biom arker. Breast Cancer Res. 2013; 15: 204. [ Crossref] [ PubMed] [ PMC]
23. Bu H, Borm ann S, Schäfer G, Horninger W, Mas-soner P, Neeb A, Lakshm anan VK, Maddalo D, Nest l A, Sültm ann H, Cato AC, Klocker H. The anter ior gradient 2 (AGR2) gene is overexpressed in prostate cancer and m ay be useful as a ur ine sedi-m ent m arker for prostate cancer detect ion. Prostate. 2011; 71: 575-587. [ Crossref] [ PubMed]
24. Hong XY, Wang J, Li Z. AGR2 expression is regulated by HI F-1 and cont r ibutes to growth and angiogen-esis of glioblastom a. Cell Biochem Biophys. 2013; 67: 1487-1495. [ Crossref] [ PubMed]
25. Xiao Z, Liu Q, Zhao B, Wu J, Lei T. Hypoxia induces hem orrhagic t ransform at ion in pituitary adenom as via the HI F-1α signaling pathway. Oncol Rep. 2011; 26: 1457-1464. [ Crossref] [ PubMed] [ PMC]
299
Turk J Endocrinol Metab. Çiftçi Doğanşen et al. 2020; 24: 293-299 AGR2 Expression in Pituitary Adenom as
2 9 9

Original Art icle Turk J Endocrinol Metab. 2020; 24: 300-307
300
The Effects of Psychological Focus Group Therapy on the Quality of Life of Fem ale Pat ients
w ith Acrom egaly Kadın Akrom egali Hastalarında Psikoloj ik Focus Grup Terapisinin
Hayat Kalitesi Üzerine Etkiler i
Özlem HALİLOĞLU, Sem a SÖZER* , Özge POLAT KORKMAZ, Serdar ŞAHİN,
Em re DURCAN, Gökhan ORAL* * , Pınar KADI OĞLU Department of Endocrinology, Metabolism and Diabetes, İstanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine, İstanbul, TURKEY
* Department of Psychology, Acıbadem Kadıköy Hospital, İstanbul, TURKEY * * Department of Forensic Medicine, İstanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine, İstanbul, TURKEY
Object ive: Chronic diseases such as acromegaly affect psycho-logical health. This study aim ed to evaluate the effects of a 1-year- long psychological focus group therapy on the qualit y of life of pat ients with acromegaly. Material and Methods: Seven fem ale pat ients with acrom egaly, followed-up at the endocrino-logy outpat ient clinic of Cerrahpasa Medical Faculty, were eva-luated. The weekly group psychotherapy sessions were conducted by a psychoanalyst and a clinical psychologist bet-ween May 2018 and May 2019. Beck Depression I nventory (BDI ) and Acrom egaly Quality of Life (AcroQoL) scales were as-sessed at baseline, 3-m onths, 6-m onths, and 1-year of group therapy. Results: The m ean age of the pat ients was 43.7 ± 6.2years, and the m edian durat ion of disease was 8 [ 3-10] years. Six pat ients were in disease rem ission. There was a sig-nificant im provem ent in the BDI (p= 0.008) and AcroQoL- total scores (p= 0.04) from the beginning t ill the end of the study. A st rong negat ive correlat ion was observed between BDI and Ac-roQoL-2 (p= 0.003; r= -0.91 vs. p= 0.04; r= -0.77) and AcroQoL-total (p= 0.03; r= -0.78 vs. p= 0.01; r= -0.85) scores at baseline and the 3-m onths of therapy, respect ively. Moreover, the psychoanalyst reported that the pat ients showed an im proved abilit y to face diff icult ies caused by their illnesses, expressed their emot ional react ions more freely, and were more capable of endur ing the disease. Conclusion: Pat ients with acrom egaly benefited from the 1-year psychological focus group therapy in terms of psychological well-being, along with improved AcroQoL and BDI scores. Psychotherapeut ic approaches, start ing with the diagnosis of the disease, m ight be a significant intervent ion that im proves the quality of life of pat ients with acrom egaly. Keyw ords: Acrom egaly; follow up studies;
psychotherapy; quality of life
Am aç: Akrom egali gibi kronik hastalık lar psikoloj ik sağlığı et -k iler. Bu çalışm anın am acı, akrom egali hastalarında 1 yıllık psi-koloj ik focus grup terapisinin hastalar ın hayat kalit esi üzer ine etkisini araşt ırm akt ı. Gereç ve Yöntem ler: Cerrahpaşa Tıp Fa-kültesi endokr inoloj i k liniğinde takip edilm ekte olan 7 kadın ak-rom egali hastası çalışm aya kat ıldı. Haft alık grup psikoterapi seanslar ı, Mayıs 2018 ile Mayıs 2019 arasında bir psikanalist ve bir k linik psikolog tarafından gerçekleşt ir ildi. Beck Depres-yon Envanter i (BDE) ve Akrom egali Hayat Kalitesi Ölçeği (Acro-QoL) t erapinin başlangıcında, 3. ve 6. ay larda ve 1. y ılda değer lendir ildi. Bulgular : Hastalar ın or talam a yaşı 43,7± 6,2 yıl, ve or tanca hastalık süresi 8 [ 3-10] yıldı. Alt ı hasta rem is-yondaydı. Çalışm anın başlangıcından sonuna doğru BDE (p= 0,008) ve Acro-QoL- total (p= 0,04) skor larında anlam lı dü-zelm e saptandı. Başlangıç ve 3. ay BDE ile AcroQoL- 2 (p= 0,003; r= -0,91 vs. p= 0,04; r= -0,77) ve BDE ile AcroQoL-total (p= 0,03; r= -0,78 vs. p= 0,01; r= -0,85) skor ları arasında kuvvet li negat if korelasyon saptandı. Ayrıca, psikanalist , has-talar ın hastalık lar ının neden olduğu zor luklar la yüzleşm ede be-lirgin bir iler lem e gösterdik ler ini, duygusal t epk iler ini daha özgürce ifade et t ik ler ini ve hastalık la daha rahat baş edebil-dik ler ini bildirdi. Sonuç: Akrom egali hastalar ında 1 yıllık psi-koloj ik focus grup t erapisi psikoloj ik iy ilik hâller i açısından fayda sağlam ış olup bu fayda BDE ve Acro-QoL skor larında iy i-leşm eye de yol açm ışt ır. Tanı anından it ibaren yapılacak psiko-terapöt ik yaklaşım lar akrom egali hastalarının yaşam kalitesini ar t t ıracak önem li bir gir işim olabilir. Anahtar kelim eler: Akrom egali; takip çalışm aları;
psikoterapi; hayat kalitesi
3 0 0
Address for Correspondence: Pınar KADI OĞLU, Division of Endocrinology, Metabolism and Diabetes, İstanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine, İstanbul, TURKEY
Phone: + 90 212 414 30 00/ 21940 E- m ail: [email protected]
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 23 Jul 2020 Received in revised form : 05 Sep 2020 Accepted: 21 Sep 2020 Available online: 19 Oct 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ )
DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
82
27

301
Turk J Endocrinol Metab. Haliloğlu et al. 2020; 24: 300-307 The Effects of Focus Group Therapy in Acromegaly
3 0 1
I nt roduct ion Acrom egaly is a rare disease that is charac-ter ized by the excessive secret ion of growth horm one (GH) from benign pituitary adeno-m as. Besides the m echanical effects of the adenom a, such as headache and/ or v isual disturbances, or the m etabolic effects of the hypersecret ion of insulin- like growth factor-1 ( I GF-1) such as glucose intolerance and hypertension, pat ients with acrom egaly are faced with som e physical changes such as the overgrowth of facial and acral bones and soft t issues (1,2) . The slow and subt le pro-gression of the disease m akes this suffer ing m ore pronounced (3) . Chronic diseases affect psychological health. Besides the physical com plaints, frequent follow-ups, and t reatm ent processes, pa-t ients with acrom egaly need to m ake per-m anent changes in both their and their relat ives’ lifestyles. Health assistance is often preferent ially pro-v ided for physical ailm ents, whereas psy-chological help is often neglected in the management of chronic diseases (4,5) . Psy-chological help is m ore im portant in acrom egaly because the pat ients are ex-posed to disease- related physical malforma-t ions apart from the psychological effects caused by the disease. Therefore, besides the ongoing m edical t reatm ents for the pa-t ients, psychological support , especially when it is given through psychological group therapy with other pat ients having the same disease, m ay be very effect ive in im proving their m ood and their abilit y to cope with the disease. Although several studies in the lit -erature have evaluated the factors that af-fect the quality of life (QoL) of pat ients with acrom egaly (6-8) , inform at ion that deals with the effect of psychological support through group therapy is scarce (9,10) . The previous study with the longest follow-up evaluated the effects of cognit ive-behavioral therapy (CBT) in pat ients with acrom egaly and reported result s over nine weeks (9) . The sam e authors also re-evaluated the pa-t ients who had at tended the 9-week group therapy after nine m onths to determ ine the long- term effects of the 9-week- long ther-apy sessions. They showed an improvement in QoL with short- term therapy and that this posit ive effect was also m aintained after nine m onths (10) .
I n this study, the effects of a 1-year- long psychological focus group therapy on the QoL and m ood of pat ients with acrom egaly were evaluated.
Materia l and Methods
Subjects and Study Design
Pat ients with acromegaly, who were followed up at the endocr inology and m etabolism outpat ient clinic at the Cerrahpasa Medical Faculty, I stanbul University-Cerrahpasa, I s-tanbul, Turkey, were inform ed about the study. Pat ients that had known depression or psychiat r ic diseases and had taken psy-choact ive m edicine were excluded. Twelve pat ients that fulf illed the inclusion cr iter ia volunteered for part icipat ion in the study. However, after two weeks, only seven fe-m ale pat ients cont inued with group therapy regular ly. The weekly group psychotherapy sessions were conducted by a therapist (psychoanalyst ) (GO) and a co- therapist ( clinical psychologist ) (SS) between May 2018 and May 2019. The part icipants were seated in a circle in a pr ivate room to create a com fortable and peaceful environm ent . The demographic and disease characterist ics of the pat ients were determ ined from the m edical f iles and the part icipants them -selves. The pat ients were considered to be “ in rem ission” if the IGF-1 levels were within the normal range for their age and sex, even under the use of drugs, and the disease was considered to be “act ive” if the I GF-1 levels were higher than the norm al range for the pat ient ’s age and sex. The part icipants were asked to com plete the Beck Depression I n-ventory (BDI ) , and Acrom egaly Qualit y of Life (AcroQoL) scales at baseline, 3-months, 6-m onths, and 1-year of the group therapy.
Beck Depression I nventory ( BDI )
The BDI is a 21- item , self- report ing scale that m easures the sym ptom s of depression. Each response has a score of 0-3 points. A score of ≥17 implies depression. The Turkish validat ion of the BDI was conducted by Hisli in 1989 (11) . Acrom egaly Quality of Life (AcroQoL) Scale AcroQoL is a 3-part QoL scale (physical status-AcroQoL-1, psychological/ appear-ance–AcroQoL-2, psychological/ social rela-t ions–AcroQoL-3) that contains 22

quest ions. I t aim s to evaluate the physical and psychological status of pat ients with acrom egaly. Each response has a score of 1–5. The total score is direct ly proport ional to the QoL of the pat ient . AcroQoL has been validated in f ive different languages by Webb et al. (12) .
Psychotherapy design
I nsight-oriented and support ive psychother-apy techniques have been used to provide relief from sym ptom s, prom ote behavioral change, and em power pat ients to adapt to their em ot ional diff icult ies that stem from liv ing with a chronic illness (13-16) . Group psychotherapy for chronically ill pat ients provides a support system am ong m em bers that have com m on problem s and exper i-ences. This enables the pat ients to express their em ot ions freely and feel understood and supported by each other. Dur ing this process, they observe other m em bers’ be-havioral changes, posit ive outcom es, and becom e capable of im itat ing their problem -solving st rategies, which result in significant behavioral changes in their lifestyle and that of their relat ives. They gain insights on the diff icult ies of having a chronic illness, how the illness and its associated emot ions affect their close relat ionships, fam ily lives, and their sense of self. I n t im e, these insights star t changing their ways of relat ing with them selves and others, which is a m anifes-tat ion of the healing process. The group process also encourages pat ients to t ry new techniques of socializat ion and talk about different aspects of the illness, and all the related difficult ies they seem ed to avoid be-fore. Changes in the m anner of com m uni-cat ing about the illness within the group prom ote sim ilar changes in the outer world. The support ive relat ional system that is built within the group enables the pat ients to for-m ulate creat ive solut ions for their com m on problem s and prom ote posit ive behavioral changes, result ing in relief from sym ptom s. All subjects gave writ ten inform ed consent . The study was approved by the local ethics com m it tee of the I stanbul Universit y Cer-rahpasa Medical Faculty, and all the proce-dures perform ed in studies involving hum an part icipants were conducted in com pliance with the ethical standards of the inst itut ional and/ or nat ional research com m it tee, the
Helsinki Declarat ion of 1964, and its subse-quent am endm ents or com parable ethical standards.
Stat ist ical analysis
The data were stat ist ically analyzed using the program “Stat ist ical Package for the So-cial Sciences” for Windows version 21.0 (SPSS, Chicago, I L) . The norm ality of dist r i-but ion was tested using the Shapiro–Wilk test . The age, m onthly incom e, durat ion of disease, and AcroQoL result s were ex-pressed as m ean± standard deviat ion and the BDI scores as m edian [ interquart ile range ( I QR) ] . The Fr iedm an test (posthoc analysis with the Wilcoxon test ) was used for com paring the AcroQoL and BDI scores of pat ients at baseline, 3-m onth, 6-m onth, and 1-year of therapy. The degree of corre-lat ion between BDI and AcroQoL scores was evaluated using Spearm an’s test . p-value of < 0.05 was considered to be stat ist ically sig-nificant .
Results The demographic and disease characterist ics of the pat ients are presented in Table 1. The m ean age of the part icipants was 43.7± 6.2 years, and all were females. The median du-rat ion of disease was eight years ( range 3–10 years) , and six of the seven pat ients were in disease rem ission.
Results of the Quest ionnaires
The t rend in scores of the BDI and Acro-QoL of each pat ient from the beginning to the end of the therapy sessions is presented in Figures 1a and 1b, respect ively. Based on the BDI scores, two pat ients had depression at the beginning of the therapy sessions, which im proved m arkedly at one year. I n the total study group, a significant difference was observed in the BDI scores at the baseline, 3-month, 6-month, and 1-year (p= 0.008) , with the posthoc analysis indi-cat ing that the difference between param e-ters at baseline and 6-m onth (p= 0.01) , and baseline and 1-year (p= 0.02) cont r ibuted largely to the difference. The total AcroQoL scores showed a signifi-cant increase from the beginning to the end of the study (p= 0.04) , which was largely at-t r ibuted to the difference between param e-ters at 3-m onth and 1-year (p= 0.02) .
302
Haliloğlu et al. Turk J Endocrinol Metab. The Effects of Focus Group Therapy in Acrom egaly 2020; 24: 300-307
3 0 2
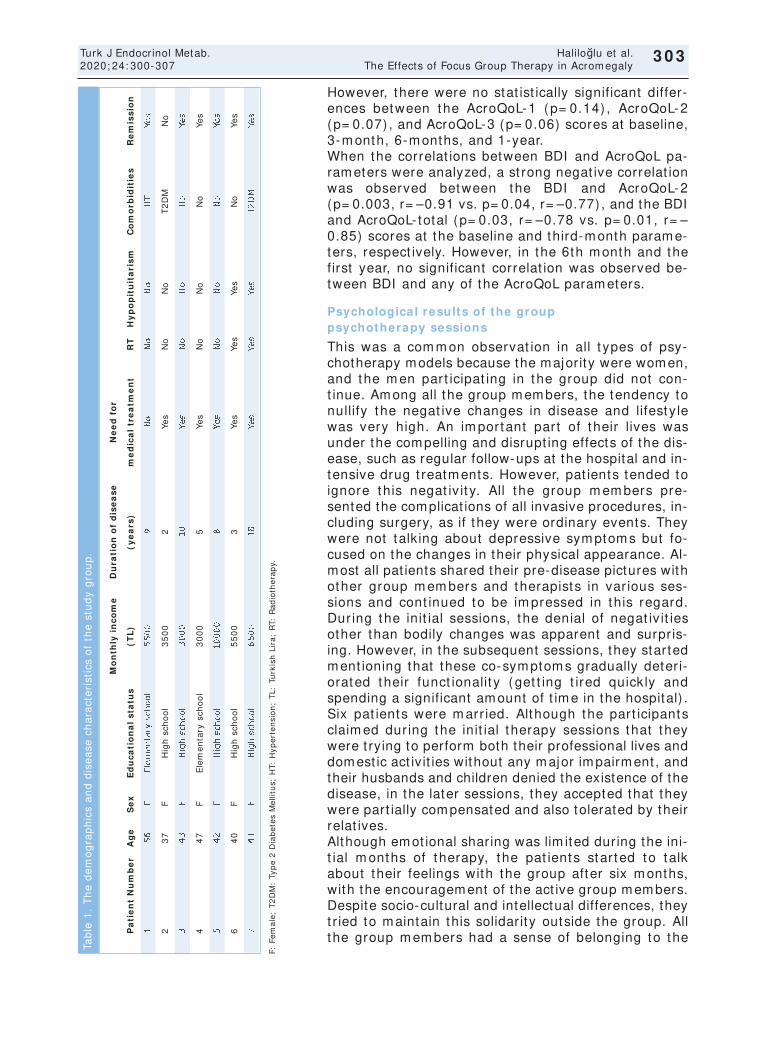
303
Turk J Endocrinol Metab. Haliloğlu et al. 2020; 24: 300-307 The Effects of Focus Group Therapy in Acromegaly
3 0 3
However, there were no stat ist ically significant differ-ences between the AcroQoL-1 (p= 0.14) , AcroQoL-2 (p= 0.07) , and AcroQoL-3 (p= 0.06) scores at baseline, 3-m onth, 6-m onths, and 1-year. When the correlat ions between BDI and AcroQoL pa-ram eters were analyzed, a st rong negat ive correlat ion was observed between the BDI and AcroQoL-2 (p= 0.003, r= –0.91 vs. p= 0.04, r= –0.77) , and the BDI and AcroQoL- total (p= 0.03, r= –0.78 vs. p= 0.01, r= –0.85) scores at the baseline and third-m onth param e-ters, respect ively. However, in the 6th m onth and the first year, no significant correlat ion was observed be-tween BDI and any of the AcroQoL param eters.
Psychological results of the group psychotherapy sessions
This was a com m on observat ion in all t ypes of psy-chotherapy models because the majority were women, and the m en part icipat ing in the group did not con-t inue. Am ong all the group m em bers, the tendency to nullify the negat ive changes in disease and lifesty le was very high. An im portant part of their lives was under the com pelling and disrupt ing effects of the dis-ease, such as regular follow-ups at the hospital and in-tensive drug t reatm ents. However, pat ients tended to ignore this negat iv it y. All t he group m em bers pre-sented the complicat ions of all invasive procedures, in-cluding surgery, as if they were ordinary events. They were not talk ing about depressive sym ptom s but fo-cused on the changes in their physical appearance. Al-most all pat ients shared their pre-disease pictures with other group m em bers and therapists in var ious ses-sions and cont inued to be im pressed in this regard. Dur ing the init ial sessions, the denial of negat iv it ies other than bodily changes was apparent and surpris-ing. However, in the subsequent sessions, they started m ent ioning that these co-sym ptom s gradually deter i-orated their funct ionalit y (get t ing t ired quickly and spending a significant am ount of t im e in the hospital) . Six pat ients were m arr ied. Although the part icipants claim ed dur ing the init ial therapy sessions that they were t rying to perform both their professional lives and domest ic act ivit ies without any major impairment , and their husbands and children denied the existence of the disease, in the later sessions, they accepted that they were part ially com pensated and also tolerated by their relat ives. Although em ot ional sharing was lim ited during the ini-t ial m onths of therapy, the pat ients star ted to talk about their feelings with the group after six m onths, with the encouragem ent of the act ive group m em bers. Despite socio-cultural and intellectual differences, they t r ied to m aintain this solidarity outside the group. All the group m em bers had a sense of belonging to the
F: F
em
ale
; T
2D
M:
Typ
e 2
Dia
be
tes
Me
llitu
s; H
T: H
yp
ert
en
sio
n;
TL:
Tu
rkis
h L
ira
; R
T: R
ad
ioth
era
py.
Mo
nth
ly i
nc
om
e
Du
rati
on
of
dis
ea
se
N
ee
d f
or
Pa
tie
nt
Nu
mb
er
Ag
eS
ex
Ed
uc
ati
on
al
sta
tus
(TL
)(y
ea
rs)
me
dic
al
tre
atm
en
tR
TH
yp
op
itu
ita
ris
mC
om
orb
idit
ies
Re
mis
sio
n
15
6F
Ele
me
nta
ry s
cho
ol
55
00
9N
oN
oN
oH
TYe
s
23
7F
Hig
h s
cho
ol
35
00
2Ye
sN
oN
oT
2D
MN
o
34
3F
Hig
h s
cho
ol
30
00
10
Yes
No
No
No
Yes
44
7F
Ele
me
nta
ry s
cho
ol
30
00
5Ye
sN
oN
oN
oYe
s
54
2F
Hig
h s
cho
ol
10
00
08
Yes
No
No
No
Yes
64
0F
Hig
h s
cho
ol
55
00
3Ye
sYe
sYe
sN
oYe
s
74
1F
Hig
h s
cho
ol
65
00
18
Yes
Yes
Yes
T2
DM
Yes
Tab
le 1
. T
he
de
mo
gra
ph
ics
an
d d
ise
ase
ch
ara
cte
rist
ics
of
the
stu
dy
gro
up
.
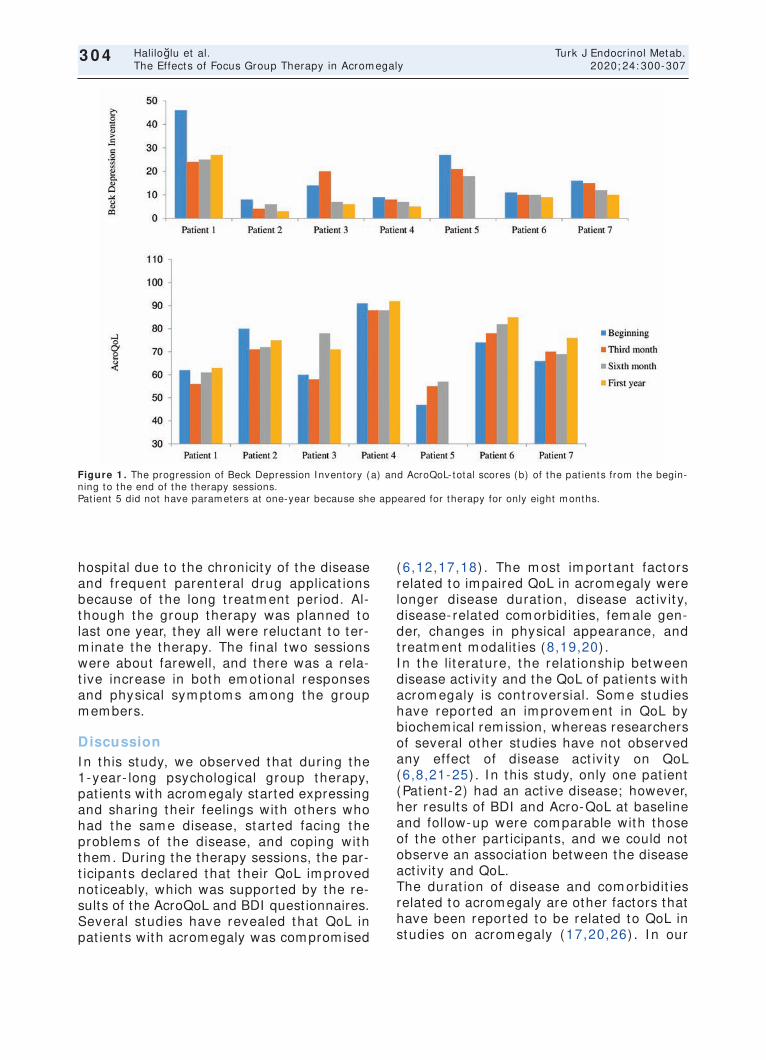
304
Haliloğlu et al. Turk J Endocrinol Metab. The Effects of Focus Group Therapy in Acrom egaly 2020; 24: 300-307
3 0 4
hospital due to the chronicity of the disease and frequent parenteral drug applicat ions because of the long t reatm ent per iod. Al-though the group therapy was planned to last one year, they all were reluctant to ter-m inate the therapy. The final two sessions were about farewell, and there was a rela-t ive increase in both em ot ional responses and physical sym ptom s am ong the group m em bers.
Discussion I n this study, we observed that dur ing the 1-year- long psychological group therapy, pat ients with acromegaly started expressing and shar ing their feelings with others who had the sam e disease, star ted facing the problem s of the disease, and coping with them . During the therapy sessions, the par-t icipants declared that their QoL im proved not iceably, which was supported by the re-sults of the AcroQoL and BDI quest ionnaires. Several studies have revealed that QoL in pat ients with acrom egaly was com prom ised
(6,12,17,18) . The m ost im portant factors related to im paired QoL in acrom egaly were longer disease durat ion, disease act iv it y, disease- related com orbidit ies, fem ale gen-der, changes in physical appearance, and t reatm ent m odalit ies (8,19,20) . I n the lit erature, the relat ionship between disease act ivity and the QoL of pat ients with acrom egaly is cont roversial. Som e studies have reported an im provem ent in QoL by biochem ical rem ission, whereas researchers of several other studies have not observed any effect of disease act iv it y on QoL (6,8,21-25) . I n this study, only one pat ient (Pat ient-2) had an act ive disease; however, her results of BDI and Acro-QoL at baseline and follow-up were com parable with those of the other part icipants, and we could not observe an associat ion between the disease act ivity and QoL. The durat ion of disease and com orbidit ies related to acrom egaly are other factors that have been reported to be related to QoL in studies on acrom egaly (17,20,26) . I n our
Figure 1 . The progression of Beck Depression I nventory (a) and AcroQoL- total scores (b) of the pat ients from the begin-ning to the end of the therapy sessions. Pat ient 5 did not have param eters at one-year because she appeared for therapy for only eight m onths.

study, no signif icant relat ionship was ob-served between the durat ion of disease or exist ing com orbidit ies with the QoL. Fem ale gender is another factor affect ing QoL in acrom egaly (8,27) . However, in the lit erature, m ale part icipat ion was low in studies where group therapy was applied due to the frequency of therapy sessions. A 9-week CBT study was conducted with ten pat ients, and only one of these pat ients was m ale. Sim ilar ly, in our study, all the part ici-pants were fem ale. Therefore, we could not evaluate the effect of sex on the QoL. Treatm ent m odalit ies can also affect QoL. Frequent requirem ents of inject ion and his-tory of radiotherapy (RT) are associated with decreased QoL in acrom egaly (8,19,28,29) . I n our study, all pat ients had undergone sur-gery, two pat ients had received RT, and six were undergoing m edical t reatm ent . Owing to the sm all study group, we could not es-tablish a correlat ion of t reatm ent m odalit ies with QoL. I ncreased anxiety and depression, changes in personality t raits, and decreased effect ive coping with difficult ies have been described in pat ients with acrom egaly (19,30,31) . Psychotherapeut ic intervent ions have been dem onst rated to be signif icant in several other chronic diseases, but the data on acrom egaly are insuff icient . Kunzler et al. designed a study to evaluate the effects of 9-week- long CBT in pat ients with acromegaly and reported improved QoL (9) . The sam e authors also re-evaluated the pa-t ients nine m onths after the CBT t r ial to evaluate the long- term effects of the ther-apy sessions and reported that the im -provem ent of QoL was sustained even then (1) . Correspondingly, we designed a psy-chological focus group therapy with a 1-year follow-up, which is the longest follow-up to date. Var ious quest ionnaires have been used to evaluate the QoL in chronic diseases. More-over, in some chronic diseases, disease-spe-cif ic QoL quest ionnaires have been developed. AcroQoL is a disease-specif ic quest ionnaire for acrom egaly. Studies that had used AcroQoL have revealed that the physical appearance was the m ost affected while personal relat ions were the least af-fected (19,32) . I n our study, we observed an im provem ent in AcroQoL- total scores,
but in the subgroup analyses, stat ist ical sig-nif icance could not be obtained, although the result s of appearance and social rela-t ions dom ains were close to signif icance. Furtherm ore, we observed st rong negat ive correlat ions between the physical appear-ance and BDI scores at the baseline and third m onth of the study, em phasizing the im portance of physical appearance in de-pression. The BDI is another scale that is used fre-quent ly in studies related to QoL. I n the 9-week CBT t r ial, Kunzler et al. observed no difference in BDI scores in ten pat ients with acrom egaly (9) . I n cont rast , we observed a significant improvement in BDI scores in our study group, which was probably due to the longer durat ion of our study.
Lim itat ions Our study has som e lim itat ions. The first is the sm all sam ple size of the study group. The once-a-week therapy sessions and the 1-year- long study period were the possible reasons for this lim itat ion. No m ale pat ients part icipated in the therapy sessions, also be-cause of the frequency of the sessions and other obligat ions such as work, which pre-vented the pat ients from part icipat ing in the study. Nevertheless, our study is im portant because, to our knowledge, this study has the longest follow-up in lit erature for the evaluat ion of psychological group therapy in pat ients with acrom egaly.
Conclusion The QoL of pat ients with acrom egaly im -proved significant ly with a 1-year- long focus group psychotherapy. The pat ients gained the abilit y to face the difficult ies caused by their illnesses, expressed their emot ional re-act ions m ore freely, and showed an im -proved abilit y to endure the disease. The support system s built within the group m em bers during the group therapy for one year enabled them to face clinically signifi-cant losses ( loss of funct ionality and physi-cal im pairm ents) to a large extent . They could accept som e of the changes in their lifestyles after the disease, such as the in-creased need for em ot ional support from fam ily m em bers, requir ing fam ily m em bers to share their burden of life, as well as the effects of changes in their appearance as a
305
Turk J Endocrinol Metab. Haliloğlu et al. 2020; 24: 300-307 The Effects of Focus Group Therapy in Acromegaly
3 0 5

result of their distor ted self- im age. Psy-chotherapeut ic approaches, start ing with the diagnosis of the disease, m ight be an im -portant intervent ion that im proves the QoL of pat ients with acrom egaly.
Acknow ledgem ents We thank Mr. David F. Chapm an for his help regarding English language edit ing.
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Author Contr ibut ions I dea/ Concept : Özlem Haliloğlu, Pınar Kadioğlu; Design: Özlem Haliloğlu, Gökhan Oral, Pınar Kadıoğlu; Cont rol/ Supervision: Özlem Haliloğlu, Sem a Sözer, Gökhan Oral, Pınar Kadıoğlu; Data Collect ion and/ or Pro-cessing: Özlem Haliloğlu, Sem a Sözer, Özge Polat Korkm az, Serdar Şahin, Em re Durcan, Gökhan Oral, Pınar Kadıoğlu; Analysis and/ or I nterpretat ion: Özlem Haliloğlu, Sem a Sözer, Gökhan Oral, Pınar Kadıoğlu; Literature Review: Özlem Haliloğlu, Sem a Sözer, Özge Polat Korkm az, Serdar Şahin, Em re Durcan, Gökhan Oral, Pınar Kadıoğlu; Writ ing the Art icle: Crit ical Review: Gökhan Oral, Pınar Kadıoğlu; References and Fund-ings: Sem a Sözer, Gökhan Oral; Materials: Özlem Haliloğlu, Sema Sözer, Özge Polat Ko-rkm az, Serdar Şahin, Em re Durcan, Gökhan Oral, Pınar Kadıoğlu.
References 1. Colao A, Ferone D, Marzullo P, Lom bardi G. Sys-
tem ic com plicat ions of acrom egaly: epidem iology, pathogenesis, and m anagem ent . Endocr Rev. 2004; 25: 102-152. [ Crossref] [ PubMed]
2. Woodhouse LJ, Mukher jee A, Shalet SM, Ezzat S. The influence of growth horm one status on physical im pairm ents, funct ional lim itat ions, and health- re-lated qualit y of life in adult s. Endocr Rev. 2006; 27: 287-317. [ Crossref] [ PubMed]
3. Ben-Shlom o A, Sheppard MC, Stephens JM, Pulgar S, Melm ed S. Clinical, quality of life, and econom ic value of acrom egaly disease cont rol. Pituitary. 2011; 14: 284-294. [ Crossref] [ PubMed] [ PMC]
4. Malhot ra S, Singh G. Psychological consequences of chronic physical illnesses in children and adoles-cents. I ndian J Pediat r. 2002; 69: 145-148. [ Cross-ref] [ PubMed]
5. Guthr ie E. Em ot ional disorder in chronic illness: psychotherapeut ic intervent ions. Br J Psychiat ry. 1996; 168: 265-273. [ Crossref] [ PubMed]
6. Kyriakakis N, Lynch J, Gilbey SG, Webb SM, Murray RD. I m paired quality of life in pat ients with t reated acrom egaly despite long- term biochem ically stable disease: Results from a 5-years prospect ive study. Clin Endocrinol (Oxf ) . 2017; 86: 806-815. [ Crossref] [ PubMed]
7. I m ran SA, Tiem ensm a J, Kaiser SM, Vallis M, Doucet te S, Abidi E, Yip CE, De Tugwell B, Siddiqi F, Clarke DB. Morphom et r ic changes correlate with poor psychological outcom es in pat ients with acrom egaly. Eur J Endocr inol. 2016; 174: 41-50. [ Crossref] [ PubMed]
8. Webb SM, Badia X. Qualit y of life in acrom egaly. Neuroendocrinology. 2016; 103: 106-111. [ Crossref] [ PubMed]
9. Kunzler LS, Naves LA, Casular i LA. Cognit ive-be-havioral therapy im proves the quality of life of pa-t ients with acromegaly. Pituitary. 2018; 21: 323-333. [ Crossref] [ PubMed]
10. Kunzler LS, Naves LA, Casular i LA. The effect of cognit ive-behavioral therapy on acrom egalics after a 9-m onth follow-up. Front Endocrinol (Lausanne) . 2019; 10: 380. [ Crossref] [ PubMed] [ PMC]
11. Hisli N. Beck Depresyon Envanter inin üniversite öğrenciler i için geçerliği, güvenir liği. Türk Psikoloj i Dergisi. 1989; 6: 3-13. [ Link]
12. Webb SM. Quality of life in acromegaly. Neuroen-docrinology. 2006; 83: 224-229. [ Crossref] [ PubMed]
13. Buchanan DC. Group therapy for chronic physically ill pat ients. Psychosom at ics. 1978; 19: 425-431. [ Crossref] [ PubMed]
14. Conte HR. Review of research in support ive psy-chotherapy: an update. Am J Psychother. 1994; 48: 494-504. [ Crossref] [ PubMed]
15. Saravay SM. Psychiatric interventions in the medically ill. Outcome and effect iveness research. Psychiatr Clin North Am. 1996; 19: 467-480. [ Crossref] [ PubMed]
16. van der Pom pe G, Duivenvoorden HJ, Antoni MH, Visser A, Heijnen CJ. Effect iveness of a short- term group psychotherapy program on endocrine and im-m une funct ion in breast cancer pat ients: an ex-ploratory study. J Psychosom Res. 1997; 42: 453-466. [ Crossref] [ PubMed]
17. Bierm asz NR, van Thiel SW, Pereira AM, Hoft ij zer HC, van Hemert AM, Sm it JW, Romijn JA, Roelfsema F. Decreased qualit y of life in pat ients with acrom egaly despite long- term cure of growth hor-m one excess. J Clin Endocr inol Metab. 2004; 89: 5369-5376. [ Crossref] [ PubMed]
306
Haliloğlu et al. Turk J Endocrinol Metab. The Effects of Focus Group Therapy in Acrom egaly 2020; 24: 300-307
3 0 6

307
Turk J Endocrinol Metab. Haliloğlu et al. 2020; 24: 300-307 The Effects of Focus Group Therapy in Acromegaly
3 0 7
18. Mat too SK, Bhansali AK, Gupta N, Grover S, Malho-t ra R. Psychosocial m orbidit y in acrom egaly: a study from I ndia. Endocr ine. 2008; 34: 17-22. [ Crossref] [ PubMed]
19. Webb SM, Crespo I , Santos A, Resm ini E, Aulinas A, Valassi E. MANAGEMENT OF ENDOCRI NE DI SEASE: Quality of life tools for the m anagem ent of pituitary disease. Eur J Endocr inol. 2017; 177(1) : R13-R26. [ Crossref] [ PubMed]
20. Webb SM, Badia X. Quality of life in growth hormone deficiency and acrom egaly. Endocr inol Metab Clin North Am . 2007; 36: 221-232. [ Crossref] [ PubMed]
21. Mat ta MP, Couture E, Cazals L, Vezzosi D, Bennet A, Caron P. I m paired qualit y of life of pat ients with acrom egaly: cont rol of GH/ I GF- I excess im proves psychological subscale appearance. Eur J En-docrinol. 2008; 158: 305-310. [ Crossref] [ PubMed]
22. Paisley AN, Rowles SV, Roberts ME, Webb SM, Badia X, Pr ieto L, Shalet SM, Trainer PJ. Treatm ent of acrom egaly im proves qualit y of life, m easured by AcroQol. Clin Endocrinol (Oxf ) . 2007; 67: 358-362. [ Crossref] [ PubMed]
23. Geraedts VJ, Andela CD, Stalla GK, Pereira AM, van Furth WR, Sievers C, Bierm asz NR. Predictors of quality of life in acrom egaly: no consensus on bio-chem ical param eters. Front Endocrinol (Lausanne) . 2017; 8: 40. [ Crossref] [ PubMed] [ PMC]
24. Gat to F, Campana C, Cocchiara F, Corica G, Albertelli M, Boschet t i M, Zona G, Crim inelli D, Giust i M, Fer-one D. Current perspect ives on the im pact of clini-cal disease and biochemical control on comorbidit ies and quality of life in acrom egaly. Rev Endocr Metab Disord. 2019; 20: 365-381. [ Crossref] [ PubMed]
25. Vandeva S, Yaneva M, Natchev E, Elenkova A, Kali-nov K, Zacharieva S. Disease cont rol and t reatm ent
m odalit ies have im pact on qualit y of life in acromegaly evaluated by Acromegaly Quality of Life (AcroQoL) quest ionnaire. Endocrine. 2015; 49: 774-782. [ Crossref] [ PubMed]
26. Kauppinen-Mäkelin R, Sane T, Sintonen H, Markka-nen H, Välim äki MJ, Löyt tyniem i E, Niskanen L, Re-unanen A, Stenm an UH. Qualit y of life in t reated pat ients with acrom egaly. J Clin Endocrinol Metab. 2006; 91: 3891-3896. [ Crossref] [ PubMed]
27. Webb SM, Badia X, Surinach NL; Spanish AcroQol Study Group. Validity and clinical applicability of the acrom egaly quality of life quest ionnaire, AcroQoL: a 6-m onth prospect ive study. Eur J Endocr inol. 2006; 155: 269-277. [ Crossref] [ PubMed]
28. Tiem ensm a J, Kaptein AA, Pereira AM, Sm it JW, Rom ijn JA, Bierm asz NR. Affected illness percep-t ions and the associat ion with im paired qualit y of life in pat ients with long- term rem ission of acrom egaly. J Clin Endocr inol Metab. 2011; 96: 3550-3558. [ Crossref] [ PubMed]
29. Johnson MD, Woodburn CJ, Vance ML. Quality of life in pat ients with a pituitary adenom a. Pituitary. 2003; 6: 81-87. [ Crossref] [ PubMed]
30. Webb SM. Pituitary tum ors: coping with 'cured' pi-tuitary tum ors. Nat Rev Endocr inol. 2011; 7: 251-252. [ Crossref] [ PubMed]
31. Tiem ensm a J, Kaptein AA, Pereira AM, Sm it JW, Rom ijn JA, Bierm asz NR. Coping st rategies in pa-t ients after t reatm ent for funct ioning or nonfunc-t ioning pituitary adenomas. J Clin Endocrinol Metab. 2011; 96: 964-971. [ Crossref] [ PubMed]
32. T'Sjoen G, Bex M, Maiter D, Velkeniers B, Abs R. Health- related qualit y of life in acrom egalic sub-jects: data from AcroBel, the Belgian regist ry on acrom egaly. Eur J Endocrinol. 2007; 157: 411-417. [ Crossref] [ PubMed]

Original Art icle Turk J Endocrinol Metab. 2020; 24: 308-313
308
Clinical Profile and Changing Et iological Spectrum of Hyperprolact inem ia
at a Tert iary Care Endocrine Facility Üçüncü Basam ak Bir Endokrin Kuruluşunda Hiperprolakt inem inin
Klinik Profili ve Değişen Et iyoloj ik Spekt rum u
Junaid Rashid DAR, Moom in Hussain BHAT* , Javaid Ahm ad BHAT, Raiz Ahm ad MI SGAR* ,
Shariq Rashid MASOODI * , Mir I ft ikhar BASHI R* , Arshad I qbal WANI *
Department of Endocrinology, GMC Srinagar, Jammu & Kashmir, INDIA * Department of Endocrinology, Sher- i-Kashmir I nst itute of Medical Sciences, Srinagar, Jammu & Kashmir, INDIA
Objective: Hyperprolact inemia is the most common disorder of the hy-pothalamic-pituitary axis. I t is most commonly caused by a pituitary ade-noma. Due to the recent easy availability of over-the-counter medication, many drugs, including herbals have commonly been related to this dis-order. Our purpose was to study the clinical presentat ion and et iology of hyperprolact inemia and to address any changing trend in the et iological profile of this disorder. Material and Methods: This study was a cross-sectional observational study on the et iologic spectrum and clinical pro-file of hyperprolact inemia. A total of 100 consecutive non-pregnant and non-lactat ing patients attending or referred to the out-patient depart-ment of Endocrinology at SKIMS, Srinagar were included. Hyperpro-lact inemia was confirmed by a serum prolact in level of > 25 ng/ mL (normal range= 1-20 ng/ mL). Patients with suspicion of drug-related hy-perprolactinemia were advised to stop drug consumption for a minimum of three days ( if medically feasible) and retest for prolact in levels as per the Institutional protocol. Hyperprolactinemia in patients whose prolactin levels normalized after stopping drug consumption was labeled as drug-induced hyperprolactinemia. Young patients with pituitary adenoma were evaluated for mult iple endocrine neoplasia syndrome (MEN 1). The re-sults were compared with those of a study conducted two decades ago at the same center. Results: Galactorrhea was the most common pre-senting symptom occurring in 64% of subjects (all females), followed by oligomenorrhea or amenorrhea in 60 patients. Both menstrual ab-normalit ies and galactorrhea were seen in 35 patients. Drug-induced hy-perprolact inemia was the most common cause seen in 59 pat ients, followed by pituitary adenoma seen in 31 patients and idiopathic cause seen in only 4% of cases. However, in the study done two decades ago at the same center, m icroprolact inoma was the most common cause (35.8% ), followed by idiopathic hyperprolactinemia (27.8% ), with drugs being responsible in only 5% of the cases. Domperidone and levosul-pride const ituted about 88% of drug- induced hyperprolact inemia. Mi-croprolact inoma was demonstrated in 15 patients, macroadenoma in 16 patients, hypothyroidism in 4% cases, and only one patient had the poly-cyst ic ovarian disease. In four patients, no apparent cause could be de-termined. Conclusion: In our study, drug-induced hyperprolact inemia was the most frequent identifiable et iology, with prokinetics being the most common cause; contrary to previous studies, where pituitary ade-noma followed by neuroleptic drugs was found to be the most common. Discontinuation of the offending drug resolved HP in all the patients. Keyw ords: Hyperprolact inem ia; galactorrhea; dom peridone;
drug- induced hyperprolact inem ia
Am aç: Hiperprolakt inem i, hipotalam us-hipofiz aksının en sık görü-len bozukluğudur. En yaygın nedeni ise hipofiz adenom udur. Son za-m anlarda reçetesiz sat ılan ilaçlar ın kolay bulunabilir liği nedeniy le, bitkiler de dahil olm ak üzere birçok ilaç bu bozuklukla ilişkilendir il-m işt ir. Burada, hiperprolakt inem inin klinik prezentasyonunun ve et i-yoloj isinin incelenm esi ve bu bozukluğun et iyoloj ik profilindeki değişen eğilim lerin ele alınması amaçlanmışt ır. Gereç ve Yöntem ler: Bu çalışm a, hiperprolakt inem inin et iyoloj ik spekt rum u ve klinik pro-fili üzerine kesitsel, gözlemsel bir çalışmadır. Srinagar'daki SKIMS en-dokrinoloj i polik liniğine gelen veya bu polikliniğe sevk edilen, gebe olm ayan ve em zirm eyen toplam 100 hasta çalışm aya dahil edilm iş-t ir. Hiperprolakt inem i, serum prolakt in seviyesinin > 25 ng/ mL olması ile doğrulanm ışt ır (norm al aralık= 1–20 ng/ m L) . İlaçla ilişkili hiperp-rolakt inem i şüphesi olan hastalara, en az üç gün süreyle ilaç kullan-m ayı bırakm aları ( t ıbbi olarak uygunsa) ve kurum protokolüne göre prolakt in seviyeler ini yeniden test et t irm eler i tavsiye edilm işt ir. İlaç kullanm ayı bırakt ıktan sonra prolakt in seviyeler i norm ale dönen has-talardaki hiperprolakt inem i, ilaca-bağlı hiperprolakt inem i olarak et i-ket lenm işt ir. Hipofiz adenom lu genç hastalar m ult ipl endokr in neoplazi sendrom u (MEN 1) açısından değerlendir ilm işt ir. Elde edilen sonuçlar, aynı m erkezde yirm i yıl önce yapılan bir araşt ırm anın so-nuçlar ıy la karşılaşt ır ılm ışt ır. Bulgular : Galaktore, kat ılım cılar ın % 64'ünde ( tüm ü kadın) gözlenen en yaygın başvuru sem ptom uydu. Bunu oligom enore veya am enore izliyordu (60 hasta) . 35 hastada hem m enst rual anom aliler hem de galaktore görüldü. İlaca bağlı hi-perprolakt inem i en sık neden iken (59 hasta) , bunu hipofiz adenom u (31 hasta) ve idiyopat ik neden (vakaların sadece % 4'ü) izlemekteydi. Oysaki, 20 yıl önce aynı m erkezde yapılan çalışm ada m ikroprolakt i-nom a en sık nedendi (% 35,8) , bunu idiyopat ik hiperprolakt inem i (% 27,8) izliyordu ve vakaların sadece % 5'inden ilaçlar sorum luydu. Dom peridon ve levosulpir id, ilaca bağlı hiperprolakt inem inin yaklaşık % 88'ini oluşturmaktaydı. 15 hastada m ikroprolakt inoma, 16 hastada m akroadenom , vakaların % 4’ünde hipot iroidizm ve sadece bir has-tada polikist ik over hastalığı tespit edildi. 4 hastada belirgin bir neden saptanamadı. Sonuç: Çalışmamızda, ilaca bağlı hiperprolakt inem i en sık saptanabilir et iyoloj iydi ve prokinet ikler en sık nedendi. Daha ön-ceki çalışm alarda ise hipofiz adenom u ve onun ardından nörolept ik ilaçlar en yaygın nedenler olarak bulunmuştu. Sorum lu olan ilacın ke-silm esiyle tüm hastalarda hiperprolakt inem i ortadan kalkt ı. Anahtar kelim eler: Hiperprolakt inem i; galaktore; dom peridon;
ilaca-bağlı hiperprolakt inem i
3 0 8
Address for Correspondence: Moom in Hussain BHAT, Departm ent of Endocrinology, Sher- i-Kashm ir I nst itute of Medical Sciences, Srinagar, Jam m u & Kashm ir, I NDI A
Phone: 8491012986 E- m ail: m oom in_48@rediffm ail.com
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 09.07.2020 Received in revised form : 12.11.2020 Accepted: 16.11.2020 Available online: 10 Dec 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
79
92

I nt roduct ion Hyperprolact inem ia (HP) is a com m on en-docr ine disorder. Apart from hypothalam o-pituitary disease, it occurs secondary to the use of drugs and chronic diseases like hy-pothyroidism , chronic hepat ic and renal dis-ease, st ress, and neurogenic disorders. I n the absence of the above-said causes, an in-crease in serum prolact in (PRL) is known as an idiopathic HP. I t affects the gonadal axis, which results in alterat ions in sexual or re-product ive funct ion and can be a m ajor t reatable cause of infert ility (1-3) . The pres-ence of galactorrhea is the single m ost im -portant clinical sign of HP, the frequency of which var ies from 30-90% in hyperpro-lact inem ic wom en (4) . With the advance-m ent in im aging, m icroprolact inom as of the size of 3 m m are easily visualized nowadays (5) . Medical management of HP provides ex-cellent results, and m ost of the pat ients do well (6) . Pituitary adenom a has been m en-t ioned in the literature to be the m ost com -m on cause of HP (7) . Recent studies have found drugs to be commonly associated with HP, which cont rasts with our previous study (8,9) . With the easy availabilit y of over- the-counter drugs as well as the use of herbal medicat ion in this part of the world and easy availabilit y of the tests for prolact in est im a-t ion, we intended to study the impact on the et iology of hyperprolact inem ia. I n the pres-ent study, we describe the clinical presenta-t ion and et iological profile of our HP pat ients and also any changing t rend in the et iology of hyperprolact inem ia.
Materia l and Methods This was a cross-sect ional observat ional study on the et iologic spect rum and clinical profile of HP. A total of 100 consecut ive non-pregnant and non- lactat ing pat ients at tend-ing or referred to the out-pat ient departm ent of Endocrinology at SKI MS, Sri-nagar with symptoms & signs of HP or eval-uat ion, and t reatm ent of HP. Hyperprolact inem ia was confirm ed by a serum prolact in level of > 25 ng/ m L (10) . Galactorrhea was defined as sponta-neous/ expressive f low of m ilk from the breast in the absence of pregnancy and nursing. Oligom enorrhea was defined as a cycle length > 35 days or less than 10 cycles per year. I nst itut ional Ethics Com m it tee ex-
em pted the study from the ethical clear-ance, as the study involved the collect ion of anonym ous data of HP pat ients. After taking consent from all pat ients, age, m ar ital status, sym ptom s along with their durat ion, and history of drug intake were noted. Pat ients with a suspicion of drug- re-lated HP were advised to stop drug con-sum pt ion for a m inim um of three days ( if m edically feasible) and repeat for prolact in levels, which is the I nst itut ional protocol. HP of pat ients whose prolact in levels norm al-ized after stopping drug was labeled as drug- induced HP. A detailed clinical exam i-nat ion was done in all the pat ients including looking for galactorrhea and gonadal func-t ion. I nvest igat ions performed included tests for serum prolact in, thyroid funct ion, and serum gonadot ropins in addit ion to rout ine com plete blood count and liver and kidney funct ion tests as per the protocol followed for hyperprolact inem ia pat ients. Serum pro-lact in levels were m easured by using DXI 800 Beckm an Coulter Chem ilum inescence random access analyzer and following the m anufacturer ’s protocol. The reference range for prolact in is 1-25 ng/ mL. The int ra-assay coefficient of var iat ion is less than 5% , and the inter-assay coefficient of varia-t ion is less than 10% . I f the above test results were normal, MRI of the pituitary gland with dynam ic cont rast scan was perform ed to look for pituitary hy-pothalam ic lesions. I f no cause was ident i-fied, then the HP was labeled as idiopathic HP.
Stat ist ical Analysis
SPSS 20 (Stat ist ical Package for Social Sci-ences) program was used for stat ist ical analysis. Numeric variables are presented as m ean ± standard deviat ion. Descript ive sta-t ist ics were perform ed for all var iables.
Results Over a period of one year, a total of 100 pa-t ients had biochemically documented HP of which, 93 part icipants were females, and 53 were m arr ied. The average age of pat ients was 30.71± 10.35 years, with the mean age of females being lower (29.87 ± 9.24 years) than that of m ales (41.85± 17.5 years; p= 0.003) . Three- fourth of the pat ients (73% ) were in the 3rd to 4th decade of life.
309
Turk J Endocrinol Metab. Dar et al. 2020; 24: 308-313 Drug I nduced Hyperprolact inem ia
3 0 9
309
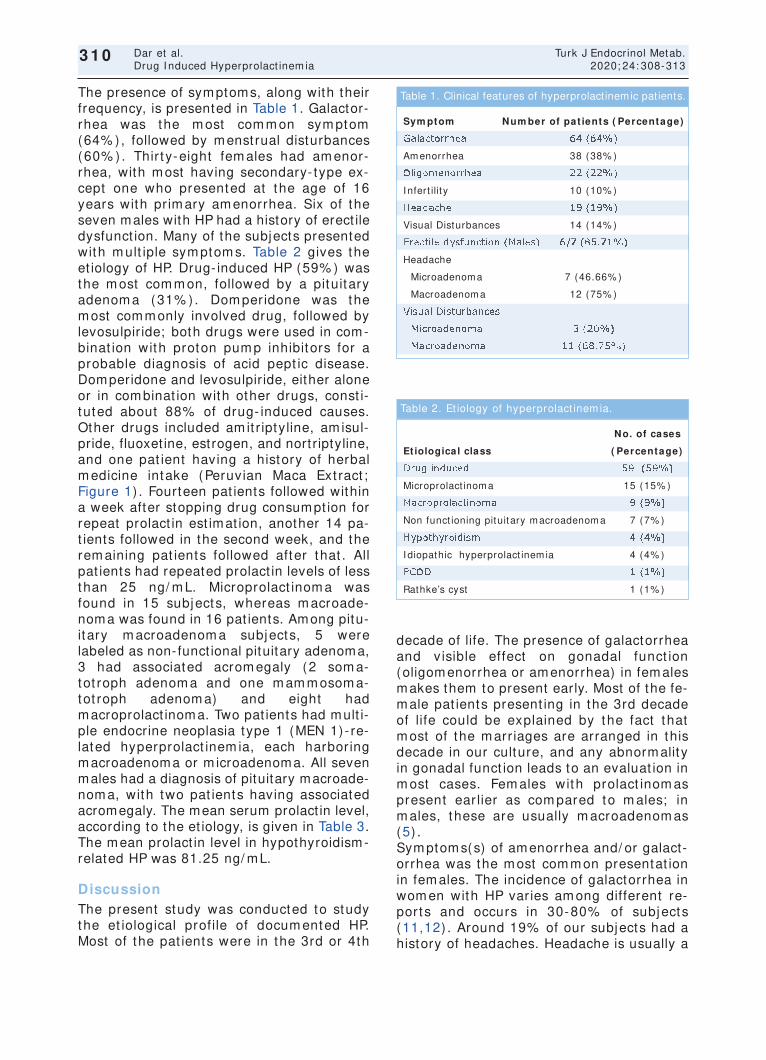
The presence of symptoms, along with their frequency, is presented in Table 1. Galactor-rhea was the m ost com m on sym ptom (64% ), followed by menst rual disturbances (60% ) . Thir ty-eight fem ales had am enor-rhea, with most having secondary- type ex-cept one who presented at the age of 16 years with pr im ary am enorrhea. Six of the seven males with HP had a history of erect ile dysfunct ion. Many of the subjects presented with m ult iple sym ptom s. Table 2 gives the et iology of HP. Drug- induced HP (59% ) was the m ost com m on, followed by a pituitary adenom a (31% ) . Dom peridone was the most commonly involved drug, followed by levosulpir ide; both drugs were used in com-binat ion with proton pum p inhibitors for a probable diagnosis of acid pept ic disease. Domperidone and levosulpir ide, either alone or in combinat ion with other drugs, const i-tuted about 88% of drug- induced causes. Other drugs included am it r iptyline, am isul-pride, fluoxet ine, estrogen, and nort riptyline, and one pat ient having a history of herbal m edicine intake (Peruvian Maca Ext ract ; Figure 1) . Fourteen pat ients followed within a week after stopping drug consumpt ion for repeat prolact in est imat ion, another 14 pa-t ients followed in the second week, and the rem aining pat ients followed after that . All pat ients had repeated prolact in levels of less than 25 ng/ m L. Microprolact inom a was found in 15 subjects, whereas m acroade-noma was found in 16 pat ients. Among pitu-itary m acroadenom a subjects, 5 were labeled as non- funct ional pituitary adenoma, 3 had associated acrom egaly (2 som a-tot roph adenom a and one m am m osom a-tot roph adenom a) and eight had macroprolact inoma. Two pat ients had mult i-ple endocrine neoplasia type 1 (MEN 1) - re-lated hyperprolact inem ia, each harbor ing macroadenoma or m icroadenoma. All seven males had a diagnosis of pituitary macroade-nom a, with two pat ients having associated acromegaly. The mean serum prolact in level, according to the et iology, is given in Table 3. The mean prolact in level in hypothyroidism-related HP was 81.25 ng/ mL.
Discussion The present study was conducted to study the et iological profile of docum ented HP. Most of the pat ients were in the 3rd or 4th
decade of life. The presence of galactorrhea and v isible effect on gonadal funct ion (oligom enorrhea or am enorrhea) in fem ales makes them to present early. Most of the fe-m ale pat ients present ing in the 3rd decade of life could be explained by the fact that m ost of the m arr iages are arranged in this decade in our culture, and any abnorm ality in gonadal funct ion leads to an evaluat ion in m ost cases. Fem ales with prolact inom as present ear lier as com pared to m ales; in m ales, these are usually m acroadenom as (5) . Sym ptom s(s) of am enorrhea and/ or galact-orrhea was the m ost com m on presentat ion in fem ales. The incidence of galactorrhea in wom en with HP varies am ong different re-ports and occurs in 30-80% of subjects (11,12) . Around 19% of our subjects had a history of headaches. Headache is usually a
310
Dar et al. Turk J Endocrinol Metab. Drug I nduced Hyperprolact inem ia 2020; 24: 308-313
3 1 0
Sym ptom Num ber of pat ients ( Percentage)
Galactorrhea 64 (64% )
Am enorrhea 38 (38% )
Oligom enorrhea 22 (22% )
I nfert ilit y 10 (10% )
Headache 19 (19% )
Visual Disturbances 14 (14% )
Erect ile dysfunct ion (Males) 6/ 7 (85.71% )
Headache
Microadenom a 7 (46.66% )
Macroadenom a 12 (75% )
Visual Disturbances
Microadenom a 3 (20% )
Macroadenom a 11 (68.75% )
Table 1. Clinical features of hyperprolact inemic patients.
No. of cases
Et iological class ( Percentage)
Drug induced 59 (59% )
Microprolact inom a 15 (15% )
Macroprolact inom a 9 (9% )
Non funct ioning pituitary m acroadenom a 7 (7% )
Hypothyroidism 4 (4% )
I diopathic hyperprolact inem ia 4 (4% )
PCOD 1 (1% )
Rathke’s cyst 1 (1% )
Table 2. Et iology of hyperprolact inem ia.
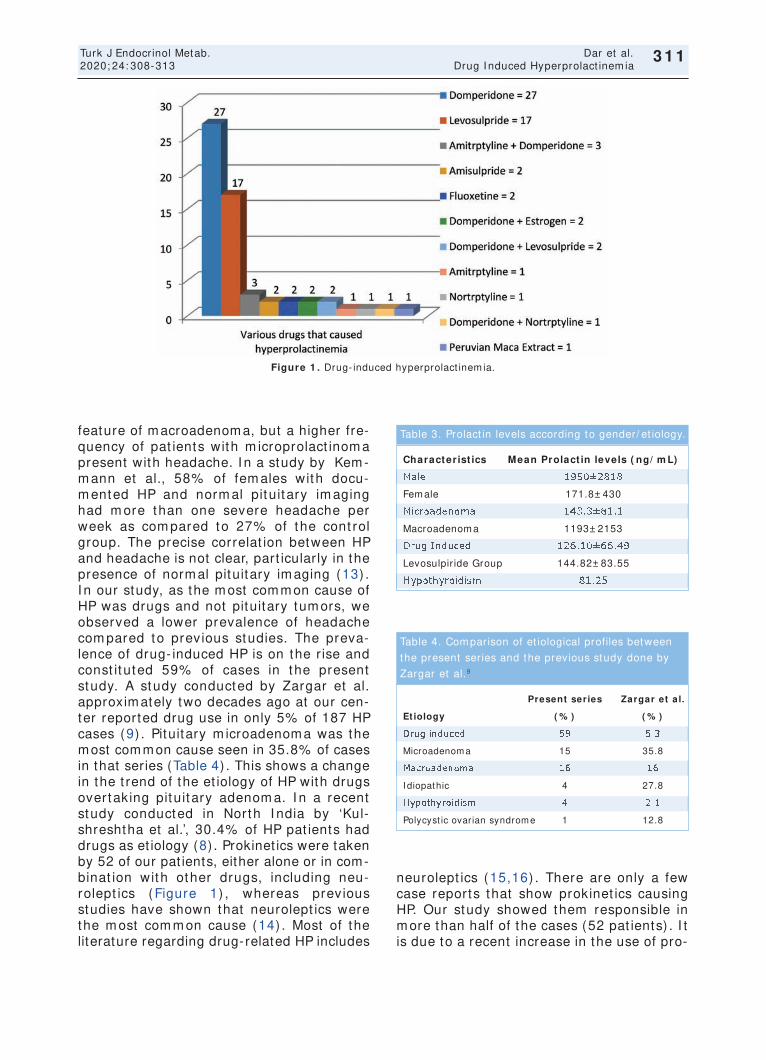
311
Turk J Endocrinol Metab. Dar et al. 2020; 24: 308-313 Drug I nduced Hyperprolact inem ia
3 1 1
feature of m acroadenom a, but a higher fre-quency of pat ients with m icroprolact inom a present with headache. I n a study by Kem -m ann et al., 58% of fem ales with docu-m ented HP and norm al pituitary im aging had m ore than one severe headache per week as com pared to 27% of the cont rol group. The precise correlat ion between HP and headache is not clear, part icular ly in the presence of norm al pituitary im aging (13) . I n our study, as the m ost com m on cause of HP was drugs and not pituitary tum ors, we observed a lower prevalence of headache com pared to previous studies. The preva-lence of drug- induced HP is on the r ise and const ituted 59% of cases in the present study. A study conducted by Zargar et al. approxim ately two decades ago at our cen-ter reported drug use in only 5% of 187 HP cases (9) . Pituitary m icroadenom a was the most common cause seen in 35.8% of cases in that series (Table 4) . This shows a change in the t rend of the et iology of HP with drugs overtaking pituitary adenom a. I n a recent study conducted in North I ndia by ‘Kul-shreshtha et al.’, 30.4% of HP pat ients had drugs as et iology (8) . Prokinet ics were taken by 52 of our pat ients, either alone or in com-binat ion with other drugs, including neu-rolept ics (Figure 1) , whereas previous studies have shown that neurolept ics were the m ost com m on cause (14) . Most of the literature regarding drug-related HP includes
neurolept ics (15,16) . There are only a few case reports that show prokinet ics causing HP. Our study showed them responsible in m ore than half of the cases (52 pat ients) . I t is due to a recent increase in the use of pro-
Figure 1 . Drug- induced hyperprolact inem ia.
Characterist ics Mean Prolact in levels ( ng/ m L)
Male 1950± 2818
Fem ale 171.8± 430
Microadenom a 143.3± 81.1
Macroadenom a 1193± 2153
Drug I nduced 126.10± 66.49
Levosulpir ide Group 144.82± 83.55
Hypothyroidism 81.25
Table 3. Prolact in levels according to gender/ et iology.
Present series Zargar et a l.
Et iology ( % ) ( % )
Drug induced 59 5.3
Microadenom a 15 35.8
Macroadenom a 16 16
I diopathic 4 27.8
Hypothyroidism 4 2.1
Polycyst ic ovarian syndrom e 1 12.8
Table 4. Com parison of et iological profiles between
the present series and the previous study done by
Zargar et al.9

kinet ics for non-specific sym ptom s and due to their easy availabilit y as an over- the-counter m edicat ion. Sim ilar to our study, Horng-Yih et al. found that the m ost com -m on offending drugs in HP are gast roin-test inal drugs such as sulpir ide (17) . I n one case in our study, HP was due to the con-sum pt ion of a herb (Peruvian Maca) ext ract , which was prescr ibed to the pat ient as an aphrodisiac in the form of capsules. I n an earlier study conducted in Southern Taiwan, herbal ext racts were reported to induce HP (17) . I n m ost of the cases of drug- induced HP, docum entat ion of levels of prolact in into the normal range after stopping/ subst itut ing the offending drug was carr ied out between week 1 and week 4 from the t im e of init ial contact with the pat ient . However, in the case of six pat ients, it took m ore than eight weeks from the point of init ial contact for the norm alizat ion of their prolact in levels due to the com pelling need for reusing the sam e or a different offending drug, m ost ly for acute m igraine episodes or bothersom e acid pept ic disorder that led to the delay in norm alizat ion. About 15% of our subjects had pituitary m i-croadenom a, and 16% had m acroadenom a on MRI together, const itut ing the second most common cause of HP in our study pop-ulat ion. Two pat ients had MEN 1- related hy-perprolact inem ia, one harbor ing m acroadenom a and the other m icroade-nom a. I diopathic HP cont inues to be an im portant cause of high prolact in. The prevalence of idiopathic HP has decreased over t im e as in our study; only 4% of pat ients represented it as com pared to 27% of pat ients repre-sent ing it in the study conducted two decades ago at the sam e center (9) . Due to the availabilit y of high- resolut ion MRI , the disorder labeled as idiopathic hyperpro-lact inem ia was later proved to be a m i-croadenom a. I t is believed that m any pat ients harbored such sm all m icroadeno-m as that were beyond the resolut ion of im -aging tools used in the past , such as hypocycloidal polysom nography, CT, and MRI (18) . Four percent of our cases had hypothy-roidism as the cause of HP. Elevat ion of the thyrot ropin- releasing horm one causes in-creased release of prolact in. The m ean pro-
lact in level in this group was 81.25 ng/ m L. Treatm ent of pr im ary hypothyroidism cor-rected hyperprolact inem ic state (19) . Vilar et al. found that 6.3% of cases of HP were due to primary hypothyroidism in their study (20) . Ear lier. Zargar et al. had found hy-pothyroidism to be responsible for 2.1% of hyperprolact inem ia cases (9) . Polycyst ic ovar ian disease (PCOD) was the sole cause of HP in one of our subjects. I n com parison, a previous study showed that PCOD was responsible for 14% of hyperpro-lact inem ia cases. The exact prevalence of HP in PCOD is not known. I ncreased pro-lact in levels lead to increased product ion of dehydroepiandrosterone sulfate (DHEAS) from adrenals, which decreases following the t reatm ent of HP (21) . Although a large num ber (13% ) of PCOD pat ients reported HP in 1984, recent data have suggested that HP does not seem to be m ore frequent in PCOD wom en than in healthy subjects (20,21) .
Conclusion HP is a com m on endocr inological problem . Every effor t should be m ade to f ind the cause of HP. Drug- induced HP was the m ost frequent ident ifiable et iology, with prokinet-ics being the m ost com m on cause in our study. This was in cont rast to the findings of previous studies as found in the literature, where pituitary adenom a followed by neu-rolept ic drugs was the m ost com m on cause of HP. Discont inuat ion of the offending drug resolves HP in all the pat ients.
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
312
Dar et al. Turk J Endocrinol Metab. Drug I nduced Hyperprolact inem ia 2020; 24: 308-313
3 1 2
313
Turk J Endocrinol Metab. Dar et al. 2020; 24: 308-313 Drug I nduced Hyperprolact inem ia
3 1 3
Authorship Contr ibut ions I dea/ Concept : Arshad I qbal Wani, Junaid Rashid Dar, Moom in Hussain Bhat ; Design: Shar iq Rashid Masoodi, Moom in Hussain Bhat ; Cont rol/ Supervision: Arshad I qbal Wani, Mir I ft ikhar Bashir, Raiz Ahm ad Mis-gar; Data Collect ion and/ or Processing: Ju-naid Rashid Dar, Javaid Ahm ad Bhat , Moom in Hussain Bhat ; Analysis and/ or I n-terpretat ion: Arshad I qbal Wani, Raiz Ahm ad Misgar; Literature Review: Moom in Hussain Bhat , Junaid Rashid Dar; Writ ing the Art icle: Moom in Hussain Bhat , Junaid Rashid Dar; Cr it ical Review: Shariq Rashid Masoodi, Mir I ft ikhar Bashir; References and Fundings: Raiz Ahm ad Misgar; Mater ials: Arshad I qbal Wani, Moom in Hussain Bhat .
References 1. Serr i O, Chik CL, Ur E, Ezzat S. Diagnosis and m an-
agem ent of hyperprolact inem ia. CMAJ. 2003; 169: 575-581. [ PubMed] [ PMC]
2. Lundberg PO, Osterm an PO, Wide L. Serum pro-lact in in pat ients with hypothalam us and pituitary disorders. J Neurosurg. 1981; 55: 194-199. [ Cross-ref] [ PubMed]
3. Zargar AH, Wani AI , Masoodi SR, Laway BA, Salahuddin M. Epidem iologic and et iologic aspects of pr im ary infert ilit y in the Kashm ir region of I ndia. Fert il Ster il. 1997; 68: 637-643. [ Crossref] [ PubMed]
4. Melm ed S. Disorders of the anter ior pituitary and hypothalam us I n: Braunwald EG, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jam eson JL, eds. Harr i-son's Principles of I nternal Medicine (15th ed) . New York: McGraw Hill; 2001; 2029-2052.
5. Lam berts SW, de Herder WW, Kwekkeboom DJ, vd Lely AJ, Nobels FR, Krenning EP. Current tools in the diagnosis of pituitary tum ours. Acta Endocr inol (Copenh) . 1993; 129 Suppl 1: 6-12. [ PubMed]
6. Molitch ME, Thorner MO, Wilson C. Managem ent of prolact inom as. J Clin Endocr inol Metab. 1997; 82: 996-1000. [ Crossref] [ PubMed]
7. Touraine P, Plu-Bureau G, Bej i C, Mauvais-Jarvis P, Kut tenn F. Long- term follow-up of 246 hyperpro-lact inem ic pat ients. Acta Obstet Gynecol Scand. 2001; 80: 162-168. [ Crossref] [ PubMed]
8. Kulshreshtha B, Pahuja I , Kothar i D, Chawla I , Sharm a N, Gupta S, Mit tal A. Menst rual cycle ab-norm alit ies in pat ients with prolact inom a and drug-induced hyperprolact inem ia. I ndian J Endocr inol Metab. 2017; 21: 545-550. [ Crossref] [ PubMed] [ PMC]
9. Zargar AH, Laway BA, Masoodi SR, Bhat MH, Wani AI , Bashir MI , Salahuddin M, Rasool R. Clinical and et iological profile of hyperprolact inem ia- -data from a ter t iary care cent re. J Assoc Physicians I ndia. 2005; 53: 288-290. [ PubMed]
10. Melm ed S, Casanueva FF, Hoffm an AR, Kleinberg DL, Montori VM, Schlechte JA, Wass JA; Endocrine Society. Diagnosis and t reatm ent of hyperpro-lact inem ia: an Endocr ine Society clinical pract ice guideline. J Clin Endocr inol Metab. 2011; 96: 273-288. [ Crossref] [ PubMed]
11. Franks S, Nabarro JD. Prevalence and presentat ion of hyperprolact inaem ia in pat ients with " funct ion-less" pituitary tum ours. Lancet . 1977; 1: 778-780. [ Crossref] [ PubMed]
12. Thorner MO, Besser GM. Brom ocript ine t reatm ent of hyperprolact inaem ic hypogonadism . Acta En-docr inol Suppl (Copenh) . 1978; 216: 131-146. [ PubMed]
13. Kem m ann E, Jones JR. Hyperprolact inem ia and headaches. Am J Obstet Gynecol. 1983; 145: 668-671. [ Crossref] [ PubMed]
14. Pet it A, Piednoir D, Germ ain ML, Trenque T. [ Drug-induced hyperprolact inem ia: a case-non-case study from the nat ional pharm acovigilance database] . Therapie. 2003; 58: 159-163. [ Crossref] [ PubMed]
15. Melkersson K. Differences in prolact in elevat ion and related sym ptom s of atypical ant ipsychot ics in schizophrenic pat ients. J Clin Psychiat ry. 2005; 66: 761-767. [ Crossref] [ PubMed]
16. Bushe C, Shaw M. Prevalence of hyperprolact i-naem ia in a naturalist ic cohort of schizophrenia and bipolar outpat ients dur ing t reatm ent with t ypical and atypical ant ipsychot ics. J Psychopharm acol. 2007; 21: 768-773. [ Crossref] [ PubMed]
17. Ou Horng-Yih, Hsiao Shu-Hwa,Yu Eugene-Hsin,Wu Ta-Jen. Et iologies and clinical m anifestat ions of hy-perprolact inem ia in a m edical cent re in Southern Taiwan. J I ntern Med Taiwan. 2004; 15: 19-24. [ Link]
18. Bronstein MD. Disorders of prolact in secret ion and prolact inom as. I n: Jam eson JL, De Groot LJ, eds. Endocrinology (6th ed) . Philadelphia: Saunders El-sevier; 2010; 333-357. [ Crossref]
19. Jacobs LS, Snyder PJ, Wilber JF, Ut iger RD, Daugh-aday WH. I ncreased serum prolact in after adm inis-t rat ion of synthet ic thyrot ropin releasing horm one (TRH) in m an. J Clin Endocr inol Metab. 1971; 33: 996-998. [ Crossref] [ PubMed]
20. Vilar L, Freitas MC, Naves LA, Casular i LA, Azevedo M, Montenegro R Jr, Barros AI , Faria M, Nascim ento GC, Lim a JG, Nóbrega LH, Cruz TP, Mota A, Ram os A, Violante A, Lam ounier Filho A, Gadelha MR, Czepielewski MA, Glezer A, Bronstein MD. Diagnosis and m anagem ent of hyperprolact inem ia: results of a Brazilian m ult icenter study with 1234 pat ients. J Endocr inol I nvest . 2008; 31: 436-444. [ Crossref] [ PubMed]
21. Thorner MO, Edwards CRW, Hanker JP, Abraham G, Besser GM. Prolact in and gonadot ropin interact ion in the m ale. I n: Troen P, Nankin HR, eds. Test is Norm I nfer t ile Men. New York: Raven Press; 1977; 351-366.
22. Luciano AA, Chapler FK, Sherm an BM. Hyperpro-lact inemia in polycyst ic ovary syndrome. Fert il Steril 1984; 41: 719-725. [ Crossref]
23. Szosland K, Pawlowicz P, Lewiński A. Prolact in se-cret ion in polycyst ic ovary syndrome (PCOS). Neuro Endocrinol Let t . 2015; 36: 53-58. [ PubMed]

Original Art icle Turk J Endocrinol Metab. 2020; 24: 314-320
314
Cardiovascular Morbidity in Diabet ic Non- Alcoholic Fat ty Liver Disease ( NAFLD) Using
NAFLD Fibrosis Score as an Early I ndicator Erken Bir Gösterge Olarak Non-Alkolik Yağlı Karaciğer Hastalığı
(NAYKH) Fibrozis Skoru Kullanılarak Diyabet ik NAYKH'de Kardiyovasküler Morbidite
Prit i SHAHAPURE, Shim pa SHARMA
Department of Medicine, D.Y. Pat il Medical College, D.Y. Pat il Educat ional Society (Deemed University) , Kolhapur, Maharashtra, INDIA
Object ive: Rising prevalence of non-alcoholic fat ty liver disease (NAFLD) , its high incidence in diabet ic pat ients, and global dia-betes prevalence, underline the need to ident ify comorbidit ies in these pat ients impact ing their quality of life and mortality.NAFL-Dis associated with increased r isk, prevalence, and com plicat i-ons of cardiovascular diseases in diabet ic and non-diabet ics alike. The study aim ed to establish a relat ionship between non-invasively assessed cardiovascular morbidity and NAFLD fibrosis score (NFS) in type 2 diabetes m ellitus with NAFLD. Materia l and Methods: After ethical approval, the study was conducted (n= 100) on pat ients < 60 years of age, havingtype 2 diabetes mellitus, and no exist ing cardiovascular disease. All pat ients un-derwent anthropological and rout ine invest igat ions, two-dim en-sion (2D) echocardiography, and ult rasonographic confirm at ion of fat ty liver disease. NAFLD was ascertained based on pat ient history and invest igat ions. Findings of cardiovascular evaluat ion on 2D-echocardiography were assessed with reference to the NFS. Results: Median age of part icipants was 53.5 years. Body m ass index (p< 0.001) , r ight carot id int im a-m edia thickness (p= 0.0124) , and left vent r icular dysfunct ion (p= 0.0024) sho-wed a significant associat ion with NAFLD. The presence of both left vent r icular diastolic dysfunct ion and significant variat ion of carot id int im a-m edia thickness am ong m ild, m oderate, and se-vere NFS groups (p= 0.0049) was observed. Pat ients with m o-derate-severe NFS had 6.38 t im es m ore r isk of developing cardiovascular m orbidit ies. Conclusion: I n pat ients with type 2 diabetes and NAFLD, the NFS helps to ident ify those at high r isk of cardiovascular disease, and pat ients needing further invest i-gat ion. I t provides clues on how non- invasive cardiovascular m arkers can be used in detect ing cardiovascular m orbidit ies. Keyw ords: Cardiovascular diseases;
carot id int im a-m edia thickness; diabetes; non-alcoholic fat ty liver disease; vent r icular dysfunct ion
Am aç: Non-alkolik yağlı karaciğer hastalığının (NAYKH) artan prevalansı, diyabet ik hastalardaki yüksek insidansı ve küresel diyabet prevalansı, bu hastalarda yaşam kaliteler ini ve m ortali-teler ini etkileyen kom orbiditeler in belir lenm esi iht iyacının alt ını çizm ektedir. NAYKH, hem diyabet ik lerde hem de diyabet ik ol-m ayanlarda artan kardiyovasküler hastalık r iski, prevalansı ve kom plikasyonları ile ilişkilidir. Bu çalışm ada, NAYKH olan Tip 2 diabetes m ellitusta noninvaziv olarak değer lendir ilen kardiyo-vasküler m orbidite ile NAYKH fibrozis skoru (NFS) arasında bir ilişki kurmak amaçlanmışt ır. Gereç ve Yöntem ler: Çalışma, et ik onay sonrası, Tip 2 diabetes m ellitusu olan ve kardiyovasküler hastalığı olm ayan 60 yaşın alt ındaki hastalar üzerinde gerçek-leşt ir ildi (n= 100) . Tüm hastalarda ant ropoloj ik ve rut in araşt ır-m alar, ik i boyut lu (2D) ekokardiyografi ve yağlı karaciğer hastalığının ult rasonografik doğrulam ası yapıldı. NAYKH, hasta öyküsü ve araşt ırm alara göre belir lendi. 2D ekokardiyografide kardiyovasküler değerlendirm e bulguları NFS referans alınarak değerlendir ildi. Bulgular: Kat ılım cıların m edyan yaşı 53,5 idi. Beden kit le indeksi (p< 0,001) , sağ karot is int im a-m edia kalın-lığı ( p= 0,0124) ve sol vent r ikül disfonksiyonu (p= 0,0024) NAYKH ile anlam lı bir ilişki gösterdi. Hafif, orta ve şiddet li NFS grupları arasında hem sol vent r ikül diyastolik disfonksiyon hem de karot is int im a-m edia kalınlığında anlam lı varyasyon gözlendi (p= 0,0049) . Orta-şiddet li NFS'li hastalarda kardiyovasküler m orbidite gelişt irm e r iski 6,38 kat daha fazlaydı. Sonuç: Tip 2 diyabet li ve NAYKH'li hastalarda NFS, yüksek kardiyovasküler hastalık r iski taşıyan ve daha fazla araşt ırm aya iht iyaç duyan hastaların belir lenmesine yardımcı olur. Non- invaziv kardiyovas-küler belirteçlerin kardiyovasküler morbiditelerin saptanmasında nasıl kullanılabileceğine dair ipuçları sağlar. Anahtar kelim eler: Kardiyovasküler hastalıklar;
karot is int im a-m edia kalınlığı; diyabet ; non-alkolik yağlı karaciğer hastalığı; vent r iküler disfonksiyon
3 1 4
Address for Correspondence: Shim pa SHARMA, Departm ent of Medicine, D.Y. Pat il Medical College, D.Y. Pat il Educat ional Society (Deem ed University) , Kolhapur, Maharasht ra, I NDI A
Phone: + 91 9820017268 E- m ail: shim pasharm a@gm ail.com
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 25 Jun 2020 Received in revised form : 29 Jul 2020 Accepted: 29 Aug 2020 Available online: 30 Sep 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
76
79

I nt roduct ion Non-alcoholic fat ty liver disease (NAFLD) is a broad term for liver diseases characterized by histological f indings of 5% or greater m acrovesicular steatosis of hepatocytes in individuals not consum ing excessive alcohol (1) . NAFLD can progress from a benign non-alcoholic fat ty liver (NAFL) to a m ore severe form known as non-alcoholic steatohepat it is (NASH) associated with lobular inflam m a-t ion and apoptosis. This further leads to fi-brosis, cirrhosis, or even hepat ic carcinom a in som e cases (2) . The prevalence of NAFLD is increasing in the world, including I ndia. I t affects around a quarter of the adult popu-lat ion, 60% of diabet ic pat ients, and 90% of obese indiv iduals (3) . The current preva-lence of NAFLD in the US and Asia isas high as 24.13% and 27.37% , respect ively(4) .I n I ndia, the prevalence of NAFLD is reported to be 9-32% (5) . I ndividuals with type 2 di-abetes mellitus (T2DM) have high incidences of NAFLD, and the current prevalence in the I ndian populat ion is 70% (6) . The m ortality rates in pat ients with T2DM due to cirrhosis have been reported to be significant ly higher than the general populat ion (7) . Evident ly, NAFLD is associated with in-creased r isk of cardiovascular diseases (CVD) , atherosclerot ic changes, and cardiac dysfunct ion such as left vent r icular diastolic dysfunct ion (LVDD) , especially in T2DM and obesity(4) . Cardiovascular events in NAFLD are found to increase by 1.87- folds in exist-ing T2DM. Also, in pat ients with T2DM, NAFLD is asso-ciated with increased carot id wall thickening, ear ly left vent r icular diastolic dysfunct ion (LVDD) , and reduced m yocardial high-en-ergy phosphate m etabolism (8) . NAFLD in-creases m icrovascular com plicat ions like chronic kidney disease in T2DM pat ients (9) . The NAFLD fibrosis score (NFS) is a score based on age, blood sugar levels, body mass index (BMI ) , platelet count , album in con-cent rat ion, and levels of aspartate and ala-nine am inot ransferases. I t independent ly ident if ies NAFLD pat ients with and without advanced fibrosis at the t im e of diagnosis (10) . Studies linking NAFLD and CVD under-pin the need for explor ing the relat ionship between cardiovascular (CV) dysfunct ion, NAFLD, and non- invasive m arkers. Non- in-vasive techniques like 2D echocardiography
are opt im al m odalit ies to assess cardiovas-cular m orbidity but are either cost ly or not available uniform ly. We aim ed to explore possible associat ions between NFS, and CV m orbidit y, by m easur ing carot id int im a-m edia thickness (CI MT) and LVDD in the T2DM pat ients with NAFLD.
Materia l and Methods This cross-sect ional, descr ipt ive study was undertaken at a tert iary care center in Ma-harasht ra, I ndia, after the approval of the I nst itut ional Ethics Commit tee in accordance withthe pr inciples of the Helsinki declara-t ion. Sim ple consecut ive sam pling was used to invest igate 154 pat ients of T2DM from whom wr it ten inform ed consent was ob-tained. Finally, a group of 100 pat ients was ident ified. Pat ients suffer ing from T2DM for m ore than five years, and < 60 years of age were included in the study (11) . Pat ients with a pr ior history of the cerebrovascular incident , m yocardial infarct ion, ischem ic heart disease,per ipheral vascular disease, hepat ic cir rhosis, pregnant wom en, sm ok-ers, pat ients with condit ions causing ather-osclerosis, pat ients on ant icancer drugs, immunosuppressants, and steroids were ex-cluded. Rout ine clinical invest igat ions ( com plete blood count , urea, creat inine, liver funct ion tests) were perform ed. Part icipants were screened for fat t y liver disease by ult ra-sonography, lipid profile (after 12-24 h of fast ing) , and viral m arkers HBsAg and ant i-HCV-ant ibodies were detected on confirm a-t ion of fat t y liver. NFS, a non- invasive scor ing system , was used to est im ate the am ount of liver scarr ing. I t is based on sev-eral laboratory tests. The form ula for calcu-lat ing NFS is [ -1.675+ 0.037× age (years) + 0.094× BMI ( kg/ m 2)+ 1.13× I FG/ diabetes ( yes= 1, no= 0) + 0.99× AST/ ALT rat io-0.013× platelet (× 109/ L) -0.66 × album in (g/ dL) . This score is evaluated as < -1.455: a predictor of the absence of significant fi-brosis (F0-F2 Fibrosis) ; ≤-1.455 to ≤0.675: interm ediate score; > 0.675: a predictor of the presence of significant fibrosis (F3-F4) (10,12) . LVDD was assessed by calculat ing the early (E) and late (A) diastolic f illing velocit ies (E/ A rat io) on M-Mode (values < 1 and > 2 considered abnorm al) . The norm al deceler-
315
Turk J Endocrinol Metab. Shahapure et al. 2020; 24: 314-320 NAFLD Fibrosis Score as an I ndicator of Cardiovascular Mobilit y
3 1 5

316
Shahapure et al. Turk J Endocrinol Metab. NAFLD Fibrosis Score as an I ndicator of Cardiovascular Mobilit y 2020; 24: 314-320
3 1 6
at ion t ime for E wave was taken in the range of 160-200 m s (values > 200 and < 160 con-sidered abnormal) . CIMT was determ ined by the carot id Doppler, and values ≥0.9 were considered abnorm al. Stat ist ical analyses, i.e., sim ple and m ult i-ple linear regression, independent sample t-test ,andchi-square test , were carr ied out for different variables to est imate the significant effects of these var iables on NAFLDand R Studio version 1.2.5001, and signif icance (p-value) was set at < 0.05.
Results The male-female ratio of part icipants was 1.17 (n= 100), with a median age of 53.5 years (Table 1). The majority of the participants were overweight or obese (median BMI= 25.91). NAFLD fibrosis cut-off was categorized as mild, moderate, and severe, as described above. Average NFS for males and females were -0.4152± 1.48 and -0.8004± 1.49, respectively, with a mean significant difference (p= .043). However, no overall association between NFS and gender was observed (p> 0.05). According to 2D-ECHO,LVDD occurred in 44 pat ients,am ong whom m ild, m oderate,or severe NFS was detected in 10, 23, and 11 pat ients, respect ively. I n pat ients without LVDD, 21, 30, and 5 pat ients had m ild, mod-erate, or severe NFS, respect ively. No sig-nif icant difference was observed in the dist r ibut ion of NFS in the presence or ab-sence of LVDD. However, a significant asso-ciat ion was observed between the presence of LVDD and NFS (p= 0.0022) . Mean CI MT showed a significant ly increas-ing t rend with respect to NFS categor ies (p= 0.0025) , and the highest m ean CI MT was found in the m oderate-severe fibrosis (F3-F4) category for the total populat ion as well as for both genders (0.81, 0.84, and 0.93 in males and 0.81, 0.93 and 0.96 in fe-males) for the m ild, indeterm inate and mod-
erate-severe groups, respect ively. Mult ino-m ial logist ic regression between CI MT and NFS (moderate and severe) with m ild NFSas the reference categorydid not revealany sig-nificant associat ion between m oderate NFS and CI MT ( r ight and left ) . However, a signif-icant associat ion (p= 0.0124) was observed between r ight CI MT and severe NFS, and no significant associat ion was observed in left CI MT and severe NFS (Table 2) . When m ild NFS and the absence of LVDD wereconsidered as the reference category, no significant associat ion between moderate NFS, CI MT (both r ight and left ) , and LVDD was observed. I n cont rast , a significant as-sociat ion was observed between severe NFS, r ight CI MT, and LVDD (p= 0.0466) , and no significant associat ion was observed be-tween severe NFS, left CI MT, and LVDD (Table 3) . Mult inom ial logist ic regression of the pres-ence of LVDD and NFS grades (m ild fibrosis as the reference category) revealed signifi-cant associat ion (p= 0.0022) , indicat ing that NAFLD related fibrosis is linked to the pres-ence of LVDD. The associat ion between anthropometric pa-ram eters, biom arkers such as fast ing blood sugar (FBS) , postprandial blood sugar test (PPBS) , hem oglobin A1c (HBA1c) , and NFS indicated a significant associat ion between BMI and NFS. However, no significant asso-ciat ion was evident between other param e-ters (Table 4) . The correlat ion between the non- invasive cardiovascular m arkers and NFS calculated by Pearson’s correlat ionrevealed a signif i-cant ly posit ive correlat ion between m ild NFS and BMI , m oderate NFS and left CI MT, and severe NFS and BMI . Although not signif i-cant , an interest ing correlat ion pat tern was not iced between m ild, moderate, and severe NFS and r ight CI MT, FBS, PPBS, and HBA1c with varying st rengths (Table 5) .
Variable Mean ± SD Minim um Median Maxim um
Age 52.81± 4.96 42 53.5 60
Height 158.03± 5.80 148 158 171
Weight 64.96± 8.62 45 65 88
BMI 25.93± 2.33 20.27 25.91 31.18
Table 1. Dem ographic dist r ibut ion of the study sam ple (n= 100) .
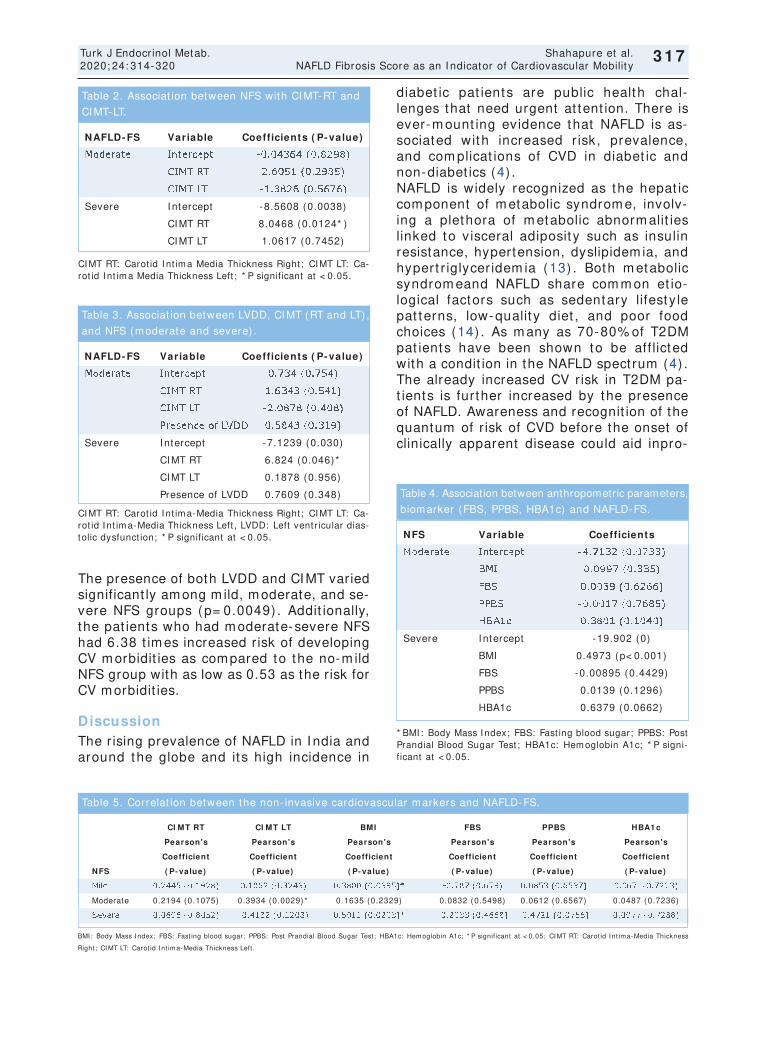
317
Turk J Endocrinol Metab. Shahapure et al. 2020; 24: 314-320 NAFLD Fibrosis Score as an I ndicator of Cardiovascular Mobilit y
3 1 7
The presence of both LVDD and CI MT varied significant ly am ong m ild, m oderate, and se-vere NFS groups (p= 0.0049) . Addit ionally, the pat ients who had m oderate-severe NFS had 6.38 t im es increased r isk of developing CV m orbidit ies as com pared to the no-m ild NFS group with as low as 0.53 as the r isk for CV m orbidit ies.
Discussion The r ising prevalence of NAFLD in I ndia and around the globe and it s high incidence in
diabet ic pat ients are public health chal-lenges that need urgent at tent ion. There is ever-m ount ing evidence that NAFLD is as-sociated with increased r isk, prevalence, and com plicat ions of CVD in diabet ic and non-diabet ics (4) . NAFLD is widely recognized as the hepat ic com ponent of m etabolic syndrom e, involv-ing a plethora of m etabolic abnorm alit ies linked to v isceral adiposit y such as insulin resistance, hypertension, dyslipidem ia, and hypert r iglycer idem ia (13) . Both m etabolic syndrom eand NAFLD share com m on et io-logical factors such as sedentary lifesty le pat terns, low-qualit y diet , and poor food choices (14) . As m any as 70-80% of T2DM pat ients have been shown to be aff licted with a condit ion in the NAFLD spect rum (4) . The already increased CV r isk in T2DM pa-t ients is further increased by the presence of NAFLD. Awareness and recognit ion of the quantum of r isk of CVD before the onset of clinically apparent disease could aid inpro-
NAFLD- FS Variable Coefficients ( P- value)
Moderate I ntercept -0.04364 (0.8298)
CI MT RT 2.6051 (0.2985)
CI MT LT -1.3826 (0.5676)
Severe I ntercept -8.5608 (0.0038)
CI MT RT 8.0468 (0.0124* )
CI MT LT 1.0617 (0.7452)
Table 2. Associat ion between NFS with CI MT-RT and
CI MT-LT.
CI MT RT: Carot id I nt im a Media Thickness Right ; CI MT LT: Ca-rot id I nt im a Media Thickness Left ; * P significant at < 0.05.
NAFLD- FS Variable Coefficients ( P- value)
Moderate I ntercept 0.734 (0.754)
CI MT RT 1.6343 (0.541)
CI MT LT -2.0878 (0.408)
Presence of LVDD 0.5843 (0.319)
Severe I ntercept -7.1239 (0.030)
CI MT RT 6.824 (0.046)*
CI MT LT 0.1878 (0.956)
Presence of LVDD 0.7609 (0.348)
Table 3. Associat ion between LVDD, CI MT (RT and LT) ,
and NFS (m oderate and severe) .
CI MT RT: Carot id I nt im a-Media Thickness Right ; CI MT LT: Ca-rot id I nt im a-Media Thickness Left , LVDD: Left vent r icular dias-tolic dysfunct ion; * P significant at < 0.05. NFS Variable Coefficients
Moderate I ntercept -4.7132 (0.0733)
BMI 0.0997 (0.335)
FBS 0.0039 (0.6266)
PPBS -0.0017 (0.7685)
HBA1c 0.3801 (0.1040)
Severe I ntercept -19.902 (0)
BMI 0.4973 (p< 0.001)
FBS -0.00895 (0.4429)
PPBS 0.0139 (0.1296)
HBA1c 0.6379 (0.0662)
Table 4. Association between anthropometric parameters,
biom arker (FBS, PPBS, HBA1c) and NAFLD-FS.
* BMI : Body Mass I ndex; FBS: Fast ing blood sugar; PPBS: Post Prandial Blood Sugar Test ; HBA1c: Hem oglobin A1c; * P signi-ficant at < 0.05.
BMI : Body Mass I ndex; FBS: Fast ing blood sugar; PPBS: Post Prandial Blood Sugar Test ; HBA1c: Hem oglobin A1c; * P significant at < 0.05; CI MT RT: Carot id I nt im a-Media Thickness
Right ; CI MT LT: Carot id I nt im a-Media Thickness Left .
CI MT RT CI MT LT BMI FBS PPBS HBA1 c
Pearson's Pearson's Pearson's Pearson's Pearson's Pearson's
Coefficient Coefficient Coefficient Coefficient Coefficient Coefficient
NFS ( P- value) ( P- value) ( P- value) ( P- value) ( P- value) ( P- value)
Mild 0.2445 (0.1928) 0.1862 (0.3243) 0.3800 (0.0395)* -0.787 (0.679) 0.0853 (0.6537) 0.067 (0.7223)
Moderate 0.2194 (0.1075) 0.3934 (0.0029)* 0.1635 (0.2329) 0.0832 (0.5498) 0.0612 (0.6567) 0.0487 (0.7236)
Severe 0.0696 (0.8052) -0.4182 (0.1208) 0.5911 (0.0203)* -0.2033 (0.4668) -0.4721 (0.0756) 0.0977 (0.7288)
Table 5. Correlat ion between the non- invasive cardiovascular m arkers and NAFLD-FS.

viding appropriate preventat ive t reatment to the cohort at r isk. The use of rout ine inves-t igat ions as a surrogate guide for CV r isk is a cost-effect ive st rategy to recom m end de-tailed invest igat ions. This is especially im -portant in count r ies like I ndia, where healthcare is plagued by lim ited resources and predom inant out-of-pocket health ex-penses. This study adds to the growing body of evidence available on NAFLD and m orbid-ity due to CVD in T2DM. Age is st rongly correlated to NAFLD owing to m echanism s that increase hepat ic fat ac-cum ulat ion, reflected in the m ean age of 52.81 years of part icipants in this study and reported by Sivabal et al.(15) . Age- related reduct ion in m uscle m ass and funct ion cou-pled with deter iorat ing efficiency of the an-t ioxidant system leads to an increase in oxidat ive st ress, thereby prom ot ing NAFLD (16) . The results of this study im ply that NFS was not influenced by gender,although fem ales had a significant ly higher NFS score as com-pared to m ales. Conflict ing t rends are seen in other studies with respect to gender predilect ion. I n studies by Koj im a et al. and Suzuki et al., m ales were found to be m ore likely to develop NAFLD (17,18) . However, in studies by Kalra et al. and Motamed et al., NAFLD was observed to be m ore prevalent in fem ales than in m ales (19,20) . I n gen-eral, invest igat ions of hum ans and anim als have shown that the female sex is protected from NAFLD, owing to the posit ive effects of est rogen. Also, young fem ales can part it ion fat ty acids towardthe product ion of ketone bodies, rather than very- low-densit y lipoprotein (VLDL) - t r iacylglycerols, fur ther bestowing protect ion against NAFLD (21) . BMI is also found to be closely linked with NAFLD, and a high m edian BMI of part ici-pants reflects this. The signif icant posit ive correlat ion of BMI with moderate and severe NFSis sim ilar to the findings of Loom is et al. and Fan et al., who dem onst rated BMI as a st rong predictor of fat t y liver disease (22,23) . They em phasized the reduct ion of obesity for the prevent ion and m anagem ent of NAFLD. I n a m eta-analysis com prising of 86 studies (8,515,431 pat ients, 22 coun-t r ies) , Younossi et al.showed 51% and 82% the prevalence of obesit y in subjects with NAFLD and NASH, respect ively (4) . Part icu-
lar ly, age and BMI are com ponents of the NFS, which probably explains the com para-t ively lower num ber of pat ients with m ild fi-brosis here. CI MT and LVDD were used as non- invasive m arkers of CVD. CI MT reflects ear ly ather-osclerot ic changes in the vascular system , while LVDD is a known m arker of CV m or-bidit ies. There is a signif icant associat ion between r ight CI MT and severe NFS, which indicates a st rong link between NAFLD, NFS, and CV r isk . The reason behind t he dif ference between left CI MT and r ight CI MT is not clear but m ay be at t r ibuted to t he dif ference in t heir anatom ical or igin, which in turn leads to a difference in f low intensit ies (24) . No signif icant associat ion between left CI MT and severe NFS can be j ust if ied t o som e extent . A study by Lankarani et al.observed t hat NAFLD pa-t ients have increased CI MT (25) . Nahandi et al. reported a signif icant associat ion be-tween the presence of NAFLD and athero-sclerosis, t he com binat ion also being a predictor of T2DM (26) . Likewise, the pres-ence of LVDD was also found to be signif i-cant ly associated with NAFLD. Bonapace et al. deciphered that in pat ients with T2DM and NAFLD, ear ly features of LVDD could be successfully detected by 2D-ECHO, sim ilar to f indings of this study (27) . I n addit ion to the t radit ional CVD r isk fac-t ors of age, BMI , and presence of T2DM, the presence of NAFLD in diabet ic pat ients adds to the burden of r isk. This study adds to the pool of knowledge by ident ify ing the signif icant ly increased CV r isk in pat ient s with m oderate- severe NFS. Using the cor-relat ion between the NFS and m easures of LVDD and CI MT, the role of NFS is postu-lated not m erely t o grade hepat ic f ibrosis but also t o ident ify pat ient s at increased CV r isk.
Strengths and lim itat ions
The cost-benefit rat io of advanced invest i-gat ions is a m at ter of both ethical and fi-nancial concerns. The psychological st ress of m erely referr ing a pat ient for advanced in-vest igat ions involvingradiological or cardio-logical assessm ents cannot be denied. Hence, it would be beneficial if invest iga-t ions such as carot id doppler or 2D-ECHO are advised after prelim inary screening. The
318
Shahapure et al. Turk J Endocrinol Metab. NAFLD Fibrosis Score as an I ndicator of Cardiovascular Mobilit y 2020; 24: 314-320
3 1 8

NFS, platelet count , and liver funct ion test ( in addit ion to age, BMI , and diabet ic status) offers a highly convenient method of screen-ing asym ptom at ic pat ients of T2DM with NAFLD with no known CVD. I n addit ion, as-sessing the correlat ion of insulin level with NFS and cardiac param eters would also be beneficial as an early indicator.
Conclusion I n T2DM pat ients with NAFLD, the NFS helps to ident ify those with CV m orbidity, ident i-fy ing pat ients who need fur ther invest iga-t ion. The highly signif icant correlat ion of cardiovascular r isk, expressed as abnorm al CI MT and/ or LVDD, with m oderate-severe NFS, offers NFS score as viable a screening tool for T2DM pat ients with NAFLD who are asym ptom at ic for CV disease. Further stud-ies on sim ilar lines, with larger sam ple size and var ied age groups,are required to de-vise a precise m odel for predict ing CV m or-bidity from NFS scores.
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions I dea/ Concept : Pr it i Shahapure, Shim pa Sharm a; Design: Pr it i Shahapure, Shim pa Sharm a; Cont rol/ Supervision: Shim pa Sharm a; Data Collect ion and/ or Processing: Prit i Shahapure; Analysis and/ or I nterpreta-t ion: Shim pa Sharm a; Literature Review: Shim pa Sharm a, Pr it i Shahapure; Writ ing the Art icle: Pr it i Shahapure, Shim pa Sharm a; Cr it ical Review: Shim pa Sharm a; References and Fundings: Shim pa Sharm a; Materials: Prit i Shahapure.
References 1. Ahm ed A, Wong RJ, Harr ison SA. Nonalcoholic fat ty
liver disease review: diagnosis, t reatment , and out-com es. Clin Gast roenterol Hepatol. 2015; 13: 2062-2070. [ Crossref] [ PubMed]
2. Machado MV, Diehl AM. Pathogenesis of nonalco-holic steatohepat it is. Gast roenterology. 2016; 150: 1769-1777. [ Crossref] [ PubMed] [ PMC]
3. Dai W, Ye L, Liu A, Wen SW, Deng J, Wu X, Lai Z. Prevalence of nonalcoholic fat ty liver disease in pa-t ients with type 2 diabetes m ellitus: a m eta-analy-sis. Medicine (Balt im ore) . 2017; 96: e8179. [ Crossref] [ PubMed] [ PMC]
4. Younossi ZM, Koenig AB, Abdelat if D, Fazel Y, Henry L, Wym er M. Global epidem iology of nonalcoholic fat t y liver disease-m eta-analyt ic assessm ent of prevalence, incidence, and outcom es. Hepatology. 2016; 64: 73-84. [ Crossref] [ PubMed]
5. Dham ija E, Paul SB, Kedia S. Non-alcoholic fat t y liver disease associated with hepatocellular carci-nom a: an increasing concern. I ndian J Med Res. 2019; 149: 9-17. [ Crossref] [ PubMed] [ PMC]
6. Dharm alingam M, Yam asandhi PG. Nonalcoholic fat ty liver disease and Type 2 diabetes m ellitus. I n-dian J Endocrinol Metab. 2018; 22: 421-428. [ Cross-ref] [ PubMed] [ PMC]
7. Li X, Jiao Y, Xing Y, Gao P. Diabetes m ellit us and r isk of hepat ic f ibrosis/ cir rhosis. Biom ed Res I nt . 2019; 2019: 5308308. [ Crossref] [ PubMed] [ PMC]
8. Targher G, Bertolini L, Rodella S, Tessari R, Zenari L, Lippi G, Arcaro G. Nonalcoholic fat ty liver disease is independent ly associated with an increased inci-dence of cardiovascular events in t ype 2 diabet ic pat ients. Diabetes Care. 2007; 30: 2119-2121. [ Crossref] [ PubMed]
9. Targher G, Lonardo A, Byrne CD. Nonalcoholic fat ty liver disease and chronic vascular com plicat ions of diabetes m ellitus. Nat Rev Endocrinol. 2018; 14: 99-114. [ Crossref] [ PubMed]
10. Angulo P, Hui JM, Marchesini G, Bugianesi E, George J, Farrell GC, Enders F, Saksena S, Burt AD, Bida JP, Lindor K, Sanderson SO, Lenzi M, Adam s LA, Kench J, Therneau TM, Day CP. The NAFLD fibrosis score: a noninvasive system that ident ifies liver fibrosis in pat ients with NAFLD. Hepatology. 2007; 45: 846-854. [ Crossref] [ PubMed]
11. American Diabetes Associat ion. 2. Classificat ion and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2018. Diabetes Care. 2018; 41: S13-S27. [ Crossref] [ PubMed]
12. Duseja A, Singh SP, Saraswat VA, Acharya SK, Chawla YK, Chowdhury S, Dhim an RK, Jayaku-m ar RV, Madan K, Misra SP, Mishra H, Modi SK, Muruganathan A, Saboo B, Sahay R, Upadhyay R. Non-alcoholic fat t y liver disease and m etabolic syndrom e-posit ion paper of the I ndian Nat ional Associat ion for the Study of the Liver, Endocrine So-ciety of I ndia, I ndian College of Cardiology and I n-dian Society of Gast roenterology. J Clin Exp Hepatol. 2015; 5: 51-68. [ Crossref] [ PubMed] [ PMC]
319
Turk J Endocrinol Metab. Shahapure et al. 2020; 24: 314-320 NAFLD Fibrosis Score as an I ndicator of Cardiovascular Mobilit y
3 1 9
320
Shahapure et al. Turk J Endocrinol Metab. NAFLD Fibrosis Score as an I ndicator of Cardiovascular Mobilit y 2020; 24: 314-320
3 2 0
13. Mendrick DL, Diehl AM, Topor LS, Dietert RR, Will Y, La Merr ill MA, Bouret S, Varm a V, Hast ings KL, Schug TT, Em eigh Hart SG, Burleson FG. Metabolic syndrom e and associated diseases: from the bench to the clinic. Toxicol Sci. 2018; 162: 36-42. [ Cross-ref] [ PubMed] [ PMC]
14. Tana C, Ballest r i S, Ricci F, Di Vincenzo A, Ticinesi A, Gallina S, Giam berardino MA, Cipollone F, Sut ton R, Vet tor R, Fedorowski A, Meschi T. Cardiovascular r isk in non-alcoholic fat ty liver disease: mechanisms and therapeut ic implicat ions. I nt J Environ Res Pub-lic Health. 2019; 16: 3104. [ Crossref] [ PubMed] [ PMC]
15. Vanj iappan S, Ham ide A, Ananthakr ishnan R, Per iyasamy SG, Mehalingam V. Nonalcoholic fat t y liver disease in pat ients with type 2 diabetes m elli-tus and its associat ion with cardiovascular disease. Diabetes Metab Syndr. 2018; 12: 479-482. [ Cross-ref] [ PubMed]
16. Golabi P, Paik J, Reddy R, Bugianesi E, Tr im ble G, Younossi ZM. Prevalence and long- term outcom es of non-alcoholic fat ty liver disease among elderly in-div iduals from the United States. BMC Gast roen-terol. 2019; 19: 56. [ Crossref] [ PubMed] [ PMC]
17. Koj im a S, Watanabe N, Num ata M, Ogawa T, Mat-suzaki S. I ncrease in the prevalence of fat ty liver in Japan over the past 12 years: analysis of clinical background. J Gast roenterol. 2003; 38: 954-961. [ Crossref] [ PubMed]
18. Suzuki A, Angulo P, Lym p J, St Sauver J, Muto A, Okada T, Lindor K. Chronological development of el-evated am inot ransferases in a nonalcoholic popula-t ion. Hepatology. 2005; 41: 64-71. [ Crossref] [ PubMed]
19. Kalra S, Vithalani M, Gulat i G, Kulkarni CM, Kadam Y, Pallivathukkal J, Das B, Sahay R, Modi KD. Study of prevalence of nonalcoholic fat t y liver disease (NAFLD) in t ype 2 diabetes pat ients in I ndia (SPRI NT) . J Assoc Physicians I ndia. 2013; 61: 448-453. [ PubMed]
20. Motam ed N, Sohrabi M, Ajdarkosh H, Hem m asi G, Maadi M, Sayeedian FS, Pirzad R, Abedi K, Aghapour S, Fallahnezhad M, Zam ani F. Fat ty liver index vs waist circum ference for predict ing non-al-
coholic fat t y liver disease. Wor ld J Gast roenterol. 2016; 22: 3023-3030. [ Crossref] [ PubMed] [ PMC]
21. Ballest r i S, Nascimbeni F, Baldelli E, Marrazzo A, Ro-magnoli D, Lonardo A. NAFLD as a sexual dimorphic disease: role of gender and reproduct ive status in the developm ent and progression of nonalcoholic fat ty liver disease and inherent cardiovascular r isk. Adv Ther. 2017; 34: 1291-1326. [ Crossref] [ PubMed] [ PMC]
22. Loomis AK, Kabadi S, Preiss D, Hyde C, Bonato V, St Louis M, Desai J, Gill JM, Welsh P, Waterworth D, Sat tar N. Body m ass index and r isk of nonalcoholic fat t y liver disease: two elect ronic health record prospect ive studies. J Clin Endocr inol Metab. 2016; 101: 945-952. [ Crossref] [ PubMed] [ PMC]
23. Fan R, Wang J, Du J. Associat ion between body m ass index and fat t y liver r isk: a dose- response analysis. Sci Rep. 2018; 8: 15273. [ Crossref] [ PubMed] [ PMC]
24. Luo X, Yang Y, Cao T, Li Z. Differences in left and r ight carot id int im a-m edia thickness and the asso-ciated r isk factors. Clin Radiol. 2011; 66: 393-398. [ Crossref] [ PubMed]
25. Lankarani KB, Mahm oodi M, Lot fi M, Zam ir i N, Hey-dar i ST, Ghaffarpasand F, Fallahzadeh MK, Babaeinejad M, Mahar louei N, Mirzaee O, Geramizadeh B, Peymani P. Common carot id int ima-m edia thickness in pat ients with non-alcoholic fat ty liver disease: a populat ion-based case-cont rol study. Korean J Gast roenterol. 2013; 62: 344-351. [ Crossref] [ PubMed]
26. Nahandi MZ, Khoshbaten M, Ram azanzadeh E, Ab-baszadeh L, Javadrashid R, Shirazi KM, Gholam i N. Effect of non-alcoholic fat ty liver disease on carot id ar tery int im a-m edia thickness as a r isk factor for atherosclerosis. Gast roenterol Hepatol Bed Bench. 2014; 7: 55-62. [ PubMed] [ PMC]
27. Bonapace S, Perseghin G, Molon G, Canali G, Bertolini L, Zoppini G, Barbier i E, Targher G. Nonal-coholic fat ty liver disease is associated with left ven-t r icular diastolic dysfunct ion in pat ients with type 2 diabetes. Diabetes Care. 2012; 35: 389-395. [ Cross-ref] [ PubMed] [ PMC]
Serum Levels of 8 - OHdG in Pat ients w ith Hashim oto’s Thyroidit is
Hashim oto Tiroidit i Olan Hastalarda Serum 8-OHdG Düzeyler i
Fatem eh ESFAHANI AN, Seyedeh Mahdieh FOTOUK KI AI E,
Roghayeh GHELI CH, Zohreh JADALI *
Department of Endocrinology, Imam Khomeini General Hospital, Tehran, IRAN * Department of Immunology, School of Public Health, Tehran University of Medical Sciences, Tehran, IRAN
3 2 1Original Art icle Turk J Endocrinol Metab. 2020; 24: 321-326
I nt roduct ion Hashimoto’s thyroidit is (HT) is characterized by diffuse lymphocyt ic infilt rat ion of the thy-roid gland and elevated level of ant ithyroid-
specific autoant ibodies. I t is m ore prevalent am ong wom en, and it s incidence has in-creased significant ly in recent years (1) . Al-though autoim m unity plays a pivotal role in
Object ive: A growing body of evidence shows a close rela-t ionship between oxidat ive st ress and autoim m une condit i-ons such as Hashim oto’s thyroidit is (HT) . Am ong different m arkers of oxidat ive dam age, 8-hydroxydeoxyguanosine (8-OHdG) is a ubiquitous m arker and broadly used in rese-arch studies. Therefore, this study aim ed to m easure the level of 8-OHdG in the sera of pat ients with HT and healthy cont rol (HC) part icipants. Materia l and Methods: I n this study, pat ients were diagnosed with clinical (n= 23) and subclinical (n= 25) hypothyroidism because of HT and com -pared with 35 healthy part icipants. 8-OHdG was m easured using enzym e- linked im m unosorbent assay in pat ients and HC part icipants. Results: No significant difference was ob-served in the m ean serum 8-OHdG levels between pat ients and HC part icipants. Conclusion: The results of this preli-m inary study do not support the fact that the serum level of 8-OHdG is a biom arker of oxidat ive st ress in pat ients with HT. However, more detailed studies are needed to reveal the exact role of 8-OHdG in this autoim m une disease of the thyroid gland. Keyw ords: 8-hydroxydeoxyguanosine;
Hashim oto’s thyroidit is; oxidat ive st ress
Am aç: Giderek artan sayıda kanıt , oksidat if st res ile Has-himoto t iroidit i (HT) gibi otoimmün durum lar arasında yakın bir ilişki olduğunu gösterm ektedir. Oksidat if hasarın farklı belir t eçler i arasında, 8-hidroksideoksiguanozin (8-OHdG) yaygın bir belir teçt ir ve araşt ırm a çalışm alarında geniş öl-çüde kullanılm aktadır. Bu nedenle, bu çalışm a HT hastala-r ının ve sağlık lı kont rol (SK) grubunun serum lar ında 8-OHdG düzeyini ölçm eyi am açlam ışt ır. Gereç ve Yön-tem ler: Bu çalışm ada hastalara HT nedeniyle klinik (n= 23) ve subklinik ( n= 25) hipot iroidizm tanısı konulm uş ve 35 sağlık lı kat ılım cı ile karşılaşt ır ılm ışt ır. 8-OHdG, hastalarda ve SK grubunda enzim e bağlı im m ünosorbent test i kullanı-larak ölçülmüştür. Bulgular: Hastalar ve SK grubu arasında ortalam a serum 8-OHdG düzeyler inde anlam lı bir fark iz-lenm em işt ir. Sonuç: Bu ön çalışm anın sonuçları, HT hasta-lar ında serum 8-OHdG düzeyinin oksidat if st resin bir biyobelir teci olduğu gerçeğini desteklememektedir. Bununla bir lik te, t iroid bezinin bu otoim m ün hastalığında 8-OHdG'nin tam rolünü ortaya çıkarm ak için daha detaylı ça-lışm alara iht iyaç vardır. Anahtar kelim eler: 8-hidroksideoksiguanozin;
Hashim oto t iroidit i; oksidat if st res
Address for Correspondence: Zohreh JADALI , Departm ent of I m m unology, School of Public Health, Tehran University of Medical Sciences, Tehran, I RAN
Phone: 6462268-6465404 E- m ail: [email protected]
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 10 Jul 2020 Received in revised form : 29 Oct 2020 Accepted: 05 Nov 2020 Available online: 10 Dec 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
76
13

t he pathogenesis of HT, the under ly ing m echanism s for the init iat ion and progres-sion of aberrant im m une responses are not com pletely understood (2) . I n recent years, several studies suggested a dynam ic relat ionship between the im m une system and oxidat ive st ress. Oxidat ive st ress has been shown to play crucial roles in the regulat ion of specific immunity and in-flam m atory responses (3,4) . Therefore, any disturbance in the oxidant-ant ioxidant bal-ance can influence im m une act iv it y. Under normal condit ions the product ion of react ive oxygen species and free radicals is neces-sary for thyroid horm onogenesis; (5) how-ever, the overproduct ion of oxygen radicals dam ages thyrocytes (6) . Oxidat ive st ress causes dam age to four m ajor m acrom olecules within the cells (pro-teins, nucleic acids, such as DNA and RNA, carbohydrates, and lipids) . The result ing ox-idat ion products from each biom olecule can then be used to assess the direct or indirect index of oxidat ive st ress. Oxidat ive dam age to DNA has been proposed as a novel and crucial factor that m ay underlie the patho-genesis of var ious autoim m une or inf lam -matory diseases. 8-hydroxydeoxyguanosine (8-OHdG) is a m ajor form of the oxidat ive DNA dam age product form ed by the at tack of oxygen radicals on 2’-deoxyguanosine. I t can pair with adenine and cause a G: CT: A t ransversion m utat ion (7) . The m ajor m am m alian enzym e for rem oving 8-OHdG from DNA is 8-oxoguanine-DNA glycosy-lase. Although this enzym e prevents the ac-cum ulat ion of ox idat ive products of DNA dam age, large delet ion m utat ions m ay also ar ise dur ing the nucleot ide excision repair pathway for rem oving 8-OHdG from DNA (8) . I n recent years, much at tent ion has been fo-cused on invest igat ing the putat ive role of oxidat ive st ress in the pathogenesis of au-toim m une thyroid disorders such as HT and Graves’ disease (GD) . Although exist ing ev-idence suggests increased oxidat ive damage in pat ients with HT, a cont roversy exists in the literature on this issue. Therefore, this study aim ed to m easure whether a differ-ence exists in the serum levels of 8-OHdG between pat ients with HT and norm al par-t icipants and assess the correlat ion between clinical and laboratory values of 8-OHdG.
Materia l and Methods
Pat ients
This is a case-control study, and the sample size was calculated using the following formula from Shin SC’s study conducted in 2001: Considering an addit ional 15% sample to pre-vent loss and withdrawal, the sample size was determined to be 28 people in each group. A total of 48 pat ients (13 m en and 35 wom en; m ean age, 42.12± 12.59 years; range, 18-75) with HT were enrolled in this study. Of the 48 consecut ive pat ients with newly diagnosed hypothyroidism seen in the endocrinology clinic, 23 had overt hypothy-roidism (OHT) , and 25 had subclinical hy-pothyroidism (SCHT) . A total of 35 healthy cont rol part icipants were included: 10 m en and 25 wom en with a m ean age of 43.71± 14.26 years ( range, 20-72) . The cont rol par t icipants were age- and sex-m atched with the pat ient group. OHT was defined as an elevated thyroid-st im ulat ing hormone (TSH, > 10 µIU/ L) with posit ive an-t it hyroid peroxidase ant ibodies (TPO, > 40 I U/ m L) . SCHT was character ized as a TSH level between 4 and 10 µI U/ L with ant i-TPO ant ibodies (> 40 I U/ m L) . The thyroid func-t ion was considered norm al when TSH fell within the norm al reference ranges. Major exclusion cr iter ia were as follows: (1) preg-nancy and lactat ion; (2) thyroid disorders or surgery; (3) m alignancy, chronic inflam m a-tory condit ions, and system ic or organ-spe-cif ic autoim m une diseases, except HT; (4) presence of acute or chronic infect ion; (5) im m unosuppressive t reatm ent , ant ithyroid drugs therapy, or m edicat ions that m ay af-fect the thyroid funct ion such as lithium or iodide; and (6) sm okers and other tobacco users. The study protocol was com pletely approved by the Ethics Commit tee of Tehran University of Medical Sciences through ref-erence no. I R.TUMS.REC.1395.00108. All part icipants had provided inform ed writ ten consent before enrollm ent in the study. Our study was conducted in accordance with the Helsinki Declarat ion pr inciples. Demographic condit ions and laboratory find-ings are shown in Table 1.
Assessm ent of Thyroid Funct ions
Peripheral venous blood sam ples were col-lected from all part icipants. The sera were
322
Esfahanıan et al. Turk J Endocrinol Metab. 8-OHdG Levels in HT 2020; 24: 321-326
3 2 2

323
separated from the cells by cent r ifugat ion and stored at -20 ° C unt il the t im e of test-ing. The serum concentrat ions of free thyroxine (FT4) and TSH were determined using an en-zyme immunoassay kit (Monobind Inc., Lake Forest , CA92630, USA) and im m unoradio-metric assay kit ( IRMA kit Radim, Pomezia, Rom e, I taly) , respect ively. I n addit ion, en-zym e im m unoassay was used to quant ify serum autoant ibodies against TPO (Monobind Inc., Lake Forest , CA92630, USA).
Quant itat ive Determ inat ion of 8 - OHdG Concentrat ions
Levels of 8-OHdG were quant ified using the enzym e- linked im m unosorbent assay k it (Zellbio Gm bH, lonsee, Germ any) according to the m anufacturer ’s inst ruct ions.
Stat ist ics
After determ ining whether num eric values were norm ally dist r ibuted, the one-way analysis of variance test was used for com -par ing m eans of three or m ore groups. Moreover, the Mann-Whitney and Kruskal-Wallis tests were used for var iables that were not norm ally dist r ibuted. A p-value of < 0.05 was considered stat ist ically signif i-cant . A correlat ion analysis was perform ed using Pearson’s test . All data analyses were perform ed using SPSS, version 11.0 (SPSS, I nc, Chicago, I L, USA) .
Results This study aim ed to assess 8-OHdG serum levels in pat ients with HT and healthy par-
t icipants. A total of 83 individuals (35 nor-m al par t icipants, 23 pat ients with SCHT, and 25 OHT pat ients) were evaluated. The m ean (standard deviat ion) age of the par-t icipants was 42.84 years (13.34) ( range, 20-75) , and 62 par t icipants were wom en (74.69% ) . The fem ale- to-m ale rat io in this study was 2.7. No stat ist ically significant difference in term s of age (p= 0.52) and sex (p= 0.46) was observed between pat ients and cont rol part icipants. I n this study, the concent rat ion of TSH was signif icant ly higher in pat ients with OHT and SCHT than healthy part ici-pants. Moreover, the level of TSH was higher in the OHT group ( range, 10-134 (about 6-fold) ) than that in the SCHT group ( range, 4.6-9.4; p< 0.001) . I n cont rast , the serum FT4 level was lower in the OHT group ( range, 0.5-1.65) than the SCHT ( range, 0.6-1.7) and cont rol groups ( range, 0.8-1.61) ; however, this difference was not sta-t ist ically significant (p> 0.06) . A significant difference was observed in the ant i-TPO an-t ibody levels in OHT ( range, 74-934 I U/ m L) and SCHT groups ( range, 75-561 I U/ m L) com pared with the cont rol group ( range, 0.6-18 I U/ m L; p< 0.001) . However, no sig-nif icant differences were observed in ant i-TPO ant ibody levels between OHT and SCHT subgroups. A posit ive correlat ion was observed between TSH and high ant i-TPO ant ibody concent rat ions in pat ients with HT ( r= 0.72, p< 0.01) . Moreover, an inverse negat ive cor-relat ion was observed between FT4 and TSH ( r= -0.24, p= 0.02) .
Turk J Endocrinol Metab. Esfahanıan et al. 2020; 24: 321-326 8-OHdG Levels in HT
3 2 3
F: Females; M: Males; TSH: thyroid st imulat ing hormone; FT4: Serum free T4; Ant i-TPO: ant ithyroid peroxidase ant ibody; 8-OHdG: 8-hydroxydeoxyguanosine. P< 0.05; * : Total hypothyroid and cont rol; †: Subclinical hypothyroid and overt hypothyroid; ∞: subclinical hypothyroid and cont rol; ‡: overt hypothyroid and cont rol.
Param eters Total hypothyroid Subclinical hypothyroid Overt hypothyroid Control
Num ber 48 25 23 34
Age(years) 42.12± 12.59 40.36± 12.4 44.04± 13.7 43.71± 14.26
Sex(F/ M) 35/ 13 20/ 5 15/ 8 27/ 8
TSH(µI U/ m L) 24.37± 30.8* 6.8± 1.33∞ 43.47± 36.11†‡ 1.95± 0.93
FT4(ng/ dL) 1.10± 0.35 1.20± 0.31 0.99± 0.36 1.13± 0.26
Ant i-TPO( I U/ m L) 321± 182.64* 314.52± 174.43∞ 328.08± 194.86‡ 6.59± 4.62
8-OHdG(ng/ m L) 12.86± 9.41 15.20± 11.87 10.31± 4.70 12.79± 8.87
Table 1. Laboratory findings and dem ographic propert ies of all pat ients with Hashim oto’s thyroidit is (subclinical
hypothyroidism and overt hypothyroidism ) and healthy cont rol part icipants.

324
Serum Levels of 8 - OHdG
Figure 1 shows the result s of 8-OHdG evaluat ion. Although the result s were not stat ist ically significant (p> 0.05) , the figure shows that the level of 8-OHdG in the sera of pat ients with SCHT ( range, 7.2-52 (15.20± 11.87) ) was higher than those with OHT ( range, 6.4-22.9 (10.31± 4.7) ) and norm al cont rol part icipants ( range, 2.7-43 (12.79± 8.87) ) . Moreover, no significant dif-ference was observed in the serum concen-t rat ion of 8-OHdG between pat ient groups and healthy part icipants. A correlat ion analysis revealed no associa-t ion between the serum levels of 8-OHdG and other clinical param eters such as TSH, FT4, and ant i-TPO within the pat ient groups.
Discussion HT is an autoim mune inflammatory disorder of the thyroid gland whose exact m olecular mechanism remains unclear. Several studies have shown that both cellular and hum oral im m unity play a role in the pathogenesis of HT. The aberrant act ivat ion of resident and circulat ing T and B cells in t issues ( the major cellular components of the adapt ive immune response) t r iggers a cascade of im m unolog-ical events, leading to increased product ion of autoant ibodies, apoptosis, and alterat ion of cytokine balance (9) . On the other hand, redox homeostasis is es-sent ial for the appropriate funct ioning of the im m une system (10) . Whereas sustained im balances in redox hom eostasis play a
m ajor role in the et iology of autoim m une disorders (11) . I t is well known that increased oxidat ive st ress affects organic m olecules. The oxida-t ion of these crucial biological molecules was confirm ed by the form at ion of oxidat ion byproducts that can serve as useful bio-markers in assessing oxidat ive st ress. I n re-cent years, great at tent ion has been focused on oxidat ive st ress- related biom arkers as their accurate evaluat ion can help in study-ing their role in disease pathogenesis and m onitor ing t reatm ent success (12) . Unt il date, different types of oxidat ive mark-ers have been ident ified in the body. 8-OHdG is one of the m ost crucial, abundant , and sensit ive biomarkers of oxidat ive DNA dam-age (13) . The removal of 8-OHdG is neces-sary for maintaining genome integrity. After excision, 8-OHdG is exported into the serum, ur ine, or other ext racellular fluids without further m etabolism (14-16) . Therefore, it can be quant ified in body fluid samples. I n this study, the levels of 8-OHdG were m easured in the sera of pat ients with HT and healthy cont rol part icipants. To the best of our knowledge, this is the first study to explore changes in 8-OHdG levels in the sera of pat ients with HT. The results showed no significant difference in the concentrat ion of 8-OHdG between pat ients and cont rol part icipants, which is in line with the results of som e previous studies. Our findings are in line with som e previous lit erature result s, showing no signif icant changes in the am ount of 8-OHdG between pat ients with HT and cont rols. For instance, in a study conducted by Hara et al., the pro-duct ion of 8-OHdG and cytochrom e c was analyzed in the culture supernatant of m ononuclear cells derived from the periph-eral blood of pat ients with GD and HT. The levels of cytochrom e c were signif icant ly higher in unt reated pat ients with GD and HT than that in healthy individuals, whereas the 8-OHdG level increased only in pat ients with GD (17) . I n cont rast , results from other studies have shown that the 8-OHdG level was signif i-cant ly increased in pat ients with HT com -pared with that in norm al cont rol part icipants. For instance, the overexpres-sion of 8-OHdG has been observed in the thyroid t issues of pat ients with HT, GD, and
Esfahanıan et al. Turk J Endocrinol Metab. 8-OHdG Levels in HT 2020; 24: 321-326
3 2 4
Figure 1 . Serum 8-OHdG levels in study groups. Each bar represents the average values of 8-OHdG levels with Stan-dard deviat ion in the four groups including total hypothy-roid (THT) , overt hypothyroid (OHT) , subclinical hypothyroid (SCHT) pat ients and healthy cont rols (HC) . There were no stat ist ically significant differences between groups.

papillary thyroid carcinoma (18) . These find-ings have also been supported by other re-search evidence indicat ing an elevated level of 8-OHdG in the ur ine of pat ients with toxic m ult inodular goiter, GD, and HT (19) . The discrepancies between these result s can part ly be associated with several possible explanat ions part icular ly related to the pa-t ient ’s t reatment status or sites/ organs from which the specim ens were obtained (20) . Therefore, a sim ultaneous t racing of 8-OHdG in the thyroid and body fluids is es-sent ial for a bet ter understanding of its role in HT. Moreover, a com par ison of 8-OHdG levels before and after t reatm ent can pro-vide valuable inform at ion regarding the role of this indicator in endogenous oxidat ive DNA dam age. Sm all sam ple size, the absence of data re-garding 8-OHdG levels in the thyroid t issue of pat ients with HT, and the lack of any ex-perim ental design for assessing t reatm ent-related alterat ions in the com posit ion of 8-OHdG were three m ajor lim itat ions of this study, which can be addressed in future studies. Moreover, sim ultaneous m easure-m ents of 8-OHdG and other m arkers of ox-idat ive st ress can provide a m ore precise interpretat ion and im prove the validity and reliabilit y of the data.
Conclusion This study does not indicate any difference in the levels of 8-OHdG between pat ients with HT and healthy part icipants. However, the role of oxidat ive st ress in HT cannot be ruled out from these findings. Therefore, m ore studies are needed to analyze the po-tent ial link between oxidat ive st ress and the pathogenesis of HT.
Financial Support and Sponsorship This study was conducted with the financial support of the Tehran University of Medical Sciences for Research through cont ract no. 34052.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions I dea/ Concept : Zohreh Jadali, Fatemeh Esfa-hanian; Design: Zohreh Jadali, Fatem eh Es-fahanian; Cont rol/ Supervision: Fatem eh Esfahanian; Data Collect ion and/ or Process-ing: Seyedeh Mahdieh Fotouk Kiaie, Roghayeh Ghelich; Analysis and/ or I nter-pretat ion: Seyedeh Mahdieh Fotouk Kiaie; Literature Review: Seyedeh Mahdieh Fotouk Kiaie; Writ ing the Art icle: Zohreh Jadali; Crit ical Review: Fatemeh Esfahanian; Refer-ences and Fundings: Tehran Universit y of Medical Sciences; Materials: Fatem eh Esfa-hanian, Seyedeh Mahdieh Fotouk Kiaie, Roghayeh Ghelich.
References 1. Saraf SR, Gadgil NM, Yadav S, Kalgutkar AD. I m -
portance of combined approach of invest igat ions for detect ion of asym ptom at ic Hashim oto Thyroidit is in ear ly stage. J Lab Physicians. 2018; 10: 294-298. [ Crossref] [ PubMed] [ PMC]
2. Li Q, Wang B, Mu K, Zhang JA. The pathogenesis of thyroid autoimmune diseases: new T lymphocytes - cytokines circuits beyond the Th1-Th2 paradigm . J Cell Physiol. 2019; 234: 2204-2216. [ Crossref] [ PubMed]
3. Weigert A, von Knethen A, Fuhrm ann D, Dehne N, Brüne B. Redox-signals and m acrophage biology. Mol Aspects Med. 2018; 63: 70-87. [ Crossref] [ PubMed]
4. Lorenzen I , Mullen L, Bekeschus S, Hanschm ann EM. Redox regulat ion of inflam m atory processes is enzym at ically cont rolled. Oxid Med Cell Longev. 2017; 2017: 8459402. [ Crossref] [ PubMed] [ PMC]
5. Brieger K, Schiavone S, Miller FJ Jr, Krause KH. Re-act ive oxygen species: from health to disease. Swiss Med Wkly. 2012; 142: w13659. [ Crossref] [ PubMed]
6. Poncin S, Gérard AC, Boucquey M, Senou M, Calderon PB, Knoops B, Lengelé B, Many MC, Colin I M. Oxidat ive st ress in the thyroid gland: from harm lessness to hazard depending on the iodine content . Endocrinology. 2008; 149: 424-433. [ Cross-ref] [ PubMed]
7. Gushim a M, Hirahashi M, Matsum oto T, Fuj ita K, Fuj isawa R, Mizum oto K, Nakabeppu Y, I ida M, Yao T, Tsuneyoshi M. Altered expression of MUTYH and an increase in 8-hydroxydeoxyguanosine are early events in ulcerat ive colit is-associated carcino-genesis. J Pathol. 2009; 219: 77-86. [ Crossref] [ PubMed]
8. Yang N, Chaudhry MA, Wallace SS. Base excision re-pair by hNTH1 and hOGG1: a two edged sword in the processing of DNA damage in gamma- irradiated hum an cells. DNA Repair (Am st ) . 2006; 5: 43-51. [ Crossref] [ PubMed]
9. Aj j an RA, Weetm an AP. The pathogenesis of Hashim oto's thyroidit is: fur ther developm ents in our understanding. Horm Metab Res. 2015; 47: 702-710. [ Crossref] [ PubMed]
325
Turk J Endocrinol Metab. Esfahanıan et al. 2020; 24: 321-326 8-OHdG Levels in HT
3 2 5

10. Gostner JM, Becker K, Fuchs D, Sucher R. Redox regulat ion of the im m une response. Redox Rep. 2013; 18: 88-94. [ Crossref] [ PubMed] [ PMC]
11. Verm a MK, Verm a P. Role of oxidant alterat ion of biom olecules in diabetes and other associated dis-eases. I nt J Life Sci Scient i Res. 2018; 4: 1542-1549. [ Crossref]
12. Liguori I , Russo G, Curcio F, Bulli G, Aran L, Della-Morte D, Gargiulo G, Testa G, Cacciatore F, Bona-duce D, Abete P. Oxidat ive st ress, aging, and diseases. Clin I nterv Aging. 2018; 13: 757-772. [ Crossref] [ PubMed] [ PMC]
13. Am es BN. Endogenous oxidat ive DNA dam age, aging, and cancer. Free Radic Res Com m un. 1989; 7: 121-128. [ Crossref] [ PubMed]
14. Shigenaga MK, Gim eno CJ, Am es BN. Urinary 8-hy-droxy-2'-deoxyguanosine as a biological m arker of in vivo oxidat ive DNA dam age. Proc Nat l Acad Sci U S A. 1989; 86: 9697-9701. [ Crossref] [ PubMed]
15. Loft S, Poulsen HE. Markers of oxidat ive dam age to DNA: ant ioxidants and m olecular dam age. Methods Enzym ol. 1999; 300: 166-184. [ Crossref] [ PubMed]
16. Suzuki J, I noue Y, Suzuki S. Changes in the ur inary excret ion level of 8-hydroxyguanine by exposure to
react ive oxygen-generat ing substances. Free Radic Biol Med. 1995; 18: 431-436. [ Crossref] [ PubMed]
17. Hara H, Sato R, Ban Y. Product ion of 8-OHdG and cytochrom e c by cultured hum an m ononuclear cells in pat ients with autoim m une thyroid disease. En-docr J. 2001; 48: 671-675. [ Crossref] [ PubMed]
18. Mseddi M, Ben Mansour R, Gouiia N, Mnif F, Bous-selaa R, Abid M, Boudaouara T, At t ia H, Lassoued S. A comparat ive study of nuclear 8-hydroxyguanosine expression in autoim m une thyroid diseases and papillary thyroid carcinoma and its relat ionship with p53, Bcl-2 and Ki-67 cancer related proteins. Adv Med Sci. 2017; 62: 45-51. [ Crossref] [ PubMed]
19. Ece H, Mehm et E, Cigir BA, Yavuz D, Muam m er K, Cum hur G, Mustafa H, Sevki C, Fusun S, Gokhan OA. Serum 8-OHdG and HI F-1α levels: do they af-fect the development of malignancy in pat ients with hypoact ive thyroid nodules? Contemp Oncol (Pozn) . 2013; 17: 51-57. [ Crossref] [ PubMed] [ PMC]
20. Bednarek J, Wysocki H, Sowiński J. Peripheral pa-ram eters of oxidat ive st ress in pat ients with infil-t rat ive Graves' ophthalm opathy t reated with cor t icosteroids. I m m unol Let t . 2004; 93: 227-232. [ Crossref] [ PubMed]
326
Esfahanıan et al. Turk J Endocrinol Metab. 8-OHdG Levels in HT 2020; 24: 321-326
3 2 6

Pneum ococcal, I nfluenza, Hepat it is B, and Tetanus Vaccinat ion Rate and Vaccine Aw areness
in Pat ients w ith Type 2 Diabetes Tip 2 Diyabet li Hastalarda Pnöm okok, İnfluenza, Hepat it B,
Tetanoz Aşılam a Oranları ve Aşı Farkındalığı
Arzu Cennet IŞI K, Seydahm et AKI N, Nazire ALADAĞ, Ersin Engin ŞİMŞEK* Clinic of I nternal Medicine, University of Health Sciences Kartal Dr. Lüt fi Kırdar City Hospital, İstanbul, TURKEY * Clinic of Family Medicine, University of Health Sciences Kartal Dr. Lüt fi Kırdar City Hospital, İstanbul, TURKEY
Original Art icle Turk J Endocrinol Metab. 2020; 24: 327-334
Object ive: This study aimed to determ ine the vaccinat ion rates and the levels of awareness on pneumococcal, influ-enza, tetanus and hepat it is B vaccinat ion am ong pat ients with Type 2 diabetes mellitus (DM). Material and Methods: The study was performed on pat ients with DM who presen-ted to the outpat ient Clinic of I nternal Disease at Kartal Dr. Lüt fi Kırdar City Hospital. Pat ients were asked to fill out a quest ionnaire regarding their vaccinat ion status, at t itude, and awareness about vaccines. Results: A total of 293 pa-t ients [ 121 (41.3% ) males and 172 (58.7% ) females] with a m ean age of 65 years were included in the study. The mean durat ion of diabetes was 15 years. Overall, 47.8% of pat ients reported awareness about the need for vaccinat ion while the rate of being unvaccinated was 52.2% . Reasons for the lack of vaccinat ion were as follows: 67.3% of pat ients were unaware of the reason for not receiving vaccines; 17.5% pat ients did not want to be vaccinated; 13.3% pat i-ents reported that their physicians did not recommend vac-cinat ion; 1.5% reported unavailability of vaccines, and 0.4% reported negligence. Among vaccinated cases, 34.1% were vaccinated against flu; 20.8% against tetanus; 9.9% against pneumonia; 7.8% against hepat it is; and 5.1% received vac-cinat ion for other diseases. Conclusion: The levels of vac-cine awareness and vaccinat ion rates are low among diabet ic pat ients. I t is essent ial to raise vaccinat ion awareness am ong this pat ient populat ion. The health authorit ies and departments need to develop effect ive st rategies to increase vaccinat ion rates across the country. Keyw ords: Diabetes m ellitus; pneum ococcal vaccine;
influenza vaccine; hepat it is B vaccine; tetanus vaccine
Am aç: Bu çalışm a, Tip 2 diabetes m ellitus (DM) hastala-rında aşılama oranlarını ve pnömokok, influenza, tetanoz ile hepat it B aşısı konusunda farkındalık düzeylerini belir lemeyi am açlam aktadır. Gereç ve Yöntem ler: Çalışm a, Kartal Dr. Lüt fi Kırdar Şehir Hastanesi İç Hastalıkları Kliniğine başvu-ran DM’li hastalar üzerinde yapıldı. Hastalardan aşı durum -lar ı, tutum ları ve aşılar la ilgili farkındalık lar ı hakkında bir anket doldurm aları istendi. Bulgular: Çalışm aya, yaş orta-lam ası 65 yıl olan toplam 293 [ 121 (% 41,3) ’i erkek, 172 (% 58,7) ’si kadın] hasta dâhil edildi. Ortalam a diyabet sü-resi 15 yıl idi. Genel olarak, hastaların % 47,8’i aşılam a iht i-yacı konusunda farkındalık bildir irken, aşı yapt ırmama oranı da % 52,2 idi. Hastaların % 67,3’ü aşı olmama nedeninin far-kında değildi. Yüzde 17,5 hasta aşı olm ak istem ediğini belir t irken; % 13,3’ü, hekim ler inin kendiler ine aşıy ı öner-m ediğini belir t t i. Ayrıca hastaların % 1,5’i aşıları bulam adı-ğını, % 0,4’ü de aşı olm ayı ihm al et t iğini bildirdi. Aşılanan olguların % 34,1’i gr ip aşısı; % 20,8’i tetanoz; % 9,9’u pnö-m oni; % 7,8’i hepat it ve % 5,1’i de diğer hastalıklara karşı aşılanm ışt ır. Sonuç: Diyabet ik hastalarda aşı farkındalığı ve aşılam a oranları düşük olarak bulundu. Bu hasta popülas-yonunda aşılam a bilincinin art ır ılm ası esast ır. Sağlık yetkili-ler i ve kuruluşlar ının, ülke genelinde aşılam a oranlar ını art ırm ak için etkili st ratej iler gelişt irm esi gerekt iği düşünül-m ektedir. Anahtar kelim eler: Diabetes m ellitus; pnöm okok aşısı;
influenza aşısı; hepat it B aşısı; tetanoz aşısı
3 2 7
Address for Correspondence: Arzu Cennet IŞI K, Clinic of I nternal Medicine, University of Health Sciences Kartal Dr. Lüt fi Kırdar City Hospital, İstanbul, TURKEY
Phone: + 905058174519 E- m ail: arzukaracelik@gm ail.com
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 05 Apr 2020 Received in revised form : 21 Jun 2020 Accepted: 23 Jul 2020 Available online: 31 Aug 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
52
88

I nt roduct ion Diabetes mellitus (DM) remains a significant cause of m orbidit y and m ortalit y (1) . Pa-t ients with DM are m ore suscept ible to de-veloping infect ions as well as m acro-and m icrovascular com plicat ions. I m m une sys-tem dysfunct ion associated with im m uno-suppression such as dysregulated or depressed phagocytosis, chem otaxis, and leukocyte binding is com m only seen in dia-betes (2) . Epidem iological data indicate that pat ients with Type 1 and Type 2 diabetes are m ore likely to be infected with pneumococcal and influenza infect ions. Diabet ic pat ients expe-rience a further severe clinical course during pneum ococcal and Haem ophilus influenzae infect ions than the non-diabet ic populat ions (3) . Mortality due to influenza infect ions is 2-4 t imes higher in diabet ic pat ients compared to the non-diabet ic populace. Pat ients with diabetes have presented higher hospitaliza-t ion rates (5.7-6.2% ) for pneumococcal in-fluenza as com pared to the non-diabet ic counterparts (4) . Pneum ococcal vaccine is associated with fewer deaths, hospitaliza-t ions, admissions to intensive care units, and higher recovery rates from respiratory fail-ure (4) . Mortality was reported in 25.7% of unvaccinated diabet ic pat ients hospitalized for pneum onia dur ing the influenza pan-dem ic between 1976 and 1978 in the Netherlands. The rates of hospitalizat ion and mortality in diabet ic pat ients are expected to decrease with pneum ococcal and influenza vaccinat ion programs (4-6) . The Am erican Diabetes Associat ion (ADA) and the Advisory Com m it tee on I m m uniza-t ion Pract ices (ACI P) recom m ends the pre-season influenza vaccine once every year and pneum ococcal vaccine at least once in a lifet im e in diabet ic pat ients. According to the current guideline of the Society of En-docrinology and Metabolism of Turkey, dia-bet ic pat ients m ust be vaccinated against influenza every year in the fall, against pneum ococcal infect ions at least once in a lifet im e, and hepat it is B vaccine should be given in 3 doses at 0, 1 and 6 m onths (7) . This study aim ed to determ ine the rates of vaccinat ion and the level of awareness for pneum ococcal, influenza, and hepat it is B vaccines in pat ients with Type 2 DM in İs-tanbul populat ion.
Materia l and Methods This cross-sect ional study included pat ients with Type 2 DM who presented to the out-pat ient Clinic of I nternal Diseases at Kartal Dr. Lüt fi Kırdar City Hospital İstanbul, Turkey between March and April 2020. Pat ients who were diagnosed with Type 2 di-abetes for at least one year were included in the study. Pat ients with Type1 diabetes, pregnant wom en, pat ients with act ive m a-lignancy, and severe neurological and psy-chiat r ic condit ions were excluded from the study. A total of 293 pat ients were included. After assessm ent at the outpat ient depart-m ent , a quest ionnaire enquir ing about the pat ient ’s vaccinat ion status, at t it ude, and awareness toward vaccinat ion for the last one year, which included item s about gen-der, age, diabetes durat ion (years) , was ob-tained. Besides dem ographic character ist ics, the pat ients were also quest ioned about previ-ous vaccinat ion, the nam e of vaccinat ion they had received ( if any) , whether a physi-cian recom m ended the vaccinat ion, and the reason for not being vaccinated. Data were recorded and analyzed using the Student ’s t - test , Mann-Whitney U test , Fisher ’s exact test , and the chi-squared test . For stat ist ical analysis, SPSS 18 software was used, and a p-value of less than 0.001 was considered significant . The Ethics Commit tee of Dr. Lüt fi Kırdar Kar-tal Cit y Hospital approved the study (26 February 2020, no 2020/ 514/ 172/ 2) . All the procedures conform ed to the ethical stan-dards of the Declarat ion of Helsinki.
Results A total of 293 [ 121 m en (41.3% ) and 172 wom en (58.7% ) pat ients; m ean age 65 years; m ean durat ion of diabetes 15 years] who presented to the outpat ient department of diabetes and m et the inclusion cr iter ia were enrolled in the study. The rate of vac-cinat ion was found to be a lit t le m ore than half, with 54.3 (n= 159) vaccinated and 45.7 (n= 134) unvaccinated pat ients (Table 1) . Am ong the unvaccinated group, the m ajor-ity of pat ients (67.3% ) stated unawareness about the vaccine to be the reason for being unvaccinated; the other reasons m ent ioned were unwillingness for vaccinat ion (17.5% ) , lack of physician’s recom m endat ion
328
Işık et al. Turk J Endocrinol Metab. Vaccinat ion Rates and Vaccine Awareness in Diabet ic I ndividuals 2020; 24: 327-334
3 2 8
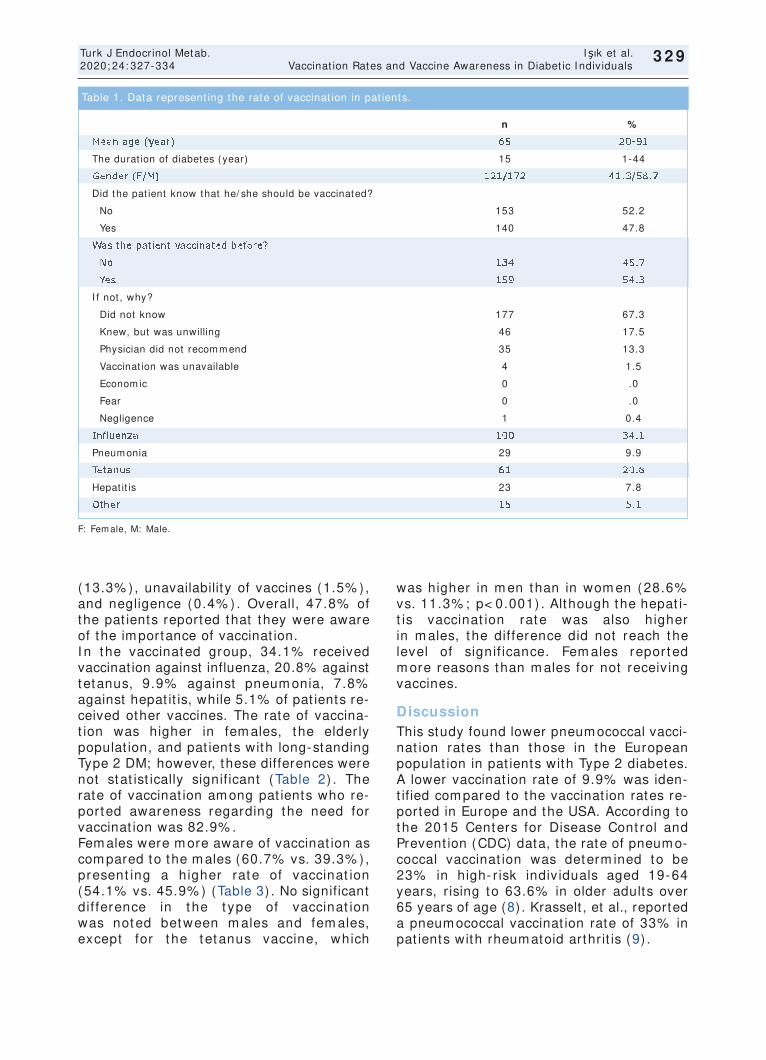
329
(13.3% ) , unavailabilit y of vaccines (1.5% ) , and negligence (0.4% ) . Overall, 47.8% of the pat ients reported that they were aware of the im portance of vaccinat ion. I n the vaccinated group, 34.1% received vaccinat ion against influenza, 20.8% against tetanus, 9.9% against pneum onia, 7.8% against hepat it is, while 5.1% of pat ients re-ceived other vaccines. The rate of vaccina-t ion was higher in fem ales, the elder ly populat ion, and pat ients with long-standing Type 2 DM; however, these differences were not stat ist ically signif icant (Table 2) . The rate of vaccinat ion am ong pat ients who re-ported awareness regarding the need for vaccinat ion was 82.9% . Fem ales were m ore aware of vaccinat ion as com pared to the m ales (60.7% vs. 39.3% ) , present ing a higher rate of vaccinat ion (54.1% vs. 45.9% ) (Table 3) . No significant dif ference in t he t ype of vaccinat ion was noted between m ales and fem ales, except for t he t etanus vaccine, which
was higher in m en than in wom en (28.6% vs. 11.3% ; p< 0.001) . Although the hepat i-t is vaccinat ion rate was also higher in m ales, the difference did not reach the level of signif icance. Fem ales repor ted m ore reasons than m ales for not receiv ing vaccines.
Discussion This study found lower pneum ococcal vacci-nat ion rates than those in the European populat ion in pat ients with Type 2 diabetes. A lower vaccinat ion rate of 9.9% was iden-t ified com pared to the vaccinat ion rates re-ported in Europe and the USA. According to the 2015 Centers for Disease Cont rol and Prevent ion (CDC) data, the rate of pneum o-coccal vaccinat ion was determ ined to be 23% in high- r isk indiv iduals aged 19-64 years, r ising to 63.6% in older adults over 65 years of age (8) . Krasselt , et al., reported a pneum ococcal vaccinat ion rate of 33% in pat ients with rheum atoid arthr it is (9) .
Turk J Endocrinol Metab. Işık et al. 2020; 24: 327-334 Vaccinat ion Rates and Vaccine Awareness in Diabet ic I ndividuals
3 2 9
F: Fem ale, M: Male.
n %
Mean age (year) 65 20-91
The durat ion of diabetes (year) 15 1-44
Gender (F/ M) 121/ 172 41.3/ 58.7
Did the pat ient know that he/ she should be vaccinated?
No 153 52.2
Yes 140 47.8
Was the pat ient vaccinated before?
No 134 45.7
Yes 159 54.3
I f not , why?
Did not know 177 67.3
Knew, but was unwilling 46 17.5
Physician did not recom m end 35 13.3
Vaccinat ion was unavailable 4 1.5
Econom ic 0 .0
Fear 0 .0
Negligence 1 0.4
I nfluenza 100 34.1
Pneum onia 29 9.9
Tetanus 61 20.8
Hepat it is 23 7.8
Other 15 5.1
Table 1. Data represent ing the rate of vaccinat ion in pat ients.

330
The rate of vaccinat ion against the flu was 34% in the present study. The CDC’s 2015 data declared the rate of vaccinat ion against influenza to be 44.8% in individuals aged 19 years and above (8) . According to the Euro-stat data, the vaccinat ion rate against in-fluenza in EU m em ber count r ies was 44.3% in 2017. Among the European Union, UK has the highest vaccinat ion rate of 72.6% against influenza (10) . A Germ an study re-ported a vaccinat ion rate of 53% against in-fluenza (9) . This study found that the level of awareness about vaccinat ion and the rate of vaccina-t ion were low in diabet ic pat ients. Unfortu-nately, the success rates seen in the adult populat ion worldwide are far from reaching those achieved for childhood vaccinat ion (5) . I n the present study, the rate of vaccine awareness was 47.8% among adult pat ients with Type 2 diabetes and a m ean age of 65.
Sim ilar to the present study, Canadian re-search on influenza vaccinat ion rates in 2009 found lower vaccinat ion rates than ex-pected in pat ients of all ages with or without diabetes, and 34-50% in the non-diabet ic populat ion (11) . A com puter-assisted tele-phonic survey in Aust ralia found low rates of immunizat ion coverage among individuals at high- r isk and chronic condit ions, being 47% for influenza and 31% for S. pneum oniae
(12) . Of the few studies on the rates of vaccina-t ion in the Turkish diabet ic populat ion, all re-ported unsat isfactory vaccinat ion rates (13,14) . I n the present study, vaccinat ion coverage included influenza in 34.1% , tetanus in 20.8% , pneumonia in 9.9% , hep-at it is in 7.8% , and other condit ions in 5.1% . Şahin, et al. docum ented the overall vacci-nat ion rates as 34% for influenza, 9.5% for pneum ococcal infect ions, and 10.6% for
Işık et al. Turk J Endocrinol Metab. Vaccinat ion Rates and Vaccine Awareness in Diabet ic I ndividuals 2020; 24: 327-334
3 3 0
Unvaccinated ( 1 0 9 ) Vaccinated ( 1 4 0 )
n % n % p
Age (year) 59.9 13.5 60.5 14.8 0.737
< 45 9 40.9 13 59.1 0.220
45-49 8 50 8 50
50-54 7 33.3 14 66.7
55-59 22 62.9 13 37.1
60-64 19 37.3 32 62.7
65-69 27 51.9 25 48.1
70-74 18 43.9 23 56.1
75-79 12 35.3 22 64.7
> 80 12 57.1 9 42.9
The durat ion of diabetes (years) 15 (1-42) 15.6 (1-15) 0.954
< 5 21 46.7 24 53.3 0.795
5-9 20 48.8 21 51.2
10-14 24 44.4 30 55.6
15-19 24 42.9 32 57.1
20-24 26 54.2 22 45.8
25-29 10 43.5 13 56.5
> 30 9 34.6 17 65.4
Gender
Male 48 39.7 73 60.3 0.81
Fem ale 86 50.0 86 50.0
Did the pat ient know that he/ she should be vaccinated?
No 110 71.9 43 28.1 < 0.001
Yes 24 26.9 116 82.9
Table 2. Character ist ics of the vaccinated and unvaccinated groups.
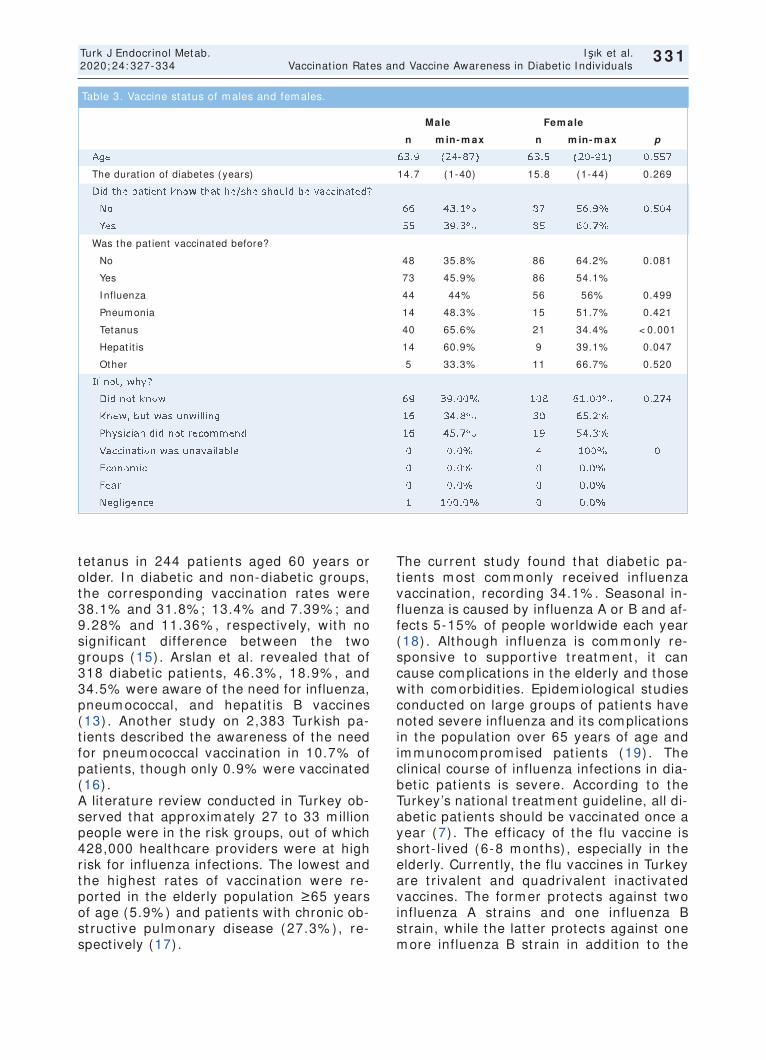
t etanus in 244 pat ients aged 60 years or older. I n diabet ic and non-diabet ic groups, the corresponding vaccinat ion rates were 38.1% and 31.8% ; 13.4% and 7.39% ; and 9.28% and 11.36% , respect ively, with no signif icant difference between the two groups (15) . Arslan et al. revealed that of 318 diabet ic pat ients, 46.3% , 18.9% , and 34.5% were aware of the need for influenza, pneum ococcal, and hepat it is B vaccines (13) . Another study on 2,383 Turkish pa-t ients described the awareness of the need for pneum ococcal vaccinat ion in 10.7% of pat ients, though only 0.9% were vaccinated (16) . A literature review conducted in Turkey ob-served that approxim ately 27 to 33 m illion people were in the r isk groups, out of which 428,000 healthcare providers were at high r isk for influenza infect ions. The lowest and the highest rates of vaccinat ion were re-ported in the elderly populat ion ≥65 years of age (5.9% ) and pat ients with chronic ob-st ruct ive pulm onary disease (27.3% ) , re-spect ively (17) .
The current study found that diabet ic pa-t ients m ost com m only received influenza vaccinat ion, recording 34.1% . Seasonal in-fluenza is caused by influenza A or B and af-fects 5-15% of people worldwide each year (18) . Although influenza is com m only re-sponsive to support ive t reatm ent , it can cause complicat ions in the elderly and those with com orbidit ies. Epidem iological studies conducted on large groups of pat ients have noted severe influenza and its complicat ions in the populat ion over 65 years of age and im m unocom prom ised pat ients (19) . The clinical course of influenza infect ions in dia-bet ic pat ients is severe. According to the Turkey’s nat ional t reatment guideline, all di-abet ic pat ients should be vaccinated once a year (7) . The eff icacy of the f lu vaccine is short - lived (6-8 m onths) , especially in the elderly. Current ly, the flu vaccines in Turkey are t r ivalent and quadr ivalent inact ivated vaccines. The form er protects against two influenza A st rains and one influenza B st rain, while the lat ter protects against one m ore influenza B st rain in addit ion to the
331
Turk J Endocrinol Metab. Işık et al. 2020; 24: 327-334 Vaccinat ion Rates and Vaccine Awareness in Diabet ic I ndividuals
3 3 1
Male Fem ale
n m in- m ax n m in- m ax p
Age 63.9 (24-87) 63.5 (20-91) 0.557
The durat ion of diabetes (years) 14.7 (1-40) 15.8 (1-44) 0.269
Did the pat ient know that he/ she should be vaccinated?
No 66 43.1% 87 56.9% 0.504
Yes 55 39.3% 85 60.7%
Was the pat ient vaccinated before?
No 48 35.8% 86 64.2% 0.081
Yes 73 45.9% 86 54.1%
I nfluenza 44 44% 56 56% 0.499
Pneum onia 14 48.3% 15 51.7% 0.421
Tetanus 40 65.6% 21 34.4% < 0.001
Hepat it is 14 60.9% 9 39.1% 0.047
Other 5 33.3% 11 66.7% 0.520
I f not , why?
Did not know 69 39.00% 108 61.00% 0.274
Knew, but was unwilling 16 34.8% 30 65.2%
Physician did not recom m end 16 45.7% 19 54.3%
Vaccinat ion was unavailable 0 0.0% 4 100% 0
Econom ic 0 0.0% 0 0.0%
Fear 0 0.0% 0 0.0%
Negligence 1 100.0% 0 0.0%
Table 3. Vaccine status of m ales and fem ales.

protect ion coverage of the t r ivalent vaccine. The protect ive effect of influenza vaccines begins 1-2 weeks after vaccinat ion and lasts for about 6-8 m onths or longer in healthy adults. This period is shorter in elderly and im m unosuppressed pat ients and is around 100 days. Since flu infect ions start to appear in Novem ber-Decem ber and cont inue unt il April-May in Turkey, vaccinat ion in October seem s to be a rat ional approach. I nternat ional author it ies such as the ADA, Wor ld Health Organizat ion, and ACI P rec-om m end influenza, hepat it is B, and pneu-m ococcal vaccines for all diabet ic pat ients. As per the New Global Vaccine Act ion Plan recom m endat ions, influenza vaccinat ion is targeted to reach 90% of the high- r isk indi-v iduals between 18 and 64 years and the ent ire populat ion above 65 years of age, in the United States. I n Turkey, the Minist ry of Health im plem ents the EPI (Expanded Pro-gram on I m m unizat ion) cam paign, em pha-sizing the im portance of vaccinat ion and providing support to high- r isk ( including DM) pat ients. Also, the 2019 Diabetes Mel-litus Diagnosis and Treatment Guideline, and the Turkish Diabetes Foundat ion 2019 Dia-betes Mellit us Diagnosis and Treatm ent Guideline recom m end vaccinat ion against influenza, pneumococcal, hepat it is B in indi-viduals with DM. The at t itude of healthcare personnel toward vaccinat ion is closely related to their ap-proach to the pat ient . Physicians who re-ceive the influenza vaccine recom m end vaccinat ion m ore often and take the vacci-nat ion procedure m ore ser iously (20) . A study in Spain reported an increm ental in-crease in vaccinat ion rates from 50.1% in 1993 to 63.7% in 2003, and 65% in 2010, for influenza. Factors that were found to in-crease vaccinat ion rates included advanced age, m ale sex, chronic diseases, and a visit to a physician in the last two weeks (21) . Low vaccinat ion rates in Turkey may be as-sociated with the ant i-vaccinat ion movement, also fueled by social media. The at t itude of health personnel, especially physicians and nurses, to diabet ic pat ients, may be benefi-cial in vaccinat ion. Health authorit ies must be more at tent ive to init iat ives and campaigns to counteract adverse media effects and pro-vide correct inform at ion to the com m unity, part icularly individual pat ients.
The pat ient ’s high response rate and per-cept ion level m ay be considered the st rength of the present study, thus providing valuable inform at ion for future nat ional im -m unizat ion st rategies. Another signif icant feature is the inclusion of elder ly (over 80 years of age) vaccinated pat ients with a reg-ular follow-up for 14-15 years. The reasons for a higher vaccinat ion rate am ong wom en m ay be at t r ibutable to m ore often hospital visits and a higher degree of willingness to vaccinate. The signif icant ly high rate of tetanus vaccinat ion am ong m ales m ay be credited to the rout ine vaccinat ion proce-dure after inj ur ies, which m en are m ore likely to sustain. The authors urge the physicians to be aware of their shortcomings before blam ing the pa-t ients. The authors deliberate that aware-ness am ong physicians m ust be raised first to do the sam e for their pat ients. I n this study, 13.3% of pat ients disclosed the lack of recom m endat ion for vaccinat ion by their physicians. Besides, increasing awareness depends st r ict ly on other sources’ engage-m ent , including health m anagers, m edia, and allied health care personnel. Nonethe-less, the authors thank the Minist ry of Health and diabetes associat ions’ keen ef-for t s for several years, because of which posit ive progress has already been achieved in adult vaccinat ions.
Lim itat ions Since the study was conducted in a tert iary health inst itut ion of the Kartal Dist r ict in İs-tanbul, it m ay not reflect the count ry’s ac-tual vaccinat ion rate. The m ajor it y of diabet ic pat ients seen in other provinces, outpat ient clinics, and fam ily health centers are likely to have low vaccinat ion rates. An-other lim itat ion of this study is the lack of integrat ion of vaccinat ion records into a na-t ional data network. Furtherm ore, pat ients who reported that they were unaware of why they had not received vaccinat ion should have been further quest ioned, which m ay have hinted to other factors affect ing vaccinat ions. Many pat ients m ight have been anxious about their responses to be negat ively evaluated by the physician if they disclosed the effect of social m edia and cul-tural m isbelieves and m ay have perhaps m isinform ed.
332
Işık et al. Turk J Endocrinol Metab. Vaccinat ion Rates and Vaccine Awareness in Diabet ic I ndividuals 2020; 24: 327-334
3 3 2

Conclusion
The level of awareness regarding vaccina-t ions is st ill a severe problem throughout t he wor ld, leading t o low vaccinat ion rates, as dem onst rated in t his study. Low vaccine awareness can be a signif icant rea-son for low vaccinat ion rat es. St udies on vaccine awareness are essent ial t o deter-m ine t he cur rent st at e of t he problem so t hat necessary st eps can be planned and init iated to raise awareness am ong indiv id-uals.
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conflicts of interest between the authors and/ or fam ily m em bers of the scient if ic and m edical com m it tee m em bers or m em -bers of the potent ial conflict s of interest , counseling, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions I dea/ Concept : Arzu Cennet Işık, Seydahmet Akın; Design: Arzu Cennet Işık, Seydahm et Akın, Nazire Aladağ; Cont rol/ Supervision: Seydahm et Akın, Ersin Engin Şimşek; Data Collect ion and/ or Processing: Arzu Cennet Işık , Seydahm et Akın; Analysis and/ or I n-terpretat ion: Seydahm et Akın; Literature Review: Arzu Cennet Işık; Writ ing the Art i-cle: Arzu Cennet Işık , Seydahm et Akın, Nazire Aladağ; Crit ical Review: Seydahm et Akın, Ersin Engin Şimşek; References and Fundings: Arzu Cennet Işık , Seydahm et Akın; Materials: Arzu Cennet Işık, Seydah-m et Akın, Nazire Aladağ.
References 1. Mahm ood SS, Levy D, Vasan RS, Wang TJ. The
Fram ingham Heart Study and the epidem iology of cardiovascular disease: a histor ical perspect ive. Lancet . 2014; 383: 999-1008. [ Crossref] [ PubMed] [ PMC]
2. Casqueiro J, Casqueiro J, Alves C. I nfect ions in pa-t ients with diabetes m ellitus: a review of pathogen-esis. I ndian J Endocr inol Metab. 2012; 16 Suppl 1: S27-S36. [ Crossref] [ PubMed] [ PMC]
3. Delam aire M, Maugendre D, Moreno M, Le Goff MC, Allannic H, Genetet B. I m paired leucocyte funct ions in diabet ic pat ients. Diabet Med. 1997; 14: 29-34. [ Crossref] [ PubMed]
4. Wang I K, Lin CL, Chang YC, Lin PC, Liang CC, Liu YL, Chang CT, Yen TH, Huang CC, Sung FC. Effec-t iveness of influenza vaccinat ion in elderly diabet ic pat ients: a ret rospect ive cohort study. Vaccine. 2013; 31: 718-724. [ Crossref] [ PubMed]
5. Giannat tasio A, Squeglia V, Lo Vecchio A, Russo MT, Barbar ino A, Car lom agno R, Guar ino A. Pneum o-coccal and influenza vaccinat ion rates and their de-term inants in children with chronic m edical condit ions. I tal J Pediat r. 2010; 36: 28. [ Crossref] [ PubMed] [ PMC]
6. Bouter KP, Diepersloot RJ, van Rom unde LK, Uit -slager R, Masurel N, Hoekst ra JB, Erkelens DW. Ef-fect of epidem ic influenza on ketoacidosis, pneum onia and death in diabetes m ellitus: a hospi-tal register survey of 1976-1979 in The Nether-lands. Diabetes Res Clin Pract . 1991; 12: 61-68. [ Crossref] [ PubMed]
7. Türkiye Diyabet Vakfı, Türk Diyabet Cem iyet i, Türkiye Endokr inoloj i ve Metabolizm a Derneği, Diyabet Hemşireliği Derneği. Diyabet ik Birey Aşılam a Rehberi. [ Link]
8. Williams WW, Lu PJ, O'Halloran A, Kim DK, Grohskopf LA, Pilishvili T, Skoff TH, Nelson NP, Harpaz R, Markowitz LE, Rodriguez-Lainz A, Fiebelkorn AP. Sur-veillance of vaccinat ion coverage among adult popu-lat ions - United States, 2015. MMWR Surveill Summ 2017; 66: 1-28. [ Crossref] [ PMC]
9. Krasselt M, I vanov JP, Baerwald C, Seifert O. Low vaccinat ion rates am ong pat ients with rheum atoid arthr it is in a Germ an outpat ient clinic. Rheum atol I nt . 2017; 37: 229-237. [ Crossref] [ PubMed]
10. EuroStat . 44% of elderly people vaccinated against influenza. 2019. (Date of Access: 31.03.2020) [ Link]
11. Quach S, Hamid JS, Pereira JA, Heidebrecht CL, Deeks SL, Crowcroft NS, Quan SD, Brien S, Kwong JC; Public Health Agency of Canada/ Canadian Inst i-tutes of Health Research Influenza Research Network Vaccine Coverage Theme Group. Influenza vaccina-t ion coverage across ethnic groups in Canada. CMAJ. 2012; 184: 1673-1681. [ Crossref] [ PubMed] [ PMC]
12. Dower J, Donald M, Begum N, Vlack S, Ozolins I . Pat terns and determ inants of influenza and pneu-m ococcal im m unisat ion am ong adults with chronic disease liv ing in Queensland, Aust ralia. Vaccine. 2011; 29: 3031-3037. [ Crossref] [ PubMed]
13. Arslan İE, Alt ınova A, Baloş Törüner F, Yalçın MM, Özkan Ç, Müjde NÇ, Arslan AM. Diyabet ik hastaların hepat it-B, influenza ve pnömokok aşı farkındalıkları. Gazi Med J. 2016; 27: 115-117. [ Link]
14. Satman I , Akalin S, Cakir B, Alt inel S; diaVAX Study Group. The effect of physicians' awareness on in-f luenza and pneum ococcal vaccinat ion rates and correlates of vaccinat ion in pat ients with diabetes in Turkey: an epidem iological Study "diaVAX". Hum Vaccin I m m unother. 2013; 9: 2618-2626. [ Crossref] [ PubMed] [ PMC]
333
Turk J Endocrinol Metab. Işık et al. 2020; 24: 327-334 Vaccinat ion Rates and Vaccine Awareness in Diabet ic I ndividuals
3 3 3
15. Sahin S, Tasar PT, Guclu YA, Sengul HS, Bozkurt N, Garip A, Dum an S, Akcicek F. Vaccinat ions rates in the elderly with diabetes m ellitus. Adv Aging Res. 2014; 3: 293-296. [ Crossref]
16. Ünal S, Durusu Tanrıöver M, Taş E, Güner İ, Çet in ÖY, Sayar İ. Aile hekim ler ine eğit im ver ilm esi ve aşilam a hedefler inin belir lenm esinin pnöm okok aşılanm a oranlar ı üzer ine etk iler i. Flora. 2015; 20: 10-15.
17. Ciblak MA; Grip Plat form u. I nfluenza vaccinat ion in Turkey: prevalence of r isk groups, current vaccina-t ion status, factors influencing vaccine uptake and steps taken to increase vaccinat ion rate. Vaccine. 2013; 31: 518-523. [ Crossref] [ PubMed]
18. Nicholson KG, Wood JM, Zam bon M. I nfluenza. Lancet . 2003; 362: 1733-1745. [ Crossref] [ PubMed]
19. Collins JP, Cam pbell AP, Openo K, Farley MM, Cum -m ings CN, Hill M, Schaffner W, Lindegren ML, Thom as A, Billing L, Bennet t N, Spina N, Bargsten
M, Lynfield R, Eckel S, Ryan P, Yousey-Hindes K, Her lihy R, Kir ley PD, Garg S, Anderson EJ. Out-com es of im m unocom prom ised adults hospitalized with laboratory-confirm ed influenza in the United States, 2011-2015. Clin I nfect Dis. 2020; 70: 2121-2130. [ Crossref] [ PubMed] [ PMC]
20. LaVela SL, Sm ith B, Weaver FM, Legro MW, Gold-stein B, Nichol K. At t itudes and pract ices regarding influenza vaccinat ion am ong healthcare workers providing services to individuals with spinal cord in-jur ies and disorders. I nfect Cont rol Hosp Epidem iol. 2004; 25: 933-940. [ Crossref] [ PubMed]
21. Jim enez-Truj illo I , López-de Andrés A, Hernández-Barrera V, Carrasco-Garr ido P, Santos-Sancho JM, Jim énez-García R. I nfluenza vaccinat ion coverage rates am ong diabetes sufferers, predictors of ad-herence and t im e t rends from 2003 to 2010 in Spain. Hum Vaccin I m m unother. 2013; 9: 1326-1332. [ Crossref] [ PubMed] [ PMC]
334
Işık et al. Turk J Endocrinol Metab. Vaccinat ion Rates and Vaccine Awareness in Diabet ic I ndividuals 2020; 24: 327-334
3 3 4

Dealing w ith COVI D- 1 9 : Through Endocrinologist ’s Eyes
Endokrinologların Gözüyle COVI D-19 ile Mücadele
Cem SULU, Pınar KADI OĞLU
Department of I nternal Medicine, Division of Endocrinology-Metabolism and Diabetes, İstanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine, İstanbul, TURKEY
Review Turk J Endocrinol Metab. 2020; 24: 335-42
I nt roduct ion Less than a year ago, none of us had heard of the novel coronavirus disease (COVID-19) and very few people were aware of the ex-istence of such v irus called “ coronavirus” ; however, today, it stays to the core of our daily lives. The World Health Organizat ion
declared COVI D-19 as pandem ic on 11 March, and since then, this global health problem cont inues to spread worldwide de-spite v igorous effor t s. Unexpectedly, this disast rous disease has united the m edical professions belonging to various specialt ies to fight against the disease in collaborat ion.
Less than a year ago, none of us had heard of novel coro-navirus disease (COVI D-19) . Today, it has become the main topic of our daily conversat ions. This disast rous disease has united the m edical professions belonging to various speci-alt ies to fight against the disease in collaborat ion. However, the exact role of endocrinologists st ill rem ains elusive. The coronavirus could potent ially infect organs other than the lungs, such as the pancreas, thyroid, adrenal glands, and pituitary, as reflected by var ious endocr inological m anife-stat ions. The direct invasion of organ system s and indirect m echanism s such as induct ion of autoim m unity could be responsible for the endocrinological consequences. A large body of literature on its pathophysiology, management , and associated condit ions is growing, and it s associat ion with endocrinological diseases is increasingly being recognized. However, data that would guide the proper m anagem ent of these endocrinological disorders during this novel pandem ic are st ill lacking. This review presented a br ief overview of the associat ion of COVI D-19 with endocrinological diseases and m ethods to ease the m anagem ent of som e frequent ly encountered endocrinological problem s. Keyw ords: COVI D-19; diabetes m ellitus; pituitary;
thyroid; adrenal insufficiency
Bir yıldan az bir süre önce hiçbir im iz yeni koronavirüs has-talığı (COVID-19) hakkında fikir sahibi değildik. Günümüzde ise bu hastalık hayat ım ızın m erkezine yerleşm iş vaziyet te. Virüsle m ücadele için çeşit li uzm anlık branşlarından hekim -ler bir araya geldiler. Bu topkeyün savaşta endokrinologlara düşen spesifik görevler henüz net değildir. Koronavirüs ak-ciğer dışında pankreas, t iroid, hipofiz bezi ve adrenal bezler gibi endokr in sistem e ait organlara da hasar vererek en-dokrinoloj ik sem ptom ve bulgulara yol açabilir. Endokrino-loj ik manifestasyonların alt ında yatan muhtemel mekanizma organ sistem lerinin virüs tarafından invazyonu ve otoimmü-nitenin tet ik lenm esi ile açıklanabilir. COVI D-19’un patofiz-yoloj isi, t edavisi ve eşlik eden kom orbit it eler hakkında literatür günden güne zenginleşm ekte, virüsün endokrino-loj ik hastalıklar ile olan ilişkiler ine ait farkındalık artm akta-dır. Buna karşın pandem inin seyr inde rast lanan endokr inoloj ik problem ler in akılcı yönet im i aydınlat ılm aya m uhtaçt ır. Bu derlem e COVI D-19 ile endokrinoloj ik hasta-lıkların arasındaki ilişkiye ışık tutmak ve COVI D-19 seyrinde sıkça rast lanılan endokrinoloj ik hastalıkların tedavisine yol gösterm ek am acıyla yazıldı. Anahtar kelim eler: COVI D-19; diabetes m ellitus; hipofiz;
t iroid; adrenal yetersizlik
3 3 5
Address for Correspondence: Pınar KADIOĞLU, Department of Internal Medicine, Division of Endocrinology-Metabolism and Diabetes, İstanbul University-Cerrahpaşa, Cerrahpaşa Faculty of Medicine, İstanbul, TURKEY
Phone: + 90 212 414 30 00 E- m ail: [email protected]
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 27 Jul 2020 Received in revised form : 23 Oct 2020 Accepted: 10 Nov 2020 Available online: 10 Dec 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
82
80

However, the part icular role of endocrinolo-gists is yet to be determ ined. The pathogenesis of COVID-19 involves the ent ry of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) into host cells through angiotensin-convert ing enzym e 2 (ACE2) . This enzyme acts as a receptor for SARS-CoV-2 and is found in various organs other than the lungs, such as the pancreas, thyroid, adrenal glands, and pituitary. The expression of ACE2 may explain endocrino-logical complicat ions of the virus. According to some but not all published data unt il date, pat ients with diabetes are apparent ly more prone to COVI D-19, and once they get in-fected, the prognosis is worse. This holds t rue for obese pat ients with COVI D-19, as they need m ore intensive care and intuba-t ion m ore readily. Moreover, the virus m ay itself locate in the thyroid gland, as the gland is st r ict ly cont iguous to the st ructures of the superior airway. I t can also cause subacute thyroidit is like any other viral infect ions. The consequent thyrotoxicosis may worsen car-diac instability, with increased morbidity. Se-r ious system ic infect ions also entail the possibilit y of the sick euthyroid syndrom e, further complicat ing the proper evaluat ion of thyroid funct ion tests. For any acute illness, COVID-19 may cause acute adrenal insuffi-ciency (AI ) , necessitat ing the im plem enta-t ion of glucocort icoids. I n addit ion to these, the virus can t r igger autoimmune processes that may have various endocrinological con-sequences. A wide spectrum of hormonal de-rangem ents caused by direct and indirect m echanism s m ay occur throughout the course of COVI D-19 and warrants endocri-nologists to take more responsibility on the front line. A large body of literature on it s pathophysiology, management , and associ-ated condit ions is growing; however, several unanswered quest ions rem ain concom i-tant ly, rendering COVID-19 st ill a hot topic. This review aim ed to present a br ief overview of the associat ion of COVI D-19 with endocrinological diseases and to guide endocrinologists encountering this disease.
COVI D- 1 9 and Diabetes Mellitus
Pat ients with diabetes are more prone to in-fect ious diseases because of mult iple pertur-bat ions of both innate and humoral immunity (1) . Previous viral pandem ics have proven
that diabetes has profound inhibitory effects on the immune system (2,3) . During SARS-CoV-1 (2002) and influenza A (2009) pan-dem ics, pat ients with diabetes m ore often suffered from complicat ions requiring hospi-talizat ion, needed more intensive care, and had a higher rate of m ortality than those without diabetes (4,5) . This will probably hold t rue for COVID-19 as more than half of severe cases have diabetes (6) . Num erous studies have reported a high prevalence of diabetes am ong pat ients with COVI D-19, with some of them reaching up to 37% (7) . Another study from I taly noted that diabetes was the second m ost com m on com orbidity associated with COVID-19 after hypertension (8) . Several postulated mechanisms exist re-garding this close relat ionship. Chronic hyperglycem ia and co-existent vis-ceral obesity induce a pro- inflam m atory m i-lieu that exerts negat ive effects on leukocyte chem otaxis and phagocytosis. Moreover, diabetes im pairs the secret ion of inflam m atory cytokines such as inter leukin 1, inter leukin 6, and tum or necrosis factor. I m m unoglobulins are glycosylated, a process that dim inishes their biological func-t ions (9) . Another possible explanat ion unique to COVID-19 can be an increased ex-pression of ACE2 because of t reatm ent with ACE inhibitors (ACEI ) and angiotensin re-ceptor blockers or de novo upregulat ion of this enzym e in pat ients with diabetes (10) . The associat ion of COVI D-19 with diabetes would be m ore com plex than expected. Ex-ocrine pancreas injury during severe COVID-19 infect ion has been speculated in 17% of pat ients as m anifested by increased serum amylase and/ or lipase (11) . Moreover, there are published data suggest ing that SARS-CoV- induced pancreat ic beta cell dam age can be responsible for the developm ent of acute diabetes in pat ients infected with SARS (12) . Although coronaviruses are not t ypically deem ed to play a role in the et iopathogenesis of type 1 diabetes mellitus, SARS-CoV and SARS-CoV-2 are potent ial environm ental t r iggers for the developm ent of type 1 diabetes m ellitus. This fact is sug-gest ive of a v icious cycle between COVI D-19 and diabetes. Drugs used for t reat ing COVI D-19 ( lopinavir and r itonavir) can in-crease insulin resistance and hence worsen glycem ic cont rol (13) .
336
Sulu et al. Turk J Endocrinol Metab. COVI D-19 and Endocrinological Disorders 2020; 24: 335-342
3 3 6
Some studies have ranked hypertension and cardiovascular diseases as the top- t ier r isk factors for a dism al prognosis of COVI D-19 (14) . Obesit y and cardiovascular diseases are well- known com orbidit ies in pat ients with diabetes (15) . Therefore, diabetes and its associated condit ions together m ake pa-t ients m ore suscept ible to COVI D-19 and worsen the outcome. Although there are hy-pothet ical concerns regarding the effects of renin angiotensin blockers and som e ant idi-abet ic t reatm ent on COVI D-19, no concrete evidence exists that suggest drug m odifica-t ion (13,16) . Met form in is protect ive against pneum onia through its im m unom odulatory and ant iproliferat ive effects in rat m odels (17) . I t also reduces the m ortality rate from COVI D-19 (18) . Pat ients with diabetes are advised to cont inue m et form in irrespect ive of their COVI D-19 status. ACE-2 has been believed to act as a recep-tor for the coronavirus (19) . Pioglitazone in-creases the expression of ACE-2. Therefore, som e clinicians avoid prescr ibing this drug in pat ients with diabetes infected with COVI D-19 (19) . I n a study that com pared sulfonylureas and thiazolidinediones, thiazo-lidinediones were found to be protect ive against pneum onia (20) . I n addit ion to pioglitazone, sodium -glucose co- t ransporter-2 inhibitors (SGLT-2i) , glucagon- like pept ide-1 receptor agonists (GLP-1Ra) , and insulin may increase the ex-pression of ACE-2 (19) . SGLT-2i and GLP-1Ra are shown to be beneficial in cardiovascular and renal complicat ions of di-abetes, which worsen the course of COVI D-19 (21,22) . The associat ion between ACE-2 expression and ant idiabet ic drugs repre-sents only a m inor it y of com plex interplay between diabetes t reatm ent and COVI D-19. I nflam m at ion plays a m ajor role during COVID-19. Dipept idyl pept idase 4 (DPP4) is expressed in various t issues, including the immune system. I t plays crucial funct ions in glucose and insulin homeostasis and in the propagat ion of inflam m at ion (23) . I n addi-t ion, it was suspected to act as a receptor for another coronavirus MERS-CoV (24) . High m ortality in pat ients with diabetes infected with MERS-CoV has been associated with DPP4-related immune dysregulat ion. Previ-ous studies have revealed their ant i- inflam-matory propert ies. However, the hypothesis
regarding their prevent ive funct ions against viral contam inat ion and at tenuated compli-cat ions remains to be established (23) . The robust relat ions between respiratory t ract in-fect ions and DPP4 inhibitors have not been completely conceptualized yet (25) . All these findings indicate a reasonable but poorly es-tablished relat ionship between DPP4 in-hibitors and COVID-19. The same is t rue for SGLT2 and pioglitazone (26,27) . Therefore, the possible role of ant idiabet ics in COVID-19 pathophysiology, course, and com plica-t ions has been suggested through various mechanisms. Some proposals are contradic-tory, as out lined above. To date, no concrete evidence exists to prefer one class of ant idi-abet ics over another. Another highly debated topic is the use of ACEI s and angiotensin I I receptor blockers (ARB) . Previous studies have indicated that the renin-angiotensin-aldosterone system (RAAS) inhibitors increase the expression of ACE2 , which acts as a receptor for coron-avirus invasion (28) . Hence, there have been concerns about the increased predis-posit ion to develop infect ion and increase the severity of COVI D-19. These drugs are essent ial in the t reatment of chronic compli-cat ions of diabetes. Several at tem pts have been m ade to elucidate the associat ions be-tween RAAS inhibitors and COVI D-19. Cur-rent data recom m end not to discont inue ACEI s or ARBs in the COVI D-19 pandem ic (29) . Further studies with a large num ber of pat ients are needed to draw definit ive con-clusions regarding COVI D-19, t reatm ent of diabetes, and its com plicat ions. Unt il then, pat ients with these condit ions should be in-st ructed to cont inue their usual care. Opt im al glycem ic cont rol is of great signifi-cance; all pat ients with COVI D-19 should have a baseline evaluat ion of glycem ic sta-tus. Am ong those with pr ior diabetes, st r ict blood glucose m onitor ing, and appropr iate intervent ions are m andatory. The “sick-day rules” need to be followed to overcom e im -m inent diabetes decom pensat ion. I f t his does not prevent the glycem ic status from get t ing worse, contact ing healthcare providers through telephone, e-m ail, or v ideo conference is recom m ended. The sam e rules of social distancing and personal hygiene for the community also met iculously apply to pat ients with diabetes.
337
Turk J Endocrinol Metab. Sulu et al. 2020; 24: 335-342 COVI D-19 and Endocrinological Disorders
3 3 7

COVI D- 1 9 and Obesity
The prevalence of obesity am ong pat ients hospitalized with COVI D-19 was 61.3% ; however, it may differ among different pop-ulat ions (30) . Hence, the effects of obesity on pat ients with COVID-19 remain to be elu-cidated. A meta-analysis confirmed that obe-sity m ight increase the r isk for hospitalizat ion, the need of invasive m e-chanical vent ilat ion, intensive care unit ad-m ission, and m ortalit y in pat ients with COVI D-19 (31) . The exact m echanism s through which obesity worsens COVI D-19 remain to be established. Moreover, severe obesity is associated with sleep apnea syn-drome and surfactant dysfunct ion that may complicate the disease course (15) . Despite unproven, chronic low-grade inflammat ion of abdominal obesity may disturb immune re-sponses through adipokines and cytokines such as tumor necrosis factor-alpha (32) . I t can also have deleterious effects on the lung parenchyma and bronchi, aggravat ing respi-ratory failure (32) . Several com orbidit ies such as diabetes mellitus, cardiovascular dis-eases, and m alignancy exist with obesity, which may increase COVID-19 severity (33) . These findings highlight the need for met ic-ulous prevent ive measures against COVI D-19 in obese people and increased awareness of the r isks that could worsen the prognosis.
COVI D- 1 9 and Thyroid Disease
Autoim m une thyroid disease is a com m on condit ion. Pat ients with both hyperact ive and hypoact ive thyroid seek m edical guid-ance irrespect ive of whether they belong to a high- r isk group. I n these pat ients, blood m onitor ing to adjust thyroid m edicat ions or ensure euthyroidism overcom es the r isk of COVI D-19 exposure. Fortunately, no firm evidence exists indicat-ing that pat ients with exist ing autoimmune thyroid disease are more prone to COVID-19 or thyroid disease itself worsens the outcome. The use of ant ithyroid drugs (ATD) dur ing COVID-19 pandemic presents a clinical chal-lenge. A precaut ionary approach should be followed while await ing further informat ion. The use of these medicat ions causes the r isk of agranulocytosis, a rare but fatal complica-t ion with an incidence rate of 2.4-15.4 cases per m illion populat ion/ year (34) . Pat ients with agranulocytosis experience severe neu-
t ropenia, which may, in turn, ease the pro-gression of COVI D-19 (35) . The symptoms of agranulocytosis, such as fever, sore throat , and m outh ulcerat ion, m ay overlap with that of COVID-19, hindering the differ-ent ial diagnoses between the two diseases. Pat ients on ATDs who exper ienced sym p-toms suggest ive of neut ropenia should dis-cont inue the drug and approach healthcare services for an urgent blood count (35) . I n these pat ients, test ing for COVID-19 should also be considered depending on the pres-entat ion. Thrombocytopenia and lymphocy-topenia are hematologic alterat ions observed throughout the COVID-19 course and do not warrant t reatm ent cessat ion (36) . I f a full blood count cannot be performed instant ly at the onset of sym ptom s suggest ive of neu-t ropenia, withdrawing ATD and restart ing after one week is recommended if the symp-tom s have disappeared (35) . I f sym ptom s reoccur, pat ients are st rongly advised to seek for urgent medical at tent ion for consid-ering alternat ive t reatments. Pat ients previously diagnosed with hypothy-roidism do not need any part icular precaut ion regarding COVI D-19. Thyroid replacem ent therapy should be cont inued as usual. I f a pat ient ’s condit ion worsen or there is signifi-cant weight change, thyroid funct ion test ing is recommended for dose modificat ion. Sim ilar to other system ic diseases, severe COVI D-19 is expected to cause low T3 syn-drom e, part icular ly if the infect ion involves the lower respiratory t ract (35,37) . This syn-drom e m ay be an adapt ive response to acute illnesses and current data are not in favor of specific intervent ion (38) . Subacute thyroidit is (SAT) is a self- lim ited thyroid disease, which is typically preceded by the upper respiratory t ract infect ion (39) . I t is character ized by neck pain, general sym ptom s, and thyroid dysfunct ion. SAT t reatm ent includes beta blockers, steroids, or nonsteroidal ant i- inflammatory drugs, de-pending on the clinical presentat ion. I nterim guidance from the World Health Organiza-t ion on the t reatm ent of COVI D-19 recom-m ends against the use of steroids if not indicated for another reason (40) . However, it is possible that thyrotoxicosis m ay nega-t ively affect COVI D-19. I n a case series, no pat ients who experienced severe discom fort and were t reated with steroids developed
338
Sulu et al. Turk J Endocrinol Metab. COVI D-19 and Endocrinological Disorders 2020; 24: 335-342
3 3 8

signs or sym ptom s suggest ive of COVI D-19 relapse during follow-up (41) . Therefore, it can be concluded that selected SAT pat ients m ay benefit from a low-dose regim en of steroid t reatm ent . This m ay overcom e neg-at ive outcom es associated with thyrotoxico-sis in pat ients with COVI D-19. Clusters of this disease were reported during outbreaks of the viral infect ion (42) ; there-fore, SAT cases may be increasingly reported in the near future. Thyrotoxicosis may cause tachycardia and impair cardiovascular func-t ions. A prompt evaluat ion of thyroid funct ion tests may allow early recognit ion and proper t reatm ent . SAT can present a few weeks after the respiratory t ract infect ion as a late complicat ion. Thus, monitoring thyroid func-t ion tests during COVID-19 follow-up is rea-sonable. As a general approach, pat ients with either hypo- and hyperthyroidism should take their medicat ions as usual. These rec-ommendat ions are based on expert opinions and not on meta-analyses or systemat ic re-views. Further studies are needed for more specific inst ruct ions about the approach to thyroid disease in pat ients with COVID-19.
COVI D- 1 9 and Adrenal I nsufficiency
Although several studies have reported that AI itself may increase the r isk of infect ion up to eight folds (43) , the current evidence does not specifically support the fact that pat ients with AI are part icularly prone to COVID-19. However, several plausible mechanisms are available, which may render pat ients with AI suscept ible to COVI D-19. AI im pairs first ly natural killer cell cytotoxicity; thus, compro-m ising ant iviral immune defense (44) . An in-crease in st ress- induced glucocort icoid plays a crucial role in the induct ion of the immune system, and the lack of this st imulant weak-ens the pr im ing of the im m une response (45) . I n cont rast , replacem ent with supra-physiologic doses of glucocort icoids leads to immunosuppression. Excess glucocort icoids m ay hinder the ident if icat ion of sym ptom s and signs of act ive infect ions, prevent ing the recognit ion of COVI D-19. Apparent ly, the causal relat ionship between AI and COVID-19 is not unidirect ional but rather bidirec-t ional. Viral sepsis m ay cause hem orrhage and thrombosis of adrenal vein and precipi-tate acute AI , which is a crucial cause of m ortalit y. Another rem arkable hypothesis
has been proposed about the m olecular m im icry between certain am ino acid se-quences by the SARS-CoV and the host adrenocort icot ropic horm one (ACTH) . Ac-cording to this hypothesis, ant ibodies pro-duced against the viral part icles will inadvertent ly dest roy the circulat ing ACTH, thereby rest r ict ing the st ress- induced cort i-sol r ise (46) . All these factors inherent ly ren-der pat ients with AI suscept ible to COVID-19 and in turn pat ients with COVID-19 to AI . I nfect ions precipitate adrenal crisis and are a major cause of death in pat ients with AI (47). Adrenal cr isis is described as a shock state and an inability of an organism to cope with acute st ress result ing from inadequate glu-cocort icoid response. Thus, all pat ients with AI should be educated appropriately to pre-vent such hazardous events. “Sick day rules” are a group of precaut ions that should be st rict ly followed during intercurrent acute ill-nesses. These include at least doubling the usual oral dose of glucocort icoids if a pat ient experiences symptoms suggest ive of COVID-19, such as cough, sputum, and fever. The doubled (or t r ipled) doses of glucocort icoids should be cont inued unt il all these symptoms resolve. I n addit ion, one needs to be ade-quately hydrated, preferably with electrolyte-containing fluids. These intervent ions are likely to prevent adrenal crisis and associated mortality. I f the clinical condit ion worsens de-spite these measures or if the oral route is com prom ised because of vom it ing or diar-rhea, pat ients should immediately reach the emergency healthcare set t ings for parenteral glucocort icoid replacement and hydrat ion. All pat ients with AI must ensure that they have enough supply of oral glucocort icoids, en-abling them to adjust the dosage properly in suspicion of COVID-19.
COVI D- 1 9 and Pituitary Diseases
COVID-19 has deeply affected the evaluat ion and treatment of pituitary disorders. Pituitary surgery, the t reatment of choice for the ma-jority of pituitary diseases, is part icularly af-fected because of diversion of healthcare resources from elect ive to urgent services. The pat ients requir ing pituitary surgery are likely to be vulnerable to COVI D-19. One possible explanat ion for this assum pt ion could be that Cushing’s disease causes im -mune suppression and diabetes. I n addit ion,
339
Turk J Endocrinol Metab. Sulu et al. 2020; 24: 335-342 COVI D-19 and Endocrinological Disorders
3 3 9

both acrom egaly and Cushing’s disease cause cardiovascular comorbidity, which are evident risk factors for more severe infect ion. The decision, t im ing, and postoperat ive fol-low-up of pat ients with pituitary diseases pose a significant clinical challenge to clini-cians even in the rout ine pract ice. Pituitary centers should cont inuously update their pro-tocols according to the rapidly evolving course of COVID-19. As a general approach, the risks must be carefully balanced against the natural history of a pituitary disease. Considering irreversible morbidity such as vi-sion loss in a pat ient with pituitary apoplexy can overcome undue delays. I n cont rast , a more flexible approach to asymptomat ic pa-t ients with prolact inoma could protect the pa-t ients from excessive exposure to COVID-19. Sim ilar to the Pituitary Society, we are in favor of st rat ify ing cases as em ergent , ur-gent , and elect ive. Decisions should be m ade on a case basis. Pituitary apoplexy and acute severe signif icant m ass effect such as vision loss or suspicion of m alignant pathology are clear indicat ions for emergent intervent ion. Urgent surgery can benefit se-lected pat ients who have slow-progressive visual com prom ise, funct ioning tum ors with aggressive clinical features, and unclear di-agnosis. Pat ients with incidental and asymp-tom at ic tum ors, nonfunct ioning adenom as, and funct ioning tum ors adequately con-t rolled with m edical therapy do not need ur-gent t reatm ent . These pat ients can be scheduled for a later t im e. For pat ients whose surgery is deferred to a later t im e and decided to be followed up with m edical t reatm ent , the choice of m ed-ical t reatm ent m ay have som e im plicat ions regarding the COVID-19. Pasireot ide, for ex-am ple, m ay act synergist ically with drugs used in COVI D-19 t reatm ent (azithromycin and hydroxychloroquine) and could prolong the corrected QT interval. Moreover, this drug m ay cause hyperglycem ia and thus re-quire close m onitor ing at the beginning of t reatm ent . This m ay expose the pat ient to COVI D-19. Hence, the decision to init iate pasireot ide should be reconsidered carefully dur ing this novel pandem ic and should be reserved for highly resistant cases. Other som atostat in receptor ligands, requir ing healthcare staff support for adm inist rat ion, m ay be allowed to be scheduled m ore fre-
quent ly for avoiding fur ther exposure, de-pending on the clinical context . The approach to the m edical t reatm ent of various pituitary diseases should be ad-dressed separately. For exam ple, pat ients with prolact inoma can be init iated and con-t inued safely with dopam ine agonists unt il they do not have com plaints necessitat ing em ergent intervent ion. The m edical m an-agement of Cushing’s disease is not as easy as a prolact inom a. These pat ients have in-herent r isk factors for COVI D-19 and the m edical t reatm ent used tem porarily m ay precipitate AI in excessive doses. Thus, ini-t ial doses should be the lowest as possible and t it rated according to the clinical response with more at tent ion on imminent AI in case of over t reatment . I t should be kept in m ind that m ild hypercort isolem ia m ay be bet ter than the adrenal crisis in the short term (48) . Pat ients should be informed about withdraw-ing the t reatment for some t ime if they ex-perience fever. I n addit ion, they should be educated about the t im ing and dosing of glu-cocort icoid adm inist rat ion when there are symptoms suggest ive of COVID-19. Hypopituitar ism is also a crucial issue. Prin-ciples of glucocort icoid and thyroid hormone replacem ent are depicted in respect ive sect ions above. Testosterone and est rogen adm inist rat ion and growth horm one re-placem ents can be delayed; however, ade-quate testosterone levels should be ensured in m en and insulin- like growth factor 1 should be m aintained within norm al lim it s whenever biochem ical test ing is feasible (49) .
Conclusion Several reports are being published about COVI D-19 and its associat ions; however, data regarding COVID-19 and endocrine dis-eases are relat ively scarce. I n addit ion to en-couraging pat ients to adhere to basic rules for protect ing themselves from the disease through social distancing and self-hygiene, endocrinologists have addit ional tasks. Avoiding unnecessary rout ine appointments and reinforcing online consultat ions are cor-nerstones of a prevent ive st rategy. The close monitoring of pat ients with AI or diabetes is crucial as COVI D-19 m ay deeply affect glycemic control and increase the risk of ad-renal cr isis. Parenteral glucocort icoid re-
340
Sulu et al. Turk J Endocrinol Metab. COVI D-19 and Endocrinological Disorders 2020; 24: 335-342
3 4 0

placement in pat ients with AI should not be delayed if a pat ient ’s clinical condit ion dete-r iorates. Educat ion on “sick day rules” can prevent disast rous consequences. Pat ients with thyroid disease should cont inue their rout ine m edicat ions. The r isk-benefit rat io should be carefully considered in pat ients with pituitary disorders, and intervent ions should be determ ined on a case basis de-pending on the severity of clinical features. Future studies on more specific aspects of the associat ion between COVI D-19 and en-docrinological diseases are warranted.
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions All authors cont r ibuted equally while this study preparing.
References 1. Singh AK, Gupta R, Ghosh A, Misra A. Diabetes in
COVI D-19: Prevalence, pathophysiology, prognosis and pract ical considerat ions. Diabetes Metab Syndr. 2020; 14: 303-310. [ Crossref] [ PubMed] [ PMC]
2. Chan-Yeung M, Xu RH. SARS: epidem iology. Respirol-ogy. 2003; 8: S9-S14. [ Crossref] [ PubMed] [ PMC]
3. Morra ME, Van Thanh L, Kam el MG, Ghazy AA, Alt ibi AMA, Dat LM, Thy TNX, Vuong NL, Mostafa MR, Ahm ed SI , Elabd SS, Fathim a S, Le Huy Vu T, Om rani AS, Mem -ish ZA, Hirayam a K, Huy NT. Clinical outcom es of cur-rent m edical approaches for Middle East respiratory syndrom e: a system at ic review and m eta-analysis. Rev Med Virol. 2018; 28: e1977. [ Crossref] [ PubMed] [ PMC]
4. Yang JK, Feng Y, Yuan MY, Yuan SY, Fu HJ, Wu BY, Sun GZ, Yang GR, Zhang XL, Wang L, Xu X, Xu XP, Chan JC. Plasm a glucose levels and diabetes are independent predictors for m ortalit y and m orbidity in pat ients with SARS. Diabet Med. 2006; 23: 623-628. [ Crossref] [ PubMed]
5. Allard R, Leclerc P, Trem blay C, Tannenbaum TN. Dia-betes and the severity of pandem ic influenza A (H1N1)
infect ion. Diabetes Care. 2010; 33: 1491-1493. [ Cross-ref] [ PubMed] [ PMC]
6. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS; China Medical Treatm ent Expert Group for Covid-19. Clinical character ist ics of coronavirus disease 2019 in China. N Engl J Med. 2020; 382: 1708-1720. [ Crossref] [ PubMed] [ PMC]
7. Rhee EJ, Kim JH, Moon SJ, Lee WY. Encounter ing COVI D-19 as endocr inologists. Endocr inol Metab (Seoul) . 2020; 35: 197-205. [ Crossref] [ PubMed] [ PMC]
8. Gent ile S, St rollo F, Cer iello A. COVI D-19 infect ion in I talian people with diabetes: Lessons learned for our fu-ture (an experience to be used) . Diabetes Res Clin Pract . 2020; 162: 108137. [ Crossref] [ PubMed] [ PMC]
9. I acobellis G. COVI D-19 and diabetes: can DPP4 inhibi-t ion play a role? Diabetes Res Clin Pract . 2020; 162: 108125. [ Crossref] [ PubMed] [ PMC]
10. Fang L, Karakiulakis G, Roth M. Are pat ients with hy-pertension and diabetes m ellit us at increased r isk for COVID-19 infect ion? Lancet Respir Med. 2020; 8(4) : e21. [ Crossref] [ PubMed] [ PMC]
11. Liu F, Long X, Zhang B, Zhang W, Chen X, Zhang Z. ACE2 expression in pancreas m ay cause pancreat ic dam age after SARS-CoV-2 infect ion. Clin Gast roenterol Hepatol. 2020; 18: 2128-2130. [ Crossref] [ PubMed] [ PMC]
12. Yang JK, Lin SS, Ji XJ, Guo LM. Binding of SARS coron-avirus to its receptor dam ages islets and causes acute diabetes. Acta Diabetol. 2010; 47: 193-199. [ Crossref] [ PubMed] [ PMC]
13. Pal R, Banerjee M. COVID-19 and the endocrine system: explor ing the unexplored. J Endocr inol I nvest . 2020; 43: 1027-1031. [ Crossref] [ PubMed] [ PMC]
14. Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, Ji R, Wang H, Wang Y, Zhou Y. Prevalence of com orbidit ies and its effects in pat ients infected with SARS-CoV-2: a system-at ic review and m eta-analysis. I nt J I nfect Dis. 2020; 94: 91-95. [ Crossref] [ PubMed] [ PMC]
15. Puig-Dom ingo M, Marazuela M, Giust ina A. COVI D-19 and endocrine diseases. A statement from the European Society of Endocr inology. Endocr ine. 2020; 68: 2-5. [ Crossref] [ PubMed] [ PMC]
16. Bassendine MF, Bridge SH, McCaughan GW, Gorrell MD. COVI D-19 and com orbidit ies: a role for dipept idyl pep-t idase 4 (DPP4) in disease sever it y? J Diabetes. 2020; 12: 649-658. [ Crossref] [ PubMed]
17. Kaj iwara C, Kusaka Y, Kim ura S, Yam aguchi T, Nanjo Y, I shii Y, Udono H, Standiford TJ, Tateda K. Met form in me-diates protect ion against Legionella pneum onia through act ivat ion of AMPK and m itochondrial react ive oxygen species. J I m m unol. 2018; 200: 623-631. [ Crossref] [ PubMed]
18. Hariyanto TI , Kurniawan A. Met form in use is associated with reduced m ortalit y rate from coronavirus disease 2019 (COVI D-19) infect ion. Obes Med. 2020; 19: 100290. [ Crossref] [ PubMed] [ PMC]
19. Pal R, Bhansali A. COVI D-19, diabetes m ellit us and ACE2: the conundrum . Diabetes Res Clin Pract . 2020; 162: 108132. [ Crossref] [ PubMed] [ PMC]
20. Gorricho J, Garjón J, Alonso A, Celaya MC, Saiz LC, Ervit i J, López A. Use of oral ant idiabet ic agents and r isk of com m unity-acquired pneum onia: a nested case-con-t rol study. Br J Clin Pharm acol. 2017; 83: 2034-2044. [ Crossref] [ PubMed] [ PMC]
341
Turk J Endocrinol Metab. Sulu et al. 2020; 24: 335-342 COVI D-19 and Endocrinological Disorders
3 4 1

21. Prat t ichizzo F, La Sala L, Rydén L, Marx N, Ferr ini M, Valensi P, Ceriello A. Glucose- lowering therapies in pa-t ients with type 2 diabetes and cardiovascular diseases. Eur J Prev Cardiol. 2019; 26: 73-80. [ Crossref] [ PubMed]
22. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao B. Clinical course and r isk factors for m ortalit y of adult inpat ients with COVI D-19 in Wuhan, China: a ret rospect ive cohort study. Lancet . 2020; 395: 1054-1062. [ Crossref] [ PubMed] [ PMC]
23. Valencia I , Peiró C, Lorenzo Ó, Sánchez-Ferrer CF, Eckel J, Rom acho T. DPP4 and ACE2 in diabetes and COVI D-19: therapeut ic targets for cardiovascular com plica-t ions? Front iers in Pharm acology. 2020; 11: 1161. [ Crossref] [ PubMed] [ PMC]
24. Raj VS, Mou H, Sm its SL, Dekkers DH, Müller MA, Dij k-m an R, Muth D, Dem m ers JA, Zaki A, Fouchier RA, Thiel V, Drosten C, Rot t ier PJ, Osterhaus AD, Bosch BJ, Haag-m ans BL. Dipept idyl pept idase 4 is a funct ional receptor for the em erging hum an coronavirus-EMC. Nature. 2013; 495: 251-254. [ Crossref] [ PubMed] [ PMC]
25. Yang W, Cai X, Han X, Ji L. DPP-4 inhibitors and r isk of infect ions: a meta-analysis of randomized cont rolled t r i-als. Diabetes Metab Res Rev. 2016; 32: 391-404. [ Cross-ref] [ PubMed]
26. Am in EF, Rifaai RA, Abdel-Lat if RG. Em pagliflozin at ten-uates t ransient cerebral ischem ia/ reperfusion injury in hyperglycem ic rats via repressing oxidat ive- inflam m a-tory-apoptot ic pathway. Fundam Clin Pharm acol. 2020; 34: 548-558. [ Crossref] [ PubMed]
27. Ceriello A. Thiazolidinediones as ant i- inflam m atory and ant i-atherogenic agents. Diabetes Metab Res Rev. 2008; 24: 14-26. [ Crossref] [ PubMed]
28. Diaz JH. Hypothesis: angiotensin-convert ing enzyme in-hibitors and angiotensin receptor blockers may increase the r isk of severe COVI D-19. J Travel Med. 2020; 27: taaa041. [ Crossref] [ PubMed] [ PMC]
29. Mehta N, Kalra A, Nowacki AS, Anjewierden S, Han Z, Bhat P, Carm ona-Rubio AE, Jacob M, Procop GW, Har-r ington S, Milinovich A, Svensson LG, Jehi L, Young JB, Chung MK. Associat ion of use of angiotensin-convert ing enzym e inhibitors and angiotensin I I receptor blockers with test ing posit ive for coronavirus disease 2019 (COVI D-19) . JAMA Cardiol. 2020; 5: 1020-1026. [ Cross-ref] [ PubMed] [ PMC]
30. Pet t it NN, MacKenzie EL, Ridgway JP, Pursell K, Ash D, Patel B, Pho MT. Obesit y is associated with increased r isk for m ortalit y am ong hospitalized pat ients with COVI D-19. Obesit y (Silver Spr ing) . 2020; 28: 1806-1810. [ Crossref] [ PubMed] [ PMC]
31. Huang Y, Lu Y, Huang YM, Wang M, Ling W, Sui Y, Zhao HL. Obesity in pat ients with COVI D-19: a systemat ic re-v iew and m eta-analysis. Metabolism . 2020; 113: 154378. [ Crossref] [ PubMed] [ PMC]
32. Zhang X, Zheng J, Zhang L, Liu Y, Chen GP, Zhang HP, Wang L, Kang Y, Wood LG, Wang G. System ic inflam -m at ion m ediates the det r im ental effects of obesity on asthm a cont rol. Allergy Asthm a Proc. 2018; 39: 43-50. [ Crossref] [ PubMed]
33. Muscogiur i G, Pugliese G, Barrea L, Savastano S, Colao A. Com m entary: obesity: the "Achilles heel" for COVI D-19? Metabolism . 2020; 108: 154251. [ Crossref] [ PubMed] [ PMC]
34. Curt is BR. Non-chem otherapy drug- induced neut rope-nia: key points to m anage the challenges. Hem atology Am Soc Hem atol Educ Program . 2017; 2017: 187-193. [ Crossref] [ PubMed] [ PMC]
35. Boelaert K, Visser WE, Taylor PN, Moran C, Léger J, Per-sani L. Endocr inology in the t im e of COVI D-19: m an-agem ent of hyperthyroidism and hypothyroidism . Eur J Endocrinol. 2020; 183: G33-G39. [ Crossref] [ PubMed]
36. Terpos E, Ntanasis-Stathopoulos I , Elalamy I , Kastrit is E, Sergentanis TN, Politou M, Psaltopoulou T, Gerotziafas G, Dim opoulos MA. Hem atological findings and com pli-cat ions of COVI D-19. Am J Hem atol. 2020; 95: 834-847. [ Crossref] [ PubMed] [ PMC]
37. Fliers E, Bianco AC, Langouche L, Boelen A. Thyroid funct ion in cr it ically ill pat ients. Lancet Diabetes En-docrinol. 2015; 3: 816-825. [ Crossref] [ PubMed] [ PMC]
38. Dworakowska D, Grossm an AB. Thyroid disease in the t im e of COVI D-19. Endocr ine. 2020; 68: 471-474. [ Crossref] [ PubMed] [ PMC]
39. Nishihara E, Ohye H, Am ino N, Takata K, Ar ishim a T, Kudo T, I to M, Kubota S, Fukata S, Miyauchi A. Clinical character ist ics of 852 pat ients with subacute thyroidit is before t reatm ent . I ntern Med. 2008; 47: 725-729. [ Crossref] [ PubMed]
40. WHO. Clinical m anagem ent of severe acute respiratory infect ion (SARI ) when COVI D-19 disease is suspected: inter im guidance, 13 March 2020. World Health Organ-izat ion; 2020. [ Link]
41. Brancatella A, Ricci D, Cappellani D, Viola N, Sgrò D, Sant ini F, Lat rofa F. I s subacute thyroidit is an underes-t imated manifestat ion of SARS-CoV-2 infect ion? Insights from a case ser ies. J Clin Endocr inol Metab. 2020; 105: dgaa537. [ Crossref] [ PubMed] [ PMC]
42. Desailloud R, Hober D. Viruses and thyroidit is: an up-date. Virol J. 2009; 6: 5. [ Crossref] [ PubMed] [ PMC]
43. Tresoldi AS, Sum ilo D, Perr ins M, Toulis KA, Prete A, Reddy N, Wass JAH, Ar lt W, Nirantharakum ar K. I n-creased infect ion r isk in Addison's disease and congen-ital adrenal hyperplasia. J Clin Endocr inol Metab. 2020; 105: 418-429. [ Crossref] [ PubMed] [ PMC]
44. Edvardsen K, Bjånesøy T, Hellesen A, Breivik L, Bakke M, Husebye ES, Brat land E. Peripheral blood cells from pa-t ients with autoimmune Addison's disease poorly respond to interferons in vit ro, despite elevated serum levels of interferon- inducible chem okines. J I nterferon Cytokine Res. 2015; 35: 759-770. [ Crossref] [ PubMed] [ PMC]
45. I sidori AM, Arnaldi G, Boscaro M, Falorni A, Giordano C, Giordano R, Pivonello R, Pofi R, Hasenm ajer V, Venneri MA, Sbardella E, Sim eoli C, Scaroni C, Lenzi A. COVI D-19 infect ion and glucocort icoids: update from the I talian Society of Endocrinology Expert Opinion on steroid re-placem ent in adrenal insufficiency. J Endocrinol I nvest . 2020; 43: 1141-1147. [ Crossref] [ PubMed] [ PMC]
46. Wheat land R. Molecular m im icry of ACTH in SARS - im -plicat ions for cort icosteroid t reatm ent and prophylaxis. Med Hypotheses. 2004; 63: 855-862. [ Crossref] [ PubMed] [ PMC]
47. Hahner S, Loeffler M, Bleicken B, Drechsler C, Milo-vanovic D, Fassnacht M, Ventz M, Quinkler M, Allolio B. Epidem iology of adrenal cr isis in chronic adrenal insuf-ficiency: the need for new prevent ion st rategies. Eur J Endocrinol. 2010; 162: 597-602. [ Crossref] [ PubMed]
48. Fleseriu M, Buchfelder M, Cetas JS, Fazeli PK, Mallea-Gil SM, Gurnell M, McCormack A, Pineyro MM, Syro LV, Tritos NA, Marcus HJ. Pituitary society guidance: pituitary disease management and pat ient care recommendat ions during the COVID-19 pandemic-an international perspective. Pi-tuitary. 2020; 23: 327-337. [ Crossref] [ PubMed] [ PMC]
49. Fleseriu M, Hashim I A, Karavitaki N, Melm ed S, Murad MH, Salvatori R, Sam uels MH. Horm onal replacem ent in hypopituitar ism in adults: an Endocrine Society Clinical Pract ice Guideline. J Clin Endocr inol Metab. 2016; 101: 3888-3921. [ Crossref] [ PubMed]
342
Sulu et al. Turk J Endocrinol Metab. COVI D-19 and Endocrinological Disorders 2020; 24: 335-342
3 4 2

Glucagon- Like Polypept ide- 1 and Brain Glukagon Benzeri Polipept id-1 ve Beyin
Okan Sefa BAKI NER, Akadlı Kürşad ÖZŞAHİN*
Department of Endocrinology and Metabolism Diseases, Başkent University Faculty of Medicine, Ankara, TURKEY * Department of Family Physician, Başkent University Faculty of Medicine, Ankara, TURKEY
Review Turk J Endocrinol Metab. 2020; 24: 343-355
I nt roduct ion Glucagon- like polypept ide-1 (GLP-1) is m ainly produced in the sm all intest inal en-tero-endocrine cells, pancreat ic alpha cells, and the nucleus t ractus solitar i (NTS) of the cent ral nervous system , using pre-proglucagon as a precursor. I t can be re-leased after conversion by prohorm one convertase, and in less than 2 m in, is broken down and inact ivated by dipept idyl pept i-dase-4 (DPP-4) . I n the circulat ion, GLP-1 can freely pass the blood-brain barr ier (BBB) , although only 20% reaches the brain
owing it s short half- life in circulat ion (hu-m oral pathway) (1,2) . I ndust r ially produced GLP-1 receptor agonists (GLP-1RA) can pass the BBB, whereas DPP-4 inhibitors cannot (3) . The im portant effects of GLP-1 in the brain have recent ly been discovered. I t was ob-served that the main sources of GLP-1 in the brain were the neurons that expressed pre-proglucagon in the NTS (4) . Unlike the in-test inal enteroendocr ine cells, which are st im ulated by food, these cells are act ivated with gast r ic distent ion, system ic cholecys-
Glucagon- like polypept ide-1 has specific effects on the cen-t ral nervous system , including regulat ion of glucose m eta-bolism , posit ive cardiovascular effects, slowing intest inal mot ility, immune modulat ion, and regulat ion of appet ite and energy expenditure. Recent ly, posit ive effects of GLP-1 on brain energy ut ilizat ion, inhibit ion and restorat ion of neuro-degenerat ion, response to st ress, and protect ion against ischem ic neuron dam age have been dem onst rated. Herein, the effects of glucagon- like polypept ide-1 on the cent ral nervous system will be discussed. Keyw ords: Glucagon- like polypept ide-1;
brain; cent ral nervous system ; neurodegenerat ion; st roke
Glukagon benzeri pept id 1’in glukoz bağım lı insülin sekres-yonu, beta hücre proliferasyonu, glukagon sekresyon inhi-biyonu ile hepat ik glukoz çıkışının azalm ası gibi m etabolik etkiler inin yanında kardiyovasküler sistem üzerine olum lu etkiler, gast rointest inal m ot ilitede yavaşlam a, im m unom o-dülasyon gibi etkiler i olduğu bilinm ektedir. Son zam anlarda sant ral sinir sistem i üzer ine de belirgin etk iler gösterdiği saptanmışt ır. Sant ral etkiler esas olarak iştah regülasyonu ve m etabolizm a üzerine olan etkiler in dışında beyin enerj i kullanım ının düzenlenm esi, nörodejenerasyonun önlenm esi ve düzelt ilmesi, iskem ik nöron hasarına karşı koruma ve or-ganizm anın st rese olan cevabının düzenlenm esi şeklinde sı-ralanabilir. Burada glukagon benzeri pept id 1’in sant ral sinir sistem i üzerine olan etkiler i tart ışılacakt ır. Anahtar kelim eler: Glukagon benzeri pept id 1;
beyin; m erkezi sinir sistem i; nörodejenerasyon; inm e
3 4 3
Address for Correspondence: Okan Sefa BAKI NER, Departm ent of Endocrinology and Metabolism Diseases, Başkent University Adana Dr. Turgut Noyan Applicat ion and Research Center, Adana, TURKEY
Phone: + 90 530 222 16 98 E- m ail: okansefabakiner@gm ail.com
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 13 Jun 2020 Received in revised form : 25 Jul 2020 Accepted: 11 Aug 2020 Available online: 30 Sep 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
73
62
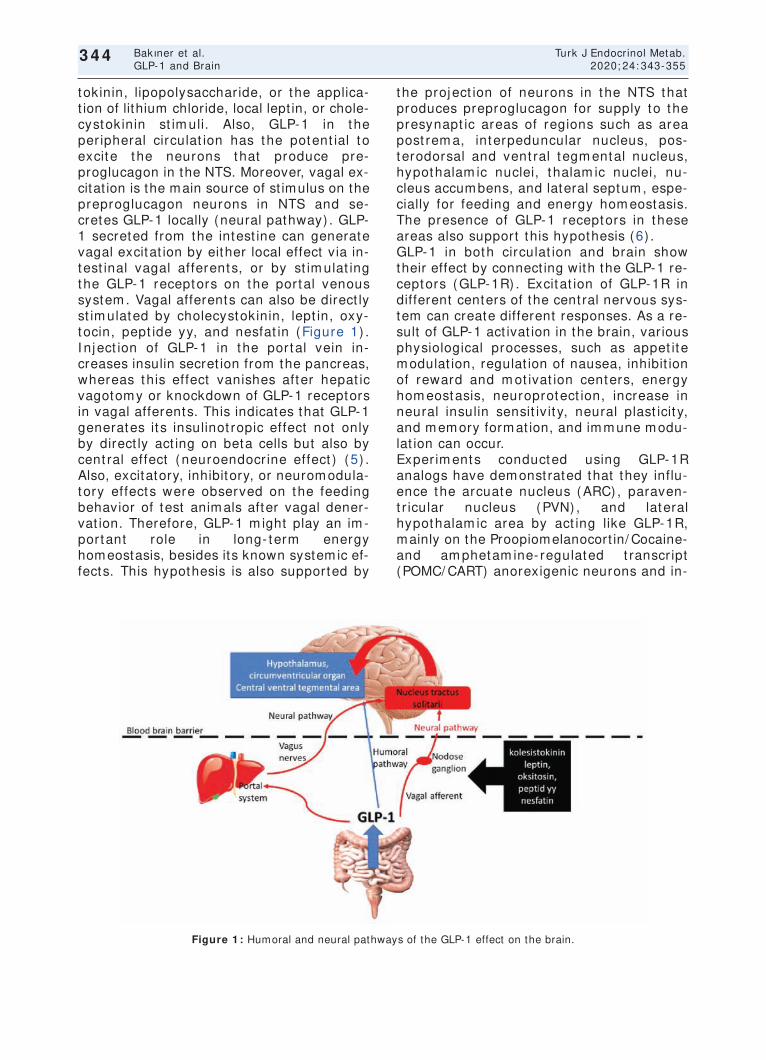
tokinin, lipopolysacchar ide, or the applica-t ion of lithium chloride, local lept in, or chole-cystokinin st im uli. Also, GLP-1 in the per ipheral circulat ion has the potent ial to excite the neurons that produce pre-proglucagon in the NTS. Moreover, vagal ex-citat ion is the main source of st imulus on the preproglucagon neurons in NTS and se-cretes GLP-1 locally (neural pathway) . GLP-1 secreted from the intest ine can generate vagal excitat ion by either local effect via in-test inal vagal afferents, or by st im ulat ing the GLP-1 receptors on the portal venous system . Vagal afferents can also be direct ly st im ulated by cholecystokinin, lept in, oxy-tocin, pept ide yy, and nesfat in (Figure 1) . I nj ect ion of GLP-1 in the portal vein in-creases insulin secret ion from the pancreas, whereas this effect vanishes after hepat ic vagotomy or knockdown of GLP-1 receptors in vagal afferents. This indicates that GLP-1 generates it s insulinot ropic effect not only by direct ly act ing on beta cells but also by cent ral effect (neuroendocr ine effect ) (5) . Also, excitatory, inhibitory, or neurom odula-tory effects were observed on the feeding behavior of test anim als after vagal dener-vat ion. Therefore, GLP-1 m ight play an im -portant role in long- term energy homeostasis, besides its known system ic ef-fects. This hypothesis is also supported by
the project ion of neurons in the NTS that produces preproglucagon for supply to the presynapt ic areas of regions such as area post rem a, interpeduncular nucleus, pos-terodorsal and vent ral tegm ental nucleus, hypothalam ic nuclei, thalam ic nuclei, nu-cleus accum bens, and lateral septum , espe-cially for feeding and energy hom eostasis. The presence of GLP-1 receptors in these areas also support this hypothesis (6) . GLP-1 in both circulat ion and brain show their effect by connect ing with the GLP-1 re-ceptors (GLP-1R) . Excitat ion of GLP-1R in different centers of the cent ral nervous sys-tem can create different responses. As a re-sult of GLP-1 act ivat ion in the brain, various physiological processes, such as appet ite m odulat ion, regulat ion of nausea, inhibit ion of reward and m ot ivat ion centers, energy hom eostasis, neuroprotect ion, increase in neural insulin sensit iv it y, neural plast icit y, and m em ory form at ion, and im m une m odu-lat ion can occur. Exper im ents conducted using GLP-1R analogs have dem onst rated that they influ-ence the arcuate nucleus (ARC) , paraven-t r icular nucleus (PVN) , and lateral hypothalam ic area by act ing like GLP-1R, mainly on the Proopiomelanocort in/ Cocaine- and am phetam ine- regulated t ranscr ipt (POMC/ CART) anorexigenic neurons and in-
344
Bakıner et al. Turk J Endocrinol Metab. GLP-1 and Brain 2020; 24: 343-355
3 4 4
Figure 1 : Humoral and neural pathways of the GLP-1 effect on the brain.

direct ly inhibit the neuropept ide Y/ Agout i-related pept ide (NPY/ AgRP) orexigenic neu-rons through GABAergic signals. Sim ilar ly, the st im ulat ion of GLP-1 in the vent ral tegm ental area, known as the reward-m ot i-vat ion center, has been observed to cont rol the m esolim bic dopam inergic signals, which decreases the pleasure of eat ing (7) . I t has also been dem onst rated that the effect of GLP-1 analogs on the vent rom edial hypo-thalam ic neurons increases the sym pathet ic act ivity, which increases the therm ogenesis with retent ion of glucose and t r iglyceride in the brown fat t issue, and causes the t rans-format ion of the white fat t issue to brown fat t issue (8) . GLP-1Rs are located in the G protein-cou-pled receptor group, and their st im ulat ion act ivates som e int racellular pathways (2) . St im ulat ion of the receptor by GLP-1 act i-vates som e pathways which can lead to acute or chronic responses. Exam ples of acute responses include insulin secret ion, exocytosis, and an increase in the int racel-lular calcium ion concent rat ion. The acute response m ainly occurs with the act ivat ion of phosphoryl k inase v ia the cyclic adeno-sine m onophosphate ( cAMP) pathway. Ex-amples of chronic effects include modulat ion of the gene expression, cell growth, cell pro-liferat ion, cell different iat ion, and ant i-apop-tot ic act iv it y. These effects occur through the phosphoinosit ide 3-kinase (PI 3K) path-way, which is sim ilar to the insulin down-st ream pathway. Act ivat ion of PI 3K t r iggers the act ivat ion of protein kinase B (AKT) . This m olecule is responsible for protein synthe-sis, an increase in ant i-apoptot ic factors, and inhibit ion of int racellular apoptot ic fac-tors. Another im portant pathway responsi-ble for the chronic effect is the m itogen-associated protein kinase/ ext racel-lular signal- regulated k inase (MAPK/ ERK) pathway. The act ivat ion of this pathway is responsible for im portant cytoprotect ive ef-fects, such as inhibit ion of apoptosis, a de-crease in oxidat ive st ress, and a decrease in the inflam m atory response.
Metabolic Basis of Neurodegenerat ive Diseases Neurodegenerat ive diseases with dem ent ia can affect memory, learning, cognit ive func-t ions, and behavior. There are approxi-
m ately 50 m illion dem ent ia pat ients world-wide, and it is t he 7 t h leading cause of death. Alzheim er ’s disease (AD) and Parkin-son’s disease (PD) account for a m ajor pro-port ion of neurodegenerat ive diseases. AD is character ized m ainly by the ext racellular accum ulat ion of amyloid β protein, with the int racellular accum ulat ion of hyperphospho-rylated τ protein in ligam entous form , neu-roinf lam m at ion, and decrease in t he ut ilizat ion of glucose by the brain. On the other hand, PD is character ized by the ac-cum ulat ion of neuronal a- synuclein and Lewy fibr ils, with the loss of dopam inergic neurons due to neuronal m itochondrial dys-funct ion. The com m on features of neurode-generat ive diseases include the format ion of neurotoxic aggregates, increased oxidat ive st ress, act ivat ion of apoptot ic pathways, neurot ransm it ter insuff iciency, and neural dif ferent iat ion failure (9) . A decrease in neuronal glucose ut ilizat ion due to cerebral insulin resistance is an im portant feature of AD (10) . I nit ially, the brain was thought to be insensit ive to insulin, but t he eventual discovery of the presence of insulin recep-tors in cer tain par t s of the brain has indi-cated that this m olecule plays an im portant role in t he m etabolic, neurot ropic, neuro-m odulatory, and neuroendocr ine regulat ion in the brain, as well as m em ory and learn-ing (11) . Glucose ut ilizat ion in the neurons occurs v ia insulin- independent glucose t ranspor ter-3 (GLUT-3) protein, whereas the forebrain, cerebral cor tex, and hip-pocam pus show coexpression of the insulin-dependent glucose t ransporter-4 (GLUT-4) protein (12) . I t is suggested that act iv it ies such as learning and rem em ber ing, which increase metabolic needs, can cause the ex-pression of the t ranslocated GLUT-4. Sim i-lar ly, expression of GLUT-4 has also been shown in the hypothalam us, which plays an im portant role in m etabolic cont rol. Besides the ut ilizat ion of cerebral glucose, insulin plays an im portant role in synapt ic plast ic-it y, neur ite m ult iplicat ion, neuroprotect ion, m em ory form at ion, cognit ive arrangem ent , m ult iplicat ion, different iat ion and myelina-t ion of oligodendrocytes, and determ inat ion of t he levels of neurot ransm it ters such as acety lcholine and norepinephr ine (13,14) . I t has been dem onst rated that insulin is synthesized in the cerebral cortex and hip-
345
Turk J Endocrinol Metab. Bakıner et al. 2020; 24: 343-355 GLP-1 and Brain
3 4 5
pocam pus in the cent ral nervous system , and that small amounts of pancreat ic insulin can pass the BBB via select ive t ransport and affect brain funct ions (15) . I nsulin levels in the cerebrospinal f luid (CSF) are correlated with those in plasm a, and it s t ranspor t through the BBB m ay be affected by obe-sit y, diabetes, inf lam m at ion, and high plasm a t r iglycer ide levels. I t was dem on-st rated that the presence of per ipheral in-sulin resistance decreased the CSF/ per ipheral insulin rat io and flow of in-sulin from blood to the CSF (16) . I n diabet ic anim al m odels, the effect of insulin in the brain decreases and is associated with de-m ent ia (17) . The Rot terdam study is am ong the pioneering research that highlighted the r isk of increased dem ent ia in t ype-2 dia-bet ic populat ion (18) . Following this, t he idea of an associat ion between AD, insulin resistance, and brain glucose ut ilizat ion was f irst hypothesized 22 years ago (19) . The r isk of dem ent ia increases by 65% in type-2 diabet ics com pared to non-diabet ics (20) . Also, per ipheral insulin resistance is associ-ated with decreased cerebral glucose ut i-lizat ion, decreased cerebral perfusion, and brain at rophy (11) . Obesity and type 2 dia-betes, which are r isk factors for AD, are as-sociated with an increase in t he fat t issue-or iginated pro- inf lam m atory adipokines and plasm a free fat t y acids. These cytokines can pass the BBB in AD and other condit ions where the cerebral circula-t ion is decreased. I n t he neurons, it can cause the phosphorylat ion of insulin recep-tor subst rate 1 ( I RS-1) via the act ivat ion of ser ine k inase. Thus, t he PI 3K pathway is blocked, and insulin resistance occurs (21) . On the other hand, insulin increases the he-pat ic clearance of neuronal amyloid β. I n the case of peripheral insulin resistance, the ac-cum ulat ion of cerebral am yloid β is in-creased due to dim inished hepat ic clearance of am yloid β ( 22) . However, som e studies advocate that the type of insulin resistance in the pathogenesis of AD is not the periph-eral insulin resistance, but the neuronal one, which is present in the cent ral nervous sys-tem (23) . The fact that t ight glycem ic con-t rol cannot help dem ent ia regression in diabet ic pat ients, and that the regression is even m ore aggravated due to frequent hy-poglycemia, also indicates that int ranasal in-
sulin should improve cognit ive funct ions and m em ory, in doses that do not cause periph-eral hypoglycem ia. These findings confirm that cent ral insulin resistance should be dif-ferent iated from per ipheral resistance. Ac-cordingly, som e researchers have nam ed the associat ion between cent ral insulin re-sistance and dem ent ia as t ype-3 diabetes (24–27) . I n cerebral insulin resistance, inhibit ion of the AKT pathway after phosphorylat ion of I RS-1 results in an increase in the levels of Glycogen Synthase Kinase-3 (GSK-3) . Fur-therm ore, the pathway causes an increase in Protein Kinase A (PKA) , and both these condit ions cont r ibute to the pathogenesis of AD by causing the phosphorylat ion of τ-pro-tein. I ncreasing GSK-3 levels cause an in-crease in the product ion of am yloid-β proteins. Neurotoxic amyloid oligom ers and plaques are created from am yloid-β pro-teins. Amyloid-β oligomers may further con-t r ibute to neuronal insulin resistance by direct ly causing an increase in the phospho-rylat ion of I RS-1, act ivat ion of TNF-α signal, or act ivat ing the glial cells to increase cy-tokine ( lL-1 β, lL-6, TNF-α) secret ion. Finally, decreased int racellular ent ry of glucose due to insulin resistance causes a decrease in neuronal ATP product ion and deter iorat ion of synapt ic act ivity. Thus, cognit ive dysfunc-t ion occurs (28) .
Effects of GLP- 1 on Alzheim er Disease GLP-1 affects the brain through basic ant i-apoptot ic, ant ioxidant , and neurot rophic im -pact on GLP-1R. PKA and PI3K pathways are act ivated upon increasing cAMP, which oc-curs due to the st im ulat ion of GLP-1R. Act i-vat ion of PKA act ivat ion increases ERK, while the act ivat ion of PI 3K increases AKT. The increase in both ERK and AKT t r iggers the t ranscr ipt ion of genes responsible for ant ioxidant , ant i-apoptot ic, neurot ropic, and ant i- inflam m atory effects (Figure 2) (29) . GLP-1 can decrease insulin resistance in the brain and reverse it . I t was dem onst rated that liraglut ide norm alized the phosphoryla-t ion of neuronal I RS-1 serine and the levels of AKT and GSK-3 β, as well as decreased the cerebral insulin levels (30) . GLP-1 was also dem onst rated to im prove cognit ive funct ions by increasing the ut ilizat ion of glu-cose in the brain (31) .
346
Bakıner et al. Turk J Endocrinol Metab. GLP-1 and Brain 2020; 24: 343-355
3 4 6
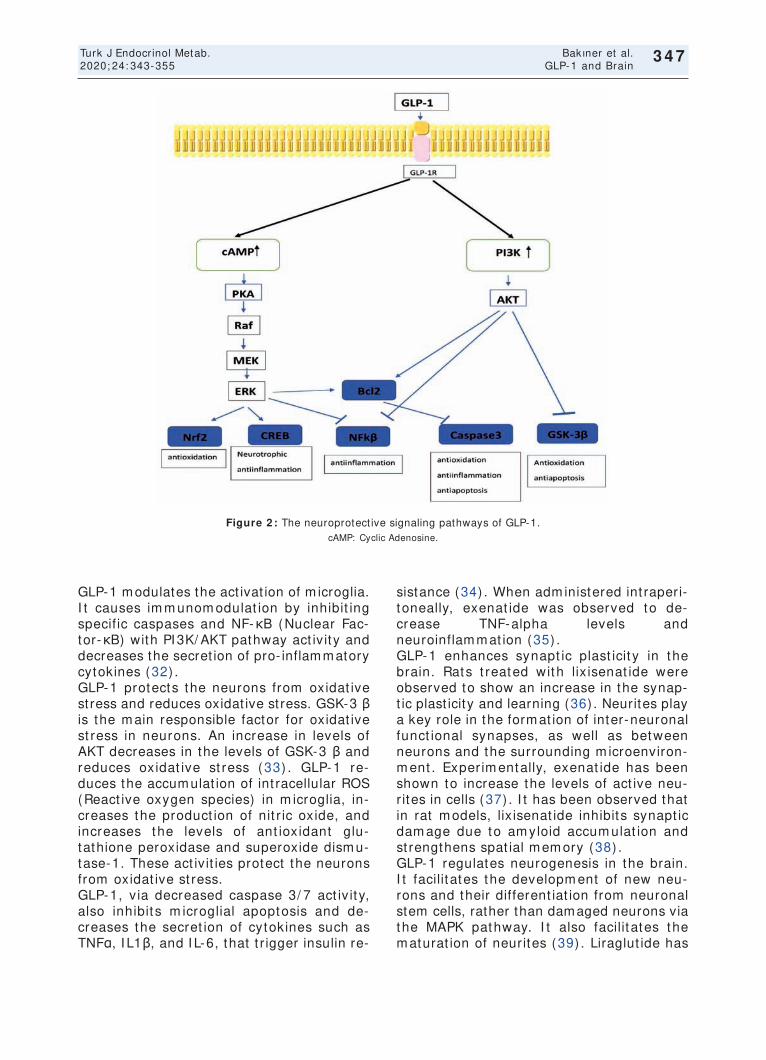
GLP-1 modulates the act ivat ion of m icroglia. I t causes im m unom odulat ion by inhibit ing specif ic caspases and NF-κB (Nuclear Fac-tor-κB) with PI 3K/ AKT pathway act ivity and decreases the secret ion of pro- inflammatory cytokines (32) . GLP-1 protects the neurons from oxidat ive st ress and reduces oxidat ive st ress. GSK-3 β is the m ain responsible factor for oxidat ive st ress in neurons. An increase in levels of AKT decreases in the levels of GSK-3 β and reduces oxidat ive st ress (33) . GLP-1 re-duces the accum ulat ion of int racellular ROS (React ive oxygen species) in m icroglia, in-creases the product ion of nit r ic oxide, and increases the levels of ant ioxidant glu-tathione peroxidase and superoxide dism u-tase-1. These act ivit ies protect the neurons from oxidat ive st ress. GLP-1, v ia decreased caspase 3/ 7 act iv it y, also inhibit s m icroglial apoptosis and de-creases the secret ion of cytokines such as TNFα, I L1β, and I L-6, that t r igger insulin re-
sistance (34) . When adm inistered int raperi-toneally, exenat ide was observed to de-crease TNF-alpha levels and neuroinflam m at ion (35) . GLP-1 enhances synapt ic plast icit y in the brain. Rats t reated with lix isenat ide were observed to show an increase in the synap-t ic plast icity and learning (36) . Neurites play a key role in the form at ion of inter-neuronal funct ional synapses, as well as between neurons and the surrounding m icroenviron-m ent . Exper im entally, exenat ide has been shown to increase the levels of act ive neu-r ites in cells (37) . I t has been observed that in rat m odels, lix isenat ide inhibits synapt ic dam age due to am yloid accum ulat ion and st rengthens spat ial m em ory (38) . GLP-1 regulates neurogenesis in the brain. I t facilit ates the developm ent of new neu-rons and their different iat ion from neuronal stem cells, rather than damaged neurons via the MAPK pathway. I t also facilit ates the m aturat ion of neurites (39) . Liraglut ide has
347
Turk J Endocrinol Metab. Bakıner et al. 2020; 24: 343-355 GLP-1 and Brain
3 4 7
Figure 2 : The neuroprotect ive signaling pathways of GLP-1. cAMP: Cyclic Adenosine.

348
been experim entally shown to increase the different iat ion of neural progenitor cells to mature neurons. I t inhibits neuron apoptosis by increasing the levels of the survival fac-tors Bcl-2 (B-cell lym phom a 2) and Bcl-XL (B-cell lym phom a-ext ra- large) through the PI 3K/ AKT pathway. I t increases cell prolifer-at ion through the sam e pathways and st im -ulates different iat ion of neurons and growth of neur ites by increasing growth factors such as brain-der ived neurot rophic factor (BDNF) and glial cell- der ived neurot rophic factor (GDNF) (31,40,41) . Liraglut ide has been shown to increase m em ory in experi-m ental anim als by prevent ing neurodegen-erat ion and synapt ic dam age (42) . GLP-1 decreases the phosphorylat ion of τ-protein and accum ulat ion of amyloid-β pro-tein. I t also decreases the product ion of GSK-3 β in the neurons via the PI 3K path-way. GSK-3 β is responsible for the phos-phorylat ion of neuronal τ-protein. Liraglut ide has been observed to prevent the hyper-phosphorylat ion of τ-protein in diabet ic db/ db rats (43) . Besides, GLP-1 reduces the levels of endogen amyloid-β protein in the brain and prevents the accum ulat ion of am yloid plaques (42) . The form at ion of amyloid plaques in exper im entally created AD in fem ale rat m odels has been shown to reduce by t reatm ent with lix isenat ide (44) . DPP-4 (dipept idyl pept idase) inhibitors are used as incret inergic agents for the t reat-m ent of diabetes, as are GLP-1 receptor analogs. These drugs inhibit the DPP-4 en-zyme and inact ivate it . They cannot pass the BBB, due to which their effect on the cent ral nervous system is associated with increas-ing endogenous GLP-1 levels. Moreover, in-hibit ion of the DPP-4 enzym e reduces the breakdown of st rom al cell-der ived factor-1 (SDF-1) . SDF-1 binds to the chem okine re-ceptor-4 (CXCR-4) on the surface of the neurons and act ivates the PI 3K/ AKT path-way, which causes cell proliferat ion and sur-v ival. DPP-4 inhibitors also posit ively influence vascular izat ion in the brain by in-creasing the expression of vascular en-dothelial growth factor (VEGF) through SDF-1 (45) . To date, no random ized prospect ive studies have been conducted on enough hum ans to study the neurocognit ive effect , which is dif-ferent from the ant idiabet ic effect , using
DPP-4 inhibitors or GLP-1 agonists. Accord-ing to a m eta-analysis, seven studies have fulfilled the inclusion cr iter ia, f ive of which are intervent ional, while two are observa-t ional (46) . An observat ional study on dia-bet ic pat ients has revealed that increased plasm a DPP-4 levels are associated with m ild loss in cognit ive funct ions (47) . I n a study on 240 cases, DPP-4 inhibitors have been shown to im prove cognit ive funct ion compared to sulfonylurea (48) . A six-month-long, random ized, placebo-cont rolled, and double-blind study has shown liraglut ide to significant ly increase brain glucose m etabo-lism com pared to placebo (49) . Sim ilar re-sults have been reported in a two-year- long, randomized study, conducted with exenat ide (50) . On the other hand, a six-m onth- long randomized double-blind study comparing li-raglut ide with placebo reported no differ-ence in the form at ion or regression of am yloid plaque in the brain (51) . Another study has dem onst rated that liraglut ide did not show a significant ly im proved effect on cognit ive funct ions over a relat ively short period of 17 days, com pared to the placebo (52) . The clinical studies on this area are sum m arized in Table 1. Therefore, the benefits of GLP-1 analogs and DPP-4 inhibitors on neurodegenerat ive dis-eases, independent of glycem ia, have not been proven com pletely. The previous stud-ies have relat ively sm all sam ple sizes, and som e individual phenotypic differences such as apo E4 carr iage m ay alter neurodegener-at ive-diabetes and associated t reatm ent (53) .
Effects of GLP-1 on Parkinson’s Disease I n preclinical studies on different exper i-m ental m odels of sim ulated Parkinson’s dis-ease, GLP-1 receptor agonists have been shown to reduce the loss of dopam inergic neurons, and regulate brain energy m etab-olism and m otor act ivity with neuroprotec-t ive effect . These effects are sim ilar to those described in AD by the act ivat ion of PKA and PI 3K/ AKT m olecular pathways through GLP-1 receptors. Exenat ide t reatm ent in rats with exper im entally induced dopam inergic neuron loss using toxic substances com -pletely decreased the toxicity and increased dopam inergic neuron v iabilit y (54) . Sim i-lar ly, another preclinical study using a neu-
Bakıner et al. Turk J Endocrinol Metab. GLP-1 and Brain 2020; 24: 343-355
3 4 8

349
Turk
J En
do
crino
l Me
tab
.B
ak
ıne
r et a
l. 2
02
0;2
4:3
43
-35
5 G
LP-1
an
d B
rain
3
49
Monophosphate; PKA: Protein kinase A; MEK: Mitogen-act ivated protein kinase; ERK: Ext racellular regulated protein kinase; PI 3K: Phosphoinosit ide 3 kinase, AKT: Protein kinase B; CREB: cAMP response elem ent-binding protein; NFKβ: Nuclear factor kappa-
beta; Bcl2: B-cell lym phom a; GSK-3β: Glycogen synthase kinase 3 beta.
I nvest igator, year, earlier studies Design Part icipants Sam ple character ist ics Results
Zheng, 2016 ( 47) Cross-sect ional, observat ional Evaluated plasm a DPP4 act ivity, I ncreased DPP4 act ivit ies are
inflam m atory m arkers, and independent ly associated with
oxidat ive st ress param eters i MCI in elderly pat ients with
n a cross-sect ional sam ple of type 2 diabetes
1,160 pat ients with type 2
diabetes aged 60 years or older in China
Tasci, 2013 (48) prospect ive and observat ional I nvest igat ion conducted in Mean follow-up t im e was Addit ion of vildaglipt in to ongoing
10 elderly type 2 diabetes m ellitus 10.9 ± 3.7 m onths. m et form in therapy in elderly with
pat ients who were started t reatm ent diabetes was accom panied by
with vildaglipt in 50 m g twice daily stable cognit ive and funct ional
to ongoing m et form in. perform ance after alm ost one
year of follow-up.
Gej l, 2016, (49) Random ized, Placebo-Cont rolled, Random ized 38 pat ients with AD to 26-week t r ial GLP-1 analog t reatm ent prevented
Double-Blind Clinical Tr ial t reatm ent with the GLP-1 analog liraglut ide the decline of glucose m etabolism in
(n = 18) , or placebo (n = 20) brain that signifies cognit ive
im pairm ent , synapt ic dysfunct ion,
and disease evolut ion.
Danielle, 2015, (50) Double-blind, random ized I n 15 m ale subjects with HbA1c of 5.7 ± 0.1% , Results dem onst rate that , a m ajor effect
The study aim was to evaluate fast ing glucose of 114 ± 3 m g/ dL, of a GLP-1RA on regulat ion of brain
the effects of a single inject ion and 2-h glucose of 177 ± 11 m g/ dL, glucose m etabolism in the absorpt ive
of the GLP-1RA exenat ide on exenat ide (5 µg) or placebo was injected state.
cerebral and peripheral
glucose m etabolism in response
to a glucose load.
Egefjord, 2012, (51) Random ized, cont rolled, AD pat ients t reated for six m onths with The prim ary outcom e is No registered drug affects the deposit ion
double-blinded intervent ion study liraglut ide (n = 20) or placebo (n = 20) . change in the deposit ion of of Aβ in the brain of AD pat ients
with AD pat ients Aβ in the cent ral nervous system
Farr, 2016, (52) Crossover, random ized, double-blind, 21 individuals with type 2 diabetes were For a total of 17 days, studied Liraglut ide alters brain act ivity related to
placebo-cont rolled t r ial t reated with placebo and liraglut ide m etabolic changes as well as highly desirable food cues.
neurocognit ive and neuroim aging
( funct ional MRI ) of responses
to food cues
Athauda, 2017, (60) Random ized, double-blind, Pat ients were aged 25–75 years, Pat ients with m oderate Exenat ide had posit ive effects on
placebo-cont rolled t r ial n: 32 to exenat ide and n: 30 to placebo. Parkinson's disease were ract ically defined off-m edicat ion
random ly assigned (1: 1) pm otor scores in Parkinson's disease
to receive subcutaneous i
nject ions of exenat ide 2 m g or
placebo once weekly for 48 weeks
in addit ion to their regular m edicat ion
Table 1. Hum an clinical t r ials describing the associat ions between GLP-1 bases therapies and dem ent ia r isk.

rotoxin observed higher levels of dopam ine in anim als adm inistered Exendin-4. This ef-fect was associated with an increase in the viability of dopaminergic neurons, and an in-crease in the levels of tyrosine hydroxylase enzym e, which produces dopam ine from its precursor, L-DOPA (55) . Cell culture studies have dem onst rated that liraglut ide and lix isenat ide also increase the act ivity of ty-rosine hydroxylase, and t r igger the ant i-apoptot ic m echanism , com pared to exendin (56) . Long- term use of liraglut ide has been shown to inhibit dopam inergic neuron loss in db- / db- diabet ic m ice models and prevent the im pairm ent of m otor funct ions and de-velopm ent of PD (57) . Exper im entally, li-raglut ide has been shown to reduce dyskinesia, which is an im portant com plica-t ion of L-DOPA t reatm ent (58) . Sem aglut ide has been shown to reduce the accum ulat ion of α-synuclein, in addit ion to the beneficial effects of other GLP-1R agonists (59) . The first random ized double-blind placebo-con-t rolled clinical study conducted on hum ans was published in 2017 on 62 cases with PD, wherein 2 m g/ week exenat ide LAR sc was com pared to placebo. Exenat ide was ob-served to show posit ive effects on clinically m onitored m otor funct ions (60) . Based on these findings, GLP-1 agonists appear to have posit ive effects on the survival and funct ions of dopam inergic cells. The field is open for addit ional clinical studies for the developm ent of an appropr iate t reatm ent st rategy.
Physiological Effects pf Central GLP- 1 on Stress Recent studies have focused on the effect of GLP-1 on the st ress response of the organ-ism . NTS has cent ral GLP-1-producing cells and receives vagal st im ulus from the pe-r iphery, as well as a st im ulus for general hom eostasis. St ress act ivates two parallel system s in the body, hypothalam o-hy-pophysioadrenal (HPA) axis and the sym pa-thet ic nervous system (SNS) . NTS is projected to hypothalam ic and autonom ic cont rol centers, which are effect ive in both these systems. GLP-1 produced by NTS neu-rons can act ivate both the HPA axis and SNS. There is no GLP-1R in the adrenal cor-tex, and the isolated adrenal cortex cells do not release cort icosterone upon GLP-1 st im -
ulus. Therefore, the effect is known to have a cent ral or igin. When adm inistered cen-t rally, exendin-4 was observed to increase cort icosterone levels in rodents. This in-crease is generated through CRH levels. The cent ral blockade of the CRH receptors elim -inates this effect (61) . On the other hand, the act ivat ion of GLP-1 receptors in the cen-t ral autonom ic system m ay st im ulate sym -pathet ic neuronal cells in the spinal cord and adrenal m edulla (62) . As a result , GLP-1 m ay regulate the st ress response of the body. Studies related to the clinical benefits of this condit ion and GLP-1RA pract ices are ongoing.
I schem ic Stroke and Glp- 1 The st roke-dam aged brain region can be di-vided into two parts, the ischem ic core and the penum bra around the ischem ic core. I n the ischem ic core, the dam age takes place rapidly and is generally irreversible. The sur-rounding penumbra provides blood flow, and therefore, the neurons in this area can be protected by well-planned, t im ely interven-t ions. These intervent ions are aim ed at the chem ical or surgical rem oval of the throm -bot ic clot . These t reatm ents are generally beneficial within the first few hours after the onset of st roke, and unfortunately, m ay not be suitable for several pat ients due to late adm ission, difficult ies in diagnosis, or con-t raindicat ions such as hypertension. I n a st roke, t he m echanism s of act ion of GLP-1-based therapies have been studied thoroughly in anim al m odels, but studies on hum an st roke pat ients have begun recent ly ( ClinicalTr ials.gov NCT02829502) . I n t he LEADER (Liraglut ide Effect and Act ion in Di-abetes) t r ial, a decrease in t he rates of nonfatal st roke was observed in the liraglu-t ide group, alt hough t he dif ference was non-signif icant (63) . I n the late SUSTAI N-6 (Tr ial to Evaluate Cardiovascular and Other Long-Term Outcom es with Sem aglut ide in Subj ect s w it h Type- 2 Diabetes) t r ial, sem aglut ide was observed to signif icant ly reduce the r isk of the sam e pr im ary com -posite endpoint as liraglut ide. Both the t r i-als dem onst rated a decrease in m aj or cardiovascular out com es; however, t here was no reduct ion in cardiovascular m ortal-it y in t he SUSTAI N-6 t r ial, as observed in t he LEADER t r ial. There was another im -
350
Bakıner et al. Turk J Endocrinol Metab. GLP-1 and Brain 2020; 24: 343-355
3 5 0

portant difference between the studies. I n t he SUSTAI N- 6 t r ial, t he reduct ion in t he m ajor CV outcom e appeared to be the re-sult of a signif icant (39% ) decrease in the rate of nonfatal st roke (64) . I n large car-diovascular safety studies using DPP-4 in-hibit ors, no decrease in t he rates of nonfatal st roke or other m ajor CV outcom es was reported (65) . GLP-1RA can cross the BBB and enter t he hypothalam ic neurons and circum vent r icular organs, whereas DPP-4 inhibitors cannot . Therefore, GLP-1R agonist s and DPP- 4 inhibit ors appear t o have different effects on the ischem ic brain t issue due to different pharm acological spe-cialt ies. I n m ice lacking GLP-1R, DPP-4 in-hibit ors were observed t o be neuroprotect ive (66) . DPP-4 inhibitors m ay affect t arget s independent of GLP- 1R. I n exper im ental m odels, Rohner t et al. showed that non-select ive DPP-4 inhibitors were related to a reduct ion in infarct vol-um e, which was not t rue for select ive DPP-4 inhibitors (67) . The m echanism s of these act ions are yet to be fully clear. The DPP-4 enzym e target s m ore act ive pept ides, in-cluding t he glucose- dependent in-sulinot ropic polypept ide ( GI P) and t he pit uit ary adeny late- cyclase-act ivat ing polypept ide (PACAP) , than the GLP-1. Han et al. have dem onst rated that a dual ago-nist target ing both GLP-1 and GI P receptors generated st ronger neuroprotect ion against ischem ic st roke than GLP-1 analog alone, indicat ing t he neuroprotect ive effect s of GI P against st roke (68) . Moreover, it was repor ted that DPP-4 inhibit ion could am e-liorate endothelium -dependent relaxat ion, and cerebrovascular dysfunct ion and re-m odeling, independent of glucose regula-t ion (69) . Previous studies on anim als have high-lighted the neuroprotect ive effect of GLP-1RAs in both diabet ic and non-diabet ic animals. I nflammat ion, oxidat ive st ress, and neuronal apoptosis due to st roke are part ic-ular ly affected by GLP-1-based therapies.
Neuroprotect ive Mechanism s of GLP- 1 - Based Therapies in I schem ic Stroke After an ischem ic st roke, GLP-1R is upregu-lated in ast rocytes, GABAergic interneurons, and m icroglia (70) . The m olecules PI 3K,
cyclic adenosine m onophosphate ( cAMP) , protein k inase-B (Akt ) , protein k inase-A (PKA) , and cAMP response elem ent-binding protein (CREB) are st im ulated after the ad-m inist rat ion of GLP-1RAs in experim entally-induced st roke. I nflam m at ion, endothelia l leakage, and excitotoxicity: The effect of GLP-1-based therapies on inflam m atory response after a st roke has been studied by several re-searchers. Both exenat ide and sitaglipt in re-duced the product ion of the pro- inflam m atory cytokine tum or necrosis factor-alpha (TNF-α) (71) . Sitaglipt in also reduced the expression of inter leukin-6 ( I L-6) and increased the product ion of the ant i-inflam m atory cytokine inter leukin-10 ( I L-10) (72) . Therapies based on GLP-1 also influence the BBB perm eabilit y. Exendin-4 signif icant ly reduced the expression of aquaporin-4 (AQ-4) and glial fibr illary acidic protein (GFAP) , which are involved in neu-roinflam m at ion, the form at ion of edem a, and ast rogliosis. Moreover, exendin-4 de-creases the intercellular adhesion m olecule-1 ( I CAM-1) and inhibits BBB leakage (73) . Expression of endothelial NOS (eNOS) , which plays a role in the m aintenance of vascular hom eostasis, is increased by re-com binant GLP-1, while exenat ide reduces the vascular ext ravasat ion of im m unoglob-ulin G ( I gG) , reducing endothelial leakage in the late inflam m atory response to ischem ia (71,74) . Product ion of brain-der ived neu-rot rophic factor (BDNF) was increased with pre- ischem ic t reatm ent with aloglipt in, which reduced the release of neurotoxic glu-tam ate and stabilized the neuroprotect ive GABAergic synapses with cont inuous expo-sure (75) . Oxidat ive st ress: Both liraglut ide and exe-nat ide decreased the product ion of react ive oxygen species (ROS) after cerebral artery occlusion in diabet ic m ice (76) . Exendin-4 decreased superoxide anion (O2) (73) . I n sitaglipt in- t reated anim als, the enzym e NADPH oxidase (NOx) , which part icipates in the generat ion of ROS, was normalized (72) . Apoptosis and neuronal dam age: To iden-t ify DNA dam age, the “ term inal deoxynu-cleot idyl t ransferase dUTP nick-end labeling’’ (TUNEL) assay is used. I n ischemic lesions, the count of TUNEL-posit ive cells was signifi-cant ly reduced by exenat ide, liraglut ide, and
351
Turk J Endocrinol Metab. Bakıner et al. 2020; 24: 343-355 GLP-1 and Brain
3 5 1

m odified GLP-1R agonists (77) . Exenat ide also reduced the act ivity of Caspase-3, which takes part in apoptosis (78) . I nfarct volum e: When administered pre- is-chem ia or post- ischem ia, GLP-1R agonists are observed to reduce infarct volum e (79) . High doses of exenat ide were observed to be neuroprotect ive when adm inistered 1.5 h and 3 h post- ischem ia, and the act ivity di-m inished upon late adm inist rat ion. Exe-nat ide adm inistered ear ly resulted in the greatest reduct ion in the infarct volum e compared to later delivery (80) . I n cont rast , the effects of DPP-4 inhibitors are more vari-able. Funct ional outcom e and cerebral blood flow : Studies on GLP-1R agonists generally reported im proved funct ional outcom es, whereas only one out of two studies using DPP-4 inhibitors dem onst rated such an ef-fect . I n the f irst study, Ma et al. reported that linaglipt in ameliorated cognit ive impair-m ent in diabet ic m ice, while the other study on aloglipt in reported no beneficial effects of the com pound on neurologic deficit s when adm inistered daily for three weeks before the st roke, to seven days post- ischem ia (75,81) . Conflict ing result s for the cere-brovascular effects of GLP-1RAs have been reported. I n one study, t reatm ent with ex-endin-4 was observed to increase blood flow, suggest ing that GLP-1RAs im paired vascular funct ion in ischem ia, while another study reported that liraglut ide did not affect the cerebral blood flow (73,82) . The effects of DPP-4I adm inist rat ion on cerebral blood flow were also variable. I n conclusion, GLP-1-based therapies have been m ainly used in diabetes and obesity, but recent studies have demonstrated their protect ive roles in the cent ral nervous sys-tem. These agents, which have experimen-tally proven benefit s both in neurodegenerat ive diseases and ischem ic neuronal injuries, should be examined in this field by clinical studies. Random ized, placebo-controlled, prospect ive, double-blind open-ended studies and system at ic m eta-analyses will indicate whether GLP-based t reatm ents have neuroprotect ive effects in clinical pract ice, regardless of the ant idia-bet ic effect . Moreover, the new GLP-1 com-binat ions, developed together with GIP and glucagon agonists, also need well-planned
clinical t r ials, even though their benefit s have been dem onst rated exper im entally (83) . I t does not appear far- fetched to use these agents as neuroprotect ive agents in di-abet ic or non-diabet ic pat ients soon.
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions I dea/ Concept : Okan Sefa Bakıner; Design: Okan Sefa Bakıner; Control/ Supervision: Akadlı Kürşad Özşahin; Data Collect ion and/ or Processing: Okan Sefa Bakıner; Analy-sis and/ or Interpretat ion: Okan Sefa Bakıner; Literature Review: Okan Sefa Bakıner; Writ-ing the Art icle: Okan Sefa Bakıner; Crit ical Review: Okan Sefa Bakıner; Other (Language edit ion) : Akadlı Kürşad Özşahin.
References 1. Campbell JE, Drucker DJ. Pharmacology, physiology, and
m echanism s of incret in horm one act ion. Cell Metab. 2013; 17: 819-837. [ Crossref] [ PubMed]
2. Sm ith NK, Hacket t TA, Galli A, Flynn CR. GLP-1: Molec-ular m echanism s and outcom es of a com plex signaling system . Neurochem I nt . 2019; 128: 94-105. [ Crossref] [ PubMed] [ PMC]
3. Fuchs H, Binder R, Greischel A. Tissue dist r ibut ion of the novel DPP-4 inhibitor BI 1356 is dom inated by saturable binding to it s target in rats. Biopharm Drug Dispos. 2009; 30: 229-240. [ Crossref] [ PubMed]
4. Holt MK, Richards JE, Cook DR, Brierley DI , Williams DL, Reim ann F, Gribble FM, Trapp S. Preproglucagon neu-rons in the nucleus of the solitary t ract are the m ain source of brain GLP-1, m ediate st ress- induced hy-pophagia, and lim it unusually large intakes of food. Di-abetes. 2019; 68: 21-33. [ Crossref] [ PubMed] [ PMC]
5. Nishizawa M, Nakabayashi H, Uehara K, Nakagawa A, Uchida K, Koya D. I nt raportal GLP-1 st im ulates insulin secret ion predom inant ly through the hepatoportal-pan-creat ic vagal reflex pathways. Am J Physiol Endocrinol Metab. 2013; 305: E376-E387. [ Crossref] [ PubMed]
352
Bakıner et al. Turk J Endocrinol Metab. GLP-1 and Brain 2020; 24: 343-355
3 5 2

6. Merchenthaler I , Lane M, Shughrue P. Dist r ibut ion of pre-pro-glucagon and glucagon- like pept ide-1 receptor m essenger RNAs in the rat cent ral nervous system . J Comp Neurol. 1999; 403: 261-280. [ Crossref] [ PubMed]
7. Alhadeff AL, Rupprecht LE, Hayes MR. GLP-1 neurons in the nucleus of the solitary t ract project direct ly to the vent ral tegm ental area and nucleus accum bens to con-t rol for food intake. Endocrinology. 2012; 153: 647-658. [ Crossref] [ PubMed] [ PMC]
8. Lockie SH, Heppner KM, Chaudhary N, Chabenne JR, Morgan DA, Veyrat-Durebex C, Ananthakr ishnan G, Rohner-Jeanrenaud F, Drucker DJ, DiMarchi R, Rah-m ouni K, Oldfield BJ, Tschöp MH, Perez-Tilve D. Direct cont rol of brown adipose t issue therm ogenesis by cen-t ral nervous system glucagon- like pept ide-1 receptor signaling. Diabetes. 2012; 61: 2753-2762. [ Crossref] [ PubMed] [ PMC]
9. Ahm ad K, Baig MH, Mushtaq G, Kam al MA, Greig NH, Choi I . Com m onalit ies in biological pathways, genet ics, and cellular m echanism between Alzheim er disease and other neurodegenerat ive diseases: an in silico-updated overview. Curr Alzheim er Res. 2017; 14: 1190-1197. [ Crossref] [ PubMed] [ PMC]
10. de la Monte SM. Brain insulin resistance and deficiency as therapeut ic targets in Alzheim er 's disease. Curr Alzheim er Res. 2012; 9: 35-66. [ Crossref] [ PubMed] [ PMC]
11. Frölich L, Blum-Degen D, Bernstein HG, Engelsberger S, Hum rich J, Laufer S, Muschner D, Thalheim er A, Türk A, Hoyer S, Zöchling R, Boissl KW, Jellinger K, Riederer P. Brain insulin and insulin receptors in aging and sporadic Alzheim er 's disease. J Neural Transm (Vienna) . 1998; 105: 423-438. [ Crossref] [ PubMed]
12. McEwen BS, Reagan LP. Glucose t ransporter expression in the cent ral nervous system : relat ionship to synapt ic funct ion. Eur J Pharm acol. 2004; 490: 13-24. [ Crossref] [ PubMed]
13. Stockhorst U, de Fries D, Steingrueber HJ, Scherbaum WA. I nsulin and the CNS: effects on food intake, m em -ory, and endocrine parameters and the role of int ranasal insulin adm inist rat ion in hum ans. Physiol Behav. 2004; 83: 47-54. [ Crossref] [ PubMed]
14. Chiu SL, Chen CM, Cline HT. I nsulin receptor signaling regulates synapse num ber, dendrit ic plast icity, and cir-cuit funct ion in vivo. Neuron. 2008; 58: 708-719. [ Cross-ref] [ PubMed] [ PMC]
15. Devaskar SU, Giddings SJ, Rajakum ar PA, Carnaghi LR, Menon RK, Zahm DS. I nsulin gene expression and in-sulin synthesis in m am m alian neuronal cells. J Biol Chem . 1994; 269: 8445-8454. [ PubMed]
16. Banks WA. The source of cerebral insulin. Eur J Phar-m acol. 2004; 490: 5-12. [ Crossref] [ PubMed]
17. Agrawal R, Zhuang Y, Cum m ings BP, Stanhope KL, Gra-ham JL, Havel PJ, Gomez-Pinilla F. Deteriorat ion of plas-t icit y and m etabolic hom eostasis in the brain of the UCD-T2DM rat m odel of naturally occurr ing type-2 dia-betes. Biochim Biophys Acta. 2014; 1842: 1313-1323. [ Crossref] [ PubMed] [ PMC]
18. Ot t A, Stolk RP, Hofm an A, van Harskam p F, Grobbee DE, Breteler MM. Associat ion of diabetes m ellitus and dem ent ia: the Rot terdam Study. Diabetologia. 1996; 39: 1392-1397. [ Crossref] [ PubMed]
19. Hoyer S. I s sporadic Alzheimer disease the brain type of non- insulin dependent diabetes m ellitus? A challenging hypothesis. J Neural Transm (Vienna) . 1998; 105: 415-422. [ Crossref] [ PubMed]
20. Arvanitakis Z, Wilson RS, Bienias JL, Evans DA, Bennet t DA. Diabetes m ellitus and r isk of Alzheim er disease and
decline in cognit ive funct ion. Arch Neurol. 2004; 61: 661-666. [ Crossref] [ PubMed]
21. Erickson MA, Dohi K, Banks WA. Neuroinflam m at ion: a com m on pathway in CNS diseases as m ediated at the blood-brain barr ier. Neuroim m unom odulat ion. 2012; 19: 121-130. [ Crossref] [ PubMed] [ PMC]
22. Tam aki C, Ohtsuki S, Terasaki T. I nsulin facilitates the hepat ic clearance of plasma amyloid beta-pept ide (1 40) by int racellular t ranslocat ion of low-density lipoprotein receptor- related protein 1 (LRP-1) to the plasm a m em -brane in hepatocytes. Mol Pharm acol. 2007; 72: 850-855. [ Crossref] [ PubMed]
23. I sik AT, Bozoglu E. Acetylcholinesterase inhibit ion and in-sulin resistance in late onset Alzheimer's disease. Int Psy-chogeriatr. 2009; 21: 1127-1133. [ Crossref] [ PubMed]
24. Areosa Sast re A, Vernooij RW, González-Colaço Har-m and M, Mart ínez G. Effect of the t reatm ent of Type 2 diabetes m ellitus on the developm ent of cognit ive im -pairm ent and dem ent ia. Cochrane Database Syst Rev. 2017; 6: CD003804. [ Crossref] [ PubMed] [ PMC]
25. Yaffe K, Falvey CM, Ham ilton N, Harr is TB, Sim onsick EM, St rotm eyer ES, Shorr RI , Met t i A, Schwartz AV; Health ABC Study. Associat ion between hypoglycem ia and dem ent ia in a biracial cohort of older adult s with diabetes m ellit us. JAMA I ntern Med. 2013; 173: 1300-1306. [ Crossref] [ PubMed] [ PMC]
26. Freiherr J, Hallschm id M, Frey WH 2nd, Brünner YF, Chapm an CD, Hölscher C, Craft S, De Felice FG, Bene-dict C. I nt ranasal insulin as a t reatm ent for Alzheim er's disease: a review of basic research and clinical evi-dence. CNS Drugs. 2013; 27: 505-514. [ Crossref] [ PubMed] [ PMC]
27. Chalichem NSS, Gonugunta C, Kr ishnam urthy PT, Du-raiswamy B. DPP4 inhibitors can be a drug of choice for t ype 3 diabetes: a m ini review. Am J Alzheim ers Dis Other Dem en. 2017; 32: 444-451. [ Crossref] [ PubMed]
28. Chen Y, Deng Y, Zhang B, Gong CX. Deregulat ion of brain insulin signaling in Alzheim er's disease. Neurosci Bull. 2014; 30: 282-294. [ Crossref] [ PubMed] [ PMC]
29. Dong D, Xie J, Wang J. Neuroprotect ive effects of brain-gut pept ides: a potent ial therapy for Parkinson's dis-ease. Neurosci Bull. 2019; 35: 1085-1096. [ Crossref] [ PubMed] [ PMC]
30. Long-Sm ith CM, Manning S, McClean PL, Coakley MF, O'Halloran DJ, Holscher C, O'Neill C. The diabetes drug liraglut ide am eliorates aberrant insulin receptor locali-sat ion and signalling in parallel with decreasing both amyloid-β plaque and glial pathology in a m ouse m odel of Alzheim er 's disease. Neurom olecular Med. 2013; 15: 102-114. [ Crossref] [ PubMed]
31. Parthsarathy V, Hölscher C. Chronic t reatm ent with the GLP1 analogue liraglut ide increases cell proliferat ion and different iat ion into neurons in an AD mouse model. PLoS One. 2013; 8: e58784. [ Crossref] [ PubMed] [ PMC]
32. Athauda D, Foltynie T. The glucagon- like pept ide 1 (GLP) receptor as a therapeut ic target in Parkinson's disease: m echanism s of act ion. Drug Discov Today. 2016; 21: 802-818. [ Crossref] [ PubMed]
33. An FM, Chen S, Xu Z, Yin L, Wang Y, Liu AR, Yao WB, Gao XD. Glucagon- like pept ide-1 regulates m itochondr-ial biogenesis and tau phosphorylat ion against advanced glycat ion end product- induced neuronal insult : Studies in v ivo and in v it ro. Neuroscience. 2015; 300: 75-84. [ Crossref] [ PubMed]
34. Spielm an LJ, Gibson DL, Klegeris A. I ncret in horm ones regulate m icroglia oxidat ive st ress, surv ival and ex-pression of t rophic factors. Eur J Cell Biol. 2017; 96: 240-253. [ Crossref] [ PubMed]
353
Turk J Endocrinol Metab. Bakıner et al. 2020; 24: 343-355 GLP-1 and Brain
3 5 3
35. Solm az V, Çınar BP, Yiğit türk G, Çavuşoğlu T, Taşkıran D, Erbaş O. Exenat ide reduces TNF-α expression and im proves hippocam pal neuron num bers and m em ory in st reptozotocin t reated rats. Eur J Pharm acol. 2015; 765: 482-487. [ Crossref] [ PubMed]
36. Lennox R, Flat t PR, Gault VA. Lix isenat ide im proves recognit ion m em ory and exerts neuroprotect ive act ions in high- fat fed m ice. Pept ides. 2014; 61: 38-47. [ Crossref] [ PubMed]
37. Luciani P, Deledda C, Benvenut i S, Cellai I , Squecco R, Monici M, Cialdai F, Luciani G, Danza G, Di Stefano C, Francini F, Peri A. Different iat ing effects of the glucagon-like pept ide-1 analogue exendin-4 in a hum an neuronal cell m odel. Cell Mol Life Sci. 2010; 67: 3711-3723. [ Crossref] [ PubMed]
38. Cai HY, Hölscher C, Yue XH, Zhang SX, Wang XH, Qiao F, Yang W, Qi JS. Lixisenat ide rescues spat ial m em ory and synapt ic plast icity from amyloid β protein- induced im pairm ents in rats. Neuroscience. 2014; 277: 6-13. [ Crossref] [ PubMed]
39. Salcedo I , Tweedie D, Li Y, Greig NH. Neuroprotect ive and neurot rophic act ions of glucagon- like pept ide-1: an em erging opportunit y to t reat neurodegenerat ive and cerebrovascular disorders. Br J Pharm acol. 2012; 166: 1586-1599. [ Crossref] [ PubMed] [ PMC]
40. Farilla L, Bulot ta A, Hirshberg B, Li Calzi S, Khoury N, Noushmehr H, Bertolot to C, Di Mario U, Harlan DM, Per-fet t i R. Glucagon- like pept ide 1 inhibit s cell apoptosis and improves glucose responsiveness of freshly isolated hum an islets. Endocr inology. 2003; 144: 5149-5158. [ Crossref] [ PubMed]
41. Li Y, Tweedie D, Mat tson MP, Holloway HW, Greig NH. Enhancing the GLP-1 receptor signaling pathway leads to proliferat ion and neuroprotect ion in hum an neurob-lastom a cells. J Neurochem . 2010; 113: 1621-1631. [ Crossref] [ PubMed] [ PMC]
42. McClean PL, Jalewa J, Hölscher C. Prophylact ic liraglu-t ide t reatm ent prevents am yloid plaque deposit ion, chronic inflam m at ion and m em ory im pairm ent in APP/ PS1 m ice. Behav Brain Res. 2015; 293: 96-106. [ Crossref] [ PubMed]
43. Ma DL, Chen FQ, Xu WJ, Yue WZ, Yuan G, Yang Y. Early in-tervention with glucagon-like peptide 1 analog liraglut ide prevents tau hyperphosphorylat ion in diabetic db/ db mice. J Neurochem. 2015; 135: 301-308. [ Crossref] [ PubMed]
44. Cai HY, Yang JT, Wang ZJ, Zhang J, Yang W, Wu MN, Qi JS. Lixisenat ide reduces amyloid plaques, neurofibrillary tangles and neuroinflam m at ion in an APP/ PS1/ tau m ouse m odel of Alzheim er's disease. Biochem Biophys Res Com m un. 2018; 495: 1034-1040. [ Crossref] [ PubMed]
45. Gault VA, Lennox R, Flat t PR. Sitaglipt in, a dipept idyl pept idase-4 inhibitor, improves recognit ion memory, ox-idat ive st ress and hippocam pal neurogenesis and up-regulates key genes involved in cognit ive decline. Diabetes Obes Metab. 2015; 17: 403-413. [ Crossref] [ PubMed]
46. Dum brill JL, Moulton CD. Effects of incret in-based ther-apies on neurocognit ive funct ion in hum ans: a system -at ic review of the lit erature. Pr im Care Diabetes. 2018; 12: 51-58. [ Crossref] [ PubMed]
47. Zheng T, Qin L, Chen B, Hu X, Zhang X, Liu Y, Liu H, Qin S, Li G, Li Q. Associat ion of plasm a DPP4 act ivity with m ild cognit ive im pairm ent in elderly pat ients with type 2 diabetes: results from the GDMD study in China. Dia-betes Care. 2016; 39: 1594-1601. [ Crossref] [ PubMed]
48. Tasci I , Naharci MI , Bozoglu E, Safer U, Aydogdu A, Yil-m az BF, Yilm az G, Doruk H. Cognit ive and funct ional in-
fluences of vildaglipt in, a DPP-4 inhibitor, added to on-going met form in therapy in elderly with type 2 diabetes. Endocr Metab I m m une Disord Drug Targets. 2013; 13: 256-263. [ Crossref] [ PubMed]
49. Gej l M, Gjedde A, Egefjord L, Møller A, Hansen SB, Vang K, Rodell A, Brændgaard H, Got t rup H, Schacht A, Møller N, Brock B, Rungby J. I n Alzheim er's disease, 6-m onth t reatm ent with GLP-1 analog prevents decline of brain glucose m etabolism : random ized, placebo-cont rolled, double-blind clinical t r ial. Front Aging Neurosci. 2016; 8: 108. [ Crossref] [ PubMed] [ PMC]
50. Daniele G, I ozzo P, Molina-Carr ion M, Lancaster J, Cio-ciaro D, Cersosim o E, Tripathy D, Triplit t C, Fox P, Musi N, DeFronzo R, Gastaldelli A. Exenat ide regulates cere-bral glucose m etabolism in brain areas associated with glucose hom eostasis and reward system . Diabetes. 2015; 64: 3406-3412. [ Crossref] [ PubMed] [ PMC]
51. Egefjord L, Gej l M, Møller A, Brændgaard H, Got t rup H, Ant ropova O, Møller N, Poulsen HE, Gjedde A, Brock B, Rungby J. Effects of liraglut ide on neurodegenerat ion, blood flow and cognit ion in Alzheim er's disease - proto-col for a cont rolled, random ized double-blinded t r ial. Dan Med J. 2012; 59: A4519. [ PubMed]
52. Farr OM, Sofopoulos M, Tsoukas MA, Dincer F, Thakkar B, Sahin-Efe A, Filippaios A, Bowers J, Srnka A, Gavrieli A, Ko BJ, Liakou C, Kanyuch N, Tseleni-Balafouta S, Mantzoros CS. GLP-1 receptors exist in the parietal cor-tex, hypothalamus and medulla of human brains and the GLP-1 analogue liraglut ide alters brain act ivity related to highly desirable food cues in indiv iduals with dia-betes: a crossover, randomised, placebo-controlled t r ial. Diabetologia. 2016; 59: 954-965. [ Crossref] [ PubMed] [ PMC]
53. Malek-Ahm adi M, Beach T, Obradov A, Sue L, Belden C, Davis K, Walker DG, Lue L, Adem A, Sabbagh MN. I n-creased Alzheim er's disease neuropathology is associ-ated with type 2 diabetes and ApoE ε.4 carr ier status. Curr Alzheim er Res. 201; 10: 654-659. [ Crossref] [ PubMed] [ PMC]
54. Kim S, Moon M, Park S. Exendin-4 protects dopam iner-gic neurons by inhibit ion of m icroglial act ivat ion and ma-t r ix m etalloproteinase-3 expression in an anim al m odel of Parkinson's disease. J Endocrinol. 2009; 202: 431-439. [ Crossref] [ PubMed]
55. Harkavyi A, Abuirmeileh A, Lever R, Kingsbury AE, Biggs CS, Whit ton PS. Glucagon- like pept ide 1 receptor st im -ulat ion reverses key deficits in dist inct rodent m odels of Parkinson's disease. J Neuroinflam m at ion. 2008; 5: 19. [ Crossref] [ PubMed] [ PMC]
56. Liu W, Jalewa J, Sharm a M, Li G, Li L, Hölscher C. Neu-roprotect ive effects of lix isenat ide and liraglut ide in the 1-m ethyl-4-phenyl-1,2,3,6- tet rahydropyr idine m ouse m odel of Parkinson's disease. Neuroscience. 2015; 303: 42-50. [ Crossref] [ PubMed]
57. Ma D, Liu X, Liu J, Li M, Chen L, Gao M, Xu W, Yang Y. Long- term liraglut ide am eliorates nigrost r iatal im pair-m ent via regulat ing AMPK/ PGC-1a signaling in diabet ic m ice. Brain Res. 2019; 1714: 126-132. [ Crossref] [ PubMed]
58. Badawi GA, Abd El Fat tah MA, Zaki HF, El Sayed MI . Sitaglipt in and liraglut ide modulate l-dopa effect and at-tenuate dyskinet ic m ovem ents in rotenone- lesioned rats. Neurotox Res. 2019; 35: 635-653. [ Crossref] [ PubMed]
59. Zhang L, Zhang L, Li L, Hölscher C. Sem aglut ide is neu-roprotect ive and reduces α- synuclein levels in the chronic MPTP m ouse m odel of Parkinson's disease. J Parkinsons Dis. 2019; 9: 157-171. [ Crossref] [ PubMed]
354
Bakıner et al. Turk J Endocrinol Metab. GLP-1 and Brain 2020; 24: 343-355
3 5 4
60. Athauda D, Maclagan K, Skene SS, Bajwa-Joseph M, Letchford D, Chowdhury K, Hibbert S, Budnik N, Zam pedri L, Dickson J, Li Y, Aviles-Olm os I , Warner TT, Lim ousin P, Lees AJ, Greig NH, Tebbs S, Foltynie T. Exe-nat ide once weekly versus placebo in Parkinson's dis-ease: a random ised, double-blind, placebo-cont rolled t r ial. Lancet . 2017; 390: 1664-1675. [ Crossref] [ PubMed] [ PMC]
61. Gil-Lozano M, Pérez-Tilve D, Alvarez-Crespo M, Mart ís A, Fernandez AM, Catalina PA, Gonzalez-Mat ias LC, Mallo F. GLP-1(7-36)-am ide and Exendin-4 st imulate the HPA axis in rodents and hum ans. Endocr inology. 2010; 151: 2629-2640. [ Crossref] [ PubMed]
62. Yam am oto H, Lee CE, Marcus JN, William s TD, Overton JM, Lopez ME, Hollenberg AN, Baggio L, Saper CB, Drucker DJ, Elm quist JK. Glucagon- like pept ide-1 re-ceptor st im ulat ion increases blood pressure and heart rate and act ivates autonom ic regulatory neurons. J Clin I nvest . 2002; 110: 43-52. [ Crossref] [ PubMed] [ PMC]
63. Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA, Nissen SE, Pocock S, Poulter NR, Ravn LS, Steinberg WM, Stockner M, Zinman B, Bergenstal RM, Buse JB; LEADER Steering Com m it tee; LEADER Trial I nvest igators. Liraglut ide and cardiovascular outcom es in t ype 2 diabetes. N Engl J Med. 2016; 375: 311-322. [ Crossref] [ PubMed] [ PMC]
64. Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jódar E, Leiter LA, Lingvay I , Rosenstock J, Seufert J, Warren ML, Woo V, Hansen O, Holst AG, Pet tersson J, Vilsbøll T; SUSTAI N-6 I nvest igators. Sem aglut ide and cardiovas-cular outcom es in pat ients with type 2 diabetes. N Engl J Med. 2016; 375: 1834-1844. [ Crossref] [ PubMed]
65. Liu D, Jin B, Chen W, Yun P. Dipept idyl pept idase 4 (DPP-4) inhibitors and cardiovascular outcom es in pat ients with type 2 diabetes m ellitus (T2DM): a system at ic re-v iew and m eta-analysis. BMC Pharm acol Toxicol. 2019; 20: 15. [ Crossref] [ PubMed] [ PMC]
66. Darsalia V, Larsson M, Lietzau G, Nathanson D, Nyst röm T, Klein T, Pat rone C. Glipt in-m ediated neuroprotect ion against st roke requires chronic pret reatm ent and is in-dependent of glucagon- like pept ide-1 receptor. Diabetes Obes Metab. 2016; 18: 537-541. [ Crossref] [ PubMed]
67. Röhnert P, Schm idt W, Emmerlich P, Goihl A, Wrenger S, Bank U, Nordhoff K, Täger M, Ansorge S, Reinhold D, St r iggow F. Dipept idyl pept idase I V, am inopept idase N and DPI V/ APN- like proteases in cerebral ischem ia. J Neuroinflam m at ion. 2012; 9: 44. [ Crossref] [ PubMed] [ PMC]
68. Han L, Hölscher C, Xue GF, Li G, Li D. A novel dual-glucagon- like pept ide-1 and glucose-dependent in-sulinot ropic polypept ide receptor agonist is neuroprotect ive in t ransient focal cerebral ischemia in the rat . Neuroreport . 2016; 27: 23-32. [ Crossref] [ PubMed]
69. Kröller-Schön S, Knorr M, Hausding M, Oelze M, Schuff A, Schell R, Sudowe S, Scholz A, Daub S, Karbach S, Kossmann S, Gori T, Wenzel P, Schulz E, Grabbe S, Klein T, Münzel T, Daiber A. Glucose- independent im prove-m ent of vascular dysfunct ion in experim ental sepsis by dipept idyl-pept idase 4 inhibit ion. Cardiovasc Res. 2012; 96: 140-149. [ Crossref] [ PubMed]
70. Lee CH, Yan B, Yoo KY, Choi JH, Kwon SH, Her S, Sohn Y, Hwang I K, Cho JH, Kim YM, Won MH. I schem ia- in-duced changes in glucagon- like pept ide-1 receptor and neuroprotect ive effect of its agonist , exendin-4, in ex-perim ental t ransient cerebral ischem ia. J Neurosci Res. 2011; 89: 1103-1113. [ Crossref] [ PubMed]
71. Kuroki T, Tanaka R, Shim ada Y, Yam ashiro K, Ueno Y, Shimura H, Urabe T, Hat tori N. Exendin-4 inhibits matrix
Metalloproteinase-9 act ivat ion and reduces infarct growth after focal cerebral ischem ia in hyperglycem ic m ice. St roke. 2016; 47: 1328-1335. [ Crossref] [ PubMed]
72. El-Sahar AE, Safar MM, Zaki HF, At t ia AS, Ain-Shoka AA. Sitaglipt in at tenuates t ransient cerebral ischemia/ reper-fusion injury in diabet ic rats: im plicat ion of the oxida-t ive- inflam m atory-apoptot ic pathway. Life Sci. 2015; 126: 81-86. [ Crossref] [ PubMed]
73. Chien CT, Jou MJ, Cheng TY, Yang CH, Yu TY, Li PC. Ex-endin-4- loaded PLGA m icrospheres relieve cerebral is-chemia/ reperfusion injury and neurologic deficits through long- last ing bioact ivity-mediated phosphorylated Akt / eNOS signaling in rats. J Cereb Blood Flow Metab. 2015; 35: 1790-1803. [ Crossref] [ PubMed] [ PMC]
74. Zhao L, Xu J, Wang Q, Qian Z, Feng W, Yin X, Fang Y. Protect ive effect of rhGLP-1 (7-36) on brain ischem ia/ reperfusion dam age in diabet ic rats. Brain Res. 2015; 1602: 153-159. [ Crossref] [ PubMed]
75. Yang D, Nakajo Y, I ihara K, Kataoka H, Yanam oto H. Aloglipt in, a dipept idylpept idase-4 inhibitor, for pat ients with diabetes m ellitus type 2, induces tolerance to focal cerebral ischem ia in non-diabet ic, norm al m ice. Brain Res. 2013; 1517: 104-113. [ Crossref] [ PubMed]
76. Li PC, Liu LF, Jou MJ, Wang HK. The GLP-1 receptor ag-onists exendin-4 and liraglut ide alleviate oxidat ive st ress and cognit ive and m ictur it ion deficits induced by m iddle cerebral artery occlusion in diabet ic m ice. BMC Neurosci. 2016; 17: 37. [ Crossref] [ PubMed] [ PMC]
77. Zhang H, Liu Y, Guan S, Qu D, Wang L, Wang X, Li X, Zhou S, Zhou Y, Wang N, Meng J, Ma X. An orally act ive alloster ic GLP-1 receptor agonist is neuroprotect ive in cellular and rodent m odels of st roke. PLoS One. 2016; 11: e0148827. [ Crossref] [ PubMed] [ PMC]
78. Zhang H, Meng J, Zhou S, Liu Y, Qu D, Wang L, Li X, Wang N, Luo X, Ma X. I nt ranasal delivery of Exendin-4 confers neuroprotect ive effect against cerebral ischem ia in m ice. AAPS J. 2016; 18: 385-394. [ Crossref] [ PubMed] [ PMC]
79. Darsalia V, Mansouri S, Ortsäter H, Olverling A, Nozadze N, Kappe C, I verfeldt K, Tracy LM, Grankvist N, Sjöholm Å, Pat rone C. Glucagon- like pept ide-1 receptor act iva-t ion reduces ischaem ic brain damage following st roke in Type 2 diabet ic rats. Clin Sci (Lond) . 2012; 122: 473-483. [ Crossref] [ PubMed] [ PMC]
80. Teram oto S, Miyam oto N, Yatom i K, Tanaka Y, Oishi H, Arai H, Hat tor i N, Urabe T. Exendin-4, a glucagon- like pept ide-1 receptor agonist , provides neuroprotect ion in m ice t ransient focal cerebral ischem ia. J Cereb Blood Flow Metab. 2011; 31: 1696-1705. [ Crossref] [ PubMed] [ PMC]
81. Ma M, Hasegawa Y, Koibuchi N, Toyam a K, Uekawa K, Nakagawa T, Lin B, Kim-Mitsuyama S. DPP-4 inhibit ion with linaglipt in am eliorates cognit ive im pairm ent and brain at rophy induced by t ransient cerebral ischemia in type 2 diabet ic m ice. Cardiovasc Diabetol. 2015; 14: 54. [ Crossref] [ PubMed] [ PMC]
82. Sato K, Kam eda M, Yasuhara T, Agari T, Baba T, Wang F, Shinko A, Wakam ori T, Toyoshim a A, Takeuchi H, Sasaki T, Sasada S, Kondo A, Borlongan CV, Matsum ae M, Date I . Neuroprotect ive effects of liraglut ide for st roke m odel of rats. I nt J Mol Sci. 2013; 14: 21513-21524. [ Crossref] [ PubMed] [ PMC]
83. Tai J, Liu W, Li Y, Li L, Hölscher C. Neuroprotect ive ef-fects of a t r iple GLP-1/ GI P/ glucagon receptor agonist in the APP/ PS1 t ransgenic mouse model of Alzheimer's dis-ease. Brain Res. 2018; 1678: 64-74. [ Crossref] [ PubMed]
355
Turk J Endocrinol Metab. Bakıner et al. 2020; 24: 343-355 GLP-1 and Brain
3 5 5

356
Giant Malignant Pheochrom ocytom a: A Unique Case Report from Turkey
Dev Malign Feokrom ositom a Vakası
Dam la TÜFEKÇİ, Yasem in E. GÜNAY, Ahm et Suat DEMİR, İr fan NUHOĞLU,
Hülya COŞKUN, Özge ÜÇÜNCÜ, Mustafa KOÇAK Department of Endocrinology and Metabolism, Karadeniz Technical University Faculty of Medicine, Trabzon, TURKEY
Case Report Turk J Endocrinol Metab. 2020; 24: 356-360
I nt roduct ion Catecholam ine-secret ing tum ors or iginat ing from chrom affin cells are of two types: pheochrom ocytom a from the adrenal m edulla and paragangliom a from the sym -pathet ic ganglia. Pheochrom ocytom as are rare neoplasm s found in less than about 0.2% of the hyper-tensive pat ients (1,2) . While classical pheochrom ocytom as are rare, giant pheochrom ocytom as are m uch less com -m on. Although m ost of such tum ors rem ain benign, about 10% becom e m alignant . Al-
though m ost cases are sporadic, som et im es they can be associated with m ult iple en-docrine neoplasia type 2 (MEN-2) , von Hip-pel-Lindau (VHL) syndrom e, and less often with neurofibrom atosis type 1 (NF-1) (3,4) . Preoperat ive diagnosis and therapeut ic t reatm ents m ay be diff icult for m alignant pheochrom ocytom a pat ients. The classic sym ptom s seen in pheochrom ocytom a pa-t ients include episodic headache, sweat ing, and tachycardia (1,5) . About half of the pa-t ients show paroxysm al hypertension; the majority of the remaining pat ients show pri-
Catecholam ine-secret ing tum ors are rare neoplasm s that occur in less than 0.2% of hypertensive pat ients. While phe-ochrom ocytom as are rare neoplasm s in the adrenal gland, giant pheochrom ocytom as are m uch less com m on. I n this report , we present the case of a 38-year-old m an who had a 29x18x12 cm giant m alignant pheochrom ocytom a. Du-r ing an exam inat ion for hem atur ia, a large m ass was de-tected incidentally in the r ight adrenal gland of the pat ient . This mass was diagnosed as pheochromocytoma and proved to be one of the largest pheochrom ocytom as reported so far; hence, its not ificat ion has been considered significant for the medical and research professionals across the world. Keyw ords: Adrenal incidentalom a; pheochrom ocytom a;
hem aturia; hypertension, m alignant ; chrom affin cells
Katekolam in salgılayan tüm örler, hipertansiyonu olan has-taların yüzde 0,2’sinden daha azında görülen nadir neopla-zilerdir. Feokrom ositom alar adrenal bezde görülen nadir neoplazilerken, dev feokrom ositom alar çok daha nadir gö-rülm ektedir. Bu vaka bildir im inde 38 yaşında 29x18x12 cm boyut lar ında dev m align feokrom ositom a tespit edilen bir erkek hasta tanım lanmışt ır. Hasta hematüri nedeni ile tetkik edilirken sağ adrenal bezinde insidental olarak kit le tespit edilm işt ir. Türkiye’de tanım lanm ış en büyük feokrom osito-m alardan bir i olarak bildir im inin önem li olabileceği düşü-nülm üştür. Anahtar kelim eler: Adrenal insidentalom; feokromositoma;
hem atüri; hipertansiyon, m align; krom afin hücreler
3 5 6
Address for Correspondence: Dam la TÜFEKÇİ, Departm ent of Endocrinology and Metabolism , Karadeniz Technical University Faculty of Medicine, Trabzon, TURKEY
Phone: + 90 545 553 77 53 E- m ail: drtufekci@gm ail.com
Peer review under responsibilit y of Turkish Journal of Endocrinology and Metabolism .
Received: 22 Jun 2020 Received in revised form : 07 Sep 2020 Accepted: 25 Sep 2020 Available online: 16 Oct 2020
1308-9846 / ® Copyright 2020 by Society of Endocrinology and Metabolism of Turkey. Publicat ion and host ing by Turkiye Klinikler i.
This is an open access art icle under the CC BY-NC-SA license (ht tps: / / creat ivecom m ons.org/ licenses/ by-nc-sa/ 4.0/ ) DO
I: 1
0.2
51
79
/tje
m.2
02
0-7
74
74

357
Turk J Endocrinol Metab. Tüfekçi et al. 2020; 24: 356-360 Giant Malignant Pheochrom ocytom a
3 5 7
m ary hypertension or norm al blood pres-sure. Most of the pheochrom ocytom a pa-t ients do not display all t hree classic sym ptom s sim ultaneously (6,7) . The first step in the diagnosis of pheochrom ocytom a is the biochem ical analysis of ur ine and plasma fract ionated metanephrines and cat-echolam ines. Radiological evaluat ion is advised after bio-chem ical confirmat ion of the diagnosis to lo-cate the tum or. Approxim ately 15% of all pheochrom ocytom asare ext ra-adrenal, but 95% of them are within the abdom en and pelvis (4) . I n order to diagnose the lesion, com puted tom ography (CT) or m agnet ic resonance im aging (MRI ) of the abdom en and pelvis is usually perform ed first ly. Once pheochrom ocytom a is diagnosed, pa-t ients should be operated after necessary m edical preparat ion. Dur ing preoperat ive preparat ion, sym pathet ic cont rol with alpha blockage followed by a beta-adrenergic blockade is required. As pheochromocytoma surgery is highly r isky, hem odynam ic var i-ables should be closely monitored during the operat ion (8) . The choice of approach in-cludes both laparoscopic and open surgery, depending on tum or character ist ics and pa-t ient factors. I n this case report , a giant m alignant pheochrom ocytom a sized 29x18x12 cm has been presented.
Case Report A 38-year-old m ale pat ient applied to the em ergency service with the com plaint of blood in the ur ine. I n the abdom inal USG perform ed for the et iology of hem atur ia, a mass of 25 cm diameter was detected in the r ight adrenal region. The pat ient was adm it-ted to the endocrinology clinic to further in-vest igate; different iate between benign and m alignant adrenal m ass, and evaluate the horm onal act iv it y. The following indicators were observed during the physical exam ina-t ion: blood pressure 150/ 90 m m Hg; pulse rate 92 beats/ m in; tem perature 36.5 ° C; the respiratory system norm al; the cardiac rhythm norm al. No addit ional voice and m urm ur were observed. I n the abdom inal exam inat ion, a m ass with regular contours of 20 cm , palpable with deep seated lesion in the r ight upper and m iddle quadrant was detected. The pat ient ’s biochem ical exam i-nat ions were norm al, but ur ine and plasm a adrenaline, noradrenaline, and norm etanephr ine levels were found to be high in the tests performed for the hormonal act ivity of the adrenal gland (Table 1) . The pat ient was diagnosed with pheochro-m ocytom a, and a Holter m onitor ing device was inserted into him ( the pat ient ) to m on-itor his 24-hour blood pressure. The fundus exam inat ion was perform ed in term s of organ dam age due to hypertension that re-
Test Pat ient ’s value Reference values
ACTH 54.3 ng/ L 6.7-22.6 ng/ L
Cort isol 22.2 µg/ dL ≤46 µg/ dL
Dexam ethasone Suppression Test (1 m g) 0.75 µg/ dL
Dehydroepiandrosterone Sulfate 61.3 µg/ dL
Testosterone 3.92 µg/ L 1.98-6.79 µg/ L
Aldosterone (ALD) 25.36 ng/ dL 7-30 ng/ dL
Plasm a Renin Act ivity (PRA) 3.68 ng/ m L/ h 0.98-4,18 ng/ m L/ h
ALD/ PRA 4,08
Plasm a Metanephrine Level 39.66 pg/ m L ≤90 pg/ m L
Plasm a Norm etanephrine Level 737.19 pg/ m L ≤180 pg/ m L
Plasm a Adrenaline 183.92 ng/ L ≤90 ng/ L
Plasm a Noradrenaline 734.93 ng/ L ≤500 ng/ L
Urine Metanephrine 158.95 µg/ 24 h 50-250 µg/ 24 h
Urine Norm etanephrine 2643.27 µg/ 24 h 100-500 µg/ 24 h
Urine Adrenaline 37.76 µg/ 24 h 0-20 µg/ 24 h
Urine Noradrenaline 114.77 µg/ 24 h 15-80 µg/ 24 h
Table 1. Table showing the pat ient ’s horm one evaluat ion with tests, and reference/ standard values.

358
Tüfekçi et al. Turk J Endocrinol Metab. Giant Malignant Pheochrom ocytom a 2020; 24: 356-360
3 5 8
vealed stage 1 hypertensive ret inopathy. Left vent r icular hypert rophy was seen on echocardiography. I n the abdominal MRI , the following features were detected. There was a m ass lesion in the r ight adrenal gland, 216 x 167 m m in size from the supe-r ior to the liver, infer ior to the r ight bound-ary pushing the portal vein anterior-superior, crossing the m idline, solid character with cyst ic-necrot ic areas, and showing heterogeneous enchantm ent of the adrenal gland (Figure 1A, B) . After t he exam inat ions and im aging, t he r ight adrenalectom y was recom m ended to the pat ient . I n order to prevent a potent ial hypertensive crisis during the operat ion, the pat ient was init iated on alpha blockade with dibenzyran and then with propranolol dur-ing the preoperat ive per iod and was oper-ated for m ass excision in March 2019 by general surgery. No hyper tensive at tack dur ing the operat ion was reported. Macro-scopic exam inat ion of the surgical specim en showed a brown color, a heterogeneous tu-m oral lesion that m easured 29x18x12 cm , weighed 1490 gram s with cyst ic cavit ies f illed with necrot ic and bleeding f luids on large areas (Figure 2) . I n the immunohistochem ical study, chromo-granin A(CgA) , synaptophysin, and S-100 protein were posit ively stained. Ki-67 label-ing index was reported as 1% .
The histopathological result confirm ed pheochrom ocytom a (Figure 3A-C) . As the m ass was evaluated as high m alig-nancy potent ial due to the pheochrom ocy-tom a of the Adrenal Gland Scaled Score (PASS) of 11, PET-CT scan was performed to detect any pathological involvem ent or m etastasis focus. The pat ient showed nor-mal levels of postoperat ive urine and plasma
Figure 1 . A) Mass lesion in heterogenous enchantm ent of the r ight adrenal gland from the superior to the liver, B) I nfe-r ior to the r ight boundary-pushing the portal vein anter ior-superior, crossing the m idline.
A B
Figure 2 . Surgical specim en: brown color shows hetero-geneous lesion (size 29x18x12 cm , weight 1490 gram s) , with the cyst ic cavity filled with necrot ic and bleeding flu-ids in adjoining areas.

359
Turk J Endocrinol Metab. Tüfekçi et al. 2020; 24: 356-360 Giant Malignant Pheochrom ocytom a
3 5 9
catecholam ines and was followed up as nor-m otensive without using any m edicat ion.
Discussion Pheochrom ocytom as are rare neoplasm s emanat ing from chromaffin cells of the sym-pathoadrenal system (9) . Eighty- f ive per-cent of the pheochromocytomas occur in the adrenal m edulla region (10) . Pheochrom o-cytom as m ay generally occur from the fourth to the f if t h decade, equally in m en and wom en. The majority of the pheochromocytomas are benign, and about 10 percent are m alignant (5) . As the size of the m ass increases, the r isk of m alignancy also increases. Malig-nancy r isk is eight t im es greater, especially in lesions larger than 6 cm . The m alignant potent ial of pheochrom ocy-tom a cannot be determ ined preoperat ively if there is no pr ior evidence of m etastases. I n our case, there was no m etastasis focus in all body im ages. Thom pson (11) evalu-ated 50 benign and 50 m alignant pheochro-m ocytom as histopathologically and found histological features such as necrosis, atypia, increased m itosis, nuclear polym or-phism , and diffuse growth to be m ore com -m on in m alignant tum ors. Each feature was scored and pheochrom ocytom a profiling by the PASS was done, 4 or m ore results were evaluated as aggressive biological features. Since the PASS in our case was 11, the m a-lignancy potent ial was considered high. Due to the low incidence of m alignant pheochrom ocytom as, there is insuff icient data regarding prognosis and survival. Five-year surv ival is generally below 50% in m etastat ic pheochrom ocytom as. These pa-t ients should be followed lifelong.
Pheochrom ocytom a is usually detected by examining asymptomat ic pat ients, detect ing an adrenal m ass incidentally, or scanning a pat ient with fam ilial disease. Fifty percent of the pat ients with pheochrom ocytom a dis-play som e typically paroxysm al sym ptom s. The classic t r iad of sym ptom s includes episodic headache, sweat ing, and tachycar-dia (1,6) . I nterest ingly, the pat ient was asym ptom at ic with an adrenal m ass of about 30 cm . I n a study in, which 20 cases of pheochrom ocytom a greater than 10 cm were presented, 13 pat ients had abdom inal pain while only five had classic sym ptom s of pheochrom ocytom a (12) . I n our case, the pat ient was diagnosed incidentally while he was being exam ined due to hem aturia. Surgery is the t reatm ent of choice in pa-t ients diagnosed with pheochrom ocytom a. I n the current case, open surgery was pre-ferred due to the large size of the mass. The pat ient was successfully operated with pre-operat ive preparat ions. Postoperat ive ur ine and plasma catecholam ine levels were found to be norm al. The average m ass size in pheochrom ocy-tom as is approxim ately 7 cm . I n the litera-ture search covering sum m aries of all giant (> 10 cm ) pheochrom ocytom as (13) , the largest tum or was reported as 45x20 cm (14) . Although, previously rare cases of av-erage size have been reported in Turkey (15) , this remarkable case showcases one of the largest pheochrom ocytom as ever re-ported in Turkey.
Source of Finance During this study, no f inancial or spir it ual support was received neither from any phar-m aceut ical com pany that has a direct con-
Figure 3 . Pheochrom ocytotom a white lesions seen in an im m unohistochem ical analysis showing staining of chrom ogranin A ( A) , Synaptophysin [ ( B) and S-100 ( C) ] .
A B C

360
Tüfekçi et al. Turk J Endocrinol Metab. Giant Malignant Pheochrom ocytom a 2020; 24: 356-360
3 6 0
nect ion with the research subject , nor from a com pany that provides or produces m ed-ical inst rum ents and m ater ials which m ay negat ively affect the evaluat ion process of this study.
Conflict of I nterest No conflicts of interest between the authors and / or fam ily members of the scient ific and medical commit tee members or members of the potent ial conflicts of interest , counsel-ing, expert ise, working condit ions, share holding and sim ilar situat ions in any firm .
Authorship Contr ibut ions I dea/ Concept : Dam la Tüfekçi; Design: Dam la Tüfekçi, Yasem in E. Günay; Con-t rol/ Supervision: Dam la Tüfekçi, İr fan Nuhoğlu; Data Collect ion and/ or Processing: Dam la Tüfekçi, Yasem in E. Günay, Ahm et Suat Dem ir; Analysis and/ or I nterpretat ion: Dam la Tüfekçi, Hülya Coşkun, İr fan Nuhoğlu, Mustafa Koçak; Literature Review: Dam la Tüfekçi; Writ ing the Art icle: Dam la Tüfekçi; Cr it ical Review: Dam la Tüfekçi, Yasem in E. Günay, İr fan Nuhoğlu; Refer-ences and Fundings: Damla Tüfekçi, Mustafa Koçak.
References 1. Stein PP, Black HR. A simplified diagnost ic approach
to pheochrom ocytom a. A review of the lit erature and report of one inst itut ion's experience. Medicine (Balt im ore) . 1991; 70: 46-66. [ Crossref] [ PubMed]
2. Pacak K, Linehan WM, Eisenhofer G, Walther MM, Goldstein DS. Recent advances in genet ics, diagno-sis, localizat ion, and t reatm ent of pheochrom ocy-tom a. Ann I ntern Med. 2001; 134: 315-329. [ Crossref] [ PubMed]
3. Neum ann HP, Berger DP, Sigm und G, Blum U, Schm idt D, Parm er RJ, Volk B, Kirste G. Pheochro-m ocytom as, m ult iple endocr ine neoplasia t ype 2, and von Hippel-Lindau disease. N Engl J Med. 1993; 329: 1531-1538. [ Crossref] [ PubMed]
4. Bravo EL. Evolving concepts in the pathophysiology, diagnosis, and t reatm ent of pheochrom ocytom a. Endocr Rev. 1994; 15: 356-368. [ Crossref] [ PubMed]
5. Bravo EL. Pheochrom ocytom a: new concepts and future t rends. Kidney I nt . 1991; 40: 544-556. [ Crossref] [ PubMed]
6. Kudva YC, Young WF, Thom pson GB, Grant CS, Van Heerden JA. Adrenal incidentalom a: an im portant com ponent of the clinical presentat ion spect rum of benign sporadic adrenal pheochrom ocytom a. The Endocrinologist . 1999; 9: 77-80. [ Crossref]
7. Baguet JP, Ham m er L, Mazzuco TL, Chabre O, Mallion JM, Sturm N, Chaffanjon P. Circum stances of discovery of phaeochrom ocytom a: a ret rospec-t ive study of 41 consecut ive pat ients. Eur J En-docrinol. 2004; 150: 681-686. [ Crossref] [ PubMed]
8. Lenders JW, Duh QY, Eisenhofer G, Gimenez-Roque-plo AP, Grebe SK, Murad MH, Naruse M, Pacak K, Young WF Jr ; Endocr ine Society. Pheochrom ocy-toma and paraganglioma: an endocrine society clin-ical pract ice guideline. J Clin Endocr inol Metab. 2014; 99: 1915-1942. [ Crossref] [ PubMed]
9. Pederson LC, Lee JE. Pheochrom ocytom a. Curr Treat Opt ions Oncol. 2003; 4: 329-337. [ Crossref] [ PubMed]
10. Dahia PL. Evolving concepts in pheochrom ocytom a and paragangliom a. Curr Opin Oncol. 2006; 18: 1-8. [ Crossref] [ PubMed]
11. Thom pson LD. Pheochrom ocytom a of the Adrenal gland Scaled Score (PASS) to separate benign from m alignant neoplasm s: a clinicopathologic and im -m unophenotypic study of 100 cases. Am J Surg Pathol. 2002; 26: 551-566. [ Crossref] [ PubMed]
12. Korgali E, Dundar G, Gokce G, Kilicli F, Elagoz S, Ayan S, Gultekin EY. Giant m alignant pheochrom o-cytom a with palpable r ib m etastases. Case Rep Urol. 2014; 2014: 354687. [ Crossref] [ PubMed] [ PMC]
13. Maharaj R, Parbhu S, Ram charan W, Baij oo S, Greaves W, Harnanan D, Warner WA. Giant cyst ic pheochrom ocytom a with low r isk of m alignancy: a case report and literature review. Case Rep Oncol Med. 2017; 2017: 4638608. [ Crossref] [ PubMed] [ PMC]
14. Gr issom JR, Yam ase HT, Prosser PR. Giant pheochrom ocytom a with sarcoidosis. South Med J. 1979; 72: 1605-1607. [ Crossref] [ PubMed]
15. Uysal E, Kırdak T, Gürer AO, İkidağ MA. Giant m ul-t icyst ic m alignant pheochrom ocytom a. Turk J Surg. 2015; 33: 296-298. [ Crossref] [ PubMed] [ PMC]
W E THANK ALL OUR REFEREES
Nam e- Surnam e The num ber of art icles he/ she review ed
AYSEN AKALI N 15
GÜZİDE GONCA ÖRÜK 13
MEDİNE NUR KEBAPÇI 10
ÖMER AZAL 9
BERRİN ÇETİNARSLAN 8
REFİK TANAKOL 8
KÜRŞAD ÜNLÜHI ZARCI 7
YUSUF ALPER SÖNMEZ 7
ZEYNEP OŞAR SİVA 7
AYŞEGÜL ATMACA 6
İNAN ANAFOROĞLU 6
MUSTAFA KULAKSI ZOĞLU 6
YALÇI N ARAL 6
ERSİN AKARSU 5
MURAT SERT 5
REYHAN ERSOY 5
AHMET ÇORAKÇI 4
AHMET KAYA 4
ERMAN ÇAKAL 4
FAHRİ BAYRAM 4
FATMA HARİKA BOZTEPE 4
FATMA TÜMAY SÖZEN 4
FÜSUN SAADET BALOŞ TÖRÜNER 4
ŞİNASİ EROL BOLU 4
ÜMİT KARAYALÇI N 4
ZELİHA FULDEN SARAÇ 4
BELGİN EFE 3
CANAN ÖZYARDI MCI ERSOY 3
CEYLA KONCA DEĞERTEKİN 3
DİDEM ÖZDEMİR 3
LÜTFİYE FÜSUN SAYGI LI 3
MEHMET ALİ EREN 3
ÖZLEM TURHAN İYİDİR 3
PI NAR KADI OĞLU 3
TANER BAYRAKTAROĞLU 3
ZELİHA HEKİMSOY 3
ASLI NAR 2
AYŞE KUBAT ÜZÜM 2
AYTEN OĞUZ 2
EMRE BOZKI RLI 2
GÖKNUR YORULMAZ 2
GÜVEN BARIŞ CANSU 2
HATİCE SEBİLA DÖKMETAŞ 2
İBRAHİM ŞAHİN 2
LEVENT ÖZSARI 2
MEHMET ERDOĞAN 2
MELEK EDA ERTÖRER 2
RAMİS ÇOLAK 2
SEMİN MELAHAT FENKÇİ 2
SERPİL SALMAN 2
SÜLEYMAN HİLMİ İPEKÇİ 2
ZÜLEYHA CİHAN ÖZDAMAR KARACA 2
ALPTEKİN GÜRSOY 1
ASLI DOĞRUK ÜNAL 1
BARIŞ AKI NCI 1
BİLGİN ÖZMEN 1
CEM HAYMANA 1
COŞKUN MERİÇ 1
FİLİZ EKŞİ HAYDARDEDEOĞLU 1
GÜZİN FİDAN YAYLALI 1
METİN GÜÇLÜ 1
MUSTAFA ÜNÜBOL 1
OKAN SEFA BAKI NER 1
ÖZLEM ÇELİK 1
RÜŞTÜ SERTER 1
SEMA ÇİFTÇİ DOĞANŞEN 1
ZEYNEP CANTÜRK 1
ISM OF TURKEYABOLITJOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND ME

ISM OF TURKEYABOLITJOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND ME
TURKJEM 3 rd PRI ZED ARTI CLE COMPETI TI ON 2 0 2 0 RESULTS
FI RST PRI ZE
Effect of Vitam in D Treatm ent on Glycem ic Control, Diastolic Funct ions, and Carot id I nt im a- Media Thickness in Pat ients w ith Type 2 Diabetes Mellitus
Mehtap EVRAN OLGUN, Gam ze AKKUŞ, Mustafa GÖK* , Çağlar Em re ÇAĞLI YAN* , İlker ÜNAL* * , Murat SERT, Tam er TETİKER
Çukurova University Faculty of Medicine, Departm ent of I nternal Medicine, Division of Endocrinology, Adana, Turkey * Çukurova University Faculty of Medicine, Departm ent of Cardiology, Adana, Turkey
* * Çukurova University Faculty of Medicine, Departm ent of Biostat ist ics, Adana, Turkey
DOI : 10.25179/ t jem .2018-63768 - Turk J Endocrinol Metab 2019; 23: 97-104
ht tp: / / www.turkjem .org/ uploads/ pdf/ 435086615789693.pdf
SECOND PRI ZE
A New Cardiovascular Risk Marker in Men w ith Hypogonadism : Alanine Am inotransferase
Murat ŞAHİN, Ayten OĞUZ, Dilek TÜZÜN, Sem iha ÇALKAYA, Kam ile GÜL
Kahram anm araş Sütçü İm am University Faculty of Medicine, Departm ent of Endocrinology and Metabolism , Kahram anm araş, Turkey
DOI : 10.25179/ t jem .2019-70493 - Turk J Endocrinol Metab 2019; 23: 197-205
ht tp: / / www.turkjem .org/ uploads/ pdf/ 634224215982064.pdf
THI RD PRI ZE
Evaluat ion of Paraoxonase1 Polym orphism s in Hypothyroid Pat ients and Their Relat ionship w ith Paraoxonase Act ivity and Serum Lipids
Ayşen CANİKLİOĞLU, Gülden BAŞKOL* , Fahri BAYRAM* * , Yusuf ÖZKUL* * * , Ferhan ELMALI * * * * , İlkay ÇAKI R* * * * * , Meral MERT* * * * * , Nahide EKİCİ GÜNAY* * * * * *
Bozok University Faculty of Medicine, Departm ent of Biochem ist ry, Yozgat , Turkey * Erciyes University Faculty of Medicine, Departm ent of Biochem ist ry, Kayseri, Turkey
* * Erciyes University Faculty of Medicine, Departm ent of Endocrinology and Metabolism , Kayseri, Turkey * * * Erciyes University Faculty of Medicine, Departm ent of Genet ic, Kayseri, Turkey
* * * * İzm ir Kat ip Çelebi University Faculty of Medicine, Departm ent of Biostat ist ics, İzm ir, Turkey * * * * * Dr. Sadi Konuk Educat ion and Research Hospital,Departm ent of Endocrinology and Metabolism , İstanbul, Turkey
* * * * * * Healthy Science University Training and Research Hospital, Departm ent of Biochem ist ry, Kayseri, Turkey
DOI : 10.25179/ t jem .2019-66617 - Turk J Endocrinol Metab 2019; 23: 213-221
ht tp: / / www.turkjem .org/ uploads/ pdf/ 628358189783382.pdf
Endocrinology andTurkish Journal of
d Metabolismf
4TH 4TH
EIZEYEAR ARTICLE PRIZE YEAR ARTICLE PRIZ
COMCOMPETITIONCOMPETITION
TL500
TL
TL000
7.500
10.
3
2
3
2
12.
tition Application Compe.II
Diseases.arch articles in the field of cOriginal rese
tititonnt of Compe Conte.I
.500 3
ess on Endocrinology ankey Congrhe 42nd Tur tat
aseor article writing rules, ple Fd.ateion and evalu will bernal of Endocrinology and Metabolism”
of Endocrinology and Metabolism of Turkey’s ntweed beblisheblication and pud for puptece
linical and experimental Endocrinology and Metabo
33
nd
olic
abolic Diseases. Metticles will be announced aThe winner ar
ntssmetition Asse Compe.III
log-in to http://www.turkjem.org/.tite compe to thrved to participatesede
scientific publication organ “Turkish Jou at the Society o202012.2020-31.01.01.
accresearch articles that weOriginal retition Application Compe.II
abolic Diseases. Met

4224442..22
EEETTT
MMMEEEE
AHHHMMMMM
AAASTATTTASSA LALIKLKLIK RILARIARRAKKKKAHAHHHASTAAATATSSAA ALIKLLKKKILLA LARIIRRRAALAL
KKKK
19 991 - 23 MM3322- - MAYISSISYYAYAMAMM S 2021212020022 1 1
NANTNA ATALYALYAT YANTNNAA TALYAAAYYLLAAT A
eeyiiküürT k yr. D
ürf
üorrP D
E.
SSo
MLİP
İ MBB Mf
L
T jolorrinkodnn ojE o, P
nır,kk
doka
e EEuri Ç. PN k ,
Ya
E YTTÇ
Euri
RN
EEK.
SELE ERr
YRTERKSLr
zzliobaatee M i v oo
bl B
to
err. E
e Mr. . D
v.
ioorrAY
.f oBoE.DfAY
ğiennrea D ğzm. M
r er
e. Dçç
ma Dolu, D .o MrDçoD, lu ş aaddee AinM ş dAAnM
eeidserp es dp31T : 0.3120.3y /
: 0ılaz
T ıK lay
trruz
şK
eM uşeM
.ggrd.omeet@tnt@@t md.orgn22 425 2 072 • F07
A2 0
R5 2
A25
K2 4
N• F
A ARAli Bdd. A
NKa
At C
/ eyy Bi A. aCt ei
me.ttwwr • w.tr • wwww emt2 4255 22 : 0.312 425 2 0
.. 29/12
31
t
: 00.3
pp
F
yy Aee 2/192tAAeB
r.tggrd.od om098
r.tr809
ağzaayy zağffi
ya O
Abeeba OSS
MR KD KN
RA
MG
DRO
A
AGRO
aaim. Mhaa rd
a M mr
mavv
Me
. Mu
M ho
Me B
acc raffi e
niul
aagBo
ge
e Offi
rrffi
ng zo g nE
rN S
e OO
ngSY
oİZAN ESNOYSAZN
oo. Nkoonn Sainr S nan SdS
yonssdaz
N
I
k
S
S
AAYYonn
Ry
TEa
EEz
RRK YAK
N
SYRETRKE
k Dolo: 21 D B DkoBD2o: D: 4444:
dmwwww dwwmhk@eet mhkt
F 0.21F : 0.212T : 00.553T : 0.53234485 •5 84434
mmoczmuurit ommr c..c
zmzm
rur
mmrttt@dmr urizm@dmr
9m c
258 50 292 258 50 2MR (R
N2 111 9 DM
AATT9 D
S 9
/ İee11
y1
r2
aa AS ATS/ İryrıS• S
rtmrr
t..t
mmmocom to
7)367)36UL
(BBN LUNN
wwwww.dm
ww
www .dwww
mhe.t mhwm
mo
em.c
.tzmuuri
wwtmr mocmzrtmrm
hk2020kr
h.tm
02020202ktm
ggr0.o grro.o

JOURNAL OF THE SOCIETY OF ENDOCRINOLOGY AND METABOLISM OF TURKEY
ISSN 1301-2193
December 2020 Volume: 24 Issue: 4
Original ArticlesDemographic and Clinical Features of Medullary Thyroid CarcinomaPınar Şişman, Buket Biçer, Hikmet Öztop, Soner Cander, Özen Öz Gül, Gökhan Ocakoğlu, Canan Ersoy, Erdinç Ertürk
The Association Between Thyroid Volume and Insulin Resistance in Patients with Non-Functional Adrenal IncidentalomaMurat Şahin, Ayten Oğuz, Dilek Tüzün, Semiha Çalkaya, Kamile Gül
Frequency of Nodular Goiter in Patients with Non-Functional Adrenal IncidentalomaMustafa Can, Melia Karaköse, Muhammet Kocabaş, İlker Çordan, Hatice Çalışkan Burgucu,Mustafa Kulaksızoğlu, Feridun Karakurt
A Slight Contribution of Retroperitoneal Fat Accumulation to the Metabolic Comorbidities of Patientswith Autonomous Cortisol ProductionMustafa M. Barış, Ahmet Peker, Ozan Bozkurt, Mustafa Seçil, Ömer Demir, Serkan Yener
Knosp and Hardy Grading Systems are Useful in Predicting Persistence of Male Hypogonadismin Prolactinomas Following Prolactin NormalizationGülay Şimşek Bağır, Aylin Güneşli, Filiz Ekşi Haydardedeoğlu, Okan Sefa Bakıner, Özlem Alkan, Melek Eda Ertörer
Role of AGR2 Expression in Specimens from Pituitary Adenoma Tissue on Tumor BehaviorSema Çiftçi Doğanşen, Ömür Günaldı, Ayla Solmaz Avcıkurt, Barış Çolluoğlu, İlhan Yılmaz, Meral Mert, Osman Tanrıverdi
The Effects of Psychological Focus Group Therapy on the Quality of Life of Female Patients with AcromegalyÖzlem Haliloğlu, Sema Sözer, Özge Polat Korkmaz, Serdar Şahin, Emre Durcan, Gökhan Oral, Pınar Kadıoğlu
Clinical Profile and Changing Etiological Spectrum of Hyperprolactinemia at a Tertiary Care Endocrine FacilityJunaid Rashid Dar, Moomin Hussain Bhat, Javaid Ahmad Bhat, Raiz Ahmad Misgar, Shariq Rashid Masoodi, Mir Iftikhar Bashir, Arshad Iqbal Wani
Cardiovascular Morbidity in Diabetic Non-Alcoholic Fatty Liver Disease (NAFLD) UsingNAFLD Fibrosis Score as an Early IndicatorPriti Shahapure, Shimpa Sharma
Serum Levels of 8-OHdG in Patients with Hashimoto’s ThyroiditisFatemeh Esfahanian, Seyedeh Mahdieh Fotouk Kiaie, Roghayeh Ghelich, Zohreh Jadali
Review ArticlesDealing with COVID-19: Through Endocrinologist’s EyesCem Sulu, Pınar Kadıoğlu
Glucagon-Like Polypeptide-1 and BrainOkan Sefa Bakıner, Akadlı Kürşad Özşahin
Case ReportGiant Malignant Pheochromocytoma: A Unique Case Report from TurkeyDamla Tüfekçi, Yasemin E. Günay, Ahmet Suat Demir, İrfan Nuhoğlu, Hülya Coşkun, Özge Üçüncü, Mustafa Koçak
253
261
270
277
284
293
308
314
335
343
356
321
300
Copyright © 2022 FDOKUMEN




















