Calcineurin inhibitors dampen humoral immunity by acting directly on naive B cells
Upload
independentCategory
view
3download
0
American Journal of Transplantation 2004; 4: 1776–1785Blackwell Munksgaard
Copyright C© Blackwell Munksgaard 2004
doi: 10.1111/j.1600-6143.2004.00627.x
De Novo Kidney Transplantation Without Use ofCalcineurin Inhibitors Preserves Renal Structure andFunction at Two Years
Stuart M. Flechnera,∗, Sunil M. Kurianb,
Kim Solezc, Daniel J. Cooka, James T. Burked,
Hank Rollina, Jennifer A. Hammondb, Thomas
Whisenantb, Caroline M. Laniganb,
Steven R. Headb and Daniel R. Salomonb
aSection of Renal Transplantation, Transplant Center, andAllogen Laboratories, The Cleveland Clinic Foundation,Cleveland, Ohio, USAbDNA Array Core Facility, and the Department ofMolecular and Experimental Medicine, The ScrippsResearch Institute, La Jolla, California, USAcDepartment of Pathology, University of Alberta,Edmonton, Alberta, CanadadTransplant Immunology, Wyeth Research, Paris, France∗Corresponding author: Stuart M. Flechner,[email protected]
We performed a randomized prospective trial compar-ing calcineurin inhibitor (CNI)-free to CNI-based im-munosuppression to determine the impact on renalfunction, structure and gene expression. Sixty-one kid-ney recipients treated with basiliximab mycopheno-late mofetil (MMF) and prednisone (P) were randomlyassigned to concentration-controlled sirolimus or cy-closporine. Two years post-transplant 55 patients un-derwent renal function studies, 48 (87%) underwenttransplant biopsies; all classified by Banff scoring and41 by DNA microarrays. Comparing sirolimus/MMF/Pto cyclosporine/MMF/P there was a significantly lowerserum creatinine (1.35 vs. 1.81 mg/dL; p = 0.008),higher Cockroft-Gault glomerular filtration rate (GFR)(80.4 vs. 63.4 mL/min; p = 0.008), iothalamate GFR(60.6 vs. 49.2 mL/min; p = 0.018) and Banff 0 (normal)biopsies (66.6 vs. 20.8%; p = 0.013). Regression anal-ysis of calculated GFRs from 1 to 36 months yielded apositive slope for sirolimus of 3.36 mL/min/year, and anegative slope for cyclosporine of −1.58 mL/min/year(p = 0.008). Gene expression profiles from kid-neys with higher Banff chronic allograft nephropa-thy (CAN) scores confirmed significant up-regulationof genes responsible for immune/inflammation andfibrosis/tissue remodeling. At 2 years the sirolimus-treated recipients have better renal function, a dimin-
Presented at the American Transplant congress, Boston, Mas-sachusetts, May 16, 2004.
ished prevalence of CAN and down-regulated expres-sion of genes responsible for progression of CAN. Allmay provide for an alternative natural history with im-proved graft survival.
Key words: Chronic allograft nephropathy, gene ex-pression, kidney transplantation, sirolimus
Received 19 May 2004, revised and accepted for publi-cation 28 July 2004
Introduction
Continued improvements in short-term graft survival forrecipients of kidney transplants have driven the demandto unprecedented levels worldwide. However, commonlyachieved 1-year graft survivals over 90%, rapidly fall to65–70% at 5 years and under 50% at 10 years (1–3). Theleading cause of late graft loss among surviving recipientsremains the non-specific process termed chronic allograftnephropathy (CAN). Clinically, this process describes theinexorable decline in renal function with time, often char-acterized histologically by renal interstitial fibrosis, tubularatrophy, vascular occlusive changes and glomerulosclero-sis(4). Retrospective analysis in both single centers andregistries have identified a number of risk factors that sta-tistically associate with CAN, which include both immuneand non-immune mechanisms (5,6). There is a strong as-sociation between CAN and the continuous use of the cal-cineurin inhibitors (CNI), cyclosporine (CsA) and tacrolimus,which have been known to be nephrotoxins since theirinitial clinical introduction (7–10). The recent report ofNankivell et al. (11), describing the longitudinal evolution ofCAN over a 10-year period, confirms the ubiquitous scar-ring of kidneys that occurs with the continuous use of CNIdrugs. In addition, Ojo et al. (12) have identified an alarm-ing prevalence of renal insufficiency and permanent renalfailure among extrarenal allograft recipients receiving con-tinuous CNI therapy.
The introduction of Target of Rapamycin (TOR) inhibitors,a new class of potent antirejection drugs, has pro-vided opportunities to develop alternative immunosuppres-sive combinations (13). The initial use of the TOR in-hibitor, sirolimus (SRL), in CNI-free regimens demonstrated
1776

Kidney Histology and Gene Expression in Sirolimus-Treated Patients
improved kidney function at 1 year (14,15). Thus, it is pos-sible that SRL in combination with the antiproliferativeagent mycophenolate mofetil (MMF) and steroids will bea regime that provides good long-term immunosuppres-sion and is less nephrotoxic. Secondly, it is possible thata CNI-free regime will prevent or delay the onset and pro-gression of CAN by minimizing immune injury and drug-induced nephrotoxicity that in turn may drive a cycle oftissue injury, interstitial fibrosis, ischemia and pathologicaltissue remodeling (16–18).
We performed a randomized, prospective trial compar-ing primary adult renal transplant recipients given eitherde novo cyclosporine-based or sirolimus-based CNI-freeimmunosuppression (19). Herein, we present the results2 years post-transplant of renal function tests, histologi-cal analysis by Banff criteria for CAN and gene expressionstudies using DNA microarrays and quantitative RT-PCR.The results are significant improvements in renal functionmatched by a significant reduction in CAN in the sirolimus-treated group. DNA microarrays successfully classified thepatients with increased Banff CAN scores by biopsy histol-ogy and that correlated with the significant up-regulation ofgenes linked to known pathways of immune/inflammatoryinjury, fibrosis, ischemia and tissue remodeling.
Methods
Patients and immunosuppression
Between March 2000 and June 2001, 61 primary kidney-only adult allo-graft recipients (age 18–70 years) were enrolled. After informed consentwas documented patients were randomized via computer-generated cardsto one of the two experimental groups. Exclusion criteria included priortransplantation or immunosuppression, HLA identical sibling donors, cancer,pregnancy or weight >105 kg. All recipients had a negative complement-dependent and flow cytometry T-cell crossmatch, and marginal donor kid-neys were avoided (age <3 or >65 years, prolonged warm or cold ischemia,etc.). Mean (range) donor age was 36.3 (6–61) years for sirolimus, and 38.3(16–65) years for CsA patients (p = ns). As previously reported (19), all pa-tients received basiliximab (Simulect, Novartis, East Hanover, NJ) 20 mginduction; mycophenolate mofetil (MMF, Cellcept, Hoffman-LaRoche, Nut-ley, NJ) 1 gm b.i.d. orally unless side effects necessitated dose reduction;and the same steroid regimen consisting of methylprednisolone 500 mg in-travenously day 0, tapered to a maintenance of 7.5 mg by 6 months. Group1 patients began sirolimus (SRL, Rapamune, Wyeth, Collegeville, PA) orallywithin 48 h of surgery and then concentration-controlled to keep 24-h wholeblood trough levels between 10–12 ng/mL (HPLC with Mass Spectroscopydetection) for 6 months, and then 5–10 ng/mL, thereafter. Group 2 patientswere given cyclosporine (CsA, Neoral, Novartis, E. Hanover, NJ) 6–8 mg/kgin divided doses, and were concentration-controlled to C0 levels of 200ng/mL the first year, and 150–175 ng/mL thereafter. (TDX monoclonal as-say, Abbott Labs, Abbott Park, IL). At 2 years, all of the SRL patients weretaking the drug, while 4 CsA patients had been switched (to tacrolimus in3, SRL in 1). At 2 years, the SRL group was receiving 3.44 mg/day with atrough level of 7.2 ng/mL, and the CsA group was receiving 3.26 mg/kg/daywith a trough level of 178 ng/mL.
Analysis of renal structure and function
Each of the 55 patients alive with a functioning transplant at 2 years had theirkidney function analyzed including a measured GFR utilizing iothalamate.After documented informed consent, 48 of 55 (87.2%) eligible patients
underwent a percutaneous kidney transplant biopsy. The reason for non-biopsy included the need for coumadin therapy in 2, and patient refusal forvarious reasons in 5, evenly divided between the groups.
Hospital Laboratory Tests: Blood and urine samples were tested forserum creatinine, calculated creatinine clearance (Cockroft-Gault For-mula) normalized to current body weight and gender (20), and 24-hurine collection for protein excretion.Dynamic Slope Analysis: Random coefficient regression analysis wasused to evaluate trends in calculated GFRs over 1–36 months. Indi-vidual estimates (intercept and slope) were made for all patients, andexpressed as the mean by treatment group (21).Measured Glomerular Filtration Rate: The clearance of 125I-sodiumiothalamate (Questcor Pharmaceuticals, Inc., Union City, CA) wasdetermined during an induced diuresis after subcutaneous injectionof 25 microCuries and subsequent collection of plasma and urinesamples. The formula GFR = UV/P, where U = counts/min in theurine collection, V = rate of urine flow in mL/min and P = counts/minin the plasma sample was used. Results were then corrected tostandard body surface area (22).
Kidney biopsies
Transplant biopsies comprised three cores obtained with 15-gauge nee-dles (ASAP Automatic Biopsy, Microvasive, Watertown, MA); two for lightmicroscopy, one for DNA microarrays. Cores for microarrays went imme-diately into 1.5 mL of RNALater (Ambion, Austin, TX), and −80◦C within4 h.
Paraffin sections were stained with hematoxylin-eosin, trichrome and peri-odic acid-Schiff. Biopsies were read by one pathologist (KS) blinded to allidentifiers and graded by Banff 1997 classification(4). Each sample had atleast 10 glomeruli and adequate cortical tissue for analysis. A Banff chronicallograft nephropathy (CAN) score was generated representing the sumof the averages of five individual lesion scores: glomerulopathy, interstitialfibrosis, tubular atrophy, increased mesangial matrix and vascular intimalthickening.
DNA microarrays
Biopsy specimens were homogenized in 1 mL of Trizol (Invitrogen, Carls-bad, CA). Total RNA was further purified using an RNeasy column (Qiagen,Valencia, CA) and quality confirmed by Agilent 2100 BioAnalyzer (Palo Alto,CA). Average total RNA yields from 15-guage-needle biopsy cores were14.9 ± 3.9 lg.
RNA labeling and hybridization Standard Affymetrix GeneChip (Santa Clara,CA) protocols were used (23). All labeled samples were hybridized toHG-U133A GeneChip arrays containing 22 283 probe sets representing over14 500 human genes.
Statistical analysis: GeneChip data were analyzed using Microarray Suite5.0 (MAS 5.0, Affymetrix) and Robust Multichip Average (RMA) (24). RMAused all Affymetrix .CEL files from this study as a training set. Probe setsabsent in all chips by Present/Absent calls (MAS 5.0) were not analyzed.BRB ArrayTools (http://linus.nci.nih.gov/BRB-ArrayTools.html) was used toperform class comparisons between the two drug treatment or Banff score-defined biopsy groups. Differentially expressed genes in biopsies of CsAand SRL-treated patients were generated by class comparison of 6682genes called as Present in >90% of at least one of the two groups (p <
0.001). Gene lists comparing Banff 0 and combined Banff 2 and 3 biopsieswere created using 15 572 genes called Present on at least one chip in thedata set. The user-defined alpha level (false positive rate) was set at p <
0.001 or p < 0.01 for these lists. Heat maps were generated using Cluster
American Journal of Transplantation 2004; 4: 1776–1785 1777

Flechner et al.
and TreeView programs (25). Groups were compared using unpaired t-testsfor continuous variables (two-sided), which were assumed to be approxi-mately normally distributed, and compared using the chi-square or Fisher’sexact test for categorical variables. Results were considered statisticallysignificant if the p-value was less than or equal to 0.05.
Quantitative RT-PCR (Q-PCR)
Q-PCR was performed on RNA from nine biopsy samples for 11 genes(Assays-on-Demand Genomic Assays, Applied Biosystems, Foster City,CA). Based on a literature review for genes associated with CAN, 8 geneswere selected from the differentially expressed genes in the class com-parison analysis between Banff 0 and the combined Banff 2 and 3 data.Three genes were selected only from the review. The signal intensities onthe GeneChips for all 11 genes validated by Q-PCR were grouped by Banffscores and compared within each class. Sample selection bias was ex-cluded by Student’s t-test. There were no significant differences betweensignal intensities of the 11 genes for samples analyzed by Q-PCR and thosethat were not. Briefly, cDNA was transcribed from 100 ng total RNA (cDNAArchive kit, Applied Biosystems). Reactions were done in 20 lL containing2 units of Amplitaq Gold® (Applied Biosystems) in an ABI Prism 7900HT. Allamplifications were done in triplicate and threshold cycle (Ct) scores wereaveraged for relative expression values. The Ct scores for candidate geneswere normalized against Ct scores for endogenous 18S rRNA. Fold-changewas determined by the following calculation (26):
Fold-change = 2−��Ct, where ��Ct
= (�Ct of experimental group) − (�Ct of calibrator group).
Power analysis
We used the t distribution rather than z because our estimates of varianceare based upon our sample values rather than a known population(27).
n = 4(ta/2 + tb )2/(d/s)2
The equation for tb was solved as follows: n = sample size. The degreesof freedom (m) was 36 by Welch’s approximate t value using Student’st degrees of freedom (28). The value for d = 1 because our calculationsare based upon log2 RMA values and 1 represents a minimum detectabledifference of 2-fold using the median standard deviation across all chips persample by gene as an indicator of the detection level for that group. Themedian standard deviations were s = 0.212 for the CsA group (n = 21) ands = 0.241 for the SRL group (n = 19). The a term = 0.001, defining a falsepositive rate of 1 in 1000 genes.
Results
Clinical outcomes
There were no statistically significant demographic differ-ences between the groups (19) with a mean follow-up of36.4 ± 9.1 months for SRL-treated and 37.3 ± 7.4 monthsfor CsA-treated. The 2-year actual patient survival, graft sur-vival and biopsy-confirmed acute rejection rates for the twogroups were not significantly different (SRL group: 93.5%,93.5% and 6.5%; CsA group: 100%, 93.3% and 16.6%). Inthe CsA group, there have been no deaths, but two graftswere lost at 9 and 14 months due to recurrent rejection,and 1 patient was switched to sirolimus. In the SRL group 2recipients died with graft function, and 1 dropped out at 3weeks for personal reasons. Thus, 55 patients were avail-able for analysis.
Renal function
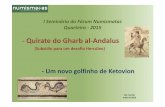
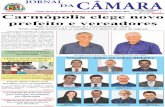
Comparing the CsA to the SRL group at 2 years, there wasa significant increase in mean serum creatinine (1.81 ±0.86 vs. 1.35 ± 0.41 mg/dL, p = 0.008), a decrease inthe Cockroft-Gault calculated GFR (63.4 ± 19.4 vs. 80.4 ±6.2 mL/min, p = 0.008) (Table 1) and a decrease in iotha-lamate clearance (CsA = 49.2 ± 17.8; SRL = 60.6 ± 18.9mL/min; p = 0.018) (Figure 1). There was no significantdifference in the 24-h urinary protein excretion compar-ing the CsA to the SRL group (0.88 ± 1.31 vs. 0.55 ±0.71 g/24 h). A comparison of the random coefficients re-gression analysis of the Cockroft-Gault-calculated GFRsfor the two groups (Figure 2) demonstrated a negativeslope of −1.58 mL/min/year for the CsA group (95% CI −4.096–0.929) and a positive slope of 3.36 mL/min/year forthe SRL group (95% CI 0.8412–5.874). The calculated dif-ference between the two slopes was 4.94 mL/min/year(p = 0.008).
Renal histology
The number of patients biopsied at 2 years was similar ineach group and represented 48 of 55 (87.2%) of those el-igible. The mean creatinine values (mg/dL) at the time ofbiopsy were 1.83 ± 0.89 for the CsA patients and 1.35 ±0.38 for the SRL patients (Table 2). The creatinines of theun-biopsied patients were lower for each group. The SRLgroup had a significantly higher frequency of the 2-yearprotocol biopsies read as normal (Banff grade 0) as com-pared to the CsA group (66.6% vs. 20.8%; p = 0.007). Notsurprisingly, 16.6% of the CsA group demonstrated spe-cific features of CNI drug nephrotoxicity, whereas noneof the SRL-treated patients demonstrated these findings.Features included hyaline arteriolar changes, tubular vac-uolization and/or interstitial calcification. The net Banff CANscores comprised individual scores for interstitial fibrosis,tubular atrophy, mesangial matrix, glomerulopathy and in-timal thickening and were also significantly different be-tween the CsA and SRL groups (3.17 ± 0.62 vs. 1.48 ±0.27; p < 0.00001). The higher net Banff CAN scores inthe CsA group were primarily due to differences in tubularatrophy and interstitial fibrosis (Figure 3). In addition, higherBanff CAN scores of grade II and III were more frequentlyobserved in the CsA group than in the SRL group (37.5%vs. 12.5%; p = 0.013) (Figure 4).
DNA microarrays
High-density DNA microarrays were used to determine aseries of gene expression profiles with the objective ofmaking two different class comparisons. The first classcomparison between the biopsies of patients treatedwith CNI-based immunosuppression (CsA/MMF/P) and thesirolimus group (SRL/MMF/P) yielded 379 differentiallyexpressed genes (p < 0.001). Importantly, 97% of thegenes are up-regulated in the CsA-treated patient biopsies(Table 3). Functional classifications of these genes basedon the Gene Ontology (GO) database and published liter-ature identified 32 groups of which the top 6 comprised
1778 American Journal of Transplantation 2004; 4: 1776–1785

Kidney Histology and Gene Expression in Sirolimus-Treated Patients
Table 1: Post-transplant renal function comparing CsA-treated and SRL-treated groups
Time post-transplant/patients (n) CsA/MMF/P1 SRL/MMF/P2 p-valuesSerum creatinine3
12 months (n = 29 and 29) 1.78 ± 0.76 1.32 ± 0.33 0.00418 months (n = 28 and 27) 1.76 ± 0.69 1.33 ± 0.34 0.00524 months (n = 28 and 27) 1.81 ± 0.86 1.35 ± 0.41 0.00830 months (n = 28 and 26) 1.91 ± 0.80 1.37 ± 0.55 0.00536 months (n = 20 and 21) 2.14 ± 1.30 1.30 ± 0.41 0.002
Cockroft-Gault GFR5
12 months (n = 29 and 29) 60.8 ± 14.4 81.1 ± 24 0.00818 months (n = 28 and 27) 63.1 ± 17.9 79.6 ± 27.2 0.00624 months (n = 28 and 27) 63.4 ± 19.6 80.4 ± 26.2 0.00830 months (n = 28 and 26) 62.8 ± 20.0 80.1 ± 27.4 0.00536 months (n = 20 and 21) 59.7 ± 21.7 83.6 ± 27.8 0.002
1Cyclosporine (CsA).2Sirolimus (SRL), mycophenolate mofetil (MMF), prednisone (P).3Serum creatinine expressed as mg/dL, Mean ± SD.4Not significant.5Glomerular filtration rate (GFR) expressed as mL/min, Mean ± SD.
Iothalamate GFR and 24 h urine protein:2 years post−transplant
0
10
20
30
40
50
60
70
80
90
100
GF
R c
c/m
in
CsA/MMF/P(n = 26)
SRL/MMF/P (n = 27)
49.2
60.6
+ 17.8
+ 18.9
p = 0.018
Up--Gm/24 h .88 + 1.31 .55 + .71 p = NS
Figure 1: Distribution and mean ± SD values for measured
iothalamate estimates of glomerular filtration rate mL/min.
Values normalized for 1.73 m2 body surface area. Results of 24-hurine collections for protein excretion mean ± SD g/24 h.
gene candidates involved in pathways for regulation oftranscription (35; 9.7%), fibrosis/tissue remodeling (27;7.1%), immunity/inflammation (25; 6.6%), intracellular pro-tein transport (23; 6.1%), signal transduction (23; 6.1%)and cell growth (18; 4.7%).
The second class comparison was done to compare geneexpression profiles of biopsies from patients with BanffCAN 0 scores (normal histology; n = 18) and those withBanff CAN scores of 2 and 3 (CAN; n = 9). We set thealpha error term at p < 0.001 such that the estimatedfalse positive error would be 1 gene call per 1000 profiled,yielding 130 candidate genes. Based on annotation of genefunction (Tables 3 and 4), we found that the largest group
Figure 2: Random coefficients regression (slope) analysis us-
ing Cockroft-Gault-calculated glomerular filtration rate values
between 1 and 36 months post-transplant.
of classified genes was immune/inflammatory responses(23; 17.3%), consistent with the same pattern of gene ex-pression in the CsA-treated group in which more Banff 2and 3 biopsies are also found. The second largest groupsare genes linked to pathways of cell adhesion and extra-cellular matrix (15; 11.3%) and genes involved in proteinsynthesis, modification and proteolysis (20; 15%). The re-sults of both class comparisons are consistent with theliterature demonstrating that genes linked to pathways ofboth immune/inflammatory and fibrosis/tissue remodelingare involved in the pathogenesis of CAN.
Based on a literature review we identified 11 genes pu-tatively involved in CAN (Table 5), only 4 of which were
American Journal of Transplantation 2004; 4: 1776–1785 1779

Flechner et al.
Table 2: Histopathologic findings in protocol renal biopsies at2-years: CsA/MMF/P vs. SRL/MMF/P1
SRL/MMF/P CsA/MMF/PPatients
Entered 31 30Eligible 28 27Biopsied (%) 24 (85.7) 24 (88.8)
DNA Microarrays (%) 19 (79) 22 (92)1-yr Acute Rejection (%) 2 (6.4) 5 (16.6)Scr2 biopsied group 1.35 ± 0.38 1.83 ± 0.893
Scr not biopsied group 1.27 ± 0.34 1.51 ± 0.54Normal histology (%) 16 (66.6) 5 (20.8)Acute rejection 0 0Allograft nephropathy (%) 8 (33.3) 17 (79.2)Drug nephrotoxicity4 (%) 0 (0) 4 (16.6)1CsA = cyclosporine, MMF = mycophenolate mofetil, P =prednisone, SRL = sirolimus.2Serum creatinine (Scr; mg/dL).3Standard deviation.4Defined by hyaline arteriolar change, tubular vacuolization orCa++ deposition.
Frequency of Banff chronic allograft nephropathyscores: CsA/MMF versus SRL/MMF
0
10
20
30
40
50
60
70
80
% p
rese
nt
Grade 0 Grade I Grade II Grade III
CsA/MMF (24)Sirolimus/MMF (24)
p=0.013, x2
Figure 3: Distribution of Banff chronic allograft nephropa-
thy (CAN) scores (0, 1, 2 and 3) at 2 years between the
sirolimus/MMF/P and cyclosporine/MMF/P groups.
included in the initial class comparison. Setting the al-pha term (false positive rate) at p < 0.001 is conserva-tive and can decrease the sensitivity of identifying dif-ferentially expressed genes. Therefore, we repeated theclass comparison with the alpha term set at p < 0.01,yielding 524 candidate genes. An additional four genecandidates identified in the literature review were dif-ferentially expressed (Table 5). The complete gene listsgenerated by all the class comparisons are provided atour website (http://www.scripps.edu/services/dna array/).Pages/AJT2 2004SD.htm.
Figure 5 represents a heat map demonstrating the correla-tions between Banff scored histology and differentially ex-pressed genes linked to immunity/inflammation and fibro-sis/tissue remodeling. Genes associated with extracellularmatrix or pro-fibrotic activity were more frequently repre-sented in the CsA biopsies as well as biopsies with higher
Sum of average Banff chronic scores (0−3) at2 years: CsA/MMF versus SRL/MMF
0
0.5
1
1.5
2
2.5
3
3.5
CsA (n = 24) Sirolimus (n = 24)
Ban
ff s
core
Vascular fibrousintimal thickeningMesangial matrix
Tubular atrophy
Interstitial fibrosis
Glomerulopathy
3.17 + .62
1.48 + . 2 7
p < .00001
Figure 4: Sums of the 5 individual histological features
that comprise the Banff chronic allograft nephropathy (CAN)
scores. Values reported as mean ± SD for the sirolimus/MMF/Pvs. the cyclosporine/MMF/P groups. The differences between thetwo groups are primarily due to scores for interstitial fibrosis andtubular atrophy.
Table 3: Biological function based on gene ontology (GO)database for class comparison of CsA/MMF/P vs. SRL/MMF/P
Numberof genes1 Percentage
Transcription regulation/DNA binding 35 9.7Fibrosis/tissue remodeling 27 7.1Immune/inflammatory responses 25 6.6Intracellular protein transport 23 6.1Signal transduction 23 6.1Cellular growth 18 4.71There were 379 differentially expressed genes (p < 0.001), 97%were up-regulated (CsA vs. SRL). The top six of 32 functionalclassification groups are listed.
Table 4: Biological function based on gene ontology (GO)database for class comparison of Banff CAN 0 vs. Banff CAN2 + 3
Numberof genes1 Percentage
Immune/inflammatory responses 23 17.3Cell adhesion/extracellular matrix 15 11.3Protein synthesis, modification 20 15.0
& proteolysisTranscription regulation/DNA binding 5 3.8Cellular metabolism 16 12.0EST and hypothetical proteins 6 4.51Total of 85 of the 133 genes in the class comparison based onshowing all groups with 5 or more genes.
Banff scores. These genes included thrombospondin 1,collagens III and IV and the matrix glycoproteins laminin,tenascin and fibronectin. Active turnover of extracellu-lar matrix is suggested by increased gene expression ofthe tissue inhibitor of matrix metalloproteinase (TIMP 1)and the matrix metalloproteinases (MMP) 2, 7 and 9, and
1780 American Journal of Transplantation 2004; 4: 1776–1785

Kidney Histology and Gene Expression in Sirolimus-Treated Patients
Table 5: Validation of DNA microarray expression data by quantitative RT-PCR (Q-PCR) based on 11 genes identified in a literature reviewas associated with CAN, 8 of which are differentially expressed by class comparison of Banff 0 vs. Banff 2 and 31
Gene names Fold change by GeneChip GeneChip p-values2 Fold change by Q-PCR Q-PCR p-values4
Matrix metalloproteinase 7 (47) 3.22 0.000001 15.01 0.026TIMP1 (48) 2.25 0.000003 3.02 0.0855
CCL5 (RANTES) (49) 1.55 0.0004 5.51 0.035VEGF (50) 1.57 0.0008 5.62 0.040Collagen III (51) 2.52 0.003 24.31 0.010MCP1/CCL2 (52) 1.36 0.003 2.82 0.043Fibronectin (38) 1.70 0.005 19.66 0.005TNF alpha (53) 1.58 0.008 189.09 0.026Angiotensin II receptor (54) 1.12 >0.013 12.80 0.006TGF beta (55) 1.28 >0.013 2.17 0.1625
PDGF (56) 1.06 >0.013 2.32 0.1775
1Alpha error level set at p ≤ 0.01 for class comparison.2p-values calculated by BRB ArrayTools for individual gene expression.3Not significant by BRB ArrayTools (p > 0.01).4Student’s t-test (one-tailed) based on assumption that CAN-associated genes should be elevated in the Banff 2 and Banff 3 biopsies.5Not significant by Student’s t-test (p > 0.05).
matrilin 1. Pro-fibrotic and cell adhesion genes such as TGFbeta, TNF alpha, PDGF, ICAM, VCAM 1 and integrin beta6 were also up-regulated. An increase in gene expressionfor CD163, human macrophage chemoattractant protein-1 (MCP-1), its receptor CCR2, macrophage inflammatoryprotein (MIP-3 beta) and class II MHC are consistent withthe presence of activated macrophage infiltrates.
Quantitative PCR
Quantitative RT-PCR (Q-PCR) for 11 genes associated withCAN was performed on nine biopsy samples comprisingthree biopsies from each of three Banff histology classes:Banff 0, 2 and 3 (Table 5). TIMP 1 is the only gene that issignificant by the class comparison based on the GeneChipdata sets that is not confirmed by Q-PCR. Angiotensin II re-ceptor expression was elevated in Banff 2 and 3 biopsies byboth Q-PCR and GeneChip data although it failed to meetstatistical significance in the GeneChip data. PDGF and TGFbeta gene expression were not significantly increased byGeneChip or Q-PCR.
We also calculated the statistical power for the gene listscreated by class comparisons with the DNA microarrays.The estimated power to detect a 2-fold change in differen-tial gene expression between the groups in this experimentis 100% based on the actual variance data for this data setand our transplant biopsy sample sizes.
Discussion
There is little debate that the demand for kidney transplan-tation worldwide far outstrips the supply of available or-gans. The need to retransplant survivors with a failed graftfrom chronic allograft nephropathy (CAN) and the growingnumbers of extrarenal organ transplant recipients that aredeveloping permanent renal failure, further exacerbatesthe need for kidneys. Therefore, approaches that diminish
the prevalence and progression of CAN, and by inferenceprolong existing kidney graft survival, will address this im-balance. Previous histological analyses have demonstratedthat some evidence of CAN is prevalent by 2 years in 75–90% of kidneys transplanted with the continuous use ofCNI drugs (cyclosporine or tacrolimus), even when renalfunction is considered stable (11,29). These changes inhistology are occurring during the current era of low acuterejection rates. In this study, despite an acute rejection rateof only 16% among the CNI-treated patients, the incidenceof CAN at 2 years was 79.2%. Retrospective analyseshave demonstrated that early renal dysfunction is a pre-dictor of CAN and diminished graft survival (6,30), as wellas a risk factor for post-transplant cardiovascular death (31).Thus, in addition to preventing acute rejection, improvingearly renal function and preventing CAN should be the fo-cus for improving immunosuppressive therapy.
Our data (Table 1) demonstrate that the CNI-free patients(SRL group) have significantly improved renal function af-ter 1 month as compared to those given CNI drugs (CsAgroup) and that observation is true 2 and 3 years after trans-plantation. This improvement is represented by approxi-mately a 0.5 mg/dL lower mean serum creatinine or a 25%higher GFR. The difference between the kidney functionof our CsA and SRL-treated patients increased between 1and 36 months post-transplant. As shown in Figure 2, thedifference in the slopes of the calculated GFRs predictsthat the CsA-treated group loses almost 5 mL/min of GFReach year post-transplant as compared to the SRL-treatedgroup. Morales et al. have also observed a similar differ-ence in renal function at 2 years between CsA-treated andpatients treated with SRL from the time of transplantation(32). The differences in GFR slopes with time are provoca-tive. The negative slope for the CsA-treated patients maybe explained by declining renal function associated withthe higher incidence of CAN and attendant renal intersti-tial fibrosis and tubular atrophy. The positive slope seen
American Journal of Transplantation 2004; 4: 1776–1785 1781

Flechner et al.
Figure 5: Heat map representing 72 genes differentially expressed comparing Banff CAN 2 and 3 vs. Banff 0 biopsies. Arrays arevertically aligned left to right by Banff scores 0, 1, 2 and 3. The majority of Banff 0 arrays were from SRL/MMF/P kidneys (black header)and the majority of higher Banff CAN score arrays were from CsA/MMF/P (blue header) kidneys. The color depth of each cell representsthe proportional range of signal intensities compared to the average signal intensity of all the chips (n = 41); blue is down-regulated, redis up-regulated and white is no change. Common gene names appear to the right.
in the SRL-treated group suggests renal compensatory hy-pertrophy. We speculate that without the CNI-driven pre-glomerular afferent arteriolar vasoconstriction (8–10), kid-neys in the CNI-free patients hypertrophy analogous to theremaining solitary kidney in the living donor (33).
A similar difference in renal function between CsA-treatedand SRL-treated kidney recipients has also been observedin a Multicenter trial in which CsA was eliminated at 3months post-transplant from a CsA/SRL/steroid mainte-nance regimen. Kreis et al. (34) reported that at 3 years the
mean calculated GFR of 59.4 mL/min for the SRL/steroidgroup was significantly better than the 47.3 mL/min ob-served in the CsA/SRL/steroid group (p = 0.001).
We were able to biopsy 87% of eligible recipients in ourstudy and here report a striking decrease in the incidence ofCAN in the patients treated with a CNI-free, SRL-based im-munosuppressive regime as measured by biopsy histologybased on Banff CAN scoring. Though we did not performimplant biopsies to establish baseline histology, recipientswere randomized prospectively and the kidney donors had
1782 American Journal of Transplantation 2004; 4: 1776–1785

Kidney Histology and Gene Expression in Sirolimus-Treated Patients
no significant differences between the two study groups.The biopsied CsA-treated patients had a mean creatinineof 1.83 mg/dL and only 20.8% had normal histology (BanffCAN grade 0). Our 79.2% rate of CAN Grade I or higherin the CsA-treated group at 2 years is about the same asthat reported by Solez et al. (72.3%) (29), and less thanthe Australian longitudinal study’s rate (94.2%) (11). In con-trast, 66.6% of our SRL-treated group had normal histology(Banff CAN 0) at 2 years correlating with better renal func-tion by calculated and measured iothalamate GFRs.
DNA microarray analysis of the 2-year biopsies for 41patients was used to determine whether there are dis-tinct profiles for gene expression associated with CAN.The first class comparison determined a profile for theCsA-treated group compared to the SRL-treated group(Table 3). This comparison yielded 379 differentially ex-pressed genes, 97% of which were up-regulated in theCsA-treated patients. Functional classifications of thesegenes demonstrated pathways for regulation of transcrip-tion, fibrosis/tissue remodeling, immunity/inflammation,intracellular protein transport, signal transduction and cellgrowth. That a major group of these classifying genes re-lated to immunity and inflammation are up-regulated inCsA-treated patients supports the hypothesis that patientsin the SRL-treated group were more adequately immuno-suppressed at the time of the 2-year protocol biopsies andthis correlates with significantly better graft function andrenal histology. On the other hand, the finding of a signif-icant number of genes involved with fibrosis and tissueremodeling supports the hypothesis that another factor inCAN is the underlying impact of CNI-induced nephrotoxi-city though the independent impact of immune-mediatedtissue injury to produce fibrosis cannot be separated bythe gene expression profiles. We propose that the inci-dence and extent of CAN is determined by complex in-teractions of both mechanisms of kidney transplant injury:rejection due to inadequate long-term immunosuppressionand drug-induced nephrotoxicity.
The second class comparison analyzed the gene expres-sion profiles of biopsies from patients with Banff CAN 0scores (normal histology) and those with Banff CAN scoresof 2 and 3 (Table 4). We found that the largest group ofclassifying genes was linked to immune/inflammatory re-sponses, a result consistent with that found in the firstcomparison of biopsies from CsA-treated and SRL-treatedpatients. Other groups are genes linked to pathways ofcell adhesion and extracellular matrix and genes involvedin protein synthesis, modification and proteolysis. Thus,whether we did our class comparisons based on treat-ment or biopsy histology groups, the fundamental resultswere the same and suggest interplay between pathwaysof immunity/inflammation and tissue injury/repair in thepathogenesis of CAN. Consistent with this hypothesis isthat specific genes identified as strongly up-regulated inthe CsA-treated kidneys with CAN include several pro-inflammatory cell chemoattractants including MCP-1, its
receptor CCR2, MIP 3 beta, CXCL6 and RANTES. The pres-ence of MCP-1 and RANTES has been localized to renaltubular epithelium in CNI-induced nephrotoxicity (35) andboth are up-regulated during rejection (36).
A number of genes up-regulated in the CAN biopsy groupare linked to the formation and deposition of extracellu-lar matrix such as collagens III and IV, and matrix glyco-proteins including laminin, tenascin and fibronectin. Theserepresent the most frequently identified extracellular ma-trix proteins in the kidney and are increased with renal injuryand scarring (16,37,38). The biopsies of the CsA-treatedgroup also suggest the remodeling of extracellular matrixincluding increased gene expression for the matrix metal-loproteinases 2, 7 and 9 as well as TIMP-1, all of whichhave been associated with renal fibrosis and CNI-inducednephrotoxicity (16,39–41).
We identified a number of pro-fibrotic and cell adhesiongenes up-regulated in the biopsies with high CAN scores,including TNF alpha, ICAM, VCAM 1 and integrin beta chain6. Expression of the pro-angiogenic growth factor, VEGF,has been reported in chronically rejecting kidneys (42) andit was significantly up-regulated in our patients with highBanff CAN scores and CsA therapy. Recently, SRL hasbeen reported to down-regulate VEGF production in an an-imal tumor model (43,44). Several reports have suggestedthat TGF beta plays a significant role in the pathogenesisof renal fibrosis linked to CAN and CNI-induced nephro-toxicity (16,40,41,45,46). In our study the expression ofTGF beta by Q-PCR and GeneChip analysis were not sta-tistically significant (Table 5). A possible explanation is thatthe combination of SRL and MMF, but not SRL alone, hasbeen shown to suppress TGF beta in a rat kidney transplantmodel (18).
In conclusion, the combination of SRL, MMF and steroidsprovides superior renal function and histological integrityof renal allografts at 2 years, compared to the continu-ous use of CsA with MMF and steroids. SRL-treated pa-tients have a decreased incidence of CAN. In contrast, the2-year transplant biopsies of the CsA-treated group demon-strate significantly higher rates of CAN histology as wellas up-regulated expression of genes linked to pathwaysof tissue injury/remodeling and immune/inflammation sug-gesting roles for both these powerful forces of kidneytransplant injury in the pathogenesis of CAN. Kidney trans-plantation without CNI drugs may provide improved graftsurvival that involves better long-term immunosuppressionand less drug-induced nephrotoxicity.
Acknowledgments
The authors would like to thank Barbara Mastroianni, RN and Kathy Savas,RN for clinical care and data collection, and Lynne Klingman, MS for biopsyprocessing and storage.
American Journal of Transplantation 2004; 4: 1776–1785 1783

Flechner et al.
This work was funded in part by a grant-in-aid from the Wyeth Pharmaceu-tical Co., Collegeville, PA who had no role in the execution of the trial, themanagement of patients or editorial decisions regarding the manuscript.This work was also supported by NIH grant M01 RR00833.
References
1. Services USDoHaH. Annual Report of the U.S. Scientific Registryfor Transplant Recipients and the Organ Procurement and Trans-plantation Network, 2001; 133: 130–133.
2. Beveridge T, Calne RY. Cyclosporine (Sandimmun) in cadavericrenal transplantation. Ten-year follow-up of a multicenter trial.European Multicentre Trial Group. Transplantation 1995; 59:1568–1570.
3. Marcen R, Pascual J, Teruel JL et al. Outcome of cadaveric re-nal transplant patients treated for 10 years with cyclosporine: ischronic allograft nephropathy the major cause of late graft loss?Transplantation 2001; 72: 57–62.
4. Racusen LC, Solez K, Colvin RB et al. The Banff 97 working classi-fication of renal allograft pathology. Kidney Int 1999; 55: 713–723.
5. Almond PS, Matas A, Gillingham K et al. Risk factors for chronicrejection in renal allograft recipients. Transplantation 1993; 55:752–756; discussion 756–757.
6. Flechner SM, Modlin CS, Serrano DP et al. Determinants ofchronic renal allograft rejection in cyclosporine-treated recipients.Transplantation 1996; 62: 1235–1241.
7. Calne RY, White DJ, Thiru S et al. Cyclosporin A in patients receiv-ing renal allografts from cadaver donors. Lancet 1978; 2: 1323–1327.
8. Pascual M, Swinford RD, Ingelfinger JR, Williams WW, CosimiAB, Tolkoff-Rubin N. Chronic rejection and chronic cyclosporintoxicity in renal allografts. Immunol Today 1998; 19: 514–519.
9. Remuzzi G, Perico N. Cyclosporine-induced renal dysfunction inexperimental animals and humans. Kidney Int Suppl 1995; 52:S70–S74.
10. de Mattos AM, Olyaei AJ, Bennett WM. Nephrotoxicity ofimmunosuppressive drugs: long-term consequences and chal-lenges for the future. Am J Kidney Dis 2000; 35: 333–346.
11. Nankivell BJ, Borrows RJ, Fung CL, O’Connell PJ, Allen RD, Chap-man JR. The natural history of chronic allograft nephropathy. NEngl J Med 2003; 349: 2326–2333.
12. Ojo AO, Held PJ, Port FK et al. Chronic renal failure after trans-plantation of a nonrenal organ. N Engl J Med 2003; 349: 931–940.
13. Sehgal SN. Rapamune (RAPA, rapamycin, sirolimus): mechanismof action immunosuppressive effect results from blockade ofsignal transduction and inhibition of cell cycle progression. ClinBiochem 1998; 31: 335–340.
14. Groth CG, Backman L, Morales JM et al. Sirolimus (rapamycin)-based therapy in human renal transplantation: similar efficacyand different toxicity compared with cyclosporine. Sirolimus Eu-ropean Renal Transplant Study Group. Transplantation 1999; 67:1036–1042.
15. Kreis H, Cisterne JM, Land W et al. Sirolimus in association withmycophenolate mofetil induction for the prevention of acute graftrejection in renal allograft recipients. Transplantation 2000; 69:1252–1260.
16. Waller JR, Nicholson ML. Molecular mechanisms of renal allograftfibrosis. Br J Surg 2001; 88: 1429–1441.
17. Jolicoeur EM, Qi S, Xu D, Dumont L, Daloze P, Chen H. Combina-tion therapy of mycophenolate mofetil and rapamycin in preven-tion of chronic renal allograft rejection in the rat. Transplantation2003; 75: 54–59.
18. Shihab FS, Bennett WM, Yi H, Choi SO, Andoh TF. Combinationtherapy with sirolimus and mycophenolate mofetil: Effects on thekidney and on transforming growth factor-beta1. Transplantation2004; 77: 683–686.
19. Flechner SM, Goldfarb D, Modlin C et al. Kidney transplantationwithout calcineurin inhibitor drugs: a prospective, randomized trialof sirolimus versus cyclosporine. Transplantation 2002; 74: 1070–1076.
20. Cockcroft DW, Gault MH. Prediction of creatinine clearance fromserum creatinine. Nephron 1976; 16: 31–41.
21. Rutter CM, Elashoff RM. Analysis of longitudinal data: randomcoefficient regression modelling. Stat Med 1994; 13: 1211–1231.
22. Israelit AH, Long DL, White MG, Hull AR. Measurement ofglomerular filtration rate utilizing a single subcutaneous injectionof 125I-iothalamate. Kidney Int 1973; 4: 346–349.
23. URL: www.affymetrix.com/support/technical/manual/expressionmanual.affx.
24. Bolstad BM, Irizarry RA, Astrand M, Speed TP. A comparison ofnormalization methods for high density oligonucleotide array databased on variance and bias. Bioinformatics 2003; 19: 185–193.
25. Eisen MB, Spellman PT, Brown PO, Botstein D. Cluster analysisand display of genome-wide expression patterns. Proc Natl AcadSci U S A 1998; 95: 14863–14868.
26. User Bulletin #2 ABI PRISM 7700 Sequence Detection System.Document 4303859B 777802-002. Relative Quantitation of GeneExpression, 1997.
27. Simon RM, Dobbin K. Experimental design of DNA microarrayexperiments. Biotechniques 2003; 34: S16–S21.
28. Zar JH. Biostatistical Analysis. Prentice Hall, Upper Saddle River,NJ, 1999.
29. Solez K, Vincenti F, Filo RS. Histopathologic findings from 2-yearprotocol biopsies from a U.S. multicenter kidney transplant trialcomparing tarolimus versus cyclosporine: A report of the FK506Kidney Transplant Study Group. Transplantation 1998; 66: 1736–1740.
30. Hariharan S, McBride MA, Cherikh WS, Tolleris CB, BresnahanBA, Johnson CP. Post-transplant renal function in the first yearpredicts long-term kidney transplant survival. Kidney Int 2002; 62:311–318.
31. Meier-Kriesche HU, Baliga R, Kaplan B. Decreased renal functionis a strong risk factor for cardiovascular death after renal trans-plantation. Transplantation 2003; 75: 1291–1295.
32. Morales JM, Wramner L, Kreis H et al. Sirolimus does not ex-hibit nephrotoxicity compared to cyclosporine in renal transplantrecipients. Am J Transplant 2002; 2: 436–442.
33. Velosa JA, Griffin MD, Larson TS et al. Can a transplanted livingdonor kidney function equivalently to its native partner? Am JTransplant 2002; 2: 252–259.
34. Kreis H, Oberbauer R, Campistol JM et al. Long-term benefitswith sirolimus-based therapy after early cyclosporine withdrawal.J Am Soc Nephrol 2004; 15: 809–817.
35. Benigni A, Bruzzi I, Mister M et al. Nature and mediators of renallesions in kidney transplant patients given cyclosporine for morethan one year. Kidney Int 1999; 55: 674–685.
36. Nadeau KC, Azuma H, Tilney NL. Sequential cytokine dynam-ics in chronic rejection of rat renal allografts: roles for cytokinesRANTES and MCP-1. Proc Natl Acad Sci U S A 1995; 92: 8729–8733.
37. Furness PN. Extracellular matrix and the kidney. J Clin Pathol1996; 49: 355–359.
38. Baboolal K, Jones GA, Janezic A, Griffiths DR, Jurewicz WA.Molecular and structural consequences of early renal allograft in-jury. Kidney Int 2002; 61: 686–696.
1784 American Journal of Transplantation 2004; 4: 1776–1785

Kidney Histology and Gene Expression in Sirolimus-Treated Patients
39. Duymelinck C, Deng JT, Dauwe SE, De Broe ME, Verpooten GA.Inhibition of the matrix metalloproteinase system in a rat model ofchronic cyclosporine nephropathy. Kidney Int 1998; 54: 804–818.
40. Shihab FS, Yamamoto T, Nast CC et al. Transforming growthfactor-beta and matrix protein expression in acute and chronicrejection of human renal allografts. J Am Soc Nephrol 1995; 6:286–294.
41. Bicknell GR, Williams ST, Shaw JA, Pringle JH, Furness PN,Nicholson ML. Differential effects of cyclosporin and tacrolimuson the expression of fibrosis-associated genes in isolatedglomeruli from renal transplants. Br J Surg 2000; 87: 1569–1575.
42. Otto K, Duchrow M, Broll R, Bruch HP, Strik MW. Expression ofvascular endothelial growth factor mRNA and protein in humanchronic renal allograft rejection. Transplant Proc 2002; 34: 3134–3137.
43. Guba M, von Breitenbuch P, Steinbauer M et al. Rapamycin in-hibits primary and metastatic tumor growth by antiangiogenesis:involvement of vascular endothelial growth factor. Nat Med 2002;8: 128–135.
44. Luan FL, Ding R, Sharma VK, Chon WJ, Lagman M, Suthanthi-ran M. Rapamycin is an effective inhibitor of human renal cancermetastasis. Kidney Int 2003; 63: 917–926.
45. Horvath LZ, Friess H, Schilling M et al. Altered expression of trans-forming growth factor-beta S in chronic renal rejection. Kidney Int1996; 50: 489–498.
46. Khanna A, Plummer M, Bromberek C, Bresnahan B, Hariharan S.Expression of TGF-beta and fibrogenic genes in transplant recipi-ents with tacrolimus and cyclosporine nephrotoxicity. Kidney Int2002; 62: 2257–2263.
47. Henger A, Kretzler M, Doran P et al. Gene expression fingerprintsin human tubulointerstitial inflammation and fibrosis as prognosticmarkers of disease progression. Kidney Int 2004; 65: 904–917.
48. Nicholson ML, Waller JR, Bicknell GR. Renal transplant fibrosiscorrelates with intragraft expression of tissue inhibitor of metal-loproteinase messenger RNA. Br J Surg 2002; 89: 933–937.
49. Segerer S, Mac KM, Regele H, Kerjaschki D, Schlondorff D. Ex-pression of the C-C chemokine receptor 5 in human kidney dis-eases. Kidney Int 1999; 56: 52–64.
50. Pilmore HL, Eris JM, Painter DM, Bishop GA, McCaughan GW.Vascular endothelial growth factor expression in human chronicrenal allograft rejection. Transplantation 1999; 67: 929–933.
51. Bakker RC, Koop K, Sijpkens YW et al. Early interstitial accumula-tion of collagen type I discriminates chronic rejection from chroniccyclosporine nephrotoxicity. J Am Soc Nephrol 2003; 14: 2142–2149.
52. Ruster M, Sperschneider H, Funfstuck R, Stein G, Grone HJ. Dif-ferential expression of beta-chemokines MCP-1 and RANTES andtheir receptors CCR1, CCR2, CCR5 in acute rejection and chronicallograft nephropathy of human renal allografts. Clin Nephrol2004; 61: 30–39.
53. Azuma H, Nadeau K, Takada M, Mackenzie HS, Tilney NL. Cel-lular and molecular predictors of chronic renal dysfunction afterinitial ischemia/reperfusion injury of a single kidney. Transplanta-tion 1997; 64: 190–197.
54. Eliahou H, Avinoach I, Shahmurov M et al. Renoprotective effectof angiotensin II receptor antagonists in experimental chronic re-nal failure. Am J Nephrol 2001; 21: 78–83.
55. Yamada K, Hatakeyama E, Arita S, Sakamoto K, Kashiwabara H,Hamaguchi K. Prediction of chronic renal allograft dysfunctionfrom evaluations of TGFBeta1 and the renin-angiotensin system.Clin Exp Nephrol 2003; 7: 238–242.
56. Weinman EJ, Lakkis J, Akom M et al. Expression of NHERF-1,NHERF-2, PDGFR-alpha, and PDGFR-beta in normal human kid-neys and in renal transplant rejection. Pathobiology 2002; 70: 314–323.
American Journal of Transplantation 2004; 4: 1776–1785 1785
Copyright © 2022 FDOKUMEN