
Cyclooxygenase2 and prostate carcinogenesis
11
Mini-review Cyclooxygenase-2 and prostate carcinogenesis Tajamul Hussain a , Sanjay Gupta b , Hasan Mukhtar a, * a Department of Dermatology, University of Wisconsin, Medical Science Center, 1300 University Avenue, Madison, WI, 53706, USA b Department of Urology, Jim & Eilleen Dicke Research Laboratory, Case Western Reserve University, 10900 Euclid Avenue, Cleveland, OH, 44106, USA Received 23 August 2002; accepted 29 August 2002 Abstract In recent years a dramatic surge has occurred on studies defining to the role of cyclooxygenase (COX)-2 in causation and prevention of cancer. Prostaglandin (PG) endoperoxidase synthase also commonly referred to as COX is a key enzyme involved in the conversion of arachidonic acid to PGs and other eicosanoids. COX exists as two isoforms, namely COX-1 and COX-2 with distinct tissue distribution and physiological functions. COX-1 is constitutively expressed in many tissues and cell types and is involved in normal cellular physiological functions whereas COX-2 is pro-inflammatory in nature and is inducible by mitogens, cytokines, tumor promoters and growth factors. A large volume of data exists showing that COX-2 is overexpressed in a large number of human cancers and cancer cell lines. The possibility of COX-2 as a candidate player in cancer development and progression evolved from the epidemiological studies which suggest that regular use of aspirin or other non-steroidal anti- inflammatory drugs could significantly decrease the risk of developing cancers in experimental animals and in humans. In our recently published study (Prostate, 42 2000 73 – 78), we provided the first evidence that COX-2 is overexpressed in human prostate adenocarcinoma. Many other studies verified our initial observation and reported that compared to normal tissue, COX-2 is overexpressed in human prostate cancer. It should be noted that some recent work has suggested that COX-2 is only up- regulated in proliferative inflammatory atrophy of the prostate, but not in prostate carcinoma. In this scenario, COX-2 inhibitors could afford their effects against prostate carcinogenesis by modulating COX-2 activity in other cells in prostate. An exciting corollary to this ongoing work is that selective COX-2 inhibitors may exhibit chemopreventive and even chemotherapeutic effects against prostate carcinogenesis in humans. q 2002 Elsevier Science Ireland Ltd. All rights reserved. Keywords: Cyclooxygenase enzyme; Prostate cancer; Non-steroidal anti-inflammatory drugs; Inflammation; Prostaglandin 1. Introduction The incidence of prostate cancer has strongly increased during the past decades and it has now become the most common malignancy of men in many Western nations [1]. In the USA, among males, prostate cancer is the second leading cause of cancer- related deaths next only to lung cancer [2]. According to projections by the American Cancer Society, a total of 189 000 men will be diagnosed with prostate cancer in the USA in the year 2002, and 30 200 prostate cancer-related deaths are predicted this year [3]. Of great concern is that fact that more than 50% of prostate cancer patients present with or develop incurable metastatic disease [4]. Although most patients with advanced prostate cancer initially respond to androgen ablation treatment, relapse to an androgen-indepen- 0304-3835/02/$ - see front matter q 2002 Elsevier Science Ireland Ltd. All rights reserved. doi:10.1016/S0304-3835(02)00524-4 Cancer Letters 191 (2003) 125–135 www.elsevier.com/locate/canlet * Corresponding author. Tel.: þ1-608-263-3927; fax: þ 1-608- 263-5223. E-mail address: [email protected] (H. Mukhtar).
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Cyclooxygenase2 and prostate carcinogenesis
Mini-review
Cyclooxygenase-2 and prostate carcinogenesis
Tajamul Hussaina, Sanjay Guptab, Hasan Mukhtara,*
aDepartment of Dermatology, University of Wisconsin, Medical Science Center, 1300 University Avenue, Madison, WI, 53706, USAbDepartment of Urology, Jim & Eilleen Dicke Research Laboratory, Case Western Reserve University, 10900 Euclid Avenue,
Cleveland, OH, 44106, USA
Received 23 August 2002; accepted 29 August 2002
Abstract
In recent years a dramatic surge has occurred on studies defining to the role of cyclooxygenase (COX)-2 in causation and
prevention of cancer. Prostaglandin (PG) endoperoxidase synthase also commonly referred to as COX is a key enzyme involved in
the conversion of arachidonic acid to PGs and other eicosanoids. COX exists as two isoforms, namely COX-1 and COX-2 with
distinct tissue distribution and physiological functions. COX-1 is constitutively expressed in many tissues and cell types and is
involved in normal cellular physiological functions whereas COX-2 is pro-inflammatory in nature and is inducible by mitogens,
cytokines, tumor promoters and growth factors. A large volume of data exists showing that COX-2 is overexpressed in a large
number of human cancers and cancer cell lines. The possibility of COX-2 as a candidate player in cancer development and
progression evolved from the epidemiological studies which suggest that regular use of aspirin or other non-steroidal anti-
inflammatory drugs could significantly decrease the risk of developing cancers in experimental animals and in humans. In our
recently published study (Prostate, 42 2000 73–78), we provided the first evidence that COX-2 is overexpressed in human
prostate adenocarcinoma. Many other studies verified our initial observation and reported that compared to normal tissue, COX-2
is overexpressed in human prostate cancer. It should be noted that some recent work has suggested that COX-2 is only up-
regulated in proliferative inflammatory atrophy of the prostate, but not in prostate carcinoma. In this scenario, COX-2 inhibitors
could afford their effects against prostate carcinogenesis by modulating COX-2 activity in other cells in prostate. An exciting
corollary to this ongoing work is that selective COX-2 inhibitors may exhibit chemopreventive and even chemotherapeutic effects
against prostate carcinogenesis in humans.
q 2002 Elsevier Science Ireland Ltd. All rights reserved.
Keywords: Cyclooxygenase enzyme; Prostate cancer; Non-steroidal anti-inflammatory drugs; Inflammation; Prostaglandin
1. Introduction
The incidence of prostate cancer has strongly
increased during the past decades and it has now
become the most common malignancy of men in many
Western nations [1]. In the USA, among males,
prostate cancer is the second leading cause of cancer-
related deaths next only to lung cancer [2]. According
to projections by the American Cancer Society, a total
of 189 000 men will be diagnosed with prostate cancer
in the USA in the year 2002, and 30 200 prostate
cancer-related deaths are predicted this year [3]. Of
great concern is that fact that more than 50% of prostate
cancer patients present with or develop incurable
metastatic disease [4]. Although most patients with
advanced prostate cancer initially respond to androgen
ablation treatment, relapse to an androgen-indepen-
0304-3835/02/$ - see front matter q 2002 Elsevier Science Ireland Ltd. All rights reserved.
doi:10.1016/S0304-3835(02)00524-4
Cancer Letters 191 (2003) 125–135
www.elsevier.com/locate/canlet
* Corresponding author. Tel.: þ1-608-263-3927; fax: þ1-608-
263-5223.
E-mail address: [email protected] (H. Mukhtar).
dent state occurs shortly leading to tumor outgrowth
[5]. Despite the clinical importance of prostate cancer,
the molecular mechanisms underlying the develop-
ment and progression of this disease are poorly
understood. Therefore, much research is needed
towards understanding the mechanisms involved in
development and progression of prostate cancer and
developing new strategies for its prevention and
treatment. The present article reviews the role of
COX-2 in prostate carcinogenesis. Based on the
evidence available, selective COX-2 inhibitors offer
promise for prevention and therapy of prostate cancer.
2. Cyclooxygenases and prostaglandins
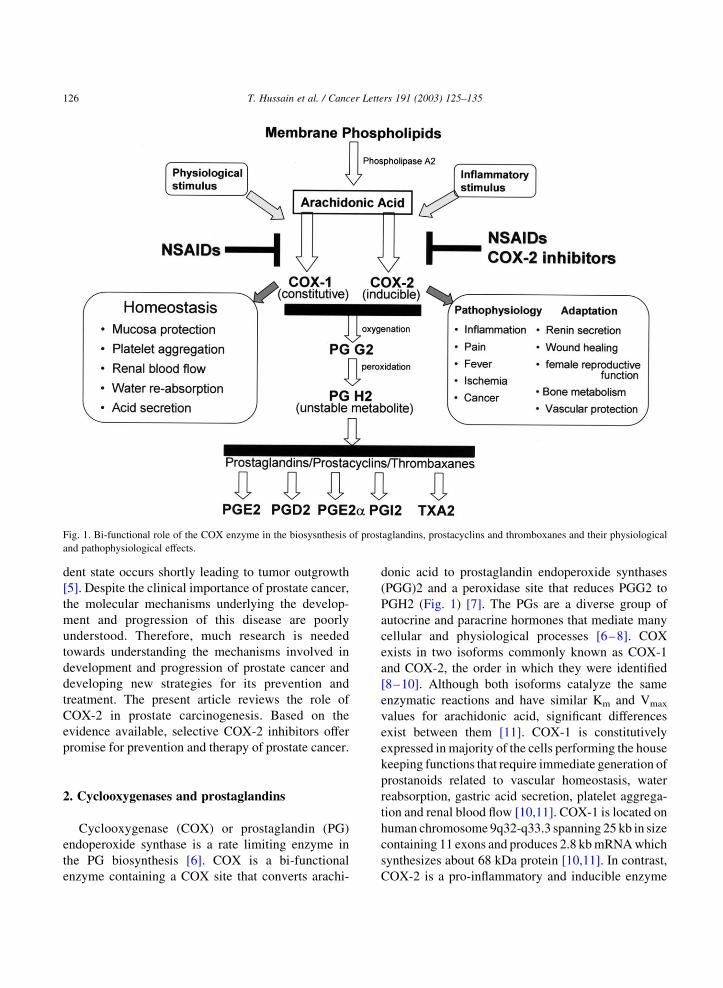
Cyclooxygenase (COX) or prostaglandin (PG)
endoperoxide synthase is a rate limiting enzyme in
the PG biosynthesis [6]. COX is a bi-functional
enzyme containing a COX site that converts arachi-
donic acid to prostaglandin endoperoxide synthases
(PGG)2 and a peroxidase site that reduces PGG2 to
PGH2 (Fig. 1) [7]. The PGs are a diverse group of
autocrine and paracrine hormones that mediate many
cellular and physiological processes [6–8]. COX
exists in two isoforms commonly known as COX-1
and COX-2, the order in which they were identified
[8–10]. Although both isoforms catalyze the same
enzymatic reactions and have similar Km and Vmax
values for arachidonic acid, significant differences
exist between them [11]. COX-1 is constitutively
expressed in majority of the cells performing the house
keeping functions that require immediate generation of
prostanoids related to vascular homeostasis, water
reabsorption, gastric acid secretion, platelet aggrega-
tion and renal blood flow [10,11]. COX-1 is located on
human chromosome 9q32-q33.3 spanning 25 kb in size
containing 11 exons and produces 2.8 kb mRNA which
synthesizes about 68 kDa protein [10,11]. In contrast,
COX-2 is a pro-inflammatory and inducible enzyme
Fig. 1. Bi-functional role of the COX enzyme in the biosysnthesis of prostaglandins, prostacyclins and thromboxanes and their physiological
and pathophysiological effects.
T. Hussain et al. / Cancer Letters 191 (2003) 125–135126
which can be induced by mitogens, tumor promoters,
cytokines and growth factors in different cell types and
controlled at both the transcriptional and post-transla-
tional levels [10–12]. COX-2 in involved in differ-
entiative processes, such as inflammation, ovulation,
and labor, in situation where only transient PG
production is required [9–11]. COX-2 is an 8 kb
gene with 10 exons located on human chromosome
1q25.2–q25.3 and transcribes a 4.1–4.5 kb mRNA
which encodes a protein of about 68 kDa [9–11].
Although, genes for COX-1and COX-2 are located on
two separate chromosomes but they are highly related
at the DNA, RNA, and protein level. COX-1 and COX-
2 consist of 576 and 587 amino acids, respectively, and
they share approximately 60% primary sequence
homology [12,13]. Both these enzymes exist as
integral membrane glycoprotein homodimers and are
found on the luminal surfaces of the endoplasmic
reticulum and nuclear envelop [14,15].
3. COX-2 and cancer
In recent years, overexpression of COX-2 has been
implicated in the progression of cancer [16,17].
Aberrant or increased expression of COX-2 has been
found in most of the cancers of the body sites [9,
16–18]. Compelling evidence from genetic and
clinical studies indicates that COX-2 upregulation is
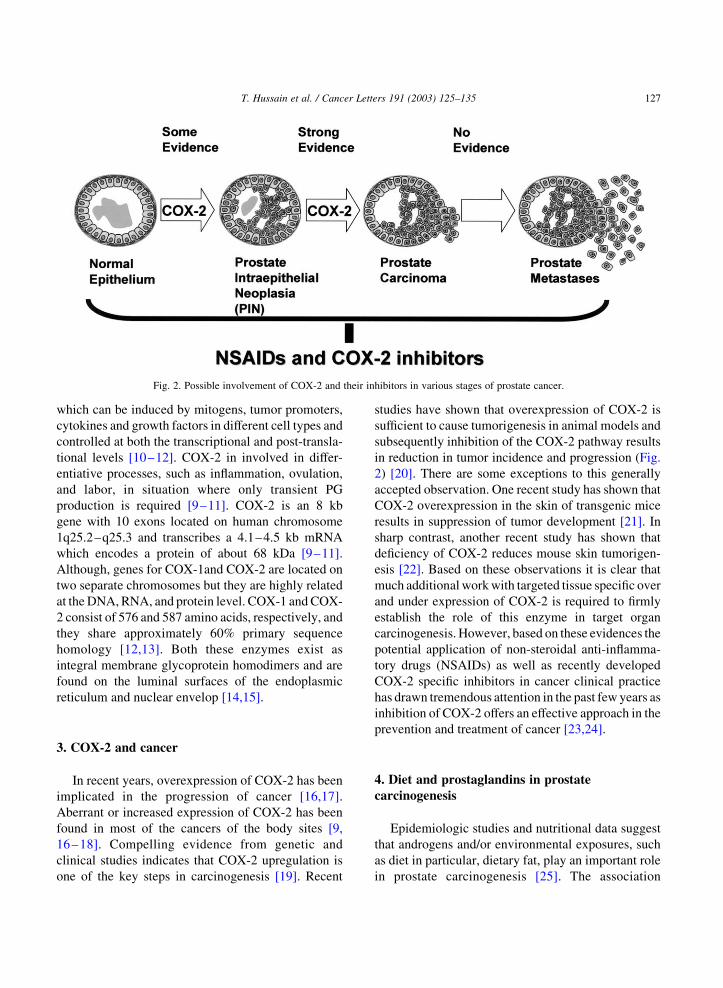
one of the key steps in carcinogenesis [19]. Recent
studies have shown that overexpression of COX-2 is
sufficient to cause tumorigenesis in animal models and
subsequently inhibition of the COX-2 pathway results
in reduction in tumor incidence and progression (Fig.
2) [20]. There are some exceptions to this generally
accepted observation. One recent study has shown that
COX-2 overexpression in the skin of transgenic mice
results in suppression of tumor development [21]. In
sharp contrast, another recent study has shown that
deficiency of COX-2 reduces mouse skin tumorigen-
esis [22]. Based on these observations it is clear that
much additional work with targeted tissue specific over
and under expression of COX-2 is required to firmly
establish the role of this enzyme in target organ
carcinogenesis. However, based on these evidences the
potential application of non-steroidal anti-inflamma-
tory drugs (NSAIDs) as well as recently developed
COX-2 specific inhibitors in cancer clinical practice
has drawn tremendous attention in the past few years as
inhibition of COX-2 offers an effective approach in the
prevention and treatment of cancer [23,24].
4. Diet and prostaglandins in prostate
carcinogenesis
Epidemiologic studies and nutritional data suggest
that androgens and/or environmental exposures, such
as diet in particular, dietary fat, play an important role
in prostate carcinogenesis [25]. The association
Fig. 2. Possible involvement of COX-2 and their inhibitors in various stages of prostate cancer.
T. Hussain et al. / Cancer Letters 191 (2003) 125–135 127

between diet and prostate cancer has been drawn from
the studies where incidence and mortality rates of
prostate cancer vary widely between different popu-
lations in various regions of the world consuming
more dietary fat [26]. Number of studies have
reported this link; countries such as the USA,
known to have high levels of fat consumption, were
also found to have a high mortality rate for prostate
cancer, whereas a country such as Japan, with one of
the lowest rates of fat consumption in the world, has a
low mortality rate for the disease [27]. In addition,
migratory studies have further confirmed this obser-
vation where it was found that Asian men migrating to
the United States acquire a higher clinical incidence
of prostate cancer, and subsequent generations of
American born Asian men have prostate cancer risks
almost equal to those of white Americans [28]. These
studies suggest that a change in dietary habits can
greatly modify prostate cancer risk. However, the
results of most case-control studies demonstrated a
significant association of prostate cancer risk with
high dietary intake of total fat while some studies did
not find a significant association [29,30].
Laboratory studies with experimental animal
models further suggest a link between fat content in
diet and the risk of prostate cancer [31]. Arachidonic
acid and its precursor, linoleic acid, are major
ingredients of animal fat and many vegetable oils
used in the regions where prostate cancer is more
common [32]. Studies have shown that treatment of
androgen-unresponsive human prostate carcinoma
cells PC-3 with linoleic acid stimulated the growth
of these cells [33].The effects of these fatty acids are
thought to be caused by their effects on PG synthesis.
A study by Hughes-Fulford et al. [34] has demon-
strated that linoleic acid, arachidonic acid and the
arachidonic acid metabolite prostaglandin (PGE)(2)
stimulate prostate tumor growth and alters gene
expression in human prostate carcinoma PC-3 cells.
Treatment of PC-3 cells with arachidonic acid was
shown to result in a dose-dependent increase in the
gene expression of c-fos, and COX-2, while the
constitutive COX-1 message was not increased.
Further effects of dietary fat was examined on the in
vivo models, where transplantation of human prostate
carcinoma cells DU145 to nude mice fed with high fat
diet was shown to result in a significant increase in
tumor growth compared to the control group of
animals fed with regular diet [35]. These studies
suggest a stimulatory effect of dietary n-6 fatty acid on
prostate cancer cell growth which may be critical for
the development and progression of prostate cancer.
Intake of unsaturated dietary fat may affect PG
synthesis, that appear to influence sex hormone levels;
this raises the possibility that increased levels of
androgens could play an important role in the
initiation of prostate cancer [36]. Studies have
shown that testosterone is capable of stimulating
oxidative stress in prostate carcinoma cells that has
been suggested to be a mechanism of initiation of
prostate carcinogenesis [37]. However, there is no
such study indicating that increase in testosterone
levels leads to an increase in COX-2 expression
during the development and progression of prostate
cancer.
5. COX-2 and prostate cancer
Studies on relationship of COX and prostate were
initiated in 1993 by O’Neill and Ford-Hutchinson [38]
who analyzed COX-1 and COX-2 mRNA expression
in various human tissues and reported the highest
levels in the prostate where COX-1 and COX-2
transcripts were found to be present in approximately
equal levels. In the year 2000, we provided the first
evidence that COX-2 is overexpressed in human
prostate adenocarcinoma [39]. Employing 12 pairs of
unique benign and prostate carcinoma tissue from the
same individuals we showed that mean levels of
COX-2 mRNA expression was significantly increased
in prostate adenocarcinoma. These results were
further verified by the COX-2 protein expression,
which was significantly higher in cancer tissue
compared to their benign counterparts. Many other
studies verified our initial observation and reported
that compared to normal tissue, COX-2 is over-
expressed in human prostate cancer.
A study by Yoshimura et al. [40] analyzed tumor
specimens obtained from 28 prostate carcinoma
patients, eight benign prostatic hyperplasia (BPH)
patients, one prostatic intraepithelial neoplasia (PIN)
patient, and eight specimens of normal prostate tissue
and showed very weak expression of COX-1 and
marked expression of immunoreactive COX-2 in
prostate tumor cells. The expression of both COX-
T. Hussain et al. / Cancer Letters 191 (2003) 125–135128
isoforms was found to be very weak in all cases of
BPH and in the normal prostate tissues. Further, the
extent and intensity of immunoreactive COX-2
polypeptides in tumor cells was statistically much
greater than those of cells from BPH. These results
were further confirmed by mRNA analysis, where
enhanced expression of COX-2, but not COX-1, was
observed in prostate cancer tissues. These results lead
to the conclusion that human prostate carcinoma cells
generated COX-2, and that COX-2 might play an
important role in the proliferation of prostate
carcinoma cells. Studies by Kirschenbaum et al. [41]
analyzed thirty-one specimens of prostate carcinoma
and 10 specimens of BPH and showed that COX-1
expression in noncancerous prostatic tissue was
predominantly (90% positive staining) seen in the
basal epithelial cells of BPH. COX-1 expression was
minimal in noncancerous luminal epithelial cells and
was found to be upregulated in prostate cancer
predominantly in the smooth muscle cells of the
prostate. COX-2 was found to be expressed in the
basal epithelial cells with 60% BPH, 94% peripheral
zone, 75% PIN, respectively. The expression of COX-
2 in prostate cancer was found to be intense and
uniform, with 87% of samples demonstrating immu-
noreactivity. The results of this study indicated that
expression of both COX-1 and COX-2 in human
prostate cancer is increased suggesting that COX-1
and COX-2 (and/or their PG products) may play a role
in the malignant transformation of the prostate. In
another study, Madaan et al. [42] have determined
COX-1 and COX-2 expression in 30 BPH and 82
prostate cancer specimens. In this study a significant
COX-2 overexpression in tumor cells was found
compared to benign glands; however, COX-1
expression in tumor cells was similar to benign
glands. A significant positive correlation between
COX-2 expression was found with increasing tumor
grade suggesting that COX-2 may play an important
role in prostate carcinogenesis. These studies are in
agreement with the study by Lee et al. [43] where
COX-2 was found to be over-expressed in 15 out of 18
(83%) prostate cancer samples and was detected in
only 22% (4/18) of paired benign tissues. Further, the
intensity of immunostaining correlated with the tumor
grading of these specimens. Another recent study by
Uotila et al. [44] has compared COX-1 and COX-2
mRNA and protein expression from 12 prostate
cancer specimens and 13 control prostates. The
intensity of COX-2 was found to be significantly
stronger in prostate cancer cells than in the non-
malignant glandular epithelium of the control pros-
tates. COX-2 was found to be clearly expressed in the
lesions of PIN in control prostates and was also
detected in the muscle fibers of the hyperplastic
stroma. No significant difference was found in COX-1
expression between control and prostate cancer. The
results of this study indicated that the expression of
COX-2 is elevated in prostatic adenocarcinoma and in
PIN. These experimental data generated from both
human prostate tumor tissue specimen and from
prostate cancer cell lines demonstrated an up-
regulation of inducible COX-2 expression and
suggested a positive role for COX-2 in prostate
carcinogenesis. However, in contrast to these obser-
vations a recent study performed immunohistochem-
ical analysis of 144 human prostate cancer cases and
found that there was no consistent overexpression of
COX-2 in established prostate cancer or high grade
PIN, as compared with adjacent normal prostate tissue
[45]. Positive staining was only seen in scattered cells
in both tumor and normal tissue regions but was much
more consistently observed in areas of proliferative
inflammatory atrophy, lesions that have been impli-
cated in prostatic carcinogenesis. Studies cited above
clearly point to the need of additional studies to
examine COX-2 expression in diverse population
groups of prostate cancer and in transgenic and
knockout models of COX-2 expression in prostate.
The expression of COX-2 in human prostate
carcinoma cells remains controversial. Either rela-
tively down modulated or undetectable levels of
COX-2 expression was observed in prostate cancer
cell lines by several investigators. For example in
LNCaP, PC-3, DU145 and tumor necrosis factor
(TSU) prostate cancer cell lines, COX-2 expression
was undetectable under basal conditions but was
found to be transiently induced in PC-3 and TSU cells
when they were subjected to phorbol ester treatment
[45]. Interestingly, in another study basal COX-2
mRNA and protein expression was found to be higher
in normal prostate epithelial cells compared to its
level of expression in PC-3, LNCaP and DU145
prostate carcinoma cells [46]. Similarly, in one study
COX-2 transcripts were found to be absent in LNCaP
and PC-3 cells [47]. In another study LNCaP and PC-
T. Hussain et al. / Cancer Letters 191 (2003) 125–135 129
3 prostate carcinoma cells were shown to exhibit trace
amounts of COX-1 and COX-2 expression as
measured by reverse transcription-polymerase chain
reaction and immunoblot analysis [48]. Therefore,
there are two significantly contrasting observations
exist, one endorsing the marked up regulation of
COX-2 and its possible involvement in prostate
cancer development and progression, while the
other, promoting a COX-2-independent mechanisms
for prostate tumor development.
6. Role of COX-2 in prostate carcinogenesis
There are multiple mechanisms through which
COX-2 may play a role in carcinogenesis and some or
all of these may be involved in prostate cancer
development and progression [49]. Number of these
mechanisms are likely to result from COX-2-induced
increase in PG synthesis. Evidence that increased PG
synthesis has both growth-promoting and positive
feedback effects in prostate cancer was provided in a
study by Tjandrawinata et al. [50] where treatment of
prostate carcinoma cells PC-3 with exogenous PGE2
wasfound to result in increasedmitogenesisandCOX-2
up-regulation. Further, treatment of PC-3 cells with 5
mM flurbiprofen in the presence of exogenous PGE2
inhibited the up-regulation of COX-2 mRNA and cell
growth. Another study has demonstrated that PGE2
stimulates PIN cell growth through activation of the
interleukin (IL)-6/GP130/signal transducers and acti-
vators of transcription (STAT)-3 signaling pathway
[51].PGE2 wasfound tostimulate soluble IL-6 receptor
(sIL-6R) release, gp130 dimerization, STAT-3 protein
phosphorylation, and DNA binding activity which led
to increased PIN cell growth. This study provides
mechanistic evidence that increased expression of
COX-2/PGE2 contributes to prostate cancer develop-
ment and progression via activation of the IL-6
signaling pathway.
COX-2 over-expression has been shown to upregu-
late Bcl2 expression with an associated decrease in
apoptosis [52]. Accordingly, in a recent study, the
human prostate carcinoma LNCaP cells, which over-
expresses COX-2, exhibits apoptosis induction and
Bcl2 down-modulation when treated with NS398, a
selective inhibitor of COX-2 enzyme function [53].
Inhibition of COX-2 by celecoxib has been shown to
induce apoptosis in both androgen-responsive LNCaP
and androgen-unresponsive PC-3 cells by blocking
Akt phosphorylation which is independent of Bcl2
[54]. In addition, COX-2 was found to be induced by
TNF-a, which underlines the inducibility of COX-2 in
response to pro-inflammatory stimulus [46]. These
experimental data demonstrate the inflammatory, anti-
apoptotic and growth stimulating nature of COX-2 in
prostate cancer and therefore suggest a positive role for
COX-2 in prostate cancer development and pro-
gression in humans. Further, Bcl2 expression has
been shown to be closely associated with the androgen-
independent prostate cancer phenotype and represents
a potential pathway through which COX-2 may induce
prostate cancer progression to an androgen-indepen-
dent state [55]. Contrary to well established exper-
imental data that NSAIDs and other COX-2 specific
inhibitors exert their chemopreventive action by
specific inhibition of COX-2 activity, several recent
studies have proposed the existence of COX-2-
independent mechanism as a mode of action of these
agents in their ability to prevent cancer. For example, it
has been shown that sulindac derivatives inhibit cell
growth and induce apoptosis in prostate cancer cells
PC-3 and LNCaP with similar sensitivity despite these
cells express COX-2 at varying levels [48]. This
similarity in sensitivity to apoptosis by sulindac
compounds led to the prediction of involvement of
COX-2-independent pathway. Similarly celecoxib, a
selective COX-2 inhibitor was reported to induce
apoptosis by interfering with functioning of Akt,
extracellular-regulated kinases and endoplasmic reti-
culum Ca2þ-adenosine triphosphatases [54,56]. Dis-
ruption of these signaling pathways led to rapid
apoptosis which was distinct from the one induced by
NSAIDs, suggesting the COX-2-independent mech-
anism in celecoxib induced apoptosis. In a recent
study, using Tet-On antisense COX-2 clones it was
demonstrated that celecoxib-induced apoptosis in PC-
3 and LNCaP prostate carcinoma cells is independent
of COX-2 inhibition [57]. Although there is a
correlation between the use of NSAIDs and the anti-
carcinogenic effects, the direct demonstration that
these agents inhibit COX-2 activity in their action both
in vitro and in vivo remains to be established.
Other effects of COX-2 overexpression that may
contribute to the malignant phenotype include
decreased E-cadherin expression with consequent
T. Hussain et al. / Cancer Letters 191 (2003) 125–135130

loss of cell-to-cell adhesion, matrix-metalloproteinase
overexpression with an associated increase in inva-
siveness, and modulated production of angiogenic
factors by cancer cells [58,59]. A correlation was
found between hypoxia-induced COX-2 expression
and up regulation of vascular endothelial growth
factor (VEGF) in PC-3 and LNCaP prostate carci-
noma cells [60]. Moreover, the COX-2-dependent
effect on VEGF up-regulation was found to be
inhibited by treatment with COX-2 specific inhibitor
NS398 and this inhibitory effect was reversed by
PGE2 treatment [61]. Since VEGF plays an important
role in angiogenesis, its up-regulation by COX-2
expression and inhibition by COX-2 specific inhibitor
suggests a positive role of COX-2 in angiogenesis, an
important event in prostate metastasis [61]. In another
study, PC-3 tumor growth in nude mice was shown to
be regressed by administration of COX-2 specific
inhibitor and the regression was found to be
associated with a significant decrease in VEGF
suggesting a role for COX-2 in prostate cancer
angiogenesis [62]. Aimed at understanding the role
of PG in invasive potential of prostate carcinoma
cells, it was been demonstrated that inhibitors of PG
synthesis inhibit invasiveness and the secretion of
matrix metalloproteinase (MMPs) [63]. This inhi-
bition of prostaglandin biosynthesis has been shown
to alter the balance between MMPs and tissue specific
inhibitors of matrix metalloproteinases thereby inhi-
biting tumor invasion in prostate cancer.
Since COX-2 reactions involve production of
reactive oxygen radicals that can potentially damage
biological macromolecules, in another study [64] the
possibility that DNA and/or nucleosides can be
oxidized during COX reactions was examined. DNA
or nucleosides incubated with COX-2 and arachidonic
acid resulted in a significant increase in the amount of
8-oxo-2’-deoxyguanosine. This increase was found to
be enzyme-dependent and could be prevented by
COX-2 inhibitors as well as by antioxidants. These
data for the first time indicated that peroxyl radicals or
other oxidized species formed during conversion of
arachidonic acid to PGG2 might be responsible for
increased oxidation of DNA bases. These results
suggested that overexpression of COX-2 in inflamma-
tory diseases like prostate cancer places an additional
burden on antioxidative defenses of the cell, which
might contribute to DNA oxidation and the induction
of mutations. Further, studies have also shown that
overexpression of COX-2 in cancer cells inhibit
immune surveillance and increase metastatic potential
[65]. These studies need validation in prostate cancer.
7. NSAIDs and prostate cancer
NSAIDs have long been known for their analgesic,
antipyretic and anti-inflammatory function [66,67].
Since inflammation is closely related to tumor pro-
motion, agents with potent anti-inflammatory activities
are anticipated to exert chemopreventive effects. These
observations led to a wide variety of investigations to
determine whether or not these drugs have an ability to
reduce the riskofprogressionof several humancancers.
NSAIDs and their mode of action in cancer chemopre-
ventionhasbeen the focusofmanyepidemiologicaland
experimental studies, which support the importance of
these drugs in cancer chemoprevention [68]. Epide-
miological studies have shown a decreased risk of some
cancers in people who regularly take aspirin or other
NSAIDs [68,69]. Many subsequent studies in several
human cancers have established the anti-tumorigenic
effectof thesedrugs.Thesestudieshaveshownthatanti-
tumorigenic action of NSAIDs is mediated by selective
inhibition of COX, particularly COX-2. Non-specific
NSAIDs such as aspirin, sulindac and indomethacin
inhibit not only the enzymatic action of inducible and
pro-inflammatory COX-2, but also the constitutively
expressed, cytoprotective COX-1 as well. Conse-
quently, non-selective NSAIDs can cause platelet
dysfunction, gastrointestinal ulceration, and kidney
damage [70–72]. For this reason, selective inhibition of
COX-2 to treatneoplasticproliferation ispreferred over
non-selective inhibition. Selective COX-2 inhibitors
such as melaxicam, celecoxib and rofecoxib are
NSAIDs that have been modified chemically to
preferentially inhibit COX-2 without affecting COX-1
[73].
The epidemiological evidence for a protective
effect of NSAIDs in prostate cancer development and
progression is equivocal. A population-based, case-
controlled study from New Zealand, reported a trend
towards reduced risk of advanced prostate cancer
associated with regular use of NSAIDs while these
associations failed to reach statistical significance [74].
Another study by Nelson and Harris [75] has demon-
T. Hussain et al. / Cancer Letters 191 (2003) 125–135 131

strated that regular daily use of ibuprofen or aspirin
was associated with a 66% reduction in prostate cancer
risk (odds ratio ¼ 0.34, 95% confidence
interval ¼ 0.23–0.58, P , 0:01). The risk of prostate
cancer was also significantly reduced in men who were
reported to be taking prescription NSAIDs (odds
ratio ¼ 0.35, 95% confidence interval ¼ 0.15–0.84,
P , 0:05). Another recent study [76] employing 1362
white men ranging from 50–79 year-old from the
Olmsted County, Minnesota using prescription and
nonprescription NSAIDs has shown that daily use of
NSAIDs may be associated with a lower incidence of
prostate cancer in men aged 60 years or older. The
stronger effect among older men suggests that NSAIDs
may prevent the progression rather than early stages of
prostate cancer from latent to clinical disease. Overall,
these results suggest that NSAIDs may have value in
the chemoprevention of prostate cancer.
Experimental studies on animal models of prostate
cancer have shown that NSAIDs exert chemopreven-
tive as well as therapeutic effects. In a study by
Pollard and Luckert [77] where treatment of trans-
plantable rat prostate adenocarcinoma III cells which
produce local tumors and osteolytic and osteoplastic
lesions and metastasize through defined lymphatic
channels to the lungs, with NSAID piroxicam resulted
in suppression of tumor growth, bone destruction, and
metastasis. In chemically-induced prostate carcino-
genesis F344 rat model supplementation with indo-
methacin in drinking water, exhibited tumor
suppressive effects and significant decrease in tissue
PGE2 levels [78]. Noble prostate cancer-bearing rats
treated with PG modulators viz. indomethacin (a
general COX inhibitor), UK 38485 (thromboxane
synthase inhibitor), and nafazatron (anti-thrombotic
agent which increases prostacyclin), had significantly
lower pulmonary metastasis than untreated controls
[79,80]. In a rat model, COX-2 inhibitors increased
tumor response to radiation treatment without increas-
ing the radiation effects on normal tissues [81].
Therefore, the role of COX-2 inhibitors in prostate
cancer prevention and treatment either alone or in
combination with chemotherapy or radiotherapy is
worthy for further exploration.
In a recent study [82] from our group we investigated
the effect of human recommended dose of celecoxib, a
specific COX-2 inhibitor against prostate carcinogen-
esis in a transgenic adenocarcinoma of the mouse
prostate (TRAMP) model. In TRAMP, expression of
theSV40earlygenes (Tandtantigen,Tag)aredrivenby
theprostate-specificpromoterprobasin that leads tocell
transformation within the prostate that histologically
resembles to human prostate cancer. The basal enzyme
activity and protein expression of COX-2 was found to
be significantly higher (,3.2-fold) in the dorso-lateral
prostate of TRAMP mice compared to their non-
transgenic littermates. This suggested that COX-2
may have a causative role in prostate cancer develop-
ment in this model. We employed 8 week old TRAMP
mice and randomly divided them in groups consuming
control diet (AIN 76A) or a custom prepared AIN 76A
diet containing 1500 ppm celecoxib ad libitum for 24
weeks. The animals fed control diet developed palpable
tumors at 12–14 weeks while at these times no palpable
tumors were observed in animals fed celecoxib-
supplemented diet. Sequential magnetic resonance
imaging analysis of celecoxib-fed mice at 16, 24, and
32 weeks of age suggested that each time point prostate
volume was lower in celecoxib-fed group compared to
control group. These results were consistent with
significant decrease in prostate and genito-urinary-
weight in celecoxib-fed mice at the termination of the
experiment. Feeding celecoxib in the diet was found to
result in significant inhibition of distant site metastases
to lymph nodes and lungs. These results were further
confirmed by the histopathological examination of the
tissue. Compared to animals consuming control diet,
celecoxib supplemented animals showed reduced
proliferation, and down-modulation of COX-2 in the
dorso-lateral prostate. Furthermore, celecoxib sup-
plementation resulted in enhanced in vivo apoptosis in
the dorso-lateral prostate. Taken together, these studies
suggest that NSAIDs and other selective COX-2
inhibitors possess chemopreventive activity against
prostate carcinogenesis.
8. Conclusions
There is ample evidence that COX-2 and its PG
products may play a critical role in prostate cancer
development and progression. Significant advances
have been made in the past 5 years in understanding
the COX-pathway in prostate, however, the relation-
ship between COX-2 and prostate carcinogenesis
remains to be more clearly elucidated. Animal models
T. Hussain et al. / Cancer Letters 191 (2003) 125–135132

of COX-2 overexpression and knockouts specifically
in prostate needs to be developed. It will be useful to
study the downstream signaling pathways and apop-
totic response for the preventive role of COX-2
inhibitors in mouse models of prostate cancer. It will
be of great interest to examine if COX-2 is sufficient
or need cooperation with other factors to induce
prostate carcinogenesis. It will be important to study
the specific roles that COX-1 and COX-2 plays during
the development of prostate cancer and to examine the
key modulator(s) for development of prostate adeno-
carcinoma: total PG production or the different PG
products derived from the COX-1 and COX-2 path-
way. Lastly, unraveling the COX-2-dependent versus
COX-2-independent effects of the COX-2 inhibitors
in prostate cancer may reveal the cellular mechanisms
of COX-2 action and its role in prostate cancer
development. Answers to these questions will provide
a molecular basis for understanding the contributing
role of COX-2 in mechanism of prostate carcinogen-
esis and the effectiveness of the use of COX-2 specific
and non-specific inhibitors in different stages of
prostate cancer treatment. However, based on avail-
able information it appears that COX-2 plays an
important role in prostate cancer development and
progression and therefore selective COX-2 inhibitors
may have promise in prostate cancer management.
Acknowledgements
Original work from authors laboratory cited in this
review is supported by the funds from United States
Public Health Service RO3 CA 89739 (to H.M. and
S.G.) and Cancer Research Foundation of America (to
S.G.).
References
[1] O.P. Kallioniemi, T. Visakorpi, Genetic basis and clonal
evolution of human prostate cancer, Adv. Cancer Res. 68
(1996) 225–255.
[2] R.T. Greenlee, M.B. Hill-Harmon, T. Murray, M. Thun,
Cancer statistics, CA Cancer J. Clin. 51 (2001) 15–36.
[3] American Cancer Society, Cancer facts and figures: Graphical
data (2002) (Available at the website http://www.cancer.org).
[4] K.J. Pienta, Etiology, epidemiology, and prevention of
carcinoma of the prostate, in: M.F. Campbell, A.B. Retik,
E.D. Vaughan (Eds.), 7th edition., Campbell’s Urology, W.B.
Saunders Company, Vol. 3, Orlando, FL, (1997), pp. 379–386.
[5] D.G. Tang, A.T. Porter, Target to apoptosis: a hopeful weapon
for prostate cancer, Prostate 32 (1997) 284–293.
[6] J.R. Vane, Y.S. Bakhle, R.M. Botting, Cyclooxygenases 1 and
2, Annu. Rev. Pharmacol. Toxicol. 38 (1998) 97–120.
[7] W.L. Smith, R.M. Garavito, D.L. DeWitt, Prostaglandin
endoperoxide H synthases (cyclooxygenases)-1 and -2,
J. Biol. Chem. 271 (1996) 33157–33160.
[8] M.E. Turini, R.N. DuBois, Cyclooxygenase-2: a therapeutic
target, Annu. Rev. Med. 53 (2002) 35–57.
[9] Y.S. Bakhle, COX-2 and cancer: a new approach to an old
problem, Br. J. Pharmacol. 134 (2001) 1137–1150.
[10] T. Hla, D. Bishop-Bailey, C.H. Liu, H.J. Schaefers, O.C.
Trifan, Cyclooxygenase-1 and -2 isoenzymes, Int. J. Biochem.
Cell Biol. 31 (1999) 551–557.
[11] M. Pairet, G. Engelhardt, Distinct isoforms (COX-1 and COX-
2) of cyclooxygenase: possible physiological and therapeutic
implications, Fundam. Clin. Pharmacol. 10 (1996) 1–17.
[12] H.R. Herschman, Prostaglandin synthase 2, Biochim. Biophys.
Acta 1299 (1996) 125–140.
[13] T. Kosaka, A. Miyata, H. Ihara, S. Hara, T. Sugimoto, O.
Takeda, E. Takahashi, T. Tanabe, Characterization of the
human gene (PTGS2) encoding prostaglandin-endoperoxide
synthase 2, Eur. J. Biochem. 221 (1994) 889–897.
[14] S.A. Kraemer, E.A. Meade, D.L. DeWitt, Prostaglandin
endoperoxide synthase gene structure: identification of the
transcriptional start site and 50-flanking regulatory sequences,
Arch. Biochem. Biophys. 293 (1992) 391–400.
[15] J.C. Otto, W.L. Smith, Prostaglandin endoperoxide synthases-
1 and -2,, J. Lipid Mediat. Cell Signal. 12 (1995) 139–156.
[16] R.N. Dubois, S.B. Abramson, L. Crofford, R.A. Gupta, L.S.
Simon, L.B. Van De Putte, P.E. Lipsky, Cyclooxygenase in
biology and disease, FASEB J. 12 (1998) 1063–1073.
[17] K.M. Leahy, A.T. Koki, J.L. Masferrer, Role of cycloox-
ygenases in angiogenesis, Curr. Med. Chem. 7 (2000)
1163–1170.
[18] P.E. Lipsky, Role of cyclooxygenase-1 and -2 in health and
disease, Am. J. Orthop. 28 (1999) 8–12.
[19] S.M. Prescott, F.A. Fitzpatrick, Cyclooxygenase-2 and
carcinogenesis, Biochim. Biophys. Acta 1470 (2000) 69–78.
[20] C.H. Liu, S.H. Chang, K. Narko, O.C. Trifan, M.T. Wu, E.
Smith, C. Haudenschild, T.F. Lane, T. Hla, Overexpression of
cyclooxygenase-2 is sufficient to induce tumorigenesis in
transgenic mice, J. Biol. Chem. 276 (2001) 18563–18569.
[21] D.K. Bol, R.B. Rowley, C.P. Ho, B. Pilz, J. Dell, M. Swerdel,
K. Kiguchi, S. Muga, R. Klein, S.M. Fischer, Cyclooxygen-
ase-2 overexpression in the skin of transgenic mice results in
suppression of tumor development, Cancer Res. 62 (2002)
2516–2521.
[22] H.F. Tiano, C.D. Loftin, J. Akunda, C.A. Lee, J. Spalding, A.
Sessoms, D.B. Dunson, E.G. Rogan, S.G. Morham, R.C.
Smart, R. Langenbach, Deficiency of either cyclooxygenase
(COX)-1 or COX-2 alters epidermal differentiation and
reduces mouse skin tumorigenesis, Cancer Res. 62 (2002)
3395–3401.
[23] A.J. Dannenberg, N.K. Altorki, J.O. Boyle, C. Dang, L.R.
T. Hussain et al. / Cancer Letters 191 (2003) 125–135 133
Howe, B.B. Weksler, K. Subbaramaiah, Cyclo-oxygenase 2: a
pharmacological target for the prevention of cancer, Lancet
Oncol. 2 (2001) 544–551.
[24] S. Gupta, L.J. Crofford, An update on specific COX-2
inhibitors: the COXIBs, Bull. Rheum. Dis. 50 (2001) 1–4.
[25] N.E. Fleshner, L.H. Klotz, Diet, androgens, oxidative stress
and prostate cancer susceptibility, Cancer Metastasis Rev. 17
(1998) 325–330.
[26] K. Griffiths, L. Denis, A. Turkes, M.S. Morton, Possible
relationship between dietary factors and pathogenesis of
prostate cancer, Int. J. Urol. 5 (1998) 195–213.
[27] L. Denis, M.S. Morton, K. Griffiths, Diet and its preventive
role in prostatic disease, Eur. Urol. 35 (1999) 377–387.
[28] A.S. Whittemore, L.N. Kolonel, A.H. Wu, E.M. John, R.P.
Gallagher, G.R. Howe, J.D. Burch, J. Hankin, D.M. Dreon,
D.W. West, Prostate cancer in relation to diet, physical
activity, and body size in blacks, whites, and Asians in the
United States and Canada, J. Natl. Cancer Inst. 87 (1995)
652–661.
[29] L.M. Fisher, High-fat diet and prostate cancer: the contro-
versial connection, Urol. Nurs. 20 (2000) 209–210.
[30] L.H. Kuller, Dietary fat and chronic diseases: epidemiologic
overview, J. Am. Diet Assoc. 97 (1997) 9–15.
[31] M.C. Bosland, I. Oakley-Girvan, A.S. Whittemore, Dietary
fat, calories, and prostate cancer risk, J. Natl. Cancer Inst. 91
(1999) 489–491.
[32] E. Giovannucci, E.B. Rimm, G.A. Colditz, M.J. Stampfer, A.
Ascherio, C.C. Chute, W.C. Willett, A. prospective, study of
dietary fat and risk of prostate cancer, J. Natl. Cancer Inst. 85
(1993) 1571–1579.
[33] R.R. Tjandrawinata, R. Dahiya, M. Hughes-Fulford, Induction
of cyclo-oxygenase-2 mRNA by prostaglandin E2 in human
prostatic carcinoma cells, Br. J. Cancer 75 (1997) 1111–1118.
[34] M. Hughes-Fulford, Y. Chen, R.R. Tjandrawinata, Fatty acid
regulates gene expression and growth of human prostate
cancer PC-3 cells, Carcinogenesis 22 (2001) 701–707.
[35] J.M. Connolly, M. Coleman, D.P. Rose, Effects of dietary fatty
acids on DU145 human prostate cancer cell growth in athymic
nude mice, Nutr. Cancer 29 (1997) 114–119.
[36] R.K. Ross, B.E. Henderson, Do diet and androgens alter
prostate cancer risk via a common etiologic pathway?, J. Natl.
Cancer Inst. 86 (1994) 252–254.
[37] X-Y. Sun, S.P. Donald, J.M. Phang, Testosterone and prostate
specific antigen stimulate generation of reactive oxygen
species in prostate cancer cells, Carcinogenesis 22 (2001)
1775–1780.
[38] G.P. O’Neill, A.W. Ford-Hutchinson, Expression of mRNA
for cyclooxygenase-1 and cyclooxygenase-2 in human tissues,
FEBS Lett. 330 (1993) 156–160.
[39] S. Gupta, M. Srivastava, N. Ahmad, D.G. Bostwick, H.
Mukhtar, Over-expression of cyclooxygenase-2 in human
prostate adenocarcinoma, Prostate 42 (2000) 73–78.
[40] R. Yoshimura, H. Sano, C. Masuda, M. Kawamura, Y.
Tsubouchi, J. Chargui, N. Yoshimura, T. Hla, S. Wada,
Expression of cyclooxygenase-2 in prostate carcinoma,
Cancer 89 (2000) 589–596.
[41] A. Kirschenbaum, A.P. Klausner, R. Lee, P. Unger, S. Yao,
X.H. Liu, A.C. Levine, Expression of cyclooxygenase-1 and
cyclooxygenase-2 in the human prostate, Urology 56 (2000)
671–676.
[42] S. Madaan, P.D. Abel, K.S. Chaudhary, R. Hewitt, M.A. Stott,
G.W. Stamp, E.N. Lalani, Cytoplasmic induction and over-
expression of cyclooxygenase-2 in human prostate cancer:
implications for prevention and treatment, BJU Int. 86 (2000)
736–741.
[43] L.M. Lee, C.C. Pan, C.J. Cheng, C.W. Chi, T.Y. Liu,
Expression of cyclooxygenase-2 in prostate adenocarcinoma
and benign prostatic hyperplasia, Anticancer Res. 21 (2001)
1291–1294.
[44] P. Uotila, E. Valve, P. Martikainen, M. Nevalainen, M. Nurmi,
P. Harkonen, Increased expression of cyclooxygenase-2 and
nitric oxide synthase-2 in human prostate cancer, Urol. Res. 29
(2001) 23–28.
[45] S. Zha, W.R. Gage, J. Sauvageot, E.A. Saria, M.J. Putzi, C.M.
Ewing, D.A. Faith, W.G. Nelson, A.M. De Marzo, W.B.
Isaacs, Cyclooxygenase-2 is up-regulated in proliferative
inflammatory atrophy of the prostate, but not in prostate
carcinoma, Cancer Res. 61 (2001) 8617–8623.
[46] V. Subbarayan, A.L. Sabichi, N. Llansa, S.M. Lippman, D.G.
Menter, Differential expression of cyclooxygenase-2 and its
regulation by tumor necrosis factor-alpha in normal and
malignant prostate cells, Cancer Res. 61 (2001) 2720–2726.
[47] S.H. Hong, I. Avis, M.D. Vos, A. Martinez, A.M. Treston, J.L.
Mulshine, Relationship of arachidonic acid metabolizing
enzyme expression in epithelial cancer cell lines to the growth
effect of selective biochemical inhibitors, Cancer Res. 59
(1999) 2223–2228.
[48] J.T. Lim, G.A. Piazza, E.K. Han, T.M. Delohery, H. Li, T.S.
Finn, R. Buttyan, H. Yamamoto, G.J. Sperl, K. Brendel, P.H.
Gross, R. Pamukcu, I.B. Weinstein, Sulindac derivatives
inhibit growth and induce apoptosis in human prostate cancer
cell lines, Biochem. Pharmacol. 58 (1999) 1097–1107.
[49] A. Kirschenbaum, X. Liu, S. Yao, A.C. Levine, The role of
cyclooxygenase-2 in prostate cancer, Urology 58 (2001)
127–131.
[50] R.R. Tjandrawinata, M. Hughes-Fulford, Up-regulation of
cyclooxygenase-2 by product-prostaglandin E2, Adv. Exp.
Med. Biol. 407 (1997) 163–170.
[51] X.H. Liu, A. Kirschenbaum, M. Lu, S. Yao, A. Klausner, C.
Preston, J.F. Holland, A.C. Levine, Prostaglandin E(2)
stimulates prostatic intraepithelial neoplasia cell growth
through activation of the interleukin-6/GP130/STAT-3 signal-
ing pathway, Biochem. Biophys. Res. Commun. 290 (2002)
249–255.
[52] M. Tsujii, R.N. DuBois, Alterations in cellular adhesion and
apoptosis in epithelial cells overexpressing prostaglandin
endoperoxide synthase 2, Cell 83 (1995) 493–501.
[53] X.H. Liu, S. Yao, A. Kirschenbaum, A.C. Levine, NS398, a
selective cyclooxygenase-2 inhibitor, induces apoptosis and
down-regulates bcl-2 expression in LNCaP cells, Cancer Res.
58 (1998) 4245–4249.
[54] A.L. Hsu, T.T. Ching, D.S. Wang, X. Song, V.M. Rangnekar,
C.S. Chen, The cyclooxygenase-2 inhibitor celecoxib induces
apoptosis by blocking Akt activation in human prostate cancer
T. Hussain et al. / Cancer Letters 191 (2003) 125–135134
cells independently of Bcl-2, J. Biol. Chem. 275 (2000)
11397–11403.
[55] K.S. Chaudhary, P.D. Abel, E.N. Lalani, Role of the Bcl-2
gene family in prostate cancer progression and its implications
for therapeutic intervention, Environ. Health Perspect. 107
(1999) 49–57.
[56] A.J. Johnson, X. Song, A. Hsu, C. Chen, Apoptosis signaling
pathways mediated by cyclooxygenase-2 inhibitors in prostate
cancer cells, Adv. Enzyme Regul. 41 (2001) 221–235.
[57] X. Song, H.P. Lin, A.J. Johnson, P.H. Tseng, Y.T. Yang, S.K.
Kulp, C.S. Chen, Cyclooxygenase-2, player or spectator in
cyclooxygenase-2 inhibitor-induced apoptosis in prostate
cancer cells, J. Natl. Cancer Inst. 94 (2002) 585–591.
[58] Z. Zhang, R.N. DuBois, Detection of differentially expressed
genes in human colon carcinoma cells treated with a selective
COX-2 inhibitor, Oncogene 20 (2001) 4450–4456.
[59] M. Tsujii, S. Kawano, S. Tsuji, H. Sawaoka, M. Hori, R.N.
DuBois, Cyclooxygenase regulates angiogenesis induced by
colon cancer cells, Cell 93 (1998) 705–716.
[60] X.H. Liu, A. Kirschenbaum, S. Yao, M.E. Stearns, J.F.
Holland, K. Claffey, A.C. Levine, Upregulation of vascular
endothelial growth factor by cobalt chloride-simulated
hypoxia is mediated by persistent induction of cyclooxygen-
ase-2 in a metastatic human prostate cancer cell line, Clin.
Exp. Metastasis 17 (1999) 687–694.
[61] J.L. Masferrer, K.M. Leahy, A.T. Koki, B.S. Zweifel, S.L.
Settle, B.M. Woerner, D.A. Edwards, A.G. Flickinger, R.J.
Moore, K. Seibert, Antiangiogenic and antitumor activities of
cyclooxygenase-2 inhibitors, Cancer Res. 60 (2000)
1306–1311.
[62] X.H. Liu, A. Kirschenbaum, S. Yao, R. Lee, J.F. Holland, A.C.
Levine, Inhibition of cyclooxygenase-2 suppresses angiogen-
esis and the growth of prostate cancer in vivo, J. Urol. 164
(2000) 820–825.
[63] F.A. Attiga, P.M. Fernandez, A.T. Weeraratna, M.J. Manyak,
S.R. Patierno, Inhibitors of prostaglandin synthesis inhibit
human prostate tumor cell invasiveness and reduce the release
of matrix metalloproteinases, Cancer Res. 60 (2000)
4629–4637.
[64] D. Nikolic, R.B. van Breemen, Oxidation DNA induced by
cyclooxygenase-2, Chem. Res. Toxicol. 14 (2001) 351–354.
[65] M. Huang, M. Stolina, S. Sharma, J.T. Mao, L. Zhu, P.W.
Miller, J. Wollman, H. Herschman, S.M. Dubinett, Non-small
cell lung cancer cyclooxygenase-2-dependent regulation of
cytokine balance in lymphocytes and macrophages: up-
regulation of interleukin 10 and down-regulation of inter-
leukin 12 production, Cancer Res. 58 (1998) 1208–1216.
[66] M.M. Taketo, Cyclooxygenase-2 inhibitors in tumorigenesis
(part I), J. Natl. Cancer Inst. 90 (1998) 1529–1536.
[67] M.M. Taketo, Cyclooxygenase-2 inhibitors in tumorigenesis
(Part II), J. Natl. Cancer Inst. 90 (1998) 1609–1620.
[68] E.M. Moran, Epidemiological and clinical aspects of non-
steroidal anti-inflammatory drugs and cancer risks, J. Environ.
Pathol. Toxicol. Oncol. 21 (2002) 193–201.
[69] X.C. Xu, COX-2 inhibitors in cancer treatment and preven-
tion, a recent development, Anticancer Drugs 13 (2002)
127–137.
[70] I. Bjarnason, J. Hayllar, A.J. MacPherson, A.S. Russell, Side
effects of nonsteroidal anti-inflammatory drugs on the small
and large intestine in humans, Gastroenterology 104 (1993)
1832–1847.
[71] D.A. Henry, Side-effects of non-steroidal anti-inflammatory
drugs, Baillieres Clin. Rheumatol. 2 (1988) 425–454.
[72] M.D. Murray, D.C. Brater, Effects of NSAIDs on the kidney,
Prog. Drug Res. 49 (1997) 155–171.
[73] I.A. Mardini, G.A. Fitzgerald, Selective inhibitors of cycloox-
ygenase-2: A growing class of anti-inflammatory drugs, Mol.
Interventions 1 (2001) 30–38.
[74] A.E. Norrish, R.T. Jackson, C.U. McRae, Non-steroidal anti-
inflammatory drugs and prostate cancer progression, Int.
J. Cancer 77 (1998) 511–515.
[75] J.E. Nelson, R.E. Harris, Inverse association of prostate cancer
and non-steroidal anti-inflammatory drugs (NSAIDs): results
of a case-control study, Oncol. Rep. 7 (2000) 169–170.
[76] R.O. Roberts, D.J. Jacobson, C.J. Girman, T. Rhodes, M.M.
Lieber, S.J. Jacobsen, Population-based A, study of daily
nonsteroidal anti-inflammatory drug use and prostate cancer,
Mayo Clin. Proc. 77 (2002) 219–225.
[77] M. Pollard, P.H. Luckert, The beneficial effects of dipho-
sphonate and piroxicam on the osteolytic and metastatic
spread of rat prostate carcinoma cells, Prostate 8 (1986)
81–86.
[78] M. Kawabe, M.A. Shibata, M. Sano, Y. Takesada, S. Tamano,
N. Ito, T. Shirai, Decrease of prostaglandin E2 and 5-bromo-
20-deoxyuridine labeling but not prostate tumor development
by indomethacin treatment of rats given 3,20-dimethyl-4-
aminobiphenyl and testosterone propionate, Jpn. J. Cancer
Res. 88 (1997) 350–355.
[79] J.R. Drago, H.A. Al-Mondhiry, The effect of prostaglandin
modulators on prostate tumor growth and metastasis, Antic-
ancer Res. 4 (1984) 391–394.
[80] J. Kaneti, D.M. Thomson, E.C. Reid, Prostaglandin E2 affects
the tumor immune response in prostatic carcinoma, J. Urol.
126 (1981) 65–70.
[81] K. Kishi, S. Petersen, C. Petersen, N. Hunter, K. Mason, J.L.
Masferrer, P.J. Tofilon, L. Milas, Preferential enhancement of
tumor radioresponse by a cyclooxygenase-2 inhibitor, Cancer
Res. 60 (2000) 1326–1331.
[82] S. Gupta, V.M. Adhami, J.S. Lewin, H. Mukhtar, Dietary
supplementation of selective COX-2 inhibitor celecoxib
suppresses prostate carcinogenesis in TRAMP Mice, Proc.
Am. Assoc. Cancer Res. 43 (2002) 671.
T. Hussain et al. / Cancer Letters 191 (2003) 125–135 135




















