Current Food Allergy Diagnostic Testing
53
1 Current Diagnostic Techniques in Food Allergy Matthew Greenhawt, MD, MBA, MSc Professor of Pediatrics Director, Food Challenge and Research Unit Section of Allergy and Immunology Children’s Hospital Colorado University of Colorado School of Medicine
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Current Food Allergy Diagnostic Testing

1
Current Diagnostic Techniques in Food Allergy
Matthew Greenhawt MD MBA MScProfessor of Pediatrics
Director Food Challenge and Research UnitSection of Allergy and Immunology
Childrenrsquos Hospital ColoradoUniversity of Colorado School of Medicine
2
Objectives
Describe the indications for when to test for diagnosing food allergy and what
test to run
Upon completion of this session the clinician should be able tohelliphellip
Review the evidence
surrounding whether
diagnostic testing can be used to
infer future reaction severity
Discuss the potential role for
component testing epitope
mapping and the basophil
activation test
3
Testing Model and Outcomes
Perform Diagnostic
Test
True PositiveDiagnosis confirmed
False PositiveOverdiagnosis
True NegativeAllergy excluded
False NegativeMissed diagnosis
bull Testing supports a clinical suspicion of a diagnosis but doesnrsquot automatically make a diagnosisbull All tests have an errormisclassification rate we must be aware ofbull We want to maximize the true positivenegative and minimize the false positivenegativebull What is the worst for our patientsmdashthe false positive or the false negative bull No matter what I tell you today no current test outperforms an OFC The rest are surrogates with an error rate
4
Trying To Find a Test To Prevent OFCshellip
5
Stop Chasing Predictive Valueshellip
bull From the analysis of ANY sample EVERY statistical package will provide SnSp PPVNPV
minus These are not special because they predict behavior ONLY in that sample and nowhere else
minus Predictive values require valid population prevalence NPV is dependent on how good a test ishellip
bull All tests are surrogates of some gold standard and by definition will have an error rate
minus OFC surrogates trade error rates and misclassification against tiny risks of severe reactions one canrsquot control
minus This instills our values in patients and forcing them to accept the health and economic detriments of misclassification
bull ldquoPredictiverdquo values from retrospective banked samplescohorts are highly biased and overspecify the accuracy of a test vs real world performancemdashselection bias timingflow are very significant issues
bull If you are avoiding doing an OFC because you are afraid of provoking a reaction you are in the wrong line of work and should also not be giving either OIT or AIT This is part of our jobs like it or nothellip
bull No test can or should ethically be marketed to ldquoreduce the necessityrdquo for a gold standard test
6
A Primer on Testing Peanut as a Case Study
7
Peanut as a Component Model
Diagram schematic courtesy Thermo Fisher 2010
bull Peanut containsbull Major allergensbull Cross-reactive allergensbull Other compounds
bull Patients can recognize multiple epitopes simultaneously
bull A ldquopositiverdquo test is a sum of all recognized parts
bull Same scenario exists for any food allergen but the issue is particularly of concern for plant-based foods such as legumes seeds nuts grains
bull Could component patter infer greater sensitivityspecificity in a diagnosis
Ara h 1
Ara h 2
Ara h 3
Ara h 6
Ara h 9 CCDAra h 8
-
8
Peanut Model of Theoretical Risk
Slide courtesy Anna-Nowak-Wegryzn Jaffe Food Allergy Institute Mount Sinai School of Medicine with permission
rAra h 1rAra h 2rAra h 3rAra h 8rAra h 9CCD
Ara h 8 Ara h 1
Ara h 26
Ara h 3
ProfilinCCD PR-10 LTP Storage Proteins
Ara h 9
Risk
Ara h 5
Pollen cross-reactive
9
Peanut Allergy Parameter Questions
1) Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
2a) In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 --would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
2b) In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
3) In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
10
GRADE Quality of Evidence
http gdtguidelinedevelopmentorgapp
Strength of RecommendationFor the Patient For the Clinician
StrongMost individuals in this situation would prefer the recommended course of action and only a small proportion would not
The attending provider should strongly consider the recommended course of action as a first-line management Formal decision aids may have less of a role to help individuals make decisions consistent with their values and preferences
ConditionalThe majority of individuals in this situation would prefer the suggested course of action but many would not
Different choices may be appropriate for different patients Decision aids may be useful in helping individuals in making decisions consistent with their values and preferences Clinicians should expect to spend more time with patients when working towards a decision
Quality of RecommendationsHigh There is high confidence that the true effect lies close to that of the estimate of the effect
Moderate There is moderate confidence in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different
LowThere is limited confidence in the effect estimate The true effect may be substantially different from the estimate of the effect
Very Low There is very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

2
Objectives
Describe the indications for when to test for diagnosing food allergy and what
test to run
Upon completion of this session the clinician should be able tohelliphellip
Review the evidence
surrounding whether
diagnostic testing can be used to
infer future reaction severity
Discuss the potential role for
component testing epitope
mapping and the basophil
activation test
3
Testing Model and Outcomes
Perform Diagnostic
Test
True PositiveDiagnosis confirmed
False PositiveOverdiagnosis
True NegativeAllergy excluded
False NegativeMissed diagnosis
bull Testing supports a clinical suspicion of a diagnosis but doesnrsquot automatically make a diagnosisbull All tests have an errormisclassification rate we must be aware ofbull We want to maximize the true positivenegative and minimize the false positivenegativebull What is the worst for our patientsmdashthe false positive or the false negative bull No matter what I tell you today no current test outperforms an OFC The rest are surrogates with an error rate
4
Trying To Find a Test To Prevent OFCshellip
5
Stop Chasing Predictive Valueshellip
bull From the analysis of ANY sample EVERY statistical package will provide SnSp PPVNPV
minus These are not special because they predict behavior ONLY in that sample and nowhere else
minus Predictive values require valid population prevalence NPV is dependent on how good a test ishellip
bull All tests are surrogates of some gold standard and by definition will have an error rate
minus OFC surrogates trade error rates and misclassification against tiny risks of severe reactions one canrsquot control
minus This instills our values in patients and forcing them to accept the health and economic detriments of misclassification
bull ldquoPredictiverdquo values from retrospective banked samplescohorts are highly biased and overspecify the accuracy of a test vs real world performancemdashselection bias timingflow are very significant issues
bull If you are avoiding doing an OFC because you are afraid of provoking a reaction you are in the wrong line of work and should also not be giving either OIT or AIT This is part of our jobs like it or nothellip
bull No test can or should ethically be marketed to ldquoreduce the necessityrdquo for a gold standard test
6
A Primer on Testing Peanut as a Case Study
7
Peanut as a Component Model
Diagram schematic courtesy Thermo Fisher 2010
bull Peanut containsbull Major allergensbull Cross-reactive allergensbull Other compounds
bull Patients can recognize multiple epitopes simultaneously
bull A ldquopositiverdquo test is a sum of all recognized parts
bull Same scenario exists for any food allergen but the issue is particularly of concern for plant-based foods such as legumes seeds nuts grains
bull Could component patter infer greater sensitivityspecificity in a diagnosis
Ara h 1
Ara h 2
Ara h 3
Ara h 6
Ara h 9 CCDAra h 8
-
8
Peanut Model of Theoretical Risk
Slide courtesy Anna-Nowak-Wegryzn Jaffe Food Allergy Institute Mount Sinai School of Medicine with permission
rAra h 1rAra h 2rAra h 3rAra h 8rAra h 9CCD
Ara h 8 Ara h 1
Ara h 26
Ara h 3
ProfilinCCD PR-10 LTP Storage Proteins
Ara h 9
Risk
Ara h 5
Pollen cross-reactive
9
Peanut Allergy Parameter Questions
1) Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
2a) In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 --would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
2b) In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
3) In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
10
GRADE Quality of Evidence
http gdtguidelinedevelopmentorgapp
Strength of RecommendationFor the Patient For the Clinician
StrongMost individuals in this situation would prefer the recommended course of action and only a small proportion would not
The attending provider should strongly consider the recommended course of action as a first-line management Formal decision aids may have less of a role to help individuals make decisions consistent with their values and preferences
ConditionalThe majority of individuals in this situation would prefer the suggested course of action but many would not
Different choices may be appropriate for different patients Decision aids may be useful in helping individuals in making decisions consistent with their values and preferences Clinicians should expect to spend more time with patients when working towards a decision
Quality of RecommendationsHigh There is high confidence that the true effect lies close to that of the estimate of the effect
Moderate There is moderate confidence in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different
LowThere is limited confidence in the effect estimate The true effect may be substantially different from the estimate of the effect
Very Low There is very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

3
Testing Model and Outcomes
Perform Diagnostic
Test
True PositiveDiagnosis confirmed
False PositiveOverdiagnosis
True NegativeAllergy excluded
False NegativeMissed diagnosis
bull Testing supports a clinical suspicion of a diagnosis but doesnrsquot automatically make a diagnosisbull All tests have an errormisclassification rate we must be aware ofbull We want to maximize the true positivenegative and minimize the false positivenegativebull What is the worst for our patientsmdashthe false positive or the false negative bull No matter what I tell you today no current test outperforms an OFC The rest are surrogates with an error rate
4
Trying To Find a Test To Prevent OFCshellip
5
Stop Chasing Predictive Valueshellip
bull From the analysis of ANY sample EVERY statistical package will provide SnSp PPVNPV
minus These are not special because they predict behavior ONLY in that sample and nowhere else
minus Predictive values require valid population prevalence NPV is dependent on how good a test ishellip
bull All tests are surrogates of some gold standard and by definition will have an error rate
minus OFC surrogates trade error rates and misclassification against tiny risks of severe reactions one canrsquot control
minus This instills our values in patients and forcing them to accept the health and economic detriments of misclassification
bull ldquoPredictiverdquo values from retrospective banked samplescohorts are highly biased and overspecify the accuracy of a test vs real world performancemdashselection bias timingflow are very significant issues
bull If you are avoiding doing an OFC because you are afraid of provoking a reaction you are in the wrong line of work and should also not be giving either OIT or AIT This is part of our jobs like it or nothellip
bull No test can or should ethically be marketed to ldquoreduce the necessityrdquo for a gold standard test
6
A Primer on Testing Peanut as a Case Study
7
Peanut as a Component Model
Diagram schematic courtesy Thermo Fisher 2010
bull Peanut containsbull Major allergensbull Cross-reactive allergensbull Other compounds
bull Patients can recognize multiple epitopes simultaneously
bull A ldquopositiverdquo test is a sum of all recognized parts
bull Same scenario exists for any food allergen but the issue is particularly of concern for plant-based foods such as legumes seeds nuts grains
bull Could component patter infer greater sensitivityspecificity in a diagnosis
Ara h 1
Ara h 2
Ara h 3
Ara h 6
Ara h 9 CCDAra h 8
-
8
Peanut Model of Theoretical Risk
Slide courtesy Anna-Nowak-Wegryzn Jaffe Food Allergy Institute Mount Sinai School of Medicine with permission
rAra h 1rAra h 2rAra h 3rAra h 8rAra h 9CCD
Ara h 8 Ara h 1
Ara h 26
Ara h 3
ProfilinCCD PR-10 LTP Storage Proteins
Ara h 9
Risk
Ara h 5
Pollen cross-reactive
9
Peanut Allergy Parameter Questions
1) Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
2a) In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 --would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
2b) In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
3) In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
10
GRADE Quality of Evidence
http gdtguidelinedevelopmentorgapp
Strength of RecommendationFor the Patient For the Clinician
StrongMost individuals in this situation would prefer the recommended course of action and only a small proportion would not
The attending provider should strongly consider the recommended course of action as a first-line management Formal decision aids may have less of a role to help individuals make decisions consistent with their values and preferences
ConditionalThe majority of individuals in this situation would prefer the suggested course of action but many would not
Different choices may be appropriate for different patients Decision aids may be useful in helping individuals in making decisions consistent with their values and preferences Clinicians should expect to spend more time with patients when working towards a decision
Quality of RecommendationsHigh There is high confidence that the true effect lies close to that of the estimate of the effect
Moderate There is moderate confidence in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different
LowThere is limited confidence in the effect estimate The true effect may be substantially different from the estimate of the effect
Very Low There is very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

4
Trying To Find a Test To Prevent OFCshellip
5
Stop Chasing Predictive Valueshellip
bull From the analysis of ANY sample EVERY statistical package will provide SnSp PPVNPV
minus These are not special because they predict behavior ONLY in that sample and nowhere else
minus Predictive values require valid population prevalence NPV is dependent on how good a test ishellip
bull All tests are surrogates of some gold standard and by definition will have an error rate
minus OFC surrogates trade error rates and misclassification against tiny risks of severe reactions one canrsquot control
minus This instills our values in patients and forcing them to accept the health and economic detriments of misclassification
bull ldquoPredictiverdquo values from retrospective banked samplescohorts are highly biased and overspecify the accuracy of a test vs real world performancemdashselection bias timingflow are very significant issues
bull If you are avoiding doing an OFC because you are afraid of provoking a reaction you are in the wrong line of work and should also not be giving either OIT or AIT This is part of our jobs like it or nothellip
bull No test can or should ethically be marketed to ldquoreduce the necessityrdquo for a gold standard test
6
A Primer on Testing Peanut as a Case Study
7
Peanut as a Component Model
Diagram schematic courtesy Thermo Fisher 2010
bull Peanut containsbull Major allergensbull Cross-reactive allergensbull Other compounds
bull Patients can recognize multiple epitopes simultaneously
bull A ldquopositiverdquo test is a sum of all recognized parts
bull Same scenario exists for any food allergen but the issue is particularly of concern for plant-based foods such as legumes seeds nuts grains
bull Could component patter infer greater sensitivityspecificity in a diagnosis
Ara h 1
Ara h 2
Ara h 3
Ara h 6
Ara h 9 CCDAra h 8
-
8
Peanut Model of Theoretical Risk
Slide courtesy Anna-Nowak-Wegryzn Jaffe Food Allergy Institute Mount Sinai School of Medicine with permission
rAra h 1rAra h 2rAra h 3rAra h 8rAra h 9CCD
Ara h 8 Ara h 1
Ara h 26
Ara h 3
ProfilinCCD PR-10 LTP Storage Proteins
Ara h 9
Risk
Ara h 5
Pollen cross-reactive
9
Peanut Allergy Parameter Questions
1) Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
2a) In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 --would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
2b) In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
3) In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
10
GRADE Quality of Evidence
http gdtguidelinedevelopmentorgapp
Strength of RecommendationFor the Patient For the Clinician
StrongMost individuals in this situation would prefer the recommended course of action and only a small proportion would not
The attending provider should strongly consider the recommended course of action as a first-line management Formal decision aids may have less of a role to help individuals make decisions consistent with their values and preferences
ConditionalThe majority of individuals in this situation would prefer the suggested course of action but many would not
Different choices may be appropriate for different patients Decision aids may be useful in helping individuals in making decisions consistent with their values and preferences Clinicians should expect to spend more time with patients when working towards a decision
Quality of RecommendationsHigh There is high confidence that the true effect lies close to that of the estimate of the effect
Moderate There is moderate confidence in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different
LowThere is limited confidence in the effect estimate The true effect may be substantially different from the estimate of the effect
Very Low There is very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

5
Stop Chasing Predictive Valueshellip
bull From the analysis of ANY sample EVERY statistical package will provide SnSp PPVNPV
minus These are not special because they predict behavior ONLY in that sample and nowhere else
minus Predictive values require valid population prevalence NPV is dependent on how good a test ishellip
bull All tests are surrogates of some gold standard and by definition will have an error rate
minus OFC surrogates trade error rates and misclassification against tiny risks of severe reactions one canrsquot control
minus This instills our values in patients and forcing them to accept the health and economic detriments of misclassification
bull ldquoPredictiverdquo values from retrospective banked samplescohorts are highly biased and overspecify the accuracy of a test vs real world performancemdashselection bias timingflow are very significant issues
bull If you are avoiding doing an OFC because you are afraid of provoking a reaction you are in the wrong line of work and should also not be giving either OIT or AIT This is part of our jobs like it or nothellip
bull No test can or should ethically be marketed to ldquoreduce the necessityrdquo for a gold standard test
6
A Primer on Testing Peanut as a Case Study
7
Peanut as a Component Model
Diagram schematic courtesy Thermo Fisher 2010
bull Peanut containsbull Major allergensbull Cross-reactive allergensbull Other compounds
bull Patients can recognize multiple epitopes simultaneously
bull A ldquopositiverdquo test is a sum of all recognized parts
bull Same scenario exists for any food allergen but the issue is particularly of concern for plant-based foods such as legumes seeds nuts grains
bull Could component patter infer greater sensitivityspecificity in a diagnosis
Ara h 1
Ara h 2
Ara h 3
Ara h 6
Ara h 9 CCDAra h 8
-
8
Peanut Model of Theoretical Risk
Slide courtesy Anna-Nowak-Wegryzn Jaffe Food Allergy Institute Mount Sinai School of Medicine with permission
rAra h 1rAra h 2rAra h 3rAra h 8rAra h 9CCD
Ara h 8 Ara h 1
Ara h 26
Ara h 3
ProfilinCCD PR-10 LTP Storage Proteins
Ara h 9
Risk
Ara h 5
Pollen cross-reactive
9
Peanut Allergy Parameter Questions
1) Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
2a) In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 --would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
2b) In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
3) In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
10
GRADE Quality of Evidence
http gdtguidelinedevelopmentorgapp
Strength of RecommendationFor the Patient For the Clinician
StrongMost individuals in this situation would prefer the recommended course of action and only a small proportion would not
The attending provider should strongly consider the recommended course of action as a first-line management Formal decision aids may have less of a role to help individuals make decisions consistent with their values and preferences
ConditionalThe majority of individuals in this situation would prefer the suggested course of action but many would not
Different choices may be appropriate for different patients Decision aids may be useful in helping individuals in making decisions consistent with their values and preferences Clinicians should expect to spend more time with patients when working towards a decision
Quality of RecommendationsHigh There is high confidence that the true effect lies close to that of the estimate of the effect
Moderate There is moderate confidence in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different
LowThere is limited confidence in the effect estimate The true effect may be substantially different from the estimate of the effect
Very Low There is very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

6
A Primer on Testing Peanut as a Case Study
7
Peanut as a Component Model
Diagram schematic courtesy Thermo Fisher 2010
bull Peanut containsbull Major allergensbull Cross-reactive allergensbull Other compounds
bull Patients can recognize multiple epitopes simultaneously
bull A ldquopositiverdquo test is a sum of all recognized parts
bull Same scenario exists for any food allergen but the issue is particularly of concern for plant-based foods such as legumes seeds nuts grains
bull Could component patter infer greater sensitivityspecificity in a diagnosis
Ara h 1
Ara h 2
Ara h 3
Ara h 6
Ara h 9 CCDAra h 8
-
8
Peanut Model of Theoretical Risk
Slide courtesy Anna-Nowak-Wegryzn Jaffe Food Allergy Institute Mount Sinai School of Medicine with permission
rAra h 1rAra h 2rAra h 3rAra h 8rAra h 9CCD
Ara h 8 Ara h 1
Ara h 26
Ara h 3
ProfilinCCD PR-10 LTP Storage Proteins
Ara h 9
Risk
Ara h 5
Pollen cross-reactive
9
Peanut Allergy Parameter Questions
1) Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
2a) In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 --would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
2b) In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
3) In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
10
GRADE Quality of Evidence
http gdtguidelinedevelopmentorgapp
Strength of RecommendationFor the Patient For the Clinician
StrongMost individuals in this situation would prefer the recommended course of action and only a small proportion would not
The attending provider should strongly consider the recommended course of action as a first-line management Formal decision aids may have less of a role to help individuals make decisions consistent with their values and preferences
ConditionalThe majority of individuals in this situation would prefer the suggested course of action but many would not
Different choices may be appropriate for different patients Decision aids may be useful in helping individuals in making decisions consistent with their values and preferences Clinicians should expect to spend more time with patients when working towards a decision
Quality of RecommendationsHigh There is high confidence that the true effect lies close to that of the estimate of the effect
Moderate There is moderate confidence in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different
LowThere is limited confidence in the effect estimate The true effect may be substantially different from the estimate of the effect
Very Low There is very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

7
Peanut as a Component Model
Diagram schematic courtesy Thermo Fisher 2010
bull Peanut containsbull Major allergensbull Cross-reactive allergensbull Other compounds
bull Patients can recognize multiple epitopes simultaneously
bull A ldquopositiverdquo test is a sum of all recognized parts
bull Same scenario exists for any food allergen but the issue is particularly of concern for plant-based foods such as legumes seeds nuts grains
bull Could component patter infer greater sensitivityspecificity in a diagnosis
Ara h 1
Ara h 2
Ara h 3
Ara h 6
Ara h 9 CCDAra h 8
-
8
Peanut Model of Theoretical Risk
Slide courtesy Anna-Nowak-Wegryzn Jaffe Food Allergy Institute Mount Sinai School of Medicine with permission
rAra h 1rAra h 2rAra h 3rAra h 8rAra h 9CCD
Ara h 8 Ara h 1
Ara h 26
Ara h 3
ProfilinCCD PR-10 LTP Storage Proteins
Ara h 9
Risk
Ara h 5
Pollen cross-reactive
9
Peanut Allergy Parameter Questions
1) Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
2a) In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 --would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
2b) In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
3) In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
10
GRADE Quality of Evidence
http gdtguidelinedevelopmentorgapp
Strength of RecommendationFor the Patient For the Clinician
StrongMost individuals in this situation would prefer the recommended course of action and only a small proportion would not
The attending provider should strongly consider the recommended course of action as a first-line management Formal decision aids may have less of a role to help individuals make decisions consistent with their values and preferences
ConditionalThe majority of individuals in this situation would prefer the suggested course of action but many would not
Different choices may be appropriate for different patients Decision aids may be useful in helping individuals in making decisions consistent with their values and preferences Clinicians should expect to spend more time with patients when working towards a decision
Quality of RecommendationsHigh There is high confidence that the true effect lies close to that of the estimate of the effect
Moderate There is moderate confidence in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different
LowThere is limited confidence in the effect estimate The true effect may be substantially different from the estimate of the effect
Very Low There is very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

8
Peanut Model of Theoretical Risk
Slide courtesy Anna-Nowak-Wegryzn Jaffe Food Allergy Institute Mount Sinai School of Medicine with permission
rAra h 1rAra h 2rAra h 3rAra h 8rAra h 9CCD
Ara h 8 Ara h 1
Ara h 26
Ara h 3
ProfilinCCD PR-10 LTP Storage Proteins
Ara h 9
Risk
Ara h 5
Pollen cross-reactive
9
Peanut Allergy Parameter Questions
1) Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
2a) In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 --would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
2b) In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
3) In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
10
GRADE Quality of Evidence
http gdtguidelinedevelopmentorgapp
Strength of RecommendationFor the Patient For the Clinician
StrongMost individuals in this situation would prefer the recommended course of action and only a small proportion would not
The attending provider should strongly consider the recommended course of action as a first-line management Formal decision aids may have less of a role to help individuals make decisions consistent with their values and preferences
ConditionalThe majority of individuals in this situation would prefer the suggested course of action but many would not
Different choices may be appropriate for different patients Decision aids may be useful in helping individuals in making decisions consistent with their values and preferences Clinicians should expect to spend more time with patients when working towards a decision
Quality of RecommendationsHigh There is high confidence that the true effect lies close to that of the estimate of the effect
Moderate There is moderate confidence in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different
LowThere is limited confidence in the effect estimate The true effect may be substantially different from the estimate of the effect
Very Low There is very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

9
Peanut Allergy Parameter Questions
1) Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
2a) In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 --would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
2b) In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
3) In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
10
GRADE Quality of Evidence
http gdtguidelinedevelopmentorgapp
Strength of RecommendationFor the Patient For the Clinician
StrongMost individuals in this situation would prefer the recommended course of action and only a small proportion would not
The attending provider should strongly consider the recommended course of action as a first-line management Formal decision aids may have less of a role to help individuals make decisions consistent with their values and preferences
ConditionalThe majority of individuals in this situation would prefer the suggested course of action but many would not
Different choices may be appropriate for different patients Decision aids may be useful in helping individuals in making decisions consistent with their values and preferences Clinicians should expect to spend more time with patients when working towards a decision
Quality of RecommendationsHigh There is high confidence that the true effect lies close to that of the estimate of the effect
Moderate There is moderate confidence in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different
LowThere is limited confidence in the effect estimate The true effect may be substantially different from the estimate of the effect
Very Low There is very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

10
GRADE Quality of Evidence
http gdtguidelinedevelopmentorgapp
Strength of RecommendationFor the Patient For the Clinician
StrongMost individuals in this situation would prefer the recommended course of action and only a small proportion would not
The attending provider should strongly consider the recommended course of action as a first-line management Formal decision aids may have less of a role to help individuals make decisions consistent with their values and preferences
ConditionalThe majority of individuals in this situation would prefer the suggested course of action but many would not
Different choices may be appropriate for different patients Decision aids may be useful in helping individuals in making decisions consistent with their values and preferences Clinicians should expect to spend more time with patients when working towards a decision
Quality of RecommendationsHigh There is high confidence that the true effect lies close to that of the estimate of the effect
Moderate There is moderate confidence in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different
LowThere is limited confidence in the effect estimate The true effect may be substantially different from the estimate of the effect
Very Low There is very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

11
InclusionExclusion Criteria
bull Literature search of Pubmed Embase and Medline for articles (1946-present) pertaining to the use of peanut allergy diagnostic testing borrowing from three recent searches and expanding these terms (Klemans et al 2015 Chaffen et al 2009 Flores Kim et al 2018)
minus Population patients with known or suspected peanut allergy
minus Intervention testing for serologic peanut specific IgE against Ara h 1-3 6 8 and whole peanut extract
minus Comparator testing for whole extract peanut specific IgE via prick skin testing and serum-specific IgE
minus Outcome peanut allergy proven through use of an oral food challenge (open single-blinded or double blinded oral food challenge) in at least 50 of the study population
bull 1314 studies identified 127 selected for full text review with 89 selected for extraction (sensspec TPFP TNFN PPVNPV) at cut-offs of 3mm035 KUL for diagnosis 2 KUL 50 KUL 10mm for severity
bull Meta-analysis of diagnostic testing run in Stata 15Rev Man (peto method random effects) with QUADAS-2 used for assessing riskapplicability of bias and GRADEpro to construct evidence profiles
bull A total of 42 studies included in the final analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

12
Search LimitsmdashWhy Only Ara h 2
bull 89 articles selected for final evidence synthesis 41 directly pertained to this question 24 had data available for extraction Had to have 50 having OFC as a criteria minimum
bull We were unable to find sufficient number of studies to analyze any other individual peanut components or pool the use of component panels
bull We can offer no comment regarding the role or significance of evaluating these other components individually or in aggregate or what the clinical implications of their use may be
bull There ware no studies identified comparing the value of the use Ara h 2 or any components used reflexively after assessment of whole peanut SPT or sIgE
bull We know that there are studies out there beginning to suggesting value of other components such as Ara h 6 or 8 but they didnrsquot meet the inclusion criteria and this is a significant limitation of data related to those tests
13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

13
Question 1
bull Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
bull Recommendation 1a We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy for both of whom shared decision-making has been employed to arrive at the final decision Conditional recommendation Certainty of evidence very low
bull Recommendation 1b We suggest against diagnostic testing in patients where there is low or very low Conditional recommendation Certainty of evidence very low
bull Not searchable no GRADE assessment
bull Comment this is a message that has been part of multiple past guidelines
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

14
Question 2
bull Question 2a In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
bull Question 2b In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
bull Recommendation 2a We suggest in favor of Ara h2 diagnostic testing (over SPT or sIgE to whole peanut) in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios Conditional recommendation Certainty of evidence moderate
bull Recommendation 2b We suggest against component testing in addition to either to skin prick test or sIgEto whole peanut to increase diagnostic accuracy Conditional recommendation Certainty of evidence moderate
bull Comment there is a knowledge gap in understanding how to use these tests in tandem with one another
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

15Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 3mm
Sensitivity 097
Specificity 046
Positive likelihood 182
Negative likelihood 005
SENSITIVITY (95 CI)
Q =17186 df = 1700 p = 000
I2 = 9011 [8660 - 9361]
097[093 - 099]
095 [085 - 099]
088 [047 - 100]
100 [095 - 100]
100 [097 - 100]
092 [062 - 100]
093 [088 - 097]
087 [076 - 094]
100 [086 - 100]
066 [051 - 079]
100 [092 - 100]
100 [083 - 100]
090 [055 - 100]
096 [078 - 100]
064 [048 - 078]
100 [098 - 100]
091 [071 - 099]
098 [087 - 100]
100 [088 - 100]100 [088 - 100]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
05 10SENSITIVITY
SPECIFICITY (95 CI)
Q =24286 df = 1700 p = 000
I2 = 9300 [9076 - 9524]
046[029 - 065]
049 [035 - 063]
099 [096 - 100]
071 [059 - 082]
008 [000 - 036]
026 [009 - 051]
063 [058 - 069]
067 [053 - 079]
044 [024 - 065]
052 [034 - 069]
040 [026 - 054]
000 [000 - 031]
027 [006 - 061]
020 [008 - 039]
081 [071 - 088]
066 [059 - 073]
030 [015 - 049]
000 [000 - 084]
044 [030 - 059]044 [030 - 059]
StudyId
COMBINED
Abrahms 2017
Begin 2017
Bernard2003
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo2015
Ludman 2013
Preece 2014
Rajput 2018
Rance2003
Sampson1997
Song 2015
Van Erp2013
00 10SPECIFICITY
16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

16
Fagan Nomogram SPT 3mm
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

17Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 035 KUL
Sensitivity 095
Specificity 038
Positive likelihood 152
Negative likelihood 014
SENSITIVITY (95 CI)
Q =70858 df = 2900 p = 000
I2 = 9591 [9506 - 9676]
095[091 - 097]
082 [066 - 092]
078 [067 - 087]
100 [063 - 100]
039 [030 - 048]
093 [085 - 098]
095 [088 - 098]
099 [096 - 100]
092 [062 - 100]
093 [087 - 097]
075 [063 - 084]
100 [087 - 100]
100 [095 - 100]
095 [090 - 098]
100 [086 - 100]
100 [094 - 100]
069 [039 - 091]
096 [079 - 100]
078 [065 - 088]
096 [085 - 099]
095 [075 - 100]
093 [087 - 097]
098 [089 - 100]
097 [082 - 100]
085 [074 - 092]
096 [078 - 100]
095 [084 - 099]
097 [093 - 099]
097 [093 - 099]
097 [092 - 099]
098 [090 - 100]098 [090 - 100]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q =40397 df = 2900 p = 000
I2 = 9282 [9105 - 9460]
038[028 - 048]
068 [055 - 080]
046 [027 - 067]
097 [092 - 099]
035 [024 - 047]
040 [019 - 064]
026 [018 - 035]
010 [000 - 045]
011 [001 - 033]
049 [043 - 056]
046 [032 - 059]
023 [010 - 041]
007 [003 - 015]
000 [000 - 012]
031 [009 - 061]
046 [031 - 063]
047 [030 - 065]
025 [010 - 047]
046 [030 - 063]
045 [032 - 060]
030 [007 - 065]
016 [008 - 028]
073 [054 - 087]
027 [016 - 041]
045 [035 - 055]
043 [025 - 063]
062 [051 - 072]
062 [055 - 069]
038 [028 - 049]
034 [026 - 044]
033 [018 - 052]033 [018 - 052]
StudyId
COMBINED
Abrahms 2017
Balmer weber 2015
Begin 2017
Beigelman 2012
Bernard2003
Beyer2015
Chinthrajah 2018
Comberiati 2016
Dang2012
DunnGalvin 2011
Ebisawa 2012
Ebisawa 2015
Eller 2013
Glaumann 2012
Guilloux 2009
Gupta2014
Johannsen 2016
Klemans Broekman2013
Klemans Otte 2013
Leo 2015
Lieberman 2013
Martinet 2016
Nicolaou 2011
Perry 2004
Preece 2014
Rajput 2018
Rance2003
Sampson 1997
Van Erp2013
Wainstein 2007
00 10SPECIFICITY
18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

18
Fagan Nomogram sIgE 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 2Post_Prob_Pos () = 3LR_Negative = 014Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 2Post_Prob_Pos () = 39LR_Negative = 014Post_Prob_Neg () = 6
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 2Post_Prob_Pos () = 78LR_Negative = 014Post_Prob_Neg () = 25
19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

19Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 035 KUL
Sensitivity 086
Specificity 084
Positive likelihood 55
Negative likelihood 017
SENSITIVITY (95 CI)
Q =12356 df = 2300 p = 000
I2 = 8139 [7458 - 8819]
086[081 - 089]
094 [083 - 099]
071 [060 - 081]
100 [088 - 100]
057 [044 - 068]
087 [070 - 096]
095 [084 - 099]
084 [074 - 092]
058 [028 - 085]
095 [086 - 099]
060 [046 - 074]
080 [071 - 087]
080 [056 - 094]
093 [088 - 097]
086 [077 - 092]
089 [083 - 093]
091 [078 - 097]
091 [071 - 099]
091 [080 - 098]
082 [063 - 094]
068 [043 - 087]
096 [080 - 100]
074 [052 - 090]
088 [070 - 098]
081 [071 - 088]081 [071 - 088]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 7598 df = 2300 p = 000
I2 = 6973 [5711 - 8235]
084[079 - 089]
100 [090 - 100]
085 [062 - 097]
096 [087 - 100]
100 [087 - 100]
067 [043 - 085]
073 [063 - 082]
078 [068 - 086]
089 [067 - 099]
073 [057 - 086]
085 [068 - 095]
092 [082 - 097]
070 [035 - 093]
100 [048 - 100]
086 [078 - 092]
060 [041 - 077]
073 [058 - 085]
100 [029 - 100]
072 [058 - 083]
090 [073 - 098]
095 [076 - 100]
085 [055 - 098]
063 [044 - 080]
071 [054 - 085]
090 [080 - 096]090 [080 - 096]
StudyId
COMBINED
Martinet 2016
Bernard2003
Nicolaou 2011
Balmer weber 2015
Schots 2016
Rajput 2018
Ebisawa 2015
Comberiati 2016
Kukkonen 2015
Klemans Broekman2013
Lieberman 2013
Leo 2015
Chinthrajah 2018
Beyer 2015
Eller 2013
Van Erp2013
Peeters2007
Klemans Otte 2013
Ebisawa 2012
Suratannon2013
Glaumann 2012
Preece 2014
Keet2013
Dang 2012
03 10SPECIFICITY
20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

20
Fagan Nomogram Ara h 2 035
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 2LR_Positive = 5Post_Prob_Pos () = 10LR_Negative = 017Post_Prob_Neg () = 0
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 30LR_Positive = 5Post_Prob_Pos () = 70LR_Negative = 017Post_Prob_Neg () = 7
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 70LR_Positive = 4Post_Prob_Pos () = 89LR_Negative = 025Post_Prob_Neg () = 36
21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

21
Question 3
bull Question 3 In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
bull Recommendation We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a reaction andor allergy phenotype or to predict the severity of a future reaction Conditional recommendation Certainty of evidence very low
bull Comment there is a knowledge gap in studies that have uniform severity criteria to evaluate the relationship between sensitization and severity
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

22Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Ara h 2 sIgE 2 KUL
Sensitivity 078
Specificity 045
SENSITIVITY (95 CI)
Q = 2875 df = 900 p = 000
I2 = 6870 [4811 - 8929]
078[069 - 085]
065 [048 - 079]
093 [082 - 098]
067 [009 - 099]
092 [064 - 100]
081 [070 - 089]
066 [055 - 076]
040 [012 - 074]
070 [035 - 093]
086 [042 - 100]
082 [048 - 098]082 [048 - 098]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
01 10SENSITIVITY
SPECIFICITY (95 CI)
Q =10703 df = 900 p = 000
I2 = 9159 [8771 - 9547]
045[028 - 063]
076 [063 - 087]
025 [015 - 036]
051 [040 - 061]
004 [000 - 021]
028 [021 - 035]
079 [049 - 095]
040 [012 - 074]
062 [032 - 086]
023 [010 - 041]
070 [059 - 080]070 [059 - 080]
StudyId
COMBINED
Balmer weber 2015
Chinthrajah 2018
Dang2012
Glaumann 2012
Klemans Blom 2015
Kukkonen 2015
Leo 2015
Preece 2014
Rajput 2018
Van Erp2013
00 10SPECIFICITY
23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

23Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
sIgE 50 KUL
Sensitivity 039
Specificity 089
SENSITIVITY (95 CI)
Q = 4943 df = 1200 p = 000
I2 = 7572 [6263 - 8881]
039[026 - 053]
072 [058 - 084]
000 [000 - 071]
027 [006 - 061]
069 [039 - 091]
028 [018 - 039]
100 [016 - 100]
027 [008 - 055]
020 [003 - 056]
040 [005 - 085]
050 [019 - 081]
021 [007 - 042]
035 [015 - 059]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q =13253 df = 1200 p = 000
I2 = 9095 [8723 - 9466]
089[075 - 095]
052 [040 - 064]
096 [091 - 099]
100 [089 - 100]
073 [052 - 088]
068 [061 - 075]
057 [034 - 077]
100 [077 - 100]
100 [075 - 100]
094 [079 - 099]
053 [035 - 071]
085 [079 - 090]
100 [090 - 100]
085 [062 - 097]085 [062 - 097]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Glaumann 2012
Klemans Blom 2015
Lewis2005
Peeters 2007
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
03 10SPECIFICITY
24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

24Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
SPT 10 mm
Sensitivity 037
Specificity 062
SENSITIVITY (95 CI)
Q = 3058 df = 1100 p = 000
I2 = 6403 [4177 - 8629]
037[022 - 055]
061 [047 - 074]
017 [000 - 064]
000 [000 - 037]
059 [039 - 076]
050 [019 - 081]
050 [007 - 093]
000 [000 - 031]
029 [004 - 071]
050 [019 - 081]
083 [036 - 100]
038 [015 - 065]
067 [022 - 096]067 [022 - 096]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
00 10SENSITIVITY
SPECIFICITY (95 CI)
Q = 9134 df = 1100 p = 000
I2 = 8796 [8236 - 9355]
062[044 - 077]
035 [024 - 048]
067 [059 - 075]
100 [090 - 100]
026 [016 - 037]
055 [023 - 083]
057 [041 - 073]
085 [055 - 098]
075 [053 - 090]
041 [024 - 059]
055 [043 - 067]
072 [055 - 085]
035 [015 - 059]035 [015 - 059]
StudyId
COMBINED
Chinthrajah 2018
Dang2012
DunnGalvin 2011
Klemans Blom 2015
Leo 2015
Lewis2005
Preece 2014
Rajput 2018
Song 2015
Van Erp2013
Wainstein 2010
Wensing 2002
02 10SPECIFICITY
25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

25
Risk of Bias Assessment
High
Unclear
Low
bull Mild to moderate risk of bias overall bull Most comes from studies where small samples
were chosen large clinic populations without an explained rationale or sample was not at random or not consecutive
bull Additional risk of bias from studies where the reference diagnostic challenge and the index diagnostic peanut test were obtained at different times
bull A lot of this is not necessarily avoidable in these studies but it does help weaken the certainty in the evidence
bull Sensitivity analysis removing studies at risk for bias for both patient selection and flowtiming revealed no significant differences in estimates
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

26
Which Test is Most Cost-effective
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
bull Diagnosis compared using each of the 3 tests at a presumed prevalence of 3 14 or 75 bull At each respective prevalence assessment use of Ara h 2 vs either SPT or peanut sIgE was associated
with larger QALY gain and lower net cost (dominated analysis)bull While we make no recommendation for or against the use of any component testing this simulation does
suggest superior health and economic benefits would be associated with preferential use of Ara h 2 as a stand-alone diagnostic test assuming these are used in populations similar to those pooled for analysis
27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

27
Sensitivity Analysis
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

28
Bottom Line Test Responsibly
SPT 3mm sIgE 035 KL Ara h 2 sIgE 035 KL
bull Testing someone with no history or risk is absolutely worthlessmdashthis means the milk allergic kid you want to also test for peanut as a common allergen has no positive value no matter which test you use
bull If this is not understood then anything in this parameter is not going to matter
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 65LR_Negative = 005Post_Prob_Neg () = 5
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 2Post_Prob_Pos () = 60LR_Negative = 014Post_Prob_Neg () = 12
0001000200050010020050102051251020501002005001000
Likelihood Ratio
01020305071235710
20304050607080
909395979899993995997998999
Post
-test
Pro
babi
lity
()
0102030507
12357
10
20304050607080
909395979899
993995997998999
Pre-
test
Pro
babi
lity
()
Prior Prob () = 50LR_Positive = 5Post_Prob_Pos () = 85LR_Negative = 017Post_Prob_Neg () = 15
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

29
Summary Recommendations
Greenhawt M Shaker M Wang J et al Peanut Allergy Diagnosis- a 2020 Practice Parameter Update Systematic Review and GRADE Analysis [published online ahead of print 2020 Aug 15] J Allergy Clin Immunol 2020S0091-6749(20)31137-4 doi101016jjaci202007031
Question Recommendation Evidence Certainty Risk of Bias
Should diagnostic testing for peanut allergy be performed in adults and children with a history of suspected peanut allergy who are requesting evaluation for peanut allergy
We suggest in favor of diagnostic (skin prick or serum sIgE) testing for peanut allergy in patients with a 1) physician-judged high pre-test probability of peanut allergy or 2) prior to an oral food challenge for patients with moderate pre-test probability of peanut allergy with whom shared decision-making has been employed to arrive at the final decision
We suggest against diagnostic testing in patients where there is low or very low pre-test probability of peanut allergy
Very Low Not Rated
In the patient presenting for evaluation of suspected peanut allergy which of the three testsmdashSPT sIgE to whole peanut or Ara h2 would provide the highest diagnostic accuracy as determined by the more optimal positivenegative likelihood ratio
We suggest in favor of Ara h2 diagnostic testing in a patient presenting for evaluation of suspected peanut allergy for which a single diagnostic test is to be used as Ara h2 would provide the best diagnostic accuracy as determined by virtue of more optimal positivenegative likelihood ratios
Moderate High
In a patient presenting for evaluation of suspected peanut allergy does testing for peanut components in addition to either SPT or sIgE to whole peanut increase the diagnostic accuracy
We suggest against component testing in addition to either to skin prick test or sIgE to whole peanut to increase diagnostic accuracy
Very Low High
In the patient presenting for evaluation of suspected peanut allergy can the results of a diagnostic test be used to predict the severity of a future allergic reaction
We suggest against the clinician using the results of a SPT sIgE to whole peanut extract or sIgE to peanut components to determine the severity of a previous reaction andor allergy phenotype or to predict the severity of a future reaction
Very Low High
30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

30
What About an Ara h 2 Cut-off Point
31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

31
Is There an Optimal Ara h 2 Cut Off Point
bull Multiple studies suggest Ara h 2 as best discriminator but cut-off points have varied and there probably is no absolute ldquopredictiverdquo level for general use
bull Generating a PPV for the parameter was a non-starter without knowing the accurate prevalence
bull We felt likelihood ratios were a better assessment which we provided instead
Beyer et al Allergy 2015 70 90-98Klemans et al Clin Exp Allergy 2015 45 720-30
Study 95 PPV Cutoff (kuL) Sensitivity Specificity
Sampson 2001 15 (peanut) 57 100
Nicolaou 2011 035 (optimal cut point) 100 96
Codreanu 2011 023 (optimal cut point) 93 97
Eller 2013 128 (not a PPV) 76 97
Dang 2012 196 96
Keet 2013 2 (75 PPV 623 NPV) 23 94
Klemans 2013 035 (74 PPV ) 91 72
Beyer 2015 42 [035 (50)144 (90)]
Kukkonen 2015 035 (PPV 91NPV 84 for severe rxn)
Leo 2015 2 (91 PPV 47 NPV) 50 90
Ballmer-Weber 2015 2 (97 prob in sample for severe rxn)
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip
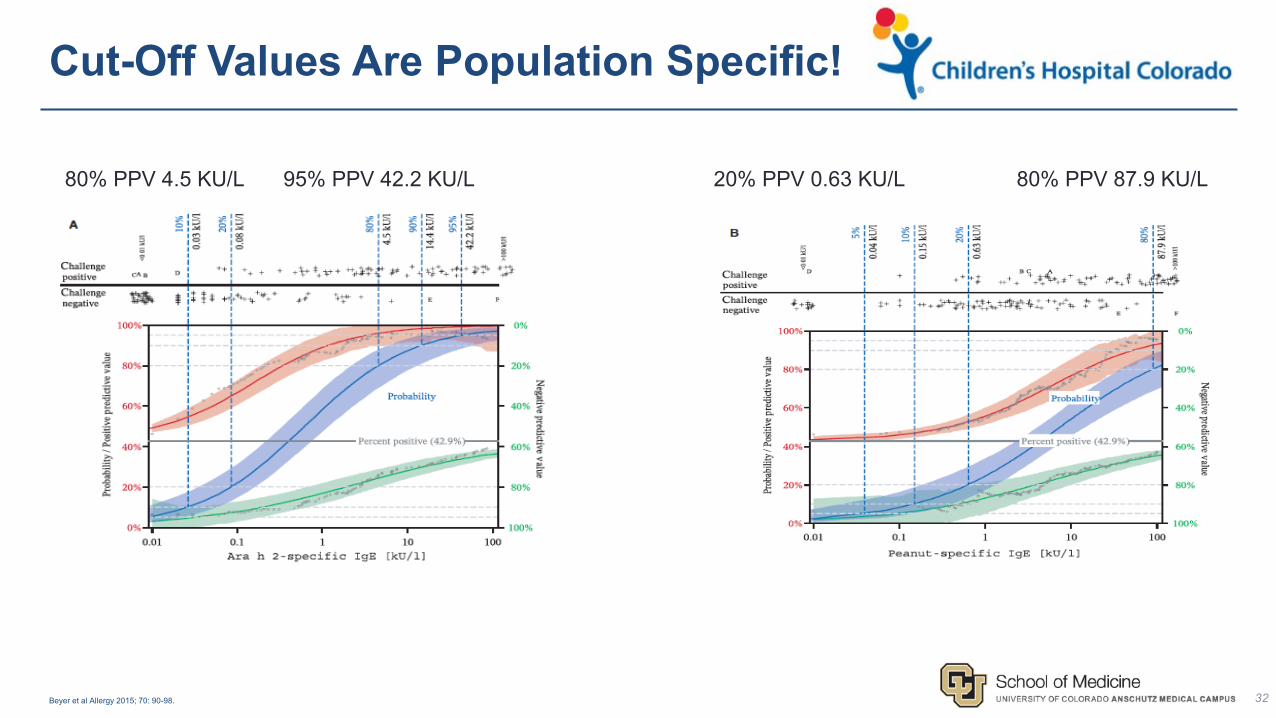
32
95 PPV 422 KUL80 PPV 45 KUL
Cut-Off Values Are Population Specific
Beyer et al Allergy 2015 70 90-98
20 PPV 063 KUL 80 PPV 879 KUL
33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

33
Beyond Peanuthellip
34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

34
Summary Slide
bull Components have been developed for a number of allergens but best studied for peanut
bull There is no evidence supporting the necessity or added utility of components for diagnosing egg milk tree nut seed or wheat allergy
bull There are emerging data from single center studies that are trying to demonstrate particular key indicator components exist for cashew walnut sesame and wheat akin to Ara h 2
bull Limitations of these data are the same as for peanut if not worse for these
bull These tests are not at the point where they are reliable and usable surrogates that approach the potential utility of Ara h 2
bull These will not ldquobeatrdquo a good history appropriate use of first order testing and an OFC
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip
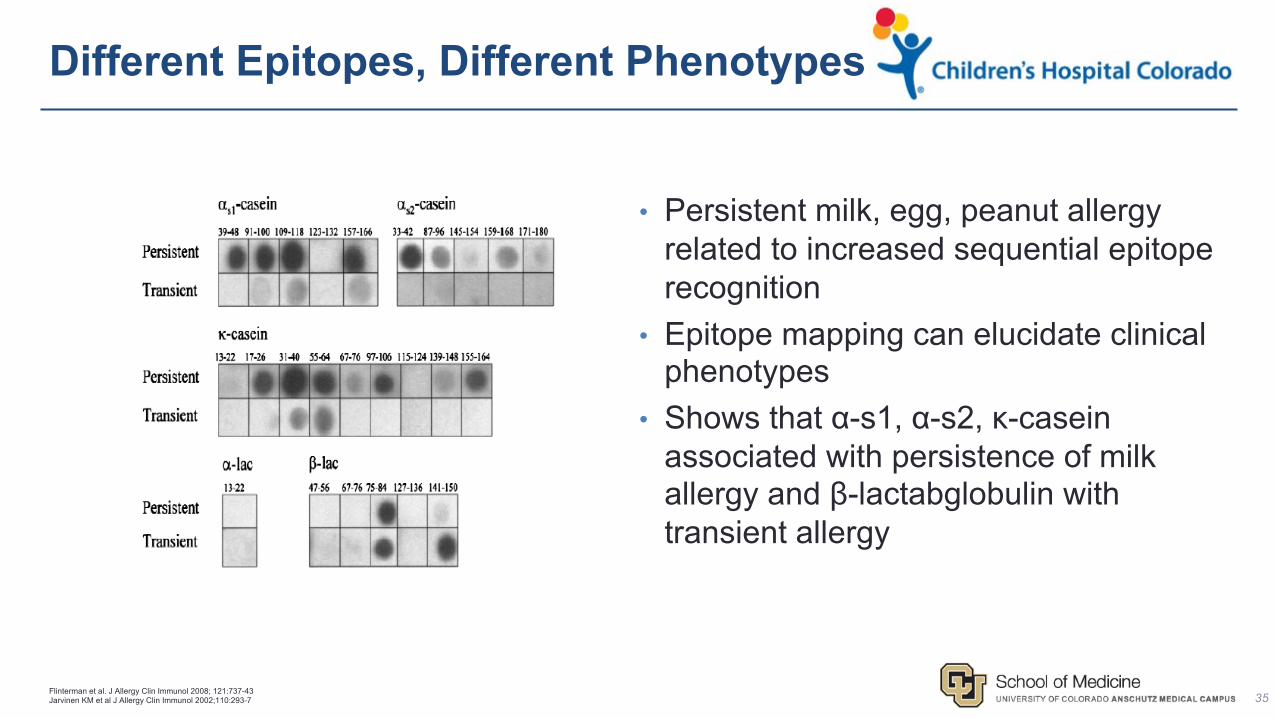
35
Different Epitopes Different Phenotypes
Flinterman et al J Allergy Clin Immunol 2008 121737-43Jarvinen KM et al J Allergy Clin Immunol 2002110293-7
bull Persistent milk egg peanut allergy related to increased sequential epitope recognition
bull Epitope mapping can elucidate clinical phenotypes
bull Shows that α-s1 α-s2 κ-casein associated with persistence of milk allergy and β-lactabglobulin with transient allergy
36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

36
Components for Milk
bull Milk proteins are casein (80) and whey
minus α-lactalbumin (bos d 4) β-lactabglobulin (bos d 6) casein (bos d 8) whey
minus 5 caseins (κ αs1-2 γ1-3) most with αs1 and κ (likely sequential)
minus 5 proteins (α-lactalb β-lactabglob BSA immunoglobulin lactoferrin)
bull Persistent allergy associated w higher number of sequential epitopes
bull Casein gt078 kUL α-lact gt 34 kUL β-lact gt 99 kUL are proposed 95 predictive decision points (single study)
minus Baked milk proposed 95 predictive decision point 5 kUL (single study)
minus These are defined in single samples and likely do not generalizemdashuse cautiously
bull No clear predictor of persistent milk allergy or who are the ~20 that donrsquot tolerate baked milk
Fiochi et al Curr Opin Allergy Clin Immunol 11216ndash221Drsquourbano et al Clin Exp Allergy 2010 401561 ndash 1570Nowak-Wegryzn et al J Allergy Clin Immunol 2008 122342 ndash 347
37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

37
Components for Egg
bull Egg white has gt 20 proteins
minus Ovomucoid heatdigestion stable dominant allergen (gal d 1)
minus Ovalbumin ovotransferrin lysozyme (gal d 2 3 4) all heatacid labile
minus Egg yolk (gal d 5)mdashseen in bird-egg syndrome
bull Ovomucoid associated with persistent allergy
minus 95 PDPrsquos of 11 30 50 and kUL for baked egg reactivity
minus 1 kUL reported as ldquosaferdquo level for bakedcooked egg
minus Persistent egg allergy seen with increased number of sequential epitopes
bull HealthNuts 80 of children failing egg challenge were baked egg TOLERANT
bull Decision points have same cautions as with milkAndo et al J Allergy Clin Immunol 2008 122 583ndash8Caubet et al Curr Opinion Allergy Immunol 2011 11210ndash215Lemon Mule J Allergy Clin Immunol 2008 122977ndash983e1Osborne et al J Allergy Clin Immunol 2011 127 668-76
Haneda et al J Allergy Clin Immunol 2012 1291681-2
38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

38
Hazelnut Components
Datema MR et al Allergy 201873549ndash559
bull Multicenter Europreval study looking at CRD use in hazelnut allergy to predict reaction severity
bull From n=731 patients with reported hazelnut allergy n=423 available sera were analyzed for hazelnut CRD with n=124 consenting for DBPCFC (~17 total sample)
bull Cor a 9 and 14 had OR 105 and 101 to predict reaction severity and Cor a 1 OR 014 for predicting reaction severity at gt035 KUAL
bull When Cor a 14 combined in a multivariate model with eczema walnut sensitization and pollen sensitization this had 92 specificity and 763 specificity but misclassified severity in a ldquolarge number of patientsrdquo per authors given a low prevalence of severe hazelnut allergy (16)
39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

39
CashewPistachio Cross-Reactivity
Savvatianos et al J Allergy Clin Immunol 2015 136 192-4
40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

40
Practical Limitations of Components
bull Necessity In a patient you clearly suspect is either allergic or suspect is non-allergic any test will
suffice and there is no proven advantage for components
bull Uncertainty Where there is low to moderate pretest probability components have higher
specificity which reduces the chances of false positive tests but the positive likelihood is not
strong enough to translate to very high post test odds and a challenge is still needed This may
be the best choice in these situations but not as good as the OFC
bull Evidence Certainty Many of the component studies have issues with selection bias flow and
timing and degree of use of OFC These have tended to characterize known allergic individuals
and have not robustly characterized non-allergic individuals or community samples
bull Use there are limited data about how to best use components in the diagnostic algorithm
highlighting the necessity and uncertainty issues
bull Consider the harm that results from a false positive diagnosismdashwhich is worse the false positive
or the false negative in the grander scheme
41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

41
Basophil Activation Testing
bull Growing importance of the role of the basophil in mediating allergic responses in mice
bull Growing body of evidence for utility of measuring basophil activation as a marker in humans as well
bull Basophils release histamine from preformed granules similar to mast cells
bull Basophils have a half-life of only one week
bull Markers
minus Advances in flow cytometry has made it possible to measure surface markers as opposed to histaminemediator release
minus Method more accessible than auto-analyzers for mediator measurement
minus Can use heparanized whole blood
minus Common markers include CD63 CD203c and CD69
MacGlashan J Allergy Clin Immunol 2013132 777-87
42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

42
Basophil Histamine Release
bull Basophils release varying degrees of histamine but is a highly individualized response
--Spontaneous release has been used in foodeczema studies
--Release can be triggered by FcER1 binding
--However other molecules can trigger histamine release such as C5a so the process can be non-specific
bull Measurement is very technical--Involves lymphocyte enrichment requires careful platelet removal
--Measurement through RIA or ELISA
--1ml blood (20000 basophils) generally sufficient
--Release from antigenFcER1 cross-linking is susceptible to dose-response effects surface receptor density and receptor reductions
MacGlashan J Allergy Clin Immunol 2013132 777-87
43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

43
Basophil Activation Test
bull CD63 (BAT) is most commonly used--Most closely associated with anaphylactic vs piecemeal degranulation
--Because degranulation processes are distinct CD63 only appears with anaphylaxis and can distinguish histamine release mechanisms
--Commercial assay available
--Assay sensitivity enhanced by IL-3
bull CD203c and CD69 expression can also be quantified--Evidence that CD203c expression is not related to histamine degranulation and can be triggered by multiple stimuli including IL-3
--CD69 is expressed by basophil cytokine expression and occurs slowly
--Expression of both is highly distinct from CD63MacGlashan J Allergy Clin Immunol 2013132 777-87
44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

44
BAT Clinical Applications
bull CD63 may have diagnostic properties--Expression not altered by anti-histamines
--Can run on blood within 1 year of exposure
bull Sensitivity for food allergy diagnosis is 77-98 and sensitivity 75-100
--Has shown enhanced accuracy vs SPT and sIgE
bull Has shown potential ability to determine --if peanut OFC is needed and how severe a reaction in an OFC was
--if baked milkegg tolerance and if have outgrown milk allergy
--if OIT subject achieved clinical desensitization
--if Omalizumab treatment had effect on food tolerance
MacGlashan J Allergy Clin Immunol 2013132 777-87Hoffmna et al Allergy 2015 70 1393-1405Santos et al J Allergy Clin Immunol 2015 134 645-52Glaumann et al Allergy 2012 67242-47Jones et al J Allergy Clin Immunol 2009 124292-300Burks et al N Engl J Med 2012 367 292-300
45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

45
BAT Limitations
bull Still mainly a research tool
bull Accessibility
bull Price (cost-effectiveness)
bull Limited data showing effectiveness
bull Is a very promising and potentially useful tool that should play a larger role going forward
46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

46
Mast Cell Activation Test
47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

47
48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

48
What is an Epitope
bull 3-D allergen binding site
--No universally common structure
bull Can bind IgE and IgG
--Can elicit cross-reactivity
--T cell epitopes exist as well
bull Conformational tertiary
--Heat labile subject to hydrolysis
bull Linear sequential
--Heat stable not alterable
Sampson HA J Allergy Clin Immunol 2004 113 805-819
49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

49
50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

50
51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

51All taken from Twitter FoodAllergy Some tweets have since been deleted by FoodAllergy
52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

52
Practical Take Home Points
1 Positive tests detect sensitization not allergymdashthese are not the same concept
minus People can have a rdquopositiverdquo test to peanut and not be allergic
2 When there is a very high or very low pre-test probability choice of test really doesnrsquot mattermdasharguably you donrsquot need testing though we do so for several reasons
minus Where there is indeterminant pre-test probability Ara h 2 offers lowest false positive risk
3 Chose to test carefully and within the most narrow contextsmdashdo not run panels or test for common allergens looking for peanut if the history does not indicate it
minus Recommend referral to specialist if considering testing due to eczema a sibling history other food allergy or the patient has never eaten peanut previously
4 Please consider the harm that results from a false positive diagnosismdashthese are hard to de-label and result in significant health and economic detriments
minus Is the false negative or the false positive the worse scenario
53
A Glimpse of Colorado Livinghellip

53
A Glimpse of Colorado Livinghellip