ALLERGIC DISEASES OF ORAL MUCOSA Allergy is the ...
60
ALLERGIC DISEASES OF ORAL MUCOSA Allergy is the perverted reaction of an organism to certain substances of the antigenic nature which in norm do not cause the painful phenomena. Endocrine and nervous systems, and also pathology of a gastroenteric tract play important role in allergy occurrence. Various substances can become the allergy reason: simple and difficult chemical compounds (iodine, bromine, proteins, polysaccharides) which getting into an organism, cause development of humoral and cellular immunologic reactions (an inflammation, a spastic stricture of bronchial muscles, a necrosis, a shock etc.). The substances causing development of allergic reactions are called allergens. The quantity of allergens in the nature is great enough, they are very various, both on structure, and on properties. According to origination the allergens are divided to exogenous and endogenous. Exogenous allergens get into an organism from the outside, and endogenous are originated in the organism and are own, but modified proteins. Thus, endogenous allergens are auto allergens. Exogenous allergens are: -Infectious - microbes, fungi, viruses, Chlamydia, protozoa -Non-infectious - vegetative, medicinal, alimentary, household, industrial etc. Endogenous allergens are: - Natural, or primary-some structures of an organism (a lens, a thyreoglobulin, etc.) which in norm do not cause the immune reaction of an organism - Acquired, or secondary - are formed in an organism during disturbances of metabolic processes under the influence of any pathological infectious or non- infectious factors (a cold, radiation, burns etc.). In a current of allergic reactions three stages are distinguished: 1) immunologic 2) biochemical (pathochemical) 3) pathophysiological The immunologic stage begins with organism and allergen contact, which result in organism sensibilization that is origination of the antibodies which are capable to co-operate with the given allergen. If after that allergen leaves from an organism no pathological reactions occur. Thus, the first penetration of allergen into an organism has sensitizing influence. In case of repeated entrance of allergen in already sensitizing organism allergen-antibody or allergen-sensitizing lymphocyte complex is formed. The stage of allergic reaction which is characterized by development or emission of biologically active substances - BAS, allergy mediators (Histamine, serotonin, etc.) begins with this moment and pathochemical. The pathophysiological stage of allergic reaction or stage of clinical features is a result of BAS influence on tissues and organism organs. It is a stage of clinical implication of an allergy: blood circulation disturbances, spasm of bronchial and intestinal muscles, changes of structure of blood serum, disturbance of coagulability of blood etc. are characteristic. Based on the development mechanism following allergic reactions are distinguished: 1) immediate type 2) cytotoxic 3) reactions of Artuse phenomenon type (immune complexes) 4) slowed down type (cellular hypersensitivity) Each of these types of allergic reaction has the special immune mechanisms, and the mediators that cause features of a clinical current of allergic diseases. 1) Allergic reactions of the first type are called also anaphylactic or atopic. They develop during interaction of an antigen with antibodies of type IgE and IgG which are called reagents. IgE and IgG are adsorbed on tissue basophiles and fat cells. Interaction of an antigen with reagents
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of ALLERGIC DISEASES OF ORAL MUCOSA Allergy is the ...

ALLERGIC DISEASES OF ORAL MUCOSA Allergy is the perverted reaction of an organism to certain substances of the antigenic nature which in norm do not cause the painful phenomena. Endocrine and nervous systems, and also pathology of a gastroenteric tract play important role in allergy occurrence. Various substances can become the allergy reason: simple and difficult chemical compounds (iodine, bromine, proteins, polysaccharides) which getting into an organism, cause development of humoral and cellular immunologic reactions (an inflammation, a spastic stricture of bronchial muscles, a necrosis, a shock etc.).
The substances causing development of allergic reactions are called allergens. The quantity of allergens in the nature is great enough, they are very various, both on structure, and on properties.
According to origination the allergens are divided to exogenous and endogenous. Exogenous allergens get into an organism from the outside, and endogenous are originated in the organism and are own, but modified proteins. Thus, endogenous allergens are auto allergens.
Exogenous allergens are: -Infectious - microbes, fungi, viruses, Chlamydia, protozoa -Non-infectious - vegetative, medicinal, alimentary, household, industrial etc. Endogenous allergens are: - Natural, or primary-some structures of an organism (a lens, a thyreoglobulin, etc.) which in
norm do not cause the immune reaction of an organism - Acquired, or secondary - are formed in an organism during disturbances of metabolic
processes under the influence of any pathological infectious or non- infectious factors (a cold, radiation, burns etc.).
In a current of allergic reactions three stages are distinguished: 1) immunologic 2) biochemical (pathochemical) 3) pathophysiological The immunologic stage begins with organism and allergen contact, which result in organism
sensibilization that is origination of the antibodies which are capable to co-operate with the given allergen. If after that allergen leaves from an organism no pathological reactions occur. Thus, the first penetration of allergen into an organism has sensitizing influence.
In case of repeated entrance of allergen in already sensitizing organism allergen-antibody or allergen-sensitizing lymphocyte complex is formed.
The stage of allergic reaction which is characterized by development or emission of biologically active substances - BAS, allergy mediators (Histamine, serotonin, etc.) begins with this moment and pathochemical.
The pathophysiological stage of allergic reaction or stage of clinical features is a result of BAS influence on tissues and organism organs. It is a stage of clinical implication of an allergy: blood circulation disturbances, spasm of bronchial and intestinal muscles, changes of structure of blood serum, disturbance of coagulability of blood etc. are characteristic.
Based on the development mechanism following allergic reactions are distinguished: 1) immediate type 2) cytotoxic 3) reactions of Artuse phenomenon type (immune complexes) 4) slowed down type (cellular hypersensitivity) Each of these types of allergic reaction has the special immune mechanisms, and the mediators
that cause features of a clinical current of allergic diseases. 1) Allergic reactions of the first type are called also anaphylactic or atopic. They develop
during interaction of an antigen with antibodies of type IgE and IgG which are called reagents. IgE and IgG are adsorbed on tissue basophiles and fat cells. Interaction of an antigen with reagents

causes degranulation of the basophiles and fat cells. As a result, in intercellular space there is an emission of mediators of an allergy being inside these cells: Histamine, heparin, serotonin, prostaglandin (PG). Clinical features of an allergy of this type begin in 15-20 minutes after contact of an organism to allergen; therefore they are called reactions of immediate type.
Anaphylactic shock, urticaria, bronchial asthma, hay fever etc concern to reactions of immediate type.
2) Allergic reactions of the second type (cytotoxic) - are characterized by formation of antibodies IgG and IgM, capable to activate a complement. In case of this type of reaction the antigen is a component of a cell or is adsorbed on it, and the antibody arrives in a tissue. Adhesion of antibody with an antigen causes complement activation, cell destruction, a phagocytosis and excision of the blasted cells and tissues.
Medicinal allergies concern to reactions of cytotoxic type. 3) Allergic reactions of the third type (immune complexes) during which neither the antigen,
nor an antibody are not a component of cells, and formation of an antigen-antibody immune complex occurs in blood and an intercellular liquid. In case of this type of reaction antibodies are IgG and IgM as well. Immune complexes settle down around vessels and in a vascular wall. It leads to disturbance of microcirculation and a secondary lesion of tissues, up to a necrosis.
Autoallergic diseases concern to reactions of immune complexes (lupus erythematosus, etc.) 4). Allergic reactions of the fourth type (slowed down type) are characterized by T-
lymphocytes co-operation with antigens. These T-lymphocytes have the receptors on the membrane capable to contact with antigen. When T-lymphocyte is joined to allergen, the mediator of cellular immunity - lymphokines is formed. About 30 various lymphokines are known by means of which T-lymphocytes become organizers of destruction of antigens by other leucocytes of blood. Lymphokines cause a clump of macrophages therefore the inflammation develops and the phagocytosis is carried out.
Allergic reactions of the slowed down type develop in 24-48 hours after contact of allergen to an organism. Reactions of such type underlie almost all virus and bacteriemic infections (tuberculosis, syphilis etc.).
Diagnosis: Diagnosis of allergic diseases is based on the allergological anamnesis, diagnostic and
laboratory tests. During subjective examination (allergological anamnesis) the contacts with various household
and industrial substances, predisposition of an organism to allergies, possible reasons of allergies should be taken into account.
Diagnostic tests should be done in 2-3 weeks after acute implication of an allergy. Dermal tests are done: to find out a medicinal allergy - by means of application on a skin, allergy of a bacteriemic or fungal origination - an intradermal method.
Reaction of basophiles degranulation (test of Sheili), and reaction of leukocytosis are concern to laboratory tests.
Anaphylactic shock Anaphylactic shock (choc anaphylacticus) is the generalized anaphylactic reaction originating during interaction of the entered antigen with cytophilous antibodies. Anaphylactic shock is the highest step of implication of allergic reaction of immediate type.
In dental practice anaphylactic shock can occur from anesthetics, analgesics, antibiotics, filling materials, including root channels sealers, impression materials etc.
Clinical features: Anaphylactic shock develops suddenly, in some minutes, and even immediately after antigen
introduction. The patient shows anxiety; has a feeling of fear, fever, and constraint in a breast. There are complicated breath, at first frequent, and then convulsive, nausea, vomiting, plentiful

diaphoresis, hyperemia of integuments, headache, pulsation in head. Pupils extend and do not react to light. These symptoms are replaced by balance loss, falling, cramps. Spontaneous urination and defecation occur. Changes of cardiovascular system: tachycardia, threadlike pulse, sharp falling of arterial pressure- are characteristic for anaphylactic shock.
Anaphylactic shock is not shown on oral mucosa. Differential diagnosis: The anaphylactic shock is necessary for differentiating from: - An acute heart insufficiency - A myocardial infarction (heart attack) - Epilepsies Treatment: The outcome of an anaphylactic shock depends on severity of symptoms less, than
on complete and on time treatment. First of all it is necessary to stop allergen introduction in an organism. Horizontal position is
given to the patient; prostheses should be removed from an oral cavity, and a mandible should be pushed forward and fixed in this position to prevent tongue asphyxia.
0,5ml of 0,1 % adrenaline solution or 2-4ml of 0,2 % epinephrine solution should be injected subcutaneously or intramuscularly (in serious cases intravenous introduction is prescribed) to increase arterial blood pressure.
For bronchospasm cupping use 5-10ml of 2,4 % euphilinum solution intravenously. In case of cramps tranquilizers and neuroleptics (Seduxenum, Elenium) are used. Angioneurotic Quincke's edema Quincke's edema (oedema angioneuroticum Quinke) is
promptly developing deep edema of the limited part of skin, connective tissue and mucosa which has a sudden onset; can spontaneously disappear and again be shown.
For the first time this disease was described by German therapist Quinke. In case of angioneurotic edema the BAS deactivation and inhibition system is broken. It
develops in case of hereditary deficiency of these inhibitors, disturbance of function of the organs deactivating BAS. Activation of BAS is very easily for these patients. This activation can be caused not only by a complex of antigen-antibody, but also by non-immune agents (for example, a cold). Under the influence of BAS there is an exit of an exudate and an edema of tissues.
Clinical features: Disease begins sharply, within several minutes there is a limited expressed edema. The edema basically is localized in the field of lips, eyelids, external genitals, tongue and a larynx. Colour of a skin in the field of an edema is not changed, tissues are strained, but the fossa is not formed during palpation which is painless. Edema presents from several hours till two days and disappears completely without any changes. In case of tongue edema it is hardly located in an oral cavity. The edema of tongue and larynxes are the most dangerous, as can lead to development of a stenosing asphyxia. If the Quincke's edema is located in cerebral covers there are neurologic disturbances (epileptic attack).
There are periodic remissions during this disease, which is not accompanied by painful sensations, patients complain of feeling of tension in tissues more often.
Differential diagnosis: Quincke's edema localized in lips is necessary to distinguish from: - A cheilitis granulomatosa (syndrome Melkersson-Rosenthal) - An erysipelatous inflammation of lips - A collateral edema of lips and a lymphostasis during periostitis In case of Melkersson-Rosenthal syndrome the edema of lips is combined by fissured tongue
and neuritis of a facial nerve. In case of erysipilatous inflammation of lips the affected part is hyperemic, and in case of
Quincke's edema - is not changed in colour. Treatment: First of all stop contact to allergen.

Antihistamine drugs (Dimedrol, Suprastinum, Tavegilum) are prescribed intramuscularly, and in easy cases in the form of tablets 2-3 times a day. For reduction of permeability of vascular walls Ascorutinum is prescribed. During edema of larynxes 25 mg of prednisolone is intramuscularly entered, and in case of need the patient should be taken in a hospital for tracheotomy carrying out. In serious cases 0,1-0,5ml of 0,1 % adrenaline solution is subcutaneously entered for blood pressure increase.

CHANGES OF ORAL MUCOSA IN CASE OF HYPO - AND AVITAMINOSIS Vitamins play the important role in organism vital activity. They accept active participation in
metabolism processes. The basic source of vitamins is food, synthesis of some of them is partially carried out by an intestine microflora, and still the part is formed from provitamins in an organism.
The hypovitaminosis is a condition which comes in case of insufficient entering of vitamin in an organism or disturbance of its absorption.
The avitaminosis is full absence of any vitamin in an organism. At present the avitaminosis practically is not met.
Depending on the mechanism of development of vitamin insufficiency we distinguish some kinds of hypo-and avitaminosis:
1) Alimentary - occurs in case of insufficient entering of vitamins with nutrition 2) Resorptive – originates in case of destruction of vitamins in gastroenteric tract, disturbance
of their absorption and synthesis by an intestinal microflora 3) Dissimilative – occurs in case of disturbance of vitamins metabolism which is a
consequence of the general metabolism. Vitamin В1 (Thiamine) - is synthesized in a human body, and also entered with nutrition. After
an absorption in thin intestine it turns to a cocarboxylase. Physiological value - regulates metabolism processes, in particular carbohydrate and protein
metabolism. Besides, vitamin В1 takes part in transfer of nervous impulses and in hemopoiesis. Daily requirement of an organism for vitamin В1 is 2-3 mg. Hypovitaminosis of В1 in an oral cavity does not cause certain specific changes. It is used
during treatment of neuritis and neuralgias of n.trigeminus, periodontal diseases, oral pathologies of various etiologies.
Producing forms: - each tablet and dragee contain 0,002 g and 0,01g - Solutions for injections- 3 % and 6 % Vitamin В2 (Riboflavin) – is entered in an organism with nutrition, and also is synthesized in
an intestine and collected in a cerebral tissue, a liver, kidneys and heart. Physiological value - participates in oxidation-reduction reactions and a metabolism. Daily requirement of an organism for vitamin В2 is 2,5 (2-3) mg. Hypovitaminosis of vit В2 causes the changes of oral mucosa and an eye. Cracks (fissures)
covered by squama (crusts) are thus formed in mouth angles. Dryness, peeling and reddening of lips, formation of vertical fissures become perceptible. Crusts occur on nose wings nasal-labial folds as well. Tongue papillae are atrophied, there are a hyperemia and the aphthous changes, patients note a burning sensation and a pain.
Changes on oral mucosa are accompanied by lesions of eyes: dacryorrhea a keratitis, cornea turbidity.
Hypovitaminosis of vit В2 is diagnosed by decrease of its quantity in urine and blood. In stomatological practice Riboflavin is used in case of glossitis, cheilitis, allergic diseases. Output forms: - each tablet contains 0,05 g - A solution for injections- 1 % Vitamin В6 (pyridoxine) - is synthesized by bacteriemic flora of an intestine. Physiological value - is a biocatalyst of metabolic processes, stimulates formation of
hemoglobin and leucocytes, promotes development of natural immunity due to increase of phagocytic activity of leucocytes.
Daily requirement of an organism for vitamin В6 is 2-4 mg. Hypovitaminosis of vit В6 causes occurrence of angular stomatitis, cheilitis and glossitis. In stomatological practice the pyridoxine is used during treatment of medicamental stomatitis,
glossitis, cheilitis. Vitamins В1 and В6 is inexpedient to prescribe together for parenteral taking as their
biological activation becomes difficult in an organism. Producing forms: - each tablet contains 0,002, 0,005 and 0,01g - Solutions for injections- 1 %, 2,5 % and 5 %

Vitamin В12 (cyanocobalamin) - is entered in an organism with nutrition where it is soaked up in a stomach with the assistance of intrinsic factor of Castle (gastromucoprotein) which is developed in a stomach.
Physiological value - provides normal maturing of bloody elements in bone marrow, and, besides, raises phagocytic activity of leucocytes, production of antibodies, activates protein synthesis.
Daily requirement of an organism for vitamin В12 is 2-3 mg. Hypovitaminosis of vit В12 causes development of Addison-Birmer anemia (В12-deficiency
anemia). The initial symptoms of this anemia are the tongue lesions: a burning sensation, a pricking, occurrence of a hyperemia and an atrophy of papillae - the "polished" tongue. Dryness in a mouth (xerostomia) simultaneously becomes perceptible. Later the pain in tongue while eating is added to these symptoms.
Anemia of Addison-Birmer is diagnosed by means of the blood analysis (blood chemistry) where reduction of quantity of erythrocytes and hemoglobin is observed. And the quantity of erythrocytes decreases faster quantity of hemoglobin; therefore this anemia has hyperchromatic character.
In dental practice cyanocobalamin is used during treatment of neuralgia of n. trigeminus, tongue paresthesia, lupus erythematosus.
Producing forms: - each tablet contains 100-200 mcg. Vitamin В12 is usually used in a complex with other B vitamins. Vitamin РР (nicotinic acid) - - is entered in an organism with nutrition. Physiological value - participates in metabolism of the carbohydrates, proteins and other kinds. Daily requirement of an organism for vitamin РР is 15-25 mg. Hypovitaminosis of vit РР is shown in the form of tongue edema in an oral cavity. Tongue is
enlarged in size, becomes bright red; papillae are hypertrophic in the beginning, then they are smoothed out.
In dental practice nicotinic acid is used during treatment of rubber lichen planus, periodontal diseases, cheilitis, etc.
Producing forms: - each tablet contains 0,05 g - Solution for injection 1 % Vitamin C (Acid ascorbic) - is entered in an organism with nutrition. Physiological value - vitamin C is necessary for normal realization of the vital processes. It
participates in collagen synthesis, protein metabolism, regulates permeability of walls of blood vessels and makes active impact on resistance of an organism to an infection.
Daily requirement of an organism for vitamin C is 70-80 mg. Hypovitaminosis of vit C in an oral cavity is shown always. First of all there is profuse gingival
bleeding and hemorrhages on oral mucosa. In case of advance of vit C hypovitaminosis gingivitis passes in the ulcerative form. The general condition of the patient suffers: there is vivid asthenia, fast fatigability, pains in calf muscles.
In dental practice vitamin C is used very widely: during treatment of periodontal diseases and oral pathologies.
Acidum ascorbinicum is desirable for prescribing with vitamin Р (Rutin) which is a synergist of vitamin C and strengthens its action.
Producing forms: - each tablet of vitamin C contains 0,05 g and 0,1g, each tablet of vitamin C and Rutin - "Ascorutin" - contains 0,05g
- Solution for injection 5 % Vitamin A (Retinol) - is entered in an organism with nutrition. Physiological value - vitamin A is necessary for growth of an organism, maintenance of a
normal condition of a skin and mucosa, raises protective properties of oral mucosa to various traumatic factors.
Daily requirement of an organism for vitamin A is 1,5mg. Hypovitaminosis of vit A in an oral cavity is shown by hyperkeratosis symptoms, dryness of
skin and oral mucosa.
In dental practice Retinol is used during treatment of Leukoplakia, rubber lichen planus, for acceleration of epithelization processes in case of many oral pathologies and as a basis for a medical bandage during periodontal diseases treatment.
Producing forms: - each dragee contains 10000-25000 ME - Solutio oleosa for intake (taking peroral) and intramuscularly injections Vitamin E (tocopherol acetate) - is entered in an organism with nutrition. Physiological value - vitamin E is an antioxidant, promotes accumulation of vitamin A and
other fat soluble vitamins, improves a fatty and mineral metabolism. Daily requirement of an organism for vitamin E is 10 - 25 mg. Hypovitaminosis of vit Е in an oral cavity is not shown by any specific signs. In dental practice tocopherol acetate is used with vitamin A during treatment of parodontitis
and for applications on erosions and ulcers in case of oral pathologies. Producing forms: - dragee and Solutio oleosa, a dragee "Aevit" - vitamins A and Е.
CHANGES OF ORAL MUCOSA DURING EXOGENOUS INTOXICATIONS Exogenous intoxications of an organism are possible during toxic action of medicines,
professional harmfulnesses. Thus intoxications from medicines are possible only during their overdosage, in the result of disturbance of function of secretary organs.
Toxic action of medicines needs to be distinguished from a medicinal allergy. In case of medicinal intoxication for each medicament the specific picture of a lesion is
characteristic, and poisoning degree depends on a medicine dose in an organism. Thus the antibodies are not developed, and during treatment antidotes, bathing are used.
In case of medicinal allergy the clinical picture and its severity do not depend on a type and a dose of medicine. In an organism antibodies are formed, and during treatment antiallergic medicines (antihistamine, etc.) are used
Intoxications from mercury and bismuth medicaments Intoxications from mercury medicaments cause the general and local changes. The general are
disturbances of nervous system and a gastroenteric tract, and local - various changes of oral mucosa from discoloration till necrotizing ulcerative lesions.
Intoxications from bismuth medicaments (biochinol, bismoverolum, etc.), cause a lesion of oral mucosa in the form of a discoloration. On gingival margins, and sometimes and on other parts of oral mucosa there is a bismuthic border of grayish or black colour.
In case of intoxications from medicaments of both mercury and bismuth painful sensations are present only in case of disturbance of integrity of a mucosa, and in case of necrotizing ulcerative lesions there is an unpleasant smell from a mouth.
Intoxications from lead Lead intoxications is met among people, in working time contacting to lead (lead extraction,
type-setters in printing house). In case of mild form while poisoning from lead there is a grey border on gums, maculae are
rarer. In more serious cases, during long contact to lead, there are hearths of an aseptic necrosis as lead, being accumulated in walls of vessels, causes blood supply disturbances.
Except of oral mucosa the skin is affected also - there are erythema and bulla on it. In serious cases anemia, neurosis, paralyses and nephropathies can develop. For treatment antidotes (Unithiolum, Succimerum, etc.), a solution of potassium iodide,
vitamins C and В1 are used. Locally: oral cavity sanitation (as presence of carious cavities and dental deposits promotes
more serious current of a poisoning) is carried out. Mucosa is processed by 1 % solution of acetic acid which dissolves a lead dust.
Intoxications from mercury Mercurial intoxications are found out among workers of mercurial manufactures and occur in
case of inhalation of steams of mercury. The general symptoms of intoxication are: irritability, depression of memory, working
capacity.

In an oral cavity the poisoning is shown in the form of a border of black colour on marginal gingiva. There are gingival bleeding, necrotizing ulcerative lesions which can extend on other sites of oral mucosa. Patients can note unpleasant metal taste in a mouth, a hypersalivation.
Treatment is referred on the termination of entering of mercury and its deducing from an organism. For this purpose prescribe plentiful alkaline drink, taking Sodium thiosulfate solution, injection of Unithiolum which forms insoluble bonds with heavy metals, polyvitamines.
Locally: oral cavity sanitation, antiseptic processing of oral mucosa is done as well, in case of ulcerative lesions- application of keratoplastics.

Condition of the OCMM during blood and hematopoietic system diseases
According to actual representations, in the etiology and pathogenesis of parodont
and oral mucosa diseases a great value have the diseases of inner organs and organism systems.
Among the general diseases, accompanied by oral cavity disorders, the diseases of hematopoietic system have a special place. All the disorders of hematopoiesis first of all are shown on the oral membrane. Hence, the stomatologist can be the first, who can diagnose the general diseases, and render a special professional approach in the treatment of such patients.
1. Diseases of red blood
Fe-deficiency anemia develops in case of disorders of Fe ions absorption, long lasting bleedings, anacid gastritis, chronic infections etc. Disease is more often observed in the age of 30-40 years, develops slowly and has a chronic current. In peripheral blood of the patient deficiency of erythrocytes within the bottom borders of norm is found out. The color indicator is less than 1(approximately 0.7).
Patients complain on weakness, dizziness, headaches, restless sleep, fast fatigue, disorders of sensitivity of separate areas of the skin, especially on fingers. Disorders of gastrointestinal and cardiovascular systems are often observed. The skin of the patient is pale. Trophy changes of the skin, nails and in the area of the scalp can be found out.
Oral mucosa is pale. Patients often complain on disorders of sense of smell and flavor. It is shown by appetite loss, use of inedible products (chalk, tooth-paste, sand etc.), and also by feeling of burning and paresthesia of tongue, especially on tip.
Salivation is decreased, which leads to dryness of the OCMM and constant requirement for drink.
Often in the mouth corners painful cracks and angular stomatitis are formed. Catarrhal gingivitis, and in heavy cases, parodontitis are observed, accompanied by
bleedings of various degrees. During objective examination tongue edema, atrophy of tongue papillae is
observed. Tongue body is hyperemic. In heavy cases all papillae of the tongue become atrophic; tongue becomes shiny (like the Gunter-Moeller’s glossitis).
The teeth are affected by chronic caries, enamel loses the shine, the teeth become fragile, pathological abrasion of tooth hard tissues is observed. В12 vitamin-deficiency anemia (Addison-Birmer’s anemia). The lack of vitamin
В12 is the reason of this disease. Disorder of synthesis of “Castly’s internal factor” leads to disorder of vitamin В12 absorption, which can cause В12 vitamin-deficiency anemia.
Generally women of more than 40 years old are affected. The quantity of erythrocytes is decreased; the color indicator is more than 1.
Patients complain on general weakness, dizziness, headaches, nausea, pains in the area of heart. The skin is pale, in some places it is pigmented.
In the oral cavity the first signs are the neurologic changes of the tongue, patients complain on feeling of burning and pain, disorder of flavor sensitivity. The tongue papillae quickly become atrophic, the tongue becomes shiny, bright red spots appeared on the tongue body (Gunter-Moeller’s glossitis). Sometimes petechias and eckchimosis appear on the cheeks and lips. Often gingivitis and parodontitis are found out, accompanied by gingival bleedings.
Caries of the teeth have fast current. Erythremia (Vakez’s disease) is characterized by hyperplasia of all cells of
hematopoietic system. The reason of the disease is not found out. People of more than 30 years old are
affected generally.
Patients complain on dizziness, insomnia, general weakness and headaches. Often there is a noise in the ears and appearance of "points" in front of the eyes.
During examination dark red color of the skin is observed. Bleedings from nose, gastrointestinal bleedings, and bleedings connected with urinogenital system are observed. The liver and the spleen are increased, arterial pressure is high.
In peripheral blood the quantity of erythrocytes, platelets and leukocytes is increased, the quantity hemoglobin is also increased. The blood volume is increased up to 10-15 liter.
The changes of the oral cavy t are generally connected with darkening of the color of mucous membrane, it gets a cherry shade. The hard palate remains pale and differs from bright red soft palate (Cooperman’s symptom). Gingival bleedings, basically, of the traumatic nature are possible.
Surgical interventions, especially removal of the teeth, can lead to hard stopped bleedings.
2. Diseases of white blood
From the diseases of white blood leukemia meets more often. Leukemia is displayed by swift hyperplasia of leukocytes. By the current leukemia
can be acute and chronic. The acuity of leukemia depends on the speed of process and qualitative signs of leukocytes in peripheral blood.
Acute leukemia. Depending on the type of the cells, the following forms of acute leukemia are
distinguished: lymphoblastic, myeloblastic, monoblastic, promyelocytic and non-differentiated. Acute leukemia generally meets at young age, till 40 years old.
Acute leukemia has unexpected beginning, fast current and is often similar to other diseases: flu, pneumonia, quinsy, etc.
Patients usually complain on general weakness, fast fatigue, pallor, bone pains, disposition to sweating, recurring sub-febrile temperature.
During objective examination displays of hemorrhagic diathesis are found out on the skin of the patients: petechias, hemorrhages, eckchimosis, nasal, uterine and gastrointestinal bleedings. Also ulcerative-necrotic complications are observed: necrotic quinsy, pleurisy, pneumonia, ulcers and areas of necrosis in the oral cavity and in the field of organs of urogenital system.
Displays of leukemia in the oral cavity can be divided into 3 groups: hemorrhagic, ulcerative-necrotic and hyperplastic.
Hemorrhagic symptom, first of all, is displayed by gingival bleedings. Very often this can be the first and the only sign of leukemia for a long time. Besides, intramucous bleedings are characteristic for leukemia: petechias, eckchimosis, hematomas and hemorrhagic spots. After bleeding erosion and ulcers are formed on their places. The bleeding can begin even from insignificant damage: cleaning of the teeth, hard food eating, medical manipulations.
Often ulcerative-necrotic processes prevail at the patients. The depth and spreading of these processes testify about exacerbation of the general process. Necrosis and ulcers begin from marginal gingiva and extend on the other areas of the oral cavity.
Depending on the depth of the affection erosion and ulcers can be: - Superficial - aphtae (erosion) with hyperemic ring around it, covered by white
fibrin membrane, which cannot be removed - Deep - clean, painful ulcers which often bleed. Erosion and ulcers are often settled down on the most traumatic areas of the
mucous: cheeks, on the line of teeth closure, lateral surfaces of tongue, in the area of incorrectly filled teeth and artificial constructions. In the tissues, surrounding ulcers, inflammatory reaction is absent. Regional lymph nodes are increased, sometimes are painful.
The hemorrhagic symptom is often combined with ulcerative-necrotic one and hypertrophy of the gums. The combination of all three symptoms (bleeding, ulcers and hypertrophy of gums) is defined as “leukemic stomatitis”.

Histollogically leukemic infiltration is defined in the mucous if gingiva. Hypertrophy is also observed in the area of lymphatic organs of the oral cavity: increase of pharyngeal and glossal tonsils.
Very often during initial stages of leukemia there are pains of healthy teeth, which can be explained by metaplasia of pulp and periodont cells.
During leukemia is often possible to observe fungal affections - candidiasis. Patients complain on dryness of the oral cavity, disorders of flavor sensitivity, pain during chewing and eating, tongue looks like a "brush". White membrane appears which covers the pale mucous membrane and does not precede the catarrhal gingivitis (difference from usual candidiasis). It is removed vary hardly, damaging the mucous.
Chronic leukemia. Chronic leukemia characterized by long current and rather poor clinical picture.
Chronic myeloleukemia and lymphatic leukemia are distinguished. Persons of more than the middle age are affected.
The displays in the oral cavity are gingival bleedings, especially after surgical intervention. Ulcerative-erosive affections meet seldom, basically during myeloleukemi. Hypertrophy of gums can be also observed.
Agranulocytosis is a clinical-hematologic syndrome which is characterized by partial or full disappearance of granulocytes in the blood.
The basic reasons are certain medical products (amidopyrine, analgin, barbiturates, sulfonamides, some antibiotics, antihistamine preparations), ionizing radiation, influence of allergic diseases on the processes of hematopoiesis. Besides quantitative changes, decrease of impellent and phagocytal activity of neutrophills is also observed.
All these lead to decrease of an organism resistibility to infections and occurrence of infectious complications.
Women more than 30-40 years old are affected more often. Acute agranulocytosis is characterized by combination of clinical symptoms of
acute sepsis and necrotic complications. Develops at once, has fast current, in several days or weeks can lead to death.
Basically develops after reception of amidopyrine. In initial stages patients complain on weakness, decreased working capacity, acute
pains in the throat and in the oral cavity. Further the body temperature raises, and necrotic changes appear on the OCMM: necrotic quinsy, ulcerative-necrotic gingivitis and stomatitis, ulceration of the tongue and the soft palate, with subsequent punching. In heavy cases gangrene of the tongue and mouth floor can develops.
Chewing and swallowing processes are broken, contracture of chewing muscles develops.
Disease can be complicated by bronchopneumonia, septic myocarditis, hepatitis, disorders of gastrointestinal system.
There were cases when the toothache was one of the first symptoms of agranulocytosis.
Chronic agranulocytosis has recurring character and long benign current. Oral cavity affections are found out during relapses and correspond to clinic of acute agranulocytosis. During remissions stable hypostasis and cyanosis of gums without necrotic processes is observed.
3. Thrombocytopenia
Hemophilia Hemophilia is a congenital, genetically caused disease. Boys are affected, because
the disease is transferred through sexual Х chromosome. The reason of the disease is congenital absence of the VIII (antihemophilic globulin) or the IX (Christmas-factor) factors in the blood, that leads to disorder of the first stage of blood clotting: formation of active plasmatic tromboplasts.
That’s why the basic clinical displays of the disease are hemorrhages in submucous and subdermal cellulose. They can be spacious at strong damages, especially in joints.
For the stomatologist it is very difficult to spend any stomatologic manipulations for these patients, especially surgical. Before starting any actions, the patient needs to be prepared for them in advance: to spend blood transfusion, to make and settle a special artificial prostesis etc. Into the alveola of the removed tooth a tampon moistened with a solution of thrombin is located.
Trombocytopenic purple (Verlhoph’s disease) Disease, basically, affects young women. Unlike hemophilia, the bleedings can arise even from insignificant damage.
Internal bleedings are possible, especially intrauterine and intracerebral bleedings are dangerous. Unlike hemophilia the intraarticular hemorrhages are absent. Plentiful nasal and gingival bleedings are characterized. Basically the gingival papilla bleeds, the gum is necrotic, and is covered by livid (bluish-grey) blood clots. Even insignificant contact with this clots leads to a bleeding. Hemorrhages are observed also on the mucous of soft palate and tongue. Patients often complain on a stench (very bad smell) from the oral cavity. All surgical manipulations of such patients are interfaced to danger and demand preliminary preparation of the patient.
Hemorrhagic vasculitis (Shenlejn-Henokh’s disease) – is displayed by bleedings, the reason can be allergic affection of small vessels. The disease meets at young age.
Intensive bleedings are not characteristic. Symmetric hemorrhagic rash is found out, which can also be on the OCMM. Intraarticular hemorrhages are especially characteristic.
Disease has a chronic current with relapses. Coagulability of blood is not broken. During manipulations in the oral cavity it is necessary to consider the general allergic background and to spend some actions for prevention of infection of the wound.
Hemorrhagic angiomatosis (Randju-Osler’s disease) - has a hereditary character and is caused by a congenital dystrophy of walls of capillaries and arterioles. Therefore local expansions of vessels are formed - teleangiectasias, both on the skin, and on the OCMM. Teleangiectasias can bleed and, further, become the reason of Fe-deficiency anemia.
Angiohemophilia (Villebrand’s disease) - has hereditary character. The reason is the disorder of capillary hemostasis and of the first phase of blood clotting.
It is displayed by intensive bleedings of the mucous membranes of the nose, oral cavity, gums, gastrointestinal system. Small surgical interventions, such as tooth removal, are accompanied by intensive bleedings, which are dangerous for life, but spacious interventions - not. Therefore preliminary preparation of the patient should precede any intervention.
Thus, it is possible to conclude, that blood diseases have their own displays in the oral cavity, which can become a base for fast and exact diagnostics.
Treatment
Treatment of complications of blood diseases in the oral is a part of the general treatment and has symptomatic character. Its efficiency depends on tactics of treatment of the general disease. Oral cavity sanitation should be spent in the period of remission of the general disease. It includes removal of destroyed teeth and roots, tooth plaque, filling of carious cavities and treatment of parodont diseases.

Acantholysis (epidermolysis) bullosa
Acantholysis (epidermolysis) bullosa is a bullous dermatosis which is characterized by
formation of intraepithelial blisters on not changed skin or mucosa as a result of acantolysis. Disease has a long chronic current with remissions. Distinguish 4 clinical forms of acantholysis (epidermolysis) bullosa:
1. pemphigus vulgaris 2. pemphigus vegetans 3. pemphigus foliaceus 4. seborrheal pemphigus.
The etiology is unknown. There are viral (virus) and autoimmune theories of this disease. Basically men and women from 40 till 60 years are ill.
Pemphigus vulgaris meets much more often other forms and almost always begins with lesion oral mucosa (75 %). Suddenly disease begins with formation of individual blisters with the serous or hemorrhagic contents, having very thin covering (operculum, tegmentum). Owing to a constant maceration in an oral cavity blisters are very quickly opened, baring an erosive surface with scraps of covering of blisters on periphery. The hypersalivation is possible. Erosions on oral mucosa can be formed and another form: in the centre of a lesion the epithelium grows turbid (dims), undergoes to maceration and easily exfoliates, forming erosion in the centre. Erosions has red colour, pure or are covered by fibrinous scurf, are painful. Extensive erosions sharply worsen the general condition of patients, and joining of a pyogenic microflora causes occurrence of specific bad smell from oral cavity. The hypersalivation is possible. Nikolsky's symptom, as a rule, is positive. The erosion epithelization occurs slowly, even at using of big doses of corticosteroids.
Pemphigus vegetans also meets frequent in an oral cavity. Blisters are small, erozions are covered by dirty-grey scurf. A bottom of erosions is rough because of fast formation of growths (vegetations) which easily bleed. Vegetations tower (elevate) over intact sites, reaching height 1-2 sm. Nikolsky's symptom is positive.
Pemphigus foliaceus begins with formation of flat flaccid blisters on face skin and on pilary part of head (scalp). Blisters, merging, form solid erosive surfaces reminding burn of a skin.. Nikolsky's symptom is well expressed. Oral cavity mucosa and other mucosas are seldom involved in process.
Seborrheal pemphigus meets seldom enough. Begins with occurrence on a face skin of rashes which are located in the form of the butterfly and represent the erythematic centers against a fat seborrhea with layering the thin or loosened crusts of yellow colour. Quite often define erosions on oral cavity mucosa . Nikolsky's symptom is well expressed.
At acantholysis (epidermolysis) bullosa eating is complicated, and sometimes it is impossible owing to erosions painfullness. On a red border of lips and on angles of oral cavity the erosion quickly cover by yellow-brown or bloody crusts. The pemphigus is characterized by a wavy current, the exacerbation periods are replaced by the periods of remission . There are 3 versions of Nikolsky's symptom.
1. If to take with forceps from blister covering or from superficial layer of erosion epithelium and to pull, occurs exfoliation of epithelium on probably not changed healthy mucosa and skin. Thin epithelium membrane is not strong very much and is easily dissected by a forceps
2. At rubbing of visibly not changed mucosa or skin between lesion areas leads to fast formation of blisters or erosions.
3. At rubing visibly not changed mucosa or skin, which are located far from lesion area also leads to fast formation of blisters or erosions.

The second and especially the third version of Nikolsky’s symptom testify to intensifying of intensity of an acantolysis.
There is so-called <<Nikolsky's false symptom>> or a symptom of perifocal subepithelial detachment. Thus blisters are located subepithelial and round them all depth of an epithelium in limits 4-8мм can easily exfoliate. The covering in such cases is thick. This symptom is observed at bullous form of lichen ruber planus, at non acantholysis bullosa, at allergies etc.
The diagnosis of pemphogus put on the basis of clinical implications, Nikolsky's positive symptom, results of cytologic research at which find out characteristic acantholytic cells (Tzanck cells); histological research at which the acantolysis, edema, and disappearance of intercellular bridge in the lower rows of spinous layer is found out.
The differential diagnosis is spent with: - herpes iris -pemphigoid
- medicinal allergy - bullous form of lichen ruber planus - dermatitis herpetiformis, Duhring's disease - benign pemphigus (only oral mucous membrane) At herpes iris blisters are surrounded by an erythema zone, they are located subepithelial,
Nikolsky's symptom is negative. For herpes iris the acute beginning, seasonal prevalence of relapses, expressed inflammation of oral mucosa are characteristic.
At pemphigoid blisters are located under the epithelium, covering (tegmentum)is thick, Nikolsky's symptom is negative, Tzanck cells are not found out. People are ill after 60 years.
The differential diagnosis with an allergic stomatitis spends on the basis of the anamnesis (data on a drug intake) and results of allergological tests. Blisters are located under the epithelium, Nikolsky's symptom is negative, at change of medicines blisters disappear, Tzanck cells are not found out.
At bullous form of lichen ruber planus blisters are subepithelial, the acantolysis is not present. Round blisters or on other sites of mucosa there are the plural papules typical for lichen ruber planus.
At Duhring's disease the isolated forms on oral mucosa are not observed. Blisters are subepithelial, located on hydropic hyperemic mucosa, formation of blister is accompanied by burning sensation and an itch. Nikolsky's symptom is negative, acantolitic cells are absent, in blood the eosinophilia is observed. Patient's sensitivity to iodine preparations is raised.
At benign pemphigus the blisters are localized only on oral mucosa, they are located under an epithelium, tegmentum of blister is thick, often has hemorrhagic contents. Tzanck cells are absent, Nikolsky's symptom is negative.
Treatment of pemphigus includes corticosteroids which are the basic agent of treatment of this disease. All other medicinal preparations, including cytostatics, use for liquidation of the complications bound to reception of glucocorticoids. Begin treatment with shock (loading) doses of corticosteroids (50-80 mg of Prednisolonum or 8-10 mg of dexamethasone a day throughout 10-15 days). After that a daily dose gradually reduce: 10-15 mg of Prednisolonum or 0,5-1 mg of dexamethasone. For reduction of complications from corticosteroid therapy restriction in nutrition of table salt, water is recommended. Protein diet is recommended. Inside prescribe potassium preparations, vitamins C, B, calcium preparations, immunodepressants. The good therapeutic effect is observed at simultaneous appointment of glucocorticoids and cytostatics (Methotrexatum). Local treatment includes anesthetics in the form of baths, antiseptic preparations in not irritating concentration, mucosa greasing by corticosteroid ointments (Flucinarum). To purification (cleansing) of erosions from scurf apply proteolytic enzymes with antibiotics. For acceleration of erosions and ulcers epithelization except application with keratoplastics, antibiotics, corticosteroids, it is shown also laserotherapy

CANCER OF THE ORAL CAVITY MUCOUS MEMBRANE AND THE RED BORDER OF LIPS Histologicaly the cancer can be: - planocellular, which develops from the cells of the aculeiform layer of epithelium - basal cellular, which develops from the cells of the basal layer of epithelium More often the planocellular keratinizing cancer meets on the OCMM and on red border of the lips, basal
cellular form meets very rare. Clinical displays of the cancer depend on the stage and growth character of the illness (exo - or
endophytic), and on previous precancer diseases. In late stages the clinical displays of the cancer are usually identical, but at early stages the papillary, infiltrative and ulcerative forms of the disease are distinguished.
Papillary form is evident as an exophytic (i.e. growing outside) formation on a leg or on a wide basis, like a mushroom. There are papillary formations on the surface, covered by keratinized mass. In the basis of this formation and around it infiltration is defined by palpation. Very quickly the tumor breaks up in the centre and becomes a cancer ulcer.
Infiltrative form is endophytic (i.e. growing inside) and the most unfavorable for treatment and forecast. A painless infiltration appears under the mucous membrane during this form, which grows very quickly, breaks up in the centre and forms a typical cancer ulcer. The ulcer also quickly increases in sizes.
The ulcerative form is also endophytic. It begins with erosion of the mucous membrane which turns into an ulcer. Gradually an infiltration appears in the basis of the ulcer and around it. The underlaying tissues are also affected, which leads to the increase of the ulcer.
Thus, at late stages of the cancer an ulcer is always formed, which has dense raised edges, rough granular bottom, covered by grey or grey-yellow necrotic film. A dense infiltration is defined in the basis and in surrounding fabrics by palpation. A cancer ulcer is not very painful. However, there are pains, unpleasant smell from the oral cavity during infection conjunction. Swallowing and chewing are complicated also.
Cancer of the red border of lips, as a rule, is the progression of precancer diseases. Thus the sign of dissemination is always the consolidation occurrence in the base of the affection centre and around it, ulceration and bleeding of its surface. There are only two forms of cancer of the red border of lips:
- papillary - develops from luekoplakia verrucosa, verruciform precancer, limited hyperkeratosis, cutaneous horn and papilloma.
- ulcerative - develops from Manganotti’s cheilitis and chronic inflammatory (more often ulcerative) processes.
Regional lymph nodes at initial stages of the cancer are not changed. However after dissemination of the cancer into the lymph nodes, they increase, become dense and motionless, as they are connected with surrounding tissues. Very often the cancer of tongue, localized in the field of its root, disseminates.
The current of cancer of the OCMM and lips can aggravate such factors, as traumas (sharp edges of the teeth, artificial prosthesis, etc.), smoking, too hot food, various cauterizations, which are dangerous at ulcers of any etiology, but especially at tumors.
Diagnosis of the cancer of the OCMM and the red border of lips is done on the base of external survey and palpation, as this cancer concerns to cancers of visual localization, which allows their evaluation without special equipments. Earlier morphological changes can be seen by stomatoscope. After statement of the clinical diagnosis, it should be confirmed by cytological and histological research methods. By the cytological method the correct diagnosis is possible to put in 90-95 % cases. The material for research is taken by scrapping or puncture. Sometimes biopsy is applied, which is desirable to spend in the clinic, where the patient must be treated.
During cytological research atypical cancer cells are found out, which differ from usual cells by the following signs:
- cancer cells easily separate from the basic tissue, often don’t have cytoplasm, "naked" nuclei are appeared
- nuclei have different sizes, often more large than normal ones, non-uniform arrangement of chromatin in nuclei is found out
- huge multinuclear cells, mitoses - there are additional inclusions, dystrophy and phagocytosis in cytoplasm and nuclei Differential diagnosis. Cancer of the OCMM and the red border of lips is necessary to differentiate from:

- leukoplakia - benign tumours - traumatic and trophic ulcers - ulcers arising during specific defeats (syphilis, tuberculosis) - ulcers arising during lichen ruber planus and other chronic inflammatory processes The cancer is confirmed or except only by histological and, especially, cytological research methods. For timely diagnosis of cancer of the OCMM and the red border of lips oncological vigilance of the
stomatologist at inspection of any patient has great value. It is necessary to eliminate local irritating factors (sharp edges of the teeth, injuring edges of artificial prosthesis) before confirming the diagnosis. Application of factors promoting growth of tumors (cauterization, physiotherapeutic procedures) is contraindicated.
Treatment. It is spent by oncologists. Cutaneous horn This is a painless limited area of epithelium hyperplasia with expressed hyperkeratosis, reminding a horn.
Cutaneous horn is appeared on the red border of lips, more often on lower lip, and also on the face skin. The cutaneous horn has diameter of 1sm and length of also 1sm. It has grey or grey-brown color. It can exist for years. We can know about dissemination from occurrence of an inflammation and consolidation around the horn basis and also from strengthening of cornification.
Treatment – is surgical (removal of the cutaneous horn within healthy tissues) with the conformation of the diagnosis by histological and cytological research methods.
Keratoacathoma Keratoacanthoma is an epidermal benign tumor with localization on the red border of lips and, rarely, on
tongue. The tumor is a dense grey-red small nodule. It has a deepening in the centre, filled by horny mass, which can be easily removed. The tumor grows quickly, reaching to 2.5sm in diameter and 1sm in height. Thus, it is painless, mobile, is not connected with surrounding tissues. After 6-8 months of existence keratoacanthoma either spontaneously decreases in sizes and disappears, or become a cancer, getting denser consistence, dense base and propensity to bleeding. Treatment. It is surgical.

CHEILITIS Cheilitis are benign inflammatory diseases of lips, which can be self-arisen or a symptom of various
OCMM diseases. Classification of cheilitis by G.Savkina (1965) 1. Exfoliative cheilitis a)dry form b)exudative form 2. Glandular cheilitis a)primary b)secondary c)purulent 3. Chronic recurring cracks of lips 4. Eczematous cheilitis a)during general eczema b)contact c)bacterial 5. Actinic cheilitis a)eczematous form b)serous form 6. Abrasive pre-cancer cheilitis (Manganotti’s cheilitis) 7. Macrocheilitis (Melkersona-Rozental’s syndrome) Classification by A.Mashkillejson and S.Kutin 1. Proper cheilitis a)exfoliative b)glandular c)contact
- simple - allergic
d)meteorological e)actinic 2. Symptomatic cheilitis a)atopic b)eczematous c)plasmocellular d)macrocheilitis (Melkersona-Rozental’s syndrome) e)cheilitis during ichthiosis f)cheilitis during hypovitaminosis
Exfoliative cheilitis Exfoliative cheilitis is a chronic disease, which affects only the red border of lips and is accompanied
by peeling. More often affects women at the age of 20-40 years old. Etiology and pathogenesis are not studied, but it is consider, that neurogenic factors are the reason of
this disease. There are data about communication of diseases of thyroid gland with exoliative cheilitis. The role of genetic and immune factors is also marked.
Pathologically during exfoliative cheilitis fibrous of connecting tissue is observed. This can be caused by inflammatory, allergic, metabolic and hereditary factors. In epithelium akantosis, parakeratosis and hyperkeratosis are observed, with formation of "empty" cells without cytoplasmatic inclusions.
Clinic. There are two forms of exfoliative cheilitis - dry and exudative. One or both lips can be affected. The defeat element is a scale. It is densely attached in the center to underlying tissues, and the edges are eliminated. The defeat zone lasts from one corner of the mouth to another, and a part of the red border from Klein's line to its middle is affected only. The corners of the mouth and a part of the red border,

contacting to the skin, are not affected. Process never passes to the skin and the OCMM. The mucous membrane around Klein's zone can sometimes be a little bit hyperemic.
The dry form is characterized by occurrence of stagnant hyperemia, on which dry semitransparent scales of grey color are formed. They are attached in the centre to the red border of lips and have eliminated edges. Lips are dry and are constantly peeled. Scales can be easily removed, exposing stagnant red surface. Erosions are not formed. Patients constantly bite the scales, but in 5-7 days they are formed again.
The dry form can turn into exudative, which is characterized by expressed pains, hypostasis and hyperemia of a lip. A lot of scales and crusts of grey-yellow color are formed in Klein's zone. Sometimes the crusts can reach to big sizes and hang down from the lip like an apron. After removal of the crusts, brightly hyperemic surface is exposed, without any erosion. Patients are disturbed by feeling of burning, pains of lips, especially during mouth closing; therefore the mouth of these patients is often slightly opened. After treatment the exudative form of exfoliative cheilitis can turn into the dry form.
Differential diagnosis. The dry form should be differentiated from: - meteorological cheilitis - inflammation affects the whole surface of the red border - atopic cheilitis - the red border, underlying skin and mouth corners are affected - contact allergic cheilitis - allergic factors are noted in anamnesis Exudative form should be differentiated from: - exudative forms of actinic cheilitis - connection with the year season is noted, the whole red border is affected - eczematous cheilitis - polymorphism of precipitation (rash) exists, the face skin is also affected - erosive-ulcerative form of lupus erithematodes – presence of expressed erythema, hyperkeratosis, erosions and ulcers - pemphigus - after the crusts removal, erosion are formed, Nikolsky's symptom is positive - Manganotti’s cheilitis - limitation of the process, current, presence of erosions Treatment should be complex. The great value has psycho-emotional influence on organism by
tranquilizers (Seduxen, Fenazepam, Relanium). During the dry form smearing of lips by indifferent creams and hygienic lipsticks are recommended. During exudative form influence by Bukki’s border beams is effective. Crusts from the red border can be removed by 2 % solution of boric acid. For increase of organism resistibility Pyrogenal is applied. Reflex and psychotherapy are also very effective.
Glandular cheilitis Glandular cheilitis is a disease of lips; generally it affects the lower one. It develops from hyperplasia
and hyperfunction of small salivary glands, in the field of the red border of lips and Klein's zone. Primary and secondary glandular cheilitis are distinguished. Development of the primary is connected
with congenital anomaly of salivary glands. Secondary arises from various diseases of lips (lichen ruber planus, lupus erythematodes, leukoplakia, etc.).
Generally men of 50 years old and more are affected. Clinic. The lower lip is affected more often, than the upper one. Glandular cheilitis has a typical clinical
picture. In the field of the red border of lips expanded ducts of salivary glands are visible in the form of red points. From these points saliva drops are escaped – the symptom of "dew drops”. There is a dryness of the red border of lips, maceration, cracks and erosion because of frequent humidifying of the lip by saliva and evaporation of it. Sometimes around the expanded ducts of salivary glands hyperkeratosis is observed, in the form of thin rings (Puente-Asevedo’s form). Because of long current and constant irritation of the lips (with cracks and hyperkeratosis occurrence), development of precancer diseases is possible. In case of infection penetration into the expanded ducts of salivary glands, glandular cheilitis can turn into the purulent form. It is characterized by pains and edema of the lip, which is covered by thick crusts of yellowish-green or black color. Purulent exudates escapes from the ducts. Occurrence of abscesses is also possible.
Treatment. Anti-inflammatory (corticosteroid) ointments are applied (Prednisolone, Hydrocortisone). Electric coagulation or excision of hypertrophied salivary glands is recommended.
Contact allergic cheilitis

This disease develops from hypersensitivity of the red border of lips during contact with various chemical substances. Generally affects women of 20-60 years old.
Etiology. More often the reason of the disease is the lipstick, tooth-paste, plastic of artificial prosthesis. Clinic. Process is usually localized on the red border of lips, sometimes affects the skin a little.
Erythema occurs in the place of contact with allergen. On inflamed surface small vials appear, which are quickly opened, forming erosion, cracks. Patients complain on itch, burning, edema of the lips. Sometimes only limited erythema and a little peeling exist.
Differential diagnosis is done from: - exfoliative cheilitis - dry form of actinic cheilitis - atopic cheilitis Treatment. First of all it is necessary to eliminate the factors, which caused the disease. For local
treatment ointments with corticosteroids are used. Desensitizing preparations (Suprastin, Tavegil) are applied per os.
Actinic cheilitis Actinic cheilitis is an inflammatory disease of the lips, which develops as an allergic reaction of the slow
type from UV-beams. It affects men of 20-60 years old. This disease has seasonal current with exacerbations during spring-summer period. Dry and exudative forms of actinic cheilitis are distinguished. Some authors carry the dry form to precancer diseases.
Clinic. The dry form is expressed by dryness of the lower lip. Defeat affects the whole surface of the red border. It becomes bright red, is covered by small, dry silver-white scales. Occurrence of hematomas, erosions is possible. Sometimes areas of hyperkeratosis are formed.
During exudative form on edematic hyperemic surfaces of the red border of the lips bright red erythemas, small vials, erosions, crusts are formed. Patients are disturbed by itch, burning, pains of the lips. In case of long existence of actinic cheilitis, its malignization is possible.
Differential diagnosis. The dry form is differentiated from: - dry form of exfoliative cheilitis - lupus erythematodes Exudative form is differentiated from: - contact allergic cheilitis - atopic cheilitis Treatment. It is necessary to avoid insolation. Nicotinic acid, vitamins B, sometimes in combination
with anti-malarial preparations (chloroquine) and small doses of corticosteroids (prednisilone) are applied. Locally ointments with corticosteroids are used.
Meteorological cheilitis Meteorological cheilitis is an inflammatory disease of lips of not allergic nature. The reasons of this
disease are different meteorological factors (wind, cold, high or low dampness). The current of this cheilitis is chronic, and does not depend on the season.
Clinic. The whole red border of the lips (usually lower) is affected. It is slightly hyperemic and infiltrated, dry, and is often covered by small scales. Patients are disturbed by dryness of lips, feeling of tightening, peeling. Occurrence of erosion and cracks is possible. The skin and the mucous membrane are not involved into the process.
Differential diagnosis is spent from: - dry form of actinic cheilitis - allergic contact cheilitis - dry form of exfoliative cheilitis Treatment is the same as for actinic cheilitis. It is necessary to apply neutral and hygienic lipsticks.

Atopic cheilitis
Atopic cheilitis is one of symptoms of atopic dermatitis or neurodermatitis, i.e. concerns to symptomatic cheilitis.
The disease more often affects children from 7 till 17 years old. In etiology an important role belongs to genetic factors which create predisposition to so-called atopic
allergies. Medicines, foodstuff, flower and household dust, microorganisms can be allergens. Clinical display is promoted by disorders of central and vegetative nervous systems.
Clinic. The red border of lips and contacting skin are amazed. The affection is more intensive in the area of the corners of the mouth. Process never passes to the oral cavity mucous membrane. The red border of lips is infiltrated, and is covered by small scales. During time radial cracks and furrows are formed on the red border. Changes of the lips are often combined with dryness and peeling of face skin. Patients are disturbed by itch and burning.
Pathohistologically parakeratosis, akantosis, lymphocyte and histiocyte infiltrations are observed. Atopic cheilitis proceeds long. Exacerbations mainly arise during the fall-winter period. Remissions
usually happen in the summer. After puberty in some cases self-treatment is observed. Differential diagnosis is done from: - actinic cheilitis - allergy to UV-beams is noted in anamnesis - exfoliative cheilitis - lip is amazed only in Klein's zone - allergic cheilitis - presence of contact to allergen - streptococcal angular stomatitis- mouth corners are amazed only - fungal angular stomatitis - mouth corners are amazed only, fungi like Candida are found out Treatment. Desensitizing preparations, corticosteroids, anti-histamine preparations (Erius, Tavegil,
Claritin) are applied.
Eczematous cheilitis
Eczematous cheilitis is a symptom of general eczematous process, in which basis is the neural-allergic inflammation of outer layers of the skin. External and internal irritants promote the disease occurrence. Various factors can be the allergens: microorganisms, food, medicines, materials for prosthesis, filling materials etc.
Pathohistologically spongiosis is observed. Clinic. Eczematous cheilitis can be acute, sub-acute or chronic. Affection of the red border of lips can be
isolated or combined with affection of the face skin. Acute stage of the disease is characterized by polymorphism: at the beginning there is hyperemia, then
vials, crusts, weeping, and scales. Process is accompanied by edema of lips. The affection elements arise not simultaneously, but consistently replace each other. Patients are disturbed by itch and burning, mouth opening is complicated.
Chronic form of the disease is characterized by reduction of the inflammation. The red border of lips is condensed, because of inflammatory infiltration, small nodules and scales appear. All described clinical symptoms of eczematous cheilitisа develop on not changed lips. Sometimes long existing bacterial angular stomatitis precede to the occurrence of this cheilitis. In these cases the developing eczema is considered as a bacterial sensitization of the red border of lips or skin. Its feature is the expressed eczematous reaction near to the bacterial centre - hyperemia, edema, occurrence of small vials, which quickly shrink, forming yellow crusts.
Differential diagnosis is done from: - atopic cheilitis - affects children, mouth corners are amazed - allergic contact cheilitis - absence of polymorphism of elements, presence of allergy - exudative forms of actinic cheilitis - seasonal prevalence of the disease is characteristic Treatment. Desensitizing and sedative preparations are used. Locally ointments and aerosols with
corticosteroids are applied.
Plasmocellular cheilitis

Plasmocellular cheilitis is a limited chronic inflammatory process which mainly arises in the area of natural apertures and is accompanied by massive plasmocellular infiltration.
In etiology and pathogenesis of the disease a big role have the chronic inflammation of lips, including microtraumas, influence of solar beams.
Clinic. Often the lower lip is involved into the process. It becomes hyperemic, "varnished". Sometimes erosions and petechias can be formed on this surface. In other cases, some areas of the red border become covered by brown crusts. Painful erosions and soft tumor-like formations are found out on the crusts.
Pathohistologically akantosis, hyperkeratosis, spongiosis are observed. The skin is edematic, dense plasmocellular infiltration is present. There is a probability of malignization.
Treatment. Surgical excision of the affected area is done.
Macrocheilitis
Macrocheilitis is the leading symptom of Melkerson-Rozental’s syndrome. In etiology of this disease an important role have constitutional and hereditary features of the person.
Some authors consider Melkerson-Rozental’s syndrome as angioneurosis. There is also an infectious-allergic theory of the disease occurrence.
Clinic. Melkerson-Rozental’s syndrome is characterized by 3 symptoms: macrocheilitis, folded tongue and paralysis of facial nerve. The disease begins suddenly. As a rule, the first symptom is the edema of one or both lips. Patients mark an itch and increase of the lips. The color of the lip is not changed, but sometimes it gets a cyanotic shade. The lip edge is often turned out and is away from the teeth a little (“a muzzle of a tapir”). Sometimes the lips become thicker in 3-4 times. Such edemas exist constantly, accruing and weakening. The edema is localized more often on lips, cheeks, eyelids, etc. The 2nd symptom is the paralysis of the facial nerve. It consists in unilateral vasomotor rhinopatia, unpleasant sensations in the oral cavity, and changes of saliva excretion. There is an omission of the mouth corner of the amazed half, expansion of the eye crack. The 3rd symptom is the folded tongue (at 60 % of patients). The edema of the tongue, leading to its non-uniform increase, is clinically marked. The combination of all 3 symptoms is not always observed.
Clinical current of Melkerson-Rozental’s syndrome is chronic. At the beginning of the disease relapses arise seldom, but at a long current of macrocheilitis and paralysis of the facial nerve they become stable.
Differential diagnosis is done from: - Kvinke’s edema - erysipelatous inflammation - lymphangioma - hemangioma
Treatment. Corticosteroids (Prednisolone, dexamethasone) in combination with antibiotics of wide spectrum (Oletetrin) and anti-malarial preparations (Delagil) are used. Anti-histamine preparations, vitamin C and B are also applied. Treatment course lasts 30-40 days.
Treatment of stable forms of the disease, in remission is spent by pyrogenic preparations (Pyrogenal, Prodigiosan). For treatment of macrocheilitis electrophoresis by heparin and dimexide is applied on affected edematic area. In case of the absence of the effect from conservative treatment, surgical methods are applied - a part of lip tissue is excised. However it does not prevent the disease relapses.
The specified courses of treatment should be repeated in 2-3 months.
Chronic cracks of the lips
In the etiology a big role have individual features of the anatomic structure of lips (deep middle fold) and
chronic traumas. Weather conditions are also important, which can be the reason of dryness, loss of elasticity of lips and occurrence of cracks on them. The bacterial flora brakes the process of healing of cracks. Avitaminosises A and B also matter in the occurrence of the disease.
Clinic. On the red border of a lip one linear deep, painful crack appears, which never passes to the skin. The chronic crack epythelizates at night and in the morning, because of lip movements, it again reveals and sometimes bleeds.
Treatment. Removal of the etiological factor should be done. Locally antibiotics, corticosteroids, keratoplastics, vitamins are applied.


Candidiasis
Candidiasis (candidosis) – is disease which causes yeast fungus of sort Candida. On oral mucous membrane and integuments live various kinds of yeast fungus in the form of saprophytes. Pathological changes more often cause Candida albicans, Candida tropicalis, Candida krusei. Localization of fungus Candida in oral cavity is various: various parts of mucosa, carious cavities, root channels. The fungus "loves" acidic environment (pH 5,8-6,5) and develops numerous enzymes, proteolytic, lipids and carbohydrates. Aetiology and pathogenesis. Implication of pathogenic properties of fungus of sort Candida depends mainly on macroorganizm condition. The leading role to develop of candidiasis is played weakening of immune system.
Candidiasis development can be promoted by serious accompanying diseases: malignant neoplasms, HIV-infection, tuberculosis, endocrinopathies, diseases of gastrointestinal tract. Development of candidiasis is promoted by long treatment by corticosteroids, cytostatics, antibiotics. At long reception of antibiotics the structure of resident microflora of oral cavity therefore the dysbacteriosis is formed is broken. There is an oppression of resident microflora of oral cavity and sharp growth virulence is conditional-pathogenic fungus Candida causing disease of oral cavity mucosa . Long reception of corticosteroids also leads to oppression of organism resistance , breaks an exchange of carbohydrates and frames favorable conditions for candidiasis occurrence. The candidiasis can arise owing to radial influences, the use of alcohol and narcotics. In rare instances an infection source the sick person can be. The leading role to develop of candidiasis is played the condition of oral cavity mucosa and its immunity. Candidiasis occurrence is promoted by chronic trauma of oral mucosa with teeth acute edges , poor-quality prostheses. The candidiasis of oral mucosa meets at newborn child and older persons is more often. Allocate some clinical forms of candidiasis (classification of Shecklacov):
- A superficial candidiasis of mucosa, skin and fingernails - A chronic generalized candidiasis of children - A visceral (systemic) candidiasis
Clinical picture. On clinical current distinguish acute and chronic forms. The acute candidiasis can proceed in the form of milkwoman (oral moniliasis, thrush) or an acute atrophic candidiasis. The chronic candidiasis also exists in two clinical forms: the chronic hyperplastic and chronic atrophic. They can develop as independent forms, or to be transformed one to another.
Acute pseudomembranous candidiasis, or the milkwoman (oral moniliasis, thrush ) - one of most often meeting forms of candidiasis. At newborn child the milkwoman(oral moniliasis, thrush) is observed often and proceeds rather easily. The mucosa of tongue back, cheeks, the sky, labiums is amazed more often. It is hyperemic and dry. Against hyperemia there is the white scurf reminding curtailed milk or cottage cheese, towering over mucosa level. Scurf consists of the epithelial cells subject to desquamation, the rests of nutrition and mycelium. In the beginning of disease he is easily taken out at scraping by spatula, under which it is found out smooth, slightly hydropic, hyperemic surface. Then the scurf becomes more dense and removes hardly, baring an erosive surface of oral mucosa.
Patients complain on burning sensation in a mouth, pain at eating, especially acute. Acute pseudomembranous glossitis differentiate from desquamative glossitis at which on tongue back there are sites
of desquamation of epithelium, migrating on tongue back and surrounded with crown of an exfoliated epithelium. Acute candidosis stomatitis differentiate from leukoplakia and lishen rubber planus. At the last whitish membrane and
nodules on mucosa surface are formed owing to hyperkeratosis and consequently are not taken out at scraping. The definitive diagnosis put on the basis of data of bacterioscopic research.
The acute atrophic candidiasis is characterized by appreciable morbidity, burning sensation, dryness in oral cavity. The mucosa is bright-red and dry. At tongue back lesion becomes pink-red color, dry, shining, thread like papillas are undergo atrophy. Scurf is absent or remains in deep cords, is taken out hardly. Acute atrophic candidiasis differentiate from allergic reaction to plastic of demountable prostheses. The important role is played in this case by clinical observation over dynamics of change of mucosa after elimination prosthesis and carrying out of bacterioscopic research.
The general condition sick of an acute candidiasis does not suffer. The chronic hyperplastic candidiasis is characterized by formation on hyperemic oral mucosa thick layer of scurf densely soldered to it in the form of nodules or plaques. Scurf usually settles down on tongue back , in the sky. In tongue the area typical for rhomboidal glossitis is more often amazed. The chronic hyperplastic candidiasis in the sky looks like papillar hyperplasia. In cases of long, persistently proceeding disease scurf becomes impregnated with fibrin, the yellow-grey membrane densely soldered to the subject mucosa are formed. At scraping scurf is taken out hardly, under it the bleeding erosive surface is bared hyperemic. Patients complain of dryness in a mouth, of burning sensation, and in the presence of erosions - on morbidity. This form should be differentiated from leukoplakia and lishen rubber planus.

The chronic atrophic candidiasis is shown by dryness in oral cavity, burning sensation, morbidity at using of demountable prosthesis. The site of mucosa corresponding to borders of prosthetic location, hyperemic, hydropic, painful, under prosthesis erosions, papillomatosis are observed.
At candidosis atrophic glossitis tongue back of pink-red color, dry, shining, thread like papillas are undergo atrophic. White-grey scurf is available in small amount only in deep cords, is taken out hardly. Under a microscope in scurf find out disputes and mycelium fungus of sort Candida. For an atrophic candidosis stomatitis the triad - an inflammation of the palat, tongue and mouth angles is very characteristic.
Differential diagnosis is spend with the lishen rubber planus, the allergic stomatitis caused by action of acrylic plastic, various forms of medicamental stomatitis, syphilitic papules. The mycotic (yeast) perleche is observed mainly at persons of advanced age with the underestimated height of an occlusion owing to the expressed deleting of teeth hard tissues or an adentia. Presence of deep cords in angles of a mouth and a constant maceration of these sites of skin a saliva is framed by favorable conditions for occurrence of candidosis perleche. Patients complain on burning sensation, morbidity in mouth angles where there are easily taken out grey transparent flakes, gentle crusts or scurf. After excision of these elements dry and weak-becoming wet erosions or cracks are bared. Process can pass to mucosa of red border of labiums, the candidosis cheilitis as a result develops. It is characterized by hyperemia, puffiness, presence of grayish color of flakes and the fine cross-section located cracks.
Differentiate from a streptococcal perleche for which the plentiful exudation is characteristic, erosion is covered by copper(Cu)-yellow crusts. Differentiate also from hard ulcer and syphilitic papules in the angles of mouth having inspissation in the basis.
The definitive diagnosis put on the basis of results of microscopic research smear from lesion site, and also a Wassermann reaction. Diagnostics. At statement of the diagnosis of candidiasis are based on typical complaints of patients, a clinical picture and datas of laboratory. Carry out microscopic research of scraped materials from oral mucosa surface and demountable prostheses. For research it is desirable to take a material in the morning on an empty stomach, before cleaning of teeth. In norm fungus of sort Candida are found out in the form of individual yeast-like cells in diameter 2-5 microns. At candidiasis tap clump of budding both not budding cells and thin branched threads pseudomicel. Treatment. For successful treatment sick of candidiasis careful inspection and treatment of accompanying diseases are important.
The general treatment - antimicotic preparations prescribe inside nystatin or levorinum. The daily dose should be not less than 4.000.000 UNITS of the tablet it is recommended to crush and, having put under tongue to suck, since they are badly soaked up in gastrointestinal tract.
The good antimicotic effect is observed at Dekaminum suction in shape caramel: on 1-2 caramel 6-8 times a day. The expressed antimicotic action renders Diflucan. It prescribe in capsules on 50-100 mg of 1 times a day. Amphoglucamin prescribe inside on 200 000 units 2 times a day after meal and local in the form of ointment.
For dryness reduction in oral cavities and influences on fungoid flora prescribe 2-3 % solution of Iodidum of potassium on 1 item of l. In 2-3 times a day after meal. Being allocated through the skin, a mucosa and mucous glands, iodine shows the fungistatic properties and stimulates sialosis.
Inside prescribe group vitamins In, РР, With. Local treatment. To applications and greasing of oral mucosa apply 0,5 % decamin ointment, Amphotericinum In (30 000 units/g), 1 % ointment and 1 % Clotrimazolum solution. A mucosa and a red border of labiums process solutions of aniline stains, first of all the violet. Agents, alkalizing in an oral cavity - rinsing 2-5 % a solution burs, 2 % r-rum of hydrocarbonate of sodium, 2 % Acidum boricum r-rum are effective medium. At yeast perleche and cheilitis Unguentum Nystatini, 5 % levorin ointment, 0,5 % decamin ointment, Clotrimazolum is effective.
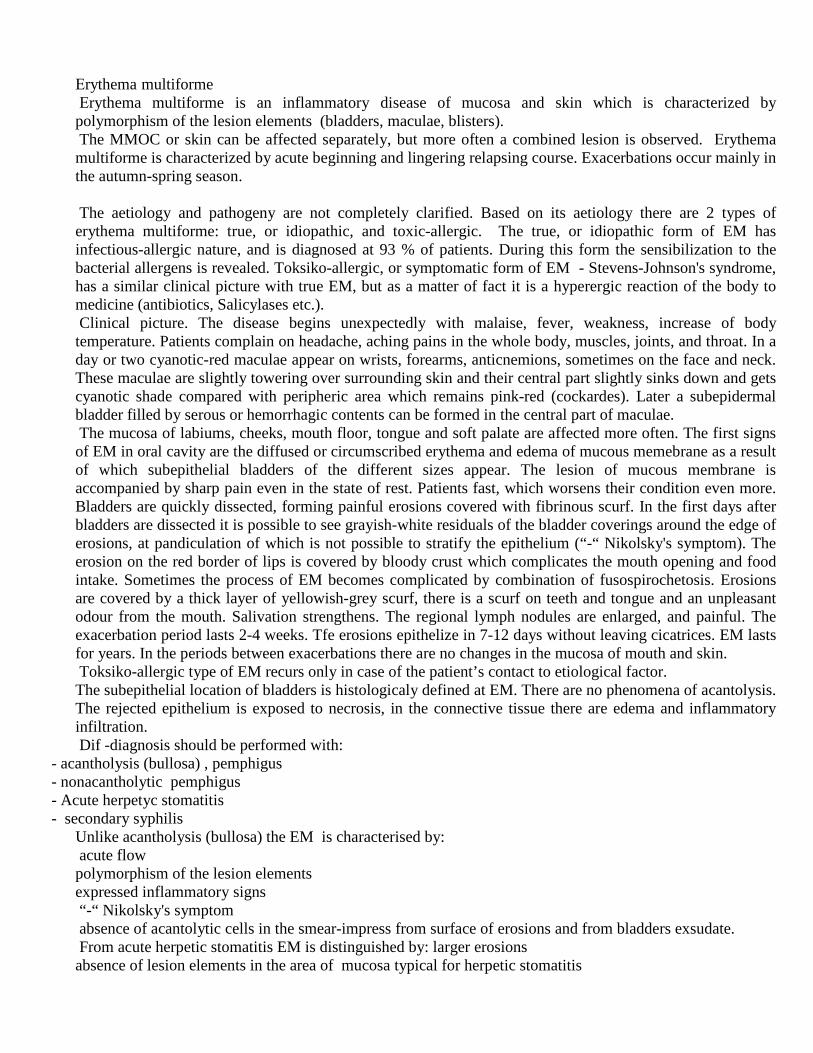
Еrythema multiforme Еrythema multiforme is an inflammatory disease of mucosa and skin which is characterized by polymorphism of the lesion elements (bladders, maculae, blisters). The MMOC or skin can be affected separately, but more often a combined lesion is observed. Еrythema multiforme is characterized by acute beginning and lingering relapsing course. Exacerbations occur mainly in the autumn-spring season. The aetiology and pathogeny are not completely clarified. Based on its aetiology there are 2 types of erythema multiforme: true, or idiopathic, and toxic-allergic. The true, or idiopathic form of EM has infectious-allergic nature, and is diagnosed at 93 % of patients. During this form the sensibilization to the bacterial allergens is revealed. Toksiko-allergic, or symptomatic form of EM - Stevens-Johnson's syndrome, has a similar clinical picture with true EM, but as a matter of fact it is a hyperergic reaction of the body to medicine (antibiotics, Salicylases etc.). Clinical picture. The disease begins unexpectedly with malaise, fever, weakness, increase of body temperature. Patients complain on headache, aching pains in the whole body, muscles, joints, and throat. In a day or two cyanotic-red maculae appear on wrists, forearms, anticnemions, sometimes on the face and neck. These maculae are slightly towering over surrounding skin and their central part slightly sinks down and gets cyanotic shade compared with peripheric area which remains pink-red (cockardes). Later a subepidermal bladder filled by serous or hemorrhagic contents can be formed in the central part of maculae. The mucosa of labiums, cheeks, mouth floor, tongue and soft palate are affected more often. The first signs of EM in oral cavity are the diffused or circumscribed erythema and edema of mucous memebrane as a result of which subepithelial bladders of the different sizes appear. The lesion of mucous membrane is accompanied by sharp pain even in the state of rest. Patients fast, which worsens their condition even more. Bladders are quickly dissected, forming painful erosions covered with fibrinous scurf. In the first days after bladders are dissected it is possible to see grayish-white residuals of the bladder coverings around the edge of erosions, at pandiculation of which is not possible to stratify the epithelium (“-“ Nikolsky's symptom). The erosion on the red border of lips is covered by bloody crust which complicates the mouth opening and food intake. Sometimes the process of EM becomes complicated by combination of fusospirochetosis. Erosions are covered by a thick layer of yellowish-grey scurf, there is a scurf on teeth and tongue and an unpleasant odour from the mouth. Salivation strengthens. The regional lymph nodules are enlarged, and painful. The exacerbation period lasts 2-4 weeks. Tfe erosions epithelize in 7-12 days without leaving cicatrices. EM lasts for years. In the periods between exacerbations there are no changes in the mucosa of mouth and skin. Toksiko-allergic type of EM recurs only in case of the patient’s contact to etiological factor. The subepithelial location of bladders is histologicaly defined at EM. There are no phenomena of acantolysis. The rejected epithelium is exposed to necrosis, in the connective tissue there are edema and inflammatory infiltration. Dif -diagnosis should be performed with:
- acantholysis (bullosa) , pemphigus - nonacantholytic pemphigus - Acute herpetyc stomatitis - secondary syphilis
Unlike acantholysis (bullosa) the EM is characterised by: acute flow polymorphism of the lesion elements expressed inflammatory signs “-“ Nikolsky's symptom absence of acantolytic cells in the smear-impress from surface of erosions and from bladders exsudate. From acute herpetic stomatitis EM is distinguished by: larger erosions absence of lesion elements in the area of mucosa typical for herpetic stomatitis

absence of multinuclear cells of herpes in the scraping from surface of erosions. The EM differs from nonacantholytic pemphiguses by: acute course expression of inflammatory reaction of mucosa, seasonal relapsing character of the course absence of disease signs in between relapsing periods. Light course of EM can have resemblance with errosiend papules at a secondary syphilis in the base of which there is always an infiltration. Hyperemia around syphilitic papules in the form of narrow border, is sharply delimited from healthy mucosa. At multiform exudative erythema a hyperemia is extensive, poured. In scrapings from a surface of syphilitic papules treponema palladium are found. Treatment. The general treatment includes prescription of desensitizing medications: Dimedrol, Tavegilum, Klaritinum etc. To provide antiinflammatory therapy salicylases (Acidum acetylsalicylicum), calcium containing medications (calcium gluconat, calcium Glycerophosphatum) are used. For the same purpose intravenously Sodium thiosulfatum is prescribed. It is necessary to prescribe vitamins of B group (В1, В2, В6). The general treatment of patients with serious flow of EM should be performed within hospital premises where patients are prescribed complex therapy - detoxing, desensitizing, antiinflammatory. In this case corticosteroids - Prednisolonum and dexamethasone are usually used. Reopolyglucin, Haemodesum, Sodium thiosulfatum are injected intravenously. In case of toksiko-allergic form of EM it is necessary to find out the causal medication-allergen and to stop its reception. Local treatment is directed to liquidation of the inflammation, puffiness and acceleration of cuticularization of the affected mucosa. Before medicamental processing the mucosa needs to be anaesthetised with 1-2% solutions of Trimecainum, Lidocaine. Antiseptic processing of a mucosa of a mouth is carried out by 0,25-0,5 % solution of peroxide of hydrogen, 0,25 % solution of Chloraminum, 0,02 % solution of Chlorhexidine. In case of necrotic scurf on the surface of erosions it is effective to apply proteolytic enzymes (Trypsinum, chimotripsinum, lizoamidazа). Then in order to acceleration the cuticularization keratoplasties (carotolinum, a dogrose and sea-buckthorn oil, solkoserilum) are used. The life forecast in case of EM is congenial and in case of Stevens-Johnson's syndrome it is rather serious.

Glossitis Independent glossitis develop only on a tongue, do not affect other parts of OMM. Acute catarrhal inflammation of tongue is the limited inflammation of a tongue mucous membrane.
An becoming principal cause is a penetration of coccal infections through damaged epithelium into the deeper layers. The damage reasons of epithelium can be sharp edges of a teeth, poor-quality metal artificial limbs, unsatisfactory hygiene of an oral cavity.
Disease begins with pain appearance in a tongue which is increased at conversation and food intake. A tongue surface is hyperemic and edemic, prints of a teeth on each side are visible, the back of tongue is covered with a scurf. Tongue is increased in size and is condensed. Especially increase fungiform papillae which are marked out on the background of a furred tongue. It is observed hypersalivation.
Treatment. Elimination of the causal factor, rinsing by warm solutions of antiseptics, decoction of medicinal herbage (a camomile, an oak bark, a yarrow) 6-8 times a day.
The tongue abscess can develop us a result of a tongue trauma or us a complication of an acute glossitis. There are superficial abscesses which is located directly under a mucous membrane, and deep ones which are formed in thickness of a tongue muscular layer.
At examination the tongue hypostasis, local hyperemia of the mucous membrane in the center of inflammation is found out. The palpation is painful, the tongue is condensed, mobility is limited, function is complicated.
At deep abscesses the general condition of patients suffers, the body temperature is raised, in blood is observed leukocytosis, ESR(erythrocyte sedimentation rate) is raised. The tongue is swelled, increased in sizes, the hypostasis passes to area of a pharyngeal aperture, is caused a dyspnea and an asphyxia. The regional lymphatic nodes are increased in size, are painful.
Surgical treatment is abscess opening, drainage, washings with antiseptics. Folded tongue is a congenital anomaly of the form and the sizes of tongue. For this anomaly presence
of deep folds on surface of the tongue, which is located symmetrically in a longitudinal and cross-section direction is characteristic. The deepest longitudinal fold usually located on a middle line of the tongue. Cross-section folds less deep and usually directed to the longitudinal fold, which unites them in uniform system. Papillae of the tongue are well expressed, are sometimes hypertrophied. It is in most cases observed moderated macroglosia and a thickening of the tongue.
Folded tongue can be one of symptoms of Melkerson-Rozental syndrome. Besides in 30-50 % of cases it is combined with desquamative glossitis, also it is marked at diseases of Down. Complaints, as a rule, are absent. At bad care of an oral cavity, decreasing of salivation, the remains of food,the microflora can cause an inflammation and complaints to a burning pain. Presence of deep folds favour to vegetation of fungoid flora.
Treatment. Local treatment is not required. Observance of an oral cavity hygiene and timely sanitation are necessary.
Desquamative glossitis (“geographical tongue”) often meets at diseases of a gastrointestinal tract , vegetative, endocrine disorders, rheumatic diseases. Assume that in appearance of this glossitis the specified role play a virus infection, hereditary factors.
Clinic. Process begins with appearance of an epithelium whitish-grey dimness area in a diameter of some mm. Then this site is bulged and in its centre the filiform papillae is desquamated, with opening of an bright-pink or red areas of the roundish form. The areas of desquamation is quickly increases, but intensity of desquamation decreases. In the area of desquamation are well visible fungiform papillae as a form of bright red points. When the centre reaches the considerable sizes, the border is blurred and in the centre starts to be restored normal cornification of the filiform papillae, in area of cornification, on the contrary, starts desquamation.
At the majority of patients this changes occur without subjective sensations. Only some patients complain of burning pain , pricking, paresthesia, pains from irritating food.
Diff. diagnosis spent with: - Lichen ruber planus - leukoplakoia - Plaques at a secondary syphilis

- hypovitaminosis В2, В6, В12 - Allergic stomatitis - candidiasis Treatment in case of complaints absence do not spend. In the presence of burning feeling, pains
antiseptic rinsings, irrigation and oral bath with solution of zithreal, applications with anaesthesine and oil solution of vitamin E, keratoplastic agents is done. Good results are given by treatment with calcium pantotenate. Revealing and treatment of accompanying diseases, timely sanitation and observance of an oral cavity hygiene are obligatory. However till now there are no full elimination of the disease.
Black ("hairy") tongue - the disease characterized by cornification and hyperplasia of the filliform papillae.
Aetiology Allocate three groups of the factors promoting occurrence of this diseases 1) physical and chemical influence (tobacco, alcohol); 2) infringement of a tongue ephitelium trophism, 3) action of the microbic factor.
Clinical picture. Complaints can not be. More often patients the unusual kind of tongue, sometimes sensation of an alien body on it an emetic reflex at conversation, an itch on the hard palate, decrease of gustatory sensitivity disturb. On a tongue back, in its back third, filiform papilae are extended, became thicken and get color from light brown to the black. Their length sometimes reaches 2 sm, and diameter to 2mm, outwardly the papillae remind hair. A characteristic sign of black tongue is its coloring which is caused by activityof chromogen bacteria.
Diff.Diagnosis is necessary to distinguish from so-called false black tongue. Deterioration of an oral cavity hygiene, an exacerbation of gastrointestinal diseases, coloring by foodstuff, using of medical products can be the reason of such pigmentation. Thus is absent expressed hyperplasia of filiform papillae, all back of tongue is painted and after cancellation of medicaments occur a normalization of color within several days. It is necessary to differentiate from "hairy" Leukoplakia at a HIV-infection, which differs from localization (lateral surfaces of language), and also more dense and diffuse lesion elements. Differentiate also from tongue changes at pipigmentopapilliar dystrophies, Adison diseases
Treatment. Spend oral cavity sanitation. For local treatment is recommended to use keratolotic - lubricating with 3-5 % solution of resorcin, 5-10 % solution of salicylic spirit the back of tongue. Injections under the lesion centre with solution of calcium chloride with novocaine 2 times a week (a course of 3-5 injections) is used. Forbid to smoke and to accept irritating food. At expressed hyperplasia of papillae is possible to remove with the cryodestruction .
Rhomboid glossitis - chronic inflammatory tongue disease with characteristic kind and localization. Aetiology. The majority of researchers assume, that rhomboid glossitis is the congenital disease
which development is caused by infringements of an embryogenesis processes. Other authors specify in a role of the microbic factor as in the lesion centre conditionally pathogenic microflora (Candida and Actinomyces) prevails. Disease meets mainly at the men smoking and abusing alcohol.
Clinical picture. Disease is shown by the rhomboid the oval form flatten or raised over the level of a mucous membrane lesions.There are slightly condensed at palpation, located strictly on an middle line anteriad from grooved papillae.
Allocate 3 forms of disease: flat (smooth), tubercular(tuberous),papillomatous (hyperplastic). At the flat form the lesion surface is smooth, polished, does not rise over surrounding mucous
membrane, pink or red color, papillae in the field of lesion are absent. The lesion parts is slightly condensed, painless.
At tubercular form the lesion consists from tubercules , separated from each other by accurately expressed folds. The surface is red with a cyanotic shade, is deprived of papillae.
At papiilomatous form the lesion foci represents the tuberous tumourous growths, rising over a surface of tongue, 3-5 sm in diameter.
At tubercular and pappiloumatous forms the surface of the lesion can become horny and get dairy white coloring.
All 3 clinical forms can proceed without subjective sensations. Complaints to burning, a roughness, and sometimes pain appear when the inflammation develops. Single instances of the rhomboid glossitis malignization are described.
Diff. diagnosis is spent with:

- desquamative glossitis - Avitaminosis - tongue tumors - A candidiasis Treatment. Spend oral cavity sanation, recommend to quit smoking. At founding ofa fungi Candida
carry out anticandidial treatment. At revealing of propensity to growth of tubercles and papillomatous forms is effective cryotherapy.

The changes of oral mucous membrane at diseases of nervous system Diseases of nervous system are more often shown in subjective unpleasant sensations in oral cavity and very rare cause
morphological changes of mucosa. The mouth and tongue mucosa is a zone in which it is form the strongest stream of afferentation in the central nervous system
(CNS). Thus many diseases of nervous system essentially influence on formation of afferentation stream and transformation the information from periphery to central nervous structures. Compensatory can arise changes of oral mucosa.
Stomalgia (glossalgia)
Stomalgia (glossalgia) or a glossodynia, tongue paresthesias, glossopirozis - the disease characterized by burning sensation,
pricking, more rare by pain of various sites of tongue without visible local changes. Less often similar sensation arises on lips, on the hard palate or on all oral mucosa. In such cases disease names stomalgia or paresthesias of mucosa of lips, oral cavitie, a syndrome of stomatic burning sensation.
Among patients with glossalgia prevail women after 40 years, men are ill in 5-6 times less often. Etiology and pathogenesis. Now there are bases to consider glossalgia as polyetiologic disease. In pathogenesis the leading
role belongs to pathology of vegetative nervous system which is supported by boring nervously-reflex chains at its various levels. These disturbances have often functional, rare organic character.
Glossalgia often develops against the diseases of gastro-enteric tract and liver, vascular lesions, diseases of central and peripheric nervous system, endocrine disturbances.
Some authors suppose that the reason of stomalgia is raised level of monomers in the acrylic bases of prostheses. More probable reasons can be mechanical boring with prostheses and parafunctional habits. The big number of chemical agents and medicinal preparations capable to cause pathological changes with oral localizations (enaloprol, captopril, izinopril) .
Clinical picture. Patients complain on constant or periodic burning sensation, smarting, tingling (prickling) in tongue, feeling of fatigue (tiredness) after conversation (talking), more rare on pain in tongue and paresthesia. At stomalgia similar sensations arise in other sites of oral mucous membrane . More than 30 % of patients complain on dryness in an oral cavity. Unpleasant sensations amplify (increased) after conversation, at excitement, in the evenings. It is characteristic, that during eating they disappear. They are localized on tip and lateral surfaces of tongue, more rare on back or on root of tongue. The site of these sensations has no exact borders, its localization can vary. Without treatment disease with various intensity lasts months - ten years, can disappear, even for long term, then come back, or, less often, disappear at all.
Many patients with stomalgia complain of taste disorder - dysgeusia, which has been detected at 68 % patients with stomalgia, especially from bitter foods. 95 % of patients with stomalgia note presence of anxiety and depressions. The women suffering with stomalgia, mainly in a period of menopause, feel a boring in the field of tongue and oral cavity mucosa.
At stomalgia (glossalgia) objective changes of mucosa are absent or are insignificant (puffiness, hypertrophy of separate papillas, varicose tongue phlebectasias).
The mental status of the majority of patients with glossalgia has the feature, which are testifying to latent or obvious (evident) mental depression.
Differential diagnostics. The glossalgia (stomalgia) is necessary to distinguish from -Organic diseases of tongue: the basic difference consists in absence at glossalgia objective changes in tongue. -pain as a result of trauma: the pain and burning sensation are constant and are localized always in the same place, with
elimination of the injuring factor the pain pass. -Neuralgia: differs from glossalgia sharp short-term attacks of a pain which almost always have unilateral character and are
localized in a zone corresponding to an innervations of a certain branch of trigeminal or glossopharyngeal nerves. -Neuritis: for neuritis the localization of the pain strictly corresponding to affected nerve, and simultaneously sensitivity
abasement in this zone are characteristic. So, at neuritis of a lingual nerve the pain is unilateral and localized in frontal 2/3 part of tongue. In the same area partially or completely loose superficial sensitivity which is detected with numbness and paresthesia. Pains at neuritis increased at tongue movement, at eating.
-odontogenic pains. Treatment. It is necessary complex - medicamental therapy, physiotherapy, acupuncture, laser therapy, hyperbaric oxygenation and psychotherapy.
The first stage is stomatologic inspection for the purpose of revealing the local pathological changes which could cause or provoking factors of development burning sensation syndrome of oral cavity. Full sanation of an oral cavity was spent if it is necessary. To patients with the diagnosed depression prescribe antidepressants - selective inhibitors of return capture of serotonin (prozac in a dose 20-40mg a day) and tricyclic antidepressant amitriptyline to 200mg a day.
To patients with effect of alarm (anxiety) prescribe tranquilizers of group benzidiazepinov-Phenazepamum in a dose of 0,25-0,5 mg 2-3 times a day.
For microcirculation improvement, especially at persons with vascular diseases and degenerate changes of cervical department of backbone (spinal column), are prescribed nicotinic acid (300-600 mg a day) and pentoxyfilin.
For reduction of xerostomia phenomena for stimulations function sialadens prescribe Pilocarpinum on 5 mg 1 time sublingual.

Taste disturbances Taste disturbances (dysgeusia) meets at facial nerve pathology, if the lesion centre is localized in the channel of facial nerve
falopiev channel. It is bound by that on the given piece of facial nerve near to it there passes cord of tympanum in which structure there are the gustatory conductors carrying the information from taste receptors of frontal 2/3 tongues in cortex of big hemispheres. In this case accordingly reveal unilateral abaissement of gustatory sensitivity on frontal 2/3 tongues.
Out of the channel facial gustatory fibers settle down as a part of lingual nerve, therefore at its lesion abaissement of gustatory sensitivity on lobbies 2/3 tongues, but in a combination to other symptoms also is observed. It is necessary to mark, that unilateral disturbance of gustatory sensitivity on posterior 1/3 tongues is caused by glossopharyngeal nerve lesion.
Full bilateral, more rare unilateral disturbance of gustatory sensitivity arises at organic lesions of the central nervous system (swelled brain, neurosyphilis).
Gustatory bulbs settle down mainly in a tongue mucosa, therefore the etiological factors amazing them causing disturbances of taste are: virus infections, allergic glosites, a radiation injury, traumas, avitaminoses A and B, Shegren syndrome, diseases of gastro-intestinal tract and etc. At the same time the desquamation of tongue threadlike papillas epithelium is diagnosed, in this connection gustatory papillas are accessible to an excessive irritation. In such cases gustatory sensitivity is restored in process of regeneration of threadlike papillas.
Acidic smack can arise at patients with the phenomena galvanism. A source of unpleasant taste in an oral cavity can be ulitis, parodontitis, periodontitis. Smack bitter, acidic can appear at hepatocholecystitis, at gastritis. Disorder of taste or its loss are possible at hysteria.
Treatment spends neuropathologist according to principles of therapy of these diseases and taking into account their etiology.
Salivation disturbance Salivation disturbance can be caused pathology of innervation of salivary glands, a lesion of salivary glands and oral
mucosa. Distinguish 2 kinds of disturbance of salivation: hypersalivation and hypoptyalism, with its extreme degree - xerostomia. Hypersalivation. The etiological factors causing hypersalivation is acute inflammatory processes of oral mucosa,
accompanied unconditioned reflex mechanism of augmentation of saliva allocation owing to sharp boring of mucosa that is protective reaction of an organism are. Sometimes the hypersalivation arises as consequence of an immediate boring of secretory cells of salivary glands salts of serious metals (mercury, lead, bismuth), iodine, etc.
Long hypersalivation observe at some organic illnesses of CNS-parkinsonizme, a bulbar and pseudobulbar paralysis, sometimes after the transferred stroke, etc.
At neurosis, obsessional conditions the false hypersalivation when patients complain of the plentiful allocation of saliva which are not proving to be true at objective inspection is possible.
Treatment in all cases should be referred on liquidation of the basic disease which has caused it status. Time depression of allocation of saliva can achieve application of preparations of atropine.
Hyposalivation the reason of hyposalivation are : an avitaminosis A, В1, В6, B 12, Е, a hyposiderosis, a diabetes, general diseases of a connecting tissue, radiation injuries, a chronic parotitis. Dryness of an oral cavity at patients with Shegren syndrome is most expressed.
At people with the broken nasal breath (polyps, a curvature of nasal septum), compelled constantly to breathe a mouth, dryness of an oral cavity is caused by the strengthened evaporation by the strengthened evaporation of a liquid from an oral cavity (a false hypoptyalism).
At a hypoptyalism, especially the xerostomias, sick complain of sensation of dryness of an oral cavity, difficulty at eating (especially acute and firm) and conversation, burning sensations, mucosa roughnesses. The hypoptyalism is often combined with dryness of other mucosas.
At objective inspection the mucosa is weakly wetted or dry, matte. It is not enough saliva, it foamy. At patients with a long hypoptyalism the quantity of a debris is enlarged, there is plural caries of a teeth, resistance of oral mucous membrane to action of traumatic factors decreases.
Treatment consists in determination and if it is possible elimination of the reason causing hypoptyalism. Oral cavity sanation, including prosthetics is obligatory. Localy recommend anti-inflammatory preparations and the agents raising resistance of a mucosa to action of stimuluses a lysozyme, Solutio oleosa of vitamins A, Е, etc.
As a rule, prescribe a vitamin therapy (Vit A, В1, В6, В12,), under indications - sexual hormones, iodine preparations inside. The good effect is given by galvanising of area of the big salivary glands. As symptomatic agents with success apply antixolonesteraze preparations, in particular 0,5 % Galantaminum solution on 1,0 ml subcutaneously, or its introduction by a method of an electrophoresis or inside daily within 1 month, 1 % solution of pilokarpinium hydrochloride on 4 drops 1-2 times a day.
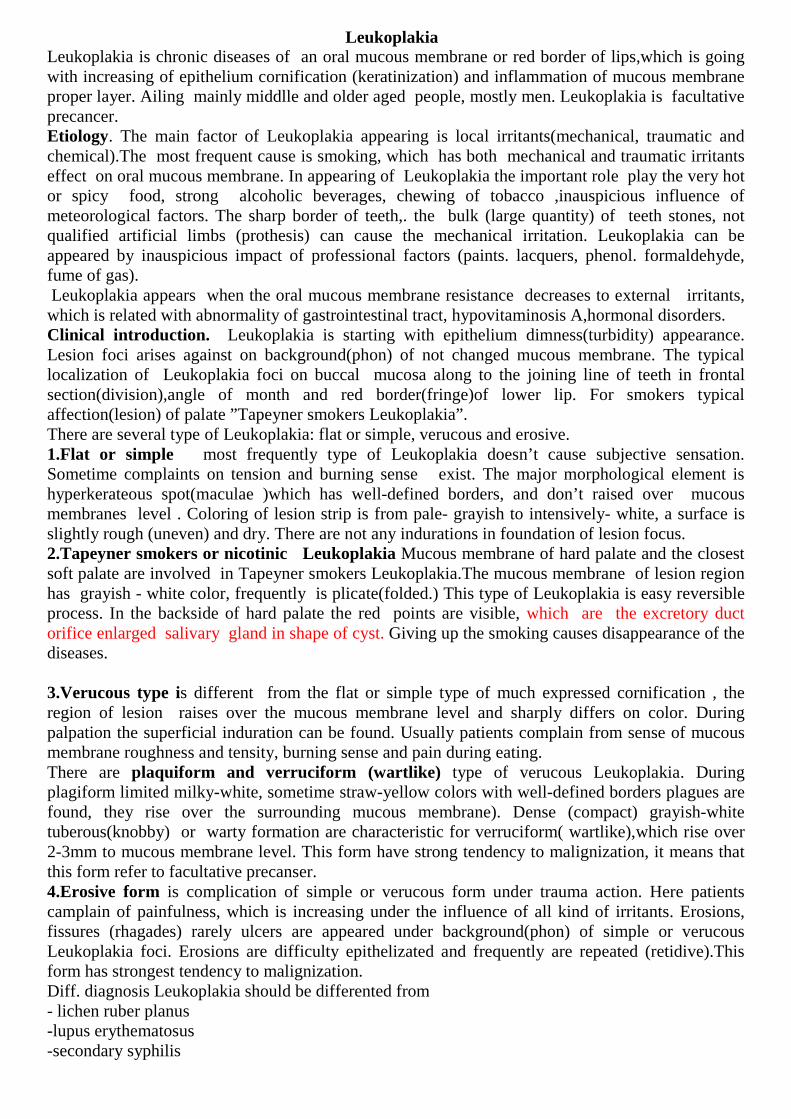
Leukoplakia Leukoplakia is chronic diseases of an oral mucous membrane or red border of lips,which is going with increasing of epithelium cornification (keratinization) and inflammation of mucous membrane proper layer. Ailing mainly middlle and older aged people, mostly men. Leukoplakia is facultative precancer. Etiology. The main factor of Leukoplakia appearing is local irritants(mechanical, traumatic and chemical).The most frequent cause is smoking, which has both mechanical and traumatic irritants effect on oral mucous membrane. In appearing of Leukoplakia the important role play the very hot or spicy food, strong alcoholic beverages, chewing of tobacco ,inauspicious influence of meteorological factors. The sharp border of teeth,. the bulk (large quantity) of teeth stones, not qualified artificial limbs (prothesis) can cause the mechanical irritation. Leukoplakia can be appeared by inauspicious impact of professional factors (paints. lacquers, phenol. formaldehyde, fume of gas). Leukoplakia appears when the oral mucous membrane resistance decreases to external irritants, which is related with abnormality of gastrointestinal tract, hypovitaminosis A,hormonal disorders. Clinical introduction. Leukoplakia is starting with epithelium dimness(turbidity) appearance. Lesion foci arises against on background(phon) of not changed mucous membrane. The typical localization of Leukoplakia foci on buccal mucosa along to the joining line of teeth in frontal section(division),angle of month and red border(fringe)of lower lip. For smokers typical affection(lesion) of palate ”Tapeyner smokers Leukoplakia”. There are several type of Leukoplakia: flat or simple, verucous and erosive. 1.Flat or simple most frequently type of Leukoplakia doesn’t cause subjective sensation. Sometime complaints on tension and burning sense exist. The major morphological element is hyperkerateous spot(maculae )which has well-defined borders, and don’t raised over mucous membranes level . Coloring of lesion strip is from pale- grayish to intensively- white, a surface is slightly rough (uneven) and dry. There are not any indurations in foundation of lesion focus. 2.Tapeyner smokers or nicotinic Leukoplakia Mucous membrane of hard palate and the closest soft palate are involved in Tapeyner smokers Leukoplakia.The mucous membrane of lesion region has grayish - white color, frequently is plicate(folded.) This type of Leukoplakia is easy reversible process. In the backside of hard palate the red points are visible, which are the excretory duct orifice enlarged salivary gland in shape of cyst. Giving up the smoking causes disappearance of the diseases. 3.Verucous type is different from the flat or simple type of much expressed cornification , the region of lesion raises over the mucous membrane level and sharply differs on color. During palpation the superficial induration can be found. Usually patients complain from sense of mucous membrane roughness and tensity, burning sense and pain during eating. There are plaquiform and verruciform (wartlike) type of verucous Leukoplakia. During plagiform limited milky-white, sometime straw-yellow colors with well-defined borders plagues are found, they rise over the surrounding mucous membrane). Dense (compact) grayish-white tuberous(knobby) or warty formation are characteristic for verruciform( wartlike),which rise over 2-3mm to mucous membrane level. This form have strong tendency to malignization, it means that this form refer to facultative precanser. 4.Erosive form is complication of simple or verucous form under trauma action. Here patients camplain of painfulness, which is increasing under the influence of all kind of irritants. Erosions, fissures (rhagades) rarely ulcers are appeared under background(phon) of simple or verucous Leukoplakia foci. Erosions are difficulty epithelizated and frequently are repeated (retidive).This form has strongest tendency to malignization. Diff. diagnosis Leukoplakia should be differented from - lichen ruber planus -lupus erythematosus -secondary syphilis

-chronic hyperplastic candidosis -Bouen diseases -soft Leukoplakia - cornificated epidermoid(planocellular) cancer Leukoplakia is different from lichen ruber planus of characteristical lesion elements. During Leukoplakia hyperkeratosis macules(spots) are charcterictical. During lichen ruber planus the multiple papulae are characteristical, which are mixed in the patterned drawing shape. During Leukoplakia there is not any inflammation and the skin covering never is involved in process, but during lichen ruber planus there are mucous membrane inflammation and the skin covering are involved in the process. Leukoplakia is different from lupus erythematosus with the absence of typical contours bright erythema , absence of atrophy and typical skin lesion. At Leukoplakia corneous mass isn’t removed during curage (abrasion), but grayish –white scurf covering syphilitic papules, is easily removed with opening the erosion. There are many Treponema pallidum on surface of erosion. The infiltration is characteristic for syphilitic papules and is not for Leukoplakia. As a rule the Vaserman reaction is positive at syphilis. In difference from Leukoplakia the whitish covering is easily removed during chronic hyperplastic candidosis, and there are many fungus Candida on the surface. In difference from Leukoplakia During Bouen diseases the grayish-white covering is easily removed and opens velvety stagnant-red color surface .There are inflammation reaction surround lesion foci. During soft Leukoplakia the grayish-white covering is removed during curage(abrasion), It is the consequence of parakeratosis. In difference from Leukoplakia cornificated epidermoid(planocellular) cancer has compaction in base .During cytological and histological examination is found atypical sells. Treatment There are several conservative methods of treatment for flat or simple Leukoplakia: General conservative methods are: - normalization of epithelium metabolic processes with using of Vit A per os(10 drops 3-4 time per day). -Giving up smoking ,stopping having hot or sharp food and strong alcoholic beverages Local conservative methods are: -elimination of local irritating factors -application with Vit A oil solution (3-4 time per day). - carrying out of oral cavity sanation by teeth sharp edges smoothening and efficient prosthetics. Conservative method of flat Leukoplakia lastes 6-8weeks. At first conservative treating of verucous and erosive Leukoplakia the same with the flat or simple one. In the presence of erosion and ulcer take part in treating of oral mucous membrane local stimulation (Vit A,E ,dogrose(rosehip) oil ,solcoseryl) and in the presence of pain sensations appoint the local anesthesia( lidocaine. trimecaine).The conservative method of erosive Leukoplakia lastes 2 weeks, at verucous Lekoplakia lasts 4 weeks. At successful conservative treating of verucous Leukolpakia it is passed in the flat form. If the erosion and ulcer does not epithelzaited during 2 weeks the surgical intervention and histological research should be done .The surgical intervention is done after unsuccessful conservative treating within 1 month at verucous Leukoplakia, and after unsuccessful conservative treating within 2 weeks at erosive Leukoplakia.

Lichen planus It is a relatively common chronic inflammatory disease of the oral mucosa and skin. 40-60 years old women are more commonly affected. Although the etiology is not well known, there are neurogen, viral, immune allergic, hereditary, intoxication theories of origination. Usually it starts in case of chronic diseases of gastrointestinal tract, diabetes, hypertonic disease, neurosis etc. Trauma (teeth sharp edges, incorrect prosthesis, galvanism etc) is important in exacerbation development of lichen planus. Clinical features: characteristic lesion of lichen planus is keratinized flat or polygonal papule in the diameter till 2mm. Skin manifestations of l. planus characterized by flat-topped, shiny pink or bluish-red papules. On oral mucosa papules are whitish-gray because of continuous maceration. Papules coalesce, forming a network of lines (lace –like, snow-flake). They rise above oral mucosa giving roughness. On dorsal and buccal surface of tongue the papules aggregate, usually forming hyperkeratotic plaques; in these areas papillae are flatten. Common placement of lichen planus is on the cheeks oral mucosa, dorsal and buccal surfaces of tongue; transitive cord is involved as well. Lips, gingiva, palate and mouth bottom are rarely affected (are the sites of predilection). Following forms of the disease are recognized on the oral mucosa: the common –typical (simple); the less common-exudative-hyperemic, erosive -ulcerative, and the rare –bullous, hyperkeratotic. Typical form: whitish mother-of-pearl papules are located separately or forming lace –like, patterned configuration, fern leaf on visibly unchanged oral mucosa. Complains are minimal, they are burning, roughness, dryness of oral mucosa. Commonly the current is symptomless. Exudative-hyperemic form: papules are located on hyperemic, swollen oral mucosa. Sensations are more expressed; burning, pain, increasing while eating spicy food, speaking. On the background of inflamed, hyperemic oral mucosa the picture loose vividness. Erosive -ulcerative form: the most severe type. This form can occur as a complication of typical or exudative-hyperemic forms in the result of erosion origination because of traumatic factors influence. In case of this form there are erosions, sometimes ulcers, which are surrounded by typical papules forming network of lines. The lesion elements are located on the hyperemic and swollen oral mucosa. Erosions and ulcers are covered with fibrin membrane, which removal causes bleeding. They can be in small number, small, slightly painful, though may be multiple, sharply painful. These erosions and ulcers will remain during months or years without epithelization. Sometimes an atrophy of oral mucosa is originated on the sites of long-term erosions and ulcers. In some cases they can turn into malignant lesions. Bullous form: is characterized by both whitish mother-of-pearl papules and bullae (with dense covering) in the diameter of 2-3 mm till 1-1,5 sm. Bullae are filled by serous or hemorrhagic exudate; soon rupture with erosions origination. Spontaneous resolution of the erosions is rather fast, that differ this type from previous one. Hyperkeratotic form: is characterized by different hyperkeratotic plaques rising over mucosal membrane. Plaques have sharp borders. Hearths of hyperkeratosis are surrounded by typical papules. The sites of predilection are cheek mucosa and dorsal surface of tongue. Lichen planus is chronic long-term illness. It can last decades with remissions and exacerbations. The oral lesions malignant transformation is common among elderly patients suffering from long-term erosive –ulcerative or hyperkeratotic types of l. planus. Pathohistologically there are hyper- and parakeratosis and akantosis. Differential diagnosis: -leukoplakia -candidiasis -LE -papullous syphilis -allergic stomatitis In case of leukoplakia (differ from l.planus) keratotic site slightly rises over oral mucosa and is continuous whitish plaque; surrounded mucosa is not changed; papules are absent. The sites of predilection are frontal parts of mouth, commonly mucosa of mouth angles and cheeks. In case of candidiasis oral lesions has not vivid picture; white plaque can be scraped partially or totally. During bacteriological examination Candida fungi are found out.

The lesions of LE (lupus erythematosus) are localized usually on the lips, cheeks, rare –on the palate. They are hyperemic, infiltrative; hyperkeratosis is only seen in the hearths of inflammation; atrophy is in the center of lesion. Papules are absent. Syphilitic papules differ by big sizes; surface is covered with grayish-white membrane, which is easily removed while scraping. Wassermann reaction is positive; treponema pallida is found out. Allergic stomatitis should be differentiated by means of anamnesis data and allergic tests. Treatment: Oral health care, elimination of traumatic factors should be carried out. Sedative drugs are prescribed during all types of the disease (valerian, tranquilizers). During typical and exudative-hyperemic forms: vit A for internal use, long-term usage of vit B, especially nicotinic acid. Vit A should be applied locally as well. Exudative-hyperemic and erosive –ulcerative forms: 1 ml of 1% nicotinic acid solution with 1% Novocain solution is injected in lesions hearths in a day, 15-20 appointments. Erosive –ulcerative and bullous forms: corticosteroids with antimalarial drugs (prednisolone or dexamethasone with delagil). If corticosteroids are contraindicated hyposensibilization should be done with histaglobuline during erosive –ulcerative form. Chonsuride, whish stimulates erosions and ulcers epithelization, has anti-inflammatory action, is used. Local treatment: in case of inflamed mucosal membrane, erosions, ulcers. Mouthwashes with solutions of chamomile, chloramine, sage; application of keratoplastics ( vit A, E, solkoseril); 0.25% lysozyme to increase resistance and regeneration of oral mucosa. Physiotherapy: laser, electrophoresis,cryodestruction.

Lupus Erythematosus Two main forms of the disease are recognized: discoid (DLE)- relatively benign clinical form and systemic (SLE) –with bad current. Both red border of the lips and oral mucosa are affected in case of these forms. Isolated affection of oral mucosa is not practically seen. Women are mostly suffer from this disease in the age of 20-40 years old. Etiology and pathogenesis: nowadays it is believed that this disease concerned to rheumatoid and autoimmune illnesses. Disease occurs as the result of organism sensibilization to infectious and non-infectious factors. Predisposal factors are: exposure to sun, cold (physical allergy) and chronic infection hearths. There are data about genetic predisposition. DLE, clinical features: Usually it starts with cutaneous lesions, commonly appear on the face (the nose, forehead, cheeks in the form of butterfly),ears, scalp, lips red borders. Lip lesions are characterized by erythema, hyperkeratosis and atrophy. Current is periodic. First (erythematous) stage is characterized by origination of small 1-2 slightly swollen, well-defined and gradually increasing in size maculae. They are reddish with teleangiectasia in the center. Lesions develop, fuse forming butterfly, which back is on the nose, and wings are on the cheeks. Macula origination can be accompanied by burning, stitching. During second stage (hyperkeratotic, infiltrative) lesions are infiltrated and originate dense discoid plaques. There are small grayish-white squamae tightly adhered to the plaques. Further plaque can be keratinized and surrounded by a border of hyperemia. Third stage (atrophic): plaque is characterized by central atrophic (cicatrical) white area; plaque is in the form of saucer. It has well-defined hyperkeratotic with multiple teleangiectasia. Plaque is tightly adhered to the underlying tissues and surrounded by a infiltration and hyper pigmentation. On oral mucosa the lesions are well-defined blue-reddish or whitish plaques with sunken rarely erosionated center. Patients complain of pain and burning sensations, increasing while eating and speaking. On the red borders of the lips 4 clinical forms are distinguished: typical, without expressed atrophy, erosive-ulcerated and deep. During typical form the oval deep red lesions with stable enlarged vessels and expressed infiltration are originated. On the surface of lesions tightly attached squamae are placed, which removal is painful and results in bleeding. Atrophy of red border and skin is seen in the center of lesion, which surrounded by dimness (discoloration) area of epithelium. Clinical form without expressed atrophy is characterized by diffusive hyperemia hyper- and parakeratotic squamae on red border. Squamae are exfoliated easier, than in case of typical form; hyperkeratosis is less expressed. In case of erosive-ulcerated type vividly expressed inflammation is seen; lesions are bright red, swollen, with erosions and fissure (rhagas), covered by blood purulent crusts. Lesions are surrounded by atrophy and hyperkeratosis in the form of squamae. Patients complain of acute pain, burning, itching. Atrophic cicatrices are stain after healing. In case of deep form of Kaposi- Urging the lesions are rarely occurred on the red border, are in the form of nodes with erythema and hyperkeratosis on its surface. Oral mucosa is rarely affected. Lesions are placed on oral mucosa of the lips, cheeks in the line of teeth closure, sometimes on tongue and palate. There are typical, exudative hyperemic, erosive-ulcerative types of LE. Typical form is characterized by hearths of hyperemia with infiltration and hyperkeratosis. Lesions are characterized by a central atrophy and peripheral hyperkeratosis in the form of whitish striae. In case of exudative hyperemic form atrophy and hyperkeratosis are slightly expressed because of acute inflammation. In the presence of traumatic factor this type is fast transformed into erosive-ulcerative type, which is characterized by lesions with painful central erosions or ulcers and peripheral irradiated whitish striae on the ground of erythema. After healing the cicatrical atrophy with treelike cicatrices and fibers is seen. Current is long-term, exacerbations are in spring and fall. Erosive-ulcerative type can be determined as facultative precancer.

Diagnostics: clinical examination, additional methods (histological, immune morphological, luminescence). During luminescence the lesions of red borders are snow blue or snow white (shiny), and lesions of oral mucosa have white or dimly white radiance in the form of spots and lines. Differential diagnostics:
- lichen planus - lupus tuberculosus - leukoplakia
In case of localization on red borders: -actinic cheilitis - abrasive precancerous cheilitis of Manganotti Treatment: quinoline drugs (plaquenol, plaquenil, delagil), corticosteroids in small doses, vitamins В2, В6, В12 , С, РР immune correctors (if immune status is abnormal) –decaris, T-activin. Local treatment: corticosteroid ointment (flucinar, lorinden), in case of erosive-ulcerative type- corticosteroid liniments with antibiotics and antimicrobial mediums (oksikort, lokakorten). SLE (acute), clinical features: SLE is an inflammatory connective tissue disease with variable features, frequently including fever, weakness and fatigability, joints pains, muscle pains, adynamia, inner organs affection. Blood picture is: leucopenia, anemia and ESR increase. Percentage of the patients with oral mucosa lesions is 60%. Oral mucosa lesions are hyperemic and swollen maculae, vesicles of different sizes with hemorrhagic exudate, vesicles rupture, leaving erosions covered by blood purulent membrane. Diagnosis: is based on found out skin lesions, condition of inner organs, and presence of “cells of red lupus” (LE-cells). Treatment is started in acute period: corticosteroids in big doses (60mg), further should be gradually decreased till 15mg during 6 months. Later the minimal individual dose should be prescribed (5-10mg). K drugs (panangin, KCl) are indicated to prevent mineral metabolic disturbances. After acute period elimination combine treatment by corticosteroids (small doses) and aminocholine (plaquenil, delagil) drugs are used.

Medicamental lesions (drug-induced) of oral mucosa The medicinal allergy (allergia medicamentosa), or a medicamental allergic
lesion of oral mucosa meets enough often. Any drug can be the reason of occurrence of a medicamental allergy practically;
however these are the antibiotics, sulfanilamide, analgesics, tranquilizers and iodine more often. Speed and degree of sensibilization depend on a way of drug introduction. If medicine is used in form of applications and inhalations the allergy is originated faster and more often. In case of intramuscular and hypodermic introduction the sensibilization is expressed less, than in case of intravenous injection. The peroral drug intake is least dangerous.
All four types of allergic reactions can participate in a pathogenesis of a medicinal allergy, but the leader always is one of them.
Diagnosis of medicamental allergy of oral mucosa is based on clinical and laboratory tests. At present there are various tests for medicinal allergy definition in vitro - test of basophiles degranulation, reaction of a sintering of leucocytes, etc.
During medicinal allergy medicamental stomatitis, cheilitis and glossitis are distinguished in an oral cavity depending on localization of pathological changes.
According to degree of expression of inflammatory reaction there are: a) Catarrhal and catarrhal-hemorrhagic stomatitis, cheilitis and glossitis b) Erosive stomatitis, cheilitis and glossitis c) Necrotizing ulcerative stomatitis, cheilitis and glossitis. Catarrhal and catarrhal-hemorrhagic stomatitis, cheilitis and glossitis It is the easiest form of a medicinal allergy. Clinical features: Patients complain of itching, burning sensation, dull pain while
eating hot and spicy food. During examination an oral mucosa is bright red, slightly swollen, disturbance of integrity of an epithelium is not present. Sometimes there are hemorrhages on hyperemic mucous. In case of pathological changes the dorsal surface of tongue gets bright red colour, the atrophy of papillae and an epithelium desquamation are observed.
Differential diagnosis: The medicamental catarrhal stomatitis is necessary to differentiate from:
- Hypovitaminosis of B and C vitamins - Diseases of a gastroenteric tract - Fungal affections In case of hypovitaminosis of vitamin C the hemorrhages are present on a skin as
well: there are general asthenia, fast fatiguability (easily tired) and pains in muscles. Hypovitaminosis of vitamin В12 have a characteristic picture of blood: reduction of quantity of erythrocytes, hemoglobin, origination of megalocytes, and decrease of quantity of leucocytes.
In case of fungal affections of oral mucosa the bacteriological analysis shows presence of funguses in a considerable quantity, their mycelium.

Treatment: cancellation of the medicinal preparation which has caused an allergy or its replacements by another. Antihistaminic, calcium containing medicaments are prescribed. In case of hemorrhages vitamins C and P are prescribed. Local treatment is not required. Gargles with infusions of medicinal herbs and not irritating diet are recommended.
Erosive stomatitis, cheilitis and glossitis It is rather serious form of a medicinal allergy. Patients complain of the pains increasing while eating and speaking. In serious
cases the general condition worsens and there are complaints of asthenia, appetite loss and high temperature.
Clinical features: On hyperemic and swollen oral mucosa there are bullae of the different sizes. They soon rupture, leaving erosions. Bullae are located on the different parts of oral mucosa; however favorite localization is the mucosa of lips, tongue, cheeks and palate. Erosions sometimes enlarge, forming the big erosive surfaces. Gingival papillae are edematous, hyperemic, easily bleed. Increase of temperature till 37,5-38oС is characteristic.
Hypovitaminosis (especially B vitamins), dysbacteriosis, unsatisfactory hygiene of an oral cavity, a considerable quantity of decayed teeth can aggravate a disease current.
Differential diagnosis: Erosive medicamental stomatitis should be differentiated from:
- Primary herpetic gingivostomatitis - Erythema multiforme - Pemphigus In case of Primary herpetic gingivostomatitis bullae of the small size and after
their rupture the small aphthae are formed having inflammatory borders and covered with inflammatory greyish-white plaque. Vesicles are intraepithelial, during allergy they are located subepithelial. In case of herpes the virus is found out in vesicles content.
In case of Erythema multiforme the general symptoms (asthenia etc.) are appeared before bullae occurrence; in case of medicamental stomatitis- after. Lesions present both on oral mucosa and skin where they have the characteristic form and colour (cyanotic-pink maculae; target or iris-like skin pattern).
In case of Pemphigus bullae are intraepithelial; Nikolsky's positive symptom and the acantolysis phenomena in an epithelium become perceptible.
During differential diagnosis of allergic medicamental lesions a communication of oral lesions with reception of a medicinal preparation and comparatively fast healing after cancellation of this medicament are important.
Treatment: cancellation of medicine which has caused an allergy or its replacements by another. Desensitizing therapy (antihistaminic, calcium containing medicines), vitamin C are prescribed. In case of severe form the corticosteroids (Prednisolone 15-20mg, dexamethason of 2-3 mg within 10-14 days) are prescribed.

Locally: anaesthetizing and corticosteroid ointments, antiseptics, proteolytic enzymes and keratoplastics are prescribed.
Necrotizing ulcerative medicamental stomatitis, cheilitis and glossitis It is the most serious form of medicinal lesions of an oral cavity. Usually
develops in case of serious general allergic reactions. Clinical features: Necrotizing ulcerative process proceeds with serious
disturbances of the general condition of an organism (fever, asthenia). Because of acute pain food intake is complicated, the hypersalivation is observed. Visual inspection: hyperemia, erosions and the necrosis hearths are present on various parts of oral mucosa. Submandibular lymph nodes are enlarged, painful, but are mobile.
Differential diagnosis: Necrotizing ulcerative medicamental stomatitis should be differentiated from:
- Necrotizing ulcerative stomatitis of Vensan - Lesions of oral mucosa in case of blood diseases (leucosis, agranulocytosis) - Trophic ulcers during cardiovascular diseases In case of stomatitis of Vensan the bacteriological analysis finds out disease
originators (spirochetes and fusobacteria). Diagnosis of blood diseases is helped by typical changes in a blood picture. For trophic ulcer longer time of the existence, weakly expressed symptoms of an
inflammation, a flaccid current on which medicinal preparation cancellation does not render any influence are characteristic.
Treatment: antihistaminic medicine, corticosteroids; intravenous injection of Sodium thiosulfate solution, and in hospital - Haemodesum.
Locally: anesthesia, processing of mucous membrane with antiseptics, proteolytic enzymes and keratoplastics.
Keeping diet is very important. The products, capable to cause an allergy (fish caviar, eggs, chocolate, coffee, etc.) and to irritate oral mucosa and mucous membrane of gastroenteric tract (salty, spicy, fried and too hot) are excluded.
Contact allergic stomatitis Except a medicinal allergy stomatologists in the practice face to allergic
reactions to dental materials as well, in particular, acrylic of prostheses, amalgams, dyes, composites and components of adhesive systems. These allergic reactions are reactions of the slowed down type.
Clinical features: The allergy is usually shown in 5-7 days, and sometimes in some months. In place of contact of mucous membrane with allergen there are hyperemia, edema, sometimes bullae, which fast rupture leads to occurrence of erosions. Patients complain of burning sensation, dryness of mucosa, disturbance of gustatory sensitivity or its full absence.
Diagnosis: is helped by lesion localization (in the field of possible allergen), and also data of allergological researches.

Treatment: consists in allergen elimination, prescription of anti-inflammatory medicine and antiseptics. In serious cases prescribe desensitizing treatment (antihistamine, calcium containing medicaments, corticosteroids).

Pemphigoid (nonacantolytic pemphigus) This group includes bullous dermatoses which unlike the true pemphigus are not accompanied by acantolisis. They are:
• Leffer`s bullous pemphigoid or non-acantolytic pemphigus • Ocular pemphigus or cicatrizant pemphigoid • Benign pemphigus of OCMM
Aetiology. It is not definitively clarified. The main role belongs to autoimmune processes. The following are characteristics for all kinds of pemphigoids:
• lack of acantolysis, • subepitelial location of bullas, • expressed inflammation, • there are no acantolytic cells, • Nikolsky's Symptom is "negative", sometimes - false positive.
Bullous pemphigoid. It usually affect people above 60 years old; the skin, mucosa of oral cavity, generative organs are affected. Clinical features. Formation of big (0,5-2 cm), tense, subepitelial vesicles on the erythematic or invariable skin and mouth mucosa is characteristic. They are often localized on the inguinal fields, on the inferior part of abdomen, in the upper limb folds. In 1/3 of coses the OCMM is affected. 5-22 mm diameter bladders filled with serous or hemorrhagic liquid appear on the swelled and hyperemic mucosa; they preserve from several hours to several days, after which erosion covered by fibrin scurf is formed on the same place. Unlike the acantolytic pemphigus, erosions are epitelized within 10-15 days, without atrophy and cicatrixes formation. But after a while the erosions can repeat. In the oral cavity their occurrence is painless, on the skin it is accompanied by itch, sense of burning and pain. Infrequently it happens on gums, the vestibular surface of which is hyperemic, swelled and bleeds. In this case the Nikolsky's symptom is "positive". Differential diagnosis:
1. Akantolitic pemphigus (Phemphigus vulgaris) 2. Duhring's dermatitis herpetiformis (Duhring's disease) 3. erythema multiforme (herpes iris) 4. bullous toxicoderma.
Akantolitic pemphigus can be differentiated from pemphigoid based on the clinical features. The following are characteristics for pemphigoid:
• arises at older age • there are big tense bullas, • arose erosions quickly epitelize, • Nikolsky's symptom is "negative", • there are no acantolytic cells.
2. Following are characteristic for Duhring's disease: • the spreading on skin is polymorphic, • it is accompanied by edema and itch, • lesion of mucosa is not typical.
3. For erythema multiforme the following are characteristic: • acute course • arises in young age, • vesicles are located on the swelled and hyperemic OCMM and skin.
4. bullous toxicoderma: • arises as a result of usage of medicine,

• spreading is polymorph. Treatment The best results are achieved by use of corticosteroids (prednisolone, 30-40 mg in day), in some cases the combined treatment gives good results: prednisolone with cytostatics. Polyvitaminums, medicines of K, Са and sedatives are also prescribed. Ocular pemphigus or cicatrizant pemphigoid. Women of 50 years old are more often affected by this disease. The oral cavity mucosa, conjunctiva are affected and in 1/3 of cases there is a rash on the body. Vesicles in the oral cavity are formed on hyperemic mucosa and are 0,2-1,5 cm in diameter. They are mostly located on the soft palate, uvula, tonsils and mucosa of cheeks. Vesicles are tense and are covered by dense membrane; contents can be serous or hemorrhagic.
Duhring's herpetiform dermatitis (Duhring's disease) Duhring's disease is a chronic disease, characterized by polymorphism of rashes. Only 10 % of patients have
OCMM lesions. Aetiology and pathogeny. Based on modern notion Duhring's disease have autoimmune nature. The
hypersensitivity to iodine has a certain role in aetiology of this disease. Duhring's herpetiform dermatitis is the polyetiological syndrome arising when people have thin intestine function disorder (malabsorption syndrome, sprue).
Clinical features. Disease usually begins with subjective sensations (itch, sense of burning, pricking), low fever, malaise which can be preceded by dermal rashes a few hours, days or even months before. Rashes are characterized by true polymorphism - combination of erythematic maculae, tense vesicles and bullas both on the edematous erythematic base and on choronomicly healthy skin; urtical erythematic elements, papulovesicules. Rashes are symmetric; more often located on the extensor surfaces of limbs, shoulders, breeches, loin and on the face.
Isolated lesion of OCMM is not observed. Papules, bullas and vesicles are formed on hyperemic and edematous OCMM. Sometimes only the bullas are formed, which are located subepitelially, have transparent contents and thick cover. This makes them similar to herpes. In 3-4 days bullas are dissected, forming bright red erosions with scallop-shape lineaments; sense of pain is weak. Nikolsky's symptom is negative, there are no acantolytic cells. Erosions epitelised in 2-3 weeks. The hypo-and hyper-pigmented maculae remain on their place. More often the lesion elements are localized on the palatal mucosa and cheeks. Cyclical course is characteristic for this disease.
The eosinophilia is observed in patients’ peripheric blood and in the contents of bullas. The diagnosis is conformed based on the clinical symptoms and lesion elements, as well as based on the fact of
allergy to iodine containing medicines and eosinophilia. Dif.diagnostics is carried out with - True acantolytic pemphigus - non-acantolityc pemphigus - Multiform exudative erythema - Bulloz toxicodermitis Treatment. Medications of sulfonal series (diaphenylsulfonal) are used. Vitamins C, Rutinum, vitamins B
series, antihistamine medicines are prescribed simultaneously. In case of serious, persistent course of the disease these medicines are combined with corticosteroids (40-50mg for 2-3 weeks and gradual reduction of dosege to 2,5-5 mg). The diet excluding products from rye and wheat is also recommended.

Precancerous (premalignant) diseases of oral mucosa and red border of lips
The term “precancer” means long-term existing chronic diseases (with the general dysplastic changes, and also independent diseases) which always or often lead to malignant neoplasms (tumors).( Precancer is a lesion from which a malignant neoplasm is believed to develop in a significant number of instances, and which may or may not be recognizable clinically or by microscopic changes in the affected tissue).
Diseases which always turn to cancer are called “obligate”, and the disease which can be a basis for malignant neoplasms development, are called facultative. In concept of precancerous disease or a condition the complex of clinical, morphological, pathological and biochemical changes are laid. Morphological changes consist of atypical growth of an epithelium, its proliferation in subject tissues (but without an invasion), cellular atypism, depolarization, occurrence of protoplasmatic nuclei etc. Biochemical changes of the tissues consist of phosphatase presence, increase of quantity of water, change of cholesteric substances, linkage of functional albuminous matters (albumen) by thiol poisons, etc.
Precancerous diseases (obligate) of oral mucosa and red border of lips have high predilection to malignancy. They are characterized by absence of objective signs of a cancer tumor, however in the presence of pathogenic factors they turn into cancer. Clinical features of this group of diseases are various enough that complicate their diagnostics. On the other hand, the prognosis depends on variety of factors: the local status and the general condition of an organism and carcinogens as well. In case of exception of unfavorable influences the lesion elements probably grow in opposite direction; stabilization of process without essential changes or the further development without predilection to degeneration are possible. Conservation of an adverse background leads to a malignancy of the lesion centre.
The following symptoms can be the basic signs of a malignant degeneration: sharp change of a clinical picture, i.e.: acceleration of development of a tumor or an ulcer, exophytic growth or ulceration of tumors. Following alarm moments are the hearth bleeding, a lesion, and occurrence of a hyperkeratosis, infiltration and inspissation. Absence of effect of conservative treatment within 7-10 days is an indication for consultation with the oncologist.
In 1976г classification of precancerous diseases of oral mucosa and a red border of lips has been confirmed.
Classification of precancerous diseases of oral mucosa: A. with high frequency of malignancy (obligate):
1) Bowen dermatosis
B. With small frequency of malignancy (facultative): 1) leukoplakia (verrucous and erosive/speckled), 2) papillomatosis
3) erosive- ulcerative and hyperkeratotic forms of lichen planus and lupus erythematosus 4) radiation(x-ray) stomatitis
Classification of precancerous diseases of red border of lips

A. with high frequency of malignancy (obligate): 1) warty precancer, 2) limited precancerous hyperkeratosis, 3) abrasive precancerous cheilitis of Manganotti
B. With small frequency of malignancy (facultative): 1) leukoplakia, 2) keratoacanthoma, 3) dermal horn, 4) papilloma with a keratinization, 5) erosive- ulcerative and hyperkeratotic forms of lichen planus and lupus erythematosus 6) radiation(x-ray) cheilitis
Diseases with low frequency of malignancy are not included in given classification (flat /homogenous/leukoplakia, median lip fissure, etc.), and also actinic and meteorological cheilitis, cicatrices and a cicatrical atrophy which are surveyed as background conditions.
Bowen dermatosis (morben Bowen) It is surveyed as a precancerous dermatosis and described in 1912. This disease possesses the greatest potential of malignancy among the precancerous diseases and keeps within concept cancer in situ. Men suffer from this dermatosis more often, mainly at the age from 40 till 70 years. Favorite localizations are on soft palate, uvula, retromolar area, tongue. On oral mucosa the clinical features of disease are various enough. One of the symptoms is found out often, two and more hearths of lesion-rarely. There is a limited, slowly enlarged spotty-nodular lesion. Sometimes the lesion has similarity to leukoplakia and lichen planus because of irregular keratinization. The surface of a lesion can be erosive or covered by papillary growths in some parts, more often is congestive-red, velvety, with fine (small) papillary growths, is smooth rarely. In case of long-time existence of a lesion a slight atrophy of mucosa is revealed and then the centre slightly sinks down. If a lesion is placed on tongue papillae disappear in a lesion place. Several hearths can fuse into plaques with incorrect outlines. Subjective sensations can be absent. However not in all cases of Bowen dermatosis there is a clear clinical picture. Descriptions are known when the disease is characterized by only hyperemia of a small part of oral mucosa or is clinically indistinguishable from leukoplakia. Sometimes implication of disease by an accurate grayish-white drawing reminds clinical features in case of lichen planus, and by plicated mucosa in the centre-leukoplakia. Such lesion can be observed in case of becomes localization on mucosa of cheeks. Disease proceeds uncertain time. In some cases invasive growth of an epithelium is occurred quickly, in other cases it remains un- changed for years. Pathological histology is characterized by weakly expressed hyper- or parakeratosis, an acanthosis and expanded epithelial outgrowth are always available, the basal layer is maintained, invasive growth is not present. In stratum spinosum there is a picture of cancer in situ, i.e. intraepithelial planocellular cancer which is not accompanied by infiltrative growth.

In stratum spinosum (prickle cell layer) there are ugly, monstrous cells, sometimes with many nuclei (polynuclear). Often there is a keratinization of separate cells of malpighian layer, true corneal pearls can develop. In corneal layer if it is available, sometimes grains and round little bodies are find out similar to ones as in case of Darier disease. Basal membrane is maintained. Disease course: Long-time, many years, usually unfavorable. Early invasive growth is observed if process is localized on oral mucosa. Prognosis: is bad without treatment. In the literature there are no mentions on possibility of spontaneous retrogressing of this process. Diagnostics is clinically difficult if lesion is placed on oral mucosa. The diagnosis should be always confirmed by results of histological research. Differential diagnostics: should be differentiated with a leukoplakia, lupus erythematosus, tubercular lupus, syphilitic papules (for Bowen dermatosis accurate contours of the pathological hearth in shape of plaque or disk, rising or sinking down in comparison with surrounding tissues are characteristic, the cherry shade of hearth is typical). Treatment consists in total removal of lesion within healthy tissues. If it is impossible, it is necessary to apply radiotherapy.
Warty (nodous) precancer of red borders of lips (precancer verrucosus)
Warty precancer is described in 1965 by A.L.Mashkillejson as an independent clinical form of precancer of red borders of lips, possessing high potential frequency of malignancy. It occurs mainly on a lower lip; basically among men above 40 years old. The percentage of meeting among all precancerous diseases of lips is about 7 %.
Clinical features: lesion has sharply limited character. Element in diameter from 4 mm to 1sm is located strictly on a red border, usually semiball-shaped form. It arises over surrounding red border on 3-5 mm and has dense consistence. Coloring of such nodule varies from colour of a normal red border to congestive-red. Often the nodule surface is covered by densely sitting thin squamae. In this case the lesion rather reminds a wart or a keratosic papilloma. Nodule palpation is painless. Warty precancer is located on outwardly unchanged red borders of lips.
Pathological histology: warty precancer is sharply limited proliferation of flattened epithelium as upwards, sometimes in the form of wide papillary formations, and is deep downwards below usual level of an epithelium. Proliferation occurs due to expansion of stratum spinosum (prickle cell layer). Small hyperkeratosis zones often alternate with parakeratosis zones; dyscomplexity and polymorphism of prickle cells are observed. There is an infiltration with a considerable quantity of lymphocytes, plasmocytes and labrocytes in connective tissue. Elastic fibers are homogenic in some parts.
Disease course: of warty precancer is fast enough, malignancy can occur in 1-2 months after the disease beginning. Clinically to establish the beginning of malignancy is almost impossible. It is necessary to pay attention to sudden augmentation of the sizes of a lesion, keratinization intensifying, erosions or element ulceration. Diagnostics is based on the clinical picture confirmed with results of histological tests.

Differential diagnostics: ordinary wart differs from a precancer by presence of threadlike papillary growths and hypertrophied cornual layer on periphery. Papilloma differs by presence of a leg, a soft consistence, and histological tests data are decisive. Keratoacanthoma differentiates from a warty precancer by presence of dense peripheric reddish roll which surrounds the central crater filled with cornual masses; after their removal a funneled excavation is formed. Piogenic granuloma differs by presence of a leg, bright red coloring and soft consistence. Treatment: Full surgical extraction of the lesion within healthy tissues with a subsequent histological test.
Limited precancerous hyperkeratosis (hyperkeratosis praecancrosa circumscripta)
Limited precancerous hyperkeratosis is described in 1965 by A.L.Mashkillejson as
an independent clinical form of precancer of red borders of lips. . It occurs mainly on a red border of lower lip (near center); basically among men above 30 years old. The percentage of meeting among all precancerous diseases of lips is about 8 %.
Clinical features: lesion is sharply limited, often it has polygonal form, in the size from 0,2х0,5 to 2х1,5 sm. Lesion surface is covered by thin firmly attached squamae(scales) which has grayish-white colour. Usually the centres of lesions are slightly sunk down. However due to accumulation of the scales the lesion can slightly rise over surrounding red border. Hearth of the limited hyperkeratosis has a flat surface and seldom develops on inflamed tissues.
Pathological histology: there is a limited proliferation of an epithelium toward underlying tissues, often accompanied by dyscomplexity of prickle cells with expressed hyperkeratosis on a surface.
Disease course of the limited hyperkeratosis is not as fast as in case of warty precancer; however its malignancy can occur in 6 months after the disease beginning. Clinical features of malignancy are: intensifying of a keratinization and inspissation occurrence in the element basis. However these signs usually appear long after the malignancy beginning. Diagnostics is based on clinical features and histological tests data. A unique reliable way of diagnostics of malignancy is a biopsy which should be carried out as soon as possible (asap).
Differential diagnostics: in case of leukoplakia there are not hyperkeratotic squamae on hearth surface; lupus erythematosus is differentiated from the limited hyperkeratosis by presence of inflammation and atrophy, the lupus erythematosus hearth usually are larger than the lesions of the limited hyperkeratosis. Lichen planus differs from limited hyperkeratosis by infiltration and inflammatory coloring in the lesion hearth. In case of lichen planus formed squamae are coarser (rougher) than during limited hyperkeratosis.
During patient evaluation in case of limited precancerous hyperkeratosis or warty precancer of red borders of lips the aim is to determine the absence or occurrence of malignancy. Clinical features of malignancy are: intensifying of a keratinization, inspissation occurrence in the element basis, erosions or ulceration. However these signs usually appear

long after the malignancy beginning, therefore unique way of diagnostics of malignancy is the biopsy which should be done as soon as possible (asap).
Treatment: Full surgical extraction of the lesion within healthy tissues with a subsequent histological test.
Abrasive precancerous cheilitis of Manganotti (cheilitis abrasiva praecancrosa
Manganotti)
In 1933 Manganotti described original erosive change of red border of the lower lip which tended to be transformed into a planocellular cancer, and named it abrasive precancerous cheilitis. It has high frequency of malignancy and concerns to obligate precancer. It occurs mainly among men at the age of 50-60 years.
Etiology and pathogenesis: In occurrence of cheilitis the following has appreciable role: age trophic changes of tissues, in particular a lower lip, which are especially expressed among patient with missing teeth (secondary adentia) or destroyed lower frontal teeth. That’s why a dystrophy of lower lip area can easily lead to destructive response to such stimuli as an insolation, acute and chronic trauma, smoking, etc. Hypovitaminosis of vit A and pathology of a gastroenteric tract has certain value in a pathogenesis of cheilitis. Clinical features of Manganotti cheilitis are various. Usually the lesion is an erosion of the oval or wrong form, often with smooth “polished” surface of deep red color. In some cases erosion is covered with transparent thin epithelium. Often the crusts are formed on an erosion surface the removal of which causes bleeding. While easy trauma of the erosions without the crusts does not cause bleeding. Usually the inspissations of tissues are not present in the basis and around erosions. Sometimes erosion is located on slightly hyperemic and infiltrated basis. Thus inflammatory reaction extends on 1-1,5 sm from erosion borders, but sometimes inflammatory process has widespread character. Inflammation is presented in the form of small congestive hyperemia and infiltration of a red border. Distinctive feature of inflammation is its instability. Usually there is one erosion, rarely - two, very rarely - three. In some cases occurred erosions exist for a long time, being a little enlarged, but more often erosions are spontaneously healed and then quickly enough recur on the same or other places.
Pathological histology: there is a defect of an epithelium filled with a dense diffusive infiltrate, consisting of lymphocytes, histiocytes, plasmocytes and labrocytes. Along the erosion edges the epithelium is proliferated, but sometimes is atrophied. In some parts the prickle cells (especially in area of proliferation) are atypical and in a condition of various degree of dyscomplexity. In depth of a derma there is a growth of a connecting tissue. Focal infiltrations, consisting of lymphocytes, histiocytes, plasmocytes and labrocytes, fibroblasts and macrophages, located around sharply expanded blood and lymph vessels.
Disease course of cheilitis is very fast, chronic, in case of proceeding action of the causal factor the process turns to a cancer in various terms (from 3 months till 30 years) after the disease beginning. Correct treatment can be effective.
Diagnostics is based on clinical data, confirmed by results of histological tests. Differential diagnostics: cheilitis of Manganotti should be differentiated from
erosive forms of lupus erythematosus, lichen planus and leukoplakia, Pemphigus, erythema
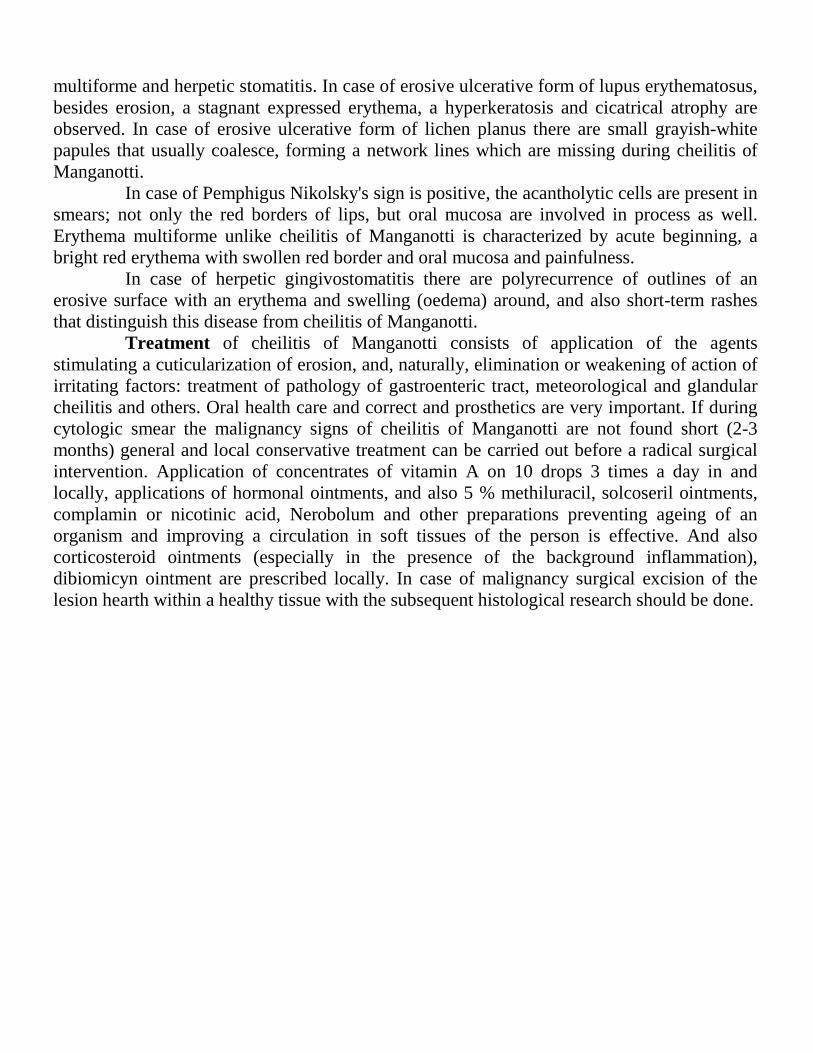
multiforme and herpetic stomatitis. In case of erosive ulcerative form of lupus erythematosus, besides erosion, a stagnant expressed erythema, a hyperkeratosis and cicatrical atrophy are observed. In case of erosive ulcerative form of lichen planus there are small grayish-white papules that usually coalesce, forming a network lines which are missing during cheilitis of Manganotti.
In case of Pemphigus Nikolsky's sign is positive, the acantholytic cells are present in smears; not only the red borders of lips, but oral mucosa are involved in process as well. Erythema multiforme unlike cheilitis of Manganotti is characterized by acute beginning, a bright red erythema with swollen red border and oral mucosa and painfulness.
In case of herpetic gingivostomatitis there are polyrecurrence of outlines of an erosive surface with an erythema and swelling (oedema) around, and also short-term rashes that distinguish this disease from cheilitis of Manganotti.
Treatment of cheilitis of Manganotti consists of application of the agents stimulating a cuticularization of erosion, and, naturally, elimination or weakening of action of irritating factors: treatment of pathology of gastroenteric tract, meteorological and glandular cheilitis and others. Oral health care and correct and prosthetics are very important. If during cytologic smear the malignancy signs of cheilitis of Manganotti are not found short (2-3 months) general and local conservative treatment can be carried out before a radical surgical intervention. Application of concentrates of vitamin A on 10 drops 3 times a day in and locally, applications of hormonal ointments, and also 5 % methiluracil, solcoseril ointments, complamin or nicotinic acid, Nerobolum and other preparations preventing ageing of an organism and improving a circulation in soft tissues of the person is effective. And also corticosteroid ointments (especially in the presence of the background inflammation), dibiomicyn ointment are prescribed locally. In case of malignancy surgical excision of the lesion hearth within a healthy tissue with the subsequent histological research should be done.

STEVENS-JOHNSON AND CHAIGRIN SYNDROMES Stevens-Johnson syndrome is the severe form of multiform complex erythema with
characteristic specific symptoms. Stevens-Johnson syndrome develops as a medicament affection. NSAID-s, sulfamides can cause this disease.
The basic changes occur in the superficial epithelium. They are presented by spongiose, ballonic dystrophy, hypostasis and infiltrations in the papillary layer of the own plate.
Clinic. The disease often begins with fever and pains in joints. Then the temperature slowly decreases, remaining subfebrilite during 3-4 weeks. The disease is accompanied by vesicle and erosive affection elements, severe affection of eyes with appearance of vials and erosion on conjoctive, rarer on cornea. The constant simptom of Stevens-Johnson syndrome is the generalized affection of the oral cavity mucous membrane (OCMM) accompanied by appearance of widespread erosions, covered with white membrane. At generalized affection vulvo-vaginite usually develops. The rash of the skin is characterized by polymorphism (erythema, papules, vials, bulles). Papules on the skin usually have depression in the centre, taking the form of a cockarde. On the red bordure of the lips, tongue, soft and hard palate bulles with serous-hemorrhagic exudate are formed. After their exposure painful erosions are appeared, covered by purulent-hemorrhagic patches, which complicates food intake, talking. The mucous membrane of the nose (rhinitis, nasal bleedings) and genitals is also affected.
Development of pneumonia and encephalomyelite with lethal outcome is possible. Treatment. For treatment of Stevens-Johnson syndrome corticoide (60-80 mg prednisolone)
and desintoxication therapy, hemosorption, antibiotics of wide spectrum, antihistamine preparations, sulfamides, salicialades are recommended. Local - anesthetics, proteolitic enzymes, inhibitors of proteolysis enzymes, Lizocim, antiseptics, immune modulators, corticoide and keratoplastic (regenerative) preparations are used.
Chaigrin syndrome is a system disease described by Chaigrin in 1933. A common opinion, concerning the reason of occurrence of this disease, does not exist. An infectious-allergic genesis, role of hormonal disturbances, hereditary predisposition of vitamin A exchange disturbance is supposed. A number of authors confirm the auto-immune nature of this disease. Clinic. The initial changes can be the reduction of quantity and increase of viscosity of saliva during a long period. Then mucous membrane changes appear: atrophy of tongue papillae, the tongue becomes hyperemic, feeling of pyrosis appears. By this time atrophic changes of the top respiratory ways mucous membrane are observed (dry tracheo-bronchitis, rhinitis). Decrease of sense of smell can occur. Achylie arises. Patients complain of dryness of the oral cavity and pain while food intake, occurrence of cracks in mouth corners, dryness of eyes, conjuctivitis, accompanied by tranchees, photophobia, absence of tears. In later stage atrophic changes of the genitals mucous membrane, dryness and desquamation of the skin, dryness and fragility of the hair appear. Changes like chronic arthritis can arise (approximately at 1/3 of patients). Occurrence of pneumosclerosis, peripheral and trigeminal neuralgia sometimes is noted. At examination, along with salivation reduction, tumor-like increase of one or both parotids and the other salivary glands is observed. Sometimes in the parotids calculi are observed. At histologic examination local lymphocyte infiltration is observed in the oral cavity mucous membrane, considerable reduction of activity of submucous (including salivary) glands is marked. Chaigrin syndrome is necessary to differentiate from xerostomie. Treatment is complex, and is spent by stomatologist, oculist and therapist. Preparations activating salivation, vitamins A, Е, B12, C are used. Corticoids, Levamisol are also applied.

BEHCET SYNDROME Behcet syndrome (Touraine’s big aphthous) - chronic system disease of mucous membranes, characterized by three basic symptoms: aphtous-ulcerative affection of the OCMM, mucous membrane of genitals and defeat of eyes (iritis, iridocyclite which can lead to blindness). For the first time the disease was described by Turkish dermatologiste Behcet in 1937. Patients with Behcet syndrome quite often have skin defeats (rash of nodular erythema, pyodermite, vasculite), affection of joints (arthralgie) and nervous system. Touraine has described other localization of this disease when not only the mucous membranes of the oral cavity, genitals, eyes, but also intestines mucous membrane is affected. Thus nodular erythemas and thrombophlebitis are noted. Persons of 20-30 years old are affected mainly. Etiologic factors of Behcet syndrome are considered viruses, infectious allergy, auto-aggressity, hereditary. Clinic. The disease is characterized by chronic current with remissions by duration from several days till several years. Behcet syndrome usually begins with general malaise, which can be accompanied by fever and myalgias. By the time aphthas appear on the OCMM and mucous membrane of external genitals. There are many aphthas 10 mm in diameter, which are very painful and have a circumscribed area of inflammation of bright red color. The surface of the aphtha is covered by yellowish white fibrin membrane. They are healed without cicatrices. At some patients deep aphthas are formed, which are not healing for a long time, and form rough cicatrices after epithelization, deforming the mucous membrane. In the area of external genitals painful aphthous-ulcerative rash appears, with dense infiltration in the basis. Elements are raised a little over the surrounding skin; the bottom of ulcers is covered by yellowish grey covering. Defeat of the eyes is appeared by severe bilateral iridocyclite, with hypopion and opacification of corps vitre. This leads to gradual formation of synechie, growing of the pupil and to progressing decrease in sight, sometimes to full blindness. At Behcet syndrome nodule erythema, pyodermal elements are appeared quite often. At 60-70% of patients in the active stage of Behcet syndrome the phenomenon of pathergia is observed - occurrence of small papule or pustule in the place of intradermal injection of sodium chloride isotonic solution. More serious is the defeat of the nervous system, which proceeds like meningo-encephalite. Among other symptoms of Behcet syndrome most often are met: affection of gastro-intestinal tract (syndrome of malabsorption, erosions, ulcers), vasculites of various localizations, with development of thromboses and aneurysms. Histologically, in the period of formation of aphthas, penetration of lymphocytes and monocytes into epithelium is observed. After epithelium destruction erosions are appeared. They have infiltrations in the basis and on the boarders. The infiltrations consist of neutrophiles, monocytes and lymphocytes. Differential diagnosis is spent with: - erosive papules at secondary syphilis - herpetic erosion - chronic reccuring aphthous stomatitis - Stevens-Johnson syndrome Treatment. There are no standard methods of treatment of Behcet syndrome nowadays. There is data of successful treatment of this syndrome by colchicine and levamosole, but these preparations were effective only for skin-mucous symptoms of the syndrome. Antibiotics of wide spectrum, plasma transfusion, gamma globulin are also applied. Use of antihistamine and detoxicative preparations is rational. Quite often application of corticoid preparations, for example

dexamethasone, is effective, which is appointed 3-6mg per day, with the subsequent transfer of the patient into supporting doses.

Syphilis
Syphilis - the chronic infectious disease which causative agent is Treponema pallidum. On a oral mucous membrane syphilitic appearance is possible to find out in all periods of a syphilis. Distinguish the congenital and acquired syphilis. Treponema pallidum penetrates into a fetus organism through a placenta from sick mother at a congenital syphilis. An obligatory condition of the acquired syphilis is infringement of a skin corneal layer or a oral mucous membrane epithelium integrity(homogenous). Infection with a syphilis can occur by direct contact (basically sexual), at various medical manipulations (injections, surgical interventions), at direct penetration of Treponema pallidum in blood, at contact with various subjects containing the causative agent, at disturbance of their sterilization process. The most dangerous source of infection is the primary or secondary syphilis. Clinical picture. The syphilis clinic is characterized by a wavy course- change of the active and latent stage periods of disease. Periods of a clinical course of syphilis are distinguished: incubative, primary, secondary and tertiary. The incubative period (from the beginning of Treponema pallidum penetration to appearance of the hard chancre) lasts on average 3-4 weeks. It can last longer at the persons taking antibiotics containing medicaments from other diseases. The primary syphilis lasts on average 6-7 weeks. It is characterized by appearance of painless inflammatory infiltration(hard chancre or primary siphiloma) on a place of Treponema pallidum penetration. In 5-7 days after its formation is appeared a secondary obligatory symptom – regional lymphadenitis(scleradenitis). Lymph nodes have densely-elastic consistation, are painless, are movable, the skin over them is not changed. During the last week of primary syphilis develops polyadenitis of the all or majority lymph nodes. In the lymph nodes is going an intensive reproduction of treponema pallidum. Hard chancre can be individual or in number of 2-3. More often it is localized on lips, gums, tongue, and tonsils. Diameter of hard chancre can be from 1-3мм (dwarfish chancre) to 1,5-2sm(gigantic chancre). Diameter of hard chancre on average is 5-10mm. The sizes, the form and depth of hard chancre lesion depend on its localization, reactivity of an organism and presence of current diseases. Development of hard chancre begins with appearance of the limited reddening in which centre for 2-3 appear a induration which is result of infiltration. In the central part of infiltration necrosis and erosion of bright red color is formed, more rarely the ulcer. It is painless, with cartilage-shape infiltration at palpation, a bottom dense, shining. The form of hard chancre depends on its localization. In tongue it looks like the turned saucer, in mouth corners – like a fissure (rhagates), on a red border of lips sometimes there are atypical forms of hard chancre, like a hat of a mushroom sharply towering over level of a red border of lips, diameter 2-3sm, more often at localization on lips the chancre looks like erosion or an ulcer covered with a crust at localization on lips. The hard chancre looks like bright red erosion which( looks like a half moon) and adjoins to a teeth on gums.It can be 3 forms on tonsils: ulcerous, anginous and combined. One side tonsils only are involved in process. It gets honey-red(copper-colored) color, is increased in size, became densely,is painless. At the ulcerous form on this background(phon) a meat-red color with well-defined borders ulcer is appeared. Process can be accompanied by painful sensations. Diagnostics. The diagnosis of hard chancre should be confirmed by detection of pale Treponema pallidum from a primary syfiloma surface or in punctate of regional lymphatic nodes. In the presence of negative result it is necessary to carry out repeated examinations. Specific serologic reactions (Vaserman reaction) become positive a little bit later, only in 3 weeks after appearance of the hard chancre. By the end of the primary period at patients the general phenomena can be observed: an indisposition, pains in bones, increasing of body temperature, a headache, leukocytosis. Differential diagnosis. The primary syphilis should be differentiated from a traumatic ulcer which is very painful and has no compaction in the basis. The hard chancre, localized on tonsils, are differentiated from tonsillitis with one side lesions, absence of a pain and
inflammatory hyperemia. A hard chancre on lips is necessary to differentiate from the erosion arising at relapsing herpes which has a slightly edematous, hyperemic basis and is painful. Herpetic erosion are characterized also by a fast course. Besides, the erosion are preceded by formation of vesicles at herpes, which never happens at a syphilis. It is differentiated also with the heavy form of recurrent aphthous stomatitis (Setons aphthae) Ulcers or aphthae are sharply painful, besides from the anamnesis it is known about recurrent character of disease. Hard chancre can have similarity to a cancer tumors. Infiltration sets down more deeply, edges dense, the bottom easily bleeds at the cancer tumor. At laboratory research find out atypical sells. The secondary syphilis lasts on the average 3-4 years. Generalization of process with lesion of mucous membranes in the form of a characteristic rash (syphilids) is appeared, in process involved condition affection of an organism, internal organs, bone and nervous systems, sight and hearing organs. Appearing on a oral mucous membrane arise simultaneously with skin affection, but sometime can be isolated. Disease has wavy character. In this stage of disease there are two type of lesion: spotty (roseolous, maculeous) and papuleous syphilids. The roseolous rash basically arise symmetrically on the palatal arch, on the soft palate, on the tonsils. They have stagnant-red color and accurate borders, in diameter of 0,5-1,0sm, can cause unpleasant sensations or morbidity, are disappeared at pressing. On a skin rashes are localized on a breast, a stomach and lateral surfaces of a body. These changes keep about 1 month without treatment. Subjective sensations are absented. At a recurrent syphilis the roseolous spots arise without the sharp inflammatory phenomena and are make the foci in the form of rings or arches.

Syphilitic roseolous spots differentiate from medicinal stomatitis which is accompanied by burning sensation, morbidity of a oral mucous membrane. All symptoms disappear after the termination of a drug intake. Syphilitic quinsy should be distinguished from banal catarrhal quinsy at which there are painful sensations, increasing of temperature, puffiness(edema). Papuleous syphilids - the most frequent form of secondary syphilis in an oral cavity. Papulous rashes can be formed in any place of a mucous membrane, but mostly are located on tonsils, on the soft palate and palatal arches. Papule are painless, dense, the roundish form, 1-1,5 sm in diameter towering over level of a mucous membrane. They roundish or oval, are not inclined to confluence. The papules are covered gy grayish-white scurf because of maceration. The surf is easily removed and under it meat-red erosion is bared. The are inflammatory borders around papules. The papules contain a considerable quantity of Treponema pallidum.. On a mouth mucous membrane papuleous sypilids are the erosive-ulcer form which is caused by maceration and the frequent traumas. Therefore the clinical picture gets similarity to Vensan stomatitis.
Papules are often localized on lateral and dorsal surfaces of tongue. On a dorsal surfaces of tongue in papules appearance places the filiform ang fungiform pappiles disappear. Quite often precipitation is arised to the posterior part of pharynx and cause hoarseness of voices (syphilitic dysphonia). The diagnosis should be confirmed by detection of Treponema pallidum from papules surfaces. The serologic reactions (For example Vaserman reaction) should be positive. Diff. diagnosis . Syphilitic papules on oral mucous membrane is necessary to differentiate from Leukoplakia, lichen ruber planus and lupus erythematosus. The whitish scurf is easily removed at papuleous syphilids, that does not occur at the listed pathologies. Besides, at Leukoplakia, lichen ruber planus and lupus erythematosus in the base of papule is absent intiltration, and along the borders of foci is not present inflammatory rim. at syphilitis after removing of the grayish-white scurf from the papule surface the erosion is bared, Treponema pallidum are found. At candidiosis after removing of white scurf is bared the hyperemic surface of a mucous membrane. Sometimes papuleous syphilids has similarity with multiform exudative erythema and an allergic stomatitis. At these diseases In the basis of erosion there is no infiltration, a mucous membrane is hyperemic at these diseases. Syphilitic papules on a dorsal surface of tongue is necessary to distinguish from desquamative glossitis. Migration of the desquamative foci and a chronic courses of disease distinguish desquamative glossitis from syphilitic foci . The tertiary syphilis begins in 4-6 years after the beginning of disease and is characterized by formation of syphilitic gummas on a mucous membrane and a skin. For this period of disease affection of internal organs, nervous and bone systems are characteristic. More often gummas are localized in the hard and soft palate and tongue . In thickness of an oral mucous membrane the painless node is formed which gradually increases in size, reaching 1,5-3sm in diameter. Then the centre of gummas is opened, the crateriform ulcer with necrotic rod in the centre arises. The ulcer painful, is surrounded with dense infiltration, has dense, equal borders, the bright red bottom covered with small granulations. Ulcer healing is finished with formation of star-shaped cicatrice. This process lasts 3-4 months and is not accompanied by subjective sensations. Gummous tongue lesions can occur like a diffuse sclerotic glossitis at which the deep diffuse infiltration in all thickness of tongue is characteristic. The sizes of tongue increase, the papillae are smoothed. Subsequently the infiltration is replaced with a cicatricial tissue, tongue decreases in sizes, becomes very dense, its mobility is limited. On a dorsal surface of tongue painful sulci and fissures are formed. The food intake is hampering and chewing function is broken at tertiary syphilisis. This form is the heaviest form of the oral mucous membrane lesion at a syphilis. At localization of gummas on the hard palate the bone tissue and periosteum is very quickly involved in process, there are bones necrosis, ,there sequestration, extensive defects, perforation of the hard palate. Gummous ulcers can be complicated joining of a streptococcal infection. Diff.diagnosis Syphilitic gummas is necessary to differentiate from a millar-ulceric tuberculosis, tumors, traumatic ulcers, the heavy form of chronic recurrent aphthous stomatitis. Treatment of a syphilis is spent in specialized venereologic medical institutions. Local treatment provides oral cavity sanation, removal of irritants, rinsing by antiseptic solutions.

Tuberculosis
Tuberculosis is a chronic infectious disease which is caused by mycobacterium tuberculosis (Kokh's rod). It panatrates in oral mucous membrane by the hematogenic, lymphogenic and exogen (air-drop or alimentary) way. Primary tuberculosis is extremely rare case, basically kids have this type of tuberculosis . The oral mucous membrane has more resistance of tubercular bacterias increasing.. However in the presence of mucous membrane damages mycobacterium can get through it and cause a primary tubercular ulcer. Infection occurs more often by air-drop way. After the incubatory period (from 8 till 30 days) on an infection place the ulcer appears with unequal borders, granular bottom and in dirty grey color. For a tubercular ulcer absence of the sharp inflammatory phenomena and the expressed morbidity are characteristic. In 2-4 weeks after formation the ulcer increases in sizes, regional lymph nodes are becoming bigger,inflemmated and are opened, it causes subfibril temperature, strong sweating.. Tubercular ulcer is differanted from primary syphilitic chancre, traumatic and trophic ulcers, a cancer of an oral cavity due to cytological research (presence of Kokh rod and gigantic Langhans sells). On oral mucous membrane the tuberculosis basically is shown again (as a consequence of a tuberculosis of lungs, joints, skin) in the form of tubercular lupus, a millar-ulcer tuberculosis and is very rare - colliquative tuberculosis (scrofulodermia). Tubercular lupus meets most often. At tubercular lupus affection of a oral mucous membrane and a red border of lips is combined with skin affection. The basic primary element is lupoma - specific tubercular tubercle red or yellow-red color, a soft consistency, with the size of 1-3mm in diameter. They are located with the groups: the fresh are formed on periphery, formed in the centre are inclined to curdled(caseous) disintegration and are joined with adjacent tubercles. In this case they are formed in the shallow(not too deep) ulcers with the soft, uneven, undermined borders, covered by the clear red or yellow- red papillomatous like a raspberry growths, covered with yellowish scurf, which easily bleed. The location of tubercular lupus predominantly on skin face (in the form of “butterfly”), spreading to upper lip, red border, rarely to the mucous membrane of the gums, hard and soft palate. The gums is infiltrated , easily bleeds, painless. The progressive parodontitis picture develops. A teeth becomes mobile and come out. On a red border of lips the ulcer is covered by bleedy-purulent scurf. The affected lip strongly swells. Ulcers on oral mucous membrane and a red border of lips can in 1-10 % of cases malignizated. A symptom of "apple jelly” and test by a probe are characteristic for a tubercular lupus. If to press on lupus with a probe it easily fails (Pospelov's symptom). There are 4 clinical type of tubercular lupus: infiltrative, tubercular, ulcerous and cicatricial. In infiltrative type a oral mucous membrane is hyperemic, primary elements are not expressed. For a tubercular type is characteristic appearance of small tubercle which are joined together. In an ulcerous type appears tubercules ulceration with formation of deep ulcers. The cicatricial stage is characteristic formation of the cicatrices, which are dense, rough, knitting together a mucous membrane of a mouth with underlying tissues. Repeated formation of lupus on a cicatrice is characteristic. A course of tubercular lupus is chronic. Regional lymph nodes are increased, soldered uneven packages.
Diagnostics. Reaction Mantu is positive. At cytological research gigantic sells of Pirogov_Langhans and epithelioid sells are found. Diff.diagnosis is spent with a tertiary syphilis (tubercles are dense, with equal borders, repeatedly are never formed on cicatrices; Pospelov's symptom negative), leprosy and lupus erythematosus (absence of lupus, presence of erythema, hyperkeratosis and a cicatricial atrophy). The milliar-ulcer tuberculosis develops against on background of an organism decreased reactivity. The patients having a heavy forms of a tuberculosis of lungs or throat, is followed with sputum discharging with big quantity of mycobacterium tuberculosis within. Micobacterium of tuberculosis penetrate to cheeks mucous membrane along of the teeth joining line , a dorsal and lateral surfaces of tongue, the soft palate. Thus the typical tubercular tubercles are developed. They are breaked up in the centre and are formed a small, with rough, uneven, soft borders, very painful ulcer. These ulcers have a creeping character. Its grow along the periphery, reaching the big sizes. The borders and bottom of ulcers have a granular character (due to the tubercles), are covered with yellow-grey scurf. On periphery of an ulcer surface is possible to reveal the small abscesses (grains or little corpuscles of Treyl ). At long existence of an ulcer the secondary infection joins, the borders and bottom of an ulcer are compacted. Diagnostics. The general condition of the patient (weakness, an exhaustion, paleness, increasing of temperature, sweating) suffers. At cytologic research huge sells of Pirogov-Langhans, and epithelial sells are found. Diff.diagnosis is spent with traumatic, decubital and trophic ulcers, gummous ulcers at a tertiary syphilis (it is painless,is crateriform with dense forked borders), stomatitisof Vensan , cancerof oral mucous membrane. Coliquative tuberculosis (scrofulodermia) - more rare form of a secondary tuberculosis. It is encountered mainly in children. A typical sign is formation of nodes in deep layersor oral mucous membrane. Nodes are break up, with forming of irregular ulcers.For these ulsers is characteristic a soft consistency, and a corroded uneven borders and flaccid granulations at the bottom. The ulcer is not painful ,with its healing "shaggy" cicatrices are formed. Diff.diagnosis is spent with a gummous ulcer (it is painless,is crateriform with dense forked borders.At healing the star-shaped cicatrices are formed);actinomycosis(for actinomycosis is characteristic wooden density of nodes, presence of fistulas, are found a radiant mushroom) at cytological research) a cancer ulcer (density, the morbidity, the turned borders , presence of atypical sells). Treatment is done together with the phthisiatrician. Locally is done the oral cavity sanation, antiseptic processing, medicaments for a necroolysis , specific antitubercular medicaments -isoniazid, ftyvazid, metazid; anesthesia, medicaments improving of reparative possibilities of sells.

VINCENT’S NECROTIZING ULCERATIVE GINGIVO-STOMATITIS Vincent’s necrotizing ulcerative gingivo-stomatitis is an inflammation of the OCMM. Two microorganisms, Bacillus fusiformis and Borelli Vincentii are responsible for this disease. In the literature it is described by various names: ulcerative gingivitis and stomatitis, necrotizing ulcerative stomatitis, ulcerative-membranous stomatitis, Plaut-Vincent’s stomatitis. At affection of only gingiva the disease is defined as Vincent’s gingivitis, at simultaneous affection of gingiva and other parts of the OCMM it is called Vincent’s stomatitis, when the palatal tonsillas are involved into the process, it is called Vincent’s angina.
Etiology. Vincent’s necrotizing ulcerative gingivo-stomatitis is caused by symbiosis of fusiform bacillus and Vincent’s Spirochetes. In usual conditions these microorganisms are representatives of resident microflora of the oral cavity and are presented in small amount at all people having teeth. Development of Vincent’s necrotizing ulcerative gingivo-stomatitis is connected with decrease of an organism resistibility, avitaminosis, stresses etc. At disturbance of specific and nonspecific mechanisms of protection of an organism, raises the virulence and quantity of fusobacterias and spirochetes, and the disturbance of integrity of the OCMM, owing to injuring factors, creates conditions for introduction of these microorganisms. The unsatisfactory hygiene of the oral cavity creates favorable conditions for development of non-aerobic infections. The disease is non-contagious.
Clinic. Persons of young age (17-30 years), generally men, are affected mainly. The disease has a seasonal nature with the greatest frequency of occurrence in autumn and spring. Clinically acute and chronic currents are distinguished, and by severity - easy, middle and severe forms.
The disease begins with fever 37.5-38°С. Regional lymph nodes are increased, condensed, become painful at palpation, but keep their mobility. Patients usually have headaches, general malaise, pains of the OCMM, amplifying at food intake, talking; gingival bleeding, hypersalivation, bad smell from the mouth. Expressed changes in hemogram can be absent, but quite often leukocytosis and moderate increase of ESR is observed.
The catarrhal changes of the oral cavity mucous membrane quickly pass into the ulcerative. Gingiva becomes edematic, hyperemic, very painful, and bleeds at touching. The epithelium of the gingiva and interdental papillae becomes turbid, and then necrotized. Its surface is covered by yellowish grey covering, which can be removed easily. Subsequently the affected part of the gingiva is not completely restored and remains deformed.
More often the area at the lower third molar is affected. The necrosis extends from the alveolar process to the mucous membrane of the cheek and retromolar area, causing trisms and pains at swallowing. Ulcers on the mucous membrane of the cheeks can reach the big sizes (to 5-6 sm) and depths. Their edges are irregular, soft. The bottom is covered by thick greenish grey necrotic membrane, having bad smell. After the covering (membrane) removal the friable bleeding bottom of the ulcer is bared. Indurations in the field of the basis and edges of the ulcer are not present. Surrounding tissues are edematic and hyperemic.
Quite often there are ulcers on lateral surfaces of tongue, on the hard and soft palate. On the hard palate the ulcer quickly leads to necrosis of all layers of the mucous membrane and to bone exposure.
The isolated affection of the pharynx (Vincent’s angina), as a rule, happens unilateral and meets seldom. Except the ulcer form of Vincent’s angina there is also it pseudomembranous or diphteroid form. In this case the process is localized only on tonsilles. There is no inflammation in the surrounding tissues.
The process can last months and years, with recedives and remissions, leading to loss of the alveolar process and loss of the teeth for rather short period. Self-healing does not happen.

In rare cases, when treatment is not spent or it is inefficient, the chronic form of Vincent’s necrotizing ulcerative gingivo-stomatitis develops, during which the general symptoms are absent. Patients complain on bleeding and pain of the gingiva, bad smell from the oral cavity. The gingiva is edematic, hyperemic, its ulcerative edge is quite often condensed, and necrotic parts are generally in the interdental area. At exploring of gingival edges bared bone tissue is defined. Lymph nodes are condensed, slightly painful. At duration of the disease of 4-8 months, they get chondroide consistence. Diagnosis of Vincent’s necrotizing ulcerative gingivo-stomatitis is done by clinical picture and by cytologic smear (in the scrape from the surface of the ulcers fusiform bacteria and spirochetes are found out in big quantities). Differential diagnosis. Vincent’s necrotizing ulcerative gingivo-stomatitis is necessary to distinguished from ulcerative defeats at blood diseases (leucosis, agranulocytosis). Along with clinical differs (pallor of the OCMM, presence of hemorrhages, leukemic infiltrations, expressed and long lasting bleedings of gingiva at blood diseases) very important value for differentiation have changes in peripheral blood at leucosis and agranulocytosis. From the allergic stomatitis Vincent’s necrotizing ulcerative gingivo-stomatitis is distinguished by anamnesis data, by clinical particularities and by results of bacteriological investigation. Necrotizing ulcerative process of the oral cavity, similar to Vincent’s stomatitis, can arise at mercury intoxication. In case of contact to mercury, the urine analysis on the mercury maintenance is carried out. Necrotizing ulcerative defeats of the OCMM can be complicated by specific infection (syphilis, HIV-infection) or malignant tumors (cancer, sarcoma). For avoidance of errors in diagnostics, it is necessary to take anamnesis very carefully. It is necessary to carry out laboratory examinations: cytological, bacteriological, histological, serological, analysis of blood. Treatment. For easy current of Vincent’s necrotizing ulcerative gingivo-stomatitis local treatment is enough. It consists of removing injuring factors, necrotic tissues, influence on microflora and activation of regeneration of the OCMM. To begin the oral cavity disinfection, applicative or injective anesthesia (benzocaine, lidocaine) should be done. Then all mechanical stimuli should be removed: preparation of sharp edges of the teeth and artificial prosthesis, dental deposit removal. Necrotic tissues should be removed from ulcer surfaces by proteolytic enzymes: trypsin, chemotrypsin, lizoamidasa. The whole oral cavity should be rinsed by warm solutions of antiseptics (0.5% solution of hydrogen peroxides, 0.25% solution of chloramines), and also antimicrobic preparations (0.02-0.06% solution of chlorhexidine, 0.5% of solution of metronidazole). On the area of the affected mucous membrane metrogil-denta gel is applied, 2 times a day for 15 minutes, 7-10 days. At home the patient should do oral rinsing with antimicrobic preparations and applications with metrogil-denta to the affected parts of the mucous membrane.
In acute stage of the disease surgical interventions are not recommended (teeth removal, etc.). In heavier cases general treatment is necessary. For antibacterial therapy metronidazole is applied per os (0.25, 2 times a day, 7-10 days). Antibiotics of wide spectrum are used: chloromycetine, sumamed. Antihistamine preparations (tavegil, suprastine) and polyvitamins are also applied. It is recommend to drink a lot, and to use high-calorific not irritating food. At correct treatment improvement of the patient’s condition comes after 24-48 hours. Epithelization of the ulcers at easy degree of the disease happens within 3-6 days.
Relapses (recidives) of Vincent’s necrotizing ulcerative gingivo-stomatitis can happen, if there are centers of chronic infection or injuring factors in the oral cavity, and also at unsatisfactory hygienic condition of the oral cavity.

RECURRENT APHTHOUS STOMATITIS Recurrent aphthous stomatitis - chronic inflammatory disease of the oral mucous membrane which is characterized by prolonged course with periodic remissions and exacerbation, forming aphthae and ulcers. Recurrent aphthous stomatitis is the one of the widespread diseases affected oral cavity mucous membrane, which prevalence fluctuated from 10 to 40 %. Middle age of the patients is 20-40 years. Aetiology and pathogenesis. The main role in the pathogenesis of this disease has the immune system. The decreasing of immune reactivity, disordering of nonspecific protection are characteristic for recurrent aphthous stomatitis, which can be result of chronic infection of the body (quinsy, pharyngitis, gastrointestinal diseases). Also, some adverse factors (chronic stressful situations, frequent change of climatic belts etc.) can be affected on developing of this disease. Microbic associations of oral cavity when Recurrent aphthous stomatitis basically are presented by coccal flora (coagulazonegative staphylococcus) and anaerobic cocci (peptococci, peptostreptococci). And their quantity increases with increasing of the amount of microbic associations. The fungi and colon bacillus are also presented. Increasing of microorganisms virulence leads to strengthening of an organism bacterial sensibilization therefore is occurring a stimulation of immunity B-system, i.e. is connected a humoral type of reaction, accelerating transition of the easy form of disease in the heavy. The autoimmune reaction is developing, which result of in acanthaceous layer are formed a microcavities,with following necrosis. Clinical introduction There are 2 clinical forms of recurrent aphthous lesions of oral cavity: easy and heavy (recurrent deep cicatrizing aphthae). Recurrent aphthous stomatitis can be one of the general aphthosis symptoms at which areas of genitals and intestines (big Touraine aphthosis) are affected. Besides of aphthous rash on oral cavity mucous membrane, there are affection of eyes, and sometimes pyodermia are occurred Recurrent aphthous stomatitis (the easy form) is characterized by occurrence of individual aphtha on the oral mucous membrane which development is preceded often by feeling of burning, short-term morbidity, mucous membrane paraesthesia in an occurrence place of aphtha. Formation process of a mucous membrane aphtha begins with appearing of a small, hyperemic, sharply delimited spot in diameter of 0,1-0,5 sm. After a while the element slightly rises over surrounding mucous membrane, and still after a while became erosive and is covered with fibrinous grayish-yellow, dense scurf. The aphtae are very painful and soft at palpation. The aphthae is surrounded sharply delimited, is very hyperemic, slightly edematous borders. Quite often it is accompanied with regional lymphadenitis. Later 2-4 days necrotic masses are torn away, and in 2-3 days aphthae is allowed ; some time for its place keeps a stagnant hyperemia. 50 % of patients have the exacerbation 1-2 times a year. If the recurrent aphthous stomatitis lasts more than 3 years ,in this case the easy form of disease transfer to heavy. The factors fastening of easy form to heavy transfer are professional harmfulness, frequent change of climatic zone,presence of chronic diseases(quinsy, gastrointestinal diseases). Histologic research of usual aphtha finds out a deep fibrinous-necrotic inflammation, which begins in proper plate and submucous base of a oral mucous membrane. After enlargment of vessels, small perivascular infiltration is occurred a hypostasis of epithelium acanthaceous layer, then is occurred a spongiosis and formation of microcavities. Process is finished by epithelium necrosis and a mucous membrane erosion. The epithelium defect is filled with fibrin which is strongly accustomed with undercovering tissues. Diff.Diagnosis is spent with:
- Traumatic erosion - Herpetic erosion - Syphilitic papules
Herpetic erosion differs from aphta with the polycyclic outlines, not so expressed morbidity more diffused inflammatory reaction around it. Erosion occurrence at a herpes is preceded by the grouped of vesicles. Syphilitic papules are characterized by small morbidity, presence of infiltration in the base, Treponema pallidum on a surface of erosion, stagnant character inflammatory borders on periphery, positive reaction of Vaserman. Recurrent aphthous stomatitis (the heavy form) or Seton aphtha. This form can have following versions of a clinical courses: - A lesion element on a mucous membrane is aphtha, its epithelization period 14-20 days, a monthly exacerbation of disease;

- On a mucous membrane arise a sharply painful, deep, crateriform ulcers, there epithelization period 25-35 days, an exacerbetion of disease 5-6 times in a year. - On a mucous membrane find out aphthae and ulcers simultaneously, there epithelization 25-35 days, an exacerbation of disease 1 times in 2-3 months. The disease exacerbation usually begins with occurrence of the limited painful compaction of a mucous membrane on which is formed at first superficial, covered with fibrinogenous scurf and then a deep, crateriform ulcer with small hyperemia around. The ulcer, as a rule, increases in sizes. Sometimes in the beginning is formed a superficial aphtha which is transformed to a deep ulcer. It epithelization occurs extremely slowly (to 1,5-2 months) . After healing of ulcers remain rough connective tissue cicatrices ,which is cases of a oral mucous membrane deformation.At location of of such ulcers in mouth corners there can case the deformations, which sometime case a microstomia. Duration of aphthae cicatrising existence varies from 2 weeks to 2 months Precipitation more often is located on lateral surfaces of tongue, a mucous membrane of lips, cheeks, pharynx. At the heavy form of recurrent aphthous stomatitis register the raised irritability, a bad dream, appetite loss (at 70 % of patients). In histological research is found the part of necrosis with full destruction of epithelium and basal membranes, and also an inflammation of proper plate of mucous membrane and submucous base. Often on lesion parts there are salivary glands with expressed periglandular infiltration, that is way Sutton give the name of this disease “recurrent necrotic periadenitis of a mucous membrane”. Diff.Diagnosis it is spent with: - Traumatic erosion - A traumatic ulcer - recurrent herpes - Bexchet diseases - ulceriuos-necrotic stomatitis of Vensan - Ulcers at specific infections (a syphilis, a tuberculosis) - malignant ulcers At Bexchet diseases are observed combination of aphthous-ulcerious lesions of a oral mucous membrane, eyes and genitals. At ulceriuos-necrotic stomatitis of Vensan are find out an abundance of fuzo-bacteria and spirochaet. The malignant ulcers are dense, little painful At cytologic research reveal atypical sells. Treatment. Before the beginning of treatment of the patient the therapist, the otolaryngologist and other experts for the purpose of revealing of accompanying diseases, first of all gastrointestinal tract diseases, the centers of a chronic infection, a status of immune system.The special attention should be given a teeth and parodont diseases treatment. For a immunocorrection are used a thymogen, and deckaris, regulating of cellular and humoral reactions. For the purpose of normalization of a cellular metabolism are used a pantothenate calcium, cocarboxylase, orotate potassium, vitamin В12, folic acid (В9) etc. Sedative preparations enter into complex therapy of a recurrent aphthous stomatitis (a root of Valerian, "small" tranquilizers – diazepam, phenotropil, ataraxia). In successful treatment the important role is played a diet. The use of sharp, spicy food, spirits, smoking is forbidden. For the factor stimulation of specific and nonspecific protection modern methods of physiotherapy (transcutaneous electric stimulator of nerves, laser therapy on reflexogenic zones, aeroionic massage on affected oral mucous membrane) are effectively used. At a heavy corse of disease the oxygenation are used. Local treatment is done with the oral cavity sanation, elimination of injuring factors and the foci of a chronic infection. In an period of exacerbation are used an anesthetics - applications of 1-2 % lidocaine, trimecaine, pyromecaine solution, 5 % pyromecaine ointment.The fibrinogenous and necrotic scurf from a surface of aphthae and ulcers is removed with the help of proteolytic enzymes (trypsin, chymotrypsin, lysoamidaza). Antiseptic processing spend with solutions of antiseptic solutions - 0,02-0,06 % chlorhexidine, 0,02 % r-or furacilin. For stimulation of ephitelization is used an oil solution of vitamin A and Е,carotolin, ointment of solcoseryl, actovegin, sea-buckthorn oil.