CT Anatomy of the Abdomen and Pelvis - Human Health ...
77
CT Anatomy of the Abdomen and Pelvis J. Antonio Obando, MD Yale university School of Medicine VA Connecticut Healthcare System
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of CT Anatomy of the Abdomen and Pelvis - Human Health ...
CT Anatomy of the Abdomen and Pelvis
J. Antonio Obando, MDYale university School of MedicineVA Connecticut Healthcare System

Objectives
• Review crossectional imaging of peritoneal and retroperitoneal spaces
• Review anatomy of the lymph nodes • Anatomy of intra abdominal organs
Outline
• Peritoneal spaces• Retroperitoneal spaces• Lymph nodes• Abdominal organs

Peritoneum
• Serosal membrane• Encases the peritoneal cavity • Composes the mesenteries,• Partially or completely covers the abdominal and pelvic viscera.

Anatomic peritoneal spaces
• Peritoneal cavity: potential space between visceral and parietal peritoneum
• Visceral peritoneum lines:– Intraperitoneal organs– Mesenteries and omenta
Anatomic peritoneal spaces
Parietal peritoneum lines:• undersurface of the hemidiaphragm• abdominal wall• anterior surface the retroperitoneum• pelvis

Peritoneal ligaments
• Double folds of peritoneum. • Suspend and support the intraperitonealorgans
• Subdivide the peritoneal cavity into interconnected compartments
• Dictate the flow of fluid and location of disease
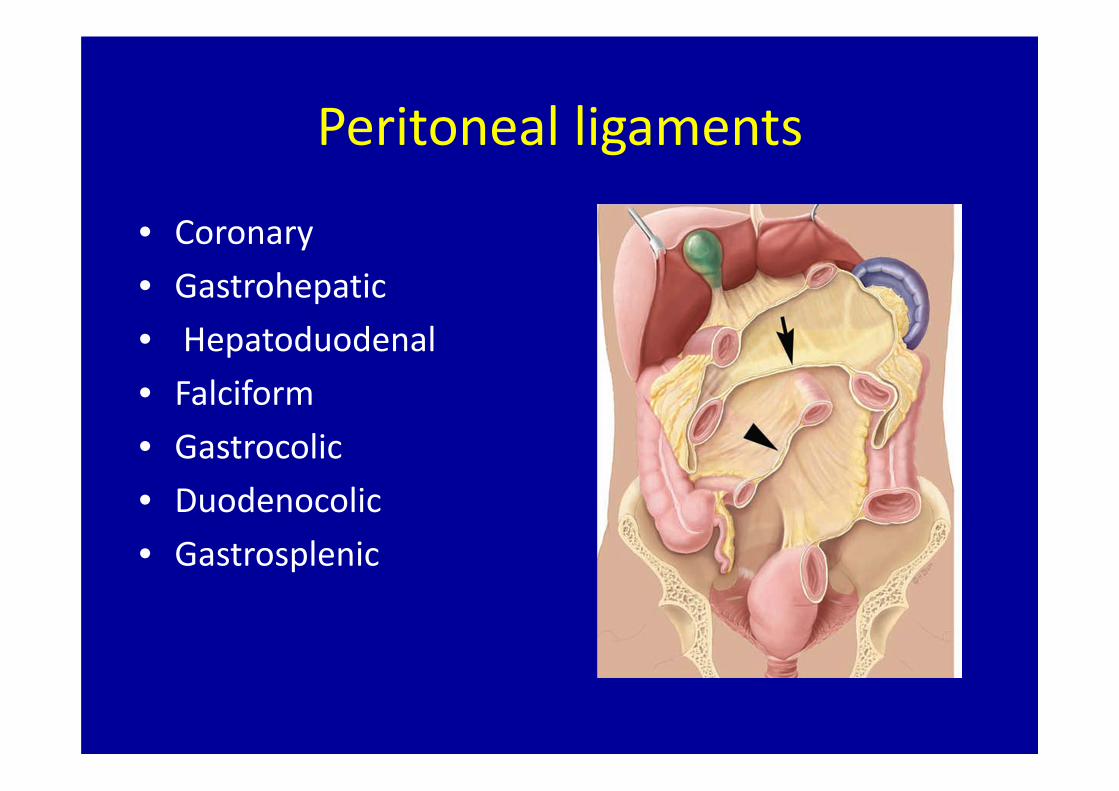
Peritoneal ligaments
• Coronary • Gastrohepatic• Hepatoduodenal• Falciform• Gastrocolic• Duodenocolic• Gastrosplenic

Peritoneal ligaments

Peritoneal fluid dynamics

Peritoneal fluid
Areas of stasis• Ileocolic region • Root of the sigmoid mesentery • Pouch of Douglas

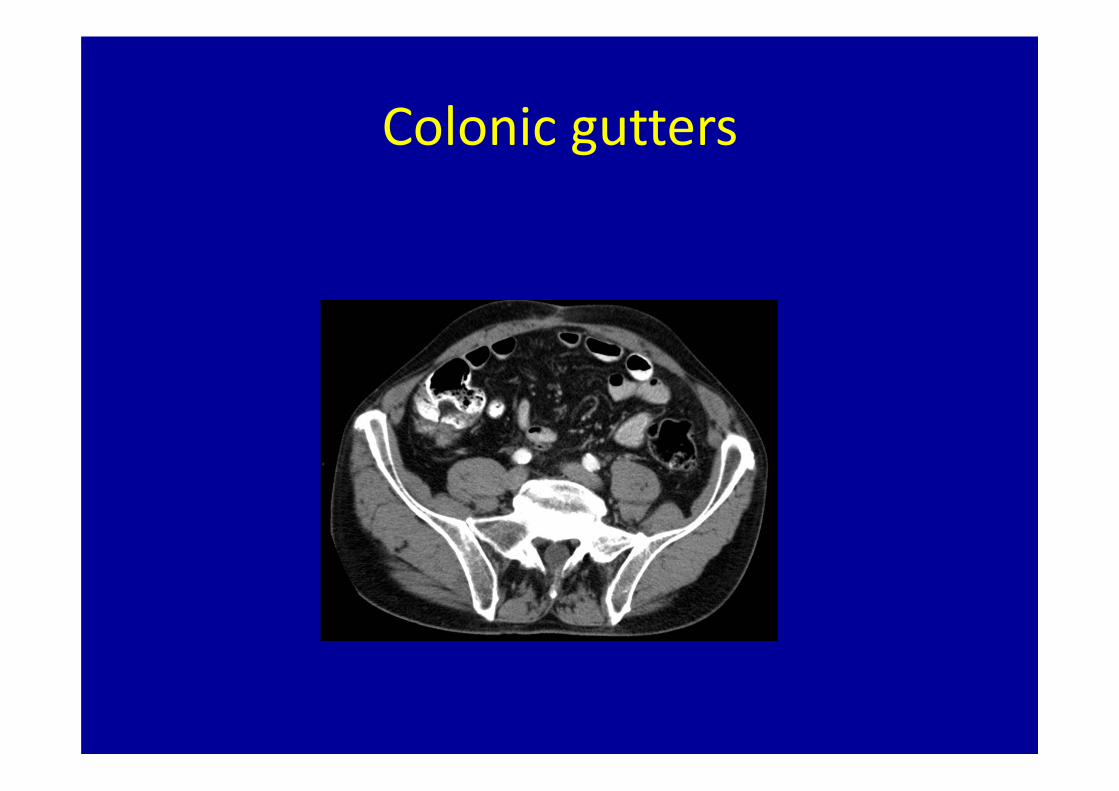
Colonic gutters

Pathologic processes of the peritoneum
• Metastatic neoplasms• Infectious and inflammatory lesions• Miscellaneous tumors and tumor‐like lesions

Pathologic processes of the peritoneum
• Metastatic neoplasms• Carcinomatosis• Pseudomyxoma peritoneiInfectious and inflammatory lesions
• Granulomatous peritonitis• Inflammatory pseudotumor• Sclerosing encapsulating peritonitis• Endometriosis• Splenosis

Pseudomyxoma peritonei

Peritoneal tuberculosis
• Thick ascitis• Terminal ileum abnormalities
• Low density lymphadenopathy

Omental caking
• Colon cancer• Ovarian• GI

Liver
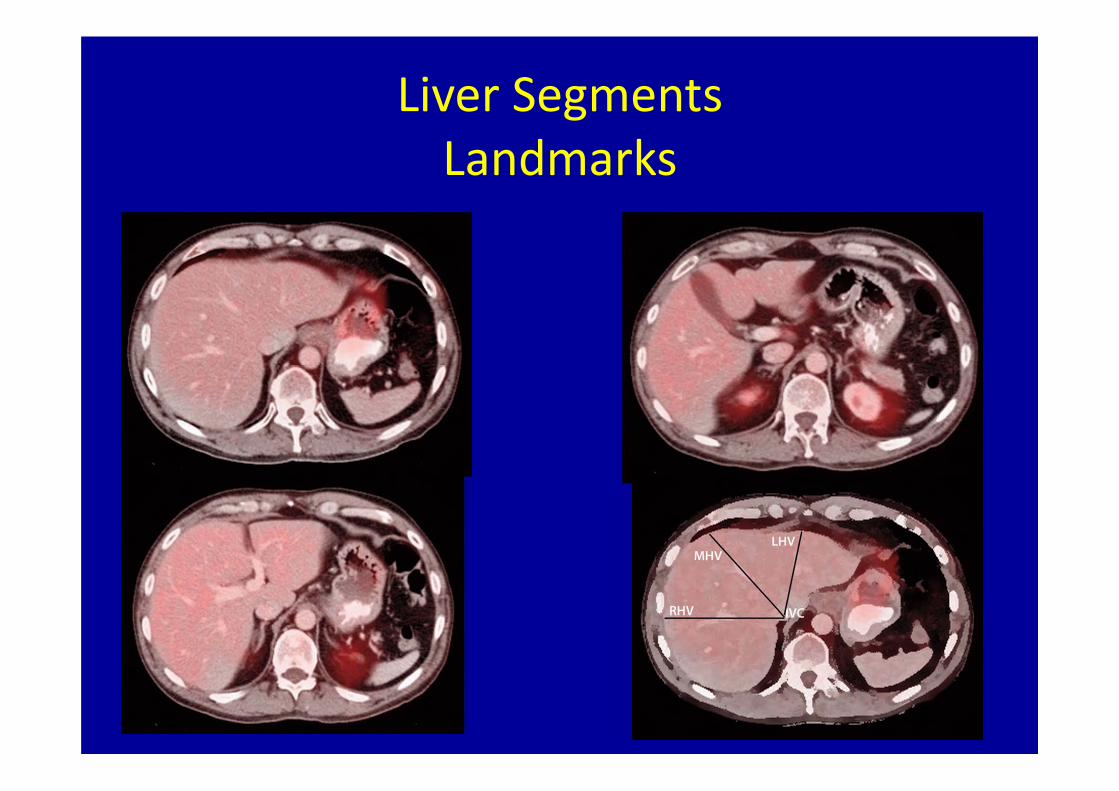
Liver SegmentsLandmarks

Liver SegmentsLandmarks
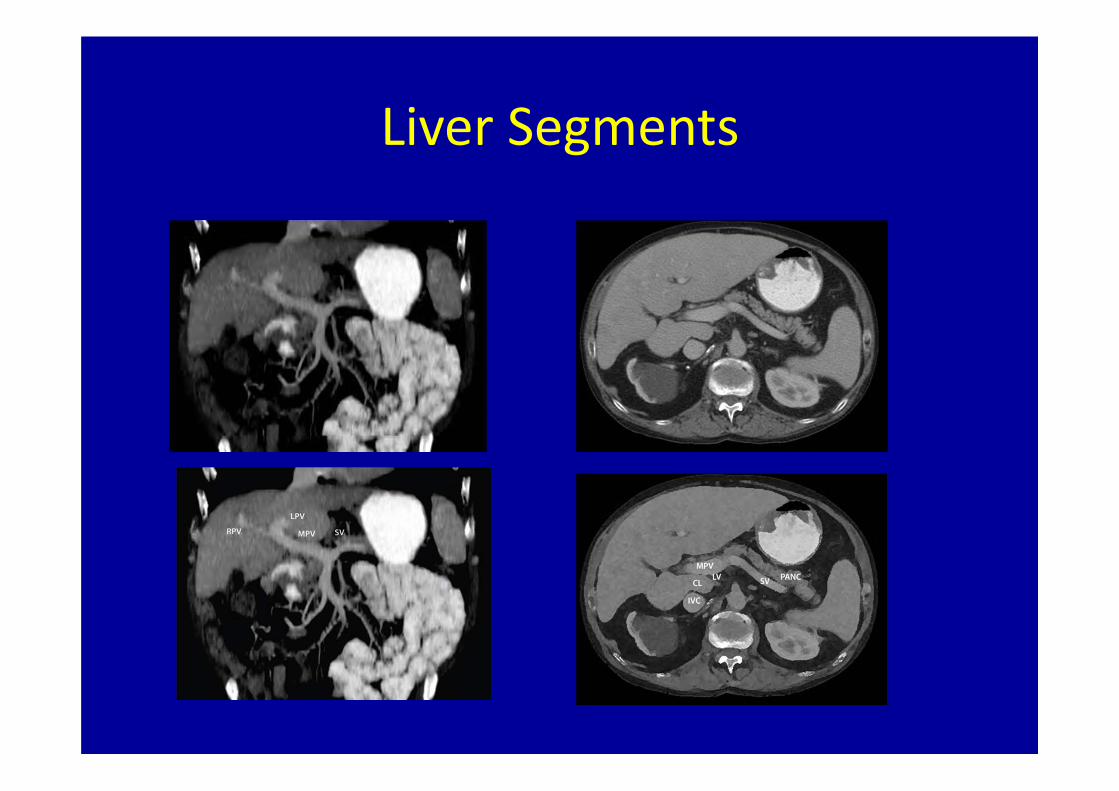
Liver Segments

Liver Segments

Liver Segments
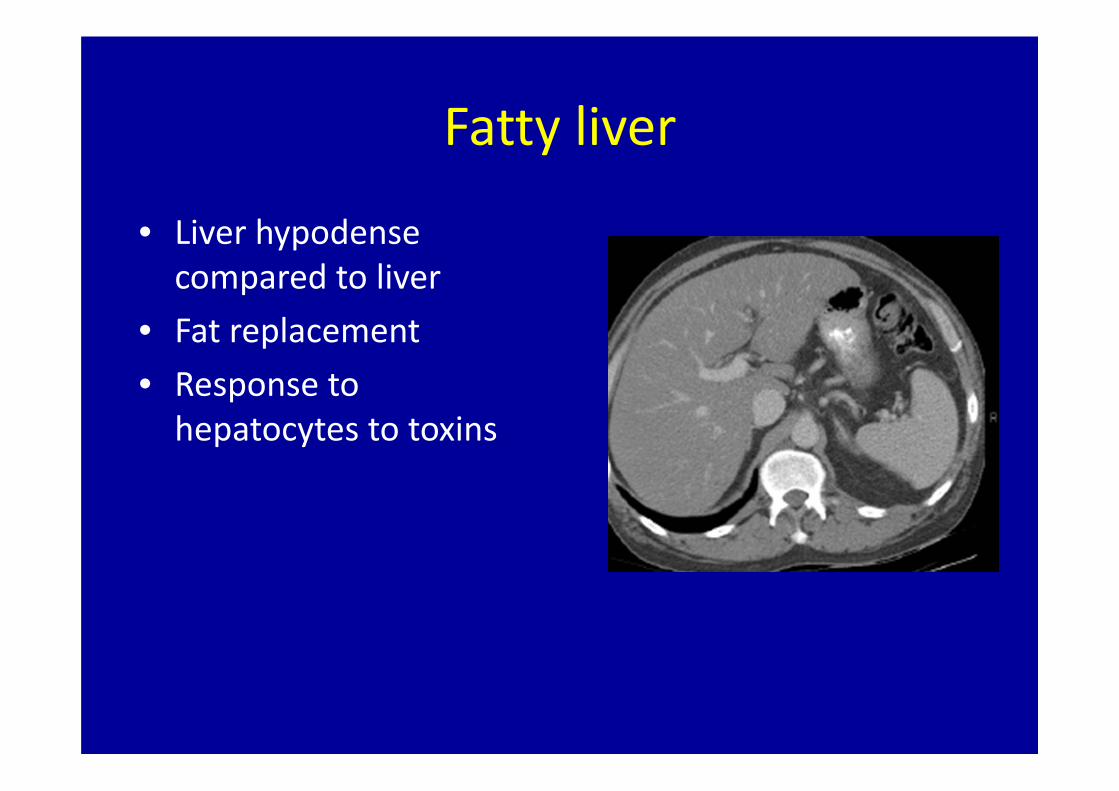
Fatty liver
• Liver hypodensecompared to liver
• Fat replacement• Response to hepatocytes to toxins

Cirrhosis
• Hepatocytesdestruction
• Inflamatory response• Nodularity• Fibrosis• Portal hypertension

Liver tumor enhancement
• Liver blood supply: 80% portal vein
– 20% hepatic artery
• Tumors 100% supply from hepatic artery– Enhance in arterial phase

Contrast phases
• Early arterial phase. FNH
• Portal venous phase. Hypovascular met
• Equilibriumcholangiocarcinoma

Hepatocelular carcinoma
Contour abnormality
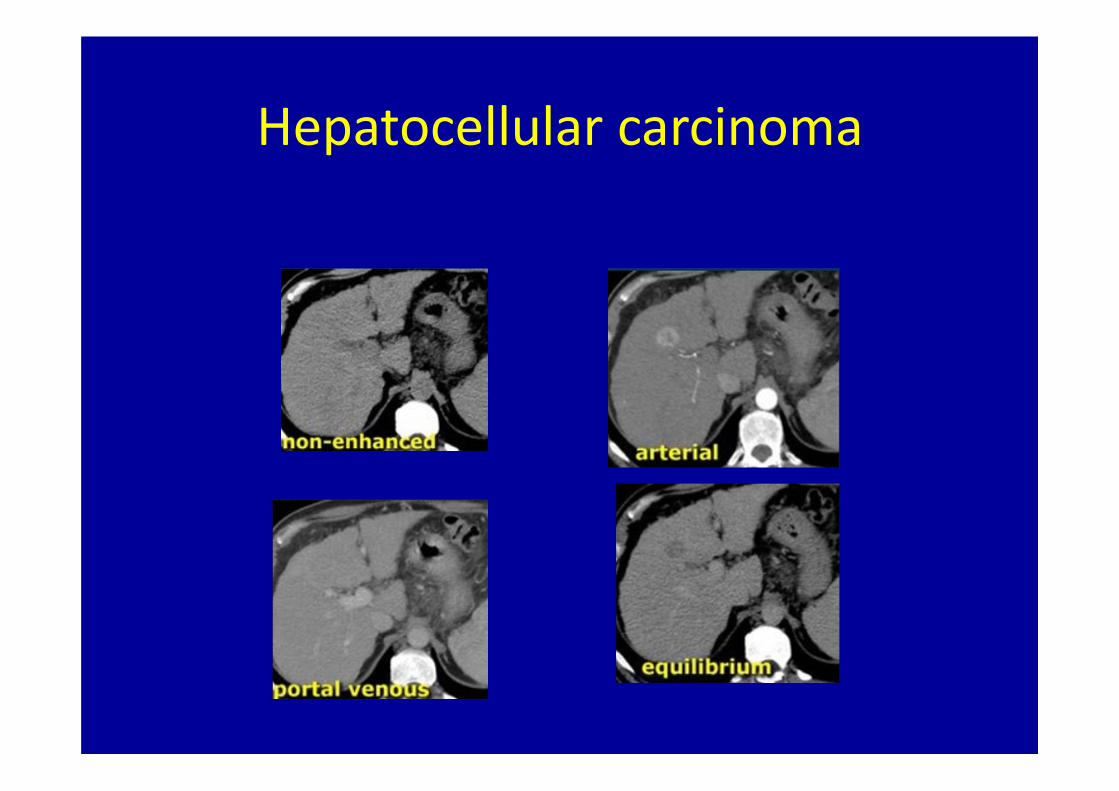
Hepatocellular carcinoma

Arterial phase imaging
• Characterisaton of a liver lesion of unknown origin
• Detection of HCC in patients with a high alpha 1 fetoprotein
• Screening of cirrhotic patients for HCC.• Detection of metastases in patients with hypervascular tumors

Hypervascular lesions?HCC Adenoma
FNH Hemangioma
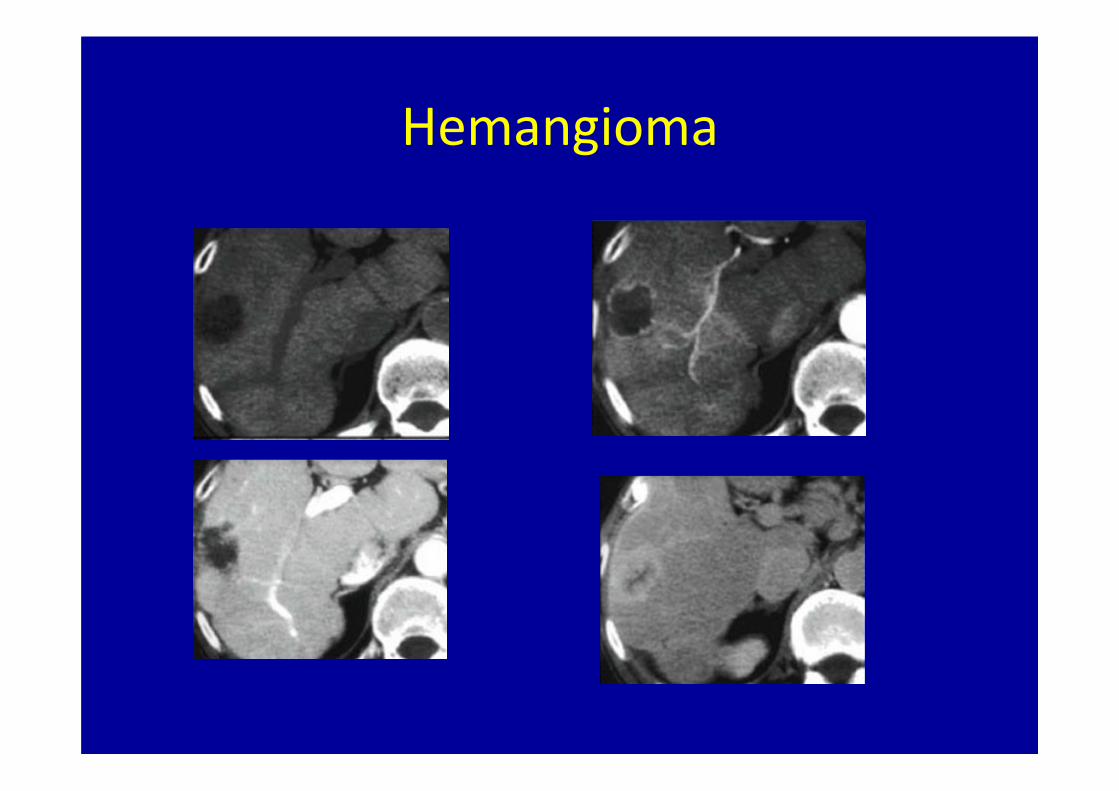
Hemangioma
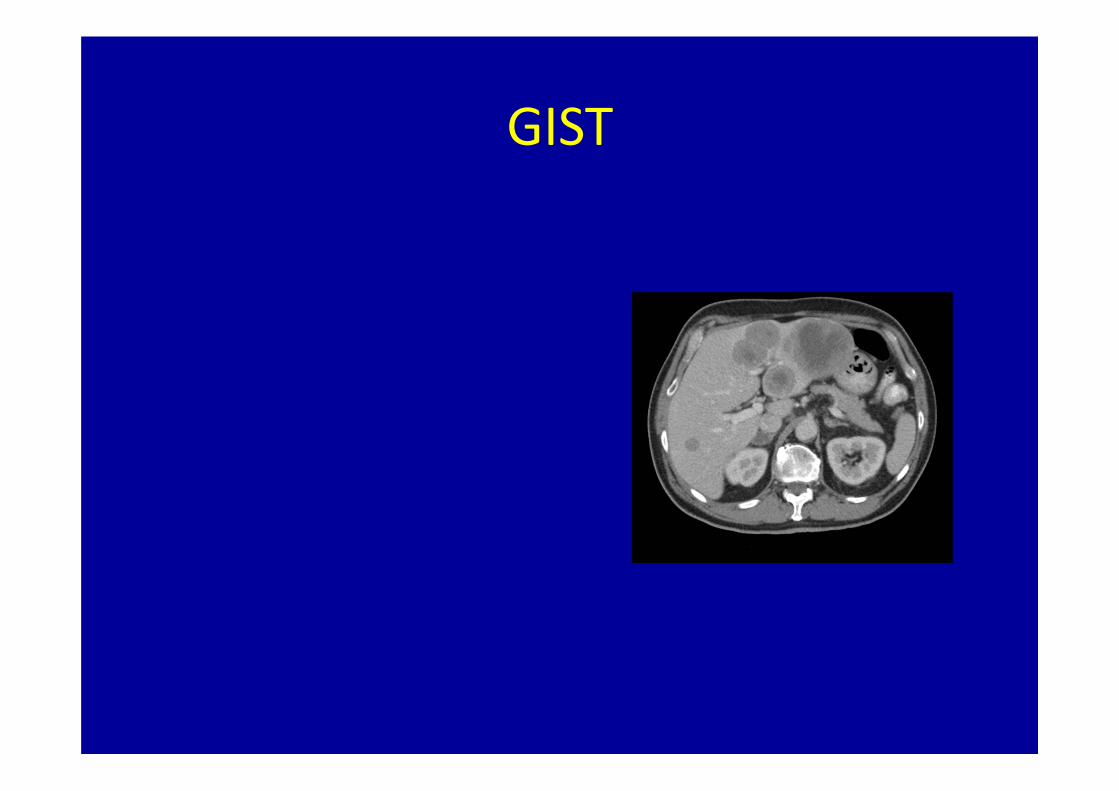
GIST

Splenosis

Retroperitoneum
• Pararenal spaces• Perirenal spaces

Kidneys

Adrenal glands

Pancreatitis

Pancreatic cancer

Stomach

Lumbar vertebral body


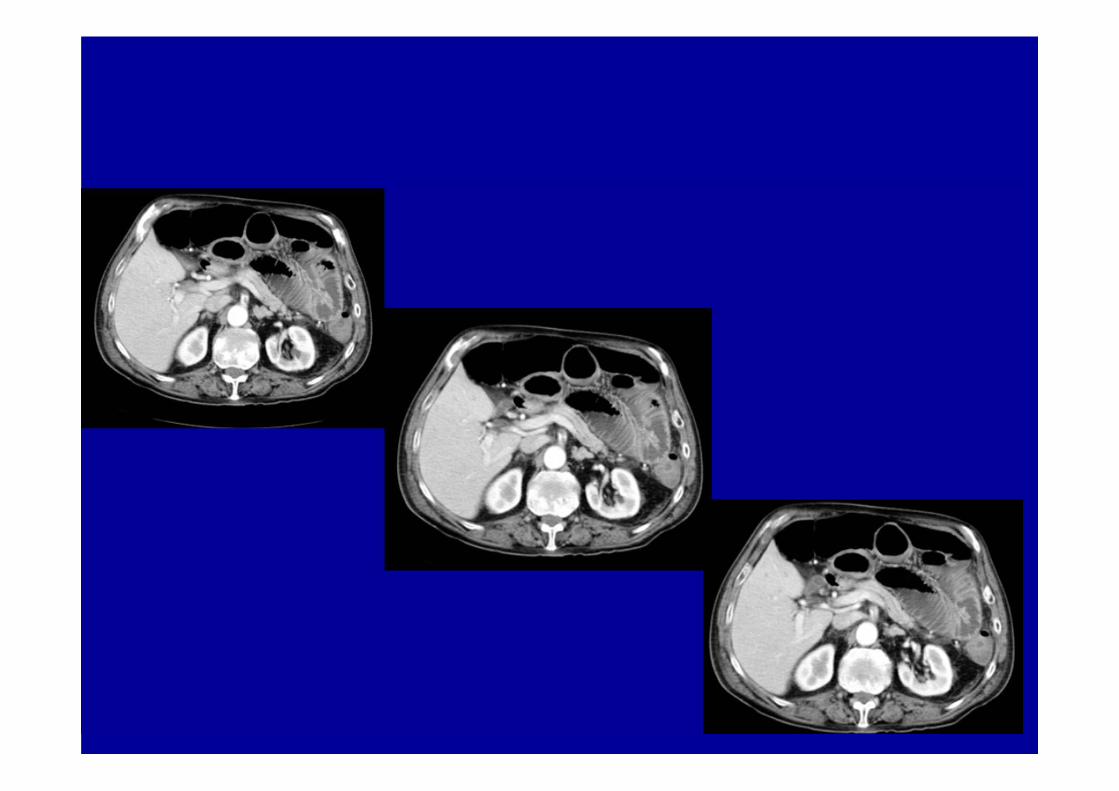
SMA

SMA thrombosis
•lack of enhancement of the lumen of the SMA•bowel wall thickening•ileus•absent mucosal enhancement•free fluid•mural gas, portal venous gas
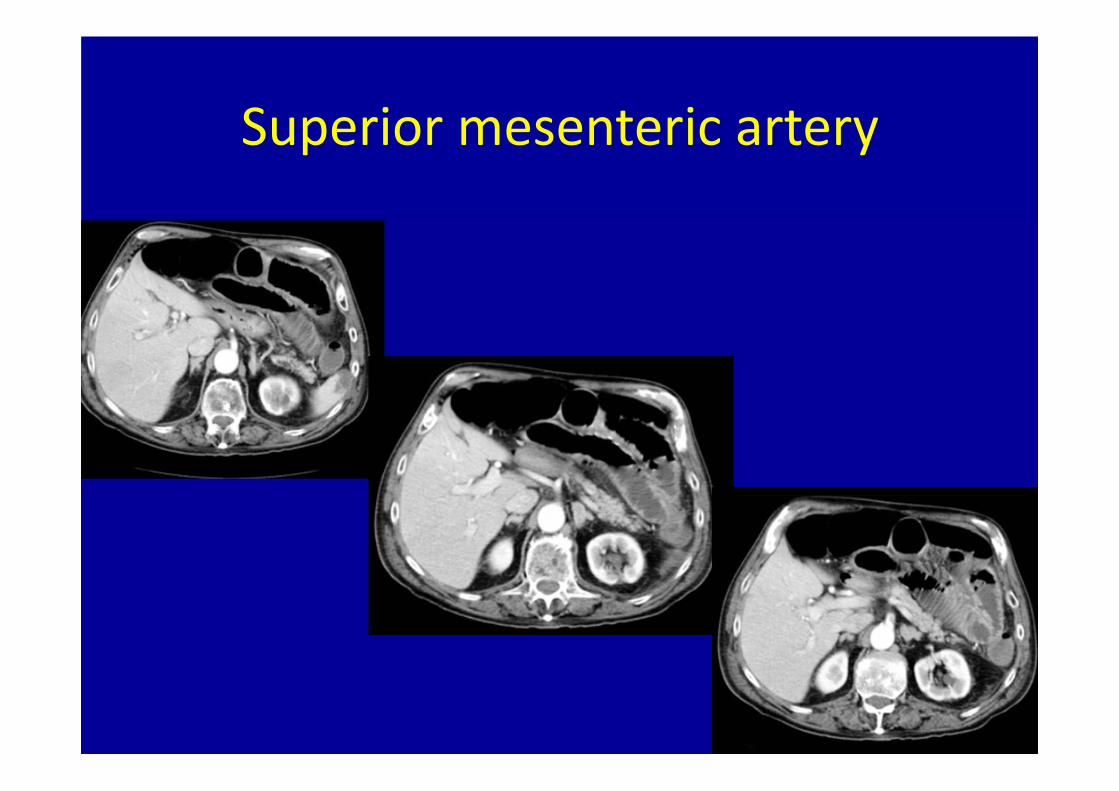
Superior mesenteric artery


Lymph nodes
• Diameter: 1cm• Porta hepatis: 6 mm• Retrocrural : 6 mm• Multiple: > 8 to 10 mm suspicious• False positives: hepatitis

Lymph nodes
• Paraaortic• Inferior mesenteric• Common iliac• Internal iliac• External iliac• Superficial inguinal• Deep inguinal• Sacral• Pararectal

Lymph nodes

Gastric ligament

Portocaval

Paraaortic

Para‐aortic
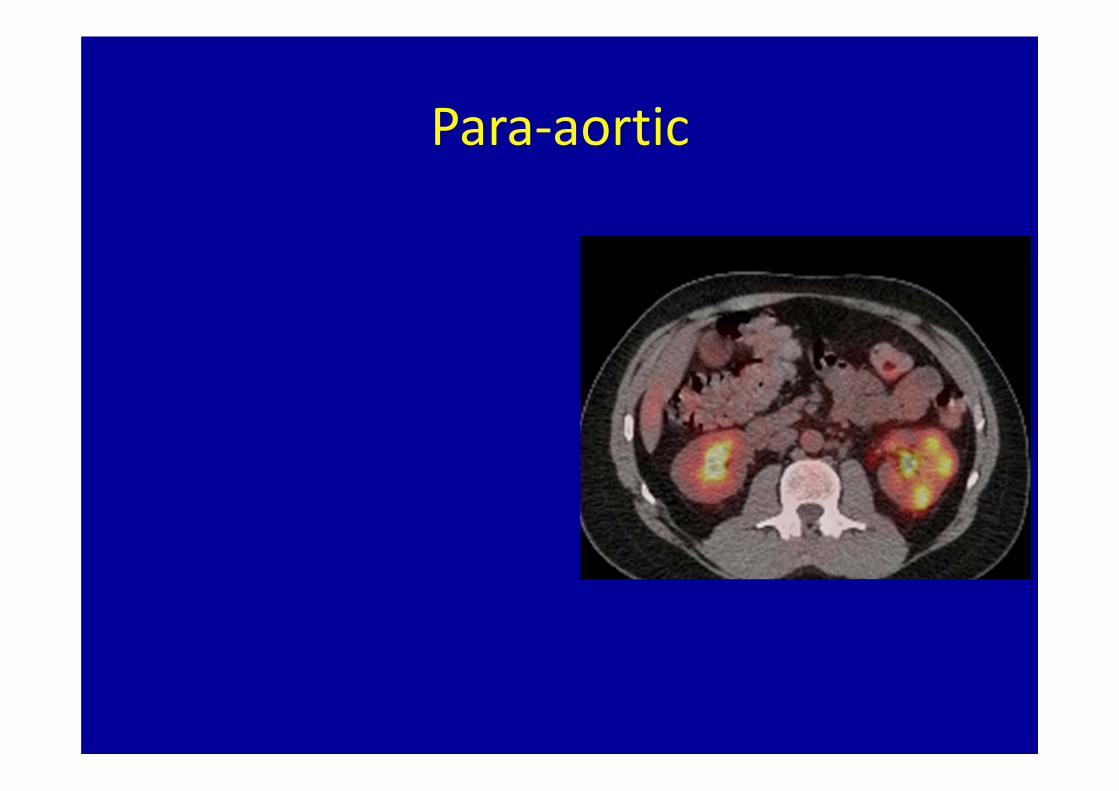
Para‐aortic

Caval aortic LN?

Diaphragmatic insertion


Aortocaval
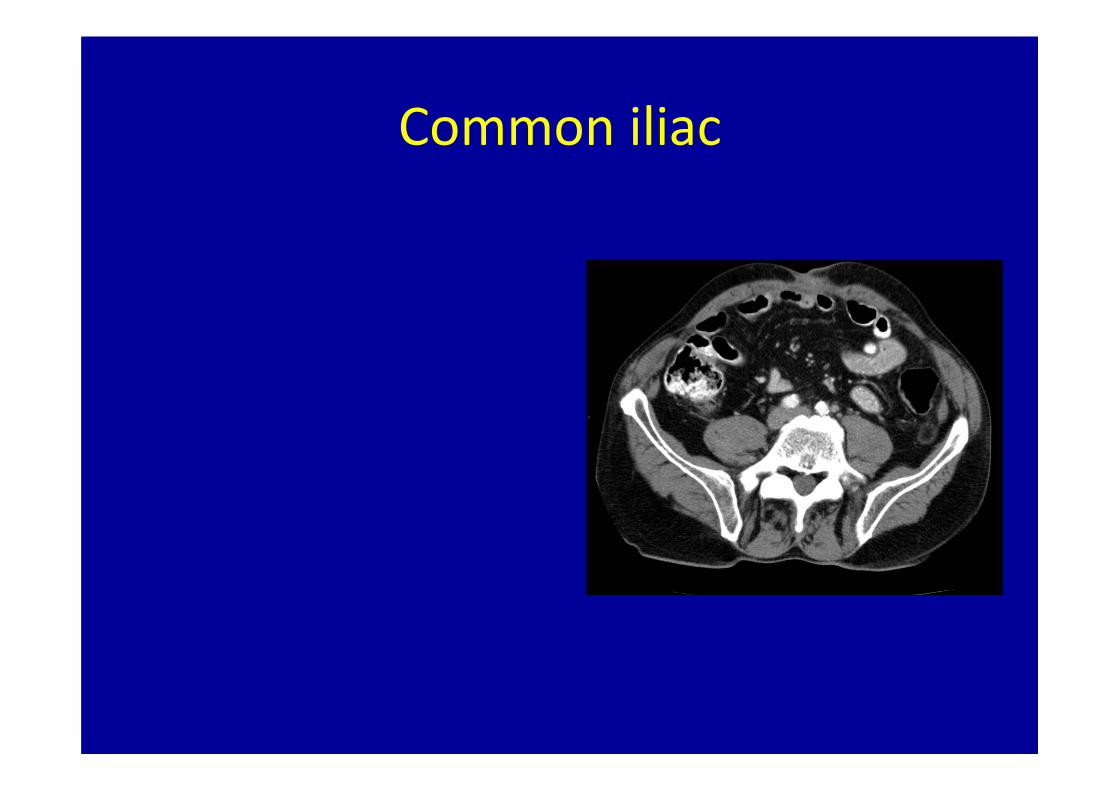
Common iliac

Internal and external iliac

Inguinal

Perirectal

Abdomen CT Questions
J. Antonio Obando, MDYale University School of MedicineVA Connecticut Healthcare System

CT Abdomen Question 1
• Hypodense lesion in the liver, seen on CT
• 1) Segment 2• 2) Segment 7• 3) Caudate lobe• 4) Segment 8• 5) Segment 6

CT Abdomen Answers Question 1• 1) Segment 2. Segment 2 is
in the left lobe• 2) Segment 7. Is the
posterior and superior segment
• 3) Caudate lobe. Is medial, and anterior to vena cava
• 4) Segment 8. Anterior to the left hepatic vein
• 5) Segment 6. Posterior and inferior segment liver segment.
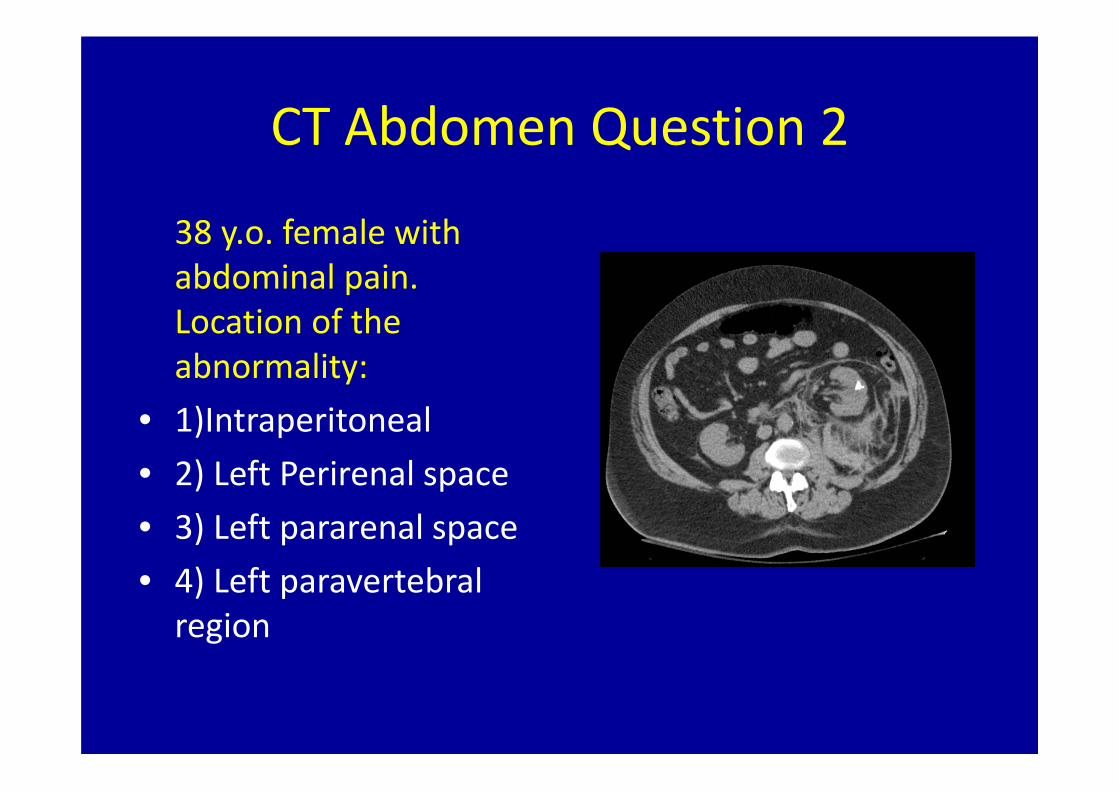
CT Abdomen Question 2
38 y.o. female with abdominal pain. Location of the abnormality:
• 1)Intraperitoneal• 2) Left Perirenal space• 3) Left pararenal space• 4) Left paravertebral region

CT Abdomen Answer Question 2
• 1)Intraperitoneal. The bleeding is retroperitoneal
• 2) Left Perirenal space.• 3) Left posterior pararenal space
• 4) Left paravertebral region.

CT Abdomen Question 3
• 72 y.o. male with hematuria. The abnormality in the right kidney is:
• 1) Simple cyst• 2) Infarct• 3) Hypervascular lesion• 4)Scar• 5) Normal variant

CT Abdomen Answer Question 3
• 1) Simple cyst. Simple cysts do not enhance• 2) Infarct. Renal infarcts are usually wedge shaped and do not enhance
• 3) Hypervascular lesion. Biopsy showed RCC• 4)Scar. Scars do not enhance• 5) Normal variant. Post contrast scan is definitely abnormal

CT Abdomen Question 4
• Hypodensity shown in the CT is located:
• 1) Segment 2• 2) Segment 3• 3) Caudate lobe• 4) Segment 4A

CT Abdomen Answers Question 4
• Hypodensity shown in the CT is located:
• 1) Segment 2• 2) Segment 3• 3) Caudate lobe• 4) Segment 4A

CT Abdomen Question 582 y.o. male with severe abdominal pain. CT image shows:
• 1) Left retroperitoneal hematoma
• 2) Ruptured AAA with retroperitoneal hematoma
• 3) Right retroperitoneal mass
• 4) Right retroperitoneal lymphadenpathy

CT Abdomen Question 5
• 1) Left retroperitoneal hematoma
• 2) Ruptured AAA with retroperitoneal hematoma
• 3) Right retroperitoneal mass
• 4) Right retroperitoneal lymphadenpathy

CT Abdomen Question 6
• 57 y.o. male history of ETOH abuse, abdominal pain.
• Diagnosis:• 1) Ascitis• 2) Pancreatitis• 3) Cirrhosis• 4) Pancreatic necrosis

CT Abdomen Answer 6
• 57 y.o. male history of ETOH abuse, abdominal pain.
• Diagnosis:• 1) Ascitis• 2) Pancreatitis• 3) Cirrhosis• 4) Pancreatic necrosis