
Cost-effectiveness of alternative methods for diabetic retinopathy screening
9
O R I G I N A L A R T I C L E Cost-Effectiveness of Alternative Methods for Diabetic Retinopathy Screening DAVID R. LAIRSON, PHD JACQUELINE A. PUGH, MD ASHA S. KAPADIA, PHD RONALD J. LORIMOR, PHD JAMES JACOBSON, MD RAMON VELEZ, MD OBJECTIVE— To assess from the perspectives of a government delivery system and patients, the cost-effectiveness of the 45-degree retinal camera compared to the standard ophthalmologist's exam and an ophthalmic exam by a physician's assistant or nurse practitioner technician, for detecting nonproliferative and proliferative diabetic retinopathy. RESEARCH DESIGN AND METHODS— Comparison of 45-degree fundus photographs with and without pharmacological pupil dilation taken by technicians and interpreted by experts, direct and indirect ophthalmoscopy by ophthalmologists, and direct ophthalmoscopy by technicians with seven-field stereoscopic fundus photography (reference standard). Costs were estimated from market prices and actual resource use. The study included 352 patients attending outpatient diabetes and general-medicine clinics at VA and DOD facilities. RESULTS— Medical system costs per true positive were: 45-degree photos with dilation, $295; 45-degree photos without dilation, $378; ophthalmologist, $390; and technician, $794. Patient costs per true positive were: 45-degree photos with dila- tion, $139; 45-degree photos without dilation, $171; ophthalmologist, $306; and technician, $1009. Cost-effectiveness is sensitive to program size due to high fixed cost of the camera methods but not to prevalence. Cost-effectiveness of the technician exam is strongly affected by its sensitivity. CONCLUSIONS— Primary-care screening with retinal photographs through pharmacologically dilated pupils for diabetic retinopathy is an appropriate and cost-effective alternative to screening by an ophthalmologist in this setting. Ophthal- mologists are scarce, primary-care physicians are extremely busy, and large clinics allow fixed equipment costs to be spread across many patients. FROM THE UNIVERSITY OF TEXAS HEALTH SCIENCE CENTER AT HOUSTON, SCHOOL OF PUBLIC HEALTH, HOUSTON; THE AUDIE L. MURPHY VA HOSPITAL, SAN ANTONIO; AND THE WILFORD HALL USAF MEDICAL CENTER, SAN ANTONIO, TEXAS. ADDRESS CORRESPONDENCE AND REPRINT REQUESTS TO DAVID R. LAIRSON, PHD, SCHOOL OF PUBLIC HEALTH, PO BOX 20186, UNIVERSITY OF TEXAS HEALTH SCIENCE CENTER, HOUSTON, TX 77225. RECEIVED FOR PUBLICATION 12 SEPTEMBER 1991 AND ACCEPTED IN REVISED FORM 30 APRIL 1992. PA, PHYSICIANS ASSISTANT; VA, VETERANS ADMINISTRATION; USAF, U.S. AIR FORCE; DOD, DE- PARTMENT OF DEFENSE. E pidemiological and health-services research has established diabetic retinopathy as a candidate for sec- ondary prevention through retinal screening. Using either excavated or computer-simulated cost estimates de- rived usually from a funding agency per- spective, studies have provided eco- nomic justification for ophthalmoscopy screening by an ophthalmologist (1,2) and, under certain cohort conditions, fundus photography through pharmaco- logically dilated pupils as a more cost- effective mode of screening for prolifera- tive diabetic retinopathy (3). Unfortunately, half of the high- risk diabetic population may be unaware of diabetic retinopathy (4), which is the leading cause of new cases of blindness in people 20-74 yr of age (5). Afflicting 5% of the U.S. population (5), diabetes is estimated to have a total economic im- pact of at least $14 billion annually (6), with diabetic blindness accounting for $75 million annually in lost income and public-welfare expense (7). Further- more, a large percentage of people with diabetes do not obtain screening exams (8-10). Cost-effective alternatives to oph- thalmologist screening that use less- expensive manpower substitutes can ease the adoption of routine screening by the VA and other public health-care organi- zations. Ophthalmoscopic examination by an ophthalmologist and stereoscopic fundus photography have been demon- strated as methods of detection and se- verity assessment (11); however, the de- velopment of a wide-angle 45-degree camera that can be used without phar- macological dilation has made primary- care and large-scale screening programs appear more feasible. Because 8-15% of all lesions and 27% of proliferative reti- nopathy cases have been observed out- side a single 45-degree field and because of a decreased ability to detect macula edema without stereoscopic photo- graphs, the application of nonstereo- scopic photography confronts an impor- DIABETES CARE, VOLUME 15, NUMBER 10, OCTOBER 1992 1369
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Cost-effectiveness of alternative methods for diabetic retinopathy screening

O R I G I N A L A R T I C L E
Cost-Effectiveness ofAlternative Methods forDiabetic Retinopathy ScreeningDAVID R. LAIRSON, PHDJACQUELINE A. PUGH, MDASHA S. KAPADIA, PHD
RONALD J. LORIMOR, PHDJAMES JACOBSON, MDRAMON VELEZ, MD
OBJECTIVE— To assess from the perspectives of a government delivery systemand patients, the cost-effectiveness of the 45-degree retinal camera compared to thestandard ophthalmologist's exam and an ophthalmic exam by a physician's assistantor nurse practitioner technician, for detecting nonproliferative and proliferativediabetic retinopathy.
RESEARCH DESIGN AND METHODS— Comparison of 45-degree fundusphotographs with and without pharmacological pupil dilation taken by techniciansand interpreted by experts, direct and indirect ophthalmoscopy by ophthalmologists,and direct ophthalmoscopy by technicians with seven-field stereoscopic fundusphotography (reference standard). Costs were estimated from market prices andactual resource use. The study included 352 patients attending outpatient diabetesand general-medicine clinics at VA and DOD facilities.
RESULTS— Medical system costs per true positive were: 45-degree photos withdilation, $295; 45-degree photos without dilation, $378; ophthalmologist, $390; andtechnician, $794. Patient costs per true positive were: 45-degree photos with dila-tion, $139; 45-degree photos without dilation, $171; ophthalmologist, $306; andtechnician, $1009. Cost-effectiveness is sensitive to program size due to high fixedcost of the camera methods but not to prevalence. Cost-effectiveness of the technicianexam is strongly affected by its sensitivity.
CONCLUSIONS— Primary-care screening with retinal photographs throughpharmacologically dilated pupils for diabetic retinopathy is an appropriate andcost-effective alternative to screening by an ophthalmologist in this setting. Ophthal-mologists are scarce, primary-care physicians are extremely busy, and large clinicsallow fixed equipment costs to be spread across many patients.
FROM THE UNIVERSITY OF TEXAS HEALTH SCIENCE CENTER AT HOUSTON, SCHOOL OF PUBLIC HEALTH,
HOUSTON; THE AUDIE L. MURPHY VA HOSPITAL, SAN ANTONIO; AND THE WILFORD HALL USAF
MEDICAL CENTER, SAN ANTONIO, TEXAS.
ADDRESS CORRESPONDENCE AND REPRINT REQUESTS TO DAVID R. LAIRSON, PHD, SCHOOL OF PUBLIC
HEALTH, PO BOX 20186, UNIVERSITY OF TEXAS HEALTH SCIENCE CENTER, HOUSTON, TX 77225.
RECEIVED FOR PUBLICATION 12 SEPTEMBER 1991 AND ACCEPTED IN REVISED FORM 30 APRIL 1992.
PA, PHYSICIANS ASSISTANT; VA, VETERANS ADMINISTRATION; USAF, U.S. AIR FORCE; DOD, DE-
PARTMENT OF DEFENSE.
E pidemiological and health-servicesresearch has established diabeticretinopathy as a candidate for sec-
ondary prevention through retinalscreening. Using either excavated orcomputer-simulated cost estimates de-rived usually from a funding agency per-spective, studies have provided eco-nomic justification for ophthalmoscopyscreening by an ophthalmologist (1,2)and, under certain cohort conditions,fundus photography through pharmaco-logically dilated pupils as a more cost-effective mode of screening for prolifera-tive diabetic retinopathy (3).
Unfortunately, half of the high-risk diabetic population may be unawareof diabetic retinopathy (4), which is theleading cause of new cases of blindnessin people 20-74 yr of age (5). Afflicting5% of the U.S. population (5), diabetes isestimated to have a total economic im-pact of at least $14 billion annually (6),with diabetic blindness accounting for$75 million annually in lost income andpublic-welfare expense (7). Further-more, a large percentage of people withdiabetes do not obtain screening exams(8-10).
Cost-effective alternatives to oph-thalmologist screening that use less-expensive manpower substitutes can easethe adoption of routine screening by theVA and other public health-care organi-zations. Ophthalmoscopic examinationby an ophthalmologist and stereoscopicfundus photography have been demon-strated as methods of detection and se-verity assessment (11); however, the de-velopment of a wide-angle 45-degreecamera that can be used without phar-macological dilation has made primary-care and large-scale screening programsappear more feasible. Because 8-15% ofall lesions and 27% of proliferative reti-nopathy cases have been observed out-side a single 45-degree field and becauseof a decreased ability to detect maculaedema without stereoscopic photo-graphs, the application of nonstereo-scopic photography confronts an impor-
DIABETES CARE, VOLUME 15, NUMBER 10, OCTOBER 1992 1369

Retinopathy screening cost-effectiveness
tant restriction (11). However, researchby Klein et al. (12) suggests that it maybe an effective alternative in routinescreening, especially where the availabil-ity of ophthalmologists and physicians islimited.
Investigations have only recentlyextended beyond issues of test accuracyand the cost-effectiveness of a singletechnology to address manpower substi-tutability and the comparative cost-effectiveness of screening alternatives un-der normal primary-care practiceconditions. Evidence from Foulds et al.(1) implied that an ophthalmoscopyscreening by either an ophthalmologistor a diabetologist is cost-effective. Usingannual incidence figures derived fromthe study's screen of all patients attend-ing a diabetic outpatient clinic, we devel-oped staff and workload projections toestimate the annual cost of undertaking ascreening program for 25,000 patientswith serious retinopathy. In U.S. dollars,the total annual cost projection for de-tection and treatment was $757/personcompared with an average annual savingin social benefits of $6994/person (4).However, resource constraints prohib-ited the use of the stereoscopic photoreference standard. More recently,Nathan et al. (13) determined that anophthalmoscopic examination by a dia-betologist was a competitive substitutefor ophthalmologist screening in terms ofaccuracy in classifying disease severity,promising savings of 10% by avoidingunnecessary ophthalmologist exams.However, only two diabetologists partic-ipated in the study, making the resultsless generalizable.
Assessed from the perspective ofthe delivery system and participating pa-tients, this paper examines the cost-effectiveness of the 45-degree retinalcamera as an alternative screeningmethod for nonproliferative and prolifer-ative diabetic retinopathy. The standardophthalmologist's exam and an oph-thalmic exam by a technician (PA ornurse practitioner) are compared withthe camera's performance with and with-
out pharmacological dilation of the pu-pils and with photos interpreted by ex-pert readers in a centralized readingcenter. Effectiveness was defined as thenumber of true-positive cases, and theaccuracy of each method was determinedby comparing the methods with the ref-erence standard of stereoscopic photos,also scored by the reading center. Thispaper focuses on the economic methodsand analysis.
RESEARCH DESIGN ANDMETHODS— The study determinedthe effectiveness by comparing perfor-mance of the four methods in identifyingtrue-positive cases of diabetic retinopa-thy among 352 individuals. About 50%were veterans receiving care at the AudieL. Murphy Memorial VA Hospital and50% were USAF personnel, dependents,or retirees receiving care at the WilfordHall USAF Medical Center, both locatedin San Antonio, Texas. Details of recruit-ment are included in a companion paperthat has been submitted for publicationQ.A.P., J.J., W.A.J. Van Heuver, J.A.Walters, M. Tuley, D.R.L., R.J.L.,A.S.K., R.V., "Screening for Diabetic Ret-inopathy: The Wide Angle Retinal Cam-era").
Description of screening exam andinterpretationFor the cost-effectiveness analysis, we as-sumed that each person screened re-sponds to an intake questionnaire andcomplies with a routine preliminaryexam consisting of intraocular pressure;visual acuity; and height, weight, andblood pressure measurements. Patientsare screened by one of four methods. The45-degree photographic method withoutpharmacological dilation includes onephotograph of each eye encompassing afield centered horizontally between theoptic disc and the macula taken by a PAor nurse practitioner with a 45-degreecamera. The photos are read by an inter-nist at the clinic and by trained readers atthe University of Wisconsin FundusPhotograph Reading Center. For the sec-
ond 45-degree photographic method,the pupils first are dilated, and threephotographs are taken of each eye en-compassing the same field as above butin stereo (achieved by moving the cam-era slightly lateral for the 2nd photo) anda third photo temporal to the maculawith the optic disc at the far nasal edge ofthe photo. Again, the 45-degree camerais operated by a PA or nurse practitioner.All positive findings are verified by pho-tographs through dilated eyes with sev-en-field stereoscopic 30-degree photo-graphs of each eye taken by a certifiedretinal photographer and read by trainedreaders at the Reading Center. The oph-thalmologist conducts both direct andindirect funduscopic exams through di-lated pupils, and the technician (PA ornurse practitioner) examines dilated eyeswith direct ophthalmoscopy. Positivefindings also are verified by the samemethod described for the photographicscreening modalities. The technicianshave minimal advanced ophthalmologi-cal training, having only completed theself-taught module of the PennsylvaniaDiabetes Academy on recognizing dia-betic retinopathy (16).
Analysis is conducted from theperspectives of the public provider ofhealth-care services (VA and DOD) andthe patient.
Accuracy of the screening meth-ods was determined by having subjectssequentially screened by the four meth-ods, testing results against the referencestandard of seven-field stereoscopic fun-dus photographs of each eye. Procedureswere adapted from the Early Treatmentof Diabetic Retinopathy Study. Slideswere mailed to the Reading Center andgraded for lesions of diabetic retinopathywith a modification of the Airlie HouseClassification (17-19). Details of de-scription of the effectiveness analysis areincluded in a companion paper that hasbeen submitted for publication Q.A.P.,J.J., W.A.J. Van Heuven, J.A. Walters, M.Tuley, D.R.L., R.J.L., A.S.K., R.V.,"Screening for Diabetic Retinopathy: TheWide Angle Retinal Camera").
1370 DIABETES CARE, VOLUME 15, NUMBER 10, OCTOBER 1992

Lairson and Associates
Assessment measuresEffectiveness. The number of true-positive tests was the chosen indicator ofeffectiveness for the alternative screeningmethods. The focus is on the intermedi-ate outcome of test accuracy, becausedecision makers have decided to recom-mend an annual screen based on previ-ous research on the final outcome ofsight-years saved and cost savings. Theissue is whether the camera methods area more efficient means of achieving thescreening goal. A true positive was de-fined as any retinopathy beyond mildnonproliferative or, more specifically, amodified Airlie House classification level>40 on the reference standard. This cutoff was chosen because this is the level atwhich it is recommended that an oph-thalmologist should follow the retinopa-thy. Up to this level, screening could takeplace in a primary-care setting on anannual basis if the screening method hada similar level of accuracy as an ophthal-mologist's exam. The Early Treatment ofDiabetic Retinopathy Study suggests that~12% of those with a modified AirlieHouse classification of 40 will progressto proliferative disease in 1 yr and 3.6%to high-risk proliferative disease. Al-though this may be a worst-case scenario(because high-risk individuals might beenrolled in treatment trials), this rate ofprogression would warrant referral to anophthalmologist if any level higher thanmild nonproliferative is found. Ungrad-able photos were counted as positive be-cause they would require referral for fur-ther evaluation.
Cost assessments. Actual resources re-quired to provide screening by the alter-native methods were identified, enumer-ated, and valued with market prices paidby the system and proxy measures ofpatient-time value. Medical system costsconsisted of personnel, equipment andsupplies, participants' time, space, over-head, and Reading Center fees. Personnelcosts were comprised of salaries andfringe benefits of ophthalmologists, pri-mary-care physicians, nurse practition-ers, PAs, and intake clerks. Time was
recorded prospectively with a stop watchat each station as the patient progressedthrough the screening process. Prices,wages, cost of capital items, space, andoverhead were obtained from VA rec-ords. Equipment included a Canon CR2-45NM camera, pneumatic chairs,Visulite base and viewer, and other asso-ciated small equipment items for viewingslides and taking photographs. Equip-ment costs were amortized over their ex-pected life (Appendix 1). Values for com-puting amortization of equipment andfacilities were obtained from medical sys-tem records and equipment manufactur-ers. The rate on long-term U.S. govern-ment bonds in 1989, 8.24%, wasselected for the interest rate to estimatethe government's cost of funds. It wasassumed that the camera and associatedequipment would be used only for thescreening. Overhead costs are estimatedat 29.7% of ambulatory care health-system costs. This rate was determinedby the local VA hospital administrationand includes administration, data pro-cessing, engineering, housekeeping, andutilities.
Patient costs included the costs oftransportation and opportunity costs(the value of time spent traveling, wait-ing, and being screened) and were calcu-lated on the basis of information re-corded at the clinic and provided by thepatient. Patient waiting and screeningtime was measured prospectively with astopwatch, whereas travel time and costwere self-reported. When employed, pa-tients' time was valued by their reportedwage rate. For those not employed, theminimum wage ($3.35/h) was used as aproxy for patient-time value.
We assumed that every positivetest would be referred for a stereoscopicphoto exam for verification. The cost ofthat exam, calculated from the perspec-tive of the medical system and the pa-tient, is therefore the estimated cost of afalse-positive test. The cost of false neg-atives, in terms of sight-years lost orother consequences, was beyond thescope of our data. However, the false
negatives are determined for eachmethod, and the implications for relativecost-effectiveness are described.
Cost-effectiveness analysisThe cost-effectiveness measure was theratio of the total cost of each screeningmethod to the number of true-positivetests achieved by that method or the costper true-positive test. The ratio may ob-scure whether the result is attributable torelatively low cost or high effectiveness,and therefore the results are presented ingraphical form with the cost of screeningon the x-axis and the effectiveness ofscreening (true positives) on the y- axis(Fig. 1). Cost-effectiveness is the inverseof the slope of a line (data not shown)between the origin and the coordinatesfor a screening method, and the incre-mental cost- effectiveness is the inverse ofthe slope of the lines between the coor-dinates of the screening methods (20).Steeper slopes represent more cost-effective modalities.
Because the camera methodshave relatively high fixed costs, the sen-sitivity of the results are examined forchanges in the number of peoplescreened. Because prevalence is an im-portant determinant of the number oftrue positives and may vary across pop-ulations, the results are examined for al-ternative levels of prevalence. Finally,limited training may have resulted in alow sensitivity for the technician exam,and those results are examined underassumptions of improved performance.
Statistical analysisThe cost data were analyzed by two-tailed Student's t tests. The four tech-niques were compared to the referencestandard of 30-degree seven-field ste-reoscopic photos read by the FundusPhotographic Reading Center. Measuresof sensitivity and specificity were com-pared for significant differences with Mc-Nemar's test for comparing proportionsof dependent samples (21).
DIABETES CARE, VOLUME 15, NUMBER 10, OCTOBER 1992 1371

Retinopathy screening cost-effectiveness
A 70
46 Deg. with DM. $ 1 3 9
6 10 16System Screening Cost x $1,000 2 4 6 8
Patient Screening Cost x $1,000
Figure 1—Cost (x-axis) and effect (y-axis) of number of true-positive cases identified from medicalsystem perspective (A) and patient's perspective (B). (45 Deg. with Dil), 45-degree camera methodwith dilation; (45 Deg. w/o Dil.), 45-degree camera method without dilation; (Ophthal), direct andindirect ophthalmoscopy by ophthalmologist; (Tech.), direct ophthalmoscopy by PA or nurse practi-tioner. Dollar figures represent cost-effectiveness ratios and are computed as inverse of slope of linefrom origin (not shown) to each coordinate. Inverse of slopes (not shown) of lines between pointsrepresent incremental cost-effectiveness ratios. Steeper slopes imply greater cost-effectiveness.
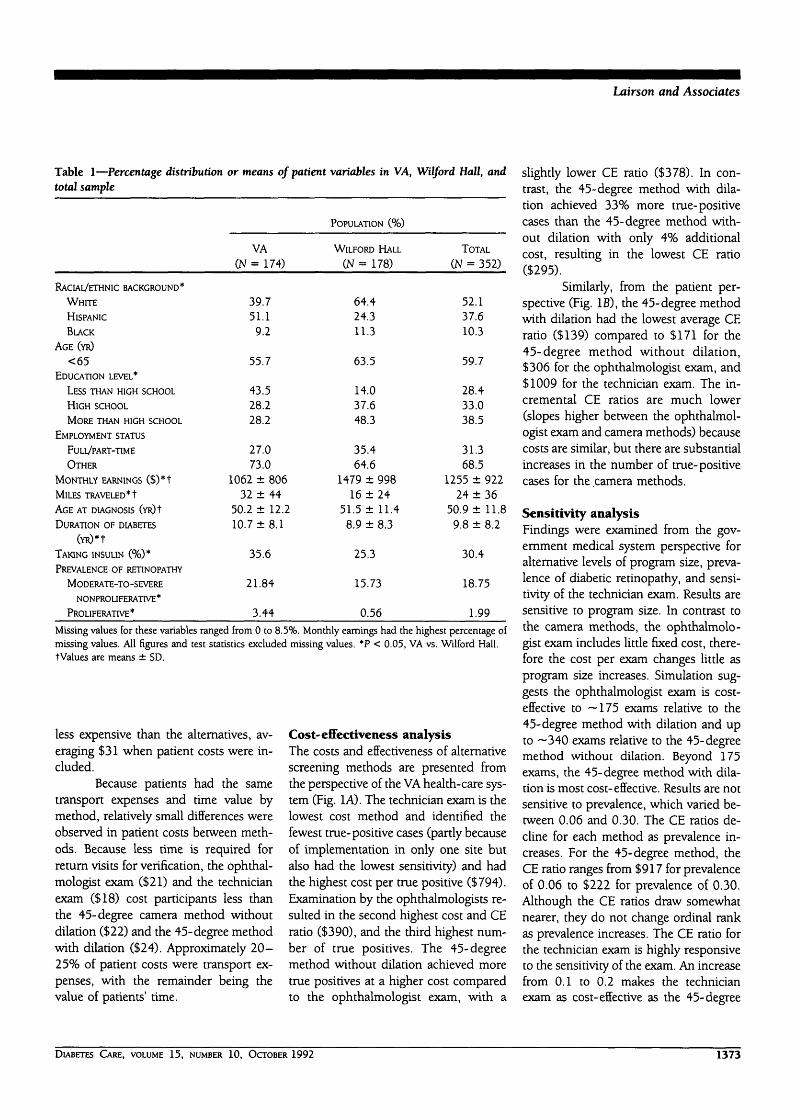
RESULTS— The VA and Wilford Hallsites served slightly different clientele(Table 1). The VA group consisted ofmore Hispanics, was older, and had lesseducation than the group studied at Wil-ford Hall. The VA patients also reportedless employment, lower monthly earn-ings, and longer average distances fromtheir home to the clinic. The mean age atwhich the two groups were first diag-nosed as diabetic did not differ. How-ever, consistent with their older age, theVA patients reported a longer duration ofdiabetes with a greater prevalence ofmoderate-to-severe nonproliferative andproliferative retinopathy, and a higherpercentage was taking insulin (35 vs.25%, respectively). Prevalence of moder-ate-to-severe nonproliferative retinopa-thy was 22% for VA and 16% for WilfordHall patients. One case of proliferativeretinopathy was identified among Wil-ford Hall patients compared with six forthe VA. Additional details on the study
populaton, including characteristics ofrespondents and nonrespondents are in-cluded in a companion paper that hasbeen submitted for publication (JAP.,J.J., W.A.J. Van Heuven, J.A. Walters, M.Tuley, D.R.L., R.J.L., A.S.K., R.V.,"Screening for Diabetic Retinopathy: TheWide Angle Retinal Camera").
EffectivenessEffectiveness results of the field study arepresented in Table 2. Results are basedon 351 cases for the camera methods,347 cases for the exam by the ophthal-mologists, and 172 cases for the techni-cian exam (Wilford Hall site only). Thetechnician exam was added midwaythrough the study and therefore was notavailable for all patients. One patient wasexcluded entirely because the stereo-scopic photographs were not gradable,and 4 other patients were excluded fromthe ophthalmologist evaluation becausethey were not examined by the ophthal-
mologist. Six patients at Wilford Hallwere not examined by the technician.
The reference standard examidentified 74, 73, and 30 cases of diseasein the populations screened by the cam-era methods, the ophthalmologists, andthe technician, respectively. The 45-degree photo method with dilation hadthe highest sensitivity (0.81) (60 truepositives and 14 false negatives). The 45-degree photo method with dilation is sig-nificantly more sensitive than all theother methods: ophthalmologist,(P < 0.0001; and 45-degree without di-lation, P < 0.002). The ophthalmologistexam ranks first in specificity (0.99),lowest in false positives (1), and highestin true negatives (273). The ophthalmol-ogist is more sensitive than the techni-cian (P < 0.02) but equally specific(P = 0.24). The ophthalmologist is sig-nificantly more specific than the 45-degree photos with dilation caused byfalse positives from ungradable photos(P = 0.011). The 45-degree photoswithout dilation are less specific than the45-degree photos with dilation (P <0.0001), primarily because of the largernumber of ungradable photos, 14.0 ver-sus 3.7% for the method with dilation.The technician exam has low sensitivity,identifying only 3 of 30 cases of disease.
CostsCosts by screening method are displayedin Table 3, and detailed estimates of per-sonnel time and cost per minute are dis-played in Appendix 2. The health-systemcost was ~$50/exam for the 45-degreecamera methods with and without dila-tion, $27 for the ophthalmologist exam,and $14 for the technician exam. Each ofthe three alternative method's costs wassignificantly different from the averageophthalmologist exam cost (P = 0.001).Including patient costs, the cost per pa-tient screened by the 45-degree methodwithout dilation was $70, with the 45-degree method with dilation being — $4more per case. In contrast, screening byan ophthalmologist cost about $48/case.The technician exam was considerably
1372 DIABETES CARE, VOLUME 15, NUMBER 10, OCTOBER 1992
Lairson and Associates
Table 1—Percentage distribution or means of patient variables in VA, Wilford Hall, andtotal sample
RACIAL/ETHNIC BACKGROUND*
WHITE
HISPANIC
BLACK
AGE (YR)
<65EDUCATION LEVEL*
LESS THAN HIGH SCHOOL
HIGH SCHOOL
MORE THAN HIGH SCHOOL
EMPLOYMENT STATUS
FULL/PART-TIME
OTHER
MONTHLY EARNINGS ($)*t
MILES TRAVELED *t
AGE AT DIAGNOSIS (YR)!
DURATION OF DIABETES
(YR)*t
TAKING INSULIN (%)*
PREVALENCE OF RETINOPATHY
MODERATE-TO-SEVERE
NONPROL1FERATIVE *
PROLIFERATE*
VA(N = 174)
39.751.1
9.2
55.7
43.528.228.2
27.073.0
1062 ± 80632 ± 4 4
50.2 ± 12.210.7 ±8.1
35.6
21.84
3.44
POPULATION (%)
WILFORD HALL
(N = 178)
64.424.311.3
63.5
14.037.648.3
35.464.6
1479 ± 99816 ± 2 4
51.5 ± 11.48.9 ± 8.3
25.3
15.73
0.56
TOTAL
(N = 352)
52.137.610.3
59.7
28.433.038.5
31.368.5
1255 ± 92224 ± 3 6
50.9 ± 11.89.8 ± 8.2
30.4
18.75
1.99
Missing values for these variables ranged from 0 to 8.5%. Monthly earnings had the highest percentage ofmissing values. All figures and test statistics excluded missing values. *P < 0.05, VA vs. Wilford Hall,tValues are means ± SD.
less expensive than the alternatives, av-eraging $31 when patient costs were in-cluded.
Because patients had the sametransport expenses and time value bymethod, relatively small differences wereobserved in patient costs between meth-ods. Because less time is required forreturn visits for verification, the ophthal-mologist exam ($21) and the technicianexam ($18) cost participants less thanthe 45-degree camera method withoutdilation ($22) and the 45-degree methodwith dilation ($24). Approximately 2 0 -25% of patient costs were transport ex-penses, with the remainder being thevalue of patients' time.
Cost-effectiveness analysisThe costs and effectiveness of alternativescreening methods are presented fromthe perspective of the VA health-care sys-tem (Fig. 1A). The technician exam is thelowest cost method and identified thefewest true-positive cases (partly becauseof implementation in only one site butalso had the lowest sensitivity) and hadthe highest cost per true positive ($794).Examination by the ophthalmologists re-sulted in the second highest cost and CEratio ($390), and the third highest num-ber of true positives. The 45-degreemethod without dilation achieved moretrue positives at a higher cost comparedto the ophthalmologist exam, with a
slightly lower CE ratio ($378). In con-trast, the 45-degree method with dila-tion achieved 33% more true-positivecases than the 45-degree method with-out dilation with only 4% additionalcost, resulting in the lowest CE ratio($295).
Similarly, from the patient per-spective (Fig. IB), the 45-degree methodwith dilation had the lowest average CEratio ($139) compared to $171 for the45-degree method without dilation,$306 for the ophthalmologist exam, and$1009 for the technician exam. The in-cremental CE ratios are much lower(slopes higher between the ophthalmol-ogist exam and camera methods) becausecosts are similar, but there are substantialincreases in the number of true-positivecases for the camera methods.
Sensitivity analysisFindings were examined from the gov-ernment medical system perspective foralternative levels of program size, preva-lence of diabetic retinopathy, and sensi-tivity of the technician exam. Results aresensitive to program size. In contrast tothe camera methods, the ophthalmolo-gist exam includes little fixed cost, there-fore the cost per exam changes little asprogram size increases. Simulation sug-gests the ophthalmologist exam is cost-effective to —175 exams relative to the45-degree method with dilation and upto ~ 3 40 exams relative to the 45-degreemethod without dilation. Beyond 175exams, the 45-degree method with dila-tion is most cost-effective. Results are notsensitive to prevalence, which varied be-tween 0.06 and 0.30. The CE ratios de-cline for each method as prevalence in-creases. For the 45-degree method, theCE ratio ranges from $917 for prevalenceof 0.06 to $222 for prevalence of 0.30.Although the CE ratios draw somewhatnearer, they do not change ordinal rankas prevalence increases. The CE ratio forthe technician exam is highly responsiveto the sensitivity of the exam. An increasefrom 0.1 to 0.2 makes the technicianexam as cost-effective as the 45-degree
DIABETES CARE, VOLUME 15, NUMBER 10, OCTOBER 1992 1373

Retinopathy screening cost-effectiveness
Table 2—Effectiveness of screening methods
METHOD
SENSITIVITY
SPECIFICITY
TRUE POSITIVE (N)
TRUE NEGATIVE (N)
FALSE NEGATIVE (N)
FALSE POSITIVE (N)
45-DEGREE
WITHOUT DILATION
(N = 351)
0.610.85
452362941
PHOTO
W I T H DILATION
(N = 351)
0.810.96
60267
1410
EXAM
OPHTHALMOLOGIST
(N = 347)
0.330.99
2427349
1
TECHNICIAN
(N = 172)
0.100.993
140432
Four patients failed to return for ophthalmologist's exam, and PA exam was evaluated in 1 site, WilfordHall.
method with dilation. If sensitivity is 0.6,the cost per true-positive test is half theCE ratio for the 45-degree camera withdilation. Even if training costs increasefivefold (to $2500) to achieve a sensitiv-ity of 0.6, the CE ratio for the technicianexam is 66% of the CE ratio for the45-degree method with dilation.
CONCLUSIONS— We compared effi-ciency of alternatives for achieving true-positive screening tests, an intermediateoutcome, in preventing the conse-quences of diabetic retinopathy. Previousstudies have provided evidence for theeconomic justification of diabetic reti-nopathy screening in terms of sight-yearssaved and net savings to government andsociety. They also have shown that the30-degree camera method of screeningwith dilation is cost-effective relative tothe 45-degree camera without dilationand the ophthalmologic exam (3).
By analyzing epidemiological andeconomic data on 352 patients in a VAand USAF population, this study foundthat, in this setting, medical care cost pertrue-positive case detected was lower forthe 45-degree camera with dilation($295) compared with the 45-degreecamera without dilation ($378), the stan-dard ophthalmologic examination($390), and direct funduscopic examina-tion by a PA or nurse practitioner ($794)for diabetic retinopathy screening. Whenpatient costs were added, the relative
rankings remained the same. Althoughthe cost of false negatives is beyond thescope of our data (and would includedisability and sight-yr lost), the relativeranking of the methods would remainthe same if the cost of false negativeswere included. A ranking of the methodsby the number of false negatives showedthe 45-degree photo method with dila-tion had the fewest false negatives, fol-lowed by the 45-degree techniquewithout dilation (29) and the ophthal-mologist exam (49).
Our findings differ from Dasbachet al.'s (3) simulation, which predictedthe 30-degree photo method with dila-tion was only marginally more cost-effective than the 45-degree photo with-out dilation and the ophthalmoscopyexam (3). In that case, choice of methodcould be determined by local conditionsof the delivery setting. This holds, intheir analysis, if sensitivity of the lattertwo methods does not fall below 0.65.We found sensitivity below 0.65, andtherefore the 45-degree photos with di-lation are preferred for our population,an older population with more difficultyachieving adequate nonpharmacologicaldilation.
Our classification of positivecases included both moderate and severestages of retinopathy. The former re-quires continued screening, and the lat-ter may require immediate treatment toavoid sight loss. A review of the cases
shows that 24 of 46 cases of nonprolif-erative disease missed by the ophthal-mologists had soft exudates as the onlyadvanced lesion beyond microaneurysm.These are difficult to identify, and theirpredictive value for progression to pro-liferative disease has been questioned(22). However, of the 7 cases of prolif-erative disease the ophthalmologistsidentified only 3. In 3 of 4 cases missed,the lesions were not on the optic disc andwould be considered low risk for loss ofvision.
This study applies data from onlytwo sites, ones with special populations,veterans and retired and active-duty mil-itary personnel, and dependents of re-tired and active-duty personnel. The re-sults, therefore, primarily apply to thesegroups. The Wilford Hall group wasyounger, better educated, had fewer eth-nic minorities, and lived closer to theclinic. The same camera technicians wereused at both sites, but the ophthalmolo-gists differed. However, sensitivity andspecificity of the screening methods var-ied little between sites. Time estimates ofthe activities were similar, although timerequired for the camera methods de-clined as the technicians gained experi-ence with the equipment and movedfrom the VA to the Wilford Hall site. Thisprobably was attributable to movementalong the learning curve and the youngerWilford Hall population. The technicianexam was conducted only at one site,and the technicians received limitedtraining before the project, possibly re-sulting in the extremely low sensitivity. Ifthis could be improved, even with a sub-stantial increase in training costs, thetechnician exam would compete favor-ably with other methods on the basis ofcost-effectiveness. Prevalence differedbetween the sites, but sensitivity analysisshowed that relative cost-effectivenesswas not affected as prevalence varied be-tween 0.06 and 0.30.
Cost differences between themethods are primarily attributable to therelatively high capital cost of the cameramethods. Although the ophthalmologist
1374 DIABETES CARE, VOLUME 15, NUMBER 10, OCTOBER 1992

Lairson and Associates
Table 3—Cost elements by screening method (in $)
RECURRENT COSTS
PERSONNEL*
READING CENTER CHARGE
O T H E R !
VERIFICATION O F POSI-
TIVES 1=
TRAINING
SYSTEM—CAPITAL AND
OVERHEAD
SPACE§
CAMERA||
OTHER EQUIPMENT^
OVERHEAD (RATE
29.7%)**TOTAL
SYSTEM COST PER EXAM
PATIENT COSTS
TRANSPORTATION
TRANSPORT TIME
SCREENING TIME
WAITING TIME
VERIFICATION t t
TOTAL
PATIENT COST PER EXAM
GRAND TOTAL COST
TOTAL COST PER EXAM
45 DEGREE
WITHOUT DILATION
(N = 351)
26081530597
4386
405
9413322
4372802
17,02849
18462011
548154217447691
2224,719
70
PHOTOS
WITH DILATION
(N = 351)
2802180111683570
405
9413322
4373136
17,67250
184620111211185114208339
2426011
74
EXAM
OPHTHALMOLOGIST
(N = 347)
5771—
1391275
—
179—
1511853
936827
1825198811831830507
733321
1670148
TECHNICIAN
(N = 172)
963—69
255
598
90—58
350
238314
540762526
1099101
302818
541131
*See table 1, in appendix, for cost elements.tOther costs include film, film processing, supplies, mailing, and camera maintenance.fAll positive tests are verified with stereographic photographs at $51 per exam.§Typical clinic space was priced at the market rental rate of $.78 per square foot per month. Space wasutilized for camera storage, camera exams, fundoscopic exams, and prorated for the time actually used forthat purpose.||The 45 degree Canon camera cost $12,000 and was amortized over an estimated 7 year life, assuming adiscount rate of .0824 and a resale value of $1,500. The annual cost of $2,157 was multiplied by 1.54(18.5/12) to represent the 18.5 month project period.HSmall equipment items included pneumatic chairs, visulite base, Donaldson viewer, Visulite Viewer, andan external fixation device.**VA accounting estimates that 29.7% of total ambulatory cost is indirect. This does not includedepreciation of VA facilities. Space costs are estimated according to footnote 4 above.ttPatient verification costs include transport cost, transport time, screening time, and waiting time. Theaverage cost was $20.28.
time is more expensive, the exam isshorter than that required for the cameramethods. The current sites, with largecentral clinics, are particularly suited toscreening projects requiring significantcapital investment. Personnel can spe-
cialize, and fixed costs can be spreadacross many patients. Use of the cameramethods in dispersed solo and smallgroup practices may result in lower cost-effectiveness, as suggested by the sensi-tivity analysis of program size. To reduce
patient costs associated with travel tocentral sites and to increase compliance,innovative methods are required to pro-vide screening in remote sites. One op-tion is the use of mobile screening unitsoperated by traveling technicians, in-cluding nurse practitioners or PAstrained to conduct screening with a cam-era. This option should be evaluated incomparison with the centralized systemsexamined in this study.
Both technicians (12) and diabe-tologists (13) can be trained to provideexams with acceptable sensitivity andspecificity. The barriers to primary-carephysicians providing such exams clearlyexist. First, these exams usually would beperformed in the context of a routinevisit with the cost (time, equipment,drugs for dilation) folded into the cost ofthe visit. They would not be reimbursedseparately. This economic disincentivecoupled with the multiplicity of otherconditions for which the primary-carephysician is being asked to screen (otherdiabetic complications, depression, alco-holism, other high-risk behaviors, livingconditions for the elderly, nutrition,breast and colon cancer risk, etc.) makeimplementation of retinopathy screeningby the primary-care physician unlikely.Second, the current recommendationsspecifically require an ophthalmologist'sexam, assuming that primary-care phy-sicians are not competent in this area. Incontrast to the primary-care physician,the ophthalmologist is reimbursed a fulloffice visit just for this exam. Finally,technicians who do not view screeningas either reducing their income or astaking away from their primary functionas a health-care provider, may in thelong run be more successful at screen-ing. However, their competence wouldhave to be monitored just as the compe-tence of the Reading Center staff is mon-itored.
The implementation of the 45-degree camera screening strategy wouldbe constrained by the resources of theindividual clinic or hospital using themand would have to be studied locally for
DIABETES CARE, VOLUME 15, NUMBER 10, OCTOBER 1992 1375

Retinopathy screening cost-effectiveness
quality control. Using the 45-degreecamera, the screening could take place asan addition to a routine visit in a prima-ry-care clinic or as a separate visit justfor screening. The person taking thepictures could be a nurse's aid, a nurse,or a physician extender (PA or nursepractitioner). Most facilities would notneed someone performing screening fulltime, so this would be only one ofmany duties. The photographs could ei-ther be read by a centralized readingcenter, or local personnel could betrained to read (each would require pe-riodic reevaluation of competency).Cut-off points for referral would be setlocally between the primary-care person-nel and ophthalmologists. Frequency ofscreening should follow national guide-lines. In VA and DOD facilities, this strat-egy has the potential of greatly increasingscreening because current screening islimited by scarce ophthalmological re-sources.
Appendix 2—Estimates of personnel time per case and cost per minute
ACTIVITY
PRELIMINARY
INTAKE/HISTORY
PHYSICAL EXAMT
DILATION f
SCREENING
45-DEGREE PHOTOS
WITHOUT DILATION
45-DEGREE PHOTOS
WITH DILATION
OPHTHALMOLOGY EXAM
TECHNICIAN EXAM
INTERPRETATION
45-DEGREE PHOTOS
WITHOUT DILATION
45-DEGREE PHOTOS
WITH DILATION
PERSON
CLERK
PA/NURSE PRACTITIONER
PA/NURSE PRACTITIONER
PA/NURSE PRACTITIONER
PA/NURSE PRACTITIONER
OPHTHALMOLOGIST
PA/NURSE PRACTITIONER
PRIMARY PHYSICIAN
PRIMARY PHYSICIAN
COST/MIN
($)*
0.16550.39140.3914
0.3914
0.3914
1.90000.3914
0.6412
0.6412
MINUTES
(MEAN ± SD)
4.41 ± 2.106.99 ± 2.68
2.00-
8.09 ± 4.17
7.26 ± 3.99
6.52 ± 5.073.44 ± 1.60
1.23 ± 0.92
1.79 ± 1.30
*Determined by dividing annual salary plus fringe benefits by 2080 h.tPhysical exam consists of visual-acuity test; height, weight, and blood pressure measurements; andintra- ocular pressure test. Dilation is done for mydriatic photos and for exams by ophthalmologist andtechnician.^Dilation time was estimated by project staff. Individual time measurements were not taken.
Acknowledgments—This work was sup-ported by the DOD and the VA.
We thank John A. Watters, MD (WilfordHall USAF Medical Center); Louis DeNino,PhD, Michael Tuley, PhD, Mary Dahl (AudieL. Murphy VA Hospital); Dima Abi-Said, andRhonda K. Ramby (Univ. of Texas School ofPublic Health) for valuable assistance.
Appendix 1—The following standardformula is used to determine annual cost ofcapital. The process is illustrated for wide-angle camera equipment (1)
AC = [RC - (SV/(1 + RT)] • A(R,N) (1)
= [$12,000 - ($1500/(1 + 0.0824)7] •0.1936
= $2156WHERE A(R,N) = [R(l + R)N]/[(1 + R)N - 1]
A ( 0 . 8 2 4 , 7 ) = [0.0824 (1 +
0.0824)7]/[(l + 0.0824)7 - 1]
A = 0.1936
AC, annualized cost; RC, replacement value; SV,scrap value; R, interest rate; N, useful life of capital.A(R,N), annuity factor (N yr at interest rate R)
References1. Foulds WS, McCuish A, Barrie T, Green
F, Scobie IN, Ghafour 1M, McClure E,Barber JH: Diabetic retinopathy in thewest of Scodand: its detection and prev-alence, and the cost-effectiveness of aproposed screening programme. HealthBull 41:318-26, 1983
2. Javitt JC, Canner JK, Sommer A: Costeffectiveness of current approaches to thecontrol of retinopathy in type 1 diabetics.Ophthalmology 96:255-64, 1989
3. Dasbach EJ, Fryback DG, Newcomb PA,Klein R, Klein BEK: Cost-effectiveness ofstrategies for detecting diabetic retinop-athy. Med Care 29:20-39, 1991
4. Porta M, Kohner E: Screening for dia-betic retinopathy in Europe. Diabetic Med8:197-98, 1991
5. National Society to Prevent Blindness,Operational Research Department: VisionProblems in the United States, 1978: A Sta-tistical Analysis. New York, National So-ciety to Prevent Blindness, 1980
6. Entmacher PS, Sinnock P, Bostic E, Har-ris MI: Economic impact of diabetes. In
Diabetes in America. Washington, DC,U.S. Dept. of Health and Human Serv-ices, 1985 (NIH publ. no. 85-1468,XXXII 1-13)
7. Klein R, Klein BEK: Vision disorders indiabetes. In Diabetes in America. Wash-ington, DC, U.S. Dept. of Health andHuman Services, 1985 (NIH publ. no.85-1468, XIII 1-36)
8. Witkin SR, Klein R: Ophdialmologic carefor persons with diabetes. JAMA 251:2534-37, 1984
9. Herman W, Halpern M, Pack VE, BeasleyJ, Callaghan C: Improving eye care forpersons with diabetes mellitus—Michi-gan. MMWR 34:697-99, 1985
10. Abi-Said D, Lorimor RJ, Lairson DR, Ja-cobsonj, PughJA: Annual retinal screen-ing for diabetic retinopathy: who gets itdone? Clin Res.
11. Owens DR, Dolben J, Young S, RyderREJ, Jones IR, VoraJ, Jones D, MorsmanD, Hayes TM: Screening for diabetic ret-inopathy (symposium). Diabetic Med8:S4-10, 1991
12. Klein R, Klein BEK, Neider MW, Hub-
1376 DIABETES CARE, VOLUME 15, NUMBER 10, OCTOBER 1992

Lairson and Associates
bard LD, Meuer SM, Brothers RJ: Dia-betic retinopathy as detected using oph-thalmoscopy, a nonmydriatic cameraand a standard fundus camera. Ophthal-mology 92:485-91, 1985
13. Nathan DM, Fogel HA, Godine JE, LouPL, D'Amico DJ, Regan CD], ToppingTM: Role of diabetologist in evaluatingdiabetic retinopathy. Diabetes Care 14:26-33, 1991
15. Diabetic Retinopathy Study ResearchGroup: Photocoagulation treatment ofproliferative diabetic retinopathy: clinicalapplication of Diabetic RetinopathyStudy (DRS) findings, DRS report num-ber 8. Ophthalmology 88:583-600, 1981
16. Brucker AJ: Module 2: visual impair-ment. In The Prevention and Treatment of
Five Complications of Diabetes: A Guide for
Primary Care Practitioners. Pennsylvania
Diabetes Academy, Ed. Philadelphia, PA,Academy, 1985
17. Klein BEK, Davis MD, Segal P, LongJA,Harris WA, Haug GA, Magli YL, SyrjalaS: Diabetic retinopathy: assessment of se-verity and progression. Ophthalmology91:10-17, 1984
18. Klein R, Klein BEK, Magli YL, Brothers RJ,Meuer SM, Moss SE, Davis MD: An alter-native method of grading diabetic retinop-athy. Ophthalmology 93:1183-87, 1986
19. Diabetic Retinopathy Study Research
Group: VIII. A modification of the AirlieHouse classification of diabetic retinopa-thy. Invest Ophthalmol Visual Sci 21:210-26, 1981
20. EisenbergJ: Clinical economics: a guideto the economic analysis of clinical prac-tices. JAMA 262:2879-86.
21. Fleiss JL: Statistical Methods for Rates andProportions. 2nd ed. New York, Wiley,1981, p. 113
22. Early Treatment Diabetic RetinopathyStudy Research Group: Fundus photo-graphic risk factors for progression ofdiabetic retinopathy: ETDRS reportnumber 12. Ophthalmology 98 (Suppl.):823-33, 1991
DIABETES CARE, VOLUME 15, NUMBER 10, OCTOBER 1992 1377




















