
Software for Reading and Grading Diabetic Retinopathy: Aravind Diabetic Retinopathy Screening 3.0
Upload
khangminh22Category
view
0download
0
Vitamin D and Diabetic Neuropathy
A thesis submitted to the University of Manchester for the degree of
Doctor of Philosophy in Medicine
in the Faculty of Medical and Human Sciences
2013
Uazman Alam
SCHOOL OF MEDICINE
Institute of Human Development, Centre for Endocrinology and Diabetes

2
Table of Contents
1 Chapter I - INTRODUCTION ......................................................................... 35 1.1 Aetiopathology of Diabetes ........................................................................... 36 1.2 Latent Autoimmune Diabetes in Adults (LADA) ........................................... 40
1.2.1 Screening and Treatment in LADA ............................................................... 40 1.2.2 Auto Antibodies in LADA .............................................................................. 43 1.2.3 Microvascular complications in LADA ........................................................... 44
1.3 Complications of Diabetes............................................................................. 45 1.3.1 Diabetic Neuropathy ..................................................................................... 46 1.3.2 Painful Diabetic Neuropathy ......................................................................... 51 1.3.3 Pathogenesis of Diabetic Neuropathy ........................................................... 53
1.4 Vitamin D deficiency ...................................................................................... 62 1.4.1 Vitamin D deficiency, Hyperlipidaemia and Hypertension ............................. 63 1.4.2 Vitamin D deficiency and Macrovascular Complications ............................... 64 1.4.3 Vitamin D and Diabetic Neuropathy .............................................................. 65 1.4.4 Vitamin D and Diabetic Retinopathy ............................................................. 67 1.4.5 Vitamin D and Diabetic Nephropathy ............................................................ 68
1.5 Clinical Evaluation and Investigations of Neuropathy ................................. 69 1.5.1 Diagnosis of Diabetic Distal Symmetrical Polyneuropathy ............................ 70
1.6 REFERENCES ................................................................................................. 79
2 CHAPTER II - METHODS ........................................................................... 113 2.1 Synopsis ....................................................................................................... 114 2.2 Hypothesis and aims.................................................................................... 114 2.3 Study Design ................................................................................................ 116 2.4 METHODS: Neuropathy Studies - Chapters 3, 4, 5 &8 ............................... 116
2.4.1 Patient Enrolment ....................................................................................... 116 2.4.2 Inclusion Criteria for Chapters 3, 4, 5 & 8 ................................................... 117 2.4.3 Exclusion Criteria for Chapters 3, 4, 5 & 8 .................................................. 118 2.4.4 Questionnaire Administration ...................................................................... 118 2.4.5 Neuropathy Disability Score (NDS) ............................................................. 119 2.4.6 Neuropad ................................................................................................... 121 2.4.7 Heart Rate Variability to Deep Breathing .................................................... 122 2.4.8 Quantitative Sensory Testing ...................................................................... 122 2.4.9 Electrophysiology ....................................................................................... 123 2.4.10 Skin Biopsies and Immuno-histology ...................................................... 125 2.4.11 Corneal sensitivity .................................................................................. 126 2.4.12 Corneal Confocal microscopy ................................................................. 127 2.4.13 Manual Image Analysis: Chapter 4,5 & 8 ................................................ 130 2.4.14 Automated Image Analysis: Chapter 3 only ............................................ 131
2.5 METHODS: Vitamin D Studies – Chapters 6, 7 & 9 .................................... 132 2.5.1 Participant Exclusion Criteria for Chapters 6, 7 & 9 .................................... 132 2.5.2 Blood pressure and Anthropometric measurements ................................... 132 2.5.3 Assessment of Demographics, Cardiovascular disease and Medications ... 133 2.5.4 Laboratory Measurements .......................................................................... 133 2.5.5 Diabetic Retinopathy Assessment .............................................................. 134 2.5.6 25(OH) Vitamin D Assay ............................................................................. 135
2.6 REFERENCES ............................................................................................... 136
3 Chapter III - Rapid Nerve Fibre Decline in patients with Type 1 diabetes can be readily detected using Corneal Confocal Microscopy. ..................... 138
3.1 ABSTRACT ................................................................................................... 139 3.2 INTRODUCTION ............................................................................................ 141 3.3 RESEARCH DESIGN AND METHODS ......................................................... 143

3
3.3.1 Selection of patients ................................................................................... 143 3.3.2 Assessment of neuropathy ......................................................................... 143 3.3.3 Corneal Confocal Microscopy ..................................................................... 144 3.3.4 Statistical analysis and Power calculation ................................................... 145
3.4 RESULTS ...................................................................................................... 147 3.4.1 Demographics ............................................................................................ 147 3.4.2 Metabolic and Anthropometric measurements ............................................ 149 3.4.3 Neuropathy evaluation ................................................................................ 151
3.5 DISCUSSION ................................................................................................. 159 3.6 REFERENCES ............................................................................................... 162
4 Chapter IV - Diagnostic Utility of Corneal Confocal Microscopy and Intra-Epidermal Nerve Fibre Density in Diabetic Neuropathy ................................ 167
4.1 ABSTRACT ................................................................................................... 168 4.2 INTRODUCTION ............................................................................................ 170 4.3 RESEARCH DESIGN AND METHODS ......................................................... 172
4.3.1 Selection of patients ................................................................................... 172 4.3.2 Definition of Neuropathy ............................................................................. 172 4.3.3 Assessment of neuropathy ......................................................................... 172 4.3.4 Corneal Confocal Microscopy ..................................................................... 173 4.3.5 Skin biopsy and immunohistochemistry ...................................................... 174 4.3.6 Statistical analysis ...................................................................................... 174
4.4 RESULTS ...................................................................................................... 176 4.4.1 Demographics, Metabolic and Anthropometric Assessment ....................... 176 4.4.2 Symptoms and deficits ............................................................................... 178 4.4.3 Neuropathy evaluation ................................................................................ 180
4.5 DISCUSSION ................................................................................................. 190 4.6 REFERENCES ............................................................................................... 194
5 Chapter V - Enhanced Small Fibre Neuropathy in Patients with Latent Autoimmune Diabetes in Adults ...................................................................... 201
5.1 ABSTRACT ................................................................................................... 202 5.2 INTRODUCTION ............................................................................................ 203 5.3 RSEARCH DESIGN AND METHODS ............................................................ 205
5.3.1 Selection of patients ................................................................................... 205 5.3.2 LADA definition ........................................................................................... 205 5.3.3 Assessment of neuropathy ......................................................................... 205 5.3.4 Corneal Confocal Microscopy ..................................................................... 206 5.3.5 Skin biopsy and immunohistochemistry ...................................................... 207 5.3.6 Statistical analysis ...................................................................................... 208
5.4 RESULTS ...................................................................................................... 209 5.4.1 Demographics and Clinical Neuropathy ...................................................... 209 5.4.2 Metabolic and Anthropometric measurements ............................................ 211 5.4.3 Neuropathy evaluation ................................................................................ 213
5.5 DISCUSSION ................................................................................................. 218 5.6 REFERENCES ............................................................................................... 220
6 Chapter VI - Marked vitamin D deficiency in patients with diabetes from secondary care: Ethnic and seasonal differences and an association with dyslipidaemia .................................................................................................... 226
6.1 ABSTRACT ................................................................................................... 227 6.2 INTRODUCTION ............................................................................................ 228 6.3 RESEARCH DESIGN AND METHODS ......................................................... 231
6.3.1 Subjects ..................................................................................................... 231 6.3.2 Blood pressure and Anthropometric measurements ................................... 231 6.3.3 Assessment of Demographics, Cardiovascular disease and Medications ... 232

4
6.3.4 Laboratory Measurements .......................................................................... 232 6.3.5 Statistical analysis ...................................................................................... 233
6.4 RESULTS ...................................................................................................... 235 6.5 DISCUSSION ................................................................................................. 241 6.6 REFERENCES ............................................................................................... 245
7 Chapter VII - Differential effects of different vitamin D replacement strategies in patients with diabetes ................................................................ 249
7.1 ABSTRACT ................................................................................................... 250 7.2 INTRODUCTION ............................................................................................ 251 7.3 RESEARCH DESIGN AND METHODS ......................................................... 253
7.3.1 Blood pressure and Anthropometric measurements ................................... 253 7.3.2 Assessment of Demographics, Cardiovascular disease and Medications ... 254 7.3.3 Laboratory Measurements .......................................................................... 254 7.3.4 Statistical analysis ...................................................................................... 255
7.4 RESULTS ...................................................................................................... 256 7.5 DISCUSSION ................................................................................................. 263 7.6 REFERENCES ............................................................................................... 267
8 Chapter VIII - Vitamin D Deficiency Contributes to Painful Diabetic Neuropathy ........................................................................................................ 272
8.1 ABSTRACT ................................................................................................... 273 8.2 INTRODUCTION ............................................................................................ 274 8.3 RESEARCH DESIGN AND METHODS ......................................................... 276
8.3.1 Selection of patients ................................................................................... 276 8.3.2 Assessment of neuropathy ......................................................................... 276 8.3.3 Corneal Confocal Microscopy ..................................................................... 277 8.3.4 Skin biopsy and immunohistochemistry ...................................................... 278 8.3.5 25(OH) Vitamin D Assay ............................................................................. 279 8.3.6 Statistical analysis ...................................................................................... 280
8.4 RESULTS ...................................................................................................... 281 8.4.1 Demographics, Metabolic and Anthropometric Assessment ....................... 281 8.4.2 Symptoms and deficits ............................................................................... 284 8.4.3 Quantitative sensory tests .......................................................................... 286 8.4.4 Electrophysiology ....................................................................................... 286 8.4.5 Autonomic function, IENFD and CCM ......................................................... 286 8.4.6 25(OH)D status .......................................................................................... 289
8.5 DISCUSSION ................................................................................................. 290 8.6 REFERENCES ............................................................................................... 294
9 Chapter IX - Vitamin D Deficiency is not associated with Diabetic Retinopathy or Maculopathy: A Cross Sectional study ................................ 300
9.1 ABSTRACT ................................................................................................... 301 9.2 INTRODUCTION ............................................................................................ 302 9.3 RESEARCH DESIGN AND METHODS ......................................................... 305
9.3.1 Subjects ..................................................................................................... 305 9.3.2 Blood pressure and Anthropometric measurements ................................... 305 9.3.3 Assessment of Demographics, Cardiovascular disease and Medications ... 306 9.3.4 25(OH) vitamin D Assay ............................................................................. 307 9.3.5 Statistical analysis ...................................................................................... 308
9.4 RESULTS ...................................................................................................... 310 9.5 DISCUSSION ................................................................................................. 320 9.6 REFERENCES ............................................................................................... 322
10 Chapter X - Discussion .......................................................................... 327

5
10.1 Rapid Nerve Fibre Decline in patients with Type 1 diabetes can be readily detected using Corneal Confocal Microscopy ........................................... 330 10.2 Diagnostic Utility of Corneal Confocal Microscopy and Intra-Epidermal Nerve Fibre Density in Diabetic Neuropathy .............................................. 330 10.3 Enhanced Small Fibre Neuropathy in Patients with Latent Autoimmune Diabetes in Adults ........................................................................................ 331 10.4 Marked vitamin D deficiency in patients with diabetes from secondary care: Ethnic and seasonal differences and an association with dyslipidaemia ............................................................................................... 332 10.5 Differential effects of different vitamin D replacement strategies in patients with diabetes. ............................................................................................... 333 10.6 Vitamin D Deficiency Contributes to Painful Diabetic Neuropathy ........... 334 10.7 Vitamin D Deficiency is not associated with Diabetic Retinopathy or Maculopathy: A Cross Sectional study ...................................................... 335 10.8 Study limitations .......................................................................................... 336 10.9 Future Work .................................................................................................. 338 10.10 Conclusion ................................................................................................ 339 10.11 REFERENCES ........................................................................................... 340
11 REFERENCES ......................................................................................... 350
12 APPENDIX 1– Study Related Documents ............................................. 403
13 APPENDIX 2 – Additional Analyses ...................................................... 413
Word count: 81807

6
List of Tables
Table 1-1 Diagnosis of DM ................................................................................... 37
Table 1-2 Details of major epidemiological studies of DSPN ................................ 49
Table 1-3 Abnormal sensations in DSPN .............................................................. 52
Table 1-4 Treatment of DSPN based on the putative pathogenetic mechanisms
and outcome of clinical trials. ................................................................................ 61
Table 1-5 Serum 25(OH) vitamin D concentrations and status ............................. 63
Table 1-6 Type of nerve fibres in the peripheral nervous system.......................... 70
Table 3-1 Participant demographics and clinical neuropathy parameters in control
subjects and patients with T1DM at baseline and 2 year follow up ..................... 148
Table 3-2 Metabolic parameters in control subjects and T1DM patients at baseline
and 2 year follow up ............................................................................................ 150
Table 3-3 Small and large fibre tests of nerve structure and function in control
subjects and diabetic patients at baseline and 2 year follow up .......................... 153
Table 3-4 T1DM subjects with Rapid Nerve Fibre Decline at baseline and 2 year
follow up .............................................................................................................. 156
Table 4-1 Participant demographics and metabolic parameters in control subjects
and diabetic patients without (T1DM) and with neuropathy (DSPN) ................... 177
Table 4-2 Neuropathy symptoms and deficits in control subjects and diabetic
patients without (T1DM) and with neuropathy (DSPN) ....................................... 179
Table 4-3 Small and large fibre tests of nerve structure and function in control
subjects and diabetic patients without (T1DM) and with neuropathy (DSPN) ..... 183
Table 4-4 Spearman’s rank correlation of CNFD, CNBD, CNFL and IENFD versus
NDS, McGill VAS, NSP, IENFD, thermal thresholds, VPT and nerve conduction
studies ................................................................................................................ 186
7
Table 4-5 ROC analysis with area under the curve, optimal cut off and respective
sensitivity and specificity with 95% confidence interval in T1DM versus DSPN for
CNFD, CNBD, CNFL, IENFD, VPT, CST and WST ............................................ 188
Table 5-1 Participant demographics in Controls, T2DM and LADA .................... 210
Table 5-2 Clinical and metabolic parameters in control subjects and patients with
T2DM and LADA ................................................................................................. 212
Table 5-3 Small and large fibre neuropathy tests in control subjects, T2DM and
LADA .................................................................................................................. 216
Table 6-1 Baseline characteristics of subjects with and without diabetes ........... 235
Table 6-2 Characteristics by categories of 25(OH)D in 563 unselected subjects
with diabetes. ...................................................................................................... 238
Table 6-3 Regression analyses of 25(OH)D and T-CHL, HDL and triglycerides in
subjects with diabetes ......................................................................................... 239
Table 6-4 Characteristics of subjects with diabetes based on ethnicity .............. 240
Table 7-1 Clinical and demographic data and Characteristics of Anti-Diabetic
therapy in all three cohorts of all three intervention cohorts ................................ 257
Table 7-2 Change in 25(OH)D status, metabolic data and anthropometric
measurements following intervention in all three cohorts .................................... 259
Table 8-1 Participant demographics and metabolic parameters in control subjects
and diabetic patients with DPN and PDN ............................................................ 282
Table 8-2 Clinical neuropathy symptoms and deficits in control subjects and
diabetic patients with DPN and PDN ................................................................... 285
Table 8-3 Small and large fibre tests of nerve structure and function in control
subjects and diabetic patients with DPN and PDN .............................................. 287

8
Table 9-1 Demographic and metabolic parameters in subgroups based on severity
of retinopathy ...................................................................................................... 312
Table 9-2 Logistic regression analyses for the relationship between retinopathy,
25(OH)D status and other confounding variables ............................................... 314
Table 9-3 Demographic and metabolic parameters in subgroups based on
maculopathy........................................................................................................ 316
Table 9-4 Logistic regression analyses for the relationship between maculopathy,
25(OH)D status and other confounding variables ............................................... 317
Table 9-5 Frequencies of retinopathy, maculopathy and photocoagulation scarring
categorised by 25(OH)D status ........................................................................... 319
Table 13-1 Baseline characteristics of the complete Control group (n=16) and the
Control group with only white European participants (n=12) ............................... 414
Table 13-2 Baseline characteristics of the complete Control group (n=27) and the
Control group with only white European participants (n=21) ............................... 415
Table 13-3 Baseline characteristics of the complete Control group (n=27) and the
Control group with participants of an older age matched to the DSPN group (n=13)
............................................................................................................................ 416

9
List of Figures
Figure 1-1 The pathogenesis of DSPN ................................................................. 56
Figure 1-2 Polyol Pathway in DSPN ..................................................................... 57
Figure 1-3 Putative effect of C-peptide on peripheral nerve structure and function
.............................................................................................................................. 60
Figure 1-4 Montage of the whole human subbasal nerve plexus .......................... 77
Figure 2-1 The Neuropathy Disability Score ....................................................... 120
Figure 2-2 Testing vibration sensation with a 128 Hz tuning fork as part of the NDS
............................................................................................................................ 120
Figure 2-3 Testing temperature sensation on the dorsum of foot as part of the NDS
............................................................................................................................ 121
Figure 2-4 The Neuropad .................................................................................... 121
Figure 2-5 The user interface for thermal threshold and pain measurement ...... 123
Figure 2-6 Electrodiagnostic studies of the peroneal and sural nerves ............... 124
Figure 2-7 Skin biopsies stained for PGP9.5 in a healthy control and subjects with
DM ...................................................................................................................... 126
Figure 2-8 Estimation of corneal sensation using NCCA .................................... 127
Figure 2-9 Corneal confocal microscopy ............................................................. 128
Figure 2-10 Positioning of the TomoCap® on the cornea ................................... 129
Figure 2-11 Image of the corneal subbasal nerves using corneal confocal
microscopy .......................................................................................................... 129
Figure 2-12 A preview of an image from the corneal subbasal nerves on the
Heidelberg eye explorer. ..................................................................................... 130
Figure 2-13 An CCM image of a control subject analysed to quantify corneal
subbasal nerve morphology in DSPN.. ............................................................... 131

10
Figure 3-1a, b & c. CNFD, CNBD and CNFL and baseline and 2 year follow up.
............................................................................................................................ 157
Figure 3-2 a & b. CCM images of a subject with RNFD at baseline and 2 year
follow up .............................................................................................................. 158
Figure 4-1a, b & c. Skin biopsy images of IENF in Controls, T1DM and DSPN ........
............................................................................................................................ 182
Figure 4-2a, b & c. CCM images in Controls, T1DM and DSPN ......................... 182
Figure 4-3 Receiver-operated characteristic (ROC) curves, based on the analysis
of CNFD and IENFD in T1DM versus DSPN ...................................................... 189
Figure 5-1 Skin biopsies stained for PGP9.5. in a healthy control, LADA patient
and T2DM patient with neuropathy ..................................................................... 214
Figure 5-2 Corneal confocal microscopy in a healthy control, LADA patient and
T2DM patient with neuropathy ............................................................................ 215
Figure 6-1 Histogram of 25(OH)D Status in subjects with diabetes .................... 237
Figure 6-2 Relationship between serum 25(OH)D and high-density lipoprotein
cholesterol (HDL) in subjects with diabetes ........................................................ 239
Figure 7-1a, b, c Box and Whisker plots for 25(OH)D pre- and post-intervention in
ECC, CCC and CC subdividing into <15ng/ml and >15ng/ml .................... 260 - 262
Figure 8-1 Graph showing 25(OH)D levels in ng/ml in C, DPN and PDN ........... 289
Figure 9-1 Frequencies of retinopathy, maculopathy and photocoagulation scarring
categorised by 25(OH)D status ........................................................................... 318
Figure 12-1Patient information sheet .................................................................. 404
Figure 12-2 Patient consent form ........................................................................ 407
Figure 12-3 Physical measurements and peripheral neuropathy assessment forms
............................................................................................................................ 408

11
Figure 12-4 Ophthalmic examination sheet ........................................................ 410

12
The University of Manchester
ABSTRACT OF THESIS submitted by Uazman Alam for the degree of Doctor of
Philosophy and entitled Vitamin D and Diabetic Neuropathy
September 2013
ABSTRACT
The accurate assessment of human diabetic somatic polyneuropathy (DSPN) is
important to define at risk patients, predict deterioration, and assess the efficacy of
pathogenetic treatments. Corneal confocal microscopy (CCM) has been proposed
as a surrogate endpoint for DSPN. Approximately 50% of patients with DSPN
experience neuropathic pain or symptoms and the underlying reasons are not
clearly elucidated. Vitamin D deficiency has been associated with diabetic
complications including DSPN and diabetic retinopathy (DR). However there is a
paucity of data regarding the interaction of vitamin D status with diabetic
complications.
This thesis shows that CCM can readily detect small fibre neuropathy prior to large
fibre involvement and assess rapidly progressive nerve fibre loss prior to
conventional thermal threshold testing. CCM has a superior diagnostic capabilities
compared to intra-epidermal nerve fibres and correlates better with nerve
conduction studies. Patients with LADA have a greater prevalence of small fibre
neuropathy compared to matched patients with type 2 diabetes. Vitamin D
deficiency is highly prevalent in patients with diabetes and despite relatively
aggressive replacement regimens are inadequate in raising vitamin D levels in a
significant proportion of patients. Vitamin D deficiency is not associated with DR
but there is a strong association between painful DSPN and vitamin D insufficiency
and more so with overt deficiency.

13
DECLARATION
No portion of the work referred to in this thesis has been submitted in support of an
application for another degree or qualification of this or any other university or other
institute of learning.
COPYRIGHT STATEMENT
i. The author of this thesis (including any appendices and / or schedules to
this thesis) owns certain copyright or related rights in it (the “Copyright”) and he
has given The University of Manchester certain rights to use such Copyright,
including for administrative purposes.
ii. Copies of this thesis, either in full or in extracts and whether in hard or
electronic copy, may be made only in accordance with the Copyright, Designs and
Patents Act 1988 (as amended) and regulations written under it or, where
appropriate, in accordance with the licensing agreements which the University has
from time to time. This page must form part of any such copies made.
iii. The ownership of certain copyright, patents, designs, trademarks and other
intellectual property (the “Intellectual Property”) and any reproductions of copyright
works in this thesis, which may be described in this thesis, may not be owned by
the author and may be owned by third parties. Such Intellectual Property and
Reproductions cannot and must not be made available for use without the prior
written permission of the owner(s) of the relevant Intellectual Property and / or
Reproductions.
iv. Further information on the conditions under which disclosure, publication
and commercialisation of this thesis, the Copyright and any Intellectual Property
and / or Reproductions described in it may take place is available in the University

14
IP Policy (see
http://www.campus.manchester.ac.uk/medialibrary/policies/intellectual-
property.pdf), in any relevant Thesis restriction declarations deposited in the
University Library, The University Library’s regulations (see
http://www.manchester.ac.uk/library/aboutus/regulations) and in the University’s
policy on presentation of Theses.
15
CONTRIBUTION
This section is to confirm that Uazman Alam, the author of this thesis, was actively
involved and had a significant contribution in all chapters/studies presented and
discussed in this thesis. Briefly, he recruited the vast majority of subjects with type
1 diabetes and latent autoimmune diabetes, a large portion of control subjects and
a smaller portion of subjects with type 2 diabetes. He consented subjects,
performed peripheral neuropathy assessments and undertook skin biopsies in the
majority of subjects in the included studies. He also partook in a portion of
laboratory skin biopsy processing and undertook intra-epidermal nerve fibre
analysis for all controls, subject with type 1 diabetes and latent autoimmune
diabetes as the dual examiner (along with Dr Maria Jeziorska). For chapters 4, 5
and 7, which are analyses of vitamin D data, he designed the studies and
undertook data extraction with co-researchers. He performed all of the statistical
analyses in this thesis with knowledge gained through an MSc in Population
Health, postgraduate certificate in statistics for clinical trials and masters level
professional development modules in advanced epidemiology. Finally, he has
written all the chapters of this thesis which have been reviewed by his supervisor,
Professor Rayaz Malik. The following tasks were performed by other members of
the research team:
Electrodiagnostic studies by Dr Andrew Marshall, consultant
neurophysiologist.
Ophthalmic examinations were performed by Dr Ioannis Petropulos, Dr.
Mitra Tavakoli and Maryam Ferdousi.
Peripheral neuropathy assessments and skin biopsies were also performed
by Dr Omar Asghar and Dr Hassan Fadavi.
16
Skin biopsy processing was undertaken by Dr Maria Jeziorska, Simon
Forman, Louisa Nelson, Aisha Meskiri, and Wendy Jones.
Skin biopsy analyses were also Dr Maria Jeziorska and Professor Rayaz
Malik.
Patient recruitment was also conducted by Georgios Ponirakis, Professor
Rayaz Malik and Dr Hassan Fadavi.
Software engineering to develop image analysis was undertaken by Dr
Mohammad A Dabbah, Dr Xin Chen and Dr James Graham.
Blood and Urine sample collections and anthropometric measurements by
the nursing staff in the Wellcome Trust Clinical Research Facility.
Haematology, immunology and clinical biochemistry analysis was performed
and reported by the relevant departments under the directorate of Laboratory
Medicine, Central Manchester University Hospitals, NHS foundation trust, UK.
Vitamin D laboratory analyses were undertaken by the vitamin D laboratory
at the Central Manchester Foundation Trust under the guidance of Dr Jacqueline
Berry.
Co-researchers assisting with trial design and data extraction on chapters 4,
5 and 7 were Professor J Kennedy Cruickshank, Dr Sara Al-Himdani, Dr Sophie
Benoliel, Dr Yasar Amjad, Dr Agnes Chan, Dr Ravinder Jugdey and Dr Osman
Najam.

17
ALTERNATIVE THESIS FORMAT
The author has been granted permission to submit this Ph.D. thesis in an
alternative format by his supervisor Professor Rayaz A. Malik approved under the
University of Manchester, Faculty of Medical and Human Sciences regulations,
including sections which are in a format suitable for submission for publication or
dissemination. The following chapters in this thesis have been published or will be
submitted for publication:
- Chapter 3: To be submitted for publication.
- Chapter 4: To be submitted for publication.
- Chapter 5: To be submitted for publication.
- Chapter 6: Published in the journal Diabetic Medicine, 2012.
- Chapter 7: Accepted for publication in the Journal of Diabetes and its
Complications, 2013.
- Chapter 8: Submitted for publication in the journal Diabetes and is currently
being revised for resubmission, 2013.
- Chapter 9: To be submitted for publication.

18
LIST OF ABBREVIATIONS
1,25(OH)2D: 1,25 vitamin D: 1,25 hydroxyvitamin D
25(OH)D: 25(OH) vitamin D: 25 hydroxyvitamin D
Ab: antibody
ACCORD: Action to Control Cardiovascular Risk in Diabetes
ACR: albumin creatinine ratio
AE: adverse event
AGE: advanced glycation end products
ALADIN: Alpha Lipoic in Diabetic Neuropathy
Alb: Albumin
ALP: Alkaline phosphatise
BDR: background diabetic retinopathy
BMI: body mass index
BP: blood pressure
CCa2+: corrected calcium
CCM: corneal confocal microscopy
CI: confidence interval
CNBD: corneal nerve branch density
CNFD: corneal nerve fibre density
CNFL: corneal nerve fibre length
CNFT: corneal nerve tortuosity coefficient
CNS: central nervous system
CBC: complete blood count
CKD: chronic kidney disease
CRGP: calcitonin gene-related peptide

19
CST: cold sensation threshold
CVA: Cerebrovascular accident
CVD: cardiovascular disease
DCCT: diabetes control and complications trial
DD: disc diameter
DM: diabetes mellitus
DNS: Diabetic Neuropathy Symptom Score
DPN: diabetic peripheral neuropathy
DR: diabetic retinopathy
DSPN: diabetic somatic polyneuropathy
EDIC: Epidemiology of Diabetes Interventions and Complications
eGFR: estimated Glomerular Filtration Rate
eNOS: endothelial nitric oxide synthase
fMRI: functional magnetic resonance imaging
GAD: anti-glutamic acid decarboxylase
HbA1c: glycated haemoglobin A1c
HDL: high density lipoprotein cholesterol
ICA: islet cell antibodies
IDF: International Diabetes Federation
IENF: intra-epidermal nerve fibre
IENFD: intra-epidermal nerve fibre density
IFN: interferon
IHD: ishaemic heart disease
IQR: interquartile range
IU: international units

20
LADA: latent autoimmune diabetes in adults
LANDMARK: Longitudinal Assessment of Opthalmic Diabetic Neuropathy
LDL: low density lipoprotein cholesterol
LFT: liver function tests
LURIC study: ludwigshafen risk and cardiovascular health study
MI: myocardial infarction
McGill VAS: McGill visual analogue score
NBF: nerve blood flow
NCCA: non-contact corneal aesthiometer
NCS: nerve conduction studies
NCV: nerve conduction velocity
NDR: no diabetic retinopathy
NDS: neuropathy disability score
NGF: nerve growth factor
NGSP: National Glycohaemoglobin Standardization Program
NHANES: National Health and Nutrition Examination study
NSP: neuropathy symptom profile
NCS: nerve conduction study
OGTT: oral glucose tolerance test
OR: odds ratio
PDR: proliferative diabetic retinopathy
PPDR: pre-proliferative diabetic retinopathy
PKC: protein kinase C
PMNCV: peroneal motor nerve conduction velocity
PMNamp: peroneal motor nerve amplitude

21
PVD: peripheral vascular disease
ROC: receiver operating characteristic
QST: quantitative sensory testing
RAGE: receptor for AGE
RAS: renin angiotensin aldosterone system
RCT: randomised clinical trial
RNFD: rapid nerve fibre decline
SD: standard deviation
SSNCV: sural sensory nerve conduction velocity
SSNAmp: sural sensory nerve amplitude
TGF-β1: transforming growth factor β1
TRIG: triglycerides
TRPV1: transient receptor potential channel V1
T-CHL: total cholesterol
UE: urea and electrolytes
VAS: visual analogue score
RDA: recommended daily allowance
UKPDS: United Kingdom prospective diabetes study
VDR: vitamin D receptor
VEGF: vascular endothelial growth factor
VITAL: Vitamin D and Omega-3 Trial
VPT: vibration perception threshold
WST: warm sensation threshold

22
In the name of Allah, the beneficent, the merciful.
La-ilaha-iLLaLLah- Muhammadur-Rasulullah.
“There is no wealth like knowledge, no poverty like ignorance”.
“There is no knowledge and science like pondering and thought; and there is
no prosperity and advancement like knowledge and science”.
Hazraat Ali bin Abu-Talib (RA), Fourth Caliph of Islam
DEDICATION
This Thesis is dedicated to my beloved mother,
my first and most important teacher.
She continues to be the most inspirational person in my life.

23
ACKNOWLEDGEMENTS
Even before I decided to practice medicine and become a physician, I always had
a clear aspiration to undertake research. The completion of this PhD has brought
together a number of years of work which started well before this project
commenced. I have thoroughly enjoyed my time undertaking this novel work. It
would not have been possible without the support of many individuals.
First and foremost, I would like to thank Professor Rayaz Malik who has been my
friend and mentor for over ten years. He has guided me from a fourth year medical
student working on peripheral nerve histology to my current role as a SpR in
endocrinology and on the cusp of completing a PhD. He has been a continual
source of personal encouragement and has a enthusiastic passion for research
and clinical excellence which he projects on all his co-workers and students. A
special mention must be given to Dr Kashif Khawaja who took an interest in me as
a medical student on a paediatric placement when I said ‘I am interested in
learning research’ and introduced Professor Malik and I in 2002.
My co-supervisor Dr Maria Jeziorska has spent much time and effort in providing
me with skills of skin biopsy processing and analysis. Her help with reviewing
chapters of the thesis and overall encouragement were invaluable. I would also like
to thank my advisor Professor Andrew J M Boulton for allowing me to gain early
research skills in the diabetic foot at the Diabetes Research Institute, University of
Miami whilst an undergraduate medical student and for all his advice and support
during the PhD.
Drs Ioannis Petropoulos, Omar Asghar, Hassan Fadavi, Maryam Ferdousi, Mitra
Tavakoli, Andrew Marshall, Ravinder Jugdey, Georgios Ponirakis, Osman Najam,
Yasar Amjad, Agnes Chan, Sara Al-Himdani, Sophie Benoliel, Cristiano Van Zeller,
24
and April Buazon have provided significant support to the series of studies
presented and I am indebted for their efforts in this work. Dr Ioannis Petropoulos
and Dr Salik Kakar require further mention, they have both provided me with
detailed technical support of Microsoft office© Word.
Both my family and close friends were very important in bringing all this together. I
must show an immense amount of gratitude to my wife, Iram who is expectant with
our first child at the time of writing this thesis. She has encouraged me throughout
the writing process and has been very patient and understanding of my work
commitments, particularly as I have combined the thesis writing with working as an
SpR. I would also like to thank my parents, my brother Kashif and two sisters,
Afshaan and Saima, eldest niece Marihah and my nephew, Danyaal for all their
support during this PhD and the many previous years.
I would like to acknowledge the significant contribution of all of the subjects who
participated in this research and without their efforts none of this work would be
possible. The support of the nursing staff at the Wellcome Trust Clinical Research
Facility was of course invaluable. The Juvenile Diabetes Research Foundation and
the National Institute of Health must be generously acknowledged for their financial
and honourable commitment to these projects. Finally, I want to thank my close
friends Ravinder Jugdey and Mohammed Qadir Hussain for their continual
personal support and guidance.
Addendum to the Acknowledgements
My daughter, Inara, was born on Sunday 20th October 2013. I hope her life is full of
happiness (with Allah’s will); she has brought immense happiness to my wife and I
and my extended family.

25
PREFACE
Uazman Alam graduated with a BSc in Medical Science from the University of St.
Andrews, Scotland, UK in 2001, before he went on to the University of Manchester,
UK in 2001 to undertake Medicine (MBChB) and graduated from this in 2005. Part
way through studying Medicine he took a year out to study for an MSc in
Population Health (MPHe) in 2003 until 2004 and graduated from this in 2005. He
has also completed other academic courses in Advanced Epidemiology and he has
advanced his knowledge of statistics by completing a Post-Graduate Certificate in
Statistics for Clinical Trials. Uazman has a plethora of work based clinical and
research experience as well as experience of academic teaching. He has been
actively involved in research from a fourth year medical student. The genesis of
Uazman’s research education began working on peripheral nerve histology in
experimental models of diabetes under the auspices of Professor Rayaz Malik.
Uazman worked as a ‘houseman’ at the Pennine Acute Hospital NHS Trust in 2005
and rotated in A&E, chest medicine and general surgery. He successfully applied
for a prestigious academic FY2 post at the North West Lung Centre, Wythenshawe
Hospital and was involved in a randomised controlled trial on cough and
inflammation which involved clinical assessment of subjects, undertaking flow
volume loops, body plethysmography and laboratory analysis of sputum. From
there, Uazman went on to complete his senior house officer training in South
Yorkshire at Rotherham General Hospital and the Northern General Hospital
(2007-2009). He is currently an SpR (ST5) in Endocrinology and Diabetes at
Pennine Acute Hospital Trust.
Uazman’s interest in Diabetes and Endocrinology has its foundations as a 4th year
medical student in 2003 working with Professor Rayaz Malik on animal models of

26
peripheral nerve histology and during his elective period at the Diabetes Research
Institute, University of Miami in 2005. Uazman became involved in diabetes during
this period of time and then advanced his interest in this speciality in 2009 when he
was awarded a National Training Number in Endocrinology and Diabetes and the
same year he took time out of programme as a Clinical Research Fellow to
undertake a PhD. He undertook both clinical work and research at the Manchester
Diabetes Centre, Manchester Royal Infirmary and Centre for Endocrinology and
Diabetes, University of Manchester. The three years he spent working and
researching at these latter two locations have allowed him to conduct research and
extrapolate data for his PhD focusing on Longitudinal Assessment of Ophthalmic
Diabetic Neuropathy Markers (LANDMARK) study and the role of vitamin D in
diabetes under the supervision of Professor Rayaz A Malik.
During his PhD, he presented his work at regional, national and international
conferences between 2010 and 2013 including the American Diabetes Association,
NeuroDiab - Diabetic Neuropathy Study Group of the EASD, Diabetes UK and at
the International Diabetes Federation’s World Diabetes Congress.
Uazman is a member of the Royal College of Physicians and a council member for
Lipids, Metabolism and Vascular risk section of the Royal Society of Medicine. He
is also an examiner for the University of Manchester Medical School and has been
the assistant lead examiner for the final MB exams from 2010-2012 at the
Manchester Royal Infirmary.
27
LIST OF PUBLICATIONS
Research Publications
1. Alam U, Chan AWS, Buazon A, Van Zeller C, Berry JL, Jugdey RS, Asghar
O, Cruickshank JK, Petropoulos IN, Malik RA. Differential effects of different
vitamin D replacement strategies in patients with diabetes. J Diabetes
Complications 2013; [Epub ahead of print]
2. Petropoulos IN, Alam U, Fadavi H, Asghar O, Green P, Ponirakis G,
Marshall A, Boulton AJ, Tavakoli M, Malik RA: Corneal Nerve Loss Detected With
Corneal Confocal Microscopy Is Symmetrical and Related to the Severity of
Diabetic Polyneuropathy. Diabetes Care 2013; [Epub ahead of print]
3. Tavakoli M, Mitu-Pretorian M, Petropoulos IN, Fadavi H, Asghar O, Alam U,
Ponirakis G, Jeziorska M, Marshall A, Efron N, Boulton AJ, Augustine T, Malik RA:
Corneal confocal microscopy detects early nerve regeneration in diabetic
neuropathy after simultaneous pancreas and kidney transplantation. Diabetes
2013;62:254-260
4. Petropoulos IN, Manzoor T, Morgan P, Fadavi H, Asghar O, Alam U,
Ponirakis G, Dabbah MA, Chen X, Graham J, Tavakoli M, Malik RA: Repeatability
of in vivo corneal confocal microscopy to quantify corneal nerve morphology.
Cornea 2013;32:e83-89
5. Alam U, Najam O, Al-Himdani S, Benoliel S, Jinadev P, Berry JL, Kew M,
Asghar O, Petropoulos IN, Malik RA: Marked vitamin D deficiency in patients with
diabetes in the UK: ethnic and seasonal differences and an association with
dyslipidaemia. Diabetic Medicine 2012;29:1343-1345

28
6. Marsden PA, Smith JA, Kelsall AA, Owen E, Naylor JR, Webster D, Sumner
H, Alam U, McGuinness K, Woodcock AA: A comparison of objective and
subjective measures of cough in asthma. J Allergy Clin Immunol 2008;122:903-907
Review Publications
1. Asghar O, Alam U, Hayat SA, Aghamohammadzadeh R, Heagerty AM,
Malik RA: Obesity, diabetes and atrial fibrillation; epidemiology, mechanisms and
interventions. Curr Cardiol Rev 2012;8:253-264
2. Alam U, Asghar O, Malik RA: Diabetic gastroparesis: Therapeutic options.
Diabetes Ther 2010;1:32-43
3. Tavakoli M, Asghar O, Alam U, Petropoulos IN, Fadavi H, Malik RA: Novel
insights on diagnosis, cause and treatment of diabetic neuropathy: focus on painful
diabetic neuropathy. Ther Adv Endocrinol Metab 2010;1:69-88
4. Rogers LC, Alam U, Tesfaye S, Malik RA. Treatment of painful diabetic
neuropathy: A review of the most efficacious pharmacological treatments. Practical
Diabetes International 2004;7(21):301-306
Editorials
1. Alam U, Asghar O, Malik RA: Are vitamin D and B deficiency relevant to the
pathogenesis and treatment of diabetic neuropathy? Future Neurology 2012;7:235-
238
2. Alam U, Asghar O, Malik RA: Vitamin D deficiency and cardiovascular
disease: the missing link. Diabetes Management 2011;1:151-155
3. Alam U, Malik RA. New NICE guidance for DPNP: Evidence based and cost
effective. The Diab Foot J 2010;13(2):56.
29
LIST OF ABSTRACTS
1. Alam U, Petropoulos IN, Fadavi H, Asghar O, Marshall A, Ponirakis G, Al-
Ahmar A, Kheyami A, Ferdousi M, Azmi S, Tavakoli M, Boulton AJM, Malik RA.
Corneal Confocal Microscopy is as Proficient as Electrophysiology and Skin Biopsy
in Detecting Neuropathy in Subjects with Type 1 Diabetes Mellitus. American
Diabetes Association conference 21th-25th June 2013. Chicago, USA (Oral)
2. Azmi S, Alam U, Fadavi H, Asghar O, Petropoulos IN, Ponirakis G, Marshall
A, Ferdousi M, Kheyami A, Al-Ahmar A, Tavakoli M, Boulton AJM, Malik RA.Early
Non-Progressive Small Fibre Neuropathy in Type 2 Diabetes. American Diabetes
Association conference 21th-25th June 2013. Chicago, USA (Poster)
3. Pritchard N, Edwards K, Vagenas D, Sampson G, Russell A, Petropoulos
IN, Alam U, Fadavi H, Asghar O, Ponirakis G, Marshall A, Tavakoli M, Malik RA,
Efron N. Corneal sensitivity and corneal confocal microscopy in a large cohort with
type 1 diabetes: the LANDmark study. Annual meeting of the Diabetic Neuropathy
Study Group of the EASD, 27th – 30th September 2012. Dresden, Germany (Oral
presentation)
4. Green P, Tavakoli M, Petropoulos IN, Marshall A, Alam U, Fadavi H,
Asghar O, Chan A, Malik RA. Neuropathy precedes retinopathy and nephropathy
in type 1 diabetes. Annual meeting of the Diabetic Neuropathy Study Group of the
EASD, 27th – 30th September 2012. Dresden, Germany (Poster presentation)

30
4. Alam U, Petropoulos IN, Asghar O, Fadavi H, Marshall A, Ponirakis G,
Boulton AJM, Tavakoli M, Malik RA. Small fibre dysfunction and vitamin D
deficiency may underlie the symptoms of painful neuropathy in subjects with IGT
and diabetes. Annual meeting of the Diabetic Neuropathy Study Group of the
EASD, 27th – 30th September 2012. Dresden, Germany (Oral presentation)
5. Ponirakis G, Petropoulos IN, Fadavi H, Alam U, Asghar O, Tavakoli M,
Malik RA. Diagnostic accuracy of the Neuropad response to assess small and
large fibre in diabetic peripheral neuropathy. Annual meeting of the Diabetic
Neuropathy Study Group of the EASD, 27th – 30th September 2012. Dresden,
Germany (Oral presentation)
6. Petropoulos IN, Ponirakis G, Green P, Chen X, Dabbah MA, Graham J,
Fadavi H, Asghar O, Alam U, Tavakoli M, Malik RA. Quantification of corneal
nerve fibre morphology using a novel automated algorithm. Annual meeting of the
Diabetic Neuropathy Study Group of the EASD, 27th – 30th September 2012.
Dresden, Germany (Poster presentation)
7. Petropoulos IN, Asghar O, Alam U, Fadavi H, Ponirakis G, Marshall A,
Tavakoli M, Boulton AJM, Malik RA. Corneal confocal microscopy detects and
tracks progression of neuropathy in subjects with impaired glucose tolerance.
Annual meeting of the Diabetic Neuropathy Study Group of the EASD, 27th – 30th
September 2012. Dresden, Germany (Oral presentation)

31
8. Buazon A, Alam U, Chan AWS, Petropoulos IN, Asghar O, Malik RA.
Endemic Vitamin D Deficiency: Inadequate Replacement Strategies. American
Diabetes Association conference 12th-18th June 2013. Philedelphia, USA (Poster)
9. Petropoulos IN, Chan AWS, Asghar O, Alam U, Malik RA. Vitamin D: a
novel risk factor for diabetic retinopathy. International Diabetes Federation World
Diabetes Congress, 4th – 8th December 2011. Dubai, United Aram Emirates (Poster
presentation)
10. Petropoulos IN, Asghar O, Fadavi H, Alam U, Ponirakis G, Marshall A,
Nelson L, Forman S, Jeziorska M, Dabbah MA, Tavakoli M, Malik RA. Corneal
confocal microscopy detects significant neuropathy in subjects with impaired
glucose tolerance. Annual meeting of the Diabetic Neuropathy Study Group of the
EASD, 8th – 11th September 2011. Porto, Portugal (Oral presentation)
11. Alam U, Fadavi H, Petropoulos IN, Ponirakis G, Asghar O, Marshall A,
Tavakoli M, Boulton AJM, Malik RA. Protection from Neuropathy: lessons from
Patients with Long Duration Type 1 Diabetes. American Diabetes Association 24th-
28th June 2011. San Diego, USA. (Poster presentation)
12. Alam U, Petropoulos IN, Fadavi H, Jinadev P, Asghar O, Ponirakis G,
Boulton AJM, Tavakoli M, Malik RA. Corneal confocal microscopy detects
neuropathy in subjects with latent autoimmune diabetes in adults. Diabetes UK,
30th March-1st April 2011. London, UK. (Poster presentation)

32
13. Asghar O, Petropoulos IN, Alam U, Fadavi H, Ponirakis G, Dabbah MA,
Marshall A, Tavakoli M, Boulton AJM, Malik RA. Corneal confocal microscopy
detects significant neuropathy in subjects with impaired glucose tolerance.
Diabetes UK, 30th-1st April 2011. London, UK. (Oral & Poster presentation)
14. Petropoulos IN, Fadavi H, Asghar O, Alam U, Ponirakis G, Dabbah M,
Marshall A, Tavakoli M, Boulton AJM, Malik RA. Corneal Confocal Microscopy
Detects minimal small nerve fibre regeneration following combined pancreas and
kidney transplantation in patients with Type 1 diabetes. Diabetes UK, 30th March-
1st April 2011. London, UK. (Poster presentation)
15. Najam O, Alam U, Petropoulos IN, Asghar O, Malik RA. Lack of placebo
worsening in trials of human diabetic neuropathy. 20th Annual meeting of the
Diabetic Neuropathy Study Group of the EASD, 17th – 19th September 2010.
Stockholm, Sweden (Oral presentation)
16. Petropoulos IN, Fadavi H, Asghar O, Alam U, Ponirakis G, Dabbah MA,
Tavakoli M, Boulton AJM, Malik RA. Corneal confocal microscopy detects minimal
neuropathy in patients with impaired glucose tolerance which progresses with
diabetes. Annual meeting of the Diabetic Neuropathy Study Group of the EASD,
17th – 19th September 2010. Stockholm, Sweden (Oral presentation)
17. Petropoulos IN, Asghar O, Alam U, Fadavi H, Dabbah MA, Marshall A,
Tavakoli M, Boulton AJM, Malik RA. Corneal Confocal Microscopy Detects
33
Neuropathy in Subjects with Impaired Glucose Tolerance. American Diabetes
Association conference 25th-29th June 2010. Orlando, USA. (Poster presentation)
18. Alam U, Jinadev P, Asghar O, Petropoulos IN, Davies R, Rutter M, Boulton
AJM, Malik RA. Marked Vitamin D Deficiency in a General Diabetic Population.
Diabetes UK, 3rd-5th March 2010. Liverpool, UK. (Oral & Poster presentation)
19. Petropoulos IN, Manzoor T, Alam U, Fadavi H, Asghar O, Dabbah MA,
Tavakoli M, Boulton AJM, Malik RA. Corneal confocal microscopy demonstrates
significant neuropathy in south Asian patients with diabetes. Diabetes UK, 3rd- 5th
March 2010. Liverpool, UK. (Poster presentation)
20. Alam U, Kelsall A, Sumner H, Donnoley I, Thompson NC, Smith JA,
Woodcock A. Voluntary Coughing and Sputum Inflammatory Markers in Healthy
Volunteers. American Thoracic Society conference, 16th – 21st May 2008.
Toronto, Canada. (Poster)
21. Alam U, Siddique I, Patel R, Chung SK, Malik RA. Sensory nerve
morphology in nitric oxide synthase-knockout and diabetic mice: relevance to
diabetic neuropathy. International Diabetes Federation Congress, 24th – 29th Aug
2003. Paris, France. (Poster)
22. Alam U, Siddique I, Patel R, Wong AKC, Boulton AJM, Chung SK, Malik
RA. Sensory nerve morphology in nitric oxide synthase-knockout and diabetic

34
mice: relevance to diabetic neuropathy. Annual meeting of the Diabetic Neuropathy
Study Group of the EASD 30th Aug – 2nd Sept 2003. St Malo, France. (Oral)
23. Patel R, Alam U, Boulton AJM, Kador P, Malik RA. Endoneurial
microangiopathy without neuropathy or apoptosis in the long duration galactosemic
dog. Annual meeting of the Diabetic Neuropathy Study Group of the EASD 30th
Aug – 2nd Sept 2003. St Malo, France. (Oral)

35
1 Chapter I - INTRODUCTION

36
Diabetes Mellitus (DM) has been recognised for millennia and an Egyptian
manuscript described a condition as “too great emptying of the urine” as early as
1550 BC. Around the same time, Indian physicians identified the disease and
classified it as ‘madhumeha’ or honey urine noting that the urine would attract ants.
However, it was not until the 18th century that Western physicians began to study
diabetes and its complications (1). The islets of Langerhans were discovered in
1869 by the anatomist Paul Langerhan. The endocrine role of the pancreas and
the existence of insulin were not fully clarified until the epochal discovery in 1921
when Frederick Banting and George Best demonstrated they could reverse
induced diabetes in dogs, by extirpating the pancreas and then administrating an
extract from the pancreatic islets of Langerhans of healthy dogs (2-3).
DM is group of disorders which are characterised by hyperglycaemia due to an
absolute or relative deficit in insulin production or action (4). The chronic
hyperglycaemia of DM is associated with end-organ damage, dysfunction and
failure, including the retina, kidney, nerves, heart and blood vessels (4). The
International Diabetes Federation (IDF) estimates an overall prevalence of DM to
be 366 million in 2011, and this is expected to rise to 552 million by 2030 (5).
1.1 Aetiopathology of Diabetes
DM is a heterogeneous group of metabolic disorders fall into two broad categories
characterised by raised plasma glucose concentrations due to absolute (type 1
DM) or relative (type 2 DM) lack of insulin secretion, action or both and thus
resulting in aberrations in fat, carbohydrate and protein metabolism. Diagnosis may
be made through glucose tolerance test, fasting and/or random plasma glucose or
glycated haemoglobin A1c (HbA1c) (Table 1-1).

37
Table 1-1 Diagnosis of DM
Diagnostic Parameter Comment
Fasting Plasma Glucose
≥7.0 mmol/l
Fasting is regarded as no caloric intake for
8 hours
2 hour plasma glucose ≥11.1 mmol/l
during an OGTT
The test should be performed according to
the World Health Organisation guidelines,
using a glucose load containing the
equivalent of 75 g anhydrous glucose
dissolved in water.
In a patient with classic symptoms of
hyperglycaemia, a random plasma glucose
≥11.1 mmol/l
HbA1C ≥6.5% / 48mmol/mol
Its role in diagnosis has been cemented by
the American Diabetes Association,
although some consider there is a further
case for discussion in its precise role (6).
The test should be performed in a
laboratory using a method that is NGSP
Certified and Standardized to the DCCT
assay.
Adapted from Diagnosis and Classification of Diabetes Mellitus (7).
Table key
OGTT – Oral Glucose Tolerance Test.
DCCT – Diabetes Control and Complication Trial.
NGSP - National Glycohaemoglobin Standardization Program.
In type 1 DM, individuals are often metabolically normal before the disease is
clinically manifest, but the process of autoimmune β-cell destruction can be
detected before overt diabetes develops. The presence of this autoimmune
disorder is characterised by the presence of auto-antibodies such as anti-glutamic
acid decarboxylase (GAD), islet (ICA) or insulin antibodies (8). Type 1 DM is
38
associated with HLA DR3 and DR4 (9-11) and it has been proposed that an
interplay of a genetic predisposition with environmental factors may lead to an
autoimmune response (12). Environmental factors implicated include viral
infections, early childhood cow’s milk administration, malnutrition, and
vaccinations, which trigger an immune cascade leading to cross reactivity with
pancreatic β-cells, however to date no definitive causal link has been identified (12-
14). Furthermore, there is a putative link of vitamin D deficiency and the
occurrence of type 1 DM (15) with a positive impact of supplementation with
cholecalciferol (vitamin D3) during the first year of life on the risk of developing type
1 DM (16) and a meta-analysis of five observational studies has confirmed this risk
reduction (17). Importantly in the Finnish Birth cohort study (16), children with
suspected rickets had a threefold increase in their risk of type 1 DM. There is a
striking geographical variation in the incidence of type 1 diabetes and seasonal
variation with the highest incidence of onset during the winter months and at
greater latitudes; thus suggesting that variations in vitamin D synthesis in the skin
and subsequent status may play a significant role in the pathogenesis (18-20). The
destruction of pancreatic β-cells is an autoimmune T-helper cell mediated disorder
and activated vitamin D (1,25(OH)2D) has immunomodulatory actions in T-cells
and leads to a reduction in the induction of Th1 cytokines such as interferon (IFN) γ
(15; 21-23).
Type 2 DM has become an epidemic in Western society and virtually no health
care professional is without patients who have the disease. The majority of patients
with DM have type 2 DM (~90%) with only a small proportion having the
monogenic forms such as maturity onset diabetes of the young (24-25). Type 2 DM
results from defects in insulin secretion, but with a major contribution from insulin

39
resistance (7). There is subsequently an inadequate compensatory insulin
secretary response resulting in hyperglycaemia. Numerous mechanisms have
been implicated, including changes in fatty acid fractions, interplay of inflammatory
cytokines and adipokines, mitochondrial dysfunction with insulin resistance, and
glucotoxicity, lipotoxicity, and amyloid formation and deposition leading to β-cell
dysfunction (26). Type 2 DM has a strong genetic component, however, only a
small number of genes have been identified to date (26). A family history confers a
2-4 fold increase for type 2 DM. The lifetime risk of type 2 DM is approximately
38% and 60% if one or both parents have the disease respectively (27-28). This
genetic predisposition is highlighted by the fact that monozygotic twins have higher
concordance rates of type 2 DM than dizygotic twins (29-30). Vitamin D may play
an important role in the pathogenesis of type 2 DM. Insulin sensitivity is improved
significantly in adults with impaired fasting glucose who were randomised to
calcium and vitamin D supplementation (31). Furthermore, baseline 25(OH) vitamin
D levels in non-diabetic subjects were shown to predict future glycaemia and
insulin resistance (32). In the meta-analysis by Parker et all (33), the risk of type 2
diabetes may be reduced by 55% in individuals with the highest levels of vitamin D.
Despite the majority of cases of diabetes falling into the two broad
aetiopathogenetic categories of type 1 and type 2 DM often classified on their
clinical presentation. In some individuals this classification is not so well defined. It
is common practice to classify individuals based on the following variables:
1. Age at onset of diabetes
2. The abruptness of hyperglycaemia
3. Presence of ketosis
40
4. Degree of obesity
5. Need for insulin at diagnosis
This however, does not always accurately classify the aetiology of diabetes.
1.2 Latent Autoimmune Diabetes in Adults (LADA)
Latent Autoimmune Diabetes in Adults (LADA) is an under diagnosed form of
diabetes. Particularly, as the age at onset is later than in classical type 1 diabetes.
The finding of auto antibodies is characteristic of type 1 DM but can be found in 10-
30% of those who have phenotypically type 2 DM (34-35). It is this subset that is
termed as LADA. Furthermore, the U.K. prospective diabetes study (UKPDS)
demonstrated that approximately 10% of adults with type 2 diabetes have LADA
(36). Although the prevalence may be as low as 3.6% of all newly diagnosed
apparent type 2 diabetic patients (37). Despite the initial lack of requirement of
exogenous insulin the underlying process is that of β-cell destruction as opposed
to the insulin resistance of type 2 DM, it does however occur slower than the
classical young onset type 1 DM (38).
1.2.1 Screening and Treatment in LADA
Insulin dependency can occur after a relatively short period of around 6 months or
up to 10 years or more (39-40). The time to insulin therapy use can vary depending
on local clinical judgement and use of laboratory GAD antibody testing (41).
However, despite the variances, the median time to failure of oral medication and
exogenous insulin use is less than 5 years (41). In fact, a clinical screening tool
has been developed which can help to identify individuals with LADA (42). These
criteria are based upon the clinical presentation of this subgroup of individuals. The
five clinical features that are more common in LADA compared to type 2 DM are:

41
a. Age of onset less than 50 years
b. Acute symptoms (polyuria, polydipsia, osmotic visual changes etc)
c. BMI ≤25kg/m2
d. Personal history of autoimmune disorders
e. Family history of autoimmune disease
In one particular study (42) the presence of at least two of these distinguishing
features (clinical risk score ≥2) had a 90% sensitivity and 71% specificity for
identifying LADA. The negative predictive value for a LADA clinical risk score ≤1
was 99% (42). The most common diagnostic test for LADA is a GAD antibody
assay (43). GAD antibodies may also be present in individuals with type 1 DM and
thus generally an initial exogenous insulin free period is often considered a
requirement for a definitive diagnosis of LADA. GAD antibodies are not found in
patients with pure type 2 DM (37).
Individuals with LADA may require insulin at an earlier in the disease compared to
those with type 2 DM. The slow process of β-cell destruction occurs to the point
that oral agents poorly control hyperglycaemia. However, a number of interventions
have been trialled to evaluate the possible beneficial effects of different classes of
diabetes medications (44). There are a paucity of data on the effects of oral agents
alone in LADA. Sulphonylurea treatments work by stimulating the β-cells to
produce endogenous insulin. This class of medication has been associated with a
more rapid progression to insulin treatment in those who are well controlled at
baseline compared to other treatment groups (44). It is possible that β-cell failure is
accelerated through the action of sulphonylureas. Furthermore, in the systematic

42
review by Brophy et al (44) individuals who were poorly controlled at baseline
progressed to insulin treatment rapidly (60% in 2 years). There may be some
beneficial effect on β-cell preservation in those with LADA who are treated with the
now withdrawn rosiglitazone (when compared to sulphonylureas) and this may
highlight the possibility that there is a degree of insulin resistance despite the
autoimmune nature of the disorder (45-46). Other interventions have also been
shown to have a protective effect on β-cell function. Li et al (47) undertook a
randomised trial of insulin versus 1-α-hydroxyvitamin D3 plus insulin and in a
subgroup of those with a duration of diabetes less than 1 year they showed a
significantly elevated fasting c-peptide and postprandial c-peptide in those who
were treated with insulin and 1-α-hydroxyvitamin D3, suggesting that β-cell function
was better preserved. Indeed there is some evidence that vitamin D deficiency may
be related to type 1 DM (48). Furthermore, vitamin D deficiency and receptor gene
polymorphisms may be a risk factor for the development of type 1 DM and other
forms of diabetes that have an autoimmune element to their pathogenesis (49-51).
There is evidence to suggest that autoimmune diabetes presents a continuum of
genetic susceptibility, which extends from a strong effect in childhood-onset type 1
DM to a more limited effect in LADA (52). The predominant imbalanced production
of T helper 1 cells in part through the production of interleukin (IL) 12 in
autoimmune diabetes is destructive to the pancreatic β-cell (52). Activated vitamin
D may inhibit the production of IFN-γ, IL-2 and IL-12 (53) and thus possibly
disrupting the T helper 1 mediated pathogenesis.
This highlights a possible opportunity to preserve β-cell function as there is a
slower rate of β-cell decline than in the classical type 1 DM. Maximising β-cell

43
function through interventions may lead to better glycaemic control and hence
reduce the rate of microvascular complications (54).
1.2.2 Auto Antibodies in LADA
Generally a diagnosis of LADA is based upon a phenotypically type 2 individual
testing positive for GAD antibodies, as this is the most common antibody present
in this cohort (55). Even in the absence of GAD antibodies some individuals may
test positive for other β-cell auto-antibodies (56) conferring a diagnosis of LADA.
Furthermore, other autoimmune markers such as ICA, and tyrosine phosphatase
auto-antibodies (anti-IA2 or anti-ICA512) have been found in LADA. A combination
of ICA and GAD antibodies and the levels of their titres have been shown by
Lohmann et al 2001 (57) to help differentiate two clinical and phenotypical variants
of LADA. Those who are ICA positive and have high titres of GAD antibodies are
clinically more similar to individuals with type 1 diabetes whereas those who are
negative for ICA and have low titres of GAD antibodies are clinically similar to
individuals with type 2 diabetes (57). The levels of GAD antibody titres are not
thought to predict disease progression (58) but a combination of thyroid peroxidase
antibodies (which one study occurred at a possible prevalence of 29% (59)), anti-
IA2 and C-peptide levels may predict β-cell failure (60).
Previous studies have shown co-existing coeliac disease in those with type1 DM
with a rate of between 1-7% (61-62) and anti-gliadin antibodies may have a high
prevalence in those with type 1 DM even without symptoms of coeliac disease
(63). It seems that there is an increased frequency of humoral markers of
autoimmunity and this is also mirrored in LADA (64). A number of non β-cell
antibodies are associated with LADA and include anti-gliadin and thyroid
44
peroxidase antibodies (64). It has been suggested that a susceptibility to anti-
gliadin antibodies may reflect changes in the mucosal barrier function and thus
cause changes in antigen exposure (64).
Defining LADA through testing for auto-antibodies itself can pose a significant
diagnostic challenge as these markers can change over time including absence of
ICA and GAD antibodies after the presenting illness. Defining cut off levels of these
antibodies for diagnosis is troublesome as there is a continuous spectrum of
distribution in both diabetic and control populations. This also highlights the
possibility of false positives, as these markers may be present in non-diabetic
populations.
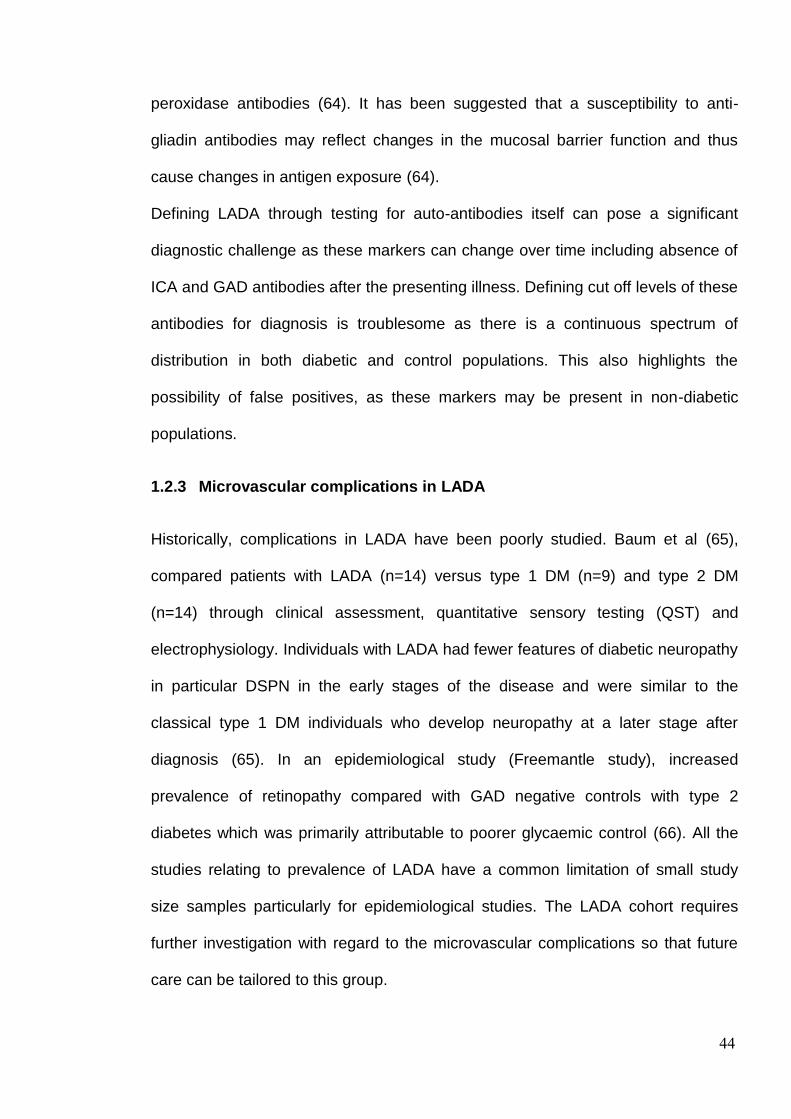
1.2.3 Microvascular complications in LADA
Historically, complications in LADA have been poorly studied. Baum et al (65),
compared patients with LADA (n=14) versus type 1 DM (n=9) and type 2 DM
(n=14) through clinical assessment, quantitative sensory testing (QST) and
electrophysiology. Individuals with LADA had fewer features of diabetic neuropathy
in particular DSPN in the early stages of the disease and were similar to the
classical type 1 DM individuals who develop neuropathy at a later stage after
diagnosis (65). In an epidemiological study (Freemantle study), increased
prevalence of retinopathy compared with GAD negative controls with type 2
diabetes which was primarily attributable to poorer glycaemic control (66). All the
studies relating to prevalence of LADA have a common limitation of small study
size samples particularly for epidemiological studies. The LADA cohort requires
further investigation with regard to the microvascular complications so that future
care can be tailored to this group.

45
1.3 Complications of Diabetes
Diabetes is a major risk factor for macro and micro-vascular complications, such as
strokes and amputations, nephropathy, retinopathy and neuropathy. These
complications are a major cause of illness and an enormous economic burden
especially with the increasing prevalence of diabetes in western society (67).
Diabetes is a leading cause of end-stage renal disease in many developed
countries accounting for up to 50% of patients receiving renal replacement therapy
(67). Kidney disease is common at the time of diagnosis of DM with a prevalence
of ~20% (68) but also accounts for 21% of deaths in type 1 DM and 11% of deaths
in type 2 DM (69). Within 20 years after disease onset, nearly all adults with type 1
DM and more than 60% of adults with type 2 DM develop the complication of DR
(70-71). In an analysis in the UK, it is believed that there is a prevalence of
blindness of 4200 and an annual incidence of blindness of 1280 people with
diabetes (72) and in a retrospective analysis (n=20,686) from 1990-2006 of
national diabetic retinopathy screening program, the first retinal examination
(baseline), 79% did not have retinopathy, 18% had non-proliferative retinopathy,
and 2.9% had pre-proliferative retinopathy (73). In this same study after 10 years,
patients without retinopathy at baseline had an increased incidence of pre-
proliferative retinopathy (cumulative incidence 16.4%), sight-threatening
maculopathy (1.2%), or proliferative retinopathy (1.5%) (73). In Wisconsin
Epidemiologic Study, the 14-year rate of progression of retinopathy was 86%,
regression of retinopathy was 17%, progression to proliferative retinopathy was
37% and incidence of macular oedema was 26% (74). Diabetic neuropathy is
discussed in more detail below.
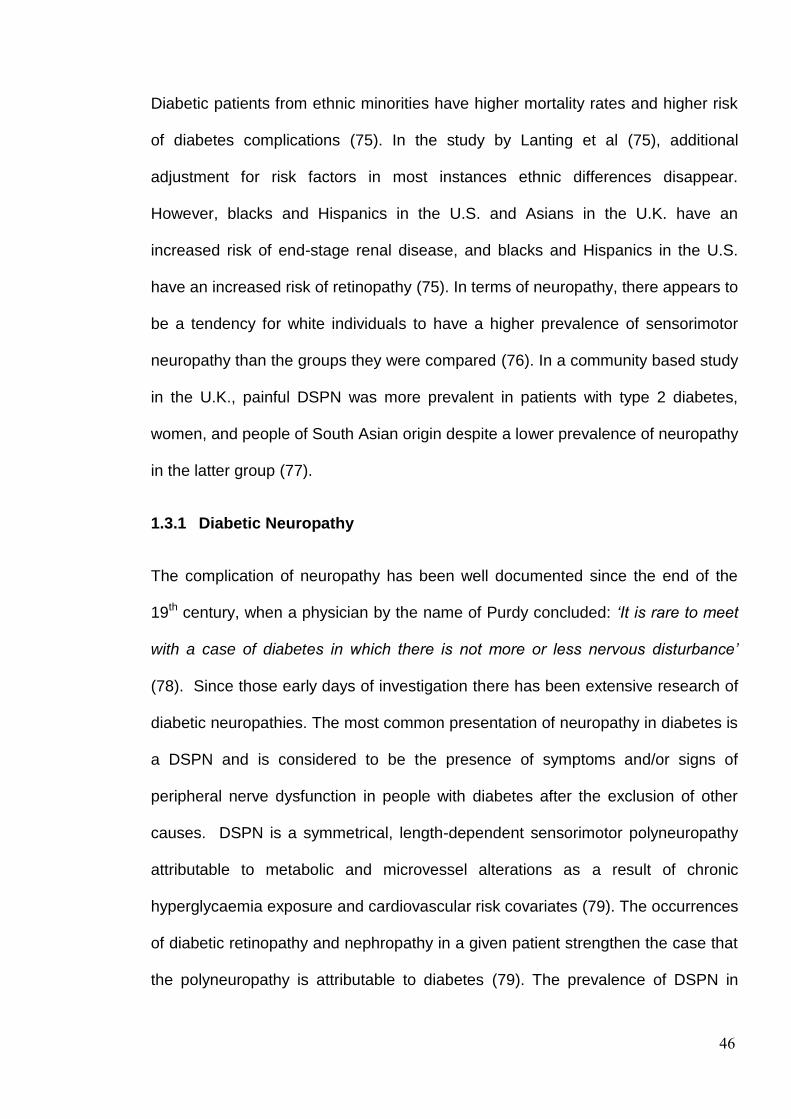
46
Diabetic patients from ethnic minorities have higher mortality rates and higher risk
of diabetes complications (75). In the study by Lanting et al (75), additional
adjustment for risk factors in most instances ethnic differences disappear.
However, blacks and Hispanics in the U.S. and Asians in the U.K. have an
increased risk of end-stage renal disease, and blacks and Hispanics in the U.S.
have an increased risk of retinopathy (75). In terms of neuropathy, there appears to
be a tendency for white individuals to have a higher prevalence of sensorimotor
neuropathy than the groups they were compared (76). In a community based study
in the U.K., painful DSPN was more prevalent in patients with type 2 diabetes,
women, and people of South Asian origin despite a lower prevalence of neuropathy
in the latter group (77).
1.3.1 Diabetic Neuropathy
The complication of neuropathy has been well documented since the end of the
19th century, when a physician by the name of Purdy concluded: ‘It is rare to meet
with a case of diabetes in which there is not more or less nervous disturbance’
(78). Since those early days of investigation there has been extensive research of
diabetic neuropathies. The most common presentation of neuropathy in diabetes is
a DSPN and is considered to be the presence of symptoms and/or signs of
peripheral nerve dysfunction in people with diabetes after the exclusion of other
causes. DSPN is a symmetrical, length-dependent sensorimotor polyneuropathy
attributable to metabolic and microvessel alterations as a result of chronic
hyperglycaemia exposure and cardiovascular risk covariates (79). The occurrences
of diabetic retinopathy and nephropathy in a given patient strengthen the case that
the polyneuropathy is attributable to diabetes (79). The prevalence of DSPN in

47
diabetes can be as high as 50% (80) and symptomatic diabetic neuropathy can
affect up to 30-40% of diabetic patients with neuropathy (81). Traditionally
symptoms have been denoted as either positive (aching, burning, sharp or
pressure pains) or negative (numbness or dead feeling). Both ‘negative and
positive symptoms’ may coexist.
1.3.1.1 Prevalence of Distal Symmetrical Polyneuropathy
The prevalence of DSPN is thought to be around 30% (80; 82) and increases with
the duration of the disease. When diabetes has been present for greater than 25
years, the prevalence rises to approximately 50% (82). The Rochester Diabetic
Neuropathy Study reported a prevalence of 54% and 45% for patients with type 1
and type 2 DM respectively, amongst 380 patients in total, with the majority
however not exhibiting neuropathic symptoms (83). The 1989 National Health
Interview Survey consisted of a representative sample of 84,572 persons in the
U.S.A. aged 18 years or over (84). Those with DM (n=2405) were identified and
administered a questionnaire to define the prevalence of symptoms of sensory
neuropathy which was found to be 30.2% among subjects with type 1 DM. This
prevalence was 36.0% for men and 39.8% for women with type 2 DM, compared
with 9.8 and 11.8% for non-diabetic men and women, respectively (84). Symptoms
of sensory neuropathy affect 30-40% of diabetic patients and the prevalence of
these symptoms increase with longer duration of diabetes; hypertension and
hyperglycaemia (84). However, importantly there was neither a clinical or
quantitative assessment of neuropathy in this study. In a survey of 10 English
practices based in the community (85), 1077 subjects with diabetes were screened
for neuropathy by eliciting two of the following five:

48
1. Neuropathic foot symptoms
2. Loss of light touch sensation
3. Impaired pin prick sensation
4. Absent ankle jerk reflexes
5. Vibration perception threshold greater than 97.5% of an age-standardised
value.
There was an age and sex matched non-diabetic control group (n=480) (85). The
prevalence of neuropathy was 16.3% in diabetic patients and 2.9 % in non-diabetic
subjects, yielding a prevalence odds of 6.75 (95% CI 3.87-11.79), p<0.001 (85).
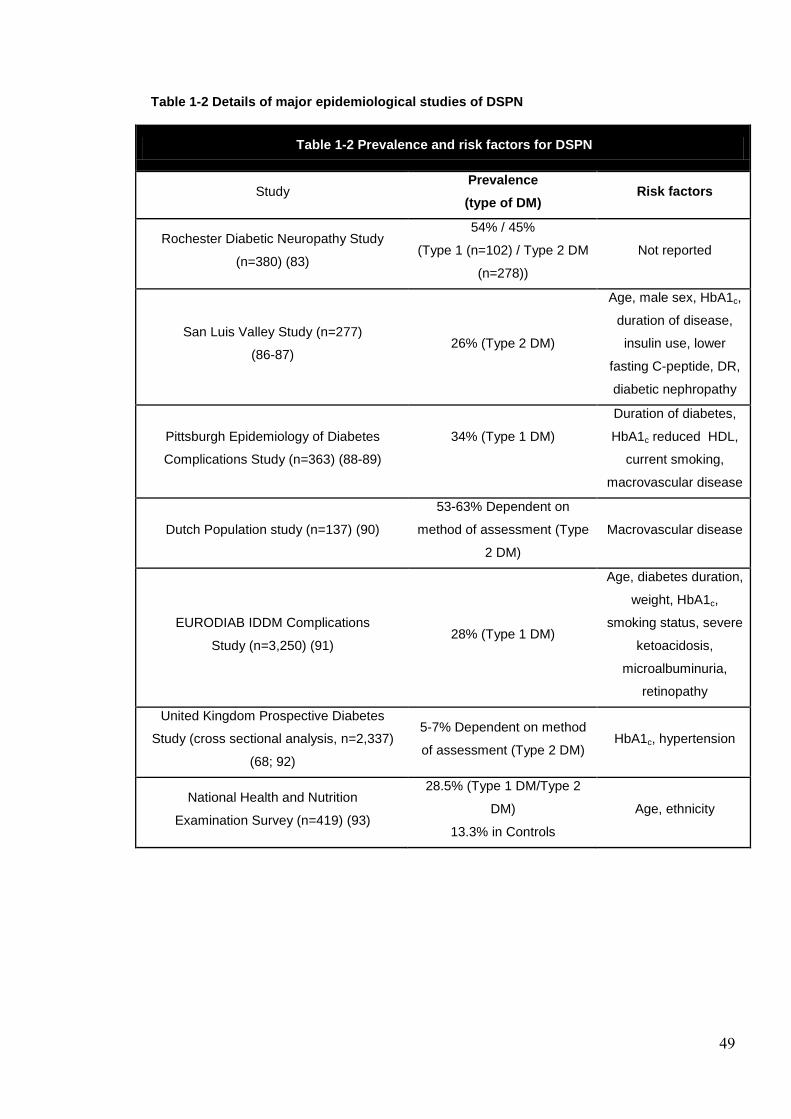
49
Table 1-2 Details of major epidemiological studies of DSPN
Table 1-2 Prevalence and risk factors for DSPN
Study Prevalence
(type of DM) Risk factors
Rochester Diabetic Neuropathy Study
(n=380) (83)
54% / 45%
(Type 1 (n=102) / Type 2 DM
(n=278))
Not reported
San Luis Valley Study (n=277)
(86-87) 26% (Type 2 DM)
Age, male sex, HbA1c,
duration of disease,
insulin use, lower
fasting C-peptide, DR,
diabetic nephropathy
Pittsburgh Epidemiology of Diabetes
Complications Study (n=363) (88-89)
34% (Type 1 DM)
Duration of diabetes,
HbA1c reduced HDL,
current smoking,
macrovascular disease
Dutch Population study (n=137) (90)
53-63% Dependent on
method of assessment (Type
2 DM)
Macrovascular disease
EURODIAB IDDM Complications
Study (n=3,250) (91) 28% (Type 1 DM)
Age, diabetes duration,
weight, HbA1c,
smoking status, severe
ketoacidosis,
microalbuminuria,
retinopathy
United Kingdom Prospective Diabetes
Study (cross sectional analysis, n=2,337)
(68; 92)
5-7% Dependent on method
of assessment (Type 2 DM) HbA1c, hypertension
National Health and Nutrition
Examination Survey (n=419) (93)
28.5% (Type 1 DM/Type 2
DM)
13.3% in Controls
Age, ethnicity

50
1.3.1.2 Diabetic Neuropathy, Glycaemia Control and other risk factors
The role of tight glycaemic control in improving microvascular outcomes is
irrefutable. The United Kingdom Prospective Diabetes Study (UKPDS)
demonstrated a significant risk reduction for cardiovascular disease (CVD) and
amputation for every 1% reduction in mean HbA1c (94). The Diabetes Control and
Complications Trial (DCCT) is another landmark study conducted in type 1 DM
(95). This prospective study evaluated 1441 subjects aged 13 to 39 years old who
were followed up for 5 years (96). 726 had type 1 DM for 1 to 5 years and had no
retinopathy at baseline (primary prevention cohort); 715 had type 1 DM for 1 to 15
years and had minimal to moderate non-proliferative retinopathy at baseline
(secondary intervention cohort) (96). Intensive therapy reduced the development of
confirmed clinical neuropathy by 64% in the combined cohorts after 5 years of
follow-up (96). This was defined as a history or physical examination consistent
with clinical neuropathy confirmed by either abnormal nerve conduction or
autonomic nervous system testing. The prevalence of abnormal nerve conduction
and abnormal autonomic nervous system function were reduced by 44% and 53%
respectively (96). The Epidemiology of Diabetes Interventions and Complications
(EDIC) Study (this assessed the 14-year cumulative benefits of prior intensive
insulin treatment in the DCCT) found a lower incidence of DSPN (22.0% vs.
28.0%) amongst patients assigned to the intensive arm compared to the
conventional arm (97). Therefore, the benefit of former intensive insulin treatment
persisted for 13-14 years after DCCT closeout (97). These data introduced the
concept of ‘metabolic memory’ in which provides significant evidence of a durable
effect of prior intensive treatment on neuropathy (98).

51
The Eurodiab study (91), assessed the risk factors for the development of distal
symmetric neuropathy in 1172 patients with type 1 DM. Neuropathy was assessed
at baseline (1989 to 1991) and at follow-up (1997 to 1999), with a follow-up of
7.3±0.6 years. A standardised protocol for the evaluation of DSPN included clinical
evaluation, quantitative sensory testing and autonomic-function tests. Serum lipids
and lipoproteins, HbA1c, and the urinary albumin excretion rate were also
measured. Duration of diabetes, HbA1c status, change in glycosylated
haemoglobin value during the follow-up period, body-mass index and smoking
were all independently associated with the incidence of neuropathy (91). Other
than glycaemic control, the incidence of neuropathy is associated with potentially
modifiable cardiovascular risk factors, including a raised triglyceride level, body-
mass index, smoking and hypertension (91).
1.3.2 Painful Diabetic Neuropathy
DSPN has an insidious onset and is often indicated by sensory symptoms that start
in the toes and then progress proximally to involve the feet and legs in a stocking
distribution. DSPN results in the loss of sensation, which may lead to foot
ulceration and eventual lower limb amputation, representing the commonest cause
of hospitalisation amongst patients with DM (99). Approximately 50% of patients
with DSPN experience neuropathic symptoms (100) and these symptoms include;
burning pain, electrical or stabbing sensations, paraesthesiae, hyperaesthesia and
a deep aching pain (Table 1.3).
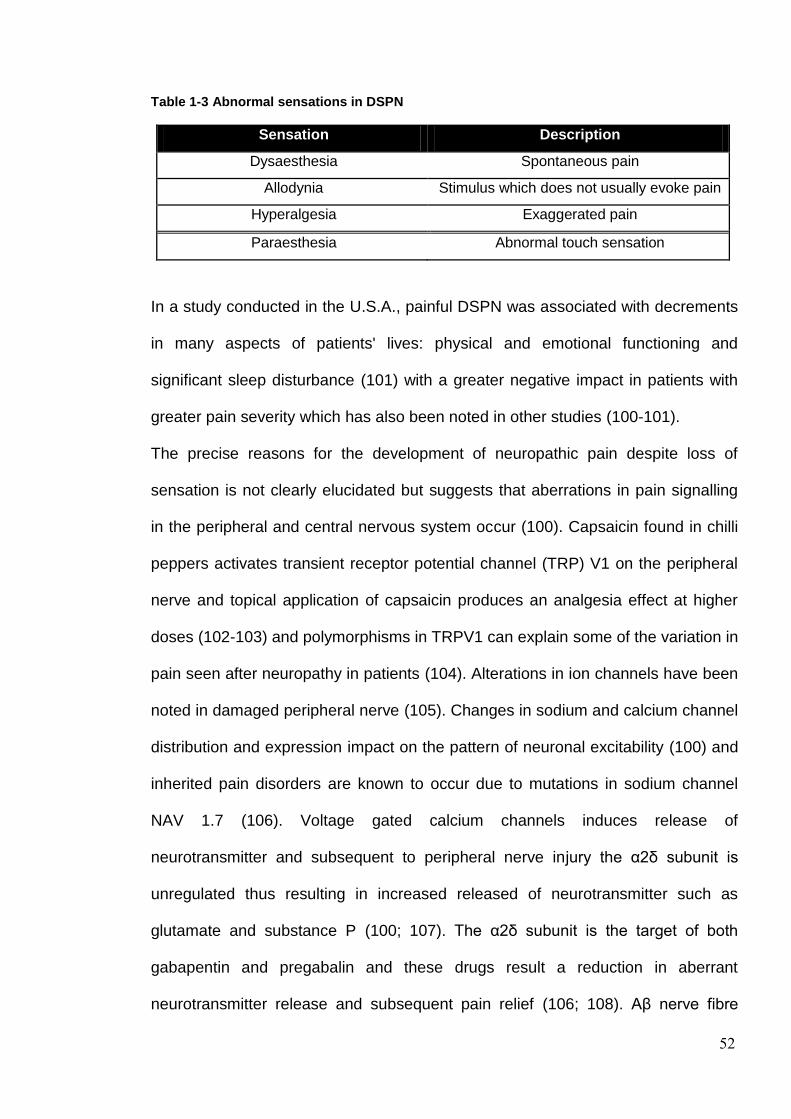
52
Table 1-3 Abnormal sensations in DSPN
Sensation Description
Dysaesthesia Spontaneous pain
Allodynia Stimulus which does not usually evoke pain
Hyperalgesia Exaggerated pain
Paraesthesia Abnormal touch sensation
In a study conducted in the U.S.A., painful DSPN was associated with decrements
in many aspects of patients' lives: physical and emotional functioning and
significant sleep disturbance (101) with a greater negative impact in patients with
greater pain severity which has also been noted in other studies (100-101).
The precise reasons for the development of neuropathic pain despite loss of
sensation is not clearly elucidated but suggests that aberrations in pain signalling
in the peripheral and central nervous system occur (100). Capsaicin found in chilli
peppers activates transient receptor potential channel (TRP) V1 on the peripheral
nerve and topical application of capsaicin produces an analgesia effect at higher
doses (102-103) and polymorphisms in TRPV1 can explain some of the variation in
pain seen after neuropathy in patients (104). Alterations in ion channels have been
noted in damaged peripheral nerve (105). Changes in sodium and calcium channel
distribution and expression impact on the pattern of neuronal excitability (100) and
inherited pain disorders are known to occur due to mutations in sodium channel
NAV 1.7 (106). Voltage gated calcium channels induces release of
neurotransmitter and subsequent to peripheral nerve injury the α2δ subunit is
unregulated thus resulting in increased released of neurotransmitter such as
glutamate and substance P (100; 107). The α2δ subunit is the target of both
gabapentin and pregabalin and these drugs result a reduction in aberrant
neurotransmitter release and subsequent pain relief (106; 108). Aβ nerve fibre

53
sprouting into dorsal horn, and reduced inhibition via descending pathways (109)
together with axonal atrophy in peripheral nerves have been demonstrated in
patients with painful diabetic neuropathy (110). Painful diabetic neuropathy has
also been associated with significantly greater autonomic dysfunction than painless
DPN (111). Central nervous system (CNS) involvement also seems to be a
hallmark of DSPN but may actually be related to nocturnal exacerbations typically
noted by suffers which impairs sleep (100). A combination of central sensitisation,
changes in inhibition of descending pathways and increased thalamic vascularity
may all play a significant role in painful DSPN and the latter has been noted in
studies of functional magnetic resonance imaging (fMRI) (112-113).
Currently there are two licenced treatments for the treatment of painful DSPN
within the UK, namely pregabalin and duloxetine with amtriptylline also commonly
used particularly within primary care. There is no definitive accepted cut off for a
reduction in pain which is deemed clinically significant. However, an end-point of
50% improvement in pain relief is generally considered an adequate response to
an intervention considering a placebo response may be as great as 35% (114).
The treatment of painful DSPN remains inadequate and in recent studies in DSPN
have shown a placebo effect which has approached and in the study by Selvarajah
et al (115), a medicinal cannabis-based product even surpassed that of the active
therapy, obscuring the precise treatment effect of the active treatment (116). There
is an urgent need for novel therapeutic agents in the treatment of painful DSPN.
1.3.3 Pathogenesis of Diabetic Neuropathy
The pathogenesis of diabetic neuropathy is yet to be fully elucidated but is known
to involve metabolic effects mediated directly and indirectly by hyperglycemia,

54
resulting in oxidative stress, accelerated polyol pathway metabolism, and
generation of advanced glycation end-products (117-118). Both metabolic and
microvascular factors are considered to play important roles (119-120). Chronic
hyperglycaemia is a pivotal mediator. Even pre-diabetic or intermittent
hyperglycaemia may be related to painful neuropathy (121). In one study, 25% of
apparent idiopathic painful neuropathy and electrodiagnostic evidence of axonal
injury with loss of epidermal nerve fibres had IGT (122). Diabetic neuropathy is
initially a predominantly small fibre neuropathy which begins at the distal
extremities moving proximally with time (123). In fact, around 56% of those
presenting with the burning feet of idiopathic small fibre neuropathy have impaired
glucose tolerance (124). Many individuals with small fibre neuropathy will only
have mild, subclinical large fibre disease (125) and thus there is a cohort of those
with small fibre neuropathy not detectable with traditional investigations.
The Diabetes Control and Complications Trial (96) and the United Kingdom
Prospective Diabetes Study (126) have demonstrated that poor glycaemic control
is related to increased prevalence of neuropathy and other microvascular
complications. Improvement in glycaemic control may even prevent or slow
elements of diabetic neuropathy (96). The results of the DCCT (96) were
particularly important; this randomised, prospective study showed a significant
reduction in the development and progression of clinical neuropathy (64%), motor
nerve conduction velocity (44%) and autonomic dysfunction in type 1 diabetic
patients with optimal glycaemic control.
After many years of research the precise mechanism of hyperglycaemia leading to
diabetic neuropathy is still to be fully explained. The numerous pathological
changes are mediated through competing or parallel pathological pathways;

55
glucose-induced activation of protein kinase C isoforms; increased formation of
advanced-glycation end-products (AGE); and increased glucose flux through the
aldose reductase pathway (127). Brief accounts of the postulated pathways which
are the focus of therapeutic interventions are described below.
Over 80% of amputations follow a foot ulcer or injury (82), early recognition of at
risk individuals and appropriate foot care may result in a reduced incidence of
ulceration and consequently amputation. However, the study by Lincon et al (128)
has challenged this notion with an observer-blind, randomised controlled trial to
assess the effect of a foot care education programme in the secondary prevention
of foot ulcers. Intervention was associated with improved foot care behaviour,
however there was no evidence that a programme of targeted education was
associated with clinical benefit over and above usual care (128). The ever
increasing prevalence of DM and consequently lower limb amputation in the
western world (80) highlights the need to understand and accurately assess DSPN.
Figure 1.1 highlights the main mechanisms contributing to DSPN. Cellular factors
derived from the bone marrow may produce chimeric cells in peripheral nerves of
diabetic animals thus elicit nerve injury and cellular components from the bone
marrow have an influence on the nerve pathology in diabetes (129).

56
Figure 1-1 The pathogenesis of DSPN
Schematic adapted from Yagihashi et al (129)
1.3.3.1 Polyol Pathway
Polyol pathway (Figure 1.2) hyperactivity has been postulated as a mechanism
linking hyperglycaemia to neuropathy (130). Animal models have consistently
demonstrated an association between increased polyol pathway flux and a
reduction in nerve conduction velocity, which may be ameliorated with aldose
reductase inhibitors (131). It is thought that hyperglycaemia leads to sorbitol
accumulation in the peripheral nerve due to increased conversion from glucose, via
the enzyme aldose reductase. This is evidenced by elevated sorbitol in diabetic
nerves (132-133) however, it is now thought that this accumulation may actually
not be as important as previously considered (134). The high rate of flux through
the pathway may contribute to oxidative stress (134). This pathway has been the
focus of much of the therapeutic interventions that have been trialled. Aldose

57
reductase inhibitors have shown an improvement in nerve conduction velocity and
some improvement in nerve fibre count (135) but have consistently failed in phase
III clinical trials (136). It is postulated that the role of the polyol pathway in humans
perhaps is not as crucial as described in animal models. Furthermore, there may
be a considerable heterogeneity in the level of the polyol pathway metabolites as
shown by numerous studies (137-140).
Figure 1-2 Polyol Pathway in DSPN
NADPH NADP+ NAD+ NADH
Glucose Sorbitol Fructose
Aldose reductase Sorbitol dehydrogenase
1.3.3.2 Non-enzymatic glycation
Glucose and other sugars can form covalent bonds with proteins (non-enzymatic
glycation) which has been documented in diabetes (141). Advanced Glycation End
products have also been identified that may contribute to oxidative stress and
interplay with other pathways (134). AGEs can quench nitric oxide and thus lead to
impaired tissue blood flow (142).
1.3.3.3 Oxidative stress
In diabetes, there is increased free radical production due to hyperglycaemia and a
reduced ability to neutralize free radicals. This is partly the result of non-enzymatic
glycation and polyol pathway hyperactivity (134). There is acceleration in free-
radical formation that may be associated with a deficiency of antioxidant and
detoxification pathways (134). With polyol pathway hyperactivity, the ability to
neutralize free radicals is reduced, as there is NADH depletion (143). Oxidative

58
stress impairs nerve function by either a direct toxic effects or by reducing nitric
oxide. This in turn may impinge on blood flow in endoneurial capillaries.
A powerful antioxidant (alpha lipoic acid) which scavenges hydroxyl radicals,
superoxide and peroxyl radicals and generates glutathione has shown some
benefit (144) and the Alpha Lipoic in Diabetic Neuropathy (ALADIN) study
demonstrated an improvement of neuropathic symptoms with 3 weeks of
intravenous treatment with alpha lipoic acid (145) although with such a short
duration of intervention a considerable placebo effect is likely. The ALADIN II study
which comprised of 5 days of intravenous treatment with alpha lipoic acid followed
by 2 years of oral treatment showed a significant improvement in sural and tibial
nerve conduction parameters (146). However, the more recent study by Nathan I
study (147), which was a 4 year randomized double-blind parallel-group trial
enrolling 460 diabetic patients with mild to moderate DSPN who were randomly
assigned to oral treatment with 600 mg alpha lipoic acid once daily (n = 233) or
placebo (n = 227) did not achieve the primary end point. However, importantly the
primary end point did not deteriorate significantly in placebo treated subjects and
brings into question the reoccurring dilemma of the lack of placebo decline in trials
of human DSPN (148).
1.3.3.4 Protein Kinase C (PKC) activation
Hyperactivity of Protein Kinase C (PKC) by 1,2-diacylglycerol inducement occurs in
diabetes and is associated with abnormalities in vascular function. It can improve
Na+-K+- ATPase activity, which is normally suppressed (134). PKC inhibitors have
been shown to correct nerve conduction velocity and perfusion deficits and to
protect endothelial dependent relaxation in animal models (149-150). A PKC-β

59
inhibitor, Ruboxistaurin, has been studied in randomised placebo controlled trials
and failed in its primary outcome measure (151-152).
1.3.3.5 Renin-Angiotensin-Aldosterone System (RAS)
A small open label study of lisinopril in hypertensive subjects (n=13) showed
improvements in nerve conduction measures over 12 weeks (153). One double
blind randomised controlled study has found benefit of trandolopril in normotensive
patients with DM and mild neuropathy over a one year period (154). The
mechanism of action is thought to be mediated through protection from nerve
hypoxia.
1.3.3.6 C-Peptide, Complications and DSPN
C-peptide deficiency is an important contributing factor to the characteristic
functional and structural abnormalities of the peripheral nerves (155). C-peptide
binds to cell membranes, resulting in stimulation of endothelial nitric oxide
synthase (eNOS) and Na+, K+ -ATPase (Figure 1.3) (156). In the Joslin 50-Year
Medallist Study (157), protection from complications (retinopathy, nephropathy and
neuropathy) was thought to be due to the presence of enriched protective factors
against microvascular complications. It was also noted that there was residual C-
peptide production (6% of subjects) which may itself play an important role (157).
In two double-blind, placebo-controlled studies in type 1 DM patients, C-peptide
replacement or placebo was given with the patients’ regular insulin therapy (158-
159). Sensory NCV assessed in the sural nerve and showed a significant
improvement. The two studies had different populations: In the first study, patients
were at an early stage of nerve dysfunction with an average age of 29 years and
approximately 10 years diabetes duration. There was an increase after 3 months

60
which amounted to 2.7 m/s, corresponding to an 80% correction of the initial
conduction velocity deficit in these patients (158). In the second study, patients
presented with sensory NCV in the sural nerve that was at baseline on average 2.6
SD below normal after correction for body height thus suggesting that some
patients had quite marked nerve conduction deficits prior to the 6 months of
intervention (159). Further detailed large randomised controlled trials of sufficient
quality and length are required to truly assess the effectiveness of C-peptide as a
therapeutic intervention. Figure 1.3 shows the postulated mechanism by which C-
peptide may exert an effect on nerve structure and function.
Figure 1-3 Putative effect of C-peptide on peripheral nerve structure and function
Adapted from Ekberg et al (156).
1.3.3.7 Treatments for DSPN based on pathogenetic mechanisms
Treatments based on the pathogenetic mechanisms of DSPN have dramatically
failed at the clinical trial stage (82; 136; 160-162). In part, the failure of these
C-Peptide
eNOS ↑ Improved
Endothelial Function
Improved Nerve function
Na+, K+ -ATPase ↑
Na+ - Retention ↓
Energy status ↑
Improved Nerve function
Amelioration of Nerve Structural
Abnormalities
Neurotrophic Factors ↑
NGF, IGF-1, NT3 ↑ Amelioration of Nerve Structural
Abnormalities

61
treatments may be due to inadequate trial design, inappropriate surrogate end
points and a lack of decline in the placebo arms of clinical trials (148). Currently,
there is a single treatment which is licensed only in Japan (163), although its
clinical effectiveness is debatable. There are no licensed treatments in the UK.
Treatments based on their putative mechanism and effects in RCTs are detailed in
Table 1.4.
1-4 Treatment of DSPN based on the putative pathogenetic mechanisms and outcome of
clinical trials.
Abnormality Compound Aim of treatment Status of RCTs
Polyol pathway↑ Aldose reductase
inhibitors Nerve sorbitol↓
Sorbinil/Tolrestat/
Zenarestat/Lidorestat Withdrawn (AE)
Zopolrestat
Withdrawn
No published clinical
trials
Ponalrestat
Ineffective
Epalrestat
Marketed in Japan
Ranirestat
In phase III trials (157)
Oxidative stress↑ α-Lipoic acid Oxygen free radicals↓
Effective in RCTs,
Nathan I (147) –
ineffective at primary
endpoint
Nerve hypoxia↑ ACE inhibitors NBF↑ Effective in one RCT
Protein kinase C↑ Protein kinase C-β
inhibitor NBF↑ RCTs ongoing,
C-peptide↓ C-peptide NBF↑ Some data available,
Studies ongoing
Neurotrophism↓ Nerve growth factor Nerve regeneration,
growth↑ Ineffective
Adapted from Boulton et al: Diabetes Neuropathies (162).
AE adverse event, NBF nerve blood flow, RCT randomised clinical trial.

62
1.4 Vitamin D deficiency
It estimated that vitamin D deficiency affects one billion people worldwide (164).
Previous estimates of vitamin D deficiency in the UK suggest it may affect up to
87% of adults, depending on the season (165). Considerable attention has recently
been focused on the role of vitamin D deficiency on cardiovascular health (161;
166-167). The vitamin D receptor (VDR) is known not only to be expressed in bone
but ubiquitously in other tissues and cells including lymphocytes, cardiomyocytes,
endothelium, pancreatic β-cells, and lipid laden macrophages (foam cells) (168).
25(OH) vitamin D is used to determine vitamin D status as it accurately represents
body stores and has a half-life of approximately 15 days (169-170), whereas the
active form (1,25(OH)2 vitamin D) has a short half life 15 hours and can alter over a
24 hour period (169).
Current ‘healthy’ or sufficient levels of 25(OH) vitamin D are suggested to be
>30ng/dl although this advice is based on data derived from bone metabolic health
(171) (Table 1.5) and there is no definitive consensus on optimal levels (164).
Vitamin D deficiency is defined by some experts as a 25(OH) vitamin D of less than
20 ng/ml (172-174), however, 25(OH) vitamin D levels are inversely associated
with parathyroid hormone levels until 25(OH) vitamin D reaches 30 to 40 ng/ml at
which point parathyroid hormone levels reach their nadir (175-177).

63
1-5 Serum 25(OH) vitamin D concentrations and status
Serum 25(OH) vitamin D concentrations and status (164)
25(OH) vitamin D Concentration 25(OH) vitamin D status
<10ng/ml Severely Deficient
10-<20ng/ml Deficient
20-<30ng/ml Insufficient
≥30ng/ml Adequate
≥150ng/ml Possible toxicity
1.4.1 Vitamin D deficiency, Hyperlipidaemia and Hypertension
1.4.1.1 Hyperlipidaemia
Vitamin D and cholesterol share a common metabolic pathway through 7-
dehydrocholesterol and this metabolite is a precursor for both. Lower levels of
25(OH) vitamin D have been associated with lower high density lipoprotein
cholesterol (HDL) and hyper triglyceridaemia (178). Statin therapy has shown to
raise vitamin D levels (179) and a study in macrophages from obese hypertensive
patients with DM established that culturing with 1,25(OH)2 vitamin D suppressed
foam cell formation by reducing oxidized low-density lipoprotein cholesterol (LDL)
uptake (180). The deletion of the vitamin D receptor in macrophages in the same
study accelerated foam cell formation induced by modified LDL (180). 25(OH)

64
vitamin D is sequestered in adipose tissue and this may partly explain the low
levels associated with obesity by reducing the release of this inactive form into the
circulation for transformation to active vitamin D (181) as well as being
independently associated with HDL and metabolic syndrome (178).
1.4.1.2 Hypertension
Vitamin D is implicated in hypertension by its role as a negative regulator of the
RAS and in experimental studies, VDR knockout mice have elevated renin,
angiotensin and aldosterone, suggesting that vitamin D may be a potent inhibitor of
the RAS axis (182). The NHANES III study (183) described a lower blood pressure
in those in the highest deciles of 25(OH) vitamin D and vitamin D3 with calcium
supplementation has been shown to reduce blood pressure compared to calcium
supplementation alone (184). However, the largest interventional study was the
Women's Health Initiative (n = 36 282), which was designed to evaluate the effects
of 400 IU of daily vitamin D3 with calcium supplementation on fracture and cancer
risk when compared to placebo showed no change in blood pressure or incident
hypertension over 7 years (185).
1.4.2 Vitamin D deficiency and Macrovascular Complications
The Framingham offspring study longitudinally followed up individuals (n=1739)
with no prior history of cardiovascular disease in this cohort (167). During the follow
up period (mean 5.4 years) a composite of cardiovascular events was assessed
and after multivariate adjustment those with 25(OH) vitamin D of <15ng/ml had a
hazard ratio of 1.62 (95% confidence interval (CI) 1.11-2.36, p=0.01) for incident
cardiovascular events compared to 25(OH) vitamin D ≥15ng/ml (167). This
increased risk was even more evident in those with hypertension (167). Vitamin D
65
deficiency has been related to cardiac disease in the form of coronary artery
calcification, myocardial infarction, stroke and congestive cardiac failure (170). The
Ludwigshafen risk and cardiovascular health study (LURIC study) assessed a
consecutive cohort of 3258 individuals scheduled for coronary angiography (186)
for their vitamin D status. Sudden cardiac death and death due to heart failure
were independently and inversely associated with 25(OH) vitamin D, and CVA was
related to both 25(OH) vitamin D and 1,25(OH)2 vitamin D levels (186).
Furthermore, the NHANES III study subgroup (n=3408) analysis supported these
findings as 25(OH) vitamin D was inversely associated with all-cause mortality over
a mean period of 7.3 year (187). Compared to individuals with 25(OH) vitamin D of
≥40ng/ml, those with 25(OH) vitamin D of <10ng/ml the adjusted risk was
approximately 83% higher (187). A study vitamin D deficiency was associated with
an increased amputation risk in veterans with peripheral arterial disease (188).
1.4.3 Vitamin D and Diabetic Neuropathy
The effective treatment of DSPN remains a major challenge and anticonvulsants
and anti-depressants remain the mainstay of symptom relief, but provide no benefit
for underlying nerve damage. However, increasing data suggest that vitamin D
may have not only comparable analgesic but also play a pivotal role in the
peripheral nervous system and in particular diabetic neuropathy (189-192).
Vitamin D deficiency may occur in a significant proportion of UK patients; with
diabetes ~90% classified as being insufficient (<30ng/ml) with severe deficiency in
over 30% (<10ng/ml) (193). Nerve Growth Factor (NGF) and neuronal Ca2+
homeostasis, both may play a neuroprotective role in the peripheral nerve have
been linked to vitamin D experimental studies through the regulation of

66
neurotrophins (194). NGF is depleted in experimental diabetes (195). Sciatic nerve
NGF was preserved in animals exposed to a vitamin D analogue (CB1093) (194)
and another vitamin D analogue (MC903) is known to increase NGF synthesis
(196). Also in the peripheral nervous system, VDR are found in predominantly
nociceptive neurons of dorsal root ganglia and their expression is influenced by
ovarian hormones and a significant increase in VDR expression has been
observed in DRG neurons of diabetic rats (197).
Observational studies have demonstrated a significant link between vitamin D
deficiency and DSPN (190-191). In the National Health and Nutrition Examination
Survey (NHANES) 2001-2004, an unweighted sample of 591 subjects with
diabetes demonstrated a significant association between vitamin D deficiency and
both paraesthesiae (odds ratio 2.12; 95% CI 1.17–3.85) and numbness (odds ratio
2.04; 95% CI 1.18–3.52) after adjusting for confounders (191). Similarly in a cross
sectional study by Shebab et al (190), vitamin D deficiency was an independent
risk factor for DSPN assessed using the neuropathy symptom score, as well as
clinical and electrophysiological measures of DSPN.
Vitamin D deficiency has been implicated in numerous pain syndromes (198-199).
Vitamin D supplementation may improve musculoskeletal pain and non-traumatic
back pain as shown in some studies (200), although the data on vitamin D
deficiency prevalence and non-specific musculoskeletal pain is not as compelling
(201). The data supporting a benefit of vitamin D treatment in painful DSPN is as
yet limited. However, in a non-randomised non-placebo controlled but prospective
study with cholecalciferol (vitamin D3) at a mean dose of 2059 IU daily for 3
months in painful DSPN an improvement of ~50% on the Visual Analogue (pain)
Scores (VAS) was observed (202). Furthermore Valensi et al (203), showed use of

67
a compound (QR-333) containing a vitamin D analogue in a double blind
randomised controlled trial reduced the severity of numbness, jolting pain, and
irritation in subjects with painful DSPN although QR-333 also contained an aldose
reductase inhibitor compound, which may have had an impact on the pathogenetic
mechanisms causing neuropathy. The largest observational study of patients with
in the community in northwest England (n = 15,692) has shown that the prevalence
of painful symptoms and painful DSPN was 34 and 21% respectively (77).
Additionally, despite a lower prevalence of neuropathy in South Asians compared
to Europeans and Afro-Caribbeans, painful symptoms were greater in South
Asians (77). These differences may partly be explained in relation to vitamin D
deficiency as these groups have been shown to have excess vitamin D deficiency
(204). Thus the role of vitamin D supplementation in painful DSPN requires further
study in terms of mechanisms but also demands good quality randomised
controlled trials.
1.4.4 Vitamin D and Diabetic Retinopathy
There is a possible direct link between vitamin D deficiency and the development
and progression of diabetic retinopathy. Not only have immunostaining in animal
models shown that vitamin D receptor (VDR) is expressed in the ganglion cells, the
inner and outer plexiform layer and the photoreceptor layer (205) but VDR
dependent calcium binding proteins have been isolated in the photoreceptor layer
of the human retina (206). In experimental models of ischaemic retinopathy,
calcitriol is a potent inhibitor of retinal neovascularisation (207). Other experimental
studies show similar findings with administration of active vitamin D having a
partially protective effect on diabetic retinopathy of diabetic rats, through a

68
mechanism which may involve inhibition of vascular endothelial growth factor
(VEGF) and transforming growth factor (TGF)-β1 expressions in the retinal tissues
(208).
Furthermore, retinoblastoma tissue expressing VDR has shown reduction of
growth with subsequent apoptosis of the retinoblastoma cells after
supplementation with vitamin D (209). VDR genotypes have been linked with the
cumulative prevalence of diabetic retinopathy (210). The VDR gene in the French
population, FokI and TaqI single nucleotide polymorphisms have been associated
with DR (211-212). In a Turkish study, there was a demonstrated inverse
correlation between worsening diabetic retinopathy and lower activated vitamin D
in a population of 66 subjects (213). Cross-sectional studies in children and adults
with DM, show positive associations with vitamin D deficiency and DR (214-216).
The NHANES III study showed an association between severity of diabetic
retinopathy and prevalence of vitamin D deficiency, but the findings were
inconclusive about the existence of a significant relationship (216). These findings
were also mirrored in a smaller cross sectional study of type 1 DM and controls
and those with proliferative diabetic retinopathy having the lowest vitamin D status
(215). Further evaluation of this possible important relationship is required.
1.4.5 Vitamin D and Diabetic Nephropathy
Vitamin D therapies for renal disease have been used for over a half century and
are likely to be utilised for many more years (217). Vitamin D has paracrine
functions through local activation by 1-alpha-hydroxylase and thus maintain
vascular function, cardiomyocyte health, and abrogate inflammation and insulin
resistance (218). Low serum 25(OH) vitamin D status is a common complication in

69
patients with chronic kidney disease (CKD) and the severity of deficiency increases
with the progression of CKD (219). The RAS plays a critical role in the
development of diabetic nephropathy, and blockade of the RAS is currently used
for treatment of diabetic nephropathy (220). Vitamin D plays a significant role as a
RAS inhibitor (220). In an experimental study, combination of vitamin D analogues
and RAS inhibitors prevented renal injury in diabetic nephropathy (220) and a
vitamin D analogue (paricalcitriol) has shown an improvement in microalbuminuria
in a human study through a mechanism related to inhibition of RAS (221).
1.5 Clinical Evaluation and Investigations of Neuropathy
The assessment of DSPN is a common clinical entity facing the general physician.
A simple approach to the assessment of neurological deficits is essential and can
be undertaken using the neuropathy disability score (NDS). Further evaluation
includes symptom questionnaires, quantitative sensory testing, electrophysiology,
autonomic tests and/or skin biopsy. Sural sensory nerve biopsy is a well
established method of accurately assessing neuropathy. However, due to the
invasive nature of the investigation it is not commonly used and is reserved for
diagnoses that are inconclusive, often when a vasculitic phenomena is a
differential (222). Sensory nerve biopsy will not be considered further in this thesis
for this reason. A thorough examination should include evaluation of large
myelinated nerve fibres (Aβ) by evaluating vibration perception, small myelinated
(Aδ) fibres by evaluating sharp pain and cold sensation and small unmyelinated (C)
nerve fibres by evaluating warm and pain perception. Types of nerve fibres in
peripheral nervous system are shown in table 1.6.

70
1-6 Type of nerve fibres in the peripheral nervous system
Motor Sensory Autonomic
Myelination Myelinated Myelinated Thinly
myelinated Unmyelinated Unmyelinated
Fibre type
Aα
Aα/Aβ
Aδ
C C
Function Motor control
Coarse Touch Proprioception
Vibration perception
Cold perception
Pain
Warm perception
Pain
Cardiovascular control (heart
rate, blood pressure),
genitourinary and sexual
function diaphoresis and gastrointestinal
control.
1.5.1 Diagnosis of Diabetic Distal Symmetrical Polyneuropathy
A number of approaches are employed to diagnose and evaluate the severity of
neuropathic deficits and painful symptoms in diabetic neuropathy. In a clinical
environment, bedside screening instruments are usually sufficient in screening for
neuropathy (136). The diagnosis of DSPN can only be made after a careful history
and clinical examination. The consensus is all patients with diabetes should be
screened annually for DSPN by examining:
1. Pinprick
2. Temperature
3. Vibration perception (using a 128-Hz tuning fork)
4. Ankle reflexes
5. 10g monofilament pressure sensation at the distal halluces.
71
A combination of more than one test has >87% sensitivity in detecting DSPN (4).
The modified neuropathy disability score (NDS) is a screening instrument for signs
of neuropathy. It comprises three sensory modalities and one assessment of
reflexes: 1) pain sensation (pin prick), 2) temperature sensation (hot and cold
rods), 3) vibration perception (128Hz tuning fork), and 4) absence/presence of
Achilles tendon reflexes. Thus the total maximum abnormal score possible is 10. A
score of 3-5 is regarded as evidence of mild neuropathic signs, 6-8 as moderate
and a score of 9 or 10 as severe signs of neuropathy. The original NDS in the
Rochester Diabetic Neuropathy study (223) and more recently a study by Abbott et
al, (224) using the modified NDS showed this evaluation to be reliable and
reproducible as a screening instrument of peripheral neuropathy. An increasing
NDS and Vibration Perception Thresholds (VPT) along with abnormal plantar foot
pressures can be used in identifying those at risk of foot ulceration (225). An NDS
>6 was an independent risk factor for diabetic foot ulceration (224). Also the loss of
vibration perception and 10g monofilament alone can accurately predict the risk for
future foot ulceration (82) which is an important factor in the morbidity that can be
associated with diabetes. A NDS of >6 has however been shown to be a better
predictor than the 10g monofilament and is only second to past or present history
of ulceration (224). The NDS does not diagnose the cohort with small fibre
neuropathy or with subclinical large fibre disease and should be used as a guide to
the risk of neuropathic ulceration.
Two major end-points are used particularly when assessing neuropathy for either
research purposes or quantifying the benefits of an intervention (81). These are:
a. Assessment of symptoms in defining efficacy of pain relief agents.
b. Assessment of neurological deficits in defining efficacy of nerve repair agents.
72
An alteration of symptoms does not necessarily constitute an improvement in nerve
function itself and changes in nerve ultrastructure may not equate to improved
nerve function. The criteria which is used to determine the effectiveness of an
intervention on symptoms is thus varied and lacks any specialist consensus.
1.5.1.1 Neuropathy Symptom Questionnaires
Diabetic patients usually find it difficult to describe the neuropathic pain they
experience and thus numerous questionnaires and scoring systems have been
developed to quantify the subjective feeling of neuropathic pain. Some of the more
commonly used questionnaires are discussed below.
Neuropathy Symptom Profile (NSP) assesses neuropathy in general but has been
validated in diabetes (226). It comprises of 38 questions with further subsections
which are subdivided on anatomy. It is useful in detecting neuropathy and staging
severity (226). The Rochester Diabetic Neuropathy Study (227) concluded that
NSP, combined with other neurological examinations is a valid means to assess
neuropathy.
The McGill Pain Questionnaire is the most frequently used questionnaire, however
is not specific for diabetic neuropathy. This questionnaire is a valid measure of
neuropathic pain symptoms (228). A more recently developed questionnaire, the
Diabetic Neuropathy Symptom Score (DNS) is a simple and easily reproducible
test in clinical practice. It is a 4-item questionnaire and the DNS score has been
shown to differentiate between individuals with and without diabetic neuropathy
(229) but is used more as a screening questionnaire. These questionnaires,
however valid at assessing symptoms are unable to differentiate accurately
between large and small nerve fibre deficit.

73
1.5.1.2 Quantitative Sensory Testing (QST)
QST involves the delivery of a stimulus which is reproducible and controlled, has
an established normal range and allows for serial evaluation of a standardised
stimuli (81). The biothesiometer is a QST of vibration and the other widely used
QST is that of thermal and pain thresholds (136). Both can track progression (230)
and predict those at risk of ulceration (231). The advantages and limitations of QST
are established. The most important advantage is that it requires little expertise to
perform and has a reasonable sensitivity, accuracy and reproducibility when
evaluating different stages of neuropathy at multiple anatomical sites (136). The
main limitations are variability and subjectivity of the test, patient motivation,
attention and expectation bias (232). Thermal testing consists of graded and
standardised warm and cold stimuli delivered through a thermode attached to the
foot. Thermal testing is able to quantify warm and cold sensation thresholds,
temperature induced pain and temporal summation. Room temperature, inter-
stimulus intervals, gender, age and lifestyle may also affect the outcomes (233).
However, QST including thermal threshold assessment for cold sensation (A
fibres) and warm sensation (C fibres) can assess small fibre dysfunction but are
subjective, lack accuracy and reproducibility (136; 232).
The San Antonio consensus (234-235) and now the Toronto consensus (79) states
that nerve conduction studies and symptoms and/or signs should be used as a
definitive diagnosis of DSPN. However, a significant limitation is that this approach
primarily assesses large myelinated nerve fibres (235) and only then the neural
activity of a specific small subset of large, myelinated fibres (236). Despite this
obvious draw back nerve electrophysiology is used as a surrogate marker in
clinical trials (237).

74
1.5.1.3 Electrophysiology
Electrophysiological procedures in the form of nerve conduction studies (NCS) are
one of the fundamental tests in the diagnosis of diabetic neuropathy and are
particularly used in clinical trials as a measure of effectiveness. Indeed the San
Antonio and now the Toronto consensus on diabetic neuropathy recommends the
use of electrophysiological testing along with other tests such as QST and
autonomic function to assess clinical deficits of neuropathy (79, 235). The
procedure is not invasive, but objective and is highly sensitive and therefore
accurately measures and classifies DSPN. The drawback is an inability to target
the fibre types most commonly affected by diabetes (small fibres) as it assesses
large myelinated fibres (238) and also has limited ability to demonstrate
regeneration and repair. Electrophysiological tests measure conduction of both
sensory and motor nerves, the amplitude of the propagating neural signal, the
density and synchrony of muscles activated by maximal nerve simulation and the
integrity of neuromuscular transmission (236). There are several factors
contributing to nerve conduction velocity (NCV) slowing: 1) stage of nerve
demyelination, 2) mean diameter of the conducting axons, 3) internodal distance in
the segment under study and 4) the nodal microenvironment (136).
In a study by Dyck et al, (239) when compared to nerve conduction studies,
individual physicians clinical diagnosis was highly variable with a propensity to over
diagnose DSPN. Although considered a ‘Gold Standard’ test, confounding factors
can lead to decreased sensitivity and specificity (240). Gender, weight, age and
height may all affect the results of NCS with the latter two variables having the
most significant effect (240). In a 10-year follow-up study of newly diagnosed
patients with type 2 DM, NCV slowing and decrease in sensory and motor

75
amplitudes were reported in 16.7% of the patients at 5 years and 41.9% at 10
years, indicating an increase in the severity of DPN with time (241). Although more
recent experimental studies have shown significant variability in measures of nerve
conduction with up to 56.4% variability in motor amplitude in serial measures over
a 4.5 month period (242).
Abnormal NCV is known to correlate with morphologic features in small fibre
neuropathy and QST (243) and is still used as an end point in
interventional/observational trials of DSPN.
1.5.1.4 Skin Biopsy
The only techniques which allow a direct examination of thinly myelinated and
unmyelinated nerve fibre damage and repair, are those of sural nerve biopsy with
electronmicroscopy (119; 244) and the newly refined skin-punch biopsy (124; 245).
This technique allows a reliable and reproducible means of assessing the small (C)
fibres which previously were limited to nerve biopsies, in particular that of the sural
nerve (246). Intraepidermal nerve fibres (IENF) are stained using
immunohistochemistry with the antibody to protein gene products 9.5 (120). The
densities are calculated in at least three sections as the number of IENF per length
of the section (IENF/mm) (247). According to the European Federation of
Neurological Societies/Peripheral Nerve Society Guideline on the use of skin
biopsy in the diagnosis of small fibre neuropathy, single IENF crossing the dermal–
epidermal junction should be counted, whereas secondary branching is excluded
from quantification (247). Intra- and inter observer variability, and inter laboratory
agreement on IENF counts has been assessed with good reliability scores
obtained (kappa values > or = 0.90) (248).
76
Previous studies have associated reduced IENF density with small fibre
neuropathy and more so with painful DSPN (123; 125) with excellent sensitivity
(123). There is increased small fibre loss at >5 years duration of diabetes with
shortening of IENF at all durations (123). Also reduced rates of nerve regeneration
have been seen in individuals with diabetes but without signs or symptoms of
disease or evidence of neuropathy (249). Unsurprisingly skin biopsy analysis may
be more sensitive than sural nerve conduction studies for diagnosing small fibre
neuropathy (250). The advantages of this method of assessing small fibres are:
1. Quantitative
2. Reproducible
3. Can be used for longitudinal assessment
4. Can be used at multiple sites
However, there are also major disadvantages as the technique is limited
significantly by its availability and is certainly not commonly used in clinical
practice, it is invasive and requires potentially intensive complicated laboratory
analysis.
1.5.1.5 Corneal Confocal Microscopy (CCM)
The cornea is one the most densely innervated organs in the body (251). Most
corneal nerves are derived from the ophthalmic branch of the trigeminal nerve and
constitute both Aδ and C fibres. Approximately 70 – 80 trunks of large diameter (~
6μm), myelinated nerves (Aδ) containing 900 – 1200 axons enter the cornea at the
stroma and run anteriorly towards the midpoint of the cornea. The nerves penetrate
the Bowman’s membrane and form the subbasal nerve plexus (Figure 1.3) in the

77
boundary between the Bowman’s layer and the epithelium and finally terminate in
the superficial layers of epithelium.
Figure 1-4 Montage of the whole human subbasal nerve plexus [Image adapted from: Patel
and McGhee (252).
78
Recently developed, CCM is a rapid, reiterative, non-invasive procedure which
allows microscopic examination of the cellular and nerve structures of the cornea.
Conventional techniques of electrophysiology and quantitative sensory testing
along with an assessment of neurological disability offer a relatively robust means
of defining neuropathic severity (136). However, they have major shortcomings
when they are employed to define therapeutic efficacy in clinical intervention trials
(253). New therapies in the treatment of diabetic neuropathy have been hampered
by the lack of clinically relevant end points (136) as historically quantification of
large nerve fibres were used to diagnose neuropathy and not in assessing nerve
regeneration or a response to an intervention (254). CCM may provide an ideal
surrogate end-point and has been shown to demonstrate corneal nerve fibre
pathology which is correlated with DSPN (255-257). Numerous studies have
looked at the relationship of corneal nerve pathology and diabetic neuropathy
suggesting it may be used as a surrogate marker of small fibre neuropathy (258-
263). Significant changes can be detected in corneal nerve fibre density,
branching, and tortuosity which relate to the severity of DSPN (256; 264). CCM has
also been shown to detect the benefits of therapeutic intervention with pancreas
transplantation after 6 months of the intervention (265) and more recently with
simultaneous pancreas and kidney transplantation after 12 months (266). This
highlights the ability of this modality to be potentially used in assessing therapeutic
interventions. It has been argued that however significant the changes to nerve
structure this may not necessarily equate to alterations in function. However,
corneal sensitivity is reduced and is directly related to the severity of the
neuropathy in diabetes (267). This modality has shown significant potential as a
surrogate test of nerve function.

79
1.6 REFERENCES
1. Vladimir S: Diabetic Neuropathy: Clinical Management. 2nd Ed ed. Veves A MR,
Ed. New Jersey, Humana Press Inc, 2007, p. 1-5
2. http://www.nobelprize.org/educational/medicine/insulin/discovery-insulin.html
[article online]. Last accessed 25/09/2013.
3. Busnardo AC, DiDio LJA, Tidrick RT, Thomford NR: History of the pancreas.
The American Journal of Surgery 1983;146:539-550
4. American Diabetes Association: clinical practice recommendations 2002.
Diabetes care 2002;25 Suppl 1:S1-147
5. Whiting DR, Guariguata L, Weil C, Shaw J: IDF Diabetes Atlas: Global estimates
of the prevalence of diabetes for 2011 and 2030. Diabetes Research and Clinical
Practice 2011;94:311-321
6. Kilpatrick ES, Bloomgarden ZT, Zimmet PZ: International Expert Committee
report on the role of the A1C assay in the diagnosis of diabetes: response to the
International Expert Committee. Diabetes Care 2009;32:e159; author reply e160
7. Diagnosis and classification of diabetes mellitus. Diabetes Care 2013;36 Suppl
1:S67-74
8. Lopez-Liuchi JV: Autoimmune diabetes: is GAD the culprit? Eur J Endocrinol
1999;141:458-459
9. Sanjeevi CB, Hook P, Landin-Olsson M, Kockum I, Dahlquist G, Lybrand TP,
Lernmark A: DR4 subtypes and their molecular properties in a population-based
study of Swedish childhood diabetes. Tissue antigens 1996;47:275-283
10. Sanjeevi CB, Kanungo A, Shtauvere A, Samal KC, Tripathi BB: Association of
HLA class II alleles with different subgroups of diabetes mellitus in Eastern India
80
identify different associations with IDDM and malnutrition-related diabetes. Tissue
antigens 1999;54:83-87
11. Sanjeevi CB, Lybrand TP, Landin-Olsson M, Kockum I, Dahlquist G, Hagopian
WA, Palmer JP, Lernmark A: Analysis of antibody markers, DRB1, DRB5, DQA1
and DQB1 genes and modeling of DR2 molecules in DR2-positive patients with
insulin-dependent diabetes mellitus. Tissue antigens 1994;44:110-119
12. Norris JM, Beaty B, Klingensmith G, Yu L, Hoffman M, Chase HP, Erlich HA,
Hamman RF, Eisenbarth GS, Rewers M: Lack of Association Between Early
Exposure to Cow's Milk Protein and {beta}-Cell Autoimmunity: Diabetes
Autoimmunity Study in the Young (DAISY). JAMA 1996;276:609-614
13. Graves PM, Barriga KJ, Norris JM, Hoffman MR, Yu L, Eisenbarth GS, Rewers
M: Lack of association between early childhood immunizations and beta-cell
autoimmunity. Diabetes care 1999;22:1694-1697
14. Hummel M, Fuchtenbusch M, Schenker M, Ziegler AG: No major association of
breast-feeding, vaccinations, and childhood viral diseases with early islet
autoimmunity in the German BABYDIAB Study. Diabetes care 2000;23:969-974
15. Hypponen E: Vitamin D and increasing incidence of type 1 diabetes-evidence
for an association? Diabetes Obes Metab 2010;12:737-743
16. Hypponen E, Laara E, Reunanen A, Jarvelin MR, Virtanen SM: Intake of
vitamin D and risk of type 1 diabetes: a birth-cohort study. Lancet 2001;358:1500-
1503
17. Zipitis CS, Akobeng AK: Vitamin D supplementation in early childhood and risk
of type 1 diabetes: a systematic review and meta-analysis. Archives of Disease in
Childhood 2008;93:512-517

81
18. Mohr SB, Garland CF, Gorham ED, Garland FC: The association between
ultraviolet B irradiance, vitamin D status and incidence rates of type 1 diabetes in
51 regions worldwide. Diabetologia 2008;51:1391-1398
19. Levy-Marchal C, Patterson C, Green A: Variation by age group and seasonality
at diagnosis of childhood IDDM in Europe. The EURODIAB ACE Study Group.
Diabetologia 1995;38:823-830
20. Mooney JA, Helms PJ, Jolliffe IT, Smail P: Seasonality of type 1 diabetes
mellitus in children and its modification by weekends and holidays: retrospective
observational study. Arch Dis Child 2004;89:970-973
21. Roep BO: The role of T-cells in the pathogenesis of Type 1 diabetes: from
cause to cure. Diabetologia 2003;46:305-321
22. Mora JR, Iwata M, von Andrian UH: Vitamin effects on the immune system:
vitamins A and D take centre stage. Nat Rev Immunol 2008;8:685-698
23. Bikle DD: Vitamin D and the immune system: role in protection against
bacterial infection. Curr Opin Nephrol Hypertens 2008;17:348-352
24. Fajans SS, Bell GI, Polonsky KS: Molecular mechanisms and clinical
pathophysiology of maturity-onset diabetes of the young. The New England journal
of medicine 2001;345:971-980
25. Shields BM, Hicks S, Shepherd MH, Colclough K, Hattersley AT, Ellard S:
Maturity-onset diabetes of the young (MODY): how many cases are we missing?
Diabetologia 2010;53:2504-2508
26. Stumvoll M, Goldstein BJ, van Haeften TW: Type 2 diabetes: principles of
pathogenesis and therapy. The Lancet 2005;365:1333-1346
27. Pierce M, Keen H, Bradley C: Risk of diabetes in offspring of parents with non-
insulin-dependent diabetes. . Diabet Med 1995;12:6-13
82
28. Tattersal RB, Fajans SS: Prevalence of diabetes and glucose intolerance in
199 offspring of thirty-seven conjugal diabetic parents. . Diabetes 1975;24:452-462
29. Kaprio J, Tuomilehto J, Koskenvuo M, Romanov K, Reunanen A, Eriksson J,
Stengard J, Kesaniemi YA: Concordance for type 1 (insulin-dependent) and type 2
(non-insulin-dependent) diabetes mellitus in a population-based cohort of twins in
Finland. Diabetologia 1992;35:1060-1067
30. Newman B, Selby JV, King MC, Slemenda C, Fabsitz R, Friedman GD:
Concordance for type 2 (non-insulin-dependent) diabetes mellitus in male twins. .
Diabetologia 1987;30:763-768
31. Pittas AG, Harris SS, Stark PC, Dawson-Hughes B: The effects of calcium and
vitamin D supplementation on blood glucose and markers of inflammation in
nondiabetic adults. Diabetes Care 2007;30:980-986
32. Forouhi NG, Luan J, Cooper A, Boucher BJ, Wareham NJ: Baseline serum 25-
hydroxy vitamin d is predictive of future glycemic status and insulin resistance: the
Medical Research Council Ely Prospective Study 1990-2000. Diabetes
2008;57:2619-2625
33. Parker J, Hashmi O, Dutton D, Mavrodaris A, Stranges S, Kandala NB, Clarke
A, Franco OH: Levels of vitamin D and cardiometabolic disorders: systematic
review and meta-analysis. Maturitas 2010;65:225-236
34. Gleichmann H, Zorcher B, Greulich B, Gries FA, Henrichs HR, Betrams J, Kolb
H: Correlation of islet cell antibodies and HLA-DR phenotypes with diabetes
mellitus in adults. Diabetologia 1984;27:90-92
35. Hagopian WA, Karlsen AE, Gottsater A, Landin Olsson M, Grubin CE,
Sundkvist G, Petersen JS, Boel E, Dyrberg T, Lernmark A: Quantitative assay
using recombinant human islet glutamic decarboxylase (GAD65)shows that 64K

83
autoantibody positivity at onset predicts diabetes type. J Clin Invest 1993;91:368-
362
36. Turner R, Stratton I, Horton V, Manley S, Zimmet P, Mackay IR, Shattock M,
Bottazzo GF, Holman R: UKPDS 25: autoantibodies to islet-cell cytoplasm and
glutamic acid decarboxylase for prediction of insulin requirement in type 2
diabetes: UK Prospective Diabetes Study Group. Lancet 1997;350:1288–1293
37. Davies H, Brophy S, Fielding A, Bingley P, Chandler M, Hilldrup I, Brooks C,
Williams R: Latent autoimmune diabetes in adults (LADA) in South Wales:
incidence and characterization. Diabetic Medicine 2008;25:1354-1357
38. Naik RG, Palmer JP: Latent Autoimmune Diabetes in Adults (LADA). Reviews
in Endocrine and Metabolic Disorders 2003;4:233-241
39. Hosszufalusi N, Vatay A, Katalin R, Prohaszka Z, Pozsonyi E, Horvath L,
Grosz A, Gero L, Madacsy L, Romics L, Karadi I, Fust G, Panczel P: Similar
Genetic Features and Different Islet Cell Autoantibody Pattern of Latent
Autoimmune Diabetes in Adults (LADA) Compared With Adult-Onset Type 1
Diabetes With Rapid Progression. Diabetes care 2003;26:452-457
40. Zimmet P, Turner R, McCarty D, Rowley M, Mackay I: Crucial points at
diagnosis. Type 2 diabetes or slow type 1 diabetes. Diabetes care 1999;22 Suppl
2:B59-64
41. Brophy S, Yderstraede K, Mauricio D, Hunter S, Hawa M, Pozzilli P,
Schernthaner G, Schloot N, Buzzetti R, Davies H, Leslie D, Williams R: Time to
insulin initiation cannot be used in defining latent autoimmune diabetes in adults.
Diabetes care 2008;31:439-441
84
42. Fourlands S, Perry C, Stein MS, Stankovich J, Harrison LC, Colman PG: A
Clinical Screening Tool Identifies Autoimmune Diabetes in Adults. Diabetes Care
2006;29:970-975
43. Raivo U, Åke L, Unanue EM, McDevitt HO: Chapter 3 GAD65 Autoimmunity--
Clinical Studies. In Advances in Immunology, Academic Press, 2008, p. 39-78
44. Brophy S, Brunt H, Davies H, Mannan S, Williams R: Interventions for latent
autoimmune diabetes (LADA) in adults. Cochrane Database of Systematic
Reviews 2007:Art.No.:CD006165. DOI:006110.001002/14651858. CD14006165
.pub14651852
45. Carlsson S, Midthjell K, Tesfamarian MY, Grill V: Age, overweight and physical
inactivity increase the risk of latent autoimmune diabetes in adults: results from the
Nord-Trøndelag health study. Diabetologia 2007;50:55-58
46. Chiu HK, Tsai EC, Juneja R, Stoever J, Brooks-Worrell B, Goel A, al. e:
Equivalent insulin resistance in latent autoimmune diabetes in adults (LADA) and
type 2 diabetic patients. Diabetes Res Clin Pract 2007;77:237–244
47. Li X, Liao L, Yan X, Huang G, Lin J, Lei M, Wang X, Zhou Z: Protective effects
of 1-alpha-hydroxyvitamin D3 on residual beta-cell function in patients with adult-
onset latent autoimmune diabetes (LADA). Diabetes/Metabolism Research and
Reviews 2009;25:411-416
48. Mathieu C, Gysemans C, Giulietti A: Vitamin D and diabetes. Diabetologia
2005;48 1247–1257
49. Hypponen E, Laara E, Reunanen A, Jarvelin MR, Virtanen SM: Intake of
vitamin D and risk of type 1 diabetes: a birth cohort study. Lancet 2001;358:1500-
1503

85
50. Pozzilli P, Manfrini S, Crino A, Picardi A, Leomanni C, Cherubini V, Valente L,
Khazrai M, Visalli N: Low levels of 25-hydroxyvitamin D3 and 1,25-
dihydroxyvitamin D3 in patients with newly diagnosed type 1 diabetes. Hormone
and metabolic research = Hormon- und Stoffwechselforschung = Hormones et
metabolisme 2005;37:680-683
51. Stene LC, Ulriksen J, Magnus P: Use of cod liver oil during pregnancy
associated with lower risk of type 1 diabetes in the offspring. Diabetologia
2000;43:1093–1098.
52. Alfonso B, Liao E, Busta A, Poretsky L: Vitamin D in diabetes mellitus—a new
field of knowledge poised for D-velopment. Diabetes/Metabolism Research and
Reviews 2009;25:417-419
53. Lemire JM: Immunomodulatory actions of 1,25-dihydroxyvitamin D3. J Steroid
Biochem Mol Biol 1995;53:599-602
54. Maruyama T, Shimada, A., Kanatsuka, A., Kasuga, A., Takei, I., Yokoyama, J.,
et al.: Multicenter prevention trial of slowly progressive type 1 diabetes with small
dose of insulin (the Tokyo study): Preliminary report. Annals of the New York
Academy of Sciences, 2003;1005,:362–369.
55. Sima A, Rosu M, Vlad A, Silberberg G, Serban V: Latent Autoimmune Diabetes
in Adults (LADA). TMJ 2003;53:241-245
56. Falorni A, Calcinaro F: Autoantibody profile and epitope mapping in latent
autoimmune diabetes in adults. Annals of the New York Academy of Sciences
2002;958:99-106
57. Lohmann T, Kellner K, Verlohren HJ, Krug J, Steindorf J, Scherbaum WA,
Seissler J: Titre and combination of ICA and autoantibodies to glutamic acid
86
decarboxylase discriminate two clinically distinct types of latent autoimmune
diabetes in adults (LADA). Diabetologia 2001;44:1005-1010
58. Desai M, Cull CA, Horton VA, Christie MR, Bonificio E, Lampasona V, Bingley
PJ, Levy JC, Mackay IR, Zimmet P, Holman RR, Clark A: GAD autoantibodies and
epitope reactivities persist after diagnosis in latent autoimmune diabetes in adults
but do not predict disease progression: UKPDS 77. Diabetologia 2007;50:2052-
2060
59. Barker JM, Yu J, Yu L, Wang J, Miao D, Bao F, Hoffenberg E, Nelson JC,
Gottlieb PA, Rewers M, Eisenbarth GS: Autoantibody “Subspecificity” in Type 1
Diabetes: Risk for organ-specific autoimmunity clusters in distinct groups. Diabetes
Care 2005;28:850-855
60. Murao S, Kondo S, Ohashi J, Fujii Y, Shimizu I, Fujiyama M, Ohno K, Takada
Y, Nakai K, Yamane Y, Osawa H, Makino H: Anti-thyroid peroxidase antibody, IA-2
antibody, and fasting C-peptide levels predict beta cell failure in patients with latent
autoimmune diabetes in adults (LADA)—A 5-year follow-up of the Ehime study.
Diabetes Research and Clinical Practice 2008;80:114-121
61. Holmes GK: Screening for coeliac disease in type 1 diabetes. Arch Dis Child
2002;87:495–499
62. Prokopova L: Celiac disease—a severe disease. Vnitr Lek 2003;49:474–481
63. Maki M, Hallstrom O, Vesikari T, Visakorpi JK: Evaluation of serum IgA–class
reticulin antibody test for detection of childhood celiac disease. J Pediatr
1984;105:901–905.
64. Kucera P, Novakova D, Behanova M, Novak J, Tlaskalova-Hogenova AM:
Gliadin, endomysial and thyroid antibodies in patients with latent autoimmune
diabetes of adults (LADA). Clin Exp Immunol 2003;133:139-143

87
65. Baum P, Hermann W, Verlohren HJ, Wagner A, Lohmann T, Grahmann F:
Diabetic neuropathy in patients with "latent autoimmune diabetes of the adults"
(LADA) compared with patients with type 1 and type 2 diabetes. J Neurol
2003;250:682-687
66. Balme M, McAllister I, Davis WA, Davis TME: Retinopathy in latent
autoimmune diabetes of adults: the Fremantle Diabetes Study. Diabetic Medicine
2002;19:602-605
67. Susan van D, Beulens JWJ, Yvonne T. van der S, Grobbee DE, Nealb B: The
global burden of diabetes and its complications: an emerging pandemic. European
Journal of Cardiovascular Prevention & Rehabilitation 2010;17:s3-s8
68. UK Prospective Diabetes Study 6. Complications in newly diagnosed type 2
diabetic patients and their association with different clinical and biochemical risk
factors. Diabetes Res 1990;13:1-11
69. Morrish NJ, Wang SL, Stevens LK, Fuller JH, Keen H: Mortality and causes of
death in the WHO Multinational Study of Vascular Disease in Diabetes.
Diabetologia 2001;44 Suppl 2:S14-21
70. Morello CM: Etiology and natural history of diabetic retinopathy: an overview.
Am J Health Syst Pharm 2007;64:S3-7
71. Fong DS, Aiello L, Gardner TW, King GL, Blankenship G, Cavallerano JD,
Ferris FL, 3rd, Klein R: Diabetic retinopathy. Diabetes Care 2003;26:226-229
72. Scanlon PH: The English national screening programme for sight-threatening
diabetic retinopathy. Journal of Medical Screening 2008;15:1-4
73. Jones CD, Greenwood RH, Misra A, Bachmann MO: Incidence and
Progression of Diabetic Retinopathy During 17 Years of a Population-Based
Screening Program in England. Diabetes Care 2012;35:592-596

88
74. Klein R, Klein BEK, Moss SE, Cruickshanks KJ: The Wisconsin epidemiologic
study of diabetic retinopathy: XVII: The 14-year incidence and progression of
diabetic retinopathy and associated risk factors in type 1 diabetes. Ophthalmology
1998;105:1801-1815
75. Lanting LC, Joung IMA, Mackenbach JP, Lamberts SWJ, Bootsma AH: Ethnic
Differences in Mortality, End-Stage Complications, and Quality of Care Among
Diabetic Patients: A review. Diabetes Care 2005;28:2280-2288
76. Sosenko JM: The prevalence of diabetic neuropathy according to ethnicity.
Curr Diab Rep 2009;9:435-439
77. Abbott CA, Malik RA, van Ross ER, Kulkarni J, Boulton AJ: Prevalence and
characteristics of painful diabetic neuropathy in a large community-based diabetic
population in the U.K. Diabetes Care 2011;34:2220-2224
78. Purdy CW: Diabetes-its causes, symptoms and treatment. FA D, Ed.
Philadelphia, Hardpress Publishing, 1890
79. Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, Lauria G,
Malik RA, Spallone V, Vinik A, Bernardi L, Valensi P: Diabetic neuropathies:
update on definitions, diagnostic criteria, estimation of severity, and treatments.
Diabetes Care 2010;33:2285-2293
80. Shaw J, Zimmet P: The epidemiology of diabetic neuropathy. Diabetes Revs
1999;7:245-252
81. Skljarevski V, Malik RA: Clinical Diagnosis of Diabetic Neuropathy. In Diabetic
Neuropathy: Clinical Management, 2nd Ed ed. Veves A MR, Ed. New Jersey,
Humana Press, 2007

89
82. Boulton AJM, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, Malik RA,
Maser RE, Sosenko JM, Ziegler D: Diabetic neuropathies: a statement by the
American Diabetes Association. Diabetes care 2005;28:956-962
83. Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM, Wilson DM,
O'Brien PC, Melton LJ, 3rd, Service FJ: The prevalence by staged severity of
various types of diabetic neuropathy, retinopathy, and nephropathy in a population-
based cohort: the Rochester Diabetic Neuropathy Study. Neurology 1993;43:817-
824
84. Harris M, Eastman R, Cowie C: Symptoms of sensory neuropathy in adults with
NIDDM in the U.S. population. Diabetes Care 1993;16:1446-1452
85. Walters DP, Gatling W, Mullee MA, Hill RD: The prevalence of diabetic distal
sensory neuropathy in an English community. Diabet Med 1992;9:349-353
86. Franklin GM, Kahn LB, Baxter J, Marshall JA, Hamman RF: Sensory
neuropathy in non-insulin-dependent diabetes mellitus. The San Luis Valley
Diabetes Study. Am J Epidemiol 1990;131:633-643
87. Franklin GM, Shetterly SM, Cohen JA, Baxter J, Hamman RF: Risk factors for
distal symmetric neuropathy in NIDDM. The San Luis Valley Diabetes Study.
Diabetes Care 1994;17:1172-1177
88. Maser RE, Steenkiste AR, Dorman JS, Nielsen VK, Bass EB, Manjoo Q, Drash
AL, Becker DJ, Kuller LH, Greene DA, et al.: Epidemiological correlates of diabetic
neuropathy. Report from Pittsburgh Epidemiology of Diabetes Complications
Study. Diabetes 1989;38:1456-1461
89. Orchard TJ, Dorman JS, Maser RE, Becker DJ, Ellis D, LaPorte RE, Kuller LH,
Wolfson SK, Jr., Drash AL: Factors associated with avoidance of severe
90
complications after 25 yr of IDDM. Pittsburgh Epidemiology of Diabetes
Complications Study I. Diabetes Care 1990;13:741-747
90. Verhoeven S, van Ballegooie E, Casparie AF: Impact of Late Complications in
Type 2 Diabetes in a Dutch Population. Diabetic Medicine 1991;8:435-438
91. Tesfaye S, Chaturvedi N, Eaton SEM, Ward JD, Manes C, Ionescu-Tirgoviste
C, Witte DR, Fuller JH: Vascular Risk Factors and Diabetic Neuropathy. New
England Journal of Medicine 2005;352:341-350
92. Tight blood pressure control and risk of macrovascular and microvascular
complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study
Group. BMJ 1998;317:703-713
93. Gregg EW, Sorlie P, Paulose-Ram R, Gu Q, Eberhardt MS, Wolz M, Burt V,
Curtin L, Engelgau M, Geiss L: Prevalence of lower-extremity disease in the US
adult population >=40 years of age with and without diabetes: 1999-2000 national
health and nutrition examination survey. Diabetes Care 2004;27:1591-1597
94. Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D,
Turner RC, Holman RR: Association of glycaemia with macrovascular and
microvascular complications of type 2 diabetes (UKPDS 35): prospective
observational study. BMJ 2000;321:405-412
95. Reichard P, Nilsson BY, Rosenqvist U: The effect of long-term intensified
insulin treatment on the development of microvascular complications of diabetes
mellitus. N Engl J Med 1993;329:304-309
96. The effect of intensive diabetes therapy on the development and progression of
neuropathy. The Diabetes Control and Complications Trial Research Group.
Annals of internal medicine 1995;122:561-568

91
97. Albers JW, Herman WH, Pop-Busui R, Feldman EL, Martin CL, Cleary PA,
Waberski BH, Lachin JM: Effect of prior intensive insulin treatment during the
Diabetes Control and Complications Trial (DCCT) on peripheral neuropathy in type
1 diabetes during the Epidemiology of Diabetes Interventions and Complications
(EDIC) Study. Diabetes Care 2010;33:1090-1096
98. White NH, Sun W, Cleary PA, Danis RP, Davis MD, Hainsworth DP, Hubbard
LD, Lachin JM, Nathan DM: Prolonged effect of intensive therapy on the risk of
retinopathy complications in patients with type 1 diabetes mellitus: 10 years after
the Diabetes Control and Complications Trial. Arch Ophthalmol 2008;126:1707-
1715
99. Boulton AJM, Malik RA: Diabetic Neuropathy. Med Clin N Amer 1998;82:909-
929
100. Tesfaye S, Boulton AJ, Dickenson AH: Mechanisms and management of
diabetic painful distal symmetrical polyneuropathy. Diabetes Care 2013;36:2456-
2465
101. Gore M, Brandenburg NA, Dukes E, Hoffman DL, Tai KS, Stacey B: Pain
severity in diabetic peripheral neuropathy is associated with patient functioning,
symptom levels of anxiety and depression, and sleep. J Pain Symptom Manage
2005;30:374-385
102. Tandan R, Lewis GA, Krusinski PB, Badger GB, Fries TJ: Topical capsaicin in
painful diabetic neuropathy. Controlled study with long-term follow-up. Diabetes
Care 1992;15:8-14
103. Kulkantrakorn K, Lorsuwansiri C, Meesawatsom P: 0.025% capsaicin gel for
the treatment of painful diabetic neuropathy: a randomized, double-blind,
crossover, placebo-controlled trial. Pain Pract 2013;13:497-503

92
104. Binder A, May D, Baron R, Maier C, Tolle TR, Treede RD, Berthele A,
Faltraco F, Flor H, Gierthmuhlen J, Haenisch S, Huge V, Magerl W, Maihofner C,
Richter H, Rolke R, Scherens A, Uceyler N, Ufer M, Wasner G, Zhu J, Cascorbi I:
Transient receptor potential channel polymorphisms are associated with the
somatosensory function in neuropathic pain patients. PLoS One 2011;6:e17387
105. Dickenson AH, Matthews EA, Suzuki R: Neurobiology of neuropathic pain:
mode of action of anticonvulsants. Eur J Pain 2002;6 Suppl A:51-60
106. Yang Y, Wang Y, Li S, Xu Z, Li H, Ma L, Fan J, Bu D, Liu B, Fan Z, Wu G, Jin
J, Ding B, Zhu X, Shen Y: Mutations in SCN9A, encoding a sodium channel alpha
subunit, in patients with primary erythermalgia. J Med Genet 2004;41:171-174
107. Bauer CS, Nieto-Rostro M, Rahman W, Tran-Van-Minh A, Ferron L, Douglas
L, Kadurin I, Sri Ranjan Y, Fernandez-Alacid L, Millar NS, Dickenson AH, Lujan R,
Dolphin AC: The increased trafficking of the calcium channel subunit alpha2delta-1
to presynaptic terminals in neuropathic pain is inhibited by the alpha2delta ligand
pregabalin. J Neurosci 2009;29:4076-4088
108. Murad MH, Smith SA: Review: TCAs, anticonvulsants, opioids, and capsaicin
cream are effective for diabetic neuropathy. Evid Based Med 2008;13:21
109. Tesfaye S, Vileikyte L, Rayman G, Sindrup S, Perkins B, Baconja M, Vinik A,
Boulton A: Painful Diabetic Peripheral Neuropathy: Consensus Recommendations
on Diagnosis, Assessment and Management. Diabetes Metab Res Rev
2011;27:629-638
110. Britland ST, Young RJ, Sharma AK, Clarke BF: Association of Painful and
Painless Diabetic Polyneuropathy With Different Patterns of Nerve Fibre
Degeneration and Regeneration. Diabetes 1990;39:898-908

93
111. Gandhi RA, Marques JL, Selvarajah D, Emery CJ, Tesfaye S: Painful diabetic
neuropathy is associated with greater autonomic dysfunction than painless diabetic
neuropathy. Diabetes Care 2010;33:1585-1590
112. Wilkinson ID, Selvarajah D, Greig M, Shillo P, Boland E, Gandhi R, Tesfaye
S: Magnetic resonance imaging of the central nervous system in diabetic
neuropathy. Curr Diab Rep 2013;13:509-516
113. Selvarajah D, Wilkinson ID, Davies J, Gandhi R, Tesfaye S: Central nervous
system involvement in diabetic neuropathy. Curr Diab Rep 2011;11:310-322
114. Quessy SN, Rowbotham MC: Placebo response in neuropathic pain trials.
Pain 2008;138:479-483
115. Selvarajah D, Gandhi R, Emery CJ, Tesfaye S: Randomized Placebo-
Controlled Double-Blind Clinical Trial of Cannabis-Based Medicinal Product
(Sativex) in Painful Diabetic Neuropathy: Depression is a major confounding factor.
Diabetes Care 2010;33:128-130
116. Tavakoli M, Asghar O, Alam U, Petropoulos IN, Fadavi H, Malik RA: Novel
insights on diagnosis, cause and treatment of diabetic neuropathy: focus on painful
diabetic neuropathy. Ther Adv Endocrinol Metab 2010;1:69-88
117. Brownlee M: The pathobiology of diabetic complications: a unifying
mechanism. Diabetes 2005;54:1615-1625
118. Malik RA: The pathology of human diabetic neuropathy. Diabetes. Diabetes
1997;46:50-53
119. Malik RA, Veves A, Walker D, Siddique I, Lye RH, Schady W, Boulton AJM:
Sural nerve fibre pathology in diabetic patients with mild neuropathy: relationship to
pain, quantitative sensory testing and peripheral nerve electrophysiology. Acta
Neuropathologica 2001;101:367-374

94
120. Ward JD, Tesfaye S: Pathogenesis of human diabetic neuropathy. . In
Textbook of Diabetes Pickup J WG, Eds., Ed. Oxford, Blackwell Science,, p. 49.41-
49.19
121. Singleton JR, Smith AG, Bromberg MB: Increased Prevalence of Impaired
Glucose Tolerance in Patients With Painful Sensory Neuropathy. Diabetes Care
2001;24:1448-1453
122. Azad N, Emanuele NV, Abraira C, Henderson WG, Colwell J, Levin SR,
Nuttall FQ, Comstock JP, Sawin CT, Silbert C, Rubino FA: The effects of intensive
glycemic control on neuropathy in the VA cooperative study on type II diabetes
mellitus (VA CSDM). J Diabetes Complications 1999;13:307-313
123. Pittenger GL, Ray M, Burcus NI, McNulty P, Basta B, Vinik AI: Intraepidermal
Nerve Fibres Are Indicators of Small-Fiber Neuropathy in Both Diabetic and
Nondiabetic Patients. Diabetes care 2004;27:1974-1979
124. Sumner CJ, Sheth S, Griffin JW, Cornblath DR, Polydefkis M: The spectrum
of neuropathy in diabetes and impaired glucose tolerance. Neurology 2003;60:108-
111
125. Lacomis D: Small-fiber neuropathy. Muscle & Nerve 2002;26:173-188
126. Intensive blood-glucose control with sulphonylureas or insulin compared with
conventional treatment and risk of complications in patients with type 2 diabetes
(UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet
1998;352:837-853
127. Malik RA: Current and future strategies for the management of diabetic
neuropathy. Treatments in endocrinology 2003;2:389-400

95
128. Lincoln NB, Radford KA, Game FL, Jeffcoate WJ: Education for secondary
prevention of foot ulcers in people with diabetes: a randomised controlled trial.
Diabetologia 2008;51:1954-1961
129. Yagihashi S, Mizukami H, Sugimoto K: Mechanism of diabetic neuropathy:
Where are we now and where to go? Journal of Diabetes Investigation 2011;2:18-
32
130. Gabbay KH, Merola LO, Field RA: Sorbitol pathway: presence in nerve and
cord with substrate accumulation in diabetes. Science (New York, NY
1966;151:209-210
131. Chung SS, Chung SK: Aldose reductase in diabetic microvascular
complications. Curr Drug Targets 2005;6:475-486
132. Greene DA, Lattimer SA, Sima AA: Sorbitol, phosphoinositides, and sodium-
potassium-ATPase in the pathogenesis of diabetic complications. The New
England journal of medicine 1987;316:599-606
133. Tomlinson DR: Polyols and myo-inositol in diabetic neuropathy--of mice and
men. Mayo Clinic proceedings 1989;64:1030-1033
134. Duby JJ, Campbell RK, Setter SM, White JR, Rasmussen KA: Diabetic
neuropathy: an intensive review. Am J Health Syst Pharm 2004;61:160-173
135. Tomlinson DR, Moriarty RJ, Mayer JH: Prevention and reversal of defective
axonal transport and motor nerve conduction velocity in rats with experimental
diabetes by treatment with the aldose reductase inhibitor Sorbinil. Diabetes
1984;33:470-476
136. Boulton AJM, Malik RA, Arezzo JC, Sosenko JM: Diabetic Somatic
Neuropathies. Diabetes care 2004;27:1458-1486

96
137. Dyck PJ, Sherman WR, Hallcher LM, Service FJ, O'Brien PC, Grina LA,
Palumbo PJ, Swanson CJ: Human diabetic endoneurial sorbitol, fructose, and
myo-inositol related to sural nerve morphometry. Ann Neurol 1980;8:590-596
138. Mayhew JA, Gillon KR, Hawthorne JN: Free and lipid inositol, sorbitol and
sugars in sciatic nerve obtained post-mortem from diabetic patients and control
subjects. Diabetologia 1983;24:13-15
139. Hale PJ, Nattrass M, Silverman SH, Sennit C, Perkins CM, Uden A, Sundkvist
G: Peripheral nerve concentrations of glucose, fructose, sorbitol and myoinositol in
diabetic and non-diabetic patients. Diabetologia 1987;30:464-467
140. Dyck PJ, Zimmerman BR, Vilen TH, Minnerath SR, Karnes JL, Yao JK,
Poduslo JF: Nerve glucose, fructose, sorbitol, myo-inositol, and fiber degeneration
and regeneration in diabetic neuropathy. N Engl J Med 1988;319:542-548
141. Brownlee M, Cerami A, Vlassara H: Advanced glycosylation end products in
tissue and the biochemical basis of diabetic complications. The New England
journal of medicine 1988;318:1315-1321
142. Cameron NE, Cotter MA: The relationship of vascular changes to metabolic
factors in diabetes mellitus and their role in the development of peripheral nerve
complications. Diabetes/metabolism reviews 1994;10:189-224
143. Giugliano D, Ceriello A, Paolisso G: Oxidative stress and diabetic vascular
complications. Diabetes care 1996;19:257-267
144. Ziegler D, Hanefeld M, Ruhnau KJ, Meissner HP, Lobisch M, Schutte K, Gries
FA: Treatment of symptomatic diabetic peripheral neuropathy with the anti-oxidant
alpha-lipoic acid. A 3-week multicentre randomized controlled trial (ALADIN Study).
Diabetologia 1995;38:1425-1433

97
145. Ruhnau KJ, Meissner HP, Finn JR, Reljanovic M, Lobisch M, Schutte K,
Nehrdich D, Tritschler HJ, Mehnert H, Ziegler D: Effects of 3-week oral treatment
with the antioxidant thioctic acid (alpha-lipoic acid) in symptomatic diabetic
polyneuropathy. Diabet Med 1999;16:1040-1043
146. Reljanovic M, Reichel G, Rett K, Lobisch M, Schuette K, Moller W, Tritschler
HJ, Mehnert H: Treatment of diabetic polyneuropathy with the antioxidant thioctic
acid (alpha-lipoic acid): a two year multicenter randomized double-blind placebo-
controlled trial (ALADIN II). Alpha Lipoic Acid in Diabetic Neuropathy. Free Radic
Res 1999;31:171-179
147. Ziegler D, Low PA, Litchy WJ, Boulton AJM, Vinik AI, Freeman R, Samigullin
R, Tritschler H, Munzel U, Maus J, Schütte K, Dyck PJ: Efficacy and Safety of
Antioxidant Treatment With α-Lipoic Acid Over 4 Years in Diabetic Polyneuropathy:
The NATHAN 1 trial. Diabetes Care 2011;34:2054-2060
148. Dyck PJ, Norell JE, Tritschler H, Schuette K, Samigullin R, Ziegler D, Bastyr
EJ, 3rd, Litchy WJ, O'Brien PC: Challenges in design of multicenter trials: end
points assessed longitudinally for change and monotonicity. Diabetes Care
2007;30:2619-2625
149. Cameron NE, Cotter MA, Jack AM, Basso MD, Hohman TC: Protein kinase C
effects on nerve function, perfusion, Na(+), K(+)-ATPase activity and glutathione
content in diabetic rats. Diabetologia 1999;42:1120-1130
150. Eichberg J: Protein kinase C changes in diabetes: is the concept relevant to
neuropathy? International review of neurobiology 2002;50:61-82
151. Brooks B, Delaney-Robinson C, Molyneaux L, Yue DK: Endothelial and neural
regulation of skin microvascular blood flow in patients with diabetic peripheral
98
neuropathy: effect of treatment with the isoform-specific protein kinase C beta
inhibitor, ruboxistaurin. Journal of diabetes and its complications 2008;22:88-95
152. Vinik AI, Bril V, Kempler P, Litchy WJ, Tesfaye S, Price KL, Bastyr EJ, null:
Treatment of symptomatic diabetic peripheral neuropathy with the protein kinase C
beta-inhibitor ruboxistaurin mesylate during a 1-year, randomized, placebo-
controlled, double-blind clinical trial. Clinical therapeutics 2005;27:1164-1180
153. Reja A, Tesfaye S, Harris ND, Ward JD: Is ACE Inhibition with Lisinopril
Helpful in Diabetic Neuropathy? Diabetic Medicine 1995;12:307-309
154. Malik RA, Williamson S, Abbott C, Carrington AL, Iqbal J, Schady W, Boulton
AJ: Effect of angiotensin-converting-enzyme (ACE) inhibitor trandolapril on human
diabetic neuropathy: randomised double-blind controlled trial. Lancet
1998;352:1978-1981
155. Sima AA: New insights into the metabolic and molecular basis for diabetic
neuropathy. Cell Mol Life Sci 2003;60:2445-2464
156. Wahren J, Ekberg K, Jornvall H: C-peptide is a bioactive peptide. Diabetologia
2007;50:503-509
157. Sun JK, Keenan HA, Cavallerano JD, Asztalos BF, Schaefer EJ, Sell DR,
Strauch CM, Monnier VM, Doria A, Aiello LP, King GL: Protection From
Retinopathy and Other Complications in Patients With Type 1 Diabetes of Extreme
Duration: The Joslin 50-Year Medalist Study. Diabetes Care 2011;34:968-974
158. Ekberg K, Brismar T, Johansson BL, Jonsson B, Lindstrom P, Wahren J:
Amelioration of sensory nerve dysfunction by C-Peptide in patients with type 1
diabetes. Diabetes 2003;52:536-541

99
159. Ekberg K, Brismar T, Johansson BL, Lindstrom P, Juntti-Berggren L, Norrby
A, Berne C, Arnqvist HJ, Bolinder J, Wahren J: C-Peptide replacement therapy and
sensory nerve function in type 1 diabetic neuropathy. Diabetes Care 2007;30:71-76
160. Schemmel KE, Padiyara RS, D'Souza JJ: Aldose reductase inhibitors in the
treatment of diabetic peripheral neuropathy: a review. Journal of diabetes and its
complications 2010;24:354-360
161. Vincent AM, Callaghan BC, Smith AL, Feldman EL: Diabetic neuropathy:
cellular mechanisms as therapeutic targets. Nat Rev Neurol 2011;7:573-583
162. Boulton AJ, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, Malik RA,
Maser RE, Sosenko JM, Ziegler D: Diabetic neuropathies: a statement by the
American Diabetes Association. Diabetes Care 2005;28:956-962
163. Schemmel KE, Padiyara RS, D'Souza JJ: Aldose reductase inhibitors in the
treatment of diabetic peripheral neuropathy: a review. Journal of diabetes and its
complications 2010;24:354-360
164. Holick MF: Vitamin D Deficiency. New England Journal of Medicine
2007;357:266-281
165. Hypponen E, Power C: Hypovitaminosis D in British adults at age 45 y:
nationwide cohort study of dietary and lifestyle predictors. Am J Clin Nutr
2007;85:860-868
166. Alam U, Asghar O, Malik RA: Vitamin D deficiency and cardiovascular
disease: the missing link. Diabetes Management 2011;1:151-155
167. Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K,
Benjamin EJ, D'Agostino RB, Wolf M, Vasan RS: Vitamin D deficiency and risk of
cardiovascular disease. Circulation 2008;117:503-511
100
168. Zittermann A, Gummert JF: Sun, vitamin D, and cardiovascular disease. J
Photochem Photobiol B 2010;101:124-129
169. Jones G: Pharmacokinetics of vitamin D toxicity. The American Journal of
Clinical Nutrition 2008;88:582S-586S
170. Aggarwal N, Reis J, Michos E: Vitamin D Deficiency and Its Implications on
Cardiovascular Disease. Current Cardiovascular Risk Reports 2010;4:68-75
171. Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, Vieth R:
Estimates of optimal vitamin D status. Osteoporos Int 2005;16:713-716
172. Holick MF: High prevalence of vitamin D inadequacy and implications for
health. Mayo Clin Proc 2006;81:353-373
173. Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes
B: Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple
health outcomes. Am J Clin Nutr 2006;84:18-28
174. Malabanan A, Veronikis IE, Holick MF: Redefining vitamin D insufficiency.
Lancet 1998;351:805-806
175. Thomas MK, Lloyd-Jones DM, Thadhani RI, Shaw AC, Deraska DJ, Kitch BT,
Vamvakas EC, Dick IM, Prince RL, Finkelstein JS: Hypovitaminosis D in medical
inpatients. N Engl J Med 1998;338:777-783
176. Chapuy MC, Preziosi P, Maamer M, Arnaud S, Galan P, Hercberg S, Meunier
PJ: Prevalence of vitamin D insufficiency in an adult normal population.
Osteoporos Int 1997;7:439-443
177. Holick MF, Siris ES, Binkley N, Beard MK, Khan A, Katzer JT, Petruschke RA,
Chen E, de Papp AE: Prevalence of Vitamin D inadequacy among
postmenopausal North American women receiving osteoporosis therapy. J Clin
Endocrinol Metab 2005;90:3215-3224

101
178. Maki KC, Rubin MR, Wong LG, McManus JF, Jensen CD, Marshall JW,
Lawless A: Serum 25-hydroxyvitamin D is independently associated with high-
density lipoprotein cholesterol and the metabolic syndrome in men and women.
Journal of Clinical Lipidology 2009;3:289-296
179. Yavuz B, Ertugrul DT, Cil H, Ata N, Akin KO, Yalcin AA, Kucukazman M, Dal
K, Hokkaomeroglu MS, Yavuz BB, Tutal E: Increased levels of 25 hydroxyvitamin
D and 1,25-dihydroxyvitamin D after rosuvastatin treatment: a novel pleiotropic
effect of statins? Cardiovasc Drugs Ther 2009;23:295-299
180. Oh J, Weng S, Felton SK, Bhandare S, Riek A, Butler B, Proctor BM, Petty M,
Chen Z, Schechtman KB, Bernal-Mizrachi L, Bernal-Mizrachi C: 1,25(OH)2 vitamin
d inhibits foam cell formation and suppresses macrophage cholesterol uptake in
patients with type 2 diabetes mellitus. Circulation 2009;120:687-698
181. Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF: Decreased
bioavailability of vitamin D in obesity. Am J Clin Nutr 2000;72:690-693
182. Vaidya A, Williams JS: The relationship between vitamin D and the renin-
angiotensin system in the pathophysiology of hypertension, kidney disease, and
diabetes. Metabolism 2012;61:450-458
183. Scragg R, Sowers M, Bell C: Serum 25-hydroxyvitamin D, ethnicity, and blood
pressure in the Third National Health and Nutrition Examination Survey. Am J
Hypertens 2007;20:713-719
184. Pfeifer M, Begerow B, Minne HW, Nachtigall D, Hansen C: Effects of a short-
term vitamin D(3) and calcium supplementation on blood pressure and parathyroid
hormone levels in elderly women. J Clin Endocrinol Metab 2001;86:1633-1637
185. Margolis KL, Ray RM, Van Horn L, Manson JE, Allison MA, Black HR,
Beresford SA, Connelly SA, Curb JD, Grimm RH, Jr., Kotchen TA, Kuller LH,

102
Wassertheil-Smoller S, Thomson CA, Torner JC: Effect of calcium and vitamin D
supplementation on blood pressure: the Women's Health Initiative Randomized
Trial. Hypertension 2008;52:847-855
186. Pilz S, Dobnig H, Fischer JE, Wellnitz B, Seelhorst U, Boehm BO, Marz W:
Low vitamin d levels predict stroke in patients referred to coronary angiography.
Stroke 2008;39:2611-2613
187. Ginde AA, Scragg R, Schwartz RS, Camargo CA, Jr.: Prospective study of
serum 25-hydroxyvitamin D level, cardiovascular disease mortality, and all-cause
mortality in older U.S. adults. J Am Geriatr Soc 2009;57:1595-1603
188. Gaddipati VC, Bailey BA, Kuriacose R, Copeland RJ, Manning T, Peiris AN:
The relationship of vitamin d status to cardiovascular risk factors and amputation
risk in veterans with peripheral arterial disease. J Am Med Dir Assoc 2011;12:58-
61
189. Holmoy T, Moen SM: Assessing vitamin D in the central nervous system. Acta
Neurol Scand Suppl 2010:88-92
190. Shehab D, Al-Jarallah K, Mojiminiyi OA, Al Mohamedy H, Abdella NA: Does
Vitamin D deficiency play a role in peripheral neuropathy in Type 2 diabetes?
Diabet Med 2012;29:43-49
191. Soderstrom LH, Johnson SP, Diaz VA, Mainous AG, 3rd: Association
between vitamin D and diabetic neuropathy in a nationally representative sample:
results from 2001-2004 NHANES. Diabet Med 2012;29:50-55
192. Alam U, Asghar O, Malik RA: Are vitamin D and B deficiency relevant to the
pathogenesis and treatment of diabetic neuropathy? Future Neurology 2012;7:235-
238

103
193. Alam U, Najam O, Al-Himdani S, Benoliel S, Jinadev P, Berry JL, Kew M,
Asghar O, Petropoulos IN, Malik RA: Marked vitamin D deficiency in patients with
diabetes in the UK: ethnic and seasonal differences and an association with
dyslipidaemia. Diabet Med 2012;29:1343-1345
194. Riaz S, Malcangio M, Miller M, Tomlinson DR: A vitamin D(3) derivative
(CB1093) induces nerve growth factor and prevents neurotrophic deficits in
streptozotocin-diabetic rats. Diabetologia 1999;42:1308-1313
195. Hellweg R, Wohrle M, Hartung HD, Stracke H, Hock C, Federlin K: Diabetes
mellitus-associated decrease in nerve growth factor levels is reversed by
allogeneic pancreatic islet transplantation. Neurosci Lett 1991;125:1-4
196. Jehan F, Neveu I, Barbot N, Binderup L, Brachet P, Wion D: MC903, an
analogue of 1,25-dihydroxyvitamin D3, increases the synthesis of nerve growth
factor. Eur J Pharmacol 1991;208:189-191
197. Filipović N, Ferhatović L, Marelja I, Puljak L, Grković I: Increased vitamin D
receptor expression in dorsal root ganglia neurons of diabetic rats. Neuroscience
Letters 2013;549:140-145
198. Gloth F, Iii, Lindsay JM, Zelesnick LB, Greenough WB: Can vitamin d
deficiency produce an unusual pain syndrome? Archives of Internal Medicine
1991;151:1662-1664
199. Arnson Y, Amital H: Is vitamin D a new therapeutic agent in autoinflammatory
and pain syndromes? Isr Med Assoc J 2011;13:234-235
200. Straube S, Andrew Moore R, Derry S, McQuay HJ: Vitamin D and chronic
pain. Pain 2009;141:10-13
104
201. Block SR: Vitamin D deficiency is not associated with nonspecific
musculoskeletal pain syndromes including fibromyalgia. Mayo Clin Proc
2004;79:1585-1586; author reply 1586-1587
202. Lee P, Chen R: Vitamin D as an analgesic for patients with type 2 diabetes
and neuropathic pain. Arch Intern Med 2008;168:771-772
203. Valensi P, Le Devehat C, Richard JL, Farez C, Khodabandehlou T,
Rosenbloom RA, LeFante C: A multicenter, double-blind, safety study of QR-333
for the treatment of symptomatic diabetic peripheral neuropathy. A preliminary
report. J Diabetes Complications 2005;19:247-253
204. Tahrani AA, Ball A, Shepherd L, Rahim A, Jones AF, Bates A: The prevalence
of vitamin D abnormalities in South Asians with type 2 diabetes mellitus in the UK.
Int J Clin Pract 2010;64:351-355
205. Craig TA, Sommer S, Sussman CR, Grande JP, Kumar R: Expression and
regulation of the vitamin D receptor in the zebrafish, Danio rerio. J Bone Miner Res
2008;23:1486-1496
206. Verstappen A, Parmentier M, Chirnoaga M, Lawson DE, Pasteels JL, Pochet
R: Vitamin D-dependent calcium binding protein immunoreactivity in human retina.
Ophthalmic Res 1986;18:209-214
207. Albert DM, Scheef EA, Wang S, Mehraein F, Darjatmoko SR, Sorenson CM,
Sheibani N: Calcitriol is a potent inhibitor of retinal neovascularization. Invest
Ophthalmol Vis Sci 2007;48:2327-2334
208. Ren Z, Li W, Zhao Q, Ma L, Zhu J: The impact of 1,25-dihydroxy vitamin D3
on the expressions of vascular endothelial growth factor and transforming growth
factor-β1 in the retinas of rats with diabetes. Diabetes Research and Clinical
Practice 2012;98:474-480

105
209. Wagner N, Wagner KD, Schley G, Badiali L, Theres H, Scholz H: 1,25-
dihydroxyvitamin D3-induced apoptosis of retinoblastoma cells is associated with
reciprocal changes of Bcl-2 and bax. Exp Eye Res 2003;77:1-9
210. Bucan K, Ivanisevic M, Zemunik T, Boraska V, Skrabic V, Vatavuk Z,
Galetovic D, Znaor L: Retinopathy and nephropathy in type 1 diabetic patients--
association with polymorphysms of vitamin D-receptor, TNF, Neuro-D and IL-1
receptor 1 genes. Coll Antropol 2009;33 Suppl 2:99-105
211. Taverna MJ, Sola A, Guyot-Argenton C, Pacher N, Bruzzo F, Slama G, Reach
G, Selam JL: Taq I polymorphism of the vitamin D receptor and risk of severe
diabetic retinopathy. Diabetologia 2002;45:436-442
212. Taverna MJ, Selam JL, Slama G: Association between a protein
polymorphism in the start codon of the vitamin D receptor gene and severe diabetic
retinopathy in C-peptide-negative type 1 diabetes. J Clin Endocrinol Metab
2005;90:4803-4808
213. Aksoy H, Akçay F, Kurtul N, Baykal O, Avci B: Serum 1,25 dihydroxy vitamin
D (1,25(OH)2D3), 25 hydroxy vitamin D (25(OH)D) and parathormone levels in
diabetic retinopathy. Clin Biochem 2000;33:47-51
214. Kaur H, Donaghue KC, Chan AK, Benitez-Aguirre P, Hing S, Lloyd M,
Cusumano J, Pryke A, Craig ME: Vitamin D deficiency is associated with
retinopathy in children and adolescents with type 1 diabetes. Diabetes Care
2011;34:1400-1402
215. Payne JF, Ray R, Watson DG, Delille C, Rimler E, Cleveland J, Lynn MJ,
Tangpricha V, Srivastava SK: Vitamin D insufficiency in diabetic retinopathy.
Endocr Pract 2012;18:185-193

106
216. Patrick PA, Visintainer PF, Shi Q, Weiss IA, Brand DA: Vitamin D and
retinopathy in adults with diabetes mellitus. Arch Ophthalmol 2012;130:756-760
217. Plum LA, Zella JB: Vitamin D compounds and diabetic nephropathy. Archives
of Biochemistry and Biophysics 2012;523:87-94
218. Agarwal R: Vitamin D, Proteinuria, Diabetic Nephropathy, and Progression of
CKD. Clinical Journal of the American Society of Nephrology 2009;4:1523-1528
219. Levin A, Bakris GL, Molitch M, Smulders M, Tian J, Williams LA, Andress DL:
Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in
patients with chronic kidney disease: results of the study to evaluate early kidney
disease. Kidney Int 2007;71:31-38
220. Zhang Z, Zhang Y, Ning G, Deb DK, Kong J, Li YC: Combination therapy with
AT1 blocker and vitamin D analog markedly ameliorates diabetic nephropathy:
blockade of compensatory renin increase. Proc Natl Acad Sci U S A
2008;105:15896-15901
221. Ireland R: Diabetic nephropathy: Paricalcitol lowers residual albuminuria in
type 2 diabetes. Nat Rev Nephrol 2011;7:62
222. Willison HJ, Winer JB: Clinical evaluation and investigation of neuropathy.
Journal of neurology, neurosurgery, and psychiatry 2003;74 Suppl 2:ii3-ii8
223. Dyck PJ, Karnes JL, O'Brien PC, Litchy WJ, Low PA, Melton LJ, 3rd: The
Rochester Diabetic Neuropathy Study: reassessment of tests and criteria for
diagnosis and staged severity. Neurology 1992;42:1164-1170
224. Abbott CA, Carrington AL, Ashe H, Bath S, Every LC, Griffiths J, Hann AW,
Hussein A, Jackson N, Johnson KE, Ryder CH, Torkington R, Van Ross ERE,
Whalley AM, Widdows P, Williamson S, Boulton AJM: The North-West Diabetes
107
Foot Care Study: incidence of, and risk factors for, new diabetic foot ulceration in a
community-based patient cohort. Diabetic Medicine 2002;19:377-384
225. Pham H, Armstrong DG, Harvey C, Harkless LB, Giurini JM, Veves A:
Screening techniques to identify people at high risk for diabetic foot ulceration: a
prospective multicenter trial. Diabetes care 2000;23:606-611
226. Dyck PJ, Karnes J, O'Brien PC, Swanson CJ: Neuropathy Symptom Profile in
health, motor neuron disease, diabetic neuropathy, and amyloidosis. Neurology
1986;36:1300-
227. Dyck PJ, Kratz KM, Lehman KA, Karnes JL, Melton LJI, O' Brien PC, Litchy
WJ, Windebank AJ, Smith BE, Low PA, Service FJ, Rizza RA, Zimmerman BR:
The Rochester Diabetic Neuropathy Study: Design, criteria for types of neuropathy,
selection bias, and reproducibility of neuropathic tests. Neurology 1991;41:799-807
228. Masson EA, Hunt L, Gem JM, Boulton AJM: A novel approach to the
diagnosis and assessment of symptomatic diabetic neuropathy. Pain 1989;38:25-
28
229. Meijer J-WG, Bosma E, Lefrandt JD, Links TP, Smit AJ, Stewart RE, van der
Hoeven JH, Hoogenberg K: Clinical Diagnosis of Diabetic Polyneuropathy With the
Diabetic Neuropathy Symptom and Diabetic Neuropathy Examination Scores.
Diabetes care 2003;26:697-701
230. Tesfaye S, Selvarajah D: The Eurodiab study: What has this taught us about
diabetic peripheral neuropathy? Current Diabetes Reports 2009;9:432-434
231. Sosenko JM, Kato M, Soto R, Bild DE: Comparison of quantitative sensory-
threshold measures for their association with foot ulceration in diabetic patients.
Diabetes care 1990;13:1057-1061

108
232. Dyck PJ, Dyck PJB, Kennedy WR, Kesserwani H, Melanson M, Ochoa J, Shy
M, Stevens JC, Suarez GA, O'Brien PC: Limitations of quantitative sensory testing
when patients are biased toward a bad outcome. Neurology 1998;50:1213
233. Hansson P, Backonja M, Bouhassira D: Usefulness and limitations of
quantitative sensory testing: Clinical and research application in neuropathic pain
states. Pain 2007;129:256-259
234. Yarnitsky D, Pud D: Quantitative sensory testing. Clinical Neurophysiology
2004;1:305-332
235. Kahn R: Report and recommendations of the san antonio conference on
diabetic neuropathy. Annals of Neurology 1988;24:99-104
236. Arezzo JC: The use of electrophysiology for the assessment of diabetic
neuropathy. Neuroscience Research Communications 1997;21:13-23
237. Diabetic polyneuropathy in controlled clinical trials: concensus report of the
peripheral nerve society: Peripheral Nerve Society. Am Neurol 1995;38:478-482
238. Arezzo JC: New developments in the diagnosis of diabetic neuropathy. The
American Journal of Medicine 1999;107:9-16
239. Dyck PJ, Overland CJ, Low PA, Litchy WJ, Davies JL, Dyck PJ, O'Brien PC,
Albers JW, Andersen H, Bolton CF, England JD, Klein CJ, Llewelyn JG,
Mauermann ML, Russell JW, Singer W, Smith AG, Tesfaye S, Vella A: Signs and
symptoms versus nerve conduction studies to diagnose diabetic sensorimotor
polyneuropathy: Cl vs. NPhys trial. Muscle & nerve 2010;42:157-164
240. Huang CR, Chang WN, Chang HW, Tsai NW, Lu CH: Effects of age, gender,
height, and weight on late responses and nerve conduction study parameters. Acta
neurologica Taiwanica 2009;18:242-249

109
241. Partanen J, Niskanen L, Lehtinen J, Mervaala E, Siitonen O, Uusitupa M:
Natural History of Peripheral Neuropathy in Patients with Non-Insulin-Dependent
Diabetes Mellitus. N Engl J Med 1995;333:89-94
242. Graham WA, Goldstein R, Mansfield K, Nesathurai S: Serial nerve conduction
studies of the tail of rhesus monkey ( Macaca mulatta ) and potential implications
for interpretation of human neurophysiological studies. Annals of Indian Academy
of Neurology 2007;10:252-254
243. Loseth S, Lindal S, Stelberg E, Mellgren SI: Intraepidermal nerve fibre
density, quantitative sensory testing and nerve conduction studies in a patient
material with symptoms and signs of sensory polyneuropathy. European Journal of
Neurology 2006;13:105-111
244. Malik RA, Tesfaye S, Newrick PG, Walker D, Rajbhandari SM, Siddique I,
Sharma AK, Boulton AJM, King RHM, Thomas PK, Ward JD: Sural nerve
pathology in diabetic patients with minimal but progressive neuropathy.
Diabetologia 2005;48:578-585
245. Smith GA, Singleton RJ: Impaired Glucose Tolerance and Neuropathy. The
Neurologist 2008;14:23-29
246. Polydefkis M: Punch Skin Biopsy in Diabetic Neuropathy. In Diabetic
Neuropathy: Clinical Management Veves A MR, Ed. New Jersey, Humana Press,
2007, p. 293-307
247. Lauria G, Hsieh ST, Johansson O, Kennedy WR, Leger JM, Mellgren SI,
Nolano M, Merkies IS, Polydefkis M, Smith AG, Sommer C, Valls-Sole J: European
Federation of Neurological Societies/Peripheral Nerve Society Guideline on the
use of skin biopsy in the diagnosis of small fibre neuropathy. Report of a joint task

110
force of the European Federation of Neurological Societies and the Peripheral
Nerve Society. Eur J Neurol 2010;17:903-912, e944-909
248. Bakkers M, Merkies IS, Lauria G, Devigili G, Penza P, Lombardi R, Hermans
MC, van Nes SI, De Baets M, Faber CG: Intraepidermal nerve fiber density and its
application in sarcoidosis. Neurology 2009;73:1142-1148
249. Polydefkis M, Hauer P, Sheth S, Sirdofsky M, Griffin JW, McArthur JC.: The
time course of epidermal nerve fiber regeneration: studies in normal controls and in
people with diabetes, with and without neuropathy. Brain 2004;127:1606-1615
250. Herrmann DN, Griffin JW, Hauer P, Cornblath DR, McArthur JC: Epidermal
nerve fiber density and sural nerve morphometry in peripheral neuropathies.
Neurology 1999;53:1634-1640
251. Muller LJ, Marfurt CF, Kruse F, Tervo TMT: Corneal nerves: structure,
contents and function. Experimental Eye Research 2003;76:521-542
252. Patel DV, McGhee CN: Mapping of the normal human corneal sub-Basal
nerve plexus by in vivo laser scanning confocal microscopy. Invest Ophthalmol Vis
Sci 2005;46:4485-4488
253. Mojaddidi M, Quattrini C, Tavakoli M, Malik RA: Recent developments in the
assessment of efficacy in clinical trials of diabetic neuropathy. Current diabetes
reports 2005;5:417-422
254. Dyck PJ, Thomas PK, Asbury AK, Winegrad AL, Porte D: Diabetic
Neuropathy. Philadelphia, Saunders, 1987
255. Malik RA, Kallinikos P, Abbott CA, van Schie CHM, Morgan P, Efron N,
Boulton AJM: Corneal confocal microscopy: a non-invasive surrogate of nerve fibre
damage and repair in diabetic patients. Diabetologia 2003;46:683-688

111
256. Quattrini C, Tavakoli M, Jeziorska M, Kallinikos P, Tesfaye S, Finnigan J,
Marshall A, Boulton AJM, Efron N, Malik RA: Surrogate Markers of Small Fiber
Damage in Human Diabetic Neuropathy. DIABETES 2007;56:2148-2154
257. Rosenberg ME, Tervo TMT, Immonen IJ, Muller LJ, Gronhagen-Riska C,
Vesaluoma MH: Corneal Structure and Sensitivity in Type 1 Diabetes Mellitus.
Invest Ophthalmol Vis Sci 2000;41:2915-2921
258. Malik RA, Kallinikos P, Abbott CA, van Schie CH, Morgan P, Efron N, Boulton
AJ: Corneal confocal microscopy: a non-invasive surrogate of nerve fibre damage
and repair in diabetic patients. Diabetologia 2003;46:683-688
259. Hossain P, Sachdev A, Malik RA: Early detection of diabetic peripheral
neuropathy with corneal confocal microscopy. Lancet 2005;366:1340-1343
260. Mehra S, Tavakoli M, Kallinikos PA, Efron N, Boulton AJ, Augustine T, Malik
RA: Corneal confocal microscopy detects early nerve regeneration after pancreas
transplantation in patients with type 1 diabetes. Diabetes Care 2007;30:2608-2612
261. Tavakoli M, Quattrini C, Abbott C, Kallinikos P, Marshall A, Finnigan J,
Morgan P, Efron N, Boulton AJ, Malik RA: Corneal confocal microscopy: a novel
noninvasive test to diagnose and stratify the severity of human diabetic
neuropathy. Diabetes Care 2010;33:1792-1797
262. Tavakoli M, Mitu-Pretorian M, Petropoulos IN, Fadavi H, Asghar O, Alam U,
Ponirakis G, Jeziorska M, Marshall A, Efron N, Boulton AJ, Augustine T, Malik RA:
Corneal confocal microscopy detects early nerve regeneration in diabetic
neuropathy after simultaneous pancreas and kidney transplantation. Diabetes
2013;62:254-260

112
263. Rosenberg ME, Tervo TM, Immonen IJ, Muller LJ, Gronhagen-Riska C,
Vesaluoma MH: Corneal structure and sensitivity in type 1 diabetes mellitus. Invest
Ophthalmol Vis Sci 2000;41:2915-2921
264. Kallinikos P, Berhanu M, O'Donnell C, Boulton AJM, Efron N, Malik RA:
Corneal Nerve Tortuosity in Diabetic Patients with Neuropathy. Invest Ophthalmol
Vis Sci 2004;45:418-422
265. Mehra S, Tavakoli M, Kallinikos PA, Efron N, Boulton AJM, Augustine T, Malik
RA: Corneal Confocal Microscopy Detects Early Nerve Regeneration After
Pancreas Transplantation in Patients With Type 1 Diabetes. Diabetes care
2007;30:2608-2612
266. Tavakoli M, Mitu-Pretorian M, Petropoulos IN, Fadavi H, Asghar O, Alam U,
Ponirakis G, Jeziorska M, Marshall A, Efron N, Boulton AJ, Augustine T, Malik RA:
Corneal Confocal Microscopy Detects Early Nerve Regeneration in Diabetic
Neuropathy After Simultaneous Pancreas and Kidney Transplantation. Diabetes
2013;62:254-260
267. Tavakoli M, Kallinikos PA, Efron N, Boulton AJM, Malik RA: Corneal
Sensitivity Is Reduced and Relates to the Severity of Neuropathy in Patients With
Diabetes. Diabetes care 2007;30:1895-1897

113
2 CHAPTER II - METHODS

114
2.1 Synopsis
The ability to define the ‘at risk’ patient, anticipate deterioration, and assess new
therapies is of paramount importance in DSPN and there is also an urgent need for
‘new’ surrogate endpoints for this condition. Current techniques lack the sensitivity
(QST), require expert assessment or target inappropriate nerve fibre types (NCS),
are invasive (skin biopsy) and are not routinely performed across health systems.
A surrogate endpoint needs to reliably reflect the activity of the underlying disease
process, which ultimately causes significant morbidity such as foot ulceration and
lower limb amputation. Vitamin D has long been linked with bone metabolic
disease however, more recently there have been postulated links to DM and it
complications. There is a subsequent need to assess the role of vitamin D in
diabetic microvascular complications, the effectiveness of therapeutic interventions
and the prevalence of vitamin D deficiency in patients with DM.
2.2 Hypothesis and aims
The primary hypothesis of this study is corneal nerve morphology using CCM is a
valid surrogate marker for human DSPN and the vitamin D status has a definitive
role in the diabetic microvascular complications of DR and DSPN. This research
aims:
i.To delineate subjects who have rapidly progressive DSPN and assess whether this
may be discerned through the novel modality of CCM. It will also aim to assess
corneal nerve fibre damage visualised with CCM and evaluate if it is progressive in
nature and in agreement with the natural history of the disease relating to clinical
(NDS, QST, NCS) and laboratory (intra-epidermal nerve fibre density) markers of
DSPN.

115
ii.To establish whether subjects with LADA have a different neuropathic phenotype
than those with type 2 DM. We aim to establish the ability of CCM to discernibly
validate small fibre changes compared to conventional small and large fibre
neurological tests.
iii.To estimate the prevalence of neuropathy measured with CCM and Non Contact
Corneal Aesthesiometry (NCCA) in a cohort of patients with type 1 DM and
compare this with the results of neurological deficits (NDS); nerve
electrophysiology, quantitative sensory testing (thermal thresholds and VPT), IENF
quantitative analysis and establish the relationship with risk factors.
iv.To establish the local prevalence of vitamin D deficiency and its association with
the constituents of metabolic syndrome and cardiovascular disease risk which may
also drive DSPN.
v.To establish the improvement in vitamin D status through the effects of 3 different
vitamin D replacement regimens (using combinations of ergocalciferol,
cholecalciferol and calcium carbonate/cholecalciferol) for the treatment of vitamin D
deficiency.
vi.To establish any phenotypic and metabolic differences between groups with mild
neuropathy with and without painful DSPN and to compare the results of
neurological deficits (NDS); nerve electrophysiology, quantitative sensory testing
(thermal thresholds and VPT), IENF quantitative analysis and vitamin D status.
vii.To establish the relationship of vitamin D status to DR alongside conventional risk
factors such as duration of diabetes, glycaemic control, lipids and blood pressure.

116
2.3 Study Design
1. Chapter III – Prospective longitudinal, investigator-masked observational
study.
2. Chapter IV, V – Prospective cross-sectional, investigator-masked
observational study.
3. Chapter VI – Retrospective cross-sectional, case-control study
4. Chapter VII – Retrospective analysis of clinical therapeutic intervention
5. Chapter VIII – Prospective cross-sectional, investigator-masked
observational study.
6. Chapter IX – Retrospective cross-sectional study
2.4 METHODS: Neuropathy Studies - Chapters 3, 4, 5 &8
Ethical approval was obtained prior to the initiation of the study by the North
Manchester and Salford and Trafford Research Ethics Committee, and written
informed consent was obtained according to the Declaration of Helsinki. This study
is conducted in accordance with the stipulations stated in the Declaration of
Helsinki and along with Good Clinical Practice guidance. All participants were
supplied with study literature at least 24 hours prior to informed consent being
obtained.
2.4.1 Patient Enrolment
Informed written consent was obtained from all subjects prior to their participation
and they were provided with the opportunity to discuss any concerns about the

117
experimental protocol and their safety with a trained member of the research team
(a copy of the patient consent and study forms can be found in Appendix 2). Upon
enrolment to the study, all control and diabetes participants underwent detailed
screening by means of personal and medical history and a set of blood and urine
tests to determine their metabolic status and ensure eligibility for this study. The
specific inclusion / exclusion criteria used are presented below. Appointments were
offered to participants during normal working hours and if a participant could not
complete the full visit assessment in a single visit, a second visit was scheduled
within a month.
Patients with type 1 and 2 DM and LADA were recruited from the Manchester
Diabetes Centre and general medical clinics at the Manchester Royal Infirmary,
Manchester, UK. Controls are recruited from the University of Manchester and via
social networks of the study investigators.
2.4.2 Inclusion Criteria for Chapters 3, 4, 5 & 8
Participants were expected to satisfy the following criteria prior to inclusion in the
study:
a) Aged 14 to 80 years
b) Signed written informed consent
c) Type 1 or 2 DM or LADA
d) Absence of diabetes for the control group
e) Be willing to participate and comply with the experimental protocol.

118
2.4.3 Exclusion Criteria for Chapters 3, 4, 5 & 8
Any of the following criteria rendered the participant ineligible for inclusion:
a) History of corneal trauma or surgery (cataract surgery does not preclude
enrolment unless surgery occurred in the 12 months prior to enrolment date)
b) History of ocular disease or systemic disease which may affect the cornea
c) Concurrent ocular disease, infection or inflammation
d) History of systemic disease (e.g. malignant disease, congestive heart failure
NYHA Grade III or IV, major psychosis (i.e. schizophrenia or bipolar), certain
autoimmune diseases – hypothyroidism, Addison’s disease, vitiligo)
e) History of neuropathy due to non-diabetic cause e.g. alcoholism,
amyloidosis, autoimmune disorders, chronic kidney failure, connective tissue
disease, infectious disease (e.g. Lyme disease, HIV/AIDS, hepatitis B, leprosy),
liver failure, radiculopathy, vitamin deficiencies (e.g. pernicious anaemia, B12
deficiency)
f) Current or active diabetic foot ulcer or infection
g) Participating in any other interventional (e.g. drug) research trial.
2.4.4 Questionnaire Administration
The NSP, DNS and McGill Pain Questionnaire were either administered by a
researcher or they were self-completed. When questionnaires were self completed,
careful instructions were provided to the patient on how to score the questionnaire
in order to avoid any misinterpretation.
119
2.4.5 Neuropathy Disability Score (NDS)
The NDS is derived from a basic neurological examination testing vibration, pin-
prick and temperature perception in addition to deep tendon reflexes. A score
ranging between 0 and 10 is calculated and the degree of neuropathy is
categorised as no neuropathy [0-2], mild neuropathy [3-5], moderate neuropathy
[6-8] and severe [9-10] (Figure 2.1).
Pain sensation (C fibres) was tested using a neurotip. Sharp and blunt ends were
applied and the patient then distinguished the sharp sensation. Vibration sensation
was tested using a 128 Hz tuning fork. The vibrating fork was first applied on the
subject’s forearm/sternum and was then applied three times to the bony
prominence of the first hallux of each foot. Two correct responses were deemed as
being normal (Figure 2.2). Temperature sensation was tested using two metal rods
separately placed in hot and cold water (Figure 2.3). The patient was then asked to
ascertain the correct sensation and two or more correct responses were deemed
as being normal. Deep tendon reflexes were assessed by the achilles tendon
reflex. If absent, subjects were asked to ‘reinforce’ the reflex. The score was then
recorded (0: normal, 1: present with reinforcement and 2: abnormal). All
procedures were repeated for the opposite foot.

120
Figure 2-1 The Neuropathy Disability Score
From Boulton, A.J.M (1).
Figure 2-2 Testing vibration sensation with a 128 Hz tuning fork as part of the NDS

121
Figure 2-3 Testing temperature sensation on the dorsum of foot as part of the NDS
2.4.6 Neuropad
The Neuropad is an early detection test to ascertain the hydrosis status (moisture
content) of the sole of the foot (Figure 2.4). Those with chrome, nickel and/or
cobalt allergy were excluded from the test. Shoes and socks were removed at least
5 minutes prior to application of the neuropad on the ball of the small toe. After 10
minutes the colour of the pad was assessed and a gross % assessment was
made. 100% pink is considered normal whilst the pad remaining blue or patchy is
considered abnormal (Figure 2.4).
Figure 2-4 Neuropad: a) 100% pink- normal response, b) no change- abnormal and c) patchy-
abnormal
122
2.4.7 Heart Rate Variability to Deep Breathing
Computer-aided sensory evaluator IV (CASE IV) was used to measure the heart
rate response to deep breathing. In this test the patient was asked to inhale and
exhale deeply six to eight times in a row in the supine position, whilst following the
rhythm of a “breathing cue” in the form on an LED light. The changes in heart rate
are displayed on an ECG monitor. One eight-cycle breathing series was completed
and then a subsequent six-cycle breathing series interspersed by two minutes of
normal breathing. The acquired data was analysed by calculating the mean
difference between the highest and lowest heart rate for five consecutive, artefact-
free cycles in each series.
2.4.8 Quantitative Sensory Testing
The patient was made comfortable in a semi-recumbent position, with heels resting
on the bed. The patient was familiarised with the sensation of vibration from the
neurothesiometer at the wrist/forearm. The tip of the neurothesiometer was rested
on the great toe (right and left). The amplitude of vibration for the probe was
increased from zero, by turning the dial slowly, whilst the patient has their eyes
closed. The patient was instructed to say “Yes” when he/she first detects the
slightest “buzzing” or vibration sensation and this is recorded as the vibration
perception threshold which was repeated three times on each test site. VPT is
measured in volts and has a range between 0-50 volts.
Thermal tests were performed with a Medoc TSA 2001 device (Medoc Ltd,
Minneapolis, MN). To avoid tactile or pressure stimulation the probe was kept in
contact with the skin for the entire duration of the test. The starting temperature
(adaptation temperature) was 32°C. The thermode is controlled by a computer
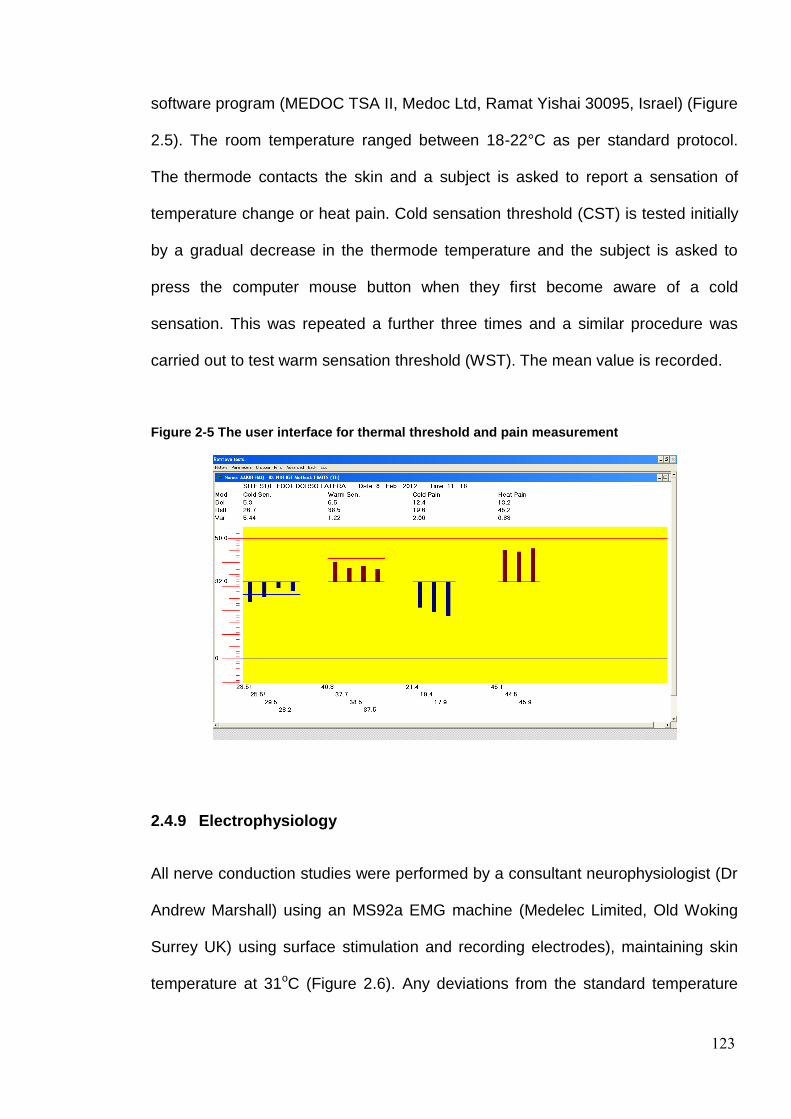
123
software program (MEDOC TSA II, Medoc Ltd, Ramat Yishai 30095, Israel) (Figure
2.5). The room temperature ranged between 18-22°C as per standard protocol.
The thermode contacts the skin and a subject is asked to report a sensation of
temperature change or heat pain. Cold sensation threshold (CST) is tested initially
by a gradual decrease in the thermode temperature and the subject is asked to
press the computer mouse button when they first become aware of a cold
sensation. This was repeated a further three times and a similar procedure was
carried out to test warm sensation threshold (WST). The mean value is recorded.
Figure 2-5 The user interface for thermal threshold and pain measurement
2.4.9 Electrophysiology
All nerve conduction studies were performed by a consultant neurophysiologist (Dr
Andrew Marshall) using an MS92a EMG machine (Medelec Limited, Old Woking
Surrey UK) using surface stimulation and recording electrodes), maintaining skin
temperature at 31oC (Figure 2.6). Any deviations from the standard temperature
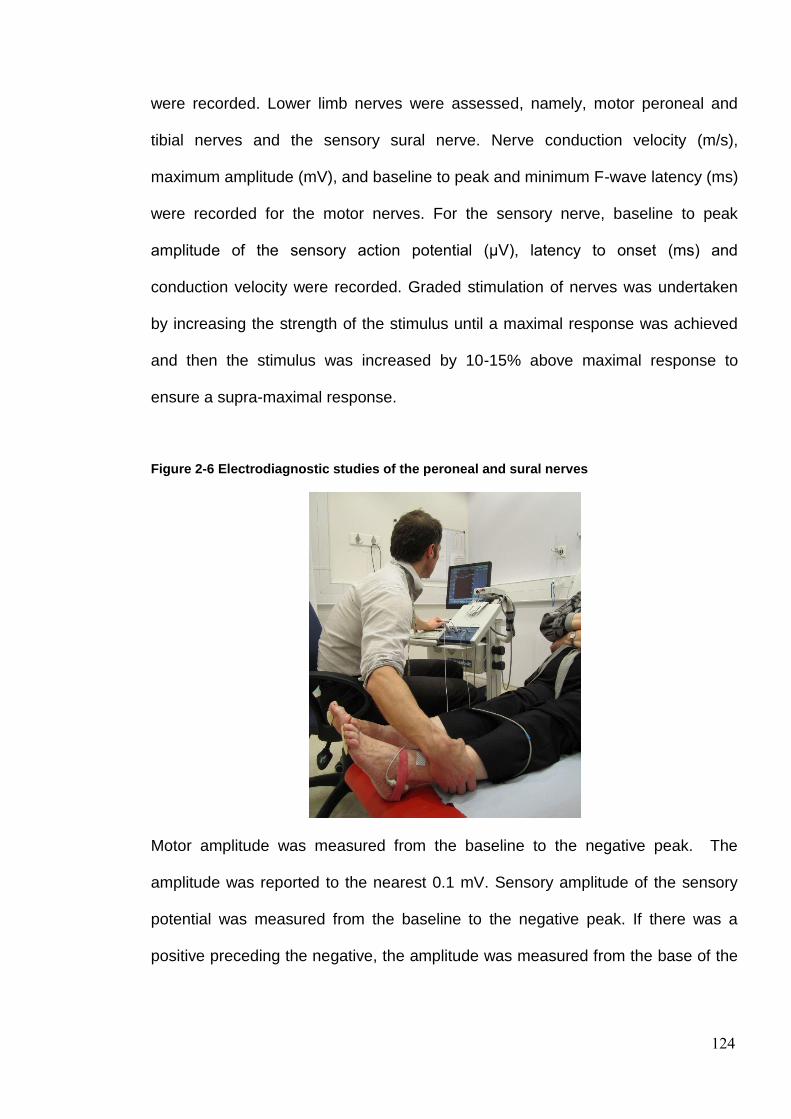
124
were recorded. Lower limb nerves were assessed, namely, motor peroneal and
tibial nerves and the sensory sural nerve. Nerve conduction velocity (m/s),
maximum amplitude (mV), and baseline to peak and minimum F-wave latency (ms)
were recorded for the motor nerves. For the sensory nerve, baseline to peak
amplitude of the sensory action potential (μV), latency to onset (ms) and
conduction velocity were recorded. Graded stimulation of nerves was undertaken
by increasing the strength of the stimulus until a maximal response was achieved
and then the stimulus was increased by 10-15% above maximal response to
ensure a supra-maximal response.
Figure 2-6 Electrodiagnostic studies of the peroneal and sural nerves
Motor amplitude was measured from the baseline to the negative peak. The
amplitude was reported to the nearest 0.1 mV. Sensory amplitude of the sensory
potential was measured from the baseline to the negative peak. If there was a
positive preceding the negative, the amplitude was measured from the base of the
125
positive peak to the negative peak. The sensory nerve action was reported to the
nearest whole number.
2.4.10 Skin Biopsies and Immuno-histology
A sub-cohort of participants underwent a 3-mm punch skin biopsy from the dorsum
of the foot; 2 cm above the second metatarsal head after local anaesthesia (1%
lidocaine). The biopsy site was closed using Steristrips, and the specimen was
immediately fixed in PBS-buffered 4% paraformaldehyde for 18-24 h, washed in
Tris-buffered saline, cryoprotected in sucrose, frozen in liquid nitrogen and stored
at -80°C and subsequently cut into 50-μm sections on a cryostat microtome. Five
floating sections per subject were immunostained for PGP 9.5 neuronal marker.
Briefly, the non-specific protein binding and endogenous peroxidase activity were
blocked by incubation in 5% goat serum and 0.3% hydrogen peroxide,
respectively. The anti-PGP9.5 antibody (Milipore 1:1000; Billerica,MA) was
followed first by goat anti-rabbit IgG and then by HRP-Streptavidin (both diluted
1:1000, both from Vector Laboratories, Peterborough, UK). Nerve fibres were
visualised by SG chromogen (Vector Laboratories). Intraepidermal nerve fibre
density (IENFD) was calculated as the number of nerve fibres crossing the
basement membrane of the epidermis and expressed per millimetre length of
epidermis (Figure 2.7).
IENFD were assessed by two independent assessors as per European Federation
of Neurological Societies/Peripheral Nerve Society Guideline on the use of skin
biopsy in the diagnosis of small fibre neuropathy (2).
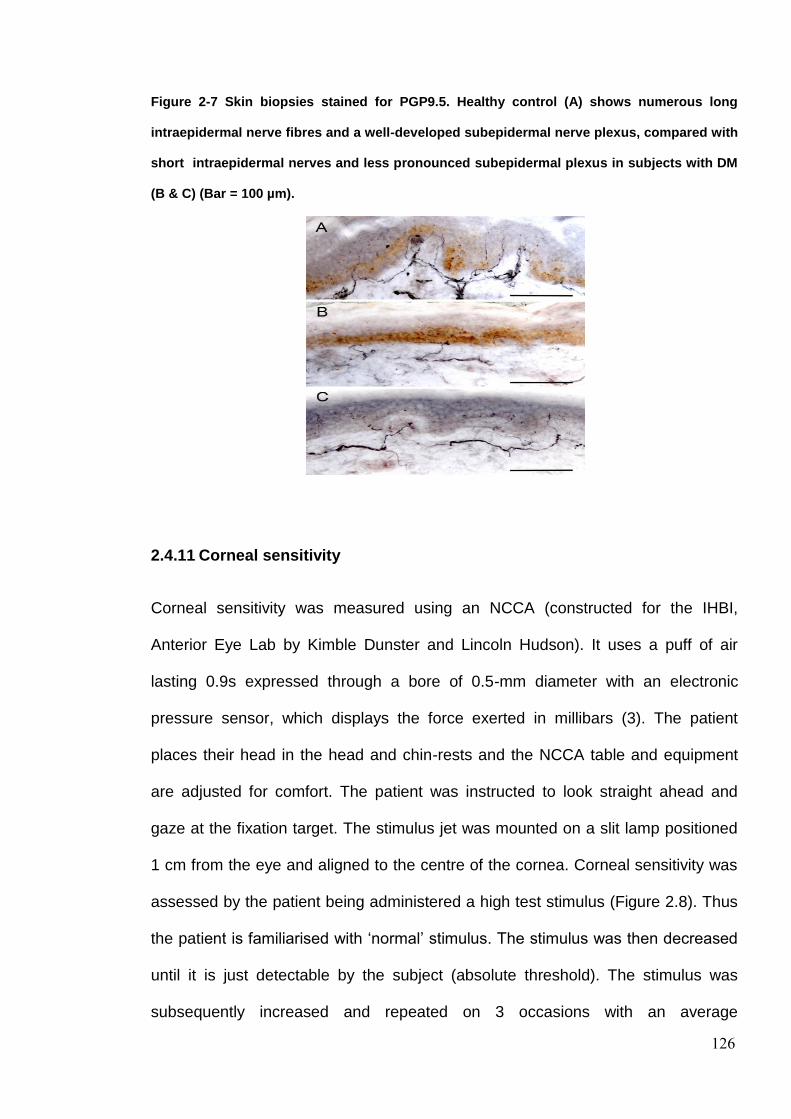
126
Figure 2-7 Skin biopsies stained for PGP9.5. Healthy control (A) shows numerous long
intraepidermal nerve fibres and a well-developed subepidermal nerve plexus, compared with
short intraepidermal nerves and less pronounced subepidermal plexus in subjects with DM
(B & C) (Bar = 100 µm).
2.4.11 Corneal sensitivity
Corneal sensitivity was measured using an NCCA (constructed for the IHBI,
Anterior Eye Lab by Kimble Dunster and Lincoln Hudson). It uses a puff of air
lasting 0.9s expressed through a bore of 0.5-mm diameter with an electronic
pressure sensor, which displays the force exerted in millibars (3). The patient
places their head in the head and chin-rests and the NCCA table and equipment
are adjusted for comfort. The patient was instructed to look straight ahead and
gaze at the fixation target. The stimulus jet was mounted on a slit lamp positioned
1 cm from the eye and aligned to the centre of the cornea. Corneal sensitivity was
assessed by the patient being administered a high test stimulus (Figure 2.8). Thus
the patient is familiarised with ‘normal’ stimulus. The stimulus was then decreased
until it is just detectable by the subject (absolute threshold). The stimulus was
subsequently increased and repeated on 3 occasions with an average

127
measurement derived. This was recorded and the procedure repeated for the
alternate eye.
Figure 2-8 Estimation of corneal sensation using NCCA
2.4.12 Corneal Confocal microscopy
Previously established indicators of corneal nerve pathology which have been
shown to be valid markers of peripheral neuropathy include corneal nerve fibre
(CNFD) and branch density (CNBD), length (CNFL) and the corneal nerve
tortuosity coefficient (CNFT):
i. CNFD: the number of main nerve fibres / mm2.
ii. CNBD: the number of main nerve branches / mm2.
iii. CNFL: the sum of the length (mm./mm2) of all nerve structures.
iv. CNFT: the tortuosity or non-linearity of the main nerve fibres.
Patients underwent examination with a corneal confocal microscope. Images are
obtained using the HRT III-RCM (Heidelberg Engineering GmBH, Heidelberg,
Germany) (Figure 2.9). The laser is a 670 nm red wavelength Helium Neon diode
laser and does not pose any danger to ocular structures. The corneal sub-basal

128
nerve plexus is determined by continuous imaging of the cornea through use of an
OCD camera.
Figure 2-9 Corneal confocal microscopy
Patient demographics were entered in the Heidelberg Eye Explorer software
(Heidelberg Engineering GmBH, Heidelberg, Germany) and the confocal
microscope is prepared for examination. One eye was selected and anesthetized
with one drop of 0.4% benoxinate hydrochloride (oxybuprocaine hydrochloride)
(Chauvin Pharmaceuticals Ltd., Essex, UK). The objective lens of the confocal
microscope was disinfected (isopropyl alcohol 70% vol/vol, swabs), and 1 drop of
Viscotears liquid gel (Carbomer 980, 0.2%; Novartis, UK) was applied onto the tip
of the lens and advanced forward until the gel touched the cornea thus allowing
visual but not physical contact between the lens and corneal epithelium (Figure
2.10). The cornea was scanned in 2 min and en face two-dimensional images were
acquired. Approximately three to five high-quality images of Bowman’s layer were
examined as it contains the main nerve plexus (Figure 2.11 and 2.12). When
enough images had been captured the procedure was repeated for the other eye.

129
Morphometric measurements of the images were undertaken and the assessors of
the images were masked with respect to the identity of the patient.
Figure 2-10 Positioning of the TomoCap® on the cornea
Figure 2-11 Image of the corneal subbasal nerves using corneal confocal microscopy

130
Figure 2-12 A preview of an image from the corneal subbasal nerves on the Heidelberg eye
explorer with a simultaneous view of the location of the image through the CCD camera.
2.4.13 Manual Image Analysis: Chapter 4,5 & 8
Images are analysed manually by the assessor using purpose built software called
“CCM image analysis tools v0p6” (CCMIATv0p6) (M.A. Dabbah, Imaging Science,
The University of Manchester). The following parameters were quantified to define
corneal nerve fibre damage and repair: 1) nerve fibre density (CNFD), the total
number of major nerves per square millimetre of corneal tissue; 2) nerve fibre
length (CNFL), the total length of all nerve fibres and branches per square
millimetre of corneal tissue; 3) nerve branch density (CNBD), the number of
branches emanating from each nerve trunk per square millimetre of corneal tissue;
and 4) nerve fibre tortuosity (CNFT), a parameter that is mathematically derived
from the images (4).

131
Figure 2-13 An CCM image of a control subject analysed to quantify corneal subbasal nerve
morphology in DSPN. The red colour corresponds to CNFD and the CNFT, the green dots
highlight CNBD at the points of junction with main nerve fibres and CNFL, the length of
nerve structures in the entire CCM image is highlighted under the red and blue colour.
2.4.14 Automated Image Analysis: Chapter 3 only
Automated corneal nerve fibre quantification consists of two steps: (1) CCM image
enhancement and nerve fibre detection and (2) quantification of CNFD, CNBD and
CNFL. The detection of nerve fibre is a challenging task, as the nerve fibres often
show poor contrast in the relatively noisy images. As described in our earlier work
(5-6), a dual-model feature descriptor combined with a neural network classifier
was used to train the computer to distinguish nerve fibres from the background
(noise and underlying connective tissue). In the nerve fibre quantification process,
all the end points and branch points of the detected nerve fibres are extracted and
used to construct a connectivity map. Each segment in the connectivity map can
then be connected and classified as main nerve fibres or branches according to the
nerve intensity, orientation and length.
132
2.5 METHODS: Vitamin D Studies – Chapters 6, 7 & 9
Studies were undertaken from a population-based cohort at the Central
Manchester University Hospitals NHS Foundation Trust, Manchester, UK of those
with Type 1 and 2 DM attending a tertiary diabetes centre. Ethical approval was not
required for this specific analysis as the data were extracted retrospectively from
clinical databases and did not extend beyond standard clinical practice.
Retrospective vitamin D studies undertaken are as follows:
a. Chapter VI: Marked vitamin D deficiency in patients with diabetes from
secondary care: Ethnic and seasonal differences and an association with
dyslipidaemia.
b. Chapter VII: Differential effects of different vitamin D replacement strategies
in patients with Diabetes
c. Chapter IX: Vitamin D Deficiency is not associated with Diabetic
Retinopathy or Maculopathy in Diabetes Mellitus
2.5.1 Participant Exclusion Criteria for Chapters 6, 7 & 9
Those with renal impairment (eGFR <30 mL/min/1.73m2 (CKD stage 4 and below),
granulomatous diseases (tuberculosis, sarcoidosis etc), malabsorption syndromes
(Coeliac disease, bacterial overgrowth, concomitant orlistat treatment), pregnant
and lactating women.
2.5.2 Blood pressure and Anthropometric measurements
Body mass index (BMI) was measured as per the standard equation (mass
(kg)/(height(m))2. Weight was measured with a digital scale (Seca 701, Seca,

133
Hamburg, Germany) to the nearest 0.1kg and height to the nearest 0.1cm. Blood
pressure (BP) measurements were obtained with the use of an automated BP
device (Dinamap pro 100v2, GE Medical Systems, Freiburg, Germany) with an
appropriate cuff size. A minimum of two measurements of systolic and diastolic BP
were made five minutes apart with the lowest reading recorded.
2.5.3 Assessment of Demographics, Cardiovascular disease and
Medications
An assessment of patient demographics, previous cardiovascular events and
medications were made through analysis of medical records and an in-hospital
medical record database (Diamond database, Hicom, Surrey, UK). The subject
demographics extracted were age, sex, ethnicity (Caucasian, South Asian, Far
East Asian and Afro-Caribbean descent), smoking status (never, previous and
current) and type (Type 1 and 2 diabetes) and duration of diabetes. Previous
cardiovascular events extracted were ischaemic heart disease (IHD), myocardial
infarction (MI), cerebrovascular accidents (CVA) and peripheral vascular disease
(PVD).
2.5.4 Laboratory Measurements
Standard assessment of 25(OH)D was instituted in the Manchester Diabetes
Centre, Manchester, UK in August 2009 as part of routine haematological and
biochemical laboratory measurements which included HbA1c, (Complete Blood
count (CBC)), Urea and Electrolytes (UE), Liver function tests (LFT), bone profile
(Corrected Calcium (CCa2+), Alkaline Phosphatase (ALP), Albumin (Alb), and
Lipid profile (Total Cholesterol (T-CHL), High Density lipoprotein Cholesterol
(HDL), Triglycerides (TRIG)). Low Density lipoprotein (LDL) analyses were not

134
undertaken and patients were routinely advised that bloods were to be collected
under fasting conditions.
2.5.5 Diabetic Retinopathy Assessment
The retinopathy data were collected according to the grading criteria set out to a
national standard by the National Screening Committee (NSC)(7-8). Previous
studies have shown acceptable levels of quality and accuracy of grading compared
to expert graders within the English NSC (9). The national guidelines do not
contain R1.5 or M0.5 grades and are categorised as Pre-Proliferative Diabetic and
Diabetic Maculopathy being present respectively. These sub-gradings are used
locally in screening centres have thus been included. The grading of retinopathy
are as follows:
R0 - No Diabetic retinopathy (NDR)
R1 - Background Diabetic Retinopathy (NDR): microaneurysms, retinal
haemorrhages, exudates
R1.5 - Moderate numbers of intra-retinal haemorrhages, hard exudates >1 disc
diameter (DD) from fovea, 3-6 cotton wool spots visible
R2 - Pre-Proliferative Diabetic Retinopathy (PPDR): Venous beading or looping,
deep haemorrhages visible, other microvascular anomaly visible.
R3 - Proliferative Diabetic Retinopathy (PDR): New vessel formation, vitreous
haemorrhage, pre- retinal haemorrhage or fibrosis and/or retinal detachment.
The outlines for maculopathy grading are as follows:
M0 - No maculopathy.
M0.5 - Hard exudates within the arcades >1DD from the centre of the fovea.

135
M1- Exudates <1DD within the centre of the fovea, retinal thickening <1DD of the
centre of the fovea.
The outlines for photocoagulation grading are as follows:
P0 – No photocoagulation scarring
P1 – Photocoagulation scarring present
2.5.6 25(OH) Vitamin D Assay
The specific laboratory used for the biochemical assay measurements (Vitamin D
Research Group Manchester Royal Infirmary, UK) was accredited to ISO
9001:2008 and ISO 13485:2003 by Lloyd’s Register Quality Assurance, certificate
number LRQ 4001542 and participated successfully in the Vitamin D quality
assurance scheme (DEQAS). Serum was separated from whole blood and stored
at -20 C until assay. The assay used was an automated platform assay
(ImmunoDiagnostic Systems Ltd, Bolden, Tyne and Wear, UK) and is based on
chemiluminescence technology. Briefly, samples were subjected to a pre-treatment
step to denature the vitamin D binding protein. The treated samples were then
neutralised in assay buffer and a specific anti-25(OH)D antibody labelled with
acridinium was added. Following an incubation step, magnetic particles linked to
25(OH)D were added. Following a further incubation step, the magnetic particles
were “captured” using a magnet. After a washing step and addition of trigger
reagents, the light emitted by the acridinium label was inversely proportional to the
concentration of 25(OH)D in the original sample. The concentration of 25(OH)D
was calculated automatically using a 4-point logistic curve. The cross reactivity for
vitamin D2 (of the assay) as per manufacturers assertion was 100% (relative to
vitamin D3) and the assay has excellent correlation to existing globally recognised
136
assays, in combination with good sensitivity and precision (10). The reportable
range of the assay was 5-140 ng/mL. Inter- and intra- assay variation of the in-
house control was 5.6% and 9.7% respectively. Vitamin D deficiency (<20ng/ml)
and insufficiency (<30ng/ml) were defined according to the Institute of Medicine
(IOM) of the National Academies (11).
2.6 REFERENCES
1. Boulton AJM: Management of Diabetic Peripheral Neuropathy. Clinical Diabetes
2005;23:9-15
2. Lauria G, Hsieh ST, Johansson O, Kennedy WR, Leger JM, Mellgren SI, Nolano
M, Merkies IS, Polydefkis M, Smith AG, Sommer C, Valls-Sole J: European
Federation of Neurological Societies/Peripheral Nerve Society Guideline on the
use of skin biopsy in the diagnosis of small fibre neuropathy. Report of a joint task
force of the European Federation of Neurological Societies and the Peripheral
Nerve Society. Eur J Neurol 2010;17:903-912, e944-909
3. Murphy PJ, Lawrenson JG, Patel S, Marshall J: Reliability of the Non-Contact
Corneal Aesthesiometer and its comparison with the Cochet–Bonnet
aesthesiometer. Ophthalmic and Physiological Optics 1998;18:532-539
4. Kallinikos P, Berhanu M, O'Donnell C, Boulton AJM, Efron N, Malik RA: Corneal
Nerve Tortuosity in Diabetic Patients with Neuropathy. Invest Ophthalmol Vis Sci
2004;45:418-422
5. Dabbah MA, Graham J, Petropoulos IN, Tavakoli M, Malik RA: Automatic
analysis of diabetic peripheral neuropathy using multi-scale quantitative
morphology of nerve fibres in corneal confocal microscopy imaging. Medical Image
Analysis 2011;15:738-747

137
6. Dabbah M, Graham J, Petropoulos I, Tavakoli M, Malik R: Dual-Model Automatic
Detection of Nerve-Fibres in Corneal Confocal Microscopy Images
Medical Image Computing and Computer-Assisted Intervention – MICCAI 2010.
Jiang T, Navab N, Pluim J, Viergever M, Eds., Springer Berlin / Heidelberg, 2010,
p. 300-307
7. Scanlon PH: The English national screening programme for sight-threatening
diabetic retinopathy. J Med Screen 2008;15:1-4
8. Jyothi S, Elahi B, Srivastava A, Poole M, Nagi D, Sivaprasad S: Compliance with
the quality standards of National Diabetic Retinopathy Screening Committee. Prim
Care Diabetes 2009;3:67-72
9. Patra S, Gomm EMW, Macipe M, Bailey C: Interobserver agreement between
primary graders and an expert grader in the Bristol and Weston diabetic
retinopathy screening programme: a quality assurance audit. Diabetic Medicine
2009;26:820-823
10. ASBMR 31st Annual Meeting MO0001–MO0445. Journal of Bone and Mineral
Research 2009;24:S370-S496
11. Rosen CJ, Gallagher JC: The 2011 IOM report on vitamin D and calcium
requirements for north america: clinical implications for providers treating patients
with low bone mineral density. J Clin Densitom 2011;14:79-84
138
3 Chapter III - Rapid Nerve Fibre Decline in patients with
Type 1 diabetes can be readily detected using Corneal
Confocal Microscopy.
Contribution: Uazman Alam contributed to the conception and design of the study
and made a major contribution to the recruitment of subjects, clinical neuropathy
assessments, all statistical analyses and writing of this chapter.
To be submitted for publication
Uazman Alam, Omar Asghar, Ioannis N Petropoulos, Hassan Fadavi, Georgios
Ponirakis, Maria Jeziorska, Andrew Marshall, Mitra Tavakoli, Andrew JM Boulton,
Nathan Efron, Rayaz A Malik.

139
3.1 ABSTRACT
Diabetic neuropathy is associated with increased morbidity and is an independent
risk factor for mortality. Defining a population which has progressive rather than
stable neuropathy would allow risk stratification and also perhaps identify those
who may respond optimally to therapeutic intervention. We have assessed whether
corneal confocal microscopy (CCM) can detect progression of neuropathy by
establishing a decline in corneal nerve morphology.
Fifty subjects with Type 1 diabetes (T1DM) and sixteen non-diabetic healthy
control subjects (C) underwent assessment of neurologic deficits; quantitative
sensory testing (QST), electrophysiology and CCM at baseline and two year follow
up.
Neuropathic symptom profile (NSP) (P<0.0006), McGill pain index (P=0.008),
neuropathy disability score (NDS) (P=0.008), HbA1c (P<0.0001), and vibration
perception threshold (VPT) (P<0.0001) were significantly increased and sural
nerve conduction velocity and amplitude (P<0.0001 and P=0.0003 respectively),
peroneal nerve conduction velocity and amplitude (P<0.0001 and P=0.0003
respectively) were significantly reduced in T1DM compared to controls. Corneal
nerve fibre density (CNFD) (P<0.0001), corneal nerve branch density (CNBD)
(P=0.007) and corneal nerve fibre length (CNFL) (P<0.0001) were significantly
reduced at baseline in T1DM compared with control subjects. There was no
significant change for: NDS, vibration perception threshold (VPT), warm sensation
threshold (WST), electrophysiology and CCM measures in both T1DM and controls
at 2 year follow up. However, we identified 11/50 T1DM patients who had a greater
than 14.4% decline in CNFL over 2 years based on a 2 standard deviation cut off
for intra-individual variation in the control group. In this cohort: sural sensory

140
(P=0.04) and peroneal motor (P=0.05) nerve conduction velocities, CNFD
(18.8±10.2 vs 11.5±9.4 no./mm2, P=0.0006), CNBD (24.1±15.6 vs 10.7±12.8
no./mm2, P=0.0002) and CNFL (12.1±5.0 vs 8.5±4.5 mm/mm2, P=0.0002) were
significantly reduced from baseline to follow up after 2 years, which was not related
to any change in HbA1c, lipids or BP.
A rapid small fibre decline is readily detectable in a subgroup of subjects with Type
1 diabetes using CCM and this novel modality provides an ideal surrogate endpoint
in defining those who at risk of progressive DPN.

141
3.2 INTRODUCTION
Diabetic peripheral neuropathy (DPN) is a distressing condition which affects
around one half of patients during the natural history of the disease (1) although
prevalence data varies (2-3). DPN is a confirmed risk factor for debilitating lower
limb amputation (4) and large nerve fibre dysfunction in diabetes is itself predicted
by cardiovascular disease (5) and is one of only three independent and significant
risk factors for mortality as confirmed through the Action to Control Cardiovascular
Risk in Diabetes (ACCORD) study (6). Risk factors for DPN include duration of
diabetes, glycaemic control and elevated triglycerides (7) and improvement of
glycaemic control as shown through the Diabetes Control and Complications Trial
(DCCT) and the Epidemiology of Diabetes Interventions and Complications (EDIC)
to improve neuropathy outcomes both in the short and long term respectively (8-9).
An analysis of a placebo control arm in a multi-centre, double-blind study showed
that short term metabolic improvements in glycaemic control and serum triglyceride
levels have an independent, additive and durable effect on restoration of nerve
function as evaluated by neurophysiology (10). We have previously shown that
improvements in corneal nerve fibre density (CNFD) occur with an improvement in
HbA1c (11) and corneal nerve fibre density (CNFD) and branch density (CNBD)
improves with simultaneous pancreas and kidney transplantation (12). Smith et al
(13) also showed that intra-epidermal nerve fibre density (IENFD) improved with
diet and exercise in a pre-diabetic group. Deterioration in small nerve fibres may
progress overtime and indeed a postulated longitudinal decline in IENFD (14) and
small fibre function with diminished axon reflex-mediated vasodilator response is
thought to occur (15). Longitudinal studies of neuropathy are limited; however, they
do show deterioration of neuropathy overtime in both Type 1 diabetes (16) and

142
Type 2 diabetes using electrophysiology (17). The progression of DPN is thought
to occur much slower than previously thought and is likely in part due to the
positive impact on the peripheral nerve from commonly prescribed agents such as
ACE inhibitors (18) and statins (19). This lack of placebo decline is of course one
of the postulated reasons for the dramatic failure of pathogenetic treatments for
DPN and Dyck et al concluded that future clinical trials should include subjects who
are developing neuropathy rather than those with established neuropathy (20).
In the current study, we evaluated a cohort of subjects with Type 1 Diabetes at
baseline and 2 year follow up in relation to their neuropathy status with the aim of
delineating subjects who have rapidly progressive DPN through the novel modality
of CCM.
143
3.3 RESEARCH DESIGN AND METHODS
3.3.1 Selection of patients
Fifty subjects with Type 1 diabetes (T1DM) (n=50) and sixteen age and sex
matched non-diabetic healthy control subjects (C) (n=16) were assessed at
baseline and two year follow up. Control subjects were selected through the
University of Manchester staff network or friends and family of diabetic participants.
Both diabetic patients and control subjects underwent full neurologic assessment
and were included in final analyses on completing the protocol of baseline and 2
year follow up visit. Retinopathy status evaluation through retinal photography was
not a part of the experimental protocol. All causes of peripheral neuropathy (except
diabetes in T1DM) and those with a history of ocular trauma or previous ocular
surgery were excluded. This study was of an observational nature only with no
active study intervention although alterations to anti-glycaemic, anti-hypertensive
and lipid modifying medication may have been instituted either in primary or
secondary care. The study was approved by the North West Research Ethics
committee, and written informed consent was obtained according to the
Declaration of Helsinki.
3.3.2 Assessment of neuropathy
All patients and control subjects underwent a detailed evaluation of neurologic
symptoms according to the neuropathy symptom profile (NSP), and the McGill
visual analogue score (VAS) was used to assess the severity of painful
neuropathy. Clinical neurologic deficits were assessed using the modified
neuropathy disability score (NDS), which includes evaluation of vibration, pin prick,
and temperature perception as well as the presence or absence of ankle reflexes

144
to establish the severity of neuropathy (21). Quantitative sensory testing included
an assessment of vibration perception threshold (VPT), measured using a
Neurothesiometer (Horwell, Scientific Laboratory Supplies, Wilford, Nottingham,
U.K.), cold sensation threshold (CST) (Aδ fibres) and warm sensation threshold
(WST) (22) (c fibres) using the method of limits with the MEDOC TSA II (Medoc,
Ramat Yishai, Israel) on the dorsum of the left foot.
Electro-diagnostic studies were undertaken using a Dantec “Keypoint” system
(Dantec Dynamics, Bristol, U.K.) equipped with a DISA temperature regulator to
keep limb temperature constantly between 32°C and 35°C. Peroneal motor and
sural sensory nerves were assessed in the right lower limb by a consultant
neurophysiologist. The motor study was performed using silver-silver chloride
surface electrodes at standardized sites defined by anatomical landmarks, and
recordings for the sural nerve were taken using antidromic stimulation over a
distance of 100 mm.
3.3.3 Corneal Confocal Microscopy
Patients underwent examination with the Heidelberg retina tomography III in vivo
corneal confocal microscope employing our established methodology for image
acquisition (23). Several scans of the entire depth of the cornea were recorded by
turning the fine focus of the objective lens backward and forward for ~2 min using
the section mode, which enables manual acquisition and storage of single images
of all corneal layers. This provides en face two-dimensional images with a lateral
resolution of ~2 mm/pixel and final image size of 400 x 400 pixels of the subbasal
nerve plexus of the cornea from each patient and control subject. Each sub-basal
nerve fibre bundle contains unmyelinated fibres, which run parallel to Bowman’s

145
layer before dividing and terminating as individual axons underneath the surface
epithelium. Five images per patient from the centre of the cornea were selected
and examined in a masked and randomised fashion (24). Three corneal nerve
parameters were quantified: 1) CNFD, the total number of major nerves per square
millimetre of corneal tissue (no.mm2); 2) corneal nerve branch density (CNBD), the
number of branches emanating from all major nerve trunks per square millimetre of
corneal tissue (no.mm2); and 3) corneal nerve fibre length (CNFL), the total length
of all nerve fibres and branches (mm/mm2) within the area of corneal tissue.
Automated corneal nerve fibre quantification (ACCMetrics software, University of
Manchester, Manchester, UK) was undertaken and consists of two steps: (1) CCM
image enhancement and nerve fibre detection and (2) quantification of three
morphometric parameters i.e. CNFD, CNBD and CNFL. In the nerve fibre
quantification process, all the end points and branch points of the detected nerve
fibres are extracted and used to construct a connectivity map. Each segment in the
connectivity map can then be connected and classified as main nerve fibres or
branches according to the nerve properties such as intensity, orientation and
length.
3.3.4 Statistical analysis and Power calculation
Previous natural history studies are lacking in assessing CCM parameters in the
progression of diabetic neuropathy and thus power calculations are based on
unpublished data. For the diabetic cohort, an assumption of paired groups was
used to calculate the sample size considering a change in CNFD over 2 years. The
standard deviation between groups is likely to be 9 nerves/mm2. Therefore,
recruiting a minimum of 28 patients for the diabetic group will provide 80% chance

146
to detect a clinically meaningful change in CNFD of 5 nerves/mm2 and an
assumption of a type 1 error (α-level) of 0.05. Considering a greater change of 7.5
nerves/mm2 at 80% power to detect a clinically meaningful change, 14 patients
would be required with an assumption of type 1 error of 0.05. Statistical analyses
were undertaken on Statsdirect (Statsdirect, Cheshire, UK). The data are
expressed as Mean ± standard deviation (SD). Paired t-test or a non-parametric
counterpart, Mann-Whitney-U were used to assess differences between baseline
and follow up data on normality of the data. Unpaired t-test or Mann-Whitney-U test
were used to assess differences between baseline control and T1DM data,
depending on normality of the data. Chi squared analyses were used to assess
frequencies of gender and ethnicity. A significant P value was considered to be
≤0.05 corrected for multiple comparison tests. A post hoc analysis was undertaken
of those showing a worsening neuropathy through assessment of decline in CNFL
defined as rapid nerve fibre decline based on a two standard deviation cut off of
CNFL variation over 2 years in the control group.

147
3.4 RESULTS
3.4.1 Demographics (Table 3.1)
The participant demographics and metabolic and anthropometric measurements in
diabetic subjects and age-matched control subjects are summarized in Table 3.1.
There were no significant differences in age (Control baseline: 41.4±11.4 vs T1DM
baseline: 48.2±15.5 years, P=NS) and duration of diabetes was 33.1±16.7 years at
baseline in the T1DM group. There were a no differences in gender between
controls and T1DM but there were a higher proportion of white Europeans in T1DM
(Chi2 P<0.0001).
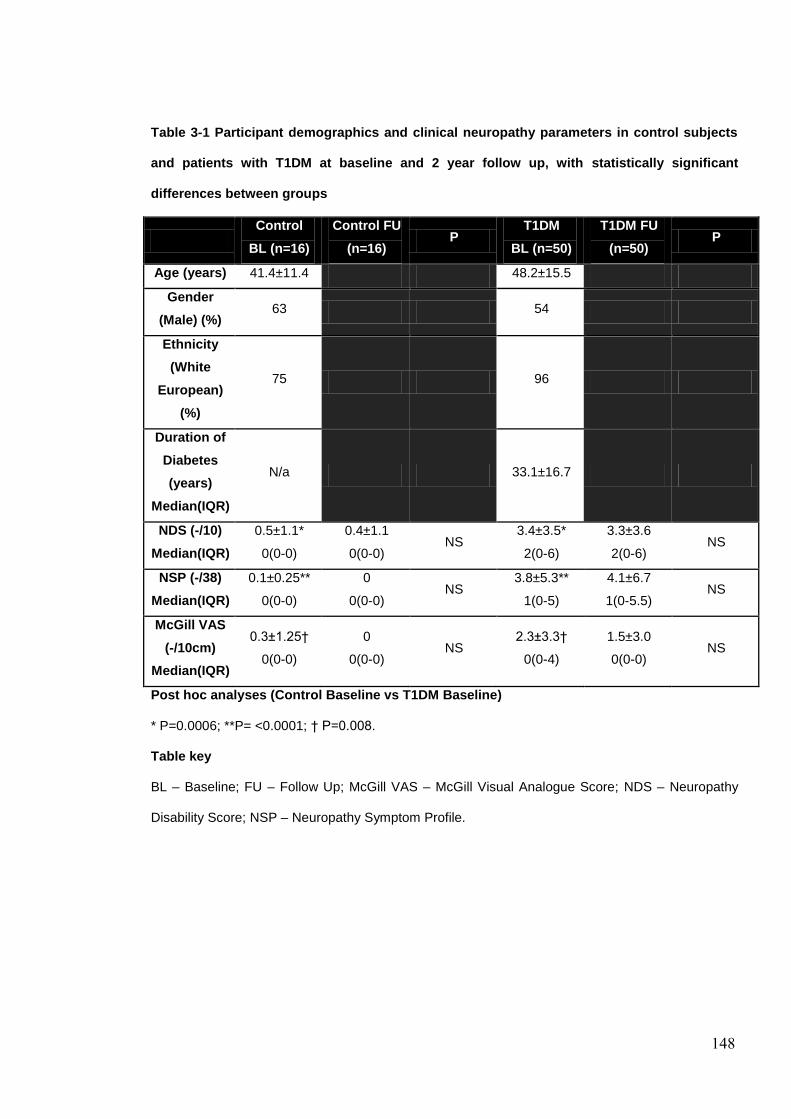
148
Table 3-1 Participant demographics and clinical neuropathy parameters in control subjects
and patients with T1DM at baseline and 2 year follow up, with statistically significant
differences between groups
Control
BL (n=16)
Control FU
(n=16) P
T1DM
BL (n=50)
T1DM FU
(n=50) P
Age (years) 41.4±11.4 48.2±15.5
Gender
(Male) (%) 63 54
Ethnicity
(White
European)
(%)
75 96
Duration of
Diabetes
(years)
Median(IQR)
N/a 33.1±16.7
NDS (-/10)
Median(IQR)
0.5±1.1*
0(0-0)
0.4±1.1
0(0-0) NS
3.4±3.5*
2(0-6)
3.3±3.6
2(0-6) NS
NSP (-/38)
Median(IQR)
0.1±0.25**
0(0-0)
0
0(0-0) NS
3.8±5.3**
1(0-5)
4.1±6.7
1(0-5.5) NS
McGill VAS
(-/10cm)
Median(IQR)
0.3±1.25†
0(0-0)
0
0(0-0) NS
2.3±3.3†
0(0-4)
1.5±3.0
0(0-0) NS
Post hoc analyses (Control Baseline vs T1DM Baseline)
* P=0.0006; **P= <0.0001; † P=0.008.
Table key
BL – Baseline; FU – Follow Up; McGill VAS – McGill Visual Analogue Score; NDS – Neuropathy
Disability Score; NSP – Neuropathy Symptom Profile.

149
3.4.2 Metabolic and Anthropometric measurements (Table 3.2)
BMI did not differ between patients with T1DM and control subjects at baseline.
HbA1c was significantly higher in T1DM (P<0.0001) compared to controls with no
significant change at 2 year follow up. Although, there was a significant reduction in
HbA1c in controls at follow up, both baseline and follow up values were in the
normal non-diabetic range. The total cholesterol was significantly lower (P<0.0001)
in diabetic patients due to greater statin use, whilst triglycerides and HDL were
comparable between T1DM and control subjects with no changes at follow up.
Systolic BP was no different in controls compared to T1DM at baseline. T1DM
(P=0.04) exhibited a mild drop in systolic BP at 2 year follow up with no change in
controls at baseline and follow up. There were no differences in the estimated
glomerular filtration rate between T1DM and controls at baseline, however, there
was a decline in eGFR in T1DM at 2 year follow up (P=0.02).

150
Table 3-2 Metabolic parameters in control subjects and T1DM patients at baseline and 2 year
follow up, with statistically significant differences between groups
Control
BL (n=16)
Control FU
(n=16) P
T1DM
BL (n=50)
T1DM FU
(n=50)
P
HbA1c (%) 5.6±0.3 5.3±0.3
0.003
8.2±1.3* 8.1±1.6
NS HbA1c
(mmol/mol) 38.0±3.3 34.8±3.4 66.2±14.3* 65.2±17.1
BMI (kg/m2) 25.7±4.2 24.7±3.8 NS 26.9±4.4 27.1±4.7 NS
T-CHL
(mmol/l) 5.1±0.9 4.8±0.7 NS 4.3±0.9** 4.3±0.9 NS
HDL (mmol/l) 1.5±0.3 1.5±0.3 NS 1.7±0.5 1.7±0.5 NS
Triglycerides 1.4±0.7 1.2±0.5 NS 1.1±0.7 1.1±0.5 NS
Systolic BP
(mmHg) 125±21 120±18 NS 132±18 127±21 0.04
Diastolic BP
(mmHg) 75±12 74±11 NS 73±8 66±9 0.004
eGFR
(ml/min/1.73) 86±7 83±7 NS 81±19 75±17 0.02
Post hoc analyses (Control Baseline vs T1DM Baseline)
*P<0.0001; ** P=0.003.
Table key
BL – Baseline; BMI – Body Mass Index; BP – Blood Pressure; eGFR – estimated Glomerular
Filtration Rate; FU – Follow Up; HbA1c – Glycated Haemoglobin A1c; HDL – High Density
Lipoprotein Cholesterol; T-CHL – Total Cholesterol.

151
3.4.3 Neuropathy evaluation (Table 3.3)
3.4.3.1 Symptoms and Deficits
Neuropathic symptoms as assessed with the NSP were significantly greater in
diabetic patients than in control subjects at baseline (P<0.0006), but there was no
significant change at 2 year follow up for either controls or T1DM. The McGill pain
index was significantly (P=0.008) greater at baseline compared with control
subjects and did not show a significant change at 2 years follow up in T1DM. The
modified NDS was significantly (P=0.008) greater at baseline compared with
control subjects, indicating a mild to moderate neuropathy, and did not change
significantly at 2 year follow up in T1DM.
3.4.3.2 Vibration Perception and Thermal Thresholds
VPT was significantly greater in T1DM (P<0.0001) compared with control subjects
at baseline with no significant change from baseline to 2 year follow up in either
controls or T1DM. CST was significantly greater in T1DM (P=0.002) compared with
control subjects at baseline and further increased at 2 year follow up in T1DM
(P=0.02) although the latter isolated change may be due to chance. WST did not
differ between T1DM and control subjects at baseline and did not change at follow
up.
3.4.3.3 Electrophysiology
Sural nerve conduction velocity and amplitude were significantly lower (P<0.0001
and P=0.0003 respectively) at baseline in T1DM compared with control subjects.
Peroneal nerve conduction velocity and amplitude were significantly lower
(P<0.0001 and P=0.0003 respectively) at baseline in T1DM compared with control

152
subjects. There were no significant changes in electrophysiology from baseline to 2
year follow up in either controls or T1DM.
3.4.3.4 Corneal sensation and structure
NCCA was significantly greater in T1DM compared to control subjects and did not
progress over 2 years of follow up in either T1DM or controls. CNFD (P<0.0001),
CNBD (P=0.007) and CNFL (P<0.0001) were reduced in T1DM compared to
controls at baseline with no significant changes at 2 year follow up in either
controls or T1DM.

153
Table 3-3 Small and large fibre tests of nerve structure and function in control subjects and
diabetic patients at baseline and 2 year follow up, with statistically significant differences
between groups.
Control
BL (n=16)
Control FU
(n=16) P
T1DM
BL
(n=50)
T1DM FU
(n=50)
P
NCCA
(mBar) 0.6±0.3 0.6±0.4 NS 1.4±2.3† 1.5±2.3 NS
CNFD
(no/mm2) 30.1±4.9 28.3±5.5 NS 19.5±9.1* 18.7±9.9 NS
CNBD
(no/mm2) 36.6±15.5 39.3±18.0 NS 23.9±15.0** 22.6±15.8 NS
CNFL
(mm/mm2) 16.9±2.8 16.6±3.0 NS 12.0±4.6*** 12.1±5.0 NS
CST (˚C) 28.6±2.1 26.8±4.8 NS 24.8±6.9˚ 22.5±8.4 0.02
WST(˚C) 37.6±3.5 38.9±3.8 NS 39.6±4.6 40.2±5.7 NS
VPT (volts) 5.3±4.8 6.0±5.2 NS 15.5±13.6ª 15.9±12.6 NS
SSNCV
(m/s) 49.4±3.9 48.1±4.7 NS 43.6±6.3
ƒ 41.3±6.4 NS
SSNAmp
(µV) 21.0±10.8 18.6±8.7 NS 10.1±6.7
ƒƒ 8.7±6.8 NS
PMNCV
(m/s) 47.8±3.6 47.3±4.2 NS 40.6±7.0^ 40.0±6.6 NS
PMNAmp
(mV) 6.0±1.6 5.8±1.2 NS 3.4±2.4^^ 3.2±2.0 NS
Post hoc analyses (Control Baseline vs T1DM Baseline)
†P=0.02; *P<0.0001; **P=0.007; ***P<0.0001; ˚P=0.002; ªP<0.0001; fP<0.0001;
ƒƒP=0.0003;
^P<0.0001; ^^P=0.0003.
Table key
BL – Baseline; CNBD – Corneal Nerve Branch Density; CNFD – Corneal Nerve Fibre Density;
CNFL – Corneal Nerve Fibre Length; CST – Cold Sensation Threshold; FU – Follow Up, PMNAmp
– Peroneal Motor Nerve Amplitude; PMNCV – Peroneal Motor Nerve Conduction Velocity;
SSNAmp – Sural Nerve Sensory Nerve Amplitude; SMNCV – Sural Nerve Conduction Velocity;
VPT – Vibration Perception Threshold; WST – Warm Sensation Threshold.

154
3.4.3.5 Rapid Nerve Fibre Decline (RNFD) in T1DM
(Table 3.4, Figures 3.1 & 3.2)
The mean intra-individual change in CNFL over the 2 year follow up in the control
group was 7.9±7.2%. A 2 standard deviation intra-individual change is therefore
14.4%. We thus used this parameter as a cut off for RNFD in the T1DM group. We
identified eleven subjects (n=11) out of fifty in the T1DM group who had a greater
than 14.4% decline in CNFL over 2 years. This analysis is based on the
unpublished data presented by Professor Bruce Perkins (at the American Diabetes
Association conference 2013) in which rapid nerve fibre decline was defined as a
change in CNFL of -14% (25). The mean intra-individual change in CNFL over 2
year follow up in the T1DM group was 27.8±32.4%.
There were no significant differences for age HbA1c, BMI, T-CHL and systolic BP
in those with RNFD. There were no significant changes in VPT (Baseline:
17.5±13.1 vs 2 yr FU: 19.7±14.2 volts, P=NS), CST (Baseline: 25.5±4.0 vs 2 year
FU: 23.3±4.4 (˚C), P=NS) and WST (Baseline: 39.2±4.2 vs 2 year FU: 40.1±4.3
(˚C), P=NS).
There were concomitant reductions at 2 year follow up in sural sensory and
peroneal motor nerve conduction velocities (P=0.04 and P=0.05 respectively) with
no change in sural and peroneal amplitudes over the same period.
All measures of CCM were significantly reduced at follow up: CNFD (Baseline:
18.8±10.2 vs 2 yr FU: 11.5±9.4 no./mm2, P=0.0006), CNBD (Baseline: 24.1±15.6
vs 2 yr FU: 10.7±12.8 no./mm2, P=0.0002) and CNFL (Baseline: 12.1±5.0 vs 2 yr
FU: 8.5±4.5 mm/mm2, P=0.0002) (Figure 3.1a, b & c). Figure 3.2a & b shows
images from a subject with RNFD at baseline and 2 year follow up. In assessing
155
subjects with reductions in peroneal motor and sural sensory nerve conduction
velocity, concomitant reductions in CNFD, CNBD and CNFL were also noted,
however data are analysed based on those with a reduction of 14.4% in CNFL or
greater.
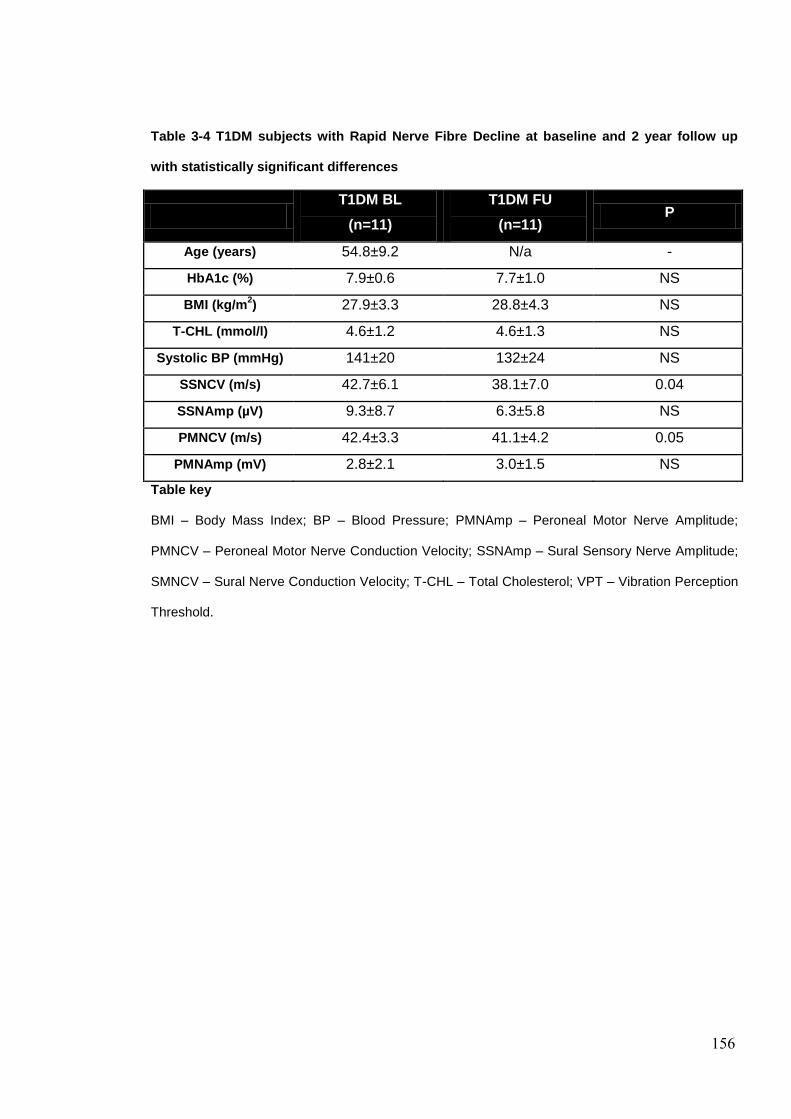
156
Table 3-4 T1DM subjects with Rapid Nerve Fibre Decline at baseline and 2 year follow up
with statistically significant differences
T1DM BL
(n=11)
T1DM FU
(n=11) P
Age (years) 54.8±9.2 N/a -
HbA1c (%) 7.9±0.6 7.7±1.0 NS
BMI (kg/m2) 27.9±3.3 28.8±4.3 NS
T-CHL (mmol/l) 4.6±1.2 4.6±1.3 NS
Systolic BP (mmHg) 141±20 132±24 NS
SSNCV (m/s) 42.7±6.1 38.1±7.0 0.04
SSNAmp (µV) 9.3±8.7 6.3±5.8 NS
PMNCV (m/s) 42.4±3.3 41.1±4.2 0.05
PMNAmp (mV) 2.8±2.1 3.0±1.5 NS
Table key
BMI – Body Mass Index; BP – Blood Pressure; PMNAmp – Peroneal Motor Nerve Amplitude;
PMNCV – Peroneal Motor Nerve Conduction Velocity; SSNAmp – Sural Sensory Nerve Amplitude;
SMNCV – Sural Nerve Conduction Velocity; T-CHL – Total Cholesterol; VPT – Vibration Perception
Threshold.

157
Figure 3-1a, b & c. CNFD, CNBD and CNFL and baseline and 2 year follow up.
C
B
A

158
Figure 3-2 a & b. CCM images of a subject with RNFD at baseline and 2 year follow up
CCM progressionBaseline (A) vs. 2 Years (B)
A B
Nerve Branches
Nerve Fibres

159
3.5 DISCUSSION
The major findings of this study are: 1) Type 1 diabetes patients show no
significant progression of neuropathy over 2 years; 2) A subgroup of patients with
Type 1 diabetes shows rapidly progressive and readily detectable decline in
corneal nerve fibre structure using CCM 2) and 3) CCM provides an ideal
surrogate endpoint for the assessment and progression of diabetic neuropathy.
These findings are both of importance in identifying those who have progression of
DPN with subsequent risk of ensuing complications such as foot ulceration and
lower limb amputation but also mortality. Furthermore, it may also be important in
identifying patients who should be recruited into clinical trials of DPN as Dyck et al
(20) concluded that future trials of DPN should include those with developing
neuropathy and also select endpoints which show a discernible worsening. CCM
provides a seemingly suitable surrogate endpoint for the assessment of DPN and
has also shown an excellent correlation with the current gold standard IENFD (26).
At 2 years there were no significant changes in the majority of our diabetic subjects
and this is in keeping with the notion that DPN progresses much slower than
previously thought (27). This may provide a partial explanation for the failure of
pathogenetic treatments in clinical trials of DPN. Nerve conduction velocity is only
gradually diminished by DPN, with estimates of a loss of ~0.5m/s/ year (28). In the
10 year natural history study by Partanen et al (17), nerve conduction velocity
deteriorated in all nerve segments evaluated with the largest deficit of 3.9 m/s for
the sural nerve. The DCCT showed a similar slow progression of change in nerve
conduction velocity over a 5 year period (29). Previously, a placebo controlled
study has shown improvements in signs and VPT in the placebo-treated arm with a
small reduction in electrophysiological measures (30) and this has also been
160
demonstrated in another placebo controlled study (31). Both the study by Partanen
et al (17) and the DCCT (16) were undertaken prior to the widespread use of ACE
inhibitors and statins, both of which are likely to impact positively on the peripheral
nerve (18-19). Electrophysiology, of course focuses on large fibre function wherein
the primary pathology lies in small fibres and predates abnormalities in nerve
conduction studies (32). Therefore a measure of small fibre damage may be the
most sensitive to detect an early abnormality and progression. Small fibre
neuropathy in particular that of sudomotor dysfunction may result in dryness
of foot skin and has been associated with foot ulceration (33) and CCM provides
an ideal surrogate marker for small fibre neuropathy.
The Toronto criteria for DPN (32) advocates electrophysiology for epidemiologic
surveys or controlled clinical trials of DPN as an early and reliable indicator of the
occurrence of neuropathy. However, our study clearly shows a lack of concomitant
reductions in nerve amplitudes particularly sural amplitude which is a considered a
particularly valid and sensitive marker of nerve damage (34). Furthermore,
variability in measurements (intra-observer variability) can be a significant concern
when interpreting electrophysiological results, particularly in multi centre trials (35)
and short term improvements in metabolic control can cause significant increases
in nerve conduction parameters (10) although whether this correlates to actual
repair or enhancement of large nerve fibre structure is unknown. Our data shows
globally reduced measures of corneal nerve structure at baseline confirming
previous studies which have shown that corneal small nerve fibre damage can be
detected prior to abnormalities in electrophysiology and quantitative sensory
testing (26). CCM also has the ability to detect nerve fibre repair and regeneration

161
as evidenced by our recently published data on subjects undergoing simultaneous
pancreas and kidney transplantation with amelioration of Type 1 diabetes (12).
We have no obvious metabolic explanation for the basis of rapid nerve fibre decline
observed in the subset of patients with T1DM as there were no significant changes
in HbA1c, lipids and blood pressure in the overall T1DM cohort. This is clearly
different from the results of the Eurodiab study which showed that the development
of neuropathy was related to a range of cardiovascular risk factors (7). However,
the control group was relatively small and the cut offs used for RNFD may be
different if derived from a larger cohort and the duration of follow up was relatively
short.
In conclusion, we have shown that CCM can identify a subcohort of patients with
T1DM with a rapid degree of small fibre decline. Furthermore, given that we have
recently shown that CCM can detect early nerve fibre repair after SPK (12) this
adds to the evidence that CCM may be an ideal surrogate endpoint for clinical trials
of new therapies in diabetic neuropathy.

162
3.6 REFERENCES
1. Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM, Wilson DM,
O'Brien PC, Melton LJ, 3rd, Service FJ: The prevalence by staged severity of
various types of diabetic neuropathy, retinopathy, and nephropathy in a population-
based cohort: the Rochester Diabetic Neuropathy Study. Neurology 1993;43:817-
824
2. Abbott CA, Malik RA, van Ross ERE, Kulkarni J, Boulton AJM: Prevalence and
Characteristics of Painful Diabetic Neuropathy in a Large Community-Based
Diabetic Population in the U.K. Diabetes Care 2011;34:2220-2224
3. Young MJ, Boulton AJ, MacLeod AF, Williams DR, Sonksen PH: A multicentre
study of the prevalence of diabetic peripheral neuropathy in the United Kingdom
hospital clinic population. Diabetologia 1993;36:150-154
4. Adler AI, Boyko EJ, Ahroni JH, Smith DG: Lower-extremity amputation in
diabetes. The independent effects of peripheral vascular disease, sensory
neuropathy, and foot ulcers. Diabetes Care 1999;22:1029-1035
5. Elliott J, Tesfaye S, Chaturvedi N, Gandhi RA, Stevens LK, Emery C, Fuller JH:
Large-fibre dysfunction in diabetic peripheral neuropathy is predicted by
cardiovascular risk factors. Diabetes Care 2009;32:1896-1900
6. Calles-Escandon J, Lovato LC, Simons-Morton DG, Kendall DM, Pop-Busui R,
Cohen RM, Bonds DE, Fonseca VA, Ismail-Beigi F, Banerji MA, Failor A, Hamilton
B: Effect of intensive compared with standard glycemia treatment strategies on
mortality by baseline subgroup characteristics: the Action to Control Cardiovascular
Risk in Diabetes (ACCORD) trial. Diabetes Care 2010;33:721-727
163
7. Tesfaye S, Chaturvedi N, Eaton SEM, Ward JD, Manes C, Ionescu-Tirgoviste C,
Witte DR, Fuller JH: Vascular Risk Factors and Diabetic Neuropathy. New England
Journal of Medicine 2005;352:341-350
8. The Effect of Intensive Treatment of Diabetes on the Development and
Progression of Long-Term Complications in Insulin-Dependent Diabetes Mellitus.
New England Journal of Medicine 1993;329:977-986
9. Albers JW, Herman WH, Pop-Busui R, Feldman EL, Martin CL, Cleary PA,
Waberski BH, Lachin JM: Effect of prior intensive insulin treatment during the
Diabetes Control and Complications Trial (DCCT) on peripheral neuropathy in type
1 diabetes during the Epidemiology of Diabetes Interventions and Complications
(EDIC) Study. Diabetes Care 2010;33:1090-1096
10. Perkins BA, Dholasania A, Buchanan RA, Bril V: Short-term metabolic change
is associated with improvement in measures of diabetic neuropathy: a 1-year
placebo cohort analysis. Diabetic Medicine 2010;27:1271-1279
11. Tavakoli M, Kallinikos P, Iqbal A, Herbert A, Fadavi H, Efron N, Boulton AJ, R
AM: Corneal confocal microscopy detects improvement in corneal nerve
morphology with an improvement in risk factors for diabetic neuropathy. Diabet
Med 2011;28:1261-1267
12. Tavakoli M, Mitu-Pretorian M, Petropoulos IN, Fadavi H, Asghar O, Alam U,
Ponirakis G, Jeziorska M, Marshall A, Efron N, Boulton AJ, Augustine T, Malik RA:
Corneal confocal microscopy detects early nerve regeneration in diabetic
neuropathy after simultaneous pancreas and kidney transplantation. Diabetes
2013;62:254-260

164
13. Smith AG, Russell J, Feldman EL, Goldstein J, Peltier A, Smith S, Hamwi J,
Pollari D, Bixby B, Howard J, Singleton JR: Lifestyle Intervention for Pre-Diabetic
Neuropathy. Diabetes Care 2006;29:1294-1299
14. Pittenger GL, Ray M, Burcus NI, McNulty P, Basta B, Vinik AI: Intraepidermal
Nerve Fibers Are Indicators of Small-Fiber Neuropathy in Both Diabetic and
Nondiabetic Patients. Diabetes Care 2004;27:1974-1979
15. Vas PRJ, Rayman G: The Rate of Decline in Small Fibre Function Assessed
Using Axon Reflex-Mediated Neurogenic Vasodilatation and the Importance of Age
Related Centile Values to Improve the Detection of Clinical Neuropathy. PLoS One
2013;8:e69920. doi:69910.61371/journal.pone.0069920
16. The effect of intensive diabetes therapy on the development and progression of
neuropathy. The Diabetes Control and Complications Trial Research Group. Ann
Intern Med 1995;122:561-568
17. Partanen J, Niskanen L, Lehtinen J, Mervaala E, Siitonen O, Uusitupa M:
Natural history of peripheral neuropathy in patients with non-insulin-dependent
diabetes mellitus. N Engl J Med 1995;333:89-94
18. Malik RA, Williamson S, Abbott C, Carrington AL, Iqbal J, Schady W, Boulton
AJ: Effect of angiotensin-converting-enzyme (ACE) inhibitor trandolapril on human
diabetic neuropathy: randomised double-blind controlled trial. Lancet
1998;352:1978-1981
19. Davis TM, Yeap BB, Davis WA, Bruce DG: Lipid-lowering therapy and
peripheral sensory neuropathy in type 2 diabetes: the Fremantle Diabetes Study.
Diabetologia 2008;51:562-566
20. Dyck PJ, Norell JE, Tritschler H, Schuette K, Samigullin R, Ziegler D, Bastyr
EJ, 3rd, Litchy WJ, O'Brien PC: Challenges in design of multicenter trials: end

165
points assessed longitudinally for change and monotonicity. Diabetes Care
2007;30:2619-2625
21. Young M, Boulton A, Macleod A, Williams D, Sonksen P: A multicentre study of
the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital
clinic population. Diabetologia 1993;36:150-154
22. Bravenboer B, van Dam PS, Hop J, vd Steenhoven J, Erkelens DW: Thermal
threshold testing for the assessment of small fibre dysfunction: normal values and
reproducibility. Diabet Med 1992;9:546-549
23. Petropoulos IN, Manzoor T, Morgan P, Fadavi H, Asghar O, Alam U, Ponirakis
G, Dabbah MA, Chen X, Graham J, Tavakoli M, Malik RA: Repeatability of in vivo
corneal confocal microscopy to quantify corneal nerve morphology. Cornea
32:e83-89
24. Tavakoli M, Malik RA: Corneal confocal microscopy: a novel non-invasive
technique to quantify small fibre pathology in peripheral neuropathies. J Vis Exp
2011; 3(47):2194. doi: 10.3791/2194.
25. Halpern EM, Lovblom LE, Orlov S, Bril V, Perkins BA: The Existence of Rapid
Small Fiber Decline in Type 1 Diabetes: A Potential Proxy for Neuropathy
Progression Using In Vivo Corneal Confocal Microscopy Orals. Diabetes
2013;62:A1-A98
26. Quattrini C, Tavakoli M, Jeziorska M, Kallinikos P, Tesfaye S, Finnigan J,
Marshall A, Boulton AJM, Efron N, Malik RA: Surrogate Markers of Small Fiber
Damage in Human Diabetic Neuropathy. Diabetes 2007;56:2148-2154
27. Boulton AJ: Whither clinical research in diabetic sensorimotor peripheral
neuropathy? Problems of end point selection for clinical trials. Diabetes Care
2007;30:2752-2753

166
28. Arezzo JC: The use of electrophysiology for the assessment of diabetic
neuropathy. Neuroscience Research Communications 1997;21:13-23
29. Effect of intensive diabetes treatment on nerve conduction in the Diabetes
Control and Complications Trial. Ann Neurol 1995;38:869-880
30. Tesfaye S, Tandan R, Bastyr EJ, 3rd, Kles KA, Skljarevski V, Price KL: Factors
that impact symptomatic diabetic peripheral neuropathy in placebo-administered
patients from two 1-year clinical trials. Diabetes Care 2007;30:2626-2632
31. Brown MJ, Bird SJ, Watling S, Kaleta H, Hayes L, Eckert S, Foyt HL: Natural
progression of diabetic peripheral neuropathy in the Zenarestat study population.
Diabetes Care 2004;27:1153-1159
32. Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, Lauria G,
Malik RA, Spallone V, Vinik A, Bernardi L, Valensi P: Diabetic neuropathies:
update on definitions, diagnostic criteria, estimation of severity, and treatments.
Diabetes Care 2010;33:2285-2293
33. Stewart JD, Low PA, Fealey RD: Distal small fiber neuropathy: results of tests
of sweating and autonomic cardiovascular reflexes. Muscle Nerve 1992;15:661-
665.
34. Freeman TL, Johnson E, Freeman ED, et al.: Nerve Conduction Studies
(NCS). S C, Ed. New York, Demos Medical Publishing, 2004
35. Keith M, Goldstein R, Nesathurai S, Graham W: Serial nerve conduction
studies of the tail of rhesus monkey Macaca mulatta and potential implications for
interpretation of human neurophysiological studies Annals of Indian Academy of
Neurology 2007; DOI:10.4103/0972-2327.37818
167
4 Chapter IV - Diagnostic Utility of Corneal Confocal
Microscopy and Intra-Epidermal Nerve Fibre Density in
Diabetic Neuropathy
Contribution: Uazman Alam contributed to the conception and design of the study
and made a major contribution to the recruitment of subjects, clinical tests including
neuropathy assessments and skin biopsies, skin biopsy analyses, all statistical
analyses and writing of this chapter.
To be submitted for publication
Uazman Alam, Maria Jeziorska, Ioannis N Petropoulos, Omar Asghar, Hassan
Fadavi, Georgios Ponirakis, Andrew Marshall, Mitra Tavakoli, Andrew JM Boulton,
Nathan Efron, Rayaz A Malik

168
4.1 ABSTRACT
Corneal confocal microscopy (CCM) is a rapid, non-invasive, reproducible
technique that quantifies small nerve fibres. We have compared the diagnostic
capability of CCM against a range of established measures of nerve damage in
patients with diabetic neuropathy.
Thirty subjects with Type 1 diabetes without neuropathy (T1DM), thirty one
subjects with Type 1 diabetes and neuropathy (DSPN) and twenty seven non-
diabetic healthy control subjects underwent detailed assessment of neuropathic
symptoms and neurologic deficits, quantitative sensory testing (QST),
electrophysiology, skin biopsy and CCM.
Comparing subjects with DSPN and T1DM, those with DSPN they were older
(P=0.0002), had a longer duration of diabetes (P<0.0001), lower eGFR (P=0.006)
and higher albumin-creatinine ratio (ACR) (P=0.03) with no significant difference
for HbA1c, BMI, lipids and blood pressure. Patients with DSPN had more
symptoms (neuropathy symptom profile (NSP) (P<0.0001), McGill visual analogue
score (McGill VAS) (P=0.01) and McGill pain score (P=0.02), higher neuropathy
disability score (NDS) (P<0.0001), CST (P=0.007), WST (P=0.0004), vibration
perception threshold (VPT) (P<0.0001) and lower peroneal motor nerve conduction
velocity (PMNCV) and amplitude (PMNAmp) (P<0.0001 and P<0.0001), sural
sensory nerve conduction velocity (SSNCV) and amplitude (SSNAmp) (P<0.0001),
intra-epidermal nerve fibre density (IENFD) (P=0.001), corneal nerve fibre density
(CNFD) (P<0.0001), corneal nerve branch density (CNBD) (P=0.02) and corneal
nerve fibre length (CNFL) (P=0.001). CNFD correlated better with PMNCV
(Spearman’s Rho= 0.60 P<0.0001) than IENFD with PMNCV (Spearman’s Rho=
0.56 P<0.0001). For the diagnosis of diabetic neuropathy the sensitivity for CNFD
169
was 0.77 and specificity was 0.79 with Wilcoxon estimate of area under the ROC
curve of 0.81. IENFD had a diagnostic sensitivity of 0.61, specificity of 0.80 and
area under the ROC curve of 0.73.
CCM is a valid accurate non-invasive method which is superior to skin biopsy in
diagnosing DPN.

170
4.2 INTRODUCTION
Diabetic peripheral neuropathy is a debilitating condition which may lead to pain,
foot ulceration and eventual amputation (1). Therefore it is important to accurately
diagnose diabetic neuropathy at the earliest stage of damage. Clinical neurological
assessment is poorly reproducible (2), and whilst QST can measure both large and
small nerve fibre function it is subjective and requires an alert and motivated
subject. Nerve conduction studies remain the mainstay for the diagnosis and
progression of diabetic neuropathy (3). However, the earliest nerve fibres to
degenerate (4-5) and regenerate (6) are the small unmyelinated fibres and indeed
they are central to the genesis of pain and the development of foot ulceration (7).
In 2005 the European Federation of Neurological Societies published guidelines on
the use of skin biopsy in the diagnosis of peripheral neuropathies (8) and more
recently the value of the technique has been further emphasized (9). Currently,
skin biopsy with an assessment of intra-epidermal nerve fibres (IENF) is
considered the gold standard for the evaluation of small fibre neuropathy and has
been advocated as measure of treatment response in clinical trials (10). Previous
studies have demonstrated good diagnostic ability of skin biopsy for small fibre
neuropathy (11-14), however, these studies have assessed mixed populations of
small fibre neuropathy and the diagnostic utility of CCM versus IENF have not
been evaluated. Hence reproducible and reliable processing and accurate
quantification methods have been established for assessing IENF pathology
against normative ranges (15). However, despite being advocated as an endpoint
in clinical trials of diabetic neuropathy there is surprisingly scarce data which have
established the diagnostic ability of skin biopsy for diabetic neuropathy (7).

171
Furthermore skin biopsy is invasive with a small but significant risk for bleeding and
infection and requires expertise in laboratory assessment (16).
CCM is a non-invasive ophthalmic application, which is rapid, non-invasive and
readily reproducible for quantifying small nerve fibres and thereby has been shown
to diagnose and track the progression of diabetic neuropathy (17-19). CCM has
been shown to have reasonable diagnostic utility in detecting DPN diagnosed
using NDS (20) with good reproducibility (21). More recently CCM has been shown
to correlate with functional measures of small nerve fibre injury (22). However, the
differential ability of CCM against currently accepted gold standard FDA approved
methods such as skin biopsy, QST and nerve conduction studies for the diagnosis
of diabetic neuropathy has not been evaluated to date. We have therefore
compared the ability of CCM, QST and skin biopsy in the diagnosis of diabetic
neuropathy using the Toronto criteria (3).

172
4.3 RESEARCH DESIGN AND METHODS
4.3.1 Selection of patients
Sixty one consecutive subjects with Type 1 diabetes were assessed and
subsequently divided into two groups based their neuropathy status. Patients were
recruited from general diabetes clinics in the Manchester Diabetes Centre, Central
Manchester Foundation Trust. Thirty subjects with Type 1 diabetes without
neuropathy (T1DM) (n=30), thirty one T1DM subjects with neuropathy (DSPN)
(n=31) and twenty seven non-diabetic healthy control subjects were studied.
Subjects with a history of neurologic conditions, ocular trauma or previous ocular
surgery were excluded. The study was approved by the North Manchester
Research Ethics committee, and written informed consent was obtained according
to the Declaration of Helsinki.
4.3.2 Definition of Neuropathy
Diabetic neuropathy was defined according to the Toronto criteria by the presence
of an abnormality of electrophysiology and a symptom or symptoms or a sign or
signs of neuropathy (3).
4.3.3 Assessment of neuropathy
All patients and control subjects underwent a detailed evaluation of neurologic
symptoms according to the NSP, and the McGill VAS was used to assess the
severity of painful neuropathy. Clinical neurologic deficits were assessed using the
modified neuropathy disability score, which includes an evaluation of vibration, pin
prick, and temperature perception as well as the presence or absence of ankle
reflexes (23). Quantitative sensory testing included an assessment of the VPT,
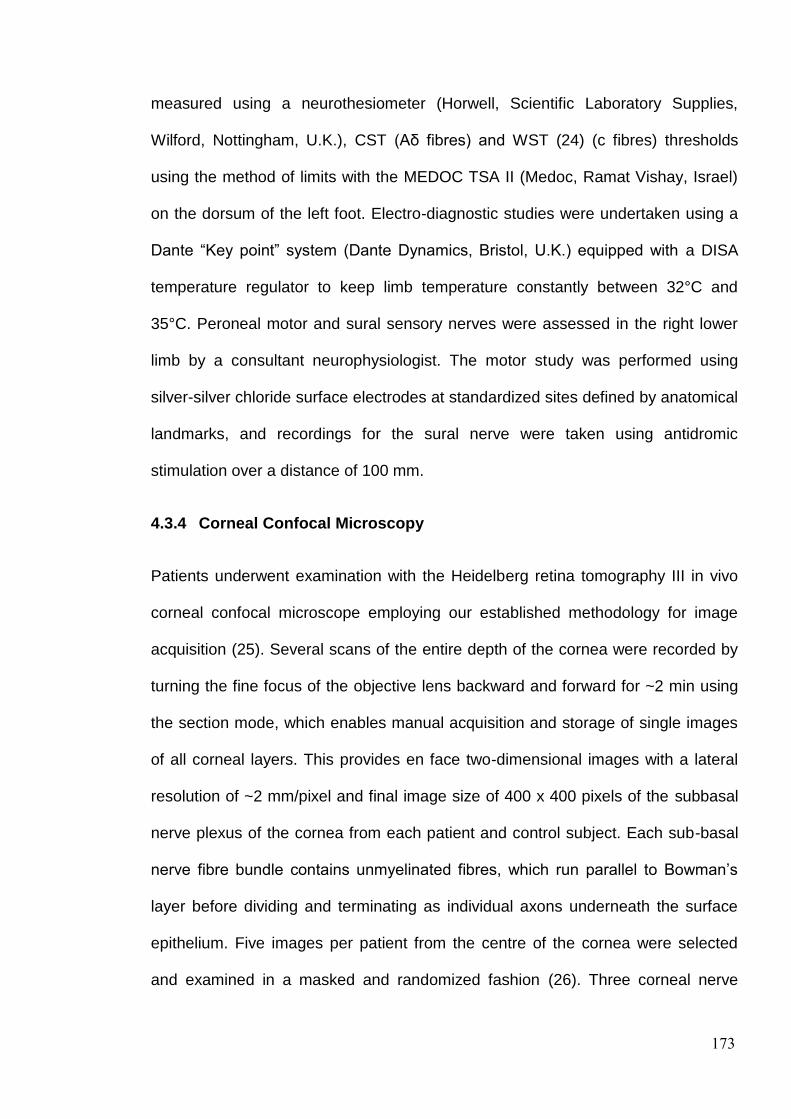
173
measured using a neurothesiometer (Horwell, Scientific Laboratory Supplies,
Wilford, Nottingham, U.K.), CST (Aδ fibres) and WST (24) (c fibres) thresholds
using the method of limits with the MEDOC TSA II (Medoc, Ramat Vishay, Israel)
on the dorsum of the left foot. Electro-diagnostic studies were undertaken using a
Dante “Key point” system (Dante Dynamics, Bristol, U.K.) equipped with a DISA
temperature regulator to keep limb temperature constantly between 32°C and
35°C. Peroneal motor and sural sensory nerves were assessed in the right lower
limb by a consultant neurophysiologist. The motor study was performed using
silver-silver chloride surface electrodes at standardized sites defined by anatomical
landmarks, and recordings for the sural nerve were taken using antidromic
stimulation over a distance of 100 mm.
4.3.4 Corneal Confocal Microscopy
Patients underwent examination with the Heidelberg retina tomography III in vivo
corneal confocal microscope employing our established methodology for image
acquisition (25). Several scans of the entire depth of the cornea were recorded by
turning the fine focus of the objective lens backward and forward for ~2 min using
the section mode, which enables manual acquisition and storage of single images
of all corneal layers. This provides en face two-dimensional images with a lateral
resolution of ~2 mm/pixel and final image size of 400 x 400 pixels of the subbasal
nerve plexus of the cornea from each patient and control subject. Each sub-basal
nerve fibre bundle contains unmyelinated fibres, which run parallel to Bowman’s
layer before dividing and terminating as individual axons underneath the surface
epithelium. Five images per patient from the centre of the cornea were selected
and examined in a masked and randomized fashion (26). Three corneal nerve

174
parameters were quantified: 1) CNFD, the total number of major nerves per square
millimetre of corneal tissue (no.mm2); 2) CNBD, the number of branches
emanating from all major nerve trunks per square millimetre of corneal tissue
(no.mm2); and 3) CNFL, the total length of all nerve fibres and branches (mm/mm2)
within the area of corneal tissue (27).
4.3.5 Skin biopsy and immunohistochemistry
Participants underwent a 3-mm punch skin biopsy from the dorsum of the foot; 2
cm above the second metatarsal head after local anaesthesia (1% lidocaine). The
biopsy site was closed using Steristrips, and the specimen was immediately fixed
in PBS-buffered 4% paraformaldehyde for 18-24 hours, washed - in Tris-buffered
saline, cryoprotected in sucrose, frozen in liquid nitrogen and stored at -80°C- and
subsequently cut into 50-μm sections on a cryostat microtome. Five floating
sections per subject were immunostained for PGP9.5 neuronal marker. Non-
specific protein binding and endogenous peroxidase activity were blocked by
incubation in 5% goat serum and 0.3% hydrogen peroxide, respectively. The anti-
PGP9.5 antibody (Milipore 1:1000; Billerica,MA) was followed first by goat anti-
rabbit IgG and then by HRP-Streptavidin (both diluted 1:1000, both from Vector
Laboratories, Peterborough, UK). Nerve fibres were visualised by SG chromogen
(Vector Laboratories). IENFD was calculated as the number of nerve fibres
crossing the basement membrane of the epidermis and expressed per millimetre
length of epidermis (28).
4.3.6 Statistical analysis
Statistical analyses were undertaken on Statsdirect (Statsdirect, Cheshire, UK).
The data are expressed as Mean ± standard deviation (SD). ANOVA method or a

175
non-parametric counterpart, Kruskal-Wallis were used to assess differences
between groups depending on normality of the data. The Mann-Whitney U test was
used to compare T1DM with DSPN for the duration of diabetes. Chi squared
analyses were used to assess frequencies of gender, and ethnicity. Overall the P
value was maintained at 0.05 for multiple comparison tests (Bonferoni adjustment
or Conover-Inmann pairwise comparison). Spearman’s rank correlation was
undertaken for CNFD, CNBD, CNFL and IENFD versus NDS, McGill VAS, NSP,
IENFD, thermal thresholds, VPT and nerve conduction studies. ROC curve
analyses were used to define the Wilcoxon estimate of area under ROC curve,
optimal cut offs with associated sensitivity and specificity for CCM parameters,
IENFD, VPT and thermal thresholds. Positive predictive value (PPV) and negative
predictive value (NPV) were calculated for the three diagnostic measures, which
had the greatest Wilcoxon estimate of area under the ROC curve.

176
4.4 RESULTS
4.4.1 Demographics, Metabolic and Anthropometric Assessment (Table 4.1)
The participant demographics and metabolic and anthropometric measurements in
diabetic patients and control subjects are summarized in Table 4.1. Those with
DSPN (53.3±11.9) were significantly older compared to controls (41.0±14.9 years,
P=0.0008) and T1DM (38.8±12.5, P<0.0001) and the duration of diabetes was
greater in DSPN compared to T1DM (P<0.0001). The non white European
ethnicities in table 4.1 were Asian with one participant of African origin in the
control and T1DM group. HbA1c (P<0.0001) was significantly higher in diabetic
patients compared with control subjects with no difference between patients with
T1DM and DSPN. Total cholesterol was significantly lower in diabetic patients with
T1DM (P=0.006) and DSPN (P=0.002) compared to control subjects. BMI, HDL,
triglycerides, systolic and diastolic blood pressure were comparable between
diabetic patients and control subjects. The estimated glomerular filtration rate
(eGFR) was lower in DSPN compared to T1DM (P=0.006), the Albumin-Creatinine
Ratio (ACR) was higher in DSPN compared to T1DM (P=0.03) and controls
(P=0.004), although median values for controls, T1DM and DSPN were all within
the normal range for ACR.

177
Table 4-1 Participant demographics and metabolic parameters in control subjects and
diabetic patients without (T1DM) and with neuropathy (DSPN), with statistically significant
differences between groups
C (n=27) T1DM (n=30) DSPN (n=31) T1DM v DSPN
Age (years) 41.0±14.9 38.8±12.5 53.3±11.9 0.0002
Gender (Male) (%) 59 43 61 -
Ethnicity (White
European) (%) 77 90 97 -
Aetiology of
Diabetes (Type 1
DM) (%)
- 100 100 NS
Duration of
Diabetes (years) - 17.2±12.0 37.2±13.1 <0.0001
HbA1c (%) 5.5±0.3 8.0±1.3 8.5±1.5 NS
HbA1c (mmol/mol) 36.9±3.4 61.0±21.0 70.0±17.0 NS
BMI (kg/m2) 26.9±4.0 26.3±4.4 27.2±4.2 NS
T-CHL (mmol/l) 5.0±0.8 4.4±0.9 4.3±0.9 NS
HDL (mmol/l) 1.6±0.4 1.6±0.4 1.6±0.5 NS
Triglycerides 1.3±0.6 1.2±0.8 1.3±0.7 NS
Systolic BP (mmHg) 128±18 126±17 132±22 NS
Diastolic BP
(mmHg) 70±10 71±10 72±9 NS
ACR (mg/mmol)
((Median)IQR)
0.4±0.4
(0.3(0.2-0.4))
0.7±0.9
(0.3(0.2-0.5)
2.8±4.8
(0.7(0.2-2.7) 0.03
eGFR (ml/min/1.73) 85±7 90±3 80±18ƒ 0.006

178
Post Hoc Analyses
Age: C vs T1DM (NS); C vs DSPN (P=0.0008); T1DM vs DSPN (P<0.0001).
Gender: Chi2 – P=0.02.
Ethnicity: Chi2 – P<0.0001.
HbA1c: C vs T1DM (P<0.0001); C vs DSPN (P<0.0001); T1DM vs DSPN (NS).
T-CHL: C vs T1DM (P=0.006); C vs DSPN (P=0.002); T1DM vs DSPN (NS).
ACR: C vs T1DM (NS); C vs DSPN (P=0.004); T1DM vs DSPN (P=0.03).
eGFR: C vs T1DM (NS); C vs DSPN (NS); T1DM vs DSPN (P=0.006).
Table key
ACR – Albumin Creatinine Ratio; BMI – Body Mass Index; BP – Blood Pressure; C – Controls,
estimated Glomerular Filtration Rate; HbA1c – Glycated Haemoglobin A1c; T-CHL – Total
Cholesterol; HDL – High Density Lipoprotein Cholesterol.
4.4.2 Symptoms and deficits (Table 4.2)
The NDS was significantly increased in patients with DSPN compared with control
subjects (P<0.0001) and T1DM (P<0.0001), with no significant difference between
controls and T1DM. The NSP was significantly higher in patients with DSPN
(P<0.0001) compared to control subjects and T1DM (P<0.0001). The McGill pain
score and McGill VAS were significantly increased in diabetic patients with DSPN
compared with control subjects (P=0.001 and P=0.0007 respectively) and patients
with T1DM (P=0.01 and P=0.02 respectively). There were no differences between
in NDS, NSP, McGill pain score and VAS between controls and T1DM.

179
Table 4-2 Neuropathy symptoms and deficits in control subjects and diabetic patients
without (T1DM) and with neuropathy (DSPN), with statistically significant differences
between groups
C (n=27) T1DM (n=30) DSPN (n=31) T1DM v DSPN
NDS (-/10)
(Median (IQR)
0.4±0.8
0(0-1)
1.2±2.0
0(0-2)
4.6±3.3
5(2-7)
<0.0001
NSP (-/38)
(Median (IQR)
0.1±0.4
0(0-0)
1.3±2.0
0(0-2)
5.0±6.2
2.5(0-6)
<0.0001
McGill VAS
(-/10cm)
(Median (IQR)
0.2±1.0
(0(0-0)
1.0±2.3
(0(0-0)
3.3±3.8
(0(0-0)
0.01
McGill Pain score
(Median (IQR)
0.1±0.4
(0(0-0)
1.9±6.5
(0(0-0)
4.2±6.5
(2(0-5) 0.02
Post Hoc Analyses
NDS: C vs T1DM (NS); C vs DSPN (P<0.0001); T1DM vs DSPN (P<0.0001).
NSP: C vs T1DM (NS); C vs DSPN (P<0.0001); T1DM vs DSPN (P<0.0001).
McGill VAS: C vs T1DM (NS), C vs DSPN (P=0.001); T1DM vs DSPN (P=0.01).
McGill Pain score: C vs T1DM (NS); C vs DSPN (P=0.0007); T1DM vs DSPN (P=0.02).
Table key
C – Controls; McGill VAS – McGill Visual Analogue Score; NDS – Neuropathy Disability Score,
NSP – Neuropathy Symptom Profile.
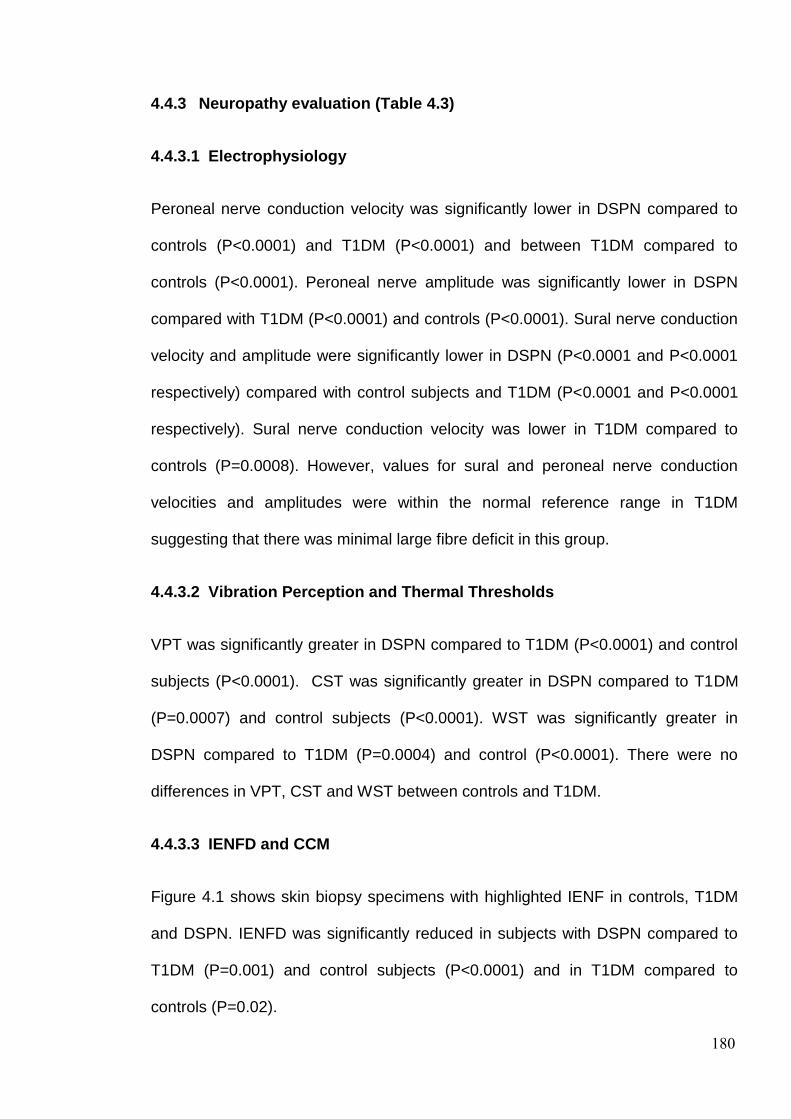
180
4.4.3 Neuropathy evaluation (Table 4.3)
4.4.3.1 Electrophysiology
Peroneal nerve conduction velocity was significantly lower in DSPN compared to
controls (P<0.0001) and T1DM (P<0.0001) and between T1DM compared to
controls (P<0.0001). Peroneal nerve amplitude was significantly lower in DSPN
compared with T1DM (P<0.0001) and controls (P<0.0001). Sural nerve conduction
velocity and amplitude were significantly lower in DSPN (P<0.0001 and P<0.0001
respectively) compared with control subjects and T1DM (P<0.0001 and P<0.0001
respectively). Sural nerve conduction velocity was lower in T1DM compared to
controls (P=0.0008). However, values for sural and peroneal nerve conduction
velocities and amplitudes were within the normal reference range in T1DM
suggesting that there was minimal large fibre deficit in this group.
4.4.3.2 Vibration Perception and Thermal Thresholds
VPT was significantly greater in DSPN compared to T1DM (P<0.0001) and control
subjects (P<0.0001). CST was significantly greater in DSPN compared to T1DM
(P=0.0007) and control subjects (P<0.0001). WST was significantly greater in
DSPN compared to T1DM (P=0.0004) and control (P<0.0001). There were no
differences in VPT, CST and WST between controls and T1DM.
4.4.3.3 IENFD and CCM
Figure 4.1 shows skin biopsy specimens with highlighted IENF in controls, T1DM
and DSPN. IENFD was significantly reduced in subjects with DSPN compared to
T1DM (P=0.001) and control subjects (P<0.0001) and in T1DM compared to
controls (P=0.02).

181
Figure 4.2 shows CCM images with highlighted corneal nerves in controls, T1DM
and DSPN from the same subjects as in Figure 4.1. CNFD, CNBD and CNFL were
significantly lower in DSPN compared with both T1DM (CNFD: P<0.0001, CNBD:
P=0.02 and CNFL: P=0.001) and controls (CNFD: P<0.0001, CNBD: P<0.0001
and CNFL: P<0.0001). These parameters were also significantly reduced in
patients with T1DM compared to controls (CNFD: P<0.0001, CNBD: P=0.0008 and
CNFL: P<0.0001) suggesting early small fibre damage.
Excluding non-white European subjects from the control group (6 participants)
(n=21) made no significant difference to any of the demographic, metabolic or
neuropathy parameters. Therefore the control group in this study had no significant
confounding effect through ethnicity (Appendix 2, Table 13.2). There were no
significant differences when analysing an older control subgroup (Age: 54.4±9.9
years, n=13) which was more closely matched in age to the DSPN group (Age:
53.3±11.9) compared to the overall complete control group. There were no
significant differences in demographic, metabolic and neuropathy parameters
between the older control subgroup (n=13) and complete control group (n=27). The
control group in this study is therefore representative sample which may be
appropriately used for comparison to both T1DM and DSPN (see appendix 2,
Table 13.3).
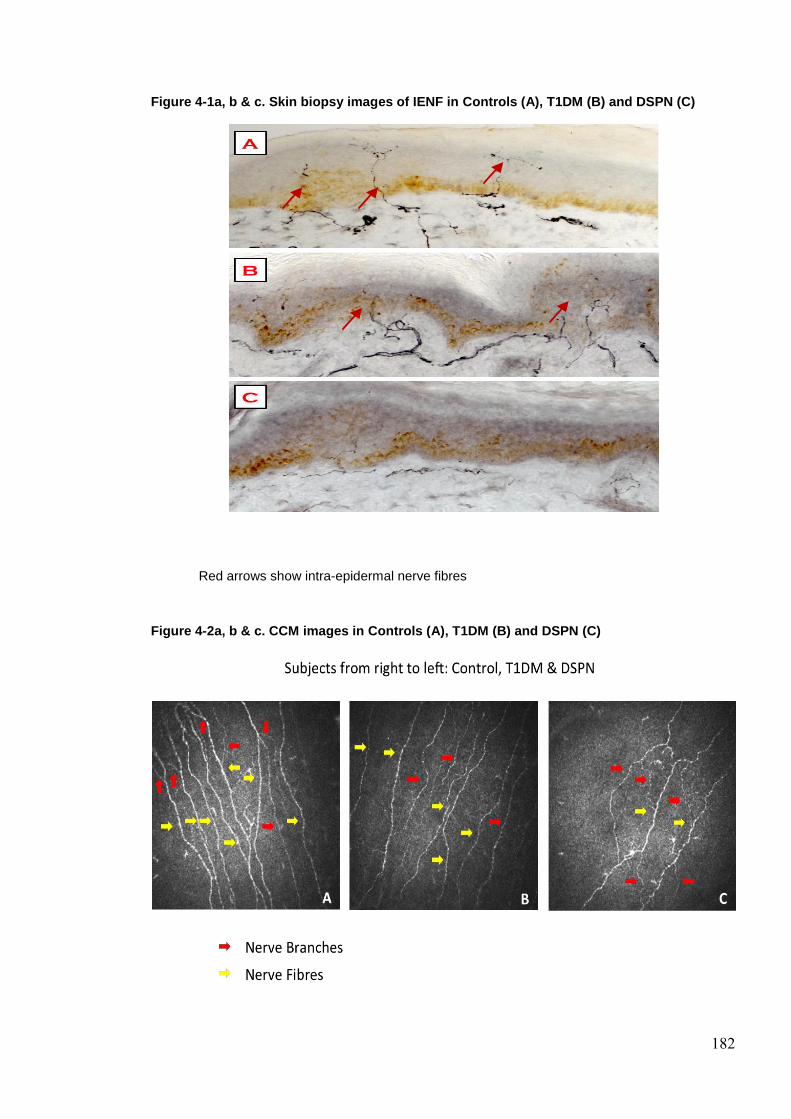
182
Figure 4-1a, b & c. Skin biopsy images of IENF in Controls (A), T1DM (B) and DSPN (C)
Red arrows show intra-epidermal nerve fibres
Figure 4-2a, b & c. CCM images in Controls (A), T1DM (B) and DSPN (C)

183
Table 4-3 Small and large fibre tests of nerve structure and function in control subjects and
diabetic patients without (T1DM) and with neuropathy (DSPN), with statistically significant
differences between groups
C (n=27) T1DM (n=30) DSPN (n=31) T1DM v DSPN
NCCA (mBar) 0.5±0.3 0.8±0.7 1.3±2.6 NS
CNFD (no/mm2) 37.2±5.1 30.1±6.7 19.8±9.2
<0.0001
CNBD (no/mm2) 92.0±36.2 60.7±27.9 45.4±32.0
0.02
CNFL (mm/mm2) 26.6±3.8 21.5±4.8 15.8±7.0
0.001
IENFD (no/mm) 10.2±3.3 8.3±5.5 4.7±4.3
0.001
CST (˚C) 28.6±2.0 27.5±2.0 21.4±9.1 0.0007
WST(˚C) 36.4±2.0 38.1±3.4 41.8±4.5 0.0004
VPT (volts) 5.3±4.1 5.6±2.5 18.4±12.2 <0.0001
SSNCV (m/s) 50.6±4.2 47.1±4.1 39.4±6.1 <0.0001
SSNAmp (µV) 20.2±8.8 15.1±6.1 5.5±4.2 <0.0001
PMNCV (m/s) 49.2±3.7 45.5±2.2 35.4±8.6 <0.0001
PMNAmp (mV) 6.1±2.4 7.3±9.7 2.4±2.1 <0.0001

184
Post hoc analyses
CNFD: C vs T1DM (P<0.0001); C vs DSPN (P<0.0001); T1DM vs DSPN (P<0.0001).
CNBD: C vs T1DM (P=0.0008); C vs DSPN (P<0.0001); T1DM vs DSPN (P=0.02).
CNFL: C vs T1DM (P<0.0001); C vs DSPN (<0.0001); T1DM vs DSPN (P=0.001).
IENFD: C vs T1DM (P=0.02); C vs DSPN (P<0.0001); T1DM vs DSPN (P=0.001).
CST: C vs T1DM (NS); C vs DSPN (P<0.0001); T1DM vs DSPN (P=0.0007).
WST: C vs T1DM (NS); C vs DSPN (P<0.0001); T1DM vs DSPN (P=0.0004).
VPT: C vs T1DM (NS); C vs DSPN (P<0.0001); T1DM vs DSPN (P<0.0001).
SSNCV: C vs T1DM (P=0.0008); C vs DSPN (P<0.0001); T1DM vs DSPN (P<0.0001).
SNAmp: C vs T1DM (NS); C vs DSPN (P<0.0001); T1DM vs DSPN (P<0.0001).
PMNCV: C vs T1DM (P<0.0001); C vs DSPN (P<0.0001); T1DM vs DSPN (P<0.0001).
PMNAmp: C vs T1DM (NS); C vs DSPN (P<0.0001); T1DM vs DSPN (P<0.0001).
Table key
C – Controls; CNFD – Corneal Nerve Fibre Density; CNBD – Corneal Nerve Branch Density; CNFL
– Corneal Nerve Fibre Length; CST – Cold Sensation Threshold; IENFD – Intra Epidermal Nerve
Fibre Density; PMNAmp – Peroneal Motor Nerve Amplitude; PMNCV – Peroneal Motor Nerve
Conduction Velocity; SSNAmp – Sural Nerve Sensory Nerve Amplitude; SSNCV – Sural Motor
Nerve Conduction Velocity; VPT – Vibration Perception Threshold; WST – Warm Sensation
Threshold.

185
4.4.3.4 Correlates of CCM & IENFD (Table 4)
To explore the relationship of CCM parameters and IENFD with other diagnostic
modalities, Spearman’s rank correlations of these measures were undertaken and
are highlighted in table 4.4. The strongest correlation was between CNFD and
peroneal motor nerve conduction velocity (Rho= 0.60, P<0.0001). Other
neurophysiology measures correlated well with CNFD (peroneal motor nerve
amplitude: Rho= 0.52 P<0.0001, sural sensory nerve conduction velocity: Rho=
0.52 P<0.0001, sural sensory nerve amplitude: Rho= 0.48 P<0.0001). IENFD
correlated less well (peroneal motor nerve conduction velocity Rho= 0.56
P<0.0001, peroneal motor nerve amplitude: Rho= 0.45 P<0.0001, sural sensory
nerve conduction velocity: Rho= 0.45 P<0.0001, sural sensory nerve amplitude:
Rho= 0.50 P<0.0001). Only a low to moderate correlation (Rho=0.3-0.49) was
found between CCM parameters and IENFD (CNFD: Rho= 0.33 P=0.001, CNBD:
Rho= 0.33 P=0.003, CNFD: Rho= 0.32 P=0.002). However, both signs (NDS) and
in particular symptoms (NSP and McGill VAS) correlated better with CNFD and
IENFD.

186
Table 4-4 Spearman’s rank correlation of CNFD, CNBD, CNFL and IENFD versus NDS, McGill
VAS, NSP, IENFD, thermal thresholds, VPT and nerve conduction studies
CNFD CNBD CNFL IENFD
NDS (-/10) Rho= -0.45
P<0.0001
Rho= -0.27
P=0.01
Rho= -0.34
P=0.001
Rho= -0.47
P<0.0001
McGill VAS
(-/10cm)
Rho= -0.43
P<0.0001
Rho= -0.34
P=0.002
Rho= -0.43
P<0.0001
Rho= -0.45
P<0.0001
NSP (-/38) Rho= -0.51
P<0.0001
Rho= -0.28
P=0.009
Rho= -0.39
P=0.0002
Rho= -0.51
P<0.0001
IENFD (no/mm) Rho= 0.33
P=0.001
Rho= 0.31
P=0.003
Rho= 0.32
P=0.002
CST (˚C) Rho= 0.37
P=0.0005
Rho= 0.23
P=0.04
Rho= 0.26
P=0.02
Rho= 0.33
P=0.002
WST(˚C) Rho= -0.39
P=0.0003
Rho= -0.35
P=0.0009
Rho= -0.33
P=0.002
Rho= -0.52
P<0.0001
VPT (volts) Rho= -0.49
P<0.0001
Rho= -0.31
P=0.004
Rho= -0.37
P=0.0004
Rho= -0.47
P<0.0001
SSNCV (m/s) Rho= 0.52
P<0.0001
Rho= 0.40
P=0.0002
Rho= 0.43
P<0.0001
Rho= 0.45
P<0.0001
SSNAmp (µV) Rho= 0.48
P<0.0001
Rho= 0.28
P=0.01
Rho= 0.34
P=0.002
Rho= 0.50
P<0.0001
PMNCV (m/s)
Rho= 0.60
P<0.0001
Rho= 0.46
P<0.0001
Rho= 0.54
P<0.0001
Rho= 0.46
P<0.0001
PMNAmp (mV) Rho= 0.52
P<0.0001
Rho= 0.40
P=0.0002
Rho= 0.52
P<0.0001
Rho= 0.45
P<0.0001
The strongest correlations are for CCM parameters and IENFD are highlighted in bold.

187
Table key
CNFD – Corneal Nerve Fibre Density; CNBD – Corneal Nerve Branch Density; CNFL – Corneal
Nerve Fibre Length; CST – Cold Sensation Threshold; IENFD – Intra Epidermal Nerve Fibre
Density; PMNAmp – Peroneal Motor Nerve Amplitude; PMNCV – Peroneal Motor Nerve
Conduction Velocity; SSNAmp – Sural Nerve Sensory Nerve Amplitude; SMNCV – Sural Motor
Nerve Conduction Velocity; VPT – Vibration Perception Threshold; WST – Warm Sensation
Threshold.
4.4.3.5 Receiver-Operating Characteristic (ROC) analysis (Table 4.5, Figure
4.3)
To assess the diagnostic ability of small and large fibre tests including optimal cut
offs, sensitivity and specificity ROC analysis was undertaken for all measures of
neuropathy. As the delineation of T1DM from DSPN was based on the nerve
conduction studies (Toronto criteria for definite diabetic neuropathy (3)) we have
used the ROC analysis for peroneal motor nerve conduction velocity as the
referent value for Wilcoxon estimate of area under ROC curve = 0.98 (95% CI:
0.49 – 1), sensitivity = 0.94 (95% CI: 0.79 - 0.99) and specificity = 1 (95% CI: 0.88
– 1). The Wilcoxon estimate of area under the ROC curve was greatest for VPT at
0.85 with an optimal cut off of 13 volts, sensitivity of 0.67, specificity of 1, PPV of
1.0 and NPV 0.75. The small fibre test with the greatest Wilcoxon estimate of area
under the ROC curve was CNFD at 0.81 (Figure 4.3), which was superior to IENFD
(Figure 4.3). The PPV and NPV for CNFD were 0.8 and 0.77 respectively for a cut
off of 25 fibres/mm. IENFD had a lower Wilcoxon estimate of area under the ROC
curve at 0.73, which was similar to CNFL (0.74), CST (0.76) and WST (0.74). The
PPV and NPV were also lower for IENFD at 0.76 and 0.67 respectively for a cut off
of 4.5 fibres/mm.

188
Table 4-5 ROC analysis with area under the curve, optimal cut off and respective sensitivity
and specificity with 95% confidence interval in T1DM versus DSPN for CNFD, CNBD, CNFL,
IENFD, VPT, CST and WST
Optimal Cut off AUC
(95% CI)
Sensitivity
(95% CI)
Specificity
(95% CI)
CNFD (no/mm2)
25.0
0.81
(0.47 – 1.0)
0.77
(0.59 - 0.90)
0.79
(0.60 - 0.92)
CNBD (no/mm2) 36.5
0.67
(0.45 - 0.90)
0.58
(0.39 - 0.75)
0.79
(0.60 - 0.92)
CNFL (mm/mm2) 16.8
0.74
(0.46 – 1.0)
0.61
(0.42 - 0.78)
0.86
(0.68 -0.96)
IENFD (no/mm) 4.5 0.73
(0.46 - 1.0)
0.61
(0.42 - 0.78)
0.80
(0.61 - 0.92)
VPT (Volts) 13 0.85
(0.74 - 0.95)
0.67
(0.47 - 0.83)
1
(0.88 – 1)
CST (˚C) 24.7 0.76
(0.46 – 1.0)
0.57
(0.37 - 0.76)
0.89
(0.72 - 0.98)
WST (˚C) 38
0.74
(0.61 - 0.88)
0.86
(0.67 - 0.96)
0.64
(0.44 - 0.81)
Table key
CNFD – Corneal Nerve Fibre Density; CNBD – Corneal Nerve Branch Density; CNFL – Corneal
Nerve Fibre Length; CST – Cold Sensation Threshold; IENFD – Intra Epidermal Nerve Fibre
Density; VPT – Vibration Perception Threshold; WST – Warm Sensation Threshold.
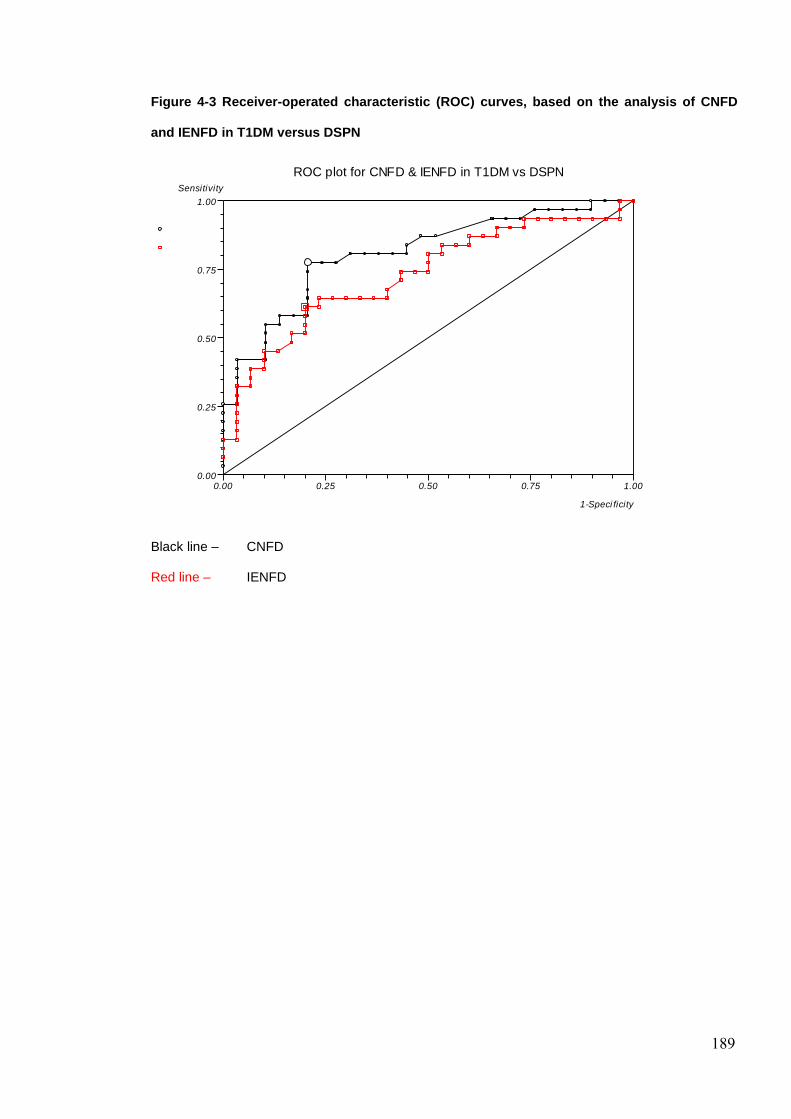
189
Figure 4-3 Receiver-operated characteristic (ROC) curves, based on the analysis of CNFD
and IENFD in T1DM versus DSPN
Black line – CNFD
Red line – IENFD
ROC plot for CNFD & IENFD in T1DM vs DSPN
0.00 0.25 0.50 0.75 1.000.00
0.25
0.50
0.75
1.00
Sensitivity
1-Speci ficity

190
4.5 DISCUSSION
There is a need for surrogate end points of diabetic neuropathy, which accurately
detect early disease, quantify disease progression and measure therapeutic
response (29). The current ‘gold’ standard for the diagnosis of neuropathy is
neurophysiology, a robust measure that also predicts foot ulceration and mortality
in diabetes (30). Other measures of neuropathy such as neurological assessment
are poorly reproducible (2), QST is subjective and more accurate measures such
as skin and nerve biopsy are invasive and require specialist analysis (3) . Small
fibre neuropathy has direct pathophysiological relevance to the main outcomes of
pain and foot ulceration (7) and therefore skin biopsy assessment of IENF has
been proposed as a valid measure of diabetic neuropathy (8). Whilst skin biopsy
detects early small nerve fibre damage even when electrophysiology and QST are
still normal (4-5), the use of this test in clinical trials is limited by its invasive nature.
CCM is a novel, rapid and readily reiterative technique, which quantifies small
nerve fibres non-invasively and shows promise (17-18; 31-34). The major findings
of this study which address major questions in relation to the diagnostic ability of
different small fibre tests in diabetic neuropathy are: 1) early subclinical small nerve
fibre decline can be detected by CCM and IENFD; 2) CNFD has higher diagnostic
utility than IENFD in the diagnosis of DPN; 3) CNFD correlates better with nerve
conduction studies than IENFD.
Early intervention with improved glycaemic control in type 1 DM can lead to a
durable reduction in DPN (35-36). Furthermore, the need for early evaluation of
subclinical small fibre neuropathy has been demonstrated by Smith et al (6) where
lifestyle intervention with diet and exercise in a pre-diabetic neuropathy group lead
to cutaneous re-innervation and improved pain. Previous studies have employed

191
ROC curve analysis of IENFD at the distal leg and shown a specificity of 95%-97%
and sensitivity of 45%- 80% (15; 37) for small fibre neuropathy but these studies
were not specifically in patients with DPN. Recently Nebuchennykh et al (13) in a
study of patients with polyneuropathy from varying causes showed a sensitivity of
35% and specificity of 95% using a cut off point of 6.7 fibres/mm for IENFD. In
another study by Vlckova-Moravcova et al (12), the diagnostic sensitivity for
detecting neuropathy was 80% and the specificity was 82% with an optimal IENFD
cut off point of ≤8.8 fibres/mm. Although, ROC curve analysis is a standard and
appropriate method for establishing diagnostic validity these studies were flawed
as they assessed a disease group against a healthy control population and thus
sensitivities and specificities will be inappropriately high and the delineation of the
optimal cut off points inaccurate. The need to identify DPN in diabetic subjects
should mean that optimal cut off points for neuropathy should be based on data
from a population with diabetes with and without neuropathy rather than a healthy
control population versus DPN. Therefore we have performed the present study in
a population of diabetic patients with and without neuropathy using the robust
Toronto criteria and utilised a best fit ROC curve analysis (38-39) to derive optimal
cut off points, sensitivities, and specificities to assess the diagnostic validity of
CCM measures and IENFD. ROC curve analysis in this study showed that IENFD
had a sensitivity of 61% and specificity of 80% at an optimal cut off point of 4.5
fibres/mm. These diagnostic validity measures are clearly lower than in the current
published literature (12-14), but we believe are more representative. Using exactly
the same population and methods we show that CNFD has a better sensitivity of
77% and an almost identical specificity of 79% at an optimal cut off point of 25.0
fibres/mm.

192
Previous studies of IENFD have found either absent or weak correlations with
nerve conduction studies (12) and sural nerve action potentials (15; 40-41). In the
present study CNFD showed a superior correlation than IENFD with peroneal
motor nerve conduction velocity and amplitude and sural sensory nerve conduction
velocity. These data support the study of Shun et al (14) which showed a
significant correlation between IENFD with sural nerve action potential and warm
sensation threshold. Thermal thresholds continue to an important psychophysical
test in evaluating small nerve fibres and our data show that the strongest
correlation was indeed between IENFD and WST. For DPN, thermal thresholds
have previously shown a sensitivity which ranges from 36%-85% (6; 42-43).
Sensitivities reported in our study are 57% and 86% respectively for CST and
WST. Furthermore, we have shown negative correlations of WST with CCM
measures and IENFD confirming a previous study (42). Interestingly CNBD, CNFD
and CNFL correlated with IENFD but the association was a low one (Spearman’s
Rho 0.33, 0.31 and 0.32 respectively). Although both CCM and skin biopsy
measure small nerve fibres, the sites of assessment are anatomically distinct.
There are no reported significant variations of IENFD calculated in adjacent
sections from the same biopsy or in adjacent biopsies from the same site (15).
However, even with IENFD differences in mean values exist between differing sites
on the lower limb (15; 44) although no direct correlations were assessed between
sites. Although DPN is considered a length dependent neuropathy, recent studies
suggest that lesions may occur in a proximal (45) multifocal fascicular pattern (46).
IENFD correlates somewhat better with NDS, McGill VAS and NSP than CNFD.
Clinical measures of neuropathy in part directly assess distal symptoms which
would be in keeping with distal measures such as IENFD. We suggest that CCM
193
measures are similar to IENFD despite assessing a distinct clinical site than
typically assessed through clinical measures of diabetic neuropathy. VPT had the
greatest AUC and specificity but this reflects the method of delineation of
neuropathy through the Toronto criteria which uses electrophysiology with signs
and/or symptoms. Both VPT and electrophysiology are large fibre measures and
therefore the ability of VPT as a diagnostic measure for diabetic neuropathy to be
high particularly as the groups were divided based on electrophysiology. However,
CNFD was still superior to IENFD despite the delineation of the groups with a large
fibre test.
The current study provides the first direct comparison between IENFD and CCM in
the assessment DPN. Both CNFD and IENFD correlated with clinical signs (NDS),
and symptoms (McGill VAS and NSP). Furthermore, CNFD had better diagnostic
utility for DPN through ROC curve analyses and correlated better with
electrophysiology than the current ‘gold’ standard of IENFD.

194
4.6 REFERENCES
1. Boulton AJ, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, Malik RA,
Maser RE, Sosenko JM, Ziegler D: Diabetic neuropathies: a statement by the
American Diabetes Association. Diabetes Care 2005;28:956-962
2. Dyck PJ, Overland CJ, Low PA, Litchy WJ, Davies JL, O'Brien PC, Albers JW,
Andersen H, Bolton CF, England JD, Klein CJ, Llewelyn JG, Mauermann ML,
Russell JW, Singer W, Smith AG, Tesfaye S, Vella A: Signs and symptoms versus
nerve conduction studies to diagnose diabetic sensorimotor polyneuropathy: Cl vs.
NPhys trial. Muscle Nerve 2010;42:157-164
3. Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, Lauria G,
Malik RA, Spallone V, Vinik A, Bernardi L, Valensi P: Diabetic neuropathies:
update on definitions, diagnostic criteria, estimation of severity, and treatments.
Diabetes Care 2010;33:2285-2293
4. Sumner CJ, Sheth S, Griffin JW, Cornblath DR, Polydefkis M: The spectrum of
neuropathy in diabetes and impaired glucose tolerance. Neurology 2003;60:108-
111
5. Singleton JR, Smith AG, Bromberg MB: Increased Prevalence of Impaired
Glucose Tolerance in Patients With Painful Sensory Neuropathy. Diabetes Care
2001;24:1448-1453
6. Smith AG, Russell J, Feldman EL, Goldstein J, Peltier A, Smith S, Hamwi J,
Pollari D, Bixby B, Howard J, Singleton JR: Lifestyle Intervention for Pre-Diabetic
Neuropathy. Diabetes Care 2006;29:1294-1299
7. Malik R, Veves A, Tesfaye S, Smith G, Cameron N, Zochodne D, Lauria G:
Small Fibre Neuropathy: Role in the diagnosis of Diabetic Sensorimotor
195
Polyneuropathy. Diabetes/Metabolism Research and Reviews 2011; 2011;27:678-
684
8. Lauria G, Cornblath DR, Johansson O, McArthur JC, Mellgren SI, Nolano M,
Rosenberg N, Sommer C: EFNS guidelines on the use of skin biopsy in the
diagnosis of peripheral neuropathy. Eur J Neurol 2005;12:747-758
9. Lauria G, Lombardi R: Small fibre neuropathy: is skin biopsy the holy grail?
Current diabetes reports 2012;12:384-392
10. Lauria G, Devigili G: Skin biopsy as a diagnostic tool in peripheral neuropathy.
Nat Clin Pract Neuro 2007;3:546-557
11. Devigili G, Tugnoli V, Penza P, Camozzi F, Lombardi R, Melli G, Broglio L,
Granieri E, Lauria G: The diagnostic criteria for small fibre neuropathy: from
symptoms to neuropathology. Brain 2008;131:1912-1925
12. Vlckova-Moravcova E, Bednarik J, Dusek L, Toyka KV, Sommer C: Diagnostic
validity of epidermal nerve fibre densities in painful sensory neuropathies. Muscle
Nerve 2008;37:50-60
13. Nebuchennykh M, Loseth S, Lindal S, Mellgren SI: The value of skin biopsy
with recording of intraepidermal nerve fibre density and quantitative sensory testing
in the assessment of small fibre involvement in patients with different causes of
polyneuropathy. J Neurol 2009;256:1067-1075
14. Shun CT, Chang YC, Wu HP, Hsieh SC, Lin WM, Lin YH, Tai TY, Hsieh ST:
Skin denervation in type 2 diabetes: correlations with diabetic duration and
functional impairments. Brain 2004;127:1593-1605
15. McArthur JC, Stocks EA, Hauer P, Cornblath DR, Griffin JW: Epidermal nerve
fibre density: normative reference range and diagnostic efficiency. Arch Neurol
1998;55:1513-1520

196
16. Hoeijmakers JG, Faber CG, Lauria G, Merkies IS, Waxman SG: Small-fibre
neuropathies--advances in diagnosis, pathophysiology and management. Nature
reviews Neurology 2012;8:369-379
17. Tavakoli M, Kallinikos P, Iqbal A, Herbert A, Fadavi H, Efron N, Boulton AJ, R
AM: Corneal confocal microscopy detects improvement in corneal nerve
morphology with an improvement in risk factors for diabetic neuropathy. Diabet
Med 2011;28:1261-1267
18. Tavakoli M, Mitu-Pretorian M, Petropoulos IN, Fadavi H, Asghar O, Alam U,
Ponirakis G, Jeziorska M, Marshall A, Efron N, Boulton AJ, Augustine T, Malik RA:
Corneal confocal microscopy detects early nerve regeneration in diabetic
neuropathy after simultaneous pancreas and kidney transplantation. Diabetes
2013;62:254-260
19. Tavakoli M, Kallinikos PA, Efron N, Boulton AJ, Malik RA: Corneal sensitivity is
reduced and relates to the severity of neuropathy in patients with diabetes.
Diabetes Care 2007;30:1895-1897
20. Petropoulos IN, Alam U, Fadavi H, Asghar O, Green P, Ponirakis G, Marshall
A, Boulton AJ, Tavakoli M, Malik RA: Corneal Nerve Loss Detected With Corneal
Confocal Microscopy Is Symmetrical and Related to the Severity of Diabetic
Polyneuropathy. Diabetes Care 2013; [Epub ahead of print]
21. Petropoulos IN, Manzoor T, Morgan P, Fadavi H, Asghar O, Alam U, Ponirakis
G, Dabbah MA, Chen X, Graham J, Tavakoli M, Malik RA: Repeatability of in vivo
corneal confocal microscopy to quantify corneal nerve morphology. Cornea
2013;32:e83-89
22. Sivaskandarajah GA, Halpern EM, Lovblom LE, Weisman A, Orlov S, Bril V,
Perkins BA: Structure-function relationship between corneal nerves and

197
conventional small-fibre tests in type 1 diabetes. Diabetes Care 2013;36:2748-
2755
23. Young M, Boulton A, Macleod A, Williams D, Sonksen P: A multicentre study of
the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital
clinic population. Diabetologia 1993;36:150-154
24. Bravenboer B, van Dam PS, Hop J, vd Steenhoven J, Erkelens DW: Thermal
threshold testing for the assessment of small fibre dysfunction: normal values and
reproducibility. Diabet Med 1992;9:546-549
25. Petropoulos IN, Manzoor T, Morgan P, Fadavi H, Asghar O, Alam U, Ponirakis
G, Dabbah MA, Chen X, Graham J, Tavakoli M, Malik RA: Repeatability of in vivo
corneal confocal microscopy to quantify corneal nerve morphology. Cornea
32:e83-89
26. Tavakoli M, Malik RA: Corneal confocal microscopy: a novel non-invasive
technique to quantify small fibre pathology in peripheral neuropathies. J Vis Exp
2011; 3(47):2194. doi: 10.3791/2194
27. Kallinikos P, Berhanu M, O'Donnell C, Boulton AJ, Efron N, Malik RA: Corneal
nerve tortuosity in diabetic patients with neuropathy. Invest Ophthalmol Vis Sci
2004;45:418-422
28. Lauria G, Bakkers M, Schmitz C, Lombardi R, Penza P, Devigili G, Smith AG,
Hsieh ST, Mellgren SI, Umapathi T, Ziegler D, Faber CG, Merkies IS:
Intraepidermal nerve fibre density at the distal leg: a worldwide normative
reference study. J Peripher Nerv Syst 2010;15:202-207
29. Dyck PJ, Norell JE, Tritschler H, Schuette K, Samigullin R, Ziegler D, Bastyr
EJ, 3rd, Litchy WJ, O'Brien PC: Challenges in design of multicenter trials: end

198
points assessed longitudinally for change and monotonicity. Diabetes Care
2007;30:2619-2625
30. Carrington AL, Shaw JE, Van Schie CHM, Abbott CA, Vileikyte L, Boulton AJM:
Can Motor Nerve Conduction Velocity Predict Foot Problems in Diabetic Subjects
Over a 6-Year Outcome Period? Diabetes Care 2002;25:2010-2015
31. Hossain P, Sachdev A, Malik RA: Early detection of diabetic peripheral
neuropathy with corneal confocal microscopy. Lancet 2005;366:1340-1343
32. Malik RA, Kallinikos P, Abbott CA, van Schie CH, Morgan P, Efron N, Boulton
AJ: Corneal confocal microscopy: a non-invasive surrogate of nerve fibre damage
and repair in diabetic patients. Diabetologia 2003;46:683-688
33. Mehra S, Tavakoli M, Kallinikos PA, Efron N, Boulton AJ, Augustine T, Malik
RA: Corneal confocal microscopy detects early nerve regeneration after pancreas
transplantation in patients with type 1 diabetes. Diabetes Care 2007;30:2608-2612
34. Quattrini C, Tavakoli M, Jeziorska M, Kallinikos P, Tesfaye S, Finnigan J,
Marshall A, Boulton AJ, Efron N, Malik RA: Surrogate markers of small fibre
damage in human diabetic neuropathy. Diabetes 2007;56:2148-2154
35. Pop-Busui R, Low PA, Waberski BH, Martin CL, Albers JW, Feldman EL,
Sommer C, Cleary PA, Lachin JM, Herman WH: Effects of prior intensive insulin
therapy on cardiac autonomic nervous system function in type 1 diabetes mellitus:
the Diabetes Control and Complications Trial/Epidemiology of Diabetes
Interventions and Complications study (DCCT/EDIC). Circulation 2009;119:2886-
2893
36. Pop-Busui R, Herman WH, Feldman EL, Low PA, Martin CL, Cleary PA,
Waberski BH, Lachin JM, Albers JW: DCCT and EDIC studies in type 1 diabetes:
199
lessons for diabetic neuropathy regarding metabolic memory and natural history.
Curr Diab Rep 2010;10:276-282
37. Chien HF, Tseng TJ, Lin WM, Yang CC, Chang YC, Chen RC, Hsieh ST:
Quantitative pathology of cutaneous nerve terminal degeneration in the human
skin. Acta Neuropathol 2001;102:455-461
38. Hanley JA: The robustness of the "binormal" assumptions used in fitting ROC
curves. Med Decis Making 1988;8:197-203
39. Hajian-Tilaki KO, Hanley JA, Joseph L, Collet JP: A comparison of parametric
and nonparametric approaches to ROC analysis of quantitative diagnostic tests.
Med Decis Making 1997;17:94-102
40. Loseth S, Lindal S, Stalberg E, Mellgren SI: Intraepidermal nerve fibre density,
quantitative sensory testing and nerve conduction studies in a patient material with
symptoms and signs of sensory polyneuropathy. Eur J Neurol 2006;13:105-111
41. Smith AG, Ramachandran P, Tripp S, Singleton JR: Epidermal nerve
innervation in impaired glucose tolerance and diabetes-associated neuropathy.
Neurology 2001;57:1701-1704
42. Scherens A, Maier C, Haussleiter IS, Schwenkreis P, Vlckova-Moravcova E,
Baron R, Sommer C: Painful or painless lower limb dysesthesias are highly
predictive of peripheral neuropathy: comparison of different diagnostic modalities.
Eur J Pain 2009;13:711-718
43. Tobin K, Giuliani MJ, Lacomis D: Comparison of different modalities for
detection of small fibre neuropathy. Clin Neurophysiol 1999;110:1909-1912
44. Umapathi T, Tan WL, Tan NC, Chan YH: Determinants of epidermal nerve fibre
density in normal individuals. Muscle Nerve 2006;33:742-746
200
45. Spectrum of High-Resolution MRI Findings in Diabetic Neuropathy. American
Journal of Roentgenology 2012;199:407-412
46. Pham M, Oikonomou D, Baumer P, Bierhaus A, Heiland S, Humpert PM,
Nawroth PP, Bendszus M: Proximal neuropathic lesions in distal symmetric
diabetic polyneuropathy: findings of high-resolution magnetic resonance
neurography. Diabetes Care 2011;34:721-723

201
5 Chapter V - Enhanced Small Fibre Neuropathy in
Patients with Latent Autoimmune Diabetes in Adults
Contribution: Uazman Alam contributed to the conception and design of the study
and made a major contribution to the recruitment of subjects, clinical tests including
neuropathy assessments and skin biopsies, skin biopsy analyses, all statistical
analyses and writing of this chapter.
To be submitted for publication
Uazman Alam, Maria Jeziorska, Ioannis N Petropoulos, Omar Asghar, Hassan
Fadavi, Georgios Ponirakis, Andrew Marshall, Mitra Tavakoli, Andrew JM Boulton,
Nathan Efron, Rayaz A Malik
202
5.1 ABSTRACT
Latent Autoimmune Diabetes in Adults (LADA) is often misdiagnosed and patients
have relatively poorer glycaemic control with a potential for an increased risk of
neuropathy. Surprisingly, few studies have been undertaken in these patients in
relation to the prevalence of neuropathy.
Subjects with LADA (LADA) (n=19), type 2 DM (T2DM) (n=22) and non-diabetic
healthy control subjects (C) (n=33) underwent detailed assessment of neurologic
deficits, quantitative sensory testing (QST), electrophysiology, skin biopsy and
corneal confocal microscopy (CCM).
There was no significant difference for age, duration of diabetes, lipids and blood
pressure, but HbA1c was higher (P<0.0001) and the BMI was lower (P=0.008) in
patients with LADA compared with T2DM. There was no significant difference in
the neuropathy disability score (NDS), vibration perception threshold (VPT) or
electrophysiology between LADA and T2DM. However, cold sensation threshold
(CST) (P=0.008), and warm sensation threshold (WST) (P=0.008), were
significantly higher and intra-epidermal nerve fibre density (IENFD) (P=0.02),
corneal nerve fibre density (CNFD) (P=0.03), corneal nerve fibre length (CNFL),
(P=0.02), and corneal nerve branch density (CNBD) (P=0.003) were significantly
lower in LADA compared to T2DM.
Despite, comparable age, duration of diabetes and cardiovascular risk factors,
subjects with LADA have a significant small fibre neuropathy compared to matched
patients with T2DM.

203
5.2 INTRODUCTION
LADA is often misdiagnosed as type 2 diabetes mellitus (DM), but
pathophysiologically is more closely related to type 1 DM. (1). Hence, these
patients present at a younger age due to a slow autoimmune destruction of
pancreatic β-cells (2-5). The prevalence of LADA in patients with type 2 DM
(T2DM) ranges from a minimum of 4% (6-7) to 10% as shown in the UKPDS (3).
Thus patients with LADA represent a significant proportion of patients with a faster
decline in C-peptide (6) and delayed treatment with insulin resulting in a significant
period of poor glycaemic control (8). Given, that early and optimal treatment of
glycaemia reduces the incidence of neuropathy in Type 1 DM as shown by the
DCCT and EDIC studies (9-10) then patients with LADA with poorer glycaemic
control may well have an increased risk of developing the long term complications
(11-12).
However, the long term complications in patients with LADA, in particular diabetic
somatic polyneuropathy (DSPN) have been poorly studied. Hence, surprisingly
individuals with LADA had a lower prevalence of diabetic neuropathy assessed
using electrophysiology, quantitative sensory testing and autonomic function,
despite having a HbA1c which was 1.1% (~12mmol/mol) higher when compared to
patients with T2DM (13). Yet in another study the prevalence of neuropathy
defined using the Michigan Neuropathy screening instrument was higher in the
LADA group (~38%) when compared to T2DM (~30%) (14). Whilst there was no
difference for neuropathy in LADA compared to Type 2 DM when assessed using
the Neuropathy Disability score (NDS) and Vibration Perception Threshold (VPT)
(15). These data reflect no clear consensus on the prevalence of DSPN in patients
with LADA and raise the important issue of the sensitivity of different tests to

204
diagnose diabetic neuropathy. Intra-epidermal nerve fibre density (IENFD) is
significantly reduced in patients with normal electrophysiology suggesting early
damage to small nerve fibres (16). Similarly, corneal confocal microscopy (CCM) is
a non-invasive technique that can detect early small sensory nerve fibre loss (17)
and repair on normalisation of glycaemia after pancreas transplantation in Type 1
diabetes (18). Therefore the assessment of small fibres may be the most sensitive
means to detect early neuropathy in diabetes (19).
We have undertaken a comprehensive study phenotyping diabetic neuropathy in
subjects with LADA to identify large and small fibre neuropathy compared to
matched patients with Type 2 DM.
205
5.3 RSEARCH DESIGN AND METHODS
5.3.1 Selection of patients
19 subjects with LADA, 22 subjects with T2DM and 33 age and sex matched non-
diabetic control subjects were studied. Subjects with a history of neurologic
conditions, ocular trauma or previous ocular surgery were excluded. The study was
approved by the North West and Salford and Trafford Research Ethics committee,
and written informed consent was obtained according to the Declaration of
Helsinki.
5.3.2 LADA definition
LADA was defined as follows: age of onset less than 50 years, anti-glutamic
decarboxylase (GAD) antibodies (GAD-Ab) positivity, exclusion of patients with
ketonuria/diabetic ketoacidosis at diagnosis and a lack of insulin treatment within
the first six months after diagnosis of diabetes mellitus, suggesting type 1 DM (1).
All subjects with LADA had elevated positive GAD-Ab titres which were consistent
with autoimmune diabetes. All subjects with T2DM had a clinical LADA screening
score of 0 or 1 and thus low risk of autoimmune diabetes as defined in the study by
Fourlanos et al (20).
5.3.3 Assessment of neuropathy
All patients and control subjects underwent a detailed evaluation of neurologic
symptoms according to the neuropathy symptom profile (NSP), and the McGill
visual analogue score (McGill VAS) VAS was used to assess the severity of painful
neuropathy. Clinical neurologic deficits were assessed using the modified
neuropathy disability score, which includes evaluation of vibration, pin prick, and

206
temperature perception as well as the presence or absence of ankle reflexes to
establish the severity of neuropathy (21). Quantitative sensory testing (QST)
included an assessment of vibration perception threshold (VPT), measured using a
Neurothesiometer (Horwell, Scientific Laboratory Supplies, Wilford, Nottingham,
U.K.), cold sensation threshold (CST) (Aδ fibres) and warm sensation threshold
(WST) (22) (c fibres) thresholds using the method of limits with the MEDOC TSA II
(Medoc, Ramat Yishai, Israel) on the dorsum of the left foot. Electro-diagnostic
studies were undertaken using a Dantec “Keypoint” system (Dantec Dynamics,
Bristol, U.K.) equipped with a DISA temperature regulator to keep limb temperature
constantly between 32°C and 35°C. Peroneal motor and sural sensory nerves
were assessed in the right lower limb by a consultant neurophysiologist. The motor
study was performed using silver-silver chloride surface electrodes at standardized
sites defined by anatomical landmarks, and recordings for the sural nerve were
taken using antidromic stimulation over a distance of 100 mm.
5.3.4 Corneal Confocal Microscopy
Patients underwent examination with the Heidelberg retina tomography III in vivo
corneal confocal microscope employing our established methodology for image
acquisition (23). Several scans of the entire depth of the cornea were recorded by
turning the fine focus of the objective lens backward and forward for ~2 min using
the section mode, which enables manual acquisition and storage of single images
of all corneal layers. This provides en face two-dimensional images with a lateral
resolution of ~2 mm/pixel and final image size of 400 x 400 pixels of the subbasal
nerve plexus of the cornea from each patient and control subject. Each subbasal
nerve fibre bundle contains unmyelinated fibres, which run parallel to Bowman’s
207
layer before dividing and terminating as individual axons underneath the surface
epithelium. Five images per patient from the centre of the cornea were selected
and examined in a masked and randomized fashion (24). Four corneal nerve
parameters were quantified: 1) CNFD, the total number of major nerves per square
millimetre of corneal tissue (no.mm2); 2) CNBD, the number of branches
emanating from all major nerve trunks per square millimetre of corneal tissue
(no.mm2); 3) CNFL, the total length of all nerve fibres and branches (mm/mm2)
within the area of corneal tissue and 4) corneal nerve fibre tortuosity (CNFT), a
parameter mathematically derived from the images (25).
5.3.5 Skin biopsy and immunohistochemistry
A sub-cohort of participants (Controls n=19, T2DM n=12, and LADA n=9)
underwent a 3-mm punch skin biopsy from the dorsum of the foot; 2 cm above the
second metatarsal head after local anaesthesia (1% lidocaine). The biopsy site
was closed using Steristrips, and the specimen was immediately fixed in PBS-
buffered 4% paraformaldehyde. After 18–24 hours, it was rinsed in Tris-buffered
saline and soaked in 33% sucrose (2–4 hours) for cryoprotection. It was then
embedded in optimal cutting temperature–embedding compound, rapidly frozen in
liquid nitrogen, and cut into 50-μm sections using a cryostat (model OTF; Bright
Instruments, Huntington, U.K.). Four floating sections per subject underwent
melanin bleaching (0.25% KMnO4 for 15 min followed by 5% oxalic acid for 3 min),
a 4-h protein block with a Tris-buffered saline solution of 5% normal swine serum,
0.5% powdered milk, and 1% Triton X-100, and overnight incubation with 1:1,200
Biogenesis polyclonal rabbit anti-human PGP9.5 antibody (Serotec, Oxford, U.K.).
Biotinylated swine anti-rabbit secondary antibody (1:300; DakoCytomation, Ely,

208
U.K.) was then applied for 1 hour; sections were quenched with 1% H2O2 in 30%
MeOH-PBS (30 min) prior to a 1 hour incubation with 1:500 horseradish
peroxidase–streptavidin (Vector Laboratories, Peterborough, U.K.). Nerve fibres
were demonstrated using 3, 3-diaminobenzidine chromogen (Sigma-Aldrich,
Manchester, U.K.). Sections were mildly counterstained with eosin to better
localize the basement membrane to identify nerve fibres passing through it.
Negative control subjects consisted of replacing the anti- PGP9.5 antibody with
rabbit immunoglobulin (DakoCytomation) at a concentration matching that of the
primary antibody, which showed no immunostaining. IENFD, i.e., the number of
fibres passing through the dermo-epidermal junction per millimetre of basement
membrane was quantified in accord with established criteria and techniques and
expressed as number per millimetre (26).
5.3.6 Statistical analysis
Statistical analyses were undertaken on Statsdirect (Statsdirect, Cheshire, UK).
The data are expressed as Mean ± standard deviation (SD). ANOVA method or a
non-parametric counterpart, Kruskal-Wallis were used to assess differences
between groups depending on normality of the data. The Mann-Whitney U test was
used to compare T2DM with LADA for the duration of diabetes. Chi squared
analyses were used to assess frequencies of gender, ethnicity and aetiology of
diabetes. Overall the P value was maintained at 0.05 for multiple comparison tests
(Bonferoni adjustment or Conover-Inmann pairwise comparison).

209
5.4 RESULTS
5.4.1 Demographics and Clinical Neuropathy (Table 5.1)
The participant demographics and clinical neuropathy measurements in subjects
with diabetes and age-matched control subjects are summarized in Table 5.1.
There were no significant differences in age (C: 53.3±9.8 vs T2DM: 54.9±6.8 vs
LADA: 50.6±11.9 years, P=NS) and duration of diabetes (T2DM: 9.8±5.4 vs LADA:
11.4±10.2 years, P=NS). There were no differences between the groups in their
ethnic mix. The NDS was significantly greater in patients with T2DM (P=0.02) and
LADA (P=0.0003) compared to control subjects, consistent with a mild neuropathy,
but did not differ between T2DM and LADA. The NSP was significantly higher in
T2DM and LADA (P<0.0001 and P=0.0002 respectively) with no differences in the
McGill VAS compared to controls. There were no significant difference in the
degree of neuropathic pain in T2DM (Median (IQR) (0.5(0-4)) compared to LADA
(0(0-0) (P=NS).

210
Table 5-1 Participant demographics in Controls, T2DM and LADA
C
(n=20)
T2DM
(n=17)
LADA
(n=19)
T2DM v LADA
Age (years) 53.3±9.8 54.9±6.8 50.6±11.9 NS
Gender (Male)
(%) 65 76 58 NS
Ethnicity (White
European) (%) 60
59
58 NS
Duration of
Diabetes (years)
Median (IQR)
- 9.8±5.4 11.4±10.2 NS
NDS (-/10)
Median(IQR)
0.5±1.0
0(0-1)
2.1±1.9*
1(0-4)
3.9±3.6**
3(1-6) NS
NSP (-/38)
Median (IQR)
0.1±0.3
0(0-0)
4.5±5.6^
2(1-4)
4.4±6.0^^
2.5(0-6) NS
McGill VAS
(-/10cm)
Median (IQR)
0.6±1.8
0(0-0)
1.9±2.5
0.5(0-4)
0.5±1.2
0(0-0)
NS
Post hoc analyses
NDS *C vs T2DM – P=0.02; **C vs LADA– P=0.0003.
NSP ^C vs T2DM – P<0.0001; ^^C vs LADA – P=0.0002.
McGill VAS C vs T2DM – P=NS; C vs LADA – P=NS.
Table Key
IQR – Inter quartile Range; McGill VAS – McGill Visual Analogue Score; NDS – Neuropathy
Disability Score; NSP – Neuropathy Symptom Profile.
211
5.4.2 Metabolic and Anthropometric measurements (Table 5.2)
Metabolic and anthropometric measurements are detailed in Table 5.2. HbA1c was
significantly higher in subjects with LADA compared to T2DM and controls
(P<0.0001). BMI was significantly higher in T2DM subjects (P=0.001 and P=0.0005
respectively) compared to subjects with LADA and control subjects. The total
cholesterol was significantly lower (P<0.0001) in diabetic patients due to greater
statin use with no difference between the patients with T2DM and LADA. HDL was
significantly lower in T2DM compared to controls (P=0.002) and subjects with
LADA (P=0.03). There were no differences between blood pressure either systolic
or diastolic in any group. There were no differences in the estimated glomerular
filtration rate (eGFR) between diabetic subjects and controls.

212
Table 5-2 Clinical and metabolic parameters in control subjects and patients with T2DM and
LADA
C
(n=20)
T2DM
(n=17)
LADA
(n=19)
T2DM v LADA
P Value
HbA1c (%) 5.7±0.4 7.0±0.7* 9.8±2.3** <0.0001
HbA1c
(mmol/mol) 38.4±4.2 52.8±7.4* 83.4±24.7** <0.0001
BMI (kg/m2) 27.5±4.5 32.8±4.6ƒ
27.1±4.0 0.001
T-CHL (mmol/l) 5.5±0.7 4.1±1.3† 4.5±1.3†† NS
HDL (mmol/l) 1.6±0.4 1.1±0.4˚ 1.4±0.4 0.03
Triglycerides 1.5±0.6 2.0±1.3 1.6±1.2 NS
Systolic BP
(mmHg) 133±16 137±25 137±22 NS
Diastolic BP
(mmHg) 76±10 79±11 76±11 NS
eGFR
(ml/min/1.73) 80±9 79±16 82±13 NS
Post hoc analyses
HbA1c: *C vs T2DM – P<0.0001; **C vs LADA – P<0.0001.
BMI: ƒC vs T2DM – P=0.0005; C vs LADA – P=NS.
T-CHL: †C vs T2DM – P<0.0001; ††C vs LADA – P=0.003.
HDL: ˚C vs T2DM – P=0.002; C vs LADA – P=NS.
Table key
ACR – Albumin Creatinine Ratio; BMI – Body Mass Index; BP – Blood Pressure; estimated
Glomerular Filtration Rate; HbA1c – Glycated Haemoglobin A1c; HDL – High Density Lipoprotein
Cholesterol; T-CHL – Total Cholesterol.

213
5.4.3 Neuropathy evaluation (Table 5.3)
5.4.3.1 Electrophysiology
Peroneal motor nerve conduction velocity was significantly lower in T2DM
(P=0.004) and LADA (P=0.0001) compared with control subjects with no difference
between the T2DM and LADA groups. Peroneal motor nerve amplitude was
significantly lower inT2DM (P=0.01) and LADA (P=0.0o2) compared with control
subjects. Sural sensory nerve conduction velocity and amplitude were significantly
lower in LADA (P=0.01 and P=0.03 respectively) with no difference in T2DM
compared with control subjects with no difference between T2DM and LADA
groups. However, values for sural sensory and peroneal motor nerve conduction
velocities and amplitudes were within the normal reference range for T2DM and
LADA groups suggesting that there was minimal large fibre deficit.
5.4.3.2 Vibration Perception, Thermal Thresholds & Neuropad
VPT was significantly greater in T2DM (P=0.009) and LADA (P=0.004) compared
with control subjects with no difference between T2DM and LADA. CST was
significantly lower in T2DM (P=0.002) and LADA (P<0.0001) compared with control
subjects and was significantly lower in LADA (P=0.03) compared to T2DM. WST
was significantly greater in T2DM (P<0.0001) and LADA (P<0.0001) compared
with control subjects and was significantly greater in LADA (P=0.02) compared to
T2DM. There were no differences between controls, T2DM and LADA in the
neuropad assessment.
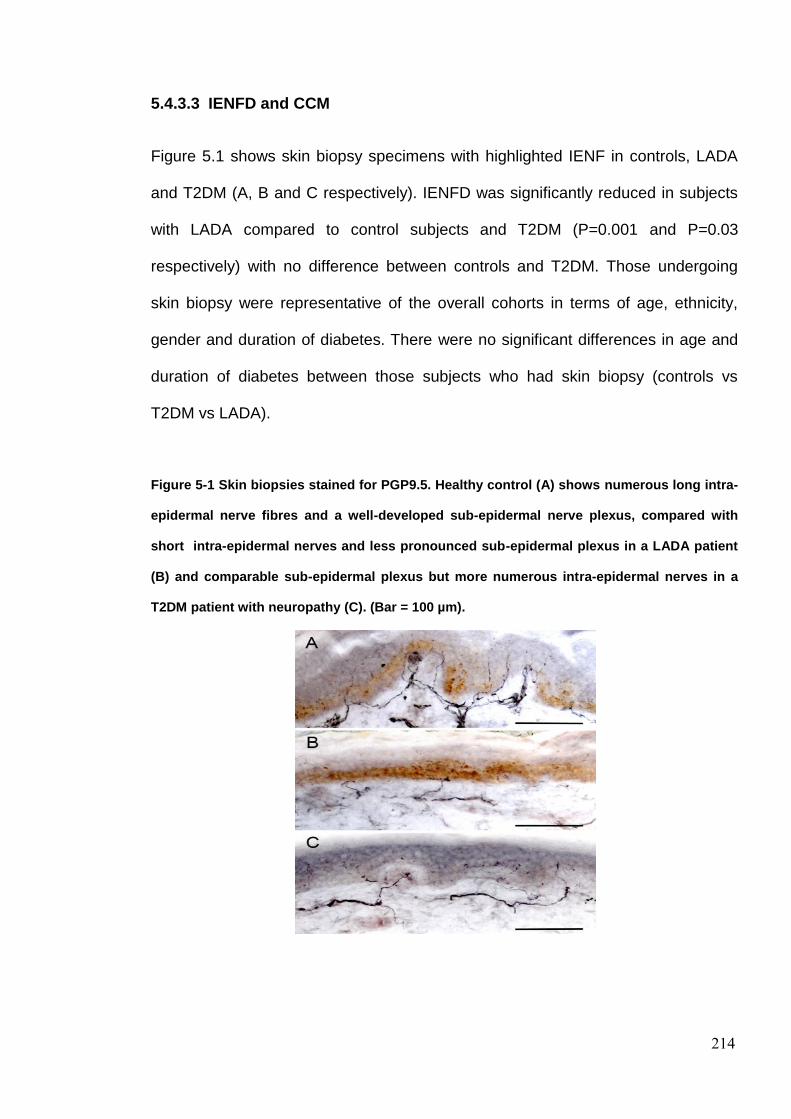
214
5.4.3.3 IENFD and CCM
Figure 5.1 shows skin biopsy specimens with highlighted IENF in controls, LADA
and T2DM (A, B and C respectively). IENFD was significantly reduced in subjects
with LADA compared to control subjects and T2DM (P=0.001 and P=0.03
respectively) with no difference between controls and T2DM. Those undergoing
skin biopsy were representative of the overall cohorts in terms of age, ethnicity,
gender and duration of diabetes. There were no significant differences in age and
duration of diabetes between those subjects who had skin biopsy (controls vs
T2DM vs LADA).
Figure 5-1 Skin biopsies stained for PGP9.5. Healthy control (A) shows numerous long intra-
epidermal nerve fibres and a well-developed sub-epidermal nerve plexus, compared with
short intra-epidermal nerves and less pronounced sub-epidermal plexus in a LADA patient
(B) and comparable sub-epidermal plexus but more numerous intra-epidermal nerves in a
T2DM patient with neuropathy (C). (Bar = 100 µm).
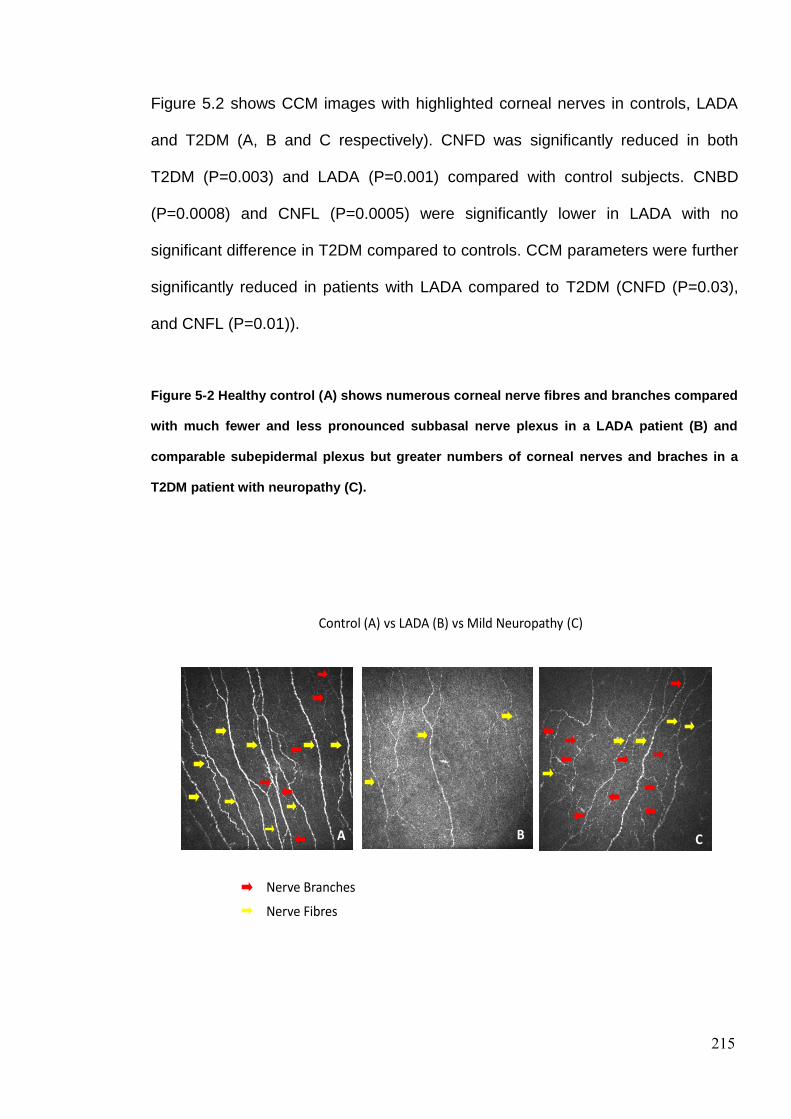
215
Figure 5.2 shows CCM images with highlighted corneal nerves in controls, LADA
and T2DM (A, B and C respectively). CNFD was significantly reduced in both
T2DM (P=0.003) and LADA (P=0.001) compared with control subjects. CNBD
(P=0.0008) and CNFL (P=0.0005) were significantly lower in LADA with no
significant difference in T2DM compared to controls. CCM parameters were further
significantly reduced in patients with LADA compared to T2DM (CNFD (P=0.03),
and CNFL (P=0.01)).
Figure 5-2 Healthy control (A) shows numerous corneal nerve fibres and branches compared
with much fewer and less pronounced subbasal nerve plexus in a LADA patient (B) and
comparable subepidermal plexus but greater numbers of corneal nerves and braches in a
T2DM patient with neuropathy (C).
Control (A) vs LADA (B) vs Mild Neuropathy (C)
BA C
Nerve Branches
Nerve Fibres
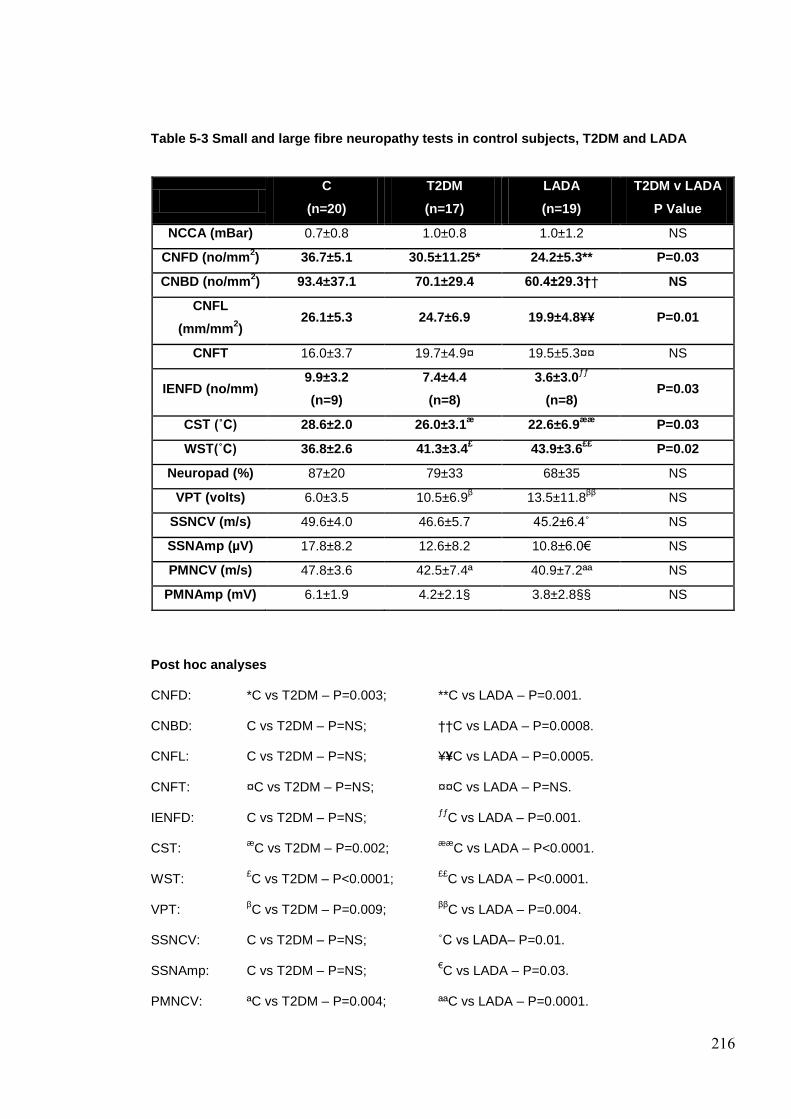
216
Table 5-3 Small and large fibre neuropathy tests in control subjects, T2DM and LADA
C
(n=20)
T2DM
(n=17)
LADA
(n=19)
T2DM v LADA
P Value
NCCA (mBar) 0.7±0.8 1.0±0.8 1.0±1.2 NS
CNFD (no/mm2) 36.7±5.1 30.5±11.25* 24.2±5.3** P=0.03
CNBD (no/mm2) 93.4±37.1 70.1±29.4 60.4±29.3†† NS
CNFL
(mm/mm2)
26.1±5.3 24.7±6.9 19.9±4.8¥¥ P=0.01
CNFT 16.0±3.7 19.7±4.9¤ 19.5±5.3¤¤ NS
IENFD (no/mm) 9.9±3.2
(n=9)
7.4±4.4
(n=8)
3.6±3.0ƒƒ
(n=8) P=0.03
CST (˚C) 28.6±2.0 26.0±3.1æ
22.6±6.9ææ
P=0.03
WST(˚C) 36.8±2.6 41.3±3.4£ 43.9±3.6
££ P=0.02
Neuropad (%) 87±20 79±33 68±35 NS
VPT (volts) 6.0±3.5 10.5±6.9β 13.5±11.8
ββ NS
SSNCV (m/s) 49.6±4.0 46.6±5.7 45.2±6.4˚ NS
SSNAmp (µV) 17.8±8.2 12.6±8.2 10.8±6.0€ NS
PMNCV (m/s) 47.8±3.6 42.5±7.4ª 40.9±7.2ªª NS
PMNAmp (mV) 6.1±1.9 4.2±2.1§ 3.8±2.8§§ NS
Post hoc analyses
CNFD: *C vs T2DM – P=0.003; **C vs LADA – P=0.001.
CNBD: C vs T2DM – P=NS; ††C vs LADA – P=0.0008.
CNFL: C vs T2DM – P=NS; ¥¥C vs LADA – P=0.0005.
CNFT: ¤C vs T2DM – P=NS; ¤¤C vs LADA – P=NS.
IENFD: C vs T2DM – P=NS; ƒƒ
C vs LADA – P=0.001.
CST: æ
C vs T2DM – P=0.002; ææ
C vs LADA – P<0.0001.
WST: £C vs T2DM – P<0.0001;
££C vs LADA – P<0.0001.
VPT: βC vs T2DM – P=0.009;
ββC vs LADA – P=0.004.
SSNCV: C vs T2DM – P=NS; ˚C vs LADA– P=0.01.
SSNAmp: C vs T2DM – P=NS; €C vs LADA – P=0.03.
PMNCV: ªC vs T2DM – P=0.004; ªªC vs LADA – P=0.0001.

217
PMNAmp: §C vs T2DM – P=0.01, §§C vs LADA – P=0.002.
Table Key
CNBD – Corneal Nerve Branch Density; CNFD – Corneal Nerve Fibre Density; CNFL – Corneal
Nerve Fibre Length; CNFT – Corneal Nerve Fibre Tortuosity; CST – Cold sensation Threshold;
IENFD – Intra Epidermal Nerve Fibre Density; NCCA- Non-Contact Corneal Aesthesiometry;
PMNAmp – Peroneal Motor Nerve Amplitude; PMNCV – Peroneal Motor Nerve Conduction
Velocity; SSNAmp – Sural Nerve Sensory Nerve Amplitude; SSNCV – Sural Sensory Nerve
Conduction Velocity; VPT – Vibration Perception Threshold; WST – Warm Sensation Threshold.

218
5.5 DISCUSSION
LADA is a slowly progressive form of autoimmune diabetes which is often
misclassified as type 2 diabetes and therefore results in a protracted period of
relatively poor glycaemic control due to a delay in the introduction of insulin (1).
Longitudinal studies in patients with LADA have found a relatively rapid decline in
insulin secretion in the first few years after diagnosis of diabetes (27-28). In a
recent study, individuals with LADA had worse glycaemic control than patients with
type 2 diabetes despite a longer time on insulin therapy (29). Two small studies
have shown beneficial effects on β-cell reserve of early insulin therapy in patients
with LADA (27; 30). Our LADA cohort also had a greater degree of hyperglycaemia
reflecting this late recognition and late introduction of insulin.
Given that poorer glycaemic control is associated with an increased risk for the
development of neuropathy in both type 1 (31-32) and type 2 diabetes (19; 33),
patients with LADA may therefore have a greater propensity for the development of
neuropathy (29). However, in subjects with LADA there are limited studies (13-15)
which have shown a varying severity of neuropathy (6; 13; 34). In a recent study
current perception thresholds and electrophysiology were found to be similar in
patients with LADA and type 1 and 2 diabetes (6). In the few other studies which
have been undertaken, the assessment of neuropathy was crude as symptoms
and clinical neurological deficits or vibration perception were assessed (14-15),
groups were not age matched. Given that small nerve fibre damage precedes large
fibre deficits (17; 35-37), and no direct assessment of small fibre function or
structure was undertaken (13; 15), neuropathy may not have been detected.
Thus in the present study we show that subjects with both T2DM and LADA have
an abnormal NDS, VPT and electrophysiology. However, patients with LADA have
219
comparable measures of large fibre neuropathy to subjects with T2DM. Cold and
warm thermal thresholds were increased, and both IENFD and corneal nerve
parameters were reduced in patients with T2DM and LADA. However, these small
fibre parameters were further significantly reduced in patients with LADA compared
to patients with T2DM. This relative more advanced pathology of small fibres may
explain the discrepant findings in previous studies where patients with LADA have
been shown to have either no abnormality or indeed mild comparable neuropathy
to patients with T2DM. However, despite less small fibre neuropathy in T2DM
compared to LADA there was no difference in levels of neuropathic pain as
demonstrated by the McGill VAS. In a previous community based study an excess
of pain was South Asian subjects with diabetes (38) although in our study, groups
were accurately matched for ethnicity.
Of potential pathogenetic relevance, GAD-Ab, which are used to diagnose LADA
have been linked to other neurological conditions such as stiff man syndrome (39),
however there has been no direct correlation of GAD-Ab status with
peripheral/autonomic neuropathy in diabetes mellitus (40-41).
In conclusion the present study shows a clear adverse consequence of LADA with
a greater degree of small fibre neuropathy compared to matched patients with
T2DM. This likely consequence is due to the poorer glycaemic control, as the other
major risk factors for neuropathy such as lipid profile were comparable and BMI
was in fact lower (32). Thus patients with LADA require assessment for small fibre
neuropathy, perhaps to enable risk stratification and earlier commencement of
insulin, limiting the progression of neuropathy. Our study also highlights the need
to undertake detailed assessment of small fibres using either skin biopsy or corneal
confocal microscopy to identify small fibre neuropathy.

220
5.6 REFERENCES
1. Fourlanos S, Dotta F, Greenbaum CJ, Palmer JP, Rolandsson O, Colman PG,
Harrison LC: Latent autoimmune diabetes in adults (LADA) should be less latent.
Diabetologia 2005;48:2206-2212
2. Tuomi T, Carlsson A, Li H, Isomaa B, Miettinen A, Nilsson A, Nissen M,
Ehrnstrom BO, Forsen B, Snickars B, Lahti K, Forsblom C, Saloranta C, Taskinen
MR, Groop LC: Clinical and genetic characteristics of type 2 diabetes with and
without GAD antibodies. Diabetes 1999;48:150-157
3. Turner R, Stratton I, Horton V, Manley S, Zimmet P, Mackay IR, Shattock M,
Bottazzo GF, Holman R: UKPDS 25: autoantibodies to islet-cell cytoplasm and
glutamic acid decarboxylase for prediction of insulin requirement in type 2
diabetes. UK Prospective Diabetes Study Group. Lancet 1997;350:1288-1293
4. Davis TM, Zimmet P, Davis WA, Bruce DG, Fida S, Mackay IR: Autoantibodies
to glutamic acid decarboxylase in diabetic patients from a multi-ethnic Australian
community: the Fremantle Diabetes Study. Diabet Med 2000;17:667-674
5. Romkens TE, Kusters GC, Netea MG, Netten PM: Prevalence and clinical
characteristics of insulin-treated, anti-GAD-positive, type 2 diabetic subjects in an
outpatient clinical department of a Dutch teaching hospital. Neth J Med
2006;64:114-118
6. Roh MO, Jung CH, Kim BY, Mok JO, Kim CH: The prevalence and
characteristics of latent autoimmune diabetes in adults (LADA) and its relation with
chronic complications in a clinical department of a university hospital in Korea. Acta
Diabetol 2013;50:129-134
7. Thunander M, Thorgeirsson H, Torn C, Petersson C, Landin-Olsson M: beta-cell
function and metabolic control in latent autoimmune diabetes in adults with early
221
insulin versus conventional treatment: a 3-year follow-up. Eur J Endocrinol
2011;164:239-245
8. Thunander M, Thorgeirsson H, Törn C, Petersson C, Landin-Olsson M: β-cell
function and metabolic control in latent autoimmune diabetes in adults with early
insulin versus conventional treatment: a 3-year follow-up. European Journal of
Endocrinology 2011;164:239-245
9. The effect of intensive diabetes therapy on the development and progression of
neuropathy. The Diabetes Control and Complications Trial Research Group. Ann
Intern Med 1995;122:561-568
10. Pop-Busui R, Herman WH, Feldman EL, Low PA, Martin CL, Cleary PA,
Waberski BH, Lachin JM, Albers JW: DCCT and EDIC studies in type 1 diabetes:
lessons for diabetic neuropathy regarding metabolic memory and natural history.
Curr Diab Rep 2010;10:276-282
11. Rolandsson O, Palmer JP: Latent autoimmune diabetes in adults (LADA) is
dead: long live autoimmune diabetes! Diabetologia 2010;53:1250-1253
12. Gale EA: Latent autoimmune diabetes in adults: a guide for the perplexed.
Diabetologia 2005;48:2195-2199
13. Baum P, Hermann W, Verlohren HJ, Wagner A, Lohmann T, Grahmann F:
Diabetic neuropathy in patients with "latent autoimmune diabetes of the adults"
(LADA) compared with patients with type 1 and type 2 diabetes. J Neurol
2003;250:682-687
14. Myhill P, Davis WA, Bruce DG, Mackay IR, Zimmet P, Davis TME: Chronic
complications and mortality in community-based patients with latent autoimmune
diabetes in adults: the Fremantle Diabetes Study. Diabetic Medicine 2008;25:1245-
1250
222
15. Isomaa B, Almgren P, Henricsson M, Taskinen MR, Tuomi T, Groop L, Sarelin
L: Chronic complications in patients with slowly progressing autoimmune type 1
diabetes (LADA). Diabetes Care 1999;22:1347-1353
16. Smith AG, Russell J, Feldman EL, Goldstein J, Peltier A, Smith S, Hamwi J,
Pollari D, Bixby B, Howard J, Singleton JR: Lifestyle Intervention for Pre-Diabetic
Neuropathy. Diabetes Care 2006;29:1294-1299
17. Quattrini C, Tavakoli M, Jeziorska M, Kallinikos P, Tesfaye S, Finnigan J,
Marshall A, Boulton AJ, Efron N, Malik RA: Surrogate markers of small fibre
damage in human diabetic neuropathy. Diabetes 2007;56:2148-2154
18. Tavakoli M, Mitu-Pretorian M, Petropoulos IN, Fadavi H, Asghar O, Alam U,
Ponirakis G, Jeziorska M, Marshall A, Efron N, Boulton AJ, Augustine T, Malik RA:
Corneal confocal microscopy detects early nerve regeneration in diabetic
neuropathy after simultaneous pancreas and kidney transplantation. Diabetes
2013;62:254-260
19. Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, Lauria G,
Malik RA, Spallone V, Vinik A, Bernardi L, Valensi P: Diabetic neuropathies:
update on definitions, diagnostic criteria, estimation of severity, and treatments.
Diabetes Care 2010;33:2285-2293
20. Fourlanos S, Perry C, Stein MS, Stankovich J, Harrison LC, Colman PG: A
clinical screening tool identifies autoimmune diabetes in adults. Diabetes Care
2006;29:970-975
21. Young M, Boulton A, Macleod A, Williams D, Sonksen P: A multicentre study of
the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital
clinic population. Diabetologia 1993;36:150-154

223
22. Bravenboer B, van Dam PS, Hop J, vd Steenhoven J, Erkelens DW: Thermal
threshold testing for the assessment of small fibre dysfunction: normal values and
reproducibility. Diabet Med 1992;9:546-549
23. Petropoulos IN, Manzoor T, Morgan P, Fadavi H, Asghar O, Alam U, Ponirakis
G, Dabbah MA, Chen X, Graham J, Tavakoli M, Malik RA: Repeatability of in vivo
corneal confocal microscopy to quantify corneal nerve morphology. Cornea
32:e83-89
24. Tavakoli M, Malik RA: Corneal confocal microscopy: a novel non-invasive
technique to quantify small fibre pathology in peripheral neuropathies. J Vis Exp
2011; 3(47):2194. doi: 10.3791/2194
25. Kallinikos P, Berhanu M, O'Donnell C, Boulton AJ, Efron N, Malik RA: Corneal
nerve tortuosity in diabetic patients with neuropathy. Invest Ophthalmol Vis Sci
2004;45:418-422
26. Lauria G, Bakkers M, Schmitz C, Lombardi R, Penza P, Devigili G, Smith AG,
Hsieh ST, Mellgren SI, Umapathi T, Ziegler D, Faber CG, Merkies IS:
Intraepidermal nerve fibre density at the distal leg: a worldwide normative
reference study. J Peripher Nerv Syst 2010;15:202-207
27. Kobayashi T, Nakanishi K, Murase T, Kosaka K: Small doses of subcutaneous
insulin as a strategy for preventing slowly progressive beta-cell failure in islet cell
antibody-positive patients with clinical features of NIDDM. Diabetes 1996;45:622-
626
28. Gottsater A, Landin-Olsson M, Fernlund P, Lernmark A, Sundkvist G: Beta-cell
function in relation to islet cell antibodies during the first 3 yr after clinical diagnosis
of diabetes in type II diabetic patients. Diabetes Care 1993;16:902-910

224
29. Andersen CD, Bennet L, Nystrom L, Lindblad U, Lindholm E, Groop L,
Rolandsson O: Worse glycaemic control in LADA patients than in those with type 2
diabetes, despite a longer time on insulin therapy. Diabetologia 2013;56:252-258
30. Maruyama T, Tanaka S, Shimada A, Funae O, Kasuga A, Kanatsuka A, Takei
I, Yamada S, Harii N, Shimura H, Kobayashi T: Insulin intervention in slowly
progressive insulin-dependent (type 1) diabetes mellitus. J Clin Endocrinol Metab
2008;93:2115-2121
31. Tesfaye S, Stevens LK, Stephenson JM, Fuller JH, Plater M, Ionescu-
Tirgoviste C, Nuber A, Pozza G, Ward JD: Prevalence of diabetic peripheral
neuropathy and its relation to glycaemic control and potential risk factors: the
EURODIAB IDDM Complications Study. Diabetologia 1996;39:1377-1384
32. Tesfaye S, Chaturvedi N, Eaton SEM, Ward JD, Manes C, Ionescu-Tirgoviste
C, Witte DR, Fuller JH: Vascular Risk Factors and Diabetic Neuropathy. New
England Journal of Medicine 2005;352:341-350
33. Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM, Wilson DM,
O'Brien PC, Melton LJ, 3rd, Service FJ: The prevalence by staged severity of
various types of diabetic neuropathy, retinopathy, and nephropathy in a population-
based cohort: the Rochester Diabetic Neuropathy Study. Neurology 1993;43:817-
824
34. Myhill P, Davis WA, Bruce DG, Mackay IR, Zimmet P, Davis TM: Chronic
complications and mortality in community-based patients with latent autoimmune
diabetes in adults: the Fremantle Diabetes Study. Diabet Med 2008;25:1245-1250
35. Umapathi T, Tan WL, Loke SC, Soon PC, Tavintharan S, Chan YH:
Intraepidermal nerve fibre density as a marker of early diabetic neuropathy. Muscle
Nerve 2007;35:591-598

225
36. Loseth S, Mellgren SI, Jorde R, Lindal S, Stalberg E: Polyneuropathy in type 1
and type 2 diabetes: comparison of nerve conduction studies, thermal perception
thresholds and intraepidermal nerve fibre densities. Diabetes Metab Res Rev
2010;26:100-106
37. Loseth S, Stalberg E, Jorde R, Mellgren SI: Early diabetic neuropathy: thermal
thresholds and intraepidermal nerve fibre density in patients with normal nerve
conduction studies. J Neurol 2008;255:1197-1202
38. Abbott CA, Malik RA, van Ross ERE, Kulkarni J, Boulton AJM: Prevalence and
Characteristics of Painful Diabetic Neuropathy in a Large Community-Based
Diabetic Population in the U.K. Diabetes Care 2011;34:2220-2224
39. Saiz A, Blanco Y, Sabater L, Gonzalez F, Bataller L, Casamitjana R, Ramio-
Torrenta L, Graus F: Spectrum of neurological syndromes associated with glutamic
acid decarboxylase antibodies: diagnostic clues for this association. Brain
2008;131:2553-2563
40. Roll U, Nuber A, Schroder A, Gerlach E, Janka HU, Ziegler AG: No association
of antibodies to glutamic acid decarboxylase and diabetic complications in patients
with IDDM. Diabetes Care 1995;18:210-215
41. Sundkvist G, Velloso LA, Kampe O, Rabinowe SL, Ivarsson SA, Lilja B,
Karlsson FA: Glutamic acid decarboxylase antibodies, autonomic nerve antibodies
and autonomic neuropathy in diabetic patients. Diabetologia 1994;37:293-299

226
6 Chapter VI - Marked vitamin D deficiency in patients with
diabetes from secondary care: Ethnic and seasonal
differences and an association with dyslipidaemia
Contribution: Uazman Alam conceived the study and subsequently designed it,
extracted data, performed statistical analyses and wrote the manuscript which
constitutes the basis for this chapter and was submitted and accepted for
publication in the journal Diabetic Medicine 2012;29:1343-1345
Uazman Alam, Osman Najam, Sarah Al-Himdani, Sophie Benoliel, Pushpa
Jinadev, Jacqueline Berry, Michelle Kew, Omar Asghar, Ioannis Petropolous,
Rayaz A Malik

227
6.1 ABSTRACT
Vitamin D deficiency has been implicated in cardiovascular disease in subjects with
diabetes. We aimed to assess the 25-hydroxyvitamin D (25(OH)D) status in
patients from a secondary care hospital.
This cross-sectional population-based cohort study assessed 25(OH)D levels in
563 unselected subjects with diabetes and 44 age and ethnicity matched subjects
without diabetes, in relation to metabolic, anthropometric and demographic factors.
The mean 25(OH)D was lower in subjects with diabetes (15.7 ± 9.1 ng/ml)
compared to age and ethnicity subjects without diabetes (21.3 ± 14.6 ng/ml)
(p=0.009) with vitamin D deficiency (<30 ng/ml) in 91% compared to 78% in the
respective groups. The severest (<10ng/ml) vitamin D deficiency occurred in South
Asian subjects (54%) compared to white Europeans (22%). There were no
significant differences in BMI, systolic and diastolic blood pressure, ALP, corrected
calcium or HbA1c between the different quartiles of 25(OH)D (<10ng/ml, 10-
19.9ng/ml, 20-29.9ng/ml, >30ng/ml). However, HDL (1.3±0.7, 1.3±0.4, 1.4±0.5,
1.6±0.6mmol/l, p=0.003) was higher and triglycerides (2.2±2.8, 1.7±1.5, 1.5±0.9,
1.6±1.3mmol/l, p=0.04) were significantly lower in subjects with diabetes with
25(OH)D >30ng/ml. There was a statistically but clinically non-significant seasonal
variation in the 25(OH)D status in the white European cohort in summer
(20.1±8.8ng/ml) versus winter (16.0±6.1ng/ml) (p=0.007), with no change in the
South Asian/Middle Eastern cohort.
There is profound vitamin D deficiency in the North West of England, particularly in
South Asians which is associated with lower HDL levels, possibly mediating
elevated cardiovascular risk. Further research is warranted to define whether
replacement of vitamin D may alter cardiometabolic risk.
228
6.2 INTRODUCTION
Over one billion people worldwide are vitamin D deficient (1). Vitamin D deficiency
is highly prevalent in the UK (2) and in a nationwide cohort study, 87.1% and
60.9% were deficient in vitamin D in the winter/spring and summer/autumn months
respectively (2) using ≥30ng/ml as a cut off for adequate levels (1; 3). At risk
groups for deficiency include those with pigmented skin (4) and severe deficiency
is highly prevalent in South Asians living in northern latitudes (5).
The role of Vitamin D is well established in the regulation of bone metabolism and
calcium homeostasis. Hence concentrations of ≥30ng/ml of vitamin D have been
identified as necessary for optimal bone health (3) by maximal suppression of
parathyroid hormone, greatest calcium absorption, and highest bone mineral
density (6). Concentrations ≥10ng/ml are sufficient to prevent the severe skeletal
manifestations leading to rickets in children and osteomalacia in adults (7). Thus a
serum concentration of ≥30 ng/ml is considered sufficient, 20 to <30ng/ml
insufficient, 10 to <20ng/ml deficient and <10ng/ml as severe deficiency (1).
Vitamin D may play a pivotal role in several chronic diseases such as diabetes and
cardiovascular disease (1; 4). The vitamin D receptor (VDR) is expressed
ubiquitously including in tissues such as cardiomyocytes, vascular endothelium
and lymphopoeitic cells (1). With regard to diabetes, the binding of the activated
hormonal form of vitamin D (1,25-hydroxyvitamin D [1,25(OH)2D]) to VDR in
pancreatic β-cells leads to the production of insulin (8). The development of both
type 1 and 2 diabetes has been causally associated with vitamin D deficiency and
has been validated in both experimental and human interventional studies (9-11).
In the Finnish birth cohort study, more than 10,000 individuals were followed over
30 years and children who were supplemented with 2000IU daily of vitamin D for

229
the first year of life had a relative risk of 0.22 (95% CI 0.05-0.89) for the
development of type 1 diabetes when compared to those who were not
supplemented (9). There is also a propensity for vitamin D deficiency, particularly
in Type 2 diabetes (12). VDR activation may be beneficial in terms of proliferation
of vascular smooth muscle and cardiomyocytes (1). Indeed two large prospective
studies have demonstrated increased cardiovascular mortality in subjects with
severe deficiency (≤10ng/ml) (13-14). The Framingham cohort study has also
shown similar results with a cut off of 15ng/ml (15) and a recent meta-analysis
showed a significant association between high levels of vitamin D and a reduction
of cardiovascular disease risk (33% reduction compared to low levels of vitamin D),
and metabolic syndrome (51% reduction) (16). The relationship of vitamin D to
cardiovascular disease is further supported considering the shared metabolic
pathway with cholesterol production, via 7-dehydrocholesterol (17). In a recent
study an approximate increase of 4.2mg/dl in HDL was associated with every
10ng/ml increase of 25(OH)D (18). Indeed, activated vitamin D inhibits foam cell
formation and an impairment of VDR signalling results in acceleration of this
process in patients with diabetes (19). This postulated link to cholesterol
metabolism and cardiovascular outcomes is further strengthened by the
demonstration that statins increase vitamin D levels (20). However, large
prospective randomised trials of vitamin D intervention assessing cardiovascular
outcomes as the primary endpoint are absent, thus the relationship may be
regarded by some as post hoc ergo propter hoc (correlation not causation).
This cross-sectional study was undertaken in a group of unselected subjects with
diabetes attending a hospital based diabetes clinic and a control group without
diabetes from a general medical clinic. We defined the prevalence of vitamin D

230
deficiency and its association with the constituents of metabolic syndrome and
cardiovascular disease risk.

231
6.3 RESEARCH DESIGN AND METHODS
Data from a population-based cohort of 563 subjects with diabetes and 44 age and
ethnicity matched subjects without diabetes from Central Manchester Foundation
Trust, Manchester, UK were analyzed. All patients attending the clinics were
assessed irrespective of a history suggestive of vitamin D deficiency. Ethical
approval was not required as the data were extracted retrospectively and did not
extend beyond standard clinical practice. All those found to be deficient in
25(OH)D, were provided with appropriate replacement therapy in accordance with
standard clinical practice.
6.3.1 Subjects
This cross sectional study was conducted in an unselected group of subjects with
and without diabetes in a general medical population. All participants were aged ≥
18 years old attending clinics at the Central Manchester Foundation Trust,
Manchester from August 2009 to July 2010. Those with renal impairment (eGFR
<30 mL/min/1.73m2 (CKD stage 4 and below), granulomatous diseases
(tuberculosis, sarcoidosis etc), malabsorption syndromes (Coeliac disease,
bacterial overgrowth, concomitant orlistat treatment), pregnant and lactating
women, and those currently on vitamin D supplementation were excluded from the
analysis. From previous prevalence studies in the UK we anticipated the proportion
of individuals with vitamin D deficiency to be greater than 50% (4).
6.3.2 Blood pressure and Anthropometric measurements
Body mass index (BMI) was measured as per the standard equation (mass
(kg)/(height(m))2. Weight was measured with a digital scale (Seca 701, Seca,
232
Hamburg, Germany) to the nearest 0.1kg and height to the nearest 0.1cm. Blood
pressure (BP) measurements were obtained with the use of an automated BP
device (Dinamap pro 100v2, GE Medical Systems, Freiburg, Germany) with an
appropriate cuff size. A minimum of two measurements of systolic and diastolic BP
were made five minutes apart with the lowest reading recorded.
6.3.3 Assessment of Demographics, Cardiovascular disease and
Medications
An assessment of patient demographics, previous cardiovascular events and
medications were made through analysis of medical records and an in-hospital
medical record database (Diamond database, Hicom, Surrey, UK). Subject
demographics extracted were age, sex, ethnicity (White European, South Asian,
Far East Asian and Afro-Caribbean descent), smoking status (never, previous and
current) and type (Type 1 and 2 diabetes) and duration of diabetes. Previous
cardiovascular events extracted were ischaemic heart disease (IHD), myocardial
infarction (MI), cerebrovascular accidents (CVA) and peripheral vascular disease
(PVD).
6.3.4 Laboratory Measurements
Standard assessment of 25(OH)D was instituted in August 2009 as part of routine
haematological and biochemical laboratory measurements which included HbA1c,
(Complete Blood count (CBC)), Urea and Electrolytes (UE), Liver function tests
(LFT), bone profile (Corrected Calcium (CCa2+), Alkaline Phosphatase (ALP),
Albumin (Alb), and Lipid profile (Total Cholesterol (T-CHL), High Density
lipoprotein Cholesterol (HDL), Triglycerides (TRIG)). Low Density lipoprotein (LDL)

233
analyses were not undertaken and patients were routinely advised that bloods
were to be collected under fasting conditions.
For 25(OH)D measurement, serum was separated from whole blood and stored at
-20 C until assay. The laboratory used for the biochemical assay measurements
(Vitamin D Research Group Manchester Royal Infirmary, UK) was accredited to
ISO 9001:2008 and ISO 13485:2003 by Lloyd’s Register Quality Assurance
certificate number LRQ 4001542 and participated successfully in the Vitamin D
quality assurance scheme (DEQAS). Serum 25(OH)D was measured using the
IDS-iSYS multi-discipline automated analyzer (Immunodiagnostic Systems Ltd,
Boldon, Tyne and Wear, UK). The assay is based on chemiluminescent technology
and was performed exactly as per the manufacturer’s instructions. Briefly, samples
were subjected to a pre-treatment step to denature the vitamin D binding protein.
The treated samples were then neutralised in assay buffer and a specific anti-
25(OH)D antibody labelled with acridinium was added. Following an incubation
step, magnetic particles linked to 25(OH)D were added. Following a further
incubation step, the magnetic particles were “captured” using a magnet. After a
washing step and addition of trigger reagents, the light emitted by the acridinium
label was inversely proportional to the concentration of 25(OH)D in the original
sample. Concentration of 25(OH)D was calculated automatically using a 4-point
logistic curve. The reportable range of the assay was 5-140 ng/mL. Inter- and
intra- assay variation of the in-house control was 5.6% and 9.7% respectively.
6.3.5 Statistical analysis
Statistical analyses were undertaken on Statsdirect (Statsdirect, Cheshire, UK).
Mean 25(OH)D ± standard deviation (SD) are presented as a whole and per

234
season and subdivided for ethnic background. ANOVA method or a non-parametric
counterpart, Kruskal-Wallis were used to assess differences between groups
depending on normality of the data. Overall the P value was maintained at 0.05 for
multiple comparison tests (Bonferoni adjustment or Dwass-Steel-Chritchlow-Fligner
pairwise comparison). Further descriptive statistics are presented for
characteristics of 25(OH)D (≥30ng/ml, 20 to <30ng/ml, 10 to <20ng/ml and
<10ng/ml). Multiple linear regression models, after assessment of normality, were
used to examine relationships between vitamin D level and lipids, adjusting for
BMI/type of diabetes and ethnicity. A P value of <0.05 was considered to be
statistically significant. All values are presented as mean ± SD.
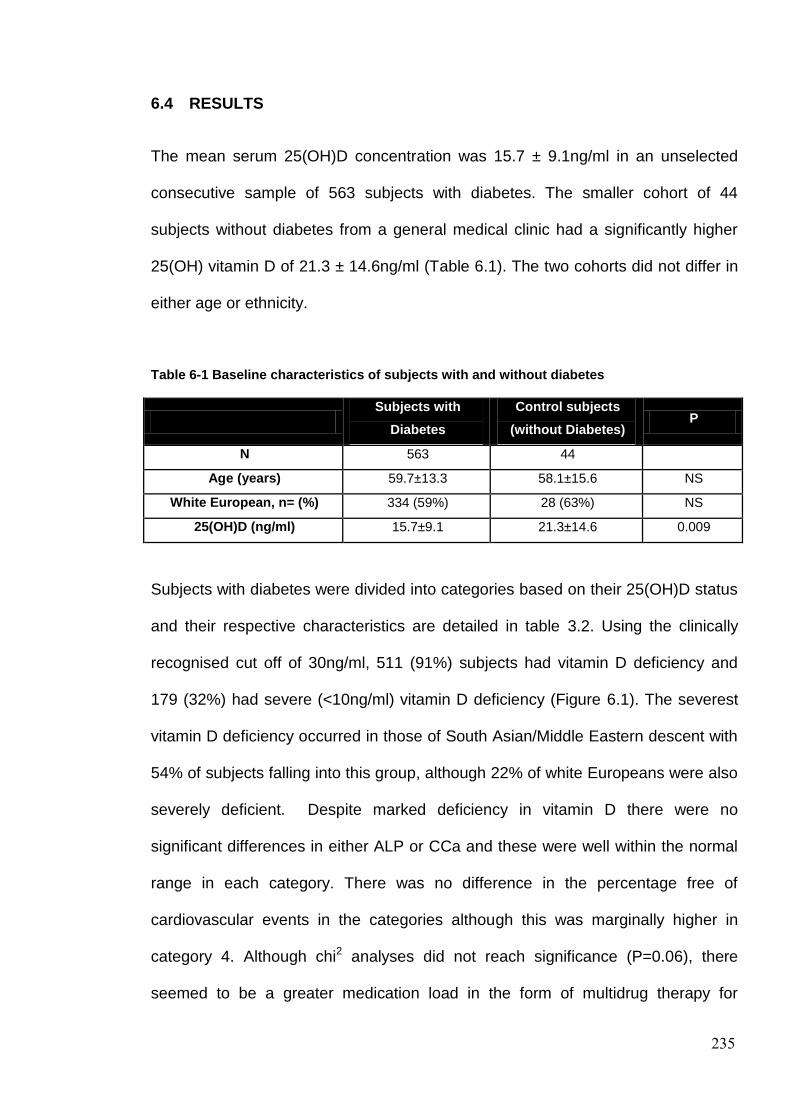
235
6.4 RESULTS
The mean serum 25(OH)D concentration was 15.7 ± 9.1ng/ml in an unselected
consecutive sample of 563 subjects with diabetes. The smaller cohort of 44
subjects without diabetes from a general medical clinic had a significantly higher
25(OH) vitamin D of 21.3 ± 14.6ng/ml (Table 6.1). The two cohorts did not differ in
either age or ethnicity.
Table 6-1 Baseline characteristics of subjects with and without diabetes
Subjects with
Diabetes
Control subjects
(without Diabetes) P
N 563 44
Age (years) 59.7±13.3 58.1±15.6 NS
White European, n= (%) 334 (59%) 28 (63%) NS
25(OH)D (ng/ml) 15.7±9.1 21.3±14.6 0.009
Subjects with diabetes were divided into categories based on their 25(OH)D status
and their respective characteristics are detailed in table 3.2. Using the clinically
recognised cut off of 30ng/ml, 511 (91%) subjects had vitamin D deficiency and
179 (32%) had severe (<10ng/ml) vitamin D deficiency (Figure 6.1). The severest
vitamin D deficiency occurred in those of South Asian/Middle Eastern descent with
54% of subjects falling into this group, although 22% of white Europeans were also
severely deficient. Despite marked deficiency in vitamin D there were no
significant differences in either ALP or CCa and these were well within the normal
range in each category. There was no difference in the percentage free of
cardiovascular events in the categories although this was marginally higher in
category 4. Although chi2 analyses did not reach significance (P=0.06), there
seemed to be a greater medication load in the form of multidrug therapy for

236
hypertension in the lower echelons (category 1 and 2) of vitamin D status
compared to category 3 and 4. A significant confounding factor is possibly the
longer duration of diabetes in category 4 and the presence of asymptomatic
undeclared CVD, thus obscuring the true cardiovascular event profile.
Nevertheless, we demonstrate a significant difference in HDL (P=0.003) and
triglycerides (P=0.04) between the categories. On post hoc analysis, HDL in
category 3 and 4 were significantly higher than category 1 (1.4±0.5mmol/l vs
1.3±0.7mmol/l, P=0.02 and 1.6±0.6mmol/l vs 1.3±0.7mmol/l, P=0.002 respectively)
and a similar relationship was found with triglycerides, with triglycerides being
significantly lower in categories 2, 3 and 4 compared to category 1 (1.7±1.5mmol/l
vs 2.2±2.8mmol/l, p=0.002, 1.5±0.9mmol/l vs 2.2±2.8mmol/l, P=0.02 and
1.6±1.3mmol/l vs 2.2±2.8mmol/l, P=0.05 respectively). However, after adjusting for
BMI, season, ethnicity and lipid medication, regression analyses between 25(OH)D
and triglycerides was no longer significant (Table 6.3 (r=-0.06, P=NS), particularly
as the lowest 25(OH)D (category 1) had a higher proportion of Asian subjects with
type 2 diabetes and features of metabolic syndrome. Table 6.3 shows a regression
analyses of lipid fractions with 25(OH)D levels and demonstrates a significant
relationship with HDL (P=0.006) after adjusting for BMI, ethnicity, season and lipid
medication. Figure 6.2 represents a scatter plot showing a positive linear trend of
25(OH)D versus HDL.

237
Figure 6-1 Histogram of 25(OH)D Status in subjects with diabetes*
*Minimal reported 25(OH)D was 5ng/ml

238
Table 6-2 Characteristics by categories of 25(OH)D in 563 unselected subjects with diabetes.
Serum 25(OH)D
Category 1 Category 2 Category 3 Category 4
<10ng/ml 10-<20ng/ml 20-<30ng/ml ≥30ng/ml
N 179 233 99 52
Men (%) 53 57 48 48
Type 2 DM (%) 85 75 69 52
White European, n (%)
71 (40) 146 (63) 73 (74) 44 (84)
South Asian/ Middle East, n
(%) 96 (54) 61 (26) 16 (16) 6 (12)
Afro-Caribbean, n (%)
8 (4) 14 (6) 8 (8) 2 (4)
Far-East Asian, n (%)
4 (2) 12 (5) 2 (2) 0 (0)
% free of Cardiovascular
events 79 80 77 84
% on CHL meds 88 85 82 81
% on BP meds (No
therapy/single therapy/multidrug
therapy)
76 (25/31/45)
76 (24/23/53)
69 (31/30/39)
76 (23/39/38)
Mean±SD P
Age (years) 58.8±13.7 59.6±13.5 61.0±12.4 60.2±13.0 NS
Duration of Diabetes (years)
15.4±9.4 17.9±11.9 19.1±11.1 22.3±15.1 0.03
BMI (kg/m2) 31.2±6.5 30.5±6.4 31.5±7.0 29.1±6.4 NS
Systolic BP (mmHg)
129±17 129±16 133±18 131±17 NS
Diastolic BP (mmHg)
69±10 70±9 69±9 71±11 NS
HbA1c (%) (IFCC (mmol/mol))
8.6±1.9, 69±24
8.4±1.7, 68±20
8.2±1.5, 66±17
8.8±1.9, 73±21
NS
T-CHL (mmol/l) 4.2±1.3 4.1±1.2 4.2±0.9 4.5±1.6 NS
HDL (mmol/l) 1.3±0.7 1.3±0.4 1.4±0.5 1.6±0.6 0.003
TRIG (mmol/l) 2.2±2.8 1.7±1.5 1.5±0.9 1.6±1.3 0.04
ALP (U/L) 94±43 86±33 85±48 85±29 NS
CCa (mmol/l) 2.3±0.1 2.3±0.1 2.4±0.1 2.4±0.1 NS
eGFR (ml/min/l) 73±20 73±19 75±16 73±21 NS
Table key
ALP – Alkaline Phosphatase; BMI – Body Mass Index; BP – Blood Pressure; CCa – Corrected
Calcium; eGFR – estimated Glomerular Filtration Rate; HDL – High-density Lipoprotein Cholesterol;
T-CHL – Total Cholesterol; TRIG – Triglycerides;

239
Table 6-3 Regression analyses of 25(OH)D and T-CHL, HDL and triglycerides in subjects with
diabetes
r
(unadjusted)
P
(unadjusted)
r *
(adjusted)
P*
(adjusted)
T-CHL 0.014 NS -0.007 NS
HDL 0.158 0.0002 0.12 0.006
TRIG -0.112 0.009 -0.06 NS
*adjusted for BMI, ethnicity, season and lipid medication.
Table key
HDL – High-density Lipoprotein Cholesterol; T-CHL – Total Cholesterol; TRIG – Triglycerides.
Figure 6-2 Relationship between serum 25(OH)D and high-density lipoprotein cholesterol
(HDL) in subjects with diabetes
*adjusted for BMI, ethnicity, season and lipid medication.
0
0.5
1
1.5
2
2.5
3
3.5
0 10 20 30 40 50
HDL-C (mmol/l)
25(OH) vit D status (ng/ml)
25(OH)D vs HDL-C
r=0.12, p=0.006

240
Table 6.4 shows ethnic differences in 25(OH)D with a further sub-categorisation for
South Asian/Middle Eastern and white European subjects. There were significant
differences between the South Asian/Middle Eastern group and white Europeans
(11.3±9.6ng/ml vs 18.0±7.0ng/ml, P<0.0001), African-Caribbean (11.3±9.6ng/ml vs
16.4±7.8ng/ml, P=0.001) and Far-East Asian groups (11.3±9.6ng/ml vs
14.5±4.5ng/ml, P=0.02). There were no differences in BMI between the ethnic
subcategories. There was a statistically significant but clinically non-significant
seasonal variation in the 25(OH)D status in the white European group in summer
(20.1±8.8ng/ml) versus winter (16.0±6.1ng/ml) (P=0.007) but there was no
seasonal variation in the South Asian/Middle Eastern group. There were
insufficient data to assess seasonal variation in either the Afro-Caribbean or the
Far-East Asian group.
Table 6-4 Characteristics of subjects with diabetes based on ethnicity
White
European
South
Asian/Middle
East
Afro-
Caribbean*
Far East
Asian*
P
for
comparison
of means
Mean 25(OH)D
(ng/ml)
18.0±7.0 11.3±9.6 16.4±7.8 14.5±4.5 <0.0001
Season Seasonal variation
Spring
(ng/ml)
17.2±9.9 10.6±6.1
Summer
(ng/ml)
20.1±8.8 11.0±5.5
Autumn (ng/ml) 17.8±9.9 10.9±6.8
Winter
(ng/ml)
16.0±6.1 12.5±8.9
P
for comparison
of means
0.009 NS
*Insufficient number to undertake seasonal analysis.

241
6.5 DISCUSSION
Vitamin D deficiency is endemic in the United Kingdom and our data confirm this
showing a pronounced severe (<10ng/ml) vitamin D deficiency in 32% of
individuals, with more than half of South Asian and Middle Eastern subjects
demonstrating severe deficiency. Whilst this highlights the need for routine testing
in patients with diabetes, the general patient population are also deficient as shown
in this study and others (2; 21). However, we have clearly shown a higher 25(OH)D
in the age and ethnicity matched subjects without diabetes in this study. Vitamin D
deficiency has not only been implicated in the causation of both type 1 and 2
diabetes, but those with type 2 diabetes are particularly prone to vitamin D
deficiency, in part due to obesity with the proposed sequestration of 25(OH)D in
adipose tissue (22). Although, a previous study has shown a propensity for vitamin
D deficiency even when adjusting for BMI (23). The reasons for this may be
multifactorial including genetic polymorphisms and variants of vitamin D binding
protein (24). The VDR is expressed on the pancreatic β-cell and activated vitamin
D affects insulin production (8). The predisposition for the development of vitamin
D deficiency may contribute to worsening glycaemic control, leading to the
development of impaired glucose tolerance and eventually diabetes. Unfortunately
most interventional studies of vitamin D have either been secondary analyses of
osteoporosis interventions or have generally had small numbers with low doses of
vitamin D replacement. This has significant implications on the guidelines for
supplementation of vitamin D particularly as the current recommended daily
allowance (RDA) of 400IU, which is less than the RDAs elsewhere, appears
woefully inadequate in the absence of adequate sunlight exposure (25).

242
Seasonal variation in levels of vitamin D are often cited as plausible reasons for
overestimation of vitamin D deficiency, particularly in South Asians, but this is a
controversial issue and previous studies have had conflicting results (26-27). In the
present study in white European subjects, the difference of 4.1 ng/ml from winter to
summer is not considered to be clinically significant. Furthermore, a lack of
seasonal variation in South Asian and Middle Eastern subjects, which may in-part
be related to lack of sunlight exposure through body attire, particularly in women of
South Asian origin, further blunts this minimal seasonal effect. Current data on the
association of vitamin D deficiency with glucose intolerance seems to be
population specific (24). Reduction in serum 25(OH)D concentration has been
noted in a UK South Asian population at risk for Type 2 diabetes compared with
subjects not at risk (28). In the same South Asian population, short-term vitamin D
supplementation increased insulin secretion (28). The data from the Third National
Health and Nutrition Examination study (NHANES) also showed an inverse
association between vitamin D status and diabetes in non-Hispanic white and
Mexican American people but not in non-Hispanic black people (29). However,
serum 25(OH)D levels have not been related to glucose status in a white European
population from the UK (30). Assessing vitamin D status in population specific
targets may an important facet in addressing poorer glycaemic control particularly
in ethnic minorities at risk of vitamin D deficiency living in the UK.
Cholesterol and vitamin D share a common metabolic pathway through 7-
dehydrocholesterol which is a precursor for both. Our study has shown a positive
but albeit weak correlation between 25(OH)D and HDL, confirming the results of
other studies (18). Our subjects are largely (approximately 80%) on statin therapy
which, of course, impacts on HDL and probably also on 25(OH)D. Atorvastatin and

243
rosuvastatin have been shown to increase levels of 25(OH)D, and statins may
require adequate levels of vitamin D to function optimally (20). However, statins
may worsen diabetes and predispose to dysglycaemia which would go against the
notion of statins increasing vitamin D levels may protect against diabetes mellitus.
However, the mechanism by which statins may cause dysglycaemia is distinct from
the vitamin D pathway and may be via inhibition of β-cell glucose transporters,
delayed ATP production, pro-inflammatory and oxidative β-cell effects of plasma-
derived cholesterol, inhibition of calcium channel-dependent insulin secretion and
β-cell apoptosis (31). In a recent study culturing macrophages from obese,
diabetic, hypertensive patients with 1,25(OH)2D suppressed foam cell formation by
reducing LDL uptake, whilst deletion of the VDR in these macrophages accelerated
foam cell formation through increased LDL uptake (19). Thus vitamin D may play
an important, perhaps even permissive role in atherosclerosis.
Whilst this cross-sectional study has limitations as it provides association and not
cause and effect a major strength is that all participants were from a single centre
and from a small geographical locality. The north west of England is known to have
lower levels of sunlight when compared to other areas of the UK (2) and this may
potentially impact on transferability of results. However, despite these
shortcomings, we are mindful that the results of this study are not dissimilar to
those of other studies in the UK (2).
In conclusion, we provide further confirmation of the epidemic of vitamin D
deficiency in diabetic patients (85% in Type 1 diabetes and 93% in Type 2
diabetes) in England. Furthermore, we provide an association with lipid
abnormalities providing a potential mechanistic link observed in the landmark
longitudinal studies such as the Framingham cohort study (15) which showed

244
approximately twice the cardiovascular risk in those with low levels of 25(OH)D
compared to higher levels. We also confirm the lower levels in those from South
Asian, Far Eastern and Afro-Caribbean ethnicity. Moreover we show that seasonal
variation contributes minimally to differences in vitamin D status, particularly in
South Asians. These data therefore highlight the need to assess 25(OH)D levels in
all patients with diabetes, not only those with symptoms of osteomalacia and also
confirms the inability of corrected calcium or alkaline phosphatase levels to target
individuals for assessment. Whether supplementation will lower cardiovascular risk
is not known and the results of the VITAL study (a randomised placebo controlled
trial of 25(OH)D and omega-3) are awaited (clinicaltrials.gov - NCT01169259).

245
6.6 REFERENCES
1. Holick MF: Vitamin D Deficiency. New England Journal of Medicine
2007;357:266-281
2. Hypponen E, Power C: Hypovitaminosis D in British adults at age 45 y:
nationwide cohort study of dietary and lifestyle predictors. Am J Clin Nutr
2007;85:860-868
3. Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, Vieth R:
Estimates of optimal vitamin D status. Osteoporos Int 2005;16:713-716
4. Pearce SH, Cheetham TD: Diagnosis and management of vitamin D deficiency.
BMJ 2010;340:b5664
5. Arya V, Bhambri R, Godbole M, Mithal A: Vitamin D status and its relationship
with bone mineral density in healthy Asian Indians. Osteoporosis International
2004;15:56-61
6. Heaney RP, Dowell MS, Hale CA, Bendich A: Calcium absorption varies within
the reference range for serum 25-hydroxyvitamin D. J Am Coll Nutr 2003;22:142-
146
7. Souberbielle JC, Friedlander G, Kahan A, Cormier C: Evaluating vitamin D
status. Implications for preventing and managing osteoporosis and other chronic
diseases. Joint Bone Spine 2006;73:249-253
8. Alvarez JA, Ashraf A: Role of vitamin d in insulin secretion and insulin sensitivity
for glucose homeostasis. Int J Endocrinol 2010;2010:351385
9. Hypponen E, Laara E, Reunanen A, Jarvelin MR, Virtanen SM: Intake of vitamin
D and risk of type 1 diabetes: a birth-cohort study. Lancet 2001;358:1500-1503

246
10. Pittas AG, Lau J, Hu FB, Dawson-Hughes B: The role of vitamin D and calcium
in type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab
2007;92:2017-2029
11. Bouillon R, Carmeliet G, Verlinden L, van Etten E, Verstuyf A, Luderer HF,
Lieben L, Mathieu C, Demay M: Vitamin D and Human Health: Lessons from
Vitamin D Receptor Null Mice. Endocr Rev 2008;29:726-776
12. Mathieu C, Gysemans C, Giulietti A, Bouillon R: Vitamin D and diabetes.
Diabetologia 2005;48:1247-1257
13. Ginde AA, Scragg R, Schwartz RS, Camargo CA, Jr.: Prospective study of
serum 25-hydroxyvitamin D level, cardiovascular disease mortality, and all-cause
mortality in older U.S. adults. J Am Geriatr Soc 2009;57:1595-1603
14. Pilz S, Dobnig H, Fischer JE, Wellnitz B, Seelhorst U, Boehm BO, Marz W:
Low vitamin d levels predict stroke in patients referred to coronary angiography.
Stroke 2008;39:2611-2613
15. Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K, Benjamin
EJ, D'Agostino RB, Wolf M, Vasan RS: Vitamin D deficiency and risk of
cardiovascular disease. Circulation 2008;117:503-511
16. Parker J, Hashmi O, Dutton D, Mavrodaris A, Stranges S, Kandala NB, Clarke
A, Franco OH: Levels of vitamin D and cardiometabolic disorders: systematic
review and meta-analysis. Maturitas 2010;65:225-236
17. Michos ED, Melamed ML: Vitamin D and cardiovascular disease risk. Curr
Opin Clin Nutr Metab Care 2008;11:7-12
18. Maki KC, Rubin MR, Wong LG, McManus JF, Jensen CD, Marshall JW,
Lawless A: Serum 25-hydroxyvitamin D is independently associated with high-

247
density lipoprotein cholesterol and the metabolic syndrome in men and women.
Journal of Clinical Lipidology 2009;3:289-296
19. Oh J, Weng S, Felton SK, Bhandare S, Riek A, Butler B, Proctor BM, Petty M,
Chen Z, Schechtman KB, Bernal-Mizrachi L, Bernal-Mizrachi C: 1,25(OH)2 vitamin
d inhibits foam cell formation and suppresses macrophage cholesterol uptake in
patients with type 2 diabetes mellitus. Circulation 2009;120:687-698
20. Perez-Castrillon JL, Abad L, Vega G, Sanz-Cantalapiedra A, Garcia-Porrero M,
Pinacho F, Duenas A: Effect of atorvastatin on bone mineral density in patients
with acute coronary syndrome. Eur Rev Med Pharmacol Sci 2008;12:83-88
21. Ford L, Graham V, Wall A, Berg J: Vitamin D concentrations in an UK inner-city
multicultural outpatient population. Ann Clin Biochem 2006;43:468-473
22. Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF: Decreased
bioavailability of vitamin D in obesity. Am J Clin Nutr 2000;72:690-693
23. Di Cesar DJ, Ploutz-Snyder R, Weinstock RS, Moses AM: Vitamin D Deficiency
Is More Common in Type 2 Than in Type 1 Diabetes. Diabetes Care 2006;29:174
24. Palomer X, Gonzalez-Clemente JM, Blanco-Vaca F, Mauricio D: Role of
vitamin D in the pathogenesis of type 2 diabetes mellitus. Diabetes Obes Metab
2008;10:185-197
25. Glerup H, Mikkelsen K, Poulsen L, Hass E, Overbeck S, Thomsen J, Charles
P, Eriksen EF: Commonly recommended daily intake of vitamin D is not sufficient if
sunlight exposure is limited. J Intern Med 2000;247:260-268
26. Mavroeidi A, O'Neill F, Lee PA, Darling AL, Fraser WD, Berry JL, Lee WT, Reid
DM, Lanham-New SA, Macdonald HM: Seasonal 25-hydroxyvitamin D changes in
British postmenopausal women at 57 degrees N and 51 degrees N: a longitudinal
study. J Steroid Biochem Mol Biol 2010;121:459-461

248
27. Gozdzik A, Barta JL, Weir A, Cole DE, Vieth R, Whiting SJ, Parra EJ: Serum
25-hydroxyvitamin D concentrations fluctuate seasonally in young adults of diverse
ancestry living in Toronto. J Nutr 2010;140:2213-2220
28. Boucher BJ, Mannan N, Noonan K, Hales CN, Evans SJ: Glucose intolerance
and impairment of insulin secretion in relation to vitamin D deficiency in east
London Asians. Diabetologia 1995;38:1239-1245
29. Scragg R, Sowers M, Bell C: Serum 25-hydroxyvitamin D, diabetes, and
ethnicity in the Third National Health and Nutrition Examination Survey. Diabetes
Care 2004;27:2813-2818
30. Wareham NJ, Byrne CD, Carr C, Day NE, Boucher BJ, Hales CN: Glucose
intolerance is associated with altered calcium homeostasis: a possible link between
increased serum calcium concentration and cardiovascular disease mortality.
Metabolism 1997;46:1171-1177
31. Sattar N, Taskinen M-R: Statins are diabetogenic – Myth or reality?
Atherosclerosis Supplements 2012;13:1-10

249
7 Chapter VII - Differential effects of different vitamin D
replacement strategies in patients with diabetes
Contribution: Uazman Alam conceived the study and subsequently designed it,
acquired data, performed statistical analysis and wrote the manuscript which
constitutes the basis for this chapter and was submitted and accepted for
publication in the Journal of Diabetes and its Complications 2013 (Epub ahead of
print).
Uazman Alam, Agnes WS Chan, April Buazon, Cristiano Van Zeller, Jacqueline L
Berry, Ravinder S Jugdey, Omar Asghar, John Kennedy Cruickshank, Ioannis N
Petropoulos, Rayaz A Malik

250
7.1 ABSTRACT
The optimal treatment regimen for correcting vitamin D insufficiency in diabetic
patients has not been established.
Two hundred and forty four adult diabetic patients with vitamin D insufficiency were
enrolled to receive: Ergocalciferol (D2) 50,000 IU daily over 10 days (500,000 IU)
followed by Calcichew D3 (calcium carbonate/Cholecalciferol) BID (~24,000IU
cholecalciferol/month) (ECC) (n=53); Cholecalciferol (D3) 40,000 IU daily over 10
days (400,000 IU) followed by Calcichew D3 BID (~24,000IU cholecalciferol/month)
(CCC) (n=94) or Cholecalciferol 40,000 IU daily over 10 days (400,000 IU) followed
by Cholecalciferol 40,000 IU monthly (CC) (n=97). The 25(OH)D, HbA1c, lipids,
blood pressure and eGFR were assessed at baseline and after a mean follow up of
8.0±4.0 months.
Treatment increased 25(OH)D concentrations significantly in ECC (17.4±13.8 vs
29.9±9.6ng/ml, P<0.0001), CCC (14.2±6.6 vs 30.9±13.1ng/ml, p<0.0001) and CC
(13.5±8.4 vs 33.9±14.4ng/ml, P<0.0001). The relative increase in 25(OH)D was
significantly lower with ECC compared to CC (+14.6±12.2 vs +20.6±15.0, P=0.01)
and the majority of subjects in the ECC group (63%) remained vitamin D deficient
(25(OH)D<30ng/ml) compared to CCC (46%) and CC (36%)(P=0.0005).
This study demonstrates that relatively aggressive treatment regimens of both
vitamin D2 and D3 increase 25(OH)D concentrations in diabetic patients, but the
ability to raise 25(OH)D status to ‘sufficient’ levels is inadequate in a large
proportion of individuals.
251
7.2 INTRODUCTION
There is an epidemic of vitamin D deficiency worldwide (1). Vitamin D has been
implicated not only in bone health but also a host of cardiovascular diseases
including diabetes, hypertension and metabolic syndrome (2). Vitamin D deficiency
poses a significant health problem in many countries irrespective of economic,
cultural or geographic diversity (3).
There is currently consensus that levels below 10ng/ml (25nmol/L) qualify as
‘deficient’ and require treatment, but beyond this there is currently no standard
definition of ‘optimal’ 25(OH)D with some sources suggesting that levels above
20ng/ml (50nmol/L) are ‘sufficient’, while 28-32ng/ml (70–80nmol/L) are ‘optimal’
(4). The Department of Health in the UK has set dietary recommendations for
children aged 6 months to 5 years, those aged 65 years and over (5), and pregnant
or lactating women and also recommends that people at risk of low sun exposure
should get 10 µg of vitamin D a day, through supplementation (6). However, the
recommended daily allowance (RDA) has not changed despite its inability to
prevent severe vitamin D deficiency and ensuing bone or metabolic complications
in the absence of adequate sunlight exposure (7-9).
Recent data confirm the high prevalence of vitamin D deficiency and no impact of
dietary vitamin D intake in the UK due to low amounts of fortification (10).
Furthermore, proposed treatment strategies recommending ‘over the counter’
vitamin D preparations have been found to be largely ineffective in correcting
vitamin D deficiency (2; 7; 11). Currently there are limited data to guide policy on
replacement strategies (2; 7). Previous studies have suggested that vitamin D2 is
2-3 times less effective at increasing serum 25-hydroxyvitamin D (25(OH)D) than

252
vitamin D3, but that vitamin D2 taken on a daily basis in high enough doses may be
as effective in maintaining 25(OH)D as vitamin D3 (12-14).
We assessed the effects of 3 different vitamin D replacement regimens (using
combinations of ergocalciferol, cholecalciferol and calcium
carbonate/cholecalciferol) dependent on the clinician’s preference for treatment of
vitamin D deficiency.

253
7.3 RESEARCH DESIGN AND METHODS
The study was undertaken at the Central Manchester University Hospitals NHS
Foundation Trust, Manchester, UK. Data from a population-based cohort of 244
patients with Diabetes (Type 1 and 2 Diabetes Mellitus) attending a tertiary
diabetes centre were analyzed. Ethical approval was not required for this analysis
as all the data were extracted retrospectively. This therefore did not extend beyond
standard clinical practice. All patients with a 25(OH)D <30ng/ml were allocated to 3
different treatment regimens based on the prescribing choice of three different
clinicians: Ergocalciferol (D2) 50,000 IU daily over 10 days (500,000 IU) followed by
Calcichew D3 (calcium carbonate/Cholecalciferol) BID (~24,000IU
cholecalciferol/month) (ECC) (n=53); Cholecalciferol (D3) 40,000 IU daily over 10
days (400,000 IU) followed by Calcichew D3 BID (~24,000IU cholecalciferol/month)
(CCC) (n=94) or Cholecalciferol 40,000 IU daily over 10 days (400,000 IU) followed
by Cholecalciferol 40,000 IU monthly (1st day of each month (CC (n=97). All
subjects were provided with vitamin D regimens as soon as vitamin D results were
made available, however, data on medication compliance were unavailable.
7.3.1 Blood pressure and Anthropometric measurements
Body mass index (BMI) was measured as per the standard equation (mass
(kg)/(height(m))2. Weight was measured with a digital scale (Seca 701, Seca,
Hamburg, Germany) to the nearest 0.1kg and height to the nearest 0.1cm with a
calibrated stadiometer. Both height and weight were taken at comparable times at
baseline and follow up. Blood pressure (BP) was assessed using an automated BP
device (Dinamap pro 100v2, GE Medical Systems, Freiburg, Germany) with an

254
appropriate cuff size. Two measurements of systolic and diastolic BP were made
five minutes apart with the lowest reading recorded.
7.3.2 Assessment of Demographics, Cardiovascular disease and
Medications
An assessment of patient demographics was made through analysis of medical
records and an in-hospital medical record database (Diamond database, Hicom,
Surrey, UK). Subject demographics extracted were age, sex, ethnicity (White
European, South Asian, Far East Asian and Afro-Caribbean descent), type
(T1DM/T2DM), duration of diabetes and current anti-diabetic therapy with any
alterations to treatment during the intervention period.
7.3.3 Laboratory Measurements
Assessment of 25(OH)D was instituted in August 2009 as part of routine
haematological and biochemical laboratory measurements which included HbA1c,
Complete Blood count (CBC), Urea and Electrolytes (UE), Liver function tests
(LFT), bone profile (Corrected Calcium (CCa2+), Alkaline Phosphatase (ALP),
Albumin (Alb), and Lipid profile (Total Cholesterol (T-CHL), High Density lipoprotein
Cholesterol (HDL), Triglycerides (TRIG)). For 25(OH)D measurement, serum was
separated from whole blood and stored at -20 C until assay. The laboratory used
for the biochemical assay measurements (Vitamin D Research Group Manchester
Royal Infirmary, UK) was accredited to ISO 9001:2008 and ISO 13485:2003 by
Lloyd’s Register Quality Assurance certificate number LRQ 4001542 and
participated successfully in the Vitamin D quality assurance scheme (DEQAS).
Serum 25(OH)D was measured using the IDS-iSYS multi-discipline automated

255
analyzer (Immunodiagnostic Systems Ltd, Boldon, Tyne and Wear, UK). The assay
is based on chemiluminescent technology and was performed exactly as per the
manufacturer’s instructions. The cross reactivity for vitamin D2 (of the assay) as per
manufacturers assertion was 100% (relative to vitamin D3) and the assay has
excellent correlation to existing globally recognised assays, in combination with
good sensitivity and precision (15). The reportable range of the assay is 5-140
ng/ml Inter- and intra- assay variation of the in-house control was 5.6% and 9.7%
respectively.
7.3.4 Statistical analysis
Statistical analyses were undertaken using Statsdirect (Statsdirect, Cheshire, UK).
ANOVA method or a non-parametric counterpart, Kruskal-Wallis were used to
assess differences between groups depending on normality of the data. Overall the
P value was maintained at 0.05 for multiple comparison tests (after Bonferoni
adjustment or Conover-Inman pairwise comparison). Paired t-tests were used for
intra-individual observations. A P value of ≤0.05 was considered to be statistically
significant. All values are presented as mean ± standard deviation (SD).

256
7.4 RESULTS
Demographics of the three cohorts are shown in Table 7.1. They did not differ in for
age, type of diabetes, sex and ethnicity and there were no differences in the period
of follow up. A significant proportion of subjects still remained deficient on ECC
regimen of supplementation (P=0.0005) compared to the other regimens (CCC and
CC). Anti-diabetic therapies used in each cohort are detailed in Table 7.1. There
were significant differences in the types of anti-diabetic regimens used (chi2
P=0.01) across the 3 groups, however, there were no significant differences in the
numbers of individuals who had intensification of their diabetes treatment in each
cohort from baseline to follow up. In those individuals requiring insulin
administration, mean doses of insulin units required per day did not differ.

257
Table 7-1 Clinical and demographic data and Characteristics of Anti-Diabetic therapy in all
three cohorts of all three intervention cohorts
ECC (n=53) CCC (n=94) CC (n=97)
Age (years) 60.7±12.1 58.2±13.3 57.0±12.2
Sex (% male) 55 57 52
Type 2 DM (%) 81 68 82
Duration of diabetes (years) 16.7±11.2 21.1±12.8 17.1±10.3
Ethnicity (% White European)
55 57 52
% on lipid lowering therapy 80 90 87
Period of follow up (months)
8.0±3.7 7.8±3.9 8.1±4.3
Insufficient after supplementation
with 25(OH)D (<30ng/ml) n (%)
32 (63)* 43 (46)* 35 (36)*
Treatment regimens^
Diet controlled n (%) 0 (0) 3 (3) 1 (1)
Single oral therapy n (%) 8 (15) 7 (7) 4 (4)
Oral combination therapy n (%)
20 (38) 22 (23) 31 (32)
Oral and/or Insulin + GLP-1 mimetic n (%)
1 (2) 8 (9) 10 (10)
Oral + Insulin therapy n (%) 15 (28) 21 (22) 30 (31)
Insulin alone n (%) 12 (23) 31 (33) 20 (21)
CSII therapy n (%) 2 (4) 2 (2) 1 (1)
Mean Insulin dose/day (mean±SD) Median(IQR)
86±81** 64(44-76)
92±149** 68.5(48-88)
84±63** 65(52-104)
Escalation in Anti diabetic Therapy n (%)
11 (19)*** 20 (21)*** 17 (18)***
No. of subjects with increase in insulin n (%)
1 (2) 10 (11) 2 (2)
Average dose increase in insulin/day (units)
(mean±SD) 6±0 4±1.3 2±0
Post hoc analyses
*P=0.0005 (Chi2 test); ^Chi
2 for treatment regimens – P=0.01; **KrusKal-Wallis – P=NS.
***Chi 2 for intensification of anti-diabetic therapy – P=NS.
Type 2 DM – Type 2 Diabetes Mellitus.
Table key
CSII – Continuous Subcutaneous Insulin Infusion, DM – Diabetes Mellitus, IQR – Interquartile
range, SD – Standard deviation.

258
25(OH)D status and metabolic data are presented in Table 7.2. The 25(OH)D
concentrations at baseline were higher in the ECC cohort when compared to CCC
and CC (17.4±13.8 vs 14.2±6.6 vs 13.5±8.4ng/ml), respectively, although this did
not reach statistical significance. After treatment 25(OH)D concentrations
increased significantly in the ECC (17.4±13.8 vs 29.9±9.6, P<0.0001), CCC
(14.2±6.6 vs 30.9±13.1, P<0.0001) and CC (13.5±8.4 vs 33.9±14.4ng/ml,
P<0.0001) cohorts, respectively. There was no difference in the increase in
25(OH)D comparing ECC to CCC (+14.6±12.2 vs +16.7±13.4ng/ml). However,
there was a significantly greater increase in CC compared to ECC (+20.6±15.0 v
+14.6±12.2, P=0.01) with no difference compared to CCC. However, 63% of
patients remained deficient (25(OH)D <30ng/ml) after treatment in the ECC cohort
compared to 46% and 36% in the CCC and CC cohorts, respectively (chi2
P=0.0005). When further subdividing the three cohorts into those with an initial
25(OH)D <15ng/ml and >15ng/ml (based on the study by Wang et al (16)) there
were significant differences between pre- and post-intervention, with a more
pronounced increase in 25(OH)D in those with a lower baseline 25(OH)D (ECC:
+21.2±8.4 vs +6.4±11.4ng/ml, p<0.0001, CCC: +20.1±13.8 vs +12.3±11.6ng/ml,
P=0.005, CC: +24.4±14.5 vs +12.1±12.9ng/ml, P=0.01)(figures 7.1a, b and c).
There were no significant changes in BMI, systolic and diastolic blood pressure,
lipid profile (T-CHL, HDL and TRIG) and eGFR after treatment in any of the
cohorts. However, there was a significant reduction in HbA1c after treatment in
ECC (-0.5% or 5.2mmol/mol, P=0.02), with no change in the CCC (8.3±1.7 vs
8.3±1.7%) or CC (8.2±1.6 vs 8.1±1.6%) cohorts.
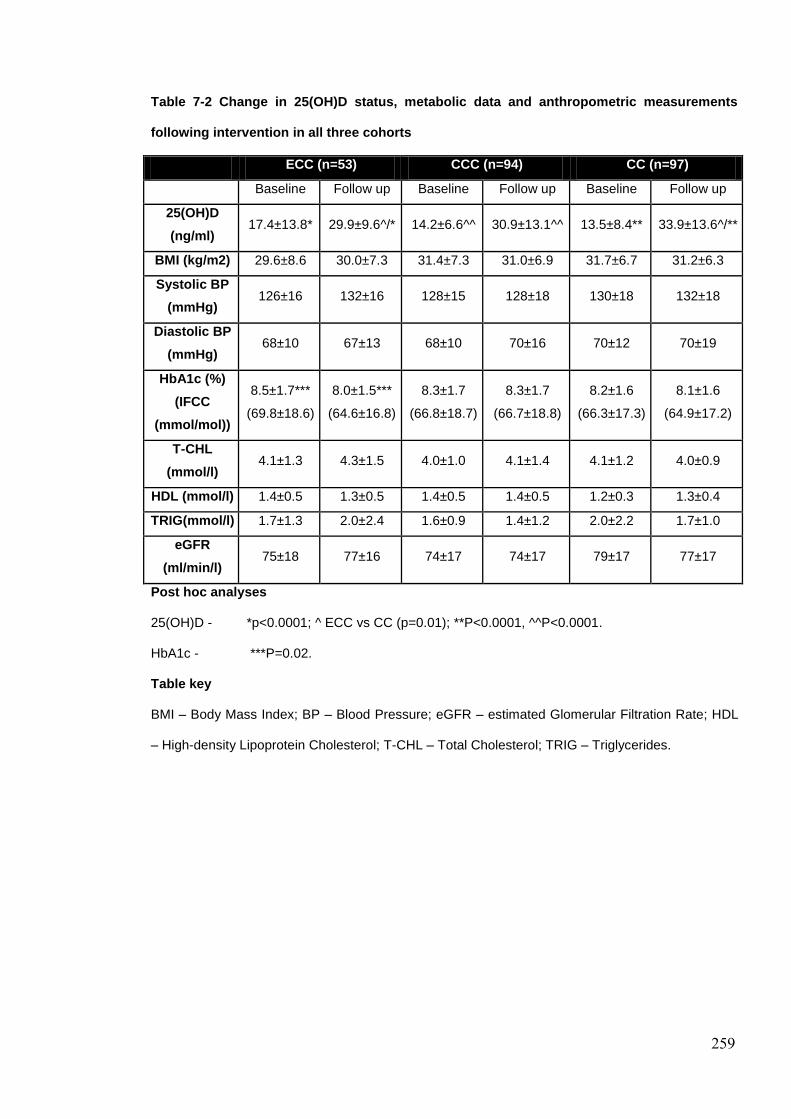
259
Table 7-2 Change in 25(OH)D status, metabolic data and anthropometric measurements
following intervention in all three cohorts
ECC (n=53) CCC (n=94) CC (n=97)
Baseline Follow up Baseline Follow up Baseline Follow up
25(OH)D
(ng/ml) 17.4±13.8* 29.9±9.6^/* 14.2±6.6^^ 30.9±13.1^^ 13.5±8.4** 33.9±13.6^/**
BMI (kg/m2) 29.6±8.6 30.0±7.3 31.4±7.3 31.0±6.9 31.7±6.7 31.2±6.3
Systolic BP
(mmHg) 126±16 132±16 128±15 128±18 130±18 132±18
Diastolic BP
(mmHg) 68±10 67±13 68±10 70±16 70±12 70±19
HbA1c (%)
(IFCC
(mmol/mol))
8.5±1.7***
(69.8±18.6)
8.0±1.5***
(64.6±16.8)
8.3±1.7
(66.8±18.7)
8.3±1.7
(66.7±18.8)
8.2±1.6
(66.3±17.3)
8.1±1.6
(64.9±17.2)
T-CHL
(mmol/l) 4.1±1.3 4.3±1.5 4.0±1.0 4.1±1.4 4.1±1.2 4.0±0.9
HDL (mmol/l) 1.4±0.5 1.3±0.5 1.4±0.5 1.4±0.5 1.2±0.3 1.3±0.4
TRIG(mmol/l) 1.7±1.3 2.0±2.4 1.6±0.9 1.4±1.2 2.0±2.2 1.7±1.0
eGFR
(ml/min/l) 75±18 77±16 74±17 74±17 79±17 77±17
Post hoc analyses
25(OH)D - *p<0.0001; ^ ECC vs CC (p=0.01); **P<0.0001, ^^P<0.0001.
HbA1c - ***P=0.02.
Table key
BMI – Body Mass Index; BP – Blood Pressure; eGFR – estimated Glomerular Filtration Rate; HDL
– High-density Lipoprotein Cholesterol; T-CHL – Total Cholesterol; TRIG – Triglycerides.

260
Figure 7-1a Box and Whisker plots for 25(OH)D pre- and post-intervention in ECC
subdividing into <15ng/ml and >15ng/ml
1st VIT D ECC <15ng/ml 2nd Vit D ECC <15ng/ml 1st VIT D ECC >15ng/ml 2nd Vit D ECC >15ng/ml
0
10
20
30
40
50
6025 (OH)D pre- and post-intervention dependent on baseline Vitamin D status
25
(O
H)D
ng
/ml
P<0.0001 +6.4 ± 11.4
ng/ml
+21.2 ± 8.4
ng/ml
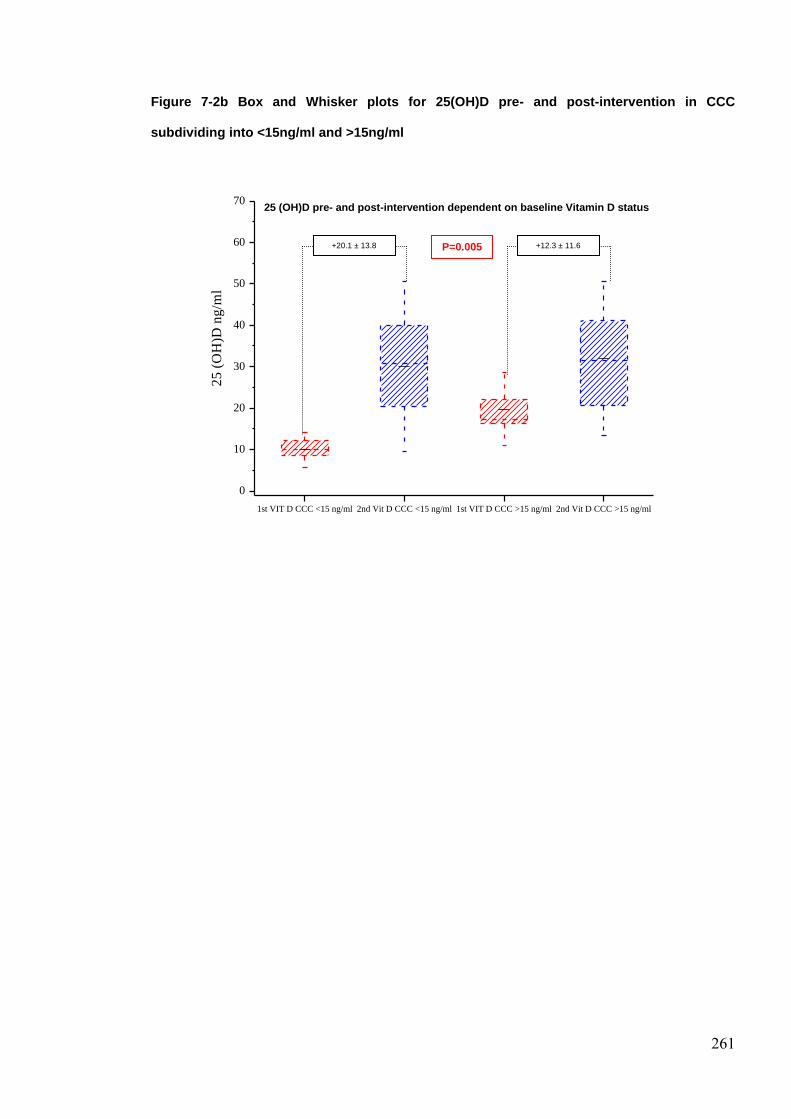
261
Figure 7-2b Box and Whisker plots for 25(OH)D pre- and post-intervention in CCC
subdividing into <15ng/ml and >15ng/ml
1st VIT D CCC <15 ng/ml 2nd Vit D CCC <15 ng/ml 1st VIT D CCC >15 ng/ml 2nd Vit D CCC >15 ng/ml
0
10
20
30
40
50
60
70
25
(O
H)D
ng
/ml
25 (OH)D pre- and post-intervention dependent on baseline Vitamin D status
+12.3 ± 11.6
ng/ml
+20.1 ± 13.8
ng/ml
P=0.005
0.)00.00
5
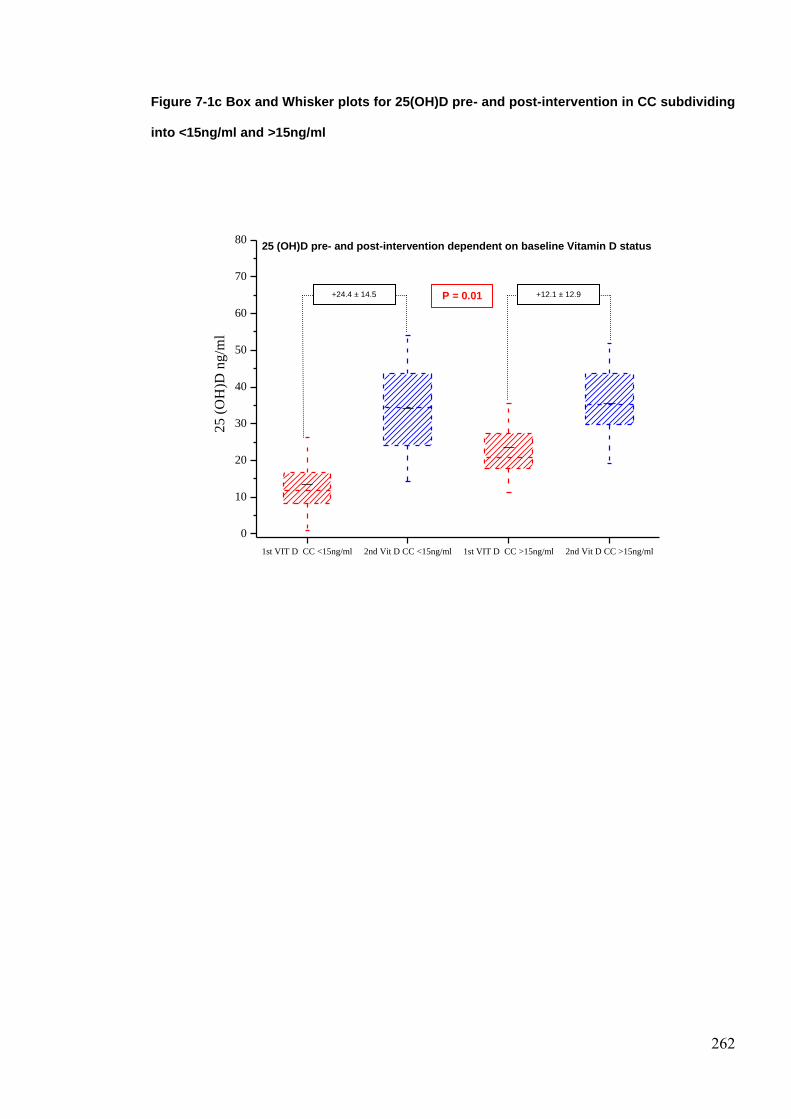
262
Figure 7-1c Box and Whisker plots for 25(OH)D pre- and post-intervention in CC subdividing
into <15ng/ml and >15ng/ml
1st VIT D CC <15ng/ml 2nd Vit D CC <15ng/ml 1st VIT D CC >15ng/ml 2nd Vit D CC >15ng/ml
0
10
20
30
40
50
60
70
8025 (OH)D pre- and post-intervention dependent on baseline Vitamin D status
25
(O
H)D
ng
/ml
P = 0.01 +12.1 ± 12.9
ng/ml
+24.4 ± 14.5
ng/ml

263
7.5 DISCUSSION
Vitamin D deficiency is highly prevalent and current guidelines recommending
replacement regimes appear inadequate (17). In 2011, the US Institute of Medicine
(IOM) Recommended Dietary Allowance (RDA) of vitamin D was 800 IU per day
for older adults. A serum 25(OH)D of 20 ng/ml is considered to be sufficient by the
IOM. However, recently the US Endocrine Society's Clinical Practice Guideline
suggest 1500-2000 IU per day for adults aged 19 years or more to maintain
25(OH)D above the optimal level of 30 ng/ml (18). Earlier data suggested that at
least 55 µg (2200IU)/day is necessary to increase 25(OH)D concentrations from
20- 40 nmol/L (8-16 ng/ml) to 80 nmol/L (32 ng/ml) (19). Yet both the UK
Department of Health and NICE continue to endorse dietary supplementation of 10
µg (400IU)/day and UK recommendations, particularly for primary care advocate
‘over the counter’ supplements or dual calcium carbonate and cholecalciferol
supplementation which only contain 100-400IU of cholecalciferol/per tablet (7; 20).
Recent guidelines by Holick et al (21) have suggested in adults that a dose of
400,000IU vitamin D2 over 8 weeks followed by a maintenance therapy of 1500-
2000IU daily is adequate in the treatment of deficiency. In a retrospective cohort
study from the US, a dosing schedule of D2 (50,000IU on alternate weeks) has
recently been shown to be effective, with a baseline 25(OH)D of 31.0 ± 10.6 ng/mL
increasing to 48.3 ± 13.4 ng/mL (22). Our treatment protocols at the Manchester
Diabetes centre consisted of a loading dose of vitamin D2 (ergocalciferol) or D3
(cholecalciferol) at non-bioequivalent doses of 500,000IU and 400,000IU
respectively, followed by a maintenance dose of cholecalciferol with or without
calcium carbonate. In our study the baseline 25(OH)D concentration was lower,
264
than the previous study, and therefore despite a higher dose replacement the
increase in 25(OH)D was not as marked (D2 ~12-13ng/ml, D3 ~20ng/ml). Most
treatment protocols do not differentiate between the therapeutic effect of vitamin D2
and D3 (7; 23), although, clearly this has implications on therapeutic effects and
monitoring of treatment. The difference in increasing the concentrations of
25(OH)D is both physiologically and pharmacologically meaningful with studies
showing that increasing 25(OH)D improves calcium absorption (2), reduces fall
frequency (24) and osteoporotic fracture risk (25). Previous studies have
suggested that 50,000IU of vitamin D2 may be biologically equivalent to ~15,000IU
of vitamin D3 (13). Of course, vitamin D2 is effective in elevating 25(OH)D
concentrations, but has been considered not to be bio-equivalent with a
suggestion for dose adjustment in treatment protocols (26). However, conclusions
regarding the biological consequence and functional effects of the D2 and D3
cannot clearly be drawn. Additional studies are needed to elucidate the
pharmacokinetic parameters and the varying vitamin D2 and vitamin D3 25(OH)D
metabolites produced which may have differing biological affinity and thus differing
physiological responses (19; 27).
Despite these differences a considerable proportion of individuals still remain
vitamin D deficient on these regimens. Thus even with doses of cholecalciferol
which were approximately equivalent to the current recommended maintenance
therapy in addition to an ‘adequate’ loading dose still resulted in around 46% of
individuals being below the target 25(OH)D of 30ng/ml. This cannot be due to
inadequate time of exposure to treatment as the time to equilibrium of vitamin D3 is
approximately 5 months (28). Our data confirm a significant disparity of effect
between those supplemented at lower compared to higher baseline levels (29). It
265
has been previously suggested that there is essentially a linear relationship up to
10000IU (4), however there are minimal data directly assessing baseline 25(OH)D
status and response to a standardised vitamin D intervention. Variations in
circulating concentrations can also be attributed to differences in the transport of
vitamin D in the circulation following exposure to the sun and oral routes (30) with
an initial rapid hepatic delivery of vitamin D via the oral route but the increase in
concentrations is not as well sustained. However, in the present study all three
interventions were oral and of sufficiently long duration to ensure a steady state
concentration. Therefore the differences can be primarily attributed to
pharmacological differences in the replacement regimens, although genetic
polymorphisms may affect the vitamin D metabolic pathway (31). Furthermore, we
show that patients with a lower baseline show the most marked rise in
concentrations of 25 (OH)D, despite equivalent doses. This may be important for
dosing considerations when establishing replacement protocols and the need for
less conservative treatment (32). In fact vitamin D shares a similar intake-response
curve as other nutrients and in persons whose baseline values differ, an identical
nutrient intake may or may not produce a measurable response (33).
Unfortunately, most of the randomized, controlled trials of vitamin D that have been
published to date have paid little attention to baseline status (33).
A range of potentially beneficial metabolic effects of vitamin D have been proposed
(34-36). Vitamin D receptors are of course expressed ubiquitously along with
vitamin D activating enzymes (2) and are also present on pancreatic β-cells (2).
Circulating 25(OH)D is inversely associated with insulin resistance and possibly
insulin secretion (37), and there is a inverse relationship between 25(OH)D
concentrations and the risk of Type 2 DM (38). Moreover, a recent study has
266
shown an improvement in HbA1c when diabetic patients were given vitamin D (39).
A recent meta-analysis, stated ‘there was a insufficient evidence of beneficial effect
to recommend vitamin D supplementation as a means of improving glycaemia or
insulin resistance in patients with diabetes, normal fasting glucose or impaired
glucose tolerance’, although the doses used for replacement were not adequate
(40). In the present study, whilst there was an overall intensification of anti-diabetic
treatment in all groups there was no significant difference between the cohorts.
Importantly the administration of D2 did not achieve adequate plasma
concentrations of 25(OH)D which was lower than CCC and CC cohorts which did
not produce significant drops in glycaemia. Therefore the improvement in blood
glucose control cannot be entirely accredited to ergocalciferol administration. This
study provides hypothesis generating data to assess any differential effect of
vitamin D2 and D3 on glycaemic control.
A major limitation of the present retrospective analysis was that it was not
randomised (to treatment groups) and there was no placebo arm and was
therefore subject to a greater degree of confounding. However, it provides
interesting hypotheses generating ‘real world’ data on the ‘correct’ dosing regimens
in vitamin D deficiency and the need for more intensive dosing regimens for
patients with vitamin D deficiency. This highlights the significant need for high
quality randomised controlled trials assessing the effectiveness of cholecalciferol
and ergocalciferol in the treatment of vitamin D deficiency and metabolic outcomes
in diabetes.

267
7.6 REFERENCES
1. Holick MF: Deficiency of sunlight and vitamin D. BMJ 2008;336:1318-1319
2. Holick MF: Vitamin D Deficiency. New England Journal of Medicine
2007;357:266-281
3. Ghazi AA, Hosseinpanah F, E MA, Ghazi S, Hedayati M, Azizi F: Effects of
different doses of oral cholecalciferol on serum 25(OH)D, PTH, calcium and bone
markers during fall and winter in schoolchildren. Eur J Clin Nutr 2010;64:1415-
1422
4. Vieth R: Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and
safety. The American Journal of Clinical Nutrition 1999;69:842-856
5. Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes B:
Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple
health outcomes. Am J Clin Nutr 2006;84:18-28
6. VITAMIN D - ADVICE ON SUPPLEMENTS FOR AT RISK GROUPS [article
online], 2012. Available from:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/1345
50/dh_132508.pdf.pdf.
7. Pearce SH, Cheetham TD: Diagnosis and management of vitamin D deficiency.
BMJ 2010;340:b5664
8. Vieth R, Bischoff-Ferrari H, Boucher BJ, Dawson-Hughes B, Garland CF,
Heaney RP, Holick MF, Hollis BW, Lamberg-Allardt C, McGrath JJ, Norman AW,
Scragg R, Whiting SJ, Willett WC, Zittermann A: The urgent need to recommend
an intake of vitamin D that is effective. Am J Clin Nutr 2007;85:649-650

268
9. Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes B:
Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple
health outcomes. The American Journal of Clinical Nutrition 2006;84:18-28
10. Darling AL, Hart KH, Macdonald HM, Horton K, Kang'ombe AR, Berry JL,
Lanham-New SA: Vitamin D deficiency in UK South Asian Women of childbearing
age: a comparative longitudinal investigation with UK Caucasian women.
Osteoporos Int 2012; 2013;24:477-488
11. Gupta K, Warner JT: Inappropriate and inconsistent modalities of treatment of
vitamin D deficiency in children. Archives of Disease in Childhood 2011;
doi:10.1136/adc.2011.214361
12. Trang H, Cole D, Rubin L, Pierratos A, Siu S, Vieth R: Evidence that vitamin D3
increases serum 25-hydroxyvitamin D more efficiently than does vitamin D2. The
American Journal of Clinical Nutrition 1998;68:854-858
13. Armas LAG, Hollis BW, Heaney RP: Vitamin D2 Is Much Less Effective than
Vitamin D3 in Humans. Journal of Clinical Endocrinology & Metabolism
2004;89:5387-5391
14. Tjellesen L, Hummer L, Christiansen C, Rodbro P: Serum concentration of
vitamin D metabolites during treatment with vitamin D2 and D3 in normal
premenopausal women. Bone Miner 1986;1:407-413
15. ASBMR 31st Annual Meeting MO0001–MO0445. Journal of Bone and Mineral
Research 2009;24:S370-S496
16. Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K, Benjamin
EJ, D'Agostino RB, Wolf M, Vasan RS: Vitamin D deficiency and risk of
cardiovascular disease. Circulation 2008;117:503-511

269
17. Alam U, Najam O, Al-Himdani S, Benoliel S, Jinadev P, Berry JL, Kew M,
Asghar O, Petropoulos IN, Malik RA: Marked vitamin D deficiency in patients with
diabetes in the UK: ethnic and seasonal differences and an association with
dyslipidaemia. Diabet Med 2012;
18. Pramyothin P, Holick MF: Vitamin D supplementation: guidelines and evidence
for subclinical deficiency. Curr Opin Gastroenterol 2012;28:139-150
19. Heaney RP: The Vitamin D requirement in health and disease. J Steroid
Biochem Mol Biol 2005;97:13-19
20. Ross AC, Manson JE, Abrams SA, Aloia JF, Brannon PM, Clinton SK, Durazo-
Arvizu RA, Gallagher JC, Gallo RL, Jones G, Kovacs CS, Mayne ST, Rosen CJ,
Shapses SA: The 2011 Report on Dietary Reference Intakes for Calcium and
Vitamin D from the Institute of Medicine: What Clinicians Need to Know. Journal of
Clinical Endocrinology & Metabolism 2011;96:53-58
21. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney
RP, Murad MH, Weaver CM: Guidelines for preventing and treating vitamin D
deficiency and insufficiency revisited. J Clin Endocrinol Metab 2012;97:1153-1158
22. Demetriou ET, Travison TG, Holick MF: Treatment with 50,000 IU vitamin D2
every other week and effect on serum 25-hydroxyvitamin D2, 25-hydroxyvitamin
D3, and total 25-hydroxyvitamin D in a clinical setting. Endocr Pract 2012;18:399-
402
23. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney
RP, Murad MH, Weaver CM: Evaluation, Treatment, and Prevention of Vitamin D
Deficiency: an Endocrine Society Clinical Practice Guideline. Journal of Clinical
Endocrinology & Metabolism 2011;96:1911-1930

270
24. Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, Staehelin HB, Bazemore
MG, Zee RY, Wong JB: Effect of Vitamin D on Falls. JAMA: The Journal of the
American Medical Association 2004;291:1999-2006
25. Lips P, Hosking D, Lippuner K, Norquist JM, Wehren L, Maalouf G, Ragi-Eis S,
Chandler J: The prevalence of vitamin D inadequacy amongst women with
osteoporosis: an international epidemiological investigation. J Intern Med
2006;260:245-254
26. Khazai NB, Judd SE, Jeng L, Wolfenden LL, Stecenko A, Ziegler TR,
Tangpricha V: Treatment and Prevention of Vitamin D Insufficiency in Cystic
Fibrosis Patients: Comparative Efficacy of Ergocalciferol, Cholecalciferol, and UV
Light. Journal of Clinical Endocrinology & Metabolism 2009;94:2037-2043
27. Houghton LA, Vieth R: The case against ergocalciferol (vitamin D2) as a
vitamin supplement. The American Journal of Clinical Nutrition 2006;84:694-697
28. Heaney RP, Davies KM, Chen TC, Holick MF, Barger-Lux MJ: Human serum
25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol.
Am J Clin Nutr 2003;77:204-210
29. Trang HM, Cole DE, Rubin LA, Pierratos A, Siu S, Vieth R: Evidence that
vitamin D3 increases serum 25-hydroxyvitamin D more efficiently than does
vitamin D2. The American Journal of Clinical Nutrition 1998;68:854-858
30. Haddad JG, Matsuoka LY, Hollis BW, Hu YZ, Wortsman J: Human plasma
transport of vitamin D after its endogenous synthesis. J Clin Invest 1993;91:2552-
2555
31. Ahn J, Yu K, Stolzenberg-Solomon R, Simon KC, McCullough ML, Gallicchio L,
Jacobs EJ, Ascherio A, Helzlsouer K, Jacobs KB, Li Q, Weinstein SJ, Purdue M,
Virtamo J, Horst R, Wheeler W, Chanock S, Hunter DJ, Hayes RB, Kraft P,

271
Albanes D: Genome-wide association study of circulating vitamin D levels. Human
Molecular Genetics 2010;19:2739-2745
32. Vieth R: Vitamin D and Cancer Mini-Symposium: The Risk of Additional
Vitamin D. Annals of Epidemiology 2009;19:441-445
33. Heaney RP: Vitamin D — Baseline Status and Effective Dose. New England
Journal of Medicine 2012;367:77-78
34. Holick MF: Evidence-based D-bate on health benefits of vitamin D revisited.
Dermatoendocrinol 2012;4:183-190
35. Holick MF: Nutrition: D-iabetes and D-eath D-efying vitamin D. Nat Rev
Endocrinol 2012;8:388-390
36. Holick MF: Vitamin D: extraskeletal health. Rheum Dis Clin North Am
2012;38:141-160
37. Peechakara SV, Pittas AG: Vitamin D as a potential modifier of diabetes risk.
Nat Clin Pract End Met 2008;4:182-183
38. Mitri J, Muraru MD, Pittas AG: Vitamin D and type 2 diabetes: a systematic
review. Eur J Clin Nutr 2011;65:1005-1015
39. Ali AM, Awad, T.G., Ali, O.M.: Effect of Short-Term Vitamin D Supplementation
On Glycemic Control In Newly-Diagnosed Type 2 Diabetics. Australian Journal of
Basic and Applied Sciences 2011;5:1235-1239
40. George PS, Pearson ER, Witham MD: Effect of vitamin D supplementation on
glycaemic control and insulin resistance: a systematic review and meta-analysis.
Diabet Med 2012;29:e142-150

272
8 Chapter VIII - Vitamin D Deficiency Contributes to
Painful Diabetic Neuropathy
Contribution: Uazman Alam contributed to the conception and design of the study
and made a major contribution to the recruitment of subjects, clinical tests including
neuropathy assessments and skin biopsies, skin biopsy analyses, all statistical
analyses and the writing of this chapter.
Submitted to Diabetes awaiting revision and resubmission
Uazman Alam, Ioannis N Petropoulos, Georgios Ponirakis, Omar Asghar, Maria
Jeziorska, Hassan Fadavi, Andrew Marshall, Mitra Tavakoli, Andrew JM Boulton,
Nathan Efron, Rayaz A Malik

273
8.1 ABSTRACT
The aetiology of painful diabetic neuropathy (PDN) is unclear. Low vitamin D levels
have been associated with a number of painful conditions. We have evaluated
vitamin D levels in diabetic patients with and without painful neuropathy.
Forty three type 1 diabetic patients subdivided into painless neuropathy (DPN)
(n=20) and painful neuropathy (PDN) (n=23) and 14 non-diabetic healthy control
subjects (C) underwent detailed assessment of neurologic deficits, quantitative
sensory testing (QST), electrophysiology, skin biopsy and corneal confocal
microscopy (CCM) together with measurement of serum 25(OH)D.
There were no significant differences for age, BMI, HbA1c, lipids, neurological
evaluation, QST, electrophysiology, intra-epidermal nerve fibre density (IENFD)
and corneal nerve morphology when comparing DPN with PDN. Both positive
(hyperalgesia and allodynia) and negative symptoms (paraesthesia and
numbness) of diabetic neuropathy were greater in PDN compared to DPN
(P=0.009 and P=0.02 respectively). Serum 25(OH)D level were significantly lower
in PDN (24.0±14.1ng/ml) compared to DPN (34.6±15.0ng/ml, P=0.01) and controls
(34.1±8.6ng/ml, P=0.03). The odds ratio in favour of painful diabetic neuropathy
was 9.8 (P=0.003 (95% CI 2.2-76.4) for vitamin D deficiency (<20ng/ml) and 4.4
(P=0.03 (95% CI 1.1-19.8)) for vitamin D insufficiency (<30ng/ml).
This study provides a novel association between vitamin D deficiency and painful
diabetic neuropathy.

274
8.2 INTRODUCTION
A large population based study has recently shown that the prevalence of painful
diabetic neuropathy is ~21% and painful symptoms are more prevalent in patients
with type 2 diabetes, females and South Asians (1). It is characterised by
symmetrical lower limb paraesthesiae, dysaesthesiae, lancinating pains and
allodynia with nocturnal exacerbation (2) which are associated with significant
sleep disturbance and reduced quality of life (3). National and international
guidelines advocate a range of therapies providing symptomatic relief (4-5).
However, the therapeutic efficacy for all recommended medications is at best
~50% pain relief and is limited due to unwanted side effects (2; 6). Apart from
peripheral and central alterations (7), metabolic alterations such as increased
glycaemic flux (8) and elevated plasma methylglyoxal levels have been implicated
in patients with painful diabetic neuropathy (9).
Two recent observational studies in diabetic patients have demonstrated a
significant association between vitamin D deficiency and both paraesthesiae and
numbness (10) and diabetic neuropathy per se, defined using the neuropathy
symptom score, neurological deficits and electrophysiology (11). However, neither
of these studies delineated negative from positive symptoms and there was no
definitive assessment of pain. There is of course an association between vitamin D
deficiency and painful symptoms in the general population (12). In relation to a
mechanistic link between vitamin D and pain, a recent study has shown that
nociceptive calcitonin gene-related peptide (CGRP)-positive neurones have a
distinct vitamin D phenotype with hormonally-regulated ligand and receptor levels
(13). Vitamin D deficiency results in increased numbers of axons containing CGRP,
and in culture vitamin D receptor (VDR) expression is increased in growth cones

275
and sprouting appears to be regulated by VDR-mediated rapid response signalling
pathways (14). Nerve Growth Factor (NGF) is known to be depleted in
experimental diabetes (15) and in a study of patients with diabetic neuropathy NGF
immunostaining on skin keratinocyte correlated with skin axon-reflex vasodilation
(16). In an experimental study a preservation of NGF expression was shown in
sciatic nerves of diabetic animals treated with a vitamin D analogue (CB1093).
Similarly Tacalcitol, an active vitamin D3 induces NGF production in human
epidermal keratinocytes (17). Given that demyelination and axonal degeneration
are the hallmarks of diabetic neuropathy (18-20), of potential relevance, treatment
with vitamin D3 has been shown to reduce demyelination in a cuprizone
experimental model of demyelination (21) and in a separate spinal cord
compression model it has been shown to induce axonal regeneration (22).
In relation to the potential therapeutic benefits of vitamin D therapy, a prospective
study by Lee et al (23) of 51 patients with Type 2 diabetes and painful neuropathy
given ~2000 IU of cholecalciferol daily for 3 months showed a ~50% decrease in
pain scores as measured by Visual Analogue Score (VAS). Similarly a dramatic
improvement in neuropathic symptoms has been described recently after treatment
with 50000U of D2 weekly in a type 1 diabetic patient who had been refractory to
treatment with tricyclics, gabapentin, pregabalin and oxycodone (24).
In the present study we have evaluated the association between the levels of
25(OH)D and painful versus painless diabetic neuropathy matched for all other
measures of neuropathy.

276
8.3 RESEARCH DESIGN AND METHODS
8.3.1 Selection of patients
Forty three type 1 diabetic patients were categorized into two groups: painless
neuropathy (DPN) (n=20) and painful neuropathy (PDN) (n=23) using the McGill
Visual Analogue Score (McGill VAS) and McGill pain score, and compared with 14
age, sex and ethnicity matched non-diabetic healthy control subjects (C). Subjects
with any history of neurologic conditions, ocular trauma or ocular surgery were
excluded. The study was approved by the North West and Salford and Trafford
Research Ethics committee, and written informed consent was obtained according
to the Declaration of Helsinki.
8.3.2 Assessment of neuropathy
All patients and control subjects underwent a detailed evaluation of neurologic
symptoms according to the neuropathy symptom profile (NSP), and the McGill VAS
was used to assess the severity of painful neuropathy. Neurologic deficits were
assessed using the modified neuropathy disability score (NDS), which includes
evaluation of vibration, pin prick, and temperature perception as well as the
presence or absence of ankle reflexes (25). Quantitative sensory testing included
an assessment of vibration perception threshold (VPT), measured using a
Neurothesiometer (Horwell, Scientific Laboratory Supplies, Wilford, Nottingham,
U.K.), cold sensation threshold (CST) (Aδ fibres) and warm sensation threshold
(WST) (26) (C fibres) thresholds using the method of limits with the MEDOC TSA II
(Medoc, Ramat Yishai, Israel) on the dorsum of the left foot. Computer-Aided
Sensory Evaluator (CASE IV) (WR Medical Electronic Ltd, Maplewood, Maine,
USA) was used to measure the heart rate response to deep breathing (HRV-DB)
277
over two 8-cycle breathing series interspersed by a 5-min period of normal
breathing. Electro-diagnostic studies were undertaken using a Dantec “Keypoint”
system (Dantec Dynamics, Bristol, U.K.) equipped with a DISA temperature
regulator to keep limb temperature constantly between 32°C and 35°C. Peroneal
motor and sural sensory nerves were assessed in the right lower limb by a
consultant neurophysiologist. The motor study was performed using silver-silver
chloride surface electrodes at standardized sites defined by anatomical landmarks,
and recordings for the sural nerve were taken using antidromic stimulation over a
distance of 100 mm.
8.3.3 Corneal Confocal Microscopy
Patients underwent examination with the Heidelberg retina tomography III in vivo
corneal confocal microscope employing our established methodology for image
acquisition (27). Several scans of the entire depth of the central cornea were
recorded by turning the fine focus of the objective lens backward and forward for
~2 min using the section mode, which enables manual acquisition and storage of
single images of all corneal layers. This provides en face two-dimensional images
with a lateral resolution of ~2 mm/pixel and final image size of 400 x 400 pixels of
the subbasal nerve plexus of the cornea. Each nerve fibre bundle contains
unmyelinated fibres, which run parallel to Bowman’s layer before dividing and
terminating as individual axons underneath the surface epithelium. Five images per
patient from the centre of the cornea were selected and examined in a masked and
randomized fashion (28). Three corneal nerve parameters were quantified: 1)
corneal nerve fibre density (CNFD), the total number of major nerves per square
millimetre of corneal tissue (no.mm2); 2) corneal nerve branch density (CNBD), the

278
number of branches emanating from all major nerve trunks per square millimetre of
corneal tissue (no.mm2); and 3) corneal nerve fibre length (CNFL), the total length
of all nerve fibres and branches (mm/mm2) within the area of corneal tissue.
8.3.4 Skin biopsy and immunohistochemistry
Intra-epidermal nerve fibre density (IENFD) was assessed in a sub-cohort of
participants (Controls n=10, DPN n=11, and PDN n=9) who agreed to undergo a 3-
mm punch skin biopsy from the dorsum of the foot; 2 cm proximal to the second
metatarsal head, after local anaesthesia (1% lidocaine). The biopsy specimen was
immediately fixed in PBS-buffered 4% paraformaldehyde and after 18–24 hours
rinsed in Tris-buffered saline and soaked in 33% sucrose (2–4 hours) for
cryoprotection. It was then embedded in optimal cutting temperature-embedding
compound, rapidly frozen in liquid nitrogen, and cut into 50- μm sections using a
cryostat (model OTF; Bright Instruments, Huntington, U.K.). Four floating sections
per subject were subjected to melanin bleaching (0.25% KMnO4 for 15 min
followed by 5% oxalic acid for 3 min), a 4-h protein block with a Tris-buffered saline
solution of 5% normal swine serum, 0.5% powdered milk, and 1% Triton X-100,
and overnight incubation with 1:1,200 Biogenesis polyclonal rabbit anti-human
PGP9.5 antibody (Serotec, Oxford, U.K.). Biotinylated swine anti-rabbit secondary
antibody (1:300; DakoCytomation, Ely, U.K.) was then applied for 1 hour; sections
were quenched with 1% H2O2 in 30% MeOH-PBS (30 min) before a 1 hour
incubation with 1:500 horseradish peroxidase–streptavidin (Vector Laboratories,
Peterborough, U.K.). Nerve fibres were demonstrated using 3, 3-diaminobenzidine
chromogen (Sigma-Aldrich, Manchester, U.K.). Sections were mildly
counterstained with eosin to better localize the basement membrane to identify

279
nerve fibres passing through it. Negative control subjects consisted of replacing the
anti-PGP9.5 antibody with rabbit immunoglobulin (DakoCytomation) at a
concentration matching that of the primary antibody and showed no
immunostaining. IENFD, i.e., the number of fibres per millimetre of basement
membrane, was quantified in accord with established criteria and techniques and
expressed as number per millimetre (29).
8.3.5 25(OH) Vitamin D Assay
The laboratory used for the biochemical assay measurements (Vitamin D
Research Group Manchester Royal Infirmary, UK) was accredited to ISO
9001:2008 and ISO 13485:2003 by Lloyd’s Register Quality Assurance certificate
number LRQ 4001542 and participated successfully in the Vitamin D quality
assurance scheme (DEQAS). Serum was separated from whole blood and stored
at -20 C until assay. The assay used was an automated platform assay
(ImmunoDiagnostic Systems Ltd, Bolden, Tyne and Wear, UK) and is based on
chemiluminescence technology. Briefly, samples were subjected to a pre-treatment
step to denature the vitamin D binding protein. The treated samples were then
neutralised in assay buffer and a specific anti-25(OH)D antibody labelled with
acridinium was added. Following an incubation step, magnetic particles linked to
25(OH)D were added. Following a further incubation step, the magnetic particles
were “captured” using a magnet. After a washing step and addition of trigger
reagents, the light emitted by the acridinium label was inversely proportional to the
concentration of 25(OH)D in the original sample. The concentration of 25(OH)D
was calculated automatically using a 4-point logistic curve. The cross reactivity for
vitamin D2 (of the assay) as per manufacturers assertion was 100% (relative to

280
vitamin D3) and the assay has excellent correlation to existing globally recognised
assays, in combination with good sensitivity and precision (30). The reportable
range of the assay was 5-140 ng/mL. Inter- and intra- assay variation of the in-
house control was 5.6% and 9.7% respectively. Vitamin D deficiency (<20ng/ml)
and insufficiency (<30ng/ml) were defined according to the Institute of Medicine
(IOM) of the National Academies (31).
8.3.6 Statistical analysis
Statistical analyses were undertaken on Statsdirect (Statsdirect, Cheshire, UK). All
values are presented as mean ± SD. ANOVA method or a non-parametric
counterpart, Kruskal-Wallis were used to assess differences between groups
depending on normality of the data. Overall the p value was maintained at 0.05 for
multiple comparison tests (Bonferoni adjustment or Dwass-Steel-Chritchlow-Fligner
pairwise comparison). Unpaired t-test or Mann-Whitney U test were used for
analysis for DPN versus PDN for the duration of diabetes and IENFD. Chi2
analyses were used to assess frequencies of gender, ethnicity and aetiology of
diabetes. Odds Ratios for painful symptoms were calculated by further delineating
DPN and PDN groups based on the cut offs for vitamin D deficiency (<20ng/ml)
and insufficiency (<30ng/ml).

281
8.4 RESULTS
8.4.1 Demographics, Metabolic and Anthropometric Assessment (Table 8.1)
The participant demographics and metabolic and anthropometric measurements in
diabetic patients and control subjects are summarized in Table 8.1. There were no
significant differences in age (C: 59.3±7.8 vs DPN: 57.1±13.5 vs PDN: 59.8±11.7
years, P=NS), duration of diabetes (DPN: 36.0±17.5 vs PDN: 35.5±14.9 years,
P=NS) gender, type of diabetes and all subjects were of white European origin.
BMI was lower in diabetic patients but this was not significant. HbA1c (P<0.0001)
was significantly higher in diabetic patients compared with control subjects with no
difference between patients with PDN and DPN. The total cholesterol was
significantly lower in diabetic patients with DPN (P=0.003) and PDN (P=0.02)
compared to control subjects, due to greater statin use. HDL, triglycerides, systolic
and diastolic blood pressure were comparable between diabetic patients and
control subjects. The estimated glomerular filtration rate was comparable between
diabetic patients and control subjects, but the Albumin-Creatinine Ratio (ACR) was
higher in the DPN (P=0.009) and PDN (P=0.002) groups versus control subjects
with no difference between DPN and PDN. Serum vitamin B12 levels were
comparable between groups.

282
Table 8-1 Participant demographics and metabolic parameters in control subjects and
diabetic patients with DPN and PDN, with statistically significant differences between groups
C (n=14) DPN (n=20) PDN (n=23) DPN v PDN
Age (years) 59.3±7.8 57.1±13.5 59.8±11.7 NS
Gender (Male) (%) 57 60 53 NS
Ethnicity (White
European) (%) 100 100 100 NS
Aetiology of
Diabetes (Type 1
DM) (%)
- 85 91 NS
Duration of
Diabetes (years) - 36.0±17.5 35.5±14.9 NS
HbA1c (%) 5.7±0.2 8.1±1.1* 8.0±1.5** NS
HbA1c (mmol/mol) 38.3±2.5 65.2±12.0* 63.7±16.3** NS
BMI (kg/m2) 31.0±4.2 28.1±4.1 26.6±4.9 NS
T-CHL (mmol/l) 5.1±1.2 4.2±1.0† 4.4±0.8†† NS
HDL (mmol/l) 1.7±0.5 1.7±0.4 1.7±0.6 NS
Triglycerides 1.6±0.7 1.2±0.5 1.3±0.8 NS
Systolic BP
(mmHg) 138±15 141±26 141±23 NS
Diastolic BP
(mmHg) 77±8 71±7 71±11 NS
ACR (mg/mmol)
((Median)IQR)
0.4±0.3
(0.2(0.2-0.7))
7.1±16.7¥
(0.2(0.2-0.7)
5.3±6.7¥¥
(2.2(0.5-10.2) NS
eGRF
(ml/min/1.73) 85±7 77±16 78±15 NS
Serum Vitamin
B12 (ng/l) 247±69 342±121 317±111 NS
283
Post hoc analyses
HbA1c: *C vs DPN (P<0.0001); **C vs PDN (P<0.0001); DPN vs PDN (NS).
T-CHL: †C vs DPN (P=0.003); ††C vs PDN (P=0.02); DPN vs PDN (NS).
ACR: ¥C vs DPN (P=0.009); ¥¥C vs PDN (P=0.002); DPN vs PDN (NS).
Table key
ACR – Albumin Creatinine Ratio; BMI – Body Mass Index; C – Controls; DPN – Diabetic Peripheral
Neuropathy; estimated Glomerular Filtration Rate; HDL – High Density Lipoprotein Cholesterol;
PDN – Painful Diabetic Neuropathy; T-CHL – Total Cholesterol.
284
8.4.2 Symptoms and deficits (Table 8.2)
The NSP was significantly higher in patients with PDN (P<0.0001) compared to
control subjects and between patients with PDN compared to DPN (P<0.0005).
Positive symptoms (out of 6) were significantly greater in PDN compared to control
subjects (P=0.05) and DPN (P=0.009). Negative symptoms (out of 4) were
significantly greater in PDN compared to control subjects (P=0.009) and DPN
(P=0.02). The McGill pain score and McGill VAS were significantly increased in
diabetic patients with PDN compared with control subjects (P<0.0001) and patients
with DPN (P<0.0001). The NDS was significantly increased in patients with DPN
(P=0.01) and PDN (P=0.002) compared with control subjects, but there were no
significant difference between DPN and PDN.

285
Table 8-2 Clinical neuropathy symptoms and deficits in control subjects and diabetic
patients with DPN and PDN, with statistically significant differences between groups
Post hoc analyses
NDS: *C vs DPN (P=0.01); **C vs PDN (P=0.002); DPN vs PDN (NS).
NSP: C vs DPN (NS); ^C vs PDN (P<0.0001); DPN vs PDN (P=0.0005).
+ve Symptoms: C vs DPN (NS); σC vs PDN (P=0.05); DPN vs PDN (P=0.009).
-ve Symptoms: C vs DPN (NS); ¥C vs PDN (P=0.009); DPN vs PDN (P=0.02).
McGill VAS: C vs DPN (NS); †C vs PDN (P<0.0001); DPN vs PDN (P<0.0001).
McGill Pain score: C vs DPN (NS); ††C vs PDN (P<0.0001); DPN vs PDN (P<0.0001).
Table key
C – Controls; DPN – Diabetic Peripheral Neuropathy; IQR – Inter Quartile Range; McGill VAS –
McGill Visual Analogue Score; NDS – Neuropathy Disability Score; NSP – Neuropathy Symptom
Profile; PDN – Painful Diabetic Peripheral Neuropathy.
C
(n=14)
DPN
(n=20)
PDN
(n=23) DPN v PDN
NDS (-/10)
(Median(IQR)
1.4±1.5
1(0-2)
3.9±3.2*
3.5(1.5-5.5)*
4.5±3.2**
4(2-6)** NS
NSP (-/38)
(Median(IQR)
1±1.5
0(0-1)
2.2±2.6
1(0.5-2.5)
6.3±5.5^
5(2-11)^ <0.0005
+ve Symptoms
on NSP (-/6)
(Median(IQR)
0.5±0.9
(0(0-1)
0.25±0.6
(0(0-0)
1.6±1.8σ
(1(0-3)σ 0.009
-ve symptoms on
NSP (-/4)
(Median(IQR)
0±0
(0(0-0)
0.3±0.4
(0.5(0-1)
1.1±1.2¥
(1(0-2)¥ 0.02
McGill VAS
(-/10cm) 0.5±1.4 0±0 5.7±2.3† <0.0001
McGill Pain score
(Median (IQR)
0.4±0.9
(0(0-0)
0±0
(0(0-0)
6.1±6.5††
(3(2-10) <0.0001

286
8.4.3 Quantitative sensory tests (Table 8.3)
VPT, CST and WST did not differ between diabetic patients and control subjects or
between patients with DPN and PDN.
8.4.4 Electrophysiology (Table 8.3)
Peroneal motor nerve conduction velocity and amplitude were significantly lower in
DPN (P=0.004 and P=0.003, respectively) and PDN (P=0.0008 and P=0.001,
respectively) compared with control subjects, but there was no difference between
patients with DPN and PDN. Sural sensory nerve conduction velocity and
amplitude were significantly lower in DPN (P=0.02 and P=0.007, respectively) and
PDN (P=0.005 and P=0.04, respectively) compared with control subjects, but there
was no significant difference between patients with DPN and PDN.
8.4.5 Autonomic function, IENFD and CCM (Table 8.3)
HRV-DB did not differ between diabetic patients and control subjects or between
patients with DPN and PDN. IENFD did not differ between patients with DPN and
control subjects but was significantly reduced in PDN compared to control subjects
(P=0.05) with no difference between DPN and PDN. CNFD was significantly
reduced in patients with DPN (P=0.0008) and PDN (P<0.0001) compared with
control subjects with no difference between DPN and PDN. CNBD was significantly
reduced only in patients with PDN (P<0.03) compared with control subjects with no
difference between DPN and PDN. CNFL was significantly reduced in patients with
DPN (P=0.03) and PDN (P<0.0009) compared with control subjects with no
difference between DPN and PDN.

287
Table 8-3 Small and large fibre tests of nerve structure and function in control subjects and
diabetic patients with DPN and PDN, with statistically significant differences between groups
C (n=14) DPN (n=20) PDN (n=23) DPN v PDN
CNFD (no/mm2) 34.6±5.4 24.5±8.4* 20.4±10.0**
NS
CNBD (no/mm2) 75.9±24.2 56.1±31.8 45.5±29.3
†
NS
CNFL (mm/mm2) 24.3±3.6 19.8±5.7
¥ 15.8±7.2
¥¥
NS
IENFD (no/mm) 7.6±3.4
(n=10)
5.2±3.7
(n=11)
3.9±2.9a
(n=9)
NS
DB-HRV (beats/min) 23±10 18±9 18±14 NS
CST (˚C) 27.2±1.9 24.0±6.6 23.5±6.8 NS
WST(˚C) 39.8±3.8 40.7±4.7 42.0±4.9 NS
VPT (volts) 10.7±6.6 17.0±14.0 19.5±13.1 NS
SSNCV (m/s) 47.7±5.1 41.9±6.2˚ 42.2±4.6˚˚ NS
SSNAmp (µV) 9.6±2.7 6.9±4.8€ 5.3±5.3
€€
NS
PMNCV (m/s) 45.9±3.3 38.3±9.3ª 38.4±8.7ªª NS
PMNAmp (mV) 4.9±1.0 2.6±1.9§ 2.6±2.5
§§
NS
Post hoc analyses
CNFD: *C vs DPN (P=0.0008); **C vs PDN (P<0.0001); DPN vs PDN (NS).
CNBD: C vs DPN (NS); †C vs PDN (P=0.03); DPN vs PDN (NS).
CNFL: ¥C vs DPN (P=0.03); ¥¥C vs PDN (P=0.0009); DPN vs PDN (NS).
IENFD: C vs DPN (NS); ªC vs PDN (P=0.05); DPN vs PDN (NS).
SSNCV: ˚ ˚C vs DPN (P=0.02); ˚˚C vs PDN (P=0.005); DPN vs PDN (P=NS).
SSNAmp: €C vs DPN (P=0.007);
€€C vs PDN (P=0.04); DPN vs PDN (NS).
PMNCV: ªC vs DPN (P=0.004); ªªC vs PDN (P=0.0008); DPN vs PDN (P=NS).
PMNAmp: §C vs DPN (P=0.003); §§C vs PDN (P=0.001); DPN vs PDN (P=NS).
288
Table Key
C – Controls; CNBD – CNFD – Corneal Nerve Fibre Density; Corneal Nerve Branch Density; CNFL
– Corneal Nerve Fibre Length; CST – Cold Sensation Threshold; DB-HRV – Deep Breathing –
Heart Rate Variability; DPN – Diabetic Peripheral Neuropathy; IENFD – Intra Epidermal Nerve Fibre
Density; PDN – Painful Diabetic Neuropathy; PMNAmp – Peroneal Motor Nerve Amplitude; PMNCV
– Peroneal Motor Nerve Conduction Velocity; SSNAmp – Sural Nerve Sensory Nerve Amplitude;
SSNCV – Sural Sensory Nerve Conduction Velocity; VPT – Vibration Perception Threshold; WST –
Warm Sensation Threshold.

289
8.4.6 25(OH)D status (Figure 8.1)
The serum 25(OH)D level was significantly lower in PDN (24.0±14.1 ng/ml)
compared to DPN (34.6±15.0 ng/ml, P=0.01) and control subjects (34.1±8.6 ng/ml,
P=0.03). The odds ratio in favour of painful diabetic neuropathy was 9.8 (P=0.003
(95% CI 2.2-76.4) for vitamin D deficiency (<20ng/ml) and 4.4, (P=0.03 (95% CI
1.1-19.8)) for vitamin D insufficiency (<30ng/ml).
Figure 8-1 Graph showing 25(OH)D levels in ng/ml in C, DPN and PDN
Post hoc analyses
C vs DPN – P=NS; *C vs DPN – P=0.03; **DPN vs PDN – P=0.01.
(Overall P for Kruskal Wallis = 0.02).
Controls DPN PDN 0
10
20
30
40
50
60
25
(OH
)D
in n
g/m
l
25(OH)D levels in C, DPN & PDN
*/** ** *

290
8.5 DISCUSSION
Painful neuropathy is an extremely disabling condition which may be present in at
least one fifth of diabetic patients (1). The treatment of this disabling condition has
remained unsatisfactory with a ‘good’ response to conventional medication rated at
between 30-50% pain relief (5). Available drugs are often moderately effective and
their use is limited by side effects.
The aetiology of painful diabetic neuropathy is not clear. Central changes
comprising of increased thalamic vascularity (32), Aβ fibre sprouting into lamina II
of the dorsal horn, and reduced inhibition via descending pathways (2) together
with axonal atrophy in peripheral nerves have been demonstrated in patients with
painful diabetic neuropathy (33). In the present study we carefully phenotyped
diabetic patients into those with painful and painless diabetic neuropathy. Painful
diabetic neuropathy has also been associated with significantly greater autonomic
dysfunction than painless DPN (34). Previously we have shown that the LDIflare, a
measure of small fibre function, is abnormal in patients with painful diabetic
neuropathy, whilst conventional quantitative sensory testing and dermal nerve fibre
density did not differ from those with painless neuropathy (35). Given the results of
these studies suggesting greater small fibre, particularly autonomic dysfunction we
undertook detailed assessment of large and small fibre neuropathy. There was no
difference for electrophysiology, quantitative sensory testing and autonomic
function between diabetic patients with painful and painless neuropathy. We have
also shown a greater reduction in both intraepidermal nerve and corneal nerve
fibre length in diabetic patients with painful neuropathy (36). A recent detailed
immunophenotyping study has shown increased axonal growth through growth
associated proteins (higher GAP43/PGP) and axonal swellings, positive for

291
tropomyosin-receptor-kinase A and substance P in patients with painful compared
to painless neuropathy (37). In the present study, although patients with painful
diabetic neuropathy had greater deficits for IENFD and corneal nerve morphology
compared to diabetic patients with painless neuropathy, this was not significantly
different between diabetic patients with painful and painless neuropathy. Although
IENFD was lower in PDN, however due to a fewer number of subjects consenting
for skin biopsy compared to the overall group this did not reach significance.
Painful neuropathic symptoms tend to vary in their severity over time and therefore
it is difficult to reconcile these ‘hard wired’ changes with the fluctuating symptoms.
Changes in sodium channel distribution and expression, altered peripheral blood
flow and glycaemic flux have also been implicated (2). Given the potential link
between vitamin D and pain, together with the high prevalence of vitamin D
deficiency in diabetic populations (38) we have explored the link with painful
diabetic neuropathy. Two recent studies have shown a relationship between
vitamin D deficiency and diabetic neuropathy (10-11), but did not assess the link
between positive and negative neuropathic symptoms in these cohorts. In the
present study we have shown a markedly increased risk of diabetic painful
neuropathy in diabetic patients with vitamin D deficiency and insufficiency. We
observed no relationship for painful diabetic neuropathy with any other risk factor
for neuropathy such as glycaemic control or severity of neuropathy, which
challenges the two recent studies showing a link between vitamin D deficiency and
diabetic neuropathy (10-11). Previous epidemiological studies have shown a
higher prevalence of painful diabetic neuropathy in South Asians despite a lower
prevalence of neuropathy (1) compared to other ethnic groups and of course South
Asian are at the highest risk of vitamin D deficiency (38). In our previous study

292
(38), 55% of our South Asian patients were severely deficient with a 25(OH)D
<10ng/ml. The cohort of subjects evaluated in this study was exclusively of white
European origin thus minimising ethnicity as a confounding factor.
Whilst vitamin D supplementation has been used to treat pain particularly in
rheumatological conditions (39) a Cochrane review (40) concluded that there was a
poor evidence base for the use of vitamin D in chronic pain. Intervention studies in
diabetic neuropathy are limited. Whilst Valensi et al (41) showed benefit for painful
symptoms with a topical compound (QR-333) containing quercetin (aldose
reductase inhibitor effects), ascorbyl palpitate and vitamin D3, with three different
compounds that may benefit painful neuropathy it is difficult to define the relative
effectiveness of vitamin D3. Lee et al (23) showed benefit with oral cholecalciferol
in painful diabetic neuropathy, however, this study had neither a placebo group nor
was it randomised. Most recently a dramatic improvement was observed in a single
type 1 patient with painful neuropathy, refractory to a range of standard therapies
(24). However given that recent studies of novel drugs in the treatment of painful
diabetic neuropathy have dramatically failed (42-43) with active treatment being
barely superior to placebo there is an urgent need to explore new mechanisms and
hence treatments for diabetic painful neuropathy.
Whilst this is a small study a major strength is the detailed phenotyping undertaken
to ensure that diabetic patients with and without painful neuropathy were absolutely
matched for all other measures of neuropathy and demographic characteristics,
except painful symptoms. The results appear unequivocally in favour of a
relationship between vitamin D deficiency and painful neuropathic symptoms. A
well constructed controlled trial of vitamin D supplementation in painful diabetic

293
neuropathy is required in order to assess the effectiveness of a potentially simple
treatment with no obvious side effects.
294
8.6 REFERENCES
1. Abbott CA, Malik RA, van Ross ERE, Kulkarni J, Boulton AJM: Prevalence and
Characteristics of Painful Diabetic Neuropathy in a Large Community-Based
Diabetic Population in the U.K. Diabetes Care 2011;34:2220-2224
2. Tesfaye S, Vileikyte L, Rayman G, Sindrup S, Perkins B, Baconja M, Vinik A,
Boulton A: Painful Diabetic Peripheral Neuropathy: Consensus Recommendations
on Diagnosis, Assessment and Management. Diabetes Metab Res Rev
2011;27:629-638
3. Sadosky A, Schaefer C, Mann R, Bergstrom F, Baik R, Parsons B, Nalamachu
S, Nieshoff E, Stacey BR, Anschel A, Tuchman M: Burden of illness associated
with painful diabetic peripheral neuropathy among adults seeking treatment in the
US: results from a retrospective chart review and cross-sectional survey. Diabetes
Metab Syndr Obes 2013;6:79-92
4. Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, Lauria G,
Malik RA, Spallone V, Vinik A, Bernardi L, Valensi P: Diabetic neuropathies:
update on definitions, diagnostic criteria, estimation of severity, and treatments.
Diabetes Care 2010;33:2285-2293
5. Bril V, England J, Franklin GM, Backonja M, Cohen J, Del Toro D, Feldman E,
Iverson DJ, Perkins B, Russell JW, Zochodne D: Evidence-based Guideline:
Treatment of Painful Diabetic Neuropathy: Report of the American Academy of
Neurology, the American Association of Neuromuscular and Electrodiagnostic
Medicine, and the American Academy of Physical Medicine and Rehabilitation.
PM&R 2011;3:345-352.e321
6. Tesfaye S, Wilhelm S, Lledo A, Schacht A, Tölle T, Bouhassira D, Cruccu G,
Skljarevski V, Freynhagen R: Duloxetine and pregabalin: High-dose monotherapy

295
or their combination? The “COMBO-DN study” – a multinational, randomized,
double-blind, parallel-group study in patients with diabetic peripheral neuropathic
pain. PAIN 2013 [Epub ahead of print].
http://dx.doi.org/10.1016/j.pain.2013.05.043.
7. Wilkinson ID, Selvarajah D, Greig M, Shillo P, Boland E, Gandhi R, Tesfaye S:
Magnetic resonance imaging of the central nervous system in diabetic neuropathy.
Curr Diab Rep 2013;13:509-516
8. Oyibo SO, Prasad YD, Jackson NJ, Jude EB, Boulton AJ: The relationship
between blood glucose excursions and painful diabetic peripheral neuropathy: a
pilot study. Diabet Med 2002;19:870-873
9. Bierhaus A, Fleming T, Stoyanov S, Leffler A, Babes A, Neacsu C, Sauer SK,
Eberhardt M, Schnolzer M, Lasitschka F, Neuhuber WL, Kichko TI, Konrade I,
Elvert R, Mier W, Pirags V, Lukic IK, Morcos M, Dehmer T, Rabbani N, Thornalley
PJ, Edelstein D, Nau C, Forbes J, Humpert PM, Schwaninger M, Ziegler D, Stern
DM, Cooper ME, Haberkorn U, Brownlee M, Reeh PW, Nawroth PP: Methylglyoxal
modification of Nav1.8 facilitates nociceptive neuron firing and causes hyperalgesia
in diabetic neuropathy. Nat Med 2012;18:926-933
10. Soderstrom LH, Johnson SP, Diaz VA, Mainous AG, 3rd: Association between
vitamin D and diabetic neuropathy in a nationally representative sample: results
from 2001-2004 NHANES. Diabet Med 2012;29:50-55
11. Shehab D, Al-Jarallah K, Mojiminiyi OA, Al Mohamedy H, Abdella NA: Does
Vitamin D deficiency play a role in peripheral neuropathy in Type 2 diabetes?
Diabet Med 2012;29:43-49
12. Hirani V: Vitamin D status and pain: analysis from the Health Survey for
England among English adults aged 65 years and over. Br J Nutr 107:1080-1084
296
13. Tague SE, Smith PG: Vitamin D receptor and enzyme expression in dorsal root
ganglia of adult female rats: modulation by ovarian hormones. J Chem Neuroanat
2011;41:1-12
14. Tague SE, Clarke GL, Winter MK, McCarson KE, Wright DE, Smith PG:
Vitamin D deficiency promotes skeletal muscle hypersensitivity and sensory
hyperinnervation. J Neurosci 2011;31:13728-13738
15. Hellweg R, Wohrle M, Hartung HD, Stracke H, Hock C, Federlin K: Diabetes
mellitus-associated decrease in nerve growth factor levels is reversed by
allogeneic pancreatic islet transplantation. Neurosci Lett 1991;125:1-4
16. Anand P, Terenghi G, Warner G, Kopelman P, Williams-Chestnut RE, Sinicropi
DV: The role of endogenous nerve growth factor in human diabetic neuropathy.
Nat Med 1996;2:703-707
17. Fukuoka M, Sakurai K, Ohta T, Kiyoki M, Katayama I: Tacalcitol, an active
vitamin D3, induces nerve growth factor production in human epidermal
keratinocytes. Skin Pharmacol Appl Skin Physiol 2001;14:226-233
18. Malik RA, Veves A, Walker D, Siddique I, Lye RH, Schady W, Boulton AJ:
Sural nerve fibre pathology in diabetic patients with mild neuropathy: relationship to
pain, quantitative sensory testing and peripheral nerve electrophysiology. Acta
Neuropathol 2001;101:367-374
19. Dyck PJ, Giannini C: Pathologic alterations in the diabetic neuropathies of
humans: a review. J Neuropathol Exp Neurol 1996;55:1181-1193
20. Malik RA, Tesfaye S, Newrick PG, Walker D, Rajbhandari SM, Siddique I,
Sharma AK, Boulton AJ, King RH, Thomas PK, Ward JD: Sural nerve pathology in
diabetic patients with minimal but progressive neuropathy. Diabetologia
2005;48:578-585

297
21. Wergeland S, Torkildsen O, Myhr KM, Aksnes L, Mork SJ, Bo L: Dietary
vitamin D3 supplements reduce demyelination in the cuprizone model. PLoS One
6:e26262
22. Bianco J, Gueye Y, Marqueste T, Alluin O, Risso JJ, Garcia S, Lavault MN,
Khrestchatisky M, Feron F, Decherchi P: Vitamin D(3) improves respiratory
adjustment to fatigue and H-reflex responses in paraplegic adult rats.
Neuroscience 2010;188:182-192
23. Lee P, Chen R: Vitamin D as an analgesic for patients with type 2 diabetes and
neuropathic pain. Arch Intern Med 2008;168:771-772
24. Bell DS: Reversal of the Symptoms of Diabetic Neuropathy through Correction
of Vitamin D Deficiency in a Type 1 Diabetic Patient. Case Rep Endocrinol 2012:
Article ID 165056. http://dx.doi.org/10.1155/2012/165056
25. Young M, Boulton A, Macleod A, Williams D, Sonksen P: A multicentre study of
the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital
clinic population. Diabetologia 1993;36:150-154
26. Bravenboer B, van Dam PS, Hop J, vd Steenhoven J, Erkelens DW: Thermal
threshold testing for the assessment of small fibre dysfunction: normal values and
reproducibility. Diabet Med 1992;9:546-549
27. Petropoulos IN, Manzoor T, Morgan P, Fadavi H, Asghar O, Alam U, Ponirakis
G, Dabbah MA, Chen X, Graham J, Tavakoli M, Malik RA: Repeatability of in vivo
corneal confocal microscopy to quantify corneal nerve morphology. Cornea
32:e83-89
28. Tavakoli M, Malik RA: Corneal confocal microscopy: a novel non-invasive
technique to quantify small fibre pathology in peripheral neuropathies. J Vis Exp
2011; 3(47):2194. doi: 10.3791/2194
298
29. Lauria G, Bakkers M, Schmitz C, Lombardi R, Penza P, Devigili G, Smith AG,
Hsieh ST, Mellgren SI, Umapathi T, Ziegler D, Faber CG, Merkies IS:
Intraepidermal nerve fibre density at the distal leg: a worldwide normative
reference study. J Peripher Nerv Syst 2010;15:202-207
30. ASBMR 31st Annual Meeting MO0001–MO0445. Journal of Bone and Mineral
Research 2009;24:S370-S496
31. Rosen CJ, Gallagher JC: The 2011 IOM report on vitamin D and calcium
requirements for north america: clinical implications for providers treating patients
with low bone mineral density. J Clin Densitom 2011;14:79-84
32. Selvarajah D, Wilkinson ID, Gandhi R, Griffiths PD, Tesfaye S: Microvascular
perfusion abnormalities of the Thalamus in painful but not painless diabetic
polyneuropathy: a clue to the pathogenesis of pain in type 1 diabetes. Diabetes
Care 2011;34:718-720
33. Britland ST, Young RJ, Sharma AK, Clarke BF: Association of Painful and
Painless Diabetic Polyneuropathy With Different Patterns of Nerve Fibre
Degeneration and Regeneration. Diabetes 1990;39:898-908
34. Gandhi RA, Marques JL, Selvarajah D, Emery CJ, Tesfaye S: Painful diabetic
neuropathy is associated with greater autonomic dysfunction than painless diabetic
neuropathy. Diabetes Care 2010;33:1585-1590
35. Krishnan ST, Quattrini C, Jeziorska M, Malik RA, Rayman G: Abnormal
LDIflare but normal quantitative sensory testing and dermal nerve fibre density in
patients with painful diabetic neuropathy. Diabetes Care 2009;32:451-455
36. Quattrini C, Tavakoli M, Jeziorska M, Kallinikos P, Tesfaye S, Finnigan J,
Marshall A, Boulton AJ, Efron N, Malik RA: Surrogate markers of small fibre
damage in human diabetic neuropathy. Diabetes 2007;56:2148-2154
299
37. Cheng HT, Dauch JR, Porzio MT, Yanik BM, Hsieh W, Smith AG, Singleton JR,
Feldman EL: Increased Axonal Regeneration and Swellings in Intraepidermal
Nerve Fibres Characterize Painful Phenotypes of Diabetic Neuropathy. The
Journal of Pain 2013;14:941-947
38. Alam U, Najam O, Al-Himdani S, Benoliel S, Jinadev P, Berry JL, Kew M,
Asghar O, Petropoulos IN, Malik RA: Marked vitamin D deficiency in patients with
diabetes in the UK: ethnic and seasonal differences and an association with
dyslipidaemia. Diabet Med 2012;29:1343-1345
39. Catalano A, Morabito N, Atteritano M, Basile G, Cucinotta D, Lasco A: Vitamin
D Reduces Musculoskeletal Pain After Infusion of Zoledronic Acid for
Postmenopausal Osteoporosis. Calcif Tissue Int 2012;90:279-285
40. Straube S, Andrew Moore R, Derry S, McQuay HJ: Vitamin D and chronic pain.
PAIN 2009;141:10-13
41. Valensi P, Le Devehat C, Richard JL, Farez C, Khodabandehlou T,
Rosenbloom RA, LeFante C: A multicenter, double-blind, safety study of QR-333
for the treatment of symptomatic diabetic peripheral neuropathy. A preliminary
report. J Diabetes Complications 2005;19:247-253
42. Selvarajah D, Gandhi R, Emery CJ, Tesfaye S: Randomized Placebo-
Controlled Double-Blind Clinical Trial of Cannabis-Based Medicinal Product
(Sativex) in Painful Diabetic Neuropathy: Depression is a major confounding factor.
Diabetes Care 2010;33:128-130
43. Ziegler D, Hidvégi T, Gurieva I, Bongardt S, Freynhagen R, Sen D,
Sommerville K, Group obotLSS: Efficacy and Safety of Lacosamide in Painful
Diabetic Neuropathy. Diabetes Care 2010;33:839-841

300
9 Chapter IX - Vitamin D Deficiency is not associated with
Diabetic Retinopathy or Maculopathy: A Cross Sectional
study
Contribution: Uazman Alam conceived the study and subsequently designed it,
extracted data, performed statistical analyses and wrote the manuscript which
constitutes the basis for this chapter.
To be submitted for publication
Uazman Alam, Yasar Amjad, Omar Asghar, Ioannis N Petropoulos, Rayaz A Malik

301
9.1 ABSTRACT
Experimental data and several small clinical studies suggest a possible association
between vitamin D deficiency and both diabetic retinopathy and maculopathy.
We have performed a cross-sectional study in adults aged 18-80 years with Type 1
and 2 Diabetes Mellitus. The relationship between the presence and severity of
diabetic retinopathy and maculopathy with serum 25-hydroxyvitamin D
concentration was evaluated using logistic regression analyses in the presence of
demographic and clinical covariates, such as age, race, gender, duration of
diabetes, anthropometric measures (Body Mass Index (BMI) and Blood Pressure
(BP)) and metabolic parameters (HbA1c and lipid fractions).
657 adults with diabetes were stratified based on retinopathy grading: No Diabetic
retinopathy (NDR) (39%), Background Diabetic Retinopathy (BDR) (37%), Pre-
Proliferative Diabetic Retinopathy (PPDR) (21%) and Proliferative Diabetic
Retinopathy (PDR) (3%), respectively. There were no differences in serum 25-
hydroxyvitamin D concentrations (25(OH)D) between the groups (15.3±9.0 vs
16.4±10.5 vs 15.9±10.4 vs 15.7±8.5ng/ml, P=NS). Logistic regression analysis
demonstrated no statistically significant relationship between the severity of
retinopathy and serum 25(OH)D. Furthermore, there was no difference in serum
25(OH)D between those with (n=94, 14%) and without (n=563, 86%) diabetic
maculopathy (16.2±10.0 vs 15.8±9.8, p=NS) and no relationship was demonstrated
by logistic regression analyses between the two variables.
This study has found no association between serum 25(OH)D concentrations and
the presence and severity of diabetic retinopathy or maculopathy.
302
9.2 INTRODUCTION
The prevalence of diabetic retinopathy (DR) approaches 93 million people
worldwide (1) and is one the leading causes of premature visual loss in the UK and
worldwide (2-3). Indeed, the World Health Organization estimates that whilst DR
accounts for approximately 5% of the global prevalence of blindness, the
prevalence rises sharply to 15-17% in developed countries (4). Several risk factors
are implicated in the aetiology of DR with hyperglycemia and hypertension showing
the strongest association (5), yet interventions aimed at correcting these risk
factors have demonstrated moderate success (6-7). Therefore the interactions
between neural and retinal vascular dysfunction and the mechanisms resulting in
retinal pathology including neovascularisation have been questioned recently (8).
Furthermore, micronutrients including Vitamin C, Vitamin E and magnesium have
been postulated to play a role in DR (9).
Vitamin D deficiency has been linked to a host of cardiovascular diseases including
diabetes and hypertension (10-11). Vitamin D receptor (VDR) genotypes have
been associated with the cumulative prevalence of diabetic retinopathy (12). In two
separate studies of the VDR gene in the French population, FokI and TaqI single
nucleotide polymorphisms have been associated with DR (13-14). In a study of
Caucasians with C-peptide-negative type 1 diabetes, there was a novel association
between the functional FokI VDR polymorphism and severe DR (13). VDR
dependent calcium binding proteins have been isolated in the human retina,
particularly in the photoreceptor layer of the cones (15) and immunostaining in
animal models has shown that VDR is expressed in the ganglion cells, the inner
and outer plexiform layer and the photoreceptor layer (16). In an in-vitro study of
303
retinoblastoma tissue expressing VDR, supplementation with vitamin D resulted in
a reduction of growth and apoptosis of the retinoblastoma cells (17). 1,25-
dihydroxyvitamin D3 (1,25(OH)2D3) closely regulates Vascular Endothelial Growth
Factor in experimental models (18) and there is an inverse correlation of 25(OH)D
with Vascular Endothelial Growth Factor, postulated to be related to tissue hypoxia
(19). In a mouse model of ischaemic retinopathy, 1,25(OH)2D3 was shown to inhibit
neovascularisation in retinal tissue (20). Vitamin D may also have a direct effect on
the renin-angiotensin-aldosterone-system (RAS) and the RAS is known to be
overexpressed in type 1 diabetic patients with retinopathy (21) and blockade of this
system reduces DR progression (22). A vitamin D analogue (paricalcitriol) has
shown an improvement in microalbuminuria through a mechanism related to
inhibition of RAS (23).
Aksoy H et al, demonstrated an inverse correlation in a Turkish cohort between
worsening diabetic retinopathy and lower 1,25-hydroxyvitamin D3 (active vitamin D)
in a population of 66 subjects (24). Furthermore, severe vitamin D deficiency has
been shown to predict not only mortality but the development of nephropathy and
retinopathy in type 1 diabetes (5). In a recent cross-sectional study of children and
adolescents with type 1 diabetes, retinopathy prevalence was higher in children
and adolescents with lower levels of vitamin D (25). Other cross-sectional studies
which have assessed vitamin D status in relation to DR in adults have either had
small numbers (26) or have been based on retrospective analysis of data collected
from the National Health and Nutrition Examination Survey between 1988 and
1994 (27). However, since then the targets for glycaemia, blood pressure and
lipids have changed and also this study made no assessment of diabetic
maculopathy (27). Therefore we have undertaken a study to establish the

304
relationship between vitamin D status and the severity of DR and maculopathy in a
large adult population with type 1 and type 2 diabetes.

305
9.3 RESEARCH DESIGN AND METHODS
All patients attending clinics were assessed for the level of 25(OH)D, irrespective
of a history suggestive of vitamin D deficiency. Ethical approval was not required
as the data were extracted retrospectively and did not extend beyond standard
clinical practice. 25(OH)D was added as a standard routine test from June 2009
due to the high levels of deficiency noted.
9.3.1 Subjects
All participants were aged ≥ 18 years old attending clinics at the Central
Manchester Foundation Trust, Manchester from August 2009 to May 2011. Those
with renal impairment (eGFR <30 mL/min/1.73m2 (CKD stage 4 and below),
granulomatous diseases (tuberculosis, sarcoidosis etc), malabsorption syndromes
(Coeliac disease, bacterial overgrowth, concomitant Orlistat treatment), pregnant
and lactating women, and those currently on vitamin D supplementation were
excluded from the analysis.
9.3.2 Blood pressure and Anthropometric measurements
BMI was measured as per the standard equation (mass (kg)/(height(m))2. Weight
was measured with a digital scale (Seca 701, Seca, Hamburg, Germany) to the
nearest 0.1kg and height to the nearest 0.1cm. Blood pressure measurements
were obtained with the use of an automated device (Dinamap pro 100v2, GE
Medical Systems, Freiburg, Germany) with an appropriate cuff size. A minimum of
two measurements of systolic and diastolic blood pressures were made five
minutes apart with the lowest reading recorded and the mean of the preceding 2
years blood pressure results were used. Metabolic variables were also recorded

306
with a mean of 2 year retrospective readings for glycosylated haemoglobin A1c
(HbA1c) and components of the lipid profile (total cholesterol (T-CHL), high density
lipoprotein cholesterol (HDL) and triglycerides). The following measurements were
taken as ‘spot readings’ at the same date as baseline 25(OH)D measurements:
BMI; bone profile markers such as corrected calcium (CCa), alkaline phosphatase
(ALP) and estimated glomerular filtration rate (eGFR).
9.3.3 Assessment of Demographics, Cardiovascular disease and
Medications
An assessment of patient demographics, previous cardiovascular events and
medications were made through analysis of medical records and an in-hospital
medical record database (Diamond database, Hicom, Surrey, UK). Subject
demographics extracted were age, sex, ethnicity (Caucasian, South Asian, Far
East Asian and Afro-Caribbean descent), smoking status (never, previous and
current) and type (type 1 and 2 diabetes) and duration of diabetes. Dates of
baseline 25(OH)D were used to obtain respective retinopathy screening data. Only
retinopathy screening data within 1 year of the baseline 25(OH)D and prior to
vitamin D supplementation were included.
Baseline 25(OH)D status and retinopathy data were collected for 657 patients who
had attended their retinopathy screening appointments. The retinopathy data were
collected according to the grading criteria of the National Screening Committee
(28-29). Previous studies have shown acceptable level of quality and accuracy of
grading compared to expert graders within the English National Screening
Committee (30). The national guidelines do not contain R1.5 or M0.5 grades and
are categorised as Pre-Proliferative Diabetic Retinopathy and Diabetic
307
Maculopathy, respectively. These sub-gradings were used locally in screening
centres and have been included. Retinopathy was graded as follows:
R0 - No Diabetic retinopathy (NDR).
R1 - Background Diabetic Retinopathy (BDR): microaneurysms, retinal
haemorrhages, exudates.
R1.5 - Moderate numbers of intra-retinal haemorrhages, hard exudates >1 disc
diameter (DD) from fovea, 3-6 cotton wool spots visible.
R2 - Pre-Proliferative Diabetic Retinopathy (PPDR): Venous beading or looping,
deep haemorrhages visible, other microvascular anomaly visible.
R3 - Proliferative Diabetic Retinopathy (PDR): New vessel formation, vitreous
haemorrhage, pre- retinal haemorrhage or fibrosis and/or retinal detachment.
M0 - No maculopathy.
M0.5 - Hard exudates within the arcades >1 disc diameter from the centre of the
fovea.
M1- Exudates <1 DD from the centre of the fovea, retinal thickening <1 disc
diameter from the centre of the fovea.
P0 – No photocoagulation scarring.
P1 – Photocoagulation scarring.
9.3.4 25(OH) vitamin D Assay
Assessment of 25(OH)D was instituted in August 2009 as part of routine
haematological and biochemical laboratory measurements which included HbA1c,
(Complete Blood count (CBC)), Urea and Electrolytes (UE), Liver function tests
(LFT), bone profile (Corrected Calcium (CCa2+), Alkaline Phosphatase (ALP),
Albumin (Alb), Phosphate (phos)), and Lipid profile (Total Cholesterol (T-CHL),

308
High Density lipoprotein Cholesterol (HDL), Triglycerides (TRIG)). Serum was
separated from whole blood and stored at -20 C until assay. The laboratory used
for the biochemical assay measurements (Vitamin D Research Group Manchester
Royal Infirmary, UK) was accredited to ISO 9001:2008 and ISO 13485:2003 by
Lloyd’s Register Quality Assurance certificate number LRQ 4001542 and
participated successfully in the Vitamin D quality assurance scheme (DEQAS).
Serum 25(OH)D was measured using the IDS-iSYS multi-discipline automated
analyzer (Immunodiagnostic Systems Ltd, Boldon, Tyne and Wear, UK). The assay
is based on chemiluminescent technology and was performed exactly as per the
manufacturer’s instructions. The cross reactivity for vitamin D2 (of the assay) as per
manufacturers assertion was 100% (relative to vitamin D3) and the assay has
excellent correlation to existing globally recognised assays, in combination with
good sensitivity and precision (31). The reportable range of the assay is 5-140
ng/ml Inter- and intra- assay variation of the in-house control was 5.6% and 9.7%
respectively.
9.3.5 Statistical analysis
Data were analysed using StatsDirect (StatsDirect, Altringham, Cheshire, UK). The
data were stratified according to retinopathy (NDR, BDR, PPDR and PDR) and
maculopathy (No maculopathy and maculopathy) status and a comparison of
means was undertaken using either ANOVA or Krus-Kal Wallis for DR data and
Unpaired t-test or Mann-Whitney U for maculopathy data. Chi Squared test were
used for aetiology of diabetes, ethnicity, gender and smoking status. Logistic
regression analyses were undertaken to assess the association between serum
25(OH)D levels and retinopathy and maculopathy status (either present (1) or not

309
present (0)), adjusting for mean values of duration of diabetes, smoking status,
HbA1c, total cholesterol, HDL, triglycerides, systolic and diastolic blood pressure.
Further assessment of the results comparing vitamin D categories (Severely
deficient (<10ng/ml), Deficient (10-<20ng/ml), Insufficient (20-<30ng/ml) and
Sufficient (>30ng/ml)) and retinopathy (NDR, BDR, PPDR and PDR), maculopathy
(No maculopathy and maculopathy) and photocoagulation status (No
photocoagulation and photocoagulation) were performed using chi2 testing.
Appropriate statistical analyses were employed depending on the normality of the
data. Overall the P value was maintained at 0.05 for multiple comparison tests
(Bonferoni adjustment or Dwass-Steel-Chritchlow-Fligner pairwise comparison).

310
9.4 RESULTS
657 patients were stratified according to their retinopathy status: NDR (n=257,
39%), BDR (n= 243, 37%), PPDR (n=135, 21%) and PDR (n=22, 3%); No Diabetic
Maculopathy (n=563, 86%) and Diabetic Maculopathy (n=94, 14%). 206 (31%) of
the patients had severe vitamin D deficiency with 25(OH)D levels below 10ng/ml,
284 (43%) were deficient with 25(OH)D of 10-<20ng/ml, 101(14%) were insufficient
with 25(OH)D of 20-<30ng/ml. Only 65 (10%) individuals had ‘adequate’ levels of
25 (OH)D at >30ng/ml. The mean 25(OH)D for the population was 15.8 ± 9.4
ng/ml.
Table 9.1 shows demographic and metabolic data based on retinopathy grading;
NDR, BDR, PPDR and PDR respectively. There were no differences in 25(OH)D
status between the groups (15.3±9.0 vs 16.4±10.5 vs 15.9±10.4 vs 15.7±8.5,
P=NS). Subjects were matched for age (59.8±13.8 vs 58.8±13.3 vs 60.8±10.9 vs
55.1±13.6 years), however, the duration of diabetes was significantly lower in NDR
(11.3±8.7 vs 18.7±11.7 vs 21.0±9.8 vs 19.7±10.0 years, P<0.0001). The median
number of metabolic and anthropometric measurements over the preceding two
year period from the baseline 25(OH)D result was 4 (Interquartile range 3-5). Two
year mean HbA1c (%) (8.2±1.6 vs 8.6±1.7 vs 8.9±1.6 vs 8.9±1.5, P<0.0006)
showed a significantly lower HbA1c, lower systolic Blood pressure (129±13 vs
131±15 vs 134±15 vs 134±11mmHg, P=0.007) and higher eGFR (76.3±16.9 vs
75.9±17.5 vs 70.9±16.9 vs 69.0±21.6, P=0.02) in NDR (Table 9.1). There was no
difference for aetiology of diabetes, ethnicity, sex, smoking status, BMI, lipid and
bone parameters and diastolic blood pressure between the grades of DR. Table
9.2 shows logistic regression analyses for DR status with Odds Ratios (OR) and
95% CI. There was no correlation of DR with 25(OH)D (OR 1.00 (95% CI 0.98-

311
1.02), P=NS), gender or ethnicity. However, lower age (OR 0.97 (95% CI 0.96-
0.99), P=0.01), longer duration of diabetes (OR 1.09 (95% CI 1.06-1.13),
P<0.0001), higher HbA1c (OR 1.22 (95% CI 1.07-1.39), P=0.003) and systolic
blood pressure (OR 1.02 (95% CI 1.00-1.04), P=0.02) were all associated with DR.

312
Table 9-1 Demographic and metabolic parameters in subgroups based on severity of
retinopathy
No Diabetic
Retinopathy
(NDR)
(n=257)
Background
Diabetic
Retinopathy
(BDR)
(n=243)
Pre-
Proliferative
Diabetic
Retinopathy
(PPDR)
(n=135)
Proliferative
Diabetic
Retinopathy
(PDR)
(n=22)
P value
Age (years) 59.8±13.8 58.8±13.3 60.8±10.9 55.1±13.6 NS
Duration of
Diabetes
(years)
11.3±8.7† 18.7±11.7† 21.0±9.8† 19.7±10.0† <0.0001
Type 2 DM (%) 88 75 80 77 NS
Ethnicity (White
European/South
Asian (%))
48/45 55/38 50/45 52/48 NS
Sex (male (%)) 51 50 48 53 NS
Current
Smokers/Past
smokers/Never
smokers (%)
14/25/61 14/33/53 14/26/60 4/23/71 NS
BMI (kg/m2) 31.6±10.6 31.1±7.1 31.9±6.4 31.1±6.9 NS
25(OH)D (ng/ml) 15.3±9.0 16.4±10.5 15.9±10.4 15.7±8.5 NS
HbA1c (%) 8.2±1.6* 8.6±1.7* 8.9±1.6* 8.9±1.5 <0.0001
T-CHL (mmol/l) 4.1±1.0 4.2±1.1 4.2±1.3 4.3±1.1 NS
HDL (mmol/l) 1.3±0.5 1.4±0.5 1.4±0.7 1.3±0.4 NS
TRIG (mmol/l) 1.8±0.9 1.8±1.5 1.8±0.9 2.5±2.9 NS
eGFR (ml/min/l) 76.3±16.9** 75.9±17.5 70.9±16.9** 69±21.6 0.02
Systolic BP
(mmHg) 129±13*** 131±14.6 134±15*** 134±11 0.007
Diastolic BP
(mmHg) 70±7 69±7 70±8 71±8 NS
ALP (u/L) 87±39 83±34 84±32 93±43 NS
CCa (mmol/l) 2.4±0.1 2.4±0.1 2.3±0.1 2.4±0.2 NS
313
Post hoc analyses
Duration of Diabetes – †NDR vs BDR (P<0.0001); NDR vs PPDR (P<0.0001);
NDR vs PDR (P=0.001).
HbA1c – *NDR vs BDR (P=0.01); NDR vs PPDR (P<0.0001).
eGFR – **NDR vs PPDR (P=0.04).
Systolic BP – ***NDR vs PPDR (P=0.008).
Table key
ALP – Alkaline Phosphatase; BMI – Body Mass Index; BP – Blood Pressure; CCa – Corrected
Calcium; eGFR – estimated Glomerular Filtration Rate; HDL – High-density Lipoprotein Cholesterol;
T-CHL – Total Cholesterol; TRIG – Triglycerides.
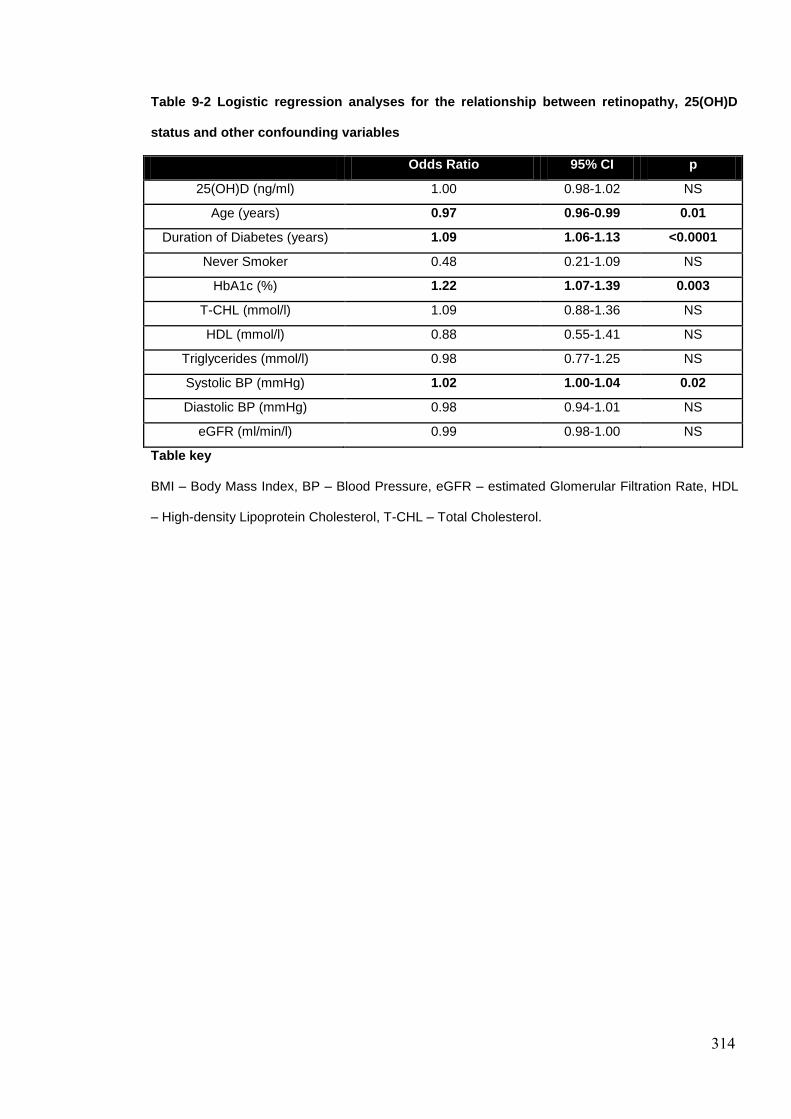
314
Table 9-2 Logistic regression analyses for the relationship between retinopathy, 25(OH)D
status and other confounding variables
Odds Ratio 95% CI p
25(OH)D (ng/ml) 1.00 0.98-1.02 NS
Age (years) 0.97 0.96-0.99 0.01
Duration of Diabetes (years) 1.09 1.06-1.13 <0.0001
Never Smoker 0.48 0.21-1.09 NS
HbA1c (%) 1.22 1.07-1.39 0.003
T-CHL (mmol/l) 1.09 0.88-1.36 NS
HDL (mmol/l) 0.88 0.55-1.41 NS
Triglycerides (mmol/l) 0.98 0.77-1.25 NS
Systolic BP (mmHg) 1.02 1.00-1.04 0.02
Diastolic BP (mmHg) 0.98 0.94-1.01 NS
eGFR (ml/min/l) 0.99 0.98-1.00 NS
Table key
BMI – Body Mass Index, BP – Blood Pressure, eGFR – estimated Glomerular Filtration Rate, HDL
– High-density Lipoprotein Cholesterol, T-CHL – Total Cholesterol.
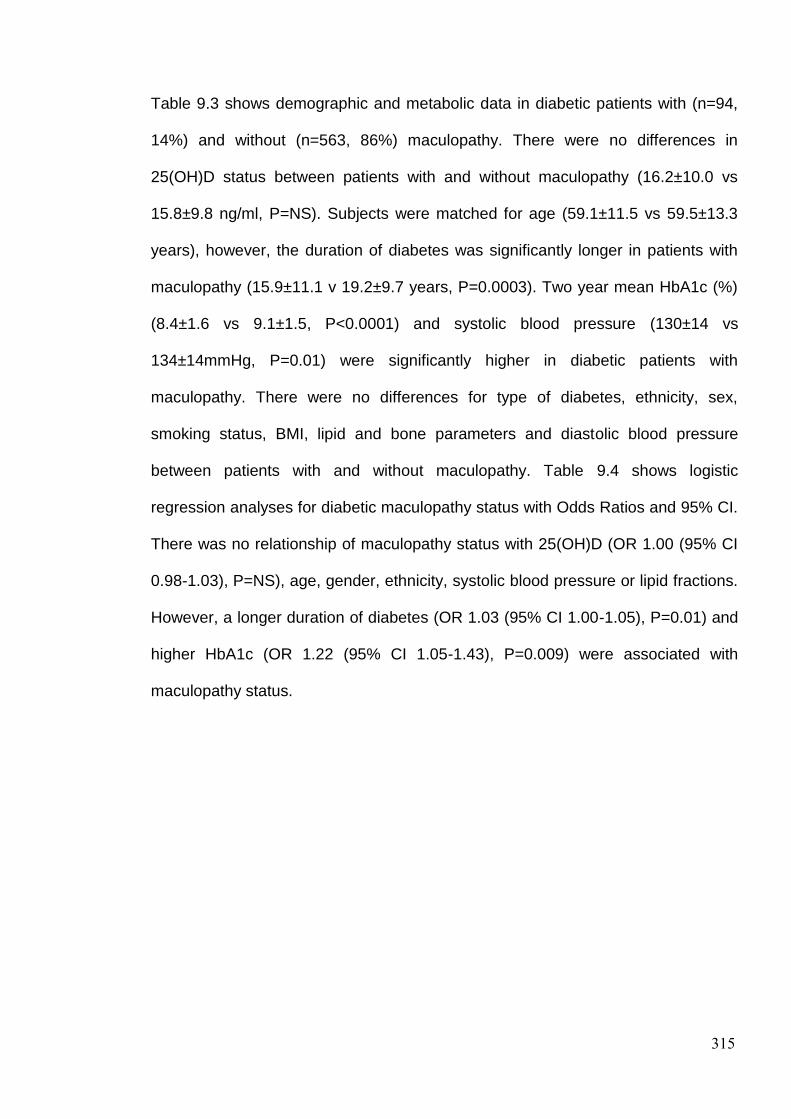
315
Table 9.3 shows demographic and metabolic data in diabetic patients with (n=94,
14%) and without (n=563, 86%) maculopathy. There were no differences in
25(OH)D status between patients with and without maculopathy (16.2±10.0 vs
15.8±9.8 ng/ml, P=NS). Subjects were matched for age (59.1±11.5 vs 59.5±13.3
years), however, the duration of diabetes was significantly longer in patients with
maculopathy (15.9±11.1 v 19.2±9.7 years, P=0.0003). Two year mean HbA1c (%)
(8.4±1.6 vs 9.1±1.5, P<0.0001) and systolic blood pressure (130±14 vs
134±14mmHg, P=0.01) were significantly higher in diabetic patients with
maculopathy. There were no differences for type of diabetes, ethnicity, sex,
smoking status, BMI, lipid and bone parameters and diastolic blood pressure
between patients with and without maculopathy. Table 9.4 shows logistic
regression analyses for diabetic maculopathy status with Odds Ratios and 95% CI.
There was no relationship of maculopathy status with 25(OH)D (OR 1.00 (95% CI
0.98-1.03), P=NS), age, gender, ethnicity, systolic blood pressure or lipid fractions.
However, a longer duration of diabetes (OR 1.03 (95% CI 1.00-1.05), P=0.01) and
higher HbA1c (OR 1.22 (95% CI 1.05-1.43), P=0.009) were associated with
maculopathy status.

316
Table 9-3 Demographic and metabolic parameters in subgroups based on maculopathy
No Diabetic
Maculopathy
(n=563)
Diabetic
Maculopathy
(n=94 )
P
Age (years) 59.5±13.3 59.1±11.5 NS
Duration of
Diabetes (years) 15.9±11.1 19.2±9.7 0.0003
Type 2 DM (%) 82 80 NS
Ethnicity (White
European/South
Asian (%))
40/50 49/48 NS
Sex (male (%)) 51 47 NS
Current/Past/Never
smokers (%) 15/28/57 16/27/57 NS
BMI 31.4±8.8 31.3±6.2 NS
25(OH)D (ng/ml) 15.8±9.8 16.2±10.0 NS
HbA1c (%) 8.4±1.6 9.1±1.5 <0.0001
T-CHL (mmol/l) 4.1±1.1 4.4±1.4 NS
HDL (mmol/l) 1.3±0.5 1.4±0.8 NS
TRIG (mmol/l) 1.8±1.2 1.9±1.6 NS
eGFR (ml/min/l) 75±18 73±20 NS
Systolic BP
(mmHg) 130±14 134±14 0.01
Diastolic BP
(mmHg) 71±7 70±7 NS
ALP (u/L) 87±53 100±129 NS
CCa (mmol/l) 2.3±0.1 2.4±0.1 NS
Table key
ALP – Alkaline Phosphatase; BMI – Body Mass Index; BP – Blood Pressure; CCa – Corrected
Calcium; eGFR – estimated Glomerular Filtration Rate; HDL – High-density Lipoprotein Cholesterol;
T-CHL – Total Cholesterol; TRIG – Triglycerides.
317
Table 9-4 Logistic regression analyses for the relationship between maculopathy, 25(OH)D
status and other confounding variables
OR 95% CI p
25(OH)D 1.00 0.98-1.03 NS
Age (years) 0.99 0.97-1.02 NS
Duration of Diabetes (years) 1.03 1.00-1.05 0.01
Never Smoker 1.24 0.73-2.12 NS
HbA1c (%) 1.22 1.05-1.43 0.009
T-CHL (mmol/l) 1.05 0.84-1.33 NS
HDL (mmol/l) 1.12 0.73-1.73 NS
Triglycerides (mmol/l) 1.19 0.77-1.25 NS
Systolic BP (mmHg) 1.01 0.99-1.04 NS
Diastolic BP (mmHg) 1.03 0.98-1.07 NS
eGFR (ml/min/l) 0.99 0.97-1.00 NS
Table key
ALP – Alkaline Phosphatase; BMI – Body Mass Index; BP – Blood Pressure; CCa – Corrected
Calcium; eGFR – estimated Glomerular Filtration Rate; HDL– High-density Lipoprotein Cholesterol;
T-CHL – Total Cholesterol.

318
The frequencies for both severity of retinopathy, maculopathy and
photocoagulation were similar between the four vitamin D categories (severely
deficient (<10ng/ml), deficient (10-<20ng/ml), insufficient (20-<30ng/ml) and
sufficient (>30ng/ml) (Figure 9.1, Table 9.5).
Figure 9-1 Frequencies of retinopathy, maculopathy and photocoagulation scarring
categorised by 25(OH)D status
0
10
20
30
40
50
60
70
80
90
100
%
Retinopathy, Maculopathy and Photocoagulation status subdivided by 25(OH)D categories
Severely Deficient (<10ng/ml)
Deficient (10-<20ng/ml)
Insufficient (20-<30ng/ml)
Sufficient (=/>30ng/ml)

319
Table 9-5 Frequencies of retinopathy, maculopathy and photocoagulation scarring
categorised by 25(OH)D status
<10ng/ml 10-<20ng/ml 20-<30ng/ml >30ng/ml p
No Diabetic
Retinopathy 37 43 39 30
NS
Background
Diabetic
Retinopathy
36 35 35 45
Pre-Proliferative
Diabetic
Retinopathy
25 19 21 23
Proliferative
Diabetic
Retinopathy
2 3 5 2
No Maculopathy 85 84 87 83 NS
Maculopathy 15 16 13 17
No
Photocoagulation 90 87 80 83
NS
Photocoagulation 10 13 20 17
320
9.5 DISCUSSION
Vitamin D deficiency has wide ranging implications for insulin resistance, beta cell
dysfunction and hypertension and therefore provides a potential link with diabetic
complications (32). Experimental studies have postulated an important link
between vitamin D deficiency and retinopathy (33) and an increased risk of diabetic
retinopathy has been demonstrated in the presence of VDR polymorphisms (13).
However, our study has shown no relationship between the vitamin D status and
the severity of diabetic retinopathy or maculopathy in a large cohort of patients with
predominantly type 2 diabetes, after correcting for glycaemic control, blood
pressure and lipids. We confirm that the ‘usual culprits’ of longer duration of
diabetes, higher HbA1c and systolic blood pressure are directly related to
retinopathy and maculopathy (1), thereby providing confidence in the validity of our
data. Furthermore, the metabolic and anthropometric measurements used in the
regression analysis were taken over an extended period of time as opposed to
‘spot’ readings taken in other studies (24; 26). A possible explanation for the lack of
relationship between vitamin D deficiency and retinopathy could be the striking
extent of vitamin D deficiency in this population, although this is consistent with our
previous data (34). Thus the majority of patients demonstrated deficiency (~90%)
and indeed severe deficiency (~31%). Therefore any relationship between
retinopathy and adequacy of vitamin D could not be explored adequately. Only a
limited number of clinical studies have investigated the role of vitamin D deficiency
in DR. In one of the earliest studies Aksoy et al showed an inverse relationship
between 1,25(OH)2D3 and worsening retinopathy, although the short half life of
1,25(OH)2D3 may limit the interpretation of any such relationship (24). Another
smaller North American study has shown that subjects with DR, in particular PDR,
321
have lower levels of 25(OH)D (26). Whilst in a recent study the percentage of
individuals with vitamin D deficiency increased with the severity of retinopathy,
regression analysis did not demonstrate a statistically significant relationship
between retinopathy severity and serum 25(OH)D concentration (27). In a
prospective observational follow-up study of a cohort of type 1 diabetic patients,
although severe vitamin D deficiency independently predicted all-cause mortality, it
was not related to the development of either retinopathy or nephropathy (5).
In conclusion, this large cross-sectional study found no association of vitamin D
status with diabetic retinopathy or maculopathy. A population with a larger spread
of vitamin D levels may provide further insight into a possible association, but this
may not be possible due to the high prevalence of vitamin D deficiency.

322
9.6 REFERENCES
1. Yau JWY, Rogers SL, Kawasaki R, Lamoureux EL, Kowalski JW, Bek T, Chen
S-J, Dekker JM, Fletcher A, Grauslund J, Haffner S, Hamman RF, Ikram MK,
Kayama T, Klein BEK, Klein R, Krishnaiah S, Mayurasakorn K, O’Hare JP, Orchard
TJ, Porta M, Rema M, Roy MS, Sharma T, Shaw J, Taylor H, Tielsch JM, Varma
R, Wang JJ, Wang N, West S, Xu L, Yasuda M, Zhang X, Mitchell P, Wong TY,
Group ftM-AfEDS: Global Prevalence and Major Risk Factors of Diabetic
Retinopathy. Diabetes Care 2012;35:556-564
2. Bunce C, Wormald R: Leading causes of certification for blindness and partial
sight in England & Wales. BMC Public Health 2006;6:58
3. Roodhooft JM: Leading causes of blindness worldwide. Bull Soc Belge
Ophtalmol 2002:19-25
4. Resnikoff S, Pascolini D, Etya'ale D, Kocur I, Pararajasegaram R, Pokharel GP,
Mariotti SP: Global data on visual impairment in the year 2002. Bull World Health
Organ 2004;82:844-851
5. Joergensen C, Hovind P, Schmedes A, Parving H-H, Rossing P: Vitamin D
Levels, Microvascular Complications, and Mortality in Type 1 Diabetes. Diabetes
Care 2011;34:1081-1085
6. Ismail-Beigi F, Craven T, Banerji MA, Basile J, Calles J, Cohen RM, Cuddihy R,
Cushman WC, Genuth S, Grimm RH, Jr., Hamilton BP, Hoogwerf B, Karl D, Katz
L, Krikorian A, O'Connor P, Pop-Busui R, Schubart U, Simmons D, Taylor H,
Thomas A, Weiss D, Hramiak I: Effect of intensive treatment of hyperglycaemia on
microvascular outcomes in type 2 diabetes: an analysis of the ACCORD
randomised trial. Lancet 2010;376:419-430

323
7. Ismail-Beigi F, Craven TE, O'Connor PJ, Karl D, Calles-Escandon J, Hramiak I,
Genuth S, Cushman WC, Gerstein HC, Probstfield JL, Katz L, Schubart U:
Combined intensive blood pressure and glycemic control does not produce an
additive benefit on microvascular outcomes in type 2 diabetic patients. Kidney Int
2012;81:586-594
8. Hammes HP, Feng Y, Pfister F, Brownlee M: Diabetic retinopathy: targeting
vasoregression. Diabetes 2011;60:9-16
9. Lee CT, Gayton EL, Beulens JW, Flanagan DW, Adler AI: Micronutrients and
diabetic retinopathy a systematic review. Ophthalmology 2010;117:71-78
10. Holick MF: Vitamin D Deficiency. New England Journal of Medicine
2007;357:266-281
11. Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K, Benjamin
EJ, D'Agostino RB, Wolf M, Vasan RS: Vitamin D deficiency and risk of
cardiovascular disease. Circulation 2008;117:503-511
12. Bucan K, Ivanisevic M, Zemunik T, Boraska V, Skrabic V, Vatavuk Z, Galetovic
D, Znaor L: Retinopathy and nephropathy in type 1 diabetic patients--association
with polymorphysms of vitamin D-receptor, TNF, Neuro-D and IL-1 receptor 1
genes. Coll Antropol 2009;33 Suppl 2:99-105
13. Taverna MJ, Selam JL, Slama G: Association between a protein polymorphism
in the start codon of the vitamin D receptor gene and severe diabetic retinopathy in
C-peptide-negative type 1 diabetes. J Clin Endocrinol Metab 2005;90:4803-4808
14. Taverna MJ, Sola A, Guyot-Argenton C, Pacher N, Bruzzo F, Slama G, Reach
G, Selam JL: Taq I polymorphism of the vitamin D receptor and risk of severe
diabetic retinopathy. Diabetologia 2002;45:436-442

324
15. Verstappen A, Parmentier M, Chirnoaga M, Lawson DE, Pasteels JL, Pochet
R: Vitamin D-dependent calcium binding protein immunoreactivity in human retina.
Ophthalmic Res 1986;18:209-214
16. Craig TA, Sommer S, Sussman CR, Grande JP, Kumar R: Expression and
regulation of the vitamin D receptor in the zebrafish, Danio rerio. J Bone Miner Res
2008;23:1486-1496
17. Wagner N, Wagner KD, Schley G, Badiali L, Theres H, Scholz H: 1,25-
dihydroxyvitamin D3-induced apoptosis of retinoblastoma cells is associated with
reciprocal changes of Bcl-2 and bax. Exp Eye Res 2003;77:1-9
18. Cardus A, Panizo S, Encinas M, Dolcet X, Gallego C, Aldea M, Fernandez E,
Valdivielso JM: 1,25-Dihydroxyvitamin D3 regulates VEGF production through a
vitamin D response element in the VEGF promoter. Atherosclerosis 2009;204:85-
89
19. Panou N, Georgopoulos S, Sergentanis TN, Papalampros A, Maropoulos M,
Tentolouris N, Sigala F, Venetsanou K, Papalambros E: Serum 25(OH)D and
VEGF in diabetes mellitus type 2: Gender-specific associations. International
Journal of Collaborative Research on Internal Medicine & Public Health
2011;3:790-795
20. Albert DM, Scheef EA, Wang S, Mehraein F, Darjatmoko SR, Sorenson CM,
Sheibani N: Calcitriol is a potent inhibitor of retinal neovascularization. Invest
Ophthalmol Vis Sci 2007;48:2327-2334
21. Kordonouri O, Wladimirowa A, Danne T: High total serum renin concentrations
are associated with the development of background retinopathy in adolescents with
type 1 diabetes. Diabetes Care 2000;23:1025-1026
325
22. Harindhanavudhi T, Mauer M, Klein R, Zinman B, Sinaiko A, Caramori ML:
Benefits of Renin-Angiotensin blockade on retinopathy in type 1 diabetes vary with
glycemic control. Diabetes Care 2011;34:1838-1842
23. Ireland R: Diabetic nephropathy: Paricalcitol lowers residual albuminuria in type
2 diabetes. Nat Rev Nephrol 2011;7:62
24. Aksoy H, Akçay F, Kurtul N, Baykal O, Avci B: Serum 1,25 dihydroxy vitamin D
(1,25(OH)2D3), 25 hydroxy vitamin D (25(OH)D) and parathormone levels in
diabetic retinopathy. Clin Biochem 2000;33:47-51
25. Kaur H, Donaghue KC, Chan AK, Benitez-Aguirre P, Hing S, Lloyd M,
Cusumano J, Pryke A, Craig ME: Vitamin D deficiency is associated with
retinopathy in children and adolescents with type 1 diabetes. Diabetes Care
2011;34:1400-1402
26. Payne JF, Ray R, Watson DG, Delille C, Rimler E, Cleveland J, Lynn MJ,
Tangpricha V, Srivastava SK: Vitamin D insufficiency in diabetic retinopathy.
Endocr Pract 2012;18:185-193
27. Patrick PA, Visintainer PF, Shi Q, Weiss IA, Brand DA: Vitamin D and
retinopathy in adults with diabetes mellitus. Arch Ophthalmol 2012;130:756-760
28. Scanlon PH: The English national screening programme for sight-threatening
diabetic retinopathy. J Med Screen 2008;15:1-4
29. Jyothi S, Elahi B, Srivastava A, Poole M, Nagi D, Sivaprasad S: Compliance
with the quality standards of National Diabetic Retinopathy Screening Committee.
Prim Care Diabetes 2009;3:67-72
30. Patra S, Gomm EMW, Macipe M, Bailey C: Interobserver agreement between
primary graders and an expert grader in the Bristol and Weston diabetic
326
retinopathy screening programme: a quality assurance audit. Diabetic Medicine
2009;26:820-823
31. ASBMR 31st Annual Meeting MO0001–MO0445. Journal of Bone and Mineral
Research 2009;24:S370-S496
32. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney
RP, Murad MH, Weaver CM: Evaluation, Treatment, and Prevention of Vitamin D
Deficiency: an Endocrine Society Clinical Practice Guideline. Journal of Clinical
Endocrinology & Metabolism 2011;96:1911-1930
33. Deluca HF, Cantorna MT: Vitamin D: its role and uses in immunology. FASEB
J 2001;15:2579-2585
34. Alam U, Najam O, Al-Himdani S, Benoliel S, Jinadev P, Berry JL, Kew M,
Asghar O, Petropoulos IN, Malik RA: Marked vitamin D deficiency in patients with
diabetes in the UK: ethnic and seasonal differences and an association with
dyslipidaemia. Diabet Med 2012;29:1343-1345
327
10 Chapter X - Discussion

328
The chronic hyperglycaemia of DM is associated with end-organ damage,
dysfunction and failure, including the retina, kidney, nerves, heart and blood
vessels (1). The IDF estimates an overall prevalence of DM to be 366 million in
2011, and this is expected to rise to 552 million by 2030 (2). The prevalence of
DSPN is thought to be around 30% (3-4) and increases with a longer duration of
the disease. When diabetes has been present for greater than 25 years the
prevalence rises to approximately 50% (4).
In the same manner that identifying and treating microalbuminuria allows the
prevention of diabetic nephropathy, identifying and treating abnormalities in small
nerve fibre function may help to prevent diabetic neuropathy and its sequelae.
Furthermore, earlier diagnosis of neuropathy would allow for the optimisation of
conventional risk factors and consequently reduce the morbidity associated with
neuropathy. The accurate detection and quantification of DSPN are important to
identify at risk patients, anticipate deterioration of nerve function, and assess
endpoints in clinical trials. Current methods lack sensitivity (QST), primarily focus
on large fibres (NCS) or are invasive and require detailed laboratory processing
(skin/nerve biopsy) and thus are not routinely performed within the health care
system. CCM has been proposed as a surrogate endpoint of DSPN and allows for
rapid, reiterative and non-invasive assessment of the corneal subbasal nerve
plexus. The evaluation of corneal subbasal nerve morphology has shown
significant diagnostic potential for a number of peripheral neuropathies and in
particular DSPN (5-8). Corneal nerve pathology correlates well with IENF loss (9)
and currently prospective natural history studies are underway will investigate the
utility of CCM to assess the status and progression of DSPN in subjects with type 1
329
and type 2 DM (9). Furthermore, recent studies using CCM have also shown nerve
fibre regeneration after simultaneous pancreatic and kidney transplant (10).
The UKPDS demonstrated a significant risk reduction for cardiovascular disease
and amputation for every 1% reduction in mean HbA1c (11). Intensive therapy
reduced the development of confirmed clinical neuropathy by 64% in the DCCT
after 5 years of follow-up (12). However, approximately 50% of patients with DSPN
experience neuropathic symptoms (13) and these symptoms include; burning pain,
electrical or stabbing sensations, paraesthesia, hyperaesthesia and a deep aching
pain. The precise reasons for the development of neuropathic pain despite loss of
sensation is not clearly elucidated but suggests that aberrations in pain signalling
in the peripheral and central nervous system occur (13). Furthermore, there is an
epidemic of vitamin D deficiency worldwide with over one billion people thought to
be affected (14). Until recently, studies of vitamin D have largely focussed on bone
health and calcium metabolism (14), however, there is an increasing body of
evidence implicating the role of vitamin D in the nervous system (15-17). In
experimental studies, vitamin D has been linked to the regulation of neurotrophins
such as Nerve Growth Factor (NGF) and neuronal Ca2+ homeostasis, both may
play a neuroprotective role in the peripheral nerve (18). Previous studies have
shown improvements in diabetic and non-diabetic nephropathy with activated
vitamin D administration through a mechanism linked to inhibition of the RAS
system (19-21). Vitamin D is a potent RAS inhibitor (22). RAS over activity impacts
on the prevalence of diabetes related complications and inhibition of this system
may have a dramatic effect on the improvement of diabetic complications including
retinopathy and neuropathy (23-24).

330
10.1 Rapid Nerve Fibre Decline in patients with Type 1 diabetes can be
readily detected using Corneal Confocal Microscopy (To be submitted)
DSPN is a confirmed risk factor for debilitating lower limb amputation (25) and is
one of only three independent and significant risk factors for mortality as confirmed
through the ACCORD study (26). Longitudinal studies show deterioration in
neuropathy overtime in both type 1 diabetes (12) and type 2 diabetes by means of
electrophysiology (27). However, the dramatic failure of pathogenetic treatments in
DSPN (28) has been considered to be related to inappropriate surrogate endpoints
and selection of patients for studies. The progression of DSPN has been shown to
occur much slower than previously thought, likely due to overall improved diabetes
care with better glycaemic control and the more prevalent use of ACE inhibitors
(24) and statins (29), which are likely to have an impact on neuropathy. Therefore it
has been proposed that subjects with deteriorating as opposed to stable nerve
function should be recruited into clinical trials of DSPN (28). Delineating this cohort
is essential in undertaking a well conducted clinical trial and also identifying the at
risk patient for timely intervention. In this study, we have shown that CCM can be
used to identify a subgroup of subjects with type 1 diabetes undergoing a more
accelerated degree of small fibre decline. Therefore, in-vivo CCM provides an ideal
surrogate endpoint in identifying those at risk of worsening DSPN and also for
recruitment into future clinical trials of pathogenetic treatments for DSPN.
10.2 Diagnostic Utility of Corneal Confocal Microscopy and Intra-Epidermal
Nerve Fibre Density in Diabetic Neuropathy (To be submitted)
DSPN is a debilitating condition which may lead to pain, foot ulceration and
eventual amputation (30). Therefore it is important to accurately diagnose diabetic

331
neuropathy at the earliest stage of damage. However, the earliest nerve fibres to
degenerate (31-32) and regenerate (33) are the small unmyelinated fibres and
indeed they are central to the genesis of pain and the development of foot
ulceration (34). CCM is a non-invasive ophthalmic application, which is rapid, non-
invasive and readily reproducible for quantifying small nerve fibres and thereby has
been shown to diagnose and track the progression of diabetic neuropathy (5; 7;
35). CNFD has a superior sensitivity and an almost identical specificity compared
to IENFD. Subsequently, CNFD had better diagnostic utility for DSPN and
correlated better with electrophysiology than the current ‘gold’ standard of IENFD.
CCM is a valid accurate non-invasive method which is superior to skin biopsy in
diagnosing DSPN.
10.3 Enhanced Small Fibre Neuropathy in Patients with Latent Autoimmune
Diabetes in Adults (To be submitted)
Latent Autoimmune Diabetes in Adults is an under recognized (~10%) form of
diabetes which is often misdiagnosed as type 2 diabetes mellitus (36). The
pathophysiology is more closely related to autoimmune destruction of β-cells rather
than the insulin resistance found in type 2 diabetes. Patients with LADA are
autoantibody positive at a younger age of presentation, with a relatively low BMI
and have an earlier loss of glycaemic control which may influence the development
of complications (37-41). The complications of LADA have been poorly phenotyped
with only a handful of studies assessing neuropathy in this group (41-44). We
clearly demonstrate a greater degree of small fibre neuropathy in subjects with
LADA who have poorer glycaemic control. This was detected using conventional
small fibre tests such as thermal thresholds and IENFD but in particular the novel

332
non-invasive test of CCM. Hyperglycaemia predisposes to microvascular
complications including DSPN (11; 45-46) and therefore poorer glycaemic control
due to continued conventional oral hypoglycaemic treatment as opposed to earlier
treatment with insulin in LADA (47) may result in the more prevalent small fibre
damage. Furthermore, given the potential link between C-peptide and neuropathy,
the faster decline in C-peptide levels may also predispose to more prevalent
neuropathy (43). Thus patients with LADA require early and accurate assessment
for neuropathy to identify those individuals who may be at greater risk for
progression to early β-cell failure and loss of glycaemic control.
10.4 Marked vitamin D deficiency in patients with diabetes from secondary
care: Ethnic and seasonal differences and an association with dyslipidaemia
(48) (Alam U, et al. Diabet Med 2012;29:1343-1345)
The purpose of this cross sectional study was to assess the prevalence of vitamin
D deficiency in a diabetic population in relation to metabolic parameters. Using
≤30ng/ml as a cut off for deficiency (49) we found that 91% of our subjects with
diabetes, compared to 78% age and ethnicity matched subjects without diabetes,
were deficient (48). Despite particularly low vitamin D concentrations there was no
association with an increase in ALP or low corrected calcium status, both of which
are considered to be good metabolic indicators of vitamin D deficiency (50-51).
This is an important observation as current local, national and international
guidelines endorse a view that vitamin D should only be assessed if there are overt
symptoms of osteomalacia or if the calcium is reduced and or ALP is elevated, in
predefined high risk groups. An association was found, albeit weak with HDL
cholesterol, suggesting an important relationship with lipids and a possible
333
explanation for the excess cardiovascular disease described in vitamin D
deficiency states. Significant ethnic differences were seen with the lowest levels in
South Asian/middle Eastern patients but the differences were not marked, again
challenging the sterotype that vitamin D deficiency occurs predominantly in South
Asians. Furthermore, there was a minimal seasonal variation in white European
patients and there were no significant variation of note in South Asian/middle
Eastern subjects. Seasonality is often cited as a reason for vitamin D insufficiency;
however with a lack of sunlight exposure in most patients in all seasons this not
likely to be a valid contributing factor. This study demonstrates an important
deficiency of vitamin D which is not routinely assessed in diabetic patients and may
play a role in cardiovascular disease states.
10.5 Differential effects of different vitamin D replacement strategies in
patients with diabetes. (Alam U et al. J Diabetes Complications 2013.
Accepted, [Epub ahead of print])
Sunlight exposure in the U.K. is insufficient in providing an adequate 25(OH)D
status (52-53) and effective replacement strategies are required particularly in high
risk groups. This study is an evaluation of vitamin D status at baseline and after
intervention with vitamin D in over two hundred and forty participants assigned to
three treatment strategies of Vitamin D2 or D3. Despite relatively aggressive
regimens of vitamin D replacement there was significant vitamin D deficiency in a
large subgroup, particularly in those treated with vitamin D2. Furthermore, there
was a significant disparity in regimens of vitamin D2 and vitamin D3 in relation to
the relative effectiveness of the improvement in 25(OH)D concentrations which has
also been suggested in previous literature (54). Current regimens do not adjust for

334
these differences (55) and the relative disparity of treatments may lead to
inadequate replacement with consequent complications. Vitamin D shares a similar
intake-response curve to other nutrients and in persons whose baseline values
differ then an identical nutrient intake may or may not produce a measurable
response (56). We have found reduced efficacy of vitamin D replacement in those
with higher baseline vitamin D status. Differences in baseline concentrations and
type of vitamin D (D2/D3) replacement need to be considered for future policies and
guidelines. We believe our data provides considerable insights to enable more
evidence based guidance to be developed.
10.6 Vitamin D Deficiency Contributes to Painful Diabetic Neuropathy (Alam
U et al. Submitted Diabetes awaiting revision)
We have undertaken a detailed assessment in forty three subjects with mild
diabetic neuropathy based on the neuropathy disability score with and without
painful neuropathy compared to a healthy age matched control group. A previous
study has shown a potential therapeutic benefit of modest intervention with vitamin
D therapy (~2000 IU cholecalciferol daily) in patients with type 2 diabetes and
painful neuropathy (57). Other than potential analgesic effects, active vitamin D3
induces NGF (58) and NGF is known to be depleted in experimental diabetes (59).
This suggests vitamin D may have a direct effect on the pathogenesis of diabetic
neuropathy, particularly when considering that vitamin D3 has been shown to
reduce demyelination in a cuprizone experimental model of demyelination (60).
The data provides a novel postulated link between vitamin D deficiency and painful
diabetic neuropathy. Despite identical severity of neuropathy and metabolic control,
the only abnormality noted was a lower level of vitamin D in a cohort of patients
335
with painful diabetic neuropathy. Furthermore, there was a significantly greater
odds ratio for painful neuropathy in those with vitamin D insufficiency and in
particular deficiency. This study provides a novel association between vitamin D
deficiency and painful diabetic neuropathy. Recent studies of novel drugs in the
treatment of painful diabetic neuropathy have dramatically failed (61-62) with active
treatment being barely superior to placebo. There is an urgent need to explore new
mechanisms and hence clinical trials assessing the efficacy of vitamin D
replacement in painful diabetic neuropathy are urgently required.
10.7 Vitamin D Deficiency is not associated with Diabetic Retinopathy or
Maculopathy: A Cross Sectional study (To be submitted).
A cross sectional evaluation of retinopathy and maculopathy in subjects with type 1
and type 2 diabetes in relation to vitamin D status, demographic, anthropometric
measurement, blood pressure and blood metabolic chemistry was undertaken in
six hundred and fifty seven participants. VDR genotypes have been associated
with the cumulative prevalence of diabetic retinopathy (63) and the VDR is
expressed in the ganglion cells, the inner and outer plexiform layer and the
photoreceptor layer of the retina as demonstrated by immunostaining in animal
models (64). Several risk factors are implicated in the aetiology of DR with
hyperglycaemia and hypertension showing the strongest association (65).
However, interventions aimed at correcting these risk factors have demonstrated
moderate success (66-67). Recent studies have suggested a link with vitamin D
status and DR in adolescents (68) and adults (69). Whilst we have shown there is
a marked vitamin D deficiency in this population, we found no association between
vitamin D status and the presence and severity of diabetic retinopathy or

336
maculopathy. However, well established risk factors such as HbA1c, age, duration
of diabetes and systolic blood pressure were significantly associated with the
severity of retinopathy. We conclude that further studies, in particular longitudinal
evaluation is required to better understand the potential interplay between vitamin
D and diabetic retinopathy and maculopathy.
10.8 Study limitations
There are several limitations to the current studies and should be acknowledged. A
major limitation in all but the first study (chapter 3) is the cross-sectional design.
Furthermore, the studies of vitamin D deficiency prevalence, differential vitamin D
intervention and vitamin D status in relation to retinopathy were retrospective
analyses of clinically derived data. Nevertheless, this work provides a real world
analysis of the extent of this significant public health problem and detailed
effectiveness of commonly used replacement regimens. This is particularly
important as there is no consensus agreement on the optimal replacement
strategies in vitamin D deficiency and many of the current proposed strategies lack
an evidence base. The study of vitamin D status in relation to painful diabetic
neuropathy provides a novel clinical association which demands further
mechanistic studies and human clinical trials. A lack of association between
vitamin D status and diabetic retinopathy and maculopathy in our study does not
exclude causation, particularly as most of the subjects had a low level of vitamin D.
Of course, epidemiological studies are liable to ecological fallacy.
We also present a prospective study evaluating the ability to predict the
development and progression of neuropathy through CCM. This builds on our
previously published data showing that CCM can accurately stratify the severity of
337
neuropathy (70) and track an improvement in nerve structure (5). A large
longitudinal study of CCM as a surrogate marker of DSPN is currently ongoing to
establish the predictive value of this novel modality (9). There was an absence of
skin biopsy data in the longitudinal study over 2 years. This therefore limits
interpretation as IENFD is the current gold standard technique in assessing small
nerve fibres and would allow direct comparison versus corneal nerve structure and
peripheral nerve function thus allowing a more accurate prediction of the ability of
CCM in the diagnosis and assessment of progression of DSPN. The
restoration/regeneration of the peripheral nerve is of paramount importance and
future studies of pathogenetic treatments that may show regression of neuropathy
detected by CCM are of key significance. For recruitment into these studies the
correct patient population and surrogate endpoints are required. CCM may indeed
be a game changer if this current data are mirrored in longitudinal studies with
accurate comparisons to IENFD and electrophysiology. It has been argued that the
human cornea is avascular and immune privileged and therefore assessment of
corneal nerves which are of course also much shorter has limited relevance to
peripheral nerves and hence a dying back sensorimotor neuropathy which affects
the most distal nerves first. However, the corneal subbasal nerve plexus is the
most distal portion of the ophthalmic branch of the trigeminal nerve with its cell
body in the trigeminal ganglion and therefore is directly comparable to the anatomy
of any peripheral nerve. Furthermore, the observed alterations in corneal nerves
appear to be the result of vascular-mediated effects which occur in the trigeminal
ganglion and accompanying neurovascular bundle (71-72).

338
10.9 Future Work
In terms of CCM, the prognostic value of the corneal nerve morphometric
parameters is currently being established through a number of longitudinal studies.
A community based study, investigating the ability of CCM as a screening tool for
DSPN would be invaluable and the rates of subsequent ‘hard’ endpoints such as
foot ulceration would provide valuable evidence on the utility of the technique.
Clearly subjects with LADA may have a significant predisposition to poorer
glycaemic control and subsequent small fibre neuropathy and this population may
require more intensive screening for diabetic complications, and CCM may provide
a unique opportunity for non-invasive, reiterative screening of small nerve fibres.
Future epidemiological studies of vitamin D status relating to diabetic complications
should be prospective and data derived, from multi-national sources consisting of a
spread of vitamin D status including a significant proportion that have sufficient
vitamin D concentrations. Of course, the definitive scientific evaluation should be
through double blinded randomised placebo controlled trials of vitamin D
supplementation for metabolic outcomes, diabetic complications and painful
diabetic neuropathy. However, a number of obstacles must be considered; the
likely effective dose as under dosing has been an issue in other studies, the type of
vitamin D preparation and metabolites and the length of treatment required with the
relevant vitamin D formulation. Vitamin D deficiency in relation to painful diabetic
neuropathy is an important avenue which clearly needs urgent scientific and
clinical trial evaluation as it represents an almost perfect treatment option with once
weekly or even monthly dosing, minimal side effects and of course the potential for
multiple other benefits.

339
10.10 Conclusion
In conclusion, this thesis provides evidence of marked vitamin D deficiency in a
population with diabetes and a novel association with DSPN but not retinopathy.
We also show that corneal nerve loss is readily detected with CCM and allows the
identification of both progressive DSPN and early small fibre neuropathy in patients
with LADA and type 1 diabetes.
340
10.11 REFERENCES
1. American Diabetes Association: clinical practice recommendations 2002.
Diabetes care 2002;25 Suppl 1:S1-147
2. Whiting DR, Guariguata L, Weil C, Shaw J: IDF Diabetes Atlas: Global estimates
of the prevalence of diabetes for 2011 and 2030. Diabetes Research and Clinical
Practice 2011;94:311-321
3. Shaw J, Zimmet P: The epidemiology of diabetic neuropathy. Diabetes Revs
1999;7:245-252
4. Boulton AJM, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, Malik RA,
Maser RE, Sosenko JM, Ziegler D: Diabetic neuropathies: a statement by the
American Diabetes Association. Diabetes care 2005;28:956-962
5. Tavakoli M, Mitu-Pretorian M, Petropoulos IN, Fadavi H, Asghar O, Alam U,
Ponirakis G, Jeziorska M, Marshall A, Efron N, Boulton AJ, Augustine T, Malik RA:
Corneal confocal microscopy detects early nerve regeneration in diabetic
neuropathy after simultaneous pancreas and kidney transplantation. Diabetes
2013;62:254-260
6. Tavakoli M, Marshall A, Pitceathly R, Fadavi H, Gow D, Roberts ME, Efron N,
Boulton AJ, Malik RA: Corneal confocal microscopy: a novel means to detect nerve
fibre damage in idiopathic small fibre neuropathy. Exp Neurol 2010;223:245-250
7. Tavakoli M, Kallinikos PA, Efron N, Boulton AJ, Malik RA: Corneal sensitivity is
reduced and relates to the severity of neuropathy in patients with diabetes.
Diabetes Care 2007;30:1895-1897
8. Quattrini C, Tavakoli M, Jeziorska M, Kallinikos P, Tesfaye S, Finnigan J,
Marshall A, Boulton AJM, Efron N, Malik RA: Surrogate Markers of Small Fibre
Damage in Human Diabetic Neuropathy. Diabetes 2007;56:2148-2154
341
9. Edwards K, Pritchard N, Vagenas D, Russell A, Malik RA, Efron N: Utility of
corneal confocal microscopy for assessing mild diabetic neuropathy: baseline
findings of the LANDMark study. Clin Exp Optom 2012;95:348-354
10. Tavakoli M, Mitu-Pretorian M, Petropoulos IN, Fadavi H, Asghar O, Alam U,
Ponirakis G, Jeziorska M, Marshall A, Efron N, Boulton AJ, Augustine T, Malik RA:
Corneal Confocal Microscopy Detects Early Nerve Regeneration in Diabetic
Neuropathy After Simultaneous Pancreas and Kidney Transplantation. Diabetes
2013;62:254-260
11. Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D,
Turner RC, Holman RR: Association of glycaemia with macrovascular and
microvascular complications of type 2 diabetes (UKPDS 35): prospective
observational study. BMJ 2000;321:405-412
12. The effect of intensive diabetes therapy on the development and progression of
neuropathy. The Diabetes Control and Complications Trial Research Group. Ann
Intern Med 1995;122:561-568
13. Tesfaye S, Boulton AJ, Dickenson AH: Mechanisms and management of
diabetic painful distal symmetrical polyneuropathy. Diabetes Care 2013;36:2456-
2465
14. Holick MF: Vitamin D deficiency. N Engl J Med 2007;357:266-281
15. Alam U, Asghar O, Malik RA: Vitamin D deficiency and cardiovascular disease:
the missing link. Diabetes Management 2011;1:151-155
16. Holmoy T, Moen SM: Assessing vitamin D in the central nervous system. Acta
Neurol Scand Suppl 2010:88-92

342
17. Alam U, Asghar O, Malik RA: Are vitamin D and B deficiency relevant to the
pathogenesis and treatment of diabetic neuropathy? Future Neurology 2012;7:235-
238
18. Riaz S, Malcangio M, Miller M, Tomlinson DR: A vitamin D(3) derivative
(CB1093) induces nerve growth factor and prevents neurotrophic deficits in
streptozotocin-diabetic rats. Diabetologia 1999;42:1308-1313
19. Tan X, He W, Liu Y: Combination therapy with paricalcitol and trandolapril
reduces renal fibrosis in obstructive nephropathy. Kidney Int 2009;76:1248-1257
20. Tan X, Li Y, Liu Y: Paricalcitol attenuates renal interstitial fibrosis in obstructive
nephropathy. J Am Soc Nephrol 2006;17:3382-3393
21. Ireland R: Diabetic nephropathy: Paricalcitol lowers residual albuminuria in type
2 diabetes. Nat Rev Nephrol 2011;7:62
22. Vaidya A, Forman JP: Vitamin D and Hypertension: Current Evidence and
Future Directions. Hypertension 2010;56:774-779
23. Hsueh WA, Wyne K: Renin-Angiotensin-Aldosterone System in Diabetes and
Hypertension. The Journal of Clinical Hypertension 2011;13:224-237
24. Malik RA, Williamson S, Abbott C, Carrington AL, Iqbal J, Schady W, Boulton
AJ: Effect of angiotensin-converting-enzyme (ACE) inhibitor trandolapril on human
diabetic neuropathy: randomised double-blind controlled trial. Lancet
1998;352:1978-1981
25. Adler AI, Boyko EJ, Ahroni JH, Smith DG: Lower-extremity amputation in
diabetes. The independent effects of peripheral vascular disease, sensory
neuropathy, and foot ulcers. Diabetes Care 1999;22:1029-1035
26. Calles-Escandon J, Lovato LC, Simons-Morton DG, Kendall DM, Pop-Busui R,
Cohen RM, Bonds DE, Fonseca VA, Ismail-Beigi F, Banerji MA, Failor A, Hamilton
343
B: Effect of intensive compared with standard glycemia treatment strategies on
mortality by baseline subgroup characteristics: the Action to Control Cardiovascular
Risk in Diabetes (ACCORD) trial. Diabetes Care 2010;33:721-727
27. Partanen J, Niskanen L, Lehtinen J, Mervaala E, Siitonen O, Uusitupa M:
Natural history of peripheral neuropathy in patients with non-insulin-dependent
diabetes mellitus. N Engl J Med 1995;333:89-94
28. Dyck PJ, Norell JE, Tritschler H, Schuette K, Samigullin R, Ziegler D, Bastyr
EJ, 3rd, Litchy WJ, O'Brien PC: Challenges in design of multicenter trials: end
points assessed longitudinally for change and monotonicity. Diabetes Care
2007;30:2619-2625
29. Davis TM, Yeap BB, Davis WA, Bruce DG: Lipid-lowering therapy and
peripheral sensory neuropathy in type 2 diabetes: the Fremantle Diabetes Study.
Diabetologia 2008;51:562-566
30. Boulton AJ, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, Malik RA,
Maser RE, Sosenko JM, Ziegler D: Diabetic neuropathies: a statement by the
American Diabetes Association. Diabetes Care 2005;28:956-962
31. Sumner CJ, Sheth S, Griffin JW, Cornblath DR, Polydefkis M: The spectrum of
neuropathy in diabetes and impaired glucose tolerance. Neurology 2003;60:108-
111
32. Singleton JR, Smith AG, Bromberg MB: Increased Prevalence of Impaired
Glucose Tolerance in Patients With Painful Sensory Neuropathy. Diabetes Care
2001;24:1448-1453
33. Smith AG, Russell J, Feldman EL, Goldstein J, Peltier A, Smith S, Hamwi J,
Pollari D, Bixby B, Howard J, Singleton JR: Lifestyle Intervention for Pre-Diabetic
Neuropathy. Diabetes Care 2006;29:1294-1299

344
34. Malik R, Veves A, Tesfaye S, Smith G, Cameron N, Zochodne D, Lauria G:
Small Fibre Neuropathy: Role in the diagnosis of Diabetic Sensorimotor
Polyneuropathy. Diabetes/Metabolism Research and Reviews 2011; 2011;27:678-
684
35. Tavakoli M, Kallinikos P, Iqbal A, Herbert A, Fadavi H, Efron N, Boulton AJ, R
AM: Corneal confocal microscopy detects improvement in corneal nerve
morphology with an improvement in risk factors for diabetic neuropathy. Diabet
Med 2011;28:1261-1267
36. Fourlanos S, Dotta F, Greenbaum CJ, Palmer JP, Rolandsson O, Colman PG,
Harrison LC: Latent autoimmune diabetes in adults (LADA) should be less latent.
Diabetologia 2005;48:2206-2212
37. Tuomi T, Carlsson A, Li H, Isomaa B, Miettinen A, Nilsson A, Nissen M,
Ehrnstrom BO, Forsen B, Snickars B, Lahti K, Forsblom C, Saloranta C, Taskinen
MR, Groop LC: Clinical and genetic characteristics of type 2 diabetes with and
without GAD antibodies. Diabetes 1999;48:150-157
38. Turner R, Stratton I, Horton V, Manley S, Zimmet P, Mackay IR, Shattock M,
Bottazzo GF, Holman R: UKPDS 25: autoantibodies to islet-cell cytoplasm and
glutamic acid decarboxylase for prediction of insulin requirement in type 2
diabetes. UK Prospective Diabetes Study Group. Lancet 1997;350:1288-1293
39. Davis TM, Zimmet P, Davis WA, Bruce DG, Fida S, Mackay IR: Autoantibodies
to glutamic acid decarboxylase in diabetic patients from a multi-ethnic Australian
community: the Fremantle Diabetes Study. Diabet Med 2000;17:667-674
40. Romkens TE, Kusters GC, Netea MG, Netten PM: Prevalence and clinical
characteristics of insulin-treated, anti-GAD-positive, type 2 diabetic subjects in an

345
outpatient clinical department of a Dutch teaching hospital. Neth J Med
2006;64:114-118
41. Myhill P, Davis WA, Bruce DG, Mackay IR, Zimmet P, Davis TM: Chronic
complications and mortality in community-based patients with latent autoimmune
diabetes in adults: the Fremantle Diabetes Study. Diabet Med 2008;25:1245-1250
42. Baum P, Hermann W, Verlohren HJ, Wagner A, Lohmann T, Grahmann F:
Diabetic neuropathy in patients with "latent autoimmune diabetes of the adults"
(LADA) compared with patients with type 1 and type 2 diabetes. J Neurol
2003;250:682-687
43. Roh MO, Jung CH, Kim BY, Mok JO, Kim CH: The prevalence and
characteristics of latent autoimmune diabetes in adults (LADA) and its relation with
chronic complications in a clinical department of a university hospital in Korea. Acta
Diabetol 2013;50:129-134
44. Isomaa B, Almgren P, Henricsson M, Taskinen MR, Tuomi T, Groop L, Sarelin
L: Chronic complications in patients with slowly progressing autoimmune type 1
diabetes (LADA). Diabetes Care 1999;22:1347-1353
45. Effect of intensive therapy on the development and progression of diabetic
nephropathy in the Diabetes Control and Complications Trial. The Diabetes Control
and Complications (DCCT) Research Group. Kidney Int 1995;47:1703-1720
46. Albers JW, Herman WH, Pop-Busui R, Feldman EL, Martin CL, Cleary PA,
Waberski BH, Lachin JM: Effect of prior intensive insulin treatment during the
Diabetes Control and Complications Trial (DCCT) on peripheral neuropathy in type
1 diabetes during the Epidemiology of Diabetes Interventions and Complications
(EDIC) Study. Diabetes Care 2010;33:1090-1096

346
47. Thunander M, Thorgeirsson H, Törn C, Petersson C, Landin-Olsson M: β-cell
function and metabolic control in latent autoimmune diabetes in adults with early
insulin versus conventional treatment: a 3-year follow-up. European Journal of
Endocrinology 2011;164:239-245
48. Alam U, Najam O, Al-Himdani S, Benoliel S, Jinadev P, Berry JL, Kew M,
Asghar O, Petropoulos IN, Malik RA: Marked vitamin D deficiency in patients with
diabetes in the UK: ethnic and seasonal differences and an association with
dyslipidaemia. Diabet Med 2012;29:1343-1345
49. Holick MF: Vitamin D Deficiency. New England Journal of Medicine
2007;357:266-281
50. Jesudason D, Need AG, Horowitz M, O'Loughlin PD, Morris HA, Nordin BE:
Relationship between serum 25-hydroxyvitamin D and bone resorption markers in
vitamin D insufficiency. Bone 2002;31:626-630
51. Need AG: Bone resorption markers in vitamin D insufficiency. Clin Chim Acta
2006;368:48-52
52. Webb AR, Kift R, Durkin MT, O’Brien SJ, Vail A, Berry JL, Rhodes LE: The role
of sunlight exposure in determining the vitamin D status of the U.K. white adult
population. British Journal of Dermatology 2010;163:1050-1055
53. Macdonald HM: Contributions of sunlight and diet to vitamin D status. Calcif
Tissue Int 2013;92:163-176
54. Armas LAG, Hollis BW, Heaney RP: Vitamin D2 Is Much Less Effective than
Vitamin D3 in Humans. Journal of Clinical Endocrinology & Metabolism
2004;89:5387-5391
55. Pearce SH, Cheetham TD: Diagnosis and management of vitamin D
deficiency. BMJ 2010;340:b5664

347
56. Heaney RP: Vitamin D — Baseline Status and Effective Dose. New England
Journal of Medicine 2012;367:77-78
57. Lee P, Chen R: Vitamin D as an analgesic for patients with type 2 diabetes and
neuropathic pain. Arch Intern Med 2008;168:771-772
58. Fukuoka M, Sakurai K, Ohta T, Kiyoki M, Katayama I: Tacalcitol, an active
vitamin D3, induces nerve growth factor production in human epidermal
keratinocytes. Skin Pharmacol Appl Skin Physiol 2001;14:226-233
59. Hellweg R, Wohrle M, Hartung HD, Stracke H, Hock C, Federlin K: Diabetes
mellitus-associated decrease in nerve growth factor levels is reversed by
allogeneic pancreatic islet transplantation. Neurosci Lett 1991;125:1-4
60. Wergeland S, Torkildsen O, Myhr KM, Aksnes L, Mork SJ, Bo L: Dietary
vitamin D3 supplements reduce demyelination in the cuprizone model. PLoS One
6:e26262
61. Selvarajah D, Gandhi R, Emery CJ, Tesfaye S: Randomized Placebo-
Controlled Double-Blind Clinical Trial of Cannabis-Based Medicinal Product
(Sativex) in Painful Diabetic Neuropathy: Depression is a major confounding factor.
Diabetes Care 2010;33:128-130
62. Ziegler D, Hidvégi T, Gurieva I, Bongardt S, Freynhagen R, Sen D,
Sommerville K, Group obotLSS: Efficacy and Safety of Lacosamide in Painful
Diabetic Neuropathy. Diabetes Care 2010;33:839-841
63. Bucan K, Ivanisevic M, Zemunik T, Boraska V, Skrabic V, Vatavuk Z, Galetovic
D, Znaor L: Retinopathy and nephropathy in type 1 diabetic patients--association
with polymorphysms of vitamin D-receptor, TNF, Neuro-D and IL-1 receptor 1
genes. Coll Antropol 2009;33 Suppl 2:99-105

348
64. Craig TA, Sommer S, Sussman CR, Grande JP, Kumar R: Expression and
regulation of the vitamin D receptor in the zebrafish, Danio rerio. J Bone Miner Res
2008;23:1486-1496
65. Joergensen C, Hovind P, Schmedes A, Parving H-H, Rossing P: Vitamin D
Levels, Microvascular Complications, and Mortality in Type 1 Diabetes. Diabetes
Care 2011;34:1081-1085
66. Ismail-Beigi F, Craven T, Banerji MA, Basile J, Calles J, Cohen RM, Cuddihy
R, Cushman WC, Genuth S, Grimm RH, Jr., Hamilton BP, Hoogwerf B, Karl D,
Katz L, Krikorian A, O'Connor P, Pop-Busui R, Schubart U, Simmons D, Taylor H,
Thomas A, Weiss D, Hramiak I: Effect of intensive treatment of hyperglycaemia on
microvascular outcomes in type 2 diabetes: an analysis of the ACCORD
randomised trial. Lancet 2010;376:419-430
67. Ismail-Beigi F, Craven TE, O'Connor PJ, Karl D, Calles-Escandon J, Hramiak I,
Genuth S, Cushman WC, Gerstein HC, Probstfield JL, Katz L, Schubart U:
Combined intensive blood pressure and glycemic control does not produce an
additive benefit on microvascular outcomes in type 2 diabetic patients. Kidney Int
2012;81:586-594
68. Kaur H, Donaghue KC, Chan AK, Benitez-Aguirre P, Hing S, Lloyd M,
Cusumano J, Pryke A, Craig ME: Vitamin D deficiency is associated with
retinopathy in children and adolescents with type 1 diabetes. Diabetes Care
2011;34:1400-1402
69. Payne JF, Ray R, Watson DG, Delille C, Rimler E, Cleveland J, Lynn MJ,
Tangpricha V, Srivastava SK: Vitamin D insufficiency in diabetic retinopathy.
Endocr Pract 2012;18:185-193

349
70. Tavakoli M, Quattrini C, Abbott C, Kallinikos P, Marshall A, Finnigan J, Morgan
P, Efron N, Boulton AJ, Malik RA: Corneal confocal microscopy: a novel
noninvasive test to diagnose and stratify the severity of human diabetic
neuropathy. Diabetes Care 2010;33:1792-1797
71. Davidson EP, Coppey LJ, Yorek MA: Early loss of innervation of cornea
epithelium in streptozotocin-induced type 1 diabetic rats: improvement with ilepatril
treatment. Invest Ophthalmol Vis Sci 2012;53:8067-8074
72. Davidson EP, Coppey LJ, Holmes A, Yorek MA: Changes in corneal
innervation and sensitivity and acetylcholine-mediated vascular relaxation of the
posterior ciliary artery in a type 2 diabetic rat. Invest Ophthalmol Vis Sci
2012;53:1182-1187
350
11 REFERENCES
351
Abbott CA, Carrington AL, Ashe H, Bath S, Every LC, Griffiths J, Hann AW,
Hussein A, Jackson N, Johnson KE, Ryder CH, Torkington R, Van Ross ERE,
Whalley AM, Widdows P, Williamson S, Boulton AJM: The North-West Diabetes
Foot Care Study: incidence of, and risk factors for, new diabetic foot ulceration in a
community-based patient cohort. Diabetic Medicine 2002;19:377-384
Abbott CA, Malik RA, van Ross ER, Kulkarni J, Boulton AJ: Prevalence and
characteristics of painful diabetic neuropathy in a large community-based diabetic
population in the U.K. Diabetes Care 2011;34:2220-2224
Adler AI, Boyko EJ, Ahroni JH, Smith DG: Lower-extremity amputation in diabetes.
The independent effects of peripheral vascular disease, sensory neuropathy, and
foot ulcers. Diabetes Care 1999;22:1029-1035
Agarwal R: Vitamin D, Proteinuria, Diabetic Nephropathy, and Progression of CKD.
Clinical Journal of the American Society of Nephrology 2009;4:1523-1528
Aggarwal N, Reis J, Michos E: Vitamin D Deficiency and Its Implications on
Cardiovascular Disease. Current Cardiovascular Risk Reports 2010;4:68-75
Ahn J, Yu K, Stolzenberg-Solomon R, Simon KC, McCullough ML, Gallicchio L,
Jacobs EJ, Ascherio A, Helzlsouer K, Jacobs KB, Li Q, Weinstein SJ, Purdue M,
Virtamo J, Horst R, Wheeler W, Chanock S, Hunter DJ, Hayes RB, Kraft P,
Albanes D: Genome-wide association study of circulating vitamin D levels. Human
Molecular Genetics 2010;19:2739-2745
Aksoy H, Akçay F, Kurtul N, Baykal O, Avci B: Serum 1,25 dihydroxy vitamin D
(1,25(OH)2D3), 25 hydroxy vitamin D (25(OH)D) and parathormone levels in
diabetic retinopathy. Clin Biochem 2000;33:47-51
Alam U, Asghar O, Malik RA: Are vitamin D and B deficiency relevant to the
pathogenesis and treatment of diabetic neuropathy? Future Neurology 2012;7:235-
238
352
Alam U, Asghar O, Malik RA: Vitamin D deficiency and cardiovascular disease: the
missing link. Diabetes Management 2011;1:151-155
Alam U, Najam O, Al-Himdani S, Benoliel S, Jinadev P, Berry JL, Kew M, Asghar
O, Petropoulos IN, Malik RA: Marked vitamin D deficiency in patients with diabetes
in the UK: ethnic and seasonal differences and an association with dyslipidaemia.
Diabet Med 2012;29:1343-1345
Albers JW, Herman WH, Pop-Busui R, Feldman EL, Martin CL, Cleary PA,
Waberski BH, Lachin JM: Effect of prior intensive insulin treatment during the
Diabetes Control and Complications Trial (DCCT) on peripheral neuropathy in type
1 diabetes during the Epidemiology of Diabetes Interventions and Complications
(EDIC) Study. Diabetes Care 2010;33:1090-1096
Albert DM, Scheef EA, Wang S, Mehraein F, Darjatmoko SR, Sorenson CM,
Sheibani N: Calcitriol is a potent inhibitor of retinal neovascularization. Invest
Ophthalmol Vis Sci 2007;48:2327-2334
Alfonso B, Liao E, Busta A, Poretsky L: Vitamin D in diabetes mellitus—a new field
of knowledge poised for D-velopment. Diabetes/Metabolism Research and
Reviews 2009;25:417-419
Ali AM, Awad, T.G., Ali, O.M.: Effect of Short-Term Vitamin D Supplementation On
Glycemic Control In Newly-Diagnosed Type 2 Diabetics. Australian Journal of
Basic and Applied Sciences 2011;5:1235-1239
Alvarez JA, Ashraf A: Role of vitamin d in insulin secretion and insulin sensitivity for
glucose homeostasis. Int J Endocrinol 2010: Article ID 351385.
http://dx.doi.org/10.1155/2010/351385
American Diabetes Association: clinical practice recommendations 2002. Diabetes
care 2002;25 Suppl 1:S1-147
353
Anand P, Terenghi G, Warner G, Kopelman P, Williams-Chestnut RE, Sinicropi
DV: The role of endogenous nerve growth factor in human diabetic neuropathy.
Nat Med 1996;2:703-707
Andersen CD, Bennet L, Nystrom L, Lindblad U, Lindholm E, Groop L, Rolandsson
O: Worse glycaemic control in LADA patients than in those with type 2 diabetes,
despite a longer time on insulin therapy. Diabetologia 2013;56:252-258
Arezzo JC: New developments in the diagnosis of diabetic neuropathy. The
American Journal of Medicine 1999;107:9-16
Arezzo JC: The use of electrophysiology for the assessment of diabetic
neuropathy. Neuroscience Research Communications 1997;21:13-23
Armas LAG, Hollis BW, Heaney RP: Vitamin D2 Is Much Less Effective than
Vitamin D3 in Humans. Journal of Clinical Endocrinology & Metabolism
2004;89:5387-5391
Arnson Y, Amital H: Is vitamin D a new therapeutic agent in autoinflammatory and
pain syndromes? Isr Med Assoc J 2011;13:234-235
Arya V, Bhambri R, Godbole M, Mithal A: Vitamin D status and its relationship with
bone mineral density in healthy Asian Indians. Osteoporosis International
2004;15:56-61
ASBMR 31st Annual Meeting MO0001–MO0445. Journal of Bone and Mineral
Research 2009;24:S370-S496
Azad N, Emanuele NV, Abraira C, Henderson WG, Colwell J, Levin SR, Nuttall FQ,
Comstock JP, Sawin CT, Silbert C, Rubino FA: The effects of intensive glycemic
control on neuropathy in the VA cooperative study on type II diabetes mellitus (VA
CSDM). J Diabetes Complications 1999;13:307-313

354
Bakkers M, Merkies IS, Lauria G, Devigili G, Penza P, Lombardi R, Hermans MC,
van Nes SI, De Baets M, Faber CG: Intraepidermal nerve fiber density and its
application in sarcoidosis. Neurology 2009;73:1142-1148
Balme M, McAllister I, Davis WA, Davis TME: Retinopathy in latent autoimmune
diabetes of adults: the Fremantle Diabetes Study. Diabetic Medicine 2002;19:602-
605
Barker JM, Yu J, Yu L, Wang J, Miao D, Bao F, Hoffenberg E, Nelson JC, Gottlieb
PA, Rewers M, Eisenbarth GS: Autoantibody “Subspecificity” in Type 1 Diabetes:
Risk for organ-specific autoimmunity clusters in distinct groups. Diabetes Care
2005;28:850-855
Bauer CS, Nieto-Rostro M, Rahman W, Tran-Van-Minh A, Ferron L, Douglas L,
Kadurin I, Sri Ranjan Y, Fernandez-Alacid L, Millar NS, Dickenson AH, Lujan R,
Dolphin AC: The increased trafficking of the calcium channel subunit alpha2delta-1
to presynaptic terminals in neuropathic pain is inhibited by the alpha2delta ligand
pregabalin. J Neurosci 2009;29:4076-4088
Baum P, Hermann W, Verlohren HJ, Wagner A, Lohmann T, Grahmann F: Diabetic
neuropathy in patients with "latent autoimmune diabetes of the adults" (LADA)
compared with patients with type 1 and type 2 diabetes. J Neurol 2003;250:682-
687
Bell DS: Reversal of the Symptoms of Diabetic Neuropathy through Correction of
Vitamin D Deficiency in a Type 1 Diabetic Patient. Case Rep Endocrinol 2012:
Article ID 165056. http://dx.doi.org/10.1155/2012/165056
Bianco J, Gueye Y, Marqueste T, Alluin O, Risso JJ, Garcia S, Lavault MN,
Khrestchatisky M, Feron F, Decherchi P: Vitamin D(3) improves respiratory
adjustment to fatigue and H-reflex responses in paraplegic adult rats.
Neuroscience 2010;188:182-192

355
Bierhaus A, Fleming T, Stoyanov S, Leffler A, Babes A, Neacsu C, Sauer SK,
Eberhardt M, Schnolzer M, Lasitschka F, Neuhuber WL, Kichko TI, Konrade I,
Elvert R, Mier W, Pirags V, Lukic IK, Morcos M, Dehmer T, Rabbani N, Thornalley
PJ, Edelstein D, Nau C, Forbes J, Humpert PM, Schwaninger M, Ziegler D, Stern
DM, Cooper ME, Haberkorn U, Brownlee M, Reeh PW, Nawroth PP: Methylglyoxal
modification of Nav1.8 facilitates nociceptive neuron firing and causes hyperalgesia
in diabetic neuropathy. Nat Med 2012;18:926-933
Bikle DD: Vitamin D and the immune system: role in protection against bacterial
infection. Curr Opin Nephrol Hypertens 2008;17:348-352
Binder A, May D, Baron R, Maier C, Tolle TR, Treede RD, Berthele A, Faltraco F,
Flor H, Gierthmuhlen J, Haenisch S, Huge V, Magerl W, Maihofner C, Richter H,
Rolke R, Scherens A, Uceyler N, Ufer M, Wasner G, Zhu J, Cascorbi I: Transient
receptor potential channel polymorphisms are associated with the somatosensory
function in neuropathic pain patients. PLoS One 2011;6:e17387
Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, Staehelin HB, Bazemore MG,
Zee RY, Wong JB: Effect of Vitamin D on Falls. JAMA: The Journal of the
American Medical Association 2004;291:1999-2006
Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes B:
Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple
health outcomes. Am J Clin Nutr 2006;84:18-28
Block SR: Vitamin D deficiency is not associated with nonspecific musculoskeletal
pain syndromes including fibromyalgia. Mayo Clin Proc 2004;79:1585-1586; author
reply 1586-1587
Boucher BJ, Mannan N, Noonan K, Hales CN, Evans SJ: Glucose intolerance and
impairment of insulin secretion in relation to vitamin D deficiency in east London
Asians. Diabetologia 1995;38:1239-1245

356
Bouillon R, Carmeliet G, Verlinden L, van Etten E, Verstuyf A, Luderer HF, Lieben
L, Mathieu C, Demay M: Vitamin D and Human Health: Lessons from Vitamin D
Receptor Null Mice. Endocr Rev 2008;29:726-776
Boulton AJ, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, Malik RA, Maser
RE, Sosenko JM, Ziegler D: Diabetic neuropathies: a statement by the American
Diabetes Association. Diabetes Care 2005;28:956-962
Boulton AJ: Whither clinical research in diabetic sensorimotor peripheral
neuropathy? Problems of end point selection for clinical trials. Diabetes Care
2007;30:2752-2753
Boulton AJM, Malik RA, Arezzo JC, Sosenko JM: Diabetic Somatic Neuropathies.
Diabetes care 2004;27:1458-1486
Boulton AJM, Malik RA: Diabetic Neuropathy. Med Clin N Amer 1998;82:909-929
Boulton AJM, Vinik AI, Arezzo JC, Bril V, Feldman EL, Freeman R, Malik RA,
Maser RE, Sosenko JM, Ziegler D: Diabetic neuropathies: a statement by the
American Diabetes Association. Diabetes care 2005;28:956-962
Boulton AJM: Management of Diabetic Peripheral Neuropathy. Clinical Diabetes
2005;23:9-15
Bravenboer B, van Dam PS, Hop J, vd Steenhoven J, Erkelens DW: Thermal
threshold testing for the assessment of small fibre dysfunction: normal values and
reproducibility. Diabet Med 1992;9:546-549
Bril V, England J, Franklin GM, Backonja M, Cohen J, Del Toro D, Feldman E,
Iverson DJ, Perkins B, Russell JW, Zochodne D: Evidence-based Guideline:
Treatment of Painful Diabetic Neuropathy: Report of the American Academy of
Neurology, the American Association of Neuromuscular and Electrodiagnostic
Medicine, and the American Academy of Physical Medicine and Rehabilitation.
PM&R 2011;3:345-352.e321

357
Britland ST, Young RJ, Sharma AK, Clarke BF: Association of Painful and Painless
Diabetic Polyneuropathy With Different Patterns of Nerve Fiber Degeneration and
Regeneration. Diabetes 1990;39:898-908
Brooks B, Delaney-Robinson C, Molyneaux L, Yue DK: Endothelial and neural
regulation of skin microvascular blood flow in patients with diabetic peripheral
neuropathy: effect of treatment with the isoform-specific protein kinase C beta
inhibitor, ruboxistaurin. Journal of diabetes and its complications 2008;22:88-95
Brophy S, Brunt H, Davies H, Mannan S, Williams R: Interventions for latent
autoimmune diabetes (LADA) in adults. . Cochrane Database of Systematic
Reviews 2007:Art.No.:CD006165.DOI:
006110.001002/14651858.CD14006165.pub14651852
Brophy S, Yderstraede K, Mauricio D, Hunter S, Hawa M, Pozzilli P, Schernthaner
G, Schloot N, Buzzetti R, Davies H, Leslie D, Williams R: Time to insulin initiation
cannot be used in defining latent autoimmune diabetes in adults. Diabetes care
2008;31:439-441
Brown MJ, Bird SJ, Watling S, Kaleta H, Hayes L, Eckert S, Foyt HL: Natural
progression of diabetic peripheral neuropathy in the Zenarestat study population.
Diabetes Care 2004;27:1153-1159
Brownlee M, Cerami A, Vlassara H: Advanced glycosylation end products in tissue
and the biochemical basis of diabetic complications. The New England journal of
medicine 1988;318:1315-1321
Brownlee M: The pathobiology of diabetic complications: a unifying mechanism.
Diabetes 2005;54:1615-1625
Bucan K, Ivanisevic M, Zemunik T, Boraska V, Skrabic V, Vatavuk Z, Galetovic D,
Znaor L: Retinopathy and nephropathy in type 1 diabetic patients--association with
358
polymorphysms of vitamin D-receptor, TNF, Neuro-D and IL-1 receptor 1 genes.
Coll Antropol 2009;33 Suppl 2:99-105
Bunce C, Wormald R: Leading causes of certification for blindness and partial sight
in England & Wales. BMC Public Health 2006;6:58
Busnardo AC, DiDio LJA, Tidrick RT, Thomford NR: History of the pancreas. The
American Journal of Surgery 1983;146:539-550
Calles-Escandon J, Lovato LC, Simons-Morton DG, Kendall DM, Pop-Busui R,
Cohen RM, Bonds DE, Fonseca VA, Ismail-Beigi F, Banerji MA, Failor A, Hamilton
B: Effect of intensive compared with standard glycemia treatment strategies on
mortality by baseline subgroup characteristics: the Action to Control Cardiovascular
Risk in Diabetes (ACCORD) trial. Diabetes Care 2010;33:721-727
Cameron NE, Cotter MA, Jack AM, Basso MD, Hohman TC: Protein kinase C
effects on nerve function, perfusion, Na(+), K(+)-ATPase activity and glutathione
content in diabetic rats. Diabetologia 1999;42:1120-1130
Cameron NE, Cotter MA: The relationship of vascular changes to metabolic factors
in diabetes mellitus and their role in the development of peripheral nerve
complications. Diabetes/metabolism reviews 1994;10:189-224
Cardus A, Panizo S, Encinas M, Dolcet X, Gallego C, Aldea M, Fernandez E,
Valdivielso JM: 1,25-Dihydroxyvitamin D3 regulates VEGF production through a
vitamin D response element in the VEGF promoter. Atherosclerosis 2009;204:85-
89
Carlsson S, Midthjell K, Tesfamarian MY, Grill V: Age, overweight and physical
inactivity increase the risk of latent autoimmune diabetes in adults: results from the
Nord-Trøndelag health study. Diabetologia 2007;50:55-58

359
Carrington AL, Shaw JE, Van Schie CHM, Abbott CA, Vileikyte L, Boulton AJM:
Can Motor Nerve Conduction Velocity Predict Foot Problems in Diabetic Subjects
Over a 6-Year Outcome Period? Diabetes Care 2002;25:2010-2015
Catalano A, Morabito N, Atteritano M, Basile G, Cucinotta D, Lasco A: Vitamin D
Reduces Musculoskeletal Pain After Infusion of Zoledronic Acid for
Postmenopausal Osteoporosis. Calcif Tissue Int 2012;90:279-285
Chapuy MC, Preziosi P, Maamer M, Arnaud S, Galan P, Hercberg S, Meunier PJ:
Prevalence of vitamin D insufficiency in an adult normal population. Osteoporos Int
1997;7:439-443
Cheng HT, Dauch JR, Porzio MT, Yanik BM, Hsieh W, Smith AG, Singleton JR,
Feldman EL: Increased Axonal Regeneration and Swellings in Intraepidermal
Nerve Fibers Characterize Painful Phenotypes of Diabetic Neuropathy. The
Journal of Pain 2013;14:941-947
Chien HF, Tseng TJ, Lin WM, Yang CC, Chang YC, Chen RC, Hsieh ST:
Quantitative pathology of cutaneous nerve terminal degeneration in the human
skin. Acta Neuropathol 2001;102:455-461
Chiu HK, Tsai EC, Juneja R, Stoever J, Brooks-Worrell B, Goel A, al. e: Equivalent
insulin resistance in latent autoimmune diabetes in adults (LADA) and type 2
diabetic patients. Diabetes Res Clin Pract 2007;77:237–244
Chung SS, Chung SK: Aldose reductase in diabetic microvascular complications.
Curr Drug Targets 2005;6:475-486
Craig TA, Sommer S, Sussman CR, Grande JP, Kumar R: Expression and
regulation of the vitamin D receptor in the zebrafish, Danio rerio. J Bone Miner Res
2008;23:1486-1496
Dabbah M, Graham J, Petropoulos I, Tavakoli M, Malik R: Dual-Model Automatic
Detection of Nerve-Fibres in Corneal Confocal Microscopy Images: In Medical

360
Image Computing and Computer-Assisted Intervention – MICCAI 2010 Jiang T,
Navab N, Pluim JW, Viergever M, Eds., Springer Berlin Heidelberg, 2010, p. 300-
307
Dabbah MA, Graham J, Petropoulos IN, Tavakoli M, Malik RA: Automatic analysis
of diabetic peripheral neuropathy using multi-scale quantitative morphology of
nerve fibres in corneal confocal microscopy imaging. Medical Image Analysis
2011;15:738-747
Darling AL, Hart KH, Macdonald HM, Horton K, Kang'ombe AR, Berry JL, Lanham-
New SA: Vitamin D deficiency in UK South Asian Women of childbearing age: a
comparative longitudinal investigation with UK Caucasian women. Osteoporosis
International 2013;24:477-488
Davidson EP, Coppey LJ, Holmes A, Yorek MA: Changes in corneal innervation
and sensitivity and acetylcholine-mediated vascular relaxation of the posterior
ciliary artery in a type 2 diabetic rat. Invest Ophthalmol Vis Sci 2012;53:1182-1187
Davidson EP, Coppey LJ, Yorek MA: Early loss of innervation of cornea epithelium
in streptozotocin-induced type 1 diabetic rats: improvement with ilepatril treatment.
Invest Ophthalmol Vis Sci 2012;53:8067-8074
Davies H, Brophy S, Fielding A, Bingley P, Chandler M, Hilldrup I, Brooks C,
Williams R: Latent autoimmune diabetes in adults (LADA) in South Wales:
incidence and characterization. Diabetic Medicine 2008;25:1354-1357
Davis TM, Yeap BB, Davis WA, Bruce DG: Lipid-lowering therapy and peripheral
sensory neuropathy in type 2 diabetes: the Fremantle Diabetes Study. Diabetologia
2008;51:562-566
Davis TM, Zimmet P, Davis WA, Bruce DG, Fida S, Mackay IR: Autoantibodies to
glutamic acid decarboxylase in diabetic patients from a multi-ethnic Australian
community: the Fremantle Diabetes Study. Diabet Med 2000;17:667-674
361
Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, Vieth R: Estimates
of optimal vitamin D status. Osteoporos Int 2005;16:713-716
Deluca HF, Cantorna MT: Vitamin D: its role and uses in immunology. FASEB J
2001;15:2579-2585
Demetriou ET, Travison TG, Holick MF: Treatment with 50,000 IU vitamin D2 every
other week and effect on serum 25-hydroxyvitamin D2, 25-hydroxyvitamin D3, and
total 25-hydroxyvitamin D in a clinical setting. Endocr Pract 2012;18:399-402
Desai M, Cull CA, Horton VA, Christie MR, Bonificio E, Lampasona V, Bingley PJ,
Levy JC, Mackay IR, Zimmet P, Holman RR, Clark A: GAD autoantibodies and
epitope reactivities persist after diagnosis in latent autoimmune diabetes in adults
but do not predict disease progression: UKPDS 77. Diabetologia 2007;50:2052-
2060
Devigili G, Tugnoli V, Penza P, Camozzi F, Lombardi R, Melli G, Broglio L, Granieri
E, Lauria G: The diagnostic criteria for small fibre neuropathy: from symptoms to
neuropathology. Brain 2008;131:1912-1925
Di Cesar DJ, Ploutz-Snyder R, Weinstock RS, Moses AM: Vitamin D Deficiency Is
More Common in Type 2 Than in Type 1 Diabetes. Diabetes Care 2006;29:174
Diabetic polyneuropathy in controlled clinical trials: concensus report of the
peripheral nerve society: Peripheral Nerve Society. Am Neurol 1995;38:478-482
Dickenson AH, Matthews EA, Suzuki R: Neurobiology of neuropathic pain: mode of
action of anticonvulsants. Eur J Pain 2002;6 Suppl A:51-60
Duby JJ, Campbell RK, Setter SM, White JR, Rasmussen KA: Diabetic
neuropathy: an intensive review. Am J Health Syst Pharm 2004;61:160-173

362
Dyck PJ, Dyck PJB, Kennedy WR, Kesserwani H, Melanson M, Ochoa J, Shy M,
Stevens JC, Suarez GA, O'Brien PC: Limitations of quantitative sensory testing
when patients are biased toward a bad outcome. Neurology 1998;50:1213
Dyck PJ, Giannini C: Pathologic alterations in the diabetic neuropathies of humans:
a review. J Neuropathol Exp Neurol 1996;55:1181-1193
Dyck PJ, Karnes J, O'Brien PC, Swanson CJ: Neuropathy Symptom Profile in
health, motor neuron disease, diabetic neuropathy, and amyloidosis. Neurology
1986;36:1300-
Dyck PJ, Karnes JL, O'Brien PC, Litchy WJ, Low PA, Melton LJ, 3rd: The
Rochester Diabetic Neuropathy Study: reassessment of tests and criteria for
diagnosis and staged severity. Neurology 1992;42:1164-1170
Dyck PJ, Kratz KM, Karnes JL, Litchy WJ, Klein R, Pach JM, Wilson DM, O'Brien
PC, Melton LJ, 3rd, Service FJ: The prevalence by staged severity of various types
of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort:
the Rochester Diabetic Neuropathy Study. Neurology 1993;43:817-824
Dyck PJ, Kratz KM, Lehman KA, Karnes JL, Melton LJI, O' Brien PC, Litchy WJ,
Windebank AJ, Smith BE, Low PA, Service FJ, Rizza RA, Zimmerman BR: The
Rochester Diabetic Neuropathy Study: Design, criteria for types of neuropathy,
selection bias, and reproducibility of neuropathic tests. Neurology 1991;41:799-807
Dyck PJ, Norell JE, Tritschler H, Schuette K, Samigullin R, Ziegler D, Bastyr EJ,
3rd, Litchy WJ, O'Brien PC: Challenges in design of multicenter trials: end points
assessed longitudinally for change and monotonicity. Diabetes Care 2007;30:2619-
2625
Dyck PJ, Overland CJ, Low PA, Litchy WJ, Davies JL, Dyck PJ, O'Brien PC, Albers
JW, Andersen H, Bolton CF, England JD, Klein CJ, Llewelyn JG, Mauermann ML,
Russell JW, Singer W, Smith AG, Tesfaye S, Vella A: Signs and symptoms versus

363
nerve conduction studies to diagnose diabetic sensorimotor polyneuropathy: Cl vs.
NPhys trial. Muscle & nerve 2010;42:157-164
Dyck PJ, Sherman WR, Hallcher LM, Service FJ, O'Brien PC, Grina LA, Palumbo
PJ, Swanson CJ: Human diabetic endoneurial sorbitol, fructose, and myo-inositol
related to sural nerve morphometry. Ann Neurol 1980;8:590-596
Dyck PJ, Thomas PK, Asbury AK, Winegrad AL, Porte D: Diabetic Neuropathy.
Philadelphia, Saunders, 1987
Dyck PJ, Zimmerman BR, Vilen TH, Minnerath SR, Karnes JL, Yao JK, Poduslo
JF: Nerve glucose, fructose, sorbitol, myo-inositol, and fiber degeneration and
regeneration in diabetic neuropathy. N Engl J Med 1988;319:542-548
Edwards K, Pritchard N, Vagenas D, Russell A, Malik RA, Efron N: Utility of
corneal confocal microscopy for assessing mild diabetic neuropathy: baseline
findings of the LANDMark study. Clin Exp Optom 2012;95:348-354
Effect of intensive diabetes treatment on nerve conduction in the Diabetes Control
and Complications Trial. Ann Neurol 1995;38:869-880
Effect of intensive therapy on the development and progression of diabetic
nephropathy in the Diabetes Control and Complications Trial. The Diabetes Control
and Complications (DCCT) Research Group. Kidney Int 1995;47:1703-1720
Eichberg J: Protein kinase C changes in diabetes: is the concept relevant to
neuropathy? International review of neurobiology 2002;50:61-82
Ekberg K, Brismar T, Johansson BL, Jonsson B, Lindstrom P, Wahren J:
Amelioration of sensory nerve dysfunction by C-Peptide in patients with type 1
diabetes. Diabetes 2003;52:536-541

364
Elliott J, Tesfaye S, Chaturvedi N, Gandhi RA, Stevens LK, Emery C, Fuller JH:
Large-fiber dysfunction in diabetic peripheral neuropathy is predicted by
cardiovascular risk factors. Diabetes Care 2009;32:1896-1900
Fajans SS, Bell GI, Polonsky KS: Molecular mechanisms and clinical
pathophysiology of maturity-onset diabetes of the young. The New England journal
of medicine 2001;345:971-980
Falorni A, Calcinaro F: Autoantibody profile and epitope mapping in latent
autoimmune diabetes in adults. Annals of the New York Academy of Sciences
2002;958:99-106
Filipović N, Ferhatović L, Marelja I, Puljak L, Grković I: Increased vitamin D
receptor expression in dorsal root ganglia neurons of diabetic rats. Neuroscience
Letters 2013;549:140-145
Fong DS, Aiello L, Gardner TW, King GL, Blankenship G, Cavallerano JD, Ferris
FL, 3rd, Klein R: Diabetic retinopathy. Diabetes Care 2003;26:226-229
Ford L, Graham V, Wall A, Berg J: Vitamin D concentrations in an UK inner-city
multicultural outpatient population. Ann Clin Biochem 2006;43:468-473
Forouhi NG, Luan J, Cooper A, Boucher BJ, Wareham NJ: Baseline serum 25-
hydroxy vitamin d is predictive of future glycemic status and insulin resistance: the
Medical Research Council Ely Prospective Study 1990-2000. Diabetes
2008;57:2619-2625
Fourlands S, Perry C, Stein MS, Stankovich J, Harrison LC, Colman PG: A Clinical
Screening Tool Identifies Autoimmune Diabetes in Adults. Diabetes Care
2006;29:970-975
Fourlanos S, Dotta F, Greenbaum CJ, Palmer JP, Rolandsson O, Colman PG,
Harrison LC: Latent autoimmune diabetes in adults (LADA) should be less latent.
Diabetologia 2005;48:2206-2212
365
Fourlanos S, Perry C, Stein MS, Stankovich J, Harrison LC, Colman PG: A clinical
screening tool identifies autoimmune diabetes in adults. Diabetes Care
2006;29:970-975
Franklin GM, Kahn LB, Baxter J, Marshall JA, Hamman RF: Sensory neuropathy in
non-insulin-dependent diabetes mellitus. The San Luis Valley Diabetes Study. Am
J Epidemiol 1990;131:633-643
Franklin GM, Shetterly SM, Cohen JA, Baxter J, Hamman RF: Risk factors for
distal symmetric neuropathy in NIDDM. The San Luis Valley Diabetes Study.
Diabetes Care 1994;17:1172-1177
Freeman TL, Johnson E, Freeman ED, et al.: Nerve Conduction Studies (NCS). S
C, Ed. New York, Demos Medical Publishing, 2004
Fukuoka M, Sakurai K, Ohta T, Kiyoki M, Katayama I: Tacalcitol, an active vitamin
D3, induces nerve growth factor production in human epidermal keratinocytes. Skin
Pharmacol Appl Skin Physiol 2001;14:226-233
Gabbay KH, Merola LO, Field RA: Sorbitol pathway: presence in nerve and cord
with substrate accumulation in diabetes. Science (New York, NY 1966;151:209-
210
Gaddipati VC, Bailey BA, Kuriacose R, Copeland RJ, Manning T, Peiris AN: The
relationship of vitamin d status to cardiovascular risk factors and amputation risk in
veterans with peripheral arterial disease. J Am Med Dir Assoc 2011;12:58-61
Gale EA: Latent autoimmune diabetes in adults: a guide for the perplexed.
Diabetologia 2005;48:2195-2199
Gandhi RA, Marques JL, Selvarajah D, Emery CJ, Tesfaye S: Painful diabetic
neuropathy is associated with greater autonomic dysfunction than painless diabetic
neuropathy. Diabetes Care 2010;33:1585-1590
366
George PS, Pearson ER, Witham MD: Effect of vitamin D supplementation on
glycaemic control and insulin resistance: a systematic review and meta-analysis.
Diabet Med 2012;29:e142-150
Ghazi AA, Hosseinpanah F, E MA, Ghazi S, Hedayati M, Azizi F: Effects of
different doses of oral cholecalciferol on serum 25(OH)D, PTH, calcium and bone
markers during fall and winter in schoolchildren. Eur J Clin Nutr 2010;64:1415-
1422
Ginde AA, Scragg R, Schwartz RS, Camargo CA, Jr.: Prospective study of serum
25-hydroxyvitamin D level, cardiovascular disease mortality, and all-cause mortality
in older U.S. adults. J Am Geriatr Soc 2009;57:1595-1603
Giugliano D, Ceriello A, Paolisso G: Oxidative stress and diabetic vascular
complications. Diabetes care 1996;19:257-267
Gleichmann H, Zorcher B, Greulich B, Gries FA, Henrichs HR, Betrams J, Kolb H:
Correlation of islet cell antibodies and HLA-DR phenotypes with diabetes mellitus
in adults. Diabetologia 1984;27:90-92
Glerup H, Mikkelsen K, Poulsen L, Hass E, Overbeck S, Thomsen J, Charles P,
Eriksen EF: Commonly recommended daily intake of vitamin D is not sufficient if
sunlight exposure is limited. J Intern Med 2000;247:260-268
Gloth F, Iii, Lindsay JM, Zelesnick LB, Greenough WB: Can vitamin d deficiency
produce an unusual pain syndrome? Archives of Internal Medicine 1991;151:1662-
1664
Gore M, Brandenburg NA, Dukes E, Hoffman DL, Tai KS, Stacey B: Pain severity
in diabetic peripheral neuropathy is associated with patient functioning, symptom
levels of anxiety and depression, and sleep. J Pain Symptom Manage
2005;30:374-385

367
Gottsater A, Landin-Olsson M, Fernlund P, Lernmark A, Sundkvist G: Beta-cell
function in relation to islet cell antibodies during the first 3 yr after clinical diagnosis
of diabetes in type II diabetic patients. Diabetes Care 1993;16:902-910
Gozdzik A, Barta JL, Weir A, Cole DE, Vieth R, Whiting SJ, Parra EJ: Serum 25-
hydroxyvitamin D concentrations fluctuate seasonally in young adults of diverse
ancestry living in Toronto. J Nutr 2010;140:2213-2220
Graham WA, Goldstein R, Mansfield K, Nesathurai S: Serial nerve conduction
studies of the tail of rhesus monkey ( Macaca mulatta ) and potential implications
for interpretation of human neurophysiological studies. Annals of Indian Academy
of Neurology 2007;10:252-254
Graves PM, Barriga KJ, Norris JM, Hoffman MR, Yu L, Eisenbarth GS, Rewers M:
Lack of association between early childhood immunizations and beta-cell
autoimmunity. Diabetes care 1999;22:1694-1697
Greene DA, Lattimer SA, Sima AA: Sorbitol, phosphoinositides, and sodium-
potassium-ATPase in the pathogenesis of diabetic complications. The New
England journal of medicine 1987;316:599-606
Gregg EW, Sorlie P, Paulose-Ram R, Gu Q, Eberhardt MS, Wolz M, Burt V, Curtin
L, Engelgau M, Geiss L: Prevalence of lower-extremity disease in the US adult
population >=40 years of age with and without diabetes: 1999-2000 national health
and nutrition examination survey. Diabetes Care 2004;27:1591-1597
Gupta K, Warner JT: Inappropriate and inconsistent modalities of treatment of
vitamin D deficiency in children. Archives of Disease in Childhood 2011;
doi:10.1136/adc.2011.214361
Haddad JG, Matsuoka LY, Hollis BW, Hu YZ, Wortsman J: Human plasma
transport of vitamin D after its endogenous synthesis. J Clin Invest 1993;91:2552-
2555

368
Hagopian WA, Karlsen AE, Gottsater A, Landin Olsson M, Grubin CE, Sundkvist
G, Petersen JS, Boel E, Dyrberg T, Lernmark A: Quantitative assay using
recombinant human islet glutamic decarboxylase (GAD65)shows that 64K
autoantibody positivity at onset predicts diabetes type. J Clin Invest 1993;91:368-
362
Hajian-Tilaki KO, Hanley JA, Joseph L, Collet JP: A comparison of parametric and
nonparametric approaches to ROC analysis of quantitative diagnostic tests. Med
Decis Making 1997;17:94-102
Hale PJ, Nattrass M, Silverman SH, Sennit C, Perkins CM, Uden A, Sundkvist G:
Peripheral nerve concentrations of glucose, fructose, sorbitol and myoinositol in
diabetic and non-diabetic patients. Diabetologia 1987;30:464-467
Halpern EM, Lovblom LE, Orlov S, Bril V, Perkins BA: The Existence of Rapid
Small Fiber Decline in Type 1 Diabetes: A Potential Proxy for Neuropathy
Progression Using In Vivo Corneal Confocal Microscopy Orals. Diabetes
2013;62:A1-A98
Hammes HP, Feng Y, Pfister F, Brownlee M: Diabetic retinopathy: targeting
vasoregression. Diabetes 2011;60:9-16
Hanley JA: The robustness of the "binormal" assumptions used in fitting ROC
curves. Med Decis Making 1988;8:197-203
Hansson P, Backonja M, Bouhassira D: Usefulness and limitations of quantitative
sensory testing: Clinical and research application in neuropathic pain states. Pain
2007;129:256-259
Harindhanavudhi T, Mauer M, Klein R, Zinman B, Sinaiko A, Caramori ML:
Benefits of Renin-Angiotensin blockade on retinopathy in type 1 diabetes vary with
glycemic control. Diabetes Care 2011;34:1838-1842

369
Harris M, Eastman R, Cowie C: Symptoms of sensory neuropathy in adults with
NIDDM in the U.S. population. Diabetes Care 1993;16:1446-1452
Heaney RP, Davies KM, Chen TC, Holick MF, Barger-Lux MJ: Human serum 25-
hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am J
Clin Nutr 2003;77:204-210
Heaney RP, Dowell MS, Hale CA, Bendich A: Calcium absorption varies within the
reference range for serum 25-hydroxyvitamin D. J Am Coll Nutr 2003;22:142-146
Heaney RP: The Vitamin D requirement in health and disease. J Steroid Biochem
Mol Biol 2005;97:13-19
Heaney RP: Vitamin D — Baseline Status and Effective Dose. New England
Journal of Medicine 2012;367:77-78
Hellweg R, Wohrle M, Hartung HD, Stracke H, Hock C, Federlin K: Diabetes
mellitus-associated decrease in nerve growth factor levels is reversed by
allogeneic pancreatic islet transplantation. Neurosci Lett 1991;125:1-4
Herrmann DN, Griffin JW, Hauer P, Cornblath DR, McArthur JC: Epidermal nerve
fiber density and sural nerve morphometry in peripheral neuropathies. Neurology
1999;53:1634-1640
Hirani V: Vitamin D status and pain: analysis from the Health Survey for England
among English adults aged 65 years and over. Br J Nutr 107:1080-1084
Hoeijmakers JG, Faber CG, Lauria G, Merkies IS, Waxman SG: Small-fibre
neuropathies--advances in diagnosis, pathophysiology and management. Nature
reviews Neurology 2012;8:369-379
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP,
Murad MH, Weaver CM: Guidelines for preventing and treating vitamin D
deficiency and insufficiency revisited. J Clin Endocrinol Metab 2012;97:1153-1158

370
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP,
Murad MH, Weaver CM: Evaluation, Treatment, and Prevention of Vitamin D
Deficiency: an Endocrine Society Clinical Practice Guideline. Journal of Clinical
Endocrinology & Metabolism 2011;96:1911-1930
Holick MF, Siris ES, Binkley N, Beard MK, Khan A, Katzer JT, Petruschke RA,
Chen E, de Papp AE: Prevalence of Vitamin D inadequacy among
postmenopausal North American women receiving osteoporosis therapy. J Clin
Endocrinol Metab 2005;90:3215-3224
Holick MF: Deficiency of sunlight and vitamin D. BMJ 2008;336:1318-1319
Holick MF: Evidence-based D-bate on health benefits of vitamin D revisited.
Dermatoendocrinol 2012;4:183-190
Holick MF: High prevalence of vitamin D inadequacy and implications for health.
Mayo Clin Proc 2006;81:353-373
Holick MF: Nutrition: D-iabetes and D-eath D-efying vitamin D. Nat Rev Endocrinol
2012;8:388-390
Holick MF: Vitamin D Deficiency. New England Journal of Medicine 2007;357:266-
281
Holick MF: Vitamin D: extraskeletal health. Rheum Dis Clin North Am 2012;38:141-
160
Holmes GK: Screening for coeliac disease in type 1 diabetes. Arch Dis Child
2002;87:495–499
Holmoy T, Moen SM: Assessing vitamin D in the central nervous system. Acta
Neurol Scand Suppl 2010:88-92
371
Hossain P, Sachdev A, Malik RA: Early detection of diabetic peripheral neuropathy
with corneal confocal microscopy. Lancet 2005;366:1340-1343
Hosszufalusi N, Vatay A, Katalin R, Prohaszka Z, Pozsonyi E, Horvath L, Grosz A,
Gero L, Madacsy L, Romics L, Karadi I, Fust G, Panczel P: Similar Genetic
Features and Different Islet Cell Autoantibody Pattern of Latent Autoimmune
Diabetes in Adults (LADA) Compared With Adult-Onset Type 1 Diabetes With
Rapid Progression. Diabetes care 2003;26:452-457
Houghton LA, Vieth R: The case against ergocalciferol (vitamin D2) as a vitamin
supplement. The American Journal of Clinical Nutrition 2006;84:694-697
Hsueh WA, Wyne K: Renin-Angiotensin-Aldosterone System in Diabetes and
Hypertension. The Journal of Clinical Hypertension 2011;13:224-237
http://www.nobelprize.org/educational/medicine/insulin/discovery-insulin.html
[article online]. Last accessed 25/09/2013.
Huang CR, Chang WN, Chang HW, Tsai NW, Lu CH: Effects of age, gender,
height, and weight on late responses and nerve conduction study parameters. Acta
neurologica Taiwanica 2009;18:242-249
Hummel M, Fuchtenbusch M, Schenker M, Ziegler AG: No major association of
breast-feeding, vaccinations, and childhood viral diseases with early islet
autoimmunity in the German BABYDIAB Study. Diabetes care 2000;23:969-974
Hypponen E, Laara E, Reunanen A, Jarvelin MR, Virtanen SM: Intake of vitamin D
and risk of type 1 diabetes: a birth-cohort study. Lancet 2001;358:1500-1503
Hypponen E, Power C: Hypovitaminosis D in British adults at age 45 y: nationwide
cohort study of dietary and lifestyle predictors. Am J Clin Nutr 2007;85:860-868
Hypponen E: Vitamin D and increasing incidence of type 1 diabetes-evidence for
an association? Diabetes Obes Metab 2010;12:737-743

372
Intensive blood-glucose control with sulphonylureas or insulin compared with
conventional treatment and risk of complications in patients with type 2 diabetes
(UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet
1998;352:837-853
Ireland R: Diabetic nephropathy: Paricalcitol lowers residual albuminuria in type 2
diabetes. Nat Rev Nephrol 2011;7:62
Ismail-Beigi F, Craven T, Banerji MA, Basile J, Calles J, Cohen RM, Cuddihy R,
Cushman WC, Genuth S, Grimm RH, Jr., Hamilton BP, Hoogwerf B, Karl D, Katz
L, Krikorian A, O'Connor P, Pop-Busui R, Schubart U, Simmons D, Taylor H,
Thomas A, Weiss D, Hramiak I: Effect of intensive treatment of hyperglycaemia on
microvascular outcomes in type 2 diabetes: an analysis of the ACCORD
randomised trial. Lancet 2010;376:419-430
Ismail-Beigi F, Craven TE, O'Connor PJ, Karl D, Calles-Escandon J, Hramiak I,
Genuth S, Cushman WC, Gerstein HC, Probstfield JL, Katz L, Schubart U:
Combined intensive blood pressure and glycemic control does not produce an
additive benefit on microvascular outcomes in type 2 diabetic patients. Kidney Int
2012;81:586-594
Isomaa B, Almgren P, Henricsson M, Taskinen MR, Tuomi T, Groop L, Sarelin L:
Chronic complications in patients with slowly progressing autoimmune type 1
diabetes (LADA). Diabetes Care 1999;22:1347-1353
Jehan F, Neveu I, Barbot N, Binderup L, Brachet P, Wion D: MC903, an analogue
of 1,25-dihydroxyvitamin D3, increases the synthesis of nerve growth factor. Eur J
Pharmacol 1991;208:189-191
Jesudason D, Need AG, Horowitz M, O'Loughlin PD, Morris HA, Nordin BE:
Relationship between serum 25-hydroxyvitamin D and bone resorption markers in
vitamin D insufficiency. Bone 2002;31:626-630
373
Joergensen C, Hovind P, Schmedes A, Parving H-H, Rossing P: Vitamin D Levels,
Microvascular Complications, and Mortality in Type 1 Diabetes. Diabetes Care
2011;34:1081-1085
Jones CD, Greenwood RH, Misra A, Bachmann MO: Incidence and Progression of
Diabetic Retinopathy During 17 Years of a Population-Based Screening Program in
England. Diabetes Care 2012;35:592-596
Jones G: Pharmacokinetics of vitamin D toxicity. The American Journal of Clinical
Nutrition 2008;88:582S-586S
Jyothi S, Elahi B, Srivastava A, Poole M, Nagi D, Sivaprasad S: Compliance with
the quality standards of National Diabetic Retinopathy Screening Committee. Prim
Care Diabetes 2009;3:67-72
Kahn R: Report and recommendations of the san antonio conference on diabetic
neuropathy. Annals of Neurology 1988;24:99-104
Kallinikos P, Berhanu M, O'Donnell C, Boulton AJ, Efron N, Malik RA: Corneal
nerve tortuosity in diabetic patients with neuropathy. Invest Ophthalmol Vis Sci
2004;45:418-422
Kaprio J, Tuomilehto J, Koskenvuo M, Romanov K, Reunanen A, Eriksson J,
Stengard J, Kesaniemi YA: Concordance for type 1 (insulin-dependent) and type 2
(non-insulin-dependent) diabetes mellitus in a population-based cohort of twins in
Finland. Diabetologia 1992;35:1060-1067
Kaur H, Donaghue KC, Chan AK, Benitez-Aguirre P, Hing S, Lloyd M, Cusumano
J, Pryke A, Craig ME: Vitamin D deficiency is associated with retinopathy in
children and adolescents with type 1 diabetes. Diabetes Care 2011;34:1400-1402
Keith M, Goldstein R, Nesathurai S, Graham W: Serial nerve conduction studies of
the tail of rhesus monkey and potential implications for interpretation of human

374
neurophysiological studies. Annals of Indian Academy of Neurology 2007;
DOI:10.4103/0972-2327.378182007
Khazai NB, Judd SE, Jeng L, Wolfenden LL, Stecenko A, Ziegler TR, Tangpricha
V: Treatment and Prevention of Vitamin D Insufficiency in Cystic Fibrosis Patients:
Comparative Efficacy of Ergocalciferol, Cholecalciferol, and UV Light. Journal of
Clinical Endocrinology & Metabolism 2009;94:2037-2043
Kilpatrick ES, Bloomgarden ZT, Zimmet PZ: International Expert Committee report
on the role of the A1C assay in the diagnosis of diabetes: response to the
International Expert Committee. Diabetes Care 2009;32:e159; author reply e160
Klein R, Klein BEK, Moss SE, Cruickshanks KJ: The Wisconsin epidemiologic
study of diabetic retinopathy: XVII: The 14-year incidence and progression of
diabetic retinopathy and associated risk factors in type 1 diabetes. Ophthalmology
1998;105:1801-1815
Kobayashi T, Nakanishi K, Murase T, Kosaka K: Small doses of subcutaneous
insulin as a strategy for preventing slowly progressive beta-cell failure in islet cell
antibody-positive patients with clinical features of NIDDM. Diabetes 1996;45:622-
626
Kordonouri O, Wladimirowa A, Danne T: High total serum renin concentrations are
associated with the development of background retinopathy in adolescents with
type 1 diabetes. Diabetes Care 2000;23:1025-1026
Krishnan ST, Quattrini C, Jeziorska M, Malik RA, Rayman G: Abnormal LDIflare
but normal quantitative sensory testing and dermal nerve fiber density in patients
with painful diabetic neuropathy. Diabetes Care 2009;32:451-455
Kucera P, Novakova D, Behanova M, Novak J, Tlaskalova-Hogenova AM: Gliadin,
endomysial and thyroid antibodies in patients with latent autoimmune diabetes of
adults (LADA). Clin Exp Immunol 2003;133:139-143
375
Kulkantrakorn K, Lorsuwansiri C, Meesawatsom P: 0.025% capsaicin gel for the
treatment of painful diabetic neuropathy: a randomized, double-blind, crossover,
placebo-controlled trial. Pain Pract 2013;13:497-503
Lacomis D: Small-fiber neuropathy. Muscle & Nerve 2002;26:173-188
Lanting LC, Joung IMA, Mackenbach JP, Lamberts SWJ, Bootsma AH: Ethnic
Differences in Mortality, End-Stage Complications, and Quality of Care Among
Diabetic Patients: A review. Diabetes Care 2005;28:2280-2288
Lauria G, Bakkers M, Schmitz C, Lombardi R, Penza P, Devigili G, Smith AG,
Hsieh ST, Mellgren SI, Umapathi T, Ziegler D, Faber CG, Merkies IS:
Intraepidermal nerve fiber density at the distal leg: a worldwide normative
reference study. J Peripher Nerv Syst 2010;15:202-207
Lauria G, Cornblath DR, Johansson O, McArthur JC, Mellgren SI, Nolano M,
Rosenberg N, Sommer C: EFNS guidelines on the use of skin biopsy in the
diagnosis of peripheral neuropathy. Eur J Neurol 2005;12:747-758
Lauria G, Devigili G: Skin biopsy as a diagnostic tool in peripheral neuropathy. Nat
Clin Pract Neuro 2007;3:546-557
Lauria G, Hsieh ST, Johansson O, Kennedy WR, Leger JM, Mellgren SI, Nolano
M, Merkies IS, Polydefkis M, Smith AG, Sommer C, Valls-Sole J: European
Federation of Neurological Societies/Peripheral Nerve Society Guideline on the
use of skin biopsy in the diagnosis of small fiber neuropathy. Report of a joint task
force of the European Federation of Neurological Societies and the Peripheral
Nerve Society. Eur J Neurol 2010;17:903-912, e944-909
Lauria G, Lombardi R: Small fiber neuropathy: is skin biopsy the holy grail? Current
diabetes reports 2012;12:384-392
Lee CT, Gayton EL, Beulens JW, Flanagan DW, Adler AI: Micronutrients and
diabetic retinopathy a systematic review. Ophthalmology 2010;117:71-78
376
Lee P, Chen R: Vitamin D as an analgesic for patients with type 2 diabetes and
neuropathic pain. Arch Intern Med 2008;168:771-772
Lemire JM: Immunomodulatory actions of 1,25-dihydroxyvitamin D3. J Steroid
Biochem Mol Biol 1995;53:599-602
Levin A, Bakris GL, Molitch M, Smulders M, Tian J, Williams LA, Andress DL:
Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in
patients with chronic kidney disease: results of the study to evaluate early kidney
disease. Kidney Int 2007;71:31-38
Levy-Marchal C, Patterson C, Green A: Variation by age group and seasonality at
diagnosis of childhood IDDM in Europe. The EURODIAB ACE Study Group.
Diabetologia 1995;38:823-830
Li X, Liao L, Yan X, Huang G, Lin J, Lei M, Wang X, Zhou Z: Protective effects of
1-alpha-hydroxyvitamin D3 on residual beta-cell function in patients with adult-
onset latent autoimmune diabetes (LADA). Diabetes/Metabolism Research and
Reviews 2009;25:411-416
Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP: 1,25-Dihydroxyvitamin D(3) is a
negative endocrine regulator of the renin-angiotensin system. J Clin Invest
2002;110:229-238
Lincoln NB, Radford KA, Game FL, Jeffcoate WJ: Education for secondary
prevention of foot ulcers in people with diabetes: a randomised controlled trial.
Diabetologia 2008;51:1954-1961
Lips P, Hosking D, Lippuner K, Norquist JM, Wehren L, Maalouf G, Ragi-Eis S,
Chandler J: The prevalence of vitamin D inadequacy amongst women with
osteoporosis: an international epidemiological investigation. J Intern Med
2006;260:245-254
377
Lohmann T, Kellner K, Verlohren HJ, Krug J, Steindorf J, Scherbaum WA, Seissler
J: Titre and combination of ICA and autoantibodies to glutamic acid decarboxylase
discriminate two clinically distinct types of latent autoimmune diabetes in adults
(LADA). Diabetologia 2001;44:1005-1010
Lopez-Liuchi JV: Autoimmune diabetes: is GAD the culprit? Eur J Endocrinol
1999;141:458-459
Loseth S, Lindal S, Stelberg E, Mellgren SI: Intraepidermal nerve fibre density,
quantitative sensory testing and nerve conduction studies in a patient material with
symptoms and signs of sensory polyneuropathy. European Journal of Neurology
2006;13:105-111
Loseth S, Mellgren SI, Jorde R, Lindal S, Stalberg E: Polyneuropathy in type 1 and
type 2 diabetes: comparison of nerve conduction studies, thermal perception
thresholds and intraepidermal nerve fibre densities. Diabetes Metab Res Rev
2010;26:100-106
Loseth S, Stalberg E, Jorde R, Mellgren SI: Early diabetic neuropathy: thermal
thresholds and intraepidermal nerve fibre density in patients with normal nerve
conduction studies. J Neurol 2008;255:1197-1202
Macdonald HM: Contributions of sunlight and diet to vitamin D status. Calcif Tissue
Int 2013;92:163-176
Maki KC, Rubin MR, Wong LG, McManus JF, Jensen CD, Marshall JW, Lawless A:
Serum 25-hydroxyvitamin D is independently associated with high-density
lipoprotein cholesterol and the metabolic syndrome in men and women. Journal of
Clinical Lipidology 2009;3:289-296
Maki M, Hallstrom O, Vesikari T, Visakorpi JK: Evaluation of serum IgA–class
reticulin antibody test for detection of childhood celiac disease. . J Pediatr
1984;105:901–905.
378
Malabanan A, Veronikis IE, Holick MF: Redefining vitamin D insufficiency. Lancet
1998;351:805-806
Malik RA, Veves A, Tesfaye S, Smith G, Cameron N, Zochodne D, Lauria G: Small
Fiber Neuropathy: Role in the diagnosis of Diabetic Sensorimotor Polyneuropathy.
Diabetes/Metabolism Research and Reviews 2011;27:678-684
Malik RA, Kallinikos P, Abbott CA, van Schie CH, Morgan P, Efron N, Boulton AJ:
Corneal confocal microscopy: a non-invasive surrogate of nerve fibre damage and
repair in diabetic patients. Diabetologia 2003;46:683-688
Malik RA, Tesfaye S, Newrick PG, Walker D, Rajbhandari SM, Siddique I, Sharma
AK, Boulton AJ, King RH, Thomas PK, Ward JD: Sural nerve pathology in diabetic
patients with minimal but progressive neuropathy. Diabetologia 2005;48:578-585
Malik RA, Veves A, Walker D, Siddique I, Lye RH, Schady W, Boulton AJM: Sural
nerve fibre pathology in diabetic patients with mild neuropathy: relationship to pain,
quantitative sensory testing and peripheral nerve electrophysiology. Acta
Neuropathologica 2001;101:367-374
Malik RA, Williamson S, Abbott C, Carrington AL, Iqbal J, Schady W, Boulton AJ:
Effect of angiotensin-converting-enzyme (ACE) inhibitor trandolapril on human
diabetic neuropathy: randomised double-blind controlled trial. Lancet
1998;352:1978-1981
Malik RA: Current and future strategies for the management of diabetic
neuropathy. Treatments in endocrinology 2003;2:389-400
Malik RA: The pathology of human diabetic neuropathy. Diabetes. Diabetes
1997;46:50-53
Margolis KL, Ray RM, Van Horn L, Manson JE, Allison MA, Black HR, Beresford
SA, Connelly SA, Curb JD, Grimm RH, Jr., Kotchen TA, Kuller LH, Wassertheil-
Smoller S, Thomson CA, Torner JC: Effect of calcium and vitamin D

379
supplementation on blood pressure: the Women's Health Initiative Randomized
Trial. Hypertension 2008;52:847-855
Maruyama T, Shimada, A., Kanatsuka, A., Kasuga, A., Takei, I., Yokoyama, J., et
al.: Multicenter prevention trial of slowly progressive type 1 diabetes with small
dose of insulin (the Tokyo study): Preliminary report. Annals of the New York
Academy of Sciences, 2003;1005,:362–369.
Maruyama T, Tanaka S, Shimada A, Funae O, Kasuga A, Kanatsuka A, Takei I,
Yamada S, Harii N, Shimura H, Kobayashi T: Insulin intervention in slowly
progressive insulin-dependent (type 1) diabetes mellitus. J Clin Endocrinol Metab
2008;93:2115-2121
Maser RE, Steenkiste AR, Dorman JS, Nielsen VK, Bass EB, Manjoo Q, Drash AL,
Becker DJ, Kuller LH, Greene DA, et al.: Epidemiological correlates of diabetic
neuropathy. Report from Pittsburgh Epidemiology of Diabetes Complications
Study. Diabetes 1989;38:1456-1461
Masson EA, Hunt L, Gem JM, Boulton AJM: A novel approach to the diagnosis and
assessment of symptomatic diabetic neuropathy. Pain 1989;38:25-28
Mathieu C, Gysemans C, Giulietti A, Bouillon R: Vitamin D and diabetes.
Diabetologia 2005;48:1247-1257
Mavroeidi A, O'Neill F, Lee PA, Darling AL, Fraser WD, Berry JL, Lee WT, Reid
DM, Lanham-New SA, Macdonald HM: Seasonal 25-hydroxyvitamin D changes in
British postmenopausal women at 57 degrees N and 51 degrees N: a longitudinal
study. J Steroid Biochem Mol Biol 2010;121:459-461
Mayhew JA, Gillon KR, Hawthorne JN: Free and lipid inositol, sorbitol and sugars
in sciatic nerve obtained post-mortem from diabetic patients and control subjects.
Diabetologia 1983;24:13-15

380
McArthur JC, Stocks EA, Hauer P, Cornblath DR, Griffin JW: Epidermal nerve fiber
density: normative reference range and diagnostic efficiency. Arch Neurol
1998;55:1513-1520
Medical Image Computing and Computer-Assisted Intervention – MICCAI 2010.
Jiang T, Navab N, Pluim J, Viergever M, Eds., Springer Berlin / Heidelberg, 2010,
p. 300-307
Mehra S, Tavakoli M, Kallinikos PA, Efron N, Boulton AJ, Augustine T, Malik RA:
Corneal confocal microscopy detects early nerve regeneration after pancreas
transplantation in patients with type 1 diabetes. Diabetes Care 2007;30:2608-2612
Meijer J-WG, Bosma E, Lefrandt JD, Links TP, Smit AJ, Stewart RE, van der
Hoeven JH, Hoogenberg K: Clinical Diagnosis of Diabetic Polyneuropathy With the
Diabetic
Neuropathy Symptom and Diabetic Neuropathy Examination Scores. Diabetes
care 2003;26:697-701
Michos ED, Melamed ML: Vitamin D and cardiovascular disease risk. Curr Opin
Clin Nutr Metab Care 2008;11:7-12
Mitri J, Muraru MD, Pittas AG: Vitamin D and type 2 diabetes: a systematic review.
Eur J Clin Nutr 2011;65:1005-1015
Mohr SB, Garland CF, Gorham ED, Garland FC: The association between
ultraviolet B irradiance, vitamin D status and incidence rates of type 1 diabetes in
51 regions worldwide. Diabetologia 2008;51:1391-1398
Mojaddidi M, Quattrini C, Tavakoli M, Malik RA: Recent developments in the
assessment of efficacy in clinical trials of diabetic neuropathy. Current diabetes
reports 2005;5:417-422

381
Mooney JA, Helms PJ, Jolliffe IT, Smail P: Seasonality of type 1 diabetes mellitus
in children and its modification by weekends and holidays: retrospective
observational study. Arch Dis Child 2004;89:970-973
Mora JR, Iwata M, von Andrian UH: Vitamin effects on the immune system:
vitamins A and D take centre stage. Nat Rev Immunol 2008;8:685-698
Morello CM: Etiology and natural history of diabetic retinopathy: an overview. Am J
Health Syst Pharm 2007;64:S3-7
Morrish NJ, Wang SL, Stevens LK, Fuller JH, Keen H: Mortality and causes of
death in the WHO Multinational Study of Vascular Disease in Diabetes.
Diabetologia 2001;44 Suppl 2:S14-21
Muller LJ, Marfurt CF, Kruse F, Tervo TMT: Corneal nerves: structure, contents
and function. Experimental Eye Research 2003;76:521-542
Murad MH, Smith SA: Review: TCAs, anticonvulsants, opioids, and capsaicin
cream are effective for diabetic neuropathy. Evid Based Med 2008;13:21
Murao S, Kondo S, Ohashi J, Fujii Y, Shimizu I, Fujiyama M, Ohno K, Takada Y,
Nakai K, Yamane Y, Osawa H, Makino H: Anti-thyroid peroxidase antibody, IA-2
antibody, and fasting C-peptide levels predict beta cell failure in patients with latent
autoimmune diabetes in adults (LADA)—A 5-year follow-up of the Ehime study.
Diabetes Research and Clinical Practice 2008;80:114-121
Murphy PJ, Lawrenson JG, Patel S, Marshall J: Reliability of the Non-Contact
Corneal Aesthesiometer and its comparison with the Cochet–Bonnet
aesthesiometer. Ophthalmic and Physiological Optics 1998;18:532-539
Myhill P, Davis WA, Bruce DG, Mackay IR, Zimmet P, Davis TM: Chronic
complications and mortality in community-based patients with latent autoimmune
diabetes in adults: the Fremantle Diabetes Study. Diabet Med 2008;25:1245-1250

382
Naik RG, Palmer JP: Latent Autoimmune Diabetes in Adults (LADA). Reviews in
Endocrine and Metabolic Disorders 2003;4:233-241
Nebuchennykh M, Loseth S, Lindal S, Mellgren SI: The value of skin biopsy with
recording of intraepidermal nerve fiber density and quantitative sensory testing in
the assessment of small fiber involvement in patients with different causes of
polyneuropathy. J Neurol 2009;256:1067-1075
Need AG: Bone resorption markers in vitamin D insufficiency. Clin Chim Acta
2006;368:48-52
Newman B, Selby JV, King MC, Slemenda C, Fabsitz R, Friedman GD:
Concordance for type 2 (non-insulin-dependent) diabetes mellitus in male twins. .
Diabetologia 1987;30:763-768
Norris JM, Beaty B, Klingensmith G, Yu L, Hoffman M, Chase HP, Erlich HA,
Hamman RF, Eisenbarth GS, Rewers M: Lack of Association Between Early
Exposure to Cow's Milk Protein and {beta}-Cell Autoimmunity: Diabetes
Autoimmunity Study in the Young (DAISY). JAMA 1996;276:609-614
Oh J, Weng S, Felton SK, Bhandare S, Riek A, Butler B, Proctor BM, Petty M,
Chen Z, Schechtman KB, Bernal-Mizrachi L, Bernal-Mizrachi C: 1,25(OH)2 vitamin
d inhibits foam cell formation and suppresses macrophage cholesterol uptake in
patients with type 2 diabetes mellitus. Circulation 2009;120:687-698
Orchard TJ, Dorman JS, Maser RE, Becker DJ, Ellis D, LaPorte RE, Kuller LH,
Wolfson SK, Jr., Drash AL: Factors associated with avoidance of severe
complications after 25 yr of IDDM. Pittsburgh Epidemiology of Diabetes
Complications Study I. Diabetes Care 1990;13:741-747
Oyibo SO, Prasad YD, Jackson NJ, Jude EB, Boulton AJ: The relationship
between blood glucose excursions and painful diabetic peripheral neuropathy: a
pilot study. Diabet Med 2002;19:870-873
383
Palomer X, Gonzalez-Clemente JM, Blanco-Vaca F, Mauricio D: Role of vitamin D
in the pathogenesis of type 2 diabetes mellitus. Diabetes Obes Metab
2008;10:185-197
Panou N, Georgopoulos S, Sergentanis TN, Papalampros A, Maropoulos M,
Tentolouris N, Sigala F, Venetsanou K, Papalambros E: Serum 25(OH)D and
VEGF in diabetes mellitus type 2: Gender-specific associations. International
Journal of Collaborative Research on Internal Medicine & Public Health
2011;3:790-795
Parker J, Hashmi O, Dutton D, Mavrodaris A, Stranges S, Kandala NB, Clarke A,
Franco OH: Levels of vitamin D and cardiometabolic disorders: systematic review
and meta-analysis. Maturitas 2010;65:225-236
Partanen J, Niskanen L, Lehtinen J, Mervaala E, Siitonen O, Uusitupa M: Natural
History of Peripheral Neuropathy in Patients with Non-Insulin-Dependent Diabetes
Mellitus. N Engl J Med 1995;333:89-94
Patel DV, McGhee CN: Mapping of the normal human corneal sub-Basal nerve
plexus by in vivo laser scanning confocal microscopy. Invest Ophthalmol Vis Sci
2005;46:4485-4488
Patra S, Gomm EMW, Macipe M, Bailey C: Interobserver agreement between
primary graders and an expert grader in the Bristol and Weston diabetic
retinopathy screening programme: a quality assurance audit. Diabetic Medicine
2009;26:820-823
Patrick PA, Visintainer PF, Shi Q, Weiss IA, Brand DA: Vitamin D and retinopathy
in adults with diabetes mellitus. Arch Ophthalmol 2012;130:756-760
Payne JF, Ray R, Watson DG, Delille C, Rimler E, Cleveland J, Lynn MJ,
Tangpricha V, Srivastava SK: Vitamin D insufficiency in diabetic retinopathy.
Endocr Pract 2012;18:185-193

384
Pearce SH, Cheetham TD: Diagnosis and management of vitamin D deficiency.
BMJ 2010;340:b5664
Peechakara SV, Pittas AG: Vitamin D as a potential modifier of diabetes risk. Nat
Clin Pract End Met 2008;4:182-183
Perez-Castrillon JL, Abad L, Vega G, Sanz-Cantalapiedra A, Garcia-Porrero M,
Pinacho F, Duenas A: Effect of atorvastatin on bone mineral density in patients
with acute coronary syndrome. Eur Rev Med Pharmacol Sci 2008;12:83-88
Perkins BA, Dholasania A, Buchanan RA, Bril V: Short-term metabolic change is
associated with improvement in measures of diabetic neuropathy: a 1-year placebo
cohort analysis. Diabetic Medicine 2010;27:1271-1279
Petropoulos IN, Alam U, Fadavi H, Asghar O, Green P, Ponirakis G, Marshall A,
Boulton AJ, Tavakoli M, Malik RA: Corneal Nerve Loss Detected With Corneal
Confocal Microscopy Is Symmetrical and Related to the Severity of Diabetic
Polyneuropathy. Diabetes Care 2013;
Petropoulos IN, Manzoor T, Morgan P, Fadavi H, Asghar O, Alam U, Ponirakis G,
Dabbah MA, Chen X, Graham J, Tavakoli M, Malik RA: Repeatability of in vivo
corneal confocal microscopy to quantify corneal nerve morphology. Cornea
32:e83-89
Pfeifer M, Begerow B, Minne HW, Nachtigall D, Hansen C: Effects of a short-term
vitamin D(3) and calcium supplementation on blood pressure and parathyroid
hormone levels in elderly women. J Clin Endocrinol Metab 2001;86:1633-1637
Pham H, Armstrong DG, Harvey C, Harkless LB, Giurini JM, Veves A: Screening
techniques to identify people at high risk for diabetic foot ulceration: a prospective
multicenter trial. Diabetes care 2000;23:606-611
Pham M, Oikonomou D, Baumer P, Bierhaus A, Heiland S, Humpert PM, Nawroth
PP, Bendszus M: Proximal neuropathic lesions in distal symmetric diabetic

385
polyneuropathy: findings of high-resolution magnetic resonance neurography.
Diabetes Care 2011;34:721-723
Pierce M, Keen H, Bradley C: Risk of diabetes in offspring of parents with non-
insulin-dependent diabetes. . Diabet Med 1995;12:6-13
Pilz S, Dobnig H, Fischer JE, Wellnitz B, Seelhorst U, Boehm BO, Marz W: Low
vitamin d levels predict stroke in patients referred to coronary angiography. Stroke
2008;39:2611-2613
Pittas AG, Harris SS, Stark PC, Dawson-Hughes B: The effects of calcium and
vitamin D supplementation on blood glucose and markers of inflammation in
nondiabetic adults. Diabetes Care 2007;30:980-986
Pittas AG, Lau J, Hu FB, Dawson-Hughes B: The role of vitamin D and calcium in
type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab
2007;92:2017-2029
Pittenger GL, Ray M, Burcus NI, McNulty P, Basta B, Vinik AI: Intraepidermal
Nerve Fibers Are Indicators of Small-Fiber Neuropathy in Both Diabetic and
Nondiabetic Patients. Diabetes care 2004;27:1974-1979
Plum LA, Zella JB: Vitamin D compounds and diabetic nephropathy. Archives of
Biochemistry and Biophysics 2012;523:87-94
Polydefkis M, Hauer P, Sheth S, Sirdofsky M, Griffin JW, McArthur JC.: The time
course of epidermal nerve fibre regeneration: studies in normal controls and in
people with diabetes, with and without neuropathy. Brain 2004;127:1606-1615
Polydefkis M: Punch Skin Biopsy in Diabetic Neuropathy. In Diabetic Neuropathy:
Clinical Management Veves A MR, Ed. New Jersey, Humana Press, 2007, p. 293-
307

386
Pop-Busui R, Herman WH, Feldman EL, Low PA, Martin CL, Cleary PA, Waberski
BH, Lachin JM, Albers JW: DCCT and EDIC studies in type 1 diabetes: lessons for
diabetic neuropathy regarding metabolic memory and natural history. Curr Diab
Rep 2010;10:276-282
Pop-Busui R, Low PA, Waberski BH, Martin CL, Albers JW, Feldman EL, Sommer
C, Cleary PA, Lachin JM, Herman WH: Effects of prior intensive insulin therapy on
cardiac autonomic nervous system function in type 1 diabetes mellitus: the
Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions
and Complications study (DCCT/EDIC). Circulation 2009;119:2886-2893
Pozzilli P, Manfrini S, Crino A, Picardi A, Leomanni C, Cherubini V, Valente L,
Khazrai M, Visalli N: Low levels of 25-hydroxyvitamin D3 and 1,25-
dihydroxyvitamin D3 in patients with newly diagnosed type 1 diabetes. Hormone
and metabolic research = Hormon- und Stoffwechselforschung = Hormones et
metabolisme 2005;37:680-683
Pramyothin P, Holick MF: Vitamin D supplementation: guidelines and evidence for
subclinical deficiency. Curr Opin Gastroenterol 2012;28:139-150
Prokopova L: Celiac disease—a severe disease. Vnitr Lek 2003;49:474–481
Purdy CW: Diabetes-its causes, symptoms and treatment. FA D, Ed. Philadelphia,
Hardpress Publishing, 1890.
Quattrini C, Tavakoli M, Jeziorska M, Kallinikos P, Tesfaye S, Finnigan J, Marshall
A, Boulton AJ, Efron N, Malik RA: Surrogate markers of small fiber damage in
human diabetic neuropathy. Diabetes 2007;56:2148-2154
Quessy SN, Rowbotham MC: Placebo response in neuropathic pain trials. Pain
2008;138:479-483
Raivo U, Åke L, Unanue EM, McDevitt HO: Chapter 3 GAD65 Autoimmunity--
Clinical Studies. In Advances in Immunology, Academic Press, 2008, p. 39-78

387
Reichard P, Nilsson BY, Rosenqvist U: The effect of long-term intensified insulin
treatment on the development of microvascular complications of diabetes mellitus.
N Engl J Med 1993;329:304-309
Reja A, Tesfaye S, Harris ND, Ward JD: Is ACE Inhibition with Lisinopril Helpful in
Diabetic Neuropathy? Diabetic Medicine 1995;12:307-309
Ren Z, Li W, Zhao Q, Ma L, Zhu J: The impact of 1,25-dihydroxy vitamin D3 on the
expressions of vascular endothelial growth factor and transforming growth factor-
β1 in the retinas of rats with diabetes. Diabetes Research and Clinical Practice
2012;98:474-480
Resnikoff S, Pascolini D, Etya'ale D, Kocur I, Pararajasegaram R, Pokharel GP,
Mariotti SP: Global data on visual impairment in the year 2002. Bull World Health
Organ 2004;82:844-851
Riaz S, Malcangio M, Miller M, Tomlinson DR: A vitamin D(3) derivative (CB1093)
induces nerve growth factor and prevents neurotrophic deficits in streptozotocin-
diabetic rats. Diabetologia 1999;42:1308-1313
Roep BO: The role of T-cells in the pathogenesis of Type 1 diabetes: from cause to
cure. Diabetologia 2003;46:305-321
Roh MO, Jung CH, Kim BY, Mok JO, Kim CH: The prevalence and characteristics
of latent autoimmune diabetes in adults (LADA) and its relation with chronic
complications in a clinical department of a university hospital in Korea. Acta
Diabetol 2013;50:129-134
Rolandsson O, Palmer JP: Latent autoimmune diabetes in adults (LADA) is dead:
long live autoimmune diabetes! Diabetologia 2010;53:1250-1253
388
Roll U, Nuber A, Schroder A, Gerlach E, Janka HU, Ziegler AG: No association of
antibodies to glutamic acid decarboxylase and diabetic complications in patients
with IDDM. Diabetes Care 1995;18:210-215
Romkens TE, Kusters GC, Netea MG, Netten PM: Prevalence and clinical
characteristics of insulin-treated, anti-GAD-positive, type 2 diabetic subjects in an
outpatient clinical department of a Dutch teaching hospital. Neth J Med
2006;64:114-118
Roodhooft JM: Leading causes of blindness worldwide. Bull Soc Belge Ophtalmol
2002:19-25
Rosen CJ, Gallagher JC: The 2011 IOM report on vitamin D and calcium
requirements for north america: clinical implications for providers treating patients
with low bone mineral density. J Clin Densitom 2011;14:79-84
Rosenberg ME, Tervo TM, Immonen IJ, Muller LJ, Gronhagen-Riska C,
Vesaluoma MH: Corneal structure and sensitivity in type 1 diabetes mellitus. Invest
Ophthalmol Vis Sci 2000;41:2915-2921
Ross AC, Manson JE, Abrams SA, Aloia JF, Brannon PM, Clinton SK, Durazo-
Arvizu RA, Gallagher JC, Gallo RL, Jones G, Kovacs CS, Mayne ST, Rosen CJ,
Shapses SA: The 2011 Report on Dietary Reference Intakes for Calcium and
Vitamin D from the Institute of Medicine: What Clinicians Need to Know. Journal of
Clinical Endocrinology & Metabolism 2011;96:53-58
Ruhnau KJ, Meissner HP, Finn JR, Reljanovic M, Lobisch M, Schutte K, Nehrdich
D, Tritschler HJ, Mehnert H, Ziegler D: Effects of 3-week oral treatment with the
antioxidant thioctic acid (alpha-lipoic acid) in symptomatic diabetic polyneuropathy.
Diabet Med 1999;16:1040-1043
Sadosky A, Schaefer C, Mann R, Bergstrom F, Baik R, Parsons B, Nalamachu S,
Nieshoff E, Stacey BR, Anschel A, Tuchman M: Burden of illness associated with
painful diabetic peripheral neuropathy among adults seeking treatment in the US:

389
results from a retrospective chart review and cross-sectional survey. Diabetes
Metab Syndr Obes 2013;6:79-92
Saiz A, Blanco Y, Sabater L, Gonzalez F, Bataller L, Casamitjana R, Ramio-
Torrenta L, Graus F: Spectrum of neurological syndromes associated with glutamic
acid decarboxylase antibodies: diagnostic clues for this association. Brain
2008;131:2553-2563
Sanjeevi CB, Hook P, Landin-Olsson M, Kockum I, Dahlquist G, Lybrand TP,
Lernmark A: DR4 subtypes and their molecular properties in a population-based
study of Swedish childhood diabetes. Tissue antigens 1996;47:275-283
Sanjeevi CB, Kanungo A, Shtauvere A, Samal KC, Tripathi BB: Association of HLA
class II alleles with different subgroups of diabetes mellitus in Eastern India identify
different associations with IDDM and malnutrition-related diabetes. Tissue antigens
1999;54:83-87
Sanjeevi CB, Lybrand TP, Landin-Olsson M, Kockum I, Dahlquist G, Hagopian
WA, Palmer JP, Lernmark A: Analysis of antibody markers, DRB1, DRB5, DQA1
and DQB1 genes and modeling of DR2 molecules in DR2-positive patients with
insulin-dependent diabetes mellitus. Tissue antigens 1994;44:110-119
Sattar N, Taskinen M-R: Statins are diabetogenic – Myth or reality? Atherosclerosis
Supplements 2012;13:1-10
Scanlon PH: The English national screening programme for sight-threatening
diabetic retinopathy. Journal of Medical Screening 2008;15:1-4
Schemmel KE, Padiyara RS, D'Souza JJ: Aldose reductase inhibitors in the
treatment of diabetic peripheral neuropathy: a review. Journal of diabetes and its
complications 2010;24:354-360
Scherens A, Maier C, Haussleiter IS, Schwenkreis P, Vlckova-Moravcova E, Baron
R, Sommer C: Painful or painless lower limb dysesthesias are highly predictive of

390
peripheral neuropathy: comparison of different diagnostic modalities. Eur J Pain
2009;13:711-718
Scragg R, Sowers M, Bell C: Serum 25-hydroxyvitamin D, diabetes, and ethnicity
in the Third National Health and Nutrition Examination Survey. Diabetes Care
2004;27:2813-2818
Selvarajah D, Gandhi R, Emery CJ, Tesfaye S: Randomized Placebo-Controlled
Double-Blind Clinical Trial of Cannabis-Based Medicinal Product (Sativex) in
Painful Diabetic Neuropathy: Depression is a major confounding factor. Diabetes
Care 2010;33:128-130
Selvarajah D, Wilkinson ID, Davies J, Gandhi R, Tesfaye S: Central nervous
system involvement in diabetic neuropathy. Curr Diab Rep 2011;11:310-322
Selvarajah D, Wilkinson ID, Gandhi R, Griffiths PD, Tesfaye S: Microvascular
perfusion abnormalities of the Thalamus in painful but not painless diabetic
polyneuropathy: a clue to the pathogenesis of pain in type 1 diabetes. Diabetes
Care 2011;34:718-720
Shaw J, Zimmet P: The epidemiology of diabetic neuropathy. Diabetes Revs
1999;7:245-252
Shehab D, Al-Jarallah K, Mojiminiyi OA, Al Mohamedy H, Abdella NA: Does
Vitamin D deficiency play a role in peripheral neuropathy in Type 2 diabetes?
Diabet Med 2012;29:43-49
Shields BM, Hicks S, Shepherd MH, Colclough K, Hattersley AT, Ellard S: Maturity-
onset diabetes of the young (MODY): how many cases are we missing?
Diabetologia 2010;53:2504-2508
Shun CT, Chang YC, Wu HP, Hsieh SC, Lin WM, Lin YH, Tai TY, Hsieh ST: Skin
denervation in type 2 diabetes: correlations with diabetic duration and functional
impairments. Brain 2004;127:1593-1605

391
Sima A, Rosu M, Vlad A, Silberberg G, Serban V: Latent Autoimmune Diabetes in
Adults (LADA). TMJ 2003;53:241-245
Sima AA: New insights into the metabolic and molecular basis for diabetic
neuropathy. Cell Mol Life Sci 2003;60:2445-2464
Singleton JR, Smith AG, Bromberg MB: Increased Prevalence of Impaired Glucose
Tolerance in Patients With Painful Sensory Neuropathy. Diabetes Care
2001;24:1448-1453
Sivaskandarajah GA, Halpern EM, Lovblom LE, Weisman A, Orlov S, Bril V,
Perkins BA: Structure-function relationship between corneal nerves and
conventional small-fiber tests in type 1 diabetes. Diabetes Care 2013;36:2748-
2755
Skljarevski V, Malik RA: Clinical Diagnosis of Diabetic Neuropathy. In Diabetic
Neuropathy: Clinical Management, 2nd Ed ed. Veves A MR, Ed. New Jersey,
Humana Press, 2007
Smith AG, Ramachandran P, Tripp S, Singleton JR: Epidermal nerve innervation in
impaired glucose tolerance and diabetes-associated neuropathy. Neurology
2001;57:1701-1704
Smith AG, Russell J, Feldman EL, Goldstein J, Peltier A, Smith S, Hamwi J, Pollari
D, Bixby B, Howard J, Singleton JR: Lifestyle Intervention for Pre-Diabetic
Neuropathy. Diabetes Care 2006;29:1294-1299
Soderstrom LH, Johnson SP, Diaz VA, Mainous AG, 3rd: Association between
vitamin D and diabetic neuropathy in a nationally representative sample: results
from 2001-2004 NHANES. Diabet Med 2012;29:50-55
Sosenko JM, Kato M, Soto R, Bild DE: Comparison of quantitative sensory-
threshold measures for their association with foot ulceration in diabetic patients.
Diabetes care 1990;13:1057-1061
392
Sosenko JM: The prevalence of diabetic neuropathy according to ethnicity. Curr
Diab Rep 2009;9:435-439
Souberbielle JC, Friedlander G, Kahan A, Cormier C: Evaluating vitamin D status.
Implications for preventing and managing osteoporosis and other chronic diseases.
Joint Bone Spine 2006;73:249-253
Spectrum of High-Resolution MRI Findings in Diabetic Neuropathy. American
Journal of Roentgenology 2012;199:407-412
Stene LC, Ulriksen J, Magnus P: Use of cod liver oil during pregnancy associated
with lower risk of type 1 diabetes in the offspring. . Diabetologia 2000;43:1093–
1098.
Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D,
Turner RC, Holman RR: Association of glycaemia with macrovascular and
microvascular complications of type 2 diabetes (UKPDS 35): prospective
observational study. BMJ 2000;321:405-412
Straube S, Andrew Moore R, Derry S, McQuay HJ: Vitamin D and chronic pain.
PAIN 2009;141:10-13
Stewart JD, Low PA, Fealey RD: Distal small fiber neuropathy: results of tests of
sweating and autonomic cardiovascular reflexes. Muscle Nerve 1992;15:661-665
Stumvoll M, Goldstein BJ, van Haeften TW: Type 2 diabetes: principles of
pathogenesis and therapy. The Lancet 2005;365:1333-1346
Sumner CJ, Sheth S, Griffin JW, Cornblath DR, Polydefkis M: The spectrum of
neuropathy in diabetes and impaired glucose tolerance. Neurology 2003;60:108-
111
Sun JK, Keenan HA, Cavallerano JD, Asztalos BF, Schaefer EJ, Sell DR, Strauch
CM, Monnier VM, Doria A, Aiello LP, King GL: Protection From Retinopathy and
393
Other Complications in Patients With Type 1 Diabetes of Extreme Duration: The
Joslin 50-Year Medalist Study. Diabetes Care 2011;34:968-974
Sundkvist G, Velloso LA, Kampe O, Rabinowe SL, Ivarsson SA, Lilja B, Karlsson
FA: Glutamic acid decarboxylase antibodies, autonomic nerve antibodies and
autonomic neuropathy in diabetic patients. Diabetologia 1994;37:293-299
Susan van D, Beulens JWJ, Yvonne T. van der S, Grobbee DE, Nealb B: The
global burden of diabetes and its complications: an emerging pandemic. European
Journal of Cardiovascular Prevention & Rehabilitation 2010;17:s3-s8
Tague SE, Clarke GL, Winter MK, McCarson KE, Wright DE, Smith PG: Vitamin D
deficiency promotes skeletal muscle hypersensitivity and sensory hyperinnervation.
J Neurosci 2011;31:13728-13738
Tague SE, Smith PG: Vitamin D receptor and enzyme expression in dorsal root
ganglia of adult female rats: modulation by ovarian hormones. J Chem Neuroanat
2011;41:1-12
Tahrani AA, Ball A, Shepherd L, Rahim A, Jones AF, Bates A: The prevalence of
vitamin D abnormalities in South Asians with type 2 diabetes mellitus in the UK. Int
J Clin Pract 2010;64:351-355
Tan X, He W, Liu Y: Combination therapy with paricalcitol and trandolapril reduces
renal fibrosis in obstructive nephropathy. Kidney Int 2009;76:1248-1257
Tan X, Li Y, Liu Y: Paricalcitol attenuates renal interstitial fibrosis in obstructive
nephropathy. J Am Soc Nephrol 2006;17:3382-3393
Tandan R, Lewis GA, Krusinski PB, Badger GB, Fries TJ: Topical capsaicin in
painful diabetic neuropathy. Controlled study with long-term follow-up. Diabetes
Care 1992;15:8-14

394
Tattersal RB, Fajans SS: Prevalence of diabetes and glucose intolerance in 199
offspring of thirty-seven conjugal diabetic parents. . Diabetes 1975;24:452-462
Tavakoli M, Asghar O, Alam U, Petropoulos IN, Fadav IN, Malik RA: Advances in
Diagnosis and Treatment of Diabetic Neuropathy. 2010;In Press
Tavakoli M, Kallinikos P, Iqbal A, Herbert A, Fadavi H, Efron N, Boulton AJ, R AM:
Corneal confocal microscopy detects improvement in corneal nerve morphology
with an improvement in risk factors for diabetic neuropathy. Diabet Med
2011;28:1261-1267
Tavakoli M, Kallinikos PA, Efron N, Boulton AJ, Malik RA: Corneal sensitivity is
reduced and relates to the severity of neuropathy in patients with diabetes.
Diabetes Care 2007;30:1895-1897
Tavakoli M, Malik RA: Corneal confocal microscopy: a novel non-invasive
technique to quantify small fibre pathology in peripheral neuropathies. J Vis Exp
2011 Jan 3;(47):2194. doi: 10.3791/2194.
Tavakoli M, Marshall A, Pitceathly R, Fadavi H, Gow D, Roberts ME, Efron N,
Boulton AJ, Malik RA: Corneal confocal microscopy: a novel means to detect nerve
fibre damage in idiopathic small fibre neuropathy. Exp Neurol 2010;223:245-250
Tavakoli M, Mitu-Pretorian M, Petropoulos IN, Fadavi H, Asghar O, Alam U,
Ponirakis G, Jeziorska M, Marshall A, Efron N, Boulton AJ, Augustine T, Malik RA:
Corneal confocal microscopy detects early nerve regeneration in diabetic
neuropathy after simultaneous pancreas and kidney transplantation. Diabetes
2013;62:254-260
Tavakoli M, Quattrini C, Abbott C, Kallinikos P, Marshall A, Finnigan J, Morgan P,
Efron N, Boulton AJ, Malik RA: Corneal confocal microscopy: a novel noninvasive
test to diagnose and stratify the severity of human diabetic neuropathy. Diabetes
Care 2010;33:1792-1797
395
Taverna MJ, Selam JL, Slama G: Association between a protein polymorphism in
the start codon of the vitamin D receptor gene and severe diabetic retinopathy in
C-peptide-negative type 1 diabetes. J Clin Endocrinol Metab 2005;90:4803-4808
Taverna MJ, Sola A, Guyot-Argenton C, Pacher N, Bruzzo F, Slama G, Reach G,
Selam JL: Taq I polymorphism of the vitamin D receptor and risk of severe diabetic
retinopathy. Diabetologia 2002;45:436-442
Tesfaye S, Boulton AJ, Dickenson AH: Mechanisms and management of diabetic
painful distal symmetrical polyneuropathy. Diabetes Care 2013;36:2456-2465
Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, Lauria G,
Malik RA, Spallone V, Vinik A, Bernardi L, Valensi P: Diabetic neuropathies:
update on definitions, diagnostic criteria, estimation of severity, and treatments.
Diabetes Care 2010;33:2285-2293
Tesfaye S, Chaturvedi N, Eaton SEM, Ward JD, Manes C, Ionescu-Tirgoviste C,
Witte DR, Fuller JH: Vascular Risk Factors and Diabetic Neuropathy. New England
Journal of Medicine 2005;352:341-350
Tesfaye S, Selvarajah D: The Eurodiab study: What has this taught us about
diabetic peripheral neuropathy? Current Diabetes Reports 2009;9:432-434
Tesfaye S, Stevens LK, Stephenson JM, Fuller JH, Plater M, Ionescu-Tirgoviste C,
Nuber A, Pozza G, Ward JD: Prevalence of diabetic peripheral neuropathy and its
relation to glycaemic control and potential risk factors: the EURODIAB IDDM
Complications Study. Diabetologia 1996;39:1377-1384
Tesfaye S, Tandan R, Bastyr EJ, 3rd, Kles KA, Skljarevski V, Price KL: Factors
that impact symptomatic diabetic peripheral neuropathy in placebo-administered
patients from two 1-year clinical trials. Diabetes Care 2007;30:2626-2632
Tesfaye S, Vileikyte L, Rayman G, Sindrup S, Perkins B, Baconja M, Vinik A,
Boulton A: Painful Diabetic Peripheral Neuropathy: Consensus Recommendations

396
on Diagnosis, Assessment and Management. Diabetes/Metabolism Research and
Reviews 2011;27:629-638
Tesfaye S, Wilhelm S, Lledo A, Schacht A, Tölle T, Bouhassira D, Cruccu G,
Skljarevski V, Freynhagen R: Duloxetine and pregabalin: High-dose monotherapy
or their combination? The “COMBO-DN study” – a multinational, randomized,
double-blind, parallel-group study in patients with diabetic peripheral neuropathic
pain. PAIN 2013 [Epub ahead of print].
http://dx.doi.org/10.1016/j.pain.2013.05.043.
The effect of intensive diabetes therapy on the development and progression of
neuropathy. The Diabetes Control and Complications Trial Research Group.
Annals of internal medicine 1995;122:561-568
Thomas MK, Lloyd-Jones DM, Thadhani RI, Shaw AC, Deraska DJ, Kitch BT,
Vamvakas EC, Dick IM, Prince RL, Finkelstein JS: Hypovitaminosis D in medical
inpatients. N Engl J Med 1998;338:777-783
Thunander M, Thorgeirsson H, Törn C, Petersson C, Landin-Olsson M: β-cell
function and metabolic control in latent autoimmune diabetes in adults with early
insulin versus conventional treatment: a 3-year follow-up. European Journal of
Endocrinology 2011;164:239-245
Tight blood pressure control and risk of macrovascular and microvascular
complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study
Group. BMJ 1998;317:703-713
Tjellesen L, Hummer L, Christiansen C, Rodbro P: Serum concentration of vitamin
D metabolites during treatment with vitamin D2 and D3 in normal premenopausal
women. Bone Miner 1986;1:407-413
Tobin K, Giuliani MJ, Lacomis D: Comparison of different modalities for detection
of small fiber neuropathy. Clin Neurophysiol 1999;110:1909-1912

397
Tomlinson DR, Moriarty RJ, Mayer JH: Prevention and reversal of defective axonal
transport and motor nerve conduction velocity in rats with experimental diabetes by
treatment with the aldose reductase inhibitor Sorbinil. Diabetes 1984;33:470-476
Tomlinson DR: Polyols and myo-inositol in diabetic neuropathy--of mice and men.
Mayo Clinic proceedings 1989;64:1030-1033
Trang H, Cole D, Rubin L, Pierratos A, Siu S, Vieth R: Evidence that vitamin D3
increases serum 25-hydroxyvitamin D more efficiently than does vitamin D2. The
American Journal of Clinical Nutrition 1998;68:854-858
Tuomi T, Carlsson A, Li H, Isomaa B, Miettinen A, Nilsson A, Nissen M, Ehrnstrom
BO, Forsen B, Snickars B, Lahti K, Forsblom C, Saloranta C, Taskinen MR, Groop
LC: Clinical and genetic characteristics of type 2 diabetes with and without GAD
antibodies. Diabetes 1999;48:150-157
Turner R, Stratton I, Horton V, Manley S, Zimmet P, Mackay IR, Shattock M,
Bottazzo GF, Holman R: UKPDS 25: autoantibodies to islet-cell cytoplasm and
glutamic acid decarboxylase for prediction of insulin requirement in type 2
diabetes: UK Prospective Diabetes Study Group. Lancet 1997;350:1288–1293
UK Prospective Diabetes Study 6. Complications in newly diagnosed type 2
diabetic patients and their association with different clinical and biochemical risk
factors. Diabetes Res 1990;13:1-11
Umapathi T, Tan WL, Loke SC, Soon PC, Tavintharan S, Chan YH: Intraepidermal
nerve fiber density as a marker of early diabetic neuropathy. Muscle Nerve
2007;35:591-598
Umapathi T, Tan WL, Tan NC, Chan YH: Determinants of epidermal nerve fiber
density in normal individuals. Muscle Nerve 2006;33:742-746
Vaidya A, Forman JP: Vitamin D and Hypertension: Current Evidence and Future
Directions. Hypertension 2010;56:774-779

398
Vaidya A, Williams JS: The relationship between vitamin D and the renin-
angiotensin system in the pathophysiology of hypertension, kidney disease, and
diabetes. Metabolism 2012;61:450-458
Valensi P, Le Devehat C, Richard JL, Farez C, Khodabandehlou T, Rosenbloom
RA, LeFante C: A multicenter, double-blind, safety study of QR-333 for the
treatment of symptomatic diabetic peripheral neuropathy. A preliminary report. J
Diabetes Complications 2005;19:247-253
Vas PRJ, Rayman G: The Rate of Decline in Small Fibre Function Assessed Using
Axon Reflex-Mediated Neurogenic Vasodilatation and the Importance of Age
Related Centile Values to Improve the Detection of Clinical Neuropathy. PLoS One
2013;8:e69920. doi:69910.61371/journal.pone.0069920
Verhoeven S, van Ballegooie E, Casparie AF: Impact of Late Complications in
Type 2 Diabetes in a Dutch Population. Diabetic Medicine 1991;8:435-438
Verstappen A, Parmentier M, Chirnoaga M, Lawson DE, Pasteels JL, Pochet R:
Vitamin D-dependent calcium binding protein immunoreactivity in human retina.
Ophthalmic Res 1986;18:209-214
Vieth R, Bischoff-Ferrari H, Boucher BJ, Dawson-Hughes B, Garland CF, Heaney
RP, Holick MF, Hollis BW, Lamberg-Allardt C, McGrath JJ, Norman AW, Scragg R,
Whiting SJ, Willett WC, Zittermann A: The urgent need to recommend an intake of
vitamin D that is effective. Am J Clin Nutr 2007;85:649-650
Vieth R: Vitamin D and Cancer Mini-Symposium: The Risk of Additional Vitamin D.
Annals of Epidemiology 2009;19:441-445
Vieth R: Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and
safety. The American Journal of Clinical Nutrition 1999;69:842-856

399
Vincent AM, Callaghan BC, Smith AL, Feldman EL: Diabetic neuropathy: cellular
mechanisms as therapeutic targets. Nat Rev Neurol 2011;7:573-583
Vinik AI, Bril V, Kempler P, Litchy WJ, Tesfaye S, Price KL, Bastyr EJ, null:
Treatment of symptomatic diabetic peripheral neuropathy with the protein kinase C
beta-inhibitor ruboxistaurin mesylate during a 1-year, randomized, placebo-
controlled, double-blind clinical trial. Clinical therapeutics 2005;27:1164-1180
VITAMIN D - ADVICE ON SUPPLEMENTS FOR AT RISK GROUPS [article
online],
2012.Availablefrom:https://www.gov.uk/government/uploads/system/uploads/attach
ment_data/file/134550/dh_132508.pdf.pdf.
Vladimir S: Diabetic Neuropathy: Clinical Management. 2nd Ed ed. Veves A MR,
Ed. New Jersey, Humana Press Inc, 2007, p. 1-5
Vlckova-Moravcova E, Bednarik J, Dusek L, Toyka KV, Sommer C: Diagnostic
validity of epidermal nerve fiber densities in painful sensory neuropathies. Muscle
Nerve 2008;37:50-60
Wagner N, Wagner KD, Schley G, Badiali L, Theres H, Scholz H: 1,25-
dihydroxyvitamin D3-induced apoptosis of retinoblastoma cells is associated with
reciprocal changes of Bcl-2 and bax. Exp Eye Res 2003;77:1-9
Wahren J, Ekberg K, Jornvall H: C-peptide is a bioactive peptide. Diabetologia
2007;50:503-509
Walters DP, Gatling W, Mullee MA, Hill RD: The prevalence of diabetic distal
sensory neuropathy in an English community. Diabet Med 1992;9:349-353
Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K, Benjamin EJ,
D'Agostino RB, Wolf M, Vasan RS: Vitamin D deficiency and risk of cardiovascular
disease. Circulation 2008;117:503-511

400
Ward JD, Tesfaye S: Pathogenesis of human diabetic neuropathy. In Textbook of
Diabetes Pickup J WG, Eds., Ed. Oxford, Blackwell Science,, p. 49.41-49.19
Wareham NJ, Byrne CD, Carr C, Day NE, Boucher BJ, Hales CN: Glucose
intolerance is associated with altered calcium homeostasis: a possible link between
increased serum calcium concentration and cardiovascular disease mortality.
Metabolism 1997;46:1171-1177
Webb AR, Kift R, Durkin MT, O’Brien SJ, Vail A, Berry JL, Rhodes LE: The role of
sunlight exposure in determining the vitamin D status of the U.K. white adult
population. British Journal of Dermatology 2010;163:1050-1055
Wergeland S, Torkildsen O, Myhr KM, Aksnes L, Mork SJ, Bo L: Dietary vitamin D3
supplements reduce demyelination in the cuprizone model. PLoS One 6:e26262
White NH, Sun W, Cleary PA, Danis RP, Davis MD, Hainsworth DP, Hubbard LD,
Lachin JM, Nathan DM: Prolonged effect of intensive therapy on the risk of
retinopathy complications in patients with type 1 diabetes mellitus: 10 years after
the Diabetes Control and Complications Trial. Arch Ophthalmol 2008;126:1707-
1715
Whiting DR, Guariguata L, Weil C, Shaw J: IDF Diabetes Atlas: Global estimates of
the prevalence of diabetes for 2011 and 2030. Diabetes Research and Clinical
Practice 2011;94:311-321
Wilkinson ID, Selvarajah D, Greig M, Shillo P, Boland E, Gandhi R, Tesfaye S:
Magnetic resonance imaging of the central nervous system in diabetic neuropathy.
Curr Diab Rep 2013;13:509-516
Willison HJ, Winer JB: Clinical evaluation and investigation of neuropathy. Journal
of neurology, neurosurgery, and psychiatry 2003;74 Suppl 2:ii3-ii8
Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF: Decreased bioavailability of
vitamin D in obesity. Am J Clin Nutr 2000;72:690-693

401
Yagihashi S, Mizukami H, Sugimoto K: Mechanism of diabetic neuropathy: Where
are we now and where to go? Journal of Diabetes Investigation 2011;2:18-32
Yang Y, Wang Y, Li S, Xu Z, Li H, Ma L, Fan J, Bu D, Liu B, Fan Z, Wu G, Jin J,
Ding B, Zhu X, Shen Y: Mutations in SCN9A, encoding a sodium channel alpha
subunit, in patients with primary erythermalgia. J Med Genet 2004;41:171-174
Yarnitsky D, Pud D: Quantitative sensory testing. Clinical Neurophysiology
2004;1:305-332
Yau JWY, Rogers SL, Kawasaki R, Lamoureux EL, Kowalski JW, Bek T, Chen S-J,
Dekker JM, Fletcher A, Grauslund J, Haffner S, Hamman RF, Ikram MK, Kayama
T, Klein BEK, Klein R, Krishnaiah S, Mayurasakorn K, O’Hare JP, Orchard TJ,
Porta M, Rema M, Roy MS, Sharma T, Shaw J, Taylor H, Tielsch JM, Varma R,
Wang JJ, Wang N, West S, Xu L, Yasuda M, Zhang X, Mitchell P, Wong TY, Group
ftM-AfEDS: Global Prevalence and Major Risk Factors of Diabetic Retinopathy.
Diabetes Care 2012;35:556-564
Yavuz B, Ertugrul DT, Cil H, Ata N, Akin KO, Yalcin AA, Kucukazman M, Dal K,
Hokkaomeroglu MS, Yavuz BB, Tutal E: Increased levels of 25 hydroxyvitamin D
and 1,25-dihydroxyvitamin D after rosuvastatin treatment: a novel pleiotropic effect
of statins? Cardiovasc Drugs Ther 2009;23:295-299
Young M, Boulton A, Macleod A, Williams D, Sonksen P: A multicentre study of the
prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic
population. Diabetologia 1993;36:150-154
Zhang Z, Zhang Y, Ning G, Deb DK, Kong J, Li YC: Combination therapy with AT1
blocker and vitamin D analog markedly ameliorates diabetic nephropathy: blockade
of compensatory renin increase. Proc Natl Acad Sci U S A 2008;105:15896-15901
Ziegler D, Hanefeld M, Ruhnau KJ, Hasche H, Lobisch M, Schutte K, Kerum G,
Malessa R: Treatment of symptomatic diabetic polyneuropathy with the antioxidant

402
alpha-lipoic acid: a 7-month multicenter randomized controlled trial (ALADIN III
Study). ALADIN III Study Group. Alpha-Lipoic Acid in Diabetic Neuropathy.
Diabetes Care 1999;22:1296-1301
Ziegler D, Hanefeld M, Ruhnau KJ, Meissner HP, Lobisch M, Schutte K, Gries FA:
Treatment of symptomatic diabetic peripheral neuropathy with the anti-oxidant
alpha-lipoic acid. A 3-week multicentre randomized controlled trial (ALADIN Study).
Diabetologia 1995;38:1425-1433
Ziegler D, Hidvégi T, Gurieva I, Bongardt S, Freynhagen R, Sen D, Sommerville K,
Group obotLSS: Efficacy and Safety of Lacosamide in Painful Diabetic Neuropathy.
Diabetes Care 2010;33:839-841
Ziegler D, Low PA, Litchy WJ, Boulton AJM, Vinik AI, Freeman R, Samigullin R,
Tritschler H, Munzel U, Maus J, Schütte K, Dyck PJ: Efficacy and Safety of
Antioxidant Treatment With α-Lipoic Acid Over 4 Years in Diabetic Polyneuropathy:
The NATHAN 1 trial. Diabetes Care 2011;34:2054-2060
Zimmet P, Turner R, McCarty D, Rowley M, Mackay I: Crucial points at diagnosis.
Type 2 diabetes or slow type 1 diabetes. Diabetes care 1999;22 Suppl 2:B59-64
Zipitis CS, Akobeng AK: Vitamin D supplementation in early childhood and risk of
type 1 diabetes: a systematic review and meta-analysis. Archives of Disease in
Childhood 2008;93:512-517
Zittermann A, Gummert JF: Sun, vitamin D, and cardiovascular disease. J
Photochem Photobiol B 2010;101:124-129

403
12 APPENDIX 1-STUDY RELATED DOCUMENTS

404
12-1Patient information sheet - Ophthalmic markers of diabetic neuropathy

405

406

407
12-2 Patient consent form
Participant Study Number:
Participant identification Number:
CONSENT FORM
Title of Project: Ophthalmic markers of diabetic neuropathy
Investigators: Prof. Rayaz. A Malik, Consultant Physician, MB ChB, FRCP, PhD.
Prof. Andrew Boulton, Consultant Physician, MBBS, MD, FRCP, DSc.
Dr. Andrew Marshall, Consultant Clinical Neurophysiologist BSc, BM CHB, MRCP
Dr. Mitra Tavakoli, Post-Doctoral Research Fellow BSc (Hons), MSc, PhD
Please initial box:
I confirm that I have read and I understand the information sheet dated…26/04/2011
(Version 5...) for the above study and have had the opportunity to ask questions.
I understand that my participation is voluntary and that I am free to withdraw at any time,
without giving any reason, without my medical care or legal rights being affected
I understand that sections of any of my medical notes may be looked at by responsible
individuals from University of Manchester and NHS Trust where it is relevant to my
taking part in research. I give permission for these individuals to have access to my records.
I agree to take part in the above study.
I agree that you may contact my GP regarding my participation in this study
I also agree that you can contact me in the future to see how my circumstances have
changed.
I understand that this study requires two small samples of skin to be removed from the
top of the foot. I agree to have this procedure undertaken.
……………………………. ……….………………. …………….... Name of Patient Signature Date
…………………………… ……….………………. …………..... Name of Person Signature Date
taking consent
1 for participant; 1 for researcher

408
12-3 Physical measurements and peripheral neuropathy assessment forms
Check List: Surrogate markers of diabetic neuropathy ( IGT- Diabetes- Transplant- JDRF) Name of Patient:
Date Notes
Travel costs
Information sheet
Consent forms
NCS
NDS
VPT
Neuropad
Medoc
Blood pressures
Blood samples
NCCA
CCM
Fundus camera
Skin biopsy
Medical history
Hypertension Stroke High cholesterol Heart problems Breathing problems
Other health issues: Medication
Beta blockers Warfarin Synthrome Aspirin Clopidogrel ACE inhibitor
A2RB Statin Fibrates
Other anti-hypertensive medication Neuropathy Exclusion criteria

409
Severe systemic diseases (e.g. congestive cardiac failure,
rheumatoid disease, SLE)
Chronic renal
impairment (serum creatinine >250 umol/l)
Known peripheral vascular
disease (e.g. previous bypass surgery, angioplasty or
claudication)
Alcohol intake >21 units
per week (males) or >14
units/week (females)
Non-diabetic peripheral
neuropathy Aspirin and Clopidrogrel
410
12-4 Ophthalmic examination sheet
Ophthalmic markers Ophthalmic record sheet
Participant’s Full Name: Date of Birth:
Date of Visit: Investigator(s): Study & Visit ID:
IF NOT PART OF A TRIAL
Patient referred from: Hospital No.:
Address details:
Medical History :
Type of Diabetes:
Duration of Diabetes:
Family History of Diabetes (quote parental/maternal side):
Other systemic disease (e.g. Heart Failure, Liver Failure, Hep B, HIV+, Vit. Deficiencies, Alcohol abuse, MS, Connective Tissue
Disease, SLE, psoriasis):
Medication (quote reason e.g. hypertension, cholesterol, diabetes, other CVD-related etc.):
Ocular History:
History of previous ocular disease (e.g. systemic, infections) / trauma:
History of operations (quote year, eye, type of operation):
History of contact lens use (quote type and frequency):
History of retinopathy (official grading):
For Transplant Study:
Date of Transplant:
Type of Transplant:
Duration on Renal Dialysis:
Smoking: per day
Drinking: units per week
Ophthalmic Examinations:
Slit Lamp Biomicroscopy (draw findings):
OD OS
Comments: Cornments:

411
Corneal Aesthesiometry: NCCA (mbar) CB-A
OD OS
Puppilometry (ensure 10 min. dark adaptation before examination):
Tear Tests:
BUT:
Schirmer Test:
Tear Sample collection:
- Schirmer strips:
- Microcappillary tubes:
Corneal Confocal Microscopy (HRT III-RCM)
Epithelium Bowman’s Layer/Nerve Plexus Stroma Endothelium
OD
OS
Corneal nerve parameters (values):
NFD (no./mm2) NBD (no./mm
2) NFL (mm/mm
2) NFT
OD
OS
Fundoscopy (Mydriatic/Non-Mydriatic) and Ophthalmoscopy (draw findings):
OD OS
Comments: Comments:
412
Additional Notes
413
13 APPENDIX 2 – Additional Analyses

414
Table 13-1 Baseline characteristics of the complete Control group (n=16) and the
Control group with only white European participants (n=12) with significant
differences.
Complete
Control BL
(n=16)
White European
Control BL
(n=12)
P value
Age (years) 41.4±11.4 42.6±12.5 NS
Gender (Male) (%) 63 58 NS
Ethnicity (White
European) (%) 75 100 NS
NDS (-/10)
Median(IQR)
0.5±1.1
0(0-0)
0.6±1.3
0(0-1)
NS
NSP (-/38)
Median(IQR)
0.1±0.25
0(0-0)
0.1±0.29
0(0-0)
NS
McGill VAS (-/10cm)
Median (IQR)
0.3±1.25
0(0-0)
0.4±1.40
(0-0)
NS
HbA1c (%) 5.6±0.3 5.6±0.3 NS
BMI (kg/m2) 25.7±4.2 24.9±4.2 NS
T-CHL (mmol/l) 5.1±0.9 5.1±1.0 NS
HDL (mmol/l) 1.5±0.3 1.5±0.3 NS
Triglycerides 1.4±0.7 1.4±0.8 NS
Systolic BP (mmHg) 125±21 127±24 NS
Diastolic BP (mmHg) 75±12 75±13 NS
eGFR (ml/min/1.73) 86±7 87±5 NS
NCCA (mBar) 0.6±0.3 0.7±0.3 NS
CNFD (no/mm2) 30.1±4.9 30.1±4.7 NS
CNBD (no/mm2) 36.6±15.5 34.1±16.1 NS
CNFL (mm/mm2) 16.9±2.8 16.6±2.9 NS
CST (˚C) 28.6±2.1 28.5±2.2 NS
WST(˚C) 37.6±3.5 38.2±3.9 NS
VPT (volts) 5.3±4.8 6.0±5.5 NS
SSNCV (m/s) 49.4±3.9 49.2±3.9 NS
SSNAmp (µV) 21.0±10.8 21.6±12.1 NS
PMNCV (m/s) 47.8±3.6 47.2±4.1 NS
PMNAmp (mV) 6.0±1.6 5.4±1.0 NS

415
Table 13-2 Baseline characteristics of the complete Control group (n=27) and the
Control group with only white European participants (n=21) with significant
differences.
Controls (n=27)
Controls White
European only
(n=21)
P value
Age (years) 41.0±14.9 42.9±16.0 NS
Gender (Male) (%) 59 57 NS
HbA1c (%) 5.5±0.3 5.5±0.3 NS
HbA1c (mmol/mol) 36.9±3.4 36.9±3.4 NS
BMI (kg/m2) 26.9±4.0 26.9±4.3 NS
T-CHL (mmol/l) 5.0±0.8 5.0±0.9 NS
HDL (mmol/l) 1.6±0.4 1.6±0.4 NS
Triglycerides 1.3±0.6 1.4±0.6 NS
Systolic BP (mmHg) 128±18 129±20 NS
Diastolic BP (mmHg) 70±10 69±9 NS
eGFR (ml/min/1.73) 85±7 85±7 NS
NDS (-/10)
Median(IQR)
0.4±0.8
0(0-1)
0.5±0.9
0(0-1) NS
NSP (-/38)
Median(IQR)
0.1±0.4
0(0-0)
0.1±0.5
0(0-0) NS
McGill VAS (-/10cm)
Median(IQR)
0.2±1.0
(0(0-0)
0.2±1.1
(0(0-0) NS
NCCA (mBar) 0.5±0.3 0.6±0.3 NS
CNFD (no/mm2) 37.2±5.1 37.7±4.8 NS
CNBD (no/mm2) 92.0±36.2 92.2±34.1 NS
CNFL (mm/mm2) 26.6±3.8 27.0±2.8 NS
IENFD (no/mm) 10.2±3.3 10.2±3.3 NS
CST (˚C) 28.6±2.0 28.5±2.1 NS
WST(˚C) 36.4±2.0 36.6±2.2 NS
VPT (volts) 5.3±4.1 5.9±4.5 NS
SSNCV (m/s) 50.6±4.2 50.4±4.6 NS
SSNAmp (µV) 20.2±8.8 19.2±9.3 NS
PMNCV (m/s) 49.2±3.7 48.8±4.0 NS
PMNAmp (mV) 6.1±2.4 5.5±2.5 NS
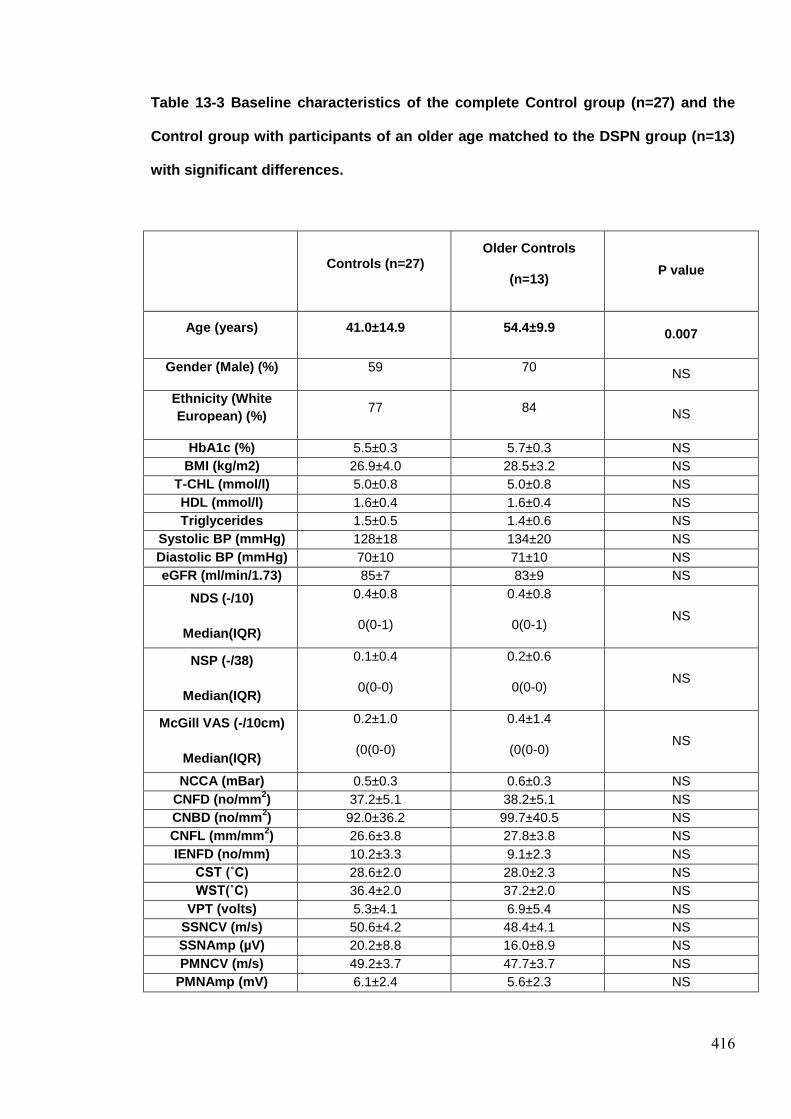
416
Table 13-3 Baseline characteristics of the complete Control group (n=27) and the
Control group with participants of an older age matched to the DSPN group (n=13)
with significant differences.
Controls (n=27) Older Controls
(n=13) P value
Age (years) 41.0±14.9 54.4±9.9 0.007
Gender (Male) (%) 59 70 NS
Ethnicity (White
European) (%) 77 84
NS
HbA1c (%) 5.5±0.3 5.7±0.3 NS
BMI (kg/m2) 26.9±4.0 28.5±3.2 NS
T-CHL (mmol/l) 5.0±0.8 5.0±0.8 NS
HDL (mmol/l) 1.6±0.4 1.6±0.4 NS
Triglycerides 1.5±0.5 1.4±0.6 NS
Systolic BP (mmHg) 128±18 134±20 NS
Diastolic BP (mmHg) 70±10 71±10 NS
eGFR (ml/min/1.73) 85±7 83±9 NS
NDS (-/10)
Median(IQR)
0.4±0.8
0(0-1)
0.4±0.8
0(0-1) NS
NSP (-/38)
Median(IQR)
0.1±0.4
0(0-0)
0.2±0.6
0(0-0) NS
McGill VAS (-/10cm)
Median(IQR)
0.2±1.0
(0(0-0)
0.4±1.4
(0(0-0) NS
NCCA (mBar) 0.5±0.3 0.6±0.3 NS
CNFD (no/mm2) 37.2±5.1 38.2±5.1 NS
CNBD (no/mm2) 92.0±36.2 99.7±40.5 NS
CNFL (mm/mm2) 26.6±3.8 27.8±3.8 NS
IENFD (no/mm) 10.2±3.3 9.1±2.3 NS
CST (˚C) 28.6±2.0 28.0±2.3 NS
WST(˚C) 36.4±2.0 37.2±2.0 NS
VPT (volts) 5.3±4.1 6.9±5.4 NS
SSNCV (m/s) 50.6±4.2 48.4±4.1 NS
SSNAmp (µV) 20.2±8.8 16.0±8.9 NS
PMNCV (m/s) 49.2±3.7 47.7±3.7 NS
PMNAmp (mV) 6.1±2.4 5.6±2.3 NS
417
Key for Table 13.1, 13.2 & 13.3
ACR – Albumin Creatinine Ratio; BMI – Body Mass Index; BP – Blood Pressure; C – Controls;
CNFD – Corneal Nerve Fibre Density; CNBD – Corneal Nerve Branch Density; CNFL – Corneal
Nerve Fibre Length; CST – Cold Sensation Threshold; estimated eGFR – Glomerular Filtration
Rate; HbA1c – Glycated Haemoglobin A1c; HDL – High Density Lipoprotein Cholesterol; IENFD –
Intra Epidermal Nerve Fibre Density; McGill VAS – McGill Visual Analogue Score; NDS –
Neuropathy Disability Score, NSP – Neuropathy Symptom Profile; PMNAmp – Peroneal Motor
Nerve Amplitude; PMNCV – Peroneal Motor Nerve Conduction Velocity; SSNAmp – Sural Nerve
Sensory Nerve Amplitude; SSNCV – Sural Motor Nerve Conduction Velocity; T-CHL – Total
Cholesterol; VPT – Vibration Perception Threshold; WST – Warm Sensation Threshold.
Copyright © 2022 FDOKUMEN




















