Contrast Sensitivity and Vision-Related Quality of Life ...
163
Contrast Sensitivity and Vision-Related Quality of Life Assessment in the Pediatric Low Vision Setting THESIS Presented in Partial Fulfillment of the Requirements for the Degree Master of Science in the Graduate School of The Ohio State University By Gregory Robert Hopkins, II Graduate Program in Vision Science The Ohio State University 2014 Master's Examination Committee: Angela M. Brown, PhD, Adviser Roanne E. Flom, OD Thomas W. Raasch, OD, PhD
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Contrast Sensitivity and Vision-Related Quality of Life ...

Contrast Sensitivity and Vision-Related Quality of Life Assessment
in the Pediatric Low Vision Setting
THESIS
Presented in Partial Fulfillment of the Requirements for the Degree Master of Science in
the Graduate School of The Ohio State University
By
Gregory Robert Hopkins, II
Graduate Program in Vision Science
The Ohio State University
2014
Master's Examination Committee:
Angela M. Brown, PhD, Adviser
Roanne E. Flom, OD
Thomas W. Raasch, OD, PhD

Copyright by
Gregory Robert Hopkins, II
2014

ii
Abstract
A new test of contrast sensitivity (CS), the Stripe Card Contrast
Sensitivity (SCCS) test, could serve as a simple and efficient means for estimating the
maximum contrast sensitivity value of a given patient without having to use multiple
spatial frequency gratings, and without knowing the spatial frequency at which maximum
sensitivity occurs. This test could be useful for a wide range of patients with various
levels of visual acuity (VA), ages, and diagnoses.
We measured VA [Bailey-Lovie (BL), Teller Acuity Cards (TAC)] and CS [Pelli-
Robson (PR), SCCS, Berkeley Discs (BD)] in counterbalanced order with subjects at the
Ohio State School for the Blind (OSSB). Thus, we tested VA and CS using letter charts
(B-L, P-R), grating cards (TAC, SCCS) and a chart with shapes (BD).
Vision-related quality of life (QoL) surveys [The Impact of Visual Impairment in
Children (IVI_C) and Low Vision Prasad Functional Vision Questionnaire (LVP-FVQ)]
were used following vision testing. Additionally, we obtained Michigan Orientation &
Mobility (O&M) Severity Rating Scale (OMSRS) severity of need scores for some
participants.
Testing was performed over a two-year period for 51 participants at OSSB. We
have organized our work into three experiments: Experiment I was performed in the
2012-13 school year and included 27 participants who were tested monocularly using the

iii
patient’s preferred eye. The following year, we returned for repeat testing of 11
participants from the first year (“Experiment IIa”) and additional testing of 24 new
participants (“Experiment IIb”). Those assessments were performed on each eye
monocularly (where possible) rather than just with the preferred eye. QoL and O&M
results were obtained during both years of testing and are detailed in Experiment III.
Vision tests on the better eyes correlated positively and significantly with one
another, except for a non-significant correlation between the B-L and SCCS. The IVI_C
correlated significantly with all vision tests, except B-L acuity, with better visual function
always correlating with higher quality of life. The LVP-FVQ correlated significantly with
all metrics employed. The OMSRS scores did not correlate significantly with any of our
metrics, except the LVP-FVQ, probably because so few subjects provided data for the
OMSRS.
Both of the grating tests (SCCS and TAC) and the BD indicated better visual
performance than the corresponding letter acuity and contrast charts for subjects with
reduced vision. For measuring contrast sensitivity in those with reduced vision, the
simpler task and bolder patterns of the SCCS and BD may make them more likely to
reveal the maximum performance that a given patient can achieve.

iv
Dedication
This document is dedicated to Katya, my wife,
and our two daughters: Adelaide and Matilda.

v
Acknowledgements
Angela Brown has been a brilliant and gentle mentor to me throughout this
process and I have been fortunate to have had the opportunity to develop a deeper
understanding of vision science as a result of her attention and support.
I am truly fortunate to join a lineage of recognized field leaders by training with
Dr. Roanne Flom. It has been a privilege to have the opportunity to discuss low vision
history, practice, and research with Dr. Thomas Raasch.
I must thank the teachers and staff at The Ohio State School for the Blind,
particularly Nurse Judith Babka, Principals Marcom and Miller, and orientation &
mobility instructors Phil Northup and Mary Swartwout.
I’d also like to acknowledge Ian L. Bailey, OD, DSc(hc), FCOptom, FAAO,
professor at the University of California, Berkeley School of Optometry for providing the
spark from which this work was lit.
Finally, I’d like to acknowledge the substantial contributions Bradley E.
Dougherty, OD, PhD has made towards the analysis of the patient-reported outcome and
quality of life measures in my study. I would also like to thank him for the overall role he
has played in development of my career from a third year optometry student up through
post-graduate advanced practice fellowship work.

vi
Vita
June 2002 .......................................................Moeller High School
2006................................................................Biology, The Ohio State University
2010................................................................O.D., The Ohio State University
2012 to present ..............................................Advanced Practice Fellow in Low Vision
Rehabilitation, College of Optometry,
The Ohio State University
Publications
Hopkins, G.R., & Flom, R.E. (2013, October). Disability Determination: More Within
Our Means Now Than Ever. Poster presented at the annual meeting of the
American Academy of Optometry, Seattle, WA.
Hopkins, G.R., & Brown, A.M. (2013, May). Contrast Sensitivity Measurement in the
Pediatric Low Vision Setting. Poster presented at the annual meeting of
Association for Research in Vision and Ophthalmology, Seattle, WA.
Fields of Study
Major Field: Vision Science

vii
Table of Contents
Abstract ............................................................................................................................... ii
Dedication .......................................................................................................................... iv
Acknowledgements ............................................................................................................. v
Vita ..................................................................................................................................... vi
List of Tables ..................................................................................................................... xi
List of Figures ................................................................................................................... xii
List of Frequently Used Abbreviations ............................................................................. xv
Introduction ......................................................................................................................... 1
Purpose ............................................................................................................................ 1
Visual Acuity Measurement ........................................................................................... 2
Significance of Acuity Measurement .......................................................................... 2
Development of Acuity Measurement ........................................................................ 2
Grating Acuity Measurement. ..................................................................................... 7
Contrast Sensitivity Measurement ................................................................................ 10
Definition .................................................................................................................. 10

viii
Development of Contrast Sensitivity Testing ........................................................... 11
Techniques for Contrast Sensitivity Measurement ................................................... 15
Significance of Contrast Sensitivity Measurement ................................................... 22
Vision-Related Quality of Life Assessment ................................................................. 23
The IVI_C ................................................................................................................. 25
The LVP-FVQ .......................................................................................................... 26
Orientation and Mobility Assessment ........................................................................... 27
The Michigan Orientation and Mobility Severity Rating Scale ............................... 28
Experiment Overview. .................................................................................................. 29
Ethics............................................................................................................................. 31
Recruitment ................................................................................................................... 31
Participant Characteristics ............................................................................................ 33
Objectives ..................................................................................................................... 37
Experiment I...................................................................................................................... 38
Study Design ................................................................................................................. 38
Study Methods .............................................................................................................. 38
Letter Acuity Procedure ............................................................................................ 39
Grating Acuity Procedure ......................................................................................... 39
Letter Contrast Procedure ......................................................................................... 40

ix
Stripe Card Contrast Sensitivity Test ........................................................................ 41
The Berkeley Discs of Contrast Sensitivity .............................................................. 42
Results for Experiment I ............................................................................................... 42
Discussion for Experiment I ......................................................................................... 58
Experiment II – Separate Eye Testing .............................................................................. 60
Introduction to Experiment II ....................................................................................... 60
Methods for Experiment II............................................................................................ 60
Results for Experiment IIa: Repeat Testing .................................................................. 61
Repeatability between Experiments I and IIa ........................................................... 71
Results for Experiment IIb: New Subjects.................................................................... 73
Discussion for Experiment II ........................................................................................ 83
Experiment III – Quality of Life and Orientation and Mobility ....................................... 89
Vision-Related Quality of Life ..................................................................................... 89
Orientation and Mobility............................................................................................. 100
Discussion for Experiment III ..................................................................................... 108
Vision-Related Quality of Life ............................................................................... 108
Orientation and Mobility......................................................................................... 114
General Discussion ......................................................................................................... 116
Test Results ................................................................................................................. 116

x
Other Considerations .................................................................................................. 117
Stated Objectives ........................................................................................................ 118
References ....................................................................................................................... 122
Appendix A: Study Materials ......................................................................................... 129

xi
List of Tables
Table 1. Complete Participant List ................................................................................... 35
Table 2. Experiment I Participants.................................................................................... 43
Table 3. Experiment I Summary Test Results .................................................................. 44
Table 4. Experiment IIa Participants ................................................................................ 62
Table 5. Experiment IIa Summary Test Results ............................................................... 63
Table 6. Experiment IIa Repeatability Statistics ............................................................... 73
Table 7. Experiment IIb Participants ................................................................................ 74
Table 8. Experiment IIb Summary Results ....................................................................... 75
Table 9. Experiment I & II Better Eye Only ..................................................................... 84
Table 10. Experiment II Summary Results ....................................................................... 85
Table 11: Test Chart Correlations ..................................................................................... 88
Table 12. QoL and O&M Correlations ........................................................................... 107

xii
List of Figures
Figure 1: The original Snellen and Sloan Charts ................................................................ 4
Figure 2. Bailey-Lovie Chart .............................................................................................. 6
Figure 3. ETDRS LogMAR Chart ...................................................................................... 7
Figure 4. Teller Acuity Cards ........................................................................................... 10
Figure 5. Campbell-Robson CSF Chart ............................................................................ 13
Figure 6. Pelli-Robson Chart ............................................................................................ 18
Figure 7. The Stripe Card Contrast Sensitivity ................................................................. 21
Figure 8. The Berkeley Discs of Contrast Sensitivity ...................................................... 22
Figure 9. All OSSB Student Visual Acuities by Chart Report ......................................... 33
Figure 10. Participant Diagnoses ...................................................................................... 34
Figure 11. Experiment I Summary Plot Statistics ............................................................. 45
Figure 12. Experiment I B-L vs Chart Report .................................................................. 47
Figure 13. Experiment I Lettered Chart Results by Diagnosis ......................................... 48
Figure 14. Experiment I Striped Chart Results by Diagnosis ........................................... 49
Figure 15. Experiment I Shaped Chart Results by Diagnosis ........................................... 50
Figure 16. : Experiment I Acuity Results ......................................................................... 51
Figure 17. Experiment I P-R & SCCS Results ................................................................. 53
Figure 18. Experiment I P-R & SCCS Bins ...................................................................... 54

xiii
Figure 19. Experiment I P-R & BD Results ..................................................................... 55
Figure 20. Experiment I P-R & BD Bins .......................................................................... 56
Figure 21. Experiment I SCCS & BD Results .................................................................. 57
Figure 22. Experiment I SCCS & BD Bins ...................................................................... 58
Figure 23. Experiment IIa Summary Plot Statistics.......................................................... 64
Figure 24. Experiment IIa Acuity Results ........................................................................ 65
Figure 25. Experiment IIa P-R & SCCS Results .............................................................. 66
Figure 26. Experiment IIa P-R & SCCS Bins................................................................... 67
Figure 27. Experiment IIa SCCS & BD Results ............................................................... 68
Figure 28. Experiment IIa P-R & BD Bins ....................................................................... 69
Figure 29. Experiment IIa SCCS & BD Results ............................................................... 70
Figure 30. Experiment IIa SCCS & BD Bins ................................................................... 71
Figure 31. Experiment IIa Lettered Chart Test-Retest ...................................................... 72
Figure 32. Experiment IIa Striped Chart Test-Retest ....................................................... 72
Figure 33. Experiment IIa Shaped Chart Test-Retest ....................................................... 73
Figure 34. Experiment IIb Summary Plot Statistics ......................................................... 76
Figure 35. Experiment IIb Acuity Results ........................................................................ 77
Figure 36. Experiment IIb P-R & SCCS Results .............................................................. 78
Figure 37. Experiment IIb P-R & SCCS Bins .................................................................. 79
Figure 38. Experiment IIb P-R & BD Results .................................................................. 80
Figure 39. Experiment IIb P-R & BD Bins....................................................................... 81
Figure 40. Experiment IIb SCCS & BD Results............................................................... 82

xiv
Figure 41. Experiment IIb SCCS & BD Bins ................................................................... 83
Figure 42. Experiment II Summary Plot Statistics ........................................................... 86
Figure 43. IVI_C v B-L Regression .................................................................................. 91
Figure 44. IVI_C vs. P-R Regression ............................................................................... 92
Figure 45. IVI_C vs. TAC Regression.............................................................................. 93
Figure 46. IVI_C vs. SCCS Regression ............................................................................ 94
Figure 47. IVI_C vs. BD Regression ................................................................................ 95
Figure 48. LVP-FVQ vs. B-L Regression ........................................................................ 96
Figure 49. LVP-FVQ vs. P-R Regression ......................................................................... 97
Figure 50. LVP-FVQ vs. TAC Regression ....................................................................... 98
Figure 51. LVP-FVQ vs. SCCS Regression ..................................................................... 99
Figure 52. LVP-FVQ vs. BD Regression ....................................................................... 100
Figure 53. O&M vs. B-L Regression .............................................................................. 101
Figure 54. O&M vs. P-R Regression .............................................................................. 102
Figure 55. O&M vs. TAC Regression ............................................................................ 103
Figure 56. O&M vs. SCCS Regression .......................................................................... 104
Figure 57. O&M vs. BD Regression ............................................................................... 104
Figure 58. Average person scores for the IVI_C (left) and the LVP-FVQ (right) ......... 110
Figure 59. Subject-Item map for the IVI_C .................................................................... 112
Figure 60. Subject-Item map for the LVP-FVQ. ............................................................ 113
Figure 61. Person Score Linear Regression of LVP-FVQ vs. IVI_C ............................. 114
Figure 62. Cutoffs for normal SCCS Performance ......................................................... 120

xv
List of Frequently Used Abbreviations
B-L Bailey-Lovie Chart
BD Berkeley Discs of Contrast Sensitivity
c/deg Cycles per degree
CSF Contrast Sensitivity Function
HM Hand Motion Only
IVI_C Impact of Visual Impairment in Children Survey
LogCS Logarithm of the contrast sensitivity
LogMAR Logarithm of the minimum angle of resolution
LP Light Perception
LVP-FVQ Low Vision Prasad Functional Vision Questionnaire
MAR Minimum Angle of Resolution
NLP No Light Perception
O&M Orientation and Mobility
OMSRS The Michigan Orientation and Mobility Severity Rating Scale
OSSB The Ohio State School for the Blind
P-R Pelli-Robson Chart
QoL Quality of Life (related to vision)
RL Right and Left eye tested individually
SCCS Stripe Card Contrast Sensitivity
TAC Teller Acuity Cards

1
Introduction
Purpose
Measuring the functional ability of patients with ocular disorders is a classic
problem in clinical vision science. While objective assessments are certainly important,
functional visual assessments often yield the most appropriate management strategies for
patients with reduced vision. The intention of this research is to develop and validate
examination methodologies that best represent the functional visual abilities of persons
with reduced vision. This is important because, even when one’s underlying disorder
cannot be treated, care can still be given to maximize one’s success in life. Said another
way, “Even though it may be true that nothing more can be done for the eye, it is almost
never true that nothing more can be done for the patient” (Tandon, 1994). Traditional
methods of visual assessment include visual acuity, contrast sensitivity, color vision, and
visual field testing, among others. Eye care practitioners’ most well recognized
assessment methodology has customarily been visual acuity. However, it has been known
from the early testing days that acuity values do not represent a complete picture of a
given patient’s ocular health let alone his or her visual functioning. My purpose is to
assist in the development of a reliable and easy-to-use test of pediatric contrast
sensitivity. My hope is that by making this test available, we will encourage eye care
practitioners to consider including contrast sensitivity measurement as one component of
the testing that they perform when examining children with visual impairment.

2
Visual Acuity Measurement
Significance of Acuity Measurement. Visual acuity measurement has become an
integral part of eye care ever since the mid 1800s, when it was first introduced. Visual
acuity is usually the first testing procedure performed during any ocular examination.
Generally, visual acuity is a measure of the spatial resolving ability of the human eye,
combined with the visual system’s ability to process images as distinct based upon the
angle that these objects subtend upon the eye. The assessment of visual acuity is useful in
many ways. Some examples include, but are not limited to: monitoring the refractive
status, health and stability of a given patient’s eyes, determining a patient’s legal
blindness status, determining his or her ability to qualify for driving privileges, and
candidacy for cataract extraction (or other medical workup).
Development of Acuity Measurement. In the mid 1800s, early medical
practitioners developed many different methods of acuity measurement in their efforts to
standardize the task (Bennett, 1965). Early normative test results suggested that most
observers have a minimum angle of resolution (MAR) that is only slightly smaller than
one arc minute. Accordingly, practitioners designed eye charts so that the smallest
appreciable detail element would subtend less than one minute of arc from a practicable
test distance so that threshold measurements could be obtained. As will be discussed
further in the next section of this thesis, a ratio between the MAR and the overall size of
the optotype containing this detail element has conventionally been a 1 to 5 ratio.
Considering the smallest letter that a patient can identify, the MAR for his or her visual
acuity is given as the reciprocal of the ratio between the height of that barely identifiable

3
letter and a letter corresponding to one arc minute. This proportion is variously expressed
by its logarithm (logMAR) or, with numerator and denominator multiplied by 20 feet or 6
meters (as a “Snellen fraction”).
Detection, Localization, Resolution, Recognition or Identification Acuity. There
are various ways to go about discovering whether an observer can perceive fine detail.
One approach is to determine the smallest object that a given observer can detect against
a uniform background (detection task). A variation on this method is to force an observer
to choose whether or not a small object is present in one defined area versus a blank
space (localization task). Two alternative forced-choice experiments are often designed
with either two spatial or two temporal intervals, with the stimulus being presented in one
of those intervals. Another method is to use closely spaced lines or dots as visual stimuli,
and then describe the test distance at which they can be resolved as spatially distinct
(resolution task). If, instead, the acuity task is to describe orientation of an object, then
visual acuity can be measured using a wide variety of stimuli such as shapes, gratings or
letters (recognition task). Alternatively, one could present an array of identifiable
symbols such as shapes, numbers or letters (identification task) (Kramer & Mcdonald,
1986; Owsley, 2003).
The identification acuity approach lends itself very well to clinical practice. A
Dutch ophthalmologist named Hermann Snellen designed the original eye chart shown in
Figure 1 and is responsible for the popularization of unrelated letter identification as the
primary method of visual acuity measurement. The use of high-contrast capital letters as
optotypes was Snellen’s key innovation. It allowed for the rapid proliferation of visual

4
acuity measurement as a technique used by medical practitioners. For a patient stated to
have exactly “20/20” visual acuity using Snellen’s notation system, the smallest letter
identifiable by this patient will subtend 5 minutes of arc. The minimum angle of
resolution of a letter at threshold size is assumed to have a 1:5 ratio of the letter height, so
their MAR is one arc minute. Eye charts with various letter fonts were developed over the
years and many of them assumed the MAR to be 1/5th the letter height—even if the
stroke widths of those letters were not uniform. Subsequently, Louise Sloan developed a
letter series with roughly equal legibility and a 5 x 5 stroke width aspect ratio to solve the
problem of inconsistent typefaces. Sloan also advocated for equally spaced optotype
arrays that scaled geometrically (Sloan, 1959).
Figure 1: The original Snellen and Sloan Charts
Left, the original Snellen chart (from www.Precision-Vision.com);
Right, Sloan’s distance acuity charts (from Sloan, 1959)

5
Bailey-Lovie Acuity Chart. Ian Bailey and Jan Lovie developed the Bailey-Lovie
Acuity Chart to better assess the participants in their studies of Australian visual acuity
and contrast sensitivity in the 1970s. They designed their acuity charts following a letter
size progression based on steps equal to 0.10 LogMAR. This design feature allows for the
chart to be used with uniformity at any practicable test distance in order to best capture a
given observer’s threshold acuity value. Many of the design concepts they introduced
were incorporated in to subsequent acuity chart designs such as: approximately equally
legible optotypes, an equal number of letters on every row, uniform letter and row
spacing, a logarithmic size progression that covers a wide range of human vision, and the
use letter-by-letter LogMAR scoring (Bailey & Lovie, 1976).
The chart we used in the present study (see Figure 2) has seventy 5x4 sans serif
British standard letters total, with five letters per row. The LogMAR scores along the
right hand column of the chart are based on a standard testing distance of 6 meters, but
the actual letter sizes (in M units) were included to facilitate testing at any practical
distance. The original Bailey-Lovie chart covered a wide range of letter sizes from 3.2 M
to 63M. Acuity measurements from 6/3 (20/10) through 1/60 (20/12,000) could be
reasonably made with appropriate adjustments in testing distance. The chart we used is
also designed to cover more than a ten-fold range of acuity: from 20/12 through 20/250
when viewed from 10 feet away.

6
Figure 2. Bailey-Lovie Chart
(from Tasman, 1992)
Later Developments in Letter Acuity Measurement. The investigators in the
Early Treatment of Diabetic Retinopathy Study (ETDRS) created a backlit light box chart
to ensure equal illumination of the 5x5 letters from the Sloan series (Ferris, Kassoff,
Bresnick, & Bailey, 1982). Their chart, shown in Figure 3 below, is the current “gold
standard” for clinical research. Future developments in visual acuity testing will likely
include a move towards computerized methodologies, which will enable examiners to test
with even greater uniformity, precision and efficiency.
Practitioners who select well-designed eye charts benefit in many ways—
including the use of efficient scoring notation. Conversion of Snellen “20/__” or other
notation to LogMAR values allows for statistical analysis of acuity data sets. Acuity
scoring can be performed in a number of ways, but letter-by-letter scoring has been
shown to be the most repeatable (Raasch, Bailey, & Bullimore, 1998).

7
Figure 3. ETDRS LogMAR Chart
(from www.Precision-Vision.com)
Grating Acuity Measurement. Measurement of visual acuity in the classical
way, i.e., via the identification of carefully selected and arranged letters, requires an
observer who is cognitively capable of reading and reporting letters. Other methods have
been developed to measure visual acuity when a patient cannot read numbers or letters, or
even identify a shape or report its orientation. Approaches such as the observation of
optokinetic nystagmus, preferential looking and visual evoked potential are some
examples. These techniques often include stripes or other patterns as a measure of
resolution acuity or cortical response. Examiners have known since at least the 1960s that
the eyes of visual observers are preferentially drawn towards visible patterns versus blank
homogenous areas (Frantz, Ordy, & Udelf, 1962). To provide a measure of resolution
acuity, examiners developed visual stimuli using striped gratings.
Teller Acuity Cards. Davida Teller developed this test with her collaborators in
the mid-1980s for the purpose of rapid estimation of acuity in infants (McDonald et al.,
1985). Prior to this time, testing was done either in a very regimented and time-

8
consuming laboratory setting, or very informally by clinicians using “fix and follow”
penlight testing techniques.
The Teller Acuity test consists of a deck of sixteen 25.5 x 55.5 cm gray cards,
each with a 4 mm round peephole in the middle and a 12 x 12 cm region of vertical black
and-white grating centered on one half. The standard testing distance is 55.5 cm, the
length of one card. The spatial frequency progression of the Teller Cards starts at about
the minimum angle of resolution for a 20/20 optotype. That is, one half of a black/white
grating cycle (one black or white stripe) covers one minute of arc from a given distance.
This pattern is printed onto the first card (see Figure 4). A single stripe is always present
on the edge of each pattern box to minimize potential edge-detection artifacts. The spatial
frequencies shown on subsequent cards are scaled up systematically until many minutes
of arc fit within one black and white grating cycle (Dobson & Teller, 1978). Specifically,
the spatial frequency of the gratings increases by a factor of two (one octave, i.e., one
base-2 log unit) after every other card. Thus, the spatial frequency of each card is higher
than its predecessor by a factor of √2. Additionally, one of the cards is left blank to serve
as a control, and another has wide stripes of 0.23 cycles per cm (0.236 cy/deg, or
20/2,540 at 55.5 cm) covering an entire half to serve as a “low vision card.” By
presenting each of these two cards at least once, the examiner can attune herself or
himself to the particular strong “looking behavior” versus “non-looking behavior” of the
subject under examination
The “grating acuity” of the participant can be estimated by observing the looking
behavior of the participant or by simply asking a capable observer to point. When a card

9
is presented containing stripes so fine as to no longer be resolvable, the participant would
either display non-looking behavior or report that they cannot ascertain whether the
stripes are present on the right or left hand side. If an examiner shows cards in octave
steps until the observer fails to find the grating, the next logical card to display would be
the one whose stripes are ½ an octave wider. The cards progress by doubling the size of a
grating cycle from initially spanning only 2 minutes of arc all the way up to covering 128
minutes of arc. This final card approximates a visual acuity of 0.32 cycles per cm
(20/1,280 at 55.5 cm). This size progression, combined with preferential looking
techniques that were refined in the mid-1980s, allow the examiner to obtain spatial visual
information with good efficiency and validity for less-sophisticated patients (McDonald
et al., 1985).
Even though measurements obtained with Teller cards can be converted into
Snellen notation, “grating acuity” measurements made by this technique are not directly
comparable to optotype identification acuity tasks. Functional visual estimations for a
given task are best performed with measurement styles that most closely relate to the
task. For example, a prudent examiner interested in reading ability would use word or
sentence acuity cards. Conversely, word reading acuity would not be expected to describe
a patient’s orientation and mobility skills. The particular utility of grating acuity may be
that, once baseline measurements have been obtained, they allow for tracking the visual
development for less-sophisticated patients over time.

10
Figure 4. Teller Acuity Cards
(from www.Precision-Vision.com)
Contrast Sensitivity Measurement
Definition. In the context of monochromatic luminance assessments (i.e., not
considering equiluminant color contrast), the term “contrast” is meant to quantify how
the luminance of a given point makes it discrete from the average luminance of the
adjacent area. Spatial contrast sensitivity can be broadly defined as one’s ability to
perceive luminance variations across visual space. Contrast itself is expressed as a
percentage and can be taken from a visual scene in three main ways: as the magnitude of
luminance variation between points in a visual scene and the average luminance of that
scene (root-mean-square contrast), as the difference between the brightest and darkest
parts of a repeating pattern divided by the sum of those extreme luminance values
(Michelson contrast), or as the brightness increment between a small object and its
background divided by the average background luminance (Weber contrast).
Calculation of contrast via the Michelson formula lends itself particularly well to
quantifying the contrast of periodic stimuli (like gratings). In the case of stripes with a

11
50:50 duty cycle, Michelson and Weber contrast values are mathematically equivalent,
and are written formulaically as 𝐶 =𝐼𝑚𝑎𝑥−𝐼𝑚𝑖𝑛
𝐼𝑚𝑎𝑥+𝐼𝑚𝑖𝑛 and 𝐶 =
Δ𝐼
𝐼𝑎𝑣𝑒, respectively. Restating
Weber Contrast components as: ∆𝐼 = 𝐼𝑚𝑎𝑥−𝐼𝑚𝑖𝑛
2 and 𝐼𝑎𝑣𝑒 =
𝐼𝑚𝑎𝑥+𝐼𝑚𝑖𝑛
2 allows for the
following rearrangement: Δ𝐼
𝐼𝑎𝑣𝑒= 𝐶 =
𝐼𝑚𝑎𝑥−𝐼𝑚𝑖𝑛
𝐼𝑚𝑎𝑥+𝐼𝑚𝑖𝑛.
Calculation of contrast for small isolated symbols on a large background is
generally done using Weber’s approach, but this situation is found less-often in real
world settings.
A pattern or scene where all the dark elements emit zero luminance has bright
elements at 100% contrast, and visual stimuli with fainter shades of gray represent
different levels of contrast up to the point where no pattern exists and the scene is entirely
uniform (0% contrast). Clinically, contrast sensitivity values are given in log10 units as an
expression of the reciprocal of the contrast threshold, the lowest percentage contrast that
a patient is able to perceive.
Development of Contrast Sensitivity Testing. The analysis of spatial vision
(i.e., the perception of borders, lines and edges) beyond the single assessment of high
contrast visual acuity has been a topic of close investigation since the 1960s. To perform
this analysis, scientists first needed to understand the optical properties of the human eye.
The modulation transfer function is one method for quantifying the clarity of an optical
system. Physicists in the 1960s were generating sine waves with cathode ray tubes to
measure optical modulation transfer functions for cameras and televisions. Sine waves
make for a convenient testing target because a sinusoidal input will always result in a

12
sinusoidal output through a linear optical system. Physiological optics researchers
modified this modulation transfer approach to measure the modulation transfer function
of the human visual system. Once the optical transfer component of the eye was generally
established, the next step was to determine the neural component of visual processing.
Psychophysicists applied cathode ray display technology to generate sine wave
gratings for contrast detection measurements at different spatial frequencies. It was then
possible to obtain s-shaped psychometric functions, where the probability of sine wave
detection was shown as a function of the contrast value. For example, the threshold value
for contrast detection at a given spatial frequency may be derived from the psychometric
curve. The threshold is the amount of contrast underlying the point on the curve with the
steepest slope. Performing this procedure over various spatial frequencies allows for the
threshold results to be combined so that contrast sensitivity, plotted as a function of
spatial frequency, forms the contrast sensitivity function (CSF). The CSF can be
considered an envelope function made up of spatial frequency tuned channels coexisting
within the visual system. The image in Figure 5 was developed by Campbell and Robson
in order to serve as a demonstration of the CSF (Shapley & Lam, 1993). The image
shows a sine wave of increasing spatial frequency from left to right and decreasing
contrast from bottom to top. Any person observing the image should be able to appreciate
the band-pass shape of his or her own contrast sensitivity function. Scientists, e.g.,
DeValois and DeValois (1988), have shown that the use of a linear model for human
spatial vision is a practicable method. This approach allows investigators to use the CSF

13
to easily predict an observer’s ability to detect other objects or patterns based upon their
size and contrast level.
The use of sine waves as visual stimuli can be traced as far back as the 1800s
when the physicist Ernest Mach designed a spinning cylindrical apparatus with movable
dark strips of paper to produce s-shaped curves along a harmonic progression known as a
Fourier series (Campbell, Howell, & Robson, 1970). Fourier’s work on heat flow in 1822
described how any periodic pattern could be broken down into composite sine waves. His
theorem was readily applied to linear systems analysis in other areas such as acoustics.
However, aside from Mach’s early work, very few references to Fourier analysis being
applied to measuring the visibility of grating stimuli can be found until the 1950s.
Figure 5. Campbell-Robson CSF Chart
(from Izumi Ohzawa)

14
Campbell and Robson understood that a typical visual scene has very few pure
sine waves to behold, so they wanted to know if Fourier analysis would allow examiners
to predict an observer’s contrast threshold for more complex visual targets. Campbell and
Robson began by generalizing from sine waves to square, saw-tooth and rectangular
wave gratings (Campbell & Robson, 1968). Each wave contains a fundamental frequency
and higher harmonic frequencies. For example, a square wave contains a fundamental
frequency (f) and combination of odd harmonic frequencies (f, 3f, 5f, 7f, etc.—much like
the tone of a clarinet). The amplitude also decreases according to the following pattern
for each harmonic: 4/π*((sin(x) + 1/3(sin(3x)) + 1/5(sin(5x)) + …). Continuing with the
square wave as an example, Fourier theory predicts a 4/π higher sensitivity relative to a
pure sine wave. This is because a square wave contains a higher amplitude fundamental
than a sine wave by a factor of a 4/π. Campbell & Robson’s threshold response data
supported this prediction, and they also demonstrated that the square wave was
distinguishable from the sine wave just when the contrast was high enough for the
harmonics to reach threshold. The following year, Blakemore and Campbell
demonstrated that if an observer adapts to a square wave, the observer’s contrast
sensitivity is relatively lowered along his/her CSF only at the frequencies of the square
wave’s fundamental and third harmonic (Blakemore & Campbell, 1969a, 1969b).
Square waves are of particular interest because the detection of straight vertical or
horizontal edges is important in daily visual functioning. Around the 1960s, examiners
were beginning to understand that the neurology of the human visual cortex leaves us
predisposed towards edge detection. Investigation of cat and primate visual cortex cells

15
by Hubel and Wiesel demonstrated the presence of center-surround receptive field
organization in these animal models. This receptor array organization enhances edge
detection by lateral inhibition (Hubel & Wiesel, 1962). An example of this edge-detection
penchant comes from one of Ernest Mach’s early discoveries: the perceptual illusion of
“Mach Bands.” Mach designed a black and white mixing disc that had sectors, similar to
Masson’s spinning discs, but with an area containing a smooth curve of increasing black
shading from the center outwards (Ratliff, 1965). He found that humans seemed to
perceive edges at the smooth white-to-black gradient created by spinning the disc, as if
the sectors had a sharper “step-wise” shading transition.
The concept of lateral inhibition between center-surround ganglion cell receptive
fields is useful in describing the band-pass nature or “inverted U-shape” of the CSF.
Investigators struggled initially to explain this phenomenon because the gradual roll-off
in contrast sensitivity at low spatial frequencies was not as readily anticipated as the high
spatial frequency roll off (which results from optical restrictions and receptor spacing
limitations within the human eye). Once technology had advanced to the point at which
the general shape and underlying properties of the CSF were well known, practitioners
began to apply this knowledge to clinical vision assessment with increasing success.
Techniques for Contrast Sensitivity Measurement. The maximum sensitivity
found on the CSF curve for most observers requires contrast presentations of less than
1%. This fact makes designing and administering tests of contrast sensitivity a challenge.
A French scientist, Pierre Bouguer, made initial attempts at measuring the human contrast
threshold in 1760. Bouguer designed an experiment in which a wooden rod cast a faint

16
shadow from a distant candle onto an illuminated white screen. The further away the
candle was placed, the fainter the shadow, until it faded out of view (Pelli & Bex, 2013).
In 1845, another Frenchman, Antoine Masson, realized that it would be very difficult to
accurately print low contrast targets so he designed black and white mixing discs that
when spun would appear gray. Varying the size of the black sectors allowed for
accurately calibrated contrast assessments. In 1918, George Young attempted to print a
contrast sensitivity testing booklet using ink spots that were precisely diluted from page
to page (Shapley & Lam, 1993).
All of these early tests were attempts at measurement via detection tasks, in which
the observer is to report the faintest detectable stimulus. Such threshold techniques are
useful, but like today’s threshold visual field tests, this approach can pose clinical
reliability challenges when false positive and false negative responses occur. Localization
(is the target in one spot or another), recognition (which way is the stimulus oriented) and
identification (what optotype was seen) tasks lend themselves much more readily to
clinical assessments. This is one factor that may explain why the visual acuity and
contrast sensitivity measurement tests most frequently used today are letter identification
charts.
As stated above, renewed interest around contrast sensitivity testing arose with the
development of cathode ray tubes in the 1960s. Finally, the technology existed to
generate reliably calibrated stimuli. More clinical tests of contrast sensitivity were
developed at that time than ever before. Early examples include: the Arden Plates, the
Cambridge Low Contrast Grating Test and the Pelli-Robson letter contrast sensitivity test

17
(Arden, 1978; Pelli, Robson, & Wilkins, 1988; Wilkins, Della Sala, Somazzi, & Nimmo-
Smith, 1988).
Pelli-Robson Contrast Chart. Denis Pelli and John Robson developed this chart
in the 1980s in order to provide a simple and reliable clinical test of contrast sensitivity
that could be adopted by practitioners in order to estimate the maximum contrast
sensitivity of a patient (Pelli et al., 1988). Prior to the development of this chart, time-
intensive measurement of the complete contrast sensitivity curve using computer-
generated sine waves was the standard practice in laboratory studies. Pelli and Robson
designed their 60 x 85 cm chart with forty-eight Sloan letters arranged in triads of
decreasing contrast value (see Figure 6). The letter triads advance in steps of 0.15 log
units from approximately 100% to 0.56% contrast (LogCS 0.00 to 2.25). All the ten letter
options are contained within the first three rows and all letters are of equal in size
throughout the chart—subtending 2.8 degrees (20/672) from the recommended 1 meter
test difference. When viewed from 1 meter, these letters are well above the acuity
threshold of most patients. If the chart were held 3 meters from a subject, the spatial
frequency of the letters would fall within the range of a normal observer’s contrast
sensitivity maximum. Testing at a closer distance ensures that results are not obtained for
spatial frequencies that would correspond to the high spatial frequency roll-off region of
an observer’s contrast sensitivity curve.

18
Figure 6. Pelli-Robson Chart
(from www.Precision-Vision.com)
Further Developments of Contrast Sensitivity Testing. Following the
development of the Pelli-Robson chart, others were designed such as: the Rabin letter
contrast sensitivity test, the Vistech Chart, the Melbourne Edge Test, and the Mars letter
contrast sensitivity test (Arditi, 2005; Eperjesi, Wolffsohn, Bowden, Napper, &
Rubinstein, 2004; Haymes et al., 2006; Rabin & Wicks, 1996; Reeves, Wood, & Hill,
1991; Wolffsohn, Eperjesi, & Napper, 2005).
For the pediatric population, there are the Hiding Heidi test and the Lea Contrast
Sensitivity booklet among others (Susan J Leat & Wegmann, 2004). A sample of novel
tests currently under development include the Stripe Card Contrast Sensitivity, the
Berkeley Discs, the PL-CS Test, the Grating Contrast Sensitivity Test, the iPad Contrast
Sensitivity Test, and the qCSF (Bailey, Chu, Jackson, Minto, & Greer, 2011; Bittner,

19
Jeter, & Dagnelie, 2011; Dorr, Lesmes, Lu, & Bex, 2013; Kollbaum, 2014; Pokusa, Kran,
& Mayer, 2013).
Stripe Card Contrast Sensitivity Test. Angela Brown, Delwin Lindsey, and I are
in the process of refining the design for this novel test of contrast sensitivity. We expect
to fill the need for reliable contrast sensitivity testing of non-verbal or otherwise
developmentally delayed patients with this test. The Stripe Card Contrast Sensitivity test
(SCCS) is similar in many respects to the Teller Acuity cards. The prototype version we
used consists of a deck of 15 gray cards sized 55.5 x 25.5 cm with one side containing a
22 x 20 cm box of horizontal stripes that start 6 cm from the central peephole and extend
to the edge of the card at a fixed spatial frequency of 1 cycle per 6.8 cm (0.15 c/deg or
20/4,000 grating acuity from 57 cm). Contrast values for the stripes decrease in 0.15 log10
unit steps from approximately 100% to 1% contrast. This progression of ½ octave steps is
similar to the Pelli-Robson chart—i.e., contrast level differs by a factor of two for every-
other letter triad on the Pelli-Robson card and for every other card on the SCCS test.
Figure 7 demonstrates two typical cards from the deck: one at full contrast and one at
about 30% contrast. In the center of the card is a peephole through which the examiner
can observe the patient’s looking behavior. The peephole is especially useful if the
patient cannot point their fingers or speak. In this case, the examiner can show the cards
to the patient with the stripes on one end, and then flipped to the other. The patient’s eyes
should be drawn to one direction for the first presentation and then reliably to the
opposite direction when presented with the opportunity for a second look. If the contrast
is high enough so that the patient can see the stripes, then his or her eyes will first be

20
drawn towards the pattern when it is presented, and then again in the other way after the
pattern has been flipped.
Similar to the Pelli-Robson test, the SCCS test does not set out to completely map
the contrast sensitivity function of a given subject. Laboratory studies that obtain
threshold values using sine waves of different spatial frequencies are the classical way to
obtain the true peak of the contrast sensitivity function (CSF), e.g., Adams’ tests for
infants and children (Adams & Courage, 2003). However, these methods are time
intensive and currently impractical for clinical application (Lennie & Hemel, 2002).
Unlike the Pelli-Robson test, the SCCS does not attempt to test with optotypes sized at
the assumed normal peak of the CSF, which lies between 3-5 c/deg. Rather, the SCCS
takes advantage of the spatial harmonic properties of square waves, which activate cells
of the human visual cortex even when the fundamental frequency is below that of the cell
(Blakemore & Campbell, 1969a, 1969b; Campbell et al., 1970; Campbell & Robson,
1968). In this way, the SCCS can test at 0.15 c/deg to be sure to avoid the steep higher
spatial frequency roll-off portion of the CSF curve, which would otherwise cause the
examiner to significantly underestimate the threshold maximum. When testing is
performed with square waves at a spatial frequency that would ordinarily be in the
gradual low spatial frequency roll-off section of the CSF, higher harmonics present in the
stimulus prevent the drop in sensitivity that would be seen in that region otherwise. This
is because at low spatial frequencies, detection is mediated by the higher harmonics and
not the fundamental frequency as would be the case in higher spatial frequencies
(Campbell et al., 1970). Measuring in the low spatial frequency region with square waves

21
means that our readings will be independent of spatial frequency and scale with the
maximum contrast sensitivity of which the subject is capable. For a channel of fixed
bandwidth, the amount of harmonic energy within that bandwidth will be constant for the
square wave no matter what its spatial frequency is (as long as the fundamental frequency
is low enough).
Figure 7. The Stripe Card Contrast Sensitivity
The Berkeley Discs of Contrast Sensitivity. Professor Ian Bailey is in the process
of refining the design for this novel test of pediatric contrast sensitivity (pictured in
Figure 8 below). The test consists of three double-sided plastic cards, with each side
containing discs of 5 cm in diameter randomly positioned within a 7.5 cm six-cell grid.
Ian Bailey has presented some of his work on this chart alongside the newly released
Berkeley Rudimentary Vision Test at the Association for Research in Vision and
Ophthalmology (“ARVO”) conference in 2011. Testing was performed with this chart on
54 subjects from the California School for the Blind, The Orientation Center for the
Blind, and the San Francisco Lighthouse. Bailey et al. found that when contrast
sensitivity was poor, generally better scores were obtained with the Berkeley Discs than

22
with the Mars chart, presumably because of the larger target size and simpler task (Bailey
et al., 2011). Measurements from 0.00 (100%) log contrast sensitivity down to 1.95
(1.1%) are possible to the nearest 0.15 log unit. The three discs printed on a given card
face are separated by 0.60 log unit (4x or two-octave) steps starting from full-contrast,
with the in-between values shifted by a 0.30 log unit (2x or one-octave) step on the
reverse side. The discs on the second card are shifted 0.15 log units towards lower
contrast from those on the first card. Printing in this manner allows for a clinician to
move immediately from a card face on which a patient failed to detect a disc directly to
the corresponding front or back card face of the second card to measure to the nearest
0.15 log unit. The first two cards cover a range of log contrast sensitivity values from
0.00 (100%) to 1.65 (2.2%).
Figure 8. The Berkeley Discs of Contrast Sensitivity
Significance of Contrast Sensitivity Measurement. Contrast sensitivity
assessments can reveal hidden losses of visual function not captured by visual acuity
testing. Diseases such as age-related macular degeneration, diabetes and glaucoma can
cause vision losses that acuity measurements may fail to reveal. Visual impairment from

23
contrast sensitivity arises when LogCS values of less than 1.50 are obtained and visual
disability is classified as LogCS less than 1.05 (Susan J Leat, Legge, & Bullimore, 1999).
From work performed by Marron in the 1980’s, it turns out that contrast sensitivity has
been shown to be better correlated than acuity with orientation and mobility in patients
with reduced vision (Marron & Bailey, 1982). Contrast sensitivity measurements are
useful for a number of clinical purposes from post-surgical outcome monitoring and
disease progression to patient-centered outcomes such as: reading, visual task
performance, orientation and mobility, driving ability, facial recognition, and vision-
related quality of life (Arden, 1978; Bochsler, Legge, Kallie, & Gage, 2012; Ginsburg,
2003; Lovie-Kitchin, Bevan, & Hein, 2001; Owsley & Sloane, 1987; Owsley, 2003).
Vision-Related Quality of Life Assessment
Medical examiners classify visual disorders along a continuum where pathology
just “outside normal anatomical limits” worsens until an impairment of visual function
arises. Increasing levels of visual impairment can cause visual disability or even total
handicapping of the individual’s ability to complete the complex visual tasks required for
daily living (The World Health Organization, 1980). Aside from the magnitude of visual
loss, the activity level and visual goals of a person modify the effect size resultant from
vision loss along this continuum. Directly asking patients questions regarding their
perceived “functional reserve” for common visual tasks is a popular method for
measuring the impact of vision loss on quality of life. Functional reserve can be defined
as the difference between a person’s ability and the ability required to perform a given
task (Kirby & Basmajian, 1984). A typical approach for this method is to provide

24
examples of specific tasks, and then ask patients how difficult they perceive each task
would be for them to complete.
One confounding aspect for the questionnaire approach lies in the “latent factors”
related to a person’s visual functioning. As will be explained further in this section, latent
factors cannot be directly observed, but only inferred. For most complex tasks performed
in daily life, there is no obviously “correct” response to concretely quantify the amount of
visual difficulty associated with that task. Therefore, the difficulty of a specific visual
task must be obtained using psychometric approaches and statistical models. While direct
measurement isn’t possible, it is possible for the items to be arranged by order of relative
difficulty for a set of survey respondents.
The other side of the questionnaire approach is the person responding to the
questionnaire, and no two people are exactly alike. Each person has a different functional
reserve available to him or her for a given task. The latent ability of a given patient
cannot be directly measured either, but sorting by perceived ability level based upon
responses to a set of survey items is possible (Massof, 2002).
Georg Rasch, a Danish mathematician, developed a set of latent variable
measurement models in the 1960s for research in educational test development (Rasch,
1960). It has since been applied in the healthcare setting. The basic premise is that the
probability of selecting a given response is equal to the difference between the ability of
the person taking the survey and the difficulty of (or ability required for) a given test
item. Relative item difficulty and person ability levels should follow a normal
distribution in most cases. The probability of obtaining a score on the extreme ends of a

25
normal curve is much lower, so logits (logarithmic odds ratios between subject ability
and survey difficulty) are used to allow for the scores to scale evenly. If a person’s
overall logit score is positive, then they perceive their ability to be relatively higher than
the average ability required across all survey items. Total quality of life scoring and
standard error values are based on the results from the performance of all subjects on the
entire questionnaire.
A well-designed survey will effectively stratify the participants’ relative ability
levels and item difficulty levels (evidenced statistically by good separation indexes) so
that differences between respondents can be measured. It is also expected that a
histogram distribution of person ability will align well with the corresponding item
difficulty histogram for a survey. This kind of comparison is generally performed on a
“subject-item map.” Each item on the survey is checked for “fit statistics” to ensure that
all questions are valid. The items analyzed together in a questionnaire should all target
the same latent trait—perception of one’s visual ability, in this case—otherwise the
measurements cannot be considered together (Massof, 1998).
The IVI_C. Researchers developed the Impact of Visual Impairment on Children
(IVI_C) questionnaire in 2008 by working with focus groups in four Australian states
(Cochrane, Lamoureux, & Keeffe, 2008). The original survey had 30 questions. The
authors used Rasch analysis in 2011 to check the quality of the survey and found it to be
psychometrically valid for use on children with visual impairment from age 8 to 18
(Cochrane, Marella, Keeffe, & Lamoureux, 2011). The Rasch-modified survey lists 24
questions with five answer choices: “always,” “almost always,” “sometimes,” “almost

26
never,” and “never”. An additional answer choice of “no, for other reasons” allows
patients to describe an item that they cannot answer for non-visual reasons. One of the
defining features of the IVI_C is that it uses positive phrasing for the majority of the
survey questions. Many of the questions follow a pattern similar to: “how confident are
you about…” instead of “how difficult is it for you to…” Six of the questions are
negatively phrased and spaced within the survey to prevent a response bias. Naturally, the
responses to these six negative questions are reverse scored. The survey includes
questions regarding social aspects of a child’s school experience in addition to questions
pertaining to vision/mobility. The IVI_C has been applied outside of Australia and found
to have good transferability. The survey does have a slight bias towards the assessment of
students with lower ability levels and is therefore susceptible to a ceiling effect when
applied elsewhere (Cochrane et al., 2011).
The LVP-FVQ. Vijaya Gothwal collaborated in 2003 with Jan Lovie-Kitchen
and Rishita Nutheti to develop the Low Vision Prasad Functional Vision Questionnaire
(LVP-FVQ) (Gothwal, Lovie-Kitchin, & Nutheti, 2003). The work was performed in
Hyderabad, India, and the survey was developed for research on eye care service-delivery
models in rural South India. Rasch analysis was employed from the beginning of survey
development. The final nineteen-item questionnaire contains four functional vision
domains: 1) distance vision, 2) near vision, 3) color vision and 4) visual field extent. The
survey was designed to assess practical problems resultant from pediatric vision loss in
developing countries. Unlike some other QoL surveys, it does not include items
pertaining to social or emotional experiences (DeCarlo, McGwin, Bixler, Wallander, &

27
Owsley, 2012). All questions are phrased according to an estimated amount of difficulty
for a given complex visual task. The response options are: “no difficulty,” “a little
difficulty,” “a moderate amount of difficulty,” “a great deal of difficulty,” and “unable to
do.” An additional response option of “not applicable” was also included. The LVP-FVQ
survey concludes with a final question that differs from the nineteen preceding questions:
“How do you think your vision is compared with that of your normal-sighted friends? Do
you think your vision is As good as your friend’s A little bit worse than your friend’s
Much worse than your friend’s?” This question was designed to assess a patient’s overall
rating of their vision to see if the personal ability levels measured via Rasch analysis
would match up to this gold standard using a receiver operating characteristic curve.
The LVP-FVQ was revised recently and now includes twenty-three questions, six
of which were retained from the original survey, and two survey questions that are
actually derived from the IVI_C. The new survey still includes the final global rating of
visual impairment question (relative to normally-sighted friends) and now incorporates
that question into the Rasch analysis. An attempt was made to introduce mobility and
orientation specific questions into the new version of the survey, but Rasch analysis
revealed that doing so would affect the one dimensional nature of the survey and
adversely affect the measurement validity (Gothwal & Sumalini, 2012).
Orientation and Mobility Assessment
The orientation and mobility training techniques that exist today were developed
as a result of the demand generated for these services by the significant number of
traumatically blinded veterans returning from World War II. The Academy for

28
Certification of Vision Rehabilitation and Education Professionals has provided
accreditation for orientation and mobility (O&M) specialists for over thirty years. O&M
instructors teach individuals with reduced vision how to gain the capacity for confident
spatial awareness and safe travel.
Many people have investigated the correlation between reduced vision and
orientation and mobility (Black et al., 1997; Geruschat, Turano, & Stahl, 1998; Goodrich
& Ludt, 2003; Kuyk, Elliot, & Fuhr, 1998; Long, Rieser, & Hill, 1990). Sheila West and
her colleagues included mobility as a primary outcome measure in their Salisbury Eye
Evaluation (SEE) Project, which they performed to determine the association between
visual impairment and everyday task performance (West, Rubin, Broman, & Mun, 2002).
They determined the level of contrast sensitivity reduction that resulted in more than 50%
of their study population to perform various tasks at 1 standard deviation below the
population mean. They found that a LogCS of 1.35 or worse affected reading speed and
facial recognition. Additionally, West et al. stated that a LogCS of 0.90 or worse had a
measurable impact on mobility. Different cutoff points for different tasks were
anticipated because the level of visual demand for a given task varies. The ability to
detect low spatial frequencies in one’s environment is important for navigation.
Preferential looking tasks such as the SCCS and others are able to measure this ability.
For this reason, we will include orientation and mobility assessments in this research
(Susan J Leat & Wegmann, 2004).
The Michigan Orientation and Mobility Severity Rating Scale. The current
version of The Michigan Orientation and Mobility Severity Rating Scale (OMSRS) was

29
completed in 2008 by a task force of the Michigan Department of Education Low
Incidence Outreach. Instructors use the OMSRS to approximate the amount of time that a
student with visual impairment may require for orientation and mobility training.
Educators find this information is valuable when formulating individualized education
plans for their students.
The OMSRS consists of eight categories: 1) Medical level of vision [central and
peripheral], 2) Functional level of vision, 3) Use/proficiency of travel tools, 4)
Discrepancy in travel skills between present and projected levels, 5) Independence in
travel in current/familiar environments, 6) Spatial/environmental conceptual
understanding, 7) Complexity or introduction of new environment, and 8) Opportunities
for use of skills outside of school. Each of these categories are scored on a scale of 1-5
using a rubric where a higher score indicates greater severity of need and more time
devoted to O&M training. The OMSRS also lists several contributing factors that may be
used to adjust the scores given for the categories above (see Appendix A).
Experiment Overview.
Our approach to aid in the care of children and others who struggle with lettered
eye charts is to design a new test of contrast sensitivity that complements testing
performed with Teller Acuity Cards. Our research was geared towards ensuring that the
results from the new test are applicable and valid. We also aim to discover how well
these results align with vision-related quality of life as reported on survey questionnaires
designed specifically for children with visual impairments.

30
To validate the Stripe Card Contrast Sensitivity (SCCS), we tested a group of
students at The Ohio State School for the Blind (OSSB). Lettered charts used were the
Bailey-Lovie and Pelli-Robson (B-L, P-R) charts. Non-lettered charts included: The
Teller Acuity Cards (TAC), SCCS, and Berkeley Discs of Contrast Sensitivity (BD). A
good outcome would be if the SCCS test results were positively correlated with the
results from the other contrast tests, and if the TAC test results correlated with the other
visual acuity test results. It would also be good if the various vision tests positively
correlated with the measures of QoL and O&M. The details of the relationships between
the various tests might indicate which tests are better for different patients.
We related the results found with these eye charts to self reports of participant
vision-related quality of life (QoL) using two questionnaires: The Impact of Visual
Impairment in Children (IVI_C) and The Low Vision Prasad Functional Vision
Questionnaire (LVP-FVQ). Additionally, we obtained O&M scores for a subset of
participants evaluated by their instructors for relation back to the eye chart test results.
The rubric used by these instructors was The Michigan Orientation and Mobility Severity
Rating Scale (OMSRS) and it can be found in the Appendix.
Research performed in the 2012-13 school year included 27 participants who
were tested monocularly using the patient’s preferred eye. We will refer to the results of
these measurements as “Experiment I” below. Ocular dominance testing was performed
using an eye sighting technique if the patient was unable to report a preferred eye. We
initially chose the dominant eye for three reasons: 1) functional vision is generally driven
by the preferred eye, 2) if performance is not driven exclusively by the better eye, then

31
using a monocular condition should remove any ambiguity regarding the relative
contribution of each eye, and 3) testing only one eye streamlines the examination process.
The following year, we returned for repeat testing of 11 participants from the first
year (“Experiment IIa”) and additional testing of 24 new participants (“Experiment
IIb”). In an effort to increase the amount of data collected with our five vision tests,
Experiment II assessments were performed on each eye monocularly (where possible)
rather than just with the preferred eye. When able to test each eye, the study was initiated
using the participant’s right eye first.
We have obtained vision-related quality of life data for all but one subject. We
have also obtained orientation and mobility scores from O&M instructors for about half
of the subjects for whom the data was potentially available. The results of these non-
visual measures fall under Experiment III below.
Ethics
The protocol for the study was approved by the Biomedical Sciences Institutional
Review Board (IRB) of The Ohio State University and followed the tenets of the
Declaration of Helsinki. Full informed consent or parental permission and child assent
were obtained before the start of all experimental work and data collection.
Recruitment
The Ohio State School for the Blind is a publicly funded educational facility for
students with visual handicaps in grade school up through high school. Students range in
age from five to twenty-one years old, with the most common age being fifteen. The
student body at OSSB is about 25% under-represented minority, and about 16% of the

32
students there have other disabilities in addition to vision loss. Around half of the
students spend the entire week at the school. These residential students leave for home by
bus at early dismissal on Friday and then returning on Sunday afternoon. The school does
not operate during the summer, but does run summer camps open to all Ohio students
with visual impairment interested in attending.
OSSB is also a clinical outreach rotation site for fourth year students at the OSU
College of Optometry. The college furnishes an exam room located within the nurse’s
station for our exclusive use. An optometry student practices under the mentorship of a
clinical preceptor (the author) on Wednesday mornings for three months. Copies of the
examination results are kept at the College of Optometry and at OSSB. Approval was
obtained from the university’s IRB for a HIPAA waiver allowing study investigators to
view the eye care and medical records kept by the school to determine which students
may have measurable vision. At the time of our research project, total enrollment at
OSSB was approximately 115 students and the author determined by chart review that
approximately fifty-three (46%) of the students were likely to have sufficient vision for
testing (see Figure 9).

33
Figure 9. All OSSB Student Visual Acuities by Chart Report
Information packets regarding the study opportunity were assembled and sent via
metered mail to the guardians of all fifty-three students with vision recorded as hand
motion or better. Sample contents of these information packets can be found in Appendix
A. Briefly, each packet contained cover letters from the school principal and our study
group, a parental consent and HIPAA form, a response checklist and a self-addressed
envelope for returning signed documents.
Participant Characteristics
Forty-three of our fifty-one participants were students with partial sight, all of
whom were examined at the Ohio State School for the Blind (OSSB). Their ages were 5-
21 years old, thirty-three were males and most (forty-two subjects) were Caucasian race.
5%
44%
5%
22%
23%
UNK
20/###
HM
LP
NLP
Unable

34
Eight participants were students in the annual summer camps put on by OSSB with ages
from 11—18 years. Four of this group were female, and seven were Caucasian race.
As shown in Figure 10, optic nerve disorders characterized the majority of
primary diagnoses in our study sample, at 43% of the total sample. Participants with
retinopathy of prematurity were the next most prevalent, comprising 13% of our sample.
Various other disorders, including congenital cataract, cortical blindness, and genetic
conditions, made up the rest of our study population
Figure 10. Participant Diagnoses

35
Participants for Experiment I Only
ID Age MF Dx Eye(s) O&M
2 8 M Retinopathy of Prematurity OD
4 17 F Optic Nerve Hypoplasia OS
5 12 F Leber's Congenital Amaurosis OS
6 15 F Optic Nerve Hypoplasia OD
8 19 F Optic Atrophy OD
11 15 M High Myopia OD
18 11 F Cone Dystrophy OS X
24 12 F Optic Atrophy OS
34 8 M Congenital Cataract and Aphakia OD X
35 12 M Retinopathy of Prematurity OD
36 18 M Optic Atrophy OS
41 16 M Glaucoma OS X
43* 11 M Microphthalmus OS
46 13 M Cortical Blindness OD
48 15 F Optic Atrophy OD
50 21 M Septo-Optic Dysplasia OS X
Experiment IIa Repeat Participants
1 17 M Optic Nerve Hypoplasia RL X
12 16 M Retinopathy of Prematurity OS X
17 14 F Microphthalmus OS
26 18 M Optic Nerve Hypoplasia RL X
28 12 F Congenital Cataract and Aphakia RL
30 18 F Optic Atrophy RL X
37 18 M Aniridia RL X
45 20 F Optic Atrophy RL X
51 13 M Optic Atrophy RL
52 15 M Optic Atrophy RL
53 16 M Cortical Blindness RL Continued
Table 1. Complete Participant List
* Number 43 was only participant unable to provide Quality of Life Data.

36
Table 1 Continued
Experiment IIb Additional Participants
31 16 M Retinoblastoma OD
54 20 M Retinopathy of Prematurity NA X
55 19 F Leber's Congenital Amaurosis NA X
56 19 M Brain Tumor NA X
57 19 M Optic Nerve Hypoplasia NA X
58 18 F Leber's Congenital Amaurosis RL X
59 20 M Retinopathy of Prematurity NA X
60 18 M Retinopathy of Prematurity RL X
61 13 M Choroideremia RL
62 11 F Blind at age 2 (unexplained) RL
63 10 F Leber's Congenital Amaurosis RL
64 13 M Optic Atrophy OS
65 16 F Marfan's Disease RL
66 17 M High Myopia OD
67 10 M Cortical Blindness OS
68 12 M Aniridia RL
69 14 M Retinopathy of Prematurity RL
70 18 M Retinitis Pigmentosa NA X
71 15 M Best's Disease RL X
72 18 F Glaucoma OS X
73 17 F Optic Atrophy NA X
74 12 M Optic Nerve Hypoplasia NA
75 12 M Retinopathy of Prematurity NA
76 6 M Retinoblastoma NA

37
Objectives
The work underlying this thesis is intended to:
Ascertain whether the Stripe Card Contrast Sensitivity (SCCS) Test is easy to
administer and can be successfully used on a wide variety of participants.
Assess the SCCS test’s capability for validly measuring contrast sensitivity levels
of children with impaired vision.
Ascertain the relationship between SCCS test results and other functional
measurements such as: visual acuity, letter contrast sensitivity, vision-related
quality of life metrics, and orientation and mobility assessments.

38
Experiment I
Study Design
To ascertain the effectiveness and validity of the SCCS Test, assessments needed
to be performed on young patients with reduced vision because this is the intended
clinical population. In order to avoid possible fatigue effects from repeat vision
assessment, a pseudo-randomization scheme was necessary. Accordingly, a five item
balanced Latin square array guided the order of test presentation for each study
encounter. Duration of testing was recorded to the nearest second for each eye on each
chart. Room and chart illumination measurements were taken periodically using an iOS
application (Megaman LuxMeter). Vision-related quality of life assessments followed
vision testing in all cases, and the IVI_C was performed prior to administering the LVP-
FVQ in each case. More will be said about these surveys in another section.
Study Methods
The school nurse (or an aide) escorted eligible subjects to the OSSB examination
room, in which most have previously had routine eye care performed. Two 18 watt/950
lumen compact fluorescent flood lamps positioned just above and behind the subject
provided additional lighting in the range of the recommended 85 cd/m2 onto the front
surface of all the eye charts. An IRB approved verbal assent or consent form was read
aloud to all participants, and their responses were noted. Participants were invited to ask
questions or discontinue participation at any time. No potential subjects declined to

39
participate when read the assent/consent materials and only one participant discontinued
the study (just before beginning the QoL assessment).
Letter Acuity Procedure. When possible, each child in our study was examined
with the same version of a Bailey-Lovie acuity chart. Refraction was not performed prior
to the initiation of vision testing. Participants wore their habitual correction. Visual acuity
assessments were performed with the Bailey-Lovie chart at 2 meters (or closer when
necessary) and scoring was calculated using total number of letters read correctly without
any substitutions. Test distance variations were taken into account so that each letter
represented a value of 0.02 LogMAR. We employed letter-by-letter scoring in our
protocol, as this method has been shown to provide better reliability (Raasch et al., 1998).
We did not permit substitutions, such as accepting the letter “C” for “O,” but we did
remind participants that the list of possible letter choices was restricted to those letters
that could be found on the top three rows. The stopping rule was enforced whenever a
subject could not identify 3/5 of the letters on a given row. While the chart is available at
two different levels of contrast, we used only the high contrast version: Chart #4. The use
of this chart version was purely arbitrary, but we intended to maintain the use of this
version across all eyes tested in the experiment to control for any small amount of
variation that could be the result of employing a different optotype set.
Grating Acuity Procedure. We used a set of Teller Acuity Cards manufactured
in 1991 by Vistech in order to avoid luminance artifacts present in some of the cards
(Teller Acuity Cards II) made by the other major manufacturer, Stereo Optical.
Normative data exist for the Vistech cards, and they incorporate some design

40
modifications from the initial prototype set of Teller Cards (Mayer et al., 1995). Many of
the subjects who participated in our research were able to reliably point towards the
stripes when they saw them. Therefore, the use of a peephole was not necessary, but the
examiner did make assessments of the patient’s looking behavior throughout the
examination. The stopping rule was whenever a patient admitted that they could not see
the stripes or the examiner was convinced that they could not. We did not need to present
an initial blank card for the purpose of calibrating the examiner to the participant’s
looking behavior. In order to screen for potential luminance artifacts, we asked subjects
to explain whether or not it was the actual stripes they saw or if, instead, they were
detecting a “box” of different luminance than the rest of the card. Adjustments in
working distance or card orientation from horizontal to vertical are possible, and a “low
vision” test distance of 38 cm has been outlined in the Teller Acuity Card user guide, but
we did not find it necessary to employ those techniques at any point. We maintained a 55
cm test distance, recording the cy/deg of the last identifiable card by patient report.
Letter Contrast Procedure. We performed calibration testing with a
SpectraScan photometer on a Pelli-Robson chart and employed only this calibrated chart.
Naturally, the purpose of using only the calibrated chart was to control for any variability
that may result due to discrepancies between the nominal contrast and the actual
measured value. Two luminance values were obtained from the center of a given letter
stroke as well as the adjacent white background. These values were averaged separately
and then the contrast percentage was calculated using Michelson’s formula. The log
contrast values on the chart were close to being linearly related to the nominal log

41
contrast values on the chart. However, the contrast levels on the chart were lower than the
nominal ones (perhaps due to gradual fading), so the nominal values underestimate the
subject’s true contrast sensitivity by 0.36 ± 0.15 LogCS on average. I fit a trend line to
the calibration results with the following formula: y = 1.18x + 0.15 so as to generate
corrected P-R values. Here, I will report the nominal values in the tables and figures
below because those are the ones that every clinician will have available for clinical use.
The results obtained on the better eye (or second measurement) of each subject remain
statistically significant. The comparison between the P-R vs. SCCS is significantly
different at the p < .01 level using the calibrated values instead of p < 0.001 for the
nominal P-R values. The difference between the results obtained for the Berkeley Discs
and the calibrated P-R values continue to be not statistically significant.
We generally tested at the recommended distance of 1 meter, only shifting to
closer than 1 meter for a few students with very poor acuity. Scoring was letter-by-letter,
and each optotype counted for 0.05 log units (Dougherty, Flom, & Bullimore, 2005). The
stopping rule was whenever a subject could not get 2/3 of a letter triad correct.
Stripe Card Contrast Sensitivity Test. Calibration was performed on our SCCS
cards in a similar manner as was performed for the Pelli-Robson chart. Our calibrated
contrast values were only slightly lower than the nominal ones, requiring a greater
sensitivity of 0.013 ± 0.03 LogCS. We calibrated our cards prior to initiation of testing
and were able to measure down to 1.65 LogCS during the first year of testing (and down
to 2.00 during the second year of testing when additional cards were produced).

42
Test presentation style and stopping criteria were the same as for Teller cards,
with the preferential looking technique was used to determine a subject’s threshold
contrast sensitivity. We tested at one card length (57 cm) from the subjects and threshold
was determined to be the point at which the subject could no longer find the stripes.
The Berkeley Discs of Contrast Sensitivity. As stated earlier, the first two cards
cover a range of log contrast sensitivity values from 0.00 (100%) to 1.65 (2.2%).
Precision-Vision provided us with calibration readings for the two cards supplied, and we
obtained our own photometry measurements prior to vision testing. An additional third
card was not available for our testing due to production difficulties experienced by the
manufacturer (Precision-Vision). Thus, we could not evaluate performance at log contrast
sensitivity levels of 1.80 (1.6%) or 1.95 (1.1%).
Berkeley discs were presented at 40 cm with a rubberized wand for subjects to use
to point to discs. All card sides were presented even when performance was perfect on
the first card. The design of the cards allows for a clinician to move immediately from a
card face on which a subject failed to detect a disc directly to the corresponding card face
(front or back) of the second card to measure to the nearest 0.15 log unit. However, we
allowed our participants to view both sides of each card even if it were possible to skip
ahead. We did not enforce a stopping rule for the Berkeley Discs since we had only a
two-card set. Most subjects were able to see discs on all card faces, so we presented every
student with the opportunity to view both sides of each card.
Results for Experiment I
Below is a summary table for the results on all students tested in Experiment I.

43
ID Age S Diagnosis Eye B-L
LogMAR
TAC
LogMAR
P-R
LogCS
SCCS
LogCS
BD
LogCS
01 17 M Optic Nerve Hypoplasia OS 1.28 0.50 0.65 1.65 1.65
02 8 M Retinopathy of Prematurity OD 0.62 0.21 1.95 1.65 1.65
04 17 F Optic Nerve Hypoplasia OS 0.48 0.08 2.10 1.65 1.65
05 12 F Leber's Congenital Amaurosis OS 1.42 1.56 1.10 0.60 1.50
06 15 F Optic Nerve Hypoplasia OD 0.74 0.38 2.00 1.65 1.65
08 19 F Optic Atrophy OD 0.88 0.21 1.45 1.65 1.50
11 15 M High Myopia OD 0.94 0.99 1.35 1.65 1.65
12 16 M Retinopathy of Prematurity OS 0.54 0.68 1.80 1.65 1.50
17 14 F Microphthalmus OS 1.40 1.56 0.85 1.20 1.05
18 11 F Cone Dystrophy OS 0.70 0.81 1.40 1.65 1.65
24 12 F Optic Atrophy OS 1.16 0.50 1.65 1.65 1.35
26 18 M Optic Nerve Hypoplasia OS 1.02 0.21 1.80 1.65 1.65
28 12 F Congenital Cataract OD 1.16 0.50 1.65 1.65 1.65
30 18 F Optic Atrophy OS 0.88 0.38 1.00 1.50 1.65
34 8 M Congenital Cataract OD 0.22 0.21 1.65 1.65 1.50
35 12 M Retinopathy of Prematurity OD 0.82 0.68 1.75 1.65 1.65
36 18 M Optic Atrophy OS 1.60 0.81 0.90 1.65 1.65
37 18 M Aniridia OD 0.66 0.68 1.75 1.65 1.65
41 16 M Glaucoma OS 1.96 2.45 0.10 1.20 0.90
43* 11 M Microphthalmus OS — 1.56 — 0.75 0.00
45† 20 F Optic Atrophy OD — 1.11 — 1.35 0.30
46† 13 M Cortical Blindness OD — 0.84 — 1.35 0.75
48 15 F Optic Atrophy OD 1.20 0.68 1.15 1.65 1.50
50 21 M Septo-Optic Dysplasia OS 1.90 0.68 0.70 1.50 0.30
51 13 M Optic Atrophy OS 1.18 0.38 0.75 1.35 0.75
52 15 M Optic Atrophy OS 2.08 0.50 0.80 1.65 1.35
53 16 M Cortical Blindness OD 2.50 0.21 0.15 1.35 1.20
Table 2. Experiment I Participants
n = 27 students (27 eyes tested)
*Subject 43 was unable to provide quality of life data, nor was he testable by lettered charts.
†These subjects were not testable via lettered charts.
Result values of all test encounters are summarized in Tables 3 and 4 below,
along with average testing times per eye. For the SCCS test, 17/24 (71%) of subjects
obtained the maximum log contrast sensitivity value that we could measure (1.65). For
the BD test, 12/24 (50%) obtained the maximum contrast sensitivity value we could
measure (also 1.65).

44
B-L TAC P-R SCCS* BD*
Mean 1.13 (20/274) 0.66 (20/92) 1.27 1.65 1.58 Median
STDev ± 0.56 ± 0.54 ± 0.57 1.50 1.35 75th %
Time (sec) 54 ± 33 97 ± 67 61 ± 42 55 ± 45 31 ± 19 Time (sec)
Table 3. Experiment I Summary Test Results
Acuity and contrast sensitivity are presented in LogMAR and LogCS units, respectively.*Unable to measure
values better than 1.65. Note: if the calibrated P-R values are used, the results would be 0.30±0.15 LogCS higher.
Two-tailed t-test comparisons of pairwise findings for the acuity and contrast
sensitivity measures are shown below. Each comparison was run independently of the
others. It is understood that our data do not likely meet all the assumptions required to
run t-test analysis. However, parametric statistics have been attempted nonetheless.

45
Figure 11. Experiment I Summary Plot Statistics
Test results are shown with contrast values in the negative direction so as to keep the direction of better vision
consistent (higher values indicate poorer vision). Average values are shown for the B-L, TAC and P-R charts,
with error bars indicating standard deviations. *The SCCS and BD tests were limited to a ceiling of 1.65 logCS,
so their bar graphs represent median values and error bars extend up to the 75th percentile contrast value. Note:
if the calibrated P-R values are used, the difference between the P-R and SCCS is no longer statistically
significant (p < 0.14).
We compared the Bailey-Lovie letter acuity values obtained through my testing
with those reported for our subjects in their charts (Figure 12A). These charted acuity
values were obtained within 1-2 years of our testing by a different optometrist in concert
with a fourth year optometry student. Values were obtained using the same physical
Bailey-Lovie chart that we used, or with a Feinbloom number chart. Our testing was done
using letter-by-letter tallying, but the values in the record were obtained using a three out
of five correct identification criterion for the last row read. In the mean-difference plot
B - L T A C
P - R S C C S * B D *
- 2 . 5
- 2
- 1 . 5
- 1
- 0 . 5
0
0 . 5
1
1 . 5
2
2 . 5
p < 0.001**
p < 0.01**
p < 0.1 1
p < 0.15

46
below (Figure 12B), the average of my value and the chart value runs along the abscissa
and the difference between the reported value and my measurement is plotted on the y-
axis (Bland & Altman, 1986). The standard deviation of our measurement differences
from those in the record was ±3 lines. These results were within acceptable tolerances for
repeatability of visual acuity measures and therefore show good agreement with the
corresponding values reported in the participant’s records (Raasch et al., 1998).

47
Figure 12. Experiment I B-L vs Chart Report
Comparison between performance on the Bailey-Lovie chart and the visual acuities reported in the subject’s
patient file. A, Direct LogMAR comparison between the two data sets. Major diagonal is the equality line. Data
above the equality line indicate better performance noted in the patient’s file. Data below the equality line
indicate better performance when measured in our study. B, Data from A presented as a Bland-Altman plot.
I have used a novel format to show individual results for acuity and contrast
sensitivity testing for each eye tested. Figure 13 shows results that are clustered by
0
0.5
1
1.5
2
2.5
3
0.00 1.00 2.00 3.00
Mea
sure
d B
-L
Reported B-L
A
ReportedBetter
MeasuredBetter
-3-2.4-1.8-1.2-0.6
00.61.21.82.4
3
0 1 2 3Me
asu
red
-R
ep
ort
ed
Average B-L Values
B

48
primary diagnosis and sorted by visual acuity within diagnoses. As in Figure 11 above,
we graph contrast threshold instead of sensitivity in order to keep the direction of better
vision consistent (higher values indicate poorer vision).
Figure 13. Experiment I Lettered Chart Results by Diagnosis
LogMAR visual acuity and Log contrast sensitivity measured using lettered charts. Each red + blue bar
represents an individual subject’s visual performance. The upper edge of the blue bar on top is the subject’s
LogMAR acuity, and the lower edge of the red bar on the bottom is the subject’s LogCS. The bar as a whole is
lower for better performance. Bars are grouped by diagnosis and within diagnoses they are sorted by visual
performance on the LogMAR chart. Subsequent charts in this format maintain subject order from this graph.
** **** **
-2.7-2.4-2.1-1.8-1.5-1.2-0.9-0.6-0.3
00.30.60.91.21.51.82.12.42.7
ROPOptic NerveHypoplasia
CongenitalCataract
OpticAtrophy Other
CorticalBlindness
Go
od
Lo
gCS
Lo
gMA
R
Po
or
** Unable
B-L Acuity
P-R Contrast Sensitivity

49
Figure 14. Experiment I Striped Chart Results by Diagnosis
Log MAR visual acuity and log contrast sensitivity using striped charts. Conventions and subject order are as in
Figure 13. Note that the SCCS test had a ceiling of 1.65 LogCS (shaded area).
It is difficult to compare Berkeley disc data directly to Teller Acuity values in the
way that the SCCS can be. The Berkeley Discs certainly require a different amount of
visual search ability than the Bailey-Lovie and Teller Acuity Cards do. The results for the
Berkeley Discs are shown in Figure 15 against the average of Bailey-Lovie letter acuity
and Teller Acuity Card grating acuity, since there is a localization element to the
Berkeley Discs that is not present in the SCCS test.
-2.7-2.4-2.1-1.8-1.5-1.2-0.9-0.6-0.3
00.30.60.91.21.51.82.12.42.7
ROPOptic NerveHypoplasia
CongenitalCataract
OpticAtrophy Other
CorticalBlindness
Go
od
L
ogC
S L
ogM
AR
P
oo
r
SCCS
TAC

50
Figure 15. Experiment I Shaped Chart Results by Diagnosis
Experiment I Shaped Chart Results by Diagnosis. Here the average between B-L and TAC are used for the
acuity value given that the BD test is neither a letter nor a stripe chart and therefore not directly comparable to
either acuity measure employed. Conventions and subject order are the same as for Figure 13. Note that the BD
had a ceiling of 1.65 LogCS (shaded area).
The Teller Acuity card values were significantly better than those using the
Bailey-Lovie chart, especially for those subjects with acuity worse than LogMAR 1.0
(20/200) (see Figure 16). However, it was clear that the TAC values and the LogMAR
values were statistically significantly correlated with one another. These correlations will
be examined in a later section of the thesis.
-2.7-2.4-2.1-1.8-1.5-1.2-0.9-0.6-0.3
00.30.60.91.21.51.82.12.42.7
ROPOptic NerveHypoplasia
CongenitalCataract
OpticAtrophy Other
CorticalBlindness
Go
od
Lo
gCS
L
ogM
AR
Po
or Ave B-L & TAC
BD
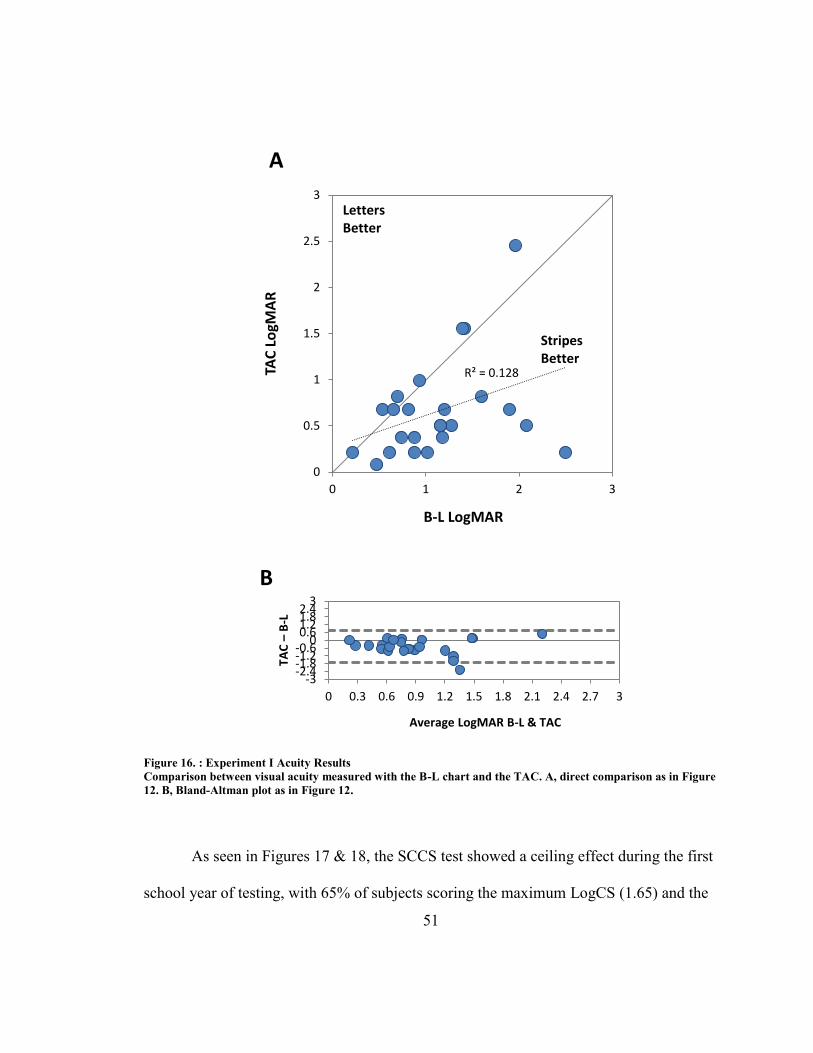
51
Figure 16. : Experiment I Acuity Results
Comparison between visual acuity measured with the B-L chart and the TAC. A, direct comparison as in Figure
12. B, Bland-Altman plot as in Figure 12.
As seen in Figures 17 & 18, the SCCS test showed a ceiling effect during the first
school year of testing, with 65% of subjects scoring the maximum LogCS (1.65) and the
R² = 0.128
0
0.5
1
1.5
2
2.5
3
0 1 2 3
TAC
Lo
gMA
R
B-L LogMAR
A
LettersBetter
StripesBetter
-3-2.4-1.8-1.2-0.6
00.61.21.82.4
3
0 0.3 0.6 0.9 1.2 1.5 1.8 2.1 2.4 2.7 3
TAC
–B
-L
Average LogMAR B-L & TAC
B

52
lower quartile scoring at least LogCS of 1.35. All contrast sensitivity plots have been
produced with negative values in order to maintain directional consistency with acuity
plots, where a lower value is indicative of better performance.

53
Figure 17. Experiment I P-R & SCCS Results
Comparisons between contrast sensitivity measured with the SCCS test and the Pelli-Robson chart. A, Direct
comparison as in Figure 12. B, Bland-Altman plot as in Figure 12.
R² = 0.2191
-2.25
-1.95
-1.65
-1.35
-1.05
-0.75
-0.45
-0.15
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S Lo
gCS
Pelli-Robson LogCS
A
LettersBetter
StripesBetter
-2.25-1.65-1.05-0.450.150.751.351.95
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S –
P-R
Average LogCS P-R & SCCS
B

54
Figure 17. Experime nt I P-R & SCC S Bins
Figure 18. Experiment I P-R & SCCS Bins
The number of subjects in each contrast sensitivity group for the Pelli-Robson and Stripe Card tests as shown in
Figure 17.
All but one of the subjects with impaired CS on the PR (according to Leat et al.,
PR<1.50) showed a better LogCS on the SCCS test than the PR test (sign test, p< 0.05, 2-
tailed; nonparametric test required because of the ceiling effect on the SCCS).
The results from the Berkeley Discs were also typically better than those found
with the Pelli-Robson chart as well, but not to the same degree as the SCCS test (as
shown in Figure 19).
0
2
4
6
8
10
12
14
16
18
2.1 1.95 1.8 1.65 1.5 1.35 1.2 1.05 0.9 0.75 0.6 0.45 0.3 0.15 0
Nu
mb
er o
f Su
bje
cts
LogCS
SCCS
P-R

55
Figure 19. Experiment I P-R & BD Results
Comparison between contrast sensitivity measured with the Berkeley Discs and the Pelli-Robson chart. A, direct
comparisons as in Figure 12. B, Bland-Altman plot as in Figure 12.
R² = 0.3637
-2.25
-1.95
-1.65
-1.35
-1.05
-0.75
-0.45
-0.15
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
BD
Lo
gCS
Pelli-Robson LogCS
A
LettersBetter
DiscsBetter
-2.25-1.65-1.05-0.450.150.751.351.95
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
BD
–P
-R
Average LogCS P-R & BD
B

56
Figure 20. Experiment I P-R & BD Bins
The number of subjects in each contrast sensitivity group for the Berkeley Discs and the Pelli-Robson chart as
shown in Figure 19.
A comparison was also possible between the results of the SCCS and Berkeley
Discs since both tests had a ceiling of 1.65 during the first year of testing. The data
corresponding to fifteen of the subjects below plot at the same location on the graph,
giving the appearance of less data than actually obtained. For this reason, bin count
figures have been generated to illustrate the level of overlap in our results.
0
2
4
6
8
10
12
14
2.1 1.95 1.8 1.65 1.5 1.35 1.2 1.05 0.9 0.75 0.6 0.45 0.3 0.15 0
Nu
mb
er o
f Su
bje
cts
LogCS
BD
P-R

57
Figure 21. Experiment I SCCS & BD Results
Comparison between contrast sensitivity measured by SCCS and BD. A, Direct comparison as in Figure 12. B,
Bland-Altman plot as in Figure 12.
R² = 0.1353
-2.25
-1.95
-1.65
-1.35
-1.05
-0.75
-0.45
-0.15
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S Lo
gCS
BD LogCS
A
DiscsBetter
StripesBetter
-2.25-1.65-1.05-0.450.150.751.351.95
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S -
BD
Average LogCS SCCS & BD
B

58
Figure 22. Experiment I SCCS & BD Bins
The number of subjects at each contrast level when tested with the Berkeley Discs and the SCCS test as shown in
figure 21.
Discussion for Experiment I
Both of the grating tests (SCCS and TAC) gave statistically significantly better
values than the corresponding letter charts. The average grating acuity value measured on
Teller cards was almost 3x better than the acuity value measured by the Bailey-Lovie
chart. Statistical analysis of our results by t-test demonstrated that the two acuity charts
gave significantly different results. Similarly, the contrast sensitivity values measured
with the SCCS were over 2x better than the Pelli-Robson values. Again, t-test results
show that the two charts give significantly different results.
Some of the inconsistency between the Pelli-Robson and SCCS test may be a
result of the LogCS 1.65 ceiling limiting the SCCS results. This fact affected our ability
0
2
4
6
8
10
12
14
16
18
2.1 1.95 1.8 1.65 1.5 1.35 1.2 1.05 0.9 0.75 0.6 0.45 0.3 0.15 0
Nu
mb
er o
f Su
bje
cts
LogCS
BD
SCCS

59
to employ a t-test without any reservations. We measured 2.4x the contrast sensitivity
despite this inability to measure lower levels of contrast during Experiment I. For
measuring contrast sensitivity in those with reduced vision, the simpler task and bolder
patterns of the SCCS may make it more likely to reveal the maximum performance that a
given patient can achieve.
The Berkeley Discs also demonstrated better results than the Pelli-Robson (a
factor of 2x), but not to the same level as the SCCS test (again, 2.4x). This was despite
the fact that both the BD and SCCS tests had the same LogCS 1.65 ceiling. Perhaps the
localization task for the BD test was more complex than for the SCCS.
There were also inconsistent BD responses by some subjects (report of seen
circles in blank areas), which make the test difficult to interpret at times. As you may
recall, we allowed our subjects to view every card face instead of skipping some.
Theoretically, the subjects should have seen every disc present on a card containing
contrast levels higher than previously detected. However, some of them failed to detect
all the discs on those card faces. In our case, we gave the participants credit for the lowest
contrast value reported, but this finding does affect the validity of our results.

60
Experiment II – Separate Eye Testing
Introduction to Experiment II
In this second phase of our study, we sought to examine each eye of our subjects
individually, whenever possible. We also opened up participation to students with no
measurable vision. These students without measurable vision were included to constrain
our vision-related quality of life data analysis, discussed under Experiment III. A second
information packet was mailed out to all students at the school in order to encourage
repeat assessments for some students, and to allow for the inclusion of students with no
measurable vision.
We also sought and obtained permission from the IRB to recruit participants from
OSSB’s summer camp activities. Angela Brown attended the registration event for
summer camp at OSSB between the first and second year of testing. She was able to
recruit interested participants by answering questions and distributing information
packets in person.
Methods for Experiment II
The methods for Experiment II were almost entirely the same as for Experiment I.
One difference was that all assessments were performed on each eye monocularly where
possible instead of just on the subject’s preferred eye. When both eyes were tested, the
right eye was tested first.

61
New SCCS cards were developed to extend our measurement range of LogCS
values from approximately 1.65 to 2.00. We calibrated the cards again prior to initiating
testing and found that our cards continue to be close enough to the nominal values for
good use.
The results below display testing performed on subjects allowing them to use each
eye to view our charts. We allowed subjects to use their “worse” eye (provided that they
had any measurable vision in that eye). Inclusion of testing for each eye, whenever
possible, for each subject in Experiment II rather than just the dominant (and presumably
better) eye as in Experiment I, was intended to increase the data at very low levels of
visual performance for comparison across the five vision tests.
Results for Experiment IIa: Repeat Testing
Table 4 below shows the re-test results for eleven subjects who also participated
in the Experiment I. Repeat testing was performed for at least one eye, and an additional
eye was measured when possible. The right eye was always tested first.

62
ID Age S Diagnosis Eye B-L
LogMAR
TAC
LogMAR
P-R
LogCS
SCCS
LogCS
BD
LogCS
01 17 M Optic Nerve Hypoplasia OD 1.58 1.11 0.85 1.95 1.05
01 17 M Optic Nerve Hypoplasia OS 1.32 0.68 1.20 2.00 1.05
12 16 M Retinopathy of Prematurity OS 0.68 0.68 1.90 2.00 1.65
17 14 F Microphthalmus OS 1.36 1.29 1.35 1.90 1.5
26 18 M Optic Nerve Hypoplasia OD 1.60 0.81 0.10 1.65 1.2
26 18 M Optic Nerve Hypoplasia OS 0.96 0.38 2.05 2.00 1.65
28 12 F Congenital Cataract OD 1.28 0.68 1.75 2.00 1.65
28 12 F Congenital Cataract OS 1.30 0.68 1.75 2.00 1.65
30 18 F Optic Atrophy OD 0.96 0.68 1.30 1.65 1.65
30 18 F Optic Atrophy OS 0.94 0.99 1.05 1.65 1.65
37 18 M Aniridia OD 0.96 0.38 1.50 1.65 1.65
37 18 M Aniridia OS 0.92 0.50 1.35 1.65 1.65
45† 20 F Optic Atrophy OD — 1.29 — 0.75 0
45† 20 F Optic Atrophy OS — 1.29 — 1.20 0.9
51 13 M Optic Atrophy OD 1.42 1.11 1.00 1.50 1.65
51 13 M Optic Atrophy OS 1.14 0.50 1.20 1.65 1.2
52 15 M Optic Atrophy OD 3.14 0.81 0.20 1.05 —
52 15 M Optic Atrophy OS 2.30 0.68 0.50 1.50 0.75
53 16 M Cortical Blindness OD 3.00 0.38 0.70 1.90 1.5
53 16 M Cortical Blindness OS 2.84 0.38 0.70 1.90 0.9
Table 4. Experiment IIa Participants
n = 11 (20 eyes tested)
†These subjects were not testable by lettered charts.
All test measurements are summarized in the table below, along with average
testing times per eye.

63
B-L TAC P-R SCCS* BD†
Mean 1.54 (20/689) 0.71 (20/101) 1.14 1.76 1.50 Median
STDev ± 0.76 ± 0.28 ± 0.56 ± 0.25 1.01 75th %
Time (sec) 65 ± 29 89 ± 67 76 ± 66 79 ± 43 57 ± 31 Time (sec)
Table 5. Experiment IIa Summary Test Results
*Unable to measure values better than 2.00
†Unable to measure values better than 1.65
Time of testing is for each individual eye. Note: if the calibrated P-R values are used, the results would be
0.30±0.15 LogCS higher.
Two-tailed t-test comparisons of findings for the acuity and contrast sensitivity
measures are shown below.

64
Figure 23. Experiment IIa Summary Plot Statistics
Conventions are as in Figure 11. The ceiling was extended for the SCCS test, so the average is reported and the
standard deviation is now shown for the SCCS error bar. The Berkeley Discs are still presented with median
and 75th percentile values. *The SCCS ceiling was LogCS 2.00 and the †Berkeley Discs ceiling was 1.65. Note: if
the calibrated values for the P-R are used, the difference between the P-R and the BD scores is no longer
statistically significant (p < .18)
Importantly, in Experiment II the SCCS test no longer had a ceiling of LogCS
1.65, but instead, we could measure up to LogCS 2.00. The Berkeley discs test continued
to have a ceiling of 1.65.

65
Figure 24. Experiment IIa Acuity Results
Comparison between acuity testing techniques of Teller Acuity and Bailey-Lovie Acuity for subjects for whom
we already have seen better-eye data in Experiment I. This plot includes repeat testing of the better eyes as well
as measurement of the worse eye where possible. All but two subjects contribute two eyes. A, Direct comparison
as in Figure 12. B, Bland-Altman plot as in Figure 12.
R² = 0.0133
0
0.5
1
1.5
2
2.5
3
0 1 2 3
TAC
Lo
gMA
R
B-L LogMAR
A
LettersBetter
StripesBetter
-3-2.4-1.8-1.2-0.6
00.61.21.82.4
3
0 0.3 0.6 0.9 1.2 1.5 1.8 2.1 2.4 2.7 3
TAC
–B
-L
Average LogMAR B-L & TAC
B

66
Figure 25. Experiment IIa P-R & SCCS Results
Comparison between contrast sensitivity values obtained by the SCCS test and the P-R chart for repeat
subjects’ better and worse eyes. All but two subjects contribute two eyes. A, Direct comparison as in Figure 12.
B, Bland-Altman plot.
R² = 0.3725
-2.25
-1.95
-1.65
-1.35
-1.05
-0.75
-0.45
-0.15
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S Lo
gCS
Pelli-Robson LogCS
A
LettersBetter
StripesBetter
-2.25-1.65-1.05-0.450.150.751.351.95
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S –
P-R
Average LogCS P-R & SCCS
B

67
Figure 26. Experiment IIa P-R & SCCS Bins
Number of subjects at each contrast sensitivity level when measured with the SCCS and P-R tests. These results
are not limited by a ceiling of 1.65 as in Experiment I. Instead, the SCCS has a ceiling of 2.00.
0
1
2
3
4
5
6
7
8
9
10
2.1 1.95 1.8 1.65 1.5 1.35 1.2 1.05 0.9 0.75 0.6 0.45 0.3 0.15 0
Nu
mb
er o
f Su
bje
cts
LogCS
SCCS
P-R

68
Figure 27. Experiment IIa SCCS & BD Results
Comparison between contrast sensitivity values measured with the BD test and the P-R chart. The BD test is
bounded by a ceiling of 1.65. A, Direct comparison as in Figure 12. B, Bland-Altman plot.
R² = 0.4349
-2.25
-1.95
-1.65
-1.35
-1.05
-0.75
-0.45
-0.15
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
BD
Lo
gCS
Pelli-Robson LogCS
A
LettersBetter
DiscsBetter
-2.25-1.65-1.05-0.450.150.751.351.95
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
BD
–P
-R
Average LogCS P-R & BD
B

69
Figure 28. Experiment IIa P-R & BD Bins
Number of subjects at various levels of contrast sensitivity when measured by BD and P-R tests. The BD test is
limited by a ceiling of 1.65.
0
1
2
3
4
5
6
7
8
9
10
2.1 1.95 1.8 1.65 1.5 1.35 1.2 1.05 0.9 0.75 0.6 0.45 0.3 0.15 0
Nu
mb
er o
f Su
bje
cts
LogCS
BD
P-R

70
Figure 29. Experiment IIa SCCS & BD Results
Comparison between contrast sensitivity measured with SCCS and BD test. Here, the SCCS is bounded by a
ceiling of 2.00, but the BD is bounded by a 1.65 ceiling. Many subjects obtained those ceiling values, resulting in
their data points plotting to the same spot on the graph. This gives the appearance of less data than was actually
obtained. A, Direct comparison as in Figure 12. B, Bland-Altman plot.
R² = 0.0068
-2.25
-1.95
-1.65
-1.35
-1.05
-0.75
-0.45
-0.15
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S Lo
gCS
BD LogCS
A
DiscsBetter
StripesBetter
-2.25-1.65-1.05-0.450.150.751.351.95
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S –
BD
Average LogCS SCCS & BD
B

71
Figure 30. Experiment IIa SCCS & BD Bins
Number of subjects at each contrast sensitivity level when measured with the BD and SCCS tests.
Repeatability between Experiments I and IIa. Since we had the opportunity to
retest eleven of our subjects, we were able to generate the graphs below. Naturally, these
subjects were a few months older during the retest than they were during the original
assessments, which may introduce some variability in test vs. retest findings. Figures 31-
33 demonstrate the value scored for the first eye tested next to the second eye(s)
examined.
0
1
2
3
4
5
6
7
8
9
10
2.1 1.95 1.8 1.65 1.5 1.35 1.2 1.05 0.9 0.75 0.6 0.45 0.3 0.15 0
Nu
mb
er o
f Su
bje
cts
LogCS
BD
SCCS

72
Figure 31. Experiment IIa Lettered Chart Test-Retest
Retest values for the better eyes of subjects who participated in Experiments I and IIa. Conventions are similar
to those in Figure 13. The fist test is shown to the left, and the repeat assessment follows to the right.
Figure 32. Experiment IIa Striped Chart Test-Retest
Retest values for the better eyes of subjects who participated in Experiments I and IIa. Conventions are similar
to those in Figure 13. The first test is shown to the left, and the repeat assessment follows to the right. The SCCS
was limited by a ceiling of 1.65 during Experiment I tests, but by 2.00 for Experiment IIa.
** **** **
-3.2-2.9-2.6-2.3
-2-1.7-1.4-1.1-0.8-0.5-0.20.10.40.7
11.31.61.92.22.52.83.1
Go
od
Lo
gCS
Lo
gMA
R
P
oo
r
** Unable
B-L Acuity
P-R Contrast Sensitivity
-3.2-2.9-2.6-2.3
-2-1.7-1.4-1.1-0.8-0.5-0.20.10.40.7
11.31.61.92.22.52.83.1
Go
od
Lo
gCS
Lo
gMA
R
P
oo
r TAC Acuity
SCCS Contrast Sensitiviy

73
Figure 33. Experiment IIa Shaped Chart Test-Retest
Retest values for the BD test shown with the average of each experiment’s acuity measurements as in Figure 15.
T-test comparisons demonstrate that the repeatability of our testing was good with
these subjects’ better eyes (Table 6).
B-L TAC P-R SCCS BD
p-value 2.11 1.20 1.90 3.60 0.121
Sig (<0.05) Not different Not different Not different Not different Not different
Table 6. Experiment IIa Repeatability Statistics
Results for Experiment IIb: New Subjects
Eight participants were students in the annual summer camps put on by OSSB.
Their subject ID numbers were #62-69. Ten of the subjects listed in the table below had
no measurable vision, but were able to provide quality of life data.
-3.2-2.9-2.6-2.3
-2-1.7-1.4-1.1-0.8-0.5-0.20.10.40.7
11.31.61.92.22.52.83.1
Go
od
Lo
gCS
Lo
gMA
R
P
oo
r Average B-L and TAC Acuity
BD Contrast Sensitivity

74
ID Age S Diagnosis Eye B-L
LogMAR
TAC
LogMAR
P-R
LogCS
SCCS
LogCS
BD
LogCS
31 16 M Retinoblastoma OD 0.98 0.68 1.75 2.00 1.65
54† 20 M Retinopathy of Prematurity — — — — — —
55† 19 F Leber's Congenital Amaurosis — — — — — —
56† 19 M Brain Tumor — — — — — —
57† 19 M Optic Nerve Hypoplasia — — — — — —
58 18 F Leber's Congenital Amaurosis OD 2.18 0.50 0.95 1.65 1.65
58 18 F Leber's Congenital Amaurosis OS 2.10 0.68 0.95 1.65 1.65
59† 20 M Retinopathy of Prematurity — — — — — —
60 18 M Retinopathy of Prematurity OD 1.56 0.99 1.00 1.50 0.6
6†0 18 M Retinopathy of Prematurity OS — 1.29 — 0.60 0.6
61 13 M Choroideremia OD 1.54 0.99 0.15 0.90 0.45
61 13 M Choroideremia OS 1.18 0.81 0.25 1.05 0.45
62 11 F Blind at age 2 (unexplained) OD 1.58 — 0.15 0.00 0.00
62 11 F Blind at age 2 (unexplained) OS 1.38 1.38 0.15 0.00 0.00
63 10 F Leber's Congenital Amaurosis OD 1.14 0.81 0.85 1.65 1.65
63 10 F Leber's Congenital Amaurosis OS 1.04 0.99 1.00 1.65 1.5
64 13 M Optic Atrophy OS 1.18 1.11 0.80 0.60 0.45
65 16 F Marfan's Disease OD 0.28 0.38 1.55 1.65 1.65
65 16 F Marfan's Disease OS 0.68 0.50 1.55 1.50 1.65
66 17 M High Myopia OD 0.08 0.21 2.00 1.50 1.65
67 10 M Cortical Blindness OS 1.79 0.99 0.90 1.20 1.35
68 12 M Aniridia OD 1.94 1.38 0.35 1.35 1.05
68 12 M Aniridia OS 1.04 0.68 1.80 2.00 1.65
69 14 M Retinopathy of Prematurity OD 0.98 0.99 1.40 1.90 1.65
69 14 M Retinopathy of Prematurity OS 0.98 0.68 1.55 2.00 1.65
70† 18 M Retinitis Pigmentosa — — — — — —
71 15 M Best's Disease OD 0.86 0.38 1.65 2.00 1.65
71 15 M Best's Disease OS 0.84 0.38 1.65 2.00 1.65
72 18 F Glaucoma OS 1.04 0.99 1.05 1.35 1.05
73† 17 F Optic Atrophy — — — — — —
74† 12 M Optic Nerve Hypoplasia — — — — — —
75† 12 M Retinopathy of Prematurity — — — — — —
76† 6 M Retinoblastoma — — — — — —
Table 7. Experiment IIb Participants
n = 34 (23 eyes tested)
†These subjects were not testable via lettered charts.

75
Result values of all test encounters with the new subjects are summarized in the
table below along with average testing times per eye. All but one student contributed two
eyes to these results.
B-L TAC P-R SCCS* BD†
Mean 1.20 (20/314) 0.79 (20/121) 1.07 1.41 1.65 Median
STDev ± 0.53 ± 0.32 ± 0.59 ± 0.59 0.71 75th %
Time (sec) 66 ± 45 86 ± 53 50 ± 26 49 ± 27 60 ± 39 Time (sec)
Table 8. Experiment IIb Summary Results
*Unable to measure values better than 2.00
†Unable to measure values better than 1.65
Time of testing is for each individual eye. Note: if the calibrated P-R values are used, the results would be
0.30±0.15 LogCS higher.
Two-tailed t-test comparisons of findings for the acuity and contrast sensitivity
measures are shown below.

76
Figure 34. Experiment IIb Summary Plot Statistics
Conventions are as in Figure 23.
The figures below are test results for new students who were added to the study in
the second year of testing and were not previously assessed.
B - L $ T A C
P - R S C C S * B D †
- 2 . 5
- 2
- 1 . 5
- 1
- 0 . 5
0
0 . 5
1
1 . 5
2
2 . 5
p < 0.01**
p < 0.71 p < 0.001**
p < 0.001**

77
Figure 35. Experiment IIb Acuity Results
Comparison of acuity measured by TAC and B-L for both eyes of new subjects during our second year of
testing. All but two subjects contribute two eyes. Conventions are as in Figure 12. A, Direct comparison, B,
Bland-Altman plot.
R² = 0.1467
0
0.5
1
1.5
2
2.5
3
0 1 2 3
TAC
Lo
gMA
R
B-L LogMAR
A
LettersBetter
StripesBetter
-3-2.4-1.8-1.2-0.6
00.61.21.82.4
3
0 0.3 0.6 0.9 1.2 1.5 1.8 2.1 2.4 2.7 3
TAC
–B
-L
Average LogMAR B-L & TAC
B

78
Figure 36. Experiment IIb P-R & SCCS Results
Comparison of contrast sensitivity values obtained by SCCS and P-R charts for new subjects. All but two
subjects contribute two eyes. Conventions are as in Figure 12. A, Direct comparison. B, Bland-Altman plot.
R² = 0.6142
-2.25
-1.95
-1.65
-1.35
-1.05
-0.75
-0.45
-0.15
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S Lo
gCS
Pelli-Robson LogCS
A
LettersBetter
StripesBetter
-2.25-1.65-1.05-0.450.150.751.351.95
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S –
P-R
Average LogCS P-R & SCCS
B

79
Figure 37. Experiment IIb P-R & SCCS Bins
Number of subjects at each contrast sensitivity level for the SCCS and P-R testing of new subjects. The SCCS is
bounded by a ceiling of LogCS 2.00.
0
1
2
3
4
5
6
7
2.1 1.95 1.8 1.65 1.5 1.35 1.2 1.05 0.9 0.75 0.6 0.45 0.3 0.15 0
Nu
mb
er o
f Su
bje
cts
LogCS
SCCS
P-R

80
Figure 38. Experiment IIb P-R & BD Results
Comparison of contrast sensitivity testing by BD and P-R chart for new subjects. The BD test is bounded by a
ceiling of 1.65. A, Direct comparison. B, Bland-Altman plot.
R² = 0.6582
-2.25
-1.95
-1.65
-1.35
-1.05
-0.75
-0.45
-0.15
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
BD
Lo
gCS
Pelli-Robson LogCS
A
LettersBetter
DiscsBetter
-2.25-1.65-1.05-0.450.150.751.351.95
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
BD
–P
-R
Average LogCS P-R & BD
B
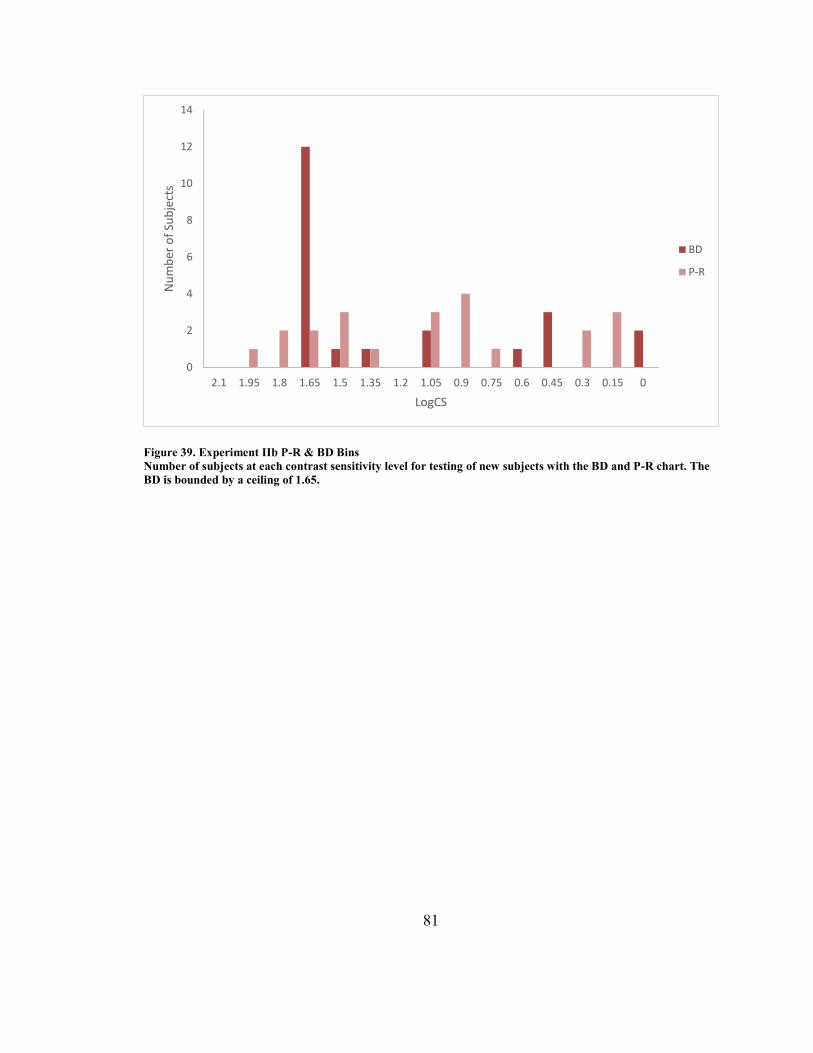
81
Figure 39. Experiment IIb P-R & BD Bins
Number of subjects at each contrast sensitivity level for testing of new subjects with the BD and P-R chart. The
BD is bounded by a ceiling of 1.65.
0
2
4
6
8
10
12
14
2.1 1.95 1.8 1.65 1.5 1.35 1.2 1.05 0.9 0.75 0.6 0.45 0.3 0.15 0
Nu
mb
er o
f Su
bje
cts
LogCS
BD
P-R

82
Figure 40. Experiment IIb SCCS & BD Results
Comparison of contrast sensitivity testing by BD and SCCS for new subjects. The BD is bounded by a 1.65
ceiling and the SCCS test by 2.00. Many subjects obtained the maximum values for each chart leading to their
data points plotting to the same location on the graphs. This gives the appearance of less data than actually
obtained. A, Direct comparison. B, Bland-Altman Plot.
R² = 0.8134
-2.25
-1.95
-1.65
-1.35
-1.05
-0.75
-0.45
-0.15
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S Lo
gCS
BD LogCS
A
DiscsBetter
StripesBetter
-2.25-1.65-1.05-0.450.150.751.351.95
-2.25 -1.95 -1.65 -1.35 -1.05 -0.75 -0.45 -0.15
SCC
S –
BD
Average LogCS SCCS & BD
B

83
Figure 41. Experiment IIb SCCS & BD Bins
Number of new subjects at each contrast sensitivity level for the BD and SCCS tests. The BD is bounded by a
ceiling of 1.65, and the SCCS has a LogCS ceiling of 2.00.
Discussion for Experiment II
Some of the data that we have obtained through the efforts of Experiment I can be
added to the better eye results from Experiment II. In order to check correlations between
the five eye charts, it was necessary to generate a table containing test results for each
subject using only one eye—the better one. In the case of students tested only in
Experiment I, the results on the only tested eye appear. In the case of students tested in
both Experiment I and Experiment II, the results on the better eye in Experiment II are
listed. In the case of students tested only in Experiment II, the results on the better eye are
listed.
0
2
4
6
8
10
12
14
2.1 1.95 1.8 1.65 1.5 1.35 1.2 1.05 0.9 0.75 0.6 0.45 0.3 0.15 0
Nu
mb
er o
f Su
bje
cts
LogCS
BD
SCCS

84
ID Exp Diagnosis Eye B-L
LogMAR
TAC
LogMAR
P-R
LogCS
SCCS
LogCS
BD
LogCS
01 IIa Optic Nerve Hypoplasia OS 1.32 0.68 1.20 2.00 1.05
02 I Retinopathy of Prematurity OD 0.62 0.21 1.95 1.65 1.65
04 I Optic Nerve Hypoplasia OS 0.48 0.08 2.10 1.65 1.65
05 I Leber's Congenital Amaurosis OS 1.42 1.56 1.10 0.60 1.50
06 I Optic Nerve Hypoplasia OD 0.74 0.38 2.00 1.65 1.65
08 I Optic Atrophy OD 0.88 0.21 1.45 1.65 1.50
11 I High Myopia OD 0.94 0.99 1.35 1.65 1.65
12 IIa Retinopathy of Prematurity OS 0.68 0.68 1.90 2.00 1.65
17 IIa Microphthalmus OS 1.36 1.29 1.35 1.90 1.50
18 I Cone Dystrophy OS 0.7 0.81 1.40 1.65 1.65
24 I Optic Atrophy OS 1.16 0.5 1.65 1.65 1.35
26 IIa Optic Nerve Hypoplasia OS 0.96 0.38 2.05 2.00 1.65
28 IIa Congenital Cataract and Aphakia OD 1.28 0.68 1.75 2.00 1.65
30 IIa Optic Atrophy OS 0.94 0.99 1.05 1.65 1.65
31 IIb Retinoblastoma OD 0.98 0.68 1.75 2.00 1.65
34 I Congenital Cataract and Aphakia OD 0.22 0.21 1.65 1.65 1.50
35 I Retinopathy of Prematurity OD 0.82 0.68 1.75 1.65 1.65
36 I Optic Atrophy OS 1.6 0.81 0.90 1.65 1.65
37 IIa Aniridia OD 0.96 0.38 1.50 1.65 1.65
41 I Glaucoma OS 1.96 2.45 0.10 1.20 0.90
45 IIa Optic Atrophy OD — 1.29 — 0.75 0.00
46 I Cortical Blindness OD — 0.84 — 1.35 0.75
48 I Optic Atrophy OD 1.2 0.68 1.15 1.65 1.50
50 I Septo-Optic Dysplasia OS 1.9 0.68 0.70 1.50 0.30
51 IIa Optic Atrophy OS 1.14 0.5 1.20 1.65 1.20
52 IIa Optic Atrophy OS 2.3 0.68 0.50 1.50 0.75
53 IIa Cortical Blindness OD 3 0.38 0.70 1.90 1.50
58 IIb Leber's Congenital Amaurosis OS 2.1 0.68 0.95 1.65 1.65
60 IIb Retinopathy of Prematurity OD 1.56 0.99 1.00 1.50 0.60
61 IIb Choroideremia OS 1.18 0.81 0.25 1.05 0.45
62 IIb Blind at age 2 (unsure) OS 1.38 1.38 0.15 0.00 0.00
63 IIb Leber's Congenital Amaurosis OS 1.04 0.99 1.00 1.65 1.50
64 IIb Optic Atrophy OS 1.18 1.11 0.80 0.60 0.45
65 IIb Marfan's Disease OD 0.28 0.38 1.55 1.65 1.65
66 IIb High Myopia OD 0.08 0.21 2.00 1.50 1.65
67 IIb Cortical Blindness OS 1.79 0.99 0.90 1.20 1.35
68 IIb Aniridia OS 1.04 0.68 1.80 2.00 1.65
69 IIb Retinopathy of Prematurity OS 0.98 0.68 1.55 2.00 1.65
71 IIb Best’s Disease OD 0.86 0.38 1.65 2.00 1.65
72 IIb Glaucoma OS 1.04 0.99 1.05 1.35 1.05
Table 9. Experiment I & II Better Eye Only
n = 36 Subjects (36 eyes) Note: Subject 43 was not included here as he did not provide any QoL data.

85
This grouping of subjects allows for us to check for correlations across all the
tests we employed.
B-L TAC P-R SCCS* BD†
Mean 1.16 (20/287) 0.75 (20/112) 1.30 1.55 1.50 Median
STDev ± 0.58 ± 0.44 ± 0.54 ± 0.44 1.05 75th %
Time (sec) 62 ± 37 86 ± 60 61 ± 38 56 ± 32 47 ± 31 Time (sec)
Table 10. Experiment II Summary Results
*Unable to measure values better than 2.00
†Unable to measure values better than 1.65
Time of testing is for each individual eye. Note: if the calibrated P-R values are used, the results would be
0.30±0.15 LogCS higher.

86
Figure 42. Experiment II Summary Plot Statistics
Conventions are as in Figure 34. Here only one eye per subject is included—the better eye (or second test if
repeat data are available). Subject number 43 is not included in this analysis since he did not provide quality of
life data. Note: if the calibrated P-R values are compared to the SCCS, then p < 0.01.
When comparing results across the better eye for all subjects, all tests were
positively correlated with one another. These correlations were statistically significant in
all but one case—the B-L and the SCCS were not significantly correlated. As can be seen
in the table below, the B-L chart was most strongly correlated with the P-R, perhaps
because it was only other letter chart. The next strongest, correlation was with the TAC,
perhaps due to the fact that they are both acuity tests. Next, the BD showed a significant
correlation with the B-L chart, perhaps because both tests include a visual search
localization component where the stimulus to be detected or identified must be localized.
B - L T A C
P - R S C C S * B D †
- 2 . 5
- 2
- 1 . 5
- 1
- 0 . 5
0
0 . 5
1
1 . 5
2
2 . 5
p < 0.001**
p < 0.001** p < 0.001**
p < 0.05*

87
For the P-R chart, the strongest correlation was found with the BD test, followed
by the B-L chart, TAC and finally the SCCS. The SCCS was most strongly correlated
with the BD, followed by P-R, and then TAC.

88
PRLogCS TACLogMAR SCCSLogCS BDLogCS O&MScore IVI_C LVP-FVQ
BLLogMAR
Pearson Correlation .692** .401* .149 .389* .540 -.197 -.594**
Sig. (2-tailed) .000 .013 .372 .016 .057 .237 .000
N 38 38 38 38 13 38 33
PRLogCS
Pearson Correlation .653** .608** .738** .166 -.481** -.738**
Sig. (2-tailed)
.000 .000 .000 .588 .002 .000
N 38 38 38 13 38 33
TACLogMAR
Pearson Correlation .539** .450** .219 -.367* -.597**
Sig. (2-tailed)
.000 .004 .453 .020 .000
N 40 40 14 40 35
SCCSLogCS
Pearson Correlation .708** .165 -.576** -.512**
Sig. (2-tailed)
.000 .574 .000 .002
N 40 14 40 35
BDLogCS
Pearson Correlation .450 -.434** -.584**
Sig. (2-tailed) .106 .005 .000
N 14 50 45
Table 11: Test Chart Correlations
**. Correlation was very significant: at the 0.01 level (2-tailed).
*. Correlation was significant: at the 0.05 level (2-tailed).
Note: The table has been shaded to help the reader quickly visualize significant correlations (or the absence of correlation).
Subject 43 was not included in this analysis since he did not provide any QoL or O&M data. Table 13 Continued

89
Experiment III – Quality of Life and Orientation and Mobility
Vision-Related Quality of Life
Quality of life surveys were administered following vision testing for each
subject. In order to facilitate testing, we modified the surveys so that they would contain
appropriate phrasing (e.g., for one LVP-FVQ question: switch the word for a “rupee”
coin to a “nickel”). Copies of the verbal scripts actually used are in Appendix A. The first
five subjects tested (#01, 02, 05, 12, and 34) did not have the opportunity to complete the
LVP-FVQ, but did complete the IVI_C questionnaire. When both tests were
administered, the IVI_C was always administered before the LVP-FVQ. Although two
examiners were used, each participant was interviewed by the same examiner for both
surveys. Angela Brown administered 38 out of 50 IVI_C surveys (76%) and Greg
Hopkins administered the remainder.
We used a 26 item IVI_C survey, which included two questions that were
dropped when the IVI_C underwent Rasch analysis because they only received answers
in 4 out of 5 response categories (“Do you get the same information as the other
students?” and “…Are you confident about asking for help that you need?”).Our
research was initiated prior to the publication of the revised LVP-FVQ II survey, so we
did not have the opportunity to apply the new version.

90
Bradley Dougherty performed Rasch analysis on the results from the two surveys
that we used. The analysis generated person scores (and standard errors around those
scores) for each subject relative to the others who took the surveys. The Rasch analysis
was performed using all five-category responses, and the response option probability
curves were not ideal. Further work may require a three or four category structure.
Testing time for the IVI_C was 8 ± 9 minutes. Linear regressions for the IVI_C
versus the results for each eye chart are below. Error bars represent the standard error
value around the person scores for each participant. There were two subjects (marked
with the ∆ symbol), who could not perform letter acuity or contrast tasks, but were
testable with other charts. Subjects without measurable vision were spread apart on the x-
axis systematically for acuity and contrast plots.

91
Figure 43. IVI_C v B-L Regression
Data are for the better eye of all subjects with measurable vision. Subjects with no measurable vision are plotted
separately using open circles (not included in the regression trend line) by adding 0.25 LogMAR to the
maximum value for partially-sighted subjects and then systematically adding 0.01 LogMAR to shift each point
along the x-axis in order of subject number. Subjects marked with the ∆ symbol could not perform letter tasks.
Note: The B-L Chart was the only vision test not significantly correlated with the IVI_C results.
R² = 0.0387
-1.00
-0.50
0.00
0.50
1.00
1.50
2.00
2.50
3.00
0 0.5 1 1.5 2 2.5 3 3.5 4
IVI_
C P
erso
n S
core
B-L LogMAR Acuity

92
Figure 44. IVI_C vs. P-R Regression
Data are for the better eye of all subjects with measurable vision. Subjects with no measurable vision are plotted
separately (not included in the regression trend line) by starting at positive 0.25 LogCS and then systematically
shifting subjects along the x-axis by adding 0.0125 logCS in order of subject ID number.
R² = 0.2312
-1.00
-0.50
0.00
0.50
1.00
1.50
2.00
2.50
3.00
-2.5 -2 -1.5 -1 -0.5 0 0.5 1
IVI_
C P
erso
n S
core
P-R LogCS

93
Figure 45. IVI_C vs. TAC Regression
Data are for all subjects with measurable vision. Two subjects on this plot are included that could not be
measured via lettered charts. Their points have been marked with a ∆ symbol. Conventions for this plot are the
same as for Figure 43. Note: The TAC test was significantly correlated with the IVI_C only at the 0.05 level (2-
tailed).
R² = 0.1343
-1.00
-0.50
0.00
0.50
1.00
1.50
2.00
2.50
3.00
0 0.5 1 1.5 2 2.5 3 3.5 4
IVI_
C P
erso
n S
core
TAC LogMAR Acuity

94
Figure 46. IVI_C vs. SCCS Regression
Data are for the better eye of all subjects with measurable vision. Two subjects on this plot are included that
could not be measured via lettered charts. Their points have been marked with a ∆ symbol. Conventions for this
plot are the same as for Figure 44.
R² = 0.3313
-1.00
-0.50
0.00
0.50
1.00
1.50
2.00
2.50
3.00
-2.5 -2 -1.5 -1 -0.5 0 0.5 1
IVI_
C P
erso
n S
core
SCCS LogCS

95
Figure 47. IVI_C vs. BD Regression
Data are for the better eye of all subjects with measurable vision. Two subjects on this plot are included that
could not be measured via lettered charts. Their points have been marked with a ∆ symbol. Conventions for this
plot are the same as for Figure 44.
Testing time for the LVP-FVQ was 6 ± 2 minutes. Linear regressions for the
LVP-FVQ versus the results for each eye chart are below. Again, there were two subjects
(marked with the ∆ symbol), who could not perform letter acuity or contrast tasks, but
were testable with other charts.
R² = 0.1884
-1.00
-0.50
0.00
0.50
1.00
1.50
2.00
2.50
3.00
-2.5 -2 -1.5 -1 -0.5 0 0.5 1
IVI_
C P
erso
n S
core
BDLogCS

96
Figure 48. LVP-FVQ vs. B-L Regression
Data are for the better eye of all subjects with measurable vision. Conventions are the same as for Figure 43.
R² = 0.3525
-2
-1
0
1
2
3
4
0 0.5 1 1.5 2 2.5 3 3.5 4
LVP
-FV
Q P
erso
n S
core
B-L LogMAR Acuity

97
Figure 49. LVP-FVQ vs. P-R Regression
Data are for the better eye of all subjects with measurable vision. Conventions are the same as for figure 44.
R² = 0.5447
-2
-1
0
1
2
3
4
-2.5 -2 -1.5 -1 -0.5 0 0.5 1
LVP
-FV
Q P
erso
n S
core
P-R LogCS

98
Figure 50. LVP-FVQ vs. TAC Regression
Data are for the better eye of all subjects with measurable vision. Conventions are the same as for figure 43.
R² = 0.3569
-2
-1
0
1
2
3
4
0 0.5 1 1.5 2 2.5 3 3.5 4
LVP
_FV
Q P
erso
n S
core
TAC LogMAR Acuity

99
Figure 51. LVP-FVQ vs. SCCS Regression
Data are for the better eye of all subjects with measurable vision. Conventions are the same as for figure 44.
R² = 0.2623
-2
-1
0
1
2
3
4
-2.5 -2 -1.5 -1 -0.5 0 0.5 1
LVP
-FV
Q P
erso
n S
core
SCCS LogCS

100
Figure 52. LVP-FVQ vs. BD Regression
Data are for the better eye of all subjects with measurable vision. Conventions are the same as for figure 44.
Orientation and Mobility
We were able to obtain orientation and mobility data for nineteen of our subjects,
seven of whom had no measurable vision. We obtained the severity-of-need scores for
each student and modified the values by subtracting out the score for central visual
acuity. All other assessments by the orientation and mobility instructors (including
peripheral vision) were maintained in the score.
Linear regression for modified O&M severity-of-need score is displayed versus
the results for each eye chart. Those subjects without any vision have their O&M scores
displayed separately from those subjects with measurable vision. There was one subject
R² = 0.3407
-2
-1
0
1
2
3
4
-2.5 -2 -1.5 -1 -0.5 0 0.5 1
LVP
-FV
Q P
erso
n S
core
BDLogCS

101
(marked with a ∆ symbol), who could not perform letter acuity or contrast tasks, but was
testable with other charts. Subjects without measurable vision were spread apart on the x-
axis systematically for acuity and contrast plots. For the acuity plots, subjects with no
measurable vision begin at LogMAR 3.0 and then an additional 0.01 LogMAR was
added in the order of subject ID number. For the contrast sensitivity plots, subjects with
no measurable vision are shown on the positive side of the x-axis starting at zero and
adding 0.0125 logCS to each subject in order of ID number. All of the O&M regressions
below were appropriately related to the vision testing results, but none of them reach
statistical significance.
Figure 53. O&M vs. B-L Regression
Data are for the better eye of subjects with measurable vision. Subjects with no measurable vision are shown
separately (not included in the regression trend line) and spread out systematically on the x-axis. One subject
who could not complete letter charts is marked with a ∆ symbol.
R² = 0.2916
0
5
10
15
20
25
30
0 0.5 1 1.5 2 2.5 3 3.5
O&
M S
core
B-L LogMAR Acuity

102
Figure 54. O&M vs. P-R Regression
Data are for the better eye of subjects with measurable vision. Subjects with no measurable vision are shown
separately. One subject who could not complete lettered charts is marked with a ∆ symbol.
R² = 0.0275
0
5
10
15
20
25
30
-2.5 -2 -1.5 -1 -0.5 0 0.5
O&
M S
core
P-R LogCS

103
Figure 55. O&M vs. TAC Regression
Data are for the better eye of subjects with measurable vision. One subject is marked with a ∆ symbol because
that subject could not read lettered charts.
R² = 0.0478
0
5
10
15
20
25
30
0 0.5 1 1.5 2 2.5 3 3.5
O&
M S
core
TAC LogMAR Acuity

104
Figure 56. O&M vs. SCCS Regression
Data are for the better eye of subjects with measurable vision. One subject (marked with a ∆ symbol) could not
complete lettered charts.
Figure 57. O&M vs. BD Regression
Data are for the better eye of subjects with measurable vision. One subject is marked with a ∆ symbol. This
subject was only able to see the first circle on the BD test (LogCS 0.00).
R² = 0.0271
0
5
10
15
20
25
30
-2.5 -2 -1.5 -1 -0.5 0 0.5
O&
MSc
ore
SCCS LogCS
R² = 0.2027
0
5
10
15
20
25
30
-2.5 -2 -1.5 -1 -0.5 0 0.5
O&
M S
core
BDLogCS

105
Correlations for vision-related quality of life and orientation & mobility and our
vision test results are summarized in Table 15, where only the better eye for subjects with
measureable vision are included. Generally, the LVP-FVQ correlated best with our vision
testing, followed by the IVI_C and then the adjusted OMSRS scores (which do not
include central visual acuity). As expected, the two QoL surveys correlated positively and
highly significantly with one another. Taken as a whole, our contrast sensitivity testing
correlated with a higher significance level to the QoL metrics than our visual acuity
testing did. The IVI_C correlated appropriately with all vision tests, demonstrating that
higher ability scores match with lower LogMAR and better LogCS values. The
correlation between the IVI_C was highly significant with all charts except the TAC test
(2-tailed 0.05 level only). The B-L acuity chart was not significantly correlated with the
IVI_C. In addition, the LVP-FVQ correlated very significantly and appropriately with all
vision testing.
We adjusted the OMSRS data by removing “central acuity” from the total score.
It appears that the relationship between the adjusted O&M scores was appropriate for our
vision testing measures, where worse visual performance was indicative of greater need
for services and a higher score. Likewise, a higher O&M score related to a lower visual
ability level on both of our QoL surveys. However, the adjusted OMSRS data correlated
only with the LVP-FVQ, and only at the 0.05 level (2-tailed). Interestingly, if we
removed all vision data from the OMSRS, then the only significant correlation was with
B-L, and only at the 0.05 level (2-tailed). Otherwise, the O&M data we have obtained did
not correlate significantly with any of our vision tests. Clearly, our small sample size (13

106
subjects for letter charts and 14 for shaped charts) affected our power to detect
statistically significant relationships.

107
O&MScore IVI_C LVP-
FVQ
BLLogMAR PRLogCS TACLogMAR SCCSLogCS BDLogCS
IVI_C
Pearson
Correlation
-.372 .651** -.197 -.481** -.367* -.576** -.434**
Sig. (2-tailed) .097
.000 .237 .002 .020 .000 .005
N 21 45 38 38 40 40 40
LVP-FVQ
Pearson
Correlation
-.573* .651** -.594** -.738** -.597** -.512** -.584**
Sig. (2-tailed) .013 .000
.000 .000 .000 .002 .000
N 18 45 33 33 35 35 35
O&MScore
Pearson
Correlation
-.372 -.573* .540 .166 .219 .165 .450
Sig. (2-tailed)
.097 .013 .057 .588 .453 .574 .106
N 21 18 13 13 14 14 14
Table 12. QoL and O&M Correlations
**. Correlation was very significant: at the 0.01 level (2-tailed).
*. Correlation was significant: at the 0.05 level (2-tailed).
Note: conventions for this table are the same as for Table 14.

108
Discussion for Experiment III
Vision-Related Quality of Life. The IVI_C and LVP-FVQ can be administered
to students at OSSB, and it appears that scores were positively correlated with measures
of vision. However, some of the IVI_C content may not be well suited to students in
these specialized settings. Rehabilitation and classroom adaptations at OSSB are quite
good. It appears that the LVP-FVQ better targets the patient population at OSSB, as the
mean ability score for the survey participants was more closely aligned with the mean
item difficulty score of the survey.
It could be that some portion of the disability paradox was in play here: people
who are visually impaired place a higher value on vision than those who are not, yet
report better quality of life than expected (Albrecht & Devlieger, 1999). Perhaps with the
IVI_C (which contains social questions) we were not truly measuring functional reserve
but instead, overall happiness or some other construct. The high results we obtained on
the IVI_C could be due to the acclimation to vision loss that the student population at
OSSB exhibits. For instance, the least difficult question on the IVI_C by Rasch analysis
was: “Do your teachers understand your special needs?” Most people want to be happy,
and if they can find a way to adapt, they will be. The functional nature of the LVP-FVQ
may be better suited to assessing these students. Other measures like classroom
productivity may be appropriate as well.
Eight of our subjects were not OSSB students, but rather, were at OSSB for
summer camps. Their average person scores from the two surveys are shown in Figure 58

109
below. Generally, OSSB students with vision performed the best on the IVI_C. This
could be due to the fact that they are well adapted in their school environment. The
summer campers out performed OSSB students on the LVP-FVQ, perhaps due to the fact
that the LVP-FVQ is more functionally oriented, and these students function in
mainstream schools. In both cases, the OSSB students without measurable vision perform
the worst, and the difference is more dramatic on the LVP-FVQ. Error bars indicate the
standard error of measurement for each group. There were two blind students on the
LVP-FVQ who perceived their abilities to be quite high, resulting in a large range of
measurement for that group. One-way ANOVA analysis revealed a significant difference
between the subject groups (OSSB Partially-Sighted, Functionally Blind, and Summer
Campers) on the IVI_C only, but the effect was not confirmed by post-hoc analysis.

110
Figure 58. Average person scores for the IVI_C (left) and the LVP-FVQ (right)
Data are separated out by vision level and enrolment at OSSB.
The location of our summer school students relative to those other students who
took the two surveys can be seen on the subject-item maps in Figures 59 and 60. These
figures back up the assertion that summer campers generally perform better on the LVP-
FVQ than OSSB partially-sighted students and worse on the IVI_C.
It is also apparent from Figures 59 and 60 that the subject mean IVI_C is well
above the item mean. This confirms the fact that the IVI_C is perhaps more appropriate
for visually impaired students at mainstream schools and not at specialized school for the
blind settings.

111
Figure 60 demonstrates that the LVP-FVQ is better targeted for the subjects we
assessed, but our results do not follow a normal distribution. It is possible that increasing
the number of subjects would improve this distribution.

112
Figure 59. Subject-Item map for the IVI_C
Demonstrates Rasch-calibrated participant locations (x’s, left) and item locations (right). At the top of the map
are participants with higher perceived visual ability and questions thought to be more difficult. This map
demonstrates the targeting of the different response levels of each question to the respondents. Summer school
students have been marked with boxes. M, Mean; S, 1 SD from the mean; T, 2 SD from the mean.

113
Figure 60. Subject-Item map for the LVP-FVQ.
Conventions are the same as for Figure 59.
Linear regression between the Rasch-adjusted person scores for each individual
survey participant is demonstrated in Figure 61. It is clear that two functionally blind
subjects rated their perceived functional ability to be quite high on the LVP-FVQ, yet fell
in the middle of the pack (close to the y-axis) for the IVI_C. Likewise, there was one
subject in the functionally blind category on the IVI_C whose perceived visual ability
level was higher than the others in that group. His or her point can be found outlying the
trend line just above the abscissa.

114
Figure 61. Person Score Linear Regression of LVP-FVQ vs. IVI_C
Subjects with no measurable vision (or unable to perform lettered charts) are plotted with their standard errors
using the same symbol conventions as in Figure 39. All subjects are included in the regression in this case.
Orientation and Mobility. It does appear that, generally, subjects with
measurable vision receive a lower severity of need score. Thus, they need less time
devoted to orientation and mobility training. However, B-L acuity was the only factor
whose correlation reaches a level of statistical significance. This was despite the fact that
we adjusted the scores so as not to include B-L acuity. This may be due to the fact that
R² = 0.2436
-2
-1
0
1
2
3
4
-1 0 1 2 3
LVP
-FV
Q P
ers
on
Sco
re
IVI_C Person Score

115
the O&M teachers are aware of the child’s acuity and this awareness colors their
impressions for other items on the OMSRS.
We were only able to obtain a relatively small set of data for orientation and
mobility severity of need scores. This may affect our power to detect significant
statistical correlations.

116
General Discussion
Test Results
Our results in the tables above show that not all participants were able to complete
every aspect of the study protocol. Some participants (who were functionally blind) were
able to provide only quality of life questionnaire responses. We included those
participants for the purposes of balancing our Rasch analysis. We wanted to see if the
vision-related quality of life of functionally blind students tested as the same as those
with vision. It appears that they did not—students who lack measurable vision generally
clustered together at lower ability levels than sighted students. They were also generally
allocated more training time for orientation and mobility than their partially-sighted
classmates.
All vision tests were significantly correlated with one another except the B-L and
SCCS. This makes sense because the two charts are the least alike in terms of
measurement outcome and test methodology. As we hoped, we were able to measure a
variety of contrast sensitivity and acuity levels in this student population. However,
ceiling effects did come into play for some of our contrast sensitivity tests. Testing with
the striped cards (TAC and SCCS) cards consistently produced better results than the
lettered charts: B-L and P-R. With the SCCS cards, the majority of our subjects hit the
1.65 LogCS ceiling during our first year of testing. When we raised the ceiling to LogCS
2.00 for our second round of testing, again, the majority of subjects were able to see the

117
stripes on that card. The distribution of results for the P-R chart was much more
stratified—subjects who performed worse on the P-R chart gathered together with high
performing P-R subjects on the SCCS and BD test result graphs.
The Berkeley disc results were also better than the P-R test results, but were
limited by a 1.65 LogCS ceiling effect at all phases of our trial. The simpler task and
bolder patterns of the SCCS and the Berkeley Discs may make those tests more likely to
reveal the maximum performance that a given patient can achieve, even with the ceiling
in place. From the results of testing with a higher ceiling using the SCCS, it appears that
at least half of the subjects measured at 1.65 LogCS on the Berkeley Discs might have
been capable of 2.00 LogCS. These results are likely to be better transferrable to some
activities, such as O&M class, life skills, and gym. Performance in other courses, such as
English, Math, and Science may be better predicted by the results of our letter
identification tests.
Other Considerations
We did not screen for VF defects, which could affect a patient’s ability to locate
the discs within the grid or find the stimulus on the SCCS test. Based on my experience
testing these children, I believe that visual field status was only a factor during the testing
of three subjects: #5, #41 and #48.
Some subjects exhibited interesting behavior such as apparent malingering on the
Berkeley Discs and SCCS tests. One subject reported detecting our stimulus with his or
her “worse” eye on the blank half of the SCCS test 100% of the time (much higher than
chance) starting at the contrast threshold of the fellow and continuing all the way down to

118
the lowest contrast card. Perhaps he or she was unaware of the fact that intentionally
selecting the area absent a stimulus reveals the ability to discern stimulus location. On the
Berkeley Discs, several other subjects incorrectly reported discs in areas where none
were present. Perhaps this was in an attempt in their minds to try and get as many stimuli
identified as possible in an effort to boost their hit rate. It has been shown by other
investigators that children are much more prone to tolerating misses when reaching their
measurement thresholds, i.e., they’re willing to guess (Susan J Leat & Wegmann, 2004).
It is our opinion that these children were not intending to malinger, but instead were
experiencing false-positives throughout the entire test. This is because, given the design
of the Berkeley Discs, their threshold stimulus may be present in any cell on the grid.
Stated Objectives
Our goal was to ascertain whether the Stripe Card Contrast Sensitivity (SCCS)
Test was easy to administer and whether it could be successfully used on a wide variety
of participants. I believe that the test performed very well in this patient population and
would be appropriate to use in pediatric low vision settings whenever grating acuity
measurements are indicated.
We also wished to assess the SCCS test’s capability for validly quantifying
contrast sensitivity levels of children with impaired vision. It appears that this chart has
no trouble detecting the very high levels of contrast sensitivity performance that some
children with visual impairment are capable of. This is important because, while contrast
sensitivity measurement isn’t more useful than other standard examination procedures at
detecting disease, it does add valuable information regarding a patient’s expected level of

119
visual function. It seems that this patient population suffers less contrast impairment than
those who have visual impairment due to diseases more prevalent in the elderly such as
macular degeneration and diabetic retinopathy. However, we have not studied the SCCS
outside of the pediatric population as of yet.
Certainly, measurements from the SCCS test cannot be easily decimalized or
broken down in to smaller increments (such as LogCS 0.05) as is possible using letter-by-
letter scoring on the Pelli-Robson chart. This may affect the repeatability of the SCCS.
However, the target population for the SCCS is likely one where measurement by means
such as letter identification tasks simply isn’t possible. Test-retest variance would be
expected to be high in this group of patients for other functional reasons (such as autism
or developmental delay) and accuracy to the nearest 0.05 LogCS would not be a
consideration for most clinical examiners. It is likely that SCCS test results translate best
to daily living tasks for children that rely on low and middle spatial frequencies only such
as mobility, household, self-care, sports, and social activities. It may be useful to run the
SCCS test whenever input about a given student’s performance potential on these types
of tasks is a consideration for parents or educators.
I have calculated the SCCS contrast sensitivity values necessary for a subject to
have a vision-related quality of life score at the level found for the 75th percentile of our
functionally blind participants for both the IVI_C and the LVP-FVQ (See Figure 62).
Their contrast sensitivity would have to be approximately LogCS 1.02 for both the IVI_C
and the LVP-FVQ.

120
Figure 62. Cutoffs for normal SCCS Performance
The 75th percentile vision-related quality of life score was calculated for the students without measurable vision
and extended horizontally across the graph. The intersection point with the trend line was drawn vertically so
that the LogCS value on the abscissa demonstrates the expected contrast sensitivity level for partially-sighted
students with the same quality of life score. A, cutoff point for the IVI_C. B, cutoff point for the LVP-FVQ.
R² = 0.3313
-1.00
-0.50
0.00
0.50
1.00
1.50
2.00
2.50
3.00
-2.5 -2 -1.5 -1 -0.5 0 0.5 1
IVI_
C P
erso
n S
core
SCCS LogCS
A
R² = 0.2623
-2
-1
0
1
2
3
4
-2.5 -2 -1.5 -1 -0.5 0 0.5 1
LVP
-FV
Q P
erso
n S
core
SCCS LogCS
B

121
This means that successfully localizing the striped pattern on the SCCS test for
the LogCS 0.90 card (or worse) would be a reasonable cutoff indicative of performance
that is definitely abnormal. Indeed, this value corresponds well with cutoffs for
significantly impaired contrast sensitivity found in the literature and described in earlier
sections of this thesis (S J Leat & Woo, 1997; Susan J Leat et al., 1999; West et al.,
2002).
The findings in this section, taken together, demonstrate the Stripe Card Contrast
Sensitivity test to be a useful clinical measure for young, non-verbal or otherwise
developmentally delayed patients with visual impairment.

122
References
Adams, R. J., & Courage, M. L. (2003). Can the visual acuity of infants be predicted
from a measurement of contrast sensitivity? J Pediatr Ophthalmol Strabismus,
40(1), 35–38. Retrieved from
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=
Citation&list_uids=12580270
Albrecht, G. L., & Devlieger, P. J. (1999). The disability paradox: high quality of life
against all odds. Social Science & Medicine (1982), 48(8), 977–88. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/10390038
Arden, G. B. (1978). The importance of measuring contrast sensitivity in cases of visual
disturbance. British Journal of Ophthalmology, 62(4), 198–209.
doi:10.1136/bjo.62.4.198
Arditi, A. (2005). Improving the design of the letter contrast sensitivity test. Investigative
Ophthalmology & Visual Science, 46(6), 2225–9. doi:10.1167/iovs.04-1198
Bailey, I. L., Chu, M. A., Jackson, A. J., Minto, H., & Greer, R. B. (2011). Assessment of
vision in severely visually impaired populations. In ARVO Fort Lauderdale. Fort
Lauderdale, FL.
Bailey, I. L., & Lovie, J. (1976). New design principles for visual acuity letter charts. …
Journal of Optometry and Physiological Optics. Retrieved from
http://europepmc.org/abstract/MED/998716
Bennett, A. G. (1965). Ophthalmic test types. A review of previous work and discussions
on some controversial questions. The British Journal of Physiological Optics, 22(4),
238–71. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/5331332
Bittner, A. K., Jeter, P., & Dagnelie, G. (2011). Grating acuity and contrast tests for
clinical trials of severe vision loss. Optometry and Vision Science, 88(10), 1153–
1163.
Black, A. A., Lovie-Kitchin, J. E., Woods, R. L., Arnold, N., Byrnes, J., & Murrish, J.
(1997). Mobility performance with retinitis pigmentosa. Clinical Experimental
Optometry Journal of the Australian Optometrical Association, 80, 1–12. Retrieved
from http://dx.doi.org/10.1111/j.1444-0938.1997.tb04841.x

123
Blakemore, C., & Campbell, F. W. (1969a). Adaptation to spatial stimuli. The Journal of
Physiology. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/5761934
Blakemore, C., & Campbell, F. W. (1969b). On the existence of neurones in the human
visual system selectively sensitive to the orientation and size of retinal images. The
Journal of Physiology, 237–260. Retrieved from
http://jp.physoc.org/content/203/1/237.short
Bland, J. M., & Altman, D. G. (1986). Statistical methods for assessing agreement
between two methods of clinical measurement. Lance (Vol. 47, pp. 307–310).
Elsevier Ltd. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2868172
Bochsler, T. M., Legge, G. E., Kallie, C. S., & Gage, R. (2012). Seeing steps and ramps
with simulated low acuity: impact of texture and locomotion. Optometry and Vision
Science, 89(9), E1299–307. doi:10.1097/OPX.0b013e318264f2bd
Campbell, F. W., Howell, E., & Robson, J. G. (1970). The appearance of gratings with
and without the fundamental Fourier component. The Journal of Physiology, 193–
201. Retrieved from http://europepmc.org/abstract/MED/5571919
Campbell, F. W., & Robson, J. G. (1968). Application of Fourier analysis to the visibility
of gratings. The Journal of Physiology, 197(3), 551. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1351748/
Cochrane, G. M., Lamoureux, E. L., & Keeffe, J. E. (2008). Defining the content for a
new quality of life questionnaire for students with low vision (the Impact of Vision
Impairment on Children: IVI_C). Ophthalmic Epidemiology, 15(2), 114–20.
doi:10.1080/09286580701772029
Cochrane, G. M., Marella, M., Keeffe, J. E., & Lamoureux, E. L. (2011). The Impact of
Vision Impairment for Children (IVI_C): validation of a vision-specific pediatric
quality-of-life questionnaire using Rasch analysis. Investigative Ophthalmology &
Visual Science, 52(3), 1632–40. doi:10.1167/iovs.10-6079
DeCarlo, D. K., McGwin, G., Bixler, M. L., Wallander, J., & Owsley, C. (2012). Impact
of pediatric vision impairment on daily life: results of focus groups. Optometry and
Vision Science : Official Publication of the American Academy of Optometry, 89(9),
1409–16. doi:10.1097/OPX.0b013e318264f1dc
Dobson, V., & Teller, D. Y. (1978). Visual acuity in human infants: a review and
comparison of behavioral and electrophysiological studies. Vision Research, 18(11),
1469–83. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/364823

124
Dorr, M., Lesmes, L. a, Lu, Z.-L., & Bex, P. J. (2013). Rapid and reliable assessment of
the contrast sensitivity function on an iPad. Investigative Ophthalmology & Visual
Science, 54(12), 7266–73. doi:10.1167/iovs.13-11743
Dougherty, B. E., Flom, R. E., & Bullimore, M. A. (2005). An evaluation of the Mars
Letter Contrast Sensitivity Test. Optometry and Vision Science, 82(11), 970–5.
Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/16317373
Eperjesi, F., Wolffsohn, J., Bowden, J., Napper, G., & Rubinstein, M. (2004). Normative
contrast sensitivity values for the back-lit Melbourne Edge Test and the effect of
visual impairment. Ophthalmic & Physiological Optics : The Journal of the British
College of Ophthalmic Opticians (Optometrists), 24(6), 600–6. doi:10.1111/j.1475-
1313.2004.00248.x
Ferris, F. L., Kassoff, A., Bresnick, G. H., & Bailey, I. L. (1982). New visual acuity
charts for clinical research. American Journal of Ophthalmology, 94(1), 91–96.
Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/7091289
Frantz, R. L., Ordy, J. M., & Udelf, M. S. (1962). Maturation of pattern vision in infants
during the first six months. Journal of Comparative and Physiological Psychology.
doi:10.1037/h0044173
Geruschat, D., Turano, K. A., & Stahl, J. (1998). Traditional Measures of Mobility
Performance and Retinitis Pigmentosa. Optometry & Vision Science, 75(7), 525–
537. Retrieved from
http://journals.lww.com/optvissci/Abstract/1998/07000/Traditional_Measures_of_M
obility_Performance_and.22.aspx
Ginsburg, A. P. (2003). Contrast sensitivity and functional vision. International
Ophthalmology Clinics, 43(2), 5–15. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/12711899
Goodrich, G. L., & Ludt, R. (2003). Assessing visual detection ability for mobility in
individuals with low vision. Visual Impairment Research, 5(2), 57–71. Retrieved
from http://informahealthcare.com/doi/abs/10.1076/vimr.5.2.57.26265
Gothwal, V. K., Lovie-Kitchin, J. E., & Nutheti, R. (2003). The Development of the LV
Prasad-Functional Vision Questionnaire: A Measure of Functional Vision
Performance of Visually Impaired Children. Investigative Ophthalmology & Visual
Science, 44(9), 4131–4139. doi:10.1167/iovs.02-1238
Gothwal, V. K., & Sumalini, R. (2012). The Second Version of the LV Prasad-Functional
Vision Questionnaire. Optometry & Vision Science, 89(11), 1601–10.
doi:10.1097/OPX.0b013e31826ca291

125
Haymes, S. A., Roberts, K. F., Cruess, A. F., Nicolela, M. T., LeBlanc, R. P., Ramsey,
M. S., … Artes, P. H. (2006). The letter contrast sensitivity test: clinical evaluation
of a new design. Investigative Ophthalmology & Visual Science, 47(6), 2739–45.
doi:10.1167/iovs.05-1419
Hubel, D., & Wiesel, T. (1962). Receptive fields, binocular interaction and functional
architecture in the cat’s visual cortex. The Journal of Physiology, 106–154.
Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1359523/
Kirby, R., & Basmajian, J. (1984). The nature of disability and handicap. In Medical
Rehabilitation (pp. 14–18). Baltimore: Williams & Wilkins.
Kollbaum, P. (2014). Validation of an iPad test of letter contrast sensitivity. Optometry
and Vision Science: 91(3), 291–296. Retrieved from
http://pdfs.journals.lww.com/optvissci/9000/00000/Validation_of_an_iPad_Test_of
_Letter_Contrast.99023.pdf
Kramer, S. G., & Mcdonald, M. A. (1986). Diagnostic and surgical techniques,
assessment of visual acuity in toddlers. Survey of Ophthalmology, 31(3), 189–210.
Kuyk, T., Elliot, J., & Fuhr, P. (1998). Visual correlates of mobility in real world settings
in older adults with low vision. Optometry & Vision Science, 75(7), 538–547.
Retrieved from
http://journals.lww.com/optvissci/abstract/1998/07000/visual_correlates_of_mobilit
y_in_real_world.23.aspx
Leat, S. J., Legge, G. E., & Bullimore, M. A. (1999). What is low vision? A re-evaluation
of definitions. Optometry & Vision Science, 76(4), 198–211. Retrieved from
http://journals.lww.com/optvissci/Abstract/1999/04000/What_Is_Low_Vision__A_
Re_evaluation_of_Definitions.23.aspx
Leat, S. J., & Wegmann, D. (2004). Clinical testing of contrast sensitivity in children:
age-related norms and validity. Optometry and Vision Science, 81(4), 245–54.
Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/15097766
Leat, S. J., & Woo, G. C. (1997). The validity of current clinical tests of contrast
sensitivity and their ability to predict reading speed in low vision. Eye (London,
England), 11 ( Pt 6)(519), 893–9. doi:10.1038/eye.1997.228
Lennie, P., & Hemel, S. B. V. (2002). Visual impairments: determining eligibility for
social security benefits. National Academy Press. Retrieved from
http://books.google.com/books?id=5QbtT8rzJcwC

126
Long, R., Rieser, J., & Hill, E. (1990). Mobility in individuals with moderate visual
impairments. Journal of Visual Impairment & Blindness, 84, 111–118.
Lovie-Kitchin, J. E., Bevan, J. D., & Hein, B. (2001). Reading performance in children
with low vision. Clinical & Experimental Optometry : Journal of the Australian
Optometrical Association, 84(3), 148–154. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/12366326
Marron, J. A., & Bailey, I. L. (1982). Visual factors and orientation-mobility
performance. American Journal of Optometry and Physiological Optics, 59(5), 413–
426.
Massof, R. W. (1998). A systems model for low vision rehabilitation II. Measurement of
vision disabilities. Optometry & Vision Science, 75(5), 349. Retrieved from
http://journals.lww.com/optvissci/Abstract/1998/05000/A_Systems_Model_for_Lo
w_Vision_Rehabilitation__II_.25.aspx
Massof, R. W. (2002). The measurement of vision disability. Optometry and Vision
Science, 79(8), 516–52. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/12199545
Mayer, D. L., Beiser, a S., Warner, a F., Pratt, E. M., Raye, K. N., & Lang, J. M. (1995).
Monocular acuity norms for the Teller Acuity Cards between ages one month and
four years. Investigative Ophthalmology & Visual Science, 36(3), 671–85. Retrieved
from http://www.ncbi.nlm.nih.gov/pubmed/7890497
McDonald, M. A., Dobson, V., Sebris, S. L., Baitch, L., Varner, D., & Teller, D. Y.
(1985). The acuity card procedure: a rapid test of infant acuity. Investigative
Ophthalmology & Visual Science, 2, 1158–1162. Retrieved from
http://www.iovs.org/content/26/8/1158.short
Owsley, C. (2003). Contrast sensitivity. Ophthalmology Clinics of North America, 16(2),
171–177. doi:10.1016/S0896-1549(03)00003-8
Owsley, C., & Sloane, M. E. (1987). Contrast sensitivity, acuity, and the perception of
“real-world” targets. The British Journal of Ophthalmology, 71(10), 791–796.
Retrieved from
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=
Citation&list_uids=3676151
Pelli, D. G., & Bex, P. (2013). Measuring contrast sensitivity. Vision Research, 90, 10–4.
doi:10.1016/j.visres.2013.04.015

127
Pelli, D. G., Robson, J. G., & Wilkins, A. J. (1988). The design of a new letter chart for
measuring contrast sensitivity. Clin Vis Sci, 2(3), 187–199. Retrieved from
http://scholar.google.com/scholar?hl=en&btnG=Search&q=intitle:THE+DESIGN+
OF+A+NEW+LETTER+CHART+FOR+MEASURING+CONTRAST+SENSITIVI
TY#0
Pokusa, J. E., Kran, B. S., & Mayer, L. (2013). A pilot study of a preferential looking
contrast sensitivity test for individuals with vision and/or multiple impairments.
Seattle, WA.
Raasch, T. W., Bailey, I. L., & Bullimore, M. A. (1998). Repeatability of visual acuity
measurement. Optometry and Vision Science Official Publication of the American
Academy of Optometry, 75, 342–348. Retrieved from
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=
Citation&list_uids=9624699
Rabin, J., & Wicks, J. (1996). Measuring resolution in the contrast domain: the small
letter contrast test. Optometry & Vision Science, 73, 398–403.
doi:10.1097/00006324-199606000-00007
Rasch, G. (1960). Probabilistic models for some intelligence and attainment tests.
Copenhagen.
Ratliff, F. (1965). Mach bands : quantitative studies on neural networks in the retina. San
Francisco, CA: Holden-Day.
Reeves, B. C., Wood, J. M., & Hill, A. R. (1991). Vistech VCTS 6500 charts--within-
and between-session reliability. Optometry and Vision Science, 68(9), 728–737.
Shapley, R. M., & Lam, D. (1993). Contrast Sensitivity. Cambridge, Mass: MIT Press.
Sloan, L. (1959). New test charts for the measurement of visual acuity at far and near
distances. American Journal of Ophthalmology, 48(Dec), 807–813.
Tandon, J. H. (1994). Nothing more can be done...a fable for our times. Ophthalmology,
(7), 203–205.
Tasman, W. (1992). Duane’s Foundations of Clinical Ophthalmology. Philadelphia, PA:
Lippincott Williams & Wilkins.
The World Health Organization. (1980). International Classification of Impairments,
Disabilities, and Handicaps (ICDH). Geneva: World Health Organization.

128
West, S. K., Rubin, G. S., Broman, A. T., & Mun, B. (2002). How does visual
impairment affect performance on tasks of everyday life?, 120(June).
Wilkins, A. J., Della Sala, S., Somazzi, L., & Nimmo-Smith, I. (1988). Age-related
norms for the Cambridge Low Contrast Gratings, including details concerning their
design and use. Clin Vis Sci, 2(3), 201–212. Retrieved from
http://www.essex.ac.uk/psychology/overlays/1988-75.pdf
Wolffsohn, J. S., Eperjesi, F., & Napper, G. (2005). Evaluation of Melbourne edge test
contrast sensitivity measures in the visually impaired. Ophthalmic & Physiological
Optics : The Journal of the British College of Ophthalmic Opticians (Optometrists),
25(4), 371–4. doi:10.1111/j.1475-1313.2005.00282.x

129
Appendix A: Study Materials

130

131
Dear Parent/Guardian,
We would like to share this invitation with you so that your child may join us (perhaps for the second time) in a
collaborative research study. As you may already know, the goal of our study will be to develop a new way to
measure a person’s ability to sense the contrast between light, gray, and dark. Unlike previous methods of measuring
the ability to sense contrast, this method will not require the patient to read the letters of an eye chart.
We would like to ask your child to take part in this study because s/he is partially sighted. If your child agrees to enter
the study, we may:
Ask your child some questions to find out how greatly his/her vision affects him/her in everyday life.
Measure his/her vision using regular lettered eye charts and charts with shapes
Measure his/her ability to see different shades of gray using letters and shapes
Give your child a $5 gift card to thank them for their help with our project.
If you give your permission for your child to participate, s/he will have the opportunity to choose not to participate. If
your child is uncomfortable answering any of the questions, s/he may just skip the questions s/he does not like. This
test does not involve eye drops of any kind. We will be testing one eye at a time, so we will ask your child to wear a
“pirate” type eye patch during testing. However, if your child prefers not to wear it, we will not insist. We do not need
to touch your child in any way, although we will be happy to help him/her put on the eye patch if s/he needs it.
If you wish to allow your child to participate, please read and sign the permission form, as well as the HIPAA form.
These are the standard forms that are used any time human subjects are involved in research projects. Please
complete and return all of the provided forms to us.
If you do NOT wish to allow your child to participate, please complete and return the response form enclosed with
this letter. On this form, you may request that we will remove your contact information from our records so that we
will not contact you again about this project.
If you have any questions or concerns about your child’s participation in this study, please do not hesitate to contact
us.
Thank you for your consideration and for potentially allowing your child to participate in our study!
Sincerely yours,
Angela M Brown, PhD Professor The OSU College of Optometry [email protected] o: 614-292-4423
Gregory R Hopkins, OD Senior Research Associate OSSB Extern Site Preceptor [email protected] o: 614-688-5542
Bradley E Dougherty, OD, MS OSU Clinical Attending Optometrist The OSU College of Optometry [email protected]
PARENTAL PERMISSION Biomedical/Cancer
IRB Protocol Number: 2011H0350
IRB Approval date: 4/4/12
Version: 2.0
132
The Ohio State University Parental Permission
For Child’s Participation in Research
Study Title: Pilot Study Pilot Study validation of the Stripe Card Contrast Sensitivity Test on
low-vision participants
Principal
Investigator: Angela M Brown, PhD
Sponsor:
The Center for Clinical and Translational Science
of the National Institutes of Health
National Eye Institute of the National Institutes of Health
This is a parental permission form for research participation. It contains important
information about this study and what to expect if you permit your child to participate. Please consider the
information carefully. Feel free to discuss the study with your friends and family and to ask questions
before making your decision whether or not to permit your child to participate.
Your child’s participation is voluntary. You or your child may refuse participation in this study.
If your child takes part in the study, you or your child may decide to leave the study at any time.
No matter what decision you make, there will be no penalty to your child and neither you nor your
child will lose any of your usual benefits.
Your decision will not affect your future relationship with The Ohio State University. If you
or your child is a student or employee at Ohio State, your decision will not affect your grades or
employment status.
Your child may or may not benefit as a result of participating in this study. Also, as explained
below, your child’s participation may result in unintended or harmful effects for him or her that
may be minor or may be serious depending on the nature of the research.
You and your child will be provided with any new information that develops during the
study that may affect your decision whether or not to continue to participate. If you permit
your child to participate, you will be asked to sign this form and will receive a copy of the form.
You are being asked to consider permitting your child to participate in this study for the reasons
explained below.
1. Why is this study being done?
This study is being done to develop a new method of measuring visual function in infants and children.
2. How many people will take part in this study?
56

PARENTAL PERMISSION Biomedical/Cancer
IRB Protocol Number: 2011H0350
IRB Approval date: 4/4/12
Version: 2.0
133
3. What will happen if my child takes part in this study?
Your child will have five vision tests: two visual acuity tests (one with letters and one with stripes) and
three contrast sensitivity tests (one with letters, one with stripes, and one with circles). Your child may also
be interviewed using a questionnaire to determine what impact his/her vision has on his/her everyday life.
This study does not involve any eye drops, and we will not be puffing your child’s eyes, or touching his/her
eyes in any way.
4. How long will my child be in the study?
For up to three sessions only, lasting no more than a half hour each.
5. Can my child stop being in the study?
Your child may leave the study at any time. If you or your child decides to stop participation in the study,
there will be no penalty and neither you nor your child will lose any benefits to which you are otherwise
entitled. Your decision will not affect your future relationship with The Ohio State University.
6. What risks, side effects or discomforts can my child expect from being in the study?
These tests are not associated with any known risks, side effects or discomforts.
7. What benefits can my child expect from being in the study?
We do not anticipate that your child will benefit from being in this study.
8. What other choices does my child have if he/she does not take part in the study?
You or your child may choose not to participate without penalty or loss of benefits to which you are
otherwise entitled.
9. Will my child’s study-related information be kept private?
Efforts will be made to keep your child’s study-related information confidential. However, there may be
circumstances where this information must be released. For example, personal information regarding your
child’s participation in this study may be disclosed if required by state law.
Also, your child’s records may be reviewed by the following groups (as applicable to the research):
Office for Human Research Protections or other federal, state, or international regulatory agencies;
U.S. Food and Drug Administration;

PARENTAL PERMISSION Biomedical/Cancer
IRB Protocol Number: 2011H0350
IRB Approval date: 4/4/12
Version: 2.0
134
The Ohio State University Institutional Review Board or Office of Responsible Research
Practices;
The sponsor supporting the study, their agents or study monitors; and
Your insurance company (if charges are billed to insurance).
If this study is related to your child’s medical care, your child’s study-related information may be placed in
their permanent hospital, clinic, or physician’s office records. Authorized Ohio State University staff not
involved in the study may be aware that your child is participating in a research study and have access to
your child’s information.
You may also be asked to sign a separate Health Insurance Portability and Accountability Act (HIPAA)
research authorization form if the study involves the use of your child’s protected health information.
10. What are the costs of taking part in this study?
There are no costs associated with participating in this study.
11. Will I or my child be paid for taking part in this study?
We will offer your child a gift card of $5.00. By law, payments to subjects are considered taxable income.
12. What happens if my child is injured because he/she took part in this study?
If your child suffers an injury from participating in this study, you should notify the researcher or study
doctor immediately, who will determine if your child should obtain medical treatment at The Ohio State
University Medical Center.
The cost for this treatment will be billed to you or your medical or hospital insurance. The Ohio State
University has no funds set aside for the payment of health care expenses for this study.
13. What are my child’s rights if he/she takes part in this study?
If you and your child choose to participate in the study, you may discontinue participation at any time
without penalty or loss of benefits. By signing this form, you do not give up any personal legal rights your
child may have as a participant in this study.
You and your child will be provided with any new information that develops during the course of the
research that may affect your decision whether or not to continue participation in the study.
You or your child may refuse to participate in this study without penalty or loss of benefits to which you
are otherwise entitled.

PARENTAL PERMISSION Biomedical/Cancer
IRB Protocol Number: 2011H0350
IRB Approval date: 4/4/12
Version: 2.0
135
An Institutional Review Board responsible for human subjects research at The Ohio State University
reviewed this research project and found it to be acceptable, according to applicable state and federal
regulations and University policies designed to protect the rights and welfare of participants in research.
14. Who can answer my questions about the study?
For questions, concerns, or complaints about the study you may contact Dr Angela M Brown, Professor,
the Ohio State University College of Optometry. 614-292-4423.
For questions about your child’s rights as a participant in this study or to discuss other study-related
concerns or complaints with someone who is not part of the research team, you may contact Ms. Sandra
Meadows in the Office of Responsible Research Practices at 1-800-678-6251.
If your child is injured as a result of participating in this study or for questions about a study-related injury,
you may contact Dr Angela M Brown.
Signing the parental permission form
I have read (or someone has read to me) this form and I am aware that I am being asked to provide
permission for my child to participate in a research study. I have had the opportunity to ask questions and
have had them answered to my satisfaction. I voluntarily agree to permit my child to participate in this
study.
I am not giving up any legal rights by signing this form. I will be given a copy of this form.
Printed name of subject
Printed name of person authorized to provide
permission for subject
Signature of person authorized to provide
permission for subject
AM/PM
Relationship to the subject Date and time

PARENTAL PERMISSION Biomedical/Cancer
IRB Protocol Number: 2011H0350
IRB Approval date: 4/4/12
Version: 2.0
136
Investigator/Research Staff
I have explained the research to the participant or his/her representative before requesting the signature(s)
above. There are no blanks in this document. A copy of this form has been given to the participant or
his/her representative.
Printed name of person obtaining consent Signature of person obtaining consent
AM/PM
Date and time

137
OSU-OSSB Contrast Sensitivity Study Response Form
Student Name: <Insert Name>
If at all possible, please use the enclosed envelope to return these forms to us within 10 days. If
we have not heard back from you after that time, you may be contacted via telephone or email
regarding this study. Thank you for your consideration regarding our collaborative research
study!
The Ohio State University College of Optometry Visual Perception Lab has contacted me to
invite my child to participate in a research project:
YES NO
I have completed and will enclose:
1. Parental Permission Form:
Filled-out/signed/dated top portion of the final page
2. Personal Health Information in Research Form:
Printed child’s name on first page
Initialed/dated bottom corner of first two pages
Signed/filled-out bottom portion of final page.
I prefer that my child
NOT participate in this study
I will return only this
form using the enclosed
envelope
Please remove our contact
information from your
records for the purpose of
this study
Parent/Guardian Signature: X ______________________________________________
Comments:
______________________________________________________________________________
______________________________________________________________________________

138
Verbal Consent Script
Pilot Study validation of the Stripe Card Contrast Sensitivity Test on Low-Vision Participants
Angela M Brown, PhD
Principal Investigator
Funded by the Center for Clinical and Translational Science and the National Eye Institute.
Hi, [student’s name]. My name is Dr/Mr/Ms [first tester’s name], and Dr/Mr/Ms [second
tester’s name] will be helping out today with this research project. If it’s OK with you, we want to test
your vision each of your eyes separately, and ask you some questions about your life (if we haven’t
already).
The goal of our study will be to develop a new way to measure a person’s ability to sense the
contrast between light, gray, and dark. The tests of your vision won’t be hard: you’ll just read five
different eye charts, two with letters and three with shapes. The questions about your life won’t be
hard at all either, since there are no “right” or “wrong” answers to any of them.
The information that you share with us will help us to learn how to do a better job testing
the vision of other students like yourself.
This project will take up to one half-hour of your time and after you finish, we will give you a $5 gift
card to say “thank you” for helping us today
There is a small risk of a breach of confidentiality, but all efforts will be made to keep everything we
learn about you in the strictest confidentiality. We will not link your name to anything that you say in
any of our publications.
There are no other expected risks of participation. Nothing bad will happen to you if you
participate. We won’t be using any eye drops at all and we won’t be puffing you in the eye. We would
like for you to put a pirate-patch while viewing the eye charts, but we will not be touching you at all,
unless you ask for help with the patch.
Participation is voluntary. If you decide not to participate, there will be no penalty or loss of
benefits to which you are otherwise entitled. You can, of course, decline to wear the pirate patch or to
answer any questions about your life that you are uncomfortable with, as well as to stop participating
at any time, without any penalty or loss of benefits to which you are otherwise entitled.
If you want to talk to your parents, teachers or friends about this before you decide, just let
us know. You can come back another day and we can test you then, if you want. We will only test you
if you say it is OK. If you have any additional questions concerning this research or your participation
in it, please feel free to contact us or our university research office at any time using the contact sheet
that we will provide you with today.
Do you have any questions for us right now before we start?
Is it OK if we do the eye tests today? Is it OK if we ask you the questions today? If everything
is OK, then let’s begin…
Student’s signature: x____________________________________ Printed name: ___________________________________
I have read this script to this student, and s/he indicated willingness to participate in this research.
First tester’s Signature: x _____________________________________ Date: ___ /___ /___
First tester’s Printed Name: ___________________________________ Time: ______ AM/PM
139
Verbal Assent Script
Pilot Study validation of the Stripe Card Contrast Sensitivity Test on Low-Vision
Participants
Angela M Brown, PhD
Principal Investigator
Funded by the Center for Clinical and Translational Science and the National Eye
Institute.
Hi, [student’s name]. My name is Dr/Mr/Ms [first tester’s name], and Dr/Mr/Ms [second tester’s
name] will be helping out today.
If it’s OK with you, we want to test your vision in each of your eyes separately, and ask you
some questions about your life (if we haven’t already). If you are under the age of 18, your parents
have already said it is OK for you to do these tests, but we want to make sure it is OK with you too.
We are doing this so we can learn how to do a better job testing the vision of students like
yourself.
The tests of your vision won’t be hard: you’ll just read five different eye charts, two with
letters and three with shapes. We would like for you to put a pirate-patch on the eye you don’t want
us to test, but if you don’t want to wear the patch, that would be OK too. If you want us to, we will
wear a pirate patch too, just for fun.
The questions about your life won’t be hard at all either, and there are no right or wrong
answers to any of them.
The tests and questions will take no more than a half hour.
You can say “No” or stop testing any time you want to. You won’t get into trouble if you say
“No” or want to stop.
Nothing bad will happen to you if you participate. We won’t be using any drops at all, and we
won’t be puffing you in the eye, and we will not be touching you at all, unless you ask for help. We
don’t expect anything good to happen either, though.
After you finish, we will give you a $5 gift card to say “thank you” for helping us today.
If you want to talk to your parents, teachers or friends about this before you decide, just let
us know. You can come back another day and we can test you then, if you want. We will only test
you if you say it is OK.
Is it OK if we do the eye tests? Is it OK if we ask you the questions?
Do you have any questions for us before we start?
Student’s signature: x______________________________ Printed name: ________________________
I have read this script to this student, and s/he indicated willingness to participate in this research.
First tester’s Signature: x _____________________________________ Date: ___ /___ /___
First tester’s Printed Name: ___________________________________ Time: ______ AM/PM

140
Testing Counterbalance No 1st Test 2nd Test 3rd Test 4th Test 5th Test 01 B-L P-R BD TAC SCCS 02 SCCS TAC BD P-R B-L 03 P-R TAC B-L SCCS BD 04 BD SCCS B-L TAC P-R 05 TAC SCCS P-R BD B-L 06 B-L BD P-R SCCS TAC 07 SCCS BD TAC B-L P-R 08 P-R B-L TAC BD SCCS 09 BD B-L SCCS P-R TAC 10 TAC P-R SCCS B-L BD 11 B-L P-R BD TAC SCCS 12 SCCS TAC BD P-R B-L 13 P-R TAC B-L SCCS BD 14 BD SCCS B-L TAC P-R 15 TAC SCCS P-R BD B-L 16 B-L BD P-R SCCS TAC 17 SCCS BD TAC B-L P-R 18 P-R B-L TAC BD SCCS 19 BD B-L SCCS P-R TAC 20 TAC P-R SCCS B-L BD 21 B-L P-R BD TAC SCCS 22 SCCS TAC BD P-R B-L 23 P-R TAC B-L SCCS BD 24 BD SCCS B-L TAC P-R 25 TAC SCCS P-R BD B-L 26 B-L BD P-R SCCS TAC 27 SCCS BD TAC B-L P-R 28 P-R B-L TAC BD SCCS 29 BD B-L SCCS P-R TAC 30 TAC P-R SCCS B-L BD 31 B-L P-R BD TAC SCCS 32 SCCS TAC BD P-R B-L 33 P-R TAC B-L SCCS BD 34 BD SCCS B-L TAC P-R 35 TAC SCCS P-R BD B-L 36 B-L BD P-R SCCS TAC 37 SCCS BD TAC B-L P-R 38 P-R B-L TAC BD SCCS 39 BD B-L SCCS P-R TAC 40 TAC P-R SCCS B-L BD 41 B-L P-R BD TAC SCCS

OSSB Vision Testing Worksheet Subject ID: ____ -______
Date: ______ /______ /______ Testing
Order #: ______
| Rx: N; Y | Eye: R; L | MM DD YY
141

OSSB Vision Testing Worksheet Subject ID: ____ -______
Date: ______ /______ /______ Testing
Order #: ______
| Rx: N; Y | Eye: R; L | MM DD YY
142

OSSB Human Subject Payment Receipt
Protocol #: 2011H0350
Subject ID: ____ -______
Date: ______ /______ /______
MM DD YY
143

144
The Impact of Visual Impairment in Children (IVI_C) Questionnaire:
I’m going to read some questions to you.
Please say which answer best describes what you do and feel most of the time.
There are no “right” or “wrong” answers.
Please answer the questions for yourself – we don’t want your family’s answers.
Please answer with one of the responses that I read out to you: Always, Almost Always,
Sometimes, Almost Never, Never.
Some things you won’t do. In this case, just answer, ‘No, for other reasons’.
These questions are all about how things are for you BECAUSE OF YOUR EYESIGHT:
01 Do you find it difficult to go down stairs or to step off the sidewalk?
02 Are you confident to make your own way to school?
03 Are you confident to use public transport (such as buses, trains, ferries) by yourself?
04 Are you confident in places you don’t know?
05 Are you confident that you can move around safely in places you don’t know in the daytime?
06 Are you confident that you can move around safely in places you don’t know at night-time?
07 Can you find your friends in the playground at lunch and play time?
08 When you are in a room, can you recognize people you know before they speak to you?
09 Can you take part in games or sports that you want to play with your friends?
10 Do you get the chance to go to activities other than sport (such as social groups)?
11 Has your eyesight stopped you from doing the things that you want to do?
12 Do other students help you when you ask them for help?
13 Do other students help you to join in with them?
14 Do you find it hard to join in with other students?
15 Do you get frustrated?
16 Do other students understand your special needs?
17 Do your teachers understand your special needs?
18 In the classroom, do you get all the same information as other students?
19 Do you get all the information at the same time as the other students?
20 Do you get enough time in school to complete the work set by the teacher?
21 When you are in the classroom, are you confident about asking for help you need?
22 When you ask for help, do people understand how much help you need?
23 Do people tell you that you can’t do the things that you want to do?
24 Do people stop you from doing the things you want to do?
25 Do you get yourself ready for school?
26 Can you recognize coins and paper money when paying for things?

145
The LV Prasad Visual Functioning Questionnaire (LVP_VFQ):
I’m going to read some questions to you.
Please say which answer best describes what you do and feel most of the time.
There are no “right” or “wrong” answers.
Please answer the questions for yourself - your family is important but we don’t want their answers, we want yours.
I will ask you how much difficulty you have with some typical activities.
Please answer with one of the responses that I read out to you: None, Little, Moderate, Great
Deal, Unable.
Some things you won’t do because you are too young or for other reasons. In this case, just
answer, ‘Does not apply’.
BECAUSE OF YOUR VISION, how much difficulty do you have with:
01 Making out whether the person you are seeing across the road is a boy or a girl (during the day)?
02 Seeing whether somebody is calling you by waving his or her hand from across the road?
03 Walking alone in the hallway at school without bumping into objects or people?
04 Walking home at night (from anywhere) without assistance when there are streetlights?
05 Copying from the blackboard while sitting on the first seat in your class?
06 Reading the bus numbers?
07 Reading the other details on the bus (such as its destination?)
08 Reading your textbooks at an arm’s length?
09 Writing along a straight line?
10 Finding the next line while reading when you take a break and then resume reading?
11 Locating dropped objects (pen, pencil, and eraser) within the classroom?
12 Threading a needle?
13 Distinguishing between a quarter and a nickel (without touching)?
14 Climbing up or down stairs?
15 Lacing your shoes?
16 Locating a ball while playing in the daylight?
17 Putting toothpaste on your toothbrush?
18 Locating food on your plate while eating?
19 Identifying colors (e.g., while coloring)?
20 How do you think your vision is compared with that of your normal-sighted friends?
As good as your friend’s? 2 A little bit worse than your friend’s? 3 Much worse than your friend’s?

146
Orientation & Mobility Severity Rating Scale (O&MSRS)
Severity of Need NONE
0 MILD
1 MODERATE
2 SEVERE
3 PROFOUND
4 SCORE
(1) Level of Vision
(Medical)
Distance Acuity
20/70 - 20/100 20/100 - 20/200 20/200 - 20/600 20/600 - LP
Light Perception to Nil
Peripheral Field
No loss No loss 30˚ - 10˚ field or
hemianopsia 10˚ field - 1˚ field
(2) Level of Vision (Functional)
Refer to Guidelines: page 4, Level of Vision
(Functional) #1
Visual impairment affects ability to travel in a few
selected environments
Visual impairment affects ability to travel in some environments
Visual impairment affects ability to travel in most environments
Visual impairment affects ability to travel
in all environments
(3) Use/proficiency of travel tool (cane/Alternate
Mobility Device)
Visual skills sufficient for safe, independent
travel w/o travel tool or
demonstrates mastery of cane skills
Travel tool used only for identification
or occasional instruction in cane
skills
Level of travel tool use moderately
impacts safe travel in some
environments
Level of travel tool use severely impacts
safe travel in most environments
Level of travel tool use profoundly impacts
safe travel in all environments
(4) Discrepancy in travel skills between present and projected levels
No discrepancy Discrepancy in a
few selected situations
Discrepancy in some situations
Discrepancy in most situations
Discrepancy in all situations
(5) Independence in travel in current/familiar
environments
Maintains & refines skills in all current
travel environments
Needs occasional instruction in current
environments to maintain travel
ability
Needs some instruction to
maintain current skills in current environments
Needs some instruction in new skills and regular
instruction to maintain current sills
Needs extensive instruction to introduce
new skills and maintain current skills in current environment
(6) Spatial/ Environmental conceptual understanding
Conceptual understanding sufficient for
development of travel skills
Progress in O&M is mildly inhibited by
conceptual understanding
Progress in O&M is moderately inhibited
by conceptual understanding
Progress in O&M is severely inhibited by
conceptual understanding
Progress in O&M is profoundly inhibited by
conceptual understanding
(7) Complexity or introduction of new
environment
Is able to learn new environment with no
specialized instruction
Learns new environment after brief introduction
Needs some instruction of skills in
new or future environments
Needs regular instruction in skills for new or future
environments
Needs extensive instruction in new or future environments
(8) Opportunities for use of skills outside of school
Student has multiple opportunities
Student has frequent
opportunities
Student has occasional
opportunities
Student has sporadic opportunities
Student rarely has opportunities
Adapted from Michigan Department of Education - Low Incidence Outreach - Revised 2012 Need Severity Score 0

147
CONTRIBUTING FACTORS TO SERVICE DELIVERY
Severity of Need Score Frequency add (.5) or subtract (-.5) points for each + or -
Total From Page 1 0 - 2 Service not indicated
Posture, gait and motor development Other physical or health impairment
2.5 - 4 1 - 5 times / year Nature of eye disease or condition Transition to new school, neighborhood, worksite, etc.
4.5 - 6 3 - 4 times / semester Recent vision loss New, hazardous, complex or difficult environment
6.5 - 12 1 - 2 times / month 20 - 60 minutes
each Potential for improvement of travel skills Age of onset of visual impairment
12.5 - 24 1 - 2 times / week 30 - 45 minutes
each Maturity and motivation Attendance
24.5 - 36 2 or more times/week 30 - 60 Team commitment for follow-up
Travel time needed to transport student to area of instruction affects frequency of instruction RECOMMENDATION OF SERVICES
Instruction in low vision aids (monocular, bioptic system) Final Severity of Need Score Frequency of Service Instruction in use of GPS
Other (explain)
Severity of Need Score
Contributing Factors + / -
Final Severity of Need Score