
Connective tissue nevi of the skinClinical, genetic, and histopathologic classification of...
21
JOURNAL of the Amesucare Acanemv OF DerMaTOLOGY VOLUME 3 NUMBER 5 NOVE"IBER, 1980 Continuing medical education Connective tissue nevi of the skin Clinical, genetic, and histopathologic classification of hamartomas of the collagen, elastin, and proteoglycan type Jouni Uitto, M.D., Ph.D.,* Daniel J. Santa Cruz, M.D., and Arthur Z. Eisen, M.D. St. LOllis, MO Connective tissue nevi of the skin are hamartomatous lesions consisting predominantly of one of the components of the extracellular matrix, namely, collagen, elastin, or glycosaminoglycans. On the basis of clinical, histopathologic, and genetic considerations, the connective tissue nevi can be classified into defined categories. Association with extracutaneous features allows further delineation of these disease entities and aids in establishing an accurate diagnosis. (J AM ACAD DERMATOL 3:441 -461, 1980.) Connective tissue nevi are hamartomas consist- ing of the various components of the dermal con- nective tissue. The predominant element of the extracellular connective tissue within an indi- vidual nevus can be collagen, elastic fibers, or glycosaminoglycans. Furthermore, lesions charac- terized by the accumulation of adipose tissue or From the Division of Dermatology, Department of Medicine, and the Division of Surgical Pathology, Department of Pathology, Wash- ington University School of Medicine. Supported in part by Grants AM-12129 and GM-28833 from the United States Public Health Service, National Institutes of Health, and by a grant from March of Dimes-the Birth Defect Foundation. requests to: Dr. Jouni Uitto, Division of Dermatology, De- partment of Medicine, Harbor-UCLA Medical Center, 1000 West Carson St.. Torrance, CA 90509/213-533-2465. 'Recipient of Research Career Development Award AM-00455 from the National Institutes of Health. 1190-9622/80/ II 0441+ 21S02 .10/0 © 1980 Am Acad Dermatol various cellular elements in the dermis have also been considered as a type of connective tissue nevus. Numerous cases reported in the literature appear to fulfill the diagnostic criteria of connec- tive tissue nevi. Classification of the connective tissue nevi in general, however, has been confus- ing because the histopathologic nature of the le- sions in most cases has not been fully delineated and the associated clinical features have been in- completely understood. In the present review, we propose a new classification for connective tissue nevi. Increased knowledge of the basic biology of the connective tissues and an advanced under- standing of the genetic role in the expression of connective tissue nevi have allowed us to formulate a classification based on clinical, genetic, and his- topathologic considerations. 441
Transcript of Connective tissue nevi of the skinClinical, genetic, and histopathologic classification of...

JOURNAL of the
Amesucare Acanemv OF
DerMaTOLOGYVOLUME 3 NUMBER 5 NOVE"IBER, 1980
Continuing medical education
Connective tissue nevi of the skin
Clinical, genetic, and histopathologic classification ofhamartomas of the collagen, elastin, and proteoglycan type
Jouni Uitto, M.D., Ph.D.,* Daniel J. Santa Cruz, M.D., andArthur Z. Eisen, M.D.St. LOllis, MO
Connective tissue nevi of the skin are hamartomatous lesionsconsisting predominantly of one of the components of theextracellular matrix, namely, collagen, elastin, orglycosaminoglycans. On the basis of clinical, histopathologic, andgenetic considerations, the connective tissue nevi can be classifiedinto defined categories. Association with extracutaneous featuresallows further delineation of these disease entities and aids inestablishing an accurate diagnosis. (J AM ACAD DERMATOL
3:441 -461, 1980.)
Connective tissue nevi are hamartomas consisting of the various components of the dermal connective tissue. The predominant element of theextracellular connective tissue within an individual nevus can be collagen, elastic fibers, orglycosaminoglycans. Furthermore, lesions characterized by the accumulation of adipose tissue or
From the Division of Dermatology, Department of Medicine, and theDivision of Surgical Pathology, Department of Pathology, Washington University School of Medicine.
Supported in part by Grants AM-12129 and GM-28833 from theUnited States Public Health Service, National Institutes of Health,and by a grant from March of Dimes-the Birth Defect Foundation.
~eprint requests to: Dr. Jouni Uitto, Division of Dermatology, Department of Medicine, Harbor-UCLA Medical Center, 1000 WestCarson St .. Torrance, CA 90509/213-533-2465.
'Recipient of Research Career Development Award AM-00455 fromthe National Institutes of Health.
1190-9622/80/ II 0441+21S02 .10/0 © 1980 Am Acad Dermatol
various cellular elements in the dermis have alsobeen considered as a type of connective tissuenevus. Numerous cases reported in the literatureappear to fulfill the diagnostic criteria of connective tissue nevi. Classification of the connectivetissue nevi in general, however, has been confusing because the histopathologic nature of the lesions in most cases has not been fully delineatedand the associated clinical features have been incompletely understood. In the present review, wepropose a new classification for connective tissuenevi. Increased knowledge of the basic biology ofthe connective tissues and an advanced understanding of the genetic role in the expression ofconnective tissue nevi have allowed us to formulatea classification based on clinical, genetic, and histopathologic considerations.
441

442 Uitto et (II
Table I. Classification of connective tissuenevi of the skin
I. Hamartomas of the collagen typeA. Inherited
I. Familial cutaneous collagenorna2. Shagreen patches in tuberous sclerosis
B. AcquiredI. Eruptive collagcnornas2. Isolated collagcnornas
II. Hamartomas of the elastin typeA. Inherited
I. Dermatofibrosis lenticularis disserninatain the Buschke-Ollendorff syndrome
2. Pseudoxanthoma clasticumB. Acquired
I. Elastosis perforans serpiginosa2. Isolated clastornas3. Pseudoxanthorna elasticurn (rare cases)
III. Hamartomas of the proteoglycan typeA. Inherited
I. Dermal nodules in mucopolysaccharidosisII (the Hunter syndrome)
B. AcquiredI. Lichen myxedcrnatosus2. Focal mucinosis
NORMAL BIOLOGY OF THE DERMALCONNECTIVE TISSUE
Collagen. The extracellular connective tissue inthe dermis consists of several biochemically distinct components whose balanced interactions andnormal quantities are required for physiologicallyfunctional skin. The major fibrillar component ofthe cutaneous connective tissue is collagen, whichcomprises about 70% of the dry weight of thedennis. (For recent reviews on collagen, see references 1-4.) Collagen appears in the form of fiberswhich are composed of thinner microfibrils. Thesemicrofibrils in turn are built of individual collagenmolecules. Each collagen molecule is a rodlikestructure of 300 nm in length and 1.5 nm in width,and consists of three polypeptide chains, thea-chains. These polypeptides are wrapped aroundeach other in a unique triple helical conformation.The a-chains of collagen are characterized by thepresence of relatively large amounts of hydroxyproline and hydroxylysine, two amino acids whichare found in few other mammalian proteins. Inaddition, collagen is rich in glycine, and sequencestudies of collagen a-chains have demonstrated
Journal of theAmerican Academy of
Dermatology
that this amino acid is evenly spaced in every thirdposition of the polypeptide. The alignment of collagen molecules along the microfibrils is stabilizedby the presence of covalent cross-links, which arederived from lysine or hydroxylysine residues ofthe collagen molecule.
It has been demonstrated that collagen is actually a family of closely related, yet geneticallydistinct proteins, which have a characteristic tissuedistribution.e" In nonnal human skin, the twomajor collagens are type I and type III. r.s Type Icollagen predominates, so that in adult skin itcomprises about 80% of the total collagen whileabout 15% is of type III. The remaining 5% or soconsists of less abundant forms, such as type IV,type l-trimer, and A-B collagens.v!' The genetically distinct collagens evidently contribute to thephysiologic requirements of any given tissue, bUIthe exact functional role of each collagen typeawaits delineation.
The biologic functions of collagen in the skirand otherconnective tissues are manyfold. In theskin, the most apparent function of collagen is tcprovide tensjle strength to the dennis. The propelsynthesis and accumulation of extracellular collagen fibers also play an essential role in the norma:wound healing and development of the tissues.Furthermore, collagen serves as an attachment sitefor a variety of cells, including fibroblasts ancepidermal cells. 12
•1:! These attachments are medi·ated through a family of so-called attachment proteins, fibronectin being the most extensively studied. H
•15 Finally, interaction of collagen with othe:connective tissue components, as, for examplewith proteoglycans.!" is apparently required fanormal function of connective tissue in the skin.
The elastic fibers. The elastic fibers, anotheiextracellular connective tissue component, anpresent in skin as highly branching structureswhich apparently are responsible for its physiologic elasticity. (For recent reviews on elastin, setreferences 17-19.) Although present in normahuman skin, the elastic connective tissue protein:represent a relatively small fraction of the dennisthese fibers are more abundant in the aorta ancother vascular connective tissues, in the lungs, ancin various tendons, such as ligamentum nuchaeand the achilles tendon. The elastic fibers consis
Volume 3Number "5November, 1980
Connective tissue nevi of skin 443
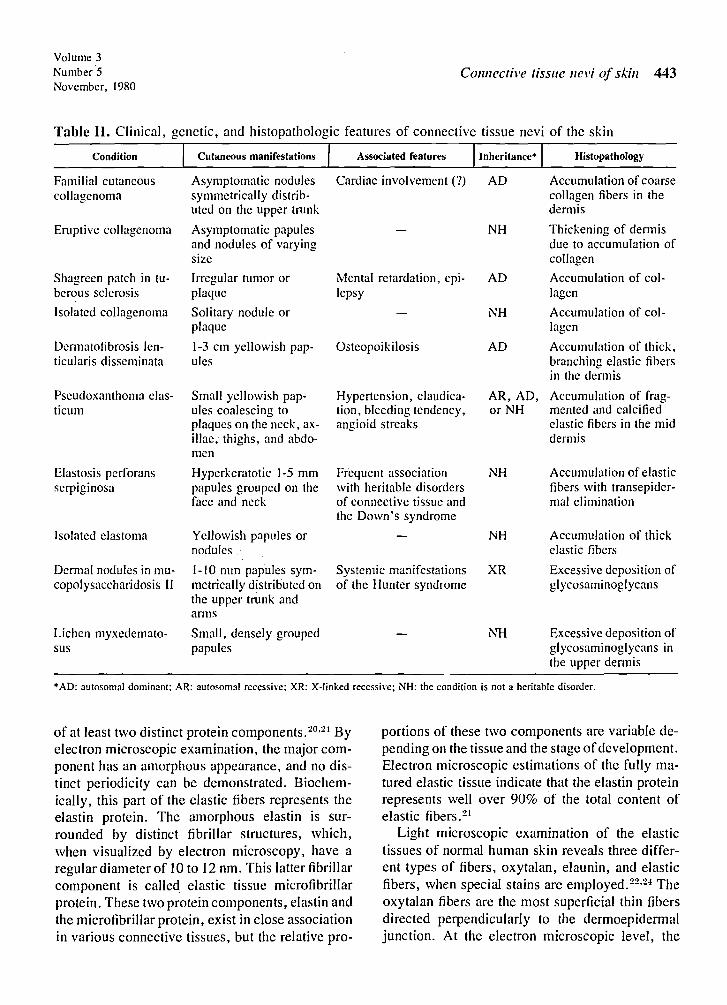
Table II. Clinical, genetic, and histopathologic features of connective tissue nevi of the skin
Condition Cutaneous manifestations Associated features Histopathology
Familial cutaneous Asymptomatic nodules Cardiac involvement (7) AD Accumulation of coarsecollagcnorna symmetrically distrib- collagen fibers in the
uted on the upper trunk dermis
Eruptive collagcnoma Asymptomatic papules NH Thickening of dermisand nodules of varying due to accumulation ofsize collagen
Shagreen patch in tu- Irregular tumor or Mental retardation, cpi- AD Accumulation of col-berous sclerosis plaque lepsy lagen
Isolated collagenoma Solitary nodule or NH Accumulation of col-plaque lagcn
Dermatofibrosis len- 1-3 ern yellowish pap- Osteopoikilosis AD Accumulation of thick,ticularis disserninata ules branching elastic fibers
in the dermis
Pseudoxanthoma elas- Small yellowish pap- Hypertension, claudica- AR, AD, Accumulation of frag-ticum ules coalescing to tion, bleeding tendency, or NH men ted and calcified
plaques on the neck, ax- angioid streaks elastic fibers in the midiliac, thighs, and abdo- dermismen
Elastosis perforans Hyperkeratotic 1-5 rnm Frequent association NH Accumulation of elasticserpiginosa papules grouped on the with heritable disorders fibers with transepider-
face and neck of connective tissue and mal eliminationthe Down's syndrome
Isolated elastoma Yellowish papules or NH Accumulation of thicknodules clastic fibers
Dermal nodules in mu- 1-10 mm papules syrn- Systemic manifestations XR Excessive deposition ofcopolysaccharidosis 11 metrically distributed on of the Hunter syndrome glycosaminoglycans
the upper trunk andanns
Lichen myxedemato- Small, densely grouped NH Excessive deposition ofsus papules glycosaminoglycans in
the upper dermis
*AD: autosomal dominant; AR: autosomal recessive; XR: X-linked recessive; NH: the condition is not a heritable disorder.
of at least two distinct protein components. 20.2t Byelectron microscopic examination, the major component has an amorphous appearance, and no distinct periodicity can be demonstrated. Biochemically, this part of the elastic fibers represents theelastin protein. The amorphous elastin is surrounded by distinct fibrillar structures, which,when visualized by electron microscopy, have aregular diameter of 10 to 12 nm. This latter fibrillarcomponent is called elastic tissue microfibrillarprotein. These two protein components, elastin andthe microfibrillar protein, exist in close associationin various connective tissues, but the relative pro-
portions of these two components are variable depending on the tissue and the stage ofdevelopment.Electron microscopic estimations of the fully matured elastic tissue indicate that the elastin proteinrepresents well over 90% of the total content ofelastic fibers."!
Light microscopic examination of the elastictissues of normal human skin reveals three different types of fibers, oxytalan, elaunin, and elasticfibers, when special stains are employed.F'<' Theoxytalan fibers are the most superficial thin fibersdirected perpendicularly to the dermoepidermaljunction. At the electron microscopic level, the

444 Uitto et (IIJournal of the
Am erican Academy ofDermatology
Fig. 1. Multiple connective tissue nevi on the back of a patient with familial cutaneouscollagenoma.
oxytalan fibers are formed of bundles of tubularmicrofibrils , IOta 12 nm in diameter, and theyappear to be similar, if not identical, to the elastictissue microfibrillar protein described abo ve. Theoxytalan fibers are connected to a plexus of fiberswhich, on the basis of their tinctorial characteristics, are termed elaunin fibers . The elaunin fibersin turn are connected with thick elastic fibers ofthe reticular dermis.
Biochemically, the elastin protein consists ofpolypeptides with an approximate molecularweight of 72,000 daltons. 17•2:;- 2 i The amino acidcomposition of elastin is similar to collagen in thatone of every three amino acids is a glycine . Sequential studies demonstrated that glycine residuesare randomly distributed along the elastin polypeptide chain, in contrast to collagen where it is inevery third position . Elastin also contains somehydroxyproline, but the relative content of thisamino acid is variable and con siderably lower thanin collagen.P" Unlike collagen, elastin contains nohydroxylysine. The amino acid composition ofelastin is also relatively rich in valine and alanine,whereas tryptophan and methionine appear to beabsent.
The elastin polypeptides form highly branched
fibers and these polypeptides are linked togetherby the formation of complex covalent cross-linksknown as desmosines.!' The microfibrillar proteinof the clastic tissues is clearly distinct from elastin, although biochemical isolation and characterization of this protein have not yet been completed.
Glycosarninoglycans. The fibrillar componentsof the dermis, collagen and elastin, are enmeshedin an extracellular material, called the groundsubstance. The major components of the groundsubstance are mucopolysaccharides, a class ofmacromolecules consisting of a polysaccharideportion , glycosaminoglycan, and a protein part.Frequently, the entire polysaccharide-protein complex is called a proteoglycan. (For review on glycosaminoglycans, see reference 29 .)
The glycosaminoglycan chains consist of hexosamine units (either glucosamine or galactosamine)alternating with a uronic acid (either glucuronicacid or iduronic acid). Thus, the glycosaminoglycans are linear chains consisting of repeatingdisaccharide units. The length of chains may varyfrom a few disaccharide units to several thousand,and, consequently , the molecular weight of eachindividual glycosaminoglycan chain can vary fromseveral thousand to several million . The glycos-

Volume 3Number 5November, 1980
. ~.-
Connective tissue nevi of skin 445
Fig. 2. Histology of the skin lesions in familial cutaneous collagenoma. The picturedemonstrates accumulation of coarse collagen fibers in the lower dermis and partialreplacement of the subcutaneous tissue by collagen . Thus, these lesions are connectivetissue nevi of the coJlagen type. (Hematoxylin-eosin stain ; original magnification , X 12.)
aminoglycan chains are linked to a protein core,fanning a proteoglycan monomer unit.
In the skin, the glycosaminoglycans compriseapproximately 0.1 % to 0.3% of the dry weight oftissue. so The predominant glycosaminoglycans inthe skin are hyaluronic acid and dermatan sulfate,while lesser amounts of chondroitin-fi-sulfate andhcparan sulfate are present. 29 The relative proportions of these different glycosaminoglycansmay vary not only among species and individuals,but also among body regions and different dermallayers .3 1- 3:1
Glycosaminoglycans in the skin have severalprobable functions. 29 For example, they contributeto the maintenance of salt and water balance byexcluding large macromolecules by lodging waterin the proteoglycan molecule itself. Glycosaminoglycans probably serve as a support for otherdermal components , and they may also regulateconnective tissue metabolism by promoting cellmigration, growth, and differentiation.
CONNECTIVE TISSUE NEVI OF THE SKIN
Definition. The term "nevus" is used in thedermatologic literature at least two differentways."! First, the term refers to lesions composedof nevus cells, such as nevocelJar nevus or pigmented nevus. Second, the term has been usedfrequently to describe lesions composed of proliferation of various mature elements of the skin .Although the term "hamartoma" would probablybe more appropriate to describe those lesionswhich do not contain nevus cells, terms such asconnective nevus are widely employed. In a strictsense , connective tissue nevi refer to lesionscharacterized by excessive deposition of one of thecomponents of the extracellular matrix , either collagen, elastic fibers, or proteoglycans. In abroader sense, the term "connective tissue nevus"could be used to describe any hamartomatoustumor consisting of other connective tissue components of the skin, such as adipose tissue or cellular elements. In this review, however, connective

446 Uitto et {If
Fig. 3. Lesions of adenoma sebaceum in a patient withtuberous sclerosis.
Fig. 4. A large shagreen patch on the back of a patientwith tuberous sclerosis.
tissue nevus will refer to tumors composed of collagen, elastic fibers, or proteoglycans. The lesionsconsisting of other components of the extracellularmatrix or of cellular elements are discussed whenconsidering the differential diagnosis of connective tissue nevi.
Journal of theAmerican Academy of
Dermatology
Classification. Previously, attempts to classifyand categorize connective tissue nevi have beenmade. :1;;-;19 Although these classifications havebeen helpful in delineating some of the clinicalconditions, it is clear that we are now at a juncturewhich allows us to formulate a more definitive anddetailed classification of connective tissue nevibased on increased knowledge of connective tissuebiology. In this study, we are proposing aclassification based on clinical, histopathologic,and genetic features of these conditions (Table I).On the basis of the histologic characteristics, theconnective tissue nevi can be classified as collagen, elastin, or proteoglycan type. On the basis ofthe mode of inheritance, or lack of it, these clinical conditions can also be categorized either asinherited or acquired ones. And finally, association of distinct extracutaneous manifestations withskin lesions can serve as a distinguishing feature.The clinical, genetic, and histopathologic featuresof the connective tissue nevi are presented inTable II.
Hamartomas of the collagen type
Familial cutaneous collagenoma. In 1968,Henderson et al described three brothers withmultiple asymptomatic cutaneous nodules on thetrunk and proximal arms. -io Histologically, thenodules showed thickening of the dermis due toincreased collagen deposition. Because of theunique clinical and histologic presentation and thepresence of the lesions in three siblings, the authors named the entity "familial cutaneous collagenoma. " Subsequently, a female patient withsomewhat similar cutaneous nodules was described.:" In this case, however, there was nofamily history of similar lesions, and it is, therefore, unclear whether she indeed had familial cutaneous collagenoma. Recently, we reported sixpatients, representing a kindred of 53, with a clinical picture similar to those described by Henderson et alY These patients presented with multipledermal nodules symmetrically distributed on thetrunk and upper arms. Most of the lesions werelocalized to the upper two thirds of the back (Fig.1). The individual lesions varied from a few millimeters to several centimeters in size, were indurated, and showed only minimal epidermal
Volume 3Number 5November, 1980
changes. Histologically, the nodules were characterized by an excessive accumulation of dense,coarse collagen fibers in the dermis (Fig. 2). Elastic fibers appeared diminished in number, perhapsrepresenting a dilution phenomenon due to excessive collagen accumulation. -12 Histologically, thelesions in these patients were connective tissuenevi of the coIlagen type .
Because of the relatively large number of patients affected and the presence of the lesions inthree subsequent generations, we were able, forthe first time, to establish the mode of inheritance'in familial cutaneous collagenoma. Examinationof the pedigree indicated that the dermal nodulesin familial cutaneous coIlagenoma were inheritedin an autosomal dominant pattern. :" Of particularinterest in these patients was the observation thatthe lesions in all patients had an onset at the ageof 15 to 19 years, and the number of lesionssignificantly increased during pregnancy. It isconceivable, therefore, that familial cutaneouscollagenoma is an inherited condition whoseexpression may be under hormonal control, andthat changes which occur during puberty andpregnancy accelerate the phenotypic expression ofthe lesions.
In familial cutaneous collagenoma, the possibility of an association of skin lesions with extracutaneous abnormalities also exists. In particular, cardiac findings, such as idiopathic progressivemyocardiopathy with congestive heart failure, andearly R wave transition in the electrocardiogram,have been encountered in some of the patients. -10,-12
On the other hand, skeletal x-ray survey revealedno evidence of osteopoikilosis, thus allowingfurther distinction of familial cutaneous collagenoma from other conditions, such as theBuschke-Ollendorff syndrome (see below).
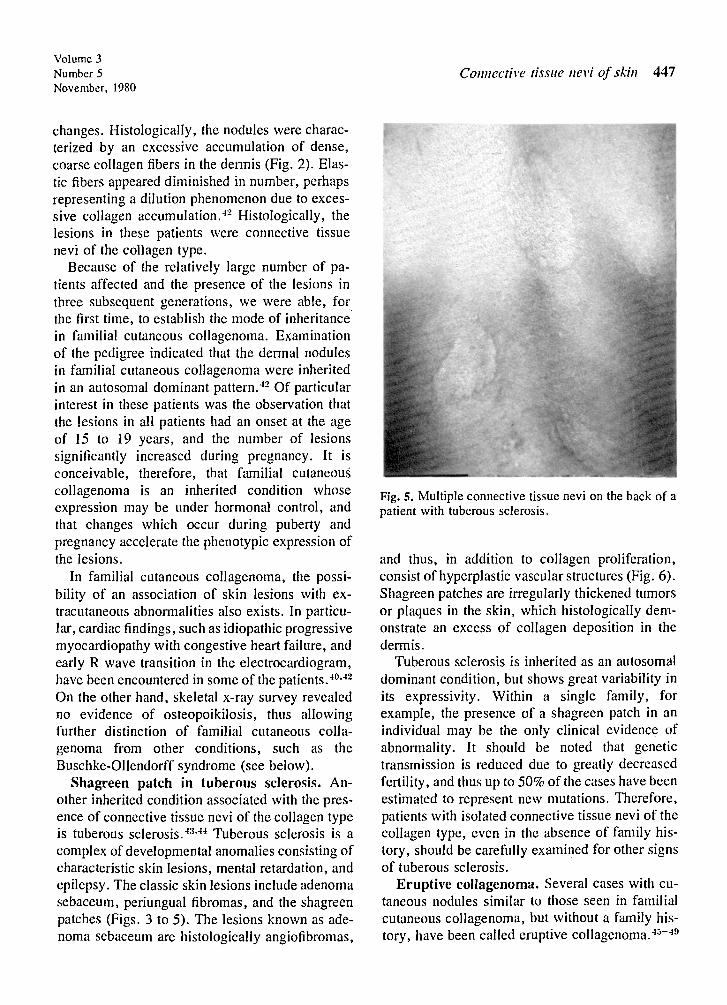
Shagreen patch in tuberous sclerosis. Another inherited condition associated with the presence of connective tissue nevi of the collagen typeis tuberous sclerosis. -13..J-1 Tuberous sclerosis is acomplex of developmental anomalies consisting ofcharacteristic skin lesions, mental retardation , andepilepsy. The classic skin lesions include adenomasebaceum, periungual fibromas , and the shagreenpatches (Figs. 3 to 5). The lesions known as adenoma sebaceum are histologically angiofibromas,
Connective tissue nevi of skin 447
Fig. s. Multiple connective tissue nevi on the back of apatient with tuberous sclerosis .
and thus, in addition to collagen proliferation,consist of hyperplastic vascular structures (Fig. 6).Shagreen patches are irregularly thickened tumorsor plaques in the skin, which histologically demonstrate an excess of collagen deposition in thedennis .
Tuberous sclerosis is inherited as an autosomaldominant condition, but shows great variability inits expressivity. Within a single family, forexample, the presence of a shagreen patch in anindividual may be the only clinical evidence ofabnormality. It should be noted that genetictransmission is reduced due to greatly decreasedfertility , and thus up to 50% of the cases have beenestimated to represent new mutations. Therefore,patients with isolated connective tissue nevi of thecollagen type, even in the absence of family history, should be carefuIly examined for other signsof tuberous sclerosis.
Eruptive collagenoma. Several cases with cutaneous nodules similar to those seen in familialcutaneous collagenoma, but without a family history , have been called eruptive collagenoma. -1:>--19

..
448 Uitto et al
•
I
,
Journal of theAmerican Academy of
Dermatology
/
I
..
Fig. 6. Histology of a lesion of adenoma sebaceum. The picture demonstrates proliferationof collagen and hyperplastic vascular structures. Thus, histologically these lesions areangiofibromas. (Hematoxylin-eosin stain; original magnification, x300.)
Careful examination of the case reports revealsthat these patients consist of at least two differentgroups which can be separated both on clinical andhistologic grounds. Some not only have cutaneouslesions resembling that of familial cutaneous collagenoma, but also the histologic picture demonstrates collagen accumulation, thus confirmingthat the lesions represent true collagenomas. Itshould be emphasized, however, that the occurrence of similar lesions in other members of the
family has not been reported. A few patients described as having eruptive collagenomas have lesions which are considerably smaller, and theirdistribution is different from those seen in familialcutaneous collagenoma in that they are located onthe extremities and the lower trunk. Histologically, the lesions also differ in that there is anaccumulation of metachromatically staining mucinous material in the dermis. ~9 These cases, therefore, seem to be closely related, if not identical, to
Volume 3Number 5November, 1980
lichen myxedematosus, and should be separatedboth on a clinical and histologic basis from truecollagenomas. In patients described as havingeruptive collagenomas and with the lesions characterized by collagen accumulation, a detailed family history is indicated to establish whether thepatients might indeed have familial cutaneous collagenoma.
Isolated collagenoma. In addition to the eruptive collagenoma syndrome, other cases withhamartomas of the collagen type and without ,afamily history have been reported. These lesionshave been described, for example, as paving stonenevi, or plantar fibromatosis. 50-52 The histology ofthese cases is also consistent with a collagenoma.Connective tissue nevi in a zosteriform patternhave also been described in one patient bySteiner.53 In this case, the collagen bundles appeared irregularly arranged and short, while theclastic fibers were also abnormal. Thus, the truenature of the zosteriform connective tissue nevussyndrome, as described by Steiner, is unclear.Several additional cases with connective tissuenevi characterized by collagen accumulation havebeen reported in patients without occurrence ofsimilar lesions in the family. 35 ,36 ,:;4-5, As indicatedabove, careful examination of these patients toexclude tuberous sclerosis is indicated. In addition, these cases can be clearly separated fromfamilial cutaneous collagenoma or eruptive collagenorna by the appearance and distribution of theindividual lesions.
Hamartomas of the elastin type
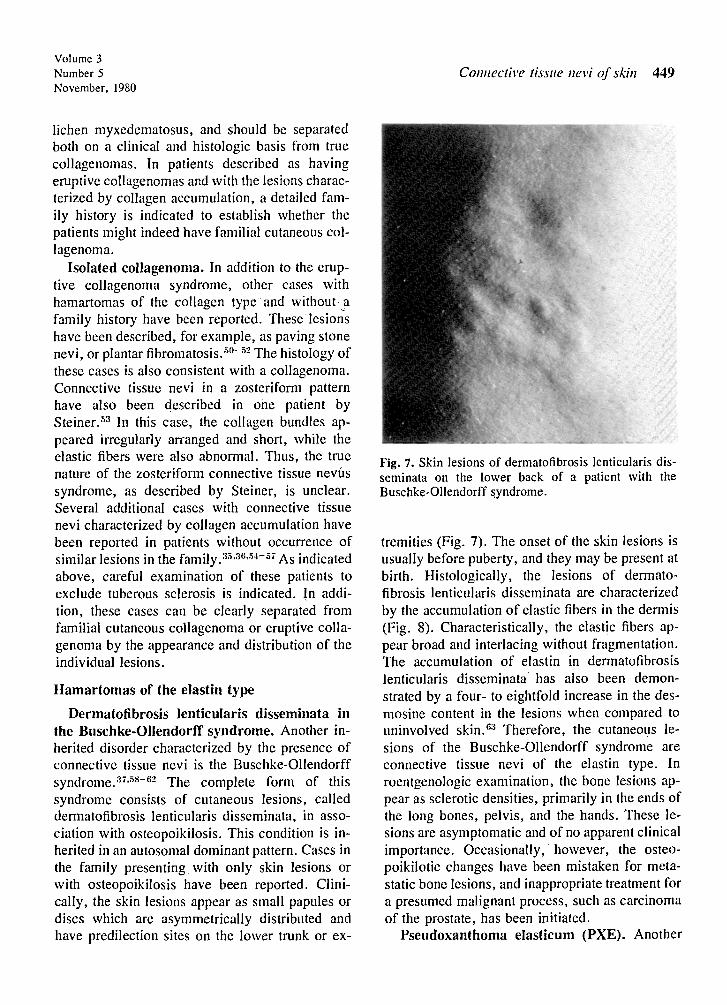
Dermatofibrosis lenticularis disseminata inthe Buschke-Ollendorff syndrome. Another inherited disorder characterized by the presence ofconnective tissue nevi is the Buschke-Ollendorffsyndrome. 3 , ,5s - 62 The complete form of thissyndrome consists of cutaneous lesions, calleddermatofibrosis lenticularis disseminata, in association with osteopoikilosis. This condition is inherited in an autosomal dominant pattern. Cases inthe family presenting .with only skin lesions orwith osteopoikilosis have been reported. Clinically, the skin lesions appear as small papules ordiscs which are asymmetrically distributed andhave predilection sites on the lower trunk or ex-
Connective tissue nevi of skin 449
Fig. 7. Skin lesions of derrnatofibrosis lenticularis dissemi nata on the lower back of a patient with theBuschke-Ollendorff syndrome.
tremities (Fig . 7). The onset of the skin lesions isusually before puberty, and they may be present atbirth. Histologically, the lesions of dermatofibrosis lenticularis disseminata are characterizedby the accumulation of elastic fibers in the dermis(Fig. 8). Characteristically, the elastic fibers appear broad and interlacing without fragmentation.The accumulation of elastin in dermatofibrosislenticularis disserninata has also been demonstrated by a four- to eightfold increase in the desmosine content in the lesions when compared touninvolved skin.?" Therefore, the cutaneous lesions of the Buschke-Ollendorff syndrome areconnective tissue nevi of the elastin type. Inroentgenologic examination, the bone lesions appear as sclerotic densities, primarily in the ends ofthe long bones, pelvis, and the hands. These lesions are asymptomatic and of no apparent clinicalimportance. Occasionally, ' however, the osteopoikilotic changes have been mistaken for metastatic bone lesions, and inappropriate treatment fora presumed malignant process, such as carcinomaof the prostate, has been initiated,
Pseudoxanthoma eIasticum (PXE). Another

450 Vitro et alJournal of the
American Academy ofDermatology
Fig. 8. Histology of the skin lesions in the Buschkc-OIIendorff syndrome. The picturedemonstrates accumulation of broad, interlacing elastic fibers in the dermis. Thus, theselesions are connective tissue nevi of the elastin type. (Verhoeff stain; original magnifica-tion, x 350.) .
Fig. 9. Typical skin lesions in a patient with pseudox anthoma clasticum, demonstrating redundant, inelastic skin in a plaque composed of yellowish papulesin the axillary fold.
skin disease affecting the elastic connective tissuesis PXE. This is a generalized disorder and includesdistinct skin lesions, ocular changes, and vasculardisturbances.Vr'V'"?" Relative severity of thesechanges can produce a wide variety of clinicalpictures. Genetically, PXE is heterogenous withboth autosomal dominant and autosomal recessiveinheritance patterns.44. 68.69 A spectrum of severityis seen, varying from a highly debilitating diseasewith severe angina, claudication , hypertension,and the development of blindness, to a relativelymild form with symptoms limited to the skin.
Typical skin lesions in PXE consist of small,1-3 mrn yellowish papules which tend to coalesceinto thickened, leathery plaques (Fig. 9). Thepredilection sites are the neck , axillary and inguinal folds, thighs, and abdomen. Yellowish lesionssomewhat similar to those seen in the skin can alsobe encountered on the buccal mucous membranes .
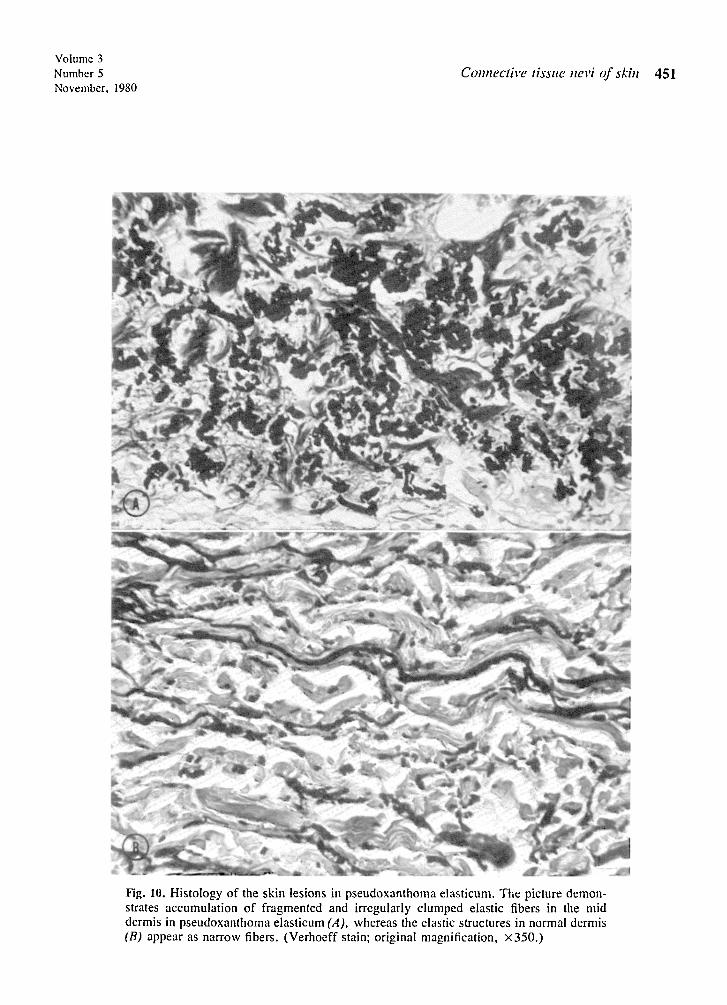
Histologic examination of the skin reveals anaccumulation of abnormal elastic fibers (Fig. 10).In contrast to the elastic fibers seen in normal skin
Volume 3Number 5November. 1980
Connective tissue nevi of skin 451
Fig. 10. Histology of the skin lesions in pseudoxanthoma elasticum. The picture demonstrates accumulation of fragmented and irregularly clumped elastic fibers in the middermis in pseudoxanthoma elasticum (A), whereas the elastic structures in normal dermis(B) appear as narrow fibers. (Verhoeff stain; original magnification, x350.)

452 Uitto et alJournal of the
American Academy ofDermatology
Fig. 11. Electron microscopy of a skin lesion in pseudoxanthoma elasticum. The picturedemonstrates an elastic fiber containing electron-dense deposits of calcium apatite. (Original magnification, X54,OOO.) (The picture was kindly provided by Dr. Lis Danielsen,University of Copenhagen, Denmark.)
or in derrnatofibrosis lenticularis disseminata, thefibers in PXE appear coarse, irregularly clumped,and show marked fragmentation and degeneration.Electron microscopic examination reveals dystrophic calcification of the elastic fibers (Fig. 11).lt appears, therefore, that in addition to proliferation, the elastic fibers undergo degenerativechanges which lead to destruction and to a loss ofphysiologic function.
In addition to the inherited forms of PXE, several acquired cases with similar clinical,· histologic, and electron microscopic picture, butwithout family history, have been presented. '()-'2
Sometimes the development of skin lesions is related to an external chemical trauma. For example, ten patients reported by Otkjaer-Nielsen etal 70 developed papular lesions on their forearmsfollowing an exposure to Norwegian saltpeter (amixture of calcium and ammonium nitrates). Thelesions showed by light and electron microscopicexamination changes indistinguishable from thoseseen in the inherited form of PXE. None of thesepatients had a family history of PXE, and nosystemic manifestations of the disease werepresent.
Recently, patients with an unusual perforating

Volume 3Number 5November, 1980
variant of PXE have been described. i:l In these .patients the lesions are confined to the abdomen,most often in a periumbical distribution (Fig.12). i:l.i~ None of these patients had a family history of PXE, suggesting that periumbilical perforating pseudoxanthoma elasticum is a distinctacquired form of the disease.
It should be noted that some studies have suggested ultrastructural abnormalities in the collagenin PXE, such as the appearance of irregularly arranged and twisted collagen fibrils. Gi These findings, however, are not specific for PXE, sincesimilar ultrastructural changes have been seen in avariety of unrelated conditions. Also, the synthesis of collagen by skin explants is normal inPXE.i5·,G
Elastosis perforans serpiginosa (EPS). Thisskin condition frequently appears in associationwith heritable connective tissue disorders, such asthe Ehlers-Danlos syndrome, the : Marfan syndrome, and osteogenesis imperfecta, but it hasalso been reported in otherwise healthy individualsand in several patients with the Down's syndrome.li.~~.ii.'8 The coexistence of inherited PXEand EPS has also been reported . Since PXE has aperforating variant histologically similar to EPS, ithas been suggested that most of the reported associations of PXE and EPS in fact represent perforating PXE.i9 Also, in general the genetic componentin the development of EPS and its possible modeof inheritance have not been delineated. It shouldbe pointed out that some patients receivingn-penicillamine, a drug interfering with elastinand collagen cross-linking, have developed clinical lesions of EPS. 1;0
The skin lesions in EPS consist of 1-5 mmpapules which appear hyperkeratotic and are typically grouped in a circular or arciform configuration (Fig. 13). The sites of predilection are on theneck and face. The histopathologic change in EPSconsists of a focal increase in the amount of elasticfibers which also appear larger than normal. i8.8I.S:!In addition, the epidermis contains several narrowchannels which contain necrotic and degeneratedelastic material being extruded through the skin .EPS, therefore, appears to be a reactive perforating dermatosis characterized by proliferation
Connective tissue nevi of skin 453
Fig. 12. Typical skin lesions in a periumbilical perforating variant of PXE.
Fig. 13. Skin lesions of EPS, demonstrating groups ofhyperkeratotic papules in an arciform configuration onthe side of the neck.
of elastic fibers in the upper dermis . For unknown reasons, this material is extruded fromthe skin.
Isolated elastomas. Several isolated cases withconnective tissue nevi of the elastin type havebeen reported previously. These have been described under various names, such as juvenileelastoma, nevus elasticus, nevu s conjunctivus ,and naevus pseudocolloide perifolliculaire. S:I-SS Inseveral patients, the skin lesions are similar, both

454 Uiuo et alJournal of the
American Academy ofDermatology
Fig. 14. Skin lesions of lichen myxedernatosus, demonstrating small papules on the back.
clinically and histologically, to those observed inthe Buschke-Ollendorff syndrome, but no detailedfamily history or radiologic investigations of thebones have been carried out. It is unclear, therefore, whether some of these patients actuallyrepresent the Buschke-Ollendorff syndrome orwhether. some of them are true isolated cases ofelastoma.
The first to use the term nevus elasticus wasLewandowsky who, in 1921, reported three casesof connective tissue nevi, using the term "naevuselasticus regionis mammariae.' '89 The lesionswere characterized as groups of small, yellowishperifol1icular papules on the pectoral region. Histologically, these lesions were found to lack elastic fibers, and thus are not nevi of the elastin type.This same condition was subsequently called byWith and Kissmeyer'" as dystrophia elastica follicularis thoracis and by Staricco and Mehregan'"as nevus anelasticus.
In 1931, Weidman et al8:l reported a young childwith numerous discrete nodules on the lower trunkand anterior aspects of the thighs. No family history of similar skin lesions was obtained. Histologically, there was a marked accumulation of
elastic fibers which appeared in relatively largeaggregations. Because of the clinical and histologic presentation, the authors called this condition juvenile elastoma. Subsequently, severalcases with a histologic presentation similar to thatof juvenile elastoma have been reported (seeabove). Since these lesions consist of hyperplasiaof normal-appearing elastic fibers, they have frequently been called nevus elasticus. Staricco andMehregan'" described four cases with a distinctaccumulation of elastic fibers in the lesions. Sinceone of the cases presented, in addition to hyperplasia of the elastic fibers, a well-developedvascular component, an additional term, "nevuse1asticus vascularis," was suggested for this particular condition. It appears then that the exactnature of the lesions described as nevus elasticus isunclear in some cases, and in subsequent studiesskin samples should be examined by adequate histopathologic procedures to establish the diagnosisof connective tissue nevus of the elastin type.
Two cases of a connective tissue nevus whichappears to be a clinically distinct entity have reocently been reported.P'<" In both studies a youngpatient with a bilateral eruption on the face leading

Volume 3Number 5November, 1980
Connective tissue nevi of skill 455
Fig. 15. Histology of the skin lesions in lichen myxedematosus. The picture demonstratesdeposition of proteoglycans in the dermis, causing widening of the spaces between collagen fibers. (Hematoxylin-eosin stain; original magnification, x90.)
to formation of plaques on both cheeks was described. Clinically the lesions were characterizedby wrinkling, furrowing, and irregular thickeningof the skin. No history of a familial occurrence ofsimilar lesions or the association with systemicabnormalities was noted. Histologically, an increase in the elastic fibers was noted in both cases.The epidermis appeared thickened . The sebaceousglands were either absent or not well developed.In one case the hair follicles were immature andappeared to be increased in number, while in theother case, deposits of perifollicular mucin werereported. Therefore, both clinically and histologically, these two cases are separate from any otherpreviously described elastoma. The role of actinicdamage, as implied in one of the reports, to theskin in these young individuals is unclear but
could be clarified when further reports of similarcases are presented.
Hamartomas of the proteoglycan type
Dermal nodules in mucopolysaccharidosis II.Although the skin in most cases of the geneticmucopolysaccharidoses shows generalized thickening, the only inherited mucopolysaccharidestorage disease demonstrating distinctive skinchanges is mucopolysaccharidosis II, the Huntersyndrome. -14.93-9;; This syndrome is classically inherited in an X-linked recessive pattern, althougha less frequent autosomal recessive form mayexist. It should be noted that all the othermucopolysaccharidoses are autosomal recessive.The biochemical defect in the Hunter syndrome isexcessive accumulation of both dermatan sulfate

456 Uitto et alJournal of the
American Academy ofDermatology
Fig. 16. Typical skin lesions of nevus lipomatosus superficialis, demonstrating multiplesoft nodules in a zonal distribution on the lower trunk.
and heparan sulfate due to iduronate sulfatasedeficiency.
The skin changes in mucopolysaccharidosis IIconsist of small, usually 1-10 mm papules, whichhave been described as a "pebbling" of the skin.The lesions are symmetrically distributed with thepredilection sites being the scapular and pectoralregions as well as the arms. By light and electronmicroscopic examination, the fibroblasts in theskin, both in normal-appearing areas and in thepapules, contain metachromatically staining cytoplasmic material and characteristic vacuoles."In addition, the papules demonstrate an extracellular accumulation of metachromatic material.Thus, the cutaneous papules encountered in theHunter syndrome are due to excessive depositionof glycosaminoglycans in the dermis.
Lichen myxedematosus. The cutaneous eruption in this acquired clinical condition and inits variant, scleromyxedema, consists of small,densely grouped papules (Fig . 14). The predilection sites are the exterior aspects of the forearmsand the axillary folds, but any part of the skin canbe affected in localized areas .?" Most patients aremiddle-aged adults, and no associated endocrineabnormalities have been demonstrated. Histologically , the lesions show a deposition of glycosaminoglycans mostly in the upper third of the dermis,causing a separation of the collagen fibers (Fig.15),uG.9; Since this material can be digested withhyaluronidase, it appears that hyaluronic acid is
the predominant component which accumulates inthe skin. These changes are accompanied by aproliferation of large stellate and elongated fibroblasts.P" Thus, the increased presence of mucopolysaccharides in the skin may be explained bythe excessive synthesis by these cells.
It should be pointed out that in several instancesscleromyxedema is associated with the presence ofa circulating monoclonal IgG, and immunofluorescence studies have shown deposition ofthe same protein in the skin." The relation ofthese observations to deposition of proteoglycansin the skin is unclear, and it may be that thesepatients represent a distinct subgroup ofscleromyxedema.
Cutaneous focal mucinosis, a condition distinctfrom lichen myxedematosus, presents with solitary asymptomatic papules or nodules.P" The lesions usually occur on the face, trunk , or extremities, but not in proximity to the joints of thehands, wrists, or feet. The pathologic changeconsists of a marked proliferation of fibroblastsand an increased production of hyaluronic acid bythese cells. Hyaluronic acid then accumulates between the collagen fibers, eventually replacingmost of the collagen. This process occasionallyresults in the formation of cystic spaces, such asseen in myxoid cysts of the fingers and toes. Itmay be that the pathogenesis of these two conditions is similar and the clinical variation might beexplained by the anatomic differences of the in-

Volume 3Number 5November, 1980
volved sites, although the myxoid cyst may beconnected to the synovial space.
Two further conditions characterized by deposition of glycosaminoglycans in the skin are diffuse myxedema and pretibial myxedema. In theformer, generalized thickening of the skin withpuffy edema and xerosis takes place. In the latter,localized edematous plaques and tumors are seenin the pretibial area. Both of these conditions areassociated with thyroid disorders. Diffuse myxedema is usually a sequela of hypothyroidism,while pretibial myxedema is associated with hyperthyroidism. The long-acting thyroid stimulator(LATS) has been implicated in the appearance ofthe pretibial lesions. Recently, the presence of aserum factor, different from LATS, which stimulates proteoglycan synthesis by human skin fibroblasts has been described; this factor has been proposed to be somatomedin.w-'?"
DIFFERENTIAL DIAGNOSIS OF THECONNECTIVE TISSUE NEVI
The term "connective tissue nevi," as employed in the present study, refers to skin lesionsconsisting predominantly of the elements of theextracelIular connective tissue, colIagen, elastin,or proteoglycans. Previously, the term has beenused more broadly, and it has been extended toinclude hamartomas consisting of other dermalcomponents, such as the adipose tissue and thecellular elements. Clinically, many of these lesions are included in the differential diagnosis ofthe connective tissue nevi, and only a histopathologic examination of the skin definitivelyallows to establish the correct diagnosis.
One of the conditions entering in the differentialdiagnosis is nevus lipomatosus superficial is. 101.103
This relatively rare malformation consists ofpapules usually occurring on the lower trunk. Twoclinically distinct types are recognized: the classictype, as originally described by Hoffmann andZurhelle;'?' consists of multiple lesions in a zonaldistribution (Fig. 16), while another form consistsof a solitary papule or nodule. 103 The characteristic histopathologic change in the skin is replacement of the dermal connective tissue by ectopicadipose tissue. The amount of ectopic fat variesmarkedly, and the lesions also show additional
Connective tissue nevi of skill 457
changes in the dermal connective tissue. 10:1 Theseinclude the presence of excess amounts of collagen as well as a proliferation of small blood vessels. Such changes probably explain the formationof elevated papules with a characteristic cerebriform outline. In addition to the superficial formof this entity, cases with folded skin associatedwith underlying, more deeply seated nevus lipomatosus have been described. 101 When generalized, this condition has been called "theMichelin tire baby. "10;;
It should be mentioned that focal dermal hypoplasia (the Goltz syndrome) shows histologicchanges similar to nevus lipomatosus superficialis. 106• lOi Clinically, however, focal dermalhypoplasia is clearly a distinct entity and can beseparated from nevus lipomatosus superficialis bythe clinical appearance of the lesions, absence offat herniation, and the presence of widespread associated anomalies of the osseous, ocular, anddental structures.
Another condition frequently entering the differential diagnosis of connective tissue nevi isleiomyoma. Clinically, leiomyomas present asfirm dermal nodules of varying size which mayoccur as a solitary lesion or, more commonly, asmultiple tumors. Many cases with multiple leiomyomas have a family history of similar lesions.Histologically, the leiomyomas are composed ofsmooth muscle cells which can be derived fromthe arrector pili muscle, the media of the bloodvessels, or from smooth muscle of the nipples or genital area. On the basis of histopathologicexamination and, in particular, when special stainsare employed, these lesions can be distinguishedfrom those consisting of collagen. Of interest is arecent report suggesting that Becker's nevus, inaddition to the characteristic epidermal changes,also has a distinct dermal component consisting ofnumerous bundles of smooth muscle cells. 108
An interesting group of patients has been recently described by Birt et al 109 as hereditary multiple fibrofolliculomas. These patients presentwith multiple, 2-4 mm fibromatous papules frequently involving the head but also seen elsewhereon the skin. These lesions are inherited in an autosomal dominant pattern. Histologically, themultiple fibrofolliculomas have in the center a

458 Uitto ct al
well-formed hair follicle which is surrounded by aproliferation of fine collagen fibers embedded inabundant ground substance. Intere stingly, thefibrofolliculomas may be associated with a largeconnective tissue nevus similar to a shagreenpatch, multiple acrochordons, and trichodiscomas, a benign skin tumor related to Haarscheibe(the hair disc) . 109-112
In addition to the lesions discussed above, a fewother hamartomas can rarely be confused withdermal connective tissue nevi. Such entities mayinclude vascular hamartomas, .as, for example,cavernous hemangioma, rubber bleb nevus, angiofibroma, lymphangioma circumscriptum, andglomus tumor. These lesions , however, havespecific histologic presentations and can be readilyseparated from connective tissue nevi. Severalother disease entities which show ectopic orhamartomatous growth of some forms of connective tissue, such as fibrous papul e of the nose,accessory tragus, or enchondromas in Maffucci'ssyndrome, can also be separated from connectivetissue nevi by their typical clinical presentation. Ineach case, however, histopathologic examinationof the skin is helpful in substantiating the clinicalimpression.
We thank Drs . Jerome Aronberg and Lis Danielsen forproviding some of the illustrations.
REFERENCES
I. Uitto J, Eisen AZ: Collagen, ill Fitzpatrick TB, EisenAZ, Wolff K, Freedberg 1M, Austen KF, editors: Dermatology in general medicine, cd. 2 . New York, 1979,McGraw-Hill Book Co., pp. 164-180.
2 . Prockop OJ, Kivirikko KI, Tuderman L, Guzman NA:The biosynthesis of collagen. N Engl J Med 301: 13-23,77-85, 1979.
3 . Gay S, Miller EJ: Collagen in the physiology andpathol ogy of connective tissue . Stuttgart , 1978, GustavFischer Verlag, pp. 1-110 .
4 . Bauer EA, Uitto J: Collagen in cut aneous diseases . Int JDerrnatol 8:251-270, 1979.
5 . Miller EJ : Biochemical characteristics and biologicalsignificance of gen eticall y-dist inct coll agens. Mol CellBiochem 13:165-192, 1976 .
6. Uitto J. Lichtenstein JR: Defects in the biochemistry ofcoll agen in diseases of connecti ve tissue . J Invest Derrnatol 66:59-79. 1976 .
7. Epstein EH , Munderloh NH: Human skin collagen .Presence of type I and type 111 at all levels of the dermis . J BioI Chem 253:1336-1337, 1978.
8. Uitto J: Collagen polymorphism: Isolation and partial
Journal of theAmerican Academy of
Dermatology
characterization of a I(I)-trimer molecules in normalhuman skin. Arch Biochem Bioph ys 192:371 -379,1979.
9. Kefalide s NA: Basement membranes: Structural andbiosynthetic considerations . J Invest Derm atol 65:8592 , 1975.
10. Burgeson RE, El Adli FA , Kaitila I , Holli ster OW:Fetal membrane collagens: Ident ificat ion of two newa-chains . Proc Natl Acad Sci USA 73:2579-2583,1976 .
II. Rhodes RK, Miller EJ: Physicochemical characterization and molecular organization of the collagen A and Bchains. Biochemistry 17:3442-3448, 1978.
12. Murray JC, Stingl G, Kleinman HK, Martin GR, KatzSI: Epidermal cells adhere preferentially to type I V
. (basement membrane) collagen. J Cell BioI 80: 197202, 1979.
13. Kleinman HK, Murray JC, ~lcGoodwin EB, MartinGR: Connective tissue structure: Cell binding to collagen. J Invest Dermatol 71:9-11, 1978 .
14. Vaheri A , Ruoslahti E, Mosher OF: Fibroblast surfaceprotein. Ann NY Acad Sci 312:1-456, 1978.
15. Yamada KM, Olden K: Fibronectins-adhesive glycoproteins of cell surface and blood. Nature 275: 179184, 1978.
16. Obr ink B: Non-agg regated tropocoll agen at physiological pH and ionic strength . A chemical and physicochemical characterization of tropocollagen isolatedfrom the skin of lathyritic rats . Eur J Biochem 25:563572, 1972 .
17. Uitto J: Biochemistry of the elastic fibers in normalconnective tissues and its alter ation s in diseases. J Invest Oermatol 72:1-10, 1979 .
18. Sandberg LB: Elastin structure in health and disease . IntRev Connective Ti ssue Res 7: 159-210, 1976.
19. Uitto J: Elastic fibers , ill Fitzp atrick TB, Eisen AZ,Wolff K, Freedberg 1M, Austen KF, editors: Dermatology in general medicine, ed . 2. New York, 1979,t\fcGraw-Hill Book Co., pp. 182-188.
20. Varadi OP: Studies on the chemistry and fine structureof clastic fibers from normal adult skin. J Invest DermatoI66:59-79, 1976.
21. Ross R, Fialkow PJ, Altman LK: The morphogenesis ofelastic fibers. Adv Exp Med BioI 79:7-17, 1977.
22 . Fullmer HM, Lillie RO: The oxytal an fiber: A previously undescribed connective tissue fiber. 1 HistochemCytochem 6:725-430 , 1958.
23 . Hasegawa J: "Oxytalan " fibers of the dermal-epidermal junction. Arch Dermatol 82:250-252, 1960 . ·
24 . Cotta-Pereira G, Guerra Rodrigo F, Bittencourt-Sampalo S: Oxytalan, elaunin, and elastic fibers in thehuman skin. J Invest Dermatol 66:143-148, 1976.
25. Sandberg LB, Weissman N. Smith OW: The purification and parti al characterization of a solubleelastin-like protein from copper-deficient porcine aorta.Biochemistry 8:2940-2945, 1969.
26. Foster lA , Bruenger E, Gray WR , Sandberg L8: Isolation and amino acid sequences of tropoelastin peptides.J BioI Chem 2-18:2876-2879, 1973 .
27 . Sykes BC, Partridge SM : Salt-soluble elastin fromlathyritic chicks. Biochem J 1~1:567-572, 1974.

Volume 3Number 5November, 1980
28 . Uitto 1, Hoffmann H-P , Prockop Dl: Synthesis of ela stin and procollagen by cells from embryonic aorta . Differences in the role of hydroxyproline and the effects ofproline analogs on the secretion of the two proteins .Arch Biochem Biophys 173:187-200, 1976.
29 . Silbert lE: Mucopolysaccharides of ground substance.ill Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg 1M,Austen KF, editors: Dermatology in general medicine,ed . 2. New York, 1979 , Mcflraw-Hill Book Co . , pp.189-195.
30 . Pearce RH: Glycosaminoglycans and glycoproteins inskin, ill Balazs EA, leanloz RW, editors: The aminosugars. New York, 1965, Academic Press, Inc., vol.IIA,pp.149-193.
31. Hoffman P, Linker A, Meyer K: The acid mucopolysaccharides of connective tissue. II. Further experiments on chondroitin sulfate B. Arch Biochern Biophys69: 435-440, 1957.
32. Loewi G: The acid mucopolysaccharides of humanskin . Biochim Biophys Acta 52:435-440, 1961.
33 . Flei schmajer R, Perlish lS, Gaisin A: Comparativestudy of dermal glycosarninoglycans. 1 Invest Dermatol61:1-6, 1973 .
34 . Lever WF, Schaumburg-Lever G: Histopathology ofthe skin, ed . 5. Philadelphia, 1975, 1. B. LippincottCo., pp. 499-500. .
35. Prakken lR: Connective tissue naevi. Br 1 Dermatol64:87-96 , 1952.
36 . Rocha G , Winkelmann RK: Connective tissue nevus.Arch Derrnatol 85:722-729, 1962.
37 . Smith JG, Sams WM, Finlayson GR: Biochemistry andpathology of cutaneous elastic tissue, ill MackennaRMB, editor: Modem trend s in dermatology. London,1966 , Butterworth & Co., pp. 110-142.
38 . Raque Cl, Wood MG : Connective tissue nevus. Dermatofibrosis lenticularis disserninata with osteopoikilo sis. Arch Dennatol 102:390-396, 1970 .
39 . Reed Rl, Clark WH, Mihm MC: The cutaneous collagenoses. Hum Pathol 4:165-186, 1973.
40 . Henderson RR, Wheeler CE, Abele DC: Familial cutaneous collagenoma. Report of cases . Arch Dermatol98:23-27, 1968.
41. Hegedus SI, Schorr WF: Familial cutaneous collagenoma. Cutis 10:283-288, 1972 .
42. Uitto 1, Santa-Cruz Dl, Eisen AZ : Familial cutaneouscoll agenoma: Genetic studies on a family. Br 1 DermatoI101:185-195, 1979.
43. Nickel WR , Reed WB: Tuberous sclerosis. Arch DermatoI85:209-226, 1962.
44 . McKusick VA: Heritable disorders of connective tissue, cd. 4. SI. Louis, 1972 , The C. V. Mosby Co.,pp. 1-878 .
45. Prieto lG, Perez PR, Cas cos MA: Uber cine in multiplen Herden auftretende, mit met achromasie verlaufende eruptive Kollagenose. Hautarzt 9:300-309,1952.
46 . Duverne 1, Condert 1, Colomb D: Tentative d 'individualisation due collagenome eruptif (a propos d'uneobservation) . Ann Dermatol 82:160-165, 1955.
47 . Loewenthal UA: Connective tissue nevi and collagenome eruptif. Dermatologica 114:81-90, 1957.
Connective tissue nevi of skill 459
48. Woerdernan MJ: Is collagenom eruptif a separate entity? Br 1 Dennatol 72:217-220, 1960.
49 . Metz 1, Schubert E: Das sog. "eruptive Kollagcnorn "-ein Lichen myxocdcrnatosus? Arch Derrnatol Forsch 240: 148-159, 1971.
50 . Lipschutz B: Uber eine bisher nicht beschriebeneNaevusform (Ptlastersteinforminger Bindegewebsnaevus) . Arch Dermatol Syph 139:477-482, 1922.
51. Cohen MM, Hayden P\V: A newly recognized hamartomatous syndrome. Birth Defects: Original ArticleSeries XV (5B):291-296, 1979 .
52. Uitto 1, Bauer EA, Santa Cruz Dl, Eisen AZ: Cerebriform connective tissue nevi of the foot : Decreasedcollagenase production by fibroblasts in culture. ClinRes. (In press.)
53. Steiner K: Connective-tissue nevus. Arch DermatolSyph 50:183-190, 1944.
54 . Terntarny SA, Rogers 10: Macrodactyly, hemihypertrophy, and connective tissue nevi: Report of a newsyndrome and review of the literature. 1 Pediatr89:924-927, 1976 .
55. Danielsen L, Kobayashi T, Krag Jacob sen G: Ultrastructural changes in dis seminated connective tissuenevi. Acta Derm Venereol (Stockh) 57:93-101, 1977.
56 . Miki T , Oka M, Tamaka S: Ostcopoikilosis associatedwith plantar fibromatosis: A case report. Orthopedics2:258-261, 1979.
57. Kop er A V, Levine N: General ized connective tissuenevi and ichthyosis in Down's syndrome. Arch Derrnatol 115:623-624, 1979.
58 . Buschke A, Ollendorff H: Ein Fall von Dermatofibrosislent icularis disseminata. Derrnatol Wochenschr 86:257-262 , 1928.
59 . Schorr WF, Optiz 1M, Reyes CN: The connective tissuenevus-osteopoikilosis syndrome. Arch Dermatol 106:208-214, 1972.
60 . Danielsen L, Mitgaard K, Christensen HE: Osteopoikilos is associated with derm atofibrosis lenticularis disserninata. Arch Dennatol 100:465-470, 1969.
61. Verbov 1: Buschkc-Ollendorff syndrome (disseminateddermatofibrosis with osteopoikilosis). Br 1 Dermatol96:87-90, 1977.
62 . Morrison lGL, Wilson Jones E, McDonald DM:luvenile elastoma and osteopoikilosis (the BuschkeOllendorff syndrome) . Br 1 Dermatol 97:417-422,1977.
63. Uitto 1, Santa-Cruz Dl, Starcher BC, Whyte MP; Murphy \VA: Biochemical and ultrastructural demonstrationof elastin accumulation in the sk in lesions of theBuschke-Ollendorff syndrome. 1 Invest Dermatol, (Inpress .)
64. Goodman RM, Smith EW, Paton D, Bergman RA,Siegel CL, Ottesen OE, Shelley WM, Pusch AL,McKusick VA: Pseudoxanthoma elasticum. A clinicaland histopathological study: Medicine (Baltimore) 42:297-334, 1963.
65 . Altm an LK, Fialkow Pl , Parker F, Sagebiel R\V: Pseudoxanthoma ela sticum. An underdiagnosed geneticallyheterogenous disorder with protean manifestations.Arch Intern Med 134: 1048-1054, 1974 .
66. McKee PH, Cameron CHS, Archer DB, Logan we: A

460 Vitia ct a!
study of four cases of pseudo xanthorna elasticum. JCutan PathoI4:146-153, 1977.
67. Danielsen L: Morphological change s in pseudoxanthorna elasticum and senile skin. Acta Derm Venereol(Stockh) 59(suppl 83): 1-79, 1979.
68 . Pope FM: Autosomal domin ant pseudo xanthoma elasticum. J Med Genet 11:152-157, 1974.
69. Pope FM: Two types of autosomal ' recessi ve pseudoxanthoma elasticum . Arch Dermatol 110:209-212,1974.
70 . Otkjaer-Nielsen AD, Christensen OB , Hentzer B,Johnson D, Kobayasi T: Saltpeter-induced dermalchange s electron-microscopically indistinguishablefrom pseudoxanthorna elasticurn. Acta Derm Venereol(Stockh) 58:323-327, 1978.
71. Christensen 0: An exogenous variety of pseudoxanthorna elasticum in old farmers. Acta DermVenereol (Stockh) 58:319-321,1978.
72. Neldner KH, Martinez-Hernandez A: Localized acquired cutaneous pseudoxanthorna elasticurn. J AMACAD DER~IATOL 1:523-530, 1979.
73 . Hicks J , Carpenter EL , Reed R: Periumbilical perforating pscudoxanthoma elasticum . Arch Dermatol 115:300-303, 1979.
74 . Auster B, Santa-Cruz DJ: Psoriasis and pseudo xanthoma elasticurn. Cutis 22:178-180, 1978.
75. Uillo J , Lindy S, Turto H, Danielsen L: Biochemicalcharacterization of pseudoxanthoma elasticum: Collagen biosynthesis in the skin. J Invest Dermatol 57:4448, 1971.
76. Blumenkrantz N, Danielsen L, Asboe-Hansen G:Biosynthe sis of collagen in pseudox anthoma elasticum.Acta Dertll Venereol (Stockh) 53:429-434, 1973.
77. Mehregan AH: Elastosis perforans serpiginosa; a review of the literature and report of II cases. Arch Derrnatol 97:381-393, 1968.
78 . Whyte HJ, Winkelmann RK: Elastosis perforans (perforating elastosis). The association of congenital anomalies, salient facts in the histology, studies of enzymedigestion and a report of necropsy in a case. J InvestDermatol 35:113-122, 1960.
79. Lund HZ, Gilbert CF: Perforating pseudoxanthornaelasticurn. Its distinction from elastosi s perforans serpiginos a, Arch Pathol Lab Med 100:544-546, 1976.
80 . Kirsch N, Hukill PB: Elastosis perforans serpiginosainduced by penicillamine. Arch DermatoI1l3:630-635,1977.
81. Hashimoto K, Hill WR: Elastosis perforans serpigi nasa. A case report with histochemical and enzyme digestion studies. J Invest Dermatol 35:7-14, 1960.
82 . Cohen AS, Hashimoto K: Electron microscopic observation on the lesion of elastosis perforan s serpiginosa. JInvest Dermatol 35:15-19, 1960.
83. Weidman FD, Anderson NP, Ayres S: Juvenile elastorna. Arch Dermatol Syph 28:182-189, 1933.
84 . Gutmann C: Bindegewebsnaevus . Zentralbl Hautkr Geschlechtskr 22:26, 1927.
85 . Guimares NA, Piva N: Nevo elastico de Lewandowsky.An Bras Dermatol SyphiloI31:95-IOI, 1936.
86 . deGr aciansky 1', Leclercq R: Le "naevus elasticus " enturncurs disseminees. Ann Dcrmatol Syphilol 87:5-25,1960.
Journal of theAmer ican Academy of
Dermatology
87. Ferreira-Marques J , Pous S: Contribucion a estudio dela etiologia, patogenia y clinica del naevus elasticus deLewandowsky, Arch argent derrnatol 9:419-441, 1951.
88. Staricco R, Mehregan AH: Nevus elasticus and nevuselasticus vascularis. Arch Dermatol 84:943-947 , 196I.
89 . Lewandowsky F: Obereinen eigentiimlichen Naevus derArustgegend. Arch Klin Exp Dermatol 131:90, 192\.
90 . With C, Kissmeyer A: Dystroph i elast ique folliculairethoracique (hereditaire") : Naevus clasticus de Lewan dowsky. Ann Dermatol Syphilol 3: 169-113, 1922.
91 . Sosis AC, Johnson WC: Connective tissue nevus. Derrnatologica 144:57-62, 1972.
92. Becke RFA, Musso LA: An unusual epithelialconnective tissue naevus with perifollicular mucinosis.Aust J DermatoI19:118-120, 1978.
93 . Pinnell SR, McKusick VA: Heritable disorders of connective tissue with skin changes, in Fitzpatrick TB,Eisen AZ, Wolff K, Freedberg 1M, Austen KF, editors:Dermatology in general medicine, cd . 2. New York,1979, McGraw-Hili Book Co., pp . 1144·1160.
94. Hambrick GW, Scheie HG: Studie s of the skin inHurler 's syndrome. Arch Dermatol 85:455-471, 1962.
95. Freeman RG: A pathological basis for the cutaneouspapules of mucopolysaccharidosis 11 (the Hunter syndrome). J Cutan PathoI4:318-328, 1977.
96 . Mongornery H, Underwood U : Lichen myxedernatosus(differentiation from cutaneous myxedemas or mucoidstates). J Invest DermatoI20:213-236, 1953.
97 . Danielsen L, Kobayasi T: Ultrastructural changes inscleromyxedema. Acta Derm Venereol (Stockh) 55:451-460 ,,1975.
98. Johnson WC, Helwig EB: Cutaneous focal mucinosis.A clinicopathological and histochemical stud y. ArchDermatol 93:13 -20, 1966.
99. Cheung HS, Nicoloff JT, Kamich MD, Spolter L,Nimni ME: Stimulation of fibroblast biosynthetic activity by serum of patient s with pretibial myxedema. JInvest Derrnatol 71:12-17, 1978.
100. Jolliffe DS, Gaylarde PM, Brock AI', Sarkany I: Pretibial myxedema: Stimulation of mucopolysaccharide production of fibroblasts by serum. Br J Derrnatol100:557 -560, 1979.
101. Hoffmann E, Zurhelle E: Uber cinen Naevus Lipomatodes cutaneus superficial is der Iinken Glutaalgegend,Arch Dermatol Syph 130:327-333, 1921.
102. Mehregan AH, Tavafoghi V, Ghandchi A: Nevuslipomatosus cutancus superfici alis (Hoffmann-Zurhelle) . J Cutan Pathol 2:307-313 , 1975.
103. Wilson Jones E, Marks R, Dongeshirum D: Naevussuperficialis lipomatosus . A clinicopathological reportof twenty cases. Br J Dermatol 93:121 -133, 1975.
1Q.l. Gardner EW, Miller HM, Lowney ED: Folded skinassociated with underlying nevus lipomatosus . ArchDerrnatol 115:978-979, 1979.
105. Ross CM: Generalized folded skin with an underlyinglipomatous nevus: "The Michelin tire baby." ArchDermatol 100:320-322, 1969.
106. Goltz RW, Henderson RR, Hitch JM , On JE: Focaldermal hypoplasia syndrome. A review of the literatureand report of two cases. Arch Derrnatol 101:1-11,1970.
107. Uillo J, Bauer EA, Santa-Cruz DJ, Loewinger RJ,

Volume 3Number 5November. 1980
Eisen A7:. Focal dermal hypoplasia: Abnormal growthcharacteristics of skin fibroblast in culture. J InvestDerrnatol 75:170-175, 1980.
108. Huneke E: The dermal component in melanosis naeviformis Becker. J Cutan Pathol 6:53-58, 1979.
109. Birt AR, Hogg GR, Dube WJ: Hereditary multiplefibrofolliculomas with trichodiscornas and acrochordons. Arch Dermatol 113:1674-1677, 1977.
Connective tissue nevi of skill 461
110. Weintraub R, Pinkus H: Multiple fibrofolliculomas(Birt-Hogg-Dube) associated with large connective tissue nevus. J Cutan Pathol 4:289-299, 1977.
III. Delacretaz J, Balsiger F: Harnartorne folliculaire multiple familial. Dermatologica 159:316-324, 1979.
112. Pinkus H. Coskey R, Burgess GH: Trichodiscorna: Abenign tumor related to Haarscheibe (hair disc). J InvestDerrnatol 63:212-218, 1974.




















