
Alterations of pulse pressure stimulate arterial wall matrix remodeling

Photochemistry and Photobiology, 2005, 81 : 457-466
ln Vivo Optical Analysis of Quantitative Changes in Collagen and Elastin During Arterial RemodelingT
Alexander Christov’+, Renee M. Korol’i2it, Erbin Dai’, Liying Liu’, Haiyan Guan’, Mark A. Bernards3, Paul B. Cavers3, David Susko3 and Alexandra L u c ~ s * ’ ’ ~ ’John P. Robarts Research Institute, London, ON, Canada ‘Department of Medical Biophysics, University of Western Ontario, London, ON, Canada 3Department of Plant Sciences, University of Western Ontario, London, ON, Canada 4Department of Microbiology and Immunology, University of Western Ontario, London, ON, Canada
Received 10 March 2004; accepted 10 November 2004
ABSTRACT
Altered collagen and elastin content correlates closely with remodeling of the arterial wall after injury. Optical analytical approaches have been shown to detect qualitative changes in plaque composition, but the capacity for detection of quantitative changes in arterial collagen and elastin content in vivo is not known. We have assessed fluorescence spectroscopy for detection of quantitative changes in arterial composition in situ, in rabbit models of angioplasty and stent implant. Fluorescence emission intensity (FEI) recorded at sites remote from the primary implant site was correlated with immunohistochemical (IH) analysis and extracted elastin and collagen. FEI was significantly decreased (P c 0.05) after treatment with anti-inflammatory agents, and plaque area decreased on comparison with saline-treated rabbits after stent implant or angioplasty (P 5 0.013). Excellent correlations for FEI with elastin and collagen I, 111 and IV content measured by IH (Rz 2 0.961) analysis were detected by multiple regression (MR) analysis. Good correlations also were found for FEI with elastin and collagen measured by high-performance liquid chromatography; MR analysis pro- vided highly predictive values for collagen and elastin (R2 ? 0.994). Fluorescence spectroscopic analysis detects quantita- tive compositional changes in arterial connective tissue in vivo, demonstrating changes at sites remote from primary angio- plasty and stent implant sites.
~~ ~~
T/Posted on the website on 23 November 2004 *To whom correspondence should be addressed: John P. Robarts Research
Institute, 100 Perth Drive. P.O. Box 5015, London, ON, Canada, N6A 5K8. Fax 5 19-663-3789; e-mail: [email protected]
?These authors have contributed equally to this study. Abbreviations: adj, adjusted CCD, charge-coupled device, FE, fluores-
cence emission; FEI, fluorescence emission intensity; FSA, fluorescence spectroscopic analysis; HPLC, high-performance liquid chromatography; E L , internal elastic lamina; IH, immunohistochemical: IVUS, in- travascular ultrasound; MR, multiple regression; MRI, magnetic resonance imaging; PITC, phenylisothiocyanate.
0 2005 American Society for Photobiology 003 1 -8655/05
INTRODUCTION Accelerated plaque growth causes narrowing of blood vessels culminating in eventual obstruction to blood flow. Rapid plaque growth contributes to vessel reocclusion after angioplasty and stent implantation. Local plaque ulceration can cause sudden thrombotic arterial occlusion in unstable clinical conditions such as unstable angina, transient ischemic attacks and myocardial and cerebrovas- cular infarction (heart attacks and strokes) (1-3). Accelerated plaque growth and unstable plaque rupture are both associated with simultaneous degradation and syntheses of connective tissues (4- 6), specifically collagen, elastin (7,8) and proteoglycans (9). Macrophages in the inflammatory response system release rnatrix- degrading enzymes (metalloproteinases) that break down collagen and elastin, allowing circulating cells to invade the arterial wall and initiate remodeling as well as plaque erosion and rupture (10.1 I) .
Native, fluorescent compounds in the arterial wall, collagen types I, 111 and IV and elastin provide natural markers for tissue analysis. Fluorescence spectroscopic analysis (FSA) of native fluorescence (autofluorescence) has been designed to probe human tissue (1 2), accurately detecting changes in atherosclerotic plaque composition in vitro and in vivo (1 3-1 7). Elastin and collagen are the main sources of autofluorescence in vascular tissues (14,18,19), and atherosclerotic plaque growth has been shown to alter the arterial fluorescence profile. Thus, FSA is predicted to provide a highly sensitive diagnostic tool for in situ quantification of changes in collagen and elastin content in the arterial wall. Fluorescence analysis has been demonstrated to detect qualitative changes in plaque composition in vivo and quantitative changes in collagen, elastin and lipids in vitro, but a clear demonstration of quantitative changes in plaque composition in vivo, in a circulating blood field, has not been reported previously. Blood components have been reported to absorb light both at excitation and emission wavelengths in FSA (20).
Arterial injury produced by percutaneous transluminal coronary angioplasty disrupts the arterial intima, exposing subendothelial connective tissue and lipids to circulating blood cells (monocytes, T lymphocytes and platelets) and their ligands (5,21). The use of endovascular stents during angioplasty is one of the most significant recent technical advances for prevention of postangio- plasty coronary occlusions, maintaining lumen patency and reducing inward remodeling, which in turn constricts the vessel lumen and reduces the incidence of recurrence (22-24). The stent
457

458 Alexander Christov eta/.
Table 1. Experimental surgical groups
Anti-inflammatory treatment
Group Angioplasty Stent type Saline control Serp-1 M-T7
- - - - Group I (n = 6) Group I1 (n = 6) Yes - - - -
-
Premounted NIR PRIMO (n = 9) Premounted NIR ROYAL (n = 12) Hand-mounted NIR
Saline (n = 4) Saline (n = 3) Saline (n = 6)
0.05 mgkg (n = 2) 0.05 mg/kg (n = 5 ) 0.05 mgkg (n = 7)
0.01 m a g (n = 3) 0.01 mg/kg (n = 4) 0.01 mg/kg (n = 7)
Group 111 (n = 21)
Group IV (n = 20)
Yes
Yes
site has initially greater cell proliferative responses, but through simple mechanical support, the stent prevents adventitial and medial scar formation (collagen and elastin) and lumen constric- tion. However, stenting also carries an additional risk of thrombosis and inflammation (22,24,25). Furthermore, neointimal hyperplasia in the stented section of the artery (23,26,27) is related closely to stent design (27-29), size (22,23,27,28) and coating (30- 32). Implanted stents have also been reported to affect blood vessel structure and function at sites adjacent to the implant site and to increase early inflammatory cell responses and invasion leading to a systemic increase in macrophage activation (33,34).
In this study, we demonstrate the use of optical analysis for detection of quantitative changes in arterial collagen and elastin content in situ in rabbit models after angioplasty injury and stent implant. Using FSA, we have detected quantitative changes in arterial elastin and collagen content produced by angioplasty injury and stent implant in the abdominal aorta of cholesterol-fed rabbits at sites remote from the stent implant.
MATERIALS AND METHODS Animal model. Fifty-three New Zealand white rabbits were fed 0.5% cholesterol/6% peanut oil for 7 days/week beginning 2 weeks before and continuing 2 weeks after balloon angioplasty and stent implant. For the purpose of this study, rabbits (3-4 kg) were divided into groups as shown in Table 1: Group I, untreated (normal) rabbits; Group II, angioplasty-alone; Group 111, rabbits with stent implant after angioplasty with premounted stent systems; Group IV, rabbits with stent implant after angioplasty with hand-mounted stents. Groups 111 and IV include rabbits with and without treatment with anti-inflammatory proteins, Serp-1, a viral serpin (33 , and M-T7, a viral chemokine-binding protein (36).
Angioplasty injury to the abdominal aorta was performed as described previously (17,35,36) using a 3.5 X 20 mm angioplasty balloon (USCI, C.R. Bard Ireland Ltd., Galway, Ireland) in rabbits under general anesthesia (40 mg/kg ketalean, 8 mg/kg xylazene and 0.5 mgikg acepromazine given by intramuscular injection). The angioplasty balloon was introduced via femoral arterial cut down under fluoroscopic control, inflated and then advanced and withdrawn three times to the level of the diaphragm. Immediately before angioplasty, 500 U heparin (Hepalen 1000 U/mL, Organon Teknika, Toronto, ON, Canada) per rabbit was administered by intra-arterial injection. SCIMED NIR PRIMO and NIR ROYAL pre- mounted stent systems as well as nonmounted NIR stents 3.0-5.0 mm diameter X 25 mm length (3.0-5.0 X 25 mm) (Boston Scientific, Galway, Ireland) hand-mounted onto 3.5 mm diameter by 32 mm length (3.5 X 32 mm) balloon catheters (Boston Scientific) were deployed in the distal abdominal aorta 1 cm above the iliac bifurcation, taking care to avoid insertion of the stent-mounted balloon above the stented site. The NIR PRIMO stents varied in length from 16 to 32 mm, all with diameter of 3.5- 4.0 mm, and were mounted on 20, 29 and 36 mm long, 3.5 mm diameter balloons. The NIR ROYAL stents were gold coated to enhance radio- opacity, with lengths ranging from 9 to 32 mm and diameter of 3 . 5 4 0 mm. Rabbits were sacrificed after follow-up in vivo FSA study by intra-arterial injection of euthanyl (8 10 mg sodium pentobarbitolhabbit) (MTC Pharmaceuticals, Cambridge, Canada). All surgical procedures and sacrifice of rabbits were performed according to the University Laboratory Animal Welfare Committee and National guidelines.
Anti-inflammatory treatment. Serp-1 , a myxoma virus serine proteinase inhibitor (serpin), was purified to 90% purity from a recombinant engineered Chinese hamster ovary cell line by affinity chromatography, using a linked monoclonal antibody as described previously (35). M-T7, a myxoma virus chemokine-binding protein that binds the C terminus of chemokines of the C, C-C and CXC chemokine classes was isolated and purified by fast-performance liquid chromatography from baby green monkey kidney cells infected with a vaccinia vector containing the M-T7 gene, as described elsewhere (36). The anti-inflammatory agents were delivered initially by intra-arterial injection immediately after stent implant and subsequently by ear vein injection as bolus doses for 10 days; daily for Serp-1 (0.05 mgkg) or on alternate days for M-T7 (0.01 mg/kg). Saline was used for control injections.
Fluorescence emission analysis. Tissue fluorescence emission (FE) was induced during argon laser light excitation (Innova 90, Coherent Laser Products, Palo Alto, CA; operating at 351-363 nm) (Fig. 1). Spectra were recorded with an EG&G Princeton Applied Research Model 1462 Optical Multichannel Analysis system (EG&G PARC, Toronto, Canada), as described previously (16), with a chopped wave output (exposure time, 0.2 ms; delay, 1.0 ms) produced by a Uniblitz shutter (Vincent Associates, Rochester, N Y 0.5-1.5 &/pulse). The laser beam was focused onto a 7F (French) laser angioplasty ring catheter (CeramOptec, Bonn, Germany). Recorded spectra are the sum of 10 individual spectra normalized to maximum intensity after background subtraction. In vivo fluorescence emission intensity (FEI) spectra were recorded in anesthetized rabbits with the laser catheter inserted retrograde through a 7F femoral sheath at 28 days follow-up after surgery. Five to 10 spectra were recorded from each of two sites in the abdominal aorta 2 cm apart starting 2 cm above the stent implant. In the control, nonstented rabbits, FSA was performed at aortic artery sites above the iliac bifurcation (2-8 cm) corresponding to the sites proximal to the stent implant (2-4 cm above the stent implant) at which FEI was measured in the stented aortas. FE spectra were recorded during infusion of 5 mL of saline through the central laser catheter lumen for 15- 20 s to reduce blood interference in the recording field. The position of the catheter was determined using a Siremobil 2 portable “C”-arm X-ray unit (Siemens, Munchen, Germany; donated by the Samia General Hospital) and by manual palpation of the arterial site from which spectra were recorded through a limited abdominal incision. After recording of FEI, sites were marked by s u ~ r e needles for later histological and compositional analysis. After sacrifice, 10 abdominal aortic specimens (each 0.5 cm in length) were harvested from the site where FEI was recorded. Five of these specimens (every other specimen) were frozen at -78°C for later extraction of elastin and collagen. The other five specimens were fixed in formalin and used later for histological analysis.
Morphometric and immunohistologic analysis. Formalin-fixed specimens from the abdominal aorta representing sites of FEI measurement were processed and stained (hematoxylin and eosin staining) as described previously for light microscopic examination (two sections per slide) (17,35-37). For morphometric analysis, cross-sectional areas of athero- sclerotic plaque defined as the area of intimal hyperplasia within the internal elastic lamina were outlined using a Sony Power HAD 3 charge- coupled device (CCD) color video camera attached to a Zeiss Axioskop using the Empix Northern Eclipse trace application program (Empix Imaging Inc., Mississauga, Canada) calibrated to the microscopic objective (17,35,36). Mean values of plaque area and vessel narrowing {[Total internal elastic lamina (EL) area - intimal area] X100Rotal IEL} were measured and calculated, respectively, for each rabbit and used for subsequent analysis.
For immunohistochemical (IH) analysis of relative collagen and elastin content, the sections were incubated with antibodies specific for collagens I,

Photochemistry and Photobiology, 2005, 81 459
Figure 1. FE analysis instrumental setup used for in vivo excitation and detection of FE in intact rabbit aorta and in tissue specimens. Arrows show light paths and signals.
111, IV (goat anti-human collagens I, 111, IV diluted 1/100; Chemicon International Inc., Temecula, CA) and elastin (mouse anti-bovine tropoelastin; Cedarlane Laboratories Ltd., Homby, ON, Canada) diluted 1/200 and then immunostained using the indirect peroxidase-labeled antibody technique (35). After incubation with primary antibody overnight, sections were incubated for 20 min with biotinylated antigoat antibody diluted 1/200 for collagen staining or antimouse immunoglobulin G diluted 1/200 for elastin staining (Vector Laboratories, Burlington, ON, Canada). Sections were then incubated with avidin-biotin-peroxidase complex for 20 min and developed with 3’3-diaminobenzidine for 5 min. Control stains lacking the primary or secondary antibodies were performed as negative controls.
Collagen- and elastin-stained areas were measured using a Sony Power HAD 3CCD color video camera attached to a Zeiss Axioscop connected to the Empix Northern Eclipse trace application program (Empix Imaging Inc.). Ratios of positively stained arterial wall area divided by the cross-sectional area of the intimal and medial arterial tissue layers examined were calculated. The analysis was limited to a depth of 350 pm on the basis of a predicted tissue penetration depth of the fluorescence excitation laser UV light of 100- 200 pm. Three high-power fields were examined per section analyzed.
Extraction of elastin and collagen. Arterial specimens were washed with saline to clear blood, the adventitia was cleaned off and samples were then blotted on filter paper and weighed. Lipid was extracted by soaking the tissue samples consecutively in acetone for 6 h and diethyl ether for 12- 15 h. Defatted samples were dried in a vacuum over CaS04. Elastin was separated from collagen and other soluble proteins by autoclaving in water (1 10°C, 15 pounds pressure for 6 h) followed by centrifugation “until clear.” This process leaves elastin as a pellet, while hydrolyzing collagen into the supernatant (38). Elastin-containing residue was heated sub- sequently in 0.1 N NaOH at 100°C for 45 min to solubilize remaining nonelastin proteins, then washed once with 0.1 N NaOH, thrice with water at 27°C and dried. Elastin was then weighed on an automatic electrobalance (CAHN Instruments Inc., Semtos, CA).
Analytical high-performance liquid chromatography measurement oj amino acid composition. To measure the collagen content, a derivatization procedure was applied to the solubilized nonelastin protein fraction. Dried protein hydrolysates from the samples were reconstituted in 20 mL water- triethylamine-MeOH (3:1:1), dried under a stream of Nz and broken down to component amino acids with 20 mL phenylisothiocyanate (PITC) reagent (water-triethylamine-PPC-MeOH, 1: 1: 1 :7) at room temperature for 20 min. Samples were dried under a stream of N2. reconstituted in 5 mM phosphate buffer (pH 7.4) containing 5.26% acetonitrile (vol/vol), centrifuged to remove insolubles and analyzed immediately by high- performance liquid chromatography (HPLC). Analytical HPLC was carried out using a Beckman System Gold Nouveau5 consisting of a Model 126 binary pump, a Model 168 diode array detector and a Model 508 autosampler (Beckman Coulter, Mississauga, ON, Canada). Samples (10 mL) were injected onto an Ultrasphere (2-18 reversed-phase column (250 X 4.6 mm, 5 mm; Beckman) fitted with a 7.5 X 4.6 mm guard column with the
same packing and eluted with a complex series of curved and linear gradients of acetonitrile-water (3:2) in 250 mM acetate buffer (pH 6.35) containing 0.5% triethylamine and 6.5% acetonitrile. The flow rate was 1 mL/min and eluant was monitored at 254 nm. Glycine, proline and hydroxyproline standards (Sigma-Aldrich, Oakville, ON, Canada) were treated similarly as above and used to calibrate the detector.
Statistics. Recorded spectra, after baseline correction, were normalized by dividing fluorescence intensity at all wavelengths by the maximum intensity, providing values ranging from 0 to 1.0 FEI units. Background fluorescence was recorded before each fluorescence measurement and subtracted from all subsequently recorded spectra. The FE spectra were calibrated with a mercury lamp before recording each day’s spectral analyses. Mean FEI at selected wavelengths for individual animals were used for atl statistical analyses. Changes in normalized FE spectra at selected wavelengths after various interventions or treatments as well as structural characteristics of plaque growth and arterial remodeling and of measured extracted elastin and collagen content (mean for individual animals) were analyzed by analysis of variance-factorial. After determining poolability (P is nonsignificant for Groups III and IV) by Student’s t-test, Groups I11 and TV were combined for these analyses. A value of P 5 0.05 was considered significant. Fisher’s least significant difference post hoc analysis was used to evaluate all possible pairwise comparisons.
The mean values for elastin and collagen I, 111 and N from IH analysis and of extracted elastin and HPLC-detected hydroxyproline, glycine and proline content (for collagen), corrected for tissue weight, were compared with normalized FEI at selected wavelengths using multiple regression (MR) analysis and simple regression analysis, as described previously (37). Selection of the wavelength ranges for the MR analysis was made on the basis of known peaks in FEI spectra for collagen and elastin and optimal representation of the differences in FEI between the treatment variants. Using formulas generated by MR analysis, predicted values for elastin and collagen derivatives (hydroxyproline, glycine and proline) were calculated as follows: measured mean values for connective tissue parameters, e.g. elastin content or collagen content, of a given treatment group were removed from the analyzed data set and MR analysis based on the remaining values was then applied. On the basis of each formula defined by MR analysis (y = a + bx, + cx: + dx: . . . where XI, XI, xg . . . represent FEI at selected wavelengths), a predicted value for the omitted parameter was calculated. This procedure was performed using wavelength ranges in the spectra, which provided the best correlation (highest adjusted [adj] R2 values) for FEI and tissue compositional characteristics. The calculated predicted values for elastin and collagen I, III and IV, as well as the amino acids hydroxyproline, glycine and proline, were compared with the corresponding measured mean values from each treatment group for these parameters using simple regression analysis. For MR analysis, the adj provides a correction for the increase in the R2 value inherent in this analysis when additional independent variables are assigned to an existing regression by applying a “penalty” to the R2 value on the basis of the numbers of the variables assigned.

460 Alexander Christov eta/.
RESULTS Histological analysis of atherosclerotic plaque
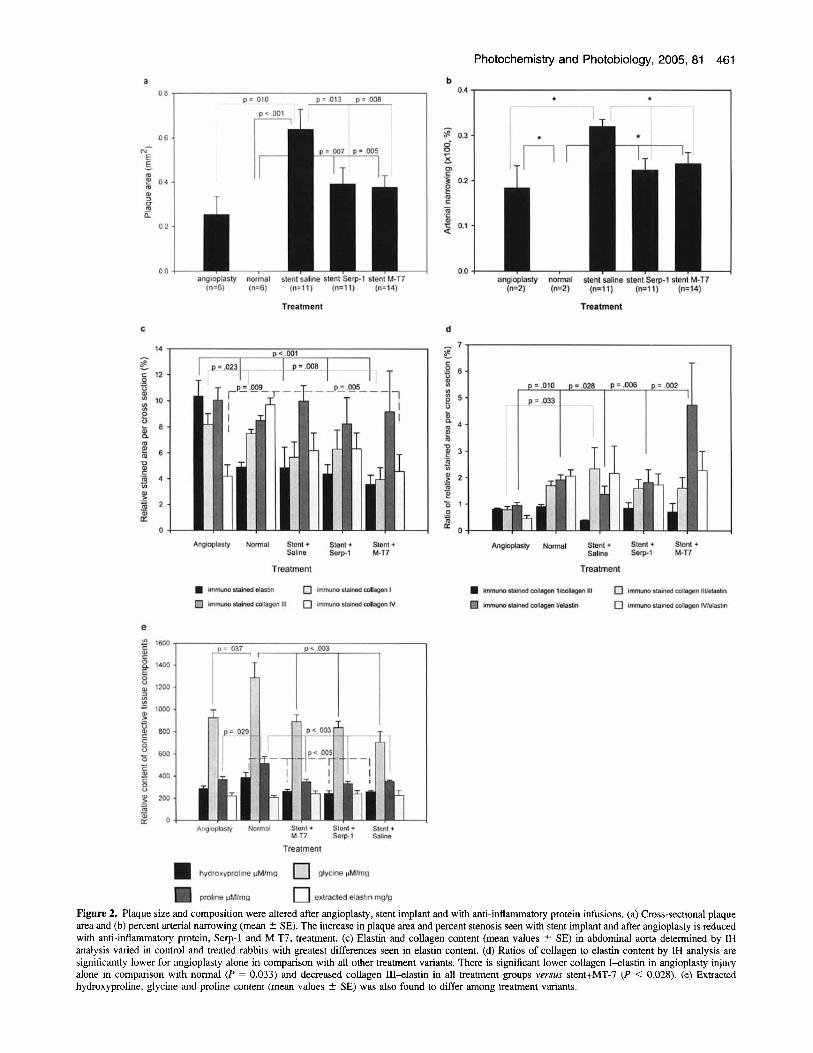
Treatment with the anti-inflammatory proteins, Serp- 1 and M-T7, significantly reduced plaque growth (P = 0.013 and P = 0.008, respectively) and arterial narrowing (P = 0.001 and P = 0.004, respectively) when compared with stented aortas with control saline infusion (Fig. 2a,b). Plaque growth was increased after either angioplasty injury or angioplasty with stent implant as expected (Fig. 2a,b) when compared with normal arteries without surgery (1,3,7,11,27-3 1). A relative increase in cross-sectional atherosclerotic plaque area (P 5 0.011) and arterial narrowing ( P 5 0.004) was also detected at sites in the abdominal aorta be- tween 2 and 4 cm proximal to the stent implant (Fig. 2a,b) on comparison with the angioplasty balloon-injured and nonstented arteries.
Altered plaque connective tissue composition was assessed similarly in individual arterial sections. IH analysis of elastin and collagen content in the intimal and medial arterial tissue layers, examined to a maximum depth of 350 vm, revealed significant differences between the treatment variants (Fig. 2c). On immunostained sections, elastin content in the abdominal aorta of rabbits from the three stent groups (saline, Serp-1 and M-T7 treated) or normal uninjured arteries had significantly lower elastin content when compared with sections taken from the rabbits after angioplasty injury alone without stent implant (P 5 0.0008). Staining for collagen I demonstrated significant reduc- tions after stent implant with M-T7 treatment (P 5 0.023) when compared with angioplasty alone; normal uninjured arteries also had reduced collagen I when compared with angioplasty (P 5 0.008). Immunostaining for collagen IV also detected significant increases in normal untreated rabbits when compared with angioplasty balloon-injured (P 5 0.009) and MT-7-treated stent implants (P 5 0.005), whereas collagen Type III was not significantly different among the variants. When ratios of collagen I, I11 and IV to elastin were compared among the treatment variants (Fig. 2d), an overall reduction in the collagen4astin ratios was seen in the angioplasty injury alone group when compared with all other treatment variants. There was a significant increase in collagen Velastin ratio in the stent implant with saline group in comparison with balloon injury alone (P 5 0.033). There was also a significant decrease in collagen IIVelastin for all treatment variants when compared with MT-7-treated stent (P 5 0.028).
Changes in extracted elastin and collagen content after angioplasty and stent implant
Proline (P 5 0.021), hydroxyproline (P 5 0.042) and glycine (P 5 0.028) were present in lower amounts in whole arterial extracts after angioplasty or stent implant (or both) at sites 2-8 cm above the iliac bifurcation after angioplasty alone and at sites 2 4 cm proximal to the stent implant when compared with sections harvested from normal, untreated rabbit aorta (Fig. 2e). The differences in the amounts of elastin extracted from the arterial wall did not reach statistical significance.
Analysis of arterial FEI recorded from rabbit aortas in vivo
Spectra recorded from pure elastin and collagen were compared initially with spectra recorded from normal rabbit aorta. Quanti- tative changes in plaque size and composition for individual
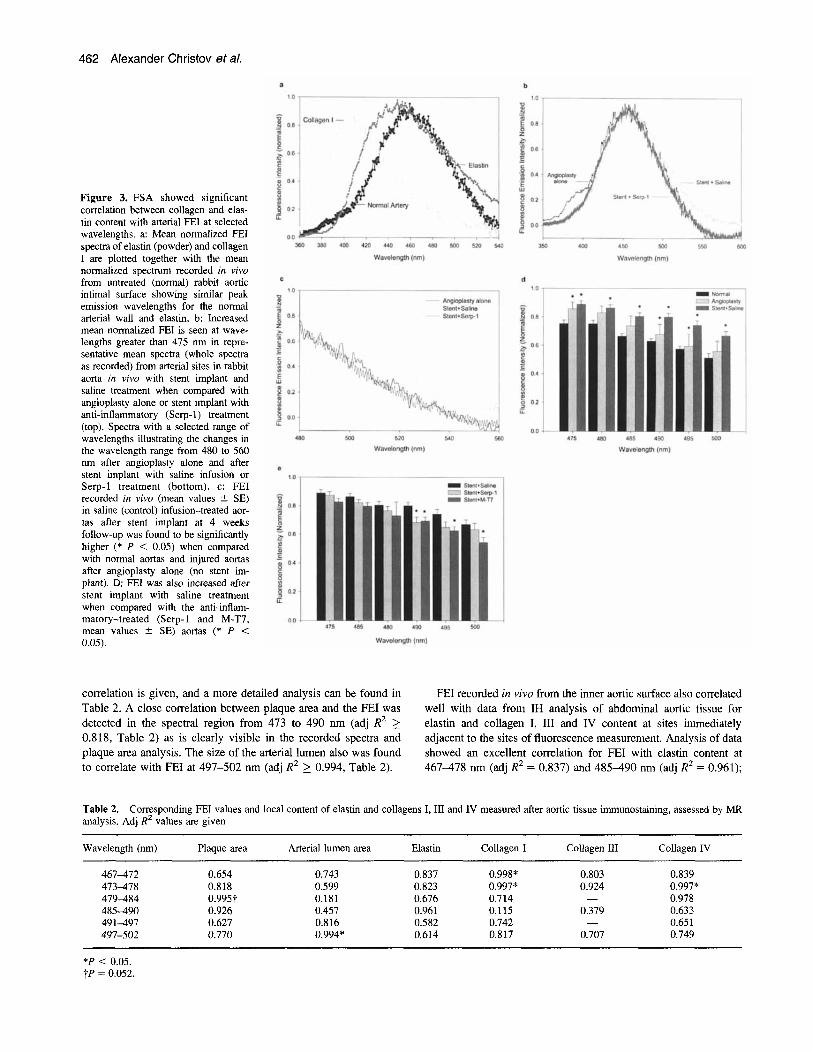
arterial sections (Fig. 2) were correlated subsequently with changes in FEI. In Fig. 3a, mean normalized FEI spectra of pure elastin (powder) (from bovine neck ligament, Sigma-Aldrich) and collagen I (from bovine Achilles tendon, Sigma-Aldrich) are plotted together with the mean normalized spectrum from the intimal surface of an untreated (normal) rabbit aorta recorded in vivo. Our results support the baseline assumption that elastin is the major natural fluorophore in the arterial intimal layer with a close correspondence between peak wavelengths for FEI at 450-510 nm. Recorded spectra demonstrated that FEI in absolute units or specific FEI (FEI per unit volume) of pure elastin is roughly two- fold higher than specific FEI of the pure collagen I and approximately four times higher than the FEI from the arterial tissue recorded in vivo (data not shown). Thus, smaller differences in the local elastin content were compared with collagen in the arterial wall and are expected to have improved expression, and hence detection, in the integral FEI spectra.
The major difference in shape for the normalized spectra recorded from powdered elastin and collagen I is seen at wavelengths from 400 to 540 nm. In this region, a close similarity in the spectral profiles of FEI from pure elastin and untreated aortic intimal surface was observed including specific changes in individual peaks of FEI (455460 nm; 465470 nm). In rabbit aortas after angioplasty injury and stent implant, plaque growth was associated with changes in FEI in this wavelength range (Fig. 3b). Decrease in fluorescence intensity was observed with anti- inflammatory treatment in the group of rabbits receiving Serp-1 after stent implant in comparison with stent group receiving saline treatment (Fig. 2b). The decreased FEI in the 480-560 nm range correlates well with the decreased plaque growth seen with stent implant with anti-inflammatory treatment when compared with stent implant with saline control treatment and a further reduction when compared with angioplasty injury alone (Fig. 2a,b). This difference in FEI at 480-560 nm was paralleled by significant increases in collagen LU-elastin content ratio (Fig. 2d) seen with M-T7 treatment and to a lesser extent with Serp-1 treatment. Thus, the FEI spectra were predictive of increased collagen III-elastin ratios and decreased fluorescence with anti-inflammatory treatment. However, the FEI was not predictive for the increase in collagen III-elastin and decreased elastin seen in saline-treated stents.
The mean FEI recorded in vivo, in rabbit aortas, after saline (control) infusion and stent implant was found to be significantly higher (P 5 0.05) when compared with normal aortas. This increase was seen throughout the wavelength range from 475 to 500 nm (analyzed at 1 nm intervals) (Fig. 3c). FEI values from the aorta of saline-treated rabbits after stent implant were higher (P 5 0.05) when compared with aortas of rabbits given anti-inflamma- tory agents, at 490 for Serp-1 and 490-500 nm for M-T7 (Fig. 3d). The presence of distal stent implants is predicted to alter tissue responses at sites adjacent to, and within, the implant site. A continuing vascular response to the foreign metal embedded in the artery wall is thus postulated readily and may upregulate system inflammatory responses.
Correlation of FEI values with tissue elastin and collagen content determined by immunostaining
FEI, recorded in viva, was correlated with the histological characteristics of atherosclerotic plaque growth in the arterial wall as measured by cross-sectional plaque area and arterial lumen size, using MR analysis. Over a range of wavelengths, the lowest
Treatment
Treatment
Photochemistry and Photobiology, 2005, 81 461
Treatment
Treatment
Treatment
Figure 2. Plaque size and composition were altered after angioplasty, stent implant and with anti-inflammatory protein infusions. (a) Cross-sectional plaque area and (b) percent arterial narrowing (mean ? SE). The increase in plaque area and percent stenosis seen with stent implant and after angioplasty is reduced with anti-inflammatory protein, Serp-1 and M-T7, treatment. (c) Elastin and collagen content (mean values If: SE) in abdominal aorta determined by IH analysis varied in control and treated rabbits with greatest differences seen in elastin content. (d) Ratios of collagen to elastin content by IH analysis are significantly lower for angioplasty alone in comparison with all other treatment variants. There is significant lower collagen I-elastin in angioplasty injury alone in comparison with normal (P = 0.033) and decreased collagen III-elastin in all treatment groups versus stent+MT-7 (P 5 0.028). (e) Extracted hydroxyproline, glycine and proline content (mean values 2 SE) was also found to differ among treatment variants.
462 Alexander Christov et a/.
Figure 3. FSA showed significant correlation between collagen and elas- tin content with arterial FEI at selected wavelengths. a: Mean normalized FEI spectra of elastin (powder) and collagen I are plotted together with the mean normalized spectrum recorded in vivo from untreated (normal) rabbit aortic intimal surface showing similar peak emission wavelengths for the normal arterial wall and elastin. b: Increased mean normalized FEI is seen at wave- lengths greater than 475 nm in repre- sentative mean spectra (whole spectra as recorded) from arterial sites in rabbit aorta in vivo with stent implant and saline treatment when compared with angioplasty alone or stent implant with anti-inflammatory (Serp-1) treatment (top). Spectra with a selected range of wavelengths illustrating the changes in the wavelength range from 480 to 560 nm after angioplasty alone and after stent implant with saline infusion or Serp-l treatment (bottom). c: FEI recorded in vivo (mean values ? SE) in saline (control) infusion-treated aor- tas after stent implant at 4 weeks follow-up was found to be significantly higher (* P < 0.05) when compared with normal aortas and injured aortas after angioplasty alone (no stent im- plant). D: FEI was also increased after stent implant with saline treatment when compared with the anti-inflam- matory-treated (Serp-1 and M-T7, mean values ? SE) aortas (* P < 0.05).
correlation is given, and a more detailed analysis can be found in Table 2. A close correlation between plaque area and the FEI was detected in the spectral region from 473 to 490 nm (adj R2 2 0.818, Table 2) as is clearly visible in the recorded spectra and plaque area analysis. The size of the arterial lumen also was found to correlate with FEI at 497-502 nm (adj R2 2 0.994, Table 2).
FEI recorded in vivo from the inner aortic surface also correlated well with data from IH analysis of abdominal aortic tissue for elastin and collagen I, I11 and IV content at sites immediately adjacent to the sites of fluorescence measurement. Analysis of data showed an excellent correlation for FEI with elastin content at 467-478 nm (adj R2 = 0.837) and 485-490 nm (adj R2 = 0.961);
Table 2. Corresponding FEI values and local content of elastin and collagens I, I11 and IV measured after aortic tissue immunostaining, assessed by MR analysis. Adj R2 values are given
Wavelength (nm) Plaque area Arterial lumen area Elastin Collagen I Collagen I11
467-472 0.654 0.743 0.837 0.998* 0.803 473478 0.818 0.599 0.823 0.997" 0.924 479-484 0.995t 0.181 0.676 0.714 - 485-490 0.926 0.457 0.961 0.115 0.379 491497 0.627 0.816 0.582 0.742 - 497-SO2 0.770 0.994* 0.614 0.817 0.707
Collagen IV
0.839 0.997" 0.978 0.633 0.651 0.749
*P < 0.05. tP = 0.052.
Photochemistry and Photobiology, 2005, 81 463
10 -
v) 8 - - 5 ,3 n 6 -
a 4 -
2 -
a Elastin (YO immunostained area)
12 I
500 -
450 - 5
'& 400 -
350 - e! 3w.
250 -
0 4 I 0 2 4 6 8 10 12
Measured Values
V = O 021 + 0 995.X. R2=0 994
Confidence ~nleryals ooefliciant 95% I m r 95% u p p i lnlercepl 0027 -0381 0441 Elastin 0995 0920 1069
C Glycine(umol/mg)
b Hydroxyproline (umollmg)
400 7
200 4 200 250 300 350
Measured Values V = -1042 + 1 002 ' X , R'=O 996
Confidence I ~ I ~ W B I S C O ~ L C I ~ I 95% l ow, 95% u w r Intercept 1042s-11 -1886 1885 hydmxypmline 1 0 0 0934 1066
d Proline (umollma)
400 600 800 1004 1200 14C
Measured Values
Y = -25 198 + 1 03 ' X, R2=0 994
conflaence in te~a is coemcient 95% i o w r 95% upper IWiUWN -252 -977 4 7 3 glYCl"e 1030 0952 1106
m 200 300 400 500
Measured Values V = - 7 8 2 5 + 1 0 2 4 ' X R2=0997
Inarc*fl -7925 -301 142 Pmlme -1 024 OW3 1084
conmsnce i"leN.lll coement 95% I-, 95% upper
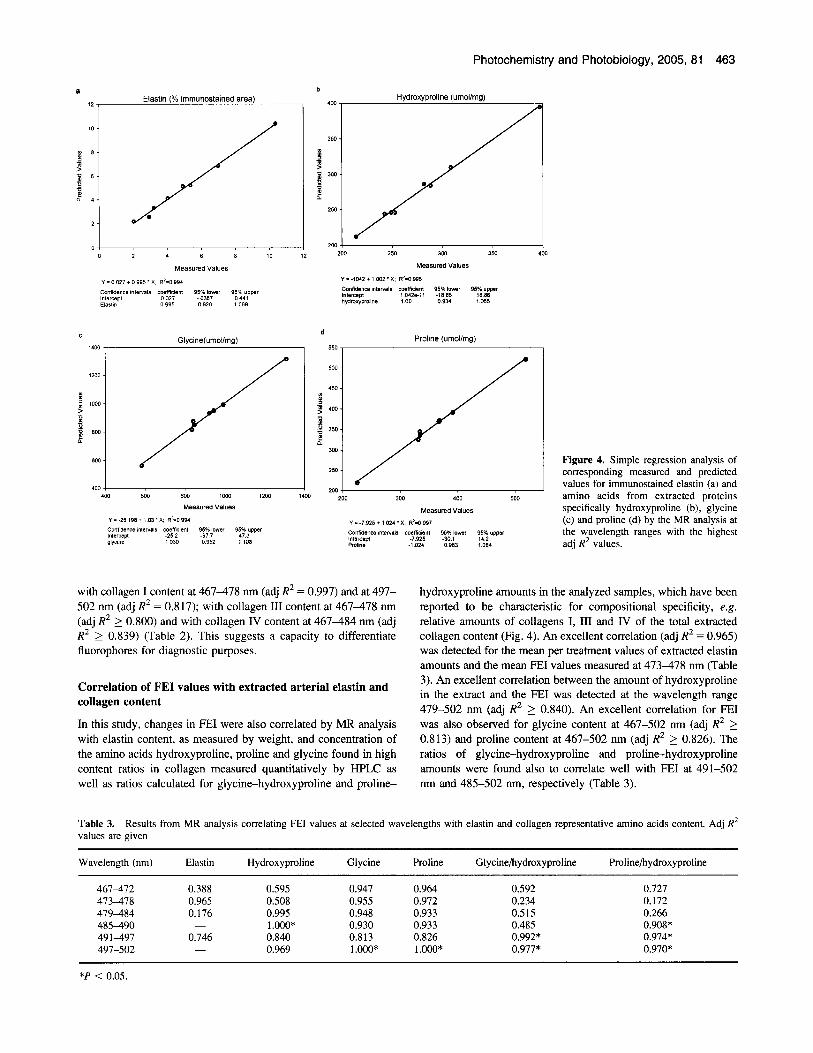
Figure 4. Simple regression analysis of corresponding measured and predicted values for immunostained elastin (a) and amino acids from extracted proteins specifically hydroxyproline (b), glycine (c) and proline (d) by the MR analysis at the wavelength ranges with the highest adj R2 values.
with collagen I content at 467-478 nm (adj R2 = 0.997) and at 497- 502 nm (adj R' = 0.817); with collagen 111 content at 467-478 nm (adj R2 2 0.800) and with collagen IV content at 467-484 nm (adj R2 L. 0.839) (Table 2). This suggests a capacity to differentiate fluorophores for diagnostic purposes.
hydroxyproline amounts in the analyzed samples, which have been reported to be characteristic for compositional specificity, e.g. relative amounts of collagens I, I11 and IV of the total extracted collagen content (Fig. 4). An excellent correlation (adj R2 = 0.965) was detected for the mean per treatment values of extracted elastin amounts and the mean FEI values measured at 473-478 nm (Table 3). An excellent correlation between the amount of hydroxyproline in the extract and the FEI was detected at the wavelength range 479-502 nm (adi R2 2 0.840). An excellent correlation for €XI
Correlation of FEI values with extracted arterial elastin and collagen content
In this study, changes in FEI were also correlated by MR analysis was also observed forglycine content at 467-502 nm (adj R2 2 with elastin content, as measured by weight, and concentration of 0.813) and proline content at 467-502 nm (adj R2 2 0.826). The the amino acids hydroxyproline, proline and glycine found in high ratios of glycine-hydroxyproline and proline-hydroxyproline content ratios in collagen measured quantitatively by HPLC as amounts were found also to correlate well with FEI at 491-502 well as ratios calculated for glycine-hydroxyproline and proline- nm and 485-502 nm, respectively (Table 3).
Table 3. values are given
Results from MR analysis correlating FEI values at selected wavelengths with elastin and collagen representative amino acids content. Adj RZ
Wavelength (nm) Elastin Hydroxyproline Glycine Proline Glycine/hydroxyproline Prolinehydroxyproline
467-472 0.388 0.595 0.947 0.964 0.592 0.727 473478 0.965 0.508 0.955 0.972 0.234 0.172 479-484 0.176 0.995 0.948 0.933 0.515 0.266 485490 - 1 .ooo* 0.930 0.933 0.485 0.908* 491497 0.746 0.840 0.813 0.826 0.992* 0.974* 497-502 - 0.969 1 .ooo* l.OOO* 0.977* 0.970*
*P < 0.05.

464 Alexander Christov eta/.
Predictive capacity of FSA for arterial elastin and collagen content
Predicted contents for elastin and collagen were calculated using formulas generated by MR analysis at the wavelength ranges with the highest adj R2 values. Corresponding measured and predicted values were then compared using simple regression analyses. An excellent correlation was detected between predicted values and measured values for collagen I (R2 = 0.999), collagen 111 (R2 = 0.989), collagen IV (R2 = 0.999) and a close correlation for elastin (R2 = 0.994) on the basis of IH analysis (Fig. 4a) and for the extracted hydroxyproline, glycine and proline (Fig. 4b-d). However, no correlation for extracted elastin content (R2 = 0.083) was found.
DISCUSSION In vivo analysis of native arterial FE provides additional information on arterial chemical composition when combined with conventional imaging techniques such as white-light, endoscopy diagnostics, X-ray angiography, magnetic resonance imaging (MRI) or intravascular ultrasound (IVUS) (39). Optical coherence tomography provides highly detailed images of atherosclerotic plaque, and this laser-based imaging technology lends itself readily to combined analysis with spectroscopy. The use of FSA for the detection of natural vascular fluorophores can yield quantitative biochemical and morphological information. Although Raman (39), fluorescence (14,39) and reflectance spectroscopy (40) have been reported to detect quantitative changes in arterial wall composition in vitro, optical (fluorescence spectroscopic) detection of quantitative changes in collagen and elastin content in vivo in a circulating blood field has not been demonstrated previously. IVUS and angiography do not provide compositional tissue analysis. MRI has the potential, as does Raman spectroscopy (39), but these techniques have yet to be tested and proven applicable in vivo. In previous studies, we have demonstrated that FSA, when applied in vivo in experiments using a rabbit model, is a sensitive and highly informative diagnostic technique for detection of stable atherosclerotic plaque trans- formation to an unstable state (17). The use of this fluorescence- based analysis system has demonstrated quantitative changes in atherosclerotic plaque and arterial wall collagen and elastin composition (19,37). However, FSA remains an experimental approach with inherent limitations. The broad-based FEI spectra are produced by overlapping FE from the various native fluorophores present in the tissue. Scattering and absorption of incident and emitted light complicate the acquired signal (39) and require specific corrections to be made to eliminate additional noise and artifacts in the recorded spectra. Thus, the exact capability for fluorescence to detect specific quantitative changes in fluorophore chemical content remains unknown.
In this study, we have used FSA to assess remote effects of stent implant on arterial remodeling and plaque growth at sites distant from the site of intervention. Stents are known to cause local cellular reactions at the sites of implantation, leading to de- velopment of “in-stent restenosis” (24). We were unable to analyze FEI from stented aortic zones because of interference produced by the metal struts with this system for optical analysis, which indicates a limitation in this optical system. However, with longer incubation times, plaque growth covering stent implants is expected to reduce FSA interference produced by reflected light. Analysis of spectra recorded from sites above and remote from the
stent implants detected unexpected significant increases in intimal arterial structure at discrete sites distant from the stent implant site (33,34). These studies are based upon multiple spectra recorded from each site and confirmed previous reports of fluorescence spectroscopic detection of plaque growth (17,19,39). A definitive correlation was detected between FEI and plaque growth, which is based upon multiple analyses of FEI recorded from individual arterial sites in a large total group of animals (53 in total with l o o t arterial sites examined). However, further study will be necessary for confirmation of these observed remote effects of stent implants on plaque growth. These findings are of great interest when considering the recent reports of generalized increases in in- flammatory responses during plaque development.
Although it is possible that the simple introduction of the stent after balloon angioplasty may have created further trauma, care was taken to place the stent only at the specified site, e.g. not to advance the stent, or the balloon on which it was mounted, to sites more proximal to the implant site. Thus, the finding that mea- sured plaque area was increased and recorded FEI spectra were significantly changed between 2 and 4 cm above the proximal stent edge appears to demonstrate a remote effect. Therefore, this generalized increase in plaque area may be the result of increased trauma because of secondary insertion of the stent mounted on a balloon after the initial simple balloon angioplasty or may be because of systemic responses to the stent implant. The response to treatment with the anti-inflammatory agents used in this study also indicates that the accelerated plaque growth above stent implant sites is driven by inflammatory responses. Furthermore, activated circulating monocytes are expected to release collagen- and elastin- degrading enzymes (matrix metalloproteinases, chymase and cathepsins) whereas activated smooth muscle cells can increase matrix synthesis; two activities predicted to alter arterial matrix composition during plaque growth.
Elastin is well recognized as a major natural fluorophore (41) in the arterial intimal surface tissue layer (42). Our previous research has demonstrated that FSA in vitro can detect and differentiate collagen species (collagen I, I11 and IV) and elastin components in the arterial wall and in cardiac valve leaflets in vitro (19,37). We demonstrate here, that FEI from natural fluorophores recorded in a living artery can be applied to directly assess arterial connective tissue composition.
In this study, close associations between FEI spectral profiles of elastin and the normal (untreated) rabbit aorta confirmed the greater contribution of tissue elastin to the total emitted fluorescence from natural fluorophores in arterial intima. Therefore, improved correlation for FEI when compared with elastin and collagen content determined by immunostaining was predicted. FE is recorded predominately from the aortic intimal and medial tissue layers, where the elastin and collagen content were measured quantitatively by immunostaining. Conversely, extracted elastin- and collagen-specific amino acids (hydroxyproline, glycine and proline) amounts provide highly quantifiable numbers for these correlation analyses but represent the extract from the total arterial wall, including both the surface tissue layers to which the laser light is expected to penetrate and also deeper arterial tissue at depths beyond FE excitation light penetration.
Despite being a major step for preventing complications after invasive cardiovascular procedures, stenting itself is known to cause not only inflammation and restenosis (26,4345) but also thrombosis (4648), shortly after implantation. Simultaneous treatment of patients with antithrombotic and antiplatelet drugs

Photochemistry and Photobiology, 2005, 81 465
during the procedure has now proven beneficial for early successful outcomes (25,3 1,35,46-55), but long-term restenosis remains a difficult problem. In this study, w e have tested the effects of two anti-inflammatory proteins, Serp-1 and M-T7, to vary the extent of plaque growth and local macrophage activation after stent implant. A constant overall reduction in FEI in the group of stent implants was observed with anti-inflammatory treatment and correlated closely with reduced plaque growth and changes in collagen and elastin, specifically increased collagen Yelastin and collagen III/elastin ratios. An unexpected finding was that although stent implant alone with saline treatment markedly increased FEI, the collagen In11 to elastin ratio was increased and elastin content decreased. This suggests that either another fluorophore was present (proteoglycan) or an absorbing species was absent and merits further investigation.
In summary, spectroscopic analysis of autofluorescence emitted from the aortic intimal surface recorded in situ was used successfully for quantitative assessment of compositional changes in arterial connective tissue in situ in the living artery. Thus, FSA detected increased plaque growth in the arterial wall after stent implant at sites remote from the implant site. Autofluorescence emission intensity was correlated with a quantitative analysis of extracted arterial elastin and collagen and demonstrated an excellent correlation between FEI and local elastin and collagen concentration. The spectral ranges with the best correlation were found to specifically match characteristic maxima in FEI spectra of pure powdered elastin and collagen I. These fluorescence maxima were also well identified in the tissue spectra, proving once again very high sensitivity for elastin and collagen detection. Using formulas generated by MR analysis, an excellent pre- dictive capacity was demonstrated for elastin and collagen in vivo. Although previous work has suggested that the absorbance of emitted fluorescence light by blood (20) would interfere with accurate optical analysis of elastin and collagen in vivo, in a circulating blood field, this work demonstrates a clear cor- relation between measured elastin and collagen content and the value of FEI.
Acknowledgements-We would like to thank the Heart and Stroke Foun- dation of Ontario, the Canadian Institutes of Health Research and The J.P. Robarts Research Institute for their ongoing support of this research.
REFERENCES 1. Libby, P., P. M. Ridker and A. Maseri (2002) Inflammation and
atherosclerosis. Circulation 106, 135-136. 2. Carr, S . C., A. Farb, W. H. Pearce, R. Virmani and J. S . Yao (1997)
Activated inflammatory cells are associated with plaque rupture in carotid artery stenosis. Surgery 122, 757-764.
3. Vink, A,, A. H. Schoneveld, W . Richard, D. P. V. de Kleijn, E. Falk, C. Borst and G. Pasterkamp (2001) Plaque burden, arterial remodeling and plaque vulnerability determined by systemic factors. J . Am. Coll. Cardiol. 38, 718-723.
4. Frishman, W . H., B. Bums, B. Atac, N. Alturk, B. Altajar and K. Lemck (1995) Novel antiplatelet therapies for treatment of patients with ischemic heart disease: inhibitors of the platelet glycoprotein IIb/IIIa integrin receptor. Am. Heart J . 130, 877-892.
5. Haverkate, F., S . G. Thompson, S . D. Pyke, J. R. Gallimore and M. B. Pepys (1997) Production of C-reactive protein and risk of coronary events in stable and unstable angina. European Concerted Action on Thrombosis and Disabilities Angina Pectoris Study Group. Lancet 349,
6. Dangas, G., J. J. Badimon, B. S. Coller, J. T. Fallon, S. K. Sharma, R. M. Hayes, P. Meraj, J. Ambrose and J. D. Marmur (1998) Administration of Abciximab during percutaneous coronary interven-
1252-1253.
tion reduces both ex vivo platelet thrombus formation and fibrin deposition. Arterioscler. Thromb. Vase. Biol. 18, 1342-1 349.
7. Davies, M. J. (1996) Stability and instability: two faces of coronary atherosclerosis. Circulation 94, 201 3-2020.
8. Shah, P. K., E. Falk, J. J. Badimon, A. Femandez-Ortiz, A. Mailhac, G. Villareal-Levy, J. T. Fallon, J. Regnstrom and V. Fuster (1995) Human monocyte-derived macrophages induce collagen breakdown in fibrous caps of atherosclerotic plaques. Potential role of matrix-degrading metalloproteinases and implications for plaque rupture. Circulation 92,
9. Bruel, A. and H. Oxlund (1996) Changes in biornechanical properties, composition of collagen and elastin, and advanced glycation end- products of the rat aorta in relation to age. Atherosclerosis 1272, 155-165.
10. Shah, P. H. (2000) Circulating markers of inflammation for vascular risk prediction: are they ready for prime time. Circulation 105,
11. Lendon, C. L., M. J. Davies, G. V. Bom and P. D. Richardson (1991) Atherosclerotic plaque caps are locally weakened when macrophage density is increased. Atherosclerosis 87, 87-90.
12. Baraga, J. J., P. R. Rava, P. Taroni, C. Kittrell, M. Fitzmaurice and M. S. Feld (1990) Laser-induced fluorescence spectroscopy of normal and atherosclerotic human aorta using 3 0 6 3 10 nm excitation. Lasers Surg. Med. 10, 245-261.
13. Garrand, T. J., M. L. Stetz, K. M. O’Brien, G. R. Gindi, L. I. Laifer and L. I. Deckelbaum (1990) Characterization of the site dependency of normal canine arterial fluorescence. Lasers Surg. Med. 10, 375-383.
14. Laifer, L. I., K. M. O’Brien, M. L. Stetz, G. R. Gindi, T. J. Garrand and L. I. Deckelbaum (1989) Biochemical basis for the difference between normal and atherosclerotic arterial fluorescence. Circulation 80, 1893-1901.
15. Sartori, M., D. Weilbaecher, G. L. Valderrama, S. Kubodera, R. C. Chin, M. J. Berry, F. K. Tittel, R. Sauerbrey and P. D. Henry (1988) Laser-induced autofluorescence of human arteries. Circ. Res. 63,
16. Deckelbaum, L. I. (1989) Laser-assisted angioplasty of inferior vena caval obstructions: what’s good for the artery is good for the vein. Hepatology 9, 338-339.
17. Christov, A,, E. Dai, M. Drangova, L. Liu, G. S . Abela, P. Nash, G. McFadden and A. Lucas (2000) Optical detection of triggered atherosclerotic plaque disruption fluorescence emission analysis. J . Photochem. Photobiol. 12, 242-252.
18. Leon, M. B., D. Y. Lu, L. G. Prevosti, W . W . Macy, P. D. Smith, M. Granovsky, F. R. Bonner and R. S . Balban (1988) Human arterial surface fluorescence: atherosclerotic plaque identification and effect of laser atheroma ablation. J . Am. Coll. Cardiol. 12, 94-102.
19. Yan, W., M. Perk, A. Chagpar, Y. Wen, S . Stratoff, W. J. Schneider, B. I. Jugdutt, J. Tulip and A. Lucas (1995) Laser-induced fluorescence: 111. Quantitative analysis of atherosclerotic plaque content. Lasers Surg. Med. 16, 164-168.
20. Lucas, A. R., T. Gauthier, R. H. Clark and J. M. Isner (1991) Angiographic contrast media interference with laser-induced fluores- cence excitation and detection in atherosclerotic human coronary arteries. Am. Heart J . 121, 110-118.
21. Le Breton, H., E. F. Plow and E. J. Topol (1996) Role of platelets in restenosis after percutaneous coronary revascularization. J . Am. Coll. Cardiol. 28, 1643-1651. [Review]
22. di Mario, C., B. Reimers, Y. Almagor, I. Moussa, L. Di Francesco, M. Farraro, M. B. Leon, K. Richter and A. Colombo (1998) Procedural and follow up results with a new balloon expandable stent in unselected lesions. Heart 79, 234-241.
23. Garasic, J. M., E. R. Edelman, J. C. Squire, P. Seifert, M. S. Williams and C. Rogers (2000) Stent and artery geometry determine intimal thickening independent of arterial injury. Circulation 101, 812-818.
24. Farb, A,, G. Sangiorgi, A. J. Carter, V. M. Walley, W . D. Edwards, R. S. Schwartz and R. Virmani (1999) Pathology of acute and chronic coronary stenting in humans. Circulation 99, 44-52.
25. Herbert, J.-M., F. Dol, A. Bemat, R. Falotico, A. Lale and P. Savi (1998) The antiaggregating and antithrombotic activity of clopidogrel is potentiated by aspirin in several experimental models in the rabbit. Thromh. Haemostasis 80, 512-5 18.
26. Kollum, M., S . Kaiser, R. Kinscherf, J. Metz, W . Kubler and C. Hehrlein (1997) Apoptosis after stent implantation compared with
1565-1569.
1758-1759.
1053-1059.
466 Alexander Christov eta/.
balloon angioplasty in rabbits. Role of macrophages. Arterioscler. Thromb. Vasc. Biol. 17, 2383-2388.
27. Costa, M. A,, M. Sabate, I. P. Kay, P. J. de Feyter, K. Kozuma, P. Serrano, V. de Valk, M. Albertal, J. M. R. Lightart, C. Disco, D. P. Foley and P. W. Sermys (2000) Three-dimensional intravascular ultrasonic volumetric quantification of stent recoil and neointimal formation of two new generation tubular stents. Am. J . Cardiol. 85,
28. Kobayashi, Y., J. De Gregorio, N. Kobayashi, B. Reimers, R. Albiero, M. Vagnetti, L. Finci, C. Di Mario and A. Colombo (1999) Comparison of immediate and follow-up results of the short and long NIR stent with the Palmaz-Schatz stent. Am. J . Cardiol. 84, 499-504.
29. Almagor, Y., S. Feld, F. Kiememeij, P. W. Sermys, M.-C. Morice, A. Colombo, C. Macaya, J. L. Guermonperez, J. Marco, R. Erbel, I. M. Penn, R. Bonan and M. B. Leon for the FINESS Investigators (1997) First international new intravascular rigid-flex endovascular stent study (FINES): clinical and angiographic results after effective and urgent stent implantation. 1. Am. Coll. Cardiol. 30, 847-854.
30. Edalman, E. R., P. Seifert, A. Groothuis, A. Morss, D. Bomstein and C. Rogers (2001) Gold-coated NIR stents in porcine coronary arteries. Circulation 103, 429434.
31. Kastrati, A., A. Schomig, M. Seyfarth, W. Koch, S. Elezi, C. Bottiger, J. Mehilli, K. Schomig and N. von Beckerath (1999) PIA poly- morphism of platelet glycoprotein IIIa and risk of restenosis after coronary stent placement. Circulation 99, 1005-1010.
32. Foo, R. S.-Y., A. H. Gershlick, K. Hogrefe, J. H. Baron, T. W. Johnston, A. J. Hussey, I. Gamer and D. P. de Bono (2000) Inhibition of platelet thrombosis using an activated protein C-loaded stent: in vitro and in vivo results. Thromb. Huemostasis 83, 496-502.
33. Miller, D. D., A. A. Karim, W. D. Edwards and R. S. Schwartz (1996) Relationship of vascular thrombosis and inflammatory leukocyte infiltration to neointimal growth following porcine coronary artery stent placement. Atherosclerosis 124, 145-155.
34. Milavetz, J. J., T. D. Miller, D. 0. Hodge, D. R. Holmes and R. J. Gibbons ( 1 998) Accuracy of single-photon emission computed tomography myocardial perfusion imaging in patients with stents in native coronary arteries. Am. J . Cardiol. 82, 857-861.
35. Lucas, A,, L. Liu, J. Macen, P. Nash, E. Dai, M. Stewart, K. Graham, W. Etches, L. Boshkov, P. N. Nation, D. Humen, M. Lundstrom- Hobman and G. McFadden (1996) Virus-encoded serine proteinase inhibitor Serp-1 inhibits atherosclerotic plaque development after balloon angioplasty. Circulation 94, 2890-2900.
36. Liu, L., A. Lalani, E. Dai, B. Seet, C. Macauly, R. Sing, L. Fan, G. McFadden and A. Lucas (2000) The viral anti-inflammatory chemo- kine-binding protein M-T7 reduces intimal hyperplasia after vascular injury. J . Clin. InvestiR. 105, 1613-1621.
37. Christov, A. M., L. Y. Liu, S. Lowe, C. Icton, J. Dunmore-Buyze, D. R. Boughner, E. Dai and A. Lucas (1999) Laser-induced fluorescence (LIF)-recognition of the structural composition of porcine heart valves. J . Photochem. Photobiol. 69, 382-389.
38. Neuman, R. E. and M. A. Logan (1950) The determination of collagen and elastin in tissues. J . Biol. Chern. 186, 549-556.
39. Christov, A,, A. Vitkin, B. C. Wilson and A. Lucas (2001) Optical analysis of atherosclerotic plaque. Recent Res. Devel. Photochem. Photobiol. 5, 95-129.
40. Jaross, W., V. Neumeister, P. Lattke and D. Schuh (1999) De- termination of cholesterol in atherosclerotic plaques using near infrared diffuse reflection spectrolscopy. Atherosclerosis 147, 327-337.
135-139.
41. Papazoglou, T. G. (1995) Malignancies and atherosclerotic plaque diagnosis-is laser induced fluorescence spectroscopy the ultimate solution? J . Photochem. Photobiol. B: Biol. 28, 3-1 1.
42. Richards-Kortum, R., R. P. Rava, M. Fitzmaurice, J. R. Kramer and M. S. Feld (1991) 476 nm excited laser-induced fluorescence spectroscopy of human coronary arteries: applications in cardiology. Am. Heart J .
43. Economou, E., D. Tousoulis, A. Katinioti, C. Stefanadis, A. Trikas, C. Pitsavos, C. Tentolouris, M. G. Toutouza and P. Toutouzas (2001) Chemokines in patient with ischemic heart disease and the effect of coronary angioplasty. Int. J. Cardiol. 80, 55-60.
44. Hojo, Y., U. Ikeda, T. Katsuki, 0. Mizuno, H. Fukazawa, H. Fujikawa and K. Shimada (2001) Chemokine expression in coronary circulation after coronary angioplasty as a prognostic factor in restenosis. Atherosclerosis 156, 165-170.
45. Cipollone, F., M. Marini, M. Fazia, B. Pini, A. Iezzi, M. Reale, L. Paloscia, G. Materazzo, E. D’Annunzio, P. Conti, F. Chiarelli, F. Cuccurullo and A. Mezzetti (2001) Elevated circulating levels of monocyte chemoattractant proteins in patients with restenosis after coronary angioplasty. Arterioscler. Thromh. Vasc. Biol. 21, 327-334.
46. Casserly, I. P., D. Hasdai, P. B. Berger, D. R. Holmes, R. S. Schwam and M. R. Bell (1998) Usefulness of abciximab for treatment of early coronary artery stent thrombosis. Am. J . Cardiol. 82, 981-984.
47. Wilson, S. H., C. S. Rihal, M. R. Bell, J. L. Velianou, D. R. Holmes and P. B. Berger (1999) Timing of coronary stent thrombosis in patients treated with ticlopidine and aspirin. Am. J . Cardiol. 83, 1006-1011.
48. Moussa, I., M. Oetgen, G. Roubin, A. Colombo, X. Wang, S. Iyer, R. Maida, M. Collins, E. Kreps and J. W. Moses (1999) Effectiveness of clopidogrel and aspirin versus ticlopidin and aspirin in preventing stent thrombosis after coronary stent implantation. Circulation 99, 2364-2366.
49. Hasdai, D., C. S. Rihal, M. R. Bell, P. B. Berger, D. E. Grill, K. N. Gmatt and D. R. Holmes (1998) Abciximab administration and outcome after intracoronary stent implantation. Am. J . Cardiol. 82,
50. The ERASER Investigators. (1999) Acute platelet inhibition with abciximab does not reduce in-stent restenosis. Circulation 100,
51. Muller, C., H. J. Buttner, J. Petersen and H. Roskamm (2000) A randomized comparison of clopidogrel and aspirin versus ticlopidin and aspirin after the placement of coronary-artery stents. Circulation 101, 590-593.
52. Cura, F. A., D. A. Bhatt, A. M. Lincoff, S. P. Kapadia, P. L. L’Allier, K. M. Ziada, K. A. Wolski, D. J. Molitemo, S. J. Brener, S. G . Ellis and E. J. Topol (2000) Pronounced benefit of coronary stenting and adjunctive platelet glycoprotein IIbAla inhibition in complex athero- sclerotic lesions. Circulation 102, 28-34.
53. Santoro, G. M. and L. Bolognese (2001) Coronary stenting and platelet glycoprotein IIb/IIIa receptor blockade in acute myocardial infarction. Am. Heart J . 141, 26-35.
54. Schuhlen, H., A. Kastrati, J. Pache, J. Dirshinger and A. Schomigg (2001) Sustained benefit over four years from an initial combined antiplatelet regimen after coronary stent placement in the ISAR trial. Am. J . Cardiol. 87, 397400.
55. Ahmed, J. A., G. Dangas, A. J. Lansky, R. Mehran, M. K. Hong, G. S. Minz, A. D. Pichard, L. F. Satler, K. M. Kent, G. W. Stone and M. B. Leon (2001) Influence of gender on early and one-year clinical outcomes after saphenous vein graft stenting. Am. J . Cardiol. 87, 401-405.
122, 1141-1 150.
705-709.
799-806.
Copyright © 2022 FDOKUMEN




















