
Computational study of oxygen concentration in human blood under low frequency disturbances
13
ISSN 2070-0482, Mathematical Models and Computer Simulations, 2009, Vol. 1, No. 2, pp. 283–295. © Pleiades Publishing, Ltd., 2009. Original Russian Text © S.S. Simakov, A.S. Kholodov, 2008, published in Matematicheskoe Modelirovanie, 2008, Vol. 20, No. 4, pp. 87–102. 283 Computational Study of Oxygen Concentration in Human Blood under Low Frequency Disturbances S. S. Simakov and A. S. Kholodov Moscow Institute of Physics and Technology Received September 8, 2006 Abstract—A complex dynamic model of the closed cardiovascular and respiratory systems including their interaction is considered. It is proposed to substitute a single-component model of the alveolar vol- ume with a multi-component one. A refined structure of the vascular network based on experimental data is suggested. Resonance properties of the alveolar volume components are investigated with the help of the proposed multi-component model. Computational results are presented showing an amplitude- dependent decrease in oxygen concentration in the venous part of the pulmonary circuit when the alve- olar volume is subject to periodic disturbances at its eigenfrequencies DOI: 10.1134/S2070048209020112 INTRODUCTION Environmental vibration impact on a human body is one of the major factors in its life activity. Such impacts are mostly anthropogenic and may be caused by heavy traffic in large cities or by various industrial vehicles and mechanisms on factory floors. High-intensity vibration impacts can disturb the functioning of vital body organs such as the liver, lungs, and cardiovascular system. This can result in headaches, dystaxia, vertigo, visual impairment, and deviant social behavior [1]. Along with other functional changes, long-term exposure to vibration substantially changes the blood flow pattern, thus causing or aggravating cardiovascular diseases [2]. The effect of noise on the function of lungs and blood flow in the minor vessels of the pulmonary system can be less evident but no less far reach- ing. Thus, the disturbance in the alveolar pressure leads to the drop in the blood oxygen during pulmonary gas exchange. The study of this process is an important task, since severe hypoxia may cause irreversible changes in vital body organs. Noise-induced functional disturbances in the human body have been studied by many researchers. At the same time, some parts of the body, such as the heart and alveolar volume, are oscillatory systems in them- selves. In this respect, exposure to moderate or even low intensity impacts, whose frequency coincides with the eigenfrequency of the corresponding organ can be at least as dangerous. It should be noted that such normal eigenfrequencies lie in the infrared range, i.e., their value does not exceed 20 Hz, which makes them still less noticeable to an ordinary person. This work presents a numerical study of the oxygen content in human blood under low-frequency impacts using the dynamic models of breathing and closed blood circulation. First, assumptions are made allowing blood flow in a vessel and air motion in the pulmonary tube to be considered within the same model and a complete mathematical statement of the problem for a complex model is provided. A multi-component model is proposed instead of the currently prevalent single-component model of alveolar volume. Then, the structure of the vascular network and conductive part of the respiratory system based on experimental data is given. After this, resonant properties of the multi-component model of alveolar volume are studied show- ing the existence of two eigenfrequencies and the air flow in the tracheal-bronchial tree under the impact of the established eigenfrequencies is considered. In conclusion, the decline in the oxygen concentration in the venous part of the pulmonary circuit is considered as a function of the amplitude of the periodic disturbances at the established eigenfrequencies. The time required for the new concentration level to be established in the entire arterial blood of the body is estimated. THEORETICAL ANALYSIS Distributed dynamic model. We assume that blood is a viscous homogenous incompressible liquid with a constant temperature; the air flow in the respiratory tract is of a laminar character; the composition of the respiratory gas in the alveolar volume is homogenous and the gas itself is incompressible. We assume also
Transcript of Computational study of oxygen concentration in human blood under low frequency disturbances
ISSN 2070-0482, Mathematical Models and Computer Simulations, 2009, Vol. 1, No. 2, pp. 283–295. © Pleiades Publishing, Ltd., 2009.Original Russian Text © S.S. Simakov, A.S. Kholodov, 2008, published in Matematicheskoe Modelirovanie, 2008, Vol. 20, No. 4, pp. 87–102.
283
Computational Study of Oxygen Concentrationin Human Blood under Low Frequency Disturbances
S. S. Simakov and A. S. Kholodov
Moscow Institute of Physics and Technology
Received September 8, 2006
Abstract
—A complex dynamic model of the closed cardiovascular and respiratory systems includingtheir interaction is considered. It is proposed to substitute a single-component model of the alveolar vol-ume with a multi-component one. A refined structure of the vascular network based on experimental datais suggested. Resonance properties of the alveolar volume components are investigated with the help ofthe proposed multi-component model. Computational results are presented showing an amplitude-dependent decrease in oxygen concentration in the venous part of the pulmonary circuit when the alve-olar volume is subject to periodic disturbances at its eigenfrequencies
DOI:
10.1134/S2070048209020112
INTRODUCTION
Environmental vibration impact on a human body is one of the major factors in its life activity. Suchimpacts are mostly anthropogenic and may be caused by heavy traffic in large cities or by various industrialvehicles and mechanisms on factory floors. High-intensity vibration impacts can disturb the functioning ofvital body organs such as the liver, lungs, and cardiovascular system. This can result in headaches, dystaxia,vertigo, visual impairment, and deviant social behavior [1].
Along with other functional changes, long-term exposure to vibration substantially changes the bloodflow pattern, thus causing or aggravating cardiovascular diseases [2]. The effect of noise on the function oflungs and blood flow in the minor vessels of the pulmonary system can be less evident but no less far reach-ing. Thus, the disturbance in the alveolar pressure leads to the drop in the blood oxygen during pulmonarygas exchange. The study of this process is an important task, since severe hypoxia may cause irreversiblechanges in vital body organs.
Noise-induced functional disturbances in the human body have been studied by many researchers. At thesame time, some parts of the body, such as the heart and alveolar volume, are oscillatory systems in them-selves. In this respect, exposure to moderate or even low intensity impacts, whose frequency coincides withthe eigenfrequency of the corresponding organ can be at least as dangerous. It should be noted that suchnormal eigenfrequencies lie in the infrared range, i.e., their value does not exceed 20 Hz, which makes themstill less noticeable to an ordinary person.
This work presents a numerical study of the oxygen content in human blood under low-frequencyimpacts using the dynamic models of breathing and closed blood circulation. First, assumptions are madeallowing blood flow in a vessel and air motion in the pulmonary tube to be considered within the same modeland a complete mathematical statement of the problem for a complex model is provided. A multi-componentmodel is proposed instead of the currently prevalent single-component model of alveolar volume. Then, thestructure of the vascular network and conductive part of the respiratory system based on experimental datais given. After this, resonant properties of the multi-component model of alveolar volume are studied show-ing the existence of two eigenfrequencies and the air flow in the tracheal-bronchial tree under the impact ofthe established eigenfrequencies is considered. In conclusion, the decline in the oxygen concentration in thevenous part of the pulmonary circuit is considered as a function of the amplitude of the periodic disturbancesat the established eigenfrequencies. The time required for the new concentration level to be established inthe entire arterial blood of the body is estimated.
THEORETICAL ANALYSIS
Distributed dynamic model.
We assume that blood is a viscous homogenous incompressible liquid witha constant temperature; the air flow in the respiratory tract is of a laminar character; the composition of therespiratory gas in the alveolar volume is homogenous and the gas itself is incompressible. We assume also

284
MATHEMATICAL MODELS AND COMPUTER SIMULATIONS
Vol. 1
No. 2
2009
SIMAKOV, KHOLODOV
that the respiratory gas supplied to the lungs from the environment is instantaneously heated and after thatits temperature remains constant, while, at the same time, it is instantaneously saturated with water vapors.These assumptions allow us later to consider the blood flow process in the vessels and the air flow throughthe bronchial tubes within the same model, representing the flow of a viscous incompressible mediumthrough the network of tubes with elastic walls [3–6].
We assume that for all the considered tubes with elastic walls, their diameter to length ratio is sufficientlysmall and the linear velocity of the flow and pressure are averaged over their cross-section and depend onlyon the coordinate counted along it. The laws of mass and momentum conservation for each tube can be,therefore, written [3] as
(1)
(2)
where
t
is the time;
x
coordinate along the tube length measured from the point of conjunction with tubesof younger generations (or from the point of junction with the heart, from the trachea inlet);
ρ
is the densityof the medium (for blood and inhaled air: 1 g/cm
3
and 1.23
×
10
–3
g/cm
3
, respectively right braket;
k
standsfor the number of vessels;
S
k
(
t
,
x
) is the area of the tube cross-section;
u
k
(
t
,
x
) denotes the linear rate of flowaveraged over the cross-section;
p
k
is the difference between the pressure in the vessel and the pressure inthe environment (atmospheric pressure);
ϕ
k
denotes a term describing the out- or inflow of matter that canbe used, e.g., for modeling blood loss in traumas of the vessel walls, blood transfusion, etc. (in this work,for all tubes it was assumed that:
ϕ
k
= 0);
ψ
k
is the term describing the outside influence (gravitation, friction,etc.);
χ
ki
are the parameters describing the
i
th impact on the
k
th tube. The viscous friction has been takeninto account as follows [3]:
,
where =
S
k
/ ;
d
k
is the tube diameter; and
µ
is the viscosity factor;
For the closure of the equation system (1) and (2), account should be taken of the elastic properties oftube walls determining the relationship between the pressure in it and its cross-section. These properties aredetermined by the so-called “constitutive equation” of the tube walls:
(3)
where
c
0
k
is the velocity of small disturbances in the wall’s tissue:
p
∗
k
is the surrounding tissues' pressureon the vessel walls. For most tubes it is assumed that
p
∗
k
= 0 and only for the small vessels of the pulmonarycircuit it is assumed equal to the alveolar pressure induced by the walls of the respective component of therespiratory system’s alveolar volume. The type of the function
f
k
(
S
k
) depends on the shape and size of theelastic tube. In the general case, it is a monotonous
S
-shaped curve whose flex point corresponds to the tran-sition from a circular to an elliptic shape of the cross-section. Here, for blood vessels it is assumed
(4)
and for respiratory tubes
(5)
where is the area of the tube cross-section at zero transmural pressure (
p
k
( ) –
p
∗
k
= 0) and at zero bloodvelocity.
Boundary conditions.
As the dynamics of the blood flow and breathing is normally a periodic pulsat-ing flow, the initial conditions in each of the considered tubes can be selected quite arbitrarily from the
∂Sk/∂t ∂ Skuk( )/∂x+ ϕk t x Sk uk χki, , , ,( ),=
∂uk/∂t ∂ uk2/2 pk/ρ+( )/∂x+ ψk t x Sk uk χki, , , ,( ),=
ψk 16µukη S̃k( )/ S̃kdk2( )–=
S̃k Sk
η S̃k( )2, S̃k 1>
S̃k 1/S̃k, S̃k+ 1≤⎩⎨⎧
=
pk Sk( ) p*k– ρc0k2 f k Sk( ),=
f k Sk( )Sk/Sk 1–( ) – 1, Skexp Sk>
Sk/Sk( ), Skln Sk,≤⎩⎨⎧
=
f k Sk( ) Sk/Sk 1,–=
Sk Sk

MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
COMPUTATIONAL STUDY OF OXYGEN CONCENTRATION 285
physiologically reasonable range, e.g.:
(6)
where is the value of the tube cross-section corresponding to its unstressed state. This value can bedirectly determined from the anatomical atlases [7, 8]. In this selection of initial conditions, computationsof several heart and breathing cycles must be performed. After this, in the absence of external impacts, aperiodic mode of medium flow corresponding to the normal state is established in all tubes. These distribu-tions can be used as the initial conditions for computational experiments.
In the statement of boundary conditions it must be taken into account that equations (1) and (2) are of ahyperbolic type. Boundary conditions for this type of equations shall be set, allowing for the behavior ofcharacteristic curves on the border of the integration domain. Namely, at any moment of time within theperiod considered, the number of boundary conditions at each point of the boundary must correspond to thenumber of characteristic curves going out of the region at this point. Simultaneously, the conditions imposedby the equations of characteristic curves entering the domain (compatibility conditions) must be included.
Therefore, it is essentialto determine the behavior of the characteristic curves of equations (1) and (2).Denoting:
we write equations (1) and (2) in a divergence form:
(7)
Then, by the scalar multiplication of (7) by the left eigenvectors wki (i = 1, 2) of the Jacobi matrix Ak =∂Fk/∂Vk, we obtain the characteristic form of (1) and (2):
(8)
where λki are the eigenvalues of the matrix Ak; (dVk/dt)i is the total derivative along the ith characteristiccurve.
Using (4) and (5), we find specific expressions for Ak, λki , and wki . First of all, by definition:
The eigenvalues of λki are found from the equation
,
where E is the identity matrix. The solution of this equation is given by
(9)
From (4) it follows that for blood vessels
and, therefore,
The left eigenvectors wki are determined except for constant factor from equation
Sk 0 x,( ) Sk, uk 0 x,( ) 0,= =
Sk
Vk Sk uk,{ }, Fk Skuk uk2/2 pk/ρ+,{ }, gk ϕk ψk,{ }= = =
∂Vk/∂t ∂Fk Vk( )/∂x+ gk.=
wki dVk/dt( )i⋅ wki ∂Vk/∂t λki∂Vk/∂x+( )⋅ wki gk, i⋅ 1 2,,= = =
Ak
uk Sk
1ρ---
∂ pk
∂Sk
-------- uk⎝ ⎠⎜ ⎟⎜ ⎟⎜ ⎟⎛ ⎞
.=
det Ak λkE–( ) 0=
λki uk 1–( )i Sk
ρ----
∂ pk
∂Sk
--------, i+ 1 2.,= =
∂ f k
∂Sk
--------1/Sk( ) Sk/Sk 1–( ), Skexp Sk>
1/Sk, Sk Sk,≤⎩⎨⎧
i 1 2,= =
λki
uk 1–( )ic0k Sk/Sk( ) Sk/Sk 1–( )exp , Sk+ Sk>
uk 1–( )ic0k, Sk Sk,≤+⎩⎨⎧
i 1 2.,= =
wki Ak λkiE–( )⋅ 0, i 1 2,= =

286
MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
SIMAKOV, KHOLODOV
and, therefore, it is possible to choose, for example:
or, allowing for (4)
Here, in the second case, vector normalization by has been performed.
For the respiratory tubes, with allowance for (5), find
The value ck = from (9) is the velocity of small disturbances. In all parts of the cardiovascular
and respiratory systems during the normal functioning and in cases of most pathologies the condition uk < ck
holds. For such flows, as follows from (9), in each point of the considered domain at any moment of time,one of the characteristic curves has a positive slope and the other has a negative slope. In the statement ofboundary conditions, therefore, only one condition should be set at the inlet and outlet of the elastic tube.Simultaneously with this condition, condition (8) at i = 2 if it is an inlet to the vessel (and condition (8) at i= 1 if it is an outlet), must hold.
For the bloodstream, there are various methods for the junction of vessels: namely, the branching (bifur-cations) of arteries, anastomoses (the branching and reconnection of arteries), and the confluence of veins.All these types of junctions can be treated as the connection of several vessels with a specific nodal point,passing through which the blood is redistributed between vessels according to their properties and bloodflow dynamics [3–6]. In the tracheobronchial tree the situation becomes even simpler, since the branchingof respiratory tubes in it always proceeds dichotomically, i.e., each tube of a younger generation is dividedinto two tubes of an older generation.
The real flow in the field of the junction of elastic tubes has a quite complex structure. For its specificdescription, a model based on at least a two-dimensional description of the blood flow in the area of bifur-cation has to be used. However, within the global model of breathing and bloodstream dynamics in the entirebody, such an approach increases drastically the computational resources required even for the evaluationof at least a few heart and breathing cycles, because the number of the junction areas to be examined mayrise to several thousands.
Let us further assume that the sizes of the junction areas of the tubes are of the same order as the diameterof the largest tube entering or going out of this area. As has been mentioned, the ratio of the tube diameterto its length is a small value:
We assume that incoming/outgoing flow overcomes the hydrodynamic resistance that results in the pres-sure difference between the end/beginning of the tube and the nodal point. Here k is the number of tubesand l is number of junction areas. This relationship can be expressed by Poiseuille’s law
(10)
where k1, k2, …, kM are the numbers of tubes coming into or going out of the junction area and pl(t) is thepressure in the nodal point; if the kth tube goes from the junction area, then = 0, εk = –1, otherwise =Lk, εk = +1 where is the Lk tube length.
A more accurate approach is to use the limiting ratios from (1) and (2) for each junction area. They canbe computed using Bernoulli’s equations [5]. The results of these numerical experiments showed that the
wki1ρ---
∂ pk
∂Sk
-------- 1–( )i Sk,⎩ ⎭⎨ ⎬⎧ ⎫
, i 1 2,= =
wki
c0k 1/Sk( ) Sk/Sk 1–( )exp 1–( )i Sk,{ }, Sk Sk>
c0k 1–( )iSk,{ }, Sk Sk,≤⎩⎨⎧
i 1 2.,= =
Sk
λki uk 1–( )ic0k Sk/Sk, i+ 1 2,,= =
wki c0k 1–( )i Sk,{ }, i 1 2.,= =
Sk
ρ----
∂ pk
∂Sk
--------
dk/Lk � 1.
Rkl
pk Sk t x̃k,( )( ) pl t( )– εkRkl Sk t x̃k,( )uk t x̃k,( ), k k1 k2 … kM,, , ,= =
x̃k x̃k

MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
COMPUTATIONAL STUDY OF OXYGEN CONCENTRATION 287
impact of terms proportional to velocity squared is small in comparison to the terms proportional to pres-sure. This fact is also validated by the results of analytical studies of linearized problems [6].
The number of equations in (10) equals the number of tubes coming into and going out of the nodal point.However, there are also pl(t), and, for closure of the system of equations in the node, an additional relation-ship is needed. It can be deduced from the equality of incoming and outgoing flows:
(11)
This implies that in every junction area, the equations for a flow in an elastic tube (1)–(3) are related toeach other by boundary conditions forming a system of equations (10) and (11). For each ki (i = 1, …, M),this system should include (8) at i = 2 if the tube ki goes out of the nodal point, and at i = 1 otherwise.
The networks of arteries and veins of greater and lesser circulation systems are connected through a net-work of small vessels (arterioles and venules) forming a zone of micro circulation. A detailed considerationof this zone is difficult, as neither the accurate structure of the vessels forming it, nor their parameters areknown. An additional difficulty is that the blood flow in the micro circulation field cannot be considered interms of Newtonian fluid, since the typical sizes of the flow range become comparable with particle sizes.In order to describe the blood flow in microcirculation, averaged characteristics are normally used. Anexample can be the model of liquid filtration in a two-dimensional porous medium [9, 10]. Such a modeldescribes the distribution of blood flow and substances transported by tissues, but does not take into accountthe changed dynamics of the blood flow and, thus, cannot be used for the set boundary conditions of thedynamic model.
For the dynamics of blood flow it is essential that the micro vessel bed has hydrodynamic resistancewhich provides a pressure difference of about 60 mm Hg in the systemic circulation and about 5 mm Hg inthe pulmonary circuit [11]. Such a difference can be reached when using Poiseuille’s law (10) with therespective value of the coefficient of hydrodynamic resistance, which is equivalent to the Darcy law.According to this, with the accuracy required for this work, it is possible to state that the particular fields ofmicrovascular bed are equivalent to the junction areas of vessels of the respective arterial and venal parts.
Under normal breathing, as a boundary condition at the inlet to the trachea the atmospheric pressure ofthe environment can be set:
which, taking into account (5), is equivalent to:
Dynamic heart model. For modeling the heart functioning, we use here an approach based on [3],according to which each heart chamber is put in relationship to a specific spherical reservoir with elasticwalls characterized by inertness. The reservoirs are connected with each other by inextensible fluid channelswith hydrodynamic resistance. Some of the channels can at certain times be closed. Some chambers canhave additional connecting channels according to atrium or interventricular defects (Fig. 1).
The cardiac cycle is divided into the following stages [11]: isovolumetrical contraction of ventricles,ejection, isovolumetrical relaxation of ventricles, and filling. During the first and third phases the inlets andoutlets of the ventricles are closed:
during the second phase the atrioventricular valves are closed:
and during the fourth phase the aortal valves are closed:
where Qij is the volumetric blood flow between the ith and jth chambers.It will be further assumed that all the valves are opened and closed instantaneously; the hydrodynamic
resistance of all channels, inlets, outlets, and chambers is constant; the walls of the chambers are homoge-nous and uniformly extensible; and changes in the form of the ventricles and lengths of the myocardiumfibers under isovolumetric compression and relaxation are not taken into consideration. The functioning of
εkSk t x̃,( )uk t x̃,( )k k1 k2 … kM, , ,=
∑ 0.=
p1 t 0,( ) pT t( ),=
S1 t 0,( ) S1 1 pT t( )/ ρc012( )+( ).=
Q51 0, Q62 0, Q14 0, Q23 0,= = = =
Q14 0, Q23 0,= =
Q51 0, Q62 0,= =

288
MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
SIMAKOV, KHOLODOV
the heart, therefore, can be described in terms of volumetrically aver-aged equations for the blood flow in heart chambers:
(12)
of the law of mass conservation for each chamber:
(13)
(14)
(15)
(16)
and of Poiseuille’s law, which is widely used in physiology for inter-chamber channels and for inlets and outlets:
(17)
I jd2V j/dt2 r jdV j/dt V /c j+ + p j t( ) P j
ext t( ),–=
dV1/dt Q51– Q14 Q12,+ +=
dV2/dt Q62– Q23 Q12,–+=
dV3/dt Q37 Q23– Q34,+=
dV4/dt Q48 Q14– Q34,–=
Qij
p j pi–( )/rij for the open valve
0 for the closed valve,⎩⎨⎧
=
where j is the index of the chamber; Ij , cj , rj is the inertness, extensibility and hydrodynamic resistance of
the chamber; pj denotes the pressure in the chamber; Vj (t) stands for the volume; (t) is given func-tion (see [3]) determining the external pressure induced by the contraction of heart muscles ( j = 1–4);Pj designates the pressure at the heart inlets and outlets (j = 5–8); and rij and Qij(t) denote the hydrodynamicresistance and blood flow in interchamber channels and in the respective inlets and outlets; then:
In selecting the physiologically it has been taken into account that the solution of equation (12) consistsof the gradually dying solution of the homogenous equation and the periodic solution of a special inhomo-geneous equation, describing the forced vibrations. Its initial conditions can be set, for example, as
where is the volume of the heart chamber at the initial moment of time.The system of equations (12)–(17) is incomplete, since it includes twenty unknowns related by only six-
teen equations. On the other hand, this system does not yet allow for the interaction with the vessels of pul-monary and systemic circulation. This interaction can be described by imposing general boundary condi-tions at the inlets to the atrium connected with the outlets from the respective veins and at the outlets fromthe ventricles connected with the inlets to the respective arteries.
Let K1 and K2 be the numbers of arteries of lesser and greater systems of circulation going out of therespective right (1) and left (2) ventricles, and let K3 and K4 be the numbers of veins of lesser and greatersystems of circulation connected with the left (3) and the right (4) atrium, respectively (Fig. 1), then
where εi = +1, xi = 0 for arteries and εi = –1, xi = for veins. The system of equations (12)–(17) must besupplemented with two compatibility conditions (8) at i = 2 for areas of artery junctions with the ventriclesand two conditions at i = 1 for areas of the junction of atria with veins.
Another possible approach to modeling the heart function with the level of detail required for this classof blood circulation models has been described, for example, in [4].
Dynamic model of the alveolar volume. The transitional and breathing zones of lungs have a detailedstructure since they consist of a highly branched network of small bronchioles and a great number of smallalveoli. At the same time, these zones compose up to 95% of the total volume of airways and it is impossibleto exclude them entirely from consideration.
For describing the dynamics of such processes, models dealing with averaged parameters are widelyused. One version of such a single-component model of the lung was proposed in [12] where the summary
P jext
i j,( ) 1 4,( ) 2 3,( ) 5 1,( ) 6 2,( ) 8 4,( ) 7 3,( ) 1 2,( ) 4 3,( ), , , , , , ,{ }.∈
V j 0( ) V j,dV j 0( )
dt----------------- 0,= =
V j
p4 i+ pKit xi,( ), i 1–4,= =
Q4 i+ i, t( ) εiSKit xi,( )uKi
t xi,( ),=
LKi
21
34
5
8
6
7
Fig. 1. Scheme of the four-cham-ber model of heart allowing fordefects of inter-chamber septa.

MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
COMPUTATIONAL STUDY OF OXYGEN CONCENTRATION 289
mass of the lungs and thorax was assumed to be distributed over the surface of the reservoir of a variablevolume. The mechanical properties of such a reservoir were described by integral characteristics includingresistance of airways, air inertness in them, and the flexibility of lungs and the thorax. The model is basedon the equation of ideal gas under isothermal conditions, the equation of the motion of the reservoir shell,and the integral equation of air motion in airways.
This model includes properties of the conductivity zone that has already been described within the dis-tributed dynamic model. For adaptation of the single-component model of lungs, therefore, a higher levelof detail should be used. Since every respiratory tube is communicated only with a limited part of the alve-olar volume, we will use the equation of the model from [12] not for the whole volume of lungs but only forits particular components, into which air enters through one of the respiratory tubes. We will assume thatone latest-generation respiratory tube can join, one and only one, component of the alveolar volume, whichis in full agreement with the anatomical data. Then the volume averaged equation for each component looksas follows:
(18)
where Nalv is the number of components of the alveolar volume (coinciding with the number of respiratorytubes in the oldest generation of the conductivity zone; for the structure of the tracheobronchial tree used in
this work Nalv = 32); is the pressure inside the alveolar component; ppl is the pleural pressure from of
the muscles of the thorax; and are constants determining the elastic and inertial properties of the jth com-ponent of the alveolar volume. According to the data in [11]
(19)
where = –0.5 kPa and = 0.1 kPa, Tresp = 4 s.The initial conditions for (18) and (12) are not so important because they do not determine the periodic
solution of the inhomogeneous equation. Therefore, it can be specified:
where is the volume of the jth component at the initial moment of time.Boundary conditions in the junction area of the alveolar volume component and the respective respira-
tory tube include the law of mass conservation and condition of equality of pressures at the end of the tubeand inside the component (the hydrodynamic resistance of the junction area can be neglected as the airvelocity is small in it):
(20)
(21)
where ki is the index of the bronchial tube connected with the ith component of the alveolar volume. Thesystem of equations (20)–(21) also shall be completed with the condition of compatibility (8) at i = 2 sincethe outlet from the bronchial tube is considered.
Model of mass transport. In the examination of the mass transport within the above models, it has beenassumed that the convective component prevails over the diffusion component and the equation of transport is
(22)
where Cjk is the specific concentration of the jth substance in the kth tube; Fjk is the source or mass outflow,or substance transformation rate as a result of a chemical reaction; uk is the velocity of the carrier phase (ofair or blood); and bjk is the coefficient regulating the convective transport of matter (for substances dissolvedin the blood plasma bjk = 1 and for macromolecules and formed elements 0 ≤ bjk < 1). This approach iswidely known. In particular, it was used in [13] for the description of the distribution of pharmaceutical sub-stances.
aijd
iV alvj
dti-------------
i 1=
4
∑ V alvj
C--------+ palv
j t( ) pplj t( ), j– 1–Nalv,= =
palvj
aij
ppl t( ) Ppl1
Ppl2
2πt/T resp( )cos 1–( ),+=
Ppl1
Ppl2
V alvj 0( ) V alv
j,
dV alvj 0( )dt
-------------------- 0,d2V alv
j 0( )dt2
---------------------- 0,d3V alv
j 0( )dt3
---------------------- 0,= = = =
V alvj
dV alvi
dt------------ Ski
t Lki,( )uki
t Lki,( ),=
pkit Lki,( ) palv
i t( ),=
∂C jk/∂t b jkuk∂C jk/∂x+ F jk t x C1k C2k … CJk, , , , ,( ),=

290
MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
SIMAKOV, KHOLODOV
The boundary conditions for (22) are imposed with allowance for the behavior of its characteristics atthe tube’s boundaries, the inclination of which is determined by the sign of flow’s linear velocity. If thevelocity of the flow at the tube’s ends is directed from it (positive at the outlet or negative at the inlet), thenthere is no need to impose boundary conditions and the respective value of concentration is calculated from(22).
Further on, only cases requiring the statement of boundary conditions will be considered. At the inlet tothe breathing system at the inhale:
(23)
In the area of the vessels' junction with the heart’s chambers and of the bronchioles with the components ofalveolar volume, the concentration of substances must coincide with the respective values inside the com-ponents:
(24)
where K are the indexes of the tubes; MK is the number of the respective chamber or component; and xK = 0for the inlet to the tube and xK = LK for the outlet.
At the points of the tubes' junction
(25)
where Qm(t, xm) = Sm(t, xm)um(t, xm); and εm = +1, xm = Lm for tubes entering the node and εm = –1, xm = 0 forthose going out of the node. The respective conditions of compatibility (8) at i = 2 for the incoming tube andat i = 1 for the outgoing one are taken into account. Here, it is assumed that (this assumption has been val-idated by computational experiments) at any moment of time there is a non-zero flow of matter directedfrom the junction point. Otherwise, this problem has no definite solution [13].
In the alveolar volume of lungs (k = Ka, xk = ), as in small vessels of the pulmonary system (k = Kp,xk = 0), the concentrations of matter transported through the alveolar septa embedded in the pulmonary cap-illaries are connected in the general case by rather complex relationships. These relationships are deter-mined by different processes of transport (membrane transfers, diffusion, etc.). In the simplest case of quasi-equilibrium by partial kinetic pressures, and can be estimated from (22) with the right parts:
(26)
(27)
Here, δj > 0 is a value regulating the rate of coming to the steady state for and that grows withits increase.
METHODS
The numerical implementation of the complex model described above involves numerous difficulties dueto the complex structure of the integration domains for its distributed parts, the great number of obscure andhighly variable parameters determining the models, and the properties of the equations considered. Partially,these problems have been solved in [3, 10, and 14–17]. In this work, some refinements were made toimprove the adequacy of the models.
In the numerical solution of the problem (1)–(3) on the motion of a viscous incompressible fluid in anelastic tube, an explicit two-step hybrid scheme was used, corresponding to the most accurate monotonousscheme of the first order and to the least oscillating scheme of the second order of accuracy [18] (pp. 103–104). As in the considered impacts, no shock waves appeared in the system, the coefficient of hybridity wasselected in such a way that the scheme could be of the second order. At the same time, the computationscarried out earlier with the use of the most accurate first-order monotonous scheme have also yielded quitesatisfactory results [14].
C j1 t 0,( ) C jT t( ).=
C jK t xK,( ) C jMKt( ),=
C jk t xk,( )
εmCmj t xm,( )Qm t xm,( )m εmum 0>( )
∑
Qm t xm,( )m εmum 0>( )
∑--------------------------------------------------------------------------,=
LKa
C jKaC jK p
F jKaδ j pa t( ) p0+( )C jka
t LKa,( ) pK p
t 0,( ) p0+( )C jkpt 0,( )–[ ],–=
F jK pδ j pa t( ) p0+( )C jka
t LKa,( ) pK p
t 0,( ) p0+( )C jkpt 0,( )–[ ].=
C jKaC jK p

MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
COMPUTATIONAL STUDY OF OXYGEN CONCENTRATION 291
The choice of the numerical method for the problem of the heart’s functioning and the component of thealveolar volume is determined primarily by the stiffness of these equations associated with the values ofparameters I, R, and C assuming values from the physiologically permissible range. For the solution of sucha system, an implicit single-step A- and L-stable method of the third order approximation [19] (pp. 35–38)was used, which made it possible to decrease the limitations of the integration step imposed by the require-ment of the method’s stability.
This work, as compared with earlier works [3, 10, 14–16], refined the structure of a one-dimensional vas-cular system. It was based on the experimental results of [20], according to which the structure of the arterialand venous parts of the pulmonary system is a tree. However, because of the vast number of vessels (about1.25 × 108), only the structure of the first four generations has been reconstructed counting from the heart.It should be noted that on assigning a vessel to a particular generation in [20] the Strahler’s ordering lowwas used, in which not only the position of the vessel in the whole structure but also its diameter was takeninto account. Under this classification, the vessels of the third and older generations can go out from a vesselof the first generation. The structure of the vessels in [20] was described by means of the connectivity matri-ces that do not yield full information on their real geometry. For this reason, the final reconstruction of thearterial and venous parts of the pulmonary system was performed by making use of widely known anatomicand physiological atlases [7, 8, 11]. Its results are given in Figs. 2 and 3.
The structure of the large vessels of the systemic circulation can be obtained from experimental obser-vations by use of MRI methods, ultrasound dopplerography, angiography, etc. In this work, for the recon-struction of the network of the vessels of the greater circulation, the results of studies given in [21, 22] andin other works on blood flow modeling [4, 23, 24] were used. The results of reconstruction are given in Fig. 4.
This structure includes the thoracic and abdominal parts of the aorta, their main branches, vessels of theupper and lower limbs, detailed vessels of the head and brain, stomach, and intestines. The parameters ofthe branches of the tracheal-bronchial tree, the structure of which is a binary tree [16], were determined ina similar way.
Fig. 2. Structure of the arterial part of the pulmonary circuit.
Fig. 3. Structure of the venous part of the pulmonary circuit.

292
MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
SIMAKOV, KHOLODOV
RESULTSBy means of the described models, computations aimed at the study of the oxygen concentration in blood
in the presence of periodic external impacts with a frequency coinciding with one of the eigenfrequenciesof the components of the alveolar volume have been performed.
The number of eigenfrequencies of the alveolar volume’s components is determined by a fourth-orderequation (18), which allows the existence of two eigenfrequencies, since its characteristic equation can havetwo pairs of complex-conjugate squares. In order to obtain these frequencies, the disturbance
was added to the right part of equation (18) and the amplitude of disturbance was assumed to be 1% of theamplitude of the compulsive pleural pressure.
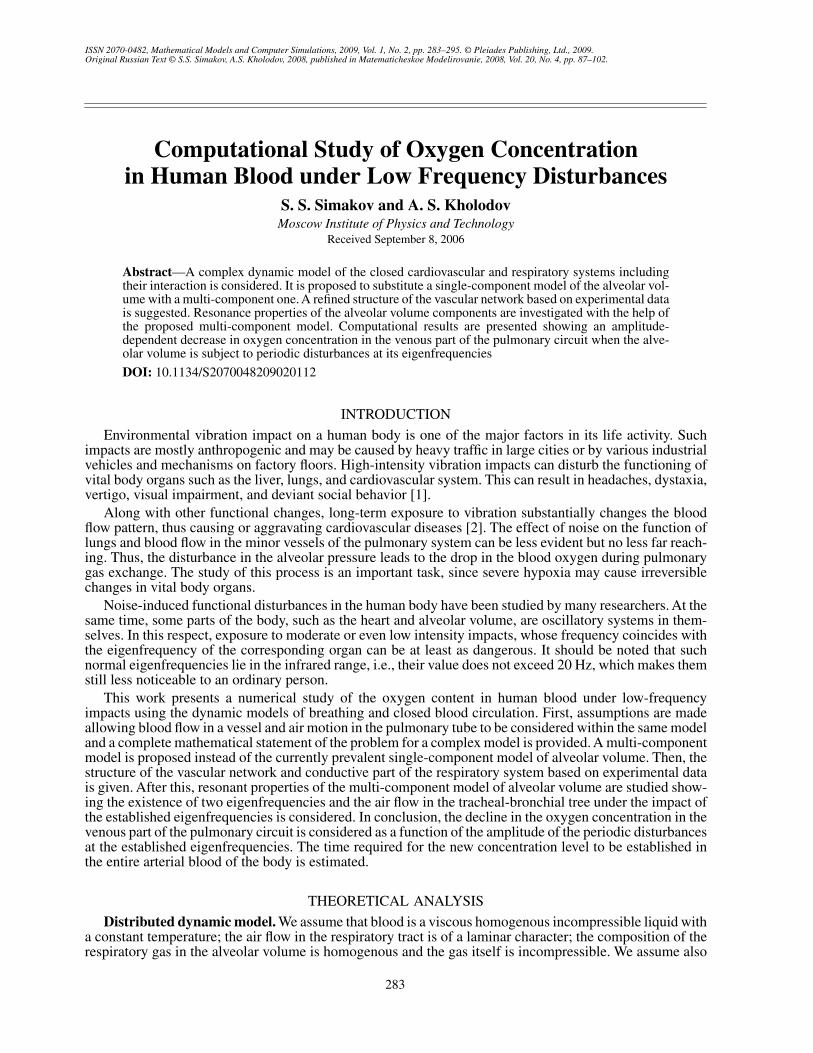
Then, a series of computational experiments were made, in the course of which the disturbance fre-quency varied from 0 to 100 Hz. In doing this, the response in the summary alveolar volume and alveolarpressure was the same for all components. The results of these experiments are presented in Fig. 5 andFig. 6, from which it is seen that the component of the alveolar volume has two proper frequencies: 7 Hz(Figs. 5, 6a) and 70 Hz (Figs. 5, 6b). The amplitude of the summary alveolar volume and alveolar pressure
Pimp P̃ ωimpt( ),sin=
(a) (b)
Fig. 4. Structure of the vessels of the systemic circulation: (a)—artery; (b)—veins.
0 5 10 15 20 25 30
0.4
0.8
1.2
kPa
Hz
(a)
40 50 60 70 90 100
46
50
54
Pa
Hz
(b)
4030 80
Fig. 5. Resonance of alveolar pressure.
MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
COMPUTATIONAL STUDY OF OXYGEN CONCENTRATION 293
5 10 15 20 25 30
3.2
3.6
4.0
Hz
(a)
40 50 60 70 90 100
2.8138
2.8146
2.8150
Hz
(b)
2.813230 80
2.8
4.4
0
2.8142
Fig. 6. Resonance of alveolar volume.
A
B
C
1.2
0.8
0.4
01 2 3 4 5 6
kPa
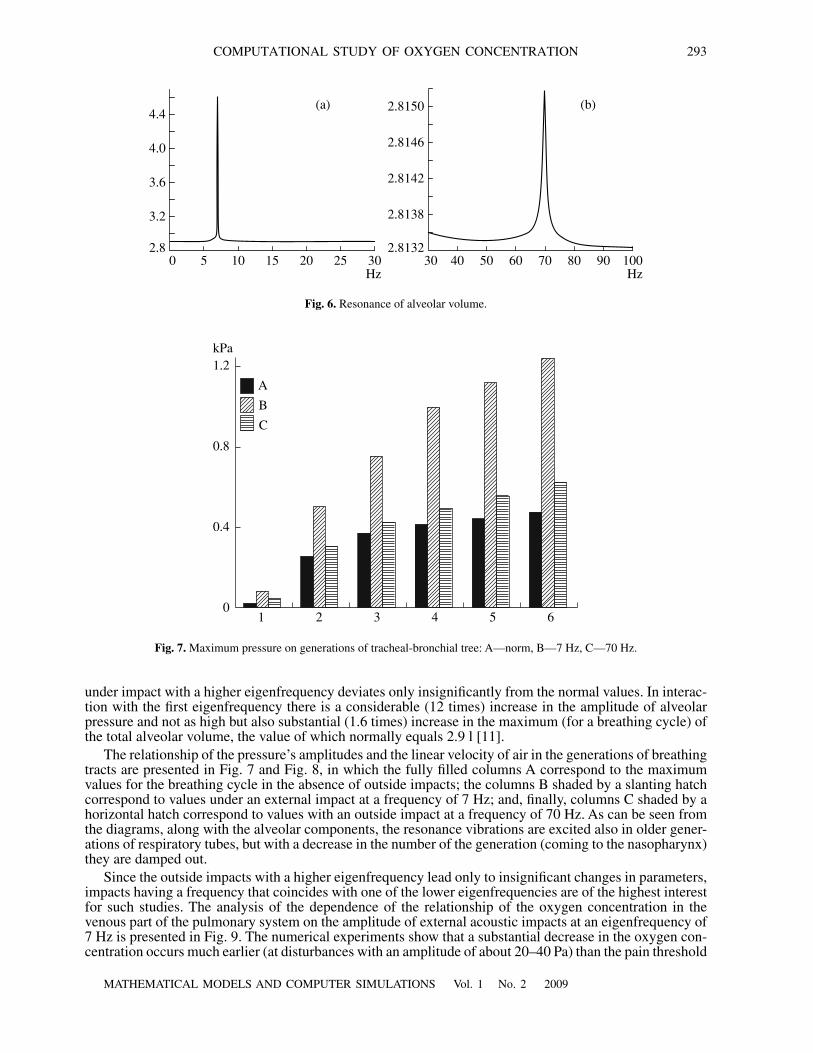
Fig. 7. Maximum pressure on generations of tracheal-bronchial tree: A—norm, B—7 Hz, C—70 Hz.
under impact with a higher eigenfrequency deviates only insignificantly from the normal values. In interac-tion with the first eigenfrequency there is a considerable (12 times) increase in the amplitude of alveolarpressure and not as high but also substantial (1.6 times) increase in the maximum (for a breathing cycle) ofthe total alveolar volume, the value of which normally equals 2.9 l [11].
The relationship of the pressure’s amplitudes and the linear velocity of air in the generations of breathingtracts are presented in Fig. 7 and Fig. 8, in which the fully filled columns A correspond to the maximumvalues for the breathing cycle in the absence of outside impacts; the columns B shaded by a slanting hatchcorrespond to values under an external impact at a frequency of 7 Hz; and, finally, columns C shaded by ahorizontal hatch correspond to values with an outside impact at a frequency of 70 Hz. As can be seen fromthe diagrams, along with the alveolar components, the resonance vibrations are excited also in older gener-ations of respiratory tubes, but with a decrease in the number of the generation (coming to the nasopharynx)they are damped out.
Since the outside impacts with a higher eigenfrequency lead only to insignificant changes in parameters,impacts having a frequency that coincides with one of the lower eigenfrequencies are of the highest interestfor such studies. The analysis of the dependence of the relationship of the oxygen concentration in thevenous part of the pulmonary system on the amplitude of external acoustic impacts at an eigenfrequency of7 Hz is presented in Fig. 9. The numerical experiments show that a substantial decrease in the oxygen con-centration occurs much earlier (at disturbances with an amplitude of about 20–40 Pa) than the pain threshold

294
MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
SIMAKOV, KHOLODOV
(100 Pa). This again emphasizes the danger of low frequency impact not perceived by the hearing apparatus,which, even if not intensive, can inflict substantial harm to the organism.
Further computational experiments with the use of the distributed model of global blood flow allow usto estimate the time, in which the new value of oxygen concentration coming with the blood from the lessercirculation is established in all parts of the arterial part of the greater circulation. The numerical studies showthat this time is about 8–10 min.
Certainly, the concrete values of eigenfrequencies can vary for different individuals since the parameterswhich determine them strongly depend on various factors (age, sex, the state of the organism at the currentmoment, etc.), but this does not influence the general relations obtained in this work as well as their practicalimportance.
REFERENCES
1. R. A. Baron and D.R. Richardson, Human Aggression (Kluwer Academic Publisher, 1994).
2. S. N. Willich, K. Wegscheider, M. Stallmann, and T. Keil, Noise Burden and the Risk of Myocardial Infraction,European Heart Journal 27 3, 276–282 (2006).
10
0 0.02 0.04 0.06 0.08 0.10kPa
15
20
%
Fig. 9. Oxygen concentration in venous blood of the pulmonary circuit at a frequency of impact of 7 Hz.
A
B
C
200
100
50
01 2 3 4 5 6
cm/s
150
Fig. 8. Maximum velocity on generations of the tracheal-bronchial tree: A—norm, B—7 Hz, C—70 Hz.

MATHEMATICAL MODELS AND COMPUTER SIMULATIONS Vol. 1 No. 2 2009
COMPUTATIONAL STUDY OF OXYGEN CONCENTRATION 295
3. A. S. Kholodov, Some Dynamical Models of External Respiration and Circulation of Blood Including Their Con-nectedness and Matter Transport, in Computer Models and Progress in Medicine, Ed. by O. M. Belotserkovskiiand A. S. Kholodov (Nauka, Moscow, 2001) [in Russian], pp. 127–163.
4. I. V. Ashmetkov, A. Ya. Bunicheva, V. A. Kukshin, et al., Mathematical Modeling of Blood Circulation on the Basisof CVSS Software Package, in Computer Models and Progress in Medicine, Eds. O. M. Belotserkovskii andA. S. Kholodov (Nauka, Moscow, 2001) [in Russian], pp. 194–218.
5. M. V. Abakumov, K. V. Gavrilyuk, N. B. Yesikov, et al., A Mathematical Model of Hemodynamics of the Cardio-vascular System, in Differential Equations (1997), vol. 33, pp. 892–218.
6. I. V. Ashmetkov, S. I. Mukhin, N. V. Sosnin, and A. P. Favorskii, Boundary Problem for LGD Equations on Graph,in Differential Equations (1997) [in Russian], vol. 40, pp. 1–11.
7. V. P. Vorobyov, Atlas of Human Anatomy (Literatura, Minsk, 1998) [in Russian].
8. S. Standring, Grey’s Anatomy. The anatomical Basis of Medicine and Surgery, 2nd ed. (Churchill-Livingstone,2004).
9. A. V. Yevdokimov and A. S. Kholodov, Quasi-stationary Spatially Distributed Model of the Closed Circulation ofBlood in Human Organism, in Computer Models and Progress in Medicine, Ed. by O. M. Belotserkovskii andA. S. Kholodov (Nauka, Moscow, 2001).
10. S. S. Simakov, A. S. Kholodov, A. V. Yevdokimov, and Y. A. Kholodov, Matter Transport Simulation Using 2DModel of Peripheral Circulation Coupled with the Model of Large Vessels, in Proceedings of the 2nd InternationalConference on Computational Bioengineering, Ed. By H. Rodrigues and M. Cerrolaza (IST Press, 2005), vol. 1,pp. 479–490.
11. Human Physiology, Ed. by R. Shmidt and G. Trevs (Mir, Moscow, 2005) [in Russian], Vol. 2.
12. A. I. Dyachenko, A Study of One-component Model of Mechanics of Lungs, in Medical Biomechanics (Riga,1986) [in Russian], vol. 1, pp. 147–152.
13. A. P. Favorskii, M. V. Abakumov, N. B. Yesikov, et al., Mathematical Model of the Cardiovascular System (MGU,Moscow, 1998) [in Russian], preprint.
14. S. S. Simakov, A.S. Kholodov, A. V. Yevdokimov, and Y. A. Kholodov, Numerical Simulations of CardiovascularDiseases and Global Matter Transport, in Advanced Information and Telemedicine Technologies for Health(Minsk, 2005) [in Russian], vol. 2, pp. 188–192.
15. S. S. Simakov, A. S. Kholodov, Y. A. Kholodov, et al., Global Dynamical Model of the Cardiovascular System,3rd European Conference on Computational Mechanics, Ed. by C. A. Mota Soares (2006), pp. 1464.1–1464.9.
16. S. S. Simakov, A. S. Kholodov, Y. A. Kholodov, et al., Computational Study of theVibrating Disturbances to theLung Function, in Proceedings of 3rd European Conference on Computational Mechanics, Ed. by S. A. MotaSoares (2006), pp. 1467.1–1467.15.
17. Y. A. Kholodov, A. S. Kholodov, N. Kovshov, et al., Computational Models on Graphs for Nonlinear Hyperbolicand Parabolic Systems of Equations, in Proceedings of the 3rd European Conference on Computational Mechan-ics, Ed. by C. A. Mota Soares (2006), pp. 2279.1–2279.19.
18. K. M. Magomedov, A. S. Kholodov, Net-characteristic Numerical Methods (Nauka, Moscow, 1988) [in Russian].
19. A. S. Kholodov, A. I. Lobanov, and A. V. Yevdokimov, Differential Schemes for Solution of Stiff Common Differ-ential Equations in the Space of Uncertain Coefficients (Moscow, 2001) [in Russian].
20. W. Huong, R. T. Yen, M. McLaurine, and G. Bledsoe, Morphometry of the Human Pulmonary Vasculature, Journalof Applied Physiology 81, 2123–2133 (1996).
21. Ultrasound Doppler Diagnostics of Vascular Diseases, Ed. By A. I. Trukhanov (Vidar, Moscow, 1998) [in Rus-sian].
22. L. N. Tarasova, T. H. Kiselyova, and A. A. Fokin, Ophthalmic Ischemic Syndrome (Meditsina, Mosocw, 2003) [inRussian].
23. Ya. A. Bunicheva, V. A. Lukshin, S. I. Mukhin, et al. Numerical Study of the Hemodynamics of the Systemic Cir-culation (MAKS-Press, Moscow, 2001) [in Russian], preprint.




















