
Story stem responses of preschoolers with mood disturbances
17
Story stem responses of preschoolers with mood disturbances CAROL BERESFORD 1 , JOANN L. ROBINSON 2 , JOHN HOLMBERG 1 ,& RANDAL G. ROSS 1 1 University of Colorado at Denver, USA, and 2 University of Connecticut at Storrs, USA Abstract Observing the young child’s affect regulation and thought processes during a clinic assessment visit is of critical importance although challenging for children referred for mood disturbance. In this study, parents reported symptoms using standardized clinical interviews and story stems narratives were administered to 20 referred and 12 typically developing preschool age children. Comparison of the referred and typically developing children in our sample showed that specific story contexts varied in eliciting responses reflecting disorganization and thought disturbance from the referred children. The experience of using story stem narratives in the clinical assessment process suggests it provides a valuable complement to parent report for children referred for mood disturbance and mania symptoms but additional development and study of the method is necessary. Keywords: Mood disturbance, mania symptoms, story stem narratives, young children, clinical research Introduction While controversy about the presence of manic depression in very young children continues, important advances are being made in the assessment of preschool children with symptoms and risks of significant mood disorders (Luby & Belden, 2006). Prevalence rates of bipolar illness in children are still being clarified in the literature but the rates of distress among preschool samples suggest a significant public health problem (Dilsaver & Akiskal, 2004). A tertiary care child psychiatry clinic reported that 12% of 1658 consecutive referrals were for preschool children with comorbid psychiatric conditions with onset dating more than 2 years prior to the initial evaluation (Wilens, Biederman, Brown, Monuteaux, Prince, & Spencer, 2002). The presence of mania symptoms has been reported in up to 25% of preschool clinical samples (Dilsaver & Akiskal, 2004) but the validity of these early symptoms to predict later disorder remains uncertain. Clinicians are faced with diagnostic decisions and must make the most of the resources available to diagnose and treat mania in preschoolers. In this paper, we present our experience of using story stem narratives in a research assessment, highlighting its level of correspondence with parent reports of symptoms and Correspondence: Carol Beresford, MD, Box C268-71, Department of Psychiatry, University of Colorado at Denver and Health Sciences Center, 4200 East 9 th Avenue, Denver, CO 80262, USA. Tel: 303 315 2155. Fax: 303 315 5347. E-mail: [email protected] Attachment & Human Development, September 2007; 9(3): 255 – 270 ISSN 1461-6734 print/ISSN 1469-2988 online Ó 2007 Taylor & Francis DOI: 10.1080/14616730701455429
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Story stem responses of preschoolers with mood disturbances

Story stem responses of preschoolers with mooddisturbances
CAROL BERESFORD1, JOANN L. ROBINSON2, JOHN HOLMBERG1, &
RANDAL G. ROSS1
1University of Colorado at Denver, USA, and 2University of Connecticut at Storrs, USA
AbstractObserving the young child’s affect regulation and thought processes during a clinic assessment visit isof critical importance although challenging for children referred for mood disturbance. In this study,parents reported symptoms using standardized clinical interviews and story stems narratives wereadministered to 20 referred and 12 typically developing preschool age children. Comparison of thereferred and typically developing children in our sample showed that specific story contexts varied ineliciting responses reflecting disorganization and thought disturbance from the referred children. Theexperience of using story stem narratives in the clinical assessment process suggests it provides avaluable complement to parent report for children referred for mood disturbance and mania symptomsbut additional development and study of the method is necessary.
Keywords: Mood disturbance, mania symptoms, story stem narratives, young children, clinical research
Introduction
While controversy about the presence of manic depression in very young children continues,
important advances are being made in the assessment of preschool children with symptoms
and risks of significant mood disorders (Luby & Belden, 2006). Prevalence rates of bipolar
illness in children are still being clarified in the literature but the rates of distress among
preschool samples suggest a significant public health problem (Dilsaver & Akiskal, 2004). A
tertiary care child psychiatry clinic reported that 12% of 1658 consecutive referrals were for
preschool children with comorbid psychiatric conditions with onset dating more than 2 years
prior to the initial evaluation (Wilens, Biederman, Brown, Monuteaux, Prince, & Spencer,
2002). The presence of mania symptoms has been reported in up to 25% of preschool
clinical samples (Dilsaver & Akiskal, 2004) but the validity of these early symptoms to
predict later disorder remains uncertain. Clinicians are faced with diagnostic decisions and
must make the most of the resources available to diagnose and treat mania in preschoolers.
In this paper, we present our experience of using story stem narratives in a research
assessment, highlighting its level of correspondence with parent reports of symptoms and
Correspondence: Carol Beresford, MD, Box C268-71, Department of Psychiatry, University of Colorado at Denver and Health
Sciences Center, 4200 East 9th Avenue, Denver, CO 80262, USA. Tel: 303 315 2155. Fax: 303 315 5347.
E-mail: [email protected]
Attachment & Human Development,
September 2007; 9(3): 255 – 270
ISSN 1461-6734 print/ISSN 1469-2988 online � 2007 Taylor & Francis
DOI: 10.1080/14616730701455429

how the emotional challenges inherent in different story stems permit a rich opportunity to
observe the child’s affect regulation and thought processes.
Parent reports of mood symptoms
Assessment of a referred child generally begins with a description from the parents or
caregivers of the child’s observable emotional and behavioral difficulties. The distress
illustrated in the parent’s retelling of periods of significant volatility in behavior and
decision-making are palpable. Examples from the literature and our own research
experience are revealing. In a case series by Tumuluru, Weller, Fristad, and Weller
(2003), the following examples are representative:
. 4½-year-old boy who was ‘‘volatile, hyperactive, hyper-verbal, and violent toward
others (e.g., hurt a puppy and set fire to his baby sibling’s crib) concomitant with a
cranky/irritable mood. During his initial evaluation (he) was noted to be expansive with
poor self-esteem. He had pressured speech and racing thoughts per parental report and
observation by one of the authors’’ (p. 491).
. A 5-year-old boy with a ‘‘one-year history of oppositionality and mood swings per
parental report. He would vacillate from being ‘sweet and loving’ one minute to violent
and aggressive the next. The aggressive outbursts were reflective of a concomitant
irritable mood. (He) had insomnia, low self-esteem, increased energy, and racing
thoughts’’ (p. 492).
In the experience of the first author, parents of preschool children referred with mood
disorder symptoms retell how these children struggle with their reactivity to stressors and
influence home life in general. A representative parent statement, in answer to diagnostic
questioning about hypertalkativeness accompanying high mood, is as follows: ‘‘She becomes
a chatterbox when she is in a high mood. She will interrupt you, and not listen when you ask
her to stop. She can talk nonsense. She seems to be blabbering. When in a calm mood, she
tells an actual account of something; she makes sense.’’ The parent-based information
reveals, in summary, a picture of young children who are highly mood-labile, and who
frequently enter mood states in which they can behave and think in extreme, unpredictable,
dangerous, and irrational ways. Given the lack of control that parents have over these
seemingly biologically determined mood states, many report the sense of walking on
eggshells within the home. Frequently, mood-disordered children come to have more and
more control over the workings of the household as parents seek to avoid the extreme mood
and behavioral episodes.
Direct child assessment
Moving beyond parent-report, child psychiatrists are faced with the dilemma of how to
evaluate the child’s own experience of psychiatric symptoms, including mood dysregulation
and in some cases psychotic ideation or sensory experiences. According to the literature
(Jensen et al., 1999), it is important to obtain information from both parents and child,
especially when the symptoms are of the type that the child experiences internally; such
symptoms would include, for instance, suicidal ideation and thought disorder including
delusional thinking and hallucinations.
To access a young child’s mental representations of their experience, including
relationships, clinicians have traditionally utilized play therapy. However, most play therapy
256 C. Beresford et al.

approaches are not standardized and rely on individual clinical experience to develop
impressions and inferences. In older children, child-informant reports of symptoms can be
vital in the identification of certain psychiatric diagnoses (Jensen et al., 1999) and bipolar
disorder specifically (Geller et al., 2001). Edelbrock, Costello, Dulcan, Conover, and Kala
(1986) conducted structured interviews with 299 psychiatrically ill children aged 6 – 18 and
their parents, and found that correlations between derived scores showed only low-to-
moderate levels of agreement. Agreement was lower on anxiety, obsessions and
compulsions, psychotic symptoms, and affective disturbance, as compared to behavioral
issues. The agreement between parents and children was found to increase sharply with age.
In this study, we evaluate children younger than represented in the Edelbrock study
(Edelbrock et al., 1986). Because such young children, and especially psychiatrically ill
young children, are difficult to interview directly, we elected to utilize a semi-structured
interaction rather than structured interview as a more reliable and valid approach. The
MacArthur Story Stem Battery (MSSB; Bretherton, Oppenheim, Emde, & the MacArthur
Narrative Working Group, 2003) is one such approach.
A substantial literature has emerged suggesting that the MSSB is able to elicit information
from the child that is both related to parent and teacher symptom reports, but also adds
qualitative information about the child’s internal experience of relationships (see Robinson,
2007 for a brief review). Prior studies of typically developing children have shown that the
child’s story incoherence as well as the content of their representations, specifically
dysregulated aggression, and the intrusion of negative atypical themes are substantially
correlated with parent reports of externalizing symptoms (e.g., von Klitzing, Kelsey, Emde,
Robinson, & Schmitz, 2000; Warren, Oppenheim, & Emde, 1996). Important contributions
by Oppenheim, Emde, and Warren (1997) also made salient children’s representations of
parent figures as nurturing, protective, and warm (i.e., positive representations), as con-
taining and limit-setting of the story child’s misbehaviors and emotional reactions (i.e.,
disciplinary representations), and hostile, ineffectual, and/or dysregulated (i.e., negative
representations). These parent representations were also associated with parent report of
externalizing symptoms; Oppenheim et al. (1997) reported associations between elevated
behavior problems and fewer positive and disciplinary and more negative parental
representations. Warren’s examinations of anxiety symptoms in typical and clinical samples
also demonstrated associations with negative emotions and emotionally incoherent res-
ponses, excessive child power, and an inability to resolve the central conflict of story stems
(Warren, 2003a; Warren, Emde, & Sroufe, 2000). Finally, a particularly significant
contribution to the clinical use of story stems has also been made by Macfie, Cicchetti, and
Toth (2001) with the validation of a scoring of children’s dissociative behaviors during story
stem responses with a teacher-reported symptom questionnaire in a sample of maltreated
children.
Although correlations of child narrative with parent- and teacher-derived information vary
across studies, most found correlations of magnitude 0.2 – 0.4 between child story stem
narrative indicators and parent and teacher report of symptoms. This is comparable to the
Edelbrock et al. study (1986) in which the correlation for global behavior/conduct scales
between parents and children (aged 6 – 18), based on structured interviews for both, is 0.51,
and the correlation for global affective/neurotic scales is 0.17. Thus, the story stem narrative
approach provides a method that allows access to a child’s internal experience in a way that
correlates with, and presumably helps explain more fully, what parents say they are
observing.
We examined parent reported symptoms of manic-like behaviors and depressive mood in
relation to the performance (including dissociation, incoherence, and distressed affects) and
Preschoolers with mood disturbance 257

content of children’s story responses (including more aggressive and fewer prosocial
themes), anticipating that there would be moderately strong associations in a sample that
included children referred for these problems. In addition, given the behavior problems
typical of the children referred for manic-like symptoms, we hypothesized that parent
representations would include less containment and disciplinary themes as well as parental
warmth and nurturance.
While previous investigations have examined performance processes and content themes
across all stories administered from the battery, individual stories evoke differing types and
degrees of stimulation and arousal in the child. The MSSB is particularly effective in the
diversity of story themes that are included in the battery, providing the possibility of
tailoring the assessment for specific purposes (Robinson & Mantz-Simmons, 2003). In
considering the context of referred children, it is very useful to consider selective use of
stories to highlight specific response tendencies and to create new story stems (Kelsay,
2003; Robinson & Kelsay, 2003). From a selected battery of eight story stems that
included two stories outside of the MSSB, we chose to focus this investigation on four
stories to illuminate children’s differentiated responses. These four stories range from
relatively less stimulating (Spilled Juice, a child spills juice at the family table) to relatively
more arousing stories: accidentally cutting one’s finger with a kitchen knife while
pretending to cook (Cooking/Bandage), watching mother and father argue (Lost Keys),
and going down the hall alone and then hearing a noise when no one is around
(Sweater). Although it was unknown at study onset which stories would be most
stimulating for the mood-disordered group, the parental argument story (Lost Keys) is
known to be highly arousing to most children (Robinson & Mantz-Simmons, 2003). The
anticipated high arousal to a story about cooking was related to comments reported by
referring parents that knives have to be hidden from their children who have mood and
psychotic disorders. The story about hearing a noise when no one is around, a potentially
very arousing event, was written for this battery with the hope that it would elicit any
experience of auditory hallucination. It was hypothesized that children’s responses to
highly arousing props and story lines would provide the context to observe clinically
meaningful differences between mood-disordered and non-referred children. Specific
hypotheses are listed below.
Hypothesis 1. Referred children will have significantly higher levels of parent reported
symptoms of mood and thought disturbances compared to typical children. In addition,
referred children’s story stem responses will show elevated levels of internal disorganization
(such as themes of danger, dysregulated aggression, and excessive child power, and
performance that includes dissociation and negative emotion) and less evidence of positive
coping that averts disorganization (such as prosocial relations, narrative coherence, and
positive affect) and reliance on warm and containing parents.
Hypothesis 2. Mania, as reflected in parent-reported child symptoms, will be positively
correlated with disorganized features of the child’s response to the narratives when observed
during high but not low challenge stories.
Hypothesis 3. In the context of high challenge but not low challenge stories, referred
children compared to typically developing non-referred children will show higher levels
of narrative features reflecting internal disorganization and lower levels of features
that reflect positive coping including reliance on warm and containing parental
representations.
258 C. Beresford et al.
Method
Subjects
Community clinicians (psychiatrists, psychologists, and pediatricians) were asked to
refer preschool children, ages 3.5 – 6.0 years, who presented with mania symptoms. Two
of the subjects were referred by parents who suspected mood symptoms, verified as
manic-like upon phone interview. Exclusion criteria for the mood-disordered group
included autism, mental retardation, physical/sexual abuse, major medical/neurological
disorder, and severe language disorder. Twenty parents of preschoolers, recruited over
20 months, agreed to participate. Sixteen typically-developing preschoolers who did not
meet exclusion criteria were recruited by advertisement. Exclusion criteria for the typical
group included: significant psychiatric symptomatology and a family history of major
psychiatric disorder in first or second degree relatives by parent report. We included one
typically-developing child in the comparison group whose second degree relative
developed a mood disorder after a head injury late in life. Four typically-developing
children were excluded due to positive family history (within first and second degree
relatives) for bipolar disorder (two children), past history of sexual abuse (one child), and
a verbal subtest score less than 2 standard deviations below the national average (one
child). The children were deemed typical if the parents did not have complaints
regarding emotional/behavioral issues with impairment. The final sample was comprised
of 32 children (20 clinically-referred, 12 non-referred); each child was accompanied by at
least one parent, the mother in all cases, with the fathers joining in five cases. Thirteen
children were female and 19 male. All participant parents were contacted and con-
sented for their child, as monitored by a local Institutional Review Board; parents were
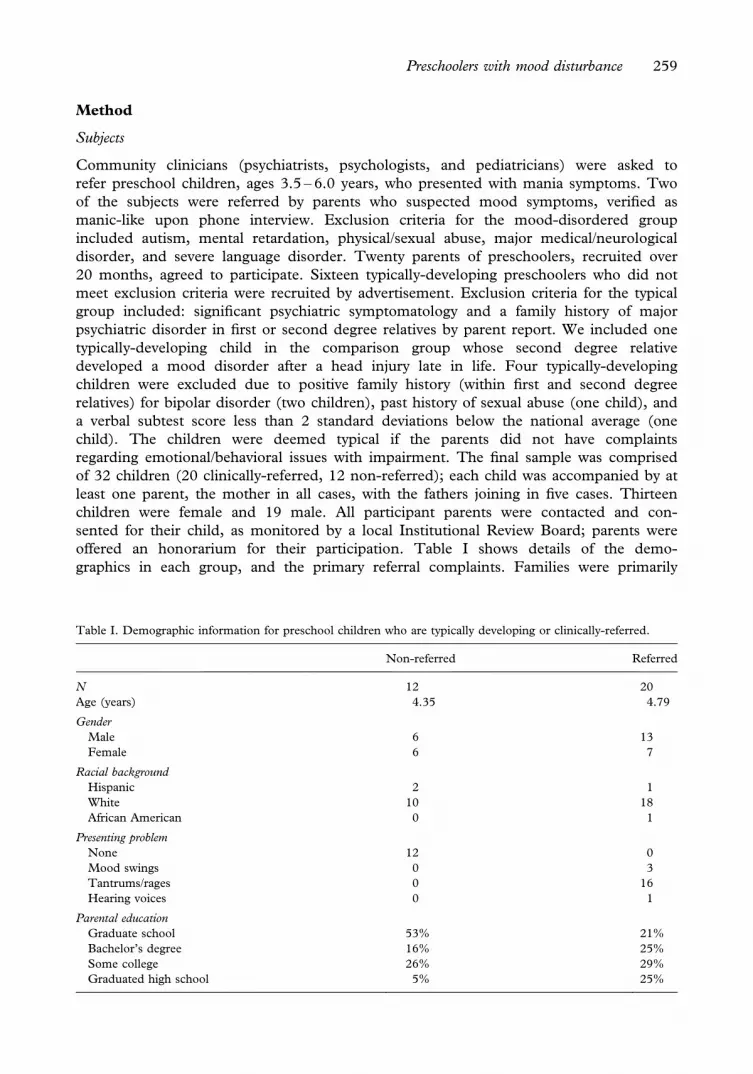
offered an honorarium for their participation. Table I shows details of the demo-
graphics in each group, and the primary referral complaints. Families were primarily
Table I. Demographic information for preschool children who are typically developing or clinically-referred.
Non-referred Referred
N 12 20
Age (years) 4.35 4.79
Gender
Male 6 13
Female 6 7
Racial background
Hispanic 2 1
White 10 18
African American 0 1
Presenting problem
None 12 0
Mood swings 0 3
Tantrums/rages 0 16
Hearing voices 0 1
Parental education
Graduate school 53% 21%
Bachelor’s degree 16% 25%
Some college 26% 29%
Graduated high school 5% 25%
Preschoolers with mood disturbance 259
white (86%); 9% were Hispanic and 5% were African American. Parents’ education
levels varied between high school completion and completion of graduate or professional
school.
Procedure
The child narrative sessions were preceded by a short free-play time, after explanation of
the consent forms to the parent. Following administration of two subtests (vocabulary and
block design) of the Wechsler Preschool and Primary Scales of Intelligence (WPPSI-III;
Wechsler, 2002) and a break, eight story stems were presented to the child in a playroom
setting with a one-way mirror, allowing non-distracting videotaping. The parent was seated
immediately outside, with the door slightly ajar if the child had separation concerns. During
a subsequent session, the parent(s) returned for the administration of semi-structured
interviews regarding mood symptoms, as well as an unstructured clinical interview. The
semi-structured interviews, administered by the first author, provided ample time for
parents to give examples of problematic behaviors. The first author was not blind to group
membership, though the coders of the MSSB tapes were blinded with the exception of one
child’s tape that was coded by the first author. Parents were given US$30 subject payments
for each visit.
Parent-reported symptoms
There were no established diagnostic interviews for mania in the preschool years at the
time this study was conducted, so two instruments were utilized: the mania and psychosis
sections from the original Preschool Age Psychiatric Assessment (PAPA) (Egger &
Angold, 1999), and a modified Section One (mood and psychosis) of the Washington
University Kiddie Schedule for Schizophrenia and Affective Disorders (KSADS; Geller
et al., 2001). PAPA is a structured diagnostic parent interview for assessing psychiatric
symptoms, disorders, and impairment in children aged 2 to 6 years old. The psychometric
reliability and validity of the PAPA is similar to those reported for interviews used with
older children or adults (Egger & Angold, 2004; Egger, Erkanli, Keeler, Potts, Walter, &
Angold, 2006). The mania section of the PAPA was since revised and used by Luby &
Belden (2006) to look at validating a bipolar diagnosis in preschool children and
discriminating bipolar from other diagnoses. KSADS is commonly used for the diagnosis
of bipolar disorder in school-age children. We have adapted it to interview parents of
preschool children by switching to third person questioning. Both the PAPA and the
KSADS provide, for each mania symptom, a score (0, 2, or 3 for the PAPA, meaning 0
for not present and 2 or 3 for present; and 1 – 7, on severity, for the KSADS) and scores
can be added across symptoms to provide an overall severity score. Reported symptom
severity on the PAPA and KSADS instruments ranged from 0 to 36 and 0 to 4.7
respectively. The PAPA mania and psychosis intensity scores that were totaled for our
composite score included the following symptoms occurring with elated or irritable mood:
expansive mood, irritability within the same day as expansive mood, depressed mood
within the same day as expansive mood, the presence of 2 months of remission of mood
symptoms in the previous year, more talkative than usual, pressure of speech, flight of
ideas, motor pressure, agitation, distractibility, decreased need for sleep, grandiosity,
poor judgment, delusions, hallucinations, thought process abnormality, idiosyncratic
behavior.
260 C. Beresford et al.

Structured interaction with the child
The MacArthur Story Stem Battery (MSSB), the instrument chosen for use in this study,
utilizes a story stem narrative method to structure interactions with the child (Bretherton
et al., 2003). The examiner, while delivering the beginning of each story, brings it to a point
of drama or conflict that the child is then invited to complete and/or resolve. The story
characters that potentially appear in each story include Grandma, Dad, Mom, and two
siblings (gender matching the gender of the subject.). The story is both told and enacted, via
small dolls and props, and is videotaped for coding.
Each child completed eight story stems, six from the MSSB and two additional stems
described below. The inclusion of eight stories allowed the examiner to intersperse more
stimulating stories with less stimulating ones, in order to provide a less intensely challenging
experience for the child. Four stories were coded for analysis, one low challenge and three
high challenge stories as described above: Spilled Juice and Lost Keys (MSSB); Cooking/
Bandage (Family Story Task; Shamir, Schudlich, & Cummings, 2002); and Sweater
(developed for this study).
Each story was rated by one of two experienced research assistants using all codes in the
MacArthur Narrative Coding System (MNCS; Robinson, Mantz-Simmons, Macfie, Kelsay,
Holmberg, & the MacArthur Narrative Working Group, 2004). Three narrative indices
were created by aggregating across codes within stories. Codes for a Negative Index that
reflected the children’s internal distress/disorganization were drawn from the content theme
area of Dysregulated Aggressive themes (including aggression weighted by severity of
behavior from 0 – 5 and personal injury rated as present/absent) and from performance
codes, including performed and verbalized emotions (anger, distress, and anxiety rated
present/absent), and codes reflecting dissociative behaviors developed by Macfie, Toth,
Rogosch, Robinson, Emde and Cicchetti (1999). If any of six dissociative behaviors from the
Macfie system occurred (intrusion of traumatic material, spacing out, fantasy proneness,
boundary confusion, fleeing painful subject, sadistic aggression) dissociation was scored
present. Several codes from the Narrative Emotion Coding Manual (Warren, 2003b) also
supplemented the Negative Index, specifically representations of danger, destruction,
inappropriate or excessive child power, and incoherent emotional sequencing. Codes for the
Positive Index reflecting children’s positive coping with story challenges were drawn from
the content theme area of Empathic Relations (including affection, affiliation, sharing,
empathy/helping each rated present/absent); performance codes, including performed and
verbalized emotion of joy (‘‘happy’’ or smiling/laughter) rated present/absent; and narrative
coherence expressed as 0 (containing incoherent story sequencing) or 1 (fully coherent story
sequencing). Codes included within the Negative Index and for the Positive Index were
averaged within each story. A Supportive Parent Index was based on the average of two
codes, positive and discipline/control, from the Parental Representations manual by
Oppenheim and colleagues (Oppenheim, Emde, & Warren, 1997) and a third code from the
MNCS, reliance on adult to resolve conflict (coded present/absent). Children’s responses to
story stems ranged from 0 to 1.0 for the Negative Index (Cronbach’s alpha¼ .72 across
stories), from 0 to .83 for the Positive Index (Cronbach’s alpha¼ .49 across stories), and
from 0 to .67 on the Supportive Parent Index (Cronbach’s alpha¼ .62 across stories).
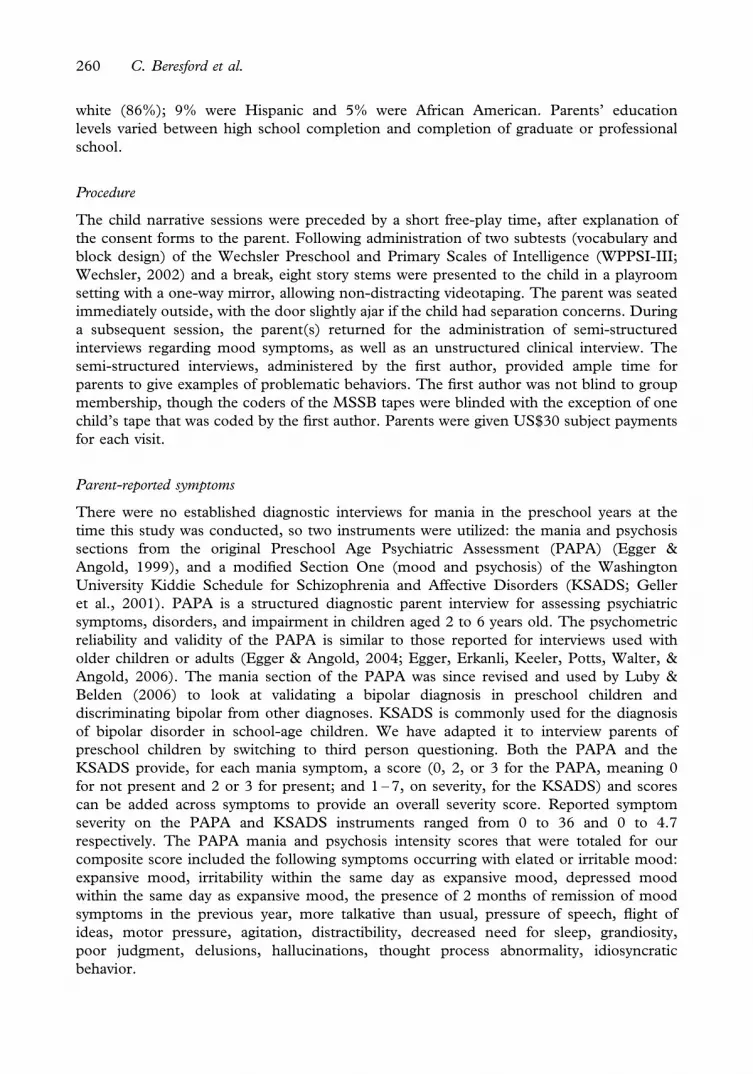
Means and standard deviations for Negative, Positive, and Supportive Parent Indices by
story stem are reported in Table II. Inter-rater reliability between the two coders and the
second author was demonstrated on a larger sample of low SES children. Based on 51
paired ratings, intraclass R for the Negative Index was .70, for the Positive Index, R¼ .84,
Preschoolers with mood disturbance 261
and for the Supportive Parent Index, R¼ .88. When coding in the current study sample was
unclear, one rater would confer with another or the second author to arrive at a consensus
rating.
Data analysis
Differences in demographic characteristics between groups of referred and typical children
were tested with chi-square or t-test and correlations between age and story stem responses
were computed. In order to test the first hypothesis, that referred children will have higher
levels of parent-reported symptoms of mania and depression, ANCOVA were computed
with child age as a covariate and results are reported in Table II using corrected means. In
order to test group differences across stories and the third hypothesis (concerning group
differences that varied by story challenge), a repeated measures analysis was conducted
(GLM routine in SPSS version 13.0) where illness group was a between subjects factor and
story stem was the repeated factor; child age was covaried following preliminary analyses of
group differences described below. For differences across illness groups for the narrative
responses (Hypothesis 1), we used multivariate results for the overall between-subjects effect
of illness group and for the averaged across-story effect for each narrative index. In order to
examine the second hypothesis that the relationship between parent reported mania
symptoms on the KSADS and PAPA interviews will be evident in the two high compared to
low challenge stories, we calculated Pearson correlations between the total KSADS and
PAPA scores and the Negative, Positive, and Supportive Parent Indices for each story,
partialling the effect of child age. No formal test of differences between correlations was
made. In order to test the third hypothesis that the narrative responses of referred (but not
typical) children will vary by story, showing elevated Negative Index and lowered Positive
Table II. Means and (standard deviations) for study variables.
Whole sample Typical Referred
PAPA mania (n¼ 30)a 11.77 (11.59) 1.82 (2.32) 18.78 (9.78)
KSADS mania (n¼28)a 2.19 (1.08) 1.17 (0.27) 2.96 (0.76)
KSADS depression (n¼29)a 0.97 (1.65) 0.0 (0.0) 1.56 (1.89)
Spilled Juice (n¼30)
Negative index 0.16 (0.18) 0.14 (0.14) 0.17 (0.20)
Positive indexa 0.28 (0.17) 0.24 (0.12) 0.30 (0.19)
Support parent 0.14 (0.18) 0.12 (0.18) 0.15 (0.18)
Lost Keys (n¼30)
Negative indexa 0.31 (0.17) 0.21 (0.09) 0.37 (0.19)
Positive indexa 0.25 (0.19) 0.30 (0.19) 0.22 (0.19)
Support parent 0.07 (0.09) 0.07 (0.10) 0.08 (0.09)
Cooking/Bandage (n¼ 31)
Negative indexa 0.32 (0.20) 0.14 (0.11) 0.41 (0.17)
Positive indexa 0.24 (0.22) 0.35 (0.28) 0.18 (0.15)
Support parent 0.19 (0.17) 0.21 (0.19) 0.18 (0.20)
Sweater (n¼30)
Negative index 0.32 (0.17) 0.30 (0.12) 0.33 (0.20)
Positive index 0.23 (0.21) 0.20 (0.16) 0.25 (0.23)
Support parent 0.17 (0.18) 0.14 (0.19) 0.19 (0.18)
asignificant difference between referred and typical children adjusted for child age.
262 C. Beresford et al.

and Supportive Parental Indexes in the higher compared to lower challenge stories, we
examined the multivariate within subjects tests for the illness group X story stem interaction
and the univariate contrasts for each narrative indicator. Stories were ordered according to
how they were presented to the child, Spilled Juice, Lost Keys, Cooking/Bandage, and
Sweater. Hence, confirmation of the hypothesis that high challenge stories would reveal
significant group differences was indicated by a significant quadratic effect.
Results
Group differences were examined and demographic information was found to differ
between the two groups (see Table I). Although referred children tended to be older than
typical children, the difference was not significant. In the referred group, there were twice as
many boys as girls and in the non-referred group gender was evenly split; the group
difference was not significant. Parents of non-referred children were better educated than
parents of referred children, with 5% versus 25% having graduated high school only and
53% versus 21% having attended graduate school. Group differences were also found for
WPPSI Vocabulary and Block Design subtests; referred children had lower Vocabulary
(Referred Mean¼ 11.6, SD¼ 2.1 vs. Non-referred Mean¼ 14.5, SD¼ 2.8; t 1,27¼ 3.18,
p5 .01) and Block Design scores (Referred Mean¼ 11.6, SD¼ 2.5 vs. Non-referred
Mean¼ 13.8, SD¼ 2.4; t 1,28¼ 2.37, p5 .05).
As can be seen in Table III, vocabulary scores were significantly negatively correlated with
parent reported symptoms (r¼7.49 and 7.51 for KSADS and PAPA reports, respectively)
but was not related to narrative indices. Within the Lost Keys story, Block Design was
significantly correlated with all three narrative indices: children with higher standard scores
had fewer negative (r¼7.38), and more positive features (r¼ .43) and parent representa-
tions (r¼ .36). Block Design was not significantly correlated with parent reported symptom
levels. Child age was not significantly correlated with symptom reports or story stem
Table III. Correlation between PAPA, KSADS symptoms, and observed representations partialling child age
(n¼24).
PAPA mania KSADS mania KSADS depression
Spilled Juice
Negative index 70.21 70.04 .01
Positive index 0.21 0.41* .21
Supportive parent 0.26 0.27 .17
Lost Keys
Negative index 0.20 0.30 .04
Positive index 70.04 70.19 .03
Supportive parent 0.34 0.20 .29
Cooking/Bandage
Negative index 0.59** 0.56** .38*
Positive index 70.04 70.22 7.19
Supportive parent 0.15 0.06 7.17
Sweater
Negative index 0.15 0.05 7.06
Positive index 0.14 0.16 .11
Supportive parent 0.19 0.12 .10
*p5 .05; **p5 .01.
Preschoolers with mood disturbance 263

responses for the whole sample or among referred children; it was, however, strongly
correlated with narrative responses of typical children. Older, compared to younger typically
developing children included more Supportive Parent representations during the Cooking/
Bandage story (r¼ .78, p5 .001) and higher Negative and lower Positive Index scores
during the Sweater story (r¼ .73 and r¼7.85, p5 .001). Models testing the main
hypotheses were run with Block Design or child age as a covariate; results were very similar
across different models. Results reported here are based on models that corrected for
child age.
In support of the first hypothesis, significantly greater parent-reported mania symptoms
were found for referred compared to typical children on the PAPA and KSADS interviews
(F 1,24¼ 40.38, p5 .001 and F 1,24¼ 56.03, p5 .001); greater depression was reported on
the KSADS (F 1,26¼ 5.04, p5 .05). See Table II. Examining group differences from the
multivariate analysis results across story stems, referred children’s responses estimated over
all three indices did not significantly differ from typicals (F 3,24¼ 1.83, p¼ .17). However,
the between subjects tests of the individual three indicators did show a significant difference
for the Negative Index (F 1,26¼ 5.51, p5 .05) suggesting elevation for referred children
across stories (Mean Referred¼ 0.31 vs. Mean Typicals¼ 0.20). Individual story univariate
statistics presented in Table II support this finding for the Spilled Juice, Lost Keys, and
Cooking/Bandage stories but not the Sweater story.
As can be seen in Table III, contrary to our hypothesis, most correlations between the
parent-reported PAPA, KSADS mania symptoms and the story stem responses were low
and non-significant. However, large and significant positive correlations were observed for
the Negative Index in the Cooking/Bandage story. An unanticipated positive correlation was
also observed between the Positive Index and the KSADS mania in the Spilled Juice story.
Support for the hypothesized differences within subjects across stories was found in the
results of the repeated measures, multivariate analysis for the Negative and Positive Indices
only. The multivariate analysis showed a significant effect for the overall within subjects
illness group by story stem interaction (F 9,18¼ 3.32, p5 .05). The repeated measures
univariate tests showed significant interaction effects for the Negative and Positive Indices
(F 3,78¼ 6.31, p5 .005 and F 3,78¼ 4.06, p5 .05). The interaction for the Supportive
Parent Index was non-significant, p4 .32). Finally, the results of the within subjects
contrasts for illness group by story stem interaction were significant for the quadratic effect
for Negative and Positive Indices (F 1,26¼ 19.96, p5 .005 and F 1,26¼ 9.14, p5 .01).
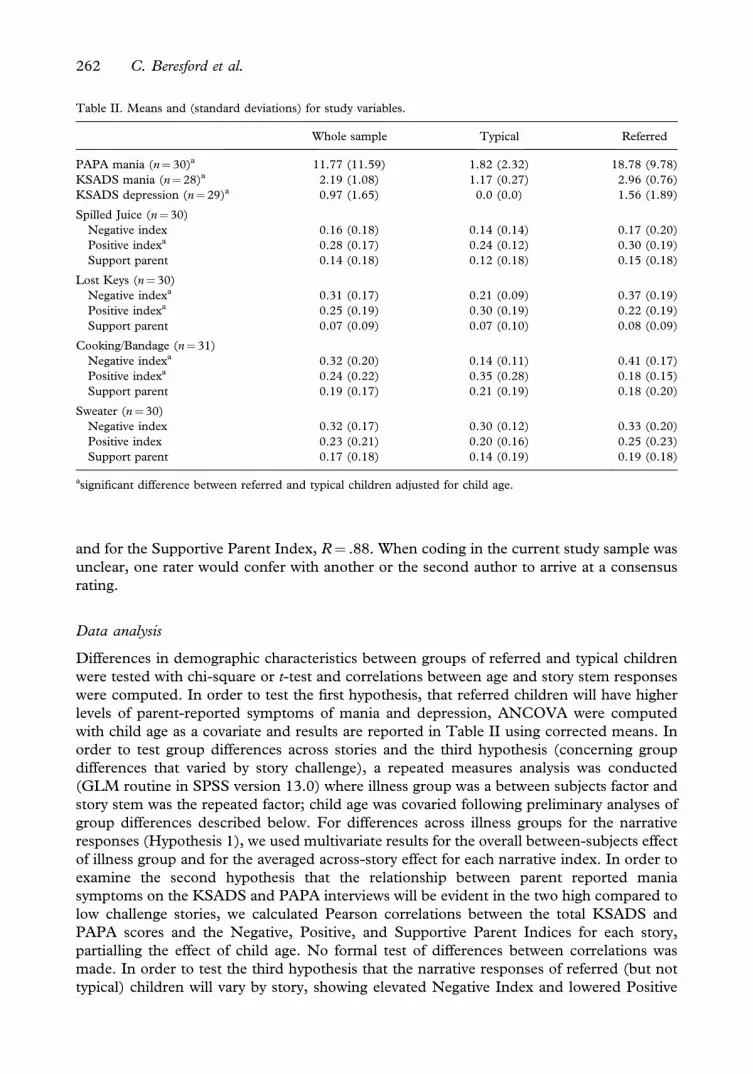
The means for the three indices within each story are displayed in Table III comparing
referred and typical children. In addition, Figure 1 illustrates the observed variations in
Negative and Positive Indices across stories. This quadratic effect refers to observed large
differences between referred and typical children in the two high challenge stories (Lost
Keys and Cooking/Bandage) that were presented to children following the Spilled Juice and
prior to the Sweater story stems. Typical children showed little variation in the Negative
Index for the first three stories, and had their strongest internally distressed/disorganized
responses to the mild fear induced in the Sweater story. Referred children showed no
elevation in the Negative Index for the Spilled Juice story compared to typicals, but marked
elevation in the Negative Index was observed in subsequent stories, especially the Lost Keys
and Cooking/Bandage. Referred and typical children had comparable internal distress/
disorganization in the Sweater story. For the Positive Index, typical children showed an
increase across stories, with markedly higher positive indicators in the more challenging
stories, Lost Keys and Cooking/Bandage. For referred children, by contrast, the Positive
Index was highest in the Spilled Juice story, exceeding the level of typical children. In the
higher challenge stories, however, the level of positive coping indicators dropped markedly
264 C. Beresford et al.
for referred children and were significantly lower than typicals in the Lost Keys and
Cooking/Bandage stories. The Positive Index in the Sweater story did not differ by illness
group.
Discussion
This study was designed as the beginning of a process of identifying and developing child
assessment processes that can augment parent report of behavior problems in young
children, especially for families with children struggling with manic-like behaviors and mood
symptoms. Preschool age children are rapidly developing a sense of self and are able to
provide, through verbalization and play, diagnostically informative details about their
experience, when clinicians provide them a non-threatening vehicle to share that
perspective. Traditional non-structured observations and play assessments fall short of
meeting the need to obtain a diagnostic picture quickly and efficiently in a managed care
environment. This evocative story stem paradigm allows clinicians to observe behaviors that
parents describe, in the child’s own voice and within a supportive context that is generally
fun and enjoyable for the child. Additionally, the MSSB method can be used in a
standardized manner, allowing comparison between patients, clinical groups, and different
research or clinical teams.
Results of this study found that, as expected and after adjusting for child age, referred
children differed significantly from normally developing children in depression and mania
symptoms by parent report. While there was not a significant multivariate main effect for
referred vs. non-referred children across the three narrative indicators, the between subjects
comparisons of the individual indicators was significant for the Negative Index. Clinic
referred children also had greater distress/internal disorganization across stories. The lack of
a robust finding here may be due to the very small samples in this study, but suggest that
large overall differences for referred children may not be seen reliably.
Figure 1. Variation in negative and positive indices for typical and referred children by story stem.
Preschoolers with mood disturbance 265

Associations between the MSSB and parent-reported symptoms on the PAPA and
KSADS were mostly low to non-significant. However, large and significant correlations
were found within the Cooking/Bandage story between the Negative Index and parent
ratings of mania symptoms and, although attenuated, for depression. Children whose
parents reported manic-like behaviors demonstrated substantially greater distress and
disorganization within this high challenge story; both the children’s experiences and the
corroboration of parent report of difficulties are important indicators for clinicians.
Obtaining this information also allows clinicians to benefit from multi-informant perspec-
tives which have been shown in clinical research to be valuable and to reduce error
associated with rater bias (Kraemer, Maeselle, Ablow, Essex, Boyce, & Kupfer, 2003).
Though not hypothesized, on the low-challenge Spilled Juice story, the study found a
significant correlation between the Positive Index and the count of PAPA mania symptoms.
Using this study’s novel repeated measures approach, applying level of challenge as the basis
for contrasting stories, effects for the ill group on the Negative and Positive Index contrasts
were found. Within subject contrasts identified differences for referred children on the
Negative and Positive Indicies in the high-challenge stories (i.e., Lost Keys and Cooking/
Bandage) but not in the lower-challenge stories (i.e., Spilled Juice and Sweater). By
contrast, typically-developing children exhibited the greatest disorganization (e.g., Negative
Index) during the fear-stimulus, Sweater story. In regard to the Positive Index, the referred
children showed elevations for the Spilled Juice story but their Positive Index scores
declined sharply on the high-challenge Lost Keys and Cooking/Bandage stories. Typically
developing children’s stories included more indicators of positive coping perhaps averting
disorganization during these high challenge stories. This more typical pattern of responses,
where distress in the story telling is seemingly managed or minimized as the child
emphasizes more positive story elements, has been found in large samples using a clustering
approach to story responses (Klute, 2004).
While not initially hypothesized, we found a correlation between mania symptoms and the
Positive Index and, as mentioned, a significant group difference (i.e., referred group mean
was nearly double that of the non-referred, typically-developing, group) for the Positive
Index within the Spilled Juice story, a low-challenge stem with a relatively simple and often
rote solution (e.g., child is reprimanded and cleans/corrects the situation). These findings
may point to a vulnerability in referred children in titrating or regulating their response to
novel stimuli. Research on offspring of parents with bipolar disorder find that those children
have an ‘‘extreme tendency to seek novelty, approach stimuli, and display uncontrolled
speech and actions—a predisposing factor’’ (Hirshfeld-Becker, Biederman, Henin, Faraone,
Cayton, and Rosenbaum, 2006). The subsequent ‘‘exhaustion’’ of positive themes for
referred children in high-arousal stems points to an interesting potential extension on this line
of research as does attempting to account for these tendencies through neuropsychological
(e.g., executive functioning) and coping (e.g., sensitivity to relationship threats) mechanisms.
The results of the current study add to a growing collection of studies (see review papers
by David Oppenheim, 2006, and Susan Warren, 2003a, for more information) suggesting
that the MSSB indeed provides insight into the child’s perspective on their life experiences
and strategies for coping with stress. The study also demonstrated that all stems are not
created equal, a point initially described by von Klitzing, Kelsey, Emde, Robinson, and
Schmitz (2003). Rather, particular utility may be found in contrasting children’s
performance in relatively low-affect stems to those with high interpersonal conflict and
rich emotional valence. While not completely analogous to valid indicators from adult
projective assessments (e.g., Rorschach Method Comprehensive System, Perceptual
Thinking Index), the atypical cognitions generated by the children with manic-like
266 C. Beresford et al.

symptoms in their story resolutions, especially during the stressful story conditions, resonate
with the flights from logical thinking seen in biologically based disorders such as bipolar,
schizoaffective, and schizophrenia spectrum disorders (Dao & Prevatt, 2006; Wood,
Nezworski, & Garb, 2003). These atypical cognitions included: bizarre aggression such as
cutting/sticking eyeballs and ears; props taking on lives of their own and floating, fighting, or
running away; invisible characters; and the escalation from one cut finger to all characters
being cut or killed, and many body parts being injured or cut off. Although hypothesized in
the development of the Sweater story, there were no auditory hallucinations reported or
observed by the children, suggesting that it did not stimulate sufficient arousal among the
children.
The crossover in pattern from high positive to high negative indicators in the context of
increasing emotional arousal, danger, and interpersonal conflict from the low-challenge
Spilled Juice to the high-challenge Cooking/Bandage stories also, with replication and
expansion, has the potential to lead to increased knowledge in terms of these children’s
symptoms and difficulties. It will be important to further explore the extent to which
behavioral observations with peers, siblings, and parents under analogous interactive
circumstances generalize these thematic differences, as it may point to etiology as well as
optimal points of entry for intervention.
Mothers and fathers describe parenting these children, with their labile mood states, as
‘‘walking on eggshells.’’ The dramatic mood swings that these children experience are
generally without physical markers that could guide a parent’s response, as would the
appearance and evident pain of a physical injury. Apparent parent – child dysynchrony that
would results from dealing with a ‘‘totally different child from one time to the next’’ puts the
parent – child relationship at great risk for distress and conflict. Despite what one would
expect, there was no significant decline in presentation of positive and available parents in
the stories of referred children. This indirectly reinforces what others have recommended in
terms of employing family therapy approaches to address the needs of children and
adolescents with manic and depressive symptoms (Kowatch et al., 2005).
In having conducted this research, the research team learned that using a standardized
assessment with this clinical population required redoubled sensitivity toward the child and
a new set of behavioral responses. In the ordinary course of an MSSB, the administration is
designed to be child responsive and the evaluator takes an active role in scaffolding the
child’s experiences, especially at the beginning and again as the child escalates in emotion.
Such structuring avoids unnecessary distress from excessive emotional arousal and
disorganization. Structuring helps the normally developing and at-risk children remain
linked to the stem at hand yet still yields rich and diagnostically informative material with
which one can use to generate hypotheses about the child’s symptoms, strengths, and
stressors. Scaffolding also allows clinicians to determine which children may be pressed to
disorganization by internal drives in contrast to children who become disorganized in
attempting to continue their line of verbalizations. The mood affected children, in this study,
required even more scaffolding and sensitivity to overload, and at times rescheduling of a
session in order to complete the brief battery. For example, one 3-year-old child became
anxious while completing the Cooking/Bandage story. During his narrative, the child said,
‘‘I cut him (Robert, the oldest brother) with the knife. Now his arm is bleeding. Now his
tummy is bleeding.’’ Then the child moved the knife toward his own hand. Then he again
poked Robert with the knife (and whispered ‘‘Cut’’). At that point, the child left the room to
rejoin mother. He was allowed to do this and take a break, and was reassured by the
examiner and his mother; he later came back to the task willingly, and did not have to leave
any other story as he did during the cooking story. This need for administration
Preschoolers with mood disturbance 267

flexibility and strategies to change administration for affected children was previously noted
by Kelsay (2003) and Robinson and Kelsay (2003) in early discussions about adapting the
story stem method to clinical populations. Also, while no direct assessment of affective
phase (i.e., hypomanic or hypodepressive) was collected, high levels of irritability for some
children led to the need for sessions to be curtailed and rescheduled. Strategies such
as tangible reinforcement (i.e., stickers) for a child giving their best effort and ready
availability of parents to reassure the children also proved to be helpful with this unique
population. Setting an initial tone of safety and openness to creativity is always important
but even more so for children with this profile of manic and mood symptoms. It may be
possible to capture the degree of scaffolding a child required in future derivations of MSSB
coding.
While the current study was a reasonable start, there are many limitations and needs in
order to move forward. First, the small sample size and limited inclusion of children from
diverse backgrounds precludes much generalizability at this stage. Second, while several
themes distinguished the ill and typically developing groups, many of these themes have also
been found to distinguish children who have been maltreated (Macfie, Toth, Rogosch,
Robinson, Emde, & Cicchetti, 1999; Toth, Cicchetti, Macfie, Rogosch, & Maughan, 2000).
Further specificity of coding may allow differential features to be more finely discerned but
for the story stem approach to become a robust clinical method these issues will need to be
addressed. We conclude, however, that the MSSB, a story stem method, has significant
potential as a clinical aid, one that is useful in evaluating the internal state of young children
with major psychiatric symptoms.
Acknowledgements
Financial support from NIMH-sponsored institutional NRSA Training program, T32
MH15442 (Martin Reite, Program Director).
References
Bretherton, I., Oppenheim, D., Emde, R. N., & the MacArthur Narrative Working Group (2003). The MacArthur
Story Stem Battery. In R. N. Emde, D. P. Wolf, & D. Oppenheim (Eds.), Revealing the inner worlds of young
children: The MacArthur Story Stem Battery and parent – child narratives (pp. 381 – 396). New York: Oxford
University Press.
Dao, T. K., & Prevatt, F. (2006). A psychometric evaluation of the Rorschach comprehensive system’s perceptual
thinking index. Journal of Personality Assessment, 86, 180 – 189.
Dilsaver, S., & Akiskal, H. (2004). Preschool-onset mania: Incidence, phenomenology and family history. Journal of
Affective Disorders, 82, S35 – S43.
Edelbrock, C., Costello, A. J., Dulcan, M. K., Conover, N. C., & Kala, R. (1986). Parent – child agreement on
child psychiatric symptoms assessed via structured interview. Journal of Child Psychology and Psychiatry, 27,
181 – 190.
Egger, H., & Angold, A. (1999). The Preschool Age Psychiatric Assessment. Durham, NC: Center for Developmental
Epidemiology, Department of Psychiatry and Behavioral Sciences, Duke University.
Egger, H., & Angold, A. (2004). The Preschool Age Psychiatric Assessment (PAPA): A Structured parent inter-
view for diagnosing psychiatric disorders in preschool children. In R. DelCarmen-Wiggins, & A. Carter (Eds.),
Handbook of infant, toddler, and preschool mental assessment (pp. 223 – 243). New York: Oxford University Press.
Egger, H., Erkanli, A., Keeler, G., Potts, E., Walter, B., & Angold, A. (2006). The test – retest reliability of the
Preschool Age Psychiatric Assessment (PAPA). Journal of the American Academy of Child and Adolescent
Psychiatry, 45, 538 – 549.
Geller, B., Zimerman, B., Williams, M., Bolhofner, K., Craney, J., Delbello, M., et al. (2001). Reliability of
the Washington University in St. Louis Kiddie Schedule for Affective Disorders and Schizophrenia (WASH-U-
KSADS) Mania and Rapid Cycling Sections. Journal of the American Academy of Child and Adolescent Psychiatry,
40, 450 – 455.
268 C. Beresford et al.

Hirshfeld-Becker, D. R., Biederman, J., Henin, A., Faraone, S. V., Cayton, G. A., & Rosenbaum, J. F. (2006).
Laboratory-observed behavioral disinhibition in the young offspring of parents with bipolar disorder: A high-risk
pilot study. American Journal of Psychiatry, 163, 265 – 271.
Jensen, P., Rubio-Stipec, M., Canino, G., Bir, H., Dulcan, M., Schwab-Stone, M., et al. (1999). Parent and child
contributions to diagnosis of mental disorder: Are both informants always necessary? Journal of Nervous and
Mental Disease, 38, 1569 – 1579.
Kelsay, K. (2003). L’utilization de complement d’histoires de MacArthur dans le clinique. Devenir, 4.
Klute, M. M. (2004). Moving toward the person: A cluster analysis of story stem responses. Paper presented at the
Biennial Meeting of the Society for Research in Human Development, Spring Meeting Park City, UT.
Kowatch, R. A., Fristad, M., Birmaher, B., Dineen-Wagner, K., Findling, R. L., Hellander, M., et al. (2005).
Treatment guidelines for child and adolescent bipolar disorder: Child Psychiatric Workgroup on Bipolar
Disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 44, 213 – 235.
Kraemer, H., Maeselle, J. R., Ablow, J. C., Essex, M. J., Boyce, W. T., & Kupfer, D. J. (2003). A new approach to
integrating data from multiple informants in psychiatric assessment and research: Mixing and matching
contexts and perspectives. American Journal of Psychiatry, 160, 1566 – 1577.
Luby, J., & Belden, A. (2006). Defining and validating bipolar disorder in the preschool period. Development and
Psychopathology, 18, 971 – 988.
Macfie, J., Cicchetti, D., & Toth, S. (2001). The development of dissociation in maltreated preschool-aged
children. Development and Psychopathology, 13, 233 – 254.
Macfie, J., Toth, S. L., Rogosch, F. A., Robinson, J., Emde, R. N., & Cicchetti, D. (1999). Effect of maltreatment
on preschoolers’ narrative representations of responses to relieve distress and of role reversal. Developmental
Psychology, 35, 460 – 465.
Oppenheim, D. (2006). Child, parent, and parent – child emotion narratives: Implications for developmental
psychopathology. Development and Psychopathology, 18, 771 – 790.
Oppenheim, D., Emde, R. N., & Warren, S. L. (1997). Children’s narrative representations of mothers: Their
development and associations with child and mother adaptation. Child Development, 68, 127 – 138.
Robinson, J. (2007). Story stem narratives with young children: Moving to clinical research and practice. Attachment
& Human Development, 9(3), 179 – 185.
Robinson, J., & Kelsay, K. (2003). Le complement d’histoires de MacArthur: Un nouvel outil clinique d’evaluation.
Devenir, 4, 401 – 414.
Robinson, J. L., & Mantz-Simmons, L. (2003). The MacArthur Narrative Coding System: One approach to
highlighting affective meaning making in the MacArthur Story Stem Battery. In R. N. Emde, D. P. Wolf, &
D. Oppenheim (Eds.), Revealing the inner worlds of young children: The MacArthur Story Stem Battery and parent –
child narratives (pp. 81 – 91). New York: Oxford University Press.
Robinson, J., Mantz-Simmons, L., Macfie, J., Kelsay, K., Holmberg, J., & the MacArthur Narrative Working
Group (2004). The MacArthur Narrative Working Group. The MacArthur Narrative Coding System. Unpublished
document, University of Colorado Health Sciences Center, Denver, Colorado.
Shamir, H., Schudlich, T., & Cummings, M. (2002). Marital conflict, parenting styles, and children’s rep-
resentations of family relationships. Parenting: Science and Practice, 1, 123 – 151.
Toth, S., Cicchetti, D., Macfie, J., Rogosch, F., & Maughan, A. (2000). Narrative representations of moral-
affiliative and conflictual themes and behavioral problems in maltreated preschoolers. Journal of Clinical Child
Psychology, 29, 307 – 318.
Tumuluru, R. V., Weller, E. B., Fristad, M. A., & Weller, R. A. (2003). Mania in six preschool children. Journal of
Child and Adolescent Psychopharmacology, 13, 489 – 494.
von Klitzing, K., Kelsey, K., Emde, R. N., Robinson, J., & Schmitz, S. (2000). Gender specific characteristics of
five-year-old’s play narratives and associations with behavior ratings. Journal of American Academy of Child and
Adolescent Psychiatry, 39, 1017 – 1023.
Warren, S. L. (2003a). Narratives in risk and clinical populations. In R. N. Emde, D. P. Wolf, & D. Oppenheim
(Eds.), Revealing the inner worlds of young children: The MacArthur Story Stem Battery and parent – child narratives
(pp. 222 – 239). New York: Oxford University Press.
Warren, S. L. (2003b). Narrative emotion coding system (NEC). In R. N. Emde, D. P. Wolf, & D. Oppenheim
(Eds.), Revealing the inner worlds of young children: The MacArthur Story Stem Battery and parent – child narratives
(pp. 92 – 105). New York: Oxford University Press.
Warren, S. L., Emde, R. N., & Sroufe, L. (2000). Internal representations: Predicting anxiety from children’s play
narratives. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 100 – 107.
Warren, S. L., Oppenheim, D., & Emde, R. N. (1996). Can emotions and themes in children’s
play predict behavior problems? Journal of the American Academy of Child and Adolescent Psychiatry, 34,
1331 – 1337.
Preschoolers with mood disturbance 269

Wechsler, D. (2002). Wechsler preschool and primary scale of intelligence—revised. New York: Psychological
Corporation.
Wilens, T., Biederman, J., Brown, S., Monuteaux, M., Prince, J., & Spencer, T. (2002). Patterns of
psychopathology and dysfunction in clinically referred preschoolers. Journal of Developmental and Behavioral
Pediatrics, 23(1 Supplement), S31 – S36.
Wood, J. M., Nezworski, M. T., & Garb, H. N. (2003). What’s right with the Rorschach? The Scientific Review of
Mental Health Practice, 2, http://www.srmhp.org/0202/focus.html
270 C. Beresford et al.





















