
Reliability of electrocardiogram interpretation in critically ill patients

DOI 10.1378/chest.100.6.1676 1991;100;1676-1684Chest
R Chioléro, J P Flatt, J P Revelly and E Jéquier patients.consumption and oxygen delivery in critically ill Effects of catecholamines on oxygen
http://chestjournal.chestpubs.org/content/100/6/1676.citation
can be found online on the World Wide Web at: The online version of this article, along with updated information and services
) ISSN:0012-3692http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(without the prior written permission of the copyright holder.reserved. No part of this article or PDF may be reproduced or distributedChest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights
ofbeen published monthly since 1935. Copyright1991by the American College is the official journal of the American College of Chest Physicians. It hasChest
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from

1676 Catecholamines and 02 Consumption in Critically III Patients (Chiolem et a!)
critical careEffects of Catecholamines on Oxygen Consumptionand Oxygen Delivery in Critically Ill Patients*Ren#{233}Chiole’ro M.D.; Jean-Pierre Flatt Ph.D.;t Jean-Pierre Revelly M.D.;
and EricJequier M.D.t
(Chest 1991; 100:1676-84)
no, = oxygen delivery; EE en�rgy expenditure; MVo,myocardial oxygen consumption; Vo, = oxygen consumption
C atecholamines are widely used in the management
ofpatients whose cardiovascular system is failing.
Indeed, they figure among the most commonly used
pharmacologic agents in critically ill patients. The
positive effects of catecholamines on cardiac function,
tissue perfusion and oxygenation are well known. ‘‘#{176}
Parallel to their effects on systemic hemodynamics,
these agents exert numerous metabolic and endocrine
effects. 11-12 The most important metabolic effects in-
dude elevation of hepatic glucose production, stimu-
lation oflipolysis, increases in plasma glucose, lactate,
potassium and free fatty acids levels, as well as
elevation of the resting metabolic rate . � � The latter is
related to a direct action of catecholamines on 02
consumption (c�o2) reflecting heat production in van-
ous tissues, which is independent of their hemody-
namic effects in normal conditions.”3 In clinical
practice, the distinction between these different ef-
fects of catecholamines on whole body V02 is often
neglected and it is commonly believed that any
increase in Vo2 is associated with improvement in
systemic hemodynamics and tissue oxygenation. This
statement is not always true.
The aim of this review is to comment on the effects
ofcatecholamines on oxygen consumption and energy
metabolism, including their implications for clinical
practice. This review has three sections devoted (1) to
an evaluation of the concept of energy utilization and
heat production, (2) to the effects of catecholamines
on 02 uptake in various tissues and its mechanisms,
and (3) to the effects of catecholamines on 02 con-
sumption in critically ill patients in whom 02 delivery
is often inadequate.
5From the Surgical Intensive Care Unit, Department of Anesthe-siology, University Hospital, Lausanne, Switzerland.
tlnstitute of Physiology, Faculty of Medicine, Lausanne.Supported by a grant from Hausmann-Vifor, Geneva, Switzerland.
Reprint requests: Dr. Chiolero, Senice de Anesthesiologie, CHU1�I�iiusanne, Switzerland 1011
ENERGY EXPENDITURE AND THERMOGENESIS
Oxygen consumption and energy expenditure are
closely correlated physiologic �4 In normal
subjects, Vo2 is usually assessed using indirect calorim-
etny, which relies on direct measurement of body gas
exchange . ‘5 In clinical conditions, �#{176}2 �S often calcu-
lated from cardiac output and anteriovenous differ-
ences in 02, by means of the Fick principle. The heat
released by the oxidative processes can then be
calculated using an energy equivalent for the con-
sumed 02, which is dependent on the respiratory
quotient, the ratio between CO2 production and V02.
In subjects in thermal equilibrium, resting energy
expenditure determined by indirect calorimetry is
equivalent to heat production measured by direct
calorimetry. ‘5
Energy Utilization
Energy is utilized in the body to perform electro-
chemical, mechanical and synthetic work. These proc-
esses maintain electrochemical gradients through cell
membranes, allow muscular activity, and the synthesis
ofmacromolecules such as proteins and glycogen. The
release of energy from substrates is coupled to ATP
synthesis, while most of the cellular energy requiring
processes are dependent on ATP hydrolysis. The
energy expended by the body is ultimately converted
into heat, which must be dissipated. Heat production
is therefore the end product of energy utilization in a
resting subject. During exercise, however, a fraction
of energy is transformed into external 16
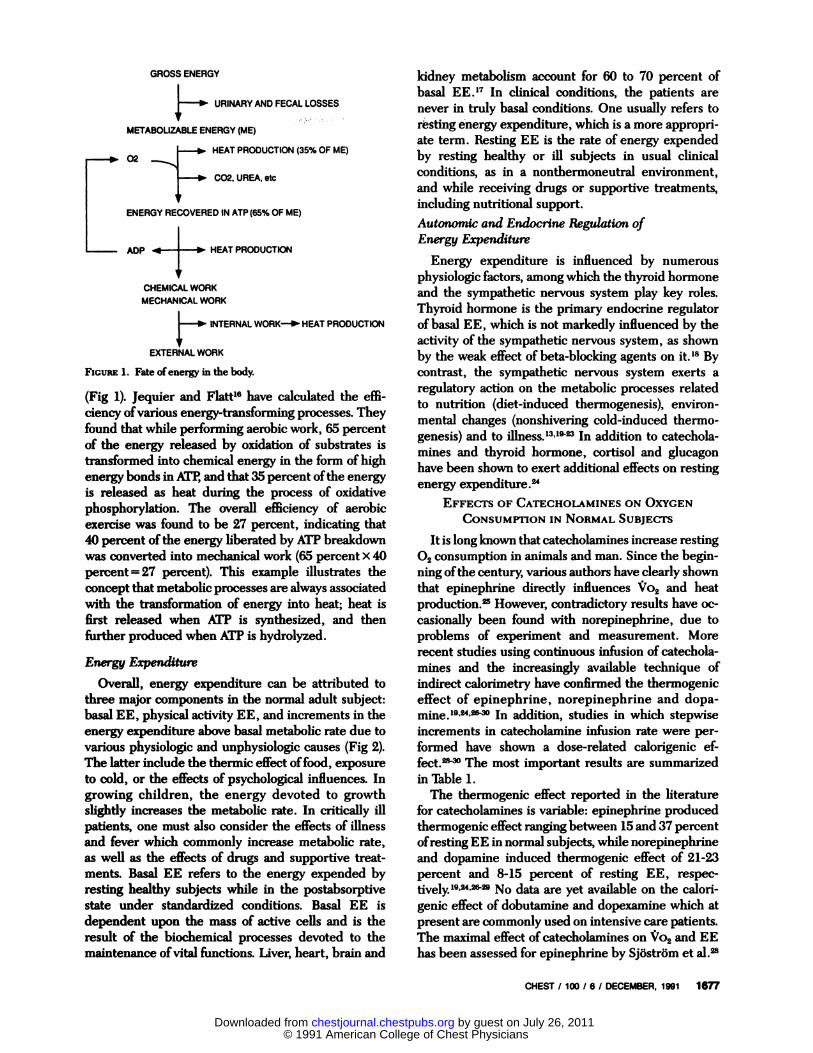
Energy utilization by the body is illustrated in
Figure 1 . Gross energy refers to the energy content
of nutrients, ie, their heat of combustion. A small part
of energy is lost in feces and urine (usually about 5
percent, except in patients with gastrointestinal or
renal diseases), leaving the metabolizable energy.
The transformation of metabolizable energy into
chemical and mechanical energy is always associated
with heat production and dissipation.’6 When discuss-
ing energy metabolism, it is useful to understand how
the energy released by substrate oxidation is utilized
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from
CHEST I 100 I 6 I DECEMBER, 1991 1677
GROSS ENERGY
F-’- URINARY AND FECAL LOSSES
METABOUZABLE ENERGY (ME)
I___.. HEAT PRODUCTION (35% OF ME)
O2��J
�-*. C02, UREA, etc
ADP 4 ! � HEAT PRODUCTION
CHEMICAL WORK
MECHANICAL WORK
t__+.INTERNAL WORK-�’ HEAT PRODUCTIONEXTERNAL WORK
Ficuan 1. Fate ofenergy in the body.
(Fig 1). Jequier and Flatt’6 have calculated the effi-
ciency ofvarious energy-transforming processes. They
found that while performing aerobic work, 65 percent
of the energy released by oxidation of substrates is
transformed into chemical energy in the form of high
energy bonds in AlP, and that 35 percent ofthe energy
is released as heat during the process of oxidative
phosphorylation. The overall efficiency of aerobic
exercise was found to be 27 percent, indicating that
40 percent ofthe energy liberated by AlT breakdown
was converted into mechanical work (65 percent X 40
percent = 27 percent). This example illustrates the
concept that metabolic processes are always associated
with the transformation of energy into heat; heat is
first released when KIT is synthesized, and then
further produced when KIT is hydrolyzed.
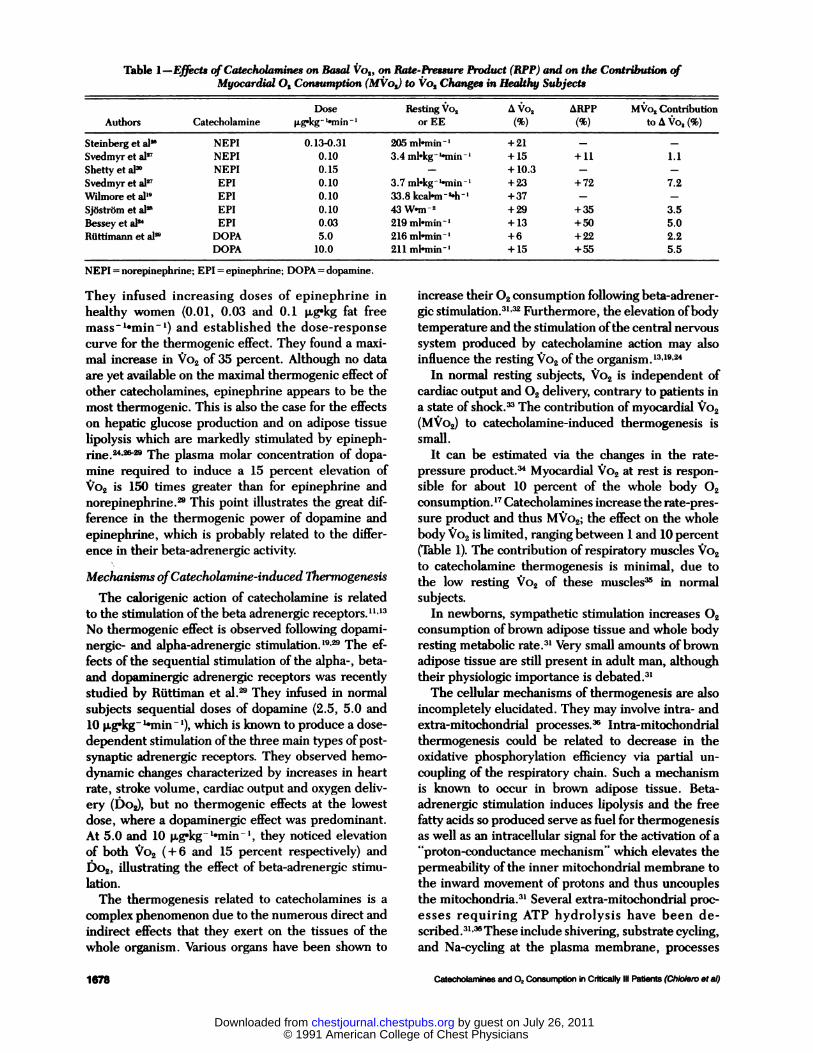
Energy Expenditure
Overall, energy expenditure can be attributed to
three major components in the normal adult subject:
basal EE, physical activity EE, and increments in the
energy expenditure above basal metabolic rate due to
various physiologic and unphysiologic causes (Fig 2).
The latter include the thermic effect offood, exposure
to cold, or the effects of psychological influences. In
growing children, the energy devoted to growth
slightly increases the metabolic rate. In critically ill
patients, one must also consider the effects of illness
and fever which commonly increase metabolic rate,
as well as the effects of drugs and supportive treat-
ments. Basal EE refers to the energy expended by
resting healthy subjects while in the postabsorptive
state under standardized conditions. Basal EE is
dependent upon the mass of active cells and is the
result of the biochemical processes devoted to the
maintenance ofvital functions. Liver, heart, brain and
ENERGY RECOVERED IN ATP(65% OF ME)
kidney metabolism account for 60 to 70 percent of
basal EE.’7 In clinical conditions, the patients are
never in truly basal conditions. One usually refers to
resting energy expenditure, which is a more appropri-
ate term. Resting EE is the rate of energy expended
by resting healthy or ill subjects in usual clinical
conditions, as in a nonthermoneutral environment,
and while receiving drugs or supportive treatments,
including nutritional support.
Autonomic and Endocrine Regulation of
Energy Expenditure
Energy expenditure is influenced by numerous
physiologic factors, among which the thyroid hormone
and the sympathetic nervous system play key roles.
Thyroid hormone is the primary endocrine regulator
ofbasal EE, which is not markedly influenced by the
activity of the sympathetic nervous system, as shown
by the weak effect of beta-blocking agents on 18 By
contrast, the sympathetic nervous system exerts a
regulatory action on the metabolic processes related
to nutrition (diet-induced thermogenesis), environ-
mental changes (nonshivering cold-induced thermo-
genesis) and to fflness.l3,l�m In addition to catechola-
mines and thyroid hormone, coi-tisol and glucagon
have been shown to exert additional effects on resting
energy expenditure .�
EFFECTS OF CATECHOLAMINES ON OXYGEN
CONSUMPTION IN NORMAL SUBJECTS
It is long known that catecholamines increase resting
02 consumption in animals and man. Since the begin-
ning ofthe century, various authors have clearly shown
that epinephrine directly influences 1�O2 and heat
production.Z However, contradictory results have oc-
casionally been found with norepinephrine, due to
problems of experiment and measurement. More
recent studies using continuous infusion of catechola-
mines and the increasingly available technique of
indirect calorimetry have confirmed the thermogenic
effect of epinephrine, norepinephrine and dopa-
mine.’9�’�”#{176} In addition, studies in which stepwise
increments in catecholamine infusion rate were per-
formed have shown a dose-related calorigemc ef-
fect.� The most important results are summarized
inTable 1.
The thermogenic effect reported in the literature
for catecholamines is variable: epinephrine produced
thermogenic effect ranging between 15 and 37 percent
ofresting EE in normal subjects, while norepinephnine
and dopamine induced thermogenic effect of 21-23
percent and 8-15 percent of resting EE, respec-
tively.’9’�� No data are yet available on the calori-
genic effect of dobutamine and dopexamine which at
present are commonly used on intensive care patients.
The maximal effect ofcatecholamines on ‘��O2 and EE
has been assessed for epinephrine by Sj#{246}str#{246}met al.�
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from
1678 Catecholamines and 02 CU�Pt�0n in CrItically III Patients (Chiolem eta!)
Table 1-Effrcts ofCateclsolamines on Basal Vo’, on Rate-&essure Product (RPP) and on the Contribution ofMyocardial O� Consumption (MVo�) to Vo, Changes in HeOJ*hIJ Subject.
Authors Catecholamine
Dose
�g.kg’.min’
Resting Vo2or EE
Vo2(%)
�RPP
(%)MVo, Contribution
to � Vo, (%)
SteinbergetaiM NEPI 0.13-0.31 205 mlmin� +21 - -Svedmyr et alv NEPI 0.10 3.4 ml#{149}kg”min’ + 15 + 11 1.1
Shettyetai’#{176} NEPI 0.15 - +10.3 - -Svedmyr et alv EPI 0.10 3.7 ml#{149}kg”min’ +23 + 72 7.2
Wilmoreetal’� EPI 0.10 33.8kcal’m’4r’ +37 - -
Sj#{246}str#{246}met al� EPI 0.10 43 W.m’ +29 +35 3.5
BesseyetaP’ EPI 0.03 219ml”min’ +13 +50 5.0
R#{252}ttimann et al� DOPADOPA
5.010.0
216 mhnin’211m}’min’
+6+15
+22+55
2.25.5
NEPI= norepinephrine; EPI = epinephrine; DOPA = dopamine.
They infused increasing doses of epinephnine in
healthy women (0.01, 0.03 and 0.1 p�g.kg fat free
mass’#{149}min�) and established the dose-response
curve for the thermogenic effect. They found a maxi-
mal increase in �‘#{176}2 of 35 percent. Although no data
are yet available on the maximal thermogenic effect of
other catecholamines, epinephrine appears to be the
most thermogenic. This is also the case for the effects
on hepatic glucose production and on adipose tissue
lipolysis which are markedly stimulated by epineph-
rine.�d�� The plasma molar concentration of dopa-
mine required to induce a 15 percent elevation of
Vo2 is 150 times greater than for epinephnne and
norepinephrine.m This point illustrates the great dii’-
ference in the thermogenic power of dopamine and
epinephrine, which is probably related to the differ-
ence in their beta-adrenergic activity.
Mechanisms ofCatecholamine-induced Thermogenesis
The calorigenic action of catecholamine is related
to the stimulation ofthe beta adrenergic receptors.”3
No thermogenic effect is observed following dopami-
nergic- and alpha-adrenergic 19,m The ef-
fects of the sequential stimulation of the alpha-, beta-
and dopaminergic adrenergic receptors was recently
studied by R#{252}ttiman et al.� They infused in normal
subjects sequential doses of dopamine (2.5, 5.0 and
10 p.g’kg ‘min ‘), which is known to produce a dose-
dependent stimulation ofthe three main types of post-
synaptic adrenergic receptors. They observed hemo-
dynamic changes characterized by increases in heart
rate, stroke volume, cardiac output and oxygen deliv-
ery (Doe), but no thermogenic effects at the lowest
dose, where a dopaminergic effect was predominant.
At 5.0 and 10 p�g.kg ‘min ‘ , they noticed elevation
of both Vo2 (+ 6 and 15 percent respectively) and
Do2, illustrating the effect of beta-adrenergic stimu-
lation.
The thermogenesis related to catecholamines is a
complex phenomenon due to the numerous direct and
indirect effects that they exert on the tissues of the
whole organism. Various organs have been shown to
increase their 02 consumption following beta-adrener-
gic stimulation.31’� Furthermore, the elevation of body
temperature and the stimulation ofthe central nervous
system produced by catecholamine action may also
influence the resting Vo2 ofthe orgaifism.’3”9”�’
In normal resting subjects, �O2 is independent of
cardiac output and 02 delivery, contrary to patients in
a state of shock.� The contribution of myocardial ‘�O2
(M�o2) to catecholamine-induced thermogenesis is
small.
It can be estimated via the changes in the rate-
pressure product.� Myocardial ��O2 at rest is respon-
sible for about 10 percent of the whole body 02
17 Catecholamines increase the rate-pres-
sure product and thus M’�o2; the effect on the whole
body ‘#{176}2 is limited, ranging between 1 and 10 percent
(Table 1). The contribution of respiratory muscles �
to catecholamine thermogenesis is minimal, due to
the low resting V02 of these muscles� in normal
subjects.
In newborns, sympathetic stimulation increases 02
consumption of brown adipose tissue and whole bodyresting metabolic rate.3’ Very small amounts of brown
adipose tissue are still present in adult man, although
their physiologic importance is debated.3’
The cellular mechanisms of thermogenesis are also
incompletely elucidated. They may involve intra- and
extra-mitochondrial processes.� Intra-mitochondrial
thermogenesis could be related to decrease in the
oxidative phosphorylation efficiency via partial Un-
coupling of the respiratory chain. Such a mechanism
is known to occur in brown adipose tissue. Beta-
adrenergic stimulation induces lipolysis and the free
fatty acids so produced serve as fuel for thermogenesis
as well as an intracellular signal for the activation of a
“proton-conductance mechanism” which elevates the
permeability ofthe inner mitochondrial membrane to
the inward movement of protons and thus uncouples
the mitochondria.3’ Several extra-mitochondrial proc-
esses requiring ATP hydrolysis have been de-
scribed.31’�These include shivering, substrate cycling,
and Na-cycling at the plasma membrane, processes
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from
0
I-
cJ
50
40
30
20
10
0
Activity
Stimulants TE
Cold TB
Food TE
Activity
Treatment TE
Cold TB
Food TB
Illness TE
CHEST I 100 I 6 I DECEMBER, 1991 1679
leading to AlT utilization and enhanced heat produc-
tion. Substrate cycling has been shown to contribute
to the increase in resting metabolic rate and thermo-
genesis in severely burned patients, bu� #{244}#{241}lyto the
extent ofa small part ofthe EE changes.�
In assessing the use of the catecholamine-induced
increment in Vo2 by the organism in a normal subject,
it is apparent that a large part leads to heat production
and dissipation (true thermogenesis), and only a small
part to extrametabolic effects, such as the elevation of
myocardial 02 and respiratory muscles’ 02 consump-
tion. The effects of catecholamine on V02 and meta-
bolic rate in normal subjects can thus be considered
the prototype ofa thermogenic process.
THE CRITICALLY ILL PATIENT
Numerous clinical studies have shown that catechol-
amines also increase Vo2 in critically ill patients (Table
2). “�‘� However, this effect is more variable than in
normal subjects and occasionally decreases in �#{176}2
have been observed in individual cases with low
cardiac output syndromes unresponsive to catechola-
mine infusion.4’7
In the critically ill, catecholamines influence body
V02 via two main mechanisms (Fig 2): (1) as in normal
subjects, they stimulate the tissue 02 consumption
directly (a thermogenic action); (2) in patients with
low 02 delivery or inadequate 02 extraction, they
affect the Vo2 via their effect on tissue 02 delivery. In
addition, they may also influence body Vo2 by altering
the regional distribution of blood flow, although no
clinical data are presently available on this point.�
Measurement of Oxygen Consumption and
Metabolic Rate
Accurate measurements of 02 consumption and
60_I
Co2 production are difficult in clinical conditions,
particularly in patients on mechanical ventilation.’#{176}
The Fick method is commonly used in intensive care
patients. It requires a pulmonary artery catheter to
measure cardiac output by thermodilution and draw
out the mixed venous blood to determine its 02
content. The accuracy of this technique of measure-
ment is ± 10 percent at best; this is due to the
cumulative measurement errors related to cardiac
output, arterial 02 content, and venous 02 content.4’
This technique does not account for the lung paren-
chyma 02 consumption, a factor which may be signif-
icant in acute lung disease. Furthermore, the Fick
method should not be used to determine the relation-
ship between V02 and Do2 because these two parain-
eters are both derived from the cardiac output and 02
arterial content values. In such conditions, the varia-
bles are not independent and there is an overestima-
tion of the correlation between these variables due to
a mathematical coupling phenomenon.’�’
The gas exchange technique measures the ‘�O2 of
the whole organism, including the lungs. It implies
that the patient is in a steady state, with identical
tissue and pulmonary gas exchange. Even brief
changes in ventilation may rapidly modify the body
gas stores and therefore invalidate this assumption. In
patients on mechanical ventilation, this technique
requires a stable inspiratory 02 concentration below
60 percent, and no gas leakage in the system . if these
requirements are satisfied, this technique has been
shown to have a fair accuracy in the 1-5 percent
range .
The difficulties and limitations in measurement of
V02 in the acutely ill patient should be taken into
consideration when analyzing the effects of agents
such as catecholamines on ‘�JO2 and metabolic rate.
Activity
Treatment TE
Cold TBFood TE
Illness TE
D02-dependent
Normal suject Critically iLl
flow dependentpatient
Critically illhypermetabolic
patient
Ficuas 2. Components of 24-h energy expenditure (EE) in normal, critically ill #{176}2delivery-dependentand critically ill hypermetabolic patients. TE = thermic effect.
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from

0
E
0
C
80
0
60 a.
0
‘.U CJ
a.
20 �
E
C
E
E
C0
0.E
InC00
0
200�
175�
150’
125�
100’
p
0 200 400 600 800 1000 1200
02 delIvery (mI.mIn1.m2)
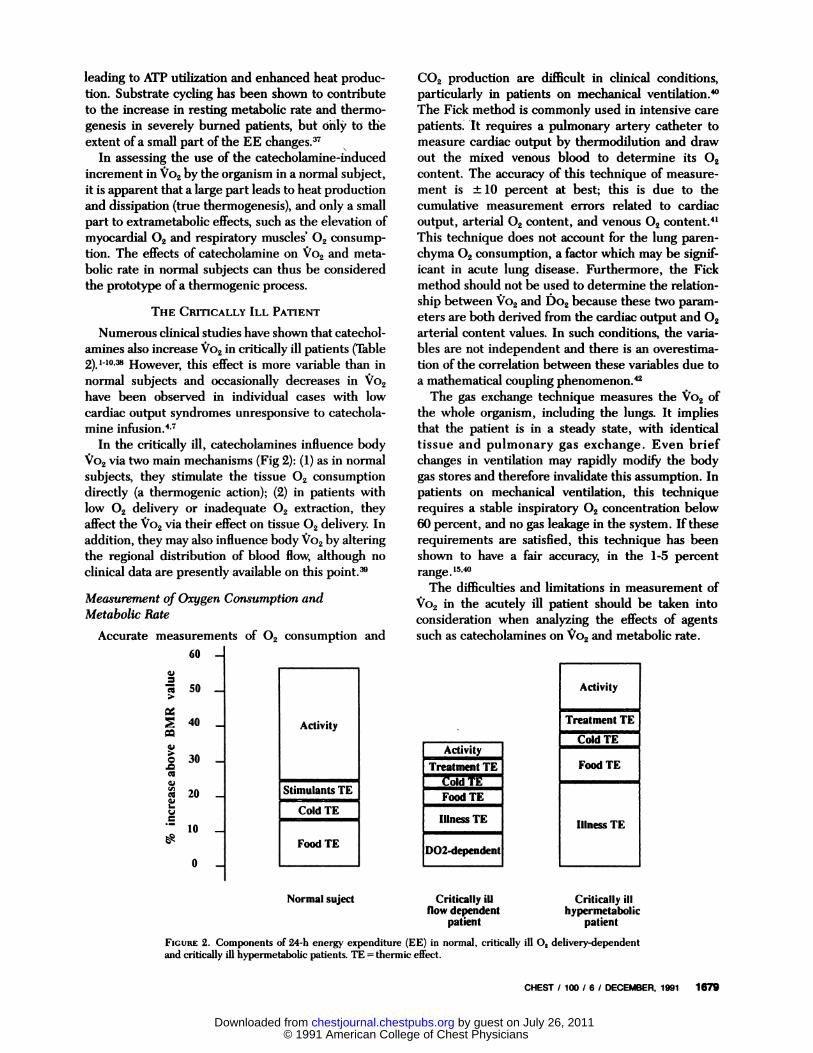
Ficuax 4. Effects ofcatecholamines or propranolol administration
on the VoJDo, relationship in normal and critically ill subjects.Normal subjects (O----O); cardiogenic shock (D-.D); pulmo-nary embolism (D-�-#{149}D); septic shock (#{149}#{149});pre and post-operative patients (A-#{149}-A); head injury (<)- <>).Sources: a) Ruttimann et al,� dopamine; b) Muller et al,’ dopamine;c, d) Richard et al,� dopamine, dobutamine; e, f, g) Jardin et al,2
dopamine; h) Jardin et al,� dobutamine; i) Mackenzie et al,’#{176}epi-
nephrine; j) Edwards et al,8 norepinephrine± dopamine± dobuta-mine; k, m) Shoemaker et al,� dopamine, dobutamine; 1) Shoemakeret al,6 dobutainine; n) Mathru et al,� dobutamine; o) Jardin et al,’dobutamine; p) Bobertson et al,’#{176}propranolol.
Effects of Catecholamines on 02 Delivery
1680 Catecholamines and 0, Consumption In Critically III Patients (chiolero eta!)
Tissue 02 delivery is dependent upon changes in car-
diac and respiratory function, and blood hemoglobin
concentration. It is calculated using the simple math-
ematical formulas: Do2 = Ca02 x QT x 10(ml#{149}min ‘) =
(Hb x Sa02 X 1 .39) + (0.003 x Pa02), where Ca02 is ar-
terial 02 content (ml#{149}100ml ‘), QT= cardiac output
(L’min - ‘), Sa02 = arterial 02 saturation (%),Hb =
hemoglobin concentration (g’lOO m1 ‘ and Pa02 =
arterial 02 partial pressure (mm Hg). Catecholamines
affect Do2 via their effects on cardiac and respiratory
functions. These are mediated via the stimulation of
the adrenergic receptors. Beta-adrenergic stimulation
causes increase in heart rate, myocardial contractility,
stroke volume, cardiac output and Do2, both in normal
subjects and in most clinical conditions. 110.29 However,
the positive action on cardiac output may be slightly
counterbalanced by the increase in intrapulmonary
shunt and the resulting decrease in Ca02, produced
by beta-adrenergic stimulation.� Moreover, moderate
increases in calculated intrapulmonary shunt fraction
have been observed following dopamine and dobuta-
mine infusion in critically ill patients,2’3’9 although
other studies have failed to find any change.4’5’6”#{176}
Effects ofCatecholamines on Oxygen Cor�umption
as Related to Oxygen Delivery
The well known relationship between oxygen de-
livery (Doe), oxygen extraction ratio (ERo2) (the per-
centage of delivered 02 extracted by the tissues) and
Vo2 in the resting subject� is shown in Figure 3.
The exact formula is as follows: �
DO,, X ERo2 = Ca02 X Q’r x ERo2. The normal values
for Do2 are in the range 500-600 ml’min ‘#{149}m2 � At
normal or high levels of Do2, Vo2 is independent of
02 delivered to tissue. When Do2 decreases, due to
failing cardiac or respiratory function or to decreased
hemoglobin concentration, there is an increase in 02
extraction which allows normal Vo2 values to be
maintained. Below a critical level, the increase in 02
extraction cannot fully compensate for the reduction
in Do2. Hence, Vo2 decreases in porportion to
Do2 below the critical Do2 threshold value, a phenom-
enon which is riot observed in normal conditions.�
The critical level at which �O2 becomes independ-
ent of Do2 varies according to species, specific organs,
and physiologic conditions. There are as yet no clear
data on the Do,/Vo2 relationship in normal human
subjects. In anesthetized dogs, the critical Do2 value
is around 10 ml#{149}kg ‘min ‘ during anemia and hypoxic
hypoxia.’� In the anesthetized man during the preby-
pass period for coronary artery surgery, the critical
Do2 value was found to be 330 ml#{149}min “-in 2 or 8.2
ml#{149}kg‘.min ‘ �‘*(� In acutely ill patients, the critical
Do2 value varies widely, according to the specific
disease, and the Do�o2 patterns are often more
0
Oxygen delivery
FIGun� 3. Oxygen consumption versus 0, delivery (-) or 02extraction ( ) in normal subjects, as well as in patients with
abnormal #{176}�extraction (-).
complex than the simple linear relationship observed
in animal studies. Furthermore, the ability of tissues
to extract oxygen may be impaired in certain acute
illnesses, such as ARDS, severe septic states, and
hypovolemic shock.�’47 In such conditions, a patho-
logic dependency on oxygen supply has been de-
scribed where, due to the inefficient tissue 02 extrac-tion, the critical Do2 value is substantially increased
(Fig 3). Critical Do2 value as high as 21 ml#{149}kg’.min’
has been found in patients with ARDS� or with severe
septic states.8’49
Numerous studies have evaluated the effects of
catecholamines on Do2 and V02. The results of some
recent studies in critically ill and normal subjects are
illustrated in Figure 4 and Table 2. The patients
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from

Table 2-Ejfrcts ofCatecholamines and Beta-Blocking Agents on 0, Consumption (Vo’) and O� Delivery (Doe)in Critically Ill Patients and in Normal Humans
VO, (mI.mini��m2) 1)02 (mhnin - ‘#{149}m�-2)
Baseline Baselinetreatment treatment
Authors Clinical Characteristics Catecholamines i� % P % P
Muller et al’ Cardiogenic shock DOPA 112 125 + 12 <0.001 287t 385t +34 <0.001
Jardin et al� Septic shock hyperdynamicSeptic shock hypodynamicSeptic shock, hypovolemic hypodynamic
DOPADOPADOPA
172 179 +4128 141 + 10122 149 + 22
NS<0.01<0.01
524 686
255 435298 536
+31+ 71
+80
<0.05
<0.01
<0.01
Jardin et al� Septic shock DOBU 132 140 +6 NS 497t 675t +36 <0.001
Richard et al� Cardiogenic shockCardiogenic shock
DOPA
DOBU
86 110 +2892 96 +4
<0.05
NS
315t 455t
333t 420t
+44
+26
<0.05
<0.05
Jardin et al’ Pulmonary embolism + shock DOBU 130 155 + 19 <0.05 228 430 + 89 <0.01
Shoemaker et al6 Critically ill surgical patients DOBU 131 157 + 20 <0.01 521 646 + 24 <0.01
Shoemaker et al� Postoperative surgical patient
Ikstoperative surgical patientDOPA
DOBU136 143 +5139 161 + 16
NS<0.05
518 630493 690
+ 22
+ 40
NS
<0.05
Edwards et al8 Septic shock NE ± DOBU ± DOPA 130 169 +30 <0.05 605 843 + 39 <0.05
Mackenzieetal’#{176} Septic shock EPI 116 133 + 15 NS 382 596 +56 <0.01ROttimann et al� Normal subjects DOPA 136 155 + 14 <0.01 790 986 + 25 <0.01
Robertson et al� Head injury PROPRA 201 164 -32 <0.05 942 697 -26 <0.05
Welle et a118 Normal subjects PROPRA 254 256 0 NS - - - -
DOPA=dopamine; DOBU =dobutamine; EPI =epinephrine; PROPRA=propranolol.
tCalculated assuming a value of 17.5 ml/100 ml for CaO,.
CHEST I 100 I 6 I DECEMBER, 1991 1681
received catecholamine therapy in the management
of cardiogenic shock,”4 septic shock,238�0 pulmonary
embolism with shock,5 penoperative or posttraumatic
circulatory failure.6’9’� The DoJ�o2 responses to
dopamine, dobutamine, epinephrine, and to norepi-
nephrine combined with dopamine ± dobutamine are
shown. In addition, the responses to dopamine in
normal subjects� and to beta-blockade in hyperdy-
namic patients with severe head injury2#{176}have also
been reported.
Keeping in mind the large individual variations, it
is clear from Figure 4 that catecholamines produced
increases in both Do2 and V02 in most ofthese studies,
whatever the baseline level of Do2 (low, normal or
high).
As expected, increases in both Do2 and �#{176}2 were
produced by catecholamines in patients with low
cardiac output syndromes”4 (Oo2<500 ml#{149}min ‘m 2).
In septic shock�’3’8”#{176} a critical condition associated
with an abnormal ability to extract 02, similar
responses were noticed in patients with normal or
elevated Do2 (Do2>500 ml.min1m2). Thus, in all
these conditions, Do2 was below the critical level, and
Vo2 was directly dependent on Do2 and thereby
enhanced by catecholamine administration.
In critically ill surgical patients,6’9’� simultaneous
changes in both Do2 and V02 were also observed in
patients with normal or elevated Do2. Many of these
patients were treated for acute illnesses associated
with a pathologic dependency of ‘�O2 on Do2, thus
explaining this relationship between these parameters.
Moreover, independent changes of V02 and Do2 did
probably also occur in others with unimpaired 02
extraction ability.
Thermogenic Effect of Catecholamines
In normal subjects and in patients with 1302 over
the critical value, the ��1O2 response to catecholamines
is not related to their effect on systemic hemodynam-
ics. In such conditions, catecholamines exert simulta-
neous and independent influences on cardiac function
and tissue metabolism. The main effect on �O2 is
caused by the thermogenic action, while the Do2
changes are produced by the stimulation of cardiac
function. This results in the disappearance of the
plateau in the Do�JVo2 response curve, as shown in
Figure 4. The simultaneous change in both V02 and
Do2 following catecholamine administration in sub-
jects with normal cardiac function is therefore not
related to a state of dependency of �‘O2 and Do2,
although this point still needs to be established clearly.
As yet, there are no data in patients with low cardiac
output states distinguishing the effects of adrenergic
agents on Vo2 due to a direct increase in the metabolic
rate from those related to Do2 enhancement. In
traumatized and in many acutely ill patients withnormal cardiovascular function, it has long been
demonstrated that sympathetic nervous system hyper-
activity plays a key role in the elevation of resting ‘�02
which is typically observed.’9’�#{176}’21’�’49 Such hypermet-
abolic patients are characterized by large increases in
plasma levels and urinary excretion of epinephrine
and norepinephrine.’� Their resting �O2 has been
found to be increased up to a maximum of200 percent
of normal resting �9 The magnitude of the
response varies according to the type of injury and its
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from

1682 Catecholamines and 02 Consumption in Critically III Patients (Oliloleto eta!)
‘9
Another way of evaluating catecholamine-induced
thermogenesis is by administrating beta-blockers. Pro-
pranolol produced a mean reduction of V02 of 12
percent in the burned patients studied by Breitenstein
et al� and a statistically nonsignificant decrease in
Vo2 in the severely burned patients reported by Wolfe
et � In the study by Wilmore et al,’� propranolol
combined with phentolamine decreased mean resting
Vo2 by 18 percent in burned patients. Robertson et
alm have evaluated the effects of beta-blockade on
systemic hemodynamics and ‘c�o2 in patients with
severe head injury. They observed a hyperdynamic
cardiovascular state characterized by tachycardia, in-
creased cardiac index and systemic vascular resis-
tances; the Do2 (725 ml’min “in 2) and ‘��o2 (173
ml”min - ‘#{149}m2) were also markedly enhanced . Pro-
pranolol produced a decrease in both Do2 (-27
percent) and Vo2 ( - 18 percent) with no apparent
detrimental effect on tissue oxygenation, as shown by
the stability of the 02 extraction ratio and the mixed
venous Po2 (Fig 4). These results demonstrate clearly
that catecholamines and sympatho-adrenergic hyper-
activity contribute to the thermogenic phenomena
which are present in the hypermetabolic critically ill
patients.
Clinical Relevance
It has been repeatedly shown that decreased body
Vo2 is associated with increased mortality among
critically ill patients under various conditions, par-
ticularly in those with low cardiac output syn-
dromes.m,m,ss Moreover, Do2 and �O2 have been shown
to be better predictors of survival than the usual
hemodynamic parameters.� Bland et ale’ have re-
cently assessed tissue 02 debt (calculated as the
measured minus the estimated Vo2) during the peri-
operative period in 100 high-risk surgical operations.
They observed a strong influence of Vo2 deficit on
survival. Nonsurvivors had a signfficantly higher mean
maximum cumulative �02 deficit (33.5 ± 36.9 (SD)
Lrn2) as compared to survivors (8.0± 10.9 L#{149}m2).
Other studies have produced evidence that supra-
physiologic increases in Do2 and in �TO2 are associated
with improved survival in some categories of pa-
flents.�
Catecholamines are widely used in the critically ill
to improve the failing systemic hemodynamics and
thereby enhance Do2. They are the mainstay of
treatment after volume resuscitation is achieved. In
patients responding to this therapy, numerous studies
have provided convincing evidence of the positive
effects of catecholamines on both 1302 and VO21’0�
particularly in the presence of increased lactate blood
levels which reflect tissue hypoxia.57 However, it is
interesting to note that in these studies catecholamines
were given primarily to correct the failing systemic
hemodynamics, while their impact on thermogenesis
was ignored. This aspect may be important in patients
with critically low cardiac output states unresponsive
to catecholamine therapy, where the catecholamine-
induced increase in energy dissipation may further
reduce an already insufficient tissue oxygenation,
although no clinical data are presently available on
this point. In these conditions, the management of the
failing cardiovascular system should rely on other
therapeutic means.
Optimal levels of Do2 and �O2 in various diseases
commonly encountered in critically patients have not
yet been specffically established and our knowledge
still remains largely empirical. Further studies are
necessary to determine the clinical importance of the
thermogenic effect of catecholamines when these
agents are used in the management of patients with
low flow states.
CONCLUSION
Catecholamines influence resting body ‘�O2 and
metabolic rate via several direct and indirect mecha-
nisms of action. In normal subjects, their main effect
on energy metabolism is related to the stimulation of
tissue 02 consumption and heat production, a complex
thermogenic phenomenon due to direct beta-adrener-
gic stimulation. In the critically ill, catecholamines
may also influence body Vo2 secondary to their effects
on systemic hemodynamics. In patients with low
cardiac output syndromes or with acute diseases
characterized by an abnormal tissue 02 extraction
capacity, 02 consumption is directly dependent and
limited by 02 delivery; catecholamines may increase
body Vo2 via their favorable effect on both cardiac
output and 02 delivery. Finally, ifthey do not improve
cardiac output and systemic 02 delivery, they may
unfavorably alter the balance between tissue 02 deliv-
ery and consumption by their calorigenic action and
thereby further reduce an already insufficient tissue
oxygenation.
ACKNOWLEDGMENTS: The authors wish to thank Dr. M.Dusmet for his helpful comments and Mrs M. Hemsch andN. Artingstall for their technical assistance.
REFERENCES
1 Mueller HS, Evans R, Ayres SM. Effect of dopamine onhemodynamics and myocardial metabolism in shock following
acute myocardial infarction in man. Circulation 1978; 57:361-65
2 Jardin F, Gurdjian F, Desfonds P. Margairaz A. Effect ofdopamine on intrapulmonary shunt fraction and oxygen trans-
port in severe sepsis with circulatory and respiratory failure.
Crit Care Med 1979; 7:273-77
3 Jardin F, Sportiche M, Bazin M, Bourokba A, Margairaz A.Dobutamine: a hemodynaimc evaluation in human septic shock.Crit Care Med 1981; 9:329-32
4 Richard C, Ricome JL, Rimailho A, Bottineau G, Auzepy P
Combined hemodynamic effects of dopamine and dobutamine
in cardiogenic shock. Circulation 1983; 67:620-26
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from

CHEST I 100 1 6 I DECEMBER, 1991 1683
5 Jardin F, Genevray B, Brun-Ney D, Margairaz A. Dobutamine:
a hemodynamic evaluation in pulmonary embolism shock. CritCare Med 1985; 13:1009-12
6 Shoemaker WC, Appel PL, Kram HB. Hemodynamic and
oxygen transport effects of dobutamine in cr!Hl#{224}llylll g#{233}h#{233}ral
s�cal patients. Crit Care Med 1986; 14:1032-37
7 Meadows D, Edwards JD, Wilkins RG, Nightingale P Reversal
of intractable septic shock with norepinephrine therapy. CritCare Med 1988; 16;663-66
8 Edwards JD, Brown GCS, Nightingale F, Slater RM, FaragherEB. Use of survivors’ cardiorespiratory values as therapeutic
goals in septic shock. Crit Care Med 1989; 17:1098-11039 Shoemaker WC, Appel PL, Kram HB, Duarte D, Harrier HD,
Ocampo HA. Comparison of hemodynamic and oxygen trans-port effects ofdopamine and dobutamine in critically ill surgical
patients. Chest 1989; 96:120-2610 Mackenzie SJ, Kapadia F, Nimmo GR, Armstrong IR, Grant IS.
Epinephrine as a first line agent in human septic shock: effect
on haemodynamics and oxygen transport. Intensive Care Med1990; 16:Suppl 1:520
11 Young JB, Landsberg L. Catecholamines and intermediarymetabolism. J Clin Endocrinol Metab 1977; 6:599-631
12 Young JB, Landsberg L. Catecholamines and the regulation of
hormone secretion. J Clin Endocrinol Metab 1977; 6:657-95
13 Landsberger L, Young JB. Autonomic regulation of thermogen-
esis. In: Girardier L, Stock MJ, eds. Mamalian thermogenesis.
London: Chapman, 1983; 99-140
14 Bursztein 5, Elwyn DH, Askanazi J, Kinney JM. Theoreticalframework of indirect calorimetry and energy balance. In:Bursztein 5, Elwyn DH, Askanazi J, Kinney JM, eds. Energymetabolism, indirect calorimetry and nutrition. Baltimore:
Williams and Wilkins, 1989; 27-84
15 J#{233}quierE, Acheson K, Schutz Y. Assessment of energy expen-
diture and fuel utilization in man. Ann Rev Nutr 1987; 7:187-
208
16 J#{233}quierB, Flail JP Recent advances in human energetics. NIPS
1986; 1:112-1417 GrandeF. Energy expenditure ofvarious organs and tissues. In:
Kinney JM, ad. Assessment ofenergy metabolism in health and
disease. Columbus, Ohio: Ross Laboratories, 1980; 89-92
18 �lle 5, Campbell RG. Stimulation of thermogenesis by car-bohydrate feeding. Evidence against sympathetic nervous sys-
tem mediation. J Cliii Invest 1983; 71:916-2519 Wilmore DW, Long JM, Mason AD, Skreen 11W, Pruitt BA.
Catecholamines: mediator of the hypermetabolic response to
thermal injury. Ann Surg 1974; 180:653-68
20 Robertson CS, Clifton GL, Taylor AA, Grossman RG. Treatmentofhypertension associated with head injury. J Neurosurg 1983;59:445-60
21 Chiol#{233}ro R, Schutz Y, Lemarchand Tb, Felber JP, De TriboletN, Freeman J et al. Hormonal and metabolic changes followingsevere head injury or noncranial injury. J Parenter Ent Nutr
1989; 13:5-12
22 Breitenstein E, Chiol#{233}roBL, J#{233}quierE, Dayer P. Krupp 5,Schutz Y. Effects ofbeta-blockade on energy metabolism follow-
ing burns. Burns 1990; 16:259-6423 Clifton CL, Ziegler MG,Grossman RG. Circulating catechola-
mines and sympathetic activity after head injury. Neumsurgery1981; 8:10-4
24 Bessey PQ, Watters JM, Aoki TF, Wilmore DW. Combined
hormonal infusion simulates the metabolic response to injury.
Ann Surg 1984; 200:264-80
25 Boothby WM, Sandiford I. The calorigenic action of adrenalin
chlorid. Am J Physiol 1923; 66:93-12226 Steinberg D, Nestel PJ, Buskirk ER, Thompson RH. Calorigenic
effect of norepinephrine correlated with plasma free fatty acidturnover and oxidation. J Clin Invest 1964; 43:167-76
27 Svedmyr N. The action of truodothyronine on some effects ofadrenaline and noradreanaline in man. Acta Pharmacol Toxicol
1966; 24:203-16
28 Sj#{246}str#{246}mL, Schutz Y, Gudinchet F, Hegnell L, Pittet PG.J#{233}quierE. Epinephrine sensitivity with respect to metabolicrate and other variables in women. AmJ Physiol 1983; 245:E431-E42
29 R#{252}ttimannY, Chiol#{233}ro R, J#{233}quier B, Breitenstein E, Schutz Y.Effects of dopamine on total oxygen consumption and oxygendelivery in healthy men. Am J Physiol 1989; 257:E541-E46
30 Shetty PS, Kurpad AV. Bole of the sympathetic nervous systemin adaptation to seasonal energy deficiency. Eur J Clin Nutr
1990; 44(Suppl 1): 47-5331 Himms-Hagen J. Thermogenesis in bmwn adipose tissue as an
energy buffer. N EngI J Med 1984; 311:1549-5832 Vasu MA, O’Keefe DD, Kapellakis GZ, Vezeridis MP, Jacobs
ML, Daggett WM, Fbwell WJ. Myocardial oxygen consumption:effects ofepinephrine, isopmterenol, dopamine, norepinephrine
and dobutamine. Am J Physiol 1978; 235:H237-H41
33 Schumacker PT, Cain SM. The concept of a critical oxygendelivery. Intensive Care Med 1987; 13:223-29
34 Kitamura K, Jorgensen CR, Cobol FL, Taylor HL, Wang Y.Hemodynamic correlates of myocardial oxygen consumptionduring upright exercise. J Appi Physiol 1972; 32:516-22
35 Campbell EJM, Westlake BK, Cherniack RM. The oxygenconsumption and efficiency of the respiratory muscles of ycongmale subjects. Clin Sci 1959; 18:55-65
36 Nicholls D, Locke R. Cellular mechanisms of heat dissipation.
In: Girardier L, Stock MJ, eds. Mammalian Thermogenesis.
London: Chapman and Hall, 1983; 8-49
37 Wolfe RR, Herndon DN, Jahoor F, Miyoshi H, Wolfe M. Effectof severe burn injury on substrate cycling by glucose and fattyacids. N Engl J Med 1987; 317:403-08
38 Mathru M, Dires DJ, Kanuri D, Blakeman B, Bao T Effect ofcardiac output on gas exchange in one-lung atelectasis. Chest1990; 97:1121-24
39 Cain SM, Chapler CK. 02 extraction by canine hindlimb duringa-adrenergic blockade and hypoxic hypoxia. J Appl Physiol1980; 48:630-35
40 Damask MC, Schwarz Y, Weissman C. Energy measurementsand requirements of critically ill patients. Crit Care Chin 1987;
3:71-96
41 Thys DM. Cardiac output. Anesthesiol Clinics of N Am 1988;
6:803-24
42 ArchieJP Mathematic couplingofdata. Ann Surg 1981; 193:296-
303
43 Porcelli RJ, Viau AT, Naftchi NE, Bergofsky EH. a-receptor
influence on lung vasoconstrictor responses to hypoxia and
humoral agents. J Appl Physiol 1977; 43:612-16
44 Cain SM. Assessment of tissue oxygenation. Crit Care Clinics
1986; 2:537-50
45 Cain SM. Oxygen delivery and uptake in dogs during anemicand hypoxic hypoxia. J Appl Physiol 1977; 42:228-34
46 Shibutani K, Komatsu T, Kubal K, Sanchala V. Kumar V. Bizzarri
DV. Critical level of oxygen delivery in anesthetized man. CritCare Med 1983; 11:640-43
47 Shoemaker WC, Appel PL, Kram HB. Measurement of tissue
perfusion by oxygen transport patterns in experimental shock
and in high-risk surgical patients. Intensive Care Med 1990;16:S135-S44
48 Schumacker P’I Samsel RW. Oxygen delivery and uptake byperipheral tissues: physiology and pathophysiology. Crit CareClin 1989; 5:255-70
49 MohsenifarZ, Goldbach P. Tashkin DP, Campisi DJ. Relationshipbteween 02 delivery and 02 consumption in the adult respiratorydistress syndrome. Chest 1983; 84:267-71
50 Wilson RF, Christensen C, LeBlanc LB Oxygen consumption
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from

1684 Catecholamlnes and 0, ConsumptIon � CrItically INPa�ei*s (ch�u .tal)
in critically-ill surgical patients. Ann Surg 1972; 176:801-04
51 Bland RD. Shoemaker WC. Common physiologic patterns ingeneral surgical patients: hemodynamic and oxygen transportchanges during and after operation in patients with and withoutassociated medical problems. Surg Clin North Am 1985; 65:793-
09
52 Shoemaker WC, Appal PL, Kram HB. T,ssue oxygen debt as a
determinant oflethal and nonlethal postoperative organ failure.Crit Care Med 1988; 16:1117-20
53 Shoemaker WC, Appal PL, Waxman K, Schwartz S, Chang PCliniCal trial of survivors’ cardiorespiratory patterns as thera-peutic goals in critically ill postoperative patients. Crit CareMed 1982; 10:398-03
54 Shoemaker WC, Appal PL, Kram HB, Waxman K, Lee TS.
Prospective trial ofsupranormal values ofsurvlvors as therapeu-
tic goals in high-risk surgical patients. Chest 1988; 94:1176-86
55 Edwards JD. Optimal levels oxygen transport in critically ill
patients. In: Vincent JL, ad. Update in Intensive Care and
Emergency Medicine. Berlin GER: Springer Verlag 989; 205-
1456 ShoemakerWC, Kram HB, AppelPL, FlemingAW. The efficacy
of central venous and pulmonary artery catheters and therapy
based upon them in reducing mortality and morbidity. ArchSurg 1990; 125:1332-38
57 VIncent JL, Roman A, De Backer D, Kahn RJ. Oxygen uptake/
supply dependency. Am Rev Bespir Dis 1990; 142:2-7
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from

DOI 10.1378/chest.100.6.1676 1991;100; 1676-1684Chest
R Chioléro, J P Flatt, J P Revelly and E Jéquiercritically ill patients.
Effects of catecholamines on oxygen consumption and oxygen delivery in
July 26, 2011This information is current as of
http://chestjournal.chestpubs.org/content/100/6/1676.citationUpdated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/100/6/1676.citation#related-urlsThis article has been cited by 1 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlonline at: Information about reproducing this article in parts (figures, tables) or in its entirety can be foundPermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the "Services" link to
Citation Alerts
slide format. See any online figure for directions. articles can be downloaded for teaching purposes in PowerPointCHESTFigures that appear in Images in PowerPoint format
© 1991 American College of Chest Physicians by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from
Copyright © 2022 FDOKUMEN




















