
Pharmacokinetic and electroencephalographic study of intravenous diazepam, midazolam, and placebo
Upload
khangminh22Category
view
1download
0
Comparative study of the effects of intravenous palonosetron versus
ondansetron and dexamethasone for prevention of postoperative
nausea and vomiting (PONV) after laparoscopic cholecystectomy: A
prospective randomized control study.
A dissertation submitted to The Tamil Nadu Dr. MGR Medical University
in part fulfillment of the degree MD ANAESTHESIA
By
Dr. Karen Lynn Lee
Christian Medical College and Hospital – Vellore
Tamil Nadu – 632004

2
CERTIFICATE
This is to certify that the dissertation titled “Comparative study of the effects of
intravenous palonosetron versus ondansetron and dexamethasone for prevention of
postoperative nausea and vomiting (PONV) after laparoscopic cholecystectomy: A
prospective randomized control study” is the bonafide work of Dr. Karen Lynn Lee
in partial fulfillment of the requirements for the M.D Anaesthesia (final)
examinations of The Tamil Nadu Dr. M.G.R medical university to be conducted in
April 2017.
Signature:
Dr. Anna B. Pulimood,
Principal,
Christian Medical College,
Vellore
Dr. Sajan Phillip George,
Head of Department,
Anaesthesia,
Christian Medical College,
Vellore
Dr. Raj Sahajanandan,
Guide,
Department of Anaesthesia,
Christian Medical College,
Vellore

3
DECLARATION
I hereby declare that this dissertation titled “Comparative study of the effects of
intravenous palonosetron versus ondansetron and dexamethasone for prevention of
postoperative nausea and vomiting (PONV) after laparoscopic cholecystectomy: A
prospective randomized control study” was prepared by me in partial fulfillment of the
regulations for the award of the degree of M.D Anaesthesia of The Tamil Nadu Dr. M.G.R
medical university, Chennai. This has not formed the basis for the award of any degree to
me before and I have not submitted this to any other university previously.
Vellore Dr. Karen Lynn Lee

4
ACKNOWLEDGEMENTS
I acknowledge God, for all guidance, mercies and support.
Dr. Raj Sahajanadan for all that he has taught me and for mentoring me.
Dr. Sajan Philip George for being supportive throughout the course.
I acknowledge all my teachers, for making this study and this course a reality.
I also thank my family for being a constant source of support and encouragement.
Finally and most importantly, I would like to express my gratitude to all the patients for
their participation.

5
TURNITIN REPORT

6
CONTENTS INTRODUCTION .................................................................................................................................... 7
AIMS AND OBJECTIVES ..................................................................................................................... 10
REVIEW OF LITERATURE ................................................................................................................. 13
DEFINITION ................................................................................................................................................... 14
CAUSES OF NAUSEA AND VOMITING ............................................................................................... 21
POSTOPERATIVE NAUSEA AND VOMITING .................................................................................. 25
MANAGEMENT OF POSTOPERATIVE NAUSEA AND VOMITING ..................................................... 32
METHODS .............................................................................................................................................. 51
RESULTS ................................................................................................................................................ 59
DISCUSSION .......................................................................................................................................... 81
LIMITATIONS ....................................................................................................................................... 85
CONCLUSION ........................................................................................................................................ 86
BIBLIOGRAPHY ................................................................................................................................... 88
ANNEXURES .......................................................................................................................................... 94
Annexure – 1 : Pro forma ............................................................................................................................ 94
Annexure – 2: Patient Information Sheet ............................................................................................. 96
Annexure – 3: Consent Form ..................................................................................................................... 98
Annexure – 4: Ethics committee approval ........................................................................................... 99
Annexure – 5: Data sheet ......................................................................................................................... 102

7
INTRODUCTION

8
INTRODUCTION
Following the inception of General anaesthesia in the first half of the nineteenth century
the phenomenon of postoperative nausea and vomiting (PONV) has challenged
postoperative care. John Snow in the 1840s recognized and pioneered the management of
this entity.(1)Despite the advances in surgical technique and anaesthetic technique the
incidence of PONV has remained high. The incidence of PONV has been higher for
certain procedures such as laparoscopic cholecystectomies and gynaecological
surgeries.(2) Unresolved PONV may result in prolonged post anesthesia care unit stay
and unanticipated hospital re-admission that result in a significant increase in overall
health care cost.(3) PONV is influenced by numerous factors, which may be patient
related, surgery related, and anesthesia related factors. Different antiemetics, a
combination of the same and even acupuncture has been in use to treat this distressing
problem. Guidelines have been published in order to better define and manage this
condition. The 2014 guidelines published by Gan et al. include risk scoring systems for
PONV; recommendations on new antiemetics; changes in recommendations from
previous guidelines based on new published information on efficacy and risk of
antiemetic drugs; recommendation on a new antiemetic combination strategy and a
multimodal prevention approach to prevent PONV and implementation of PONV
prevention and treatment strategies in the clinical setting.(4)

9
A wide variety of prophylactic antiemetic regimens have been used for the prevention of
PONV. Many of the traditional antiemetics produce undesirable side effects and have
limited efficacy. Therefore, the search for more ideal compounds has continued.
Ondansetron is considered as the “gold standard” of treatment when compared with the
other antiemetics. The combination of ondansetron with dexamethasone has been found
to be highly effective in the reduction of PONV.(5)(6) However, ondansetron has to be
administered thrice daily when used alone and the addition of dexamethasone may be
deleterious in diabetics as this may hamper optimum glycemic control. Palonosetron, a
newer 5-hydroxytryptamine 3 (5-HT3) receptor antagonist that has recently been
introduced and has a longer half-life and a better safety profile when compared to the
older generation of 5-HT3 receptor antagonists such as ondansetron.(7) There is limited
literature comparing the efficacy of palonosetron with ondansetron and dexamethasone,
especially when comparing laparoscopic operations.
Our study was designed to assess and compare the efficacy of two drug regimens,
palonosetron and ondansetron with dexamethasone in patients undergoing laparoscopic
cholecystectomy. A prospective randomized trial comparing the above-mentioned drugs
was therefore constructed. The primary outcome that was studied was to compare the
incidence of PONV between the two arms. Secondary objectives such as need for rescue
antiemetic, dosage time of administering the same and the complications if any were
studied.

10
AIMS AND OBJECTIVES
11
Aim of the study
To compare the efficacy of palonosetron vs. a combination of dexamethasone and
ondansetron in preventing postoperative nausea and vomiting in patients undergoing
laparoscopic cholecystectomy.

12
Primary objectives
To compare the efficacy of a single dose palonosetron vs. a combination of ondansetron and
dexamethasone for the prevention of postoperative nausea and vomiting after laparoscopic
cholecystectomy.
Secondary Objective
1. To study the requirement for rescue anti-emetic medications
2. To observe the side effects of the drugs administered, if any.

13
REVIEW OF LITERATURE

14
DEFINITION
Vomiting is defined as the expulsion of contents of the gastrointestinal tract through the
oral cavity. This forceful expulsion of gastrointestinal contents is the end product of
contraction of the upper gastrointestinal musculature and synchronous contraction of the
muscles of the thoracoabdominal wall. This must be differentiated from regurgitation,
which is generally used to define a condition where the passage of stomach contents into
the mouth is in a passive manner. The term retching can be described as the presence of
only the forceful muscular events present in vomiting without the actual expulsion of
gastric contents. Nausea is described as a painless unpleasant feeling that vomiting is
imminent(8)(9). This is a subjective sensation and the patient that feels nauseated may
not actually retch or vomit. Vomiting may actually ease the sensation of nausea. This is
differentiated from dyspepsia, which presents as epigastric burning pain, bloating or
discomfort. Nausea may be present along with dyspepsia however they are two distinct
events(10).
The vomiting reflex consists of two phases. The first phase is known as the pre-ejection
phase that is characterized by a feeling of nausea. This is associated with sweating,
salivation, pupillary dilation and tachycardia and the parasympathetic as well as
sympathetic nerves mediate it. The second phase is known as the ejection phase that is
comprised of the process of retching followed by expulsion of gastric contents(1).

15
The complex mechanisms present in nausea include the CNS, the endocrine system, the
autonomic nervous system, psychological states, and gastric dysrhythmias.
The medulla oblongata houses the vomiting center, which is comprised of the nucleus
tractus solitaries and the reticular formation. Activation of this center causes motor
efferents to descend to the upper gastro intestinal tract within cranial nerves V, VII, IX, X
and XII, to the lower gastro intestinal tract via the vagal and sympathetic nerves and to
the diaphragm and abdominal muscles via the spinal nerves.
Noxious stimuli arising from higher centers of the cortex and thalamus, viscera,
chemoreceptor trigger zone and vestibular system activate this pathway and result in
nausea and vomiting. The stimuli from the viscera and chemoreceptor trigger zone are
mediated by dopamine - serotonin and from the vestibular system are mediated by
histamine – acetylcholine. The current recommended pharmacological treatment for
vomiting and nausea is based on the ability of the drug to block these receptor sites(11).

16
DA2 – dopamine NK1 – Neurokinin, substance P mu/kappa – Opioids
Cortex Thalamus
[Anxiety, Pain]
Gastro Intestinal
Tract [5-HT3]
Vestibular [H1, M1]
VOMITING CENTER
[H1, M1, NK1, 5-HT3]
CHEMORECEPTOR TRIGGER ZONE
[DA2, NK1, mu, kappa]
H1 – histamine M1 – acetylcholine 5-HT3 – serotonin
Fig 1: Pathway of vomiting

17
The Central Nervous system
Although the neurocircuitry in the process of vomiting has been better illustrated, the
central mechanism that results in nausea is yet to be clearly explained(12). Autonomic
responses such as sweating or salivation may be seen during nausea or vomiting. These
are brought about by the medulla oblongata. The chemoreceptor trigger zone (CTRZ) is
found between the floor of the IV ventricle and the medulla oblongata. This receptor,
unlike other centers in the brain is not shielded by the blood-brain barrier. This implies
that due to lack of the surrounding glial cells, emetic irritants directly permeate the
endothelium of its capillaries irrespective of the size of the molecule or its lipid
solubility. They then relay information to the nucleus tractus solitarius. Afferent fibers
from the gastro intestinal tract are carried by the vagus nerve. They detect the gastric
contents as well as the gastric tone, which is also projected to the nucleus tractus
solitarius. From the nucleus tractus solitarius the neurons carry impulses to a central
pattern generator that coordinates the many actions that result in vomiting(13).
Several studies have suggested the involvement of the cerebral cortex in the pathway of
nausea(14)(15). Napadow et al in 2013 used the functional MRI to study healthy human
adults and inferred that regions of the brain that are involved in cognitive function and
emotions such as the medial part of the prefrontal cortex and the pre-genual anterior
cingulate cortex and are correlated with an increased heart rate during nausea(15). This
suggests the importance of emotional and cognitive centers in mediating the
parasympathetic to sympathetic shift seen in nausea.

18
The Autonomic Nervous system
The physiological changes seen before vomiting such as pallor, tachycardia, increased
blood pressure, cutaneous vasoconstriction, sweating and decreased gastrointestinal
motility are directed by the autonomic nervous system. Afferent signals arise from vagal
inputs that are a result of chemical or mechanical stimuli(16). Many studies now show
that an increased perception of nausea is seen with increased sympathetic and decreased
parasympathetic modulation(17)(18). This explains the presence of the symptoms
mentioned earlier. Therefore autonomic outflows as well as the CNS network that
controls it may in fact determine the overall intensity of nausea that is perceived.
Understanding these in detail could have therapeutic importance.
The Endocrine System
Research has been done on the role of various hormones in the pathogenesis of nausea
and vomiting. Many studies suggest that vasopressin plays a significant role is this.
During emetogenic situations it has been noted that vasopressin secretion is increased.
This shows clearly that rise in vasopressin levels occur before vomiting and not as a
response to hyperosmolarity or volume depletion that occurs after emesis(19). Although
various studies have shown that the severity of nausea and the levels of serum
vasopressin are related, the relationship of cause and effect is not clear yet(20)(21). Apart
from Vasopressin, Corticotropin releasing factor has been recognized as a brain – gut

19
mediator in the functioning of the foregut. It stimulates the inhibitory motor nerves that
are present in the dorsal motor nucleus of the vagal nerve and causes delayed gastric
emptying along with nausea(22).
Gastric dysrhythmias
The myoelectrical activity of the stomach can be measured by various techniques, as it is
a neuromuscular organ. A balance of the enteric nervous system, the autonomic nervous
system, the intrinsic activity of the stomach, smooth muscles and hormone levels result in
normal gastric myoelectrical activity(19). Many studies have demonstrated the
relationship between nausea and the onset of gastric dysrhythmias in pregnant women,
those with motion sickness and also in drug induced nausea(23). However it is unclear if
activation of sympathetics occurs before the onset of dysrhythmias or vice versa.
Interventions and medications that cause gastric myoelectric activity to normalize have
been shown to decrease nausea(18,23).

20
PATHOGENESIS OF NAUSEA – in summary
Cerebral cortex and limbic system – providing cognitive and emotional input
Cerebellar and Vestibular signals from motion induced nausea
Area prostema recognizes the presence of emetic agents in blood
Nucleus Tractus Solitarius receives afferent information from various parts of the body including the Vagus
Increase in Vasopressin level Autonomic nervous system response
Gastric Dysrhythmias
Nausea
Vagus mediated
CENTRAL
PERIPHERAL

21
CAUSES OF NAUSEA AND VOMITING MEDICATIONS AND TOXIC ETIOLOGIES(24)
Cancer chemotherapy Antibiotics/antivirals
Mild -fluorouracil, vinblastine, tamoxifen Erythromycin
Moderate - etoposide, methotrexate, cytarabine Tetracycline
Severe - cisplatinum, dacarbazine Sulfonamides
Analgesics Antituberculous drugs
Aspirin Acyclovir
Nonsteroidal antiinflammatory drugs Gastrointestinal medications
Antigout drugs Sulfasalazine
Cardiovascular medications Azathioprine
Digoxin CNS active drugs
Antihypertensives Narcotics
Antiarrhythmics Antiparkinsonian drugs
Calcium channel antagonists Anticonvulsants
Beta blockers Antiasthmatics
Diuretics Theophylline
Hormonal preparations/therapies Radiation therapy
Oral anti diabetics Ethanol abuse
Oral contraceptives Hypervitaminosis

22
INFECTIOUS CAUSES
Gastroenteritis Nongastrointestinal infections
Viral Otitis media
Bacterial
DISORDERS OF THE GUT AND PERITONEUM
Mechanical obstruction Organic gastrointestinal disorders
Gastric outlet obstruction Pancreatic adenocarcinoma
Small bowel obstruction Inflammatory intraperitoneal disease
Functional gastrointestinal disorders Peptic ulcer disease
Gastroparesis Cholecystitis
Chronic intestinal pseudo-obstruction Pancreatitis
Nonulcer dyspepsia Hepatitis
Irritable bowel syndrome Crohn disease
Mesenteric ischemia
Retroperitoneal fibrosis
Mucosal metastases

23
CNS CAUSES
Migraine Psychiatric disease
Increased intracranial pressure Psychogenic vomiting
Malignancy Anxiety disorders
Hemorrhage Depression
Infarction Pain
Abscess Anorexia nervosa
Meningitis Bulimia nervosa
Congenital malformation Labyrinthine disorders
Hydrocephalus Motion sickness
Pseudotumor cerebri Labyrinthitis
Seizure disorders Tumors
Demyelinating disorders Ménière disease
Emotional responses Cranial radiation

24
ENDOCRINOLOGIC AND METABOLIC CAUSES
Pregnancy
Other endocrine and metabolic
Uremia
Diabetic ketoacidosis
Hyperparathyroidism
Hypoparathyroidism
Hyperthyroidism
Addison's disease
Acute intermittent porphyria
MISCELLANEOUS CAUSES
Postoperative nausea and vomiting
Cyclic vomiting syndrome
Cardiac disease
Myocardial infarction
Heart failure
Radiofrequency ablation of the liver
Starvation

25
POSTOPERATIVE NAUSEA AND VOMITING
Nausea and vomiting are one of the most common complaints that follow surgery under
general anaesthesia. It has been described as “the big little problem” that complicates
postoperative recovery(25). 18 months after the introduction of chloroform to
anaesthesia, Sir John Snow in 1848 was the first to extensively describe the phenomenon
of PONV(1). Older inhalational anaesthetics such as chloroform and ether were used
before the 1960s; the incidence of postoperative vomiting at that time was as high as
60%(26). Advances in the field of anaesthesia with better techniques as well as the
development of newer anti-emetics and shorter acting anaesthetic drugs has decreased the
overall incidence of PONV in the first 24hours to around 30%(27)(28). However high
risk patients have an incidence of up to 80% following surgery(29). Therefore nausea and
vomiting that follows surgery is known to be multifactorial as it includes anaesthetic
factors, surgical factors as well as individual patient risk factors(30)(31).
Preoperative surveys often rate PONV as the outcome that patients would like to avoid
the most and are often willing to pay, up to even 100$ in order to avoid this unpleasant
complication(32). In Netherlands a survey done showed 22.7% of patients expressed fear
of postoperative nausea(33). Vomiting following surgery can result in dehydration and
electrolyte imbalance. Surgical wound dehiscence, esophageal tear, esophageal rupture,
aspiration of vomitus, and other complications that are associated with retching and
vomiting following surgery may be rare but can result in delay in discharge from the

26
postoperative care unit, cause an increase unanticipated hospital admission in out-patients
and also significantly increase overall costs of health care(3)(34).
There are numerous anti-emetic drugs that are available in the market today that have
been proven to be safe. However there is no drug that is available that does not have side
effects. These side effects can be mild, for example headache may occur with
ondansetron or can even be severe, for example QT prolongation that is also seen with
ondansetron. Therefore it is important to identify those individuals who are at risk of
developing nausea and vomiting after surgery and reduce it with appropriate anti-emetic
prophylaxis without the unnecessary risk of side effects of medications(29).
The etiology of postoperative nausea and vomiting is often multifactorial. These factors
can be classified under the following -
1. Patient factors
2. Intraoperative factors
a. Anaesthetic factors
b. Surgical factors
3. Postoperative factors

27
Patient Factors
Gender:
The female gender has been consistently noted as the strongest risk factor for developing
postoperative nausea and vomiting. Women in the reproductive age group are three time
more likely to suffer from PONV than men thereby suggesting the involvement of
hormones(28)(2).
Smoking Status:
Non-smokers have double the risk of developing PONV. Although the protective
mechanism is unknown, it has been suggested that cytochrome P450 enzyme is induced
by the polycyclic aromatic hydrocarbons found in cigarette smoke. This increases the
metabolism of the emetogenic anaesthetic agents(35).
History of PONV or motion sickness:
Patients who suffer from motion sickness, past history of nausea or vomiting following
surgery or both are 2-3 times more likely to develop PONV(36).
Age:
Although clinically not very significant, it has been found that in adults there is decrease
in the incidence of postoperative nausea and vomiting with increasing age of the patient.
However in children above the age of 3 it is noted that there is and increased risk of
vomiting in the postoperative period when compared to children under the age of 3.(29)

28
Delayed gastric emptying:
Those patients with diabetes mellitus, pregnancy, hypothyroidism, intra abdominal
pathologies such as pyloric stenosis, and increased intra cranial tension that have delay in
gastric emptying are also at the risk of developing PONV.
Obesity:
Although several studies have suggested that an increased BMI may predispose the
patient to develop nausea and vomiting after surgery, a systematic review done in 2001
showed no correlation.(37)
Anesthesia Factors
Inhalational agents:
The use of volatile anaesthetic agents during surgery has the highest risk of developing
PONV (38). Newer volatile agents such as halothane, sevoflurane and desflurane have a
lower incidence of nausea and vomiting in the postoperative period when compared to
the older agents such as ether and cyclopropane. Nitrous oxide when used has also been
known to cause PONV. A meta-analysis done in 2010, suggested that by avoiding nitrous
oxide, the overall risk of PONV is reduced, this has been noted especially in women(39).
However it is less of an effect than previously believed.

29
Opioid use:
The use of opioids in the intraoperative and the postoperative period also increases the
risk of developing postoperative nausea and vomiting, in a dose dependent manner.
Opioids reduce the muscle tone and the peristaltic activity, causing delayed gastric
emptying and inducing gastric distension. This triggers the vomiting reflex.
Duration of Anesthesia:
The duration of surgery and thereby anaesthesia can also predict the risk of developing
nausea and vomiting in the postoperative period. The duration of exposure to emetogenic
stimuli such as intraoperative opioids and volatile anaesthetics is also increased with
prolonged duration of surgery.
Neostigmine:
Due to insufficient evidence it is not possible to conclude whether the dose of
neostigmine causes an increase in the risk of nausea and vomiting following surgery.
Method of Anesthesia:
Some studies have suggested that an increased duration of facemask ventilation may
increase the risk of PONV. However the data available is conflicting.

30
Surgical factors Whether the type of surgery has an impact on the risk of developing of postoperative
nausea and vomiting still remains controversial. There are some studies that have shown
that ophthalmological, otological, cholecystectomies, gynaecological and thyroid
surgeries increase the risk of postoperative nausea and vomiting. (40)(41)(2). There is a
very high incidence of vomiting after intra abdominal surgeries like gall bladder and
intestinal surgeries, ear surgeries, head and neck surgeries, ovum retrieval procedures,
laminectomies, mitral valve replacements and kidney procedures. Intra abdominal
surgeries are more emetic than extra abdominal surgeries irrespective of the patient
gender. Stimulation of the mechanoreceptors and the release of 5hydroxy tryptamine
(5HT) from the enterochromaffin cells of intestine have been implicated. Laparoscopic
surgeries in particular have a higher incidence of postoperative nausea and vomiting. The
incidence of PONV following laparoscopic cholecystectomies varied from 50 to
70%.(42) In laparoscopic gynecology surgery up to 80% of patients developed nausea
and vomiting postoperatively.(43)Post operative nausea and vomiting is one of the main
complaints after laparoscopic surgeries including gall bladder surgeries and is the most
important factor determining the length of hospital stay after ambulatory anesthesia. The
etiology of nausea and vomiting after laparoscopic cholecystectomy is not fully
understood. Risk factors such as long periods of co2 insufflations, gall bladder surgery,
intraoperative use of isoflurane, fentanyl, glycopyrrolate, female sex, phase of menstrual
cycle, and postoperative use of PCA morphine may contribute to these episodes.

31
Postoperative Factors
Early intake of food, postoperative pain, early ambulation and dizziness are said to be
associated with increased incidence of nausea and vomiting.
Although various factors seem to determine the incidence of developing post operative
nausea and vomiting, the data available is sometimes conflicting or of no clinical
relevance. As per the consensus guidelines from 2014, the risk factors were classified
based on the level of evidence as well as the clinical implication. (4)
RISK FACTORS FOR PONV – IN ADULTS EVIDENCE RISKFACTORS
POSITIVE OVERALL
Female sex (B1) History of PONV or motion sickness (B1) Nonsmoking (B1) Younger age (B1) General versus regional anesthesia (A1) Use of volatile anesthetics and nitrous oxide (A1) Postoperative opioids (A1) Duration of anesthesia (B1) Type of surgery (cholecystectomy, laparoscopic, gynecological) (B1)
CONFLICTING
ASA physical status& BMI (B1) Menstrual cycle (B1) Level of anesthetist’s experience (B1) Muscle relaxant antagonists (A2)
DISPROVEN OR OF LIMITED RELEVANCE
Anxiety (B1) Nasogastric tube (A1) Supplemental oxygen (A1) Perioperative fasting (A2) Migraine (B1)

32
MANAGEMENT OF POSTOPERATIVE NAUSEA AND VOMITING The goal of prophylaxis is to decrease the incidence of nausea and vomiting that follows
surgery and thereby reduce the distress caused as well as the cost of health care. There
are several guidelines that have been published on the management of postoperative
nausea and vomiting. As per the most recent guidelines published in 2014, by Gan et al,
the first step in management is to identify the patient’s risk of developing PONV. As
discussed earlier, various risk factors are said to influence the incidence of developing
PONV. However not all play a significant role as the data available is sometimes
conflicting or of limited clinical relevance. In adults, the patient specific risk factors that
were identified include a younger age, the female sex, and a past history of PONV or
motion sickness and non-smoking status.
As seen with all drugs that are available, antiemetics also carry some risk of adverse
effects that may occur. Therefore it is important to objectively assess the individual’s risk
of developing postoperative nausea or vomiting and thereby decide on the need for
antiemetic prophylaxis. Therefore it is essential to objectively assess the baseline risk for
developing PONV by using a validated risk score. Although there are certain risk factors
for PONV that have strong evidence, no single predictor is used to clinically decide on
the need for antiemetic prophylaxis.(44) There are 2 risk scores that are commonly used
in adults, the Apfel score and Koivuranta score.(45)
The risk of developing nausea and vomiting postoperatively may be objectively assessed
using risk scores, however they are known to have a sensitivity and sensitivity between
65% and 70%. Also, it is important to make a decision for antiemetic prophylaxis based
33
on the implications of vomiting in certain clinical scenarios such as oesophageal or
gastric surgeries, increased intracranial pressures or in patients after facial surgeries with
wired jaws.
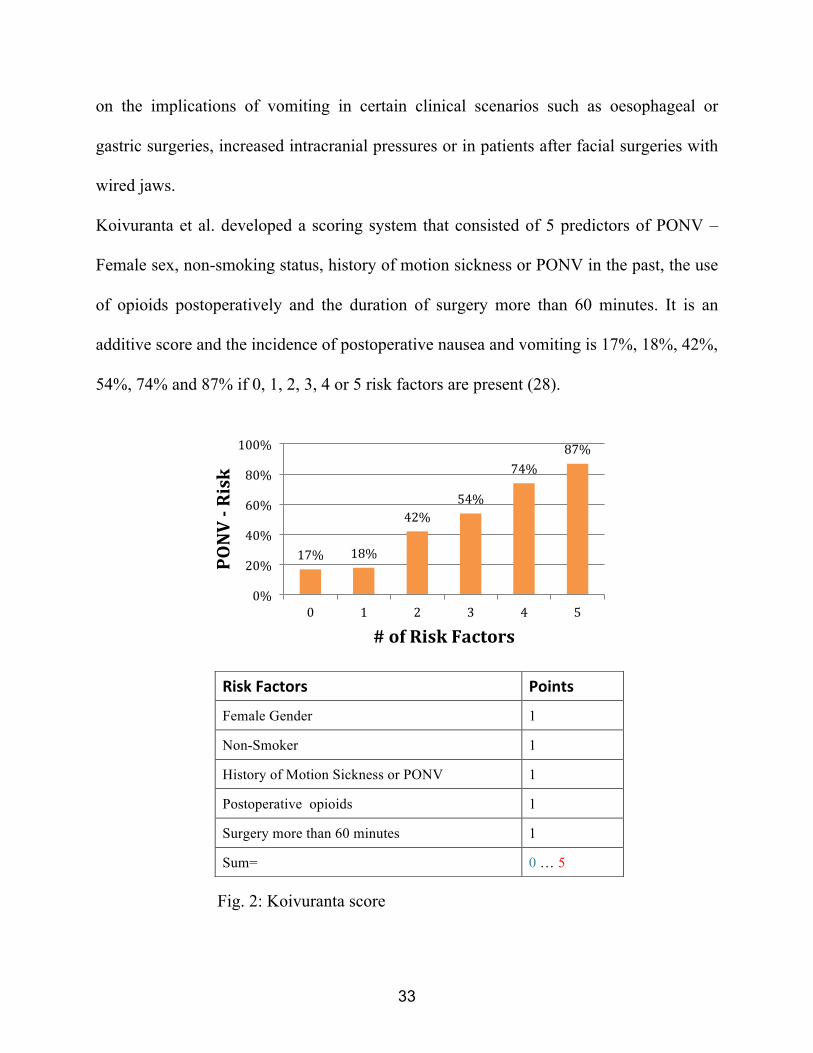
Koivuranta et al. developed a scoring system that consisted of 5 predictors of PONV –
Female sex, non-smoking status, history of motion sickness or PONV in the past, the use
of opioids postoperatively and the duration of surgery more than 60 minutes. It is an
additive score and the incidence of postoperative nausea and vomiting is 17%, 18%, 42%,
54%, 74% and 87% if 0, 1, 2, 3, 4 or 5 risk factors are present (28).
Fig. 2: Koivuranta score
Risk Factors Points
Female Gender 1
Non-Smoker 1
History of Motion Sickness or PONV 1
Postoperative opioids 1
Surgery more than 60 minutes 1
Sum= 0 … 5
17% 18%
42% 54%
74% 87%
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5
PONV -‐ Risk
# of Risk Factors

34
Subsequently Apfel et al developed a simplified scoring system that reduced the number
risk factors in the scoring system from five to four, based on the data from Koivuranta et
al. as well as their own previous data. As per the Apfel simplified score, 4 risk factors
were taken into consideration for the prediction of PONV. Nonsmoking status, the female
sex, history of motion sickness/ PONV and the use of postoperative opioids are included
in this score. The presence of 0, 1, 2, 3 or 4 risk factors implies that the risk of PONV is
10%, 20%, 40%, 60% or 80% respectively.
Fig. 3: Apfel Score

35
In children, postoperative vomiting (POV) can be predicted using a simple score
described by Eberhart et al., which identifies 4 risk factors of developing POV – age of
the child more than 3 years; duration of surgery more than 30 minutes; history of
vomiting after surgery in the patient, sibling or parent; and strabismus surgery. The risk
of postoperative vomiting was 9%, 10%, 30%, 55% and 70% with a risk score of 0, 1, 2,
3 or 4.
Fig. 4: Eberhart Score

36
As per the 2014 guidelines, patients were categorized as “low”, “medium” or “high” risk
based on their Apfel scores of 0 – 1, 2 – 3 and 4 respectively. Depending on which
category the patient belonged to, antiemetic prophylaxis as well as anaesthetic
management guidelines were suggested to prevent the occurrence of PONV.
It is also important to minimize the baseline risk factors for developing PONV. Strategies
that were suggested include the preference of regional anaesthesia over general
anaesthesia. The incidence of developing PONV after regional anaesthesia was almost 9
times less than after general anaesthesia. When it was necessary to give general
anaesthesia, induction and maintenance of anaesthesia with propofol decreased the
incidence of nausea and vomiting in the early postoperative period. According to the
IMPACT study, which evaluated 6 strategies to reduce postoperative nausea and
vomiting, it was found that total intravenous anaesthesia (TIVA) with propofol reduced
the risk of PONV by 25% (46). Reducing the dose of intraoperative as well as
postoperative opioids by using alternative methods of pain relief decrease the risk of
PONV as well as hyperalgesia (27)(47) . Another simple strategy suggested was adequate
hydration, which has also shown to decrease PONV (48).
There are 3 main classes of antiemetic drugs that are widely used in the prevention of
nausea and vomiting (49)(50). These are serotonin antagonists, corticosteroids and
dopamine antagonists, which have a similar efficacy and cause a 25% decrease in the
relative risk of developing PONV. They have different mechanisms of action, therefore
when use together they have an additive effect.

37
5-‐Hydroxytryptamine (5-‐HT3) Receptor Antagonists Radioligand binding studies have demonstrated a high density of 5HT3 receptors in areas
known to be involved in the emetic reflex, including vagal afferent terminals in gastric
mucosa, the brainstem dorsovagal nucleus, the nucleus tractus solitarius and the area
postrema. It is possible that anesthetic agents may stimulate neurons within the area
postrema and activate the vomiting reflex via 5 HT mediated pathway. Anesthetics can
disrupt mucosal enterochromaffin cells and induce the release of paracrine transmitters,
including 5HT, resulting in afferent vagal firing and this initiate the vomiting reflex.
Gastrointestinal distension caused by diffusion of nitrous oxide, laparotomy and
manipulation of gastro intestinal tract, can activate vagal afferents via mucosal 5HT
release.
5HT3 antagonists belong to the class of antiemetics that act by blocking the 5HT3
receptor. The pathway involved in emesis consists of several sites, at which the 5HT3
receptors are present, such as the vagal afferents, the nucleus tractus solitarius and also
the area postrema. These drugs prevent the binding of serotonin to the 5HT3 receptor and
thereby suppress nausea and vomiting. Based on their chemical structure they may be
classified further into 3 classes. (51)
• Carbazole derivatives:
• Indole derivatives
• Indazole derivative

38
Fig.5: Chemical structure of 5HT3 antagonists
Carbazole derivatives:
Ondansetron belongs to this class of 5HT3 receptor antagonist. It is one of the most
researched amongst its class of drugs and is often considered as the “gold standard” of
antiemetics. Ondansetron is a selective antagonist at the 5HT3 receptor and is the first
drug in the class of 5HT3 antagonist to be introduced for the clinical management of
vomiting associated with chemotherapy and radiotherapy. Ondansetron has been in
Name Structure
Ondansetron
Granisetron
Dolasetron
Ramosetron
Palonosetron

39
clinical development for the prevention and treatment of PONV since 1988. The initial
literature recommended dose is 0.1 to 0.15 mg/kg and effective blood levels are attained
30-60 minutes after administration. The elimination half-life of ondansetron is
approximately 3.5-4 hours in adults. Due to its relatively short half-life it may be relevant
to administer the drug intraoperatively towards the end of the surgical procedure,
especially those surgeries of more than 2 hours duration. Large multicenter studies have
demonstrated that intravenously administered ondansetron 4 mg is effective in preventing
and treating established PONV. This is confirmed in the 2014 consensus guidelines in the
management of PONV by Gan etal The recommended intravenous dose of ondansetron is
4mg, usually at the end of surgery(4).
Farhat etal compared 4 mg ondansetron with 10 mg metoclopramide for prevention of
PONV after laparoscopic cholecystectomy and found that prophylactic ondansetron was
more effective with fewer side effects. Hemley compared ondansetron with droperidol
and metoclopramide for laparoscopic cholecystectomy under propofol TIVA and found
that PONV in the ondansetron group was significantly less in the 1 -4 hours, but similar
in the rest of the 24 hours.
The adverse effects that are seen with the use of ondansetron include headache, diarrhea
or constipation, dry mouth, and even QT prolongation.
Indole derivatives:
Dolansetron has shown to effectively prevent PONV at a dose of 12.5mg given
intravenously(51). Due to concerns regarding QT interval prolongation and torsade de
pointes, in certain countries it is not available for use (52).

40
Indazole derivatives
Granisetron was found be as effective in the treatment of nausea and vomiting when
compared to the other first generation 5HT3 receptor blockers. The dose needed was 0.3
to 3mg given intravenously. When compared to 8mg of dexamethasone, a 3mg dose of
IV granisetron was found to be equally effective but when used as a combination it was
found to be better than using each drug alone.(53)
Ramosetron has a higher affinity for the 5HT3 receptors than the older drugs in this class.
The antiemetic property of this drug is present for more than 2 days. At a dose of 0.3mg
IV, it is effective in preventing nausea and vomiting in patients that are on patient
controlled analgesia (PCA) with fentanyl. It is available only in certain South East Asian
countries. (54)
Palonosetron is the newest of this class of drugs and it belongs to the second-generation
5HT3 receptor blockers. This drug has a significantly longer half-life of up to 40hours,
which is 4 – 5 times longer than that of ondansetron, granisetron or dolasetron. It is also
more potent and has and increased binding affinity to the 5HT3receptors. Palonosetron is
usually given at the beginning of surgery. The most effective dose for intravenous
palonosetron was found to be 0.075mg given intravenously (55). Palonosetron was also
found to have a better safety profile as studies have shown that it does not cause QT
prolongation (56)(57).

41
5HT3 receptor antagonists are usually well tolerated. Minor side effects of these
medications include mild headaches seen in 15 to 20% of patient population or
constipation that occurs in 5 – 10% of the population. Electrocardiogram interval
changes, QT prolongation is seen in the first – generation 5HT3 receptor antagonists.
Corticosteroids
In 1980 methyl prednisolone was first reported to be an effective antiemetic in
chemotherapy patients. Since 1981, dexamethasone has been reported to be more
effective than metoclopramide in controlling chemotherapy induced nausea and vomiting
and was preferred by the patients’ treated. The antiemetic effect of dexamethasone was
reported to be equal or better than the 5HT3 receptor antagonists such as ondansetron and
granisetron. Dexamethasone has also been reported to effective in reducing the incidence
of postoperative nausea and vomiting (PONV) in paediatric patients undergoing
strabismus repair, tonsillectomy, adenoidectomy, thyroidectomy, cholecystectomy, and
women undergoing major gynecological surgery.
The mechanism of action of dexamethasone is not well understood, but central
inhibition of prostaglandin synthesis, and decrease in 5HT turnover in the central nervous
system or changes in the permeability of blood CSF barrier to serum proteins may be
involved. Corticosteroids may reduce levels of 5HT, (5hydroxytryptophan) in neural
tissue by depleting its precursor tryptophan. Also, the anti-inflammatory properties of
corticosteroids may prevent the release of serotonin in the gut. It causes release of

42
endorphins; this results in mood elevation, a feeling of well-being and also an appetite. It
may potentiate the main effect of other antiemetics by sensitizing the pharmacological
receptor. Dexamethasone has a biological half life of 36-72 hours, so delayed emesis
following chemotherapy is better controlled with dexamethasone compared with classic
antiemetics. Dexamethasone, when administered immediately before the induction of
anesthesia, provided an effective decreases in nausea and vomiting throughout the first 24
hours of the postoperative period. On the contrary, when dexamethasone was given at the
end of anesthesia, it did not provide an effective antiemetic effect during the immediate
postoperative period of 0-2 hours. Since more than 50% of the patients experienced
nausea and vomiting in this early postoperative period it is very essential that a
prophylactic antiemetic should be effective during this period. It was suggested that the
onset time of dexamethasone’s antiemetic effect might be approximately two hours. It
was concluded that the prophylactic administration of dexamethasone immediately before
the induction of anesthesia was more effective than at the end of anesthesia for
preventing PONV. A wide range of dose of dexamethasone (8-32mg) has been used in
the prophylaxis of emesis related to chemotherapy and after pediatric and gynecological
surgery. Liu and his colleagues have suggested a dose of 0.15 mg/kg of dexamethasone
up to a maximum dose of 10mg for prevention of postoperative nausea and vomiting. The
minimum effective dose of dexamethasone for the prevention of PONV was suggested to
be 2.5mg in a recent study. Adverse effects related to a single dose of dexamethasone are
extremely rare. However single dose intravenous dexamethasone has been implicated in
the etiology of perineal irritation.

43
Dexamethasone when given as a prophylactic dose of 4mg intravenously is seen to
effectively decrease nausea and vomiting following surgery (58)(59)(60). It is
preferentially given after the induction of anaesthesia than at the end of surgery. A 4mg
dose of dexamethasone IV is considered to be as efficacious as a 4mg IV dose of
ondansetron or 1.25mg IV dose of droperidol.
Apart from addressing the problem of postoperative nausea and vomiting, dexamethasone
also has a dose dependent effect on the quality of recovery. De Oliveira et al. compared a
dose of 0.1mg/kg of dexamethasone with 0.05mg/kg and showed that with a higher dose
there was less opioid requirement, less nausea, sore throat and muscle pain and thereby
decreasing the time for discharge readiness(60).
The data available on the safety of using dexamethasone in the perioperative period is
inconclusive. They may have other detrimental or beneficial effects on patient recovery.
Therefore most of the available literature suggests the use of a single dose of
dexamethasone in the perioperative period as this does not seem to increase the risks of
wound infection(61)(60). An editorial published in 2013 has suggested that a single 4 to
8mg dose of dexamethasone was considered safe after considering the risks as well as the
benefits(62). Recent studies have shown an increase in the levels of blood glucoses after
an 8mg dose of dexamethasone. Therefore it is best avoided in labile diabetic patients.
Wang, Ho and Liu evaluated the antiemetic effect of dexamethasone 8 mg in prevention
of postoperative nausea and vomiting in 90 ASA l or ll patients, aged 30-55years, and
undergoing general anesthesia for elective laparoscopic cholecystectomy in a randomized

44
double blind study. They concluded that dexamethasone was effective in the prevention
of nausea and vomiting after laparoscopic cholecystectomy.(63)
Bianchin etal had similar results when he compared placebo vs 8 mg dexamethasone
for prevention of PONV after laparoscopic cholecystectomy.
Dopamine Antagonists
Drugs belonging to this class, which exhibit antiemetic properties act on the D2
receptors. They are often used as rescue antiemetics. They may be classified into three-
• Phenothyazines (e.g. Promethazine)
• Butyrophenones (e.g. Droperidol)
• Benzamides (e.g. Metoclopromide)
Other Antiemetics
Neurokinin – 1 (NK-1) receptor antagonist
Aprepitant was found to have a greater antiemetic effect when compared with
ondansetron. When used in combination with dexamethasone it was also found to be
more effective in decreasing postoperative vomiting than the combination of ondansetron
in a study done on patients undergoing craniotomy (64).
The current guidelines do not support the use of antiemetics in all patients that
undergo surgery. It is necessary to determine the risk of developing nausea and vomiting
postoperatively, based on which antiemetic prophylaxis is decided. An algorithm
suggested in the 2014 consensus guidelines for the management of postoperative nausea
and vomiting is as follows (4)–

45
Consensus Guidelines for the Management of PONV
January 2014 Volume 118 Number 1 www.anesthesia-analgesia.org 91
(5-HT3) receptor antagonists (ondansetron, dolasetron, granisetron, tropisetron, ramosetron, and palonosetron), neurokinin-1 (NK-1) receptor antagonists (aprepitant, casopitant, and rolapitant), corticosteroids (dexametha-sone and methylprednisolone), butyrophenones (droperi-dol and haloperidol), antihistamines (dimenhydrinate and meclizine), and anticholinergics (transdermal scopolamine [TDS]). While PONV prevention is recommended in a sub-set of patients, current evidence does not support giving
prophylactic antiemetics to all patients who undergo surgi-cal procedures. However, with more inexpensive generics becoming available, properly conducted cost-effectiveness (C/E) studies need to be done to support the more uni-versal use of prophylactic antiemetics. Ondansetron 4 mg, droperidol 1.25 mg, and dexamethasone 4 mg were equally effective, and each independently reduced PONV risk by approximately 25%.47 The recommended doses and timing of these drugs are listed in Table 3. Recommendations given
Adult Risk Factors Children Risk FactorsPatient Related Environmental Surgery > 30 minHistory of PONV/motion sickness Postop opioids Age > 3 yearsFemale gender Emetogenic surgery Strabismus surgeryNon-smoker (type and duration) History of POV/relative with PONV
Cost-effectiveness
Consider
LowWait and See
High>2 Interventions/
Multimodal Approach
Dexa-methasone
5-HT3 antagonist
NonPharmacological:
Acupuncture
ScopolaminePerphenazine Dimen-
hydrinate
Propofol subhypnotic dose infusion or
Propofol in PACU (rescue only)
NK-1 receptor antagonists
Droperidol†Haloperidol
Regional Anesthesia
Propofol Anesthesia
Portfolio ofprophylaxis
and treatmentstrategies
Treatment Options• If prophylaxis fails or was not received: use
antiemetic from different class than prophylactic drug
• Readminister only if >6 hours after PACU; • Do not readminister dexamethasone or
scopolamine
† Use droperidol in children only if other therapy has failed and patient is being admitted to hospital;Haloperidol for adults only
Patient preferencesFear of PONVFrequency of PONV causing headaches/migraine
Reducing baseline risksAvoidance/minimization of:Nitrous oxideVolatile anestheticsPost-op opioids
Medium
Pick 1 or 2 Interventions
Patient risk
Figure 4. Algorithm for management of postoperative nausea and vomiting. PONV = postoperative nausea and vomiting.

46
Ondansetron is generally considered as the gold standard in treating PONV (4). The
efficacy of ondansetron in reducing PONV was proven with different anaesthetic agents
as well (65). Since the early 1990s large randomized controlled studies and multi
centered studies have established the efficacy of 4mg of IV ondansetron in treating and
preventing PONV. Eight mg of ondansetron has also been proven to also reduce the
incidence of PONV in high-risk patients such as those with prior PONV history.
However a metaanalysis done by Tramer et al highlighted some of the limitations of
monotherapy for the management of PONV. Fifty-three trials studied proved the efficacy
of ondansetron in reducing PONV was 20% at best. Therefore although ondansetron was
the treating drug of choice newer drugs or combined therapy with other drugs needed to
be explored (66).
With this in mind, literature emerged about the use of combination therapy of
ondansetron and dexamethasone for PONV prophylaxis and treatment. Many studies
have shown the superiority of ondansetron plus dexamethasone.
Dexamethasone as monotherapy has been proven to be inferior to the combination of
ondansetron and dexamethasone. In a study published in 2008 by Bano et al, one hundred
patients undergoing laparoscopic cholecystectomy were randomly allocated either to
ondansetron alone or ondansetron plus dexamethasone. The authors concluded that
combination of ondansetron plus dexamethasone was better than dexamethasone alone in
preventing postoperative nausea and vomiting. A recent metaanalysis done in 2015
included 7 trials, it concluded that it was safe to use dexamethasone as an alternative to
ondansetron as prophylaxis for PONV as they were both found to be equally effective. .
47
Dexamethasone was found to have more effect than ondansetron in the late postoperative
period (63). Combination antiemetic therapy has been seen to have better results in the
prevention of PONV than using a single drug. Ondansetron has been compared with a
combination of ondansetron and dexamethasone. Song et al outlined the superiority of the
above-mentioned combination over ondansetron alone in a randomized control trial
involving one hundred and thirty patients who received patient controlled analgesia with
fentanyl. Four milligrams of ondansetron was administered to all patients undergoing
thoracoscopic surgery and 12 mg was administered as boluses through patient controlled
analgesic devices, the trial arm received 8 mg dexamethasone whereas the comparator
arm did not receive dexamethasone. The combination of ondansetron with
dexamethasone was reported to be better in preventing and treating PONV over a 48-hour
period (5). This was also confirmed by Ahsan et al in an RCT published in 2014. One
hundred patients that underwent laparoscopic cholecystectomy were randomly assigned
to receive ondansetron or ondansetron plus dexamethasone. The authors observed that
the combination of dexamethasone and ondansetron was superior to ondansetron alone
(6).Kumar et al compared a combination of ondansetron plus dexamethasone (4mg plus
8mg) vs either drug alone in the same dose and placebo in patients undergoing
laparoscopic cholecystectomy and found that the incidence was 85% in the placebo group
30% in dexamethasone group, 35% in ondansetron group and only 10% in the
combination group which was statistically significant.(67)
The current literature supporting the use of palonosetron is robust. Chun et al in a
randomized controlled trial involving over two hundred ASA I and II patients compared

48
the efficacy of palonosetron with a placebo undergoing various surgeries. This double-
blinded placebo controlled study divided patients into two arms, in one arm 0.075 mg of
palonosetron was given and in the second arm normal saline was used. At 72 hours post
operatively various parameters were assessed and the authors found PONV reduced
significantly in the arm where palonosetron was used, 33% versus 47% at 0-24 hours and
6% versus 11% at 24 -72 hours. The study also proved that severity and intensity of
nausea in the initial 24 hour period following the operation was reduced in the group that
palonosetron was administered, however this difference although clinically significant
did not show statistical significance (P value - 0.08) This has been corroborated by
various other RCTs. Kovac et al in a study published in 2008 demonstrated the efficacy
of palonosetron versus placebo in a randomized controlled trial involving over five
hundred patients undergoing either gynaecological or breast surgery. Patients were
randomly allocated to one of four groups – placebo vs. 0.025 mg of palonosetron vs.
0.050 mg palonosetron vs. 0.075 mg palonosetron. The primary end point analyzed was
the ability to prevent vomiting with various doses. They concluded that a dose of
0.075mg was required for prevention of PONV(55).
Various studies have compared the efficacy of palonosetron versus ondansetron. Park et
al in 2014 published a randomized controlled trial comparing the efficacy of 0.075 mg of
palonosetron and 8 mg of ondansetron in patients undergoing gynaecological surgery. A
total of ninety patients were randomly allotted to either of the two arms. The incidence
of PONV and the severity of nausea were assessed using a visual analogue score. The

49
study results confirmed that the incidence of PONV was significantly lower in the arm
where palonosetron was given (42.2 percent versus 66.7 percentage). The severity of
nausea as assessed by the visual analogue score was statistically equal between the two
arms. The study suggested that palonosetron was better than ondansetron in preventing
nausea and vomiting in the postoperative period (68).
The efficacy of a single dose palonosetron versus ondansetron was also studied by Kim et
al. This study from Korea, randomly allotted one hundred patients to receive
palonosetron as a single IV bolus of 0.075 mg versus ondansetron which was
administered as a bolus dose of 8 mg intravenously following which 16 mg was added to
the IV – PCA. The study revealed that a bolus of ondansetron followed by an infusion
was equal in efficacy to a single dose of palonosetron in the prevention of PONV after
laparoscopic gynaecological surgery (69). In a study done by Bhattacharjee et al,
palonosetron or granisetron was administered as PONV prophylaxis in patients
undergoing laparoscopic cholecystectomy. It was found that palonosetron was more
effective in the prevention of PONV in the 24 to 48 hour postoperative period rather than
the first 24 hours.(70)Laha etal compared palonosetron with ondansetron for prevention
of PONV after laparoscopic cholecystectomy and found that both drugs are comparable.
This result was against the pharmacokinetic (t1/2 and receptor affinity) and expected
pharmacodymamic effect of palonosetron. Researchers have compared palonosetron vs.
palonosetron plus dexamethasone in various surgical populations and found that a
combination of palonosetron plus dexamethasone is superior.(71) However the 2014

50
consensus guidelines do not suggest the combination of palonosetron and
dexamethasone, as both the drugs are long acting (24 hours) and it doesn’t offer any
additional advantage.
The use of dexamethasone alone as PONV prophylaxis was also studied in patients
undergoing laparoscopic cholecystectomies. Bianchin et al in 2007 published an RCT
done on 80 patients that received either 8mh of dexamethasone or normal saline as
placebo. The study showed that there was significant decrease in the incidence of PONV
in the dexamethasone group with no side effects noted. (72)
The literature comparing palonosetron versus a combination of ondansetron and
dexamethasone in laparoscopic surgery is sparse; therefore we have conducted a
randomized controlled trial comparing these two regimens.

51
METHODS

52
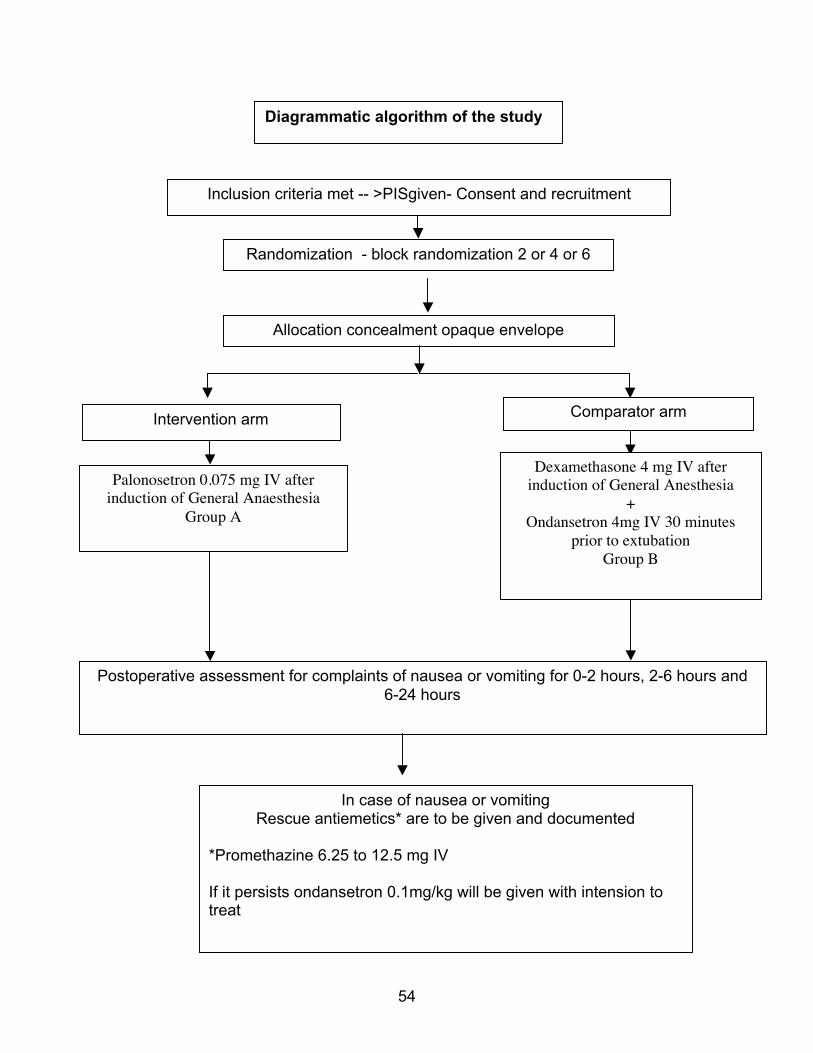
Design: A prospective blinded randomized controlled trial was designed.
There were two arms in the study:
The patients were randomly allotted to either the ‘palonosetron group’ or ‘ondansetron
plus dexamethasone group’.
Randomized groups -
Intervention: Palonosetron 0.075 mg IV
Comparator Agent: Dexamethasone 4 mg IV with Ondansetron 4mg IV
Inclusion and exclusion criteria
Inclusion Criteria:
-ASA grade I/II patients within the age group of 18 to 60 years scheduled to undergo
laparoscopic cholecystectomy, under general anaesthesia.
Exclusion Criteria:
-Pregnant and lactating patients
-Patient with hypersensitivity to palonosetron, dexamethasone or ondansetron
-Patients with history of motion sickness
-Patients on steroid therapy, antiemetics or on treatment with other medication known to
produce nausea and vomiting.

53
Recruitment:
All patients who consented for the study and fulfilled the inclusion criteria were recruited
by the principal investigator for the study.
Institutional review board clearance and ethics committee approval was obtained before
the start of the study.
Method of randomization:
The patients were be randomized to one of two groups by a computer generated random
assignment.
Method of allocation concealment:
Sequentially numbered, sealed, opaque envelopes opened in the operation theatre after
the patient is anaesthetized.
Blinding and masking:
A double blinded study was conducted. The participant and outcome assessors were
blinded to treatment allocation. The anesthetist after administering the drug documents as
either study drug A (palonosetron) or drug B (ondansetron plus dexamethasone). Even
though ondansetron can be repeated after 6 hours according to recommendations we did
not do it to keep the study blinded and as there is no role of giving ondansetron to
patients who have received palonosetron.
54
Allocation concealment opaque envelope
Intervention arm Comparator arm
Postoperative assessment for complaints of nausea or vomiting for 0-2 hours, 2-6 hours and 6-24 hours
Palonosetron 0.075 mg IV after induction of General Anaesthesia
Group A
Dexamethasone 4 mg IV after induction of General Anesthesia
+ Ondansetron 4mg IV 30 minutes
prior to extubation Group B
Inclusion criteria met -- >PISgiven- Consent and recruitment
Randomization - block randomization 2 or 4 or 6
In case of nausea or vomiting Rescue antiemetics* are to be given and documented
*Promethazine 6.25 to 12.5 mg IV If it persists ondansetron 0.1mg/kg will be given with intension to treat
Diagrammatic algorithm of the study

55
Sample size:
Sample size calculated was 77 patients in each arm of the study. With expected
difference in PONV % as 20% between the two arms, the minimum required samples
needed for this study is 77 in each arm. The sample size was calculated using the
following formula (Non-inferiority - Two Groups - Parallel - Two propotions - Equal
Allocation).

56
Proportion in the standard treatment 0.5
Proportion in the new treatment 0.5
Observed/Expected difference in proportions 0
Non-inferiority margin 0.2
Power (1- beta) % 80
Alpha Error % 5
Required sample size in each group 77
Statistical Analyses:
Statistical methods used for the primary outcome; include description of methods to
estimate the strength of the effect (e.g.: Odds ratios, relative risks, etc.).
The comparison of the post-operative nausea and vomiting (primary outcome) were done
using a chi-square test. The bootstrap 95% confidence interval was used to calculate the
difference of proportions between the two methods. Risk estimates were calculated with
95% confidence interval.
All patients were explained about the study after giving them the information sheet
(Annexure 2).
Informed consent (Annexure 3) was taken.
Those who did not give consent were not recruited in the study.

57
After informed consent, the details required as per the pro forma (Annexure 1) were
collected.
They were all followed up during their stay in hospital.
67 patients were randomized into one of the 2 arms
Six patients had to be excluded due to logistical reasons such as lost randomization
envelope and rescheduled surgeries.
Of the remaining 61 patients in the study, 2 were converted to open surgeries and 4 had
protocol violation. Therefore55 patients were analyzed, 27 in the ‘palonosetron’ arm and
28 in the ‘ondansetron with dexamethasone’ arm.
Phase of trial: Phase 3
Duration of trial: 1 year
The study had no provision for interim analysis or premature stoppage

58
*Grp 1 = Palonosetron Grp 2 = Ondansetron with dexamethasone
Lost to follow-up (n= 0) Lost to follow-up (n=0)
Follow-‐Up
Analysed (n=27)
Analysed (n=28)
Analysis
Excluded (n=6) (n=2)envelope was misplaced due to
logistical reasons and n = 4 excluded as surgeries were
rescheduled}
Randomized (n=61)
Enrollment
Assessed for eligibility (n=67))
Allocation
Allocated to intervention (Grp 1*) (n=30) ♦ Received allocated intervention (n= 30) ♦ Protocol violation (n = 3)
Allocated to intervention (Grp 2*) (n=31) ♦ Received allocated intervention (n= 28) ♦ Did not receive allocated intervention (n= 3)
♦ Protocol violation (n = 1) • Converted to open cholecystectomy
(n=2)

59
RESULTS

60
CATEGORICAL VARIABLES:
Sex distribution: Out of the total of 55 patients, 10 were male and 45 were females.
9
18
1
27
0
5
10
15
20
25
30
Male Female
Grp 1(P)
Grp 2(O+D)
Fig. 6 showing sex distribution in both groups

61
SEX DISTRIBUTION BETWEEN THE TWO ARMS:
In the intervention (Palonosetron) group 9 patients were males and 18 patients were
females.
In the comparator (Ondansetron + Dexamethasone) group, 1 were males and 27 were
females

62
AGE DISTRIBUTION:
The mean age of patients undergoing laparoscopic cholecystectomy was 44.7
years
AGE DISTRIBUTION:
The mean age between the two arms was comparable.
N Mean Std. Deviation Std. Error Mean
Palonosetron 27 46.08 16.2 2.29
Dexamethasone + Ondansetron 28 43.28 15.38 2.29
Table 1 shows the mean ages in the two arms along with the standard deviation

63
BODY MAS DISTRIBUTION:
The mean body mass index of patients having laparoscopic cholecystectomy was 20.4
kg/m2
BODY MASS INDEX DISTRIBUTION:
The body mass index in both groups was comparable.
N Mean Std. Deviation Std. Error Mean
Palonosetron 27 26.7 3.95 0.61
Dexamethasone + Ondansetron 28 28.1 4.22 0.71
Table 2 shows the mean BMI in the two arms along with the standard deviation

64
DISTRIBUTION BETWEEN TWO ARMS ACCORDING TO THE PRESENCE OF
COMORBID ILLNESSES
The following comorbidities were analyzed to ascertain the baseline characteristics in
both groups
1. Diabetes mellitus
(P= 0.16)
3
24
5
23
0
5
10
15
20
25
30
Diabetes mellitus No diabetes mellitus
Grp1 P
Grp 2 O+D
Fig. 7 showing distribution of diabetes mellitus among the two arms.

65
2. Hypertension
(P= 0.9)
4
23
5
23
0
5
10
15
20
25
Hypertension No hypertension
Palonosetron
Ondansetron+Dexamethasone
Fig. 8 showing distribution of hypertension between the two arms.

66
3. Smoking
P=0.093
3
24
1
27
0
5
10
15
20
25
30
Smoker Non smoker
Palonosetron
Dexamethasone + Ondansetron
Fig. 9 showing distribution of smoking between the two arms.

67
4. COPD or Asthma
1
26
2
26
0
5
10
15
20
25
30
COPD No COPD
Palonosetron
Ondansetron + dexamethasone
Fig.10 showing distribution of COPD or asthma between the two arms.

68
5. Hypothyroidism
The baseline characteristics between the two groups were comparable.
3
24
1
27
0
5
10
15
20
25
30
Hypothyroidism No hypothyroidism
Palonosetron
Ondansetron+Dexamethasone
Fig.11 showing distribution of hypothyroidism between the two arms.

69
The Apfel score comparison between the two groups
Palonosetron group
Score n(%)
1 3(11.1%)
2 6 (22.2%)
3 16 (59.3%)
4 2 (7.4%)
Ondansetron + dexamethasone group
Score n(%)
1 4(7.3%)
2 7(12.7%)
3 20(69.1%)
4 4(10.9%)

70
We did not analyze the relationship between Apfel score and the incidence of PONV.
Since the data collection is not complete, our numbers are not big enough for a
meaningful interpretation.
3
1
6
1
16
22
2
4
0
5
10
15
20
25
Palonosetron Ondansetron+Dexamethasone
Num
ber of patients
1
2
3
4
Fig.12 showing distribution of patients based onApfel score in the two groups

71
Nausea over a period of 24 hours
Nausea Palonosetron Dexamethasone+Ondansetron p value
n(%) n(%)
Yes 7(29) 10(42) 0.365
No 17(71) 14(58)
The above graph shows if a patient had nausea at any given point in time.
Fig.13 showing occurrence of nausea in the two arms
29
42
71
58
0
10
20
30
40
50
60
70
80
Palonosetron Dexamethasone+Ondansetron
Percentage of cases
Yes
No

72
The occurrence of nausea at intervals of 0-2, 2 -6 and 6 – 24 hours
Palonosetron Dexamethasone+Ondansetron p value
n n
0-2hrs 0 5 0.182
2-6hrs 4 5
6-24hrs 4 5
0
4 4 5
5 5
0
1
2
3
4
5
6
7
8
9
10
0-‐2hrs 2-‐6hrs 6-‐24hrs
Ondansetron+Dexamethasone
Palonosetron
Fig.14 showing occurrence of nausea in the two arms at three time intervals

73
Vomiting over a period of 24 hours
Vomiting Palonosetron Dexamethasone+Ondansetron
p value n(%) n(%)
Yes 6(22.2) 10(35.7) 0.525
No 21(77.8) 18(64.3)
Fig.15 showing occurrence of vomiting in the two arms
22.2
35.7
77.8
64.3
0
10
20
30
40
50
60
70
80
90
Palonosetron Ondansetron+Dexamethasone
% of Cases
Vomiting
No Vomiting

74
The occurrence of vomiting at intervals of 0-2, 2 -6 and 6 – 24 hours
Palonosetron Dexamethasone+Ondansetron
p value n n
0-2hrs 1 0
0.2854 2-6hrs 3 3
6-12hrs 3 8
1
3 3 0
3
8
0
2
4
6
8
10
12
0-‐2hrs 2-‐6hrs 6-‐24hrs
Num
ber of patients
Ondansetron+Dexamethasone
Palonosetron
Fig.16 showing occurrence of vomiting in the two arms at three time intervals

75
Occurrence of nausea in relation to opioid use
38.70%
29.40%
36.60%
28.60%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
NAUSEA %
Title
FENTANYL <=2.5mg/kg
FENTANYL >2.5mg/kg
MORPHINE <=.1mg/kg
MORPHINE >.1mg/kg
NAUSEA N(%) P VALUE
FENTANYL
.519 <=2.5mg/kg 12 (38.7%)
>2.5mg/kg 5(29.4%)
MORPHINE
>.999 <=.1mg/kg 15 (36.6%)
>.1mg/kg 2 (28.6%)
Fig.17 showing occurrence of nausea in relation to the dose of opioid used

76
The occurrence of vomiting in relation to opioid use
VOMITING N (%) P VALUE
FENTANYL
>.999 <=2.5mg/kg 9 (29%)
>2.5mg/kg 5 (29.4%)
MORPHINE
>.999 <=.1mg/kg 12 (29.3%)
>.1mg/kg 2 (28.6%)
With increasing intra operative opioid dose no increase was seen in the incidence of
vomiting postoperatively in both groups.
29%
29.40% 29.30%
28.60%
28%
28%
29%
29%
29%
29%
29%
30%
VOMITING %
Percentgae of cases
FENTANYL <=2.5mg/kg
FENTANYL >2.5mg/kg
MORPHINE <=.1mg/kg
MORPHINE >.1mg/kg
Fig.18 showing occurrence of vomiting in relation to the dose of opioid used

77
Table 3: Correlation between Pain and Nausea at three time intervals 0 to 2hrs, 2 to 6 hrs
and 6 to 24 hrs.
Time intervals n Correlation Coefficient p value
0 to 2 54 .279 .041
2 to 6 55 .126 .361
6 to 24 55 .241 .076
The Spearman’s Rank correlation coefficient was calculated here. The Pain and Nausea is
correlated at 0 to 2hrs. The graphical representation is given below:
There was weak correlation that was noted between nausea and pain at 0 to 2 hours and 6 to 24 hour time period.

78
Table 4: Correlation between Pain and Vomiting at three time intervals 0 to 2hrs, 2 to hrs
and 6 to 24 hrs.
Time intervals n Correlation Coefficient p value
0 to 2 54 0.077 .582
2 to 6 55 -0.003 .980
6 to 24 55 -0.060 .663
The above table shows that no correlation was found on the incidence of vomiting and
the severity of pain at various time points.

79
RESULTS As depicted by the consort diagram twenty-seven patients were randomized to the
palonosetron arm and 28 patients were randomized to ondansetron and dexamethasone
arm after the protocol violators were excluded.
Of the fifty-five patients, ten were male and forty-five were female. The mean age of
patients assessed was 44.7 years.
The baseline demographics between the two groups were identical except for uneven
gender distribution between the two groups (figure 6).
The distribution of patients based on comorbid illnesses such as diabetes mellitus,
hypertension, COPD, smoking history and hypothyroidism were comparable.
The primary objective studied was to compare the efficacy of palonosetron versus
ondansetron and dexamethasone in preventing PONV. There was no significant
difference between the two groups studied(6 patients in the palonosetron arm versus 8 in
the arm which received dexamethasone with ondansetron)(0.525).
This was studied across different time periods 0-2 hours, 2-6 and 6 – 24 hours. However
the results found were almost similar and there was no statistical significance in the
outcomes for nausea (p = 0.182) or vomiting (p = 0.2854).

80
The analysis also showed that the occurrence of nausea and vomiting was not
significantly affected by the amount of fentanyl (nausea p = 0.519 and vomiting p>0.999)
and morphine (nausea p >.0.999 and vomiting p= >0.99) used intraoperatively.
The correlation between pain represented by VAS and nausea as well as vomiting was
studied. Weak correlation between pain and nausea was noticed at 0 to 2 hours and 6 to
24 hours. There was no correlation between pain and vomiting that was noted.

81
DISCUSSION The problem of postoperative nausea and vomiting has troubled surgeon and anaesthetist
alike since the advent of general anaesthesia in the early 1800s. With the advent of
modern anaesthetic agents such as sevoflurane and desflurane; newer surgical techniques
such as laparoscopy and robotic surgery and newer antiemetics, this wheel unfortunately
needs to be re-invented and the question re-answered.
As more centers push towards doing laparoscopic cholecystectomy as a day care
procedure with a same day discharge system the use of a efficacious anti-emetic agent
may well answer most of the above mentioned questions.
Ondansetron has generally been considered as the gold standard in preventing and
managing PONV. The addition of dexamethasone has further enhanced the efficacy of
ondansetron. This has been recommended as a treatment recommendation in patients with
moderately high risk of PONV.(4) Palonosetron because of the long t ½ has been
suggested as the alternative choice by the consensus guideline published in 2014. We
wanted to compare a combination of ondansetron plus dexamethasone vs single dose IV
palonosetron for prevention of PONV after laparoscopic cholecystectomy.
The patients with history of motion sickness are thought to have a well-developed reflex
arc for vomiting and are more prone to develop PONV. Therefore they were excluded.
Safety of drugs under study is not clearly established in pregnancy and lactation. Hence
these patients were also excluded. The patients who received antiemetics or drugs with

82
emetic effects, 48 hours before surgery were also excluded, as they would have interfered
with the actions of the study drugs. Patients with known hypersensitivity to palonosetron,
ondansetron or dexamethasone and in whom the surgical procedure was converted to
open cholecystectomy were also excluded due to obvious reasons. All the patients
underwent laparoscopic cholecystectomy by the same team of anesthetists and surgeons.
The anesthetic procedure, except for the test drug, was similar in all the three groups.
Our study was not designed to find out the incidence of PONV after laparoscopic
cholecystectomy. We thought it was unethical to have a placebo arm as the side effect of
PONV is quite distressing and the established guidance clearly recommends prophylactic
anti emetic therapy.(73)
Even though a wide variety of doses of study drugs have been described in literature and
various dose finding studies suggesting the optimal doses as 0.15 mg/kg of
dexamethasone, 0.1 mg/kg of ondansetron and 0.075 mg of palonosetron, we followed
the 2014 consensus guideline for PONV and used 4 mg ondansetron, 4 mg
dexamethasone and 0.075mg of palonosetron.
The baseline demographic data were comparable except for these distribution. The
percentage of females was more in the ondansetron with dexamethasone group. This may
be explained by the fact that this is an interim analysis of the data and may equalize once
the sample size is reached.

83
Our study has shown that the incidence of PONV between the two drugs regimens is
similar during the 1st 24 hours with no statistical difference. The use of rescue antiemetic
was also similar between the two groups. There was no adverse event or drug side effect
documented in either group. The sub group analysis shows similar incidence at 0-2 hours,
2-6 hours and 6-24 hours confirming that the faster onset of iv ondansetron combined
with the longer duration of action of dexamethasone offers similar duration of anti emetic
action of palonosetron.
Our results show good agreement with the consensus guidelines that palonosetron is an
alternative to ondansetron and dexamethasone. The fact that palonosetron can be
administered as a single dose during the surgery and that it can be administered to
patients with endocrine abnormalities such as diabetes (dexamethasone may impair
glycemic control) is an added benefit. It is also known to have a better safety profile than
ondansetron as QT prolongation is not seen with this newer drug.
Palonosetron is available as a 5ml solution with 0.25mg per ml and it costs
Rs.119.Ondansetron costs Rs.8.55 for a 4mg vial and dexamethasone costs Rs.5.23 for
8mg vial. The cost of palonosetron is more than a single dose of ondansetron, which has
recently come out of the patency rules and has become cheap. However it probably
worthwhile due to its better safety profile (no QT prolongation). Even though our study
was not designed to find out the incidence of hyperglycemia and the requirement of
insulin therapy/ risk of wound infection resulting in additional costs it is well proven as a

84
complication of dexamethasone. This indirect effect may be an added financial burden to
the patient.
The analysis also showed weak correlation between PONV and pain. However as
laparoscopic cholecystectomies are usually not very painful procedures it may not be
possible to show accurate correlation as well
The BMI of patients in our study is lower than most western populations so we could not
find a correlation between obesity and PONV.
Two patients in the palonosetron group and 4 patients in the ondansetron plus
dexamethasone group had Apfel score of 4 which indicated high risk of PONV and the
anesthetists should have adopted total intravenous anesthesia with propofol as per the
recommendation of 2014 consensus guidelines. We agree with the statement in the
recommendation that a major problem is the lack of compliance among anesthetists to
follow the PONV guidelines.
In our study we could not find any association between PONV and the dose of opioids.
Similarly we could not find the association between PONV and postoperative pain.

85
LIMITATIONS
As this is a postgraduate dissertation and the study had to be done within a fixed time
frame of one year, the target sample size was not reached. The sample size that was
targeted prior to the start of the study was 77 patients in each arm. This number was not
reached.
Deviation from protocol was another challenge due to pre-existing bias towards
ondansetron from surgeon and anesthetist alike. Six patients were excluded from
analysis as there was significant protocol violation. Protocol violation were for the
following reasons – unwilling to give promethazine as rescue anti-emetic by the
surgeon(1), the consultant anaesthetist preferring to use succinylcholine over rocuronium
for anticipated difficult airway(1), conversion of laparoscopic cholecystectomies to open
procedures (2) and surgical registrar accidentally writing round the clock ondansetron
orders in the ward(2).
Blood glucose levels as well as delay in wound healing were not studied to see if
dexamethasone had any negative effect on these.
We did not document the incidence of wound infection in the study groups.
None of the patients in study groups developed life-threatening arrhythmia. However we
didn’t do an ECG routinely and looked for long QT prolongation

86
CONCLUSION
The aim of constructing a RCT and doing this study was to assess the efficacy of
palonosetron a combination of ondansetron and dexamethasone. Even though we could
not complete the study, the results from the analysis of 55 patients suggest that
palonosetron is as efficacious as ondansetron and dexamethasone in preventing post
operative nausea and vomiting. The single pre-induction dosing schedule without the
need of repeating post operatively and better safety profile makes it a cost effective
proposition in patients undergoing laparoscopic cholecystectomy.

87
Future direction and scope for further research
The study will be continued in the department of anesthesia of Christian Medical College
till sample size will be reached.
The single center RCT confers a certain bias, which needs to be mitigated through a well
constructed multi-centered RCT.

88
BIBLIOGRAPHY
1. Islam S, Jain P. Post-operative nausea and vomiting (PONV). Indian J Anaesth. 2004 Jul 1;48(4):253–253.
2. Apfel CC, Heidrich FM, Jukar-Rao S, Jalota L, Hornuss C, Whelan RP, et al. Evidence-based analysis of risk factors for postoperative nausea and vomiting. Br J Anaesth. 2012 Nov 1;109(5):742–53.
3. Fortier J, Chung F, Su J. Unanticipated admission after ambulatory surgery--a prospective study. Can J Anaesth J Can Anesth. 1998 Jul;45(7):612–9.
4. Gan TJ, Diemunsch P, Habib AS, Kovac A, Kranke P, Meyer TA, et al. Consensus guidelines for the management of postoperative nausea and vomiting. AnesthAnalg. 2014 Jan;118(1):85–113.
5. Song JW, Park EY, Lee JG, Park YS, Kang BC, Shim YH. The effect of combining dexamethasone with ondansetron for nausea and vomiting associated with fentanyl-based intravenous patient-controlled analgesia. Anaesthesia. 2011 Apr;66(4):263–7.
6. Ahsan K, Abbas N, Naqvi SMN, Murtaza G, Tariq S. Comparison of efficacy of ondansetron and dexamethasone combination and ondansetron alone in preventing postoperative nausea and vomiting after laparoscopic cholecystectomy. JPMA J Pak Med Assoc. 2014 Mar;64(3):242–6.
7. Chun HR, Jeon IS, Park SY, Lee SJ, Kang SH, Kim SI. Efficacy of palonosetron for the prevention of postoperative nausea and vomiting: a randomized, double-blinded, placebo-controlled trial. Br J Anaesth. 2014 Mar;112(3):485–90.
8. Hasler WL, Chey WD. Nausea and vomiting. Gastroenterology. 2003 Dec;125(6):1860–7.
9. Singh P, Yoon SS, Kuo B. Nausea: a review of pathophysiology and therapeutics. TherAdvGastroenterol. 2016 Jan;9(1):98–112.
10. Becker DE. Nausea, Vomiting, and Hiccups: A Review of Mechanisms and Treatment. AnesthProg. 2010;57(4):150–7.
11. Chepyala P, Olden KW. Nausea and vomiting. Curr Treat Options Gastroenterol. 2008 Apr;11(2):135–44.
12. Kowalski A, Rapps N, Enck P. Functional cortical imaging of nausea and vomiting: a possible approach. AutonNeurosci Basic Clin. 2006 Oct 30;129(1–2):28–35.
13. Hornby PJ. Central neurocircuitry associated with emesis. Am J Med. 2001 Dec 3;111 Suppl 8A:106S–112S.

89
14. Kim J, Napadow V, Kuo B, Barbieri R. A combined HRV-fMRI approach to assess cortical control of cardiovagal modulation by motion sickness. ConfProcAnnuIntConf IEEE Eng Med BiolSoc IEEE Eng Med BiolSocAnnu Conf. 2011;2011:2825–8.
15. Napadow V, Sheehan JD, Kim J, LaCount LT, Park K, Kaptchuk TJ, et al. The Brain Circuitry Underlying the Temporal Evolution of Nausea in Humans. Cereb Cortex. 2013 Apr 1;23(4):806–13.
16. Horn CC. Why is the neurobiology of nausea and vomiting so important? Appetite. 2008 May;50(2–3):430–4.
17. LaCount LT, Barbieri R, Park K, Kim J, Brown EN, Kuo B, et al. Static and dynamic autonomic response with increasing nausea perception. Aviat Space Environ Med. 2011 Apr;82(4):424–33.
18. Muth ER. Motion and space sickness: intestinal and autonomic correlates. AutonNeurosci Basic Clin. 2006 Oct 30;129(1–2):58–66.
19. Koch KL. A noxious trio: nausea, gastric dysrhythmias and vasopressin. NeurogastroenterolMotil Off J EurGastrointestMotil Soc. 1997 Sep;9(3):141–2.
20. Page SR, Peterson DB, Crosby SR, Ang VT, White A, Jenkins JS, et al. The responses of arginine vasopressin and adrenocorticotrophin to nausea induced by ipecacuanha. ClinEndocrinol (Oxf). 1990 Dec;33(6):761–70.
21. Caras SD, Soykan I, Beverly V, Lin Z, McCallum RW. The effect of intravenous vasopressin on gastric myoelectrical activity in human subjects. NeurogastroenterolMotil Off J EurGastrointestMotil Soc. 1997 Sep;9(3):151–6.
22. Taché Y. Cyclic vomiting syndrome: the corticotropin-releasing-factor hypothesis. Dig Dis Sci. 1999 Aug;44(8 Suppl):79S–86S.
23. Koch KL. Gastric dysrhythmias: a potential objective measure of nausea. Exp Brain Res. 2014 Aug;232(8):2553–61.
24. Quigley EMM, Hasler WL, Parkman HP. AGA technical review on nausea and vomiting. Gastroenterology. 2001 Jan;120(1):263–86.
25. Kapur PA. Editorial: The Big “Little Problem”. AnesthAnalg [Internet]. 1991;73(3). Available from: http://journals.lww.com/anesthesia-analgesia/Fulltext/1991/09000/Editorial__The_Big__Little_Problem__.1.aspx
26. Smessaert A, Schehr CA, Artusio JF. Nausea and vomiting in the immediate postanesthetic period. J Am Med Assoc. 1959 Aug 22;170(17):2072–6.
27. Apfel CC, Läärä E, Koivuranta M, Greim C-A, Roewer N. A Simplified Risk Score for Predicting Postoperative Nausea and Vomiting Conclusions from Cross-validations between Two Centers. J Am SocAnesthesiol. 1999 Sep 1;91(3):693–693.

90
28. Koivuranta M, Läärä E, Snåre L, Alahuhta S. A survey of postoperative nausea and vomiting. Anaesthesia. 1997 May 1;52(5):443–9.
29. Pierre S, Whelan R. Nausea and vomiting after surgery. ContinEducAnaesthCrit Care Pain. 2012 Aug 11;mks046.
30. Camu F, Lauwers MH, Verbessem D. Incidence and aetiology of postoperative nausea and vomiting. Eur J Anaesthesiol Suppl. 1992 Nov;6:25–31.
31. Watcha MF, White PF. Postoperative nausea and vomiting. Its etiology, treatment, and prevention. Anesthesiology. 1992 Jul;77(1):162–84.
32. Gan T, Sloan F, Dear G de L, El-Moalem HE, Lubarsky DA. How much are patients willing to pay to avoid postoperative nausea and vomiting? AnesthAnalg. 2001 Feb;92(2):393–400.
33. van Wijk MG, Smalhout B. A postoperative analysis of the patient’s view of anaesthesia in a Netherlands’ teaching hospital. Anaesthesia. 1990 Aug;45(8):679–82.
34. Gold BS, Kitz DS, Lecky JH, Neuhaus JM. Unanticipated admission to the hospital following ambulatory surgery. JAMA. 1989 Dec 1;262(21):3008–10.
35. Sweeney BP. Editorial II Why does smoking protect against PONV? Br J Anaesth. 2002 Dec 1;89(6):810–3.
36. Kenny GN. Risk factors for postoperative nausea and vomiting. Anaesthesia. 1994 Jan;49 Suppl:6–10.
37. Kranke P, Apfel CC, Papenfuss T, Rauch S, Löbmann U, Rübsam B, et al. An increased body mass index is no risk factor for postoperative nausea and vomiting. ActaAnaesthesiol Scand. 2001 Feb 1;45(2):160–6.
38. Apfel CC, Stoecklein K, Lipfert P. PONV: a problem of inhalational anaesthesia? Best Pract Res ClinAnaesthesiol. 2005 Sep;19(3):485–500.
39. Fernández-Guisasola J, Gómez-Arnau JI, Cabrera Y, del Valle SG. Association between nitrous oxide and the incidence of postoperative nausea and vomiting in adults: a systematic review and meta-analysis. Anaesthesia. 2010 Apr;65(4):379–87.
40. Sinclair DR, Chung F, Mezei G. Can Postoperative Nausea and Vomiting Be Predicted? J Am SocAnesthesiol. 1999 Jul 1;91(1):109–18.
41. Apfel CC, Kranke P, Eberhart LHJ. Comparison of surgical site and patient’s history with a simplified risk score for the prediction of postoperative nausea and vomiting. Anaesthesia. 2004 Nov 1;59(11):1078–82.
42. Thune A, Appelgren L, Haglind E. Prevention of postoperative nausea and vomiting after laparoscopic cholecystectomy. A prospective randomized study of metoclopramide and transdermal hyoscine. Eur J SurgActaChir. 1995 Apr;161(4):265–8.

91
43. Lee W-S, Lee K-B, Lim S, Chang YG. Comparison of palonosetron, granisetron, and ramosetron for the prevention of postoperative nausea and vomiting after laparoscopic gynecologic surgery: a prospective randomized trial. BMC Anesthesiol [Internet]. 2015 Sep 3 [cited 2016 Sep 20];15. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4558835/
44. Apfel CC, Kranke P, Katz MH, Goepfert C, Papenfuss T, Rauch S, et al. Volatile anaesthetics may be the main cause of early but not delayed postoperative vomiting: a randomized controlled trial of factorial design. Br J Anaesth. 2002 May 1;88(5):659–68.
45. Pierre S, Benais H, Pouymayou J. Apfel’s simplified score may favourably predict the risk of postoperative nausea and vomiting. Can J Anesth. 49(3):237.
46. Apfel CC, Korttila K, Abdalla M, Kerger H, Turan A, Vedder I, et al. A Factorial Trial of Six Interventions for the Prevention of Postoperative Nausea and Vomiting. N Engl J Med. 2004 Jun 10;350(24):2441–51.
47. Polati E, Verlato G, Finco G, Mosaner W, Grosso S, Gottin L, et al. Ondansetron versus metoclopramide in the treatment of postoperative nausea and vomiting. AnesthAnalg. 1997 Aug;85(2):395–9.
48. Goodarzi M, Matar MM, Shafa M, Townsend JE, Gonzalez I. A prospective randomized blinded study of the effect of intravenous fluid therapy on postoperative nausea and vomiting in children undergoing strabismus surgery. PaediatrAnaesth. 2006 Jan;16(1):49–53.
49. Carlisle JB, Stevenson CA. Drugs for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. 2006;(3):CD004125.
50. Fero KE, Jalota L, Hornuss C, Apfel CC. Pharmacologic management of postoperative nausea and vomiting. Expert OpinPharmacother. 2011 Oct 1;12(15):2283–96.
51. Graczyk SG, McKenzie R, Kallar S, Hickok CB, Melson T, Morrill B, et al. Intravenous Dolasetron for the Prevention of Postoperative Nausea and Vomiting After Outpatient Laparoscopic Gynecologic Surgery. AnesthAnalg [Internet]. 1997;84(2). Available from: http://journals.lww.com/anesthesia-analgesia/Fulltext/1997/02000/Intravenous_Dolasetron_for_the_Prevention_of.15.aspx
52. Commissioner O of the. Safety Alerts for Human Medical Products - Anzemet (dolasetron mesylate): Drug Safety Communication - Reports of Abnormal Heart Rhythms [Internet]. [cited 2016 Aug 15]. Available from: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm237341.htm?utm_campaign=Google2&utm_source=fdaSearch&utm_medium=website&utm_term=dolasetron&utm_content=2
53. Sodhi K, Mohindra BK, Sodhi GS, Kumar M. A comparative study of granisetron, dexamethasone, and granisetron plus dexamethasone as prophylactic antiemetic therapy in

92
female patients undergoing breast surgery. J AnaesthesiolClinPharmacol. 2007 Oct 1;23(4):373.
54. Choi YS, Shim JK, Yoon DH, Jeon DH, Lee JY, Kwak YL. Effect of ramosetron on patient-controlled analgesia related nausea and vomiting after spine surgery in highly susceptible patients: comparison with ondansetron. Spine. 2008 Aug 1;33(17):E602-606.
55. Kovac AL, Eberhart L, Kotarski J, Clerici G, Apfel C, Palonosetron 04-07 Study Group. A randomized, double-blind study to evaluate the efficacy and safety of three different doses of palonosetron versus placebo in preventing postoperative nausea and vomiting over a 72-hour period. AnesthAnalg. 2008 Aug;107(2):439–44.
56. Kim HJ, Lee H-C, Jung YS, Lee J, Min JJ, Hong D-M, et al. Effect of palonosetron on the QTc interval in patients undergoing sevoflurane anaesthesia. Br J Anaesth. 2014 Mar;112(3):460–8.
57. Gonullu G, Demircan S, Demirag MK, Erdem D, Yucel I. Electrocardiographic findings of palonosetron in cancer patients. Support Care Cancer Off J MultinatlAssoc Support Care Cancer. 2012 Jul;20(7):1435–9.
58. Pham A, Liu G. Dexamethasone for antiemesis in laparoscopic gynecologic surgery: a systematic review and meta-analysis. Obstet Gynecol. 2012 Dec;120(6):1451–8.
59. Sekhavat L, Davar R, Behdad S. Efficacy of prophylactic dexamethasone in prevention of postoperative nausea and vomiting. J Epidemiol Glob Health. 2015 Jun;5(2):175–9.
60. De Oliveira GS, Castro-Alves LJS, Ahmad S, Kendall MC, McCarthy RJ. Dexamethasone to prevent postoperative nausea and vomiting: an updated meta-analysis of randomized controlled trials. AnesthAnalg. 2013 Jan;116(1):58–74.
61. Henzi I, Walder B, Tramèr MR. Dexamethasone for the prevention of postoperative nausea and vomiting: a quantitative systematic review. AnesthAnalg. 2000 Jan;90(1):186–94.
62. Ali Khan S, McDonagh DL, Gan TJ. Wound complications with dexamethasone for postoperative nausea and vomiting prophylaxis: a moot point? AnesthAnalg. 2013 May;116(5):966–8.
63. Habib AS, Keifer JC, Borel CO, White WD, Gan TJ. A comparison of the combination of aprepitant and dexamethasone versus the combination of ondansetron and dexamethasone for the prevention of postoperative nausea and vomiting in patients undergoing craniotomy. AnesthAnalg. 2011 Apr;112(4):813–8.
64. Zhang D, Shen Z, You J, Zhu X, Tang Q-F. Effect of ondansetron in preventing postoperative nausea and vomiting under different conditions of general anesthesia: A preliminary, randomized, controlled study. Ups J Med Sci. 2013 May;118(2):87–90.

93
65. Tramèr MR, Moore RA, Reynolds DJ, McQuay HJ. A quantitative systematic review of ondansetron in treatment of established postoperative nausea and vomiting. BMJ. 1997 Apr 12;314(7087):1088–92.
66. Wang X-X, Zhou Q, Pan D-B, Deng H-W, Zhou A-G, Huang F-R, et al. Dexamethasone versus ondansetron in the prevention of postoperative nausea and vomiting in patients undergoing laparoscopic surgery: a meta-analysis of randomized controlled trials. BMC Anesthesiol [Internet]. 2015 Aug 15 [cited 2016 Aug 16];15. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4536735/
67. Park SK, Cho EJ. A randomized, double-blind trial of palonosetron compared with ondansetron in preventing postoperative nausea and vomiting after gynaecological laparoscopic surgery. J Int Med Res. 2011;39(2):399–407.
68. Kim YY, Moon SY, Song DU, Lee KH, Song JW, Kwon YE. Comparison of palonosetron with ondansetron in prevention of postoperative nausea and vomiting in patients receiving intravenous patient-controlled analgesia after gynecological laparoscopic surgery. Korean J Anesthesiol. 2013 Feb;64(2):122–6.
69. Bianchin A, De Luca A, Caminiti A. Postoperative vomiting reduction after laparoscopic cholecystectomy with single dose of dexamethasone. Minerva Anestesiol. 2007 Jun;73(6):343–6.
70. Aspinall RL, Goodman NW. Denial of effective treatment and poor quality of clinical information in placebo controlled trials of ondansetron for postoperative nausea and vomiting: a review of published trials. BMJ. 1995 Sep 30;311(7009):844–6.

94
ANNEXURES Annexure – 1 : Pro forma Pro forma
Department of Anesthesia
Christian Medical College and Hospital
Serial no: Name: Age : Sex: Hospital No.: Weight(in Kg): Height(in cm): Body mass index(wt/ht2): ASA I / II / III / IV Comorbidities – Diabetes Mellitus / Hypertension / COPD / Asthma / Others- History of -
- Smoking Y / N - PONV Y / N - Motion sickness Y / N
Pre operative fasting (in hours): Apfel Score - Intraoperative: Duration of General anaesthesia: (in minutes) Duration of Surgery: (in minutes) Use of Nitrous: Y / N Anesthesia ( MAC) Fentanyl dose- ___mcg Morphine dose- ___mg Reversal Dose: Neostigmine - __mg Glycopyrolate - __mg Anesthetist experience (in years) - Post operative: Opioid used (mg/kg) Post operative: 0 to 2 hours Nausea Retching Vomiting Pain score VAS score - Yes / No Episodes - 1/ 2 / > 2 /
None VAS
Rescue anti emetic used –

95
2 to 6 hours Nausea Retching Vomiting Pain score VAS score - Yes / No Episodes - 1/ 2 / > 2 /
None VAS
Rescue anti emetic used – 6 to 24 hours Nausea Retching Vomiting Pain score VAS score - Yes / No Episodes - 1/ 2 / > 2 /
None VAS
Rescue anti emetic used - Overall satisfaction - unsatisfied/ neutral/ fully satisfied
Visual Analogue Score

96
Annexure – 2: Patient Information Sheet Christian Medical College, Vellore Department of Anaesthesia Comparative study of the effects of intravenous palonosetronversus ondansetron and dexamethasone for prevention of postoperative nausea and vomiting (PONV) after laparoscopic cholecystectomy: a prospective randomized controlled study Information sheet You are invited to be part of a study to improve the current knowledge regarding the role of anti-emetics during the operation. This study will help other patients who later come to hospital for the same operation. By agreeing to be a part of this study, you will contribute to scientific knowledge. The information collected from you will include
1. History – This includes details regarding your general health and the disease for which you are undergoing the operation.
2. Clinical examination – Besides the regular doctors rounds, the primary investigator will examine you regularly.
You will be examined post operatively by the primary investigator in the ward and data will be collected and analysed.
Whether you accept or decline to be a part of this study will not affect your further treatment at this hospital Although you may not directly benefit by enrolling in the study, you will be contributing to scientific knowledge. You are scheduled to undergo laparoscopic cholecystectomy under general anaesthesia. Considering the type of surgery anesthesia and your risk factors you have a moderate high risk of suffering from nausea and vomiting at the end of surgery. The current recommendations of therapy involves a combination of two drugs dexamethasone and ondansetron. The former has side effects such as bleeding, infection and cause high blood sugars. However it offers protection from nauea and vomiting for 24 hours. The later offers good prophylaxis with side effects like head ache, constipation and rarely arrhythmia. An alternate option will be a drug called palonosetron which has a slightly better safety profile than ondansetron and a long duration of action of 24 to 48hrs. By being a part of the study you will be randomly allotted into two groups. In one group, patients will receive inj. Palenosetron and in the second group patients will receive inj. Ondansetron + dexamethasone. Both of these regimens are well studied and are routinely used during the operation to prevent post operative nausea and vomiting. The operative technique and all other anaesthetic approaches will be similar. If you develop nausea or vomiting at any time you will be treated with droperidol/ promethazine as a rescue medication according to the standard guidelines. We wished to study this in detail and are therefore conducting a scientific study.

97
All details including personal data, assessment of the doctor during and after the operation will be kept confidential. We aim to include about 60 people from this hospital in this study in the next one years. Participation in this study is purely voluntary, and you can withdraw from the study at any time and that refusal to participate will not involve any penalty or loss of benefits to which you are otherwise entitled.

98
Annexure – 3: Consent Form Informed consent form to participate in a clinical trial
Consent to take part in a clinical trial
Study Title: Comparative study of the effects of intravenous palonosetronversus ondansetron and dexamethasone for prevention of postoperative nausea and vomiting (PONV) after laparoscopic cholecystectomy: a prospective randomized controlled study Study Number: Participant’s name: Date of Birth / Age (in years): I_____________________________________________________________ ___________, son/daughter of ___________________________________ (Please tick boxes) Declare that I have read the information sheet provide to me regarding this study and have clarified any doubts that I had. [ ] I also understand that my participation in this study is entirely voluntary and that I am free to withdraw permission to continue to participate at any time without affecting my usual treatment or my legal rights [ ] I also understand that neither I, nor my doctors, will will know which anti-emetic I will receive(palonosetron or ondansetron + dexamethasone)[ ] I understand that I will receive free treatment for any study related injury or adverse event but I will not receive and other financial compensation [ ] I understand that the study staff and institutional ethics committee members will not need my permission to look at my health records even if I withdraw from the trial. I agree to this access [ ] I understand that my identity will not be revealed in any information released to third parties or published [ ] I agree to pay for any investigation routinely warranted for my treatment [ ] I voluntarily agree to take part in this study [ ] Name: Signature: Date: Name of witness: Relation to participant: Date: Name and Signature of the Doctor

99
Annexure – 4: Ethics committee approval

100

101

102
Annexure – 5: Data sheet
sno group age sex wt ht BMI ASA DiabetesMellitusHypertensionHypothyroidCOPD_AsthmaSmoking PONV MotionSicknessFasting_hrs Apfel_ScoreDuration_of_GA_mins
Duration_of_surgery_mins
1 2 23 1 66 166 24 2 2 2 2 2 2 2 2 14 2 220 1902 1 37 2 38 162 22.1 1 2 2 2 2 2 1 2 12 4 105 803 1 23 2 64 155 26.6 2 2 2 2 1 2 2 2 3 210 1654 25 1 38 2 74 160 28.9 2 2 2 1 2 2 2 2 9 3 165 1406 2 31 2 44 142 21.8 1 2 2 2 2 2 2 2 12 3 195 1507 18 29 110 2 61 2 67 148 30.6 2 1 1 2 2 2 2 2 12 3 300 27011 2 50 2 59 161 32.8 1 2 2 2 2 2 2 2 7.5 3 60 4512 113 1 48 2 55 153 23.5 2 2 1 2 2 2 2 2 7 3 180 15014 1 48 1 81 179 25.3 2 1 2 2 2 1 2 2 18 1 120 10015 2 44 2 65 158 26 2 1 1 2 2 2 2 2 3 120 10016 2 26 2 55 148 25.1 1 2 2 2 2 2 2 2 4 317 2 43 2 43 159 17 1 2 2 2 2 2 2 2 10 318 2 42 2 65 156 26.7 1 2 2 2 2 2 2 2 3 105 7519 1 41 2 53 154 22.3 1 2 2 2 2 2 2 2 18.5 3 105 9020 1 45 2 87 150 38.7 2 2 2 1 2 2 2 2 8.5 3 160 14021 2 57 2 65 148 29.7 2 1 1 2 2 2 2 2 3 120 12022 1 44 1 60 170 20.8 1 2 2 2 2 2 2 2 13.5 2 90 9023 1 24 2 55 152 23.8 1 2 2 2 2 2 2 2 14 3 120 12024 2 47 2 55 145 26.2 1 2 2 2 2 2 2 2 3 255 21025 2 39 2 58 151 25.4 1 2 2 2 2 2 2 1 4 180 15026 1 38 2 50 153 21.4 1 2 2 2 2 2 2 2 15 3 210 17527 2 2 57 145 27.1 1 2 2 2 2 2 2 2 14 3 190 16528 1 38 2 74 162 28.2 1 2 2 2 2 2 2 2 8 3 190 17029 2 38 2 69 152 29.9 1 2 2 2 2 2 2 2 9 3 240 19530 1 50 1 70 175 22.9 2 2 1 2 2 2 2 2 3 140 12031 1 42 1 55 170 19 1 2 2 2 2 1 2 2 16.5 2 110 6032 2 21 2 85 162 32.4 1 2 2 2 2 2 1 1 9 4 150 12033 1 48 2 75 149 33.8 2 1 1 2 2 2 2 2 19.5 3 220 17034 2 26 2 75 167 26.9 1 2 2 2 2 2 2 2 12 3 190 16035 1 41 2 58 153 24.8 1 2 2 2 2 2 1 2 4 90 7036 2 39 2 70 155 29.1 1 2 2 2 2 2 2 2 3 75 6037 2 48 2 52 153 22.2 1 2 2 2 2 2 2 2 9.5 3 187 14538 1 36 2 65 163 24.5 1 2 2 2 2 2 2 2 10.5 3 180 15039 1 47 2 63 146 29.6 1 2 2 2 2 2 2 2 12.75 3 135 10540 2 42 2 59 150 26.2 1 2 2 2 2 2 2 2 10 3 120 7541 1 51 1 75 173 25.1 1 2 2 2 2 2 2 1 17 2 110 9042 1 31 1 84 171 28.7 1 2 2 2 2 2 2 2 13 2 240 21043 2 56 2 65 155 27.1 2 1 1 1 2 2 2 2 3 80 11044 2 44 2 65 155 27.1 2 2 1 2 2 2 2 2 14 3 120 9045 1 28 1 60 170 20.5 2 2 2 2 2 2 2 2 11 2 135 9046 1 51 1 90 175 29.4 2 1 2 2 2 1 2 2 15 1 130 10047 2 36 2 60 154 25.3 1 2 2 2 2 2 2 2 348 2 44 2 75 155 31.2 2 1 2 2 2 2 2 2 11 3 200 17049 1 35 2 38 158 15.2 1 2 2 2 2 2 2 2 19 3 180 14550 2 32 2 80 160 31.3 2 2 2 2 1 2 2 2 9 3 165 14051 1 50 2 44 152 19 2 2 1 2 2 2 2 2 3 125 10052 2 50 2 62 148 28.3 1 2 2 2 2 2 2 2 14 3 190 15053 2 45 1 74 157 30 1 2 2 2 2 1 2 2 10 154 1 46 2 76 151 33.3 2 2 2 1 2 2 2 2 10 3 130 11555 156 2 41 2 36 139 18.6 1 2 2 2 2 2 2 2 11 3 240 22057 2 21 2 54 158 21.6 1 2 2 2 1 2 2 2 10 2 150 10558 1 23 2 50 156 20.5 1 2 2 2 2 2 2 2 17 3 120 9059 1 58 1 45 145 21.4 1 2 2 2 2 2 2 2 9.5 1 270 23060 1 29 2 70 168 24.8 2 2 2 2 2 2 2 2 12.5 2 120 10061 2 37 2 50 147 23.1 2 2 2 2 2 2 2 1 10.5 4 235 19062 263 2 35 2 53 154 22.3 1 2 2 2 2 2 1 2 11 4 180 150

103
Nitrous MAC FentanylFentany_mcg_per_kg Morphine
Morphine_mg_per_kg NeostigmineGlycopyrolateExperiecne_yrsPostop_opioidsNausea_t1_VASRetching_t1Vomiting_t1Pain_t1_VASRescue_med_t1Nausea_t2_VAS
2 1 140 2.121212121 5 0.0757575762 0.9 160 4.210526316 6 0.157894737 2.5 0.4 1 2 0 2 4 6 2 02 1 120 1.875 0 2.5 0.4 2 0 2 4 0 2 1
2 1 180 2.432432432 6 0.081081081 3 0.6 2 2 0 2 4 3 2 02 1 100 2.272727273 4 0.090909091 2.5 0.4 1 0 2 4 0 2 0
#DIV/0!2 1 120 1.791044776 9 0.134328358 2.5 0.4 7 2 0 2 4 0 2 02 1.5 200 3.389830508 4 0.06779661 2.5 1.2 2 0 1 4 0 1 0
2 1 100 1.818181818 6 0.109090909 2.5 0.4 1 2 0 2 4 0 2 02 0.8 200 2.469135802 7 0.086419753 2.5 0.4 1 2 0 2 4 0 2 02 0.9 200 3.076923077 6.5 0.1 2.5 0.4 2 2 0 2 4 3 2 02 0.9 0 5.5 0.1 2.5 0.4 2 1 0 2 4 0 2 82 1 140 3.255813953 0 0 2 0.3 17 1 0 2 4 0 2 02 0.9 120 1.846153846 0 2.5 0.4 1 2 2 2 4 3 2 02 1 160 3.018867925 6 0.113207547 2.5 0.4 18 2 0 2 4 0 2 02 1 200 2.298850575 5 0.057471264 3.5 0.6 18 1 0 2 4 0 2 02 0.9 200 3.076923077 8 0.123076923 2.5 0.4 1 0 2 4 0 2 02 0.8 120 2 5 0.083333333 2.5 0.4 2 0 2 4 0 2 02 0.9 200 3.636363636 6 0.109090909 2.5 0.4 9 2 0 2 4 0 2 32 1 260 4.727272727 5 0.090909091 2.5 0.4 2 0 2 4 0 2 22 1 150 2.586206897 5 0.086206897 2.5 0.4 2 0 2 4 0 2 32 1 175 3.5 5 0.1 2.5 0.4 6 2 0 2 2 0 1 12 1 150 2.631578947 6 0.105263158 2.5 0.4 2 0 2 4 0 2 02 0.9 100 1.351351351 4 0.054054054 2.5 0.4 12 2 0 2 4 0 2 02 0.9 170 2.463768116 4 0.057971014 2.5 0.4 2 0 2 4 0 2 02 1 150 2.142857143 5 0.071428571 2.5 0.4 2 0 2 4 0 2 02 1 140 2.545454545 5 0.090909091 2.5 0.4 2 0 2 4 0 2 02 0.9 200 2.352941176 7 0.082352941 2.5 0.4 1 7 1 4 2 2 02 1 150 2 5 0.066666667 2.5 0.4 6 1 0 2 4 0 2 12 1 150 2 0 0 2.5 0.4 3 2 0 2 4 2 2 02 1 120 2.068965517 4 0.068965517 2 0.4 2 0 2 4 0 2 02 1 140 2 0 2.5 0.4 6 2 5 1 4 6 2 62 1 100 1.923076923 4.5 0.086538462 2.5 0.4 1 0 2 4 0 2 02 1 100 1.538461538 5 0.076923077 2.5 0.4 4 2 0 2 4 0 2 02 1 100 1.587301587 5 0.079365079 2.5 0.4 4 2 0 2 4 0 2 02 0.9 100 1.694915254 4 0.06779661 3 0.5 5 1 0 2 4 4 2 02 0.7 100 1.333333333 3 0.04 2.5 0.4 15 2 0 2 4 0 2 02 1 150 1.785714286 7 0.083333333 2.5 0.4 2 2 0 2 4 0 2 02 0.9 150 2.307692308 5 0.076923077 2.5 0.4 2 0 2 4 0 2 02 1 150 2.307692308 0 0 3.5 0.5 1 2 0 2 4 0 2 02 1 100 1.666666667 0 0 2.5 0.4 1 2 0 2 4 0 2 02 0.9 100 1.111111111 5 0.055555556 2.5 0.4 8 2 0 2 4 0 2 0
0 0 2 0 2 4 0 2 02 0.9 130 1.733333333 4 0.053333333 2.5 0.4 8 2 0 2 4 0 2 02 1 120 3.157894737 0 2 0.4 8 2 0 2 4 2 2 02 0.8 200 2.5 8 0.1 2.5 0.4 26 2 0 2 4 2 2 32 0.8 130 2.954545455 3 0.068181818 2.5 0.4 1.5 2 0 2 4 2 2 02 1 140 2.258064516 4 0.064516129 2.5 0.4 2 0 2 4 2 2 02 0.8 160 2.162162162 0 2.5 0.4 0 2 4 0 2 02 0.8 140 1.842105263 4 0.052631579 2.5 0.4 2 2 0 2 4 2 0
#DIV/0! #DIV/0!2 1 100 2.777777778 3 0.083333333 2 0.4 6 2 0 2 4 2 2 02 1 150 2.777777778 0 2.5 0.4 5 2 0 2 4 0 2 02 1 100 2 5 0.1 2.5 0.4 1 0 2 4 0 2 02 0.9 100 2.222222222 4 0.088888889 2.5 0.4 10 1 0 2 4 0 2 02 0.9 100 1.428571429 5 0.071428571 2.5 0.4 2 2 0 2 4 0 2 02 0.9 140 2.8 4 0.08 2.5 0.4 3 2 6 2 4 0 1 0
2 0.9 140 2.641509434 5 0.094339623 2.5 0.4 2 7 2 4 0 1 0

104
Retching_t2 Vomit_t2 Pain_t2_VASRescu_t2 Nausea_t3_VASRetching_t3 Vomit_t3 Pain_t3_VASRescu_t3 Satisfaction
2 4 7 2 0 1 4 4 1 20 1 1 2 0 2 4 1 2
2 4 1 2 0 2 4 0 22 4 1 2 0 2 4 4 2
2 4 3 2 0 2 4 0 2 32 4 0 2 0 2 1 0 1 3
2 4 0 2 2 2 4 2 2 32 4 0 2 0 2 4 1 2 32 4 2 2 0 2 4 2 21 2 2 1 0 2 1 3 12 4 2 2 0 2 4 0 2 32 4 4 2 0 2 1 2 2 32 4 2 2 0 2 4 2 2 32 4 4 2 0 2 4 3 2 32 4 2 2 0 1 3 3 1 22 4 2 2 2 2 1 2 2 32 2 2 1 0 2 4 2 2 22 4 2 2 0 2 4 3 2 31 1 3 1 0 2 4 3 2 22 4 2 2 0 2 4 2 2 32 4 2 2 0 2 4 2 22 4 0 2 0 2 4 2 2 32 4 3 2 0 2 4 2 22 4 2 2 0 2 4 1 2 32 4 0 2 0 1 1 2 22 4 2 2 8 2 4 4 22 1 2 2 1 2 1 3 1 22 4 2 2 0 2 4 2 2 32 4 3 2 0 2 4 2 2 32 4 6 2 6 2 4 6 2 22 4 2 2 0 2 2 2 22 4 0 2 0 2 4 0 2 32 4 1 2 0 2 4 2 22 4 2 2 3 1 1 2 1 22 4 3 2 0 2 4 2 2 32 4 1 2 0 2 4 1 2 32 4 3 2 3 2 1 2 1 32 4 0 2 0 2 4 0 2 32 4 2 2 0 2 4 8 2 32 4 2 2 2 1 4 2 2 22 4 2 2 0 2 4 3 2 32 4 2 2 3 1 2 3 1 12 4 2 2 0 2 4 2 2 31 2 0 1 0 2 4 2 2 32 4 2 2 0 2 4 1 2 32 4 2 4 0 2 4 2 2 32 4 1 2 0 2 4 2 2 32 4 2 2 0 2 4 2 2 3
2 4 2 2 0 2 4 2 2 32 4 0 2 0 2 4 2 0 22 4 1 2 0 2 4 4 2 32 4 0 2 0 2 4 5 2 32 4 1 2 0 2 4 2 2 32 4 2 2 0 2 4 3 2 3
2 4 0 2 0 2 4 2 2 3

105
Copyright © 2022 FDOKUMEN




















