Intravenous iron exposure and mortality in patients on hemodialysis
10
Article Intravenous Iron Exposure and Mortality in Patients on Hemodialysis Dana C. Miskulin, Navdeep Tangri, Karen Bandeen-Roche, Jing Zhou, Aidan McDermott, Klemens B. Meyer, Patti L. Ephraim, Wieneke M. Michels, Bernard G. Jaar, Deidra C. Crews, Julia J. Scialla, Stephen M. Sozio, Tariq Shafi, Albert W. Wu, Courtney Cook, and L. Ebony Boulware for The Developing Evidence to Inform Decisions about Effectiveness (DEcIDE) Network Patient Outcomes in End Stage Renal Disease Study Investigators Abstract Background and objectives Clinical trials assessing effects of larger cumulative iron exposure with outcomes are lacking, and observational studies have been limited by assessment of short-term exposure only and/or failure to assess cause-specific mortality. The associations between short- and long-term iron exposure on all-cause and cause-specific mortality were examined. Design, setting, participants, & measurements The study included 14,078 United States patients on dialysis initiating dialysis between 2003 and 2008. Intravenous iron dose accumulations over 1-, 3-, and 6-month rolling windows were related to all-cause, cardiovascular, and infection-related mortality in Cox proportional hazards models that used marginal structural modeling to control for time-dependent confounding. Results Patients in the 1-month model cohort (n=14,078) were followed a median of 19 months, during which there were 27.6% all-cause deaths, 13.5% cardiovascular deaths, and 3% infection-related deaths. A reduced risk of all-cause mortality with receipt of .150–350 (hazard ratio, 0.78; 95% confidence interval, 0.64 to 0.95) or .350 mg (hazard ratio, 0.79; 95% confidence interval, 0.62 to 0.99) intravenous iron compared with .0–150 mg over 1 month was observed. There was no relation of 1-month intravenous iron dose with cardiovascular or infection- related mortality and no relation of 3- or 6-month cumulative intravenous iron dose with all-cause or cardio- vascular mortality. There was a nonstatistically significant increase in infection-related mortality with receipt of .1050 mg intravenous iron in 3 months (hazard ratio, 1.69; 95% confidence interval, 0.87 to 3.28) and .2100 mg in 6 months (hazard ratio, 1.59; 95% confidence interval, 0.73 to 3.46). Conclusions Among patients on incident dialysis, receipt of #1050 mg intravenous iron in 3 months or 2100 mg in 6 months was not associated with all-cause, cardiovascular, or infection-related mortality. However, nonstatistically significant findings suggested the possibility of infection-related mortality with receipt of .1050 mg in 3 months or .2100 mg in 6 months. Randomized clinical trials are needed to assess the safety of exposure to greater cumulative intravenous iron doses. Clin J Am Soc Nephrol 9: ccc–ccc, 2014. doi: 10.2215/CJN.03370414 Introduction Intravenous (IV) iron use in the United States hemo- dialysis (HD) population has increased (1) in recent years after changes in product labeling (2) and bun- dling of erythropoiesis-stimulating agents (ESAs) into dialysis per-treatment payments (3). The amount of iron that can be safely administered over the short and long term is unknown. In experimental studies, ex- cess iron has been shown to impair phagocytosis and enhance bacterial virulence, increasing risk for infection (4–7). However, the iron concentrations achieved in these experiments greatly exceed the plasma iron levels achieved in clinical practice. Iron, a potent oxidant, may also play a role in atherosclerosis (8–11). Addition- ally, recent studies show hepatic iron content to be se- verely elevated in some patients on HD (12–14), although the clinical significance of this finding is unclear. Clinical trials assessing the safety of more aggressive iron repletion on patient-centered outcomes have not been conducted, and observational studies have yielded inconsistent results (9,15–19). In a prevalent 1997–1998 HD population, receipt of a cumulative iron dose ex- ceeding 1800 mg in 6 months was not associated with mortality (16). A more recent study found an increase in infection-related mortality and hospitalizations with receipt of .200 mg IV iron in 1 month and bolus as opposed to maintenance iron therapy (15). Exposures .1 month were not examined in the first study (16), and cause-specific mortality was not examined in the second study (16). Furthermore, both of these studies were conducted on prevalent populations and therein, may have been subject to survivor bias. Studies examining the association of administering varying doses of IV iron with clinical outcomes assessed Due to the number of contributing authors, the affiliations are provided in the Supplemental Material. Correspondence: Dr. Dana C. Miskulin, Tufts Medical Center, Box 391, Division of Nephrology, 800 Washington Street, Boston, MA 02111. Email: dmiskulin@ tuftsmedicalcenter.org www.cjasn.org Vol 9 November, 2014 Copyright © 2014 by the American Society of Nephrology 1 . Published on October 15, 2014 as doi: 10.2215/CJN.03370414 CJASN ePress
-
Upload
johnshopkins -
Category
Documents
-
view
1 -
download
0
Transcript of Intravenous iron exposure and mortality in patients on hemodialysis

Article
Intravenous Iron Exposure and Mortality in Patients onHemodialysis
Dana C. Miskulin, Navdeep Tangri, Karen Bandeen-Roche, Jing Zhou, Aidan McDermott, Klemens B. Meyer,Patti L. Ephraim, Wieneke M. Michels, Bernard G. Jaar, Deidra C. Crews, Julia J. Scialla, Stephen M. Sozio, Tariq Shafi,Albert W. Wu, Courtney Cook, and L. Ebony Boulware for The Developing Evidence to Inform Decisions aboutEffectiveness (DEcIDE) Network Patient Outcomes in End Stage Renal Disease Study Investigators
AbstractBackground and objectives Clinical trials assessing effects of larger cumulative iron exposure with outcomes arelacking, and observational studies have been limited by assessment of short-term exposure only and/or failure toassess cause-specific mortality. The associations between short- and long-term iron exposure on all-cause andcause-specific mortality were examined.
Design, setting, participants, & measurements The study included 14,078 United States patients on dialysisinitiating dialysis between 2003 and 2008. Intravenous iron dose accumulations over 1-, 3-, and 6-month rollingwindows were related to all-cause, cardiovascular, and infection-related mortality in Cox proportional hazardsmodels that used marginal structural modeling to control for time-dependent confounding.
Results Patients in the 1-month model cohort (n=14,078) were followed a median of 19 months, during whichthere were 27.6% all-cause deaths, 13.5% cardiovascular deaths, and 3% infection-related deaths. A reduced riskof all-cause mortality with receipt of.150–350 (hazard ratio, 0.78; 95% confidence interval, 0.64 to 0.95) or.350mg (hazard ratio, 0.79; 95% confidence interval, 0.62 to 0.99) intravenous iron compared with.0–150 mg over 1month was observed. There was no relation of 1-month intravenous iron dose with cardiovascular or infection-related mortality and no relation of 3- or 6-month cumulative intravenous iron dose with all-cause or cardio-vascular mortality. There was a nonstatistically significant increase in infection-related mortality with receipt of.1050mg intravenous iron in 3months (hazard ratio, 1.69; 95% confidence interval, 0.87 to 3.28) and.2100mg in6 months (hazard ratio, 1.59; 95% confidence interval, 0.73 to 3.46).
ConclusionsAmong patients on incident dialysis, receipt of#1050 mg intravenous iron in 3 months or 2100 mgin 6 months was not associated with all-cause, cardiovascular, or infection-related mortality. However,nonstatistically significant findings suggested the possibility of infection-relatedmortalitywith receipt of.1050mgin 3 months or.2100 mg in 6 months. Randomized clinical trials are needed to assess the safety of exposure togreater cumulative intravenous iron doses.
Clin J Am Soc Nephrol 9: ccc–ccc, 2014. doi: 10.2215/CJN.03370414
IntroductionIntravenous (IV) iron use in the United States hemo-dialysis (HD) population has increased (1) in recentyears after changes in product labeling (2) and bun-dling of erythropoiesis-stimulating agents (ESAs) intodialysis per-treatment payments (3). The amount ofiron that can be safely administered over the shortand long term is unknown. In experimental studies, ex-cess iron has been shown to impair phagocytosis andenhance bacterial virulence, increasing risk for infection(4–7). However, the iron concentrations achieved inthese experiments greatly exceed the plasma iron levelsachieved in clinical practice. Iron, a potent oxidant,may also play a role in atherosclerosis (8–11). Addition-ally, recent studies show hepatic iron content to be se-verely elevated in some patients on HD (12–14), althoughthe clinical significance of this finding is unclear.
Clinical trials assessing the safety of more aggressiveiron repletion on patient-centered outcomes have notbeen conducted, and observational studies have yieldedinconsistent results (9,15–19). In a prevalent 1997–1998HD population, receipt of a cumulative iron dose ex-ceeding 1800 mg in 6 months was not associated withmortality (16). A more recent study found an increasein infection-related mortality and hospitalizations withreceipt of .200 mg IV iron in 1 month and bolus asopposed to maintenance iron therapy (15). Exposures.1 month were not examined in the first study (16),and cause-specific mortality was not examined in thesecond study (16). Furthermore, both of these studieswere conducted on prevalent populations and therein,may have been subject to survivor bias.Studies examining the association of administering
varying doses of IV ironwith clinical outcomes assessed
Due to the number ofcontributing authors,the affiliations areprovided in theSupplementalMaterial.
Correspondence:Dr. Dana C. Miskulin,Tufts Medical Center,Box 391, Division ofNephrology, 800Washington Street,Boston, MA 02111.Email: [email protected]
www.cjasn.org Vol 9 November, 2014 Copyright © 2014 by the American Society of Nephrology 1
. Published on October 15, 2014 as doi: 10.2215/CJN.03370414CJASN ePress

over differing lengths of time among patients on HD withsimilar dialysis history could help better elucidate the safetyof IV iron administration in clinical practice. Furthermore, itis possible that IV iron administration could decrease ESArequirements, leading to improvements in clinical outcomes,such as mortality. We examined associations of higherversus lower IV iron doses accumulated over 1, 3, and 6months with all-cause, cardiovascular (CV), and infection-related mortality in an entirely incident HD population us-ing analytic methods to account for potential time-varyingconfounders.
Materials and MethodsStudy PopulationThe study, described in detail previously (20,21), included
patients who initiated HD at dialysis units from a medium-sized national dialysis provider, Dialysis Clinic, Inc. (DCI),between January 1, 2003, and December 31, 2008, and hadMedicare as the primary payer.
Data SourcesThe electronic medical information system of DCI was
the primary source of information about ESA and IV irondoses and laboratory test results. Data were linked to theUS Renal Data System to obtain additional informationabout IV iron and ESA doses andMedicare claims. Cause ofdeath was on the basis of the National Death Index. Thestudy was conducted with adherence to the Declaration ofHelsinki. The Johns Hopkins Medicine Institutional ReviewBoard approved the study.
OutcomesThe primary outcome was all-cause mortality. We cen-
sored patients at the time of the switch from in-center HDto peritoneal or home HD, kidney transplant, transfer to an-other dialysis unit, loss to follow-up, December 31, 2008, or 4years of follow-up. For analyses of infection-related and CVmortality, patients were censored for other causes of death.
IV Iron ExposureOur primary exposure of interest was cumulative IV iron
dose calculated as the sum of IV iron in milligrams (allformulations) administered over 1-, 3-, and 6-month rollingwindows. We categorized IV iron doses into four mutuallyexclusive levels (no iron, low dose, moderate dose, or highdose) on the basis of the distribution of the data, previousanalyses, and our clinical experience. Before 2009, IV ironwas not administered by a protocol at DCI.
CovariatesWe defined baseline comorbidity from inpatient and out-
patient claims and diagnoses entered in the DCI databaseduring the first 90 days after starting dialysis. We scoredcomorbidity using a previously validated ESRD-specific co-morbidity index (22). We converted erythropoietin dosesto average daily doses and summed doses across 30-dayanalytic periods. Then, we created an average weekly dosefor the month by dividing by four. We used the percentsaturation of transferrin (TSat) and serum ferritin mea-sured closest to but not .90 days before the start of the
iron exposure window. To replicate decision-making inpractice, we considered the joint values of serum ferritinand TSat. We created a five-category variable reflecting thelikelihood that iron would be prescribed. We defined vas-cular access type as the access in use on the first day of themonth preceding the iron exposure window. We definedinfection as (1) the use of IV antibiotics as recorded in DCIor Medicare claims or (2) a hospitalization with a primarydiagnosis of infection within 21 days before the start of theiron exposure window. We defined noninfection-relatedhospitalizations as hospitalizations with a primary diag-nosis other than infection occurring within 21 days beforethe start of the iron exposure window.
Statistical AnalysesWe used marginal structural modeling (23,24) as our
primary methodology for analyzing associations of IViron dose with mortality, because prescribing decisionsare affected by characteristics that reflect past prescribingdecisions and also affect risk for death. We calculatedmonthly inverse probability weights to address time-varying confounding from the inverse of the predictedprobability that each subject belonged to the dosing cate-gory in which his or her own observed iron dose at eachfollow-up month fell conditional on their histories of priortreatment and time-varying confounders deemed to affectboth treatment choices and subsequent outcomes. Becausetreatment was defined by four levels of IV iron dose, wefitted multinomial logistic regression models for treatmentprobabilities. Treatment propensities were modeled beforethe start of the iron exposure window to avoid prediction oftreatment by future information (Figure 1). For each 30-dayinterval, we calculated the inverse of the probability of re-ceiving the treatment (e.g., treatment weight) and the inverseprobability of dropping out of the study (e.g., censoringweight). We calculated final weights as the product of thetreatment and censoring weights up to the month preced-ing the outcome assessment with stabilization using base-line demographic characteristics and comorbidity (23).We fit outcome models (separately) for 1-, 3-, and 6-month
rolling window cohorts using iron exposure averaged over asingle preceding interval as the primary predictor. Theywereimplemented as discrete time proportional hazards modelstaking person-months as observations (25). Because we hy-pothesized that the effect of iron on CV disease death wasdelayed, although the effect on infection-related death wasmore immediate, we imposed a 30-day lag between ironexposure and CV mortality, with no lag for all-cause andinfection-related mortality in our primary analyses. In sen-sitivity analyses, we also used similar models without thetime lag.In marginal structural modeling analyses, a few people
with very unusual treatment patterns may have extremelylarge weights (corresponding to small probabilities of theiroccurrence in the sample). Although disproportionateweighting is necessary to give them adequate representa-tion in analyses, these few individuals may then greatlyinfluence the analytic findings—a particularly troublingoutcome when one considers that very large weights tendto be imprecisely estimated. A common remedy is to applytruncation—that is, set all weights higher than a specifiedlevel to that level. We truncated weights at a level of
2 Clinical Journal of the American Society of Nephrology

10 (e.g., any weights.10 were reset to 10), a value selecteda priori to conform with commonly invoked truncation thresh-olds and limit undue influence while not diverging too widelyfrom a percentile-based truncation criterion of 1% of observa-tions (23,24). At a weight truncation of 10, approximately2%–5% of extreme weights were truncated. We conductedsensitivity analyses and truncated weights at 3, 5, 20, and 100.We accounted for outcome clustering by dialysis facilities
using generalized estimating equations (26) and estimatedrobust SEMs. We performed statistical analyses using SAS9.2 (SAS Institute Inc., Cary, NC). Detailed methods are pro-vided in the Supplemental Appendix.
ResultsCharacteristics of Study CohortsOf 21,233 patients who initiated dialysis between January
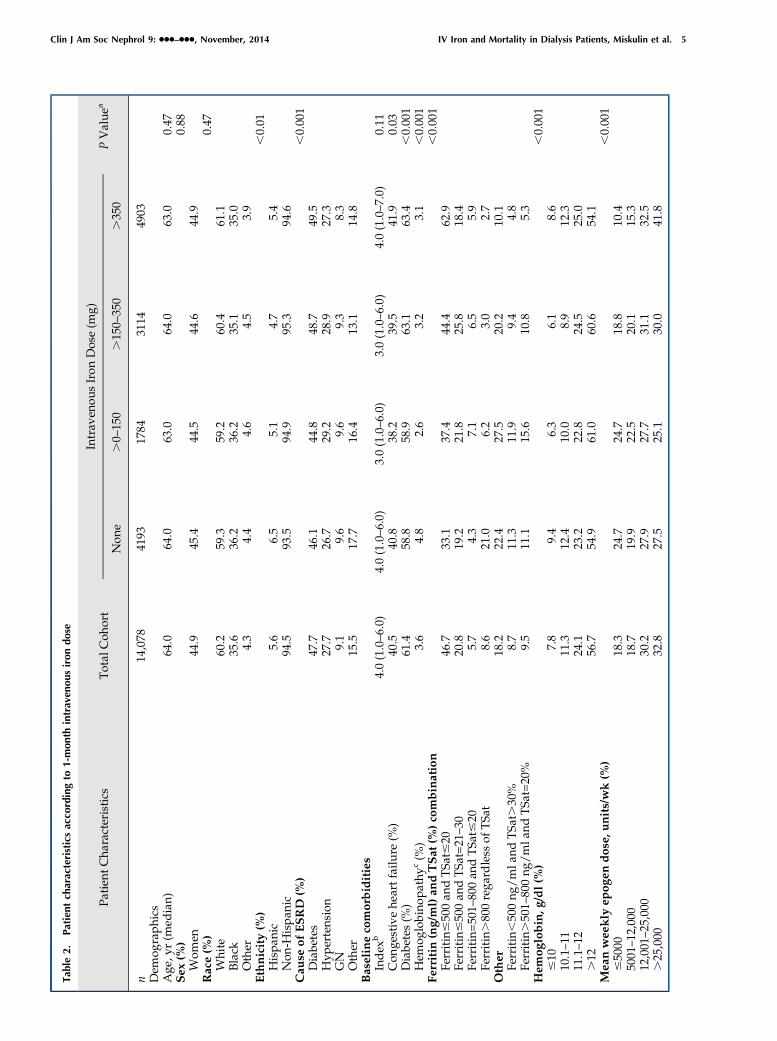
1, 2003, and December 31, 2008, at DCI, 66.3%, 59.6%, and51.3% met eligibility criteria (Figure 2) for the 1-, 3-, and6-month cumulative iron dose analyses, respectively (Table1). Patients receiving larger cumulative IV iron doses over 1(Table 2), 3, or 6 months were more likely to be white andhave diabetes; they had higher comorbidity index, lowerserum albumin, and lower TSat and serum ferritin, and theywere less likely to have a hemoglobin.12 g/dl (Supplemen-tal Tables 2 and 3) The vast majority (86%, 85%, and 87%) ofpatients who received the highest IV iron doses over 1, 3,and 6 months, respectively, had serum ferritin#500 ng/ml.
Association of IV Iron with Mortality in Weighted ModelsOne-Month Cohort. In fully adjusted models, receipt of
.150–350 mg and .350 mg IV iron were statistically sig-nificantly associated with 2% and 21%, respectively, lowerhazards of all-cause mortality compared with the refer-ence range (global test P=0.01). Findings for CV- andinfection-related mortality were not statistically signifi-cant (Table 3).Three-Month Cohort. There was no association of cu-
mulative IV iron dose over 3 months with all-cause or CVmortality. Findings for infection-related mortality were notstatistically significant, and point estimates differed in di-rection (,1.0 and .1.0) for the dose ranges .450–1050 and.1050 mg relative to the reference dose (Table 3).
Six-Month Cohort. There were no associations of cumu-lative iron doses over 6 months with all-cause or CV mor-tality. Similar to infection-related mortality in the 3-monthmodel, we observed a higher hazard of infection-related mor-tality for the highest dose category (.2100 mg for.6 months)but a lower hazard with the moderate dose category (900–2100 mg) compared with the reference (.0–900 mg), andthese associations were not statistically significant (Table 3).
Sensitivity AnalysesInfluence of Imposing Lag on CV Disease Deaths
When we eliminated the 30-day lag for ascertainment ofCV disease deaths, the categories of .150–350 and .350mg IV iron were associated with 27% and 26%, respectively,lower hazards of CV mortality (global test P=0.06), whichcontrasted with the lagged model in which the hazard ratioswere close to one and not significant (Supplemental Table 4).Models of 3- and 6-month iron exposure and CV mortalitywithout a lag did not differ from the lagged models.AlteringWeight Truncations Results using weight trun-
cations of 3, 5, 10, 20, and 100 in the weighted models werethe same for all except two models (Supplemental Tables7–15). The lower hazards of all-cause mortality with the.150–350 and .350 mg 1-month iron dose ranges thatwere found at a weight truncation of 10 were no longerstatistically significant at a weight truncation of 20 or 100(Supplemental Table 7). Point estimates were similar at alltruncation levels, which may implicate amplified variabilityaccompanying incorporation of extreme weights rather thanresidual confounding. In the 3-month model of infection-related death, the relationship of the .1050-mg IV irondose range with infection-related mortality at weight trun-cations ,20 was not significant, but .20, it was significant(Supplemental Table 12). The difference in result may re-flect better control for confounding by giving individualsmore representative weights.20 or that these rare individ-uals with unusual treatment patterns are exerting undueinfluence on the model.
DiscussionWe assessed the associations of short- and longer-term
cumulative IV iron doses with mortality in an incident HD
Figure 1. | Timing of predictor, exposure, and outcome windows. Iron was accumulated during exposure windows of 30, 90, or 180 days.Time-dependent confounders were defined during 90 days before the exposure window, and the outcomewas defined during 30 days after theexposure window (with a 30-day lag for the all-cause mortality model). Longitudinal analyses were conducted on the basis of parametersdefined in successive 1-month increments of this series of windows from the start to end of follow-up for each individual. Details are inMaterials and Methods and Supplemental Appendix.
Clin J Am Soc Nephrol 9: ccc–ccc, November, 2014 IV Iron and Mortality in Dialysis Patients, Miskulin et al. 3
population. We observed no evidence of increased all-causeor cause-specific mortality with administration of larger irondoses .1 month. Larger IV iron dose accumulations over 3and 6 months were also not associated with all-cause or CVmortality, but there was a nonsignificant trend toward anincrease in infection-related mortality. Results of this studywould suggest that dose accumulations#1050 mg IV iron in3 months and#2100 mg in 6 months are not associated withall-cause, CV, or infection-related mortality. However, find-ings suggest higher IV iron doses may increase infection-related mortality.Previous studies have produced conflicting results regard-
ing the association of IV iron dose with clinical outcomes.
Studies with no or minimal adjustment for time-dependentconfounding have shown increased mortality with cumula-tive IV iron doses .1000 mg in 6 months (17), .840 mg in 6months (9), or .400 mg in 13 weeks (18). In a subsequentstudy, receipt of .1800 mg in 6 months at baseline was alsoassociated with mortality, but the association was no longersignificant after adjustment for time-dependent confounders(15). Our findings are consistent with that study. Our resultsfor infection-related mortality are also consistent with a re-cent study that examined 1-month exposure in a mostlyprevalent population and showed an increase in infection-related deaths and hospitalizations with higher short-termIV iron exposures (.200 mg IV iron per month) as well as
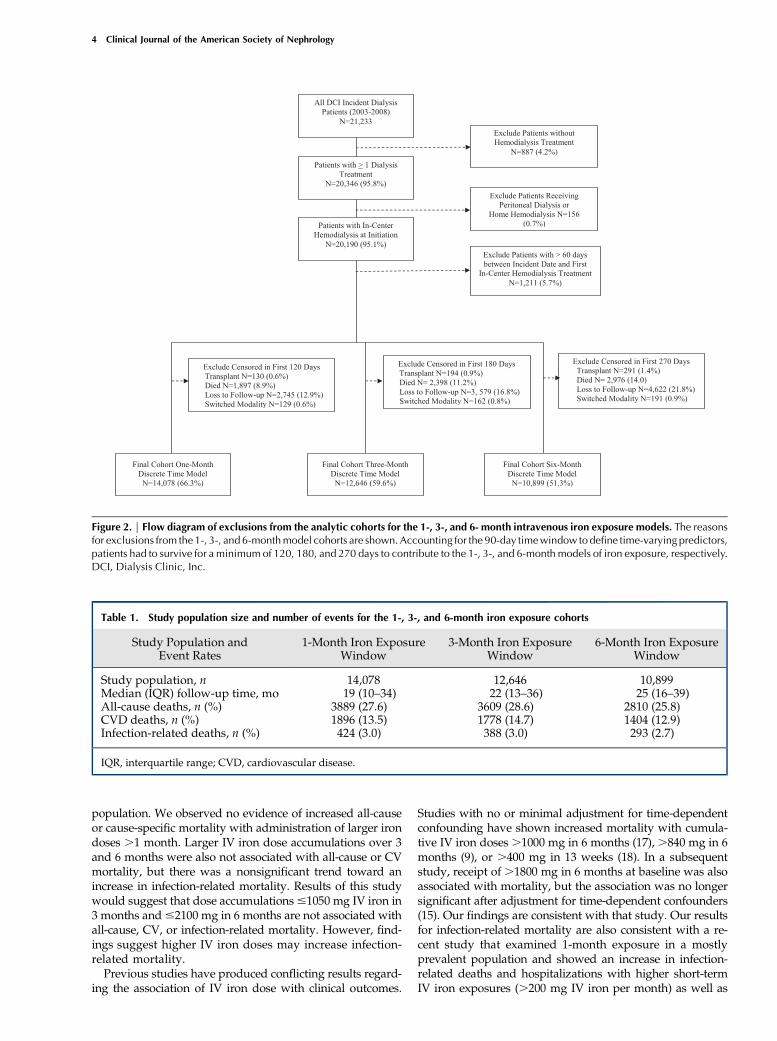
Figure 2. | Flow diagram of exclusions from the analytic cohorts for the 1-, 3-, and 6- month intravenous iron exposure models. The reasonsfor exclusions from the 1-, 3-, and 6-monthmodel cohorts are shown. Accounting for the 90-day timewindow todefine time-varying predictors,patients had to survive for a minimum of 120, 180, and 270 days to contribute to the 1-, 3-, and 6-month models of iron exposure, respectively.DCI, Dialysis Clinic, Inc.
Table 1. Study population size and number of events for the 1-, 3-, and 6-month iron exposure cohorts
Study Population andEvent Rates
1-Month Iron ExposureWindow
3-Month Iron ExposureWindow
6-Month Iron ExposureWindow
Study population, n 14,078 12,646 10,899Median (IQR) follow-up time, mo 19 (10–34) 22 (13–36) 25 (16–39)All-cause deaths, n (%) 3889 (27.6) 3609 (28.6) 2810 (25.8)CVD deaths, n (%) 1896 (13.5) 1778 (14.7) 1404 (12.9)Infection-related deaths, n (%) 424 (3.0) 388 (3.0) 293 (2.7)
IQR, interquartile range; CVD, cardiovascular disease.
4 Clinical Journal of the American Society of Nephrology
Tab
le2.
Patientch
arac
teristicsac
cordingto
1-m
onth
intrav
enousirondose
Patien
tCha
racteristics
Total
Coh
ort
Intrav
enou
sIron
Dose(m
g)PValue
a
Non
e.0–
150
.15
0–35
0.35
0
n14
,078
4193
1784
3114
4903
Dem
ographics
Age
,yr(m
edian)
64.0
64.0
63.0
64.0
63.0
0.47
Sex
(%)
0.88
Wom
en44
.945
.444
.544
.644
.9Race(%
)0.47
White
60.2
59.3
59.2
60.4
61.1
Black
35.6
36.2
36.2
35.1
35.0
Other
4.3
4.4
4.6
4.5
3.9
Ethnicity(%
),0.01
Hispa
nic
5.6
6.5
5.1
4.7
5.4
Non
-Hispan
ic94
.593
.594
.995
.394
.6Cau
seof
ESRD
(%)
,0.00
1Diabe
tes
47.7
46.1
44.8
48.7
49.5
Hyp
ertens
ion
27.7
26.7
29.2
28.9
27.3
GN
9.1
9.6
9.6
9.3
8.3
Other
15.5
17.7
16.4
13.1
14.8
Baselinecomorbidities
Index
b4.0(1.0–6.0)
4.0(1.0–6.0)
3.0(1.0–6.0)
3.0(1.0–6.0)
4.0(1.0–7.0)
0.11
Con
gestivehe
artfailu
re(%
)40
.540
.838
.239
.541
.90.03
Diabe
tes(%
)61
.458
.858
.963
.163
.4,0.00
1Hem
oglobino
pathyc
(%)
3.6
4.8
2.6
3.2
3.1
,0.00
1Fe
rritin
(ng/ml)an
dTSat
(%)co
mbination
,0.00
1Fe
rritin#50
0an
dTSa
t#20
46.7
33.1
37.4
44.4
62.9
Ferritin#50
0an
dTSa
t=21
–30
20.8
19.2
21.8
25.8
18.4
Ferritin=50
1–80
0an
dTSa
t#20
5.7
4.3
7.1
6.5
5.9
Ferritin.80
0rega
rdless
ofTSa
t8.6
21.0
6.2
3.0
2.7
Other
18.2
22.4
27.5
20.2
10.1
Ferritin,50
0ng
/mla
ndTSa
t.30
%8.7
11.3
11.9
9.4
4.8
Ferritin.50
1–80
0ng
/mla
ndTSa
t=20
%9.5
11.1
15.6
10.8
5.3
Hem
oglobin,g
/dl(%)
,0.00
1#10
7.8
9.4
6.3
6.1
8.6
10.1–11
11.3
12.4
10.0
8.9
12.3
11.1–12
24.1
23.2
22.8
24.5
25.0
.12
56.7
54.9
61.0
60.6
54.1
Mea
nwee
kly
epog
endos
e,units/wk(%
),0.00
1#50
0018
.324
.724
.718
.810
.450
01–12
,000
18.7
19.9
22.5
20.1
15.3
12,001
–25
,000
30.2
27.9
27.7
31.1
32.5
.25
,000
32.8
27.5
25.1
30.0
41.8
Clin J Am Soc Nephrol 9: ccc–ccc, November, 2014 IV Iron and Mortality in Dialysis Patients, Miskulin et al. 5

bolus ($100 mg for two or more consecutive treatments in1 month) versus maintenance therapy (15).Although two studies, including our study, suggest a re-
lation between IV iron and greater risk of infection-relatedoutcomes, inconsistencies in findings should be considered.The discordance in our findings for infection-related mor-tality and all-cause mortality, wherein we found an in-crease in infection-related deaths with higher cumulativeIV iron dose but no effect on all-cause mortality, is coun-terintuitive. If iron truly increased infections, we wouldhave expected an increase in all-cause mortality, consider-ing that this population is an older, frail population (50% ofpatients had diabetes). A prior study linking higher short-term iron exposure to infection-related outcomes in pa-tients on HD (15) did not report on all-cause mortality. Arecent meta-analysis examining outcomes associated withadministering IV iron versus oral iron or no iron in variousclinical trials involving iron-deficient (including HD) pop-ulations (27), also found an increased risk of infections butno effect on mortality. Discordance in findings regardinginfection-related mortality and all-cause mortality couldreflect bias caused by unmeasured confounders or, possi-bly, that IV iron increases infection-related deaths whiledecreasing noninfection-related deaths. We found no dose-response relationship of IV iron with infection-related mor-tality, calling into question the validity of a possible causalrelation between IV iron and infection-related mortality. Theincreased risk for infection-related death was only seenamong the highest dose category of the 3- and 6-month ex-posure models, whereas the hazard ratios of the next highestdose categories in both models are ,1. Additionally, theprior study reported a modest 5% increased hazard ofinfection-related deaths and hospitalizations with the ad-ministration of bolus or high-dose IV iron compared withnonbolus or lower-dose IV iron (28). It is possible that theassociation that we observed between higher-dose IV ironmay only indicate that patients who survived long enoughto incur these higher doses were actually more ill, becausethey required more iron because of ineffective use or someother reason.Considering that blood is lost with each HD treatment
(29), iron is used in ESA-stimulated erythropoiesis, andiron absorption is impaired (30), most patients on HDwould be expected to be deficient in iron if iron were notrepleted. Indeed, studies consistently show that administer-ing IV iron increases hemoglobin and reduces ESA doses(31–36), even among patients with serum ferritin=500–1200ng/ml (37,38). Given the range of documented and specu-lated toxicities of ESAs (39–41), it is possible that avoidinghigher ESA doses by giving more IV iron may be of netbenefit to patients, even if there were a modest increase inthe risk of infection. Beyond its role in erythropoiesis, ad-ministering iron may increase or improve the function ofother heme-containing proteins, specifically the cytochromes(42,43), which are integral to energy production and manymetabolic processes. It has been speculated that iron defi-ciency itself may induce cardiomyopathies and CV-relateddeaths. Studies have shown left ventricular dilation and mi-tochondrial swelling as well as normal sarcomere structurein rats fed an iron-deficient diet for 12 weeks (44). Random-ized control trials of administering IV iron in heart failurepopulations have shown reductions in inflammatory
Tab
le2.(Continued
)
Patien
tCha
racteristics
Total
Coh
ort
Intrav
enou
sIron
Dose(m
g)PValue
a
Non
e.0–
150
.15
0–35
0.35
0
Vascu
laraccess
(%)
,0.01
Arteriove
nousfistula
17.7
16.1
17.9
18.5
18.4
Arteriove
nousgraft
9.4
10.3
8.5
9.8
8.7
Cen
tral
veno
uscatheter
72.9
73.6
73.6
71.6
72.9
Serum
albu
min
(g/dl)b
3.6(3.3–3.9)
3.6(3.3–3.9)
3.6(3.3–3.9)
3.6(3.3–3.9)
3.6(3.3–3.9)
0.04
Serum
creatinine
(g/dl)b
6.1(4.6–8.1)
6.1(4.6–8.1)
6.2(4.5–8.2)
6.1(4.6–8.0)
6.1(4.6–8.1)
0.72
Bod
ymassindex
(kg/
m2 )b
27.2
(23.1–
32.6)
26.6
(22.8–
31.7)
26.6
(22.8–
32.0)
27.2
(23.4–
32.7)
27.9
(23.5–
33.5)
,0.00
1Infectionin
past
21d(%
)19
.120
.219
.018
.818
.30.14
Non
infection-relatedho
spitalizationin
past21
d(%
)6.5
7.0
6.1
6.3
6.5
0.52
Iron
(mg)
over
thepa
st3mob
1000
(300
–16
00)
0(0–15
0)11
00(500
–15
00)
1200
(650
–16
00)
1250
(800
–17
00)
,0.00
1
TSa
t,saturation
oftran
sferrin.
a Com
parisonacross
subg
roups
of1-mon
thcu
mulativeintrav
enou
siron
dose.
bMed
ianan
dinterqua
rtile
rang
e.c Inc
ludes
sick
lecell,
hereditarysp
herocy
tosis,mye
lodysplasia,multiplemye
loma,an
dothe
rane
miano
tcau
sedby
erythrop
oietin
oriron
defi
cien
cy;m
eanserum
albu
min
find
ings
areroun
ded
.Value
swere3.55
,3.55,
3.58
,and
3.57
forintrav
enou
siron
doses
ofno
ne,.
0–15
0mg,
.15
0–35
0mg,
and.35
0mg,
resp
ective
ly.
6 Clinical Journal of the American Society of Nephrology

Tab
le3.
Associationofintrav
enousirondose
withtimeto
all-ca
use,ca
rdiovascular,an
dinfection-related
death
Doses
(mg)
n(patient-m
o)Pe
rcen
tAll-Cau
seMortality
Cardiova
scular
Mortality
Infection-Related
Mortalitya
HR(95%
CI)
PValue
bHR(95%
CI)
PValue
bHR(95%
CI)
PValue
b
One-mon
thiron
exposure
Non
e90
,178
34.32
0.98
(0.79to
1.22
)0.01
1.11
(0.84to
1.48
)0.66
0.92
(0.54to
1.57
)0.43
.0–
150
53,302
20.16
Referen
ceReferen
ceReferen
ce.15
0–35
063
,327
23.96
0.78
(0.64to
0.95
)1.08
(0.80to
1.44
)0.77
(0.47to
1.26
).35
056
,993
21.56
0.79
(0.62to
0.99
)0.95
(0.70to
1.29
)1.26
(0.75to
2.12
)Three-mon
thiron
exposure
Non
e45
,247
19.17
1.19
(0.90to
1.57
)0.41
1.06
(0.72to
1.54
)0.49
0.86
(0.38to
1.96
)0.24
.0–
450
60,407
25.59
Referen
ceReferen
ceReferen
ce.45
0–10
5081
,396
34.48
0.99
(0.81to
1.20
)0.87
(0.67to
1.14
)0.99
(0.56to
1.74
).10
5049
,038
20.77
1.09
(0.84to
1.42
)1.02
(0.74to
1.41
)1.69
(0.87to
3.28
)Six-m
onth
iron
exposure
Non
e18
,555
9.19
1.24
(0.92to
1.69
)0.31
1.46
(0.98to
2.16
)0.28
0.75
(0.29to
1.95
)0.48
.0–
900
62,845
31.14
Referen
ceReferen
ceReferen
ce.90
0–21
0095
,058
47.10
0.98
(0.80to
1.21
)1.15
(0.85to
1.56
)0.98
(0.53to
1.81
).21
0025
,375
12.57
1.12
(0.81to
1.57
)1.17
(0.76to
1.79
)1.59
(0.73to
3.46
)
The
weigh
ting
oncu
mulativeiron
doses
received
was
ontheba
sisof
iron
history,
age,sex,
race,ethnicity,b
aselinecomorbidityat
90day
s,ba
selin
ebo
dymassindex
,cau
seof
ESR
D,y
earof
starting
dialysis,ba
selin
eiron
doses,h
emog
lobino
pathies,saturation
oftran
sferrin(TSa
t)/ferritin
catego
ries,h
emog
lobincatego
ries,w
eeklyerythrop
oietin
(EPO)d
oses
catego
ries,cha
ngein
EPO
,interaction
ofTSa
t/ferritin
catego
ries
andhe
mog
lobincatego
ries,album
in,creatinine,pred
ialysissystolicBP,
bodyweigh
t,ch
ange
inweigh
t,va
scular
access
type
,non
infection-related
hosp
italization,
andinfection.
Dem
ographics
andba
selin
ecomorbiditywereinclud
edin
theou
tcom
emod
els.HR,h
azardratio;
95%
CI,95
%confi
den
ceinterval.
a Mod
elsweread
justed
forallcov
ariatesinclud
edin
all-cause
andcard
iova
scularmoralitymod
els,exceptrecen
tinfection
.bGloba
ltests
ofiron
expo
sure.
Clin J Am Soc Nephrol 9: ccc–ccc, November, 2014 IV Iron and Mortality in Dialysis Patients, Miskulin et al. 7

markers and improvements in functional classification, exer-cise capacity, and quality of life, regardless of the continuedpresence of anemia (45,46), which may suggest a role foriron independent of effects on hemoglobin. A recent studyfound increased CV events and reduced survival associatedwith a TSat,20% relative to TSat=20%–40%, independent ofhemoglobin level (47). A reduction in platelets is anotherpostulated mechanism for a reduction in CV events withIV iron replacement (48).There are several unique strengths of our study. To date,
this study is the only observational study relating IV irondose to outcomes that has (1) been conducted on an en-tirely incident population, (2) assessed both short- andlong-term exposures to IV iron, (3) examined effects onall-cause, infection-related, and CV deaths, and (4) exam-ined iron doses and outcomes as early as 120 days afterdialysis initiation, a time period during which larger dosesof IV iron tend to be given (49) and the potential for harmmay be greater because of greater central venous catheteruse.Our study also had limitations. Althoughwe adjusted for
many potential confounders and used marginal structuralmodeling to attempt to control for time-dependent con-founding, the potential for residual confounding remains.This concern may be particularly relevant to our analyseson infection-related mortality, for which our power to de-tect subtle associations was limited. The timing of adverseevents relative to iron exposure is uncertain, and the dif-ference between lagged and unlagged models for 1-monthiron exposure and CV mortality further highlights the needfor a prospective trial, in which adverse events are mea-sured immediately after and over a longer period after ironexposure. Our study ended on December 31, 2008. Sincethat time, larger cumulative iron doses have been morefrequently prescribed, potentially limiting the generaliz-ability of our findings to current practice. The safety ofadministering higher doses of IV iron in patients with se-rum ferritin.500 ng/ml also may not have been assessedadequately, because it was an infrequent practice duringthe time course of this study. Our study was not designedto explore the influence of the pattern of iron administra-tion on outcomes, which may be important, in addition tocumulative dose. It is possible that risk may be on the basisof iron preparations, which were not analyzed separatelyin this study. Nonetheless, our study represents one of thefirst studies to rigorously explore the potential associationof cumulative IV iron use over shorter and longer periodsand cause-specific mortality.In conclusion, we did not observe consistent findings of
an association between higher cumulative IV iron dosesover 1, 3, or 6 months with all-cause mortality or CV mor-tality, but there was a nonsignificant increase in infection-related mortality with receipt of .1050 mg IV iron in 3months or .2100 mg in 6 months. Associations on thebasis of observational data may be biased. Because a ma-jority of patients on HD receives IV iron therapy, rigor-ously conducted and adequately powered clinical trialsstudying iron administration patterns reflective of present-day practice are greatly needed to provide definitive evi-dence about the safety of exposure to greater cumulativeIV iron doses in patients on HD.
AcknowledgmentsThe authors express their gratitude to the staff and patients of
Dialysis Clinic Inc.The Developing Evidence to Inform Decisions about Effective-
ness (DEcIDE) Network Patient Outcomes in ESRD Study was sup-ported by Agency for Healthcare Research and Quality ContractHHSA290200500341I (Task Order 6). W.M.M. was supported byDutch Kidney Foundation (Nierstichting) Postdoctoral Full Fel-lowship Abroad Grant (KFB 11.005). D.C.C. was supported by theAmos Medical Faculty Development Program of the Robert WoodJohnson Foundation. J.J.S. was supported by National Institute forDiabetes, Digestive and Kidney Diseases (NIDDK) Grant K23-DK095949. T.S. was supported by NIDDK Grant K23-DK083514.Parts of this manuscript were previously presented as a poster at
the Annual American Society of NephrologyMeeting in San Diego,CA (October 30 to November 4, 2012).Identifiable information, on which this report, presentation, or
other form of disclosure is based, is confidential and protected byfederal law: Section 903(c) of the Public Health Service Act, 42 USC299a-1(c). Any identifiable information that is knowingly disclosedis disclosed solely for the purpose forwhich it has been supplied.Noidentifiable information about any individual supplying the in-formation or described in it will be knowingly disclosed exceptwiththe prior consent of that individual. The data reported here havebeen supplied by the US Renal Data System. The interpretation andreporting of these data are the responsibility of the author(s) and innoway shouldbe seen as anofficial policy or interpretation of theUSGovernment.The DEcIDE Network Patient Outcomes in ESRD Study Team
consists ofmembers from JohnsHopkinsUniversity (K.B.-R., J.Z.,A.M., P.L.E.,W.M.M., B.G.J., D.C.C., S.M.S., T.S.,A.W.W.,C.C., L.E.B.,Josef Coresh, JeonyongKim, Yang Liu, Jason Luly, andPaul Scheel),UniversityofCalifornia, SanFrancisco (Neil Powe),ChronicDiseaseResearch Group (Allan Collins, Robert Foley, David Gilbertson,Haifeng Guo, Brooke Heubner, Charles Herzog, Jiannong Liu,and Wendy St. Peter), Cleveland Clinic Foundation (Joseph Nally,Susana Arrigain, Stacey Jolly, Vicky Konig, Xiaobo Liu, SankarNavaneethan, and Jesse Schold), University of NewMexico (PhilipZager), Tufts University (D.C.M. and K.B.M.), University of Miami(J.J.S.),University ofManitoba (N.T.), andAcademicMedicalCenter(W.M.M.).
DisclosuresNone.
References1. Fuller DS, Pisoni RL, Bieber BA, Gillespie BW, Robinson BM: The
DOPPS Practice Monitor for US dialysis care: Trends throughDecember 2011. Am J Kidney Dis 61: 342–346, 2013
2. FDA Drug Safety Communication: Modified dosing recom-mendations to improve the safe use of Erythropoiesis-StimulatingAgents (ESAs) in chronic kidney disease. Available at: http://www.fda.gov/Drugs/DrugSafety/ucm259639.htm. Accessed July 2,2012
3. The Federal Register 42 CFR Parts 410, 413 and 414 MedicareProgram; End-Stage Renal Disease Prospective Payment System;Final Rule and Proposed Rule. Available at: http://www.gpo.gov/fdsys/pkg/FR-2010-08-12/pdf/2010-18466.pdf. AccessedJuly 2, 2013
4. Boelaert JR, Daneels RF, Schurgers ML, Matthys EG, Gordts BZ,Van Landuyt HW: Iron overload in haemodialysis patients in-creases the risk of bacteraemia: A prospective study. NephrolDial Transplant 5: 130–134, 1990
5. Payne SM: Iron and virulence in the family Enterobacteriaceae.Crit Rev Microbiol 16: 81–111, 1988
8 Clinical Journal of the American Society of Nephrology

6. Seifert A, von Herrath D, Schaefer K: Iron overload, but nottreatment with desferrioxamine favours the development ofsepticemia in patients on maintenance hemodialysis. Q J Med65: 1015–1024, 1987
7. Sunder-Plassmann G, Patruta SI, Horl WH: Pathobiology of therole of iron in infection. Am J Kidney Dis 34[Suppl 2]: S25–S29,1999
8. Drueke T,Witko-Sarsat V, Massy Z, Descamps-Latscha B, GuerinAP, Marchais SJ, Gausson V, London GM: Iron therapy, advancedoxidation protein products, and carotid artery intima-mediathickness in end-stage renal disease. Circulation 106: 2212–2217, 2002
9. Kuo K-L, Hung S-C, Lin Y-P, Tang C-F, Lee T-S, Lin C-P, Tarng DC:Intravenous ferric chloride hexahydrate supplementation in-duced endothelial dysfunction and increased cardiovascular riskamong hemodialysis patients. PLoS ONE 7: e50295, 2012
10. Reis KA, Guz G, Ozdemir H, Erten Y, Atalay V, Bicik Z, OzkurtZN, Bali M, Sindel S: Intravenous iron therapy as a possiblerisk factor for atherosclerosis in end-stage renal disease. Int HeartJ 46: 255–264, 2005
11. Rooyakkers TM, Stroes ES, Kooistra MP, van Faassen EE, HiderRC, Rabelink TJ, Marx JJ: Ferric saccharate induces oxygenradical stress and endothelial dysfunction in vivo. Eur J Clin Invest32[Suppl 1]: 9–16, 2002
12. Ferrari P, Kulkarni H, Dheda S, Betti S, Harrison C, St Pierre TG,Olynyk JK: Serum iron markers are inadequate for guiding ironrepletion in chronic kidney disease. Clin J Am Soc Nephrol 6:77–83, 2011
13. Rostoker G, Griuncelli M, Loridon C, Couprie R, Benmaadi A,Bounhiol C, Roy M, Machado G, Janklewicz P, Drahi G, DahanH, Cohen Y:Hemodialysis-associated hemosiderosis in the era oferythropoiesis-stimulating agents: A MRI study. Am J Med 125:991–999, 2012
14. Canavese C, Bergamo D, Ciccone G, Longo F, Fop F, Thea A,Martina G, Piga A: Validation of serum ferritin values by mag-netic susceptometry in predicting iron overload in dialysis pa-tients. Kidney Int 65: 1091–1098, 2004
15. Brookhart MA, Freburger JK, Ellis AR,Wang L,WinkelmayerWC,Kshirsagar AV: Infection risk with bolus versus maintenanceiron supplementation in hemodialysis patients. J AmSocNephrol24: 1151–1158, 2013
16. Feldman HI, Joffe M, Robinson B, Knauss J, Cizman B, Guo W,Franklin-Becker E, FaichG: Administration of parenteral iron andmortality among hemodialysis patients. J Am Soc Nephrol 15:1623–1632, 2004
17. Feldman HI, Santanna J, Guo W, Furst H, Franklin E, Joffe M,Marcus S, Faich G: Iron administration and clinical outcomes inhemodialysis patients. J Am Soc Nephrol 13: 734–744, 2002
18. Kalantar-Zadeh K, Regidor DL, McAllister CJ, Michael B,Warnock DG: Time-dependent associations between iron andmortality in hemodialysis patients. J Am Soc Nephrol 16: 3070–3080, 2005
19. Kshirsagar AV, Freburger JK, Ellis AR, Wang L,WinkelmayerWC,Brookhart MA: Intravenous iron supplementation practicesand short-term risk of cardiovascular events in hemodialysispatients. PLoS ONE 8: e78930, 2013
20. Boulware LE, Tangri N, Ephraim PL, Scialla JJ, Sozio SM, CrewsDC, Shafi T, Miskulin DC, Liu J, St Peter W, Jaar BG, Wu AW,Powe NR, Navaneethan SD, Bandeen-Roche K; DEcIDE ESRDPatient Outcomes in Renal Disease Study Investigators: Com-parative effectiveness studies to improve clinical outcomes inend stage renal disease: The DEcIDE patient outcomes in endstage renal disease study. BMC Nephrol 13: 167–177, 2012
21. Miskulin DC, Zhou J, Tangri N, Bandeen-Roche K, Cook C,Ephraim PL, Crews DC, Scialla JJ, Sozio SM, Shafi T, Jaar BG,Boulware LE; DEcIDE Network Patient Outcomes in End StageRenal Disease Study Investigators: Trends in anemia manage-ment in US hemodialysis patients 2004-2010. BMC Nephrol 14:264, 2013
22. Liu J, Huang Z, GilbertsonDT, Foley RN, Collins AJ: An improvedcomorbidity index for outcome analyses among dialysis patients.Kidney Int 77: 141–151, 2010
23. HernanMA, Brumback B, Robins JM:Marginal structural modelsto estimate the causal effect of zidovudine on the survival of HIV-positive men. Epidemiology 11: 561–570, 2000
24. Robins JM, HernanMA, Brumback B:Marginal structural modelsand causal inference in epidemiology. Epidemiology 11: 550–560, 2000
25. Prentice RL, Gloeckler LA: Regression analysis of grouped sur-vival data with application to breast cancer data. Biometrics 34:57–67, 1978
26. Liang K-Y, Zeger SL: Longitudinal data analysis using generalizedlinear models. Biometrika 73: 13–22, 1986
27. Litton E, Xiao J, Ho KM: Safety and efficacy of intravenous irontherapy in reducing requirement for allogeneic blood trans-fusion: Systematic review and meta-analysis of randomisedclinical trials. BMJ 347: f4822, 2013
28. Monson R: Occupational Epidemiology, 2nd Ed., Boca Raton,FL, CRC Press Inc., 1990
29. Sargent JA, Acchiardo SR: Iron requirements in hemodialysis.Blood Purif 22: 112–123, 2004
30. Kidney Disease: Improving Global Outcomes (KDIGO) AnemiaWork Group: KDIGO clinical practice guideline for anemia inchronic kidney disease. Kidney Int Suppl 2: 295–296, 2012
31. Besarab A, Kaiser JW, Frinak S: A study of parenteral iron regi-mens in hemodialysis patients. Am J Kidney Dis 34: 21–28, 1999
32. Chang CH, Chang CC, Chiang SS: Reduction in erythropoietindoses by the use of chronic intravenous iron supplementation iniron-replete hemodialysis patients. Clin Nephrol 57: 136–141,2002
33. DeVita MV, Frumkin D, Mittal S, Kamran A, Fishbane S, MichelisMF: Targeting higher ferritin concentrations with intravenousiron dextran lowers erythropoietin requirement in hemodialysispatients. Clin Nephrol 60: 335–340, 2003
34. Fishbane S, Frei GL, Maesaka J: Reduction in recombinant hu-man erythropoietin doses by the use of chronic intravenous ironsupplementation. Am J Kidney Dis 26: 41–46, 1995
35. Macdougall IC, Tucker B, Thompson J, Tomson CR, Baker LR,Raine AE: A randomized controlled study of iron supplementa-tion in patients treated with erythropoietin. Kidney Int 50: 1694–1699, 1996
36. Sunder-Plassmann G, Horl WH: Importance of iron supply forerythropoietin therapy.Nephrol Dial Transplant 10: 2070–2076,1995
37. Coyne DW, Kapoian T, Suki W, Singh AK, Moran JE, Dahl NV,Rizkala AR; DRIVE Study Group: Ferric gluconate is highly effi-cacious in anemic hemodialysis patients with high serum ferritinand low transferrin saturation: Results of the Dialysis Patients’Response to IV Ironwith Elevated Ferritin (DRIVE) Study. J AmSocNephrol 18: 975–984, 2007
38. Kapoian T, O’Mara NB, Singh AK, Moran J, Rizkala AR,Geronemus R, Kopelman RC, Dahl NV, Coyne DW: Ferric glu-conate reduces epoetin requirements in hemodialysis patientswith elevated ferritin. J Am Soc Nephrol 19: 372–379, 2008
39. Injection Epogen (Recombinant Epoetin Alpha) Prescribing In-formation. Available at: http://www.epogen.com/. Accessed July11, 2014
40. Unger EF, Thompson AM, Blank MJ, Temple R: Erythropoiesis-stimulating agents—time for a reevaluation. N Engl J Med 362:189–192, 2010
41. Szczech LA, Barnhart HX, Inrig JK, Reddan DN, Sapp S, CaliffRM, Patel UD, Singh AK: Secondary analysis of the CHOIR trialepoetin-alpha dose and achieved hemoglobin outcomes. KidneyInt 74: 791–798, 2008
42. Dallman PR: Biochemical basis for the manifestations of irondeficiency. Annu Rev Nutr 6: 13–40, 1986
43. Dallman PR, SchwartzHC:Myoglobin and cytochrome responseduring repair of iron deficiency in the rat. J Clin Invest 44: 1631–1638, 1965
44. Dong F, Zhang X, Culver B, Chew HG Jr., Kelley RO, Ren J: Di-etary iron deficiency induces ventricular dilation, mitochondrialultrastructural aberrations and cytochrome c release: In-volvement of nitric oxide synthase and protein tyrosine nitration.Clin Sci (Lond) 109: 277–286, 2005
45. Anker SD, Comin Colet J, Filippatos G, Willenheimer R,Dickstein K, Drexler H, Luscher TF, Bart B, Banasiak W,Niegowska J, Kirwan B-A,Mori C, von Eisenhart Rothe B, PocockSJ, Poole-Wilson PA, Ponikowski P; FAIR-HF Trial Investigators:Ferric carboxymaltose in patients with heart failure and irondeficiency. N Engl J Med 361: 2436–2448, 2009
Clin J Am Soc Nephrol 9: ccc–ccc, November, 2014 IV Iron and Mortality in Dialysis Patients, Miskulin et al. 9

46. Comin-Colet J, Lainscak M, Dickstein K, Filippatos GS, Johnson P,Luscher TF, Mori C, Willenheimer R, Ponikowski P, Anker SD: Theeffect of intravenous ferric carboxymaltose on health-related qualityof life in patients with chronic heart failure and iron deficiency:A subanalysis of the FAIR-HF study. Eur Heart J 34: 30–38, 2013
47. Koo HM, Kim CH, Doh FM, Lee MJ, Kim EJ, Han JH, Han JS, OhHJ, Park JT, Han SH, Yoo T-H, Kang S-W: The relationship of initialtransferrin saturation to cardiovascular parameters and outcomesin patients initiating dialysis. PLoS ONE 9: e87231, 2014
48. Streja E,KovesdyCP,GreenlandS,Kopple JD,McAllisterCJ,NissensonAR, Kalantar-Zadeh K: Erythropoietin, iron depletion, and relativethrombocytosis: A possible explanation for hemoglobin-survivalparadox in hemodialysis. Am J Kidney Dis 52: 727–736, 2008
49. USRDS: Assessment of the new bundled dialysis payment systemand overview of the ESRD program. Presented at the AnnualMeeting of the American Society of Nephrology, San Diego, CA,October 30-November 4, 2012
Received: April 2, 2014 Accepted: July 18, 2014
Published online ahead of print. Publication date available at www.cjasn.org.
This article contains supplemental material online at http://cjasn.asnjournals.org/lookup/suppl/doi:10.2215/CJN.03370414/-/DCSupplemental.
10 Clinical Journal of the American Society of Nephrology