
Membrane topology of human NPC1L1, a key protein in enterohepatic cholesterol absorption
Upload
independentCategory
view
1download
0
Article
Cholesterol Synthesis, Cholesterol Absorption, andMortality in Hemodialysis Patients
Kyrill S. Rogacev,* Tobias Pinsdorf,† Oliver Weingartner,‡ Markus K. Gerhart,* Elena Welzel,* Kai van Bentum,*Julius Popp,§ Andreas Menzner,| Danilo Fliser,* Dieter Lutjohann,† and Gunnar H. Heine*
SummaryBackground and objectives Recent clinical trials on cholesterol-lowering in patients with CKD yielded conflictingresults, which might have resulted from different treatment strategies. Serum cholesterol levels are determinedby endogenous synthesis and intestinal absorption, which are differentially influenced by various classes ofcholesterol-lowering agents. Assessing markers of cholesterol metabolism has thus been proposed for guidanceof lipid-lowering therapy. This study analyzed surrogate markers of cholesterol absorption and synthesis inhemodialysis (HD) patients.
Design, setting, participants, & measurements In 113 HD patients, lathosterol was measured as a markerof cholesterol synthesis and cholestanol was measured as a marker of cholesterol absorption via gas chroma-tography. Controls were 229 healthy persons. Overall survival in HD patients was recorded over 3.4-yearfollow-up.
Results Compared with controls, HD patients had lower lathosterol and higher cholestanol levels (P,0.001 forboth). During follow-up, 58 patients died; higher cholestanol (indicating higher cholesterol absorption) predictedpoor outcome among HD patients in multivariate Cox regression analysis after adjustment for potential con-founders (hazard ratio for cholestanol above median, 2.24 [95% confidence interval (CI), 1.29–3.89]; P=0.004),whereas lower lathosterol (indicating lower cholesterol synthesis) did not (hazard ratio for lathosterol belowmedian, 1.43 [95% CI, 0.81–2.50]; P=0.22).
Conclusions This analysis of markers of cholesterol metabolism characterizes HD patients as cholesterolabsorbers. In longitudinal analysis, higher levels of cholestanol were associated with all-cause mortality.
Clin J Am Soc Nephrol 7: 943–948, 2012. doi: 10.2215/CJN.05170511
IntroductionPatients undergoing hemodialysis (HD) suffer from amortality rate that reaches approximately 20% per year(1). Although this enormous death toll is prominentlydriven by high cardiovascular mortality, traditionalpathways of atherogenesis can only partly explainthis phenomenon (2).
In the course of progressive loss of renal function,derangements in lipid metabolism occur (3), andrecent data revealed surprisingly low LDL choles-terol levels in HD patients (4–6). In two previouslarge-scale trials—4D (Die Deutsche Diabetes Dia-lyse Studie) and AURORA (A Study to Evaluatethe Use of Rosuvastatin in Subjects on RegularHemodialysis)—statin monotherapy failed to show asurvival benefit (4,6) despite leading to an LDL choles-terol reduction of a magnitude shown to significantlyreduce cardiovascular morbidity and mortality in thegeneral population (7). In contrast, SHARP (the Studyof Heart and Renal Protection) achieved for the firsttime a significant, albeit modest, reduction of cardio-vascular events in patients with CKD by combininginhibition of cholesterol synthesis via statin treatment
and inhibition of intestinal cholesterol absorption viaezetimibe (8).The different results obtained in 4D (6) andAURORA
(4) versus SHARP (8) remain elusive but might bepartly due to the differing treatment strategies used.Notably, serum cholesterol levels are determined byboth endogenous synthesis and intestinal absorptionof exogenous cholesterol. Both components of choles-terol metabolism can be assessed by measurement oflathosterol, an established surrogate marker that re-flects hepatic synthesis, and cholestanol, an acceptedmarker of exogenous absorption (9). Because individ-uals with high cholesterol absorption are less likely tobenefit from statin treatment (10), it has been suggestedfor the general population to stratify patients accordingto their pattern of cholesterol metabolism as “synthe-sizer type,” “mixed type,” and “absorber type” in orderto guide cholesterol-lowering therapy (11).However, a comprehensive assessment of cholesterol
metabolism has not been performed in HD patients. Inour opinion, such an analysis is needed because itsimplications might be similar to those for the generalpopulation.
*Department ofInternal Medicine IV,Nephrology andHypertension, and‡Department ofInternal Medicine III,Cardiology, Angiologyand Intensive CareMedicine, SaarlandUniversity MedicalCenter, Homburg,Germany; †Instituteof Clinical Chemistryand ClinicalPharmacology and§Department ofPsychiatry, UniversityHospital Bonn, Bonn,Germany; and|Department ofInternal Medicine III,Nephrology, SHG-Kliniken Volklingen,Saarland, Germany
Correspondence: Dr.Gunnar H. Heine,Department ofInternal Medicine IV,Nephrology andHypertension,Saarland UniversityMedical Center,Homburg, Germany.Email: [email protected]
www.cjasn.org Vol 7 June, 2012 Copyright © 2012 by the American Society of Nephrology 943
Materials and MethodsStudy PopulationWe recruited 159 HD patients in four outpatient dialy-
sis practices throughout the Federal State of Saarland,Germany, in April 2008. Comorbidity and medication weredetermined by chart review and standardized interviewsat baseline. Patients taking ezetimibe or statin medicationwere excluded from the analysis (n=46), leaving 113 patientsfor further analysis. Median vintage of dialysis treatmentwas 3.4 years (interquartile range, 1.7–5.8 years). Patientswith a history of diabetes mellitus, a spontaneous plasmaglucose level of $200 mg/dl, hypoglycemic treatment, orself-reported diabetes mellitus were categorized as dia-betic. Patients were defined as active smokers if they werecurrent smokers or had stopped smoking less than 1 monthbefore entry into the study. Body mass index was calculatedas body weight in kg/height in m2 (2).Before an HD session, systolic and diastolic BP were
measured and mean BP was calculated as follows:
ðdiastolic BPþ ½systolic BP2 diastolic BP�=3Þ:
Informed consent was obtained from all patients, and thestudy design was approved by the local ethics committee.All participants were followed from the baseline examina-tion until death or August 31, 2011. Complete follow-updata were available for 112 of 113 patients.To compare measures of cholesterol metabolism in HD
patients with those in individuals with intact renal function,229 persons from a previously described cohort (12) withoutmanifest cardiovascular disease, known diabetes mellitus, orintake of statins or ezetimibe served as controls.
Biochemical AnalysisBlood samples were taken from all participants before
the start of an HD session. To recruit patients from theafternoon HD sessions, no effort was made to collect fastingblood samples. However, we are certain that collection ofnonfasting samples does not interfere with our analysis:Markers of cholesterol synthesis and absorption are mostlybound to LDL cholesterol (13), which is not affected bytiming of meals.Plasma concentrations of cholesterol were measured by
gas chromatography–flame ionization detection (GC-FID).Fifty micrograms 5a-cholestane (Serva) (50 ml from a stocksolution of 5a-cholestane in cyclohexane; 1 mg/ml) and1 mg epicoprostanol (Sigma) (10 ml from a stock solutionepicoprostanol in cyclohexane; 100 mg/ml) were added to100 ml of plasma. After addition of 1 ml NaOH (1 M) in90% ethanol, alkaline hydrolysis was performed for 120minutes at 50°C, the solution was neutralized with phos-phoric acid (50%, vol/vol), and the sterols were extractedtwice with 4 ml of cyclohexane. The organic solvents wereevaporated and the residual sterols were derivatized totrimethylsilyl (TMSi) ethers by adding 1 ml TMSi-reagent(pyridine:hexamethylsisilazane:trimethylchlorosilane, 9:3:1,by volume; all reagents were from Merck) and incubationfor 1 hour at 64°C. The derivatization reagent was evaporatedunder nitrogen and the silyl sterol ethers from plasma weredissolved in 160 ml n-decane. Eighty microliters of the solu-tion was transferred into microvials for gas chromatography-mass spectrometry–selected ion monitoring (GC-MS-SIM)
of cholesterol precursors. The residual 80 ml was dilutedwith 400 ml n-decane for analysis of cholesterol by GC-FID.Plasma cholesterol was quantified by GC-FID on a
Hewlett-Packard 6890 series II plus gas chromatograph(Agilent Technologies, Böblingen, Germany) using 5a-cholestane as an internal standard. An aliquot of 1 ml wasinjected in a splitless mode at 280°C by an automated sam-pler and injector (Hewlett-Packard 7683). Hydrogen wasused as the carrier gas with an inlet pressure of 9.9 psi, re-sulting in a total gas flow of 1.1 ml/min; the temperature ofthe FID was kept at 280°C. The sterols were separated on across-linked methyl silicone DB-XLB 122-1232 fused silicacapillary column (J&W, Folsom, CA) (30 m 3 0.25 mm [i.e.,30.25-mm film thickness]) in a Hewlett-Packard 6890) gaschromatograph. The oven temperature was initially kept at
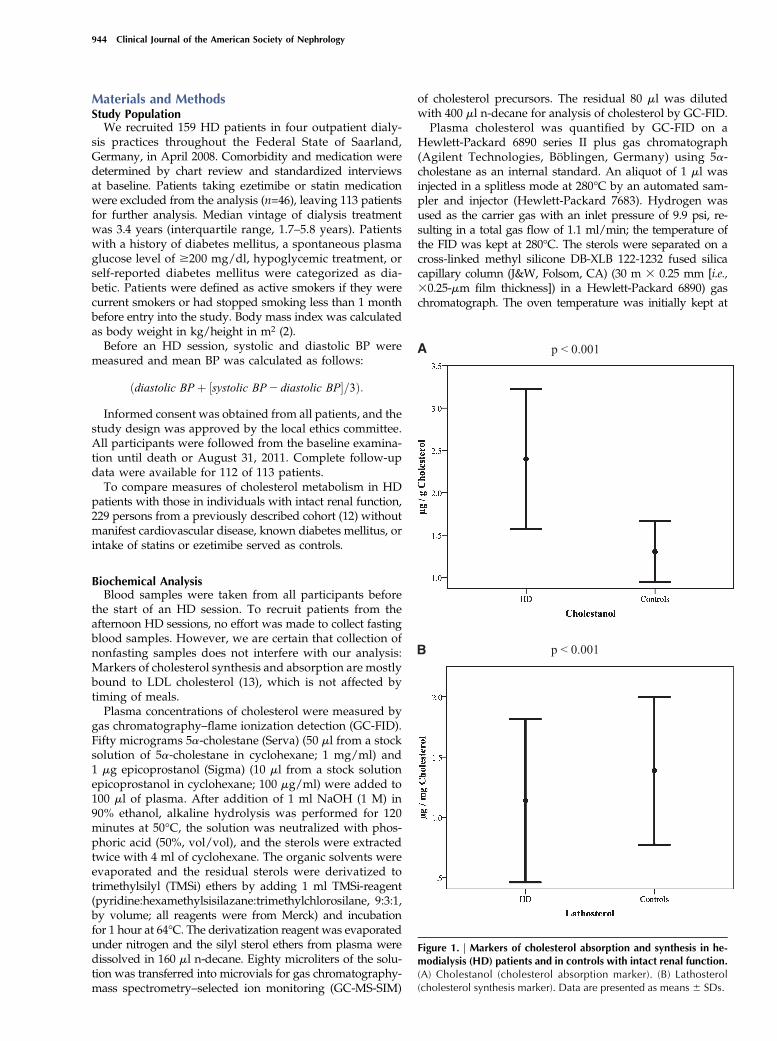
Figure 1. | Markers of cholesterol absorption and synthesis in he-modialysis (HD) patients and in controls with intact renal function.(A) Cholestanol (cholesterol absorption marker). (B) Lathosterol(cholesterol synthesis marker). Data are presented as means 6 SDs.
944 Clinical Journal of the American Society of Nephrology
150°C for 3 minutes and was then increased at 30°C incre-ments to a final temperature of 290°C. The ratios of thecholesterol areas to the area of internal standard were cal-culated and multiplied by the added amount of the inter-nal standard (50 mg 5a-cholestane) to reveal absolutecholesterol concentrations.GC-MS-SIM was performed on a Hewlett-Packard
GC-mass selective detector system (5890 series II GC) com-bined with a 5971 mass selective detector (Agilent Tech-nologies) equipped with a DB-XLB 122-1232 fused silicacapillary column (J&W) (30 m 3 0.25 mm [i.e., 30.25-mmfilm thickness]) in the splitless mode using helium (1 ml/min)as the carrier gas. The temperature program was as follows:150°C for 1 minute, followed by 20°C increases per minuteup to 260°C, and 10°C increases per minute up to 280°C(for 15 minutes). Neutral sterols were monitored as theirTMSi derivatives in the selected ion monitoring mode us-ing the following masses: epicoprostanol (internal stan-dard) mass-to-charge ratio (m/z) 370 (M+-OTMSi),cholesterol at m/z 458 (M+), cholestanol at m/z 306(M+-OTMSi-CH3-C3H9), and lathosterol at m/z 458(M+). Peak integration was performed manually and ste-rols were quantified from selected ion monitoring analy-ses against internal standard (epicoprostanol) usingstandard curves for the listed sterols. Identity of all sterolswas proven by comparison with the full-scan mass spectraof authentic compounds (range, m/z 50–500). Additionalqualifier (characteristic fragment) ions were used forstructural identification. All the preceding determinedprecursors were sufficiently separated on the columnfrom additional precursors, such as 7-dehydrocholesterol,methyl precursors, or plant sterols, present in plasmasamples. The intra- and interday coefficients of variationfor all sterols were less than 3%. Accuracy of the methodwas established by recovery experiments, day-to-dayvariation (below 3%), limit of detection, and limit ofquantification below the present concentrations for eachsterol.In line with common practice (14), serum cholestanol and
lathosterol levels are expressed as cholestanol-to-cholesterolratios and lathosterol-to-cholesterol ratios.
Statistical AnalysesCategorical variables are presented as percentage of
patients and were compared using the Fisher exact test.Continuous data are expressed as means 6 SDs and werecompared using the Mann-Whitney test (variables thatwere not normally distributed are expressed as medians[interquartile ranges]). Spearman correlation coefficientswere calculated for analyzing the relationship betweencontinuous data. To analyze the association of cholesterolmetabolism with total survival, we stratified patients bymedian levels of lathosterol and cholestanol, respectively,into two groups. Kaplan-Meier curves were drawn, andevent-free survival was compared using the log-rank test.Subsequently, Cox proportional hazards models were calcu-lated that include clinical variables that predicted survival inunivariate analysis. To illustrate the association of cholesterolmetabolism with patient survival after adjustment for poten-tial confounders, Cox regression survival plots were drawnwith separate lines for patients stratified by median values ofcholestanol and lathosterol, respectively.Statistical analyses were performedwith SPSS 18.0.2. The
level of significance was set at P#0.05.
ResultsMean age of HD patients was 64.6615.3 years; controls
were slightly but statistically significantly younger(59.7613.4 years; P=0.002). Gender distribution waseven (HD group: 63 men and 50 women; control group:108 men and 121 women; P=0.17).We found strikingly higher levels of cholestanol (Figure
1A), indicating high cholesterol absorption, and lowerlathosterol levels (Figure 1B), reflecting cholesterol synthe-sis, in HD patients than in controls.Baseline cholestanol was associated with low body mass
index (r = 20.18; P=0.06) and high C-reactive protein lev-els (r = 0.31; P=0.001), whereas lathosterol was associatedwith high body mass index (r = 0.34; P,0.001) and low C-reactive protein levels (r = 20.21; P=0.03). No associationwas found between either lathosterol or cholestanol andage, mean BP, or serum albumin.
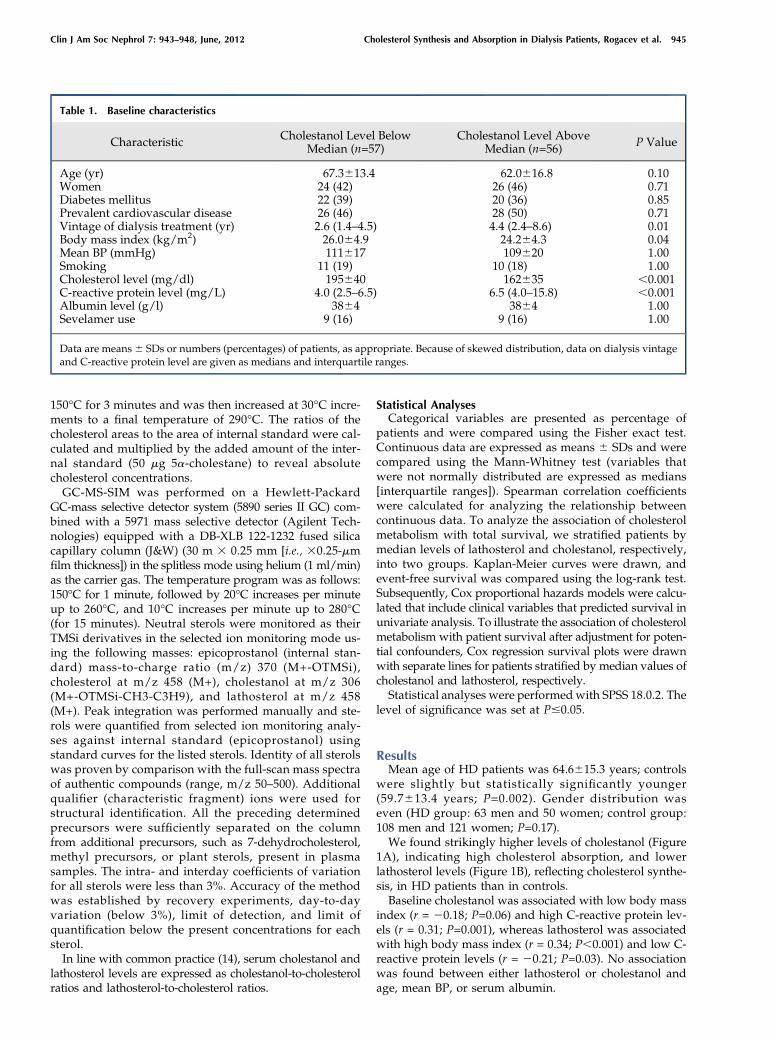
Table 1. Baseline characteristics
Characteristic Cholestanol Level BelowMedian (n=57)
Cholestanol Level AboveMedian (n=56) P Value
Age (yr) 67.3613.4 62.0616.8 0.10Women 24 (42) 26 (46) 0.71Diabetes mellitus 22 (39) 20 (36) 0.85Prevalent cardiovascular disease 26 (46) 28 (50) 0.71Vintage of dialysis treatment (yr) 2.6 (1.4–4.5) 4.4 (2.4–8.6) 0.01Body mass index (kg/m2) 26.064.9 24.264.3 0.04Mean BP (mmHg) 111617 109620 1.00Smoking 11 (19) 10 (18) 1.00Cholesterol level (mg/dl) 195640 162635 ,0.001C-reactive protein level (mg/L) 4.0 (2.5–6.5) 6.5 (4.0–15.8) ,0.001Albumin level (g/l) 3864 3864 1.00Sevelamer use 9 (16) 9 (16) 1.00
Data are means6 SDs or numbers (percentages) of patients, as appropriate. Because of skewed distribution, data on dialysis vintageand C-reactive protein level are given as medians and interquartile ranges.
Clin J Am Soc Nephrol 7: 943–948, June, 2012 Cholesterol Synthesis and Absorption in Dialysis Patients, Rogacev et al. 945
During follow-up, 58 of 113 patients died. Patientswho diedwere older (age, 72.5611.5 years in those who died and56.3614.5 years in those who did not; P,0.001), had lowerserum albumin (3764 g/L and 4064 g/L, respectively;P=0.03), and had lower mean BP (106618 mmHg and116618 mmHg, respectively; P=0.002). No significant differ-ences existed at baseline between survivors and nonsurvivorsregarding gender distribution, prevalent diabetes mellitus,prevalent cardiovascular disease, vintage of dialysis treat-ment, body mass index, smoking status, cholesterol level,C-reactive protein level, and sevelamer use. Table 1 showsbaseline characteristics stratified by median cholestanol level.In univariate analysis, a trend for higher mortality was
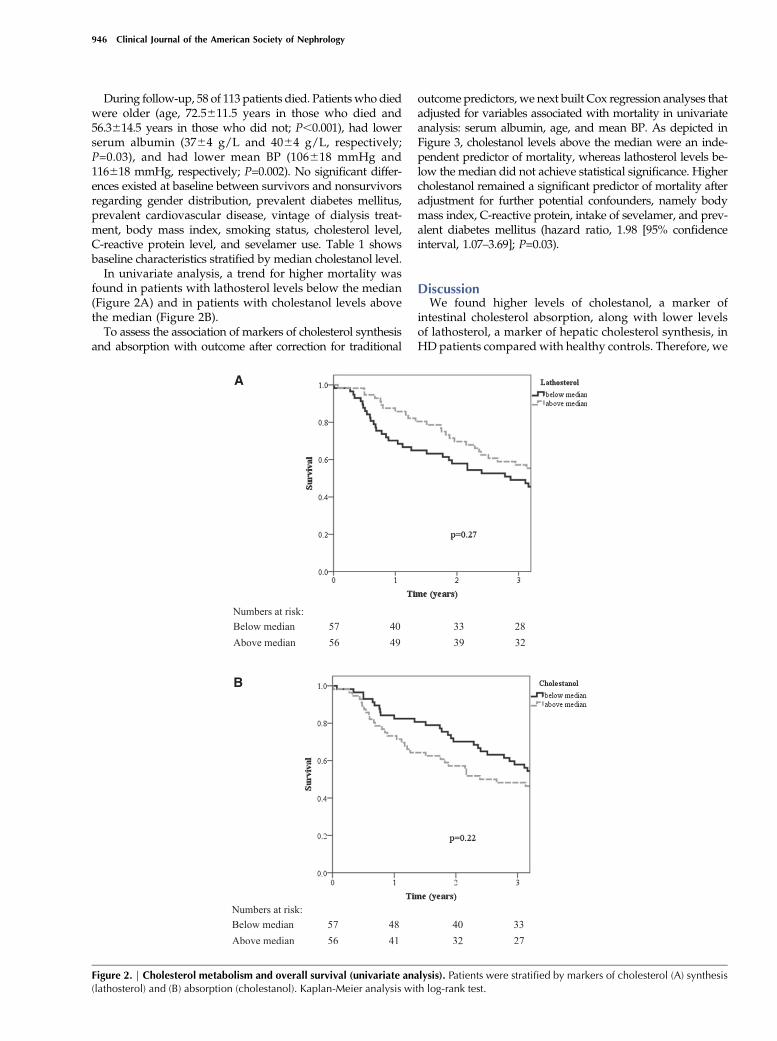
found in patients with lathosterol levels below the median(Figure 2A) and in patients with cholestanol levels abovethe median (Figure 2B).To assess the association of markers of cholesterol synthesis
and absorption with outcome after correction for traditional
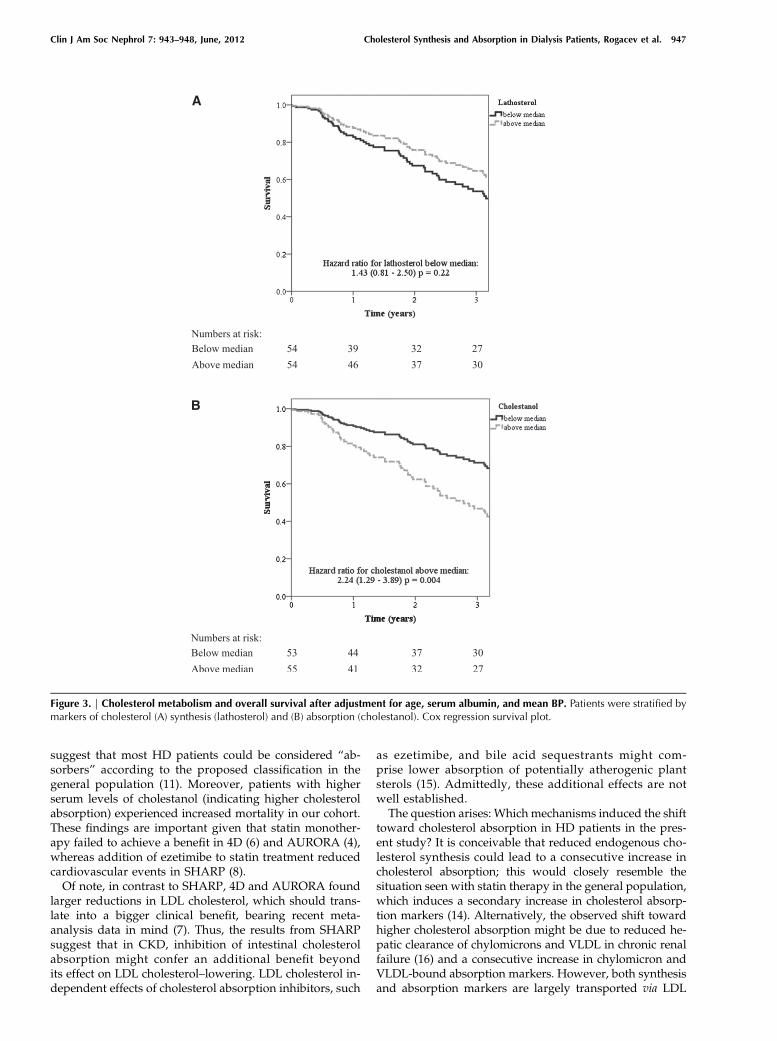
outcome predictors, we next built Cox regression analyses thatadjusted for variables associated with mortality in univariateanalysis: serum albumin, age, and mean BP. As depicted inFigure 3, cholestanol levels above the median were an inde-pendent predictor of mortality, whereas lathosterol levels be-low the median did not achieve statistical significance. Highercholestanol remained a significant predictor of mortality afteradjustment for further potential confounders, namely bodymass index, C-reactive protein, intake of sevelamer, and prev-alent diabetes mellitus (hazard ratio, 1.98 [95% confidenceinterval, 1.07–3.69]; P=0.03).
DiscussionWe found higher levels of cholestanol, a marker of
intestinal cholesterol absorption, along with lower levelsof lathosterol, a marker of hepatic cholesterol synthesis, inHD patients compared with healthy controls. Therefore, we
Figure 2. | Cholesterol metabolism and overall survival (univariate analysis). Patients were stratified by markers of cholesterol (A) synthesis(lathosterol) and (B) absorption (cholestanol). Kaplan-Meier analysis with log-rank test.
946 Clinical Journal of the American Society of Nephrology
suggest that most HD patients could be considered “ab-sorbers” according to the proposed classification in thegeneral population (11). Moreover, patients with higherserum levels of cholestanol (indicating higher cholesterolabsorption) experienced increased mortality in our cohort.These findings are important given that statin monother-apy failed to achieve a benefit in 4D (6) and AURORA (4),whereas addition of ezetimibe to statin treatment reducedcardiovascular events in SHARP (8).Of note, in contrast to SHARP, 4D and AURORA found
larger reductions in LDL cholesterol, which should trans-late into a bigger clinical benefit, bearing recent meta-analysis data in mind (7). Thus, the results from SHARPsuggest that in CKD, inhibition of intestinal cholesterolabsorption might confer an additional benefit beyondits effect on LDL cholesterol–lowering. LDL cholesterol in-dependent effects of cholesterol absorption inhibitors, such
as ezetimibe, and bile acid sequestrants might com-prise lower absorption of potentially atherogenic plantsterols (15). Admittedly, these additional effects are notwell established.The question arises: Which mechanisms induced the shift
toward cholesterol absorption in HD patients in the pres-ent study? It is conceivable that reduced endogenous cho-lesterol synthesis could lead to a consecutive increase incholesterol absorption; this would closely resemble thesituation seen with statin therapy in the general population,which induces a secondary increase in cholesterol absorp-tion markers (14). Alternatively, the observed shift towardhigher cholesterol absorption might be due to reduced he-patic clearance of chylomicrons and VLDL in chronic renalfailure (16) and a consecutive increase in chylomicron andVLDL-bound absorption markers. However, both synthesisand absorption markers are largely transported via LDL
Figure 3. | Cholesterol metabolism and overall survival after adjustment for age, serum albumin, and mean BP. Patients were stratified bymarkers of cholesterol (A) synthesis (lathosterol) and (B) absorption (cholestanol). Cox regression survival plot.
Clin J Am Soc Nephrol 7: 943–948, June, 2012 Cholesterol Synthesis and Absorption in Dialysis Patients, Rogacev et al. 947

(13). As opposed to chylomicrons and VLDL, the LDL se-rum concentration is determined by LDL biosynthesis, ex-cretion via bile acids, and tissue uptake (16).Taken together, a true increase of cholesterol absorption
in HD patients rather than a secondary increase due to re-duced hepatic clearance of carrier proteins is more likelyto be responsible for our results. However, no experimen-tal data are available to underscore our observation, andclinical information on markers of cholesterol metabolismin HD patients has been restricted so far to a single cross-sectional study comprising 8 dialysis patients and 16controls (17). A major limitation of our study is its rathersmall sample size. This limitation partly results from thenecessary exclusion of patients receiving lipid-loweringmedication because both statin and ezetimibe treatmentinterferes with plasma sterol levels. In parallel, the exclu-sion of patients taking lipid-lowering drugs inevitably re-sulted in underrepresentation of patients with overthypercholesterolemia. As a further limitation, the use ofcholestanol and lathosterol as markers of cholesterol ab-sorption and synthesis is derived from the general popula-tion because their use has not formally been validated indialysis patients.In summary, we found that compared with healthy con-
trols, HD patients have higher serum levels of cholestanol, amarker of cholesterol absorption. Moreover, HD patients withhigher cholestanol levels faced worse clinical outcome. Bysuggesting that HD patients are “cholesterol absorbers,” ourdata might provide new information to improve under-standing of the differing results of cholesterol-loweringtrials in patients with CKD. We hope that our reportinstigates a replication in a larger cohort because a confir-mation of our results would probably have an importanteffect on clinical decision-making.
AcknowledgmentsWe are grateful to Martin Marx, Rainer Bo§let, Dieter Stolz,
Susanne Brückner, and Herbert Tarrach for recruitment of patientsand to Martina Wagner for excellent technical work.
This data set has been presented as an oral presentation atAmerican Society of Nephrology Kidney Week, November 8–13,2011, Philadelphia, Pennsylvania, and as a poster at the EuropeanRenal Association–European Dialysis and Transplant AssociationCongress, June 23–26, 2011, Prague, Czech Republic.
DisclosuresD.L. received lecturing fees from Danone and Unilever. O.W.
received lecture fees from Daichii-Sankyo, MSD, Essex, and RaisioNutrition Ltd. The other authors have no competing interests todeclare.
References1. US Renal Data System: Annual Data Report: Atlas of Chronic
Kidney Disease and End-Stage Renal Disease in the UnitedStates, National Institutes of Health, National Institute of Di-abetes and Digestive and Kidney Diseases, 2010
2. SarnakMJ, Coronado BE,Greene T,Wang SR, Kusek JW, BeckGJ,Levey AS: Cardiovascular disease risk factors in chronic renalinsufficiency. Clin Nephrol 57: 327–335, 2002
3. Uhlig K, Levey AS, Sarnak MJ: Traditional cardiac risk factors in in-dividualswith chronickidneydisease.SeminDial16: 118–127, 2003
4. FellstromBC, Jardine AG, Schmieder RE,HoldaasH, Bannister K,Beutler J, Chae DW, Chevaile A, Cobbe SM, Gronhagen-Riska C,
De Lima JJ, Lins R, Mayer G, McMahon AW, Parving HH,Remuzzi G, Samuelsson O, Sonkodi S, Sci D, Suleymanlar G,Tsakiris D, Tesar V, Todorov V, Wiecek A, Wuthrich RP, GottlowM, Johnsson E, Zannad F; AURORA Study Group: Rosuvastatinand cardiovascular events in patients undergoing hemodialysis.N Engl J Med 360: 1395–1407, 2009
5. Sharp Collaborative G. Study of Heart and Renal Protection(SHARP): Randomized trial to assess the effects of loweringlow-density lipoprotein cholesterol among 9,438 patientswith chronic kidney disease. Am Heart J 160: 785–794.2010
6. Wanner C, Krane V, MarzW,Olschewski M,Mann JF, Ruf G, RitzE; German Diabetes and Dialysis Study Investigators: Atorvastatinin patients with type 2 diabetes mellitus undergoing hemodialysis.N Engl J Med 353: 238–248, 2005
7. Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, BhalaN, Peto R, Barnes EH, Keech A, Simes J, Collins R; CholesterolTreatment Trialists’ (CTT) Collaboration: Efficacy and safety ofmore intensive lowering of LDL cholesterol: A meta-analysis ofdata from 170,000 participants in 26 randomised trials. Lancet376: 1670–1681, 2010
8. Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC,Tomson C, Wanner C, Krane V, Cass A, Craig J, Neal B, Jiang L,Hooi LS, Levin A, Agodoa L, Gaziano M, Kasiske B, Walker R,Massy ZA, Feldt-Rasmussen B, Krairittichai U,Ophascharoensuk V, Fellstrom B, Holdaas H, Tesar V,Wiecek A,GrobbeeD, de ZeeuwD,Gronhagen-Riska C, Dasgupta T, LewisD, HerringtonW,MafhamM,MajoniW,Wallendszus K, GrimmR, Pedersen T, Tobert J, Armitage J, Baxter A, Bray C, Chen Y,Chen Z, Hill M, Knott C, Parish S, Simpson D, Sleight P, Young A,Collins R; SHARP Investigators: The effects of lowering LDLcholesterol with simvastatin plus ezetimibe in patients withchronic kidney disease (Study of Heart and Renal Protection):A randomised placebo-controlled trial. Lancet 377: 2181–2192,2011
9. Miettinen TA, Tilvis RS, Kesaniemi YA: Serum plant sterols andcholesterol precursors reflect cholesterol absorption and syn-thesis in volunteers of a randomly selectedmale population.Am JEpidemiol 131: 20–31, 1990
10. Miettinen TA, Gylling H, Strandberg T, Sarna S: Baseline serumcholestanol as predictor of recurrent coronary events in subgroupof Scandinavian simvastatin survival study. Finnish 4S Inves-tigators. BMJ 316: 1127–1130, 1998
11. Hoenig MR, Rolfe BE, Campbell JH: Cholestanol: A serummarker to guide LDL cholesterol-lowering therapy. Atheroscle-rosis 184: 247–254, 2006
12. Kolsch H, Heun R, Jessen F, Popp J, Hentschel F, Maier W,Lutjohann D: Alterations of cholesterol precursor levels inAlzheimer’s disease. Biochim Biophys Acta 1801: 945–950,2010
13. Miettinen TA, Gylling H: Synthesis and absorption markers ofcholesterol in serum and lipoproteins during a large dose of statintreatment. Eur J Clin Invest 33: 976–982, 2003
14. van Himbergen TM, Matthan NR, Resteghini NA, Otokozawa S,AiM, Stein EA, Jones PH, Schaefer EJ: Comparison of the effects ofmaximal dose atorvastatin and rosuvastatin therapy on choles-terol synthesis and absorption markers. J Lipid Res 50: 730–739,2009
15. Weingartner O, Lutjohann D, Bohm M, Laufs U: Relationshipbetween cholesterol synthesis and intestinal absorption is asso-ciated with cardiovascular risk. Atherosclerosis 210: 362–365,2010
16. Vaziri ND: Dyslipidemia of chronic renal failure: The nature,mechanisms, and potential consequences. Am J Physiol RenalPhysiol 290: F262–F272, 2006
17. Igel-Korcagova A, Raab P, Brensing KA, Poge U, Klehr HU, IgelM, von Bergmann K, Sudhop T: Cholesterol metabolism in pa-tients with chronic renal failure on hemodialysis. J Nephrol 16:850–854, 2003
Received: May 28, 2011 Accepted: February 24, 2012
Published online ahead of print. Publication date available at www.cjasn.org.
948 Clinical Journal of the American Society of Nephrology
Copyright © 2022 FDOKUMEN




















