
Comparison of nalbuphine and buprenorphine in total intravenous anaesthesia
24
FORUM Thoracic epidural anaesthesia for coronary artery bypass graft surgery Effects on postoperative complications D. J. Turfrey, 1 D. A. A. Ray, 1 N. P. Sutcliffe, 1 P. Ramayya, 1 G. N. C. Kenny 2 and N. B. Scott 1 * 1 HCI International Medical Centre, Beardmore Street, Clydebank, Glasgow G81 4HX, UK 2 University Department of Anaesthetics, Glasgow Royal Infirmary, 8–16 Alexandra Parade, Glasgow G31 2ER, UK Summary We have performed a retrospective analysis of the peri-operative course of 218 consecutive patients who underwent routine coronary artery bypass graft surgery in this institution. All patients received a standardised general anaesthetic using target-controlled infusions of alfentanil and propofol. One hundred patients also received thoracic epidural anaesthesia with bupivacaine and clonidine, started before surgery and continued for 5 days after surgery. The remaining 118 patients received target-controlled infusion of alfentanil for analgesia for the first 24h after surgery, followed by intravenous patient-controlled morphine analgesia for a further 48 h. Using computerised patient medical records, we analysed the frequency of respiratory, neurological, renal, gastrointestinal, haematological and cardiovascular complications in these two groups. New arrhythmias requiring treatment occurred in 18% of the thoracic epidural anaesthesia group of patients compared with 32% of the general anaesthesia group (p 0.02). There was also a trend towards a reduced incidence of respiratory complications in the thoracic epidural anaesthesia group. The time to tracheal extubation was decreased in the epidural group, with the tracheas of 21% of the patients being extubated immediately after surgery compared with 2% in the general anaesthesia group (p 0.001). There were no serious neurological problems resulting from the use of thoracic epidural analgesia. Keywords Anaesthetic techniques, regional ; epidural, thoracic. Surgery ; coronary artery bypass grafts. Complications ; postoperative. ...................................................................................... Correspondence to: Dr N. B. Scott Accepted: 2 March 1997 In recent years there has been a growing interest in the use of thoracic epidural anaesthesia for coronary artery bypass surgery. Its potential advantages include excellent analgesia [1], improved pulmonary function [2], early tracheal extubation [2, 3] and cardiac protection as a result of sympathetic blockade [4]. Thoracic epidural anaesthesia decreases the stress response to sternotomy and cardiopulmonary bypass. Increased sympathetic activ- ity may lead to an increase in arterial pressure, tachycardia and an imbalance between the myocardial oxygen demand and supply, with increased myocardial oxygen extraction and the possibility of ischaemic episodes. Moore et al. showed that plasma concentrations of adrenaline and noradrenaline did not increase in the first 24 h after cardiac surgery in patients receiving thoracic epidural anaesthesia compared with a conventional anaesthetic technique [5]. Other studies have shown that haemodynamic stability was maintained during and after surgery using thoracic epidural anaesthesia [6–9]. Thoracic epidural anaesthesia has been shown to decrease pain and improve the endocardial to epicardial blood flow ratio, thereby decreasing the number of ischaemic episodes [10–12]. Thoracic epidural anaesthesia has also been shown to decrease infarct size after coronary artery occlusion in dogs [13] and has been used in patients with unstable angina [11]. However, several concerns have been raised about the use of thoracic epidural anaesthesia in cardiac surgery, including the risk of haemodynamic Anaesthesia, 1997, 52, 1090–1113 ................................................................................................................................................................................................................................................ 1090 Q 1997 Blackwell Science Ltd
Transcript of Comparison of nalbuphine and buprenorphine in total intravenous anaesthesia

FORUM
Thoracic epidural anaesthesia for coronary artery bypassgraft surgery Effects on postoperative complications
D. J. Turfrey,1 D. A. A. Ray,1 N. P. Sutcliffe,1 P. Ramayya,1 G. N. C. Kenny2 and N. B.Scott1*
1 HCI International Medical Centre, Beardmore Street, Clydebank, Glasgow G81 4HX, UK2 University Department of Anaesthetics, Glasgow Royal Infirmary, 8–16 Alexandra Parade, Glasgow G31 2ER, UK
SummaryWe have performed a retrospective analysis of the peri-operative course of 218 consecutive patientswho underwent routine coronary artery bypass graft surgery in this institution. All patientsreceived a standardised general anaesthetic using target-controlled infusions of alfentanil andpropofol. One hundred patients also received thoracic epidural anaesthesia with bupivacaine andclonidine, started before surgery and continued for 5 days after surgery. The remaining 118patients received target-controlled infusion of alfentanil for analgesia for the first 24 h after surgery,followed by intravenous patient-controlled morphine analgesia for a further 48 h. Usingcomputerised patient medical records, we analysed the frequency of respiratory, neurological, renal,gastrointestinal, haematological and cardiovascular complications in these two groups. Newarrhythmias requiring treatment occurred in 18% of the thoracic epidural anaesthesia group ofpatients compared with 32% of the general anaesthesia group (p� 0.02). There was also a trendtowards a reduced incidence of respiratory complications in the thoracic epidural anaesthesiagroup. The time to tracheal extubation was decreased in the epidural group, with the tracheas of21% of the patients being extubated immediately after surgery compared with 2% in the generalanaesthesia group (p< 0.001). There were no serious neurological problems resulting from the useof thoracic epidural analgesia.
Keywords Anaesthetic techniques, regional ; epidural, thoracic. Surgery ; coronary artery bypass grafts.Complications ; postoperative.
......................................................................................Correspondence to: Dr N. B. ScottAccepted: 2 March 1997
In recent years there has been a growing interest in theuse of thoracic epidural anaesthesia for coronary arterybypass surgery. Its potential advantages include excellentanalgesia [1], improved pulmonary function [2], earlytracheal extubation [2, 3] and cardiac protection as aresult of sympathetic blockade [4]. Thoracic epiduralanaesthesia decreases the stress response to sternotomyand cardiopulmonary bypass. Increased sympathetic activ-ity may lead to an increase in arterial pressure, tachycardiaand an imbalance between the myocardial oxygen demandand supply, with increased myocardial oxygen extractionand the possibility of ischaemic episodes. Moore et al.showed that plasma concentrations of adrenaline andnoradrenaline did not increase in the first 24 h after cardiac
surgery in patients receiving thoracic epidural anaesthesiacompared with a conventional anaesthetic technique [5].Other studies have shown that haemodynamic stabilitywas maintained during and after surgery using thoracicepidural anaesthesia [6–9].
Thoracic epidural anaesthesia has been shown todecrease pain and improve the endocardial to epicardialblood flow ratio, thereby decreasing the number ofischaemic episodes [10–12]. Thoracic epidural anaesthesiahas also been shown to decrease infarct size after coronaryartery occlusion in dogs [13] and has been used in patientswith unstable angina [11]. However, several concerns havebeen raised about the use of thoracic epidural anaesthesiain cardiac surgery, including the risk of haemodynamic
Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1090 Q 1997 Blackwell Science Ltd

instability and the risk of epidural haematoma formation inpatients who may be receiving aspirin and who will befully heparinised during cardiopulmonary bypass [1].
Methods
A retrospective analysis of the peri-operative course of allpatients who underwent routine coronary artery bypassgraft surgery over a 9-month period was performed. Therewere 118 patients who received general anaesthesia alone(GA group) and 100 patients who received general anaes-thesia together with thoracic epidural anaesthesia (TEAgroup). The decision to perform thoracic epidural anaes-thesia was left to the individual anaesthetist. The patientswere not formally randomised into either group. Writtenconsent for surgery and anaesthesia was obtained from allpatients and the anaesthetic technique was fully explainedbefore surgery. Approval for the study was acquiredfrom the local ethics committee. Premedication for allpatients consisted of ranitidine 150 mg, metoclopramide10 mg and temazepam 30 mg given orally on the eveningbefore surgery and again 2 h before surgery. The samecardiac surgeon performed all of the procedures.
Thoracic epidural anaesthesia was performed immedi-ately before induction of anaesthesia using an 18G epiduralneedle. The catheter was sited at the T2–3 or T3–4 inter-space with the patient in the left lateral position. Allpatients had routine coagulation studies as part of thepre-operative investigation screen but bleeding time wasnot measured. Patients with abnormal coagulation studieswere not given thoracic epidural anaesthesia but patientswho were receiving aspirin were not excluded from thestudy. A block to the first thoracic dermatome wasinstituted using 4–12 ml of bupivacaine 0.5% and follow-ing induction of anaesthesia an infusion of bupivacaine0.125% with clonidine 0.6 mg.mlÿ1 was started. Thisinfusion was continued for 5 days after surgery and theblock height was maintained between the first and secondthoracic dermatomes by adjusting the infusion rate.
General anaesthesia was then induced and maintainedusing target-controlled infusions of propofol and alfen-tanil, achieving initial plasma concentrations of 1.5–3 mg.mlÿ1 and 100–200 ng.mlÿ1, respectively. The targetconcentrations were adjusted as necessary. The patients’lungs were ventilated following the administration ofpancuronium 8 mg intravenously. Additional pancuro-nium was given as necessary.
The GA group of patients continued with a target-controlled alfentanil infusion after surgery (target bloodconcentration 80 ng.mlÿ1) until they were able to use apatient-controlled target-controlled alfentanil infusionsystem. After 24 h this was changed to patient-controlledintravenous morphine with the following settings: 1 mg
bolus, 5 min lockout period, no background infusion. Allpatients in this series received regular coproxamol andibuprofen given orally for 7 days after surgery provided theplasma creatinine was normal and bleeding from the drainswas minimal.
The fully computerised hospital patient medical recordsystem was used to obtain the pre-operative and post-operative data for each patient. Data from the patientmonitoring system (Tramscope 12C, Marquette, USA)were stored automatically during surgery by the Anaes-thesia Information Management System (RECALL, Ver-sion 2, Informatics, UK) and later retrieved and analysedusing Microsoft Excel Version 5.0. Postoperative dataand patient demographic data were stored on the elec-tronic hospital medical record (Cerner Corporation,Kansas, USA).
Age, sex, weight, New York Heart Association(NYHA) classification, pre-operative arrhythmias,number of grafts performed and ischaemic time onbypass were recorded. After surgery, we assessed thefrequency of new arrhythmias, the time until trachealextubation, the use of intra-aortic balloon pumps andventricular assist devices, inotrope use and complicationsaffecting the renal, gastrointestinal, neurological andrespiratory systems. All patients underwent continuousECG monitoring for the first 5 days after surgery. Extuba-tion criteria were standardised and are shown in Table 1.
All complications during the first five postoperative dayswere recorded. Respiratory complications were dividedinto proven lower respiratory tract infection (i.e. withpositive sputum culture), atelectasis or collapse assessed onpostoperative chest X-ray, adult respiratory distress syn-drome or respiratory failure requiring intervention such asre-intubation. Arrhythmias were classified as atrial flutteror fibrillation, conduction defects and ventricular arrhyth-mias. Postoperative myocardial infarction was diagnosedusing a combination of ECG analysis and serum creatininekinase levels. Renal failure was defined as oliguria com-bined with an increase in the serum creatinine to greaterthan twice the pre-operative value. Significant bleedingwas defined as that which required treatment with blood
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1091Q 1997 Blackwell Science Ltd
Table 1 Extubation criteria following routine coronary arterybypass graft surgery.
1. Cardiovascular stability without inotropes – systolic bloodpressure of > 90 mmHg
2. Core temperature over 36.5 8C3. Spontaneous ventilation with PaO2> 12 kPa on FiO2 of<0.4
and PaCO2< 7 kPa4. Blood loss from chest drains <60 ml.hÿ1
5. Urine output >1 ml.kgÿ1. hÿ1
6. No sedation and patient not in pain or agitated

products or a return to the operating theatre in order tocontrol the haemorrhage surgically.
The data were analysed with the Chi-squared test andFisher’s exact test using Minitab software (Minitab Ltd,UK).
Results
The two groups of patients were similar when comparedfor age, sex, NYHA score, weight, ejection fraction andthe number of grafts performed (Table 2). There were nodifferences between the duration of bypass and ischaemictime. There was no difference between the two groups inthe use of inotropes or intra-aortic balloon pump devices.No patients in the study period required a ventricular assistdevice. One patient in the TEA group and two in the GAgroup died whilst in the operating theatre as a result ofintra-operative complications.
New arrhythmias requiring treatment occurred in 18%of patients in the TEA group compared with 32% in theGA group (p� 0.02). The majority of these arrhythmiaswere supraventricular in origin (Fig. 1). Respiratorycomplications occurred in 21% of the GA group and in16% of the TEA group. Immediate extubation was definedas extubation within 1 h of return to ITU and wasachieved in 21% of the TEA group compared with 2%of the GA group (p< 0.002) (Fig. 2). The median time toextubation was 12 h after arrival in the intensive care unitin both groups. Two patients in the TEA group and one inthe GA group who were extubated immediately requiredre-intubation within the next 24 h.
There were no significant differences in the incidenceof renal, haematological, neurological or wound com-plications between the two groups in the postoperativeperiod (Table 3). Of the neurological complications thatoccurred, none was serious or caused long-term problems.In the TEA group six complications occurred. These
included one transient ischaemic attack in the postopera-tive period, one brachial plexus lesion resulting in tem-porary weakness in the C7–8 distribution, one acuteconfusional state, one recurrent laryngeal nerve palsy,one frontal headache and one episode of weakness in theleft leg. In the GA group of patients, nine neurologicalcomplications occurred. Five of these were acute confu-sional states, there was one brachial plexus lesion and threecerebrovascular accidents. There was no occurrence ofepidural haematoma following epidural insertion in any
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1092 Q 1997 Blackwell Science Ltd
Figure 1 Frequency and type of postoperative arrhythmia in thetwo groups studied.
Figure 2 Percentage of patients undergoing tracheal extubationin four time periods after surgery.
Table 2 Patient demographic data, duration of bypass and cardiacischaemia and ejection fraction in the two groups of patientsstudied. Values are given as median (range) or mean (SD) whereappropriate.
TEA group GA group(n� 100) (n�118)
Number of grafts 3 (1–5) 3 (1–5)Age; years 58.7 (16.9) 61.3 (14.2)Sex ratio; M : F 6 : 1 5.7 : 1NYHA Class 3 (2–4) 3 (2–4)Weight; kg 77.4 (14.7) 71.3 (12.2)Bypass time; min 84.8 (23.7) 84.3 (26.9)Ischaemic time; min 47.6 (15.7) 53.1 (20.1)Ejection fraction; % 45 (35–65) 45 (35–65)

patient. The patient with the weak left leg in the TEAgroup received urgent magnetic resonance imaging toexclude cord compression. No abnormality was foundand the weakness resolved when the epidural infusion wasdiscontinued.
In the TEA group, four patients required resiting of theepidural in the postoperative period because of inadequateblock. One patient had a unilateral block, one epidural‘fell out’ and the other two patients had no demonstrableblock despite repeated bolus doses of bupivacaine. Inaddition, supplementary doses of intravenous morphinewere required in 22 patients in the TEA group to provideanalgesia either for leg wounds or for pain related to thechest drains. No patient who received morphine for chestdrain pain had more than 10 mg up to the point at whichthe drains were removed. In all cases the removal of thedrains led to relief of the pain. Four patients had acutetorticollis on return from the operating theatre, presum-ably due to sternal retraction, which responded well to a100 mg diclofenac suppository.
Discussion
Thoracic epidural anaesthesia following coronary arterysurgery was first used in our hospital at the beginning of1996 to provide rescue analgesia for four patients within24 h of surgery in whom standard intravenous opioidanalgesia was resulting in excessive sedation and poorrespiratory function. None of these patients requiredre-intubation and we were encouraged to increase gradu-ally the usage of the technique. All of the consultants in thedepartment are now experienced in the technique and itspostoperative management and we have reviewed all 218patients who have undergone coronary artery surgery in1996 in order to determine the need for a more compre-hensive, large, prospective, randomised study.
Our retrospective data suggest that thoracic epiduralanaesthesia is a safe adjunct to general anaesthesia forpatients undergoing routine coronary artery bypass graftsurgery. This technique may have significant benefits interms of decreased postoperative morbidity, as demon-strated in this study by the decrease in new arrhythmias anda trend towards a decreased incidence of respiratory com-plications. Thoracic epidural anaesthesia has been shownpreviously to be associated with excellent cardiovascularstability [6–8] and our study showed no significant increasein the use of inotropic agents and intra-aortic balloonpump devices in the TEA group of patients, although amore powerful study may demonstrate an increase.
The data demonstrate a significant reduction in theincidence of arrhythmias in patients receiving thoracicepidural anaesthesia. This may be a result of the blockadeof cardiac accelerator fibres, improvement of regionalmyocardial blood flow and attenuation of the stressresponse during surgery, in conjunction with postopera-tive sensory blockade preventing endocrine and auto-nomic responses to pain and trauma [5, 14]. The datasupport the view that patients receiving thoracic epiduralanaesthesia are more likely to undergo early trachealextubation. This has been shown previously by Joachim-son et al. [15] and Liem et al. [2]. Earlier studies haveshown that patients receiving thoracic epidural anaesthesiaalso have an increased PaO2 and lower pain and sedationscores in the postoperative period [2, 16]. Sedation andpain scores were not formally assessed in the present study.
The patients remained in ICU for a median of 2 daysand were then transferred to a high-dependency area for amedian of 2 days. They were then returned to a generalward for the remainder of the epidural infusion period andwere supervised by our Acute Pain Service throughouttheir hospital stay. All patients in this series received regularcoproxamol and ibuprofen orally for 7 days once thepostoperative creatinine was normal, usually within 24 hof surgery. Any pain which developed in the epiduralgroup during the 5 days was treated either by an epiduraltop-up of 4 ml bupivacaine 0.25%, with 2.5 mg morphineintravenously or 100 mg diclofenac orally or rectally.
The Peri-operative Ischaemia Randomised AnaesthesiaTrial Study Group has shown that patients undergoingperipheral vascular surgery who required re-operation forgraft thrombosis had high levels of circulating noradrena-line in the postoperative period [17]. A recent editorial byDesborough suggests similar effects may be seen in cardiacsurgery [1]. In our study, the incidence of postoperativemyocardial infarction was 1% (n� 1) in the TEA groupand 4.2% (n� 5) in the GA group. Although only smallgroups of patients were studied, we consider this differencealso warrants further investigation in prospective studies.
There was no significant difference in the frequency of
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1093Q 1997 Blackwell Science Ltd
Table 3 Number and incidence (%) of postoperative complica-tions in the two groups studied.
TEA group GA group(n�100) (n�118)
Arrhythmias 18 (18%) *38 (32%)Intra-aortic balloon pump 3 (3%) 7 (6%)Postoperative myocardial infarction 1 (1%) 5 (4%)Lower respiratory tract infection 7 (7%) 11 (9%)Other infection 2 (2%) 7 (6%)Neurological complication 6 (6%) 9 (8%)Acute renal failure 6 (6%) 6 (6%)Dialysis 0 (0%) 2 (2%)Respiratory complication 16 (16%) 25 (21%)Gastrointestinal tract complication 3 (3%) 3 (3%)Significant bleeding 8 (8%) 10 (9%)
* Significantly different from GA group, p<0.02.

atelectasis and lower respiratory tract infection betweenthe two groups, although the trend was for these compli-cations to be decreased in the TEA group.
The use of thoracic epidural anaesthesia in anticoagu-lated patients undergoing cardiac surgery is controversialbecause of the risk of epidural haematoma formation.There are currently no accepted guidelines for the safetime period between insertion of thoracic epidural anaes-thesia and full anticoagulation. In studies by Liem et al. andJoachimsson et al. [6, 15] the epidural catheter was sited24 h before surgery in an attempt to decrease the risk.Kirno et al. sited the thoracic epidural anaesthesia 12 hbefore surgery in 10 patients with no complications noted[18]. El Baz & Goldin sited thoracic epidural anaesthesiacatheters in 30 patients immediately before induction ofanaesthesia with no neurological complications noted [19].In our series, 100 catheters were sited immediately beforesurgery and we have noted no serious neurological com-plications. Furthermore, epidural analgesia has been usedin 1000 anticoagulated patients with no permanent neuro-logical complications [20]. A recent literature reviewnoted that the frequency of haematoma formation associ-ated with either spinal or epidural insertion in obstetricpatients was 17 per 180 000 (< 1 in 10 000) [21]. Theauthor of this review comments that as the frequency is sorare, the coincidental occurrence of spontaneous haema-toma must be considered even when a neuraxial blockadehas been performed.
In the postoperative setting, it is generally believed thatoutcome can be improved by good pain management andthe beneficial effects of sympathetic blockade can alsoreduce morbidity [22, 23]. This study appears to supportthis belief. Surgery for coronary artery disease is performedin a high-risk population and carries a significant mor-tality, in excess of 2%. Thus, on an individual basis, sincethe exact risk of epidural haematoma is unknown andthe published incidence is less than 0.01%, it seemsinappropriate to deny patients the benefits of this tech-nique provided that the putative benefits can be establishedin a large, prospective, randomised study.
References
1 Desborough JP. Thoracic epidural analgesia in cardiacsurgery. Anaesthesia 1996; 51: 805–7.
2 Liem TH, Hasenbos MA, Booij LH, Gielen MJ. Coronaryartery bypass grafting using two different anaesthetictechniques. Part II. Postoperative outcome. Journal ofCardiothoracic and Vascular Anesthesia 1992; 6: 156–61.
3 Swenson JD, Hullander RM, Wingler K, Leivers D. Earlyextubation after cardiac surgery using combined intrathecalsufentanil and morphine. Journal of Cardiothoracic andVascular Anesthesia 1994; 8: 509–14.
4 Kock M, Blomberg S, Emanuelsson H, Lomsky M,Stromblad SO, Ricksten SE. Thoracic epidural anesthesiaimproves global and regional left ventricular functionduring stress - induced myocardial ischaemia in patientswith coronary artery disease. Anesthesia and Analgesia 1990;71: 625–30.
5 Moore CM, Cross MH, Desborough JP, Burrin JM,Macdonald IA, Hall GM. Hormonal effects of thoracicextradural analgesia for cardiac surgery. British Journal ofAnaesthesia 1995; 75: 387–93.
6 Liem TH, Booij LH, Hasenbos MA, Gielen MJ. Coronaryartery bypass grafting using two different anesthetictechniques: Part I. Hemodynamic results. Journal ofCardiothoracic and Vascular Anesthesia 1992; 6: 148–55.
7 Stenseth R, Berg EM, Bjella L, Christensen O,Levang OW, Gisvold SE. Effects of thoracic epiduralanalgesia on coronary haemodynamics and myocardialmetabolism in coronary artery bypass surgery. Journal ofCardiothoracic and Vascular Anesthesia 1995; 9: 503–9.
8 Stenseth R, Bjella EM, Christensen O, Levang OW,Gisvold SE. Thoracic epidural analgesia in aortocoronarybypass surgery I. Haemodynamic effects. ActaAnaesthesiologica Scandinavica 1994; 38: 826–33.
9 Liem TH, Booij LHDJ, Gielen MJM, Hasenbos MAWM,Van Egmond J. Coronary artery bypass grafting using twodifferent anesthetic techniques: Part 3: Adrenergicresponses. Journal of Cardiothoracic and Vascular Anesthesia1992; 6: 162–7.
10 Toft P, Jorgensen A. Continuous thoracic epidural analgesiafor the control of pain in myocardial infarction. IntensiveCare Medicine 1987; 13: 388–9.
11 Blomberg S, Curelaru I, Emanuelsson H. Thoracic epiduralanaesthesia in patients with unstable angina pectoris.European Heart Journal 1989; 10: 437–44.
12 Blomberg S, Emanuelsson H, Kvist H. Effects of thoracicepidural anaesthesia on coronary arteries and arterioles inpatients with coronary artery disease. Anesthesiology 1990;73: 840–7.
13 Davis RF, Deboer LWV, Maroko PR. Thoracic EpiduralAnesthesia reduces myocardial infarct size after coronaryartery occlusion in dogs. Anesthesia and Analgesia 1986; 65:711–7.
14 Stenseth R, Bjella L, Berg EM, Christensen O,Levang OW, Gisvold SE. Thoracic epidural analgesia inaortocoronary bypass surgery II. Effects on the endocrinemetabolic response. Acta Anesthesiologica Scandinavica 1994;38: 834–9.
15 Joachimsson PO, Nystrom SO, Tyden H. Early extubationafter coronary artery surgery in efficiently rewarmedpatients: a postoperative comparison of opioid anesthesiaversus inhalational anaesthesia and thoracic epiduralanalgesia. Journal of Cardiothoracic and Vascular Anesthesia1989; 3: 444–54.
16 Hasenbos M, Van Egmond J, Gielen M. Postoperativeanalgesia by epidural versus intramuscular nicomorphineafter thoracotomy. Part I and II. Acta AnaesthesiologicaScandinavica 1985; 29: 572–82.
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1094 Q 1997 Blackwell Science Ltd

17 Rosenfeld BA, Beattie C, Christopherson R, et al. Theeffects of different anesthetic regimens on postoperativearterial thrombosis. Anesthesiology 1993; 79: 435–43.
18 Kirno K, Friberg P, Grzegorczyk A, Milocco I, RickstenS-E, Lundin S. Thoracic epidural anesthesia duringcoronary artery bypass surgery: effects on cardiacsympathetic activity, myocardial blood flow and metabolismand central hemodynamics. Anesthesia and Analgesia 1994;79: 1075–81.
19 El-Baz N, Goldin M. Continuous epidural infusionof morphine for pain relief after cardiac operations.Journal of Cardiothoracic and Vascular Surgery 1987; 93:878–83.
20 Odoom JA, Sih IL. Epidural analgesia and anticoagulanttherapy. Experience with one thousand cases of continuousepidurals. Anaesthesia 1983; 38: 254–9.
21 Sage DJ. Epidurals, spinals and bleeding disorders inpregnancy: a review. Anaesthesia and Intensive Care 1990;18: 319–26.
22 Kehlet H. General versus regional anaesthesia. In: RogersMC, Tinker JH, Covino BG, Longnecker DE, eds.Principles and Practice of Anesthesiology, Vol. 2. London:Mosby Year Book Inc., 1992.
23 Scott NB. The effects of pain and its treatment. In:McClure JH, Wildsmith JAW, eds. Conduction Blockade forPostoperative Analgesia. London: Edward Arnold, 1991.
FORUM
Comparison of nalbuphine and buprenorphine in totalintravenous anaesthesia
F. A. Khan, A. Zaidi and R. S. Kamal
Department of Anaesthesia, The Aga Khan University Hospital, Stadium Road, PO Box 3500, Karachi-74800, Pakistan
SummaryNalbuphine (0.3 mg.kgÿ1 ) and buprenorphine (2.5 mg.kgÿ1 ) were compared as part of a totalintravenous anaesthesia regimen using a propofol infusion in 60 patients undergoing laparoscopiccholecystectomy in a randomised double-blind study. Changes in haemodynamic variables greaterthan 20% from the baseline were noted. No difference was observed in blood pressure but theheart rate was significantly lower in the buprenorphine group. Intra-operative bradycardia (heartrate <60 beat.minÿ1 ) occurred more often in the buprenorphine group. Recovery was fast andcomparable with both drugs and no patient reported awareness. Quality of analgesia was similar inboth groups. Both drugs provide suitable analgesic supplementation to total intravenousanaesthesia.
Keywords Anaesthetics, intravenous ; propofol. Analgesics; nalbuphine, buprenorphine.
......................................................................................Correspondence to: F. A. KhanAccepted: 9 April 1997
Total intravenous anaesthesia (TIVA) is becoming increas-ingly popular, mainly because of the availability of neweranaesthetic drugs with short half-lives and advances ininfusion pump technology which has made the admin-istration of these drugs easier. Currently propofol isregarded as the most suitable anaesthetic agent for TIVAowing to its short duration of action, minimal side-effectsand rapid recovery [1, 2]. It has been used in combination
with fentanyl, alfentanil and sufentanil [3, 4] but littlework has been done with propofol and partial agonist–antagonist narcotic combinations [5].
The objective of this study was to compare nalbuphineand buprenorphine in TIVA using propofol in patientsundergoing laparoscopic cholecystectomy, comparing anal-gesic efficacy, haemodynamic stability, intra-operative com-plications and recovery profile in the two groups.
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1095Q 1997 Blackwell Science Ltd

Methods
The study was approved by the Ethics Committee of theAga Khan University Hospital and informed consent wasobtained from the patients. The study was randomised anddouble-blinded. Sixty patients aged 20–60 years, ASAstatus 1 and 2, undergoing laparoscopic cholecystectomywere included in the trial. Patients with a history ofhypertension, morbid obesity or possible difficult trachealintubation were not studied. Those enrolled in the trialwere randomly divided into two groups; group 1 receivednalbuphine 0.3 mg.kgÿ1, and group 2 received buprenor-phine 2.5 mg.kgÿ1, both intravenously, 5 min beforeinduction of anaesthesia. The investigator was blinded tothe analgesic drug by the use of coded syringes. The rest ofthe anaesthetic technique was standardised.
All patients received 7.5 mg of oral midazolam as pre-medication approximately 1 h prior to surgery. On arrivalin the operating room, base-line observations were takenand the trial drug was administered. Five minutes later pre-oxygenation was started. Anaesthesia was induced withpropofol 2 mg.kgÿ1 over 30 s followed by vecuronium0.1 mg.kgÿ1 over 15 s. An infusion of propofol was startedimmediately after induction according to the followingregimen: 10 mg.kgÿ1.hÿ1 for the first 10 min, 8 mg.kgÿ1.hÿ1 for the next 10 min and 6 mg.kgÿ1.hÿ1 thereafter,using an Imed-Gemini PC-1 infusion pump. Trachealintubation was performed 3 min after vecuronium.Patients’ lungs were ventilated with an air–oxygen mix-ture maintaining an FIO2 of 0.4. A nasogastric tube wasroutinely inserted in all patients following tracheal intu-bation and removed before reversal of neuromuscularblockade.
Depth of anaesthesia was assessed intra-operatively byrelying on signs of sympathetic and parasympathetic stimu-lation. Any variation of more than 20% above or below thebaseline in systolic blood pressure or heart rate was noted.Lacrimation, sweating and any movements during anaes-thesia were also noted. If any two of the above signs wereobserved, a supplemental bolus of propofol 10 mg wasgiven. If the signs persisted for more than 3 min aftergiving the bolus, the rate of infusion was increased again to8 mg.kgÿ1.hÿ1 for another 10 min. If the signs still per-sisted, half the pre-induction dose of analgesic wasrepeated from a coded syringe. Vecuronium supplemen-tation was given as required, after the use of a nervestimulator (Ministim). A train-of-four count of two wasmaintained during the surgical procedure. The ECG wasmonitored throughout using the CM5 lead. Noninvasiveblood pressure, oxygen saturation, FIO2 and end-tidal CO2
were all monitored using the Datex Cardiocap monitor.The infusion of propofol was stopped at the time of thelast suture and muscle relaxation was reversed with
neostigmine 0.05 mg.kgÿ1 and atropine 0.02 mg.kgÿ1
given intravenously.Blood pressure and heart rate were noted 5 min before
and 5 min after the study drug, 1, 2 and 3 min afterinduction, every minute for 5 min after tracheal intuba-tion, 1 and 2 min after decreasing the dose of propofol to8 mg.kgÿ1.hÿ1 and then to 6 mg.kgÿ1.hÿ1, 1, 2 and 3 minafter incision, and after reversal and extubation. The timeinterval between reversal and extubation was also noted.
In the immediate recovery period, time to eye openingto verbal command and time to correctly stating ownname was noted. Patients were kept in the recovery roomuntil they fulfilled our routine discharge criteria, i.e. stablevital signs for at least 30 min, maintaining a good airway,able to breathe deeply and cough, rousable or awake andmoving purposefully. Any untoward effects were noted.The time of the first dose of analgesic required in thepostoperative period was also noted.
All patients were visited the next day by one of theprincipal investigators and any complaints noted. At thepostoperative visit every patient was questioned specific-ally regarding recall of operative events. Awareness wasassessed by asking three specific questions: What is the lastthing you remember before going to sleep? What is thefirst thing you remember after waking up? Do youremember anything between these events? Patients werealso asked to give their opinion about the anaesthetic.
Variables were analysed using the Epi-info-6 statisticalpackage. Analysis of variance was used to compare themean changes in systolic, diastolic and mean blood pres-sure and heart rate The incidence of untoward effects andother qualitative data was assessed by Chi-squared analysis.A p value of less than 0.05 was taken as significant.
Results
Demographic dataBoth groups were comparable for age, weight, pre-induction blood pressure, heart rate and duration ofanaesthesia (Table 1).
Haemodynamic dataFigure 1 shows the changes in systolic blood pressure(SBP) and diastolic blood pressure (DBP) in relation totime. Both groups showed a decrease in SBP and DBP inthe first 3 min after induction which returned to nearbaseline values 1 min after intubation. This decrease wasless than 20% of baseline, except with DBP in thenalbuphine group.
The maximum negative change seen was at 3 min afterinduction (19% drop in SBP in nalbuphine group and 16%in buprenorphine group). The fall in DBP was slightlymore exaggerated, especially in the pre-intubation period
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1096 Q 1997 Blackwell Science Ltd

in the nalbuphine group (24% vs. 17% in the bupre-norphine group). No significant rise was associated withtracheal intubation, and the blood pressures remained 10–15% below the pre-induction baseline values during themaintenance period including directly after the surgicalincision. No significant difference was observed at anytime between the two groups.
Figure 2 shows the changes in heart rate whichremained within 2–8% of the baseline values after induc-tion. Tracheal intubation and surgical incision wereaccompanied by an insignificant rise (less than 5% inboth groups). The maximum fall in heart rate was seenin the unstimulated intubated patient before surgical inci-sion. A significant difference was observed in the heart ratebetween the two groups at 2, 3, 4 and 5 min after trachealintubation (p < 0.1), in the unstimulated patient beforeincision (p < 0.01) and also in the readings taken after thesurgical incision (p < 0.01), with the heart rate beinglower in the buprenorphine group.
Intra-operative sedative and analgesic drugrequirementsFour patients in the nalbuphine group and three patientsin the buprenorphine group required additional bolusesof 10 mg of propofol. The same four patients in thenalbuphine group required a further increase in infusionrate compared to only two patients in the buprenorphinegroup. Only one patient in the nalbuphine group requireda further analgesic top-up. These differences were notstatistically significant.
Untoward effects seen intra-operativelyBradycardia was predefined as a heart rate below 60 beat.minÿ1. Twenty per cent of patients in the nalbuphinegroup had bradycardia compared to 46% of patients in thebuprenorphine group (p < 0.05). Three patients receivingbuprenorphine required intravenous atropine for severebradycardia (<50 beat.minÿ1 ) accompanied by hypoten-sion (systolic blood pressure <90 mmHg).
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1097Q 1997 Blackwell Science Ltd
Figure 1 Mean (SD) systolic (S) anddiastolic (D) blood pressures duringintravenous infusions of propofol/nalbuphine (X) or propofol/buprenorphine(W) at various times during anaesthesia.* Statistical significance (p < 0.05).
Table 1 Demographic and baseline haemodynamic data. Mean (SD).
Pre-induction values
n Age (years) Weight (kg) Sex M:F SBP DBP MAP HR
Nalbuphine 30 39 (10) 64 (10) 7:23 127 (17) 83 (10) 95 (12) 88 (16)Buprenorphine 30 42 (10) 65 (12) 7:23 126 (14) 81 (8) 95 (12) 82 (10)
SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; HR, heart rate.

Recovery profileRecovery profile is shown in Table 2. No significantdifference was observed between the groups.
Untoward effects seen in the recovery roomTwo patients in the buprenorphine group had heart ratesbetween 50 and 60 beat.minÿ1 in the recovery room butdid not require any treatment. No patient in the nalbu-phine group had heart rate below 60 beat.minÿ1. Onepatient in the nalbuphine group complained of nausea andanother vomited compared to one patient in the bupre-norphine group who vomited. One patient in the nalbu-phine group complained of vertigo during the recoveryroom stay. No significant difference was observed betweenthe groups.
Extubation to first analgesic dose intervalAnalgesia in the postoperative period was given on patientdemand. After extubation analgesia was required after amean period of 352 min in the nalbuphine group and385 min in the buprenorphine group. This difference was
not statistically significant. One patient in the nalbuphinegroup and five in the buprenorphine group did not requireany postoperative analgesia.
Patient feedbackNone of the patients complained of awareness in the intra-operative period at their postoperative interview. Forty percent of patients in both groups graded anaesthesia asexcellent and 60% graded it as good or satisfactory. Four-teen patients in each group (46%) experienced nausea orvomiting postoperatively, with the majority having oneepisode only.
Discussion
Combined infusions of propofol and an opioid were firstreported in 1985 by DeGrood et al. [6] using fentanyl. Thetechnique can be used in modern sophisticated situationsor in places with the bare minimum of facilities and mayhave particular advantages in developing countries wherethere may be problems with availability of compressed
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1098 Q 1997 Blackwell Science Ltd
Reversal toextubation
Extubation toeye opening
Extubation totelling name
Extubation tofirst analgesicdose
Nalbuphine 3.2 (2.5) 5.0 (9.9) 22.9 (16.7) 352 (354)Buprenorphine 3.36 (2.6) 4.46 (7.2) 29.4 (20.6) 385 (260)
Table 2 Recovery profile. Values are mean(SD) times (min).
Figure 2 Mean (SD) heart rate duringintravenous infusions of propofol/nalbuphine (X) or propofol/buprenorphine(W) at various times during anaesthesia.* Statistical significance (p < 0.05).

gases [7]. It also obviates the need for calibrated vaporisersand Rotameters [8] and helps to achieve a rapid andeffortless turnover of surgical lists [9]. Although expensiveinfusion pumps may be required, where cost is paramount,these may be replaced by simpler alternatives such aspaediatric infusion sets or manual flow control devices.
The current group of drugs being favoured for TIVAare a combination of a hypnotic with a short half-life suchas propofol combined with a short-acting narcotic likefentanyl, sufentanil or alfentanil [3, 4, 10, 11]. One of theproblems faced by anaesthetists practising in less developedcountries is the unpredictable availability of these shorteracting narcotics. Agonist–antagonist narcotics have beenused as alternatives to short-acting narcotics in bothdeveloped and less affluent countries. Their use has beenreported by a number of investigators [12–15] and theyhave been shown to have both advantages and disadvan-tages in balanced anaesthesia. Nalbuphine is chemicallyrelated to naloxone. When tested in rats via the subcuta-neous route the ED50 was found to be 1.2 mg.kgÿ1
compared to 0.98 mg.kgÿ1 for morphine, indicating itspotency to be 0.7–0.8 times that of morphine [16].Higher dose requirements were needed for use in balancedanaesthesia in humans [17]. It has been used in dosesvarying between 0.15 and 2 mg.kgÿ1 in clinical anaesthe-sia [15, 17].
Buprenorphine is considered to be 30–40 times morepotent than morphine [18]. Its intra-operative use duringanaesthesia has been reported with doses varying from2.5 to 15 mg.kgÿ1 [13, 19, 20]. Most of the studiesinvolving the higher dosages did not use inhalationalsupplementation. In our previous work using buprenor-phine as a component in both balanced anaesthesia and inTIVA we found that 2.5 mg.kgÿ1 gave good haemo-dynamic stability with minimal side-effects in recovery[5, 19]. The doses of nalbuphine and buprenorphine usedin our study were not equipotent but were based on therecommended dosage requirements in clinical anaesthesiapractice.
Buprenophine has been used as the narcotic componentin TIVA [5]. Raftery has commented that its use maypresent difficulties in TIVA because of its poor response toopioid antagonists and its propensity for causing nausea[21]. Nalbuphine has been used in TIVA only for minorcases in patients undergoing procedures such as cystoscopyor dilatation and curettage [22].
Different regimens have been recommended for the useof propofol in TIVA. A blood propofol concentration of3 mg.mlÿ1 combined with an opioid is said to provideadequate anaesthesia [1, 23]. We used Robert’s regimenwith the slight alteration of a 2 mg.kgÿ1 induction doseinstead of 1 mg.kgÿ1.
No difference was observed by us in the blood pressure
response in the two groups, although the heart rate wassignificantly lower in the buprenorphine group. Thismight be of significance in patients with underlyingischaemic heart disease undergoing noncardiac surgery.The effect of buprenorphine on the heart rate may beexaggerated when it is combined with drugs such aspropofol [24]. Tempia et al. found a 52% incidence ofbradycardia with buprenorphine compared to 32% withfentanyl, probably due to buprenorphine’s morphine-likeeffect on the vagal nucleus [25]. In our study 46% ofpatients in the buprenorphine group experienced a fall inheart rate to below 60 beat.minÿ1 compared to only 20%in the nalbuphine group.
Supplemental doses of narcotic or propofol haveboth been found to be equally effective in controllingacute haemodynamic and hormonal responses to surgicalstimuli during TIVA [26, 27]. In our study, a supplementalpropofol bolus was required in 27% of patients inthe nalbuphine group compared to 17% of patients inthe buprenorphine group. One patient in the nalbuphinegroup required a further narcotic bolus. Buprenorphinetherefore provided more profound intra-operative analge-sia. To our knowledge no other study has comparedbuprenorphine and nalbuphine for intra-operative usein TIVA. This difference might be explained by thedifference in the potency of the two drug dosagesused. However, in a study by Pugh et al. comparingpostoperative requirements for nalbuphine and buprenor-phine with a conventional anaesthetic technique, moreadditional analgesia was required in patients givennalbuphine [28].
The recovery profile was the same in both groups, withno patient needing treatment for respiratory depression. Inthe recovery room symptomatic bradycardia (heart rate<60 beat.minÿ1 associated with SBP <90 mmHg) had tobe treated with atropine in three patients in the bupre-norphine group (10%). The other complication seen inthe recovery room was nausea and vomiting. None of thepatients had been given a prophylactic anti-emetic. A highincidence of nausea and vomiting has been reported inboth laparoscopic and biliary procedures [29], which canbe reduced by avoiding nitrous oxide. An incidence ofnausea of 30–35% has been reported with buprenorphineanaesthesia by Carl [30], with a figure of 2–22% reportedfor nalbuphine [31]. The incidence of nausea and vomit-ing in the recovery room in our study was quite low, andno difference was observed in the emetogenic properties ofthe two drugs. One of the reasons for the low incidence ofnausea and vomiting seen in the recovery room could havebeen the routine insertion of a nasogastric tube intra-operatively on surgical request. The tube was removedbefore reversal of anaesthesia. The use of propofol couldalso have contributed to this low incidence of vomiting.
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1099Q 1997 Blackwell Science Ltd

Forty-six per cent of patients in each group vomited oneor more times in the 24 h following surgery. All of thesepatients had received pethidine for postoperative analgesiaon the ward. Seventeen per cent of patients in thenalbuphine group and 20% in the buprenorphine grouphad nausea/vomiting prior to receiving any pethidine. Inthe rest of the patients the contribution of pethidine to thishigh incidence cannot be ruled out.
Awareness was not reported by any of our patients,although we used indirect criteria for monitoring lightanaesthesia. These indirect methods have been criticised[32] but no entirely reliable method or monitor for routineuse has yet come into standard practice. Although aware-ness is a problem particularly highlighted in TIVA it hasbeen pointed out that it is not specifically related to TIVAbut to the use of muscle relaxants in general [30]. Thereported incidence in TIVA is comparable to that reportedwith standard balanced anaesthesia techniques using musclerelaxants [33].
In conclusion, both drugs were found to be satisfactoryfor use in TIVA, in situations where short-acting narcoticswhich are used as an infusion are not available, and areable to provide adequate analgesia in combination withpropofol. The major side-effect seen was intra-operativeand postoperative bradycardia requiring treatment withatropine in the buprenorphine group.
References
1 Schuttler J, Kloos S, Schwilden H, Stoeckel H. TIVA withpropofol and alfentanil by computer assisted infusion.Anaesthesia 1988; 43 (Suppl): 2–7.
2 Dundee JW, Wyant GM. Propofol In: Dundee, JW, WyantGM, eds. Intravenous Anaesthesia. New York: ChurchillLivingstone, 1988; 172–83.
3 Jenstrup M, Nielsen J, Fruergard K. TIVA with propofol/alfentanil or propofol/fentanyl. British Journal of Anaesthesia1990; 64: 717–22.
4 Mustola ST, Baer GA, Metasa-Ketela T, Laippala P.Haemodynamic and plasma catecholamine responses duringTIVA for laryngomicroscopy. Anaesthesia 1995; 50:108–13.
5 Kamal RS, Khan FA, Khan FH. TIVA with propofol andbuprenorphine. Anaesthesia 1990; 45: 865–70.
6 De Grood PMRM, Ruys AHC, Van Egmond J, BooijLHDJ, Crul JF. Propofol (Diprivan) emulsion for totalintravenous anaesthesia. Postgraduate Medical Journal (Suppl.)1985; 61: 65–9.
7 Dobson MB. Anaesthesia with ketamine and thiopentonefor short surgical procedures, with reference to anaesthesiain developing countries. Anaesthesia 1978; 33: 268–70.
8 Knell PJW. Total intravenous anaesthesia by an intermittenttechnique. Use of methoheitone, ketamine and a musclerelaxant. Anaesthesia 1983; 38: 586–7.
9 Holmes C, McK. Midazolam/fentanyl. A total intravenous
technique for short procedures. Anaesthesia 1982; 37:761–5.
10 Phillips AS, McMurray TJ, Mirakhur RK, Gibson FM,Elliot P. Propofol fentanyl anaesthesia in cardiac surgery: acomparison in patients with good and impaired ventricularfunction. Anaesthesia 1993; 48: 661–3.
11 Steegers PA, Foster PA. Propofol in total intravenousanaesthesia without nitrous oxide. Anaesthesia 1988;43(Suppl.): 94–7.
12 Dobkin AB, Arandia HY, Byles PH, Africa BF, Caruso FS,Noveck RJ. Safety and efficacy of butorphanol tartrate inbalanced anaesthesia. Canadian Anaesthetists Society Journal1976; 23: 601–8.
13 Kay B. A double blind comparison between fentanyl andbuprenorphine in analgesic supplemented anaesthesia.British Journal of Anaesthesia 1980; 52: 453–6.
14 Green DW, Sinclair JR, Mikhael MC. Buprenorphineversus morphine – A comparison of intraoperative and postoperative analgesia. Anaesthesia 1985; 40: 371–5.
15 Fahmy NR. Nalbuphine in balanced anaesthesia, itsanalgesic efficacy and haemodynamic effects. Anesthesiology1980; 53: s56.
16 Schmidt WK, Tam SW, Shotzberger GS, Smith DH, ClarkR, Vernier VG. Nalbuphine: Drug and Alcohol Dependence.Ireland: Elsevier Scientific Publishers, 1985.
17 Magruper MR, Christofforetti R, Difazio CA. Balancedanaesthesia with nalbuphine hydrochloride. AnesthesiologyReview 1980; 9: 25–9.
18 Downing JW, Leary WP, White ES. Buprenorphine a newpotent long-acting synthetic analgesic. Comparison withmorphine. British Journal of Anaesthesia 1977; 49: 251–4.
19 Khan FA, Kamal RS. A comparison of buprenorphine andpethidine in analgesic supplemented anaesthesia withreference to anaesthesia in developing countries. SingaporeMedical Journal 1990; 31: 345–9.
20 Abrahamsson J, Niemand D, Olsson AK, Tornebrandt K.Buprenorphine (Temgesic) als peroperative Analgetikum.Anesthetist 1983; 32: 75–9.
21 Raftery S. Total intravenous anaesthesia. Current Opinion inAnaesthesiology 1991; 4: 522–9.
22 Kay B. Opioid supplements in total intravenous anaesthesia.In: Kay B, ed. Total Intravenous Anaesthesia. Netherlands:Elsevier Science Publishers, 1991: 103–24.
23 Roberts FL, Dixon J, Lewis GTR, Tackeey RM,Prys-Roberts C. Induction and maintenance of propofolanaesthesia. Anaesthesia 1988; 43 (Suppl): 14–7.
24 Claeys MA, Gepts E, Camu F. Haemodynamic changesduring anaesthesia induced and maintained with propofol.British Journal of Anaesthesia 1988; 60: 3–9.
25 Tempia A, Cerutti F, Fiore G, Balagna R, Lusso C,Pattona R. Use of propofol in association with fentanyl orbuprenorphine in long lasting anaesthesia. MinervaAnaesthesiol 1991; 57: 123–30.
26 Monk CR, Coates DP, Prys Roberts C, Turtle M,Spelina K. Haemodynamic effects of a prolonged infusionof propofol as a supplement to nitrous oxide. Anaesthesia1987; 59: 954–60.
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1100 Q 1997 Blackwell Science Ltd

27 Monk TG, Ding Y, White PF. Total intravenousanaesthesia: effects of opioid versus hypnoticsupplementation on automatic responses and recovery.Anesthesia and Analgesia 1992; 75: 798–804.
28 Pugh GC, Drummond GB, Elton RA, Macintyre CCA.Constant i/v infusions of nalbuphine or buprenorphine forpain after abdominal surgery. British Journal of Anaesthesia1987; 59: 1364–74.
29 Watcha M, White P. Postoperative nausea and vomiting(review article). Anesthesiology 1992; 77: 162–84.
30 Carl P, Crawford ME. A comparison betweenbuprenorphine, fentanyl, and pentazocine in analgesicsupplemented flunitrazepam nitrous oxide anaesthesia. In:
Paul L, Bevan T, Firth M, eds. Royal Society of MedicineInternational Congress and Symposium series No. 65. London:Royal Society of Medicine, 1984: 71–6.
31 Ernest H, Foster K, Gordon R, Hew E. A comparison ofnalbuphine and meperidine in treatment of post operativepain. Canadian Journal of Anaesthesia 1987; 34: 462–5.
32 Jones JG. Perception and memory during generalanaesthesia. British Journal of Anaesthesia 1994; 73: 31–7.
33 Barclay A, Houlton PC, Downing JW. Total intravenousanaesthesia: a technique using flunitrazepam, ketamine,muscle relaxants and controlled ventilation of the lung.Anaesthesia 1980; 35: 287–90.
FORUM
Analgesic and respiratory effect of nalbuphine andpethidine for adenotonsillectomy in children withobstructive sleep disorder
W. Habre1 and B. McLeod2
1 Division of Paediatric Anaesthesia, Hopital des Enfants, 6, rue Willy Donze, 1211 Geneva 14, Switzerland2 Department of Anaesthesia, Princess Margaret Hospital for Children, GPO Box D184, Perth WA 6001,Western Australia
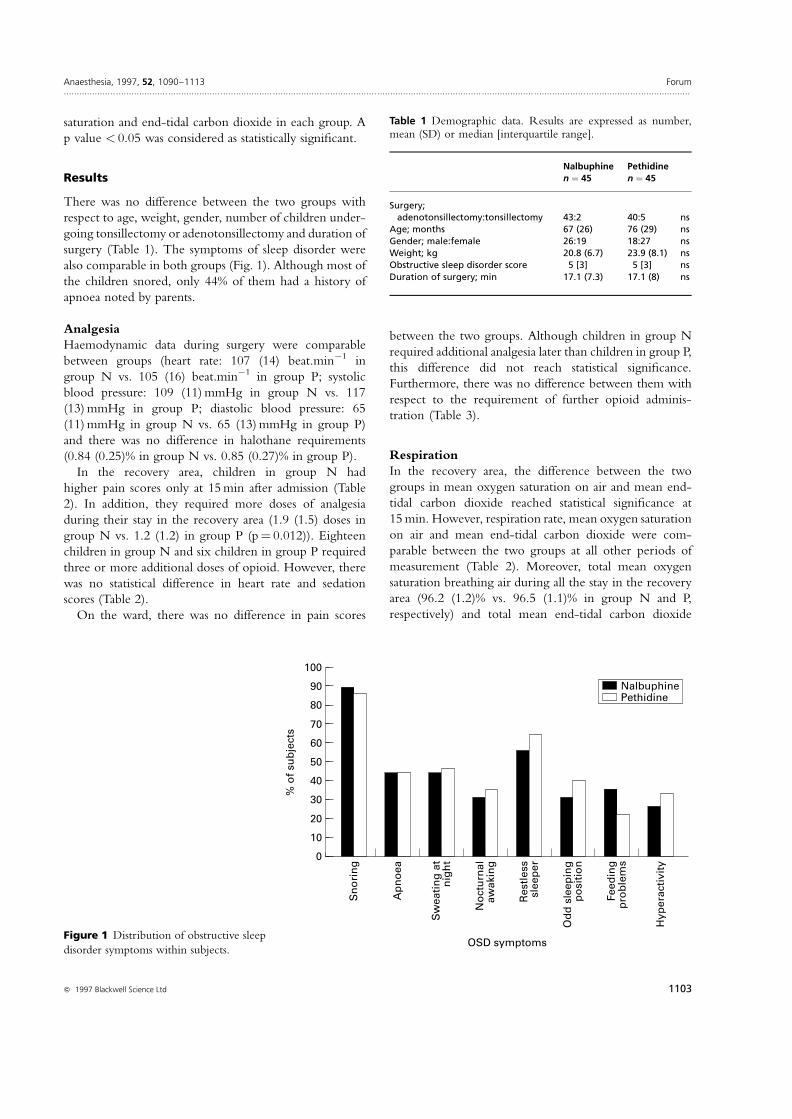
SummaryOpioids may depress respiration and contribute to airway obstruction after adenotonsillectomy forobstructive sleep disorder. We compared the respiratory and analgesic effects of nalbuphine, whichhas a ceiling effect for respiratory depression, and pethidine in 90 children (aged 2–12 years) witha history of obstructive sleep disorder undergoing adenotonsillectomy. Children were scored fortheir obstructive sleep disorder history and were randomly allocated to receive intravenously atinduction of anaesthesia either nalbuphine 0.1 mg.kgÿ1 (group N) or pethidine 1 mg.kgÿ1 (groupP). End-tidal carbon dioxide was measured in the recovery period using a nasopharyngeal catheterand oxygen saturation whilst breathing air; pain and sedation scores were recorded for 6 hpostoperatively. Both groups were similar with respect to the demographic data and respiratorymeasurements: mean (SD) oxygen saturation on air in the recovery area (96.2% (1.2) vs. 96.5%(1.1) in group N and P, respectively) and mean (SD) end-tidal carbon dioxide (46.4 (5.5) mmHgvs. 47.7 (4) mmHg in group N and P, respectively). High obstructive sleep disorder score, historyof apnoea, hyperactivity and loud snoring were found to be the best predictors of earlypostoperative oxygen desaturation in both groups.
Keywords Analgesics; nalbuphine; pethidine. Complications; sleep apnoea syndromes. Surgery;paediatric; adenotonsillectomy.
......................................................................................Correspondence to: Dr W. HabreAccepted: 14 April 1997
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1101Q 1997 Blackwell Science Ltd

Tonsillectomy or adenotonsillectomy in children for thetreatment of obstructive sleep disorder is increasing [1].The most common serious postoperative complicationfollowing this procedure is upper airway obstruction[2, 3]. Many factors may contribute including mechanicalswelling, disruption of pharyngeal receptors from surgeryand the effects of general anaesthesia [4]. There is alsoconcern that opioids may depress respiration and precipi-tate airway obstruction after surgery. Nalbuphine, anagonist/antagonist opioid analgesic, has been shown toprovide effective analgesia [5] and to possess a ceiling effectfor respiratory depression [6, 7]. These properties maymake nalbuphine a useful and safe analgesic for childrenundergoing tonsillectomy or adenotonsillectomy forobstructive sleep disorder.
We compared the analgesic and respiratory depressanteffects of intravenous pethidine and nalbuphine fortonsillectomy or adenotonsillectomy in children with ahistory of obstructive sleep disorder.
Methods
After institutional Ethics Committee approval andparental informed written consent, we studied 90 children(ASA physical status 1 or 2), aged 2–12 years. Allchildren were in-patients scheduled for tonsillectomy oradenotonsillectomy with a history of varying degrees ofobstructive sleep disorder. Children with craniofacialabnormalities, previous upper airway trauma, failure tothrive or cor pulmonale were not studied.
Parents were questioned about their child’s symptoms.Severity of obstructive sleep disorder was scored using thepresence or absence of each of the following symptoms:snoring, apnoea, nocturnal sweating, nocturnal awaken-ing, restlessness during sleep, odd sleeping position, feed-ing problems or daytime hyperactivity. A score of 0 wasgiven if the symptom was absent. Snoring was scored aseither 1 and considered as minor (when the parents mustbe in the same room to hear it), or scored 2 and con-sidered as loud (when the parents can hear it from outsidetheir child’s bedroom). All other symptoms were scored as1, if present. Apnoea was defined as the occurrence ofbreath-holding during the child’s sleep which was ofconcern to the parents. Odd sleeping position wasrecorded if the child’s head was noted to be in hyperexten-sion during sleep.
All children were given paracetamol 15 mg.kgÿ1 orallyand had topical anaesthetic cream (EMLA ) applied toboth hands 1 h before surgery. Anaesthesia was inducedwith thiopentone 5 mg.kgÿ1 intravenously and maintainedwith halothane and nitrous oxide 70% in oxygen. Atra-curium 0.5 mg.kgÿ1 was given to facilitate trachealintubation. Children were then randomly assigned to
receive on induction either nalbuphine 0.1 mg.kgÿ1 intra-venously (Group N) or pethidine 1 mg.kgÿ1 intravenously(Group P). These opioids were prepared by anotheranaesthetist who was not involved in the procedure.Further intra-operative analgesic supplements were notgiven and muscle relaxation was reversed prior to trachealextubation with atropine 0.02 mg.kgÿ1 and neostigmine0.05 mg.kgÿ1. At the end of the procedure, and prior totracheal extubation, the surgeon introduced a 10F feedingtube in the nasopharynx to allow end-tidal carbon dioxidemeasurement in the recovery period. The tube tip waspositioned under direct vision to be visible in theoropharynx just below the soft palate.
Heart rate, arterial blood pressure and administeredhalothane concentration were recorded every 3 minduring the surgical procedure. In the recovery area,oxygen saturation on air, end-tidal carbon dioxide, respira-tion rate, heart rate and sedation score (1� agitated,weeping, 2� alert, calm, 3� drowsy, sleeping but easilyawake and 4� asleep, no response to minor stimuli) wererecorded on arrival and every 15 min. Oxygen saturationand end-tidal carbon dioxide were recorded on a regularlycalibrated gas analyser (OSCAROXYTM, Datex) whichdisplays a capnograph. The same monitor was used for allchildren. End-tidal carbon dioxide was sampled continu-ously in the recovery area and values were recorded after1 min of a steady-state capnograph trace. Pain was alsoassessed at the same intervals using our institution painscoring system (PMH pain score), which is based on fourcriteria (facial expression, position in bed, vocalisation andnurse’s assessment) [8]. Each criterion was scored 0–2making a maximum pain score of 8. A total score of lessthen 4 was considered to indicate adequate analgesia. Ifanalgesia was required, children received the same opioidas given on induction from a syringe labelled with theirname. Recovery nursing staff were therefore blinded tothe choice of opioid. The children thus received eithernalbuphine 25 mg.kgÿ1 or pethidine 250 mg.kgÿ1 intra-venously every 3 min if required.
On the ward, the same variables, except end-tidalcarbon dioxide, were recorded every 30 min for the first2 h then hourly for a further 4 h. The incidence ofvomiting and the time of first analgesic administrationwere also recorded.
Groups of 45 subjects can been shown to have, respec-tively, 80% and 90% power to detect a 30% difference inpain score less or more than 4 and a 1% difference in meanoxygen saturation breathing air in the recovery areabetween the two groups. Parametric data were comparedusing unpaired two-tailed t-tests. Chi-squared analysis wasused to compare sedation scores at each time. Linearregression analysis was used to compare the effect ofobstructive sleep disorder scores on postoperative oxygen
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1102 Q 1997 Blackwell Science Ltd
saturation and end-tidal carbon dioxide in each group. Ap value < 0.05 was considered as statistically significant.
Results
There was no difference between the two groups withrespect to age, weight, gender, number of children under-going tonsillectomy or adenotonsillectomy and duration ofsurgery (Table 1). The symptoms of sleep disorder werealso comparable in both groups (Fig. 1). Although most ofthe children snored, only 44% of them had a history ofapnoea noted by parents.
AnalgesiaHaemodynamic data during surgery were comparablebetween groups (heart rate: 107 (14) beat.minÿ1 ingroup N vs. 105 (16) beat.minÿ1 in group P; systolicblood pressure: 109 (11) mmHg in group N vs. 117(13) mmHg in group P; diastolic blood pressure: 65(11) mmHg in group N vs. 65 (13) mmHg in group P)and there was no difference in halothane requirements(0.84 (0.25)% in group N vs. 0.85 (0.27)% in group P).
In the recovery area, children in group N hadhigher pain scores only at 15 min after admission (Table2). In addition, they required more doses of analgesiaduring their stay in the recovery area (1.9 (1.5) doses ingroup N vs. 1.2 (1.2) in group P (p� 0.012)). Eighteenchildren in group N and six children in group P requiredthree or more additional doses of opioid. However, therewas no statistical difference in heart rate and sedationscores (Table 2).
On the ward, there was no difference in pain scores
between the two groups. Although children in group Nrequired additional analgesia later than children in group P,this difference did not reach statistical significance.Furthermore, there was no difference between them withrespect to the requirement of further opioid adminis-tration (Table 3).
RespirationIn the recovery area, the difference between the twogroups in mean oxygen saturation on air and mean end-tidal carbon dioxide reached statistical significance at15 min. However, respiration rate, mean oxygen saturationon air and mean end-tidal carbon dioxide were com-parable between the two groups at all other periods ofmeasurement (Table 2). Moreover, total mean oxygensaturation breathing air during all the stay in the recoveryarea (96.2 (1.2)% vs. 96.5 (1.1)% in group N and P,respectively) and total mean end-tidal carbon dioxide
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1103Q 1997 Blackwell Science Ltd
Table 1 Demographic data. Results are expressed as number,mean (SD) or median [interquartile range].
Nalbuphine Pethidinen � 45 n � 45
Surgery;adenotonsillectomy:tonsillectomy 43:2 40:5 ns
Age; months 67 (26) 76 (29) nsGender; male:female 26:19 18:27 nsWeight; kg 20.8 (6.7) 23.9 (8.1) nsObstructive sleep disorder score 5 [3] 5 [3] nsDuration of surgery; min 17.1 (7.3) 17.1 (8) ns
100
0
% o
f su
bje
cts
OSD symptoms
50
60
40
30
20
10
NalbuphinePethidine
70
80
90
Sn
ori
ng
Hyp
era
cti
vit
y
Feed
ing
p
rob
lem
s
Od
d s
leep
ing
po
sit
ion
Restl
ess
sle
ep
er
No
ctu
rnal
aw
akin
g
Sw
eati
ng
at
nig
ht
Ap
no
ea
Figure 1 Distribution of obstructive sleepdisorder symptoms within subjects.

(46.4 (5.5) mmHg vs. 47.7 (4) mmHg in group N and P,respectively) were comparable (p� 0.2 and p� 0.24,respectively).
Using a linear regression analysis, low oxygen saturationbreathing air in the recovery period (less than 95%) wasstrongly associated with a high obstructive sleep disorderscore in both groups (p< 0.01). Low oxygen saturation onair in the recovery period was significantly associated onlywith a history of loud snoring, apnoea and hyperactivity(Table 4). However, there was no correlation betweenhigh values of end-tidal carbon dioxide and obstructivesleep disorder score. There was also no correlationbetween high end-tidal carbon dioxide and low oxygensaturation. Both were comparable in children whoreceived three or more doses of opioids and those whodid not.
On the ward, there was no statistical difference in meanoxygen saturation breathing air and respiration rate (Table3). We did not observe any obstructive event or need forsupplemental oxygen during the study period.
SedationSedation scores were comparable on arrival and for eachperiod of measurements in the recovery area and on theward. Tables 2 and 3 show the mean sedation score
observed in both groups in the recovery area and on theward. Two patients in group N may have experiencedpsychotomimetic effects, one child appeared to befrightened and another complained of bad dreams. Theincidence of postoperative vomiting was identical in bothgroups (58%) during the study period.
Discussion
This study shows that nalbuphine and pethidine havesimilar respiratory effects in children with a history ofobstructive sleep disorder undergoing tonsillectomy oradenotonsillectomy. Furthermore, this study providesinformation on the effect of the different obstructivesleep symptoms on the risk of postoperative oxygendesaturation. The ideal study would have included pre-operative polysomnography to confirm and document theseverity of the obstructive sleep disorder and correlate thiswith the patient’s history and the postoperative measure-ments. However, a role for routine polysomnographyprior to adenotonsillectomy in children has yet to beestablished and the economic impact of such a practice
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1104 Q 1997 Blackwell Science Ltd
T0 T15 T30
Heart rate; beat.minÿ1 Nalbuphine 102 (19) 100 (15) 101 (19)Pethidine 98 (19) 97 (19) 95 (21)
Respiratory rate; Nalbuphine 20.7 (6) 20.5 (4.9) 20.2 (3.9)breath.minÿ1 Pethidine 20.4 (6) 18.7 (4.9) 18.6 (3.5)
Oxygen saturation; % Nalbuphine 95.6 (2.4) 96.4 (1.5) 96.7 (1.4)Pethidine 95.1 (2.8) 97 (1.1)* 97.2 (1.3)
End-tidal carbon Nalbuphine 47.4 (8.7) 45.1 (5.9) 45.9 (4.8)dioxide; mmHg Pethidine 49.3 (6.6) 47.5 (3.6)* 46 (3.5)
Pain score Nalbuphine 1.2 (2.2) 1.8 (2.3) 1.5 (1.9)Pethidine 1 (2.1) 0.7 (1.5)* 0.9 (1.7)
Sedation score Nalbuphine 3.1 (1.2) 2.4 (1.2) 2.1 (1)Pethidine 3.3 (1.1) 2.8 (1.1) 2.4 (1)
* p < 0.05.
Table 2 Postoperative respiratory, analgesicand sedative effects of nalbuphinecompared to pethidine as observed atadmission to the recovery area (T0) and 15and 30 min later (T15 and T30). Resultsare expressed as mean (SD).
Table 3 Postoperative respiratory variables, analgesic and sedativeeffects of nalbuphine compared to pethidine as observed on theward. Results are expressed as mean (SD).
Nalbuphine Pethidine
Respiratory rate; breath.minÿ1 21 (2) 20 (2) nsOxygen saturation; % 97.3 (1) 97.6 (1) nsHeart rate; beat.minÿ1 101 (12) 97 (13) nsPain score 5.5 (5) 4.7 (4.7) nsSedation score 2.5 (0.4) 2.5 (0.3) nsTime of first medication; h 4.12 (2.7) 3.1 (3.2) ns
Table 4 Linear regression analysis for single variable models ofobstructive sleep disorder risk factors associated with oxygensaturation on air less than 95% in the recovery area.
Risk factor Coefficient SE Significance
Hyperactivity ÿ 0.68 0.27 p� 0.012Apnoea ÿ 0.55 0.25 p� 0.028Loud snoring ÿ 0.54 0.27 p� 0.046Odd sleeping position – 0.43 0.26 p� 0.1Feeding problems ÿ 0.41 0.27 p� 0.14Nocturnal awaking ÿ 0.37 0.26 p� 0.16Sweating ÿ 0.35 0.25 p� 0.17Restless sleeping ÿ 0.26 0.26 p� 0.32Overall: obstructive
sleep disorder score ÿ 0.17 0.05 p� 0.002

would be significant. In practice, most doctors rely on datasuch as medical history, physical examination and intra-operative findings to assess risk and determine anaesthetictechnique and postoperative management.
Postoperative respiratory complications after tonsillec-tomy or adenotonsillectomy are multifactorial and opioidsmay further compromise respiratory patterns [4]. A ceilingeffect for respiratory depression has been demonstrated fornalbuphine [7] which could have been of importance inchildren with obstructive sleep disorder, as they may alreadyhave impaired ventilatory responses to carbon dioxide [9].
We used a dose of nalbuphine 0.1 mg.kgÿ1 at theinduction of anaesthesia which is considered to be equi-analgesic to morphine 0.1 mg.kgÿ1 [10] and pethidine1 mg.kgÿ1. The mean blood pressure, heart rate andhalothane requirements during the procedure were com-parable in both groups, further suggesting that nalbuphine0.1 mg.kgÿ1 is equipotent to pethidine 1 mg.kgÿ1. How-ever, although respiratory and heart rates were compar-able, pain scores were different 15 min after arrival in therecovery area and children in the nalbuphine grouprequired more analgesia despite comparable sedationscores. Furthermore, the number of patients who requiredfurther analgesia in the recovery area was comparable inboth groups (31 in group N vs. 26 in group P).
Pain was assessed using the routine pain tool at ourinstitution [8] and our policy is to give intravenousanalgesia if the pain score is 4 or more in the recoveryarea. The reasons for higher pain scores at one stage in thenalbuphine group may be multifactorial. These mayinclude the possible psychotomimetic effects of nalbu-phine, the higher incidence of intolerance to the naso-pharyngeal catheter and the possibility that nalbuphine at adose of 0.1 mg.kgÿ1 was less potent than expected.
The monitoring of end-tidal carbon dioxide through anasal cannula and its correlation to arterial carbon dioxidetension has already been validated in children [11]. How-ever, this method could be limited by entrainment of roomair or by mouth breathing particularly in the presence of aGuedel airway. We modified this technique by using anasopharyngeal catheter which samples the gas from theposterior nasopharynx [12]. This decreases dead space andalso allows suction of the airway if postoperative bleedingoccurs. Thirteen out of the 90 children were upset by thepresence of the nasopharyngeal catheter; two of thempulled out their catheter immediately on arrival in therecovery area and 11 after 20 min. However, in theremaining children, we were able to obtain a normalcapnograph tracing with consistent measurements within1 min. We observed, 15 min after arrival in the recoveryarea, a significant difference between the two groups inthe mean value of end-tidal carbon dioxide. However,this slight difference could not be considered as clinically
relevant, and similarly for the difference in oxygen satura-tion. Furthermore, there was no correlation between theseverity of the symptoms of obstructive sleep disorder andthe values of end-tidal carbon dioxide in the recovery area.Although airway obstruction or alveolar hypoventilationmay induce an elevation in arterial carbon dioxide, ourmeasurements through a nasopharyngeal catheter wouldhave detected it, as demonstrated during polysomno-graphy in children [13]. Recently, children with sleep-induced respiratory obstruction were shown to havehigher end-tidal carbon dioxide then nonobstructersbefore surgery, but this difference disappeared afteradenotonsillectomy [14]. In our study, mean end-tidalcarbon dioxide in the recovery area was also similar inchildren with and without a history of loud snoring andapnoea.
A ceiling effect for respiratory depression has beenreported after repeated doses of nalbuphine [6]. Eighteenpatients in group N required three or more doses ofanalgesic in the recovery area compared with only six ingroup P. Despite this small number, we did not find adifference in end-tidal carbon dioxide and oxygen satura-tion on air in the recovery area between children whoreceived repeated doses of opioids and those who did not.
A simple linear regression analysis was carried out usingthe medical history of obstructive sleep disorder as a riskfactor for low values of oxygen saturation in the recoveryarea (less than 95%). In our model including all symptomsof obstructive sleep disorder a high score was significantlyassociated with postoperative oxygen desaturation. Thesymptoms of obstructive sleep disorder considered in ourstudy were similar to those found in selected patients withsleep apnoea [15, 16]. Considering each symptom, wefound only apnoea, loud snoring and hyperactivity to besignificantly associated with low oxygen saturation in therecovery area.
Stradling et al. found pre-operative hyperactivity in 60%of the children with obstructive sleep disorder whichsignificantly decreased to less than 10% 6 months afterthe operation [15]. In our study, 30% of the children wereconsidered by their parents to have pre-operative daytimehyperactivity. Children less than 4 years old were found tobe at high risk of postoperative respiratory compromisebecause of anatomical factors such as small mandible andlarge tongue [3]. Although 25% of the children in ourstudy were 4 years old or younger, only three of themhad oxygen saturation on air in the recovery area of lessthan 95%.
In conclusion, this study shows that postoperativesedation and respiratory patterns were similar after nalbu-phine or pethidine. In addition, our model showed thatthe severity of obstructive sleep disorder could be sug-gested by the medical history and predict a risk of
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1105Q 1997 Blackwell Science Ltd

postoperative oxygen desaturation. Among all risk factors,a history of apnoea, loud snoring and daytime hyperactiv-ity should be considered when assessing these patients asthese symptoms were more important determinants ofpostoperative respiratory problems than the choice ofopioid. Pre- and postoperative polysomnography in aselected group of children could more accurately delineatethe risk factors for postoperative oxygen desaturation.
References
1 Suen JS, Arnold JE, Brooks LJ. Adenotonsillectomy fortreatment of obstructive sleep apnoea in children. Archivesof Otolaryngology - Head and Neck Surgery 1995; 12: 525–30.
2 Richmond KH, Wetmore RF, Boronak CC. Postoperativecomplications following tonsillectomy and adenoidectomy-who is at risk? International Journal of PediatricOtorhinolaryngology 1987; 13: 117–24.
3 McColley SA, April MM, Carroll JZ, Naderio RM,Loughlin GM. Respiratory compromise afteradenotonsillectomy in children with obstructive sleepapnea. Archives of Otolaryngology - Head and Neck Surgery1992; 118: 940–3.
4 Helfaer MA, Wilson MD. Obstructive sleep apnea, controlof ventilation and anesthesia in children. Pediatric Clinics ofNorth America 1994; 41: 131–51.
5 Krishnan A, Tolhurst-Cleaver CL, Kay B. Controlledcomparison of nalbuphine and morphine for post-tonsillectomy pain. Anaesthesia 1985; 40: 1178–81.
6 Gal TJ, Difazio CA, Moscicki J. Analgesic and respiratorydepressant activity of nalbuphine: a comparison withmorphine. Anesthesiology 1982; 57: 367–74.
7 Rommagnoli A, Keats AS. Ceiling effect for respiratory
depression by nalbuphine. Clinical Pharmacology andTherapeutics 1980; 27: 478–85.
8 Robertson J. Pediatric pain assessment: validation of amultidimensional tool. Pediatric Nursing 1993; 19:209–13.
9 Ingram RI, Bishop JB. Ventilatory response to carbondioxide after removal of chronic airway obstruction.American Review of Respiratory Disease 1970; 102: 645–7.
10 Wandless JG. A comparison of nalbuphine with morphinefor post-orchidopexy pain. European Journal ofAnaesthesiology 1987; 4: 127–32.
11 Tobias JD, Flanagan JFK, Wheeler TJ, Garrett JS, BurneyC. Noninvasive monitoring of end-tidal CO2 via nasalcannulas in spontaneously breathing children during theperioperative period. Critical Care Medicine 1994; 22:1805–8.
12 Bongard F, Wu Y, Lee TS, Klein S. Capnographicmonitoring of extubated postoperative patients. Journal ofInvestigative Surgery 1994; 7: 259–64.
13 Morielli A, Desjardins D, Brouillette RT. Transcutaneousand end-tidal carbon dioxide pressures should be measuredduring pediatric polysomnography. American Review ofRespiratory Disease 1993; 148: 1599–604.
14 Smith TC, Hutton P. Effect of respiratory obstruction onpeak carbon dioxide concentrations in sleeping childrenusing nasal capnography. British Journal of Anaesthesia 1995;75: 655P.
15 Stradling JR, Thomas G, Warley ARH, Williams P,Freeland A. Effect of adenotonsillectomy on nocturnalhypoxaemia, sleep disturbance, and symptoms in snoringchildren. Lancet 1990; 335: 249–53.
16 Ahlqvist-Rastad J, Hultcrantz E, Svanholm H. Childrenwith tonsillar obstruction: indications for and efficacy oftonsillectomy. Acta Paediatrica 1988; 77: 831–5.
FORUM
The site of airway irritation during induction ofanaesthesia
A. K. Dashfield, S. E. Bree, A. M. Weiss and J. A. Langton*
Department of Anaesthesia, Derriford Hospital, Derriford, Plymouth PL6 8DH, UK
SummaryThe aim of this investigation was to study the role of the nasal airway in mediating upper airwayreflexes during induction of anaesthesia when the commonly used irritant inhalational anaestheticagent enflurane is used. In a prospective randomised study, 40 ASA 1 & 2 day-case patientsundergoing body surface surgery were recruited. Following intravenous induction using propofol,
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1106 Q 1997 Blackwell Science Ltd

20 patients received enflurane administered via a laryngeal mask airway (LMA), the anaestheticvapour therefore bypassing the nasal airway. In the other group, 20 patients received enfluraneanaesthesia administered using a face mask, the nasal airway therefore being exposed to inhalationanaesthetic. We were unable to demonstrate any significant (p< 0.05) differences between the twogroups in relation to upper airway complications (cough, breath holding, laryngeal spasm,bronchospasm and excitement). Previous work has identified the nose as a possible importantreflexogenic site for upper airway reflexes in humans during anaesthesia. We have been unable todemonstrate any difference in upper airway complications when the nasal airway was included orexcluded from exposure to irritant anaesthetic vapours, when administered in a clinical setting.
Keywords Complications; airway irritation. Anaesthesia; induction.
......................................................................................Correspondence to: Dr J. A. LangtonAccepted: 26 April 1997
It is generally accepted that inhalational anaesthetic agentsmay cause irritation to the upper airway when inhaled, asdemonstrated by coughing, laryngospasm and breathholding [1]. This may impair the smooth induction ofanaesthesia and lead to airway obstruction and associatedhypoxaemia and hypercarbia, which may in some cases beassociated with serious complications.
A recent study [2] has proposed that the site involved inmediating upper airway reflexes to inhaled anaestheticvapours is located within the nasal airway. Previous workhas shown that stimulation of the nasal mucosa can causevarious airway reflexes in humans [3–6]. Nasal irritationmore commonly causes apnoea rather than a sneeze underexperimental conditions. The apnoeic reflex is part of thecomplex diving response [7], the physiological stimulusbeing water applied to the face or into the nose. Associatedwith the apnoea are cardiovascular changes and completelaryngeal closure occurs as part of the diving response [8].The receptors that initiate the apnoeic reflex have notbeen identified but probably include nerve endings in thenasal mucosa. It is unlikely, however, that the diving reflexis initiated by a single modality of receptor. Nasal irritantstimuli that mimic the diving response also close the larynxby the same nervous pathways [9]. The nature and strengthof the stimulus used determines to some extent the type ofreflex response obtained.
Enflurane has been found to be especially irritant to theupper airway causing an increase in laryngeal wall tensionand prolongation of expiratory time during nasal insuffla-tion [2]. If the site which modulates upper airway reflexesduring induction of anaesthesia were to be identified,therapies could be designed to reduce and eliminate theseproblems. It may also be possible to identify particularchemical structures involved in causing irritation to theupper airway during induction of anaesthesia. This may beof particular importance in paediatric anaesthesia, where
the incidence of upper airway complications is knownto be higher and may rapidly lead to life-threateningcomplications.
To investigate this question, we performed a prospectiverandomised, controlled study of enflurane anaesthesiaadministered via a laryngeal mask airway (LMA), thusbypassing the nasal airway compared with enflurane anaes-thesia administered using a face mask and Guedel airway,therefore including the nasal airway.
Methods
Following local Ethics Committee approval, patients pre-senting for routine day-case, body surface surgery wererecruited into this study. They were ASA 1 or 2, aged 18–65 years, nonsmokers and had no history of asthma, nasalpolyps or upper respiratory tract infection within the pre-vious 2 weeks. Patients with risk factors for regurgitationof gastric contents were not studied. Written informedconsent was obtained prior to participating in the study.No premedication was administered and, prior to anaes-thesia, patients were randomly allocated to one of twogroups according to a sealed envelope random numbersystem.
A standardised general anaesthetic technique was used.Anaesthesia was induced using propofol administered viaan Ohmeda 9000 syringe pump (Ohmeda, Steeton, WestYorks., UK) set at an infusion rate of 1200 ml.hÿ1 follow-ing formal pre-oxygenation for 2 min. The end-point ofinduction was judged to be when the patient dropped a20 ml water-filled syringe [10] held between thumb andindex finger of the right hand. In the laryngeal maskairway (LMA) group the airway was then inserted in therecommended manner [11] and anaesthesia was main-tained using 2% enflurane in 66% nitrous oxide inoxygen using a Mapleson D breathing system. The
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1107Q 1997 Blackwell Science Ltd

concentration of enflurane was increased by 0.5% every30 s in the spontaneously breathing patient until 5% wasreached. In the face mask group a Guedel airway wasinserted following intravenous induction and anaesthesiawas maintained in the same manner using a close-fittingblack rubber Ohmeda anaesthetic face mask.
The anaesthetic induction was scored for upper airwaycomplications until 5% enflurane with 66% nitrous oxidein oxygen was reached. The incidence and severity of thefollowing upper airway complications were scored: (i)coughing, (ii) breath holding after spontaneous ventilationhad commenced, (iii) laryngeal spasm, (iv) bronchospasmand (v) excitement. We defined excitement as spontaneousmovement of the head, arms or legs by the patient duringinduction. Breath holding was defined as periods of apnoeain the absence of upper airway obstruction measured fromafter the commencement of spontaneous ventilation, asinitial apnoea postinduction was likely to have been due tothe respiratory depressant effect of propofol.
These complications were each scored using a four-point scale, none, occasional, frequent and continuous,and then pooled to obtain a total score. We defined occa-sional coughing as up to two coughs, frequent up to 10coughs and continuous more than 10 coughs during theinduction period. Mild laryngospasm was defined as last-ing 15 s or less with the patient able to maintain adequatespontaneous ventilation. Moderate laryngospasm lastedgreater than 15 s but could be overcome with continuouspositive airways pressure. Complete laryngospasm wasdefined as inability to ventilate the patients’ lungs requir-ing muscle relaxation to restore a clear airway. The totalcomplication score could therefore range from a minimum
of 5 to a maximum of 20 points (Table 1). This scoringsystem has been used in previous work [12] investigat-ing upper airway complications during induction ofanaesthesia.
In a previous study [2] nasal insufflation of enfluranetriggered upper airway reflexes in 46% of patients. Wecalculated that 20 patients would be required in eachgroup to give the study a power of <0.75 [13]. Statisticalanalysis of our nonparametric data was performed usingthe Macintosh Instat version 2.01 statistical computersoftware program. The Chi-squared test was applied toindividual upper airway complication scores and theMann–Whitney U-test to total upper airway complicationscores between both groups. A p value of < 0.05 wasconsidered statistically significant.
Results
Forty patients were successfully enrolled into the study.Table 2 shows the demographic data, both groups beingclosely matched for weight, age and gender.
Statistical analysis revealed that there were no significantdifferences between the two groups in relation to indivi-dual upper airway complications (cough, breath holding,laryngeal spasm, bronchospasm or excitement) or in thetotal upper airway complication scores (Table 3).
The mean (SD) induction doses of propofol (mg.kgÿ1)used were 3.32 (0.55) for the LMA group and 3.39 (0.90)for the face mask group.
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1108 Q 1997 Blackwell Science Ltd
Table 1 Scoring system for upper airway complications during induction of anaesthesia.
1 2 3 4
Cough None Occasional Frequent ContinuousBreath holding None < 15 s 15–30 s >30 sLaryngeal spasm None Mild laryngospasm Moderate laryngospasm Complete laryngospasmBronchospasm None Expiration only Inspiration and expiration Difficult to ventilateExcitement None < 30 s 30–60 s >60 s
Table 2 Demographic data.
Laryngeal maskgroup
Face maskgroup
Number of patients 20 20Age [median (range)]; years 41.8 (18–59) 40.5 (19–65)Sex (M/F) 12/8 9/11Weight [mean (SD)]; kg 75.4 (14.1) 72.1 (13.3)
Table 3 Upper airway complication scores for individual airwaycomplications and total scores for each group. Median (range).
Laryngeal maskgroup (n� 20)
Face maskgroup (n� 20)
Cough 1 (1–3) 1 (1–4)Breath holding 1 (1–4) 2 (1–3)Airway obstruction 1 (1–2) 1 (1–3)Bronchospasm 1 (1) 1 (1)Excitement 1 (1–3) 2 (1–4)Total score 122 151

Discussion
In recently published work by Nishino and co-workers, ithas been suggested that the nasal airway plays an importantrole in mediating the reflex response of the upper airway toirritant anaesthetic vapours [2]. The aim of this study wasto investigate this hypothesis in the clinical setting. Theinvestigation was designed to exclude the nasal airway inone group from exposure to anaesthetic vapour duringinduction by the use of the laryngeal mask airway. Thelaryngeal mask airway, by conducting the anaesthetic gasesdirectly to the larynx, effectively excludes the nasal airwayfrom exposure to anaesthetic vapours. In the face maskgroup the nasal airway will be exposed to anaestheticvapour. It was not possible to blind this study as therewas no means of disguising whether the laryngeal mask orface mask was being used whilst observing the patient andscoring upper airway complications.
Although the laryngeal mask may have caused directphysical stimulation during insertion we felt that this wasnot significantly greater than the stimulation caused byinsertion of a Guedel airway. Previous work found nodifference in the cardiovascular response of laryngealmask insertion when compared with Guedel airwayinsertion [14].
We attempted to standardise the induction as far aspossible and we chose to use enflurane as this had beenpreviously identified as the most irritant anaesthetic vapourto the nasal airway [2]. It would therefore have been mostlikely to reveal any differences between the two groups.Patients with blocked noses resulting from upper respira-tory tract infections or polyps were excluded from enter-ing the trial. Although the percentage of fresh gas flowtaken through the nose in the Guedel airway and face maskgroup is unknown it is likely that, during the 3 min trialperiod, anaesthetic gas containing enflurane will havediffused into the nasal passages. Previous work identifiedthe position of an apparently well positioned Guedelairway to be very variable with a high incidence of partialor complete obstruction [15]. It seems likely that the ratioof nasal to oral fresh gas flow will similarly vary.
Our results did not demonstrate a difference betweenthe two groups in relation to upper airway complicationsoccurring during induction of anaesthesia. The possibilityof a type 2 error cannot be discounted, however, as ourstudy only had a relatively low power of 0.75.
There were several important differences in methodol-ogy between our study and that employed in previouswork. The previous workers utilised a double-cuffedtracheal tube designed to measure laryngeal and trachealcuff pressures. We chose to measure clinical indicators ofupper airway complications and not solely movement ofvocal cords, tidal volume, inspiratory time and expiratory
time. There were also differences in the method of deliver-ing enflurane. We introduced a relatively low concen-tration of anaesthetic vapour, which was increased in astandardised incremental manner. This is in keeping withthe techniques most frequently employed in clinical anaes-thetic practice.
In the previous work the nasal airway was exposed bydirect insufflation of 5% enflurane in oxygen. This mayhave produced very high local concentrations of inhala-tional agent within the nasal airway.
In the LMA group in our investigation the larynx andlaryngeal inlet would have been exposed to anaestheticvapour directly. The larynx is richly supplied with sensoryreceptors mediating upper airway complications includinglaryngospasm and coughing. It is possible that this area ofthe upper airway provides an equal contribution to airwayproblems occurring during induction of anaesthesia.
In our investigation we used propofol as the inductionagent. This is in contrast to the previous work [2] whereflunitrazepam (0.04 mg.kgÿ1) and pentazocine (0.03 mg.kgÿ1) were used. It is known that propofol has a depressanteffect on upper airway reflexes [16–20]. However, in thisstudy propofol was used in both groups and thereforewould be expected to exert an equal effect.
In conclusion, although previous work has proposedthat the nasal airway may be an important reflexogenic sitemediating upper airway reflexes in humans during anaes-thesia, we have been unable to demonstrate a difference inthe incidence of upper airway complications when thenasal airway was included or excluded from exposure toinhalational anaesthetic agents in a clinical setting.
References
1 Eger E III. Isoflurane: a review. Anaesthesiology 1981; 55:559–76.
2 Nishino T, Tanaka A, Ishikawa T, Hiraya K. Respiratory,laryngeal and tracheal responses to nasal insufflation ofvolatile anaesthetics in anaesthetised humans. Anaesthesiology1991; 75: 441–4.
3 Admur MO, Melvin WW, Drinker P. Effects of inhalationof sulphur dioxide by man. Lancet 1953; 2: 758–9.
4 Allen WF. Effects of various inhaled vapors on respirationand blood pressure in anaesthetized, unanaesthetized,sleeping and anosmic subjects. American Journal of Physiology1929; 88: 620–32.
5 Sato T. Effects of nasal irritation on airway resistance. AurisNasus Larynx 1980; 7: 39–50.
6 Kaufman J, Wright GW. The effect of nasal andnasopharyngeal irritation on airway resistance in man.American Review of Respiratory Disease 1969; 100: 626–30.
7 Elsner R, Gooden B. Diving and asyphyxia. Monographs ofthe Physiological Society, 1983; 40, Cambridge, UK:Cambridge University Press.
8 Banting FG, Hall GE, James JM, et al. Physiological studies
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1109Q 1997 Blackwell Science Ltd

in experimental drowning. Canadian Medical AssociationJournal 1938; 39: 226–8.
9 Szereda-Przestaszewska M, Widdicombe JG. Reflex effectsof chemical irritation of the upper airways on the laryngeallumen in cats. Respiratory Physiology 1973; 18: 107–15.
10 Cummings C, Dixon J, Kay NH, et al. Dose requirementsof ICI 35868 (Propofol,’Diprivan’) in a new formulationfor induction of anaesthesia. Anaesthesia 1991; 46: 312–13.
11 Brimacombe JR, Brain AIJ, Berry AM. The Laryngeal MaskAirway Instruction Manual, 3rd edn. Intavent Research Ltd,1996.
12 Levy L, Pandit UA, Randel GI, Lewis IH, Tait AR. Upperrespiratory tract infections and general anaesthesia inchildren. Anaesthesia 1992; 47: 678–82.
13 Miller DK, Homan SM. Graphical aid for determiningpower of clinical trials involving two groups. British MedicalJournal 1988; 297: 672–6.
14 Hickey S, Cameron AE, Asbury AJ. Cardiovascularresponse to Brain’s laryngeal mask. Anaesthesia 1990; 45:629–33.
15 Marsh AM, Nunn JF, Taylor SJ, Charlesworth CH. Airwayobstruction associated with the use of the Guedel airway.British Journal of Anaesthesia 1991; 67: 517–23.
16 Szneke P. Oral airway tolerance: a study comparingthiopentone and propofol. Journal of the American Associationof Nurse Anesthetists 1989; 57: 41–4.
17 Mulholland D, Carlisle RJT. Intubation with propofolaugmented with intravenous lignocaine. Anaesthesia 1991;46: 312–13.
18 Brown GW, Patel N, Ellis FR. Comparison of propofoland thiopentone for laryngeal mask insertion. Anaesthesia1991; 46: 771–2.
19 Barker P, Langton JA, Wilson IG, Smith G. Movements ofthe vocal cords on induction of anaesthesia withthiopentone or propofol. British Journal of Anaesthesia 1992;69: 23–5.
20 McKeating K, Bali IM, Dundee JW. The effects ofthiopentone and propofol on upper airway integrity.Anaesthesia 1988; 43: 638–40.
FORUM
Comparison of caudal block using bupivacaine andketamine with ilioinguinal nerve block for orchidopexy inchildren
D. Findlow, L. M. Aldridge and E. Doyle
Department of Anaesthesia, Royal Hospital for Sick Children, Sciennes Road, Edinburgh EH9 1LF, UK
SummaryForty boys weighing less than 25 kg undergoing unilateral orchidopexy were randomly allocated toreceive one of two analgesic regimens. Group C received a caudal epidural block with 0.25%bupivacaine 1 ml.kgÿ1 and preservative-free ketamine 0.5 mg.kgÿ1; Group L received anilioinguinal nerve block with 0.25% bupivacaine 0.5 ml.kgÿ1 and infiltration of the wound with0.25% bupivacaine 0.5 ml.kgÿ1. All subjects received diclofenac sodium 1–2 mg.kgÿ1 as a rectalsuppository. Postoperative pain was assessed by means of a modified Objective Pain Score andanalgesia was administered if this exceeded a value of 4. The median duration of analgesia was 10 h(range 2.6 to >24 h) in Group C and 2.9 h (range 0.7 to >24 h) in Group L (p < 0.05). Therewere no differences between groups in the incidence of motor block, urinary retention,postoperative vomiting or postoperative sedation. Subjects in Group L required significantly moredoses of postoperative analgesia than those in Group C (p < 0.05).
Keywords Anaesthesia; paediatric. Pain; postoperative. Anaesthetic techniques, regional; caudal,ilioinguinal nerve block.
......................................................................................Correspondence to: Dr D. FindlowAccepted: 14 April 1997
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1110 Q 1997 Blackwell Science Ltd

Caudal epidural blockade is a common local anaesthetictechnique in paediatric anaesthesia. When used for caudalanalgesia in children, bupivacaine 2.0–2.5 mg.kgÿ1 has aduration of action of 2–4 h. Over 60% of children under-going orchidopexy with this technique require furtheranalgesia during the postoperative period [1].
It has previously been demonstrated that the addition ofketamine 0.5 mg.kgÿ1 to bupivacaine for caudal epiduralblockade in children prolongs the duration of postopera-tive analgesia and reduces the requirement for analgesics toa greater extent than the addition of adrenaline or cloni-dine [2–4]. Ketamine produces potent analgesia whengiven in subanaesthetic doses. It exerts its anaesthetic andanalgesic actions by binding to a subset of glutamatereceptors stimulated by the agonist N-methyl D-aspar-tate (NMDA receptors). These are found throughout thecentral nervous system including the lumbar spinal cord.As well as a general analgesic effect produced by systemicadministration, ketamine exerts profound analgesic actionsat a spinal cord level in animal preparations [5, 6]. Inclinical practice ketamine injected into the lumbar epi-dural space after abdominal surgery has been shown tohave a potent analgesic effect [7, 8].
Surgical procedures in the inguinal region are commonin paediatric surgery and analgesia may be provided eitherby a caudal epidural block or by an ilioinguinal nerveblock. These techniques have been shown to have similarefficacy in orchidopexy [9] and in inguinal hernia repair[10]. Ilioinguinal nerve block is free of the side-effects oflower limb motor block and urinary retention [10, 11]which may be caused by caudal blockade and, for thisreason, an ilioinguinal nerve block is often the preferredanalgesic technique. This study was designed to comparethese two techniques when ketamine is used to prolongthe duration of the caudal epidural block and to determinethe duration of analgesia and incidence of side-effectswhen they are used to provide analgesia after orchidopexy.Ilioinguinal nerve blocks were supplemented by infiltra-tion of the wound under direct vision by the surgeon in abid to improve efficacy and diclofenac was used in bothgroups since it has been shown to prolong the effects ofboth caudal epidural and ilioinguinal nerve blockade inpaediatric practice [12].
Methods
The study was approved by the local Ethics Committeeand written informed parental consent was obtained foreach subject. The study group comprised 40 boys weigh-ing up to 25 kg undergoing unilateral orchidopexy as daycases. Children in whom there were contraindications tocaudal blockade and/or whose parents were unable orunwilling to perform objective pain assessments were not
studied. At the time of recruitment, parents wereinstructed in the use of the modified Objective PainScore [1, 9, 13] for the assessment of postoperative painand the requirement for analgesia. This is an observationalpain scoring system which has been validated for use byparents [13]. The score uses five criteria: crying, agitation,movement, posture and localisation of pain. Each criterionscores from 0 to 2 to give a total score of 0–10.
Premedication was not used but EMLA cream wasapplied at least 1 h pre-operatively. Anaesthesia wasinduced with propofol 3–4 mg.kgÿ1 followed by place-ment of a laryngeal mask. Anaesthesia was maintained withhalothane 0.5%–2% with 70% nitrous oxide in oxygen.
After induction of anaesthesia, patients were allocated,by a computer-generated randomisation scheme, to receiveeither caudal epidural blockade (Group C) (n � 20) orilioinguinal nerve block and local infiltration (Group L)(n � 20). Children in Group C were positioned on theirside and a caudal injection was performed by a consultantanaesthetist using an aseptic technique. This consisted of0.25% bupivacaine 1 ml.kgÿ1 with preservative-free ket-amine (10 mg.mlÿ1 ) 0.5 mg.kgÿ1 to a maximum volumeof 20 ml. In Group L, an ilioinguinal nerve block wasperformed by a consultant anaesthetist using a 22Gshort-bevelled regional block needle to inject 0.25%bupivacaine 0.5 ml.kgÿ1. At the end of the operationthe surgeon infiltrated the wound with 0.25% bupivacaine0.5 ml.kgÿ1 to a maximum volume of 20 ml. All boys hadocclususive dressings placed over both of the possible sitesof local anaesthetic injection before leaving the operatingtheatre. A suppository containing diclofenac sodium 1–2 mg.kgÿ1 was inserted after instituting the regional blockand before the start of surgery.
Anaesthetic agents were discontinued at skin closureand the time from discontinuation of anaesthesia tospontaneous eye opening was noted. Before discharge,analgesia was requested by parents (who were unaware ofthe local anaesthetic technique employed) when theirestimate of the Objective Pain Score reached 4 or more.This consisted of paracetamol 15 mg.kgÿ1 by mouth four-hourly as required. The duration of motor blockade wasassessed by determining when the children began to movetheir legs. The time of first micturition was noted. Thedegree of sedation was assessed at 1 and 4 h postoperativelyusing an objective score based on eye opening (eyes openspontaneously � 0; eyes open in response to verbalstimulation � 1; eyes open in response to physicalstimulation � 2).
After discharge home, parents were asked to assess thechild regularly and to give analgesia if the Objective PainScore reached 4 or more. Parents were contacted bytelephone the morning following surgery to determinethe requirement for analgesia after discharge from hospital,
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1111Q 1997 Blackwell Science Ltd

the timing of micturition and any evidence of nightmares,hallucinations or odd behaviour. The total requirement forpostoperative analgesia in the first 24 h was recorded.
Statistical analysis was performed using Student’st-testing for normally distributed data and the Mann–Whitney U-test and Chi-squared test for nonpara-metric data.
Results
Two subjects in Group C and two in Group L were notincluded in the analysis. In two cases the subject did notundergo the scheduled surgery and in two it provedimpossible to obtain follow up data. The two groupswere similar in respect of physical characteristics andoperative details (Table 1).
The median duration of action of the techniqueemployed, as indicated by the time to first analgesia, wassignificantly longer in Group C (10 h) than in Group L(2.9 h) (p < 0.05) (Fig. 1).
The number of subjects pain free (OPS < 4) at hourlyintervals up to 24 h is shown for each group. Significantdifferences between the two groups occurred between 3and 8 h (p < 0.01) (Fig. 2). Significantly fewer doses ofanalgesia were required over the first postoperative 24 h by
subjects in Group C compared with Group L (p < 0.05)(Fig. 3).
There were no significant differences between thegroups either in the time taken to spontaneous eye open-ing after the cessation of anaesthesia or in sedation scores4 h postoperatively. The times to first micturition andspontaneous leg movements were similar in the twogroups. One subject in Group C and none in Group Lvomited during the postoperative period (Table 2). Therewere no reports of nightmares, hallucinations or oddbehaviour in any subject.
Discussion
This study was designed to compare the efficacy andincidence of side-effects of caudal epidural analgesic
Forum Anaesthesia, 1997, 52, 1090–1113................................................................................................................................................................................................................................................
1112 Q 1997 Blackwell Science Ltd
Table 1 Physical characteristics and relevant operative details inboys undergoing orchidopexy with caudal (group C) or ilio-inguinal (group L) methods of pain relief. Values are mean (SD)where appropriate.
Group C Group L
Weight; kg 18 (3.8) 17 (4.2)Age; months 50 (16.8) 54 (25.2)Side of operation; L/R 11/7 5/13Median [range] duration of operation; min 35 [20–25] 41 [17–70]
16
0Group C
Tim
e t
o f
irst
an
alg
esia
(h
)
6
14
12
10
8
4
2
Group L
*
Figure 1 Median time to first analgesia in patients receivingcaudal (group C) (n� 18) or ilioinguinal (group L) (n� 18)methods of pain relief for orchidopexy. * p < 0.05 comparedto Group L.
24
18
00
Time post surgery (h)
Nu
mb
er
of
su
bje
cts
pa
in f
ree
(n
)
8
10
16
14
12
10
6
4
2
12 14 16 182 4 6 8 20 22
Group L Group C
Figure 2 Number of subjects pain free during the period shownin patients receiving caudal (group C) (n � 18) or ilioinguinal(group L) (n � 18) methods of pain relief for orchidopexy.p < 0.01 from 3 to 8 h. Not significant at other times.
18
0Onedose
Nu
mb
er
of
su
bje
cts
Two ormoredoses
8
16
14
12
10
6
4
2
*
*
Group C
Group L
Figure 3 Requirement for analgesia (paracetamol) in the first24 h postoperatively in patients receiving caudal (group C)(n � 18) or ilioinguinal (group L) (n � 18) methods of painrelief for orchidopexy. Two boys in each group required noanalgesia. * p < 0.05 between groups.

technique for orchidopexy with nonepidural analgesictechnique. Our findings support those of other workersand confirm that ketamine supplementation of bupi-vacaine prolongs the duration of caudal epidural blockade[2, 3]. Our study has also shown a significant difference inthe duration of postoperative analgesia and the require-ment for subsequent analgesia between the two tech-niques. There was no difference in postoperative sedationbetween the groups as shown by the time to spontaneouseye opening and sedation scores at 4 h postoperatively. Wefound no evidence of prolonged motor block in Group C.Although some degree of motor block occurred in thisgroup this was of little clinical importance. Previous workhas shown that the degree of block with ketamine supple-mentation is no greater than when bupivacaine is usedalone [3]. It was notable that postoperative vomiting onlyoccurred in one child in group C. Although hallucinationsor nightmares have been reported after the use of epiduralketamine they appear to be very rare when a dose of0.5 mg.kgÿ1 is used compared with 1 mg.kgÿ1 when theincidence is higher [4]. Parents’ assessments of pain and theneed for analgesia using the Objective Pain Score has beenshown to be comparable to pain assessments made by adoctor [13].
In summary, when ketamine 0.5 mg.kgÿ1 is used toprolong the duration of caudal epidural blockade withbupivacaine in children, the duration of analgesia is longerand the requirement for postoperative analgesia less thanthat seen with ilioinguinal nerve block with bupivacainesupplemented by wound infiltration. The incidence ofside-effects is very low in both groups.
Acknowledgment
Dr Findlow was supported by the Sir Jules ThornCharitable Trust.
References
1 Wolf AR, Hughes D, Wade A, Mather SJ, Prys-Roberts C.Postoperative analgesia after paediatric orchidopexy:evaluation of a bupivacaine–morphine mixture. BritishJournal of Anaesthesia 1990; 64: 430–5.
2 Naguib M, Sharif A, Seraj M, El Gammel M, DawlatlyAA. Ketamine for caudal analgesia in children: comparisonwith caudal bupivacaine. British Journal of Anaesthesia 1991;67: 559–64.
3 Cook B, Grubb DJ, Aldridge LA, Doyle E. Assessment ofthe effects of adrenaline, clonidine and ketamine on theduration of caudal analgesia in children. British Journal ofAnaesthesia 1995; 75: 698–701.
4 Semple D, Findlow D, Aldridge LM, Doyle E. The optimaldose of ketamine for caudal epidural blockade in children.Anaesthesia 1996; 51: 1170–2.
5 Brockmeyer DM, Kendig JJ. Selective effects of ketamineon amino-acid mediated pathways in neonatal rat spinalcord. British Journal of Anaesthesia 1995; 74: 79–84.
6 Kristensen JG, Hartvig P, Karlsten R, Gordh T, Halldin M.CSF and plasma pharmacokinetics of the NMDA receptorantagonist CPP after intrathecal, extradural and i.v.administration in anaesthetized pigs. British Journal ofAnaesthesia 1995; 74: 193–200.
7 Islas J, Astorga J, Laredo M. Epidural ketamine for controlof postoperative pain. Anesthesia and Analgesia 1985; 64:1161–2.
8 Naguib M, Adu-Gyamfi Y, Absood GH, Farag H, GyasiHK. Epidural ketamine for postoperative analgesia.Canadian Anaesthetists’ Society Journal 1986; 33: 16–21.
9 Hannallah RS, Broadman LM, Belman AB, AbramowitzMD, Epstein BS. Comparison of caudal and ilioinguinal/iliohypogastric nerve blocks for control of post-orchidopexy pain in pediatric ambulatory surgery.Anesthesiology 1987; 66: 832–4.
10 Splinter WM, Bass J, Komocar L. Regional anaesthesia forhernia repair in children: local versus caudal anaesthesia.Canadian Journal of Anaesthesia 1995; 42: 197–200.
11 Fisher QA, McComiskey CM, Hill JL, et al. Postoperativevoiding interval and duration of analgesia followingperipheral or caudal nerve blocks in children. Anesthesia andAnalgesia 1993; 76: 173–7.
12 Mannion D, Armstrong C, O’Leary G, Casey W. Paediatricpost orchidopexy analgesia – effect of diclofenac combinedwith ilioinguinal/iliohypogastric nerve block. PaediatricAnaesthesia 1994; 4: 327–30.
13 Wilson G, Doyle E. Validation of three paediatric painscores for use by parents. Anaesthesia 1996; 51: 1005–7.
Anaesthesia, 1997, 52, 1090–1113 Forum................................................................................................................................................................................................................................................
1113Q 1997 Blackwell Science Ltd
Table 2 Recovery characteristics in boys undergoing orchido-pexy with caudal (group C) or ilioinguinal (group L) methods ofpain relief. Values are median [range] where appropriate.
Group C(n � 18)
Group L(n � 18)
Spontaneous eye opening; min 29 [17–50] 27 [4–45]4 h sedation score 0 [0] 0 [0]Micturition; h 4.8 [2.5–8.3] 3.7 [1.5–7.0]Leg movements; h <1 [0–5] <1 [0–5]Postoperative vomiting; n 1 0




















