
A longitudinal study of male buprenorphine addicts attending an addiction clinic in India
10
Addiction (2000) 95(9), 1363 – 1372 RESEARCH REPORT A longitudinal study of male buprenorphine addicts attending an addiction clinic in India DEBASISH BASU, SURENDRA K. MATTOO, ANIL MALHOTRA, NITIN GUPTA & RAMA MALHOTRA Drug De-addiction and Treatment Centre, Department of Psychiatry, Postgraduate Institute of Medical Education and Research, Chandigarh, India Abstract Aim. There is a lack of longitudinal studies of buprenorphine dependence, an important opioid dependence in several countries. We investigated the course and outcome of buprenorphine dependence in an Indian clinic-attending cohort. Design. Retrospective longitudinal study. Setting. An addiction clinic in northern India. Participants. Ninety-four male patients with buprenorphine dependence, registered for treatment between 1987 and 1993. Follow-up analyses were conducted for the 52 patients (55% of the index cohort) who completed more than a year of follow-up. In 48% of these 52 patients data were obtained from their clinical records of follow-up, while 52% were contacted speci cally to obtain the required data on follow up. Measurement. Baseline demographic and clinical variables; time spent in various phases of use or abstinence; outcome at the latest follow up; transition to other drugs during follow-up period. Findings. Over an average follow-up duration of 3 years, 56% of the time was spent in dependent use, 12% in non-dependent use and 32% in abstinence. By the end of follow-up, 6% of patients were dead (annual death rate 1.9%), 33% were unchanged and 61% were classi ed as “improved”. The proportion of patients with “improved” outcome increased over the years. Patients with poor outcome had shorter follow-up and hospital stay, and had used pentazocine and/or antihistaminic injections in the buprenorphine “cocktail” more often than those with better outcome. Thirty-two patients shifted to other drugs over the years, notably heroin or polydrug use. These “transition” patients had a family history of drug use more often, started their drug career earlier, had marital and legal complications more often, spent more time in dependent phase of drug use, underwent multiple hospital admissions but stayed for a shorter period and faced more deaths, when compared to those who did not shift. Conclusion. In clinic-attending male patients with buprenorphine dependence who were followed-up although dependent pattern of use of the drug continued for a long time in their career, there was a slow but progressive improvement. Transition to other drugs was associated with a worse course and outcome as compared to being stable on buprenorphine. Introduction Drug dependence has been viewed as a chronic disease with a uctuating course marked by peri- ods of improvement, exacerbation and relapse (Vaillant, 1966). Short-term follow-up studies tend to provide a restrictive myopic view of this variegated rubric. Thus, “the treatment of drug and alcohol addiction, like the treatment of dia- Correspondence to: Dr D. Basu, Department of Psychiatry, Pgimer, Chandigarh-160012, India. Fax: 1 91 172 744401, 745078; Tel: 1 91 172 746128 (Off.), 706618 (Res.); e-mail: [email protected] Submitted 29th January 1999; initial review completed 6th May 1999; nal version accepted 7th January 2000. ISSN 0965–2140 print/ISSN 1360-0443 online/00/091363– 10 Ó Society for the Study of Addiction to Alcohol and Other Drugs Carfax Publishing, Taylor & Francis Ltd
Transcript of A longitudinal study of male buprenorphine addicts attending an addiction clinic in India
Addiction (2000) 95(9), 1363–1372
RESEARCH REPORT
A longitudinal study of male buprenorphineaddicts attending an addiction clinic in India
DEBASISH BASU, SURENDRA K. MATTOO, ANIL MALHOTRA,NITIN GUPTA & RAMA MALHOTRA
Drug De-addiction and Treatment Centre, Department of Psychiatry, Postgraduate Institute ofMedical Education and Research, Chandigarh, India
AbstractAim. There is a lack of longitudinal studies of buprenorphine dependence, an important opioid dependencein several countries. We investigated the course and outcome of buprenorphine dependence in an Indianclinic-attending cohort. Design. Retrospective longitudinal study. Setting. An addiction clinic in northernIndia. Participants. Ninety-four male patients with buprenorphine dependence, registered for treatmentbetween 1987 and 1993. Follow-up analyses were conducted for the 52 patients (55% of the index cohort)who completed more than a year of follow-up. In 48% of these 52 patients data were obtained from theirclinical records of follow-up, while 52% were contacted speci� cally to obtain the required data on follow up.Measurement. Baseline demographic and clinical variables; time spent in various phases of use orabstinence; outcome at the latest follow up; transition to other drugs during follow-up period. Findings. Overan average follow-up duration of 3 years, 56% of the time was spent in dependent use, 12% in non-dependentuse and 32% in abstinence. By the end of follow-up, 6% of patients were dead (annual death rate 1.9%),33% were unchanged and 61% were classi� ed as “improved”. The proportion of patients with “improved”outcome increased over the years. Patients with poor outcome had shorter follow-up and hospital stay, andhad used pentazocine and/or antihistaminic injections in the buprenorphine “cocktail” more often than thosewith better outcome. Thirty-two patients shifted to other drugs over the years, notably heroin or polydrug use.These “transition” patients had a family history of drug use more often, started their drug career earlier, hadmarital and legal complications more often, spent more time in dependent phase of drug use, underwentmultiple hospital admissions but stayed for a shorter period and faced more deaths, when compared to thosewho did not shift. Conclusion. In clinic-attending male patients with buprenorphine dependence who werefollowed-up although dependent pattern of use of the drug continued for a long time in their career, there wasa slow but progressive improvement. Transition to other drugs was associated with a worse course and outcomeas compared to being stable on buprenorphine.
IntroductionDrug dependence has been viewed as a chronicdisease with a � uctuating course marked by peri-ods of improvement, exacerbation and relapse
(Vaillant, 1966). Short-term follow-up studiestend to provide a restrictive myopic view of thisvariegated rubric. Thus, “the treatment of drugand alcohol addiction, like the treatment of dia-
Correspondence to: Dr D. Basu, Department of Psychiatry, Pgimer, Chandigarh-160012, India. Fax: 1 91 172744401, 745078; Tel: 1 91 172 746128 (Off.), 706618 (Res.); e-mail: [email protected]
Submitted 29th January 1999; initial review completed 6th May 1999; � nal version accepted 7th January 2000.
ISSN 0965–2140 print/ISSN 1360-0443 online/00/091363–10 Ó Society for the Study of Addiction to Alcohol and Other Drugs
Carfax Publishing, Taylor & Francis Ltd
1364 Debasish Basu et al.
betes and hypertension, requires that clinicianstake a long range view” (Vaillant, 1988, italicsadded). Herein lies the rationale for longitudinalstudies in the � eld of substance use disorders, inorder to delineate the patterns of course andoutcome.
India has been grappling with the problem ofdrug abuse for quite some time. Abuse of newersemisynthetic and other opioids has becomeprominent over the last decade. Of these,buprenorphine has recently assumed a menacingproportion (Basu et al., 1990; Chowdhury &Chowdhury, 1990; Lal, 1991; Singh et al., 1992;Umesh Babu & Chaturvedi, 1995; Kumar &Singh, 1996; Sharma & Mattoo, 1999). Al-though its abuse potential had been reportedabroad (Harper, 1983; Strang, 1985; O’Connoret al., 1988), buprenorphine was introduced inIndia as a “safe” analgesic in 1986. The � rstreported cases of buprenorphine abuse in Indiawere seen from 1987 onwards (Basu et al.,1990), and then its abuse gained rapid momen-tum (Umesh Babu & Chaturvedi, 1995; Kumar& Singh, 1996).
Buprenorphine is available in India as injec-tion ampoules of 2 ml (containing 0.6 mg ofbuprenorphine, which is equianalgesic to 20 mgmorphine sulphate) and also as 0.2 mg sublin-gual tablets. The injectable form is abused inIndia, mainly through the intravenous and, lessoften, the intramuscular route. Although someuse only buprenorphine injection, most peoplecombine it with injectable diazepam, antihis-taminic agents (pheniramine, promethazine) andoccasionally pentazocine, mainly in the samesyringe in order to enhance the quality and dur-ation of the “kick” (Singh et al., 1992; Sharma &Mattoo, 1999). Dependence develops fast, usu-ally within months of starting use, with an opi-oid-like withdrawal of moderate severity andintense craving. Drug use continues even afterdeveloping severe injection-related complica-tions.
A longitudinal study of buprenorphine depen-dence is of interest for several reasons. First ofall, it is imperative to know the course andoutcome of a relatively new drug dependence. Inthe only published abstract of a paper on 22-month follow-up of 26 treated buprenorphinepatients, Chavan, Tripathi & Lal (1995)reported that the vast majority of their patientswere either still actively abusing buprenorphineor had shifted to heroin. Only a longer-term
study with larger sample size can put these pre-liminary � ndings into a proper perspective.
Secondly, the abusers are exposed to the risksof injectable drug abuse, such as HIV infection(Malhotra et al., 1993), other infections and eventraumatic pseudoaneurysm (Basu et al., 1994).
Finally, the other important question thatmerits an answer is: what happens to thebuprenorphine dependence itself in thelongterm? Does it continue, exacerbate, “matureout” or get shifted to abuse of other drugs? Inthis regard, it is important to note that manybuprenorphine patients originally start fromheroin (Basu et al., 1990; Singh et al., 1992;Chavan et al., 1995; Kumar & Singh, 1996).How many of them would eventually go back toheroin or other drugs? How do these “transition”patients fare vis-a-vis those “stable” onbuprenorphine? In a nutshell, what are the roots,the stem and the branches of the “tree” ofbuprenorphine dependence?
These are some of the questions thatprompted us to undertake a longitudinal study ofbuprenorphine dependent patients attending ourDe-addiction Clinic.
Objectives
(1) To characterize buprenorphine dependentpatients with respect to socio-demographicand other background features, antecedentdrug use pro� le and buprenorphine usepro� le at intake.
(2) To chart the course and outcome ofbuprenorphine dependence over the years offollow-up.
(3) To study the differences between the poor-outcome and the better-outcome patientswith respect to demographic and clinicalvariables.
(4) To study the differences between“transition” patients (those who shift frombuprenorphine to other drugs later in theircareer) and “stable” patients in terms of theabove-mentioned variables and also thecourse and outcome.
Material and methodsThe study was conducted at the Drug De-addic-tion and Treatment Centre (DDTC) of theInstitute at Chandigarh in Northern India. The
Buprenorphine cohort study 1365
Table 1. Follow-up of buprenorphine cohort: years of follow-up with outcome categories (indexcohort n 5 94)
N (%)1 in each outcome category
Years of follow-up N (% of 94) Improved Unchanged Dead†
up to 1 42* (45) – – –
. 1, up to 2 13 (14) 5 (38) 7 (54) 1 (8). 2, up to 3 12 (13) 7 (58) 4 (33) 1 (8). 3, up to 5 10 (11) 7 (70) 3 (30) 0 (0). 5, up to 11 17 (18) 13 (76) 3 (18) 1 (6)Total . 1–11 52 (55) 32 (61) 17 (33) 3 (6)(mean & median:approx. 3 years)
*These 42 patients were not considered for outcome analyses in view of their short lengthof follow-up. Further analyses were carried out for the remaining 52 patients (55% of theindex cohort). 1 These are % of total N in the respective years of follow-up. †1st death: at15 months of � rst contact (traf� c accident); 2nd death: at 36 months of � rst contact (drugoverdose); 3rd death: at 90 months of � rst contact (cause unknown).
DDTC has a large catchment area comprising ofthe Union Territory of Chandigarh and thestates of Punjab, Haryana, Himachal Pradesh,Jammu and Kashmir, and parts of Uttar Pradeshand Rajasthan. Patients are often referred fromother hospitals or departments of the Institute,but many come on their own. DDTC offers thefollowing services and facilities: outpatient, inpa-tient, laboratory, aftercare, liaison with othergovernmental and non-governmental agenciesand self-help groups, and community outreachprogramme.
The index cohort for this study consisted of allconsecutive patients registered at DDTCbetween January 1987 and September, 1993with a diagnosis of buprenorphine dependence.Psychoactive substance dependence was diag-nosed as per ICD-9 (WHO, 1978) until Decem-ber 1992, and later, using ICD-10 criteria(WHO, 1992) as established after direct inter-view with the patient and his relatives by aconsultant psychiatrist. Since we were interestedin the overall course and outcome of the entirecohort there were no exclusion criteria.
Following detailed evaluation, treatment con-sisted of detoxi� cation using clonidine, symp-tomatic treatment, treatment of medicalcomplications, if any, and psychosocial coun-selling of patients and their families. After this,regular (usually monthly) follow-up was under-taken for all patients by a psychiatrist. Duringfollow-up interviews, patients’ drug use pro� le,social and occupational functioning and physicaland psychological problems were monitored and
documented. This large database formed themajor source of the current study data.
A total of 94 patients with buprenorphinedependence were registered during the intakeperiod, i.e. January 1987 – September 1993.Their case records and follow-up notes werereviewed in September 1998, when it was seenthat, out of the index cohort of 94 patients, 42patients had follow-up notes available for lessthan or up to 1 year. These 42 patients, becauseof their short duration of follow-up, were deletedfrom analysis of course and outcome which wasthus restricted to the remaining 52 patients (i.e.55% of the index cohort). These 52 patientsconstituted the “outcome cohort”. An effort wasthen made to know the latest status (i.e. as ofSeptember 1998) of these 52 patients by � rstposting them an interview call letter, followed bytelegram or telephone call and, � nally, forpatients residing within the Union Territory ofChandigarh, by personal home visit by apsychiatric social worker specially trained inde-addiction work. In this way, 27 patients (52%of the outcome cohort) could be contactedspeci� cally to obtain the required data. For theother 25 patients (48% of the outcome cohort),data were obtained from the follow-up notes inthe patient � les for whatever period they wereavailable. Table 1 shows the basic follow-up datathus obtained.
The main problem here was how to tackle thedata for subjects lost to follow-up after a certainnumber of years. The problem was compoundedby the fact there was a long intake period span-
01-2
% o
f pat
ient
s
10
20
2-3
Years after intake
3 +
3848
80
30
40
50
60
70
80
90
1008 8 7
54 44
33
Improved Unchanged Dead
1366 Debasish Basu et al.
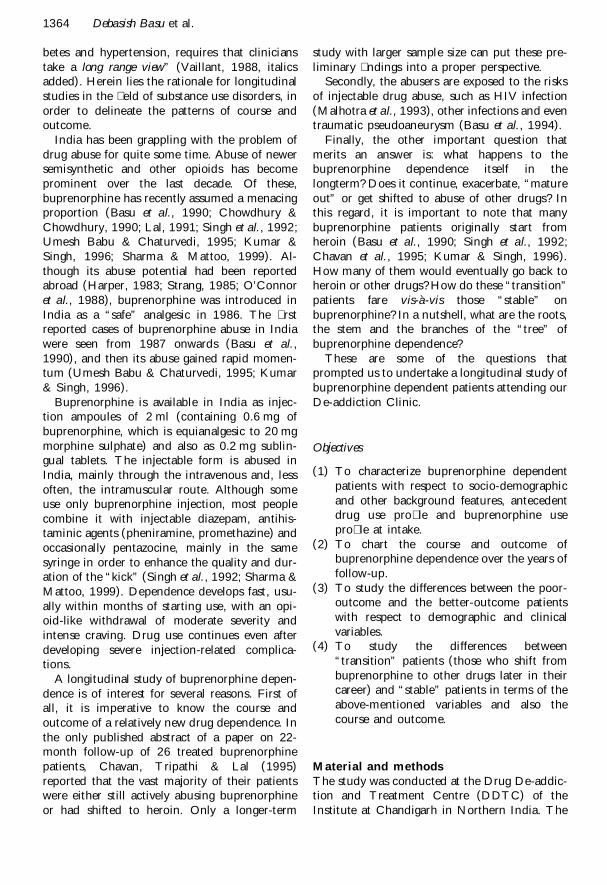
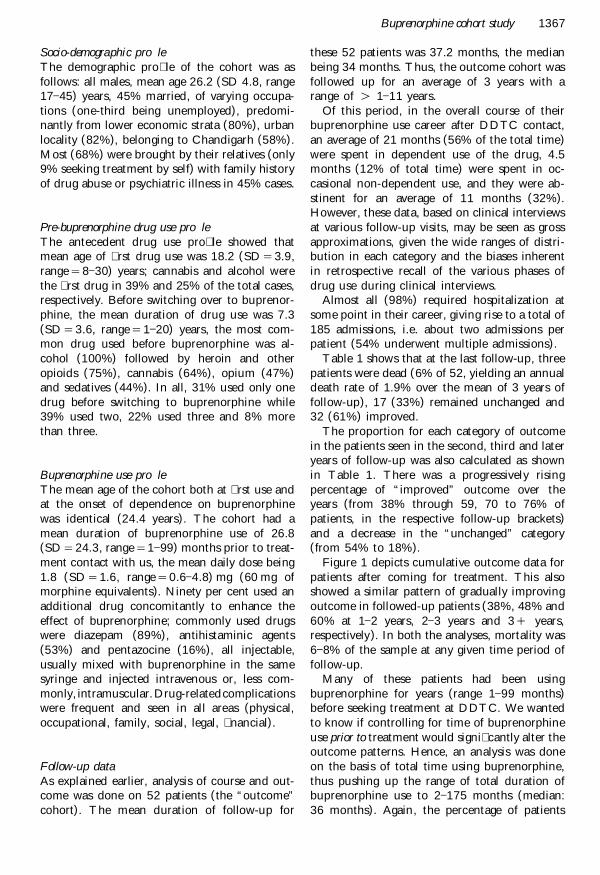
Figure 1. Cumulative outcome of buprenorphine cohort: intent-to-trea t analysis (n 5 52).
ning over 6 years (January 1987–September1993) whereas the follow-up data were collectedat a � xed point in time (September, 1998).Thus, a patient entering into our treatment con-tact in 1993 would yield a maximum 5 years offollow-up data in 1998 even if he was regularlyattending the clinic till 1998. This was one rea-son why the percentage of patients with morethan 5 years of follow-up was so low (18%,Table 1).
To mitigate this problem an “intent-to-treat”analysis was undertaken, where the previousyear’s outcomes were added onto the next year,assuming the last outcome noted in a particularpatient to be stable when carried forward. Wethus had cumulative outcome following treat-ment over the years, otherwise known as a“cumulative survival curve” (Fig. 1). In this, thepercentages of patients in different outcome cat-egories for 1–2 years’ follow-up remained thesame as that shown in Table 1 (38%, 54% and8% for improved, unchanged and dead, respect-ively). However, for the next follow-up bracket(2–3 years), the last noted outcomes in the pre-vious bracket (1–2 years) were carried forward(i.e. added on) to the next bracket. Thus, con-sulting Table 1, 12 patients (5 1 7) were nowconsidered to be improved, 11 (7 1 4) un-changed and 2 (1 1 1) dead out of a total 25(13 1 12) patients. These proportions (48%,
44% and 8%, respectively) were then plotted inFig. 1. A similar exercise was then performed for3 1 years.
A particular mention needs to be made of thecategories of outcome and their operationalde� nition. Investigators have de� ned outcome inmany ways (Haastrup & Jepsen, 1988; Taylor,1994). It has been felt that while charting pat-terns of outcome over long periods, an importantmethodological issue is realizing “the importanceof keeping the categorisations … few and sim-ple” (Taylor et al., 1985). Accordingly, we keptjust three categories of outcome: dead,unchanged and improved. “Unchanged” wouldmean active addiction and poor psychosocial/occupational functioning. The category of“improved” was deliberately kept loose andbroad. It included either of the following: (a)abstinent, (b) occasional use, or (c) regular usebut not following a dependence pattern, andwith unimpaired social functioning.
ResultsThe demographic and drug use pro� les arebased on the index cohort (n 5 94), whereas thefollow-up data are based on the outcome cohort(n 5 52). The latter did not differ signi� cantlyfrom the other 42 patients in terms of demo-graphic and drug-use variables (data not shown).
Buprenorphine cohort study 1367
Socio-demographic pro� leThe demographic pro� le of the cohort was asfollows: all males, mean age 26.2 (SD 4.8, range17–45) years, 45% married, of varying occupa-tions (one-third being unemployed), predomi-nantly from lower economic strata (80%), urbanlocality (82%), belonging to Chandigarh (58%).Most (68%) were brought by their relatives (only9% seeking treatment by self) with family historyof drug abuse or psychiatric illness in 45% cases.
Pre-buprenorphine drug use pro� leThe antecedent drug use pro� le showed thatmean age of � rst drug use was 18.2 (SD 5 3.9,range 5 8–30) years; cannabis and alcohol werethe � rst drug in 39% and 25% of the total cases,respectively. Before switching over to buprenor-phine, the mean duration of drug use was 7.3(SD 5 3.6, range 5 1–20) years, the most com-mon drug used before buprenorphine was al-cohol (100%) followed by heroin and otheropioids (75%), cannabis (64%), opium (47%)and sedatives (44%). In all, 31% used only onedrug before switching to buprenorphine while39% used two, 22% used three and 8% morethan three.
Buprenorphine use pro� leThe mean age of the cohort both at � rst use andat the onset of dependence on buprenorphinewas identical (24.4 years). The cohort had amean duration of buprenorphine use of 26.8(SD 5 24.3, range 5 1–99) months prior to treat-ment contact with us, the mean daily dose being1.8 (SD 5 1.6, range 5 0.6–4.8) mg (60 mg ofmorphine equivalents). Ninety per cent used anadditional drug concomitantly to enhance theeffect of buprenorphine; commonly used drugswere diazepam (89%), antihistaminic agents(53%) and pentazocine (16%), all injectable,usually mixed with buprenorphine in the samesyringe and injected intravenous or, less com-monly, intramuscular.Drug-relatedcomplicationswere frequent and seen in all areas (physical,occupational, family, social, legal, � nancial).
Follow-up dataAs explained earlier, analysis of course and out-come was done on 52 patients (the “outcome”cohort). The mean duration of follow-up for
these 52 patients was 37.2 months, the medianbeing 34 months. Thus, the outcome cohort wasfollowed up for an average of 3 years with arange of . 1–11 years.
Of this period, in the overall course of theirbuprenorphine use career after DDTC contact,an average of 21 months (56% of the total time)were spent in dependent use of the drug, 4.5months (12% of total time) were spent in oc-casional non-dependent use, and they were ab-stinent for an average of 11 months (32%).However, these data, based on clinical interviewsat various follow-up visits, may be seen as grossapproximations, given the wide ranges of distri-bution in each category and the biases inherentin retrospective recall of the various phases ofdrug use during clinical interviews.
Almost all (98%) required hospitalization atsome point in their career, giving rise to a total of185 admissions, i.e. about two admissions perpatient (54% underwent multiple admissions).
Table 1 shows that at the last follow-up, threepatients were dead (6% of 52, yielding an annualdeath rate of 1.9% over the mean of 3 years offollow-up), 17 (33%) remained unchanged and32 (61%) improved.
The proportion for each category of outcomein the patients seen in the second, third and lateryears of follow-up was also calculated as shownin Table 1. There was a progressively risingpercentage of “improved” outcome over theyears (from 38% through 59, 70 to 76% ofpatients, in the respective follow-up brackets)and a decrease in the “unchanged” category(from 54% to 18%).
Figure 1 depicts cumulative outcome data forpatients after coming for treatment. This alsoshowed a similar pattern of gradually improvingoutcome in followed-up patients (38%, 48% and60% at 1–2 years, 2–3 years and 3 1 years,respectively). In both the analyses, mortality was6–8% of the sample at any given time period offollow-up.
Many of these patients had been usingbuprenorphine for years (range 1–99 months)before seeking treatment at DDTC. We wantedto know if controlling for time of buprenorphineuse prior to treatment would signi� cantly alter theoutcome patterns. Hence, an analysis was doneon the basis of total time using buprenorphine,thus pushing up the range of total duration ofbuprenorphine use to 2–175 months (median:36 months). Again, the percentage of patients

1368 Debasish Basu et al.
Table 2. Comparison of poor vs. better outcome patients (n 5 52)†
Unchanged/ Improveddead (N 5 20) (N 5 32) v 2/u
Residence: N (%) v 2
Chandigarh 9 (45) 26 (81) 5.79*Others 11 (55) 6 (19)
Months of follow-up uMean 29.3 40.8 7.90**SD 26.9 27.2
Months of hospital stay: N (%) v 2
, 1 9 (45) 5 (16) 6.83*1–2 7 (35) 11 (34). 2 4 (20) 16 (50)
Additional drug for“cocktail” combination: N (%) v 2
Pentazocine 7 (35) 0 (0) 10.11**Antihistamine agents 14 (70) 13 (41) 3.85*
v 2
*p , 0.05; **p , 0.01. †Only data for statistically signi� cant differences areshown.
showing “improved” outcome at 1–5 years, 5–10years and 10–15 years of dependence were 50%,57% and 60%, respectively, which againcon� rmed the slowly but gradually increasingpattern of “improved” outcome.
Next, to meet the third objective of our study,the “improved” patient subgroup was comparedwith the “unchanged/dead” subgroup on all thedemographic, clinical and course-related vari-ables (Table 2). More patients residing inChandigarh had improved outcome, due poss-ibly to the signi� cantly better follow-up duration.They had a longer average hospital stay. Interest-ingly, signi� cantly more patients with poor out-come had abused pentazocine and/orantihistaminic injections as a “cocktail” combi-nation with buprenorphine.
The � nal objective of the study was to com-pare the patients who later shifted to anotherdrug (the “transition” group) with those who didnot (the “stable” group—stable in the sense ofnon-transition).
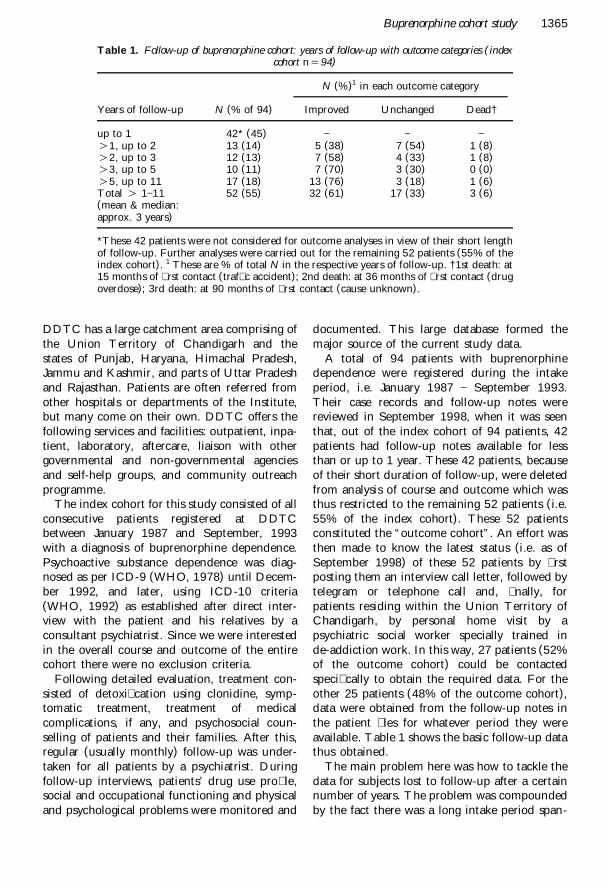
During the follow-up period, 32 patients hadshifted to abuse of other drugs (62% of theoutcome cohort). Figure 2 depicts that maxi-mum patients had their transition between 7–8years after starting buprenorphine, althoughsome had shifted much earlier (range: 14–175months; median 74 months). The most commondrug they shifted to was heroin (in 50% ofcases). A large number of other substances, how-ever, were used for transition, often in combi-
nation: alcohol (40%), cannabis (18%), opiumand/or poppy husk (9%), synthetic opioids(25%) and sedative–hypnotic agents (22%).
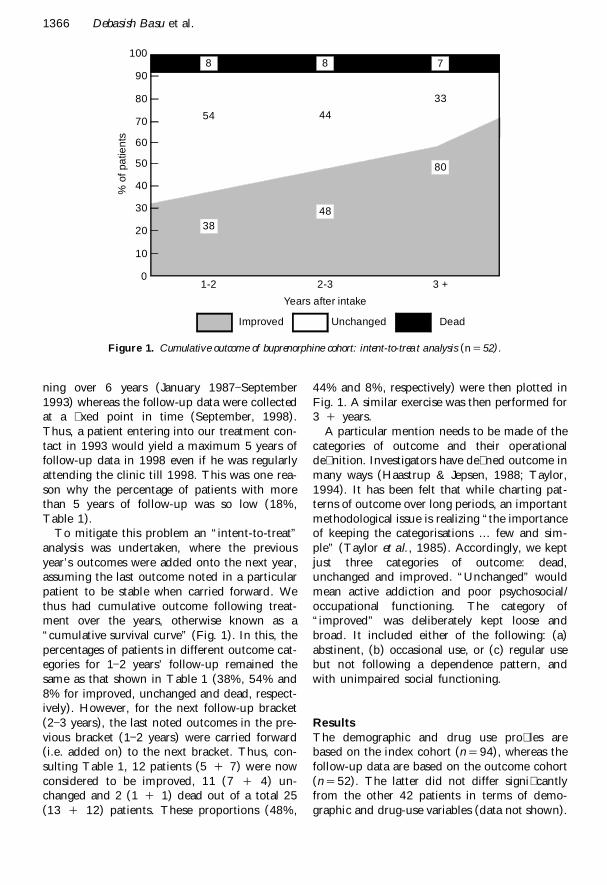
Ten patients of these 32 made a second tran-sition; � ve re-started buprenorphine, and othersused substances different from their � rst tran-sition. The pattern of transition is shown in Fig.3, where the drug use patterns have been lumpedas predominantly heroin (11 patients), predomi-nantly alcohol (six patients), and polydrug abuse(15 patients). By the second transition, heroinand buprenorphine abuse had increased at thecost of alcohol and polydrug abuse.
Lastly, Table 3 shows the comparison betweenthe “transition” and the “stable” groups. Incomparison with the stable group, the transitiongroup had lower monthly income, were moreoften from an urban locality, were more oftenbrought in by relatives than by self or frommedical referrals and had a signi� cantly higherfamily history of drug abuse. They had startedtheir drug career at a younger age. Interestingly,they sought treatment signi� cantly earlier thanthe stable group, possibly because of a muchhigher prevalence of marital and, especially, legaldrug-related complications at intake. The courseof their drug taking career was marked by asigni� cantly greater length of time spent in de-pendent phase. They were hospitalized more of-ten but spent lesser time in hospital due possiblyto a higher abscond rate. All the three deathsreported in this cohort occurred from the tran-

> 8
0Number of patients
Year
s
Range: 14-175 monthsMedian: 74 months
7-8
5-6
3-4
1-2
2 4 6 8 10 12
8
10
3
6
5
01st
Nu
mb
er
4
8
Transition 2nd
65
3
10
14
15
11
12
16
20
24
28
32
Heroin Polydrug Alcohol Buprenorphine
Buprenorphine cohort study 1369
Figure 2. Time taken for transition from buprenorphine to other drugs (n 5 32).
sition group and none from the stable group.The causes of death were heroin overdose, traf� caccident and unknown in one case each.
DiscussionBefore we interpret and discuss the results, somemethodological caveats are warranted. First, ours
was a cohort of patients who attended treatmentand hence may not be representative of theentire population of buprenorphine-dependentpatients. On the other hand, however, the socio-demographic and clinical pro� les of our patientswere very similar to those presented earlier byother authors from different parts of India(Chowdhury & Chowdhury, 1990; Singh et al.,
Figure 3. Pattern of transitions (n 5 32).

1370 Debasish Basu et al.
Table 3. “Transition” vs. “stable” groups of buprenorphine†
Transition Stable v 2 for %group group or U for
(N 5 32) (N 5 20) means
Income (Rs)Nil 25 (78) 9 (45), 1000/- 2 (6) 3 (15) 23.00**. 1000–2000 5 (16) 7 (35). 2000 0 (0) 1 (5)
LocalityUrban 29 (91) 15 (75) 7.97**Rural 3 (9) 5 (25)
Referral sourceSelf 2 (6) 2 (10)Relatives 25 (78) 13 (65) 14.93**Medical 1 (3) 3 (15)Others 4 (13) 2 (10)
Family h/o drug usePresent 15 (47) 6 (30) 5.41*Absent 17 (53) 14 (70)
Age at � rst use (years)Mean 22.8 24.7 2.11*SD 3.8 5.3
Duration of dependent use beforeseeking Rx (months)
Mean 24.6 28.0SD 25.2 23.9 2.85**
Drug-related complications atintake
Marital 19 (60) 8 (40) 7.22**Legal 11 (34) 3 (15) 8.76**
% Time spent in each phaseDependence 22 (68) 5 (25)Occasional use 6 (19) 2 (10) 27.34**Abstinence 4 (13) 13 (65)
No. of hospital admissionsNone 7 (22) 7 (35)Single 9 (28) 9 (45) 19.78**Multiple 16 (50) 4 (20)
Duration of hospital stay, 1 month 23 (72) 10 (50) 9.27**$ 1 month 9 (28) 10 (50)
Status at last follow-upDead 3 (9) 0 (0)Unchanged 9 (28) 8 (40) 11.19**Improved 20 (63) 12 (60)
All � gures, unless otherwise stated, refer to N (%). † Only data for statistically signi� cant differences are shown.*p , 0.05; **p , 0.01.
1992; Lal, 1991; Umesh Babu & Chaturvedi,1995; Chavan et al., 1995; Kumar & Singh,1996).
Secondly the outcome categories may be ques-tioned, especially the “improved” category whichwas kept somewhat broad. This was according toTaylor et al.’s (1985) suggestion. The term“improved” in our study would become moremeaningful when seen in a longitudinal compar-
ative perspective: e.g., a patient would be con-sidered improved from his own baseline conditionduring � rst clinic attendance even if he continuedto take drugs in a less severe fashion later.
A � nal important consideration is dealing withthe drop-outs and data handling. In spite of ourbest efforts, only 18% of patients were followed-up for more than 5 years. To tackle this problem,we conducted an analysis including all the 52

Buprenorphine cohort study 1371
patients who were followed-up for more than ayear. This method although certainly not fool-proof (Moncrieff & Drummond, 1997), hassome bene� ts in treatment outcome research insubstance abuse (Chick, 1997). Further, by car-rying out different types of outcome analysis allshowing a similar trend, the con� dence placed inthe results does increase.
In this retrospective cohort study over anintermediate-term follow-up period, the twomain questions asked were: what happens to thebuprenorphine abusers? What happens to thebuprenorphine abuse? Regarding the � rst, it isseen that although the buprenorphine patientsspent more than half of their time in dependenceand only one-third in abstinence at an individuallevel, at a collective level the cumulative outcomebecame progressively better over the years. The20-year follow-up results of 100 intravenousheroin addicts in the classic study by Vaillant(1973, 1988) are very similar regarding thecumulative outcome: as time passed, the numberof patients with “active narcotic addiction”(“unchanged” in our study) steadily decreasedand the number of subjects achieving “stableabstinence” (abstinence for 3 years or more)increased steadily. Our � gures, although obvi-ously not exactly comparable to Vaillant’s study,show similar trends. The trends seen in the otherimportant studies such as Stimson et al. (1978)and Haastrup & Jepsen (1988) are somewhatdifferent, but they dealt with very different popu-lations and sample characteristics, such as muchyounger age (Haastrup & Jepsen, 1988), and nospeci� c or intensive treatment (Stimson et al.,1978). Comparing the poor versus better out-come patients, the interesting new � nding was amuch higher use of pentazocine and/or antihis-taminic injections in the drug cocktail by thepoor outcome patients.
The other question, that of the fate ofbuprenorphine use, yielded the fact that at leastone-third of the index cohort (and nearly two-thirds of the outcome cohort) showed a patternof transition to other drugs. One-third of thesepatients went back to heroin use. Half of thesetransition patterns, however, involved polydrugabuse with a wide variety of available substances.One-third of these � rst transition patients evenmade a second transition, generally back tobuprenorphine. Thus, in a subgroup of patients,buprenorphine use was found to be unstable.This subgroup also fared worse compared to the
“stable” patients with respect to severity, courseand outcome of the dependence. These � ndings,if replicated, have important implications formanagement and prognosis of buprenorphinedependence.
This study, in spite of its methodological limi-tations and caveats, has generated data whichmay be useful in understanding and, perhaps,controlling buprenorphine abuse in India. Indi-vidually, patients spent a large proportion oftheir drug career in a dependent pattern of use,in spite of often multiple hospitalizations foraddiction treatment; many of them shifted toother drugs, notably heroin, and did worse.Nevertheless, the fact remains that the collectivepattern of follow-up of these patients show atleast some improvement over the years withtreatment, albeit slowly.
AcknowledgementThis study was funded by an Institute ResearchGrant for the PGI Research Scheme entitled“Long-term course and outcome of substancemisuse in patients attending a de-addictionclinic”.
ReferencesBASU, D., MATTOO, S. K., ARORA, A., MALHOTRA, A. &
VARMA, V. K. (1994) Pseudoaneurysm in injectingdrug abusers: cases from India, Addiction, 89, 1697–
1699.BASU, D., MALHOTRA, A. K. & VARMA, V. K. (1990)
Buprenorphine dependence: a new addiction inIndia, Disabilities and Impairments, 3, 142–146.
CHAVAN, B. S., TRIPATHI, B. M. & LAL, R. (1995)Outcome of parenteral buprenorphine abuse (ab-stract), Indian Journal of Psychiatry, 37 (suppl), 24.
CHICK, J. (1997) Pitfalls and possibilities in evaluatingpharmacotherapies for alcohol dependence, Addic-tion, 92, 953–956.
CHOWDHURY, A. N. & CHOWDHURY, S. (1990)Buprenorphine abuse: report from India, BritishJournal of Addiction, 85, 1349–1350.
HAASTRUP, S. & JEPSEN, P. W. (1988) Eleven-yearfollow-up of 300 young opioid addicts, Acta Psychi-atrica Scandinavica, 77, 22–26.
HARPER, I. (1983) Temgesic abuse, New Zealand Medi-cal Journal, 96, 777.
KUMAR, V. & SINGH, B. K. (1996) Reasons behindincreasing buprenorphine abuse (abstract), IndianJournal of Psychiatry, 38 (suppl.), 82.
LAL, R. (1991) Buprenorphine dependence: analysis ofseven cases, Indian Journal of Psychiatry, 33, 62–65.
MALHOTRA, A., BALAJI, M., BASU, D., MATTOO, S. K.,VARMA, V. K. & SEHGAL, S. (1993) HIV screeningand risk behaviour in psychoactive substance users,Indian Journal of Medical Research, 97 (A), 231–233.
1372 Debasish Basu et al.
MONCRIEFF, J. & DRUMMOND, D. C. (1997) Newdrugs for alcoholism problems: a critical appraisal,Addiction, 92, 939–946.
O’CONNOR, J. J., MALONEY, E., TRAVERS, R. &CAMPBELL, A. (1988) Buprenorphine abuse amongopiate addicts, British Journal of Addiction, 83, 1085–
1087.SHARMA, Y. & MATTOO, S. K. (1999) Buprenorphine
abuse in India: an update, Indian Journal of Psy-chiatry, 41, 154–159.
SINGH, R. A., MATTOO, S. K., MALHOTRA, A. &VARMA, V. K. (1992) Cases of buprenorphine abusein India, Acta Psychiatrica Scandinavica, 86, 46–48.
STIMSON, G., V. OPPENHEIMER, E. & THORLEY, A.(1978) Seven year follow-up of heroin addicts: druguse and outcome, British Medical Journal, i, 1190–
1192.STRANG, J. (1985) Abuse of buprenorphine, Lancet, ii,
725.TAYLOR, C., BROWN, D., DUCKITT, A., EDWARDS, G.,
OPPENHEIMER, E. & SHEEHAN, M. (1985) Patterns ofoutcome: drinking histories over ten years among agroup of alcoholics, British Journal of Addiction, 80,45–50.
TAYLOR, C. (1994) What happens over the long-term?British Medical Bulletin, 50, 50–66.
UMESH BABU, S. B. & CHATURVEDI, S. K. (1995)Changing patterns of opiate abuse with a focus onbuprenorphine (abstract), Indian Journal of Psy-chiatry, 37 (suppl.), 23.
VAILLANT, G. E. (1973) A 20-year follow-up of of NewYork narcotic addicts, Archives of General Psychiatry,29, 237–241.
VAILLANT, G. E. (1988) what can long-term follow-upteach us about relapse and prevention of relapse inaddiction? British Journal of Addiction, 83, 1147–
1157.VAILLANT, G. E. (1966) A 12-year follow-up of New
York narcotic addicts: II. The natural history of achronic disease, New England Journal of Medicine,275, 1282–1288.
WORLD HEALTH ORGANIZATION (1992) The ICD-10Classi� cation of Mental and Behavioural Disorders,clinical description and diagnostic guidelines(Geneva, WHO).
WORLD HEALTH ORGANIZATION (1978) The Inter-national Classi� cation of Diseases, 9th edn (Geneva,WHO).




















