Comfort and discomfort of dental trauma splints ^ a ...
6
Comfort and discomfort of dental trauma splints ^ a comparison of a new device (TTS) with three commonly used splinting techniques Traumatically loosened, displaced or avulsed perma- nent teeth are normally splinted. The splinting method used for stabilization should support period- ontal healing. Many di¡erent types of splinting tech- niques have been described in the literature (1^4). Today, an ideal splint should be passive and £exible to allow physiologic tooth mobility. The duration of splinting should be as short as possible. Usually, the periodontal ligament reaches most of its normal strength 7^14 days following trauma. Both prolonged and rigid splinting may lead to adverse e¡ects, such as ankylosis and replacement resorption (5^8). In addition, trauma splints should have optimal proper- ties for handling, application and removal. Commonly used splinting techniques have been investigated in vitro and in vivo (9^13). In a recent study, parameters such as tooth mobility (Periotest values), probing depths, plaque accumulation, bleeding on probing and the chair time needed for splint applica- tion and removal were evaluated. The investigated splinting methods included the wire-composite splint (WCS), the button-bracket splint (BS), the resin splint (RS) and the new titanium trauma splint (TTS) (14). It could be shown that all four tested splints main- tained normal tooth mobility: TTS and WCS allow- ed a more physiologic and RS a critically reduced tooth mobility (horizontal Periotest values). Period- ontal parameters remained unchanged, re£ecting Dental Traumatology 2002; 18: 275–280 Copyright # Blackwell Munksgaard 2002 Printed in Denmark. All rights reserved DENTAL TRAUMATOLOGY ISSN 1600–4469 275 Filippi A, von ArxT, Lussi A. Comfort and discomfort of dental trauma splints ^ a comparison of a new device (TTS) with three commonly used splinting techniques. DentTraumatol 2002;18: 275^280. # Blackwell Munksgaard, 2002. Abstract ^ The present experimental study compared four dental trauma splints in 10 volunteers. The evaluated splints included a wire-composite splint (WCS), a button-bracket splint (BS), a resin splint (RS), and the newly developed titanium trauma splint (TTS). All splints were bonded to the labial surfaces of the maxillary lateral and central incisors and left in place for 1week. After splint removal, the next splint was placed after a 1-week rest period.The sequence of splint application was randomized for each individual. The following subjective parameters were assessed using a visual analogue scale: sensitiveness of splinted teeth, irritation of the gingival margin, irritation of the lips, impairment of speech, eating and oral hygiene. The results show that the application of BS leads to a signi¢cantly higher irritation of the lips and greater impairment of speech compared to other splints (P < 0.05). The RS leads to an increased and signi¢cantly higher irritation of the gingiva (P < 0.05) owing to a signi¢cant increase in cleaning di⁄culties (P < 0.05). In conclusion, WCS and TTS appear to be more accepted splints according to a subjective assessment by 10 volunteers. Andreas Filippi 1 , Thomas von Arx 2 , Adrian Lussi 3 1 Department of Oral Surgery, Oral Radiology and Oral Medicine, University of Basel, Basel, Switzerland, 2 Department of Oral Surgery and Stomatology, 3 Department of Operative Dentistry, University of Berne, Berne, Switzerland Key words: dental trauma splint; splinting method; discomfort; subjective assessment Dr Andreas Filippi, Department of Oral Surgery, Oral Radiology and Oral Medicine, University of Basle, Hebelstrasse 3, CH-4056 Basle, Switzerland Tel.: þ4161267 2609 Fax: þ4161267 2607 e-mail: andreas.filippi@unibas.ch Accepted 21 March, 2002
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Comfort and discomfort of dental trauma splints ^ a ...
Comfort and discomfort of dental traumasplints ^ a comparison of a new device (TTS)with three commonly used splintingtechniques
Traumatically loosened, displaced or avulsed perma-nent teeth are normally splinted. The splintingmethod used for stabilization should support period-ontal healing. Many di¡erent types of splinting tech-niques have been described in the literature (1^4).Today, an ideal splint should be passive and £exibleto allow physiologic tooth mobility. The duration ofsplinting should be as short as possible. Usually, theperiodontal ligament reaches most of its normalstrength 7^14 days following trauma. Bothprolongedand rigid splinting may lead to adverse e¡ects, suchas ankylosis and replacement resorption (5^8). Inaddition, trauma splints should have optimal proper-ties for handling, application and removal.
Commonly used splinting techniques have beeninvestigated in vitroand in vivo (9^13). Ina recent study,parameters such as tooth mobility (Periotest values),probing depths, plaque accumulation, bleeding onprobing and the chair time needed for splint applica-tion and removal were evaluated. The investigatedsplinting methods included thewire-composite splint(WCS), thebutton-bracket splint (BS), the resin splint(RS) and the new titanium trauma splint (TTS)(14). Itcouldbe shownthat all four tested splintsmain-tained normal tooth mobility: TTS andWCS allow-ed a more physiologic and RS a critically reducedtooth mobility (horizontal Periotest values). Period-ontal parameters remained unchanged, re£ecting
Dental Traumatology 2002; 18: 275–280 Copyright # Blackwell Munksgaard 2002Printed in Denmark. All rights reserved DENTAL TRAUMATOLOGY
ISSN 1600–4469
275
Filippi A, von ArxT, Lussi A. Comfort and discomfort of dentaltrauma splints ^ a comparison of a new device (TTS) with threecommonly used splinting techniques. DentTraumatol 2002;18:275^280.# Blackwell Munksgaard, 2002.
Abstract ^ The present experimental study compared four dentaltrauma splints in10 volunteers.The evaluated splints included awire-composite splint (WCS), a button-bracket splint (BS), a resinsplint (RS), and the newly developed titanium trauma splint(TTS). All splints were bonded to the labial surfaces of themaxillary lateral and central incisors and left in place for1week.After splint removal, the next splint was placed after a1-week restperiod.The sequence of splint applicationwas randomized for eachindividual.The following subjective parameters were assessedusing a visual analogue scale: sensitiveness of splinted teeth,irritation of the gingival margin, irritation of the lips, impairmentof speech, eating and oral hygiene.The results show that theapplication of BS leads to a signi¢cantly higher irritation of the lipsand greater impairment of speech compared to other splints(P< 0.05).The RS leads to an increased and signi¢cantly higherirritation of the gingiva (P< 0.05) owing to a signi¢cant increase incleaning di⁄culties (P< 0.05). In conclusion,WCS andTTSappear to be more accepted splints according to a subjectiveassessment by10 volunteers.
Andreas Filippi1, Thomas von Arx2,Adrian Lussi31Department of Oral Surgery, Oral Radiology and OralMedicine, University of Basel, Basel, Switzerland,2Department of Oral Surgery and Stomatology,3Department of Operative Dentistry, University ofBerne, Berne, Switzerland
Key words: dental trauma splint; splinting method;discomfort; subjective assessment
Dr Andreas Filippi, Department of Oral Surgery, OralRadiology and Oral Medicine, University of Basle,Hebelstrasse 3, CH-4056 Basle, SwitzerlandTel.:þ4161267 2609Fax:þ4161267 2607e-mail: [email protected]
Accepted 21 March, 2002
the excellent oral hygiene by the study subjects. Thechair time used for ¢xation and removal was signi¢-cantly lower forTTS.From the patient’s perspective, it is important that
these splints are comfortable anddonot interferewithoral hygiene, speaking and eating. In addition, thesplints should not irritate adjacent tissues (gingiva,lips).The objective of this experimental study was tocompare and evaluate TTS,WCS, RS and BS withrespect to the subjective assessment by the patient.
Materials and methods
The study was conducted in 10 volunteers recruitedfrom the sta¡ of the Department of Oral Surgeryand Stomatology, University of Berne. All subjectswere femalewith ameanage of 21years and 6months(range 17 years and 6months to 34 years and9months).The studydesignwasapprovedbytheEthi-cal Commission of the Canton Berne (study-number:ZMK-OC1/2000) and the clinical study was carriedout according to the Helsinki declaration.The samestudydesign hasbeenused inapreviouspaperanalys-ing di¡erent clinical parameters, such as tooth mobi-lity, periodontal status, working time (9). All fourmaxillary incisors in all volunteers were free of cariesand periodontal diseases. All subjects were healthyand presented no medical contraindications for theplanned procedures.Four di¡erent splinting methods were evaluated in
each individual, resulting in a total of 40 splints.Thesequence of splint applicationwas determined at ran-dom. Each splint was left in situ for 7 days. Afterremoval, the next splint was placed after waiting forat least 1week.All splints were bonded to the labial aspect of all
maxillary incisors. By placing the splints coronally,they were kept away from the gingival margin andthe papillae. After drying the teeth, etching of theenamel surface was performedwith 35%phosphoricacid gel for 30 s. Subsequently, the gel was rinsed o¡with water and the etched surfaces were dried again.Athin layerof bondingagentwas applied. Afterpoly-merization, the splints were placed with the techni-ques described below.
Titanium trauma splint (TTS)
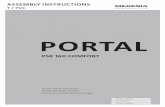
After cutting to the desired length, theTTSwas bentto the labial aspects of the incisors. Per tooth, onerhombus of theTTSwas ¢lledwith light-curing com-posite (Tetric1 Flow Chroma, Vivadent, Schaan,Liechtenstein) (Fig.1) with 30 s of polymerization.
Wire-composite splint (WCS)
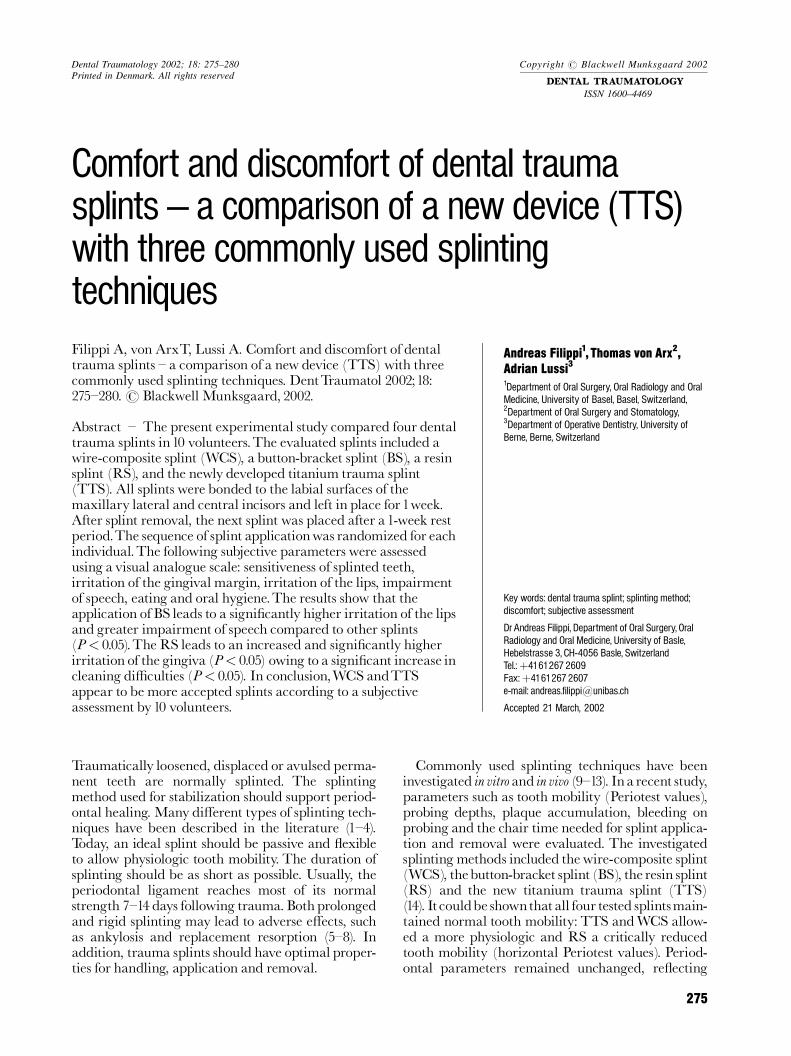
An 0.16 in.�0.22 in. orthodontic wire was cut to thedesired length, adaptedtothecurvatureof theincisors
using a plier and secured with identical composite(Fig.2).
Button-bracket splint (BS)
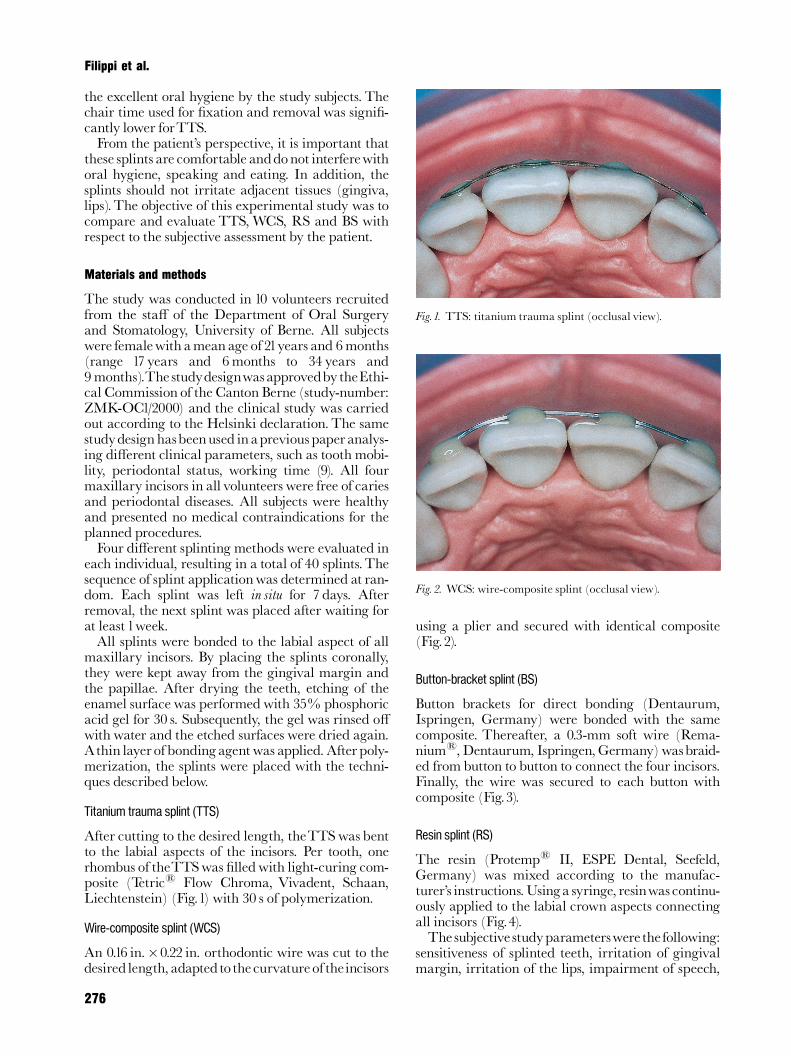
Button brackets for direct bonding (Dentaurum,Ispringen, Germany) were bonded with the samecomposite. Thereafter, a 0.3-mm soft wire (Rema-nium1, Dentaurum, Ispringen,Germany)wasbraid-ed frombutton to button to connect the four incisors.Finally, the wire was secured to each button withcomposite (Fig.3).
Resin splint (RS)
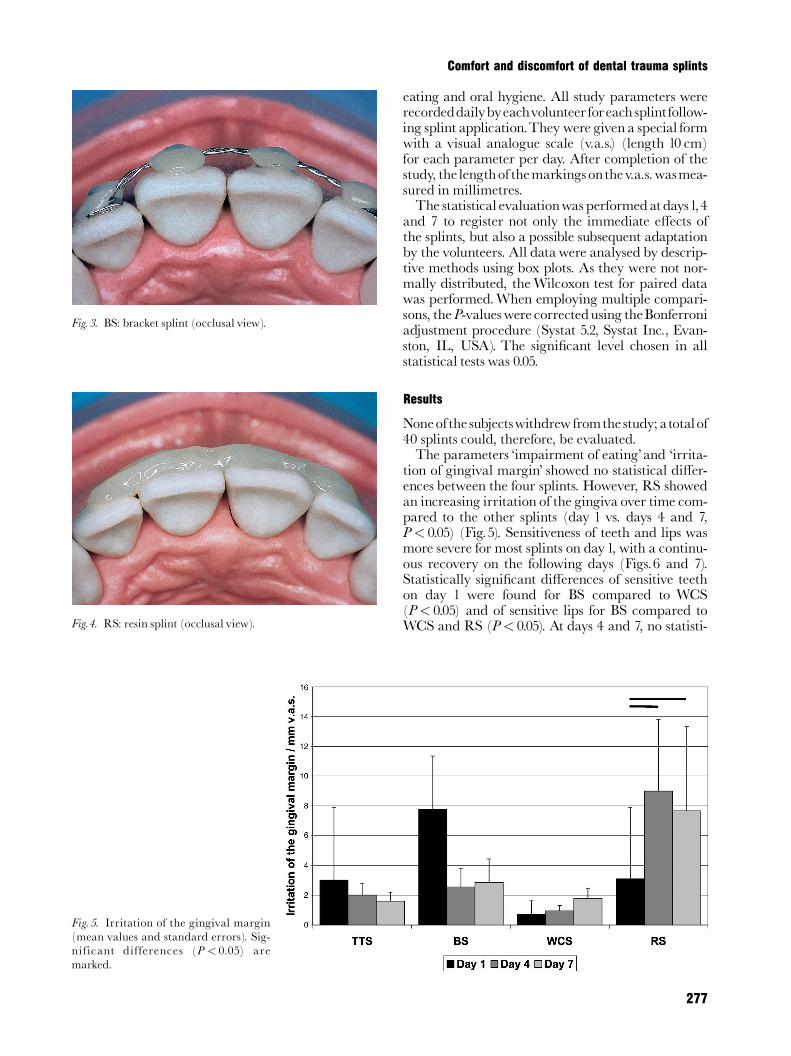
The resin (Protemp1 II, ESPE Dental, Seefeld,Germany) was mixed according to the manufac-turer’s instructions.Usinga syringe, resinwascontinu-ously applied to the labial crown aspects connectingall incisors (Fig.4).The subjective studyparameterswerethe following:
sensitiveness of splinted teeth, irritation of gingivalmargin, irritation of the lips, impairment of speech,
Fig. 1. TTS: titanium trauma splint (occlusal view).
Fig. 2. WCS: wire-composite splint (occlusal view).
Filippi et al.
276
eating and oral hygiene. All study parameters wererecordeddailybyeachvolunteer foreach splintfollow-ing splint application.They were given a special formwith a visual analogue scale (v.a.s.) (length 10 cm)for each parameter per day. After completion of thestudy, the lengthof themarkingsonthev.a.s.wasmea-sured in millimetres.The statistical evaluationwas performedatdays1,4
and 7 to register not only the immediate e¡ects ofthe splints, but also a possible subsequent adaptationby the volunteers. All datawere analysed by descrip-tive methods using box plots. As they were not nor-mally distributed, theWilcoxon test for paired datawas performed.When employing multiple compari-sons, theP-valueswere correctedusing theBonferroniadjustment procedure (Systat 5.2, Systat Inc., Evan-ston, IL, USA). The signi¢cant level chosen in allstatistical tests was 0.05.
Results
Noneofthe subjectswithdrew fromthe study;atotalof40 splints could, therefore, be evaluated.The parameters ‘impairment of eating’and ‘irrita-
tion of gingival margin’ showed no statistical di¡er-ences between the four splints. However, RS showedan increasing irritation of the gingiva over time com-pared to the other splints (day 1 vs. days 4 and 7,P< 0.05) (Fig.5). Sensitiveness of teeth and lips wasmore severe for most splints on day1, with a continu-ous recovery on the following days (Figs.6 and 7).Statistically signi¢cant di¡erences of sensitive teethon day 1 were found for BS compared to WCS(P< 0.05) and of sensitive lips for BS compared toWCS and RS (P< 0.05). At days 4 and 7, no statisti-
Fig. 3. BS: bracket splint (occlusal view).
Fig. 4. RS: resin splint (occlusal view).
Fig. 5. Irritation of the gingival margin(mean values and standard errors). Sig-nificant differences (P < 0.05) aremarked.
277
Comfort and discomfort of dental trauma splints
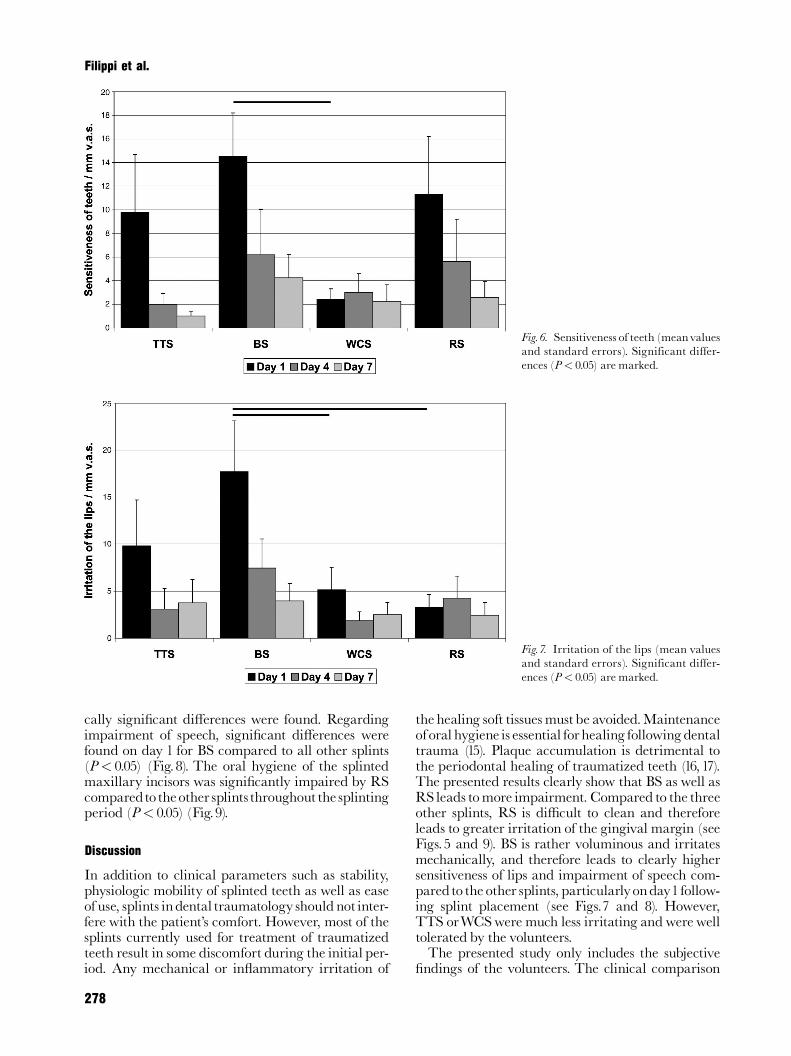
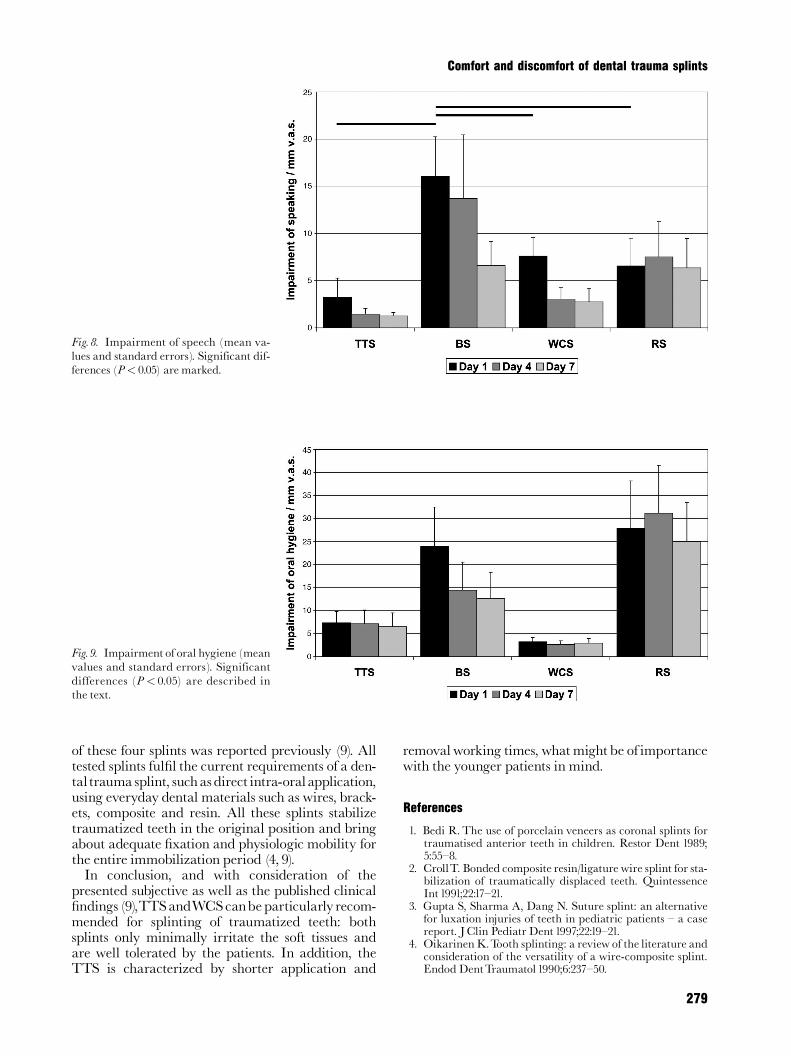
cally signi¢cant di¡erences were found. Regardingimpairment of speech, signi¢cant di¡erences werefound on day 1 for BS compared to all other splints(P< 0.05) (Fig.8). The oral hygiene of the splintedmaxillary incisors was signi¢cantly impaired by RScomparedtotheother splintsthroughoutthe splintingperiod (P< 0.05) (Fig.9).
Discussion
In addition to clinical parameters such as stability,physiologic mobility of splinted teeth as well as easeof use, splints indental traumatology should not inter-fere with the patient’s comfort. However, most of thesplints currently used for treatment of traumatizedteeth result in some discomfort during the initial per-iod. Any mechanical or in£ammatory irritation of
the healing soft tissuesmustbe avoided.Maintenanceoforal hygiene is essential forhealing followingdentaltrauma (15). Plaque accumulation is detrimental tothe periodontal healing of traumatized teeth (16,17).The presented results clearly show that BS as well asRS leads tomore impairment. Compared to the threeother splints, RS is di⁄cult to clean and thereforeleads to greater irritation of the gingival margin (seeFigs.5 and 9). BS is rather voluminous and irritatesmechanically, and therefore leads to clearly highersensitiveness of lips and impairment of speech com-paredtothe other splints, particularlyonday1follow-ing splint placement (see Figs.7 and 8). However,TTS orWCSwere much less irritating andwere welltolerated by the volunteers.The presented study only includes the subjective
¢ndings of the volunteers. The clinical comparison
Fig. 6. Sensitiveness of teeth (meanvaluesand standard errors). Significant differ-ences (P< 0.05) are marked.
Fig. 7. Irritation of the lips (mean valuesand standard errors). Significant differ-ences (P< 0.05) are marked.
278
Filippi et al.
of these four splints was reported previously (9). Alltested splints ful¢l the current requirements of a den-taltrauma splint, suchasdirect intra-oralapplication,using everyday dental materials such as wires, brack-ets, composite and resin. All these splints stabilizetraumatized teeth in the original position and bringabout adequate ¢xation and physiologic mobility forthe entire immobilization period (4, 9).In conclusion, and with consideration of the
presented subjective as well as the published clinical¢ndings (9),TTSandWCScanbeparticularly recom-mended for splinting of traumatized teeth: bothsplints only minimally irritate the soft tissues andare well tolerated by the patients. In addition, theTTS is characterized by shorter application and
removalworking times, whatmight be of importancewith the younger patients in mind.
References
1. Bedi R. The use of porcelain veneers as coronal splints fortraumatised anterior teeth in children. Restor Dent 1989;5:55^8.
2. CrollT. Bonded composite resin/ligature wire splint for sta-bilization of traumatically displaced teeth. QuintessenceInt1991;22:17^21.
3. Gupta S, Sharma A, Dang N. Suture splint: an alternativefor luxation injuries of teeth in pediatric patients ^ a casereport. JClin Pediatr Dent 1997;22:19^21.
4. OikarinenK.Tooth splinting: a review of the literature andconsideration of the versatility of a wire-composite splint.Endod DentTraumatol 1990;6:237^50.
Fig. 8. Impairment of speech (mean va-lues and standard errors). Significant dif-ferences (P< 0.05) are marked.
Fig. 9. Impairment of oral hygiene (meanvalues and standard errors). Significantdifferences (P< 0.05) are described inthe text.
279
Comfort and discomfort of dental trauma splints

5. Andreasen JO. The effect of splinting upon periodontalhealing after replantation of permanent incisors in mon-keys. Acta Odontol Scand1975;33:313^23.
6. Berude JA, Hicks ML, Sauber JJ, Li SH. Resorption afterphysiological and rigid splinting of replanted permanentincisors in monkeys. J Endod1988;14:592^600.
7. Kristerson L, Andreasen JO. The effect of splinting uponperiodontal and pulpal healing after autotransplantationof mature and immature permanent incisors in monkeys.IntJOral Surg1983;12:239^49.
8. Nasjleti CE, CastelliWA, Caffesse RG.The effects of differ-ent splinting times on replantation of teeth in monkeys.Oral Surg1982;53:557^66.
9. von ArxT, Filippi A, Lussi A. Comparison of a new dentaltrauma splint device (TTS) with three commonly usedsplinting techniques. DentTraumatol 2001;17:266^74.
10. Filippi A. Reimplantation nachTrauma. Einfluss der Schie-nung auf die Zahnbeweglichkeit. Z Zahna« rztl Implantol2000;16:8^10.
11. Ebeleseder KA, Glockner K, Pertl C, Staedler P. Splintsmade of wire and composite: an investigation of lateral
tooth mobility in vivo. Endod Dent Traumatol 1995;11:288^93.
12. Oikarinen K. Comparison of the flexibility of varioussplinting methods for tooth fixation. Int J Oral MaxillofacSurg1988;17:125^7.
13. Oikarinen K, Andreasen JO, Andreasen FM. Rigidity ofvarious fixation methods used as dental splints. EndodDentTraumatol1992;8:113^9.
14. von Arx T, Filippi A, Buser D. Splinting of traumatizedteeth with a new device: TTS (titanium trauma splint).DentTraumatol 2001;17:180^4.
15. Andreasen JO, Andreasen FM. Luxation injuries. In:AndreasenJO, Andreasen FM, editors.Textbook and coloratlas of traumatic injuries to the teeth. Copenhagen:Munksgaard;1994. p. 315^82.
16. Ne RF, Witherspoon DE, Gutman JL. Tooth resorption.Quintessence Int1999;30:9^25.
17. Trope M. Root resorption of dental and traumatic origin:classification based on etiology. Pract Periodont AesthetDent1998;10:515^22.
280
Filippi et al.