Clinico-Pathologic Conference: - DOST ScINet-Phil
7
Clinico-Pathologic Conference: Fever, Dyspnea, Chest and Abdominal Pains h'difcri by Adelaida E. Dalmacio-Cruz, MD. Hospital Ca!;!.' 1\0. l02jR:10 Ko. l1i:}4.ii Case History The patient is an IS-real'-olc! f('nullt', who {'amI.' in because of chest pain and cliffJ('ulty of breath- ing. Four and one-half months previously, the patient began to experience easy fatigue. This pI'ogresse(1 su('h that in a month's time, she did not only have dyspnea on eXl'I-tion but also at rest. Some time dul'inlt this ]lel"iod, she developed fever, jaundice :llld pallor. There was also persistent abdominal pain, located in the uppe!' abdomen, unrelated to food intak(' The pain is of such severity requil'ing her to doub) ... up. A week after the onset of the fever, she had uilateral pedal edema which gradually progressed UI' to the thighs. For these complaints, she entered another hospital. Here she was told that her illness was a "disease of the lungs and kidneys," She stayed for three months, tl'eated, and discharged asympto- matic, Upon discharge, she was maintained on th(' following medications: Streptomycin injections, Isoniazid tahlets and methenamine mandelate cap!"lIles, Two weeks prior to entry, she had recurrence of the symptoms, Aside from the exertional dyspnea. she now had orthopnea. Fever was noticed to occur at night and was associated with sweating, Generalized muscle aches were bothersome but there was no ac- companying al'thralgia, In addition to the abdominal pain, chest pain appeared. This was aggravated by deep respiration. A week after the onset of the recul'- rence, she had couj!'h which was slightly productive of whitish mucoid ('xp('ctol'ation. Insomnia and ano- I'exia were profound. Th('r(' were no bladdel' 01' bowel distul'hances. W('ight loss was not apparent. For two we('ks, she had been vomiting every time the abdominal pain became severe, On admission, she could not tol(,l'atc solid foods, In the past, she claimed to have seven episodes of "malaria", an illness chal'acterized by chills, followed by fever and profusc diaphol'esis, Thl're was no past history of jaundice. During childhood, she had epi- sodes of fevel' associated with symmetrical joint pains. APRIL·JUNE. 1966 Tht' wl'ists and tbe knees whi(·h wer(' involn·t\ were h'ndel' but not swollt'n. She also ha(\ frequl'nt bouts of epistaxis. Menarche was at 1:; real's of :ll:"e. Thereuftel', nU'lISl'S came rl'l:"ul:ll'ly e\'l'IT month until rOUI' mOllth" prim' to admission, when she became amenonht'ie, history was 1l0n-l·ontl'ibutoI'Y. On admission, she had a fevel' of 3!:\.f. 'C, pulse !'illl' of 120 per minute, respiratory rilte of per minute, blood Jll'essure of 1·\0 mill. Hg. systolic, 110 mill. Hg diastolk. She was dcveloped, poody nourished, dyspneic and ol·thopnl'i(', conscious and ('Uhel'ent, Ther(' WHS pallor of the conjunctivae. The sl'lerae wcre 1I0n-ktel'ilo. The lll'l'k veins were not ('llgorged. Regional was not noted. Chest expansion WilS equa\. There wel'e some cre- pit:lnt rales at the bases on both sides. Percussiop. note and vocal frlc'mitus wel'E' not imp;lired. The apex hellt of the heal't W;lS palpated lit the 5th ICS LMCL. :->he had a gallop rhrthm lI'ith a I'at<.' of 120 pel' mi- Ilutl'. TherE' was no murmur appl'edated. The liver ('t\g'(' was tendel'. doug-hy and extE'ndcd ·1 l'm. below the right ('ostal an'h. Thl' splenic tip was not appre- dated. There wa'> tendel'n('ss of the upper half of the abdomell. Rebound and muscle guard- inl:" were however absl'nt. Pedal edema and ('yanosis A l,h('st X-rayon admission was interpreted as "the loaJ'(\iac borders cannot be delineated becaUSE of the pulmonary shadows. There art' in both lunK fields with generalized haziness in the right lung field and fluid in the right pleural spaces, The left l)l'onchus ;lppears uplifted. The findings are wlllilatible with PUhl\OIWI'Y edema and congestion, bilateral hl'onl'hopneumonia and right pleul'al effu- sion." The plain abdomen was I'ead as "the edges of the !i\'l'r and spleen are pl'ominent, Other soft tissues are not visualized. There are no opaque lithiasis along the KC'B tracts." The patient stayed for eight days in the ward. On the second hospital she was still dehydl'ated, '>wl'atinl:", pale and sever('\y orthopneic assuming a sitting down position with the face down. There 211
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Clinico-Pathologic Conference: - DOST ScINet-Phil

Clinico-Pathologic Conference:
Fever, Dyspnea, Chest and Abdominal Pains
h'difcri by
Adelaida E. Dalmacio-Cruz, MD.
Hospital Ca!;!.' 1\0. l02jR:10 Autops~' Ko. l1i:}4.ii
Case History
The patient is an IS-real'-olc! f('nullt', sin~dl" who {'amI.' in because of chest pain and cliffJ('ulty of breathing.
Four and one-half months previously, the patient began to experience easy fatigue. This pI'ogresse(1 su('h that in a month's time, she did not only have dyspnea on eXl'I-tion but also at rest. Some time dul'inlt this ]lel"iod, she developed fever, jaundice :llld pallor. There was also persistent abdominal pain, located in the uppe!' abdomen, unrelated to food intak(' The pain is of such severity requil'ing her to doub) ... up. A week after the onset of the fever, she had uilateral pedal edema which gradually progressed UI' to the thighs. For these complaints, she entered another hospital. Here she was told that her illness was a "disease of the lungs and kidneys," She stayed for three months, tl'eated, and discharged asymptomatic, Upon discharge, she was maintained on th(' following medications: Streptomycin injections, Isoniazid tahlets and methenamine mandelate cap!"lIles, Two weeks prior to entry, she had recurrence of the symptoms, Aside from the exertional dyspnea. she now had orthopnea. Fever was noticed to occur at night and was associated with sweating, Generalized muscle aches were bothersome but there was no accompanying al'thralgia, In addition to the abdominal pain, chest pain appeared. This was aggravated by deep respiration. A week after the onset of the recul'rence, she had couj!'h which was slightly productive of whitish mucoid ('xp('ctol'ation. Insomnia and anoI'exia were profound. Th('r(' were no bladdel' 01' bowel distul'hances. W('ight loss was not apparent. For two we('ks, she had been vomiting every time the abdominal pain became severe, On admission, she could not tol(,l'atc solid foods,
In the past, she claimed to have seven episodes of "malaria", an illness chal'acterized by chills, followed by fever and profusc diaphol'esis, Thl're was no past history of jaundice. During childhood, she had episodes of fevel' associated with symmetrical joint pains.
APRIL·JUNE. 1966
Tht' wl'ists and tbe knees whi(·h wer(' involn·t\ were h'ndel' but not swollt'n. She also ha(\ frequl'nt bouts of epistaxis.
Menarche was at 1:; real's of :ll:"e. Thereuftel', nU'lISl'S came rl'l:"ul:ll'ly e\'l'IT month until rOUI' mOllth" prim' to admission, when she became amenonht'ie,
l~amily history was 1l0n-l·ontl'ibutoI'Y.
On admission, she had a fevel' of 3!:\.f. 'C, pulse !'illl' of 120 per minute, respiratory rilte of 5;~ per minute, blood Jll'essure of 1·\0 mill. Hg. systolic, 110 mill. Hg diastolk. She was fairl~' dcveloped, poody nourished, dyspneic and ol·thopnl'i(', conscious and ('Uhel'ent, Ther(' WHS pallor of the conjunctivae. The sl'lerae wcre 1I0n-ktel'ilo. The lll'l'k veins were not ('llgorged. Regional i~'m]lhadenopathy was not noted. Chest expansion WilS equa\. There wel'e some crepit:lnt rales at the bases on both sides. Percussiop. note and vocal frlc'mitus wel'E' not imp;lired. The apex hellt of the heal't W;lS palpated lit the 5th ICS LMCL. :->he had a gallop rhrthm lI'ith a I'at<.' of 120 pel' miIlutl'. TherE' was no murmur appl'edated. The liver ('t\g'(' was tendel'. doug-hy and extE'ndcd ·1 l'm. below the right ('ostal an'h. Thl' splenic tip was not appredated. There wa'> tendel'n('ss of the upper half of the abdomell. Rebound t('nderne~s and muscle guardinl:" were however absl'nt. Pedal edema and ('yanosis
A l,h('st X-rayon admission was interpreted as "the loaJ'(\iac borders cannot be delineated becaUSE of the pulmonary shadows. There art' ehan~es in both lunK fields with generalized haziness in the right lung field and fluid in the right pleural spaces, The left l)l'onchus ;lppears uplifted. The findings are wlllilatible with PUhl\OIWI'Y edema and congestion, bilateral hl'onl'hopneumonia and right pleul'al effusion." The plain abdomen was I'ead as "the edges of the !i\'l'r and spleen are pl'ominent, Other soft tissues are not visualized. There are no opaque lithiasis along the KC'B tracts."
The patient stayed for eight days in the ward. On the second hospital da~o, she was still dehydl'ated, '>wl'atinl:", pale and sever('\y orthopneic assuming a sitting down position with the face down. There
211
User
Typewritten Text
110047
User
Typewritten Text
ACTA MF.[)[CA PUn.II'PI:-;A
was tenderness in the (·o.st.o\·ert.ebral areas. The goal· lOll I'hythm was still there. Blood examination duo rill)! thi~ time revealed an anemia with II. hematocrit of 2-1 volume~ '" hcmo~lobin of 7.5 j!rams '.f. The white cell count was 17,250':cu.mm with the followin~ :khillinj!s ('ount: B·O, E-O, M-O, J-::I, St·3, Seg·BO, Ly.U, Mo·O. The amylase was 112 units. The blood ~U)!UI' was 2·13 mg. ',. (The specimen was taken whilst ;J DSNSS infusion solution was l'unning through her vein). Total NPN was 38.5 Ill!!"'; with a creatinine of 1.7 mg'.;. The sel'urn total pI'l)tein was 6.85 I{l"nms ,; with a.3 gmms " of albumin and 3.S!", grams ,; of globulin. The liver function tests in· duded CCF . + + -, TTT - 14 units, TFT - + +, Alkaline phosphatase· o.B King and Armstron!!" units. A blood culture taken dUrin!!" this time did not grow any pathogen. The electrocardiogram was intel'pI'eted as: "sinus tach~'cardia, pulmonary hypoxia, biventl"icular enlal·gement. diffuse myocardial ischemia, and/or llIyocarditis. Associated hepatic and cel'ebrlll hypoxia have to bl' ruled out." The patient from this tillle on was digitalized and antibiotic thenlpy was instituted in the fOI'm of penicillin and streptomycin injections. The severe l"ight hypochondl"iac pain which radiated to the back, and the vomiting were controlled by Meperidine, atl'opine and chlorpromazine.
On the third hospital day, a pulnlOnary consultant remarked that the absence 01' little amount of ex, pe{"toration in spite of the X-ray picture suggestive of IlIleumonia was rathel' stl·iking. To diminish dead space, a tracheostomy was sugj!ested but was not done due to the failure to get a consent. She WIIS still febrile. Her blood pressure was 140/100. The abdominal pain still bothered her. A urinalysis done durin~ this time showed a specific gl"llVity of LOla. It was deep yellow in color, Albumin was plus I. The specimen was neg-ative for sugal", red blood (."ells, ('asts and crystals. Pus cells were found in the amount of 0 to 2 per low field. A follow up chest X-ray showed "a definite clearing of the infiltration especiall~' on the right thoracic cage." A fe("alysis showed ascaris ova; occult blood was negative,
On the foul·th hospital day, she was noted to ha\"(' ('eL'vical \'enous enj!OI'gement, She was still orthopneic and dyspneic. A venous preSSUI'e determination during this time showed a value of 220 mm. of water. The 1('Ucocyte l'ount was repeated and it went down a bit to 13 .. J:;0, cu. mm. with the following differential smellr: H·O, E·O, M·O, J ·0, St-1, Seg·84, 1.y.15, Mo·O. A Widal test was negative. 500 ('1' of compatihll' blood was transfused.
On the 5th day, the dyspnea and orthopnea remained. The intern heal'd crepitant l'ales at the right base with a pleural rub on the same al·ea. The gallop rhythm Ilel·sisted. Diuretic thenpy was instituted and 7.2 g"1'lIms of IIcetyisalicylic acid was given per Ol'em daily. A C·reactive pl'otein was positive. Blood pH was i.:ln. A sputum smear showed gram-negative bacilli
212
with few pus {"(,lis. The ('ulture grew out Aerobllcter
On the lith hospital day, maculopapulal' rashes de· veloped over the anterior abdominal wall. Aside from the right hypochondriac and costo·vel·tehl·al tender· ness, positive Rovsin's sign was elicited. Dul"ing this time, there was also rebound tenderness with muscle gual"(ling over the l"ight hypochondl"iac re!!"ion and ilial' Ul·~as. The possibility of psoas abscess or l'Uptured app~ndix was entertained. She was then afeb· rill' with a blood pressure of IGO/110, and a puisI' L'ate of 100 I)er lllinute. A gynecologic c\ea\"ance was sought during this time. The labin majol'a we\"e noted to be vel'Y edematous. Internal examinHtion was essentially ne!ruth'e. There was tendel"lless ovel' the right paral'ectal al'ea on rectal examination. The opinion of the examiner was that the patient was !!"yne· mlogically dear, Post-transfusion blood studies showed a hematocrit of 28 vols.';, hemoglobin of 9..1 )!1'alllS ,; and a leucocyte count of 16,(;00 per cU.mm.
Because of the alarmin!!" abdominHI complaints, u sUI'j!ical consult was made. On the 7th day, the sur· geon found right costo-vertebral and l"ight lowel quadrant tendel'ness and pain but no muscle guardinf:( 01' ril!"idity. Bowel sounds were norma\. The clinical ('onsidentions then included intestinal obstl'uction se· condary to ascaris bolus, mesenteric thromhosis, perinephl"ic abscess and acute appendicitis. Conserv· ative management in the form of antibiotics, :\nal· gesics and fluids was suggested. A repeat udnalysis done during this time showed a slightly turbid, deep yellow specimen, with plus two albuminuria, negative fOI' sugar, red blood cells, and cl·ystals. There were few pus cells, 0 to 1 per low power field. Granular ('ash were also seen, fl'om 0 to 1 per low power field.
On the Bth day, the patient's condition became worse The orthopnea and dyspnea became more severe. Shl' started expectcll'ating red fl'Othy material. A con· sultant during this time remarked that "the dyspnea rnd tachypnea is out of proportion to the pulmonary findings by physical examination which showed only basal crepitant rales. Cyanosis is also absent." The. blood pressure then was 170/100 with an irregulal"ly irregular pulse rate of 86 pel' minute. Respiration was fast and shallow with a rate of 44 to 00 pel' minute. Terminally, the intern-on-duty noted in the observation sheet "the patient is markedly dyspneic, gasping, respil'ation gradually becoming shallower until it ceased. Heart beats still fail·Jy audible but becoming fainter and slower, eventually the heart stopped."
Clinical Discussion
DR. YOLANDO Q, M, SULlT: This morning I am privileged to discuss a very fascinating and intriguing case which was seen by a wide array of residents and consultants, was heard by some of the best auscultatory ears in town,
YOLo 2. SER. 2, No.4
CLI!>:I("O-I'ATHO!.O(;[C C():-OH:[[~::-on'
in which the clinical impression~ ranu:ed from a collagen disease, to an ascaris bolus, to an ncute appendicitis. This will gh·e us an inkling of the problems which this patient pre~ented diagnostically and much more therapeutically. May I call on the radiologist for an~r
thing which might be of help?
DR. PRUDE:-';CIO AVENDANO: The first chest X-my wa~ taken' on admission (December 14th). It shows the trachea to be deviated to the right, probably this wa~ just positional. The lung field~ show a generalized hazine~s which is more prominent on the right side. Dne to this hazines~, the border~ of the heart cannot be delineated. Thi~ was interpreted as con~istent with bilateral pulmonary congestion, edema and bronchopneumonia; right pleural effusion. The second chest X-ray was t.aken 3 days later. The g-eneralized hazines~ has disappeared revealing nn apparently enlarged heart and just some residual haziness in the right base. The computed cardiothoracic ratio is 0.64. There is a wide right supra-hilar shadow, interpreted as a dilated superior vena cava. The third che~t X-ray. taken 2 days later shows again some generalized haziness, which was thought to be due to pulmonary congestion and edema. The sudden disappearance of this haziness ruled out H
bronchopneumonic process. All these three chest films were taken in the recumbent po~ition.
The plain abdomen shows no op~\que stones in the areas of the kidneys, ureters, and urinary bladder. The right kidney is smaller than the left by 1.7 cm. The edges of the li\'er and spleen are prominent.
DR. SULIT: Would you comment on the left main bronchus, please?
DR. AVENDANO: The left bronchus is uplifted. However, there are no other findings as straightening of the cardiac waistline to favor a mitral heart disease. Probably this uplifting may just be positional. The configuration of the heart is more left ventricular.
DR. SULIT: I am sure that there is an involvement of the heart, probably a pl"imary involvement either by way of a myocarditis: that the lun~s at one time or another were
APIIII.-Jl':-OE. 1966
im'olved-that this could be a primary or secondary involvement. It is very hard to think of a lesion in the lungs which disappeared in thl·ee day:,; and was back again t\VO days latel·. I would m;e this as an important clue in ruling out a lot of things whieh ShOlild otherwise be considered. The liver was probably involved particularly during her ho:,;pitalization at the F.E.V. Hospital, when she \vas jaundiced. The kidneys bothered me, although there was no evidence of renal insufficiency. The joints were incriminated at least by history. There was abdominal pain and tenderness which bothered the patient. We .are faced with the problem of multiple organ involvement-the heart, lungs, liwr, the intestines, the kidneys and the joints.
One of the major consideratiuns would b~
an infectious process. Tuberculosis should b(: considered especially in the Philippines. However, dne to the phantom lung lesion by X.my. this is ruled out. A subacute bacterial endocarditis has to be considered as the patient presented evidences of carditis with gallop rhythm. However, the blood culture waR negative though it has been reported that as much as 20~; of blood culture in proved case::: of endocarditis may be negative. done under the best conditions in the best institutions There was also paucity of evidences of renal involvement. True there was some albuminuria, but there were no red blood cells. Typhoid becomes a consideration \vith rashe:-; confined to the abdomen. But these rasheR were maculo-papular, not the typical rosespots in typhoid fever. Typhoid could pregem terminally as an l"Icute abdomen due to II perforated gut, might present some problem::: of myocarditis and pneumonitis due to toxemia or septicemia. However, the negative \Vidal test done beyond the second week of illnes:-; would eliminate this entity. An intestinai pm'asitism with oyerwhelming larval migl'atioll to the lungs must be mentioned bec.ause thh, is a CPC. Howe\'er, there was only minimal ascaris o\'a in the feces, so that it is not so tenable.
('auld this patient at this young age of 18 have a diffuse carcinomatosis? If so, where was the primary fOCllS? There was nothing
213
ACTA ;\h:IlH'A Pllll.IPPI:->A
to incriminate a carcinoma either of the stomach, liver, and certainly not the lunl!s with the phantom X-ray lesion,
The rule in medicine is-if there is a vague ('ase with fe\'er, malaise. a slow but pl'ol!ressiye deteriomtion, one is safe with the diagnosis of a ,'ague clinical entity known as collagen diseuse. Could this be rheumatic fever? A earclitis is computible, The pneumonitis-mayhe, The episodes of pulmonary edema could be secondary to left-sided failure, The performance of- a throat swab and anti-streptolysin 0 titel' determination might have helped us in this aspect. The ECG did not show sil!ns of actiyit;r of rheumatic carditis.
('ould this be sy::;temic lupus erythematosus? The mshes are there, though they are on 1 he abdomen and not on the face. The carditis is compatible. Howeyel', in a patient with systemic lupus erythematoslIs, dying in a period of 41:! months. a more disturbing involvement of the kidney is usually present. This patient's exeretory function was apparently all right, The blood non-protein nitrogen, though done only once was 38 mg',,;. The blood pH and CO, combining power were within normal. So It metabolic acidosis-a renal death was out of the picture. Death was probably cardiac; this may be the mode of exit but is usuall}, rare in lupus erythematosus.
Could this be one of those rare systemic I'heumatoid disease , .... ith interstitial pulmonary fibrosis? I don't think so, based again on the phantom lesion on X-my. This usually involves a problem of pel'sistent, progressive respiratory h-act symptoms, especially cough and ha~ permanent lesions.
Could this be a polyarteritis nodosa? Recently, the British Council on Collagen Diseases and Hypersensiti\'ity States recommended th.lt polyartedtis nodosa (PA~) should be divided into two groups; those , ... ithout lung involvement and those with lung involvement. Clinically, those ,vithout lung invoh'ement consillt 2/3 of all casel' of polyarteritis nodosa and has a 3:1 sex ratio in fa"or of males. Patients under this group, however, invariably at one time 01' .another have a history of an acute upper respiratory tract infection or a pneumonitis. Later the true picture of PAN becomes
21~
manifest by way of hypertension and the patient may classically die in uremia or in se,'ere hypertensive state.
The second group, those with lung findings l'on!lists of 1/3 of all cases of PAK, There nrc few case reports of this type. The authors claim that this is more common in the 4th and 5th decudes of life; this is characterized by a rapid, progressi\'e course within months, lIslmlly presenting as a chronic respiratory problem, The pulmonary lesions that have been reported are those called by various names-'Vagener's gmnulomatosis, Loeffler's lesion, etc. It is manifested as II chronic respiratory disease, not infrequently characterized by asthma, occasional hemoptysis, with fever im'ariably, and almost always with eosinophilia. The differential count of this patient on two oceasions did not show any eosinophilia.
It is very inviting to make a diagnosis of 'PAK in this case. There was a progressively mild though persistent hypertension. It was possible the phantom lesion in the lungs was due to episodes of left-sided failure-the regimen of diuretics, digitalis, and rest could have mobilized this pulmonary edema, only to recur. Therefore, PAN without Wagener's granulomatosis is a very pertinent consideration in this case.
The last entity I will consider is a myxom.a. Some would consider thill a neoplasm-constituting 50~,; of all primary heart tumors. Some think this is just a pseudo-tumor, that these are thrombi in various stages of organization. In Husten's series of 86 myxomas, the left atrium was involved in 71. the right Huricle in 9, the right ventricle in 3, and the left ventricle in 3. Majority of myxomas are not diagnosed clinically; they present perplexing cardiac cases of intermittent mitrul block, associated with position, resulting in intermittent pulmonary edema, This is due to a ballvalve obstruction. Hemodynamically. they are akin to mitral stenosis. Before I say that this is probably a case of myxoma, may I voice some disturbing thoughts? Allide from my interpretation of probable left atrial hypertrophy, and insinuation radiologically of a probable uplifting of the left main bronchus, there was nothing significant auscultotal'ywise.
VOl .. 2. S£R. 2, No.4
CI.I~I('O_PATHOJ.OG](" CONn:RENn:
Of course, this i!l not unu!lllal in n patient with an acute overloading of the right ventricle secondary to an acute plugging of the mitral valve. One may not hear the classical murmurs of stenosis. In fact this patient presented findings more classic of myocarditis. However, a left atrial myxoma could explain the disappearance and recurrence of pulmonary edema. The episode of severe abdominal pains in the terminal stay of the patient-a pictllre of acute abdomen was probably due to embolism in the mesenteric vessels, with pos!lible gangrene of the intestines.
My fir!lt conRideration therefore i!l a left atrial myxoma. 1 cannot definitely rule out a polyarteritis nodosa. If this was PAN, the ves~el!\ im'olved would be the coronarieg, the hep:ltk, splenic, mesenteric and perhap!l the I'enal arteries.
DR. ELIAS S. IMPERIAL: The discus!lant of any epc is limited with the data he has in the protocol. Dr. Sulit ascribed the on and off pulmonary changes to edema. But if he !law this patient as I saw her on the morning of death-she was quite tachypneic, was really in respiratory embarrassment, so I considered the possibility of acido!lis at that time. I a!lked Dr. Rorromeo to do certain laboratory tests which probably were not performed as the patient was quite deteriorating. Dr. Sulit ha!l referred to the tests which were done three days before death in trying to minimize the in\'olvement of the kidneys, which would not be quite rational.
DR. BENJAMIN D. C'ANLAS, JR.: According to the abstl'acted protocol, the patient became more orthopneic and dyspneic on the 8th hospital (lay and !ltarted expectorating red frothy material. I thought thi!l wa!l very suggestive of pulmon.ary edema.
DR. ESTE~AN PINEDA: The history stated that since about fOlll' months or RO priOl' to admi!lsion the patient had already perRistent abdominal pain, related to food intake, and of such a severity requiring her to double up. Do you think she was already having embolism at that time?
DR. SULIT: I am seriously considering an embolic phenomE!non in thE" mesenteric ve~sell'"
APRlJ.·JV~E, HHi6
to explain the condition on the 7th hospital day, when there were llnque~tionable ~igns
of an ucute abdomen by way of severe pain and tenderness. It is probable that the abdominal pains in the past were due to small emboli of terminal mesenteric arteries, not significantly occluding a major vessel as to cause gangrene. These have caused insufficiency of blood flow to the segments of intestines, causing intestinal angina. The pain is aggravated after meals since the demand for blood is relatively greater at these times.
DR. RAMON DE JESUS: I saw this patient with one of our residents. The !\triking finding at that time was a right lumbn.r tendernes!l. Dr. BOiTomeo suspected this case to be one of the collagen diseases, probably rheumati{' heart diseuse. Foremost consideration therefore in this light, together with leucocytosi!l and fe\'er were showers of mycotic emboli to the right kidney. The possibility of acute appendicitis was al!\o entertained. However, as this case wus followed up, I was not so impressed of its being a I'eal surgical abdomen.
DR. ANDRES MAKALiNAO: When I was called, o"!e of the complaints was abdominal pain and the patient was jaundiced. However, I was more impressed of this case being more of a cardio-pulmonary pathology. Because the patient was also anemic, we were considering rheumatic heart with subacute bacterial endocarditis. At th~lt time we did not know that the patient was hypertensive, which of course can not be explained by a rheumatic heart disease.
Clinical Diagnosis
Rhellmatic Heart Disease with myocarditis; pulmonary edema. ?Acl1te appendicitis or perinephric abscess.
Dr. Sulit's Diagnosis
Left atl'ial myxoma; pulmonary edema; embolism to mesenteric arteries. ?Polyarteriti~
nodosa.
Pathologic Discussion
DR. RgNJAMIN D. CANLAS, JR.: When the body was opened, there was bilateral hydrotho-
215
A('TA MEDI('A PHIUPPISA
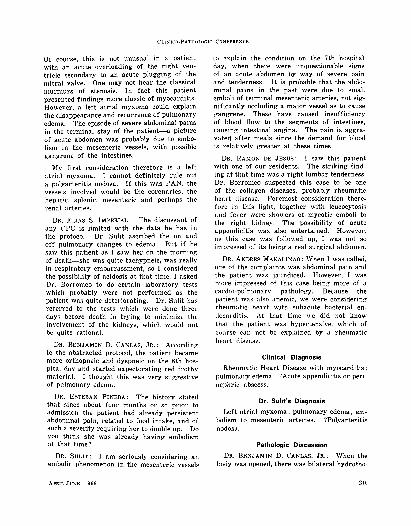
Figure 1. Cross section of a medium sized renal artery with markedly thick fibrotic wall with some lymphocytes. The lumen is almost occluded. This is a chronic lesion of PAN.
rax. :200 cc. in the right and 100 cc. of strawcolored fluid in th€ left pleural cavities. Minimal pleural adhe~ions were in the right side. The lungs were heavy and indurated. The j..!.TOf>S appearance suggested edema, congestion, as well as bronchopneumonia. The heart was enlarged \\"ith a weight of 330 grams. The enlargement was mainly due to a left ventrkular hypertrophy, which sug-gested that the hrperten~ion of the patient was quite of ;\ fairly long (Juration. The valvular orifices were normal and no scarrings were noted in any of the leaflets. There were nodulations aIOl!g" both left and right coronaries, which "'ere firm. some showing hemorrhagic discolorations. On cross-sections of these nodules of the l"oronarie~, the lumina were found to be narrowed 01' almost completely obliterated. The myocardium, however, showed no eYidence of infardion gTossly. No myxoma was preso:!nt. There were no congenital anomalies.
The kidneys were normal in size. On stripping off the capsule, the cortical surfaces were characterized by red depressed areas and . ";lI1TOlmding non-depressed pale areas. On cut sections. nodulations and luminal narrowing of the medium-sized branchefl of the renal al·teries were revealed. The depressed red areas were further verified to be multiplc- infarcts of quite recent nature. Based on these large and multiple infarcts of both kidney);, it would be consistent to expect an
2Ui
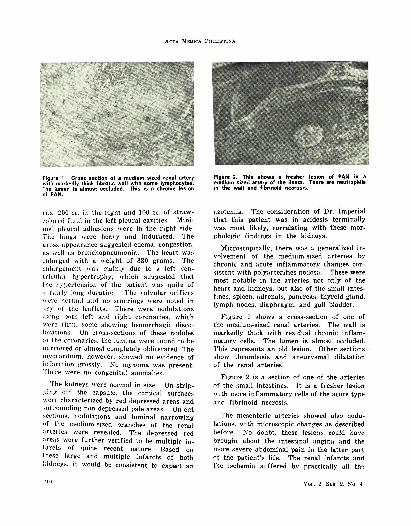
Figure 2. This shows a fresher lesion of PAN In a medium sized artery of the ileum. There are neutrophlls in the wall and fibrinoid necrosIs.
azotemia. The consideration of Dr. Imperial that this patient was in acidosis terminally
. was most likely, correlating with these morphologic findings in the kidneys.
:'iicroscopically, there was a generalized inyolvement of the medium-sized arteries by chronic and acute inflammatory changes consistent with polyarterities nodosa. These were most notable in the arteries not only of the heart and kidneys, but also of the small intestines, spleen, adrenals, pancreas, thyroid gland, lymph nodes, diaphragm, and gall bladder.
Figure 1 shows a cross-section of one of the medium-sized renal arteries. The wall is markedly thick with residual chronic inflammatory cells. The lumen is almost occluded. This represents an old lesion. Other sections show thrombosis and aneurysmal dilatation of the renal arteries.
Figure 2 is a section of one of the arteries of the small intestines. It is a fresher le~ion with more inflammatory cells of the acute type and fibrinoid necrosis .
The meflenteric arteries showed also nodulations. with microscopic changes as described before. :t\'o doubt, these lesio:ls could have brought about the intestinal angina and the more severe abdominal pain in the latter part of the patient's life. The renal infarcts and the ischemLa suffered by practically all th~··
\'01.. 2 SEM 2. ~o. "
CLI/>;ICO-PATHOI.OGIC C(l~rErn::-<n:
organs in the abdominal cavity could have contributed to the abdominal pain.
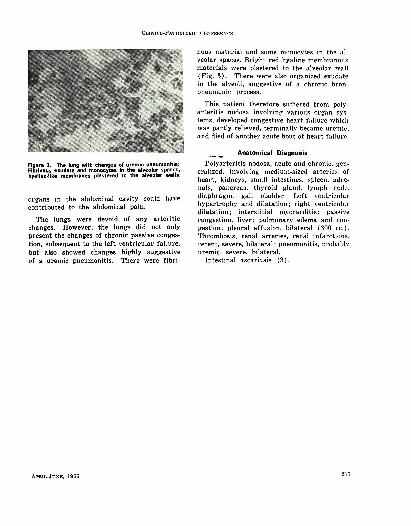
The lungs were devoid of any arteritic changes. However. the lungs did not only present the changes of chronic passive congestion. subsequent to the left ventricular failure, but also showed changes highly suggestive of a uremic pneumonitis. There were fibri-
A PRIL-JUNE, 1966
notH; material <lnd some monocytes in the alveolar spaces. Bright red hyaline membranolls materials were plastered to the alveolar 'wall (Fig. 3). There were also organized exudate in the alveoli, suggestive of a chronic bronpneumonic process.
This patient therefore suffered from polyarteritis nodosa involving various organ systems, developed congestive heart f.ailure which was partiy relieved, terminally became uremic. and died of another acute bout of heart failure.
Anatomical Diagnosis
Polyarteritis nodosa. acute and chronic, generalized, involving medium-sized arteries of heart. kidneys, small intestines, spleen. adrena1s. pancreas, thyroid gland. lymph node. diaphragm, gall bladder. Left ventricular hypertrophy and dilatation; right ventricular dilatation; interstitial myocarditis; passive congestion. liver; pulmonary edema and congestion; pleural effusion. bilateral (300 cc.). Thrombosis. renal arteries, renal infarctions. recent, severe, bilateral; pneumonitis. pl'ob<.lbl.\· uremic, severe, bilateral.
Intestinal ascariasis (3).
217