
Clinical Usefulness of Urine-based Enzyme-linked Immunosorbent Assay for Detection of Antibody to...
11
Volume 5 • Number 2 • 2000 HELICOBACTER © Blackwell Science, Inc. 1083-4389/00/$15.00/109 109–119 109 Clinical Usefulness of Urine-based Enzyme-linked Immunosorbent Assay for Detection of Antibody to Helicobacter pylori: A Collaborative Study in Nine Medical Institutions in Japan Mototsugu Kato,* Masahiro Asaka,* Masao Saito, † Hitoshi Sekine, ‡ Shuichi Ohara, ‡ Takayoshi Toyota, ‡ Taiji Akamatsu, § Taimei Kaneko,** Kendo Kiyosawa,** Osamu Nishizawa, †† Toshiko Kumagai, ‡‡ Tsutomu Katsuyama, ‡‡ Masahiro Abe, §§ Masaaki Kosaka, §§ Shojiro Hariya,*** Kunihiro Minami, ††† Yasuhiro Sanai, ‡‡‡ Masayuki Sawamura, §§§ and Tetsuya Tachikawa**** *Third Department of Internal Medicine, Hokkaido University School of Medicine, Sapporo; † Department of Digestive Tract Medicine, Sapporo Hokuyu Hospital; ‡ Third Department of Internal Medicine, Tohoku University School of Medicine, Sendai; § Endoscopy Unit, **Second Department of Internal Medicine, †† Department of Urology, ‡‡ Clinical Laboratory, Shinshu University School of Medicine, Matsumoto; §§ First Department of Internal Medicine, Tokushima University School of Medicine, Tokushima; ***Hokkaido Prefectural Faculty Examination Center, Sapporo; ††† Department of Obstetrics and Gynecology, Sapporo Toho Hospital, Sapporo; ‡‡‡ Department of Obstetrics and Gynecology, Keiai Hospital, Obihiro; §§§ Shinjuku Sakura Urology Clinic, Tokyo; and ****Department of Diagnostic ABSTRACT Reagents, Otsuka Pharmaceutical Co., Ltd., Tokushima Background. A urine-based enzyme-linked immunosor- bent assay (ELISA) kit for detection of antibody to Helicobacter pylori has been developed in Japan. Urine samples can be obtained noninvasively and are easier and safer to handle than are serum samples. The aim of this study was to examine the clinical usefulness of this urine-based ELISA kit. Materials and Methods. A pair of random, single-void urine and serum samples was collected from each of 1,061 subjects, including 238 patients with gastro- duodenal disease. The sensitivity and specificity of the urine-based ELISA was compared with those of three commercially available serum-based ELISA kits. For those patients with gastroduodenal disease, the urine- and serum-based ELISA results were also compared with those for other diagnostic methods using endo- scopic biopsy specimens, such as culture, histology, and rapid urease tests. Results. Based on the three serum-based ELISA results, the sensitivity, specificity, and accuracy of the urine-based ELISA were 97.7%, 95.6%, and 96.8%, respectively. On the basis of the biopsy test results, the sensitivity (96.2%), specificity (78.9%), and accuracy (91.0%) of the urine-based ELISA were almost equivalent or supe- rior to all three serum-based ELISAs tested. In addition, 10 of the 12 false-positive cases for urine-based ELISA were confirmed to be true positives for antibodies to H. pylori by Western blot analysis and inhibition ELISA. Conclusions. The urine-based ELISA (URINELISA H. pylori Antibody) is very accurate and should be useful as an alternative to serum-based ELISAs for screening of H. pylori infection. H elicobacter pylori, a gram-negative bacte- rium, was first identified by Warren and Marshall in 1983 [1]. H. pylori infects the gastric mucosa in humans and plays important roles in development of gastritis, peptic ulcer, gastric can- cer, and gastric mucosa-associated lymphoid tis- sue (MALT) lymphoma [2–5]. Methods of sample collection for detection of H. pylori infection can be classified into those that are invasive (e.g., mi- crobiological culture observation [culture], histo- logical observation [histology], and rapid urease test [RUT]) [6] and those that are noninvasive (i.e., serological test and urea breath test [UBT]) [7,8]. Diagnostic methods can also be classified as direct methods (culture and histology) for detect- ing H. pylori itself and indirect methods for de- tecting the urease activity derived from H. pylori (RUT and UBT) or for detecting antibody to H. pylori (serological test). The invasive methods re- quire endoscopy and gastric biopsy and are also focal tests of biopsy specimens. The 13 C-labeled UBT ( 13 C-UBT)is a safe in vivo diagnostic method and is considered the most accurate method for di- agnosing H. pylori [8,9]. However, 13 C-UBT is dif- Reprint requests to: Dr. Tetsuya Tachikawa, Department of Diagnostic Reagents, Otsuka Pharmaceutical Co. Ltd., 463–10 Kagasuno Kawauchi-cho, Tokushima 771–0192 Japan. E-mail: [email protected]
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Clinical Usefulness of Urine-based Enzyme-linked Immunosorbent Assay for Detection of Antibody to...

Volume 5 • Number 2 • 2000HELICOBACTER
© Blackwell Science, Inc. 1083-4389/00/$15.00/109 109–119
109
Clinical Usefulness of Urine-based Enzyme-linked Immunosorbent Assay for Detection of Antibody to Helicobacter pylori: A Collaborative Study in Nine Medical Institutions in Japan
Mototsugu Kato,* Masahiro Asaka,* Masao Saito,
†
Hitoshi Sekine,
‡
Shuichi Ohara,
‡
Takayoshi Toyota,
‡
Taiji Akamatsu,
§
Taimei Kaneko,** Kendo Kiyosawa,** Osamu Nishizawa,
††
Toshiko Kumagai,
‡‡
Tsutomu Katsuyama,
‡‡
Masahiro Abe,
§§
Masaaki Kosaka,
§§
Shojiro Hariya,*** Kunihiro Minami,
†††
Yasuhiro Sanai,
‡‡‡
Masayuki Sawamura,
§§§
and Tetsuya Tachikawa****
*Third Department of Internal Medicine, Hokkaido University School of Medicine, Sapporo;
†
Department of Digestive Tract Medicine, Sapporo Hokuyu Hospital;
‡
Third Department of Internal Medicine, Tohoku University School of Medicine, Sendai;
§
Endoscopy Unit, **Second Department of Internal Medicine,
††
Department of Urology,
‡‡
Clinical Laboratory, Shinshu University School of Medicine, Matsumoto;
§§
First Department of Internal Medicine, Tokushima University School of Medicine, Tokushima; ***Hokkaido Prefectural Faculty Examination Center, Sapporo;
†††
Department of Obstetrics and Gynecology, Sapporo Toho Hospital, Sapporo;
‡‡‡
Department of Obstetrics and Gynecology, Keiai Hospital, Obihiro;
§§§
Shinjuku Sakura Urology Clinic, Tokyo; and ****Department of Diagnostic
A B S T R A C T
Reagents, Otsuka Pharmaceutical Co., Ltd., Tokushima
Background.
A urine-based enzyme-linked immunosor-bent assay (ELISA) kit for detection of antibody to
Helicobacter pylori
has been developed in Japan. Urinesamples can be obtained noninvasively and are easierand safer to handle than are serum samples. The aim ofthis study was to examine the clinical usefulness of thisurine-based ELISA kit.
Materials and Methods.
A pair of random, single-voidurine and serum samples was collected from each of1,061 subjects, including 238 patients with gastro-duodenal disease. The sensitivity and specificity of theurine-based ELISA was compared with those of threecommercially available serum-based ELISA kits. Forthose patients with gastroduodenal disease, the urine-and serum-based ELISA results were also comparedwith those for other diagnostic methods using endo-
scopic biopsy specimens, such as culture, histology, andrapid urease tests.
Results.
Based on the three serum-based ELISA results,the sensitivity, specificity, and accuracy of the urine-basedELISA were 97.7%, 95.6%, and 96.8%, respectively.On the basis of the biopsy test results, the sensitivity(96.2%), specificity (78.9%), and accuracy (91.0%) ofthe urine-based ELISA were almost equivalent or supe-rior to all three serum-based ELISAs tested. In addition,10 of the 12 false-positive cases for urine-based ELISAwere confirmed to be true positives for antibodies to
H.pylori
by Western blot analysis and inhibition ELISA.
Conclusions.
The urine-based ELISA (URINELISA
H.pylori
Antibody) is very accurate and should be usefulas an alternative to serum-based ELISAs for screeningof
H. pylori
infection.
H
elicobacter pylori
, a gram-negative bacte-rium, was first identified by Warren and
Marshall in 1983 [1].
H. pylori
infects the gastricmucosa in humans and plays important roles indevelopment of gastritis, peptic ulcer, gastric can-cer, and gastric mucosa-associated lymphoid tis-sue (MALT) lymphoma [2–5]. Methods of samplecollection for detection of
H. pylori
infection canbe classified into those that are
invasive
(e.g., mi-crobiological culture observation [culture], histo-
logical observation [histology], and rapid ureasetest [RUT]) [6] and those that are
noninvasive
(i.e., serological test and urea breath test [UBT])[7,8]. Diagnostic methods can also be classified as
direct
methods (culture and histology) for detect-ing
H. pylori
itself and
indirect
methods for de-tecting the urease activity derived from
H. pylori
(RUT and UBT) or for detecting antibody to
H.pylori
(serological test). The invasive methods re-quire endoscopy and gastric biopsy and are alsofocal tests of biopsy specimens. The
13
C-labeledUBT (
13
C-UBT)is a safe in vivo diagnostic methodand is considered the most accurate method for di-agnosing
H. pylori
[8,9]. However,
13
C-UBT is dif-
Reprint requests to:
Dr. Tetsuya Tachikawa, Departmentof Diagnostic Reagents, Otsuka Pharmaceutical Co. Ltd.,463–10 Kagasuno Kawauchi-cho, Tokushima 771–0192Japan. E-mail: [email protected]

110
Kato et al.
ficult to use for screening of large populations,since the sample collection procedure required issomewhat complicated and
13
C-labeled urea is notinexpensive. The enzyme-linked immunosorbentassay (ELISA) method has been widely used fordetection of
H. pylori
infection and is useful forscreening and epidemiological investigations [10],owing to its cost-effectiveness.
It has been reported that antibodies to
H. pylori
are present in saliva [11–14] and urine [15–17] aswell as in serum, and detection of the antibodieshas been demonstrated to be useful for diagnosisof
H. pylori
infection. In a preliminary study, theurine-based ELISA kit (URINELISA
H. pylori
An-tibody: Otsuka Pharmaceuticals, Tokyo, Japan),which was employed in our clinical study, exhib-ited excellent sensitivity (99%) and specificity(100%) with the assumption that
13
C-UBT resultswere 100% accurate [17]. To examine the clinicalusefulness of this urine-based ELISA kit, our clini-cal study was conducted in multiple centers with alarge number of patients having various diseases(e.g., gastroduodenal diseases) and with pregnantwomen and healthy subjects.
Materials and Methods
Subjects
This study was performed from April 1, 1997, toFebruary 27, 1998, with written informed consentobtained from all the subjects prior to initiation.The total number of subjects was 1,061: 455 healthysubjects; 238 patients who had gastroduodenaldisease but had not undergone antibacterial eradi-cation therapy and had not received any antibiot-ics or proton pump inhibitors for other reasonsduring a 4-week period prior to endoscopic exam-ination; 93 patients with urogenital disease; 65 pa-tients with diabetes; 55 patients with hepatitis; 52pregnant women; 31 patients with autoimmunedisease; and 72 patients with various other dis-eases.
Samples
A pair of random single-void urine samples (50ml) and serum samples (2 ml) was obtained fromeach subject. Sodium azide (0.1 wt/vol percentageat final concentration) was added to the urinesamples, which then were stored at 2
8
to 8
8
C, andthe serum samples were stored at
2
20
8
C until use.
Reagents
To examine interference with assay performanceby substances possibly present in urine, the fol-
lowing substances were obtained or prepared:creatine, creatinine, acetone, L-cystine, L-leucine, cal-cium oxalate, D-glucose, urea, 5-aminolevulinic acid,L-ascorbic acid, uric acid, acetylsalicylic acid, ace-taminophen, caffeine, and sodium chloride (allpurchased from Wako Pure Chemicals, Osaka, Ja-pan). 3-Hydroxybutyric acid, norephedrine, andatropine were obtained from Aldrich (Milwaukee,WI). Human serum albumin, hemoglobin, andurobilin were obtained from Sigma (St. Louis, MO).Hemoglobin and bilirubin (free and conjugated)were obtained from Kokusai-Shiyaku (Kobe, Japan),myoglobin came from Oriental Yeast (Shiga, Japan),and mucoprotein came from Otsuka Pharmaceuti-cals. The
g
-globulin used for this study was puri-fied by affinity chromatography using protein Agel (Repligen, Cambridge, MA) from serum ob-tained from an
H. pylori
–negative subject.
Escher-ichia coli
–extracted proteins were prepared ac-cording to the method described previously [17].
ELISA Method for Urinary Antibody to H. pylori
Urinary antibodies to
H. pylori
were determinedusing the URINELISA
H. pylori
Antibody (Ot-suka Pharmaceuticals). The assay protocol was de-scribed previously [17]. Briefly, 25
m
l of 0.2 M TRIS(hydroxymethyl) aminomethane chloride buffer(pH 7.3), containing 0.14 M sodium chloride, 2%casein, 0.5% bovine serum albumin (SeikagakuKogyo, Tokyo, Japan), 0.05% Tween 20, 0.001%
E. coli
–extracted proteins, and 0.1% sodium azide,and 100
m
l of urine samples were incubated on
H.pylori
antigen–coated plates at 37
8
C for 1 hour.The plates then were rinsed with Dulbecco’s phos-phate-buffered saline (pH 7.0) containing 0.05%Tween 20 (PBST) and were incubated with 100
m
lof horseradish peroxidase (HRP)–conjugated anti-human IgG (Jackson, West Grove, PA) at 37
8
C for 1hour. The plates were rinsed with PBST and incu-bated with 100
m
l of substrate solution containing3,3
9
,5,5
9
-tetramethylbenzidine (TMB: Scytek Lab-oratories, Logan, UT) at room temperature for 15minutes for color development. The reaction wasstopped by adding 100
m
l of stop solution forTMB. Optical density (OD) was measured at 450nm using a plate reader (at 650 nm as a reference).Cutoff index was calculated by the formula—ab-sorbance of sample tested/cutoff value in each as-say—and used for evaluation of the examinationsin this study.
Preparation of Control Samples
To evaluate reproducibility of results obtained withthe urine-based ELISA kit, the following control
Usefulness of Urine-Based ELISA for
H. pylori
111
samples were prepared. Phosphate-buffered salinecontaining 0.1% bovine serum albumin (BSA) and0.1% sodium azide was used as a negative control(N-control). Serum samples positive for
H. pylori
were collected and pooled with sodium azide at afinal concentration of 0.1%, and the samples werestored at
2
80
8
C. The pooled serum was dilutedwith N-control (approximately 1 : 20,000) to pre-pare a strong positive control (H-control) andthen diluted three more times with N-control toprepare a weak positive control (L-control). Allthe controls were aliquoted (2 ml, each tube) andstored at
2
80
8
C until use.
Interfering Substances
To examine interference by substances possiblypresent in urine, various substances were added tothree positive and three negative urine specimensat different concentrations and assayed with theurine-based ELISA kit, with the exception that
g
-globulin purified from a subject negative for
H.pylori
was added only to a negative urine sampleat different concentrations. The maximum con-centrations of substances added to the urine sam-ples are shown in Table 1.
ELISA Method for Serum Antibody to H. pylori
Anti–
H. pylori
antibodies in serum were measuredusing the manufacturer’s instructions, with threecommercially available kits: (1) the HM-CAP kit(HM-CAP) named the DETERMINER
H. pylori
antibody in Japan (Enteric Products, West Burg,NY); (2) the HEL-p TEST kit (HEL-p), namedthe Sumai Test ELISA [Helicobacter] in Japan(AMRAD Biotech, Victoria, Australia); and (3)the GAP-G kit (GAP-G), named the Pylica-plate GHelicobacter II in Japan (Biomerica, NewportBeach, CA). Each assay result was assigned to apositive, negative, or indeterminate group accord-ing to kit instructions.
Overall Assessment Criteria for the Serum Antibody Assays
All subjects were classified into three groups: anoverall serum antibody–positive group, an overallserum antibody–negative group, and an overall se-rum antibody–indeterminate group, in accordancewith the overall assessment criteria for the serumantibody assays. The criteria were as follows: Theoverall serum antibody–positive group (n
5
549)was composed of subjects who were positive for atleast two of the three serum ELISAs (HM-CAP,
HEL-p, and GAP-G). The overall serum antibody–negative group (n
5
404) was composed of sub-jects who were negative for at least two of thethree serum ELISAs. The overall serum antibody-indeterminate group (n
5
108) was composed ofall other subjects, and the subjects in this groupwere excluded from the analysis on the basis ofthe overall assessment for the serum antibody as-says.
Methods of Biopsy Diagnosis
Culture, RUT, and histological tests were per-formed using endoscopic biopsy specimens ob-tained from the greater curvature of the antrum orthe body of the stomach from the patients withgastroduodenal disease. These tests were performedby standard protocols that have been adopted ineach participating institution.
Overall Assessment Criteria for Biopsy Diagnostic Tests
The patients with gastroduodenal disease wereclassified into three groups: an overall biopsytests–positive group, an overall biopsy tests–nega-
Table 1
Materials added to urine
Materials added Maximum concentration added
Human serum 1.0 vol/vol
a
Human serum albumin 1,000 mg/dlHuman
g
-globulin 10,000
m
g/dl
b
Mucoprotein 80 mg/dlHemoglobin 1.0 mg/dlMyoglobin 10
m
g/dl
b
2
-microglobin 270
m
g/dlCreatine 130 mg/dlCreatinine 1.0 gm/dlFree bilirubin 22.7 mg/dlConjugated bilirubin 18.8 mg/dlUrobilin 10.0 mg/mlAcetone 5.0 mg/dll-Cystine 180
m
mol/dll-Leucine 73
m
mol/dlCalcium oxalate 24 mg/dld-Glucose 1,000 mg/dlUrea 280 mmol/dl3-Hydroxybutyric acid 0.1 mmol/dl5-Aminolevulinic acid 1.87 mg/dll-Ascorbic acid 10 mg/dlUric acid 400 mg/dlAcetylsalicylic acid 20 mg/dlAcetaminophen 20 mg/dlCaffeine 20 mg/dlNorephedrine 20 mg/dlAtropine 20 mg/dlSodium chloride 1.5 gm/dl
a
Negative specimens determined to be positive at the concentrationof 1.0 vol/vol.
b
Negative specimens determined to be positive at the concentrationof 3000
m
g/dl.
112
Kato et al.
tive group, and an overall biopsy tests–indetermi-nate group, in accordance with the overall assess-ment criteria for biopsy diagnostic tests established,referring to the guidelines for clinical study of H.pylori of the Food and Drug Administration(FDA) [18] (with some modifications). The crite-ria were as follows: The overall biopsy tests–posi-tive group was composed of subjects who werepositive for culture, subjects who were negativefor culture but positive for both histology andRUT, and subjects who did not undergo culturetesting but who were positive for both histologyand RUT. The overall biopsy tests–negative groupwas composed of subjects who were tested with atleast two biopsy methods and were negative for allthe biopsy methods tested. The overall biopsytests–indeterminate group was composed of allother subjects and was excluded from the follow-ing analysis.
SDS-PAGE and Western Blot AnalysisBriefly, 100 ml of sample solution, including 100mg of H. pylori extract, was separated by sodiumdodecyl sulfate–polyacrylamide gel electrophoresis(SDS-PAGE) using a gradient gel (10%–20%; Bio-Clafuto, Tokyo, Japan). The proteins that under-went electrophoresis in the gel then were electropho-retically transferred to a nitrocellulose membrane(0.45 mm) for 4 hours. The membrane was cutinto 16 strips and blocked with 5% skim milk(Wako Pure Chemicals) for 4 hours at room tem-perature. Each strip was washed with PBST (pH7.4) and was incubated overnight with 0.5 ml ofurine samples with 0.5 ml of the assay buffer forthe urinary ELISA kit on a shaker at room temper-ature. The membrane was then washed five timeswith PBST and incubated with HRP-conjugatedantihuman IgG (Fc) goat antibody in the diluentfor HRP conjugates in the urinary ELISA kit for 2hours at room temperature. The membrane waswashed with PBST five times, and HRP activitybound on the membrane was detected with 4-chloro-1-naphthol (Wako Pure Chemicals).
Inhibition ELISA MethodTo examine the specificity of positive results on uri-nary ELISA, urine samples were assayed with reac-tion buffer containing H. pylori–extracted antigens(50 mg/well) or the extraction buffer as a control,according to the assay protocol for URINELISA,to inhibit specific antibodies to H. pylori in thesamples.
Results
ReproducibilityUsing three control samples (N-, L-, and H-con-trols), the reproducibility of the urine-based ELISAkit on the same day (n 5 5), on different days (n 55), with different operators (n 5 5), and for differ-ent lots of manufacture (n 5 4) were examined(Table 2). Each of the tests showed excellent re-producibility (less than 11%) except for reproduc-ibility on the same day using N-control.
To examine reproducibility for different sites oftesting, 10 negative and 15 positive urine speci-mens were assayed blind in four institutions. Com-plete agreement on test results (positive or nega-tive) was obtained among the four institutions(data not shown).
Effects on Interfering SubstancesAs shown in Table 1, none of the substances excepthuman serum and g-globulin affected assay perfor-mance. However, human serum and the g-globulinaffected the assay results at final concentrations of1.0 vol/vol and 3 mg/dl, respectively, with nega-tive specimens determined to be positive (false-positive; data not shown).
Stability of Urinary AntibodyStability of urinary H. pylori antibodies againstfreezing and thawing cycles and heat treatmentwas examined using three positive and three nega-tive urine specimens. Urinary H. pylori antibodieswere stable against at least five cycles (nonsignifi-cance by Friedman test) and heat treatment at 56–768C for 30 minutes (nonsignificance by Wilcoxonsigned-rank test). In addition, no significant differ-ence was observed between mixed urine samplesand the supernatant after centrifugation at 3,000
Table 2 Reproducibility of urine-based enzyme-linked immunosorbent assay (ELISA)
Reproducibility No. N-control L-control H-control
On the same day 5 Mean 0.044 3.575 8.908SD 0.013 0.274 0.577
CV (%) 29.4 7.6 6.5On different days 5 Mean 0.042 3.492 8.413
SD 0.004 0.097 0.872CV (%) 9.6 2.8 10.4
With different operators
5 Mean 0.034 3.648 9.193SD 0.003 0.169 0.158
CV (%) 7.8 4.6 1.74 Mean 0.035 3.468 8.543
For different lots of manufacture
SD 0.001 0.167 0.22CV (%) 3.6 4.8 2.6
N, negative; L, weak positive; H, strong positive; SD, standard deviation; CV,coefficient of valiation.

Usefulness of Urine-Based ELISA for H. pylori 113
rpm for 15 minutes to remove crystals (nonsignifi-cance by Wilcoxon signed-rank test).
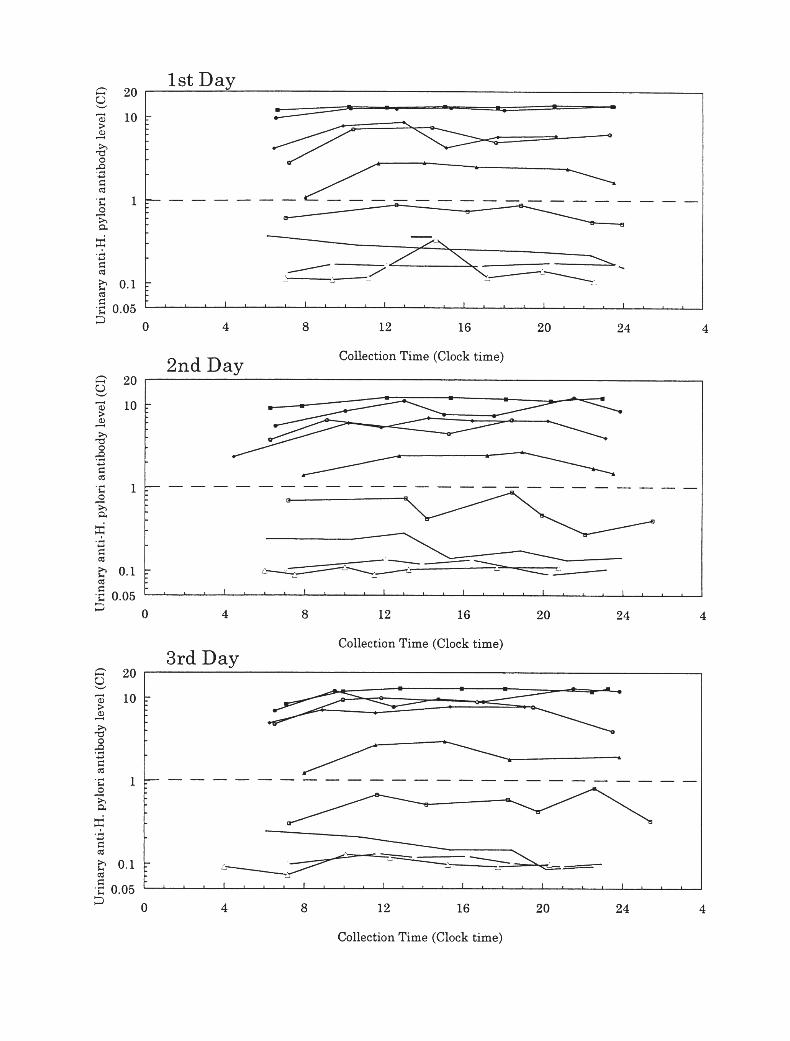
Variations in Urinary Antibody Activity to H. pylori During One Day and on Different DaysAll the random single-void urine samples obtainedduring one day were collected from nine healthyvolunteers (five positive and four negative for anti–H. pylori antibody) and assayed with the urine-based ELISA kit. This examination was repeatedtwice on different days using the same volunteers.All the urine samples collected during the 3 dayswere determined as, respectively, positive or nega-tive (Fig. 1). These findings indicate that randomsingle-void urine samples can be used to detecturinary antibody to H. pylori.
Establishment of Cutoff ValueIn our previous study [17], serum antibody test re-sults completely agreed with the results of the 13C-UBT when patients who were positive or negativefor all three serum ELISAs were evaluated. There-fore, we decided to establish the cutoff value forthe urine-based ELISA using the assay results forthe healthy subjects who were positive (n 5 137)or negative (n 5 176) for all three serum ELISAs.The cutoff value was calculated by the formula:mean absorbance of two positive controls ob-tained from each assay/the given value (hereinafterreferred to as the a-value) 1 mean absorbance ofthree negative controls obtained from the assay.
The assay results (absorbances) for the anti-body-positive and -negative groups were analyzedby the receiver operating characteristics (ROC)method to determine the cutoff value. At an a-valueof 8.5, the accuracy was highest (97.8%, 308/315),and the sensitivity and specificity were 98.6%(137/139) and 97.2% (171/176), respectively. Thecutoff value for urine-based ELISA therefore wasdetermined as the value calculated by the follow-ing formula: mean absorbance of two positivecontrols)/8.5 1 (mean absorbance of three nega-tive controls).
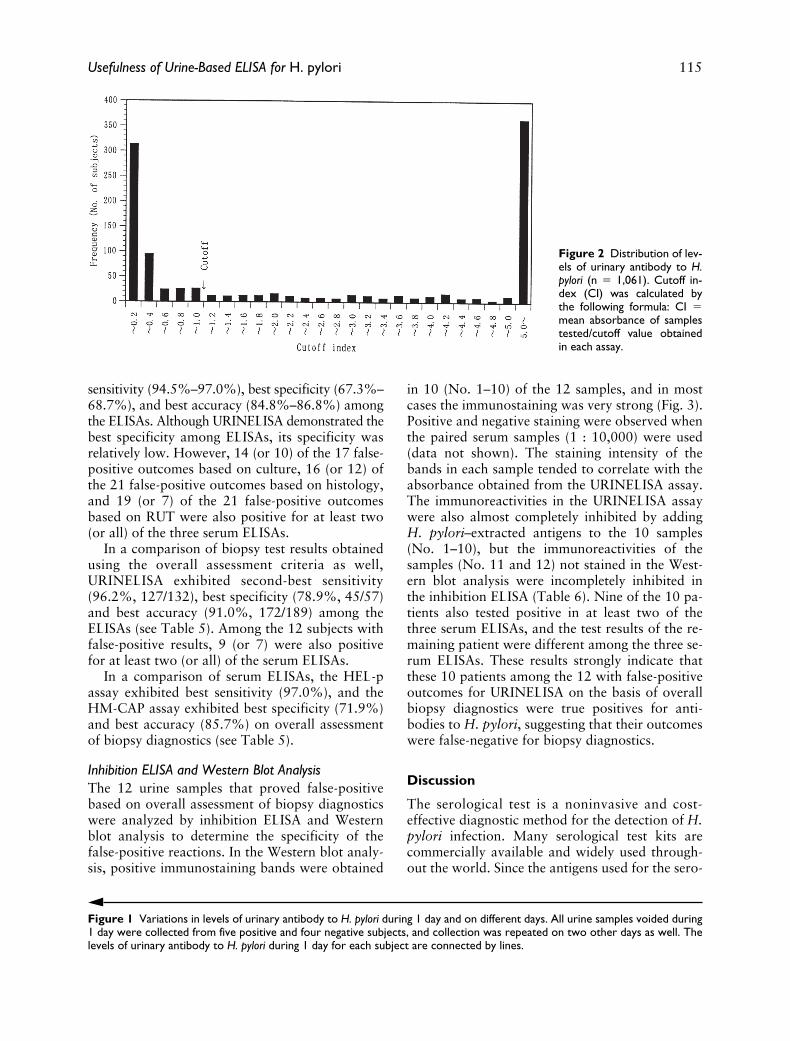
Distribution of Urinary Antibody Activity to H. pyloriThe frequency distribution of urinary antibodylevels (cutoff index, CI) is shown in Figure 2.Most of the samples exhibited sufficiently high CIsor low CIs, and only a small number of sampleswere distributed around the cutoff value (CI 5 1).
Comparison with Serum-Based ELISAsThe overall agreements (coincidence ratios) be-tween the test results of URINELISA and those of
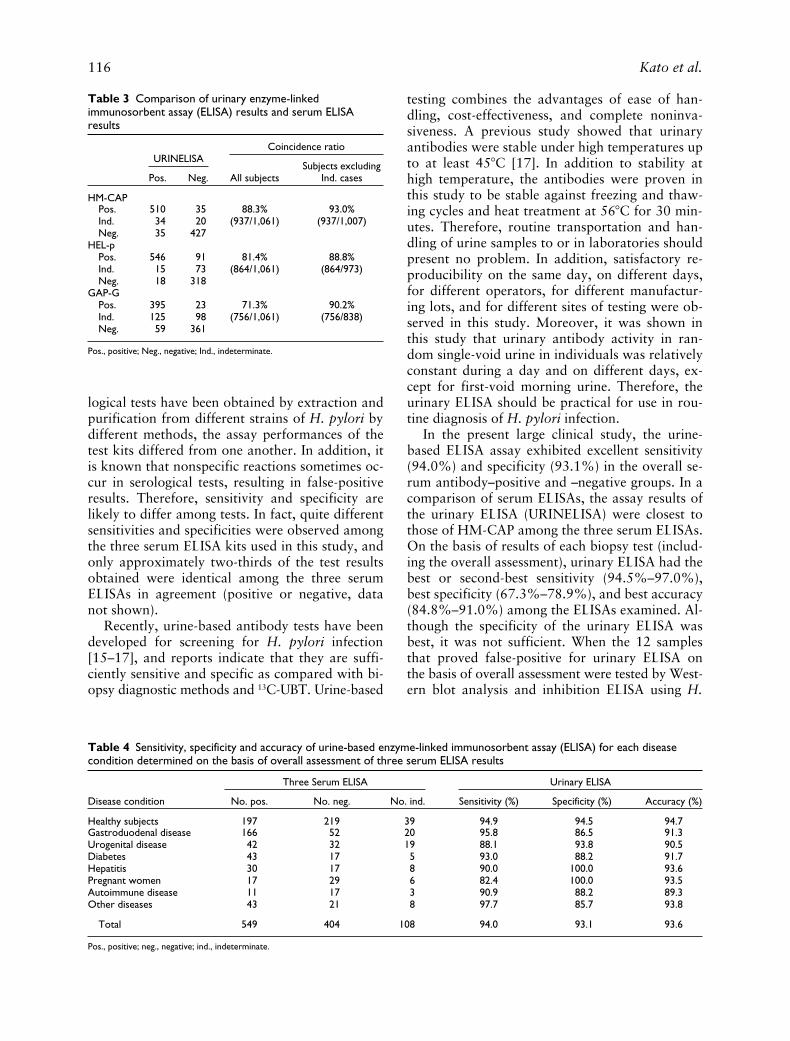
HM-CAP, HEL-p, and GAP-G ELISA were88.3% (937/1,061), 81.4% (864/1,061), and 71.3%(756/1,061), respectively (Table 3). Therefore, thetest results of URINELISA were most strongly cor-related with those of HM-CAP. The coincidenceratios were equivalent to or better than thoseamong the three serum ELISAs (70.2%–81.1%;data not shown). Each of the three serum ELISAsyielded results in the indeterminate range. Whenthe indeterminate results obtained by each serumELISA were omitted from analysis, the overallagreements with HM-CAP, HEL-p, and GAP-GELISA results were 93.0% (937/1,007), 88.8%(864/973), and 90.2% (756/838), respectively.
All subjects (N 5 1061) were classified into theoverall serum antibody–positive (n 5 549), –nega-tive (n 5 404) and –indeterminate groups (n 5108), in accordance with the overall assessmentcriteria for the serum antibody assay. With the as-sumption that this classification was 100% accu-rate, the sensitivity, specificity, and accuracy of theurine-based ELISA were 94.0% (516/549), 93.1%(376/404), and 93.6% (892/953), respectively (Ta-ble 4). For the patients with gastroduodenal dis-ease, excellent sensitivity (95.8%, 159/166), specific-ity (86.5%, 45/52) and accuracy (91.3%, 204/218)were observed. Six of the seven patients with false-negative results had undergone biopsy diagnosis,and three of the six patients also had negative bi-opsy diagnostic results (overall assessment). Fourof the seven patients with false-positive results hadundergone biopsy diagnosis, and two of the fourpatients also had positive biopsy diagnostic results(overall assessment). For the patients with otherdiseases, healthy subjects, and pregnant women,the accuracy was excellent (. 90%) except for au-toimmune disease (89.3%).
Comparison with Biopsy Diagnostic MethodsTwo-hundred two of 238 gastroduodenal diseasepatients were tested with at least one of the threebiopsy diagnostic methods using endoscopic bi-opsy specimens, such as culture (n 5 151), his-tology (n 5 200), and RUT (n 5 181). Five testresults for histology and three for RUT were inde-terminate. These test results were therefore ex-cluded from analysis. Using the remaining test re-sults, the results of urinary and serum ELISAswere compared with those for each biopsy diag-nostic result, with the assumption that the diag-nostic results for each biopsy method were 100%accurate (Table 5).
In a comparison of biopsy diagnostic methods,the URINELISA demonstrated best or second-best
114 Kato et al.
Usefulness of Urine-Based ELISA for H. pylori 115
sensitivity (94.5%–97.0%), best specificity (67.3%–68.7%), and best accuracy (84.8%–86.8%) amongthe ELISAs. Although URINELISA demonstrated thebest specificity among ELISAs, its specificity wasrelatively low. However, 14 (or 10) of the 17 false-positive outcomes based on culture, 16 (or 12) ofthe 21 false-positive outcomes based on histology,and 19 (or 7) of the 21 false-positive outcomesbased on RUT were also positive for at least two(or all) of the three serum ELISAs.
In a comparison of biopsy test results obtainedusing the overall assessment criteria as well,URINELISA exhibited second-best sensitivity(96.2%, 127/132), best specificity (78.9%, 45/57)and best accuracy (91.0%, 172/189) among theELISAs (see Table 5). Among the 12 subjects withfalse-positive results, 9 (or 7) were also positivefor at least two (or all) of the serum ELISAs.
In a comparison of serum ELISAs, the HEL-passay exhibited best sensitivity (97.0%), and theHM-CAP assay exhibited best specificity (71.9%)and best accuracy (85.7%) on overall assessmentof biopsy diagnostics (see Table 5).
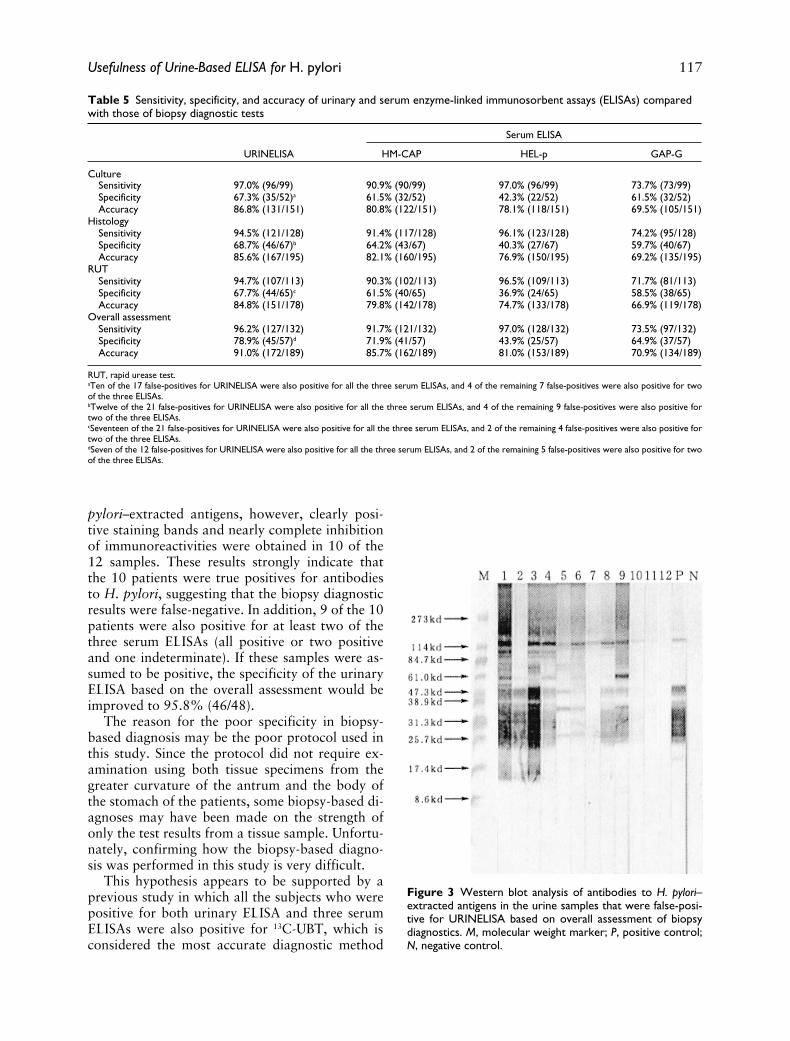
Inhibition ELISA and Western Blot AnalysisThe 12 urine samples that proved false-positivebased on overall assessment of biopsy diagnosticswere analyzed by inhibition ELISA and Westernblot analysis to determine the specificity of thefalse-positive reactions. In the Western blot analy-sis, positive immunostaining bands were obtained
in 10 (No. 1–10) of the 12 samples, and in mostcases the immunostaining was very strong (Fig. 3).Positive and negative staining were observed whenthe paired serum samples (1 : 10,000) were used(data not shown). The staining intensity of thebands in each sample tended to correlate with theabsorbance obtained from the URINELISA assay.The immunoreactivities in the URINELISA assaywere also almost completely inhibited by addingH. pylori–extracted antigens to the 10 samples(No. 1–10), but the immunoreactivities of thesamples (No. 11 and 12) not stained in the West-ern blot analysis were incompletely inhibited inthe inhibition ELISA (Table 6). Nine of the 10 pa-tients also tested positive in at least two of thethree serum ELISAs, and the test results of the re-maining patient were different among the three se-rum ELISAs. These results strongly indicate thatthese 10 patients among the 12 with false-positiveoutcomes for URINELISA on the basis of overallbiopsy diagnostics were true positives for anti-bodies to H. pylori, suggesting that their outcomeswere false-negative for biopsy diagnostics.
Discussion
The serological test is a noninvasive and cost-effective diagnostic method for the detection of H.pylori infection. Many serological test kits arecommercially available and widely used through-out the world. Since the antigens used for the sero-
Figure 1 Variations in levels of urinary antibody to H. pylori during 1 day and on different days. All urine samples voided during1 day were collected from five positive and four negative subjects, and collection was repeated on two other days as well. Thelevels of urinary antibody to H. pylori during 1 day for each subject are connected by lines.
Figure 2 Distribution of lev-els of urinary antibody to H.pylori (n 5 1,061). Cutoff in-dex (CI) was calculated bythe following formula: CI 5mean absorbance of samplestested/cutoff value obtainedin each assay.
116 Kato et al.
logical tests have been obtained by extraction andpurification from different strains of H. pylori bydifferent methods, the assay performances of thetest kits differed from one another. In addition, itis known that nonspecific reactions sometimes oc-cur in serological tests, resulting in false-positiveresults. Therefore, sensitivity and specificity arelikely to differ among tests. In fact, quite differentsensitivities and specificities were observed amongthe three serum ELISA kits used in this study, andonly approximately two-thirds of the test resultsobtained were identical among the three serumELISAs in agreement (positive or negative, datanot shown).
Recently, urine-based antibody tests have beendeveloped for screening for H. pylori infection[15–17], and reports indicate that they are suffi-ciently sensitive and specific as compared with bi-opsy diagnostic methods and 13C-UBT. Urine-based
testing combines the advantages of ease of han-dling, cost-effectiveness, and complete noninva-siveness. A previous study showed that urinaryantibodies were stable under high temperatures upto at least 458C [17]. In addition to stability athigh temperature, the antibodies were proven inthis study to be stable against freezing and thaw-ing cycles and heat treatment at 568C for 30 min-utes. Therefore, routine transportation and han-dling of urine samples to or in laboratories shouldpresent no problem. In addition, satisfactory re-producibility on the same day, on different days,for different operators, for different manufactur-ing lots, and for different sites of testing were ob-served in this study. Moreover, it was shown inthis study that urinary antibody activity in ran-dom single-void urine in individuals was relativelyconstant during a day and on different days, ex-cept for first-void morning urine. Therefore, theurinary ELISA should be practical for use in rou-tine diagnosis of H. pylori infection.
In the present large clinical study, the urine-based ELISA assay exhibited excellent sensitivity(94.0%) and specificity (93.1%) in the overall se-rum antibody–positive and –negative groups. In acomparison of serum ELISAs, the assay results ofthe urinary ELISA (URINELISA) were closest tothose of HM-CAP among the three serum ELISAs.On the basis of results of each biopsy test (includ-ing the overall assessment), urinary ELISA had thebest or second-best sensitivity (94.5%–97.0%),best specificity (67.3%–78.9%), and best accuracy(84.8%–91.0%) among the ELISAs examined. Al-though the specificity of the urinary ELISA wasbest, it was not sufficient. When the 12 samplesthat proved false-positive for urinary ELISA onthe basis of overall assessment were tested by West-ern blot analysis and inhibition ELISA using H.
Table 3 Comparison of urinary enzyme-linked immunosorbent assay (ELISA) results and serum ELISA results
URINELISACoincidence ratio
All subjectsSubjects excluding
Ind. casesPos. Neg.
HM-CAPPos. 510 35 88.3% 93.0%Ind. 34 20 (937/1,061) (937/1,007)Neg. 35 427
HEL-pPos. 546 91 81.4% 88.8%Ind. 15 73 (864/1,061) (864/973)Neg. 18 318
GAP-GPos. 395 23 71.3% 90.2%Ind. 125 98 (756/1,061) (756/838)Neg. 59 361
Pos., positive; Neg., negative; Ind., indeterminate.
Table 4 Sensitivity, specificity and accuracy of urine-based enzyme-linked immunosorbent assay (ELISA) for each disease condition determined on the basis of overall assessment of three serum ELISA results
Three Serum ELISA Urinary ELISA
Disease condition No. pos. No. neg. No. ind. Sensitivity (%) Specificity (%) Accuracy (%)
Healthy subjects 197 219 39 94.9 94.5 94.7Gastroduodenal disease 166 52 20 95.8 86.5 91.3Urogenital disease 42 32 19 88.1 93.8 90.5Diabetes 43 17 5 93.0 88.2 91.7Hepatitis 30 17 8 90.0 100.0 93.6Pregnant women 17 29 6 82.4 100.0 93.5Autoimmune disease 11 17 3 90.9 88.2 89.3Other diseases 43 21 8 97.7 85.7 93.8
Total 549 404 108 94.0 93.1 93.6
Pos., positive; neg., negative; ind., indeterminate.
Usefulness of Urine-Based ELISA for H. pylori 117
pylori–extracted antigens, however, clearly posi-tive staining bands and nearly complete inhibitionof immunoreactivities were obtained in 10 of the12 samples. These results strongly indicate thatthe 10 patients were true positives for antibodiesto H. pylori, suggesting that the biopsy diagnosticresults were false-negative. In addition, 9 of the 10patients were also positive for at least two of thethree serum ELISAs (all positive or two positiveand one indeterminate). If these samples were as-sumed to be positive, the specificity of the urinaryELISA based on the overall assessment would beimproved to 95.8% (46/48).
The reason for the poor specificity in biopsy-based diagnosis may be the poor protocol used inthis study. Since the protocol did not require ex-amination using both tissue specimens from thegreater curvature of the antrum and the body ofthe stomach of the patients, some biopsy-based di-agnoses may have been made on the strength ofonly the test results from a tissue sample. Unfortu-nately, confirming how the biopsy-based diagno-sis was performed in this study is very difficult.
This hypothesis appears to be supported by aprevious study in which all the subjects who werepositive for both urinary ELISA and three serumELISAs were also positive for 13C-UBT, which isconsidered the most accurate diagnostic method
Table 5 Sensitivity, specificity, and accuracy of urinary and serum enzyme-linked immunosorbent assays (ELISAs) compared with those of biopsy diagnostic tests
Serum ELISA
URINELISA HM-CAP HEL-p GAP-G
CultureSensitivity 97.0% (96/99) 90.9% (90/99) 97.0% (96/99) 73.7% (73/99)Specificity 67.3% (35/52)a 61.5% (32/52) 42.3% (22/52) 61.5% (32/52)Accuracy 86.8% (131/151) 80.8% (122/151) 78.1% (118/151) 69.5% (105/151)
HistologySensitivity 94.5% (121/128) 91.4% (117/128) 96.1% (123/128) 74.2% (95/128)Specificity 68.7% (46/67)b 64.2% (43/67) 40.3% (27/67) 59.7% (40/67)Accuracy 85.6% (167/195) 82.1% (160/195) 76.9% (150/195) 69.2% (135/195)
RUTSensitivity 94.7% (107/113) 90.3% (102/113) 96.5% (109/113) 71.7% (81/113)Specificity 67.7% (44/65)c 61.5% (40/65) 36.9% (24/65) 58.5% (38/65)Accuracy 84.8% (151/178) 79.8% (142/178) 74.7% (133/178) 66.9% (119/178)
Overall assessmentSensitivity 96.2% (127/132) 91.7% (121/132) 97.0% (128/132) 73.5% (97/132)Specificity 78.9% (45/57)d 71.9% (41/57) 43.9% (25/57) 64.9% (37/57)Accuracy 91.0% (172/189) 85.7% (162/189) 81.0% (153/189) 70.9% (134/189)
RUT, rapid urease test.aTen of the 17 false-positives for URINELISA were also positive for all the three serum ELISAs, and 4 of the remaining 7 false-positives were also positive for twoof the three ELISAs.bTwelve of the 21 false-positives for URINELISA were also positive for all the three serum ELISAs, and 4 of the remaining 9 false-positives were also positive fortwo of the three ELISAs.cSeventeen of the 21 false-positives for URINELISA were also positive for all the three serum ELISAs, and 2 of the remaining 4 false-positives were also positive fortwo of the three ELISAs.dSeven of the 12 false-positives for URINELISA were also positive for all the three serum ELISAs, and 2 of the remaining 5 false-positives were also positive for twoof the three ELISAs.
Figure 3 Western blot analysis of antibodies to H. pylori–extracted antigens in the urine samples that were false-posi-tive for URINELISA based on overall assessment of biopsydiagnostics. M, molecular weight marker; P, positive control;N, negative control.

118 Kato et al.
for H. pylori infection [17]. In addition, 9 of the10 patients also tested positive for at least two ofthe three serum ELISAs (all positive or two posi-tive and one indeterminate).
To develop URINELISA, 20 clinical isolates dif-ferent from those established in Japanese patientswith disorders of the upper digestive tract werecultivated and extracted using different methods,and the most suitable strain (cagA-positive, vacA-positive) and extraction methods for the urinaryELISA were selected. In addition, Escherichia coliextracts are added to reaction buffer to preventantibodies to E. coli or common structures amongbacteria from binding H. pylori antigens immobi-lized on wells of microtiter plates (17). On theother hand, the serum ELISAs used in this studywere manufactured outside Japan. Therefore, H.pylori strains used in the serum ELISAs must beestablished from patients in the original countries.The superiority of performance of URINELISA tothat of the serum ELISA may have resulted fromthe established assay conditions and the character-istics of the H. pylori strain.
In conclusion, urinary antibodies to H. pyloriare extremely stable against freezing and thawingcycles and even heat treatment, and random sin-gle-void urine samples are extremely easy to col-lect, particularly from infants and children. Theurine-based ELISA protocol also is simple and re-quires no pretreatment of samples such as dilutionor concentration prior to set-up. In addition toease of handling, the sensitivity, specificity, andaccuracy of the urine-based ELISA were almostequivalent or even superior to the serum-based
ELISAs tested. Therefore, the urine-based ELISA(URINELISA H. pylori Antibody) should be use-ful for screening H. pylori infection as an efficientalternative to serum-based assays.
References
1 Warren JR, Marshall B. Unidentified curved bacillion gastric epithelium in active chronic gastritis.Lancet 1983;1:1273–5.
2 Blaser MJ. Helicobacter pylori and the pathogene-sis of gastroduodenal inflammation. J Infect Dis1990;161:626–33.
3 Morris A, Nicholson G. Ingestion of Campylo-bacter pyloridis causes gastritis and raised fastinggastric pH. Am J Gastroenterol 1987;82:192–9.
4 Graham DY, Lew GM, Klein PD, Evans DG,Evans DJ Jr, Saeed ZA, Malaty HM. Effect oftreatment of Helicobacter pylori infection on thelong-term recurrence of gastric or duodenal ulcer.Ann Intern Med 1992;116:705–8.
5 Genta RM, Graham DY. Primary gastric MALTlymphoma: trivial condition or serious disease?Helicobacter 1997;2:56–60.
6 McNulty CAM, Dent JC, Uff JS, Gear MWL,Wilkinson SP. Detection of Campylobacter pyloriby the biopsy urease test: an assessment in 1445patients. Gut 1989;30:1058–62.
7 Evans DJ Jr, Evans DG, Graham DY, Klein PD. Asensitive and specific serologic test for detection ofCampylobacter pylori infection. Gastroentrol 1989;96:1004–8.
8 Graham DY, Klein PD, Evans DJ Jr, Evans DG,Alpert LC, Opekum AR, Boutton TW. Campylo-bacter pylori detected noninvasively by the 13C-urea breath test. Lancet 1987;1:1174–7.
Table 6 Summary of test results of gastroduodenal patients with false-positive results on URINELISA
Sample
Biopsy diagnostics Serum ELISA
URINELISA
Inhibition ELISA (OD at 450 nm)
H. pylori antigen addedReduction
(%)Culture Histology RUT HM-CAP HEL-p GAP-G 0 mg/well 50 mg/well
Negative control 0.017 0.016Positive control 1.748 0.032 98.21 2 2 2 1 1 1 1 4.000 0.130 96.82 2 ND 2 1 1 1 1 1.340 0.037 97.23 2 2 2 6 1 2 1 3.899 0.124 96.84 2 2 2 1 1 1 1 2.474 0.043 98.35 ND 2 2 1 1 1 1 3.228 0.061 98.16 ND 2 2 1 1 1 1 3.452 0.133 96.17 ND 2 2 1 1 6 1 0.501 0.026 94.88 2 2 2 1 1 6 1 1.377 0.026 98.19 2 2 2 1 1 1 1 2.380 0.077 96.810 2 2 2 1 6 1 1 0.303 0.024 92.111 2 2 ND 2 2 6 1 0.323 0.140 56.712 2 2 2 2 6 2 1 0.869 0.689 79.3
RUT, rapid urease test; OD, optical density; ND, not done.The sample number is the same as in Figure 3.1, positive; 2, negative; 6 indeterminate.
Usefulness of Urine-Based ELISA for H. pylori 119
9 Ohara S, Kato M, Asaka M, Toyota T. Studies of13C-urea breath test for diagnosis of Helicobacterpylori infection in Japan. J Gastroenterol 1998;33:6–13.
10 Breslisn NP, O’Morain CA. Noninvasive diagnosisof Helicobacter pylori infection: A review. Helico-bacter 1997;2:111–7.
11 Luzza F, Maletta M, Biancone L, Imeneo G, Mon-teleone G, Doldo P, Pallone F. Isotypic analysis ofspecific antibody response in serum, saliva andgastric homogenates of Helicobacter pylori in-fected patients. Gastroenterology 1994;106:A724.
12 Patel P, Mendall MA, Khulusi S, Molineaux N,Levy J, Maxwell JD, Northfield TC. Salivary anti-bodies to Helicobacter pylori: Screening dyspepticpatients before endoscopy. Lancet 1994;344:511–2.
13 Doldo P, Marasco R, Biancone L, Pallone F. Sal-ivary specific IgG is a sensitive indicator of thehumoral immune response to Helicobacter py-lori. FEMS Immunol Med Microbiol 1995;10:281–4.
14 Luzza F, Maletta M, Imeneo M, Marcheggiano A,
Iannoni C, Biancone L, Pallone F. Salivary specificimmunoglobulin G in the diagnosis of Helico-bacter pylori infection in dyspeptic patients. Am JGastroenterol 1995;90:1820–3.
15 Alemohammad MM, Foley TJ, Dooley CP. Isurine a suitable specimen for the detection of anti-H. pylori IgG? Am J Gastroenterol 1991;86:A71.
16 Alemohammad MM, Foley TJ, Cohen H. Detec-tion of immunoglobulin G antibodies to Helico-bacter pylori in urine by an enzyme immunoassaymethod. J Clin Microbiol 1993;31:2174–7.
17 Katsuragi K, Noda A, Tachikawa T, Azuma A,Mukai F, Murakami K, Fujioka T, Kato M, AsakaM. Highly sensitive urine-based enzyme-linked im-munosorbent assay for detection of antibody toHelicobacter pylori. Helicobacter 1998;3:289–95.
18 FDA Center for Drug Evaluation and Research,Division of Anti-Infective Drug Products. DAIDPpoints to consider document: Helicobacter pylori–associated peptic ulcer disease. Indication no. 25.United States Department of Agriculture, Rock-ville, MD, March 15, 1995.




















