7 - Urine Cytology - Amazon AWS
43
7 Urine Cytology DAVID G. BOSTWICK CHAPTER OUTLINE Introduction 322 Utility of Urine Cytology 322 Indications 322 Sources 322 Specimen Adequacy 323 Reporting and Classification 323 The Paris System 2013 324 Normal Components of the Urinary Sediment 326 Superficial (Umbrella) Cells 326 Cells Originating From the Deeper Layers of the Urothelium 326 Columnar Cells 327 Mucus-Containing Epithelial Cells 327 Squamous Cells 327 Renal Epithelial Cells 328 Other Benign Cells 329 Noncellular Components of the Urinary Sediment 329 Diagnostic Criteria 330 Infections 330 Reactive Cytologic Changes 333 Other Benign Conditions 336 Benign Tumors and Tumor-Like Processes 337 Atypical Urothelial Cells 338 Suspicious 342 Low-Grade Urothelial Carcinoma 342 High-Grade Carcinoma 343 Correlation of Urine Cytology and Biopsy Findings (Diagnostic Accuracy) 346 Urinary Cells Originating From Other Sites 346 Anticipatory Positive Cytology 348 Other Types of Carcinoma 348 Major Diagnostic Pitfalls 349 Ancillary Studies and Immunocytology 350 Digital Image Analysis and Morphometry 350 Cytochemical Stains 351 Immunocytochemical Stains 351 Fluorescence In Situ Hybridization 354 The Problem of Hematuria 354 Routine Laboratory Investigation of Hematuria 355 Dysmorphic Red Blood Cells Indicate Glomerular Disease 356 Comprehensive Analysis of Urine for Evaluation of Hematuria 356 Introduction Examination of urine is one of the oldest medical tests, used by Samarians, Babylonians, Egyptians, Indians, and Greeks in their traditional medicine. It was not until after Papanicolaou and Mar- shall published the first article in 1945 that urine cytology was used to detect urothelial carcinoma. 1 Subsequently, Koss, Melamed, and colleagues characterized urine cytology and histology in 1960. 2-5 Numerous classification systems have been introduced, and those before 2013 are nicely reviewed by Owens et al. 6 The greatest contemporary issues with urine cytology are low sensitivity detection of low-grade cancer, poor interobserver agree- ment (especially with atypia), and lack of standardized diagnostic criteria. Recent efforts described in this chapter offer great promise in resolving these concerns. This chapter discusses the spectrum of cytologic abnormalities in voided urine samples and washings to allow comparison with biopsy findings described in Chapters 5 and 6, and presents clas- sifications published after the last edition of this text. The clinically significant and common problem of hematuria is also addressed from the perspective of the cytopathologist. Utility of Urine Cytology Indications Cytologic examination of the urine sediment is of value in the diag- nosis of a wide variety of benign and malignant diseases of the blad- der, urethra, ureter, and kidney. 7-10 The chief indications for the use of cytology in disorders of the urinary tract include: 1. Screening and diagnosis of carcinoma in situ and high-grade carcinoma 2. Follow-up of patients with atypical cytology evaluation or urothelial tumor, regardless of grade 3. Monitoring of patients with urothelial tumor undergoing or after treatment, including active surveillance 8,11,12 4. Evaluation of hematuria, including separation of kidney (upper tract disease) and nonkidney (lower tract) causes Sources The sources of urologic cytology specimens include voided urine, catheterized urine, bladder washing (barbotage), brushing, ureteral and renal pelvic brushing and washing, and neobladder urine from 322
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of 7 - Urine Cytology - Amazon AWS

7Urine CytologyDAVID G. BOSTWICK
CHAPTER OUTLINE
Introduction 322
Utility of Urine Cytology 322Indications 322Sources 322Specimen Adequacy 323
Reporting and Classification 323The Paris System 2013 324
Normal Components of the Urinary Sediment 326Superficial (Umbrella) Cells 326Cells Originating From the Deeper Layers of the Urothelium 326Columnar Cells 327Mucus-Containing Epithelial Cells 327Squamous Cells 327Renal Epithelial Cells 328Other Benign Cells 329Noncellular Components of the Urinary Sediment 329
Diagnostic Criteria 330Infections 330Reactive Cytologic Changes 333Other Benign Conditions 336Benign Tumors and Tumor-Like Processes 337Atypical Urothelial Cells 338Suspicious 342Low-Grade Urothelial Carcinoma 342High-Grade Carcinoma 343Correlation of Urine Cytology and Biopsy Findings (Diagnostic
Accuracy) 346Urinary Cells Originating From Other Sites 346Anticipatory Positive Cytology 348Other Types of Carcinoma 348Major Diagnostic Pitfalls 349
Ancillary Studies and Immunocytology 350Digital Image Analysis and Morphometry 350Cytochemical Stains 351Immunocytochemical Stains 351Fluorescence In Situ Hybridization 354
The Problem of Hematuria 354Routine Laboratory Investigation of Hematuria 355Dysmorphic Red Blood Cells Indicate Glomerular Disease 356Comprehensive Analysis of Urine for Evaluation of
Hematuria 356
322
Introduction
Examination of urine is one of the oldest medical tests, used bySamarians, Babylonians, Egyptians, Indians, and Greeks in theirtraditional medicine. It was not until after Papanicolaou and Mar-shall published the first article in 1945 that urine cytology was usedto detect urothelial carcinoma.1 Subsequently, Koss, Melamed,and colleagues characterized urine cytology and histology in1960.2-5 Numerous classification systems have been introduced,and those before 2013 are nicely reviewed by Owens et al.6
The greatest contemporary issues with urine cytology are lowsensitivity detection of low-grade cancer, poor interobserver agree-ment (especially with atypia), and lack of standardized diagnosticcriteria. Recent efforts described in this chapter offer great promisein resolving these concerns.
This chapter discusses the spectrum of cytologic abnormalitiesin voided urine samples and washings to allow comparison withbiopsy findings described in Chapters 5 and 6, and presents clas-sifications published after the last edition of this text. The clinicallysignificant and common problem of hematuria is also addressedfrom the perspective of the cytopathologist.
Utility of Urine Cytology
IndicationsCytologic examination of the urine sediment is of value in the diag-nosis of a wide variety of benign and malignant diseases of the blad-der, urethra, ureter, and kidney.7-10 The chief indications for theuse of cytology in disorders of the urinary tract include:1. Screening and diagnosis of carcinoma in situ and high-grade
carcinoma2. Follow-up of patients with atypical cytology evaluation or
urothelial tumor, regardless of grade3. Monitoring of patients with urothelial tumor undergoing or
after treatment, including active surveillance8,11,12
4. Evaluation of hematuria, including separation of kidney (uppertract disease) and nonkidney (lower tract) causes
SourcesThe sources of urologic cytology specimens include voided urine,catheterized urine, bladder washing (barbotage), brushing, ureteraland renal pelvic brushing and washing, and neobladder urine from

323CHAPTER 7 Urine Cytology
an ileal conduit or colonic pouch.13,14 Initial morning first-voidurine includes exfoliated cells, debris, and impurities that have col-lected in the urinary tract and urethral opening during the night,and may optimize yield of potential pathogens such as human pap-illomavirus.15,16 Ureteral washings and other instrumented speci-mens require caution because they may produce artifactuallyclustered urothelium.17
The specimen source is critically important for diagnosis. Forexample, upper urinary tract washings were superior to voided sam-ples in detection of upper tract high-grade carcinoma (90% versus50% yield, respectively).18 Similarly, urinary diversion cytologyspecimens from patients who undergo radical cystectomy are oftensubmitted for screening for recurrent urothelial carcinoma, andthose with carcinoma (2% to 6% incidence rate) revealed scant,well-preserved urothelial cells either alone or in clusters withhigh-grade features, including eccentrically located, enlarged,hyperchromatic nuclei; irregular nuclear borders; and highnuclear-to-cytoplasmic (N/C) ratios, often with an inflammatorybackground.19,20 The sensitivity, specificity, positive predictivevalue, and negative predictive value of cytology for high-grade car-cinoma in diversion remnants were 82%, 97%, 75%, and 98%,respectively; 21% of patients with atypia were eventually diagnosedwith carcinoma.21 In another study, bladder washing specimenswere more predictive of high-grade cancer than voided urinespecimens.22
Specimen AdequacyAdequacy is a reflection of how representative the specimen isbased chiefly on cellularity, although the presence of obscuring ele-ments is also important.23 Regardless of the specimen type (voidedurine or instrumented), an unsatisfactory or inadequate specimenis one that is poorly cellular, completely obscured, or predomi-nantly degenerate. Obscuring elements include neutrophils, lubri-cants, other foreign debris, crystals, bacteria, squames, andspermatozoa. Conversely, according to one group, if there areany atypical cells, regardless of the overall cellularity, this representsa satisfactory specimen.24 Brief exposure to contrast agents doesnot influence adequacy; thus, contrast washings of the urinary tractcan be sent for cytologic diagnosis if fixed within a short time.25
Inadequate voided specimens were defined by Bastacky et al.and the Papanicolaou Society of Cytopathology as those that con-tained fewer than 15 intermediate or basal urothelial cells, obscur-ing blood or inflammation, or poor cellular preservation.26,27
Prather et al. defined adequacy as the presence of a total of 2600cells or 20 urothelial cells in 10 consecutive high-power fields(hpf) in instrumented urine specimens processed using the Thin-Prep method.28 The Paris System 2013 included a category ofunsatisfactory/nondiagnostic, but provided no qualifications fordifferent specimen sources (voided, instrumented) and preparationtypes.29
Adequacy is based on multiple features, including: (1) volume,(2) collection method, (3) processing method, (4) underlyingpatient condition, (5) operator-dependent factors, and (6) logisticfactors. Volume is an important determinant of adequacy of voidedurine specimens. Adequacy increased linearly for each increment ofurine volume submitted to the laboratory up to 30 mL, after whichthe correlation was nonlinear, and low-volume specimens were lesslikely to harbor suspicious or malignant cells.23 Collectionmethods are also significantly associated with specimen adequacyand cellularity.30 Comparison of voided urine and bladder wash-ings revealed concordance in more than 99% of cases, indicating
equivalence of these collection techniques.31 Conversely, in aseries of patients with biopsy-proven low-grade carcinoma onfollow-up, 56% of urine cytology specimens demonstrated atypicalfeatures, including the presence of tissue fragments, cytoplasmictails, and eccentric and enlarged nuclei, and these features weresignificantly more common in washings than in voided urinespecimens.32
Contemporary processing methods include conventional cytos-pin, Meiers improved filter method, ThinPrep, and SurePathmethods (Table 7.1); direct smear has been largely abandoned.The cytospin method was superior to direct smear, Thin Prep,and SurePath in a comparative study of voided urine specimens;the rate of unsatisfactory preparations was quite low (0.30%),and the overall sensitivity, specificity, and positive and negativepredictive values for urothelial carcinoma were 0.72, 0.92, 0.97,and 0.46, respectively.33 Cytospin was also superior to ThinPrepfor evaluation of nuclear detail and background material in speci-mens with nonurothelial malignancies.34 Conversely, Kim andKim found similar sensitivity and specificity for cytospin and Thin-Prep in a large series of bladder washings (61% versus 60% and95% versus 95%, respectively).35 Metaanalysis showed that therewas similar sensitivity with cytospin and liquid-based cytologymethods.36 Using the Paris System 2013, cytospin and ThinPrephad similar sensitivity and specificity for the diagnosis of suspiciousor high-grade urothelial carcinoma.37 The filter method was supe-rior to cytospin by decreasing the number of false-negative casesbecause of higher cellularity and improved detection of atypicalor malignant epithelial cells.38 ThinPrep increased the numberof nonatypical urothelial cell clusters compared with cytospin(13% to 21% versus 7%, respectively).39
The patient’s underlying condition and his or her indication forcytologic evaluation influences specimen adequacy. Increased cel-lularity is observed in specimens from patients with cancer, calculi,or infection compared with those with only hematuria or irritativevoiding symptoms.29 Other adequacy factors include level ofhydration, micturition before specimen acquisition, the use ofdiuretics or other medications, the presence of obstructive condi-tions such as benign prostatic hyperplasia, with consequent reduc-tion of bladder capacity, and medical problems resulting inoliguria.
Operator-dependent factors refer to expertise of the examinerand the potential for human bias and error. Logistic factors thatinfluence adequacy include length of time from collection to pro-cessing, container leakage with potential drying artifacts, and manyothers.
Reporting and Classification
Several reporting and classification systems for urine cytology havebeen published, each of which has relative strengths and weak-nesses. Unlike cervical cytology, there has not been widespreadacceptance and use of any single reporting system for urine cytol-ogy studies. Thus, terminology and criteria for urine cytologyreporting are not uniform among pathologists.6 The major diag-nostic categories that we use at our laboratory are presented inTable 7.2.
Recently two international consensus conferences publishedtheir classifications: the Paris System 2013 and the InternationalConsultation on Urologic Disease–European Association of Urol-ogy 2015 (Table 7.2). Both were based on expert consensus bysmall, self-selected academic groups with minimal input from othercytopathologists, urologists, oncologists, or others.

TABLE 7.1 Comparison of Processing Methods of Urine Cytology Processing
Method Description
Cytospin smear (two-stepcentrifugation/fixation method)
Urine samples are sedimented at 700 g for 10 minutes. The supernatant is removed to within approximately 1-2 mL ofthe cell pellet, and the pellet is then resuspended and rinsed with 10 mL of hypotonic solution (0.075 M potassiumchloride) for 10 minutes. The cells are resedimented at 600 g for 10 minutes, and the supernatant is removed to within0.5 mL of the pellet. The pellet is then gently vortexed and resuspended in 10 mL 3:1 methanol/glacial acetic acidfixative. Fixed specimens are left at room temperature for 30 minutes. The urinary cells are then sedimented at 600 gfor 5 minutes, aspirated, and transferred to a 2-mL microfuge tube. The final cell pellet is left in approximately 100-500μL of residual methanol/glacial acetic acid fixative, depending on the size of the cell pellet. A total of 10 μL of cellsediment is placed on the slide, and the specimen is allowed to dry.261
Meiers improved filter method Urine samples are fixed in ethanol and drawn up into a 60-mL syringe threaded with a Luer lock tip. An 8.0-μM filtermounted in a filter holder is subsequently attached to the syringe tip. The urine sample is then pushed gently throughthe filter until complete. The membrane filter is placed on a positively charged glass slide. Gauze is placed over themembrane and slight pressure applied with the palm of the hand to transfer the cell filtrate. The cell filtrate is placed ona slide in a manner similar to Cytospin. The membrane is discarded and the filter holder was deposited in a 10% bleachsolution overnight until next use.261
ThinPrep (Hologic, Bedford, MA) ThinPrep test is performed with a proprietary automated liquid-based monolayer cell preparation system. Urinesamples are immersed in a buffered preservative solution, transferred to a bowl, and a cylinder with a filtrationmembrane is then placed in the bowl to ensure that the cells are homogeneously distributed. Using negative pressure,the erythrocytes and mucus penetrate the filtration membrane, leaving only the filtration membranes for the diagnosticprocedure. This maneuver is repeated until an appropriate number of cells (2000-50,000) is collected. Thereafter thecylinder is removed from the bowl; cells left on the filtration membrane are attached to the slide and then fixed in 95%alcohol.
SurePath (BD Diagnostics,Burlington, NC)
The SurePath test is performed with a proprietary liquid-based monolayer cell preparation system densitygradient-based cell enrichment. Urine samples are immersed in ethanolic preservative solution and a device is placedinto the vial to ensure that cells are homogenously distributed. A polysaccharide-based density gradient reagent isused to filter debris, centrifuged, resuspended, and centrifuged again. The PrepStain processor creates and stains theslides.
324 CHAPTER 7 Urine Cytology
It should be noted that evidence-based guidelines have sup-planted such expert panels and simple consensus conference-basedconclusions, and are now considered to be the contemporary stan-dard for defining the practice of medicine; thus it is surprising thatthese recent efforts failed to abide by even the most basic tenets ofevidence-based medicine, instead resorting to “biology by democ-racy.” All proper methods of systematic review and guideline gen-eration share certain core concepts, including careful selection ofthe guideline topic, thorough structured review of the evidencewith grading and synthesis, creation of recommendations,consultation and peer review, dissemination and implementation,revision, and updating. According to the U.S. Agency for Health-care Research andQuality, three key principles are required for suc-cessful conduct of systematic reviews: (1) the review must berelevant and timely, focusing on the most important issues andthe optimal time to initiate a review; (2) the review must be objec-tive and scientifically rigorous, free from conflicts of interest; and(3) the review must include public participation and transparencyto ensure confidence and credibility, and provide for accountabil-ity.40 Thus the recent cytopathology consensus statements shouldbe considered below the standards of current practice of evidence-based medicine. Nonetheless, any efforts to create standardized ter-minology are laudable and generate renewed interest in refinementof diagnostic criteria, continuing the work of the PapanicolaouSociety at creation of uniformity in cytopathology practice.27
In Paris System 2013, the recommended diagnostic words arealso problematic. The words “negative for high-grade urothelialcarcinoma” on a report could easily be mistyped or misinterpretedby the transcriptionist, cytopathologist, or urologist if the wordnegative is overlooked while the word carcinoma registers,
potentially resulting in serious consequences for the patient.Reasonable alternatives include “negative for high-grade malig-nancy,” “negative for high-grade neoplasia,” and “no definiteevidence of malignancy.”
The Paris System 2013The Paris System 2013 focused chiefly on accuracy of identifica-tion of high-grade carcinoma, requiring five criteria for a definitivediagnosis: at least 5 malignant cells (10 cells for upper tract cancer),elevated N/C ratio (�0.7), markedly atypical nuclear borders,moderate to severe hyperchromasia, and coarse chromatin(Tables 7.2 and 7.3). However, malignant specimens often containdegenerative changes, and this may limit the number of diagnosticcells; consequently, about half of positive cases failed to fulfill thiscriterion in a report from Johns Hopkins University.41 Further-more less than 20% of cells present in positive specimens fulfilledall five of the criteria. The second most restrictive criterion, N/Cratio �0.7, was present in only 78% of positive specimens. None-theless, the Paris System 2013 upgraded about 40% of indetermi-nate specimens and did not change the frequency of diagnosis ofhigh-grade carcinoma.41
N/C ratio is a critical component of the Paris System, but justhow reliable is it? Hang et al. confirmed the importance of the�0.5 cut point for the diagnosis of atypical urothelial cells usingdigital image analysis; receiver operating characteristic analysisdemonstrated that the maximum N/C ratio alone was highly pre-dictive of high-grade carcinoma on follow-up (area under the curve[AUC], 79%), with a sensitivity of 73% and a specificity of 85%.42
However, visual quantitation of N/C ratio showed only a fair
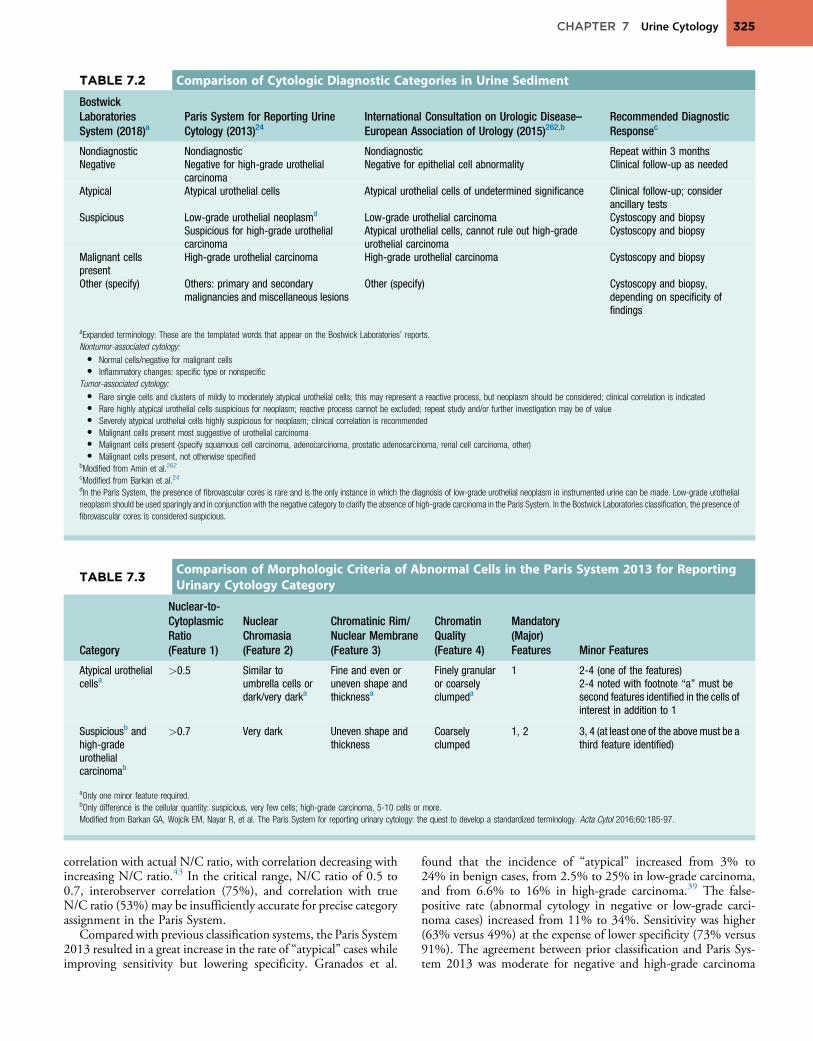
TABLE 7.2 Comparison of Cytologic Diagnostic Categories in Urine Sediment
BostwickLaboratoriesSystem (2018)a
Paris System for Reporting UrineCytology (2013)24
International Consultation on Urologic Disease–European Association of Urology (2015)262,b
Recommended DiagnosticResponsec
Nondiagnostic Nondiagnostic Nondiagnostic Repeat within 3 monthsNegative Negative for high-grade urothelial
carcinomaNegative for epithelial cell abnormality Clinical follow-up as needed
Atypical Atypical urothelial cells Atypical urothelial cells of undetermined significance Clinical follow-up; considerancillary tests
Suspicious Low-grade urothelial neoplasmd Low-grade urothelial carcinoma Cystoscopy and biopsySuspicious for high-grade urothelialcarcinoma
Atypical urothelial cells, cannot rule out high-gradeurothelial carcinoma
Cystoscopy and biopsy
Malignant cellspresent
High-grade urothelial carcinoma High-grade urothelial carcinoma Cystoscopy and biopsy
Other (specify) Others: primary and secondarymalignancies and miscellaneous lesions
Other (specify) Cystoscopy and biopsy,depending on specificity offindings
aExpanded terminology: These are the templated words that appear on the Bostwick Laboratories’ reports.Nontumor-associated cytology:• Normal cells/negative for malignant cells• Inflammatory changes: specific type or nonspecific
Tumor-associated cytology:• Rare single cells and clusters of mildly to moderately atypical urothelial cells; this may represent a reactive process, but neoplasm should be considered; clinical correlation is indicated• Rare highly atypical urothelial cells suspicious for neoplasm; reactive process cannot be excluded; repeat study and/or further investigation may be of value• Severely atypical urothelial cells highly suspicious for neoplasm; clinical correlation is recommended• Malignant cells present most suggestive of urothelial carcinoma• Malignant cells present (specify squamous cell carcinoma, adenocarcinoma, prostatic adenocarcinoma, renal cell carcinoma, other)• Malignant cells present, not otherwise specified
bModified from Amin et al.262cModified from Barkan et al.24dIn the Paris System, the presence of fibrovascular cores is rare and is the only instance in which the diagnosis of low-grade urothelial neoplasm in instrumented urine can be made. Low-grade urothelialneoplasm should be used sparingly and in conjunction with the negative category to clarify the absence of high-grade carcinoma in the Paris System. In the Bostwick Laboratories classification, the presence offibrovascular cores is considered suspicious.
TABLE 7.3Comparison of Morphologic Criteria of Abnormal Cells in the Paris System 2013 for ReportingUrinary Cytology Category
Category
Nuclear-to-CytoplasmicRatio(Feature 1)
NuclearChromasia(Feature 2)
Chromatinic Rim/Nuclear Membrane(Feature 3)
ChromatinQuality(Feature 4)
Mandatory(Major)Features Minor Features
Atypical urothelialcellsa
>0.5 Similar toumbrella cells ordark/very darka
Fine and even oruneven shape andthicknessa
Finely granularor coarselyclumpeda
1 2-4 (one of the features)2-4 noted with footnote “a” must besecond features identified in the cells ofinterest in addition to 1
Suspiciousb andhigh-gradeurothelialcarcinomab
>0.7 Very dark Uneven shape andthickness
Coarselyclumped
1, 2 3, 4 (at least one of the above must be athird feature identified)
aOnly one minor feature required.bOnly difference is the cellular quantity: suspicious, very few cells; high-grade carcinoma, 5-10 cells or more.Modified from Barkan GA, Wojcik EM, Nayar R, et al. The Paris System for reporting urinary cytology: the quest to develop a standardized terminology. Acta Cytol 2016;60:185-97.
325CHAPTER 7 Urine Cytology
correlation with actual N/C ratio, with correlation decreasing withincreasing N/C ratio.43 In the critical range, N/C ratio of 0.5 to0.7, interobserver correlation (75%), and correlation with trueN/C ratio (53%) may be insufficiently accurate for precise categoryassignment in the Paris System.
Compared with previous classification systems, the Paris System2013 resulted in a great increase in the rate of “atypical” cases whileimproving sensitivity but lowering specificity. Granados et al.
found that the incidence of “atypical” increased from 3% to24% in benign cases, from 2.5% to 25% in low-grade carcinoma,and from 6.6% to 16% in high-grade carcinoma.39 The false-positive rate (abnormal cytology in negative or low-grade carci-noma cases) increased from 11% to 34%. Sensitivity was higher(63% versus 49%) at the expense of lower specificity (73% versus91%). The agreement between prior classification and Paris Sys-tem 2013 was moderate for negative and high-grade carcinoma

326 CHAPTER 7 Urine Cytology
cases (κ ¼ 0.42 and 0.56, respectively) and weak for low-gradetumors (κ ¼ 0.35). Conversely, Hassan et al. found fewer caseswere diagnosed as “atypical” with the Paris System compared withtheir original diagnoses (26% versus 39%), whereas the correlationof “atypical” with subsequent high-grade cancer increased from33% to 53%.44 The new system also resulted in a higher numberof low-grade carcinomas diagnosed as “negative” (40%) rather than“atypical” (22%). In another study, 70% of cases of “atypical” caseswere reclassified by Paris System 2013 as “negative”; however, 18%of these were found to have high-grade cancer.45 The sensitivityand specificity of fluorescence in situ hybridization (FISH)with Paris System 2013 were 86% and 33%, respectively, in the“atypical” group and 63% and 100%, respectively, in the“negative” group.
The category of “atypical urothelial cells” no longer includescellular changes attributed to the BK polyomavirus cytopathiceffect, according to the Paris System 2013. Reclassification of suchcases as “negative” decreased the rate of “atypical” from 25% to21%, although the high rate of subsequent “high-grade cancer”among nonsurveillance patients suggested that the reclassificationmay be “inappropriate.”46
In Paris System 2013, nonatypical urothelial cell groups areclassified as “negative for high-grade carcinoma” except in casesthat display fibrovascular cores that are now diagnosed as “low-grade urothelial neoplasm.” However, because of the correlationof nonatypical urothelial cells with high-grade carcinoma (highspecificity and negative predictive value [87.1% and 94%, respec-tively]) despite low sensitivity (30.4%), Granados et al. concludedthat the presence of nonatypical urothelial cell clusters in voidedurine (even without fibrovascular cores) should not be diagnosedas “negative.”39
The predictive values of “suspicious” and “high-grade carci-noma” diagnoses were unchanged (94% each) after reclassificationwith Paris System 2013 despite the new exclusion criterion of cel-lular degeneration for “suspicious.”44 Joudi et al.22 found that“high-grade carcinoma” with the Paris System 2013 yielded ahigher predictive value for carcinoma than the cytologic diagnosisof “suspicious” (79% versus 55%, respectively), similar to resultswith the Bostwick Laboratories Classification (74% versus 54%,respectively).22,47
Addition of anisonucleosis and India ink nuclei (but not tumordiathesis, ragged edge of urothelial cells, apoptotic bodies, or pleo-morphism) significantly improved the predictive accuracy of theParis System 2013 according to Suh et al.48 With their modifica-tion the reporting rate of “atypical” decreased from 25% in theiroriginal system to 15% in Paris System 2013 and 11% in Suh’sproposed modification; likewise, sensitivity increased from 59%to 71% and 90.0%, respectively.48
Interobserver agreement with the Paris System 2013 was ade-quate for the category of “negative for high-grade carcinoma,”but not for the other categories, with mean absolute agreementof 65% and a mean expected agreement of 44%; the meanchance-corrected agreement (κ) was only 0.32.49 Approximately15% of disagreements were classified as high clinical impact.The authors concluded that this low level of diagnostic precisionmay negatively impact the applicability of Paris System 2013 forwidespread clinical application.
Normal Components of the Urinary Sediment
Themost common cellular elements are benign superficial urothelialcells, followed by intermediate and basal urothelial cells that are
more commonly observed in instrumented specimens. Superficialsquamous cells from the female genital tract often outnumberurothelial cells. Benign glandular cells (from cystitis glandularis),squamous cells originating in squamous metaplasia of urotheliumor external genital tract skin, and, rarely, benign seminal vesical cellsalso fall into this category. Clusters or fragments of urothelial cellsthat may be seen in both instrumented and noninstrumented urinespecimens should be classified as “negative” unless the cytomorphol-ogy of the cells forming the group fulfills the criteria for “atypical.”Similarly, changes associated with urolithiasis, treatment-relatedchanges, and polyomavirus cytopathic changes should all be classi-fied as “negative,” according to Paris System 2013.
Urothelial cells are the most variably sized cells in the urinarysediment, ranging from 20 μm in diameter for intermediate andbasal cells up to 100 μm for typical “umbrella” or superficial cells.Urothelial cells typically have single round to oval nuclei withabundant, homogenous, predominately basophilic cytoplasm.Cells from the basal urothelium are smaller, round, and displaywell-defined thickened cytoplasmic membranes. Chromocentersand multiple eosinophilic micronucleoli may be prominent, espe-cially in cases with accompanying inflammation.
Fragments of urothelial cells are commonly found in catheter-ized specimens, as well as bladder washes; however, it is abnormalto see urothelial fragments in spontaneously voided urine, and theirpresence may be associated with papilloma or low-grade urothelialcancer. Occasionally large urothelial fragments may display cyto-plasmic vacuoles containing neutrophils. Multinucleation, nuclearenlargement, and hyperchromasia can be found in inflammatoryprocesses within the lower urinary tract.
Superficial (Umbrella) CellsRegardless of the type of sample and collection technique used,superficial urothelial cells are a common component of the urinesediment. These cells have one or more nuclei that are large, mea-suring up to 3 μm in diameter, comparable with superficial squa-mous cells (Fig. 7.1A).8 Binucleate and multinucleate cells arecommon. Such cells are often larger than the mononucleate super-ficial cells, and their nuclei are somewhat smaller. Large multi-nucleate superficial cells are by far the most striking componentof the urinary sediment, particularly in washings or brushings ofthe bladder or ureter. Multinucleate superficial cells are particularlylarge and may be mistaken for giant cells. A potential error in diag-nosis is misinterpretation of large superficial cells as macrophagesor tumor cells. The DNA content of superficial cells may bepolypoid.50,51
The chromatinic rim of the nucleus is thick and sharply demar-cated. The chromatin is finely granular, often with a “salt and pep-per” appearance, and may contain one or more prominentchromocenters. The structure of the nucleus is better preservedin bladder washings than in voided urine. In women there maybe a sex chromatin body attached to the nuclear membrane.The cytoplasm of these cells is usually basophilic, often finelygranular, and sometimes vacuolated. The cell border is convex(luminal) and concave (deep).
Cells Originating From the Deeper Layers of theUrotheliumAll other urothelial cells are smaller than the superficial cells, andoften exfoliate in clusters, particularly in instrumented specimens.Single small urothelial cells are observed in voided urine. Clusters

Fig. 7.1 Normal superficial (umbrella) cells. (A) Superficial cells in voided urine. (B) Deeper layer cells (parabasal cells).
Fig. 7.2 Columnar cells in bladder wash.
Fig. 7.3 Squamous cells in the urine.
327CHAPTER 7 Urine Cytology
of urothelial cells may be tightly packed and assume spherical“pseudopapillary” configurations with sharp borders. Such clustersare often misinterpreted as low-grade papillary carcinoma.52,53
When deep (basal) cells are removed by instrument, they oftenappear in loose clusters. These cells are polygonal or elongate,sometimes columnar, and almost always display cytoplasmic exten-sions in contact with other cells. The amount of basophilic cyto-plasm in such cells depends on the layer of origin and is moreabundant in cells derived from upper layers. Single cells resembleparabasal squamous cells in size and configuration. These cells areoften spherical or round, particularly in voided urine, but may alsoshow cytoplasmic extensions.8 The nuclei of the smaller urothelialcells are approximately the same size, measuring about 2 to 5 μm indiameter (Fig. 7.1B). They are usually finely granular and benignappearing, containing one or rarely two small chromocenters. Invoided urine the nuclei may be pale or opaque and occasionallysomewhat darker.
Columnar CellsColumnar urothelial cells are common, particularly in specimensobtained by instrumentation.54 Columnar cells often derive fromcystitis cystica or the urethra. They can be single or in small groups,often with a tail by which they are attached to the basement mem-brane (Fig. 7.2).
Mucus-Containing Epithelial CellsOccasionally urine specimens contain mucus-secreting columnarepithelial cells with peripheral nuclei and distended clear cyto-plasm. These cells may be ciliated. Such cells often derive fromcystitis cystica or cystitis glandularis but may represent cells fromurachal remnant, nephrogenic metaplasia, or M€ullerian rest (endo-metriosis or endocervicosis).
Squamous CellsSquamous cells of varying size and degrees of maturation are com-mon in urine sediment, particularly in voided specimens (Fig. 7.3).Such cells are more abundant in female than male patients.8 In

A
C
B
Fig. 7.4 (A) Proximal and distal convoluted cells from the nephron.(B) Necrotic proximal and distal convoluted cells. (C) Collecting duct cells.
328 CHAPTER 7 Urine Cytology
women these cells originate in the urethral squamous epitheliumand in the trigone of the urinary bladder, and are often glycoge-nated. Voided urine sediment may also contain squamous cellsderived from the vulva, vagina, or uterine cervix. In men the originof the squamous cells is the terminal portion of the urethra or, inrare cases, vaginal type of squamous metaplasia with bladder origin.Among the benign squamous cells, there may be superficial cells,intermediate cells, and small parabasal cells. Navicular cells areintermediate squamous cells with abundant cytoplasmic glycogencontent and peripheral nuclei; these cells stain yellow with Papani-colaou stain. Such cells may be observed during pregnancy, earlymenopause, and sometimes in women or men receiving hormonaltherapy (androgen deprivation therapy for prostate cancer). Squa-mous cells may also be anucleate and fully keratinized. In suchcases these should be reported, because the presence of such“ghost” cells may be of considerable significance, representing leu-koplakia or squamous cell carcinoma of the bladder.7
Renal Epithelial CellsCells derived from renal tubules sometimes appear in the urine sed-iment. These cells are small and usually poorly preserved, withpyknotic, hyperchromatic, condensed, spherical nuclei, and gran-ular eosinophilic cytoplasm. Occasionally the tubular cells formsmall clusters or casts. The significance of tubular cells in urine sed-iment remains uncertain. In patients after kidney transplant thepresence of renal tubular cells may indicate rejection of theallograft.55
Convoluted Tubular CellsCells from the convoluted tubular epithelium are the largest cells inthe nephron, present at the entrance to the Bowman capsule andextending to the beginning of the loop of Henle. These cells arerarely seen in healthy individuals but are shed in large numbersin cases of renal toxicity and renal ischemia caused by a wide varietyof drugs, heavy metals, immunosuppressant, and other toxins.
Proximal tubular cells in urine are easily identified by theirlarge size (20 to 60 μm in diameter); irregular, elongate, orcigar-like appearance; and coarsely granular basophilic cytoplasm(Fig. 7.4A). Cytoplasmic borders are indistinct and may be raggedor torn. The granular cytoplasm contains large numbers of mito-chondria by ultrastructure. Nuclei are slightly larger than erythro-cytes and may occasionally be multinucleate. Interestingly,proximal and distal tubular cells appear singly, never in fragmentsor clusters. These cells are often mistaken for granular casts inunstained bright-field microscopy. Proximal and distal renal tubu-lar cells slough from their basement membranes and can be foundin urine as intact preserved cells or as “ghost” or necrotic forms thatretain their size and cytoplasmic characteristics (Fig. 7.4B).
Collecting Duct CellsRenal tubular cells lining the proximal and distal collecting ductsare small (12 to 18 μm in diameter), and each contains a singleslightly eccentric nucleus with coarse and evenly distributed chro-matin. There may be an occasional prominent nucleolus, becausethese cells may be reactive, but they are never multinucleate. Thecytoplasm is polygonal to columnar, finely granular, and uniform

329CHAPTER 7 Urine Cytology
basophilic, with distinct borders (Fig. 7.4C). Vacuolization mayoccasionally be seen, especially in reactive states. The cells mayphagocytize castlike material, crystals, and pigments.
Collecting duct cells in urine may be present in very low num-bers in normal individuals, but are significant when found withrenal casts or as fragments. An abnormal number (greater thanone per hpf) may be found in a wide variety of clinical conditions,including shock, trauma, burn, and exposure to toxins; also, anincreased number of cells in renal transplant patients heraldsclinical rejection up to 48 hours early.56
Renal epithelial cell fragments in urine indicate a severe form ofrenal tubular injury (“ischemic necrosis”) and are exclusively fromthe collecting duct. This reflects loss of blood flow (ischemic injury)to the renal tubules and subsequent sloughing of entire segments orportions of the renal tubules with regeneration of lost epithelium, aprocess similar to repair in cervical smears. There are five typesof fragments, and these are classified according to morphology:(1) spindle fragments; (2) fragments attached to or surrounding castmaterial; (3) pavement or “en face” fragments; (4) fragments withreactive cellular or noncellular inclusions (castlike, crystal, or pig-mented [bile] inclusions); and (5) cylindrical, tubelike fragments.
Other Benign CellsOccasionally cells of prostatic and seminal vesicle (Fig. 7.5) originmay be present in the urinary sediment. Such cells accompanyspermatozoa and are common after prostatic massage.57,58 Eryth-rocytes are a frequent component of the urinary sediment, partic-ularly in patients with clinical evidence of hematuria (see later).7
Inflammatory CellsMacrophages are often observed in inflammatory reactions of theurinary tract. The cells may be mononucleate or multinucleate andcontain fine cytoplasmic vacuoles, sometimes with phagocyticdebris. Normal urine sediment contains very few lymphocytes orneutrophils. The presence of large numbers of such cells may pre-cede clinical evidence of inflammation. For example, when therewere more than 12.5 white blood cells/μL by image analysis,sensitivity and specificity for predicting Chlamydia infection were87% and 89%, respectively, in first voided urines in men at highrisk.59
Fig. 7.5 Seminal vesicle cells and sperm in voided urine.
Noncellular Components of the Urinary SedimentIn addition to viral inclusions, a variety of intracellular and extra-cellular findings may be diagnostically valuable in the urinesediment.
Pigment and Pigmented CellsNumerous normal and pathologic processes result in extracellularpigmented material in the urine and pigmented cells (Table 7.4).60
Cytoplasmic Eosinophilic Inclusions (Melamed-WolinskaBodies)Nonspecific cytoplasmic inclusions may appear as products ofdegenerating cells in multiple body fluids and can be seen withcareful examination in 43% of urine samples.61 There is no rela-tionship with any disease. The round, opaque bodies are 12 to15 μm in diameter, and may be single or multiple, with eosino-philia standing in contrast with the pale-staining urothelial cyto-plasm. Nuclei are usually degenerate, with hyperchromasia,karyorrhexis, or pyknosis, but may also be intact.
Nonspecific cytoplasmic eosinophilic inclusions should bedistinguished from acid-fast–positive nuclear inclusions in renaltubular cells associated with lead poisoning, as well as nonspecificacid-fast–negative red nuclear inclusions of uncertain significancein older women.62,63
CrystalsPolygonal transparent crystalline precipitates of urates are commonin voided urine. Their presence results from changes in the acidityof urine after collection but has no diagnostic significance. Crystalsderived from true uric acid are rare, and other crystals are rarely ofdiagnostic value.64 Voided urine and occasional specimensobtained by instrumentation may contain contaminants and renalcasts. For a complete review, refer to other texts.
Casts and Other Findings Attributable to RenalDiseases in UrineRenal casts are observed in urine sediment in patients with glomer-ular and renal parenchymal diseases. Casts are composed of Tamm-Horsfall protein and originate in the distal tubules and collectingducts. In healthy individuals hyaline and rare granular casts may
TABLE 7.4Pigmented Cells in Urine: Differen-tial Diagnosis
Finding Description
Lipofuscin pigment Granular yellow-brown pigment scattered aroundnuclei, often obscured by degenerative changes
Hemosiderin Coarse golden-brown, brown, or black pigmentusually in the cytoplasm of macrophages or rarelyin urothelium; often observed in the setting ofinjury, blood transfusions, calculi, or foreignbodies; may be mistaken for melanin
Melanin Dusty brown pigment found in melanosis, nevi, ormelanoma; the greatest difficulty is when melaninpigment is associated with atypical urothelial cells;distinguishing urothelial cells from melanoma cellsmay require biopsy; with uncertainty, biopsy isindicated

330 CHAPTER 7 Urine Cytology
occasionally appear because of dehydration, fever, exercise, andother factors; these casts are considered physiologic. Conversely,nonphysiologic casts made of abnormal urine protein and thosethat contain cells of various types are easily identified. The typeof cells contained within the cast matrix, the width of the casts,and the number of casts is indicative of the severity of the under-lying disease. The presence of abnormal amounts of protein, blood,leukocytes, nitrites, and bilirubin all correlate with the type of cast.
“Round cells” are recently described cells in patients withend-stage renal failure that appear to be predictive of early hemo-dialysis.65 They are distinct from known cells in sediment and aresimilar to proximal convoluted tubule-derived cells based on mor-phology and molecular marker expression (GGT1, but not podo-calyxin). These cells also express PAX2, Wilms tumor 1 (WT1),OSR1, and SIX2. The number of round cells correlates with theseverity of chronic kidney disease.
The severity of lupus nephritis correlates strongly with voidedurine cytology findings, including erythrocytes (isomorphic anddysmorphic), acanthocytes, and leukocytes (0.65 for each); classi-fication tree has an accuracy rate of 84.3%.66
Dysmorphic red blood cells may be indicative of urologic or glo-merular diseases (see later).
Diagnostic Criteria
InfectionsBacteriaA wide variety of bacteria may affect the epithelium of the urinarytract. Most are coliforms and other gram-negative rods. Cystitismay be acute or chronic. Acute cystitis is usually associated withsymptoms that rarely require confirmatory tissue biopsy or cyto-logic examination. The sediment may contain numerous exfoliatedurothelial cells, necrotic material, and inflammatory cells, with apredominance of neutrophils (Fig. 7.6A to C). Marked necrosisand inflammation may also occur in the presence of necrotictumors, particularly high-grade urothelial carcinoma and squa-mous cell carcinoma.
The sediment in chronic cystitis usually contains a backgroundof chronic inflammation with macrophages and erythrocytes.7
Urothelial cells may be abundant and poorly preserved, occasion-ally forming small clusters. The cytoplasm in these cells tends to begranular and vacuolated; when the cells are degenerate, thecytoplasm contains spherical eosinophilic inclusions (Melamed-Wolinska bodies) (Fig. 7.7).67 There may be slight nuclear
Fig. 7.6 (A) Acute cystitis, consisting of marked inflammation, degenerateurothelial cells, and scattered superficial cells. (B) Necrosis and macro-phages in tuberculosis of bladder. (C) Acid-fast bacilli in urine (Ziehl-Neelsen stain).

Fig. 7.7 Degenerate urothelial cells with cytoplasmic inclusions (Melamed-wolinska bodies).
331CHAPTER 7 Urine Cytology
enlargement and hyperchromasia, but the contours of the nucleiare usually regular and the chromatin texture is finely granularwithout the coarse granularity of cancer cells. There may be necro-sis of urothelial cells, with nuclear pyknosis and marked cytoplas-mic vacuolization. In ulcerative cystitis, large sheets of urothelialcells may exfoliate.
Interstitial cystitis, a form of chronic cystitis associated withchronic inflammation, displays nonspecific cytologic changes.8
Eosinophilic cystitis has a predominance of eosinophils, a patternthat may be seen in patients with allergic disorders, previous biop-sies, or after mitomycin C treatment.68
Tuberculous cystitis may be observed in patients with AIDSand those receiving treatment for urothelial carcinoma with bacil-lus Calmette–Gu�erin (BCG). In such patients the urine has inflam-matory cells, necrosis (Fig. 7.6B), and rarely contains fragmentsof tubercles consisting of clusters of elongate carrot-shapedepithelioid cells, sometimes accompanied by multinucleatedLanghans-type giant cells, and reactive atypia of urothelialcells.69-71 Ziehl-Neelsen staining may reveal acid-fast bacilli
Fig. 7.8 Candida albicans in the urinary sediment. (A) Distinctive branching fungathat stand in contrast with the urothelial cells.
(Fig. 7.6C). The sediment occasionally contains “decoy” cells withglassy hyperchromatic nuclei.70 Similar findings may occur inpatients with tuberculosis of the bladder.
FungiFungi occasionally affect the lower urinary tract, particularly theurinary bladder, and Candida albicans is the most common, usuallyseen in pregnant women, diabetics, and those with impairedimmunity such as patients with AIDS, those undergoing chemo-therapy for cancer, and bone marrow transplant recipients. Inthe sediment the fungi may appear as yeast forms, with small ovalbodies, or pseudohyphae, with oblong branching nonencapsulatedfilaments (Fig. 7.8A and B). Other fungi are uncommon, includingBlastomyces dermatitidis, Aspergillus, and mucormycosis. A fungus ofthe species Alternaria is a common laboratory contaminant.8
VirusesSeveral important viruses cause significant morphologic changes inthe urothelial cells, many of which may be confused with malig-nancy. The dominant feature of viral infection is the formationof nuclear and cytoplasmic inclusions (Table 7.5).
Herpes simplex is an obligate intracellular virus, and florid infectionwith permissive replication of the virus causes abnormalities inurothelial cells that are readily recognized. In the early stages of viralreplication the nuclei of infected cells appear hazywith a ground-glassappearance. Multinucleation is commonly observed in such cells.Multiple nuclei are often densely packed, with nuclear moldingand tightly fitting contoured nuclei (Fig. 7.9). In later stages of infec-tion the viral particles concentrate in the center of the nuclei, formingbright eosinophilic inclusions with a narrow clear zone or halo at theperiphery. Infected cells may contain single or multiple nuclei.8,64
Cytomegalovirus is usually seen in newborn infants withimpaired immunity. The infection is common in adults with AIDS.The characteristic changes are readily recognized in the sediment,including large cells with prominent basophilic nuclear inclusionssurrounded by an abundant peripheral clear zone (Fig. 7.10). Thereis a distinct outer band of condensed nuclear chromatin.
Polyomavirus infection is widespread, according to serologicstudies of adults. The BK polyomavirus may cause hemorrhagiccystitis in patients with allogeneic hematopoietic stem cell
l hyphae are abundant in this routine specimen. (B) Note the small oval bodies

Fig. 7.9 Herpes infection.
Fig. 7.10 Cytomegalovirus infection.
TABLE 7.5Characteristic Cytologic ChangesAssociated with Viruses
Cytomegalovirus• Enlarged cells• High N/C ratio• Basophilic intranuclear inclusion with “owl’s-eye” appearance; occa-
sionally small, dark intracytoplasmic inclusions
Herpesvirus• Enlarged, multinucleated cells with “ground-glass” chromatin• High N/C ratio• Opaque, structureless chromatin• Eosinophilic intranuclear inclusion
Polyomavirus• Enlarged cells• High N/C ratio• Opaque, structure-less chromatin, chromatinic membrane is common• Nuclei stain with a magenta hue• Intranuclear inclusion fills almost the entire nuclear area
Papillomavirus• Perinuclear clear cytoplasmic zones (koilocytosis)• Nuclear enlargement and homogeneous hyperchromasia
N/C, Nuclear-to-cytoplasmic.
332 CHAPTER 7 Urine Cytology
transplant and virus-associated nephritis in patients with renaltransplant. The occult virus can become activated and recognizedin voided urine sediment. Polyomavirus plays a major role in urinecytology because it produces cell abnormalities that may be readilyconfused with cancer; these cells are also known as “decoy” cells(Fig. 7.11A).72 In permissive infections, the virus produces largehomogeneous basophilic nuclear inclusions that occupy almostthe entire volume of the nuclei with only a thin chromatinicrim.73,74 The background usually contains abundant inflammatoryand cellular debris. Infected cells are often enlarged and usuallycontain a single nucleus, but binucleation and occasional largemultinucleated cells may be seen.75 Elongate cells are referred to
as “comet” cells. Nonspecific eosinophilic inclusions (Melamed-Wolinska bodies) may be present in the cytoplasm.67 Late infec-tions may contain pale-staining degenerated inclusion-bearing cellsin cases in which the virus may be detected in voided urine.76
When the inclusions regress, the chromatin acquires a distinctive,coarsely clumped appearance. Clearance of decoy cells from urine isclosely related to histologic remission of polyomavirus nephropa-thy.77 The cytologic picture in some cases may be quite dramaticand has led to misdiagnosis of carcinoma.78 Decoy cells do notexhibit aneuploidy by FISH, and acid hematoxylin stain appearedto be superior to Papanicolaou stain in identifying and confirmingthe presence of infection (Fig. 7.11B).79 Decoy cells occurred in14% of samples from patients with histologically proven viralnephropathy, with a sensitivity of 67%, specificity of 89%, positivepredictive value of 12%, and negative predictive value of 99%.80
Quantification of decoy cells improved the positive predictive valueto 32% (threshold 10 � cells). Immunohistochemical staining ofurinary exfoliated cells for SV40T improved sensitivity to 86% fordetecting atypical or degenerate infected cells (specificity of 93%and positive predictive value of 33%).
More than 70 types of human papillomavirus have been identi-fied, and types 6 and 11 are associated with condyloma acuminatum.Condyloma may also appear in the urethra and invariably induceskoilocytosis. Urothelial carcinoma exhibits a low incidence ofhuman papillomavirus types 16 and 18 infection (Fig. 7.12).81
Trematodes and Other ParasitesThe most common urine parasite is Schistosoma haematobium (Bil-harzia). There are two important cytologic manifestations of infec-tion with S. haematobium: recognition of the ova and the malignanttumors that may be associated with it.68 The ova are elongate struc-tures with a thick transparent capsule and a sword-shaped protru-sion known as the terminal spine located at the narrow end ofthe ovum. Fresh or calcified ova may be readily recognized in thesediment. The embryonal form of the parasite, known as miracid-ium, is released in human stool and urine, retaining the shape of theovum with its terminal spine. Other common intestinal parasitesthat affect the bladder include Ascaris lumbricoides, Enterobius vermi-cularis, and agents of filariasis. Trichomonas vaginalis is a sexuallytransmitted parasite that is rarely found in urine (0.1% incidence),appearing as round to oval organisms with eccentric nuclei and cyto-plasmic granules; acute inflammation is usually present.82 Hassanet al. described microfilariae of Wuchereria bancrofti in an18-year-old boy in India who presented with chylous hematuria.273

Fig. 7.11 Decoy cells in polyomavirus infection. (A) These may be mistaken for malignant cells. (B) Nuclear details of polyomavirus infection(acid hematoxylin stain).
Fig. 7.12 Koilocytes (Human papillomavirus infection) in urine.
TABLE 7.6Differential Diagnosis of UrothelialAtypia Found in Urinary Sediment
Urinary tract conditionsUrethral catheterizationUrinary calculiChronic cystitis and cystitis glandularisPolyoma (BK) virus infectiona
Cellular changes resulting from radiation therapy and chemotherapyReactive and/or hyperplastic urothelium (e.g., cystitis, inflammation, etc.)Papillary urothelial tumor of low malignant potential and low-grade
urothelial carcinomaRenal parenchymal conditions
Acute tubular necrosisPapillary necrosisRenal infarctionAcute allograft rejection with ischemic necrosis
aNot considered within the category of “atypical” in Paris System 2013 (categorized as“negative”).
333CHAPTER 7 Urine Cytology
Reactive Cytologic ChangesNumerous reactive changes involving the urothelium may be mis-interpreted as “atypical” or “suspicious/malignant” (Table 7.6).
LithiasisAbout 40% of patients with calculi have abnormal cytologic find-ings in voided urine.52 These patients have numerous large,smooth-bordered clusters of benign urothelial cells with an abun-dance of superficial cells (Fig. 7.13A). These changes may overlapwith the spectrum of findings with low-grade urothelial carci-noma, but the cells tend to cluster, with fewer single cells.52 Cal-culi are abrasive to the mucosa when present in the renal pelvis,ureter, or urinary bladder, and the resultant cytologic specimensclosely resemble the effects of instrumentation. Significant atypiaof urothelial cells due to lithiasis is uncommon, and the clustershave smooth borders (Fig. 7.13B and C).8 Nonetheless, lithiasisremains a major diagnostic pitfall in urine cytologyinterpretation.
Drug EffectsIntravesically administered agents and drugs, including BCG (seeearlier Bacteria section), mitomycin C, and thiotepa, are com-monly used for treatment of primary and recurrent bladder tumors(Figs. 7.14A and B and 7.15). They may induce cell enlargement,cytoplasmic vacuolization, and other reactive changes, includingnuclear enlargement of cells, wrinkled nuclear membranes, mildhyperchromasia, pleomorphism, abnormal nuclear morphology,disordered orientation of the urothelium, and eosinophilicinflammation.83 Intravesical chemotherapy can contribute tofalse-positive results in urine cytology.84
Systemically administered drugs, such as the alkylating agentscyclophosphamide and busulfan, have a marked effect on theurothelium, inducing significant cytologic abnormalities(Fig. 7.16A to C). These drugs may cause changes that includebizarre urothelial cells with marked nuclear and nucleolar enlarge-ment, mimicking poorly differentiated carcinoma.8,85,86 Largedoses of cyclophosphamide have been shown to induce urothelialcarcinoma, leiomyosarcoma, and carcinosarcoma.87,88
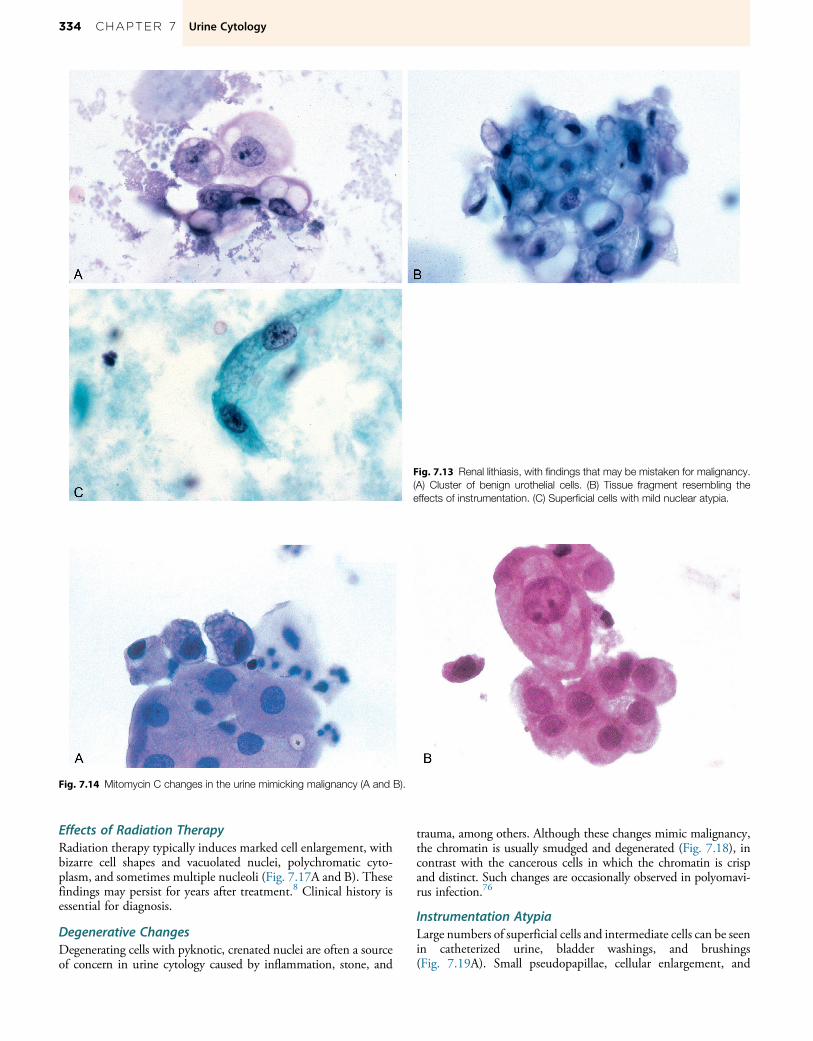
Fig. 7.14 Mitomycin C changes in the urine mimicking malignancy (A and B).
Fig. 7.13 Renal lithiasis, with findings that may be mistaken for malignancy.(A) Cluster of benign urothelial cells. (B) Tissue fragment resembling theeffects of instrumentation. (C) Superficial cells with mild nuclear atypia.
334 CHAPTER 7 Urine Cytology
Effects of Radiation TherapyRadiation therapy typically induces marked cell enlargement, withbizarre cell shapes and vacuolated nuclei, polychromatic cyto-plasm, and sometimes multiple nucleoli (Fig. 7.17A and B). Thesefindings may persist for years after treatment.8 Clinical history isessential for diagnosis.
Degenerative ChangesDegenerating cells with pyknotic, crenated nuclei are often a sourceof concern in urine cytology caused by inflammation, stone, and
trauma, among others. Although these changes mimic malignancy,the chromatin is usually smudged and degenerated (Fig. 7.18), incontrast with the cancerous cells in which the chromatin is crispand distinct. Such changes are occasionally observed in polyomavi-rus infection.76
Instrumentation AtypiaLarge numbers of superficial cells and intermediate cells can be seenin catheterized urine, bladder washings, and brushings(Fig. 7.19A). Small pseudopapillae, cellular enlargement, and
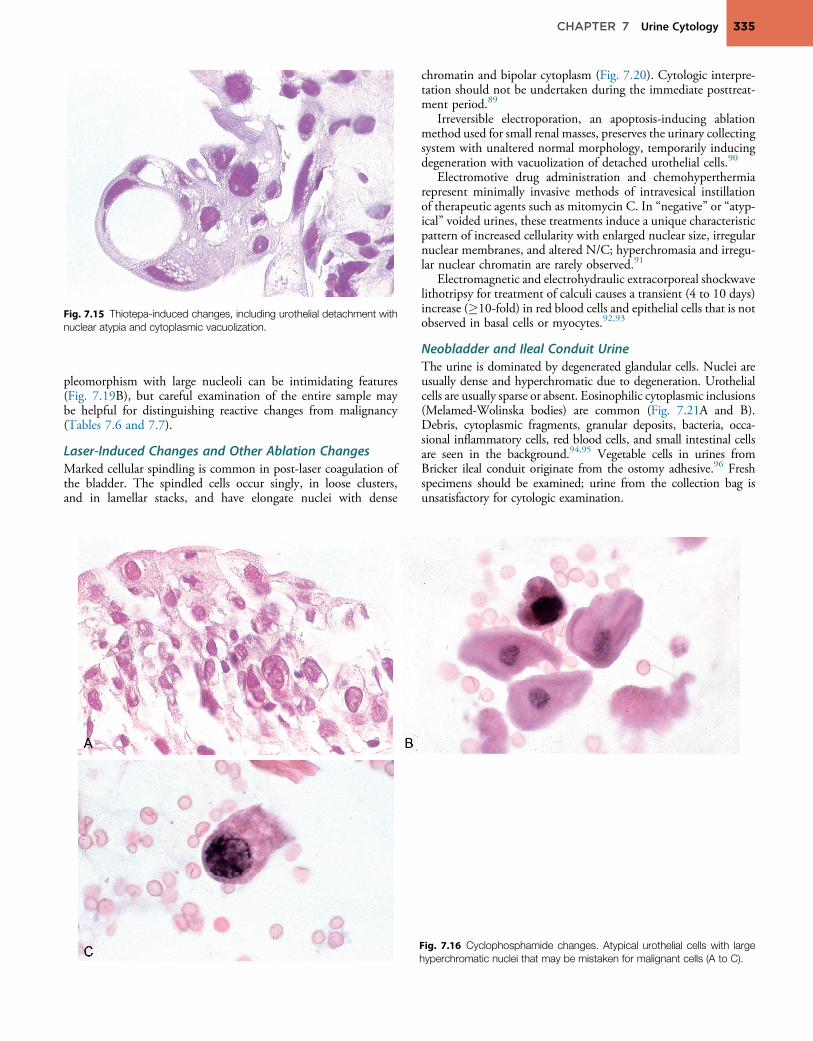
Fig. 7.15 Thiotepa-induced changes, including urothelial detachment withnuclear atypia and cytoplasmic vacuolization.
335CHAPTER 7 Urine Cytology
pleomorphism with large nucleoli can be intimidating features(Fig. 7.19B), but careful examination of the entire sample maybe helpful for distinguishing reactive changes from malignancy(Tables 7.6 and 7.7).
Laser-Induced Changes and Other Ablation ChangesMarked cellular spindling is common in post-laser coagulation ofthe bladder. The spindled cells occur singly, in loose clusters,and in lamellar stacks, and have elongate nuclei with dense
chromatin and bipolar cytoplasm (Fig. 7.20). Cytologic interpre-tation should not be undertaken during the immediate posttreat-ment period.89
Irreversible electroporation, an apoptosis-inducing ablationmethod used for small renal masses, preserves the urinary collectingsystem with unaltered normal morphology, temporarily inducingdegeneration with vacuolization of detached urothelial cells.90
Electromotive drug administration and chemohyperthermiarepresent minimally invasive methods of intravesical instillationof therapeutic agents such as mitomycin C. In “negative” or “atyp-ical” voided urines, these treatments induce a unique characteristicpattern of increased cellularity with enlarged nuclear size, irregularnuclear membranes, and altered N/C; hyperchromasia and irregu-lar nuclear chromatin are rarely observed.91
Electromagnetic and electrohydraulic extracorporeal shockwavelithotripsy for treatment of calculi causes a transient (4 to 10 days)increase (�10-fold) in red blood cells and epithelial cells that is notobserved in basal cells or myocytes.92,93
Neobladder and Ileal Conduit UrineThe urine is dominated by degenerated glandular cells. Nuclei areusually dense and hyperchromatic due to degeneration. Urothelialcells are usually sparse or absent. Eosinophilic cytoplasmic inclusions(Melamed-Wolinska bodies) are common (Fig. 7.21A and B).Debris, cytoplasmic fragments, granular deposits, bacteria, occa-sional inflammatory cells, red blood cells, and small intestinal cellsare seen in the background.94,95 Vegetable cells in urines fromBricker ileal conduit originate from the ostomy adhesive.96 Freshspecimens should be examined; urine from the collection bag isunsatisfactory for cytologic examination.
Fig. 7.16 Cyclophosphamide changes. Atypical urothelial cells with largehyperchromatic nuclei that may be mistaken for malignant cells (A to C).

Fig. 7.18 Crenated (Degenerating) cells.
Fig. 7.17 Radiation changes (A and B). Note bizarre enlarged urothelial cells with numerous vacuolations.
Fig. 7.19 Instrumentation atypia. (A) Ureteric wash with mild increase in nuclearpillae) with slightly irregular outline and normal nuclear membrane (bladder was
336 CHAPTER 7 Urine Cytology
Urine Cytology in Renal Transplant RecipientsUrine cytology is an effective screening method for monitoringpatients with renal transplant, with high sensitivity and high negativepredictive value, and can be routinely used in follow-up.97 The epi-thelial cells of collecting tubules are well preserved. The cells thatappear in urine specimens have scant vacuolated cytoplasm withspherical and somewhat opaque nuclei. A feature of impending rejec-tion is the presence of numerous T lymphocytes and erythrocytes inthe urine. The erythrocytes have a thick outer border and clear centersuggestive of renal origin. In rejection, tissue fragments may be pre-sent, including necrotic renal tubules and hyaline casts.55
Other Benign ConditionsA wide variety of benign conditions induce unique findings in theurine. Partial or complete keratinization of the squamous epithe-lium, referred to clinically as leukoplakia, often replaces the urothe-lium, resulting in a cystoscopic gray-white appearance of themucosa. In the urinary sediment, anucleated keratinized cells,
-to-cytoplasmic ratio and prominent nucleoli. (B) Cluster of cells (pseudopa-h sample).

TABLE 7.7Features of Reactive Changes and Urothelial Carcinoma (World Health Organization 1973Classification)
Feature Reactive Changes Grade 1 Carcinoma Grades 2 and 3 Carcinoma and Carcinoma InSitu
Cell arrangements Pseudopapillae Papillae and tight clusters Single cells and loose clustersCell configuration Flat groups Papillary Variable
Size Enlarged, pleomorphic Slightly enlarged, uniform Markedly enlarged, pleomorphicNumbers Few cells Few groups Variable
Cytoplasm Vacuolated Homogeneous Variable, vacuolatedNucleus Central, uniform Eccentric, enlarged Eccentric, pleomorphic
Nuclear-to-cytoplasmicratio
Normal to slightlyincreased
Increased Moderate to markedly increased
Size Slightly enlarged Enlarged EnlargedBorder Smooth, thick Slightly irregular, one or two notches, thin Moderate to markedly irregular, thinChromatin Fine, evenly distributed Granular, evenly distributed Coarse, unevenly distributedNucleoli Often large Small, absent Large, variable
DNA content Diploid Usually diploid Aneuploid
Fig. 7.20 Laser-induced changes.
Fig. 7.21 Ileal conduit urine. (A) Cellular sample with many degenerating cells (lomelamed-wolinska bodies.
337CHAPTER 7 Urine Cytology
so-called ghost cells, may be present. When these cells are present,one should exclude the possibility of squamous cell carcinoma.7,8
Cystitis glandularis may shed ciliated mucus-containing epithelialcells that contain peripheral nuclei and clear cytoplasm. Such cellsmay bemistaken for adenocarcinoma. Endometriosis of the bladdermay result in urine shedding of diagnostic glandular and spindlecells.98 Large numbers ofmacrophagesmay be present in urine sam-ples in patients withmalakoplakia, but the release of such inflamma-tory cells usually occurs after biopsy and is detected in the urinestream (Fig. 7.22A). The spherical, intracytoplasmic, eosinophilic,or calcifiedMichaelis-Guttmann bodies associated with malakopla-kia in the cytoplasmof themacrophages are usually readily identified(Fig. 7.22B). Urinary mulberry cells indicate Fabry disease, a lyso-somal storage disorder caused by a deficiency ofα-galactosidase A.99
Benign Tumors and Tumor-like ProcessesThere are no cell changes that are characteristic of inverted papil-loma (Fig. 7.23A and B) or nephrogenic adenoma, and cytologic
w magnification). (B) Columnar cells, degenerating cells, red blood cells, and
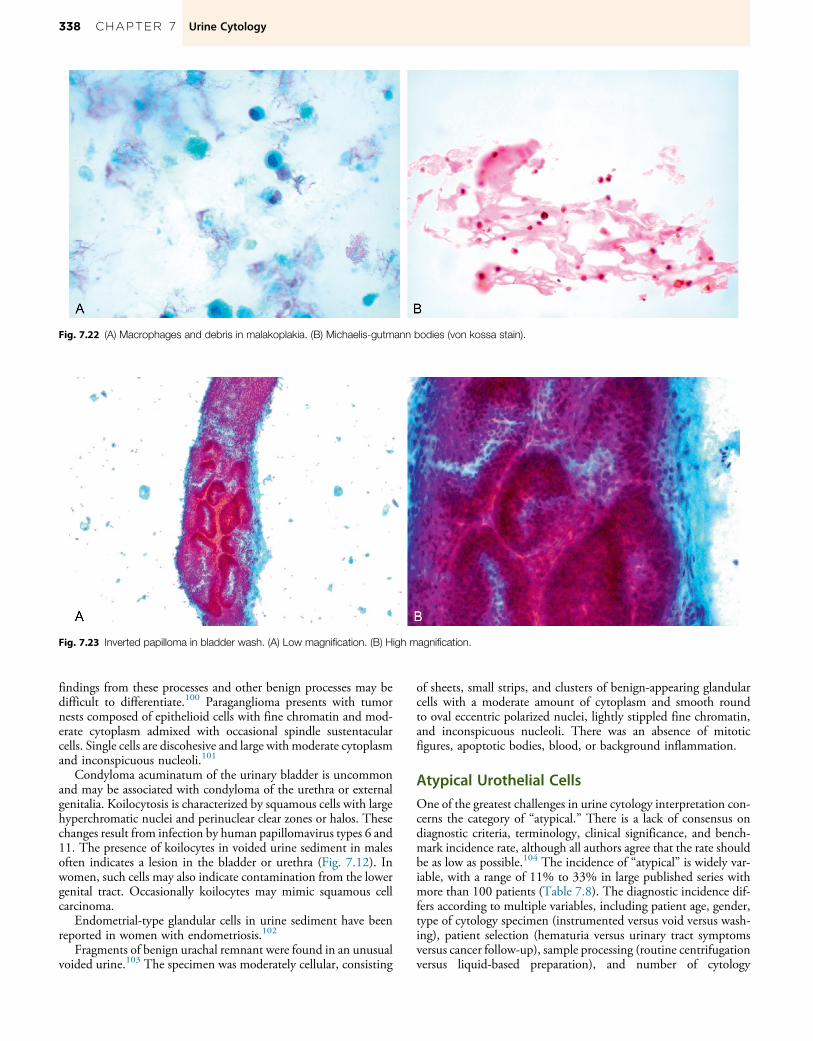
Fig. 7.22 (A) Macrophages and debris in malakoplakia. (B) Michaelis-gutmann bodies (von kossa stain).
Fig. 7.23 Inverted papilloma in bladder wash. (A) Low magnification. (B) High magnification.
338 CHAPTER 7 Urine Cytology
findings from these processes and other benign processes may bedifficult to differentiate.100 Paraganglioma presents with tumornests composed of epithelioid cells with fine chromatin and mod-erate cytoplasm admixed with occasional spindle sustentacularcells. Single cells are discohesive and large with moderate cytoplasmand inconspicuous nucleoli.101
Condyloma acuminatum of the urinary bladder is uncommonand may be associated with condyloma of the urethra or externalgenitalia. Koilocytosis is characterized by squamous cells with largehyperchromatic nuclei and perinuclear clear zones or halos. Thesechanges result from infection by human papillomavirus types 6 and11. The presence of koilocytes in voided urine sediment in malesoften indicates a lesion in the bladder or urethra (Fig. 7.12). Inwomen, such cells may also indicate contamination from the lowergenital tract. Occasionally koilocytes may mimic squamous cellcarcinoma.
Endometrial-type glandular cells in urine sediment have beenreported in women with endometriosis.102
Fragments of benign urachal remnant were found in an unusualvoided urine.103 The specimen was moderately cellular, consisting
of sheets, small strips, and clusters of benign-appearing glandularcells with a moderate amount of cytoplasm and smooth roundto oval eccentric polarized nuclei, lightly stippled fine chromatin,and inconspicuous nucleoli. There was an absence of mitoticfigures, apoptotic bodies, blood, or background inflammation.
Atypical Urothelial CellsOne of the greatest challenges in urine cytology interpretation con-cerns the category of “atypical.” There is a lack of consensus ondiagnostic criteria, terminology, clinical significance, and bench-mark incidence rate, although all authors agree that the rate shouldbe as low as possible.104 The incidence of “atypical” is widely var-iable, with a range of 11% to 33% in large published series withmore than 100 patients (Table 7.8). The diagnostic incidence dif-fers according to multiple variables, including patient age, gender,type of cytology specimen (instrumented versus void versus wash-ing), patient selection (hematuria versus urinary tract symptomsversus cancer follow-up), sample processing (routine centrifugationversus liquid-based preparation), and number of cytology

TABLE 7.8 Incidence and Cancer Yieldd of “Atypical Urine Cytology”a and Other Categories
Authors (Date)
Total Casesof Atypical(n)
AtypicalRate (%)
Cases ofAtypical withFollow-upBiopsy (n)
Time Intervalto Biopsy(months) Negative
All Atypical, Excluding“Favor Neoplasm” and“Favor High-GradeCarcinoma” “Suspicious” “Positive”
Deshpandeand McKee(2005)104
238 N/A 102 �12 N/A 23.4 N/A N/A
Raab et al.(2007)109
710 11.1 133 �14 42 65.4 81.8 79.7
Voss et al.(2008)263
b b 128b �12 56.9 60.9 73.8 90.7
Brimo et al.(2009)107
691 23.2 110 �12 68.9 78 87 N/A
Siddappa et al.(2012)250
464 32.5 464 N/A N/A 11.5 N/A N/A
Dimashkiehet al. (2013)264
296 16.1 296 �36 8.3 32.1 N/A N/A
Bostwick andHossain(2014)47
1074 10.2 1074 �12 13.5 31.1 54.3 75.1
Muus Ubagoet al. (2013)265
1320 8.1 N/A �138 N/A 21.0c N/A N/A
Chau et al.(2015)110
159 22.8 159 �24 41.9 61.3 78.3 83.7
Virk et al.(2017)232
377 N/A 377 �12 N/A 16.5 N/A N/A
The atypical rate may be misleading because many articles reported only cases with matched cytology–histology pairs, and most negative biopsies would be excluded because they do not trigger subsequentbiopsy.N/A, Data not available.aExcludes studies with less than 100 “atypical” cytologies with follow-up biopsy.45,266-269 Excludes upper tract cases and renal cell carcinoma.52 Excludes Piaton et al. (2011)271 and (2014)270 with an“atypical” rate of 0.8% to 2%.bThis study126 included an additional category of cellular “clusters” that accounted for 579 cases, so the results cannot be directly compared with other studies.cPositive includes 44 cases diagnosed by subsequent positive cytology only (no biopsy) and 17 secondary (nonurothelial) carcinomas.dCancer yield on biopsy includes suspicious for malignancy and diagnostic of malignancy because both categories require immediate clinical intervention.
339CHAPTER 7 Urine Cytology
specimens obtained.105 Further, it is compounded by variance insubsequent predictive accuracy of “atypical” for carcinoma. The“atypical” category encompasses findings that may include fromlow- to intermediate-grade dysplasia (an uncommon histologicfinding) (Figs. 7.24 through 7.28) at the low end of the spectrum,
Fig. 7.24 Atypical, favor reactive. (A) Atypical cells with mild hyperchromatic n(B) Atypical cells, same case as in (A) with nuclear chromatin details and smoot
although it is difficult, if not impossible, to recognize specific cyto-logic changes corresponding to histologic low- to intermediate-grade dysplasia.8,106 High-grade (severe) dysplasia and carcinomain situ are considered to be equivalent, and the findings in urinemay be underinterpreted as “atypical” when they are best classified
uclei, slightly overlapping cells, and smooth outlines (Papanicolaou stain).h nuclear membrane (acid hematoxylin stain).

Fig. 7.25 Atypical, uncertain. (A) Groups of atypical cells with mildly hyperchromatic nuclei and mild nuclear membrane irregularity (Papanicolaou stain). (B)Same case as in (A) depicting nuclear details (acid hematoxylin stain).
Fig. 7.26 Atypical cells in bladder wash. (A) Papanicolaou stain. (B) Acid hematoxylin stain.
Fig. 7.27 Atypical cells in voided urine. (A) Papanicolaou stain. (B) Acid hematoxylin stain.
340 CHAPTER 7 Urine Cytology
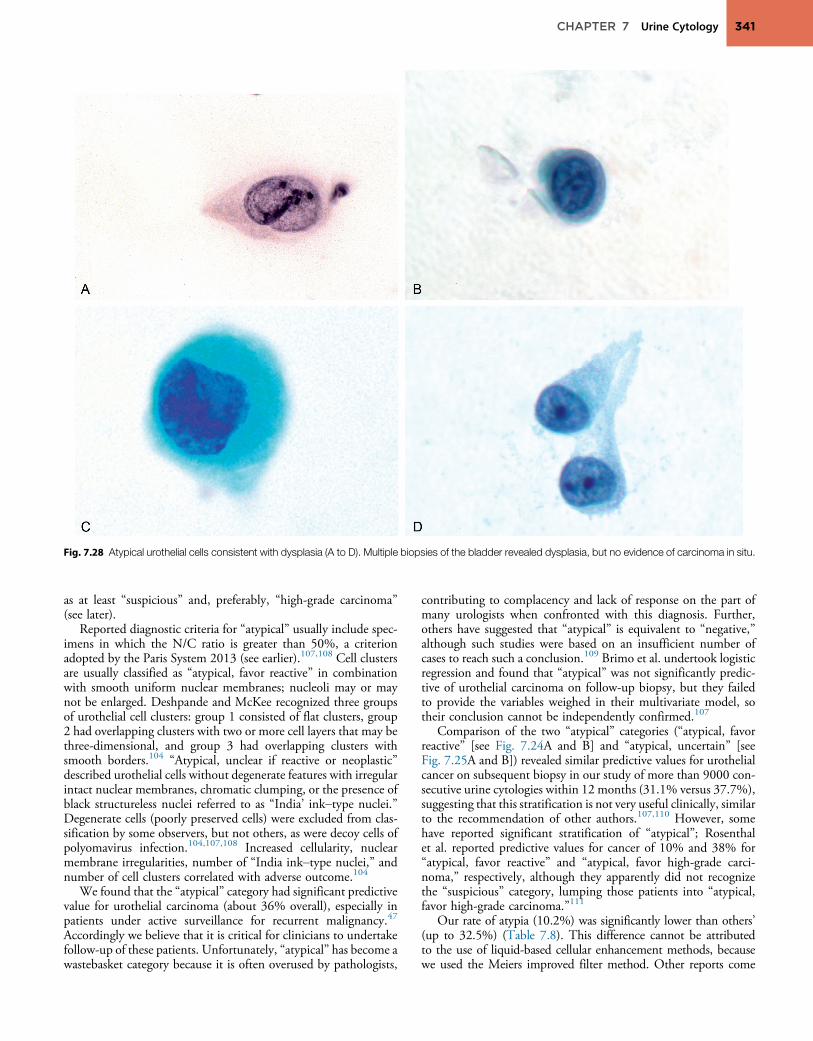
Fig. 7.28 Atypical urothelial cells consistent with dysplasia (A to D). Multiple biopsies of the bladder revealed dysplasia, but no evidence of carcinoma in situ.
341CHAPTER 7 Urine Cytology
as at least “suspicious” and, preferably, “high-grade carcinoma”(see later).
Reported diagnostic criteria for “atypical” usually include spec-imens in which the N/C ratio is greater than 50%, a criterionadopted by the Paris System 2013 (see earlier).107,108 Cell clustersare usually classified as “atypical, favor reactive” in combinationwith smooth uniform nuclear membranes; nucleoli may or maynot be enlarged. Deshpande and McKee recognized three groupsof urothelial cell clusters: group 1 consisted of flat clusters, group2 had overlapping clusters with two or more cell layers that may bethree-dimensional, and group 3 had overlapping clusters withsmooth borders.104 “Atypical, unclear if reactive or neoplastic”described urothelial cells without degenerate features with irregularintact nuclear membranes, chromatic clumping, or the presence ofblack structureless nuclei referred to as “India’ ink–type nuclei.”Degenerate cells (poorly preserved cells) were excluded from clas-sification by some observers, but not others, as were decoy cells ofpolyomavirus infection.104,107,108 Increased cellularity, nuclearmembrane irregularities, number of “India ink–type nuclei,” andnumber of cell clusters correlated with adverse outcome.104
We found that the “atypical” category had significant predictivevalue for urothelial carcinoma (about 36% overall), especially inpatients under active surveillance for recurrent malignancy.47
Accordingly we believe that it is critical for clinicians to undertakefollow-up of these patients. Unfortunately, “atypical” has become awastebasket category because it is often overused by pathologists,
contributing to complacency and lack of response on the part ofmany urologists when confronted with this diagnosis. Further,others have suggested that “atypical” is equivalent to “negative,”although such studies were based on an insufficient number ofcases to reach such a conclusion.109 Brimo et al. undertook logisticregression and found that “atypical” was not significantly predic-tive of urothelial carcinoma on follow-up biopsy, but they failedto provide the variables weighed in their multivariate model, sotheir conclusion cannot be independently confirmed.107
Comparison of the two “atypical” categories (“atypical, favorreactive” [see Fig. 7.24A and B] and “atypical, uncertain” [seeFig. 7.25A and B]) revealed similar predictive values for urothelialcancer on subsequent biopsy in our study of more than 9000 con-secutive urine cytologies within 12 months (31.1% versus 37.7%),suggesting that this stratification is not very useful clinically, similarto the recommendation of other authors.107,110 However, somehave reported significant stratification of “atypical”; Rosenthalet al. reported predictive values for cancer of 10% and 38% for“atypical, favor reactive” and “atypical, favor high-grade carci-noma,” respectively, although they apparently did not recognizethe “suspicious” category, lumping those patients into “atypical,favor high-grade carcinoma.”111
Our rate of atypia (10.2%) was significantly lower than others’(up to 32.5%) (Table 7.8). This difference cannot be attributedto the use of liquid-based cellular enhancement methods, becausewe used the Meiers improved filter method. Other reports come

342 CHAPTER 7 Urine Cytology
from academic medical centers with a high level of experience incytopathology, especially urine cytology, so this is an unlikely sourceof significant variation. Further, our comparison group did not relyon expert re-review of cases, but rather used the real-life method ofreviewing existing diagnoses from reports. Rodgers et al. found thaturine cytology was unable to rule out malignancy or exclude patientsfrom further investigation despite ability to confirm the presence ofcancer.112 Interobserver disagreement was “moderate to good” usingKappa statistics, but there were considerable differences in accuracyaccording to the level of expertise and reporting bias.113
It is probable that the improvement in the atypical rate is due tothe use of two stains: the acid hematoxylin stain in combination withthe Papanicolaou stain. Nuclear details are critical for diagnosis, andthe acid hematoxylin provides significant new information beyondthat of the routine Papanicolaou stain or routine hematoxylin stain(see later). Examples of atypia in the bladder wash (Fig. 7.26A and B)and atypia in voided urine (Fig. 7.27A and B) are shown to comparePapanicolaou and acid hematoxylin stains.
SuspiciousThe reported rate of “suspicious” urine cytology ranges from 1.9%to 28.7%, reflecting variability in definitions and diagnostic cutpoints.47,109,114-116 The Paris System 2013 limited this categoryto “suspicious for high-grade urothelial carcinoma” in recognitionof the clinical importance of high sensitivity for detection of high-grade carcinoma at the expense of lower specificity, excluding fromconsideration suspicion of low-grade carcinoma.24,39,117 The pre-dictive value of “suspicious” for all grades of cancer before publi-cation of Paris System 2013 varied from 54% to 87%(Table 7.9). Using criteria employed in the Paris System 2013,the predictive value of “suspicious for all cancers” increased to92%, with high-grade carcinoma found in 79%.118
Low-Grade Urothelial CarcinomaThe low-grade urothelial carcinoma category accounts for the urinefindings from papillary neoplasm of low malignant potential,World Health Organization (WHO) 1973 grade 1 and 2 carcino-mas, low-grade papillary carcinoma, and, likely, papilloma. Thediagnosis of low-grade urothelial carcinoma in the WHO 1999and WHO/International Society of Urologic Pathology 2004
TABLE 7.9 Incidence and Cancer Yield of “Suspiciou
Authors (Date)Cases of Suspicious WithFollow-up Biopsy (n)
IncidencSuspicio
Voss et al. (2008)263 96 4.1Siddappa et al. (2012)250,b 28 2.0Vandenbussche et al. (2013)272 62 6.5Bostwick and Hossain (2014)47 593 4.1Piaton et al. (2014)270 185 2.0Ton Nu et al. (2014)118 191 2.5Joudi et al. (2016)22 150 N/A
N/A, Data not available.aSuspicious is reported by some as “atypical urothelial cells, cannot exclude high-grade urothelial carcinomwith “suspicious.” The suspicious rate may be misleading because many articles only reported cases with mtrigger subsequent biopsy.bThis series included only cases of hematuria.cHigh-grade carcinoma only (excluded low-grade carcinoma).
overlaps with WHO 1973 grade 1 and 2 carcinomas, as well aspapillary neoplasm of low malignant potential, compounding con-fusion among pathologists and clinicians (Table 7.10).
It may also be difficult cytologically to separate WHO grade 1urothelial carcinoma (papillary urothelial neoplasm of low malig-nant potential) from papilloma in urine cytology specimens.119,120
The urothelial cell clusters are often arranged in a papillary config-uration and are difficult to distinguish from those shed from nor-mal benign urothelium after palpation, instrumentation, orirritation by calculi or inflammation (Figs. 7.29 and 7.30).52,53
In voided urine, spontaneously shed complex clusters of morpho-logically benign urothelial cells may be suggestive of a papillarytumor, provided that trauma is excluded clinically. Diagnostic fea-tures of WHO grade 1 carcinoma (papillary neoplasm of lowmalignant potential) include the presence of tumor fragments withconnective tissue stalks or central capillary vessels (Tables 7.7 and7.10).121 Numerous attempts to define the precise microscopicfeatures of tumor fragments that separate benign urothelial cellclusters fromWHO grade 1 carcinoma have met with limited suc-cess.122 Some authors claim that low- to intermediate-grade pap-illary urothelial tumors shed recognizable cells in the urinarysediment; they note that the characteristic features includeincreased N/C ratio, enlarged and eccentric nuclei, and inconspic-uous nucleoli, features present in 70% of such tumors.123,124 Maiet al. found that low-grade urothelial carcinoma in urine frequentlycontained three-dimensional cell clusters with disordered nucleiand cellular dyscohesion, findings that collectively had sensitivityof 70% and specificity of 94%.125 Scant cellularity was observedin 20% of cases. Others reported correct cytologic diagnosis in33% of such cases.122
Differentiation of WHO grade 1 carcinoma (papillary urothelialneoplasmof lowmalignantpotential) from instrumentation artifact isbased on the presence of cell clusters with ragged borders, unlike thesmooth borders lined by densely stained cytoplasm at the edge ofbenign cell clusters.53 Grade 1 carcinoma can be identified with45% sensitivity and 98% specificity based on cytologic criteria ofincreased N/C ratio, irregular nuclear borders, and cytoplasmichomogeneity.126 In one study, overall observer accuracy was 76%,with a sensitivity of 82% for a definitive negative diagnosis and spec-ificity for a definitive positive diagnosis of 96%.127 In another study,sensitivity of 90% and specificity of 65% for grade 1 carcinoma wasbased on the absence of inflammation, the presence of single and
s”a in Recent Reports
e ofus (%)
Time Interval to Biopsy(months)
Cancer Yield on Biopsy (%)
Negative Suspicious
�12 56.9 73.8N/A 0 036-60 11 89c
�12 16.6 53.64-56 N/A 38c
>6 6.3 93.7�6 N/A 55.3
a”; the similarity of incidence rates and described criteria suggest that these groups are comparableatched cytology–histology pairs, and most negative biopsies would be excluded because they do not

Fig. 7.29 Examples of grade 1 (of 3) papillary urothelial carcinoma (A and B). In each case the diagnosis was confirmed by biopsy.
TABLE 7.10 Criteria for Cytologic Grading of Urothelial Cancer
MorphologicFeatures Carcinoma In Situ
Grade 1 Carcinoma (PapillaryNeoplasm of Low MalignantPotential)
Grade 2 Carcinoma(Low-Grade UrothelialCarcinoma)
Grade 3 Carcinoma(High-Grade UrothelialCarcinoma)
Background Clean Clean Clean Dirty, tumor diathesis
Cellular arrangement Numerous single cells, rarefragments
Large fragments of urothelium Large fragments ofurothelium and single cells
Large fragments andnumerous single cells
Nuclear features Syncytia,a cannibalism Slightly enlarged Nuclear crowding and overlap Syncytia,a cannibalism
Nuclear membrane Marked membraneirregularity
Regular, round or oval Minimal membraneirregularity
Marked membraneirregularity
Chromatin Increased chromatin,coarsely granular, evenlydistributed
Finely granular, vesicular Finely granular, evenlydistributed
Increased chromatin,coarsely granular, unevenlydistributed
Nucleolus Rare nucleoli Occasional micronucleoli Variable micronucleoli Macronucleoli
Cytoplasmic features Variable maturation Cell maturation present Moderate degree ofmaturation
Maturation absent,squamoid and/or glandularfeatures
aLoss of cell borders.Modified from Shenoy UA, Colby TV, Schumann GB. Reliability of urinary cytodiagnosis in urothelial neoplasms. Cancer 1985;56:2041-2045.
343CHAPTER 7 Urine Cytology
overlapping groups of cells with high N/C ratio, hyperchromasia,nuclear grooves and notches, and small nucleoli.84 A third studyshowed 26% sensitivity for grade I urothelial carcinoma, and a fourthshowed37%sensitivity (suspicious ormalignant diagnoses) and94%specificity; 48% of these cytology specimens were classified as atypi-cal.26,128WHO grade 1 carcinoma is a major source of false-negativeresults in urine cytology.84 Chung et al. reported that five distinctivecytologic criteria were helpful in cases in which other conventionalcriteria for low-grade carcinoma were insufficient for diagnosis (lossof polarity of papillaroid clusters, irregular contours, absence ofcolumnar cells, hobnail features, and hyperchromasia).129 Stepwiselogistic regression analysis revealed that four features distinguishedlow-grade carcinoma fromreactiveurothelial cells: increasednumbersof monotonous single (nonumbrella) cells, increased N/C ratio,hyperchromasia, and presence of small and large urothelial cells.130
The Paris System 2013 recognizes the diagnosis of low-gradeurothelial neoplasm (not low-grade carcinoma) based on the
presence of fibrovascular cores in urothelial cell groups and anabsence of cytologic atypia.24 However, in a series of select histo-logically proven low-grade carcinomas and negative control urines,McCroskey et al. found low sensitivity (21% to 53%) but relativelyhigh specificity (81% to 95%), resulting in poor-to-fair accuracyfor the diagnosis of low-grade urothelial carcinoma; overall agree-ment was fair (κ ¼ 0.30).131
Ancillary techniques (see later) that may be valuable for separat-ing benign and neoplastic urothelial cells include FISH, immuno-cytochemical tests, and DNA ploidy analysis.123,132-139 Digitalimage analysis of voided urine was superior to bladder wash cytol-ogy for prediction of tumor recurrence.140
High-Grade Carcinoma“High-grade carcinoma” includes the findings from urothelial car-cinoma in situ, characterized by the presence of malignant cells that

Fig. 7.30 Examples of grade 2 (of 3) papillary urothelial carcinoma (A to H). In each case the diagnosis was confirmed by biopsy.

Fig. 7.31 Carcinoma in situ. Carcinoma in situ in association with atypicalcells of dysplasia (A and B). (C) Cluster of cells of carcinoma in situ. (D) Multi-nucleated cell of carcinoma in situ. (E) Small cell variant of carcinoma in situ.
345CHAPTER 7 Urine Cytology
that look like high-grade urothelial carcinoma and are often uni-form in size and may be small or large (Fig. 7.31A to E;Table 7.10).86,141,142 The cells show markedly enlarged nucleiwith high N/C ratio, coarse and dark chromatin, and irregularnuclear membranes. Nucleoli may or may not be present. Thebackground is often clean, free of necrotic debris, and lacks inflam-mation. Occasionally the cells may be heterogeneous and large,particularly after biopsies. When there is prominent inflammationpresent, it is often prudent not to attempt to separate carcinomain situ from invasive carcinoma. Microinvasive carcinoma maynot be recognizable in cytologic samples, particularly when carci-noma in situ is present. Carcinoma in situ may persist after intra-vesical therapy such as BCG (Fig. 7.32A and B).
This category also accounts for the urine findings from WHO1973 grade 2 (intermediate- to high-grade) carcinoma, WHO1973 grade 3 (high-grade) carcinoma, and carcinoma in situ. Itmay be difficult to separate grades 2 (Fig. 7.30A to H) and 3(Fig. 7.33A to F) carcinoma from carcinoma in situ in urine sam-ples (Table 7.10). Unlike benign urothelial cells, these cells havesubstantial nuclear and cytoplasmic abnormalities. The principalvalue of urine cytology is the diagnosis and monitoring of high-grade tumors that may not be evident cystoscopically, includingcarcinoma in situ and occult invasive carcinoma.142,143
In voided urine, low-grade and high-grade urothelial carcinomacells vary in size and shape, and may be small or large. The nucleiare enlarged, with coarsely granular chromatin, hyperchromasia,

Fig. 7.32 Carcinoma in situ resistant to bacillus calmette–gu�erin therapy, with clusters of hyperchromatic neoplastic cells (A and B).
346 CHAPTER 7 Urine Cytology
abnormal nuclear contours, and prominent nucleoli. Multinucle-ate cancer cells and mitotic figures are often readily identified.144
In washings, urothelial carcinoma may demonstrate a lowerdegree of nuclear hyperchromasia, perhaps resulting in more prom-inent large nucleoli. The cells may be poorly preserved, particularlywhen there is inflammation or necrosis, and a variety of changesmay be present, including frayed or vacuolated cytoplasm, nonspe-cific eosinophilic cytoplasmic inclusions, and pyknotic nuclei. Insome high-grade papillary tumors the dominant cytologic findingmay be the presence of isolated cancer cells, either singly or ingroups of two or three.
Grade 2 carcinoma may present a diagnostic challenge becauseit is often similar cytologically to grade 1 carcinoma.8,128,143,145
Fortunately, in most cases, atypical urothelial cells are observed,alerting the clinician of the need for cystoscopic examination.For high-grade urothelial carcinoma, digital image analysis andbladder wash cytology are equally predictive.140
Correlation of Urine Cytology and BiopsyFindings (Diagnostic Accuracy)The diagnostic accuracy of urine cytology is generally high inpatients who are symptomatic or being managed after treatmentfor bladder cancer. However, reported results vary considerably,especially in different patient cohorts. For example, most seriesof bladder tumors indicate that papilloma and papillary urothelialneoplasm of low malignant potential cannot be reliably diagnosedby urine cytology despite inclusion of several key cytologic find-ings. Reported sensitivity of urine cytology for grade 1 urothelialcarcinoma varied from 26% to 90%.26,84 The sensitivity increasedto 80% for grade 2 and 95% for grade 3.
Carcinoma in situ is usually diagnosed as “suspicious” or “posi-tive” in almost all instances. The overall sensitivity of urine cytologyfor primary carcinoma of the bladder ranges from 45% to 97%. In arecent report, urine cytology predicted 82% of all recurrent tumorsin the bladder.146 Two major drawbacks of urinary cytology arethe high rate of false-positive results in patients receiving intravesicalchemotherapy and the high rate of false-negative results in those withgrade 1 carcinoma. Scarcity of diagnostic or malignant cells is argu-ably the greatest single limitation of urine cytology, according toFrost and colleagues.147 Urine cytology findings, cystoscopy, andpossible diagnostic outcomes are summarized in Table 7.11.
False-negative diagnosis of high-grade carcinoma can be attrib-uted to underdiagnosis as “negative,” “atypical,” or “suspicious”;interestingly, in about 20% of cases, false-negative result was
attributed to overdiagnosis on biopsy of high-grade carcinoma.148
If poor preservation and obscured samples were considered non-diagnostic, the sensitivity and specificity of cytology for high-gradecancer would be as high as 94% and 71%, respectively.148
“Positive” voided urine predicted progression and cancer-specificmortality for non–muscle-invasive carcinoma, independent ofand outperforming histologic grade on biopsy.149 The 5-year cumu-lative progression and cancer-specific mortality rates for patientswith “positive” cytology were 20% and 15%, respectively, comparedwith 2% and 2%, respectively, for those with “negative” results.
Urine cytology after BCG therapy had sensitivity and specificityof 56% and 56% for cancer recurrence; when combined with cys-toscopy, results were 88% and 82%, respectively, obviating theneed in many patients for routine biopsy.150 Urine cytology afterradical cystectomy is an early indicator of cancer recurrence,preceding radiographic evidence by a mean of 2.1 years.151
Urinary Cells Originating From Other SitesProstateProstatic adenocarcinoma (Fig. 7.34) may yield cells in voidedurine spontaneously or after prostatic massage, particularly whenthe carcinoma is high grade. Cancer cells in the urine sedimentare usually small, often spherical, and columnar, sometimes insmall clusters. The cytoplasm is usually basophilic with open vesic-ular nuclei and prominent nucleoli.
UrethraPrimary cancer of the urethra is rare, and may be urothelial,squamous cell, or adenocarcinoma. Other rare cancers includemalignant melanoma and clear cell adenocarcinoma.
Cytologic examination of the urethra after cystectomy for blad-der cancer sometimes reveals carcinoma in situ or early invasivecarcinoma.142
Upper TractUrine cytology is usually diagnostic when there is urothelial carci-noma of the renal pelvis and ureter, particularly when the cancersare high grade. With low-grade urothelial malignancies, the samediagnostic problems are encountered as in the bladder. Urine cytol-ogy rarely identifies renal cell carcinoma. When malignant cells arepresent, they are large, with clear or vacuolated cytoplasm and dis-tinct nucleoli.
Among patients with clinical suspicion of upper tract malig-nancy with positive urine cytology, 42% experienced upper

Fig. 7.33 Grade 3 (of 3) papillary urothelial carcinoma with marked cytologic abnormalities (A to F). In (D), note cell cannibalism.
347CHAPTER 7 Urine Cytology
tract cancer and an additional 33% had cancer limited to thebladder.152 Voided urine, selective urine cytology, ureteralwashings, and computed tomography (CT) scan predictedupper tract cancer with a sensitivity and specificity of 63%and 67%, 76% and 73%, 50% and 95%, and 95% and26%, respectively.17,153 Patients who had combined abnormalCT and “positive” voided urine had cancer in 83% of cases,whereas 100% of those with combined normal CT and “nega-tive” voided urine (investigated for ongoing symptoms) were
cancer free. FISH hypertetrasomy showed sensitivity and spec-ificity for diagnosis of upper tract carcinoma of 50% and 89%,respectively.17 Urine cytology alone cannot differentiate uppertract cancer from bladder involvement.
Preoperative “positive” voided urine cytology was predictive ofintravesical recurrence after radical nephroureterectomy for uppertract carcinoma. Recurrence-free survival at 1 and 3 years after sur-gery was 61% and 46% in patients with “positive” urine and 71%and 52% in those with “negative” urine, respectively. Multivariate
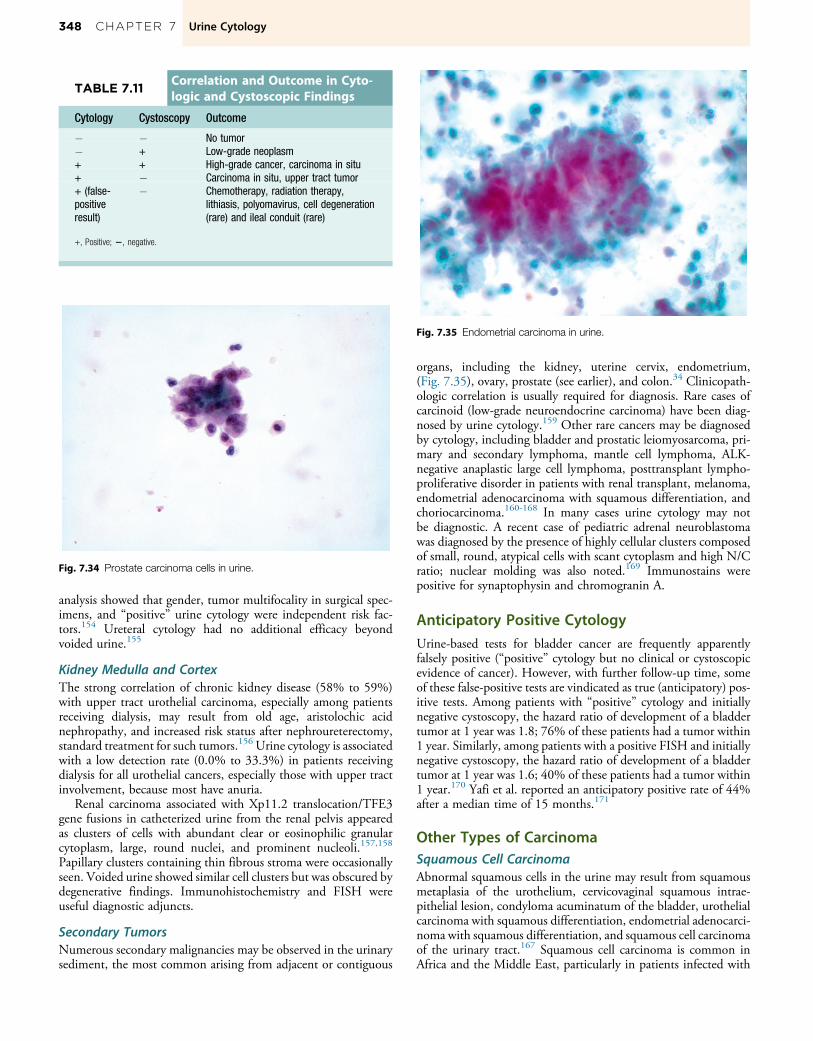
TABLE 7.11Correlation and Outcome in Cyto-logic and Cystoscopic Findings
Cytology Cystoscopy Outcome
� � No tumor� + Low-grade neoplasm+ + High-grade cancer, carcinoma in situ+ � Carcinoma in situ, upper tract tumor+ (false-positiveresult)
� Chemotherapy, radiation therapy,lithiasis, polyomavirus, cell degeneration(rare) and ileal conduit (rare)
+, Positive; 2, negative.
Fig. 7.34 Prostate carcinoma cells in urine.
Fig. 7.35 Endometrial carcinoma in urine.
348 CHAPTER 7 Urine Cytology
analysis showed that gender, tumor multifocality in surgical spec-imens, and “positive” urine cytology were independent risk fac-tors.154 Ureteral cytology had no additional efficacy beyondvoided urine.155
Kidney Medulla and CortexThe strong correlation of chronic kidney disease (58% to 59%)with upper tract urothelial carcinoma, especially among patientsreceiving dialysis, may result from old age, aristolochic acidnephropathy, and increased risk status after nephroureterectomy,standard treatment for such tumors.156 Urine cytology is associatedwith a low detection rate (0.0% to 33.3%) in patients receivingdialysis for all urothelial cancers, especially those with upper tractinvolvement, because most have anuria.
Renal carcinoma associated with Xp11.2 translocation/TFE3gene fusions in catheterized urine from the renal pelvis appearedas clusters of cells with abundant clear or eosinophilic granularcytoplasm, large, round nuclei, and prominent nucleoli.157,158
Papillary clusters containing thin fibrous stroma were occasionallyseen. Voided urine showed similar cell clusters but was obscured bydegenerative findings. Immunohistochemistry and FISH wereuseful diagnostic adjuncts.
Secondary TumorsNumerous secondary malignancies may be observed in the urinarysediment, the most common arising from adjacent or contiguous
organs, including the kidney, uterine cervix, endometrium,(Fig. 7.35), ovary, prostate (see earlier), and colon.34 Clinicopath-ologic correlation is usually required for diagnosis. Rare cases ofcarcinoid (low-grade neuroendocrine carcinoma) have been diag-nosed by urine cytology.159 Other rare cancers may be diagnosedby cytology, including bladder and prostatic leiomyosarcoma, pri-mary and secondary lymphoma, mantle cell lymphoma, ALK-negative anaplastic large cell lymphoma, posttransplant lympho-proliferative disorder in patients with renal transplant, melanoma,endometrial adenocarcinoma with squamous differentiation, andchoriocarcinoma.160-168 In many cases urine cytology may notbe diagnostic. A recent case of pediatric adrenal neuroblastomawas diagnosed by the presence of highly cellular clusters composedof small, round, atypical cells with scant cytoplasm and high N/Cratio; nuclear molding was also noted.169 Immunostains werepositive for synaptophysin and chromogranin A.
Anticipatory Positive CytologyUrine-based tests for bladder cancer are frequently apparentlyfalsely positive (“positive” cytology but no clinical or cystoscopicevidence of cancer). However, with further follow-up time, someof these false-positive tests are vindicated as true (anticipatory) pos-itive tests. Among patients with “positive” cytology and initiallynegative cystoscopy, the hazard ratio of development of a bladdertumor at 1 year was 1.8; 76% of these patients had a tumor within1 year. Similarly, among patients with a positive FISH and initiallynegative cystoscopy, the hazard ratio of development of a bladdertumor at 1 year was 1.6; 40% of these patients had a tumor within1 year.170 Yafi et al. reported an anticipatory positive rate of 44%after a median time of 15 months.171
Other Types of CarcinomaSquamous Cell CarcinomaAbnormal squamous cells in the urine may result from squamousmetaplasia of the urothelium, cervicovaginal squamous intrae-pithelial lesion, condyloma acuminatum of the bladder, urothelialcarcinoma with squamous differentiation, endometrial adenocarci-noma with squamous differentiation, and squamous cell carcinomaof the urinary tract.167 Squamous cell carcinoma is common inAfrica and the Middle East, particularly in patients infected with

Fig. 7.36 Squamous cell carcinoma in urine.
349CHAPTER 7 Urine Cytology
S. haematobium, but it is relatively uncommon in developed coun-tries, accounting for no more than 3% of bladder tumors.68 Squa-mous cell carcinoma has been observed with increasing frequencyin long-term survivors with severe spinal cord injury and neuro-genic bladder.
Squamous cell carcinoma may display varying degrees of differ-entiation (Fig. 7.36). In well-differentiated cases, the cytologicfindings in voided urine are distinctive, often consisting of kerati-nized cells with thick, yellow or orange cytoplasm and large, irreg-ular, dark pyknotic nuclei. Squamous pearls, characterized by cellaggregates concentrically arranged around a core of keratin, may beobserved.8 The background often shows evidence of marked necro-sis, and ghost cells may be present. A mixture of cancer cells isobserved in the urine of the patients with poorly differentiatedsquamous cell carcinoma, including sharply demarcated cells witheosinophilic cytoplasm and large nuclei.7,8 Most cases areaneuploid.172
AdenocarcinomaIn colonic-type adenocarcinoma of the bladder, the sediment con-tains columnar cancer cells with large hyperchromatic nuclei andlarge nucleoli, sometimes in clusters.173 In poorly differentiatedmucus-producing carcinoma, the cancer cells are small, sphericalor cuboidal in shape, and contain large hyperchromatic nuclei,often with prominent nucleoli. The cytoplasm is usually baso-philic, often scant, and sometimes poorly preserved. When thereare large cytoplasmic vacuoles containing mucus, the nuclei maybe pushed to the periphery of the cell, features suggestive of or diag-nostic of signet ring cell carcinoma.
In clear cell adenocarcinoma the cancer cells are large, withabundant finely vacuolated or granular cytoplasm, open vesicularnuclei, and prominent nucleoli. Such cells usually form round pap-illary clusters.7 Most cases are aneuploid.174
When numerous mucin-producing goblet cells are present,another consideration is villous adenoma.175
Small Cell Undifferentiated Carcinoma (Oat CellCarcinoma)In small cell carcinoma, the cancer cells are small and round to oval,about four times the size of lymphocytes, contain compact andfinely granular chromatin, often with pyknotic nuclei, high N/C
ratio, and scant basophilic cytoplasm, and are set in a backgroundof inflammatory and necrotic material.176,177 Nuclear moldingmay be prominent; nucleoli are not visible. The presence of smallclusters of tightly packed tumor cells with nuclear molding is diag-nostically helpful.8 The presence of cell clusters without prominentnucleoli is useful in differentiating these cells from malignant lym-phoma; in the latter, cells do not cluster and usually contain smallnucleoli. The demonstration of neuroendocrine differentiation insmall cell carcinoma may require immunocytologic or ultrastruc-tural studies.178,179
Mixed CarcinomaUrothelial cancer may contain foci with more than one histologictype, including squamous cell carcinoma, adenocarcinoma, andsmall cell carcinoma. The cytologic findings in such tumors rarelyallow the diagnosis of mixed carcinoma. Usually one pattern isdominant, although a mixed population of cancer cells may beobserved, including some of the rare variants.
Rare Variants of Urothelial CarcinomaSignet ring cell, micropapillary, plasmacytoid, urothelial carcinomawith oncocytic features, and sarcomatoid variants have beenreported in the cytology literature, mostly as case reports.180-184
Recognition of variants is critical because many are associated withdifferent clinical outcomes or therapeutic approaches.
Signet ring cell carcinoma consists of scattered malignant epi-thelial cells displaying distinct cell borders, abundant cytoplasmwith single large, discrete mucin vacuoles, and eccentric irregularnuclei with prominent nucleoli.180 In contrast, metastatic colonicsignet ring cell carcinoma displayed predominantly single dispersedmalignant cells containing eccentrically placed, oval nuclei withoccasional small nucleoli and a moderate amount of vacuolatedcytoplasm.
Micropapillary urothelial carcinoma is rarely identified, appear-ing as numerous small, cohesive groups and single neoplasticcells.183,185 Pseudopapillae were present in 17 of 20 cases, andin 9 they were a relevant finding; morules were present in 15 cases;isolated microacini were seen in 14 cases; cellular atypia was prom-inent in 17 cases.185 In 15 cases a cytologic diagnosis of urothelialcarcinoma was made, 1 case was diagnosed as adenocarcinoma, andthe remaining 4 cases were considered suspicious of malignancy.
Plasmacytoid carcinoma contains single cells with eosinophiliccytoplasm and characteristic eccentric hyperchromatic nuclei.Immunoreactivity for CD138 is helpful but represents a pitfallbecause it is also positive in plasma cell dyscrasias.186
Urothelial carcinoma with oncocytic features appeared asdelicate papillae with cells displaying oncocytic cytoplasm andrelatively low N/C ratio; immunostains showed strong p53 immu-noreactivity and low Ki-67 labeling.184
Major Diagnostic PitfallsMost errors in urine cytology are overdiagnosis of benign cellularchanges as malignant (Table 7.12). Knowledge of these changes isfundamental to the practice of cytology. The College of AmericanPathologists Interlaboratory Comparison project of more than46,000 pathologists found that participants performed well inaccurately classifying cases as benign or malignant (overall92.4% concordance) (Table 7.13).187 However, the greatest diffi-culties were with correct identification of adenocarcinoma andsquamous cell carcinoma cases, and with overinterpretation of ilealloop and polyomavirus as high-grade carcinoma.187

TABLE 7.13
Concordance with the Urine Cytol-ogy Reference Standard in theCollege of American PathologistsInterlaboratory ComparisonProgram 2000 to 2010187,a
ReferenceDiagnosis
No. ofResponses
ConcordanceRate (%)
False Responses (%)
High-gradeurothelialcarcinoma
71,581 83.8 Atypical urothelial cells(4.1), reactive (3.2),adenocarcinoma (3.1),negative for malignancy(1.3), squamous cellcarcinoma (1.1),polyomavirus (0.9),inflammation (0.7), andother (1.8)
Negative formalignancy
2852 73.9 a
Polyomavirus 3535 71.7 Reactive (6.4), high-grade carcinoma (6.2),and cytomegalovirus/herpes (3.1)
Ileal loop urine 5291 55.8 a
Squamous cellcarcinoma
756 49.1 a
Adenocarcinoma 1667 42.9 a
Treatment-related changes
1293 36.3 a
aNot provided.
TABLE 7.12Major Diagnostic Pitfalls in LowerUrinary Tract Cytology
Overdiagnosis of normal and degenerated urothelium as malignantOverdiagnosis of human polyomavirus infection as malignantOverdiagnosis of effects of cyclophosphamide as malignantUnderdiagnosis of grade 1 or 2 urothelial carcinoma (papillary urothelial
neoplasia of low malignant potential or low-grade urothelial carcinoma)as benign
350 CHAPTER 7 Urine Cytology
Following is a summary of some of the most vexing problems,which are also described and illustrated elsewhere in this chapter.
Trauma or InstrumentationThe normal urothelium tends to exfoliate in the form of tissue frag-ments that are round or oval, commonly designated as papillaryclusters. Vigorous palpation, catheterization, or any form of instru-mentation may result in the formation of such epithelial clusters.When present in large numbers, these clusters may be misinter-preted as carcinoma.53 Another source of error is the presence ofnumerous superficial urothelial cells that may be mistaken forcancer because of their variable nuclear features.86 Careful consid-eration of chromatin pattern, N/C ratio, and nuclear membraneirregularity should enable differentiation of benign and malignantprocesses in the vast majority of cases.
Cell PreservationCells in voided urine sediment, particularly in the first morningvoid, are often poorly preserved, compounding the diagnostic
difficulty. The diagnosis of cancer in voided urine should beavoided unless the findings are unequivocal.8
Human PolyomavirusPolyomavirus (BK virus) infection creates large intranuclear inclu-sions that may mimic cancer nuclei. However, the inclusions arehomogeneous and lack the coarse chromatin granularity of malig-nancy. This is an important source of diagnostic errors that can con-tribute to costly and lengthy patient investigations.78 Polyomavirus-infected cells and malignant cells may coexist in urine cytology.188
LithiasisCalculi in the lower urinary tract are abrasive, dislodging epithelialfragments that may be quite large and display papillary appearancemimicking low-grade carcinoma.52 The presence of numeroussuperficial cells may also create diagnostic difficulty because ofnuclear abnormalities.8,84,86
Drugs and Other Therapeutic ProceduresUrothelial cell changes may result from a wide variety of incitingagents, including chemotherapy, radiotherapy, and other interven-tions. Intravesical chemotherapy is responsible for a high rate offalse-positive results.84 A further source of diagnostic difficultymay be synchronous infection with polyomavirus in patientswho are immunocompromised.8 It should be remembered thaturothelial carcinoma or sarcoma may develop in patients whoare receiving cyclophosphamide for treatment of lymphoma.87,88
Ancillary Studies and Immunocytology
This section is limited to discussion of cell-based assays that may beused in the anatomic pathology/cytology laboratory, including dig-ital image analysis, cytochemical and immunocytochemical stains,and FISH. Excluded are clinical laboratory methods such as meta-bolomics, microRNA and DNA assays, deep sequencing, andserum-based methods of soluble biomarkers.
Digital Image Analysis and MorphometryDigital image analysis was superior to flow cytometry for DNAploidy analysis, with sensitivities of 83% to 91% and 71%, respec-tively, and was even higher in carcinoma in situ, grade 3 cancer,and stages T2 and T3 cancer (all nearly 100%).134,189
Digital image analysis can be combined with flow cytometry toidentify subpopulations of urothelial cells. The diagnosis of canceris strongly suspected in cases with abundant aneuploid cells or 16%or more of measured cells with hyperdiploid DNA (greater thantwice the DNA content). A specimen is less likely to be malignantif no aneuploid stemline is detected and fewer than 11% of the cellsare hyperdiploid. If 11% to 16% of the cells measured are hyper-diploid and no aneuploid stemline is detected, the samples are con-sidered “suspicious.”
Recurrent cancer can be detected with the combination of urinecytology and image analysis.190,191 Digital image analysis by itselfwas superior to cytologic examination for prediction of tumorrecurrence after negative findings by cystoscopic examinationand was equivalent to cytology for detection of high-grade can-cer.140 Muralidaran et al. demonstrated the utility of an artificialneural network for urine cytology diagnosis based on nuclear area,diameter, perimeter, standard deviation of nuclear area, and inte-grated gray density.192
Apoptotic index was found to be diagnostically useful. Exclud-ing ileal conduit specimens, the finding of a high apoptotic index

351CHAPTER 7 Urine Cytology
with the presence of pyknosis or karyorrhexis in the urine corre-lated with high-grade cancer.193
Quantitative phase imaging is a new method that measures thenuclear mass and entropy of cells, and showed significant differ-ences between “negative” and “positive.”194 There was a progres-sive increase in patients with “negative” diagnosis compared withthose with “atypical,” “suspicious,” and “positive” cytologic diag-noses that was predictive of subsequent biopsy results.
Nuclear/nucleolar volume ratio creates an index for discrimina-tion of benign and malignant urothelial cells with sensitivity of56%, specificity of 89%, positive predictive value of 85%, andnegative predictive value of 64% (cut point of 1.5%).195
Digital image telepathology is feasible. Specificity and sensitiv-ity regarding categorized diagnoses were 83% to 92% and 85% to93%, respectively; overall accuracy rate was 88% to 90%.196 Inter-observer agreement was substantial (κ¼ 0.791). The lowest rate ofconcordance was with the identification of benign lesions.
Cytochemical StainsAcid Hematoxylin StainAddition of nuclear staining such as the acid hematoxylin stain toPapanicolaou staining increased sensitivity in one laboratory byabout 28% by eliminating background debris and improvingdetection of mitotic figures and other changes in chromatin thatmay be obscured.197 The combination of Papanicolaou stainingwith nuclear staining and image analysis achieved 90% sensitivityfor diagnosis of urothelial carcinoma in one report.198 DNA ploidyanalysis was equivalent with the two methods. Both stains weresuperior to Papanicolaou stain for examination of nuclear chroma-tin texture and content. These findings indicate that acid hematox-ylin is a satisfactory substitute for Feulgen staining in cytologicpreparation for DNA ploidy studies and provides additional tech-nical advantages.
In addition to Papanicolaou stain, we routinely use acid hema-toxylin stain for urine cytology. This inexpensive, nontoxic, andeasily performed stain enhances nuclear chromatin pattern (surro-gate Feulgen stain), removes unwanted background debris, andoptimizes cellular adherence to the slide. Acid hematoxylin com-plements Papanicolaou stain for diagnosis of malignant cells(Fig. 7.37A and B) and is superior to Papanicolaou stain for differ-entiating “decoy” cells from malignant cells (Fig. 7.38A and B).79
Fig. 7.37 Carcinoma in situ in urine. (A) Papanicolaou stain. (B) Acid hematoxy
Acid hematoxylin stain can also be used for DNA ploidy analysiswith the aid of an image analyzer.199,200 The increased accuracy ofdiagnosis is cost effective, obviating the need for unnecessary cys-toscopies and other invasive and expensive techniques. Acid hema-toxylin provided superior cellular yield compared with Feulgenstains, as well as more consistent staining and better preservationof nuclear size (Fig. 7.39A and B).79
CellDetectCellDetect is a unique histochemical panel consisting of a propri-etary plant extract and three dyes that enables color discriminationbetween benign (green) and malignant (red) cells based on specificmetabolic alterations exclusive to the latter. It was superior to stan-dard cytology (sensitivity of 94% versus 46%, respectively, andspecificity of 89% for both), particularly for sensitivity withlow-grade tumors (88% versus 17%, respectively).201,202
Immunocytochemical StainsTelomeraseThe ribonucleoprotein telomerase is a reverse transcriptase enzymethat adds repeat sequences to the 30 end of telomeres, a region ofrepetitive sequences at each end of eukaryotic chromosomes. Telo-meres protect the ends of the chromosomes from DNA damage oralteration. Telomerase is active in normal stem cells and most can-cer cells but is normally absent from, or at very low levels in, mostsomatic cells. Expression of the hTERT protein has also been ana-lyzed by immunocytochemistry using anti-hTERT antibodies.
The telomeric repeat amplification protocol polymerase chainreaction assay has been most widely used to assay telomeraseactivity, but it creates false-positive results in the presence ofinflammation and nonbladder epithelial cells. The availability ofpolyclonal and monoclonal antibodies for nuclear and cytoplasmichTERT protein expression allows cell-specific microscopic visual-ization of different cell components in urine and other tissues, min-imizing the influence of false-positive results (Fig. 7.40).203-205
Inflammatory cells serve as internal positive controls.
HER2 and CytokeratinsImmunocytologic expression of HER and high-molecular-weightcytokeratin in cells from voided urine predicted bladder cancer recur-rence.206 HER was expressed in 7% of cases without recurrence
lin stain.
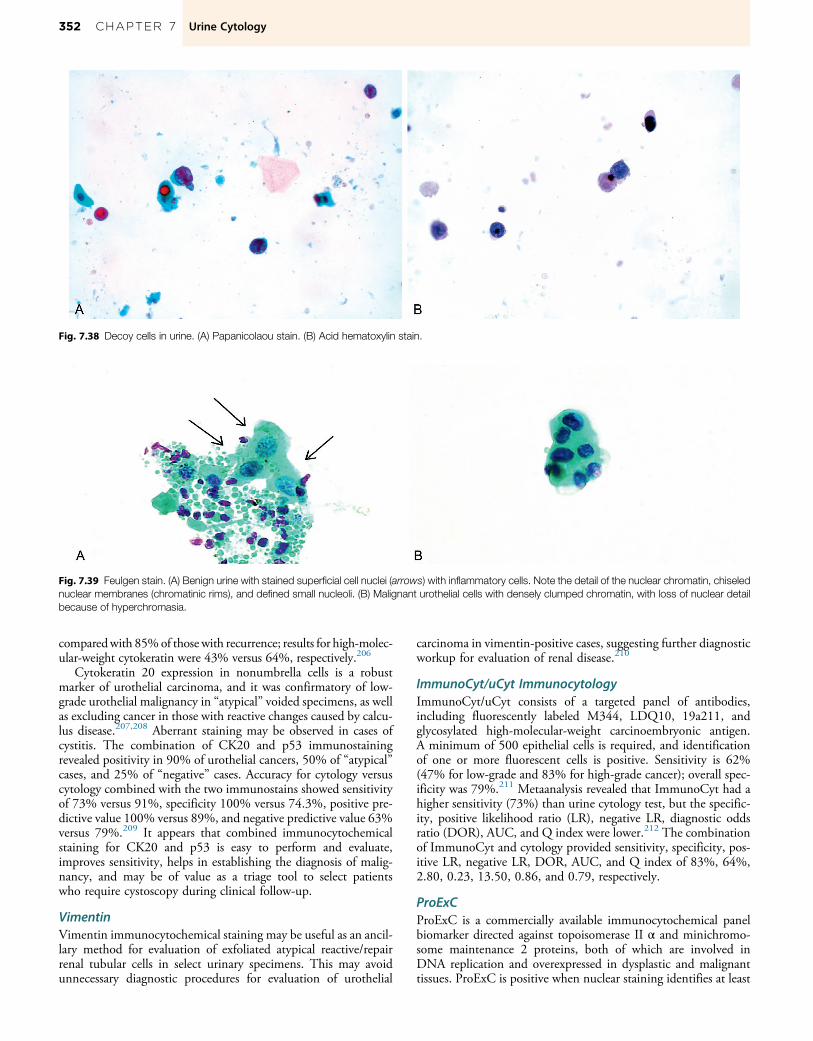
Fig. 7.39 Feulgen stain. (A) Benign urine with stained superficial cell nuclei (arrows) with inflammatory cells. Note the detail of the nuclear chromatin, chiselednuclear membranes (chromatinic rims), and defined small nucleoli. (B) Malignant urothelial cells with densely clumped chromatin, with loss of nuclear detailbecause of hyperchromasia.
Fig. 7.38 Decoy cells in urine. (A) Papanicolaou stain. (B) Acid hematoxylin stain.
352 CHAPTER 7 Urine Cytology
comparedwith 85%of those with recurrence; results for high-molec-ular-weight cytokeratin were 43% versus 64%, respectively.206
Cytokeratin 20 expression in nonumbrella cells is a robustmarker of urothelial carcinoma, and it was confirmatory of low-grade urothelial malignancy in “atypical” voided specimens, as wellas excluding cancer in those with reactive changes caused by calcu-lus disease.207,208 Aberrant staining may be observed in cases ofcystitis. The combination of CK20 and p53 immunostainingrevealed positivity in 90% of urothelial cancers, 50% of “atypical”cases, and 25% of “negative” cases. Accuracy for cytology versuscytology combined with the two immunostains showed sensitivityof 73% versus 91%, specificity 100% versus 74.3%, positive pre-dictive value 100% versus 89%, and negative predictive value 63%versus 79%.209 It appears that combined immunocytochemicalstaining for CK20 and p53 is easy to perform and evaluate,improves sensitivity, helps in establishing the diagnosis of malig-nancy, and may be of value as a triage tool to select patientswho require cystoscopy during clinical follow-up.
VimentinVimentin immunocytochemical staining may be useful as an ancil-lary method for evaluation of exfoliated atypical reactive/repairrenal tubular cells in select urinary specimens. This may avoidunnecessary diagnostic procedures for evaluation of urothelial
carcinoma in vimentin-positive cases, suggesting further diagnosticworkup for evaluation of renal disease.210
ImmunoCyt/uCyt ImmunocytologyImmunoCyt/uCyt consists of a targeted panel of antibodies,including fluorescently labeled M344, LDQ10, 19a211, andglycosylated high-molecular-weight carcinoembryonic antigen.A minimum of 500 epithelial cells is required, and identificationof one or more fluorescent cells is positive. Sensitivity is 62%(47% for low-grade and 83% for high-grade cancer); overall spec-ificity was 79%.211 Metaanalysis revealed that ImmunoCyt had ahigher sensitivity (73%) than urine cytology test, but the specific-ity, positive likelihood ratio (LR), negative LR, diagnostic oddsratio (DOR), AUC, and Q index were lower.212 The combinationof ImmunoCyt and cytology provided sensitivity, specificity, pos-itive LR, negative LR, DOR, AUC, and Q index of 83%, 64%,2.80, 0.23, 13.50, 0.86, and 0.79, respectively.
ProExCProExC is a commercially available immunocytochemical panelbiomarker directed against topoisomerase II α and minichromo-some maintenance 2 proteins, both of which are involved inDNA replication and overexpressed in dysplastic and malignanttissues. ProExC is positive when nuclear staining identifies at least

Fig. 7.40 Telomerase Immunocytology. (A) Benign urine nuclei have scant fine dusty staining of nuclei, easily distinguished from (B to D) intense but variablenuclear immunoreactivity in high-grade carcinoma.
353CHAPTER 7 Urine Cytology
one morphologically atypical urothelial cell. Sensitivity and speci-ficity were 85% and 69%, respectively, compared with 85% and31% for ImmunoCyt, and 93% and 23% for the combinationof tests; prediction of high-grade urothelial carcinoma had sensitiv-ity of 92% for ProExC, 86% for ImmunoCyt, and 92% for thecombination.213 ProExC was superior to FISH for prediction ofcancer, with sensitivity of 89% and 56%, specificity of 78% and44%, positive predictive value of 89% and 67%, and negativepredictive value of 78% and 33%, respectively.214
Other ImmunostainsUbiquilin-2, a ubiquitin-related protein, is expressed in the nuclei ofurothelial carcinoma cells, but not benign cells.215 Overall sensitivitywas 88%, specificity was 99%, positive predictive value was 98%,and negative predictive value was 93% for detection of carcinoma.
ERG immunocytochemistry has sensitivity and specificity forprostate cancer in urine of 23% and 100%, respectively; it shouldbe noted that up to half of prostate cancers are ERG� in prostatic tis-sues, so the expected sensitivity inurinewill beaccordingly limited.216
WT1 antibody recognizes a podocyte marker that can distin-guish normal and nonrenal urinary tract disease from kidney dis-ease.217 WT1+ cells were found in 50% of voided urine samples,
whereas no positive cells were found in patients with lower urinarytract disease or in healthy volunteers.
Immunostains for p53 or Ki-67 (optimal cutoffs were 5% for p53and 3% forKi-67) in combinationwith cytology increased specificitywithout penalizing sensitivity for detection of carcinoma; sensitivityand specificity for the detection of all cancers were 86% and 77% forcytology alone, 81% and 93% for cytology and p53, 76% and 88%for cytology andKi-67, and69%and98%for the full combinationofcytology, p53, and Ki-67, respectively.218
PAX8 is a useful immunostain to diagnose nephrogenic ade-noma in voided specimens; however, care must be taken to avoidmisinterpretation of positive staining in lymphocyte nuclei.219
Epidermal growth factor receptor positivity was an independentrisk factor for recurrence after intravesical chemotherapy.220
Polyomavirus-infected cells were categorized as SV40+/S100P+
and SV40+/S100P� by immunostains.221
Calreticulin, annexin A2, and annexin A3 were overexpressed inupper tract carcinoma.222
In patients with bladder cancer independent of stage, TERTmutations were found in 55%, FGFR3 mutations in 30%,PIK3CA in 14%, and TP53 mutations in 12%, with 70% sensi-tivity and 97% specificity.223

354 CHAPTER 7 Urine Cytology
Fluorescence In Situ HybridizationMultitarget FISH using probes for chromosomes 3, 7, 17, and9p21 has high sensitivity and specificity for detecting urothelialcarcinoma (Fig. 7.41A to E). A positive result is defined as polys-omy in four or more cells, which also includes tetrasomy. The sen-sitivity of FISH for detecting cancer was superior to cytology,despite similar specificity, irrespective of cancer grade and stage:overall, 81% versus 33%; low grade, 76% versus 12%; high grade,85% versus 50%; nonmuscle invasive, 81% versus 28%; and mus-cle invasive, 80% versus 45%, respectively.224 Sensitivity rangedfrom 55% to 98% and specificity from 55% to 100%. 9p21 loss(>12%) was an independent prognostic factor for recurrence.225
About 27% of patients under surveillance for recurrent bladdercancer with no immediate clinical evidence of recurrence had pos-itive FISH, and about 65% of these anticipatory positive patientshad recurrent cancer within 29 months.135,226-231
FISH may be useful in decreasing the rate of atypia, but it islimited by high false-positive incidence. Carcinoma was diagnosedmore frequently in patients with positive than in those with neg-ative FISH results (49% versus 9%, respectively). Sensitivity, spec-ificity, positive predictive value, negative predictive value, andaccuracy of FISH were 45%, 82%, 47%, 80%, and 72% for allcancers and 48%, 79%, 28%, 90%, and 74% for high-grade car-cinoma, respectively. FISH showed a high false-positive rate (53%)
Fig. 7.41 Fluorescence in situ hybridization (FISH) in voided urine cytology.(A) Normal urothelium showing two copies of chromosome 3 (red), two cop-ies of chromosome 7 (green), two copies of chromosome 17 (aqua), and twocopies of LSI 9p21 (gold) by FISH. (B) Aneusomic urothelial cell showing fivecopies of chromosome 3 (red), three copies of chromosome 7 (green), fivecopies of chromosome 17 (aqua), and no copies of LSI 9p21 (gold) by FISH.(C) Aneusomic urothelial cell showing five copies of chromosome 3 (red),seven copies of chromosome 7 (green), and four copies of chromosome17 (aqua) by FISH. (D) Aneusomic urothelial cell showing four copies of chro-mosome 3 (red), two copies of chromosome 7 (green), two copies of chro-mosome 17 (aqua), and two copies of LSI 9p21 (gold) by FISH. (E) Urothelialcarcinoma cell showing gains of chromosomes 3 (red), 7 (green), and 17(aqua) by FISH.
that remained high even after extended follow-up, arguing against“anticipatory positive” results.232
The combination of FISH and cytology, FISH and Immuno-Cyt, or cytology and ImmunoCyt all showed negative predictivevalue of 99% of recurrence in patients with a prior history ofhigh-grade carcinoma.233
For upper tract cancer, FISH was superior to voided cytology,with sensitivity of 77% to 84% and specificity of 90% to 95%(64% versus 29% for low-grade urothelial carcinoma and 87% ver-sus 27% for high-grade urothelial carcinoma, respectively).18,234,235
Comparison revealed that cytology was more suitable for identifica-tion of high-grade cancer, FISH was superior for identifying low-grade cancer, and immunostains for p16/Ki-67 were useful for dis-tinguishing high-grade from low-grade cancer.236
Alternative evaluation methods may offer superior diagnosticperformance compared with the manufacturer’s algorithm. Mod-ification of UroVysion scoring criteria with gain of at least onechromosome (3, 7, or 17) or heterozygous or homozygous deletionof 9p21 resulted inmoderate increased sensitivity (81%) and only aslight decrease in specificity.237 In our experience, 9p21 deletionwas present in 12% of FISH-positive cases and always occurredwith other chromosomal anomalies, rarely if ever a solitary find-ing.238 Modification by addition of cytologic prescreening anduse of positive results defined as at least one copy number changeof a probe target resulted in an increase in sensitivity from to 68%to 81% and a slight decrease in specificity from 84% to 82%.237
Zellweger et al. found that sensitivity of FISH to predict recurrencewas significantly improved by considering specimens with rare(�10) tetraploid cells as negative, and this observation was laterconfirmed.239,240 Zhou and colleagues determined that exclusionof tetrasomy from the polysomy category changed the thresholdfrom 8.5 to 4.5 cells, increased specificity (59% to 79%), butreduced sensitivity (70% to 66%).241 The introduction of specificcutoffs for tetraploid cells improved specificity.
Molecular grading with FISH increased the accuracy of predic-tion for both recurrence and progression in patients withintermediate-risk non–muscle-invasive bladder cancer. Lowmolecular grading was defined as diploid chromosomal patternor only a loss of p16 or chromosome 3 aneuploidy, and high molec-ular grading as aneuploidy of chromosome 7 or 17.242 Withmedian follow-up of 67 months, 57% of tumors were classifiedas low molecular grading. The 2- and 5-year recurrence-free sur-vival rates were 68% and 49% for low molecular grading, and47% and 30% for high molecular grading, respectively. The2- and 5-year progression-free survival rates were 95% and 84%for low molecular grading, and 79% and 58% for high moleculargrading tumor patients, respectively. Cancer severity score andmolecular grading independently and positively predicted progres-sion in multivariable models.
FISH for AURKA gene copy number in urine yielded a speci-ficity of 79.7% and sensitivity of 79.6%, with an AUC of 0.90.243
The Problem of Hematuria
Hematuria is present in about 21% of Americans, including up to2% of children.244,245 It is most commonly microscopic, usuallydiscovered incidentally during laboratory studies accompanyingphysical examination, or gross and typically apparent to patient.Only 1 mL of red blood cells per liter is sufficient to noticeablychange the color of urine. Microscopic hematuria is defined asat least three red blood cells per hpf in freshly voided centrifugedurine, preferably documented on three separate occasions.246 Upto 3% of adults normally excrete small numbers of red blood cells

355CHAPTER 7 Urine Cytology
(up to two red blood cells per hpf, or the equivalent of 1000 redblood cells/mL), so it is important in such cases to avoid overdiag-nosis. Gross hematuria is the visible discoloration of urine second-ary to blood.
Hematuria may be symptomatic or asymptomatic, transient orpersistent, but is often accompanied by other physical findingsincluding proteinuria, edema, and hypertension. A thorough his-tory and physical examination is mandatory. Current guidelinesaround the world recommend against the use of routine urine
TABLE 7.14Causes of Hematuria in Children andAdults (%)
Causes
CHILDREN245 ADULTS251
MicroscopicHematuria
GrossHematuria
MicroscopicHematuria
GrossHematuria
Idiopathic 38 80 43 0Malignancy 0 0 5 23Calculi 0 1 5 11Urinary tractinfection
0 0 4 33
Renal disease 3 34 2 0Hypercalciuria 16 22 0 0
TABLE 7.15 Site-Specific Causes of Hematuria
Lower Urinary Tract Bleeding
Tumors (urethra, bladder, prostate, ureters, renal pelvis)Obstructive uropathyBenign prostatic hyperplasiaLithiasis (stones)Infections (cystitis, prostatitis, schistosomiasis, tuberculosis, condyloma acuminatCoagulopathyTraumaRadiation therapyInstrumentationVigorous exerciseMenstrual contaminationEndometriosis
cytology for evaluation of asymptomatic microscopic hematu-ria.247,248 Metaanalysis revealed an overall pooled urinary tractcancer rate for hematuria of 3.3%.249
Hematuria may originate anywhere in the urinary tract, fromthe glomeruli to the distal urethra. Causes of hematuria are numer-ous and may be benign or malignant (Table 7.14 throughTable 7.16). “Atypical urothelial cells” are present in 33% of casesof gross or microscopic hematuria, with 10% of these predictive ofcarcinoma (3% of all cases of hematuria).250 The commonestcauses of gross hematuria in adults are urinary tract infection(33%), malignancy (23%), and urolithiasis (11%). The most com-mon causes of hematuria in adults are idiopathic (43% of cases ofmicroscopic hematuria) and urinary tract infection (33% of casesof gross hematuria (Table 7.14).251 Among children the most com-mon causes are idiopathic (80% of cases of microscopic hematuria)and renal disease (34% of cases of gross hematuria).245 It is criticalthat the source of persistent hematuria be identified, according tothe Best Practice Policy of the American Urologic Association.251
Such patients should be referred for appropriate urologic workup.
Routine Laboratory Investigation of HematuriaRoutine urinalysis combines the macroscopic reagent strip (dip-stick) test with microscopic examination of the sediment to detectdisorders of the urinary tract. Dipsticks detect 0.05 to 0.3 mg of
Upper Urinary Tract (Renal) Bleeding
um)
Primary glomerulopathies
Immunoglobulin A nephropathyPostinfectious glomerulonephritisMembranoproliferative glomerulonephritisFocal glomerular sclerosis
Secondary glomerulopathies
Lupus nephritisHenoch-Sch€onlein syndromeVasculitis (polyarteritis nodosa)Wegener granulomatosisHemolytic-uremic syndromeEssential mixed cryoglobulinemiaInterstitial nephritis
Familial conditions
Hereditary nephritis (Alport syndrome)HemoglobinopathiesMetabolic disorders (hypercalcuria)Polycystic kidney
Infections
Pyelonephritis (acute or chronic)TuberculosisCytomegalovirusPolyomavirus
Nephrolithiasis
Light chain deposition
Diabetic nephropathy
Amyloid
Renal tumors (renal cell carcinoma)

TABLE 7.16Etiologic Classification of Causes ofHematuria by Ingestion andPigments
Drugs andMedications Pigments Other
Antibiotics
PenicillinCephalosporinRifampinErythromycinSulfonamidesAminoglycosidesTetracycline
Nonsteroidalantiinflammatorydrugs
AcetaminophenAcetylsalicylic acidNaproxenIbuprofenIndomethacinPhenylbutazoneTolmetinMefenamic acidFenoprofen
Other drugs
CaptoprilCimetidinePhenobarbitalDilantinInterferonLithium
Rhabdomyolysis(myoglobin)
Hemoglobin(transfusionreaction)
Heme pigment(hemolysis)
Diuretics
ThiazidesFurosemideTriamtereneChlorthalidone
Other
Radiocontrast agentsCisplatinumHeavy metals (gold,
cadmium, mercury)Organic solvents
356 CHAPTER 7 Urine Cytology
hemoglobin per deciliter of urine. The sensitivity of dipstick exam-ination to detect three or more red blood cells per hpf is around90%. Myoglobin is also detected by screening reagent strips, soconfirmatory testing by an appropriate reagent strip and micro-scopic examination is necessary. The degree of hematuria bearsno relation to the severity of underlying disease and should beconsidered evidence of disease until proven otherwise.
Dysmorphic Red Blood Cells Indicate GlomerularDiseaseRed blood cell morphology is useful for determining the site of ori-gin (glomerular or nonglomerular) of hematuria. Dysmorphic redblood cells are associated with hematuria caused by glomerularinjury.252 Two distinct types of dysmorphic red blood cells havebeen described: (1) target cells containing a distinct central inclu-sion of heme pigment surrounded by a clear zone, and (2) cells withmultiple cytoplasmic blebs (Fig. 7.42A to D). How dysmorphicred blood cells are formed has not been definitively elucidated,although some suggest that causes include mechanical damage tothe red blood cell within the glomerulus followed by osmotic injurysustained during passage through the renal tubules.253,254 In con-trast with dysmorphic red blood cells, isomorphic red blood cellssuggest nonglomerular hematuria.
We analyzed 146 patients (Table 7.17) who had diagnostic renalbiopsies and prior cytologic examination of urine sediment, includ-ing detailed analysis of red blood cell morphology (unpublished
data). Of 108 patients with histologically confirmed glomerulopa-thy, 67 had dysmorphic red blood cells in urine. One of 38 patientswith no glomerulopathy diagnosed at renal biopsy had dysmorphicred blood cells. Using histologically confirmed glomerulopathy asthe end point for analysis of dysmorphic red blood cells and glomer-ulopathy, sensitivity was 70%, specificity was 97%, positive predic-tive value was 99%, and the negative predictive value was 54%.
Red blood cell morphology alone is not sufficient to categorizepatients with hematuria. Although the specificity of dysmorphicred blood cells is high, their absence does not entirely excludethe possibility of glomerulopathy, nor does their presence guaran-tee renal disease. The evaluation of red cell morphology is mostuseful when accompanied by evaluation of all components of urinesediment, including urothelial cell morphology, urinalysis withurine chemistry, and serum chemistries.
Studies have evaluated various percentages of dysmorphic redblood cells in patients with known glomerular disease. Increasingthe percent required for the diagnosis of glomerular bleedingincreases the specificity of the test.255,256 Among patients exhibiting�40 dysmorphic red blood cells, 34% had urologic diseases and29% had glomerular diseases.257 Urologic diseases included 27%with malignancies and 52% with conditions requiring immediatetreatment. For predicting glomerular disease, the presence of pro-teinuria was more accurate than the number of dysmorphic cells.
Comprehensive Analysis of Urine for Evaluationof HematuriaComprehensive quantitative evaluation of the sediment, alsoknown as optimal cytodiagnostic urinalysis, is useful to help dis-criminate inflammatory, infectious, degenerative, or neoplasticconditions of the kidney and the lower urinary tract, and can oftendiscriminate glomerular and tubular injury.64,258 This methodincorporates routine urinalysis, urine chemistries, and detailedcytologic examination of urothelial and renal cellular elements.Enhanced cytologic preparation improves cell recovery to maxi-mize microscopic visualization and quantitative assessment of dys-morphic and isomorphic red blood cells, inflammatory cells, renalcasts, and renal tubular elements. Diagnostic findings are corre-lated with serum findings, providing the clinician with the fullspectrum of chemical and morphologic abnormalities, and allow-ing triage of patients to the appropriate specialist (e.g., nephrolo-gist, urologist). There are six components in comprehensiveanalysis of urine for evaluation of hematuria:1. Patient history2. Physical examination of the urine sample, including color, char-
acter, and specific gravity3. Chemical examination, consisting of multiparameter reagent
dipstick testing and confirmatory tests; albumin, β2 microglo-bulin, and protein are reported quantitatively
4. Microscopic urine sediment examination using standardizedsediment recovery and high-contrast Papanicolaou stain
5. Quantitative microscopic examination of the sediment entitiesand 10 specific morphologic categories: background, cellularity,epithelial fragments, inclusion-bearing cells, red blood cells, neu-trophils, eosinophils, lymphocytes, renal tubular cells, and casts
6. Diagnostic interpretationThere is a high level of intraobserver and interobserver agree-
ment in determination of origin of renal cells (glomerular, tubular,interstitial, or vascular cells).258 Similarly, the correlation is highwith biopsy findings: 89% correlation in native kidneys and77% in transplant kidneys. Sensitivity and specificity for glomer-ular lesions alone in native and transplant kidneys was 91% and

Fig. 7.42 (A) Isomorphic red blood cells. Note the smooth membranes and uniform amount of hemoglobin. Compare with (B), dysmorphic red blood cells,“target cell type.” Note the central inclusion of heme pigment. (C) Dysmorphic red blood cells with prominent “blebs” or protrusions of red cell membrane.(D) Dysmorphic red blood cell “target cell type” with cytoplasmic bleb.
TABLE 7.17Patient Correlation of Urine Red CellMorphology and Glomerulopathy
GlomerulopathyNegative forGlomerulopathy
Dysmorphic red bloodcells (n)
76 1
Isomorphic red bloodcells (n)
32 37
357CHAPTER 7 Urine Cytology
85%, respectively. Severity scores showed good correlationbetween optimal cytodiagnostic urinalysis results and renal biopsyin native and transplanted kidneys, and correlated well withincreased creatinine concentration. In cases with biopsy-provenglomerular lesions, more severe changes were found by optimalcytodiagnostic urinalysis when the biopsy showed a proliferativelesion than when only normal glomeruli were found by light
microscopy. Optimal cytodiagnostic urinalysis has an advantageover renal biopsy in that it can be repeated as often as necessary,thereby providing data regarding a renal lesion over time.258
A study of 201 patients demonstrated that the presence of morethan five lymphocytes/hpf correlated with a 4.3 increased odds ratioof acute rejection among patients after antithymocyte globulininduction; the association was lost, however, with alemtuzumabinduction. In addition, the study showed that a demonstrationof polyomavirus infection was associated with polyomavirusnephropathy.259
Data from quantitative measurement of marker proteins (e.g.,albumin, transferrin, IgG, α1-microglobulin, retinol binding pro-tein, α2-macroglobulin, Bence Jones proteins) have challenged thedominant role of microscopy. Renal biopsy abnormalities wereidentified in all cases by marker protein excretion, but in only41% of cases by sediment.260
References are available at expertconsult.com

357.e1 CHAPTER 7 Urine Cytology
References
1. Papanicolaou GN, Marshall VF. Urine sediment smears as a diag-nostic procedure in cancers of the urinary tract. Science.1945;101:519–520.
2. Koss LG, Melamed MR, Ricci A, Melick WF, Kelly RE. Carcino-genesis in the human urinary bladder: observations after exposureto para-aminodiphenyl. N Engl J Med. 1965;272:767–770.
3. Melamed MR, Koss LG. Developments in cytological diagnosis ofcancer. Med Clin North Am. 1966;50:651–666.
4. Melamed MR, Koss LG, Ricci A. Cytohistological observations ondeveloping carcinoma of the urinary bladder in man. Cancer.1960;13:67–74.
5. Melamed MR, Voutsa NG, Grabstald H. Natural history and clin-ical behavior of in situ carcinoma of the human urinary bladder.Cancer. 1964;17:1533–1545.
6. Owens CL, Vandenbussche CJ, Burroughs FH, Rosenthal DL. Areview of reporting systems and terminology for urine cytology.Can-cer Cytopathol. 2013;121:9–14.
7. Fracchia JA, Motta J, Miller LS, Armenakas NA, Schumann GB,Greenberg RA. Evaluation of asymptomatic microhematuria. Urol-ogy. 1995;46:484–489.
8. Koss LG. Errors and pitfalls in cytology of the lower urinary tract.Monogr Pathol. 1997;60–74.
9. Ooms EC, Veldhuizen RW. Cytological criteria and diagnostic ter-minology in urinary cytology. Cytopathology. 1993;4:51–54.
10. Potts SA, Thomas PA, Cohen MB, Raab SS. Diagnostic accuracyand key cytologic features of high-grade transitional cell carcinomain the upper urinary tract. Mod Pathol. 1997;10:657–662.
11. Badalament RA, Gay H, Cibas ES, et al. Monitoring endoscopictreatment of superficial bladder carcinoma by postoperative urinarycytology. J Urol. 1987;138:760–762.
12. Schwalb DM, Herr HW, Fair WR. The management of clinicallyunconfirmed positive urinary cytology. J Urol. 1993;150:1751–1756.
13. Matzkin H, Moinuddin SM, Soloway MS. Value of urine cytologyversus bladder washing in bladder cancer. Urology.1992;39:201–203.
14. Bian Y, Ehya H, Bagley DH. Cytologic diagnosis of upper urinarytract neoplasms by ureteroscopic sampling. Acta Cytol.1995;39:733–740.
15. Van Keer S, Pattyn J, Tjalma WAA, et al. First-void urine: a poten-tial biomarker source for triage of high-risk human papillomavirusinfected women. Eur J Obstet Gynecol Reprod Biol. 2017;216:1–11.
16. Tshomo U, Franceschi S, Tshokey T, et al. Evaluation of the perfor-mance of human papillomavirus testing in paired urine andclinician-collected cervical samples among women aged over 30 yearsin Bhutan. Virol J. 2017;14:74.
17. Reynolds JP, Voss JS, Kipp BR, et al. Comparison of urine cytologyand fluorescence in situ hybridization in upper urothelial tract sam-ples. Cancer Cytopathol. 2014;122:459–467.
18. Zhang ML, Rosenthal DL, VandenBussche CJ. Upper urinarytract washings outperform voided urine specimens to detect uppertract high-grade urothelial carcinoma. Diagn Cytopathol. 2017;45:700–704.
19. Shanmugam V, Geraghty B, DeSimone RA, Hoda RS. Diagnosticvalue of positive urinary cytology in the detection of recurrenturothelial carcinoma: 10-Year Experience at the Papanicolaou Cytol-ogy Laboratory. Diagn Cytopathol. 2016;44:975–979.
20. Xing J, Roy S, Monaco SE, Pantanowitz L. Cytohistologic correla-tion of recurrent urothelial carcinoma detected in urinary diversionspecimens. Cancer. 2017;125:120–127.
21. Chen H, Liu L, Pambuccian SE, Barkan GA, Quek ML,Wojcik EM. Urine cytology in monitoring recurrence in urothelialcarcinoma after radical cystectomy and urinary diversion. CancerCytopathol. 2016;124:273–278.
22. Joudi AM, Pambuccian SE, Wojcik EM, Barkan GA. The positivepredictive value of “suspicious for high-grade urothelial carcinoma”
in urinary tract cytology specimens: A single-institution study of 665cases. Cancer Cytopathol. 2016;124:811–819.
23. VandenBussche CJ, Rosenthal DL, Olson MT. Adequacy in voidedurine cytology specimens: the role of volume and a repeat void uponpredictive values for high-grade urothelial carcinoma. Cancer Cyto-pathol. 2016;124:174–180.
24. Barkan GA,Wojcik EM, Nayar R, et al. The Paris System for report-ing urinary cytology: the quest to develop a standardized terminol-ogy. Acta Cytol. 2016;60:185–197.
25. Frees S, Bidnur S, Metcalfe M, et al. Effect of contrast media on uri-nary cytopathology specimens. Can Urol Assoc J. 2016;10:228–233.
26. Bastacky S, Ibrahim S, Wilczynski SP, Murphy WM. The accuracyof urinary cytology in daily practice. Cancer. 1999;87:118–128.
27. Layfield LJ, Elsheikh TM, Fili A, Nayar R, Shidham V. Review ofthe state of the art and recommendations of the Papanicolaou Soci-ety of Cytopathology for urinary cytology procedures and reporting:the Papanicolaou Society of Cytopathology Practice Guidelines TaskForce. Diagn Cytopathol. 2004;30:24–30.
28. Prather J, Arville B, Chatt GU. Evidence-based adequacy criteria forurinary bladder barbotage cytology. J Am Soc Cytopathol. 2015;4:57–62.
29. Barkan GA. Enough is enough: adequacy of voided urine cytology.Cancer Cytopathol. 2016;124:163–166.
30. Hundley AF, Maygarden S, Wu JM, Visco AG, Connolly A. Ade-quacy of urine cytology specimens: an assessment of collection tech-niques. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18:997–1001.
31. Keller AK, Jensen JB. Voided urine versus bladder washing cytologyfor detection of urothelial carcinoma: which is better? Scand J Urol.2017;51:290–292.
32. Zhang ML, Rosenthal DL, VandenBussche CJ. The cytomorpholo-gical features of low-grade urothelial neoplasms vary by specimentype. Cancer Cytopathol. 2016;124:552–564.
33. Toyonaga Y, Yamazaki K, Koyama Y, Yamada M, Ishida Y. A mod-ified direct-smear processing technique employing two-step centri-fugation/fixation is useful for detecting high-grade urothelialcarcinoma. Acta Cytol. 2017;61:447–454.
34. Savant D, Bajaj J, Gimenez C, et al. Urine cytology of nonurothelialmalignancies: a 10-year experience in a large multihospital health-care system. Diagn Cytopathol. 2017;45:22–28.
35. Kim JY, Kim HJ. A comparison between thinprep monolayer andcytospin cytology for the detection of bladder cancer. Korean J Urol2014;55:390–394.
36. Luo Y, She DL, Xiong H, Yang L, Fu SJ. Diagnostic value of liquid-based cytology in urothelial carcinoma diagnosis: a systematic reviewand meta-analysis. PLoS One. 2015;10: e0134940.
37. Straccia P, Bizzarro T, Fadda G, Pierconti F. Comparison betweencytospin and liquid-based cytology in urine specimens classifiedaccording to the Paris System for Reporting Urinary Cytology. Can-cer Cytopathol. 2016;124:519–523.
38. Sekita N, Shimosakai H, Nishikawa R, et al. Comparison of the con-ventional centrifuged and filtrated preparations in urine cytology.Hinyokika Kiyo. 2016;62:111–116.
39. Granados R, Butron M, Santonja C, et al. Increased risk of malig-nancy for non-atypical urothelial cell groups compared to negativecytology in voided urine. Morphological changes with LBC. DiagnCytopathol. 2016;44:582–590.
40. Agency for Healthcare Research and Quality. Methodology.Evidence-based Reports. Available from URL: https://www.ahrq.gov/research/findings/evidence-based-reports/technical/methodology/index.html.
41. CowanML, Rosenthal DL, VandenBussche CJ. Improved risk strat-ification for patients with high-grade urothelial carcinoma followingapplication of the Paris System for Reporting Urinary Cytology.Cancer. 2017;125:427–434.
42. Hang JF, Charu V, Zhang ML, VandenBussche CJ. Digital imageanalysis supports a nuclear-to-cytoplasmic ratio cutoff value of 0.5for atypical urothelial cells. Cancer. 2017;125:710–716.

357.e2CHAPTER 7 Urine Cytology
43. Layfield LJ, Esebua M, Frazier SR, et al. Accuracy and reproducibil-ity of nuclear/cytoplasmic ratio assessments in urinary cytology spec-imens. Diagn Cytopathol. 2017;45:107–112.
44. Hassan M, Solanki S, Kassouf W, et al. Impact of implementing theParis System for reporting urine cytology in the performance of urinecytology: a correlative study of 124 cases. Am J Clin Pathol.2016;146:384–390.
45. Miki Y, Neat M, Chandra A. Application of The Paris System toatypical urine cytology samples: correlation with histology and Uro-Vysion(R) FISH. Cytopathology. 2017;28:88–95.
46. Allison DB, Olson MT, Lilo M, Zhang ML, Rosenthal DL,VandenBussche CJ. Should the BK polyomavirus cytopathic effectbe best classified as atypical or benign in urine cytology specimens?Cancer Cytopathol. 2016;124:436–442.
47. Bostwick DG, Hossain D. Does subdivision of the “atypical” urinecytology increase predictive accuracy for urothelial carcinoma?DiagnCytopathol. 2014;42:1034–1044.
48. Suh J, Go H, Sung C, et al. Modification of The Paris System forurinary tract washing specimens using diagnostic cytological fea-tures. Cytopathology. 2017;28:516–523.
49. Long T, Layfield LJ, Esebua M, Frazier SR, Giorgadze DT,Schmidt RL. Interobserver reproducibility of The Paris System forReporting Urinary Cytology. Cytojournal. 2017;14:17.
50. Amberson JB, Laino JP. Image cytometric deoxyribonucleic acidanalysis of urine specimens as an adjunct to visual cytology in thedetection of urothelial cell carcinoma. J Urol. 1993;149:42–45.
51. Kline MJ, Wilkinson EJ, Askeland R, Given RW, Stephen C,Hendricks JB. DNA tetraploidy in Feulgen-stained bladder washingsassessed by image cytometry. Anal Quant Cytol Histol. 1995;17:129–134.
52. Highman W, Wilson E. Urine cytology in patients with calculi. JClin Pathol. 1982;35:350–356.
53. Kannan V, Bose S. Low grade transitional cell carcinoma and instru-ment artifact. A challenge in urinary cytology. Acta Cytol. 1993;37:899–902.
54. Harris MJ, Schwinn CP, Morrow JW, Gray RL, Browell BM.Exfoliative cytology of the urinary bladder irrigation specimen. ActaCytol. 1971;15:385–399.
55. Roberti I, Reisman L, Burrows L, Lieberman KV. Urine cytologyand urine flow cytometry in renal transplantation—a prospectivedouble blind study. Transplantation. 1995;59:495–500.
56. Eggensperger D, Schweitzer S, Ferriol E, O’Dowd G, Light JA. Theutility of cytodiagnostic urinalysis for monitoring renal allograftinjury. A clinicopathological analysis of 87 patients and over1,000 urine specimens. Am J Nephrol. 1988;8:27–34.
57. Gutmann EJ. Seminal vesicle cell in a spontaneously voided urine.Diagn Cytopathol. 2006;34:824–825.
58. RuppM,O’Hara B,McCullough L, Saxena S, Olchiewski J. Prostaticcarcinoma cells in urine specimens.Cytopathology. 1994;5:164–170.
59. Ito S, Horie K, Seike K, et al. Usefulness of quantifying leukocytes infirst-voided urine to predict positivity for Chlamydia trachomatis inasymptomatic men at high risk for chlamydial infection. J Infect Che-mother. 2014;20:748–751.
60. Kagan JA, Wu S, Bardarov S. Significance of pigmented urothelialand non-urothelial cells in voided urine specimens: A case report andreview. J Cytol. 2017;34:101–103.
61. Melamed MR, Wolinska WH. On the significance of intracytoplas-mic inclusions in the urinary sediment. Am J Pathol.1961;38:711–719.
62. Landing BH, Nakai H. Histochemical properties of renal lead-inclusions and their demonstration in urinary sediment. Am J ClinPathol. 1959;31:499–503.
63. Rouse BA, Donaldson LD, Goellner JR. Intranuclear inclusions inurinary cytology. Acta Cytol. 1986;30:105–109.
64. Marcussen N, Schumann J, Campbell P, Kjellstrand C. Cytodiag-nostic urinalysis is very useful in the differential diagnosis of acuterenal failure and can predict the severity. Ren Fail.1995;17:721–729.
65. Shukuya K, Ogura S, Tokuhara Y, et al. Novel round cells in urinesediment and their clinical implications. Clin Chim Acta. 2016;457:142–149.
66. Martinez-Martinez MU, Llamazares-Azuara LM,Martinez-Galla D,et al. Urinary sediment suggests lupus nephritis histology. Lupus.2017;26:580–587.
67. Rashidi B, Tongson-Ignacio JE. Melamed-Wolinska bodies in urinecytology an interesting aggregate in a degenerated urothelial cell.Diagn Cytopathol. 2011;39:117.
68. Eltoum IA, Suliaman SM, Ismail BM, Ismail AI, Ali MM,Homeida MM. Evaluation of eosinophiluria in the diagnosis ofschistosomiasis hematobium: a field-based study. Am J Trop MedHyg. 1992;46:732–736.
69. Betz SA, See WA, Cohen MB. Granulomatous inflammation inbladder wash specimens after intravesical bacillus Calmette-Guerintherapy for transitional cell carcinoma of the bladder. Am J ClinPathol. 1993;99:244–248.
70. BhanR, Pisharodi LR,GudlaugssonE, BedrossianC.Cytological, his-tological, and clinical correlations in intravesical Bacillus Calmette-Guerin immunotherapy. Ann Diagn Pathol. 1998;2: 55–60.
71. Schwalb MD, Herr HW, Sogani PC, Russo P, Sheinfeld J, Fair WR.Positive urinary cytology following a complete response to intrave-sical bacillus Calmette-Guerin therapy: pattern of recurrence. J Urol.1994;152:382–387.
72. Crabbe JG. “Comet” or “decoy” cells found in urinary sedimentsmears. Acta Cytol. 1971;15:303–305.
73. Burgos D, Lopez V, Cabello M, et al. Polyomavirus BK nephropa-thy: the effect of an early diagnosis on renal function or graft loss.Transplant Proc. 2006;38:2409–2411.
74. Maghrabi M, Marwan D, Osoba AO. BK virus infection in a renaltransplant Saudi child. Saudi Med J. 2007;28:121–124.
75. Koss LG, Sherman AB, Eppich E. Image analysis and DNA contentof urothelial cells infected with human polyomavirus. Anal QuantCytol. 1984;6:89–94.
76. Ranzi AD, Introini GO, Prolla JC, et al. Correlation between thepresence of degenerated inclusion-bearing cells in voided urine sam-ples and the occurrence of polyomavirus infection. Cytopathology.2017;28:103–108.
77. Matsukuma Y, Masutani K, Tsuchimoto A, et al. Early disappear-ance of urinary decoy cells in successfully treated polyomavirusBK nephropathy. Transplant Proc. 2014;46:560–563.
78. Seftel AD, Matthews LA, Smith MC, Willis J. Polyomavirusmimicking high grade transitional cell carcinoma. J Urol.1996;156:1764.
79. Hossain D, Hull D, Kalantarpour F, Maitlen R, Qian J,Bostwick DG. Does polyoma virus infection interfere with bladdercancer fluorescence in situ hybridization (FISH)? Diagn Cytopathol.2014;42(3):225–229.
80. Nankivell BJ, Renthawa J, Jeoffreys N, et al. Clinical utility of uri-nary cytology to detect BK viral nephropathy. Transplantation.2015;99:1715–1722.
81. Lopez-Beltran A, Escudero AL, Carrasco-Aznar JC, Vicioso-Recio L.Human papillomavirus infection and transitional cell carcinoma ofthe bladder. Immunohistochemistry and in situ hybridization.Pathol Res Pract. 1996;192:154–159.
82. Doxtader EE, Elsheikh TM. Diagnosis of trichomoniasis in men byurine cytology. Cancer. 2017;125:55–59.
83. Guler Simsek G, Vargol E, Simsek H. Cytomorphological effects ofmitomycin C on urothelial cells: eosinophils may be clue to the drug-induced changes. Cell J. 2014;16:375–376.
84. Maier U, Simak R, Neuhold N. The clinical value of urinary cytol-ogy: 12 years of experience with 615 patients. J Clin Pathol.1995;48:314–317.
85. Forni AM, Koss LG, Geller W. Cytological study of the effect ofcyclophosphamide on the epithelium of the urinary bladder inman. Cancer. 1964;17:1348–1355.
86. MurphyWM. Current status of urinary cytology in the evaluation ofbladder neoplasms. Hum Pathol. 1990;21:886–896.

357.e3 CHAPTER 7 Urine Cytology
87. Travis LB, Curtis RE, Boice JD, Jr., Fraumeni JF Jr. Bladder cancerafter chemotherapy for non-Hodgkin’s lymphoma. N Engl J Med.1989;321:544–545.
88. Wall RL, Clausen KP. Carcinoma of the urinary bladder inpatients receiving cyclophosphamide. N Engl J Med.1975;293:271–273.
89. Fanning CV, Staerkel GA, Sneige N, Thomsen S, Myhre MJ, VonEschenbach AC. Spindling artifact of urothelial cells in post-lasertreatment urinary cytology. Diagn Cytopathol. 1993;9:279–281.
90. Wendler JJ, PechM, Kollermann J, et al. Upper-urinary-tract effectsafter irreversible electroporation (IRE) of human localised renal-cellcarcinoma (RCC) in the IRENE pilot phase 2a ablate-and-resectstudy. Cardiovasc Intervent Radiol. 2018;41(3):466–476.
91. Pierconti F, Straccia P, Emilio S, et al. Cytological and histologicalchanges in the urothelium produced by electromotive drug admin-istration (EMDA) and by the combination of intravescical hyper-thermia and chemotherapy (thermochemotherapy). Pathol ResPract. 2017;213:1078–1081.
92. Mustafa M, Aburas H, Helo FM, Qarawi L. Electromagnetic andelectrohydraulic shock wave lithotripsy-induced urothelial damage:is there a difference? J Endourol. 2017;31:180–184.
93. Grabsky AM,Manukyan EV, Muradyan AA. Cytological evaluationof urothelial damage in extracorporeal shock-wave lithotripsy. Uro-logiia. 2016;(5):4–9.
94. Ajit D, Dighe SB, Desai SB. Cytology of lleal conduit urine in blad-der cancer patients: diagnostic utility and pitfalls. Acta Cytol.2006;50:70–73.
95. Wolinska WH, Melamed MR. Urinary conduit cytology. Cancer.1973;32:1000–1006.
96. Planinsek T, Kladnik A, Pohar-Marinsek Z, Flezar MS. Vegetablecells in urinary samples of patients with bricker ileal conduit. DiagnCytopathol. 2014;42:120–124.
97. Pillai KR, Jayasree K, Pisharody R, Abraham EK. Decoy cells in theurine cytology of a renal transplant recipient: an immunohistochem-ical study. Indian J Pathol Microbiol. 2010;53:347–350.
98. Brady PC, Missmer SA, Laufer MR. Bladder involvement in stage Iendometriosis. J Pediatr Adolesc Gynecol. 2017;30:503–504.
99. Shimohata H, Ogawa Y, Maruyama H, Hirayama K, Kobayashi M.A renal variant of Fabry disease diagnosed by the presence of urinarymulberry cells. Intern Med. 2016;55:3475–3478.
100. Stilmant M,Murphy JL, Merriam JC. Cytology of nephrogenic ade-noma of the urinary bladder. A report of four cases. Acta Cytol.1986;30:35–40.
101. Lee J, Park S, Cho MS, Sung SH, Kim KH. Urine cytology findingsof primary paraganglioma of the urinary bladder: case report. DiagnCytopathol. 2017;45:350–353.
102. Schneider V, Smith MJ, Frable WJ. Urinary cytology in endometri-osis of the bladder. Acta Cytol. 1980;24:30–33.
103. ChaumpM, Giorgadze T, Schreiner AM. Urine cytology: pitfall dueto a “remnant” lesion. Cytojournal. 2015;12:16.
104. Deshpande V, McKee GT. Analysis of atypical urine cytology in atertiary care center. Cancer. 2005;105:468–475.
105. Planz B, Jochims E, Deix T, Caspers HP, Jakse G, Boecking A. Therole of urinary cytology for detection of bladder cancer. Eur J SurgOncol. 2005;31:304–308.
106. Murphy WM, Soloway MS. Urothelial dysplasia. J Urol.1982;127:849–854.
107. Brimo F, Vollmer RT, Case B, Aprikian A, Kassouf W, Auger M.Accuracy of urine cytology and the significance of an atypical cate-gory. Am J Clin Pathol. 2009;132:785–793.
108. Renshaw AA. Subclassifying atypical urinary cytology specimens.Cancer. 2000;90:222–229.
109. Raab SS, Grzybicki DM, Vrbin CM, Geisinger KR. Urine cytologydiscrepancies: frequency, causes, and outcomes. Am J Clin Pathol.2007;127:946–953.
110. Chau K, Rosen L, Coutsouvelis C, et al. Accuracy and risk of malig-nancy for diagnostic categories in urine cytology at a large tertiaryinstitution. Cancer Cytopathol. 2015;123:10–18.
111. Rosenthal DL, Vandenbussche CJ, Burroughs FH,Sathiyamoorthy S, Guan H, Owens C. The Johns Hopkins Hospitaltemplate for urologic cytology samples: part I—creating the tem-plate. Cancer Cytopathology. 2013;121:15–20.
112. Rodgers M, Nixon J, Hempel S, et al. Diagnostic tests and algo-rithms used in the investigation of haematuria: systematic reviewsand economic evaluation. Health Technol Assess. 2006;10:iii–ivxi-259.
113. RaitanenMP, Aine R, Rintala E, et al. Differences between local andreview urinary cytology in diagnosis of bladder cancer. an interobser-ver multicenter analysis. Eur Urol. 2002;41:284–289.
114. Mokhtar GA, Al-Dousari M, Al-Ghamedi D. Diagnostic signifi-cance of atypical category in the voided urine samples: a retrospectivestudy in a tertiary care center. Urol Ann. 2010;2:100–106.
115. Matsumoto K, IkedaM,Hirayama T, et al. Clinical value of dividingfalse positive urine cytology findings into three categories: atypical,indeterminate, and suspicious of malignancy. Asian Pac J CancerPrev. 2014;15:2251–2255.
116. Kapur U, Venkataraman G, Wojcik EM. Diagnostic significance of‘atypia’ in instrumented versus voided urine specimens. Cancer.2008;114:270–274.
117. Granados R, Duarte JA, Corrales T, Camarmo E, Bajo P. Applyingthe Paris System for reporting urine cytology increases the rate ofatypical urothelial cells in benign cases: a need for patient manage-ment recommendations. Acta Cytol. 2017;61:71–76.
118. Ton Nu TN, Kassouf W, Ahmadi-Kaliji B, Charbonneau M,Auger M, Brimo F. The value of the “suspicious for urothelial car-cinoma” cytology category: a correlative study of 4 years including337 patients. Cancer Cytopathol. 2014;122:796–803.
119. Renshaw AA, Nappi D,Weinberg DS. Cytology of grade 1 papillarytransitional cell carcinoma. A comparison of cytologic, architecturaland morphometric criteria in cystoscopically obtained urine. ActaCytol. 1996;40:676–682.
120. Wolinska WH, Melamed MR, Klein FA. Cytology of bladder pap-illoma. Acta Cytol. 1985;29:817–822.
121. Green LK MH. Dramatically increased specificity and sensitivity indetecting low grade papillary TCC via a combination of cytospinand cell blocking techniques (abstract). Mod Pathol. 1995;8.
122. Wiener HG, Vooijs GP, van’t Hof-Grootenboer B. Accuracy of uri-nary cytology in the diagnosis of primary and recurrent bladder can-cer. Acta Cytol. 1993;37:163–169.
123. Sack MJ, Artymyshyn RL, Tomaszewski JE, Gupta PK. Diagnosticvalue of bladder wash cytology, with special reference to low gradeurothelial neoplasms. Acta Cytol. 1995;39:187–194.
124. Murphy WM, Soloway MS, Jukkola AF, Crabtree WN, Ford KS.Urinary cytology and bladder cancer. The cellular features of transi-tional cell neoplasms. Cancer. 1984;53:1555–1565.
125. Mai KT, Ball CG, Kos Z, Belanger EC, Islam S, Sekhon H. Three-dimensional cell groups with disordered nuclei and cellular discohe-sion (3DDD) are associated with high sensitivity and specificity forcystoscopic urine cytopathological diagnosis of low-grade urothelialneoplasia. Diagn Cytopathol. 2014;42:555–563.
126. Raab SS, Lenel JC, Cohen MB. Low grade transitional cell carci-noma of the bladder. Cytologic diagnosis by key features as identi-fied by logistic regression analysis. Cancer. 1994;74:1621–1626.
127. Raab SS, Slagel DD, Jensen CS, et al. Low-grade transitional cell car-cinoma of the urinary bladder: application of select cytologic criteriato improve diagnostic accuracy [corrected]. Mod Pathol. 1996;9:225–232.
128. Whisnant RE, Bastacky SI, Ohori NP. Cytologic diagnosis of low-grade papillary urothelial neoplasms (low malignant potential andlow-grade carcinoma) in the context of the 1998 WHO/ISUP clas-sification. Diagn Cytopathol. 2003;28:186–190.
129. Chung YR, Won JK, Park IA, et al. Cytomorphological character-istics of low-grade papillary urothelial carcinoma for differentialdiagnosis from benign papillary urothelial lesions: logistic regressionanalysis in SurePath(TM) liquid-based voided urine cytology. Cyto-pathology. 2016;27:83–90.

357.e4CHAPTER 7 Urine Cytology
130. Cakir E, Kucuk U, Pala EE, Sezer O, Ekin RG, Cakmak O. Cyto-pathologic differential diagnosis of low-grade urothelial carcinomaand reactive urothelial proliferation in bladder washings: a logisticregression analysis. APMIS. 2017;125:431–436.
131. McCroskey Z, Pambuccian SE, Kleitherms S, et al. Accuracy andinterobserver variability of the cytologic diagnosis of low-gradeurothelial carcinoma in instrumented urinary tract cytology speci-mens. Am J Clin Pathol. 2015;144:902–908.
132. Bubendorf L, Dalquen P, Savic S. Cytology of the urinary tract:between uncertainty and clarity. Pathologe. 2009;30(Suppl2):173–178.
133. Bubendorf L, Grilli B, Sauter G, Mihatsch MJ, Gasser TC,Dalquen P. Multiprobe FISH for enhanced detection of bladdercancer in voided urine specimens and bladder washings. Am J ClinPathol. 2001;116:79–86.
134. Cajulis RS, Haines GK, 3rd, Frias-Hidvegi D, McVary K,Bacus JW. Cytology, flow cytometry, image analysis, and interphasecytogenetics by fluorescence in situ hybridization in the diagnosis oftransitional cell carcinoma in bladder washes: a comparative study.Diagn Cytopathol. 1995;13:214–223; discussion 224.
135. Halling KC, King W, Sokolova IA, et al. A comparison of cytologyand fluorescence in situ hybridization for the detection of urothelialcarcinoma. J Urol. 2000;164:1768–1775.
136. Skacel M, Fahmy M, Brainard JA, et al. Multitarget fluorescencein situ hybridization assay detects transitional cell carcinoma inthe majority of patients with bladder cancer and atypical or negativeurine cytology. J Urol. 2003;169:2101–2105.
137. Fradet Y, Lockhard C. Performance characteristics of a new mono-clonal antibody test for bladder cancer: ImmunoCyt trade mark.Can J Urol. 1997;4:400–405.
138. Lodde M, Mian C, Negri G, et al. Role of uCyt+ in the detectionand surveillance of urothelial carcinoma. Urology.2003;61:243–247.
139. Olsson H, Zackrisson B. ImmunoCyt a useful method in the follow-up protocol for patients with urinary bladder carcinoma. Scand JUrol Nephrol. 2001;35:280–282.
140. van der Poel HG, Boon ME, van Stratum P, et al. Conventionalbladder wash cytology performed by four experts versus quantitativeimage analysis. Mod Pathol. 1997;10:976–982.
141. Friedell GH, Soloway MS, Hilgar AG, Farrow GM. Summary ofworkshop on carcinoma in situ of the bladder. J Urol. 1986;136:1047–1048.
142. Gamarra MC, Zein T. Cytologic spectrum of bladder cancer. Urol-ogy. 1984;23:23–26.
143. Rife CC, Farrow GM, Utz DC. Urine cytology of transitional cellneoplasms. Urol Clin North Am. 1979;6:599–612.
144. Shenoy UA, Colby TV, Schumann GB. Reliability of urinarycytodiagnosis in urothelial neoplasms.Cancer. 1985;56:2041–2045.
145. Curry JL, Wojcik EM. The effects of the current World HealthOrganization/International Society of Urologic Pathologists bladderneoplasm classification system on urine cytology results. Cancer.2002;96:140–145.
146. Loh CS, Spedding AV, Ashworth MT, Kenyon WE, Desmond AD.The value of exfoliative urine cytology in combination with flexiblecystoscopy in the diagnosis of recurrent transitional cell carcinoma ofthe urinary bladder. Br J Urol. 1996;77:655–658.
147. Shield PW, Frost F, Finnimore JL, Wright RG, Cummings MC.External quality assurance in nongynecologic cytology: The Austral-asian experience. Cancer. 2017;125:349–361.
148. Lee PJ, Owens CL, Lithgow MY, Jiang Z, Fischer AH. Causes offalse-negative for high-grade urothelial carcinoma in urine cytology.Diagn Cytopathol. 2016;44:994–999.
149. Koga F, Kobayashi S, Fujii Y, et al. Significance of positive urinecytology on progression and cancer-specific mortality of non–mus-cle-invasive bladder cancer. Clin Genitourin Cancer. 2014;12:e87–e93.
150. Guy L, Savareux L, Molinie V, Botto H, Boiteux JP, Lebret T.Should bladder biopsies be performed routinely after bacillus
Calmette-Guerin treatment for high-risk superficial transitional cellcancer of the bladder? Eur Urol. 2006;50:516–520; discussion 520.
151. Raj GV, Bochner BH, Serio AM, et al. Natural history of positiveurinary cytology after radical cystectomy. J Urol. 2006;176:2000–2005; discussion 2005.
152. Sasaki K, Wada K, Araki M, et al. Diagnostic ureteroscopy for casesclinically suspected of carcinoma in situ of the upper urinary tract.Acta Med Okayama. 2017;71:227–232.
153. Dev HS, Poo S, Armitage J, Wiseman O, Shah N, Al-Hayek S.Investigating upper urinary tract urothelial carcinomas: a single-centre 10-year experience. World J Urol. 2017;35:131–138.
154. Tanaka N, Kikuchi E, Kanao K, et al. The predictive value of pos-itive urine cytology for outcomes following radical nephroureterect-omy in patients with primary upper tract urothelial carcinoma: amulti-institutional study. Urol Oncol. 2014;32: 48 e19-26.
155. Sakano S, Inamoto T, Inoue R, et al. Positive voided urine cytologypredicts worse pathological findings of nephroureterectomy speci-mens in patients with upper tract urothelial carcinoma: does selectiveureteral cytology have an additional efficacy? Jpn J Clin Oncol.2015;45:968–972.
156. Wang LJ, Lee SY, Teh BT, Chuang CK, Nortier J. Upper tracturothelial carcinomas in patients with chronic kidney disease: rela-tionship with diagnostic challenge. Biomed Res Int. 2014;2014:989458.
157. Kuwamoto S, Murai Y, Endo Y, Masago T, Kuroda N, Horie Y.Cytologic features of renal carcinoma associated with Xp11.2 translo-cations/ TFE3 gene fusions: a case report with voided and catheterizedurine cytology and a literature review. Acta Cytol. 2014;58:406–412.
158. Moltrasio F, Brenna A, Bovo G, et al. Pathological features of Xp11translocation renal cell carcinoma using urine liquid-based cytologywith FISH. Cytopathology. 2015;26:325–328.
159. Rudrick B, Nguyen GK, Lakey WH. Carcinoid tumor of therenal pelvis: report of a case with positive urine cytology.Diagn Cyto-pathol. 1995;12:360–363.
160. Mitra S, Kaur G, Kakkar N, Singh P, Dey P. Sarcoma in urine cytol-ogy; an extremely rare entity: a report of two cases. J Cytol.2017;34:171–173.
161. Tanaka T, Yoshimi N, Sawada K, et al. Ki-1-positive large cell ana-plastic lymphoma diagnosed by urinary cytology. A case report. ActaCytol. 1993;37:520–524.
162. Hamele-Bena D, Gonzalez AA. Urinary tract involvement of mantlecell lymphoma diagnosed by urine cytology. Diagn Cytopathol.2017;45:1125–1127.
163. Lobo J, Henrique R, Monteiro P, Lobo C. ALK-negative anaplasticlarge cell lymphoma with urinary bladder involvement diagnosed inurine cytology: a case report and literature review. Diagn Cytopathol.2017;45:354–358.
164. LuM,Ho J, Azordegan N, Perry AM, Gibson IW, Baker P. Atypicalcells in a voided urine cytology specimen in a renal transplant recip-ient. Diagn Cytopathol. 2017;45:69–72.
165. Bartone FF. Metastatic melanoma of the bladder. J Urol. 1964;91:151–155.
166. Hori T, Kato T, Komiya A, et al. Primary melanoma of the urinarybladder identified by urine cytology: a rare case report. Diagn Cyto-pathol. 2014;42:1091–1095.
167. Wang Y, Otis CN, Florence RR. Atypical squamous cells in theurine revealing endometrioid adenocarcinoma of the endometriumwith squamous cell differentiation: a case report. Diagn Cytopathol.2015;43:49–52.
168. Hajdu SI, Nolan MA. Exfoliative cytology of malignant germ celltumors. Acta Cytol. 1975;19:255–260.
169. Nishikawa S, Noguchi H, Tokumitsu T, et al. Diagnosis of pediatricneuroblastoma by urine cytology: a case report. Diagn Cytopathol.2018;46(3):280–283.
170. Gopalakrishna A, Fantony JJ, Longo TA, et al. Anticipatory positiveurine tests for bladder cancer. Ann Surg Oncol. 2017;24:1747–1753.
171. Yafi FA, Brimo F, Auger M, Aprikian A, Tanguay S, Kassouf W. Isthe performance of urinary cytology as high as reported historically?

357.e5 CHAPTER 7 Urine Cytology
A contemporary analysis in the detection and surveillance of bladdercancer. Urol Oncol. 2014;32: 27 e21–26.
172. Shaaban AA. Tribukait B, el-Bedeiwy AF, GhoneimMA. Character-ization of squamous cell bladder tumors by flow cytometric deoxyr-ibonucleic acid analysis: a report of 100 cases. J Urol.1990;144:879–883.
173. Mitra S, Chatterjee D, Gupta K, Dass Radotra B, Dey P. Urinecytology of urothelial carcinoma with villoglandular differentiation.Diagn Cytopathol. 2016;44:653–656.
174. Tribukait B. Clinical DNA flow cytometry.Med Oncol Tumor Phar-macother. 1984;1:211–218.
175. Ishikawa R, Kadota K, Hayashi T, et al. Cytopathological features ofvillous adenoma of the urinary bladder in urine: a rare case report.Diagn Cytopathol. 2016;44:632–635.
176. Rollins S, Schumann GB. Primary urinary cytodiagnosis of a bladdersmall-cell carcinoma. Diagn Cytopathol. 1991;7:79–82.
177. Yoshida K, Ishida M, Kagotani A, Iwamoto N, Iwai M, Okabe H.Small cell carcinoma of the urinary bladder and prostate: cytologicalanalyses of four cases with emphasis on the usefulness of cytologicalexamination. Oncol Lett. 2014;7:369–372.
178. Yeung HM, Jeurkar C, Pompa T, Styler M. Small cell cancer of thegenitourinary tract: a case report and review of the literature. CaseRep Oncol. 2017;10:489–492.
179. Sharma A, Sharma S, Patnaik N, et al. Cytomorphologic and immu-nophenotypic profile of a cohort of small cell carcinoma of the uri-nary bladder. Acta Cytol. 2016;60:475–480.
180. Guan H, Tatsas AD, Ali SZ. Signet ring cell carcinoma in urinecytology: cytomorphologic findings and differential diagnosis. ActaCytol. 2012;56:177–182.
181. Chow NH, Tzai TS, Cheng HL, Chan SH, Lin JS. Urinary cyto-diagnosis: can it have a different prognostic implication than a diag-nostic test? Urol Int. 1994;53:18–23.
182. Sakuma T, Furuta M, Mimura A, Tanigawa N, Takamizu R,Kawano K. Urine cytological findings of plasmacytoid urothelial car-cinoma of urinary bladder: report of two cases. Cytopathology.2009;20:264–267.
183. Zhu B, Rohan SM, Lin X. Urine cytomorphology of micropapillaryurothelial carcinoma. Diagn Cytopathol. 2013;41:485–491.
184. Tajima S. Urothelial carcinoma with oncocytic features: anextremely rare case presenting a diagnostic challenge in urine cytol-ogy. Int J Clin Exp Pathol. 2015;8:8591–8597.
185. Gonzalez-Peramato P, Jimenez-Heffernan JA, Vicandi B, et al. Micro-papillary carcinoma of the urinary tract: a cytologic study of urine andfine-needle aspirate samples. Acta Cytol. 2014;58:269–274.
186. Olsen DL, Anderson SR. Metastatic plasmacytoid urothelial carci-noma: a case report and review of the literature. Acta Cytol.2014;58:108–112.
187. Barkan GA, Laucirica R, Auger M, et al. Performance characteristicsof urinary tract cytology: observations from the college ofAmerican pathologists interlaboratory comparison program in non-gynecologic cytopathology. Arch Pathol Lab Med. 2015;139:1009–1013.
188. Galed-Placed I, Valbuena-Ruvira L. Decoy cells and malignant cellscoexisting in the urine from a transplant recipient with BK virusnephropathy and bladder adenocarcinoma. Diagn Cytopathol.2011;39:933–937.
189. Borkowski T, Monika Dulewicz A, Borkowski A, Pietka D,Radziszewski P. Clinical value of digital image analysis in the diag-nosis of urinary bladder cancer, particularly in aggressive tumors: apreliminary report. Pol J Pathol. 2016;67:122–129.
190. de la Roza GL, Hopkovitz A, Caraway NP, et al. DNA imageanalysis of urinary cytology: prediction of recurrent transitional cellcarcinoma. Mod Pathol. 1996;9:571–578.
191. Mora LB, Nicosia SV, Pow-Sang JM, et al. Ancillary techniquesin the followup of transitional cell carcinoma: a comparison ofcytology, histology and deoxyribonucleic acid image analysiscytometry in 91 patients. J Urol. 1996;156:49–54; discussion54–45.
192. Muralidaran C, Dey P, Nijhawan R, Kakkar N. Artificial neural net-work in diagnosis of urothelial cell carcinoma in urine cytology.Diagn Cytopathol. 2015;43:443–449.
193. Yang CS, Chen S, Cramer HM, Wu HH. High apoptotic index inurine cytology is associated with high-grade urothelial carcinoma.Cancer Cytopathol. 2016;124:546–551.
194. Pham HV, Pantanowitz L, Liu Y. Quantitative phase imagingto improve the diagnostic accuracy of urine cytology. CancerCytopathol. 2016;124:641–650.
195. Tone K, Kojima K, Hoshiai K, Kumagai N, Kijima H, Kurose A. Anancillary method in urine cytology: nucleolar/nuclear volume ratiofor discrimination between benign and malignant urothelial cells.Diagn Cytopathol. 2016;44:483–491.
196. Dalquen P, Savic Prince S, Spieler P, et al. Making cytological diag-noses on digital images using the iPath network. Acta Cytol.2014;58:453–460.
197. Website U. Oklahoma City, OK: Urocor, Inc.; 2011. http://urocor.com/UROLOGICAL_PRODUCTS/DiagnosticServices/BBladder/B1Bladder_Diagnostics/B1bBladderCytology/b1b2Feulgenstain.htmWeb page last accessed 2011.
198. Shabaik AS, Pow-Sang JM, Lockhart J, Nicosia SV. Role ofDNA image cytometry in the follow-up of patients with urinary tracttransitional cell carcinoma. Anal Quant Cytol Histol. 1993;15:115–123.
199. Valkov N, Voyles R, Kulikowski, et al. Acid hematoxylin is an alter-native to Feulgen staining for cytology specimens and DNA ploidyanalysis. Mod Pathol. 2013;26:502A
200. Schulte EK, Fink DK. Hematoxylin staining in quantitative DNAcytometry: an image analysis study. Anal Cell Pathol. 1995;9:257–268.
201. Davis N, Mor Y, Idelevich P, et al. A novel urine cytology stain forthe detection and monitoring of bladder cancer. J Urol.2014;192:1628–1632.
202. Davis N, Shtabsky A, Lew S, et al. A novel urine-based assay forbladder cancer diagnosis: multi-institutional validation study. EurUrol Focus. 2016 Oct 31. pii: S2405-4569(16)30149-3. doi:10.1016/j.euf.2016.10.004. [Epub ahead of print].
203. Volpi A, Bravaccini S, Medri L, Cerasoli S, Gaudio M, Amadori D.Usefulness of immunological detection of the human telomerasereverse transcriptase. Cell Oncol. 2005;27:347–353.
204. Soldateschi D, Bravaccini S, Berti B, et al. Development and charac-terization of amonoclonal antibody directed against human telomerasereverse transcriptase (hTERT). J Biotechnol. 2005;118: 370–378.
205. Sanchini MA, Bravaccini S, Medri L, et al. Urine telomerase: animportant marker in the diagnosis of bladder cancer. Neoplasia.2004;6:234–239.
206. Raica M, Zylis D, Cimpean AM. Cytokeratin 20, 34betaE12 andoverexpression of HER-2/neu in urine cytology as predictors ofrecurrences in superficial urothelial carcinoma. Rom J MorpholEmbryol. 2005;46:11–15.
207. Wadhwa N, Diwaker P, Lotha N, Arora VK, Singh N. Cytokeratin20 immunocytochemistry on urine sediments: a potential low-costadjunct to cytology in the diagnosis of low-grade urothelial carci-noma. Cytopathology. 2017;28:531–535.
208. Negri S, Biavati P, Bondi A. The diagnostic value of cytohistologicalurine analysis and cytokeratin 20 in malignant and atypical urothe-lial cells. Pathologica. 2016;108:130–135.
209. Lenos M, Katafigiotis I, Vrettou K, et al. Evaluation of doubleimmunocytochemical staining for CK20 and P53 as a potentialadjunct to cytology for urothelial cancer diagnosis. Cytopathology.2017;28:96–102.
210. Strojan Flezar M, Srebotnik-Kirbis I, Gutnik H. Use of vimentinimmunocytochemical staining for evaluation of atypical cells invoided urine samples. Diagn Cytopathol. 2017;45:85–90.
211. Yafi FA, Brimo F, Steinberg J, Aprikian AG, Tanguay S, Kassouf W.Prospective analysis of sensitivity and specificity of urinary cytologyand other urinary biomarkers for bladder cancer. Urol Oncol.2015;33: 66 e25–31.

357.e6CHAPTER 7 Urine Cytology
212. He H, Han C, Hao L, Zang G. ImmunoCyt test compared to cytol-ogy in the diagnosis of bladder cancer: a meta-analysis. Oncol Lett.2016;12:83–88.
213. Vergara-Lluri ME, Hu E, Rao JY, Levin M, Apple SK,Moatamed NA. Comparative evaluation of ProEx C and Immuno-Cyt/uCyt assays in atypical urine cytology. Arch Pathol Lab Med.2014;138:1215–1222.
214. Chang S, Smith E, Levin M, Rao JY, Moatamed NA. Comparativestudy of ProEx C immunocytochemistry and UroVysion fluores-cent in-situ hybridization assays on urine cytology specimens.Cytojournal. 2015;12;2.
215. Shimada K, Fujii T, Tatsumi Y, Anai S, Fujimoto K, Konishi N.Ubiquilin2 as a novel marker for detection of urothelial carcinomacells in urine. Diagn Cytopathol. 2016;44:3–9.
216. Pal RP, Kockelbergh RC, Pringle JH, et al. Immunocytochemicaldetection of ERG expression in exfoliated urinary cells identifieswith high specificity patients with prostate cancer. BJU Int.2016;117:686–696.
217. Ohsaki H, Sofue T, Kawakami K, et al. WT1 immunoenzyme stain-ing using SurePath() processed urine cytology helps to detect kidneydisease. Cytopathology. 2016;27:43–49.
218. Courtade-Saidi M, Aziza J, d’Aure D, et al. Immunocytochemicalstaining for p53 and Ki-67 helps to characterise urothelial cells inurine cytology. Cytopathology. 2016;27:456–464.
219. McCroskey Z, Pambuccian SE, Wojcik EM, Barkan GA. Can weidentify nephrogenic adenoma in urine cytology specimens? A studyevaluating previously described cytomorphologic features in correla-tion with PAX8 immunohistochemical staining results. Am J ClinPathol. 2016;145:373–378.
220. Long X, Zu X, Li Y, et al. Epidermal growth factor receptor and Ki-67 as predictive biomarkers identify patients who will be more sen-sitive to intravesical instillations for the prevention of bladder cancerrecurrence after radical nephroureterectomy. PLoS One. 2016;11.e0166884.
221. Ariyasu S, Yanai H, Sato M, et al. Simultaneous immunostainingwith anti-S100P and anti-SV40 antibodies revealed the originof BK virus-infected decoy cells in voided urine samples.Cytopathology. 2015;26:250–255.
222. Lu CM, Lin JJ, Huang HH, et al. A panel of tumor markers, calre-ticulin, annexin A2, and annexin A3 in upper tract urothelial carci-noma identified by proteomic and immunological analysis. BMCCancer. 2014;14:363.
223. Ward DG, Baxter L, Gordon NS, et al. Multiplex PCR and nextgeneration sequencing for the non-invasive detection of bladder can-cer. PLoS One. 2016;11: e0149756.
224. Lin T, Liu Z, Liu L, et al. Prospective evaluation of fluorescencein situ hybridization for diagnosing urothelial carcinoma. Oncol Lett2017;13:3928–3934.
225. Matsuyama H, Ikemoto K, Eguchi S, et al. Copy number aberra-tions using multicolour fluorescence in situ hybridization (FISH)for prognostication in non-muscle-invasive bladder cancer(NIMBC). BJU Int. 2014;113:662–667.
226. Halling KB, Ellison GW, Armstrong D, et al. Evaluation of oxida-tive stress markers for the early diagnosis of allograft rejection infeline renal allotransplant recipients with normal renal function.Can Vet J. 2004;45:831–837.
227. Halling KC. Vysis UroVysion for the detection of urothelial carci-noma. Expert Rev Mol Diagn. 2003;3:507–519.
228. Halling KC, King W, Sokolova IA, et al. A comparison of BTA stat,hemoglobin dipstick, telomerase and Vysis UroVysion assays for thedetection of urothelial carcinoma in urine. J Urol. 2002;167:2001–2006.
229. Halling KC, Kipp BR. Bladder cancer detection using FISH (Uro-Vysion assay). Adv Anat Pathol. 2008;15:279–286.
230. Sokolova IA, Halling KC, Jenkins RB, et al. The development of amultitarget, multicolor fluorescence in situ hybridization assay forthe detection of urothelial carcinoma in urine. J Mol Diagn.2000;2:116–123.
231. Yoder BJ, Skacel M, Hedgepeth R, et al. Reflex UroVysion testing ofbladder cancer surveillance patients with equivocal or negative urinecytology: a prospective study with focus on the natural history ofanticipatory positive findings. Am J Clin Pathol. 2007;127:295–301.
232. Virk RK, Abro S, de Ubago JMM, et al. The value of the UroVysion(R) FISH assay in the risk-stratification of patients with “atypicalurothelial cells” in urinary cytology specimens. Diagn Cytopathol.2017;45:481–500.
233. Todenhofer T, Hennenlotter J, Esser M, et al. Stepwise applicationof urine markers to detect tumor recurrence in patients undergoingsurveillance for non-muscle-invasive bladder cancer. Dis Markers.2014;2014:973406.
234. Yu J, Xiong H,Wei C, Cui Z, Jin X, Zhang J. Utility of fluorescencein situ hybridization analysis for detecting upper urinary tract-urothelial carcinoma. J Cancer Res Ther. 2017;13:647–650.
235. Yu Q, Li Y, Li G, et al. Prospective evaluation of FISH for detectingupper tract urothelial carcinoma in voided urine specimens. OncolLett. 2016;12:183–188.
236. Sun X, Liu X, Xia M, et al. The combined application of urinaryliquid-based cytology with fluorescence in situ hybridization andp16/Ki-67 dual immunostaining is valuable for improving the earlydiagnosis of upper tract urothelial carcinomas. Diagn Cytopathol.2017;45:895–902.
237. Huysentruyt CJ, Baldewijns MM, Ruland AM, et al. Modified Uro-Vysion scoring criteria increase the urothelial carcinoma detectionrate in cases of equivocal urinary cytology. Histopathology.2011;58:1048–1053.
238. Qian J, Medina M, Crewell K, Weber D, Hossain D, Bostwick DG.Deletion of 9p21 is a rare finding in urine specimens collected frompatients with a history of hematuria and bladder cancer. AmericanSociety of Clinical Oncology, ASCO, annual meeting. 2009. Orlando,FL:2009.
239. Zellweger T, Benz G, Cathomas G, et al. Multi-target fluorescencein situ hybridization in bladder washings for prediction of recurrentbladder cancer. Int J Cancer. 2006;119:1660–1665.
240. Mischinger J, Guttenberg LP, Hennenlotter J, et al. Comparison ofdifferent concepts for interpretation of chromosomal aberrations inurothelial cells detected by fluorescence in situ hybridization. J Can-cer Res Clin Oncol. 2017;143:677–685.
241. Zhou AG, Liu Y, Cyr MS, et al. Role of tetrasomy for the diagnosisof urothelial carcinoma using UroVysion fluorescent in situ hybrid-ization. Arch Pathol Lab Med. 2016;140:552–559.
242. Lodde M, Mian C, Mayr R, et al. Recurrence and progression inpatients with non-muscle invasive bladder cancer: prognostic modelsincluding multicolor fluorescence in situ hybridization moleculargrading. Int J Urol. 2014;21:968–972.
243. Mobley A, Zhang S, Bondaruk J, et al. Aurora kinase A is a bio-marker for bladder cancer detection and contributes to its aggressivebehavior. Sci Rep. 2017;7:40714.
244. McDonald MM, Swagerty D, Wetzel L. Assessment of microscopichematuria in adults. Am Fam Physician. 2006;73:1748–1754.
245. Bergstein J, Leiser J, Andreoli S. The clinical significance of asymp-tomatic gross and microscopic hematuria in children. Arch PediatrAdolesc Med. 2005;159:353–355.
246. Grossfeld GD, Wolf JS, Jr., Litwan MS, et al. Asymptomaticmicroscopic hematuria in adults: summary of the AUA bestpractice policy recommendations. Am Fam Physician.2001;63:1145–1154.
247. Linder BJ, Bass EJ, Mostafid H, Boorjian SA. Guidelineof guidelines:asymptomatic microscopic haematuria. BJU Int. 2018;121(2):176–183.
248. Schmitz-Drager BJ, Kuckuck EC, Zuiverloon TC, et al. Microhe-maturia assessment an IBCN consensus: Based upon a critical reviewof current guidelines. Urol Oncol. 2016;34:437–451.
249. Davis R, Jones JS, Barocas DA, et al. Diagnosis, evaluation andfollow-up of asymptomatic microhematuria (AMH) in adults:AUA guideline. J Urol. 2012;188:2473–2481.

357.e7 CHAPTER 7 Urine Cytology
250. Siddappa S, Mythri K, Kowsalya R. Cytological findings in routinevoided urine samples with hematuria from a tertiary care center insouth India. J Cytol. 2012;29:16–19.
251. Sutton JM. Evaluation of hematuria in adults. JAMA. 1990;263:2475–2480.
252. Schramek P, Schuster FX. Persistent microhematuria: localization ofthe source of bleeding by the evaluation of erythrocyte morphology.Urologe A. 1985;24:216–220.
253. Kitamoto Y, Yide C, Tomita M, Sato T. The mechanism of glomer-ular dysmorphic red cell formation in the kidney. Tohoku J Exp Med.1992;167:93–105.
254. Rath B, Turner C, Hartley B, Chantler C. What makes red cells dys-morphic in glomerular haematuria? Pediatr Nephrol.1992;6:424–427.
255. de Metz M, Schiphorst PP, Go RI. The analysis of erythrocyte mor-phologic characteristics in urine using a hematologic flow cytometerand microscopic methods. Am J Clin Pathol. 1991;95:257–261.
256. Gyory AZ. Diagnostic value of dysmorphic urinary red cells. N EnglJ Med. 1996;335:1323.
257. Koo KC, Lee KS, Choi AR, Rha KH, Hong SJ, Chung BH. Diag-nostic impact of dysmorphic red blood cells on evaluating micro-scopic hematuria: the urologist’s perspective. Int Urol Nephrol.2016;48:1021–1027.
258. Marcussen N, Schumann JL, Schumann GB, Parmar M,Kjellstrand C. Analysis of cytodiagnostic urinalysis findings in 77patients with concurrent renal biopsies. Am J Kidney Dis.1992;20: 618–628.
259. Mehta T, Sanaei-Ardekani M, Farooqi A, et al. The utility of cyto-diagnostic urinalysis as a tool to diagnose kidney allograft dysfunc-tion in the era lymphocyte-depleting induction therapy. TransplantProc. 2011;43:3679–3685.
260. Ottiger C, Savoca R, Yurtsever H, Huber AR. Increased sensitivityin detecting renal impairments by quantitative measurement ofmarker protein excretion compared to detection of pathological par-ticles in urine sediment analysis. Clin Chem Lab Med. 2006;44:1347–1354.
261. Meiers I, Singh H, Hossain D, et al. Improved filter method forurine sediment detection of urothelial carcinoma by fluorescencein situ hybridization. Arch Pathol Lab Med. 2007;131:1574–1577.
262. Amin MB, Smith SC, Reuter VE, et al. Update for the practicingpathologist: The International Consultation on Urologic Disease:European Association of Urology consultation on bladder cancer.Mod Pathol. 2015;28:612–630.
263. Voss JS, Kipp BR, Krueger AK, et al. Changes in specimen prepa-ration method may impact urine cytologic evaluation. Am J ClinPathol. 2008;130:428–433.
264. Dimashkieh H, Wolff DJ, Smith TM, Houser PM, Nietert PJ,Yang J. Evaluation of urovysion and cytology for bladder cancerdetection: a study of 1835 paired urine samples with clinical and his-tologic correlation. Cancer Cytopathol. 2013;121:591–597.
265. Muus Ubago J, Mehta V, Wojcik EM, Barkan GA. Evaluationof atypical urine cytology progression to malignancy. CancerCytopathol. 2013;121:387–391.
266. Roy M, Kaushal S, Jain D, Seth A, Iyer VK, Mathur SR. An insti-tutional experience with The Paris System: a paradigm shift fromambiguous terminology to more objective criteria for reporting urinecytology. Cytopathology. 2017;28:509–515.
267. Malviya K, Fernandes G, Naik L, Kothari K, Agnihotri M. Utility ofthe Paris System in reporting urine cytology. Acta Cytol. 2017;61:145–152.
268. Glass R, Cocker R, Rosen L, et al. The impact of subdividing the“atypical” category for urinary cytology on patient management.Diagn Cytopathol. 2016;44:477–482.
269. Glass RE, Coutsouvelis C, Sheikh-Fayyaz S, et al. Two-tiered sub-division of atypia on urine cytology can improve patient follow-upand optimize the utility of UroVysion.Cancer Cytopathol. 2016;124:188–195.
270. Piaton E, Decaussin-Petrucci M, Mege-Lechevallier F,Advenier AS, Devonec M, Ruffion A. Diagnostic terminologyfor urinary cytology reports including the new subcategories ‘atyp-ical urothelial cells of undetermined significance’ (AUC-US) and‘cannot exclude high grade’ (AUC-H). Cytopathology. 2014;25:27–38.
271. Piaton E, Advenier AS, Benaim G, Petrucci MD, Lechevallier FM,Ruffion A. Atypical urothelial cells (AUC): a Bethesda-derived word-ing applicable to urinary cytopathology. Ann Pathol. 2011;31:11–17.
272. Vandenbussche CJ, Sathiyamoorthy S, Owens CL, Burroughs FH,Rosenthal DL, Guan H. The Johns Hopkins Hospital template forurologic cytology samples: parts II and III—Improving the predict-ability of indeterminate results in urinary cytologic samples: an out-comes and cytomorphologic study. Cancer Cytopathol. 2013;121:21–28.
273. Hassan MJ, Jairajpuri ZS, Jetley S, et al. Microfilariae of wuchereriabancrofti in a patient of chylous haematuria: report of an unusualfinding in urine cytology. J Clin Diagn Res. 2014;8:153–154.