
Usefulness of ultrasonography in children with right iliac fossa ...
12
Radiología. 2012;54(2):137---148 www.elsevier.es/rx UPDATE IN RADIOLOGY Usefulness of ultrasonography in children with right iliac fossa pain L. Raposo Rodríguez a,∗ , G. Anes González a , J.B. García Hernández a , S. Torga Sánchez b a Servicio de Radiodiagnóstico, Hospital Universitario Central de Asturias, Oviedo, Asturias, Spain b Servicio de Radiodiagnóstico, Hospital El Bierzo, Ponferrada, León, Spain Received 14 February 2011; accepted 23 May 2011 KEYWORDS Abdominal ultrasonography; Right iliac fossa; Pediatrics; Acute abdomen; Appendicitis; Crohn’s disease Abstract Acute pain in the right iliac fossa (RIF) is common in children. It can arise from a wide variety of gastrointestinal and genitourinary processes that make up the differential diagnosis with acute appendicitis (AA). In this article, we describe the most representative findings of these processes on ultrasonography (US). We emphasize the characteristics that enable these processes to be differentiated from AA. © 2011 SERAM. Published by Elsevier España, S.L. All rights reserved. PALABRAS CLAVE Ecografía abdominal; Fosa ilíaca derecha; Pediatría; Abdomen agudo; Apendicitis; Enfermedad de Crohn Utilidad de la ecografía en ni˜ nos con dolor en la fosa ilíaca derecha Resumen El dolor agudo en la fosa ilíaca derecha es un cuadro frecuente en la infancia. Su origen puede ser secundario a un amplio abanico de procesos gastrointestinales y genitourinarios que constituyen el diagnóstico diferencial de la apendicitis aguda. En el presente artículo se describen los hallazgos ecográficos más representativos de tales procesos, insistiendo en las características que permiten diferenciarlos de la apendicitis aguda. © 2011 SERAM. Publicado por Elsevier España, S.L. Todos los derechos reservados. Please cite this article as: Raposo Rodríguez L, et al. Utilidad de la ecografía en ni˜ nos con dolor en la fosa ilíaca derecha. Radiología. 2012;54:137---48. ∗ Corresponding author. E-mail address: [email protected] (L. Raposo Rodríguez). Introduction Acute pain in the RIF is common in pediatric patients. Although AA and intestinal intussusception are the typical causes, RIF pain can also be caused by multiple gastrointesti- nal and genitourinary disorders that should be considered in the differential diagnosis of AA. US represents the ideal diagnostic modality in children with abdominal pain. Its excellent anatomic resolution in the pediatric population has helped reduce the negative 2173-5107/$ – see front matter © 2011 SERAM. Published by Elsevier España, S.L. All rights reserved. Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Usefulness of ultrasonography in children with right iliac fossa ...

Document down
Radiología. 2012;54(2):137---148
www.elsevier.es/rx
UPDATE IN RADIOLOGY
Usefulness of ultrasonography in children with right iliac fossapain�
L. Raposo Rodrígueza,∗, G. Anes Gonzáleza, J.B. García Hernándeza,S. Torga Sánchezb
a Servicio de Radiodiagnóstico, Hospital Universitario Central de Asturias, Oviedo, Asturias, Spainb Servicio de Radiodiagnóstico, Hospital El Bierzo, Ponferrada, León, Spain
Received 14 February 2011; accepted 23 May 2011
KEYWORDSAbdominalultrasonography;Right iliac fossa;Pediatrics;Acute abdomen;Appendicitis;Crohn’s disease
Abstract Acute pain in the right iliac fossa (RIF) is common in children. It can arise from a widevariety of gastrointestinal and genitourinary processes that make up the differential diagnosiswith acute appendicitis (AA). In this article, we describe the most representative findings ofthese processes on ultrasonography (US). We emphasize the characteristics that enable theseprocesses to be differentiated from AA.© 2011 SERAM. Published by Elsevier España, S.L. All rights reserved.
PALABRAS CLAVEEcografía abdominal;
Utilidad de la ecografía en ninos con dolor en la fosa ilíaca derecha
Resumen El dolor agudo en la fosa ilíaca derecha es un cuadro frecuente en la infancia. Su
loaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Fosa ilíaca derecha;Pediatría;Abdomen agudo;Apendicitis;Enfermedad de Crohn
origen puede ser secundario a un amplio abanico de procesos gastrointestinales y genitourinariosque constituyen el diagnóstico diferencial de la apendicitis aguda. En el presente artículo sedescriben los hallazgos ecográficos más representativos de tales procesos, insistiendo en lascaracterísticas que permiten diferenciarlos de la apendicitis aguda.
or El
© 2011 SERAM. Publicado p� Please cite this article as: Raposo Rodríguez L, et al. Utilidad dela ecografía en ninos con dolor en la fosa ilíaca derecha. Radiología.2012;54:137---48.
∗ Corresponding author.E-mail address: [email protected]
(L. Raposo Rodríguez).
I
AAcnt
wt
2173-5107/$ – see front matter © 2011 SERAM. Published by Elsevier Esp
sevier España, S.L. Todos los derechos reservados.
ntroduction
cute pain in the RIF is common in pediatric patients.lthough AA and intestinal intussusception are the typicalauses, RIF pain can also be caused by multiple gastrointesti-al and genitourinary disorders that should be considered in
he differential diagnosis of AA.US represents the ideal diagnostic modality in childrenith abdominal pain. Its excellent anatomic resolution in
he pediatric population has helped reduce the negative
aña, S.L. All rights reserved.

1
aespocrimsd
apAie
T
T1anttssff
psictcila
rs
N
TctwtUcaa(
tio2
oitswcof
ptIsl
A
AcTmwnspfTiasif
srtautHfwaflca
eiTdfcbpa
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
38
ppendectomy rate.1 Technological advances in US allowxamination of the layers of the intestinal wall andurrounding mesentery with high spatial resolution. Thisrovides new clinical applications such as the assessmentf acute inflammatory activity, response to treatment andomplications of Crohn’s disease, US evaluation of acuteecurrent appendicitis, follow-up of intestinal involvementn Schönlein---Henoch purpura (SHP), preoperative assess-ent of the viability in cases of ovarian torsion, or
upport for the decision of performing a biopsy in celiacisease.
The objective of this study is to describe the US findingsnd the key diagnostic findings of those conditions that mayresent with acute RIF pain in children, with an emphasis onA, since this is the most common disease in children requir-
ng surgery2,3 and the most common source of diagnosticrrors.
echnique
he graded compression technique described by Puylaert in986 is based on the fact that gradual compression on thenterior abdominal wall eliminates bowel gas and intralumi-al fluid from the bowel loops, reduces the distance betweenransducer and appendix, and displaces bowel loops out ofhe RIF.4 This compression allows visualization of iliac ves-els and psoas muscle, since the appendix is anterior to thesetructures (Fig. 1A). In addition to be ineffective and painful,ast compression may result in rupture of an appendix at riskor perforation.2
The exam is performed in the longitudinal and transverselanes. The ascending colon appears as a nonperistaltictructure containing fluid and gas. Inferiorly, the terminalleum, compressible and peristaltic, can be identified. Theecal base, where the appendix arises, is 2---3 cm below theerminal ileum. While the base of the appendix is at a fairlyonstant location, its end may move freely, and its locations therefore very variable; however, this does not trans-ate into a statistically significant difference in the rate ofppendicitis.5,6
The topology of the superior mesenteric vessels and theirelationship with the aorta and inferior vena cava should beystematically identified.
ormal right iliac fossa
he digestive tract comprises four concentric layers thatan be differentiated histologically. The layers from deepo superficial are the mucosa----consisting of an epitheliumith underlying lamina propria and the muscularis mucosa----,
he submucosa, the muscularis propria and the adventitia.S shows a penta-stratified pattern where the first (superfi-ial mucosa), third (submucosa) and fifth (adventitia) layersre hyperechogenic, and the second (muscularis mucosa)nd fourth (muscularis propria) layers are hypoechoic6---8
Fig. 1B).In adults, the thickness in any segment of the digestive
ract is ≤3 mm. In children, it ranges between 1.5 and 3 mmn the terminal ileum and <2---3 mm in the colon, dependingn the age.8 Valvulae conniventes are <2 mm in width and---5 mm in length, being more numerous in the jejunum (two
att
L. Raposo Rodríguez et al.
r three per cm) than in the ileum (two per cm). Given itsntestinal origin, the appendix exhibits similar characteris-ics to the digestive tract, therefore, its maximum diameterhould not exceed 6 mm in the transverse plane and itsall should not exceed 3 mm.3,4,6,9 Nonetheless, histologi-ally normal appendixes > 6 mm can also be found in casesf accumulation of secretions in the lumen, hyperplasia orecal impaction.10
The normal appendix is oval-shaped in the transverselane and easily compressible. Conversely, in appendicitis,he appendix walls are inflamed, rigid and noncompressible.ts lumen may contain air or fluid, or be collapsed with adhe-ion of the mucosal layers, giving rise to a central echogenicine.
Lastly, the mesentery appears slightly echogenic.
cute appendicitis
A is the most common condition requiring surgery inhildren and the one leading to more diagnostic errors.raditionally, AA has been described to occur when fecalatter or appendicoliths obstruct the appendiceal lumen,hich is usually followed by infection. However, we knowow that AA is not always secondary to obstruction and thateveral causes may lead to AA: lymphoid follicular hyper-lasia obstructing the cecal---appendiceal junction, inflamedollicles in infectious processes, foreign bodies, or trauma.hese factors lead to inflammation and an increase in
ntraluminal pressure. As a result, the appendix enlargesnd induces inflammatory changes in the surrounding tis-ues, such as the pericecal fat and peritoneum.2 Ultimately,schemia occurs and the inflamed appendix, eventually, per-orates.
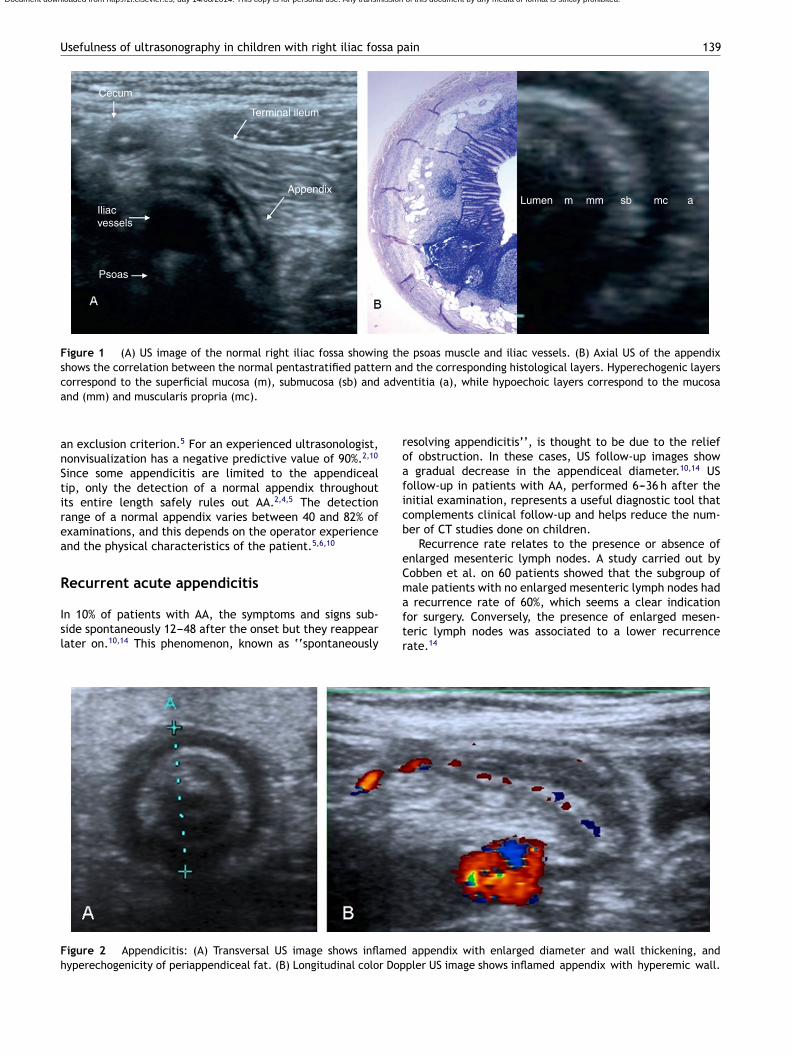
Sensitivity and specificity of sonography for the diagno-is of AA vary greatly between studies (up to 100 and 98%,espectively).2---12 The appendiceal diameter is consideredhe most relevant morphologic criteria (sensitivity > 98%)nd, traditionally, the threshold diameter > 6 mm has beensed for diagnosis of appendicitis. On transverse images,he appendix appears fixed, round and noncompressible.yperechogenicity of the pericecal fat is common. This
at may increase in volume and surround the appendix,hich represents the inflamed omentum that migrates to theppendiceal area in case perforation occurs (Fig. 2A). Freeuid and mesenteric lymph nodes are frequent but unspe-ific. In up to 30% of cases, appendicoliths are seen in theppendiceal lumen.2
Doppler signal varies depending on the stage of the dis-ase. Although it might increase in the acute phase (Fig. 2B),t may diminish in case of appendiceal perforation.2---4,9
herefore, Doppler examination alone cannot reliablyistinguish between normal and abnormal appendix. Per-oration can be suspected in the presence of an irregularontour of the appendix, fluid or collections, and dilatedowel loops with thickened walls2---4,7,10,13 (Fig. 1E). Aftererforation occurs, the appendix is usually decompressednd it is visible only in 30---60% of cases.4,9,13
Acute pain, gas and severe obesity may complicate visu-lization of the appendix. Therefore, the nonvisualization ofhe appendix does not allow us to rule out AA despite the facthat the first studies considered the nonvisualization on US
Usefulness of ultrasonography in children with right iliac fossa pain 139
Cecum
Iliacvessels
Psoas
AppendixLumen m mm sb mc a
Terminal ileum
Figure 1 (A) US image of the normal right iliac fossa showing the psoas muscle and iliac vessels. (B) Axial US of the appendixshows the correlation between the normal pentastratified pattern and the corresponding histological layers. Hyperechogenic layers
adve
roaficb
eCm
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
correspond to the superficial mucosa (m), submucosa (sb) andand (mm) and muscularis propria (mc).
an exclusion criterion.5 For an experienced ultrasonologist,nonvisualization has a negative predictive value of 90%.2,10
Since some appendicitis are limited to the appendicealtip, only the detection of a normal appendix throughoutits entire length safely rules out AA.2,4,5 The detectionrange of a normal appendix varies between 40 and 82% ofexaminations, and this depends on the operator experienceand the physical characteristics of the patient.5,6,10
Recurrent acute appendicitis
In 10% of patients with AA, the symptoms and signs sub-side spontaneously 12---48 after the onset but they reappearlater on.10,14 This phenomenon, known as ‘‘spontaneously
aftr
Figure 2 Appendicitis: (A) Transversal US image shows inflamedhyperechogenicity of periappendiceal fat. (B) Longitudinal color Dop
ntitia (a), while hypoechoic layers correspond to the mucosa
esolving appendicitis’’, is thought to be due to the relieff obstruction. In these cases, US follow-up images show
gradual decrease in the appendiceal diameter.10,14 USollow-up in patients with AA, performed 6---36 h after thenitial examination, represents a useful diagnostic tool thatomplements clinical follow-up and helps reduce the num-er of CT studies done on children.
Recurrence rate relates to the presence or absence ofnlarged mesenteric lymph nodes. A study carried out byobben et al. on 60 patients showed that the subgroup ofale patients with no enlarged mesenteric lymph nodes had
recurrence rate of 60%, which seems a clear indicationor surgery. Conversely, the presence of enlarged mesen-eric lymph nodes was associated to a lower recurrenceate.14
appendix with enlarged diameter and wall thickening, andpler US image shows inflamed appendix with hyperemic wall.

1 L. Raposo Rodríguez et al.
spe
C
Ptsbbiiptilana
A
AaTmatditca(
Li
Fbltccn
oainmn
M
Mwn
Figure 3 Mucocele. Hypoechoic mass arising from the cecum,with ‘‘skin onion’’ structure (*), thin walls and no associatedi
ropnsfli
A
Atipswi
I
Sjttsiia
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
40
The term used to name this entity is also controver-ial. Some authors use the term ‘‘appendiceal disease’’ inatients with long-standing symptoms; however, to date thisntity has not been satisfactorily described.
ystic fibrosis
atients with cystic fibrosis (CF) usually show markedly dis-ended appendixes secondary to the presence of inspissatedecretions with associated pain.15 These cases are not toe confused with AA since in CF the appendix is distendedut not inflamed. Additionally, there is no wall thicken-ng and the concentric layer structure is intact, with nonflammation of the mesenteric fat16,17 (Fig. 2E). It has beenostulated as a possible protective role of these secre-ions against AA considering the lower rate of occurrencen patients with CF (1---2%) compared with the normal popu-ation (7---8%).14,16 Nonetheless, the rate of perforations andbscess formation is higher, probably due to a delay in diag-osis because symptoms are often masked by the use ofntibiotics.16,17
ppendiceal mucocele
ppendiceal mucocele is characterized by distension of theppendix secondary to intraluminal accumulation of mucus.o date, four pathological processes leading to appendicealucocele have been described: obstruction at the cecal
ppendiceal junction; mucosal hyperplasia; mucinous cys-adenoma and mucinous cystadenocarcinoma. US shows aistended appendix with no wall thickening and no regionalnflammatory signs, with abundant echogenic content inhe interior and the ‘‘onion skin’’ structure,18---20 a signonsidered to be characteristic of mucoid material thatllows differential diagnosis with appendiceal abscesses21
Fig. 3).
ymphoid hyperplasia related to viralnfections
ollicular lymphoid hyperplasia is a histopathologic findingased on the enlargement of the lymphoid follicles in theamina propria of the appendiceal mucosa, without infil-ration of polymorphonuclear leukocytes. It is common inhildhood, and according to some authors, it may be theause of acute RIF pain in children.7 It also relates to intesti-al intussusception.
Only on rare occasions does US allow for the diagnosisf this condition. In such cases, US findings include dilatedppendix and thickening of the appendiceal mucosa andleocecal valve, secondary to the presence of hypoechogenicodules. Mesenteric lymph nodes are a constant. Cecum,esenteric echogenicity and mobility of the distal ileum are
ormal.7
esenteric lymphadenitis
esenteric lymphadenitis (ML) is a controversial entity, ande frequently resort to this diagnosis in patients in whomormal appendices have been removed. The term is used to
tl
a
nflammatory changes.
efer to enlargement of some mesenteric lymph nodes, withr without ileitis.9,10 However, some papers describe theresence of enlarged (>10 mm in the short axis) mesentericodes in asymptomatic children.22 Increased color Dopplerignal in the mesenteric vessels and minimal amount of freeuid may be seen (Fig. 3E). The nonvisualization of the
nflamed appendix is more indicative of ML than AA.9
cute gastroenteritis
cute gastroenteritis (AGE) is the most common inflamma-ory disease in children. It usually has a viral origin and theliocecal region is the most frequently affected. The classicresentation of AGE does not require imaging studies. UShows dilated, hyperperistaltic fluid-filled small bowel loopsith thin walls, where it is not uncommon to see transient
ntussusception9 (Fig. 4E).
nfectious ileitis or iliocecitis
ome bacteria----such as Salmonella, Campylobacterejuni, Yersinia and, more rarely, Mycobacteriumuberculosis----have a strong affinity for the lymphoidissue of the terminal ileum and give rise to enteritis whoseymptoms may simulate those of AA. US findings includentestinal wall thickening and hypogenicity----usually withntact wall layers----, transmural or mucosal hypervascularitynd enlargement of mesenteric lymph nodes.9,10 In contrast
o AA, the mesentery is normal and the thickened boweloops do not form a conglomerate around the appendix.Tuberculous ileitis is rare in developed countries. Itppears as asymmetrical, non-stratified thickening of the

Usefulness of ultrasonography in children with right iliac fossa pain 141
Figure 4 (A and B) Patient with tuberculosis and pain in right iliac fossa. (A) Chest radiograph shows patchy lesions of alveolarcharacteristics with bilateral distributions and diffuse secondary to tuberculous bronchopneumonia. (B) US images of the right flankshow diffuse hypoechoic thickening, with loss of normal stratification, secondary to tuberculous ileitis. Note the similarity to the
Ssctrl5
CAnan
S
Stmpa
thimdr
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
characteristic thickening of Crohn’s disease (see Fig. 5A and B).
ileocecal walls23---25 (Fig. 4A and B). Its clinical course issimilar to that of chronic diseases with US findings similarto those of Crohn’s disease, but always with considerableinvolvement of the cecum.9 The microorganism inducesan inflammatory process that eventually leads to ulcerformation with subsequent healing, as well as extensiveinfiltration of peritoneum, omentum and mesentery associ-ated with centrally hypodense lymph nodes.24---26 There areno pathognomonic findings. Biopsy during colonoscopy andculture of lesions is the diagnostic technique of choice, whilenegative histologic results do not preclude tuberculosis.26
Crohn’s disease
In 25% of cases, Crohn’s disease (CD) begins in child-hood, with involvement of the iliocecal region in 55% ofpatients.8 Acute abdominal symptoms simulating AA are notunusual. CD causes transmural inflammation that extendsto the surrounding mesentery. On US this translates intocircumferential wall thickening that may be segmental ormultifocal, and finally, loss of wall stratification.8---10,27,28
The wall appears hypoechoic with an echogenic cen-tral line that represents the superficial mucosa (Fig. 5Aand B). The mesentery is hyperechogenic and there isno motion of bowel loops with transducer pressure.10
Enlarged lymph nodes are found in approximately 15% of CDpatients.29
CD is associated with intestinal neovascularization. Incontrast with what happens in areas of fibrotic scarring,
in active disease there is mesenteric hypervascularity and‘‘comb sign’’, indicative of increased blood flow in the vasarecta (Fig. 5B). This finding may help differentiate CD frominfectious or eosinophilic ileitis or ileitis associated withC
Up
HP, where vascular proliferation is less conspicuous. Ves-el density, assessed by Doppler US in affected bowel loops,orrelates with disease activity and is used as a non-invasiveechnique for monitoring the course of the disease and theesponse to treatment.8,28,30 Vessel density is classified asow, moderate and high if there are 0---2, 3---5, or more than
Doppler signals per cm,2 respectively.30
Appendiceal involvement appears in 23% of patients withD, manifesting as appendiceal hyperemia similar to that ofA. However, thickening > 5 mm and hyperemia of the termi-al ileum support the diagnosis of CD. US findings in cecumnd appendix are similar in both entities and therefore can-ot be used for differentiation.28
chönlein---Henoch purpura
HP is a small-vessel vasculitis that may affect the intestinalract. In some patients (10---30%), the intestinal involvementay precede skin lesions, simulating AA. The episodes ofaroxysmal pain are secondary to edema in the subserosand submucosa and hemorrhagic infiltration.8,31
Characteristic US findings include diffuse, circumferen-ial thickening of the bowel wall, with focal intramuralematomas that appear as hyperechogenic areas, giving anrregular appearance to the thickened wall.2,8,31 Associatedesenteric adenopathy and free fluid are common. The duo-enum and jejunum are the initially involved sites but, withecurrent episodes, the disease extends to the ileum.
eliac disease
p to 25% of children with celiac disease initiallyresent with acute abdomen. US may help make an

142 L. Raposo Rodríguez et al.
Figure 5 Crohn’s disease. (A) Color Doppler US shows marked wall thickening of the terminal ileum mainly due to a hyperechogenicsubmucosa, a finding characteristic of Crohn’s disease, and mural hypervascularity. (B) Presence of multiple enlarged lymph nodesof inflammatory appearance (*) and mesenteric hyperechogenicity and hypervascularity.
iabTc
ttjc
T
TlcmmatbrrmaufaUc
bat
combined with the fact that pediatric patients are not goodcandidates for surgery, makes the surgical management ofthese children, who present with appendiceal thickeningand RIF pain, controversial.39
Intussusception
Intussusception involves invagination of a segment ofintestine into the lumen of an immediately distal seg-ment. Intussusception is usually idiopathic, associated withlymphoid hyperplasia, secondary to viral infections. Approx-imately 90% of patients with intussusception are youngerthan two years.3 Findings on abdominal radiograph may be
Figure 6 Typhlitis in an 8-year-old child treated for leukemia,
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
nitial diagnosis and institute an early treatment. Char-cteristic findings include abnormally dilated fluid-filledowel loops and reversal of the jejuno-ileal fold pattern.here is hyperperistalsis and minimal ascites in 82% ofases.32,33
Intestinal intussusception is a common complication andhe presence of underlying celiac disease should be inves-igated in case of recurrent intussusception. Ulcerativeejuno-ileitis should be suspected in adult patients witheliac disease and acute abdomen.34
US findings may confirm the need for biopsy.35
yphlitis
yphlitis occurs more typically in patients with hemato-ogic malignancies who are neutropenic as a result ofhemotherapy. In the pediatric population, typhlitis isore frequently seen in pre-adolescent children with acuteyeloid leukemia. The most commonly affected portions
re the ascending colon and the cecum----hence the termyphlitis----although any segment of the intestinal tract maye involved. For this reason, the term ‘‘neutropenic ente-ocolitis’’ seems more appropriate. Histologic examinationeveals bowel wall necrosis and hemorrhage, without inflam-atory or tumoral infiltration. Imaging features include
symmetrical thickening of the cecal wall (>3 mm) that issually hyperechogenic and heterogeneous with areas of dif-erent echogenicity secondary to necrosis or hemorrhage,nd redundant mucosa (Fig. 6). In most cases, DopplerS shows hypervascularity and surrounding inflammatoryhanges, as well as free fluid.36---38
In same patients, in addition to the findings compati-le with typhlitis, there might also be thickening of theppendix, possibly due to the same causative factors ofyphlitis, and surgery may therefore not be indicated. This,
with RIF pain and fever. Axial US image of the RIF shows abnor-mal thickening of the wall of the cecum (thick arrows), with lossof stratification, and of the terminal ileum to a lesser extent (i).Appendiceal caliber appears normal (arrow).

Usefulness of ultrasonography in children with right iliac fossa pain 143
Figure 7 Axial US image of an ileocolic intussusception showsthree layers of loops and the mesentery. The outer layer isthe receptor loop or intussuscipiens, which contains the cen-tral entering limb of the intussusceptum (i), located at thecenter of the intussusception next to the mesentery (M) drag-ging some lymph nodes (*). The receptor loop also contains
Figure 8 Ileal duplication cyst. Transversal view of the RIFshows hypoechoic mass with an inner echogenic layer corre-sponding to the mucosa, surrounded by an outer hypoechoicl
swtv
R
Rtpdlrdots
E
Erotadl
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
the everted returning limb of the intussusceptum, which isthicker, constituting the outer hypoechoic ring of the doughnut(arrows).
non-specific and the use of conventional enema to makethe diagnosis is no longer justified.3 US is the test of choicebecause it provides a diagnostic accuracy of 97---100%, allowsfor the detection of the causes and predictive factors ofirreducibility, and can be used for follow-up and assessmentof response to treatment.40
Approximately 90% of intussusceptions are ileocolic.The diagnostic image of intussusception is located atthe receptor bowel loop, which would explain why thelesion is not detected in the RIF, but in the subhepaticregion (Fig. 5E). The ‘‘doughnut’’ sign refers to thetransverse section of the intussusception that shows athick hypoechoic ring and an echogenic center.9,41 Thetarget sign consists of concentric hypo- and hyperechogenicrings, whose number varies depending on the extensionof the edema (Fig. 7). The pseudokidney sing refers tothe kidney-like appearance of the loop inside the recep-tor loop, in the longitudinal section (Fig. 5E), usuallyexceeding 5 cm in length.42 The main prognostic indicatorsfor irreducibility and ischemia on US include presence ofliquid trapped inside the intussusception,43 absence offlow on Doppler US, enlarged lymph nodes, thickening ofthe outer ring of the doughnut and presence of gas in theintussusceptum.3,44
Meckel diverticulum
Meckel diverticulum, related to a persistent omphalome-senteric duct, occurs on the antimesenteric border of theileum. Meckel diverticulum is a true diverticulum com-posed of all layers of the intestinal wall. It should be
fiihi
ayer corresponding to the muscle wall.
uspected in children with inflammatory signs of RIF inhom a normal appendix and a lesion connected to the
erminal ileum with similar appearance to that of AA areisualized.2,5,10,45
ight-sided diverticulitis
ight-sided diverticulitis is an unusual inflammatory condi-ion that can mimic AA. It should be considered in youngatients with RIF pain and normal appendix. Right-sideiverticula are true diverticula, composed of all intestinalayers, and are usually congenital and solitary. US findings ofight-sided diverticulitis include direct visualization of theiverticulum in the right wall of the colon, focal thickeningf the colonic wall at the diverticulum site and inflamma-ion of the adjacent fat.10,25,11,46 This condition is usuallyelf-limited and does not require surgery.47
nteric duplication cysts
nteric duplication cysts are congenital abnormalities thatesult in duplication of a normal bowel loop. They normallyccur on the mesenteric border of the bowel, usually onhe ileum. The walls are composed of all intestinal layersnd most lesions do not communicate with the lumen of theigestive tract. They may contain ectopic gastric mucosa orymphoid tissue. US examination shows a well-defined, fluid-lled mass with tubular or spherical shape and an echogenic
nner mucosal layer48 (Fig. 8). In some cases, the content iseterogeneous as a result of hemorrhage or thick materialn the interior.
144 L. Raposo Rodríguez et al.
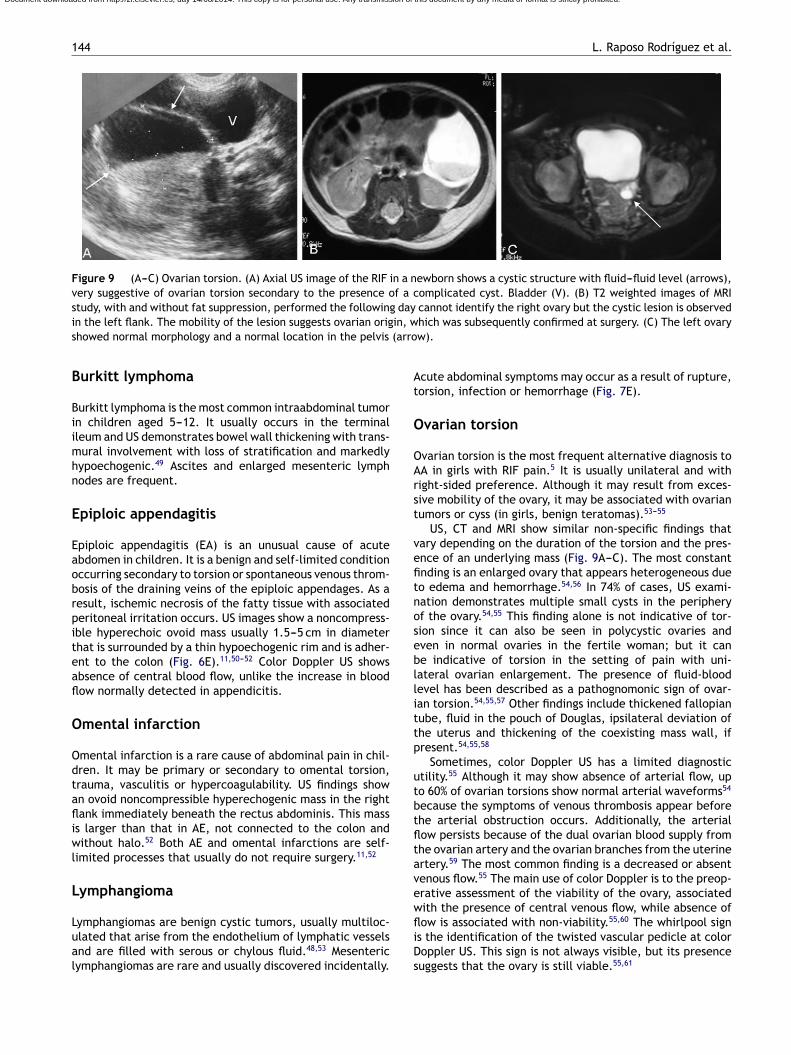
Figure 9 (A---C) Ovarian torsion. (A) Axial US image of the RIF in a newborn shows a cystic structure with fluid---fluid level (arrows),very suggestive of ovarian torsion secondary to the presence of a complicated cyst. Bladder (V). (B) T2 weighted images of MRIstudy, with and without fat suppression, performed the following day cannot identify the right ovary but the cystic lesion is observedi in, ws (arro
B
Biimhn
E
Eaobrpiteafl
O
Odtafliwl
L
Lual
At
O
OArst
vefitnosebllittp
utbtfltavew
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
n the left flank. The mobility of the lesion suggests ovarian orighowed normal morphology and a normal location in the pelvis
urkitt lymphoma
urkitt lymphoma is the most common intraabdominal tumorn children aged 5---12. It usually occurs in the terminalleum and US demonstrates bowel wall thickening with trans-ural involvement with loss of stratification and markedly
ypoechogenic.49 Ascites and enlarged mesenteric lymphodes are frequent.
piploic appendagitis
piploic appendagitis (EA) is an unusual cause of acutebdomen in children. It is a benign and self-limited conditionccurring secondary to torsion or spontaneous venous throm-osis of the draining veins of the epiploic appendages. As aesult, ischemic necrosis of the fatty tissue with associatederitoneal irritation occurs. US images show a noncompress-ble hyperechoic ovoid mass usually 1.5---5 cm in diameterhat is surrounded by a thin hypoechogenic rim and is adher-nt to the colon (Fig. 6E).11,50---52 Color Doppler US showsbsence of central blood flow, unlike the increase in bloodow normally detected in appendicitis.
mental infarction
mental infarction is a rare cause of abdominal pain in chil-ren. It may be primary or secondary to omental torsion,rauma, vasculitis or hypercoagulability. US findings shown ovoid noncompressible hyperechogenic mass in the rightank immediately beneath the rectus abdominis. This mass
s larger than that in AE, not connected to the colon andithout halo.52 Both AE and omental infarctions are self-
imited processes that usually do not require surgery.11,52
ymphangioma
ymphangiomas are benign cystic tumors, usually multiloc-lated that arise from the endothelium of lymphatic vesselsnd are filled with serous or chylous fluid.48,53 Mesentericymphangiomas are rare and usually discovered incidentally.
fliDs
hich was subsequently confirmed at surgery. (C) The left ovaryw).
cute abdominal symptoms may occur as a result of rupture,orsion, infection or hemorrhage (Fig. 7E).
varian torsion
varian torsion is the most frequent alternative diagnosis toA in girls with RIF pain.5 It is usually unilateral and withight-sided preference. Although it may result from exces-ive mobility of the ovary, it may be associated with ovarianumors or cyss (in girls, benign teratomas).53---55
US, CT and MRI show similar non-specific findings thatary depending on the duration of the torsion and the pres-nce of an underlying mass (Fig. 9A---C). The most constantnding is an enlarged ovary that appears heterogeneous dueo edema and hemorrhage.54,56 In 74% of cases, US exami-ation demonstrates multiple small cysts in the peripheryf the ovary.54,55 This finding alone is not indicative of tor-ion since it can also be seen in polycystic ovaries andven in normal ovaries in the fertile woman; but it cane indicative of torsion in the setting of pain with uni-ateral ovarian enlargement. The presence of fluid-bloodevel has been described as a pathognomonic sign of ovar-an torsion.54,55,57 Other findings include thickened fallopianube, fluid in the pouch of Douglas, ipsilateral deviation ofhe uterus and thickening of the coexisting mass wall, ifresent.54,55,58
Sometimes, color Doppler US has a limited diagnostictility.55 Although it may show absence of arterial flow, upo 60% of ovarian torsions show normal arterial waveforms54
ecause the symptoms of venous thrombosis appear beforehe arterial obstruction occurs. Additionally, the arterialow persists because of the dual ovarian blood supply fromhe ovarian artery and the ovarian branches from the uterinertery.59 The most common finding is a decreased or absentenous flow.55 The main use of color Doppler is to the preop-rative assessment of the viability of the ovary, associatedith the presence of central venous flow, while absence ofow is associated with non-viability.55,60 The whirlpool sign
s the identification of the twisted vascular pedicle at color
oppler US. This sign is not always visible, but its presenceuggests that the ovary is still viable.55,61
Usefulness of ultrasonography in children with right iliac fossa pain 145
Figure 10 Persistent urachus. Child with abdominal pain, fever and mictional syndrome. Echogenic tubular structure connected
hp
Ovarian tumors
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
to the umbilicus (*) in contact with the bladder dome (v).
Hemorrhagic ovarian cyst
Ovarian cysts may cause pain due to hemorrhage orrupture.9 Classically they appear as avascular complex cys-
tic lesions, with a thin reticular pattern, fluid-detritus levelsand/or hyperechogenic areas in relation to coagulated blood(Fig. 8E).9 The absence of involvement of the adjacent fatMo
Differential diagnosis of acute pain in the rig
UROLOGIC PATHOLOGY
Acute right pyelonephritisInfected urachal cystUreterohydronephrosisVesicoureteral reflux
ILIOCECAL PATHOLOGY
APPENDICEAL PATHOLOGY
M
Crohn's diseaseInfectious ileitisTyphlitisBurkitt lymphomaIntussusceptionDuplication cyst
Acute appendicitisMucoceleDistension related to cystic fibrosisLymphoid hyperplasia
R
UROLOGIC PATHOLOGY
Acute right pyelonephritisInfected urachal cystUreterohydronephrosisVesicoureteral reflux
LIOCECAL PATHOLOGY
APPENDICEAL PATHOLOGY
M
Crohn's diseaseInfectious ileitisTyphlitisBurkitt lymphomaIntussusceptionDuplication cyst
Acute appendicitisMucoceleDistension related to cystic fibrosisLymphoid hyperplasia
R
Figure 11 Diagram depicting the anatomy of RIF and
elps differentiate it from an abscess. The presence of freeeritoneal fluid is common.
ost ovarian tumors in girls are benign and painless but,n occasions, they may cause pain due to compression of
ht iliac fossa in children
GYNECOLOGIC PATHOLOGY
ESENTERIC/OMENTAL PATHOLOGY
LOOP PATHOLOGY
Ovarian torsionHemorrhagic cystOvarian tumors
Meckel diverticulum
Mesenteric lymphadenitisLymphangiomaOmental infarctionAppendagitis
Schönlein-HenochAcute gastroenteritis Celiac disease
ight diverticulitis
GYNECOLOGIC PATHOLO
ESENTERIC/OMENTAL PATHOLOGY
LOOP PATHOLOGY
Ovarian torsionHemorrhagic cyst
Meckel diverticulum
Mesenteric lymphadenitisLymphangiomaOmental infarctionAppendagitis
Schönlein-HenochAcute gastroenteritis Celiac
ight diverticulitis
the possible disorders arising from its structures.

1
aisp(cl
A
Inelpih
U
Uoptctcwi
l(is
C
Up(bioi
A
1
C
T
R
1
1
1
1
1
1
1
1
1
1
2
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
46
djacent structures or increase in size. Cystic teratomas the most common ovarian tumor. US shows a complexolid-cystic mass with echogenic or hypoechogenic com-onent depending on the amount of fat, fluid or calciumFig. 9E).54,62 The rest of benign ovarian tumors are usuallyystadenomas that usually present as large unilocular cysticesions with thin septa that may show solid poles.
cute pyelonephritis
n most cases of acute pyelonephritis, US findings areormal, but there might be focal or generalized renalnlargement, areas of hypo- or hyperechogenicity (Fig. 10E),oss of corticomedullary differentiation, thickening of theelvic and/or ureteral urothelium, and/or perinephricnflammatory changes.9,63 Color Doppler US shows corticalypoperfusion.64
rachal anomalies
rachal anomalies are caused by incomplete persistencef patency of the urachus. Urachal sinus refers to theersistence of the urachus at the umbilical end. At US,he persistent urachus and the urachal sinus are small-aliber tubular structures, which appear as a fluid-filled longube or as an echogenic cord (Fig. 10). Diverticulum andyst are fluid-filled masses, with or without communicationith the bladder, respectively. Internal echoes result from
nfection.65
In addition to acute pyelonephritis and urachal anoma-ies, other urinary disorders such as ureterohydronephrosisFig. 11E) and vesicoureteral reflux may also cause acute andntermittent abdominal pain.9 For this reason, the urinaryystem must also be assessed during US examination.
onclusion
S is a useful technique for the evaluation of acute RIFain in children. Multiple conditions may cause RIF painFig. 11). The high spatial resolution of US in children, evenetter than that of CT, provides relevant information regard-ng these disorders and may help confirm or rule out AA,r establish an alternative diagnosis, without the need ofnvasive techniques.
uthorship
1. Responsible for the integrity of the study (original ideaof the study): GAG.
2. Conception of the study: GAG, LRR.3. Design of the study: LRR.4. Acquisition of data: GAG, JBGH.5. Analysis and interpretation of data: LRR, GAG, JBGH.6. Statistical analysis: N/A.7. Bibliographic search: LRR.
8. Drafting of the paper: LRR, STS.9. Critical review with intellectually relevant contribu-tions: GAG, JBGH and STS.0. Approval of the final version: LRR, GAG, JBGH, STS.
2
L. Raposo Rodríguez et al.
onflict of interest
he authors declare not having any conflict of interest.
eferences
1. Hernández JA, Swischuk LE, Ángel CA, Chandler R, Lee S. Imag-ing of acute appendicitis: US as the primary imaging modality.Pediatr Radiol. 2005;35:392---5.
2. Rybkin AV, Thoeni RF. Current concepts in imaging of appendici-tis. Radiol Clin North Am. 2007;45:411---22.
3. Vasavada P. Ultrasound evaluation of acute abdominal emer-gencies in infants and children. Radiol Clin North Am.2004;42:445---56.
4. Sivit C, Siegel M, Kimberly E, Applegate K, Newman K.When appendicitis is suspected in children. Radiographics.2001;21:247---62.
5. Peletti A, Baldisserotto M. Optimizing US examination to detectthe normal and abnormal appendix in children. Pediatr Radiol.2006;36:1171---6.
6. Sandoval E, Alonso JM. Diagnóstico ecográfico de la apen-dicitis aguda. A propósito de 226 casos. Radiología. 1998;40:299---306.
7. Galindo M, Calleja S, Nieto MA, Fadrique B, González AM, Man-zanares J. Valor diagnóstico de la ecografía en la apendicitis delnino. An Esp Pediatr. 1998;48:28---32.
8. Alison M, Kheniche A, Azoulay R, Roche S, Sebag G, Belarbi N.Ultrasonography of Crohn disease in children. Pediatr Radiol.2007;37:1071---82.
9. Quillin P, Siegel M. Color Doppler US of children with acute lowerabdominal pain. Radiographics. 1993;13:1281---93.
0. Puylaert J. Ultrasonography of the acute abdomen: gas-trointestinal conditions. Radiol Clin North Am. 2003;41:1227---42.
1. Macari M, Balthazar E. Acute right lower quadrant: CT evalua-tion. Radiol Clin North Am. 2003;41:1117---36.
2. Del Cura JL, Oleaga L, Grande D, Farina MA, Isusi M.Comparación de la ecografía y la tomografía computa-rizada en el diagnóstico de la apendicitis aguda. Radiología.2001;43:175---86.
3. Sonanvane S, Siegel M. Sonography of the surgical abdomen inchildren. Ultrasound Clin. 2008;3:67---82.
4. Cobben L, De Mol van Otterlo, Puylaert J. Spontaneously resolv-ing appendicitis: frequency and natural history in 60 patients.Radiology. 2000;215:349---52.
5. Robertson MB, Choe KA, Joseph PM. Review of the abdominalmanifestations of cystic fibrosis in the adult patient. Radio-graphics. 2006;26:679---90.
6. Lardeyone S, Puylaert J, Smit M, Holscher H. Appendixin children with cystic fibrosis: US features. Radiology.2004;232:187---9.
7. Chaudry G, Navarro O, Levine DS, Oudjhane K. Abdominalmanifestations of cystic fibrosis in children. Pediatr Radiol.2006;36:233---40.
8. Pérez Fuentes DA, Cortegoso González M, Punal Pereira A,Cimadevila García A, Novás Castro S, Blanco Parra M. Muco-cele apendicular confundido con quiste de uraco infectado:un diagnóstico diferencial a tener en cuenta. Actas Urol Esp.2009;33:205---8.
9. Macek D, Jafri SZ, Madrazo BL. Ultrasound case of the day.Mucocele of the appendix. Radiographics. 1992;12:1247---9.
0. Madwed D, Mindelzun R, Jeffrey Jr. Mucocele of the appendix:
imaging findings. AJR Am J Roentgenol. 1992;159:69---72.1. Blanc E, Ripollés T, Jesús M, Delgado F, Agramunt M. Ecografía yTC del mucocele apendicular: hallazgos que sugieren etiologíamaligna. Radiología. 2003;45:79---84.

sa p
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Usefulness of ultrasonography in children with right iliac fos
22. Watanabe M, Ishii E, Hirowatari Y, Hayashida Y, Koga T,Akazawa K, et al. Evaluation of abdominal lymphadenopa-thy in children by ultrasonography. Pediatr Radiol. 1997;27:860---4.
23. Fernández Sarabia MT, Cardenal Escarcena A, Roldán Lora FA,Rivero Cruz MA, Encinas Tobajas VM. Perforación intestinal:complicación inusual de la tuberculosis mesentérica que sim-ulaba enfermedad de Crohn. Rev Esp Enferm Dig. 2005;97:536---7.
24. Harisinghani MG, McLoud TC, Shepard JO, Ko JO, Shroff MM,Mueller PR. Tuberculosis from head to toe. Radiographics.2000;20:449---70.
25. Andronikou S, Welman CJ, Kader E. The CT features ofabdominal tuberculosis in children. Pediatr Radiol. 2002;32:75---81.
26. Ruiz Marín M, González Valverde FM, Benavides BulejeJA, Escamilla Segade C, Candel Arenas MF, Terol GarauletE, et al. Perforación intestinal secundaria a tubercu-losis intestinal. Rev Esp Enferm Dig. 2009;101:443---4.doi:10.4321/S1130-01082009000600015 Available from:http://scielo.isciii.es/scielo.php?script=sci arttext&pid=S1130-01082009000600015&lng=es.
27. Ripollés T, Martínez MJ, Morote V, Errando J. Appendicealinvolvement in Crohn’s disease: gray-scale sonography andcolor Doppler flow features. AJR Am J Roentgenol. 2006;186:1071---8.
28. Ripollés T, Martínez MJ. Técnicas seccionales de imagen en laenfermedad de Crohn: ecografía, tomografía computarizada yresonancia magnética. Radiologia. 2007;49:97---108.
29. Talens A, Vernetta ML, Gil de Ramales V, Tomé A, del ValA, García JR, et al. Utilidad de la ecografía en el diagnós-tico y seguimiento de la enfermedad de Crohn. Radiologia.1999;41:655---60.
30. Spalinger J, Patriquin H, Miron MC, Marx G, Herzog D, DuboisJ, et al. Doppler US in patients with Crohn disease: vessel den-sity in the diseased bowel reflects disease activity. Radiology.2000;217:787---91.
31. Couture A, Verac C, Baud C, Galifer RB, Armelin I. Eval-uation of abdominal pain in Henoch---Schönlein syndromeby high frequency ultrasound. Pediatr Radiol. 1992;22:12---7.
32. Riccabona M, Rossipal E. Use of sonography in the diagnosis ofceliac disease. Ultraschall Med. 1996;17:31---3.
33. Riccabona M, Rossipal E. Sonographic findings in celiac disease.J Pediatr Gastroenterol Nutr. 1993;17:198---200.
34. Méndez Sánchez JM, García Fernández G, Pereda SalgueroT, González Chamorro A, Obispo Entrenas A, RiveraIrigoin R, et al. Abdomen agudo en la enfermedad celi-aca: yeyunoileitis ulcerativa. Rev Esp Enferm Dig. 2007;6:359---67.
35. Micetic-Turk D, Umek-Bradac S, Dolinsek J, Gorenjak M,Turk Z, Skalicky M. Ultrasonographic assessment of celiacdisease in children: comparison with antiendomysium anti-bodies and histology. Wien Klin Wochenschr. 2001;113:27---31.
36. McCarville MB, Thompson J, Li C, Adelman CS, Lee MO, Alsam-marae D, et al. Significance of appendiceal thickening inassociation with typhlitis in pediatric oncology patients. PediatrRadiol. 2004;34:245---9.
37. Dietrich C, Hermann S, Klein S, Braden B. Sonographicsigns of neutropenic enterocolitis. World J Gastroenterol.2006;12:1397---402.
38. Muro D, Sangüesa C, Bermúdez M, Verdeguer A. Utilidadde la ecografía en el diagnóstico precoz de la enterocoli-
tis neutropénica en la edad pediátrica. Radiologia. 1999;41:105---10.39. McCarville MB. Evaluation of typhlitis in children: CT versus US.Pediatr Radiol. 2006;36:890---1.
6
ain 147
0. Hryhorczuk AL, Strouse PJ. Validation of US as a first-linediagnostic test for assessment of pediatric ileocolic intussus-ceptions. Pediatr Radiol. 2009;39:1075---9.
1. del Pozo G, Albillos JC, Tejedor D. Intussusception: US find-ings with pathologic correlation. The crescent-in-doughnut sign.Radiology. 1996;199:688---92.
2. del Pozo G, Albillos JC, Tejedor D, Calero R, Rasero M, de laCalle U, et al. Intussusception in children: current conceptsin diagnosis and enema reduction. Radiographics. 1999;19:299---312.
3. del Pozo G, González-Spinola J, Gómez-Ansón B, SerranoC, Miralles M, González de Orbe G, et al. Intussuscep-tion: trapped peritoneal fluid detected with US-relation-ship to reducibility and ischemia. Radiology. 1996;201:379---86.
4. Stranzinger E, Dipietro MA, Yarram S, Khalatbarri S, Strouse PJ.Intramural and subserosal echogenic foci on US in large-bowelintussusceptions: prognostic indicator for reducibility? PediatrRadiol. 2009;39:42---6.
5. Costa S, Jesús M, Ripollés T, Delgado F. Diverticulítis deMeckel: hallazgos en ecografía y TC. Radiología. 2004;46:101---6.
6. Agramunt M, Ripollés T, Blanc E, Jesús M, Gómez-Abril S. Diver-ticulitis del colon derecho. Hallazgos en ecografía y tomografíacomputarizada. Radiologia. 2004;46:151---8.
7. Bogue C, Mann E. Imaging findings in right side diverticulitis ina child. Pediatr Radiol. 2008;38:1125---7.
8. Buonomo C, Griscom NT. Cystic lymphangioma (omental cyst).Radiographics. 1991;11:1146---8.
9. Toma P, Granata C, Rossi A, Garaventa A. Multimodality imag-ing of Hodgkin disease and non-Hodgkin lymphomas in children.Radiographics. 2007;27:1335---54.
0. Teijo Núnez C, Raimunde Seoane E, Álvarez Álvarez S, OlcozGoni JL. Epiploitis aguda: una causa inusual de abdomen agudomédico. An Med Interna. 2006;10:507---8.
1. Castro Garcia FJ, Santos Sánchez JA, García Inigo P, DíezHernández JC. Apendicitis epiploica. Rev Esp Enferm Dig.2006;2:140---1.
2. Miguel A, Ripollés T, Martínez MJ, Morote V, Ruiz A.Apendicitis epiploica e infarto omental. Hallazgos enecografía y tomografía computarizada. Radiología. 2001;43:395---401.
3. Servaes S, Zurakowsky D, Laufer MR, Feins N, Chow JS. Sono-graphic findings of ovarian torsion in children. Pediatr Radiol.2007;37:446---51.
4. Garel L, Dubois J, Grignon A, Filiatrault D, Van Vliet G. Us of thepediatric female pelvis: a clinical perspective. Radiographics.2001;21:1393---407.
5. Chang HC, Bhatt S, Dogra VS. Continuing medical education:pearls and pitfalls in diagnosis of ovarian torsion. Radiographics.2008;28:1355---68.
6. Surratt JT, Siegel MJ. Imaging of pediatric ovarian masses.Radiographics. 1991;11:533---48.
7. Kiech-Kohlendorfer U, Maurer K, Unsin KM, Gassner I. Fluiddebris level in follicular cysts: a pathognomonic sign of ovariantorsion. Pediatr Radiol. 2006;36:421---5.
8. Harmon JC, Binkovitz LA, Stephens J. Utterine positionin adnexal torsion: specificity and sensitivity of ipsilat-eral deviation of the uterus. Pediatr Radiol. 2009;39:354---8.
9. Rha SE, Byun JT, Jung SE, Jung JI, Choi BG, Kim BS, et al.CT and MR imaging features of adnexal torsion. Radiographics.2002;22:283---94.
0. Shandinger LL, Andreotti RF, Kurian RL. Preoperative sono-
graphic and clinical characteristics as predictors of ovariantorsion. J Ultrasound Med. 2008;27:7---13.1. Vijayaraghavan SB. Sonographic whirlpool sign in ovarian tor-sion. J Ultrasound Med. 2004;23:1643---9.

1
6
6
6
ics. 2008;28:255---76.
Document downloaded from http://zl.elsevier.es, day 14/08/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
48
2. Sisler CL, Siegel MJ. Ovarian teratomas: a comparison of sono-graphic appearance in prepubertal and postpubertal girls. AJRAm J Roentgenol. 1990;154:139---41.
3. Dacher JN, Avni F, Francois A, Rypens F, Monroc M, EurinD, et al. Renal sinus hyperechogenicity in acute pyelonephri-tis: description and pathological correlation. Pediatr Radiol.1999;29:179---82.
6
L. Raposo Rodríguez et al.
4. Craig W, Wagner B, Travis M. From the archives of theAFIP: pyelonephritis radiologic---pathologic review. Radiograph-
5. Avni EF, Matos G, Diard F, Schulman CC. Midline omphalovesicalanomalies in children: contribution of ultrasound imaging. UrolRadiol. 1988;10:189---94.




















