MORPHOLOGY OF THE CAUDAL FOSSA IN CAVALIER KING CHARLES SPANIELS
10
MORPHOLOGY OF THE CAUDAL FOSSA IN CAVALIER KING CHARLES SPANIELS , SOFIA CERDA-GONZALEZ,NATASHA J. OLBY,SUSAN MCCULLOUGH,ANTHONY P. PEASE, RICHARD BROADSTONE,JASON A. OSBORNE Chiari malformations and syringohydromyelia are an important disease complex in Cavalier King Charles Spaniels. Although abnormalities in caudal fossa morphology are considered major contributors to the de- velopment of this disease, limited information exists on the range of morphologies in Cavalier King Charles Spaniels and on the relationship of these to clinically evident disease. Sixty-four Cavalier King Charles Spaniels were studied. Each underwent a neurologic examination and magnetic resonance imaging of the cervical spine and brain. T2-weighted sagittal images were used to determine both the morphologic characteristics and volume of the caudal fossa in each dog. This volume was also analyzed as a percentage of total cranial cavity volume. Each attribute was correlated with neurological grade and presence of syringohydromyelia. Fifteen dogs had neurologic signs, and 59 had morphologic abnormalities of the craniocervical junction. While 27 dogs had syringohydromyelia, 13 of these were clinically normal. Cerebellar herniation and occipital dysplasia were common findings but were not associated with syringohydromyelia. Dorsal compressive lesions were noted at the first and second cervical vertebral junction. Factors associated with the presence of neurologic signs included syringohydromyelia and the ratio of caudal fossa/total cranial cavity volume; dogs with signs had significantly larger syringohydromyelia than asymptomatic dogs. Caudal fossa size was not associated with syringohydro- myelia. A positive association was identified between foramen magnum size and length of cerebellar herniation. The prevalence of craniocervical junction abnormalities is high in Cavalier King Charles Spaniels. While several factors are associated with neurologic signs, occipital hypoplasia appears to be the most important factor. Veterinary Radiology & Ultrasound, Vol. 50, No. 1, 2009, pp 37–46. Key words: chiari-like, occipital hypoplasia, syringomyelia, MRI. Introduction A BNORMALITIES IN CAUDAL fossa morphology are in- creasingly recognized as a cause of morbidity in many small breed dogs, especially in the Cavalier King Charles Spaniel. Specifically, Chiari-like malformations and syrin- gohydromyelia have become a serious health concern for this breed. 1–9 Dogs affected with Chiari-like malformation and/or syringohydromyelia have clinical signs including occasional to constant scratching of the head and neck re- gion, severe neck pain, scoliosis and gait changes. 7,9–13 In humans, type I Chiari malformations are character- ized as a developmental failure of the occipital bone re- sulting in occipital hypoplasia. The hypoplastic occipital bone creates an abnormally small caudal fossa, while the structures contained within it are unchanged in size. This causes crowding of the cerebellum and medulla with her- niation of the cerebellar tonsils, medullary kinking, and development of syringohydromyelia. 14–23 The syndrome in dogs has many similarities to the human type I Chiari malformation, and has been called caudal occipital mal- formation syndrome, Chiari-like malformation, and syr- ingohydromyelia. 2,3,8,24,25 A working group round table has recently agreed on the term Chiari-like malformation and syringomyelia for the canine disorder. 26 Although there has been much discussion of Chiari-like malformation in Cavalier King Charles Spaniels, there is limited understanding of the range of caudal fossa mor- phologies and the clinical implications of abnormalities detected on magnetic resonance (MR) images. Moreover, there are no data available on the relative size of the caudal fossa in affected vs. unaffected Cavalier King Charles Spaniels. There may be a trend toward smaller caudal fossa size relative to total cranial cavity size in smaller dogs. 27 This highlights the need to evaluate skull morphology in Funding for this study was provided by the American Cavalier King Charles Spaniel Club Charitable Trust and a grant from the Department of Clinical Sciences of the North Carolina State University College of Veterinary Medicine. This work was presented in abstract form at the American College of Veterinary Internal Medicine 24th Annual Forum, Louisville, KY, May 31–June 3, 2006. Address correspondence and reprint requests to Sofia Cerda-Gonzalez, at the above address. E-mail: [email protected] Received February 4, 2008; accepted for publication May 16, 2008. doi: 10.1111/j.1740-8261.2008.01487.x From the College of Veterinary Medicine, Cornell University, Ithaca, NY (Cerda-Gonzalez), College of Veterinary Medicine, North Carolina State University, Raleigh, NC (Olby, Pease), IAMS Pet Imaging Center, Raleigh, NC (McCullough, Broadstone), and Department of Statistics, North Carolina State University, Raleigh, NC (Osborne). 37
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of MORPHOLOGY OF THE CAUDAL FOSSA IN CAVALIER KING CHARLES SPANIELS

MORPHOLOGY OF THE CAUDAL FOSSA IN CAVALIER
KING CHARLES SPANIELS,
SOFIA CERDA-GONZALEZ, NATASHA J. OLBY, SUSAN MCCULLOUGH, ANTHONY P. PEASE,RICHARD BROADSTONE, JASON A. OSBORNE
Chiari malformations and syringohydromyelia are an important disease complex in Cavalier King Charles
Spaniels. Although abnormalities in caudal fossa morphology are considered major contributors to the de-
velopment of this disease, limited information exists on the range of morphologies in Cavalier King Charles
Spaniels and on the relationship of these to clinically evident disease. Sixty-four Cavalier King Charles Spaniels
were studied. Each underwent a neurologic examination and magnetic resonance imaging of the cervical spine
and brain. T2-weighted sagittal images were used to determine both the morphologic characteristics and volume
of the caudal fossa in each dog. This volume was also analyzed as a percentage of total cranial cavity volume.
Each attribute was correlated with neurological grade and presence of syringohydromyelia. Fifteen dogs had
neurologic signs, and 59 had morphologic abnormalities of the craniocervical junction. While 27 dogs had
syringohydromyelia, 13 of these were clinically normal. Cerebellar herniation and occipital dysplasia were
common findings but were not associated with syringohydromyelia. Dorsal compressive lesions were noted at the
first and second cervical vertebral junction. Factors associated with the presence of neurologic signs included
syringohydromyelia and the ratio of caudal fossa/total cranial cavity volume; dogs with signs had significantly
larger syringohydromyelia than asymptomatic dogs. Caudal fossa size was not associated with syringohydro-
myelia. A positive association was identified between foramen magnum size and length of cerebellar herniation.
The prevalence of craniocervical junction abnormalities is high in Cavalier King Charles Spaniels. While several
factors are associated with neurologic signs, occipital hypoplasia appears to be the most important factor.
Veterinary Radiology & Ultrasound, Vol. 50, No. 1, 2009, pp 37–46.
Key words: chiari-like, occipital hypoplasia, syringomyelia, MRI.
Introduction
ABNORMALITIES IN CAUDAL fossa morphology are in-
creasingly recognized as a cause of morbidity in many
small breed dogs, especially in the Cavalier King Charles
Spaniel. Specifically, Chiari-like malformations and syrin-
gohydromyelia have become a serious health concern for
this breed.1–9 Dogs affected with Chiari-like malformation
and/or syringohydromyelia have clinical signs including
occasional to constant scratching of the head and neck re-
gion, severe neck pain, scoliosis and gait changes.7,9–13
In humans, type I Chiari malformations are character-
ized as a developmental failure of the occipital bone re-
sulting in occipital hypoplasia. The hypoplastic occipital
bone creates an abnormally small caudal fossa, while the
structures contained within it are unchanged in size. This
causes crowding of the cerebellum and medulla with her-
niation of the cerebellar tonsils, medullary kinking, and
development of syringohydromyelia.14–23 The syndrome
in dogs has many similarities to the human type I Chiari
malformation, and has been called caudal occipital mal-
formation syndrome, Chiari-like malformation, and syr-
ingohydromyelia.2,3,8,24,25 A working group round table has
recently agreed on the term Chiari-like malformation and
syringomyelia for the canine disorder.26
Although there has been much discussion of Chiari-like
malformation in Cavalier King Charles Spaniels, there
is limited understanding of the range of caudal fossa mor-
phologies and the clinical implications of abnormalities
detected on magnetic resonance (MR) images. Moreover,
there are no data available on the relative size of the caudal
fossa in affected vs. unaffected Cavalier King Charles
Spaniels. There may be a trend toward smaller caudal fossa
size relative to total cranial cavity size in smaller dogs.27
This highlights the need to evaluate skull morphology in
Funding for this study was provided by the American Cavalier KingCharles Spaniel Club Charitable Trust and a grant from the Departmentof Clinical Sciences of the North Carolina State University College ofVeterinary Medicine.
This work was presented in abstract form at the American College ofVeterinary Internal Medicine 24th Annual Forum, Louisville, KY, May31–June 3, 2006.
Address correspondence and reprint requests to Sofia Cerda-Gonzalez,at the above address. E-mail: [email protected]
Received February 4, 2008; accepted for publication May 16, 2008.doi: 10.1111/j.1740-8261.2008.01487.x
From the College of Veterinary Medicine, Cornell University, Ithaca,NY (Cerda-Gonzalez), College of Veterinary Medicine, North CarolinaState University, Raleigh, NC (Olby, Pease), IAMS Pet Imaging Center,Raleigh, NC (McCullough, Broadstone), and Department of Statistics,North Carolina State University, Raleigh, NC (Osborne).
37

each specific breed of interest. There is no association be-
tween cerebellar size and clinical signs in affected Cavalier
King Charles Spaniels, suggesting that maldevelopment of
the cerebellum was not the underlying problem.8 Additional
studies specifically investigating the caudal fossa size in the
Cavalier King Charles Spaniel are needed to provide doc-
umentation of occipital hypoplasia in affected dogs.
As an attempt to improve the understanding of the as-
sociation between morphology of the caudal fossa and
clinical disease, we investigated the morphology of the
caudal fossa and craniocervical junction in clinically nor-
mal and symptomatic Cavalier King Charles Spaniels and
related these morphologic findings to the presence of
syringohydromyelia and of clinical signs.
Materials and Methods
Cavalier King Charles Spaniels were recruited from the
general population in the USA by advertising at the breed
society’s national dog shows and from Cavalier King
Charles Spaniels that were evaluated by our neurology
service. To be eligible, dogs had to be between 1 and 6
years of age, have an available pedigree and have an un-
remarkable complete blood cell count and serum biochem-
istry panel within 7 days before participating. Dogs with
medical conditions that contraindicated the use of general
anesthesia were excluded, including dogs with a heart
murmur greater than a grade three out of six. Owners were
questioned about signs of scratching, history of skin prob-
lems, and signs of pain. A neurologic grade was assigned to
each dog based on the history and the examination findings
(Table 1).
Sixty-four Cavalier King Charles Spaniels fulfilled the
inclusion criteria. There were 30 females and 34 males. The
mean age was 2.7 years, ranging from 1 to 5.7 years; me-
dian age was 2.5 years.
Each dog was premedicated with fentanyl followed by
anesthesia induction with propofol and maintenance with
sevoflurane. Mean arterial blood pressure, end tidal CO2,
ventilatory rate, temperature, and heart rate were main-
tained within physiologic limits.
Imaging was performed on each dog using a 1.5Tesla
unit.� Dogs were positioned with their craniocervical junc-
tion in a flexed position with the head angle between 1001
and 1401 to mimic a normal standing posture, except in five
clinical patients where the neck was not flexed. Spine
curvature was assessed in the dorsal localizer image and
corrected if possible. Any residual curvature was the re-
sult of scoliosis.
Sequences obtained included a sagittal T2-weighted 3D
SPACE (Sample Perfection with Application optimized
Contrasts using different flip angle Evolution) sequence
with a time to repeat (TR) of 3500ms, a time to echo (TE)
of 356ms, an echo train (ET) length of 149ms, slice thick-
ness of 3mm, and an interslice gap of 0mm using a matrix
size of 256 � 256 interpolated to 512 � 512. The flip angle
varied throughout the echo train length from 1401 to 1801.
The voxel size was 0.9mm � 0.9mm � 3mm and the ac-
quisition time was approximately 3min. On selected pa-
tients, standard T2-weighted sagittal spin echo and dual
echo T2 and proton density (PD) weighted transverse (axial)
spin echo images of the cervical spinal cord and brain were
obtained if there was evidence of a compressive lesion or to
further investigate the presence of syringohydromyelia.
MR images were analyzed by two of the authors (S.C.G.
and N.J.O.). Subjective assessments included presence or
absence of occipital dysplasia assessed as an abnormally
large foramen magnum,28,29 occipital hypoplasia assessed
as presence of indentation of the cerebellum by the supra-
occipital bone and crowding of the foramen magnum,7
cerebellar herniation,8 syringohydromyelia,30,31 medul-
lary kinking defined as an elevation of the medulla at
the cervicomedullary junction,7,9,24 scoliosis,12 ventriculo-
megaly,30,32,33 and iso- to hyperintense material in the
middle ear, presumed to be primary secretory otitis media
in the absence of clinical signs relating to this finding.34,35
Dilation of the central canal was noted as hydromyelia if
it was o1mm in height. The number of vertebral lengths
affected with syringohydromyelia assessed as an accumu-
lation of cerebrospinal fluid (CSF) within the spinal cord
parenchyma was recorded, but the thoracolumbar spine was
not imaged and therefore the full extent of syringohydro-
myelia was probably underestimated in some dogs. Lastly,
Table 1. Neurologic Grade Classifications
NeurologicGrade Clinical Signs Number of Dogs
0 Normal 491 Scratching neck/head o50% of the time observed by the owner. No evidence of skin disease 42 Scratching neck/head450% of the time observed by the owner. Owner observed signs consistent with neck pain at
home. No evidence of skin disease2
3 Scratching observed by the owner and neck pain consistently elicited on neurological examination 64 Scratching reported observed the owner and ataxia detected on neurological examination 35 Scratching reported observed the owner and paresis detected on neurological examination 0
�Siemens Medical Solutions USA Inc., Malvern, PA.
38 CERDA-GONZALEZ ET AL. 2009

any other abnormalities detected within the brain and/or
cervical spine were noted and described.
MR images were loaded into OsiriX Medical Imaging
Software (open source software—http://www.osirix-viewer.
com) for objective measurements including the height
of the foramen magnum, measured from the ventral-most
aspect of the supraoccipital bone to the caudal basis-
phenoid bone, as described previously,8 the length of cer-
ebellar herniation, measured from the level of the foramen
magnum caudally (Fig. 1) and maximum syrinx height.
The height of the spinal cord was measured at the same
level as the measurement of syrinx height, and the syrinx
height was expressed as a percentage of spinal cord height
at that point.
The volumes of the caudal fossa and the cranial fossa
were measured. Caudal fossa volume was reported as an
absolute value and as a percent of total cranial cavity vol-
ume. All measurements were obtained by tracing the inner
border of the cranial cavity on sagittal T2 SPACE brain
images. Landmarks that defined the limits of the caudal
fossa included the caudal extent of the dorsum sellae ros-
trally, the caudal-most extent of the basisphenoid bone and
the ventral and dorsal borders of the foramen magnum
caudally, and the tentorium cerebelli dorsally. Measure-
ments of the cranial fossa were made by following the inner
border of the cranial cavity as far rostrally as the cribiform
plate and caudally to the cranial extent of the caudal fossa.
These area measurements were made on each MR image
that included the cranial cavity. The final volume was cal-
culated by multiplying the sum of the area by the slice
thickness, as described previously.27
The relationship between each of the morphologic and
volumetric findings and the presence or absence of neuro-
logic signs, the neurologic grade, and the presence and
severity of syringohydromyelia was examined. The same
analysis was repeated only on dogs that had syringohydro-
myelia to determine whether there was an association
between neurologic signs and morphologic factors in dogs
with syringohydromyelia. For factors that were ordinal,
contingency tables were created and chi-square tests for
association were conducted. Associations between disease
severities and categorical factors were investigated using
chi-square tests. Associations between severity and contin-
uous factors were investigated using Spearman correlation
coefficients. An ROC curve was constructed to determine
whether the ratio of caudal fossa volume to total cranial
cavity volume could be used to predict the presence of
clinical signs. For all analyses, a P-value of o0.05 was
taken as statistically significant. Statistical analyses were
performed using JMP software (SAS Institute, Cary, NC).
Results
Fifteen dogs, of which eight were female, were clinically
affected (neurologic grade range 1–4, median 3) and 49, of
which 22 were female, were clinically normal (neurologic
grade of 0) (Table 1).
As inclusion in this study was based on voluntary par-
ticipation, our population cannot be considered random.
Forty-six of 49 clinically normal dogs were owned by
members of the breeding community, while clinically
affected dogs were owned by a more diverse client base.
Neurologic signs included scratching of the head and neck
region ranging in severity from mild and intermittent to
near-constant scratching, neck pain ranging from vocal-
ization when palpating the neck to regular pain episodes at
home during play or excitement, scoliosis, and repeatable
vocalization if pressure was applied to the cranial thoracic
region when being picked up by the owners. One dog had a
wide-based stance and ataxia following short periods of
exercise. Decreased daily interaction with the owners and/
or littermates was noted as a clinical sign in five dogs. This
change in interaction was speculated to represent neck pain
and/or head pain, as this sign improved significantly in
these patients following treatment with pain medications.
Analgesics being used at the time of the study included
gabapentinw, tramadolz, methocarbamoly, carprofenw, andprednisonez. All dogs were graded according to their signs
before receiving medications. Age and gender were not
significantly associated with either clinical signs or
syringohydromyelia. One dog had previously undergone
a suboccipital craniectomy, C1 dorsal laminectomy, and
durotomy overlying the cerebellum 1 year before partici-
pation in this study.
Although 49 of 64 dogs were clinically normal, 59 (92%)
had at least one craniocervical morphologic abnormality
detected in MR images. Abnormalities included cerebellar
indentation, crowding of the foramen magnum with oblit-
Fig. 1. T2-weighted 3D SPACE sequence mid-sagittal image of the brainof a Cavalier King Charles Spaniel with cerebellar herniation and syringohyd-romyelia. The method of measuring the height of the foramen magnum (A)and the length of cerebellar herniation are demonstrated (B) (TR¼ 3500mm,TE¼ 356mm, slice thickness¼ 3mm, interslice gap¼ 0mm).
wPfizer Inc., New York, NY.zMylan Laboratories Inc., Morgantown, WV.yQualitest Pharmaceuticals, Huntsville, AL.zWestward Pharmaceutical Inc., Eatontown, NJ.
39CAUDAL FOSSA MORPHOLOGY IN CAVALIERSVol. 50, No. 1

eration of the subarachnoid space, cerebellar herniation,
occipital dysplasia, medullary kinking, syringohydromyelia,
and dorsal compression of the cervical spinal cord at the
level of the first and second cervical vertebrae. Fifty-nine of
the dogs (87.5%) had occipital hypoplasia based on the
parameters described earlier (Fig. 2). Syringohydro-
myelia was found in 27/64 dogs (42%), with severities
ranging from small fluid accumulations to syringohyd-
romyelia occupying more than two-thirds of the height of
the cervical spinal cord (Fig. 3), and extending over a single
cervical vertebra to the entire length of the cervical spinal
cord and into the thoracic spinal cord. Fourteen of 49
(27%) normal dogs had syringohydromyelia compared
with 13 of 15 dogs with neurologic signs (88%). Cerebellar
herniation was present in 49/63 (77.8%) dogs, ranging from
mild to severe in nature (Table 2 and Fig. 4). Occipital
dysplasia was found in 56 dogs (56/64 [87.5%]) (Fig. 5).
However, in view of the lack of objective guidelines for
identifying occipital dysplasia, foramen magnum size was
also measured and used for statistical analysis (Table 2).
Upon comparison of the subjective assessments and the
measurements, dogs with a foramen magnum 41.5 cm in
height were classified as dysplastic. Medullary kinking was
identified in 42 of 64 (66%) dogs (Fig. 6). Lastly, a dorsal
compressive lesion at the interspace of the first and second
cervical vertebrae was noted in 27 of 64 (42.2%) dogs (Fig.
7). This lesion ranged in severity from causing a mild im-
pingement on the subarachnoid space to inducing spinal
cord compression. In eight dogs, syringohydromyelia began
immediately caudal to this point.
Abnormalities identified that did not directly involve the
craniocervical junction were hydrocephalus and material
within the tympanic bulla. Lateral ventriculomegaly was
present in 19 of 64 (29.7%) dogs. T2-hyperintense material
was noted within the tympanic bulla in 17 of 64 (26.6%)
dogs, unilaterally in 12 dogs and bilaterally in five dogs.
None of these dogs had signs of otitis media or externa and
none had inflammation of the external ear canal on otic
examination.
There was no statistically significant difference between
affected and normal Cavalier King Charles Spaniel with
respect to age or sex. Factors positively associated with the
presence of neurological signs were syringohydromyelia
and the ratio of caudal fossa/total cranial cavity volume.
Fig. 2. T2-weighted 3D SPACE mid-sagittal images of a normal Cavalier King Charles Spaniel (A) and one with occipital hypoplasia (B) evidenced bycerebellar crowding and indentation as well as crowding of the foramen magnum (TR¼ 3500mm, TE¼ 356mm, slice thickness¼ 3mm, interslice gap¼ 0mm).In comparison with normal dogs of other breeds, the cerebellum in the normal Cavalier King Charles Spaniel (A) appears relatively crowded.
Fig. 3. T2-weighted mid-sagittal (left) and transverse (right) images of the cranial aspect of the cervical spinal cord of a Cavalier King Charles Spaniel withsyringohydromyelia (TR¼ 3800ms, TE¼ 132ms, slice thickness¼ 3mm, interslice gap¼ 0.3mm).
40 CERDA-GONZALEZ ET AL. 2009

Factors for which there was no significant evidence of
association with neurological signs were subjective assess-
ment of the presence of occipital hypoplasia, cerebellar
herniation, foramen magnum size, medullary kinking, and
the presence of a dorsal compressive lesion at C1/2.
There was a significant association between the presence
of neurological signs and syringohydromyelia (Po0.0001).
Moreover, dogs with clinical signs had a significantly larger
syrinx than normal dogs (Po0.0001) (Table 2 and Fig. 8).
Finally, there was a significant association between neuro-
logic grade and the maximum percentage height of the
spinal cord occupied by syringohydromyelia (Spearman
correlation 0.96, Po0.0001).
The caudal fossa volume and ratio of caudal fossa
to total cranial cavity volume for clinically normal and
affected Cavalier King Charles Spaniel are given in Table
2. Caudal fossa volume did not differ significantly between
clinically affected and normal dogs, but male dogs had a
significantly larger caudal fossa volume than female
dogs (P¼ 0.018). The ratio of the caudal fossa to the to-
tal cranial cavity volume did not differ between genders,
but was significantly smaller in clinically affected Cavalier
King Charles Spaniels (P¼ 0.0005) (Fig. 9). In addition,
the association between assigned neurologic grade and the
ratio of caudal fossa volume to total cranial cavity volume
was significant (r¼�0.36, P¼ 0.0038). Based on ROC
analysis, a caudal fossa to cranial cavity ratio of 13.3%
was associated with a sensitivity of 70% and specificity
of 92% at differentiating between normal and affected
dogs.
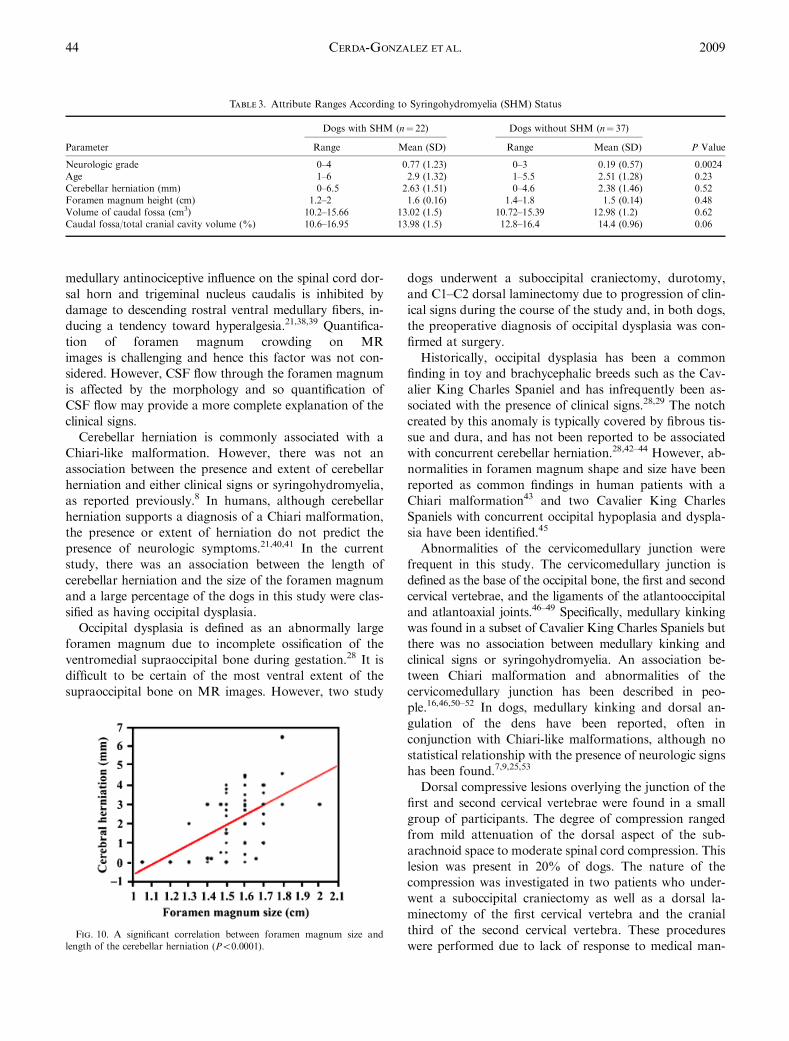
There was no relationship between the presence or se-
verity of syringohydromyelia and any morphologic quan-
tity that was measured (Table 3). The only other significant
association identified was between foramen magnum size
and length of cerebellar herniation (Po0.0001); the larger
the foramen magnum, the greater is the length of cerebellar
herniation (Fig. 10).
Discussion
In the Cavalier King Charles Spaniel population eval-
uated in this study, the caudal fossa volume was signifi-
cantly larger in male vs. female dogs, but did not differ
between affected and normal dogs. In contrast, the ratio of
the caudal fossa to cranial cavity volume was consistent in
male and female dogs, but was significantly smaller in
affected dogs than in normal dogs. These findings support
the role of occipital hypoplasia in the development of clin-
ical signs in Cavalier King Charles Spaniels affected with
Chiari-like malformations. A caudal fossa to cranial cavity
Table 2. Attribute Ranges According to Clinical Status
Attribute
Affected Cavalier King CharlesSpaniel (n¼ 15)
Unaffected Cavalier King CharlesSpaniel (n¼ 49)
P ValueRange Mean (SD) Range Mean (SD)
Age (years) 1–5 2.76 (1.18) 1–6 2.65 (1.35) 0.77Cerebellar herniation (mm) 0–6.5 2.12 (2.05) 0–4.6 2.37 (1.33) 0.58Foramen magnum height (cm) 1.05–2.0 1.56 (0.23) 1.2–1.8 1.58 (0.14) 0.73Maximum syringohydromyelia/spinal cord height (%) 0–75.00 52.33 (23.96) 0–76.92 17.5 (28.02) o0.0001Volume of caudal fossa (cm3) 10.06–15.6 12.33 (1.87) 10.47–15.5 13.08 (1.2) 0.07Caudal fossa/total cranial cavity volume (%) 10.62–16.3 13.2 (1.64) 12.04–16.95 14.46 (0.93) o0.0005
Fig. 4. T2-weighted 3D SPACE mid-sagittal images of the caudal fossa of Cavalier King Charles Spaniels with mild (A) and severe (B) cerebellar herniation(TR¼ 3500ms, TE¼ 356ms, slice thickness¼ 3mm, interslice gap¼ 0mm).
41CAUDAL FOSSA MORPHOLOGY IN CAVALIERSVol. 50, No. 1

volume of 13.3% had the highest sensitivity and specificity
for the association between neurological signs and occipital
hypoplasia. In spite of the relationship between relative
caudal fossa volume and clinical signs, there was no asso-
ciation between relative caudal fossa volume and
syringohydromyelia.
It is common to detect Chiari-like malformations in dogs
presenting for other problems, and there is a need to define
the clinical significance of these MRI findings. The inci-
dence of morphologic abnormalities of the craniocervical
junction was high in this population of dogs in which only
23% (15/64) exhibited clinical signs. In particular, occipital
dysplasia, cerebellar herniation, obliteration of the sub-
arachnoid space at the foramen magnum, and syringo-
hydromyelia were common findings. These abnormalities
make a subjective assessment of occipital hypoplasia in
91% of the dogs. Additionally, many normal dogs had
middle ear disease but no associated clinical signs.
Symptomatic Cavalier King Charles Spaniels have a
high frequency of morphologic changes in the caudal fossa,
including a high incidence of cerebellar herniation and an
abnormal shape of the cerebellum.1,7,8,24,27 Establishing a
relationship between morphometric parameters and clini-
cal signs has not always been possible.8 Similarly, the only
parameter in our study that was associated with the pres-
ence of clinical signs, other than relative caudal fossa vol-
ume, was syringohydromyelia.
Although only 15 dogs in our population had clinical
signs associated with Chiari-like malformation and/or
syringohydromyelia, all 15 had phantom scratching and/
or signs of pain, which are the predominant clinical find-
ings in dogs with this disorder.36 Although signs of brain-
stem and cerebellar involvement have been seen in Cavalier
King Charles Spaniels thought to have Chiari-like malfor-
mation,8 we did not observe this, possibly because of the
inclusion of normal dogs in our study.
Syringohydromyelia has been thought to play an im-
portant role in the manifestation of clinical signs,7,8,24,36,37
although correlating clinical signs and syringohydromyelia
has been problematic. The relationship between syringo-
hydromyelia and clinical signs is complex and difficult to
analyze. The most appropriate method of quantifying
syringohydromyelia is not known. In view of the theory
that signs associated with syringohydromyelia result from
compression of the spinothalamic tracts7,9 or involvement
of the dorsal horn gray matter causing abnormal process-
ing of sensory information,36,38 maximum syrinx height,
width or cross-sectional area appear to be logical choices.
Maximum height was chosen in this study because it could
be measured in all dogs from the sagittal images, and
would reflect the potential involvement of both white and
Fig. 5. T2-weighted 3D SPACE mid-sagittal images of the caudal fossa of a Cavalier King Charles Spaniel with an apparently normal supraoccipital bone(A) and one with occipital dysplasia (B). Arrows denote the ventral-most extent of the supraoccipital bone at the level of the foramen magnum (TR¼ 3500ms,TE¼ 356ms, slice thickness¼ 3mm, interslice gap¼ 0mm).
Fig. 6. T2-weighted 3D SPACE mid-sagittal image of the caudal fossaand cranial cervical spinal cord of a Cavalier King Charles Spaniel withmedullary kinking, seen as an elevation of the medulla at the cervicomedul-lary junction. Cerebellar herniation and mild attenuation of the dorsal aspectof the subarachnoid space at the junction between the first and second cer-vical vertebrae are also present (TR¼ 3500ms, TE¼ 356ms, slice thick-ness¼ 3mm, interslice gap¼ 0mm).
42 CERDA-GONZALEZ ET AL. 2009

gray matter. Assessment of the severity of signs of pain in
dogs is also difficult. In this study all affected dogs had
phantom scratching but quantifying its severity and fre-
quency was subjective and based on information provided
by the owner. In addition, it was extremely difficult to
quantify and even appreciate the full range of manifesta-
tions of pain in affected dogs. For example, several owners
accurately guessed their dogs would have a Chiari-like
malformation and/or syringohydromyelia because those
dogs were quieter than their littermates, had less appetite
or were less inclined to jump or play. These dogs appeared
completely normal on neurological examination; it was
only by comparison with littermates that their behavior
seemed atypical. Regardless, we found that syringohyd-
romyelia was associated with the presence of clinical signs,
that affected dogs had a larger syrinx, and that the greater
the relative height of the spinal cord occupied by a syrinx,
the more severe are the clinical signs.
Others have found a relationship between pain and max-
imal syrinx diameter,36 but severity of syringohydromyelia
has not always been found to be associated with clinical
signs.8 In our population, just over 25% of clinically normal
dogs had syringohydromyelia and two symptomatic Cav-
alier King Charles Spaniel did not, although both of these
dogs had morphologic abnormalities consistent with occip-
ital hypoplasia. If syringohydromyelia is the only cause of
clinical signs, all affected dogs should have evidence of a
syrinx. Moreover, when dogs lacking a syrinx were ex-
cluded, syrinx height was not associated with the presence
or severity of signs. Alternative theories for the develop-
ment of clinical signs in such patients is that they result
from crowding of the foramen magnum causing compres-
sion of the first cervical nerve with radiating pain, or that
Fig. 7. T2-weighted sagittal (A) and transverse (B–D) images of the cervical spinal cord of a Cavalier King Charles Spaniel. There is focal dorsalcompression of the spinal cord at the interspace between the first and second cervical vertebrae (A, C), eliminating the subarachnoid space at this level.Syringohydromyelia is apparent immediately caudal to the compressive lesion (D). In a transverse image obtained cranial to the site of compression there isearly syrinx formation with an enlarged central canal (B). Arrows denote the location of transverse slices (TR¼ 3800ms, TE¼ 132ms, slice thickness¼ 3mm,interslice gap¼ 0.3mm).
Fig. 8. Comparison of the maximum height of syringohydromyelia (ex-pressed as a percentage of the spinal cord at the same level) in affected andunaffected dogs. The syrinx in affected dogs is significantly larger than inunaffected dogs (Po0.0001).
Fig. 9. Caudal fossa volume expressed as a percentage of total cranialcavity volume in affected and normal Cavalier King Charles Spaniels.Affected dogs had a significantly smaller relative caudal fossa volume(P¼ 0.0005).
43CAUDAL FOSSA MORPHOLOGY IN CAVALIERSVol. 50, No. 1
medullary antinociceptive influence on the spinal cord dor-
sal horn and trigeminal nucleus caudalis is inhibited by
damage to descending rostral ventral medullary fibers, in-
ducing a tendency toward hyperalgesia.21,38,39 Quantifica-
tion of foramen magnum crowding on MR
images is challenging and hence this factor was not con-
sidered. However, CSF flow through the foramen magnum
is affected by the morphology and so quantification of
CSF flow may provide a more complete explanation of the
clinical signs.
Cerebellar herniation is commonly associated with a
Chiari-like malformation. However, there was not an
association between the presence and extent of cerebellar
herniation and either clinical signs or syringohydromyelia,
as reported previously.8 In humans, although cerebellar
herniation supports a diagnosis of a Chiari malformation,
the presence or extent of herniation do not predict the
presence of neurologic symptoms.21,40,41 In the current
study, there was an association between the length of
cerebellar herniation and the size of the foramen magnum
and a large percentage of the dogs in this study were clas-
sified as having occipital dysplasia.
Occipital dysplasia is defined as an abnormally large
foramen magnum due to incomplete ossification of the
ventromedial supraoccipital bone during gestation.28 It is
difficult to be certain of the most ventral extent of the
supraoccipital bone on MR images. However, two study
dogs underwent a suboccipital craniectomy, durotomy,
and C1–C2 dorsal laminectomy due to progression of clin-
ical signs during the course of the study and, in both dogs,
the preoperative diagnosis of occipital dysplasia was con-
firmed at surgery.
Historically, occipital dysplasia has been a common
finding in toy and brachycephalic breeds such as the Cav-
alier King Charles Spaniel and has infrequently been as-
sociated with the presence of clinical signs.28,29 The notch
created by this anomaly is typically covered by fibrous tis-
sue and dura, and has not been reported to be associated
with concurrent cerebellar herniation.28,42–44 However, ab-
normalities in foramen magnum shape and size have been
reported as common findings in human patients with a
Chiari malformation43 and two Cavalier King Charles
Spaniels with concurrent occipital hypoplasia and dyspla-
sia have been identified.45
Abnormalities of the cervicomedullary junction were
frequent in this study. The cervicomedullary junction is
defined as the base of the occipital bone, the first and second
cervical vertebrae, and the ligaments of the atlantooccipital
and atlantoaxial joints.46–49 Specifically, medullary kinking
was found in a subset of Cavalier King Charles Spaniels but
there was no association between medullary kinking and
clinical signs or syringohydromyelia. An association be-
tween Chiari malformation and abnormalities of the
cervicomedullary junction has been described in peo-
ple.16,46,50–52 In dogs, medullary kinking and dorsal an-
gulation of the dens have been reported, often in
conjunction with Chiari-like malformations, although no
statistical relationship with the presence of neurologic signs
has been found.7,9,25,53
Dorsal compressive lesions overlying the junction of the
first and second cervical vertebrae were found in a small
group of participants. The degree of compression ranged
from mild attenuation of the dorsal aspect of the sub-
arachnoid space to moderate spinal cord compression. This
lesion was present in 20% of dogs. The nature of the
compression was investigated in two patients who under-
went a suboccipital craniectomy as well as a dorsal la-
minectomy of the first cervical vertebra and the cranial
third of the second cervical vertebra. These procedures
were performed due to lack of response to medical man-
Table 3. Attribute Ranges According to Syringohydromyelia (SHM) Status
Parameter
Dogs with SHM (n¼ 22) Dogs without SHM (n¼ 37)
P ValueRange Mean (SD) Range Mean (SD)
Neurologic grade 0–4 0.77 (1.23) 0–3 0.19 (0.57) 0.0024Age 1–6 2.9 (1.32) 1–5.5 2.51 (1.28) 0.23Cerebellar herniation (mm) 0–6.5 2.63 (1.51) 0–4.6 2.38 (1.46) 0.52Foramen magnum height (cm) 1.2–2 1.6 (0.16) 1.4–1.8 1.5 (0.14) 0.48Volume of caudal fossa (cm3) 10.2–15.66 13.02 (1.5) 10.72–15.39 12.98 (1.2) 0.62Caudal fossa/total cranial cavity volume (%) 10.6–16.95 13.98 (1.5) 12.8–16.4 14.4 (0.96) 0.06
Fig. 10. A significant correlation between foramen magnum size andlength of the cerebellar herniation (Po0.0001).
44 CERDA-GONZALEZ ET AL. 2009

agement. In both dogs, the dorsal compression was found
to be caused by fibrosis and proliferation of the ligament-
um flavum and dura. Expansion of the subarachnoid space
was noted just cranial to the level of compression through
the dorsal laminectomy. In both patients, this dilation
resolved and pulsatile CSF flow returned with resection of
the abnormal fibrous tissue at this level. Such dural band
formation has been reported to occur in dogs with Chiari-like
malformations and syringohydromyelia at the atlantooccip-
ital joint.5,13,54,55 Upon histopathologic examination of this
tissue, an irregular pattern of collagen fascicles with hyali-
nous nodules and occasional areas of calcification and/or
ossification was found.56 In the current study, no relationship
was found between this dorsal compressive lesion and clinical
signs or syringohydromyelia. However, the C1–C2 compres-
sive lesion was frequently found along with syringohyd-
romyelia beginning just caudal to the site of compression.
Our findings support the role of occipital hypoplasia in
the development of clinical signs in dogs affected with
Chiari-like malformation, and highlights the link between
clinical signs of pain and scratching and the presence and
relative height of syringohydromyelia. However, although
rare, classic signs of pain and phantom scratching can be
present in dogs that do not have syringohydromyelia but
do have a Chiari-like malformation. Occipital hypoplasia
and cerebellar herniation do not individually have a sig-
nificant role in the development of syringohydromyelia.
The population of Cavalier King Charles Spaniels evalu-
ated had a high prevalence of morphologic abnormalities
associated with Chiari-like malformations. Morphologic
abnormalities of both the caudal fossa and the craniocer-
vical junction were seen in these dogs, demonstrating the
multifactorial nature of this disease complex. The preva-
lence of occipital dysplasia, finding a large syrinx in clin-
ically normal dogs, and the frequency of the dorsal
compressive lesion at C1/2 were unexpected. The role of
dorsal compressive cervical spinal lesions in the formation
of syringohydromyelia must be further investigated and
considered in surgical planning for affected Cavalier King
Charles Spaniels.
REFERENCES
1. Rusbridge C. Canine syringomyelia: a painful problem in man’s bestfriend. Br J Neurosurg 2007;21:468–469.
2. Rusbridge C. Syringomyelia. UK Vet Companion Anim 2003;8:59–62.
3. Rusbridge C, Knowler SP. Inheritance of occipital bone hypoplasia(Chiari type I malformation) in Cavalier King Charles Spaniels. J Vet InternMed 2004;18:673–678.
4. Rusbridge C, Knowler P, Rouleau GA, Minassian BA, Rothuizen J.Inherited occipital hypoplasia/syringomyelia in the cavalier King Charlesspaniel: experiences in setting up a worldwide DNA collection. J Hered2005;96:745–749.
5. Rusbridge C. Chiari-like malformation with syringomyelia in theCavalier King Charles spaniel: long-term outcome after surgical manage-ment. Vet Surg 2007;36:396–405.
6. Rusbridge C. Neurological diseases of the Cavalier King Charlesspaniel. J Small Anim Pract 2005;46:265–272.
7. Rusbridge C, MacSweeny JE, Davies JV, et al. Syringohydromyeliain Cavalier King Charles Spaniels. J Am Anim Hosp Assoc 2000;36:34–41.
8. Lu D, Lamb CR, Pfeiffer DU, Targett MP. Neurological signs andresults of magnetic resonance imaging in 40 Cavalier King Charles Spanielswith Chiari type 1-like malformations. Vet Rec 2003;153:260–263.
9. Churcher RK, Child G. Chiari 1/syringomyelia complex in a KingCharles Spaniel. Aust Vet J 2000;78:92–95.
10. Rusbridge C. Persistent scratching in Cavalier King Charles Span-iels. Vet Rec 1997;140:239–240.
11. Rusbridge C. Persistent scratching in Cavalier King Charles Span-iels. Vet Rec 1997;141:179.
12. Child G, Higgins RJ, Cuddon PA. Acquired scoliosis associated withhydromyelia and syringohydromyelia in two dogs. J Am Vet Med Assoc1986;189:909–912.
13. Tagaki S, Kadosawa T, Ohsaki T, Hoshino Y, Okumura M, Fu-jinaga T. Hindbrain decompression in a dog with scoliosis associated withsyringomyelia. J Am Vet Med Assoc 2005;226:1359–1363.
14. Atlas SW, Lavi E. Disorders of brain development. In: Atlas SW,Lavi E (eds): MRI of the brain and spine, 2nd ed. Philadelphia: Lippincott-Raven Publishers, 1996;183–188.
15. Huang PP, Constantini S. ‘‘Acquired’’ Chiari I malformation.J Neurosurg 1994;80:1099–1102.
16. Tubbs RS, Lyerly MJ, Loukas M, Shoja MM, Oakes WJ. Thepediatric Chiari I malformation: a review. Childs Nerv Syst 2007;23:1239–1250.
17. Green AJ. Update on Chiari malformation: clinical manifestations,diagnosis, and treatments. Pediatr Nurs 2003;29:331–335.
18. Levine DN. The pathogenesis of syringomyelia associated withlesions at the foramen magnum: a critical review of existing theories andproposal of a new hypothesis. J Neurol Sci 2004;220:3–21.
19. Oldfield EH, Muraszko K, Shawker TH, Patronas NJ. Pathophys-iology of syringomyelia associated with Chiari I malformation of the cer-ebellar tonsils. J Neurosurg 1994;80:3–15.
20. Nash J, Cheng JS, Meyer GA, Remler BF. Chiari type Imalformation: overview of diagnosis and treatment. WMJ 2002;101:35–40.
21. Milhorat TH, ChouMW, Trinidad EM, et al. Chiari I malformationredefined: clinical and radiographic findings for 364 symptomatic patients.Neurosurgery 1999;44:1005–1017.
22. Nishikawa M, Sakamoto H, Hakuba A, Nakanishi N, Inoue Y.Pathogenesis of Chiari malformation: a morphometric study of the posteriorcranial fossa. J Neurosurg 1997;86:40–47.
23. Bejjani GK. Definition of the adult Chiari malformation: a briefhistorical overview. Neurosurg Focus 2001;11:1–8.
24. Dewey CW, Berg JM, Stefanacci JD, Barone G, Marino DJ. Caudaloccipital malformation syndrome in dogs. Compend Contin Educ Pract Vet2004;26:886–895.
25. Bynevelt M, Rusbridge C, Britton J. Dorsal dens angulation and achiari type malformation in a Cavalier King Charles spaniel. Vet RadiolUltrasound 2000;41:521–524.
26. Cappello R, Rusbridge C. Report from the Chiari-like malformationand syringomyelia working group round table. Vet Surg 2007;36:509–512.
27. Garcia-Real I, Kass PH, Sturges BK, Wisner ER. Morphometricanalysis of the cranial cavity and caudal cranial fossa in the dog: a com-puterized tomographic study. Vet Radiol Ultrasound 2004;45:38–45.
45CAUDAL FOSSA MORPHOLOGY IN CAVALIERSVol. 50, No. 1

28. Watson AG, de Lahunta A, Evans HE. Dorsal notch of foramenmagnum due to incomplete ossification of supraoccipital bone in dogs.J Small Anim Pract 1989;30:666–673.
29. Wright JA. A study of the radiographic anatomy of the foramenmagnum in dogs. J Small Anim Pract 1979;20:501–508.
30. Schmahl W, Kaiser E. Hydrocephalus, syringomyelia, and spinalcord angiodysgenesis in a Lhasa-apso dog. Vet Pathol 1984;21:252–254.
31. Bagley RS, Gavin PR, Silver GM, Moore MP, Kippenes H, Con-nors R. Syringomyelia and hydromyelia in dogs and cats. Compend ContinEduc Pract Vet 2000;22:471–479.
32. Yamada H, Yokota A, Harakate J. Morphological study of exper-imental syringomyelia with kaolin-induced hydrocephalus in a canine model.J Neurosurg 1996;84:999–1005.
33. Itoh T, Nishimura R, Matsunaga S, Kadosawa T, Mochizuki M,Sasaki N. Syringomyelia and hydrocephalus in a dog. J Am Vet Med Assoc1996;209:934–936.
34. OwenMC, Lamb CR, Lu D, Targett MP. Material in the middle earof dogs having magnetic resonance imaging for investigation of neurologicsigns. Vet Radiol Ultrasound 2004;45:149–155.
35. Stern-Bertholtz W, Sjostrom L, Hakanson NW. Primary secretoryotitis media in the Cavalier King Charles spaniel: a review of 61 cases.J Small Anim Pract 2003;44:253–256.
36. Rusbridge C, Carruthers H, Dube MP, Holmes M, Jeffery ND.Syringomyelia in Cavalier King Charles Spaniels: the relationship betweensyrinx dimensions and pain. J Small Anim Pract 2007;48:432–436.
37. Rusbridge C, Greitz D, Iskandar BJ. Syringomyelia: current con-cepts in pathogenesis, diagnosis, and treatment. J Vet Intern Med2006;20:469–479.
38. Thimineur M, Kitaj M, Kravitz E, Kalizewski T, Pardeep S. Func-tional abnormalities of the cervical cord and lower medulla and their effectson pain: observations in chronic pain patients with incidental mild Chiari Imalformation and moderate to severe spinal cord compression. Clin J Pain2002;18:171–179.
39. Taylor FR, Larkins MV. Headache and Chiari I malformation:clinical presentation, diagnosis, and controversies in management. Curr PainHeadache Rep 2002;6:331–337.
40. Panigrahi M, Reddy BP, Reddy AK, Reddy JJM. CSF flow study inChiari I malformation. Childs Nerv Syst 2004;20:336–340.
41. Haughton VM, Korosec FR, Medow JE, Dolar MT, Iskandar BJ.Peak systolic and diastolic CSF velocity in the foramen magnum in adultpatients with Chiari I malformations and in normal control participants.AJNR: Am J Neuroradiol 2003;24:169–176.
42. Goel A. Chiari I malformation redefined: clinical and radiographicfindings for 364 symptomatic patients. Neurosurgery 1999;45:1497–1499.
43. da Silva JA, Holanda MM. Basilar impression, Chiari malforma-tion, and syringomyelia: a retrospective of 53 surgically treated patients. ArqNeuropsiquiatr 2003;61:368–375.
44. Simoens P, Poels P, Lauwers H. Morphometric analysis of the for-amen magnum in Pekingese dogs. Am J Vet Res 1994;55:34–39.
45. Rusbridge C, Knowler SP. Coexistence of occipital dysplasia andoccipital hypoplasia/syringomyelia in the Cavalier King Charles Spaniel.J Small Anim Pract 2006;47:603–606.
46. Erbengi A, Oge HK. Congenital malformations of the cranioverte-bral junction: classification and surgical treatment. Acta Neurochir (Wien)1994;127:180–185.
47. Barnes PD, Kim FM, Crawley C. Developmental anomalies of thecraniocervical junction and cervical spine. MRI ClinNorth Am 2000;8:651–674.
48. Kumar A, Mafee M, Jafar J, Glick R. Diagnosis and management ofanomalies of the craniocervical junction. Ann Otol Rhinol Laryngol1986;95:487–497.
49. Rao PV, Mbajiorgu EF, Levy LV. Bony abnormalities of thecraniocervical junction. Cent Afr J Med 2001;48:17–23.
50. Tubbs RS, Wellons JC, Blount JP, Grabb PA, Oakes WJ. Inclina-tion of the odontoid process in the pediatric Chiari I malformation. J Ne-urosurg 2003;98:43–49.
51. Royo-Salvador MB. Platibasia, impresion basilar, retroceso odon-toideo y kinking del tronco cerebral, etiologia comun con la siringomielia,escoliosis y malformacion de Arnold-Chiari idiopaticas. Rev Neurol 1996;24:1241–1250.
52. Kyoshima K, Kakizawa Y, Tokushige K, Akaishi K, Kanaji M,Kuroyanagi T. Odontoid compression of the brainstem without basilar im-pression—‘‘odontoid invagination’’. J Clin Neurosci 2005;12:565–569.
53. Gibson KL, Ihle SL, Hogan PM. Severe spinal cord compressioncaused by a dorsally angulated dens. Progr Vet Neurol 1995;6:55–57.
54. Vermeersch K, Van Ham L, Caemaert J, et al. Suboccipital craniec-tomy, dorsal laminectomy of C1, durotomy and dural graft placement as atreatment for syringohydromyelia with cerebellar tonsil herniation in Cav-alier King Charles spaniels. Vet Surg 2004;33:355–360.
55. Dewey CW, Berg JM, Barone G, Marino DJ, Stefanacci JD. Foramenmagnum decompression for treatment of caudal occipital malformationsyndrome in dogs. J Am Vet Med Assoc 2005;227:1270–1275, 1250–1251.
56. Nakamura N, Iwasaki Y, Hida K, Abe H, Fujioka Y, Nagashima K.Dural band pathology in syringomyelia with Chiari type I malformation.Neuropathology 2000;1:38–43.
46 CERDA-GONZALEZ ET AL. 2009