ANTERIOR IMPLANT RESTORATIONS –CHALLENGE AND COMPROMISE. A CASE REPORT
Upload
independentCategory
view
5download
0
Cr
Sa
b
c
a
A
R
R
8
A
K
A
C
C
A
C
F
M
h0
d e n t a l m a t e r i a l s 3 1 ( 2 0 1 5 ) 481–495
Available online at www.sciencedirect.com
ScienceDirect
jo ur nal home p ag e: www.int l .e lsev ierhea l th .com/ journa ls /dema
linical effectiveness of direct anteriorestorations—A meta-analysis
iegward D. Heintzea,∗, Valentin Roussonb, Reinhard Hickel c
R&D, Ivoclar Vivadent AG, Schaan, LiechtensteinBiostatistics Unit, Institute for Social and Preventive Medicine, University of Lausanne, SwitzerlandDepartment of Operative Dentistry and Periodontology, Ludwig-Maximilian-University, Munich, Germany
r t i c l e i n f o
rticle history:
eceived 1 August 2013
eceived in revised form
April 2014
ccepted 28 January 2015
eywords:
nterior restorations
lass III, Class IV
omposite resin
dhesive system
olor
racture
arginal integrity
a b s t r a c t
Objectives. This is the first meta-analysis on the efficacy of composite resin restorations
in anterior teeth. The objective of the present meta-analysis was to verify whether spe-
cific material classes, tooth conditioning methods and operational procedures influence
the result for Class III and Class IV restorations.
Material and methods. The database SCOPUS and PubMed were searched for clinical trials
on anterior resin composites without restricting the search to the year of publication. The
inclusion criteria were: (1) prospective clinical trial with at least 2 years of observation; (2)
minimal number of restorations at last recall = 20; (3) report on drop-out rate; (4) report of
operative technique and materials used in the trial, and (5) utilization of Ryge or modified
Ryge evaluation criteria. For the statistical analysis, a linear mixed model was used with
random effects to account for the heterogeneity between the studies. p-Values smaller than
0.05 were considered to be significant.
Results. Of the 84 clinical trials, 21 studies met the inclusion criteria, 14 of them for Class
III restorations, 6 for Class IV restorations and 1 for closure of diastemata; the latter was
included in the Class IV group. Twelve of the 21 studies started before 1991 and 18 before 2001.
The estimated median overall success rate (without replacement) after 10 years for Class III
composite resin restorations was 95% and for Class IV restorations 90%. The main reason
for the replacement of Class IV restorations was bulk fractures, which occurred significantly
more frequently with microfilled composites than with hybrid and macrofilled compos-
ites. Caries adjacent to restorations was infrequent in most studies and accounted only for
about 2.5% of all replaced restorations after 10 years irrespective of the cavity class. Class
III restorations with glass ionomer derivates suffered significantly more loss of anatomical
form than did fillings with other types of material. When the enamel was acid-etched and
no bonding agent was applied, significantly more restorations showed marginal staining
and detectable margins compared to enamel etching with enamel bonding or the total etch
technique; fillings with self-etching systems were in between of these two outcome vari-
ables. Bevelling of the enamel was associated with a significantly reduced deterioration of
∗ Corresponding author at: Ivoclar Vivadent, Bendererstr. 2, 9494 Schaan, Liechtenstein. Tel.: +423 235 3570; fax: +423 233 1279.E-mail address: [email protected] (S.D. Heintze).
ttp://dx.doi.org/10.1016/j.dental.2015.01.015109-5641/© 2015 Academy of Dental Materials. Published by Elsevier Ltd. All rights reserved.

482 d e n t a l m a t e r i a l s 3 1 ( 2 0 1 5 ) 481–495
the anatomical form compared to no bevelling but not with less marginal staining or less
detectable margins. The type of isolation (absolute/relative) had a statistically significant
influence on marginal caries which, however, might be a random finding.
© 2015 Academy of Dental Materials. Published by Elsevier Ltd. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4822. Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 483
2.1. Selection of clinical trials on class III/IV restorations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4833. Statistical analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4844. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 486
4.1. Study search . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4864.2. Structure of included studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4864.3. Outcome variables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 487
5. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4916. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 493
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 494
1. Introduction
Perfect anterior restorations act as an advertisement for theskills of the dental professional. Most operative interventionsin anterior teeth are accomplished with the direct placementof composite resins. The skill of the dentist in achieving anatural anatomical shape and color match with the adja-cent teeth are prerequisites to achieving a pleasing aestheticresult, which can also be assessed easily by the patients them-selves. Type of composite resin, methods and materials tocondition the tooth structure (enamel etching, self-etching,no etching) as well as the operative procedure (bevellingof enamel margin, rubber dam application) may also influ-ence both the aesthetic results and the longevity of therestoration.
Before the development of composite resins and the acid-etch technique of the enamel, carious lesions in anterior teethwere mainly restored with silicate cement, which required aretentive preparation pattern [1]. Restorations that involve theproximal part of an anterior tooth but not the incisal edge aredefined as Class III restorations.
In the early days, the building up of fractured teeth wasonly possible with indirect restorations, such as full-coveragecrowns, because bonding to the remaining tooth substancehad not yet been established as an operative procedure.Already in the nineteen-fifties, the enamel etch techniquewith phosphoric acid was developed by Buonocore [2]. How-ever, it took about 20 years until this technique has beenintroduced into clinical dentistry. This technique made itpossible to directly restore fractured anterior teeth with com-posite resin, to close diastemata or to build up worn teeth.
the etched enamel or whether high-viscosity resin compos-ites could be placed directly on the etched enamel. Theoperative procedures have been gradually simplified and thematerials improved since then. First, the application timesof both enamel etching and rinsing were reduced from 60to 30 s [3], dentin bonding agents made liners superfluousand increased the bonding strength to the tooth structure[4]. Then, self-etching adhesive systems were introduced[5]. Capable of establishing a bond to both the enamel anddentin, these materials streamlined the operative procedurebecause they eliminated the need for a separate rinsingstep.
Most contemporary dental composite resins still con-tain a monomer which was already developed in the late1950s of the last century by M. Bowen [6]: it is calledBisphenol-A glycidylmethacrylate or simply Bis-GMA orBowen’s resin Microfilled composites and later hybrid andnano-hybrid composites replaced the macrofilled compos-ites, which were the first dental resins on the market [7].Polymerization curing lights were first introduced at the endof 1970s of last century [8]. They allowed these materialsto be cured on demand, which facilitated the customiza-tion of anterior restorations, because they could be built upstep-by-step with several layers that have different opticalproperties.
With the reduction of caries prevalence in most countries,the prevalence of Class III restorations due to proximalcaries has also dropped. However the prevalence of traumaticinjuries to anterior teeth has significantly increased over thelast 20 years due to an increase in sports activities undertakenduring leisure time. In some countries, particularly in Scandi-
Restorations that involve a part of the incisal edge are definedas Class IV restorations.
At that time, there was a dispute as to whether it isnecessary to place an unfilled resin bonding material on
navia, children and adolescents have nowadays more teethdamaged by traumatic injuries than by caries [9]. The restora-tion of fractured teeth (Class IV) with composite is usually thefirst treatment option.

3 1
iSofpHot
ptt
t
----
c
-
----
1
2
3
4
5
6
7
8
2 = enamel etch + no bonding3 = enamel etch–3 steps
d e n t a l m a t e r i a l s
The question arises as to how effective such a treatment isn terms of aesthetics, function and longevity. In the databasesCOPUS and PubMed no meta-analysis or systematic reviewn the efficacy of Class III or Class IV restorations has beenound. There are several systematic reviews on posterior com-osite restorations [10–15] and cervical restorations [16,17].owever, it is inadequate to extrapolate from the longevityf posterior composite restoration to that of anterior restora-ions.
The aim of this review was to systematically evaluaterospective clinical trials on anterior resin composite restora-ions without restricting the search to the publication year orhe type of resin or adhesive system used.
The following factors affecting the clinical outcome wereo be specifically evaluated:
type of cavity (Class III, Class IV) type of enamel/dentin conditioning type of resin composite operative techniques:• bevelling of enamel• absolute versus relative isolation
These factors were to be assessed by the following outcomeriteria:
time elapsed until replacement and reason for replacement(marginal caries, fracture of filling, retention loss, etc.)
color match and surface texture marginal integrity and marginal staining anatomical form (shape) chipping and fracture
The following hypotheses were examined:
. Class IV restorations mostly suffer from chippings and frac-tures and have a reduced longevity compared to Class IIIrestorations.
. The type of composite resin does not influence the overalllongevity of Class III restorations.
. Class IV restorations with hybrid composites show a betterlongevity than Class IV restorations with microfilled com-posites.
. Restorations based on glass ionomer derivates have areduced longevity compared to composite resin restora-tions and compomers.
. Enamel etching with phosphoric acid reduces the numberof restorations that show marginal discoloration and defec-tive marginal integrity compared to self-etching systemsand compared to those restorations that were placed withenamel etching but without bonding agent.
. The type of isolation or bevelling of the enamel does notinfluence the clinical outcome.
. Hybrid and microfilled composites show a better color
match than macrofilled composites.. Hybrid composites maintain their anatomical form moreeffectively than microfilled composites, compomers andglass ionomer derivates.
( 2 0 1 5 ) 481–495 483
2. Materials and methods
2.1. Selection of clinical trials on class III/IVrestorations
Prospective clinical studies on Class III/IV restorations in per-manent teeth were searched in the databases PubMed (searchperiod 1966–2012, search time December 2012). The searchterms were “anterior” (or “Class III”) or “anterior” (or “ClassIV” or “trauma”) and “composite” and “clinical trial”.
The inclusion criteria were as follows:
1. Prospective clinical trial for Class III or Class IV cavities ordiastema closures.
2. Minimal duration of 2 years.3. Minimal sample size at last recall: 15 restorations per mate-
rial.4. The study had to report on the following outcome vari-
ables: marginal discoloration, marginal integrity, cariesadjacent to restorations, material fractures, color matchand anatomical form. The variables “surface texture”, “sur-face staining” were optional variables.
5. The study had to report on the materials and hard tissueconditioning technique used (etching of enamel with phos-phoric acid yes/no, dentin/enamel bonding agent).
6. The study had to report on the operative technique (bev-elling of enamel, preparation, isolation technique, type ofcuring).
Clinical studies on direct composite veneers and studiesthat used composite materials to correct the vertical dimen-sion were not included in the meta-analysis. Studies withexperimental materials that were never launched on the mar-ket were not taken into account. There was no restriction withregard to the publication year.
As far as the materials are concerned, studies withpolyacid-modified resin composites (compomers or PAMRC)and resin-modified glass ionomer cements (RMGIC) were alsoincluded.
The restorative materials and adhesive systems (AS) weregrouped as follows:
Restorative material (RM)1 = macrofiller2 = microfiller3 = hybrid4 = polyacid-modified resin composite (compomer)5 = resin-modified glass ionomer cements (RMGIC)
Adhesive system (AS)1 = enamel etch + enamel bonding
4 = enamel etch–2 steps5 = self-etch–2 steps6 = self-etch–1 step7 = no etch + no bond

l s 3
484 d e n t a l m a t e r i aTo further reduce the number of categories and to increasethe statistical power, four adhesive classes were defined:
1 = enamel etch with phosphoric acid + bonding2 = enamel etch with phosphoric acid + no bonding3 = self-etch4 = no etch + no bond
The following binary variables were considered, where thepercentage of the category given in brackets will be analyzedin what follows:
1. MD marginal discoloration (not visible).2. MI marginal integrity (no clinically detectable margins
(with explorers).3. CAR caries adjacent to restorations (no caries).4. F material fracture (no chipping, no bulk fracture; alterna-
tively with slight chipping or fracture).5. AF anatomical form (good/very good).6. C color match (good/very good).7. ST surface texture (good/very good).8. R retained restoration.
For most of these variables (MD, MI, F, C, ST and AF) the datawere originally graded into three categories (1 = good or verygood, corresponds to Ryge criterion “Alpha”; 2 = acceptableor repairable, corresponds to Ryge criteria “Beta” or “Char-lie”; 3 = inacceptable which needs replacement, correspondsto Ryge criterion “Delta”), but since the category 3 occurredonly rarely, the variables were dichotomized for the analysis,as given above. However, category 3 was taken into account
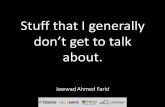
when defining and analyzing the longevity of a restoration.The percentage of restorations still in function refers to thoserestorations which did not have to be replaced due to one (ormore) of the following reasons:Fig. 1 – Estimated median percentage of restorations across the smatch in relation to the type of restorative material and to the ob
1 ( 2 0 1 5 ) 481–495
1. CAR = caries adjacent to restorations (secondary ormarginal caries)
2. F = material fracture3. R = loss or partial loss of restoration4. C = inacceptable color match5. MI = inacceptable marginal integrity6. AF = inacceptable anatomical form
To assess the possible influence of the polishing system,the various polishing methods were categorized in the follow-ing way:
1 = disc2 = silicone instrument3 = stone4 = disc + glaze5 = etch + bonding
3. Statistical analysis
All the clinical outcomes could be expressed as percentagesof restorations retaining a given property across the definedperiod of time, for example the percentage of restorationswithout a visible marginal discoloration, the percentage ofrestorations with a good or a very good anatomical form, orthe percentage of restorations which did not need replace-ment, as defined above. To permit a comparison of the rateof deterioration among the various experiments, the percent-ages observed at the various points of time were divided by thepercentage observed at baseline for those experiments wherethe latter was below 100%.
Let Y(t) be a percentage measured at time t (expressed
in years). To model the rate of deterioration, we werelooking for a model where Y(t) is a decreasing functionof t ranging from Y(0) = 100% down to 0% for large val-ues of t. A linear model of the form Y(t) = 100 − beta × ttudies and experiments with good or very good colorservation time. (Left) Class III, (right) Class IV.

d e n t a l m a t e r i a l s 3 1 ( 2 0 1 5 ) 481–495 485
Fig. 2 – Estimated median percentage of Class IIIrestorations across the studies and experiments with goodor very good surface texture in relation to the type ofr
wbsowlb
fm
+
Fig. 3 – Estimated median percentage of Class IIIrestorations across the studies and experiments withadequate anatomical form in relation to the type of
Ft
estorative material and to the observation time.
ould for example not be convenient since it would haveecome negative for large values of t, which was notensible in our context. We considered instead a deteri-ration model of the form Y = 100 × exp(−lambda × tˆalpha)ith positive values of alpha and lambda, which is equiva-
ent to stating that Log(−Log Y/100) = beta + alpha × Log(t), witheta = Log(lambda).
To study how the deterioration process depends on a given
actor of interest, we then considered the following statisticalodel for our empirical percentages Y(t):Log(−Log(Y(t)/100)) = beta j + alpha × Log(t) + study effect
experiment effect + random error.
ig. 4 – Estimated median percentage of restorations across the so the restoration in relation to the type of restorative material. (L
restorative material and to the observation time.
In this model, beta j is a fixed parameter characterizing therate of deterioration for the level j of the factor of interest, suchthat the higher the parameter, the faster the deterioration (avalue of beta j = −2 indicates for example a faster deteriorationthan a value of beta j = −3). The parameter alpha characterizesthe shape of the deterioration which does not depend on thefactor of interest. A random experiment effect was includedto account for the obvious dependencies among the repeated
percentages observed in the same experiment along time,while a random study effect was included to account for thefact that the subjects involved in different experiments fromthe same study were partly the same (split-mouth design).tudies and experiments without material chipping/fractureeft) Class III, (right) Class IV.

486 d e n t a l m a t e r i a l s 3
Fig. 5 – Estimated percentage of restorations across thestudies and experiments based on all data without cariesadjacent to the restoration in relation to the type of cavitycategory (Class III/IV).
Fig. 6 – Estimated median percentage of Class IIIrestorations across the studies and experiments withoutcaries adjacent to the restoration in relation to the type of
Out of the 58 experiments, enamel was bevelled in 31 exper-
isolation.
In our model, the deterioration curve is thus assumedto be different from study to study and from exper-iment to experiment. Figs. 1–9 below show some ofour fitted models as Y = 100 × exp(−lambda j × tˆalpha), withlambda j = exp(beta j), which can be interpreted as a median
deterioration curve for the level j of the factor of interest (esti-mated over all studies and experiments).Such a linear mixed model could be fitted using therestricted maximum likelihood method implemented in the
1 ( 2 0 1 5 ) 481–495
routine lme, which can be found in the package nlme from thestatistical software R. In this routine, it was also possible toweight each empirical percentage by the corresponding num-ber of restorations (the denominator of the percentage). Totest for the statistical significance of the factor of interest, amaximum likelihood ratio test was used, with the number oflevels of the factor of interest minus one as number of degreesof freedom. p-Values smaller than 0.05 were considered to besignificant.
4. Results
4.1. Study search
The initial search revealed 85 clinical studies on Class III/IVanterior restorations. However, only 21 studies met the criteriato be included in the review, 14 of them for Class III restora-tions, 6 for Class IV and 1 for diastema closure; the latter wasincluded in the group of Class IV restorations (Table 1). Fur-thermore, prospective studies that missed to report on one orseveral of the clinical outcome variables listed above, e.g. colormatch or marginal staining, were also included, which led tomore statistical power.
The most frequent reasons for exclusion were (in descen-ding order according to frequency):
1. No differentiation between restorations of Class III, IV, V (I,II)
2. Short duration (less than 2 years)3. Retrospective study4. Pooled data for different materials5. Other indication (e.g. restoration of worn incisors)6. Case reports
The specific characteristics of each clinical trial that isincluded in the final analysis are listed in Table 1.
4.2. Structure of included studies
The 21 studies included in the review contain 53 in vivo exper-iments with 22 different composites, 3 compomers and 2glass ionomer derivates. Fifteen different adhesive systemswere used to fabricate the restorations. Twelve of the included21 studies started before 1991 and 18 before 2001. The typeof adhesive and composite/restorative material is listed inTable 1. Eighty-five per cent of the experiments had an obser-vation period of 2–5 years. For 27 experiments data on theratio of maxillary versus mandibular anterior restorations arereported; the mean ratio was 96% with a range from 88 to 100%.In Tables 2 and 3 the frequency of studies as well as the num-ber of restorations at baseline in relation to the hard tissueconditioning method and the different groups of restorativematerials are listed.
iments, and absolute isolation (rubber dam) was applied in 29experiments (Tables 2 and 3). For 13 experiments there was nodescription on the type of isolation.

d e n t a l m a t e r i a l s 3 1 ( 2 0 1 5 ) 481–495 487
Fig. 7 – Estimated median percentage of restorations across the studies and experiments without marginal staining inr to t
4
TmetIrCcab
Fm
elation to the adhesive technique and adhesive system and
.3. Outcome variables
he curves presented in the figures below refer to the esti-ated median percentage of deterioration (across studies and
xperiments) for the binary outcomes, in relation to time ando various factors of interest, and differentiated between ClassII and Class IV restorations. If there is no graph for Class IVestorations, there were not enough data to run the model.urves were plotted for the longest observation time of the
orresponding factor levels. The parameters alpha and beta j,s well as the number of experiments (nexp) and the num-er of observed percentages (nobs) are also provided for eachig. 8 – Estimated median percentage of Class III restorations acrargins in relation to the composite material (left) and the adhe
he observation time. (Left) Class III, (right) Class IV.
factor level, together with a p-value from a maximum likeli-hood ratio test. As usual in a statistical study, the result mightnot be statistically significant despite large differences amongthe curves, due to a high between-study variability and/or tothe small number of studies involved. On the other hand,statistical significance might have been achieved despite aseemingly small difference among the curves in case of a lowbetween-study variability.
The decrease of restorations with good or very good color
match was dependent on the type of composite material.Compomers and hybrid composites showed a better colormatch than microfilled and macrofilled composites in Classoss the studies and experiments without detectablesive technique (right).

488 d e n t a l m a t e r i a l s 3 1 ( 2 0 1 5 ) 481–495
Fig. 9 – Estimated median percentage of restorations across the studies and experiments that were not replaced in relations IV.
to the type of restorative material. (Left) Class III, (right) ClasIII restorations (Fig. 1); the difference, however, was not sta-tistically significant. Class III restorations with glass ionomerderivates exhibited the most rapid deterioration in colormatch compared to the other materials; the difference to theother materials was, however, not statistically significant. InClass IV restorations hybrid composites showed a significantlybetter color match than microfilled composites (p = 0.002),which performed significantly better than macrofilled com-posites (p = 0.022). The type of polishing system did not have asignificant influence on the color match.
As far as surface texture is concerned, Class III restorationswith hybrid composites and compomers showed a statis-tically significant less rapid deterioration than restorationswith microfilled and macrofilled composites (p = 0.017) (Fig. 2).Restorations with glass ionomer derivates demonstrated theworst deterioration in surface texture. The deterioration wassignificantly worse than that of compomers (p = 0.001). Thetype of polishing system did not have a significant influenceon the surface texture.
The loss of anatomical form was material-dependent. ClassIII restorations with macrofilled and hybrid composites wereaffected to a lower degree by impaired anatomical form thanrestorations that were fabricated with other restorative mate-rials (Fig. 3); the difference, however, was only significantbetween macrofilled and microfilled composites (p = 0.003) aswell as between macrofilled or hybrid composites and glassionomer cements (p = 0.006 and p = 0.003 respectively). Thebevelling of the cavity was associated with a significant reduc-tion in the deterioration of the anatomical form compared tonot bevelling the margins (p = 0.039).
Significantly more Class IV restorations showed chippingsand fractures that resulted in the replacement of the restora-
tion than did Class III restorations (p = 0.0001). Class IVrestorations with hybrid composites showed significantly lessfractures than Class IV restorations with macrofilled compos-ites and microfilled composites (p = 0.0001) (Fig. 4); the lattershowed significantly more chippings/fractures than macro-filled composites (p = 0.0001). For Class III restorations therewas no statistically significant difference between the mate-rials.
The frequency of caries adjacent to restorations (CAR) waslow in most studies with a median prevalence of about 2.5%after 10 years in both Class III and Class IV restorations andthis rate did not differ very much across the studies (Fig. 5).The occurrence was not dependent on the type of compos-ite material, the type of enamel and dentin conditioning orthe bevelling of the cavity. However, Class III restorations thatwere placed without a rubber dam were associated with a sig-nificantly higher frequency of caries adjacent to restorationsthan those restorations that were placed with a rubber dam(p = 0.024) (Fig. 6).
The decrease of restorations with no marginal staining wasdependent on the tooth conditioning technique. Restorationswith etched enamel and treated with either an enamel ora dentin bonding agent showed less marginal discolorationthan all the other groups, including those restorations whoseenamel was etched but not coated with a bonding agent(Fig. 7). The difference was, however, only statistically signifi-cant between the groups “enamel etch and bond” and “no etchand no bond” (p = 0.008). The variables “bevelling of enamel”and “type of isolation” did not influence the result signifi-cantly.
As far as the outcome variable marginal integrity is con-cerned there was a significant more rapid decrease in nodetectable margins for Class III microfilled composite restora-tions than for Class III macrofilled restorations (p = 0.001)(Fig. 8). The type of tooth conditioning method was not statis-tically significant. The variables “bevelling of enamel” or “type
of isolation” did not influence the result significantly.The reasons for restoration replacement were predomi-nantly bulk fractures of Class IV restorations and caries atthe restorative margins. A very small number of restorations

d e n t a l m a t e r i a l s 3 1 ( 2 0 1 5 ) 481–495 489
Table 1 – Clinical studies and their characteristics that are included in the meta-analysis.
First author Reference Publicationyear
Number ofrestorationsat baseline
Number ofrestorationsat last recall
Observationperiod (years)
Bevelling
Class IIIOsborne [37] 1990 50 46 3 No
[37] 1990 50 47 3 noSchlapbach [38] 1982 111 97 2 yes
[38] 1982 43 39 2 yes[38] 1982 61 53 2 yes
van Dijken [39] 1986 29 29 6 yes[39] 1986 28 28 6 yes[39] 1986 20 20 6 yes[39] 1986 28 28 6 yes[39] 1986 47 47 6 yes
Qvist [40] 1993 52 37 11 yes[40] 1993 52 38 11 no
Davis [41] 1986 28 17 3 yes[41] 1986 28 17 3 yes[41] 1986 28 17 3 yes
Crumpler [42] 1988 28 17 5 no[42] 1988 28 16 5 no[42] 1988 28 15 5 no[42] 1988 28 18 5 no
Osborne [43] 1990 24 22 3 no[43] 1990 24 22 3 no[43] 1990 24 22 3 no
van Dijken [44] 1999 53 49 5 yes[44] 1999 49 44 5 yes[44] 1999 49 44 5 yes
van Dijken [45] 1999 52 50 5 no[45] 1999 45 42 5 no[45] 1999 57 52 5 yes
Araujo [46] 1998 21 21 2 yes[46] 1998 21 21 2 no
Reusens [47] 1999 28 23 2 yes[47] 1999 28 23 2 yes
Demirci [48] 2006 62 57 5 noDemirci [49] 2008 32 29 2 yes
[49] 2008 32 29 2 no[49] 2008 32 29 2 no
Ermis [50] 2010 51 40 3 yes[50] 2010 51 40 3 yes
Class IVSheykholeslam [51] 1977 33 33 2 No
[51] 1977 31 30 2 NoDogon [52] 1980 161 27 4 Yes
[52] 1980 161 27 4 YesRoberts [53] 1978 52 37 2 Yes
[53] 1978 52 38 2 Yes[53] 1978 52 29 2 Yes
Shey [54] 1979 25 19 2 Yes[54] 1979 25 19 2 Yes
Tyas [25] 1990 25 15 3 No[25] 1990 29 17 3 No[25] 1990 22 21 3 No[25] 1990 26 24 3 No
Peumans [55,56] 1997 61 61 5 Yesvan Dijken [28] 2010 43 40 12 Yes

490 d e n t a l m a t e r i a l s 3 1 ( 2 0 1 5 ) 481–495
Table 1 – (Continued )
Adhesive Restorative material Material class
no bonding Adaptic Macrofillerno bonding Adaptic Radiopaque Macrofillerenamel bonding Silar Microfillerno bonding Isopast Microfillerenamel bonding Concise Macrofillerno bonding Adaptic Macrofillerno bonding Silar Microfillerno bonding Isopast Microfillerno bonding Durafill Microfillerno bonding DRS Hybrid fillerno bonding Silar MicrofillerCosmic Bond Silar MicrofillerConcise enamel bond Concise Macrofillerenamel bonding Silar Microfillerenamel bonding Prisma-fil Hybrid fillerno bonding Concise Macrofillerno bonding Miradapt Hybrid fillerno bonding Silar Microfillerno bonding Superfil MicrofillerAdaptic Bonding agent Adaptic MacrofillerPolyacrylic Acid Chelon-Fil Glass ionomerPolyacrylic Acid Ketac-Fil Glass ionomerGluma2000 Pekafill Hybrid fillerGluma 4 Sealer Pekafill Hybrid fillerGluma 4 Sealer Pekafill Hybrid fillerPSA Primer/Adhesive Dyract CompomerPolyacrylic Acid Fuji II LC Glass ionomerGluma 4 Sealer Pekafill Hybrid fillerXR Primer/Bond Herculite XRV Hybrid fillerPolyacrylic Acid Chelon-Fil Glass ionomerScotchbond2 Silux Plus MicrofillerXR Primer/Bond Herculite XRV Hybrid fillerPSA Primer/Adhesive Dyract CompomerNRC + Prime&Bond NT Dyract AP CompomerPrime&Bond NT Dyract AP CompomerSingle Bond Filtek 110 MicrofillerClearfil SE Bond Clearfil AP-X Hybrid fillerClearfil SE Bond Clearfil AP-X Hybrid fillerNuva Seal Nuva-Fil MacrofillerAdaptic Bonding agent Adaptic MacrofillerConcise enamel bond Concise MacrofillerNuva Seal Nuva-Fil Macrofillerenamel bonding Exact Macrofillerno bonding Restodent MacrofillerNuva Seal Nuva-Fil MacrofillerAdaptic Bonding agent Adaptic MacrofillerAdaptic Bonding agent Adaptic Radiopaque Macrofillerenamel bonding Estic MF Microfillerenamel bonding Durafill Microfillerenamel bonding Estilux Hybrid fillerenamel bonding Miradapt Hybrid fillerScotchbond2 Herculite XRV Hybrid fillerGluma2000 Pekafill Hybrid filler
was replaced due to retention loss, inacceptable colormatch or inacceptable marginal integrity. The replacementrate for Class III fillings with glass ionomer cements and
microfilled composites was significantly higher compared tomacrofilled and hybrid composites (p = 0.014 and p = 0.017respectively) (Fig. 9). For Class IV restorations significantlymore restorations were replaced when microfilled compos-ites were used compared to macrofilled and hybrid composites(p = 0.0001).
The overall median success rate of composite restorations(excluding glass ionomer) after 10 years was about 95% forClass III restorations and 90% for Class IV restorations.

d e n t a l m a t e r i a l s 3 1 ( 2 0 1 5 ) 481–495 491
Table 2 – Number of experiments and sample size at baseline in relation to the tooth conditioning technique and thecavity class (*number of experiments).
Number ofexperiments
Number of restorationsat baseline
Rubber dam Bevelling of enamel*
Yes No Yes No
Class IIIEnamel etching + enamel bonding 9 459 7 0 7 2Enamel etching–3 steps 4 130 2 0 4 0Enamel etching–2 steps 3 115 1 2 1 2Enamel etching + no bonding 12 387 6 5 8 4Self-etch–2 steps 2 83 1 1 2 0Self-etch–1 step 2 114 0 1 0 2Glass ionomer 4 113 3 0 0 4No etch + no bond 2 100 0 0 0 2
Class IVEnamel etching + enamel bonding 12 642 6 2 6 6Enamel etching–3 steps 2 104 2 0 2 0Enamel etching + no bonding 1 52 1 0 1 0
Table 3 – Number of experiments and sample size at baseline in relation to the type of restorative material and the cavityclass (*number of experiments).
Number ofexperiments
Number of restorationsat baseline
Rubber dam* Bevelling of enamel*
Yes No Yes No
Class IIIMacrofiller 7 270 4 1 3 4Microfiller 12 478 5 4 8 4Hybrid 11 462 8 1 10 1Compomer 4 178 0 3 1 3Glass ionomer 4 113 3 0 0 4
Class IVMacrofiller 9 592 7 2 7 2Microfiller 2 54 0 0 0 2Hybrid 4 152 2 0 2 2
exp
tc
do
Note: Some studies did not report on rubber dam placement, whichnumber of experiments with rubber dam yes/no.
The type of tooth conditioning, bevelling of the enamel orhe type of isolation (absolute/relative) did not have a signifi-ant influence on the investigated outcome variables.
Table 4 summarizes the clinical performance of the fiveifferent groups of restorative materials in relation to certainutcome variables specified above.
Table 4 – Clinical performance of composite resin materials in r
Composite resin Number ofexperiments
Color match Surfacetexture
Class IIIMacrofiller 7 − +/−
Microfiller 12 +/− +
Hybrid 11 + +
Compomer 4 + +
Glass ionomer 4 - - −
Class IVMacrofiller 9 − +
Microfiller 2 +/− +
Hybrid 4 + +
++ = very good, + = good, +/− = acceptable, − = bad, - - = very bad.
lains the difference between total number of experiments and the
5. Discussion
Meta-analyses are considered a valid method to combinethe results from clinical trials that were selected accordingto predefined criteria and to extract data in order to draw
elation to the type of resin material.
Anatomicalform
Materialchipping
Material fracture(replacement)
+ ++ ++ ++ +− −
++ + −− - - - -+ +/− +−

l s 3
492 d e n t a l m a t e r i aconclusions about the efficacy of a therapeutic intervention- in this case the longevity of restorative materials and theiroperative technique to restore anterior teeth. However, thereis no consensus as to which statistical method should beapplied to conduct a meta-analysis. In the present study, alinear mixed model with random effects was considered toaccount for both the heterogeneity between the studies andthe repeated observations across time within an experimentto be the most appropriate approach.
This is the first meta-analysis on the efficacy of anteriorrestorations. However, most of the included studies were car-ried out between 1980 and 2000 and there were only 6 studieson Class IV restorations. As this is the first systematic reviewor meta-analysis of that kind, also studies that evaluated resinmaterials that are no longer available on the market, such asmacrofilled materials, had been included. Likewise, studiesthat did not use an enamel or dentin conditioning agent, hadalso been taken into consideration as the clinical result of thiskind of study may shed light on the correlation of marginalgap and marginal caries. A similar approach has been carriedout in a recent meta-analysis on the effectiveness of posteriorClass I/II resin restorations [15].
Hybrid composite restorations demonstrated the bestoverall performance (good color match, small number of frac-tures). Macrofilled composites exhibited a significantly lessfavourable color match and microfilled composites showedsignificantly more fractures in Class IV restorations and a sig-nificant loss of anatomical shape. Especially glass ionomerderivates were marred by several shortcomings and may notbe the first choice as permanent filling material to restoredefects of the anterior teeth.
Some of the clinical phenomena can be explained bymaterial-inherent properties. The rapid deterioration of thecolor match of the self-curing macrofilled materials (e.g.Concise and Adaptic) is related, first, to the initiators of theself-curing mechanism (e.g. amines), which are not verycolor-stable, and second to the higher amount of monomerscontained in them compared to the hybrid and microfilledcomposites [18,19]. The fact that the early macrofilled andmicrofilled composites were available in only a limited rangeof shades explains why in some experiments a significantpercentage of restorations did not show a good color matcheven at baseline (see Table 1). Contemporary micro-hybrid andnano-hybrid composites are available in a variety of differentshades with different degrees of opacity and translucencyand are ideal for aesthetic restorations of anterior teeth.However, studies that evaluate these more recent generationsof composite resins in anterior teeth do not appear to havebeen published.
Composite resin materials that are used to build up incisaledges must be very fracture-resistant as high shear forces dur-ing chewing stress the restoration. The meta-analysis showedthat significantly more Class IV restorations exhibited chip-pings and fractures that required the replacement of therestoration than Class III restorations. In fact the medianreplacement frequency was twice for Class IV than for Class
III after 10 years (10% versus 5%). Class IV restorations withmicrofilled composites showed significantly more chippingsand fractures than those with hybrid and macrofillled com-posites. The overall success rate of Class IV restorations,1 ( 2 0 1 5 ) 481–495
however, would have been increased only partly if the micro-filled restorations had been excluded, as three times morerestorations with hybrid composites were included in themeta-analysis than restorations with microfilled composites(see Table 2). The flexural strength of self-curing macrofilledcomposites is comparable to that of contemporary hybridcomposites (>100 MPa) [20,21] and explains why these twotypes of materials exhibited a similar fracture frequency. Sim-ilar to the composites for posterior Class II restorations, a lowflexural strength of the resin material is correlated with a highincidence of chipping and fractures of incisal edgebuild-ups(Class IV). For Class II restorations the ISO standard requires aminimum flexural strength of 80 MPa after 1 week of waterstorage [22]. Clinical studies on Class II restorations with amaterial that had a flexural strength of about 60 MPa showedmore than 20% fractures after only 2 years [23,24]. A min-imum value of flexural strength has not been specified forClass IV restorations. A clinical trial [25], whose results arealso included in this meta-analysis, has shown that materialswith a flexural strength of about 70 MPa such as Durafill [21,26]produced about 30–35% more fractures in Class IV restorationswithin 3 years than materials with a flexural strength of wellabove 100 MPa such as Estilux MF [27]. It appears reasonable todemand that materials for Class IV restorations should offera flexural strength of at least 100 MPa. Microfilled compositesfall short of this value by far [21] and are therefore not suitablefor this indication, as has been demonstrated in the presentmeta-analysis. Also resin-modified glass ionomer cementsand most compomers do not have the mechanical strengthto withstand the shear forces in Class IV cavities. A long-term clinical study, whose data on glass ionomer derivates andcompomers were not included in the present analysis due tothe low number of restorations in each material group, hasshown high fractures rates for these materials in Class IV cav-ities [28]. Fracture toughness is another important physicalparameter that needs to be considered and is closely relatedto flexural strength. Materials in stress-bearing regions shouldhave a fracture toughness of at least 1.2 MPa
√m [25].
Marginal discoloration and detectable margins are the onlyclinically measurable signs for the evaluation of the marginalseal of direct restorations. As most often 100% of the visiblemargin of Class III/IV restorations is located in the enamel, thebonding to enamel is crucial for the prevention of marginaldiscoloration and for a good seal. Enamel etching with 37%phosphoric acid is the best method to establish a microreten-tive pattern that allows a good bonding to ground enamel:the bond strength to cut enamel conditioned with a phos-phoric acid etching systems is superior to self-etching systems[29]. Besides the conditioning method, the orientation of theenamel prisms is of importance. A study has shown that themicro-shear bond strength was higher if enamel was cut in anoblique direction to the orientation of the prisms compared toa parallel direction [30]. The bevelling of the enamel marginprior to conditioning, however, did not significantly influencethe frequency of marginal discoloration in the present meta-analysis, even though there was a tendency of less marginal
staining when the enamel had been bevelled. For all subgroupsthere was a rapid increase in the restorations with stainedmargins. The reason for the insignificant difference betweenbevelled and non-bevelled margin in relation to marginal
3 1
sbpfaobrttb
wrdttsbccettnob
pfietMmameb
rsaatnspiomm
cartfpit
d e n t a l m a t e r i a l s
taining might be the fact that in most studies only a shortevel was prepared. Nowadays, it is often recommended torepare a very broad (=long) bevel, especially on the labial sur-ace, to make the transition between restoration and enamellmost invisible. The broad bevel may also reduce the numberf restorations with marginal staining in the long run. A broadevel may also increase the fracture resistance of Class IV resinestorations as a laboratory study has shown [31]. But no sys-ematic clinical trials have addressed these topics so far. Yet,he advantages of a broad bevel in anterior restorations haseen questioned recently [32].
Another interesting and unexpected result of this reviewas that the overall longevity of the anterior composite resin
estorations included in these studies did not significantlyepend on the type of enamel and dentin conditioning sys-em used, at least not over a period of 5 years. If, however,he enamel was not etched with either phosphoric acid or aelf-etching primer, there was a rapid increase in the num-er of restorations that showed marginal staining as it thease with posterior restorations that do not include an enamelonditioning agent according to a meta-analysis [15]; how-ver, marginal gaps alone are apparently no risk indicator forhe development of caries at the restorative margin Restora-ions that included the application of an enamel etchant butot an enamel bonding agent showed more marginal stainingver time than restorations with enamel etching and enamelonding.
There was a clear tendency that fillings with self-etchingrimers had a higher prevalence of marginal staining thanllings with enamel etching. General practitioners are in gen-ral advised to use phosphoric acid etching on enamel as thisechnique helps to reduce the occurrence of marginal staining.arginal discoloration is usually linked to irregularities in theargin such as gaps, cracks, ditching, etc. Therefore, it is more
ppropriate to clinically evaluate marginal adaptation thanarginal fractures, marginal gaps, etc, as considerable differ-
nces exist between the assessments of marginal adaptationy different evaluators [33–35].
As the median prevalence of marginal discoloration inestorations with enamel etching and bonding was abouteven times higher than that of marginal caries after 5 yearsnd as the existence of marginal gaps or imperfections is usu-lly necessary for the development of marginal discoloration,his is an indication that (1) small marginal gaps per se areot responsible for causing marginal caries and (2) marginaltaining is not indicative of marginal caries. Nevertheless,ractitioners should try to reduce the risk for marginal stain-
ngby etching the enamel with 37% phosphoric acid. Thisperative procedure contributes to a less premature replace-ent of restorations as general practitioners often associatearginal staining with caries at the margins [34–36].The placement of rubber dam was related to less marginal
aries of direct anterior restorations. This is, however, prob-bly a random finding as the number of included studies iselatively low and the individual results might be biased byhe fact that marginal discoloration could have been con-
ounded with marginal caries in some cases. In a recentlyublished meta-analysis on the longevity of Class II compos-te resin restorations there was not less marginal caries inhose studies that used rubber dam [15]. However, significantly
( 2 0 1 5 ) 481–495 493
less bulk fractures were observed in restorations placed withrubber dam compared to those placed without. It has beenspeculated as to whether contamination during placementcould have resulted in a mechanically compromised compos-ite material or the overall quality of the restoration was higherin those studies where dentists used rubber dam. The presentmeta-analysis on anterior restorations did not yield such aninfluence of rubber dam on the occurrence of fractures. Bulkfractures occurred almost invariably in Class IV restorations(s. Fig. 4). As only in 5 of the 7 included studies of Class IVrestorations rubber dam has been placed the influence of rub-ber dam cannot be thoroughly assessed. Also moisture controlis easier in the anterior region than in the posterior region.
The marginal integrity did not depend on the tooth con-ditioning system or method, which confirms the fact thatdetectable margins are not necessarily combined with stainedmargins. There was not even a difference between acid etch-ing and no etching in Class III restorations. As, however, thesetwo methods were not evaluated in the same study, this resultmay be explained by different levels of calibration, which alsomay explain differences between studies that used the sametooth conditioning method.
This variability with regard to the outcome variablesbetween different studies when applying the same opera-tional procedures and materials may be explained by (1)differences between different operators, and/or (2) differenceswhen applying the evaluation criteria. Usually the very grossRyge criteria or modifications of these criteria were appliedor are still applied in clinical trials. In 2007, more refinedand better structured clinical assessment criteria were pub-lished and approved by the FDI [34,35]. The Ryge criteria donot take into account the extension of certain outcome crite-ria, e.g. the percentage of margin with staining or caries, orthe extension of fractures. Therefore, the FDI criteria includeda semi-quantitative approach for certain criteria to be able tobetter differentiate between clinical phenomena.
6. Conclusions
- The absolute failure rate of anterior restorations in generalwas relatively low.
- Class IV restorations showed more fractures than ClassIII restorations, which confirms hypothesis No. 1. Class IVrestorations with hybrid composites showed less fracturesthan microfilled composites, which confirms hypothesis No.3.
- The overall performance of hybrid composites was betterthan that of microfilled composites.
- There was a consistent decrease in color match independentof the type of material. Therefore, hypothesis No. 7 had tobe rejected.
- When the enamel was etched with phosphoric acid, lessdiscoloration at the restorative margins was observed com-pared to restorations that involved other conditioning
systems. Caries adjacent to the restoration was infrequentand not related to any factor evaluated except for the type ofisolation: restorations that were placed with a rubber damshowed less caries at the margins than restorations that
l s 3
r
494 d e n t a l m a t e r i a
were placed without a rubber dam which, however, may becaused by additional confounding factors (staining, etc.).
- Bevelling of enamel had no significant influence on the out-come variables except for the anatomical form, which mightbe a random finding.
- As most of the studies were carried out between 1980 and2000 and as there are only few studies on Class IV restora-tions, more clinical trials with contemporary resin materialsespecially in Class IV cavities are warranted.
For clinicians the implications of the present meta-analysisare as follows:
1. Adhesive system: The dentist should select an adhesivesystem which includes or allows the inclusion of enamelconditioning with 37% phosphoric acid. This reduces theoccurrence of marginal discoloration which, in turn, mayreduce the temptation to prematurely replace restorationse.g. due to the confusion between stained margin andcaries at the margin or due to aesthetic reasons.
2. Restorative material: Hybrid composites can be used forboth Class III and Class IV restorations, while micro-filled composites, compomers and glass ionomer cementsshowed more shortcomings (fractures, impaired esthetics).
Operative procedures: The additional bevelling of theenamel did not result in less marginal staining or improvedmarginal integrity. Whether a (long) bevel improves aestheticsor increases the fracture resistance of Class IV restorations hasnot been systematically investigated. Absolute isolation witha rubber dam is not a prerequisite for long-lasting anteriorrestorations if adequate relative isolation can be ensured.
e f e r e n c e s
[1] Phillips RW. An evaluation of anterior restorative materials.Alumni Bull Sch Dent Indiana Univ 1970:38–42.
[2] Buonocore MG. A simple method of increasing the adhesionof acrylic filling materials to enamel surfaces. J Dent Res1955;34:849–53.
[3] Gilpatrick RO, Ross JA, Simonsen RJ. Resin-to-enamel bondstrengths with various etching times. Quintessence Int1991;22:47–9.
[4] Swift Jr EJ, Perdigao J, Heymann HO. Bonding to enamel anddentin: a brief history and state of the art, 1995.Quintessence Int 1995;26:95–110.
[5] Perdigão J, Duarte Jr S, Lopes MM. Advances in dentinadhesion. Compend Contin Educ Dent 2003;24:10–6.
[6] Bowen RL. Synthesis of silica-resin filling material: progressreport. J Dent Res 1958;37:90.
[7] Roulet J-F. Degradation of dental polymers. Basel: Karger;1987.
[8] Bassiouny MA, Grant AA. A visible light-cured compositerestorative. Clinical open assessment. Br Dent J1978;145:327–30.
[9] Glendor U. Epidemiology of traumatic dental injuries–a 12year review of the literature. Dent Traumatol 2008;24:603–11.
[10] Chadwick B, Dummer P, Dunstan F. A systematic review ofthe longevity of dental restorations. York: NHS Centre forReviews and Dissemination: University of York; 1999.
1 ( 2 0 1 5 ) 481–495
[11] Hickel R, Manhart J. Longevity of restorations in posteriorteeth and reasons for failure. J Adhes Dent 2001;3:45–64.
[12] Brunthaler A, König F, Lucas T, Sperr W, Schedle A. Longevityof direct resin composite restorations in posterior teeth. ClinOral Investig 2003;7:63–70.
[13] Manhart J, Chen H, Hamm G, Hickel R. Buonocore MemorialLecture. Review of the clinical survival of direct and indirectrestorations in posterior teeth of the permanent dentition.Oper Dent 2004;29:481–508.
[14] El Mowafy OM, Lewis DW, Benmergui C, Levinton C.Meta-analysis on long-term clinical performance ofposterior composite restorations. J Dent 1994;22:33–43.
[15] Heintze SD, Rousson V. Clinical effectiveness of direct ClassII restorations–a meta-analysis. J Adhes Dent 2012;14:407–31.
[16] Peumans M, Kanumilli P, De Munck J, Van Landuyt K,Lambrechts P, Van Meerbeek B. Clinical effectiveness ofcontemporary adhesives: a systematic review of currentclinical trials. Dent Mater 2005;21:864–81.
[17] Heintze SD, Ruffieux C, Rousson V. Clinical performance ofcervical restorations—a meta-analysis. Dent Mater2010;26:993–1000.
[18] Cook WD, Chong MP. Colour stability and visual perceptionof dimethacrylate based dental composite resins.Biomaterials 1985;6:257–64.
[19] Tyas MJ. Colour stability of composite resins: a clinicalcomparison. Aust Dent J 1992;37:88–90.
[20] Peutzfeldt A, Asmussen E. Modulus of resilience as predictorfor clinical wear of restorative resins. Dent Mater1992;8:146–8.
[21] Ilie N, Hickel R. Investigations on mechanical behaviour ofdental composites. Clin Oral Investig 2009;13:427–38.
[22] ISO. Dentistry - Polymer-based filling, restorative and lutingmaterials. International Standard 2009;No. 4049:1–27.
[23] Ernst CP, Martin M, Stuff S, Willershausen B. Clinicalperformance of a packable resin composite for posteriorteeth after 3 years. Clin Oral Investig 2001;5:148–55.
[24] Krämer N, Garcia Godoy F, Frankenberger R. Evaluation ofresin composite materials. Part II: in vivo investigations. AmJ Dent 2005;18:75–81.
[25] Tyas MJ. Correlation between fracture properties and clinicalperformance of composite resins in Class IV cavities. AustDent J 1990;35:46–9.
[26] Cobb DS, Vargas MA, Rundle T. Physical properties ofcomposites cured with conventional light or argon laser. AmJ Dent 1996;9:199–202.
[27] Peutzfeldt A, Asmussen E. Mechanical properties of threecomposite resins for the inlay/onlay technique. J ProsthetDent 1991;66:322–4.
[28] van Dijken JW, Pallesen U. Fracture frequency and longevityof fractured resin composite, polyacid-modified resincomposite, and resin-modified glass ionomer cement classIV restorations: an up to 14 years of follow-up. Clin OralInvestig 2010;14:217–22.
[29] De Munck J, Van Meerbeek B, Satoshi I, Vargas M, Yoshida Y,Armstrong S, Lambrechts P, Vanherle G. Microtensile bondstrengths of one- and two-step self-etch adhesives tobur-cut enamel and dentin. Am J Dent 2003;16:414–20.
[30] Shimada J, Tagami J. Effects of regional enamel and prismorientation on resin bonding. Oper Dent 2003;28:20–7.
[31] Tan DE, Tjan AH. Margin designs and fracture resistance ofincisal resin composite restorations. Am J Dent 1992;5:15–8.
[32] Baratieri LN, Ritter AV. Critical appraisal, to bevel or not inanterior composites. J Esthet Restor Dent 2005;17:264–9.
[33] Tobi H, Groen HJ, Kreulen CM, van Amerongen WE. Observervariation in the assessment of resin composite. Dent Mater1998;14:1–5.

3 1
d e n t a l m a t e r i a l s[34] Hickel R, Peschke A, Tyas M, Mjör I, Bayne S, Peters M, HillerKA, Randall R, Vanherle G, Heintze SD. FDI World DentalFederation - clinical criteria for the evaluation of direct andindirect restorations. Update and clinical examples. J AdhesDent 2010;12:259–72.
[35] Hickel R, Roulet JF, Bayne S, Heintze SD, Mjör IA, Peters M,Rousson V, Randall R, Schmalz G, Tyas M, Vanherle G.Recommendations for conducting controlled clinical studiesof dental restorative materials (Science Committee Project2/98 - FDI World Dental Federation). J Adhes Dent2007;9(Supplement 1):121–47.
[36] Sarrett DC. Prediction of clinical outcomes of a restorationbased on in vivo marginal quality evaluation. J Adhes Dent2007;9(Supplement 1):117–20.
[37] Osborne JW, Norman RD, Gale EN. A 12-year clinicalevaluation of two composite resins. Quintessence Int1990;21:111–4.
[38] Schlapbach T, Hotz P, Roulet JF. Ein klinischer Vergleichkonventionell und mikrogefüllter Komposits für KlasseIII-Füllungen - Resultate nach zwei Jahres. SSO SchweizMonatsschr Zahnheilkd 1982;92:667–80.
[39] van Dijken JW. A clinical evaluation of anterior conventional,microfiller, and hybrid composite resin fillings. A 6-yearfollow-up study. Acta Odontol Scand 1986;44:357–67.
[40] Qvist V, Strom C. 11-year assessment of Class-III resinrestorations completed with two restorative procedures.Acta Odontol Scand 1993;51:253–62.
[41] Davis RD, Mayhew RB. A clinical comparison of threeanterior restorative resins at 3 years. J Am Dent Assoc1986;112:659–63.
[42] Crumpler DC, Heymann HO, Shugars DA, Bayne SC,Leinfelder KF. Five-year clinical investigation of oneconventional composite and three microfilled resins inanterior teeth. Dent Mater 1988;4:217–22.
[43] Osborne JW, Berry TG. 3-year clinical evaluation of glassionomer cements as Class III restorations. Am J Dent1990;3:40–3.
[44] Van Dijken JW, Olofsson AL, Holm C. Five year evaluation ofclass III composite resin restorations in cavities pre-treatedwith an oxalic- or a phosphoric acid conditioner. J OralRehabil 1999;26:364–71.
( 2 0 1 5 ) 481–495 495
[45] Van Dijken JW. Longevity of new hybrid restorative materialsin class III cavities. Eur J Oral Sci 1999;107:215–9.
[46] de Araujo MA, Araujo RM, Marsilio AL. A retrospective lookat esthetic resin composite and glass-ionomer Class IIIrestorations: a 2-year clinical evaluation. Quintessence Int1998;29:87–93.
[47] Reusens B, D’Hoore W, Vreven J. In vivo comparison of amicrofilled and a hybrid minifilled composite resin in ClassIII restorations: 2-year follow-up. Clin Oral Investig1999;3:62–9.
[48] Demirci M, Ersev H, Sancakli HS, Topcubasi M. Clinicalevaluation of a polyacid-modified resin composite (Dyract)in Class III cavities: 5-year results. Am J Dent 2006;19:293–6.
[49] Demirci M, Yildiz E, Uysal O. Comparative clinical evaluationof different treatment approaches using a microfilled resincomposite and a compomer in Class III cavities: two-yearresults. Oper Dent 2008;33:7–14.
[50] Ermis RB, Temel UB, Cellik EU, Kam O. Clinical performanceof a two-step self-etch adhesive with additional enameletching in Class III cavities. Oper Dent 2010;35:147–55.
[51] Sheykholeslam Z, Oppenheim M, Houpt MI. Clinicalcomparison of sealant and bonding systems in therestoration of fractured anterior teeth. J Am Dent Assoc1977;95:1140–4.
[52] Dogon IL, Nathanson D, Van Leeuwen MJ. A long-termclinical evaluation of class IV acid-etched composite resinrestorations. Compend Contin Educ Dent 1980;1:385–90.
[53] Roberts MW, Moffa JP, Jenkins WA. Clinical evaluation ofthree acid-etch composite resin systems: two-year report. JAm Dent Assoc 1978;97:829–32.
[54] Shey Z, Oppenheim M. A clinical evaluation of a radiopaquematerial in the restoration of anterior and posterior teeth. JAm Dent Assoc 1979;98:569–71.
[55] Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. The5-year clinical performance of direct composite additions tocorrect tooth form and position I. Esthetic qualities. ClinOral Investig 1997;1:12–8.
[56] Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. The5-year clinical performance of direct composite additions tocorrect tooth form and position. II. Marginal qualities. ClinOral Investig 1997;1:19–26.
Copyright © 2022 FDOKUMEN