
Clinical and Dosimetric Predictors of Late Rectal Syndrome After 3D-CRT for Localized Prostate...
6
Prostate radiotherapy Clinical and dosimetric predictors of late rectal toxicity after conformal radiation for localized prostate cancer: Results of a large multicenter observational study Gianni Fellin a , Claudio Fiorino b, * , Tiziana Rancati c , Vittorio Vavassori d , Micaela Baccolini g , Carla Bianchi d , Emanuela Cagna e , Pietro Gabriele f , Floranna Mauro g , Loris Menegotti a , Angelo Filippo Monti e , Michele Stasi f , Riccardo Valdagni c a Radiotherapy and Medical Physics, Ospedale Santa Chiara, Trento, Italy; b Medical Physics, Ospedale San Raffaele, Milano, Italy; c Prostate program, Scientific Directorate, Fondazione IRCCS Istituto Nazionale dei Tumori, Milano, Italy; d Radiotherapy and Medical Physics, Ospedale di Circolo, Varese, Italy; e Department of Radiotherapy and Medical Physics, Ospedale ‘‘S. Anna”, Como, Italy; f Department of Radiotherapy and Medical Physics, Institute for Cancer Research and Treatment, Candiolo, Italy; g Department of Radiotherapy and Medical Physics, Ospedale Villa Maria Cecilia, Lugo, Italy article info Article history: Received 9 February 2009 Received in revised form 9 September 2009 Accepted 12 September 2009 Available online 12 October 2009 Keywords: Prostate Radiotherapy Rectal toxicity Dose–volume effects abstract Purpose: Assessing the predictors of late rectal toxicity after high-dose conformal radiotherapy for pros- tate cancer. Methods: One thousand one hundred thirty-two patients entered a prospective observational multicen- tric study; late rectal toxicity was evaluated by a self-reported questionnaire. Results concerning bleeding and faecal incontinence of 718/1132 patients with a complete follow-up at 36 months were analysed. The correlation between a number of clinical–dosimetric parameters and moderate/severe toxicity was inves- tigated by univariate and multivariate logistic analyses. Results: Fifty-two (7.2%) and 57/718 (7.9%) patients were scored as moderate/severe bleeders and faecal incontinents, respectively; 19/57 incontinent patients showed persistent incontinence at 36 months. Bleeding was mainly correlated with V75 Gy while severe bleeding was mainly correlated with the pre- vious abdominal/pelvic surgery; a different rectal dose–volume relationship in the two groups of patients (with/without surgery) was found. Moderate/severe acute toxicity was weakly correlated to late bleed- ing. The best predictor of faecal incontinence was acute toxicity (OR = 4 and 7 for chronic and actuarial incontinence, respectively). Conclusion: The application of rectal dose–volume constraints limited the incidence of rectal bleeding. The risk of bleeding may be further reduced by limiting V75 Gy < 5% and, in the case of patients previ- ously submitted to abdominal/pelvic surgery, V70 Gy < 15–20%. Faecal incontinence seems to be mainly a consequential effect after acute toxicity. Ó 2009 Elsevier Ireland Ltd. All rights reserved. Radiotherapy and Oncology 93 (2009) 197–202 Late rectal injury is a major concern in prostate cancer radio- therapy and many studies have been dedicated to the analysis of volume effects searching for a significant correlation between the rectal dose–volume parameters and late toxicity [1–14]. A previ- ously completed retrospective Italian cooperative study (AIRO- PROS 0101) revealed a strong correlation between grades 2 and 3 bleeding and both high and intermediate doses [4,7]. In order to confirm and/or adjust these findings, the National Working Group on Prostate Radiotherapy within the Italian Association of Radia- tion Oncology (AIRO) started a prospective multicenter trial in 2002 (AIROPROS 0102). This prospective trial focused not only on bleeding but also on the whole rectal syndrome, including other ef- fects such as faecal incontinence [15]. In a previously published study, acute toxicity was evaluated [16] and more recently preli- minary findings on late toxicity were reported [17]. In this study, we report the 3-year follow-up results of AIROPROS 0102 and eval- uate the relation between early rectal post-radiation syndrome and late rectal post-radiation syndrome, focusing on a consequential component of late damage [18–20]. Materials and methods Protocol aims, technical procedures and patient data In total, 1132 patients entered the study; the selection criteria were (a) histologically confirmed prostate adenocarcinoma; (b) participating centers using three-dimensional conformal radio- therapy (3DCRT) with prescription doses P70 Gy, at 1.8–2 Gy/fr. Co-morbidities, previous abdominal/pelvic surgery, use of drugs and previous/concomitant loco-regional diseases were registered 0167-8140/$ - see front matter Ó 2009 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.radonc.2009.09.004 * Corresponding author. Address: Medical Physics Department, San Raffaele Institute, Via Olgettina 60, 20132 Milano, Italy. E-mail address: fi[email protected] (C. Fiorino). Radiotherapy and Oncology 93 (2009) 197–202 Contents lists available at ScienceDirect Radiotherapy and Oncology journal homepage: www.thegreenjournal.com
-
Upload
uninsubria -
Category
Documents
-
view
1 -
download
0
Transcript of Clinical and Dosimetric Predictors of Late Rectal Syndrome After 3D-CRT for Localized Prostate...

Radiotherapy and Oncology 93 (2009) 197–202
Contents lists available at ScienceDirect
Radiotherapy and Oncology
journal homepage: www.thegreenjournal .com
Prostate radiotherapy
Clinical and dosimetric predictors of late rectal toxicity after conformal radiationfor localized prostate cancer: Results of a large multicenter observational study
Gianni Fellin a, Claudio Fiorino b,*, Tiziana Rancati c, Vittorio Vavassori d, Micaela Baccolini g, Carla Bianchi d,Emanuela Cagna e, Pietro Gabriele f, Floranna Mauro g, Loris Menegotti a, Angelo Filippo Monti e,Michele Stasi f, Riccardo Valdagni c
a Radiotherapy and Medical Physics, Ospedale Santa Chiara, Trento, Italy; b Medical Physics, Ospedale San Raffaele, Milano, Italy; c Prostate program, Scientific Directorate, FondazioneIRCCS Istituto Nazionale dei Tumori, Milano, Italy; d Radiotherapy and Medical Physics, Ospedale di Circolo, Varese, Italy; e Department of Radiotherapy and Medical Physics, Ospedale‘‘S. Anna”, Como, Italy; f Department of Radiotherapy and Medical Physics, Institute for Cancer Research and Treatment, Candiolo, Italy; g Department of Radiotherapy and MedicalPhysics, Ospedale Villa Maria Cecilia, Lugo, Italy
a r t i c l e i n f o
Article history:Received 9 February 2009Received in revised form 9 September 2009Accepted 12 September 2009Available online 12 October 2009
Keywords:Prostate RadiotherapyRectal toxicityDose–volume effects
0167-8140/$ - see front matter � 2009 Elsevier Irelandoi:10.1016/j.radonc.2009.09.004
* Corresponding author. Address: Medical PhysicInstitute, Via Olgettina 60, 20132 Milano, Italy.
E-mail address: [email protected] (C. Fiorino).
a b s t r a c t
Purpose: Assessing the predictors of late rectal toxicity after high-dose conformal radiotherapy for pros-tate cancer.Methods: One thousand one hundred thirty-two patients entered a prospective observational multicen-tric study; late rectal toxicity was evaluated by a self-reported questionnaire. Results concerning bleedingand faecal incontinence of 718/1132 patients with a complete follow-up at 36 months were analysed. Thecorrelation between a number of clinical–dosimetric parameters and moderate/severe toxicity was inves-tigated by univariate and multivariate logistic analyses.Results: Fifty-two (7.2%) and 57/718 (7.9%) patients were scored as moderate/severe bleeders and faecalincontinents, respectively; 19/57 incontinent patients showed persistent incontinence at 36 months.Bleeding was mainly correlated with V75 Gy while severe bleeding was mainly correlated with the pre-vious abdominal/pelvic surgery; a different rectal dose–volume relationship in the two groups of patients(with/without surgery) was found. Moderate/severe acute toxicity was weakly correlated to late bleed-ing. The best predictor of faecal incontinence was acute toxicity (OR = 4 and 7 for chronic and actuarialincontinence, respectively).Conclusion: The application of rectal dose–volume constraints limited the incidence of rectal bleeding.The risk of bleeding may be further reduced by limiting V75 Gy < 5% and, in the case of patients previ-ously submitted to abdominal/pelvic surgery, V70 Gy < 15–20%. Faecal incontinence seems to be mainlya consequential effect after acute toxicity.
� 2009 Elsevier Ireland Ltd. All rights reserved. Radiotherapy and Oncology 93 (2009) 197–202
Late rectal injury is a major concern in prostate cancer radio-therapy and many studies have been dedicated to the analysis ofvolume effects searching for a significant correlation between therectal dose–volume parameters and late toxicity [1–14]. A previ-ously completed retrospective Italian cooperative study (AIRO-PROS 0101) revealed a strong correlation between grades 2 and 3bleeding and both high and intermediate doses [4,7]. In order toconfirm and/or adjust these findings, the National Working Groupon Prostate Radiotherapy within the Italian Association of Radia-tion Oncology (AIRO) started a prospective multicenter trial in2002 (AIROPROS 0102). This prospective trial focused not only onbleeding but also on the whole rectal syndrome, including other ef-fects such as faecal incontinence [15]. In a previously published
d Ltd. All rights reserved.
s Department, San Raffaele
study, acute toxicity was evaluated [16] and more recently preli-minary findings on late toxicity were reported [17]. In this study,we report the 3-year follow-up results of AIROPROS 0102 and eval-uate the relation between early rectal post-radiation syndrome andlate rectal post-radiation syndrome, focusing on a consequentialcomponent of late damage [18–20].
Materials and methods
Protocol aims, technical procedures and patient data
In total, 1132 patients entered the study; the selection criteriawere (a) histologically confirmed prostate adenocarcinoma; (b)participating centers using three-dimensional conformal radio-therapy (3DCRT) with prescription doses P70 Gy, at 1.8–2 Gy/fr.
Co-morbidities, previous abdominal/pelvic surgery, use of drugsand previous/concomitant loco-regional diseases were registered
198 Predictors of late rectal toxicity after prostate cancer radiotherapy
in a questionnaire filled in before radiotherapy. Information onquality and duration of hormonal therapy, when prescribed, wasalso recorded.
Information concerning volume definition, planning and treat-ment modalities as well as the distribution of the main clinicalparameters of the whole population has previously been reportedin detail [16,17]. Of particular importance is the delineation ofthe rectum: an anatomically based definition (from the anus tothe point where it turns into the sigmoid) was used by the partic-ipating centers and validated by a dummy run investigation [18].The dose–volume histogram (DVH) of the solid rectum was consid-ered, as discussed elsewhere [4,7,17].
The current analysis refers to 718 patients with a 36-monthcomplete follow-up.
For each patient the prescribed dose for each irradiated volume(pelvis, seminal vesicles, and prostate), maximum and mean rectaldoses were considered; rectal DVHs of the whole treatment wererecorded for all patients and the percent fractions of rectum receiv-ing more than 20, 30, 40, 50, 60, 70, 75 Gy (named V20 Gy–V75 Gy)were considered. Tables 1 and 2 show the distribution of clinical,dosimetric and technical parameters in the subset of patients con-sidered in the present analysis.
Self-assessed questionnaire-scored toxicity: endpoints
A self-administrated questionnaire was used to score rectal andintestinal toxicities: it had to be filled by the patient before thetreatment (basal), within 1 month from the end of the therapyand then every 6 months up to 3 years after completion of thetherapy.
The basal and the first post-treatment questionnaires were alsoused to analyse acute toxicity and the results have been previouslypublished [16]. The questionnaire (the English version is reportedin Appendix 1 of the paper by Fiorino et al. [17]) was previously
Table 1Patient’s characteristics.
Yes No Missing
Diabetes 45 (6.3%) 668(93.7%)
5
Hormonal therapy 558(77.9%)
158(22.1%)
2
Haemorrhoids 151(21.2%)
561(78.8%)
6
Use of anti-coagulants/anti-aggregants
150 (21.0%) 563 (79.0%) 5
Use of anti-hypertensives 334(46.8%)
379(53.2%)
5
Previous abdominal surgery 69 (9.7%) 644 (90.3%) 5Pelvic node irradiation 39 (5.4%) 679
(94.6%)0
Seminal vesicles irradiation 547(76.5%)
168(23.5%)
3
Table 2Distribution of dosimetric parameters.
Minimum Maximum
Dose to pelvic nodes (Gy) 39.6 52.0Dose to seminal vesicles (Gy) 19.8 81.0ICRU dose (Gy) 70.0 81.6Mean rectal dose (Gy) 11.6 69.1Maximum rectal dose (Gy) 63.6 85.2V50 Gy (%) 7.1 100.0V60 Gy (%) 3.7 89.0V70 Gy (%) 0 68.5V75 Gy (%) 0 40.3
validated in a pilot study with a subset of 50 patients previouslyscored with the SOMA/LENT, checking if the results of the ques-tionnaires were consistent with the previously physician-assessedscores.
For the current analysis we focused on moderate/severe (grade2–3) faecal incontinence and late rectal bleeding and we groupedsymptoms as follows:
Late rectal bleeding (lrb)Question 9: grade 2 if bleeding >2 times/week (and the basal
questionnaire indicated no bleeding) and grade 3 if daily bleedingwas experienced (and the basal questionnaire indicates no bleed-ing or bleeding 62 time/week).
Questions 12 and 13 were used to define grade 3 lrb using twodifferent definitions:
(a) grade 2 if the patient underwent 1 or 2 blood transfusionsand/or laser coagulations and grade 3 if more than 2 proce-dures were necessary (in the following we will refer to thisdefinition as ‘‘G3a lrb”);
(b) grade 3 if any number of blood transfusions and/or lasercoagulations was necessary (in the following we will referto this definition as ‘‘G3b lrb”).
We defined as bleeders those patients showing this event at anytime 5 months after 3DCRT completion, even if they recovered, asshown by the questionnaires. This was aimed at better comparingthe results with the ‘‘actuarial” definition of bleeding reported inmost studies.
Late faecal incontinenceQuestions 5 and 6: grade 2 if unintentional stool/mucous dis-
charge was ‘‘often” experienced (and the basal questionnaire indi-cated no unintentional stool discharge) and grade 3 ifunintentional stool/mucous discharge was reported as happeningevery day.
Question 7: grade 2 if using sanitary pads 62 times/week (andthe basal questionnaire indicated no use of sanitary pads) andgrade 3 if sanitary pads were used more than 2 times/week (andthe basal situation was no use of sanitary pads).
Concerning late faecal incontinence, two endpoints wereanalysed:
(a) patients showing grade 2 or grade 3 faecal incontinence atany time 5 months after 3DCRT completion, even if theyrecovered (G2–G3 ‘‘actuarial” faecal incontinence);
(b) patients showing grade 2 or grade 3 faecal incontinence atany time 5 months after 3DCRT completion and who nevercompletely recovered (i.e. after a G2–G3 event, at least G1incontinence was recorded till 36 month follow-up, G2–G3‘‘chronic” faecal incontinence).
I quartile Median III quartile
45.0 45.0 50.060.0 66.6 74.072.0 74.0 76.045.2 51.5 56.272.7 74.8 77.037.5 49.3 63.026.8 36.0 46.911.3 18.3 25.0
0 0.6 7.0
LATE G2-G3 RECTAL BLEEDING
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0 2 4 6 8 10 12 14 16 18 20 22 24
Rectal V75 Gy
Co
mp
licat
ion
Pro
bab
ility
experimental incidence, all patients
logistic regression, all patients
2/17
9/667/608/82
4/62
5/120
17/311
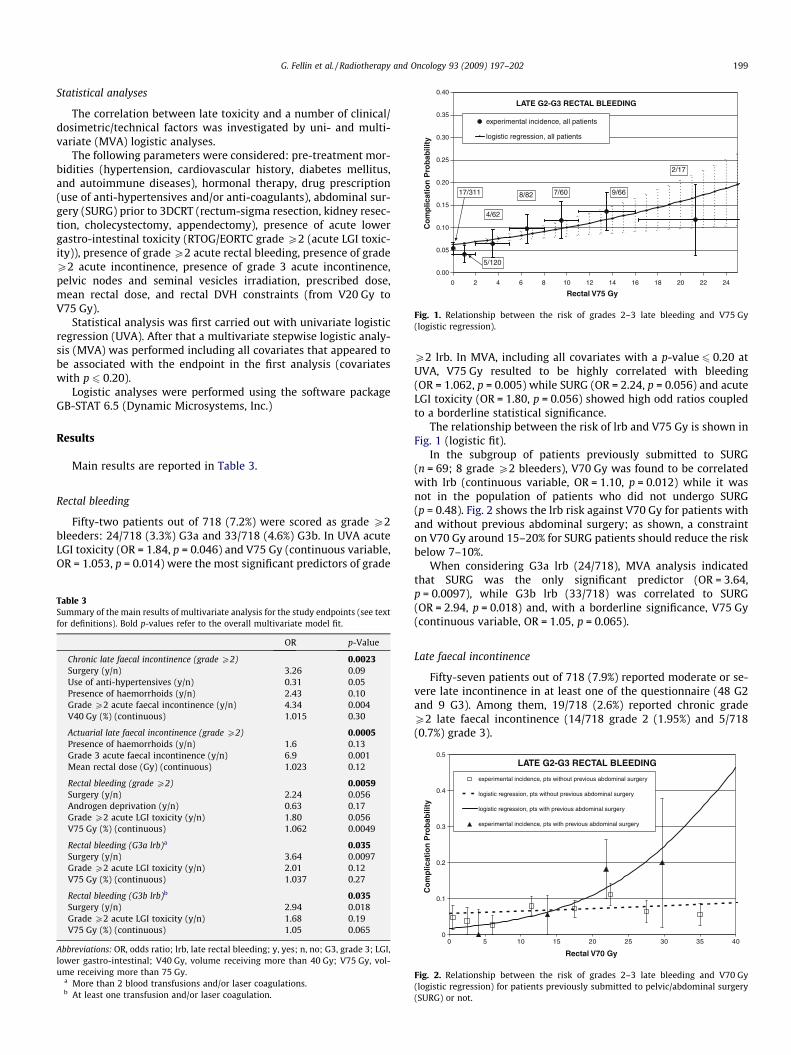
ig. 1. Relationship between the risk of grades 2–3 late bleeding and V75 Gyogistic regression).
G. Fellin et al. / Radiotherapy and Oncology 93 (2009) 197–202 199
Statistical analyses
The correlation between late toxicity and a number of clinical/dosimetric/technical factors was investigated by uni- and multi-variate (MVA) logistic analyses.
The following parameters were considered: pre-treatment mor-bidities (hypertension, cardiovascular history, diabetes mellitus,and autoimmune diseases), hormonal therapy, drug prescription(use of anti-hypertensives and/or anti-coagulants), abdominal sur-gery (SURG) prior to 3DCRT (rectum-sigma resection, kidney resec-tion, cholecystectomy, appendectomy), presence of acute lowergastro-intestinal toxicity (RTOG/EORTC grade P2 (acute LGI toxic-ity)), presence of grade P2 acute rectal bleeding, presence of gradeP2 acute incontinence, presence of grade 3 acute incontinence,pelvic nodes and seminal vesicles irradiation, prescribed dose,mean rectal dose, and rectal DVH constraints (from V20 Gy toV75 Gy).
Statistical analysis was first carried out with univariate logisticregression (UVA). After that a multivariate stepwise logistic analy-sis (MVA) was performed including all covariates that appeared tobe associated with the endpoint in the first analysis (covariateswith p 6 0.20).
Logistic analyses were performed using the software packageGB-STAT 6.5 (Dynamic Microsystems, Inc.)
Results
Main results are reported in Table 3.
Rectal bleeding
Fifty-two patients out of 718 (7.2%) were scored as grade P2bleeders: 24/718 (3.3%) G3a and 33/718 (4.6%) G3b. In UVA acuteLGI toxicity (OR = 1.84, p = 0.046) and V75 Gy (continuous variable,OR = 1.053, p = 0.014) were the most significant predictors of grade
Table 3Summary of the main results of multivariate analysis for the study endpoints (see textfor definitions). Bold p-values refer to the overall multivariate model fit.
OR p-Value
Chronic late faecal incontinence (grade P2) 0.0023Surgery (y/n) 3.26 0.09Use of anti-hypertensives (y/n) 0.31 0.05Presence of haemorrhoids (y/n) 2.43 0.10Grade P2 acute faecal incontinence (y/n) 4.34 0.004V40 Gy (%) (continuous) 1.015 0.30
Actuarial late faecal incontinence (grade P2) 0.0005Presence of haemorrhoids (y/n) 1.6 0.13Grade 3 acute faecal incontinence (y/n) 6.9 0.001Mean rectal dose (Gy) (continuous) 1.023 0.12
Rectal bleeding (grade P2) 0.0059Surgery (y/n) 2.24 0.056Androgen deprivation (y/n) 0.63 0.17Grade P2 acute LGI toxicity (y/n) 1.80 0.056V75 Gy (%) (continuous) 1.062 0.0049
Rectal bleeding (G3a lrb)a 0.035Surgery (y/n) 3.64 0.0097Grade P2 acute LGI toxicity (y/n) 2.01 0.12V75 Gy (%) (continuous) 1.037 0.27
Rectal bleeding (G3b lrb)b 0.035Surgery (y/n) 2.94 0.018Grade P2 acute LGI toxicity (y/n) 1.68 0.19V75 Gy (%) (continuous) 1.05 0.065
Abbreviations: OR, odds ratio; lrb, late rectal bleeding; y, yes; n, no; G3, grade 3; LGI,lower gastro-intestinal; V40 Gy, volume receiving more than 40 Gy; V75 Gy, vol-ume receiving more than 75 Gy.
a More than 2 blood transfusions and/or laser coagulations.b At least one transfusion and/or laser coagulation.
F(l
P2 lrb. In MVA, including all covariates with a p-value 6 0.20 atUVA, V75 Gy resulted to be highly correlated with bleeding(OR = 1.062, p = 0.005) while SURG (OR = 2.24, p = 0.056) and acuteLGI toxicity (OR = 1.80, p = 0.056) showed high odd ratios coupledto a borderline statistical significance.
The relationship between the risk of lrb and V75 Gy is shown inFig. 1 (logistic fit).
In the subgroup of patients previously submitted to SURG(n = 69; 8 grade P2 bleeders), V70 Gy was found to be correlatedwith lrb (continuous variable, OR = 1.10, p = 0.012) while it wasnot in the population of patients who did not undergo SURG(p = 0.48). Fig. 2 shows the lrb risk against V70 Gy for patients withand without previous abdominal surgery; as shown, a constrainton V70 Gy around 15–20% for SURG patients should reduce the riskbelow 7–10%.
When considering G3a lrb (24/718), MVA analysis indicatedthat SURG was the only significant predictor (OR = 3.64,p = 0.0097), while G3b lrb (33/718) was correlated to SURG(OR = 2.94, p = 0.018) and, with a borderline significance, V75 Gy(continuous variable, OR = 1.05, p = 0.065).
Late faecal incontinence
Fifty-seven patients out of 718 (7.9%) reported moderate or se-vere late incontinence in at least one of the questionnaire (48 G2and 9 G3). Among them, 19/718 (2.6%) reported chronic gradeP2 late faecal incontinence (14/718 grade 2 (1.95%) and 5/718(0.7%) grade 3).
LATE G2-G3 RECTAL BLEEDING
0
0.1
0.2
0.3
0.4
0.5
0 5 10 15 20 25 30 35 40
Rectal V70 Gy
Co
mp
licat
ion
Pro
bab
ility
experimental incidence, pts without previous abdominal surgery
logistic regression, pts without previous abdominal surgery
logistic regression, pts with previous abdominal surgery
experimental incidence, pts with previous abdominal surgery
ig. 2. Relationship between the risk of grades 2–3 late bleeding and V70 Gyogistic regression) for patients previously submitted to pelvic/abdominal surgeryURG) or not.
F(l(S
100
200 Predictors of late rectal toxicity after prostate cancer radiotherapy
In UVA, actuarial late incontinence was highly correlated to se-vere acute faecal incontinence (i.e. use of sanitary pads for acute fae-cal incontinence, OR = 7.6, p = 0.00001), with mean rectal dose(OR = 1.03, p = 0.064) and presence of haemorrhoids (OR = 1.8,p = 0.045) being less significant. At MVA, acute severe incontinenceconfirmed to be the most predictive parameter (OR = 6.9, p = 0.001).
In UVA, chronic late incontinence was highly correlated to gradeP2 acute faecal incontinence (OR = 4.97, p = 0.0011), while use ofanti-hypertensives (OR = 0.39, p = 0.06), presence of haemorrhoids(OR = 1.2, p = 0.11) and V40 Gy (OR = 1.018, p = 0.16) play a minorrole. SURG was not statistically significant (OR = 1.8, p = 0.37),nonetheless it was included in the MVA, due to its high odd ratioand its strength in predicting lrb. At MVA the most predictiveparameters was found to be grade P2 acute incontinence(OR = 4.34, p = 0.004), while SURG (OR = 3.26, p = 0.09), the pres-ence of haemorrhoids (OR = 2.43, p = 0.10) and the use ofanti-hypertensives (protective factor, OR = 0.31, p = 0.05) were ofborderline significance.
Grade 3 chronic late faecal incontinence (5 events) was corre-lated only with grade P2 acute incontinence (OR = 4.56, p = 0.097).
Discussion
Bleeding: dose–volume relationships
In the recent years a number of consistent results on the dose–volume effect of rectal bleeding appeared in the literature, mostdata confirming the prevalently serial behaviour of the rectum[9,12,13,21,22]; this means that relatively small fractions of rec-tum irradiated at ‘‘high” dose are the main cause of bleeding. Ourfindings confirm that the ‘‘high” dose region of the DVH clearly cor-related with bleeding: the most predictive parameter was V75 Gy.(Fig. 3 shows the mean cumulative DVH for the bleeder and non-bleeder groups.)
The poor correlation between the remaining portion of the DVHand lrb may appear to be in contrast with some recently reportedresults [1,2,5,7–11,17]; however, this is not surprising if weconsider that all institutions participating to the study applieddose–volume constraints derived by our previous retrospectivestudy [4,7,9], limiting a priori the value of V40 Gy–V70 Gy.
The strict application of DVH constraints is also the main causeof the reduction of the number of bleeding events compared to thepast; the actual suggestion of a ‘‘reliable” constraint for V75 Gy(<5%) may help in further reducing this risk.
It is important to underline that, even when optimal constraintsare applied, bleeding can occur due to genetic susceptibility [23,24]and/or concomitant clinical factors, as surgery (discussed later),potentially associated to a higher radiosensitivity and/or reducedrepair capacity.
0
5
10
15
20
25
30
35
40
45
50
50 55 60 65 70 75 80 85 90
Dose (Gy)
% V
olu
me
mean cumulative dose-volume histogramfor G2-G3 BLEEDING PATIENTS
mean cumulative dose-volume histogramfor NON-BLEEDING PATIENTS
Fig. 3. Mean cumulative dose–volume histogram (DVH) for patients with (contin-uous line) and without (dotted line) G2–G3 late rectal bleeding. Thick lines: meanDVH in the group, thin line: one-standard deviation area for DVHs in the group.
Even the differences between the current 3-year results on 718patients and the 2-year ad-interim analysis [17] on about 500 pa-tients of the same trial should be considered in this view. In theprevious analysis V40 Gy–V70 Gy were predictors of bleedingwhile this correlation is much poorer in current analysis (dataunreported, p-values between 0.1 and 0.2 for V65 Gy–V70 Gy).On the other hand, the result concerning surgery was substantiallyconfirmed, including the different dose–volume effect (V70 Gy) be-tween SURG and non-SURG patients. One of the possible explana-tion of these differences is the increased presence of patients withV75 Gy > 5–10% in the current population compared to the previ-ous ad-interim analysis; this probably enhanced the role ofV75 Gy (and of SURG) over V70 Gy compared to the populationanalysed in the ad-interim analysis.
Faecal incontinence: dose–volume relationships
The incidence of moderate/severe faecal incontinence appearsto be slightly higher than bleeding. This relatively high figurecompared to the risk of bleeding is in agreement with a recentlypublished study taking specifically incontinence into consider-ation [12].
On the other hand, the poor knowledge of this relatively rare ef-fect may also be due to the difficulty in claiming radiation as thecause of this impairment in an aged population, especially outsidecontrolled questionnaire-based prospective studies.
From the point of view of dose–volume relationship, our re-sults are consistent with the findings of our previous ad-interimanalysis and with the work of Peeters et al. [12,17] that showeda prevalently parallel behaviour of the rectum for this end point.Mean dose was found to be the most predictive dosimetric factoralthough not reaching statistical significance at multivariate anal-ysis (Fig. 4 shows the mean DVH for patients experiencing chroniclate faecal incontinence and for patients not reporting thistoxicity).
The existence of ‘‘spatial” effects (i.e. some portions of the rec-tum exhibiting enhanced sensitivity with respect to others) hasbeen demonstrated in the induction of incontinence [11,25–27]and could be the cause of the weak correlation between DVHs ofthe whole rectum and incontinence.
More information will be available when the rectal dose mapanalysis currently in progress, which includes spatial effects, isaccomplished.
Impact of clinical variables
The impact of previous abdominal/pelvic surgery on both rectalbleeding and incontinence was also reported in our previous anal-
0
10
20
30
40
50
60
70
80
90
20 30 40 50 60 70 80 90Dose (Gy)
% V
olum
e
mean cumulative dose-volume histogram forG2-G3 FECAL INCONTINENCE PATIENTS
mean cumulative dose-volume histogram forNON-INCONTINENCE PATIENTS
ig. 4. Mean cumulative dose–volume histogram (DVH) for patients with (contin-ous line) and without (dotted line) G2–G3 chronic late faecal incontinence. Thicknes: mean DVH in the group, thin line: one-standard deviation area for DVHs ine group.
Fulith

G. Fellin et al. / Radiotherapy and Oncology 93 (2009) 197–202 201
ysis [17] considering 518 patients with a 2-year follow-up and it isconsistent with few other reports [12,14,28].
Previous surgery appears to be the best predictor of severe latebleeding suggesting that for patients who underwent abdominal/pelvic surgery before 3DCRT an impairment of the repair capacityof the rectum due to regional (neurological and/or vascular) effectsmight be expected. Interestingly, surgery is also a predictor of per-sistent incontinence (OR � 3). These findings are in quite goodagreement with those of Peeters et al. [12].
Two recent clinical studies described a possible consequentialeffect in prostate cancer radiation therapy [20,25]. In our dataset,the consequential effect between acute and late toxicities is moreevident for incontinence (OR � 4–5) rather than for bleeding(OR � 2).
On the other hand, in our previous report on acute toxicity [16],the main predictors of acute severe faecal incontinence and in-creased stool frequency were assessed; a set of nomograms to pre-dict these symptoms was developed [29] and it can be used toreduce the risk of acute incontinence with the potential of reducingthe risk of late incontinence, seeing the prevalently consequentialnature of this effect.
Concerning androgen deprivation, no clear correlation wasdemonstrated; this issue is quite controversial in the literature[20,30,31].
The presence of haemorrhoids has been rarely consideredamong the risk factors of late rectal toxicity: from our study haem-orrhoids seem to play some role in the risk of late faecal inconti-nence. Interestingly, the use of anti-hypertensive agents was aprotective factor for persistent faecal incontinence; in our reporton acute toxicity [16] we found a correlation between the use ofanti-hypertensive agents and less diarrhea. These results are inagreement with some vascular protective effect of anti-hyperten-sive drugs, as suggested by Liu et al. [30].
The impact of diabetes was nearly irrelevant in the presentstudy although a number of reports have shown some correlationbetween bleeding and diabetes [29,32,33]. Perhaps the relativelysmall fraction of diabetic patients and the practice of reducingthe prescribed dose for these patients did not help in better clari-fying this point.
Conclusions
In summary, the main results of this study are:
– The application of previously assessed dose–volume constraints[4,6,7,9] was efficient in reducing the risk of late bleeding; as aconsequence, no clear volume effect could be found in this seriesin the range of doses 670 Gy.
– The rectum acts as a prevalently ‘‘serial” organ when consid-ering late bleeding: combining the previously suggested con-straints (V50 < 55%, V60 < 40%, V70 < 25%) with V75 Gy < 5%is expected to be associated with a small risk of late bleeding.
– Previous abdominal/pelvic surgery is correlated to rectal toxic-ity; in particular a different dose–volume effect for bleedingcan be appreciated in patients having experienced surgery ornot experienced surgery before radiotherapy.
– Acute toxicity was independently correlated to late inconti-nence, suggesting the existence of a consequential componentfor this endpoint.
– The rectum seems to act as a more parallel organ when consid-ering incontinence, although the statistical power of DVHparameters (i.e. Dmean; V40 Gy) was quite poor.
– Now, we are working on these results to build user-friendlytools, like nomograms, that might support clinicians in predict-ing and estimating late radiation toxicities [29,34].
Acknowledgements
Fondazione Monzino is gratefully acknowledged for its supportto the AIRO Working Group on Prostate Radiotherapy. T. Magnaniis acknowledged for her technical assistance. All institutions in-volved in the study are gratefully acknowledged for their enthusi-astic support.
Varese
Ospedale di Circolo V. Vavassori C. Bianchi Lugo Villa Maria Cecilia F.A. Mauro M. Baccolini Candiolo IRCCS P. Gabriele M. Stasi Como Ospedale Sant’Anna E. Cagna A. Monti Trento Ospedale Santa Chiara G. Fellin L. Menegotti Catania REM C. Greco G. Sabini Bologna Osp. Sant’OrsolaMalpighi
B. Iacopino F. RomaniBologna
Ospedale Bellaria G. Frezza S. Boni Ivrea Ospedale Civile ASL9 G. Girelli M. Pasquino Monza Policlinico G. Nava M. Mapelli Firenze Casa di Cura S. Chiara F.Casamassima
L. MasiGenova
IST S. Barra F. Foppiano Monza Ospedale San Gerardo S. Meregalli E. DePonti Carrara Civico Ospedale A.Tagliagambe
M. LuxardoRoma
Osp. Fatebenefratelli F. Tortoreto S.DelleCanneCatanzaro
Ospedale P. Ciaccio E. Mazzei M. Licandro Lecco Ospedale A. Manzoni A. Colombo F. Declich BustoArsizio
Ospedale Civile A. Storace D. CorlettoMilano
Istituto S. San Raffaele C. Cozzarini C. Fiorino Bologna Ospedale Galvani F. Bunkheila F. Romani Udine Osp. Santa Maria M. M. Signor E. MorettiReferences
[1] Boersma LJ, van den Brink M, Allison M, et al. Estimation of the incidence oflate bladder and rectum complications after high-dose (70–78 Gy) conformalradiotherapy for prostate cancer, using dose–volume histograms. Int J RadiatOncol Biol Phys 1998;41:83–92.
[2] Skwarchuk MW, Jackson A, Zelefsky MJ, et al. Late rectal toxicity afterconformal radiotherapy of prostate cancer (I): multivariate analysis and doseresponse. Int J Radiat Oncol Biol Phys 2000;47:103–13.
[3] Storey MR, Pollack A, Zagars G, et al. Complications from radiotherapy doseescalation in prostate cancer: preliminary results of a randomized trial. Int JRadiat Oncol Biol Phys 2000;48:635–42.
[4] Fiorino C, Cozzarini C, Vavassori V, et al. Relationships between DVHs and laterectal bleeding after radiotherapy for prostate cancer: analysis of a large groupof patients pooled from three institutions. Radiother Oncol 2002;64:1–12.
[5] Huang EH, Pollack A, Levy L, et al. Late rectal toxicity: dose–volume effects ofconformal radiotherapy for prostate cancer. Int J Radiat Oncol Biol Phys2002;54:1009–19.
[6] Cozzarini C, Fiorino C, Ceresoli GL, et al. Significant correlation between rectalDVH and late rectal bleeding in patients treated after radical prostatectomywith conformal or conventional radiotherapy (66.6–70.2 Gy). Int J Radiat OncolBiol Phys 2003;55:688–94.
[7] Fiorino C, Sanguineti G, Cozzarini C, et al. Rectal dose–volume constraints inhigh-dose conformal radiotherapy for localized prostate cancer. J Radiat OncolBiol Phys 2003;57:953–62.
[8] Zapatero A, Garcia-Vicente F, Modolell I, et al. Impact of mean rectal dose onlate rectal bleeding after conformal radiotherapy for prostate cancer: dose–volume effect. Int J Radiat Oncol Biol Phys 2004;59:1343–51.
[9] Rancati T, Fiorino C, Gagliardi G, et al. Fitting late rectal bleeding data usingdifferent NTCP models: results from an Italian multi-centric study(AIROPROS0101). Radiother Oncol 2004;73:21–32.
[10] Vargas C, Martinez A, Kestin LL, et al. Dose–volume analysis of predictors forchronic rectal toxicity after treatment of prostate cancer with adaptive image-guided radiotherapy. Int J Radiat Oncol Biol Phys 2005;62:1297–308.
[11] Peeters STH, Lebesque JV, Heemsbergen WD, et al. Localized volume effects forlate rectal and anal toxicity after radiotherapy for prostate cancer. Int J RadiatOncol Biol Phys 2006;64:1151–61.
[12] Peeters STH, Hoogeman M, Heemsbergen WD, et al. Rectal bleeding, fecalincontinence and high stool frequency after conformal radiotherapy for

202 Predictors of late rectal toxicity after prostate cancer radiotherapy
prostate cancer: normal tissue complication probability modeling. Int J RadiatOncol Biol Phys 2006;66:11–9.
[13] Söhn M, Yan D, Liang J, Meldolesi E, Vargas C, Alber M. Incidence of late rectalbleeding in high-dose conformal radiotherapy of prostate cancer usingequivalent uniform dose-based and dose–volume-based normal tissuecomplication probability models. Int J Radiat Oncol Biol Phys2007;26:1066–73.
[14] Van der Laan HP, van der Bergh A, Schilstra C, et al. Grading-system-dependentvolume effects of late radiation induced rectal toxicity after curativeradiotherapy for prostate cancer. Int J Radiat Oncol Biol Phys 2008;70:1138–45.
[15] Denham JW, O’Brien PC, Dunstan R, et al. Is there more than one late radiationproctitis syndrome? Radiother Oncol 1999;51:43–53.
[16] Vavassori V, Fiorino C, Rancati T, et al. Predictors for rectal and intestinal acutetoxicities during prostate cancer high-dose 3D-CRT: results of a prospectivemulticenter study. Int J Radiat Oncol Biol Phys 2007;66:1401–10.
[17] Fiorino C, Fellin G, Rancati T, et al. Clinical and dosimetric predictors of laterectal syndrome after 3DCRT for localized prostate cancer: preliminary resultsof a multicenter prospective study. Int J Radiat Oncol Biol Phys2008;70:1130–7.
[18] Foppiano F, Fiorino C, Frezza G, et al. The impact of contouring uncertainty onrectal 3D dose–volume data: results of a dummy run in a multicenter trial(AIROPROS01-02). Int J Radiat Oncol Biol Phys 2003;57:573–9.
[19] Heemsbergen WD, Peeters STH, Koper PCM, et al. Acute and lategastrointestinal toxicity after radiotherapy in prostate cancer patients:consequential late damage. Int J Radiat Oncol Biol Phys 2006;66:3–10.
[20] Zelefsky M, Levin E, Hunt M, et al. Incidence of late rectal and urinary toxicitiesafter three-dimensional conformal radiotherapy and intensity-modulatedradiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys2008;70:1124–9.
[21] Tucker SL, Dong L, Bosch WR, et al. Fit of a generalized Lyman normal tissuecomplication probability (NTCP) model to grade P2 late rectal toxicity datafrom patients treated on protocol RTOG 94-06. Int J Radiat Oncol Biol Phys2007;69:S8–9.
[22] Rancati T, Fiorino C, Valvassori V, et al. Late rectal bleeding after conformalradiotherapy for prostate cancer: NTCP modeling. Radiother Oncol2008;88:S332–3.
[23] Cesaretti JA, Stock RG, Atencio DP, et al. A genetically determined dose–volume histogram predicts for rectal bleeding among patients treated withprostate brachytherapy. Int J Radiat Oncol Biol Phys 2007;68:1410–6.
[24] Valdagni R, Rancati T, Ghilotti M, et al. To bleed or not to bleed. A predictionbased on individual gene profiling combined with dose–volume histogramshapes in prostate cancer patients undergoing three-dimensional conformalradiation therapy. Int J Radiat Oncol Biol Phys 2009;74:1431–40.
[25] Heemsbergen WD, Hoogeman MS, Hart GA, et al. Gastrointestinal toxicity andits relation to dose distributions in the anorectal region of prostate cancerpatients treated with radiotherapy. Int J Radiat Oncol Biol Phys 2005;61:1011–8.
[26] Vordemark D, Schwab M, Ness-Duurdoumas R, et al. Association of anorectaldose–volume histograms and impaired fecal continence after 3D conformalradiotherapy for carcinoma of the prostate. Radiother Oncol 2003;69:209–14.
[27] al Abany M, Helgason AR, Agren Cronqvist AK, et al. Dose to the anal-sphincterregion and risk of fecal leakage. Acta Oncol 2004;43:117–8.
[28] Smit WG, Helle Pa, van Putten WL, et al. Late radiation damage in prostatecancer patients treated by high dose external radiotherapy in relation to rectaldose. Int J Radiat Oncol Biol Phys 1990;18:23–9.
[29] Valdagni R, Rancati T, Fiorino C, et al. Development of a set of nomograms topredict acute lower gastrointestinal toxicity for prostate cancer 3D-CRT. Int JRadiat Oncol Biol Phys 2008;71:1065–173.
[30] Liu M, Pickles T, Agranovich A, et al. Impact of neoadjuvant androgen ablationand other factors on late toxicity after external beam radiotherapy. Int J RadiatOncol Biol Phys 2004;58:59–67.
[31] Peeters STH, Hoogeman MS, Heemsbergen WD, et al. Volume and hormonaleffects for acute side effects of rectum and bladder during conformalradiotherapy for prostate cancer. Int J Radiat Oncol Biol Phys 2005;63:1142–52.
[32] Herold DM, Hanlon AL, Hanks GE. Diabetes mellitus: a predictor for lateradiation morbidity. Int J Radiat Oncol Biol Phys 1999;43:475–9.
[33] Denham JW, Hauer-Jensen M. The radiotherapeutic injury – a complex‘‘wound”. Radiother Oncol 2002;63:129–45.
[34] Valdagni R, Rancati T, Fiorino C. Predictive models of toxicity in prostatecancer external radiotherapy: clinical issues. Cancer 2009;115:3141–9.




![[Magnetic resonance and extramural vascular invasion in patients with rectal cancer and liver metastases]](https://static.fdokumen.com/doc/165x107/63379f4e65077fe2dd042c38/magnetic-resonance-and-extramural-vascular-invasion-in-patients-with-rectal-cancer.jpg)















