
Herbal remedies used for the treatment of infertility in males ...
Upload
khangminh22Category
view
1download
0
Umeå University Medical DissertationsNew Series No 1255 ISSN 0346-6612 ISBN 978-91-7264-759-6
Chlamydia trachomatis as a risk factor for infertility in women and men, and ovarian tumor development
Annika Idahl2009
Department of Clinical Sciences, Obstetrics and GynecologyDepartment of Medical Biosciences, PathologyUmeå University, SE-901 87 Umeå, Sweden

Detta verk skyddas enligt lagen om upphovsrätt (URL 1960:729)© Annika Idahl 2009New Series No 1255ISBN 978-91-7264-759-6ISSN 0346-6612Produced by Print & Media, Umeå University, Umeå 2009: 2006271
Umeå, Sweden 2009

To my familywith love


“Research is to see what everybody else has seen, and to think what nobody else has thought”Albert Szent-Gyorgyi1937 Nobel laureate, Medicine


Abstract
Background: Chlamydia trachomatis in women is a risk factor for tubal factor infertility and extra uterine pregnancies, but the impact of a C. trachomatis infection on male fertility is unclear. It is also hypothesized that persistent infection with C. trachomatis, or other mi-croorganisms, might initiate/promote ovarian tumor development. The aims of the thesis were to study whether C. trachomatis serum antibodies in women and men had an impact on in-fertility diagnoses, semen characteristics, pregnancy rates and pregnancy outcomes; further-more, to explore associations of C. trachomatis, and Mycoplasma genitalium, plasma anti-bodies with epithelial ovarian cancer and borderline ovarian tumors, as well as the presence of C. trachomatis bacteria, and other microorganisms, in ovarian tissues.
Materials and methods: Papers I and II: 244/226 infertile couples were tested for serum C. trachomatis IgG, IgA, IgM and chlamydial Heat Shock Protein 60 (cHSP60) IgG antibodies. C. trachomatis IgG positive couples were also tested for C. trachomatis DNA in a urine sample. The follow-up period was 14-54 months. 244 spontaneously pregnant women were also tested for serum C. trachomatis IgG antibodies. Papers III and IV: Plasma samples from 291 women with epithelial ovarian cancer, borderline ovarian tumors and benign conditions, and plasma samples from 271 healthy controls, were analyzed for C. trachomatis IgG, IgA and cHSP60-1 IgG and M. genitalium IgG antibodies. Ovarian tissues from 186 women with benign ovaries, borderline ovarian tumors and epithelial ovarian cancer, as well as tissues from the contra lat-eral ovary in 126 women, were analyzed for the presence of C. trachomatis, M. genitalium, Neisseria gonorrhoeae, HPV and the polyoma viruses BKV and JCV with nucleic acid ampli-fication tests.
Results: Papers I and II: The prevalence of C. trachomatis IgG antibodies was higher among infertile than fertile women, and there were 9 couples with ongoing C. trachomatis infections. In men, C. trachomatis IgG and IgA antibodies were associated with a reduced likelihood to achieve pregnancy for the couple, as well as lower sperm concentration, reduced sperm motil-ity and vitality, increased teratozoospermia index and the occurrence of leukocytes. C. tracho-matis IgG and cHSP60 IgG antibodies in infertile women were associated with tubal factor infertility, but not with reduced pregnancy rates or outcomes. Paper III: cHSP60-1 IgG anti-bodies were associated with ovarian cancer belonging to the postulated type II pathogenetic pathway, when plasma samples obtained more than one year prior to diagnosis were analyzed. M. genitalium IgG antibodies were associated with borderline ovarian tumors; however a sta-tistical type 1 error cannot be excluded. Paper IV: None of the microorganisms studied were found in the ovarian tissue samples.
Conclusions: C. trachomatis IgG and IgA antibodies in the man substantially decreases the chances of the infertile couple to achieve pregnancy, and are associated with subtle negative changes in semen characteristics. C. trachomatis IgG and cHSP60 IgG antibodies in the wom-an are risk factors for tubal factor infertility. Prospective plasma cHSP60-1 IgG antibodies are associated with type II ovarian carcinomas, but C. trachomatis bacteria, or the other micro-organisms studied, could not be detected in benign, borderline or malignant ovarian tissues.
Keywords: Antibodies; borderline tumors; Chlamydia trachomatis; cHSP60; DNA; infertil-ity; ovarian cancer; pregnancy rate; RNA; semen characteristics.


Original papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals:
I: Idahl, A., Boman, J., Kumlin, U. and Olofsson, J. I. Demonstration of Chlamydia tracho-matis IgG antibodies in the male partner of the infertile couple is correlated with a reduced likelihood of achieving pregnancy. Human Reproduction 2004 19:1121-1126
II: Idahl, A., Abramsson, L., Kumlin, U., Liljeqvist, J. A., Olofsson, J. I. Male serum Chlamy-dia trachomatis IgA and IgG, but not heat shock protein 60 IgG, correlates to negatively affected semen characteristics and lower pregnancy rates in the infertile couple. Interna-tional Journal of Andrology 2007 30:99-107.
III: Idahl A, Lundin E, Jurstrand M, Kumlin U, Elgh F, Ohlson N, Ottander U (2009) Chla-mydia trachomatis and Mycoplasma genitalium plasma antibodies in relation to epithe-lial ovarian tumors. Submitted.
IV: Idahl A, Lundin E, Jurstrand M, Møller JK, Elgh F, Marklund I, Lindgren P, Ottander U. Chlamydia trachomatis, Mycoplasma genitalium, Neisseria gonorrhoeae, HPV and polyoma virus are not detectable in human tissues of epithelial ovarian cancer, borderline tumors and benign conditions. Submitted.


Abbreviations
AIH artificial insemination, husband spermAID artificial insemination, donor spermART assisted reproductive techniqueASA antisperm antibodiesBMI body mass indexBOT borderline ovarian tumorcHSP60 chlamydial Heat Shock Protein 60C. pneumoniae Chlamydia pneumoniaeC. trachomatis Chlamydia trachomatisDNA deoxyribonucleic acidEB elementary bodyEIA enzyme immuno assayELISA enzyme linked immuno sorbent assayEOC epithelial ovarian cancerFSH follicle stimulating hormoneHPV human papilloma virusH. pylori Helicobacter pyloriHRT hormone replacement therapyHSS hystero salpingo sonographyIg immunoglobulinICSI intracytoplasmic sperm injectionIVF in vitro fertilizationLAMP-EIA Lipid associated membrane protein – Enzyme immuno assayLGV lymphogranuloma venerumM. genitalium Mycoplasma genitaliumMgRT-PCR Mycoplasma genitalium Real time - PCRMIF microimmunofluorescenceMOMP major outer membrane proteinNAAT nucleic acid amplification testNAFA/ESHRE Nordic Association for Andrology/European Society of Human Reproduction and EmbryologyN. gonorrhoeae Neisseria gonorrhoeaeNPV negative predictive valueNSHDC Northern Sweden Health and Disease CohortOD optical densityOR odds ratioPCR polymerase chain reactionPID pelvic inflammatory diseasePPV positive predictive valueRB reticulate bodyRNA ribonucleic acidRR relative risk, risk ratioSSPC serous surface papillary carcinomaSTD sexually transmitted disease

STI sexually transmitted infectionTFI tubal factor infertilityTIC tubal intraepithelial carcinomaTMA transcription mediated amplificationTZI teratozoospermia index

Table of contentsAbstract
Original Papers
Abbreviations
Table of contents
Introduction ...........................................................................................................................1 Chlamydia trachomatis ..............................................................................................1 Chlamydia trachomatis – the bacterium ..........................................................................2 Developmental cycle ...........................................................................................................3 Persistence ......................................................................................................................... 4 Chlamydial Heat Shock Proteins....................................................................................... 4 Clinical manifestations of genital C. trachomatis .............................................................5 C. trachomatis diagnostic methods ...................................................................................5 Test specimen ..............................................................................................................5 Culture ........................................................................................................................ 6 Immunofluorescence (IF) and antigen detection enzyme immunoassays (EIA) .... 6 Nucleic acid amplification assays – NAATs ............................................................. 6 Serology .......................................................................................................................7 Effect of antibiotic treatment ........................................................................................... 8 Subfertility/infertility .................................................................................................. 9 Definition and prevalence ................................................................................................. 9 Psychosocial aspects .......................................................................................................... 9 Chlamydia trachomatis and infertility .................................................................. 9 C. trachomatis and female infertility ................................................................................ 9 C. trachomatis and male infertility ..................................................................................10 Ovarian tumors ............................................................................................................10 Prevalence and risk factors ..............................................................................................10 Ovarian tumor biology ..................................................................................................... 11 Pathogenesis of serous ovarian and pelvic carcinomas – a new model ..........................12 Chronic infection and inflammation in the pathogenesis of ovarian tumors .............................................................................................................12 Other types of cancer ........................................................................................................12 C. trachomatis and ovarian cancer ..................................................................................13 Previous studies ................................................................................................................13 Other genital infections as possible tumor promoters/initiators ...................................13
Aims ........................................................................................................................................15
Materials and Methods .......................................................................................................17 Ethics ................................................................................................................................17 Papers I and II: Infertility study .............................................................................. 17 Study population .............................................................................................................. 17 Clinical investigation ........................................................................................................ 17 Follow-up ..........................................................................................................................19 Fertile controls..................................................................................................................19

Papers III and IV: Ovarian tumor study ................................................................19 Study population ..............................................................................................................19 Clinical characteristics and histopathologic diagnosis ....................................................19 C. trachomatis analyses ............................................................................................ 20 C. trachomatis serology .................................................................................................. 20 DNA and RNA extraction .................................................................................................21 C. trachomatis DNA and RNA analyses ..........................................................................21 Additional analyses .....................................................................................................21 Paper III: M. genitalium serology ....................................................................................21 Paper IV: N. gonorrhoeae, M. genitalium, HPV and polyoma virus BKV and JCV detection.............................................................................................................21 Statistics ........................................................................................................................ 22
Results and Discussion .................................................................................................... 23 Papers I and II: Infertility study ............................................................................. 23 Prevalence of C. trachomatis antibodies and DNA ........................................................ 23 C. trachomatis antibodies and female infertility .............................................................25 C. trachomatis antibodies and male infertility ............................................................... 26 Methodological considerations ....................................................................................... 29 Different antibodies – different mechanisms? ............................................................... 30 Papers III and IV: Ovarian tumor study ............................................................... 30 Prevalence of C. trachomatis and M. genitalium antibodies ......................................... 30 C. trachomatis and M. genitalium antibodies in relation to ovarian tumors ............... 32 C. trachomatis, N. gonorrhoeae, M. genitalium, HPV, and polyoma virus BKV and JCV in ovarian tissues (paper IV). ....................................................................33 Methodological considerations ........................................................................................33 Suggested model of C. trachomatis in the pathogenesis of ovarian cancer ....................35 When does C. trachomatis initiate/promote ovarian carcinogenesis? ..................35 Where is the site for ovarian carcinogenic C. trachomatis infections? ................. 36 How does the C. trachomatis infection initiate/promote malignant transformation? ....................................................................................................... 36
Summary and Conclusions ............................................................................................. 39
Suggestions for future research .....................................................................................41
Acknowledgements ........................................................................................................... 43
References ............................................................................................................................45
Papers I–IV

1
introduction
C hlamydia trachomatis (C. trachomatis), the most prevalent sexually transmitted
bacteria worldwide, is a known risk factor for pelvic inflammatory disease (PID), tubal fac-tor infertility (TFI) and ectopic pregnancies, but the impact of a C. trachomatis infection on male fertility is unclear. It is also recently hypothesized that chronic infections with for example C. trachomatis might initiate/pro-mote ovarian tumor development.
In this thesis known consequences of C. trachomatis on female fertility in terms of TFI will be confirmed. Furthermore, data to sup-port that C. trachomatis infections have neg-ative effects on male fertility, as well as a pos-sible tumor promoting/initiating role of C. trachomatis in ovarian tumor pathogenesis, will be presented.
Chlamydia trachomatisThe effects of infection with C. trachomatis were first described in ancient Chinese writ-ing in the Ebers papyrus (1500 B.C.) as tra-choma of the eye.1 The name “trachoma” was first introduced in A.D. 60 and referred to the “roughness of the conjunctiva” that character-izes the ocular disease. The disease eventu-ally became endemic but during the last cen-tury, the disease has disappeared from many parts of the world. The disappearance has been attributed to improvements in the stand-ard of living and of hygienic practices. In hot, dry climates it still persists, and is a major cause of blindness in developing countries.
The developmental cycle, which is the uni-fying property that defines the genus, was first clearly described for the psittacosis agents after they had been isolated in the early 1930s. However, T’ang and colleagues (1957) in Chi-na are usually credited to have been the first to isolate the trachoma agent, which was at that time considered to be a virus.2 This find-ing boosted research on Chlamydia and by 1975 C. trachomatis was suggested to be the most common sexually transmitted bacterial pathogen worldwide.3 C. trachomatis was by then already recognized as a very common cause of urethritis in men and cervical infec-tion in women. In 1977 Mårdh and colleagues stated that C. trachomatis was a major cause of pelvic inflammatory disease (PID),4 and subsequent studies found that this organism could be associated with tubal factor infertil-ity5 and ectopic pregnancy.6 It was in the early 1980´s that C. trachomatis was divided into two groups causing primarily either ocu-lar disease or genital disease. Since then there has been a rapid progress in the knowledge of C. trachomatis and its effects and diseases in humans.
C. trachomatis is considered the worlds leading preventable cause of blindness, with about 6 million people blinded as a result of this disease.7 It is also the most common sex-ually transmitted bacteria in the world, with approximately 90 million new cases occurring each year.8 In Sweden, the incidence has raised nearly three-fold since 1997 (Figure 1)
Introduction

introduction
2
despite intensive preventive measures such as screening, partner-tracing and informa-tion. In 2008 42 000 new C. trachomatis infections were reported.9 The raise in inci-dence is most pronounced in the ages 15 – 24 years.
Chlamydia trachomatis – the bacteriumChlamydiae are obligate intracellular bacteria with a unique developmental cycle. They have
been placed in their own order, Chlamydiales, with one family, Chlamydiaceae, and a single genus, Chlamydia. There has been some dis-agreement in the scientific community wheth-er Chlamydia should be divided into two genera, Chlamydia and Chlamydophila, based on apparent differential clustering of the 16S rRNA gene,10 however this separation has not been commonly accepted.11 The genus Chlamydia consists of four major species, Chlamydia trachomatis, Chlamydia psittaci,
Chlamydia
C. trachomatis C. psittaci C. pneumoniae C. pecorum
Trachoma LGV-
lymphogranulomavenerum
Murine(mouse
pneumonitis)
Serovar A-C Serovar D-K
Figure 2. Simplified dendrogram relating genital C. trachomatis (serovar D-K) to other closely related bacteria within the genus Chlamydia.
4,000
3,500
3,000
2,500
2,000
1,500
1,000
500
0
1995
1996
1997
1998
1999
200
0
200
1
200
2
200
3
200
4
200
5
200
6
200
7
200
8
1995
1996
1997
1998
1999
200
0
200
1
200
2
200
3
200
4
200
5
200
6
200
7
200
8
Women Men
15–19
25–29
35–39
20–24
30–34
Num
ber
of
case
s p
er 1
00
,00
0 in
hab
itan
ts
Figure 1. Incidence of genital C. trachomatis infections per sex and age group, 1995–2008 in Sweden. Data from the Swedish Institute for Infectious Disease Control.

3
introduction
Chlamydia pneumoniae and Chlamydia pe-corum (Figure 2). C. trachomatis has been divided into three biovariants (biovar): tra-choma, lymphogranuloma venerum (LGV) and murine (mouse pneumonitis [MoPn] agent). The trachoma and LGV biovars are distinguished by different clinical features. LGV readily cause systemic infections and proliferate in lymph nodes, whereas growth of the trachoma biovar has been believed to be limited to columnar epithelial cells at mu-cosal surfaces. However, chlamydial antigen and nucleic acid is also found in macrophag-es and smooth muscle cells deep within the lamina propria,1 and electron microscopic investigation has revealed C. trachomatis el-ementary bodies within spermatozoa.12
The trachoma biovar consists of prototyp-ical serovariants (serovars), determined by the serological immune response, and desig-nated by the letters A through K. The serov-ariants A through C give rise to trachoma of the eye, whereas serovariant D through K in
adults give rise to genital manifestations and in newborns pneumonia and conjunctivitis.
Developmental cycleThe developmental cycle of Chlamydia con-sists of a small (0.3µm) extracellular, infec-tious elementary body (EB), and a larger (1µm) dividing intracellular reticulate body (RB)1 (Figure 3). The EB has an osmotically stable and poorly permeable cell envelope and a much reduced surface area compared to the RB. The EB are also metabolically inactive, but have the capability to recognize and enter the host cell, and to reorganize and grow 30-fold in volume to the division-capable RB form. The intracellular cycle all takes place in an inclusion, a membrane-limited vacuole. Within a few hours after inclusion, EBs dif-ferentiate into the larger, metabolically active RBs. As the chlamydiae multiply, the inclu-sion increases in size to accommodate the multiplying bacteria, which eventually turn into EBs that accumulate within the inclusion.
Infection (EBs)
Replication (RBs)
Aberrant RBs
Host cell
Nucleus
Inclusion
Transformationof RB to EB
ImmunosuppressionAntibiotic withdrawalResolved co-infection
CHSP60expression
MOMPexpression
Immune-response Antibiotics Nutrient depletion Co-infection
Transformationof EB to RB
EBs and RBs
Lysis
EB, elementary bodyRB, reticulate body
Persistence
Figure 3. Chlamydia developmental cycle.

introduction
4
The RBs continue to multiply until the cell lyses at 40 to 48 hours (C. trachomatis) postinfection, and the infectious EBs are re-leased.
PersistencePersistence of infection is the continuous presence of viable but non-infectious and non-cultivable bacteria.13 Today there is abundant evidence that chlamydiae are capa-ble of causing enduring infections for months and years. Less is known in which develop-mental form chlamydiae survive long-term within the body, the susceptibility of such forms to antibiotic treatment, or the role of persistent chlamydial infection in disease. In vitro studies have shown that chlamydiae might have an abnormal development after exposure to antibiotics, developing aberrant RBs that enlarge, but resume normal devel-opmental cycle after withdrawal of the anti-biotic14 (Figure 3). Exposure to a nutrient depleted environment has shown to give sim-ilar results, as well as cytokines, particularly gamma interferon, monocyte infection, con-tinuous infection,15 co-infection with herpes simplex virus type 2 (HSV-2)13 or sustained antibiotic treatment.16 In vivo, chlamydial DNA and antigen have been detected in cul-ture negative subjects in tubal, ovarian and endometrial tissues as well as in prostatic tis-sue and semen samples.17-19 Morphologically aberrant chlamydial forms resembling those observed in vitro have been visualized by elec-tron microscopy.20 Chlamydial RNA has been detected in the absence of cultivability in ex-perimental trachoma of primates21 as well as in synovial biopsy samples of patients with reactive arthritis or Reiter’s syndrome,22 and in the fallopian tubes of seven women with ectopic pregnancy who were DNA positive for C. trachomatis.23 Since RNA is highly labile this indicates viable, metabolically active, but non-cultivable organisms. In animal infection models mice infected with either C. tracho-matis24, 25 or C. pneumoniae,26 infections that
had become asymptomatic, reactivated after immunosuppression with cortisone or cyclo-phosphamide. Similarly, topical therapy with corticosteroids of inclusion conjunctivitis has long been considered to lead to flare-up of trachoma disease, presumably because local immunosuppression resulted in the reactiva-tion of clinically inapparent infection.27
Several studies addresses the question of persistent infections in the female genital tract, with a maximum follow-up period of five years (for review see Golden, 2000).28 The persistence rate varies between 29 and 87% depending on length of follow-up period, subjects included, detection method, test specimen etc. In a more recent study the per-sistence rate was 55% at one year,29 and in another 46% at 1 year, 18% at 2 years and 6% at 4 years.30 A C. trachomatis serovar-specif-ic analysis was done and 53 out of 55 women were found to be infected by the same sero-var at all occasions indicating persistence rather than re-infection. Oral contraceptive pill use and older age at first sexual inter-course was associated with increased clear-ance rate. In men, the duration of the follow-up period has lasted up to six months. Eight of nine (89%) men eligible for follow-up were still C. trachomatis positive by PCR testing in a urine specimen after six months.31
Chlamydial Heat Shock ProteinsHeat Shock Proteins (HSPs) are a group of highly conserved cellular proteins that acts as chaperones, with a key role in intracellular folding and refolding, assembly, and translo-cation of proteins. The expression of HSPs was initially found to be elevated in reaction to heat stress but is also expressed as well in reaction to proteolytic, mechanical or chemi-cal stress.32 There are four main groups of HSPs based on their molecular weights: HSP90, HSP70, HSP60 and the small HSPs. During persistent infection the HSP60 pro-duction is up-regulated while the production of other proteins is down-regulated.13, 33, 34

5
introduction
Chlamydial HSP60 is suggested to inhibit the apoptotic pathway of the host-cell supporting persistence of chlamydial infection.35 Human and chlamydial HSP60 share an approxi-mately 50% amino acid homology36 and de-spite this homology, chlamydial HSP60s are highly immunogenic and are the HSPs most extensively studied in relation to infertility. The humoral immune response to cHSP60 is in several studies associated with tubal dam-age and subsequent infertility.37-43 An autoim-mune cross-reaction between human and chlamydial HSP60, making the woman’s im-mune system attack autologus HSP60, or a delayed hypersensitivity reaction, is suggest-ed to be the mechanism for the inflammation and scarring of the tubes.36 More recent re-search have demonstrated that chlamydia-infected cells produce pro-inflammatory chemokines, cytokines, growth factors and other cellular modulators, sufficient to ac-count chronic and intense inflammation and the promotion of cellular proliferation, tissue remodeling and scarring in itself.32, 44
It is also suggested that chronic infection and inflammation, and inhibition of apoptosis by cHSP60, might have tumor promoting/initiating effects, increasing the risk for geni-tal cancers such as cervical cancer.45 Further-more, epithelial ovarian cancer is also sug-gested to be associated with C. trachomatis infections.46, 47
Clinical manifestations of genital C. trachomatisUp to as many as 85 to 90 percent of C. tra-chomatis infections in men and women are asymptomatic48, 49 and can persist for sev-eral months and years. The complications encountered by the female are many different such as urethritis, bartholinitis, cervicitis, en-dometritis, pelvic inflammatory disease (PID) sometimes with intraabdominal spread caus-ing periappendicitis and perihepatitis, and in rare cases proctitis. Symptoms range from pain when urinating to lower abdominal pain,
modest fever and adnexal and uterine tender-ness on pelvic examination, but often there is only a midcycle bleeding or no symptoms at all. Late sequels are infertility, ectopic preg-nancy, chronic pelvic pain and probably also uterine cervix squamous cell carcinoma.50
In men the spectrum of disease covers ure-thritis, prostatitis, orchitis and epididymitis.51 The role of C. trachomatis in male infertility is a matter of debate and will be discussed more extensively in a separate section (C. tracho-matis and male infertility). Arthritis and con-junctivitis are described in both women and men, and among those who practice anal in-tercourse also proctitis.52 In the neonate, ver-tical transmission might cause conjunctivitis or neonatal pneumonia. A very early onset of disease in some cases, suggests that the infec-tion may start as an intrauterine chlamydial infection.53
C. trachomatis diagnostic methodsTest specimenTo get valid test information it is important to have the right test specimen, but in C. tra-chomatis diagnosis this is not always easily achieved. The infection might be localized in the endometrium, fallopian tubes, ovaries or the prostatic tissue18 which are not easily ac-cessible, and it requires invasive procedures to get tissue samples from these locations. The common routine diagnosis involves a first void urine sample or a cervical or urethral swab. Lately vaginal swabs have been intro-duced with good accuracy for detection of lower genital tract infections.54 However, C. trachomatis antigen or DNA has been found in endometrium, fallopian tubes, ovaries, se-men or prostatic tissue without being able to detect any bacteria in urine specimens or cer-vical secretions.18 Chlamydia serology, utiliz-ing a blood sample, might in some instances be an alternative diagnostic method with an easily accessible test specimen giving infor-mation on the immune reaction to a chlamy-dial infection at any site of the body.

introduction
6
CultureCulture was for many years the only method available for the diagnosis of C. trachomatis, but has in the light of newer methods such as nucleic acid amplification tests (NAAT) been abandoned for routine diagnosis in large-scale laboratories. The sensitivity is approximately 60-70% which makes it a poor diagnostic tool, but the specificity is 100%.55 In brief, clinical material is inoculated onto tissue culture cells, cultured for three days and thereafter chlamy-dial inclusions are detected by staining with iodine or Giemsa stain, fluorochromelabelled poly- or mono-clonal antibody or by immuno-histochemistry. There are many different con-ditions that can reduce the sensitivity of cul-ture such as type of clinic, how well-trained the health care providers are, and the quality of the specimens they collect, the transport systems being used, the laboratory tissue cul-ture system, the type of stain being used, the speed of centrifugation, etc.
Immunofluorescence (IF) and antigen detection enzyme immunoassays (EIA)The key to this entire process is the ability to visualize an antibody attached to an antigen. The direct immunofluorescence method uses a fluorescent dye that is covalently attached to the antibody. When a light illuminates the fluorescent dye, it absorbs the light and emits a different color light which is visible to the investigator and can be photographed. This was the first method not dependent on viable C. trachomatis, but had sensitivities and spe-cificities lower than culture. In the early 1980s, monoclonal antibody technology made the immunofluorescence technique more spe-cific and led to the elucidation of the relation-ship between the newly discovered major outer membrane proteins (MOMP) and the serotypes of C. trachomatis. In enzyme im-munoassays, the attached enzyme-tagged antibody is detected by adding a substrate indicator that produces a color reaction. The
optical density of the enzyme is read by a spectrophotometer.
Nucleic acid amplification assays – NAATsNAATs are widely used for C. trachomatis diagnosis today and have proven to be more sensitive and specific than previous diagnos-tic tests (culture, IF and EIA) because they don’t need viable chlamydiae (more tolerant to transports) and due to the amplification process. A further advantage is that they can be used in non-invasive specimens such as a first-void urine or vaginal swabs with nearly identical sensitivity and specificity to those in cervical or urethral samples.56 Principally NAATs amplify either a) the target nucleic acid, DNA (polymerase chain reaction, PCR; strand displacement assay, SDA) or ribos-omal RNA (rRNA) (transcription mediated amplification, TMA); or b) the probe after it has annealed to the target nucleic acid (ligase chain reaction, LCR). The major targets for amplification based tests against C. tracho-matis are generally multiple-copy gene prod-ucts, such as the cryptic chlamydial plasmid (PCR, LCR, SDA) which is present in EBs with 7 to 10 copies, or rRNA (TMA) which may have several thousands of copies per bacte-rial cell. The high number of target copies in TMA might theoretically be advantageous with respect to sensitivity.
The first step in the PCR process is dena-turation of the DNA double stranded cryptic plasmid by heating, followed by the annealing of a specific primer. Thereafter synthesis of new DNA in a polymerase dependent process takes place where after the cycle starts over again with denaturation. These steps occur at different temperature optima, and by thermal cycling multiple copies, also called amplicons, of the target sequence are produced. The am-plicons are detected by peroxidase labeled oligonucleotide probes complementary to the amplicon, which will give a colorimetric reac-tion when peroxidase substrate is added.

7
introduction
In TMA, a primer binds to an rRNA target, a DNA copy is synthesized, a second primer binds to the new DNA copy and yet another DNA copy is made. Thereafter, RNA polymer-ase initiates transcription of 100-1000 copies of RNA amplicons from which new DNA cop-ies can be created, and finally double-strand-ed DNA. The cycle will be repeated over and over resulting in a billion-fold amplification. The amplicons are detected by adding an acridium ester labeled DNA probe that will emit light, detected by a luminometer, from hybridized probes.
Other NAATs have a principally similar way of working with a gene probe that at-taches to a target gene, amplification and de-tection.
Specificities and sensitivities among the different NAATs are reported to be similar ranging from 95% to 100% for specificity and 80% to 93% for sensitivity.56, 57 Different spec-imens can in some instances affect sensitivity due to inhibitors to the amplification process. In commercial kits there are usually several different procedures to avoid inhibition.
SerologyThe method of measuring antibodies to a mi-croorganism in serum is widely used for re-search purposes to compare sample popula-tions for prior or current exposure to an infection. There are, for example, a large number of studies which show that women with tubal factor infertility have a higher prevalence of antibodies to C. trachomatis than fertile women.58 Regarding C. pneumo-niae, associations of serum antibodies with atherosclerosis and heart disease are being evaluated.59-62 Sensitivity and specificity for serological tests, as for all diagnostic methods, are dependent on how accurate the method detects serum antibodies and what the sero-logical method is compared to. Concerning C. trachomatis and infertility, the serological methods are often compared as to how well they can detect tubal pathology. However, C.
trachomatis is not the only factor that gives rise to tubal pathology. Inherently, sensitiv-ity for the disease one wants to detect will decrease. On the other hand all C. trachoma-tis infections causing antibody production do not lead to tubal factor infertility (TFI), hence specificity is reduced.
Several commercial methods are today available, among them the MIF test, once considered the “golden standard” for C. tra-chomatis serology, and the ELISA method. The draw-back of the MIF-test is that it is la-borious. The MIF test uses chlamydial EBs treated in a process to remove the group spe-cific lipopolysaccharide (LPS) of the outer membrane. The residual major outer mem-brane protein (MOMP) has species and sero-type specific antigens and constitutes ap-proximately 60% of the organism’s outer membrane. The MIF method used in this the-sis utilizes MOMP from eight serotypes of C. trachomatis, D-K, which are known to cause genital disease. The EBs are attached to a slide to which patient sera is added and incubated. Thereafter the slide is washed to remove un-bound serum antibodies. In the next stage the slide is incubated with fluorescein-labeled antibodies that react with bound human IgG or IgA. Afterwards the slide is washed, dried, mounted and examined using fluorescence microscopy. Positive reactions appear as bright apple-green fluorescent dots/EBs (spe-cific fluorescence) (Figure 4), and can be dis-tinguished from non-specific fluorescence, which is a homogenous green coloring of the slide. Semi-quantitative endpoint titers are obtained by testing serial dilutions of positive specimens.
The principle of the ELISA method is sim-ilar but with a different detection system. In the ELISA method detecting cHSP60 IgG an-tibodies, a plate is covered with recombinant cHSP60 proteins from genital C. trachomatis. Antibodies from the serum specimen that are directed towards cHSP60 bind to the antigen. Thereafter peroxidise-conjugated anti-human

introduction
8
IgG antibodies bind to the cHSP60 bound IgG antibodies. Finally a substrate for the per-oxidase is added and the light absorption is read photometrically.
Effect of antibiotic treatment Doxycycline 100mg twice daily for 7 days, or a single dose of azithromycin 1g, are the most rigorously investigated treatment regimens for uncomplicated chlamydial infections,63 but doxycycline 200 mg on the first day with 6-9 subsequent doses of 100 mg daily is also studied. All regimens have microbial cure rates of >95% at 2-5 week follow up with cul-ture, immunofluorescence or, lately, NAAT.64 When patients are followed up for longer pe-riods of time following treatment, and tested with NAATs, more than 10% will be chlamydia positive on retesting.65 This has been consid-ered a result of re-infection but there is now emerging evidence that this may be the result of re-emergence of persistent latent (non de-tectable) infection as well as re-infection.63,
65, 66 There is some evidence that latent infec-tion might not be detectable, even using NAAT, if only cells shed from the mucosal surface are sampled.67 At high loads (high number of bacteria) persistence has been shown in vitro (heterotypic resistance). The subsequently recovered isolates do not pos-sess antimicrobial resistance at low loads
(homotypic resistance).68 One explanation for the apparent lack of homotypic antimicrobial resistance in C. trachomatis might be the unique developmental cycle. Since gene rep-lication occurs within an intracellular inclu-sion in an infected cell, acquisition of antibi-otic resistance genes from other organisms would be difficult.68 These observations sug-gest that the increased failure rate with long-er follow up could be due not only to reinfec-tion, but also to re-activation of persistent infections as a result of heterotypic resistance associated with high chlamydial loads.
By genotyping subsequent culture-positive C. trachomatis episodes, which were treated with doxycycline or azithromycin, in 7 wom-en over a two to five year period, identical genotypes for the subsequent infections were detected indicating persistence. However, re-infection by the same untreated partner could not be ruled out.66 The women had culture negative cervical samples, however positive with ligase chain reaction (LCR), in between the positive cultures, supporting that C. tra-chomatis bacteria may not have been eradi-cated by the antibiotic regimen. Similarly, an 8% infection rate three to six months after treatment with azithromycin, in women re-porting no sexual intercourse after initial treatment, has been found.65
Inflammation, scaring and fibrosis are the main pathological findings in the upper gen-ital tract after chlamydial infection, causing tubal damage, ectopic pregnancy and infertil-ity. In one experimental study on macaques, there was a significant difference both in eradicating C. trachomatis and preventing inflammatory changes after treatment with azithromycin once daily for seven days, com-pared to doxycycline once daily for 14 days, or placebo.69 In clinically apparent salpingitis and PID, anaerobic bacteria are also believed to be involved. This has resulted in the wide application of metronidazole in addition to a chlamydia specific drug.70
Figure 4. Fluorescein-labelled C. trachomatis elementary bodies (green dots) detected by the MIF-method. MIF, micro immuno fluorescence (Reprinted with permission from Focus Diagnostics Inc.)

9
introduction
Subfertility/infertilityDefinition and prevalenceSubfertility/infertility is an important medi-cal and social problem in both magnitude and impact on well-being. An often used definition is that the couple is regarded subfertile after one year of unprotected sexual intercourse without conception.71 According to the defini-tion by the World Health Organization (WHO) 2 years of unprotected sexual inter-course is required.72 Infertility is the most common used term for this condition, how-ever in fact refers to a couple that can not at all achieve pregnancy. Infertility affects ap-proximately 5-26% of couples in the repro-ductive age-group, a figure that is fairly simi-lar between less and more developed countries.73 An estimated 70 million couples are at the present experiencing infertility. This figure could, however, rise in the near future as increasing numbers of women delay child-bearing, resulting in decreased oocyte quality, raised chance of exposure to sexually trans-mitted diseases, and a secular decline in sperm counts.74 The causes of infertility are in slightly more than 1/3 due to female fac-tors, in 1/3 male factors and in 1/3 there is a combination of male and female factors.75 In 5-10% a cause can not be established despite thorough investigation.
Psychosocial aspectsFor many couples, the inability to bear children is a tragedy.76 There is both a biological and social loss that to most people is shocking and often leads to a psychological crisis following the well-known traumatic crisis, however often more prolonged.77 Childless couples are also excluded from taking leading roles in impor-tant family events such as birthdays, christen-ings, confirmations and weddings of their chil-dren.76 Even though infertility is a common problem to the couple, the man and the wom-an might have different feelings and reactions, affecting their marital and social lives in dif-ferent ways. A feeling of despair, anxiety, grief,
lack of self-esteem, and sexual inadequacy are common in the infertility situation78 and does not seem to be related to socio-economic class, race or culture. It is essentially “human” to re-spond to childlessness even though the nature of concern may differ.78
Chlamydia trachomatis and infertilityC. trachomatis and female infertilityC. trachomatis is known to cause damage to the female reproductive tract, primarily due to adhesions or obstructions of the fallopian tubes secondary to the inflammatory re-sponse. Reduced chances to achieve an in-trauterine pregnancy is the result.79 TFI is the main cause of infertility in 10-30% of cases in developed countries80, 81 and C. trachomatis is the most common causative agent to PID and TFI in the developed world,82-84 while the rate of Neisseria gonorrhoeae is low.8 In de-veloping countries the proportion of tubal factor infertility among subfertile couples is up to 85%85 and the spectrum of causative agents somewhat different with a higher pro-portion of N. gonorrhoeae and genital tuber-culosis. For example, in women in India with a history of genital tuberculosis, the rate of infertility was 58%, and among women with TFI the incidence of genital tuberculosis was 41%.86
There is today plenty of evidence that C. trachomatis serum antibodies are associated with tubal factor infertility (TFI), an associa-tion that was first discovered by Punnonen and co-workers.87 Repeated episodes of pelvic inflammatory disease, as well as the severity of PID, increase the risk for ectopic pregnan-cy and infertility.88 Since it is widely accepted that there is an association of serum C. tra-chomatis IgG with TFI, the research has shifted towards how clinically useful C. tra-chomatis antibody testing is in the infertility work-up, but also if IgA and cHSP60 IgG an-tibodies has any additional value in diagnos-ing TFI.38, 39, 41-43, 89-92

introduction
10
In-vitro fertilization was originally de-signed to overcome and by-pass damaged tubes93 and TFI has ever since the introduc-tion of the method constituted one of the main infertility causes of couples receiving IVF treatment.94 However, TFI is in itself found to be associated with a poor prognosis of IVF treatment compared with other infertility di-agnoses, particularly when a fallopian tube dilated by fluid (hydrosalpinx) is present.95 How the negative effect is mediated is still unknown96 but salpingectomy of ultra-sound visible hydrosalpinx prior to IVF is shown to increase pregnancy rates.97, 98
C. trachomatis antibodies are also pro-posed to be associated with a reduced success rate when IVF treatment is carried out. Chlamydial HSP60 IgG99 or IgA100 antibodies in follicular fluid, or cHSP60 IgA antibodies in the cervix,101 were associated with a re-duced implantation rate after IVF treatment. Suggested mechanisms are either that cHSP60 IgG antibodies indicate a persistent infection causing an inflammatory reaction undermining embryo implantation. Alterna-tively, cHSP60 IgG antibodies cross-react with human HSP60, expressed at vital stages of embryogenesis,36 and may induce destruc-tion of the embryo.
In recent years, the role of genetic traits of the host immune system for the development of tubal pathology in C. trachomatis genital infections has received increasing attention. Several markers have been identified such as HLA-A31 that has been correlated with acute chlamydial pelvic inflammatory disease,102 variants at IL10 (encoding interleukin-10) promoter positions with higher IL-10 concen-trations in cervical secretions associated with recurrent Chlamydia infection,103 HLA-DQ alleles combined with IL10 promoter poly-morphism associated with TFI,104 and multi-ple SNPs (single nucleotide polymorphisms) in the pattern recognition receptors (PRRs) involved in sensing bacterial components that
are associated with tubal pathology following a C. trachomatis infection.105
C. trachomatis and male infertilityC. trachomatis is a well-known pathogen causing damage to the female reproductive tract leading to reduced fertility. Less is known about the possible effects on fertility in men apart from causing postinflammatory strictures to the epididymis/vas, in rare cases, leading to a mechanical hinder for the sperm to reach the female reproductive tract. There are several previous reports on C. trachoma-tis antibodies in serum or semen in men in relation to reduced pregnancy rates, and im-paired semen characteristics, some showing an association42, 106-111 while others did not.112-
122 Sexual transmission of C. trachomatis bacteria to the female partner, thereby caus-ing damage to the female reproductive tract leading to reduced pregnancy rates, has been one possible explanation as to why C. tracho-matis antibodies in the man are related to reduced pregnancy rates. Lately, C. tracho-matis bacteria in semen has been associated with impaired semen characteristics,123-126 and in in-vitro, studies co-incubating human sperm with C. trachomatis, a direct negative effect of C. trachomatis on the spermatozoa has been found.127, 128 Reduced motility, vital-ity, blunted acrosome reaction and sperm DNA fragmentation are among the effects re-ported.
Ovarian tumorsPrevalence and risk factorsOvarian cancer is the sixth most common cancer among females and the most lethal gynaecologic malignancy with a 16-51% five year survival rate globally.129 The incidence is higher in the developed world compared to the developing countries (Figure 5). No firm conclusions are established on the etiology of ovarian cancer, while 5-10% is attributable to genetic predisposition.130, 131 Nulliparity, in-

11
introduction
fertility, hormone replacement therapy, en-dometriosis, high BMI and selected aspects of diet are established or proposed risk factors while child-bearing, oral contraceptive pill use, tubal ligation, hysterectomy and breast-feeding are protective factors.132, 133 “Inces-sant ovulation”, “gonadotropin stimulation” and “retrograde transportation” hypotheses have been proposed to explain the etiology of epithelial ovarian cancer.134-136 However, the high risk-reduction by for example one preg-nancy, a few years of oral contraceptive pill use, or a late menopause does not correspond to the small reduction in numbers of ovula-tions or the short duration of diminished lev-els of gonadotropins.131, 137, 138 Apparently, there must be some other biological mecha-nisms.
Ovarian tumor biologyAccording to the cell types from which ovar-ian tumors are assumed to originate, they are divided into three major groups: surface ep-ithelial-stromal tumors, germ cell tumors and sex cord-stromal tumors.139 The surface epithelial-stromal tumors account for ap-
proximately 60% of all ovarian tumors and 90% of malignant ovarian tumors and are commonly addressed as epithelial ovarian cancer (EOC). Fifteen percent of epithelial ovarian neoplasms exhibit exuberant cellular proliferation but no invasive behavior and are accordingly classified as borderline ovarian tumors (BOT), sometimes also called “of low malignant potential” or “atypically prolifer-ating”. Epithelial ovarian tumors can be sub-divided into five major subtypes designated as follows: serous, mucinous, endometrioid, clear cell, and transitional cell (or Brenner type). Highly malignant epithelial tumors lacking specific differentiation are classified as undifferentiated. BOT are mostly of serous or mucinous subtypes.
Serous tumors are tumors formed by cells that resemble those of the internal lining of the fallopian tube, are often cystic, and the malignant serous tumors are in a majority of cases widely disseminated at the time of di-agnosis. Serous or mucinous tumors identical to those in the ovary may arise in multiple locations within the pelvic region and the ab-dominal cavity. When there are simultaneous
Figure 5. Incidence of ovarian cancer (age-standardized) per 100 000 women and year (Sankaranarayanan, R. and Ferlay, J., Best Pract Res Clin Obstet Gynaecol, 2006).129
< 4.3 < 5.9 < 7.4 < 10.1 < 17.0

introduction
12
tumors in the ovary and elsewhere in the ab-domen, it’s often difficult to determine which tumor represents a de novo malignancy and which represents seedlings or implants.
Mucinous tumors are formed by cells that resemble either those of the endocervical epithelium or those of the intestinal epithe-lium. It is sometimes difficult to distinguish between primary ovarian tumors and tumors of intestinal origin, for example the appendix, metastasized to the ovaries.
Endometrioid tumors are formed by cells that resemble the internal lining of the uterus – the endometrium, while clear-cell tumors consist of clear, hobnail-like cells. Both of these tumors are often associated with en-dometriosis or cancer of the endometrium.
The cell type of transitional cell (Brenner) tumors resembles those of the internal lining of the bladder presumably due to transforma-tion of ovarian epithelium, urothelial meta-plasia. Undifferentiated tumors have highly malignant features, including high nuclear grade, and no cytoplasmic differentiation.
Pathogenesis of serous ovarian and pelvic carcinomas – a new modelIn 2004 Shih and Kurman first proposed a new model for carcinogenesis of the ovary dividing the tumors into two groups, type I and type II, with different pathogenetic path-ways.140 The model is based on clinical, path-ological and molecular genetic studies. Type I tumors are slow growing, generally confined to the ovary at diagnosis and develop from well-defined pre cursor lesions. They include low-grade micropapillary serous carcinoma, mucinous, endometrioid and clear-cell carci-nomas. Type II tumors, approximately 75% of ovarian carcinomas, are on the other hand rapidly growing, highly aggressive neoplasms. They lack well-recognized precursor lesions and are almost always discovered after peri-toneal or serosal involvement has taken place. Type II tumors include moderate or high-grade serous carcinomas, malignant mixed
mesodermal tumors, and undifferentiated carcinomas. Type I tumors are genetically stable and have mutations in a number of dif-ferent genes including KRAS, BRAF, PTEN and beta-catenin, while type II tumors are characterized by p53 mutations with p53 pro-tein over-expression and a high level of ge-netic instability.141
The precursor lesions of the type I tumor group are cystadenomas, serous borderline tumors, mucinous borderline tumors and en-dometriosis, which are often associated with their corresponding carcinoma. Tubal in-traepithelial carcinoma (TIC) is an emerging candidate precursor for the type II tumor group, and has been found associated with high-grade serous ovarian and pelvic carci-nomas. The identical p53 mutations have been identified in TIC and serous carcinomas of the same patient, and also in adjacent “p53 signatures”.142 p53 signatures are areas, pref-erably in benign mucosa in the tubal fimbriae, with strong p53 immunostaining, targeting the secretory cells.
Chronic infection and inflammation in the pathogenesis of ovarian tumorsOther types of cancerMicrobes causing chronic inflammatory dis-ease have in the last decade become increas-ingly investigated as possible cancer initia-tors/promoters and infectious etiologies have been identified for some cancers. Helico-bacter pylori colonization of the stomach may lead to gastric cancer, particular subtypes of HPV may initiate cervical cancer and chronic inflammation induced by Hepatitis B and C virus infections can cause liver cancer.143 C. trachomatis is considered a cofactor in cervical cancer and is primarily associated with squamous cell carcinoma of the cervix.50,
144-146

13
introduction
C. trachomatis and ovarian cancerThe role of persistent infection, leading to chronic inflammation, in the pathogenesis of ovarian cancer has received very little consid-eration, although a history of pelvic inflam-matory disease (PID), adjusted for age, parity, duration of oral contraceptive use and infertil-ity, is in a case-control study associated with higher risk for ovarian cancer.147 C. tracho-matis, the most common cause of PID in the developed world,82-84 is one of the genital in-fectious agents that has been addressed as a possible tumor initiator/promoter of the ova-ries.148 It is recently hypothesized that the origin of ovarian cancer might be the junction between the oviductal epithelium and the ovarian surface epithelium, an area of transi-tional epithelia with increased susceptibility to neoplastic progression.149 In parallel with cervical cancer occurring at the squamos co-lumnar junction and gastroesophagic cancer occurring at the esophagogastric junction, this might be a conflict area where chronic infec-tion with for example C. trachomatis might cause cellular damage and proliferation, lead-ing to cancer development.150 This is also the area where the type II tumors of the ovary are suggested to originate.
Persistence of infections are thought to play a key role in the possible association be-tween bacteria and cancer, and there is evi-dence that C. trachomatis can become per-sistent, and express high levels of chlamydial Heat Shock Protein 60 (cHSP60) during per-sistent infections.35, 151 Chlamydial HSP60 is suggested to have an anti apoptotic effect de-veloped to facilitate the survival of the bacte-ria within the host.35 The inflammatory reac-tion in chronic infection causes production of cytotoxic substances that might cause damage to the DNA. Increased cell-turnover is also part of the inflammatory reaction, while cHSP60, by having an anti-apoptotic effect, facilitates the survival of DNA-damaged cells leading to increased risk for cancer initia-tion.46 As C. trachomatis is especially adept
at maintaining a long-term relationship with its hosts, modulating and evading the immune system, and is shown to cause infertility (which in itself is a suggested risk factor for ovarian cancer), there is a possibility that C. trachomatis infections might play a role in carcinogenesis of the ovary.15, 47, 152
Previous studiesNess et al. have found an association of C. tra-chomatis IgG antibodies with ovarian cancer, and a non-significant monotonic trend towards increased ovarian cancer risk associated with cHSP60-1 IgG antibodies, but no associations of cHSP60-2 or cHSP60-3 IgG antibodies.153 However, in a second study no associations of C. trachomatis antibodies and ovarian cancer risk were found,154 rather a negative associa-tion in the younger age groups. Neither did Wong et al. find any associations of serum IgG, IgA or IgM antibodies to Chlamydia spp. How-ever, a serological method detecting antibodies to all Chlamydia species including C. pneumo-niae was used,155 which might have diluted a possible association.
Other genital infections as possible tumor promoters/initiatorsMycoplasma genitalium (M. genitalium), the smallest self-replicating organism known, is another sexually transmitted microorganism that in recent years has been associated with PID, TFI156, 157 and infertility.158 In vitro, M. genitalium can cause inflammatory changes of the epithelium of the human fallopian tubes.159 Similar to C. trachomatis infections, disease caused by M. genitalium is often asymptomatic, or reveals only mild to moder-ate symptoms and it often remains undetec-ted.160 M. genitalium is not previously studied in relation to ovarian cancer, however Myco-plasma DNA (PCR targeting DNA from 15 different species) has been found in 59% of ovarian cancer tissues.161 Other Mycoplasma species have been associated with various cancers such as renal cell carcinoma162 and

introduction
14
cervical intraepithelial neoplasia (CIN),163 and Mycoplasma hyorhinis with gastric and colon cancer.164
The incidence of N. gonorrhoeae in Swe-den is considerably lower than for C. tracho-matis and has from the 1980´s showed a steady decline with an incidence of 2.4 per 100 000 inhabitants in 1996. From 1997 the incidence has risen slightly and was in 2008 7.8 per 100 000 (compared with 454.1 per 100 000 for C. trachomatis).165 N. gonor-rhoeae is known to cause PID and TFI and the infection remains asymptomatic in up to 80% of women.8 In men, N. gonorrhoeae is linked to prostate cancer in several meta-analyses.166, 167 However, it is not previously studied in relation to ovarian cancer.
HPV is a well established cause of cervical cancer and the high-risk types are present in more than 95% of cervical cancer biopsies.168 Regarding HPV in ovarian tissues there are, today, a great number of reports focusing on a possible tumor initiating/promoting role of the virus. Some have detected HPV in ovarian carcinoma tissues169-179 while others have not.180-187 Serum HPV antibodies were not as-sociated with ovarian cancer in one study.188
Polyomaviruses were originally discovered in 1953 but not until 1971 the identification of two new polyoma viruses infecting humans were reported.189 BK virus (BKV) was isolated from the urine of a renal transplant patient with the initials B.K., while JC virus (JCV) was first discovered in the brain of a Hodgkin lymphoma patient who suffered from progres-sive multifocal leukoencephalopathy and whose initials were J.C. The polyoma viruses BKV and JCV have been found in several dif-ferent human tumors (urinary tract, kidney, bone, pancreatic islet, a wide variety of brain tissues and skin tumors – Merkel cell carci-noma) but a causal link has not been estab-lished.190 In vitro BKV and JCV are known to cause transformation of human cells, and they can induce different types of tumors in sev-eral rodent species.191 The presence of these
viruses in ovarian tumors is not previously explored. Recently, findings of a new polyo-mavirus in Merkel Cell carcinomas are strong-ly suggestive of an oncogenic role of the vi-rus.192, 193

15
AiMS
The overall aim of this thesis was to further investigate the effects of Chlamydia tra-
chomatis infection on fertility in men as well as in women, and Chlamydia trachomatis as a possible risk factor for developing ovarian cancer. The specific questions that needed to be answered were:
Does a • C. trachomatis infection in the man or the woman, detected by serum C. trachomatis antibodies, affect the chances of the couple to achieve pregnancy and have a child?Can a • C. trachomatis infection exert a di-rect effect on male fertility, and do semen characteristics differ between serum C. trachomatis antibody positive and nega-tive men of infertile couples?
Is infection with • C. trachomatis, detected by plasma antibodies, associated with epi-thelial ovarian cancer or borderline ovar-ian tumors? Can • C. trachomatis bacteria be detected in ovarian tissues from women with epi-thelial ovarian cancer, borderline ovarian tumors or benign conditions?Are • M. genitalium plasma antibodies as-sociated with ovarian tumors, or can M. genitalium, N. gonorrhoeae, HPV or poly-oma viruses BKV and JCV, be detected in ovarian tissues?
Aims

16

17
MAteriAlS And MethodS
EthicsAll studies were approved of by the Human Ethics Committee of the Medical Faculty, Umeå University, Sweden. Women and men were included after informed consent and the investigations and treatments were uninflu-enced by the study. Screening for C. tracho-matis among infertile couples may however, if positive, raise questions about unfaithful-ness and extramarital sexual activity that could be difficult to handle within the rela-tionship. Professional counseling was offered to all. No tissue in excess to what was clini-cally relevant was removed. An inconvenience to the women and men included was an extra blood sample for some. Control persons from the Antenatal Care program and the Northern Sweden Health and Disease cohort had previ-ously donated blood for research purposes.
Papers I and II: Infertility studyPaper I was a prospective cohort study. As-sociations of C. trachomatis IgG with diagno-sis, pregnancy rate and pregnancy outcome were analyzed comparing exposed and non-exposed within the cohort. The prevalence of C. trachomatis IgG antibodies in the cohort of infertile women was compared to the prev-alence in spontaneously pregnant women. Paper II was based on the same cohort. How-ever, additional serum C. trachomatis anti-bodies were analyzed retrospectively using frozen serum samples, and details of the se-men characteristics were reviewed.
Study populationDuring October 1997 to February 2001, 244 consecutive couples attending the gyneco-logical outpatient clinic at the Department of Obstetrics and Gynecology, University Hos-pital of Northern Sweden, due to infertility (one year of unprotected sexual intercourse without conception) were included (Figure 6). Blood was drawn upon their first visit and tested for C. trachomatis IgG antibodies, while the testing of C. trachomatis IgA and IgM, and cHSP60 IgG, antibodies was done retrospectively. Both partners were also test-ed for HIV and hepatitis B and C, and the women for rubella immunity and for ovula-tion using a mid-luteal serum progesterone according to routine infertility work-up. Se-men analysis of the man (according to the World Health Organization as modified by NAFA/ESHRE194) was undertaken, described in detail in paper II. If either one of the part-ners had C. trachomatis IgG antibodies, a first-void urine sample for detection of C. tra-chomatis DNA was collected from both. If at least one of the partners of the couple had detectable C. trachomatis DNA, they were both treated with doxycycline 100 mg x 2 the first day and thereafter doxycycline 100 mg x 1 for 9 more days.
Clinical investigationOne to three months later, when the test re-sults were available, a consultation according to routine infertility work-up was conducted,
Materials and Methods

MAteriAlS And MethodS
18
including clinical examination and ultra-sonography. Thereafter further investigations such as hysterosalpingosonography (HSS), laparoscopy or additional hormonal assays were planned. The couples were advised about treatment according to the findings. If both tubes were patent without dilation on HSS, no further tubal investigation was carried out. Else, a laparoscopy with chromoperturbation
was planned. The occurrence of an interval spontaneous pregnancy before tubal assess-ment was considered a surrogate marker for the absence of tubal pathology. However mi-nor degrees of tubal pathology may have been present.
In paper I, the clinical diagnosis of male factor, as reported in the medical records, was analyzed. In paper II, details of the semen
244 subfertile couples
C. trachomatis IgG
Achieved active treatmenta 126
Pregnancy data obtainablee 238
Details of semen characteristicsavailableg 226
C. trachomatis IgA and IgMChlamydial HSP60 IgG
C. trachomatis IgG pos
Conceivedf 7Discontinued investigationf 5
Moved away 4Unknown drop-out cause 2
Infertility investigation completedc
170
C. trachomatis PCR testb
(74 women, 70 men)
Tubal assessmentd 173
Figure 6. Study cohort originating from couples attending the gynecologic outpatient clinic due to unfulfilled desire for pregnancy for more than 1 year.
All 244 couples were included in the serum C. trachomatis IgG antibody analyses in paper I.a Ovulation induction (n=49), in vitro fertilization (n=32), intracytoplasmic sperm injection (n=25), insemination with husband or donor sperm (n=20). 118 couples did not get active treatment.b A first-void urine specimen was analyzed.c 74 couples did not have a complete investigation because they conceived before investigation was completed (n=58), and some chose to cancel the investigation (n=15).d Laparoscopy (n=66), hysterosalpingosonography (HSS) (n=87) or both (n=20).e Included in the pregnancy outcome analysis in paper I.f Number of couples who conceived or chose to cancel the investigation before semen analysis.g Couples included in paper II.

19
MAteriAlS And MethodS
characteristics were included in the analyses. Furthermore, male factor was defined as a sperm concentration below 20 millions/mL195 and/or teratozoospermia index (TZI) >1.79 and/or proportion motile spermatozoa <40%. Hence, a reclassification of male factor had to be done.
Follow-upAfter a follow-up period of 14-54 months (mean 37 months) the medical records of all couples included were studied with respect to findings at HSS and laparoscopy, clinical di-agnoses, treatments and reported pregnan-cies. Pregnancy outcome was classified as either past 28 weeks of gestation, spontane-ous abortion or ectopic pregnancy. Treatment related pregnancies were screened by ultra-sound soon after a positive pregnancy test, and all pregnancies were routinely screened by ultrasound at gestation week 15-17. Cou-ples that had not achieved pregnancy by the time the medical records were reviewed, were subjected to a structured telephone interview (carried out by A.I.). They were asked about treatments not found in the medical records (some couples were treated elsewhere), and pregnancies and pregnancy outcome that had not previously been recorded. Pregnancy data were available in 238 of 244 (97.5%) of the couples.
Fertile controlsTo compare the prevalence of C. trachomatis IgG antibodies in women from infertile cou-ples with the prevalence in proven fertile women (paper I), banked sera from women attending the Antenatal Care program at the local health care centers, caring for women in the same geographic area as the women at-tending the gynecologic outpatient clinic, were analyzed (n=244). Women were matched with respect to age (birth year) and the year when blood samples were collected. Only women with spontaneous pregnancies (as recorded in the medical records) were included.
Papers III and IV: Ovarian tumor studyStudy populationPaper III was a case-control study while paper IV was a cross-sectional study.
From 1993 to 2001, 430 women who un-derwent surgery at the Department of Obstet-rics and Gynecology, University Hospital of Northern Sweden, Umeå, Sweden, due to sus-pected ovarian pathology were included in the study after oral and written informed consent. In total, plasma samples (paper III) were available for 291 women (Figure 7), whereof in 238 cases blood was drawn in connection with surgery. For another 53 cases prospec-tive plasma samples (maximum 5.1 years prior to diagnosis) from the Northern Sweden Health and Disease Cohort (NSHDC) were obtainable and included in the analysis. NSH-DC, described in detail elsewhere,196 is a pop-ulation based health survey cohort in Väster-botten County and serves the same population as the University Hospital of Northern Swe-den regarding ovarian tumor surgery. In cases of BOT, EOC and other pelvic malignan-cies, control plasma samples from the NSHDC were matched with respect to age and date of plasma sampling. Control subjects were alive and without a cancer diagnosis (except non-melanoma skin cancer) at the time of diagno-sis of the index case. Four controls per case were analyzed. Ovarian tissue (paper IV) was obtainable in 186 women, and also from the contralateral ovary in 126 women (Figure 7). In 128 women, both plasma and ovarian tis-sue were available.
Clinical characteristics and histopathologic diagnosisInformation on histopathologic diagnosis, ac-cording to the World Health Organization classification,197 as well as data on clinical characteristics, was extracted from the medi-cal records. Histopathologic diagnoses were reviewed by a specialist in gynecologic pathol-ogy (E.L.). For paper III a reclassification ac-

MAteriAlS And MethodS
20
cording to the proposed hypothesis of a type I and a type II pathogenetic pathway,141 de-scribed in the Introduction section, was done. The type I tumors consisted of low-grade se-rous carcinomas and mucinous, endometrio-id and clear cell carcinomas. The type II tumors, that were of particular interest, con-sisted of ovarian moderate and high-grade serous carcinomas, malignant mixed meso-dermal tumors and undifferentiated carcino-mas, including also serous high-grade or un-differentiated peritoneal or fallopian tube cancer since they are suggested to have a com-mon origin.
C. trachomatis analysesC. trachomatis serologyThe principles for C. trachomatis serology are described in the Introduction section. A com-mercial MIF test (MRL Diagnostics/Focus, Cypress, CA, USA) was used according to the instructions of the manufacturer to detect serum C. trachomatis IgG and IgA antibodies. A weak specific immunofluorescence signal in the 1/40 (IgG) and 1/16 (IgA) dilutions were reported as positive in 1/20 and 1/8 respec-tively. A low cut-off value was chosen to in-crease the sensitivity of the test, despite the risk of a decreased specificity. This was done since the infections of interest for these stud-ies were not the acute infections but rather
430 womenunderwent
ovariansurgery
Benignconditions
290
Borderlineovariantumors
29
Epithelialovariancancer
89
Othermalignantconditions
22
48 healthycontrols
180 healthycontrols
43 healthycontrols
11 withmatchedcontrolsa
45 withmatchedcontrolsa
12 withmatchedcontrolsa
12 withplasmasample
54 withplasmasample
16 withplasmasample
TissueA: 110C: 65
TissueA: 4C: 3
TissueA: 52C: 42
TissueA: 20C: 16
209 withplasmasample
Figure 7. Study cohort originating from women who underwent surgery due to suspected ovarian pathology.Orange boxes show number of women with plasma sample obtainable, and yellow boxes the number of matched controls from the NSHDC (Northern Sweden Health and Disease Cohort) matched with respect to age and time of plasma sampling (paper III).Blue boxes show number of women with ovarian tissue obtainable (paper IV). A: Number of tissues from primarily affected ovaries. C: Number of tissues from contra lateral ovaries. All women with tissue from the contra lateral ovary had tissue obtainable from the primarily affected ovary as well.a Number of women for whom 4 matched controls per case were obtainable.

21
MAteriAlS And MethodS
previous, persistent or chronic infections. C. trachomatis IgG titers at the beginning of an acute infection raise rapidly, where after the titer levels decrease to a lower level.1 Chlamy-dial HSP60 IgG antibodies were analyzed with a commercial ELISA kit specific for detection of cHSP60 type 1 (cHSP60-1) IgG antibodies. Genomic studies have demonstrated that the chlamydial genome encodes three versions of HSP60, and type 1 is being expressed in the largest amounts198 and has been associated with cervical cancer.45 Cut off was defined as the mean optical density (OD) value of the negative control plus 0.350. Plasma with OD values ±10% of the cut off value were inter-preted as indeterminant and were excluded from analysis.
DNA and RNA extractionTissue, 25-30 mg for each extraction, was cut frozen in a clean area with a sterile knife. RNA was extracted with RNeasy Mini Kit (Qiagen, Hilden, Germany) and DNA was extracted with QIAamp Blood Mini Kit (Qiagen, Hilden, Germany) according to the instructions of the manufacturer. In principle, a lysis buffer is added to the tissue sample to lyse the proteins. Thereafter DNA/RNA is bound to a mem-brane and the residual contaminants are washed away. Finally, the purified DNA/RNA is eluted from the membrane and is ready to be used in a NAAT. Since human, as well as bacterial or viral, DNA and RNA are purified, the human β-globin gene (two copies per cell) was used as a positive extraction control.
C. trachomatis DNA and RNA analysesThe principles of NAATs are described in the Introduction section. For the infertility stud-ies (paper I and II) a commercially available PCR test (COBAS AMPLICOR C. trachomatis test; Roche Diagnostics, Basel, Switzerland) was used to analyze the presence of C. tracho-matis DNA in first-void urine samples. In an
attempt to increase the chance of finding C. trachomatis, that might be present at very low loads in the ovarian tissue samples (paper IV), we chose to use a commercially available TMA test (Aptima Combo 2, Gen-Probe Inc., USA)199 for paper IV. TMA has a theoreti-cally higher sensitivity due to the target gene, which is the rRNA present in thousands of copies in each cell. Positive and negative con-trols were included in each run.
The RNA-extraction, transportation and test method (paper IV) were validated by spik-ing ovarian tissue samples from 4 different women with 10, 100, 1000, 10 000 and 100 000 C. trachomatis, serovar D-K, bacte-ria respectively. RNA was similarly extracted, added to collection tubes, transported and analyzed with the Aptima Combo 2 test. Fur-ther, urine samples positive or negative for C. trachomatis with the Becton Dickinson ProbeTec (BD Diagnostics, Sparks, Massa-chusetts, USA) were also tested with the same RNA extraction method and Aptima Combo 2, with the expected results.
Additional analysesPaper III: M. genitalium serologyM. genitalium IgG antibodies were detected in plasma samples from cases and controls using a M. genitalium Lipid associated mem-brane protein – Enzyme immuno assay (LAMP – EIA) as previously described.200
Paper IV: N. gonorrhoeae, M. genitalium, HPV and polyoma virus BKV and JCV detectionThe presence of N. gonorrhoeae rRNA in ovarian tissue samples was analyzed by the TMA method (Aptima Combo 2). M. genital-ium DNA was analyzed using a M. genitalium realtime PCR (MgRT – PCR) method as pre-viously described.201, 202 HPV, polyoma virus BKV and JCV, and the human beta-globin gene were detected by PCR. For further de-tails, see paper IV.

MAteriAlS And MethodS
22
StatisticsStatistical analyses were performed using the SPSS software. A majority of the data analyzed are dichotomous why Pearson Chi-square, and when the expected frequency was <5, Fisher’s exact test was used. Spearman’s rank correlation was used for calculating correla-tions (Paper I: C. trachomatis IgG titers and positive PCR test, C. trachomatis IgG titer levels between the partners). Mann-Whitney U test was applied to analyze continuous data not normally distributed (Paper II: semen characteristics; Paper III: Clinical character-istics with continuous data). Ordinal data were analyzed using the Mantel-Haenszel test. Relative risk and 95% confidence inter-vals (CI) were calculated to estimate the strength and precision of the associations (Paper II). Odds ratios (OR) and 95% confi-dence intervals (CI) were calculated using binary logistic regression analysis (Paper I and III), and a multivariate analysis control-ling for possible confounding factors was done in papers I-III. A 2-sided P-value of less than 0.05 was considered significant. To minimize the risk of getting a type 1 error when making multiple comparisons, a sequentially rejective multiple tests procedure according to Bonfer-roni-Holm203 was performed (Paper I and III).

23
reSultS And diScuSSion
Papers I and II: Infertility studyPrevalence of C. trachomatis antibodies and DNAThe prevalence of serum C. trachomatis IgG, IgA and IgM, and cHSP60 IgG antibodies are given in Figure 8. We found a raised preva-lence of serum C. trachomatis IgG antibodies among infertile women compared with prov-en fertile women (24% vs. 16%, P = 0.02). However, in the group of infertile women without TFI the prevalence was only 19% com-pared with 44% among women with TFI (P<0.001) (Table 1). This is in the same range as other Scandinavian studies.110, 200, 204 The prevalence of the antibodies analyzed was also generally higher among women than men,
which is in agreement with the studies by Ka-rinen et. al.110, 205 Similarly the reported inci-dence rates in Sweden indicate higher inci-dence among women, at least in younger age groups, than men165 (Figure 1) possibly result-ing in higher antibody prevalence. On the other hand, in this cohort of infertile men and women, it might reflect that women may be more prone to have a negative effect on fertil-ity of a C. trachomatis infection than men, or have a more pronounced humoral immune response to a C. trachomatis infection. In several cross-sectional population-based studies the prevalence rates of C. trachomatis infection are similar in women and men.51 There is abundant evidence of the negative
Results and Discussion
IgG+
Women
Men
Fertile women
IgA+ IgM+ cHSP60IgG+
IgG+/IgA+ DNA+(% of IgG+)
25
20
15
10
5
0
Per
cent
Paper I: C. trachomatis IgG (n = 244) and DNA. Paper II: C. trachomatis IgA, IgM, cHSP60 IgG (n = 226) and IgG/IgAIgG+/IgA+ percentage refers to women and men in whom both C. trachomatis IgG and IgA antibodies were present.DNA (% of IgG+): C. trachomatis in a first-void urine specimen was present in 11% of IgG+ women and 14% of IgG+ men, thus in 5 women and 5 men. In only one couple both partners were positive.
Figure 8. Prevalence of C. trachomatis serum antibodies and DNA, among infertile men and women, and fertile control women.

reSultS And diScuSSion
24
Table 1. C. trachomatis serum antibodies in women from infertile couples (n=226), in relation to infertility diagnoses.
Diagnoses and C. trachomatis antibodies
No (%) with diagnose with antibody
No (%) without di-agnose with anti-body RR 95% CI
TFI 45 181 IgG+ 20 (44) 35 (19) 2.5 1.5-4.2 IgA+ 10 (22) 24 (13) 1.6 0.88-2.9 cHSP60 IgG+a 12 (27) 24 (14) 1.9 1.08-3.3
Male factor 72 154 IgG+ 8 (11) 47 (30) 0.39 0.20-0.76 IgA+ 7 (10) 27 (17) 0.61 0.30-1.3 cHSP60 IgG+a 8 (12) 28 (19) 0.67 0.35-1.3
Endometriosis 41 185 IgG+ 13 (32) 42 (23) 1.4 0.80-2.6 IgA+ 7 (17) 27 (15) 1.1 0.56-2.5 cHSP60 IgG+a 5 (13) 31 (17) 0.74 0.31-1.8
Anovulation 52 174 IgG+ 9 (17) 46 (26) 0.65 0.34-1.3 IgA+ 5 (10) 29 (17) 0.60 0.25-1.5 cHSP60 IgG+a 4 (8) 32 (19) 0.45 0.17-1.2
Unexplained 25 201 IgG+ 7 (28) 48 (24) 1.2 0.53-2.8 IgA+ 5 (20) 29 (14) 1.4 0.56-3.6 cHSP60 IgG+a 5 (20) 31 (16) 1.3 0.50-3.2
a217 women had valid data in cHSP60 IgG analysis. 7 women had indeterminant results and were excluded from analysis. RR, relative risk (for disease if antibody positive); CI, confidence interval; TFI, tubal factor infertility.
effects of C. trachomatis infections on female fertility, while the results of studies on the ef-fects of C. trachomatis infection on male fer-tility diverge.206 The cohort of proven fertile women was an easy accessible control group since serum, drawn at the beginning of each pregnancy, is prospectively banked within the Northern Sweden Maternity Cohort. The C. trachomatis IgG antibody analysis of the proven fertile women was done retrospec-tively for paper I. There is no corresponding Biobank with blood from proven fertile men, but serum from healthy blood donors from the same time period may have served the purpose as a fertile control group. Regarding semen characteristics, men with C. tracho-matis IgG and IgA antibodies were compared with men from other infertile couples who
might have reduced sperm quality for other reasons. Using proven fertile men as a control group might have resulted in larger differ-ences in semen characteristics.
C. trachomatis DNA was detected by PCR in a first-void urine sample in 5 women and 5 men. In only one couple both the man and the woman were C. trachomatis DNA positive by PCR test. In a recent study, C. trachomatis infections detected by both NAAT and culture or direct fluorescent antibody were concord-ant within sexual relationships in 75%.207 If detected by NAAT only, the concordance rate was 45%, compared to 20% in this study. The low concordance rate if detected with NAAT only might indicate lower bacterial load, low-er transmissibility and persistent infections that are non-infectious.13 Additionally, ex-

25
reSultS And diScuSSion
plaining the low concordance rate in this study, the cohort consisted of infertile couples with no signs or symptoms of acute C. tracho-matis infection. The concordance between C. trachomatis serum IgG in this study was higher; if the man was IgG pos the woman was also IgG pos in 59% of cases and if the woman was IgG pos the man was IgG pos in 47% of cases (P = 0.0005.).
C. trachomatis antibodies and female infertilityThe relative risks (RR) and 95% confidence intervals (95% CI) for the different infertility diagnoses, chance to achieve pregnancy and chance to have a baby (passed 28 weeks of gestation) if pregnant, depending on antibody status are given in table 1 and 2. C. trachoma-tis IgM antibodies are not presented in this or the following tables, since no pattern of asso-ciations were found for this antibody in either the men or the women, not even with a posi-tive PCR test. IgM antibodies are known to reflect acute infections while the couples in this cohort were more likely to have chronic infections. Consistent with the findings of sev-eral previous studies C. trachomatis IgG and
cHSP60 IgG were associated with an increased risk for TFI. However after a multivariate analysis, adjusting for cHSP60 IgG antibodies, age, male factor infertility, male serum C. tra-chomatis IgG and cHSP60 IgG antibodies, only C. trachomatis IgG was significantly as-sociated with TFI. Interestingly, C. trachoma-tis IgG in the woman was negatively associ-ated with a reduced risk of male factor infertility, probably because IgG antibodies in the woman were associated with TFI, and hence, the most probable cause for the infer-tility of the couple. If the woman had TFI the likelihood for a male factor infertility tended to decrease (RR = 0.57, 95% CI 0.31 - 1.1).
One might expect that the negative effect of C. trachomatis on female fertility would have been, at least partially, overcome by IVF treatment since it bypasses the requirement for patent fallopian tubes. However, a slight-ly reduced pregnancy rate was found among IVF treated couples (n = 32), and couples with TFI as their main diagnosis (n = 37) if the woman was C. trachomatis IgG positive (RR = 0.55, 95% CI 0.27 - 1.2, and RR = 0.56, 95% CI 0.29 - 1.05 respectively). The numbers in each group are too small to adjust for possible
Table 2. C. trachomatis serum antibodies in women from infertile couples (n=226), in relation to pregnancy rate and pregnancy outcome.
Pregnancy resultsa and C. trachomatis antibod-ies
No (%) of pregnant with antibody
No (%) of not preg-nant with antibody RR 95% CI
Achieved pregnancy 143 83 IgG+ 30 (21) 25 (30) 0.82 0.63-1.1 IgA+ 20 (14) 14 (17) 0.92 0.68-1.3 cHSP60 IgG+b 21 (15) 15 (19) 0.89 0.66-1.2
Passed 28 weeksc 109 34 IgG+ 23 (21) 7 (30) 1.0 0.80-1.3 IgA+ 17 (16) 3 (9) 1.1 0.92-1.4 cHSP60 IgG+b 16 (15) 5 (15) 1.0 0.77-1.3
aAfter 14-54 months (mean 37 months) of follow-up.b217 women had valid data in cHSP60 IgG analysis. 7 women had indeterminant results and were excluded from analysis. cNumber of women that passed 28 weeks of gestation out of the 143 women that achieved pregnancy.RR, relative risk (or chance to achieve pregnancy and have a child if antibody positive); CI, confidence interval.

reSultS And diScuSSion
26
confounding by C. trachomatis antibodies in the male partner. In some IVF treated cohorts chlamydial antibodies were not associated with reduced pregnancy rates.208-213 In one study all C. trachomatis IgG positive women were treated with doxycycline prior to IVF possibly masking an association.214 In sev-eral others, C. trachomatis IgG antibodies have been a predictor of negative IVF out-come.215-217 Similarly, cHSP60 IgA antibodies in the cervix101 or cHSP60 IgG or IgA antibod-ies in follicular fluid99 100 have been associ-ated with impaired embryo implantation rates after IVF. One possible explanation for a re-duced pregnancy rate is that there still is a chronic C. trachomatis infection causing an inflammatory reaction which prevents suc-cessful embryo implantation. Another, is the suggested auto-immune cross-reaction of cHSP60 IgG antibodies to human HSP60 due to the structural similarities of human and chlamydial HSP60.36 Since HSP60 is ex-pressed at unique developmental stages of embryogenesis,218 cHSP60 IgG antibodies will exert a negative effect on embryo devel-opment and implantation resulting in de-creased reproductive outcome.
One way to evaluate the clinical usefulness of a diagnostic test is to estimate the positive predictive value (PPV) and the negative pre-dictive value (NPV) which are, apart from sensitivity and specificity of the test, also de-pendent on the prevalence of the disease in the population of interest. In this cohort of infertile women the PPV of C. trachomatis IgG in diagnosing TFI was 36% and the NPV was 85%, indicating that the test alone is mediocre in discriminating between women with TFI and those without. Combining the test for C. trachomatis IgG antibodies with cHSP60 IgG antibodies did not improve the PPV or NPV.
C. trachomatis has been associated with ectopic pregnancy, preterm labor, premature rupture of the membranes (PROM) and pre-term delivery.219 In this study the rate of ec-topic pregnancy was somewhat higher in the
IgG pos group (3/32, 9.4%) than in the nega-tive group (3/118, 2.5%) but the numbers are too small to draw any conclusions. Since not all pregnancies were followed until term the rate of preterm labor, premature rupture of the membranes or neonatal infections could not be estimated. However, no difference in the number of antibody positive and negative women passing 28 weeks of gestation was found.
C. trachomatis antibodies and male infertilityThe relative risks (RR) and 95% confidence intervals (95% CI) for the different infertility diagnoses, chance to achieve pregnancy and chance to have a baby (passed 28 weeks of gestation) if pregnant, depending on antibody status in the man are given in table 3 and 4. C. trachomatis IgG and IgA antibodies in the man were associated with a slightly increased risk for male factor infertility. None of the an-tibodies in the man were significantly associ-ated with TFI in the woman even though a tendency can be noticed. C. trachomatis IgG and IgA antibodies in the man were associ-ated with reduced pregnancy rates (table 4). Interestingly the chances to achieve pregnan-cy were further reduced if the man was positive in both C. trachomatis IgG and IgA. When combining the IgG and IgA results into four different groups (i. e. IgG-/IgA-, IgG+/IgA-, IgG-/IgA+ and IgG+/IgA+) only the IgG+/IgA+ remained a statistically significant pre-dictor of reduced pregnancy rates (paper II, Table 4). The combination of IgG and IgA an-tibodies apparently increased specificity for detecting an effect on male fertility. Stratifica-tion for antibody status in the woman, TFI, or age of the man or the woman (below 35 years, 35 years or older), did not change the results. The mean follow-up time did not differ be-tween the four groups (3.1, 3.0, 3.0 and 3.2 years respectively). IVF or ICSI treatment did not seem to overcome the negative effects on pregnancy rates associated with C. trachoma-
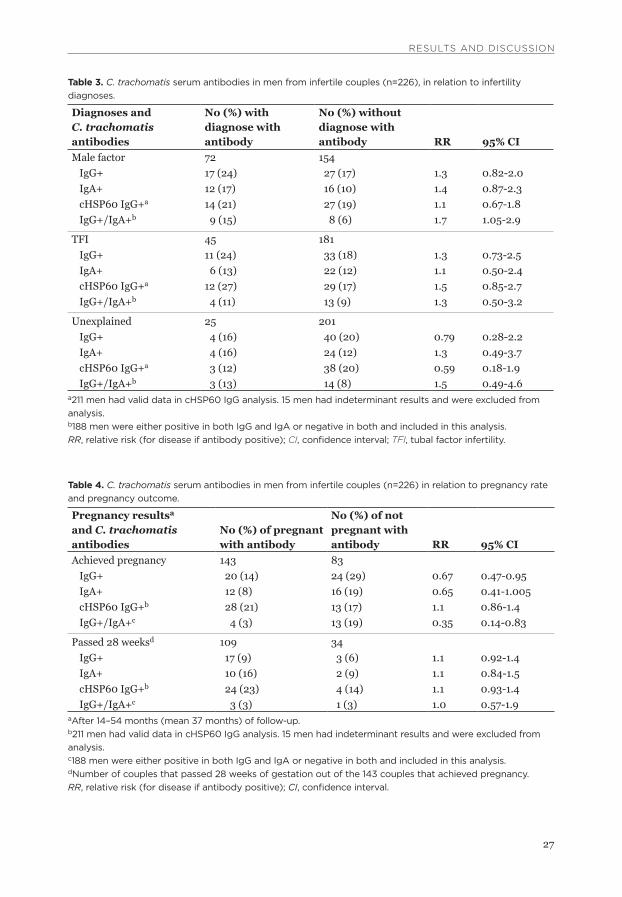
27
reSultS And diScuSSion
Table 3. C. trachomatis serum antibodies in men from infertile couples (n=226), in relation to infertility diagnoses.
Diagnoses and C. trachomatis antibodies
No (%) with diagnose with antibody
No (%) without diagnose with antibody RR 95% CI
Male factor 72 154 IgG+ 17 (24) 27 (17) 1.3 0.82-2.0 IgA+ 12 (17) 16 (10) 1.4 0.87-2.3 cHSP60 IgG+a 14 (21) 27 (19) 1.1 0.67-1.8 IgG+/IgA+b 9 (15) 8 (6) 1.7 1.05-2.9
TFI 45 181 IgG+ 11 (24) 33 (18) 1.3 0.73-2.5 IgA+ 6 (13) 22 (12) 1.1 0.50-2.4 cHSP60 IgG+a 12 (27) 29 (17) 1.5 0.85-2.7 IgG+/IgA+b 4 (11) 13 (9) 1.3 0.50-3.2
Unexplained 25 201 IgG+ 4 (16) 40 (20) 0.79 0.28-2.2 IgA+ 4 (16) 24 (12) 1.3 0.49-3.7 cHSP60 IgG+a 3 (12) 38 (20) 0.59 0.18-1.9 IgG+/IgA+b 3 (13) 14 (8) 1.5 0.49-4.6
a211 men had valid data in cHSP60 IgG analysis. 15 men had indeterminant results and were excluded from analysis. b188 men were either positive in both IgG and IgA or negative in both and included in this analysis.RR, relative risk (for disease if antibody positive); CI, confidence interval; TFI, tubal factor infertility.
Table 4. C. trachomatis serum antibodies in men from infertile couples (n=226) in relation to pregnancy rate and pregnancy outcome.
Pregnancy resultsa and C. trachomatis antibodies
No (%) of pregnant with antibody
No (%) of not pregnant with antibody RR 95% CI
Achieved pregnancy 143 83 IgG+ 20 (14) 24 (29) 0.67 0.47-0.95 IgA+ 12 (8) 16 (19) 0.65 0.41-1.005 cHSP60 IgG+b 28 (21) 13 (17) 1.1 0.86-1.4 IgG+/IgA+c 4 (3) 13 (19) 0.35 0.14-0.83
Passed 28 weeksd 109 34 IgG+ 17 (9) 3 (6) 1.1 0.92-1.4 IgA+ 10 (16) 2 (9) 1.1 0.84-1.5 cHSP60 IgG+b 24 (23) 4 (14) 1.1 0.93-1.4 IgG+/IgA+c 3 (3) 1 (3) 1.0 0.57-1.9
aAfter 14–54 months (mean 37 months) of follow-up.b211 men had valid data in cHSP60 IgG analysis. 15 men had indeterminant results and were excluded from analysis. c188 men were either positive in both IgG and IgA or negative in both and included in this analysis.dNumber of couples that passed 28 weeks of gestation out of the 143 couples that achieved pregnancy.RR, relative risk (for disease if antibody positive); CI, confidence interval.

reSultS And diScuSSion
28
tis antibodies (table 5), however the numbers were too small in that group to draw any firm conclusions. The association of C. trachoma-tis antibodies in the man with reduced preg-nancy rates is similar to those of some110 but not to others.111, 117, 118, 122 In one study, high titers of C. trachomatis antibodies in the man were associated with reduced pregnancy rates,112 however also with TFI in the female partner. The authors concluded that the neg-ative effect was probably based on sexual transmission to the female partner thereby causing damage to the female reproductive tract.
Semen characteristics in relation to C. tra-chomatis antibodies are described in table 6 (for details see paper II, table 5). There were subtle negative changes in semen character-istics associated with C. trachomatis IgG and
IgA. If both serum C. trachomatis IgG and IgA were positive in the man there was reduced sperm concentration and percentage motile spermatozoa, increased teratozoospermia in-dex (TZI), reduced sperm vitality and occur-rence of leukocytes in seminal fluid. Whether there is a direct effect on spermatozoa has un-til recently been controversial. There is accru-ing evidence of detrimental effects of C. tra-chomatis on semen characteristics. Reduced motility,124, 125, 127, 220 sperm DNA fragmenta-tion,128, 221 reduced survival of spermatozoa,127,
220 lowered sperm concentration,106, 111 blunt-ed acrosome reaction107 and an increased amount of leukocytes113, 116, 126 are among the findings. Others have not found any associa-tions between serum or semen IgG or IgA and semen characteristics.112-122 In an in vivo study on infertile men (n = 143) the effect of a C.
Table 5. Pregnancy rates in the subgroup of IVF and ICSI treated couples according to C. trachomatis IgG and IgA antibody status in the man.
C. trachomatis antibody status Pregnancy No pregnancyIVF IgG+/IgA+ 1 (50%) 1 (50%) IgG-/IgA- 19 (63%) 11 (37%)
ICSI IgG+/IgA+ 0 (0%) 3 (100%) IgG-/IgA- 10 (59%) 7 (41%)
IVF, in vitro fertilization; ICSI, intracytoplasmic sperm injection
Table 6. Simplified table of C. trachomatis serum antibodies, in men from the infertile couples, in relation to key parameters from semen analysis (n=226). P-values. Details of the semen characteristics are given in paper II.
C. trachomatis antibody
Volume(mL)
Concentra-tion(x106/mL)
Motile sperma- tozoa (%)
Teratozoo-spermia index
Sperm vitality (%)
Leuco-cytes
IgG+ ns ns ns ns ns 0.035IgA+ ns ns 0.023 ns 0.014 0.005cHSP60 IgG+a ns ns 0.033 ns ns nsIgG+/IgA+b ns 0.033 0.030 0.010 0.040 0.012
a211 men had valid data in cHSP60 IgG analysis. 15 men had indeterminant results and were excluded from analysis. b188 men were either positive in both IgG and IgA or negative in both and included in this analysis.ns, not significant

29
reSultS And diScuSSion
trachomatis infection was greatest, in relative terms, on sperm DNA fragmentation as com-pared to standard semen parameters.221 A subgroup (n = 95) of patients were evaluated after antibiotic treatment and showed a sig-nificant improvement in sperm DNA fragmen-tation and also in sperm morphology. The follow-up in terms of clinical pregnancies was somewhat irregular and considered only a very small subgroup; out of 14 couples attempting pregnancy 3-6 months after antibiotic therapy, 12 (86%) achieved pregnancy. Sperm DNA fragmentation has in meta-analyses been as-sociated with reduced pregnancy rates222 and increased risk of pregnancy loss223 after IVF and ICSI. There was in this study no associa-tion of C. trachomatis antibodies in either the man or the woman with pregnancy outcome/loss.
Even though the above mentioned impli-cates that there might be a direct effect of C. trachomatis on sperm quality, and male fer-tility, it cannot be ruled out that the effect is a result of a factor(s) that covariates with C. trachomatis serum antibodies and is as yet unknown. One of many plausible factors could be a concurrent undiagnosed infection with M. genitalium, that is also sexually transmit-ted and is an established cause of non-gono-coccal urethritis224 and is shown to attach to human spermatozoa.225 The Practice Com-mittee of the American Society for Reproduc-tive Medicine has reviewed available data on cigarette smoke and effect on fertility and conclude that there is reduced sperm concen-tration, motility and morphology in men that are cigarette smokers, but the effects on preg-nancy rates have been difficult to discern.226 Data on smoking was not available for the women and men in this study, neither was serum cotinine, a nicotine metabolite used to determine the amount of cigarette smoke ex-posure,227 analyzed. The decreased pregnan-cy rates might also, in part, be an effect of sexual transmission to the female partner causing damage to the female reproductive
tract. C. trachomatis may also, by causing epididymitis, damage the canalicular system of the male genital tract thereby causing ob-structive azoospermia, although this is prob-ably a rare event and cannot account for the results herein. Another theory is that C. tra-chomatis may induce an autoimmune cross-reaction with antisperm antibodies or autoan-tibodies based on immune activation.106, 228 There was no association of serum C. tracho-matis antibodies in the man and seminal an-tisperm antibodies in this study.
Methodological considerationsStrengths of this study were the homogenous cohort of 244 (reduced to 226 in paper II) consecutive couples where both the man and the woman were included in the analysis. There was a long follow-up period with a small number of drop-out. The serum antibody tests used are specific for C. trachomatis serovar D–K known to cause genital disease. How-ever, tubal assessment might have been more accurate if all women had undergone lapar-oscopy with chromo-perturbation where also peritubal adhesions could have been detected. Laparoscopy was carried out only if hystero-salpingosonography (HSS) did not show pat-ent, un-dilated tubes bilaterally, or if indi-cated for other reasons like suspicion of endometriosis. This should give a fairly ac-curate diagnosis of TFI since sensitivity of HSS for tubal occlusion/dilation is shown to be more than 88%.229, 230 It would also be an ethical dilemma to subject women to lapar-oscopy if HSS is sufficient. C. trachomatis DNA testing on a first-void urine specimen was performed only if one of the partners of the couple was positive in serum C. tracho-matis IgG. Testing all would have resulted in a more reliable estimate of the prevalence in the infertile cohort. Theoretically, though, not many persons would have been positive if negative in IgG testing since there was a sig-nificant correlation of C. trachomatis IgG titer levels and the finding of C. trachomatis

reSultS And diScuSSion
30
DNA (r = 0.3, P = 0.026). Since bacteria might be present in semen231, 232 or prostatic tis-sue,233 even though not evident in urine spec-imens, it would have been plausible to test also semen samples for C. trachomatis DNA. The results of couples treated by insemination should have been divided in two groups; in-semination with husband sperm (AIH) or donor sperm (AID), since the treatments are different, analyzing the impact of C. tracho-matis in the male partner regarding preg-nancy rates. Data on cigarette smoking is lacking in both women and men why possible confounding from this factor could not be ac-counted for. To be able to draw any conclu-sions on whether the negative effects of C. trachomatis can be overcome with IVF/ICSI a larger cohort of IVF/ICSI treated couples is needed.
Different antibodies – different mechanisms?Serum cHSP60 IgG antibodies are consist-ently associated with sequels of chlamydial infection in women, such as PID, TFI, and ec-topic pregnancies.37-40, 42, 43, 102, 234-239 Chlamy-dial HSP60 IgG antibodies were also associ-ated with a subgroup of ovarian tumors in the women in paper III, while C. trachomatis IgA antibodies were unrelated to any kind of ovar-ian tumors as well as infertility parameters in the women of the present studies. On the con-trary, cHSP60 IgG antibodies were not associ-ated with male infertility either in this study or the study by Karinen et al.205 Instead, a stronger association with both reduced preg-nancy rates and impaired semen characteris-tics was found when the man was positive in both serum C. trachomatis IgG and IgA anti-bodies. It is intriguing to speculate how the difference in antibodies translates into differ-ent mechanisms of disease. In women tissue damage of the fallopian tubes is the main char-acteristic of C. trachomatis induced infertility, caused by persistent or repeated C. trachoma-tis infections. When C. trachomatis enters a
persistent state it produces predominantly cHSP60 proteins thereby inducing the produc-tion of cHSP60 antibodies. If the tissue damage is caused by the bacteria itself and the inflam-matory reaction surrounding it, or by an auto-immune cross-reaction of cHSP60 antibodies to human HSP60 thereby attacking “self” tis-sue, or both, is not clearly understood.
In the man, serum cHSP60 IgG antibodies were unrelated to pregnancy rates and did not add any extra information regarding semen characteristics. Tissue damage by persistent C. trachomatis infections is probably not the main component of the negative effects on fertility. IgA antibodies, that were more in-formative regarding the effects on male fertil-ity, are more likely to reflect an active on-going phase of the infection as compared to cHSP60 IgG antibodies. A combination of both IgG and IgA antibodies seemed to increase the spe-cificity in detecting decreased fertility poten-tial and impaired semen characteristics. Hence, indicating that it is chronic (or acute) infection with C. trachomatis, and bacteria present in the male reproductive tract, exert-ing its effects directly to the spermatozoa, that impair male fertility. This is supported by in-vitro studies where co-incubation of human sperm with C. trachomatis bacteria results in increased phosphatidylserine externalization (a sign of apoptosis) and sperm DNA fragmen-tation,128 and reduced motility and vitality.127 In vivo C. trachomatis has been associated with sperm DNA fragmentation221 as well as blunted acrosome reaction.107
Papers III and IV: Ovarian tumor studyPrevalence of C. trachomatis and M. genitalium antibodiesThe prevalence of plasma antibodies among cases and controls are given in Figure 9A-C, but are also presented in paper III (table 2) including the P - value of the association be-tween a specific antibody and ovarian tumors. The prevalence of plasma C. trachomatis IgG,

31
reSultS And diScuSSion
33
23 22
24 23
22 23
0
5
10
15
20
25
30
35
Benign conditions BOT, P = 0.36 EOC, P = 0.50 Other malignancies, P = 0.67
Per
cent
Cases
Controls
Figure 9B. Prevalence of plasma cHSP60 IgG antibodies.
33
8,5
0
8,1
4,2 3,7
0 0
5
10
15
20
25
30
35
Benign conditions BOT, P = 0.012 EOC, P = 0.16 Other malignancies
Per
cent
Cases
Controls
Figure 9C. Prevalence of plasma M. genitalium IgG antibodies.
Benign conditions, n = 209; BOT, borderline ovarian tumors, n = 12/matched controls n = 48; EOC, epithelial ovarian cancer, n = 47/matched controls n = 188; other malignancies n = 9/matched controls n = 35.
33
19
11
24
19
16
11
0
5
10
15
20
25
30
35
Benign conditions BOT, P = 0.21 EOC, P = 0.37 Other malignancies, P = 0.73
Per
cent
Cases
Controls
Figure 9A. Prevalence of plasma C. trachomatis IgG antibodies.
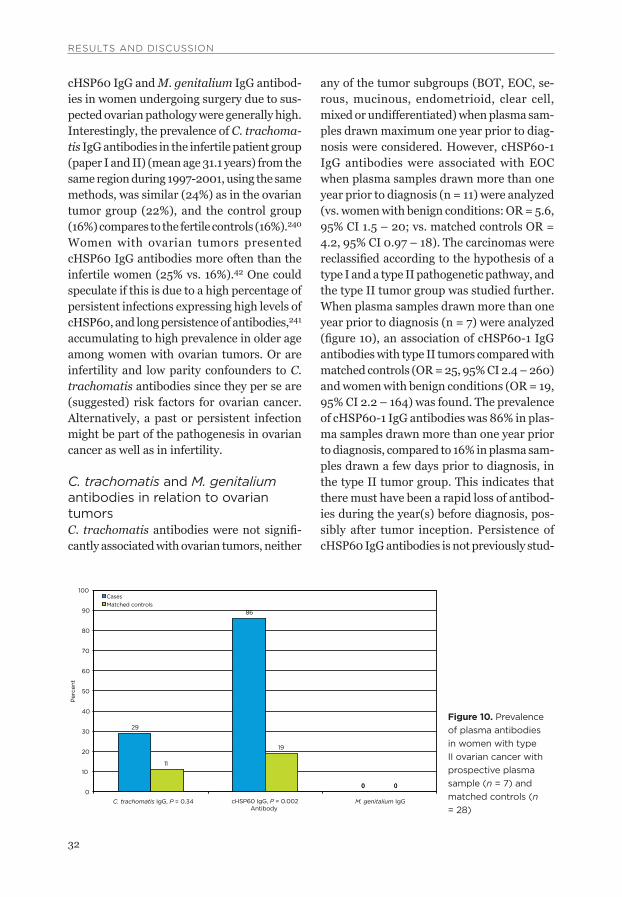
reSultS And diScuSSion
32
cHSP60 IgG and M. genitalium IgG antibod-ies in women undergoing surgery due to sus-pected ovarian pathology were generally high. Interestingly, the prevalence of C. trachoma-tis IgG antibodies in the infertile patient group (paper I and II) (mean age 31.1 years) from the same region during 1997-2001, using the same methods, was similar (24%) as in the ovarian tumor group (22%), and the control group (16%) compares to the fertile controls (16%).240 Women with ovarian tumors presented cHSP60 IgG antibodies more often than the infertile women (25% vs. 16%).42 One could speculate if this is due to a high percentage of persistent infections expressing high levels of cHSP60, and long persistence of antibodies,241 accumulating to high prevalence in older age among women with ovarian tumors. Or are infertility and low parity confounders to C. trachomatis antibodies since they per se are (suggested) risk factors for ovarian cancer. Alternatively, a past or persistent infection might be part of the pathogenesis in ovarian cancer as well as in infertility.
C. trachomatis and M. genitalium antibodies in relation to ovarian tumors C. trachomatis antibodies were not signifi-cantly associated with ovarian tumors, neither
any of the tumor subgroups (BOT, EOC, se-rous, mucinous, endometrioid, clear cell, mixed or undifferentiated) when plasma sam-ples drawn maximum one year prior to diag-nosis were considered. However, cHSP60-1 IgG antibodies were associated with EOC when plasma samples drawn more than one year prior to diagnosis (n = 11) were analyzed (vs. women with benign conditions: OR = 5.6, 95% CI 1.5 – 20; vs. matched controls OR = 4.2, 95% CI 0.97 – 18). The carcinomas were reclassified according to the hypothesis of a type I and a type II pathogenetic pathway, and the type II tumor group was studied further. When plasma samples drawn more than one year prior to diagnosis (n = 7) were analyzed (figure 10), an association of cHSP60-1 IgG antibodies with type II tumors compared with matched controls (OR = 25, 95% CI 2.4 – 260) and women with benign conditions (OR = 19, 95% CI 2.2 – 164) was found. The prevalence of cHSP60-1 IgG antibodies was 86% in plas-ma samples drawn more than one year prior to diagnosis, compared to 16% in plasma sam-ples drawn a few days prior to diagnosis, in the type II tumor group. This indicates that there must have been a rapid loss of antibod-ies during the year(s) before diagnosis, pos-sibly after tumor inception. Persistence of cHSP60 IgG antibodies is not previously stud-
Figure 10. Prevalence of plasma antibodies in women with type II ovarian cancer with prospective plasma sample (n = 7) and matched controls (n = 28)
29
86
0
11
19
0 0
10
20
30
40
50
60
70
80
90
100
Per
cent
Cases Matched controls
0 0
C. trachomatis IgG, P = 0.34 cHSP60 IgG, P = 0.002Antibody
M. genitalium IgG

33
reSultS And diScuSSion
ied but C. trachomatis IgG antibodies are in some studies shown to decrease in a high per-centage of cases242, 243 but not in others.241,
244 Since the type II tumor group with pro-
spective plasma samples was small, concern is raised that the high prevalence is due to chance alone. Furthermore, the possibility to correct for potential confounders was limited. However, data on clinical characteristics in the subgroup of type II tumors was well-doc-umented and the group was not extreme in any other respect than the prevalence of cHSP60-1 IgG antibodies (paper III, table 4). A rule of thumb is that a multiple logistic re-gression model needs at least 10 cases for each variable to be included in the analysis, and a minimum requirement is twice as many sub-jects as independent variables.245 None of the potential confounders (age at menarche, age at menopause, parity, oral contraceptive pill use, HRT use, smoking and BMI) changed the significance of the association between cHSP60-1 IgG antibodies and type II tumors in a multivariate analysis. Due to the small number of cases precision of the estimate of the association is poor and no conclusion on the strength of the relative risk associated with cHSP60-1 IgG antibodies can be inferred from this data. Nonetheless, a significant as-sociation of cHSP60-1 IgG antibodies with type II ovarian/pelvic cancer was present.
Furthermore, plasma M. genitalium IgG was associated with BOT (n = 12) (vs. matched controls: OR = 11, 95% CI 1.7 – 74; vs. benign conditions: OR = 3.8, 95% CI 1.09 - 13). C. trachomatis IgG and cHSP60-1 IgG antibod-ies were only slightly raised in the BOT sub-group. This subgroup was also small leading to poor precision in the estimates. The asso-ciation of M. genitalium IgG antibodies with BOT might represent a type 1 error since a correction for multiple comparisons accord-ing to Bonferroni-Holm,203 defining the tests performed on BOT, EOC and other pelvic ma-lignancies (paper III, table 2) as one family,
eliminates the significance of the results. Pos-sible mechanisms by which Mycoplasma might act as a tumor initiator/promoter (be-sides chronic inflammatory changes) are not known, but the Mycoplasma membrane lipo-protein p37 of M. hyorhinis is suggested to promote malignant changes in mammalian cells.246-248 The gene expression profile is al-tered during Mycoplasma-induced malignant cell transformation249 and Mycoplasma caus-es inhibition of p53 tumor suppression func-tion and activation of nuclear factor κB (NF-κB) in rodent fibroblasts.250 If this applies to M. Genitalium and BOT remains unknown.
C. trachomatis, N. gonorrhoeae, M. genitalium, HPV, and polyoma virus BKV and JCV in ovarian tissues (paper IV).All 312 ovarian tissue samples analyzed were positive for the human ß-globin gene and con-sidered to have sufficient DNA quality. None of the tissue samples were positive for M. genitalium, HPV, JCV or BKV DNA.
Urine samples positive or negative for C. trachomatis with the Becton Dickinson ProbeTec PCR method were confirmed posi-tive and negative as expected with the Aptima Combo 2 test. Likewise the ovarian tissue bi-opsies spiked with C. trachomatis bacteria were all, after RNA-extraction, transportation and handling as with the test tissues, con-firmed positive. None of the 312 ovarian tissue samples were positive for C. trachomatis or N. gonorrhoeae rRNA.
Methodological considerationsThe study population represented all cases in a well-defined geographic area during a spec-ified time period. However, plasma and tissue samples were lacking in a considerable number of cases (Figure 7). Women without plasma or tissue samples did not differ in terms of age or diagnoses from the women with plasma or tissue eligible for analysis though. Furthermore, data on general, gyne-

reSultS And diScuSSion
34
cologic and reproductive health were not complete, particularly among women with benign conditions, since they were extracted from the medical records. Plasma samples drawn within a few days prior to diagnosis were analyzed in a majority of cases. Consid-ering the results of this study, and others con-cerning C. trachomatis and cervical cancer and H. pylori and gastric cancer251, 252 (will be discussed in Suggested model of C. tracho-matis in the pathogenesis of ovarian cancer), analyzing plasma samples drawn several years prior to diagnosis would have been a more plausible approach.
We chose to compare the antibody preva-lence among the women with BOT, EOC and other malignancies with the prevalence among women with benign conditions. How-ever, women going through surgery due to benign conditions might have bleeding ir-regularities, pain, infertility, etc. Sexually transmitted infections, especially C. tracho-matis, are known to be a possible cause of many of these conditions, rendering the pos-sibility of a high prevalence of antibodies in this patient group. Using them as controls might have lead to an underestimation of the possible association of C. trachomatis and M. genitalium antibodies with ovarian tumors. The women with benign conditions were also younger than the women with carcinomas. Therefore, an external control group of wom-en without a cancer diagnosis and alive at the time of the diagnosis of the index case was also analyzed. The control plasma samples were collected as part of the Northern Sweden Health and Disease Cohort196 (NSHDC) which is a population based, prospective health sur-vey cohort, in Västerbotten County, serving the same geographic area as the cases were recruited from. Four controls per case were matched with respect to age and date of plas-ma sampling. This is important as the preva-lence of sexually transmitted infections (STI´s) is known to vary over time and the incidence and prevalence are different in dif-
ferent age groups.204, 253-255 The participation rate of the Västerbotten Intervention Project (VIP), the part of NHSDC from which a vast majority of the controls were recruited, has varied between 55% and 60% of all the eligible persons invited during the course of the pro-gram. The participants have been compared with the non-participants and no obvious so-cial differences have been found.256 By using two control populations we attempted to in-crease the basis for the interpretation of data. There was a difference in C. trachomatis IgG antibody prevalence among women with be-nign conditions compared with controls from the NSHDC (24% vs. 16%, OR 1.7, 95% CI 1.08 – 2.7). No differences in cHSP60-1 IgG or M. genitalium IgG antibodies were detected.
The prevalence of cHSP60-1 IgG antibodies in this study was relatively high compared with the prevalence of C. trachomatis IgG antibod-ies, particularly in the subgroup of women with type II carcinoma. This is different from the findings in most other studies and might reflect differences in laboratory methods. It also raises the question if there was a high number of false positive tests, i.e. poor spe-cificity. Another explanation is that the C. tra-chomatis infections that will eventually lead to carcinomatous changes produce higher amounts of cHSP60 or produces cHSP60 for a more protracted period of time, e.g. persist-ent infections for a long period of time, induc-ing the production of cHSP60 IgG antibodies. Alternatively, there is a difference in the host immune system that puts C. trachomatis bac-teria in a persistent state, leading both to the continuous production of cHSP60 IgG anti-bodies and renders the host more susceptible to carcinomatous changes. This might be the case if for example an autoimmune cross-re-action to the human HSP6036 plays a patho-logical role. Differences in host immunological traits have been associated with development of PID,102 TFI,104 recurrent infections,103 and tubal pathology.257

35
reSultS And diScuSSion
Since none of the microorganisms analyzed were found in any of the tissue samples one is reluctant to think that the methods used were insufficient. The nucleic acid extraction methods used are well-documented commer-cial kits, and the presence of human DNA was tested in all extractions. RNA quality, though, was not examined by targeting a human RNA gene in the tissue samples. However, RNA integrity in snap-frozen tissues stored at -80°C subjected to repeated freeze-thaw pro-cedures is shown to be intact.258, 259 The ex-traction, transportation and analysis of RNA were validated both by running positive C. trachomatis urine samples and C. trachoma-tis spiked ovarian biopsies through the same process with the expected results. Nonethe-less, concern might be raised if RNA was de-graded in these tissue samples, or if targeting rRNA is the right method for detecting a per-sistent C. trachomatis infection. However, rRNA is shown to be continuously expressed in experimentally induced persistent infec-tions.13, 16, 33, 260, 261 Analyzing the presence of human RNA in the tissue samples or using a NAAT method targeting C. trachomatis and N. gonorrhoeae DNA could have helped solve the question.
M. genitalium, HPV and polyoma virus were analyzed with NAATs using DNA as tar-get and with a target length shorter than the human β-globin gene used as a positive extrac-tion control. The NAATs used are well-docu-mented. All together this indicates that there is a true absence of M. genitalium, HPV or polyoma virus in the ovarian tissue samples.
Does the absence of bacteria and virus in the ovarian tissue mean that they are not part of the pathogenesis in ovarian tumor develop-ment? Wallin et al. found all tumor biopsies from cervical cancer at diagnosis to be nega-tive for C. trachomatis. However, C. tracho-matis DNA in cervical pap smears several years prior to the diagnosis was associated with cervical cancer.262 Furthermore, the se-rological association is stronger the longer the
lag time is between blood sampling and cervi-cal cancer diagnosis.45, 145, 146, 263 Concerning gastric cancer the association between H. py-lori infection and cancer is strongest when the interval between serum collection and cancer diagnosis is longer than 15 years.251 When atrophic gastritis and intestinal meta-plasia occur (precursors of gastric adenocar-cinoma), biopsies taken from these areas yields no H. pylori bacteria.251 However, H. pylori is often identified in nonatrophic loca-tions of the same stomach where intestinal metaplasia occurs, but C. trachomatis bacte-ria could not be detected in any ovarian tis-sues (malignant, benign or from the contral-ateral ovary) in this study. No tissue from the fallopian tubes or the tubal fimbriae were analyzed which might have been a more plau-sible approach considering the hypothesis that type II ovarian/pelvic cancer arises in the tubal fimbriae, with a rapid spread to the ova-ries soon after inception.
Suggested model of C. trachomatis in the pathogenesis of ovarian cancerThe results in this study will be put into the context of the present knowledge of C. tra-chomatis infections and ovarian tumor patho-genesis, suggesting a hypothesis for an asso-ciation by trying to answer three questions. When, where and how could possibly a C. trachomatis infection contribute to ovarian carcinogenesis?
When does C. trachomatis initiate/promote ovarian carcinogenesis?Chlamydial HSP60-1 IgG antibodies were as-sociated with ovarian cancer only when plas-ma samples drawn more than one year prior to diagnosis were analyzed, and the bacteria were not present in ovarian tumors at diag-nosis. Similar to this, the association of H. pylori infection with gastric cancer (which are etiologically linked) is stronger the longer the interval between serum collection and cancer

reSultS And diScuSSion
36
diagnosis,252 and H. pylori bacteria are not found in gastric adenocarcinoma tissue.251
The results herein have similarities also with the findings concerning C. trachomatis and cervical cancer. Naucler et al. observed a positive correlation between C. trachomatis IgG antibodies and cases observed during follow-up, but not with cases identified at baseline;263 cHSP60-1 IgG antibodies have been associated with cervical cancer in cases with lag time more than 3.5 years between serum sampling and cancer diagnosis;45 an increasing risk has been associated with in-creased lag time145 and if the lag time was more than 12 months there was an association between antibodies and cervical carcinoma.146 Furthermore, prediagnostic smears and cer-vical cancer tissue were devoid of C. tracho-matis even though the bacteria were present in Pap smears several years before cancer di-agnosis.262 No C. trachomatis DNA was iden-tified in Pap smears from control women.
C. trachomatis antibodies were not associ-ated with ovarian cancer in a study where retrospectively drawn plasma samples were analyzed154 but an association of borderline-significance was found in another study.153 A conceivable explanation for this is that anti-bodies might decline over time242, 243 and new infections occur that will dilute a possible as-sociation. Alternatively, the ovarian cancer treatment influences C. trachomatis antibody prevalence.
Where is the site for ovarian carcinogenic C. trachomatis infections?C. trachomatis is known to cause damage to the distal fallopian tube but the bacteria have been detected in many cell types of the human body. However, in experimentally induced infections of mice264 as well as pig-tailed mon-keys,265 where the histopathologic changes were characteristic of the damage observed in women with TFI,266 chlamydial inclusions were observed only in the secretory cells both
by immunoperoxidase staining and by trans-mission electron microscopy. C. trachomatis bacteria have not been identified in the ovar-ian tissues in this study. Are the secretory cells the main target of C. trachomatis in the fal-lopian tubes? If so, it coincides with the target of the p53 signatures that are associated with tubal intraepithelial carcinoma (TIC),142 the suggested precursor of type II ovarian/pelvic carcinomas.267 The mucosa of the tubal fim-briae have shown to be resistant to implanta-tion from carcinomas at other sites of the abdomen, whereas the ovarian surface is a well-known target for metastases from the gastro-intestinal region.268 By using protocols for the examination of the tubal fimbriae that maximize the exposure of the mucosa in se-rous ovarian, primary peritoneal and tubal carcinomas, foci of coexisting TIC were iden-tified in 20 of 30, 4 of 6 and 5 of 5 carcinomas respectively.267 In the same study, the p53 mutations of the TIC and serous ovarian can-cer were analyzed in five cases, and found to be identical in the coexisting TIC and the ovar-ian tumor mass in all five. This supports the possibility that the carcinomas considered ovarian in origin actually have its site for car-cinogenesis in the secretory cells of the tubal fimbriae, known to be damaged by C. tracho-matis infections.
How does the C. trachomatis infection initiate/promote malignant transformation?Persistent C. trachomatis infections are known to have an altered steady-state level of chlamydial antigens, with the predominance of cHSP60 protein compared to the level of the major outer membrane protein (MOMP).13,
33, 260 This is a feature believed to be part of the survival strategy for the bacteria since cHSP60 is suggested to have anti-apoptotic properties.35 It is of vital importance to the C. trachomatis bacteria that the host cell does not undergo apoptotic changes due to the ob-ligate intracellular developmental cycle. At the

37
reSultS And diScuSSion
same time the inflammatory reaction causes production of toxic oxidants, cytokines, pros-taglandins and growth factors that might cause damage to the DNA. Increased cell-turnover is also part of the inflammatory reaction with potential for replication errors and mutations, while cHSP60, by having an anti-apoptotic effect, facilitates the survival of DNA-damaged cells leading to increased risk for malignant transformation.46
Chlamydial HSP60-1 IgG was associated with type II carcinomas in this study when prospective plasma samples were analyzed, indicating that the carcinomas might have been preceded by a chlamydial infection dom-inated by cHSP60 production. Since cHSP60 is suggested to have anti-apoptotic properties and type II tumors are characterized by a high level of p53 mutations (a marker of apoptosis related genetic instability), cHSP60 might act as a tumor promoter by facilitating the sur-vival of cells with p53 mutations. In 16 of the BOT and EOC cases in this study where cHSP60-1 IgG antibodies were analyzed, the extent of p53 mutations had previously been semi-quantitatively (0, 1, 2, 3) determined by immunohistochemistry.269 Interestingly, the level of p53 staining was associated with the presence of cHSP60-1 IgG antibodies (P = 0.002, Mantel-Haenszel test).
Even though in this study the number of cases showing an association of C. trachoma-tis antibodies and type II ovarian cancer was small, and need to be confirmed in larger studies, the answers to the when, where and how questions could be summarized in the following hypothesis: C. trachomatis might initiate/promote ovarian cancer development by persistently infecting the secretory cells of the tubal fimbriae many years, or decades, before the tumor is overt. The tumor promot-ing/initiating effect can be caused by C. tra-chomatis bacteria inducing chronic inflam-mation, directly and/or by an auto-immune cross-reaction to human HSP60, with the production of cytotoxic substances. Further-
more, cHSP60 mediated inhibition of apop-tosis of DNA-damaged cells can lead to ma-lignant transformation of the secretory cells of the tubal fimbriae, followed by rapid spread to the ovaries and the peritoneal lining in close proximity. Soon, there is manifest epithelial ovarian carcinoma.

38

39
SuMMAry And concluSion
C hlamydia trachomatis is suggested to have a broad spectrum of effects in the
human body. To facilitate an intracellular de-velopmental cycle C. trachomatis has devel-oped tools to modify the regulatory mecha-nisms of the host cell, at the same time causing effects that are unwanted by the host. In this thesis, data on possible effects on fe-male fertility, male fertility and ovarian tumor development is presented.
C. trachomatis IgG and IgA antibodies in combination in the man were independently associated with substantially reduced preg-nancy rates for the infertile couple, and subtle negative effects on semen characteristics. Lately, papers supporting a direct negative effect by C. trachomatis on male fertility, and spermatozoa, are accumulating. Regarding female fertility, C. trachomatis is known to have negative effects, increasing the risk for TFI, which was supported by data in this study. A tendency, however not significant, to reduced pregnancy rates after IVF-treatment if the woman was C. trachomatis IgG antibody positive was also found.
It has been hypothesized that C. tracho-matis might increase the risk for ovarian can-cer. However, it is not previously studied whether C. trachomatis antibodies are asso-ciated with the recently hypothesized type II tumor subgroup. In this thesis a novel finding of an association of cHSP60-1 IgG antibodies with type II ovarian/pelvic carcinoma is pre-sented along with a suggested model of how
C. trachomatis might act as a tumor initiator/promoter. Since the subgroup of type II tu-mors was small, the results have to be con-firmed in future studies.
The principal findings of the present thesis can be itemized as follows:
C. trachomatis • seems to exert a direct effect on male fertility. Serum C. tracho-matis IgG and IgA antibodies in the man were associated with reduced pregnancy rates for the infertile couple, as well as subtle negative changes in semen char-acteristics.In the woman • C. trachomatis infections, as detected by serum C. trachomatis IgG and cHSP60 IgG antibodies, increased the risk for TFI, but did not significantly reduce pregnancy rates in this cohort of infertile couples.Pregnancy outcome, up to 28 weeks of • gestation, did not differ between couples with serum C. trachomatis antibodies in either of the partners, and couples without C. trachomatis antibodies.Type II ovarian/pelvic carcinomas were • associated with cHSP60-1 IgG antibodies in women with plasma samples obtained more than one year prior to diagnosis. Using TMA, • C. trachomatis rRNA could not be detected in ovarian tissues from women with epithelial ovarian cancer, borderline ovarian tumors or benign con-ditions.
Summary and Conclusions

SuMMAry And concluSion
40
M. genitalium • plasma antibodies were associated with BOT; however a statisti-cal type 1 error cannot be excluded. M. genitalium, N. gonorrhoeae, HPV and polyomaviruses BKV and JCV could not be detected in ovarian tissues.

41
SuggeStionS for future reSeArch
Suggestions for future research
The finding, in this study, of impaired fer-tility of the man if he is C. trachomatis
IgG and IgA positive has to be confirmed in other settings. To further elucidate how C. trachomatis affects male fertility, IVF and ICSI treated couples could be studied regard-ing C. trachomatis antibody status, semen characteristics, sperm DNA fragmentation, fertilization rates, embryo development and pregnancy rates. A randomized controlled trial, evaluating if antibiotic treatment can increase pregnancy rates in couples where the man is C. trachomatis IgG and IgA positive, would be of great value.
Do C. trachomatis infections have an effect on female infertility beyond causing tubal damage? Larger samples of IVF and ICSI treated couples with detailed information re-garding C. trachomatis IgG and cHSP60 IgG antibodies as well as tubal status, fertilization rate, embryo development and pregnancy rates could help solve this question. It is im-portant in future studies that both partners are evaluated regarding C. trachomatis anti-bodies to avoid confounding of the effects between the partners.
M. genitalium is another microorganism suggested to cause TFI in women and urethri-tis in men. The effect on fertility, and possible confounding, of this microorganism in both women and men should be further evaluat-ed.
Studies using plasma samples obtained more than one year prior to ovarian cancer diagnosis, focusing type II tumors in relation to cHSP60-1 IgG and C. trachomatis IgG an-tibodies, and with sufficient data on possible confounding factors, have to be carried out to verify or reject the results of the present study. Furthermore a larger number of women with BOT should be studied to confirm or reject a possible role of M. genitalium in the develop-ment of BOT.
If the association of cHSP60-1 IgG antibod-ies and type II tumors can be confirmed, the next step could be to carefully examine tubal fimbriae mucosa concerning the presence of C. trachomatis antigen, cHSP60 proteins and the suggested type II tumor precursors (p53 signatures and TIC), preferably before ovar-ian cancer is established. This could be done in women who undergo prophylactic salpin-go-oophorectomy due to hereditary increased ovarian cancer risk, or in women who under-go salpingectomy due to cervical or endome-trial cancer, or for benign conditions.
Research on a vaccine directed towards C. trachomatis is accumulating. If C. trachoma-tis in the future becomes an established risk factor for male infertility and ovarian cancer, in addition to female reproductive sequels, the impetus for vaccine development will in-crease greatly.

42

43
AcknowledgMentS
There are many people involved in the process to complete a thesis. To share
thoughts, ideas and find the joy in solving problems together are some of the best things with the research process. I would like to thank all of you who in one or another way have contributed to help me realize the dream of writing this book. In particular I would like to express my sincere gratitude to:
All the women and men that have contrib-uted to, and are the basis for, these studies. Without your benevolence this work would have been impossible.
My supervisor Ulrika Ottander, thank you for your scientific guidance and all the sup-port, encouragement and understanding dur-ing the years that have passed. Thank you also for being my friend, colleague and mentor. You have an amazing way of knowing what’s important, in research and writing, as well as in life.
Jan Olofsson, my initial supervisor, for your enthusiasm, scientific expertise and con-structive criticism. Thank you for introducing me to the world of research and getting me interested in Chlamydia trachomatis as an important pathogen in human reproductive organs.
Eva Lundin, my assistant supervisor, for all your support, scientific guidance and en-couragement, and for all the inspiring discus-sions on a broad variety of topics.
Fredrik Elgh, my assistant supervisor, for your scientific experience in the cross-road of
pathology and virology, and for constructive criticism.
Ann Lalos, head of Obsterics and Gynecol-ogy, Umeå University, you have created an atmosphere in which I have been able to car-ry through this work and to grow in many aspects… Thank you for all your support, and for believing in me.
Torbjörn Bäckström, former head of Ob-sterics and Gynecology, Umeå University for sharing your scientific experience and for your brilliant ideas for research.
Per-Åke Holmgren, Birgit Nilsson, Inga Sjöberg and Mats-Göran Damber, present and former Directors of the clinical division of Obstetrics and Gynecology, University Hos-pital of Northern Sweden, for your under-standing that time for research is a necessary component to carry through a doctoral project.
Urban Kumlin, my co-author, for your en-thusiasm with research in general and chlamydial serology in particular. Thanks for many imaginative discussions and construc-tive criticism.
Margaretha Jurstrand, for co-authorship, constructive criticism and sharing your knowledge about Mycoplasma genitalium.
Peter Lindgren for co-authorship and all your previous work with the cohort of women with ovarian tumors.
Jens Boman, Leif Abramsson, J. A. Liljeqvist, Jens K Møller, Nina Ohlson and Ingrid Marklund for co-authorship, construc-
Acknowledgements

AcknowledgMentS
44
tive criticism and readily sharing your knowl-edge in your different areas of expertise.
Åsa Hampusson. Thanks for coordinating and enrolling the infertile couples that are part of this project. Barbro Lundgren and Barbro Sandqvist for teaching me how to deal with spermatozoa…
Iréne Eriksson, Nitesh Mistry, Elisabeth Dahlberg, Birgitta Ekblom, Pernilla Anders-son, Lena Jansson and Anders Bäckman for all the laboratory work you have carried out.
Carina, Birgit, Birgitta, Margareta, Mar-gareta, Meta, Anneli, Helena, Ingrid, Mari-anne, Mats, Marie, Anna, Anna-Carin and all others that have been “rooming” in “en-hetskorridoren” during these years. Tank you for the jolly and supportive atmosphere, in happiness and in sorrow. You have been my “bollplankor” in almost every aspect of life.
All the staff at “Fertilitetscentrum” for your interest in, and support of, this project.
Everyone that I have met at the Depart-ment of Clinical Microbiology/Virology, De-partment of Medical Bioscienses/Pathology and Clinical Division of Gynecologic Oncol-ogy for your cooperation and willingness to help.
Everyone at UNC for all intellectual discus-sions and seminars, and supportive feed-back.
All my colleagues and other staff at Obstet-rics and Gynecology for your support despite my absence in every day patient counsel-ling.
My mother, Birgitta Hellgren, thank you for everything. I wish that you would have been here to share the joy with me today.
Alrik Hellgren, pappa, du gav mig en av de viktigaste egenskaperna som forskare – nyfi-kenhet.
My brother, Thomas Hellgren, you have always been my big-brother, and always will be…
Ulla Söderström, thanks for all the help and support during all the shifting aspects of life. Thank you also Lars-Åke and Lotta Idahl for all your support.
Per, my husband, you have always sup-ported me and my desire for research. Thank you also for taking care of “everything” at critical points during my doctoral education. I love you.
Joar, Alva och Saga – ni har visat vad som är viktigast här i livet för mig. Tack!
All of you not mentioned, but nevertheless not forgotten, who have supported and en-couraged me during this work – my deepest thanks.
This work was supported by grants from the Swedish Medical Research Council 1314, the Medical Faculty at Umeå University, Sweden; Lion’s Cancer Research Foundation at Umeå University, Sweden; Kempe Foundation, Umeå, Sweden; Organon Research Foundation, Swe-den; Anna Cederbergh Foundation for Medical Research, Sweden.

45
referenceS
1. Stephens RS. Chlamydia. Intracellular Biology, Pathogenesis, and Immunity. Washington, D.C.: ASM Press, 1999.
2. Ripa KT. Microbiology Diagnosis of Chlamydia trachomatis infection. In-fection 1982;10 Suppl 1:S19-24.
3. Schachter J, Hanna L, Hill EC, et al. Are chlamydial infections the most prevalent venereal disease? Jama 1975;231:1252-5.
4. Mårdh PA, Ripa T, Svensson L, Weström L. Chlamydia trachomatis infection in patients with acute salpingitis. N Engl J Med 1977;296:1377-9.
5. Mårdh PA, Svensson L. Chlamydial salpingitis. Scand J Infect Dis Suppl 1982;32:64-72.
6. Svensson L, Mårdh PA, Ahlgren M, Nor-denskjöld F. Ectopic pregnancy and anti-bodies to Chlamydia trachomatis. Fertil Steril 1985;44:313-7.
7. Thylefors B, Negrel AD, Pararajasegaram R, Dadzie KY. Global data on blindness. Bull World Health Organ 1995;73:115-21.
8. WHO. Global Prevalence and Incidence of Selected Curable Sexually Transmit-ted Infections. Overview and Estimates. Geneva: World Health Organization, 2001.
9. Velicko I, Boman J. EPI-aktuellt, vol 8, nr 11. Klamydiainfektion i Sverige år 2008.: Swedish Institute for Infectious Disease Control, 2009.
10. Everett KD, Bush RM, Andersen AA. Emended description of the order Chla-mydiales, proposal of Parachlamy-diaceae fam. nov. and Simkaniaceae fam. nov., each containing one monotyp-ic genus, revised taxonomy of the family Chlamydiaceae, including a new genus and five new species, and standards for the identification of organisms. Int J Syst Bacteriol 1999;49 Pt 2:415-40.
11. Stephens RS, Myers G, Eppinger M, Bavoil PM. Divergence without differ-ence: phylogenetics and taxonomy of Chlamydia resolved. FEMS Immunol Med Microbiol 2009;55:115-9.
12. Erbengi T. Ultrastructural observations on the entry of Chlamydia trachomatis into human spermatozoa. Hum Reprod 1993;8:416-21.
13. Deka S, Vanover J, Dessus-Babus S, et al. Chlamydia trachomatis enters a vi-able but non-cultivable (persistent) state within herpes simplex virus type 2 (HSV-2) co-infected host cells. Cell Microbiol 2006;8:149-62.
14. Wolf K, Fischer E, Hackstadt T. Ul-trastructural analysis of developmental events in Chlamydia pneumoniae-infect-ed cells. Infect Immun 2000;68:2379-85.
15. Hogan RJ, Mathews SA, Mukhopadhyay S, Summersgill JT, Timms P. Chlamydial persistence: beyond the biphasic para-digm. Infect Immun 2004;72:1843-55.
References

referenceS
46
16. Mpiga P, Ravaoarinoro M. Effects of sus-tained antibiotic bactericidal treatment on Chlamydia trachomatis-infected epithelial-like cells (HeLa) and mono-cyte-like cells (THP-1 and U-937). Int J Antimicrob Agents 2006;27:316-24.
17. Patton DL, Askienazy-Elbhar M, Henry-Suchet J, et al. Detection of Chlamydia trachomatis in fallopian tube tissue in women with postinfectious tubal infer-tility. Am J Obstet Gynecol 1994;171:95-101.
18. Toth M, Patton DL, Campbell LA, et al. Detection of chlamydial antigenic material in ovarian, prostatic, ectopic pregnancy and semen samples of cul-ture-negative subjects. Am J Reprod Immunol 2000;43:218-22.
19. Barlow RE, Cooke ID, Odukoya O, et al. The prevalence of Chlamydia tracho-matis in fresh tissue specimens from patients with ectopic pregnancy or tubal factor infertility as determined by PCR and in-situ hybridisation. J Med Micro-biol 2001;50:902-8.
20. Nanagara R, Li F, Beutler A, Hudson A, Schumacher HR, Jr. Alteration of Chlamydia trachomatis biologic behav-ior in synovial membranes. Suppression of surface antigen production in reactive arthritis and Reiter’s syndrome. Arthritis Rheum 1995;38:1410-7.
21. Holland SM, Hudson AP, Bobo L, et al. Demonstration of chlamydial RNA and DNA during a culture-negative state. Infect Immun 1992;60:2040-7.
22. Gerard HC, Branigan PJ, Schumacher HR, Jr., Hudson AP. Synovial Chlamy-dia trachomatis in patients with reactive arthritis/Reiter’s syndrome are viable but show aberrant gene expression. J Rheumatol 1998;25:734-42.
23. Gerard HC, Branigan PJ, Balsara GR, Heath C, Minassian SS, Hudson AP. Viability of Chlamydia trachomatis in fallopian tubes of patients with ectopic pregnancy. Fertil Steril 1998;70:945-8.
24. Yang YS, Kuo CC, Chen WJ. Reactivation of Chlamydia trachomatis lung infec-tion in mice by cortisone. Infect Immun 1983;39:655-8.
25. Cotter TW, Miranpuri GS, Ramsey KH, Poulsen CE, Byrne GI. Reactivation of chlamydial genital tract infection in mice. Infect Immun 1997;65:2067-73.
26. Malinverni R, Kuo CC, Campbell LA, Grayston JT. Reactivation of Chlamydia pneumoniae lung infection in mice by cortisone. J Infect Dis 1995;172:593-4.
27. Mohsenine H, Darougar S. The provoca-tive effect of cortisone on trachoma. Rev Int Trach 1957;34:336-48.
28. Golden MR, Schillinger JA, Markowitz L, St Louis ME. Duration of untreated genital infections with Chlamydia tra-chomatis: a review of the literature. Sex Transm Dis 2000;27:329-37.
29. Morre SA, van den Brule AJ, Rozendaal L, et al. The natural course of asymptom-atic Chlamydia trachomatis infections: 45% clearance and no development of clinical PID after one-year follow-up. Int J STD AIDS 2002;13 Suppl 2:12-8.
30. Molano M, Meijer CJ, Weiderpass E, et al. The natural course of Chlamydia trachomatis infection in asymptomatic Colombian women: a 5-year follow-up study. J Infect Dis 2005;191:907-16.
31. van den Brule AJ, Munk C, Winther JF, et al. Prevalence and persistence of as-ymptomatic Chlamydia trachomatis in-fections in urine specimens from Danish male military recruits. Int J STD AIDS 2002;13 Suppl 2:19-22.
32. Pockley AG. Heat shock proteins as regu-lators of the immune response. Lancet 2003;362:469-76.
33. Dreses-Werringloer U, Padubrin I, Zei-dler H, Köhler L. Effects of azithromycin and rifampin on Chlamydia trachoma-tis infection in vitro. Antimicrob Agents Chemother 2001;45:3001-8.

47
referenceS
34. Beatty WL, Byrne GI, Morrison RP. Repeated and persistent infection with Chlamydia and the development of chronic inflammation and disease. Trends Microbiol 1994;2:94-8.
35. Dean D, Powers VC. Persistent Chlamy-dia trachomatis infections resist apoptot-ic stimuli. Infect Immun 2001;69:2442-7.
36. Neuer A, Spandorfer SD, Giraldo P, Diet-erle S, Rosenwaks Z, Witkin SS. The role of heat shock proteins in reproduction. Hum Reprod Update 2000;6:149-59.
37. Dieterle S, Wollenhaupt J. Humoral im-mune response to the chlamydial heat shock proteins hsp60 and hsp70 in Chlamydia-associated chronic salpin-gitis with tubal occlusion. Hum Reprod 1996;11:1352-6.
38. Claman P, Honey L, Peeling RW, Jessa-mine P, Toye B. The presence of serum antibody to the chlamydial heat shock protein (CHSP60) as a diagnostic test for tubal factor infertility. Fertil Steril 1997;67:501-4.
39. Ault KA, Statland BD, King MM, Dozier DI, Joachims ML, Gunter J. Antibod-ies to the chlamydial 60 kilodalton heat shock protein in women with tubal fac-tor infertility. Infect Dis Obstet Gynecol 1998;6:163-7.
40. Dadamessi I, Eb F, Betsou F. Combined detection of Chlamydia trachomatis-specific antibodies against the 10 and 60-kDa heat shock proteins as a diag-nostic tool for tubal factor infertility: Re-sults from a case-control study in Cam-eroon. FEMS Immunol Med Microbiol 2005;45:31-5.
41. Tiitinen A, Surcel HM, Halttunen M, et al. Chlamydia trachomatis and chla-mydial heat shock protein 60-specific antibody and cell-mediated responses predict tubal factor infertility. Hum Re-prod 2006;21:1533-8.
42. Idahl A, Abramsson L, Kumlin U, Lil-jeqvist JA, Olofsson JI. Male serum Chlamydia trachomatis IgA and IgG, but not heat shock protein 60 IgG, cor-relates with negatively affected semen characteristics and lower pregnancy rates in the infertile couple. Int J Androl 2007;30:99-107.
43. den Hartog JE, Land JA, Stassen FR, Kessels AG, Bruggeman CA. Serological markers of persistent C. trachomatis infections in women with tubal factor subfertility. Hum Reprod 2005;20:986-90.
44. Stephens RS. The cellular paradigm of chlamydial pathogenesis. Trends Micro-biol 2003;11:44-51.
45. Paavonen J, Karunakaran KP, Noguchi Y, et al. Serum antibody response to the heat shock protein 60 of Chlamydia trachomatis in women with developing cervical cancer. Am J Obstet Gynecol 2003;189:1287-92.
46. Di Felice V, David S, Cappello F, Farina F, Zummo G. Is chlamydial heat shock protein 60 a risk factor for oncogenesis? Cell Mol Life Sci 2005;62:4-9.
47. Quirk JT, Kupinski JM. Chronic in-fection, inflammation, and epithe-lial ovarian cancer. Med Hypotheses 2001;57:426-8.
48. Cecil JA, Howell MR, Tawes JJ, et al. Features of Chlamydia trachomatis and Neisseria gonorrhoeae infection in male Army recruits. J Infect Dis 2001;184:1216-9.
49. Peipert JF. Clinical practice. Genital chlamydial infections. N Engl J Med 2003;349:2424-30.
50. Smith JS, Bosetti C, Munoz N, et al. Chlamydia trachomatis and invasive cervical cancer: a pooled analysis of the IARC multicentric case-control study. Int J Cancer 2004;111:431-9.
51. Cunningham KA, Beagley KW. Male genital tract chlamydial infection: im-

referenceS
48
plications for pathology and infertility. Biol Reprod 2008;79:180-9.
52. Hamlyn E, Taylor C. Sexually transmitted proctitis. Postgrad Med J 2006;82:733-6.
53. Mårdh PA. Influence of infection with Chlamydia trachomatis on pregnancy outcome, infant health and life-long se-quelae in infected offspring. Best Pract Res Clin Obstet Gynaecol 2002;16:847-64.
54. Hobbs MM, van der Pol B, Totten P, et al. From the NIH: proceedings of a work-shop on the importance of self-obtained vaginal specimens for detection of sexu-ally transmitted infections. Sex Transm Dis 2008;35:8-13.
55. Schachter J. Which test is best for chlamy-dia? Curr Opin Infect Dis 1999;12:41-5.
56. Cook RL, Hutchison SL, Østergaard L, Braithwaite RS, Ness RB. Systematic re-view: noninvasive testing for Chlamydia trachomatis and Neisseria gonorrhoe-ae. Ann Intern Med 2005;142:914-25.
57. Hadgu A, Dendukuri N, Hilden J. Evalu-ation of nucleic acid amplification tests in the absence of a perfect gold-stand-ard test: a review of the statistical and epidemiologic issues. Epidemiology 2005;16:604-12.
58. Land JA, Evers JL. Chlamydia infection and subfertility. Best Pract Res Clin Ob-stet Gynaecol 2002;16:901-12.
59. Paldanius M, Leinonen M, Virkkunen H, et al. Chlamydia pneumoniae anti-body levels before coronary events in the Helsinki Heart Study as measured by different methods. Diagn Microbiol Infect Dis 2006;56:233-9.
60. Pesonen E, Andsberg E, Ohlin H, et al. Dual role of infections as risk factors for coronary heart disease. Atherosclerosis 2007;192:370-5.
61. Roivainen M, Viik-Kajander M, Palosuo T, et al. Infections, inflammation, and the risk of coronary heart disease. Cir-culation 2000;101:252-7.
62. Wong BY, Gnarpe J, Teo KK, et al. Does chronic Chlamydia pneumoniae infec-tion increase the risk of myocardial in-jury? Insights from patients with non-ST-elevation acute coronary syndromes. Am Heart J 2002;144:987-94.
63. Horner P. The case for further treat-ment studies of uncomplicated genital Chlamydia trachomatis infection. Sex Transm Infect 2006;82:340-3.
64. Lau CY, Qureshi AK. Azithromycin ver-sus doxycycline for genital chlamydial infections: a meta-analysis of random-ized clinical trials. Sex Transm Dis 2002;29:497-502.
65. Golden MR, Whittington WL, Handsfield HH, et al. Effect of expedited treatment of sex partners on recurrent or persis-tent gonorrhea or chlamydial infection. N Engl J Med 2005;352:676-85.
66. Dean D, Suchland RJ, Stamm WE. Evi-dence for long-term cervical persistence of Chlamydia trachomatis by omp1 genotyping. J Infect Dis 2000;182:909-16.
67. Patton DL, Sweeney YC, Bohannon NJ, et al. Effects of doxycycline and antiin-flammatory agents on experimentally induced chlamydial upper genital tract infection in female macaques. J Infect Dis 1997;175:648-54.
68. Suchland RJ, Geisler WM, Stamm WE. Methodologies and cell lines used for antimicrobial susceptibility testing of Chlamydia spp. Antimicrob Agents Chemother 2003;47:636-42.
69. Patton DL, Sweeney YT, Stamm WE. Significant reduction in inflammatory response in the macaque model of chla-mydial pelvic inflammatory disease with azithromycin treatment. J Infect Dis 2005;192:129-35.
70. Haggerty CL, Ness RB. Newest ap-proaches to treatment of pelvic inflam-matory disease: a review of recent ran-domized clinical trials. Clin Infect Dis 2007;44:953-60.

49
referenceS
71. Evers JL. Female subfertility. Lancet 2002;360:151-9.
72. The epidemiology of infertility. Report of a WHO scientific group. World Health Organ Tech Rep Ser 1975;582:1-37.
73. Boivin J, Bunting L, Collins JA, Nygren KG. International estimates of infer-tility prevalence and treatment-seek-ing: potential need and demand for infertility medical care. Hum Reprod 2007;22:1506-12.
74. Andersson AM, Jørgensen N, Main KM, et al. Adverse trends in male repro-ductive health: we may have reached a crucial ‘tipping point’. Int J Androl 2008;31:74-80.
75. Adamson GD, Baker VL. Subfertil-ity: causes, treatment and outcome. Best Pract Res Clin Obstet Gynaecol 2003;17:169-85.
76. Rutstein SO, Iqbal HS. Infecundity, In-fertility, and Childlessness in Developing Countries. DHS Comparative Reports No. 9. Calverton, Maryland, USA: ORC Macro and the World Health Organiza-tion, 2004.
77. Lalos A. Psychological and Social Aspects of Tubal Infertility. A longitudinal study of infertile women and their men. Thesis. Umeå: Umeå University, 1985.
78. Wirtberg I. His and her childlessness. Thesis.Department of Psychiatry and Psychology. Stockholm: Karolinska In-stitutet, 1992.
79. Ankum WM, Mol BW, Van der Veen F, Bossuyt PM. Risk factors for ectopic pregnancy: a meta-analysis. Fertil Steril 1996;65:1093-9.
80. Hull MG, Glazener CM, Kelly NJ, et al. Population study of causes, treatment, and outcome of infertility. Br Med J (Clin Res Ed) 1985;291:1693-7.
81. Snick HK, Snick TS, Evers JL, Collins JA. The spontaneous pregnancy prog-nosis in untreated subfertile couples: the Walcheren primary care study. Hum Reprod 1997;12:1582-8.
82. Weström L, Wølner-Hanssen P. Patho-genesis of pelvic inflammatory disease. Genitourin Med 1993;69:9-17.
83. Tubal infertility: serologic relationship to past chlamydial and gonococcal in-fection. World Health Organization Task Force on the Prevention and Man-agement of Infertility. Sex Transm Dis 1995;22:71-7.
84. Barrett S, Taylor C. A review on pelvic inflammatory disease. Int J STD AIDS 2005;16:715-20.
85. Infections, pregnancies, and infertil-ity: perspectives on prevention. World Health Organization. Fertil Steril 1987;47:964-8.
86. Tripathy SN. Infertility and pregnancy outcome in female genital tuberculosis. Int J Gynaecol Obstet 2002;76:159-63.
87. Punnonen R, Terho P, Nikkanen V, Meurman O. Chlamydial serology in in-fertile women by immunofluorescence. Fertil Steril 1979;31:656-9.
88. Weström LV. Sexually transmitted dis-eases and infertility. Sex Transm Dis 1994;21:S32-7.
89. Paukku M, Närvänen A, Puolakkainen M, et al. Detection of Chlamydia tra-chomatis antibodies by 2 novel tests: rELISA and peptide EIA. Int J STD AIDS 1998;9:604-7.
90. den Hartog JE, Lardenoije CM, Seve-rens JL, Land JA, Evers JL, Kessels AG. Screening strategies for tubal factor sub-fertility. Hum Reprod 2008;23:1840-8.
91. Land JA, Gijsen AP, Kessels AG, Slob-be ME, Bruggeman CA. Performance of five serological chlamydia antibody tests in subfertile women. Hum Reprod 2003;18:2621-7.
92. Dabekausen YA, Evers JL, Land JA, Stals FS. Chlamydia trachomatis antibody testing is more accurate than hysteros-alpingography in predicting tubal factor infertility. Fertil Steril 1994;61:833-7.

referenceS
50
93. Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lan-cet 1978;2:366.
94. Templeton A, Morris JK, Parslow W. Factors that affect outcome of in-vitro fertilisation treatment. Lancet 1996;348:1402-6.
95. Strandell A, Waldenström U, Nilsson L, Hamberger L. Hydrosalpinx reduces in-vitro fertilization/embryo transfer preg-nancy rates. Hum Reprod 1994;9:861-3.
96. Strandell A. Treatment of hydrosalpinx in the patient undergoing assisted re-production. Curr Opin Obstet Gynecol 2007;19:360-5.
97. Strandell A, Lindhard A, Waldenström U, Thorburn J, Janson PO, Hamberger L. Hydrosalpinx and IVF outcome: a pro-spective, randomized multicentre trial in Scandinavia on salpingectomy prior to IVF. Hum Reprod 1999;14:2762-9.
98. Strandell A, Lindhard A, Waldenström U, Thorburn J. Hydrosalpinx and IVF outcome: cumulative results after sal-pingectomy in a randomized controlled trial. Hum Reprod 2001;16:2403-10.
99. Jakus S, Neuer A, Dieterle S, Bongio-vanni AM, Witkin SS. Antibody to the Chlamydia trachomatis 60 kDa heat shock protein in follicular fluid and in vitro fertilization outcome. Am J Reprod Immunol 2008;59:85-9.
100. Cortinas P, Munoz MG, Loureiro CL, Pujol FH. Follicular fluid antibodies to Chlamydia trachomatis and human heat shock protein-60 kDa and infertility in women. Arch Med Res 2004;35:121-5.
101. Witkin SS, Sultan KM, Neal GS, Jeremias J, Grifo JA, Rosenwaks Z. Unsuspected Chlamydia trachomatis infection and in vitro fertilization outcome. Am J Obstet Gynecol 1994;171:1208-14.
102. Kimani J, Maclean IW, Bwayo JJ, et al. Risk factors for Chlamydia trachomatis pelvic inflammatory disease among sex
workers in Nairobi, Kenya. J Infect Dis 1996;173:1437-44.
103. Wang C, Tang J, Geisler WM, Crowley-Nowick PA, Wilson CM, Kaslow RA. Human leukocyte antigen and cytokine gene variants as predictors of recur-rent Chlamydia trachomatis infection in high-risk adolescents. J Infect Dis 2005;191:1084-92.
104. Kinnunen AH, Surcel HM, Lehtinen M, et al. HLA DQ alleles and interleukin-10 polymorphism associated with Chla-mydia trachomatis-related tubal factor infertility: a case-control study. Hum Reprod 2002;17:2073-8.
105. den Hartog JE, Ouburg S, Land JA, et al. Do host genetic traits in the bacterial sensing system play a role in the de-velopment of Chlamydia trachomatis-associated tubal pathology in subfertile women? BMC Infect Dis 2006;6:122.
106. Witkin SS, Kligman I, Bongiovanni AM. Relationship between an asymptomatic male genital tract exposure to Chla-mydia trachomatis and an autoimmune response to spermatozoa. Hum Reprod 1995;10:2952-5.
107. Jungwirth A, Straberger A, Esterbauer B, Fink K, Schmeller N. Acrosome reac-tion in Chlamydia-positive and negative patients. Andrologia 2003;35:314-6.
108. Segnini A, Camejo MI, Proverbio F. Chlamydia trachomatis and sperm lipid peroxidation in infertile men. Asian J Androl 2003;5:47-9.
109. Jakiel G, Robak-Cholubek D, Wieczorek P, Bokiniec M. Evaluation of some pa-rameters of human semen with positive chlamydial reaction. Ann Univ Mariae Curie Sklodowska [Med] 2004;59:61-4.
110. Karinen L, Pouta A, Hartikainen AL, et al. Association between Chlamydia tra-chomatis antibodies and subfertility in the Northern Finland Birth Cohort 1966 (NFBC 1966), at the age of 31 years. Epi-demiol Infect 2004;132:977-84.

51
referenceS
111. Joki-Korpela P, Sahrakorpi N, Halttunen M, Surcel HM, Paavonen J, Tiitinen A. The role of Chlamydia trachomatis in-fection in male infertility. Fertil Steril 2008.
112. Eggert-Kruse W, Gerhard I, Naher H, Tilgen W, Runnebaum B. Chlamydial in-fection--a female and/or male infertility factor? Fertil Steril 1990;53:1037-43.
113. Bjercke S, Purvis K. Chlamydial serology in the investigation of infertility. Hum Reprod 1992;7:621-4.
114. Dieterle S, Mahony JB, Luinstra KE, Stibbe W. Chlamydial immunoglobulin IgG and IgA antibodies in serum and se-men are not associated with the presence of Chlamydia trachomatis DNA or rRNA in semen from male partners of infertile couples. Hum Reprod 1995;10:315-9.
115. Munoz MG, Witkin SS. Autoimmunity to spermatozoa, asymptomatic Chlamydia trachomatis genital tract infection and gamma delta T lymphocytes in seminal fluid from the male partners of couples with unexplained infertility. Hum Re-prod 1995;10:1070-4.
116. Weidner W, Floren E, Zimmermann O, Thiele D, Ludwig M. Chlamydial an-tibodies in semen: search for “silent” chlamydial infections in asymptom-atic andrological patients. Infection 1996;24:309-13.
117. Eggert-Kruse W, Buhlinger-Gopfarth N, Rohr G, et al. Antibodies to Chlamydia trachomatis in semen and relationship with parameters of male fertility. Hum Reprod 1996;11:1408-17.
118. Eggert-Kruse W, Rohr G, Demirakca T, et al. Chlamydial serology in 1303 asymptomatic subfertile couples. Hum Reprod 1997;12:1464-75.
119. Ochsendorf FR, Ozdemir K, Rabenau H, et al. Chlamydia trachomatis and male infertility: chlamydia-IgA antibodies in seminal plasma are C. trachomatis specific and associated with an inflam-
matory response. J Eur Acad Dermatol Venereol 1999;12:143-52.
120. Habermann B, Krause W. Altered sperm function or sperm antibodies are not associated with chlamydial antibodies in infertile men with leucocytosperm-ia. J Eur Acad Dermatol Venereol 1999;12:25-9.
121. Penna Videau S, Cermeno Vivas J, Sala-zar N. IgA antibodies to Chlamydia tra-chomatis and seminal parameters in as-ymptomatic infertile males. Arch Androl 2001;46:189-95.
122. de Barbeyrac B, Papaxanthos-Roche A, Mathieu C, et al. Chlamydia trachoma-tis in subfertile couples undergoing an in vitro fertilization program: a prospective study. Eur J Obstet Gynecol Reprod Biol 2006;129:46-53.
123. Cengiz T, Aydoganli L, Baykam M, et al. Chlamydial infections and male infertil-ity. Int Urol Nephrol 1997;29:687-93.
124. Gdoura R, Keskes-Ammar L, Bouzid F, Eb F, Hammami A, Orfila J. Chlamydia trachomatis and male infertility in Tu-nisia. Eur J Contracept Reprod Health Care 2001;6:102-7.
125. Veznik Z, Pospisil L, Svecova D, Zaji-cova A, Unzeitig V. Chlamydiae in the ejaculate: their influence on the quality and morphology of sperm. Acta Obstet Gynecol Scand 2004;83:656-60.
126. Hosseinzadeh S, Eley A, Pacey AA. Se-men quality of men with asymptom-atic chlamydial infection. J Androl 2004;25:104-9.
127. Hosseinzadeh S, Brewis IA, Eley A, Pacey AA. Co-incubation of human spermato-zoa with Chlamydia trachomatis serovar E causes premature sperm death. Hum Reprod 2001;16:293-9.
128. Satta A, Stivala A, Garozzo A, et al. Ex-perimental Chlamydia trachomatis infection causes apoptosis in human sperm. Hum Reprod 2006;21:134-7.

referenceS
52
129. Sankaranarayanan R, Ferlay J. World-wide burden of gynaecological cancer: the size of the problem. Best Pract Res Clin Obstet Gynaecol 2006;20:207-25.
130. Berchuck A, Schildkraut JM, Marks JR, Futreal PA. Managing hereditary ovarian cancer risk. Cancer 1999;86:2517-24.
131. La Vecchia C. Epidemiology of ovarian cancer: a summary review. Eur J Cancer Prev 2001;10:125-9.
132. Riman T, Nilsson S, Persson IR. Review of epidemiological evidence for repro-ductive and hormonal factors in rela-tion to the risk of epithelial ovarian ma-lignancies. Acta Obstet Gynecol Scand 2004;83:783-95.
133. Mulholland HG, Murray LJ, Cardwell CR, Cantwell MM. Dietary glycaemic index, glycaemic load and endometrial and ovarian cancer risk: a systematic review and meta-analysis. Br J Cancer 2008;99:434-41.
134. Fathalla MF. Incessant ovulation--a factor in ovarian neoplasia? Lancet 1971;2:163.
135. Stadel BV. Letter: The etiology and pre-vention of ovarian cancer. Am J Obstet Gynecol 1975;123:772-4.
136. Riman T, Dickman PW, Nilsson S, et al. Risk factors for invasive epithelial ovarian cancer: results from a Swed-ish case-control study. Am J Epidemiol 2002;156:363-73.
137. Riman T, Persson I, Nilsson S. Hormonal aspects of epithelial ovarian cancer: re-view of epidemiological evidence. Clin Endocrinol (Oxf) 1998;49:695-707.
138. Parazzini F, Chatenoud L, Chiantera V, Benzi G, Surace M, La Vecchia C. Popula-tion attributable risk for ovarian cancer. Eur J Cancer 2000;36:520-4.
139. Chen VW, Ruiz B, Killeen JL, Cote TR, Wu XC, Correa CN. Pathology and clas-sification of ovarian tumors. Cancer 2003;97:2631-42.
140. Shih Ie M, Kurman RJ. Ovarian tum-origenesis: a proposed model based on morphological and molecular genetic analysis. Am J Pathol 2004;164:1511-8.
141. Kurman RJ, Visvanathan K, Roden R, Wu TC, Shih Ie M. Early detection and treatment of ovarian cancer: shifting from early stage to minimal volume of disease based on a new model of carcinogenesis. Am J Obstet Gynecol 2008;198:351-6.
142. Lee Y, Miron A, Drapkin R, et al. A candi-date precursor to serous carcinoma that originates in the distal fallopian tube. J Pathol 2007;211:26-35.
143. Moss SF, Blaser MJ. Mechanisms of dis-ease: Inflammation and the origins of cancer. Nat Clin Pract Oncol 2005;2:90-7.
144. Madeleine MM, Anttila T, Schwartz SM, et al. Risk of cervical cancer associated with Chlamydia trachomatis antibodies by histology, HPV type and HPV cofac-tors. Int J Cancer 2007;120:650-5.
145. Koskela P, Anttila T, Bjørge T, et al. Chlamydia trachomatis infection as a risk factor for invasive cervical cancer. Int J Cancer 2000;85:35-9.
146. Anttila T, Saikku P, Koskela P, et al. Sero-types of Chlamydia trachomatis and risk for development of cervical squamous cell carcinoma. Jama 2001;285:47-51.
147. Risch HA, Howe GR. Pelvic inflamma-tory disease and the risk of epithelial ovarian cancer. Cancer Epidemiol Bio-markers Prev 1995;4:447-51.
148. Paavonen J. Chlamydia trachomatis and cancer. Sex Transm Infect 2001;77:154-6.
149. Auersperg N, Woo MM, Gilks CB. The origin of ovarian carcinomas: a developmental view. Gynecol Oncol 2008;110:452-4.
150. Carvalho JP, Carvalho FM. Is Chlamy-dia-infected tubal fimbria the origin of ovarian cancer? Med Hypotheses 2008;71:690-3.

53
referenceS
151. Beatty WL, Byrne GI, Morrison RP. Morphologic and antigenic character-ization of interferon gamma-mediated persistent Chlamydia trachomatis in-fection in vitro. Proc Natl Acad Sci U S A 1993;90:3998-4002.
152. Byrne GI, Ojcius DM. Chlamydia and apoptosis: life and death decisions of an intracellular pathogen. Nat Rev Micro-biol 2004;2:802-8.
153. Ness RB, Goodman MT, Shen C, Brun-ham RC. Serologic evidence of past in-fection with Chlamydia trachomatis, in relation to ovarian cancer. J Infect Dis 2003;187:1147-52.
154. Ness RB, Shen C, Bass D, et al. Chlamyd-ia trachomatis serology in women with and without ovarian cancer. Infect Dis Obstet Gynecol 2008;2008:219672.
155. Wong A, Maclean AB, Furrows SJ, Ridgway GL, Hardiman PJ, Perrett CW. Could epithelial ovarian cancer be asso-ciated with chlamydial infection? Eur J Gynaecol Oncol 2007;28:117-20.
156. Clausen HF, Fedder J, Drasbek M, et al. Serological investigation of Mycoplasma genitalium in infertile women. Hum Re-prod 2001;16:1866-74.
157. Svenstrup HF, Fedder J, Kristoffersen SE, Trolle B, Birkelund S, Christiansen G. Mycoplasma genitalium, Chlamydia trachomatis, and tubal factor infertil-ity--a prospective study. Fertil Steril 2008;90:513-20.
158. Grzesko J, Elias M, Maczynska B, Kasprzykowska U, Tlaczala M, Goluda M. Occurrence of Mycoplasma genita-lium in fertile and infertile women. Fertil Steril 2008.
159. Baczynska A, Funch P, Fedder J, Knud-sen HJ, Birkelund S, Christiansen G. Morphology of human Fallopian tubes after infection with Mycoplasma geni-talium and Mycoplasma hominis--in vitro organ culture study. Hum Reprod 2007;22:968-79.
160. Falk L, Fredlund H, Jensen JS. Signs and symptoms of urethritis and cervicitis among women with or without Myco-plasma genitalium or Chlamydia tra-chomatis infection. Sex Transm Infect 2005;81:73-8.
161. Chan PJ, Seraj IM, Kalugdan TH, King A. Prevalence of mycoplasma conserved DNA in malignant ovarian cancer detect-ed using sensitive PCR-ELISA. Gynecol Oncol 1996;63:258-60.
162. Pehlivan M, Pehlivan S, Onay H, Koyun-cuoglu M, Kirkali Z. Can mycoplasma-mediated oncogenesis be responsible for formation of conventional renal cell carcinoma? Urology 2005;65:411-4.
163. Kidder M, Chan PJ, Seraj IM, Patton WC, King A. Assessment of archived paraffin-embedded cervical condyloma tissues for mycoplasma-conserved DNA using sensitive PCR-ELISA. Gynecol Oncol 1998;71:254-7.
164. Huang S, Li JY, Wu J, Meng L, Shou CC. Mycoplasma infections and different hu-man carcinomas. World J Gastroenterol 2001;7:266-9.
165. SMI. Epidemiologisk årsrapport 2007: Swedish Institute for Infectious Disease Control, 2007.
166. Taylor ML, Mainous AG, 3rd, Wells BJ. Prostate cancer and sexually transmit-ted diseases: a meta-analysis. Fam Med 2005;37:506-12.
167. Dennis LK, Dawson DV. Meta-analysis of measures of sexual activity and prostate cancer. Epidemiology 2002;13:72-9.
168. zur Hausen H. Papillomaviruses in the causation of human cancers - a brief his-torical account. Virology 2009;384:260-5.
169. Lai CH, Hsueh S, Lin CY, et al. Human papillomavirus in benign and malignant ovarian and endometrial tissues. Int J Gynecol Pathol 1992;11:210-5.
170. Kaufman RH, Bornstein J, Gordon AN, Adam E, Kaplan AL, Adler-Storthz K.

referenceS
54
Detection of human papillomavirus DNA in advanced epithelial ovarian carcino-ma. Gynecol Oncol 1987;27:340-9.
171. Li T, Lu ZM, Guo M, et al. p53 codon 72 polymorphism (C/G) and the risk of hu-man papillomavirus-associated carcino-mas in China. Cancer 2002;95:2571-6.
172. Atalay F, Taskiran C, Taner MZ, Pak I, Or M, Tuncer S. Detection of human papil-lomavirus DNA and genotyping in pa-tients with epithelial ovarian carcinoma. J Obstet Gynaecol Res 2007;33:823-8.
173. Wu QJ, Guo M, Lu ZM, Li T, Qiao HZ, Ke Y. Detection of human papillomavi-rus-16 in ovarian malignancy. Br J Can-cer 2003;89:672-5.
174. Ip SM, Wong LC, Xu CM, Cheung AN, Tsang PC, Ngan HY. Detection of hu-man papillomavirus DNA in malignant lesions from Chinese women with carci-nomas of the upper genital tract. Gynecol Oncol 2002;87:104-11.
175. Zimna K, Poreba E, Kedzia W, Gozdz-icka-Jozefiak A, Kedzia H. Human pap-illomavirus (HPV) in upper genital tract carcinomas of women. Eur J Gynaecol Oncol 1997;18:415-7.
176. Kuscu E, Ozdemir BH, Erkanli S, Haber-al A. HPV and p53 expression in epithe-lial ovarian carcinoma. Eur J Gynaecol Oncol 2005;26:642-5.
177. Kedzia WM, Gozdzicka-Jozefiak A, Ked-zia H. Human papillomavirus type 16 in ovarian serous surface papilloma. Eur J Gynaecol Oncol 1996;17:354-6.
178. Lai CH, Wang CY, Lin CY, Pao CC. De-tection of human papillomavirus RNA in ovarian and endometrial carcinomas by reverse transcription/polymerase chain reaction. Gynecol Obstet Invest 1994;38:276-80.
179. Giordano G, D’Adda T, Gnetti L, Froio E, Merisio C, Melpignano M. Role of human papillomavirus in the develop-ment of epithelial ovarian neoplasms in Italian women. J Obstet Gynaecol Res 2008;34:210-7.
180. Anwar K, Nakakuki K, Imai H, Shi-raishi T, Inuzuka M. Infection of hu-man papillomavirus (HPV) and p53 over-expression in human female geni-tal tract carcinoma. J Pak Med Assoc 1996;46:220-4.
181. Beckmann AM, Sherman KJ, Saran L, Weiss NS. Genital-type human papillo-mavirus infection is not associated with surface epithelial ovarian carcinoma. Gynecol Oncol 1991;43:247-51.
182. McLellan R, Buscema J, Guerrero E, Shah KV, Woodruff JD, Currie JL. In-vestigation of ovarian neoplasia of low malignant potential for human papillo-mavirus. Gynecol Oncol 1990;38:383-5.
183. Leake JF, Woodruff JD, Searle C, Daniel R, Shah KV, Currie JL. Human papillo-mavirus and epithelial ovarian neopla-sia. Gynecol Oncol 1989;34:268-73.
184. Trottier AM, Provencher D, Mes-Mas-son AM, Vauclair R, Coutlee F. Absence of human papillomavirus sequences in ovarian pathologies. J Clin Microbiol 1995;33:1011-3.
185. Chen TR, Chan PJ, Seraj IM, King A. Absence of human papillomavirus E6-E7 transforming genes from HPV 16 and 18 in malignant ovarian carcinoma. Gyne-col Oncol 1999;72:180-2.
186. Anttila M, Syrjänen S, Ji H, Saarikoski S, Syrjänen K. Failure to demonstrate hu-man papillomavirus DNA in epithelial ovarian cancer by general primer PCR. Gynecol Oncol 1999;72:337-41.
187. Quirk JT, Kupinski JM, DiCioccio RA. Analysis of ovarian tumors for the pres-ence of human papillomavirus DNA. J Obstet Gynaecol Res 2006;32:202-5.
188. Hisada M, van den Berg BJ, Strickler HD, et al. Prospective study of antibody to human papilloma virus type 16 and risk of cervical, endometrial, and ovarian cancers (United States). Cancer Causes Control 2001;12:335-41.

55
referenceS
189. Moens U, Johannessen M. Human polyomaviruses and cancer: expand-ing repertoire. J Dtsch Dermatol Ges 2008;6:704-8.
190. Lee W, Langhoff E. Polyomavirus in hu-man cancer development. Adv Exp Med Biol 2006;577:310-8.
191. Moens U, Van Ghelue M, Johannessen M. Oncogenic potentials of the human polyomavirus regulatory proteins. Cell Mol Life Sci 2007;64:1656-78.
192. Wetzels CT, Hoefnagel JG, Bakkers JM, Dijkman HB, Blokx WA, Melchers WJ. Ultrastructural proof of polyomavirus in merkel cell carcinoma tumour cells and its absence in small cell carcinoma of the lung. PLoS ONE 2009;4:e4958.
193. Feng H, Shuda M, Chang Y, Moore PS. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science 2008;319:1096-100.
194. Kvist U, Björndahl L. Manual on Basic Semen Analysis. Oxford, UK: ESHRE Monographs. Oxford University Press, 2002.
195. WHO laboratory manual for the exami-nation of human semen and sperm-cer-vical mucus interaction. Cambridge, UK: Cambridge University Press, 1999.
196. Palmqvist R, Hallmans G, Rinaldi S, et al. Plasma insulin-like growth factor 1, insulin-like growth factor binding pro-tein 3, and risk of colorectal cancer: a prospective study in northern Sweden. Gut 2002;50:642-6.
197. Tavassoli FA, Devilee P. World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of the Breast and Female Genital Organs. Lyon: IARC Press, 2003.
198. Karunakaran KP, Noguchi Y, Read TD, et al. Molecular analysis of the multiple GroEL proteins of Chlamydiae. J Bacte-riol 2003;185:1958-66.
199. Møller JK, Pedersen LN, Persson K. Comparison of Gen-probe transcription-
mediated amplification, Abbott PCR, and Roche PCR assays for detection of wild-type and mutant plasmid strains of Chlamydia trachomatis in Sweden. J Clin Microbiol 2008;46:3892-5.
200. Jurstrand M, Jensen JS, Magnuson A, Kamwendo F, Fredlund H. A serological study of the role of Mycoplasma genita-lium in pelvic inflammatory disease and ectopic pregnancy. Sex Transm Infect 2007;83:319-23.
201. Jensen JS, Björnelius E, Dohn B, Lid-brink P. Use of TaqMan 5’ nuclease real-time PCR for quantitative detection of Mycoplasma genitalium DNA in males with and without urethritis who were at-tendees at a sexually transmitted disease clinic. J Clin Microbiol 2004;42:683-92.
202. Edberg A, Jurstrand M, Johansson E, et al. A comparative study of three different PCR assays for detection of Mycoplas-ma genitalium in urogenital specimens from men and women. J Med Microbiol 2008;57:304-9.
203. Holm S. A Simple Sequentially Rejective Multiple Test Procedure. Scand J Statist 1979;6:65-70.
204. Lyytikäinen E, Kaasila M, Koskela P, et al. Chlamydia trachomatis seropreva-lence atlas of Finland 1983-2003. Sex Transm Infect 2008;84:19-22.
205. Karinen L, Pouta A, Hartikainen AL, et al. Antibodies to Chlamydia tracho-matis heat shock proteins Hsp60 and Hsp10 and subfertility in general popu-lation at age 31. Am J Reprod Immunol 2004;w52:291-7.
206. Gonzales GF, Munoz G, Sanchez R, et al. Update on the impact of Chlamydia trachomatis infection on male fertility. Andrologia 2004;36:1-23.
207. Rogers SM, Miller WC, Turner CF, et al. Concordance of Chlamydia trachomatis infections within sexual partnerships. Sex Transm Infect 2008;84:23-8.
referenceS
56
208. Claman P, Amimi MN, Peeling RW, Toye B, Jessamine P. Does serologic evi-dence of remote Chlamydia trachoma-tis infection and its heat shock protein (CHSP 60) affect in vitro fertilization-embryo transfer outcome? Fertil Steril 1996;65:146-9.
209. Tasdemir I, Tasdemir M, Kodama H, Sekine K, Tanaka T. Effect of chlamyd-ial antibodies on the outcome of in vitro fertilization (IVF) treatment. J Assist Reprod Genet 1994;11:104-6.
210. Torode HW, Wheeler PA, Saunders DM, McPetrie RA, Medcalf SC, Ackerman VP. The role of chlamydial antibodies in an in vitro fertilization program. Fertil Steril 1987;48:987-90.
211. Osser S, Persson K, Wramsby H, Lied-holm P. Dose previous Chlamydia tra-chomatis infection influence the preg-nancy rate of in vitro fertilization and embryo replacement? Am J Obstet Gy-necol 1990;162:40-4.
212. Lessing JB, Kletter Y, Amster R, Amit A, Peyser MR, Berger S. Success rates in in vitro fertilization treatment and its correlation with high titer antibodies for Chlamydia trachomatis. Isr J Med Sci 1991;27:546-9.
213. Lunenfeld E, Sarov B, Sarov I, et al. Chla-mydial IgG and IgA in serum and follicu-lar fluid among patients undergoing in vitro fertilisation. Eur J Obstet Gynecol Reprod Biol 1990;37:163-73.
214. Sharara FI, Queenan JT, Jr., Springer RS, Marut EL, Scoccia B, Scommegna A. Elevated serum Chlamydia trachomatis IgG antibodies. What do they mean for IVF pregnancy rates and loss? J Reprod Med 1997;42:281-6.
215. Rowland GF, Forsey T, Moss TR, Steptoe PC, Hewitt J, Darougar S. Failure of in vitro fertilization and embryo replace-ment following infection with Chlamyd-ia trachomatis. J In Vitro Fert Embryo Transf 1985;2:151-5.
216. Lunenfeld E, Shapiro BS, Sarov B, Sa-rov I, Insler V, Decherney AH. The as-sociation between chlamydial-specific IgG and IgA antibodies and pregnancy outcome in an in vitro fertilization pro-gram. J In Vitro Fert Embryo Transf 1989;6:222-7.
217. Sharara FI, Queenan JT, Jr. Elevated serum Chlamydia trachomatis IgG an-tibodies. Association with decreased im-plantation rates in GIFT. J Reprod Med 1999;44:581-6.
218. Neuer A, Mele C, Liu HC, Rosenwaks Z, Witkin SS. Monoclonal antibodies to mammalian heat shock proteins impair mouse embryo development in vitro. Hum Reprod 1998;13:987-90.
219. Baud D, Regan L, Greub G. Emerging role of Chlamydia and Chlamydia-like organisms in adverse pregnancy out-comes. Curr Opin Infect Dis 2008;21:70-6.
220. Hosseinzadeh S, Pacey AA, Eley A. Chla-mydia trachomatis-induced death of human spermatozoa is caused primarily by lipopolysaccharide. J Med Microbiol 2003;52:193-200.
221. Gallegos G, Ramos B, Santiso R, Goya-nes V, Gosalvez J, Fernandez JL. Sperm DNA fragmentation in infertile men with genitourinary infection by Chlamydia trachomatis and Mycoplasma. Fertil Steril 2008;90:328-34.
222. Collins JA, Barnhart KT, Schlegel PN. Do sperm DNA integrity tests predict preg-nancy with in vitro fertilization? Fertil Steril 2008;89:823-31.
223. Zini A, Boman JM, Belzile E, Ciampi A. Sperm DNA damage is associated with an increased risk of pregnancy loss after IVF and ICSI: systematic re-view and meta-analysis. Hum Reprod 2008;23:2663-8.
224. Taylor-Robinson D. Mycoplasma geni-talium -- an up-date. Int J STD AIDS 2002;13:145-51.
57
referenceS
225. Svenstrup HF, Fedder J, Abraham-Peskir J, Birkelund S, Christiansen G. Mycoplasma genitalium attaches to human spermatozoa. Hum Reprod 2003;18:2103-9.
226. Smoking and infertility. Fertil Steril 2008;90:S254-9.
227. Florescu A, Ferrence R, Einarson T, Selby P, Soldin O, Koren G. Methods for quantification of exposure to cigarette smoking and environmental tobacco smoke: focus on developmental toxicol-ogy. Ther Drug Monit 2009;31:14-30.
228. Dimitrova D, Kalaydjiev S, Hristov L, Nikolov K, Boyadjiev T, Nakov L. Anti-chlamydial and antisperm antibodies in patients with chlamydial infections. Am J Reprod Immunol 2004;52:330-6.
229. Schlief R, Deichert U. Hysterosalpingo-contrast sonography of the uterus and fallopian tubes: results of a clinical trial of a new contrast medium in 120 pa-tients. Radiology 1991;178:213-5.
230. Bulletti C, Panzini I, Borini A, Coccia E, Setti PL, Palagiano A. Pelvic factor infertility: diagnosis and prognosis of various procedures. Ann N Y Acad Sci 2008;1127:73-82.
231. Fujisawa M, Nakano Y, Matsui T, Okada H, Arakawa S, Kamidono S. Chlamydia trachomatis detected by ligase chain reaction in the semen of asymptomatic patients without pyospermia or pyuria. Arch Androl 1999;42:41-4.
232. Bollmann R, Engel S, Petzoldt R, Gobel UB. Chlamydia trachomatis in andro-logic patients--direct and indirect detec-tion. Infection 2001;29:113-8.
233. Krieger JN, Riley DE, Roberts MC, Berg-er RE. Prokaryotic DNA sequences in pa-tients with chronic idiopathic prostatitis. J Clin Microbiol 1996;34:3120-8.
234. Sziller I, Witkin SS, Ziegert M, Csapo Z, Ujhazy A, Papp Z. Serological responses of patients with ectopic pregnancy to epitopes of the Chlamydia trachomatis
60 kDa heat shock protein. Hum Reprod 1998;13:1088-93.
235. Dutta R, Jha R, Gupta S, Gupta R, Salhan S, Mittal A. Seroprevalence of antibod-ies to conserved regions of Chlamydia trachomatis heat shock proteins 60 and 10 in women in India. Br J Biomed Sci 2007;64:78-83.
236. Eckert LO, Hawes SE, Wølner-Hanssen P, et al. Prevalence and correlates of antibody to chlamydial heat shock pro-tein in women attending sexually trans-mitted disease clinics and women with confirmed pelvic inflammatory disease. J Infect Dis 1997;175:1453-8.
237. Peeling RW, Kimani J, Plummer F, et al. Antibody to chlamydial hsp60 pre-dicts an increased risk for chlamydial pelvic inflammatory disease. J Infect Dis 1997;175:1153-8.
238. Money DM, Hawes SE, Eschenbach DA, et al. Antibodies to the chlamydial 60 kd heat-shock protein are associated with laparoscopically confirmed perihepati-tis. Am J Obstet Gynecol 1997;176:870-7.
239. Persson K, Osser S, Birkelund S, Chris-tiansen G, Brade H. Antibodies to Chla-mydia trachomatis heat shock proteins in women with tubal factor infertility are associated with prior infection by C. trachomatis but not by C. pneumoniae. Hum Reprod 1999;14:1969-73.
240. Idahl A, Boman J, Kumlin U, Olofsson JI. Demonstration of Chlamydia tracho-matis IgG antibodies in the male partner of the infertile couple is correlated with a reduced likelihood of achieving preg-nancy. Hum Reprod 2004;19:1121-6.
241. Gijsen AP, Land JA, Goossens VJ, Slobbe ME, Bruggeman CA. Chlamydia anti-body testing in screening for tubal fac-tor subfertility: the significance of IgG antibody decline over time. Hum Reprod 2002;17:699-703.

referenceS
58
242. Chaim W, Edelstein Z, Sarov B, Sarov I. The long term follow-up of asymptomat-ic women with Chlamydia trachomatis. Arch Gynecol Obstet 1992;251:159-64.
243. Puolakkainen M, Vesterinen E, Purola E, Saikku P, Paavonen J. Persistence of chlamydial antibodies after pelvic inflammatory disease. J Clin Microbiol 1986;23:924-8.
244. Piura B, Sarov B, Sarov I. Persistence of antichlamydial antibodies after treat-ment of acute salpingitis with doxycy-cline. Eur J Obstet Gynecol Reprod Biol 1993;48:117-21.
245. Dawson-Saunders B, Trapp RG. Basic & Clinical Biostatistics. Connecticut: Appleton & Lange, 1994.
246. Liu W, Ren T, Jiang B, Gong M, Shou C. Mycoplasmal membrane protein p37 promotes malignant changes in mamma-lian cells. Can J Microbiol 2007;53:270-6.
247. Gong M, Meng L, Jiang B, et al. p37 from Mycoplasma hyorhinis promotes cancer cell invasiveness and metastasis through activation of MMP-2 and followed by phosphorylation of EGFR. Mol Cancer Ther 2008;7:530-7.
248. Goodison S, Nakamura K, Iczkowski KA, Anai S, Boehlein SK, Rosser CJ. Exog-enous mycoplasmal p37 protein alters gene expression, growth and morphol-ogy of prostate cancer cells. Cytogenet Genome Res 2007;118:204-13.
249. Zhang S, Tsai S, Lo SC. Alteration of gene expression profiles during mycoplasma-induced malignant cell transformation. BMC Cancer 2006;6:116.
250. Logunov DY, Scheblyakov DV, Zubkova OV, et al. Mycoplasma infection sup-presses p53, activates NF-kappaB and cooperates with oncogenic Ras in rodent fibroblast transformation. Oncogene 2008;27:4521-31.
251. Parsonnet J. Bacterial infection as a cause of cancer. Environ Health Perspect 1995;103 Suppl 8:263-8.
252. Mbulaiteye SM, Hisada M, El-Omar EM. Helicobacter Pylori associated global gastric cancer burden. Front Biosci 2009;14:1490-504.
253. Kucinskiene V, Sutaite I, Valiukeviciene S, Milasauskiene Z, Domeika M. Preva-lence and risk factors of genital Chla-mydia trachomatis infection. Medicina (Kaunas) 2006;42:885-94.
254. Lyytikäinen E, Kaasila M, Hiltunen-Back E, et al. Chlamydia trachomatis Incidence and Prevalence Trends in Finland 1983-2003. BMC Infect Dis 2008;8:169.
255. SMI. Epidemiologisk årsrapport 2005: Swedish Institute for Infectious Disease Control, 2005.
256. Weinehall L, Hallgren CG, Westman G, Janlert U, Wall S. Reduction of selection bias in primary prevention of cardio-vascular disease through involvement of primary health care. Scand J Prim Health Care 1998;16:171-6.
257. den Hartog JE, Morre SA, Land JA. Chla-mydia trachomatis-associated tubal fac-tor subfertility: Immunogenetic aspects and serological screening. Hum Reprod Update 2006;12:719-30.
258. Micke P, Ohshima M, Tahmasebpoor S, et al. Biobanking of fresh frozen tissue: RNA is stable in nonfixed surgical speci-mens. Lab Invest 2006;86:202-11.
259. Jochumsen KM, Tan Q, Dahlgaard J, Kruse TA, Mogensen O. RNA quality and gene expression analysis of ovarian tumor tissue undergoing repeated thaw-freezing. Exp Mol Pathol 2007;82:95-102.
260. Gérard HC, Köhler L, Branigan PJ, Zei-dler H, Schumacher HR, Hudson AP. Viability and gene expression in Chla-mydia trachomatis during persistent infection of cultured human monocytes. Med Microbiol Immunol 1998;187:115-20.

59
referenceS
261. Gussmann J, Al-Younes HM, Braun PR, Brinkmann V, Meyer TF. Long-term ef-fects of natural amino acids on infection with Chlamydia trachomatis. Microb Pathog 2008;44:438-47.
262. Wallin KL, Wiklund F, Luostarinen T, et al. A population-based prospective study of Chlamydia trachomatis infec-tion and cervical carcinoma. Int J Cancer 2002;101:371-4.
263. Naucler P, Chen HC, Persson K, et al. Seroprevalence of human papillomavi-ruses and Chlamydia trachomatis and cervical cancer risk: nested case-control study. J Gen Virol 2007;88:814-22.
264. Patton DL, Landers DV, Schachter J. Experimental Chlamydia trachomatis salpingitis in mice: initial studies on the characterization of the leukocyte re-sponse to chlamydial infection. J Infect Dis 1989;159:1105-10.
265. Patton DL, Halbert SA, Kuo CC, Wang SP, Holmes KK. Host response to pri-mary Chlamydia trachomatis infection of the fallopian tube in pig-tailed mon-keys. Fertil Steril 1983;40:829-40.
266. Patton DL, Moore DE, Spadoni LR, Soules MR, Halbert SA, Wang SP. A comparison of the fallopian tube’s re-sponse to overt and silent salpingitis. Obstet Gynecol 1989;73:622-30.
267. Kindelberger DW, Lee Y, Miron A, et al. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: Evidence for a causal relationship. Am J Surg Pathol 2007;31:161-9.
268. Crum CP, Drapkin R, Miron A, et al. The distal fallopian tube: a new model for pelvic serous carcinogenesis. Curr Opin Obstet Gynecol 2007;19:3-9.
269. Lindgren PR, Cajander S, Bäckström T, Gustafsson JA, Mäkelä S, Olofsson JI. Estrogen and progesterone receptors in ovarian epithelial tumors. Mol Cell En-docrinol 2004;221:97-104.

60
Copyright © 2022 FDOKUMEN




















