
Carboplatin synergistically triggers the efficacy of photodynamic therapy via caspase 3-, 8-, and...
13
ORIGINAL ARTICLE Carboplatin synergistically triggers the efficacy of photodynamic therapy via caspase 3-, 8-, and 12-dependent pathways in human anaplastic thyroid cancer cells Raktim Biswas & Phil-Sang Chung & Jeong Hwan Moon & Seung-Ha Lee & Jin-Chul Ahn Received: 13 June 2013 /Accepted: 23 September 2013 # Springer-Verlag London 2013 Abstract Anaplastic thyroid cancer is one of the most ag- gressive forms of malignancies which grow very rapidly. Several conventional methods have been applied for the treat- ment of anaplastic thyroid cancer, but most of them were not successful in complete recovery of the patients. Therefore, a combination of two or more conventional modalities is being applied nowadays for the treatment of this type of cancer. In this present study, the combination of photodynamic therapy (PDT) and chemotherapy has been studied in anaplastic thy- roid cancer. Human anaplastic thyroid cancer cells FRO were treated with a chemotherapy drug, carboplatin (cis -diammine- 1,1-cyclobutanedicarboxyl-ateplatinum II (CBDCA)), and radachlorin-mediated PDT individually and in combination. Several parameters like cytotoxicity assay by MTT, apoptosis study by annexin V and propidium iodide, cell cycle analysis by flow cytometry, confocal microscopic study, and Western blot analysis for different apoptosis-related proteins like Bax, cytochrome c, caspases 3, 9, 8, and 12, etc. were studied to check the efficacy of the combination treatment as well as to find out the mechanism of this enhanced efficacy. Results showed that both PDT and CBDCA can induce apoptosis in FRO cells. However, a synergistic efficacy was observed when the cells were treated with CBDCA and PDT in combi- nation. Changes in mitochondrial membrane potential and an increase in reactive oxygen species generation were observed in combination treatments. The enhanced expression of dif- ferent apoptotic pathway-related proteins like Bax, cyto- chrome c, caspase 3, caspase 8, caspase 12, etc. also con- firmed the higher efficacy of combination treatment. There- fore, with this combination treatment, not only a higher effi- cacy can be achieved but also the effective dose of the che- motherapy drug can be reduced, and hence, the adverse side effects of the chemotherapy drugs can also be controlled. Keywords Anaplastic thyroid cancer . PDT . Carboplatin . Synergism . Apoptosis . Caspases Introduction Anaplastic thyroid carcinoma is an undifferentiated and rare form of thyroid cancer. Though it is responsible for only 1– 2 % of all thyroid cancer cases, it is considered as the most aggressive form of cancers in thyroid gland [1, 2]. It spreads very quickly to other parts of the body, and therefore, patients with anaplastic thyroid cancer can survive only a few months after the diagnosis of the disease [3–5]. Because of its aggres- sive nature and resistance to various chemotherapy drugs, the prognosis of the disease is also very poor. In addition to this, the treatment of ATC is also very challenging because it spreads widely within the body, hence the incidence of distant metastases is also very high. A wide range of conventional therapeutic approaches including surgery, chemotherapy, ra- diotherapy, or varying combinations of different treatment modalities have been proposed over the years, but the results of those therapies are still far from satisfaction [5, 6]. One of the promising options for the treatment of thyroid cancer and other forms of cancer is photodynamic therapy [7–9]. Photo- dynamic therapy (PDT) mainly uses some nontoxic drugs, R. Biswas : P.<S. Chung : J. H. Moon : J.<C. Ahn (*) Beckman Laser Institute Korea, Dankook University, 29-1, Anseo-dong, Cheonan, Chungnam, Republic of Korea 330-714 e-mail: [email protected] P.<S. Chung : J. H. Moon Department of Otolaryngology-Head and Neck Surgery, College of Medicine, Dankook University, Cheonan, Republic of Korea S.<H. Lee : J.<C. Ahn Department of Biomedical Engineering, Dankook University, Cheonan, Chungnam 330-714, Republic of Korea Lasers Med Sci DOI 10.1007/s10103-013-1452-9
Transcript of Carboplatin synergistically triggers the efficacy of photodynamic therapy via caspase 3-, 8-, and...
ORIGINAL ARTICLE
Carboplatin synergistically triggers the efficacyof photodynamic therapy via caspase 3-, 8-, and 12-dependentpathways in human anaplastic thyroid cancer cells
Raktim Biswas & Phil-Sang Chung & Jeong Hwan Moon &
Seung-Ha Lee & Jin-Chul Ahn
Received: 13 June 2013 /Accepted: 23 September 2013# Springer-Verlag London 2013
Abstract Anaplastic thyroid cancer is one of the most ag-gressive forms of malignancies which grow very rapidly.Several conventional methods have been applied for the treat-ment of anaplastic thyroid cancer, but most of them were notsuccessful in complete recovery of the patients. Therefore, acombination of two or more conventional modalities is beingapplied nowadays for the treatment of this type of cancer. Inthis present study, the combination of photodynamic therapy(PDT) and chemotherapy has been studied in anaplastic thy-roid cancer. Human anaplastic thyroid cancer cells FRO weretreated with a chemotherapy drug, carboplatin (cis -diammine-1,1-cyclobutanedicarboxyl-ateplatinum II (CBDCA)), andradachlorin-mediated PDT individually and in combination.Several parameters like cytotoxicity assay by MTT, apoptosisstudy by annexin V and propidium iodide, cell cycle analysisby flow cytometry, confocal microscopic study, and Westernblot analysis for different apoptosis-related proteins like Bax,cytochrome c, caspases 3, 9, 8, and 12, etc. were studied tocheck the efficacy of the combination treatment as well as tofind out the mechanism of this enhanced efficacy. Resultsshowed that both PDT and CBDCA can induce apoptosis inFRO cells. However, a synergistic efficacy was observedwhen the cells were treated with CBDCA and PDT in combi-nation. Changes in mitochondrial membrane potential and an
increase in reactive oxygen species generation were observedin combination treatments. The enhanced expression of dif-ferent apoptotic pathway-related proteins like Bax, cyto-chrome c, caspase 3, caspase 8, caspase 12, etc. also con-firmed the higher efficacy of combination treatment. There-fore, with this combination treatment, not only a higher effi-cacy can be achieved but also the effective dose of the che-motherapy drug can be reduced, and hence, the adverse sideeffects of the chemotherapy drugs can also be controlled.
Keywords Anaplastic thyroid cancer . PDT . Carboplatin .
Synergism . Apoptosis . Caspases
Introduction
Anaplastic thyroid carcinoma is an undifferentiated and rareform of thyroid cancer. Though it is responsible for only 1–2 % of all thyroid cancer cases, it is considered as the mostaggressive form of cancers in thyroid gland [1, 2]. It spreadsvery quickly to other parts of the body, and therefore, patientswith anaplastic thyroid cancer can survive only a few monthsafter the diagnosis of the disease [3–5]. Because of its aggres-sive nature and resistance to various chemotherapy drugs, theprognosis of the disease is also very poor. In addition to this,the treatment of ATC is also very challenging because itspreads widely within the body, hence the incidence of distantmetastases is also very high. A wide range of conventionaltherapeutic approaches including surgery, chemotherapy, ra-diotherapy, or varying combinations of different treatmentmodalities have been proposed over the years, but the resultsof those therapies are still far from satisfaction [5, 6]. One ofthe promising options for the treatment of thyroid cancer andother forms of cancer is photodynamic therapy [7–9]. Photo-dynamic therapy (PDT) mainly uses some nontoxic drugs,
R. Biswas : P.<S. Chung : J. H. Moon : J.<C. Ahn (*)Beckman Laser Institute Korea, Dankook University, 29-1,Anseo-dong, Cheonan, Chungnam, Republic of Korea 330-714e-mail: [email protected]
P.<S. Chung : J. H. MoonDepartment of Otolaryngology-Head and Neck Surgery, College ofMedicine, Dankook University, Cheonan, Republic of Korea
S.<H. Lee : J.<C. AhnDepartment of Biomedical Engineering, Dankook University,Cheonan, Chungnam 330-714, Republic of Korea
Lasers Med SciDOI 10.1007/s10103-013-1452-9

known as photosensitizer, and light of a specific wavelengthwhich activates the photosensitizer to generate singlet oxygenas well as reactive oxygen species (ROS) that eventuallyinduces cell death [10–12]. The major advantage of PDT isits localized effect, and therefore, it can kill malignant cellswithout causing any damage to surrounding normal healthycells. Though some damages may occur in the surroundingtissue due to photodynamic effect, it has no long-term effectand can be targeted very precisely. Unlike radiation therapy,PDT can be used many times at the same cancer site ifrequired. Beside this, PDT may destroy the blood vessels thatfeed the cancer cells and thus can reduce the malignant tumors[13–15]. In PDT, chlorin e6 and its derivates have been widelyused as a photosensitizer. One of the popular chlorin e6photosensitizers is known as radachlorin [16]. It was foundto be effective against different types of malignancies likeskin, cervical, and esophageal cancer [16–19]. Thus,radachlorin is being used as a potential photosensitizer inPDT for years. On the other hand, the platinum-based drugshave played a very important role in cancer therapy [20, 21].One of the platinum-based second-generation drugs, knownas carboplatin (cis -diammine-1,1-cyclobutanedicarboxyl-ateplatinum II, CBDCA), has been widely used as an antican-cer chemotherapeutic agent. It has been used for malignanttumors, including head and neck, ovarian, esophageal, andnon-small lung cell cancers [22–25]. In recent days, PDT incombination with other chemotherapy agents was found tobe effective against different types of cancer [26–31].Carboplatin has also been used in combination with otherconventional or alternative methods for the treatment ofcancer [32–35]. Therefore, multimodal treatment with che-motherapy drug CBDCA, and PDT can be expected toachieve a better result in combating anaplastic thyroidcancer. Beside this, with this combination therapy, not onlythe efficacy of treatment can be increased, but the adverseside effects of the chemotherapeutic drugs can also becontrolled by reducing the dose of individual drugs withoutcompromising its efficacy.
In this present study, the efficacy of PDT in combinationwith carboplatin was studied against human anaplastic thyroidcancer cells, FRO. Cells were treated with radachlorin-mediated PDT and carboplatin individually and in combina-tion to investigate whether carboplatin can trigger the efficacyof PDT. Several parameters were studied to confirm the syn-ergistic efficacy in combination therapy. Besides this, thedifferent cell death pathways were studied to find out thepossible mechanism of this synergistic activity. We also in-vestigated the possibility of reducing the effective dosage ofthe chemotherapy drug to control their side effects on normalcells. Therefore, this study has a broad potential for the man-agement of anaplastic thyroid cancer by enhancing the effica-cy of treatment as well as controlling the side effects ofchemotherapy drugs in combination with PDT.
Materials and methods
Cell culture and treatments
FRO cell is an undifferentiated human anaplastic thyroid can-cer cells. It has been derived from a patient with a large cellundifferentiated thyroid carcinoma. FRO cells were grown inRPMI 1640 with 10 % fetal bovine serum and 1 % penicillinand streptomycin (Hyclone, Thermo Scientific, South Logan,UT, USA) at 37 °C in a humidified atmosphere of 5 % CO2 inair. The cells were incubated with different concentrations ofradachlorin (0–50 μg/ml) (Rada Pharma, Russia) and/orCBDCA (0–20 mg/ml) (Sigma, Saint Louis, MO, USA) indark. After 3 h of incubation at 37 °C and 5 % CO2 atmo-sphere, the media containing radachlorin were discarded, andthe cells were washed with Dulbecco’s phosphate-bufferedsaline (DPBS) (Welgene, Daegu, South Korea). The cells werethen irradiated by placing the experimental flasks under a setof a 660-nm diode laser with an energy density of 7.8 J/cm2 for15 min. The laser system was an array of LED with a dimen-sion of 13.5×8.5 cm. The laser power of the system wascalibrated by a laser power energy meter (Gentec EO, OR,USA). Treated cells were incubated in 37 °C for different timeintervals 3, 6, 12, and 24 h for further experiments.
MTT assay
The cells were seeded into 96-well cell culture plates at adensity of 5×104 cells/ml and were treated with differentconcentrations of radachlorin (0–50 μg/ml) and/or CBDCA(0–20 mg/ml) and irradiated with laser as described before.After incubation at 37 °C, 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) solution (0.2 mg/ml)(Sigma, Saint Louis, MO, USA) was added to each well,and the absorbance was measured at 540 nm using AsysUVM340 Microplate Reader, Biochrom (Cambridge, CB40FJ, UK). From the results of MTT assay, concentrations ofCBDCA and radachlorin and incubation time after laser irra-diation were selected for further experiments. Two concentra-tions, 0.4 and 1.6 μg/ml, of radachlorin and 0.05 mg/ml ofCBDCA for 6 h of incubation after laser irradiation werechosen for single as well as combined treatments withCBDCA and radachlorin PDT.
Determination of synergism
According to the median effect equation of Chou [36, 37],combination index can be expressed as a function of dose orconcentrations of two drugs and their corresponding percent-age of cell inhibition. Therefore, combination index (CI) can
be expressed as; CI ¼ Dð Þ1Dxð Þ1 þ Dð Þ2
Dxð Þ2 , where (Dx) is the indi-
vidual dose of the drug that inhibits a system x% of cells and
Lasers Med Sci

D is the dose of the drug in combination treatment that alsoinhibits a system x% of cells. Synergy was quantified by thevalue of CI where CI<1 indicates synergism, CI>1 indicatesantagonism, and CI=1 indicates additivity. To study whetherthe efficacy of this combination treatment has any synergisticeffect in FRO cells, data from cell viability assay were ana-lyzed according to Chou and Talalay method [36]. Briefly,FRO cells were seeded in 96-well plates and treated withincreasing concentrations of radachlorin (0–50 μg/ml) and aconstant concentration of carboplatin (0.05 mg/ml) as de-scribed before and the MTT assay was performed. Synergisticeffect was analyzed using CompuSyn Version 1.0 software(ComboSyn Inc., NJ) by calculating the CI.
One of the major objectives of having a synergistic drugcombination is to reduce the dose of the drug used, therebyreducing the toxicity while maintaining efficacy. Therefore,the dose reduction index (DRI) was introduced. The dosereduction index was determined by comparing the ratio ofthe concentrations required to obtain a given degree of growthinhibition for carboplatin and PDT individually and in combi-nation. For the combination of two drugs, CI ¼ 1
DRIð Þ1 þ 1DRIð Þ2
. Therefore, we can calculate the value of DRI by the dose ofdrugs in individual treatments and in combination treatmentfollowing the rule of median effect equation as mentioned [36].The magnitude of decrease was expressed in fold changebeyond the expected dose when the combination treatment isused. A greater DRI value indicates a greater dose reduction,and thus, DRI >1 is considered as a favorable condition for thereduction of dose of the drugs.
Flow cytometric analysis
Annexin V-FITC/PI analysis
FRO cells were treated with CBDCA and PDT, and theapoptotic cells were determined by fluorescein isothiocyanate(FITC) annexin V/Dead Cell Apoptosis kit (MolecularProbes, OR, USA) according to the manufacturer’s instruc-tions. Briefly, FRO cells were treated with CBDCA and PDTas described and were harvested. Cells were washed twicewith DPBS and then resuspended in 100 μl of binding buffercontaining annexin V-FITC and 100 μg/ml propidium iodide(PI) solution (Molecular Probes Inc., OR, USA) and incubatedin the dark for 15min. The cells were then washed with DPBSagain and the annexin V(+) PI(+) and annexin V(+) PI(−) cellswere analyzed by a dot plot using a flow cytometer (BDFACSCalibur, BD Biosciences, CA, USA). The numbers ofcells in the quadrants of each plot indicate the percentage ofannexin V(+) (apoptotic) and PI-(+) cells (left bottom = nor-mal cells, right bottom = early apoptotic cells, left top =necrotic cells, right top = late apoptotic cells). Annexin V-FITC and PI-positive cells were detected in FL1 (Ex-Max
494 nm/Em-Max 520 nm) and FL2 (Ex-Max 535/Em-Max617 nm), respectively, and the histogram was plotted from thevalue of percentage of events of 10,000 cells.
Cell cycle analysis
Six hours after the treatment, cells were harvested and fixedwith ice-cold 70 % (v /v ) ethanol by adding dropwise to thecells while vortexing and incubated for 30 min, and then, thecells were stored at 4 °C for 24 h [38]. After centrifugation at5,000 rpm for 3 min, the cell pellets were washed with DPBS(pH 7.4) and resuspended in 0.5 ml PBS containingpropidium iodide (50 μg/ml) (Sigma, St. Louis, USA). Thecells were then incubated at room temperature for 30 min,and DNA content was determined by flow cytometry (BDFACSCalibur, CA, USA) and analyzed with Flowing soft-ware, Finland. The percentages of viable and dead cells weredetermined as 10,000 events per sample. Fluorescence wasmeasured at an excitation wavelength of 480 nm through aFL-2 filter (585 nm).
Measurement of mitochondrial membrane potential
After treatment as described, the FRO cells were washed twicewith PBS and were centrifuged at 1,500 rpm for 5 min. Thecells were then incubated with 10 μM of rhodamine 123(Molecular Probes Inc., OR, USA) at 37 °C for 30 min andagain washed twice with DPBS. The intensities of fluores-cence of 10,000 cells were measured by flow cytometry (BDFACSCalibur, CA, USA) at an excitation wavelength of480 nm through a FL-1 filter (530 nm). Flow cytometric datawas analyzed by Cell Quest Pro software (BD Biosciences,CA, USA). A histogram was prepared to compare the de-crease in the fluorescence in different treatment groups.
Measurement of reactive oxygen species
The cells were exposed to 0.05 mg/ml of CBDCA and/or 0.4and 1.6 μg/ml of radachlorin for PDT. Six hours after laserirradiation, the cells were harvested and washed with PBS andthen were treated with 10 μM H2DCFDA (Molecular ProbesInc., OR, USA) for 30min at 37 °C. Cells were then collected,washed twice with DPBS again, and analyzed for the gener-ation of ROS using a flow cytometer (BD FACSCalibur, CA,USA) through a FL-1 filter. The data from flow cytometry wasanalyzed by Cell Quest Pro software (BD Biosciences, CA,USA), and the relative increase in the generation of ROS indifferent treatment groups was represented in a histogram.
Study of protein expressions by Western blots
The expressions of different proteins in the treated cells wereanalyzed using the Western blot techniques. After treatment,
Lasers Med Sci

the cells were washed with cold DPBS twice and then theproteins were extracted in RIPA buffer (Sigma, St. Louis,USA). An equivalent amount of proteins was loaded ontopolyacrylamide gels and was subjected to electrophoresis.The proteins were then transferred to a PVDF membrane(Immun-Blot PVDF, BioRad Laboratories, Hercules, USA).Electrophoresis and blotting were both performed using thePowerPac200 electrophoresis system (BioRad Laboratories,Hercules, USA). After transferring the proteins, the mem-branes were blocked with 5 % non-skimmed milk for 1 hand then incubated with primary antibodies (Santa Cruz Bio-technology, Inc. CA, USA) overnight on a multishaker at4 °C. The membranes were then probed with anti-mouseIgG or anti-rabbit IgG antibody (Santa Cruz Biotechnology,Inc., CA, USA) for 1 h. The protein band was detected byECL Western blotting detection reagents (GE Healthcare,Buckinghamshire, UK), and the pictures were taken byKodakin vivo image analyzer.
Statistical analysis
All the data are expressed with the mean ± S.E. of at least threeindependent experiments. Statistical analysis was performed,
and differences between two groups were analyzed using thetwo-tailed Student’s t test; a =p <0.05, b =p <0.01, and c =p <0.001 were considered statistically significant.
Results
Cell viability assay
The effects of CBDCA, PDT alone, and CBDCA in combi-nation with PDT were analyzed by MTT assay. As shown inFig. 1a, FRO cells were treated with different concentrationsof radachlorin (0–50 μg/ml) for PDT and incubated for 3, 6,12, and 24 h. The percentage of cell viability was decreasedwith increasing concentrations of radachlorin in PDT. On theother hand, percentage of cell viability was also decreasedwith time of incubation after laser irradiation. From Fig. 1a,after 3 h of incubation, approximately 7.98±2.28 and 14.79±1.42% cells were dead at the concentrations of 0.4 and 1.6 μg/ml of radachlorin, respectively. Again, after 6 h of incubation,approximately 13.86±2.73 and 25.45±2.72% cells were deadwhen the cells were treated with radachlorin–PDT at concen-trations of 0.4 and 1.6 μg/ml respectively. Further,
Fig. 1 Study of cell viability by MTT assay of FRO cells treated withdifferent concentrations of radachlorin (0–50 μg/ml) in PDT and incu-bated for different time interval (a). MTTassay to determine cell viabilityof FRO cells treated with different concentrations of carboplatin from 0 to
20 μg/ml (b). Cytotoxicity study in FRO cells treated with 0.05 mg/mlcarboplatin and increasing concentrations of radachlorin from 0 to 50 μg/ml (c). Data are shown as mean ± S.E.
Lasers Med Sci

approximately 26.66±1.53, 65.29±1.51, 78.17±2.46, and87.62±0.61 % cells were dead at the same concentrations ofradachlorin at 12 and 24 h of incubation, respectively. On theother hand, from Fig. 1b, it can be stated that the viability ofFRO cells was decreased with increasing concentrations ofCBDCA also. Approximately 20.99±3.65 % cells were deadwhen the cells were treated with CBDCA at a concentration of0.05 mg/ml. Therefore, 0.05 mg/ml of CBDCA and 6 h ofincubation after PDT treatment were selected for combinationstudy. When the cells were treated with 0.05 mg/ml ofCBDCA in combination with varying concentrations ofradachlorin (0–50 μg/ml) in PDT, the percentage of cellviability was significantly decreased compared to theirrespective individual treatments (Fig. 1c). The viability ofthe cells was inhibited up to 71.07±1.51 and 79.04±1.61 % when the cells were treated with 0.05 mg/ml ofCBDCA and PDT with radachlorin concentrations of 0.4and 1.6 μg/ml, respectively. However, there were no no-ticeable changes in cell viability when the cells were treat-ed with radachlorin only (without any laser irradiation) atthe respective concentrations. From the MTT assay, twodifferent concentrations of radachlorin (0.4 and 1.6 μg/ml)were selected for further studies.
Determination of synergism
The evaluation of CI values indicated that combination ofcarboplatin and PDT was synergistic at higher concentrationof radachlorin. According to the Fa-log (CI) plot, the CI wasplotted against the fraction of affected cells (Fa) by corre-sponding doses of drugs. Therefore, in Fa-log (CI) plot, syn-ergism is indicated by a negative value [i.e., log (CI) <0].From Fig. 2a, effective synergism was not observed for theradachlorin concentrations up to 0.4 μg/ml in combinationtreatment with CBDCA at a concentration of 0.05 mg/ml.
However, synergistic effect can be observed when the cellswere treated with radachlorin PDT at a concentration above0.8 μg/ml. The CI value for combination therapy withradachlorin PDT (0.8 μg/ml) and CBDCA (0.05 mg/ml) is0.66 (log CI<0). For combination treatment with radachlorinconcentration 1.6 μg/ml in PDT, the CI value is 0.29 which isa clear indication of strong synergism (log CI<0). From thelog (CI)-Fa plot (Fig. 2a), it can be clearly stated that the CIvalue was increased with the increasing concentration ofradachlorin in combination treatment indicating a strongsynergism.
The DRI curve shows that the DRI values for the bothradachlorin and CBDCA are greater than 1 (DRI>1; therefore,log DRI>0) which indicates that the same efficacy of theindividual treatments can be achieved by reducing the con-centration of both radachlorin and CBDCA in combinationtreatment. From Fig. 2b, DRI values for radachlorin andCBDCAwere 1.9 and 0.33, respectively at Fa=0.117. Again,the DRI value for CBDCAwas increased with the increasingconcentrations of radachlorin. At Fa=0.388, DRI values forradachlorin PDTand CBDCAwere 2.68 and 3.38, respective-ly, which therefore indicates that the concentrations ofCBDCA can be reduced at higher concentrations ofradachlorin in combination treatment.
Annexin V-FITC/PI analysis
From the flow cytometric analysis of apoptosis with annexinV-FITC and PI, the percentages of early and late apoptoticcells in CBDCA treated cells were approximately 11.2±1.1and 1.2±0.36 %, respectively. For PDT with radachlorinconcentration of 0.4 μg/ml, percentages of early and lateapoptotic cells were 16.4±1.8 and 1.6±2.6 %, respectively.Again for PDT with radachlorin concentration of 1.6 μg/ml,the respective percentages of early and late apoptosis were
Fig. 2 a Combination index (CI) was plotted against the fraction ofinhibition of FRO cells in combination treatment for determination ofsynergism. Cells were treated with different concentrations of CBDCAand radachlorin PDT and their corresponding fraction of inhibition wascalculated. b Dose reduction index (DRI)–fraction of inhibition (Fa)
curve for the study of dose reduction of CBDCA and radachlorin inPDT. FRO cells were treated with different concentrations of CBDCAand radachlorin in PDT, and their corresponding DRI values and fractionof inhibition were calculated
Lasers Med Sci
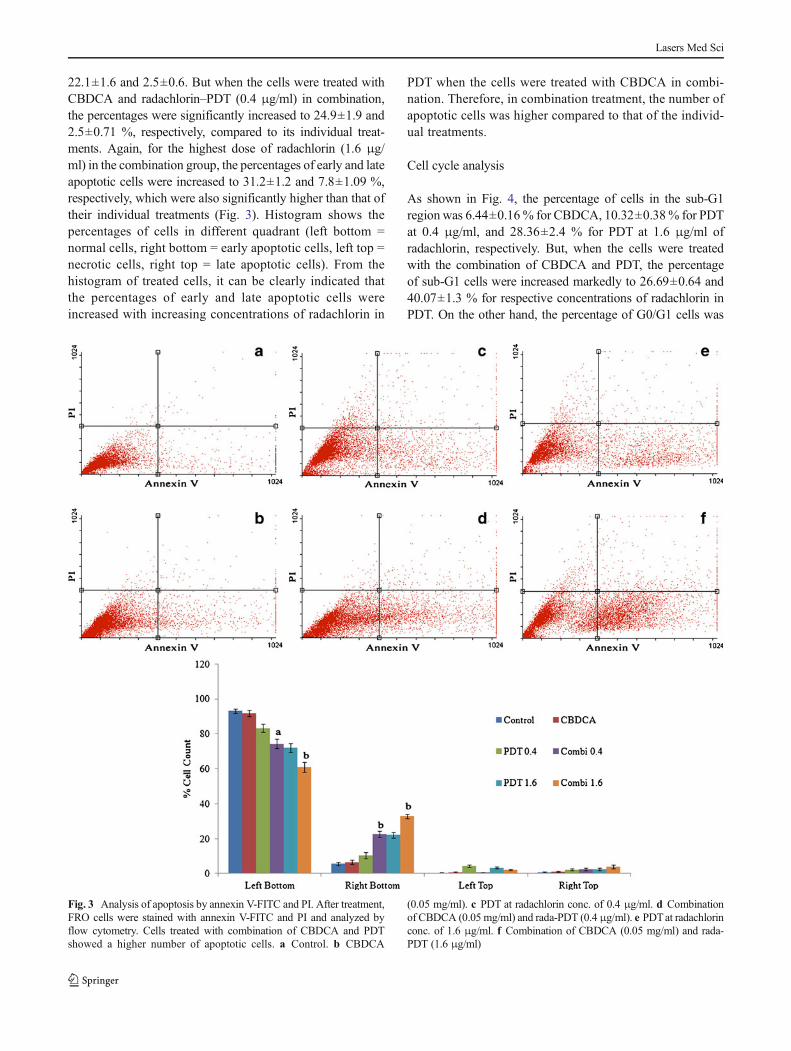
22.1±1.6 and 2.5±0.6. But when the cells were treated withCBDCA and radachlorin–PDT (0.4 μg/ml) in combination,the percentages were significantly increased to 24.9±1.9 and2.5±0.71 %, respectively, compared to its individual treat-ments. Again, for the highest dose of radachlorin (1.6 μg/ml) in the combination group, the percentages of early and lateapoptotic cells were increased to 31.2±1.2 and 7.8±1.09 %,respectively, which were also significantly higher than that oftheir individual treatments (Fig. 3). Histogram shows thepercentages of cells in different quadrant (left bottom =normal cells, right bottom = early apoptotic cells, left top =necrotic cells, right top = late apoptotic cells). From thehistogram of treated cells, it can be clearly indicated thatthe percentages of early and late apoptotic cells wereincreased with increasing concentrations of radachlorin in
PDT when the cells were treated with CBDCA in combi-nation. Therefore, in combination treatment, the number ofapoptotic cells was higher compared to that of the individ-ual treatments.
Cell cycle analysis
As shown in Fig. 4, the percentage of cells in the sub-G1region was 6.44±0.16% for CBDCA, 10.32±0.38% for PDTat 0.4 μg/ml, and 28.36±2.4 % for PDT at 1.6 μg/ml ofradachlorin, respectively. But, when the cells were treatedwith the combination of CBDCA and PDT, the percentageof sub-G1 cells were increased markedly to 26.69±0.64 and40.07±1.3 % for respective concentrations of radachlorin inPDT. On the other hand, the percentage of G0/G1 cells was
Fig. 3 Analysis of apoptosis by annexin V-FITC and PI. After treatment,FRO cells were stained with annexin V-FITC and PI and analyzed byflow cytometry. Cells treated with combination of CBDCA and PDTshowed a higher number of apoptotic cells. a Control. b CBDCA
(0.05 mg/ml). c PDT at radachlorin conc. of 0.4 μg/ml. d Combinationof CBDCA (0.05 mg/ml) and rada-PDT (0.4 μg/ml). e PDTat radachlorinconc. of 1.6 μg/ml. f Combination of CBDCA (0.05 mg/ml) and rada-PDT (1.6 μg/ml)
Lasers Med Sci

decreased in the combination group. There was a significantreduction in cell number at G0/G1 stage in combinationgroups. From Fig. 4f, for the highest dose of radachlorin inthe combination group, the percentage of sub-G1 cells wassignificantly higher than that of the cells in the PDT-treatedgroups with the same concentrations of radachlorin. The his-togram shows the percentages of cell count in different sub-populations. It also indicates that the number of apoptotic cellsin sub-G1 region was significantly higher in combinationgroup compared to their individual treatments. This increasein the sub-G1 cells in all the combination groups also indicatesthat the incidence of apoptosis was increased with increasingconcentrations of radachlorin in PDT.
Measurement of mitochondrial membrane potential (ΔΨm)
Mitochondrial membrane potential is an important indicatorof mitochondrial function and dysfunction. The role of mito-chondria in signaling, cell injury, and cell death is very
important. From the flow cytometric study, fluorescence ofthe treated cells was compared to the control cells and indi-vidual treatments, and the decrease in the cell fluorescencewas quantified by Cell Quest Pro software. Fluorescence ofrhodamine 123 in the combination group was decreased morecompared to that of their respective PDT treatments at thesame concentrations of radachlorin. For the treatments withCBDCA, and PDT with 0.4 and 1.6 μg/ml of radachlorin,percentages of cells undergoing mitochondrial membrane de-polarization were 6.06±3.02, 36.96±3.35, and 66.40±2.5 %,respectively. On the other hand, in the combination group, thepercentages were 65.48±2.4 and 85.38±1.4 % for respectiveconcentrations of radachlorin in PDT (Fig. 5). Histogram alsoshows a significant decrease in mitochondrial membrane po-tential in the combination group compared to the individualtreatment groups. Therefore, the depolarization in mitochon-drial membrane potential was much higher in the cells treatedwith CBDCA and PDT in combination compared to the cellswith individual treatments.
Fig. 4 Cell cycle analysis of FRO cells treated with CBDCA withradachlorin for PDT. a Control. b CBDCA. c PDT at radachlorin conc.of 0.4 μg/ml. d Combination of CBDCA (0.05 mg/ml) and rada-PDT
(0.4 μg/ml). e PDT at radachlorin conc. of 1.6 μg/ml. f Combination ofCBDCA (0.05 mg/ml) and rada-PDT (1.6 μg/ml)
Lasers Med Sci

Measurement of reactive oxygen species
Reactive oxygen species have an important role in a numberof cellular processes. ROS can lead to cellular damage, oxi-dative stress, and DNA damage that can lead to apoptosis ofthe cells. From the flow cytometric study, fluorescence of thetreated cells in combination group was higher compared totheir respective individual treatments. Figure 6 shows that thecell fluorescence was increased much higher in combinationgroups compared to the PDT-treated cells at the same concen-trations of radachlorin. Approximately 54.52±2.88 and 69.03±3.53% cells showed an increase in fluorescence in PDTwith0.4 and 1.6 μg/ml of radachlorin. On the other hand, thepercentages fluorescent cells were increased further up to69.03±3.53 and 89.03±2.35 %, respectively, in the respectivecombination groups. From the histogram of the percentage ofgeneration of ROS in the treated cells, it can be stated thatpercentages of fluorescent cells, i.e., generation of ROS, were
significantly increased in the combination groups compared tothe individual treatments.
Western blot analysis of proteins
Figures 7 and 8 show the expressions of different proteinsrelated to apoptosis. From Fig. 7, the expressions of Bax,cytochrome c, and caspase 9 were upregulated and the expres-sion of Bcl-2 was downregulated in the individual treatmentswith CBDCA and PDT. The expressions of caspase 3 and polyADP ribose polymerase (PARP) were also upregulated leadingto the apoptosis of the cells. But all these mitochondrialpathway-related proteins were expressed much higher whenthe cells were treated with CBDCA in combination with PDT.From the histograms of percentage of expression level of theproteins, it can be stated that the expressions of Bax, cyto-chrome c, caspase 9, caspase 3, and PARP were upregulatedin combination groups. On the other hand, the expression of
Fig. 5 Flow cytometric analysis of mitochondrial membrane potential ofthe cells treated with CBDCA and PDT. Cells were stained with rhoda-mine 123 and mitochondrial membrane depolarization was studied byflow cytometry. a Control. b CBDCA. c PDT at radachlorin conc. of
0.4 μg/ml. d Combination of CBDCA (0.05 mg/ml) and rada-PDT(0.4 μg/ml). e PDT at radachlorin conc. of 1.6 μg/ml. f Combination ofCBDCA (0.05 mg/ml) and rada-PDT (1.6 μg/ml)
Lasers Med Sci

caspase 8 was regulated in CBDCA-treated groups as well as incombination groups (Fig. 8). But in combination groups, thecaspase 8 was expressed higher compared to their individualtreatments. There was also an increase in the expressions ofcaspase 12 in the cells treated with PDT individually and incombination. The expression of caspase 12 in combination-treated cells was much higher than that of PDT only- orCBDCA only-treated cells. Beside this, a higher expression ofapoptosis-inducing factor (AIF) was also observed in combina-tion group at higher concentrations of radachlorin (Fig. 8).From the histograms of the relative band intensities of differenttreatment groups, it can be stated that significantly higherexpressions of proteins can be observed at higher concentra-tions (1.6 μg/ml) of radachlorin in combination groups. Thus,the proteins related to different apoptosis pathways were mod-ulated simultaneously in combination treatment which there-fore increases the efficacy of the treatment.
Discussion
Anaplastic thyroid carcinoma is so aggressive that in mostcases patients die within 6 to 8 months from the time ofdiagnosis. Different therapeutic approaches have been studiedto combat this disease, but the results are still disappointingand the prognosis has not yet been changed over the pastdecades [39, 40]. Carboplatin has been used as a chemother-apy drugs for the treatment of various malignancies. As pervarious clinical reports, CBDCA shows some toxicity to thehuman body and leads to inevitable side effects such as dose-dependent cumulative myelosuppression, nausea, andvomiting [32, 41]. PDT may also have some side effects likeskin phototoxicity on normal cells. In addition to this, hyper-sensitive skin reactions, local edema, nausea, and liver toxicityare the most frequent side effects of PDT [42]. Thus, a newtherapeutic approach is required to overcome these adverse
Fig. 6 Flow cytometric analysis of reactive oxygen species of the cellstreated with CBDCA and PDT individually or in combination. Cells werestained with H2DCFDA to study generation of ROS. a Control. bCBDCA. c PDT at radachlorin conc. of 0.4 μg/ml. d Combination of
CBDCA (0.05 mg/ml) and rada-PDT (0.4 μg/ml). e PDT at radachlorinconc. Of 1.6 μg/ml. f Combination of CBDCA (0.05 mg/ml) and rada-PDT (1.6 μg/ml)
Lasers Med Sci

effects. One of the ways to reduce these side effects is toreduce the dose of the chemotherapy drug, but that may alsocompromise the efficacy of the treatment. Therefore, we
proposed a treatment method in which CBDCA and PDTcan be applied in combination. In this present study, combinedeffect of carboplatin- and radachlorin-mediated photodynamic
Fig. 7 Western blot analysis of different mitochondrial pathway-relatedproteins in FRO cells treated with carboplatin- and radachlorin-mediatedPDT. Cells were treated with CBDCA and radachlorin PDT individually
and in combination, and the expressions of Bax, Bcl-2, cytochrome c,caspase 9, caspase 3, and PARP were studied. Histograms show thepercentage of expression level in the proteins in different treatment groups
Fig. 8 Western blot analysis of different ER stress and extrinsic pathway-related proteins like caspase 12 and caspase 8, respectively. Expression ofAIF was also studied in FRO cells treated with carboplatin- and
radachlorin-mediated PDT. Histograms show the percentage of expres-sion level of each protein in different treatment groups
Lasers Med Sci
therapy has been evaluated to combat anaplastic thyroid can-cer. Several parameters have been studied which confirmedthat the synergistic efficacy can be achieved through thecombination of CBDCA and PDT. Therefore, the combinationtreatment was not only expected to reduce the effective doseof CBDCA, but also can enhance the efficacy synergistically.Therefore, the adverse effects of carboplatin and PDT can becontrolled without compromising the efficacy of treatment.
From the MTT assay results, it can be stated that bothcarboplatin and PDT can induce apoptosis in FRO cells, butthe efficacy of inhibition of cell growth was significantly (p <0.05) higher in combination treatment compared to the indi-vidual treatments with PDTor CBDCA. The synergism of thecombination treatment was also studied, and from the CIvalue, a synergistic effect can be observed at a concentrationof 0.8 μg/ml of radachlorin in combination treatment. Thesynergism was then gradually increased with the increasingconcentration of radachlorin. Again, from the DRI plot, re-duction of dose of carboplatin can also be suggested. Acondition for reducing the dose of CBDCA was more favor-able at the higher concentration of radachlorin. Therefore, thisreduction in carboplatin dose may play an important role incontrolling the adverse side effects of chemotherapy drugs.The synergistic efficacy was also confirmed by the flowcytometric analysis with annexin V-FITC and PI where anincreased number of apoptotic cells were observed in combi-nation groups. From cell cycle analysis, it was observed thatmost of the cells were in the sub-G1 region after 6 h oftreatment in combination groups, and this is a clear indicationof enhanced apoptosis in combination groups compared totheir respective individual treatments. Changes in mitochon-drial membrane potential were more distinct in combinationtreatment which indicated that mitochondrial membrane de-polarization occurred in a higher extent in combination treat-ment. On the other hand, generation of ROS in the treated cellswas observed to be much higher than that of the individualtreatments which also confirmed the enhanced efficacy of thecombination treatment. To find out the possible pathway ofthis enhanced apoptosis in combination group, the expressionlevel of different apoptotic proteins was studied. From theWestern blot analysis, there was an increase in expressions ofmitochondrial pathway-related proteins like Bax, cytochromec, caspase 9, caspase 3, AIF, and PARP in combination group.The expressions of ER stress-related protein caspase 12 werealso expressed more in the combination group. On the otherhand, the extrinsic pathway-related protein caspase 8 was alsoexpressed in combination groups. Therefore, from the resultsof the Western blot study, it can be concluded that multipleapoptotic pathways were activated simultaneously in combi-nation treatment which therefore enhances the efficacy oftreatment. Previous studies show that carboplatin can induceapoptosis by mitochondrial pathways as well as caspase 8-dependent pathways [43–45]. On the other hand, PDT can
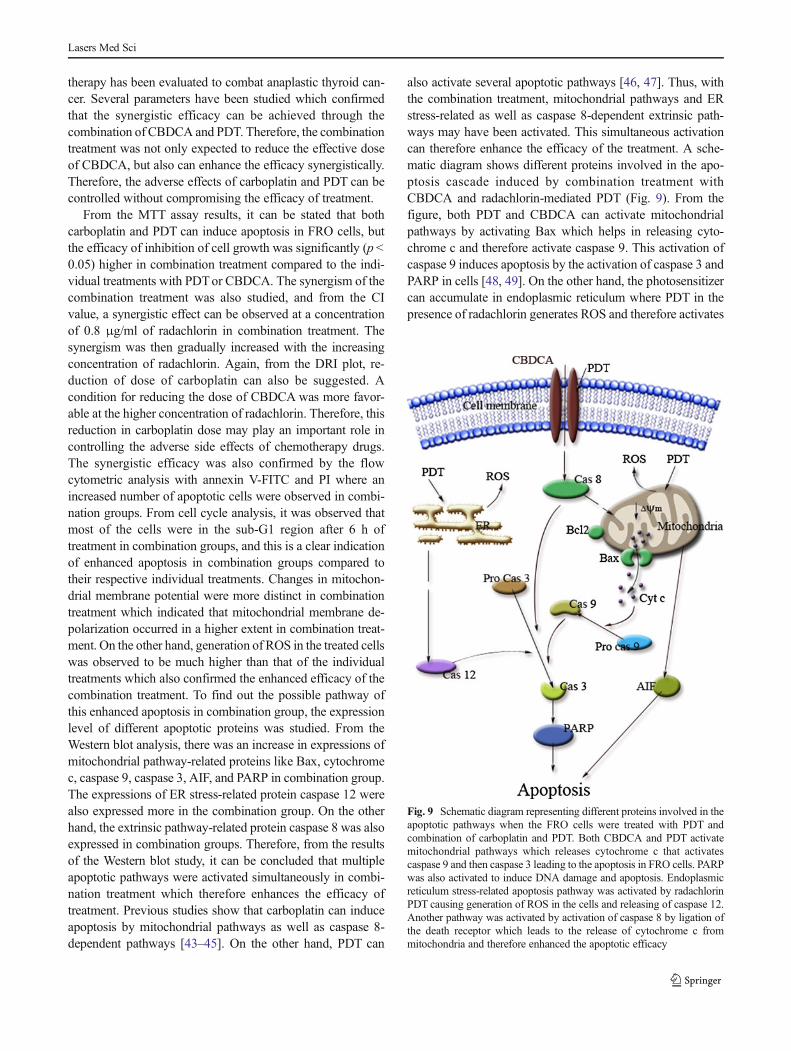
also activate several apoptotic pathways [46, 47]. Thus, withthe combination treatment, mitochondrial pathways and ERstress-related as well as caspase 8-dependent extrinsic path-ways may have been activated. This simultaneous activationcan therefore enhance the efficacy of the treatment. A sche-matic diagram shows different proteins involved in the apo-ptosis cascade induced by combination treatment withCBDCA and radachlorin-mediated PDT (Fig. 9). From thefigure, both PDT and CBDCA can activate mitochondrialpathways by activating Bax which helps in releasing cyto-chrome c and therefore activate caspase 9. This activation ofcaspase 9 induces apoptosis by the activation of caspase 3 andPARP in cells [48, 49]. On the other hand, the photosensitizercan accumulate in endoplasmic reticulum where PDT in thepresence of radachlorin generates ROS and therefore activates
Fig. 9 Schematic diagram representing different proteins involved in theapoptotic pathways when the FRO cells were treated with PDT andcombination of carboplatin and PDT. Both CBDCA and PDT activatemitochondrial pathways which releases cytochrome c that activatescaspase 9 and then caspase 3 leading to the apoptosis in FRO cells. PARPwas also activated to induce DNA damage and apoptosis. Endoplasmicreticulum stress-related apoptosis pathway was activated by radachlorinPDT causing generation of ROS in the cells and releasing of caspase 12.Another pathway was activated by activation of caspase 8 by ligation ofthe death receptor which leads to the release of cytochrome c frommitochondria and therefore enhanced the apoptotic efficacy
Lasers Med Sci

caspase 12 which may also be responsible for inducing apo-ptosis in the treated cells. Activation of caspase 8 by ligationof death receptor can also lead to mitochondrial release ofcytochrome c which activates caspase 9 and can also enhancethe apoptotic signal [50]. Thus, this activation of multiplepathways may play an important role in the synergistic effi-cacy in combination treatment by enhancing the expressionsof different apoptotic proteins.
Therefore, this study indicates that the efficacy of chemo-therapy drugs can be increased synergistically by combinationtreatment with PDT. In addition to this, the adverse side effectsof chemotherapy drugs can also be controlled withoutcompromising its efficacy. Since the overall prognosis ofanaplastic thyroid cancer was very poor for several years, thisstudy suggests the feasibility of combined modality and there-fore may be a promising option to treat anaplastic thyroidcancer.
Acknowledgments This research was supported by Leading ForeignResearch Institute Recruitment Program through the National ResearchFoundation of Korea funded by the Ministry of Education, Science andTechnology (2012K1A4A3053142).
Conflict of interest The authors have no conflict of interest to declare.
References
1. Nagaiah G, Hossain A, Mooney CJ, Parmentier J, Remick SC (2011)Anaplastic thyroid cancer: a review of epidemiology, pathogenesis,and treatment. J oncol 2011:542358. doi:10.1155/2011/542358
2. Are C, Shaha A (2006) Anaplastic thyroid carcinoma: biology,pathogenesis, prognostic factors, and treatment approaches. AnnSurg Oncol 13(4):453–464. doi:10.1245/aso.2006.05.042
3. Ain KB (1998) Anaplastic thyroid carcinoma: behavior, biology, andtherapeutic approaches. Thyroid off j Am Thyroid Assoc 8(8):715–726
4. Nagaiah G, Hossain A, Mooney CJ, Parmentier J, Remick SC (2011)Anaplastic thyroid cancer: a review of epidemiology, pathogenesis,and treatment. J oncol. doi:10.1155/2011/542358
5. Pasieka JL (2003) Anaplastic thyroid cancer. Curr opin oncol 15(1):78–83
6. Shaha AR, Ferlito A, Rinaldo A (2001) Distant metastases fromthyroid and parathyroid cancer. ORL j oto-rhino-laryngol relat spec63(4):243–249
7. Dolmans DE, Fukumura D, Jain RK (2003) Photodynamic therapyfor cancer. Nat rev Cancer 3(5):380–387. doi:10.1038/nrc1071
8. Dolmans DEJGJ, Fukumura D, Jain RK (2003) Photodynamic ther-apy for cancer. Nat rev Cancer 3(5):380–387
9. Wilson BC (2002) Photodynamic therapy for cancer: principles. Canj gastroenterol 16(6):393–396
10. Dougherty TJ, Gomer CJ, Henderson BW, Jori G, Kessel D, KorbelikM,Moan J, Peng Q (1998) Photodynamic therapy. J Natl Cancer Inst90(12):889–905
11. Henderson BW, Dougherty TJ (1992) How does photodynamictherapy work? Photochem photobiol 55(1):145–157
12. Lam M, Oleinick NL, Nieminen AL (2001) Photodynamic therapy-induced apoptosis in epidermoid carcinoma cells. Reactive oxygen
species and mitochondrial inner membrane permeabilization. J biolchem 276(50):47379–47386. doi:10.1074/jbc.M107678200
13. Brown SB, Brown EA,Walker I (2004) The present and future role ofphotodynamic therapy in cancer treatment. lancet oncol 5(8):497–508. doi:10.1016/S1470-2045(04)01529-3
14. Hopper C (2000) Photodynamic therapy: a clinical reality in thetreatment of cancer. lancet oncol 1:212–219
15. Huang Z (2005) A review of progress in clinical photodynamictherapy. Technol cancer res treat 4(3):283–293
16. Douillard S, Lhommeau I, Olivier D, Patrice T (2010) In vitroevaluation of radachlorin sensitizer for photodynamic therapy. Jphotochem photobiol B Biol 98(2):128–137. doi:10.1016/j.jphotobiol.2009.11.011
17. Bae SM, Kim YW, Lee JM, Namkoong SE, Han SJ, Kim JK,Lee CH, Chun HJ, Jin HS, Ahn WS (2004) Photodynamiceffects of Radachlorin on cervical cancer cells. Cancer res treatoff j Korean Cancer Assoc 36(6):389–394. doi:10.4143/crt.2004.36.6.389
18. Filonenko EV, Sokolov VV, Chissov VI, Lukyanets EA, VorozhtsovGN (2008) Photodynamic therapy of early esophageal cancer.Photodiagn photodyn ther 5(3):187–190. doi:10.1016/j.pdpdt.2008.06.001
19. Kochneva EV, Filonenko EV, Vakulovskaya EG, Scherbakova EG,Seliverstov OV, Markichev NA, Reshetnickov AV (2010) Photosen-sitizer Radachlorin(R): skin cancer PDT phase II clinical trials.Photodiagn photodyn ther 7(4):258–267. doi:10.1016/j.pdpdt.2010.07.006
20. Kelland L (2007) The resurgence of platinum-based cancer chemo-therapy. Nat rev Cancer 7(8):573–584
21. Decatris MP, Sundar S, O’Byrne KJ (2004) Platinum-based chemo-therapy in metastatic breast cancer: current status. Cancer treat rev30(1):53–81. doi:10.1016/s0305-7372(03)00139-7
22. Forastiere A, Koch W, Trotti A, Sidransky D (2001) Head and neckcancer. N Engl j med 345(26):1890–1900. doi:10.1056/NEJMra001375
23. Kelly K, Crowley J, Bunn PA Jr, Presant CA, Grevstad PK,Moinpour CM, Ramsey SD, Wozniak AJ, Weiss GR, Moore DF,Israel VK, Livingston RB, Gandara DR (2001) Randomized phaseIII trial of paclitaxel plus carboplatin versus vinorelbine plus cisplatinin the treatment of patients with advanced non-small-cell lung cancer:a Southwest Oncology Group trial. J clin oncol off j Am Soc ClinOncol 19(13):3210–3218
24. du Bois A, Luck HJ, Meier W, Adams HP, Mobus V, Costa S,Bauknecht T, Richter B, Warm M, Schroder W, Olbricht S, Nitz U,Jackisch C, Emons G, Wagner U, Kuhn W, Pfisterer J (2003) Arandomized clinical trial of cisplatin/paclitaxel versus carboplatin/paclitaxel as first-line treatment of ovarian cancer. J Natl Cancer Inst95(17):1320–1329
25. Wheate NJ, Walker S, Craig GE, Oun R (2010) The status ofplatinum anticancer drugs in the clinic and in clinical trials. DaltonTrans 39(35):8113–8127. doi:10.1039/c0dt00292e
26. Bhuvaneswari R, Gan YY, Soo KC, OlivoM (2009) Targeting EGFRwith photodynamic therapy in combination with Erbitux enhancesin vivo bladder tumor response. Mol cancer 8:94. doi:10.1186/1476-4598-8-94
27. Bhuvaneswari R, Yuen GY, Chee SK, Olivo M (2011)Antiangiogenesis agents avastin and erbitux enhance the efficacyof photodynamic therapy in a murine bladder tumor model. Laserssurg med 43(7):651–662. doi:10.1002/lsm.21109
28. Compagnin C, Mognato M, Celotti L, Canti G, Palumbo G, Reddi E(2010) Cell proliferation and cell cycle alterations in oesophagealp53-mutated cancer cells treated with cisplatin in combination withphotodynamic therapy. Cell prolif 43(3):262–274. doi:10.1111/j.1365-2184.2010.00673.x
29. Datta SN, Allman R, Loh C, Mason M, Matthews PN (1997) Effectof photodynamic therapy in combination with mitomycin C on a
Lasers Med Sci

mitomycin-resistant bladder cancer cell line. Br j cancer 76(3):312–317
30. Ma LW, Moan J, Steen HB, Iani V (1995) Anti-tumour activity ofphotodynamic therapy in combination with mitomycin C in nudemice with human colon adenocarcinoma. Br j cancer 71(5):950–956
31. Ahn J-C, Biswas R, Chung P-S (2012) Combination with genisteinenhances the efficacy of photodynamic therapy against human ana-plastic thyroid cancer cells. Lasers surg med 44(10):840–849. doi:10.1002/lsm.22095
32. Skirnisdottir I, Lindborg K, Sorbe B (2007) Adjuvant chemotherapywith carboplatin and taxane compared with single drug carboplatin inearly stage epithelial ovarian carcinoma. Oncol rep 18(5):1249–1256
33. Gervais R, Robinet G, Clement-Duchene C, Denis F, Kouri CE,Martin P, Chouaki N, Bourayou N, Morere JF (2013) Pemetrexedand carboplatin, an active option in first-line treatment of elderlypatients with advanced non-small cell lung cancer (NSCLC): a phaseII trial. Lung Cancer. doi:10.1016/j.lungcan.2013.01.008
34. Fury MG, Sherman E, Ho A, Katabi N, Sima C, Kelly KW,Nwankwo O, Haque S, Pfister DG (2012) A phase I study oftemsirolimus plus carboplatin plus paclitaxel for patients with recur-rent or metastatic (R/M) head and neck squamous cell cancer(HNSCC). Cancer chemother pharmacol 70(1):121–128. doi:10.1007/s00280-012-1894-y
35. Rizvi I, Celli JP, Evans CL, Abu-Yousif AO, Muzikansky A, PogueBW, Finkelstein D, Hasan T (2010) Synergistic enhancement ofcarboplatin efficacy with photodynamic therapy in a three-dimensional model for micrometastatic ovarian cancer. Cancer res70(22):9319–9328. doi:10.1158/0008-5472.CAN-10-1783
36. Chou TC (2010) Drug combination studies and their synergy quan-tification using the Chou-Talalay method. Cancer res 70(2):440–446.doi:10.1158/0008-5472.CAN-09-1947
37. Chou TC (2006) Theoretical basis, experimental design, and com-puterized simulation of synergism and antagonism in drug combina-tion studies. Pharmacol rev 58(3):621–681. doi:10.1124/pr.58.3.10
38. Pozarowski P, Darzynkiewicz Z (2004) Analysis of cell cycle by flowcytometry. Methods Mol Biol 281:301–311. doi:10.1385/1-59259-811-0:301
39. Elisei R (2012) Anaplastic thyroid cancer therapy: dream or reality?Endocrine. doi:10.1007/s12020-012-9785-x
40. Yu GP, Li JC, Branovan D, McCormick S, Schantz SP (2010)Thyroid cancer incidence and survival in the National Cancer Insti-tute surveillance, epidemiology, and end results race/ethnicitygroups. Thyroid off j Am Thyroid Assoc 20(5):465–473. doi:10.1089/thy.2008.0281
41. Rajeswaran A, Trojan A, Burnand B, Giannelli M (2008) Efficacyand side effects of cisplatin- and carboplatin-based doublet chemo-therapeutic regimens versus non-platinum-based doublet chemother-apeutic regimens as first line treatment of metastatic non-small celllung carcinoma: a systematic review of randomized controlled trials.Lung Cancer 59(1):1–11. doi:10.1016/j.lungcan.2007.07.012
42. Ofner JG, Schlogl H, Kostron H (1996) Unusual adverse reaction in apatient sensitized with Photosan 3. J photochem photobiol B Biol36(2):183–184
43. Chen H-H, Chen T-W, Lin H (2010) Pravastatin attenuatescarboplatin-induced nephrotoxicity in rodents via peroxisomeproliferator-activated receptor α-regulated heme oxygenase-1. MolPharmacol 78(1):36–45. doi:10.1124/mol.109.061101
44. Sharma A, Bhat MK (2011) Enhancement of carboplatin- andquercetin-induced cell death by roscovitine is Akt dependent andp53 independent in hepatoma cells. Integr cancer ther 10(4):NP4–NP14. doi:10.1177/1534735411423922
45. Bevis KS, McNally LR, Sellers JC, Della Manna D, Londono JoshiA, Amm H, Straughn JM Jr, Buchsbaum DJ (2011) Anti-tumoractivity of an anti-DR5monoclonal antibody, TRA-8, in combinationwith taxane/platinum-based chemotherapy in an ovarian cancer mod-el. Gynecol oncol 121(1):193–199. doi:10.1016/j.ygyno.2010.11.046
46. Panzarini E, Inguscio V, Dini L (2011) Timing the multiple cell deathpathways initiated by Rose Bengal acetate photodynamic therapy.Cell death dis 2:e169. doi:10.1038/cddis.2011.51
47. Granville DJ, Carthy CM, Jiang H, Shore GC, McManus BM, HuntDWC (1998) Rapid cytochrome c release, activation of caspases 3, 6,7 and 8 followed by Bap31 cleavage in HeLa cells treated withphotodynamic therapy. FEBS Lett 437(1–2):5–10. doi:10.1016/S0014-5793(98)01193-4
48. Singh S, Chhipa RR, Vijayakumar MV, Bhat MK (2006) DNAdamaging drugs-induced down-regulation of Bcl-2 is essentialfor induction of apoptosis in high-risk HPV-positive HEp-2 andKB cells. Cancer lett 236(2):213–221. doi:10.1016/j.canlet.2005.05.024
49. Lee CS, Kim YJ, Jang ER, Myung SC, Kim W (2010) Akt inhibitorenhances apoptotic effect of carboplatin on human epithelial ovariancarcinoma cell lines. Eur j pharmacol 632(1–3):7–13. doi:10.1016/j.ejphar.2010.01.004
50. Robertson CA, Evans DH, Abrahamse H (2009) Photodynamictherapy (PDT): a short review on cellular mechanisms and cancerresearch applications for PDT. J Photochem Photobiol B Biol 96(1):1–8. doi:10.1016/j.jphotobiol.2009.04.001
Lasers Med Sci




















