Calpain mediates cardiac troponin degradation and contractile dysfunction in atrial fibrillation
Upload
independentCategory
view
1download
0
E v I E w s
Calpain inhibition: an overview of its therapeutic potential K&n II. W. Wang and Po-Wai Yuen
lncreasmg evidence now suggests that excessive
activation of the Ca*+-dependent protease calpain
could play a key or contributory role in the pathology of
s variety of disorders, including cerebral ischaemia.
cataract, myocardial isehaemia, muscular d~~ophy
and platelet aggregation. In this review, Kevin Wang
and Po-Wai Yuen discuss the evidence linking these
disorders to celpain overactivation. At present, it is
difficultto confirm the exact role of calpain in these
disorders because of the lack of potent, selective and
cell-permeable calpain inhibitors. However, given the
multiple therapeutic indications for calpain, it appears
that achievement of selective calpain inhibition is an
impo~a~ pha~acological goal.
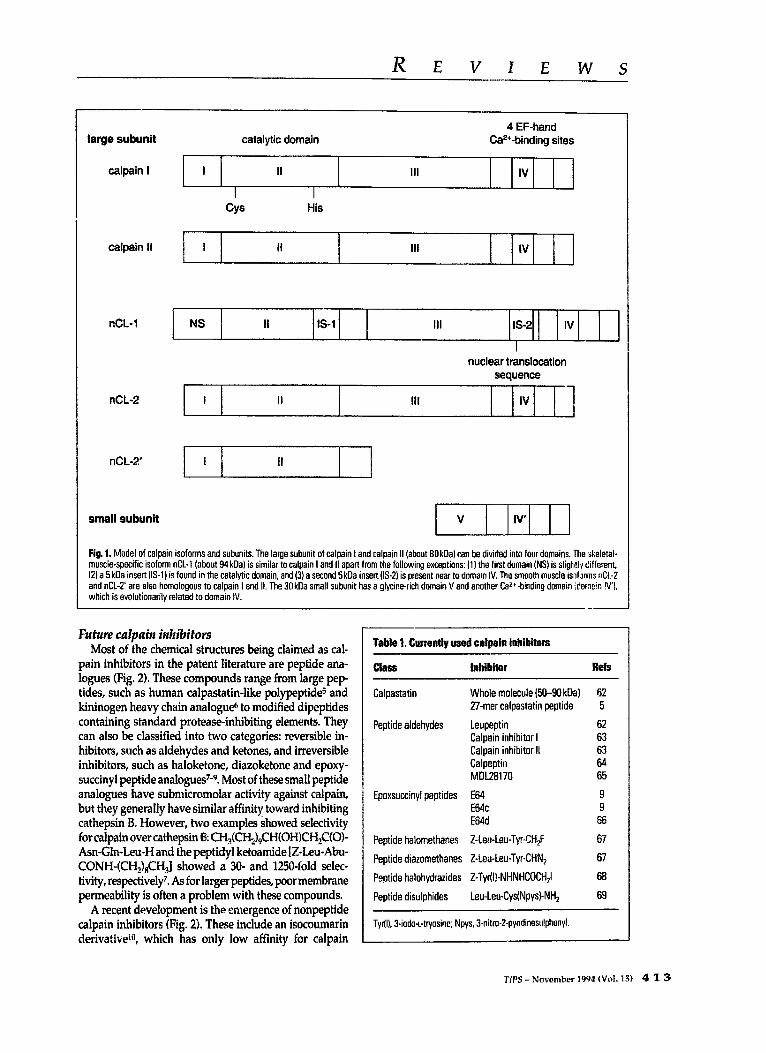
One of the many cellular proteins involved in Cal* signalling in mammalian cells is the Ca*+-activated neutral protease calpair+. There are two major isoforms: calpain 1 (or k-calpain) and calpain 11 (or m-calpain), which require low and high micromolar Ca*+ concen- trations for activation, respectively. Calpain consists of two subunits of about 8OkDa and 29kDa (Fig. 1). The large subunit can be further divided into four domains. Domain II is the catalytic domain homologous to other cysteine proteases, especially in regions that cover the two catalytic residues (His and Cys) (Fig. 1). Domain 111 has unknown function and is not homologous to other proteins. Domain IV has four EF-hand Caz+-binding sites. The N-terminal half of the small subunit appears to be important for interaction with phospholipids [for example, phosphatidy~ositol (4,5)-bisphosphatel, which lower its Caz+ r~u~rernent. The C-terminal half has another four EF-hand structures It is assumed that these Ca*+-binding sites impose a strict Ca*+ requirement on the catalytic activity, but the number of occupied Ca*--binding sites required for activity remains debatable.
Following the addition of Ca*+, calpain autolyzes by truncating an N-terminal portion of domain I and most of domain V. The catalytic activity of this truncated form (76 kDa and 18 kDa) is still Ca*+-dependent. It is uncertain whether this step is eSsentia1 before calpain can hydrolyze other substrates. Recently, cDNA clones for a skeletal- muscle- and a stomach-specific form of the large subunit were identified (nCL-1 and nCL-2, respectively), Interest-
4 1 2 TiPS - November 1994 (Vol. 15)
ingly, nCL-1 contains a nuclear translocation-like se- quence (Lys-Lys-Lys-Lys-X-Pro) in its catalytic domain, while nCL-2 can be alternatively spliced to generate a form that totally lacks the Cal+-binding domain2 (ACL-2’;
Fig. 1). Calpain appears to be selective for a subset of cellu-
lar protein@. These include cytoskele~l proteins (for example, spectrin), membrane receptors (for example, epidermal growth factor receptor), calmodulir,+binding proteins, G proteins, enzymes involved in signal trans- duction [such as protein kinase C (PKC)I and many tran- scription factors. Calpain prefers Leu or Val as the second residue on theN-terminal side of thecleavage sit&. How- ever, this rule is not strictly followed when the cleavage sites of endogenous protein substrates are examined. It was also proposed that a secondary ~~o~~A sequence may come into play. Hyd~p~~c sequences enriched in Pro, Glu, Asp, Ser and Tlu for PEST sequences) appear to exist in most calpain substrates and are usually located near the cleavage sites3.
Calpain inhibitory agents Current calpain inhibitors
There have been a number of calpain inhibitory agents described in theliterature that are ~mer~ally available (Table 1). The most potent of all is the na~mlly occurring endogenous calpain inhibitor protein, calpastatin. It inhibits both calpain 1 and 11 specifically, but not other proteases such as cathepsin B or papain. A 27 amino acid peptide based on a repeated region of calpastatin also retained the calpain inhibitory activity (Table 1).
Almost all of the calpain inhibitors reported in the literature are active-site-targeted peptide inhibitors. Many of these compounds were used in studies to deter- mine the role of calpain in a disorder. The caveat is that none of them are highly selective for calpain, making data ~te~~tation sometimes difficult. The most widely used are leupeptin, CaIpeptin, calpain inhibitor I and MDL28170, which belong to the peptide aldehyde class of inhibitors (Table 11. The latter three have demon- strated cell permeability”. Urforhmately, this class of compound will also inhibit other cysteine proteases. E64 and E64c are members of the epoxysuccinyl peptides, which are capable of formig irreversible sulphide linkage with the active-s& Cys thiol. mile E64 does not inhibit serine proteases,_ it does inhibit papain, cathepsin B and L (Table 1). The membrane permeability of E64 and E64c are relatively poor, but this prohlem can be overcome by converting the free carboxylic acid group ir. E64c into an ethyl ester (E64d). Once entering cells, E64d can be readily hydrolyzed by cellular e&erases back to the more active precursor E64c. Other classes of caIpain inhibitors included peptide halo- methanes, peptide diaz~me~hanes and peptide hale hydrazides. The d~zorne~~n~ and halohydrazid~ (Table 1) were claimed to, be more selective for inhibiting CySteiAe PrOteaSeS over serine proteases, but are not commercially available.
Q 1994, Elwvier Science ttd 0165 -6147/94/$07.00
REVIEWS
large subunit
calpain I
4 EF-hand catalytic domain Ca*+-binding sites
I II Ill IV
I
CYS His
calpain II I II Ill IV
nCL-1 NS II IS-l Ill IS-2 IV
nCL-2 I II Ill
sequence
IV I
&L-2 I I
I
small subunit
Fig. 1. Model of calpain isoforms and subunits. The large subunit of calpain I and calpain II (about 80kDal can be divided into four domains, The skeletal- muscle-specific isoform nCL-1 (about 94kDa) is similar to calpain I and II apart from the following exceptions: (1) the first domain (NS) is slightly different. 12) a 5 klla insert (IS-l) is found in the catalytic domain, and (3) a second 5 kOa insert (IS4 is present near to domain IV. The smooth muscle isnforms nCL-2 and nCL-2’ are also homologous to calpain I and II. The 3OkDa small subunit has a glycine-rich domain V and another Cart-binding domain ;dornein I\(‘). which is evolutionarily related to domain IV.
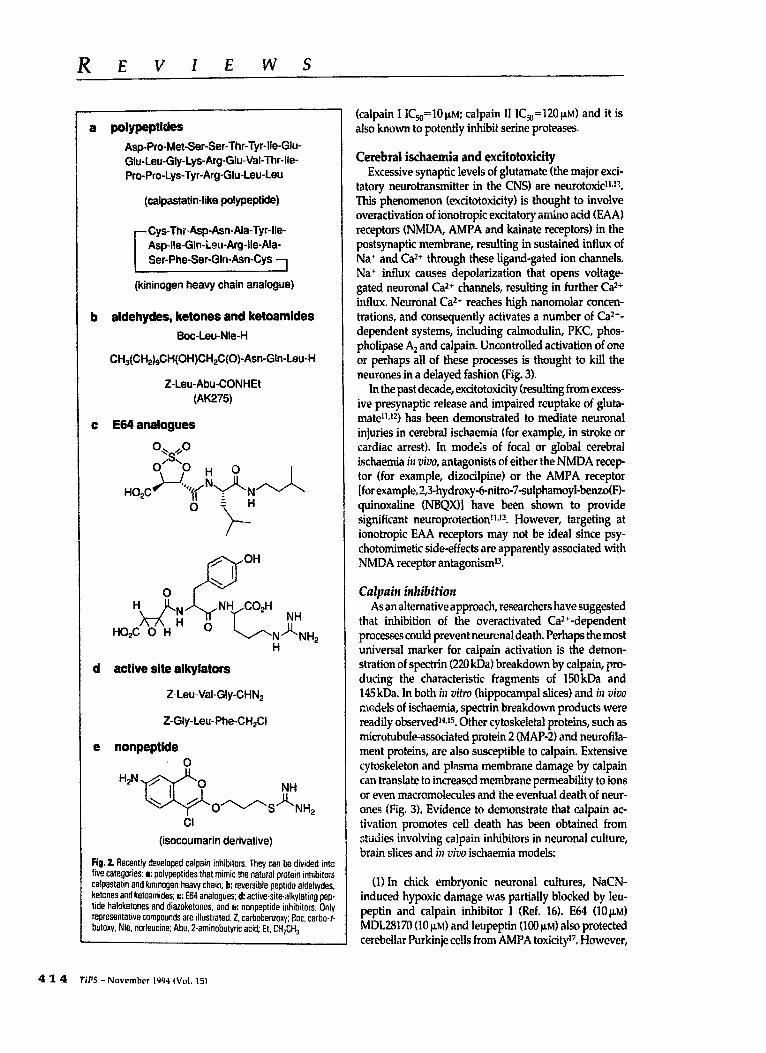
Most of the chemical structures being claimed as cal- pain inhibitors in the patent literature are peptide ana- logues (Fig. 2). These compounds range from large pep tides, such as human calpastatin-like polypeptidg and kininogen heavy chain analog& to modified dipeptides containing standard protease-inhibiting elements. They can also be classified into two categories: reversible in- hibitors, such as aldehydes and ketones, and irreversible inhibitors, such as haloketone, diazoketone and epoxy- succinyl peptide analogues’-9. Most of these smaI1 peptide analogues have submicromoiar activity against calpain, but they generally have similar affix toward orbiting cathepsin B. However, two examples showed selectivity for calpain over cathepsin 8: ~~(CH~)~CH(OH)CH~C(O)- Asn-Gin-Leu-H and the peptidyl ketoamide [Z-I.eu-Abu- CONH-(CH,),CHJ showed a 30- and 12!iO-fold selec- tivity, respectively7. As for larger peptides, poor membrane permeability is often a problem with these compounds.
A recent development is the emergence of nonpeptide calpain inhibitors (Fig. ii. These include an isocoumarin derivativei”, which has only low affinity for calpain
Table 1. Cn~em~ ilsed catpain inhi~to~
CISSS Inhibitor ltefs
Calpastatin
Peptide aldehydes
Whole molecule @I-90kDal 27-mer calpastatin peptide
Leupeptin Calpain inhibitor I Calpain inhibitor II Calpeptin MD128170
Epoxsuccinyl peptides E64 E64c E64d
Peptide halomet~nes Z-Leu-Le~Tyr-CH*F
Peptide diazomethanes Z-teu-Leu-Tyr-CHN,
Peptide halohydrazides Z-Tyr(l]-NHNHCOCH,I
Peptide disulphides Leu-Leu-Cvs(Npysl-NH,
62 5
62 63 63 64 65
9 9 66
67
67
68
69
Tyr(l). 3-iodo-t-tryosine; Npys, 3.nitro+pyridinesulphenyi.
TPS - November 1994 Wd. 151 4 1 3
REVIEWS
a polypeptides
ASPS-Met-Ser-Ser-Thr-Tyr-lie-Glu- Glu-Leu-Gly-Lys-Arg-Glu-Val-Thr-lle- Pro-Pro-Lys-Tyr-Arg-Glu-Leu-Leu
b aldehydes, ketones and ketoamides
Boc-Leu-Nle-H
GH~(CH~)~CH(~H)CH*C(O)-in-Gin-Leu-H
Z-Leu-Abu-CONHEt (AK275)
c E64 analogues
d active site alkylators
Z-Leu-Val-Gly-CHN,
Z-Gly-Leu-Phe-CHILI
e nonpeptide
fig, 2. Recently developed caipain inhibitors. They can be divided into five categories: L poiv~ptides that rmmic !he natural protein inhibit~s calpastatin and kininogen heavy chain; b: reversible peptide aldehydes, ketones and ketoamides; o: E64 analogues; d: active-site-alkylating pep tide haloketones and diazoketones. and a,: nonpeptide inhibitors. Only representativecompoundsare dlustrated.2. carbobemoq; Boc, carbo-f- butoxy; Nle. norleucine; Abu. 2-aminobutyric acid. Et. CH,CH,.
(calpain I IC,,=~O~M; caipain 11 I&,=120 PM) and it is also known to potently inhibit serine proteases.
Cerebral ischaemia and excitotoxicity Excessive synaptic levels of glutamate (the major exci-
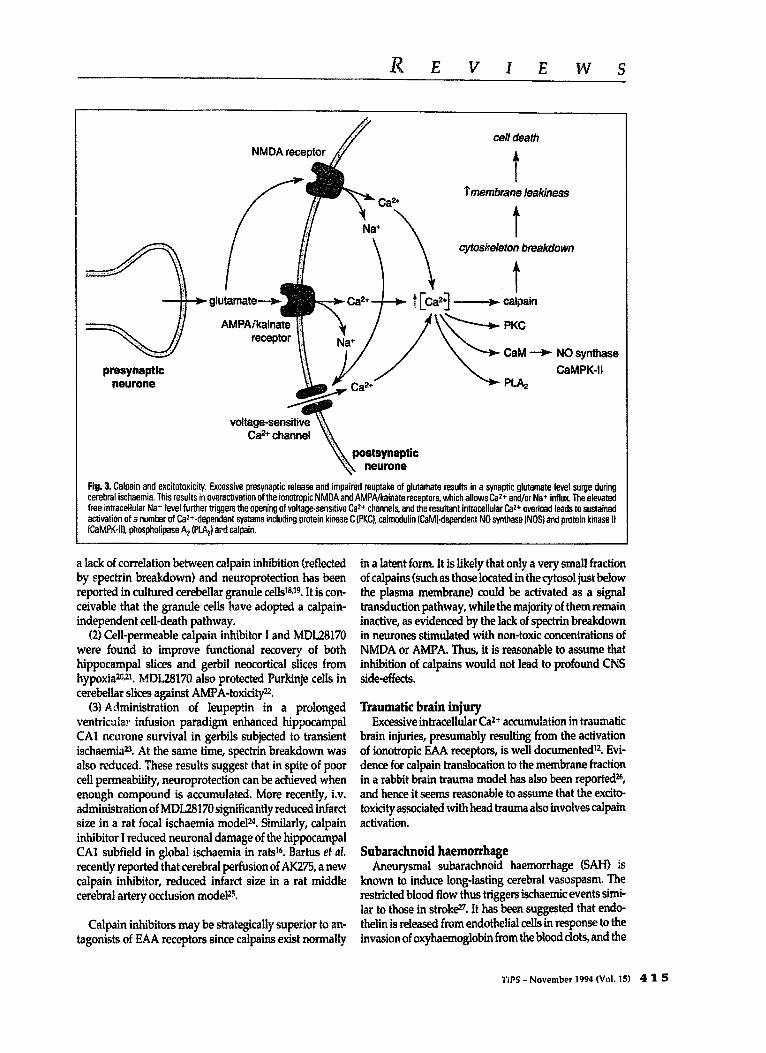
tatory neurotransmitter in the CNS) are neurotoxiP>?. This phenomenon (excitotoxicity) is thought to involve ove~ctivation of iono~opic excitatory amino acid (EAAI receptors (NMDA, AMPA and kainate receptors) in the postsynaptic membrane, resulting in sustained influx of Na’ and Ca2+ through these ligand-gated ion channels. Na+ influx causes depoIarization that opens voitage- gated neuronal Car+ channels, resulting in further Ca2+ influx. Neuronai Ca2+ reaches high nanomolar concen- trations, and consequently activates a number of Ca2+- dependent systems, including calmodulin, PKC, phos- pholipase A, and calpain. Uncontrolled activation of one or perhaps all of these processes is thought to kill the neurones in a delayed fashion (Fig. 3).
In the past decade, excitotoxicity (resulting from excess- ive presynaptic release and impaired reuptake of giuta- mateV has been demonstrated to mediate neuronai injuries in cerebral ischaemia (for example, in stroke or cardiac arrest). In models of focal or global cerebral ischaemia in vizv, antagonists of either the NMDA recep tor (for example, dizocilpine) or the AMPA receptor [for example, 2,3-hydroxy-6-nitro-7-sulphamoyl-benzoO% quinoxaiine UNIX)] have been shown to provide significant neuroprotectiorW2. However, targeting at ionotropic EAA receptors may not be ideal since psy- chotomimetic side-effects are apparently associated with NMDA receptor antagonismlJ.
As an aitema tive approach, researchers have suggested that inhibition of the overactivated Caz+-dependent processes could prevent neuronal death. Perhaps the most universal marker for caipain activation is the demon- stration of spectrin (220 kDa) breakdown by caipain, pro- ducing the characteristic fragments of 150kDa and 145 kDa. In both irz vitro (hippocampal slices) and k uiuo mcdeis of ischaemia, spectrin breakdown products were readily observedl4J5. Other cytoskeietai proteins, such as microtubule-associated protein 2 (MAP-21 and neurofila- ment proteins, are also susceptible to caipain. Extensive cytoskeleton and plasma membrane damage by caipain can translate to increased membrane permeability to ions or even macromole~i~ and the eventual death of neur- ones (Fig. 3). Evidence to demonstrate that calpain ac- tivation promotes ceil death has been obtained from studies involving calpain inhibitors in neuronal culture, brain slices and ill uivo ischaemia models:
01 In chick embryonic neuronai cultures, NaCN- induced hypoxic damage was partially blocked by leu- peptin and caipain inhibitor I (Ref. 16). E64 (10~~) MDL28170 (10 JLM) and leupeptin WJ PN) also protected cerebeiiar Purkinje cells from AMPA toxicityl7. However,
4 1 4 fiPS - November 1994 (Vol. 15)
REVIEWS
%nembrane feafdness
cyloskeferon breafrdowrt
presynaptic neurone
CaM + NO synthase
CaMPK-II
Fig. Calpain and excitotoxicity. Excessive prasynaptic release and impaired reuptake of glutamate results in a synaptic glutamate level surge during cerebral ischaemia. This results in overactivatian of theionotropic NMDA and AMPA/kainate receptors. which allows W+ and/or Na+ influx. The elevated free intracellular Na+ level further triggers the opening of voltage-sensitive Caz+ channels, and the resultant intracellular Caz+ overload leads to sustained activation of a number of Caz+-dependent systems including protein kinase C (PKC), calmodulin fCaMt-dependent NO synthase lNO.5) and pmtein kinase II {CaMPK~ilt, ph~phoiipase AZ (PLAJ ard calpain.
a lack of correlation between calpain inhibition (reflected by spectrin breakdown) and neuroprotection has been reported in cultured cerebellar granule celWJ9. It is con- ceivable that the granule cells have adopted a calpain- indrependent cell-death pathway.
(2) Cell-permeable calpain inhibitor I and MDL28170 were found to improve functional recovery of both ~p~carn~ slices and gerbil neocortical slices from hypoxiazO+*l. ~~L281~ also protected Purkinje cells in cerebellar slices against AMPA-toxicity=.
(3) Administration of leupeptin in a prolonged ventricular infusion paradigm enhanced hippocampal CA1 neurone survival in gerbils subjected to transient ischaemia23. At the same time, spectrin breakdown was also reduced. These results suggest that in spite of poor cell pe~~bili~, neuroprote~on can be achieved when enough ~rn~und is accumulated. More recently, i.v. administration of MDL28170 significantly reduced infarct size in a rat focal ischaemia modelz4. Similarly, calpain inhibitor I reduced neuronal damage of the hippocampal CA1 subfield in global ischaemia in rat+. Bartus et al. recently reported that cerebral perfusion of AK275, a new calpain inhibitor, reduced infarct size in a rat middle cerebral artery occlusion modelzs.
Calpain inhibitors may be strategically superior to an- tagonists of EAA receptors since calpains exist normally
in a latent form. It is likely that only a very small fraction of calpains (such as those located in the cytosoi just below the plasma membrane) could be activated as a signal transduction pathway, while the majority of them remain inactive, as evidenced by the lack of spectrin breakdown in neurones stimulated with non-toxic concentrations of NMDA or AMPA. Thus, it is reasonable to assume that ambition of calpains would not lead to profound Cl% side-effects.
Traumatic brain injury Excessive intracellular Ca2+ accumulation in traumatic
brain injuries, presumably resulting from the activation of ionotropic EAA receptors, is well documentedl? Evi- dence for calpain translocation to the membrane fraction in a rabbit brain trauma model has also been reported26, and hence it seems reasonable to assume that the excito- toxicity associated with head trauma also involves calpain activation.
Subarachnoid haemorrhage Aneurysmal subarachnoid haemorrhage (SAI-I) is
known to induce long-lasting cerebral vasospasm. The restricted blood flow thus triggers ischaemic events simi- lar to those in &ok@. It has been suggested that endo- thelin is released from endothelial cells in response to the invasion of oxyhaemoglobin from the blood clots, and the
UPS - November 1994 (Vol. 15) 4 1 5

REVIEWS
416
subsequent endothelin receptor activation in vascular smooth muscle cells leads to the long-lasting spastic response.
In a canine SAH model, vasospasm can be induced by successive intracistemal injection of autologous blood near the basilar artery. The resulting blood clot induces a spastic response on the blood vessel within a few day52*. In this model, topical application of calpeptin dilated the exposed spastic basilar artery”. Although the mechanism is unclear, the involvement of proteolytic activation of PKC by calpain has been suggested since the PKC inhibitor H7 also had the same vasodilating effect. The involvement of calpain was further supported by the observed increase of spectrin breakdown in the smooth muscle of spastic basilar artery in a rabbit mode1 of SAH (Ref. 29). Cerebra1 vasospasm has also been shown to cause ischaemic strokp0, and therefore it appears that calpain inhibitors could further provide beneficial effects at the vasculature level.
Other neurological disorders Chronic neurwdegenerution
In several chronic neurodegenerative disorders such as Huntington’s disease, Parkinson’s disease and amyo- trophic lateral sclerosis, there is evidence to suggest that glutamate toxicity contributes at least in part to the neurodegenerationl’J~. It is conceivable that calpain inhibitors may ameliorate the accompanying excito- toxicity in these disorders.
Alzheimer’s disease The pathogenesis of Alzheimer’s disease has been
linked to the abnormal processing of the amyloid precur- sor protein (API’) to produce the P-amyloid peptide, which, by self-aggregation, forms the major component of senile plaques in the brain over decades. Together with other proteases, calpain is capable of fragmenting APP (Ref. 31). It appears to cleave APP at three different sites. Since all cleavages are located extracellularly, if calpain were to attack API’, it is likely that internalized APP has been cleaved. The cleavage that occurs nearest to the C- terminus would produce a fragment that contains the whole of the P-amyloid peptide (amyloidogenic) if it is further processed by another protease. Incidentally, cal- pain immunoreactivity was also found in senile plaquesJ2. There is also evidence of calpain activation in the brain of Alzheimer’s patients, as judged by the increased ratio of the activated 76 kDa form to the inactive 80 kDa form of the calpain I large subunitx3.
Spinal cord injury Calpain is capable of degrading myelin sheath pro-
teins” and was found co-localized with fragmented myelin in myelinated nerve fibres from rabbiP. It is tempting to suggest that calpain may be mediating myelin degradation as seen in demyelination disorders such as Wailerian degeneration, multiple sclerosis and peripheral nervous neuropathy. In experimental spinal cord injury,
Ca?+ accumulates within the injured axons, resulting in the activation of calpain and hence contributing to the degeneration of axons and myelin+. Leupeptin has also been found to reduce axonal damage in an experimental spinal cord injury modeP7.
Cardiac ischaemia The injury sustained by cardiomyocytes during
ischaemic myocardiac infarction is likely similar to that observed in neurones in cerebra1 ischaemia. However, cardiomyocytes appear to suffer from a secondary form of injury during coronary reperfusion. The involvement of calpain is suggested from the demonstration that myo- fibrillar proteins including myosin heavy chain, troponin T and I, tropomyosin a and rx-actinin are susceptible to calpain%. In freshly isolated neonatal rat myocytes, cal- pain activity has been shown to be elevated during hypoxia, as evidenced by the presence of spectrin break- down products 3’JJ”. Furthermore, spectrin breakdown could be prevented by 10 pM of calpain inhibitor 1 or E64, and while hypoxia alone caused about 60% cell death in six hours, the presence of either inhibitor reduced cell death to slightly above the normoxic level.
The isolated heart can be subjected to a temporary (for example, 15min) global ischaemia followed by reper- fusion; this is known as myocardial stunnix@‘. Generally, this reversible insult leads to compromised mechanical myocardial functions, which can be measured by par- ameters such as developed pressure. Matsumura et al.” showed that leupeptin significantly enhanced myocardium functional recovery following stunning.
E64c was used as a potential protective agent in a dog model where acute myocardial infarction was induced by occlusion of the left anterior descending artery*‘. The combination of E64c and reperfusion was found to sig- nificantly reduce infarct size but E64c alone did not show significant reduction of infarct size.
The evidence provided by these models indicate that calpain is activated during myocardial ischaemia and several cysteine protease inhibitors that inhibit calpain showed beneficial effects. However, this area is still in its infancy.
Muscular dystrophy Dystrophin is a protein located in the sarcolemma that
regulates the stretch-sensitive Ca*+ ‘leak’ channel@, and is absent in Duchenne muscular dystrophy patients as well as mdx mice as a result of a genetic defect. In mdx mice, intracellular Ca2+ levels in skeletal muscle fibres were found to be significantly raised with a concomitant increase in the rate of protein degradation*l. The rate of protein degradation could be reduced to normal levels by leupeptin45. As noted above, myofibrillar protein turn- over, both normal and abnormal, is probably mediated by calpain*h. It has also been observed that the calpain II level is apparently higher in dystrophic hamster skeletal muscles47. Interestingly, mdx mouse myotubes cultured continuously in the presence of leupeptin (50 PM) did not
REVIEWS
experience the elevation of intracellufar Ca** levels that is normally seen in mdx muscles45. Hence, it can be pos- tulated that calpain degrades a sarcolemmal protein that leads to further increased opening of the Ca*+ leak chan- nels, and if this hypothesis is correct, calpain inhibition should have the dual benefit of reducing myofibrillar protein degradation and restoring Car+ homeostasis.
ageing, chemical toxins. //
Cataract The mammalian lens is a layer of growing epithehal
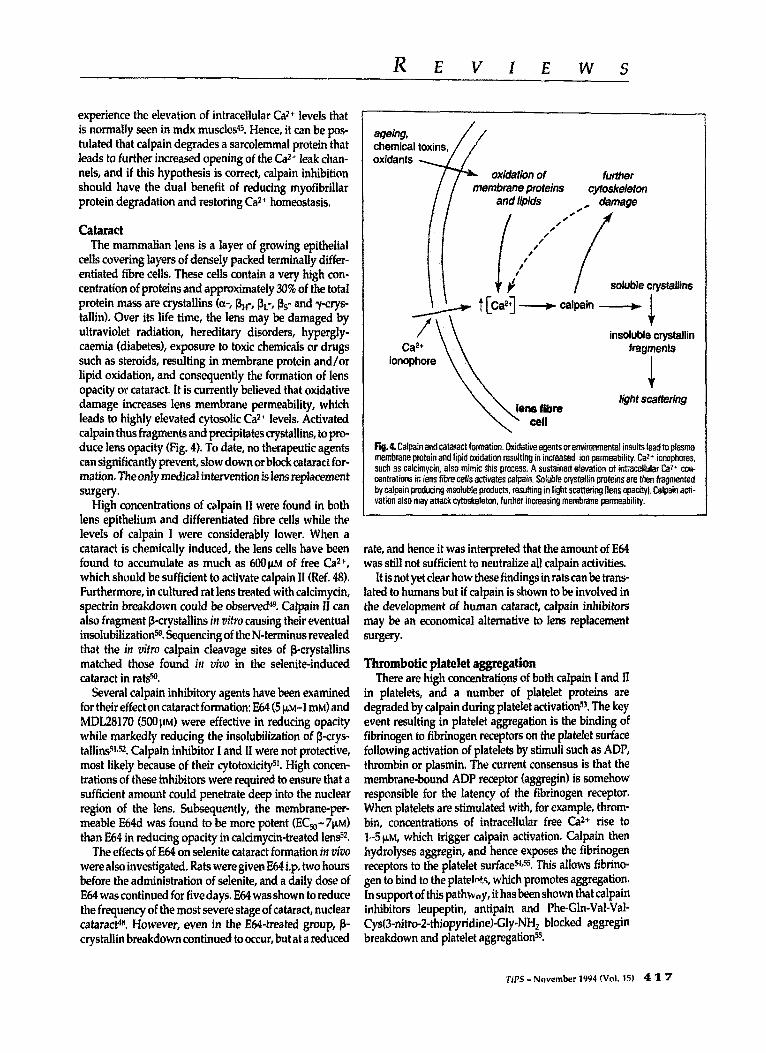
cells covering layers of densely packed terminally differ- entiated fibre cells. These cells contain a very high con- cen~ation of proteins and app~ximateiy 30% of the total protein mass are crystallins to-, I$,-, fit-, Ss- and ysrys- tallinl. Over its life time, the lens may be damaged by ultraviolet radiation, hereditavj disorders, hypergly caemia (diabetes), exposure to toxic chemicals or drugs such as steroids, resulting in membrane protein and/or lipid oxidation, and consequently the formation of lens opacity or cataract. It is currently believed that oxidative damage increases lens membrane permeability, which leads to highly elevated cytosolic Ca*+ levels. Activated calpain thus fragments and precipitates crystaIlins, to pro- duce lens opacity (Fig. 41. To date, no therapeutic agents can si~ificantly prevent, slow down or block cataract for- mation Theonly medicaf inte~ention is lens replacement surgery.
/ Ca*+
ionophore
insoluble crystallin fragments
1 tight scattering
High concentrations of calpain II were found in both lens epithelium and differentiated fibre cells while the levels of calpain 1 were considerably lower. When a cataract is chemically induced, the lens cells have been found to accumulate as much as 600~~ of free Ca*+, which should be sufficient to activate calpain II (Ref. 48). Furthermore, in cultured rat lens treated with calcimycin, spectrin breakdown could be observed49. Calpain II can also fragment ~~ysta~ins in vitro causing their eventual ~soIu~Iization5#. ~uen~ng of the N-te~inus revealed that the in vitro calpain cleavage sites of ~~stall~s matched those found irt vive in the selenite-induced cataract in rats?
fig. 4 Calpain and cataract fade. Oxi&t~ag~ts or environm~~i insults lead to plasma ~mb~oe protein and lipid oxidation resulting in increased ion ~~~~1~~. Ca2+ Iowans, such as calc~m~in~ also mimic this prows. A sustained elation of in~llolar Caz+ con- centrations in lens fibre cells activates calpain. Soluble ~~~allin proteins are then f~gmented by calpain producing insoluble products, resulting in light scattering {lens opacity). Calpain acti- vation also may attackcytaskeleton, further increasing membrane permeability.
rate, and hence it was interpreted that the amount of E64 was still not sufficient to neutralize all calpain activities.
It is not yet clear how these findings in ratscan be trans- lated to humans but if calpain is shown to be involved in the devefopment of human cataract, calpain inhibitors may be an economical alternative to lens replacement surges.
Thrombotic platelet aggregation
Several calpain inhibitory agents have been examined for their effect on cataract formation: E64 (5 FM-1 mM) and MDL28170 (5OOp~l were effective in reducing opacity while markedly reducing the insolubilization of P_crys- tallins51? Calpain inhibitor I and II were not protective, most likely because of their cytotoxicitysi. High concen- trations of these inhibitors were required to ensure that a sufficient amount could penetrate deep into the nuclear region of the lens. Subs~uentiy, the membran~~r- meable E64d was found to be more potent (Et&- 7pMf than E64 in reducing opacity in ~l~rny~n-beats Ien@.
The effects of E64 on selenite cataract formation in z&o were also investigated. Rats were given E64 i.p. two hours before the administration of selenite, and a daily dose of E64 was continued for five days. E64 was shown to reduce the frequency of the most severe stage of cataract, nuclear cataracP. However, even in the EM-treated group, p- crystaliin breakdown continued to occur, but at a reduced
There are high concentratipns of both calpain I and II in platelets, and a number of platelet proteins are degraded by calpain during platelet activationss. The key event resulting in platelet aggregation is the binding of fibrinogen to fibrinogen receptors on the platelet surface following activation of platelets by stimuli such as ADP, thrombin or plasmin. The current consensus is that the membrane-bound ADP receptor taggreginl is somehow responsible for the latency of the fibrinogen receptor. When platelets are stimulated with, for example, throm- bin, concentrations of intracelIuIar free Ca2+ rise to M~LM, which trigger calpain activation. Calpain then hydrolyses aggregin, and hence exposes the fibrinogen receptors to the piatelet surfaceXss, This allows fibrino- gen to bind to the platelnts, which promotes aggregation. In support of this pathway, it has been shown that calpain inhibitors leupeptin, antipain and Phe-Gln-Val-Val- Cys(3-nitro-Z-thiopyridinel-Gly-NH, blocked aggregin breakdown and platelet aggregation”.
7X’S - Nnvember 1994 (Vol. 15) 4 3 7

REVIEWS
Table L Therapeutic areas in which calpain overactivation is implicated
Diirdws
Stroke
Brain trauma
Subarachnoid haemorrhage
Alzheimer’s disease
Spinal cord injury
Cardiac ischaemia
Muscular dystmphy
Cataract
Thrombotic platelet aggregation
Restenosis
Arthritis
Proposed mechanism
Degradation of cytoskeletal pmteins and other cellular proteins lead to neuronal cell death and permanent tissue damage
Similar mechanism to stroke
Calpain proteolytically activates protein kinase C. leading to sustained cerebral vasospasm
Abnormal processing of amyloid precursor protein by calpain
Degradation of myelin proteins
Calpain activation leads to breakdown of myofibril proteins causing cardiac myocyte shrinkage, cell death and tissue damage
In Duchenne muscular dystrophy, genetic deletion of the dystrophin gene leads to compromised Caz+ homeostssis allowing calpain to break aown myofibril proteins
Lens protein (ctystallins) breakdown by calpain in ageing lens leads to precipitation that causes lens opacity
Thrombin increases intracellular Ca2+ levels in platelets, thus activating calpain-mediated proteolysis of aggregin and promoting platelet aggregation
Aenarrowing of blood vessel after angioplasty owing to calpain-mediated proliferation and migration of smooth muscle cells
Calpain is found in synovial fluid and is capable of breaking down cartilage and the extracellular matrix component proteoglycan
ReIs
16-25
26
2El.zg
31-33
34-37
39-42
44-47
48-52
54.55
57.58
5961
Restenosis Percutaneous trartsh.uninal coronary angioplasty is a
widely accepted medical procedure to expand the inner diameter of clotted arteries in patients with athfm- sclerotic coronary artery disease. However, the success rate of this procedure is dampened by the spontaneous, slow renarrowing of the arteries (restenosi+. Recently, it has been shown that calpeptin (100~~) and calpain inhibitor I 60 pM) blocked the cell cycle at the G2-M phase and prevented the proliferation of cultured aortic smooth muscle cell@. The same agents were shown to inhibit angioplastic restenosis 58. It is likely that the calpain inhibitors retard restenosis by controlling proliferation and migration of smooth muscle cells to the neoinitimal layer of the blood vessels.
Joint inflammation and arthritis Both calpain I and II were found extracellularly in the
synovial fluid of the knee joint, especially in patients with rheumatoid arthrWqfl. Furthermore, the major cartilage matrix component, proteoglycan, is reported to be a cal- pain substraW. It is hypothesized that externalized cal- pain damages the extracellular matrix and contributes to the inflammation process, together with other cysteine proteases and metalloproteases. However, it is not yet known if calpain inhibitors have any beneficial effects when applied to inflamed joints.
Perspectives In summary, it is evident that calpain overactivation
may be a key component in a number of disorders
4 1 8 TiPS - November 1994 (VOI. 15)
(Table 3, and the common theme for most of these dis- orders is cellular Caz+ overload. The physiological roles of calpains are not yet defined, but they are thought to be involved in specific unidirectional cellular processes (such as mitosis and membrane fusion). Since a sustained increase of intracellular Caz+ concentrations is required for calpain to be activated, calpain largely exists in a latent form in resting cells. Therefore, it would appear that cal- pain is an ideal pharmacological target since this protease is most active at the time of pathology. Furthermore, acute side-effects are not anticipated as a result of calpain inhi- bition since calpain is rarely activated under physiologi- cal conditions. This will particularly be the case if a selec- tive calpain inhibitor can be identified.
Selected references 1 Croall, D. E. and Demartino, C. N. (1991) Physiol. Rm 71,813-847 2 Sido, T. C., Sorimachi, H. asd Suzuki, K. (1994) FASEB J. 8,
814-822 3 Wang, K. K. W., Villalobo. A. and Roufogalis, B. D. (1989) Biochetu.
j. 262,693-706 4 Wang, K. K. W. (1990) Trends Phumacol. Sci. 11,139-142 5 Maki, M. et RI. (1989) 1. Biol. Chenr. 264,18866-18869 6 Bradford, H. N., Jameson, 8. A., Adam, A. A., Wassell, R. P. and
Colman, R. W. (1993) J. Biol. Chcm. 268,26546-26551 7 Li, 2. el al. (1993) J. Med. Chem. 36,3472-3480 8 Hall, A. etaI. (1992) J, Enzym. hlhib. 6,113-123 9 McGowan, E. B., Becker, E. and Detwiler, T. C. (1989) Biochenl.
Biophys. Ra. Cortrmn~~. 158,432-435 10 Foreman, 1. E., Lou, N. T., Powers, J. D. and Eveleth, D. D. (1993)
FASEB 1.7, Al;&3 11 Meldrum, B. and Garthwaite, J. (1990) Trevds Plmrtnacol. Sci. 11,
379-387 12 LiFton, S. A. and Rosenberg, P. A. (1994) Nmct EIIX. J. Med. 330,
613-622 13 Olney, 1. W. ef al. (1991) Scbtcc254,151!5-1518
REVfEWS
14 Arai, A., Vanderklish. P, Kneeler, M., Lee, K. and Lynch, G. (1991) Bmbt Res. 555,276-280
49 Marcantonio, J. M. and Duncan, G. (1991) Biachem. Sm. Traas. 19, 1148-1150
15 Sirnan, R. and Noszek, J. C. (198% Neuron 1,279-287 16 Rami, A. and Krieglstein, I. (1993) Brain Res. 6G9,67-70
50 David, L. L, Shearer, T. R. and Sahih, M. (1993) J. Biof. Chem. 268, 1937-1940
17 Brorson, J. R., M&olilIo; P. A. and Miller, R. L. (1994) /. Neurosci. 14,187-197
18 Manev, H., Favaron, M., Siman, R., Guidotti, A. and Costa, E, (19911 J. Neamchetn. 57,1288-1295
19 Di Stasi, A. M., Gallo, V., Ceccarini, M. and Petrucci, T. C. (1991) Neuron 6,445&4
20 Arlinghaus, L., Mehdi, S. and Lee, K. S. (1991) Eur. 1. Pharmacaf. 209, 123-12s
21 Hiramatsu, K-I., KasseIl, N. F. and Lee, K. S. (1993) St&e 24, 1725-1728
22 Caner, H, Coilins, J. L., Harris, S. M., KzsseU, N. F. and Lee, K. S. (1993) Brain Res. 607,~356
23 Lee, K., Frank, S., Vanderkiish, P, Arat A. and Lynch,G. 11991 f Proc. NaH Acad. Sri’. USA eS, 7233-7237
24 Hong, SC. ef al. (19941 Sfroke 25,663-669 25 Eartus, R. T. ef al. 0994) J Cereb. Hood Flow Mefab. 14,537~544 26 Arrigoni, E. and Cohadon, F. (1991) Neumcbem. Res. 16,48%487 27 Kassell, N. F., Sasaki, T.,Colohan, A. R. T.and Nazar,C. (1985) Stroke
16,562-!?2 28 Minami, N., Tani, E., Maeda, Y., Tamaura, I. and Fukami, M. (1992)
J. Netrrosq. 76, !ll-118
33 Saito, K-I., Eke, J. S., Hamos, J. E. and Nixon, R. A. (19931 Pmt. Nafl Acad. Sri. ff SA 90,2628-2632
34 Ban&, N. L, McAlhaney, W. W. and Hogan, E. L. (198511. NeJlmc~.
29 Foley, P. L.ef al. (1993) Sot. I\irrcr&. Phsfr. 19,500.7 30 Findlay, J. M., Macdonald, R. L. and Weir, 6. K. ii991) Cerebrouasc.
Bmin Mefab. Rev. 3,336-361 31 Siman, R.,Card, J. P. and Davis, L.G. (l990)J.Nexmsci. 10,2400-2411 32 Iwamoto, N.,~angnipon, W.,Crawford,C. and Emson, l? C. (19911
Bra% Res. S61,177-180
51 Lampi. K. J., Kadoya, K., Azuma, M., David, L. L. and Shea=, T. R. (1992) Tax. Appf. Pharm. 117,~57
52 Azuma, M., Ovid, L. L. and Sheanz, T. R. (1992) Biochim. Biophys. Acfu 1180.21%!20
53 Colman, k. W. and Hoffman, I. (1991) in Infrace#alar Cafcim- Dependent Profealysis (Mellgren, R. L. and Murachi, T., eds), PP. 211-224, CRC Prass
54 tidassara,i. J., @shian, S., Knipp, M. A. and Fisher, G. J. (1985) J. Biof. cbem. 260,30531-10535
55 puri R. N., Zhou, F., Colman, R. F. and Colman, R W. (1998) Am. j. Parse. 259, c862-c&%
56 McBride, W, Lange, R. A. and Hi&s, L. D. (19881 Net0 Eiig. 1. Med. 318.1734-1737
57 March, K. L.. Witensky, R L., Roe&e, R. W. and Hathaway, D. R. (19931 Circ. Res. 72,413-423
58 Wilensky,R. L.,M&h, K. L. and Hathaway, D. R. (1991) J. Am Coil. Cardiof. 17.26XA
59 Suzuki, K. ef al. (1990) Arfhrifis RIleurn. 33,728-732 60 Fukui, I., Tanaka, K. and Murachi, T. (1989) Biochem. B~ophys. Res.
corn1nrn. X2.559-566 61 Suzuki, K. et al. (1992) Bioclm. I; 2&,857-862 62 Murachi, T. (1989) Bioch?m. hf. 18.263-294 63 Shenoy, A. M. and Brahmi, 2. (19911 Cell Imtmmaol. 138,X-34 64 Tsujir;ah, T. :f of. f1?86) S;ocktr~. Bi~$~ys. Res. Comaun. 153,
1201-1208
66 Huang 2, t%&owan, E. 8. and &hviIer, T. C. (1992) J. Med. Cbem. 35,2048-2054
67 Anf&er, H., Ana& I. and Shaw, E. (1992) 1. Med. Cheer. 35,2X&220
65 Mehdi, S, Angela&o, M. R., Wiseman, J. S. and Bey, P. (19881 refry. Bio~. Res. Cmnrmm. 157.1117-1123
45,581~588 _ 68 Gi&dano, C. t-f af.‘i1&3) Eur. J. Med. Clte,n,~28,297-311 35 Persson, H. and Karlsson, J-O. (1991) Neuroscf. tiff. 130,81-84 69 Matsueda, R. eJ al. WOf C/rear. f&f. 191-194 36 Banik, N. L., Hogan, E. L., Powers, J. M. and Smith, K. P. (1986)
J. Nenrolog. Sri. 73,245-256 37 lizuka, H., Iwasaki, Y., Yamamoto. T. and Kadova, S. (1986) 1
J, Nerr&surg. 65,92-98 ,
38 Ishiura, S., Nonaka, I. and Sugita, H. (1980) in hfascldar Dystrophy (Ebashi, S., ed.), pp, 265-282, University of Tokyo Press
39 lizuka, K., Kawaguchi, H. and Yasuda, H. WJl) Biochem. Med. Mefab. Biol. 46,427431
Chemical names
40 lizuka, K., Kawaguchi, H. and Kitabatake, A. (1993) J. Mol. Cell cardiol* w, 1101-1109
41 Matsumura, Y., Kusuoka, H., Inoue, M., Hori, M. and Kamada, T. (19931 J. Car&vasc. Pf~~na#f. 22< 135-142
42 Toda, G, ef al. (1989) &au Hearf [. 30,375-386 43 France, A., Jr and Lansman, J. 6. (19901 ~JJ~re 344,670-673 44 Tu~r,P.R.,W~~~,T.,Regen,C.M.~S~~ardt,R.A.(l~)
Nafrlre 335,73S-738 45 Turner, P. R., Schultz, R., Canguly, B. and Steinhardt, R. A. (1993)
J. Merrtbr. Biof. 133,243-251 46 van der Westhuyzen, D., Matsumoto, K. and Etlinger, J. D. (1981)
J, Eiol. C/rear. 256,11791-11797 47 Johnson, P. and Hammer, J. L. (1988) hf. j. B~OCJJ~WJ. 20,1227-1230 48 Azuma, M., David, L. L. and Shearer,T. R. (19911 Qrr. Eye Res. IO,
AK275z Z-Leu-Abu-CONHCH,CH,
EC& trurrs-epoxysuccinyb+leucylamido-4-guan- idinolbutane
E6k (2s,3s)-t~ns-epoxysuccinyl-L-feu~Ja~d~~ methylbutane
E&&k (2s,~)-tranfspoxysu~nyl-L-leu~~mido-~ m~hyIbu~e ethyl ester
H7: l-CGoquinolinylsulphonyl~Z-methylpiperazine
MDl.28170: Z-Val-Phe-H
MK801: (5R,lOs)-(+)-5-methyl-lO,ll-dihydro-5H- dibenzo[a&yclohepten-5,10-imine
65766 1
Postscript
P~sf~r~pf is a new section that publishes news (such as scientific awards and ap~intrnents) from national pharmacological societies and other learned societies. Announcement are free of charge and should be addressed to TiPS Posfscripf, Elsevier Trends Journals, 68 Hills Road, Cambridge, UK CBZ ILA.
Subscription queries
The Editorial Office deals with scientific matters only. Subscription queries cannot be dealt with at this office and should be sent to the appropriate address indicated on the ccnknts page.
I 1
Tips - November 1994 <Vol. 15) 4 1 9
Copyright © 2022 FDOKUMEN