
Immunomodulatory and therapeutic activity of curcumin
11
Review Immunomodulatory and therapeutic activity of curcumin Raghvendra M. Srivastava a , Sarvjeet Singh b , Shiv K. Dubey c , Krishna Misra d , Ashok Khar e, ⁎ a Department of Otolaryngology, Hillman Cancer Centre, University of Pittsburgh Cancer Institute, Pittsburgh, PA 15213, USA b Department of Internal Medicine, Division of Cardiology, University of Texas Southwestern Medical Center, Dallas, Texas 75390, USA c Department of Internal Medicine, Division of Hematology-Oncology, University of Michigan Medical School, Ann Arbor, Michigan 48109, USA d Division of Bioinformatics, Indian Institute of Information Technology, Allahabad, India e CMBRC, Apollo Hospitals Educational and Research Foundation, Apollo Health City, Jubilee Hills, Hyderabad 500033, India abstract article info Article history: Received 1 July 2010 Accepted 22 August 2010 Available online 8 September 2010 Keywords: Curcumin Anti-inflammatory Anti-cancerous Immune and metabolic diseases Inflammation is a disease of vigorous uncontrolled activated immune responses. Overwhelming reports have suggested that the modulation of immune responses by curcumin plays a dominant role in the treatment of inflammation and metabolic diseases. Observations from both in-vitro and in-vivo studies have provided strong evidence towards the therapeutic potential of curcumin. These studies have also identified a plethora of biological targets and intricate mechanisms of action that characterize curcumin as a potent ‘drug’ for numerous ailments. During inflammation the functional influence of lymphocytes and the related cross-talk can be modulated by curcumin to achieve the desired immune status against diseases. This review describes the regulation of immune responses by curcumin and effectiveness of curcumin in treatment of diseases of diverse nature. © 2010 Elsevier B.V. All rights reserved. Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 331 2. Immunomodulatory action of curcumin on T lymphocytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 332 3. Immunoinhibitory action of curcumin on dendritic cells (DCs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 333 4. Immunomodulatory effect of curcumin on natural killer (NK) cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334 5. Immunomodulatory effect of curcumin on monocytes and macrophages (Mϕ) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334 6. Immunomodulatory effect of Curcumin on B cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 335 7. Immunomodulatory effect of curcumin on neutrophils and eosinophils and mast cells and its anti-oxidant properties . . . . . . . . . . . . 336 8. Curcumin in health and disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336 8.1. Role of curcumin in the neoplastic diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336 8.2. Curcumin in cardiovascular disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 337 8.3. Curcumin in neurodegenerative disease. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 338 8.4. Immunomodulatory action of curcumin in the prevention of inflammatory diseases . . . . . . . . . . . . . . . . . . . . . . . . . 338 9. Concluding remarks and future perspectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 339 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 339 1. Introduction Turmeric is a mixture of compounds related to curcumin known as curcuminoids consisting of curcumin [i.e.diferuloylmethane or 1,7-bis (4-hydroxy-3-methoxy-phenyl) hepta-1, 6-diene-3, 5-dione)] as the major component, demethoxycurcumin, bisdemethoxycurcumin and cyclocurcumin [1] (Fig. 1). Curcumin has been in use for its medicinal benefits since centuries but the first documented case of its use as a drug emerged only in 1937 when it was utilized to treat biliary disease. Since then its therapeutic potential has been explored in International Immunopharmacology 11 (2011) 331–341 Abbreviations: Ag, antigen; Ab, antibody; NO, nitric oxide; LPS, lipopolysaccharide; ConA, concanavalin A; AP-1, activator protein 1; NF-κB, nuclear factor-kappaB; NF-AT, nuclear factor of activated T cells; PMA, phorbol 12-myristate 13-acetate; PHA, phytohaemagglutinin; ROS, reactive oxygen species; ROIs, reactive oxygen intermedi- ates; COX-2, cyclooxygenase-2; APC, antigen presenting cells; DCs, dendritic cells; IDO, indoleamine 2,3-dioxygenase. ⁎ Corresponding author. E-mail address: [email protected] (A. Khar). 1567-5769/$ – see front matter © 2010 Elsevier B.V. All rights reserved. doi:10.1016/j.intimp.2010.08.014 Contents lists available at ScienceDirect International Immunopharmacology journal homepage: www.elsevier.com/locate/intimp
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Immunomodulatory and therapeutic activity of curcumin
International Immunopharmacology 11 (2011) 331–341
Contents lists available at ScienceDirect
International Immunopharmacology
j ourna l homepage: www.e lsev ie r.com/ locate / in t imp
Review
Immunomodulatory and therapeutic activity of curcumin
Raghvendra M. Srivastava a, Sarvjeet Singh b, Shiv K. Dubey c, Krishna Misra d, Ashok Khar e,⁎a Department of Otolaryngology, Hillman Cancer Centre, University of Pittsburgh Cancer Institute, Pittsburgh, PA 15213, USAb Department of Internal Medicine, Division of Cardiology, University of Texas Southwestern Medical Center, Dallas, Texas 75390, USAc Department of Internal Medicine, Division of Hematology-Oncology, University of Michigan Medical School, Ann Arbor, Michigan 48109, USAd Division of Bioinformatics, Indian Institute of Information Technology, Allahabad, Indiae CMBRC, Apollo Hospitals Educational and Research Foundation, Apollo Health City, Jubilee Hills, Hyderabad 500033, India
Abbreviations: Ag, antigen; Ab, antibody; NO, nitricConA, concanavalin A; AP-1, activator protein 1; NF-κB,nuclear factor of activated T cells; PMA, phorbol 1phytohaemagglutinin; ROS, reactive oxygen species; ROates; COX-2, cyclooxygenase-2; APC, antigen presentingindoleamine 2,3-dioxygenase.⁎ Corresponding author.
E-mail address: [email protected] (A. Khar).
1567-5769/$ – see front matter © 2010 Elsevier B.V. Aldoi:10.1016/j.intimp.2010.08.014
a b s t r a c t
a r t i c l e i n f oArticle history:Received 1 July 2010Accepted 22 August 2010Available online 8 September 2010
Keywords:CurcuminAnti-inflammatoryAnti-cancerousImmune and metabolic diseases
Inflammation is a disease of vigorous uncontrolled activated immune responses. Overwhelming reports havesuggested that the modulation of immune responses by curcumin plays a dominant role in the treatment ofinflammation and metabolic diseases. Observations from both in-vitro and in-vivo studies have providedstrong evidence towards the therapeutic potential of curcumin. These studies have also identified a plethoraof biological targets and intricate mechanisms of action that characterize curcumin as a potent ‘drug’ fornumerous ailments. During inflammation the functional influence of lymphocytes and the related cross-talkcan be modulated by curcumin to achieve the desired immune status against diseases. This review describesthe regulation of immune responses by curcumin and effectiveness of curcumin in treatment of diseases ofdiverse nature.
oxide; LPS, lipopolysaccharide;nuclear factor-kappaB; NF-AT,2-myristate 13-acetate; PHA,Is, reactive oxygen intermedi-cells; DCs, dendritic cells; IDO,
l rights reserved.
© 2010 Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3312. Immunomodulatory action of curcumin on T lymphocytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3323. Immunoinhibitory action of curcumin on dendritic cells (DCs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3334. Immunomodulatory effect of curcumin on natural killer (NK) cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3345. Immunomodulatory effect of curcumin on monocytes and macrophages (Mϕ) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3346. Immunomodulatory effect of Curcumin on B cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3357. Immunomodulatory effect of curcumin on neutrophils and eosinophils and mast cells and its anti-oxidant properties . . . . . . . . . . . . 3368. Curcumin in health and disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 336
8.1. Role of curcumin in the neoplastic diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3368.2. Curcumin in cardiovascular disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3378.3. Curcumin in neurodegenerative disease. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3388.4. Immunomodulatory action of curcumin in the prevention of inflammatory diseases . . . . . . . . . . . . . . . . . . . . . . . . . 338
9. Concluding remarks and future perspectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 339References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 339
1. Introduction
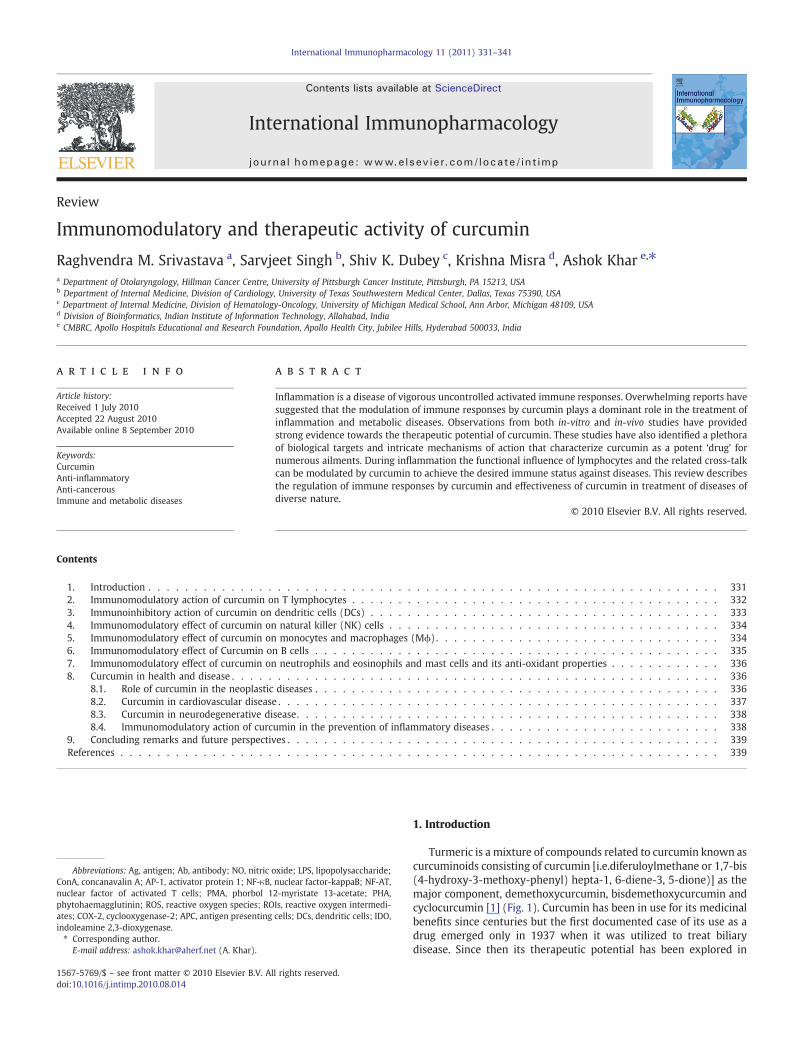
Turmeric is a mixture of compounds related to curcumin known ascurcuminoids consisting of curcumin [i.e.diferuloylmethane or 1,7-bis(4-hydroxy-3-methoxy-phenyl) hepta-1, 6-diene-3, 5-dione)] as themajor component, demethoxycurcumin, bisdemethoxycurcumin andcyclocurcumin [1] (Fig. 1). Curcumin has been in use for its medicinalbenefits since centuries but the first documented case of its use as adrug emerged only in 1937 when it was utilized to treat biliarydisease. Since then its therapeutic potential has been explored in
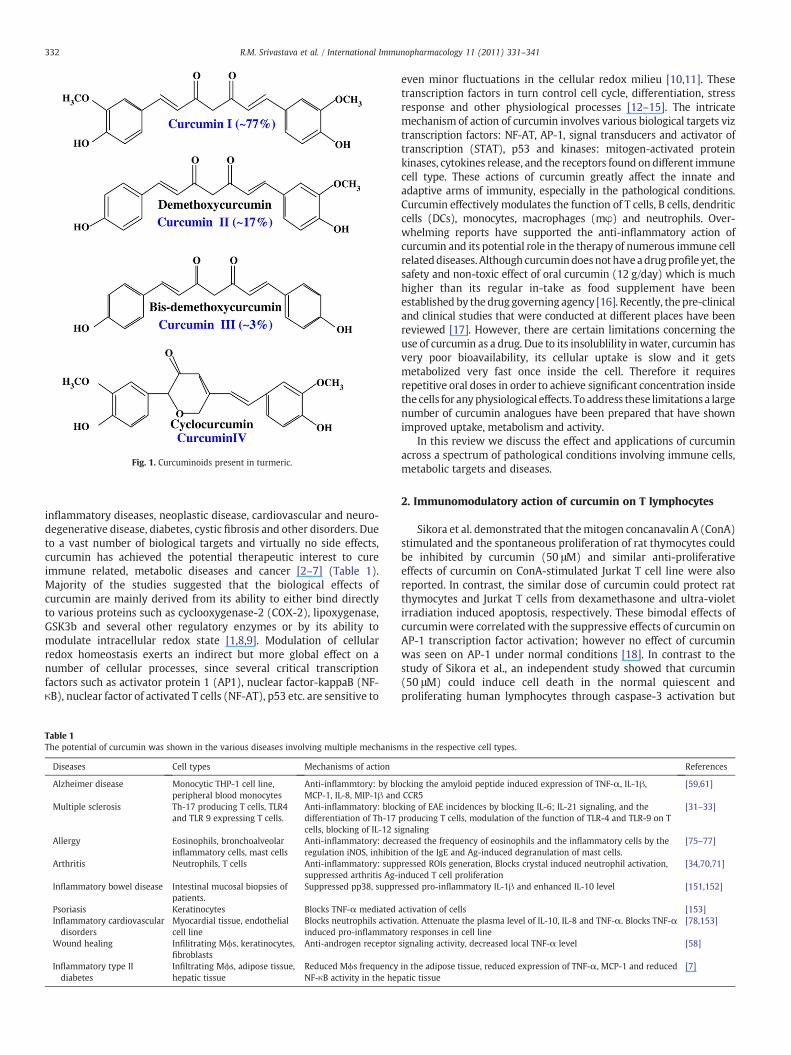
Fig. 1. Curcuminoids present in turmeric.
332 R.M. Srivastava et al. / International Immunopharmacology 11 (2011) 331–341
inflammatory diseases, neoplastic disease, cardiovascular and neuro-degenerative disease, diabetes, cystic fibrosis and other disorders. Dueto a vast number of biological targets and virtually no side effects,curcumin has achieved the potential therapeutic interest to cureimmune related, metabolic diseases and cancer [2–7] (Table 1).Majority of the studies suggested that the biological effects ofcurcumin are mainly derived from its ability to either bind directlyto various proteins such as cyclooxygenase-2 (COX-2), lipoxygenase,GSK3b and several other regulatory enzymes or by its ability tomodulate intracellular redox state [1,8,9]. Modulation of cellularredox homeostasis exerts an indirect but more global effect on anumber of cellular processes, since several critical transcriptionfactors such as activator protein 1 (AP1), nuclear factor-kappaB (NF-κB), nuclear factor of activated T cells (NF-AT), p53 etc. are sensitive to
Table 1The potential of curcumin was shown in the various diseases involving multiple mechanism
Diseases Cell types Mechanisms of action
Alzheimer disease Monocytic THP-1 cell line,peripheral blood monocytes
Anti-inflammtory: by bloMCP-1, IL-8, MIP-1β and
Multiple sclerosis Th-17 producing T cells, TLR4and TLR 9 expressing T cells.
Anti-inflammatory: blocdifferentiation of Th-17cells, blocking of IL-12 s
Allergy Eosinophils, bronchoalveolarinflammatory cells, mast cells
Anti-inflammatory: decrregulation iNOS, inhibiti
Arthritis Neutrophils, T cells Anti-inflammatory: suppsuppressed arthritis Ag-
Inflammatory bowel disease Intestinal mucosal biopsies ofpatients.
Suppressed pp38, suppr
Psoriasis Keratinocytes Blocks TNF-α mediatedInflammatory cardiovasculardisorders
Myocardial tissue, endothelialcell line
Blocks neutrophils activainduced pro-inflammato
Wound healing Infilitrating Mϕs, keratinocytes,fibroblasts
Anti-androgen receptor
Inflammatory type IIdiabetes
Infiltrating Mϕs, adipose tissue,hepatic tissue
Reduced Mϕs frequencyNF-κB activity in the hep
even minor fluctuations in the cellular redox milieu [10,11]. Thesetranscription factors in turn control cell cycle, differentiation, stressresponse and other physiological processes [12–15]. The intricatemechanism of action of curcumin involves various biological targets viztranscription factors: NF-AT, AP-1, signal transducers and activator oftranscription (STAT), p53 and kinases: mitogen-activated proteinkinases, cytokines release, and the receptors found on different immunecell type. These actions of curcumin greatly affect the innate andadaptive arms of immunity, especially in the pathological conditions.Curcumin effectively modulates the function of T cells, B cells, dendriticcells (DCs), monocytes, macrophages (mφ) and neutrophils. Over-whelming reports have supported the anti-inflammatory action ofcurcumin and its potential role in the therapy of numerous immune cellrelateddiseases. Although curcumindoesnot haveadrugprofile yet, thesafety and non-toxic effect of oral curcumin (12 g/day) which is muchhigher than its regular in-take as food supplement have beenestablished by the drug governing agency [16]. Recently, the pre-clinicaland clinical studies that were conducted at different places have beenreviewed [17]. However, there are certain limitations concerning theuse of curcumin as a drug. Due to its insolublility inwater, curcumin hasvery poor bioavailability, its cellular uptake is slow and it getsmetabolized very fast once inside the cell. Therefore it requiresrepetitive oral doses in order to achieve significant concentration insidethe cells for anyphysiological effects. To address these limitationsa largenumber of curcumin analogues have been prepared that have shownimproved uptake, metabolism and activity.
In this review we discuss the effect and applications of curcuminacross a spectrum of pathological conditions involving immune cells,metabolic targets and diseases.
2. Immunomodulatory action of curcumin on T lymphocytes
Sikora et al. demonstrated that themitogen concanavalin A (ConA)stimulated and the spontaneous proliferation of rat thymocytes couldbe inhibited by curcumin (50 μM) and similar anti-proliferativeeffects of curcumin on ConA-stimulated Jurkat T cell line were alsoreported. In contrast, the similar dose of curcumin could protect ratthymocytes and Jurkat T cells from dexamethasone and ultra-violetirradiation induced apoptosis, respectively. These bimodal effects ofcurcuminwere correlated with the suppressive effects of curcumin onAP-1 transcription factor activation; however no effect of curcuminwas seen on AP-1 under normal conditions [18]. In contrast to thestudy of Sikora et al., an independent study showed that curcumin(50 μM) could induce cell death in the normal quiescent andproliferating human lymphocytes through caspase-3 activation but
s in the respective cell types.
References
cking the amyloid peptide induced expression of TNF-α, IL-1β,CCR5
[59,61]
king of EAE incidences by blocking IL-6; IL-21 signaling, and theproducing T cells, modulation of the function of TLR-4 and TLR-9 on Tignaling
[31–33]
eased the frequency of eosinophils and the inflammatory cells by theon of the IgE and Ag-induced degranulation of mast cells.
[75–77]
ressed ROIs generation, Blocks crystal induced neutrophil activation,induced T cell proliferation
[34,70,71]
essed pro-inflammatory IL-1β and enhanced IL-10 level [151,152]
activation of cells [153]tion. Attenuate the plasma level of IL-10, IL-8 and TNF-α. Blocks TNF-αry responses in cell line
[78,153]
signaling activity, decreased local TNF-α level [58]
in the adipose tissue, reduced expression of TNF-α, MCP-1 and reducedatic tissue
[7]

333R.M. Srivastava et al. / International Immunopharmacology 11 (2011) 331–341
without DNA degradation. This study also highlighted that curcuminaffects the viability of proliferating T cells much severely thanquiescent T cells [19,20]. Furthermore Deters et al. demonstratedthat curcumin (2.8–10 μM) can significantly abrogate the prolifera-tion of peripheral blood mononuclear cells (PBMC) induced by OKT3mAb (a human TCR/CD3 complex Ab) [21]. The concentration range ofcurcumin used by Deters et al. was similar to the concentrations thatwas shown to significantly affect human T cell proliferation inducedby various distinct stimuli viz. phorbol 12-myristate 13-acetate(PMA), CD28, phytohaemagglutinin (PHA) [22]. Although directsuppressive effects of curcumin on superantigen induced proliferationof T cells were demonstrated in several studies as described before,few studies also demonstrated that T cells fail to get appropriateamount of co-stimulatory signals from curcumin-treated Ag present-ing cells (APCs), as curcumin (20–30 μM) aborted the upregulation ofCD86 and CD83 in response to the APC maturation stimuli. Thisinhibitory effect of curcumin on T cells was independent of the HLA-DR levels on the respective APCs as the HLA-DR level was notdownregulated by the curcumin. Curcumin, however, could alsoreduce the DCs' dependent allogenic CD4+ T cell proliferation in amixed lymphocyte reaction assay at 1:16 ratio of DCs to T cells. In thisstudy a probable affect of curcumin on the cytoskeleal elements of DCswas argued in this context, which may be attributed to its inhibitoryanti-proliferative effects [23]. Another study demonstrated a signif-icant increase in ConA-stimulated proliferation of splenic cells at6.25 μM curcumin and a significant decrease in proliferation at12.5 μM and a complete blockage of proliferation with 25 μMcurcumin, which confirmed the distinct function of curcumin atvariable concentrations. Also, curcumin irreversibly inhibited theinduction of lymphoproliferation by other mitogens and alloantigens.
As the in-vivo effects of curcumin are highly dependent on thebioavailable concentration of curcumin, it is indeed a daunting agendato correlate the in-vitro activities of curcumin and in-vivo responses inthe pathological conditions, especially in the localized pathologicalconditions like non-metastatic tumors of different origins [24]. Ashighlighted in the review so far, a variety of results indicated the in-vitro T cell immunosuppressive properties of curcumin in terms of Tcell death, as well as blocking the proliferation capacity of T cells.Nevertheless curcumin has been in use since centuries and itsconsumption has not been associated with any immunocompromiseddisorders; seriously arguing the significance of its immunosuppres-sive properties on T cells that have been reported under in-vitroconditions. We had demonstrated that T cells that were harvestedfrom the curcumin-injected (40 mg/kg/day; i.p) animals showedenhanced lymphoproliferation and a similar proliferative effect ofcurcumin was also observed when T cells were stimulated with ConAand PHA in conjunction with curcumin. Our study also providedevidence of specific lymphoproliferative effect of curcumin in-vivo, byusing cyclosporine A, a potent immunosuppressant drug. Interesting-ly, the enhanced Antigen (Ag)-specific T cell proliferation was alsoobserved in curcumin-injected rats that had received a highlyimmunogenic AK-5 histiocytoma cells as a source of tumor Ag [25].The evidence for the enhanced frequency of CD4+T cells wasfurthermore reported in another spontaneously generated tumormodel of adenoma in C57BL/6J-Min/+ (Min/+) mouse that were fedwith 0.1% dietary curcumin. In a statistically controlled lymphocyteinfiltration setup, this study reported an enhanced number of CD8+,CD4+ and CD3+ T cells in the curcumin fed animals. In this model thespontaneous polyp formation in themucosa was significantly reducedby the curcumin administration and the anti-tumor mechanism wascorrelated with the enhanced cytokine level due to the increasednumber of activated CD4+ T cells, although no direct evidence forsuch a conclusion was described in this study. Also, this study showedenhanced level of B cells in the intestinal mucosa, but no role orincrease in the number of monocytes was found in this spontaneoustumor model system [26]. In another elegant tumor model, in which
tumor growth could disintegrate the thymus morphology, curcumin(50 mg/kg bodyweight) restored the thymic integrity including CD3+
T cell frequency and served as immunoprotective compound duringcarcinogenesis. This effect of curcumin was attributedmechanisticallyto the anti-oxidant properties of curcumin because this tumorinduced oxidative stress in thymic T cells [27]. As an extension ofthis work the same group demonstrated that curcumin could preventthe tumor induced apoptosis of thymocytes as well as restoration ofthe frequency of CD4+ T/CD8+ T cells in the same tumor modelsystem with the same dose of curcumin. Mechanistically it was alsoshown that curcumin modulated Jak-3/Stat-5 activity to restore theimmune cell frequency and activity [28,29]. Curcumin decreased IL-12-induced STAT4 phosphorylation but enhanced the (interferon)IFN-β-induced STAT4 phosphorylation; curcumin decreased IL-12induced IFN-γ production and IL-12 Rβ1 and β2 expression, whereasit enhanced IL-10 production and IFN receptor (IFNAR) subunits 1 and2 expression. Curcumin also increased IFN-α-induced IL-10 andIFNAR1 expression. Pretreatment with curcumin decreased IFN-α-induced IFNAR2 expression and failed to modify the level of IFN-α-induced phospho-STAT4 activation. These findings favour the distinctmode of action of curcumin when T cells get activated with differentstimuli and also confirmed the multifarious targets of curcumin in theactivated T cells [30]. It was recently acknowledged that IL-17producing Th1 cells play an instrumental role in the establishedmodel of experimental autoimmune encephalomyelitis (EAE), whichmimics multiple sclerosis. Oral curcumin (100 or 200 mg/kg bodyweight) administration in the rats suppressed the frequency ofinflammatory cells in the spinal cord along with lowering thefrequency of paralytic incidences, which was the disease marker inthis model. The decreased level of IL-17, transforming growth factorbeta (TGF-β), IL-6, IL-21, STAT3 expression and STAT3-phosphoryla-tion was reported in curcumin-treated groups. Also, it was shown thatcurcumin blocks the differentiation of Th-17 cells by blocking STAT-3transcription in T cells. Moreover curcumin inhibited neural Ag-MBP68–86 peptide specific lymphocytes responses and IL-17 mRNAexpression. These recent evidences furthermore proved the signif-icance of curcumin in the IL-17 mediated disorders [31]. Bright andcolleague reported that T cells expressing Toll-like receptors-4 and 9(TLR4 and TLR9) play an instrumental role in the pathogenesis of EAEmodel. Curcumin treatment led to the decrease in the expression ofPLPp139–151 and MOGp35–55 Ag-induced TLR4 and TLR9 on theCD4+ T cells and CD8+ T cells, which also ameliorated this disease. Itwas found that TLR 4 and TLR9 acted as co-stimulatory receptors toenhance the proliferation and cytokine production in response to thespecific agonists [32]. Previously Bright's group had also reportedthat curcumin can inhibit IL-12 production in spleen cells, Mϕ andmicroglia and curcumin can inhibit EAE by blocking IL-12 signaling inT lymphocytes [33]. Curcumin also inhibited the proliferation ofmouse splenic T cells that were stimulated with ConA and in a modelof type II collagen (CII)-induced arthritis (CIA) in which T cellproliferation was induced by bovine type II collagen Ag. Moreover,curcumin reduced anti-CII IgG2a Ab in the serum of CIA mouse [34].
3. Immunoinhibitory action of curcumin on dendritic cells (DCs)
Being at the centre of various immunological responses, DCscontrol various pathogenic conditions and recently several groupshave investigated the action of curcumin on DCs' function. In adetailed study Kim et al. reported for the first time that curcumin, at adose of up to 25 μM, inhibits DC maturation and the relatedimmunostimulatory function. They also showed that more than50 μM concentration was toxic for DCs. Surprisingly however variousstudies have used 50 μM concentration in different immune cells asdescribed elsewhere in this review and the discrepancy between theuses of different concentration of curcumin reflects the variable dosesensitivities of different immune cells and cell lines to curcumin.

334 R.M. Srivastava et al. / International Immunopharmacology 11 (2011) 331–341
However, it remains to be investigated if curcumin dose sensitivity ofimmature andmature DCs results in distinct biological outcomes. Kimet al. also showed that curcumin could suppress the lipopolysaccaride(LPS) mediated surface overexpression of CD86, CD80 and MHCIIexpression in murine DCs during maturation but at the same timecurcumin treatment increased the FITC-dextran particle uptakesignificantly. These observations provided the evidence to modulateDC mediated specific immune response in the autoimmune disordersfor regulating the function of T cells [35]. Park and colleagues reportedthat the pretreatment with curcumin (1–25 μM) could also suppressthe LPS (200 ng/ml) induced indoleamine 2,3-dioxygenase (IDO)production in bone marrow derived-DCs (BMDCs). However, curcu-min enhanced the COX-2 expression by three fold and prostaglandinE2 production by two fold in the LPS treated DCs. The enhancedprostaglandin E2 level by curcumin was attributed to the suppressionof LPS-induced IDO production in this study. The curcumin orprostaglandin E2 treated DCs showed reduced proliferation of OVA-specific CD8+ T cells that was induced by LPS [36]. Althoughintravenous LPS (3 μg) injection reduces the splenic blood flow by31% and reduces the access of Ag to themouse spleen [37], a high doseof LPS (1.5 mg/kg body weight, i.p.) induced heavy IDO in splenic DCsand pre-injection of curcumin (50 mg/kg body weight, i.p.) inhibitedthe LPS-induced IDO production in the splenic DCs [36]. In contrast tothe effect of curcumin on BMDCs showing enhanced COX-2expression, another study showed the dose dependent (2–16 μM)inhibiton of the production of LPS (0.2 ng/ml) induced COX-2 in theBV2 microglial cells. This contrasting results on the COX-2 level in theBV2 microglial cells and BMDCs may be due to a very high differencein the LPS concentration (0.2 vs 200 ng/ml) or LPS serotype that wereused in these studies. Moreover, a distinct cellular response to LPScould not be ruled out in different cell types that may greatly differ inthe density of LPS receptor or co-receptors [38]. IFN-γ regulatesmultiple elements of DCs response and since it is being used formonocyte derived-DCs (MoDCs) conditioning in cancer therapy, it candrive DCs for potent Th1 polarizing activities. Although IFN-γ (5 to500 IU/ml) treatment was shown to upregulate CD86, CD38, CCR7 onMoDCs in 48 h [39], no significant increase in CD86 and CD80 levelwas found at 24 h after 200 IU/ml of IFN-γ treatment in murineBMDCs. However, IFN-γ (100 IU/ml) upregulated IDO production inBMDCs and curcumin (1–25 μM) inhibited the functions as well aslevel of IDO in IFN-γ stimulated murine BMDCs. Thus curcuminreversed the IDO-mediated reduced T cell proliferation function. Thisstudy also showed that curcumin can modulate IFN-γ induced IDOexpression by affecting Janus kinase 1 (JAK) and protein kinase C δ(PKC) signaling [40]. In a similar direction, additional data showedthat curcumin-treated DCs led to the development of anergic CD4+Tcells and curcumin-treated DCs could also induce regulatory T cells(Tregs) development. More interestingly, curcumin-treated DCs alsopromoted the production of IL-10 and αAlDHAa1 (α retinaldehydrogensae). These retinoids function as the regulators of mucosalimmune responses. Curcumin induced Treg cells inhibited Ag-specificT cell activation in-vitro and could inhibit colitis caused by Ag-specificpathogenic T cells in-vivo. These findings supported the importantrole of curcumin in the modulation of DCs' function to achievetolerogenic responses [41]. Curcumin (1 μM) itself could suppress theLPS-induced IL-12/23p40 production in-vitro, whereas IL-10 (2.5 ng/ml) and curcumin (0.1 μM) at their suboptimal concentrations actedsynergistically to suppress the LPS-induced IL-12/23p40 productionfrom DCs. However, no appreciable therapeutic effect of the dieterycurcumin was noticed in the IL10-deficient mice having Th1mediatedcolitis. Also, no significant improvement in the colitis was observed ascurcumin failed to modify the pathogenic T cells in IL-10 deficientmouse. These results comprehensively confirmed the dependence ofcurcumin on IL-10 for its immunoinhibitory actions. Nevertheless itprovided the evidence that a very little bioavailable concentration ofcurcumin might effectively modify the overall immune response in
combination with IL-10. Curcumin and IL-10 also acted synergisticallyto inhibit the NF-κB activity in intestinal epithelial cells and thus couldprovide the additional benefits without influencing the function ofimmune cells. These results also provoke the possibility of acombinatorial approach to investigate the immunohibitory action ofcurcumin with other immunohibitory molecules viz. TGF-β, prosta-glandins etc. [42]. Such investigations will be valuable to specify theaction of curcumin in various pathogenic conditions in future.
4. Immunomodulatory effect of curcumin on natural killer(NK) cells
NK cells directly participate in the killing of tumor cells after therecognition of stress inducible ligands and killing involves theinduction of cell death by perforin and granzyme B. Variousinvestigators have directly measured the NK cell activity againsttumor cells both, in-vitro and in-vivo. In the initial studies, curcuminfeeding (1, 20 or 40 mg/kg) up to five weeks showed no effect on theNK cell activity in rats but enhanced the antibody (Ab) responses inrats [43]. In another study, Yadav et al. showed that curcumintreatment can augment NK cell cytotoxicity in-vitro that can furtherbe enhanced by IFN-γ treatment [44]. The generation of IL-2 inducednon-specific cytotoxic LAK cells (similar to cytotoxic NK cells) in thepresence of curcumin (at 10–20 μM/l) was evaluated by Gau et al. andthe cytotoxic activity of LAK cells was determined against NK sensitiveYAC-1 lymphoma cells. The results showed little effect on thegeneration of LAK cell-mediated cytotoxicity, whereas higher dose(30 μM/l) of curcumin inhibited the cytotoxic LAK cell generation [24].Few serious concerns for the use of curcumin in the melanomatreatment were however raised, which were based on the facts thatNK cells from healthy donors treated with curcumin (10 or 20 μM/l)and IL-12 (10 or 50 ng/ml) secreted less amount of IFN-γ. Moreover,curcumin-treated NK cells also showed reduced granzyme B to killK562 and A375 melanoma cell lines and curcumin slightly reducedproduction of IFN-γ by NK cells in the presence of A375 melanomaand K562 target cell lines. Although this study found the direct effectof curcumin on tumor cells it could not provide appreciable reasonsfor the use of curcumin as the ‘modifiers of NK mediated immuneresponses’ in favour of its use in anti-tumor therapies [45]. Similarly,our previous study had shown that curcumin injections for prolongedduration had no effect on the NK cell activity in-vivo, during theprogression of ascites tumor [25]. However, we observed larger solidtumor with curcumin in the transplanted subcutaneous AK-5 tumorthat interestingly underwent rapid spontaneous regression. Also, anenhanced activation of NK cells was observed after curcumintreatment that correlated with the response of curcumin on thetumor in-vivo [46]. Such an effect clearly describes the effect ofcurcumin as ‘NK cells modifier’, however its in-vivo effects may behighly dependent on the specific pathology of the diseases. Recently,tumor derived exosomes attracted much attention as they caneffectively modulate the anti-tumor immune responses. Zhang et al.showed that curcumin enhanced the proteasomal degradation oftumor derived exosomal proteins that inhibit IL2-induced NK cellactivity against breast carcinoma, partially restoring the NK cellactivity against tumor. Such an action of curcumin displayed thatcurcumin can also target the immune escape strategies that arecritical for the immune responses [47].
5. Immunomodulatory effect of curcumin on monocytes andmacrophages (Mϕ)
Monocyte recruitment at the inflammatory site plays a vital role inthe inflammatory response. Curcumin inhibited the tumor necrosisfactor α (TNF-α) induced adhesion of monocytes on humanendothelial cells. The TNF-α induced upregulation of Inter-CellularAdhesion Molecule 1 (ICAM-1), vascular cell adhesion molecule-1

335R.M. Srivastava et al. / International Immunopharmacology 11 (2011) 331–341
(VCAM-1) and endothelial cell leukocyte adhesion molecule-1(ELAM-1) on monocytes was completely inhibited by curcumin. Thecurcumin mediated blocking of these adhesion molecules wasattributed to the inhibitory effect on NF-κB activation. These resultsshowed the promising activities of curcumin in the local inflammatoryresponses like arthritis as well as in metastasis [48]. PMA or LPS-induced production of inflammatory cytokines viz. TNF-α, IL-8,macrophage inflammatory protein 1 alpha (MIP-1α), monocytechemoattractant protein (MCP-1) and IL-1β in monocytes andalveolar Mϕs was significantly inhibited by curcumin in a dosedependent manner [49]. Lim et al. also showed that curcumin blockedthe enhanced expression and secretion of PMA induced inflammatorycytokine MCP-1 in U937 monocytic cell line [50]. Although curcumincompletely blocked LPS mediated NO production in RAW264.7 cellline, it enhanced the phagocytosis of fluorescent beads and the surfaceexpression of CD14. The enhancement of pahgocytic activity and thesurface expression of CD14 followed a similar pattern, however nodirect role of curcumin mediated enhanced CD14 surface expressionwas described for the phagocytic capcity [51]. Previously, anindependent study had also shown a significant increase in Mϕphagocytic activity in curcumin-treated animals. These actions ofcurcumin on Mϕs also described the enhanced scavenging capacityunder non-inflammatory conditions [52]. Prolonged alcohol treat-ment led to oxidative stress and the mononuclear cells obtained fromalcoholic animals showed lesser capacity for collagen surfaceattachment; however alcohol in conjunction with curcumin showednormal adhesion potential of mononuclear cells. This study showedthe reduction in the toxic effect of alcohol by curcumin in theprolonged duration [53]. Pretreatment with curcumin inhibited theLPS-induced TLR-2 mRNA and NF-κB level in RAW264.7 cells [54].Treatment with bisdemethoxycurcumin inhibited the LPS-inducedNO production in RAW264.7 cells, which was abrogated by blockingthe activity or the expression level of heme oxygenase-1. It was alsoshown that anti-inflammatory effects mediated by bisdemethoxy-curcumin signaling to heme oxygenase-1 involve **Ca2+/calmodulin-CaMKII-ERK1/2-Nrf2 cascade in RAW264.7Mϕ cells [55]. Sumanont etal. have furthermore reported that curcumin manganese complex(CpCpx) and diacetylcurcumin manganese complex (AcylCpCpx)have greater NO radical scavenging activity than their parentcompounds, curcumin and acetylcurcumin, respectively [56].
In diabetic condition, a massive increase in the inflammatorycytokines has been reported. To evaluate the anti-inflammatory effectof curcumin under high glucose mediated inflammatory responses,Jain et al. studied the effect of curcumin and placebo supplementationon plasma level of TNF-α, IL-6, MCP-1, glucose and oxidative stress instreptozotocin-treated diabetic rats [57]. Curcumin treatment signif-icantly reduced the high glucose mediated upregulation of inflam-matory cytokines along with increasing the lipid peroxidation.However curcumin had no effect on the reduced insulin level underdiabetic conditions. In this study, the anti-inflammatory action ofcurcumin on the high glucose induced IL-8, TNF-α, IL-6, MCP-1 wasalso shown by using human promonocytic U937 cell line.
Androgen receptor is a nuclear receptor that translocates to thenucleus following ligand binding and modulates the function ofvarious genes. In the healing skin androgen receptor were detected ininfilitrating Mϕs, keratinocytes and in dermal fibroblasts thatindicated its possible function in the healing process. Androgenreceptor activity in the presence of 5α-dihydrotestosterone inducedTNF-α promoter activity in Mϕs. The curcumin derivative ASC-J9disrupts the androgen receptor and its co-regulator interactionresulting in the increased androgen receptor degradation and thedecreased androgen receptor transactivation. The topical applicationof ASC-J9 cream in mouse resulted in quick wound healing and alsodecreased local TNF-α expression. This study concluded that thecurcumin derivative ASC-J9, which acts by inhibiting androgenreceptor activity, could be utilized in wound healing as an anti-
inflammatory agent [58]. Alzheimer's disease is a complex disordermainly characterized by deposition of large amount of amyloid-β (Aβ)peptide and subsequent massive inflammatory response. Heavyinfilitration of monocytes and Mϕ has been observed in the affectedtissue with Aβ deposition. Giri et al. demonstrated that both Aβ1–40
and fibrilar Aβ1–42 peptide are abundantly present in the plasma ofpatients along with the increase in the level of cytokines TNF-α andIL-1β and chemokines MCP-1, IL-8 and MIP-1β. Activation oftranscription factors AP-1 and EGR-1 regulates the level of cytokinesand chemokines in THP-1 monocytic cells and in peripheral bloodmonocytes [59]. Based on the ability of curcumin to block inflamma-tion as well as to modulate the activities of β-secretase andacetylcholinesterase, in-vitro and in-vivo studies with curcumin ledto suppressed Aβ deposition and aggregation in experimental animals[60]. In the evaluation study on the role of curcumin in Alzheimerdisorder Giri et al. furthermore showed that curcumin could block theAβ1–40-induced expression of TNF-α, IL-1β, MCP-1, IL-8, MIP-1β andCCR5. Also, it was reported that curcumin could inhibit Aβ-inducedEgr-1 DNA-binding activity. These results provided the mechanism ofthe anti-inflammatory action of curcumin in this disease [61].
6. Immunomodulatory effect of Curcumin on B cells
Decoté-Ricardo et al. evaluated the effects of curcumin on murinespelnic B cells. LPS-induced IgM secretion as well as CpG and TLR4-induced proliferation of B cells was inhibited following curcumintreatment. However curcumin failed to exert anti-proliferative effectwhen the B cell prolifearion was induced by the T-independent type 2stimuli anti-delta-dextran or by the anti-IgM Ab. Moreover curcumin(10 μM) had no effect on the calcium mobilization induced by anti-IgM (10 μg/ml) Ab. Interestingly, however, curcumin inhibited theTLR ligand and anti-IgM induced phosphorylation of ERK, Iκ-B andp38 kinase along with inhibiting NF-κB activation. These observationsindicated the anti-inflammatory effects of curcumin in the B cellresponse [62]. Another study described that the mitogen-LPS-inducedproliferation of B cells can be dose dependently inhibited by curcumin(1–20 μM); additionally the LPS-induced secretion of IgG1 and IgG2awas inhibited by curcumin. However, the curcumin mediatedinhibition of IgG1 secretion was more pronounced than the inhibitionof IgG2a secretion [63]. An independent study also described thatcurcumin (10 μM) can also inhibits the production of IgE from ratsplenocytes [64]. Epstein barr virus (EBV) can immortalize human Blymphocytes in-vitro and immortalization is promoted by theoxidative stress induced by potent immunosuppressive drug cyclo-sporine A andwith hydrogen peroxide. Curcumin (20 μM) aborted theEBV induced B cell immortalization process. This effect of curcuminmay be exploited to prevent post-transplant lymphoproliferativedisorders in patient receiving cyclosporine A, which otherwise maypromote EBV induced B cell immortalization [65]. Later on, it wasfound that the curcumin modulates this immortalization process byenhanced apoptosis in the virus infected B cells [66]. In animals withspontaneous polyps in the intestinal mucosa, curcumin treatmentresulted in 40% increase in B cell numbers in the intestinal mucosa,suggesting the therapeutic responses to curcumin [26].
B cell receptor (BCR) signaling regulates the induction of apoptosisin chronic lymphocytic lymphoma. The central mediator of BCR-signaling is the spleen tyrosine kinases, that govern the function andsurvival of B cells, and a high level of phosphorylated spleen tyrosinekinase was found in lymphoma cells in comparison to healthy B cells[67]. Curcumin differentially modulated the cytotoxicity of primarychronic lymphocytic lymphoma in comparison to healthy B cells [67].Rats that received 1, 20 or 40 mg/kg curcumin for 5 weeks showedsignificantly enhanced IgG only at 40 mg/kg levels whereas animalsreceiving lower dietary concentrations (1 or 20 mg/kg) of curcuminhad same IgG level as that of control with no dietary curcumin. Theseobservations suggest that a threshold level of bioavailable curcumin is

336 R.M. Srivastava et al. / International Immunopharmacology 11 (2011) 331–341
also needed to modulate the IgG mediated responses [43]. A recentstudy showed that curcumin (6 to 50 μM) could suppress theexpression of division dependent upregulation of activation-inducedcytosine deaminase, which plays pivotal role in the Ig class switchrecombination and somatic hyper-mutation and participates intumorigenesis. Also the decrease in the recovery of IgG+class-switched B cells within the divided population was observed. Theseobservations suggest the potential of curcumin in the treatment of Bcell autoimmune disease [68].
7. Immunomodulatory effect of curcumin on neutrophils andeosinophils and mast cells and its anti-oxidant properties
Several independent studies have provided the evidence thatcurcumin can act on various aspects of neutrophil function, in astimulus specific manner and may thus dampen the neutrophilmediated inflammatory response [69]. Chemotactic peptide N-formyl-methionyl-leucyl-phenylalanine (FMLP) and zymosan acti-vated plasma induced aggregation of the monkey neutrophils couldbe inhibited by the curcumin (1 mM). FMLP peptide, zymosan andarachidonic acid induced production of oxygen radical was attenuatedby the curcumin treatment. Calcium ionophore A23187 could nullifythe curcumin effect by interfering with the effect of curcumin inneutrophils [69]. Neutrophils play significant role in the damage ofjoint tissue in the rheumatoid arthritis. A recent study demonstratedthe reduced level of oxygen radical generation by neutrohphils upontreatment with curcumin both in-vitro and in-vivo. Adjuvant inducedarthritis enhanced the neutrophil frequency in the blood that remainunaltered by curcumin. The stimulation of neutrophils by PMA led toincreased level of PKC isozymes, α and β II, which was abrogated bycurcumin treatment without interfering with neutrophils vitalfunctions [70]. Similarly, the crystal induced neutrophil activationthat served as a model of induced arthritis or rheumatoid arthritiscondition was inhibited by curcumin [71]. Oral administration ofcurcumin (40–60 mg/kg body weight) increased survival of mice by70% in response to heavy dose of LPS (40 mg/kg body weight).Moreover curcumin suppressed the LPS mediated neutrophil infiltra-tion in liver that was the primary cause of liver damage. However, thereduction of infiltrationwas limited to the liver only, because whereashepatic venules had same frequency of neutrophils as that of withoutcurcumin. The reduction of LPS-induced infiltration of neutrophilswas also correlated with the reduced levels of ICAM-1 and VCAM-1 inthe liver tissue that influence neutrophil adhesion [72]. Withoutaffecting the viability, curcumin (100 μM) significantly reduced the IL-8 induced chemotactic activity of neutrophils in dose dependentmanner and curcumin modulated this chemotaxis by dampening theIL-8 induced Ca++ ion mobilization. Surface CXCR1 and CXCR2 wereinternalized upon IL-8 treatment and curcumin treatment enhancedthe intracellular level of CXCR1 and CXCR2 in conjunction with IL-8,which indicated that the effect of curcumin on the reduced migrationof neutrophils might be attributed to the reduced IL-8 receptors.However, curcumin itself downregulated surface IL-8 receptor CXCR1and CXCR2 and also blocked the recycling of these receptors onneutrophils. The Rab GTPase family (Ras superfamily of monomeric Gproteins) plays pivotal role in the cellular transport mechanism.Interestingly, both CXCR1 and CXCR2 showed enhanced binding withRab11 upon curcumin treatment, which could potentially block therecovery of IL-8 to cell surface. This study revealed the intricatemechanism that curcumin triggers to achieve anti-inflammatoryresponses meadiated by neutrophils [73]. LPS induced lung damageand reduction in lung and bronchoalveolar lavage fluid proteincontent, which was accompanied by enhanced numbers of neutro-phils and elevated myeloperoxidase activity in cell-free lavage.Elevation in the cytokine-induced neutrophil chemoattractant-Iprotein level was seen in response to LPS in the lung tissue, whichwas significantly reduced by the pretreatment with curcumin. This
shows an important protective response of curcumin by dampeningneutrophil function in lung injury [74].
In a murine model of asthama, which was induced by OVA-Ag andwhich had airway hyper-responsiveness to allergens, curcumin (i.p,10 or 20 mg/kg body weight) decreased the frequency of eosinophilsand the inflammatory cells, inhibited iNOS (inducible nitric oxidesynthase) expression in lungs and also suppressed the level of IL-4and IL-5 in bronchoalveolar lavage fluid [75]. An interesting studyinvolving the action of curcumin on mast cells indicated thatcurcumin reversibly inhibits the degranulation of mast cells alongwith inhibiting secretion of IL-4 and TNF-α. The evaluation of the anti-allergic affect of curcumin was performed by utilizing passivecutaneous anaphylaxis in the mouse ear model. Oral administrationof curcumin (50 mg/kg) suppressed the mast cell dependent IgE andAg-induced local passive cuataneous anaphylaxis [76,77]. Effect ofcurcumin during myocardial ischemia/reperfusion injury with cardi-oplegia was also investigated [78]. The postoperative increase in theIL-8, IL-10, TNF-α levels in the plasma was decreased by curcumin.Also curcumin inhibited the activation of neutrophils in myocardiumthat was estimated by the myloperoxidase activity assay [78].
8. Curcumin in health and disease
Due to the fact that curcumin has been shown to be associatedwith a number of physiological processes and that it has a widevariety of cellular targets, its therapeutic role has been studied inseveral inflammatory and non-inflammatory disorders. In this section,we discuss most recent findings related to its direct application inhealth and disease.
8.1. Role of curcumin in the neoplastic diseases
Curcumin has received maximum attention owing to its anti-tumor properties. Several hundred reports in the last two decadeshave shown its ability to selectively kill transformed cells acrossalmost all types of tumors. Curcumin can exert its anti-tumor effectsat two levels, (i) at the level of tumorigenesis or (ii) in selectivelyinducing apoptosis in tumor cells. Huang et al. have discussed theanti-carcinogenic effects of curcumin in duodenal and colon cancer inmice. In this study, dietary curcumin could significantly reduce tumorload during both pre initiation and post initiation of chemical inducedcarcinogenesis [79]. Similarly, curcumin application inhibited theinduction of epidermal DNA synthesis and the tumor promotion inskin following 12-0-tetradecanoyl phorbol-13-acetate (TPA) treat-ment [80] as well as benzopyrene induced DNA adducts and skintumors and DMBA induced skin tumors [79]. Rao et al. have shownthat curcumin (200 ppm) in the diet could significantly suppressazoxymethane-induced colonic aberrant crypt foci formation, whichare early preneoplastic lesions, and colon tumor incidence and tumormultiplicity [81]. These effects of curcumin in inhibiting tumorigen-esis involve inhibition of arachidonic acid metabolism; decrease inTPA induced ornithine decarboxylase activity and inhibition of DNAsynthesis. It was thought that metabolites of arachidonic acid such asHPETEs, HETEs, leukotrienes and prostaglandins play an importantrole in TPA induced inflammation and tumor promotion [82,83].Similarly ornithine decarboxylase (ODC) is a rate limiting enzyme inpolyamine synthesis [81] and its overexpression has been linked withcell transformation and carcinogenesis in skin, breast and colon. Thus,it is logical to speculate that inhibiting arachidonic acid metabolismand/or ODC activity shall result in an inhibition of tumorigenesis. Inaddition, curcumin has also been shown to cleave β-catenin, whichimpairs Wnt signaling and cell–cell adhesion pathways, which arecritical in the development and promotion of many types of tumorsincluding colorectal cancer [84]. Curcumin also induced downregula-tion of cyclin D1 expression and CDK-4 activity in breast andsquamous cell carcinoma cell lines [85]. The suppression of cyclin
337R.M. Srivastava et al. / International Immunopharmacology 11 (2011) 331–341
D1 by curcumin led to inhibition of CDK-4 mediated phosphorylationof retinoblastoma, which is a crucial step for the cell to pass throughthe G1 phase of cell cycle and become transformed [86].
In addition to its inhibitory effects on neoplastic transformation,curcumin has been shown to induce apoptosis in tumor cells byvarious mechanisms, which include impairment of the ubiquitinproteasome pathway, upregulation of proto-oncoprotein Bax, activa-tion of caspases and induction of Fas receptor aggregation in a Fasligand dependent manner and the generation of free radicals [87–90].One of the several possible mechanisms of apoptosis induction bycurcumin involves the inhibition of proteasome complex. In mouseneuro 2a cells, exposure to curcumin revealed a dose dependentdecrease in the proteasome activity and an increase in theubiquitinated proteins. Curcumin also decreased the turnover of thedestabilized enhanced green fluorescent protein suggesting aninhibition of the cellular proteasome machinery [90]. Another modeof apoptosis induction by curcumin involves the upregulation of p53in tumor cells. In human basal cell carcinoma, apoptosis induction bycurcumin resulted in induction of p53 and its downstream targets,p21 waf1/cip1 and GADD45, which are known to regulate apoptosisunder stress conditions [91]. Work in our laboratory has shown thatcurcumin induced apoptosis involves the production of reactiveoxygen intermediates (ROIs) and involves activation of caspase-3[87]. A large number of reports confirm that curcumin induced typicalapoptotic mode of cell death in a wide variety of tumors completewith mitochondrial depolarization and caspase-3 activation. Howev-er, some studies suggest that apoptosis induced by curcumin isindependent of caspase-3 [92,93]. Curcumin has also been reported toinduce an apoptosis like pathway, which is independent of not onlycaspases but mitochondria as well [93]. These effects of curcumin inJurkat T cells were accompanied by DNA fragmentation into high butnot low molecular weight fragments and the frequency of opening ofthe mitochondrial permeability transition pores in curcumin-treatedcells was decreased compared to the control untreated cells. However,one of the most commonly shown effects of curcumin on tumors is itsability to induce the opening of mitochondrial permeability transitionpore, which in turn induces the collapse of the mitochondrialmembrane potential, respiration impairment ultimately leading tocell death [94,95]. This observed difference in curcumin's action withrespect to the opening of permeability transition pore could beattributed to the large difference in its concentrations that were usedduring these studies.
8.2. Curcumin in cardiovascular disease
The therapeutic effects of curcumin in the development andprogression of cardiovascular disease have been studied to somedepth in the last decade. Owing to its ability to regulate oxidant stress,curcumin has been shown to be effective against cardiac hypertrophy,cardiomyocyte apoptosis following myocardial infarction and ische-mia/reperfusion injury [96–98]. Cardiac hypertrophy is the remodel-ing of the left ventricle following pressure or volume overload thatresults in ventricular wall thickening and an increase in overallcardiac dimensions. It begins as a compensatory process that becomesmaladaptive over time and leads to heart failure [99,100]. Develop-ment of hypertrophy involves activation of the calcium and redoxsensitive transcription factor NF-AT that brings about the metabolicand biochemical changes within the cardiomyocyte [101]. Transcrip-tional activation associated with hypertrophy has been recentlyshown to be regulated by acetylation and deacetylation events athistone lysine tails [102]. Acetylation and deacetylation of histones iscarried out by enzymes called histone acetyl transferases (HATs) andhistone deacetylases (HDACs), respectively. Various HDACs have beenimplicated in the pathogenesis of cardiac hypertrophy. For example,loss of class 2 HDAC results in development of hypertrophy while lossof class-1 HDAC confers resistance to hypertrophic growth [102,103].
Morimoto et al. studied the effects of curcumin on HAT andprogression of hypertrophy and subsequent decompensated heartfailure. They have shown that exposure of isolated neonatal ratcardiomyocytes (NRCMs) to 5 or 10 μM curcumin completelysuppressed the induction of hypertrophic response following phen-ylephrine treatment, a known inducer of cardiac hypertrophy [97]. Inan in-vivo setting also, administration of curcumin prevented thedevelopment of hypertension induced heart failure in salt sensitiveDahl rat model of hypertension [97]. These data strongly suggest thatcurcumin possesses anti-hypertrophic properties both in-vitro and in-vivo. It has been proposed that curcumin may inhibit hypertrophicremodeling by two mechanisms (i) by inhibition of histoneacetylation through inhibition of HATs and (ii) by disrupting p300/GATA4 transcriptional complex through a completely independentmechanism. Curcumin has also been shown to inhibit p300 mediatedacetylation of p53, both in-vitro as well as in-vivo [104]. Similarly,inhibition of NF-κB by curcumin could also be involved in the anti-hypertrophic effects of curcumin since NF-κB signaling is involved incardiomyocyte hypertrophy [105].
Oxidative stress is a major outcome determinant in myocardialinfarction and ischemia/reperfusion and curcumin's anti-oxidantproperty has been shown to prevent isoproterenol induced myocar-dial necrosis in rats [106]. In models of experimentally inducedmyocardial infarctions such as isoproterenol treatment, decrease inlysosomal stability leading to increase in lysosomal autolytic enzymeshas been reported [107,108]. Curcumin has been shown to stabilizemembranes and thereby suppress the infarct induced increase inmyocardial lysosomal enzymes [109,110]. Besides, the generation offree radicals following ischemia/reperfusion can also be controlled bycurcumin due to its strong anti-oxidant properties.
The cardiotoxicity associated with doxorubicin, a potent drug fortreatment of a broad array of cancers, is a major concern for cancerpatients [111]. Animal studies have shown that doxorubicin treatmentinduces free radical generation and p53 activation, decreases glutathi-one and increases serum peroxidase and catalase [96,112]. Curcumintreatment significantly attenuated the cardiotoxic effects of doxorubicin[113]. The beneficial effect of curcumin in blockade of doxorubicincardiotoxicity can be linked to modulation of intracellular redox statusby curcumin. In a study by Feng et al., curcumin completely abrogatedthe induction of glucose induced hypertrophy in cardiomyocytes [114].Glucose induced cardiomyocyte hypertrophy is mediated by p300upregulation and subsequent activation of p300 dependent transcrip-tion factors. Since, curcumin can inhibit p300, exposure to curcuminprevented the induction of p300 mediated hypertrophic response incardiomyocytes [114]. In human patients curcumin could markedlyreduce the generation of glucose induced reactive oxygen species (ROS)in red blood cells. Myocardial tissue from diabetic rats exhibited higherlevels of eNOS and iNOS mRNA and curcumin treatment considerablyinhibited the upregulation in both eNOS and iNOS transcript levels[115]. Collectively, these studies have established the usefulness ofcurcumin in the treatment of various cardiovascular ailments. However,caution need to be exercised while reproducing curcumin's anti-tumoreffects in the cardiovascular system due to the extremely differentmetabolic and biochemical nature of the two cell types. The molecularpathways targeted by curcumin in tumor cellsmay not be targeted at allin the cardiomyocytes or may be modulated in a markedly differentmanner so as to drastically change the physiological outcome. One ofmost important difference between the two cell types is the metabolicsignature; tumor cells have a higher dependence on glycolysis whilecardiomyocytes mainly depend on lipid oxidation for their metabolicneeds. Similarly, the proteome and the transcriptome within cardio-myocytes are regulated quite differently than in a transformed cell type.This calls for a careful examination and analysis of curcumin dosagealong with mechanistic details of its physiological effects withindifferent cell types before establishing curcumin in any independentor combinatorial drug regimen.
338 R.M. Srivastava et al. / International Immunopharmacology 11 (2011) 331–341
8.3. Curcumin in neurodegenerative disease
Brain is perhaps the most susceptible organ to oxidative damagedue to the highly oxidative intracellular environment of the neuronsand glial cells [116]. Oxidative stress has been shown to increase bothwith normal brain ageing as well as with brain injury [117,118]. ROSgeneration in the brain can enhance the production of nitric oxide byactivating neuronal nNOS and iNOS. Nitric oxide is a known mediatorof glutamatergic transmission and has been shown to be involved inageing and age related neurodegenerative disorders [117]. Accumu-lation of redox active metals such as iron, copper and zinc, due to highlevels of ascorbic acid in the brain that facilitates redox metalreactions, aggravates the oxidative load in the brain [119]. Anelevation in the free radicals and oxidative stress in turn inducesthe activation of NF-κB and other inflammatory molecules such as IL-1β and TNF-α [120,121]. The neuroprotective effects of curcuminhave been described in a variety of stress models. In an oxidativedamage induced neurodegeneration model, Guangwei et al. haveshown the ability of curcumin to attenuate acrylonitrile inducedoxidative damage in the brain [122]. In this study, curcumin dose of100 mg/kg of body weight prevented lipid peroxidation and gluta-thione depletion in response to acrylonitrile exposure. In anotherstudy, curcumin could increase the cholinergic activity of neurons andfree radical scavenging in streptozotocin induced dementia in rats[123]. The ability of curcumin to increase cholinergic activity in thebrain is mediated by an increase in the acetylcholinesterase enzyme. Ithas been previously reported that curcumin attenuated diabeticencephalopathy by a similar free radical scavenging effect andincrease in acetylcholinesterase activity [124].
Acute traumatic brain injury results in a widespread ‘secondarybrain damage’ following the primary mechanical damage. One of themost critical mediators of the rather chronic secondary brain injury isthe oxygen derived free radical species. Kontos and Povlishock haveshown upregulation of the superoxide radical (O2−) in the brainmicrovasculature immediately following acute injury [125,126]. Thesuperoxide radical can be generated from various enzymatic reactionssuch as arachidonic acid cascade, oxidation of amine neurotransmit-ters, mitochondrial leakage and xanthine oxidase activity [127]. Theability of curcumin to sacavenge oxygen derived free radicals has beenimplicated in its potential as a neuroprotective agent. Dietarycurcumin supplementation has been shown to maintain energyhomeostasis after brain trauma [128]. Cerebral edema, a cause ofincreased intracranial pressure and poor clinical outcome after acutebrain injury, was significantly controlled by pretreatment (75–150 mg/kg body weight) as well as post treatment (300 mg/kg bodyweight) with curcumin [129]. The protective effects of curcumin wereassociated with inhibition of IL-1β expression and inhibition ofaquaporin-4 induction. Wakade et al. have shown that curcumin canattenuate vascular inflammation following subarachnoid hemorrhagewhile another study by Zhao et al. has described neuroprotectionconferred by curcumin after cerebral ischemia [130,131]. Thesefindings support the notion that intervention with curcumintreatment at any point during the brain injury can change the clinicaloutcome.
Effects of curcumin on the pathophysiology of Alzheimer's diseasehave been studied somewhat extensively and several groups haveshown its ability to inhibit Aβ-plaque formation [132,133]. In a mousemodel of Alzheimer's disease, low doses of curcumin (160 ppm)decreased the plaque burden and reduced the soluble as well asinsoluble forms of Aβ by about 50% [134]. Yang et al. have describedthe ability of curcumin to inhibit the formation of Aβ-oligomers. Theyhave also shown that curcumin can bind to the amyloid plaques andsignificantly reduce in-vivo plaque formation [135]. They have earliershown the efficacy of curcumin in reducing CNS lipid peroxidationand iNOS [136], which in turn can lower the oxidative stress. One ofthe possible mechanisms suggested in curcumin's ability to inhibit
plaque formation is the high affinity with which it binds redoxreactive metals such as copper and iron and therefore may act as apotent anti-oxidant by chelating redox reactive metals [137]. Amyloidplaque burden has been associated with depolarizing of the neuronalmembrane and enhanced glutamate-mediated excitotoxicity[138,139] that results in impaired electrical firing of the neurons.Curcumin administration has been shown to prevent misfiring ofneurons following Aβ burden in embryonic hippocampal neurons[140]. In nitrosourea induced neurotoxicity, curcumin administrationprevented increase in the activity of glucose metabolic pathwayenzymes including hexokinase, LDH and SDH [141]. Similarly, inmercury induced neurotoxicity, pretreatment with curcumin abro-gated the increase in metallothinine mRNA and suppressed the toxicand oxidative stress load following mercury exposure in rats [142].Cumulatively, these studies suggest that curcumin can help inmaintaining the oxidative intraneuronal environment and therebyprotect brain from a variety of oxidative, toxic and mechanicalinjuries.
8.4. Immunomodulatory action of curcumin in the prevention ofinflammatory diseases
Curcumin administration has been shown to be associated with apositive outcome in a large number of chronic inflammatory diseasesdue to its ability to inhibit NF-κB activation and subsequent inflamma-tory pathways. Starting with its use in biliary disease in 1937, curcuminhas now been shown to ameliorate almost all kinds of liver toxicity anddisease. Curcumin can inhibit the increase in serum ALT and ASTenzymes following iron induced liver toxicity [143]. The biochemicaland histopathological changes induced by ethanol toxicity wereabrogated by curcumin administration [144]. Curcumin could alsoprotect against thiodoacetamide induced hepatitis and cirrhosis in rats.It also protected against carbon tetrachloride induced livertoxicity andreversed carbon tetrachloride induced cirrhosis [145]. The underlyingmechanism for the effects of curcumin on liver involves its ability to actas an oxidant and inhibit NFκB activation thereby inhibiting theinflammatory signaling cascade. Curcumin could protect againstdinitrobenzene sulfonic acid induced model of murine colitis bysuppressing p38 kinase and IL-1β activation [146]. In a similar murinemodel of inflammatory bowel disease, intragastric administration ofcurcumin inhibted the increase in intestinal neutrophil infiltration andserine protease activity, suggesting its promising therapeutic potentialin the treatment of inflammatory bowel disease [147]. Rheumatoidarthritis is another chronic pro-inflammatory disease that has beenshown to be targeted by curcumin. Several studies have reported thephysiologically beneficial effects of curcumin in the management ofrheumatoid arthritis [148,149]. These studies have shown the ability ofcurcumin to inhibit the increase in serum acidic glycoproteins andmatrix metalloproteinase expression that is generally associated withthe progression of disease in rheumatoid arthritis patients. Decreasedapoptosis of synovial fibroblasts is one of causes for joint inflammationand stiffness in rheumatoid arthritis patients and Park et al. have shownthat curcumin could induce apoptosis in synovial fibroblast byupregulation of proapoptotic genes including bax and a simultaneousdownregulation of anti-apoptotic genes including bcl-2 and XIAP [150].
Chronic inflammatory bowel disease is a life threatening diseasethat affects children and adults. Elevated level of pp38 kinase wasseen in the intestinal mucosa of ulcerative colitis and Crohn's diseasebiopsies, which was inhibited by curcumin (5–20 μM) ex-vivo.Curcumin suppressed the production of pro-inflammatory cytokineIL-1β and enhanced the production of IL-10 in the ex-vivo culturedmucosal biopsies. However, it had modest yet consistent effect on thereduction of IL-1β level [151]. Due to its strong inhibitory effects oncyclooxygenases1 and cyclooxygeanse-2, lipoxygenase, TNF-α, IFN-γ,iNOS and NF-κB, curcumin (360 mg/dose; 3 or 4 times/day for threemonths) showed promising response in patients and could reduce

339R.M. Srivastava et al. / International Immunopharmacology 11 (2011) 331–341
clinical relapse in patientswith quiescent inflammatory bowel disease[152]. TNF-α plays instrumental role in the pathogenesis of inflamma-tory skin disorder psoriasis and since curcumin is a strong anti-inflammatory agent, its action in the HaCa T keratinocytes wasinvestiagted. Curcumin (20 μM) aborted the TNF-α induced expressionof IL-1β, IL-6, IL-8 and TNF-α in keratinocytes. Curcumin also blockedthe activation of NF-κBp65, pJNK, pp38 kinase activation and down-regulated Cyclin E level. Without modulating the TNF receptor I and IIexpression, TNF-α induced activation of NF-κB in human umbilical veinendothelial cells was blocked by curcumin. Also, curcumin inhibited thepJNK level, pP38 kinase level and STAT-3 activation alongwith loweringthe intracellular ROS level. The expression of ICAM-1, MCP-1, and IL-8 was attenuated by curcumin at both mRNA and protein level. Thesestudies indicate the protective effect of curcumin in the treatment ofvarious pro-inflammatory diseases [153].
9. Concluding remarks and future perspectives
Immunomodulatory properties of curcumin are mostly immuno-suppressive, but in some cases immunostimulative effects have beenreported. Although studies with inflammatory disease might directthe investigators towards the exploration of only immunosuppressiveproperties of curcumin, caution shall be exercised regarding theimmunostimulative effect of curcumin. Due to the potent neoplastic,anti-inflammatory and immunoactivating properties, studying themechanism of the action of curcumin is an intriguing challenge.Defining the basis of the appropriate concentration in the host for theeffective therapeutic response, synthesis of curcumin analogues withimproved properties and the effect of curcumin on the cross-talkamong activated lymphocytes are some of the direct questions thatremain to be answered.
References
[1] Singh S, Khar A. Biological effects of curcumin and its role in cancerchemoprevention and therapy. Anticancer Agents Med Chem 2006;6(3):259–70.
[2] Egan ME, Pearson M, Weiner SA, Rajendran V, Rubin D, Glockner-Pagel J, et al.Curcumin, amajor constituent of turmeric, corrects cystic fibrosis defects. Science2004;304(5670):600–2.
[3] Mall M, Kunzelmann K. Correction of the CF defect by curcumin: hypes anddisappointments. Bioessays 2005;27(1):9–13.
[4] Fiala M, Liu PT, Espinosa-Jeffrey A, Rosenthal MJ, Bernard G, Ringman JM, et al.Innate immunity and transcription of MGAT-III and Toll-like receptors inAlzheimer's disease patients are improved by bisdemethoxycurcumin. ProcNatl Acad Sci USA 2007;104(31):12849–54.
[5] Hsu CH, Cheng AL. Clinical studies with curcumin. Adv Exp Med Biol 2007;595:471–80.
[6] Miriyala S, Panchatcharam M, Rengarajulu P. Cardioprotective effects ofcurcumin. Adv Exp Med Biol 2007;595:359–77.
[7] Weisberg SP, Leibel R, Tortoriello DV. Dietary curcumin significantly improvesobesity-associated inflammation and diabetes in mouse models of diabesity.Endocrinology 2008;149(7):3549–58.
[8] Gafner S, Lee SK, Cuendet M, Barthelemy S, Vergnes L, Labidalle S, et al. Biologicevaluation of curcumin and structural derivatives in cancer chemopreventionmodel systems. Phytochemistry 2004;65(21):2849–59.
[9] Hong J, Bose M, Ju J, Ryu JH, Chen X, Sang S, et al. Modulation of arachidonic acidmetabolism by curcumin and related beta-diketone derivatives: effects oncytosolic phospholipase A(2), cyclooxygenases and 5-lipoxygenase. Carcinogen-esis 2004;25(9):1671–9.
[10] Coronella-Wood J, Terrand J, Sun H, Chen QM. c-Fos phosphorylation induced byH2O2 prevents proteasomal degradation of c-Fos in cardiomyocytes. J Biol Chem2004;279(32):33567–74.
[11] Bykov VJ, Lambert JM, Hainaut P, Wiman KG. Mutant p53 rescue and modulationof p53 redox state. Cell Cycle 2009;8(16):2509–17.
[12] Sabapathy K, Klemm M, Jaenisch R, Wagner EF. Regulation of ES celldifferentiation by functional and conformational modulation of p53. EMBO J1997;16(20):6217–29.
[13] Shaulian E, Karin M. AP-1 in cell proliferation and survival. Oncogene 2001;20(19):2390–400.
[14] Shaulian E, KarinM.AP-1as a regulator of cell life anddeath.Nat Cell Biol 2002;4(5):E131–6.
[15] Burhans WC, Heintz NH. The cell cycle is a redox cycle: linking phase-specifictargets to cell fate. Free Radic Biol Med 2009;47(9):1282–93.
[16] Lao CD, Ruffin MTt, Normolle D, Heath DD, Murray SI, Bailey JM. Dose escalationof a curcuminoid formulation. BMC Complement Altern Med 2006;6:10.
[17] Jurenka JS. Anti-inflammatory properties of curcumin, a major constituent ofCurcuma longa: a review of preclinical and clinical research. Altern Med Rev2009;14(2):141–53.
[18] Sikora E, Bielak-Zmijewska A, Piwocka K, Skierski J, Radziszewska E. Inhibition ofproliferation and apoptosis of human and rat T lymphocytes by curcumin, a currypigment. Biochem Pharmacol 1997;54(8):899–907.
[19] Magalska A, Brzezinska A, Bielak-Zmijewska A, Piwocka K, Mosieniak G, SikoraE. Curcumin induces cell death without oligonucleosomal DNA fragmentationin quiescent and proliferating human CD8+ cells. Acta Biochim Pol 2006;53(3):531–8.
[20] Sikora E, Bielak-Zmijewska A, Magalska A, Piwocka K, Mosieniak G, KalinowskaM, et al. Curcumin induces caspase-3-dependent apoptotic pathway but inhibitsDNA fragmentation factor 40/caspase-activated DNase endonuclease in humanJurkat cells. Mol Cancer Ther 2006;5(4):927–34.
[21] Deters M, Knochenwefel H, Lindhorst D, Koal T, Meyer HH, Hansel W, et al.Different curcuminoids inhibit T-lymphocyte proliferation independently oftheir radical scavenging activities. Pharm Res 2008;25(8):1822–7.
[22] Ranjan D, Johnston TD, Wu G, Elliott L, Bondada S, Nagabhushan M. Curcuminblocks cyclosporine A-resistant CD28 costimulatory pathway of human T-cellproliferation. J Surg Res 1998;77(2):174–8.
[23] Shirley SA, Montpetit AJ, Lockey RF, Mohapatra SS. Curcumin prevents humandendritic cell response to immune stimulants. Biochem Biophys Res Commun2008;374(3):431–6.
[24] Gao X, Kuo J, Jiang H, Deeb D, Liu Y, Divine G, et al. Immunomodulatory activity ofcurcumin: suppression of lymphocyte proliferation, development of cell-mediated cytotoxicity, and cytokine production in vitro. Biochem Pharmacol2004;68(1):51–61.
[25] Varalakshmi C, Ali AM, Pardhasaradhi BV, Srivastava RM, Singh S, Khar A.Immunomodulatory effects of curcumin: in-vivo. Int Immunopharmacol 2008;8(5):688–700.
[26] Churchill M, Chadburn A, Bilinski RT, Bertagnolli MM. Inhibition of intestinaltumors by curcumin is associated with changes in the intestinal immune cellprofile. J Surg Res 2000;89(2):169–75.
[27] Bhattacharyya S, Mandal D, Sen GS, Pal S, Banerjee S, Lahiry L, et al. Tumor-induced oxidative stress perturbs nuclear factor-kappaB activity-augmentingtumor necrosis factor-alpha-mediated T-cell death: protection by curcumin.Cancer Res 2007;67(1):362–70.
[28] Bhattacharyya S, Mandal D, Saha B, Sen GS, Das T, Sa G. Curcumin preventstumor-induced T cell apoptosis through Stat-5a-mediated Bcl-2 induction. J BiolChem 2007;282(22):15954–64.
[29] Bhattacharyya S, Md Sakib Hossain D, Mohanty S, Sankar Sen G, Chattopadhyay S,Banerjee S, et al. Curcumin reverses T cell-mediated adaptive immunedysfunctions in tumor-bearing hosts. Cell Mol Immunol 2010;7(4):306–15.
[30] Fahey AJ, Adrian Robins R, Constantinescu CS. Curcumin modulation of IFN-betaand IL-12 signalling and cytokine induction in human T cells. J Cell Mol Med2007;11(5):1129–37.
[31] Xie L, Li XK, Funeshima-Fuji N, Kimura H, Matsumoto Y, Isaka Y, et al.Amelioration of experimental autoimmune encephalomyelitis by curcumintreatment through inhibition of IL-17 production. Int Immunopharmacol2009;9(5):575–81.
[32] Chearwae W, Bright JJ. 15-deoxy-Delta(12, 14)-prostaglandin J(2) and curcuminmodulate the expression of toll-like receptors 4 and 9 in autoimmune Tlymphocyte. J Clin Immunol 2008;28(5):558–70.
[33] Natarajan C, Bright JJ. Curcumin inhibits experimental allergic encephalomyelitisby blocking IL-12 signaling through Janus kinase-STAT pathway in T lympho-cytes. J Immunol 2002;168(12):6506–13.
[34] Moon DO, Kim MO, Choi YH, Park YM, Kim GY. Curcumin attenuatesinflammatory response in IL-1beta-induced human synovial fibroblasts andcollagen-induced arthritis in mouse model. Int Immunopharmacol 2010;10(5):605–10.
[35] Kim GY, Kim KH, Lee SH, Yoon MS, Lee HJ, Moon DO, et al. Curcumin inhibitsimmunostimulatory function of dendritic cells: MAPKs and translocation of NF-kappa B as potential targets. J Immunol 2005;174(12):8116–24.
[36] Jung ID, Jeong YI, Lee CM, Noh KT, Jeong SK, Chun SH, et al. COX-2 and PGE2signaling is essential for the regulation of IDO expression by curcumin inmurine bone marrow-derived dendritic cells. Int Immunopharmacol 2010;10(7):760–8.
[37] Platt CD, Ma JK, Chalouni C, Ebersold M, Bou-Reslan H, Carano RA, et al. Maturedendritic cells use endocytic receptors to capture and present antigens. Proc NatlAcad Sci USA 2010;107(9):4287–92.
[38] Kang G, Kong PJ, Yuh YJ, Lim SY, Yim SV, Chun W, et al. Curcumin suppresseslipopolysaccharide-induced cyclooxygenase-2 expression by inhibiting activatorprotein 1 and nuclear factor kappab bindings in BV2 microglial cells. J PharmacolSci 2004;94(3):325–8.
[39] Frasca L, Nasso M, Spensieri F, Fedele G, Palazzo R, Malavasi F, et al. IFN-gammaarms human dendritic cells to perform multiple effector functions. J Immunol2008;180(3):1471–81.
[40] Jeong YI, Kim SW, Jung ID, Lee JS, Chang JH, Lee CM, et al. Curcumin suppressesthe induction of indoleamine 2, 3-dioxygenase by blocking the Janus-activatedkinase-protein kinase Cdelta-STAT1 signaling pathway in interferon-gamma-stimulated murine dendritic cells. J Biol Chem 2009;284(6):3700–8.
[41] Cong Y, Wang L, Konrad A, Schoeb T, Elson CO. Curcumin induces the tolerogenicdendritic cell that promotes differentiation of intestine-protective regulatory Tcells. Eur J Immunol 2009;39(11):3134–46.
[42] Larmonier CB, Uno JK, Lee KM, Karrasch T, Laubitz D, Thurston R, et al. Limitedeffects of dietary curcumin on Th-1 driven colitis in IL-10 deficient mice suggest

340 R.M. Srivastava et al. / International Immunopharmacology 11 (2011) 331–341
an IL-10-dependent mechanism of protection. Am J Physiol Gastrointest LiverPhysiol 2008;295(5):G1079–91.
[43] South EH, Exon JH, Hendrix K. Dietary curcumin enhances antibody response inrats. Immunopharmacol Immunotoxicol 1997;19(1):105–19.
[44] Yadav VS, Mishra KP, Singh DP, Mehrotra S, Singh VK. Immunomodulatory effectsof curcumin. Immunopharmacol Immunotoxicol 2005;27(3):485–97.
[45] Bill MA, Bakan C, Benson Jr DM, Fuchs J, Young G, Lesinski GB. Curcumin inducesproapoptotic effects against human melanoma cells and modulates the cellularresponse to immunotherapeutic cytokines. Mol Cancer Ther 2009;8(9):2726–35.
[46] Bhaumik S, Jyothi MD, Khar A. Differential modulation of nitric oxide productionby curcumin in host macrophages and NK cells. FEBS Lett 2000;483(1):78–82.
[47] Zhang HG, Kim H, Liu C, Yu S, Wang J, Grizzle WE, et al. Curcumin reverses breasttumor exosomes mediated immune suppression of NK cell tumor cytotoxicity.Biochim Biophys Acta 2007;1773(7):1116–23.
[48] Kumar A, Dhawan S, Hardegen NJ, Aggarwal BB. Curcumin (Diferuloylmethane)inhibition of tumor necrosis factor (TNF)-mediated adhesion of monocytes toendothelial cells by suppression of cell surface expression of adhesion moleculesand of nuclear factor-kappaB activation. Biochem Pharmacol 1998;55(6):775–83.
[49] Abe Y, Hashimoto S, Horie T. Curcumin inhibition of inflammatory cytokineproduction by human peripheral blood monocytes and alveolar macrophages.Pharmacol Res 1999;39(1):41–7.
[50] Lim JH, Kwon TK. Curcumin inhibits phorbol myristate acetate (PMA)-inducedMCP-1 expression by inhibiting ERK and NF-kappaB transcriptional activity. FoodChem Toxicol 2010;48(1):47–52.
[51] Bisht K, Choi WH, Park SY, Chung MK, Koh WS. Curcumin enhances non-inflammatory phagocytic activity of RAW264.7 cells. Biochem Biophys ResCommun 2009;379(2):632–6.
[52] Antony S, Kuttan R, Kuttan G. Immunomodulatory activity of curcumin. ImmunolInvestig 1999;28(5–6):291–303.
[53] Rajakrishnan V, Shiney SJ, Sudhakaran PR, Menon VP. Effect of curcumin onethanol-induced stress on mononuclear cells. Phytother Res 2002;16(2):171–3.
[54] Matsuguchi T, Musikacharoen T, Ogawa T, Yoshikai Y. Gene expressions of Toll-like receptor 2, but not Toll-like receptor 4, is induced by LPS and inflammatorycytokines in mouse macrophages. J Immunol 2000;165(10):5767–72.
[55] Kim AN, Jeon WK, Kim BC. Up-regulation of heme oxygenase-1 expressionthrough CaMKII-ERK1/2-Nrf2 signaling mediates the anti-inflammatory effect ofbisdemethoxycurcumin in LPS-stimulated macrophages. Free Radic Biol Med2010;49(3):323–31.
[56] Sumanont Y, Murakami Y, Tohda M, Vajragupta O, Matsumoto K, Watanabe H.Evaluation of the nitric oxide radical scavenging activity of manganesecomplexes of curcumin and its derivative. Biol Pharm Bull 2004;27(2):170–3.
[57] Jain SK, Rains J, Croad J, Larson B, Jones K. Curcumin supplementation lowersTNF-alpha, IL-6, IL-8, and MCP-1 secretion in high glucose-treated culturedmonocytes and blood levels of TNF-alpha, IL-6, MCP-1, glucose, and glycosylatedhemoglobin in diabetic rats. Antioxid Redox Signal 2009;11(2):241–9.
[58] Lai JJ, Lai KP, Chuang KH, Chang P, Yu IC, Lin WJ, et al. Monocyte/macrophageandrogen receptor suppresses cutaneous wound healing in mice by enhancinglocal TNF-alpha expression. J Clin Invest 2009;119(12):3739–51.
[59] Giri RK, Selvaraj SK, Kalra VK. Amyloid peptide-induced cytokine and chemokineexpression in THP-1 monocytes is blocked by small inhibitory RNA duplexes forearly growth response-1 messenger RNA. J Immunol 2003;170(10):5281–94.
[60] Hamaguchi T, Ono K, Yamada M. Curcumin and Alzheimer's Disease. CNSNeurosci Ther 2010;16(5):285–97.
[61] Giri RK, Rajagopal V, Kalra VK. Curcumin, the active constituent of turmeric,inhibits amyloid peptide-induced cytochemokine gene expression and CCR5-mediated chemotaxis of THP-1 monocytes by modulating early growthresponse-1 transcription factor. J Neurochem 2004;91(5):1199–210.
[62] Decote-Ricardo D, Chagas KK, Rocha JD, Redner P, Lopes UG, Cambier JC, et al.Modulation of in vitro murine B-lymphocyte response by curcumin. Phytome-dicine 2009;16(10):982–8.
[63] Sharma S, Chopra K, Kulkarni SK, Agrewala JN. Resveratrol and curcuminsuppress immune response through CD28/CTLA-4 and CD80 co-stimulatorypathway. Clin Exp Immunol 2007;147(1):155–63.
[64] Kuramoto Y, Yamada K, Tsuruta O, Sugano M. Effect of natural food colorings onimmunoglobulin production in vitro by rat spleen lymphocytes. Biosci BiotechnolBiochem 1996;60(10):1712–3.
[65] Ranjan D, Siquijor A, Johnston TD, Wu G, Nagabhuskahn M. The effect ofcurcumin on human B-cell immortalization by Epstein–Barr virus. Am Surg1998;64(1):47–51 discussion-2.
[66] Ranjan D, Johnston TD, Reddy KS, Wu G, Bondada S, Chen C. Enhanced apoptosismediates inhibition of EBV-transformed lymphoblastoid cell line proliferation bycurcumin. J Surg Res 1999;87(1):1–5.
[67] Buchner M, Fuchs S, Prinz G, Pfeifer D, Bartholome K, Burger M, et al. Spleentyrosine kinase is overexpressed and represents a potential therapeutic target inchronic lymphocytic leukemia. Cancer Res 2009;69(13):5424–32.
[68] Haque S, Lee H, Waqas B, Chiorazzi N, Mongini P. Anti-inflammatory curcumininhibits AID expression within cycling human B cells. J Immunol 2010;184(Apr):96.21.
[69] Srivastava R. Inhibition of neutrophil response by curcumin. Agents Actions1989;28(3–4):298–303.
[70] Jancinova V, Perecko T, Nosal R, Kostalova D, Bauerova K, Drabikova K. Decreasedactivity of neutrophils in the presence of diferuloylmethane (curcumin) involvesprotein kinase C inhibition. Eur J Pharmacol 2009;612(1–3):161–6.
[71] Jackson JK, Higo T, Hunter WL, Burt HM. The antioxidants curcumin andquercetin inhibit inflammatory processes associated with arthritis. Inflamm Res2006;55(4):168–75.
[72] Madan B, Ghosh B. Diferuloylmethane inhibits neutrophil infiltration andimproves survival of mice in high-dose endotoxin shock. Shock 2003;19(1):91–6.
[73] Takahashi M, Ishiko T, Kamohara H, Hidaka H, Ikeda O, Ogawa M, et al. Curcumin(1, 7-bis(4-hydroxy-3-methoxyphenyl)-1, 6-heptadiene-3, 5-dione) blocks thechemotaxis of neutrophils by inhibiting signal transduction through IL-8 receptors. Mediat Inflamm 2007;2007:10767.
[74] Lian Q, Li X, Shang Y, Yao S, Ma L, Jin S. Protective effect of curcumin onendotoxin-induced acute lung injury in rats. J Huazhong Univ Sci Technolog MedSci 2006;26(6):678–81.
[75] Moon DO, KimMO, Lee HJ, Choi YH, Park YM, Heo MS, et al. Curcumin attenuatesovalbumin-induced airway inflammation by regulating nitric oxide. BiochemBiophys Res Commun 2008;375(2):275–9.
[76] Lee JH, Kim JW, Ko NY, Mun SH, Her E, Kim BK, et al. Curcumin, a constituent ofcurry, suppresses IgE-mediated allergic response and mast cell activation at thelevel of Syk. J Allergy Clin Immunol 2008;121(5):1225–31.
[77] Kurup VP, Barrios CS. Immunomodulatory effects of curcumin in allergy. MolNutr Food Res 2008;52(9):1031–9.
[78] Yeh CH, Chen TP, Wu YC, Lin YM, Jing Lin P. Inhibition of NFkappaB activationwith curcumin attenuates plasma inflammatory cytokines surge and cardio-myocytic apoptosis following cardiac ischemia/reperfusion. J Surg Res 2005;125(1):109–16.
[79] Huang MT, Wang ZY, Georgiadis CA, Laskin JD, Conney AH. Inhibitory effectsof curcumin on tumor initiation by benzo[a]pyrene and 7,12-dimethylbenz[a]anthracene. Carcinogenesis 1992;13(11):2183–6.
[80] Berger AL, Randak CO, Ostedgaard LS, Karp PH, Vermeer DW, Welsh MJ.Curcumin stimulates cystic fibrosis transmembrane conductance regulator Cl−
channel activity. J Biol Chem 2005;280(7):5221–6.[81] Rao CV, Simi B, Reddy BS. Inhibition by dietary curcumin of azoxymethane-
induced ornithine decarboxylase, tyrosine protein kinase, arachidonic acidmetabolism and aberrant crypt foci formation in the rat colon. Carcinogenesis1993;14(11):2219–25.
[82] Hammarstrom S, Hamberg M, Samuelsson B, Duell EA, Stawiski M, Voorhees JJ.Increased concentrations of nonesterified arachidonic acid, 12 L-hydroxy-5, 8,10, 14-eicosatetraenoic acid, prostaglandin E2, and prostaglandin F2alpha inepidermis of psoriasis. Proc Natl Acad Sci USA 1975;72(12):5130–4.
[83] Higgs GA, Salmon JA, Spayne JA. The inflammatory effects of hydroperoxy andhydroxy acid products of arachidonate lipoxygenase in rabbit skin. Br JPharmacol 1981;74(2):429–33.
[84] Jaiswal AS, Marlow BP, Gupta N, Narayan S. Beta-catenin-mediated transactiva-tion and cell–cell adhesion pathways are important in curcumin (diferuyl-methane)-induced growth arrest and apoptosis in colon cancer cells. Oncogene2002;21(55):8414–27.
[85] Mukhopadhyay A, Banerjee S, Stafford LJ, Xia C, Liu M, Aggarwal BB. Curcumin-induced suppression of cell proliferation correlates with down-regulation ofcyclin D1 expression and CDK4-mediated retinoblastoma protein phosphoryla-tion. Oncogene 2002;21(57):8852–61.
[86] Sherr CJ. D-type cyclins. Trends Biochem Sci 1995;20(5):187–90.[87] Khar A, Ali AM, Pardhasaradhi BV, Begum Z, Anjum R. Antitumor activity of
curcumin is mediated through the induction of apoptosis in AK-5 tumor cells.FEBS Lett 1999;445(1):165–8.
[88] Bush JA, Cheung Jr KJ, Li G. Curcumin induces apoptosis in humanmelanoma cellsthrough a Fas receptor/caspase-8 pathway independent of p53. Exp Cell Res2001;271(2):305–14.
[89] Pal S, Choudhuri T, Chattopadhyay S, Bhattacharya A, Datta GK, Das T, et al.Mechanisms of curcumin-induced apoptosis of Ehrlich's ascites carcinoma cells.Biochem Biophys Res Commun 2001;288(3):658–65.
[90] Jana NR, Dikshit P, Goswami A, Nukina N. Inhibition of proteasomal function bycurcumin induces apoptosis through mitochondrial pathway. J Biol Chem2004;279(12):11680–5.
[91] Jee SH, Shen SC, Tseng CR, Chiu HC, Kuo ML. Curcumin induces a p53-dependentapoptosis in human basal cell carcinoma cells. J Invest Dermatol 1998;111(4):656–61.
[92] Samejima K, Tone S, Kottke TJ, Enari M, Sakahira H, Cooke CA, et al. Transitionfrom caspase-dependent to caspase-independent mechanisms at the onset ofapoptotic execution. J Cell Biol 1998;143(1):225–39.
[93] Piwocka K, Zablocki K, Wieckowski MR, Skierski J, Feiga I, Szopa J, et al. A novelapoptosis-like pathway, independent of mitochondria and caspases, induced bycurcumin in human lymphoblastoid T (Jurkat) cells. Exp Cell Res 1999;249(2):299–307.
[94] Crompton M. The mitochondrial permeability transition pore and its role in celldeath. Biochem J 1999;341(Pt 2):233–49.
[95] Morin D, Barthelemy S, Zini R, Labidalle S, Tillement JP. Curcumin induces themitochondrial permeability transition pore mediated by membrane protein thioloxidation. FEBS Lett 2001;495(1–2):131–6.
[96] Yeh PY, Chuang SE, Yeh KH, Song YC, Chang LL, Cheng AL. Phosphorylation of p53on Thr55 by ERK2 is necessary for doxorubicin-induced p53 activation and celldeath. Oncogene 2004;23(20):3580–8.
[97] Morimoto T, Sunagawa Y, Kawamura T, Takaya T, Wada H, Nagasawa A, et al. Thedietary compound curcumin inhibits p300 histone acetyltransferase activity andprevents heart failure in rats. J Clin Invest 2008;118(3):868–78.
[98] Wongcharoen W, Phrommintikul A. The protective role of curcumin incardiovascular diseases. Int J Cardiol 2009;133(2):145–51.
[99] Frey N, Olson EN. Cardiac hypertrophy: the good, the bad, and the ugly. Annu RevPhysiol 2003;65:45–79.
[100] Hill JA, Olson EN. Cardiac plasticity. N Engl J Med 2008;358(13):1370–80.
341R.M. Srivastava et al. / International Immunopharmacology 11 (2011) 331–341
[101] Heineke J, Molkentin JD. Regulation of cardiac hypertrophy by intracellularsignalling pathways. Nat Rev Mol Cell Biol 2006;7(8):589–600.
[102] Backs J, Olson EN. Control of cardiac growth by histone acetylation/deacetylation.Circ Res 2006;98(1):15–24.
[103] Zhang CL, McKinsey TA, Chang S, Antos CL, Hill JA, Olson EN. Class II histonedeacetylases act as signal-responsive repressors of cardiac hypertrophy. Cell2002;110(4):479–88.
[104] Balasubramanyam K, Varier RA, Altaf M, Swaminathan V, Siddappa NB, Ranga U,et al. Curcumin, a novel p300/CREB-binding protein-specific inhibitor ofacetyltransferase, represses the acetylation of histone/nonhistone proteins andhistone acetyltransferase-dependent chromatin transcription. J Biol Chem2004;279(49):51163–71.
[105] Purcell NH, Tang G, Yu C, Mercurio F, DiDonato JA, Lin A. Activation of NF-kappa Bis required for hypertrophic growth of primary rat neonatal ventricularcardiomyocytes. Proc Natl Acad Sci USA 2001;98(12):6668–73.
[106] Manikandan P, Sumitra M, Aishwarya S, Manohar BM, Lokanadam B, Puvanak-rishnan R. Curcumin modulates free radical quenching in myocardial ischaemiain rats. Int J Biochem Cell Biol 2004;36(10):1967–80.
[107] Decker RS, Poole AR, Griffin EE, Dingle JT, Wildenthal K. Altered distribution oflysosomal cathepsin D in ischemic myocardium. J Clin Invest 1977;59(5):911–21.
[108] Takahashi S, Barry AC, Factor SM. Collagen degradation in ischaemic rat hearts.Biochem J 1990;265(1):233–41.
[109] Nirmala C, Puvanakrishnan R. Protective role of curcumin against isoproterenolinduced myocardial infarction in rats. Mol Cell Biochem 1996;159(2):85–93.
[110] Nirmala C, Puvanakrishnan R. Effect of curcumin on certain lysosomal hydrolasesin isoproterenol-induced myocardial infarction in rats. Biochem Pharmacol1996;51(1):47–51.
[111] Doroshow JH. Doxorubicin-induced cardiac toxicity. N Engl J Med 1991;324(12):843–5.
[112] Rajagopalan S, Politi PM, Sinha BK, Myers CE. Adriamycin-induced free radicalformation in the perfused rat heart: implications for cardiotoxicity. Cancer Res1988;48(17):4766–9.
[113] Venkatesan N. Curcumin attenuation of acute adriamycin myocardial toxicity inrats. Br J Pharmacol 1998;124(3):425–7.
[114] Feng B, Chen S, Chiu J, George B, Chakrabarti S. Regulation of cardiomyocytehypertrophy in diabetes at the transcriptional level. Am J Physiol EndocrinolMetab 2008;294(6):E1119–26.
[115] Farhangkhoee H, Khan ZA, Chen S, Chakrabarti S. Differential effects of curcuminon vasoactive factors in the diabetic rat heart. Nutr Metab (Lond) 2006;3:27.
[116] Halliwell B. Reactive oxygen species and the central nervous system. JNeurochem 1992;59(5):1609–23.
[117] Beal MF. Aging, energy, and oxidative stress in neurodegenerative diseases. AnnNeurol 1995;38(3):357–66.
[118] Lu T, Pan Y, Kao SY, Li C, Kohane I, Chan J, et al. Gene regulation and DNA damagein the ageing human brain. Nature 2004;429(6994):883–91.
[119] Zecca L, Youdim MB, Riederer P, Connor JR, Crichton RR. Iron, brain ageing andneurodegenerative disorders. Nat Rev Neurosci 2004;5(11):863–73.
[120] Sarkar D, Fisher PB. Molecular mechanisms of aging-associated inflammation.Cancer Lett 2006;236(1):13–23.
[121] Zipp F, Aktas O. The brain as a target of inflammation: common pathways linkinflammatory and neurodegenerative diseases. Trends Neurosci 2006;29(9):518–27.
[122] Guangwei X, Rongzhu L, Wenrong X, Suhua W, Xiaowu Z, Shizhong W, et al.Curcumin pretreatment protects against acute acrylonitrile-induced oxidativedamage in rats. Toxicology 2010;267(1–3):140–6.
[123] Agrawal R, Mishra B, Tyagi E, Nath C, Shukla R. Effect of curcumin on brain insulinreceptors and memory functions in STZ (ICV) induced dementia model of rat.Pharmacol Res 2010;61(3):247–52.
[124] Kuhad A, Chopra K. Curcumin attenuates diabetic encephalopathy in rats:behavioral and biochemical evidences. Eur J Pharmacol 2007;576(1–3):34–42.
[125] Kontos HA, Wei EP. Superoxide production in experimental brain injury. JNeurosurg 1986;64(5):803–7.
[126] Kontos HA, Povlishock JT. Oxygen radicals in brain injury. Cent Nerv Syst TraumaFall 1986;3(4):257–63.
[127] Hall ED, Vaishnav RA, Mustafa AG. Antioxidant therapies for traumatic braininjury. Neurotherapeutics 2010;7(1):51–61.
[128] Sharma S, Zhuang Y, Ying Z, Wu A, Gomez-Pinilla F. Dietary curcuminsupplementation counteracts reduction in levels of molecules involved inenergy homeostasis after brain trauma. Neuroscience 2009;161(4):1037–44.
[129] Laird MD, Sukumari-Ramesh S, Swift AE, Meiler SE, Vender JR, Dhandapani KM.Curcumin attenuates cerebral edema following traumatic brain injury in mice: apossible role for aquaporin-4? J Neurochem 2010;113(3):637–48.
[130] Zhao J, Zhao Y, Zheng W, Lu Y, Feng G, Yu S. Neuroprotective effect of curcuminon transient focal cerebral ischemia in rats. Brain Res 2008;1229:224–32.
[131] Wakade C, King MD, Laird MD, Alleyne Jr CH, Dhandapani KM. Curcuminattenuates vascular inflammation and cerebral vasospasm after subarachnoidhemorrhage in mice. Antioxid Redox Signal 2009;11(1):35–45.
[132] Smith DG, Cappai R, Barnham KJ. The redox chemistry of the Alzheimer's diseaseamyloid beta peptide. Biochim Biophys Acta 2007;1768(8):1976–90.
[133] Aksenov MY, Markesbery WR. Changes in thiol content and expression ofglutathione redox system genes in the hippocampus and cerebellum inAlzheimer's disease. Neurosci Lett 2001;302(2–3):141–5.
[134] Lim GP, Chu T, Yang F, BeechW, Frautschy SA, Cole GM. The curry spice curcuminreduces oxidative damage and amyloid pathology in an Alzheimer transgenicmouse. J Neurosci 2001;21(21):8370–7.
[135] Yang F, Lim GP, Begum AN, Ubeda OJ, Simmons MR, Ambegaokar SS, et al.Curcumin inhibits formation of amyloid beta oligomers and fibrils, binds plaques,and reduces amyloid in vivo. J Biol Chem 2005;280(7):5892–901.
[136] Cole GG, Kentridge RW, Gellatly AR, Heywood CA. Detectability of onsets versusoffsets in the change detection paradigm. J Vis 2003;3(1):22–31.
[137] Baum L, Ng A. Curcumin interaction with copper and iron suggests one possiblemechanism of action in Alzheimer's disease animal models. J Alzheimers Dis2004;6(4):367–77 discussion 443-9.
[138] Mattson MP, Rydel RE. Beta-amyloid precursor protein and Alzheimer's disease:the peptide plot thickens. Neurobiol Aging 1992;13(5):617–21.
[139] Lipton SA. Paradigm shift in neuroprotection by NMDA receptor blockade:memantine and beyond. Nat Rev Drug Discov 2006;5(2):160–70.
[140] Varghese K, Molnar P, Das M, Bhargava N, Lambert S, Kindy MS, et al. A newtarget for amyloid beta toxicity validated by standard and high-throughputelectrophysiology. PLoS ONE 2010;5(1):e8643.
[141] Singla N, Dhawan DK. Modulation of carbohydrate metabolism during N-methylN-nitrosourea induced neurotoxicity in mice: role of curcumin. Neurochem Res2010;35(4):660–5.
[142] Agarwal R, Goel SK, Behari JR. Detoxification and antioxidant effects of curcuminin rats experimentally exposed to mercury. J Appl Toxicol 2010, doi:10.1002/jat.1517.
[143] Reddy AC, Lokesh BR. Effect of curcumin and eugenol on iron-induced hepatictoxicity in rats. Toxicology 1996;107(1):39–45.
[144] Rajakrishnan V, Viswanathan P, Rajasekharan KN, Menon VP. Neuroprotective roleof curcumin from curcuma longa on ethanol-induced brain damage. Phytother Res1999;13(7):571–4.
[145] Rivera-Espinoza Y, Muriel P. Pharmacological actions of curcumin in liverdiseases or damage. Liver Int 2009;29(10):1457–66.
[146] Salh B, Assi K, Templeman V, Parhar K, Owen D, Gomez-Munoz A, et al. Curcuminattenuates DNB-induced murine colitis. Am J Physiol Gastrointest Liver Physiol2003;285(1):G235–43.
[147] Ukil A, Maity S, Karmakar S, Datta N, Vedasiromoni JR, Das PK. Curcumin, themajor component of food flavour turmeric, reduces mucosal injury intrinitrobenzene sulphonic acid-induced colitis. Br J Pharmacol 2003;139(2):209–18.
[148] Joe B, Rao UJ, Lokesh BR. Presence of an acidic glycoprotein in the serum ofarthritic rats: modulation by capsaicin and curcumin. Mol Cell Biochem1997;169(1–2):125–34.
[149] Onodera S, Kaneda K, Mizue Y, Koyama Y, Fujinaga M, Nishihira J. Macrophagemigration inhibitory factor up-regulates expression of matrix metalloproteinasesin synovial fibroblasts of rheumatoid arthritis. J Biol Chem 2000;275(1):444–50.
[150] Park C, Moon DO, Choi IW, Choi BT, Nam TJ, Rhu CH, et al. Curcumin inducesapoptosis and inhibits prostaglandin E(2) production in synovial fibroblasts ofpatients with rheumatoid arthritis. Int J Mol Med 2007;20(3):365–72.
[151] Epstein J, Docena G, MacDonald TT, Sanderson IR. Curcumin suppresses p38mitogen-activated protein kinase activation, reduces IL-1beta and matrixmetalloproteinase-3 and enhances IL-10 in the mucosa of children and adultswith inflammatory bowel disease. Br J Nutr 2010;103(6):824–32.
[152] Hanai H, Sugimoto K. Curcumin has bright prospects for the treatment ofinflammatory bowel disease. Curr Pharm Des 2009;15(18):2087–94.
[153] Kim YS, Ahn Y, Hong MH, Joo SY, Kim KH, Sohn IS, et al. Curcumin attenuatesinflammatory responses of TNF-alpha-stimulated human endothelial cells. JCardiovasc Pharmacol 2007;50(1):41–9.




















