Bronchovascular Reconstruction for Lung Cancer: Does Induction Chemotherapy Influence the Outcomes?
9
DOI: 10.1016/j.athoracsur.2012.05.050 2012;94:907-913 Ann Thorac Surg Petrella, Alessandro Pardolesi and Lorenzo Spaggiari Domenico Galetta, Piergiorgio Solli, Alessandro Borri, Roberto Gasparri, Francesco Influence the Outcomes? Bronchovascular Reconstruction for Lung Cancer: Does Induction Chemotherapy http://ats.ctsnetjournals.org/cgi/content/full/94/3/907 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2012 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by Domenico Galetta on January 26, 2013 ats.ctsnetjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Bronchovascular Reconstruction for Lung Cancer: Does Induction Chemotherapy Influence the Outcomes?

DOI: 10.1016/j.athoracsur.2012.05.050 2012;94:907-913 Ann Thorac Surg
Petrella, Alessandro Pardolesi and Lorenzo Spaggiari Domenico Galetta, Piergiorgio Solli, Alessandro Borri, Roberto Gasparri, Francesco
Influence the Outcomes?Bronchovascular Reconstruction for Lung Cancer: Does Induction Chemotherapy
http://ats.ctsnetjournals.org/cgi/content/full/94/3/907located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2012 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by Domenico Galetta on January 26, 2013 ats.ctsnetjournals.orgDownloaded from

Bronchovascular Reconstruction for Lung Cancer: DoesInduction Chemotherapy Influence the Outcomes?Domenico Galetta, MD, PhD, Piergiorgio Solli, MD, PhD, Alessandro Borri, MD,Roberto Gasparri, MD, Francesco Petrella, MD, Alessandro Pardolesi, MD, andLorenzo Spaggiari, MD, PhD
Division of Thoracic Surgery, European Institute of Oncology; and University of Milan School of Medicine, Milan, ItalyGEN
ERA
LT
HO
RA
CIC
Background. Bronchoangioplastic interventions (BAIs)for lung cancer are challenging procedures associatedwith a high risk of postoperative morbidity and mortal-ity. The role of induction chemotherapy (IC) in thesepatients is debated.
Methods. We reviewed clinical records of patients whounderwent a BAI between 1998 and 2009 using a prospec-tive clinical and operative database.
Results. Among 47 patients (39 men; mean age, 66years) who underwent BAI, 26 (55.3%) received IC for N2disease or for locally advanced lung cancer. We per-formed 35 pulmonary artery (PA) sleeve resections (31partial and 4 circumferential), 10 PA reconstructions witha pericardial patch (8 autologous, and 2 heterologous),and 2 PA reconstructions using heterologous conduit.The 30-day mortality rate was 4.2% (n � 2). Morbidityoccurred in 19 (40.4%) patients; 5 patients (10.6%) had
major complications (3 [6.4%] patients with fatal bron-European Institute of Oncology, Via Ripamonti, 435, Milan, Italy; e-mail:[email protected].
© 2012 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
by Dats.ctsnetjournals.orgDownloaded from
chovascular fistulas and 1 patient each with cardiacdislocation and acute respiratory distress syndrome)(2.2%). Fourteen patients (29.8%) had minor complica-tions: 6 (12.7%) cardiac, 7 (14.9%) pulmonary, and 1 (2.2%)stroke. IC did not influence the complication rate. Over-all 5-year survival and disease-free survival was 39.2%and 36.9%, respectively. Early pathologic stage and theabsence of nodal involvement significantly influencedsurvival (p � 0.005 and p � 0.002, respectively). Patientsreceiving IC had a better prognosis (62.7% versus 10.7%;p � 0.0003). At multivariate analysis, IC influenced long-term survival (p � 0.003 [95% CI, 2.92–8.56]).
Conclusions. BAIs are feasible and effective surgicalprocedures with acceptable morbidity and mortality. ICdoes not influence morbidity and allows good long-termoutcomes.
(Ann Thorac Surg 2012;94:907–13)
© 2012 by The Society of Thoracic SurgeonsSince the first 1-stage pneumonectomy reported byGraham and Singer in 1933 [1], this procedure re-
mained the preferred therapy for lung cancer for nearly 2decades, becoming the standard treatment for central orlocally advanced non–small-cell lung cancer (NSCLC). Inthe following years, improved definition of the pulmo-nary anatomy [2] permitted anatomic lobar and sublobarresections. By the mid-1950s, lobectomy was accepted asthe gold standard of resection for lung cancers limited toa single anatomic lobe [3, 4]. Since the mid-1970s, con-servative techniques (sleeve lobectomies) have beenwidely accepted in the management of lung cancer, withbest long-term results compared with those reportedafter pneumonectomy [5–8].
In addition, when lung tumors involve the airway aswell as the central vascular structures, in particular thePA, sleeve lobectomy concomitant with PA reconstruc-tion (double sleeve) remains the only alternative topneumonectomy. However this procedure has been lesswidely used compared with bronchial reconstruction
Accepted for publication May 11, 2012.
Presented at the Forty-seventh Annual Meeting of The Society of ThoracicSurgeons, San Diego, CA, Jan 31–Feb 2, 2011.
Address correspondence to Dr Galetta, Division of Thoracic Surgery,
alone, probably because of the discouraging results interms of complications [9] and to the heterogeneity ofpopulations and varying surgical techniques reported inthese studies. To date there are only a few reports onBAIs in the literature, which may in part be due to highrisk, complicated surgical procedures, and decreasedlong-term survival [10].
Since the introduction of neoadjuvant therapy for pa-tients with clinically advanced disease, the safety ofsleeve lobectomy remains a concern. It is thought thatneoadjuvant radiation, either alone or with chemother-apy with its attendant adverse effects on the bronchialblood supply, may lead to a higher risk of anastomoticcomplications after sleeve resections. Therefore the pur-pose of this study was to retrospectively review ourexperience with BAI by analyzing the surgical results,long-term outcome, prognostic factors, and the impact ofIC on patients who underwent these procedures.
Patients and Methods
We performed a retrospective analysis of a prospectivedatabase of patients with lung cancer who underwentBAI from September 1998 to August 2009 at the Divisionof Thoracic Surgery of the European Institute of Oncol-
ogy in Milan, Italy. Institutional review board approval0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2012.05.050
omenico Galetta on January 26, 2013

908 GALETTA ET AL Ann Thorac SurgCOMBINED BRONCHOANGIOPLASTY FOR LUNG CANCER 2012;94:907–13
GEN
ERA
LT
HO
RA
CIC
was obtained in order to perform this retrospectiveinvestigation.
The following data were collected from the clinicalcharts and operating reports: sex, age, induction therapy,type of sleeve resection (right upper sleeve lobectomy[RUSL] versus left upper sleeve lobectomy [LUSL] versusupper sleeve bilobectomy [USBil]), indication and extentof resection, type and material used for angioplasty,tumor histologic type, pathologic stage, and postopera-tive morbidity and mortality. Possible postoperativetreatments were also recorded. Information and fol-low-up were obtained from the hospital database, officerecords, referring physicians, and direct contact with thepatients or patients’ relatives. Permission to performsuch an outcome analysis was included in the informedconsents signed before surgical treatment.
Preoperative EvaluationPatients demonstrating radiographic and clinical signs ofNSCLC scheduled to undergo surgical resection receivedthe following preoperative clinical evaluation: patienthistory and physical examination with evaluation ofperformance status, complete blood count and hemato-chemical tests, bronchoscopy, pulmonary function tests,arterial blood gas analysis, lung perfusion scan, electro-cardiography, and echocardiography. Computed tomog-raphy (CT) of the chest, abdomen, and brain, as well aspositron emission tomography (PET), were performed toexclude metastatic dissemination and to stage the diseaseaccording to the Mountain revision of the internationalsystem for staging lung cancer [11]. Diagnosis of NSCLCwas performed with fine-needle aspiration biopsy, endo-bronchial biopsy, or bronchoscopic brushing or washing.Mediastinal lymph node involvement was confirmed bycervical mediastinoscopy. Mediastinoscopy was carriedout only when there was clinical N2 involvement by CTor CT/PET. The presence of extrathoracic metastases aswell as histologically confirmed pN3 (contralateral), sta-tion 2 (upper mediastinal lymph nodes), and bulky N2disease or the presence of more than 1 level of N2involvement were definitive contraindications to surgicalresection; these patients received definitive chemoradio-
Abbreviations and Acronyms
ARDS � acute respiratory distress syndromeBAI � bronchoangioplastic interventionCT � computed tomographyFEV1 � forced expiratory volume in 1 secondIC � induction chemotherapyLUSL � left upper sleeve lobectomyNSCLC � non–small-cell lung cancerPA � pulmonary arteryPET � positron emission tomographyppoFEV1 � postoperative forced expiratory
volume in 1 secondRUSL � right upper sleeve lobectomyUSBil � upper sleeve bilobectomy
therapy. Patients with pN2 disease (R4 or 7, or both)
by Dats.ctsnetjournals.orgDownloaded from
received induction therapy, and those with an objectiveresponse or at least stable disease were selected forsurgical intervention. IC was also received by somepatients with T4 NSCLC, and this decision in many caseswas made by the referring medical oncologist. Preoper-ative radiotherapy is not routinely used at our institutionand none of the patients in this series received it. In casesof progressive disease, surgical intervention was denied.
Resection was considered functionally feasible if thepredictive postoperative forced expiratory volume in 1second (ppoFEV1), calculated on the basis of spirometryand lung perfusion scan, was greater than 40% of thepredicted value and provided that no major hypoxemia(�60 mm Hg) or hypercapnia (�46 mm Hg) existed,whereas it was contraindicated if the ppoFEV1 was lessthan 30%. When FEV1 values were between 30% and40%, patients were considered at relative high risk, and adefinitive decision was based on an evaluation of multi-ple parameters (ppoFEV1, partial pressure of oxygen,partial pressure of carbon dioxide, carbon monoxidetransfer factor, age, associated comorbidities, and resultsof exercise tests (stair climbing and 6-minute walking).
Perioperative ManagementThe standard surgical approach to the thoracic cavity wasa modified muscle-sparing lateral thoracotomy (sparingthe serratus muscle) in the fourth or fifth intercostalspace. Double-lumen intubation was used preferentially.Mediastinal lymph node dissection was routinely per-formed at the beginning of the procedure.
Indications for BAI were the presence of a tumor ormetastatic nodes infiltrating the right or left upper bron-chus or its origin or the presence of tumor or metastaticlymph nodes infiltrating the PA. Sometimes a bronchialand vascular plasty was associated with an upper bilo-bectomy. Our policy in case of locally advanced lungcancer was to preserve as much lung parenchyma astechnically and oncologically possible. Thus arterialsleeve resection was carried out when possible and notonly in cases of respiratory impairment contraindicatingpneumonectomy.
The surgical technique for PA resection includes thefollowing steps. Proximal control of the main PA isusually obtained extrapericardially. On the right side,proximal control is obtained posterior to the superiorvena cava; on the left side, it is obtained just distal to theligamentum arteriosum, avoiding left recurrent laryngealnerve damage. Distal control of the PA is usually ob-tained in the pulmonary fissure. The pulmonary vein ofthe lobe to be removed is encircled and then dividedusing a vascular stapler. Systemic anticoagulation isinitiated (3000–5000 IU heparin sodium) and not reversedby protamine at the end of the procedure. The PA isoccluded at its origin with a vascular clamp and distally,in the pulmonary fissure, with another vascular clamp orbulldog vascular clamp, or both, allowing sufficient roomfor the operating surgeon. Thereafter, resection of thetargeted lobe is carried out en bloc with the invadedportion of the PA. Separate frozen section margins of the
bronchus and the PA should be sent for analysis. In allomenico Galetta on January 26, 2013

909Ann Thorac Surg GALETTA ET AL2012;94:907–13 COMBINED BRONCHOANGIOPLASTY FOR LUNG CANCER
GEN
ERA
LT
HO
RA
CIC
cases of bronchial and vascular reconstruction, we preferto perform the arterial resection and reconstruction first,which decreases the clamp time, followed by the bron-chial reconstruction. The resected PA is now evaluated todetermine the type of arterial reconstruction: if the resid-ual arterial caliber is 50% or greater, a direct suture iscarried out. Otherwise, application of an autologous orheterologous (bovine) pericardial patch is performed. If acircumferential resection of the PA is required, an end-to-end vascular anastomosis or the interposition of aconduit (autologous or heterologous) is performed. Su-turing is carried out using 5-0 polypropylene suture. Justbefore tying the arterial suture, the distal clamp is takenoff to help remove the air from the PA. The proximalvascular clamp is then removed to ensure hemostasis ofthe sutured line. Postoperatively, the patient receivesantithrombotic prophylaxis with low-molecular-weightheparin at preventive doses for about 2 weeks. Prolongedanticoagulation is administered to patients only if apolytetrafluoroethylene prosthesis was used. In everycase, a pedicled flap (pericardial fat pad or parietalpleural) was interposed between the 2 anastomoses. Inparticular, the pedicled flap was used for circumferen-tially wrapping the bronchial anastomosis and in thisway separating the bronchial anastomosis from the PAclosure (primary closure, patch, or circumferentialreconstruction).
In case of local invasion, additional structures—such aspericardium (intrapericardial resection), vena cava, chestwall, and others—were resected to get clear margins.
SurvivalSurvival and tumor recurrence were assessed by patientfollow-up. Patients were to be followed monthly for thefirst 3 months, every 3 months for the next 2 years, every6 months for the following 3 years, and annually there-after. Investigations included interim history, physicalexamination, and laboratory tests. CT of the chest, abdo-men, and brain was carried out every 3 months for thefirst year, every 6 months for the following 3 years, andyearly thereafter or when clinical signs of recurrencedeveloped. Recurrence was classified as locoregional(inside the ipsilateral thorax excluding parenchymal nod-ules, always classified as M) or distant (outside theipsilateral thorax), or both.
Statistical AnalysisThe survival probabilities were calculated using the Ka-plan-Meier method from the data of the operation untildeath or loss to follow-up. Operative mortality was cal-culated by taking into account all the deaths occurringwithin 30 days of the operation or during the hospital-ization. Disease-free survival was calculated from thefirst day of operation until any event, such as tumorrecurrence, incidence of second cancer, or secondarycondition. Statistical differences between the individualcurves were assessed with the log-rank test. A value ofp � 0.05 was considered to indicate statistical significanceand all resulting p values were 2-tailed. Age, sex, tumor
stage and N status, histologic type, type of bilobectomy,by Dats.ctsnetjournals.orgDownloaded from
extent of resection, and induction treatment were evalu-ated using univariate and multivariate (Cox proportionalhazards multivariate regression model) analyses to de-termine the prognostic relevance.
Results
Forty-seven patients with lung cancer underwent bron-chovascular resection and reconstruction during thestudy period. The study population included 39 male and7 female patients with a median age of 66 years (range,26–80 years) (Table 1).
Ten patients (21.3%) were older than 70 years, and 83%(n � 39) were current or former smokers. Twelve patients(25.5%) had a history of cardiovascular disease, and 11(23.4%) had a history of pulmonary disease.
Mean preoperative FEV1 was 77.40% � 18.81%; 20patients (42.5%) had a FEV1 less than 70%.
Primary tumor histologic type included 20 squamouscell carcinomas, 18 adenocarcinomas, 3 adenosquamouscarcinomas, 4 pleomorphic carcinomas, and 2 large-cellcarcinomas.
Twenty-two procedures were performed on the rightside and 25 on the left side. RUSL was performed on 14patients (29.8%), LUSL on 25 (53.2%) patients, and 8patients underwent USBil.
A partial PA resection was performed in 43 patients(91.5%) and circumferential resection in 4 (8.5%) patients.Vascular reconstruction was carried out with runningsuture in 33 patients (70.3%), with a pericardial patch in10 (21.2%) patients (8 patients [17.0%] with autologous
Table 1. Demographics
VariableIC
(n � 26)No IC
(n � 21) p Value
Age (y, median) 66.4 66.2 0.53Sex 21 M/5 F 18 M/3 F 0.54FEV1 (% predicted, mean) 77.91 77.44 0.43Histologic (%)
Squamous 10 (38.4) 10 (47.6) 0.68Adenocarcinoma 12 (46.2) 6 (28.6) 0.45Othera 4 (15.4) 5 (23.8) 0.54
Surgical resection (%)RUSL 10 (38.4) 4 (19.0) 0.28LUSL 12 (46.2) 13 (62.0) 0.55USBil 4 (15.4) 4 (19.0) 0.78
Type of PA resection (%)Partial 24 (92.3) 19 (90.5) 0.96Circumferential 2 (7.7) 2 (9.5) 0.83
Comorbidities (%)Pulmonary 2 (7.7) 9 (42.8) 0.02Cardiovascular 4 (15.4) 8 (38.1) 0.17
a Other includes large-cell carcinoma, adenosquamous carcinoma, andpleomorphic carcinoma.
FEV1 � forced expiratory volume in 1 second; IC � induction chemo-therapy; LUSL � left upper sleeve lobectomy; no IC � no induc-
tion chemotherapy; PA � pulmonary artery; RUSL � right uppersleeve lobectomy; USBil � upper sleeve bilobectomy.omenico Galetta on January 26, 2013

910 GALETTA ET AL Ann Thorac SurgCOMBINED BRONCHOANGIOPLASTY FOR LUNG CANCER 2012;94:907–13
GEN
ERA
LT
HO
RA
CIC
tissue and 2 patients [4.2%] with bovine pericardium),and by the interposition of conduit in 4 patients (8.5%) (2polytetrafluoroethylene and 2 handmade conduits ofbovine pericardium).
In 4 patients, superior vena cava resection and recon-struction was also required. A carinal resection and achest wall resection were performed in 1 patient each.
Postoperative OutcomeNo intraoperative mortality occurred. Overall, the mor-bidity rate was 40.4% (n � 19). Major complication ratewas 10.6% (n � 5) (Table 2) and included 1 case of acuterespiratory distress syndrome requiring prolonged me-chanical ventilation; 1 cardiac dislocation requiring reop-eration and reparation of an excessive pericardial win-dow, and 3 fatal bronchovascular fistulas (6.4%). Of theselast patients, 2 (4.2%) died on the 30th postoperative dayand both received IC, and 1 patient died on the 36thpostoperative day and did not receive IC. IC did notstatistically influence the bronchovascular fistula rate(Table 2). These 3 patients underwent RUSL in 2 casesand USBil in 1 case and all received partial PA resection.The PA was reconstructed by a running suture in 1 caseand by a patch closure in 2 cases (autologous pericardiumand bovine pericardium, respectively). Autopsy was notperformed on any of these patients.
Fourteen patients had minor complications (Table 1),including pulmonary (n � 7), cardiac (n � 6), andneurologic (n � 1) complications. Pulmonary complica-tions included prolonged air leak in 3 patients (6.4%) andatelectasis in 4 (8.5%) patients. Cardiac complicationsincluded ischemic events in 2 patients (4.2%) and atrialfibrillation in 4 (8.5%) patients. In our series there was nolate bronchial anastomotic stenosis.
Median postoperative hospitalization was 8 days(range, 5–78 days). Thirty-five patients (74.5%) requiredpostoperative intensive care unit stay, and the medianintensive care unit stay was 2 days (range, 0–67 days). ICdid not influence either postoperative morbidity or post-operative mortality. Two patients (4.2%) had a complete
Table 2. Postoperative Complications
ComplicationsIC
(n � 26)No IC
(n � 21) p Value
Overall Mortality (%) 3 (11.5) 0 0.12Morbidity (%) 11 (42.3) 8 (38.1) 0.84
Major 4 (15.4) 1 (4.7) 0.28ARDS 1 (3.8) 0 0.37Cardiac dislocation 0 1 (4.7) 0.20Bronchovascular fistula 2 (7.7) 1 (4.7) 0.70
Minor 7 (26.9) 7 (33.3) 0.72Prolonged air leak 2 (7.7) 1 (4.7) 0.70Atelectasis 1 (3.8) 3 (14.3) 0.24Atrial fibrillation 3 (11.5) 1 (4.7) 0.44Ischemic event 1 (3.8) 1 (4.7) 0.88Stroke 1 (3.8) 0 0.37
ARDS � acute respiratory distress syndrome; IC � induction chemo-therapy; no IC � no induction chemotherapy.
by Dats.ctsnetjournals.orgDownloaded from
pathologic response after IC. Pathologic stages werestage I in 7 patients (14.9%), stage II in 14 (29.8%) patients,stage IIIA in 17 (36.2%) patients, and stage IIIB in 7(14.9%) patients. A pathologic complete resection wasachieved in 46 patients (97.8%). Two patients had mac-roscopic incomplete resection of the bronchus despitenegative systematic frozen section results. Except forpatients with incomplete resection in whom a clearindication of adjuvant therapy was present, the decisionto administer adjuvant therapy in the remaining patientswas made by referred medical oncologists.
SurvivalNo patient was lost to follow-up. Median follow-up forthe entire population was 24 months. At the completionof the study and including all patients, 19 patients (40.4%)are alive (16 disease free; 3 with disease), and 28 (59.6%)are dead.
Recurrence was diagnosed in 20 (42.5%) patients: lo-coregional relapse was registered in 4 patients (8.5%),distant recurrence in 7 (14.9%) patients, and multiorgandisease in 9 (19.1%) patients.
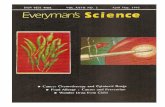
Median overall survival was 22 months (range, 0–128months). The calculated 5-year Kaplan-Meier survivalrate in all 47 patients was 39.2% (Fig 1A). The 5-yeardisease-free interval in the entire population was 36.9%(Fig 1B). The 5-year survival rate was significantly higherfor early-stage disease (p � 0.005) (Fig 2), no nodalinvolvement (p � 0.002) (Fig 3), and for patients receivingIC (62.7% versus 10.7%; p � 0.0003) (Fig 4).
On multivariate analysis, IC was significantly associ-ated with overall survival (p � 0.003; 95% CI, 2.92–8.56).
Comment
Despite the advances that have been made in the multi-modal therapy of lung cancer, surgical therapy stillremains the most important tool if cure is attempted.Complete resection of NSCLC, if possible, not onlyremoves all malignant tissue but also improves long-term survival. The completeness and extent of resectiondirectly correlates with the probability of tumor recur-rence and survival [12] as well as with perioperativemorbidity and mortality [12, 13].
The preservation of pulmonary tissue is a standardpractice in lung operations. One of the most commonlyused techniques to preserve lung tissue is lobectomywith bronchial reconstruction. Since sleeve lobectomyyields survival results that are at least equal to those ofpneumonectomy but provides better functional results, ithas become an accepted procedure for patients who havelung cancer and anatomically suitable tumors, regardlessof pulmonary function [14, 15]. As the technique ofangioplasty has been introduced into the field of pulmo-nary surgery, sleeve lobectomy with PA reconstructionhas become feasible.
Parenchyma-sparing bronchovascular sleeve resec-tions were primarily intended to offer a surgical alterna-tive to those individuals who would not tolerate a pneu-
monectomy because of impairment of pulmonaryomenico Galetta on January 26, 2013

911Ann Thorac Surg GALETTA ET AL2012;94:907–13 COMBINED BRONCHOANGIOPLASTY FOR LUNG CANCER
GEN
ERA
LT
HO
RA
CIC
reserve. Initial reports indicated that this form of resec-tion was associated with an increased mortality andmorbidity associated with the bronchial and vascularanastomosis [16, 17]. There has been additional concernof a possibly higher risk of tumor recurrence with in-creased mortality [18, 19].
Several series have been published in recent yearsindicating that bronchial sleeve resection applied irre-spective of pulmonary function was associated with amortality risk lower than that of pneumonectomy and inmost instances was comparable to standard lobe resec-tion [20–22]. The incidence of bronchial anastomoticcomplications has been consistently lower than that ofpneumonectomy [20–22]. The published 5-year survivaland disease-free interval data have not been inferior tothose after pneumonectomy.
Although the use of bronchial sleeve resections isgaining wider acceptance, concern continues regardingthe routine application of bronchovascular sleeve resec-tions for the treatment of central lung cancer involving
Fig 1. (A) Overall 5-year survival curve including postoperativedeaths (n � 47). (B) Five-year disease-free interval of the overall
population. (Pts � patients.)by Dats.ctsnetjournals.orgDownloaded from
the PA. In a series of 37 sleeve resections of the PA,Vogt-Moykopf and colleagues [16, 23] reported accept-able long-term results but an operative mortality of up to14%. Major complications of the vascular anastomosishave been described [16, 23]. Apparently many surgeonshave been reluctant to use this technique, having theimpression that angioplasty was not a safe procedure. Ithas become apparent only recently that angioplasticresections can be performed with favorable early [24, 25]and late [26] results. In addition, lessons learned fromlung transplantation not only pointed out potential pit-falls of the vascular anastomosis but also showed ways toavoid them [25, 27].
In a recent meta-analysis [28] evaluating whethersleeve lobectomy with or without PA reconstruction hadfavorable results for NSCLC compared with pneumonec-tomy, the surgical outcomes of PA resection were notonly comparable to sleeve lobectomy—with 3.3% opera-tive mortality, 32.4% postoperative complications, and38.7% 5-year survival—but better than those of pneumo-
Fig 2. Survival curves according to the pathologic stage. Stage I in-cludes the 2 complete pathologic responses. (Pts � patients.)
Fig 3. Survival curves according to the N status: N0 (n � 10) versus
N1 (n � 20) versus N2 (n � 17). (Pts � patients.)omenico Galetta on January 26, 2013

912 GALETTA ET AL Ann Thorac SurgCOMBINED BRONCHOANGIOPLASTY FOR LUNG CANCER 2012;94:907–13
GEN
ERA
LT
HO
RA
CIC
nectomy. These data indicate that BAI is as safe as sleevelobectomy for the treatment of NSCLC.
Our current results indicate that bronchovascularsleeve resections for the treatment of central lung carci-nomas can be performed with low perioperative risk.Most importantly, the long-term data regarding survivaland tumor recurrence are identical to those of bronchialsleeve resection and pneumonectomy in our patientpopulation. Thus we believe that this surgical optiondoes not compromise oncologic treatment success. Adefinitive conclusion regarding oncologic treatment re-sults is, however, hampered by the relatively limitednumber of individuals in our study. In a recent meta-analysis, an increased risk of local tumor recurrence wasfound after sleeve lobectomy compared with pneumo-nectomy. Interestingly, this increase in tumor recurrencedid not affect long-term results [29]. It is unclear whetherroutine application of adjuvant radiotherapy for all pa-renchyma-sparing operations could be of benefit.
Our long-term survival is in line with that observed forpatients with NSCLC of similar stage who do not requirevascular reconstructions. The overall and disease-freesurvivals are encouraging, and the local recurrence rateis low; however the N status, and in particular the N2stage, has a significant effect on outcome. Also the ad-ministration of induction therapy had a significant prog-nostic value in our experience. Although our finding thatpatients who received IC had markedly improved sur-vival (62.7% versus 10.7%) could sound strange andinconsistent with the survival according to the pathologicN status, this result is explained by the fact that survivalin patients with N2 disease was improved if they receivedchemotherapy.
Our data demonstrated that PA reconstruction can beperformed safely after IC, in line with previous reports ofbronchial sleeve resection. In fact, the lower survivalobserved in this group of patients reflects the stage of thetumor rather than the incidence of postoperative compli-cations. The low rate of bronchovascular fistula in ourexperience (7.7% in those receiving IC versus 4.7% in
Fig 4. Survival according to induction chemotherapy (IC). (Pts �patients.)
those who did not receive IC; p � not significant) con-
by Dats.ctsnetjournals.orgDownloaded from
firmed the low negative effect of IC on the postoperativeoutcome.
An important issue is the use of a vascularized pedi-cled flap (intercostal, pleural, fat pad) for wrapping thebronchial anastomosis and separating the PA reconstruc-tion to reduce the risk of bronchovascular fistulas. Al-though this technique was adopted in all patients in ourseries, an overall rate of bronchovascular fistula of 6.4%occurred, which may be considered in the reportedranges of the literature even if a vascular intercostal flapwas used.
We therefore conclude that bronchovascular sleeveresections are as safe as bronchial sleeve resections forthe treatment of central lung cancer. Both procedureshave comparable early and long-term results, which aresimilar to those of pneumonectomy. Thus it appearsreasonable to also apply bronchovascular sleeve resec-tions more liberally.
References
1. Graham EA, Singer JJ. Successful removal of an entire lungfor carcinoma of the bronchus. JAMA 1933;101:1371–4.
2. Boyden EA. Segmental Anatomy of the Lungs. A Study ofthe Patterns of the Segmental Bronchi and Related Pulmo-nary Vessels. New York, NY: McGraw-Hill; 1955.
3. Robinson JC, Jones JC, Meyer BW. Indication for lobectomyin the treatment of carcinoma of the lung. J Thorac Cardio-vasc Surg 1956;32:500–7.
4. Belcher JR. Lobectomy for bronchial carcinoma. Lancet 1956;270:349–52.
5. Deslauriers J, Gaulin P, Beaulieu M, Piraux M, Bernier R,Cormier Y. Long-term clinical and functional results ofsleeve lobectomy for primary lung cancer. J Thorac Cardio-vasc Surg 1986;92:871–9.
6. Ludwig C, Stoelben E, Olschewski M, Hasse J. Comparisonof morbidity, 30-day mortality, and long-term survival afterpneumonectomy and sleeve lobectomy for non-small celllung carcinoma. Ann Thorac Surg 2005;79:968–73.
7. Takeda S, Maeda H, Koma M, et al. Comparison of surgicalresults after pneumonectomy and sleeve lobectomy for non-small cell lung cancer: trends over time and 20-year institu-tional experience. Eur J Cardiothorac Surg 2006;29:276–80.
8. Parissis H, Leotsinidis M, Hughes A, McGovern E, Luke D,Young V. Comparative analysis and outcomes of sleeveresection versus pneumonectomy. Asian Cardiovasc ThoracAnn 2010;17:175–82.
9. Shrager JB, Lambright ES, McGrath CM, et al. Lobectomywith tangential pulmonary artery resection without regardto pulmonary function. Ann Thorac Surg 2000;70:234–9.
10. Kim YT, Kang CH, Sung SW, Kim JH. Local control ofdisease related to lymph node involvement in non-small celllung cancer after sleeve lobectomy compared with pneumo-nectomy. Ann Thorac Surg 2005;79:1153–61.
11. Mountain CF. Revisions in the international system forstaging lung cancer. Chest 1997;111:1710–7.
12. Suzuki K, Nagai K, Yoshida J, et al. Conventional clinico-pathologic prognostic factors in surgically resected non-small cell lung carcinoma. Cancer 1999;86:1976–84.
13. Bernard A, Ferrand L, Hagry O, et al. Identification ofprognostic risk factors determining risk groups for lungresection. Ann Thorac Surg 2000;70:1161–71.
14. Gaissert HA, Mathisen DJ, Moncure AC, Hilgenberg AD,Grillo HC, Wain JC. Survival and function after sleevelobectomy for lung cancer. J Thorac Cardiovasc Surg 1996;
111:948–53.omenico Galetta on January 26, 2013

913Ann Thorac Surg GALETTA ET AL2012;94:907–13 COMBINED BRONCHOANGIOPLASTY FOR LUNG CANCER
ENER
AL
TH
OR
AC
IC
15. Khargi K, Duurkens VA, Verzijibergen FF, Huysmans HA,Knaepen PJ. Pulmonary function after sleeve lobectomy.Ann Thorac Surg 1994;57:1302–4.
16. Vogt-Moykopf I, Fritz TH, Meyer G, Bulzerbruck H, DaskosG. Bronchoplastic and angioplastic operation in bronchialcarcinoma: long-term results of a retrospective analysis from1973 to 1983. Int Surg 1986;71:211–20.
17. Faber JP, Jensik RJ, Kittle CF. Results of sleeve lobectomy forbronchogenic carcinoma in 101 patients. Ann Thorac Surg1984;37:279–85.
18. Fadel E, Yildizeli B, Chapelier AR, Dicenta I, Mussot S,Dartevelle P. Sleeve lobectomy for bronchogenic cancer:factors affecting survival. Ann Thorac Surg 2002;74:851–9.
19. Tedder M, Anstadt MP, Tedder SD, Lowe JE. Currentmorbidity, mortality, and survival after bronchoplastic pro-cedures for malignancy. Ann Thorac Surg 1992;54:387–91.
20. Suen HG, Meyers BF, Guthrie T, et al. Favorable results aftersleeve lobectomy or bronchoplasty for bronchial malignan-cies. Ann Thorac Surg 1999;67:1557–62.
21. Tronc F, Gregoire J, Rouleau J, Deslauriers J. Long-termresults of sleeve lobectomy for lung cancer. Eur J Cardiotho-rac Surg 2000;17:550–6.
22. Lausberg HF, Greater TP, Wendler O, et al. Bronchial and
bronchovascular sleeve resection for treatment of centrallung tumors. Ann Thorac Surg 2000;70:36–72.artery reducing the risk of bronchopulmonary fistula.
by Dats.ctsnetjournals.orgDownloaded from
23. Vogt-Moykopf I, Fritz TH, Bulzerbruck H, Merkle N, DaskosG, Meyer G. Bronchoplastic and angioplastic operation inbronchial carcinoma. Langenbecks Arch Chir 1987;371:85–101.
24. Rendina EA, Venuta F, Ciriaco P, Ricci C. Bronchovas-cular sleeve resection. J Thorac Cardiovasc Surg 1993;106:73–9.
25. Rendina EA, Venuta F, De Giacomo T, et al. Sleeve resectionand prosthetic reconstruction of the pulmonary artery forlung cancer. Ann Thorac Surg 1999;68:995–1002.
26. Venuta F, Ciccone AM, Anile M, et al. Reconstruction of thepulmonary artery for lung cancer: long-term results. J Tho-rac Cardiovasc Surg 2009;138:1185–91.
27. Griffith BP, Magee MJ, Gonzales IF, et al. Anastomoticpitfalls in lung transplantation. J Thorac Cardiovasc Surg1994;107:743–54.
28. Ma Z, Dong A, Fan J, Cheng H. Does sleeve lobectomyconcomitant with or without pulmonary artery reconstruc-tion (double sleeve) have favorable results for non-small celllung cancer compared with pneumonectomy? A meta-analysis. Eur J Cardiothorac Surg 2007;32:20–8.
29. Ferguson MK, Lehman AG. Sleeve lobectomy or pneumo-
nectomy: optimal management strategy using decision anal-ysis techniques. Ann Thorac Surg 2003;76:1782–8.G
DISCUSSION
DR JOSEPH FRIEDBERG (Philadelphia, PA): That was a greattalk.
I’ve never used Gore-Tex on the pulmonary artery. Do youuse any sort of anticoagulation after you do that?
DR GALETTA: We don’t use Gore-Tex. We use autologous orheterologous bovine pericardium. During the intervention, weheparinize the patient just before clamping the pulmonaryartery, and postoperatively usually we use, as for all patients,low-molecular-weight heparin.
DR FRIEDBERG: How long do you use that, just while they’re inthe hospital?
DR GALETTA: Sorry?
DR FRIEDBERG: Just while they’re in the hospital? Do you sendthem out on anything?
DR GALETTA: Yes.
DR FRIEDBERG: How long, or it’s just in the hospital?
DR GALETTA: We usually use low-molecular-weight heparinfor a few weeks after patient’s discharge.
DR MICHAEL LANUTI (Boston, MA): Do you interpose anytissue between your bronchovascular reconstruction?
DR GALETTA: Yes. Every time we perform a sleeve lobectomyassociated or not to a vascular angioplastic procedure, weinterpose some tissue. Usually we use fat pad tissue or apedicled parietal pleural flap, and usually we encircle with thistissue the bronchial anastomosis; in this way we protect thebronchial anastomosis and separate it from the pulmonary
DR JOSEPH B. SHRAGER (Stanford, CA): It’s interesting thatItalians seem to be most interested in this problem—more thananyone else. Most of us would be more concerned aboutinduction chemoradiation than induction chemotherapy withthese patients. Are you specifically choosing chemo alone asyour induction therapy when you think there is a likelihood thatthere is going to be a sleeve, or is chemo your induction therapyacross the board?
DR GALETTA: In this series we have only patients who receivedchemotherapy and not chemoradiation therapy. In a neoadju-vant setting, for patients with pN2 and/or cT4, our policy is toperform chemotherapy. We rarely perform radiotherapy associ-ated with chemotherapy.
DR STEVEN D. HERMAN (Brooklyn, NY): I, too, was interestedin whether you used radiation prior to resection. As you per-formed only a partial resection of pulmonary artery in the videothat you showed, in that that type of particular case, do you alsoutilize postoperative chemotherapy and/or radiation to helpcontrol local disease?
DR GALETTA: Yes. Adjuvant chemotherapy was administeredto those patients with pathological N2 disease who didn’treceive induction therapy. In some cases some patients receivedadjuvant radiotherapy.
DR ABEL GOMEZ-CARO (Barcelona, Spain): Congratulations,Domenico. It was a great presentation.
When you discharge the patient, do you use antiplatelettherapy?
DR GALETTA: Usually for a few weeks we use low-molecular-weight heparin, but only for a few weeks.
DR GOMEZ-CARO: No aspirin at all?
DR GALETTA: No.
omenico Galetta on January 26, 2013

DOI: 10.1016/j.athoracsur.2012.05.050 2012;94:907-913 Ann Thorac Surg
Petrella, Alessandro Pardolesi and Lorenzo Spaggiari Domenico Galetta, Piergiorgio Solli, Alessandro Borri, Roberto Gasparri, Francesco
Influence the Outcomes?Bronchovascular Reconstruction for Lung Cancer: Does Induction Chemotherapy
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/94/3/907including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/94/3/907#BIBL
This article cites 28 articles, 19 of which you can access for free at:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/lung_cancer Lung - cancer
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by Domenico Galetta on January 26, 2013 ats.ctsnetjournals.orgDownloaded from