Phase I/II Trial of Induction Chemotherapy Followed by Concurrent Chemoradiotherapy and Surgery for...
11
Phase I/II Trial of Induction Chemotherapy Followed by Concurrent Chemoradiotherapy and Surgery for Locoregionally Advanced Pancreatic Cancer Jennifer L. Marti, MD, 1 Howard S. Hochster, MD, 2 Spiros P. Hiotis, MD, PhD, 1 Bernadine Donahue, 3,4 Theresa Ryan, MD, 2 and Elliot Newman, MD 1 1 Division of Surgical Oncology, Department of Surgery, NYU Cancer Institute, New York University School of Medicine, 160 East 34th Street, 9th Floor, New York, NY 10016, USA 2 Division of Medical Oncology, Department of Medicine, NYU Cancer Institute, New York University School of Medicine, New York, NY, USA 3 Department of Radiation Oncology, NYU Cancer Institute, New York University School of Medicine, New York, NY, USA 4 Department of Radiation Oncology, Maimonides Cancer Center, 6300 8th Avenue, Brooklyn, NY 11220, USA Background: We used a novel combination of induction chemotherapy with gemcitabine (GEM) and cisplatin (CDDP), followed by concurrent chemoradiotherapy (CCRT) with the same agents in patients with locoregionally advanced pancreatic cancer. Surgery or additional chemotherapy followed on the basis of response. Methods: Patients with borderline resectable or locally advanced pancreatic cancer received induction weekly with GEM (1000 mg/m 2 ) or CDDP (30 g/m 2 ). Patients without progression of disease then underwent surgery or CCRT, including four cohorts of escalating GEM/ CDDP doses combined with full-dose radiotherapy. After CCRT, patients deemed resectable underwent surgery; patients with disease that remained unresectable and that did not progress received additional GEM/CDDP for 2 months. Results: A mean 76% of intended GEM dose and 75% of CDDP dose was delivered during induction (n = 26). There were three incidences of grade 4 toxicity (fever or neutropenia). After induction, five patients progressed and one patient underwent resection. Eighteen patients received CCRT, and three patients underwent resection. After CCRT, disease of 10 patients progressed, and in 5 patients, it remained unresectable without progression, and the patient received additional GEM/CDDP. Dose-limiting toxicity was at dose level IV (thrombocytopenia). Median overall and disease-specific survival was 13 months. Conclusion: GEM/CDDP induction chemotherapy followed by CCRT is well tolerated and rendered the disease of 4 of 26 patients resectable in this study. The recommended phase II dose for GEM and CDDP in combination with full-dose radiotherapy (5040 cGy) is 300 mg/ m 2 and 10 mg/m 2 weekly for 5 weeks. Median survival in this group was 13 months. This neoadjuvant combined modality approach is both feasible and active; further studies are warranted. Pancreatic adenocarcinoma is the 11th most com- mon cancer and the 4th leading cause of cancer death, resulting in the deaths of 30,000 Americans each year and 190,000 worldwide. 1 Overall median survival is 3 to 4 months, 2 1-year survival is 24%, and 5-year survival is < 5%. 2 Long-term survival is only possible with resection; however, only 10% to 20% of Published online October 2, 2008. Address correspondence and reprint requests to: Elliot Newman, MD; E-mail: [email protected] Publishedby Springer Science+Business Media, LLC Ó 2008 The Society of Surgical Oncology, Inc. Annals of Surgical Oncology 15(12):3521–3531 DOI: 10.1245/s10434-008-0152-3 3521
Transcript of Phase I/II Trial of Induction Chemotherapy Followed by Concurrent Chemoradiotherapy and Surgery for...

Phase I/II Trial of Induction Chemotherapy Followedby Concurrent Chemoradiotherapy and Surgeryfor Locoregionally Advanced Pancreatic Cancer
Jennifer L. Marti, MD,1 Howard S. Hochster, MD,2 Spiros P. Hiotis, MD, PhD,1
Bernadine Donahue,3,4 Theresa Ryan, MD,2 and Elliot Newman, MD1
1Division of Surgical Oncology, Department of Surgery, NYU Cancer Institute, New York University School of Medicine,160 East 34th Street, 9th Floor, New York, NY 10016, USA
2Division of Medical Oncology, Department of Medicine, NYU Cancer Institute, New York University School of Medicine,New York, NY, USA
3Department of Radiation Oncology, NYU Cancer Institute, New York University School of Medicine, New York, NY, USA4Department of Radiation Oncology, Maimonides Cancer Center, 6300 8th Avenue, Brooklyn, NY 11220, USA
Background: We used a novel combination of induction chemotherapy with gemcitabine(GEM) and cisplatin (CDDP), followed by concurrent chemoradiotherapy (CCRT) with thesame agents in patients with locoregionally advanced pancreatic cancer. Surgery or additionalchemotherapy followed on the basis of response.
Methods: Patients with borderline resectable or locally advanced pancreatic cancer receivedinduction weekly with GEM (1000 mg/m2) or CDDP (30 g/m2). Patients without progressionof disease then underwent surgery or CCRT, including four cohorts of escalating GEM/CDDP doses combined with full-dose radiotherapy. After CCRT, patients deemed resectableunderwent surgery; patients with disease that remained unresectable and that did not progressreceived additional GEM/CDDP for 2 months.
Results: A mean 76% of intended GEM dose and 75% of CDDP dose was delivered duringinduction (n = 26). There were three incidences of grade 4 toxicity (fever or neutropenia).After induction, five patients progressed and one patient underwent resection. Eighteenpatients received CCRT, and three patients underwent resection. After CCRT, disease of 10patients progressed, and in 5 patients, it remained unresectable without progression, and thepatient received additional GEM/CDDP. Dose-limiting toxicity was at dose level IV(thrombocytopenia). Median overall and disease-specific survival was 13 months.
Conclusion: GEM/CDDP induction chemotherapy followed by CCRT is well tolerated andrendered the disease of 4 of 26 patients resectable in this study. The recommended phase IIdose for GEM and CDDP in combination with full-dose radiotherapy (5040 cGy) is 300 mg/m2 and 10 mg/m2 weekly for 5 weeks. Median survival in this group was 13 months. Thisneoadjuvant combined modality approach is both feasible and active; further studies arewarranted.
Pancreatic adenocarcinoma is the 11th most com-mon cancer and the 4th leading cause of cancerdeath, resulting in the deaths of 30,000 Americanseach year and 190,000 worldwide.1 Overall mediansurvival is 3 to 4 months,2 1-year survival is 24%, and5-year survival is <5%.2 Long-term survival is onlypossible with resection; however, only 10% to 20% of
Published online October 2, 2008.Address correspondence and reprint requests to: Elliot Newman,
MD; E-mail: [email protected]
Published by Springer Science+Business Media, LLC � 2008 The Society ofSurgical Oncology, Inc.
Annals of Surgical Oncology 15(12):3521–3531
DOI: 10.1245/s10434-008-0152-3
3521

patients manifest local disease, i.e., confined to thepancreas, and as such deemed resectable.3–5
Approximately 25% to 30% of patients manifestregional disease or disease that extends outside thepancreas, without distant metastases. However, theterm for this extent of disease, locally advanced, isactually often used in the literature to refer to twogroups of patients: those with borderline resectabledisease, who are actually in a distinct groupcompared with those categorized as having locallyadvanced unresectable disease by National Compre-hensive Cancer Network (NCCN) criteria. The dif-ference between these groups relates to how much ofthe regional vasculature (superior mesenteric artery,portal vein–superior mesenteric vein confluence, orceliac axis) are involved by tumor. The specific defi-nitions, which define involvement, abutment, orencasement of these vessels, can be found in currentNCCN guidelines.6,7
For patients with locoregionally advanced disease,median survival is 8 to 12 months.2 Treatment forthis group is challenging because in this group,resection can often lead to a microscopically positivemargin of resection, which does not seem to confer asurvival benefit compared with no resection.8 For thisreason, therapeutic options for this group havefocused on multimodality therapy, combiningchemotherapy, radiation, and possibly surgery toimprove outcome.9–11
Studies have shown that combined chemoradio-therapy (RT) is better than either modality alone andhas shown promise in improving survival.12,13
Chemoradiation treatment may also downstage bor-derline resectable or locally advanced disease in thehopes of making the disease resectable.14–16 However,the success of chemoradiation in this setting is highlyvariable17 and often relates to whether the clinician isdealing with borderline resectable disease or locallyadvanced, unresectable disease.5-Fluorouracil (5FU) and RT have historically
been the standard therapy for locally advanced pan-creatic cancer, with reported 1-year survival of 17%to 28%.2,18–26 Gemcitabine (difluoro-deoxycytidine;GEM) is a nucleoside analog that has been shown tobe more active than 5FU in advanced disease forpalliation of symptoms.27 Numerous studies haveinvestigated combination regimens with GEM, and asynergistic relationship with cisplatin (CDDP) hasbeen demonstrated. GEM is thought to augmentCDDP-induced DNA cross-linking and inhibit DNArepair.2 CDDP also inhibits catabolism of GEM.28
Preclinical studies have also shown that GEMradiosensitizes pancreas cell lines.27,29,30
Building on the synergism of GEM and CDDP as achemotherapy combination and as radiation sensi-tizers, we designed a novel multimodality regimen ofinduction chemotherapy (IND) with GEM andCDDP followed by concurrent chemoradiotherapy(CCRT). Because we did not know the activity of thechemotherapy regimen, we began with a 2-monthinduction cycle, with the option for surgical resectionif possible. This was followed by a dose escalationphase I portion of the study, escalating doses of thechemotherapy agents in a 3 9 3 design with full-doseRT. Surgery or additional chemotherapy followed onthe basis of response. We studied the toxicity of thisregimen, as well as the effect of this therapy onradiologic response, the ability to render the diseaseresectable, and the overall survival of this patientgroup.
PATIENTS AND METHODS
Eligibility and Evaluation
Between November 1997 and February 2004, atotal of 26 patients with locoregionally advancedpancreatic carcinoma were enrolled. Patients weretreated in New York City at New York UniversityMedical Center, Bellevue Hospital Center or theManhattan Veteran’s Affairs Medical Center. Insti-tutional review board (IRB) approval was obtainedat each site, and each patient signed an IRB-approved informed consent documents. Eligibilitycriteria included histopathologic diagnosis of pan-creatic adenocarcinoma, locoregionally advanced,nonmetastatic disease on pretreatment computedtomographic (CT) imaging, and Eastern CooperativeOncology Group (ECOG) performance status 0 or 1.When the study was initiated, the current NCCN
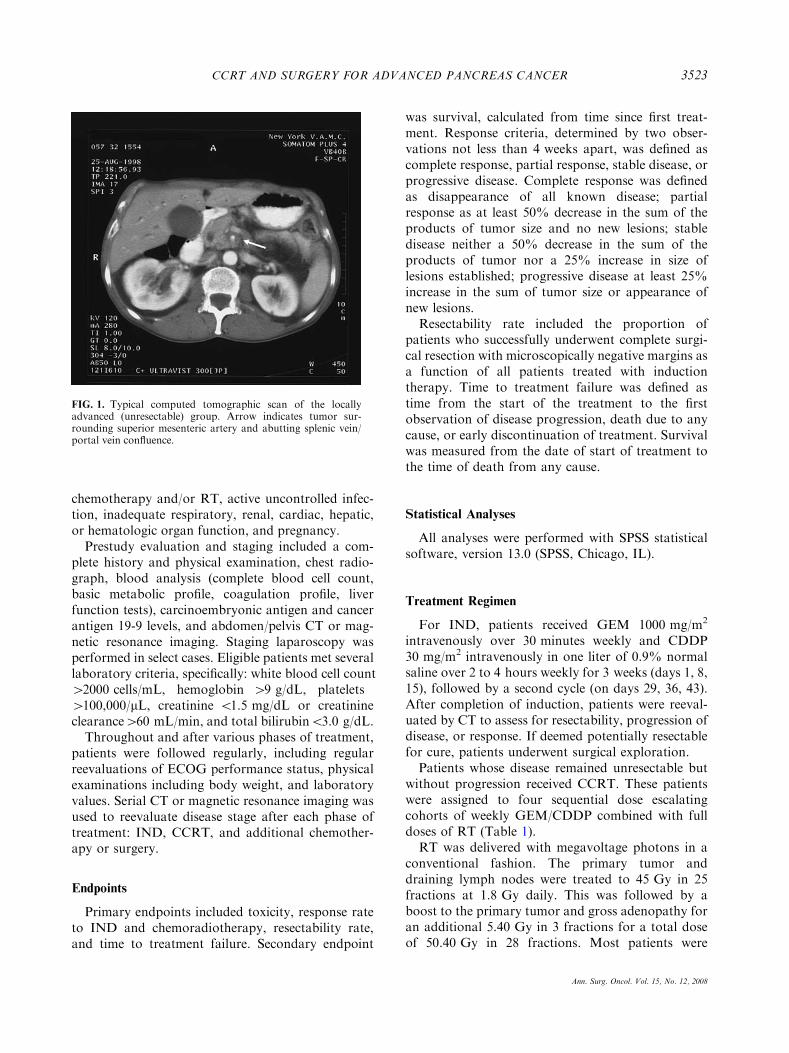
guidelines to define resectability status were notestablished. Our definition at that time for locore-gionally advanced disease was disease that wasdeemed unresectable with negative microscopic mar-gins by the surgical oncology consultant on the basisof involvement of the mesenteric vessels, i.e., thesuperior mesenteric artery, celiac axis, or portal vein–superior mesenteric vein confluence. In retrospectivelyreviewing the patients with current NCCN guidelines,the disease of most patients (n = 23) would be definedas locally advanced unresectable and three defined asborderline resectable.7 A representative CT scan of apatient with locally advanced unresectable disease isshown in Fig. 1. Exclusion criteria included histologyother than adenocarcinoma, metastatic disease, prior
J. L. MARTI ET AL.3522
Ann. Surg. Oncol. Vol. 15, No. 12, 2008
chemotherapy and/or RT, active uncontrolled infec-tion, inadequate respiratory, renal, cardiac, hepatic,or hematologic organ function, and pregnancy.Prestudy evaluation and staging included a com-
plete history and physical examination, chest radio-graph, blood analysis (complete blood cell count,basic metabolic profile, coagulation profile, liverfunction tests), carcinoembryonic antigen and cancerantigen 19-9 levels, and abdomen/pelvis CT or mag-netic resonance imaging. Staging laparoscopy wasperformed in select cases. Eligible patients met severallaboratory criteria, specifically: white blood cell count>2000 cells/mL, hemoglobin >9 g/dL, platelets>100,000/lL, creatinine <1.5 mg/dL or creatinineclearance>60 mL/min, and total bilirubin<3.0 g/dL.Throughout and after various phases of treatment,
patients were followed regularly, including regularreevaluations of ECOG performance status, physicalexaminations including body weight, and laboratoryvalues. Serial CT or magnetic resonance imaging wasused to reevaluate disease stage after each phase oftreatment: IND, CCRT, and additional chemother-apy or surgery.
Endpoints
Primary endpoints included toxicity, response rateto IND and chemoradiotherapy, resectability rate,and time to treatment failure. Secondary endpoint
was survival, calculated from time since first treat-ment. Response criteria, determined by two obser-vations not less than 4 weeks apart, was defined ascomplete response, partial response, stable disease, orprogressive disease. Complete response was definedas disappearance of all known disease; partialresponse as at least 50% decrease in the sum of theproducts of tumor size and no new lesions; stabledisease neither a 50% decrease in the sum of theproducts of tumor nor a 25% increase in size oflesions established; progressive disease at least 25%increase in the sum of tumor size or appearance ofnew lesions.Resectability rate included the proportion of
patients who successfully underwent complete surgi-cal resection with microscopically negative margins asa function of all patients treated with inductiontherapy. Time to treatment failure was defined astime from the start of the treatment to the firstobservation of disease progression, death due to anycause, or early discontinuation of treatment. Survivalwas measured from the date of start of treatment tothe time of death from any cause.
Statistical Analyses
All analyses were performed with SPSS statisticalsoftware, version 13.0 (SPSS, Chicago, IL).
Treatment Regimen
For IND, patients received GEM 1000 mg/m2
intravenously over 30 minutes weekly and CDDP30 mg/m2 intravenously in one liter of 0.9% normalsaline over 2 to 4 hours weekly for 3 weeks (days 1, 8,15), followed by a second cycle (on days 29, 36, 43).After completion of induction, patients were reeval-uated by CT to assess for resectability, progression ofdisease, or response. If deemed potentially resectablefor cure, patients underwent surgical exploration.Patients whose disease remained unresectable but
without progression received CCRT. These patientswere assigned to four sequential dose escalatingcohorts of weekly GEM/CDDP combined with fulldoses of RT (Table 1).RT was delivered with megavoltage photons in a
conventional fashion. The primary tumor anddraining lymph nodes were treated to 45 Gy in 25fractions at 1.8 Gy daily. This was followed by aboost to the primary tumor and gross adenopathy foran additional 5.40 Gy in 3 fractions for a total doseof 50.40 Gy in 28 fractions. Most patients were
FIG. 1. Typical computed tomographic scan of the locallyadvanced (unresectable) group. Arrow indicates tumor sur-rounding superior mesenteric artery and abutting splenic vein/portal vein confluence.
CCRT AND SURGERY FOR ADVANCED PANCREAS CANCER 3523
Ann. Surg. Oncol. Vol. 15, No. 12, 2008
treated with a four-field technique with CT planningto limit dose to critical structures.After a second evaluation, patients whose disease
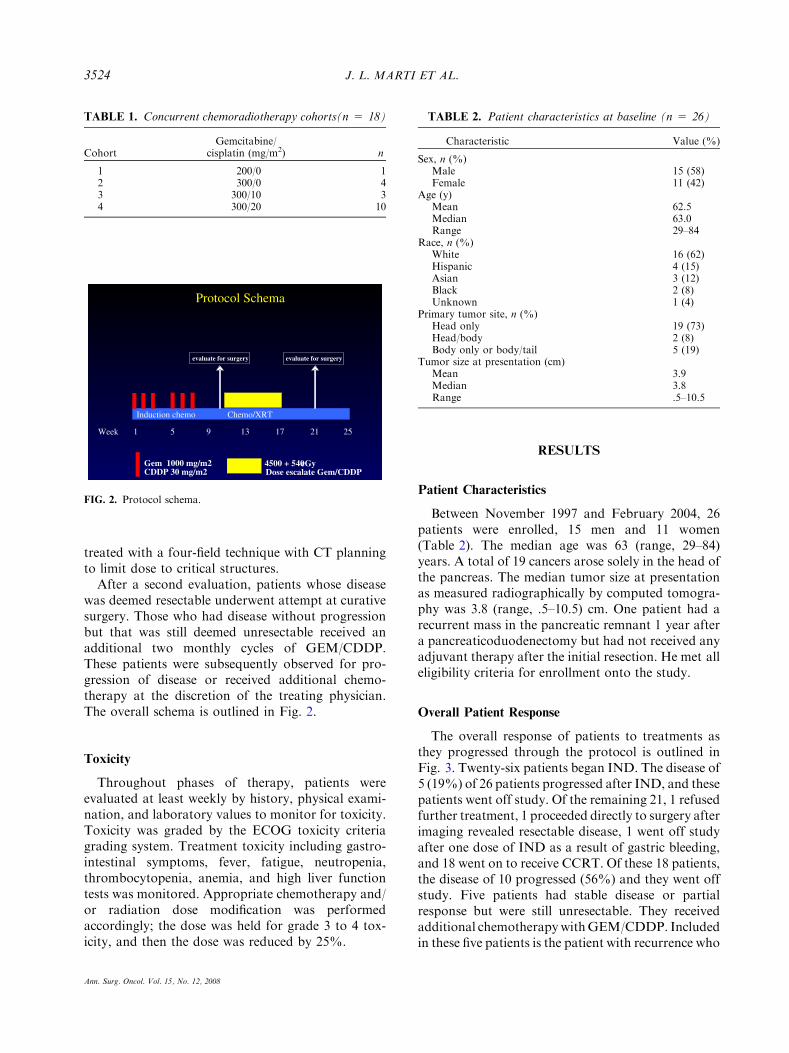
was deemed resectable underwent attempt at curativesurgery. Those who had disease without progressionbut that was still deemed unresectable received anadditional two monthly cycles of GEM/CDDP.These patients were subsequently observed for pro-gression of disease or received additional chemo-therapy at the discretion of the treating physician.The overall schema is outlined in Fig. 2.
Toxicity
Throughout phases of therapy, patients wereevaluated at least weekly by history, physical exami-nation, and laboratory values to monitor for toxicity.Toxicity was graded by the ECOG toxicity criteriagrading system. Treatment toxicity including gastro-intestinal symptoms, fever, fatigue, neutropenia,thrombocytopenia, anemia, and high liver functiontests was monitored. Appropriate chemotherapy and/or radiation dose modification was performedaccordingly; the dose was held for grade 3 to 4 tox-icity, and then the dose was reduced by 25%.
RESULTS
Patient Characteristics
Between November 1997 and February 2004, 26patients were enrolled, 15 men and 11 women(Table 2). The median age was 63 (range, 29–84)years. A total of 19 cancers arose solely in the head ofthe pancreas. The median tumor size at presentationas measured radiographically by computed tomogra-phy was 3.8 (range, .5–10.5) cm. One patient had arecurrent mass in the pancreatic remnant 1 year aftera pancreaticoduodenectomy but had not received anyadjuvant therapy after the initial resection. He met alleligibility criteria for enrollment onto the study.
Overall Patient Response
The overall response of patients to treatments asthey progressed through the protocol is outlined inFig. 3. Twenty-six patients began IND. The disease of5 (19%) of 26 patients progressed after IND, and thesepatients went off study. Of the remaining 21, 1 refusedfurther treatment, 1 proceeded directly to surgery afterimaging revealed resectable disease, 1 went off studyafter one dose of IND as a result of gastric bleeding,and 18 went on to receive CCRT. Of these 18 patients,the disease of 10 progressed (56%) and they went offstudy. Five patients had stable disease or partialresponse but were still unresectable. They receivedadditional chemotherapywithGEM/CDDP. Includedin these five patients is the patient with recurrence who
TABLE 1. Concurrent chemoradiotherapy cohorts(n = 18)
CohortGemcitabine/
cisplatin (mg/m2) n
1 200/0 12 300/0 43 300/10 34 300/20 10
Protocol Schema
Week 1 5 9 13 17 21 25
Induction chemo
Gem 1000 mg/m2 CDDP 30 mg/m2
4500 + 540 cGyDose escalate Gem/CDDP
evaluate for surgery evaluate for surgery
Chemo/XRT
FIG. 2. Protocol schema.
TABLE 2. Patient characteristics at baseline (n = 26)
Characteristic Value (%)
Sex, n (%)Male 15 (58)Female 11 (42)
Age (y)Mean 62.5Median 63.0Range 29–84
Race, n (%)White 16 (62)Hispanic 4 (15)Asian 3 (12)Black 2 (8)Unknown 1 (4)
Primary tumor site, n (%)Head only 19 (73)Head/body 2 (8)Body only or body/tail 5 (19)
Tumor size at presentation (cm)Mean 3.9Median 3.8Range .5–10.5
J. L. MARTI ET AL.3524
Ann. Surg. Oncol. Vol. 15, No. 12, 2008
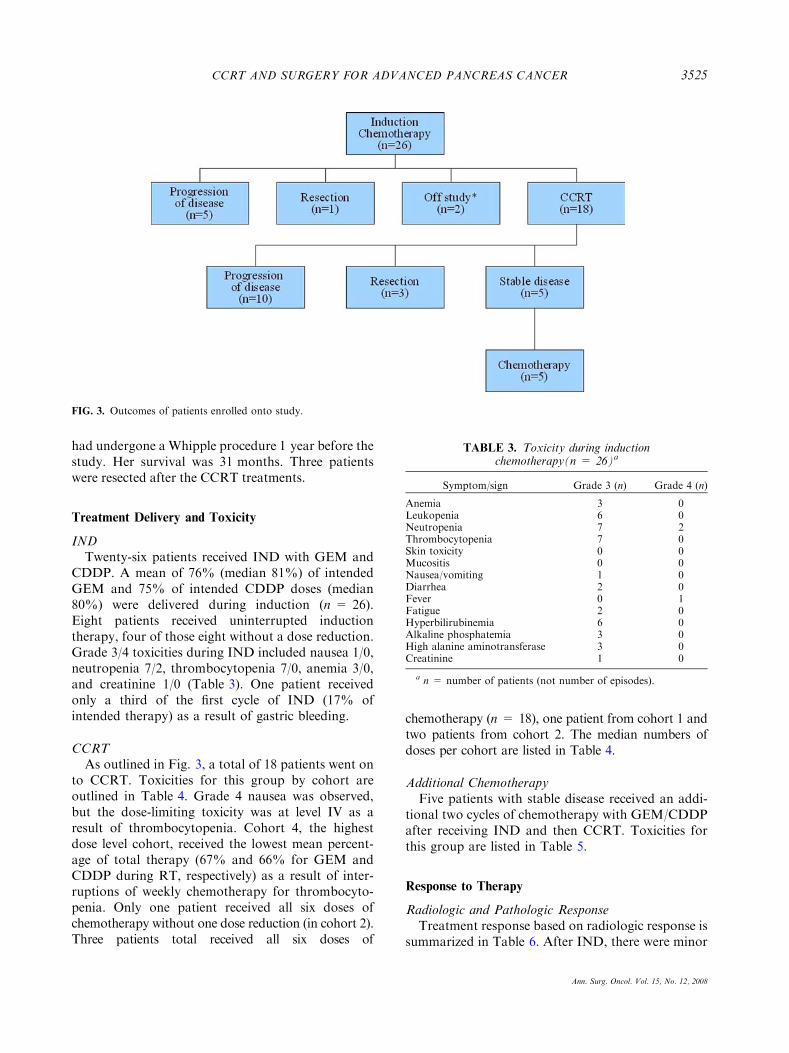
had undergone a Whipple procedure 1 year before thestudy. Her survival was 31 months. Three patientswere resected after the CCRT treatments.
Treatment Delivery and Toxicity
INDTwenty-six patients received IND with GEM and
CDDP. A mean of 76% (median 81%) of intendedGEM and 75% of intended CDDP doses (median80%) were delivered during induction (n = 26).Eight patients received uninterrupted inductiontherapy, four of those eight without a dose reduction.Grade 3/4 toxicities during IND included nausea 1/0,neutropenia 7/2, thrombocytopenia 7/0, anemia 3/0,and creatinine 1/0 (Table 3). One patient receivedonly a third of the first cycle of IND (17% ofintended therapy) as a result of gastric bleeding.
CCRTAs outlined in Fig. 3, a total of 18 patients went on
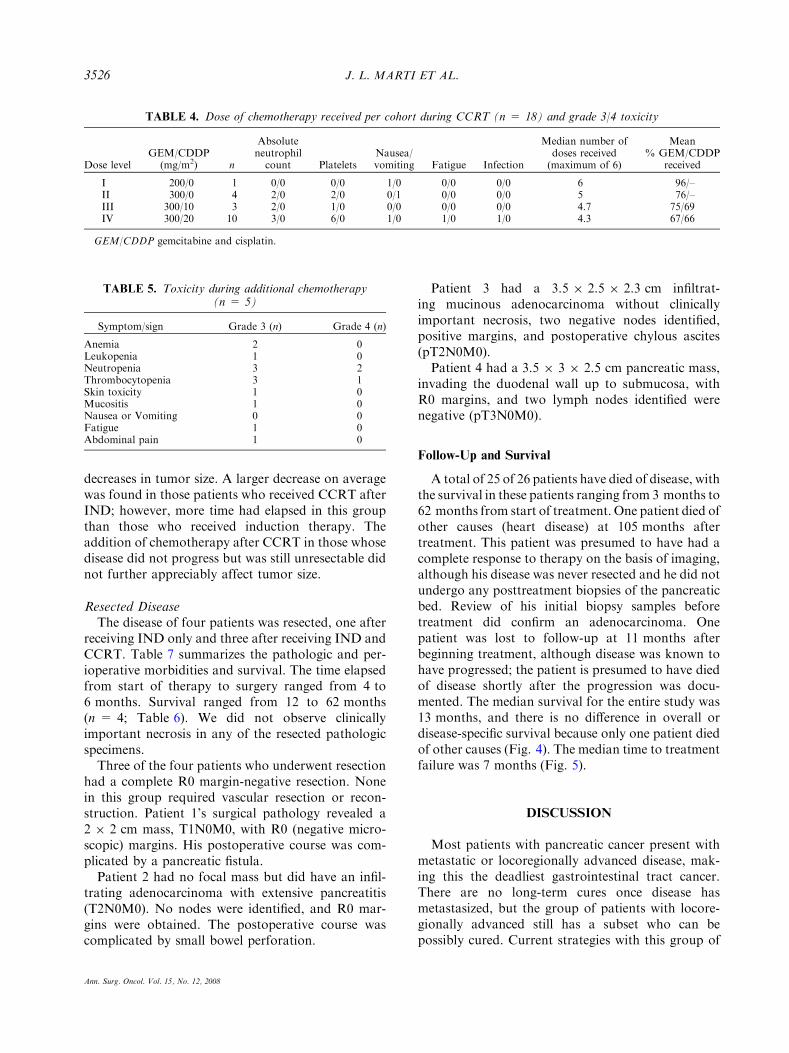
to CCRT. Toxicities for this group by cohort areoutlined in Table 4. Grade 4 nausea was observed,but the dose-limiting toxicity was at level IV as aresult of thrombocytopenia. Cohort 4, the highestdose level cohort, received the lowest mean percent-age of total therapy (67% and 66% for GEM andCDDP during RT, respectively) as a result of inter-ruptions of weekly chemotherapy for thrombocyto-penia. Only one patient received all six doses ofchemotherapy without one dose reduction (in cohort 2).Three patients total received all six doses of
chemotherapy (n = 18), one patient from cohort 1 andtwo patients from cohort 2. The median numbers ofdoses per cohort are listed in Table 4.
Additional ChemotherapyFive patients with stable disease received an addi-
tional two cycles of chemotherapy with GEM/CDDPafter receiving IND and then CCRT. Toxicities forthis group are listed in Table 5.
Response to Therapy
Radiologic and Pathologic ResponseTreatment response based on radiologic response is
summarized in Table 6. After IND, there were minor
FIG. 3. Outcomes of patients enrolled onto study.
TABLE 3. Toxicity during inductionchemotherapy(n = 26)a
Symptom/sign Grade 3 (n) Grade 4 (n)
Anemia 3 0Leukopenia 6 0Neutropenia 7 2Thrombocytopenia 7 0Skin toxicity 0 0Mucositis 0 0Nausea/vomiting 1 0Diarrhea 2 0Fever 0 1Fatigue 2 0Hyperbilirubinemia 6 0Alkaline phosphatemia 3 0High alanine aminotransferase 3 0Creatinine 1 0
a n = number of patients (not number of episodes).
CCRT AND SURGERY FOR ADVANCED PANCREAS CANCER 3525
Ann. Surg. Oncol. Vol. 15, No. 12, 2008
decreases in tumor size. A larger decrease on averagewas found in those patients who received CCRT afterIND; however, more time had elapsed in this groupthan those who received induction therapy. Theaddition of chemotherapy after CCRT in those whosedisease did not progress but was still unresectable didnot further appreciably affect tumor size.
Resected DiseaseThe disease of four patients was resected, one after
receiving IND only and three after receiving IND andCCRT. Table 7 summarizes the pathologic and per-ioperative morbidities and survival. The time elapsedfrom start of therapy to surgery ranged from 4 to6 months. Survival ranged from 12 to 62 months(n = 4; Table 6). We did not observe clinicallyimportant necrosis in any of the resected pathologicspecimens.Three of the four patients who underwent resection
had a complete R0 margin-negative resection. Nonein this group required vascular resection or recon-struction. Patient 1’s surgical pathology revealed a2 9 2 cm mass, T1N0M0, with R0 (negative micro-scopic) margins. His postoperative course was com-plicated by a pancreatic fistula.Patient 2 had no focal mass but did have an infil-
trating adenocarcinoma with extensive pancreatitis(T2N0M0). No nodes were identified, and R0 mar-gins were obtained. The postoperative course wascomplicated by small bowel perforation.
Patient 3 had a 3.5 9 2.5 9 2.3 cm infiltrat-ing mucinous adenocarcinoma without clinicallyimportant necrosis, two negative nodes identified,positive margins, and postoperative chylous ascites(pT2N0M0).Patient 4 had a 3.5 9 3 9 2.5 cm pancreatic mass,
invading the duodenal wall up to submucosa, withR0 margins, and two lymph nodes identified werenegative (pT3N0M0).
Follow-Up and Survival
A total of 25 of 26 patients have died of disease, withthe survival in these patients ranging from 3 months to62 months from start of treatment. One patient died ofother causes (heart disease) at 105 months aftertreatment. This patient was presumed to have had acomplete response to therapy on the basis of imaging,although his disease was never resected and he did notundergo any posttreatment biopsies of the pancreaticbed. Review of his initial biopsy samples beforetreatment did confirm an adenocarcinoma. Onepatient was lost to follow-up at 11 months afterbeginning treatment, although disease was known tohave progressed; the patient is presumed to have diedof disease shortly after the progression was docu-mented. The median survival for the entire study was13 months, and there is no difference in overall ordisease-specific survival because only one patient diedof other causes (Fig. 4). The median time to treatmentfailure was 7 months (Fig. 5).
DISCUSSION
Most patients with pancreatic cancer present withmetastatic or locoregionally advanced disease, mak-ing this the deadliest gastrointestinal tract cancer.There are no long-term cures once disease hasmetastasized, but the group of patients with locore-gionally advanced still has a subset who can bepossibly cured. Current strategies with this group of
TABLE 4. Dose of chemotherapy received per cohort during CCRT (n = 18) and grade 3/4 toxicity
Dose levelGEM/CDDP
(mg/m2) n
Absoluteneutrophil
count PlateletsNausea/vomiting Fatigue Infection
Median number ofdoses received(maximum of 6)
Mean% GEM/CDDP
received
I 200/0 1 0/0 0/0 1/0 0/0 0/0 6 96/–II 300/0 4 2/0 2/0 0/1 0/0 0/0 5 76/–III 300/10 3 2/0 1/0 0/0 0/0 0/0 4.7 75/69IV 300/20 10 3/0 6/0 1/0 1/0 1/0 4.3 67/66
GEM/CDDP gemcitabine and cisplatin.
TABLE 5. Toxicity during additional chemotherapy(n = 5)
Symptom/sign Grade 3 (n) Grade 4 (n)
Anemia 2 0Leukopenia 1 0Neutropenia 3 2Thrombocytopenia 3 1Skin toxicity 1 0Mucositis 1 0Nausea or Vomiting 0 0Fatigue 1 0Abdominal pain 1 0
J. L. MARTI ET AL.3526
Ann. Surg. Oncol. Vol. 15, No. 12, 2008

patients focus on multimodality treatments andidentifying those who can be brought to resection foran attempt at cure. In this study, we introduced anovel treatment regimen for these patients: inductionGEM/CDDP, followed by concurrent chemoradia-tion, followed by either surgery or further chemo-therapy, depending on tumor response. We found theregimen to be feasible with expected toxicities ofcombined chemoradiation, with an overall survivalthat is on the higher end of other comparable studies.Most importantly, resectability for cure was
attempted in four patients in this study, with threehaving negative margins (R0 resections). Of particu-lar note is that all four patients had pathologicallynegative nodes at the time of resection.When discussing locoregionally advanced pancre-
atic cancer, and assessing the literature and otherstudies, two key issues arise. One is defining the natureof the disease being dealt with, and the second isdefining resectability. The term locally advanced pan-creas cancer has been used in many publications todefine disease that abuts, involves, or encases the
TABLE 6. Radiologic response at varying phases of therapy
CharacteristicAt presentation
(n = 26)After IND(n = 26)
After CCRT(n = 18)
After additionalCT (n = 5)
Mean 3.9 cm 3.8 cma 3.3 cmb 3.1 cmMedian 3.8 cm 3.8 cma 3.65 cmb 3.0 cmRange .5–10.5 cm .4–9.0 cma 0 (NED) to 6.5 cmb 1.0 to 5.0 cmProgression of disease 19% (n = 5) 56% (n = 10) 0% (n = 0)Stable disease or partial response 81% (n = 21) 44% (n = 8) 100% (n = 5)
IND induction chemotherapy, CCRT concurrent chemoradiotherapy, CT chemotherapy.a n = 23; size not measured by radiologist for 3.b n = 16; size not measured by radiologist for 2.
TABLE 7. Summary of patients who underwent pancreaticoduodenectomy
Patient Preoperative therapy Stage Margin Postoperative morbiditySurvival(months)
1 IND T1NOMO R0 Pancreatic fistula 202 IND and CCRT (cohort 1) T2N0M0 R0 Small bowel perforation 123 IND and CCRT (cohort 2) T3N0MX R1 Chylous ascites 144 IND and CCRT (cohort 4) T2N0MX R0 None 62
IND induction chemotherapy, CCRT concurrent chemoradiotherapy.
Overall SurvivalNYU 97-03
Months from start of treatment
12010896847260483624120
Ove
rall
Sur
viva
l
1.0
.8
.6
.4
.2
0.0
Survival Function
Censored
FIG. 4. Overall survival.
Time to Treatment Failure
NYU 97 - 03
Months from start of treatment to falure
12010896847260483624120
Cum
Sur
viva
l
1.0
.8
.6
.4
.2
0.0
Survival Function
Censored
FIG. 5. Time to treatment failure.
CCRT AND SURGERY FOR ADVANCED PANCREAS CANCER 3527
Ann. Surg. Oncol. Vol. 15, No. 12, 2008
regional mesenteric vessels for varied lengths leadingto a heterogeneous population of patients beingreported on under this same descriptor. Yet if we lookat the current NCCN guidelines that define resect-ability, there is a clear distinction between borderlineresectable (e.g., superior mesenteric vein impinge-ment, superior mesenteric artery abutment) andlocally advanced unresectable (e.g., superior mesen-teric vein occlusion, superior mesenteric arteryencasement).7 Therefore, it is important to clarifywhich patient population is being studied. We haveused the term locoregionally advanced disease in abroad sense to encompass both the patients withborderline resectable disease and those with locallyadvanced unresectable disease that we described inthis study. Clearly one would expect more patients inthe former group to possibly come to resection asopposed to in the latter group (as we showed in ourstudy). We would suggest that the current, commonuse of the term locally advanced for studies of thisnature49–52,54,55,57 should be restricted only to studiesthat meet the NCCN guidelines for unresectable dis-ease.7 Ultimately, however, regardless of how weattempt to define resectability by imaging, the onlytrue definition of a resectable lesion must relate to agross and microscopic negative resection margin.Patients with locoregionally advanced disease under-going margin-positive resection do not seem to havebetter survival outcomes than the unresected group.8
Because our study was started before the publica-tion of the NCCN guidelines, we only includedpatients with disease that was considered unresec-table by initial surgical evaluation with close surgicalconsultation during the course of therapy. We spe-cifically retrospectively reviewed our cases to moreaccurately define our population of patients. Wefound that 23 of our 26 patients with locoregionallyadvanced disease had locally advanced, unresectabledisease as defined by the NCCN guidelines.7 Of these23 patients, none were resected for cure (one wasresected but had a positive margin). Three of 26patients had NCCN-defined borderline resectabledisease, and all 3 were able to undergo curativemargin-negative resection. Although clearly thesenumbers are too small to make any definitive state-ments, it certainly supports the concept that whendealing with locoregionally advanced pancreaticcancer, the borderline resectable group is more likelyto have a chance for curative resection as opposed toa truly defined locally advanced group. Our curative(R0) resectability rate was 12% (3 of 26)—compa-rable to the 13% of patients undergoing resection inthe study of Ammori et al.14 of GEM/RT, anothergroup that used NCCN criteria to differentiatebetween borderline resectable and locally advancedunresectable.7
Our resectability rate was not as favorable as the28% of patients who obtained R0 resections in
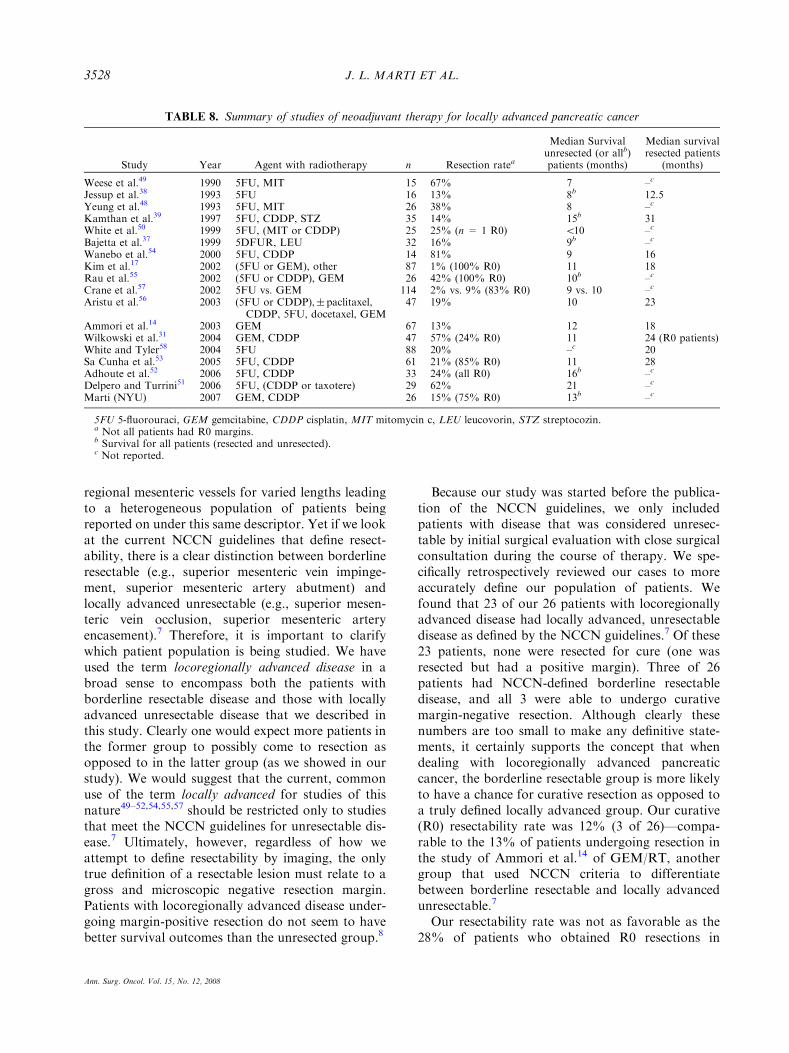
TABLE 8. Summary of studies of neoadjuvant therapy for locally advanced pancreatic cancer
Study Year Agent with radiotherapy n Resection ratea
Median Survivalunresected (or allb)patients (months)
Median survivalresected patients
(months)
Weese et al.49 1990 5FU, MIT 15 67% 7 –c
Jessup et al.38 1993 5FU 16 13% 8b 12.5Yeung et al.48 1993 5FU, MIT 26 38% 8 –c
Kamthan et al.39 1997 5FU, CDDP, STZ 35 14% 15b 31White et al.50 1999 5FU, (MIT or CDDP) 25 25% (n = 1 R0) <10 –c
Bajetta et al.37 1999 5DFUR, LEU 32 16% 9b –c
Wanebo et al.54 2000 5FU, CDDP 14 81% 9 16Kim et al.17 2002 (5FU or GEM), other 87 1% (100% R0) 11 18Rau et al.55 2002 (5FU or CDDP), GEM 26 42% (100% R0) 10b –c
Crane et al.57 2002 5FU vs. GEM 114 2% vs. 9% (83% R0) 9 vs. 10 –c
Aristu et al.56 2003 (5FU or CDDP),±paclitaxel,CDDP, 5FU, docetaxel, GEM
47 19% 10 23
Ammori et al.14 2003 GEM 67 13% 12 18Wilkowski et al.31 2004 GEM, CDDP 47 57% (24% R0) 11 24 (R0 patients)White and Tyler58 2004 5FU 88 20% –c 20Sa Cunha et al.53 2005 5FU, CDDP 61 21% (85% R0) 11 28Adhoute et al.52 2006 5FU, CDDP 33 24% (all R0) 16b –c
Delpero and Turrini51 2006 5FU, (CDDP or taxotere) 29 62% 21 –c
Marti (NYU) 2007 GEM, CDDP 26 15% (75% R0) 13b –c
5FU 5-fluorouraci, GEM gemcitabine, CDDP cisplatin, MIT mitomycin c, LEU leucovorin, STZ streptocozin.a Not all patients had R0 margins.b Survival for all patients (resected and unresected).c Not reported.
J. L. MARTI ET AL.3528
Ann. Surg. Oncol. Vol. 15, No. 12, 2008
the study by Wilkowski et al.31; however, theirresectability criteria were more loosely defined anddid not strictly adhere to differentiating betweenthose that were borderline resectable initially andthose that were locally advanced unresectable.31
The benefit of combined modality therapy forlocally advanced pancreatic cancer has been demon-strated in previous trials12,13,32–35 (Table 8). Asshown in our study, at times chemoradiotherapy mayrender a subset of patients resectable.14–16,36–39
However, direct comparisons often cannot be madebetween studies as a result of differing protocols andvarying definitions, as explained above.Earlier studies have relied on a 5FU- or CDDP-
based mode of therapy. The use of GEM in advancedpancreas cancer was shown to be superior to 5FU byBurris et al.27 as well as others40,41 both in terms ofsurvival and toxicity. GEM, a nucleoside analogue ofdeoxycytidine, works as an antimetabolite and RTsensitizer.29,30,42–44 GEM has also been shown to besynergistic with CDDP in a number of cell lines,including pancreatic cell lines. It is approved by theU.S. Food and Drug Administration for use withCDDP in the treatment of non-small-cell lung cancerand pancreatic cancer. Randomized studies of GEMalone versus GEM and CDDP or oxaliplatin haverevealed improved progression-free survival but notoverall survival with combined therapy,33 although arecent meta-analysis of these two large randomizedstudies did show borderline survival advantage.In this phase I/II trial, the regimen was well
tolerated. At least approximately two-thirds of thedose of GEM/CDDP was administered in all fourdose levels; this compares favorably to prior stud-ies.10,11,16,45,46 It is also noteworthy that the disease inone patient in this group completely responded totherapy. Two complete responses occurred in oneprior study of concurrent GEM with RT.47 This hasnot been observed with 5FU. In the present study,many patients had either stable disease or a partialresponse after IND and CCRT.In terms of survival outcomes, our data are com-
parable to other studies assessing combined modalitytherapy for locoregionally advanced pancreas cancer(Table 8).48–58 As would be expected, those whocome to resection have better survival than those whodo not, which was consistent with findings in ourstudy. The four patients who underwent resection inour study had a range of survival from 12 to62 months (Table 7), which is comparable to otherreports. Our overall median survival of 13 months(n = 26) for this group of locoregionally advancedpancreas cancer patients is comparable to the median
survivals in the studies cited above (Table 8), where itranged from 7 to 21 months.This induction GEM/CDDP and concurrent che-
moradiation regimen is well tolerated, with mediantolerated dose of CCRT at dose level 3 (GEM200 mg/m2; CDDP 10 mg/m2) with median survivalin this trial in the upper limit of reported results forlocoregionally advanced pancreatic carcinoma. Fourof 26 patients were resected, three with negativemargins, allowing for prolonged survival, under-scoring the potential of neoadjuvant regimens toimprove outcome in this group of patients. However,more work and novel approaches are needed to trulyimprove outcome in those with locoregionallyadvanced pancreas cancer.
REFERENCES
1. Jemal A, Thomas A, Murray T, et al. Cancer Statistics. CACancer J Clin 2002; 52:23–47.
2. Heinemann V, Quietzsch D, Gieseler F, et al. RandomizedPhase III trial of gemcitabine pulse cisplatin compared withgemcitabine alone in advanced pancreatic cancer. J Clin Oncol2006; 24:3946–52.
3. Bramhall SR, Allum WH, Jones AG, et al. Treatment andsurvival in 13,560 patients with pancreatic cancer, and inci-dence of disease, in the west midlands: an epidemiologicalstudy. Br J Sur 1985; 82:111–5.
4. Parker S, Tong T, Bolden S, et al. Cancer statistics. CA CancerJ Clin 1997; 47:5–27.
5. Trede M, Schwal G, Saeger H, et al. Survival after pancreati-coduodenectomy. Ann Surg 1990; 211:447–58.
6. National Cancer Institute: Surveillance, Epidemiology, andEnd Results (SEER) *Stat 6.1 Database: Incidence—SEER 9Regs Public Use, Bethesda, MD, National Cancer Institute,DCCPS, Surveillance Research Program, Cancer StatisticsBranch. Nov 2004 Sub (1973–2002).
7. National Comprehensive Cancer Network (NCCN). Pancreaticadenocarcinoma. Practice Guidelines in Oncology. v.1.2008.Fort Washington, PA. http://www.nccn.org/professionals/physician_gls/PDF/pancreatic.pdf.
8. Massuco P, Capussotti L, Magnino A, et al. Pancreaticresections after chemotherapy for locally advanced ductaladenocarcinoma: analysis of perioperative outcome and sur-vival. Ann Surg Oncol 2006; 13:1201–8.
9. Talamonti M, Small W, Mulcahy M, et al. A Multi-institu-tional Phase II trial of preoperative full-dose gemcitabine andconcurrent radiation for patients with potentially resectablepancreatic carcinoma. Ann Surg Oncol 2005; 13:150–8.
10. Spitz FR, Abbruzzese JL, Lee JE, et al. Preoperative andpostoperative chemoradiation strategies in patients treatedwith pancreaticoduodenectomy for adenocarcinoma of thepancreas. J Clin Oncol 1997; 15:928–37.
11. Hoffman J, Lipsitz S, Pisansky T, et al. Phase II trial of pre-operative radiation therapy and chemotherapy for patientswith localized, resectable adenocarcinoma of the pancreas: anEastern Cooperative Oncology Group study. J Clin Oncol1998; 16:317–23.
12. Moertel CG, Frytak S, Hahn RG, et al. Therapy of locallyunresectable pancreatic carcinoma: a randomized comparisonof high dose (6000 rads) radiation alone, moderate dose radi-ation (4000 rads + 5-fluorouracil), and high dose radiation +5-fluorouracil. Cancer 1981; 48:1075–10.
CCRT AND SURGERY FOR ADVANCED PANCREAS CANCER 3529
Ann. Surg. Oncol. Vol. 15, No. 12, 2008
13. Gastrointestinal Tumor Study Group Treatment of locallyunresectable carcinoma of the pancreas: comparison ofcombined-modality therapy (chemotherapy plus radiotherapy)to chemotherapy alone. J Natl Cancer Inst 1988; 80:751–5.
14. Ammori JB, Colletti LM, Zalupski MM, et al. Surgicalresection following radiation therapy with concurrent gemcit-abine in patients with previously unresectable adenocarcinomaof the pancreas. J Gastrointest Surg 2003; 7:766–72.
15. Chao C, Hoffman J, Ross E, et al. Pancreatic carcinomadeemed unresectable at exploration may be resected for cure:an institutional experience. Am Surg 2000; 66:378–87.
16. White RR, Hurwitz HI, Morse MA, et al. Neoadjuvant che-moradiation for localized adenocarcinoma of the pancreas.Ann Sur Oncol 2001; 8:758–65.
17. Kim HJ, Czischke K, Brennan MF, et al. Does neoadjuvantchemoradiation downstage locally advanced pancreatic cancer?J Gastrointest Surg 2002; 6:763–9.
18. Berlin JD, Catalano P, Thomas JP, et al. Phase III study ofgemcitabine in combination with fluorouracil versus gemcita-bine alone in patients with advanced pancreatic carcinoma:Eastern Cooperative Oncology Group Trial E2297. J ClinOncol 2002; 20:3270–5.
19. Moore MJ, Hamm J, Dancey J, et al. Comparison of gemcit-abine versus the matrix metalloproteinase inhibitor BAY 12-9566 in patients with advanced or metastatic adenocarcinomaof the pancreas: a phase III trial of the National CancerInstitute of Canada Clinical Trials Group. J Clin Oncol 2003;21:3296–302.
20. Rocha L, Green M, Roche R, et al. Irinotecan plus gemcita-bine results in no survival advantage compared with gemcita-bine monotherapy in patients with locally advanced ormetastatic pancreatic cancer despite increased tumor responserate. J Clin Oncol 2004; 22:3776–83.
21. Bramhall SR, Schultz J, Nemunaitis J, et al. A double-blindplacebo-controlled, randomised study comparing gemcitabineand marimastat with gemcitabine and placebo as first linetherapy in patients with advanced pancreatic cancer. Br JCancer 2002; 87:161–7.
22. Bramhal SR, Rosemurgy A, Brown PD, Marimastat Pancre-atic Cancer Study Group. Marimastat as first-line therapy forpatients with unresectable pancreatic cancer: a randomizedtrial. J Clin Oncol 2001; 19:3477–55.
23. Van Cutsem E, van de Velde H, Karase P, et al. Phase III trial ofgemcitabine plus tipifarnib compared with gemcitabine plus pla-cebo in advanced pancreatic cancer. JClinOncol 2004; 22:1430–8.
24. O’Reilly EM, Abou-Alfa GK, Letorneau R, et al. A random-ized phase III trial of DX-8951f (exatecan mesylate) andgemcitabine vs gemcitabine alone in advanced pancreatic can-cer. Proc Am Soc Clin Oncol 2004; 23:abstr 4006.
25. Richards DA, Kindler HL, Oettle H, et al. A randomizedphase III study comparing gemcitabine + pemetrexed versusgemcitabine in patients with locally advanced and metastaticpancreas cancer. Proc Am Soc Clin Oncol 2004; 23:abstr 4007.
26. Louvet C, LabiancaR,Hammel P, et al. GemOx (gemcitabine+oxaliplatin) versus Gem (gemcitabine) in non-resectable pancre-atic adenocarcinoma: final results of the GERCOR/GISCADIntergroupphase III.ProcAmSocClinOncol2004; 23:abstr 4008.
27. Burris HA, Moore MJ, Anderson J, et al. Improvements insurvival and clinical benefit with gemcitabine as first-linetherapy for patients with advanced pancreas cancer: a ran-domized trial. J Clin Oncol 1997; 15:2403–13.
28. Bergman A, van Ruiz Haperen V, Veerman G, et al. Syner-gistic interaction between cisplatin and gemcitabine in vitro.Clin Cancer Res 1996; 2:521–30.
29. Lawrence T, Chang E, Hahn T, et al. Radiosensitization ofpancreatic cancer cells by 20,-difluoro-20deoxycytidine. Int JRadiat Oncol Biol Phys 1996; 34:867–72.
30. Pauwels B, Korst A, Lardon F, et al. Combined modality ther-apy of gemcitabine and radiation. Oncologist 2005; 10:34–51.
31. Wilkowski R, Thoma M, Schauer R, et al. Effect of chemo-radiotherapy with gemcitabine and cisplatin on locoregionalcontrol in patients with primary inoperable pancreatic cancer.World J Surg 2004; 28:1011–8.
32. Haller DG. Chemotherapy for advanced pancreatic cancer. IntJ Radiat Oncol Biol Phys 2003; 56:16–23.
33. Heinemann V. Gemcitabine based combination treatment ofpancreatic cancer. Semin Oncol 2002; 29:25–35.
34. Reni M, Cordio S, Milandri C, et al. Gemcitabine versus cis-platin epirubicin, fluorouracil, and gemcitabine in advancedpancreatic cancer: a randomised controlled multicentre phaseIII trial. Lancet Oncol 2005; 6:369–76.
35. Gastrointestinal Tumor Study Group. A multi-institutionalcomparative trial of radiation therapy alone and in combina-tion with 5-FU for locally unresectable pancreatic cancer. AmSurg 1979;189:205–11.
36. Cora L, Coffman L, Sher R, et al. Preoperative chemoradia-tion for adenocarcinoma of the pancreas and duodenum. Int JRadiat Oncol Biol Phys 1994; 30:161–7.
37. Bajetta E, Di Bartolomeo M, Stani SC, et al. Chemotherapy aspreoperative treatment in locally advanced unresectable pan-creatic cancer patients: results of a feasibility study. J RadiatOncol Biol Phys 1999; 45:285–9.
38. Jessup JM, Steele, Mayer RJ, et al. Neoadjuvant therapy forunresectable pancreatic adenocarcinoma. Arch Surg 1993;128:559–64.
39. Kamthan AG, Morris J, Dalton J, et al. Combined modalitytherapy for stage II and stage III pancreatic carcinoma. J ClinOncol 1997; 15:2920–7.
40. Poplin E, Corbett T, Flaherty L, et al. Difluorodeoxycytidine(dFDC)-gemcitabine: a phase I study. Invest New Drugs 1992;10:165–70.
41. Rothenberg M, Moore M, Cripps M, et al. A phase II trial ofgemcitabine in patients with 5-FU refractory pancreas cancer.Ann Oncol 1996; 7:347–53.
42. McGinn C, Smith D, Ozark’s C, et al. A phase I study ofgemcitabine in combination with radiation therapy in patientswith localized, unresectable pancreatic cancer. Proc ASCO1998; 17:264a.
43. McGinn C, Zalupski M, Shureiqi I, et al. A phase I trial ofradiation dose escalation with concurrent weekly full dosegemcitabine in patients with advanced pancreatic cancer. J ClinOncol 2001; 19:4202–8.
44. Eisbruch A, Shewach D, Bradford C, et al. Radiation con-current with gemcitabine for locally advanced head and neckcancer: a phase I trial and intracellular drug incorporationstudy. J Clin Oncol 2001; 19:792–9.
45. Evans D, Rich T, Byrd D. Preoperative chemoradiation andpancreaticoduodenectomy for adenocarcinoma of the pan-creas. Arch Surg 1992; 127:1335–9.
46. Pisters PW, Abbruzzese JL, Janjan NA, et al. Rapid-frac-tionation preoperative chemoradiation, pancreaticoduodenec-tomy and intraoperative radiation therapy for resectablepancreatic adenocarcinoma. J Clin Oncol 1998; 16:3843–50.
47. Abou-Alfa GK, Letourneau R, Harker G, et al. O’Reilly EM.Randomized phase III study of exatecan and gemcitabinecompared with gemcitabine alone in untreated advanced pan-creatic cancer. J Clin Oncol 2006; 4:4441–7.
48. Yeung R, Weese J, Hoffman J, et al. Neoadjuvant chemora-diation in pancreatic and duodenal carcinoma. A phase IIstudy. Cancer 1993; 72:2124–33.
49. Weese JL, Nussbaum ML, Paul AR. Increased resectability oflocally advanced pancreatic and periampullary carcinoma withneoadjuvant chemoradiotherapy. Int J Pancreatol 1990; 7:177–85.
50. White R, Lee C, Anscher M, et al. Preoperative chemoradia-tion for patients with locally advanced adenocarcinoma of thepancreas. Ann Surg Oncol 1999; 6:38–45.
J. L. MARTI ET AL.3530
Ann. Surg. Oncol. Vol. 15, No. 12, 2008
51. Delpero JR, Turrini O. Locally advanced pancreatic adeno-carcinoma. Chemoradiotherapy, reevaluation and secondaryresection. Cancer Radiother 2006; 10:462–70.
52. Adhoute X, Smith D, Vendrely V, et al. Subsequent resectionof locally advanced pancreatic carcinoma after chemoradio-therapy. Gastroenterol Clin Biol 2006; 30:224–30.
53. Sa Cunha A, Rault A, Laurent C, et al. Surgical resection afterradiochemotherapy in patients with unresectable adenocarci-noma of the pancreas. Am Coll Surg 2005; 201:359–65.
54. Wanebo HJ, Glicksman AS, Vezeridis MP, et al. Preoperativechemotherapy, radiotherapy, and surgical resection of locallyadvanced pancreatic cancer. Arch Surg 2000; 135:81–7.
55. Rau HG, Wichmann MW, Wilkowski R, et al. Surgical ther-apy of locally advanced and primary inoperable pancreatic
carcinoma after neoadjuvant preoperative radio chemother-apy. Chirurg 2002; 73:132–7.
56. Aristu J, Canon R, Pardo F, et al. Surgical resection afterpreoperative chemoradiotherapy benefits selected patients withunresectable pancreatic cancer. Am J Clin Oncol 2003; 26:30–6.
57. Crane CH, Abbruzzeze JL, Evans DB, et al. Is the therapeuticindex better with Gemcitabine-based chemoradiation than with5-FU-based chemoradiation in LAPC? Int J Radiat Oncol BiolPhys 2002; 52:1293–302.
58. White RR, Tyler DS. Neoadjuvant therapy for pancreaticcancer: the Duke experience. Surg Oncol Clin N Am 2004;13:675–84.
CCRT AND SURGERY FOR ADVANCED PANCREAS CANCER 3531
Ann. Surg. Oncol. Vol. 15, No. 12, 2008