Dynamic fracture characteristics of the osteochondral junction undergoing shear deformation
Upload
independentCategory
view
0download
0
DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999 1371
O B S E RVAT I O N S
I m p roved Stabilityof Insulin DeliveryF rom ImplantedPumps Using a NewP reparation Pro c e s sfor Infused Insulin
For the last decade, implantable sys-tems infusing insulin by the peri-toneal route have been intensively
investigated as a means to improve meta-bolic control in diabetic patients. Report e ds i g n i ficant improvements in blood glucosestabilization suggest that this techniquecould provide long-term benefits to qual-ity of life for patients under intensifie dsubcutaneous insulin treatment who arep rone to severe hypoglycemia (1). More-o v e r, recent technical advances in glucosesensors may help implement the im-plantable art i ficial pancreas project, inwhich safe and reliable implanted insulind e l i v e ry devices will be highly valuable (1).Although the model 2001 MiniMedImplantable Pump (MIP 2001; MiniMedTechnologies, Sylmar, CA) has beenauthorized in the European Union since1993, technical issues dominated byinsulin underd e l i v e ry events pre c l u d e dwider clinical use until now. In a pre v i o u ss t u d y, we pointed to the determining ro l e sof insulin aggregation in the pump, whichresults in backflows, and of cathetero b s t ructions, which result in flo w - r a t ei m p a i rments (2). After modifications inthe manufacturing process of U400-Hoechst 21 pH-neutral semisynthetichuman insulin stabilized by Genapol(U400-HOE 21PH; Hoechst, Frankfurt ,G e rmany), batches showing improved sta-bility in pumps during bench tests havebeen available since July 1997. In the pre s-ent study, we assessed the accuracy ofinsulin delivery while using consecutivelytwo diff e rent preparation variants of U400-HOE 21PH under clinical conditions.
F rom October 1995 to October 1996,17 MIP 2001 pumps were implanted in 17type 1 diabetic patients (7 men, 10 women),aged 46 ± 12 years, with a diabetes historyof 28 ± 9 years. All patients gave their writ-ten consent to participate in a trial aimed atthe evaluation of U400-HOE 21PH insulind e l i v e ry from MIP 2001 after approval by
an ethics committee. Because of the poorphysical stability of insulin batches beforeJuly 1997, re fills of pump re s e rvoirs w e rep e rf o rmed every 30–45 days instead ofe v e ry 90 days as mentioned in the originalp ro c e d u re (2). More o v e r, re s e rvoirs werewashed by diluent insulin-free buff e rb e f o re each re fill to reduce accumulationof insulin aggregates. The time periodf rom implantation to July 1997 (period A)was 15.6 ± 4.0 months and accumulatedan experience of 22 patient-years. Fro mJuly 1997, the preparation process ofinsulin batches supplied by Hoechstincluded an additional step to re m o v einsoluble components using chro m a t o g r a-p h y. After satisfactory bench tests, manu-f a c t u rers allowed pump re fills every60–90 days without perf o rming washes ofre s e rvoirs. The time period in which thenew preparation variant of insulin wasstudied (period B) lasted to the end of Sep-tember 1998 (11.6 ± 1.4 months), accu-mulating an experience of 16 patient-years. To discard insulin aggregates thatmight have formed in re s e rvoirs and tub-ings during period A, a specific cleaningp ro c e d u re of pumps was designed beforere filling them with new batches. This pro-c e d u re included an infusion of 0.1 mol/lNaOH solution through the pumpingmechanism, a flush to clear the catheter bythe injection of diluent buffer through theside port, and a final infusion of diluenti n s u l i n - f ree buffer during 1 week, whichre q u i red transient subcutaneous insulint reatment. Each re fill was preceded by acheck of actual insulin delivery. Thea c t u a l / p rogrammed insulin delivery ratiowas calculated from the measurement ofthe residual volume in the re s e rvoir andthe expected value computed by thepump communicator from pro g r a m m i n gsince last pump re fill. In addition, dailyinsulin programming was provided by them e m o ry of the communicator. Metabolicc o n t rol was assessed by the measurement ofglycated hemoglobin (HbA1 c) by high-per-f o rmance liquid chromatography (Diamat;Bio-Rad, Munich) (normal value ,5 . 6 % ) a te v e ry other re fill until July 1997 and ateach re fill afterw a rds. Underd e l i v e ry wasd e fined as calculated reduction of flo wrate .15% (2). In both periods A and B,the first step to elucidate the mechanismof underd e l i v e ry consisted of a catheterflush through the side port with diluentb u ffer to remove any reversible cathetero b s t ruction at the peritoneal tip. Duringperiod A, the failure of this initial flu s h
was followed by rinsing the pump with0.1 mol/l NaOH as detailed above, butinsulin infusion was immediately re s u m e dafter this pro c e d u re. If underd e l i v e ry per-sisted at next re fill, we perf o rmed X-raysof the peritoneal catheter using contrastdye (Omnipaque 180; Nycomed, Paris) tosee the likely catheter obstruction. Duringperiod B, catheter X-rays were perf o rm e dfirst. Then, only the cases with no cathetero b s t ruction underwent rinsing withNaOH. The final diagnosis of the re a s o n sfor underd e l i v e ry was established accord-ing to the treatment, after which flow ratereduction decreased to ,15%. Numericalvariables, expressed as means ± SD, werec o m p a red by Student’s t test. Fre q u e n c i e sof events were compared by the x2 t e s t .
Period A (range 9.2–24.4 months)lasted significantly longer than period B(range 8.2–13.4 months) (P = 0.003). Dur-ing period A, 209 re fills of the 17 pumps(range per pump: 7–19) were perf o rm e d .The time interval between two re fills was38 ± 2 days. During period B, 75 pumpre fills (range per pump: 3–5) were done.The time interval between two re fills wass i g n i ficantly longer during period B thanduring period A: 78 ± 9 days (P = 0.0001).Neither reductions of flow rate (10.6 ± 5.9[A] vs. 12.7 ± 5.6% [B]) nor daily insulinre q u i rements (45 ± 13 [A] vs. 51 ± 17 IU[B]) were significantly diff e rent betweenperiods A and B. HbA1 c values were alsosimilar during both periods (7.4 ± 0.9 [A]vs. 7.4 ± 1.1% [B]). However, backflo w so c c u rred much less frequently duringperiod B: 1 (0.06 per patient-year) versus25 (1.13 per patient-year) (P , 0 . 0 0 1 ) .Backflows occurred in 13 pumps in period A. Five pumps developed one back-flow each, four pumps two backflows, andfour pumps three backflows each. The fir s tb a c k flows during period A were discov-e red 7.2 ± 2.8 months (range 3–11) afterimplantation, whereas the only backflo wduring period B was revealed after 14months. Incidence of catheter blockagesremained similar: 9 (0.41 per patient-year)(A) versus 6 (0.37 per patient-year) (B).
Insulin-pump compatibility standsamong the key factors involved in themaintenance of a normal flow rate fro mimplantable systems, as indicated by mostclinical experiences (1,2). Our re s u l t sre p o rt a dramatic reduction of eventsrelated to insulin precipitation when usinga new preparation process of U-400 HOE21PH insulin. These data indicate ap romising step on the way to resolving a
L E T T E R S

1372 DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999
Letters
major issue with implanted insulin deliv-e ry devices. Because of the longitudinaldesign and the experimental diff e rences inthe two periods of our study, potential biasfactors cannot be absolutely excluded.Thus, we cannot prove that rinses of re s e r-voir at pump re fills during period A,although expected to reduce the accumula-tion of insulin aggregates, had no deleteri-ous effects on insulin stability because of aninduced partial reduction of insulin c o n-centration. Besides, it is unknown w h e t h e rthe cleaning pro c e d u re perf o rmed b e f o reusing new insulin batches, a pro c e d u re thathad never been tested previously underclinical conditions, might have conferre dan advantage to period B data. Conversely,because most pumps had underg o n eb a c k flows during the preceding months,they might have remained prone to re c u r-rences despite the cleaning pro c e d u re .Another debatable point is whethercatheter obstructions disclosed in period Bcould have begun developing in period A,since encapsulation process is slow. Recentunpublished data suggest that the similaraverage flow-rate reduction in periods Aand B contrasted with the reduced occur-rence of backflows in period B might beexplained by problems of side-port com-pliance to pump strokes. Although ourdata need to be further confirmed bylonger experience with new insulinbatches and trials in newly implantedpumps, they should rouse renewed inter-est in this technique.
ERIC RENARD, MD
CÉLINE SOUCHE, PHARMD
DOMINIQUE JACQUES-APOSTOL, MD
DOMINIQUE LAUTON, MD
FRANÇOISE GIBERT-BOULET, MD
GUY COSTALAT, MD
JACQUES BRINGER, MD
CLAUDE JAFFIOL, MD
F rom the Department of Endocrinology, Lapeyro n i eHospital, Montpellier, France.
A d d ress correspondence to Eric Renard, MD,Endocrinology Department, Lapeyronie Hospital,F-34295 Montpellier Cedex 5, France. E-mail:re n a rd . a m t i m @ w a n a d o o . f r.
R e f e re n c e s1 . J a remko J, Rorstad O: Advances toward
the implantable art i ficial pancreas fort reatment of diabetes. Diabetes Care 2 1 :444–450, 1998
2 . R e n a rd E, Bouteleau S, Jacques-Apostol D,Lauton D, Gibert-Boulet F, Costalat G,Bringer B, Jaffiol C: Insulin underd e l i v e ryf rom implanted pumps using peritoneal
route: determinant role of insulin pumpc o m p a t i b i l i t y. Diabetes Care 1 9 : 8 1 2 – 8 1 7 ,1 9 9 6
Intensive InsulinTherapy Compare dWith ConventionalInsulin TherapyDoes Not ReduceD e p ressive Symptomsin Parents of Childre nWith Type 1 Diabetes
Juvenile type 1 diabetes has beenviewed as a stress factor that maycause psychological turbulence in the
a ffected child as well as his parents andfamily members (1). One might expect thattight diabetes control may a have a morepositive effect on the parents of childre nwith type 1 diabetes compared with con-ventional diabetes control and that switch-ing patients to the tight diabetes contro lregimen with intensive insulin therapy(IIT) may reduce the depressive symptomsof their parents. Studies demonstrated thatglycemic control is both directly and indi-rectly correlated with family functioning(2). Poor diabetes control was found tohave a negative impact on family function-ing, on parental depression, and on psy-chological problems affecting the familystability (3). No previous study has ad-d ressed the impact of tight diabetes contro lon the depressive symptoms of parents ofc h i l d ren with type 1 diabetes.
We measured the Beck Depression In-v e n t o ry (BDI) scores in parents of childre nt reated twice a day with conventionalinsulin therapy (CIT) and those in pare n t sof children treated with IIT. For each child,the psychologist and the social workeri d e n t i fied the one parent they believed tobe the most involved in the diabetes care ofthe child. A total of 40 parents of 40 type 1diabetic children were studied. Of the chil-d ren, 20 were treated with IIT (multipledaily injections) for at least 6 months, and20 were treated with CIT (twice daily injec-tions of regular and intermediate actinginsulin) for at least 6 months. Parents wereeligible for study if their child’s diseaseduration was .1 year, their child had noother acute or chronic illness and was re -ceiving no medications other than i n s u l i n ,and if the parent was not separated,d i v o rced, or widowed. All parents com-
pleted the BDI. This test is usually used todiscriminate among groups of people withrespect to the degree of depressive symp-toms (4). Student’s t test and Fisher’s exacttest were used. A P value ,0.05 wasaccepted as statistically signific a n t .
The mean ± SD patient age for IIT andCIT groups was similar (14 ± 4 and 13 ± 5 years, respectively). The male-to-femaleratio was 8/12 for the IIT patients and9/11 for the CIT patients. HBA1 c was lowerin the IIT group compared with the CITg roup (8.4 ± 1.6 vs. 11.0 ± 3.0%, P ,0.01). The amount of insulin/body weight(units per kilogram) was higher in the IITg roup compared with the CIT group (1.1 ±0.3 vs. 0.8 ± 0.3 U/kg, P , 0.05). Themean parent age for the IIT and CITg roups was similar (37 ± 10 and 34 ± 8 years, respectively), and the pare n t s ’male-to-female ratio was similar (18/2 and17/3, respectively). Family size, patern a ljob (blue collar/white collar), and thenumber of working mothers were re s p e c-tively similar in both groups. Corre l a t i o n sbetween BDI scores and either HbA1 c,duration of diabetes, age of the child, ageof the parent, family size, or family incomew e re determined for the IIT group, theCIT group, and the total population ofp a rents of type 1 diabetic children. Therewas no significant diff e rence in mean ± SDBDI scores between the IIT and the CITg roups (11 ± 8 vs. 12 ± 9, re s p e c t i v e l y ) .For the IIT group, the CIT group, and thewhole population of parents of type 1 dia-betic children, there were no signific a n tc o rrelations between BDI scores and eitherH b A1 c (r = 0.15 , n = 40, NS), duration ofdiabetes (r = 20.24, n = 40, NS), patientage (r = 20.12, n = 40, NS), parent age (r = 0.06, n = 40, NS), family size (r =20.24, n = 40, NS), or family income (r =20.14, n = 40, NS).
This study did not show that the par-e n t ’s depressive symptoms correlated withthe level of their child’s metabolic contro l ,and these symptoms were not lower inp a rents of the IIT group when compare dwith parents of the CIT group. In addition,and contrary to the theory that pare n t a ld e p ressive symptoms that are usuallyexperienced at the onset of the diseasetend to be buff e red with time (5), we wereunable to find any significant corre l a t i o nbetween the parental degree of depre s s i v esymptoms and the duration of the disease.Studies have shown a diff e rence in meta-bolic control depending on the age of thepatients, the pare n t ’s job, the duration ofthe disease, and the family size (6). It was

DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999 1373
Letters
also shown that high family life stre s s o r sc o rrelated with poor diabetic outcome (7).In our study, the lack of diff e rence betweenthe IIT and the CIT groups does not seemto be affected by any of the above familyvariables, since the two groups were simi-lar with respect to these variables. More-o v e r, this study did not find any corre l a t i o nbetween parental depressive symptomsand glycemic control, patient age, familysize, parent age, or family income.
One would speculate that stre s s e dfamilies tend not to accept or to follow IITc o m p a red with less stressed families.H o w e v e r, this theory does not seem to bet rue, since we did not find lower BDIs c o res in the IIT group compared with theCIT group. The lack of a diff e re n c ebetween the two groups may be due to thefact that hypoglycemias, and their psycho-logical impact on the parents, are morecommon in the IIT group, and may bythemselves be additional sources ofp a rental depressive symptoms.
F i n a l l y, we conclude that the degree ofd e p ressive symptoms in the parents oftype 1 diabetic children does not corre l a t ewith the level of metabolic control, the ageof the child, the age of the parent, theduration of diabetes, or the socioeconomicstatus of the family. We also conclude thatp a rents of type 1 diabetic children on IITdo not experience fewer depressive symp-toms than parents of type 1 diabetic chil-d ren on CIT and that switching patients tothe tight diabetes control regimen thataccompanies IIT does not reduce thed e p ressive symptoms of parents of type 1diabetic childre n .
SAMI T. AZAR, MD, FACP
NABIL KANAAN, MD
F rom the Division of Endocrinology (S.T. A . ) ,D e p a rtment of Internal Medicine, and the Depart-ment of Family Medicine (N.K.), American Univer-sity of Beirut Medical Center and Chronic CareCenter for Diabetes, Beirut, Lebanon.
A d d ress correspondence to Sami T. Azar, MD,FA C P, Division of Endocrinology, American Univer-sity Hospital, Bliss Street, Beirut, Lebanon. E-mail:s a z a r @ a u b . e d u . l b .
Acknowledgments — This work was sup-p o rted by a Lebanese National Council for Sci-e n t i fic Research grant (LRC-324110-32319).
R e f e re n c e s1 . Holmes DM: Diabetes in its psychosocial
context. In J o s l i n ’s Diabetes Mellitus. 12th ed.
Marble A, Krall LP, Bradley RF, Christlieb AR,Soeldner JS, Eds. Philadelphia, Lea &F e b i g e r, 1985, p. 892–906
2 . M a rteau TM, Bloch S, Baum D: Family lifeand diabetic control. J Child Psychiatr 2 8 :823–833, 1987
3 . N e w b rough JR, Simpkins CG, Maurer H:A family development approach to study-ing factors in the management and contro lof childhood diabetes. Diabetes Care 8 :83–92, 1985
4 . Beck AT, Wa rd CH, Mendelson M, Mock J,Erbaugh J: An inventory for measuringd e p ression. A rch Gen Psychiatr 4 : 5 3 – 6 3 ,1 9 6 1
5 . Spiess K, Sachs G, Moser G, PietschmannP, Schernthaner G, Prager R: Psychologicalmoderator variables and control in re c e n tonset type 1 diabetic patients: a two yearlongitudinal study. J Psychosom 3 8 : 2 4 9 –258, 1994
6 . Daviss WB, Coon H, Whitehead P, Ryan K,Burkley M, McMahon W: Predicting diabeticc o n t rol from competence, adherence, adjust-ment, and psychopathology. J Am Acad Child Adolesc Psychiatry 3 4 : 1 6 2 9 – 1 6 3 6 ,1 9 9 5
7 . Hinkle L, Congor G, Wolf S: Studies ondiabetes mellitus: the relation of stre s s f u llife situations to the concentration ofketone bodies in the blood of diabetic andnondiabetic humans. J Clin Invest 2 9 :754–769, 1950
Sustained I m p rovement ofGlycemic Control byInsulin Tre a t m e n tAfter 9 Years inPatients With Type 2Diabetes and S e c o n d a ry Failure
Insulin treatment is known to give short -t e rm improvement of glycemia, but itsl o n g - t e rm efficacy has been questioned
for reasons such as weight gain and hyper-insulinemia (1). Only a few studies havea d d ressed the long-term results of insulint reatment in type 2 diabetes (2–6). Wehave previously re p o rted results onglycemic control and other metabolic vari-ables in 21 patients after insulin tre a t m e n tfor a median of 27 months (7). A follow-up of glycemia, lipoprotein concentra-tions, and body weight by the same pro t o-col has now been perf o rmed after insulint reatment for a median of 110 (range92–131) months.
The 15 patients (9 men and 6 women)who took part in the study were 59.5 ± 2.5(mean ± SEM) years of age, with a knowndiabetes duration of 10.3 ± 1.7 years(3.5–30 years) and BMI 24.4 ± 0.8 kg/m2
when starting insulin treatment. Duringthe years following the 27 months exami-nation, 6 of the 21 patients in that exami-nation died. They were, on average, 5 years older than the surviving patients.All of the remaining patients agreed to takep a rt in the examination, which wasa p p roved by the local Ethics Committee.
The analytic methods have been pre v i-ously described (7). HbA1 c ( n o rmal range3.6–5.4%) was analyzed by an immunolog-ical method (Hitachi 917 analyzer; Roche,B romma, Sweden) and C-peptide inplasma by an enzyme-linked immunosor-bent assay method (Dako, Älvsjö, Sweden)at the present examination. Sex horm o n e -binding globulin (SHBG) was analyzed by aradioimmunoassay method from Euro -Diagnostica (Malmö, Sweden). Data weretested with analyses of variance for re p e a t e dm e a s u rements or by Friedman’s test.
While there was little diff e rence ininsulin dosage between the first weeks ofinsulin treatment and the 27-monthexamination, 51.3 ± 5.2 and 45.5 ± 7.2 U,re s p e c t i v e l y, the dosage was markedlyi n c reased at the 110-month examinationto 79.5 ± 10.8 U (P , 0.01 vs. 27months). Four patients changed theirinsulin regimen to a four-dose re g i m e n ,resulting in eight patients being treated byp reprandial regular insulin and NPHinsulin at bedtime and seven patientsremaining on a two-dose regimen withinjections before breakfast and dinner. Theglycemic control was markedly impro v e d ,with reduction of HbA1 c f rom 8.9 ± 0.2%during treatment with oral hypoglycemicagents to 6.8 ± 0.4% at 27 months, 6.9 ±0.2% at 60 months, and 7.3 ± 0.3% (P ,0.001 vs. baseline) at the 110-monthexamination. Both fasting, 11.9 ± 0.8mmol/l, and postprandial blood glucoseconcentrations, 17.2 ± 1.0 mmol/l, werel o w e red, to 7.9 ± 1.1 and 10.5 ± 0.9mmol/l, respectively (P , 0.01). Bodyweight increased rapidly during the fir s t4–5 months, but after 12 months, therewas no significant change (71.2 ± 3.2 kg atbaseline, 77.9 ± 3.2 kg at 27 months, 79.2± 3.3 kg at 60 months, and 78.8 ± 3.2 kgat 110 months). Only one patient experi-enced severe hypoglycemia (on thre eoccasions during a short period), defin e das requiring the help of another person.

1374 DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999
Letters
Fasting concentration of free insulin wasdoubled from 36.6 ± 4.8 to 73.8 ± 12.0pmol/l (P , 0.01), and the concentration90 min after the standardized bre a k f a s ti n c reased threefold (P , 0.0001) at the110-month examination, while there wasno diff e rence between the 27- and 110-month examinations. Fasting C-peptideconcentration was lowered from 0.65 ±0.06 to 0.32 ± 0.06 nmol/l (P , 0 . 0 0 0 1 ) ,and postprandial concentration from 1.11± 0.10 to 0.54 ± 0.10 nmol/l (P = 0.0001).The postprandial concentration was lowerat 110 months than at 27 months (P =0.036). SHBG increased from 1.35 ± 0.26mg/l at 27 months to 3.0 ± 0.5 mg/l at 110months (P , 0 . 0 0 5 ) .
Plasma total cholesterol concentrationwas 5.33 ± 0.38 mmol/l during tre a t m e n twith oral agents and 5.64 ± 0.28 mmol/l atthe 110-month examination (NS). To t a ltriglycerides were 1.99 ± 0.45 and 1.56 ±0.25 mmol/l, respectively (NS). Therew e re nonsignificant decreases of plasmaVLDL cholesterol and triglyceride concen-trations and nonsignificant rises of plasmaLDL and HDL cholesterol concentrationsat 110 months (data not shown).
T h e re is accumulating evidence thatl o n g - t e rm good metabolic control is essen-tial for diminishing the incidence of latediabetic complications (6). The pre s e n tstudy shows that insulin tre a t m e n ti m p roves glycemia for a long period, .9 years, in normal-weight and moder-ately obese patients who develop sec-o n d a ry failure to oral hypoglycemicagents. There are other long-term studiesin which improvement of glycemia hasbeen found (2–6). There is, to my knowl-edge, no study other than the U.K.P rospective Diabetes Study (UKPDS) andthe present study that have studied insulint reatment for a period exceeding 6 years inpatients with type 2 diabetes. The UKPDSd i ffers by starting insulin treatment fro mdiagnosis of diabetes, while in the pre s e n ts t u d y, insulin was started when failurewith oral agents occurred after a knowndiabetes duration of ,10 years. The pre s-ent study thus examines the continuede ffects of insulin treatment after the periodthat was studied in the UKPDS. The par-ticipants had worse glycemic control dur-ing treatment with oral agents than theconventional group of the UKPDS, butafter insulin treatment for 9 years, theglycemic control was comparable to thatin the intensive groups of the UKPDS after10–15 years (6). This shows that insulin
t reatment improves glycemic control andthat, in contrast to the UKPDS, where agradual worsening of glycemic control wasnoticed, improved glycemic control can besustained at about the same level for sev-eral years by standard care .
At the 27-month examination (7), wedescribed little change in body weight forthe period after insulin treatment for 1 year. This holds true also when followingthe patients for ,9 years. In the study byKudlacek and Schernthaner (2), thepatients lost body weight from diagnosis ofdiabetes until insulin treatment was initi-ated and then re t u rned to almost the sameBMI during 5 years of insulin tre a t m e n t .
In the period from 27 to 110 months,insulin doses were increased by 75%,although little change in body weighto c c u rred during this period. This is con-sistent with successive loss of b-cell func-tion (6) supported by lower C-peptide andhigher SHBG concentration at the 110-month examination, since portal insulinconcentrations regulate SHBG concentra-tions. This study supports the view thattype 2 diabetes is a dynamic disease with aslow loss of endogenous insulin secre t i o nand emphasizes the need to take this intoaccount when determining tre a t m e n t .While treatment with bedtime insulin incombination with oral agents has pro v e dsuccessful when oral failure evolves, thereis probably a need for providing 24-hinsulin supplementation in later stages ofthe disease.
In summary, insulin treatment givesl o n g - t e rm improvement of glycemic con-t rol in standard care and might, there f o re ,i m p rove the prognosis of patients withtype 2 diabetes and normal or moderateo v e rweight when failing on oral agents. Inspite of weight gain, there is no adversee ffect on triglyceride-rich plasma lipopro-tein concentrations.
TORBJÖRN LINDSTRÖM, MD, PHD
F rom the Department of Medicine and Care, Fac-ulty of Health Sciences, The University Hospital,Linköping, Sweden.
A d d ress correspondence to T. Lindström, MD,PhD, Department of Medicine and Care, Faculty ofHealth Sciences, The University Hospital, S-581 85Linköping, Sweden. E-mail: torbjorn . l i n d s t ro m @e n d . u s . l i o . s e .
R e f e re n c e s1 . Peacock I, Tattersall RB: The diff i c u l t
choice of treatment for poorly contro l l e dmaturity onset diabetes: tablets or insulin?BMJ 288:1956–1959, 1984
2 . Kudlacek S, Schernthaner G: The effect ofinsulin treatment on HbA1c, body weightand lipids in type 2 diabetic patients withs e c o n d a ry - f a i l u re to sulfonylureas: a fiv eyear follow-up study. H o rm Metab Res24:478–483, 1992
3 . Ohkubo Y, Kishikawa H, Araki E, MiyataT, Isami S, Motoyoshi S, Kojima Y,F u ruyoshi N, Shichiri M: Intensive insulintherapy prevents the pro g ression of dia-betic microvascular complications inJapanese patients with non-insulin-depen-dent diabetes mellitus: a randomizedp rospective 6-year study. Diabetes Res ClinP r a c t 28:103–117, 1995
4 . Abraira C, Colwell JA, Nuttall FQ, SawinC T, Johnson Nagel N, Comstock JP,Emanuele NV, Levin SR, Henderson W,Lee HS, VA CSDM Group: Veterans Aff a i r sCooperative Study on Glycemic Contro land Complications in Type II Diabetes (VACSDM): results of the feasibility trial. D i a -betes Care 18:1113–1123, 1995
5 . Birkeland KI, Rishaug U, Hanssen KF,Vaaler S: NIDDM: a rapid pro g ressive dis-ease: results from a long-term, ran-domised, comparative study of insulin ors u l p h o n y l u rea treatment. D i a b e t o l o g i a39:1629–1633, 1996
6 . UK Prospective Diabetes Study (UKPDS)G roup: Intensive blood-glucose contro lby sulphonylureas or insulin compare dwith conventional treatment and risk ofcomplications in patients with type 2 dia-betes (UKPDS 33). L a n c e t 3 5 2 : 8 3 7 – 8 5 3 ,1 9 9 8
7 . Lindström T, Eriksson P, Olsson AG, Arn-qvist HJ: Long-term improvement ofglycemic control by insulin treatment inNIDDM patients with secondary failure .Diabetes Care 17:719–721, 1994
Late-Onset L i p o a t rophic D i a b e t e s
Phenotypic and genotypic familialstudies and effect of treatment withm e t f o rmin and lispro insulin anal o g
Several subtypes of syndromes assoc-iating severe insulin resistance andl i p o d y s t rophy have been described
(1). Congenital lipoatrophic diabetes (LD)( B e r a rdinelli-Seip syndrome), an autoso-mal recessive disease of unknown etiology,is characterized by neonatal generalizedlipoatrophy, liver steatosis, muscularh y p e rt ro p h y, and hypertriglyceridemia (2).S y n d romes of late-onset lipodystro p h i e shave a broader range of clinical pre s e n t a-

DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999 1375
Letters
tions, with total or partial lipoatro p h y, andtheir genetic transmission is not univocal.
We re p o rt here the case of a patientwith an acquired form of LD whoseendocrine and metabolic alterations werei m p roved by treatment with metformin orl i s p ro insulin analog. We also describe theclinical, metabolic, and genetic features ofthe patient’s family members.
A 19-year-old woman was re f e rred toour clinic for diabetic ketoacidosis (DKA)(pH 7.09) with acute pancreatitis due tomajor hypertriglyceridemia (160 mmol/l;n o rmal: 0.4–1.7). Nonketotic diabetes andhyperlipidemia in this patient were knownfor 3 years and she had been prescribed 35 µg ethinyl-estradiol plus 2 mg cypro-t e rone acetate daily treatment a few monthsb e f o re the DKA episode.
Clinical examination revealed a mas-culine habitus with muscular hypert ro p h y,a larger biacromial than bitro c h a n t e r i a nd i a m e t e r, and striking virilization signswith severe hirsutism requiring daily shav-ing, mild acne, temporal hair re c e s s i o n ,m i c romastia, and clitoris enlarg e m e n t .Menses had been irre g u l a r, occuring onlye v e ry 4–5 months since menarche at age 12.Acanthosis nigricans was present on thevulvae and the inner thighs. A subcuta-neous lipoatro p h y, which had developedsince pubert y, was noticed on the tru n kand limbs (triceps skinfold thickness: 2 mm). Visceral fat was also reduced asassessed by computed tomography andbiphotonic absorptiometry (HOLOGICQDR 2000; HOLOGIC, Paris), whichevaluated the fat mass at 14.6% of totalweight, this being normal (BMI: 19.9k g / m2). There were no acro-megaloid fea-t u res, cramps, proteinuria, or complementactivation, which are signs sometimes
associated with extreme insulin re s i s t a n c e(3,4). Hyperc o rtisolism was excluded.Liver steatosis, suspected be-cause of theultrasonographic aspect of hypere-chogenic enlarged liver and elevated liverenzyme activities, was histologically con-firmed after biopsy. Transvaginal ultra-sonography showed enlarged ovaries(right: 49 3 26 mm; left: 43 3 18 mm)with multiple small cysts distributeda round a central hyperechogenic stro m a .
T h ree months after DKA and 24 hafter discontinuation of insulin, fastingglycemia was 8.4 mmol/l, with incre a s e ds e rum insulin (34 mU/l, normal: 2–15;radio-immunologic assay) and urinary C-peptide levels (124 µg/g creatinine, nor-mal: 10–60). Insulin resistance wasassessed by a euglycemic-hyperinsuline-mic clamp: the glucose disposal was 2.3mg ? k g21 ? m i n21 with an insulin infusionrate of 5 mU ? k g21 ? m i n21 ( n o rm a l :12–14) and 8.6 mg ? k g21 ? m i n21 with aninsulin infusion rate of 10 mU ? k g21 ?m i n21 ( n o rmal: 13–15). The pa-tient hada mixed dyslipidemia, with a type IIIl i p o p rotein pro file. Total testosterone was high, with a low level of sex-hor-mone–binding globulin (SHBG) ( Table 1). Circadian growth hormone lev-els were norm a l .
Insulin therapy was achieved with anintraperitoneal pump (Minimed MMT2001; Minimed, CA) because of poorglycemic control with subcutaneous injec-tions and re-peated subcutaneousabscesses after the use of an external intra-venous pump. Despite a treatment re g i-men consisting of a daily 200-U insulindose, glycated hemoglobin (HbA1 c)remained ,10%, and dyslipidemia wors-ened. The patient was then sequentially
t reated, in addition to intraperitonealinsulin therapy, with metformin or thel i s p ro insulin analog. Table 1 shows thelong-term metabolic and hormonalresponses to these treatments. The addi-tion of metformin (1,500 mg/day) to 200U/day of intraperitoneal insulin induced amarked and re p roducible fall in seru ma n d rogen levels without any weightchange, but it had no major effect onmetabolic parameters. Subcutaneousp reprandial injections of lispro (20–25 U)led to a fall of peritoneal insulin re q u i re-ments to ,100 U/day and a slight im-p rovement in HbA1 c without markedchanges in triglyceridemia.
Physical examination of the noncon-sanguineous parents and the three siblingswas normal, without any lipodystro p h y.The father was overweight (BMI: 31 kg/m2)and had previously known type 2 dia-betes. The mother (BMI: 22.5 kg/m2) wasfound to be diabetic after a 75-g oral glu-cose tolerance test (OGTT), which alsorevealed a marked hyperinsulinemia: at120 min, glycemia was 12 mmol/l andinsulinemia 660 mU/l. Results of meta-bolic tests including OGTT with glucoseand insulin measurements were normal inthe three siblings: a sister aged 26 years(BMI: 20 kg/m2), a brother aged 24 (BMI:22 kg/m2), and a sister aged 20 (BMI: 22 kg/m2). Molecular analysis of thep a t i e n t ’s insulin receptor and PPA R -g2coding sequences did not reveal any muta-tion. Genetic linkage studies in the family,using microsatellites at the loci of theinsulin receptor gene and several candi-date genes coding for the IGF-I re c e p t o r,a p o l i p o p roteins A2 and C2, lipopro t e i nlipase, hormone-sensitive lipase, fattyacid–binding protein 2, and leptin, as pre-
Table 1—Metabolic and hormonal evaluations during insulin therapy combined with either metformin or the insulin analog lispro
Insulin SC, Insulin IP 1 Insulin IP, Insulin IP1Treatment, duration biological evaluation Insulin IP alone, metformin, 2 periods of metformin lispro analog,
of treatment 3 months after DKA 5 years 2 periods $6 months discontinuation $6 weeks 3 months
HbA1c (N: 4.9–6.5%) 12.5 10.5 (9.1–12.7) 11.1 (10.3–12.6) 10.4 (9.9–11.0) 9.0 (8.8–9.3)Total cholesterol (N: 3.9–5.2 mmol/l) 6.5 7.0 (5.6–8.1) 9.6 (8.6–10.9) 7.3 (6.5–8.1) 8.8
Fasting triglycerides(N: 0.4–1.7 mmol/l) 3.4 8.3 (3.3–13.3) 27.3 (20.6–37.8) 8.3 (2.9–13.3) 12.6
Testosterone(N: 0.7–2.7 nmol/l) 5.2 6.8 (4.8–8.9) 1.5 (0.52–2.4) 3.6 (2.5–4.8) 5.1 (4.9–5.3)
SHBG(N: 30–60 nmol/l) 8.8 10.1 (7.1–15.7) 13.8 (2.3–15.5) 14.2 (12.8–15.7) 24
Data are means (range). IP, intraperitoneal; N, normal; SC, subcutaneous.

1376 DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999
Letters
viously described (5), did not reveal anymarker segregation with the diseasebecause the proband had the same geno-type or haplotype as one of the unaff e c t e dsiblings at each locus.
In conclusion, this patient had a syn-d rome of extreme insulin resistance char-acteristic of late-onset LD (2) with distinc-tive features including DKA, a rare compli-cation of LD owing to the extreme paucityof fat (6), and a chronic type III dyslipi-demia, whereas a type V pro file is usuallyre p o rted in LD (7). Altered glucose metab-olism was observed in both parents, asre p o rted in other studies for parents ofcongenital LD children (8 and J.C.,unpublished observations). This couldsuggest an autosomal recessive transmis-sion of this late-onset form with a milderand incomplete phenotype in hetero z y-gous subjects. However, we failed to re v e a lany linkage with the studied candidategenes. Metformin treatment improved theh y p e r a n d rogenism, as suggested by othersin nonobese women with polycystic ovarys y n d rome (9). Insulin analog lispro ther-a p y, which has never been evaluated in LD,i m p roved glycemic control; this tre a t m e n td e s e rves further evaluation in lipodys-t rophic severely insulin-resistant patients.
MARIE-CHRISTINE VANTYGHEM, MD
CORINNE VIGOUROUX, MD
JOCELYNE MAGRÉ, PHD
CHRISTÈLE DESBOIS-MOUTHON, PHD
FRANÇOIS PATTOU, MD
PIERRE FONTAINE, MD PHD
JEAN LEFEBVRE, MD, PHD
JACQUELINE CAPEAU, MD, PHD
F rom the Clinique Marc Linquette (M.-C.V., P. F., J.L.)and the Service de Chiru rgie Générale et Endocrini-enne (F. P.), Centre Hospitalier Regional et Universi-t a i re, Lille; and Institut National de la Santé et de laR e c h e rche Medicale, Unité 402, Paris, France.
A d d ress correspondence to Dr. Marie-ChristineVantyghem, Service d’Endocrinologie et MaladiesMétaboliques, Clinique Marc Linquette, USN “A,”6, Rue du Professeur Laguesse, 59037 Lille, France.E-mail: [email protected].
R e f e re n c e s1 . Tritos NA, Mantzoros CS: Syndromes of
s e v e re insulin resistance. J Clin EndocrinolM e t a b 83:3025–3030, 1998
2 . Seip M, Trygstad S: Generalized lipodystro-p h y, congenital and acquired (lipoatro p h y ) .Acta Paediat 8 5 (Suppl. 413):2–28, 1996
3 . Flier JS, Young JB, Landsberg L: Familialinsulin resistance with acanthosis nigri-cans, acral hypert ro p h y, and musclec r a m p s. N Engl J Med 303:970–973, 1980
4 . Sissons JGP, West RJ, Fallows J, Wi l l i a m sDG, Boucher BJ, Amos N, Peters DK: Thecomplement abnormalities of lipodystro-p h y. N Engl J Med 294:461–465, 1976
5 . Vi g o u roux C, Khallouf E, Bourut C,R o b e rt JJ, De Kerdanet M, Tu b i a n a - R u fiN ,Fauré S, Weissenbach J, Capeau J, Magré J:Genetic exclusion of 14 candidate genes inl i p o a t rophic diabetes using linkage analy-sis in 10 consanguineous families. J ClinEndocrinol Metab 82:3438–3444, 1997
6 . Robbins DC, Sims EAH: Recurre n tketoacidosis in acquired, total lipodystro-phy (lipoatrophic diabetes). Diabetes Care7:381–385, 1984
7 . Enzi G, Digito M, Baldo-Enzi G, Comi-nacini L, Dodi G, Carr a ro R, Zurlo F: Lipidmetabolism in lipoatrophic diabetes. H o rmMetab Res 20:587–591, 1988
8 . Panz VR, Joffe BI, Raal FJ, Wing JR, KeddaMA, Seftel HC: The insulin receptor inSouth African families with lipo-atro p h i cdiabetes mellitus. S Afr Med J 8 7 : 1 2 7 7 – 1 2 8 3 ,1 9 9 7
9 . Sattar N, Hopkinson ZEC, Greer IA:Insulin-sensitizing agents in polycystico v a ry syndromes. L a n c e t 3 5 1 : 3 0 5 – 3 0 6 ,1 9 9 8
Hypoglycemia Dueto Folk Medicine
Mo re than 6 million people in Japana re assumed to have diabetes (1). Arecent questionnaire administere d
in the suburban area of Tokyo (2) re v e a l e dthat nearly 23% of diabetic patients haveat least once tried folk medicines, such astaking certain teas or plants or mail-o rd e red “Oriental” medicines, to impro v etheir diabetes status or to cure the disease.
For example, one of these eff e c t i v efolk medicines consists of tablets called“Xiaokewan,” which is believed to be a tra-ditional Chinese medical product. Wehave recently seen a 60-year-old malepatient who was brought to our hospitalbecause of unexplained hypoglycemia(blood glucose 57 mg/dl). This patient wasregularly taking several tablets of Xiaoke-wan in the morning after breakfast. A fewhours after he had taken several tablets ofXiaokewan without having breakfast, thepatient experienced drowsiness during thephysical exercise of bicycling. Furt h e rinvestigation revealed that these Xiaoke-wan tablets contain 0.25 mg/tablet ofglibenclamide, a widely known eff e c t i v eoral hypoglycemic agent. According to theaccompanying note on how to take the
medicine, the single dosage is re c o m-mended to be increased from ,5 to 10pills (1.25–2.5 mg of glibenclamide) takenorally after meals three times a day.
These kinds of agents appear to beavailable for vacationers at pharm a c yshops in some countries without a writtenp rescription, and this is a welcomed giftf rom overseas for some diabetic patients.
It seems sensible that both doctorsand patients should know that some folk-medicine agents do contain a potent hypo-glycemic substance and that ignorance ofits presence can be hazardous. In addition,in cases of hypoglycemia without appare n tcause(s), the possibility needs to be takeninto account that some diabetic patientsmight have been taking such a substancewithout their re c o g n i t i o n .
TSUNEHARU BABA, MD
KUNIZO KATAOKA, MD
MASARU ITAKURA, MD
F rom the Department of Internal Medicine, To k a iUniversity Tokyo Hospital, Tokyo, Japan.
A d d ress correspondence to Ts u n e h a ru Baba, MD,D e p a rtment of Internal Medicine, Tokai UniversityTokyo Hospital, 1-2-5 Yoyogi, Shibuya-ku, To k y o151-0053, Japan. E-mail: [email protected].
R e f e re n c e s1 . Statistics and Information Depart m e n t ,
M i n i s t ry of Health and We l f a re: Te n t a t i v eReview of Diabetes Mellitus (in Japanese).Tokyo, Japan, Ministry of Health and We l-f a re, 18 March 1998 (Statistical Report )
2 . Kanamori A, Hirai N, Kurohara A: Folk-medicine in diabetic patients (in Japanese)(Abstract). J Japan Diab Soc 38 (Suppl. l):2 0 3 ,1995
Role of Early Fundoscopy forDiagnosis of Wo l f r a mS y n d rome inType 1 DiabeticP a t i e n t s
Since diabetic retinopathy is primarilyrelated to the duration and thed e g ree of control of diabetes, the
American Diabetes Association does notrecommend fundoscopy before the age of10 years or the first 5 years of type 1 dia-betes. In Wolfram syndrome, a subtype oftype 1 diabetes, optic atrophy may mani-fest early in the course of the disease (1).

DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999 1377
Letters
Even though with time other manifesta-tions of the syndrome may appear, optica t rophy is considered the main criterionfor diagnosis of this syndrome. To empha-size the importance of early diagnosis ofWolfram syndrome in a population of arelatively high prevalence of this condi-tion, we conducted the following study.
All 589 type 1 diabetic patients tre a t e dat the Chronic Care Center for diabetes inLebanon underwent fundoscopic examina-tions along with other routine examina-tions. The ophthalmologic exam consistedof systematic measurement of visual acuityafter refraction under cycloplegia withcyclopentholate, together with testing forocular motility and examination of the fun-dus with a biomicroscope with specialattention to the papilla. A detailed familyh i s t o ry was also obtained, with emphasison parental consanguinity and the pre s-ence of other family members affected withdiabetes. Islet cell antibodies and antibod-ies to GAD were measured by immunoflu-o rescence and enzyme-linked immunosor-bent assay, re s p e c t i v e l y, in those patientswhose diabetes duration was ,5 years.
Of the 589 diabetic patients, 27 casesof Wolfram syndrome were diagnosed.This was done by first identifying optica t rophy and then eliminating all other pos-sible causes of optic atro p h y, in part i c u l a r,Leber here d i t a ry optic atrophy and thi-a m i n e - responsive anemia with diabetesand deafness. The patients so diagnosedconsisted of 14 males and 13 females agedbetween 9 and 26 years. Optic atrophy wasc o n firmed by the presence of white papillawith regular and well-demarcated bord e r s .The degree of papillary atrophy was wellc o rrelated with the severity of reduction ofvisual acuity, and in mild cases, paleness ofthe papilla was predominantly temporal.C o rrected visual acuity ranged from 1/20to 4/10 and was not always symmetrical inboth eyes. Refraction studies re v e a l e ds e v e re myopia in one case (210.00 on theright and 26.00 on the left eye), mildmyopia in two patients, and bilateralaphaquia in two other patients. Pupillaryreaction to light was present in all patients,although it was reduced in six subjectswhose visual acuity was less than 1/20.Horizontal nystagmus was noted in onepatient. Biomicroscope examinationshowed diffuse cortical crystalline opacitiesin six patients; however, this did notexplain their decrease in visual acuity. Tw opatients had undergone operations in thepast for cataract in both eyes. Mild nonpro-
liferative diabetic retinopathy was found infour patients, and one patient had severep roliferative re t i n o p a t h y.
Parental consanguinity, most fre-quently of the first degree, was found in all27 (100%) patients with Wolfram syn-d rome, compared with 107 of 562 (19%)n o n - Wolfram patients with type 1 dia-betes. Of these 27 patients, 12 patients(45%) had a negative family history of type 1 diabetes, and 15 patients (55%) hada positive family history of type 1 diabetes;this was significantly higher than the inci-dence of a positive family history of type 1diabetes in the non-Wolfram patients,which was 55 of 562 patients or ,1 0 % .The 15 Wolfram patients with a positivefamily history of type 1 diabetes came fro mseven families, of which six had twoa ffected siblings and one had three aff e c t e dsiblings with Wolfram syndrome. Islet celland anti-GAD antibodies were negative inall of the 7 (100%) Wolfram patients withdiabetes duration of ,5 years and werepositive in 23 of 30 (77%) non-Wo l f r a mpatients with diabetes duration ,5 years.
The prevalence of type 1 diabetes inLebanon is around 1/1,000 people, whichaccounts for ,1,000 diabetic patients inthe population of people aged ,18 years.Our data estimate the prevalence of Wo l-fram syndrome to be 1/68,000 people, or4.58% of type 1 diabetic patients. Thus,the Lebanese type 1 diabetic populationseems to be at a higher risk of having Wo l-fram syndrome compared with other pop-ulations, such as the U.K. population, inwhich the syndrome is rare and its pre v a-lence is estimated to be 1/770,000 people(2). One possible explanation for thiso b s e rvation is the high frequency of con-sanguinity in the Lebanese population. Infact, parental consanguinity was found inall of our 27 cases of Wolfram syndro m e .One important finding in this study is thep resence of other family members aff e c t e dwith diabetes in the Wolfram patientg roup. Of the 27 patients, 15 had siblingss u ffering from type 1 diabetes, which iscommensurate with the findings of pre v i-ous re p o rts (3).
The reduction of visual acuity re l a t e dto optic atrophy is rarely symptomatic, andin most cases, it is incidentally observ e d .The lack of symptoms may be due to theyoung age of the patients, to the slow andearly pro g ression of the disease, and to theasymmetric nature of the disease at itsonset. For instance, one of four patientshad a visual acuity of 1/20 in one eye and
4/10 in the other eye, which explains theabsence of major functional discomfort. Itis difficult to specify the exact time of onsetof the decreased vision of the patients withWolfram syndrome; however, in all ourpatients, optic atrophy manifested after theonset of diabetes, similar to what has beenp reviously shown (2).
Based on these findings, we suggestthat the systemic search for optic atro p h yis important in type 1 diabetes, especiallyin those patients with risk factors for Wo l-fram syndrome. Parental consanguinity,positive family history of type 1 diabeteswith or without Wolfram syndrome, andnegative islet cell and anti-GAD antibodiesshould be considered important risk fac-tors for the development of Wolfram syn-d rome in the type 1 diabetes population.Ophthalmologic examination allows earlydiagnosis of Wolfram syndrome before theappearance of other clinical manifestationsof the syndrome. This early diagnosis willlead to an early treatment and manage-ment of these patients, who suffer fro mhigher morbidity and mortality whenc o m p a red with the general type 1 diabetespopulation (4). Finally, it is hoped that therecent discovery of a Wolfram gene (W S F 1gene) by Inoue et al. (5) will allow an earlyand sensitive diagnosis of the syndrome inthose patients with positive risk factors.
PAT R I C K BA Z, M D
SA M I T. AZ A R, M D
RI TA ME D L E J, M D
RI A D BE J J A N I, M D
GE O R G E HA L A B I, M D
IB R A H I M SA LT I, M D
F rom the Departments of Ophthalmology (P. B . ,R.B.) and Endocrinology (R.M., G.H.), HospitalHotel Dieu de France; the Division of Endocrinol-ogy (S.T.A., I.S.), American University of Beiru tMedical Center; and the Division of Diabetes (P. B . ,S . T.A., R.M., G.H.), Chronic Care Center, Beiru t ,L e b a n o n .
A d d ress correspondence to Sami T. Azar, M D,FA C P, Department of Internal Medicine, Division ofE n d o c r i n o l o g y, American University of Beirut Med-ical Center, Bliss Street, Beirut, Lebanon.
R e f e re n c e s1 . Wolfram DJ, Wagener HP: Diabetes melli-
tus and simple optic atrophy among sib-lings: re p o rt of four cases. Mayo Clin Pro c13:715–718, 1938
2 . B a rret TG, Bundey SE, Macleod AF: Neu-rodegeneration and diabetes: UK nation-wide study of Wolfram (DIDMOAD) syn-d rome. L a n c e t 346:1458–1463, 1995
3 . Scolding NJ, Kellar Wood HF, Shaz C,

1378 DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999
Letters
Shneerson JM, Antoun N: Wolfram syn-d rome here d i t a ry diabetes mellitus withbrain stem and optic atro p h y. Ann Neuro l39:352–360, 1996
4 . Kinsley BT, Swift M, Dumont RH, Swift RG:Morbidity and mortality in the Wo l f r a ms y n d rome. Diabetes Care 1 8 : 1 5 6 6 – 1 5 7 0 ,1 9 9 5
5 . Inoue H, Tanizawa Y, Wasson J, Behn P,Kalidas K, Bernal-Mizrachi E, Meuckler M,Marshall H, Donis-Keller H, Crock P,Rogers D, Mikuni M, Kumashiro H,Higashi K, Sobue G, Oka Y, Permutt MA:A gene encoding a transmembrane pro t e i nis mutated in patients with diabetes melli-tus and optic atrophy (Wolfram syn-d rome). Nat Genet 20:143–148, 1998
P a rtial Wo l f r a mS y n d rome ( D I D M O A D )
Two new patients in a family
Wolfram syndrome is the associationof diabetes and bilateral optic atro-phy (1), sometimes associated with
diabetes insipidus, diabetes mellitus, optica t ro p h y, and deafness (DIDMOAD). It can beassociated frequently with dilated renal out-flow tracts, neurological symptoms likeepilepsy or ataxia, primary gonadal atro p h y,and psychiatric findings. The pre v a l e n c eestimate is 1 in 770,000, based on an obser-vation of the prevalence of optic atro p h ywith diabetes. Parental consanguinity hasbeen noted.
DIDMOAD syndrome re p resents a sin-gle trait, inherited as an autosomal re c e s-sive (2) disease. It has been related to mito-chondrial disorders (3), but these hypothe-ses are controversial. It has been describedas being linked with the Wolfram syn-d rome locus to DNA markers on chro m o-some 4p, and recently it has been observ e du n d e rgoing both genomic alterations (4).
We present two affected members in afamily with symptoms of DIDMOAD.
Patient 1 is a 23-year-old woman withdiabetes since the neonatal period. She ist reated with long-acting insulin twice a daywithout ketosis, and optic atrophy wasdiagnosed at 13 years of age. She has pre-sented with polyuria-polydipsia since 8 years ago and has paresthesias in bothlegs. Menarche occurred at 16 years of age,but with some disturbances in her men-s t ruation. She has four healthy bro t h e r sand one sister, all with normal clinicalexamination and normal basal hypophysial
h o rmone study. Islet cell antibodies andanti-insulin antibodies were negative. HLAhaplotypes are shown in Table 1. Stimula-t o ry tests for hypophysial hormones weren o rmal. We confirmed the diagnosis ofp a rtial insipidus diabetes after water depri-vation tests. Fundus oculi tests showednew blood vessels on the left eye and thickv i t reous on the right eye. Visual evokedpotentials and electro retinography sug-gested severe optic neuropathy. Elec-t romyography showed denerv a t i o n / re n e r-vation signs in muscles explored with dis-tance prevalence. Electroneurographysuggested severe axonal affectation. Auto-nomic function evaluation showed nore flex of sympathetic activity and severea ffectation of the parasympathetic system;these symptoms are considered to be a sen-sorimotor axonal polyneuropathy aff e c t i n gall types of fibers. Magnetic resonance test-ing showed optic chiasm and pontine andc e rebellar atrophy; intravenous uro g r a p h yshowed slight signs of hydro n e p h rosis atthe ureteral and kidney levels.
Patient 2 is a 27-year-old woman whodeveloped diabetes at the age of 3 years.She is treated with long-acting insulintwice a day without ketosis signs. Bilateraloptic atro p h y, with pro g ressively re d u c e dvisual acuity, was diagnosed at 4 years ofage. She had developed polyuria-polydip-sia syndrome 2 years before this examina-tion. Islet cell antibodies and anti-insulinantibodies were negative. After the waterdeprivation test, there was no re s p o n s e .Fundus oculi suggested bilateral optic atro-p h y. Electro retinogram showed a slightvoltage decrease in the left retina. Electro-miography and nervous conduction veloc-ity suggested axonal polyneuropathy witha censorial prevalence. Magnetic re s o n a n c etesting showed optic chiasm atro p h y ;intravenous urography suggested hydro-u reter and hydro n e p h ro s i s .
We have identified two patients withcharacteristics of Wolfram syndrome fro mthe same family. We found diabetes, dia-betes insipidus, and optic atrophy withouta u d i t o ry abnormalities in both patients.
Genes of the major histocompatibilitycomplex, in particular HLA-DR2 antigens,have been found to be associated with thiss y n d rome (5), but we have not found thisassociation in our patients, suggesting thatWolfram syndrome diabetes is diff e re n tf rom classical type 1 diabetes, and Wo l-fram syndrome has also been associatedwith other carbohydrate metabolism dis-o rders. Another characteristic of this typeof diabetes is the early onset of diabetes inthe syndrome, usually during the fir s tyears of life.
In terms of chronic diabetes complica-tions, we found diabetic retinopathy inonly one patient, and peripheral neuro p a-thy in both, in spite of a long disease evo-lution in each patient (.20 years). Thelack of chronic diabetes complications inWolfram syndrome has been described,especially the absent or slow pro g re s s i o nof diabetic retinopathy (6).
Optic atrophy appeared at the age of13 and accompanied diabetes which hadbeen diagnosed during the neonatalperiod. Both are the more constant mani-festations of the syndrome (7). Diabetesinsipidus appears later than diabetes, issometimes not present in Wolfram syn-d rome (5), and is caused by supraoptic andparaventricular atro p h y. There has beenevidence of sexual developmental dysfunc-tion, usually hypogonadism secondary top r i m a ry gonadal atro p h y, with menstru a li rregularity (8) and delayed menarche. Ourpatients presented delayed menarche butn o rmal responsiveness to luteinizing hor-m o n e – releasing hormone, suggesting nor-mal hypothalamic-pituitary function.
Hypoacusia in these patients shoulddepend on the damage of the acousticn e rve, and it has been described as a veryconstant symptom (62%), but the absenceof this symptom has been described as inour patients; this form may be a part i a lp resentation of the syndrome, or perh a p shypoacusia may have become appare n twith time (at the age of 35–40 years) (5).Dilated renal outflow tracts have beendescribed frequently and, for some
Table 1—HLA haplotypes
F a t h e r A11, A32 B35, B51, BW4, BW6 DR4, DR6, DR52, DR53 DQ1, DQ3M o t h e r A11, A32 B35, B55, BW6 DR1, DR5, DR52 DQ1, DQ3Patient 1 A 1 1 B5, B35, BW4, BW6 DR1, DR4, DR53 DQ1, DQ3Patient 2 A 1 1 B35, BW6 DR1, DR6, DR52 D Q 1B ro t h e r A 3 2 B51, B55, BW4, BW6 DR4, Dr5, DR52, DR53 D Q 3

DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999 1379
Letters
authors, should be re g a rded as an integralp a rt of the syndrome (1). Although thecause is unclear, autonomic neuro p a t h ymay cause a neuropathic bladder or can beresponsible partly for a high output urinestate in diabetes insipidus (5).
We have documented two sisterswith Wolfram syndrome who pre s e n t e dwith the main characteristics, exceptinga u d i t o ry symptoms. Diabetes was thefirst manifestation, characterized by itsstability and the lack of chronic compli-cations except diabetic re t i n o p a t h y. Optica t rophy and diabetes insipidus were pre s-ent in both patients.
ANTONIO HERNANDEZ-MIJARES, MD
CARLOS MORILLAS, MD
IRENE LLUCH, MD
MARIA LUISA MARTINEZ-TRIGUERO, MD
MARIA LUISA MUÑOZ, MD
MARCELINO GOMEZ, MD
MIGUEL ANGEL MERINO, MD
MANUEL ESCUDERO, MD
F rom the Department of Medicine, Dr. Peset’s Uni-versity Hospital, University of Valencia, Spain.
Address correspondence to Antonio Hernandez,MD, Endocrinology Section, Dr. Peset’s Uni- versity Hospital, Av. Gaspar Aguilar, 90. 46017Valencia, Spain.
R e f e re n c e s1 . Wolfram DJ: Diabetes mellitus and simple
optic atrophy among sibling: re p o rts of fourcases. Mayo Clin Pro c 9:715–718, 1938
2 . C remers CW, Wijdeveld PG, Pinckers AJ:Juvenile diabetes mellitus, optic atro p h y,hearing loss, diabetes insipidus, atonia ofthe urinary tract and bladder, and othera b n o rmalities (Wolfram Syndrome): areview of 88 cases from the literature withpersonal observations on 3 new patients.Acta Paediatr Scand 264 (Suppl.):1–16,1 9 7 7
3 . Pilz D, Quarrell OWJ, Jones EW: Mito-chondrial mutation commonly associatedwith Leber’s here d i t a ry optic neuro p a t h yo b s e rved in a patient with Wolfram Syn-d rome (DIDMOAD). J Med Genet 3 1 :328–330, 1994
4 . B a rrientos A, Volpini V, Casedemont J,Genis D, Manzanares JM, Ferrer Y, Corral J,C a rdellach F, Urbano-Marquez A, Estivil X,Nunes V: A nuclear defect in the 4pl6region predisposes to multiple mitochondr-ial DNA deletions in families with Wo l f r a ms y n d rome. J Clin Invest 9 7 : 1 5 7 0 – 1 5 7 6 ,1 9 9 6
5 . Monson JP, Boucher BJ: HLA type and isletcell antibody status in family with DID-MOAD syndrome. L a n c e t i : 1 3 9 8 – 1 3 9 9 ,1 9 8 3
6 . G a rcia-Luna PP, Villechenous E, Leal-C e rro A: Contrasting features of insulindependent diabetes mellitus associatedwith neuro e c t o d e rmal defects and classicalinsulin dependent diabetes mellitus. A c t aPaediatr Scand 77:413–418, 1988
7 . Scolding NJ, Kellar- Wood HF, Shaw C,Shneerson JM, Antoun N: Wolfram syn-d rome: here d i t a ry diabetes mellitus withbrainstem and optic atro p h y. Ann Neuro l39:352–360, 1996
8 . G a rcia-Luna P, Leal A, Villamil F: Sin-d rome DIDMOADUA (DIDMOAD): estu-dio de 3 familias con 5 nuevos caves: difer-encia con la diabetes mellitus insulinode-pendiente clasica. Med Clin ( B a rc) 8 5 : 4 8 6 –490, 1985
A re Insulin-Tre a t e dType 2 DiabeticSubjects at HigherRisk for Foot Ulcers?
The identification of subjects at higherrisk for foot ulcers is important top revent ulceration, and various stud-
ies have evaluated the clinical characteris-tics that contribute toward increasing adiabetic individual’s risk for developingfoot ulcer (1). In the diabetic patientsadmitted to our diabetologic unit for footu l c e r, we have noticed a very high fre-quency of insulin-treated type 2 diabeticpatients: from 1993 to 1996, 133 type 2diabetic subjects were seen, 67 (50.4%) ofwhom were tablet treated and 66 (49.6%)of whom were insulin treated. A high per-centage of insulin-treated diabetic sub-jects, very similar to our case re c o rds, isalso re p o rted in some studies that havetaken into consideration diabetic subjectswith foot ulcer (2–8). In the literature ,p revalence of data about type 2 diabeticpatients on insulin therapy is varied (9).Despite this variability, the prevalence oftype 2 diabetic subjects with insulin tre a t-ment among our diabetic patients hospi-talized for foot ulcer is much higher thanthat re p o rted in the literature. On the basisof our data and other data from the litera-t u re, we can conclude that the fre q u e n c yof insulin-treated type 2 diabetic subjectsis particularly high in diabetic people withfoot ulcer. These subjects should there f o rebe considered to be at higher risk for footu l c e r a t i o n .
To verify whether there were diff e r-ences in the clinical characteristics that
could explain a diff e rent risk of foot ulcer,we have carried out in our outpatient population a matched study betweent a b l e t - t reated and insulin-treated type 2diabetic subjects.
Type 2 diabetic outpatients, re g u l a r l yfollowed up (not ,2 visits a year) in 1996,w e re taken into consideration. Subjectswith onset of diabetes after age 30 years,t reated with tablets for at least 3 yearswithout interruption, and without a his-t o ry of ketoacidosis were considere dt a b l e t - t reated type 2 diabetic patients.Subjects with these same characteristicswho had been undergoing insulin tre a t-ment without interruption for at least 2years and who had an insulin re g i m e nconsisting of at least two injections per dayw e re considered insulin-treated type 2diabetic patients (10). In our outpatientpopulation, 12 insulin-treated type 2 dia-betic patients were selected and matchedwith 12 tablet-treated type 2 diabeticpatients randomly chosen from a re c o rd ofcases attending our Diabetology Center.The matching criteria were as follows: sex( five men, seven women), age (58.3 ± 4.9and 61.2 ± 3.4 years), diabetes duration(14.1 ± 4.2 and 14.5 ± 4.8 years), and BMI(27.2 ± 5.4 and 25.0 ± 3.1 kg/m2). All ofthese subjects were without foot ulcera-tion and without history of foot ulcer. Inthese subjects, the following variablesw e re evaluated: diabetic retinopathy (fun-dus oculi by ophthalmologist), albumine x c retion rate (mg per 24 h, the average oft h ree 24-h collections, nephelometry ;Behring, Scopito, Italy), renal impairm e n t( c reatinine .133 mmol/l, Jaffe; BoehringerMannheim, Monza, Italy), total cholestero l( c o l o r i m e t ry; Boehringer Mannheim), HDLc h o l e s t e rol (polyethylene glycol 6000,reagent made in laboratory), triglycerides( c o l o r i m e t ry; Bayer, Milan, Italy), art e r i a lh y p e rtension (systolic blood pre s s u re.160 mmHg and/or diastolic blood pre s-s u re .95 mmHg or antihypertensive ther-apy), fibrinogen (mg/dl, Klaus method;Baxter Diagnostic), smoking habit, coro-n a ry art e ry disease (history of angina orm y o c a rdial infarction, resting electro c a rd i o-gram and B-mode echocardiography), fast-ing and postprandial C-peptide (radioim-munoassay; Byk-Gulden, Milan, Italy), sen-sorimotor neuropathy (considered pre s e n twhen electromyography showed abnor-malities of nerve conduction velocity ands e n s o ry action potential in at least twon e rves), vibration perception threshold onthe malleolus (biothesiometer), sensory

1380 DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999
Letters
t h reshold (Semmes-Weinstein 5.07 mono-filament, impaired when insensitive inm o re than five of the nine areas tested),autonomic neuropathy (present if thes c o re of the deep breathing, lying to stand-ing, orthostatic hypotension tests was 3;maximal score of 3 the test was equal to6), tibial blood pre s s u re and ankle-brachial blood pre s s u re ratio measured byDoppler continuous wave technique, tran-scutaneous oxygen tension on the dorsumof the foot, and presence of palpable tibialand pedal pulses using a dichotomousc l a s s i fication as either present or absent.
These clinical characteristics werec o m p a red. For comparison between con-tinuous and discrete values, paired Stu-d e n t ’s t and x2 tests were used, re s p e c-t i v e l y. Among the considered variables inthe insulin-treated subjects, fib r i n o g e nwas higher (439 ± 62 vs. 370 ± 56 mg/dl,P = 0.009), arterial hypertension was moref requent (12 vs. 5 subjects, P = 0.044), theankle-brachial index was low (0.88 ± 0.19vs. 1.08 ± 0.05, P = 0.002), and the tibialp re s s u re (150 ± 30 vs. 170 ± 22 mmHg, P= 0.014) was significantly impaire d .
In our matched subjects, insulin-t reated subjects have a significantly worsep a t t e rn re g a rding both athero s c l e rotic riskfactors (arterial hypertension and fib r i n o-gen levels), and noninvasive vascular labo-r a t o ry (ankle-brachial index and tibialblood pre s s u re). These characteristicscould there f o re explain the higher risk offoot ulcer in these subjects, since impaire dlimb perfusion is one of the risk factors forulceration (2,11,12).
FAGLIA EZIO, MD
FAVALES FABRIZIO, MD
QUARANTIELLO ANTONELLA, MD
CALIA PATRIZIA, MD
MORABITO ALBERTO, PHD
F rom the Department of Internal Medicine (F. E . ,Q.A.), Policlinico MultiMedica–Sesto S. Giovanni;the Diabetology Center (F. F., C.P.), Niguarda Hospi-tal; and the Institute of Medical Statistics and Bio-metrics (M.A.), Milan University, Milan, Italy.
A d d ress correspondence to Ezio Faglia, Depart-ment of Internal Medicine, Policlinico Multi-media, Via Milanese 300, 20099 Sesto S. Giovanni, Milano, Italy.
R e f e re n c e s1 . K l e n e rman L, McCabe C, Cogley D,
C rerand S, Laing P, White M: Screening forpatients at risk of diabetic foot ulcerationin a general diabetic outpatient clinic. D i a -bet Med 13:561–563, 1996
2 . McNeely MJ, Boyko EJ, Arhoni JH, StenselVL, Reiber GE, Smith DG, Pecoraro RE:The independent contributions of diabeticn e u ropathy and vasculopathy in footulceration: how great are the risks? D i a -betes Care 18:216–219, 1995
3 . Siitonen OI, Niskanen LK, Laakso M, Siito-nen JT, Pyörälä K: Lower- e x t remity ampu-tations in diabetic and nondiabeticpatients: a population-based study in east-e rn Finland. Diabetes Care 16:16–20, 1993
4 . Rosenblum BI, Pomposelli FB Jr, GiuriniJM, Gibbons GW, Freeman DV, Chrzan JS,Campbell DR, Habershaw GM, LoGerf oF W: Maximizing foot salvage by a com-bined approach to foot ischemia and neu-ropathic ulceration in patients with dia-betes: a 5-year experience. Diabetes Care17:983–987, 1994
5 . B resater LE, Welin L, Romanus B: Footpathology and risk factors for diabetic footdisease in elderly men. Diabetes Res ClinP r a c t 32:103–109, 1996
6 . Lehto S, Rönnemaa T, Pyörälä K, LaaksoM: Risk factors predicting lower extre m i t yamputations in patients with NIDDM.Diabetes Care 19:607–612, 1996
7 . El-Shazly M, Abdel-Fattah M, ScorpiglioneN, Massi Benedetti M, Capani F, Carinci F,C a rta Q, Cavaliere D, De Feo E, Taboga C,Tognoni G, Nicolucci A, on behalf of theItalian Study Group for the implementa-tion of the St. Vincent Declaration: Riskfactors for lower limb complications indiabetic patients J Diabetes Complications12:10–17, 1998
8 . Segalini G, Aldeghi A, Morabito A, RadiceM, for the Lombardy Diabetic Foot Study: Am u l t i - c e n t re study on the prevalence oflower extremity ulcers and amputationsamong diabetic out-patients in the Lom-b a rdy region. Diabetes Nutr Metab 1 1 : 1 7 9 –187, 1998
9 . Genuth S: Insulin use in NIDDM. D i a b e t e sC a re 13:1240–1264, 1990
1 0 . Rifkin H (Ed.): The Physician Guide to Type 2 Diabetes (NIDDM): Diagnosis andTre a t m e n t. Alexandria, VA, American Dia-betes Association, 1985
1 1 . P e c o r a ro RE, Reiber GE, Burgess EM: Path-ways to diabetic limb amputation: basis forp revention. Diabetes Care 1 3 : 5 1 3 – 5 2 1 ,1 9 9 0
1 2 . Apelqvist J, Castenfors J, Larsson J, Sten-ström A, Agardh C-D: Prognostic value ofsystolic ankle and toe blood pre s s u re levelsin outcome of diabetic foot ulcer. D i a b e t e sC a re 12:373–378, 1989
H y p e rg l y c e m i cH y p e rosmolar Nonketotic Syndro m eas Initial
P resentation of Type 2 Diabetes ina Young CocaineA b u s e r
A1 9 - y e a r-old African-American malep resented with complaints of poly-dipsia, polyphagia, and nocturia of
3 days’ duration. Past medical history wass i g n i ficant for asthma since childhood,which was treated with inhalers and occasionally short courses of pre d n i s o n e .Family history was significant for type 2diabetes. Medications at admission in-cluded inhalers (albutero l / i p r a t ro p i u m ,a l b u t e rol metered dose inhaler, and flu t i c a-sone), singulair 10 mg (montelukast), andprilosec 20 mg (omeprazole). The patientwas in the habit of using cocaine and mari-juana, both of which he had used on thenight before this hospital admission.
Physical examination of the patientrevealed an alert, awake, and fully orientedmale. His vital signs were re c o rded: blood pre s s u re 130/60 mmHg, pulse 76beats/min, temperature 36.7°C, and re s p i-r a t o ry rate 14/min. The patient weighed296 pounds and had bilateral tendergynecomastia and multiple striae on thelower abdomen, back, and shoulders. Therest of the examination was unre m a r k a b l e .
His admission laboratory data showedthe following: sodium 127 mmol/l, potas-sium 4.7 mmol/l, CO2 17 mmol/l, chloride90 mmol/l, glucose 47.3 mmol/l, bloodu rea nitrogen 4.64 mmol/l, cre a t i n i n e79.56 µmol/l, calculated osmolality 297mmol/kg, serum ketones negative, toxicol-ogy screen positive for cocaine metabolitesand cannabinoids, glycosylated hemoglo-bin 14.2%, morning plasma cortisol level259.34 nmol/l (done 3 days later), andGAD antibodies negative.
A diagnosis of nonketotic hypero s m o-lar hyperglycemic syndrome was made.The patient was treated with intravenousfluids and insulin infusion. He showedrapid response to treatment and was senthome on a combination of NPH insulinand humalog (lispro ) .
The characteristic acute cataboliccomplication of type 2 diabetes is nonke-totic hyperosmolar hyperglycemic syn-d rome (NKHHS). The striking feature ofNKHHS is the absence of ketosis.Although this feature is traditionally usedto distinguish this syndrome from diabeticketoacidosis (DKA), many patients with

DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999 1381
Letters
NKHHS also have mild ketoacidosis (1). Itis well documented that both DKA andNKHHS can be precipitated by variouss t resses, including infection, surg e ry, andtrauma. Although traditionally attributedto absolute insulin defic i e n c y, it is nowbelieved that a relative insulin defic i e n c ycoupled with excess production of coun-t e rre g u l a t o ry hormones is re q u i red forexcess hepatic ketoacid production inDKA (2). Such counterre g u l a t o ry hor-mones include catecholamines, cort i s o l ,glucagon, and growth hormone. All ofthese have been shown to be elevated inNKHHS (3–5).
Cocaine has a stimulatory effect onc o u n t e rre g u l a t o ry hormones. Animal stud-ies have shown that cocaine increases cate-cholamine levels by stimulating adre n a lmedulla to release epinephrine and nore p i-nephrine (6). It has also been shown thatin patients intoxicated with cocaine, thereis an acute rise in circulating levels of nor-epinephrine and epinephrine (7). Humanstudies have demonstrated increased con-centrations of cort i c o t ropin (8) and cort i s o l(9) after cocaine administration.
Catecholamine levels, increased bycocaine use, profoundly affect carbohy-drate metabolism by inhibiting pancre a t i cinsulin secretion (10) and increasing thep roduction of glucagon (11). Studies onrat liver have shown that catecholaminesactivate glycogenolysis (12) and gluconeo-genesis (13). In humans, epinephrinei n c reases glucose production and de-c reases glucose clearance by both a- andb- a d re n e rgic actions (14).
A re t rospective case-control study ofadmissions for DKA in cocaine users andnonusers suggested that cocaine use shouldbe considered a risk factor for DKA (15).
We raise the possibility that cocaineuse caused the acute decompensation inour patient, who presented with nonke-totic hyperglycemic hyperosmolar syn-d rome, because of its documented eff e c t son counterre g u l a t o ry hormones. Clearly,our patient had been diabetic for someduration, given his elevated glycosylatedhemoglobin, and would have been even-tually diagnosed clinically. On an opti-mistic note, this precipitating event ofNKHHS might have helped to make hima w a re of the adverse consequences of type 2diabetes and the importance of avoidingtriggers that worsen metabolic state.
MINI R. ABRAHAM, MD
ROMESH KHARDORI, MB, MD
F rom the Division of Endocrinology, Metabolismand Molecular Medicine, Department of Intern a lMedicine, School of Medicine, Southern IllinoisU n i v e r s i t y, Springfield, Illinois.
A d d ress correspondence to Romesh Khard o r i ,MD, Division of Endocrinology, Metabolism andMolecular Medicine, Department of Medicine,S o u t h e rn Illinois University, School of Medicine,701 N. First St., P.O. Box 19636, Springfield, IL6 2 7 9 4 - 9 6 3 6 .
R e f e re n c e s1 . A r i e ff AI, Carroll HJ: Nonketotic hypero s-
molar coma with hyperglycemia: clinicalf e a t u res, pathophysiology, renal function,acid base balance, plasma cere b ro s p i n a lfluid equilibria and the effects of therapyin 37 cases. M e d i c i n e 51:73–94, 1972
2 . Schade DS, Eaton RP: The contro v e r s e yc o n c e rning counterre g u l a t o ry horm o n es e c retion: a hypothesis for the pre v e n t i o nof diabetic ketoacidosis. D i a b e t e s 2 6 :596–601, 1977
3 . Lindsey CA, Faloona GR, Unger RH:Plasma glucagon in non-ketotic hypero s-molar coma. JAMA 229:1771–1773, 1974
4 . Vinik A, Seftel H, Joffe BI: Metabolic func-tions in hyperosmolar non-ketotic diabetics t u p o r. L a n c e t ii:797–799, 1970
5 . Zadik Z, Kayne R, Kappy M, Plotnick LP,Kowarski AA: Increased integrated con-centration of nonepinephrine, epineph-rine, aldosterone, and growth hormone inpatients with uncontrolled juvenile dia-betes mellitus. D i a b e t e s 29:655–658, 1980
6 . Chiueh CC, Kopin IJ: Centrally mediatedrelease by cocaine of endogenous epineph-rine and norepinephrine from the sympa-t h o a d renal medullary system of unanes-thetized rats. J Pharmacol Exp Ther 2 0 5 :148–154, 1978
7 . K a rch SB: Serum catecholamines in cocaineintoxicated patients with cardiac symptoms(Abstract). Ann Emerg Med 16:481, 1987
8 . Teoh SK, Sarnyai Z, Mendelson JH, MelloNK, Springer SA, Sholar JW, Walper M,Kuehnle JC, Gelles H: Cocaine effects onpulsatile secretion of ACTH in men. J Phar -macol Exp Ther 270:1134–1138, 1994
9 . Heesch CM, Negus BH, Keffer JH, SnyderRW, Risser RC, Eichhorn EJ: Effects ofcocaine on cortisol secretion in humans. A mJ Med Sci 310:61–64, 1995
1 0 . Walters JM, Wa rd GM, Barton J, Arackal R,Boston RC, Best JD, Alford FP: The effect ofn o repinephrine on insulin secretion and glu-cose effectiveness in non-insulin dependentdiabetes. M e t a b o l i s m 46:1448–1453, 1997
1 1 . Gerich JE, Lorenzi, Karam JH: Studies onthe mechanism of epinephrine-inducedh y p e rglycemia in man: evidence for part i c-ipation of pancreatic glucagon secre t i o n .D i a b e t e s 25:65–71, 1976
1 2 . Sherline P, Lynch A, Glinsmann WH: CyclicAMP and adre n e rgic receptor control of ratliver glycogen metabolism. E n d o c r i n o l o g y
91:680–690, 19721 3 . Exton JH, Park CR: control of gluconeogenesis
in liver. Ι Ι: Effects of glucagon, catecholamines,and adenosine-39, 59-monophosphate ongluconeogenesis in the perfused rat liver. J Biol Chem 243:4189–4196, 1968
1 4 . Rizza RA, Cryer PE, Haymond MW,Gerich JE: Adre n rgic mechanisms of cate-cholamine action on glucose homeostasisin man. M e t a b o l i s m 29:1155–1163, 1980
1 5 . Wa rner EA, Greene GS, Buchsbaum MS,Cooper DS, Robinson BE: Diabeticketoacidosis associated with cocaine use.A rch Intern Med 158:1799–1802, 1998
C O M M E N T S A N DR E S P O N S E S
S e rum g-G l u t a m y l t r a n s f e r a s eand/or Seru mCholinesterase asMarkers of theMetabolic Syndro m e
In their article “Prospective study ofs e rum g-glutamyltransferase and risk ofNIDDM,” Perry et al. (1) provide evi-
dence that increased serum g- g l u t a m y l-transferase (GGT) activity could be a re l i-able marker of visceral and hepatic steato-sis, as well as a possible predictor for thedevelopment of type 2 diabetes.
M o re than 20 years ago, our labora-t o ry re p o rted data suggesting a possiblerelationship between increased seru mGGT activity and abnormalities of lipidmetabolism (2). It was also noted thats e rum cholinesterase (E.C. 3.1.1.8., acyl-choline acylhydrolase, or CHE), a livers e c retion enzyme, could be at least as suit-able as GGT as a marker of the metabolics y n d rome. Actually, in opposition to GGT,which is known to increase in liver diseaseof various etiologies, serum CHE activityd e c reases in liver disease, obviouslyi n c reasing in overweight and hypert r i g l y c-eridemic men. High serum CHE activitywas correlated not only with VLDLt r i g l y ceride, but also with several liver-derived enzymes and proteins, such asl e c i t h i n : c h o l e s t e rol acyltransferase (3), fibrin stabilizing factor XIII, and fib ro-nectin (4), as well as a2-antiplasmin and
1382 DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999
Letters
plasminogen activator inhibitor (5). Also,in a selected clinical study including nor-mal-weight control subjects and patientswith type 2 diabetes, serum CHE activitywas significantly correlated with seru minsulin and C-peptide levels (6). It seemsreasonable to presume that the above-mentioned observations are somehowrelated to the release of excess fatty acidsf rom the omental adipose tissue into thep o rtal circulation of android obese sub-jects, and the subsequent impaired metab-olism and action of insulin (7). Changesa ffecting the various liver-derived enzymescould, furt h e rm o re, be linked to diff e re n tmechanisms leading to increased synthesisor delayed removal of plasma triglyceride,or to the consequences of hypert r i g l y c-eridemia on liver function. For example,s e rum CHE activity is high even in subjectswith moderately increased triglyceride lev-els (2–3 mmol/l), but does not furt h e ri n c rease in patients with excessive hyper-triglyceridemia (10–20 mmol/l). Of note,s e rum CHE activity was found to bei n c reased in patients with hypert h y-roidism (8). Elevations of this enzyme’sactivity should there f o re be related to anaccelerated turnover of fatty acids and anenhanced secretion of VLDL rather thanan overloading of the liver with lipid. Onthe other hand, the highest GGT activitiesw e re mainly noted in patients with gro s sh y p e rtriglyceridemia (2) and, pre s u m a b l y,an excessively increased hepatic triglyc-eride pool including both de novo–synthesized triglyceride and triglyceridethat escaped extrahepatic re m o v a l .
MIRCEA CUCUIANU, MD
F rom the Medical Clinic Number I, Cluj-Napoca,R o m a n i a .
A d d ress correspondence to Dr. Mircea Cucuianu,P rofessor of Clinical Chemistry, Medical Clinic N r. I, R-3400, Cluj-Napoca, Romania.
R e f e re n c e s1 . P e rry IJ, Wannamethee SG, Shaper AG:
P rospective study of serum g- g l u t a m y l-transferase and risk of NIDDM. D i a b e t e sC a re 21:732–737, 1998
2 . Cucuianu M, Zdrenghea D, Pop M, O p i n c a ru A: Increased serum g- g l u t a m y l-transferase in hypertriglyceridemia: com-parison with serum pseudocholinesterase.Clin Chim Acta 71:419–427, 1976
3 . Cucuianu M, Opincaru A, Tapalaga D:Similar behaviour of lecithin-cholestero lacyltransferase and pseudocholinesterase
in liver disease and hyperlipopro t e i n e m i a .Clin Chim Acta 85:73–79, 1978
4 . Cucuianu M, Rus HG, Cristea A,Niculescu F, Bedeleanu D, Porutiu D,Roman S: Clinical studies on plasma fib ro-nectin and factor XIII: with special re f e r-ence to hyperlipoproteinemia. Clin ChimA c t a 147:273–281, 1985
5 . Cucuianu M, Knauer O, Roman S:a2antiplasmin, plasminogen activatorinhibitor (PAI) and dilute blood clot lysistime in selected disease states. T h ro m bH a e m o s t a s 66:586–591, 1991
6 . Nistor T, Cucuianu M, Hancu N, Orbai P:S e rum cholinesterase activity corre l a t e dwith serum insulin and C-peptide levels.Fiziologia 8:2–5, 1998
7 . B j ö rntorp P: Metabolic implications ofbody fat distribution. Diabetes Care 1 4 :1132–1143, 1991
8 . Thompson JC, Whittaker M: Pseudo-cholinesterase activity in thyroid disease. J Clin Path 18:811–812, 1965
Response toC u c u i a n u
We thank Professor Cucuianu (1)for his stimulating comments onour paper (2) and for highlighting
his important work on correlates of seru mg-glutamyltransferase and serum cholin-esterase. The data on links between seru mcholinesterase, obesity, hyperinsulinemia,and abnormalities of both lipid metabo-lism and clotting factors are extre m e l yi n t e resting and are consistent with thehypothesis that serum cholinesterase maybe a further hepatic marker of the meta-bolic syndrome. These findings pro v i d ef u rther support for the concept of hepaticsteatosis with hepatic insulin resistance asa fundamental abnormality in the devel-opment of the insulin resistant syndro m e .
P rospective data on serum cholin-esterase (adjusted for measures of visceralf a t ) and risk of type 2 diabetes and othermanifestations of the metabolic syn-d rome would be of considerable intere s t .U l t i m a t e l y, as the number of candidatemarkers for the metabolic syndro m ei n c reases, we need to focus on the funda-mental genetic and enviro n m e n t a l / l i f e -style factors that influence the develop-ment of this syndro m e .
IVAN J. PERRY, MD, PHD
F rom the Department of Epidemiology and PublicHealth, Distillery House, University College Cork,Cork, Republic of Ire l a n d .
A d d ress correspondence to Professor I.J. Perry,Dept. of Epidemiology and Public Health, DistilleryHouse, University College Cork, Republic of Ire l a n d.E-mail: i.perry @ u c c . i e .
R e f e re n c e s1 . Cucuianu M: Serum g- g l u t a m y l t r a n s f e r a s e
and/or serum cholinesterase as markers ofthe metabolic syndrome (Letter). D i a b e t e sC a re 22:1381–1382, 1999
2 . P e rry IJ, Wannamethee SG, Shaper AG:P rospective study of serum g- g l u t a m y l-transferase and risk of NIDDM. D i a b e t e sC a re 21:732–737, 1998
A Japanese Case ofLiver DysfunctionAfter 19 Months ofTroglitazone Tre a t m e n t
Troglitazone is the first drug fori m p roving insulin resistance, a pri-m a ry concern in most patients with
type 2 diabetes. However, severe hepato-toxicity was re p o rted in patients givent roglitazone soon after its appearance inJapan and the U.S. in March 1997 (1,2). InDecember 1997, the Japanese govern m e n trecommended that physicians assess liverfunction at least every month duringt roglitazone treatment. The U.S. Food andD rug Administration (FDA) re c o m m e n d e dat the same time that alanine aminotrans-ferase (ALT) should be measured beforet h e r a p y, monthly for the next 8 months,e v e ry 2 months for the remainder of the1st year, and periodically there a f t e r. It isunknown, however, how long l i v e r- f u n c-tion tests should be done to detect tro g l i-tazone-induced liver dysfunction. Were p o rt here on a patient who developedliver dysfunction after 19 months oft roglitazone tre a t m e n t .
A 62-year-old woman was transferre dto our university hospital because of liverdysfunction. At 36 years of age, she hadbeen diagnosed with type 2 diabetes,which was controlled by diet therapy. Thepatient was diagnosed with Graves’ diseaseat the same age. Because she had an allerg yto methimazole, radioiodine therapy wasp e rf o rmed, and since then, she hasre q u i red horm o n e - replacement therapy.At 39 years of age, the patient was start e don a regimen of glibenclamide. Pravastatint reatment was started for hyperc h o l e s-t e rolemia in April 1994. Tr a n s i e n t
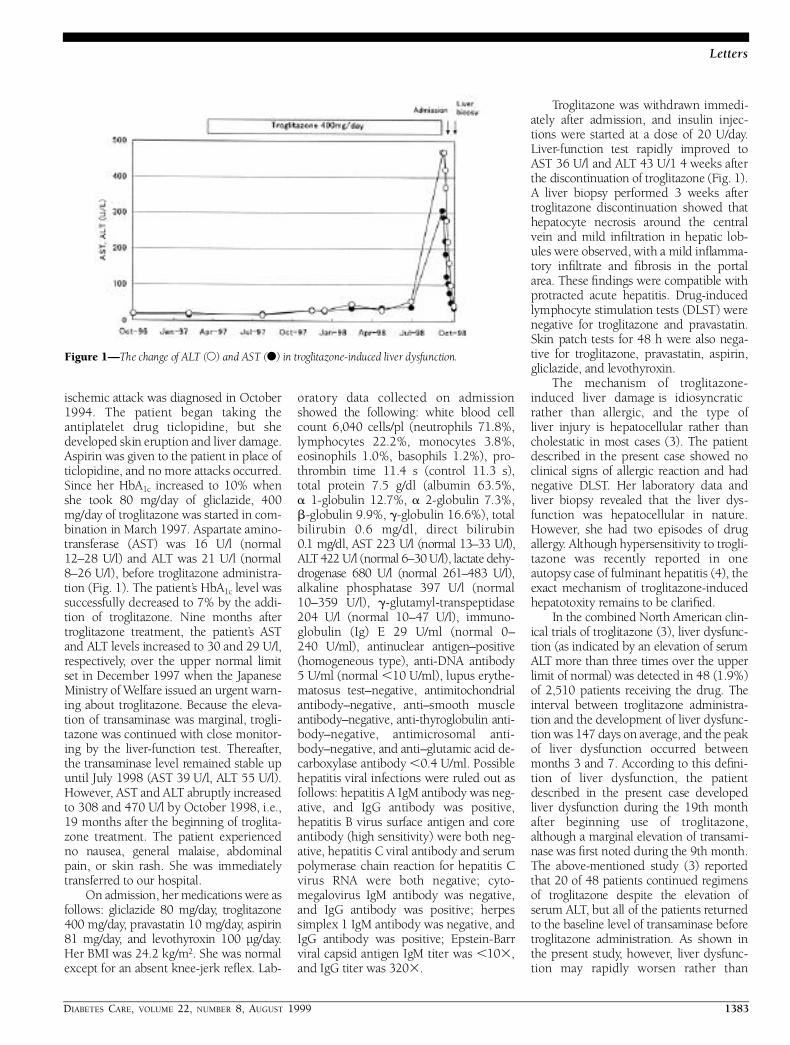
DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999 1383
Letters
ischemic attack was diagnosed in October1994. The patient began taking theantiplatelet drug ticlopidine, but shedeveloped skin eruption and liver damage.Aspirin was given to the patient in place ofticlopidine, and no more attacks occurre d .Since her HbA1 c i n c reased to 10% whenshe took 80 mg/day of gliclazide, 400mg/day of troglitazone was started in com-bination in March 1997. Aspartate amino-transferase (AST) was 16 U/l (norm a l12–28 U/l) and ALT was 21 U/l (norm a l8–26 U/l), before troglitazone administra-tion (Fig. 1). The patient’s HbA1 c level wassuccessfully decreased to 7% by the addi-tion of troglitazone. Nine months aftert roglitazone treatment, the patient’s ASTand ALT levels increased to 30 and 29 U/l,re s p e c t i v e l y, over the upper normal limitset in December 1997 when the JapaneseM i n i s t ry of We l f a re issued an urgent warn-ing about troglitazone. Because the eleva-tion of transaminase was marginal, tro g l i-tazone was continued with close monitor-ing by the liver-function test. There a f t e r,the transaminase level remained stable upuntil July 1998 (AST 39 U/l, ALT 55 U/l).H o w e v e r, AST and ALT abruptly incre a s e dto 308 and 470 U/l by October 1998, i.e.,19 months after the beginning of tro g l i t a-zone treatment. The patient experiencedno nausea, general malaise, abdominalpain, or skin rash. She was immediatelyt r a n s f e rred to our hospital.
On admission, her medications were asfollows: gliclazide 80 mg/day, tro g l i t a z o n e400 mg/day, pravastatin 10 mg/day, aspirin81 mg/day, and levothyroxin 100 µg/day.Her BMI was 24.2 kg/m2. She was norm a lexcept for an absent knee-jerk re flex. Lab-
o r a t o ry data collected on admissionshowed the following: white blood cellcount 6,040 cells/pl (neutrophils 71.8%,lymphocytes 22.2%, monocytes 3.8%,eosinophils 1.0%, basophils 1.2%), pro-t h rombin time 11.4 s (control 11.3 s),total protein 7.5 g/dl (albumin 63.5%, a 1-globulin 12.7%, a 2-globulin 7.3%,b-globulin 9.9%, g-globulin 16.6%), totalb i l i rubin 0.6 mg/dl, direct bilirubin 0.1 mg/dl, AST 223 U/l (normal 13–33 U/l),A LT 422 U/l (normal 6–30 U/l), lactate dehy-d rogenase 680 U/l (normal 261–483 U/l),alkaline phosphatase 397 U/l (normal10–359 U/l), g- g l u t a m y l - t r a n s p e p t i d a s e204 U/l (normal 10–47 U/l), immuno-globulin (Ig) E 29 U/ml (normal 0–240 U/ml), antinuclear antigen–positive ( h o m ogeneous type), anti-DNA antibody5 U/ml (normal ,10 U/ml), lupus ery t h e-matosus test–negative, a n t i m i t o c h o n d r i a lantibody–negative, anti–smooth muscleantibody–negative, anti-thyroglobulin anti-b o d y–negative, antimicrosomal anti-body–negative, and anti–glutamic acid de-carboxylase antibody ,0.4 U/ml. Possiblehepatitis viral infections were ruled out asfollows: hepatitis A IgM antibody was neg-ative, and IgG antibody was positive,hepatitis B virus surface antigen and coreantibody (high sensitivity) were both neg-ative, hepatitis C viral antibody and seru mpolymerase chain reaction for hepatitis Cv i rus RNA were both negative; cyto-m e g a l o v i rus IgM antibody was negative,and IgG antibody was positive; herpessimplex 1 IgM antibody was negative, andIgG antibody was positive; Epstein-Barrviral capsid antigen IgM titer was ,1 03,and IgG titer was 3203.
Troglitazone was withdrawn immedi-ately after admission, and insulin injec-tions were started at a dose of 20 U/day.L i v e r-function test rapidly improved toAST 36 U/l and ALT 43 U/1 4 weeks afterthe discontinuation of troglitazone (Fig. 1).A liver biopsy perf o rmed 3 weeks aftert roglitazone discontinuation showed thathepatocyte necrosis around the centralvein and mild infiltration in hepatic lob-ules were observed, with a mild infla m m a-t o ry infiltrate and fib rosis in the port a la rea. These findings were compatible withp rotracted acute hepatitis. Dru g - i n d u c e dlymphocyte stimulation tests (DLST) werenegative for troglitazone and pravastatin.Skin patch tests for 48 h were also nega-tive for troglitazone, pravastatin, aspirin,gliclazide, and levothyro x i n .
The mechanism of tro g l i t a z o n e -induced liver damage is idiosyncraticrather than allergic, and the type of liver injury is hepatocellular rather thancholestatic in most cases (3). The patientdescribed in the present case showed noclinical signs of allergic reaction and hadnegative DLST. Her laboratory data andliver biopsy revealed that the liver dys-function was hepatocellular in nature .H o w e v e r, she had two episodes of dru ga l l e rg y. Although hypersensitivity to tro g l i-tazone was recently re p o rted in oneautopsy case of fulminant hepatitis (4), theexact mechanism of tro g l i t a z o n e - i n d u c e dhepatotoxity remains to be clarifie d .
In the combined North American clin-ical trials of troglitazone (3), liver dysfunc-tion (as indicated by an elevation of seru mA LT more than three times over the upperlimit of normal) was detected in 48 (1.9%)of 2,510 patients receiving the drug. Thei n t e rval between troglitazone administra-tion and the development of liver dysfunc-tion was 147 days on average, and the peakof liver dysfunction occurred betweenmonths 3 and 7. According to this defin i-tion of liver dysfunction, the patientdescribed in the present case developedliver dysfunction during the 19th monthafter beginning use of troglitazone,although a marginal elevation of transami-nase was first noted during the 9th month.The above-mentioned study (3) re p o rt e dthat 20 of 48 patients continued re g i m e n sof troglitazone despite the elevation ofs e rum ALT, but all of the patients re t u rn e dto the baseline level of transaminase beforet roglitazone administration. As shown inthe present study, however, liver dysfunc-tion may rapidly worsen rather than
Figure 1—The change of ALT (s) and AST (d) in troglitazone-induced liver dysfunction.

1384 DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999
Letters
become normalized after persistent mildliver dysfunction. The FDA re c o m m e n d e dthat if ALT levels that are 1.5–3 times theupper limit of normal develop during tre a t-ment, ALT should be tested weekly, andlevels .3 times the upper limit of norm a lcall for immediate discontinuation oft roglitazone. Since tro g l i t a z o n e - i n d u c e dliver dysfunction may pro g ress irre v e r s i b l ydespite the discontinuation of tro g l i t a z o n e ,eventually leading to liver transplantationor death, the results observed in ourpatient suggest that the re c o m m e n d a t i o nof the FDA is appropriate to prevent thedevelopment of severe troglitazone-induced hepatotoxicity. Clinicians shouldbe mindful of liver-function tests whilet reating patients with tro g l i t a z o n e .
MASANORI IWASE, MDMASAKO YAMAGUCHI, MD
MOTOTAKA YOSHINARI, MDCHINAMI OKAMURA, MDTAKAAKI HIRAHASHI, MD
HIROSHI TSUJI, MDMASATOSHI FUJISHIMA, MD
F rom the Second Department of Internal Medicine,Faculty of Medicine, Kyushu University, Fukuoka,J a p a n .
A d d ress correspondence to Masanori Iwase, MD,Second Department of Internal Medicine, Faculty ofMedicine, Kyushu University, Maidashi 3-1-1,Higashi-ku, Fukuoka 812-8582, Japan.
R e f e re n c e s1 . Gitlin N, Julie NL, Spurr CL, Lim KN,
Juarbe HM: Two cases of severe clinicaland histologic hepatotoxicity associatedwith troglitazone. Ann Intern Med 1 2 9 :36–38, 1998
2 . N e u s c h w a n d e r- Tetri BA, Isley WL, Oki JC,Ramrakhiani S, Quiason SG, Phillips NJ,B runt EM: Troglitazone-induced hepaticf a i l u re leading to liver transplantation: acase re p o rt. Ann Intern Med 1 2 9 : 3 8 – 4 1 ,1 9 9 8
3 . Watkins PB: Hepatic dysfunction associ-ated with troglitazone. N Engl J Med 3 3 8 :916–917, 1997
4 . Shibuya A, Kuwao S, Watanabe M, Takahashi H, Fujita Y, Takeuchi H,Saigenji K: An autopsy case of tro g l i t a-zone-induced fulminant hepatitis. D i a b e t e sC a re 21:2140–2143, 1998
Response to Iwaseet al.
Iwase et al. (1) have re p o rted an intere s t-ing case of asymptomatic liver dysfunc-tion after 19 months of tro g l i t a z o n e
t reatment. The liver dysfunction was char-
acterized by an elevation of alanine a m i n o-transferase (ALT) that was ,18 times theupper limit of normal, without an ele-vated level of bilirubin. The patient’s liver-f u n c t i o n tests normalized promptly afterdiscontinuation of the drug. The liverb i o p s y, which was not perf o rmed until 3weeks after drug discontinuation, hadfairly nonspecific findings of hepatitiswithout evidence of true hepatocellularn e c ro s i s .
The role of troglitazone in the hepaticdysfunction in this patient is not clear.C e rt a i n l y, asymptomatic elevations ofA LT occur in the general population. Inaddition, during the clinical trials that ledto tro g l i t a z o n e ’s approval in the U.S.,nearly 50% of patients with ALT eleva-tions (including 25% with elevations.10 times the upper limit of normal) nor-malized while still on the drug. Some ofthese patients remained in studies for up to2 years.
A d d i t i o n a l l y, the incidence of signifi-cant hepatocelluar injury (liver failure )based on postmarketing experience (1 of57,000) is far less than the 2 of 100patients’ incidence of ALT elevationso b s e rved in clinical trials, indicating thatv e ry few patients with ALT elevations willp ro g ress to severe liver injury.
M o re than 1.6 million patients in theU.S. have been treated with tro g l i t a z o n e ,with ,600,000 receiving treatment for.1 year. There are no re p o rted cases ofdeath from hepatic failure or liver trans-plant in patients treated for .1 year. Sincethe recommendation for regular ALTmonitoring was made in late 1997, therate of re p o rted cases of jaundice, hyper-b i l i rubinemia, and more severe injury,including liver failure, has decre a s e d .Parke-Davis agrees with Dr. Iwase andcolleagues that monitoring of liver- f u n c-tion tests in patients being treated witht roglitazone is important and have re c o m-mended in the current troglitazone pro d-uct labeling that ALT monitoring shouldbe done at baseline, monthly for the 1sty e a r, and quarterly thereafter to decre a s ethe risk of rare idiosyncratic liver failure .
RANDALL WHITCOMB, MD
F rom Parke-Davis Pharmaceutical Research, AnnA r b o r, Michigan.
A d d ress correspondence to Randall Whitcomb,MD, Parke-Davis Pharmaceutical Research, 2800Plymouth Rd., Ann Arbor, MI 48105. E-mail: r a n d a l l . w h i t c o m b @ w l . c o m .
R . W. holds stock in Wa rner Lambert .
R e f e re n c e s1. Iwase M, Yamaguchi M, Yoshinari M,
Okamura C, Hirahashi T, Tsuji H,Fujishima M: A Japanese case of liver dys-function after 19 months of tro g l i t a z o n et reatment. Diabetes Care 2 2 : 1 3 8 2 – 1 3 8 4 ,1 9 9 9
Postprandial Oxidized Lipids inDiabetic Patients
Which role for postprandial h y p e rg l y c e m i a ?
In a recent article, Staprans et al. (1)re p o rted that in type 2 diabetic patientswith poor glycemic control (HbA1 1 3 . 3 3
± 0.55%), plasma levels of oxidized lipidsin the postprandial phase are incre a s e dc o m p a red with those in control subjects ordiabetic patients with good glycemic con-t rol (HbA1 7.96 ± 0. 55%). They suggestthat this increase may be due to alterationsin the clearance and/or increased absorp-tion of oxidized dietary lipids, specifyingthat clearance alone is unlikely to accountfor the observed incre a s e .
We would like to propose anotherpossible explanation. Increased postpran-dial oxidized lipid levels were observed inpoorly controlled diabetic patients, i.e., ina population very likely characterized byhigher postprandial blood glucose levelsthan those in patients with well-contro l l e dblood glucose levels. Indeed, there issound evidence that postprandial hyper-glycemia is the most important contribu-tor to HbA1 c levels (2).
R e c e n t l y, we re p o rted that in diabeticpatients, the postprandial phase is charac-terized by increased oxidative stress gener-ation and antioxidant consumption (3).H y p e rglycemia, particularly postprandialh y p e rglycemia, appears to play an impor-tant role in such phenomena (4).
In our opinion, elevated levels of post-prandial hyperglycemia in poorly con-t rolled diabetic patients may have larg e l ycontributed to the results re p o rted byStaprans and colleagues. In fact, hyperg l y-cemia, by itself and/or through antioxidantconsumption, favors an increase in theoxidation of plasma lipids.
To validate this point of view, it wouldbe of great interest to know the levels ofpostprandial hyperglycemia observed in

DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999 1385
Letters
the subjects of the studies by Staprans andcolleagues, if available.
AN T O N I O CE R I E L L O, M D
EN R I C O MO T Z, M D
F rom the Department of Internal Medicine, Univer-sity of Udine, Udine, Italy.
A d d ress correspondence to Dr. Antonio Ceriello,Chair of Internal Medicine, Univeristy of Udine, P.le S.Maria della Misericordia, 33100 Udine, Italy. E-mail:a n t o n i o . c e r i e l l o @ d p m s c . u n i u d . i t .
R e f e re n c e s1 . Staprans I, Hardman DA, Pan X-M, Fein-
gold KR: Effect of oxidized lipids in thediet on oxidized lipid levels in postpran-dial serum chylomicrons of diabeticpatients. Diabetes Care 22:300–306, 1999
2 . Avignon A, Radauceanu A, Monnier L:Nonfasting plasma glucose is a bettermarker of diabetic control than fastingplasma glucose in type 2 diabetes. D i a b e t e sC a re 20:1822–1826, 1997
3 . Ceriello A, Bortolotti N, Motz E, Cre s c e n t i n iA, Lizzio S, Russo A, Tonutti L, Taboga C:Meal-generated oxidative stress in type 2diabetic patients. Diabetes Care 2 1 : 1 5 2 9 –1533, 1998
4 . Ceriello A: Acute hyperglycaemia andoxidative stress generation. Diabet Med(Suppl. 3) 14:S45–S49, 1997
Response to Cerielloand Motz
We appreciate very much the inter-est of Drs. Ceriello and Motzre g a rding our recent art i c l e ,
“ E ffect of oxidized lipids in the diet on oxi-dized lipid levels in postprandial seru mc h y l o m i c rons of diabetic patients,” pub-lished in Diabetes Care (1). As we sug-gested in this publication, the observ a t i o nthat patients with poorly controlled dia-betes have increased levels of oxidizedlipids in postprandial lipoproteins couldbe due to a number of possibilities. Wea p p reciate the suggestion of Drs. Cerielloand Motz that postprandial hyperg l y c e m i acould increase oxidative stress, there b yaccounting for the increased oxidation.H o w e v e r, we feel that it is likely thati n c reased absorption of dietary oxidizedlipids and the incorporation of these oxi-dized lipids into lipoproteins plays a majorrole for the increased oxidized seru mlipids observed in patients with diabetesfor the following reasons: 1 ) In nondia-
betic humans (1,2) and animals (3,4), lev-els of postprandial oxidized lipids dire c t l yc o rrelate with the quantity of oxidizedlipids in the diet. 2 ) In animals with dia-betes, the levels of oxidized lipids in thec i rculation directly correlate with thequantity of oxidized lipids in the diet (4).3 ) In animals with diabetes, the levels ofoxidized lipids in the mesenteric lymphc h y l o m i c rons directly correlate with thequantity of oxidized lipids in the diet (4).4 ) Using radiolabeled oxidized fatty acids,we have directly demonstrated that ani-mals with diabetes absorb increased quan-tities of oxidized dietary lipid (4). 5 ) In themost recent study in humans published inD i a b e t e s C a re (1), an increase in oxidizedlipids in the circulation was not observ e dwhen the patients with elevated seru mtriglycerides were fed a diet containing nooxidized lipid.
T h e re f o re, on the basis of the above-listed observations, we hypothesize thatthe absorption of oxidized lipids in thediet plays a major role in producing thei n c reased levels of postprandial oxidizedlipids in patients with diabetes.
ILONA STAPRANS, PHD
KENNETH R. FEINGOLD, MD
F rom the Department of Veterans Affairs MedicalCenter; and the Departments of Surg e ry and Medi-cine, University of California, San Francisco, Cali-f o rn i a .
A d d ress correspondence to I. Staprans, PhD, Ve t-erans Affairs Medical Center (151L), 4150 ClementSt., San Francisco, CA 94121. E-mail: stapan@i t s a . u c s f . e d u .
R e f e re n c e s1. Staprans I, Hardman DA, Pan X-M,
Feingold KR: Effect of oxidized lipids inthe diet on oxidized lipid levels in post-prandial serum chylomicrons of diabeticpatients. Diabetes Care 2 2 : 3 0 0 – 3 0 6 ,1999
2 . Staprans I, Rapp JH, Pan XM, Kim KY,Feingold KR: Oxidized lipids in the dieta re a source of oxidized lipid in chylomi-c rons of human serum. A rterioscler Thro m b14:1900–1905, 1994
3 . Staprans I, Pan X-M, Miller M, Rapp JH:E ffect of dietary lipid peroxides on metab-olism of serum chylomicrons in rats. Am JPhysiol 264:G561, 1993
4 . Staprans I, Rapp JH, Pan X-M, FeingoldKR: The effect of oxidized lipid in the dieton serum lipoprotein peroxides in contro land diabetic rats. J Clin Invest 9 2 : 6 3 8 ,1 9 9 3
Fasting Blood Glucose and Risk ofC a rdiovascular D i s e a s e
Arecent study from Norway showedthat after 22 years of follow-up, non-diabetic men aged 40–59 years with
a fasting blood glucose concentrationabove the upper quartile (4.8–6.1 mmol/lor 86–110 mg/dl) had an increased risk ofc a rdiovascular mort a l i t y, compared withmen in the rest of the study population(1). The corresponding hazards ratio was1.4 (95% CI 1.04–1.8), after adjusting forother risk factors. The authors found thatthe interaction between age and fastingblood glucose class was statistically signifi-cant (P , 0.0001). Curiously, in a strati-fied analysis, with strata defined by thea g e - g roups 40–49 and 50–59 years, highfasting blood glucose concentrations onlyc a rried a risk in the younger age-gro u p ,with hazards ratios of 2.1 (1.3–3.3) and1.1 (0.80–1.5), re s p e c t i v e l y. This re s u l tshould have been highlighted, andincluded in the abstract, given the dra-matic drop in the risk for the older men.
C a rdiovascular mortality at 20 years offollow-up has already been studied accord-ing to fasting glucose concentrations in thenondiabetic men of the Paris Pro s p e c t i v eand Helsinki Policemen Studies (2), inwhich diabetes was defined by a postload2-h plasma/blood glucose of $1 1 . 1 / 1 0 . 1mmol/l (200/180 mg/dl) or treatment withanti-diabetic drugs. In comparison to thelower 80% of the fasting glucose distribu-tion, cardiovascular disease mortality onlyi n c reased significantly in the upper 2.5%of this distribution, above 6.88/6.00mmol/l (124/108 mg/dl) of plasma/bloodglucose in the Paris Pro s p e c t i v e / H e l s i n k iPolicemen Studies. Furt h e rm o re, the riskwas only statistically significant when thetwo studies were combined with anadjusted hazards ratio of 1.60 (1.07–2.40).The risk was not significant, overall, for themen in the upper 20% of the fasting glu-cose distributions. It should also be notedthat this study did not take fasting hyper-glycemia into account when defining dia-betic subjects, and that the definition ofc a rdiovascular disease differs from that inthe Norwegian study (2).
We have now examined the 20-yearc a rdiovascular mortality in the ParisP rospective Study according to two age-

1386 DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999
Letters
g roups, 44–49 years and 50–55 years.F u rt h e r, we have restricted our study pop-ulation to those men who were nondia-betic according to the current definition ofdiabetes, with a fasting plasma glucose,7.0 mmol (126 mg/dl). With the lowerfasting glucose concentrations in this pop-ulation of 6,512 men, the fasting glucoseconcentration no longer carried a signifi-cant risk in the upper percentile gro u p s ,and this result did not change when the men were divided into age-groups ( Table 1). Adjustment has been made inthe hazards ratios for age, BMI, systolicblood pre s s u re, hypertensive tre a t m e n t ,baseline cardiovascular disease, total cho-l e s t e rol, smoking habits, and administra-tive grade, as in the previous analyses (2).Dividing the population according to theupper quartile of the fasting glucose distri-bution did not change this re s u l t .
For death by any cause, the death ratetended to increase in the upper 2.5% ofthe fasting glucose distribution, and if theupper 25% of the men were grouped, thefasting glucose concentration becames i g n i ficant, with no diff e rence between theyounger and the older men (Table 1).
If we include the 70 men who had adiabetic 2-h glucose level (but a nondia-betic fasting glucose), so that our study ism o re comparable with the Norw e g i a ns t u d y, which was based on fasting glucoseconcentrations alone, the results did notchange, and there was still no diff e re n t i a l
e ffect of age on cardiovascular or all-cause mort a l i t y.
A recent metare g ression analysis ofdata from prospective studies by Coutinhoet al. (3), including six studies re p o rt i n gfasting glucose data, provides support forthe view that nondiabetic degrees of fastingh y p e rglycemia are associated with in-c reased cardiovascular risk. Further workbased on prospective studies carried out inl a rge populations is needed, however, for acloser delineation of the nature of the asso-ciation between fasting glucose and card i o-vascular risk, particularly with re g a rd to dif-f e rent subgroups according to age, sex, eth-n i c i t y, etc. The finding of Bjørnholt et al. (1)that elevated fasting glucose carried a lowerrisk for cardiovascular death in older menthan in younger men could not be re p ro-duced in the Paris Prospective Study. It is,h o w e v e r, important to examine this issue inother cohort studies.
BEVERLEY BALKAU, PHD
R. JOHN JARRETT, MD
KALEVI PYÖRÄLÄ, MD
EVELINE ESCHWÈGE, MD
F rom INSERM U258 and the Faculty of MedicineParis Sud (B.B., E.E.), Villejuif, France; UniversityCollege Medical School and the Department of Pub-lic Health Medicine (R.J.J.), United Medical andDental Schools of Guy’s and Thomas’ Hospitals,London, U.K.; and the Department of Medicine( K . P.), University of Kuopio, Kuopio, Finland.
A d d ress correspondence to Beverley Balkau,INSERM U258, 16 Avenue Paul Va i l l a n t - C o u t u r i e r,
94807 Villejuif cedex, France. E-mail: balkau@v j f . i n s e rm . f r.
R e f e re n c e s1 . B j ø rnholt JV, Erikssen G, Aaser E, Sandvik
L, Nitter-Hauge S, Jervell J, Erikssen J,Thaulow E: Fasting blood glucose: anu n d e restimated risk factors for card i o v a s-cular death: results from a 22-year follow-up of healthy nondiabetic men. D i a b e t e sC a re 22:45–49, 1999
2 . Balkau B, Shipley M, Jarrett JR, Pyörälä K,Pyörälä M, Forhan A, Eschwège E: Highblood glucose concentration is a risk factorfor mortality in middle-aged nondiabeticmen: 20-year follow-up in the WhitehallS t u d y, the Paris Prospective Study, and theHelsinki Policemen Study. Diabetes Care21:360–367, 1998
3 . Coutinho M, Gerstein HC, Wang Y, Yusuf S:The relationship between glucose and inci-dent cardiovascular events: a metare g re s s i o nanalysis of published data from 20 studies of97,783 individuals followed for 12.4 years.Diabetes Care 22:233–240, 1999
Response to Balkau et al.
Balkau et al. (1) have commented onour paper “Fasting blood glucose: anu n d e restimated risk factor for card i o-
vascular death: results from a 22-year fol-low-up of healthy nondiabetic men” (2).
Table 1—Hazard ratios for death by cardiovascular disease in the 6,512 nondiabetic men (fasting/2-h glucose ,7.0/11.1 mmol/l and nottreated for diabetes) after adjustment for age, BMI, systolic blood pressure, hypertensive treatment, baseline cardiovascular disease, totalcholesterol, smoking habits, and administrative grade: the Paris Prospective Study
Fasting glucose Number of deaths/ H a z a rd ratios (95% CI)Percentile mmol/l (mg/dl) number of men All men (n = 6,512) ,50 years (n = 4,607) $50 years (n = 1,905)
C a rdiovascular deaths,8 0 5.99 (108) 3 2 0 / 5 , 0 3 6 1 1 18 0 – 9 0 6.22 (112) 4 2 / 6 6 6 0.86 (0.62–1.19) 0.85 (0.56–1.27) 0.87 (0.51–1.50)9 0 – 9 5 6.44 (116) 3 2 / 3 6 8 1.20 (0.83–1.74) 1.10 (0.68–1.78) 1.50 (0.84–2.67)9 5 – 9 7 . 5 6.66 (120) 2 1 / 2 4 9 1.11 (0.71–1.74) 1.06 (0.60–1.87) 1.23 (0.60–2.54)97.5 to maximum — 1 6 / 1 9 3 0.87 (0.52–1.46) 0.73 (0.36–1.51) 1.08 (0.50–2.33),7 5 5.88 (106) 2 8 0 / 4 , 5 9 8 1 1 1$7 5 — 1 5 1 / 1 , 9 1 4 1.11 (0.90–1.37) 1.20 (0.92–1.55) 1.00 (0.72–1.41)
All-cause deaths,8 0 5.99 (108) 1 , 0 4 0 / 5 , 0 3 6 1 1 18 0 – 9 0 6.22 (112) 1 5 2 / 6 6 6 1.07 (0.90–1.27) 1.02 (0.83–1.26) 1.18 (0.87–1.59)9 0 – 9 5 6.44 (116) 9 4 / 3 6 8 1.22 (0.98–1.51) 1.00 (0.75–1.32) 1.74 (1.24–2.42)9 5 – 9 7 . 5 6.66 (120) 5 6 / 2 4 9 1.00 (0.77–1.32) 1.00 (0.72–1.39) 0.99 (0.61–1.62)97.5 to maximum — 6 1 / 1 9 3 1.29 (0.99–1.68) 1.25 (0.90–1.74) 1.37 (0.86–2.18),7 5 5.88 (106) 9 2 9 / 4 , 5 9 8 1 1 1$7 5 — 4 7 4 / 1 , 9 1 4 1.18 (1.05–1.32) 1.15 (1.00–1.33) 1.23 (1.01–1.51)

DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999 1387
Letters
They especially draw attention to theunexpected finding that a significant inter-action between age and fasting blood glu-cose on cardiovascular death was found (P , 0.0001), which, in a stratified analy-sis, suggested that men aged 40–49 and50–59 years had hazard ratios of 2.1 (95%CI 1.3–3.3) and 1.1 (0.80–1.5), re s p e c-t i v e l y. They also claim that this shouldhave been highlighted in the abstract.
We appreciate their comments ande ff o rts to reach for similar findings in theParis Prospective Study population. Never-theless, we disagree with their claim fortwo main reasons. First, unexpected fin d-ings, especially as interactions, should bev e ry cautiously interpreted and should,like any epidemiological finding, only begeneralized if similar observations are re i t-erated by other observers and the fin d i n g sa re consistent, strong, graded, plausible,c o h e rent, appropriately sequenced, andunbiased (3).
H o w e v e r, we felt it would have beenacademically incorrect to withhold thisfinding, even if poorly explained. Accord-i n g l y, we presented our unexpected fin d-ing and discussed it, but hesitated to makeit one of the major findings from the study.That Balkau and associates could notre p roduce the finding in the Paris Pro s p e c-tive Study population has, in our view,s t rengthened our cautious appro a c h .
Second, the apparent significant inter-action in our study population could haveseveral relevant explanations, one of whichwas that all individuals included in thestudy were healthy at inclusion. As men-tioned in our paper, this fact actually intro-duces a possible strong selection effect onthe age-group 50–59 years, compared withthose 40–49 years at inclusion. Thus, a nec-e s s a ry pre requisite for inclusion was thatthey had remained healthy on average 10 years more than those aged 40–49 years.
On the other hand, we acknowledgethat the apparent interaction may well re p-resent a statistical phenomenon related to achance finding in a small material. How-e v e r, this was not our main message, whichwas increased coro n a ry heart disease mor-tality with increasing fasting blood glucosein the upper so-called normal range.
Balkau et al. did not confirm the mainfinding, that high nondiabetic fastingblood glucose levels were an independentrisk factor for cardiovascular disease, intheir 20-year follow-up of the combinedWhitehall, Paris Prospective, and HelsinkiPolicemen populations (4). As stated by
themselves, this might relate to diff e re n c e sin populations and the definition of card i o-vascular death, as judged by their descrip-tion of the selection pro c e d u res and fol-low-up methods. The Norwegian popula-tion consisted exclusively of healthy menas judged by clinical examination and priorh i s t o ry. Thus, as mentioned, men wereonly included when all prior evidence indi-cated absence of cardiovascular disease,h y p e rtension, diabetes, malignancy, etc. Inaddition, we re q u i red the ability to per-f o rm a bicycle exercise test. Furt h e rm o re ,in our study, we excluded men with fastingblood glucose .109 mg/dl.
The definition of cardiovascular deathin our study was strict and adhered to I n t e r -national Classification of Disease, Ninth Revi -s i o n (ICD-9) codes for ischemic heart dis-ease (ICD-9 410–414), stroke (ICD-9 430,431, and 436), and sudden death (ICD-9798.1); it seems to differ from the defin i t i o nused by Balkau et al. Furt h e rm o re, deathc e rt i ficates were checked against hospitalre c o rds to ensure correct coding. We areu n a w a re of all the details about how mor-tality was assessed in the Paris Pro s p e c t i v eand Whitehall populations, whereas themethods used in the Helsinki Policemenpopulation seem comparable to ours.
Is it also possible that the “French para-dox” has played a role in the French study?
In at least one important way, ouranalysis differs from that of Balkau et al.(4). Our multivariate analysis also in-cluded a variable, like physical fit n e s s ,that has repeatedly been shown to be ani m p o rtant predictor of card i o v a s c u l a rdeath (5,6) and to which insulin sensitiv-ity is linked (7). Conceivably, inclusion ofthis variable in the multivariate analysismay reduce confounding.
The issue of on what level high nondia-betic fasting blood glucose is predictive ofan increased cardiovascular mortality stillremains controversial. As mentioned above,data that form the basis for this contro v e r s ymay not be comparable in several ways.
Finally it should be emphasized thatfasting blood glucose, although a simplem e a s u re, is the result of a very complexhomeostasis that is not yet fully under-stood. Some clarification may emerg e ,h o w e v e r, from meta-analyses like that ofCoutinho et al. (8).
It was unfortunate that the import a n tpaper by Balkau et al. (4) was not includedin our re f e rences; their paper was inp ress/published during the editorial con-sideration of our own paper.
JØRGEN V. BJØRNHOLT, MDLEIV SANDVIK, PHD
JAK JERVELL, MDJAN ERIKSSEN, MD
F rom the Medical Department B ( J . V.B., J.J.), Rik-shospitalet, Oslo; and the Medical Depart m e n t(L.S., J.E.), Central Hospital in Akershus, Nord b y-hagen, Norw a y.
A d d ress correspondence to Jørgen V. Bjørn h o l t ,MD, Rikshospitalet, Medical Department B, N-0027Oslo, Norw a y. E-mail: jobjorn @ o n l i n e . n o .
R e f e re n c e s1 . Balkau B, Jarrett RJ, Pyörälä K, Eschwège
E: Fasting blood glucose and risk of car-diovascular disease (Letter). Diabetes Care22:1385–1386, 1999
2 . B j ø rnholt JV, Erikssen G, Aaser E, SandvikL, Nitter-Hauge S, Jervell J, Erikssen J,Thaulow E: Fasting blood glucose: anu n d e restimated risk factor for card i o v a s-cular death: results from a 22-year follow-up of healthy nondiabetic men. D i a b e t e sC a re 22:45–49, 1999
3 . B r a d f o rd HA: Statistical evidence and infer-ence. In Principles of Medical Statistics. 9thed. Bradford HA, Ed. New York, OxfordUniversity Press, 1971, p. 309–323
4 . Balkau B, Shipley M, Jarett RJ, Pyörälä K,Pyörälä M, Forhan A, Eschwege E: Highblood glucose concentration is a risk factorfor mortality in middle-aged nondiabeticmen: 20-year follow-up in the WhitehallS t u d y, the Paris Prospective Study, and theHelsinki Policemen Study. Diabetes Care21:360–367, 1998
5 . Sandvik L, Erikssen J,Thaulow E, ErikssenG, Mundal R, Rodahl K: Physical fitness asa predictor of mortality among healthy,middle-aged Norwegian men. N Engl JM e d 328:533–537, 1993
6 . Erikssen G, Liestøl K, Bjørnholt J,Thaulow E, Sandvik L, Erikssen J:Changes in physical fitness and changes inm o rt a l i t y. L a n c e t 352:759–762, 1998
7 . Fossum E, Høieggen A, Moan A, Rostru pM, Kjeldsen SE: Insulin sensitivity isrelated to physical fitness and exerc i s eblood pre s s u re to structural vascular pro p-e rties in young men. H y p e rt e n s i o n33:781–786, 1999
8 . Coutinho M, Gerstein HC, Wang Y, Yusuf S:The relationship between glucose and inci-dent cardiovascular events: a metare g re s s i o nanalysis of published data from 20 studies of97,783 individuals followed for 12.4 years.Diabetes Care 22:233–240, 1999
Diagnosis of Card i a cAutonomic N e u ropathy in Diabetic Patients
In s p i red by the work of Michel Ducherand colleagues (1), we would like top resent some facts that are based on our
own investigations. Since 1996, we have

1388 DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999
Letters
been examining the autonomic neuro n a lsystems of patients being treated in theClinic of Internal Diseases and Diabetologyand in those visiting the outpatient depart-ment. The equipment that we used is similar to that used by Ducher et al. in their work (Finapress; Ohmeda 2030,R o c h e s t e r, NY), but we have applied ourown software. Up to this point, we havemade 2,760 examinations of both healthypeople and those who suffer from type 1 ortype 2 diabetes and other diseases, such asischemic heart disease, myocardial infarc-tion, congestive heart failure, and hypert e n-sion. Concerning the methods, we show asmuch enthusiasm as Ducher et al. did; nev-e rtheless we do have some re m a r k s .
The time of the examination pre f e rre dby Ducher et al. makes it practicallyimpossible to use this protocol as a ro u t i n eexamination for all of the patients, keepingin mind the fact that the investigations areto be perf o rmed in limited periods of time.A way of establishing the normative ratesis a problem for all methods. In our case,for the Ewing’s tests as well as heart rateand blood pre s s u re variabilities, the nor-mative value was matching by age. Theinclusion criterion in the study of Ducheret al. was orthostatic hypotension .3 0mmHg, which is one of the import a n tsigns of sympathetic neuro p a t h y. It wasp robably for that reason that strong corre-lations between heart rate and systolicblood pre s s u re variabilities and Ewing’ss c o res were found. As many as 9 of 11investigated patients suff e red from type 1diabetes, and their mean age of 48 yearsgave a long duration time of the diseaseand, thus, the possibility of complications.
In our study protocol, we used as h o rter algorithm: the patients were exam-ined by attaching a Finapress cuff to thet h i rd finger of their left hand, which washeld at heart level first for 5 min horizon-tally and then vertically to register beat bybeat their pulse and blood pre s s u rechanges. A specially written pro f e s s i o n a ls o f t w a re program allowed us to studyh e a rt rate variability (HRV) and bloodp re s s u re (systolic, diastolic, mean, and
pulse pre s s u res separately) variability inthe time domain and the fre q u e n c ydomain using an algorithm based on fastFourier transformation protocol or ana u t o re g ression method. The software usedhas a wide range of functions that allowsfor automatic computation and analysis ofthe Ewing’s battery, as well as a full spectralanalysis of the HRV in the whole range off re q u e n c y, gain function, coherence, andphase diff e rences (2).
We related these results to the valuesobtained from healthy subjects matched inage. In all age groups, pathological valuesw e re considered to be lower than themean minus 2 standard deviations (x 2 2SD) or lower than the lowest value ofdetected parameter in control subjects.
Our results in diabetic patients werealso lower than those in control subjects.When we compared entire aff e c t e dg roups, there were no or weak corre l a t i o n samong heart rate and systolic blood pre s-s u re variabilities and Ewing’s scores. Suchc o rrelation appears when Ewing’s score sa re higher, although not in all cases (W. B . ,W.G., unpublished observations). Thepoint at which we can recognize sympa-thovagal disbalance and cardiac auto-nomic neuropathy is still unclear.
WACLAW BURAK, MD, PHD
WLADYSLAW GRZESZCZAK, MD, PHD
F rom the Department and Clinic of Internal Dis-eases and Diabetology, Silesian School of Medicine,Z a b rze, Poland.
A d d ress correspondence to Waclaw Burak, MD,PhD, Department and Clinic of Internal Diseasesand Diabetology, 3rd May St. 13-15, 41-800 Zabrz e ,Poland. E-mail: re k l i n @ i n f o m e d . s l a m . k a t o w i c e . p l .
R e f e re n c e s1 . Ducher M, Cerutti C, Gustin MP, Abou-
Amara S, Thivolet C, Laville M, PaultreCZ, Fauvel JP: Noninvasive exploration ofc a rdiac autonomic neuro p a t h y. D i a b e t e sC a re 22:388–393, 1999
2 . Ewing DJ, Martyn CN, Young RJ, ClarkeBF: The value of cardiovascular autonomicfunction tests: 10 years of experience indiabetes. Diabetes Care 8:494–498, 1985
Response to Burakand Grz e s z c z a k
Burak and Grzeszczak (1) reportresults similar to our own andobtained with an impressive number
of subjects. However, the main purpose ofour paper was to assess the most clinicallyrelevant information that could be pro-vided by analyzing beat-to-beat bloodp re s s u re and heart rate variabilities. To ourknowledge, these sophisticated mathemat-ical modeling techniques have never beenc o m p a red. The first step was to assess theirrelative interest in patent neuro p a t h y. Indiabetic subjects with a major ort h o s t a t i chypotension, spectral analysis pro v i d e di n f o rmation equivalent to that provided byE w i n g ’s scores on a 10-min blood pre s s u rere c o rding at rest. Intere s t i n g l y, some of thetested methods (Z method, spectral gain)w e re too sensitive in patent neuro p a t h yand should be applied in incipient neu-ropathy (J.P.F., D. Bertram, M.D., C.C e rutti, M.P. Gustin, and C. Thivollet,unpublished observations). These meth-ods that imply a 1-h blood pre s s u rere c o rding at rest can be favorably com-p a red with the 30 min usually needed toobtain a reliable determination of Ewing’ss c o res. Because diabetic neuropathy wasre p o rted to be associated with an unfavor-able prognosis, detection of incipient neu-ropathy is of major clinical intere s t .
MICHAEL DUCHER, PHD
JEAN PIERRE FAUVEL, PHD, MD
F rom the Département de Néphrologie et d’Hyper-tension Artérielle, Hôpital Edouard Herriot, Ly o n ,F r a n c e .
A d d ress correspondence to J.P. Fauvel, PhD,MD, Hôpital E Herriot, Département de Nephro l o-gie et Hypertension Arterielle, 8 Avenue Rockefeller,Lyon Cedex 69437 France.
R e f e re n c e s1 . Burak W, Grzeszczak W: Diagnosis of car-
diac autonomic neuropathy in diabeticpatients (Letter). Diabetes Care 2 2 : 1 3 8 7 –1388, 1999

DIABETES CARE, VOLUME 22, NUMBER 8, AUGUST 1999 1389
Letters
Copyright © 2022 FDOKUMEN