Mechanisms of drug resistance in chemotherapy for urogenital carcinoma
13
International Journal of Urology (1999) 6, 427–439 Review Article Mechanisms of drug resistance in chemotherapy for urogenital carcinoma SEIJI NAITO, 1 AKIRA YOKOMIZO 1,2 AND HIROFUMI KOGA 1 1 Department of Urology, Faculty of Medicine, Kyushu University, Fukuoka and 2 The Japanese Society for the Promotion of Science, Tokyo, Japan Abstract Cancer chemotherapy is the principal approach for urogenital cancers. However, the acquisition of resistance to anticancer agents is a critical factor that limits the successful treatment of malig- nancies. The multidrug resistant (MDR) phenotype has been widely recognized in cancer chemotherapy in urogenital tumors and the mechanisms underlying MDR have also been exten- sively studied. One of the principle mechanisms in MDR is caused by the overexpression of P-glycoprotein (P-gp), encoded by the multidrug resistance gene (MDR1). It functions as an ATP- dependent active efflux pump of chemotherapeutic agents in human cancer cells. Recently, other drug resistance proteins, including multidrug resistance-associated protein (MRP1) and cMOAT (or MRP2), were also identified from multidrug resistant cells. A functional analysis of MRP1 has shown that MRP1 may have the potential to act as a transporter of glutathione conjugates, which has been known as a central detoxification pathway in anticancer agents. Furthermore, several other resistance-related proteins (e.g. glutathione S-transferase, metallothionein, thioredoxin, topoi- somerase I, II, O 6 -alkylguanine-DNA methyltransferase, etc.) have been found to be up- or down- regulated in resistant cells and these molecules are believed to contribute to the resistant phenotype as well. Based on the molecular characteristics identified in MDR, several experimental and clini- cal approaches have been studied to overcome MDR. One of these strategies is to reverse MDR by using such P-gp inhibitors as verapamil and cyclosporine A. In this review, we summarize the recent advances in MDR-related molecules and clinical trials to circumvent MDR in urogenital carcinomas. Key words multidrug resistance, urogenital cancer, anticancer drug, chemotherapy, review. Introduction Chemotherapy for neoplasms has become an effective and widely used treatment in urogenital cancers. In testicular tumors, cisplatin-based chemotherapy has become an accepted modality for curing cancer. Presently, more than 90% of all newly diagnosed patients and 70–80% of patients with metastatic dis- ease can be cured. 1 However, the remaining patients are at risk of relapse and death because of diseases resistant to chemotherapy. 2 In metastatic bladder can- cer, the initial responses by chemotherapy may reach 70%, however, long-term survival does not exceed 5– 15%. 3 In cases of renal cell carcinoma and prostate cancer, the effect of chemotherapy has been far from satisfactory, although numerous efforts have been made to develop an effective chemotherapeutic regi- men. Generally, drug resistance can be classified into two categories: intrinsic drug resistance and acquired drug resistance. Renal and prostate cancers are known as intrinsic drug resistant cancers, which already have a relatively resistant phenotype to anticancer agents without drug-selection. In contrast to intrinsic drug resistance, acquired resistance is characterized by the acquisition of a resistant phenotype after being exposed to cytotoxic agents. Acquired drug resistance in recurrent tumors is the most critical and dangerous occurrence for patients treated by chemotherapy. Fur- thermore, once drug resistance is developed, cancer Correspondence: Dr Seiji Naito, Department of Urology, Faculty of Medicine, Kyushu University 71, 3-1-1 Maid- ashi, Higashi-ku, Fukuoka 812-8582, Japan. Email: <[email protected]> Received 26 April 1999; accepted 26 April 1999.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Mechanisms of drug resistance in chemotherapy for urogenital carcinoma

International Journal of Urology (1999) 6, 427–439
Review Article
Mechanisms of drug resistance in chemotherapy for urogenital carcinoma
SEIJI NAITO,1 AKIRA YOKOMIZO1,2 AND HIROFUMI KOGA1
1Department of Urology, Faculty of Medicine, Kyushu University, Fukuoka and 2The JapaneseSociety for the Promotion of Science, Tokyo, Japan
Abstract Cancer chemotherapy is the principal approach for urogenital cancers. However, the acquisition of resistance to anticancer agents is a critical factor that limits the successful treatment of malig-nancies. The multidrug resistant (MDR) phenotype has been widely recognized in cancerchemotherapy in urogenital tumors and the mechanisms underlying MDR have also been exten-sively studied. One of the principle mechanisms in MDR is caused by the overexpression of P-glycoprotein (P-gp), encoded by the multidrug resistance gene (MDR1). It functions as an ATP-dependent active efflux pump of chemotherapeutic agents in human cancer cells. Recently, otherdrug resistance proteins, including multidrug resistance-associated protein (MRP1) and cMOAT(or MRP2), were also identified from multidrug resistant cells. A functional analysis of MRP1 hasshown that MRP1 may have the potential to act as a transporter of glutathione conjugates, whichhas been known as a central detoxification pathway in anticancer agents. Furthermore, severalother resistance-related proteins (e.g. glutathione S-transferase, metallothionein, thioredoxin, topoi-somerase I, II, O6-alkylguanine-DNA methyltransferase, etc.) have been found to be up- or down-regulated in resistant cells and these molecules are believed to contribute to the resistant phenotypeas well. Based on the molecular characteristics identified in MDR, several experimental and clini-cal approaches have been studied to overcome MDR. One of these strategies is to reverse MDR byusing such P-gp inhibitors as verapamil and cyclosporine A. In this review, we summarize therecent advances in MDR-related molecules and clinical trials to circumvent MDR in urogenitalcarcinomas.
Key words multidrug resistance, urogenital cancer, anticancer drug, chemotherapy, review.
Introduction
Chemotherapy for neoplasms has become an effectiveand widely used treatment in urogenital cancers. In testicular tumors, cisplatin-based chemotherapy hasbecome an accepted modality for curing cancer.Presently, more than 90% of all newly diagnosedpatients and 70–80% of patients with metastatic dis-ease can be cured.1 However, the remaining patientsare at risk of relapse and death because of diseasesresistant to chemotherapy.2 In metastatic bladder can-
cer, the initial responses by chemotherapy may reach70%, however, long-term survival does not exceed 5–15%.3 In cases of renal cell carcinoma and prostatecancer, the effect of chemotherapy has been far fromsatisfactory, although numerous efforts have beenmade to develop an effective chemotherapeutic regi-men. Generally, drug resistance can be classified intotwo categories: intrinsic drug resistance and acquireddrug resistance. Renal and prostate cancers are knownas intrinsic drug resistant cancers, which already havea relatively resistant phenotype to anticancer agentswithout drug-selection. In contrast to intrinsic drugresistance, acquired resistance is characterized by theacquisition of a resistant phenotype after beingexposed to cytotoxic agents. Acquired drug resistancein recurrent tumors is the most critical and dangerousoccurrence for patients treated by chemotherapy. Fur-thermore, once drug resistance is developed, cancer
Correspondence: Dr Seiji Naito, Department of Urology,Faculty of Medicine, Kyushu University 71, 3-1-1 Maid-ashi, Higashi-ku, Fukuoka 812-8582, Japan. Email: <[email protected]>
Received 26 April 1999; accepted 26 April 1999.

428 S Naito et al.
cells often obtain cross-resistance, that is, resistance isachieved not only to an applied single drug, but also to a variety of chemically and functionally unrelateddrugs. This phenomenon is called multidrug resist-ance. To improve the survival rate by cancer chemo-therapy, numerous studies have thus focused on theidentification of molecules that are responsible fordrug resistance. In 1986, the multidrug resistance gene(MDR1) was cloned and recognized as the first mole-cule to explain the multidrug resistance phenome-non.4,5 The development of the MDR phenotype incancer cells is often associated with an enhancedexpression of the MDR1 gene; the MDR1 geneencodes membranous P-glycoprotein (P-gp) which catalyzes the ATP-dependent outwards transport ofanticancer agents. However, recent studies have alsoreported that the MDR phenomena could not beexplained by the overexpression of the MDR1 genealone. Recently, several other candidate genes havebeen isolated and characterized, such as MRP16 andcMOAT.7,8 These reports support the hypothesis thatmultiple resistance-associated genes may contribute tothe occurrence of drug resistance, sometimes in a cell-specific or organ-specific manner.
This paper deals with the theoretical backgroundand basic features of the molecules related to drugresistance in urogenital carcinomas. We also discuss
the inhibitors and clinical significance of overcomingMDR.
Molecular structure related to drug resistance
ATP-binding cassette transporters(ABC family)
P-glycoprotein
The earliest discovered drug efflux pump, P-gp, wasfirst isolated and characterized based on the molecularbiological findings. Its gene, MDR1, encodes a mem-brane glycoprotein of 1280 amino acids with 12 trans-membrane domains and two intracellular ATPase sites(Fig. 1).4,5 The MDR1 gene belongs to the ATP-bindingcassette superfamily (ABC family), which is known to be a transporter.9,10 P-glycoprotein is an ATP-dependent active transporter of widely used, natural-derivative anticancer agents such as vinca alkaloids,anthracyclins, epipodophyllotoxins and taxanes but notcisplatin (Table 1).11 P-glycoprotein is supposed to bethe most responsible molecule in the MDR phenotype.P-glycoprotein can extrude not only anticancer agents,but also other chemicals such as immune suppressive
Table 1 Lists and characteristics of anticancer agents widely used in urogenital cancer chemotherapy
Name Category Mechanism of Cytotoxicity Related drug resistant molecules
Cisplatin Platinum derivative DNA inter-/intra-calator, SO GSH, MT, DNA repair enzyme, cMOAT?Carboplatin Platinum derivative DNA inter-/intra-calator, SO GSH, MT, DNA repair enzymesDoxorubicin Anthracycline TopoII inhibitor, SO GSH, P-gp, MRP, TopoIIEpirubicin Anthracycline TopoII inhibitor, SO GSH, P-gp, MRP, TopoIIMitoxantrone Anthracenedione TopoII inhibitor, GSH, P-gp, MRP, TopoIIEtoposide Epipodophyllotoxin TopoII inhibitor MRP, TopoII, P-gpTeniposide Epipodophyllotoxin TopoII inhibitor MRP, TopoII, P-gpCamptothecin Topoisomerase TopoI inhibitor TopoI
interactive agentsMethotrexate Antimetabolites Follic acid antagonist Amplification of dihydrofolate reductase
(DHFR)Vincristine Vinca alkaloid Tubulin polymerization inhibitor P-gp, MRPVinblastine Vinca alkaloid Tubulin polymerization inhibitor P-gp, MRPPaclitaxel Taxanes Microtuble assembly and P-gp, altered a/b tubulin
tubulin disassembly inhibitorMitomycin C Aziridines DNA alkylation, SO DT-diaphorase, GSHBleomycin Glycopeptide DNA strand break, SO DNA repair enzyme, DNA polymerases,
antibiotics GSHCyclophosphamide Mustards DNA alkylation GSHIfosfamide Mustards DNA alkylation GSH
SO, superoxides and free radicals; GSH, glutathione; MT, metallothionein; cMOAT, multispecific organic anion trans-porter; P-gp, P-glycoprotein; MRP, multidrug resistance-associated protein; TopoI, topoisomerase I; TopoII, topoisomeraseII.

Drug resistance in urogenital carcinoma 429
cyclosporinee A and FK506; cardiac glycoside;digozin; antibiotics like rifampicin; and theanthelminitic pesticide, ivermectin.11 Some of the sub-stances were evaluated to determine whether or notthey could overcome and reverse MDR both in vitroand in vivo. The detailed results are discussed in thefollowing sections. The physiological function of P-gphas not yet been determined but it is considered to actas a steroid transporter, a blood–brain barrier in nor-mal human tissues.12,13 The MDR1 gene is highlyexpressed in several normal tissues including theadrenal cortex, renal proximal tubules, bile duct, capil-lary endothelial cells in both the brain and intestinalmucosa.10
Multidrug resistance-associated protein
In 1992, another MDR-related protein was clonedfrom a doxorubicin selected, multidrug resistanthuman small cell lung cancer cell line and the proteinwas designated multidrug resistance-associated protein(MRP).6 The open reading frame of the mRNA en-coded a 1531 amino acid polypeptide that containedtwo potential ATP-binding domains and multiplepotential membrane spanning helices (Fig. 1). The predicted amino acid sequence and the presence ofcharacteristic sequence motifs in both ATP-bindingsites indicated that MRP was a member of the ABCSuperfamily the same as MDR1. However, the similar-ity of the amino acid arrangement between MRP and
P-gp was very low (15%) and it was restricted to gen-erally conserved regions of the two ATP-bindingdomains (Walker A,B domain). As MRP is overex-pressed in doxorubicin resistant cells6,14 and in etopo-side (VP16) selected cells,15 MRP appeared to beresponsible for the preferential drug resistance totopoisomerase II inhibitors. In 1994, MRP1 wasrevealed to act as a transporter of glutathione (GSH)drug conjugates and it was thus determined to be thelong sought after GS-X pump.16–18 When it is overex-pressed in cultured cells, they display increased resis-tance to vinca alkaloids, epipodophyllotoxins and cer-tain anthracyclines. The increase in resistance is alsoassociated with a decrease in drug accumulation andan increase in drug efflux.19–21 Notably, MRP is lesseffective than P-gp at conferring resistance to taxoland mitoxantrone and the MRP expression levels didnot affect the cisplatin sensitivity.19–21 Therefore, MRPcannot be the only molecule to transport GSH-drugconjugates. Expanded molecular analyses are neces-sary to resolve what kinds of substrate MRP transfersand how it exports the anticancer agents outward.Recently, MRP2, 3, 4, 5, 6 were identified and some ofthem showed altered expressions in resistance cellscompared with wild type cell lines, although no pre-cise analyses have been performed.7,22 One of the MRPfamily molecules, MRP 6 has recently been reportedregarding its relationship to drug resistance.23 TheMRP6 gene is located on chromosome 16, immediate-ly next to MRP1 and it is coamplified with MRP1,however, MRP6 does not play an important role indrug resistance because its overexpression was iden-tified in only a few of the resistant cells they ana-lyzed.23 Moreover, Miyake et al.24 cloned the MXR1,2gene, another ABC family gene, from mitoxantrone-resistant sublines. They found this gene to be overex-pressed and coamplified in doxorubicin resistant cells,which suggests this new gene is possibly associatedwith mitoxantrone and doxorubicin resistance.24
Canalicular multispecific organic anion transporter
Human multispecific organic anion transporter gene(cMOAT) was first isolated by degenerative PCR methods which focused on the highly conserved ATP-binding domain of ABC transporters (Fig. 1).8 Thefull-length cDNA sequence revealed this gene to be ahomolog of the rat canalicular multispecific organicanion transporter gene (cMOAT). The rat cMOAT waspreviously isolated from mutated rat strains thatimpaired the biliary excretion of bilirubin glucuronidesand GSH conjugates.25 The mutation of human cMOAT
Fig. 1 Topological map of P-glycoprotein (P-gp), multidrug resistance-associated protein (MRP) and multi-specific organic anion transporter (cMOAT). The organi-zations in the cell membrane are estimated based on itsprimary sequences. Two ATP-binding domains are highlyconserved among the three molecules.

430 S Naito et al.
causes rare congenital hyperbilirubinemia, Dubin–Johnson syndrome.25,26 The human cMOAT was over-expressed in several cisplatin resistant cells,8,22 andantisense transfection increased the sensitivity to cisplatin, vincristine, doxorubicin and camptothecinderivatives,27 thus suggesting a possible associationbetween cMOAT and MDR. Unfortunately, the over-expression of functional cMOAT in cultured cells runs into experimental problems in several indepen-dent laboratories, probably caused by insufficient protein transportation to apical (luminal) membrane.7
It is not yet clear how cMOAT is related to MDR inhuman cancers. Recently, another cMOAT/MRP familygene, cMOAT2/MRP3, was identified and found to beexpressed mainly in the liver and to a lesser extent inthe colon, small intestine and prostate, however, nooverexpression was observed in cisplatin resistantcells.28
Lung resistance protein
Lung resistance protein (LRP) was identified as a pro-tein highly expressed in many non-P-gp MDR celllines.29 Lung resistance protein is one of four vaultproteins that make barrel-like structures in a perinu-clear lesion.29 The transfection of LRP cDNA did notresult in drug resistance, however, an elevated level ofLRP was a good drug resistance-related predictor ofadverse clinical outcome in leukemia, better than anelevated level of either P-gp or MRP1.30 This proteinmay thus possibly be an indicator of resistance causedby an up-regulation of other proteins, rather than adrug transporter itself.
Thiols
Reduced glutathione S and its metabolic enzymes
Intracellular non-protein sulfhydryl reduced GSH is atripeptide of glycine, glutamate and cysteine and it hasmultiple functions in catalysis, transport and reductivephenomena.31–33 Moreover, it reacts with toxic endoge-nous and exogenous substances, including free radicalsand anticancer agents. Reduced glutathione S conjuga-tion is catalyzed by glutathione S-transferases (GST),which belong to the phase II detoxification enzymefamily (Fig. 2). Glutathione S-transferases consist offive isozymes including Alfa, Mu, Pi, Theata andmicrosomal, and conjugate many different biologicalactive and potential carcinogenic compounds toGSH.34,35 The GSH detoxification functions are impor-tant in drug resistance treated by nitrogen mustards,nitrosourea, cisplatin and anthracyclines.34,35 Acquiredresistance to these agents is frequently accompanied byan elevation in the GSH content and in GST activity,especially GSTP1 (used to be called pi class).36 How-ever, overexpression experiments with the GSTP1 genehave resulted in controversial observations. Miyazakiet al.37 demonstrated the introduction of GSTP1 cDNAto make the recipient CHO cells 1.4- to 3.0-fold moreresistant to cisplatin. In contrast, Nakagawa et al.38
showed that transfected NIH3T3 cells were more resis-tant to adriamycin and ethacrynic acid, but not to mel-phalan and cisplatin. These findings thus suggest thatincreased GST levels play a role in determining thesensitivity to some drugs, including alkylating agents,
Fig. 2 Glutathione (GSH)-relateddetoxification pathway. Glu-tathione is synthesized intracellu-lary by two enzymes, g-glutamyl-cysteine synthetase (g-GCS, ratelimiting reaction) and glutathionesynthetase. While, GSH conjuga-tions are catalyzed by glutathionetransferases (GST). Anticancerdrugs are bound to GSH by theaction of GST and excreted into bile acids or urine. Glu-tathione also reduces hydroxyperoxide (H
2O
2) by the action of
glutathione peroxidase.

Drug resistance in urogenital carcinoma 431
but that the selectivity of these drugs appears to differ according to the origin of the cell line.33 TheGSH synthesis pathways are also important in drugresistance. Glutathione S is synthesized intracellularlyby the action of two enzymes: g-glutamylcysteine synthetase (g-GCS) and GSH synthetase (Fig. 2). g-Glutamylcysteine synthetase is a heterodimer of cat-alytic, heavy subunit (g-GCSh, 73 kDa) and regulatory,light subunit (g-GCSl, 31 kDa), functioning as a ratelimiting enzyme in GSH synthesis.39,40 The overexpres-sion of a heavy subunit of the g-GCS gene increasedthe intracellular GSH content, activated the GSH-conjugated export pump and changed the cell pheno-type resistant to melphalan and cisplatin.40,41
Furthermore, lowering the GSH levels by treatmentwith a g-GCS inhibitor, namely buthionine sulfox-imine, can increase the cytotoxic activities of melpha-lan, cisplatin and other anticancer agents in vitro aswell as in vivo.36 These observations emphasize theimportance of the g-GCS gene in GSH detoxification,especially regarding the anticancer drug metabolisms.
Recently MRP1 and cMOAT were identified as can-didate molecules of GSH-conjugate transporters asdescribed above. At present, several intensive studiesare underway to reveal the molecular interactionsamong them.
Thioredoxin
Thioredoxin (TRX), an abundant cellular thiol similarto GSH, functions as a self-defence mechanism inresponse to environmental stimuli, including oxidativestress. We first determined that increased levels ofthioredoxin contributed to cisplatin resistance. Anti-sense DNA transfection of TRX into human bladdercancer T24 cells sensitized the cells to superoxide-generating agents such as cisplatin, doxorubicin, mito-mycin C and etoposide, thus suggesting that TRXappeared to limit sensitivity to various superoxide-generating anticancer drugs.42 We also observed TRXexpression to be closely associated with tumor sensi-tivity to cisplatin in clinically resected hepatocellularcarcinomas.43 Similar evidence was reported fromindependent laboratories on adult T-cell leukemiacells,44,45 while controversy remains regarding ovaryand colon cancers.46
Metallothionein
Metallothionein (MT) is a cysteine-rich low moleculethiol that has a high affinity for heavy metals. Severalreports have demonstrated that cellular MT expression
correlates with drug sensitivity, especially with cis-platin,47–49 thus implying the role of MT in drug resis-tance. According to these reports, a special chelatingaffinity to heavy metals is considered to contribute tocisplatin resistance in cancer cells. Recent evidencesupports another role for MT as an antioxidant mol-ecule underlying the interception of free radicals, com-plexation of redox sensitive transition metals, alteredzinc homeostasis or interaction with GSH.47 Therefore,the resistant mechanism includes not only a chelatingaffinity with heavy metals but also an inactivationcapacity to superoxide generated by anticancer drugs.
Other enzymes
Topoisomerase
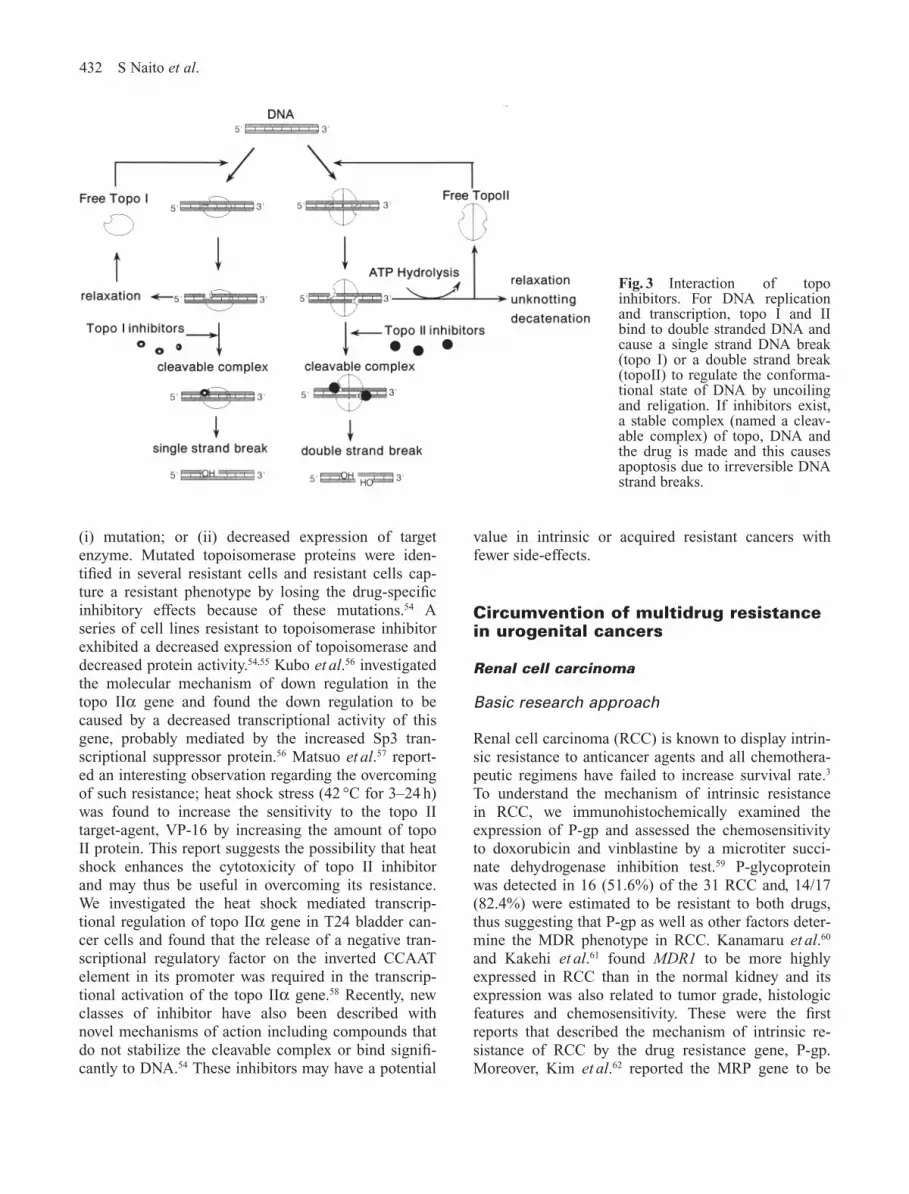
DNA topoisomerases (topo) are nuclear enzymes thatalter the topological (conformational) state of DNAthrough DNA strand cleavage, strand passage and reli-gation.50,51 Topoisomerases bind to double-strandedDNA and induce single-strand breaks (by topo I) ordouble-stranded breaks (by topo II) to uncoil thehypercoiled DNA (Fig. 3). These processes are essen-tial for DNA replication and transcription.52 Only oneform of topo I (100 kDa protein) has been identified,whereas two isoenzymes of topo II have beendescribed; the alpha form (170 kDa protein) and thebeta form (180 kDa protein).53 Both topo II isoenzymeshave distinct nuclear localization, are regulated inde-pendently, differ in their responsiveness to inhibitorsand are differentially expressed in drug resistant celllines.54 Several clinically active anticancer drugs (Table1) inhibit these enzymes by stabilizing a putative intermediate reaction intermediatory called the cleav-able complex where the topoisomerase remains at-tached to either one strand of DNA (topo I) or bothstrands of double helix (topo II) after strand cleavage(Fig. 3). The DNA cleavage sites appear unique for dif-ferent classes of inhibitor and are probably critical fordefining cytotoxicity. The formation of the cleavablecomplex are considered to cause cell death either bycolliding with replication forks, by promoting illegiti-mate genomic-DNA recombination, by arresting thecells in the G2-phase of the cell cycle or by inducingapoptosis.54
Drug resistant mechanisms in topoisomeraseinhibitors are partially caused by an overexpression ofMDR1 and MRP as described above. Further importantfactors that determine chemosensitivity are the alterations in the topoisomerases themselves. These alterations are clearly classified into two patterns,
432 S Naito et al.
(i) mutation; or (ii) decreased expression of targetenzyme. Mutated topoisomerase proteins were iden-tified in several resistant cells and resistant cells cap-ture a resistant phenotype by losing the drug-specificinhibitory effects because of these mutations.54 Aseries of cell lines resistant to topoisomerase inhibitorexhibited a decreased expression of topoisomerase anddecreased protein activity.54,55 Kubo et al.56 investigatedthe molecular mechanism of down regulation in thetopo IIa gene and found the down regulation to becaused by a decreased transcriptional activity of thisgene, probably mediated by the increased Sp3 tran-scriptional suppressor protein.56 Matsuo et al.57 report-ed an interesting observation regarding the overcomingof such resistance; heat shock stress (42 °C for 3–24 h)was found to increase the sensitivity to the topo II target-agent, VP-16 by increasing the amount of topoII protein. This report suggests the possibility that heatshock enhances the cytotoxicity of topo II inhibitorand may thus be useful in overcoming its resistance.We investigated the heat shock mediated transcrip-tional regulation of topo IIa gene in T24 bladder can-cer cells and found that the release of a negative tran-scriptional regulatory factor on the inverted CCAATelement in its promoter was required in the transcrip-tional activation of the topo IIa gene.58 Recently, newclasses of inhibitor have also been described withnovel mechanisms of action including compounds thatdo not stabilize the cleavable complex or bind signifi-cantly to DNA.54 These inhibitors may have a potential
value in intrinsic or acquired resistant cancers withfewer side-effects.
Circumvention of multidrug resistancein urogenital cancers
Renal cell carcinoma
Basic research approach
Renal cell carcinoma (RCC) is known to display intrin-sic resistance to anticancer agents and all chemothera-peutic regimens have failed to increase survival rate.3
To understand the mechanism of intrinsic resistance in RCC, we immunohistochemically examined theexpression of P-gp and assessed the chemosensitivityto doxorubicin and vinblastine by a microtiter succi-nate dehydrogenase inhibition test.59 P-glycoproteinwas detected in 16 (51.6%) of the 31 RCC and, 14/17(82.4%) were estimated to be resistant to both drugs,thus suggesting that P-gp as well as other factors deter-mine the MDR phenotype in RCC. Kanamaru et al.60
and Kakehi et al.61 found MDR1 to be more highlyexpressed in RCC than in the normal kidney and itsexpression was also related to tumor grade, histologicfeatures and chemosensitivity. These were the firstreports that described the mechanism of intrinsic re-sistance of RCC by the drug resistance gene, P-gp.Moreover, Kim et al.62 reported the MRP gene to be
Fig. 3 Interaction of topoinhibitors. For DNA replicationand transcription, topo I and IIbind to double stranded DNA andcause a single strand DNA break(topo I) or a double strand break(topoII) to regulate the conforma-tional state of DNA by uncoilingand religation. If inhibitors exist,a stable complex (named a cleav-able complex) of topo, DNA andthe drug is made and this causesapoptosis due to irreversible DNAstrand breaks.

Drug resistance in urogenital carcinoma 433
overexpressed in RCC compared with the normal kid-ney and Volm et al.63 found that the majority of unse-lected RCC already exhibited the drug resistance phe-notype mediated by P-gp, GSTP1 and Topo II. Thesereports suggested that multiple drug resistance mole-cules possibly contributed to the intrinsic MDR inRCC as well as in the normal kidney.
The combination of reversal agents targeting suchdrug resistance markers may be a way to improve theoutcome of chemotherapy for RCC. Regarding thepresently available reversal agents, however, clinicallyrelevant chemosensitizing doses cannot be given tohumans without inducing significant toxicity. Thedevelopment of new reversal agents that can be usedwithout inducing significant toxicity is thus greatlyneeded. We recently developed newly synthesizedimmidazothiazole derivatives which could reverse themultidrug resistance in P-gp overexpressing humanepidermoid and bladder carcinoma cell lines withoutinducing significant toxicity.64 These novel reversalagents also remarkably enhanced the sensitivity to vin-blastine and doxorubicin in both P-gp- and MRP-over-expressing RCC cell line. Further studies on the toxi-cology, pharmacology and drug metabolism of theseagents are now under way.
Clinical trials
A radical nephrectomy or partial nephrectomy stillremains the only curable option for localized RCC.Metastatic RCC is highly resistant to the many sys-temic therapies that have been extensively investigated.To reverse MDR in RCC, many clinical trials havebeen attempted using modulators or inhibitors of P-gptogether in chemotherapy. Combination regimens ofdexverapamil with vinblastine,65 cyclosporinee andvinblastine,66 quinidine and vinblastine,67 acrivastineand vinblastine,68 and dipyridamole and vinblastine69
have also been evaluated, however, all of them provedto be unsuccessful. The emergence of side-effects pre-vent the use of clinically relevant doses of such modu-lators in systemic chemotherapy.
Bladder cancer
Basic research approach
To investigate the drug resistant mechanisms in blad-der cancer, we established several sublines selected byclinically used anticancer agents.70 The doxorubicin-resistant cell line, KK47/ADM, exhibited cross-resistance to vinca alkaloids (vinblastine, vincristine)and etoposide. We observed KK47/ADM cells ex-
pressed P-gp and acquired resistance, mainly due to alower accumulation of the drugs. Although verapamil,a P-gp inhibitor, enhanced the doxorubicin sensitivityof KK47/ADM, a complete overcoming of the resis-tance could not be obtained. Therefore, we concludedthat the overexpression of P-gp was partially responsi-ble for the MDR phenotype in KK47/ADM. Sub-sequently, we observed the overexpression of MRP inthe same cell lines, thus MRP also seemed to con-tribute to drug resistance.14 For further investigations,we established another doxorubicin-resistant bladdercancer cell line, T24/ADM.14 Interestingly, T24/ADMoverexpressed MRP but not P-gp,14 and also exhibiteddecreased expression of topo II.71 These differentobservations in doxorubicin-resistant bladder cancercell lines suggest that cancer cells have a multiplepotential to develop drug resistance even when theyoriginate from the same organ.
In cisplatin resistant KK47/DDP cells, decreasedintracellular platinum accumulation and increased GSH detoxification activity (overexpression of GSTP1and g-GCSh) are considered to be responsible for theresistant mechanism.72 Another cisplatin-resistant cellline T24/DDP, showed an interesting phenotype that had never been seen in other cells. T24/DDP showedcollateral sensitivity to CPT-11, an inhibitor of topo Iand we concluded that this collateral sensitivity wascaused by increased expression of the topo I gene.73 Thisin vitro observation indicated that CPT-11 might beeffective in overcoming cisplatin resistance and thusmight enhance its cytotoxicity. Rowinsky et al.74 empha-sized the effectiveness of a combined therapy of cis-platin and topotecan in clinical trials and this protocolmay thus be a good example in which basic researchfindings could be effectively applied to clinical trials.
To identify other underlying genes in cisplatin resis-tance, we applied differential display techniques in various cisplatin-resistant cell lines.75 Twenty-four geneswere confirmed by a Northern blot analysis to be differentially expressed between resistant and the cor-responding sensitive cells. Partial DNA sequencesrevealed one of them to be T-plastin. Transfection intoT24/DDP10 cells with an antisense vector demonstratedreduced T-plastin expression to be associated with anincreased sensitivity to cisplatin and thus confirmed theassociation between T-plastin and cisplatin sensitivity.Interestingly, T-plastin was also independently isolatedfrom a cisplatin resistant renal cell carcinoma cell lineby the differential display method (Ueda K et al. pers.comm., 1997). Further research is necessary to revealhow this molecule interacts with cisplatin.
Moreover, our previous report49 and another76 alsoinvestigated the close correlation between metalloth-

434 S Naito et al.
ionein expression and cisplatin sensitivity in bladdercancers. Summarizing these data, bladder cancer cellsacquire drug resistance with changing several targetmolecules including P-gp, MRP, GSH, topoisomerasesand metallothionein.
Clinical trials
Most (80%) transitional cell carcinomas of the bladderare superficial at diagnosis and can be removed by atransurethral resection.77 However, approximately 50%of patients develop recurrent disease within a fewyears. To prevent recurrence, prophylactic intravesicalinstillation chemotherapy using doxorubicin (DXR),mitomycin C, thiotepa or epirubicin has been per-formed. Many studies have shown the advantages ofadjuvant treatment after transurethral resection indecreasing the recurrence rate of bladder cancers or inprolonging the disease free interval of patients.78 Toimprove this intravesical instillation therapy, we treatedpatients with DXR combined with verapamil (VR), aninhibitor of P-gp.79 The patients (available number was157) were randomized into two groups: one groupreceived an intravesical instillation of DXR (30 mg)plus VR (15 mg) after a transurethral resection ofsuperficial bladder cancer (19 times over 1 year) andthe other group received DXR alone on the same treat-ment schedule. As a result, the DXR plus VR instilla-tion group showed a significantly higher non-recurrence rate than the DXR-alone instillation group.Furthermore, the side-effects were not significantlydifferent between the two groups. Lukkarinen et al.80
also studied the randomized comparison of epirubicinand epirubicin plus VR instillation therapy. The recur-rent rate was 37% in epirubicin plus VR group, whileit was 50% in the epirubicin alone group and thuswithout statistical significance. Nakagawa et al.81 inves-tigated the P-gp and MRP expression before and afterthe instillation chemotherapy and found that P-gp wasexpressed in 67% of the bladder cancers before theinstillation chemotherapy and that P-gp may be up-regulated after the instillation chemotherapy. Thesedistributions of P-gp may explain the effectiveness ofVR in superficial bladder cancers.
In localized muscle invasive bladder cancer,definitive treatment has consisted of radical cystectomyor external radiotherapy. Despite improvements in surgical techniques and radiotherapy, the survival ofpatients has not changed, up to 50% of patients devel-op metastases and die within 5 years.77 Metastatic blad-der cancer is currently treated with multidrug regimensincluding methotrexate, vinblastine, DXR and cisplatin(CM, CISCA, CMV or M-VAC), however, long-term
survival usually does not exceed 5–15%.77 To improvethe classic chemotherapy, neoadjuvant methods wereintroduced. The neoadjuvant chemotherapy is an alter-native regimen performed before a radical cystectomyor definitive radiotherapy, in contrast to adjuvantchemotherapy which is given after radical treatment.Although neoadjuvant M-VAC achieves a completeremission in some patients, the impact of such treat-ment on a large proportion of patients with bladdercancer is still minimal.77 Therefore, improved or newlydesigned strategies must be applied in invasive bladdercancer chemotherapy. A better understanding of theMDR-related molecules is therefore needed to makeany breakthroughs in this area. Furthermore, the mol-ecular prediction of effectiveness in response tochemotherapy can be performed based on the expres-sion of MDR related molecules, growth factors, onco-genes and the mutational status in tumor suppressorgenes.
Testicular germ cell tumor
Basic research approach
It was recognized in the 1960s that testicular germ celltumors (TGCT) were curable with chemotherapeuticdrugs. Since then, newer drugs including cisplatin haveincreased the cure rate of these tumors to over 80%,even in the patients with metastatic disease. Patientswho relapse after initial treatment can be salvaged withsecond-line chemotherapy.3 However, molecular deter-minations on drug resistance are still necessary inrecurrent or relapsed TGCT. In non-seminomatousgerm cell tumors, cancer cells are more resistant tochemotherapy and the prognosis of teratocarcinomasand choriocarcinomas is thus relatively poor.3 The normal testis clearly express P-gp and it is supposed to function as a part of blood–testis barrier.13 This evidence seems controversial when we consider thehigh sensitivity of TGCT to chemotherapeutic agents.Katagiri et al.82 identified a high expression of P-gpand pi-class glutathione S-transferase (GSTP1–1)which were thought to be correlated with multipledrug resistance in non-seminomatous TGCT, which are more refractory than seminomas to anticancerchemotherapy. This may support the possibility that P-gp contributes to the drug resistance phenotype evenwhen it is expressed normally. Masters et al.83 charac-terized cisplatin-resistant germ cell tumors and foundthat increased GSH and metallothionein contents arepossibly related to the sensitivity of anticancer agentsin testicular tumors. Other approaches were performedon apoptosis-related genes in TGCT. Eid et al.84 exam-

Drug resistance in urogenital carcinoma 435
ined the expression of p53 immunohistochemically inTGCG and found that high levels of p53 expressioncorrelated with the clinical stage and clinical chemo-sensitivity in TGCT. Houldsworth et al.85 identified themutations of p53 only in cisplatin-resistant cells withreduced expression of bax, an agonist of apoptosis.These two reports explain that the cisplatin-resistantphenotype is caused by the inability to respond toapoptotic signals by a functionally inactivating p53mutation. However, few molecular analyses have beendone in poor-prognosis, recurrent TGCT subgroups.Recently, Rao et al.86 performed comparative genomichybridization analysis between chemotherapy-resistantTGCT and sensitive tumors to search for genetic alteration underlying drug resistance. They identifiedeight amplified regions (1q31–32, 2p23–24, 7q21,7q31, 9q22, 9q32–34, 15q23–24 and 20q11.2–12) infive resistant tumors, which could possibly involvegenes responsible for resistance. In future, chemothera-py related or prognosis-related genes will be identifiedand these findings will make a great contributiontoward the selection of patients, the prediction of prog-nosis and the design of new drugs in testicular canceras well as other cancers.
Clinical trials
Despite the success of cisplatin based chemotherapy inthe treatment of metastatic TGCT, further modificationof the chemotherapeutic regimen is necessary in sev-eral subgroups, i.e. (1) metastatic disease having poor prognosis classification on IGC-CCG criteria,87
(2) relapsed diseases after successful chemotherapyand (3) non-responded diseases in cisplatin based-chemotherapy.88 For these subgroups, cisplatin-basedhigh dose chemotherapy has been intensively studiedand approximately a 40% cure rate has been achieved,while standard-dose salvage yielded a rate of only a20%.88 The high-dose chemotherapy with peripheralblood stem cell transplantation is expected to allowlonger term cure rates and lower treatment-related lateside-effects in the treatment for high-risk groups.88 Theincorporation of a new active drug, paclitaxel and newalkylating agent ifosfamide may thus improve theresults in poor prognosis patients.89
Prostate cancer
Basic research approach
Clinically localized prostate cancer can be removed bya radical prostatectomy or treated by radiation therapy.The 10-year actuarial survival rate after a radical
prostatectomy is excellent (> 80%) if the disease isconfined to the organ.90 In metastatic prostate cancer,tumors initially respond to androgen-ablation therapy,however, many prostate cancers become hormonerefractory, progress further and eventually becomefatal. Intensive basic research approaches have beendone to reveal the molecular mechanism underlyingandrogen insensitivity in prostate cancer. Recentadvances have revealed that androgen independence is caused by several molecular alterations includingmutations in the androgen receptor (AR), amplifica-tion of the AR gene and alteration of AR-mediated transcriptional signaling pathway.91 Prostate cancer isgenerally considered to consist of a heterogeneouspopulation of cells regarding hormone sensitivity.Therefore, hormone refractory prostate cancer is alsolikely to develop due to the selective proliferation ofandrogen-insensitive clones during androgen-abrationtherapy.92
Unfortunately, hormone-independent metastaticprostate cancer is resistant to a broad range of anti-cancer agents.3,93 Several studies using a basic researchapproach have revealed the drug resistant mechanismsin prostate cancer as follows:
1. prostate cancer cells grow very slowly, with a highnumber of cells resting in G
0phase of the cell
cycle;93
2. hormone-insensitive prostate cancer cells have losttheir commitment to apoptosis in response to andro-gen ablation and these molecular alterations inapoptosis can help them to escape from apoptosispathways caused by anticancer agents as well;94
and 3. the overexpression of drug resistant genes con-
tributes to the intrinsic resistance in prostate cancer.
For example, Siegsmund et al.95 reported P-gp wasoverexpressed in hormone-insensitive mouse cellscompared with hormone-sensitive cells. Izbicka E etal.96 identified the overexpression of both MDR1 andMRP in metastatic human prostate tissues but not inprimary tumors in limited clinical samples. Nakagawaet al.97 established cisplatin resistant cells from a hor-mone refractory prostate cancer cell line, PC-3, andestimate that decreased drug accumulation was respon-sible for cisplatin resistant phenotype. Recently,Taniguchi et al.8 found cMOAT overexpression in thesecell lines, thus suggesting that cMOAT might functionas a transporter of cisplatin in these cells. As we alsoobserved the overexpression of an antioxidant mol-ecule, thioredoxin, in these cells, we therefore believethat thioredoxin partially contributes to cisplatin resis-tance in PC-3 cells.42

436 S Naito et al.
Clinical trials
According to the review article by Yagoda et al.93 theoverall response rate of chemotherapy in prostate can-cer was only 8.7% in 26 trials organized between 1987and 1991. However, a new modulated and renewedchemotherapeutic regimen is now emerging for hor-mone refractory, metastatic prostate cancer. The appli-cation of estramustine is one of the promising proto-cols for prostate cancer. Estramustine is a conjugate ofnitrogen mustard and estradiol, whose mechanism ofaction is likely to be antimitotic, particularly by bind-ing to microtuble-associated proteins.98 Eighteen phaseII trials (634 patients) of single agent estramustineresulted in only a 19% measurable response rate, butthe synergic effects of estramustine were obtained inseveral clinical trials when it was combined with vin-blastine, paclitaxel or etoposide.99 Speicher et al.100
reported another pharmacological character of estra-mustine, that it interacts with P-gp by changing theintracellular drug accumulation. The inhibitory effectof estramustine on P-gp may thus have a synergiceffect when used with anticancer agents.
Other novel combinations and new drugs currentlybeing tested include mitoxantrone with hydrocorti-sone100 and topoisomerase inhibitors, including camp-tothecin, topotecan, irinotecan and b-lapachone.3
These regimens are expected to improve the prognosisof prostate cancer.
Conclusion
Recent research has provided us with a better under-standing of the mechanisms underlying drug resistancein cancer chemotherapy. The identification of P-gp andMRP had a great impact on intrinsic or acquired drugresistance in genitourinary cancers and it has alsoresulted in new approaches to overcome MDR byusing inhibitors. Moreover, other multiple moleculeshave been identified and characterized in relation todrug resistance. Summarizing these data, cancer cellscan acquire the drug resistance phenotype by sharingvarious molecular alterations with some moleculescontributing to a major part of resistance, while otherscontribute to only a small part of such resistance. Toovercome drug resistance in these multipotential can-cer cells, further molecular analyses to determine themost responsible molecules will be necessary in eachorgan or even in each patient. Moreover, a furthercharacterization of each responsible protein will helpus to eventually identify the specific inhibitors andoverlapping inhibitors against drug resistance.
Acknowledgments
We thank Professor Michihiko Kuwano and Dr Manabu Furukawa (Department of Biochemistry, Fac-ulty of Medicine, Kyushu University) and Drs ShujiKoth and Michitaka Nakashima (Department of Urolo-gy, Faculty of Medicine, Kyushu University) for theirfruitful discussions. This work was supported in partby a Grant-in-Aid of The Japan Medical Associationand a Grant-in-Aid for Scientific Research (B) fromthe Ministry of Education, Science, Sports and Cultureof Japan.
References
1 Bosl GJ, Motzer RJ. Testicular germ-cell cancer. N.Engl. J. Med. 1997; 337: 242–53.
2 Rao PH, Houldsworth J, Palanisamy N et al. Chromo-somal amplification is associated with cisplatin resis-tance of human male germ cell tumors. Cancer Res.1998; 58: 4260–3.
3 van Brussel JP, Mickisch GH. Circumvention of mul-tidrug resistance ingenitourinary tumors. Int J. Urol.1998; 5: 1–15.
4 Roninson IB, Chin JE, Choi KG et al. Isolation ofhuman mdr DNA sequences amplified in multidrug-resistant KB carcinoma cells. Proc. Natl Acad. Sci.USA 1986; 83: 4538–42.
5 Chen CJ, Chin JE, Ueda K, Clark DP, Pastan I, Gottesman MM, Roninson IB. Internal duplication andhomology with bacterial transport proteins in the mdr1(P-glycoprotein) gene from multidrug-resistant humancells. Cell 1986; 47: 381–9.
6 Cole SP, Bhardwaj G, Gerlach JH et al. Overexpres-sion of a transporter gene in a multidrug-resistanthuman lung cancer cell line. Science 1992; 258:1650–4.
7 Borst P, Kool M, Evers R. Do cMOAT (MRP2), otherMRP homologues, and LRP play a role in MDR?Semin.. Cancer Biol. 1997; 8: 205–13.
8 Taniguchi K, Wada M, Kohno K et al. A humancanalicular multispecific organic anion transporter(cMOAT) gene is overexpressed incisplatin-resistanthuman cancer cell lines with decreased drug accumu-lation. Cancer Res. 1996; 56: 4124–9.
9 Lomri N, Fitz JG, Scharschmidt BF. Hepatocellulartransport: Role of ATP-binding cassette proteins.Semin. Liver Dis. 1996; 16: 201–10.
10 Aszalos A, Ross DD. Biochemical and clinical aspectsof efflux pump-related resistance to anti-cancer drugs.Anticancer Res. 1998; 18: 2937–44.
11 Schinkel AH. The physiological function of drug-transporting P-glycoproteins. Semin. Cancer Biol.1997; 8: 161–70.
12 Ueda K, Okamura N, Hirai M et al. Human P-glyco-protein transports cortisol, aldosterone, and dexam-ethasone, but not progesterone. J. Biol. Chem 1992;267: 24 248–52.

Drug resistance in urogenital carcinoma 437
13 Schinkel AH, Smit JJ, van Tellingen O et al. Disrup-tion of the mouse mdr1a P-glycoprotein gene leads toa deficiency in the blood–brain barrier and toincreased sensitivity to drugs. Cell 1994; 77: 491–502.
14 Hasegawa S, Abe T, Naito S et al. Expression of mul-tidrug resistance-associated protein (MRP), MDR1and DNA topoisomerase II in human multidrug-resistant bladder cancer cell lines. Br. J. Cancer 1995;71: 907–13.
15 Schneider E, Horton JK, Yang CH, Nakagawa M,Cowan KH. Multidrug resistance-associated proteingene overexpression and reduced drug sensitivity oftopoisomerase II in a human breast carcinoma MCF7cell line selected for etoposide resistance. Cancer Res.1994; 54: 152–8.
16 Jedlitschky G, Leier I, Buchholz U, Center M, KepplerD. ATP-dependent transport of glutathione S-conjugates by the multidrug resistance-associated pro-tein. Cancer Res. 1994; 54: 4833–6.
17 Leier I, Jedlitschky G, Buchholz U, Cole SP, DeeleyRG, Keppler D. The MRP gene encodes an ATP-dependent export pump for leukotriene C4 and struc-turally related conjugates. J. Biol. Chem 1994; 269: 27807–10.
18 Muller M, Meijer C, Zaman GJ et al. Overexpressionof the gene encoding the multidrug resistance-associated protein results in increased ATP-dependent-glutathione S-conjugate transport. Proc. Natl Acad.Sci. USA 1994; 91: 13033–7.
19 Grant CE, Valdimarsson G, Hipfner DR, AlmquistKC, Cole SP, Deeley RG. Overexpression of multidrugresistance-associated protein (MRP) increases resis-tance to natural product drugs. Cancer Res. 1994; 54:357–61.
20 Cole SP, Sparks KE, Fraser K et al. Pharmacol-ogical characterization of multidrug resistant MRP-transfected human tumor cells. Cancer Res. 1994; 54:5902–10.
21 Deeley RG, Cole SP. Function, evolution and structureof multidrug resistance protein (MRP). Semin. CancerBiol. 1997; 8: 193–204.
22 Kool M, de Haas M, Scheffer GL et al. Analysis ofexpression of cMOAT (MRP2), MRP3, MRP4, andMRP5, homologues of the multidrug resistance-associated protein gene (MRP1), in human cancer celllines. Cancer Res. 1997; 57: 3537–47.
23 Kool M, van der Linden M, de Haas M, Baas F, BorstP. Expression ofhuman MRP6, a homologue of themultidrug resistance protein gene MRP1, in tissuesand cancer cells. Cancer Res. 1999; 59: 175–82.
24 Miyake K, Mickley L, Litman T et al. Molecularcloning of cDNAs which are highly overexpressed inmitoxantrone-resistant cells: Demonstration of homol-ogy to ABC transport genes. Cancer Res. 1999; 59:8–13.
25 Paulusma CC, Kool M, Bosma PJ et al. A mutation inthe human cMOAT gene causes the Dubin–Johnsonsyndrome. Hepatology 1997; 25: 1539–42.
26 Wada M, Toh S, Taniguchi K et al. Mutations in thecanilicular multispecific organic anion transporter(cMOAT) gene, a novel ABC transporter, in patientswith hyperbilirubinemia II/Dubin–Johnson syndrome.Hum. Mol. Genet. 1998; 7: 203–7.
27 Koike K, Kawabe T, Tanaka T, Toh S, Uchiumi T,Wada M, Akiyama S, Ono M, Kuwano M. A canalicu-lar multispecific organic anion transporter (cMOAT)antisense cDNA enhances drug sensitivity in humanhepatic cancer cells. Cancer Res. 1997; 57: 5475–9.
28 Uchiumi T, Hinoshita E, Haga S et al. Isolation of anovel human canalicular multispecific organic aniontransporter, cMOAT2/MRP3, and its expression in cisplatin-resistant cancer cells with decreased ATP-dependent drug transport. Biochem. Biophys. Res.Commun. 1998; 252: 103–10.
29 Scheffer GL, Wijngaard PLJ, Flens MJ et al. The drugresistance-related protein LRP is the human majorvault protein. Nat. Med. 1995; 1: 578–82.
30 List AF, Spier CS, Grogan TM et al. Overexpressionof the major vault transporter protein lung-resistanceprotein predicts treatment outcome in acute myeloidleukemia. Blood 1996; 87: 2464–9.
31 Meister A, Anderson M. Glutathione. Annu. Rev.Biochem. 1983; 52: 711–60.
32 Ziegler DM. Role of reversible oxidation-reduction ofenzyme thiols-disulfides in metabolic regulation.Annu. Rev. Biochem. 1985; 54: 305–29.
33 Yokomizo A, Kohno K, Wada M et al. Markedlydecreased expression of glutathione S-transferase pigene in human cancer cell lines resistant to buthioninesulfoximine, an inhibitor of cellular glutathione syn-thesis. J. Biol. Chem 1995; 270: 19451–7.
34 Tew KD. Glutathione-associated enzymes in anti cancerdrug resistance. Cancer Res. 1994; 54: 4313–20.
35 Meister A. Glutathione, ascorbate, and cellular protec-tion. Cancer Res. 1994; 54: 1969s–75s.
36 Ozols RF, Hamilton TC, Masuda H, Young RC. Noveldrugs that affect glutathione metabolism. In: WoolleyPV III, Tew KD (eds). Mechanisms of Drug Resis-tance in Neoplastic Cells. Academic Press, New York,1988; 289–306.
37 Miyazaki M, Kohno K, Saburi Y et al. Biochem. Bio-phys. Res. Commun. 1990; 166: 1358–64.
38 Nakagawa K, Saijo N, Tsuchida S et al. Glutathione-S-transferase pi as a determinant of drug resistance intransfectant cell lines. J. Biol. Chem. 1990; 265:4296–301.
39 Richman PG, Meister A. Regulation of gamma-glutamyl-cysteinesynthetase by non-allosteric feed-back inhibition by glutathione. J. Biol. Chem 1975;250: 1422–6.
40 Mulcahy RT, Bailey HH, Gipp JJ. Transfection ofcomplementary DNAs for the heavy and light sub-units of human gamma-glutamylcysteine synthetaseresults in an elevation of intracellular glutathione andresistance to melphalan. Cancer Res. 1995; 55: 4771–5.
41 Kurokawa H, Ishida T, Nishio K et al. Gamma-glutamylcysteine synthetase gene overexpressionresults in increased activity of the ATP-dependent glu-tathione S-conjugate export pump and cisplatin resis-tance. Biochem. Biophys. Res. Commun 1995; 216:258–64.
42 Yokomizo A, Ono M, Nanri H et al. Cellular levels ofthioredoxin associated with drug sensitivity to cis-platin, mitomycin C, doxorubicin, and etoposide. Can-cer Res. 1995; 55: 4293–6.

438 S Naito et al.
43 Kawahara N, Tanaka T, Yokomizo A et al. Enhancedcoexpression of thioredoxin and high mobility groupprotein 1 genes in human hepatocellular carcinomaand the possible association with decreased sensitivityto cisplatin. Cancer Res. 1996; 56: 5330–3.
44 Sasada T, Iwata S, Sato N et al. Redox control of resis-tance to cis-diamminedichloroplatinum (II) (CDDP):Protective effect of humanthioredoxin against CDDP-induced cytotoxicity. J. Clin. Invest 1996; 97: 2268–76.
45 Wang J, Kobayashi M, Sakurada K, Imamura M,Moriuchi T, Hosokawa M. Possible roles of an adult T-cell leukemia (ATL) -derived factor/thioredoxin in thedrug resistance of ATL to adriamycin. Blood 1997; 89:2480–7.
46 Yamada M, Tomida A, Yoshikawa H, Taketani Y, Tsuruo T. Overexpression of thioredoxin does not con-fer resistance to cisplatin in transfected human ovarianand colon cancer cell lines. Cancer Chemotherphar-macol. 1997; 40: 31–7.
47 Lazo JS, Kuo SM, Woo ES, Pitt BR. The protein thiolmetallothionein as an antioxidant and protectantagainst antineoplastic drugs. Chem Biolinteract 1998;24: 255–62.
48 Kasahara K, Fujiwara Y, Nishio K et al. Metalloth-ionein content correlates with the sensitivity of humansmall cell lung cancer cell lines to cisplatin. CancerRes. 1991; 51: 3237–42.
49 Kotoh S, Naito S, Sakamoto N, Goto K, Kumazawa J.Metallothionein expression is correlated with cisplatinresistance in transitional cell carcinoma of the urinarytract. J. Urol. 1994; 152: 1267–70.
50 Berger JM, Gamblin SJ, Harrison SC, Wang JC. Struc-ture and mechanism of DNA topoisomerase II. Nature1996; 379: 225–32.
51 Wang JC. DNA topoisomerases. Annu. Rev. Biochem.1996; 65: 635–69.
52 Sinha BK. Topoisomerase inhibitors. A review of theirtherapeutic potential in cancer. Drugs 1995; 49:11–19.
53 Jenkins JR, Ayton P, Jones T, Davies SL, Simmons DL,Harris AL, Sheer D, Hickson ID. Isolation of cDNAclones encoding the beta isozyme of human DNA topoi-somerase II and localisation of the gene to chromosome3p24. Nucl. Acids Res. 1992; 20: 5587–92.
54 Cummings J, Smyth JF. DNA topoisomerase I and IIas targets for rational design of new anticancer drugs.Ann. Oncol. 1993; 4: 533–43.
55 Matsuo K, Kohno K, Takano H, Sato S, Kiue A,Kuwano M. Reduction of drug accumulation andDNA topoisomerase II activity in acquired teniposide-resistant human cancer KB cell lines. Cancer Res.1990; 50: 5819–24.
56 Kubo T, Kohno K, Ohga T et al. DNA topoisomeraseII alpha gene expression under transcriptional controlin etoposide/teniposide-resistant human cancer cells.Cancer Res. 1995; 55: 3860–4.
57 Matsuo K, Kohno K, Sato S et al. Enhanced expres-sion of the DNA topoisomerase II gene in response toheat shock stress in human epidermoid cancer KBcells. Cancer Res. 1993; 53: 1085–90.
58 Furukawa M, Uchiumi T, Nomoto M et al. The role ofan inverted CCAAT element in transcriptional activa-
tion of the human DNA topoisomerase II alpha geneby heat shock. J. Biol. Chem 1998; 273: 10 550–5.
59 Naito S, Sakamoto N, Kotoh S, Goto K, Matsumoto T,Kumazawa J. Expression of P-glycoprotein and mul-tidrug resistance in renal cell carcinoma. Eur. Urol.1993; 24: 156–60.
60 Kanamaru H, Kakehi Y, Yoshida O, Nakanishi S, Pastan I, Gottesman MM. MDR1 RNA levels inhuman renal cell carcinomas: Correlation with grade-and prediction of reversal of doxorubicin resistance byquinidine in tumor explants. J. Natl Cancer Inst. 1989;81: 844–9.
61 Kakehi Y, Kanamaru H, Yoshida O et al. Measurementof multidrug-resistance messenger RNA in urogenitalcancers; elevated expression in renal cell carcinoma isassociated with intrinsic drug resistance. J. Urol. 1988;139: 862–5.
62 Kim WJ, Kakehi Y, Kinoshita H, Arao S, FukumotoM, Yoshida O. Expression patterns of multidrug-resistance (MDR1), multidrug resistance-associatedprotein (MRP), glutathione-S-transferase-pi (GST-pi)and DNA topoisomerase II (Topo II) genes in renalcell carcinomas and normal kidney. J. Urol. 1996; 156:506–11.
63 Volm M, Mattern J, Efferth T, Pommerenke EW.Expression of several resistance mechanisms inuntreated human kidney and lung carcinomas. Anti-cancer Res. 1992; 12: 1063–7.
64 Naito S, Koike K, Ono M et al. Development of novelreversal agents, Imidazothiazole derivatives, targetingMDR1- and MRP-mediated multidrug resistance.Oncol. Res. 1998; 10: 123–32.
65 Motzer RJ, Lyn P, Fischer P et al. Phase I/II trial ofdexverapamil plus vinblastine for patients withadvanced renal cell carcinoma. J. Clin. Oncol. 1995;13: 1958–65.
66 Warner E, Tobe SW, Andrulis IL, Pei Y, TrachtenbergJ, Skorecki KL. Phase I-II study of vinblastine andoral cyclosporin A in metastatic renal cell carcinoma.Am. J. Clin. Oncol. 1995; 18: 251–6.
67 Agarwala SS, Bahnson RR, Wilson JW, Szumowski J,Ernstoff MS. Evaluation of the combination of vin-blastine and quinidine in patients with metastatic renalcell carcinoma: A phase I study. Am. J. Clin. Oncol.1995; 18: 211–15.
68 Berlin J, King AC, Tutsch K, Findlay JW, Kohler P,Collier M, Clendeninn NJ, Wilding G. A phase IIstudy of vinblastine in combination with acrivastine inpatients with advanced renal cell carcinoma. Invest.New Drugs 1994; 12: 137–41.
69 Murphy BR, Rynard SM, Pennington KL, Grosh W,Loehrer PJ. A phase II trial of vinblastine plus dipyri-damole in advanced renal cell carcinoma: A HoosierOncology Group Study. Am. J. Clin. Oncol. 1994; 17:10–13.
70 Kimiya K, Naito S, Soejima T et al. Establishment andcharacterization of doxorubicin-resistant human blad-der cancer cell line, KK47/ADM. J. Urol. 1992; 148:441–5.
71 Naito S, Hasegawa S, Yokomizo A et al. Non-P-glyco-protein-mediated atypical multidrug resistance in ahuman bladder cancer cell line. Jpn. J. Cancer Res.1995; 86: 1112–18.

Drug resistance in urogenital carcinoma 439
72 Kotoh S, Naito S, Yokomizo A, Kohno K, Kuwano M,Kumazawa J. Enhanced expression of gamma-glutamyl cysteine synthetase and glutathioneS-trans-ferase genes in cisplatin-resistant bladder cancer cellswith multidrug resistance phenotype. J. Urol. 1997;157: 1054–8.
73 Kotoh S, Naito S, Yokomizo A et al. Increased expres-sion of DNA topoisomerase I gene and collateral sen-sitivity to camptothcin in human cisplatin-resistantbladder cancer cells. Cancer Res. 1994; 54: 3248–52.
74 Rowinsky EK, Kaufmann SH, Baker SD et al.Sequences of topotecan and cisplatin: Phase I, phar-macologic, and in vitro studies to examine sequencedependence. J. Clin. Oncol. 1996; 14: 3074–84.
75 Hisano T, Ono M, Nakayama M, Naito S, Kuwano M,Wada M. Increased expression of T-plastin gene in cis-platin-resistant human cancer cells: Identification bymRNA differential display. FEBS Lett 1996; 397:101–7.
76 Satoh M, Cherian MG, Imura N, Shimizu H. Modula-tion of resistance to anticancer drugs by inhibition ofmetallothionein synthesis. Cancer Res. 1994; 54:5255–7.
77 van der Meijden AP. Bladder cancer. BMJ 1998; 317:1366–9.
78 Herr HW, Loudone VP, Whitmore WF Jr An overviewof intravesical therapy for superficial tumours. J. Urol.1987; 138: 1363–8.
79 Naito S, Kotoh S, Omoto T et al. Prophylactic intra-vesical instillation chemotherapy against recurrenceafter a transurethral resection of superficial bladdercancer: A randomized controlled trial of doxorubicin-plus verapamil versus doxorubicin alone: The KyushuUniversity Urological Oncology Group. CancerChemother. Pharmacol. 1998; 42: 367–72.
80 Lukkarinen O, Paul C, Hellstrom P et al. Intravesicalepirubicin with and without verapamil for the prophy-laxis of superficial bladder tumours. Scand. J. UrolNephrol. 1991; 25: 25–8.
81 Nakagawa M, Emoto A, Nasu N et al. Clinicalsignificance of multi-drug resistance associated pro-tein and P-glycoprotein in patients with bladder can-cer. J. Urol. 1997; 15: 1260–5.
82 Katagiri A, Tomita Y, Nishiyama T, Kimura M, SatoS. Immunohistochemical detection of P-glycoproteinand GSTP1–1 in testis cancer. Br. J. Cancer 1993; 68:125–9.
83 Masters JR, Thomas R, Hall AG, Hogarth L, MathesonEC, Cattan AR, Lohrer H. Sensitivity of testis tumourcells to chemotherapeutic drugs: Role of detoxifyingpathways. Eur. J. Cancer 1996; 32: 1248–53.
84 Eid H, Van der Looij M, Institoris E et al. Is p53expression, detected by immunohistochemistry, animportant parameter of response to treatment in testiscancer? Anticancer Res. 1997; 17: 2663–9.
85 Houldsworth J, Xiao H, Murty VV et al. Human malegerm cell tumor resistance to cisplatin is linked toTP53 gene mutation. Oncogene 1998; 16: 2345–9.
86 Rao PH, Houldsworth J, Palanisamy N et al. Chromo-somal amplification is associated with cisplatin resis-tance of human male germ cell tumors. Cancer Res.1998; 58: 4260–3.
87 International Germ Cell Cancer Collaborative Group.International Germ Cell Consensus Classification. Aprognostic factor-based staging system for metasta-tic germ cell cancers. J. Clin. Oncol. 1997; 15:594–603.
88 Bokemeyer C, Harstrick A, Beyer J et al. The use ofdose-intensified chemotherapy in the treatment ofmetastatic non-seminomatous testicular germ celltumors. German Testicular Cancer Study Group.Semin. Oncol. 1998; 25 (Suppl. 4): 24–32.
89 Haas N, Hudes GR. Genito-urinary malignancy. Can-cer Chemother Biol. Response Modif. 1997; 17:504–35.
90 Petrovich Z, Baert L, Bagshaw MA et al. Adenocarci-noma of the prostate: Innovations in management. Am.J. Clin. Oncol. 1997; 20: 111–19.
91 Koivisto P, Kolmer M, Visakorpi T, Kallioniemi OP.Androgen receptor gene and hormonal therapy failureof prostate cancer. Am. J. Pathol. 1998; 152: 1–9.
92 Arai Y, Yoshida O. A heterogeneous pattern of pro-gression in endocrine-treated patients with prostatecancer. Eur. Urol. 1996; 29: 331–6.
93 Yagoda A, Petrylak D. Cytotoxic chemotherapy foradvanced hormone-resistant prostate cancer. Cancer.1993; 71 (Suppl. 3): 1098–109.
94 Berges RR, Furuya Y, Remington L, English HF,Jacks T, Isaacs JT. Cell proliferation, DNA repair, and p53 function are not required for programmeddeath of prostatic glandular cells induced by androgenablation. Proc. Natl Acad. Sci. USA 1993; 90: 8910–14.
95 Siegsmund MJ, Kreukler C, Steidler A, Nebe T,Kohrmann KU, Alken P. Multidrug resistance inandrogen-independent growing rat prostate carcinomacells is mediated by P-glycoprotein. Urol. Res. 1997;25: 35–41.
96 Izbicka E, Dalton WS, Troyer D, Von Hoff DD.Expression of two multidrug resistance genes inhuman prostatic carcinomas. J. Natl Cancer Inst.1998; 90: 166–7.
97 Nakagawa M, Nomura Y, Kohno K et al. Reduction ofdrug accumulation in cisplatin-resistant variants ofhuman prostatic cancer PC-3 cell line. J. Urol. 1970;1993: 150–3.
98 Hudes G. Estramustine-based chemotherapy. Semin.Urol. Oncol. 1997; 15: 13–19.
99 Oh WK, Kantoff PW. Management of hormone refrac-tory prostate cancer:current standards and futureprospects. J. Urol. 1998; 160: 1220–9.
100 Speicher LA, Barone LR, Chapman AE et al. P-glyco-protein binding and modulation of the multidrug-resistant phenotype by estramustine. J. Natl CancerInst. 1994; 86: 688–94.