Exploring the work of nurses who administer chemotherapy
11
Exploring the work of nurses who administer chemotherapy to children and young people Faith Gibson a, b, * , Lisa Shipway a , Susie Aldiss b , Jeanette Hawkins c , Wendy King d , Margaret Parr e , Deborah Ridout f , Rebecca Verity g , Rachel M. Taylor b, h a Great Ormond Street Hospital for Children NHS Trust, London, UK b Department of Children’s Nursing, London South Bank University, UK c Birmingham Children’s Hospital, Birmingham, UK d The Whittington Hospital, London, UK e Children’s Hospital, Queens Medical Centre Campus, Nottingham, UK f UCL Institute of Child Health, London, UK g Health & Social Care, King’s College London, London, UK h Cancer Institute, University College London, London, UK Keywords: Chemotherapy Nursing Education Competence abstract Purpose of the research: To explore the knowledge, attitudes and beliefs of nurses who administer chemotherapy to children and young people. Methods and sample: A national postal survey of nurses working within the 21 cancer centres in the United Kingdom and Ireland. The questionnaire included 25-items addressing the attitudes, beliefs and concerns regarding nurses’ roles, support mechanisms and educational preparation related to admin- istration of chemotherapy. Results: In total 286/507 (56%) questionnaires were returned. The majority of nurses worked in inpatient þ/-outpatient (78%) settings and most gave chemotherapy on a daily basis (61%). The median time working in oncology was 10 [range 0.5e32] years and time administering chemotherapy was 8 [0.1e32] years. Aspects of administration that caused the most worry included treatment side- effects, extravasation, dealing with allergic/anaphylactic reactions and knowledge deficits in colleagues. There was no significant difference in worry according to level of nurse education but those with an oncology qualification had less Knowledge-related worry (p ¼ 0.05). There was no difference in attitude according to level of education or having an oncology qualification. There were significant correlations between time qualified, time working in oncology and the number of years administering chemotherapy and the worry domains (ranging from r ¼0.14 to r ¼0.24, p < 0.05); and attitude to chemotherapy (ranging from r ¼ 0.12 to r ¼ 0.26, p < 0.001). Conclusion: As anticipated nurses new to chemotherapy administration were initially anxious about the role and they worried about making a drug error. Education and support from colleagues appears to have a positive effect on reducing worry and increasing competence. Ó 2012 Elsevier Ltd. All rights reserved. Introduction Children and young people with cancer are currently cared for in the 21 Childhood Cancer and Leukaemia Group (CCLG) centres and around 60 shared care units (care closer to home) within the United Kingdom (UK) and Ireland. Throughout these centres chemotherapy remains the primary treatment modality for hae- matological malignancies and many solid tumours, when it is Abbreviations: CCLG, Children’s Cancer and Leukaemia Group; CIVAS, Central Intravenous Additive Service; DH, Department of Health; NCAG, National Chemotherapy Advisory Group; NCAT, National Cancer Action team; NCIG, National Chemotherapy Implementation Group; NPSA, National Patient Safety Agency; PONF, Paediatric Oncology Nurse’s Forum; RCN, Royal College of Nursing; SRS, Stress-Response-Sequence. * Corresponding author. Clinical Professor of Children and Young People’s Cancer Care, Great Ormond Street Hospital NHS Trust and London South Bank University, Department of Children’s Nursing London South Bank University 103 Borough Road, London SE1 0AA, United Kingdom. Tel.: þ44 0207 813 8543. E-mail addresses: [email protected], [email protected] (F. Gibson), [email protected] (L. Shipway), [email protected] (S. Aldiss), Jeanette.hawkins@ bch.nhs.uk (J. Hawkins), [email protected] (W. King), [email protected] (M. Parr), [email protected] (D. Ridout), [email protected] (R. Verity), [email protected] (R.M. Taylor). Contents lists available at SciVerse ScienceDirect European Journal of Oncology Nursing journal homepage: www.elsevier.com/locate/ejon 1462-3889/$ e see front matter Ó 2012 Elsevier Ltd. All rights reserved. doi:10.1016/j.ejon.2012.01.006 European Journal of Oncology Nursing 17 (2013) 59e69
Transcript of Exploring the work of nurses who administer chemotherapy

at SciVerse ScienceDirect
European Journal of Oncology Nursing 17 (2013) 59e69
Contents lists available
European Journal of Oncology Nursing
journal homepage: www.elsevier .com/locate/ejon
Exploring the work of nurses who administer chemotherapy to children andyoung people
Faith Gibson a,b,*, Lisa Shipwaya, Susie Aldiss b, Jeanette Hawkins c, Wendy King d, Margaret Parr e,Deborah Ridout f, Rebecca Verity g, Rachel M. Taylor b,h
aGreat Ormond Street Hospital for Children NHS Trust, London, UKbDepartment of Children’s Nursing, London South Bank University, UKcBirmingham Children’s Hospital, Birmingham, UKd The Whittington Hospital, London, UKeChildren’s Hospital, Queens Medical Centre Campus, Nottingham, UKfUCL Institute of Child Health, London, UKgHealth & Social Care, King’s College London, London, UKhCancer Institute, University College London, London, UK
Keywords:ChemotherapyNursingEducationCompetence
Abbreviations: CCLG, Children’s Cancer and LeukaAdvisory Group; NCAT, National Cancer Action team; NNurse’s Forum; RCN, Royal College of Nursing; SRS, S* Corresponding author. Clinical Professor of Child
Department of Children’s Nursing London South BankE-mail addresses: [email protected], faith.g
bch.nhs.uk (J. Hawkins), [email protected](R. Verity), [email protected] (R.M. Taylor).
1462-3889/$ e see front matter � 2012 Elsevier Ltd.doi:10.1016/j.ejon.2012.01.006
a b s t r a c t
Purpose of the research: To explore the knowledge, attitudes and beliefs of nurses who administerchemotherapy to children and young people.Methods and sample: A national postal survey of nurses working within the 21 cancer centres in theUnited Kingdom and Ireland. The questionnaire included 25-items addressing the attitudes, beliefs andconcerns regarding nurses’ roles, support mechanisms and educational preparation related to admin-istration of chemotherapy.Results: In total 286/507 (56%) questionnaires were returned. The majority of nurses worked ininpatient þ/-outpatient (78%) settings and most gave chemotherapy on a daily basis (61%). Themedian time working in oncology was 10 [range 0.5e32] years and time administering chemotherapywas 8 [0.1e32] years. Aspects of administration that caused the most worry included treatment side-effects, extravasation, dealing with allergic/anaphylactic reactions and knowledge deficits incolleagues. There was no significant difference in worry according to level of nurse education but thosewith an oncology qualification had less Knowledge-related worry (p ¼ 0.05). There was no difference inattitude according to level of education or having an oncology qualification. There were significantcorrelations between time qualified, time working in oncology and the number of years administeringchemotherapy and the worry domains (ranging from r ¼ �0.14 to r ¼ �0.24, p < 0.05); and attitude tochemotherapy (ranging from r ¼ 0.12 to r ¼ 0.26, p < 0.001).Conclusion: As anticipated nurses new to chemotherapy administration were initially anxious about therole and they worried about making a drug error. Education and support from colleagues appears to havea positive effect on reducing worry and increasing competence.
� 2012 Elsevier Ltd. All rights reserved.
Introduction
Children and young peoplewith cancer are currently cared for inthe 21 Childhood Cancer and Leukaemia Group (CCLG) centres
emia Group; CIVAS, Central IntravCIG, National Chemotherapy Impletress-Response-Sequence.ren and Young People’s Cancer CUniversity 103 Borough Road, [email protected] (F. Gibson), ship.uk (W. King), margaret.parr@nott
All rights reserved.
and around 60 shared care units (care closer to home) within theUnited Kingdom (UK) and Ireland. Throughout these centreschemotherapy remains the primary treatment modality for hae-matological malignancies and many solid tumours, when it is
enous Additive Service; DH, Department of Health; NCAG, National Chemotherapymentation Group; NPSA, National Patient Safety Agency; PONF, Paediatric Oncology
are, Great Ormond Street Hospital NHS Trust and London South Bank University,ndon SE1 0AA, United Kingdom. Tel.: þ44 0207 813 [email protected] (L. Shipway), [email protected] (S. Aldiss), [email protected] (M. Parr), [email protected] (D. Ridout), [email protected]

F. Gibson et al. / European Journal of Oncology Nursing 17 (2013) 59e6960
usually used in combination with surgery with or without radio-therapy. The delivery of chemotherapy to children and youngpeople, particularly small children, is recognised to be especiallydifficult, with more potential for errors more than in chemotherapyadministration in adults (National Institute for Health and ClinicalExcellence, 2005).
Background
Over the past twenty years the important task of administeringchemotherapy has become an integral part of the role of thechildren’s cancer nurse. The overall aim of nurses administeringchemotherapy is to ensure that patients receive it safely andprovide support for children, young people and their families toenable them to manage the physical and psychological conse-quences of their treatments (Hooker and Palmer, 1999). Nursesmust be confident about their knowledge, competence and tech-nical skills in order for them to effectively fulfil this role. Thisconfidence should not only come from clinical experiencebut also education (Pike and Gibson 1991; Price and McShane,2002). However, the education programmes undertaken toprepare nurses for this role are often delivered within a clinicalservice and developed locally to meet the needs of the workforce.Wide variation is known throughout the UK in terms of educa-tional preparation: this is disconcerting given the implicationsand current concerns regarding chemotherapy administration(Department of Health [DH], 2007; National ChemotherapyAdvisory Group [NCAG], 2009; National Confidential Enquiry intoPatient Outcome and Death, 2008).
Many of the education programmes are similar in content andassessment strategies but there are no nationally agreed educa-tional standards to be attained (Royal College of Nursing [RCN],2005). Additionally, little is known about the needs and compe-tence of practitioners in this area. This resulted in a group of chil-dren’s cancer nurses leading on the production of a key document,the Integrated Competency Framework for Training Programmes inthe Safe Administration of Chemotherapy to Children and YoungPeople (RCN, 2005). This was revised in 2010 and incorporated aspart of a set of generic competencies for practice: An integratedcareer and competence framework for nurses working in the fieldof children and young people’s cancer care (RCN, 2010). Althoughdisseminated throughout the UK CCLG centres, and referenced inthe Children’s Cancer Measures (National Cancer Action Team[NCAT], 2011), it is not known how far this framework has beenimplemented, and where it has, its impact on education andpractice. More will be known following peer review of the CCLGunits using the measures; this should be reported from across theUK in 2013. Additional information will result from a focus on thechemotherapy workforce by the National Chemotherapy Imple-mentation Group (NCIG; www.ncat.nhs.uk/our-work/ensuring-better-treatment/chemotherapy), but until then, the nationalprofile of how education is provided, the support available tonurses and the effect this has on competence and confidence hasyet to be described prior to this survey.
Nurses’ informal accounts of their work suggests that some findthe chemotherapy role to be a stressful and all-consuming part oftheir work. There is often anticipation of this extension to their role,a role some nurses look forward to taking on and others remainanxious and uncertain about. There is a desire to deliver holisticcare, including chemotherapy administration, yet there areconcerns about what it means to be a ‘chemo-giver’. Although thereis a natural progression towards developing this aspect of their role,little is known about how nurses experience this transition; theirattitudes, concerns and feelings surrounding this role extensionhave yet to be explored. It is argued that to give quality emotional
and physical support to the individual with cancer and theirfamilies, the nurse’s perception and experience of work in this fieldof care needs to be explored in depth (McCray, 1997).
Some of these issues have been explored by Verity and a team atKing’s College London (Wiseman et al., 2005) in a multi-methodstudy, incorporating both a survey and ethnographic design toexplore the role of nurses in adult cancer care. The first componentof the study utilised the Chemotherapy: Education, Worries andAttitudes Questionnaire, which was sent to 526 nurses workingwith adults within London hospitals providing chemotherapyservices. Staff education and experience, pressures of time andworkload, nurses receiving regular updated knowledge andworking with more experienced and knowledgeable role modelswere found to be factors that influenced nurses’ perspectives ofadministering chemotherapy. Although this information is helpful,we would suggest that while there are some similarities, such assafe handling of chemotherapy, there are differences in this specificrole between nurses who care for adults and those who care forchildren and young people for the findings to be translated into ourpractice. For example, variation in educational preparation, localissues around training and support for nurses in the role. Addi-tionally, the nature of the work itself we might anticipate thatvery different worries and concerns might be raised aboutadministration of chemotherapy to children, particularly the veryyoung. Despite these differences we feel that the similarities aresufficient to adopt the same research design, and benefit from theexperience of this research team to benefit our study throughcollaboration. We believe that there is much to be gained fromcollaboration within profession but across specialty (Ream andGibson, 2007).
Aims
The principle research question was: What is the knowledge,attitudes and beliefs of nurses who administer chemotherapy tochildren and young people?
Specific aims of the study were to:
� Explore attitudes, feelings and beliefs of nurses’ administeringchemotherapy;
� Ascertain the nature and extent of educational preparation andsources of support that nurses who administer chemotherapyare in receipt of and whether they perceive this to be sufficient;
� Determine whether experience and/or education have animpact on nurses’ attitudes or concerns.
Methods
Study design
This was a national survey collecting a combination of quanti-tative and qualitative data.
Theoretical framework for the study
The theoretical framework for this study draws on the work ofHinds who sought to explore role-related stress and role meaningin paediatric oncology nursing (Hinds et al., 1990). The field ofchildren’s and young people’s cancer care is undoubtedly stressful.Nurses can easily become overwhelmed in providing care toyoung patients and their families. The nature of the work itselfand the work environment can impact on a nurses’ performance. Ithas been suggested that one of the main reasons for oncologynurses experiencing stress and burnout is associated with

F. Gibson et al. / European Journal of Oncology Nursing 17 (2013) 59e69 61
chemotherapy administration (Delvaux et al., 1988). The modifiedStress-Response-Sequence (SRS) model offers a description of therelationship between stressors and individual’s reactions tothe stressors. It has been used to determine relationships betweenrole-related stress, coping and work consequences in paediatriconcology nursing (Hinds et al., 2003).
Participants
The target population was the total number of nurses whoadminister chemotherapy in all 21 CCLG centres, both in theinpatient and outpatient setting.
Data collection
Descriptive, quantitative data were obtained through self-completion of a postal questionnaire: referred to as the Chemo-therapy Education, Worries and Attitudes Questionnaire. This wasoriginally developed by (Verity, 2002) and evaluated further ina study involving 253 nurses involved in adult cancer care acrossthe London Cancer Network (Verity et al., 2008). The questionnairewas adapted by the project team to reflect the nature of children’scancer nursing. This 25-item questionnaire addressed the attitudes,beliefs and concerns regarding the nurse’s role, their supportmechanisms and educational preparation. It used various ques-tioning techniques including both closed and open questions. Themajority of the closed questions required a nominal responsechoice. The section of the questionnaire concerned with worriesand attitudes towards chemotherapy administration required anordinal response via a 4-point Likert scale (see Table 1 for anexample).
A pilot study of the questionnaire was undertaken to determinethe acceptability, appropriateness and feasibility of the revisedquestionnaire. Ten pilot test questionnaires were distributed tomembers of the RCN Paediatric Oncology Nursing Forum’s (PONF)1
education group. These nurses were predominately involved insupervising practice and educating nurses about chemotherapy.These nurses were not included in the main study; however,no changes were made to the questionnaire so these data wereincluded in the analysis.
Recruitment & procedure
A multi-stage approach was employed to recruit participants,similar to Verity et al. (2008), see Fig. 1. Once the list of names wasreceived from the named link nurse (a list of link nurses for eachCCLG centre is maintained by the speciality), questionnaires wereposted to the individual nurses at their work address. A uniquestudy identification number and centre code was assigned to eachquestionnaire to maintain confidentiality. In order to increase theresponse rate: i) a short piece was written for NewsLink (The RCNForum Newsletter) informing members about the survey; ii) thestudy was presented to PONF link nurses at one of their regularmeetings; and iii) and a series of reminders were sent to follow upnon-response at 3e4 weeks and again at 6e8 weeks to nurses withoutstanding responses.
Ethical considerations
The study was approved by an NHS Research Ethics Committee(study reference 08/H0703/114) and local R&D approval was
1 At the time of study the RCN group was referred to as PONF but now it is calledChildren’s and Young People’s Community of Practice.
obtained from 20 Trusts (R&D approval was not required in Eire).Consent to participate was assumed through return of thequestionnaire.
Data analysis
Data were entered into an SPSS (version 15.0) database foranalysis. Descriptive statistics, such as frequency distributionswere used to describe and summarise the characteristics of thesample and the variation in response. The items in the worry andattitudes section of the questionnaire were reduced to threedomains through consensus by three members of the project team(FG, SA, LS). These were confirmed as appropriate through reviewfrom other members of the project team (JH, WK). The worrydomains were titled knowledge, safety and child support, and theattitude scales were titled education, emotion and communica-tion. A sum of the responses for each domain was calculated tofacilitate further analysis. Differences due to level of education(BSc and above; specialist cancer course) and frequency ofchemotherapy administration were analysed using Mann Whit-ney U test and KruskaleWallis test for the comparison of morethan 2 groups. Relationship between degree of worry/attitudeand time (since qualification, working on oncology, givingchemotherapy) were assessed using Spearman’s rank correlation.To explore the strength of importance of frequency, the educationand time variables, on the three worry domains, multipleregression analyses were conducted. Data are presented asmedian (range).
The findings from the open questions were entered verbatim intoan Excel spread sheet and analysed using content analysis. This wasconducted by four members of the project team (FG, SA, LS, RT).
Results
Sample characteristics
Five hundred and seven nurses who were administeringchemotherapy agreed to receive a questionnaire, which werereturned by 288 (57%). There was wide variation according tocancer centre ranging from 38 to 82% (Fig. 2). Seven questionnaireshad been completed in the pilot study and therefore analysis wasconducted on 295 completed questionnaires.
The demographic details of participants are shown in Table 2.Nurses were qualified for a median of 14 (range 2e40) years, hadbeen working in oncology for 10 (range 0.5e32) years andadministering chemotherapy for 8 (0.1e32) years. Of the 277 nurseswho specified their professional qualifications, only one did nothave a children’s nursing qualification. One hundred and twenty-five (43%) nurses were qualified to degree level or above and 22(8%) held a higher degree. An oncology/chemotherapy course wasobtained by 187 (64%) nurses: diploma (n¼ 11; 4%), degree (n¼ 26;9%), higher degree (n ¼ 4; 1%), ENB or equivalent (n ¼ 158; 55%)2.The majority of nurses (n ¼ 131; 79%) worked in inpatientsettings (� outpatients) and gave chemotherapy on a daily basis(n ¼ 176; 60%).
Education
Only 49 (17%) nurses recalled receiving any pre-registrationeducation about chemotherapy; however, 291 (99%) had under-taken post-registration education, typically for >10 h (n ¼ 176;
2 Number of responses >180 due to multiple qualifications held by somerespondents.

Table 1Examples of questions included in the survey.
Example question Question type Response format
Think back t when you first started to administer chemotherapy.Please describe how it felt.
Open Free text.....................................................................
How much teaching did you receive on chemotherapy? Closed Nominal response:Less than 1 h ,
1e5 h ,
>5e10 h ,
Over 10 h ,
Uncertain ,
Are there times when you think it is NOT safe to handle chemotherapy? Closed 4-point Likert scaleNever , Occasionally , Often , Always ,
F. Gibson et al. / European Journal of Oncology Nursing 17 (2013) 59e6962
62%). Education had been received in a variety of formatsincluding study days (n ¼ 223; 78%), informal clinical teaching(n ¼ 217; 76%) and lectures as part of a course (n ¼ 157; 55%).Seven nurses (from different units) reported not receivingformal education as they were qualified before nurses routinelyadministered chemotherapy. However, they were responsible fordeveloping education, practice and policy for nursing chemo-therapy administration.
A chemotherapy workbook had been completed by 253 (88%)respondents, typically >5 years previously (n ¼ 159, 63%). While102 (36%) nurses stated they had not had any education updates,126 (45%) underwent yearly updates. This was mostly as study days(n ¼ 106; 37%) or informally in the clinical setting (n ¼ 69; 23%). Aworkbook update had only been completed by 67 (27%). Onehundred and eighty five (65%) nurses were aware of the RCN PONFcompetency framework. Eighty-five (30%) nurses reported thatthey had undergone a formal assessment either in their initialtraining or after updates. This included formal exams, assessmentdocuments and competencies.
The areas where nurses had received education andwhere they felt more education would be beneficial are shown
Fig. 1. Flowchart illustrating the multi-stage approach utilised for ascertaining andaccessing sample. CCLG: Children’s Cancer and Leukaemia Group; PONF: PaediatricOncology Nursing Forum; R&D: Research and Development.
in Fig. 3. Very few had received any education on reconstitutingchemotherapy on the ward (n ¼ 63; 23%), although it was noted asan area where education could be beneficial (n ¼ 106; 40%). Areaswhere more education was required included psychological(n ¼ 166; 59%) and long-term consequences (n ¼ 195; 61%), anddevelopments in chemotherapy treatment (n¼ 248; 87%). Overall,nurses responded positively to undertaking updates and furthertraining:
On-going training is essential as regimens and drugs usedare constantly evolving and changing. I am a confident practi-tioner with a sound knowledge base but realise that there isalways more to learn on all aspects of chemotherapy (Participant620)
Nurses were asked to state the three most important issuesto be included in chemotherapy education. The suggestedtopics related to five main themes: safety (n ¼ 257); side-effects(n ¼ 195); specific knowledge (n ¼ 83); child/family (n ¼ 62);and miscellaneous (n ¼ 20). The sub-themes and additional detailsare outlined in Table 3. The preferred format for further educationwas study days (n ¼ 162; 57%) and informal clinical teaching(n ¼ 143; 50%).
Feelings
Two hundred and twenty-four (76%) nurses felt their feelingshad changed about giving chemotherapy. Most described this usingnegative terms, such as ‘anxious’, ‘scary’, ‘terrified’, and ‘appre-hensive’. Examples of nurse’s initial feelings are shown in Table 4.The majority of nurses described a positive change in their feelingstowards giving chemotherapy (n ¼ 215), with most stating thatthey feel more confident:
Confident in my abilities and knowledge. Ability to recogniseproblems and navigate protocols has increased (Participant 1710)Have been doing it a long time so am more confident, no longernervous and assist with clinical assessments of new staff (Partici-pant 1804)
While nurses expressed more confidence, there was an aware-ness of the responsibilities associated with giving chemotherapy(n¼ 64), particularly of the effects on the child and issues related tosafety:
I fear for the many things I know can go wrong but also haveconfidence in my knowledge and techniques (Participant 403)Confident, but also very aware of how potentially dangerouschemotherapy is and how devastating if administered incorrectlyor unsafely (Participant 2016)
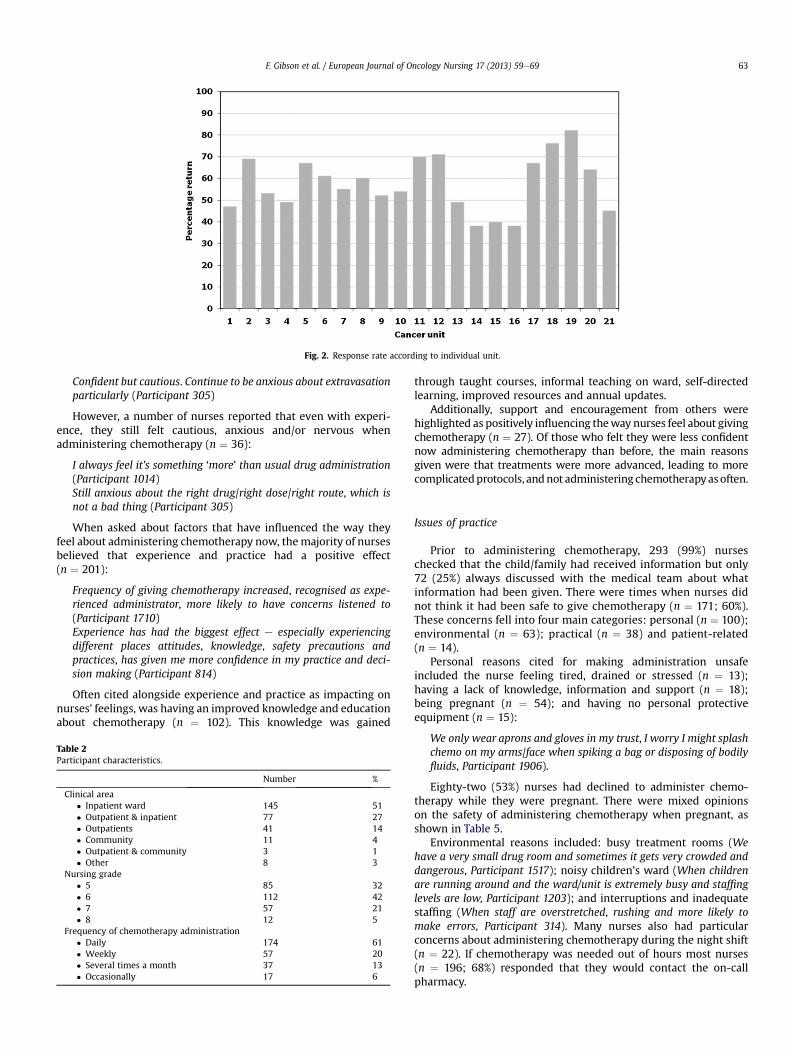
Fig. 2. Response rate according to individual unit.
F. Gibson et al. / European Journal of Oncology Nursing 17 (2013) 59e69 63
Confident but cautious. Continue to be anxious about extravasationparticularly (Participant 305)
However, a number of nurses reported that even with experi-ence, they still felt cautious, anxious and/or nervous whenadministering chemotherapy (n ¼ 36):
I always feel it’s something ‘more’ than usual drug administration(Participant 1014)Still anxious about the right drug/right dose/right route, which isnot a bad thing (Participant 305)
When asked about factors that have influenced the way theyfeel about administering chemotherapy now, themajority of nursesbelieved that experience and practice had a positive effect(n ¼ 201):
Frequency of giving chemotherapy increased, recognised as expe-rienced administrator, more likely to have concerns listened to(Participant 1710)Experience has had the biggest effect e especially experiencingdifferent places attitudes, knowledge, safety precautions andpractices, has given me more confidence in my practice and deci-sion making (Participant 814)
Often cited alongside experience and practice as impacting onnurses’ feelings, was having an improved knowledge and educationabout chemotherapy (n ¼ 102). This knowledge was gained
Table 2Participant characteristics.
Number %
Clinical area� Inpatient ward 145 51� Outpatient & inpatient 77 27� Outpatients 41 14� Community 11 4� Outpatient & community 3 1� Other 8 3
Nursing grade� 5 85 32� 6 112 42� 7 57 21� 8 12 5
Frequency of chemotherapy administration� Daily 174 61� Weekly 57 20� Several times a month 37 13� Occasionally 17 6
through taught courses, informal teaching on ward, self-directedlearning, improved resources and annual updates.
Additionally, support and encouragement from others werehighlighted as positively influencing theway nurses feel about givingchemotherapy (n ¼ 27). Of those who felt they were less confidentnow administering chemotherapy than before, the main reasonsgiven were that treatments were more advanced, leading to morecomplicatedprotocols, andnot administering chemotherapyasoften.
Issues of practice
Prior to administering chemotherapy, 293 (99%) nurseschecked that the child/family had received information but only72 (25%) always discussed with the medical team about whatinformation had been given. There were times when nurses didnot think it had been safe to give chemotherapy (n ¼ 171; 60%).These concerns fell into four main categories: personal (n ¼ 100);environmental (n ¼ 63); practical (n ¼ 38) and patient-related(n ¼ 14).
Personal reasons cited for making administration unsafeincluded the nurse feeling tired, drained or stressed (n ¼ 13);having a lack of knowledge, information and support (n ¼ 18);being pregnant (n ¼ 54); and having no personal protectiveequipment (n ¼ 15):
We only wear aprons and gloves in my trust, I worry I might splashchemo on my arms/face when spiking a bag or disposing of bodilyfluids, Participant 1906).
Eighty-two (53%) nurses had declined to administer chemo-therapy while they were pregnant. There were mixed opinionson the safety of administering chemotherapy when pregnant, asshown in Table 5.
Environmental reasons included: busy treatment rooms (Wehave a very small drug room and sometimes it gets very crowded anddangerous, Participant 1517); noisy children’s ward (When childrenare running around and the ward/unit is extremely busy and staffinglevels are low, Participant 1203); and interruptions and inadequatestaffing (When staff are overstretched, rushing and more likely tomake errors, Participant 314). Many nurses also had particularconcerns about administering chemotherapy during the night shift(n ¼ 22). If chemotherapy was needed out of hours most nurses(n ¼ 196; 68%) responded that they would contact the on-callpharmacy.
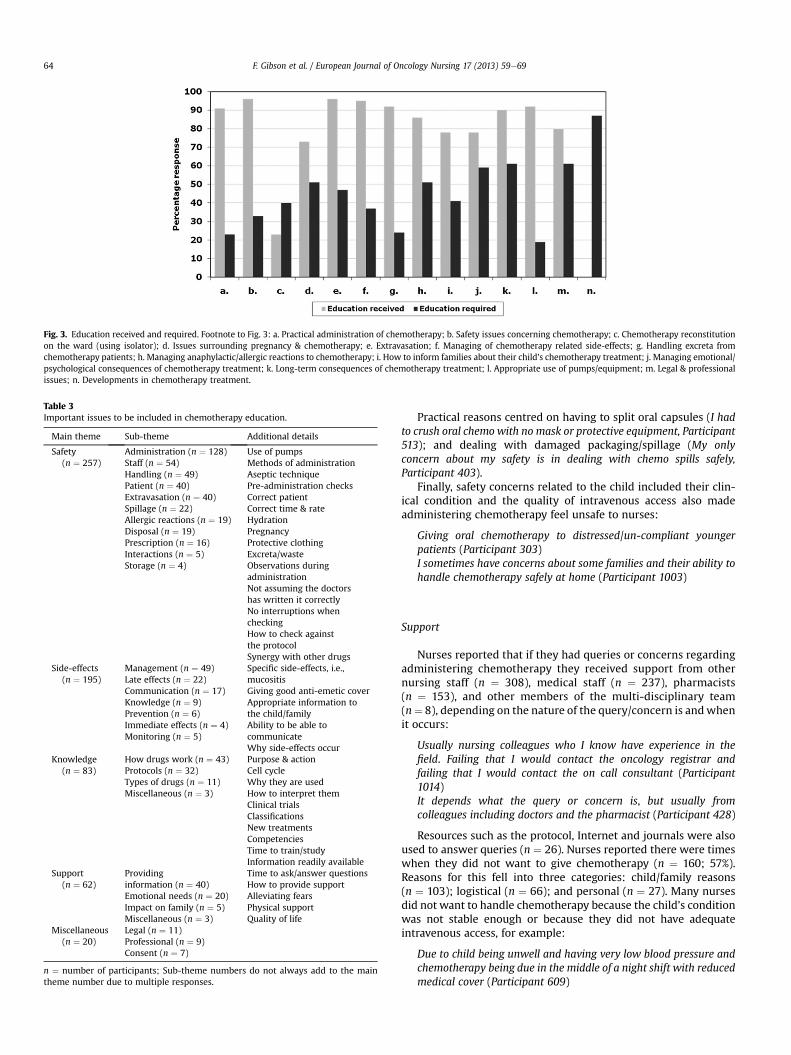
Fig. 3. Education received and required. Footnote to Fig. 3: a. Practical administration of chemotherapy; b. Safety issues concerning chemotherapy; c. Chemotherapy reconstitutionon the ward (using isolator); d. Issues surrounding pregnancy & chemotherapy; e. Extravasation; f. Managing of chemotherapy related side-effects; g. Handling excreta fromchemotherapy patients; h. Managing anaphylactic/allergic reactions to chemotherapy; i. How to inform families about their child’s chemotherapy treatment; j. Managing emotional/psychological consequences of chemotherapy treatment; k. Long-term consequences of chemotherapy treatment; l. Appropriate use of pumps/equipment; m. Legal & professionalissues; n. Developments in chemotherapy treatment.
Table 3Important issues to be included in chemotherapy education.
Main theme Sub-theme Additional details
Safety(n ¼ 257)
Administration (n ¼ 128)Staff (n ¼ 54)Handling (n ¼ 49)Patient (n ¼ 40)Extravasation (n ¼ 40)Spillage (n ¼ 22)Allergic reactions (n ¼ 19)Disposal (n ¼ 19)Prescription (n ¼ 16)Interactions (n ¼ 5)Storage (n ¼ 4)
Use of pumpsMethods of administrationAseptic techniquePre-administration checksCorrect patientCorrect time & rateHydrationPregnancyProtective clothingExcreta/wasteObservations duringadministrationNot assuming the doctorshas written it correctlyNo interruptions whencheckingHow to check againstthe protocolSynergy with other drugs
Side-effects(n ¼ 195)
Management (n ¼ 49)Late effects (n ¼ 22)Communication (n ¼ 17)Knowledge (n ¼ 9)Prevention (n ¼ 6)Immediate effects (n ¼ 4)Monitoring (n ¼ 5)
Specific side-effects, i.e.,mucositisGiving good anti-emetic coverAppropriate information tothe child/familyAbility to be able tocommunicateWhy side-effects occur
Knowledge(n ¼ 83)
How drugs work (n ¼ 43)Protocols (n ¼ 32)Types of drugs (n ¼ 11)Miscellaneous (n ¼ 3)
Purpose & actionCell cycleWhy they are usedHow to interpret themClinical trialsClassificationsNew treatmentsCompetenciesTime to train/studyInformation readily available
Support(n ¼ 62)
Providinginformation (n ¼ 40)Emotional needs (n ¼ 20)Impact on family (n ¼ 5)Miscellaneous (n ¼ 3)
Time to ask/answer questionsHow to provide supportAlleviating fearsPhysical supportQuality of life
Miscellaneous(n ¼ 20)
Legal (n ¼ 11)Professional (n ¼ 9)Consent (n ¼ 7)
n ¼ number of participants; Sub-theme numbers do not always add to the maintheme number due to multiple responses.
F. Gibson et al. / European Journal of Oncology Nursing 17 (2013) 59e6964
Practical reasons centred on having to split oral capsules (I hadto crush oral chemowith no mask or protective equipment, Participant513); and dealing with damaged packaging/spillage (My onlyconcern about my safety is in dealing with chemo spills safely,Participant 403).
Finally, safety concerns related to the child included their clin-ical condition and the quality of intravenous access also madeadministering chemotherapy feel unsafe to nurses:
Giving oral chemotherapy to distressed/un-compliant youngerpatients (Participant 303)I sometimes have concerns about some families and their ability tohandle chemotherapy safely at home (Participant 1003)
Support
Nurses reported that if they had queries or concerns regardingadministering chemotherapy they received support from othernursing staff (n ¼ 308), medical staff (n ¼ 237), pharmacists(n ¼ 153), and other members of the multi-disciplinary team(n¼ 8), depending on the nature of the query/concern is andwhenit occurs:
Usually nursing colleagues who I know have experience in thefield. Failing that I would contact the oncology registrar andfailing that I would contact the on call consultant (Participant1014)It depends what the query or concern is, but usually fromcolleagues including doctors and the pharmacist (Participant 428)
Resources such as the protocol, Internet and journals were alsoused to answer queries (n ¼ 26). Nurses reported there were timeswhen they did not want to give chemotherapy (n ¼ 160; 57%).Reasons for this fell into three categories: child/family reasons(n ¼ 103); logistical (n ¼ 66); and personal (n ¼ 27). Many nursesdid not want to handle chemotherapy because the child’s conditionwas not stable enough or because they did not have adequateintravenous access, for example:
Due to child being unwell and having very low blood pressure andchemotherapy being due in the middle of a night shift with reducedmedical cover (Participant 609)

Table 4Nurses feelings when they began administering chemotherapy.
Negative comments (n ¼ 233) Positive comments (n ¼ 23)
Examples: Examples:Very cautious and nervous of the impact the chemotherapy would have
upon a patient and also psychologically their family (Participant 303)I felt that I could provide holistic care to the child based ontheir needs/routine etc. I felt more in control (Participant 201)
Nervous about getting things wrong even though deemed competent.Often back then only one on a shift giving chemo (Participant 327)
Fine, felt comfortable. I had experienced the side-effects prior toadministering chemo. I was comfortable with the protocol wherethe child was in treatment and the prescription to be used. Chemowas always checked with a senior member of staff (Participant 208)
Absolutely petrified! I double, triple & quadruple checkedeverything e patient route, drug hydration fluid (Participant 332)
Excited! In 1978 giving chemo for solid tumours was very new.Fascinating and keen to learn more (Participant 629)
Scary!! Seems ironic that you are in effect harming the patient by killingoff good cells in order to target the cancerous cells (Participant 429)
Confident and felt ready to administer chemotherapy but withobvious and sensible caution (Participant 1012)
It was a kind of scary experience to understand protocols and so muchstuff to keep in mind like patients’ blood results etc. But once used toit was easy to follow (Participant 705)
n ¼ total number of participants who made comments (some made both negative and positive comments).
F. Gibson et al. / European Journal of Oncology Nursing 17 (2013) 59e69 65
If the peripheral cannula or Hickman line failed to bleed back(Participant 1914)When administering a vesicant into a peripheral line in a very smalland squirmy child (Participant 1003)
Children being non-compliant or distressed and families beingunprepared for chemotherapy were also an issue:
Situation rushed. Did not know child or family, e.g. on PICU(Intensive Care) or another ward within unit when no chemo giveravailable. Family not fully prepared (Participant 1308)
Many nurses were concerned about quality of life issues, espe-cially the debate of palliation versus cure:
When patients are palliative but still receiving non-palliativetreatment that you know will make them sick and require inpa-tient treatment (Participant 1821)Concerned that family had been pressurised into agreeing to thechild receiving chemotherapy in the palliative phase of illnesse butstill gave the drugs as prescribed (Participant 2001)
The main logistical reasons for not wanting to administerchemotherapy involved inadequate paperwork, prescriptions,incomplete pre-chemotherapy checks, and the child not being ready:
Unable to find written consent for treatment or inadequate proof ofrequired investigations (Participant 0416)
Table 5Have you administered chemotherapy whilst you were pregnant?
Yes (n ¼ 49) Didn’t mind, happy that our practiceI felt satisfied that I was adequatelyIt was part of my job, I followed theHappy as only bolus via luer-lock sywouldn’t have liked even taking bedI think it should be the individual nuProbably more risk emptying urine p
No (n ¼ 33) Glad not to be administering it (PartI chose not to give chemo but I waswaste. I preferred not to give it, I felspillage (Participant 332)I felt that although no definite problWorried about the effects on my unb
‘Yes, but., No, but.’ (n ¼ 45) Did not want to risk handling chemoI had no choice, the ward was too bNo real issue about drugs already prrisk (Participant 1301)I did not give chemo drugs that needI would administer it if I had to but
Query about dose, confusion in notes about what chemo to give(Participant 1316)
Poor staffing and out of hour’s administration were alsohighlighted as reasons for not wanting to give chemotherapy. Thefinal logistical reason for not wanting to give chemotherapy wasdue to the drug having expired, precipitated or not beenreconstituted.
Personal reasons cited for not giving chemotherapy included:being pregnant, unsure and being unfamiliar with the treatmentprotocol. Most (n ¼ 291, 99%) would not administer chemotherapyif they did not want to. Only 62 (23%) always felt supported withthis decision. Colleagues who were reported as providing mostsupport were nursing staff (n ¼ 115), mainly from the nurse incharge, other chemotherapy givers and other nurses who were onthe same shift. Medical (n ¼ 75) and pharmacy (n ¼ 16) staff werealso identified as providing support.
Even though nurses stated that they felt supported in theirdecisions not to give chemotherapy, some made additionalcomments:
People won’t support you in not giving chemo unless you arepregnant and even then it depends which trust you work for(Participant 1906)Other nurses supported me. However response from specialistpharmacist and more senior nurses was scathing (Participant312)
was safe (Participant 720)protected by the PPE I used (Participant 117)safety guidelines and had no negative feelings regarding this (Participant 314)ringes and non-touch technique; wouldn’t have been so keen if ward based but thenpans etc. away (Participant 918)rses’ choice but also believe with good practice the risk is very small.ots.” (Participant 403)icipant 509)a second checker, i.e. didn’t handle cytotoxic product. I also did not handle cytotoxict I was ‘protecting’ my unborn child by not exposing my body to the risk of chemo
ems listed about administering when pregnant, it was safer not to (Participant 813)orn baby (Participant 210)but at times no option as no one else to do it (Participant 510)
usy and chemo had to be given, I just got on with it (Participant 632)epared. Avoided crushing tablets and making up chemo to prevent any
ed to be reconstituted e.g. capsules (Participant 1339)if other staff available to do so, I’d ask them (Participant 2103)

F. Gibson et al. / European Journal of Oncology Nursing 17 (2013) 59e6966
Many nurses also stated that not administering chemotherapywas not their decision to make:
I will make it clear that I have never not given chemo even though Isometimes disagree with it being given e it is my job (Participant1005)
Worries about chemotherapy
Nurses were asked to identify the areas of chemotherapyadministration that caused them most worry (Fig. 4). Nursesidentified a number of other worries regarding their chemotherapyrole such as making an error, the potential risks to themselves andwhether their chemotherapy knowledge was adequate and up-to-date. Being the only person on shift trained to administer chemo-therapy also led to worries as they felt unsupported and underpressure:
When lots of chemotherapy patients and chemotherapy adminis-tration and I am the only chemotherapy trained, no other chemo-therapy trained colleagues to support me (Participant 109)
There was no difference in the amount of worry according tofrequency of chemotherapy administration or level of educationbut nurses with an oncology/chemotherapy course had lessknowledge- and family support-worry (Table 6). The longernurses had been working in oncology the less knowledge-worry(rs ¼ �0.15, p ¼ 0.01), safety-worry (rs ¼ �0.28, p < 0.001), andfamily support-worry (rs ¼ �0.21, p < 0.001); and the longer theyhad been administering chemotherapy the less knowledge-worry(rs ¼ �0.19, p ¼ 0.001), safety-worry (rs ¼ �0.25, p < 0.001), andfamily support-worry (rs ¼ �0.23, p < 0.001). Frequency, educa-tion and the time factors were entered into stepwise multipleregression analysis to create models to explain the variance in the3 worry domains. The only factor that best predicted worry waslength of time delivering chemotherapy: Knowledge-worry,b ¼ �0.197, adjusted R2 ¼ 0.035 (df ¼ 275, p ¼ 0.001); safety-worry, b ¼ �0.232, adjusted R2 ¼ 0.05 (df ¼ 275, p < 0.001); andfamily support-worry, b ¼ �0.229, adjusted R2 ¼ 0.049 (df ¼ 275,p < 0.001).
Fig. 4. Frequency of worry. Footnote to Fig. 4: a. Your understanding of chemotherapy prescward; d. The risk of exposure to yourself; e. The risk of exposure on fertility/pregnancy;anaphylactic reactions; j. Accidental spillage; k. Disposal of cytotoxics; l. Giving informationemotionally; o. Patient distress about their treatment; p. Giving chemotherapy to a child on
Attitudes
Table 7 outlines the responses to the 21 statements related toattitude to chemotherapy practice. Most responded that givingchemotherapy did not make them feel guilty (n ¼ 199; 71%), thatthey knew the precautions to prevent risks (n ¼ 175; 63%) and thatpatients should be informed of their treatment (n ¼ 267; 95%).
The respondents were given an opportunity to add furthercomments about the above statements relating to attitudes.Fifty-nine nurses made a further comment regarding handling/administering chemotherapy when pregnant. Many were unsurewhether there was a risk to the unborn baby, with some com-menting that more research should be carried out in this area andthat they would not want to handle chemotherapy if they werepregnant:
I feel this is unknown quantity and more research needs to be donein this area. Although safety measures are in place for safe handlingof cytotoxics, there are always risks and most mothers would notwant to take any risk with an unborn baby (Participant 806)
Others thought that there was not a risk as long as the rightprecautions were taken:
If an individual follows hospital policy then there should be noharmful effects to the unborn baby (Participant 413)
There was no difference in attitude according to frequency ofchemotherapy administration (education: H ¼ 1.53, p ¼ .68;emotion: H ¼ 3.06, p ¼ .38; communication: H ¼ 2.37, p ¼ 0.50);level of education (education: U ¼ 9443.5, p ¼ 0.63; emotion:U¼ 9447, p¼ 0.63; communication:U¼ 9839.5, p¼ 0.98) or havinga specialist oncology/chemotherapy course (education: U ¼ 8524,p ¼ 0.21; emotion: U ¼ 8966.5, p ¼ 0.55; communication:U ¼ 9050.5, p ¼ 0.59). However, the longer nurses had beenworking in oncology the more positive attitude to education(rs ¼ 0.24, p < 0.001), emotional issues (rs ¼ 0.20, p ¼ 0.001), andcommunication (rs ¼ 0.22, p < 0.001); and the longer nurses hadbeen administering chemotherapy, the more positive attitudetowards education (rs¼ 0.23, p< 0.001), emotional issues (rs¼ 0.17,p ¼ 0.005) and communication (rs ¼ 0.23, p < 0.001).
Frequency, education and the time factors were entered intostepwise multiple regression analysis to create models to explainthe variance in the attitude domains. The only factor that best
riptions/protocols; b. Handling cytotoxic drugs; c. Reconstituting chemotherapy on thef. Extravasation; g. Treatment of side-effects; h. Patient allergic reactions; i. Patientabout treatments; m. Giving information about side-effects; n. Supporting the familyanother ward in your hospital; q. Education/knowledge deficits of other nursing staff.

Table 6A comparison of worry according to frequency of chemotherapy administration and level of education.
Frequency of chemotherapyadministration
Level of educationa Specialist qualificationb
H P value U P value U P value
Knowledge-worry 4.13 0.25 9644.5 0.23 8363.5 0.02Safety-worry 3.17 0.37 10 154.5 0.63 8833.5 0.12Family support-worry 5.28 0.152 10 262.5 0.74 8569 0.05
a Degree level or below.b Formal oncology or chemotherapy course; either ENB (or equivalent), diploma, degree or higher degree.
F. Gibson et al. / European Journal of Oncology Nursing 17 (2013) 59e69 67
predicted attitude to education was the number of years adminis-tering chemotherapy: b ¼ 0.199, adjusted R2 ¼ 0.036 (df ¼ 267,F ¼ 10.9, p ¼ 0.001). Only the number of years working in oncologypredicted attitudes to emotional issues: b ¼ 0.169, adjustedR2 ¼ 0.005 (df ¼ 267, F ¼ 7.8, p ¼ 0.005); but a two-factor modelbest predicted attitudes to communication: number of yearsworking in oncology (b ¼ 0.228; p ¼ 0.05) and number of yearsadministering chemotherapy (b ¼ 0.187; p ¼ 0.07), adjustedR2 ¼ 0.060 (df ¼ 268, F ¼ 6.7, p < 0.001).
Discussion
We report the results of a national survey of nurses’ experiences,attitudes and worries when administering chemotherapy to chil-dren. The current survey was based on a previous study with adultcancer nurses (Verity et al., 2008). We found striking similaritiesbetween the nurses’ experiences, whether they cared for children/young people or adults. Nurses in both studies described howscared theywerewhen first taking on this role, how theywere overcautious and nervous about making a mistake even though theyhad been assessed as competent in the role. Experience and prac-tice had a positive effect, with nurses reporting increased confi-dence, and amove away from the task itself tomore concerns aboutthe system and overall safety, and the effects on the child. This shiftin perspective has been described by Hinds (2004) as a feature thatdistinguishes new and experienced children’s cancer nurses.Benner (2001) also noted that more experienced nurses knew thatthe most relevant task in clinical care is to relieve suffering. While
Table 7Attitude towards chemotherapy administration.
Attitude statements
a. When presented with complications caused by chemotherapy I feel confident in myb. It causes me distress when I see patients affected by chemotherapy I have given thec. I know enough about chemotherapy to answer patients’ questions alreadyd. When presented with emergencies caused by chemotherapy I do not feel confidente. Chemotherapy causes more harm than goodf. I handle and administer chemotherapy without hurryingg. I handle and administer chemotherapy without interruptionsh. Giving chemotherapy to patients makes me feel guiltyi. I know that all precautions are taken to ensure that I am not at risk from chemotherj. Patients should always be informed about their treatmentk. I know that when I administer chemotherapy patients have understood as much asl. I always feel that I have supported patients during their chemotherapy treatmentm. Giving chemotherapy impedes communication with patientsn. It is easy to inform patients about their treatment but harder to help them emotiono. I focus entirely on the practical aspects of the task when giving/handling chemothep. Administering/handling chemotherapy is no different than administering/handlingq. Talking with children/young people about their treatments is stressfulr. Children/young people and their family know more about their chemotherapy thans. Administering/handling chemotherapy is a satisfying part of the rolet. I do not find administering/handling chemotherapy a challenging part of my roleu. Handling/administering chemotherapy when pregnant is harmful to the unborn bab
anxiety alleviated over time for many nurses, seeing the effects ofchemotherapy on patients remained a distressing aspect of the role.More research is needed to understand the reasons for this, whichmight then lead to interventions tailored to the specific stressor.
Knowledge for qualified nurses is derived through a range ofpost-qualifying and on-going continuing education. Ninety-nineper cent of nurses in this survey had undertaken post-qualifyingeducation related to chemotherapy. While only 64% had attendeda specific oncology course, in some this was a course focusing onadults with cancer rather than children. Andam and Silva (2008)described the development of a competency-based educationprogramme for children’s cancer nurses in North America. Whenthey attended the Oncology Nursing Society’s oncology course theyfound it did not address issues related to protocols used withchildren, growth and development concerns or communicationwith the family. This was the driving force for developing specificeducation for thosewho care for children and young people. Nurseswho had only undertaken adult cancer training may therefore nothave comprehensive enough knowledge to be competent in look-ing after children receiving chemotherapy. However, the currentstudy did not find a relationship between level of education, atti-tude or worry. This may reflect the simplistic way in which weclassified level of education rather than delineating the on-goingnature of education in nursing.
Even with baseline oncology education, the continual advancesin medication and treatment regimens necessitate regular knowl-edge updates, especially as protocols become increasingly complex.‘On the job’ learning (the preferred mode of learning by 50% nurses
n Number and percentage ofrespondents
Always/often Occasionally/never
competency 279 269 (92) 20 (8)m 283 54 (19) 229 (81)
283 263 (93) 20 (7)in my competency 283 20 (7) 263 (93)
280 11 (4) 269 (97)283 247 (88) 36 (13)283 194 (68) 89 (31)283 4 (1.4) 279 (99)
apy 282 258 (91) 24 (9)283 283 (100) 0
wish about their treatment 278 274 (96) 10 (4)284 276 (49) 8 (3)281 20 (7) 261 (92)
ally 281 162 (58) 119 (42)rapy 279 133 (47) 146 (53)intravenous antibiotics 276 50 (18) 226 (82)
281 63 (23) 238 (78)I do 280 14 (5) 266 (96)
279 79 (29) 200 (71)278 72 (26) 206 (74)
y 254 79 (31) 175 (69)

F. Gibson et al. / European Journal of Oncology Nursing 17 (2013) 59e6968
in our survey) does not guarantee correctness or relevance ofknowledge. Similarly, making a protocol available on the ward doesnot guarantee nurses are reading and understanding them(Bradshaw, 1998). It is important therefore that there is a formalstructure for ensuring competency is maintained. Our surveyindicated only 36% of nurses had completed an updated workbookand only 45% had done so yearly. This suggests there may be nursesadministering chemotherapy in the UK without up-to-dateknowledge. The Children’s Cancer Measures (NCAT, 2011) arequite specific that the RCN competencies shape chemotherapyrelated education, however they are less specific about how regularthis knowledge should be updated.
In results similar to those of Verity et al. (2008), the currentstudy found a major worry expressed by nurses was administrationof chemotherapy at night when minimal support was available ifsomething went wrong. Nurses reported that interruptions whileadministering chemotherapy was also a worry in case distractionled to medication errors. The need for concentration whenadministering medications has been central to current changes inpolicy dictated by the National Patient Safety Agency (NPSA). Thisdetailed howmedications must be dispensed on the ward, with thespecific aim to reducing error caused by distractions (NCAG, 2009).In England themajority of chemotherapy is prepared by CentralisedIntravenous Additive Service (CIVAS) teams, which has reduced thenumber of medication errors (NCAG, 2009). However, on rareoccasions nursesmay be required to prepare chemotherapy. In suchsituations most nurses (68%) responded that they would contactthe on-call pharmacy. Despite this, many nurses reported that theyneeded more education about preparing chemotherapy implyingthat out of hours support was not always available.
While wards must provide a dedicated area so chemotherapycan be dispensed safely, an additional anxiety expressed by nurseswas administration of chemotherapy outside the haematology/oncology unit, such as intensive care. Nurses expressed that theywere unfamiliar with the environment and patient, and were oftenuncertain about the child’s safety, e.g., nurses in non-oncology unitsknowing how to manage spillages and excreta. However, attemptsto train non-oncology nurses to be competent to deliver chemo-therapy are challenged by nurses not wanting to develop a skill thatis not going to be utilised, and hence updated, on a regular basis.Often the education courses available are considered too detailedfor need (Andam and Silva, 2008). The Children’s Cancer Measures(National Cancer Action Team [NCAT], 2011) have been helpful herein recommending four levels of training for nurses working withchildren receiving chemotherapy. The levels identify how differentelements of training are required in different settings, such assenior nurses in a cancer centre who may also have a role inteaching, to nurses administering approved low-risk treatments inthe community. Level 3 training is aimed at those nurses who donot need to administer chemotherapy but who need to understandfor example the safety aspects, side-effects and patient/carerinformation required to support the care of those on treatment.This level may be suitable for supporting smaller teams ofchemotherapy trained nurses in a shared care unit.
The current study identified times when nurses did not want togive chemotherapy. The most frequently cited reason being whenthe child is too sick. This may reflect the dichotomy associated withchemotherapy administration: trained to heal but to do so requireadministration of a highly toxic substance. Logically nurses knowchemotherapy is beneficial but emotionally it is difficult, anda cause of role-related stress, to see the child experience the arrayof side-effects that inevitably accompanies chemotherapy (Hinds,2000). Education and experience enables nurses to becomecompetent but it seems the emotional aspect of the role remains.Similar to Hinds, 2004, the more experienced nurses learnt to
manage the emotional stressors of the role and initiate copingresponses that diminished these stressors.
Limitations
A limitation of our study is we only evaluated the experiencesof nurses working in principal treatment centres and not thosewho administer chemotherapy in shared care units. It couldbe hypothesised that nurses who do not give chemotherapyas regularly as those in the current study (lower frequency ofadministration was often in more senior nurses, i.e., more experi-enced) and do not have experienced colleagues available forsupport, would report a different experience, express more worryand have a less positive attitude. Themethod of recruitment used inthe current survey was chosen to maximise response rates but thisprecluded shared care units due to the regulatory approval thatwould be required. Future work exploring the work of nurses whoadminister chemotherapy needs to adopt a different strategy toreflect the role-related stress of shared care nurses. Some of theattitude statements and response choices were found difficult andconfusing to complete: this may have affected responses.
Implications
The results from the current study have a number of clinicalimplications. Anecdotally, junior nurses are reluctant to developand take on the chemotherapy role. While the reasons for this areunclear, our study shows a relationship between worry and expe-rience. It will be important to acknowledge the concerns of nursesnew to this role, and assure them that experience will help toreduce their anxiety. Being introduced to the role early in theircancer career, in terms of knowledge required, observing practiceand becoming gradually introduced to what the role will requirewill have benefits. Competency-based training, as recommended inthe Children’s Cancer Measures (NCAT, 2011), and experience, arecombined approaches to reducing anxiety. It is important that thenovice chemo administrator is given appropriate levels of support.Support from senior colleagues, and pharmacists was highlightedas being crucial by all nurses in this survey, and would suggest thatthis would need to be provided in any clinical unit where chemo-therapy is administered to children and young people. Educationand training was in place for the study participants, but the timingof updateswas less clear, and no specific guidance on this is given inthe Children’s Cancer Measures although it is specified in Chemo-therapy Measures for those working in adult practice. Nationalclarification on this and standardisation of practice would be ofvalue to support children’s nurses throughout their professionalnursing career.
Conclusion
Ensuring quality and safety in relation to drug treatments wasa key strand of the UK Cancer Reform Strategy (DH, 2007). Thedevelopment of services in a sustainable way for the future toensure quality and safety is assured will be determined by col-lecting evidence on changes in the chemotherapy workforce,including education, training and assessment of clinical compe-tence. Knowing more about how nurses experience this aspect oftheir role, and about the environments they work in, will enableeducational programmes to remain current and responsive.
Funding
This study was funded by CLIC Sargent.

F. Gibson et al. / European Journal of Oncology Nursing 17 (2013) 59e69 69
Conflict of interest statement
No conflict of interest has been declared by the author(s).
Acknowledgements
Thanks to Rachel Hollis and Wendy McNally for reviewing ourmanuscript and providing constructive comments.
References
Andam, R., Silva, M., 2008. A journey to pediatric chemotherapy competence.Journal of Pediatric Nursing 23 (4), 257e268.
Benner, P., 2001. From Novice to Expert: Excellence and Power in Clinical NursingPractice, Commemorative Edition ed. Prentice Hall Health, Upper Saddle River, NJ.
Bradshaw, A., 1998. Defining ’competency’ in nursing (Part II): an analytical review.Journal of Clinical Nursing 7 (2), 103e111.
Delvaux, N., Razavi, D., Farvacques, C., 1988. Cancer careea stress for healthprofessionals. Social Science & Medicine 27 (2), 159e166. 1982.
Department of Health, 2007. The Cancer Reform Strategy. The Stationery Office,London.
Hinds, P.S., 2000. Fostering coping by adolescents with newly diagnosed cancer.Seminars in Oncology Nursing 16 (4), 317e334.
Hinds, P.S., 2004. Adolescent-focused oncology nursing research. Oncology NursingForum 31 (2), 281e287.
Hinds, P.S., Fairclough, D.C., Dobos, C.L., Greer, R.H., Herring, P.L., Mayhall, J., et al.,1990. Development and testing of the stressor scale for pediatric oncologynurses. Cancer Nursing 13 (6), 354e360.
Hinds, P.S., Srivastava, D.K., Randall, E.A., Green, A., Stanford, D., Pinlac, R., et al.,2003. Testing the revised stress-response sequence model in pediatric oncologynurses. Journal of Pediatric Oncology Nursing 20 (5), 213e232.
Hooker, L., Palmer, S., 1999. Administration of chemotherapy. In: Gibson, F.,Evans, M. (Eds.), Paediatric Oncology Nursing: Acute Care Nursing. WhurrPublishers, London, pp. 22e58.
McCray, N.D, 1997. Psychosocial and quality of life issues. In: Otto, S. (Ed.), OncologyNursing. St Louis, Mosby.
National Cancer Action Team, 2011. Manual for Cancer Services: Children’s CancerMeasures Version 2.0. National Cancer Peer Review Programme. DH, London.
National Chemotherapy Advisory Group, 2009. Chemotherapy Services in England:Ensuring Quality and Safety. Department of Health, London.
National Confidential Enquiry into Patient Outcome and Death, 2008. For Better, forWorse? NCEPOD, London.
National Institute for Health and Clinical Excellence, 2005. Guidance on CancerServices: Improving Outcomes in Children and Young People with Cancer. NICE,London.
Pike, S., Gibson, F., 1991. A programme to support your extended role. Chemo-therapy training for paediatric nurses. Professional Nurse 6 (7), 362e364.
Price, J., McShane, B., 2002. Administration of chemotherapy: evaluating a frame-work for developing practice. Paediatric Nursing 14 (8), 14e18.
Ream, E., Gibson, F., 2007. Collaboration: working together or cooperating with theenemy? European Journal of Oncology Nursing 11 (2), 104e105.
Royal College of Nursing, 2005. Competencies: an Integrated Framework forTraining Programmes in the Safe Administration of Chemotherapy to Childrenand Young People. RCN, London.
Royal College of Nursing, 2010. RCN Competences: an Integrated Career andCompetence Framework for Nurses Working in the Field of Children and YoungPeople’s Cancer Care. Royal College of Nursing, London.
Verity, R., 2002. Administring Cytotoxic Chemotherapy: the Nurses Perspective.University of Surrey.
Verity, R., Wiseman, T., Ream, E., Teasdale, E., Richardson, A., 2008. Exploring thework of nurses who administer chemotherapy. European Journal of OncologyNursing 12 (3), 244e252.
Wiseman, T., Verity, R., Ream, E., Alderman, E., Richardson, A., 2005. Exploring theWork of Nurses Who Administer Chemotherapy; a Multi-method Study. King’sCollege London, London.