Filipino Nurses' Spirituality and Provision of ... - CiteSeerX
19
Clinical Nursing Research 1–19 © The Author(s) 2015 Reprints and permissions: sagepub.com/journalsPermissions.nav DOI: 10.1177/1054773815590966 cnr.sagepub.com Article Filipino Nurses’ Spirituality and Provision of Spiritual Nursing Care Leodoro J. Labrague, MAN, BSN, RN 1 , Denise M. McEnroe-Petitte, PhD, MSN, BSN, AS, RN 2 , Romeo H. Achaso Jr., BSN, RN 3 , Geifsonne S. Cachero, BSN, RN 3 , and Mary Rose A. Mohammad, BSN, RN 3 Abstract This study was to explore the perceptions of Filipino nurses’ spirituality and the provision of spiritual nursing care. A descriptive, cross-sectional, and quantitative study was adopted for this study. The study was conducted in the Philippines utilizing a convenience sample of 245 nurses. Nurses’ Spirituality and Delivery of Spiritual Care (NSDSC) was used as the main instrument. The items on NSDSC with higher mean scores related to nurses’ perception of spirituality were Item 7, “I believe that God loves me and cares for me,” and Item 8, “Prayer is an important part of my life,” with mean scores of 4.87 (SD = 1.36) and 4.88 (SD = 1.34), respectively. Items on NSDSC with higher mean scores related to the practice of spiritual care were Item 26, “I usually comfort clients spiritually (e.g., reading books, prayers, music, etc.),” and Item 25, “I refer the client to his/her spiritual counselor (e.g., hospital chaplain) if needed,” with mean scores of 3.16 (SD = 1.54) and 2.92 (SD = 1.59). Nurse’s spirituality correlated significantly with their understanding of spiritual nursing care (r = .3376, p ≤ .05) and delivery of spiritual nursing care (r = .3980, p ≤ .05). Positive significant correlations 1 Sultan Qaboos University, Muscat, Sultanate of Oman 2 Kent State University at Tuscarawas, New Philadelphia, OH, USA 3 Samar Provincial Hospital, Samar, Philippines Corresponding Author: Leodoro J. Labrague, Department of Fundamentals and Administration, College of Nursing, Sultan Qaboos University, Muscat, Sultanate of Oman. Email: [email protected] 590966CNR XX X 10.1177/1054773815590966Clinical Nursing ResearchLabrague et al. research-article 2015 at PENNSYLVANIA STATE UNIV on February 20, 2016 cnr.sagepub.com Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Filipino Nurses' Spirituality and Provision of ... - CiteSeerX

Clinical Nursing Research 1 –19
© The Author(s) 2015Reprints and permissions:
sagepub.com/journalsPermissions.navDOI: 10.1177/1054773815590966
cnr.sagepub.com
Article
Filipino Nurses’ Spirituality and Provision of Spiritual Nursing Care
Leodoro J. Labrague, MAN, BSN, RN1, Denise M. McEnroe-Petitte, PhD, MSN, BSN, AS, RN2, Romeo H. Achaso Jr., BSN, RN3, Geifsonne S. Cachero, BSN, RN3, and Mary Rose A. Mohammad, BSN, RN3
AbstractThis study was to explore the perceptions of Filipino nurses’ spirituality and the provision of spiritual nursing care. A descriptive, cross-sectional, and quantitative study was adopted for this study. The study was conducted in the Philippines utilizing a convenience sample of 245 nurses. Nurses’ Spirituality and Delivery of Spiritual Care (NSDSC) was used as the main instrument. The items on NSDSC with higher mean scores related to nurses’ perception of spirituality were Item 7, “I believe that God loves me and cares for me,” and Item 8, “Prayer is an important part of my life,” with mean scores of 4.87 (SD = 1.36) and 4.88 (SD = 1.34), respectively. Items on NSDSC with higher mean scores related to the practice of spiritual care were Item 26, “I usually comfort clients spiritually (e.g., reading books, prayers, music, etc.),” and Item 25, “I refer the client to his/her spiritual counselor (e.g., hospital chaplain) if needed,” with mean scores of 3.16 (SD = 1.54) and 2.92 (SD = 1.59). Nurse’s spirituality correlated significantly with their understanding of spiritual nursing care (r = .3376, p ≤ .05) and delivery of spiritual nursing care (r = .3980, p ≤ .05). Positive significant correlations
1Sultan Qaboos University, Muscat, Sultanate of Oman2Kent State University at Tuscarawas, New Philadelphia, OH, USA3Samar Provincial Hospital, Samar, Philippines
Corresponding Author:Leodoro J. Labrague, Department of Fundamentals and Administration, College of Nursing, Sultan Qaboos University, Muscat, Sultanate of Oman. Email: [email protected]
590966 CNRXXX10.1177/1054773815590966Clinical Nursing ResearchLabrague et al.research-article2015
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

2 Clinical Nursing Research
were found between understanding of spiritual nursing care and delivery of spiritual nursing care (r = .3289, p ≤ .05). For nurses to better provide spiritual nursing care, they must care for themselves through self-awareness, self-reflection, and developing a sense of satisfaction and contentment.
Keywordsspirituality, spiritual care, Filipino nurses, holistic care
Introduction
The provision of spiritual nursing care is considered a professional mandate for all nurses (McSherry, 2006; McSherry & Jamieson, 2011; McSherry & Ross, 2010; Narayanasamy, 2010, 2006) and an important aspect of nursing care (American Nurses Association, 2001; Catholic Health Association of Canada and the Canadian Association for Pastoral Practice and Education, 2000; International Council of Nurses, 2012; Joint Commission on Accreditation of Healthcare Organizations, 2005; Philippine Nurses Association, 2003; United Kingdom Central Council for Nurses, Midwives, and Health Visitors, 2000). Mounting evidence has shown that nurses are likely to provide spiritual nursing care effectively, tend to have favorable attitudes toward spiritual care, and are more sensitive to the spiritual needs of patients if they have a deep understanding about their own spirituality (Belcher & Griffiths, 2005; Cavendish et al., 2006; Chan, 2010; Chung, Wong, & Chan, 2007). Spirituality is not only important in coping with dis-ease but also has the potential to improve the quality of life. Such areas would include that of one’s resolutions; meaning and purpose in life; relief of dis-ease-related symptoms; decreased symptoms of depression, anxiety, and overall distress; enhanced pain management; improved surgical outcomes; reduced risks of substance abuse and suicide; and lower mortality rates in patients (Gaskamp, Sutter, & Meraviglia, 2006; George, Larson, Koenig, & McCullough, 2000; Hart, 2008; Koenig, George, & Titus, 2004; Larson & Larson, 2003; McSherry & Jamieson, 2011; Narayanasamy, 2007). It is therefore paramount that nurses integrate spirituality into their nursing prac-tice while being aware of and at ease with their own spirituality.
Review of Literature
Nurse researchers in particular have affirmed and considered spirituality and spiritual care to be fundamental aspects of a holistic nursing care approach (Hart, 2008; McSherry, 2006; McSherry & Jamieson, 2011; McSherry &
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

Labrague et al. 3
Ross, 2010; Narayanasamy, 2006, 2010). In this approach, nurses ascend that spirituality is an integrative element of people and believe that many patients have spiritual needs. In addition, numerous nursing and health care organiza-tions locally and internationally recognize the essential role of spirituality and spiritual nursing care. Internationally, the United Kingdom Central Council for Nurses, Midwives, and Health Visitors’ (2000), the American Nurses Association (2001), and the International Council of Nurses (2012) stated that a practicing nurse must provide nursing care that promotes an environment in which human rights, values, customs, and spiritual beliefs of patients are respected. Locally, the Philippine Nurses Association (2003) emphasized the provision of a spiritual environment and spiritual care as a vital component for nursing care and responsibilities of the nurse. Multiple health care organizations such as the Joint Commission on Accreditation of Healthcare Organizations (2005) and the Catholic Health Association of Canada and the Canadian Association for Pastoral Practice and Education (2000) required the health care team to consider patients’ physical, mental, spiritual, and emotional beliefs, and to respect patients’ cultural and spiritual practices.
A plethora of empirical approaches in the nursing literature attempt to define spirituality; however, although considered as universal phenomenon, this concept remains ambiguous and difficult to define (Chan, 2010; Chung et al., 2007; McSherry, 2006; McSherry & Jamieson, 2011; Narayanasamy, 2010). Chung, Wong & Chan (2007) argued that although there is increasing amount of research exploring characteristics of spirituality, the focus has not been directed at defining what is meant by spirituality and spiritual care. Nevertheless, spirituality, according to O’Brien (2013), is an individual’s atti-tude and beliefs related to transcendence or/and of nature. It goes beyond religion and religious practices (MacLaren, 2004); usually is perceived as being personal and subjective (McSherry, 2006; McSherry & Ross, 2010), intangible, and multi-dimensional (Tanyi, 2002); and is influenced by culture (Baldacchino, 2006; Chan, 2010). Chung et al. (2007) defined spirituality as a relationship with the self and with dimensions beyond ourselves. In a more recent study, Weathers, McCarthy, and Coffey (2015) defined spirituality as “a way of being in the world in which a person feels a sense of connectedness to self, others, and/or a higher power or nature; a sense of meaning in life; and transcendence beyond self, everyday living, and suffering” (p. 15).
Studies have shown that the way a nurse relates to his or her own spiritual-ity is an important predictor to the quality of the spiritual nursing care he or she will provide (Belcher & Griffiths, 2005; Cavendish et al., 2006; Chan, 2010; Chan et al., 2006; Chung et al., 2007; Hart, 2008). Nurses’ spirituality is influenced by their personal values, experiences, beliefs, and practices
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

4 Clinical Nursing Research
(MacLaren, 2004). It is therefore paramount for nurses to have a deep under-standing of themselves, their own spiritual beliefs, values, and convictions. This understanding allows the nurse to remain focused on the patient and remain nonjudgmental when dealing with their specific spiritual concerns. It can be especially important when the patient’s spiritual beliefs vary from those of the health care professional (Anandarajah & Hight, 2001). Several authors support the claim that the nurses’ own spirituality is essential when providing spiritual care to patients (Belcher & Griffiths, 2005; Cavendish et al., 2004; Chan, 2010; Chung et al., 2007). For instance, Chung et al. (2007) showed that Hong Kong nurses’ perceptions of their own spirituality seemed to influence the delivery of spiritual nursing care to their patients. Similarly, Cavendish et al. (2004) and Belcher and Griffiths (2005) asserted that nurses’ spirituality and their knowledge base of spiritual nursing care are important factors that support the delivery of spiritual care to patients and their families.
Spiritual care is a dynamic concept that demonstrates the integration of unique aspects of providing care to others (Ramezani, Ahmadi, Mohammadi, & Kazemnejad, 2014). Spiritual care, in the context of nursing shows con-cern for the care a nurse delivers relative to the religious, existential, and spiritual needs of their patients, including their questions and experiences of its meaning and purpose (Pesut, 2006; Ross, 2006). Qualities of spiritual nursing care include developing of a caring relationship, establishing con-nectedness with the recipient, showing concern or through sharing of com-mon experiences and/or similar spiritual beliefs (Carr, 2008; Grant, 2004; McSherry, 2011; Tanyi, 2002). However, spiritual nursing care is not neces-sarily about doing; it is also, or more importantly, about being—being pres-ent, being respectful, being loving (Grant, 2004; Tuck, Wallace, & Pullen, 2001).
The review of the literature on spirituality suggests that spirituality and spiritual care are important aspects of health and nursing care (McSherry & Jamieson, 2011; Ramezani et al., 2014). Literature review by Visser, Garssen, and Vingerhoets (2010) showed that spirituality was highly associated with a higher well-being. Evidence also links spiritual and religious practices to the reduced onset of physical and mental illnesses, reduced mortality, and the likelihood of recovery from or adjustment to physical and mental illness (George et al., 2000). In one study among low-income men who were expe-riencing metastatic prostate cancer, the presence and practice of spirituality was associated with perceptions of a better quality of life and psychosocial function (Zavala, Maliski, Kwan, Fink, & Litwin, 2009). In another study among patients with schizophrenia, spirituality and religiosity additionally had an important influence on their overall quality of life (Shah et al., 2011).
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from
Labrague et al. 5
Spirituality has been associated with high levels of physical, psychologi-cal, and social health and well-being. Specifically, spirituality may be seen as a powerful source of coping among patients with health-related problems such as chronic illness and advanced diseases (Narayanasamy, 2007). Spirituality may provide hope and aid for adaptation to illness for individuals of all ages (Gaskamp et al., 2006), and a decrease in symptoms of depression, anxiety, and overall distress (Koenig et al., 2004). Other studies have sug-gested that spirituality is not only important in coping with disease, but also has the potential to improve the quality of life, relieve symptoms, lower mor-tality rates, and provide a high patient satisfaction rate (Clark, Drain & Malone, 2003; McSherry & Jamieson, 2011). Research by Labrague (2012) has suggested that spirituality could be an essential part of a patients’ journey to overall recovery and well-being.
Nurses are the largest group of health care professionals who undertake administering patient care, including that of spiritual care (Baldacchino, 2008, Narayanasamy, 2004). Moreover, the very nature of nursing practice places nurses in vital positions to foster peaceful resolutions in their patients’ lives by assisting them with their spiritual needs (Tanyi, 2002). Recent studies have shown that there is a lack of knowledge and general confusion regarding nurses’ perceptions of and delivery of spiritual care and spirituality (Chan et al., 2006; Christensen & Turner, 2008; McSherry & Jamieson, 2011; Narayanasamy & Owens, 2001; Ozbasaran, Ergul, Temel, Aslan, & Coban, 2011). The need for nurses to provide spiritual care has been emphasized in research, consequently, little is known in the literature highlighting spirituality and provision of spiritual care among Filipino nurses. Given the paucity of research there is a need to explore the views of nurses about spirituality and spiritual care. Gaining insights into how Filipino nurses perceive this integral dimension of nursing care could help to improve and shape nursing practice.
Philippine Nursing Education
Nursing in the Philippines started in the 1880s and the “Philippine Nursing Act” has specifically defined the scope of nursing (Philippine Board of Nursing, 2009; Tupas, 1952). Currently, the Philippine nursing program is a 4-year program consisting of general education and professional courses. Within the context of the curriculum, nursing education focuses on caring as its foundation. The program subscribes to the following core values, which are vital components in the development of a professional nurse and are emphasized in the bachelor of science in nursing (BSN) program: (a) love of God, (b) caring as the core of nursing, (c) love of the people, and (d) love of the country (Philippine Board of Nursing, 2009).
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

6 Clinical Nursing Research
Spirituality Among Filipino Culture
The Philippines is the fifth largest Christian country, with about 87% of the population being adherents (Pew Research and Religion and Public Life Project, 2011). It is also one of two predominantly Roman Catholic nations in Asia and is the third largest Catholic country in the world. Based on the Pew Research and Religion and Public Life Project (2011), an estimated 87% of Filipinos are Christians of whom 80.9% are Roman Catholic, while more than 6 million Filipinos, or about 7% of the population, are non-Christians, most of whom are Muslim. The majority of Filipinos believe that praying is a way of communicating between a person and the Supreme Creator. Other spiritual practices among Filipinos include daily Eucharist or attendance at mass and the use of sacramental or religious aids in the spiritual life, such as rosary beads/prayer, holy images, or candles.
Aim of the Study
The aim of this study was to determine the perceptions and correlations of Filipino nurses of their own spirituality and their understanding of, and provi-sion of, spiritual nursing care.
Method
Research Design
A descriptive, cross-sectional, and quantitative study was adopted for this study. Cross-sectional studies involved a single examination of phenomena in a certain population at a given time (Polit & Beck, 2013). This study design was appropriate as the main objective of the investigation was to explore a certain group of nurses’ spirituality and spiritual care.
Study Participants
The study was conducted at six hospitals in the western part of Samar, Philippines. Utilizing convenience sampling, 300 nurses were invited partici-pants in the investigation and 245 responded (81.67% response rate). Participants had to be currently working, understand and speak English, and be willing to participate in the study.
Measurements
The Nurses’ Spirituality and Delivery of Spiritual Care (NSDSC) scale devel-oped by Chung et al. (2007) was the primary instrument for the study. This
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from
Labrague et al. 7
27-item questionnaire captured nurses’ spirituality and their understanding and practice of spiritual care, which was rated on a 5-point Likert-type scale ranging from strongly agree to strongly disagree. Permission had been obtained for use of the instrument from the author.
The NSDSC is subdivided into four subscales namely, Beyond Dimension (Items 7-9), Self-Dimension (1-6, 15-21), Understanding of Spiritual Care (10-14), and Practice of Spiritual Care (22-27). In this study, the first two subscales (the Self-Dimension and Dimension Beyond Self) were combined because they form the area of nurses’ spirituality after being reviewed by three experts on spirituality research. In scoring, the higher the scores indi-cated a higher perception of spirituality and understanding and practice of spiritual care. In the current study, the original English version of the tool was utilized because English is one the official languages of the country.
The Cronbach’s alpha coefficient of the NSDSC was .80, which showed a reasonable level of reliability based on the previous study (Chung et al., 2007). The alpha coefficient reported for this study was .91.
Ethical Considerations
The Health Ethics Committee of Samar State University reviewed and approved the study protocol. To ensure confidentiality and anonymity of the participants, codes were used instead of their names in the demographic forms and survey instruments. Moreover, the purpose, nature, and risks of the study were fully disclosed to the participants and they were asked to sign an informed consent. Data were collected over a period of 5 months from January 8 to May 7, 2013.
Data Analysis
Data collected were entered in Microsoft Excel and were analyzed with SPSS using version 16 (SPSS Inc., Chicago, IL, USA) for descriptive and inferen-tial statistics. Descriptive statistics used included percentages, means, and frequencies. Pearson’s correlation coefficient was utilized to test the relation-ships between the samples’ of spirituality, understanding of spirituality, and providing of spiritual care. Fisher’s t test was utilized to determine the sig-nificance of correlations. A p value of equal to or less than .05 was considered statistically significant.
Results
More than half of the respondents (n = 162, 66.12%) were female and about three fourths (n = 177, 72.24%) were between 21 and 29 years old. Most were
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

8 Clinical Nursing Research
Table 1. Respondents’ Characteristics (n = 245).
Characteristics Frequency %
Sex Male 83 33.87 Female 162 66.12Age 21-29 177 72.24 30-39 19 7.75 40-49 21 8.57 50-59 23 9.39 60-69 5 2.04Religion Roman Catholic 208 84.89 Born again Christians 26 10.61 Iglesia Ni Kristo 11 4.49Work duration (in years) Less than 1 year 145 59.18 1-5 66 26.94 6-10 7 2.86 11-25 24 9.79 26-40 3 1.22Working position Staff nurse 213 86.94 Head nurse 32 13.06Received spiritual care training No 245 100 Yes 0 0
Roman Catholic (n = 208, 84.89%) while 15.10% (n = 37) belonged to other religions. The amount of experience revealed that more than half of the respondents (n = 145, 59.18%) were employed for less than year. Of the 245 participating nurses, 86.94% (n = 213) were employed in a staff nurse posi-tion while the remaining 32 participating nurses were employed as head nurses (see Table 1).
The mean scores for the NSDSC are presented in Table 2. The items with the higher mean scores related to the nurses’ perception of spirituality. Item 7, “I believe that God loves me and cares for me,” and Item 8, “Prayer is an important part of my life,” revealed mean scores of 4.87 (SD = 1.36) and 4.88 (SD = 1.34), respectively. The Item 5, “I don’t feel any relationship between my values and what I do,” and Item 20, “I feel fragmented and have no energy
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

Labrague et al. 9
Table 2. Responses on the NSDSC Tool.
Items Minimum Maximum M SD
Factor 1: Perception of spirituality 1. I’m satisfied with my life when I
achieved my set goals.1.00 5.00 4.59 1.67
2. I still feel life is positive when I’m facing uncertainties.
1.00 5.00 4.40 1.98
3. I find real purpose for my life. 1.00 5.00 4.41 1.34 4. I set goals for myself even in times
of difficulty.1.00 5.00 4.54 1.35
5. I don’t feel any relationship between my values and what I do.a
1.00 5.00 2.03 1.76
6. I still feel disturbed when I think about bad experiences I’ve had.a
1.00 5.00 2.73 1.45
7. I believe that God loves me and cares for me.
1.00 5.00 4.87 1.36
8. Prayer is an important part of my life. 1.00 5.00 4.88 1.34 9. Spiritual reading gives me direction
in life.1.00 5.00 4.68 1.76
15. I welcome change and perceive it as an opportunity for growth.
1.00 5.00 4.69 1.67
16. I review my life periodically to search for and/or confirm my pursuits.
1.00 5.00 4.27 1.44
17. I always have inner energy to pursue my goals in life.
1.00 5.00 4.61 1.78
18. I believe I live up to my potentials. 1.00 5.00 4.45 1.65 19. I do something to show love for
myself.1.00 5.00 4.49 1.32
20. I feel fragmented and have no energy for finding interest in things.a
1.00 5.00 1.92 1.99
21. I regard my spiritual health as good. 1.00 5.00 4.35 2.01Factor 2: Understanding of spiritual care 10. Spiritual strength can be drawn
on to promote the healing of the physical body.
1.00 5.00 4.38 1.44
11. I believe nurses can provide spiritual care only by arranging the client’s own religious leader if requested.
1.00 5.00 2.69 1.65
12. I don’t believe nurses can provide spiritual care by showing concern when giving care.a
1.00 5.00 1.59 1.83
(continued)
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from
10 Clinical Nursing Research
Items Minimum Maximum M SD
13. I believe nurses can provide spiritual care by listening to the client’s concerns, discussing and exploring their fears, anxieties, and troubles.
1.00 5.00 4.63 1.32
14. I don’t believe nurses can help a client to find meaning in his/her illness.a
1.00 5.00 1.79 1.56
Factor 3: Practice of spiritual care 22. I usually explore the client’s
religious practices.1.00 5.00 3.27 1.43
23. I usually explore the client’s spiritual values.
1.00 5.00 3.23 1.61
24. I usually explore the client’s hopes and sources of strength.
1.00 5.00 3.53 1.42
25. I refer the client to his/her spiritual counselor (e.g., hospital chaplain) if needed.
1.00 5.00 2.92 1.59
26. I usually comfort clients spiritually (e.g., reading books, prayers, music, etc.).
1.00 5.00 3.16 1.54
27. I will sit with the client if needed. 1.00 5.00 3.66 1.67
Note. NSDSC = Nurses’ Spirituality and Delivery of Spiritual Care.aReversed for the purpose of computing the grand mean.
Table 2. (continued)
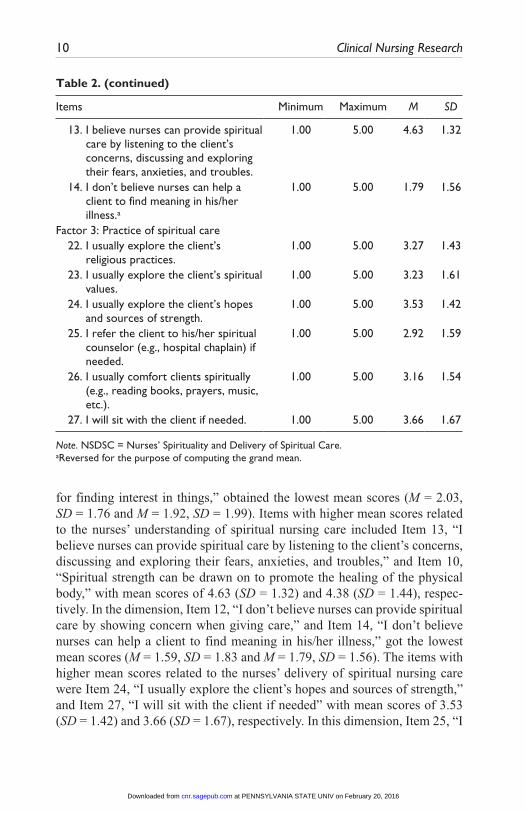
for finding interest in things,” obtained the lowest mean scores (M = 2.03, SD = 1.76 and M = 1.92, SD = 1.99). Items with higher mean scores related to the nurses’ understanding of spiritual nursing care included Item 13, “I believe nurses can provide spiritual care by listening to the client’s concerns, discussing and exploring their fears, anxieties, and troubles,” and Item 10, “Spiritual strength can be drawn on to promote the healing of the physical body,” with mean scores of 4.63 (SD = 1.32) and 4.38 (SD = 1.44), respec-tively. In the dimension, Item 12, “I don’t believe nurses can provide spiritual care by showing concern when giving care,” and Item 14, “I don’t believe nurses can help a client to find meaning in his/her illness,” got the lowest mean scores (M = 1.59, SD = 1.83 and M = 1.79, SD = 1.56). The items with higher mean scores related to the nurses’ delivery of spiritual nursing care were Item 24, “I usually explore the client’s hopes and sources of strength,” and Item 27, “I will sit with the client if needed” with mean scores of 3.53 (SD = 1.42) and 3.66 (SD = 1.67), respectively. In this dimension, Item 25, “I
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

Labrague et al. 11
refer the client to his/her spiritual counselor (e.g., hospital chaplain) if needed,” and Item 26, “I usually comfort clients spiritually (e.g., reading books, prayers, music, etc.),” received the lowest mean scores (M = 2.92, SD = 1.59 and M = 3.16, SD = 1.54).
Pearson’s correlation coefficients were calculated to determine the rela-tionship between the nurses’ perception of spirituality, understanding of, and delivery of spiritual nursing care (see Table 3). Nurse’s spirituality correlated significantly with their understanding of spiritual nursing care (r = .3376, p ≤ .05) and delivery of spiritual nursing care (r = .3980, p ≤ .05). Weak posi-tive, significant correlations were found between understanding of spiritual nursing care and the delivery of spiritual nursing care (r = .3289, p ≤ .05).
Study Limitations
Although the results of this study are important as it is the first study of its kind conducted in the Philippines, nevertheless it has some limitations need-ing to be addressed. First, the majority of the respondents were Christian, and nurses from other religious affiliations may have different responses or views on this topic. Second, although the response rate in this study is sufficient, the use of convenience sampling may weaken the generalization of the study. Third, data were collected from one country (Philippines), thus caution should be made when interpreting the results. The views among Filipino nurses may be different from nurses’ views from other countries. Future stud-ies examining spiritual views and the extent to which nurses share the same view across countries must be conducted. Fourth, spirituality is a concept considered to be ambiguous and difficult to define, thus the use of a self-reporting questionnaire may limit the respondents’ choices. Spiritual research that is qualitative in nature may be conducted to further allow for the freedom
Table 3. Correlation Matrix of Spirituality, Understanding of and Delivery of Spiritual Care.
Nurses’ spiritualityUnderstanding of
spiritual care
Variable r p r p
Understanding of spiritual care
.3376 <.05*
Provision of spiritual care
.3986 <.05* .3289 <.05*
*p < .05.
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from
12 Clinical Nursing Research
of additional responses and views of the respondents than those responses designated in the statements utilized in the NSDSC.
Discussion
Findings of this study revealed a general agreement on Item 8, “Prayer is an important part of my life”; Item 7, “I believe that God loves me and cares for me”; and Item 9, “Spiritual reading gives me direction in life.” These items combine to form a part of the nurses’ spirituality (Dimension Beyond the Self). This finding indicated a strong connection with the God/Supreme Being. With more than 87% Christian and a predominantly Roman Catholic nation, as the Philippines is designated, this finding is not surprising. In addition, in this study, all respondents (100%, n = 245) are Christian. In the Philippines, Catholicism is the predominant religion with a significant Spanish Christian tradition and practice, and this Spanish-style Christianism is highly embedded in the culture. Prayer is a common Filipino tradition instilled by colonial Spanish priests and still currently practiced.
Further analysis revealed that there are some minor disagreements on Items 5, 6, and 20 of the NSDSC, which is valuable in the formation of the nurses’ spirituality (self-dimension). According to Chung et al. (2007), spiri-tuality is a relationship or connection that we have with ourselves and beyond ourselves to include connectedness to our Supreme Being. Finding meaning and purpose of life is regarded as the existential aspect and a core component of spirituality (Fawcett & Noble, 2004), and holistic nursing care is only pos-sible when the nurse is conscious about oneself (Chung et al., 2007). Chung et al. (2007) argued that a fragmented nurse cannot bring a sense of harmony to his or her patient. This result indicated a need to continuously improve oneself because only through serenity, self-awareness, wholeness, and sense of satisfaction the nurse will come to realize how to relate to oneself and beyond while connecting with the patient spiritually.
The study results indicated a high mean score on factor 2 for Item 13, “I believe nurses can provide spiritual care by listening to the client’s concerns, discussing and exploring their fears, anxieties, and troubles.” This finding supported claims of previous authors which demonstrated establishing con-nectedness and caring relationships, and showing concern and sharing com-mon experiences as hallmarks of nurses providing quality spiritual nursing care (Grant, 2004; McSherry, 2010; Tanyi, 2002). Other studies identified the most frequent forms of spiritual care offered by nurses such as acceptance and nonjudgmental attitude, nurses presence, listening, giving respect, instill-ing hope, maintaining privacy and dignity, and the use of religious objects
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

Labrague et al. 13
(Grant, 2004; McSherry, 2006; Narayanasamy, 2007; Tanyi, 2002; van Leeuwen & Cusveller, 2004)
Spiritual forms of nursing care are not always well understood by nurses and for some, although they are committed to providing spiritual care, can find it complex and difficult (Chan et al., 2006; Christensen & Turner 2008). Empirical evidences consistently showed a lack of the nurse’s awareness of the spiritual dimension as an essential component of nursing care (Chan, 2009; McSherry, 2006; Ozbasaran et al., 2011). For instance, in the study by McSherry (2006), most of the nurse participants did not consider spiritual care as part of their patient care duties. In another study conducted in Turkey by Ozbasaran et al. (2011), it was observed that the Turkish nurses’ percep-tion of spiritual care was inconclusive, meaning they tend to be confused about what constitutes spiritual care. Such differences according to previous authors may be attributed to a lack of knowledge, lack of general conceptual clarity, and general consensus regarding a nurse’s perceptions related to spiri-tuality and spiritual care (McSherry, 2010; Narayanasamy, 2007).
Factor 3, Item 25, “I refer the client to his/her spiritual counselor (e.g., hospital chaplain) if needed,” scored low among all items, which indicated that nurses need to acknowledge the fundamental role of hospital chaplains in providing spiritual care to their patients. Nurses need to be aware that the provision of spiritual care requires collaboration from other health care pro-fessionals such as chaplains and religious leaders. In the study by McSherry and Jamieson (2011), the majority of respondents felt that aside from nurses, chaplains, patients, families, and other health care professionals were addi-tionally responsible for providing spiritual care. Ideally, hospitals employ hospital chaplains who are available to offer various services focusing on spiritual care to all patients, their caregivers, friends and family, as well as staff members. These job duties may include praying with patients and the hospital staff, as well as offering spiritual guidance. Their presence is to serve, support, and encourage grieving families, as well as individuals who are experiencing a crisis. In addition, they assist with expanding the provision of spiritual care through modeling, mentoring, and even in facilitating educa-tional programs relative to spirituality (Tiew & Drury, 2012). However, in many countries (to include the Philippines), chaplaincy remains not well established and is not well understood by many in the area of hospital admin-istration. This could be the reason why nurses in the study rated this item low.
Nurse’s spiritual perceptions are vital when providing spiritual care (Belcher & Griffiths, 2005; Cavendish et al., 2006; Chan, 2010; Chan et al., 2006; Chung et al., 2007; Hart, 2008). In this study, positive correlations were found between the nurse’s spirituality, their understanding of, and provision of spiritual nurs-ing care. This implies that high perceptions of spirituality may be an important
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

14 Clinical Nursing Research
factor in increasing the understanding of and in the actual provision of the spiri-tual care. Several authors supported this claim that the nurses’ own spirituality is essential when providing spiritual care to patients (Cavendish et al. 2006; Chan, 2010; Chan et al., 2006; Chung et al., 2007; Belcher & Griffiths, 2005). For instance, Chung et al. (2007) reported that Hong Kong nurses’ perceptions of their own spirituality seem to influence the delivery of spiritual nursing care to their patients. Similarly, Cavendish et al. (2006) and Belcher and Griffiths (2005) asserted that the nurses’ spirituality and a knowledge base of spiritual nursing care were important factors that supported the delivery of spiritual care. In another study conducted by Chan (2009), the study findings revealed a posi-tive correlation between spiritual care perceptions and spiritual care practice among nurses. This meant that the greater the nurse’s spiritual care perceptions, the more frequently that spiritual care is included in that nurse’s individual practice. Results indicated the need for nurses to further improve oneself through self-care or personal care (Cavendish et al., 2001). Wu and Lin (2011) suggested that self-care or personal care is essential to be considered when exploring or defining one’s own spirituality.
Several studies suggested that providing spiritual training/courses to nurses has a positive impact on the nurse’s perceptions of spirituality and spiritual care (Wu & Lin, 2011). In this study, 100% of nurses received no training on spirituality. This result was similar to that of Çetinkaya, Azak, and Dundar’s (2013) study, where 96.9% of the nurses included in the study had not received spiritual training. This finding is alarming considering the very nature of the nursing profession. If nurses are to provide holistic care to patients, spiritual aspects of care must not be underestimated. In agreement with previous authors (Chan, 2009; McSherry, 2006; Ozbasaran et al., 2011; Wu & Lin, 2011), educational training programs for nurses must be strength-ened and should incorporate and adequately address the spiritual dimension of nursing care. These training programs, in turn, would promote the nurse’s ability to deepen and expand their own understanding of spirituality and spir-itual care (Christensen & Turner, 2008).
Conclusion
This study is the only study conducted in the Philippines that explored nurse’s spirituality and provision of spiritual care. The study findings provided insights on the Filipino nurses’ perception of spirituality and the provision of spiritual nursing care while contributing to the understanding of the univer-sality of the subject matter. Correlations between the nurses’ perceptions of spirituality, understanding of spiritual care, and provision of spiritual care indicated that for nurses to better provide spiritual nursing care, the nurse
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

Labrague et al. 15
must care for oneself through self-awareness, self-reflection, and developing a sense of satisfaction and contentment. In turn, the nurse will be able to relate themselves to others, to the Supreme Being, to the environment, and eventually to the patient.
Research resulted in providing implications to both the areas of nursing academe and nursing administration. In agreement to previous researchers’ findings, both nursing academe and nursing administration roles play a criti-cal role in focusing and shaping of nurses and students spirituality through evidence-based strategies that would allow them to grow spiritually and prac-tice spiritual care effectively (Cavendish et al., 2006; Chung et al., 2007). For instance, the findings derived from this study would be able to be imple-mented by nursing administrators in identifying and planning effective strate-gies, interventions, and programs to improve spirituality among nurses and eventually the care offered to patients. This may include the formulation of activities that would allow nurses to identify and clarify their own spirituality through self-awareness workshops/activities and spirituality assessments and strengthen nurses commitment to the value of spiritual care through periodic assessment on their personal integration of spiritual care.
In the academic platform, nurse educators may consider the integration of concepts of spirituality in nursing education and training. According to Narayanasamy and Narayanasamy (2010), nurse education is an ideal place where issues relative to spirituality could be explored. Student engagement in learning spirituality may be fostered through non-traditional learning strate-gies such as simulation activities, role-playing, games, and the use of reflec-tive journals. Nurse educators may also require students to submit a written journal, Nursing Care Plans, and anecdotal records of demonstration of spiri-tual care provided and summative self-assessment on integration of spiritual care during clinical exposure.
Acknowledgments
The authors express their heartwarming thanks and gratitude to all nurses who partici-pated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publi-cation of this article.
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from

16 Clinical Nursing Research
References
American Nurses Association. (2001). Code of ethics for nurses with interpretive statements. Silver Spring, MD: Nursesbooks.org.
Anandarajah, G., & Hight, E. (2001). Spirituality and medical practice. American Family Physician, 63, 81-88.
Baldacchino, D. R. (2006). Nursing competencies for spiritual care. Journal of Clinical Nursing, 15, 885-896.
Baldacchino, D. R. (2008). Spiritual care: Is it the nurse’s role? Spirituality and Health International, 9, 270-284.
Belcher, A., & Griffiths, M. (2005). The spiritual care perspectives and practices of hospice nurses. Journal of Hospice & Palliative Nursing, 7, 271-279.
Carr, T. (2008). Mapping the processes and qualities of spiritual nursing care. Qualitative Health Research, 18(5), 686-700.
Catholic Health Association of Canada and the Canadian Association for Pastoral Practice and Education. (2000). Standards of spiritual and religious care for health services in Canada. Retrieved from http://www.chac.ca/alliance/online/docs/brochure_standards_en.pdf
Cavendish, R., Konecny, L., Naradovy, L., Luise, B. K., Como, J., Okumakpeyi, P., . . . Lanza, M. (2006). Patients’ perceptions of spirituality and the nurse as a spiri-tual care provider. Holistic Nursing Practice, 20, 41-47.
Cavendish, R., Luise, B. K., Bauer, M., Gallo, M. A., Horne, K., Medefindt, J., & Russo, D. (2001). Recognizing opportunities for spiritual enhancement in young adults. International Journal of Nursing Terminologies and Classifications, 12, 77-91.
Çetinkaya, B., Azak, A., & Dundar, S. A. (2013). Nurses’ perceptions of spirituality and spiritual care. Australian Journal of Advanced Nursing, 31(1), 5-10.
Chan, M. F., Chung, L. Y. F., Lee, A. S. C., Wong, W. K., Lee, G. S. C., Lau, C. Y., . . . Ng, J. W. S. (2006). Investigating spiritual care perceptions and practice pat-terns in Hong Kong nurses: Results of a cluster analysis. Nurse Education Today, 26, 139-150.
Chan, M. F. (2010). Factors affecting nursing staff in practicing spiritual care. Journal of Clinical Nursing, 19, 2128-2136.
Christensen, K. H., & Turner, de. S. (2008). Spiritual care perspectives of Danish registered nurses. Journal of Holistic Nursing, 26, 7-14.
Chung, L. Y. F., Wong, F. K. Y., & Chan, M. F. (2007). Relationship of nurses’ spiri-tuality to their understanding and practice of spiritual care. Journal of Advanced Nursing, 58, 158-170.
Clark, P. A., Drain, M., & Malone, M. P. (2003). Addressing patients’ emotional and spiritual needs. Joint Commission Journal on Quality and Patient Safety, 29(12), 659-670.
Fawcett, T. N., & Noble, A. (2004). The challenge of spiritual care in a multi-faith society experienced as a Christian nurse. Journal of Clinical Nursing, 13, 136-142.
Gaskamp, C., Sutter, R., Meraviglia, M., Adams, S., & Titler, M. G. (2006). Evidence-based guideline: Promoting spirituality in the older adult. Journal of gerontologi-cal nursing, 32(11), 8-13.
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from
Labrague et al. 17
George, L. K., Larson, D. B., Koenig, H. G., & McCullough, M. E. (2000). Spirituality and health: What we know, what we need to know. Journal of Social & Clinical Psychology, 19, 102-116.
Grant, D. (2004). Spiritual interventions: How, when, and why nurses use them. Holistic Nursing Practice, 18, 36-41.
Hart, J. (2008). Spirituality and health. Alternative and Complementary Therapies, 14(4), 189-193.
International Council of Nurses. (2012). International council of nurses code of ethics for nurses. Retrieved from http://www.icn.ch/images/stories/documents/about/icncode_english.pdf
Joint Commission on Accreditation of Healthcare Organizations. (2005). Evaluating your spiritual assessment. Retrieved from http://www.professionalchaplains.org/files/resources/reading_room/evaluating_your_spiritual_assessment_process.pdf
Koenig, H. G., George, L. K., & Titus, P. (2004). Religion, spirituality, and health in medically ill hospitalized older patients. Journal of the American Geriatrics Society, 52, 554-562.
Labrague, L. J. (2012). Caring competencies of baccalaureate nursing students of Samar State University. Journal of Nursing Education and Practice, 2(4), 105-113.
Larson, D. B., & Larson, S. S. (2003). Spirituality’s potential relevance to physi-cal and emotional health: A brief review of quantitative research. Journal of Psychology and Theology, 31(1), 37-51.
MacLaren, J. (2004). A kaleidoscope of understandings: Spiritual nursing in a multi-faith society. Journal of Advanced Nursing, 45, 457-462.
McSherry, W. (2006). Making sense of spirituality in nursing and health care prac-tice: An interactive approach. London, England: Jessica Kingsley.
McSherry, W., & Jamieson, S. (2011). An online survey of nurses’ perceptions of spirituality and spiritual care. Journal of Clinical Nursing, 20, 1757-1767.
McSherry, W., & Ross, L. (Eds.). (2010). Spiritual assessment in healthcare practice. Keswick, England: M&K Update Ltd.
Narayanasamy, A., & Owens, J. (2001). A critical incident study of nurses’ responses to the spiritual needs of their patients. Journal of Advanced Nursing, 33, 446-455.
Narayanasamy, A. (2004). The puzzle of spirituality for nursing: A guide to practical assessment. British Journal of Nursing, 13, 1140-1144.
Narayanasamy, A. (2006). The impact of empirical studies of spirituality and culture on nurse education. Journal of clinical nursing, 15(7), 840-851.
Narayanasamy, A. (2007). Palliative care and spirituality. Indian Journal of Palliative Care, 13(2), 32.
Narayanasamy, A. (2010). Recognizing spiritual needs. In L. Ross & W. McSherry (Eds.), Spiritual assessment in healthcare practice (pp. 37-55). Keswick, England: M&K Update Ltd.
Narayanasamy, A., & Narayanasamy, M. (2010). Spiritual journey board game as an educational tool for teaching spirituality in higher education. Discourse, 9, 59-79.
O’Brien, M. E. (2013). Spirituality in nursing. Burlington, MA: Jones & Bartlett.Ozbasaran, F., Ergul, S., Temel, A. B., Aslan, G. G., & Coban, A. (2011). Turkish
nurses’ perceptions of spirituality and spiritual care. Journal of Clinical Nursing, 20, 3102-3110.
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from
18 Clinical Nursing Research
Pesut, B. (2006). Fundamental or foundational obligation? Problematizing the ethical call to spiritual care in nursing. Advances in Nursing Science, 29, 125-133.
Pew Research and Religion and Public Life Project. (2011). Regional distribution of Christians. Retrieved from http://www.pewforum.org/2011/12/19/global- christianity-regions/
Philippine Board of Nursing. (2009). Philippines Nursing Act of 2002. Retrieved from http://www.prc.gov.ph/uploaded/documents/NURSING%20LAW.PDF
Philippine Nurses Association. (2003). Philippine Nurses Association Code of Ethics. Retrieved from http://www.pna-ph.org/downloads/Code%20of%20Ethics%20for%20Nurses.pdf
Polit, D. F., & Beck, C. T. (2013). Essentials of nursing research. Philadelphia, PA: Lippincott Williams & Wilkins.
Ramezani, M., Ahmadi, F., Mohammadi, E., & Kazemnejad, A. (2014). Spiritual care in nursing: A concept analysis. International Nursing Review, 61, 211-219.
Ross, L. (2006). Spiritual care in nursing: An overview of the research to date. Journal of Clinical Nursing, 15, 852-862.
Shah, R., Kulhara, P., Grover, S., Kumar, S., Malhotra, R., & Tyagi, S. (2011). Contribution of spirituality to quality of life in patients with residual schizophre-nia. Psychiatry Research, 190, 200-205.
Tanyi, R. A. (2002). Towards clarification of the meaning of spirituality. Journal of Advanced Nursing, 39, 500-509.
Tiew, L. H., & Drury, V. (2012). Singapore nursing students’ perceptions and atti-tudes about spirituality and spiritual care in practice: A qualitative study. Journal of Holistic Nursing, 30(3), 160-169.
Tuck, I., Wallace, D., & Pullen, L. (2001). Spirituality and spiritual care provided by parish nurses. Western Journal of Nursing Research, 23, 441-453.
Tupas, A. G. (1952). History of nursing in the Philippines. Manila, Philippines: Rex Bookstore.
United Kingdom Central Council for Nurses, Midwives, and Health Visitors. (2000). United Kingdom Central Council for Nurses, Midwives, and Health Visitors’ Code of Professional Conduct. Retrieved from http://www.legislation.gov.uk/uksi/2000/2554/pdfs/uksi_20002554_en.pdf
Van Leeuwen, R., & Cusveller, B. (2004). Nursing competencies for spiritual care. Journal of Advanced Nursing, 48, 234-246..
Visser, A., Garssen, B., & Vingerhoets, A. (2010). Spirituality and well-being in can-cer patients: A review. Psycho-Oncology, 19, 565-572.
Weathers, E., McCarthy, G., & Coffey, A. (2015). Concept analysis of spiritual-ity: An evolutionary approach. In Nursing forum. Advance online publication. doi:10.1111/nuf.12128
Wu, L. F., & Lin, L. Y. (2011). Exploration of clinical nurses’ perceptions of spiritu-ality and spiritual care. Journal of Nursing Research, 19, 250-256.
Zavala, M. W., Maliski, S. L., Kwan, L., Fink, A., & Litwin, M. S. (2009). Spirituality and quality of life in low-income men with metastatic prostate cancer. Psycho-Oncology, 18, 753-761.
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from
Labrague et al. 19
Author Biographies
Leodoro J. Labrague, MAN, BSN, RN, is a lecturer at Sultan Qaboos University, College of Nursing, Sultanate of Oman. He teaches nursing administration course. His research interest include: health promotion, mobile health, eLearning, comple-mentary therapy, nursing education, caring, genetics, disaster nursing, and use of social media.
Denise M. McEnroe-Petitte, PhD, MSN, BSN, AS, RN, is an associate professor at Kent State University Tuscarawas, USA. She teaches content in the Medical - Surgical areas. In addition, other areas of research include: heart failure, nursing education, curriculum development, caring, and critical care.
Romeo H. Achaso Jr., BSN, RN, is a registered nurse at Samar Provincial Hospital.
Geifsonne S. Cachero, BSN, RN, is a registered nurse at Samar Provincial Hospital.
Mary Rose A. Mohammad, BSN, RN, is a registered nurse at Samar Provincial Hospital.
at PENNSYLVANIA STATE UNIV on February 20, 2016cnr.sagepub.comDownloaded from