
Beneficial effects of dalteparin on haemostatic function and local tissue oxygenation in patients...
9
REGULAR ARTICLE Beneficial effects of dalteparin on haemostatic function and local tissue oxygenation in patients with diabetes, severe vascular disease and foot ulcers Majid Kalani a, ⁎ , Angela Silveira b , Margareta Blombäck c , Jan Apelqvist d , Björn Eliasson e , Jan W. Eriksson f , Bengt Fagrell g , Ole Torffvit h , Anders Hamsten b , Gun Jörneskog a a Karolinska Institutet, Department of Clinical Sciences, Danderyd Hospital, Stockholm, Sweden b Atherosclerosis Research Unit, King Gustaf V Research Institute, Karolinska University Hospital Solna, Karolinska Institutet, Stockholm, Sweden c Department of Molecular Medicine and Surgery/Coagulation Research, Karolinska University Hospital Solna, Karolinska Institutet, Stockholm, Sweden d Department of Endocrinology, University Hospital in Malmö, University of Lund, Göteborg, Sweden e Department of Medicine, Sahlgrenska University Hospital, Göteborg, Sweden f Department of Medicine, University Hospital in Umeå, Göteborg, Sweden g Department of Internal Medicine, Karolinska University Hospital Solna, Karolinska Institutet, Stockholm, Sweden h Department of Internal Medicine, University Hospital in Lund, University of Lund, Göteborg, Sweden Received 11 July 2006; received in revised form 15 November 2006; accepted 11 December 2006 Available online 2 February 2007 Abstract Introduction: A state of hypercoagulation and fibrinolytic dysfunction is present in individuals with diabetes, which may contribute to disturbed skin microcirculation and impaired ulcer healing. We have previously reported an improved outcome of chronic diabetic foot ulcers during treatment with dalteparin. In the present study we investigated the effects of dalteparin on skin microcirculation and haemostatic function. KEYWORDS Blood coagulation; Diabetes mellitus; Fibrinolysis; Fibrin gel; Low molecular weight heparin; Microcirculation Abbreviations: PAOD, peripheral arterial obliterative disease; TcPO 2 , transcutaneous oxygen tension; LDF , laser Doppler fluxmetry; Ks, fibrin gel permeability coefficient; μ, fiber mass – length ratio; F1+2, prothrombin fragment 1 + 2; PAI-1, plasminogen activator inhibitor-1; tPA, tissue plasminogen activator; hsCRP , high sensitive C-reactive protein; SAA, serum amyloid A. ⁎ Corresponding author. Microcirculatory Laboratory, Department of Clinical Sciences, Danderyd Hospital, SE-182 88 Stockholm, Sweden. Tel.: +46 70 5620374; fax: +46 8 6301165. E-mail address: [email protected] (M. Kalani). intl.elsevierhealth.com/journals/thre 0049-3848/$ - see front matter © 2007 Elsevier Ltd. All rights reserved. doi:10.1016/j.thromres.2006.12.006 Thrombosis Research (2007) 120, 653–661
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Beneficial effects of dalteparin on haemostatic function and local tissue oxygenation in patients...

intl.elsevierhealth.com/journals/thre
Thrombosis Research (2007) 120, 653–661
REGULAR ARTICLE
Beneficial effects of dalteparin on haemostaticfunction and local tissue oxygenation inpatients with diabetes, severe vasculardisease and foot ulcers
Majid Kalani a,⁎, Angela Silveirab, Margareta Blombäckc, Jan Apelqvist d,Björn Eliassone, Jan W. Eriksson f, Bengt Fagrell g, Ole Torffvit h,Anders Hamstenb, Gun Jörneskoga
a Karolinska Institutet, Department of Clinical Sciences, Danderyd Hospital, Stockholm, Swedenb Atherosclerosis Research Unit, King Gustaf V Research Institute, Karolinska University Hospital Solna,Karolinska Institutet, Stockholm, Swedenc Department of Molecular Medicine and Surgery/Coagulation Research, Karolinska University Hospital Solna,Karolinska Institutet, Stockholm, Swedend Department of Endocrinology, University Hospital in Malmö, University of Lund, Göteborg, Swedene Department of Medicine, Sahlgrenska University Hospital, Göteborg, Swedenf Department of Medicine, University Hospital in Umeå, Göteborg, Swedeng Department of Internal Medicine, Karolinska University Hospital Solna,Karolinska Institutet, Stockholm, Swedenh Department of Internal Medicine, University Hospital in Lund, University of Lund, Göteborg, Sweden
Received 11 July 2006; received in revised form 15 November 2006; accepted 11 December 2006Available online 2 February 2007
Abbreviations: PAOD, peripheral arKs, fibrin gel permeability coefficient;inhibitor-1; tPA, tissue plasminogen ac⁎ Corresponding author. Microcircula
Sweden. Tel.: +46 70 5620374; fax: +4E-mail address: [email protected]
0049-3848/$ - see front matter © 200doi:10.1016/j.thromres.2006.12.006
Abstract
Introduction: A state of hypercoagulation and fibrinolytic dysfunction is present inindividuals with diabetes, which may contribute to disturbed skin microcirculationand impaired ulcer healing. We have previously reported an improved outcome ofchronic diabetic foot ulcers during treatment with dalteparin. In the present study weinvestigated the effects of dalteparin on skin microcirculation and haemostaticfunction.
KEYWORDSBlood coagulation;Diabetes mellitus;Fibrinolysis;Fibrin gel;Low molecular weightheparin;Microcirculation
terial obliterative disease; TcPO2, transcutaneous oxygen tension; LDF, laser Doppler fluxmetry;μ, fiber mass – length ratio; F1+2, prothrombin fragment 1+2; PAI-1, plasminogen activatortivator; hsCRP, high sensitive C-reactive protein; SAA, serum amyloid A.tory Laboratory, Department of Clinical Sciences, Danderyd Hospital, SE-182 88 Stockholm,6 8 6301165.(M. Kalani).
7 Elsevier Ltd. All rights reserved.

654 M. Kalani et al.
Materials and methods: 87 patients with diabetes, peripheral arterial obliterativedisease and chronic foot ulcers were investigated in a prospective, randomised,double-blind and placebo-controlled study. They were randomised to treatment withsubcutaneous injections of 5000 U dalteparin (n=44) or placebo (n=43), once dailyuntil ulcer healing or for a maximum of six months. Plasma fibrinogen, fibrin gelstructure [permeability coefficient (Ks) and fiber mass/length ratio (μ)], prothrombinfragment 1+2 (F1+2) antigen, plasminogen activator inhibitor-1 (PAI-1) activity andtissue plasminogen activator (tPA) antigen were analysed before randomization(baseline value), and at the end of the treatment period. The skin microcirculation ofthe foot was investigated by transcutaneous oxygen tension (TcPO2) and laser Dopplerfluxmetry (LDF).Results: The changes (Δ-values) of Ks, μ, tPA and TcPO2 were higher (pb0.05) duringtreatment with dalteparin, as compared to the changes during treatment withplacebo. At baseline, plasma fibrinogen and Ks were significantly correlated to TcPO2.Conclusions: Local skin oxygenation improved and a less thrombogenic fibrin gelstructure was formed in patients treated with dalteparin. Beneficial effects onhaemostatic function are likely to contribute to the improved skin oxygenationobserved during treatment with dalteparin.© 2007 Elsevier Ltd. All rights reserved.
Introduction
Hypercoagulation and impaired fibrinolysis arecommon findings in diabetic patients [1–4] whichmay be exacerbated in patients with reducedperipheral perfusion pressure due to peripheralarterial obliterative disease (PAOD). PAOD is animportant factor in the development of chronic footulcers, a severe and expensive complication indiabetic patients [5,6]. In diabetic patients withPAOD, the nutritive skin capillary circulation isseverely impaired [7], which may have negativeconsequences on local tissue oxygenation andnutrition. Hemorheological disturbances, as elevat-ed levels of plasma fibrinogen, are common inpatients with diabetes and may contribute tochanges in vascular function [8]. During bloodcoagulation, upon activation with thrombin, fibrin-ogen forms fibrin monomers which polymerize andform a network of fibrin. Abnormal architectures ofthe fibrin network, i.e. a dense fibrin network, withthin fibers and small pores, have been described indiabetes mellitus [9,10]. The architecture of thefibrin network is an important determinant of thefibrinolysis rate [11,12], and, in turn, of theoccurrence of thrombosis [12].
In a prospective, randomised, double-blind andplacebo-controlled study, we have previously shownthat treatment with the low molecular weightheparin (LMWH) compound dalteparin (Fragmin®,Pharmacia Corporation/Pfizer) improves the out-come of neuro-ischaemic foot ulcers in patientswith diabetes [13]. The reason for the betteroutcome in the dalteparin treated patients isunclear but the beneficial effects of dalteparin on
haemostatic function may have contributed to animproved skin microvascular function. Treatmentwith dalteparin was reported to persistently depresscoagulation activity in patients with unstablecoronary disease [14]. Based on an ancillary studywe here report the effect of dalteparin on local skinmicrocirculation, markers of coagulation and fibri-nolysis, and the relations of haemostatic param-eters to skin microcirculation in the feet of patientswith diabetes, PAOD and chronic foot ulcers.
Materials and methods
Patients
Eighty-seven consecutive patients with diabetes,chronic foot ulcers and PAOD were enrolled in thestudy [13]. Inclusion criteria were a toe/arm bloodpressure index ≤0.6, foot ulcer duration of morethan 2 months, ulcer stage I and II according to theWagner classification [15], and a daily dose of 75 mgaspirin since at least four weeks before randomisa-tion and throughout the whole study period [13].Exclusion criteria included vascular reconstructionor angioplasty less than three months beforerandomisation; renal insufficiency defined as aserum creatinine level≥200 μmol/L; and treatmentwith anticoagulants. All patients have been evalu-ated for vascular surgery, as described [13].
Study design and objective
The studywas designedas a prospective, randomised,double-blind and placebo-controlled multicenter

655Haemostasis and microcirculation in diabetes
study to evaluate the effect of dalteparin (Fragmin®)on peripheral macro- and microcirculation, andhaemostatic function in patients with diabetes,PAOD and chronic foot ulcers. Eligible patients wererandomised to treatment with subcutaneous injec-tions of 0.2 ml dalteparin (Fragmin®, 25000 U/ml,n=44) or 0.2ml physiological saline (n=43) once dailyuntil ulcer healing, or for a maximum of six months.The randomisation list was prepared by an indepen-dent statistician by the method of computer-gener-ated random numbers for each treatment. Ulceroutcome was defined as: healed with intact skin,improved (≥50% reduction of the ulcer area),unchanged (decreased or increased ulcer areab50%), impaired ulcer area (≥50% increase of theulcer area) or amputation above or below the ankle.Further data on study design and results on ulceroutcome have been reported in reference [13].
Peripheral circulation
All investigations were performed in the morning, inthe supine position after 20 min of rest. Patientswere asked to refrain from coffee and smoking for atleast 8 h before the investigations. Room temper-ature was kept between 22–24 °C. Peripheralmacro- and microcirculation were investigated atbaseline, after 3 and 6 months, or earlier in case ofdiscontinuation of treatment. Systolic toe bloodpressure (TBP) was assessed [16], and the toe to armblood pressure index was determined. Peripheralneuropathy was evaluated by investigation ofpressure sensation of the foot skin to a 5.07 nylonmonofilament and by vibration sensation using atuning fork 128 Hz [13].
Local skin microcirculation
Total skin microcirculation, at two sites close to thefoot ulcer, was measured by laser Doppler fluxmetry(LDF; PeriFlux 4001 Master, Perimed®, Järfälla,Sweden). LDF measures mainly blood circulation indeeper skin microcirculation and over 90% of thelaser Doppler flux is generated by flow in non-nutritional, sub-papillary vessels [17–19]. Peak LDFand time to peak LDF were measured following a4 min arterial occlusion at the ankle with a cuffpressure of 250 mmHg. The remaining LDF signalduring an arterial occlusion was considered to bethe biological zero value and was subtracted fromthe total LDF signal [20]. When the LDF signals hadreturned towards baseline levels, the skin under theLDF-probes was heated to 44 °C (PeriTemp 4005with thermostatic probe PF 457, Perimed®) during6 min. The hyperemic responses to arterial occlu-sion and local heating, respectively, were calculat-
ed as percent increase of resting LDF. Day-to-daycoefficient of variation (CV) for peak LDF duringpostocclusive reactive hyperemia was investigatedin 6 healthy subjects and was b26%, whereas CV forpeak LDF during local heating of skin to 44 °C at thefoot level was b20%.
Local skin oxygenation was evaluated by mea-surement of transcutaneous oxygen tension (TcPO2)(Oxykapnomonitor, SMK 363; Hellige®, Freiburg imBreisgau, Germany) [21] at the dorsum of the foot inthe first intermetatarsal space. TcPO2 is a non-invasive method reflecting local arterial skin bloodflow and oxygenation [22] and has been used as apredictor of ulcer healing in patients with PAOD [23–26]. A calibration period of 10–15 min was used andthe TcPO2 signal was continuously recorded on a PCand analysed with the Perisoft software (Peri-med®). Day-to-day variability of TcPO2 has beeninvestigated and the results show a strong linearrelation between measures of TcPO2 performed onthree different days, indicating good reproducibilityof the method [27].
Blood samples
For determination of haemostatic parameters,venous blood was taken between 8 and 9 am aftera 10-h fast. Blood samples were collected withoutstasis, or when necessary, with minimal stasis on theforearm after 20 min supine rest. The first 2 ml werediscarded and blood was drawn into 10 ml vacuumtubes containing trisodium citrate (0.13 mol/L, pH7.5). The tubes were immediately centrifuged for20 min (2200 g, room temperature), and plasma wasdispensed into plastic tubes and frozen at −70 °Cwithin one hour.
Laboratory analyses
Total plasma fibrinogen was analysed with asyneresis method [28], which measures theamount of clottable protein incorporated into theclot, after addition of thrombin to the plasmasample. Thrombin generation was estimatedthrough determination of prothrombin fragment1+2 (F1+2) with an ELISA (Enzygnost F1+2 μ, DadeBehring, Marburg GmbH, Marburg, Germany). PAI-1activity was determined by a bioimmunoassay(Chromolize PAI-1), and tPA antigen with an ELISA(TintElize tPA), both from Biopool International,Umeå, Sweden.
Fibrin gel structure was assessed by determina-tion of the permeability coefficient (Ks), whichreflects fibrin clot porosity, and fiber mass – lengthratio (μ), as described in detail [29]. In brief, Ks andμ are determined in assays in which a buffer is
Table 1 Baseline characteristics of 85 diabetic patientswith chronic foot ulcers and peripheral arterial diseasewho were randomised to treatment with dalteparin orplacebo and completed the study
Dalteparin(n=43)
Placebo(n=42)
Age (years) 73±8 72±11Sex (male/female) 29/14 31/11Body mass index (kg/m2) 27±5 26±4Type 1/type 2 diabetes (n) 5/38 7/35Diabetes duration (years) 20±13 21±14Smokers/ex-smokers/non-smokers (n)
5/10/28 6/17/19
Treatment with insulin/tabl/diet(n)
33/8/2 33/6/3
HbA1c (%) 6.9±1.6 6.9±1.2
Peripheral neuropathy (n) 43 42Toe blood pressure (mmHg) 53±23 53±20Toe to arm blood pressure index 0.33±0.14 0.35
±0.12C-reactive protein (mg/L) 17±24 15±24Serum amyloid A (mg/L) 44±132 32±71
Data are given as number of subjects in group or mean±SD.There were no statistically significant differences betweenthe groups.
656 M. Kalani et al.
percolated through clots formed in special cuvetteswith recalcified plasma samples, using five differenthydrostatic pressures, under standardized condi-tions. Ks and μ values are derived from the volumesof the flow through buffer in equations as describedby Blombäck [29]. The coefficient of variation for Kswas 13.4%.
Statistical analysis
Continuous normally distributed data are reportedas mean±SD. Skewed data are reported as geomet-ric mean (interquartile range). Paired and unpaired
Table 2 Baseline values, and comparisons of changes (Δpatients with chronic foot ulcers and peripheral arterial ocdalteparin or placebo
Dalteparin (n=43)
Baseline Δ-value
TcPO2 (mmHg) 25±19 8.55 (14.6Resting LDF (PU) 65±48 −8.0 (45.0Biological zero (PU) 3.8±2.1 0.00 (1.70Peak LDF% 78±85 0.00 (96.0Time to peak LDF (s) 151±97 −12.8 (55.0hp-LDF% † 204±197 25.5 (256.
TcPO2, transcutaneous oxygen tension; LDF, laser Doppler fluxmetrend-of-study and baseline values) are median (interquartile range);groups; †percent increase in LDF during heating of the skin to 44 °C
Student's t-tests were used to evaluate differencesin coagulation and fibrinolysis variables, and othercontinuous variables between and within groups.Mann–Whitney and Wilcoxon sign rank tests wereused to evaluate differences in macro- and micro-circulation variables between and within groups.The associations between different variables wereinvestigated by linear correlation analyses. In caseof death or interruption of treatment because ofadverse events, the last investigation was used inthe analysis. A value of pb0.05 was consideredstatistically significant.
Ethical considerations
The protocol of this trial was approved by the localEthics Committee of each centre, and the SwedishMedical Products Agency. Written informed consentwas obtained from all patients.
Results
Two patients, one in each group, were excludedearly during the study period: one patient rando-mised to placebo suffered an acute arterial throm-boembolism before having the first injection ofstudymedication. The other patient was randomisedto dalteparin and was excluded after two weekstreatment due to a painful trochanteritis. Theremaining 85 patients completed the study protocol[13]. As published [13], baseline clinical character-istics of the treatment groups were comparable. Theselected characteristics are presented in Table 1.Analyses performed at baseline and at the end of thestudy revealed that circulating glucosylated hemo-globin (HbA1c) concentrations at the end-of-studydecreased (pb0.05) in the placebo group while itwas not significantly changed in the dalteparingroup, compared with baseline levels [13]. Of
-values) in microcirculatory variables, in 85 diabeticclusive disease, randomly assigned to treatment with
Placebo (n=42) P
Baseline Δ-value
) 32±19 0.00 (14.8) 0.015) 62±45 0.00 (44.8) 0.264) 4.2±1.9 0.00 (2.1) 0.772) 70±87 1.00 (76.0) 0.344) 168±117 0.00 (89.0) 0.5230) 295±481 40.5 (232.0) 0.552
y. Baseline data are mean±SD; Δ-values (=difference betweenP values refer to differences in Δ-values between the treatment.
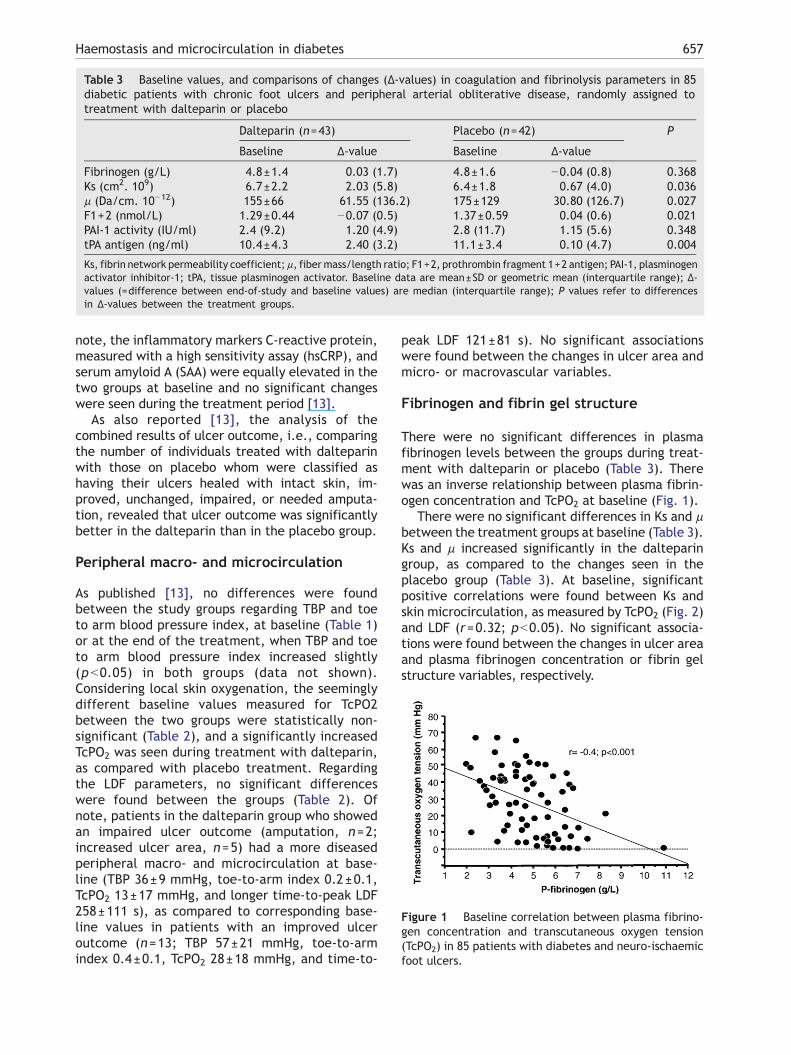
Table 3 Baseline values, and comparisons of changes (Δ-values) in coagulation and fibrinolysis parameters in 85diabetic patients with chronic foot ulcers and peripheral arterial obliterative disease, randomly assigned totreatment with dalteparin or placebo
Dalteparin (n=43) Placebo (n=42) P
Baseline Δ-value Baseline Δ-value
Fibrinogen (g/L) 4.8±1.4 0.03 (1.7) 4.8±1.6 −0.04 (0.8) 0.368Ks (cm2. 109) 6.7±2.2 2.03 (5.8) 6.4±1.8 0.67 (4.0) 0.036μ (Da/cm. 10−12) 155±66 61.55 (136.2) 175±129 30.80 (126.7) 0.027F1+2 (nmol/L) 1.29±0.44 −0.07 (0.5) 1.37±0.59 0.04 (0.6) 0.021PAI-1 activity (IU/ml) 2.4 (9.2) 1.20 (4.9) 2.8 (11.7) 1.15 (5.6) 0.348tPA antigen (ng/ml) 10.4±4.3 2.40 (3.2) 11.1±3.4 0.10 (4.7) 0.004
Ks, fibrin network permeability coefficient; μ, fibermass/length ratio; F1+2, prothrombin fragment 1+2 antigen; PAI-1, plasminogenactivator inhibitor-1; tPA, tissue plasminogen activator. Baseline data are mean±SD or geometric mean (interquartile range); Δ-values (=difference between end-of-study and baseline values) are median (interquartile range); P values refer to differencesin Δ-values between the treatment groups.
Figure 1 Baseline correlation between plasma fibrino-gen concentration and transcutaneous oxygen tension(TcPO2) in 85 patients with diabetes and neuro-ischaemicfoot ulcers.
657Haemostasis and microcirculation in diabetes
note, the inflammatory markers C-reactive protein,measured with a high sensitivity assay (hsCRP), andserum amyloid A (SAA) were equally elevated in thetwo groups at baseline and no significant changeswere seen during the treatment period [13].
As also reported [13], the analysis of thecombined results of ulcer outcome, i.e., comparingthe number of individuals treated with dalteparinwith those on placebo whom were classified ashaving their ulcers healed with intact skin, im-proved, unchanged, impaired, or needed amputa-tion, revealed that ulcer outcome was significantlybetter in the dalteparin than in the placebo group.
Peripheral macro- and microcirculation
As published [13], no differences were foundbetween the study groups regarding TBP and toeto arm blood pressure index, at baseline (Table 1)or at the end of the treatment, when TBP and toeto arm blood pressure index increased slightly(pb0.05) in both groups (data not shown).Considering local skin oxygenation, the seeminglydifferent baseline values measured for TcPO2between the two groups were statistically non-significant (Table 2), and a significantly increasedTcPO2 was seen during treatment with dalteparin,as compared with placebo treatment. Regardingthe LDF parameters, no significant differenceswere found between the groups (Table 2). Ofnote, patients in the dalteparin group who showedan impaired ulcer outcome (amputation, n=2;increased ulcer area, n=5) had a more diseasedperipheral macro- and microcirculation at base-line (TBP 36±9 mmHg, toe-to-arm index 0.2±0.1,TcPO2 13±17 mmHg, and longer time-to-peak LDF258±111 s), as compared to corresponding base-line values in patients with an improved ulceroutcome (n=13; TBP 57±21 mmHg, toe-to-armindex 0.4±0.1, TcPO2 28±18 mmHg, and time-to-
peak LDF 121±81 s). No significant associationswere found between the changes in ulcer area andmicro- or macrovascular variables.
Fibrinogen and fibrin gel structure
There were no significant differences in plasmafibrinogen levels between the groups during treat-ment with dalteparin or placebo (Table 3). Therewas an inverse relationship between plasma fibrin-ogen concentration and TcPO2 at baseline (Fig. 1).
There were no significant differences in Ks and μbetween the treatment groups at baseline (Table 3).Ks and μ increased significantly in the dalteparingroup, as compared to the changes seen in theplacebo group (Table 3). At baseline, significantpositive correlations were found between Ks andskin microcirculation, as measured by TcPO2 (Fig. 2)and LDF (r=0.32; pb0.05). No significant associa-tions were found between the changes in ulcer areaand plasma fibrinogen concentration or fibrin gelstructure variables, respectively.
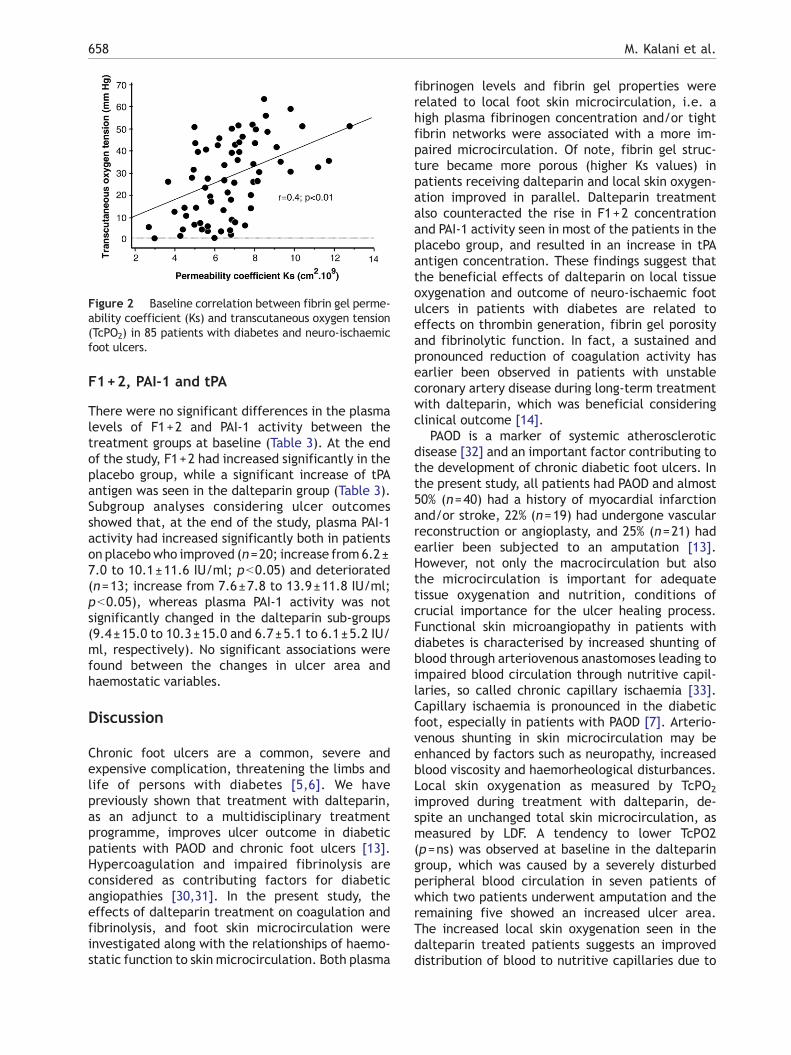
Figure 2 Baseline correlation between fibrin gel perme-ability coefficient (Ks) and transcutaneous oxygen tension(TcPO2) in 85 patients with diabetes and neuro-ischaemicfoot ulcers.
658 M. Kalani et al.
F1+2, PAI-1 and tPA
There were no significant differences in the plasmalevels of F1+2 and PAI-1 activity between thetreatment groups at baseline (Table 3). At the endof the study, F1+2 had increased significantly in theplacebo group, while a significant increase of tPAantigen was seen in the dalteparin group (Table 3).Subgroup analyses considering ulcer outcomesshowed that, at the end of the study, plasma PAI-1activity had increased significantly both in patientson placebowho improved (n=20; increase from 6.2±7.0 to 10.1±11.6 IU/ml; pb0.05) and deteriorated(n=13; increase from 7.6±7.8 to 13.9±11.8 IU/ml;pb0.05), whereas plasma PAI-1 activity was notsignificantly changed in the dalteparin sub-groups(9.4±15.0 to 10.3±15.0 and 6.7±5.1 to 6.1±5.2 IU/ml, respectively). No significant associations werefound between the changes in ulcer area andhaemostatic variables.
Discussion
Chronic foot ulcers are a common, severe andexpensive complication, threatening the limbs andlife of persons with diabetes [5,6]. We havepreviously shown that treatment with dalteparin,as an adjunct to a multidisciplinary treatmentprogramme, improves ulcer outcome in diabeticpatients with PAOD and chronic foot ulcers [13].Hypercoagulation and impaired fibrinolysis areconsidered as contributing factors for diabeticangiopathies [30,31]. In the present study, theeffects of dalteparin treatment on coagulation andfibrinolysis, and foot skin microcirculation wereinvestigated along with the relationships of haemo-static function to skin microcirculation. Both plasma
fibrinogen levels and fibrin gel properties wererelated to local foot skin microcirculation, i.e. ahigh plasma fibrinogen concentration and/or tightfibrin networks were associated with a more im-paired microcirculation. Of note, fibrin gel struc-ture became more porous (higher Ks values) inpatients receiving dalteparin and local skin oxygen-ation improved in parallel. Dalteparin treatmentalso counteracted the rise in F1+2 concentrationand PAI-1 activity seen in most of the patients in theplacebo group, and resulted in an increase in tPAantigen concentration. These findings suggest thatthe beneficial effects of dalteparin on local tissueoxygenation and outcome of neuro-ischaemic footulcers in patients with diabetes are related toeffects on thrombin generation, fibrin gel porosityand fibrinolytic function. In fact, a sustained andpronounced reduction of coagulation activity hasearlier been observed in patients with unstablecoronary artery disease during long-term treatmentwith dalteparin, which was beneficial consideringclinical outcome [14].
PAOD is a marker of systemic atheroscleroticdisease [32] and an important factor contributing tothe development of chronic diabetic foot ulcers. Inthe present study, all patients had PAOD and almost50% (n=40) had a history of myocardial infarctionand/or stroke, 22% (n=19) had undergone vascularreconstruction or angioplasty, and 25% (n=21) hadearlier been subjected to an amputation [13].However, not only the macrocirculation but alsothe microcirculation is important for adequatetissue oxygenation and nutrition, conditions ofcrucial importance for the ulcer healing process.Functional skin microangiopathy in patients withdiabetes is characterised by increased shunting ofblood through arteriovenous anastomoses leading toimpaired blood circulation through nutritive capil-laries, so called chronic capillary ischaemia [33].Capillary ischaemia is pronounced in the diabeticfoot, especially in patients with PAOD [7]. Arterio-venous shunting in skin microcirculation may beenhanced by factors such as neuropathy, increasedblood viscosity and haemorheological disturbances.Local skin oxygenation as measured by TcPO2
improved during treatment with dalteparin, de-spite an unchanged total skin microcirculation, asmeasured by LDF. A tendency to lower TcPO2(p=ns) was observed at baseline in the dalteparingroup, which was caused by a severely disturbedperipheral blood circulation in seven patients ofwhich two patients underwent amputation and theremaining five showed an increased ulcer area.The increased local skin oxygenation seen in thedalteparin treated patients suggests an improveddistribution of blood to nutritive capillaries due to

659Haemostasis and microcirculation in diabetes
a decreased shunting of blood through arteriove-nous channels. This phenomenon might be anexplanation for the demonstrated trend towardimproved ulcer outcome in patients treated withdalteparin [13].
Factors enhancing thrombus formation includehigh-grade stenosis, low blood flow, hyperfibrino-genemia, increased thrombin generation and highplasma PAI-1 activity which generally results indecreased fibrinolysis. In the present study, wefound strikingly high levels of plasma fibrinogen,F1+2 and PAI-1 in both treatment groups, indicat-ing hypercoagulation and impaired fibrinolysis.Serum concentrations of the acute phase reactantsCRP and SAA were equally elevated in the twotreatment groups, both at baseline and at studytermination, indicating a similar degree of inflam-mation in the two treatment groups. A significantinverse association was found between the plasmafibrinogen concentration and local skin oxygena-tion, as measured by TcPO2. TcPO2 may partlyreflect local nutritive capillary circulation, andhave been suggested for evaluation of PAOD [23],prediction of ulcer outcome [24,26], and amputa-tion level [25]. The association between plasmafibrinogen and local skin microcirculation mostprobably reflects effects of high blood viscosity,the latter being even higher in vessels with lowperfusion pressure as in patients with PAOD [34].Also an elevated plasma fibrinogen concentrationmight be secondary to advanced vascular diseasegenerating a vicious circle as suggested by Yamadaet al. [35].
There was a significant positive correlation be-tween fibrin gel porosity (Ks) and local skinmicrocirculation as measured by both TcPO2 andLDF, which was largely independent of fibrinogenlevels. Ks and μ increased significantly with dalte-parin treatment. Increased fibrin gel porosity duringtreatment with dalteparin may positively influencemicrovascular function by decreasing the propensityto microthrombosis and/or improving the rheologi-cal properties of the blood. The properties of fibringel structure are influenced by various factors, suchas metabolic control [36,37] and treatment withaspirin [38]. Since the metabolic control, as mea-sured by HbA1c, was remarkably good in bothtreatment groups throughout the study, and allpatients were treated with a daily dose of 75 mgaspirin, these factors are unlikely to have influencedthe results.
Plasma F1+2 increased significantly in theplacebo group, and PAI-1 increased in most of thepatients receiving placebo whereas these variableswere not significantly changed in the dalteparingroup. This is probably due to the inhibitory effect
of dalteparin on coagulation activation and itsprofibrinolytic properties [14]. The increase in tPAantigen in dalteparin treated patients was notaccompanied by a rise in PAI-1 activity, whichmight indicate enhanced fibrinolytic activity.
Despite no statistically significant correlationsbetween changes in ulcer area and microvascular(tcPO2) or haemostatic variables, the improve-ments of these variables were all seen in thedalteparin group. No significant improvementswere seen in any of these variables in the placebogroup. Several factors contribute to the impairedulcer healing process in this severely diseasedpatient group (off loading of the foot ulcer,inflammation, metabolic control, neuropathy, oxy-genation, coagulation and fibrinolysis) and thesefactors most probably work in concert. Thus, theincreased tcPO2 level and improved haemostaticfunction during treatment with dalteparin mostprobably provide a better healing capacity as alsoindicated by the better ulcer outcome in thisgroup. Of note, only two amputations wereperformed in the dalteparin group as compared toeight in the placebo group. These findings mostlikely indicate that dalteparin has beneficialeffects on the healing process of diabetic neuro-ischemic foot ulcers.
A limitation of the present study is the highnumber of patients with previous arterial recon-struction and amputation [13], who could possiblyhave a different endothelial function and coagula-tion profile compared with patients without ampu-tations. However, there were no differencesbetween the study groups with respect to thenumber of patients who had undergone previousarterial reconstruction and amputation [13]. Inaddition there were no differences in plasmaconcentrations of haemostatic variables betweenthe patients who have undergone percutaneoustransluminal angioplasty and/or by-pass surgery andthose who have not.
In conclusion, the present study demonstrates anassociation between skin microvascular functionand haemostatic factors, i.e. plasma fibrinogenconcentration and fibrin gel structure in patientswith diabetes, vascular disease and chronic footulcers. Treatment with dalteparin exerted aninhibitory effect on thrombin generation, increasedfibrin gel porosity, which, in turn, favoured fibrino-lysis. In addition, dalteparin improved fibrinolyticfunction by increasing tPA antigen and blunting agradual increase in plasma PAI-1 activity. Thesefindings may constitute likely mechanisms for thebeneficial effects of dalteparin on local skinoxygenation and outcome of neuro-ischaemic footulcers in patients with diabetes.

660 M. Kalani et al.
Acknowledgements
We thank Perimed AB, Stockholm, Sweden, for sup-porting the study with equipment for measurementsof laser Doppler fluxmetry, and Radiometer MedicalA/S, Copenhagen, Denmark for transcutaneousoxygen tension equipment.
The study was supported by grants from thePharmacia Corporation, the Swedish Heart–LungFoundation, the Swedish Research Council, and theStockholm County Council.
References
[1] Carr ME. Diabetes mellitus: a hypercoagulable state.J Diabetes Complications 2001;15:44–54.
[2] Sobel BE, Woodcock-Mitchell J, Schneider DJ, Holt RE,Marutsuka K, Gold H. Increased plasminogen activatorinhibitor type 1 in coronary artery atherectomy specimensfrom type 2 diabetic compared with nondiabetic patients: apotential factor predisposing to thrombosis and its persis-tence. Circulation 1998;97:2213–21.
[3] Aso Y, Matsumoto S, Fujiwara Y, Tayama K, Inukai T,Takemura Y. Impaired fibrinolytic compensation for hyper-coagulability in obese patients with type 2 diabetes:association with increased plasminogen activator inhibi-tor-1. Metabolism 2002;51:471–6.
[4] Anand SS, Yi Q, Gerstein H, Lonn E, Jacobs R, Vuksan V, et al.Relationship of metabolic syndrome and fibrinolytic dys-function to cardiovascular disease. Circulation 2003;108:420–5.
[5] Apelqvist J, Ragnarson Tennvall G, Persson U, Larsson J.Diabetic foot ulcers in a multidisciplinary setting. Aneconomical analysis of primary healing or healing withamputation. J Intern Med 1994;235:463–71.
[6] Apelqvist J. Diabetic foot ulcers: the importance of clinicalcharacteristics and prognostic factors for the outcome[dissertation]. Lund, Sweden: University of Lund; 1991.
[7] Jörneskog G, Brismar K, Fagrell B. Skin capillary circulationis more impaired in toes of diabetic than non-diabeticpatients with peripheral vascular disease. Diabet Med1995;12:36–41.
[8] Ganda OP, Arkin CF. Hyperfibrinogenemia. An important riskfactor for vascular complications in diabetes. Diabetes Care1992;15:1245–50.
[9] Jörneskog G, Egberg N, Fagrell B, Fatah K, Hessel B,Johnsson H, et al. Altered properties of the fibrin gelstructure in patients with IDDM. Diabetologia 1996;39:1519–23.
[10] Dunn EJ, Ariens RA, Grant PJ. The influence of type 2diabetes on fibrin structure and function. Diabetologia2005;48:1198–206.
[11] Gabriel DA, Muga K, Boothroyd EM. The effect of fibrinstructure on fibrinolysis. J Biol Chem 1992;267 (34):24259–63.
[12] Collet JP, Allali Y, Lesty C, Tanguy ML, Silvain J, Ankri A, et al.Altered fibrin architecture is associated with hypofibrino-lysis and premature coronary atherothrombosis. Arterios-cler Thromb Vasc Biol 2006;26 (11):2567–73.
[13] Kalani M, Apelqvist J, Blombäck M, Brismar K, Eliasson B,Eriksson JW, et al. Effect of dalteparin on healing of chronicfoot ulcers in diabetic patients with peripheral arterialocclusive disease: a prospective, randomised, double-blind
and placebo-controlled study. Diabetes Care 2003;26:2575–80.
[14] Oldgren J, Fellenius C, Boman K, Jansson JH, Nilsson TK,Wallentin L, et al. Influence of prolonged dalteparintreatment on coagulation, fibrinolysis and inflammation inunstable coronary artery disease. J Intern Med 2005;258:420–7.
[15] Wagner FW. The dysvascular foot: a system for diagnosis andtreatment. Foot Ankle 1981;2:64–122.
[16] Wahlberg E, Gush R. A new automated toe blood pressuremonitor for assessment of limb ischemia. Eur J VascEndovasc Surg 2002;24:304–8.
[17] Fagrell B. Problems using laser Doppler on the skin in clinicalpractice. In: Belcaro G, Hoffman U, Bollinger A, NicolaidesA, editors. Laser Doppler. London: MED-ORION Publ. Co.;1994. p. 49–54. Chapter 4.
[18] Hirata K, Nagasaka T, Noda Y. Partional measurement ofcapillary and arteriovenous anastomotic blood flow in thehuman finger by laser Doppler flowmeter. Eur J Appl Physiol1988;57:616–21.
[19] Nilsson GE, Tenland T, Öberg PA. Evaluation of a laserDoppler flowmeter for measurement of tissue blood flow.IEEE Trans Biomed Eng 1980;27:597–604.
[20] Caspary L, Creutzig A, Alexander K. Biological zero inlaser Doppler fluxmetry. Int J Microcirc Clin Exp 1988;7:367–71.
[21] Huch A, Huch R, Arner B, Rooth G. Continuous transcuta-neous oxygen measured with a heated electrode. Scand JClin Lab Invest 1973;31:269–75.
[22] Sheffield PJ. Measuring tissue oxygen tension: a review.Undersea Hyperb Med 1998;25:179–88.
[23] Howd A, Proud G, Chamberlain J. Transcutaneous oxygenmonitoring as an indication of prognosis in critical ischaemiaof the lower limb. Eur J Vasc Surg 1988;2:27–30.
[24] Kalani M, Brismar K, Fagrell B, Östergren J, Jörneskog G.Transcutaneous oxygen tension and toe blood pressure aspredictors for outcome of diabetic foot ulcers. DiabetesCare 1999;22:147–51.
[25] Harward TR, Volny J, Golbranson F, Bernstein EF, Fronek A.Oxygen inhalation-induced transcutaneous PO2 changes as apredictor of amputation level. J Vasc Surg 1985;2:220–7.
[26] Bacharach JM, Rooke TW, Osmundson PJ, Gloviczki P.Predictive value of transcutaneous oxygen pressure andamputation success by use of supine and elevationmeasurements. J Vasc Surg 1992;15:558–63.
[27] Jörneskog G, Djavani K, Brismar K. Day-to-day variability oftranscutaneous oxygen tension in patients with diabetesmellitus and peripheral arterial occlusive disease. J VascSurg 2001;34:277–82.
[28] Blombäck B, Blombäck M. Purification of human and bovinefibrinogen. Arkiv Kemi 1956;10:415–43.
[29] Blombäck B, Carlsson K, Hessel B, Liljeborg A, Procyk R,Aslund N. Native fibrin gel networks observed by 3Dmicroscopy, permeation and turbidity. Biochim BiophysActa 1989;997:96–110.
[30] Panahloo A, Yudkin JS. Diminished fibrinolysis in diabetesmellitus and its implication for diabetic vascular disease.J Cardiovasc Risk 1997;4:91–9.
[31] Lapolla A, Piarulli F, Sartore G, Rossetti C, Martano L,Carraro P, et al. Peripheral artery disease in type 2 diabetes:the role of fibrinolysis. Thromb Haemost 2003;89:91–6.
[32] Aronow WS, Ahn C. 62 years of age. Am J Cardiol1994;74:64–5.
[33] Fagrell B, Jörneskog G, Intaglietta M. Disturbed microvas-cular reactivity and shunting — a major cause for diabeticcomplications. Vasc Med 1999;4:125–7.

661Haemostasis and microcirculation in diabetes
[34] Lowe GD. Virchow's triad revisited: abnormal flow.Pathophysiol Haemost Thromb 2003 Sep-2004 Dec; 33:455–457.
[35] Yamada T, Sato A, Nishimori T, Mitsuhashi T, Terao A, SagaiH, et al. Importance of hypercoagulability over hypergly-cemia for vascular complication in type 2 diabetes. Dia-betes Res Clin Pract 2000;49:23–31.
[36] Nair CH, Azhar A, Wilson JD, Dhall DP. Studies on fibrinnetwork structure in human plasma Part II — Clinicalapplication: diabetes and antidiabetic drugs. Thromb Res1991;64:477–85.
[37] Jörneskog G, Hansson LO, Wallen NH, Yngen M, Blombäck M.Increased plasma fibrin gel porosity in patients with type Idiabetes during continuous subcutaneous insulin infusion.J Thromb Haemost 2003;1:1195–201.
[38] Jörneskog G, Fatah K, Blombäck M. Fibrin gel structure indiabetic patients before and during treatment with acet-ylsalicylic acid: a pilot study. Fibrinolysis Proteolysis1998;12:360–5.




















