
Systematic Review of the Effectiveness of Hyperbaric Oxygenation Therapy in the Management of...
10
Systematic Review of the Effectiveness of Hyperbaric Oxygenation Therapy in the Management of Chronic Diabetic Foot Ulcers Rui Liu, PhD; Ling Li, MD; Mengliu Yang, MD; Guenther Boden, MD; and Gangyi Yang, PhD Abstract Objective: To assess the efficacy and safety of hyperbaric oxygenation (HBO) therapy as adjunctive treatment for diabetic foot ulcers with a systematic review and meta-analysis of the literature. Methods: MEDLINE, EMBASE, and the Cochrane Library were searched to find relevant articles pub- lished up to April 20, 2012, without restriction as to language or publication status. All controlled trials that evaluated adjunctive treatment with HBO therapy compared with treatment without HBO for chronic diabetic foot ulcers were selected. A meta-analysis was performed to assess the efficacy and safety of hyperbaric oxygen in managing foot ulcers. Results: Thirteen trials (a total of 624 patients), including 7 prospective randomized trials, performed between January 1, 1966, and April 20, 2012, were identified as eligible for inclusion in the study. Pooling analysis revealed that, compared with treatment without HBO, adjunctive treatment with HBO resulted in a significantly higher proportion of healed diabetic ulcers (relative risk, 2.33; 95% CI, 1.51-3.60). The analysis also revealed that treatment with HBO was associated with a significant reduction in the risk of major amputations (relative risk, 0.29; 95% CI, 0.19-0.44); however, the rate of minor amputations was not affected (P¼.30). Adverse events associated with HBO treatment were rare and reversible and not more frequent than those occurring without HBO treatment (P¼.37). Conclusions: This meta-analysis reveals that treatment with HBO improved the rate of healing and reduced the risk of major amputations in patients with diabetic foot ulcers. On the basis of these effects, we believe that quality of life could be improved in selected patients treated with HBO. ª 2013 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2013;88(2):166-175 T he worldwide epidemic of type 2 diabetes mellitus has brought increased attention to some of its common complications, such as foot ulcers, secondary infections, and limb amputations. 1,2 The development of dia- betic foot ulcers is driven primarily by the effects of peripheral sensory neuropathy on foot biome- chanics (foot deformity being associated with high pressures in specific weight-bearing areas). 3 Lower extremity ulcers are responsible for 20% of diabetes-related hospital admissions and are a major source of morbidity and loss of income for patients with diabetes mellitus. 4,5 Treatment is often prolonged and is sometimes unsuccessful, and the patients are prone to serious complications. Traditional management is based on cleansing, debridement, and elimi- nating infections. 6-9 Many different interven- tions have been proposed to accelerate the healing process, but few have been subjected to strict evaluation. Hyperbaric oxygenation (HBO) has been proposed as an adjunctive treatment for dia- betic foot ulcers 9-11 and has been reported to reduce the incidence of major amputations in diabetic patients with ischemic foot ulcers. 12 The value of HBO therapy, however, remains controversial because of conflicting data in the literature. 13-18 We believe that a system- atic review of the literature, comparing treat- ment of chronic diabetic foot ulcers with and without HBO, would help clinicians and policymakers decide whether HBO therapy should be more widely used. Therefore, this review analyzes peer-reviewed medical publications that have reported results of HBO as an adjunctive treatment for diabetic foot ulcers. From the Department of Endocrinology, the Second Affiliated Hospital (R.L., M.Y., G.Y.), and Key Laboratory of Diagnostic Medicine (Ministry of Education) and Department of Clinical Biochemistry, Division of Laboratory Medicine (L.L.), Chongqing Medical University, Chongqing, China; and the Division of Endocrinology/ Diabetes/Metabolism and the Clinical Research Center, Temple University School of Medicine, Philadelphia, PA (G.B.). 166 Mayo Clin Proc. n February 2013;88(2):166-175 n http://dx.doi.org/10.1016/j.mayocp.2012.10.021 www.mayoclinicproceedings.org n ª 2013 Mayo Foundation for Medical Education and Research ORIGINAL ARTICLE
Transcript of Systematic Review of the Effectiveness of Hyperbaric Oxygenation Therapy in the Management of...

ORIGINAL ARTICLE
From the Department oEndocrinology, the SecoAffiliated Hospital (R.L.,G.Y.), and Key LaboratoDiagnostic Medicine (Mof Education) andDepartment of ClinicalBiochemistry, Division oLaboratory Medicine (LChongqing Medical UnivChongqing, China; and tDivision of EndocrinoloDiabetes/Metabolism anClinical Research CenteTemple University SchoMedicine, Philadelphia, P(G.B.).
166
Systematic Review of the Effectiveness ofHyperbaric Oxygenation Therapy in the
Management of Chronic Diabetic Foot Ulcers
Rui Liu, PhD; Ling Li, MD; Mengliu Yang, MD; Guenther Boden, MD;and Gangyi Yang, PhD
Abstract
Objective: To assess the efficacy and safety of hyperbaric oxygenation (HBO) therapy as adjunctivetreatment for diabetic foot ulcers with a systematic review and meta-analysis of the literature.Methods: MEDLINE, EMBASE, and the Cochrane Library were searched to find relevant articles pub-lished up to April 20, 2012, without restriction as to language or publication status. All controlled trialsthat evaluated adjunctive treatment with HBO therapy compared with treatment without HBO for chronicdiabetic foot ulcers were selected. A meta-analysis was performed to assess the efficacy and safety ofhyperbaric oxygen in managing foot ulcers.Results: Thirteen trials (a total of 624 patients), including 7 prospective randomized trials, performedbetween January 1, 1966, and April 20, 2012, were identified as eligible for inclusion in the study. Poolinganalysis revealed that, compared with treatment without HBO, adjunctive treatment with HBO resulted ina significantly higher proportion of healed diabetic ulcers (relative risk, 2.33; 95% CI, 1.51-3.60). The analysisalso revealed that treatment with HBO was associated with a significant reduction in the risk of majoramputations (relative risk, 0.29; 95% CI, 0.19-0.44); however, the rate of minor amputations was not affected(P¼.30). Adverse events associated with HBO treatment were rare and reversible and not more frequent thanthose occurring without HBO treatment (P¼.37).Conclusions: This meta-analysis reveals that treatment with HBO improved the rate of healing andreduced the risk of major amputations in patients with diabetic foot ulcers. On the basis of these effects,we believe that quality of life could be improved in selected patients treated with HBO.
ª 2013 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2013;88(2):166-175
fndM.Y.,ry ofinistry
f.L.),ersity,hegy/d ther,ol ofA
T he worldwide epidemicof type2diabetesmellitus has brought increased attentionto some of its common complications,
such as foot ulcers, secondary infections, andlimb amputations.1,2 The development of dia-betic foot ulcers is driven primarily by the effectsof peripheral sensory neuropathy on foot biome-chanics (foot deformity being associated withhigh pressures in specific weight-bearing areas).3
Lower extremity ulcers are responsible for 20%of diabetes-related hospital admissions andare a major source of morbidity and loss ofincome for patients with diabetes mellitus.4,5
Treatment is often prolonged and is sometimesunsuccessful, and the patients are prone toserious complications. Traditional managementis based on cleansing, debridement, and elimi-nating infections.6-9 Many different interven-tions have been proposed to accelerate the
Mayo Clin Proc. n February 2013www.mayoclinicproceedings.org n
healing process, but few have been subjected tostrict evaluation.
Hyperbaric oxygenation (HBO) has beenproposed as an adjunctive treatment for dia-betic foot ulcers9-11 and has been reported toreduce the incidence of major amputations indiabetic patients with ischemic foot ulcers.12
The value of HBO therapy, however, remainscontroversial because of conflicting data in theliterature.13-18 We believe that a system-atic review of the literature, comparing treat-ment of chronic diabetic foot ulcers with andwithout HBO, would help clinicians andpolicymakers decide whether HBO therapyshould be more widely used. Therefore,this review analyzes peer-reviewed medicalpublications that have reported results ofHBO as an adjunctive treatment for diabeticfoot ulcers.
;88(2):166-175 n http://dx.doi.org/10.1016/j.mayocp.2012.10.021ª 2013 Mayo Foundation for Medical Education and Research
François
Zone de texte
FB 325.1302
François
Zone de texte
Oui, mais il faut savoir quantifier le degré d'ischémie et stratifier, ça marche sur les cas qui ne sont pas en ICC consensus 1991, il faut savoir faire les amputations mineures à temps avant que l'infection ne dérape (d'ailleurs ici bénéfice sur les amputations majeures, mais pas sur les mineures ...)
François
Texte surligné
HBO THERAPY IN DIABETIC FOOT ULCERS
METHODS
Data Sources and SearchWe conducted a systematic literature search ofMEDLINE (1966 to April 20, 2012), EMBASE(1974 to April 20, 2012), and the CochraneLibrary (2012) for studies reporting on HBOtherapy of diabetic foot ulcers. In addition, wesearched the reference lists of relevant publica-tions, reviewed the abstracts of selected scien-tific meetings (American Diabetes Association,the Society for Research on HBO, and othermajor diabetes and endocrinology or plasticsurgery scientific meetings) from 2003 to April20, 2012. Other completed but still unpublishedtrials were identified and retrieved from thewww.clinicaltrials.gov, www.novonordisk-trials.com, and www.clinicalstudyresults.org websites.For these electronic searches, we used versions ofMedical Subject Headings and main keywords(diabetic foot, diabetic lower extremity ulcers, dia-betic leg ulcers, diabetic wounds, diabetes andchronic foot ulcer, and hyperbaric oxygenation ORhyperbar*OR oxygen) but limited them to clinicaltrial and human.
Study SelectionThe identification of relevant abstracts and theselection of studies on the basis of the criteriadescribed in this article were performed inde-pendently by 2 of the authors (R.L. and M.Y.),and any discrepancy was resolved by a thirdinvestigator (G.Y.).
Clinical trials were included if they met allthe following criteria: (1) randomized controlledtrials (RCTs) or unrandomized controlled trialsusing either crossover or parallel designs, con-ducted in humans and published in anylanguage; (2) inclusion of patients with type 1or type 2 diabetes with chronic lower extremityulcers; (3) regular interventions performed forcontrol of glycemia, revascularization, debride-ment, off-loading, and metabolic and infectioncontrols assessed as outcome; (4) full-text articlesof controlled trials examining HBO plus tra-ditional therapy vs therapy without HBO; (5)reporting of proportion of healed ulcers, majoror minor amputations, adverse events, qualityof life, and cost-effectiveness from baseline toend of trial and the corresponding variances;and (6) inclusion of both prospective and retro-spective studies. Studies that assessed the efficacyand safety of HBO therapy in managing foot
Mayo Clin Proc. n February 2013;88(2):166-175 n http://dx.doi.orgwww.mayoclinicproceedings.org
ulcers attributable to causes other than diabetes,that did not report the outcomes of interest, inwhich it was impossible to assess the outcomesfrom the published results, or that lacked a con-trol group were excluded.
Data Extraction and Quality AssessmentThe primary clinical outcome of interest wasthe effect of HBO therapy on ulcer healing de-fined as complete epithelialization of the wound.Secondary outcomes included major or minoramputations. Furthermore, data on adverseevents, quality of life, and cost-effectivenesswere evaluated and tabulated along with deathfrom any cause. Two reviewers independentlyextracted data from each study, including studytitle, first author, publication year, institution,population demographics, study design, follow-up period, inclusion and exclusion criteria, andmain outcomes (healing percentages, major orminor amputations, adverse events, quality oflife, and cost-effectiveness). Duplicate reportsweremerged. If outcomes from the same patientswere published in multiple articles with differentfollow-up periods, we extracted the outcomesfrom the first study and the outcomes of thefollow-up studies from the later reports. Whenstudies from the same institution reported thesame outcomes at similar follow-up periods,either the better quality or the most informativereports were selected.
The quality of the included RCTs wasassessed by 3 categories, ranging from A (highquality) to C (low quality).18 These categoriesincluded the randomization procedure, theuse of intention-to-treat analysis, dropout rate,allocation concealment, and the extent to whichvalid outcomes were described (Table 1). Anydisagreement regarding study quality wasresolved by discussion among the authors.
Statistical AnalysesThe RCTs in this meta-analysis were includedaccording to the QUOROM guidelines.24,25
For categorical variables, the relative risk (RR)was used to compare the event ratio betweenthe study group (HBO therapy) and the controlgroup (no HBO therapy). In the case of adverseevents, an RR of less than 1 favored the studygroup. Statistical significance was assumed atthe P<.05 level. A fixed-effects model waschosen on the presumption that variation inthe individual trial results occurred around
/10.1016/j.mayocp.2012.10.021 167
François
Texte surligné
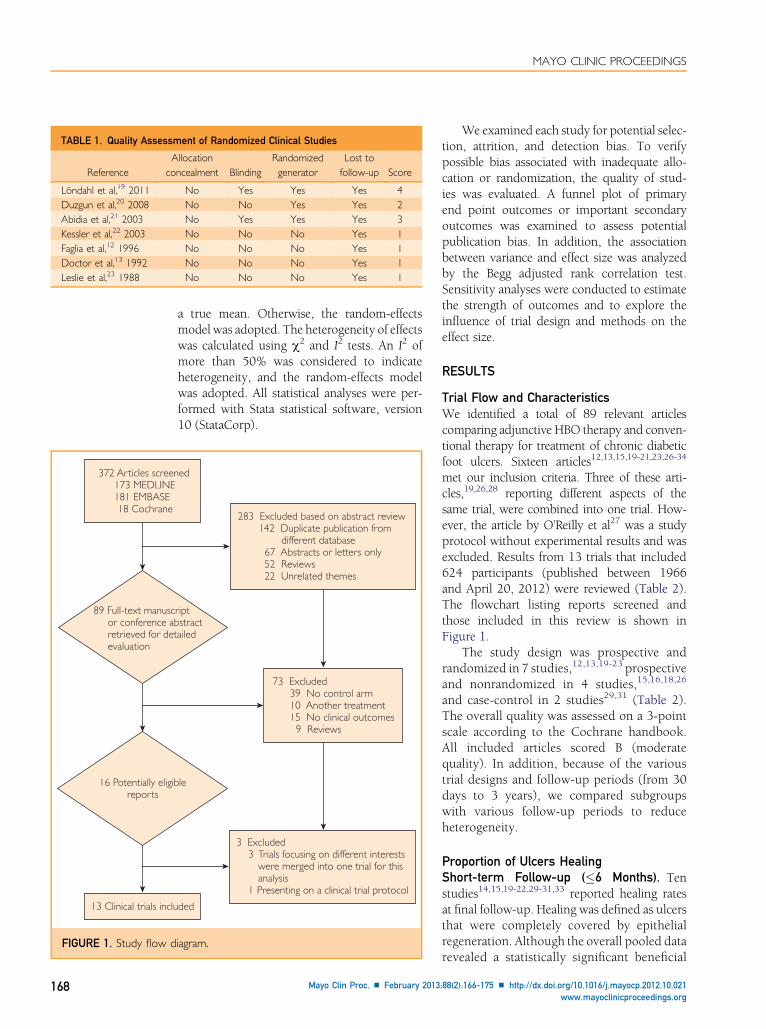
TABLE 1. Quality Assessment of Randomized Clinical Studies
ReferenceAllocation
concealment BlindingRandomizedgenerator
Lost tofollow-up Score
Löndahl et al,19 2011 No Yes Yes Yes 4Duzgun et al,20 2008 No No Yes Yes 2Abidia et al,21 2003 No Yes Yes Yes 3Kessler et al,22 2003 No No No Yes 1Faglia et al,12 1996 No No No Yes 1Doctor et al,13 1992 No No No Yes 1Leslie et al,23 1988 No No No Yes 1
13 Clinical trials inclu
372 Articles screen 173 MEDLINE 181 EMBASE 18 Cochrane
89 Full-text manusc or conference ab retrieved for det evaluation
16 Potentially eligibreports
FIGURE 1. Study flow d
MAYO CLINIC PROCEEDINGS
168
a true mean. Otherwise, the random-effectsmodel was adopted. The heterogeneity of effectswas calculated using c2 and I2 tests. An I2 ofmore than 50% was considered to indicateheterogeneity, and the random-effects modelwas adopted. All statistical analyses were per-formed with Stata statistical software, version10 (StataCorp).
ded
ed
283 Excluded based on abstract review 142 Duplicate publication from different database 67 Abstracts or letters only 52 Reviews 22 Unrelated themes
3 Excluded 3 Trials focusing on different interests were merged into one trial for this analysis 1 Presenting on a clinical trial protocol
riptstractailed
le
73 Excluded 39 No control arm 10 Another treatment 15 No clinical outcomes 9 Reviews
iagram.
Mayo Clin Proc. n February 2013
We examined each study for potential selec-tion, attrition, and detection bias. To verifypossible bias associated with inadequate allo-cation or randomization, the quality of stud-ies was evaluated. A funnel plot of primaryend point outcomes or important secondaryoutcomes was examined to assess potentialpublication bias. In addition, the associationbetween variance and effect size was analyzedby the Begg adjusted rank correlation test.Sensitivity analyses were conducted to estimatethe strength of outcomes and to explore theinfluence of trial design and methods on theeffect size.
RESULTS
Trial Flow and CharacteristicsWe identified a total of 89 relevant articlescomparing adjunctive HBO therapy and conven-tional therapy for treatment of chronic diabeticfoot ulcers. Sixteen articles12,13,15,19-21,23,26-34
met our inclusion criteria. Three of these arti-cles,19,26,28 reporting different aspects of thesame trial, were combined into one trial. How-ever, the article by O’Reilly et al27 was a studyprotocol without experimental results and wasexcluded. Results from 13 trials that included624 participants (published between 1966and April 20, 2012) were reviewed (Table 2).The flowchart listing reports screened andthose included in this review is shown inFigure 1.
The study design was prospective andrandomized in 7 studies,12,13,19-23 prospectiveand nonrandomized in 4 studies,15,16,18,26
and case-control in 2 studies29,31 (Table 2).The overall quality was assessed on a 3-pointscale according to the Cochrane handbook.All included articles scored B (moderatequality). In addition, because of the varioustrial designs and follow-up periods (from 30days to 3 years), we compared subgroupswith various follow-up periods to reduceheterogeneity.
Proportion of Ulcers HealingShort-term Follow-up (�6 Months). Tenstudies14,15,19-22,29-31,33 reported healing ratesat final follow-up. Healing was defined as ulcersthat were completely covered by epithelialregeneration. Although the overall pooled datarevealed a statistically significant beneficial
;88(2):166-175 n http://dx.doi.org/10.1016/j.mayocp.2012.10.021www.mayoclinicproceedings.org

TABLE 2. Characteristics of 13 Clinical Controlled Trials of Diabetic Foot Ulcers Treated With or Without Hyperbaric Oxygenation
Reference Study design Inclusion criteria Follow-up
Patients undergoing HBO therapy/therapy without HBO
No. ofpatients
Age (y),mean � SD
No. withIUDM
Löndahl et al,19 2011 Randomized prospective Chronic DFU >3 mo 12 mo 38/37 67�8.5/71�7 26/32Blackman et al,33 2010 Nonrandomized prospective Chronic DFU 24 mo 17/11 62.4�9.7/63.4�9.6 NADuzgun et al,20 2008 Randomized prospective DFU >4 wk 92�12 wk 50/50 58.1�11.03/63.3�9.15 NAAlbuquerque and
Sousa,29 2005 Retrospective DFU >6 mo 55 mo 55/41 61.1�12.9/64.2�13.7 18/17.1Abidia et al,21 2003 Randomized prospective Ischemic DFU >6 wk 12 mo 8/8 72�12.6/70�6.6 NAKessler et al,22 2003 Randomized prospective Nonischemic DFU >3 mo 1 mo 14/13 60.2�9.7/67.6�10.5 14/15Kalani et al,30 2002 Nonrandomized prospective Chronic DFU >2 mo 3 y 17/21 54�14/65�11 65/43Zamboni et al,15 1997 Nonrandomized prospective Nonhealing DFU 4-6 mo 5/5 63.6�3.96/53.8�3.50 NAFaglia et al,12 1996 Randomized prospective Ischemic DFU >1 mo 3 mo 35/33 61.7�10.4/65.6�9.1 60/66.7Doctor et al,13 1992 Randomized prospective Chronic DFU 2 mo 15/15 56.2/59.8 15/20Oriani et al,14 1992 Nonrandomized prospective Diabetic foot gangrene 3 mo 62/18 52.7�12.4/58.2�8.2 NALeslie et al,23 1988 Randomized prospective DFU 2 wk 12/16 52.8�8.6/46.2�8.5 0/33Baroni et al,31 1987 Retrospective Diabetic foot gangrene NA 18/10 67�8.5/71�7 NA
DFU ¼ diabetic foot ulcer; HBO ¼ hyperbaric oxygenation; IUDM ¼ insulin-using diabetes mellitus; NA ¼ not available.
HBO THERAPY IN DIABETIC FOOT ULCERS
effect in HBO-treated cases (RR, 2.33; 95% CI,1.51-3.6), there was a great deal of heteroge-neity (I2¼50.4%) (Figure 2, A). Because healingof diabetic ulcers might be influenced by thelength of treatment, a random-effects modelanalysis was adopted to assess the proportionof healed ulcers, and subgroup analyses wereperformed to assess results of trials with short-term follow-up (�6 months). The results re-vealed that even short-term HBO treatment(�6 months) improved healing rates (RR, 1.50;P¼.02) without heterogeneity (I2¼0).
Long-term Follow-up (�1 Year). Seven trials(366 participants), representing 58.6% of allpatients in this review,19-21,29-31,33 had follow-up periods of 1 year or more. There was a sta-tistically significant increase in the proportion ofhealed ulcers after HBO therapy, and the long-term follow-up results demonstrated a largerRR (2.97) compared with the RR (1.50) of theshort-term subgroup results (P<.01).
RCT Subanalysis. A total of 300 patients in 4RCTs were assessed for wound healing as theprimary outcome. There were large heterogene-ities in the subanalysis (I2¼79.4%) and in thetotal population (Figure 2, B). To strengthenthe power of the meta-analysis and to decreaseheterogeneity, the study by Duzgun et al20 wasexcluded because it reported healing only with
Mayo Clin Proc. n February 2013;88(2):166-175 n http://dx.doi.orgwww.mayoclinicproceedings.org
conservative therapy without surgical interven-tion. Exclusion of the data of Duzgun et al im-proved the beneficial effects of adjunctive HBOtherapy (RR, 2.13; 95%CI, 1.392-3.259;P¼.04).
Major and Minor AmputationMajor Amputation. The most serious compli-cation (ie, major amputations, defined as ampu-tations above the ankle joint) was assessed in11 trials, which found that there were signifi-cantly fewer major amputations in patientsundergoing HBO therapy compared with con-ventional therapy without HBO. The pooledRR (Mantel-Haenszel) was 0.29 (95% CI, 0.19-0.44; P<.01). No heterogeneity was detected(P¼.26; Figure 3). As seen in Figure 3, the re-sults of subgroup analyses with only RCTs alsodemonstrated reduced risk of major amputation(RR, 0.24; 95% CI, 0.12-0.48; P<.01).
Minor Amputation. Five trials, including 4RCTs, provided data on minor amputationsdistal to the ankle joint with outcome assessmentfor up to 55 months. Pooled analysis of thesedata resulted in an RR of 1.24 (95% CI, 0.83-1.85; P¼.30), revealing identical minor amputa-tion rates between HBO and conventionaltherapy and no evidence to suggest statisticalheterogeneity (P¼.37) (Figure 4, A). Sub-group analysis with RCTs revealed similarrates of minor amputations (RR, 1.55; 95%
/10.1016/j.mayocp.2012.10.021 169
François
Texte surligné
François
Texte surligné

Reference
A
Proportion healed
Long-term follow-up
Löndahl et al,19 2011
Blackman et al,33 2010
Duzgun et al,20 2008
Albuquerque and Sousa et al,29 2005
Abidia et al,21 2003
Kalani et al,30 2002
Baroni et al,31 1987
Subtotal (I2 = 58.6%, P=.025)
Long-term follow-up z=3.41, P>.001
Short-term follow-up
Kessler et al,22 2003
Zamboni et al,15 1997
Oriani et al,14 1992
Short-term follow-up z=2.44, P=.02
Subtotal (I2 = 0.0%, P=.41)
Overall (I2 = 50.4%, P=.33)Overall z=3.83, P<.001
NOTE: Weights are from random-effects analysis
.00094 1 1064
Favors control Favors HBO therapy
RR (95% CI)
4.67 (0.24-88.96)
4.00 (0.66-24.37)
1.43 (1.02-1.99)
1.50 (1.08-2.07)
2.33 (1.51-3.60)
1.82 (1.05-3.16)
1.81 (0.91-3.59)
67.00 (4.22-1064.23)
13.18 (1.84-94.53)
11.00 (0.71-170.98)
1.61 (0.95-2.70)
8.89 (1.37-57.47)
2.97 (1.59-5.54)
Events, oxygen
2/14
4/5
59/82
65/81
185/273
25/48
14/17
33/50
14/34
5/8
13/17
16/18
120/192
Events, control
0/13
1/5
12/18
13/36
42/210
12/42
5/11
0/50
1/32
0/8
10/21
1/10
29/174
2.01
4.77
24.14
30.92
100.00
19.35
16.54
2.26
4.13
2.29
20.00
4.52
69.08
Weight(%)
Reference
B
RCTLöndahl et al,19 2011
Duzgun et al,20 2008
Abidia et al,21 2003
Kessler et al,22 2003
Subtotal (I2 = 79.4%, P=.002)
RCT z=1.71 P=.09
Non-RCT
Blackman et al,33 2010
Albuquerque and Sousa et al,29 2005
Kalani et al,30 2002
Zamboni et al,15 1997
Oriani et al,14 1992
Baroni et al,31 1987
Subtotal (I2 = 63.9%, P=.02)
Non-RCT z=2.77 P=.006
Overall (I2 = 74.5%, P<.001)
Overall z=3.43 P=.001
NOTE: Weights are from random-effects analysis
.00094 10641
Favors control Favors HBO therapy
RR (95% CI)
1.82 (1.05-3.16)
67.00 (4.22-1064.23)
11.00 (0.71-170.98)
4.67 (0.24-88.96)
7.64 (0.74-78.93)
1.81 (0.91-3.59)
13.18 (1.84-94.53)
1.61 (0.95-2.70)
4.00 (0.66-24.37)
1.43 (1.02-1.99)
8.89 (1.37-57.47)
2.22 (1.26-3.89)
2.92 (1.58-5.39)
15.67
6.45
17.07
7.22
18.43
6.93
71.76
100.00
16.83
3.91
3.96
3.53
28.24
Weight(%)
FIGURE 2. Forest plots for meta-analyses comparing the healing rate of foot ulcer treated with or withouthyperbaric oxygenation (HBO). A, Subgroup analyses with short-term (6 months) or long-term (�1 year)follow-ups. B, Subgroup analyses only including randomized controlled trials (RCTs). Ulcer healing wasdefined as complete epithelial regeneration. RR ¼ relative risk.
MAYO CLINIC PROCEEDINGS
170 Mayo Clin Proc. n February 2013;88(2):166-175 n http://dx.doi.org/10.1016/j.mayocp.2012.10.021www.mayoclinicproceedings.org

Reference Major amputation
RR (95% CI)
2.63 (0.28-24.29)
0.03 (0.00-0.46)
1.00 (0.07-13.37)
0.26 (0.08-0.84)
0.29 (0.07-1.16)
(Excluded)
0.24 (0.12-0.48)
0.44 (0.22-0.88)
0.35 (0.08-1.48)
0.15 (0.04-0.52)
0.28 (0.06-1.26)
(Excluded)
0.33 (0.20-0.56)
0.29 (0.19-0.44)
Weight (%)
1.40
22.99
1.31
14.88
9.20
0.00
49.78
23.01
8.23
12.22
6.76
50.22
100.00
0.00
RCT
Löndahl et al,19 2011
Duzgun et al,20 2008
Abidia et al,21 2003
Faglia et al,12 1996
Doctor et al,13 1992
Kessler et al,22 2003Subtotal (I2 = 49.2%, P=.010)
RCT z=4.06, P<.001
Non-RCT
Albuquerque and Sousa,29 2005
Kalani et al,30 2002
Oriani et al,14 1992
Baroni et al,31 1987Zamboni et al,15 1997
Non-RCT z=4.16, P<.001
Subtotal (I2 = 0.0%, P=.51)
Overall (I2 = 20.2%, P=.26)
Overall z=5.82, P<.001
.00177 567
Favors controlFavors HBO therapy
1
FIGURE 3. Forest plot for meta-analyses comparing major amputations in diabetic foot ulcer treated withor without hyperbaric oxygenation (HBO). Subgroup analysis including only randomized controlled trials(RCTs). Major amputation was defined as amputation above the ankle joint. RR ¼ relative risk.
HBO THERAPY IN DIABETIC FOOT ULCERS
CI, 0.97-2.47; P¼.78; Figure 4, B). Finally, wefound that HBO therapy demonstrated a lowerrisk in total amputation rate compared withconventional therapy (13.63% vs 30.07%).
Adverse EventsFour studies, including 3 RCTs and 1 prospec-tive study, reported adverse events related toHBO therapy, including barotraumatic lesions,oxygen toxicity, confinement anxiety, and oc-ular effects. Overall, no statistically significantdifference was found in adverse event ratesbetween the HBO-treated and the controlgroups (RR, 1.41; 95% CI, 0.66-2.98; P¼.37)(Figure 5). Moreover, the pooling analysis of 4RCTs also found no significant difference inadverse events between the 2 groups (RR,1.41; 95% CI, 0.66-2.98; P¼.37).
Quality of LifeOnly 106 patients in 2 trials provided infor-mation on quality of life on the basis of self-
Mayo Clin Proc. n February 2013;88(2):166-175 n http://dx.doi.orgwww.mayoclinicproceedings.org
reported questionnaires. The most recent RCT19
provided some evidence to suggest that HBOtreatment might improve long-term quality oflife, although another trial21 implied that it didnot produce significant improvements in qualityof life.
Infection-Related IssuesOne RTC13 investigated treatment of infection asthe outcome end point. When compared withindividuals treated without HBO, individualstreatedwithHBOhad fewer infections, indicatedby lower bacterial colony counts. Although footinfection was not investigated as an end point inmost trials, these trials indirectly demonstratedbetter infectious outcomes, such as ulcers healed,reduced ulcer size, and amputations.
Cost-effectiveness AnalysisOnly one study evaluated cost-effectiveness.This double-blindRCTdemonstrated a potentialsaving in total cost of treatment for each patient
/10.1016/j.mayocp.2012.10.021 171

Löndahl et al,19 2011
Albuquerque and Sousa,29 2005
Abidia et al,21 2003
Faglia et al,12 1996
Doctor et al,13 1992
Overall (I2 = 6.7%, P=.37)
.0156 64.31
0.88 (0.23-3.28)
0.66 (0.29-1.52)
3.00 (0.14-64.26)
1.65 (0.97-2.79)
2.00 (0.43-9.32)
1.24 (0.83-1.85)
RR (95% Cl)
4/48
7/34
1/8
21/35
4/15
37/140
Events,HBOReference
Test of RR=1: z=1.04, P=.30
Minor amputation
Favors HBO therapy Favors controlA
1
14.50
35.02
1.70
41.98
6.80
100.00
Weight(%)
4/42
10/32
0/8
12/33
2/15
28/130
Events ,control
Löndahl et al,19 2011
Abidia et al,21 2003
Faglia et al,12 1996
Doctor et al,13 1992
Overall (I2 = 0.0%, P=.79)
.0156 64.3
RCT: RR=1: z=1.84, P=.07
Favors HBO therapy Favors control
Reference
B
0.88 (0.23-3.28)
3.00 (0.14-64.26)
1.65 (0.97-2.79)
2.00 (0.43-9.32)
1.55 (0.97-2.47)
RR (95% Cl)
4/48
1/8
21/35
4/15
30/106
Events,HBO
22.32
2.62
64.61
10.46
100.00
Weight(%)
0/8
4/42
12/33
2/15
18/98
Events ,control
FIGURE 4. Forest plot for meta-analyses comparing minor amputation in diabetic foot ulcer treated withor without hyperbaric oxygenation (HBO). A, Overall analyses. B, Subgroup analyses including onlyrandomized controlled trials (RCTs). Minor amputation was defined as amputation below ankle joint.RR ¼ relative risk.
MAYO CLINIC PROCEEDINGS
172
treated with HBO.21 Because the healing ofulcers takes place during a long period, itpossibly results in a higher cost for HBO-treated patients compared with those under-going a conventional therapy or amputation.
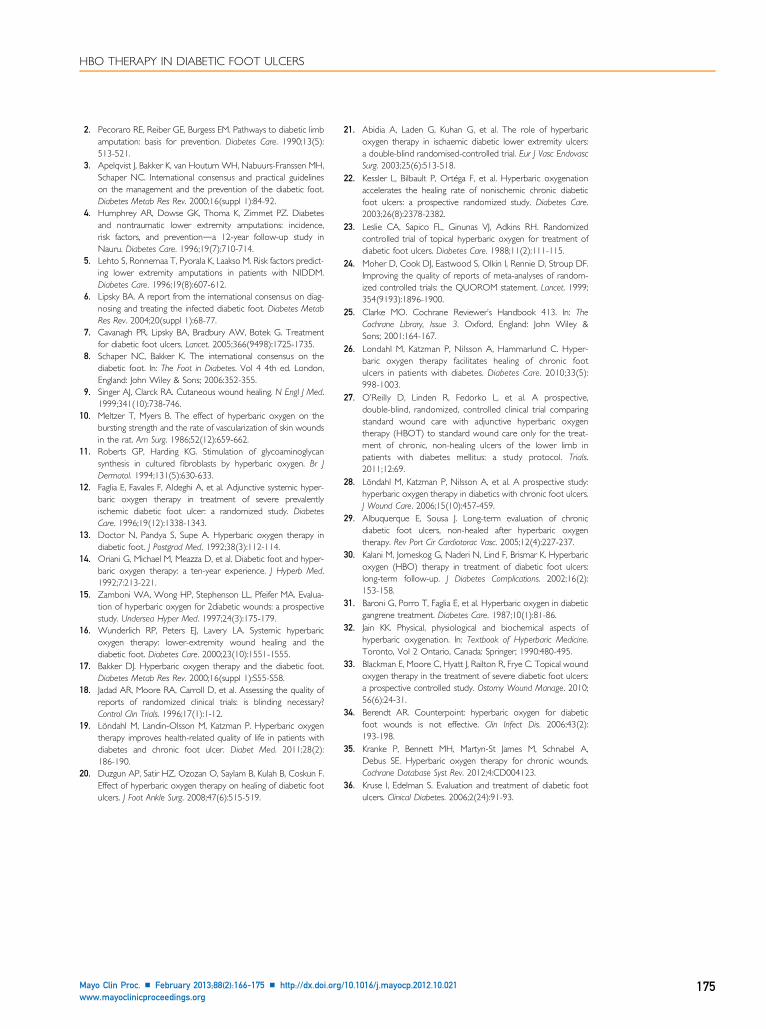
Publication Bias Assessment and SensitivityAnalysisWe assessed publication bias using the Beggrank correlation analysis. The Begg linear
Mayo Clin Proc. n February 2013
regression test was performed for the quantita-tive evaluation of the symmetry of the meta-analysis funnel plot. P values of the Begg testwere greater than .99, and their 95% CIs ofintercept included zero in the Begg publicationbias plots. This result indicates that the meta-analysis funnel plots were symmetrical withoutpublication bias. Simultaneous sensitivity anal-ysis was performed by using different samplesizes or effect models. We did not identify
;88(2):166-175 n http://dx.doi.org/10.1016/j.mayocp.2012.10.021www.mayoclinicproceedings.org
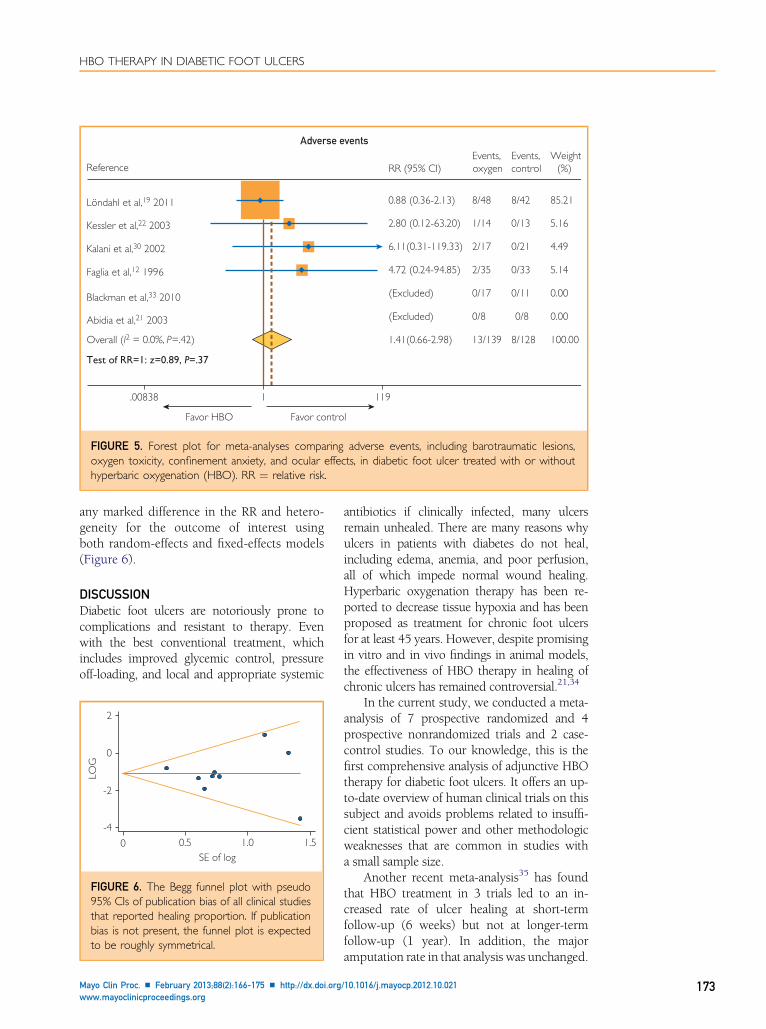
Reference
Löndahl et al,19 2011
Kessler et al,22 2003
Kalani et al,30 2002
Faglia et al,12 1996
Blackman et al,33 2010
Abidia et al,21 2003
Adverse events
RR (95% CI)
0.88 (0.36-2.13)
2.80 (0.12-63.20)
6.11(0.31-119.33)
4.72 (0.24-94.85)
1.41(0.66-2.98)
(Excluded)
(Excluded)
Events, oxygen
0/17
0/8
8/48
2/17
2/35
13/139
1/14
0/8
Events, control
8/42
0/21
0/33
8/128
0/11
0/13
85.21
4.49
5.14
0.00
0.00
100.00
5.16
Overall (I2 = 0.0%, P=.42)
Test of RR=1: z=0.89, P=.37
.00838 1191
Favor controlFavor HBO
Weight(%)
FIGURE 5. Forest plot for meta-analyses comparing adverse events, including barotraumatic lesions,oxygen toxicity, confinement anxiety, and ocular effects, in diabetic foot ulcer treated with or withouthyperbaric oxygenation (HBO). RR ¼ relative risk.
HBO THERAPY IN DIABETIC FOOT ULCERS
any marked difference in the RR and hetero-geneity for the outcome of interest usingboth random-effects and fixed-effects models(Figure 6).
DISCUSSIONDiabetic foot ulcers are notoriously prone tocomplications and resistant to therapy. Evenwith the best conventional treatment, whichincludes improved glycemic control, pressureoff-loading, and local and appropriate systemic
2
0
-2
-4
0 0.5 1.0 1.5SE of log
LOG
FIGURE 6. The Begg funnel plot with pseudo95% CIs of publication bias of all clinical studiesthat reported healing proportion. If publicationbias is not present, the funnel plot is expectedto be roughly symmetrical.
Mayo Clin Proc. n February 2013;88(2):166-175 n http://dx.doi.orgwww.mayoclinicproceedings.org
antibiotics if clinically infected, many ulcersremain unhealed. There are many reasons whyulcers in patients with diabetes do not heal,including edema, anemia, and poor perfusion,all of which impede normal wound healing.Hyperbaric oxygenation therapy has been re-ported to decrease tissue hypoxia and has beenproposed as treatment for chronic foot ulcersfor at least 45 years. However, despite promisingin vitro and in vivo findings in animal models,the effectiveness of HBO therapy in healing ofchronic ulcers has remained controversial.21,34
In the current study, we conducted a meta-analysis of 7 prospective randomized and 4prospective nonrandomized trials and 2 case-control studies. To our knowledge, this is thefirst comprehensive analysis of adjunctive HBOtherapy for diabetic foot ulcers. It offers an up-to-date overview of human clinical trials on thissubject and avoids problems related to insuffi-cient statistical power and other methodologicweaknesses that are common in studies witha small sample size.
Another recent meta-analysis35 has foundthat HBO treatment in 3 trials led to an in-creased rate of ulcer healing at short-termfollow-up (6 weeks) but not at longer-termfollow-up (1 year). In addition, the majoramputation rate in that analysis was unchanged.
/10.1016/j.mayocp.2012.10.021 173

MAYO CLINIC PROCEEDINGS
174
Therefore, it seemed that our results differedfrom those of the Cochrane analysis by Krankeet al.35 The reason for the differences may bethe different characteristics of the 2 studiesand sample sizes. Only 7 RCTs were used inthe meta-analysis by Kranke et al,35 whereas 7RCTs, 4 prospective trials, and 2 case-controlstudies were represented in our meta-analysis.Our larger sample size likely decreased publica-tion bias and strengthened the power of anal-ysis. Furthermore, in the study by Krankeet al,35 only 2 trials assessed ulcer healing within1 year. This causes problems with forest plotsand assessing publication bias. More impor-tantly, comparing healing rates of ulcers be-tween HBO and conventional therapy, therewas significant heterogeneity in the study byKranke et al35 (I2¼50%).
Our review provides evidence that HBOtherapy in patients with diabetic ulcers decreasesthe overall risk of amputations, especially majoramputation, when compared with therapywithout HBO (13.63% vs 30.07%; RR, 0.29;95% CI, 0.13-0.71).
The RR ratio revealed a significant effect infavor of adjunctive HBO therapy in patientswith short-term follow-up (�6 months). Al-though there was more heterogeneity in the sub-analysis for patients with follow-up ofmore than12 months, we found a tendency toward evenlarger positive effects of HBO treatment com-pared with those seen within 6 months. Theseresults are consistent with a report by Kalaniet al30 in which 76% of the patients treatedwith HBO had healed ulcers after 3 years,compared with only 48% of patients treatedwithout HBO. Furthermore, Albuquerque andSousa29 reported that long HBO treatment(mean, 45 months) increased significantly (ap-proximately 13-fold) the healing rate of chroniclower limb ulcers in diabetic patients.
Both efficacy and safety ofHBO therapywereassessed in this meta-analysis. Six studies thatcontained safety data found no significant differ-ences between therapy with or without HBO.The incidence of adverse events was low andinvolved middle ear and nasal sinus problems.All these adverse events could be treated easilyand rarely resulted in termination of the HBOtherapy. Therefore, HBO therapy can be consid-ered as a useful adjunct in the treatment ofdiabetic foot ulcers with an acceptable com-plication rate as long as safety guidelines
Mayo Clin Proc. n February 2013
concerning preexaminations, contraindica-tions, therapeutic schemes, and monitoringof the patients are followed.
Cost-effectiveness needs to be considered byphysicians and patients. The cost ofHBO therapyvaries, depending on region, setup costs, ongoingcosts, and the number of treated patients. Theonly economic analysis included in this meta-analysis revealed that despite the extra cost ofthe equipment, the total cost for each patienttreated with HBO was probably reduced in thelong run. For example, in 2006 in the UnitedStates,36 the mean cost of therapy for an infectedfoot ulcerwas $17,000 andwas increased 2- to 3-fold by a major amputation. Considering theincreased ulcer healing, the reduction of majoramputations, and the reduced frequency ofoffice visits, HBO treatment appears to havethe potential of providing cost savings for thetreatment of diabetic foot ulcers.
CONCLUSIONThismeta-analysis demonstrates that adjunctivetreatment with HBO increases the likelihood ofhealing in diabetic foot ulcers and reducesthe need for major amputations. In addition,adverse events are rare and acceptable. There-fore, we believe that the long-term quality oflife of patients treated with HBO therapy couldbe improved by its judicious application.
ACKNOWLEDGMENTSDrs Liu and Li contributed equally to this work.
Abbreviations and Acronyms: HBO = hyperbaric oxygen-ation; RCT = randomized controlled trial; RR = relative risk
Grant Support: This work was supported by researchgrants 30871199, 81270913, 81070640, 30971388 and30771037 from the National Natural Science Foundationof China, grants 20105503110002 and 20125503110003from the Doctoral Fund of Ministry of Education of China,and grant cstc2012 jjB10022 from the Natural ScienceFoundation Key Project of CQ cstc (G.Y.) and AmericanDiabetes Association grant 1-10-CT06 (G.B.).
Correspondence: Address to Gangyi Yang, PhD, Depart-ment of Endocrinology, the Second Affiliated Hospital,Chongqing Medical University, 400010 Chongqing, China([email protected]).
REFERENCES1. Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The
global burden of diabetic foot disease. Lancet. 2005;366(12):1719-1724.
;88(2):166-175 n http://dx.doi.org/10.1016/j.mayocp.2012.10.021www.mayoclinicproceedings.org
François
Texte surligné
HBO THERAPY IN DIABETIC FOOT ULCERS
2. Pecoraro RE, Reiber GE, Burgess EM. Pathways to diabetic limbamputation: basis for prevention. Diabetes Care. 1990;13(5):513-521.
3. Apelqvist J, Bakker K, van Houtum WH, Nabuurs-Franssen MH,Schaper NC. International consensus and practical guidelineson the management and the prevention of the diabetic foot.Diabetes Metab Res Rev. 2000;16(suppl 1):84-92.
4. Humphrey AR, Dowse GK, Thoma K, Zimmet PZ. Diabetesand nontraumatic lower extremity amputations: incidence,risk factors, and preventionda 12-year follow-up study inNauru. Diabetes Care. 1996;19(7):710-714.
5. Lehto S, Ronnemaa T, Pyorala K, Laakso M. Risk factors predict-ing lower extremity amputations in patients with NIDDM.Diabetes Care. 1996;19(8):607-612.
6. Lipsky BA. A report from the international consensus on diag-nosing and treating the infected diabetic foot. Diabetes MetabRes Rev. 2004;20(suppl 1):68-77.
7. Cavanagh PR, Lipsky BA, Bradbury AW, Botek G. Treatmentfor diabetic foot ulcers. Lancet. 2005;366(9498):1725-1735.
8. Schaper NC, Bakker K. The international consensus on thediabetic foot. In: The Foot in Diabetes. Vol 4 4th ed. London,England: John Wiley & Sons; 2006:352-355.
9. Singer AJ, Clarck RA. Cutaneous wound healing. N Engl J Med.1999;341(10):738-746.
10. Meltzer T, Myers B. The effect of hyperbaric oxygen on thebursting strength and the rate of vascularization of skin woundsin the rat. Am Surg. 1986;52(12):659-662.
11. Roberts GP, Harding KG. Stimulation of glycoaminoglycansynthesis in cultured fibroblasts by hyperbaric oxygen. Br JDermatol. 1994;131(5):630-633.
12. Faglia E, Favales F, Aldeghi A, et al. Adjunctive systemic hyper-baric oxygen therapy in treatment of severe prevalentlyischemic diabetic foot ulcer: a randomized study. DiabetesCare. 1996;19(12):1338-1343.
13. Doctor N, Pandya S, Supe A. Hyperbaric oxygen therapy indiabetic foot. J Postgrad Med. 1992;38(3):112-114.
14. Oriani G, Michael M, Meazza D, et al. Diabetic foot and hyper-baric oxygen therapy: a ten-year experience. J Hyperb Med.1992;7:213-221.
15. Zamboni WA, Wong HP, Stephenson LL, Pfeifer MA. Evalua-tion of hyperbaric oxygen for 2diabetic wounds: a prospectivestudy. Undersea Hyper Med. 1997;24(3):175-179.
16. Wunderlich RP, Peters EJ, Lavery LA. Systemic hyperbaricoxygen therapy: lower-extremity wound healing and thediabetic foot. Diabetes Care. 2000;23(10):1551-1555.
17. Bakker DJ. Hyperbaric oxygen therapy and the diabetic foot.Diabetes Metab Res Rev. 2000;16(suppl 1):S55-S58.
18. Jadad AR, Moore RA, Carroll D, et al. Assessing the quality ofreports of randomized clinical trials: is blinding necessary?Control Clin Trials. 1996;17(1):1-12.
19. Löndahl M, Landin-Olsson M, Katzman P. Hyperbaric oxygentherapy improves health-related quality of life in patients withdiabetes and chronic foot ulcer. Diabet Med. 2011;28(2):186-190.
20. Duzgun AP, Satir HZ, Ozozan O, Saylam B, Kulah B, Coskun F.Effect of hyperbaric oxygen therapy on healing of diabetic footulcers. J Foot Ankle Surg. 2008;47(6):515-519.
Mayo Clin Proc. n February 2013;88(2):166-175 n http://dx.doi.orgwww.mayoclinicproceedings.org
21. Abidia A, Laden G, Kuhan G, et al. The role of hyperbaricoxygen therapy in ischaemic diabetic lower extremity ulcers:a double-blind randomised-controlled trial. Eur J Vasc EndovascSurg. 2003;25(6):513-518.
22. Kessler L, Bilbault P, Ortéga F, et al. Hyperbaric oxygenationaccelerates the healing rate of nonischemic chronic diabeticfoot ulcers: a prospective randomized study. Diabetes Care.2003;26(8):2378-2382.
23. Leslie CA, Sapico FL, Ginunas VJ, Adkins RH. Randomizedcontrolled trial of topical hyperbaric oxygen for treatment ofdiabetic foot ulcers. Diabetes Care. 1988;11(2):111-115.
24. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF.Improving the quality of reports of meta-analyses of random-ized controlled trials: the QUOROM statement. Lancet. 1999;354(9193):1896-1900.
25. Clarke MO. Cochrane Reviewer’s Handbook 413. In: TheCochrane Library, Issue 3. Oxford, England: John Wiley &Sons; 2001:164-167.
26. Londahl M, Katzman P, Nilsson A, Hammarlund C. Hyper-baric oxygen therapy facilitates healing of chronic footulcers in patients with diabetes. Diabetes Care. 2010;33(5):998-1003.
27. O’Reilly D, Linden R, Fedorko L, et al. A prospective,double-blind, randomized, controlled clinical trial comparingstandard wound care with adjunctive hyperbaric oxygentherapy (HBOT) to standard wound care only for the treat-ment of chronic, non-healing ulcers of the lower limb inpatients with diabetes mellitus: a study protocol. Trials.2011;12:69.
28. Löndahl M, Katzman P, Nilsson A, et al. A prospective study:hyperbaric oxygen therapy in diabetics with chronic foot ulcers.J Wound Care. 2006;15(10):457-459.
29. Albuquerque E, Sousa J. Long-term evaluation of chronicdiabetic foot ulcers, non-healed after hyperbaric oxygentherapy. Rev Port Cir Cardiotorac Vasc. 2005;12(4):227-237.
30. Kalani M, Jorneskog G, Naderi N, Lind F, Brismar K. Hyperbaricoxygen (HBO) therapy in treatment of diabetic foot ulcers:long-term follow-up. J Diabetes Complications. 2002;16(2):153-158.
31. Baroni G, Porro T, Faglia E, et al. Hyperbaric oxygen in diabeticgangrene treatment. Diabetes Care. 1987;10(1):81-86.
32. Jain KK. Physical, physiological and biochemical aspects ofhyperbaric oxygenation. In: Textbook of Hyperbaric Medicine.Toronto, Vol 2 Ontario, Canada: Springer; 1990:480-495.
33. Blackman E, Moore C, Hyatt J, Railton R, Frye C. Topical woundoxygen therapy in the treatment of severe diabetic foot ulcers:a prospective controlled study. Ostomy Wound Manage. 2010;56(6):24-31.
34. Berendt AR. Counterpoint: hyperbaric oxygen for diabeticfoot wounds is not effective. Clin Infect Dis. 2006;43(2):193-198.
35. Kranke P, Bennett MH, Martyn-St James M, Schnabel A,Debus SE. Hyperbaric oxygen therapy for chronic wounds.Cochrane Database Syst Rev. 2012;4:CD004123.
36. Kruse I, Edelman S. Evaluation and treatment of diabetic footulcers. Clinical Diabetes. 2006;2(24):91-93.
/10.1016/j.mayocp.2012.10.021 175




















