Australasian resuscitation of sepsis evaluation (ARISE): A multi-centre, prospective, inception...
8
Resuscitation 80 (2009) 811–818 Contents lists available at ScienceDirect Resuscitation journal homepage: www.elsevier.com/locate/resuscitation Clinical paper Australasian resuscitation of sepsis evaluation (ARISE): A multi-centre, prospective, inception cohort study Sandra L. Peake a,b,∗ , Michael Bailey c , Rinaldo Bellomo d,e,f , Peter A. Cameron g , Anthony Cross h , Anthony Delaney i,j , Simon Finfer k,l,m , Alisa Higgins c , Daryl A. Jones c , John A. Myburgh l,n,o , Gillian A. Syres c , Steven A.R. Webb p,q , Patricia Williams b , the ARISE Investigators, for the Australian and New Zealand Intensive Care Society Clinical Trials Group a University of Adelaide, Adelaide, South Australia, Australia b Department of Intensive Care Medicine, The Queen Elizabeth Hospital, Adelaide, South Australia, Australia c Australian and New Zealand Intensive Care Research Centre, Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Victoria, Australia d Monash University, Melbourne, Australia e Howard Florey Institute, Melbourne University, Australia f Department of Intensive Care, Austin Hospital, Heidelberg, Victoria, Australia g Department of Epidemiology and Preventive Medicine, Monash University, Alfred Hospital, Melbourne, Australia h Intensive Care Unit, Emergency Department, Box Hill Hospital, Melbourne, Australia i Royal North Shore Hospital, Sydney, Australia j Northern Clinical School, University of Sydney, New South Wales, Australia k Faculty of Medicine, University of Sydney, Australia l Critical Care and Trauma, The George Institute for International Health, Sydney, Australia m Royal North Shore Hospital, Sydney, Australia n University of New South Wales, Department of Intensive Care Medicine, Australia o Department of Intensive Care Medicine, St George Hospital, Sydney, Australia p Department of Intensive Care Medicine, Royal Perth Hospital, Australia q School of Medicine and Pharmacology and School of Public Health, University of Western Australia, Perth, Western Australia, Australia article info Article history: Received 8 February 2009 Received in revised form 27 February 2009 Accepted 4 March 2009 Keywords: Critical illness Sepsis Early goal-directed therapy Resuscitation Mortality Emergency department abstract Aim: Determine current resuscitation practices and outcomes in patients presenting to the emergency department (ED) with sepsis and hypoperfusion or septic shock in Australia and New Zealand (ANZ). Methods: Three-month prospective, multi-centre, observational study of all adult patients with sepsis and hypoperfusion or septic shock in the ED of 32 ANZ tertiary-referral, metropolitan and rural hospitals. Results: 324 patients were enrolled (mean [SD] age 63.4 [19.2] years, APACHE II score 19.0 [8.2], 52.5% male). Pneumonia (n = 138/324, 42.6%) and urinary tract infection (n = 98/324, 30.2%) were the common- est sources of sepsis. Between ED presentation and 6 hours post-enrolment (T6hrs), 44.4% (n = 144/324) of patients received an intra-arterial catheter, 37% (n = 120/324) a central venous catheter and 0% (n =0/324) a continuous central venous oxygen saturation (ScvO 2 ) catheter. Between enrolment and T6hrs, 32.1% (n =104/324) received a vasopressor infusion, 7.4% (n = 24/324) a red blood cell transfusion, 2.5% (n = 8/324) a dobutamine infusion and 18.5% (n = 60/324) invasive mechanical ventilation. Twenty patients (6.2%) were transferred from ED directly to the operating theatre, 36.4% (n = 118/324) were admit- ted directly to ICU, 1.2% (n = 4/324) died in the ED and 56.2% (n = 182/324) were transferred to the hospital floor. Overall ICU admission rate was 52.4% (n = 170/324). ICU and overall in-hospital mortality were 18.8% (n = 32/170) and 23.1% (n = 75/324) respectively. In-hospital mortality was not different between patients admitted to ICU (24.7%, n =42/170) and the hospital floor (21.4%, n = 33/154). Conclusions: Management of ANZ patients presenting to ED with sepsis does not routinely include proto- colised, ScvO 2 -directed resuscitation. In-hospital mortality compares favourably with reported mortality in international sepsis trials and nationwide surveys of resuscitation practices. © 2009 Elsevier Ireland Ltd. All rights reserved. “A Spanish translated version of the summary of this article appears as Appendix in the final online version at doi:10.1016/j.resuscitation.2009.03.008.” ∗ Corresponding author at: Australian and New Zealand Intensive Care Research Centre, Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Victoria, Australia. Tel.: +61 3 99030247; fax: +61 3 99030071. E-mail address: [email protected] (S.L. Peake). 0300-9572/$ – see front matter © 2009 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.resuscitation.2009.03.008
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Australasian resuscitation of sepsis evaluation (ARISE): A multi-centre, prospective, inception...

Resuscitation 80 (2009) 811–818
Contents lists available at ScienceDirect
Resuscitation
journa l homepage: www.e lsev ier .com/ locate / resusc i ta t ion
Clinical paper
Australasian resuscitation of sepsis evaluation (ARISE): A multi-centre,prospective, inception cohort study�
Sandra L. Peakea,b,∗, Michael Baileyc, Rinaldo Bellomod,e,f, Peter A. Camerong, Anthony Crossh,Anthony Delaneyi,j, Simon Finferk,l,m, Alisa Higginsc, Daryl A. Jonesc, John A. Myburghl,n,o,Gillian A. Syresc, Steven A.R. Webbp,q, Patricia Williamsb, the ARISE Investigators, for the Australian andNew Zealand Intensive Care Society Clinical Trials Groupa University of Adelaide, Adelaide, South Australia, Australiab Department of Intensive Care Medicine, The Queen Elizabeth Hospital, Adelaide, South Australia, Australiac Australian and New Zealand Intensive Care Research Centre, Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Victoria, Australiad Monash University, Melbourne, Australiae Howard Florey Institute, Melbourne University, Australiaf Department of Intensive Care, Austin Hospital, Heidelberg, Victoria, Australiag Department of Epidemiology and Preventive Medicine, Monash University, Alfred Hospital, Melbourne, Australiah Intensive Care Unit, Emergency Department, Box Hill Hospital, Melbourne, Australiai Royal North Shore Hospital, Sydney, Australiaj Northern Clinical School, University of Sydney, New South Wales, Australiak Faculty of Medicine, University of Sydney, Australial Critical Care and Trauma, The George Institute for International Health, Sydney, Australiam Royal North Shore Hospital, Sydney, Australian University of New South Wales, Department of Intensive Care Medicine, Australiao Department of Intensive Care Medicine, St George Hospital, Sydney, Australiap Department of Intensive Care Medicine, Royal Perth Hospital, Australiaq School of Medicine and Pharmacology and School of Public Health, University of Western Australia, Perth, Western Australia, Australia
a r t i c l e i n f o
Article history:Received 8 February 2009Received in revised form 27 February 2009Accepted 4 March 2009
Keywords:Critical illnessSepsisEarly goal-directed therapyResuscitationMortalityEmergency department
a b s t r a c t
Aim: Determine current resuscitation practices and outcomes in patients presenting to the emergencydepartment (ED) with sepsis and hypoperfusion or septic shock in Australia and New Zealand (ANZ).Methods: Three-month prospective, multi-centre, observational study of all adult patients with sepsis andhypoperfusion or septic shock in the ED of 32 ANZ tertiary-referral, metropolitan and rural hospitals.Results: 324 patients were enrolled (mean [SD] age 63.4 [19.2] years, APACHE II score 19.0 [8.2], 52.5%male). Pneumonia (n = 138/324, 42.6%) and urinary tract infection (n = 98/324, 30.2%) were the common-est sources of sepsis. Between ED presentation and 6 hours post-enrolment (T6hrs), 44.4% (n = 144/324)of patients received an intra-arterial catheter, 37% (n = 120/324) a central venous catheter and 0%(n = 0/324) a continuous central venous oxygen saturation (ScvO2) catheter. Between enrolment andT6hrs, 32.1% (n = 104/324) received a vasopressor infusion, 7.4% (n = 24/324) a red blood cell transfusion,2.5% (n = 8/324) a dobutamine infusion and 18.5% (n = 60/324) invasive mechanical ventilation. Twentypatients (6.2%) were transferred from ED directly to the operating theatre, 36.4% (n = 118/324) were admit-ted directly to ICU, 1.2% (n = 4/324) died in the ED and 56.2% (n = 182/324) were transferred to the hospitalfloor. Overall ICU admission rate was 52.4% (n = 170/324). ICU and overall in-hospital mortality were 18.8%(n = 32/170) and 23.1% (n = 75/324) respectively. In-hospital mortality was not different between patientsadmitted to ICU (24.7%, n = 42/170) and the hospital floor (21.4%, n = 33/154).
Conclusions: Management of ANZ patients presenting to ED with sepsis does not routinely include proto-colised, ScvO2-directed resuscitation. In-hospital mortality compares favourably with reported mortalityin international sepsis trials and nationwide surveys of resuscitation practices.© 2009 Elsevier Ireland Ltd. All rights reserved.
� “A Spanish translated version of the summary of this article appears as Appendix in the final online version at doi:10.1016/j.resuscitation.2009.03.008.”∗ Corresponding author at: Australian and New Zealand Intensive Care Research Centre, Department of Epidemiology and Preventive Medicine, Monash University,
Melbourne, Victoria, Australia. Tel.: +61 3 99030247; fax: +61 3 99030071.E-mail address: [email protected] (S.L. Peake).
0300-9572/$ – see front matter © 2009 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.resuscitation.2009.03.008

8 citatio
1
wdrpp((sSpotstt
smisarti
2
2
Imb(OmhICft
i
123
4
h
2
d
12 S.L. Peake et al. / Resus
. Introduction
Despite international guidelines for the resuscitation of patientsith severe sepsis,1,2 there is variation between countries in theegree to which these guidelines have been implemented.3,4 Indi-ect evidence suggests that the routine management of sepsisatients in Australia and New Zealand (ANZ) does not incor-orate protocolised, ScvO2-directed, early goal-directed therapyEGDT).5,6 In 2006, 1864 patients were admitted to intensive careICU) from the emergency department (ED) with sepsis or septichock (data from the Australian and New Zealand Intensive Careociety Adult Patient Database, ANZICS APD). However, in the sameeriod, only 197 “Presep®” central venous catheters (CVCs) capablef measuring continuous ScvO2 were sold. Moreover, a retrospec-ive analysis of 7649 patients admitted to ICU from ANZ EDs withepsis or septic shock between 1997 and 20057 suggests that hospi-al mortality may be considerably lower than that observed in bothhe standard care and EGDT arms of the Rivers’ trial.6
There are no prospective studies examining how patients pre-enting to the ED with sepsis and septic shock in ANZ are currentlyanaged and accurate mortality estimates are unknown. Accord-
ngly, we conducted a prospective, multi-centre, inception cohorttudy in patients presenting to the ED of ANZ hospitals to: (1) char-cterise current resuscitation practices, including whether patientseceived EGDT; (2) determine patient outcomes and; (3) establishhe feasibility of undertaking a randomised, controlled trial of EGDTn ANZ and obtain information critical to the design of such a trial.
. Methods
.1. Study population
A prospective, observational study was performed in 32 ANZ-CS Clinical Trials Group (ANZICS CTG)-affiliated, tertiary-referral,
etropolitan and regional hospitals (Appendix A) between Septem-er 1, 2006 and January 31, 2007. All sites screened for 3 monthsindividual sites commenced screening between September 1 andctober 1, 2006). Screening methods included prospective assess-ent by ED personnel and review of daily ED presentation and
ospital admission databases. The study was endorsed by the ANZ-CS CTG and was undertaken in collaboration with the ANZ Intensiveare Research Centre. Approval to conduct the study was obtainedrom local institutional ethics committees at participating sites andhe need for patient consent was waived.
All adult patients (≥18 years) present in ED at the time of fulfill-ng the following entry criteria were enrolled:
) Presumed or confirmed infection) Two or more systemic inflammatory response criteria8AND EITHER) Blood pressure (BP) criteria (one or more of the following): (i) sys-
tolic BP <90 mmHg OR >40 mmHg fall below premorbid systolicBP OR mean arterial pressure (MAP) <65 mmHg, after ≥500 mlintravenous fluid challenge over 30–60 min; (ii) requirementfor vasoactive infusion (adrenaline, noradrenaline, dopamine,dobutamine, vasopressin, metaraminol) for ≥30 min to maintainBP OR
) Metabolic acidosis criteria (one or more of the following): arterial orvenous: (i) blood lactate >4.0 mmol/L; (ii) anion gap >20 mEq/L;(iii) serum bicarbonate <16.0 mmol/L.
Patients meeting the above criteria are herein referred to asaving either sepsis with hypoperfusion or septic shock.
.2. Data collection
The following data were recorded: demographic data (age, gen-er, weight); APACHE II score using the baseline physiological
n 80 (2009) 811–818
variables obtained closest in time, but prior, to meeting the finalstudy inclusion criterion; concurrent medical conditions (definedas an acute disease process present during the current ED pre-sentation) and co-morbidities (defined as conditions known to bepresent prior to the current ED presentation)9; source of sepsis,microbiological specimens, causative organisms and type, timing,choice and appropriateness of anti-microbial therapy; dispositionpost-ED (e.g. hospital floor, ICU); length of invasive ventilation andvasoactive agent support; ED, ICU and hospital length of stay (LOS)and; ICU and hospital mortality.
Physiological variables (HR, BP, central venous pressure [CVP],RR, arterial oxygen saturation (SaO2), urine output [UO]), vasoactiveinfusions and crystalloid, colloid and blood product administra-tion were recorded at the time of meeting the final entry criterionfor sepsis with hypoperfusion or septic shock (defined as T0hrs).Thereafter, measurements were recorded hourly between T0hrsand T6hrs and at 72 h. Laboratory data at T0hrs, T6hrs and T72hrswas also recorded. Given the observational nature of the study,physiological and laboratory measurements were not mandatedand data was only available if measurement at the specific studytime-points was performed.
In addition, through the time periods T0–T6hrs and T6–T72hrsthe following data were collected: type and timing of insertion ofinvasive cardiovascular monitoring; frequency of measuring resus-citation “goals” (UO, BP, CVP, cardiac output, arterial blood gasanalysis, blood lactate and central or mixed venous oxygen satura-tion) and; type and timing of therapeutic interventions (vasoactiveagents, mechanical ventilation, drotrecogin alfa, corticosteroids,intensive insulin therapy and renal replacement therapy).
2.3. Outcome measures
All patients were followed until hospital discharge and ICU(where appropriate) and in-hospital mortality recorded. Secondaryoutcomes included: time-to-antimicrobial therapy, requirementfor, and duration of, invasive ventilation; use of vasoactive infusionsand duration of administration; ED, ICU and hospital LOS.
2.4. Statistical analysis
Variables are tabulated and/or reported as mean (standard devi-ation, SD) or median (interquartile range, IQR) as appropriate. Noassumptions were made about missing data. Multivariate analysisof changes over time (T0–T6hrs) was performed using repeat mea-sures analysis of variance adjusting for age and gender. Results aredisplayed graphically with means and standard error bars. Com-parisons between physiological variables at T6hrs and T72hrs wereconducted using paired t-tests. A two-sided p-value of 0.05 was con-sidered statistically significant. All analyses were performed usingSAS 9.1 (SAS Institute Inc., Carey, NC, USA).
3. Results
3.1. Patients
A total of 324 patients with sepsis and hypoperfusion or sep-tic shock were enrolled over a 3-month period in 32 sites. Duringthe same 3-month period, the total number of patients (mean, SD)presenting to the ED at each site was 10,974 (3525). Age, weightand APACHE II score were 63.4 (19.2) years, 76.3 (24.2) kg and19.0 (8.2) respectively. One hundred and seventy patients (52.5%)
were male. Baseline demographics, co-morbidities and concurrentmedical conditions are given in Table 1. The incidence of patientsmeeting the BP and metabolic acidosis inclusion criteria was 64.5%(n = 209/324) and 50.0% (n = 162/324) respectively. Only 15.1% ofpatients (n = 47/324) fulfilled both the BP and metabolic acidosis
S.L. Peake et al. / Resuscitation 80 (2009) 811–818 813
Table 1Baseline demographics, co-morbidities and concurrent medical conditions.
Variable
Age (years) 63.4 (19.2)Weight (kg) 76.3 (24.2)Males, % (n) 170 (52.5)APACHE II score 19.0 (8.2)
Chronic co-morbidities, n (%)Congestive cardiac failure 38 (11.7)Chronic lung disease 38 (11.7)Chronic renal failure 33 (10.2)Chronic liver disease 16 (4.9)Diabetes 74 (22.8)Cancer 48 (14.8)Immunosuppression 42 (13.0)
Concurrent acute medical conditions, n (%)Acute coronary syndrome 12 (3.7)Acute pulmonary oedema 5 (1.5)Arrhythmia 40 (12.3)Status asthmaticus 1 (0.3)Active gastrointestinal bleed 8 (2.5)Acute cerebrovascular accident 7 (2.2)Status epilepticus 2 (0.6)Drug overdose 1 (0.3)Burn injury 1 (0.3)Pregnancy 1 (0.3)Contra-indication to central venous catheterisation 1 (0.3)
D
cfia
3
d((adw
Fig. 1. Study entry criteria. Each bar represents the % of patients fulfilling each ofthe study entry criteria for sepsis with hypoperfusion or septic shock in the emer-gency department. “BP criteria” refers to the total number of patients meeting one ormore of the blood pressure criteria; “Acidosis criteria” refers to the total number ofpatients meeting one or more metabolic acidosis criteria and “Vasoactives” refers tothe infusion of one or more vasoactive agents to maintain blood pressure (adrenaline,noradrenaline, dopamine, vasopressin, metaraminol). SIRS, Systemic Inflammatory
TP
V
THMCRSSUCLpBHW
0Hac
v
Requirement for immediate surgery 24 (7.4)Do-not-resuscitate order 51 (15.7)
ata presented as mean (SD) or number (%).
riteria (Fig. 1). The time between ED presentation and meeting thenal inclusion criterion (T0hrs) was 1.6 (0.7,16.5) h. Physiologicalnd laboratory variables at T0hrs are given in Table 2.
.2. Microbiology
At study entry, 420 suspected or proven infection sources wereetermined to be present by the treating clinician. Of those, 82.1%
n = 345/420) were considered to be medical in origin and 14.6%n = 61/420) were surgical. Overall, pneumonia (n = 138/324, 42.6%)nd urinary tract infection (n = 99/324, 30.6%) were the commonestiagnoses at presentation. Abdominal infection (n = 45/324, 13.9%)as the commonest surgical source.able 2hysiological and laboratory data at enrolment (0 h) and at 6 and 72 h after meeting inclu
ariable 0 h
Mean (SD) n
emperature (◦C) 37.8 (2.1) 240R (beats/min) 120 (20) 276AP (mmHg) 68 (20) 232
VP (mmHg) 11 (8) 12R (breaths/min) 31 (9) 247aO2 (%) 96 (5) 281cvO2 (%)a 0O (ml/h) 96 (116) 128reatinine (�mol/L) 223 (209) 267actate (mmol/L) 6.9 (3.6) 93Hb 7.28 (0.52) 220ase deficit 7.7 (6.6) 212aematocrit (%) 37.1 (8.0) 273CC (×109/L) 18.3 (10.9) 220
h refers to the time the patient satisfies the final entry criterion for sepsis with hypoperR, heart rate; MAP, mean arterial pressure; CVP, central venous pressure; RR, respiratoryrterial blood gas analysis or pulse oximetry); ScvO2, central venous oxygen saturation; Ureatinine and WCC data not collected at 6 and 72 h.
a Continuous or intermittent ScvO2 measurement not performed at 0, 6 and 72 h.b For pH, measurement was obtained from arterial blood in 70.1% (n = 155), 95.1% (n = 1
enous pH was measured.
Response Syndrome; BP, blood pressure; SBP, systolic blood pressure; Premorbid,>40 mm Hg fall below premorbid SBP; MAP, mean arterial pressure.
Blood cultures were obtained in the majority of patients(n = 250/324, 77.2%) prior to T0hrs. Additional microbiological spec-imens (e.g. sputum, urine) were collected in 55.2% of patients(n = 179/324) prior to T0hrs. A positive culture(s) from any sourcewas subsequently identified in 67.9% of patients (n = 221/324) withgram-negative (n = 144/324, 44.4%) and gram-positive (n = 92/324,28.4%) bacteria being the most common isolates. Blood cultureswere positive in 119 patients (36.7%). Gram-negative bacteria werethe commonest blood culture isolates (n = 72/119, 60.5%).
Antimicrobial therapy was commenced 2.2 h (1.1, 3.8) after ED
presentation. Twenty-eight patients (n = 28/309, 9%) did not receiveantimicrobial therapy either before T0hrs or in the following 6 h(time-to-antimicrobial therapy not available for 15 patients). Mostpatients (n = 300/324, 92.6%) were subsequently deemed by the sitesion criteria for sepsis with hypoperfusion or septic shock.
6 h 72 h
Mean (SD) n Mean (SD) n
NA NA NA NA100 (22) 237 93 (20) 24175 (13) 225 86 (14) 23014 (5) 56 13 (7) 7521 (8) 212 19 (5) 21497 (7) 221 96 (3) 225
0 081 (83) 183 105 (99) 170NA NA NA NA3.2 (2.6) 128 2.1 (2.1) 897.26 (0.14) 144 7.38 (0.08) 959.4 (6.3) 141 4.4 (3.5) 9332.8 (6.3) 133 30.4 (5.2) 118NA NA NA NA
fusion or septic shock.rate; SaO2, arterial oxygen saturation (includes measurements obtained via eitherO, urine output; WCC, white cell count; SD, standard deviation; NA, temperature,
37) and 96.0% (n = 94) of cases at 0, 6 and 72 h respectively. In the remaining cases,
814 S.L. Peake et al. / Resuscitation 80 (2009) 811–818
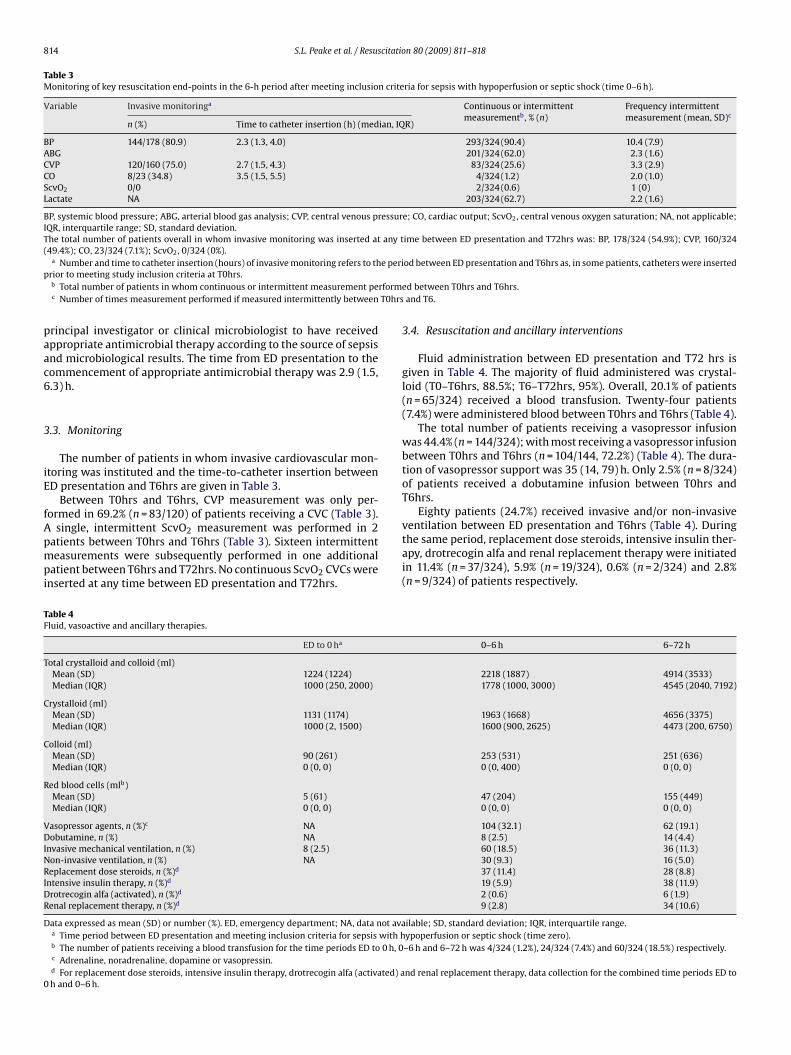
Table 3Monitoring of key resuscitation end-points in the 6-h period after meeting inclusion criteria for sepsis with hypoperfusion or septic shock (time 0–6 h).
Variable Invasive monitoringa Continuous or intermittentmeasurementb, % (n)
Frequency intermittentmeasurement (mean, SD)c
n (%) Time to catheter insertion (h) (median, IQR)
BP 144/178 (80.9) 2.3 (1.3, 4.0) 293/324 (90.4) 10.4 (7.9)ABG 201/324 (62.0) 2.3 (1.6)CVP 120/160 (75.0) 2.7 (1.5, 4.3) 83/324 (25.6) 3.3 (2.9)CO 8/23 (34.8) 3.5 (1.5, 5.5) 4/324 (1.2) 2.0 (1.0)ScvO2 0/0 2/324 (0.6) 1 (0)Lactate NA 203/324 (62.7) 2.2 (1.6)
BP, systemic blood pressure; ABG, arterial blood gas analysis; CVP, central venous pressure; CO, cardiac output; ScvO2, central venous oxygen saturation; NA, not applicable;IQR, interquartile range; SD, standard deviation.The total number of patients overall in whom invasive monitoring was inserted at any time between ED presentation and T72hrs was: BP, 178/324 (54.9%); CVP, 160/324(49.4%); CO, 23/324 (7.1%); ScvO2, 0/324 (0%).
a e perip
rformT0hrs
paac6
3
iE
fApmpi
TF
T
C
C
R
VDINRIDR
D
0
Number and time to catheter insertion (hours) of invasive monitoring refers to thrior to meeting study inclusion criteria at T0hrs.b Total number of patients in whom continuous or intermittent measurement pec Number of times measurement performed if measured intermittently between
rincipal investigator or clinical microbiologist to have receivedppropriate antimicrobial therapy according to the source of sepsisnd microbiological results. The time from ED presentation to theommencement of appropriate antimicrobial therapy was 2.9 (1.5,.3) h.
.3. Monitoring
The number of patients in whom invasive cardiovascular mon-toring was instituted and the time-to-catheter insertion betweenD presentation and T6hrs are given in Table 3.
Between T0hrs and T6hrs, CVP measurement was only per-
ormed in 69.2% (n = 83/120) of patients receiving a CVC (Table 3).single, intermittent ScvO2 measurement was performed in 2atients between T0hrs and T6hrs (Table 3). Sixteen intermittenteasurements were subsequently performed in one additional
atient between T6hrs and T72hrs. No continuous ScvO2 CVCs werenserted at any time between ED presentation and T72hrs.
able 4luid, vasoactive and ancillary therapies.
ED to 0 ha
otal crystalloid and colloid (ml)Mean (SD) 1224 (1224)Median (IQR) 1000 (250, 2000)
rystalloid (ml)Mean (SD) 1131 (1174)Median (IQR) 1000 (2, 1500)
olloid (ml)Mean (SD) 90 (261)Median (IQR) 0 (0, 0)
ed blood cells (mlb)Mean (SD) 5 (61)Median (IQR) 0 (0, 0)
asopressor agents, n (%)c NAobutamine, n (%) NA
nvasive mechanical ventilation, n (%) 8 (2.5)on-invasive ventilation, n (%) NAeplacement dose steroids, n (%)d
ntensive insulin therapy, n (%)d
rotrecogin alfa (activated), n (%)d
enal replacement therapy, n (%)d
ata expressed as mean (SD) or number (%). ED, emergency department; NA, data not avaa Time period between ED presentation and meeting inclusion criteria for sepsis with hb The number of patients receiving a blood transfusion for the time periods ED to 0 h, 0c Adrenaline, noradrenaline, dopamine or vasopressin.d For replacement dose steroids, intensive insulin therapy, drotrecogin alfa (activated) ah and 0–6 h.
od between ED presentation and T6hrs as, in some patients, catheters were inserted
ed between T0hrs and T6hrs.and T6.
3.4. Resuscitation and ancillary interventions
Fluid administration between ED presentation and T72 hrs isgiven in Table 4. The majority of fluid administered was crystal-loid (T0–T6hrs, 88.5%; T6–T72hrs, 95%). Overall, 20.1% of patients(n = 65/324) received a blood transfusion. Twenty-four patients(7.4%) were administered blood between T0hrs and T6hrs (Table 4).
The total number of patients receiving a vasopressor infusionwas 44.4% (n = 144/324); with most receiving a vasopressor infusionbetween T0hrs and T6hrs (n = 104/144, 72.2%) (Table 4). The dura-tion of vasopressor support was 35 (14, 79) h. Only 2.5% (n = 8/324)of patients received a dobutamine infusion between T0hrs andT6hrs.
Eighty patients (24.7%) received invasive and/or non-invasive
ventilation between ED presentation and T6hrs (Table 4). Duringthe same period, replacement dose steroids, intensive insulin ther-apy, drotrecogin alfa and renal replacement therapy were initiatedin 11.4% (n = 37/324), 5.9% (n = 19/324), 0.6% (n = 2/324) and 2.8%(n = 9/324) of patients respectively.0–6 h 6–72 h
2218 (1887) 4914 (3533)1778 (1000, 3000) 4545 (2040, 7192)
1963 (1668) 4656 (3375)1600 (900, 2625) 4473 (200, 6750)
253 (531) 251 (636)0 (0, 400) 0 (0, 0)
47 (204) 155 (449)0 (0, 0) 0 (0, 0)
104 (32.1) 62 (19.1)8 (2.5) 14 (4.4)60 (18.5) 36 (11.3)30 (9.3) 16 (5.0)37 (11.4) 28 (8.8)19 (5.9) 38 (11.9)2 (0.6) 6 (1.9)9 (2.8) 34 (10.6)
ilable; SD, standard deviation; IQR, interquartile range.ypoperfusion or septic shock (time zero).–6 h and 6–72 h was 4/324 (1.2%), 24/324 (7.4%) and 60/324 (18.5%) respectively.
nd renal replacement therapy, data collection for the combined time periods ED to

citatio
3
gCHaaUdr
7ao“t9(
Fat
S.L. Peake et al. / Resus
.5. Clinical progress
Haemodynamic and laboratory data at T6hrs and T72hrs areiven in Table 2. There was a progressive increase in MAP (P < 0.001),VP (P = 0.02) and SaO2 (P = 0.06) and a progressive decrease inR (P < 0.001), RR (P < 0.001) and UO (P = 0.02) between T0hrsnd T6hrs (RMANOVA). Over the subsequent T6–T72hrs, MAPnd SaO2 continued to increase (P < 0.001 for both) and HR andO decreased (P ≤ 0.001 for both). Lactate and haematocrit alsoecreased significantly over the same period (P = 0.002 and P = 0.03espectively).
In patients in whom physiological data was available at T6hrs,1.1% (n = 160/225) and 91.1% (n = 51/56) respectively achieved
MAP of 65–90 mmHg and a CVP ≥8 mmHg at the endf the 6-h period. The time to achieving these resuscitation
end-points” was 2.0 (1.0, 3.0) and 4.0 (2.0, 6.0) h respec-ively. Most patients also achieved a SaO2 ≥93% (n = 206/221,3.2%), UO ≥0.5 ml/kg/h (n = 110/159, 69.8%) and haematocrit ≥30%n = 92/133, 69.2%).ig. 2. Outcome of 324 patients presenting to the Emergency Department with sepsis anddmissions includes direct admissions to the hospital floor (n = 121) or other clinical areransfer to the operating theatre (n = 20) and deaths in ED (n = 4). ED, Emergency departm
n 80 (2009) 811–818 815
3.6. Outcomes
Following ED discharge, 36.4% (n = 118/324) of patients weretransferred directly to ICU and 56.2% (n = 182/324) were transferredto the hospital floor (n = 121/324, 37.5%) or other clinical areas (highdependency, ED observation ward) (Fig. 2). Twenty patients werealso transferred from ED directly to the operating theatre (6.2%) and4 patients (1.2%) died in ED. ED LOS was 6.7 (4.2, 9.9) h and the timebetween T0hrs and ED discharge was 4.2 (2.0, 7.1) h.
An additional 52 index patients were subsequently transferredfrom the hospital floor to ICU during the hospital admission (totalICU admission rate 52.4%). Overall, 98 patients (30.2%) requiredinvasive ventilation. Length of ventilation was 74 (21, 156) h. ICU andhospital LOS were 3.7 (1.7, 7.4) and 9.1 (4.1, 16.4) days respectively.
Overall in-hospital mortality was 23.1% (n = 75/324). For patients
meeting either the BP or lactate (>4.0 mmol/L) criteria, hospitalmortality was 23.0% (n = 48/209) and 26.9% (25/93) respectively(P = 0.56). Thirty-three percent (n = 70/209) of patients meeting theBP criterion received ≥20 ml/kg fluid bolus prior to study entry.hypoperfusion or septic shock in 32 Australian and New Zealand hospitals. Non-ICUas (e.g. high dependency unit, ED observation ward, coronary care) (n = 61), directent; ICU, Intensive Care Unit.

8 citatio
H≥22irfdolt
Em4O
3
twnisEdoco
svcBroWMamvu
ic(oteSfS
nCtttst
oaT
16 S.L. Peake et al. / Resus
ospital mortality for patients with hypotension unresponsive to20 ml/kg fluid and/or meeting the lactate entry criterion was2.7% (n = 34/150). For non-ICU patients, in-hospital mortality was1.4% (n = 33/154) and for patients admitted to ICU, overall ICU andn-hospital mortality were 18.8% (n = 32/170) and 24.7% (n = 42/170)espectively; odds ratio and 95% confidence intervals (OR, 95%CI)or mortality 1.20 (0.72, 2.02) (P = 0.48). For patients not admittedirectly to ICU from ED (e.g. ICU admission via the hospital floor,perating theatre) (n = 52), in-hospital mortality (n = 9/52, 17%) wasower but not significantly different to patients transferred directlyo ICU from ED (n = 33/118, 28%); OR 0.54 (95%CI 0.24, 1.23) (P = 0.14).
Fifty-one patients (15.7%) had a “do-not-resuscitate” order atD presentation, with 11.8% (n = 6/51) admitted to ICU. In-hospitalortality for patients designated “not-for-resuscitation” (n = 24/51,
7.1%) was higher than for remaining patients (n = 51/273, 18.7%);R 3.8 (95%CI 2.06, 7.25) (P < 0.0001).
.7. Discussion
This prospective, multi-centre, observational study of resuscita-ion practices and outcomes in a cohort of patients presenting to EDith sepsis and hypoperfusion or septic shock suggests that EGDT isot currently practised in ANZ. In particular, routine management
n the first 6 h after meeting the criteria for sepsis with hypoperfu-ion or septic shock did not incorporate integral components of theGDT algorithm such as continuous ScvO2 monitoring and ScvO2-irected blood transfusion and dobutamine infusion.6 Moreover,verall in-hospital mortality was considerably lower than standardare mortality in both randomised11 and non-randomised studiesf goal-directed resuscitation.10–12
Traditional resuscitation practices, as exemplified in the currenttudy, characteristically involve early antimicrobial therapy, fluids,asoactive agents and source control, with the intensity of resus-itation typically being determined by clinical end-points such asP, UO and CVP. The institution of protocolised early, goal-directedesuscitation does not appear to be integral to the resuscitationf patients with sepsis and hypoperfusion or septic shock in ANZ.hilst most patients achieved the physiological “EGDT goals” (e.g.AP, SaO2, UO), no patients received a continuous ScvO2 catheter
nd only two patients had a single intermittent ScvO2 measure-ent in the first 6 h after meeting the study entry criteria. Mixed
enous oxygen saturation via a pulmonary artery catheter was alsoncommon.
A similar lack of implementation of EGDT has been observedn a multi-centre, observational study of 92 ICU patients withommunity-acquired severe sepsis or septic shock in FinlandFinnsepsis study).3 Only 6.5% of patients received all elementsf the Surviving Sepsis Campaign early, goal-directed resuscita-ion bundle of care. Despite the introduction of a Spanish nationalducation programme directed at implementation of the Survivingepsis Campaign 6-h resuscitation and 24-h management bundlesor severe sepsis, compliance with the resuscitation guidelines inpain is also low (10%).4
Our study is unable to inform as to the reasons why EGDT hasot been incorporated into current resuscitation practices in ANZ.oncerns about the considerable financial and resource implica-ions of EGDT,13 the internal and external validity of the Rivers’rial and the potential risks associated with various elements ofhe EGDT resuscitation protocol such as dobutamine,14,15 aggres-ive fluid resuscitation16,17 and the liberal use of red cell transfusion
o achieve a haematocrit >30%18 may be important factors.Overall in-hospital mortality in our study, despite the lackf early goal-directed resuscitation, was only 23.1%. For patientsdmitted directly to ICU from ED, in-hospital mortality was 28%.he observed mortality is consistent with data from the ANZICS
n 80 (2009) 811–818
APD in which overall in-hospital mortality for medical ICU patientspresenting to ED with sepsis or septic shock between 1997 and2005 was 27.6%.7 A single-centre, retrospective Australian studyof >3000 ED patients with severe sepsis also reported that in-hospital mortality, in the absence of EGDT, was <30%.19 By wayof comparison, reported in-hospital mortality in before–after tri-als of EGDT ranges from 27 to 44% pre-implementation and 18 to21% post-introduction.12,20,21 In the Finnsepsis study, in-hospitalmortality for patients transferred from ED to ICU with septic shockwas 35%.3 However, differences in factors such as time to presen-tation, co-morbidities, incidence and duration of hypotension andvariations in treatment practices limit the ability to draw valid com-parisons of outcomes between our study and other single-centre orpopulation-based cohorts.
The third aim of our observational study was to confirm the fea-sibility of undertaking a randomised controlled trial of EDGT in ANZ.Given the lack of implementation of ScvO2-directed resuscitation,the number of patients meeting study entry criteria and the over-all in-hospital mortality, a large, multi-centre study examining theeffectiveness of EGDT in ANZ is necessary and achievable.
Our study has certain limitations. The participating sites wereself-selected, ANZICS CTG-affiliated sites and not all ANZ hospi-tals with an ED were included. Accordingly, the results may notaccurately reflect clinical practice in the whole population. How-ever, the observed hospital mortality is similar to data from theANZICS APD which contains information from the majority of ICUsin ANZ.22,23 Moreover, the 32 participating sites included a mix oftertiary-referral, metropolitan, and rural hospitals.
Secondly, although identification and recruitment of all poten-tially eligible patients may be incomplete or non-representative,the total number of patients admitted directly to ICU in our surveyis similar to the number of patients admitted directly to ICU from EDwith sepsis or septic shock in the ANZICS APD7 (3.7 patients/site/3months vs. 4.7 patients/site/3 months in the 101 ICUs contributingdata to the APD in 2005); suggesting that the number of potentiallymissing patients is limited. Hospital mortality is also similar (23.1%vs. 21.2% respectively).
Thirdly, although the study involves prospective data collection,missing data are inevitable as the time at which measurement wasdeemed necessary by the treating clinician did not necessarily cor-relate with the specific study time points (e.g. T6hrs) Nonetheless,hospital outcome was available in 100% of patients and, for mostof the physiological variables, data were available in approximately70% of patients at each of the time points specified over the 72 hstudy period.
Finally, it is important to note that the study entry criteria arebroader than those of the Rivers’ trial and direct comparisons arelimited.6 There were no exclusion criteria in our study and the vol-ume of fluid required to meet the BP criterion was considerablysmaller than previous sepsis studies. Given that one of the aims ofour study was to fully characterise the extent and variety of ANZresuscitation practices in patients with sepsis, liberal inclusion andexclusion criteria were essential. Nonetheless, in-hospital mortalityof patients meeting the BP inclusion criterion (23.0%) is similar tothe mortality of all patients admitted to ICU from the ED with sep-sis or septic shock in the ANZICS APD for 2005. Moreover, for thosepatients receiving a larger fluid bolus challenge prior to study entry(≥20 ml/kg) and/or with a lactate ≥4.0 mmol/L, hospital mortalitywas also similar (22.7%). Whilst it is possible that patients withconcurrent acute medical conditions may not have had sepsis asthe primary diagnosis, patients had to have a presumed infection
to be enrolled, nearly 70% subsequently had a positive microbiolog-ical culture, and the incidence of most of the individual concurrentmedical conditions was <1%. The three commonest concurrent con-ditions (“do-not resuscitate order” [15.7%], arrhythmia [12.3%] andrequirement for immediate surgery [7.4%]) are not unexpected in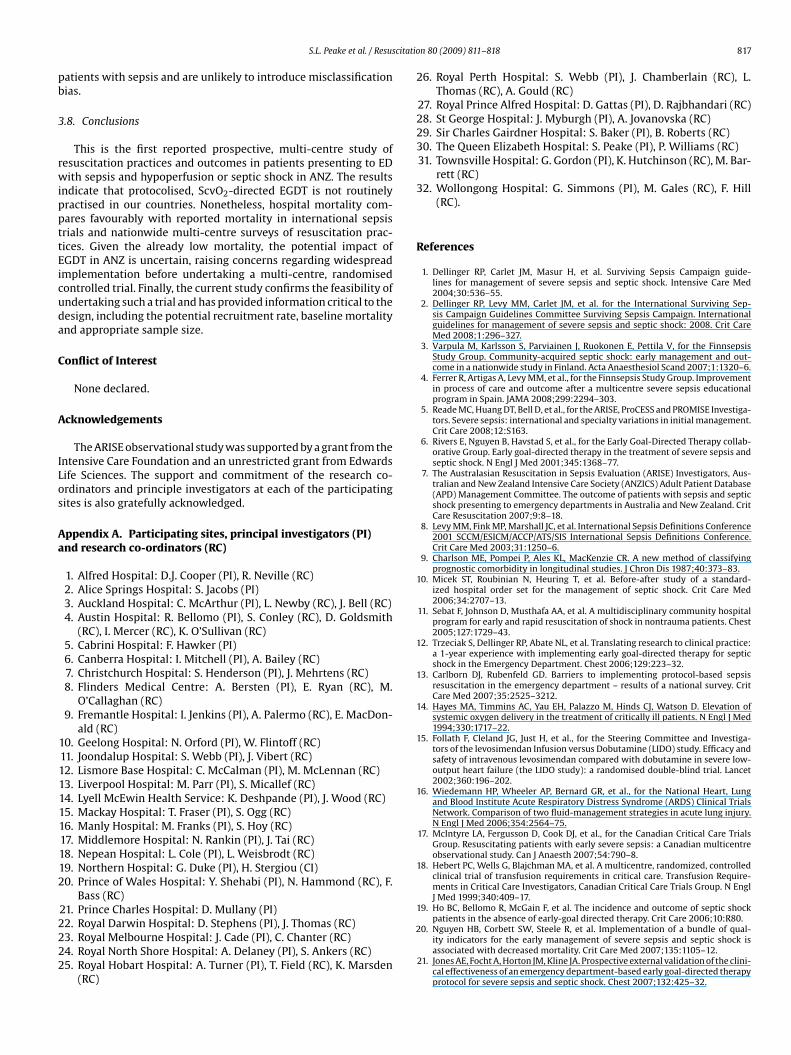
citatio
pb
3
rwippttEicuda
C
A
ILos
Aa
2
2222
1
S.L. Peake et al. / Resus
atients with sepsis and are unlikely to introduce misclassificationias.
.8. Conclusions
This is the first reported prospective, multi-centre study ofesuscitation practices and outcomes in patients presenting to EDith sepsis and hypoperfusion or septic shock in ANZ. The results
ndicate that protocolised, ScvO2-directed EGDT is not routinelyractised in our countries. Nonetheless, hospital mortality com-ares favourably with reported mortality in international sepsisrials and nationwide multi-centre surveys of resuscitation prac-ices. Given the already low mortality, the potential impact ofGDT in ANZ is uncertain, raising concerns regarding widespreadmplementation before undertaking a multi-centre, randomisedontrolled trial. Finally, the current study confirms the feasibility ofndertaking such a trial and has provided information critical to theesign, including the potential recruitment rate, baseline mortalitynd appropriate sample size.
onflict of Interest
None declared.
cknowledgements
The ARISE observational study was supported by a grant from thentensive Care Foundation and an unrestricted grant from Edwardsife Sciences. The support and commitment of the research co-rdinators and principle investigators at each of the participatingites is also gratefully acknowledged.
ppendix A. Participating sites, principal investigators (PI)nd research co-ordinators (RC)
1. Alfred Hospital: D.J. Cooper (PI), R. Neville (RC)2. Alice Springs Hospital: S. Jacobs (PI)3. Auckland Hospital: C. McArthur (PI), L. Newby (RC), J. Bell (RC)4. Austin Hospital: R. Bellomo (PI), S. Conley (RC), D. Goldsmith
(RC), I. Mercer (RC), K. O’Sullivan (RC)5. Cabrini Hospital: F. Hawker (PI)6. Canberra Hospital: I. Mitchell (PI), A. Bailey (RC)7. Christchurch Hospital: S. Henderson (PI), J. Mehrtens (RC)8. Flinders Medical Centre: A. Bersten (PI), E. Ryan (RC), M.
O’Callaghan (RC)9. Fremantle Hospital: I. Jenkins (PI), A. Palermo (RC), E. MacDon-
ald (RC)10. Geelong Hospital: N. Orford (PI), W. Flintoff (RC)11. Joondalup Hospital: S. Webb (PI), J. Vibert (RC)12. Lismore Base Hospital: C. McCalman (PI), M. McLennan (RC)13. Liverpool Hospital: M. Parr (PI), S. Micallef (RC)14. Lyell McEwin Health Service: K. Deshpande (PI), J. Wood (RC)15. Mackay Hospital: T. Fraser (PI), S. Ogg (RC)16. Manly Hospital: M. Franks (PI), S. Hoy (RC)17. Middlemore Hospital: N. Rankin (PI), J. Tai (RC)18. Nepean Hospital: L. Cole (PI), L. Weisbrodt (RC)19. Northern Hospital: G. Duke (PI), H. Stergiou (CI)0. Prince of Wales Hospital: Y. Shehabi (PI), N. Hammond (RC), F.
Bass (RC)21. Prince Charles Hospital: D. Mullany (PI)
2. Royal Darwin Hospital: D. Stephens (PI), J. Thomas (RC)3. Royal Melbourne Hospital: J. Cade (PI), C. Chanter (RC)4. Royal North Shore Hospital: A. Delaney (PI), S. Ankers (RC)5. Royal Hobart Hospital: A. Turner (PI), T. Field (RC), K. Marsden(RC)
2
n 80 (2009) 811–818 817
26. Royal Perth Hospital: S. Webb (PI), J. Chamberlain (RC), L.Thomas (RC), A. Gould (RC)
27. Royal Prince Alfred Hospital: D. Gattas (PI), D. Rajbhandari (RC)28. St George Hospital: J. Myburgh (PI), A. Jovanovska (RC)29. Sir Charles Gairdner Hospital: S. Baker (PI), B. Roberts (RC)30. The Queen Elizabeth Hospital: S. Peake (PI), P. Williams (RC)31. Townsville Hospital: G. Gordon (PI), K. Hutchinson (RC), M. Bar-
rett (RC)32. Wollongong Hospital: G. Simmons (PI), M. Gales (RC), F. Hill
(RC).
References
1. Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaign guide-lines for management of severe sepsis and septic shock. Intensive Care Med2004;30:536–55.
2. Dellinger RP, Levy MM, Carlet JM, et al. for the International Surviving Sep-sis Campaign Guidelines Committee Surviving Sepsis Campaign. Internationalguidelines for management of severe sepsis and septic shock: 2008. Crit CareMed 2008;1:296–327.
3. Varpula M, Karlsson S, Parviainen J, Ruokonen E, Pettila V, for the FinnsepsisStudy Group. Community-acquired septic shock: early management and out-come in a nationwide study in Finland. Acta Anaesthesiol Scand 2007;1:1320–6.
4. Ferrer R, Artigas A, Levy MM, et al., for the Finnsepsis Study Group. Improvementin process of care and outcome after a multicentre severe sepsis educationalprogram in Spain. JAMA 2008;299:2294–303.
5. Reade MC, Huang DT, Bell D, et al., for the ARISE, ProCESS and PROMISE Investiga-tors. Severe sepsis: international and specialty variations in initial management.Crit Care 2008;12:S163.
6. Rivers E, Nguyen B, Havstad S, et al., for the Early Goal-Directed Therapy collab-orative Group. Early goal-directed therapy in the treatment of severe sepsis andseptic shock. N Engl J Med 2001;345:1368–77.
7. The Australasian Resuscitation in Sepsis Evaluation (ARISE) Investigators, Aus-tralian and New Zealand Intensive Care Society (ANZICS) Adult Patient Database(APD) Management Committee. The outcome of patients with sepsis and septicshock presenting to emergency departments in Australia and New Zealand. CritCare Resuscitation 2007;9:8–18.
8. Levy MM, Fink MP, Marshall JC, et al. International Sepsis Definitions Conference2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference.Crit Care Med 2003;31:1250–6.
9. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifyingprognostic comorbidity in longitudinal studies. J Chron Dis 1987;40:373–83.
10. Micek ST, Roubinian N, Heuring T, et al. Before-after study of a standard-ized hospital order set for the management of septic shock. Crit Care Med2006;34:2707–13.
11. Sebat F, Johnson D, Musthafa AA, et al. A multidisciplinary community hospitalprogram for early and rapid resuscitation of shock in nontrauma patients. Chest2005;127:1729–43.
2. Trzeciak S, Dellinger RP, Abate NL, et al. Translating research to clinical practice:a 1-year experience with implementing early goal-directed therapy for septicshock in the Emergency Department. Chest 2006;129:223–32.
13. Carlborn DJ, Rubenfeld GD. Barriers to implementing protocol-based sepsisresuscitation in the emergency department – results of a national survey. CritCare Med 2007;35:2525–3212.
14. Hayes MA, Timmins AC, Yau EH, Palazzo M, Hinds CJ, Watson D. Elevation ofsystemic oxygen delivery in the treatment of critically ill patients. N Engl J Med1994;330:1717–22.
15. Follath F, Cleland JG, Just H, et al., for the Steering Committee and Investiga-tors of the levosimendan Infusion versus Dobutamine (LIDO) study. Efficacy andsafety of intravenous levosimendan compared with dobutamine in severe low-output heart failure (the LIDO study): a randomised double-blind trial. Lancet2002;360:196–202.
16. Wiedemann HP, Wheeler AP, Bernard GR, et al., for the National Heart, Lungand Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical TrialsNetwork. Comparison of two fluid-management strategies in acute lung injury.N Engl J Med 2006;354:2564–75.
17. McIntyre LA, Fergusson D, Cook DJ, et al., for the Canadian Critical Care TrialsGroup. Resuscitating patients with early severe sepsis: a Canadian multicentreobservational study. Can J Anaesth 2007;54:790–8.
18. Hebert PC, Wells G, Blajchman MA, et al. A multicentre, randomized, controlledclinical trial of transfusion requirements in critical care. Transfusion Require-ments in Critical Care Investigators, Canadian Critical Care Trials Group. N EnglJ Med 1999;340:409–17.
19. Ho BC, Bellomo R, McGain F, et al. The incidence and outcome of septic shockpatients in the absence of early-goal directed therapy. Crit Care 2006;10:R80.
0. Nguyen HB, Corbett SW, Steele R, et al. Implementation of a bundle of qual-ity indicators for the early management of severe sepsis and septic shock isassociated with decreased mortality. Crit Care Med 2007;135:1105–12.
21. Jones AE, Focht A, Horton JM, Kline JA. Prospective external validation of the clini-cal effectiveness of an emergency department-based early goal-directed therapyprotocol for severe sepsis and septic shock. Chest 2007;132:425–32.

8
2
18 S.L. Peake et al. / Resuscitatio
2. Hicks P, Cooper DJ, for the Australian and New Zealand Intensive Care Society(ANZICS) Board and Clinical Trials Group Executive Committee. The SurvivingSepsis Campaign: International guidelines for management of severe sepsis andseptic shock: 2008. Crit Care Resusc 2008;10:8.
2
n 80 (2009) 811–818
3. Stow PJ, Hart GK, Higlett T, et al., for the ANZICS Database Management Commit-tee. Development and implementation of a high-quality clinical database: theAustralian and New Zealand Intensive Care Society Adult Patient Database. J CritCare 2006;21:133–41.