
Ashkenazi Jewish population screening for Tay-Sachs disease: The International and Australian...
30
Title: Ashkenazi Jewish population screening for Tay-Sachs disease (TSD): A systematic review of the literature and the Australian experience. Authors Raelia M Lew 1 , Leslie Burnett 2, 3 , Anné L Proos 3 , Kristine Barlow-Stewart 2, 4 , Martin B Delatycki 5, 6 , Agnes Bankier 5 , Harry Aizenberg 7 , Michael J Field 8 , Yemima Berman 8 , Ronald Fleischer 8 , Michael Fietz 9 Institutional Affiliations 1. Department of Obstetrics and Gynaecology, QEII Research Institute for Mothers and Infants, The University of Sydney, NSW 2006 Australia. 2. Sydney Medical School -Northern, Royal North Shore Hospital E25, University of Sydney, Sydney NSW 2065, Australia. 3. Pacific Laboratory Medicine Services (PaLMS), NSW Health Pathology North, Royal North Shore Hospital, St Leonards NSW 2065, Australia. 4. NSW Centre for Genetics Education. Royal North Shore Hospital, St Leonards NSW 2065, Australia. 5. Department of Clinical Genetics, Austin Health, Heidelberg, VIC 3084, Australia 6. Bruce Lefroy Centre for Genetic Health Research, Murdoch Childrens Research Institute, Parkville, VIC 3052, Australia. 7. Wolper Jewish Hospital, Woollahra NSW 2025, Australia.
Transcript of Ashkenazi Jewish population screening for Tay-Sachs disease: The International and Australian...

Title:
Ashkenazi Jewish population screening for Tay-Sachs disease (TSD): A systematic
review of the literature and the Australian experience.
Authors
Raelia M Lew1, Leslie Burnett 2, 3, Anné L Proos 3, Kristine Barlow-Stewart 2, 4,
Martin B Delatycki 5, 6, Agnes Bankier 5 , Harry Aizenberg 7, Michael J Field 8,
Yemima Berman 8, Ronald Fleischer 8, Michael Fietz 9
Institutional Affiliations
1. Department of Obstetrics and Gynaecology, QEII Research Institute for Mothers and
Infants, The University of Sydney, NSW 2006 Australia.
2. Sydney Medical School -Northern, Royal North Shore Hospital E25, University of
Sydney, Sydney NSW 2065, Australia.
3. Pacific Laboratory Medicine Services (PaLMS), NSW Health Pathology North, Royal
North Shore Hospital, St Leonards NSW 2065, Australia.
4. NSW Centre for Genetics Education. Royal North Shore Hospital, St Leonards NSW 2065,
Australia.
5. Department of Clinical Genetics, Austin Health, Heidelberg, VIC 3084, Australia
6. Bruce Lefroy Centre for Genetic Health Research, Murdoch Childrens Research Institute,
Parkville, VIC 3052, Australia.
7. Wolper Jewish Hospital, Woollahra NSW 2025, Australia.

8. Department of Clinical Genetics, Royal North Shore Hospital, St Leonards NSW 2065,
Australia.
9. Department of Biochemical Genetics, SA Pathology, North Adelaide, SA 5006, Australia.
Corresponding author:
Dr Raelia Lew
Email: [email protected]
Postal Address: 183 Glenalmond Avenue, Cambridge UK CB28DH
Contact telephone: +4407455557698
Conflict of Interest:
Raelia M Lew, Leslie Burnett, Anné L Proos, Kristine Barlow-Stewart,
Martin B Delatycki, Agnes Bankier, Harry Aizenberg, Michael J Field,
Yemima Berman, Ronald Fleischer and Michael Fietz declare no conflict of interest.
Abstract:
Internationally, Tay-Sachs disease (TSD) preconception screening of Ashkenazi Jewish (AJ)
individuals and couples has led to effective primary prevention of TSD. In Australia,
adolescent preconception genetic screening programs operate mainly in Jewish community
high schools. These existing programs offer an effective means of primary prevention of TSD,
are cost effective and safe. However, in the broader Australian community TSD screening is
not systematically performed; cases still occur in unscreened AJ individuals. There is a need
for definitive guidelines for healthcare professionals to facilitate extension of the proven
benefits of preconception TSD screening to all AJ individuals at risk in the broader
community. We performed a systematic review of the relevant literature relating to AJ pre-
conception and antenatal screening for TSD. The evidence was assessed using an established
National Health and Medical Research Council evidence grading system. Evaluations of
efficacy of TSD screening programs design and execution, cost-benefit and cost-utility health
economic evaluation, and population outcomes were undertaken. The results have been used
to propose a model for universal AJ TSD preconception and antenatal screening for the
primary care setting.

Figure Legend
Tables
Table 1: Grades of recommendations for bodies of evidence
Table 2: Evidence summary
Table 3: Recommendations for TSD screening in primary care
Figures
Figure 1. Two-step screening
Figure 2. One-step couple screening
Figure 3. One step couple screening (ultra-orthodox unmarried couple)

1
Introduction
Tay-Sachs disease (TSD)
TSD is a due to congenital deficiency of ß-hexosaminidase enzyme, caused by mutations of
HEXA OMIM *606869 (gene map locus 15q23-q24). TSD has autosomal recessive
inheritance, in which heterozygous genetic carriers are phenotypically normal. In a couple
where both partners are carriers, 25% of pregnancies will be affected. Most infants with TSD
appear healthy at birth.(Kaback et al. 1993) After a three to six month period of normal
development, TSD-affected infants regress neurologically secondary to neuronal
accumulation of sphingolipid GM2 gangliosides. Most motor and social skills are lost by 18
months of age. Children rarely survive beyond 5 years of age. No effective treatment
exists.(Gravel 1995) (Okada and O'Brien 1969; Sandhoff 1969) In Ashkenazi Jews (Jews of
Central/Eastern European descent) TSD incidence is 1 in 2,500 (carrier frequency 1 in
25).(Lew et al. 2011) 93.1 to 99.1% of Jewish TSD carriers are found to have one of three
common HEXA mutations: c.1278insTATC, c.1421+1G>C and c.805G>A.(Kaback 2000;
Kaback et al. 1993; Bach et al. 2001; Myerowitz and Costigan 1988; Arpaia et al. 1988;
Myerowitz 1988; Ohno and Suzuki 1988; Navon and Proia 1989; Triggs-Raine et al. 1990;
Landels et al. 1991) In general (non-AJ) populations TSD incidence is 1 in 250,000 (carrier
frequency 1 in 250).(Control of Hereditory Diseases 1996)

2
Principles of population genetic screening
Classic principles of population genetic screening were defined by Wilson &
Jungner.(Wilson J. 1968) A World Health Organization (WHO) review synthesised
additional principles for the genomic age proposed over the last 40 years.(Andermann et al.
2008)
International practice
Strong international consensus supports universal TSD AJ preconception/antenatal
screening.(Committee 2006; Genetics 2009; Langlois et al. 2006; Monaghan et al. 2008) In
the United States,(Kaback et al. 1993) Canada(Kaback et al. 1993; Kaplan 1998) and
Israel(Zlotogora 2009) TSD screening of Ashkenazi Jewish individuals has resulted in >90%
reduction in TSD incidence.
The following international bodies recommend that TSD preconception/antenatal screening
should be offered to all individuals with Ashkenazi Jewish heritage:
1. The American Congress of Obstetricians and Gynecologists (ACOG)(Genetics 2009)
2. The American College of Medical Genetics (ACMG)(Monaghan et al. 2008)
3. Society of Obstetricians and Gynaecologists of Canada (SOGC)(Langlois et al. 2006)
4. United Kingdom National Screening Committee (UK NSC)(Committee 2006)
5. State of Israel Ministry of Health(State of Israel 2013)

3
Australian practice
Despite strong international support of universal AJ preconception TSD screening, no
Australian guideline exists and AJ TSD screening is not publicly funded.
Cost-benefit and ethical considerations
In terms of direct monetary cost, pre-conception or antenatal screening for TSD is superior to
retrospective identification of carrier parents following the birth of an affected infant. The
direct tangible monetary costs have been analysed in an Australian cost-utility study, which
found in favour of screening.(Warren et al. 2005) Important ethical benefits of TSD carrier
screening include informed reproductive choice(Metcalfe 2012) and a net increase in health
of carrier couples and families by preventing the profound psychological costs of having a
TSD affected infant. These additional benefits are difficult to quantify in terms of monetary
value.(Shabat 1999; Tsukahara and Kadota 1977)

4
Objective
Australia is a good model for evaluating the effectiveness of high school TSD screening
programs. Australia has a relatively static Jewish population strongly concentrated to two
major centres (Sydney and Melbourne).(Rutland 2005; Rubinstein 1995) Australian
screening programs are well funded, have high uptake of services by AJ high school students
targeted (>8000 student participants to date) and are highly collaborative with ongoing
analysis of more than 17 years of data.(Lew et al. 2012)
This paper aims to systematically review the international evidence-base supporting universal
preconception TSD screening for Ashkenazi Jewish individuals, to present the Australian
experience and to argue the case for supporting universal AJ TSD screening in Australia. Our
data and resultant conclusions may be of assistance for screening AJ communities in other
countries.

5
Australian Tay-Sachs disease population genetic screening programs
Based on international best-practice principles(Kaback 2000; Ekstein and Katzenstein 2001;
Bach et al. 2001; Mitchell et al. 1996) Australian genetic screening programs for
TSD(Burnett et al. 1995) have targeted senior Jewish high school students in Sydney and
Melbourne since 1995.(Lew et al. 2012) The design of the Sydney program, on which the
Melbourne program is based, has been described.(Barlow-Stewart et al. 2003) Screening
programs were developed in consultation with the local communities and consist of
mandatory onsite education followed by voluntary on-site genetic carrier testing (originally
by venepuncture, but more recently by mouthwash sampling). Participants may request
immediate or deferred disclosure of results.(Burnett L 2013) Screening is cost free to
participants (philanthropically funded) and participation rates are high (99.6%).(Ioannou et al.
2010)
An alternative approach to screening is that of Dor Yeshorim,(Ekstein and Katzenstein 2001)
an international Jewish genetic screening program accessible to Australians. Dor Yeshorim
targets ultra-orthodox Jewish communities worldwide. The program is accessed prior to
marriage to advise on the genetic compatibility of a proposed match. Individuals’ results
remain anonymous. A small minority of Jewish Australians identify as ultra-orthodox. Dor
Yeshorim is unaffiliated with Australian TSD screening programs. Dor Yeshorim screening
records were unavailable to authors of this paper.

6
In addition to TSD, both Australian Jewish genetic screening programs and Dor Yeshorim
now offer testing for other conditions relevant to the target community.(Ioannou et al. 2010;
Lew et al. 2011; Ekstein and Katzenstein 2001)
TSD population genetic screening programs have proved a successful strategy for primary
prevention of TSD.(Lew et al. 2012; Kaback et al. 1993; Mitchell et al. 1996; Chemke and
Zlotogora 1997) Over the 17 years so far evaluated in health outcome studies, no Australian
TSD screening program participant has had an affected child – representing complete
prevention in the 7756 screened between 1995 and 2011.(Lew et al. 2012) In 5 to 11 year
post high school follow up analysis, screening program participants were supportive of the
program, retained good knowledge of TSD and were happy with the timing of
screening.(Curd et al. 2013)
Two AJ cases of TSD have occurred since the introduction of Australian screening programs.
In both these cases, none of the four parents had accessed TSD screening. (Lew et al. 2012)
Access to TSD screening in Australia is incomplete
The most frequent route of access to TSD screening in Australia is by participation in
organised screening programs in senior high schools and associated outreach programs.
However, even taking into account those who have accessed these programs, the majority of
Australians with AJ heritage of reproductive age have not accessed TSD screening.(Lew et al.
2012). From Australian Bureau of Statistics and Australian Jewish Community data it is
estimated that approximately 50% of current Australian Jewish high school students attend

7
schools that do not currently participate in TSD screening programs. (Eckstein G.
Demography of the Sydney Jewish community: an overview of information from the 2006
Census. Unpublished report commissioned by the Jewish Community Appeal (JCA); copies
available on request from http://www.jca.org.au). AJ individuals who completed high school
prior to 1995 in Sydney and 1998 in Melbourne (predating TSD screening programs) did not
have access to any TSD population genetic screening; a cohort of this group remains in the
reproductive age bracket.
Outside of screening programs, TSD genetic preconception screening can in theory be
accessed through primary care clinician referral.(Metcalfe 2012) In the Australian context,
the primary care clinician is usually a patient’s General Practitioner, or
Obstetrician/Gynaecologist. In practice, such referral for TSD screening is uncommon (Anné
L Proos - unpublished data). Barriers include lack of clinician education, omission of genetic
risk identifying enquiry during medical history taking,(Hill and Schorr 2001; Shapiro and
Shapiro 1989) lack of patient knowledge,(D'Souza et al. 2000) cost of testing(Stark et al.
2013) and unplanned pregnancy (accounting for 30 to 50% of all pregnancies in developed
countries).(Black et al. 2010)

8
Methods:
Identification of studies
A Medline-Pubmed advanced search was conducted using MeSH topics “Tay Sachs disease”
AND (“screening” OR “genetic counselling” OR “cost” OR “GM2” OR “genetic diseases” or
“Ashkenazi Jewish”). A manual review of abstracts identified articles relevant to genetic
screening for TSD in individuals with AJ heritage. These were subsequently reviewed in full.
No language restrictions were applied.
Inclusion criteria: all research and review articles reporting experience of AJ TSD screening,
including clinical, laboratory, cost analysis and psychological aspects of TSD screening.
Exclusion criteria: Articles related to non-human subjects, experimental laboratory methods,
genetic screening in non-Jewish populations.
Formulation of evidence based recommendations
The evidence supporting the proposed guidelines was appraised with reference to the
Australian National Health and Medical Research Council (NHMRC) evidence grading
system.(NHMRC 1999)

9
Results:
The Medline-Pubmed advanced search identified 288 articles. A manual review of abstracts
identified 85 relevant articles relevant to AJ TSD preconception and antenatal screening of
which all were reviewed in full. No randomised controlled trials relating to TSD carrier
screening were identified. Some papers had findings relevant to more than one body of
evidence. Grades of recommendations for bodies of evidence are reported in Table 1. The
evidence summary is reported in Table 2.
Based on the results of this review recommendations for TSD screening in primary care are
outlined in Table 3.
Alternative models of TSD screening are depicted in Figures 1-3.

10
Discussion
Evidence from 17 years experience of TSD screening programs in Australian Jewish high
schools has shown screening to be both effective in TSD primary prevention(Lew et al. 2012)
and also cost effective.(Warren et al. 2005) Reliance solely on high school based programs is
an inadequate strategy for population wide screening; less than half the at-risk target
population (AJ individuals of reproductive age) is within this screened cohort (Eckstein G.
Demography of the Sydney Jewish community: an overview of information from the 2006
Census. Unpublished report commissioned by the Jewish Community Appeal (JCA); copies
available on request from http://www.jca.org.au). Currently, cases that could be prevented
are missed.(Lew et al. 2012)
Primary care clinician referral for TSD screening is the pragmatic solution to reach this
remaining community sector and to facilitate universal access. Challenges to implementation
of this strategy include improving clinician and patient education(Shapiro and Shapiro 1989;
Garber et al. 1993; Clarke 1978) and funding of supporting laboratory testing and health
infrastructure.(Stark et al. 2013) Creation of Australian guidelines for AJ preconception
genetic screening in the primary care context would assist in realizing universal access and
the process of developing such guidelines is underway (Human Genetics Society of
Australasia, Joint Human Genetics Society of Australasia/Royal Australian and New Zealand
College of Obstetricians and Gynaecologists Prenatal Diagnosis and Screening Committee).
Performing this screening prior to pregnancy should be considered the gold standard as
prospective diagnosis allows carrier couples access to a wider range of reproductive

11
options.(Sutton 2002; Strom 2004) As many pregnancies are unplanned(Black et al. 2010),
clinicians should consider and offer TSD screening opportunistically when at-risk patients
present for other reasons (e.g. general or sexual health check).(Shapiro and Shapiro 1989)
Presentation for screening may commonly occur in early pregnancy.(Shapiro and Shapiro
1989) Where an at-risk couple is identified during pregnancy, prompt referral for appropriate
genetic counseling and maternal fetal medical review should be undertaken. Management
may include fetal diagnostic testing.(Genetics 2009)
Good pre-test education is imperative to achieve informed consent. In Australian TSD
screening programs, pre-test education is delivered by a qualified genetic counsellor.(Barlow-
Stewart et al. 2003; Ioannou et al. 2010) Sessions include the delivery of written and
multimedia presentations. Multimedia educational presentations are highly effective in
conveying pre-test information in the context of TSD screening programs.(Gason et al. 2004)
On-line education tools made freely available to primary care clinicians and patients may
cost-effectively achieve consistent and quality-assured patient education.(Andermann and
Blancquaert 2010)
Figures 1-3 summarise the recommended screening pathways applicable to AJ individuals
and their partners. These pathways are derived from international best-practice screening
strategies (Kaback 2000; Ekstein and Katzenstein 2001; Bach et al. 2001; Mitchell et al.
1996; Barlow-Stewart et al. 2003; Ioannou et al. 2010) and offer alternative approaches to
different preconception and antenatal scenarios. The Dor Yeshorim model was designed to
12
provide culturally acceptable access to screening for an ultra-orthodox Jewish demographic.
(Ekstein and Katzenstein 2001)
Current practice recommends DNA based testing for common AJ mutations as the most cost
effective method to identify AJ TSD carriers.(Triggs-Raine et al. 1990; Bach et al. 2001)
Partners of AJ carriers should also be offered TSD preconception screening, with any such
non-AJ individuals being tested with enzyme-based assays (Natowicz and Prence 1996)
rather than DNA based testing, due to the wider range of HEXA variants found in non-AJ
heterozygote carriers.(Park et al. 2010)
Genetic laboratory testing methodology is rapidly advancing. In the immediate future
massively parallel (“Next Generation”) DNA sequencing will likely replace conventional
testing methods for conditions screened in AJ preconception programs including
TSD.(Kingsmore 2012; Bell et al. 2011; Srinivasan et al. 2010) This will expand the scope
and menu of preconception genetic screening exponentially and pose challenges for the
traditional notions of informed consent.(Harris et al. 2013) Evidence regarding the safety and
ethical impact of these developments is currently lacking.
Referral of clients to a local national and regional genetic services may be appropriate; within
Australia a directory of such resources is offered by the Centre for Genetics Education
(www.genetics.edu.au), and similar referral directories have been established in many other
regions and countries.

13
Conclusion
TSD screening programs targeting an adolescent AJ population are a highly effective and
cost-effective primary prevention strategy. Routine implementation of recommendations
summarized in Table 3 by primary care clinicians would optimize informed reproductive
choice in AJ individuals and would result in near complete TSD case prevention. The
recommendations in Table 3 have been developed through evidence-based review of all
published studies irrespective of country of origin, and should be portable and applicable to
other national jurisdictions. Universal access to TSD genetic screening for all AJ Australians
is clinically achievable in the primary care setting using simple practice workflows (Figs 1-3).
The conclusions reached based on this Australian data are likely to be transferrable and
applicable to other countries and communities.
Acknowledgements
Martin B Delatycki is an NHMRC Practitioner Fellow
References
Andermann A, Blancquaert I (2010) Genetic screening: A primer for primary care. Canadian family physician Medecin de famille canadien 56 (4):333-339
Andermann A, Blancquaert I, Beauchamp S, Dery V (2008) Revisiting Wilson and Jungner in the genomic age: a review of screening criteria over the past 40 years. Bull World Health Organ 86 (4):317-319
Arpaia E, Dumbrille-Ross A, Maler T, Neote K, Tropak M, Troxel C, Stirling JL, Pitts JS, Bapat B, Lamhonwah AM, et al. (1988) Identification of an altered splice site in Ashkenazi Tay-Sachs disease. Nature 333 (6168):85-86. doi:10.1038/333085a0
Bach G, Tomczak J, Risch N, Ekstein J (2001) Tay-Sachs screening in the Jewish Ashkenazi population: DNA testing is the preferred procedure. Am J Med Genet 99 (1):70-75

14
Barlow-Stewart K, Burnett L, Proos A, Howell V, Huq F, Lazarus R, Aizenberg H (2003) A genetic screening programme for Tay-Sachs disease and cystic fibrosis for Australian Jewish high school students. J Med Genet 40 (4):e45
Bell CJ, Dinwiddie DL, Miller NA, Hateley SL, Ganusova EE, Mudge J, Langley RJ, Zhang L, Lee CC, Schilkey FD, Sheth V, Woodward JE, Peckham HE, Schroth GP, Kim RW, Kingsmore SF (2011) Carrier testing for severe childhood recessive diseases by next-generation sequencing. Sci Transl Med 3 (65):65ra64. doi:10.1126/scitranslmed.3001756
Black KI, Gupta S, Rassi A, Kubba A (2010) Why do women experience untimed pregnancies? A review of contraceptive failure rates. Best Pract Res Clin Obstet Gynaecol 24 (4):443-455. doi:10.1016/j.bpobgyn.2010.02.002
Burnett L PA, Barlow-Stewart K, Aizenberg H (2013) Evaluation of deferred selection of result reporting strategies in community genetic screening for autosomal recessive disorders.
Burnett L, Proos AL, Chesher D, Howell VM, Longo L, Tedeschi V, Yang VA, Siafakas N, Turner G (1995) The Tay-Sachs disease prevention program in Australia: Sydney pilot study. Med J Aust 163 (6):298-300
Chemke J, Zlotogora J (1997) Genetic services in Israel. Eur J Hum Genet 5 Suppl 2:105-111
Clarke JT (1978) Screening for carriers of Tay-Sachs disease: two approaches. Can Med Assoc J 119 (6):549-550
Committee UNS (2006) NHS Policy database, Tay Sachs disease NHS, http://www.screening.nhs.uk/taysachs
Control of Hereditory Diseases (1996). World Health Organisation Technical Report Series 865. World Health Organization, Geneva
Curd H, Lewis S, Macciocca I, Sahhar M, Petrou V, Bankier A, Lieberman S, Levy-Lahad E, Delatycki MB (2013) High school Tay-Sachs disease carrier screening: 5 to 11-year follow-up. Journal of community genetics. doi:10.1007/s12687-013-0163-z
D'Souza G, McCann CL, Hedrick J, Fairley C, Nagel HL, Kushner JD, Kessel R (2000) Tay-Sachs disease carrier screening: a 21-year experience. Genet Test 4 (3):257-263. doi:10.1089/10906570050501470
Ekstein J, Katzenstein H (2001) The Dor Yeshorim story: community-based carrier screening for Tay-Sachs disease. Adv Genet 44:297-310
Garber AP, Platt LD, Wang SJ, Jam K, Carlson DE, Rotter JI (1993) Determinants of utilization of Tay-Sachs screening. Obstet Gynecol 82 (3):460-463
Gason AA, Aitken M, Delatycki MB, Sheffield E, Metcalfe SA (2004) Multimedia messages in genetics: design, development, and evaluation of a computer-based instructional resource for secondary school students in a Tay Sachs disease carrier screening program. Genet Med 6 (4):226-231. doi:10.109701.GIM.0000132681.36771.63

15
Genetics ACo (2009) ACOG Committee Opinion No. 442: Preconception and prenatal carrier screening for genetic diseases in individuals of Eastern European Jewish descent. Obstet Gynecol 114 (4):950-953. doi:10.1097/AOG.0b013e3181bd12f4
Gravel RA, Clarke JTR, Kaback MM et al (1995) The GM2 gangliosidoses. In: Scriver CR, Beaudet AL, Sly WS, Valle D (ed) The Metabolic and Molecular Basis Of Inherited Disease. 7 edn. McGraw-Hill, New York, pp 2839–2879
Harris A, Kelly SE, Wyatt S (2013) Counseling customers: emerging roles for genetic counselors in the direct-to-consumer genetic testing market. J Genet Couns 22 (2):277-288. doi:10.1007/s10897-012-9548-0
Hill LW, Schorr SJ (2001) Prenatal screening for Tay-Sachs disease by Louisiana obstetricians: a survey study. South Med J 94 (9):910-912
Ioannou L, Massie J, Lewis S, Petrou V, Gason A, Metcalfe S, Aitken MA, Bankier A, Delatycki MB (2010) Evaluation of a multi-disease carrier screening programme in Ashkenazi Jewish high schools. Clin Genet 78 (1):21-31. doi:10.1111/j.1399-0004.2010.01459.x
Kaback M, Lim-Steele J, Dabholkar D, Brown D, Levy N, Zeiger K (1993) Tay-Sachs disease--carrier screening, prenatal diagnosis, and the molecular era. An international perspective, 1970 to 1993. The International TSD Data Collection Network. JAMA : the journal of the American Medical Association 270 (19):2307-2315
Kaback MM (2000) Population-based genetic screening for reproductive counseling: the Tay-Sachs disease model. Eur J Pediatr 159 Suppl 3:S192-195
Kaplan F (1998) Tay-Sachs disease carrier screening: a model for prevention of genetic disease. Genet Test 2 (4):271-292
Kingsmore S (2012) Comprehensive carrier screening and molecular diagnostic testing for recessive childhood diseases. PLoS Curr:e4f9877ab9878ffa9879. doi:10.1371/4f9877ab8ffa9
Landels EC, Ellis IH, Fensom AH, Green PM, Bobrow M (1991) Frequency of the Tay-Sachs disease splice and insertion mutations in the UK Ashkenazi Jewish population. J Med Genet 28 (3):177-180
Langlois S, Wilson RD, Genetics Committee of the Society of O, Gynaecologists of C, Prenatal Diagnosis Committee of the Canadian College of Medical G (2006) Carrier screening for genetic disorders in individuals of Ashkenazi Jewish descent. J Obstet Gynaecol Can 28 (4):324-343
Lew R, Burnett L, Proos A (2011) Tay-Sachs disease preconception screening in Australia: self-knowledge of being an Ashkenazi Jew predicts carrier state better than does ancestral origin, although there is an increased risk for c.1421 + 1G > C mutation in individuals with South African heritage. J Community Genet 2 (4):201-209. doi:10.1007/s12687-011-0057-x

16
Lew RM, Proos AL, Burnett L, Delatycki M, Bankier A, Fietz MJ (2012) Tay Sachs disease in Australia: reduced disease incidence despite stable carrier frequency in Australian Jews. Med J Aust 197 (11):652-654
Metcalfe SA (2012) Carrier screening in preconception consultation in primary care. J Community Genet 3 (3):193-203. doi:10.1007/s12687-011-0071-z
Mitchell JJ, Capua A, Clow C, Scriver CR (1996) Twenty-year outcome analysis of genetic screening programs for Tay-Sachs and beta-thalassemia disease carriers in high schools. Am J Hum Genet 59 (4):793-798
Monaghan KG, Feldman GL, Palomaki GE, Spector EB, Ashkenazi Jewish Reproductive Screening Working G, Molecular Subcommittee of the ALQAC (2008) Technical standards and guidelines for reproductive screening in the Ashkenazi Jewish population. Genet Med 10 (1):57-72. doi:10.1097/GIM.0b013e31815f6eac
Myerowitz R (1988) Splice junction mutation in some Ashkenazi Jews with Tay-Sachs disease: evidence against a single defect within this ethnic group. Proc Natl Acad Sci U S A 85 (11):3955-3959
Myerowitz R, Costigan FC (1988) The major defect in Ashkenazi Jews with Tay-Sachs disease is an insertion in the gene for the alpha-chain of beta-hexosaminidase. J Biol Chem 263 (35):18587-18589
Natowicz MR, Prence EM (1996) Heterozygote screening for Tay-Sachs disease: past successes and future challenges. Curr Opin Pediatr 8 (6):625-629
Navon R, Proia RL (1989) The mutations in Ashkenazi Jews with adult GM2 gangliosidosis, the adult form of Tay-Sachs disease. Science 243 (4897):1471-1474
NHMRC (1999) How to review the evidence: systematic identification and review of the scientific literature. National Health and Medical Research Council Australia (NHMRC). Accessed 11/12/2013 2013
Ohno K, Suzuki K (1988) A splicing defect due to an exon-intron junctional mutation results in abnormal beta-hexosaminidase alpha chain mRNAs in Ashkenazi Jewish patients with Tay-Sachs disease. Biochem Biophys Res Commun 153 (1):463-469
Okada S, O'Brien JS (1969) Tay-Sachs disease: generalized absence of a beta-D-N-acetylhexosaminidase component. Science 165 (3894):698-700
Park NJ, Morgan C, Sharma R, Li Y, Lobo RM, Redman JB, Salazar D, Sun W, Neidich JA, Strom CM (2010) Improving accuracy of Tay Sachs carrier screening of the non-Jewish population: analysis of 34 carriers and six late-onset patients with HEXA enzyme and DNA sequence analysis. Pediatr Res 67 (2):217-220. doi:10.1203/PDR.0b013e3181c6e318
Rubinstein WD (1995) Judaism in Australia. Religious Community Profiles Australian Govt. Pub. Service

17
Rutland SD (2005) The Jews in Australia. Cambridge University Press, Port Melbourne
Sandhoff K (1969) Variation of beta-N-acetylhexosaminidase-pattern in Tay-Sachs disease. FEBS Lett 4 (4):351-354
Shabat S (1999) Economics of screening programs for Tay-Sachs disease. Health Policy 47 (2):183-184
Shapiro DA, Shapiro LR (1989) Pitfalls in Tay-Sachs carrier detection: physician referral patterns and patient ignorance. N Y State J Med 89 (6):317-319
Srinivasan BS, Evans EA, Flannick J, Patterson AS, Chang CC, Pham T, Young S, Kaushal A, Lee J, Jacobson JL, Patrizio P (2010) A universal carrier test for the long tail of Mendelian disease. Reprod Biomed Online 21 (4):537-551. doi:10.1016/j.rbmo.2010.05.012
Stark Z, Massie J, McClaren B, Ioannou L, Cousens N, Lewis S, Metcalfe S, Delatycki MB (2013) Current Practice and Attitudes of Australian Obstetricians Toward Population-Based Carrier Screening for Inherited Conditions. Twin Res Hum Genet:1-7. doi:10.1017/thg.2012.152
State of Israel MoHS (2013) Genetic Inquiries and Pregestation tests or Tests during Pregnancy. http://www.health.gov.il/English/Services/Citizen_Services/Pages/Genetic_tests.aspx
Strom CM (2004) Population-based carrier screening and prenatal diagnosis. MLO Med Lab Obs 36 (8):12-17; quiz 20-11
Sutton VR (2002) Tay-Sachs disease screening and counseling families at risk for metabolic disease. Obstet Gynecol Clin North Am 29 (2):287-296
Triggs-Raine BL, Feigenbaum AS, Natowicz M, Skomorowski MA, Schuster SM, Clarke JT, Mahuran DJ, Kolodny EH, Gravel RA (1990) Screening for carriers of Tay-Sachs disease among Ashkenazi Jews. A comparison of DNA-based and enzyme-based tests. N Engl J Med 323 (1):6-12. doi:10.1056/NEJM199007053230102
Tsukahara T, Jr., Kadota RL (1977) Economic considerations in genetic screening programs for Tay-Sachs disease. Prog Clin Biol Res 18:319-327
Warren E, Anderson R, Proos AL, Burnett LB, Barlow-Stewart K, Hall J (2005) Cost-effectiveness of a school-based Tay-Sachs and cystic fibrosis genetic carrier screening program. Genet Med 7 (7):484-494. doi:10.109701.gim.0000178496.91670.3b
Wilson J. JG (1968) Principles and Practice of Screening for Disease. World Health Organization Public Health Papers, No 34
Zlotogora J (2009) Population programs for the detection of couples at risk for severe monogenic genetic diseases. Hum Genet 126 (2):247-253. doi:10.1007/s00439-009-0669-y

18

Table 1: Grades of recommendations for bodies of evidence Number Body of
evidence Papers Volume
of evidence
Consistency of results
Clinical impact
Ability to generalize to target population
Applicability to the Australian healthcare context
Summary grade Level of evidence
1 Ethical and Health economic aspects of TSD screening
17 B B C A A B III-3
2 Jewish TSD screening programs
34 B B B B A B III-3
3 Timing of TSD screening
24 B B C A A B III-3
4 TSD Genetic counselling/education
21 B B B B B B III-3
5 Management of TSD carriers and carrier couples
15 B B B A A B III-3
6 Laboratory testing methodology
18 B B B A A B III-3
References 1 (Barlow-Stewart et al. 2003; Leib et al. 2005; Zeesman et al. 1984; Scriver 2001; Schneiderman et al. 1978; Sutton 2002; Scriver and Clow 1990a; Nelson et al.
1978; Kinzler et al. 2002; Gason et al. 2005; Delatycki 2008; Childs et al. 1976; Tsukahara and Kadota 1977; Shabat 1999; Warren et al. 2005; Bach et al. 2001; Kaback 2001)
2 (Lew et al. 2011; Lew et al. 2012; Schneider et al. 2009; Langlois et al. 2006; Gason et al. 2005; Warren et al. 2005; Strom 2004; Gason et al. 2004; Gason et al. 2003; Barlow-Stewart et al. 2003; Sutton 2002; Ekstein and Katzenstein 2001; Scriver 2001; Kaback 2001; Bach et al. 2001; D'Souza et al. 2000; Zlotogora 2009; Kaplan 1998; Kronn et al. 1998; Edelson 1997; Natowicz and Prence 1996; Mitchell et al. 1996; Kaback et al. 1993; Broide et al. 1993; Yoo et al. 1993; Blitzer and McDowell 1992; Fernandes et al. 1992; Paw et al. 1990; Clarke et al. 1989; Zeesman et al. 1984; Krischer et al. 1982; Burnett et al. 1995; Ioannou et al. 2010; Curd et al. 2013)
3 (Langlois et al. 2006; Gason et al. 2005; Genetics 2009; Barlow-Stewart et al. 2003; Gason et al. 2003; Ekstein and Katzenstein 2001; Zlotogora 2009; Mitchell

et al. 1996; Scriver and Clow 1990a; ten Kate and Tijmstra 1990; Scriver and Clow 1990b; Clarke et al. 1989; Krischer et al. 1982; Burnett et al. 1995; Shapiro and Shapiro 1989; Sutton 2002; Edwards et al. 2004; Brundage and Strossner 2002; Lipsitz et al. 1986; Lew et al. 2011; Lew et al. 2012; Hill and Schorr 2001; Garber et al. 1993; Clarke 1978)
4 (Schneider et al. 2009; Langlois et al. 2006; Gason et al. 2005; Genetics 2009; Gason et al. 2004; Sutton 2002; Ekstein and Katzenstein 2001; Kaback 2000; Schneiderman et al. 1978; Barlow-Stewart et al. 2003; Ioannou et al. 2010; European Society of Human Genetics 2003; Marteau and Dormandy 2001; van den Berg et al. 2005, 2006; Norton 2008; Edwards et al. 2004; Brundage and Strossner 2002; Kinzler et al. 2002; Steiner-Grossman and David 1993; Kaback 1982)
5 (Langlois et al. 2006; Genetics 2009; Schneider et al. 2009; Sutton 2002; Ekstein and Katzenstein 2001; Bach et al. 2001; Kaback et al. 1993; Monaghan et al. 2008; Delatycki 2008; European Society of Human Genetics 2003; Frumkin et al. 2011; Ensenauer et al. 2005; Kaplan 1998; E99 2010; Eckstein 2008; Strom 2004; Sagi and Uhlmann 2013)
6 (Schneider et al. 2009; Langlois et al. 2006; Genetics 2009; Sutton 2002; Bach et al. 2001; DeMarchi et al. 1996; Landels et al. 1991; Paw et al. 1990; Triggs-Raine et al. 1990; Myerowitz and Costigan 1988; Arpaia et al. 1988; Myerowitz 1988; Ohno and Suzuki 1988; Monaghan et al. 2008; Lew et al. 2012; Ensenauer et al. 2005; Park et al. 2010; Vallance and Ford 2003)
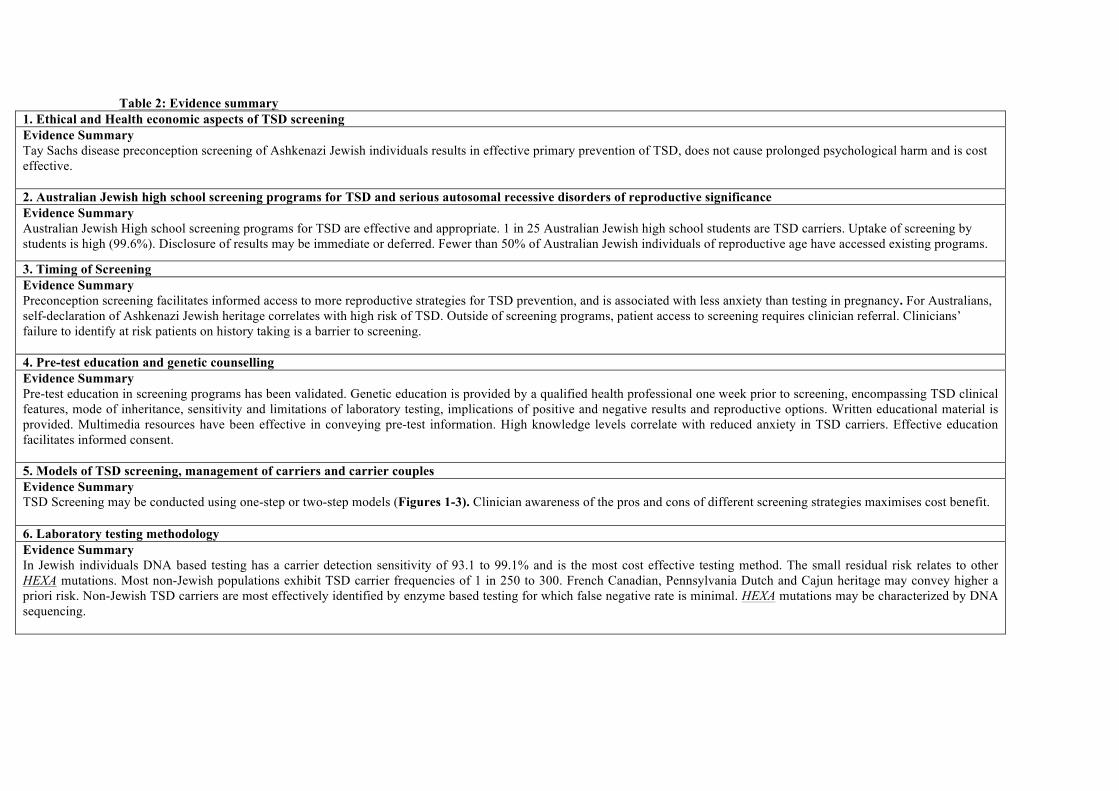
Table 2: Evidence summary 1. Ethical and Health economic aspects of TSD screening Evidence Summary Tay Sachs disease preconception screening of Ashkenazi Jewish individuals results in effective primary prevention of TSD, does not cause prolonged psychological harm and is cost effective. 2. Australian Jewish high school screening programs for TSD and serious autosomal recessive disorders of reproductive significance Evidence Summary Australian Jewish High school screening programs for TSD are effective and appropriate. 1 in 25 Australian Jewish high school students are TSD carriers. Uptake of screening by students is high (99.6%). Disclosure of results may be immediate or deferred. Fewer than 50% of Australian Jewish individuals of reproductive age have accessed existing programs.
3. Timing of Screening Evidence Summary Preconception screening facilitates informed access to more reproductive strategies for TSD prevention, and is associated with less anxiety than testing in pregnancy. For Australians, self-declaration of Ashkenazi Jewish heritage correlates with high risk of TSD. Outside of screening programs, patient access to screening requires clinician referral. Clinicians’ failure to identify at risk patients on history taking is a barrier to screening. 4. Pre-test education and genetic counselling Evidence Summary Pre-test education in screening programs has been validated. Genetic education is provided by a qualified health professional one week prior to screening, encompassing TSD clinical features, mode of inheritance, sensitivity and limitations of laboratory testing, implications of positive and negative results and reproductive options. Written educational material is provided. Multimedia resources have been effective in conveying pre-test information. High knowledge levels correlate with reduced anxiety in TSD carriers. Effective education facilitates informed consent. 5. Models of TSD screening, management of carriers and carrier couples Evidence Summary TSD Screening may be conducted using one-step or two-step models (Figures 1-3). Clinician awareness of the pros and cons of different screening strategies maximises cost benefit.
6. Laboratory testing methodology Evidence Summary In Jewish individuals DNA based testing has a carrier detection sensitivity of 93.1 to 99.1% and is the most cost effective testing method. The small residual risk relates to other HEXA mutations. Most non-Jewish populations exhibit TSD carrier frequencies of 1 in 250 to 300. French Canadian, Pennsylvania Dutch and Cajun heritage may convey higher a priori risk. Non-Jewish TSD carriers are most effectively identified by enzyme based testing for which false negative rate is minimal. HEXA mutations may be characterized by DNA sequencing.

Table 3. Recommendations for TSD screening in primary care 1. Carrier screening should be offered to Ashkenazi Jewish individuals of reproductive age in order to provide informed reproductive choice.
(Mitchell et al. 1996; Childs et al. 1976; Delatycki 2008; Gason et al. 2005; Kinzler et al. 2002; Nelson et al. 1978; Warren et al. 2005; Scriver 2006; Shabat 1999;
Tsukahara and Kadota 1977; Sutton 2002; Schneiderman et al. 1978; Scriver 2001; Zeesman et al. 1984)
2. Jewish high school screening programs for TSD should be supported, but should not be relied on as the sole means of education or access to screening.
(Barlow-Stewart et al. 2003; Ioannou et al. 2010; Lew et al. 2012; Gason et al. 2003; Burnett et al. 1995; Lew et al. 2011)
3. Primary care clinicians’ inquiry of ethnic background is required on history taking to identify AJ individuals who will be at high risk of having children
with TSD.
(Lew et al. 2011; Lew et al. 2012; Metcalfe 2012; Sutton 2002; Edwards et al. 2004; Brundage and Strossner 2002; Lipsitz et al. 1986; Garber et al. 1993)
4. Referral for pre-conception screening is recommended for all Jewish adults of reproductive age, while recognizing that at-risk couples may first present
during pregnancy.
(Lew et al. 2012; Mitchell et al. 1996; Burnett et al. 1995; Barlow-Stewart et al. 2003; Metcalfe 2012; Hill and Schorr 2001; Shapiro and Shapiro 1989) (Stark et al.
2013; Sutton 2002; Gason et al. 2005; Gason et al. 2003; Clarke et al. 1989; Garber et al. 1993; Frumkin and Zlotogora 2008)
5. Pre-test education encompassing the clinical features of disease, mode of inheritance and reproductive options should be delivered by a qualified health
professional. Voluntary informed consent should be obtained from the patient and documented.
(Barlow-Stewart et al. 2003; Ioannou et al. 2010; Gason et al. 2004; Gason et al. 2005; European Society of Human Genetics 2003; Marteau and Dormandy 2001;
van den Berg et al. 2005, 2006; Sutton 2002; Delatycki 2008; Schneiderman et al. 1978; Edwards et al. 2004; Brundage and Strossner 2002)

6. Primary health providers should be aware of different strategies of TSD screening. Partners of TSD carriers should also be offered screening, regardless
of heritage. In pregnancy, one-step screening (Fig 2) is recommended.
(Zlotogora 2009; Ioannou et al. 2010; Zeesman et al. 1984; Warren et al. 2005; Frumkin et al. 2011; Ekstein and Katzenstein 2001; Sutton 2002; Shapiro and
Shapiro 1989; Kaback et al. 1993; European Society of Human Genetics 2003; Monaghan et al. 2008; Langlois et al. 2006; Genetics 2009; Ensenauer et al. 2005;
Kaplan 1998; E99 2010)
7. DNA based testing is preferred for Ashkenazi Jewish individuals. Enzyme testing is recommended for non-Ashkenazi Jewish individuals. Testing
laboratories should comply with international best-practice standards and quality assurance procedures.
(Vallance and Ford 2003; Park et al. 2010; Schneider et al. 2009; Sutton 2002; Zlotogora 2009; Landels et al. 1991; Triggs-Raine et al. 1990; Bach et al. 2001;
Myerowitz and Costigan 1988; Myerowitz 1988; Arpaia et al. 1988; Ohno and Suzuki 1988; Navon and Proia 1989; Monaghan et al. 2008; Langlois et al. 2006;
Lew et al. 2012; Ensenauer et al. 2005; NATA Accreditation Requirement (NAR) Packages 2013; council 2007; Kaback 2001)

Test Partner A(usually female)
Is Partner A TSD carrier?
Two-step screening model
Offer Partner B TSD testingDiscuss cascade screening of A's relatives
Is Partner B Jewish?
HEXA enzyme
HEXADNA
mutations
Is Partner B TSD carrier?
YES
YES No
Negligible residual risk of TSD for offspring(Ensure couple understands that negligible TSD risk
applies ONLY in current partnership;Future partnerships will need to be retested:
note that the risk in a different future partnership remains low for the individual who has tested negative)
No referral for genetic counselling requiredNo referral for specialist reproductive medicine required
No
No
Each pregnancy of this partnership has 25% risk of TSD
As appropriate, refer for:- Genetic counselling advice or Clinical Geneticist opinion
- Specialist reproductive medicine opinionDiscuss:
- Access to educational resources- Cascade screening of relatives
YES

Test both Partner A and B simultaneously
Are both A and B TSD carriers?
One-step screening model(suitable for antenatal screening)
Negligible residual risk of TSD for offspring(Ensure couple understands that low TSD risk applies ONLY in
current partnership)
No referral for genetic counselling requiredNo referral for specialist reproductive medicine required
Each pregnancy of this partnership has 25% risk of TSD
Explain results and, as appropriate, refer for:- Genetic counselling advice or Clinical Geneticist opinion
- Specialist reproductive medicine opinionDiscuss:
- Access to educational resources- Cascade screening of relatives
YES
Is exactly ONE of
A or B TSD carrier?
(Only if consented):- Disclose individual results
- Cascade screening of relatives
No
YES
Nothing further indicatedNo

Test both prospective Partners A and B simultaneously
Are both A and B TSD carriers?
One-step screening model(ultraorthodox unmarried potential couple)
Negligible residual risk of TSD for offspring (in this partnership)(Ensure couple [or agreed 3rd party] understands that low TSD risk
applies ONLY in current partnership)
No referral for genetic counselling requiredNo referral for specialist reproductive medicine required
Each pregnancy of this partnership has 25% risk of TSDCouple may be deemed unsuitable for introduction/marriage
If non-disclosure of results requested, nothing further is indicated.Note that deidentified risk for couple may be disclosed to 3rd parties
Only if consented: As appropriate, refer for:- Genetic counselling advice or Clinical Geneticist opinion
- Specialist reproductive medicine opinionDiscuss:
- Access to educational resources- Cascade screening of relatives
YES
Is exactly ONE of
A or B TSD carrier?
If non-disclosure of results requested, nothing further is indicated.
Otherwise, and only if consented:- Disclose individual results
- Cascade screening of relatives
No
YES
Nothing further indicatedNo




















