Pyrimethamine increases β-hexosaminidase A activity in patients with Late Onset Tay Sachs
8
Pyrimethamine increases β-hexosaminidase A activity in patients with Late Onset Tay Sachs Etty Osher a , Aviva Fattal-Valevski b , Liora Sagie b , Nataly Urshanski a , Yifat Amir-Levi a , Sara Katzburg a , Leah Peleg e,f , Tally Lerman-Sagie d , Ari Zimran g , Deborah Elstein g , Ruth Navon f , Naftali Stern a, ⁎, Avi Valevski c a Institute of Endocrinology, Metabolism and Hypertension, Tel Aviv-Sourasky Medical Center, Israel b Pediatric Neurology Unit, Tel Aviv-Sourasky Medical Center, Israel c Geha Mental Health Center, Sackler School of Medicine, Tel Aviv University, Israel d Pediatric Neurology Unit, Wolfson Medical Center, Sackler School of Medicine, Tel Aviv University, Israel e Sheba Medical Center, Sackler School of Medicine, Tel Aviv University, Israel f Department of Human Genetics, Sackler School of Medicine, Tel Aviv University, Israel g Shaare Zedek Medical Center, Hadassa School of Medicine, Hebrew University, Jerusalem, Israel abstract article info Article history: Received 21 November 2010 Accepted 21 November 2010 Available online 4 December 2010 Keywords: Late Onset Tay Sachs Pyrimethamine β-hexosaminidase A Objective: To assess whether or not pyrimethamine (PMT) can be used to enhance β-hexosaminidase A activity (HexA) in subjects with Late Onset Tay Sachs (LOTS), we studied the effect of incremental doses of PMT in vivo in 9 LOTS patients carrying the αG269S/c.1278insTACT mutations. Methods: PMT treatment was initiated at a dose of 6.25 mg, increasing gradually up to a maximal allowable dose of 75 mg daily at 4–6 weeks intervals for a total of up 10 months. Mean patients' age was 37.9 ± 16.1 yrs (range 20–67 years). Results: Lymphocyte HexA activity rose in all subjects, peaking at 78 ± 30% over baseline activity (mean ± SD; range 36–114%). The optimal PMT dose varied considerably, averaging at 30 ± 24.1 mg (range—6.25–75 mg, daily). Further increase in PMT beyond the optimal dose was associated with gradual loss of effect on lymphocyte HexA. Improvement in speech was seen within several weeks in 4 out of 9 subjects, mostly paralleling the initial increment in HexA. Mood stabilization was also perceived in 3 subjects, but this was more difficult to assess due to the concomitant use of psychotropic/mood stabilizing agents. Reversible decline in motor activity manifesting predominantly in more frequent falls was seen in 3 subjects when the PMT dose was increased beyond the peak effect generating dose. Conclusions: PMT therapy can increase HexA activity in LOTS in vivo. Optimal doses should be tailored individually to avoid loss of biochemical effects. Clear cut neurological and psychiatric effects are difficult to discern at this time, mostly due to short term study follow up and large inter-individual variability. © 2010 Elsevier Inc. All rights reserved. 1. Introduction Late Onset Tay Sachs disease (LOTS) is a rare variant of the better known infantile Tay–Sachs disease, which results from mutations in the gene encoding the α subunit of β-hexosaminidase A (HexA), a lysosomal enzyme in charge of normal degradation of the ganglioside GM2. Human cells express two major β-hexosaminidase (Hex) isozymes, HexA and HexB. HexA is a heterodimer made up of α and β subunits, whereas HexB is a homodimer of two identical β-subunits [1]. Based on correlations between HexA activity and phenotype, it has been estimated that preservation of only 10% of the normal HexA activity may provide just enough GM2 degrading capacity to avoid clinically evident disease [2] In the classical infantile form, severe mutations in the α subunit gene lead to severe HexA deficiency leaving b 0.5% of the normal enzyme activity, which allows rapid intracellular accumulation of GM2 in brain neurons, inducing accelerated neural cell distortion and apoptosis and early onset of a rapidly progressive neurodegenerative disease, culminating in death during infancy [1] In contrast, LOTS occurs in individuals harboring compound heterozygote or mild homozygote α subunit gene mutations and is linked to higher residual HexA catalytic efficacy amounting to 2–5% of normal activity. This results in a more gradual course, with delayed onset, slower decline in motor, cerebral and spinocerebellar function and the evolution of psychiatric disorders such as depression, bipolar disorder and psychosis [3]. At the present time, no effective treatment for LOTS exists. Enzyme replacement therapy is impractical, predominantly due to the inability to deliver large molecules across the blood brain barrier Molecular Genetics and Metabolism 102 (2011) 356–363 ⁎ Corresponding author. Institute of Endocrinology, Metabolism and Hypertension, Tel Aviv Sourasky Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Israel. 1096-7192/$ – see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.ymgme.2010.11.163 Contents lists available at ScienceDirect Molecular Genetics and Metabolism journal homepage: www.elsevier.com/locate/ymgme
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Pyrimethamine increases β-hexosaminidase A activity in patients with Late Onset Tay Sachs

Molecular Genetics and Metabolism 102 (2011) 356–363
Contents lists available at ScienceDirect
Molecular Genetics and Metabolism
j ourna l homepage: www.e lsev ie r.com/ locate /ymgme
Pyrimethamine increases β-hexosaminidase A activity in patientswith Late Onset Tay Sachs
Etty Osher a, Aviva Fattal-Valevski b, Liora Sagie b, Nataly Urshanski a, Yifat Amir-Levi a, Sara Katzburg a,Leah Peleg e,f, Tally Lerman-Sagie d, Ari Zimran g, Deborah Elstein g, Ruth Navon f,Naftali Stern a,⁎, Avi Valevski c
a Institute of Endocrinology, Metabolism and Hypertension, Tel Aviv-Sourasky Medical Center, Israelb Pediatric Neurology Unit, Tel Aviv-Sourasky Medical Center, Israelc Geha Mental Health Center, Sackler School of Medicine, Tel Aviv University, Israeld Pediatric Neurology Unit, Wolfson Medical Center, Sackler School of Medicine, Tel Aviv University, Israele Sheba Medical Center, Sackler School of Medicine, Tel Aviv University, Israelf Department of Human Genetics, Sackler School of Medicine, Tel Aviv University, Israelg Shaare Zedek Medical Center, Hadassa School of Medicine, Hebrew University, Jerusalem, Israel
⁎ Corresponding author. Institute of Endocrinology, MTel Aviv Sourasky Medical Center, Sackler Faculty ofIsrael.
1096-7192/$ – see front matter © 2010 Elsevier Inc. Aldoi:10.1016/j.ymgme.2010.11.163
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 21 November 2010Accepted 21 November 2010Available online 4 December 2010Keywords:Late Onset Tay SachsPyrimethamineβ-hexosaminidase A
Objective: To assess whether or not pyrimethamine (PMT) can be used to enhance β-hexosaminidase Aactivity (HexA) in subjects with Late Onset Tay Sachs (LOTS), we studied the effect of incremental doses ofPMT in vivo in 9 LOTS patients carrying the αG269S/c.1278insTACT mutations.Methods: PMT treatment was initiated at a dose of 6.25 mg, increasing gradually up to a maximal allowabledose of 75 mg daily at 4–6 weeks intervals for a total of up 10 months. Mean patients' age was 37.9±16.1 yrs(range 20–67 years).Results: Lymphocyte HexA activity rose in all subjects, peaking at 78±30% over baseline activity (mean±SD;range 36–114%). The optimal PMT dose varied considerably, averaging at 30±24.1 mg (range—6.25–75 mg,
daily). Further increase in PMT beyond the optimal dose was associated with gradual loss of effect onlymphocyte HexA. Improvement in speech was seen within several weeks in 4 out of 9 subjects, mostlyparalleling the initial increment in HexA. Mood stabilization was also perceived in 3 subjects, but this wasmore difficult to assess due to the concomitant use of psychotropic/mood stabilizing agents. Reversibledecline in motor activity manifesting predominantly in more frequent falls was seen in 3 subjects when thePMT dose was increased beyond the peak effect generating dose.Conclusions: PMT therapy can increase HexA activity in LOTS in vivo. Optimal doses should be tailoredindividually to avoid loss of biochemical effects. Clear cut neurological and psychiatric effects are difficult todiscern at this time, mostly due to short term study follow up and large inter-individual variability.© 2010 Elsevier Inc. All rights reserved.
1. Introduction
Late Onset Tay Sachs disease (LOTS) is a rare variant of the betterknown infantile Tay–Sachs disease, which results from mutations inthe gene encoding the α subunit of β-hexosaminidase A (HexA), alysosomal enzyme in charge of normal degradation of the gangliosideGM2. Human cells express two major β-hexosaminidase (Hex)isozymes, HexA and HexB. HexA is a heterodimer made up of α andβ subunits, whereas HexB is a homodimer of two identical β-subunits[1]. Based on correlations between HexA activity and phenotype, ithas been estimated that preservation of only 10% of the normal HexAactivity may provide just enough GM2 degrading capacity to avoid
etabolism and Hypertension,Medicine, Tel Aviv University,
l rights reserved.
clinically evident disease [2] In the classical infantile form, severemutations in the α subunit gene lead to severe HexA deficiencyleaving b0.5% of the normal enzyme activity, which allows rapidintracellular accumulation of GM2 in brain neurons, inducingaccelerated neural cell distortion and apoptosis and early onset of arapidly progressive neurodegenerative disease, culminating in deathduring infancy [1] In contrast, LOTS occurs in individuals harboringcompound heterozygote or mild homozygote α subunit genemutations and is linked to higher residual HexA catalytic efficacyamounting to 2–5% of normal activity. This results in a more gradualcourse, with delayed onset, slower decline in motor, cerebral andspinocerebellar function and the evolution of psychiatric disorderssuch as depression, bipolar disorder and psychosis [3].
At the present time, no effective treatment for LOTS exists. Enzymereplacement therapy is impractical, predominantly due to theinability to deliver large molecules across the blood brain barrier

Table 1Clinical and demographic characteristics of the study group.
Patient Gender Age Age at firstsymptom
Symptoms at diagnosis AmbulationIndex
ALSFR Currenttreatment
Affected familymembers
1 Male 33 15 Depression,hypersomnia
3 30 MiglustatLithiumSertralineCarbamazepine,Propanolol,L-thyroxine
None
2 Male 20 10 Attention deficit 2 39 None One male brother3 Male 36 15 Walking difficulties 3 34 Carbamazepine One male brother4 Male 28 15 Psychotic episodes 36 Olanzapine
CarbamazepineOne female sister
5 Male 32 24 Speech problems 2 34 None None6 Female 62 38 Proximal weakness 5 28 Carbamazepine,
BiperidenClothiapineCarbamazepineLithiumSimvastatin,Enlapril,Metformin
None
7 Male 29 9 Speech problems 3 29 OlanzapineDuloxetine
None
8 Male 67 18 Proximal weakness 3 31 BimatoprostTimololMaleateCombigan
Three female sisters,one deceased and a sondied from infantile TS
9 Female 33 17 Unexplained falls 5 20 FluoxetineCarbamazepinePropranolol
None
357E. Osher et al. / Molecular Genetics and Metabolism 102 (2011) 356–363
(BBB) [4].Attempts to decrease the accumulation of GM2 viapharmacological inhibition of its synthesis, by blocking ceramideglucosyltransferase, have yielded promising results in a mouse modelof Sandhoff's disease, but failed to provide appreciable relief in humansubjects afflicted with LOTS [5,6].
Recently, Mahuran's group [7] has explored the possibility thatpharmacological chaperones can augment HexA. Chaperones aresmall molecules that can assist the folding of mutant misfoldedproteins retaining partial catalyic function and thus allow betteraccess of such partially functional enzymes to the lysosome, resultingin an increase in total enzyme activity. Following extensive screeningof candidate molecules, pyrimethamine (PMT), an FDA approvedanti-marial/anti-toxoplasmosis agent already used in humans [8–11]which is capable of entering the central nervous system (CNS), wasshown to enhance HexA activity in vitro in human fibroblasts carryingsome (e.g., αG269S), but not all LOTS related mutations [12].
Here we examined the effect of PMT in LOTS in a cohort of Israelipatients, all of whomwere of Jewish Ashkenazi extraction. All patientswere compound heterozygotes carrying the αG269S/c.1278insTACTmutations. We present the initial biochemical effect on HexA activity
Table 2HexA activity in the study patients.
Patient Baselineactivitynmole/h/mgprotein
HexA activity,substrate MUGS(% of wild type)baseline
HexA activity ,calculated substrateMUGS (% of wild type)peak
HexAactivityincrease(%)
1 92.1 1.33 2.18 632 84.8 1.23 2.2 78.83 96.7 1.4 1.98 414 63.31 0.92 1.25 365 134.47 1.94 3.58 856 108.6 1.57 2.65 697 48.25 0.7 0.97 388 97.35 1.4 2.92 108.59 53.38 0.77 1.61 100
HexA activity in lymphocyte preparation from unaffected healthy subjects (“wildtype”): 6900±996 nmole/h/mg protein (n=3).
and preliminary results of the clinical effects of PMT in 9 LOTSpatients, in an open label trial which included active PMT treatmentfor the duration of up to 10 months.
2. Methods
2.1. Patient recruitment and study design
Inclusion criteria for participation in this study were a geneticallyand clinically confirmed diagnosis of LOTS, and interest in closesurveillance at the study center. Exclusion criteria for participation inthis study were any serious medical illness, cardiac disease orhematologic abnormalities including bleeding diathesis and activeuncontrolled bleeding. The presence of contraindications to the use ofPMT was also excluded in each case prior to inclusion in this trial,including a history of cancer of any type, folate deficiency or the use ofantifolate drugs or drugs associated with myelosuppression, evidenceof systemic infection, history of convulsive disorders, pregnancy,lactation or child-bearing potential not using reliable means ofcontraception.
Table 3The frequency of neurological manifestations of disease (n=9).
Manifestation Frequency
Dysarthria 9Ambulation difficulties 9Dysmetria 8Adiadochokinesis 8Skeletal Muscle cramps 8Ataxia 7Muscle weakness 6Tremor 5Startle response 5Learning difficulties 4Dementia 4Swallowing difficulties 2Dystonia 2
358 E. Osher et al. / Molecular Genetics and Metabolism 102 (2011) 356–363
Eleven out of the 14 subjects diagnosed with LOTS in Israel werefound eligible but two patients withdrew in the pre-treatment phasedue to the inability to follow study protocol.
Subjects were first assessed on two separate occasions 4–6 weeksapart by a multidisciplinary team including specialists in internalmedicine, neurology and psychiatry. Initial assessment includedcomplete medical history and physical examination, neurologicaland psychiatric evaluation as detailed below and extensive laboratorytesting including CBC, serum glucose, electrolytes, calcium, phosphor,complete renal, liver and thyroid panels, folic acid, vitamin B12 andurinalysis, ECG as well as lymphocyte HexA activity. PMT wasprescribed at a starting dose of 6.25 mg/day, increasing gradually,whenever possible, at 4–6 week intervals, in a stepwise manner to12.5, 25, 37.5, 50 and 75 mg/day. Patients were then re-examined atmonthly intervals. Drug escalation was contingent on the absence ofclinical or biochemical unacceptable side effects and lack of HexAsuppression in excess of 25%. Folic acid (5 mg/day) was added withthe initiation of PMT. Duration of the active PMT treatment was up to10 months.
The primary outcome measures were the changes in HexA activityin peripheral lymphocytes and safety and tolerability of PMT therapyin LOTS patients. The secondary outcomemeasures included potentialchanges in neurological and psychomotor status of PMT-treated LOTSpatients as defined by the itemized assessment below.
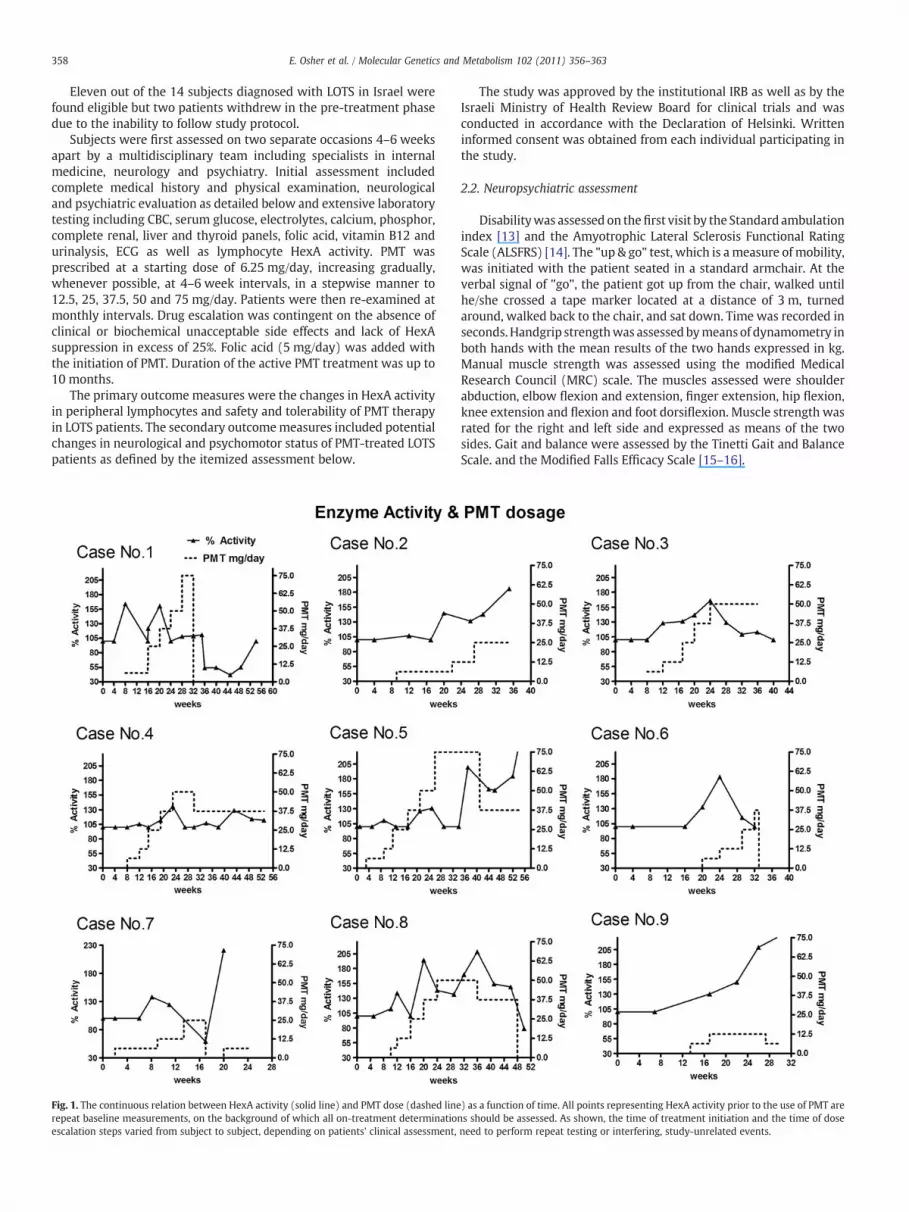
Fig. 1. The continuous relation between HexA activity (solid line) and PMT dose (dashed linerepeat baseline measurements, on the background of which all on-treatment determinatioescalation steps varied from subject to subject, depending on patients' clinical assessment,
The study was approved by the institutional IRB as well as by theIsraeli Ministry of Health Review Board for clinical trials and wasconducted in accordance with the Declaration of Helsinki. Writteninformed consent was obtained from each individual participating inthe study.
2.2. Neuropsychiatric assessment
Disabilitywas assessed on thefirst visit by the Standard ambulationindex [13] and the Amyotrophic Lateral Sclerosis Functional RatingScale (ALSFRS) [14]. The "up & go" test, which is ameasure of mobility,was initiated with the patient seated in a standard armchair. At theverbal signal of "go", the patient got up from the chair, walked untilhe/she crossed a tape marker located at a distance of 3 m, turnedaround, walked back to the chair, and sat down. Time was recorded inseconds.Handgrip strengthwas assessedbymeans of dynamometry inboth hands with the mean results of the two hands expressed in kg.Manual muscle strength was assessed using the modified MedicalResearch Council (MRC) scale. The muscles assessed were shoulderabduction, elbow flexion and extension, finger extension, hip flexion,knee extension and flexion and foot dorsiflexion. Muscle strength wasrated for the right and left side and expressed as means of the twosides. Gait and balance were assessed by the Tinetti Gait and BalanceScale. and the Modified Falls Efficacy Scale [15–16].
) as a function of time. All points representing HexA activity prior to the use of PMT arens should be assessed. As shown, the time of treatment initiation and the time of doseneed to perform repeat testing or interfering, study-unrelated events.

359E. Osher et al. / Molecular Genetics and Metabolism 102 (2011) 356–363
Psychiatric evaluation was carried out by patient interview oneach visit by the same psychiatrist. Diagnosis was made accordingDSM IV-R criteria. A Hamilton questionnaire (HAM-21) was used fordepression rating and the PANSS questionnaire was used for psychosisevaluation.
2.3. HexA activity
Lymphocyte HexA enzymatic activity was determined with 4-methylumbelliferyl-6-sulfo-N-acetyl-ß-D-glucosaminide (MUGS) asa fluorogenic substrate as previously described [17]. Cell extracts wereprepared on the day of blood collection fromwhole blood by standardmethods [19] and stored in aliquots at −20 °C. The term "lympho-cyte" in this context is somewhat general, since although lymphocytescomprised the largest fraction of the harvested population, somemononuclear cells, granulocytes and red blood cells were also present.To determine HexA activity, 4 μg of lymphocyte extract protein wereincubated with MUGS (0.7 mM; Melford Laboratories, Suffolk, UK) ina 50 mM citrate buffer (pH 4.5; 37 °C) over 1.5 h [18]. Fluorescence ofthe liberated 4-methylumbelliferone was measured by Synergy 2fluorometer (BioTek Instruments, Inc Winooski, US; excitation335 nm, emission 442 nm) and normalized for protein content. Tominimize inter-assay variations, each determination of each patientthroughout the study also included extracts from the baseline sample
Fig. 2. The continuous relation between the hand grip strength in Kg. (solid line) and PMTpeak(s) HexA activity was reached.
and at least one additional sample from the intervention period. Asvariations in the ratio between this "historical" and baseline activityon repeat measurements did not exceed ±10%, assessment of thecurrent (treatment) sample relative to baseline activity for eachsample could be safely made within the same assay. Extracts werestable in terms of enzyme activity for at least one year. Calculatedintra-assay imprecision was 10.5% and inter-assay imprecision was26 %. Biological variation in heterozygotes was 2.1%.
3. Results
3.1. Baseline clinical assessment
All patients were Ashkenazi Jews with the αG269S/c.1278insTACTmutation in the HexA gene and their baseline demographic andclinical characteristics are presented in Table 1. Mean patients' agewas 37.9±16.1 (±SD) years and the mean duration of the pre-trialsymptomatic disease was 20.2±11.9 years.
All patients had the same mutation in the HexA gene, but therewas a considerable variability in the clinical phenotype as subjects hadneurological manifestations at a different degree of severity. The mostcommon deficits were dysarthria and lower limb muscle weakness(Table 3). The ambulation index of the study group ranged at grades2–3 in all subjects, with the exception of patient 9 (grade 5). The
dose (dashed line) as a function of time. The arrows indicate the time point at which

360 E. Osher et al. / Molecular Genetics and Metabolism 102 (2011) 356–363
ALSFR score ranged at 20–39 with a mean of 31.2±5.5 and a medianscore of 31. Seven patients had a history of active neuropsychiatricmanifestation of GM2 gangliosidosis including depression in threepatients, bipolar disorder in three patients and psychosis withoutaffective symptomatology in five patients.
3.2. Effects of Pyrimethamine on HexA activity
Mean baseline HexA activity was 80.47±35.52 nmole/h/mg pro-tein (±SD) (range 8.54 to 134.47 nmole/h/mg protein). This activityamounted to 1.163±0.52% (±SD) [range 211 0.13 to 1.57 %] of theactivity in an unaffected normal human subject.
Overall, PMT increased peripheral lymphocyte HexA activity witha mean peak increase of 78%±30 (range 36%–114%). Hence, whilestatistically significant, this increment peaked, on the average, to just~2% of normal activity in unaffected healthy subjects. Fig. 1 depictsindividual HexA activity throughout the study period relative tobaseline activity. Although the effect was loosely dose-related (e.g.,patients 2, 9), the dose eliciting the maximal increase variedconsiderably among the study subjects. Further increase in the dosebeyond this patient-specific dose did not further enhance enzymeactivity and was often associated with a subsequent decline in HexAtowards pre-treatment activity. Hence, although the maximal dailydose by protocol was 75 mg, peak activity was observed at an average
Fig. 3. The continuous relation between the up & go test in seconds (solid line) and PMTdoseHexA activity was reached.
dose of 30±24.1 (±SD) mg/day, with a range of 6.25–75 mg/day.Patient 5 showed some marginal rise in HexA activity on low PMTdoses, with subsequent suppression to baseline levels while on a dailydose of 75 mg of PMT. HexA rose again, showing a sustained increaseof 60–80% over baseline when PMT dose was later titrated down to37.5 mg/day. Due to the nature of the study's protocol it is impossibleto determine whether the maximal response was truly dose-relatedor, rather, time-related. In two patients who completed the study,HexA activity declined to less than 70% of pre-treatment activity4–6 weeks following discontinuation of PMT.
3.3. Neuropsychiatric outcome
The results of the consecutive neurological examinations and thedosage of PMT are presented in Figs. 2–5. In general, there was largevariability among the repeated assessments for all tests. Improvementin hand grip strength (Fig. 2) was noted in case 2 and partially in case 1,andwas possibly associatedwith dosage increase or enzyme activity. Incase 1, a further increase in dosage resulted in reduction of hand gripstrengthwhichwas associatedwith enzyme level decline. In the up& gotest (Fig. 3) therewas a slight improvement in case 1 and case 2. Furtherincrease in PMT dosage resulted in worsening of performance. In allother patients there was no improvement in task performance, and aslight worsening was noted in case 4 concomitant with the increase in
(dashed line) as a function of time. The arrows indicate the time point at which peak(s)

Fig. 4. The continuous relation between the Tinetti balance & gait score (solid line) and PMT dose (dashed line) as a function of time. The arrows indicate the time point at whichpeak(s) HexA activity was reached.
361E. Osher et al. / Molecular Genetics and Metabolism 102 (2011) 356–363
PMT dose. The Tinetti balance & gait assessment (Fig. 4) showed similarresults, e.g., increase in dosage individually resulted in worsening ofbalance ability (cases 1 and 8). In most patients a slight improvementwas noted with a low dose. The falls efficacy assessment (Fig. 5), whichreflects patients' self report, also showed inconclusive results. However,two patients reportedmore falls on the highest PMT dose they received,which was reversed within weeks when the dose was reduced to thedose at which the peak HexA effect was seen previously. A parallelsecondary increase in enzyme activity was then seen (patients 4 and 5).Themanual muscle strength tests did not show significant change frombaseline (data not shown).We noted a subjective early improvement inspeech in 4 patients, which could not be quantified but appearedconcomitant with a rise in HexA. In the most extreme example of thiseffect, a patient whose speech was entirely impossible to follow ondirect interviewwith the study physicians then became understandableeven on the phone.
Two patients experienced hypo-manic episodes at the beginning ofthe study (cases 6 and 8), but were euthymic at the end of study period.Two patients required a change of psychiatric treatment due todepression (cases 2 and 4). Patient 4 suffered from amanic state duringtreatment, followed by psychotic depression (PANSS score worsenedfrom 30 to 60) which eventually improved with the addition of lithiumand thioridazine. Patient 8 who was hypomanic at the beginning of the
study was stabilized during the study without psychiatric treatment.However he then suffered from mild to moderate depression and wastreated successfully with Venaflaxine. Another patient (case 6), whowas hypomanic at the beginning of the study became euthymicwithoutany change in her psychiatric treatment. One patient (case 1) requiredminor changes in anti-depressive treatment. Eventually this patientsuffered from lessmoodswings as compared to theperiodpreceding thestudy. Although there was no clear effect of PMT on psychiatricmanifestations, some stabilization of mood swings was seen in fourpatients (cases 1, 3, 6, 8). This change was not temporally associatedwith enzyme activity.
3.4. Adverse events
Onepatient developeddehydration anddoublingof serumcreatininefollowing several days of vomiting of unknown etiology while on a PMTdose of 37.5 mg/day (3 weeks). She fully recovered following fluid andelectrolyte replacement. One subject experienced transient uppergastrointestinal symptoms (nausea) and another patient experiencedvertigo with doses in excess of 12.5 mg daily. Weight loss was a rathervisible outcomeof PMT: only onepatient gainedweight (+4%),whereas5 patients lostweight (mean−6.8%±7.35 of bodyweight; range−0.82to−16.7%). In the patientwith the largestweight loss, no specific reason

}
Fig. 5. The continuous relation between the Modified Falls Efficacy Scale (solid line) and PMT dose (dashed line) as a function of time. The arrows indicate the time point at whichpeak(s) HexA activity was reached.
362 E. Osher et al. / Molecular Genetics and Metabolism 102 (2011) 356–363
was initially identified, but a large frontalmeningiomawas subsequentlydiagnosed, whose removal resulted in rapid clinical improvement.
4. Discussion
The key finding in this study is that PMT can enhance HexA activityin patients with LOTS, in association with some limited clinicalbenefits. The observed short- to mid-term effects of PMT on HexA inLOTS are small to moderate in magnitude and fall far from thetheoretically desirable increase in HexA to "10% of normal HexA",above which a disease-free phenotype has been documented despitethe presence of LOTS mutations [20]. Very recently, after thesubmission of our paper for publication, Clarke et al [21] reportedthat PMT increased leukocyte activity up to ~4 folds in 8 patients withLOTS. Our report, then, is in agreement with this finding, although themagnitude of the response is more modest in our study. There areseveral important differences, however, between the former articleand the present report. First, our study population was geneticallyhomogenous in terms of the HexA mutation profile whereas Clarke etal studied LOTS patients with heterogonous genotype. As shown byMegawa et al [12] in vitro, genetically different HexA variants can varyin their response to PMT. In patients apparently carrying the G269Smutation Clarke et al [20] also reported a 2 fold enhancement in HexAactivity, which is close to the mean 1.7 increase seen in our study.
Second, our study utilized very low doses of PMT at the initiationphase, with gradual increments thereafter. Finally, the treatmentperiod lasted up to 10 months in our patients, which is considerablylonger than in the study by Clarke et al [20].
Although wewere able to maintain LOTS patients on PMT for up to10 months, the attainment of both clinical tolerability and biochemicalefficacy with such prolonged use required meticulous individualizeddose tailoring. This was reflected in several aspects of the presenttrial's outcome. First, although PMT induced a clear increase in HexAactivity in each of the 9 treated LOTS patients, the dose and treatmenttime necessary to elicit this increment as well as the actual achievedrise in the enzyme's function varied significantly from subject tosubject. Second, the increment in HexA activity was not linearlyrelated to the PMT dose. For example, in several subjects HexA activityrose initially with the escalation in PMT dose, but subsequentlydeclined with further dose increments, or even with continued use ofthe same dose which at first induced an increase in enzyme activity.
Notably, Clarke et al [20] observed a significant correlationbetween the PMT dose and plasma PMT concentration. Because it isunlikely that plasma PMT declines with continued use of the samedose, let alone with further increase in the PMT dose applied, it wouldappear that such initial correlation does not necessarily persist in thelong run. This, however, must await direct investigation. The effects ofthe PMT dose per se, duration of treatment and the influence of

363E. Osher et al. / Molecular Genetics and Metabolism 102 (2011) 356–363
concomitant medications on HexA activity and their clinical implica-tions remain subject to future examination.
Third, the highest dose allowed by the protocol (75 mg/day) couldbe actually reached in only two subjects, in whom it had to be thendecreased due severe vertigowithdecline inHexAactivity all theway tobaseline levels (case 1) and an intolerable increase in thenumber of falls(case 5). Even a daily PMT dose of 50 mg was impossible to adhere toover time and had to be reduced due to increased number of falls in onesubject and general malaise in the other. In all of the above cases, sideeffects entirely subsided with dose reduction or PMT discontinuation.Fourth, dose reduction (from75 to 37.5 mg/day and from37.5 to 25 mg/day) was associated with a clear rise in HexA activity in two patients.Fifth, in two patients who completed the approved study period anddiscontinued PMT due to apparent loss of effect on HexA, enzymeactivity declined to 40% and 70% of baseline activity after discontinu-ation. In the first subject, post-study assessment showed continuedsuppression of activity for 6–8 weeks, with a subsequent and gradualrise, eventually returning to baseline after 2.5 months. Collectively,these results suggest that PMT administered at either low doses or overa short period is capable of raising HexA activity in LOTS. Under theseconditions, doubling of enzyme activity was not unusual. Higher dosesand/or longer periods of therapy exerted the opposite effect andinduced suppression, which could be profound, long lasting and/ orassociated with clinical intolerance and neurological side effects. In thiscontext, Clarke et al [20] reported that the daily use of 50–75 mg PMTwas associated with a high rate of side effects in LOTS patients.
While lymphocyte HexA activity may correlate, to some extent,with brain HexA activity, it is unlikely to accurately reflect the CNSenzyme function. In favor of some association between peripherallymphocyte HexA and brainHexA is thefinding that high doses of PMTtended to both suppress lymphocyte enzyme activity and elicitneurological side effects, some of which appeared as aggravation oftypical symptoms of LOTS (e.g., falls). Nevertheless, lymphocytes areshort living cells and their exposure time to PMT is much shorter thanthat of the neurons positioned permanently in the brain. Further, PMTis rather lipophylic [21] and may be preferentially stored in CNS cells.The suppression of HexA activity by high PMT dose, which persistedand even worsened after its discontinuation, is consistent not onlywith the known effect of PMT as an HexA inhibitor, but also with itslong half-life in humans (t1/2=96 h) [12]. Hence PMTmight be storedand released, inside and/or outside the CNS for quite some time, evenwhen the drug is no longer administered. Such considerations shouldbe carefully weighed in the planning of future dosing in LOTS, perhapsallowing the use of PMT for only 2–3 days in aweek in order to preventits inhibitory effect. The measurement of circulating PMT, which wasnot carried out in the present study, could be also helpful under thesecircumstances, although plasma PMTdoes not necessarily reflect braintissue PMT levels. Additionally, the possibility that observed neuro-logical side effects were related to PMT per se, independent of HexA, isobviously difficult to exclude base on the current study.
The obviously limited gross neuropsychiatric benefits seen withPMT in LOTS may be related to not only to dosing difficulties but alsoto inherent limitations of assessing a slowly progressive condition alsocomplicated by swings of mood within a short time frame [6]. Someexisting neurological deficits may be already irreversible in thislifelong pathological process. The small number of patients studied,the open-label design of the trial and the variable HexA responsecomprise additional limitations of this study. These limitations shouldbeweighed in light of the extreme care taken in our study tominimizeinter-assay variation and the rarity of this condition.
In conclusion, as assessed by enzyme activity in peripherallymphocytes, PMT can enhance HexA function in LOTS patients for aperiod of several weeks to several months. However, the judicious useof low doses with gradual dose escalation of PMT under closemonitoring of clinical status and HexA activity appear desirable.Whether or not such increases in HexA can be further augmented by
more sophisticated modes of PMT therapy and translated intosustainable clinical benefits in LOTS remains to be determined. Thispreliminary report provides a clear impetus to better exploit the abilityto raise HexA activity in vivo towards the design of amoremature formof PMT–or some other chaperone–based therapy in LOTS.
Acknowledgment
This studywas supported, in part, by a grant from the Chief Scientistof the Ministry of Health, Israel.
References
[1] R. Gravel, M. Kaback, R. Proia, K. Sandhoff, K. Suzuki, K. Suzuki, The GM2, in: C.R.Scriver, A.L. Beaudet, D. Valle, W.S. Sly (Eds.), The Metabolic and Molecular Basisof Inherited Disease, 8th Ed, McGraw-Hill, New York, 2001, pp. 3827–3876.
[2] P. Leinekugel, S. Michel, E. Conzelmann, K. Sandhoff, Quantitative correlationbetween the residual activity of beta-hexosaminidase A and arylsulfatase A and theseverity of the resulting lysosomal storage disease, Hum. Genet. 88 (1992) 513–523.
[3] O. Neudorfer, G.M. Pastores, B.J. Zeng, J. Gianutsos, C.M. Zaroff, E.H. Kolodny, Late-onset Tay-Sachs disease: phenotypic characterization and genotypic correlationsin 21 affected patients, Genet. Med. 7 (2005) 119–123.
[4] R.J. Desnick, E.H. Schuchman, Enzyme replacement and enhancement therapies:lessons from lysosomal disorders, Nat. Rev. Genet. 3 (2002) 954–966.
[5] M. Jeyakumar, T.D. Butters, M. Cortina-Borja, V. Hunnam, R.L. Proia, V.H. Perry, R.A.Dwek, F.M. Platt, Delayed symptom onset and increased life expectancy inSandhoff disease mice treated with Nbutyldeoxynojirimycin, Proc. Natl Acad. Sci.USA 96 (1999) 6388–6393.
[6] B.E. Shapiro, G.M. Pastores, J. Gianutsos, C. Luzy, E.H. Kolodny, Miglustat in late-onset Tay-Sachs disease: a 12-month, randomized, controlled clinical study with24 months of extended treatment, Genet. Med. 11 (2009) 425–433.
[7] M.B. Tropak, D. Mahuran, Lending a helping hand, screening chemical libraries forcompounds that enhance beta-hexosaminidase A activity in GM2 gangliosidosiscells, FEBS J. 274 (2007) 4951–4961.
[8] C. Leport, G. Chene, P. Morlat, B.J. Luft, F. Rousseau, S. Pueyo, R. Hafner, J. Miro, J.Aubertin, R. Salamon, J.L. Vildé, Pyrimethamine for primary prophylaxis oftoxoplasmic encephalitis in patients with human immunodeficiency virusinfection: a double-blind, randomized trial. ANRS 005-ACTG 154 GroupMembers.Agence Nationale de Recherche sur leSIDA. AIDS Clinical Trial Group, J. Infect. Dis.173 (1996) 91–97.
[9] L.M. Weiss, B.J. Luft, H.B. Tanowitz, M. Wittner, Pyrimethamine concentrations inserum during treatment of acute murine experimental toxoplasmosis, Am. J. Trop.Med. Hyg. 46 (1992) 288–291.
[10] I.L.O. Buxton, Pharmacokinetics and pharmacodynamics:the dymamics of drugabsorption, distribution, action and elimination, Goodman and Gilman's thePharmacological Basis of Therapeutics Brunton LL, editor, McGraw-Hill Books,New York, 2006.
[11] L.M. Weiss, C. Harris, M. Berger, H.B. Tanowitz, M. Wittner, Pyrimethamineconcentrations in serum and cerebrospinal fluid during treatment of acuteToxoplasma encephalitis in patients with AIDS, J. Infect. Dis. 157 (1988) 580–583.
[12] G.H. Maegawa, M. Tropak, J. Buttner, T. Stockley, F. Kok, J.T. Clarke, D.J. Mahuran,Pyrimethamine as a potential pharmacological chaperone for late-onset forms ofGM2 gangliosidosis, J. Biol. Chem. 282 (2007) 9150–9161.
[13] S.L. Hauser, D.M. Dawson, J.R. Lehrich, M.F. Beal, S.V. Kevy, R.D. Propper, J.A. Mills,H.L. Weiner Intensive, immunosuppressant in progressive multiple sclerosis. Arandomized, three arm study of high-dose intravenous cyclophosphamide,plasma exchange, and ACTH, N. Engl. J. Med. 308 (1983) 173–180.
[14] B.R. Brooks, M. Sanjak, S. Ringel, ALS CNTF Treatment Study (ACTS) Phase I–IIStudy Group. The Amyotrophic Lateral Sclerosis Functional Rating Scale.Assessment of activities of daily living in patients with Amyotrophic LateralSclerosis, Arch. Neurol. 53 (1996) 141–147.
[15] M.E. Tinetti, Performance-oriented assessment of mobility problems in elderlypatients, J. Am. Geriatr. Soc. 34 (1986) 119–126.
[16] M. Tinetti, D. Richman, L. Powell, Falls efficacy as a measure of fear of falling, J.Gerontol 45 (1990) 239–243.
[17] H. Kresse, W. Fuchs, J. Glössl, D. Holtfrerich, W. Gilberg, Liberation of N-acetylglucosamine-6-sulfate by human beta-N-acetylhexosaminidase A, J. Biol.Chem. 256 (1981) 12926–12932.
[18] A. Bøyum, Isolation of mononuclear cells and granulocytes from human blood,Scand. J. Clin. Lab. Invest. 21 (1968) 77–89.
[19] Z. Cao, E. Petroulakis, T. Salo, B. Triggs-Raine, Benign HEXA mutations, C739T(R247W) and C745T(R249W), cause beta-hexosaminidase A pseudodeficiency byreducing the alpha-subunit protein levels, J. Biol. Chem. 272 (1997) 14975–14982.
[20] J.T. Clarke, D.J. Mahuran, S. Sathe, E.H. Kolodny, B.A. Rigat, J.A. Raiman, M.B.Tropak, An open-label Phase I/II clinical trial of pyrimethamine for the treatmentof patients affected with chronic GM2 gangliosidosis (Tay-Sachs or Sandhoffvariants), Mol. Genet. Metab. (2010)8 Epub ahead of print.
[21] H. Sprecher, H.M. Barr, J.I. Slotky, M. Tzukerman, G.D. Eytan, Y.G. Assaraf,Alteration of mitochondrial gene expression and disruption of respiratoryfunction by the lipophilic antifolate pyrimethamine in mammalian cells, J. Biol.Chem. 282 (2007) 9150–9161.