Fractional-order Modeling of the Arterial Compliance - arXiv
Upload
independentCategory
view
1download
0
●
scsCbbaTffpe1uis©
Ia
Alvuftdddtahn
U
M
o
f
vvE
8
Arterial Steal Syndrome: A Modest Proposal for an Old Paradigm
Arif Asif, MD, Carlos Leon, MD, Donna Merrill, RN, Bhagwan Bhimani, MD, Renee Ellis, MD,Marco Ladino, MD, and Florin N. Gadalean, MD
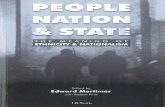
Background: Access ligation has been considered to be the treatment for patients presenting with arterial stealyndrome by many nephrologists. We report results of a prospective study using comprehensive arteriographyoupled with percutaneous transluminal balloon angioplasty (PTA) or surgical intervention to evaluate and manageteal syndrome. Methods: Twelve consecutive patients referred for symptoms of steal syndrome were examined.omprehensive arteriography of the extremity to diagnose arterial stenoses and delineate anatomy was performedy advancing a diagnostic catheter into the subclavian artery. Findings of arteriography and degrees of stenosisefore and after PTA also were documented. Resolution of symptoms after PTA and surgical interventions, as wells complications, were recorded. Results: Angiography showed arterial stenotic lesions in 10 of 12 patients (83%).he degree of stenosis was 66% � 14% (SD). Eight patients (80%) with stenotic lesions underwent PTA success-ully. The degree of stenosis after PTA was 13% � 10%. The remaining 2 patients were not considered candidatesor PTA and were referred to surgery with arteriography images. One patient underwent ligation and the otheratient required an axillary loop fistula using the same outflow vein. The 2 patients without stenoses showedxcessive steal through the anastomosis and underwent lengthening procedures by insertion of a vein segment. All2 patients are symptom free with a mean follow-up of 8.3 � 4 months, and 11 of 12 patients (92%) are dialyzingsing the same access. There were no procedure-related complications. Conclusion: We suggest that complete
maging of the arterial circulation of the extremity be considered in patients presenting with symptoms of stealyndrome to properly assess the arterial anatomy and develop a treatment strategy. Am J Kidney Dis 48:88-97.2006 by the National Kidney Foundation, Inc.
NDEX WORDS: Arterial steal syndrome; arterial stenosis; arteriovenous fistula; interventional nephrology; balloon
ngioplasty.mmip
ssrihrernmsd
cpiiircms
RTERIAL STEAL SYNDROME is an im-portant complication in patients receiving
ong-term hemodialysis (HD) using an arterio-enous access. Depending upon the definitionsed, the prevalence of this complication variesrom 1% to 20%.1-5 It is more common in pa-ients with proximal (brachial artery–based) thanistal (radial artery–based) accesses.2 The syn-rome usually manifests as hand pain (on and offialysis) and, less frequently, loss of distal func-ion and tissue death. Although it results inccess loss, ligation of the arteriovenous accessas been considered to be the treatment by manyephrologists. At a conceptual level, the goal for
From Interventional Nephrology, Division of Nephrology,niversity of Miami Miller School of Medicine, Miami, FL.Received December 13, 2005; accepted in revised formarch 28, 2006.Originally published online as doi:10.1053/j.ajkd.2006.03.077
n June 5, 2006.Support: This project was not supported by any grants or
unding agencies. Potential conflicts of interest: None.Address reprint requests to Arif Asif, MD, Director, Inter-
entional Nephrology, Associate Professor of Medicine, Uni-ersity of Miami Miller School of Medicine, Miami, FL.-mail: [email protected]© 2006 by the National Kidney Foundation, Inc.0272-6386/06/4801-0010$32.00/0
idoi:10.1053/j.ajkd.2006.03.077
American Journ8
anaging this complication must focus on aug-enting blood flow distal to the access to relieve
schemia while preserving the lifeline of theatient.Pathophysiologic mechanisms governing
teal syndrome are complex and poorly under-tood. Whereas shunting of blood to a lowesistance area (arteriovenous access) result-ng in hypoperfusion distal to the anastomosisas been suggested to be the cause, increasedesistance to blood flow offered by the pres-nce of arterial stenosis also can have a criticalole.2,6 Recent data have emphasized that sig-ificant (�50%) arterial stenoses are seen com-only in dialysis patients presenting with
ymptoms of arterial steal6-8 or vascular accessysfunction.9-11
Although many reports have accentuated surgi-al interventions, including access ligation, banding/lication, tapered graft insertion, distal revascular-zation-interval ligation, and revision using distalnflow procedure,6,12-17 only a few mentioned themportance of stenotic lesions in patients with arte-ial steal.6-8 This study presents a systematic appli-ation of a percutaneous approach in the manage-ent of patients with arterial steal syndrome and
uggests an algorithm to manage patients present-
ng with this complication.al of Kidney Diseases, Vol 48, No 1 (July), 2006: pp 88-97

S
lboiCatpiaswpmo
fas
P
cptas
D
ttdapasctiolw
nmftprp
P
ac
pr
tm6tHebs4htafipec
cTaepd
NAS
R
T
SC
n
MANAGEMENT OF ARTERIAL STEAL 89
METHODS
ettings and Study DesignFrom July 2004 to November 2005, a total of 12 of 372
ong-term HD patients (3.2%; receiving HD on an outpatientasis) presented with symptoms of arterial steal (hand painn and/or off dialysis). Physical examination was performedn all patients before and after the corrective intervention.omplete arteriography was performed to document arterialnatomy and to ascertain the presence of stenotic lesions onhe arterial side. Percutaneous transluminal balloon angio-lasty (PTA) was performed to treat the stenosis, whenndicated. Those who were not considered candidates forngioplasty based on imaging were referred to a vascularurgeon. A hard copy of images and the arteriography reportere sent to the surgeon. The plan and findings of arteriogra-hy for each patient were discussed with the surgeon. Theanagement plan also was shared with the referring nephrol-
gy team. All patients were followed up prospectively.Local institutional review board approval was obtained
or this study. All study procedures were carried out inccordance with the Declaration of Helsinki regarding re-earch involving human subjects.
hysical ExaminationPhysical examination included inspection for trophic
hanges and determination of extremity temperature byalpation. In addition, pulse volume by using simple palpa-ion was recorded both with and without occlusion of therteriovenous access and compared with the contralateralide. Finally, capillary refill was also determined.
escription of Angiography and AngioplastyDiagnostic arteriography was performed by cannulating
he access in a retrograde direction and advancing a diagnos-ic catheter into the subclavian artery. Positioning of theiagnostic catheter in the subclavian artery to image therterial circulation of the upper extremity was based onrevious descriptions by Khan and Vesely.10 Complete evalu-tion of the extremity arteries was performed from theubclavian artery to the palmar arch. Images were re-orded by using digital subtraction angiography in mul-iple planes, including orthogonal views. Angiographicmages with and without occlusion of the access werebtained. Stenosis of 50% or greater narrowing of theuminal diameter compared with adjacent normal segmentas considered significant.Angioplasty was performed by using a standard tech-
ique.18 Low-pressure balloons (Classique; ultrathin dia-ond; Boston Scientific, Natick, MA) were used to per-
orm angioplasty. The size of the balloon never exceededhe size of the artery in which angioplasty was beingerformed. A brachial artery approach to perform angiog-aphy or angioplasty was not needed and never waserformed.
arameters RecordedDemographic characteristics of the 12 study patients were
nalyzed. Locations of arterial stenoses were recorded. Pro-
edure success, defined by disappearance of symptoms, and arocedure-related complications were recorded. Data areeported as mean � SD.
RESULTS
Demographic characteristics of the study pa-ients show that more than 60% of patients wereen. Mean age was 52 � 11 years (range, 31 to
6 years; Table 1). African Americans and Hai-ians comprised 81% of the study population.ypertension was the most common cause of
nd-stage renal disease (45%), followed by dia-etes (36%). Eight patients were receiving dialy-is therapy using an arteriovenous fistula, whereaspatients had an arteriovenous graft. No patient
ad a radiocephalic fistula. Additionally, no pa-ient in this study had duplex brachial/radialrtery or forearm pressure measurements beforestula creation, and no records of simple bloodressure measurements to compare the differ-nce between the upper extremities before accessreation were available.
Physical examination showed a cold extremityompared with the other side in all 12 patients.rophic changes were found in no patient. Brachialrterial pulses examined at midarm level werequal on both sides in all patients. Radial arteryulse was absent in all patients with steal syn-rome without occlusion of the arteriovenous
Table 1. Demographic Characteristics of PatientsWith Arterial Steal Syndrome
o. of patients 12ge (y) 52 � 11exMales 7 (64)ace/ethnicityAfrican American 7 (58)Hispanic 3 (25)Haitian 2 (17)
ype of accessArteriovenous fistula
Brachiocephalic 8 (67)Arteriovenous graft
Brachiobasilic loop 4 (33)moking 7 (58)ause of end-stage renal diseaseHypertension 6 (50)Diabetes 3 (25)Glomerulonephritis 2 (17)Polycystic kidney disease 1 (8)
NOTE. Results expressed as mean � SD, number, orumber (percent).
ccess, except for 1 patient. With occlusion, 10
ofal(o
T
A
1wsFmmsElo
P
tcnas
ASIF ET AL90
f the 11 patients with absent pulse showed aeeble pulse, whereas 1 patient did not developradial pulse even after this maneuver. Capil-
ary refill was difficult to assess and delayed�4 seconds) in all patients with or withoutcclusion of the access.
echnical Success
Arteriography results are shown in Fig 1.ngiography showed arterial stenotic lesions in
Completearteriography
Arterial stenosis
Presentn=10*
Interventions
ercutaneous Interventionn= 8
S
ReResolution of symptoms n=8
Access preservation n=8
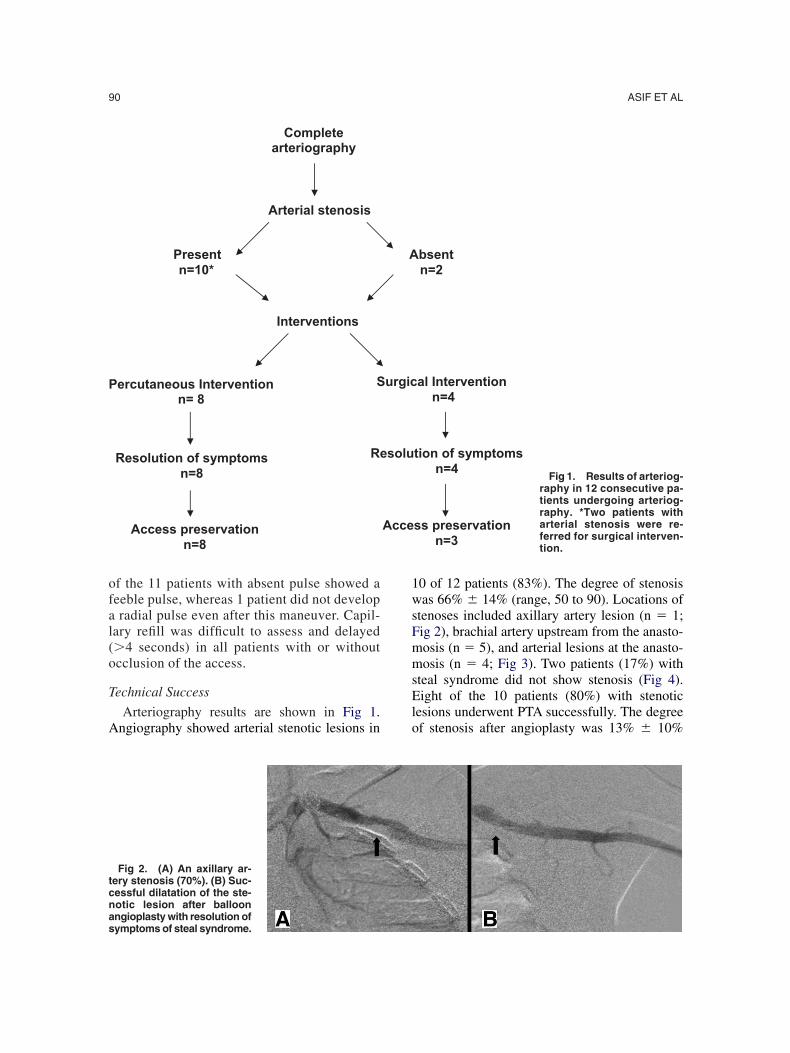
Fig 2. (A) An axillary ar-ery stenosis (70%). (B) Suc-essful dilatation of the ste-otic lesion after balloon
ngioplasty with resolution ofymptoms of steal syndrome.0 of 12 patients (83%). The degree of stenosisas 66% � 14% (range, 50 to 90). Locations of
tenoses included axillary artery lesion (n � 1;ig 2), brachial artery upstream from the anasto-osis (n � 5), and arterial lesions at the anasto-osis (n � 4; Fig 3). Two patients (17%) with
teal syndrome did not show stenosis (Fig 4).ight of the 10 patients (80%) with stenotic
esions underwent PTA successfully. The degreef stenosis after angioplasty was 13% � 10%
bsentn=2
al Intervention n=4
tion of symptomsn=4
ss preservation n=3
Fig 1. Results of arteriog-raphy in 12 consecutive pa-tients undergoing arteriog-raphy. *Two patients witharterial stenosis were re-ferred for surgical interven-tion.
A
urgic
solu
Acce

(liap
aptatfiewoTi
C
spsdimr(w
psptss
fistst
cRdpUt
MANAGEMENT OF ARTERIAL STEAL 91
range, 0 to 40). Five patients showed residualesions ranging from 10% to 40%. The remain-ng 2 patients were not considered candidates forpercutaneous approach. One patient had a com-lete occlusion of the brachial artery distal to the
Fig 3. Brachiocephalicstula with (A) critical steno-is of the brachial artery inhe anastomotic area and (B)uccessful angioplasty ofhe lesion.
Fig 4. (A) A patient with a brachial artery (arrow) toephalic vein fistula with symptoms of arterial steal.etrograde flow into the fistula was seen through theistal portion of the brachial artery. No flow distallyast the arrowhead was seen on angiography. (B, C)
tpon occlusion, antegrade flow was established into
he forearm arteries (arrows).
nastomosis and underwent an access ligationrocedure. This patient had fistula creation onhe contralateral side. The remaining patient hadvariant brachial artery (Fig 5) and was referred
o the surgeon for creation of an axillary loopstula. The 2 patients without stenoses showedxcessive flow through the anastomosis coupledith severe retrograde flow from a distal portionf the brachial artery into the fistula (Fig 4A).hese patients successfully underwent lengthen-
ng procedures by insertion of a vein segment.
linical Success
Overall, 8 of 12 patients (67%) were treateduccessfully with percutaneous balloon angio-lasty, whereas 4 of 12 patients (33%) requiredurgical intervention. Symptoms of arterial stealisappeared in all 12 patients immediately afterntervention. At a mean follow-up of 8.3 � 4
onths (range, 3 to 18 months), these patientsemain symptom free. Eleven of the 12 patients92%) are dialyzing using the same access. Thereere no procedure-related complications.
DISCUSSION
Previous investigators have documented theresence of underlying obstructive arterial steno-es as a cause of peripheral ischemia in HDatients.6-8 Using comprehensive arteriography,hese studies reported the incidence of arterialtenosis to range from 62% to 100%.6-8 In 1tudy,7 complete arteriography from the aortic to
he palmar arch was performed to assess the
piIesslpiwaiwpatrcaia
p
ftdpttdamapsbw1dpscura
bssrs is casee r artery
ASIF ET AL92
resence of arterial stenosis in HD patients present-ng with symptoms of peripheral ischemia (n � 13).n this analysis, 62% of the 13 patients referred forvaluation of symptoms of steal syndrome showedignificant (�50%) arterial stenosis. Conversely, aeparate report6 found stenosis in the inflow circu-ation in 100% of patients who underwent com-lete arteriography (n � 5). In the current study, thencidence of significant (�50%) arterial stenosisas 10 of 12 patients (83%). These results are in
greement with a recent study that reported an 80%ncidence of arterial disease in patients presentingith arterial steal syndrome.8 Only a minority ofatients (2 of 12 patients; 17%) with symptoms ofrterial steal showed absence of arterial lesions inhe present report. However, in this study, arteriog-aphy was performed by advancing a diagnosticatheter into the subclavian artery. The incidence ofrterial stenosis might have been even greater if themaging catheter was advanced into the aortic archrea to visualize proximal arteries.
The presence of arterial stenosis can have a
Fig 5. (A-F) Arteriography in a patient with symptomlood flow. Bold arrow (short) indicates 60% stenosis ofhows a juxta-anastomotic venous stenosis. Even thisyndrome. Retrograde flow was noted through the radialetrograde filling of the radial artery by occluding the ulnahowed a good radial artery on physical examination. Thxisting fistula. Abbreviations: RA, radial artery; UA, ulna
rofound effect on the surgical procedure per- i
ormed to correct arterial steal. Recognition ofhese stenoses before planning a surgical proce-ure can be very important. For example, in theresence of significant arterial stenosis proximalo the anastomosis, a banding procedure appliedo correct arterial steal can result in a criticalecrease in access blood flow, culminating inccess thrombosis. Such a scenario was docu-ented by DeCaprio et al.6 In a retrospective
nalysis, these investigators reported 18 dialysisatients who presented with symptoms of arterialteal. Eleven of 18 patients (61%) underwent aanding procedure without a prior arteriography,ith a 6-month patency rate of only 9%. Five of8 patients (28%) underwent arteriography andocumented an arterial inflow lesion. Of these 5atients, 2 patients underwent angioplasty andtent insertion, with resolution of symptoms andontinued patency of the access. One patientnderwent graft ligation because of multiple arte-ial lesions. Of the remaining 2 patients, axillaryrtery stenosis could not be opened successfully
rterial steal syndrome. Arrows indicate the direction ofery just proximal to the anastomosis. Bold arrow (long)sis was not able to protect the patient against steal
into the access. Physical examination could confirm they and performing palpation of the radial artery. The patientrequired an axillary loop fistula using the outflow of the; CVAVF, cephalic vein arteriovenous fistula.
s of athe art
stenoarteryr arter
n 1 patient and the graft thrombosed. The last

pbtwtmcv
nlaaawcawdtwadc
lpu
aeTtmtsdiatp
ocNdcnmvidptap
ts
MANAGEMENT OF ARTERIAL STEAL 93
atient with an arterial inflow lesion underwent aanding procedure without angioplasty. This grafthrombosed 2 days later. One of the 18 patientsas lost to follow-up. This study highlights that
he presence of unsuspected arterial stenosisight explain, at least in part, the dismal suc-
ess6,12 of banding procedures performed to alle-iate steal syndrome.In the present series, a combination of percuta-
eous and surgical interventions resulted in reso-ution of symptoms in 100% of patients, withccess preservation in more than 90%. We treatedrterial lesions, including arterial stenosis in thenastomotic area (Fig 3), with PTA. Lesionsere approached through the arteriovenous ac-
ess itself. Brachial artery puncture to performngioplasty was not needed. Only the patientith complete occlusion of the brachial arteryistal to the anastomosis required an access liga-ion procedure. Choice of the surgical procedureas based on the surgeon’s discretion. All 11
ccesses are patent, and the patients are receivingialysis therapy successfully using the same ac-ess with a mean follow-up of 8.3 � 4 months.
In the present report, patients with stenoticesions did not automatically qualify for angio-lasty. Similarly, not all patients referred for steal
Consider PTA
Arterial s
Stenoses amenable t
Yes
Fig 6. A simple algorithmo manage patients withymptoms of arterial steal.
nderwent surgical intervention. Nevertheless, s
ll patients with symptoms of arterial steal werevaluated first by using arteriography (Fig 6).he management approach was based solely on
he findings of arteriography. Instead of the com-on approach of focusing on limiting the flow
hrough the access system and risking thrombo-is, treatment strategies converged on improvingistal perfusion, as well as preserving the exist-ng access. Patients underwent either ligation orlengthening procedure to increase resistance in
he outflow of the fistula or angioplasty to im-rove overall inflow to the extremity.It is important to note that in a great majority
f forearm and proximal arteriovenous accesses,linically silent retrograde flow can be seen.19,20
evertheless, demonstration of retrograde flowoes not predict or indicate the existence of alinical steal syndrome.2,19 Likewise, hemody-amic evidence of arterial steal can be found inost patients; however, ischemic symptoms de-
elop in only a minority. A variety of noninvasivenvestigations, such as digital blood pressure (DBP),igital/brachial index (DBI) measurement, digitallethysmography, duplex ultrasonography, andranscutaneous oxygen saturation determination,re available to assist in the management ofatients with symptoms of arterial steal.21-26 In 1
out other causes of hand pain: el tunnel, diabetic neuropathy,
etc
Symptoms of arterial steal
is present Arterial stenosis absent
rform complete arteriography
oplasty
Surgical Intervention
RuleCarp
tenos
Pe
o angi
No
tudy (n � 35), DBI less than 0.6 reasonably

pda0aloaiopsmpts
oeftapsvoosdvpevrmt
tsigsthcpot
is
aswftAfpmfltostiaeplohAostsrcfp
stfsVmlpsditWirtvm
ASIF ET AL94
redicted, but still was not diagnostic for, theevelopment of symptoms of arterial steal.21 Innother report of 109 patients,22 DBI less than.6 to predict steal had specificity of only 59%nd a positive predictive value of 18%. An abso-ute DBP or DBI value below which symptomsf steal were inevitable has not been validatednd standardized in a prospective fashion.23 Us-ng pulse oximeter, Halevy et al24 found anxygen saturation of only 42% to 63% in 5atients presenting with symptoms of arterialteal. Postintervention, these investigators docu-ented an increase in oxygen saturation in all 5
atients (80% to 100%), with resolution of symp-oms. However, the small sample size of thetudy is a major limitation of this study.
Sumner26 has emphasized that measurementf DBP, DBI, and oxygen saturation requiresxtreme caution. Such studies should be per-ormed in a warm (25°C) draft-free room withhe patient relaxed. All efforts should be made tollay apprehension. Even in this scenario, someatients may remain vasoconstricted and requireoaking the hand in warm water. In this way,asoconstriction that can make the interpretationf results very difficult can be avoided. Theperator must consider performing digital pres-ure in all fingers to localize the problem toigital versus palmar arch. Although noninvasiveascular laboratories are the correct place for theerformance of most hemodynamic tests, thisnvironment is not always present in most inter-entional suites. However, when performed accu-ately, hemodynamic evaluation can assist in theanagement of patients presenting with symp-
oms of arterial steal syndrome.Although all these interventions can assist in
he management of patients presenting withymptoms of arterial steal, for the most part,ndication to intervene is based solely on clinicalrounds (ie, hand pain on and or off dialy-is).25,27 In this context, this report has a limita-ion in that we did not perform these objectiveemodynamic parameters before or after the pro-edure. Conversely, the current report deals withatients presenting with established symptomsf arterial steal and largely converges on resolu-ion of symptoms postintervention.
Intuitively, one could imagine that by perform-ng physical examination, the cause of arterial
teal would be disclosed. In this context, the appearance of a radial pulse with access occlu-ion would indicate that the arteriovenous accessas stealing too much blood away from the
orearm, creating ischemia, and flow reductionhrough the large anastomotic orifice was needed.lthough logical, findings of the present study
ail to support this notion. A majority (91%) ofatients showed pulse with occlusion, yet only ainority (18%) of patients were candidates for aow-reduction procedure through the access. In-
erestingly, 1 patient had a radial pulse withoutcclusion and, despite this, had symptoms ofteal syndrome. This patient had retrograde flowhrough the radial artery to the fistula (Fig 3). Ofnterest, pulse examination in the patient withxillary artery stenosis did not indicate a differ-nce in volume of the brachial artery pulse com-ared with the other side. We did not find capil-ary refill to be helpful. In retrospect, pulseximetry compared with visual inspection mightave been a better test to assess capillary refill.lthough physical examination is emerging asne of the most valuable tools in the diagnosis oftenoses in dialysis access, its utility to differen-iate between patients with and without arterialtenosis was less than optimal in the presenteport. However, the small sample size of theurrent series does not allow a firm conclusionor or against the use of physical examination inatients with arterial steal syndrome.In addition to arterial stenosis and excessive
teal through the anastomosis, vascular calcifica-ion causing distal arteriopathy is an importantactor that may contribute to the development ofymptoms of arterial steal syndrome (Fig 7).28
ascular calcification affects both intimal andedia layers.29 Disturbances in mineral metabo-
ism in the uremic milieu, calcium-containinghosphate binders and vitamin D treatment ofecondary hyperparathyroidism, increased oxi-ized low-density lipoprotein cholesterol levels,ncreased oxidative stress, and hyperhomocys-einemia may contribute to the pathogenesis.28
hereas PTA and surgical interventions offer anmportant role in the management of ischemiaelated to stenosis and excessive steal throughhe fistula, there is no definite therapy for thisascular calcification. Avoidance of treatmentodalities that lead to calcium overload and
chievement of good mineral metabolic balance

am
lChtit1sdrabtaSitcte
maopdfsmwt
cdlbndDbltdtttlfh
diocaAit
CHH
a
MANAGEMENT OF ARTERIAL STEAL 95
nd optimal dialysis are the mainstay of treat-ent for vascular calcification.Symptoms of arterial steal have been high-
ighted to be common in patients with diabetes.onversely, in this study, only 36% of patientsad diabetes. However, 7 of 12 patients (58%) inhe current report gave a history of active smok-ng, whereas 4 of 12 patients (34%) indicatedhey had not smoked for at least 6 months. Onlypatient (8%) never smoked. Current and former
moking are associated with peripheral arterialisease.30,31 In addition, smoking increases theisk for amputation in patients with claudication32
nd decreases patency rates after lower-extremityypass.33 Foley et al34 showed in dialysis patientshat current smoking was predictive of peripheralrterial disease and future cardiovascular events.moking cessation seems to result in an increase
n exercise tolerance and ankle pressure in pa-ients with intermittent claudication.35 In thisontext, smoking remains a modifiable risk fac-or. Consequently, smoking cessation should bencouraged strongly.
Time from access creation to steal develop-ent generally is short, with steal immediately
pparent after access creation. However, time ofnset of symptoms of arterial steal in our studyatients (who were already receiving long-termialysis on an outpatient basis) was 8 � 2 monthsrom the time of access creation. Duration ofymptoms was 2 � 0.5 months. Although mostild cases of steal would resolve on their ownith the development of collateral circulation, in
Fig 7. A patient with a ra-iocephalic fistula. (A) Arrows
ndicate vascular calcificationf forearmarteries. (B)Thebra-hial artery of the same patientlso shows calcification.nastomosis (double arrow),
maging catheter into the fis-ula (arrowhead).
his analysis, patients reported that symptoms o
rogressively increased in severity. Hand painuring dialysis was the most critical symptomound in this study (Table 2).
In addition to arterial insufficiency, hand painan be caused by carpal tunnel syndrome, ten-opathies, and arthropathies, which can occur inong-term HD patients and mainly are influencedy �2-microglobulin amyloidosis.36 Carpal tun-el syndrome, caused by entrapment of the me-ian nerve, is seen in a majority of patients.iagnostic clues include pain in both handsecause median nerve entrapment is bilateral in aarge proportion of cases. Wasting of the lateralhenar muscles often is present at diagnosis,enoting advanced nerve compression.36-38 Elec-romyogram showing a decrease in motor conduc-ion can help establish the diagnosis.37 Destruc-ive arthropathy of the hands is common inong-term HD patients.39 This condition differsrom deposition of amyloid in the joint becauseistological studies of the synovial membrane
Table 2. Symptoms of Arterial Steal
Symptom of ArterialSteal Severity of Symptoms
No. ofPatients
old hand Moderate 12and pain at rest Moderate to severe* 8and pain duringdialysis† Moderate to severe* 12
*Patient reported progressive worsening of hand pain onnd off dialysis.†Patients required early termination of dialysis because
f hand pain frequency.

apdmoircDlassdvpbmttpadcrspTahnuatrodsv
vhdtbap
dra
itaaps
Ai7
eV
o7
ct
s1
Hd
Bao
Mlr
it
wt1
MvD
bdUg
oav
s
ASIF ET AL96
nd subchondral bone found no amyloid, even inatients with clinical or roentgenographic evi-ence of amyloidosis at other sites. Electronicroscopy studies also failed to show crystals
r amyloid.39 Destructive arthropathy of the handsn HD patients is not a manifestation of dialysis-elated amyloidosis. The pathophysiological pro-ess of the condition remains poorly understood.eformities of phalangeal joints, instability, and
ocalized tenderness are some of the features thatssist in making the diagnosis of this entity. Jointpace obliteration and subchondral erosions areeen on radiographic examination. Another con-ition that can result in hand pain after arterio-enous access creation is reflex sympathetic dystro-hy syndrome.40 This syndrome is characterizedy pain and swelling of an affected extremity,ost commonly seen after trauma. Reflex sympa-
hetic dystrophy syndrome should be included inhe differential diagnosis of unexplained limbain coupled with swelling after arteriovenousccess placement. Although mostly symmetrical,iabetes can involve isolated limb nerves andause pain.41 However, ischemic monomelic neu-opathy is a complication of vascular access ob-erved almost exclusively in patients with diabetes,articularly those with preexisting neuropathy.20,42
he entity is characterized by the development ofcute pain, weakness, and paralysis of forearm andand muscles. There often is sensory loss accompa-ied with motor. The condition occurs soon (min-tes to hours) after creation of an arteriovenousccess. The condition results from ischemic infarc-ion of the vasa nervosa. Ischemic monomelic neu-opathy can be diagnosed clinically based on acutenset of pain after access creation with a history ofiabetes and dominant neurological symptoms andigns. The hand is warm, and the radial pulseariably is present.
Good vascular surgery support is critical. Thealue of working with a vascular surgeon whoas a full repertoire of surgical skills and proce-ures that allow the application of highly innova-ive solutions to difficult anatomic problems cannote overemphasized. The surgeon, interventionalist,nd referring nephrologist must work together tolan an optimal strategy for a given situation.In conclusion, significant arterial stenoses in
ialysis patients with an arteriovenous access are aeality. We suggest that complete imaging of the
rterial circulation of the extremity be considered pn long-term dialysis patients presenting with symp-oms of arterial steal. We propose that planning andpplication of corrective procedures must take intoccount the findings of arteriography. A team ap-roach among nephrologists, interventionalists, andurgeons would only improve patient care.
REFERENCES
1. Morsy A, Kulbaski M, Chen C, Isiklar H, LumsdenB: Incidence and characteristics of patients with hand
schemia after a hemodialysis access procedure. J Surg Res4:8-10, 19982. Tordoir JHM, Dammers R, van der Sande FM: Upper
xtremity ischemia and hemodialysis vascular access. Eur Jasc Endovasc Surg 27:1-5, 20043. Haimov M, Baez A, Neff M, Sliftin R: Complications
f arteriovenous fistulae for hemodialysis. Arch Surg 110:08-712, 19754. Rinnaert P, Struyvan J, Mathieu J: Intermittent claudi-
ation of the hand after creation of an arteriovenous fistula inhe forearm. Am J Surg 139:838-843, 1980
5. Miles AM: Upper limb ischemia after vascular accessurgery: Differential diagnosis and management. Semin Dial3:312-315, 20006. DeCaprio JD, Valentine RJ, Kakish HB, Awad R,
agino RT, Claggett GP: Steal syndrome complicating hemo-ialysis access. Cardiovasc Surg 5:648-653, 19977. Valji K, Hye RJ, Roberts AC, Oglevie SB, Ziegler T,
ookstein JJ: Hand ischemia in patients with hemodialysisccess grafts: Angiographic diagnosis and treatment. Radiol-gy 196:697-701, 19958. Guerra A, Raynaud A, Beyssen B, Pagny JY, Sapoval, Angel C: Arterial percutaneous angioplasty in upper
imbs with vascular access devices for haemodialysis. Neph-ol Dial Transplant 17:843-851, 2002
9. Asif A, Gadalean FN, Merrill D, et al: Inflow stenosisn arteriovenous fistulas and grafts: A multicenter, prospec-ive study. Kidney Int 67:1986-1992, 2005
10. Khan FA, Vesely TM: Arterial problems associatedith dysfunctional hemodialysis grafts: Evaluation of pa-
ients at high risk for arterial disease. J Vasc Interv Radiol3:1109-1114, 200211. Lockhart ME, Robbin ML, McNamara MM, Allon: Association of pelvic arterial calcification with arterio-
enous thigh graft failure in haemodialysis patients. Nephrolial Transplant 9:2564-2569, 200412. Odland MD, Kelly PH, Ney AL, Andersen RC, Bu-
rick MP: Management of dialysis-associated steal syn-rome complicating upper extremity arteriovenous fistulas:se of intraoperative digital photoplethysmography. Sur-ery 110:664-669, 199113. Schild AF, Pruett CS, Newman MI, et al: The utility
f the VCS clip for creation of vascular access for hemodi-lysis: Long-term results and intraoperative benefits. Cardio-asc Surg 9:526-530, 200114. Rivers SP, Scher LA, Veith FJ: Correction of steal
yndrome secondary to hemodialysis access fistulas: A sim-
lified quantitative technique. Surgery 112:593-597, 1992
Tw7
rtS
id
Pm
ss
maD
Lu3
cp
ts3
ifi
aa
mEp
aS
u6
lu
ch
AC(8
sp1
sl
cS1
p2
Vp
t
r1
arR
pv4
P
Jr
MANAGEMENT OF ARTERIAL STEAL 97
15. Schanzer H, Schwartz M, Harrington E, Haimov M:reatment of ischemia due to “steal” by arteriovenous fistulaith distal artery ligation and revascularization. J Vasc Surg:770-773, 198816. Berman SS, Gentile AT, Glickman MH, et al: Distal
evascularization-interval ligation for limb salvage and main-enance of dialysis access in ischemia steal syndrome. J Vascurg 26:393-404, 199717. Minion DJ, Moore E, Endean E: Revision using distal
nflow: A novel approach to dialysis-associated steal syn-rome. Ann Vasc Surg 19:625-628, 200518. Beathard GA, Arnold P, Jackson J, Litchfield T, for the
hysician Operators Forum of RMS Lifeline: Aggressive treat-ent of early fistula failure. Kidney Int 64:1487-1494, 200319. Duncan H, Ferguson L, Faris I: Incidence of the radial
teal syndrome in patients with Brescia fistula for hemodialy-is: Its clinical significance. J Vasc Surg 4:144-147, 1986
20. Miles AM: Vascular steal syndrome and ischaemiconomelic neuropathy: Two variants of upper limb isch-
emia after haemodialysis vascular access surgery. Nephrolial Transplant 14:297-300, 199721. Papasavas PK, Reifsnyder T, Birdas TJ, Caushaj PF,
eers S: Prediction of arteriovenous access steal syndrometilizing digital pressure measurements. Vasc Endovasc Surg7:179-184, 200322. Goff CD, Sato DT, Bloch PH, et al: Steal syndrome
omplicating hemodialysis access procedures: Can it beredicted? Ann Vasc Surg 14:138-144, 200023. Valentine RJ, Bouch CW, Scott DJ, et al: Do preopera-
ive finger pressures predict early arterial steal in hemodialy-is access patients? A prospective analysis. J Vasc Surg6:351-356, 200224. Halevy A, Halpern Z, Negri M, et al: Pulse oximetry
n the evaluation of the painful hand after arteriovenousstula creation. J Vasc Surg 14:537-539, 199125. Lazarides MK, Staramos DN, Panagopoulos GN, et
l: Indications for surgical treatment of angioaccess-inducedrterial “steal.” J Am Coll Surg 187:422-426, 1998
26. Sumner DS: Noninvasive vascular laboratory assess-ent, in Machleder HI (ed): Vascular Disorders of Upperxtremity, Revised (ed 2). Mount Kisco, NY, Futura, 1989,p 9-5727. Schanzer H, Skladany M, Haimov M: Treatment of
ngioaccess-induced ischemia by revascularization. J Vascurg 16:861-864, 199228. Derici U, El Nahas AM: Vascular calcifications in
remia: Old concepts and new insights. Semin Dial 19:60-
8, 2006 u29. Goldsmith DJ, CovicA, Sambrook PA,Ackrill P: Vascu-ar calcification in long-term haemodialysis patients in a singlenit: A retrospective analysis. Nephron 77:37-43, 1997
30. Murabito JM, Evans JC, Nieto K, et al: Prevalence andlinical correlates of peripheral arterial disease in the Framing-am Offspring Study. Am Heart J 143:961-965, 2002
31. Newman AB, Siscovick DS, Manolio TA, et al:nkle-arm index as a marker of atherosclerosis in theardiovascular Health Study. Cardiovascular Heart Study
CHS) Collaborative Research Group. Circulation 88:837-45, 199332. Juergens JL, Barker NW, Hines EA Jr: Arteriosclero-
is obliterans: Review of 520 cases with special reference toathogenic and prognostic factors. Circulation 21:188-195,96033. Myers KA, King RB, Scott DF, et al: The effect of
moking on the late patency of arterial reconstructions in theegs. Br J Surg 65:267-271, 1978
34. Foley RN, Herzog CA, Collins AJ: Smoking andardiovascular outcomes in dialysis patients: The Unitedtates Renal Data System Wave 2 Study. Kidney Int 63:1462-467, 200335. Quick CR, Cotton LT: The measured effect of stop-
ing smoking on intermittent claudication. Br J Surg 69:24-6, 1982.36. Vellani G, Dallari D, Fatone F, Martella D, Bonomini
, Gualtieri G: Carpal tunnel syndrome in hemodialyzedatients. Chir Organi Mov 78:15-18, 199337. Bartova V, Zima T: Diagnosis and treatment of carpal
unnel syndrome. Ren Fail 15:533-537, 199338. Asencio G, Rigout C, Ramperez P, et al: Hemodialysis-
elated lesions of the hand. Rev Rhum Engl Ed 62:233-240,99539. Flipo RM, Le Loet X, Siame JL, et al: Destructive
rthropathy of the hands in chronic hemodialysis patients. Aeport of seven cases with pathological documentation. Revhum Engl Ed 62:241-247, 199540. Weise WJ, Bernard DB: Reflex sympathetic dystro-
hy syndrome of the hand after placement of an arterio-enous graft for hemodialysis. Am J Kidney Dis 18:406-08, 199141. Bansal V, Kalita J, Misra UK: Diabetic neuropathy.
ostgrad Med J 82:95-100, 200642. Riggs JE, Moss AH, Labosky DA, Liput JH, Morgan
J, Gutmann L: Upper extremity ischemic monomelic neu-opathy: A complication of vascular access procedures in
remic diabetic patients. Neurology 39:997-998, 1989Copyright © 2022 FDOKUMEN