
A Critique of Flow-directed Pulmonary Arterial Catheterization
11
Anest hesiolo)l)' -17:455-4ti5, 1977 Medical Intelligence JOHN D. MICHENFELDER, M.D., Editor A Critique of Flow-directed Pulmonary Arterial Catheterization Nathan Leon Pace, M.D. • IN I 9:13, Lategola and Rahn reported the use in clogs of a hand-fashioned, balloon-tipped, self'..guiding catheter for cardiac and pulmonary arterial cathe- terization and occlusion.• During the following 15 years, several self'..guiding right-heart catheters were developed for human use, but none was balloon- guicled, and none became well known. 2 - 5 In 1970, Swan ,•t al. 0 reported I heir initial ex pcriencc with a 111ultih1111en, balloon-Lipped, radiopaquc, extruded pol}'\'inyl chloride catheter (with adequate frequency response) that met three criteria: I) reliable, prompt passage to the pulmonary artery, 2) minimal ar- rhythmias, and 3) passage without fluoroscopy. The catheter may be introduced either by cutdown or percutaneously in one of several veins (femoral, antecubital, axillary, subclavian, external jugular, proximal basilic or internal jugular). 1 1-1 11 Placement is optimally performed by continuous pressure moni- toring with electronic transduction and oscilloscopic display. 11 - 13 After the catheter tip is advanced into the thorax (detected by respiratory fluctuations in the pressure trace), the balloon is inflated and the catheter is further advanced, relying on blood flow lo direct the catheter Lip through the tricuspid and pulmonic valves into the pulmonary artery. Details of tech- niques of cat hctcr passage and of care of the catheter arc straightforward and widely reprinted. 0 ,H-IH Since the initial report, a family of balloon-tipped catheters has been developed to allow: I) in-vivo oximetry, tu 2) pulmonary angiography,21 1 3) pediatric cardiac catheterization, 21 4) transvenous cardiac pacing, 22 5) His-bu ml le elcctrocardiogra ph y, 23 6) thermocl ii ution cardiac output dctcrmination,2' 1 and 7) artifact-free cardiac monitoring. 25 The catheter has been used in enormously diverse clinical situations. 7 • 11 • 14 • 211 -:m In general, the indications * Assistalll Professor, Department of Anesthesiology, Uni\'ersity of Utah College of i\leclidne, Salt Lake Cily, Utah tH 132. Accepted for publication June 23, 1977. 455 for its use appear to be: I) continuous hcmoclynamic monitoring following complicated acute myocardial infarction, 2) managemclll of fluid balance in non- canliogenic pulmonary edema, in non-canliogenic shock, and following cardiopulmonary bypass, and 3) evaluation of therapeutic interventions with mechan- ical ventilation, vasoactive drugs, hemodialysis and assisted circulation. Swan has recommernled that a pulmonary-artery catheter should be used when one thinks that a central venous pressure (CVP) measure- ment is needcd. 37 Several review articles detailing Swan Ganz (S-G) catheter use are available. 17 ·a 8 -~ 2 This article critically examines certain limitations inherent in pulmonary arterial moniroring and dis- cusses its use in clinical anesthesia. Pulmonary "Capillary" Pressure Pulmonary "capillary" pressure refers to the pres- sure measured through a cardiac catheter impacted into a branch of the pulmonary artery in such a fashion that there is a free communication between the catheter tip and the capillary-venous compart- ment of the lung. This pressure has been called pulmonary wedge pressure (PWP), pulmonary-artery wedge pressure (PA WP), pulmonary capillary pres- sure (PCP), and more recently, pulmonary-artery occlusion pressure (PAOP). Three criteria ha\'e been thought necessary for a true wedge prcssure:~a I) blood withdrawn from wedge position should be fully saLUrated with oxygen, 2) the pulmonary-artery phasic contour should change Lo a left atrial trace on wedging, and 3) mean wedge pressme should be less than mean pulmonary arterial pressure; it has been observed that a wedged catheter blood sam pie may or may not be I 00 per cent oxygen-saturated in patients who have pulmonary shunts and during positive end-expiratory pressure (PEEP). 0 • 44 ·~ 5 Thus, only the latter two criteria now apply. 44 Initial studies in both animal and man confirmed the
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of A Critique of Flow-directed Pulmonary Arterial Catheterization
A nest hesiolo)l)' -17:455-4ti5, 1977
Medical Intelligence JOHN D. MICHENFELDER, M.D., Editor
A Critique of Flow-directed Pulmonary Arterial Catheterization
Nathan Leon Pace, M.D. •
IN I 9:13, Lategola and Rahn reported the use in clogs of a hand-fashioned, balloon-tipped, self'..guiding catheter for cardiac and pulmonary arterial catheterization and occlusion.• During the following 15 years, several self'..guiding right-heart catheters were developed for human use, but none was balloonguicled, and none became well known. 2- 5 In 1970, Swan ,•t al. 0 reported I heir initial ex pcriencc with a 111ultih1111en, balloon-Lipped, radiopaquc, extruded pol}'\'inyl chloride catheter (with adequate frequency response) that met three criteria: I) reliable, prompt passage to the pulmonary artery, 2) minimal arrhythmias, and 3) passage without fluoroscopy. The catheter may be introduced either by cutdown or percutaneously in one of several veins (femoral, antecubital, axillary, subclavian, external jugular, proximal basilic or internal jugular). 1
1-1 11 Placement is optimally performed by continuous pressure monitoring with electronic transduction and oscilloscopic display. 11- 13 After the catheter tip is advanced into the thorax (detected by respiratory fluctuations in the pressure trace), the balloon is inflated and the catheter is further advanced, relying on blood flow lo direct the catheter Lip through the tricuspid and pulmonic valves into the pulmonary artery. Details of techniques of cat hctcr passage and of care of the catheter arc straightforward and widely reprinted. 0,H-IH Since the initial report, a family of balloon-tipped catheters has been developed to allow: I) in-vivo oximetry, tu
2) pulmonary angiography,211 3) pediatric cardiac catheterization, 21 4) transvenous cardiac pacing, 22 5) His-bu ml le elcctrocardiogra ph y, 23 6) thermocl ii ution cardiac output dctcrmination,2' 1 and 7) artifact-free cardiac monitoring. 25
The catheter has been used in enormously diverse clinical situations. 7•11•14•211-:m In general, the indications
* Assistalll Professor, Department of Anesthesiology, Uni\'ersity of Utah College of i\leclidne, Salt Lake Cily, Utah tH 132.
Accepted for publication June 23, 1977.
455
for its use appear to be: I) continuous hcmoclynamic monitoring following complicated acute myocardial infarction, 2) managemclll of fluid balance in noncanliogenic pulmonary edema, in non-canliogenic shock, and following cardiopulmonary bypass, and 3) evaluation of therapeutic interventions with mechanical ventilation, vasoactive drugs, hemodialysis and assisted circulation. Swan has recommernled that a pulmonary-artery catheter should be used when one thinks that a central venous pressure (CVP) measurement is needcd. 37 Several review articles detailing Swan Ganz (S-G) catheter use are available. 17·a8-~ 2
This article critically examines certain limitations inherent in pulmonary arterial moniroring and discusses its use in clinical anesthesia.
Pulmonary "Capillary" Pressure
Pulmonary "capillary" pressure refers to the pressure measured through a cardiac catheter impacted into a branch of the pulmonary artery in such a fashion that there is a free communication between the catheter tip and the capillary-venous compartment of the lung. This pressure has been called pulmonary wedge pressure (PWP), pulmonary-artery wedge pressure (PA WP), pulmonary capillary pressure (PCP), and more recently, pulmonary-artery occlusion pressure (PAOP). Three criteria ha\'e been thought necessary for a true wedge prcssure:~a I) blood withdrawn from wedge position should be fully saLUrated with oxygen, 2) the pulmonary-artery phasic contour should change Lo a left atrial trace on wedging, and 3) mean wedge pressme should be less than mean pulmonary arterial pressure; it has been observed that a wedged catheter blood sam pie may or may not be I 00 per cent oxygen-saturated in patients who have pulmonary shunts and during positive end-expiratory pressure (PEEP). 0•44·~5 Thus, only the latter two criteria now apply. 44 Initial studies in both animal and man confirmed the
456 NATIIAN L. !'ACF. AneMhf'!\h,1,,~V •17, No !'i, N,w IH77
validity or the pulmonary-artery wedge pressure as an index or pulmonary venous pressure and left atrial pressure (LAP).43
Balloon-tipped and ordinary pulmonary-arterr catheters have been shown to give identical PAOP reaclings. 11 Whereas pulmonary-artery catheters without a balloon tip must be manually advanced to measure PAOP and then withdrawn, the S-G catheter requires onl)' intermittent inflation or the balloon to let blood flow pull the catheter tip out into a wedge position; tlrns, catheter manipulation is avoided and long-term monitoring becomes more feasible. Artifactual PAOP readings can be produced by an overinflated balloon occluding the catheter tip or an eccentrically inflated balloon not producing complete occlusion or the vessel lumen; inflating the balloon with the minimum volume of air sufficient to yield a PAOP trace and maintaining a central position or the catheter tip will avoid these problcms:12,·1t1-4K Analysis of PAOP (by S-G) as a measure of' LAP has shown very good correlation in most st11clics.41H 1 LAP has also been estimated from measurements of' pulmonary arterial encl-diastolic pressure (PAEDP). PAEIW is usually only 1-2 torr higher than PAOP ancl LAP; however, in critically ill patients, the correlation between PAEDP and PAOP is unreliable because of either pre-existing pulmonary hypertension or increased pulmonary vascular resistance secondary to acute cardiopulmonary failure. 1uo- 54 Normal hemoclynamic values in the pulmonary artery are 20/12 (torr), with a mean of 13 torr and a mean PAOP of 6-12 torr. Caution must always be used in interpreting a single reading; sequential readings are thus necessary. The frequency of readings will, of course, depend on the instability of the patient, and might be as often as every 30 seconds, but certainly no less often than every 15 minutes.
The widespread availability of S-G catheters prom pt eel a re-evaluation of central venous pressure measurements. Previously accepted as an adequate guideline for managing shock and hypovolemia, 5~-su poor or absent correlation was found in comparing PAOI>, PAEDP, or LAP with CVP in seriously ill patients. 0•211- 3 i. 51 •57-u 3 In the absence of cardiopulmonary dysfunction, CVP remains a reliable assessment of right and left heart filling,3 '·
58 but in serious illness right ventricular function and left ventricular function are so disparate that not only the absolute CVP but even CVP changes are unreliable and misleading estimates of left heart filling.57·60
Some controversy does remain. First, a recent large series showed a good correlation of PAOP and LAP al pressures of' IO torr or less, but as PAOP increased
the prediction of LAP from PAOP was su~ject to considerable error 64; at PAO P's greater than 15 torr the 95 per cent confidence interval for predicting LAP was at least ±5 torr. This was auributed to a change in the ratio of pulmonary arterial Lo pulmonary venous compliance. Second, evidence has been found for a pulmonary venous waterfall effect at the exit of the large pulmonary veins from the surface of the lung. 65 A pulmonary vascular waterfall effect is said Lo occur in a collapsible vascular segment when the intra vascular downstream pressure is less than the pressure surrounding the collapsible section. 66 Under these conditions the vessels exposed to the surrounding pressure partially collapse and blood flow becomes independent of the more negative downstream pressure. Under no-flow conditions, a wedged upstream pressure will fall lo the level of the pressure around the collapsible segment and not to the more negative downstream pressure. With a waterfall effect in the pulmonary veins and al very low LAP's, PAOP will be higher than LAP. This work65 was clone in the clog with an open thorax; the conditions under which it might apply to man arc unknown.
Whether PAOP reflects LAP during mechanical ventilation with PEEP is in doubt; PEEP raises alveolar pressure and creates a waterfall effect al the alveolar level, thus keeping PAOP higher than LAP.45·67•68 The presence or absence of a PAOP-toLAP discrepancy during PEEP will depend on the complex relationship of: l) the height of the S-G catheter tip above the left atrium during wedging, 2) the lel'L atrial pressure, and 3) the level of PEEP; if the catheter tip wedges in a region of hmg where alveolar pressure excedes pulmonary venous pressure, PAOP will reflect alveolar pressure and not LAP.45·66 (The recent suggestion of Benumof el al. m, that a PAOP-to-LAP discrepancy will arise only when alveolar pressure excedes pulmonary arterial pressure appears in error. 611) Since the S-G catheter tip can distribute to peripheral regions of lung, 69 it is easily conceivable that a change in patient position (supine LO sitting or lateral decubilus) would produce a sudden, unexpected error in PAOP estimates of LAP. Equally, a change in the level of PEEP or LAP or a random migration of the S-G catheter tip during wedging would produce or eliminate an alveolar waterfall effect without a change in patient position. Unfortunately, the presence or absence of an alveolar waterfall effect during PEEP is not discernible with only an S-G catheter.
In addition, PEEP increases intrathoracic pressure and thus all imravascular and intracarcliac pressures. The true distending pressure of a vessel or of a
A11t.·~1 ht.·~ic,lc1M) \' ·17. :-.:or,, Nm· IH77 PULMONARY ARTERIAL MONITORING 457
cardiac chamber under these conditions is the intraluminal pressure minus the surrounding pressure. Calculation of' transmural pressures (PAOP - intrapleural or esophageal pressure) has been recommended to preserve the accuracy of PAOP in estimating distending pressures charing PEEP. Surrounding pressures have been taken with an esophageal balloon 711 and with a fluid-filled intrapleural cat hcter.7 1 The laller technique has been criticized by Craig 72 as measuring pleural liquid pressure, which can be quite clifferelll from pleural surface pressure. It is pleural surface pressure that determines expansion of the lung and is transmitted to intraI horacic extra pulmonary structures. Use of an esophageal balloon pressure must be taken with reservation owing to the possible artifacts introduced by the esophagus and surrounding structures. 73 Even if pleural surface pressure is measured accurately, calculation of transmural filling pressures is potentially in error, as the pressure around the heart is more negative than pleural surface pressure and varies with hmg volume. 73
Some have ol~jected that in patients with chronic ohst ructivc pulmonary disease (COPD) an elevated PAOP may be an artifact of the pulmonary abnormality and docs not necessarily indicate left ventricular l'ailure (LVF).74 In general, however, elevated PAOP's in COPD have been shown to reflect true LVF.15
- 77 In patients who have severe obstructive pulmonary disease, the wide swings in intrathoracic pressure during "active expiration" can influence PAOP interpretation; ideally, in this circumstance transmural PAOP should again be used 78 ; however, this technique is not routinely employed as it requires an esophageal balloon.
How, then, should PAOP be measured during elevated or rapidly changing intrathoracic pressure? The following suggestions might be useful. Pulmonary arterial pressures should be taken as the average over several heart beats at end-expiration with the transducer at the mid-axillary line and referenced to atmospheric pressure. For the mechanically ventilated patient who has a respiratory rate so rapid that a stable end-expiratory trace cannot be seen, the ventilator should be momentarily disconnected during the measurement. During vigorous spontaneous respiration, the patient with COPD or severe respiratory distress should be instructed to hold his breath at encl-expiration; if this is not possible, transmural pressures must be taken or apnea induced.
Positive end-expiratory pressure of modest amounts (perhaps to as high as 10-12 cm H20) appears to induce clinically unimportant errors in endexpiratory PAOP estimates of LAP.67•68 Temporary
withdrawal of PEEP during wedging would also appear valid. 14•30 During higher levels of PEEP (> 10-12 cm H20) no consistently reliable measurement protocol exists; it is possible that further experience comparing PAOP with LAP or LVEDP in patients with severe acute respiratory failure will confirm one report showing no PAOP to LVEDP discrepancy charing PEEP to as high as 30 cm H20. 79
Left Ventricular Filling
It is widely accepted that the Frank-Starling law applies to the intact human heart; i.e., at any given functional state the force of ventricular contraction is dependent upon its end-diastolic volume or enddiastolic wall tension. For want of a technique for routine ventricular volume determination, investigators and clinicians have relied on ventricular enddiastolic pressure as an index of' end-diastolic volume and tension. Two questions arise: I) how reliable is left ventricular end-diastolic pressure (LVEDP) in assessing left ventricular end-diastolic volume (LVEDV), and 2) how reliable is PA WP in estimating LVEDP.
During diastole the left ventricle fills passively and the pressure developed is exponentially related lo the volume. An elevated LVEDP is commonly taken to signify the presence of LVF: a normal LVEDP is assumed to be evidence against its presence. In fact, apparent left ventricular (LV) function as reflected by LVEDP can change in many ways.80 Among them arc a true change in the LV contractile state, a change in the diastolic properties of the L V, and hypervolemia. 57
•81
•82 Particularly following acute myo
cardial infarction (AMI) or acute hemodynamic inter-
ABBREVIATIONS
AMI = acute myocardial infarction C(a - v)0, = arterial-venous oxygen content difference
COPD = chronic obstructive pulmonary disease CVP = central venous pressure LAP = left atrial pressure
L V = left ventricle L VEDP = left ventricular end-diastolic pressure LVEDV = left ventricular end-diastolic volume
L VF = left ventricular failure L VSWI = left venaricular stroke work index PAEDP = pulmonary arterial end-diastolic pressure
PAOP = pulmonary-artery occlusion pressure PA WP = pulmonary-artery wedge pressure
PCP = pulmonary capillary pressure PEEP = positive end-expira1ory pressure
Pv0 , = mixed venous oxygen tension PWP = pulmonary wedge pressure S-G = Swan-Ganz Sv0 , = mixed venous oxygen saturation

458 NATHAN L. PACE Anr:sthcsi«tlngy V 47, !'.o 5, il:m· 1!177
ventions (vasopressor and vasodilator infusions), impaired ventricular relaxation and decreased diastolic ventricular compliance may account in part for an elevation in LVEDP without any change in L VEDV. "2
·" 3 Under these conditions it may be incorrect to assume that an elevated LVEDP represents an impairment of myocardial contractility.Ht.H3 A systematic study of the relationships of LVEDV, LVEDP. ventricular relaxation and ventricular diastolic compliance in many forms of cardiovascular dysfunction (anesthesia, trauma, sepsis, burns) is not available.
Second, the relationship between PAOP and LVEDP is complex . In subjects who have normal cardiovascular systems, PAOP, LAP and LVEDP arc essentially interchangeable. Following myocardial infarction, atrial contraction makes a greater contribution to left ventricular filling (probably clue to changes in ventricular compliance) and raises LVEDP 1nuch higher than mean PAOP 17·" 4-
86; LVEDPisoften
10 torr or more greater than LAP or PAOP. One study ol' anesthetized patients with coronary-artery disease also showed LVEDP greater than PAOP." 7
PAOP 11m,· reflects the left ventricular diastolic pressure prior to atrial contraction and is a poor estimate ol' left ventricular filling, but still provides reliable information about pulmonary venous hypertension and pulmonary edema. The lower the cardiac output, the more important is atrial contraction for ventricular filling and the less reliable is mean PAOP for estimating L V EDP. 115 During severe respiratory f'ailu re, PAOP has been shown in a few patients both to equal LVEDP 711 and to underestimate LVEDP. 1111
But the relationship of PAOP and LVEDP during cardiopulmonary failure has not been systematically investigated.
A11empts to get a better estimate of LVEDP than that given by PAOP have been madc," 4•80-ot and the pulmonary-artery occlusion "a" wave appears most valid. The wedge pressure trncc is a reflection ol' the lefr at rial phasic events and can show prominent "a" and "v" waves. 1\·lcasurcment of the "a" wave pressure ol' the wedged pressure trace (rather than mean PAOP) seems to correlate very well with LVEDP.112 Unfortunately, the "a" wave is rarely distinctly seen in the wedge trace, and the "a" wave pressure has not been widely used.
Ventricular Function
An early modification of the S-G catheter was a multiple-lumen, thermistor-tipped S-G unit that
permitted thermodilution determination of cardiac output. 24
•93 The principles of measurement are as
follows: If a known quantity of cold solution is introduced into the circulation and adequately mixed, recording of the resulting cooling curve at a downstream site allows calculation of net blood flow. In practice 10 ml ol' 5 per cent dextrose at O C or room temperature arc injected into the superior vcna cava or right atrium via the proximal lumen of the S-G. The thermistor allows recording of the baseline pulmonary-artery blood temperature and the subsequent temperature change. The resulting curve may be analyzed manually by simple planimelric methods or by computer.
Validation studies of the thcrmodihnion technique using S-G catheters show both good reproducibility and good correlation with the dye dilution methods of measuring cardiac output. 24 •114•95 However, large variations in baseline pulmonary-artery temperature related to cardiac and respiratory cycling may occur, especially in mechanically ventilated critically ill patients, which lessens precision and accuracy 94 ·1lf1; such errors may be minimized by repeating the cold i1~jcctions during the same point in the respiratory cyclc.911 Only a modest correlation between thermodilution and Fick oxygen methods has been found in one study. 117
Perhaps this is not too surprising, as patients in the operating room or intensive care unit are rarely in a steady hcmodynamic stale and the thermodilution method is an average over 4-10 heart beats, while the Fick method averages over 2-3 minutes. In addition, there arc other potential errors in both meth()(ls. Ultimately, there is no standard by which to compare accuracy. Each method must be consiclcrecl an estimate, but the lhermodilution methods appear particularly simple and efficicnt. 98
With lhc easy availability of frequent cardiac output determinations in critically ill patients, construction of ventricular function curves has been recommcnded.114
•1111 Left ventricular stroke work indcxt is plotted versus left ventricular filling pressure; filling pressure is altered by such maneuvers as administering fluid challenges, diuretics and vasoprcssors, or by varying mechanical ventilation, PEEP and assisted circulation; Starling curves may then be constructed. Because of the previously mentioned disparity between PAOP and LVEDP, Starling curves so constructed from PAOP must be considered critically. It is easily seen that since trnc left ventricular filling pressure may be 8-10 torr greater than
cardiac output in I/min X (mean arterial pressure in torr - occlusion pressure in torr) t LVSWI (in gram-meters/1112 ) = _________ ...,_ ____ --'------ x 13.6.
heart rme in bemsJmin x body surface area in 1112
At1t•Ml1r,inl••)O: \' ·17, So !",, So,· I !l77 l'Ul.MONARY ARTERIAL MONITORING 459
PAOP in certain patient groups, all points clerivecl using PAOP may be eri·oncously plouccl leftward and upward, thus creating a left-shif"tecl Starling curve and suggesting left ventricular function better rhan in f"acl.
Crexclls 1•t al.911 constructed Starling curves for the left vent ride with volume cfo,llcnges i11 patients following A l\H and found maximum LVSWI at PAOP 14-18 torr: this, then, was considered t.o be the optimal filling pressure for adequate cardiac performance without risk of pulmonary congestion. 1111-rn2
However, since it is well demonstrated that pulmonary edema can develop in association with low colloid oncotic pressure or increased pulmonary capillary permeability at normal PAOP's, 27·2K,in3-rn5
PAOP's of 14-18 torr may not be tolerable for adequate gas exchange in all patients. Whether survival following AM I is enhanced by manipulating PAOP to 14-18 torr is not proven. Others have not found an optimal left ventricular filling pressure following AMl. 11111
Swan and co-workers, using hemodynamic data obtained by S-G catheter, divided patients with AM I into subsets and suggested specific therapies. 107 The therapies arc clepcnclent on continual reassessment of hcmodynamics with pulmonary-artery catheters. Although classificalion of patients within these groups is of prognostic value, little evidence that overall morbidity or mortality may be changed by the suggested manipulations is yet available. 1117
Rapid diagnosis of certain complicatioi1s of AM I and open-heart surgery (ruptured inierventricular septum, acute mitral insufficiency, and cardiac tamponade) 1°K-III and serial hemodynamics during intra-aortic balloon pumping 112·113 have been facilitated by pulmonary-artery monitoring. However, it was recently found that cardiac tamponade is probably better detected by CVP monitoring. 114
Analysis of Mixed Venous Blood
As a simpler method of assessing effective tissue perfusion or oxygenation in seriously ill patients, serial sampling for determination of blood oxygen saturation in the right atrium, right ventricle, or pulmonary artery has been used, since mixed venous blood oxygen saturation is directly proportional to cardiac output when arterial oxygen content and oxygen consumption remain constan1.m-llK Normal mixed venous blood 0 2 saturation is 70- 75 per cent: values less than 60 per cent have been associated with heart failure and values less than 40 per cent with shock. 118 Only true mixed venous blood from the right ventricle or pulmonary artery can be used in seriously ill patients, as right atrial samples are poorly
mixed and may give falsely elevated whole-body \'enous oxygen saturat ions. 115·118·119 Fiberopt ic S-G catheter oximeters have been developed to monitor mixed venous blood oxygen saturation (S,•0 ,) continuously. rn,120-122 Also, serial measurements of mixed venous blood oxygen tension (Pv02 ) have been used to assess circulation a11d oxygen therapy (normal 38-42 torr), 123- 125 and the arterial-venous oxygen content difference [C(a-v)02 ] (normal 3.5-5 vol per cent .) has been used to detect and differentiate co-existent cardiac failure and respiratory failure. 128
Clinical decisions based on C(a-v)02 • P,•02 , and S,•02
must . be made cautiously. It is important to remember that a single C(a-v)0 ,, Sv02 , or P,1
02 is, strictly speaking, uninterpretable without a simultaneous cardiac output determination,' 27 but a very low P,•0 ,
( <20 t.oiT) or s,,02 ( <40 per cent) or a very high C(a-v)02 (>9 vol per cent) by itself docs confirm a very severe derangement of oxygen transport. There is another possible error. As contamination of desaturated mixed venous blood by saturated pulmhnary capillary blood is possible during aspiration through the non-wedged S-G, withdrawal of blood should be slow and abnormally high values suspect. •2K-120
Other Uses
Measurement of PAOP has proved essential to cliscriniinate LVF in tile presence of acute respiratory failure as traditional signs of L VF (tachycardia, engorged jugular veins, hepatomegaly, gallop rhythm) become nonspecific and insensitive. 136•131
The use of S-G catheters in severe acute respiratory failure has also revealed the almost universal presence of pulmonary hypertension and elevated pulmonary vascular resistance. 711 Calculation of right ventricular stroke work index shows a threefold elevation over normal values: but afterload reduction to prevent right heart failure docs not appear jmssible. Pulmonary angiography has been facilitated in critically ill patients by use of an indwelling S-G catheter. 132
Complications
Initial reports of S-G catheter use mentioned frequent minor problems 6
•211
•133; these included: transient
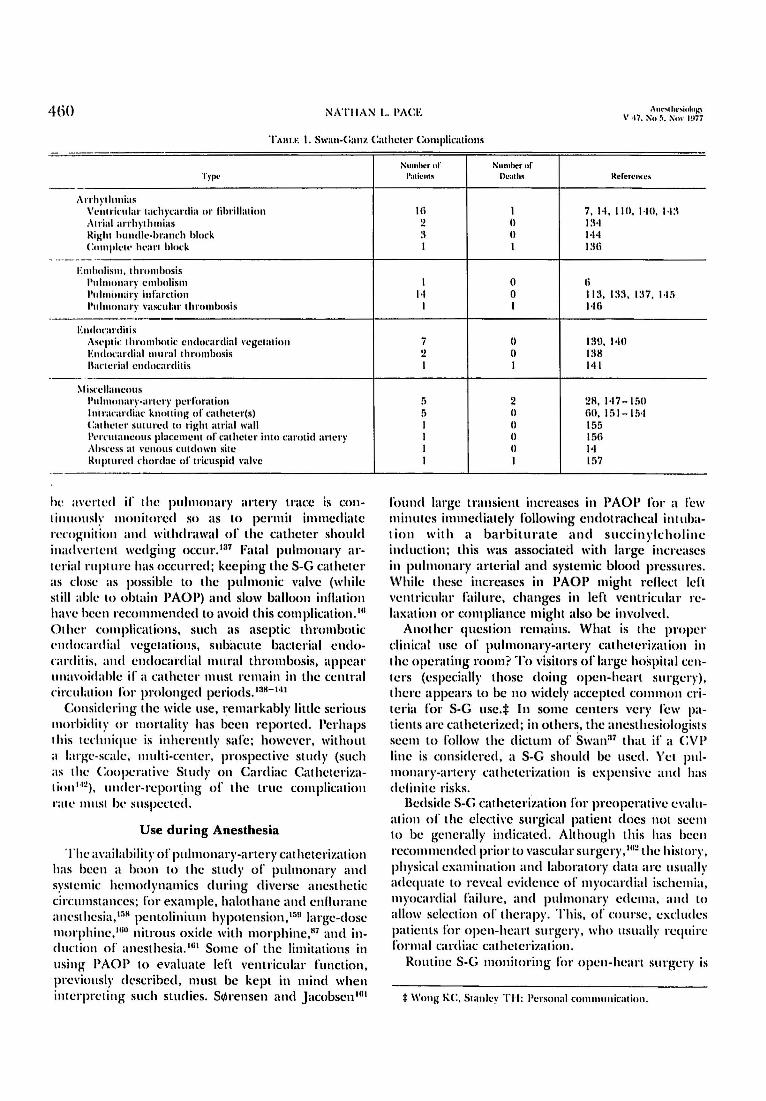
arrhythmias during passage, balloon rupture, catheter thrombosis, catheter coiling in the right ventricle, and local infection at the cutaneous insertion site. More serious complications have also been reported (table I); some of these arc preventable or treatable. Rhythm disturbances may usually be terminated by withdrawal of the catheter, 134,t:15 but deaths have resulted. 136 Pulmonary infarction can probably
460 NATIIAN I.. PACE Am·~• ht·~ioluh~· \' ·17, !'\o !i, :'\n\ · 1Hi7
TAnu: I. Swan-C:;mz Ca1hc1cr Complica1ions
Type
·- --,\rrh1 ·1h111ias
V1'.i11rirnlar 1achycardia Ill' lihrillation :\1rial arrhy1h111ias Rii:111 hundle -hrand1 hlm:k Cn111ple1t• hearl hlock
- - - -- · E111h11lis111, I hromhosis
1'11lm1111an· embolism 1'11lm1111,ir)' infarction l'nlmonary l'ascnlar 1hrn111bosis
.
En,J,,rnrdi1is As1•p1k 1hrn111ho1ic endocardial l'ege1a1ion E111locardial mural 1hromhosis llac1erial cndocarcli1is
--- -~lisrellaneous
l'nln111nary-ar1cry perforntion ln 1rarnrd iac knolling of ca1he1er(s) Ca1he1er s11111recl lo rigl11 airial wall 1'1·1Tn1aneous placemen! of ca1he1cr into carotid artery :\hsrl'SS at 1·cnous cutclown silc Rup111red d10rclae of tricuspicl ,·ah-c
··-~- ·
he averted if the pulmonary artery tmcc is conti1111ously monitored so as to permit immediate nxog-11it ion and withdrawal of the catheter should inad\'ertelll wedging occur. t:17 Fatal pulmonary arterial rnp1urc has occurred; keeping the S-G catheter as close as possible to the pulmonic valve (while still able Lo obtain PAOP) and slow balloon inflation ha\'c been recommended to avoid this complication. 111
Other complications, such as aseptic thrombotic c11cloca n I ial vegetations, sub;1cute bacterial cmlocarcl it is. and cndocardial mural thrombosis, appear unarniclahlc if a catheter must remain in the central l'irc11latio11 for prolonged pcriods. •:iH-i.tt
Considering the wide use, remarkably little serious morbidity or mortality has been reported . Perhaps this 1cd111iquc is i11hcrc111ly safe ; however, without a larg-e-scalc, nHtlti-ccntcr, prnspcctivc study (such as the Cooperative Study on Cardiac Cathclcrizat ion ,..2), 1111cler-rcport.ing of the true complication rate must be suspected.
Use during Anesthesia
The availability of pulmonary-artery cathetcrizatio11 has been a boon to the study of pulmonar) ' and systemic he mod ynamics during diverse anesthetic circumstances ; for example, halothane and enllurane anesthesia , tr.K pentolinium hypmension, 159 large-close morphine,1 1111 nitrous oxide with morphinc,K 7 and induction of anesthesia." 11 Some of the limitations in using PAOP to evaluate left ventricular function, previously described, must be kept in mind when interpreting such studies. S~rensen and Jacobsenlll 1
Numhcl'ol' Number of l'a1ic11t!I llea1h, Rcl'erc11l'l'!i
Iii I 7, 1-1, 110, HO , 1·1:\ 2 (I I :\.I :1 () J.1-1 I I t:lti
I 0 Ii J.I 0 113, 1:1:1. 1:n. 1-1r, I I 146
7 () 139, 140 2 () 138 I I 141
5 2 28 , 147-1:,0 5 () till, 151- 15,f I (I 155 I () 15ti I () 14 I I 157
found large transient increases in PAOP for a few minutes immediately following endotrachcal int ubat ion with a barbiturate and succinylcholine induction; this was associated with large increases in pulmonary arterial and systemic blood pressures . While these increases in PAOP might rellect left ,·e111ricular failure, changes in left ventricular relaxation or compliance might also be involved.
Another question remains. What is the proper clinical use of pulmonary-artery cathetcrization in the operating room? To visitors orlarge hospital centers (especially those doing open-heart surgery), there appears to be no widely accepted common criteria for S-G use.i In some centers very l'cw patienls arc catheterized; in others, the anesthesiologists seem to follow the dictum of' Swan 37 that if a CV P line is considered, a S-G should be used. Yet pulmonary-artery cathetcrization is expensive and has dclinitc risks.
Bedside S-G cathctcrization for preoperative evaluation of the elective surgical patient docs not seem to be generally indicated. Although this has been rccom mended prior to vascular su rgcry, rn2 the history, ph ysical examination and laboratory data arc usually adequate to reveal evidence of' myocardial ischemia, myocardial failure , and p11lmonar}' edema, and to allow selection of therapy. This, of course, excludes patients for open-hcarL surgery , who usually require formal cardiac cathcterizat ion.
Routine S-G monitoring for open-heart surgery 1s
:I: Wong KC, Stanley TJ-1: Personal rnmm1111icatio11.
A1u·Mlwsi1,l1•KY \' •17, ~u !i, !\:o\ ' 1!177
l'UI.MONAlff ARTERIAi. :\IONITORING 461
probably an unnecessary expense, hazard, and inconvenience for 111ost patients, with the exception ol" those with very severely impaired left atrial or lcli ventricular !'unction. Anesthesia may be induced and maintained with arterial and central venous pressure monitoring; after cardiopul111onary bypass, direct LAP is easily and frequently used lo a<Uust lcli heart lilting. It is possible that certain patients who have coronary-artcr)' disease will bcnclit by pharmacologic unloading or I.he left ventricle during hypertensive episodes 111
=1 prior to cardiopulmonary
bypass to alleviate myocardial ischcmia, 1114 and that this will be facilitated by S-G monitoring. This ap 'proach needs validation.
One situation where S-G 111onitoring should be routinely employed has been identiliecl. lnfrarcnal aortic cross-cla111ping during repair of abdominal aortic a11eurys111s or during aortofcmoral bypass surgery in patients with severe coronary artery disease frequently produces severe hemodynamic disturham:cs and myocardial ischemia. 1115•
11111 Observation ol" PAOP and ECG seems necessary to detect and ameliorate these changes.
Early detection or venous air embolism during si11i111,{ intracranial surgery was rcportcd 1117
; however, I real IIICIII of such embolism by withdrawal of air through I he S-G docs not appear superior to use ol" com•c111ional right atrial lincs. 111K Since other sensitive met hods for detecting air e111bolism exist (prccordial Doppler monitoring and end-tidal CO 2 sa111pling), the rout inc use or pulmonarr-artery catheterization for siu ing craniotomies docs not appear warranted.
Certainly, the critically ill patient (in partirnlar, I hose with cardiogenic and septic shock and acute respiratory failure) whose care is dependent 011 pulmonary-artery catheterization will also benefit by its use during emergency surgical procedures. The anesthesiologist should be prepared to initiate S-G cathcterization in these patients (by himself or by others) ii" the need has not been perceived.
Swan-Ganz catheters have been placed during many 01 her types or surgical procedures but except for the operations mentioned above, it is the cardiopul111011ary status or the patient that should determine cathcterization. Overall, pulmonary-artery cathctcrization should never become a m11ti11e technique for most anesthesia care .
Conclusion
Pulmonary arterial monitoring with Swan-Ganz catheters must be considered one or the most important advances in the care of the critically ill. As I have detailed, a more critical attitude should be adopted in evaluating data derived from the
catheter because or the inherent limitations in pulmonary arterial monitoring and unresolved details of cardiovascular dysfunction. Fault' tf,, 111i1•11x, its use should be encouraged in appropriate patient groups.
References
I. l.:11egola M, Rahn 1-1: A sell~g11idi11g ca1he1er for cardiac and pulmonary ar!erial ca1he1erization and occlusion . l'rnc Soc Exp l\iol Med 84 :titi7-lili8, 1!15:l
2. 1'radley RD: piagnos1ic righ1-hear1 catheterizatim1 with miniature catheters in sc\'crcly ill patients. Lancet 2:!M I -!142, l!lli4
:I. Fife WP, Lee BS: Construction and use of sell~guiding right heart ;md pulmonar)' artery catheter. J A1>pl Physiol :!II: 1-18-14!1, l!lli5
·I. Schcinman l\lM, A~lmtt JA, Rapaport E: Clinical uses of a llow-directcd right heart catheter. Arch Intern l\lcd I 24: 1!1-24, l!lli!I
.:i. Arhorclius l\l Jr, Li!ja I\, Wcnnhcrg 1-1\1: N1111-tra11mati1.ing pcrrntanconsright heart catheter. Br Heart J :15:855-857, 1!17:1
li. Swan I-I.JC, Ganz W, Forrester .J, cl al: Cathcterization nf the heart in man with the use of a flow-directed hallrnmtipped catheter. N Engl J l\led 283:447-451. 1!171l
7. Eilertson l)G, McGnugh EC, Rasmussen B, ct al: l'ulmnnar\' artery monitoring in critical!)' ill surgical patients . Am '.I Surg 128:7!11- 7!lli, 1!174
8. Rodman GH Jr, Ci\'ctta.)l\l: Bedside pnlmnmlr)' artery cathcterization. Arch Surg IO!l:B.Jll-841, 1!174
!I. Cil'cttaJl\l, Gabel.JC: Flow-directed pulmonary artery rntheterizatinn in surgical patients: Indications and modilication~ of tcchnic . Ann Surg 176:753-756, 1!172
Ill. Mmulel S, l\arash I': The proximal basilic vein: A new approach for introduction ofa llow-gniilcd catheter into the pulmouary art er)' . .I Thorne Cardiol'asc Smg 71 ::171i-:177. 1!17ti
11. Bennett KR, Cibulski AA, l\lul\'ihill J, ct al: l'uhnonaryartcry pressure in myocardial iufarctiou. N Engl J :\led 28·1: 11142, 1!171
12. Cil'ctta J M: Pulmonary-artery-pressure determination: electronic: snpcrinr to m;momcfric. N Engl J Med 28:1: 1145-11-l(i, 1971
13. Rcctra EH. Lamb FD: Flow-directed balloon-tipped t:athctcrizatiun under clectrocardiographic monitoring. N Engl J :\led 285:57!1, I !171
14. Archer G, Cobb I.A: Long term pulmon;1ry artery pressure monitoring in the management of the criticalll' ill. Aun Surg 18():747-752, 1!174 '
15. l\olognini \I: The Swan-Ganz pulmonary artery catheter: Implications for nursing. 1-leart Lung 3:!171i-!18 I, I !17-1
Iii. Swan I-I.JC, Gam . W: Guidelines for use of balloon-tip11e1l catheter. Am J Canliol 34: 119-120, 1!174
17. Swan I-I.JC, Ganz W: Use of balloon flotation catheters in critically ill patients. Surg Clin North Am 55:5() I -:121l, 1!175
IH. Gernert CF, Schwart1. S: l'ulmonary artery catheteri1 .atio11. Am.J Nurs 7:l: 1182-1185, 1!173
l!I. Cole JS, l\lartin WE, Cheung l'W, cl al: Clinical studies with a solid state lihcrnptic oximetcr. Am .J Cardin( 2!1::183-:~HH, I !172
21l. Wilson JE Ill, 1'y11um LJ: An imprm ·ed pulmonary a11giographic tcchni11ne using a balloon-tipped catheter. Am Rev RcspirDis 114:1137-1144, 1976
462 NATHAN L. l'AC:E Am•!!illlt'!iic1l,1~y V •17. So 5, NuY 1Hi7
2 I. l\lack IFS: Floating a c.nhctcr into the puhnonary artery in transposition of the grcal arlerics. Am 1-lcal'I .I 8":7(il-71i:1, 1!172
22. :'llcistcr SG. Banka \IS, l-lelfan1 RI-I: Translcmoral pacing wilh halloou-1ippcd rn1he1crs. JAMA 225:712-714, I !17:1
2:1. :\leis1er SC. Banka VS. C:hadda KD, cl al: A halloon lipped ca1hcll 0 r for oht;1ining 1-lis h111111lc clcctrograms without lhmrosropy. Cin :11la1ion ·1!1:·12-·lli, I !17-1
2·1. Forreslcr JS, Ganz W, Diamond G, ct al: Thcrmmlihuion cardiac outpul dc1enniua1ion wilh a single llow-dirccted rnlhctcr. Am I lcart .J !l:l::IOli-:111, I !172
25. C:hattl'l:jccc K, Swan I-I.JC:. Ganz \\', cl ;11: Use of a lmllooulippcd llotatiou elcrtnulc catheter for cardiac monitmiug. Am J C:ariliol 3(i:5li-li I. I !175
2li. Cerra F, Milch R, l.ajos TZ: Pulmonary aricry ca1hctcriza· lion in critirallr ill surgical pa1ien1s. Ann S11rg 177:37-:1!), 1!17:1
27. Fishhciu MC, S1a1e D, 1-lirosc F, cl al: Capillary leak syudromc wi1h massive in1cstinal cdctm, alicr appc111lcc10111y. Am J Surg 127:7,f0-7"4. 1974
28. German .JC, Allyu PA. Bar1lc11 RI-I: Pulmonary artery pressure monitoring iu acute hum management. Arch Surg I Oli: 788- 7!11, I !17:1
2!1. Jaml'S PM Jr. Bevis A, Myers RT: Expcricuces with central vcnm1s and pulmon;lt"y artery pressure in a series of 3500 11.11icn1s. South l\le,I .J li!i: 12!1!1-t:107, 1!172
:111. Sharl'l'kin J B, l\larAr1l111r J l): l'ulmonarr arlcrial pressure as a guide to 1he ht•modynamk statns of surgical palicnls. Arch Surg IO:,:li!l!l-7lM, 1!172
:11. Toussaint C:Pl\l, Burgess.fl -I. 1-lampsou l.G: Central vemms pressure aml pulmonary wedge pressure in crilical surgic;tl illness. Arch Surg IO!l:2ti:,-2ti!I, 1!17-1
:12. Ruhenlire 1\1, EvangclistaJ. W;!jszczuk W.J, cl al: lmplica1ion of a persis1cn1 lefl superior \'cna cava in lransvenous pacemaker therapy and cardiac hemodynamic monitoring. Chesl (i:,: 145-147. 1!17-1
3:1. Barhcrn-Marcial 1\1, Verginelli G, Arie S. cl al: lntrapulmon.U"y balloon for temporary relief of pulmonary hyper· tension. J Thorac Cardim•asc Surg li!l:!142-!146, I !175
:H. Rosenbaum RW. 1-laycs 1\1 F Jr. l\lorcllo nc, cl al: The imporiance of pulmonary ar1ci·y pressure monitoring. Surg Gy11ccol Obstcl 13li:2lil-2ti4, 1!173
:15. l.aks Ml\l, Garner D, Bcazell .J. cl al: A new method for iuternal calibraliou of left ventricular cineaugiography. Am J Physiol 232:IH3-t-1-M3li, 1!177
:Hi. Zapol \\'l\l, Snider l\lT, Schneider RC: Ex1racorporeal memhrauc oxygeuatiou for acme respira1ory failure. Ast:sT11t:s1<11.0tlY -lli:272-285, I !177
:17. Swau I-I.JC: Cen1ral veuous pressure monitori11g is au 11111-motkd procedure of limited practical value, Controversy in lntt•rnal l\lcdiciue II. Edited by lugcllingcr I-], Eberl RV, Fiulaml 1\1, cl al. l'hilailelphia, W. B. Saunders, 1\174. pp 185-l!l:1
:111. Swau l·IJC: Balloo11 llotaliou cathclcrs: Their use in hcmodyuamic 111011itoring in clinical prat:ticc . .)Al\lA 2:13:8li5-81i7, 1!175
:l!I. Swan HJC: The role of hcmmlynamic moni1oring in the mauagcmcm of the critically ill. Cril Care l\lcd :1:lt1-8!1, 1!175
40. Gilbcr1son AA: Pulmouary artery ca1hc1criza1iou aud wc,lgc pressure mcas11rcmcn1 iu 1hc general in1ensivc therapy 11ni1. llr J Anaesth 46:!17-111-1, l!l74
·11. Del Guercio LRM, Cohn .JD: l\louitoring : Methods aml significance. Surg Clin North Am 5li:!177-9!l-l, I !lili
·12. Buchbinder N, Ganz W: 1-lemodynamic monitoring: lnvasi\'c lcchniqucs. ANESTHESIOLOGY 45: I 4li- I 55, I !17li
•1:1. Rapaport E. llcxler l.: 1'11lmon;1ry "capillary" 1>rcssurc. Mt•th Mccl Res 7:85-!1:-\, 1!158
<1-1. l\rcws1n 1-1, l\kllror MB: l\lood gas 1cnsions and /'1-1 of pulmonary "wedge·· samples in paiicnts wi1h heart disease. .J Appl Physiol ,14 :4 I :1-4 lli. 1!17:1
•15. Sdtarf SM. Caldini I'. Ingram RI-I .Jr: Cardiovascular cffi.·c1s of innc;1sing airway pressure in the dog. Am .I l'hysiol 2:{2:1135-tf.l:I, 1!177
"(i. Shiu B. McAslau TC, Ayella R.J: Problems with measurement using 1hc Swan-Ganz ca1hc1cr. ANt:ST11t:s1<>1.oc;y 43:47·1-47li. 1!175
47. l'\lcister SG. Engel TR, Fisdtcr I-IA. ct al: 1'01c11tial ar1ifac1 in measurement ol'lcli \·cn1ric11lar filling pressure with llowdircctccl rn1hc1crs. C;11hc1 Canliovasc Diagn 2: I 7r>-17!1, I !17li
48. Shin II, Ayclla RJ, l\kAslan TC: Pitfalls of Swan-Ganz ca1hc1criza1ion. Cril Care Med 5:125-127, 1!177
4!1. Balson GA. Chandrasekhar KP, l'ay;1s \', cl al: Mcasurcmeut of pulmonan wedge pressure hy the flow-directed SwanC:anz ca1hc1cr. Cardim·asc Res li:748- 752, 1!172
50. Fi1zpa1rick C:F. Hampson LG. Burgess JI-I: Bedside dctcrmina1im1 of lcli atrial pressure. Can l\lcd Assoc .J lllli: I 2!l3- I 2!l8, I !172
:,I. 1-lmnphrcy CB, Oury JI -I. Virgilio RW. cl al: An analysis of dirccl amt indirect mcasuremellls of left atrial filling pressure . .J Thor;1c Canliovasc Surg 71 :li43-lH7. I !17fi
52. Jenkins BS, Bradley RD, Bran1hwai1c l\lA: Evaluation of puhnonary ar1crial end-diastolic pressure as ;m indirecl cslimatc of lcli atrial mcau pressure. Circulation 42:75-78, 1!170
53. Lappas n. I.ell WA, Gabel JC, ct al: Indirect mcas11rcme11t orlcli-at rial pressure in surgical pa1icn1s-Pulmonarycapillary wedge and pulmonar)·-arlery diastolic pressures rnmpared with lcl"t-atrial pressure. ANt:sTm:s101.oG\" 38: 3!14-3!17, 1!173
54. I lcrhcrl WI-I: l.imi1a1ions of pulmonary artery cnd-di;1s101ic pressure as the rcllec1im1 of lcli ventricular end-diastolic pressure . N\' Slate .J Med 72:22!1-232. 1!172
55. Cohn JN. Tristani FE. Khatri 11\1: S1udics in clinical shock and hnm1cnsion. VI. Relationship between lcli and riglu ventricular function. J Clin lnvesl 48:2008-2018, l!IH!I
!iii. Weil 1\11·1. Shubin 1-1. Rosoff L: Fluid repletion in circulalory shock: Cemral \'Cnous pressure and other prnctical guides. JAMA l\l2:Hli8-H74 , Hlli5
57. Foncslcr .JS, Diamond G, l\kl-hagh 'I], Cl al: Filling pressures in 1hc riglll and left sides of 1hc heart in acute myocanlial infarction. A reappraisal of cc111ral-vcnous-prcssurc monitoring. N Engl .I l\lccl 285: I !10-1 !12, I !171
58. Ch ·c11a JM. Gabel JC, Laver MB: Disparate vcn1ricular func1iou in surgical patients. Surg Forum 22: I 3li- 13!1, 1!171
59 . .James PM.Jr. Myers RT: Cc111ral \•cnous pressure monitoring: Misin1crprc1a1ions, abuses, indications and a new tcdmk. Ann Surg 175:fi!l:1-701, 1972
lill. De l.a11rcn1is DA. 1-laycs M, Ma1s11ms10 T, cl al: Docs ccn1ral ,·c11011s pressure arcurately reflect hcmodynamic aud lluid volume pallt·rns in the critiral surgical pa1icn1? Am.) Surg 12lHl5-·118, l!ln
ti I.
(.,, '-·
li:I.
Bell 1-1, Stubbs D, Pugh D: Rcliahili1y of central venous pressure as an indirntor of lefl a1rial pressure. A suuly iu pa1icn1s wi1h mi1ral valve disease. Chcsl 5!1:lli!l-173, l!l71
Sarin CL, Yahl\· E. Clemen! A.J. t't al: The necessity for mcasurcmclll of leli atrial prt·ssurc alicr rnnliac surgery . Thorax 25: 185-18!1. I !170
Back Sl\l, Makabali GG. Bryan-Brown CW. cl al: Plasma expansion in surgical palicnts with high cenlral \·cnous
A11eMheii11lnK)' V 47, ~o 5, ~o, · IU77 PUU\IONARY ARTERIAL :\IONITORING 463
pressure (CVI'); the relationship of blood rnlumc to hcma10-cri1, CVP, pulmonary wedge pressure and cardiorcspirawry changes. Surgery 78:304-315, 1975
(i4. Walston A II, Kendall ME: Comparison of pulmonary wedge and left atrial pressure in man. Am Heart J 81i: 15!1-lli4, 1!17!{
ti5. Smith HC, Butler J: Pulmonary ,·cnous waterfall and pcri\'cnous pressure in the lh·ing clog. J Appl Ph)·siol 38: 304-!108, I !!75
lili. Lopez-Muniz R, Stephens NL, Brombcrgcr-Barnca B, ct al: Critical closure of pulmonary \'csscls analyzed in terms of' Starling resistor model. J Appl Physiol 24:ti25-635, 1!168
li7. l.m.111;111 J, Powers SR Jr, Older T, ct al: Correlation of pulmonary wedge and left atrial pressures. A study in the patient rccci\'ing posili\'c end expiratory pressure ventilation. Arch Surg I O!l:270-277, 1974
68. Hobclmann CF Jr, Smith DE, Virgilio RW, ct al: Left atrial and pulmonary artery wedge pressure difference with positi\'c end-expiratory pressure. Surg Fornm 25:232-234, 1!!74
li9. IknumofJL, Saiclman LJ, Arkin DB, cl al: Where pulmonary artery catheters go: lntrathoracic distribution. ANt:sTm:stoLOG\' 4(i:331i-338, 1977
70. Q,•isl J. Ponloppidan H, Wilson RS, ct al: Hcmoclynamic responses lo mechanical \'Clllilation with PEEP: The effect of hypcr\'olcmia. ANt:STIIESIOI.OG\' 42:45-55, 1975
71. Downs JU: A 1cchni11uc for direct measurement of i111raplcnral pressure. Cril Care Med 4:207-2 IO, 1976
72. Craig t>U, in discussion, Downs JU, Douglas l\lE, Sanlclippo l'M, ct al: Vcntilatory pallcrn, intraplcural pressure and canliac output. Anacslh Analg (Cleve) 51i:88-91i, 1!!77
73. Agosloni E: l\lcchanics of' the pleural space. Physiol Re\' 52: 57-128. 1!172
74. Hcrlcs F: The pulmonary artery wedge pressure. lls origin and value in assessing pulmomtr)' hacmoclynamics in emphysema. Cor Vasa 8: Iii 1- llili, l!llili
75. Lockhart A, Tzarc\'a 1\1, Nader F, cl al: Elevated pulmonary artery wedge pressure al rest .t11<l cl uring exercise in chronic bronchitis: Fact or fanq. Clin Sci 37:f>0!{-517, Hl6!l
76. Rao BS, Cohn KE, Ehlriclgc FL, cl al: Lcli ventricular failure secondary to chronic puhnonar)' disease. Am J Med 45:22!)-24 I, l!l(i8
77. Bahler RC: Assessment oflcli \'cntricular function in chronic ubstrncti\'c pulmonary disease. Chest 68: 132-133, 1975
78. Rice DL, Awe RJ, Gaasch WH, cl al: Wedge pressure mcasurcmclll in obstructive puhnonary disease. Chest (iii: li28-li32, I !l74
7!1. Zapol WM, Snider MT: Pulmonary hypertension in sc\'crc acute respiratory failure. N Engl J l\lccl 2!1(i:471i-480, Hl77
80. Gorlin R: Current concepts in cardiology: Practical cardiac hcmmlynamics . N Engl J Med 2!lli:203-205, 1977
81. Braunwalcl E, Ross J Jr: The \'cntricular end-diastolic pressure. Appraisal of' its value in the recognition of ,·c111ricular failure in man. Am J Med 34: 147-150, 1!)63
82. Grossman W, Mclaurin LP: Diastolic properties of' the left \'Clllridc. Ann llllcrn Med 84:316-326, 1976
83. Alderman EL, Glantz SA: Acute hcmodynamic intcn ·e111ions shift the diastolic pressure-\'olumc cur\'c in man. Circulation 54:662-671, 1976
84. Rahimtoola SH: Left \'entricular end-diastolic and filling pressures in assessment of \'entricular function. Chest 63:858-860, 1973
85. Rahimtoola SH, Ehsani A, Si11110 MZ, et al: Left atrial transport function in myocardial infarction: Importance of its booster pump function. Am J Med 59:686-694, 1975
86. Rahimtoola SH, Loeb HS, Ehsani A, et al: Relationship of
puhnonarr artcrr Ill lcli \'cntricular diastolic pressures in acute myocardial infarction. Circulation 41i:283-290, I !l72
87. Lappas DG, Buckley MJ, La\'cr :\IB, cl al: Left ,·cntricular performance and puhnonarr circulation following addition of' nitrous oxide lO morphine during coronary-artery surgery. Ast:STIIESIOI.OG\' 43:li 1-(i9, 1975
88. Eberhart RC, Lamy M, Dietrich HP, cl al: Hemmlynamk aspects of' prolonged cxtracorporcal oxrgcnation. Trans Am Soc Artif Intern Organs 20:4!ll-4!l7, l!li4
8!l. Forsberg SA: Relations between pressure in pulmonarr arterr, lcli atrium and leli ,·enlriclc with special reference to c\'ents at encl-diastole. Br Heart J 33:4!H-4!l!l, l!l7 I
!lO. Schcinman l\l, Evans GT, Weiss A, ct al: Relationship between pulmonary ancry encl-diastolic pressure and lcli ,·cntricular filling pressure in patients in shock. Circulation 47:317-324, 1!!73
!JI. Falicm· RE, Rcsncko\' L: Relationship of' the pulmonar)' artery cncl-cliaslolic pressure lo the left \'entricular enddiastolic ;uul mean lilling pressures in patients with and without lcli ,·cntricular clysf'unclion. Circulation 42:li5-7 !{, I !170
92. Fisher ~IL, DcFclicc CE, Parisi AF: Assessing lcli ,·cntrirnlar pressure with llow-clircctccl (Swan-Ganz) catheters: l>clcclion of' snclclcn changes in patients with lcli ,·cnlricular dysfunction. Chest li8:542-547, 1!175
!)3. Ganz W, Donoso R, Marcus HS, cl al: A new 1crhni11uc for mcasurcmcnl of canliac output by 1hcrmmlih11ion in man. Am J Canliol 27:3!l2-3!11i, I !!71
!14. Weisel RD, Berger RL, Hcchtman HB: Measurement of cardiac ontpul by thermmlilution. N Engl J l\lcd 2!12: (i82-li84, 1!)75
!15. Weisel RI>, Vito L, Dennis RC, cl al: Clinical applications of' thcnnoclilntion cardiac ntllptll dc1cr111ina1ions. Am J Snrg 12!!:+l!l-454, I !!75
!l(i. Woods M, Scull RN, Harken AH: Practical considerations for the use of a pnlmonary artery thermistor catheter. Surgery 7!1:4ti!l-475, 1!171i
!J7. Hmlgcs M, Downs Jl\, l\li1chell LA: Thermmlihniun and Fick cardiac index dc1er111ina1ions following ranliac surgery. Cril Care Med !1:182-184, 1!175
!18. Weil l\l 1·1: l\lcasurcmclll of cardiac out put. Crit Care :\!eel 5: 117-11!1, 1!)77
99. Crcxclls C, Cha11c1:jcc K, Forrester JS, cl al: Optim.il lc\'el of filling pressure in the lcli side of the heart in acute myocardial infarction. N Engl J l\lcd 28!1: I 21i:1-I 21i(i, I !17:{
IOO. Uiclcllc TL, Khanua PK, Yu PN, cl al: Lung water in patients with acute myocardial infarction. Cirrnlation 4!1: 115-123, 1!174
I 01. l\lcl-lugh 'I], Forrester JS, Adler L, ct al: Pulmouary \'ascular congestion in acute myocanlial infarction : Hemodynamic and radiologic correlations. Ann Intern l\lccl 71i: 2!l-33, I !!72
102. Biddle TL, Yu PN, Hodges M, cl al: Hypoxcmia aud hmg water in acute myocardial infarction. Am Hearl J !l2: 692-699, 1976
103. Robin ED, Carey LC, Grcn\'ik A, ct al: Capillarr leak syndrome with pulmonary edema. Arch llllcrn Med 130: 66-71, 1972
104. Stein L, Bcraud JJ, Morissclle l\l, ct al: Pulmonary edema during \'olumc infusion. Circulatiou 52:483-48!1, 1975
105. Stein L, Bcraud JJ, Ca\'anillcs J, cl al: Pulmonary cdcum during fluid iufusion in the absence of heart failure . JAl\lA 229:65-68, 1974
106. Enrico JF, Reynacrt :\I, Grimbert F, ct al: Hacmodrriamic response to slow plasma \'olume expansion in uncompli-
464 NATHAN L. PACE A11t'\llll'\it1lt1~y V ·17, Su 5, ~o\· l!li7
rated myocardial infarction. Eur J I111ensive C.:are Med I: 145-151, 1975
107. Foncstcr JS, Diamond G, Clmttctjcc K, ct al: Medical therapy of acute myocardial infarction by application of hcmrnl)'namic subsets. N EnglJ Med 295: I 351i- I 362, I 4lM-141 ,1, 1!171i
ll18. Foncstcr JS, Diamond GA, Swan HJC.:: Bedside diagnosis of latent cardiac complications in acutely ill patients. JAMA 222:5!!-ll:I, 1972
lll\1. Meister SG, 1-lelfant RI-I: Rapid bedside differentiation of ruptured i111crvcntricular septum from acute mitral insuflidcncy. N Engl.) Med 287:1024-1025, 1972
I Ill. Moncl IIG, l-lunt D, Sloman G: Haemodynamic monitoring in the rnronary care unit using the Swan-Ganz right heart catheter. Br l-lcart .J 35:635-642, 1973
111. Weeks KR, C.:hattctjcc K, Block S, et al: Bedside hcmmlynamic monitoring: Its \•aluc in the diagnosis of tamponadc complicating cardiac surgcr)', J Thorac C.:anliovasc Surg i I: 250-252, 1976
112. Dilley RB, Ross .J Jr, Bernstein EF: Serial hemmlynamics during i111ra-aortic balloon counter pulsation for cardiogcnic shock. C.:irculation 47 and 48 (suppl lll):99-lll4, 1973
11,{. lhmkman WB, Leinbach RC.:, Buckley MJ, et al: Clinical and hcmodynamic results of intraaortic balloon pumping and surgery for cardiogcnic shock. Circulation 46:465-477, 1972
I H. Fidel J. Shiroff RA, Zclis RF, ct al: Limitations in the use or I he pulmonary capillary wedge pressure: Cardiac tamponaclc. Chest 70:451-453, 1976
11!",. l.l'l' .J, Wright F, Barber R, ct al: Central venous oxygen saturation in shock. A study in man. ANESTHt:SIOLllG\' ,11i: ·172-•178, 1!172
11 li. Sd1cinman MM, Brown MA, Rapaport E: Critical assessment of use of central venous oxygen saturation as a minor or mixed venous oxygen in severely ill cardiac patients. Circulation ·IO: lli5-172, 1969
117. Ashley WW, Bhaduri U, Pietras R.J, ct al: Pulmonary arterial oxygen saturation during treadmill exercise. A discriminative index of functional dass. Am Heart.) 90:463-41i7, 1975
I 18. Goldman RI-I, Kluglmupt M, MetcalfT, ct al: Measurement or ccmral venous oxygen saturation in patients with myornrclial infarction. Circulation 38:!141-946, I 91i8.
I l!J. Horovitz JI-I, C.:arrirn CJ, Shires GT: Venous sampling sites for pulmonary shunt determinations in the injured paticlll. .I Trauma I l:!Jl l-914, 1971
120. Martin WE. Cheung PW, Johnson CC, cl al: Co111inuous monitoring of mixed venous oxygen saturation in man. Ancsth Analg (Clc\•c) 52:784- 793, 1973
121. Krauss XI-I, Vcrclouw PD, l-lugcnholtz PG, ct al: On-line monitoring of mixed venous oxygen saturntion :lficr carcliothoradc surgery. Thorax 30:636-643, 1975
122. Trcmolicrcs F, Lecompte F, Sinct M, ct al: Ill vivo mcasurcmcuts oroxyhacmoglobin saturation by a liberoptic catheter. The effects ol'variations in pH and hacmatocrit. EurJ llllensivc Care Med 2:177-180, 1976
123. ~lithocfcr JC, Holford FD, Keighley JFH: The effect of oxygen admiuistration on mixed venous oxygenation in chronic obstructive pulmonary disease. Chest 66: 122-132, 1974
124. Stanley TH, Iscrn-Amaral J: Periodic analysis of mixed vcuous oxygen tcusion to monitor the adequacy of perfusion during and afrer cardiopulmonary bypass. Can Anaesth Soc.J 21:454-460, 1974
125. Block A.J, Burrows B, Kanner RE, et al: Oxygen administration in the home. Am Rev Rcspir Dis 115:897-899, 1977
126. Stevens PM: Assessment or acute respiratory failure: Cardiac versus pulmonary causes. Chest li7: 1-2, l!li!i
127. Zierlcr KL: Theory of the use or artcrim·cnous rnuccntration differences for measuring metabolism in steady and non-steady states. J Clin Invest 40:2111-2125, l!lli I
128. Shapiro HM, Smith G, Pribble Al-I, ct al: Errors in sampling pulmonary arterial blood with a Swan-Gan,. catheter. ANESTHESIOLOGY 40:2!) ( -295, 1974
129. Suter PM, Lindauer Jl\l, Fairley I-IB, ct al: Errors in data derived from pulmonary artery blood gas values. Crit Can• Med 3:175-181, 1!175
130. Civetta JM, Gabel JC: "Pscudocanliogcnic" pulmonary edema. J Trauma 15:143-149, 1975
131. Unger KM, Shibel EM, Moser KM: Dctcclion of lcl'I ventricular failure in patients with adult respiratory distress syndrome. Chest 67:8-13, 1975
132. Alsbrook EH, Comer PB, Gibson RL, cl al: Pulmonary angiography via an indwelling fimr-channcl Swan-Ganz catheter. Crit Care Med 4:320-322, l!lili
133. Scott ML, Webre DR, Arens .JF, ct al: Clinical application of a flow-directed balloon-tipped cardiac catheter. Am Surg 38:690-696, 1972
134. Geha DG, Davis NJ, Lappas DG: Persistent atrial arrhythmias associated with placement or a Swan-Ganz cat hctcr. ANESTHESIOLOGY 39:651-653, I 973
135. Voukydis PC, Cohen SI: Cathctcr-imlucccl anhythmias. Am Heart J 88:588-592, I 974
131i. Abernathy WS: Complete heart block caused hy the SwanGanz catheter. Chest 65:349, I !174
137. Foote GA, Schabel SI, Hodges M: Pulmonary complications of the flow-directed balloon-tipped catheter. N Engl J ~led 290:927-931, 1974
138. Goodman DJ, Rider AK, Billingham ME, cl al: Thrombocmbolic complications with the indwelling balloon-tipped pulmonary arterial catheter. N Engl .J Med 2!11 :777, 1!174
139. Greene .JF Jr, Cummings KC: Aseptic thrombotic c111locanlial vegetations. A complication of indwelling pulmonary artery catheters. JAMA 225: 1525-152li, l!l7:I
140. Pace NL, Horton W: lnclwclling pulmonary artery catheters: Their relationship to aseptic thrombotic cmlocanlial vegetations. JAMA 233:893-894, 1!175
141. Greene JF Jr, Fitzwater JE, Clemmer Tl': Septic t•ndocarditis and indwelling pulmonary artery catheters. JAMA 233:891-892, 1975
142. Cooperative Study on Cardiac Cathctcrization. Circulation ,Ii (suppl lll):1-113, 1968
143. Cairns JA, Holder D: Vc111ricular librilla1ion clue lo passage of a Swan-Ganz catheter. Am .J Carcliol ,15:58!1, I !li5
144. Luck JC, Engel TR: Transient right bundle branch block with "Swan-Ganz" cathctcrization. Am I-Icar1.J !12:2li:l-21H, 1976
145. Colvin MP, Savcgc TM, Lewis C.:T: Pulmonary damagc from a Swan-Ganz catheter. Br J Anacsth 4 7: 11 Oi -1 I O!l, I !l7 5
146. Yorra FH, Oblath R, Jaffe I-I, ct al: ~lassi\'c thrombosis associated with use of the Swan-Ganz catheter. Chest li5: 682-684, 1974
147. Chun GM, Ellestad l\lI-1: Perforation of the pulmonary artery by a Swan-Ganz catheter. N Engl J Med 28·1: I(),( I -1042, 1971
148. Lapin ES, Murray JA: l-lcmoptysis with flow-directed cardiac cathetcrization. JAMA 220: 1246, 1972
149. Golden MS, PindcrT.Jr, Anderson WT, ct al: Fatal pulmonary hemorrhage complicating use of a llow-clircctcd balloontipped catheter in a patient receiving anticoagulant therapy. AmJ Cardiol 32:865-867, 1973
AIH!slhcsic,loK)' V ·17, No !i, Nu\' 1977 l'ULi\lONARY ARTERIAL MONITORING 465
150. Page DW, Tcrcs D, Hartshorn JW: Fatal hemorrhage from Swan-Ganz catheter. N Engl J Med 2!11 :2ti0, I !174
151. Lipp 1-1, O'Donughuc K, Rcsncko,· L: lnlnu:anliac knolling of a flow-directed halluun catheter. N Engl J Med 284: 220, 1971
152. Swaroup S: Knolling of two central venous monitoring catheters. Am J Med 53:386-388, 1!172
15,1. Daum S, Sdmpira M: lntracanliac knot li.mnation in a Swan-Ganz catheter. Ancsth Analg (Cleve) 52:862-863, 1!17,1
154. Mond 1-IG, Clark DW, Ncshill SJ, ct al: A technique for unknolling an intracardiac flow-directed balloon catheter. Chest ll7:731-732, 1!175
155. Block PC: Snaring of a Swan-Ganz catheter. J Thorne Cardiovasc Surg 71 :!117-!ll 9, 1976
15ti. McNabb TG, Green LH, Parker FL: A potentially serious complication with Swan-Ganz catheter placement by the percutaneous internal jugular route. Br J Anacsth 4 7:895-897, 1!175
157. Smith WR, Glauser FL.Jemison P: Ruptured chordae of the tricuspid valve: The consequence of flow-directed SwanGanz cathctcrization. Chest 70:790-7!12, 1 !17ti
158. Filncr BE, Karlincr JS: Alterations of normal left ventricular performance b)' general anesthesia. ANESTHESIOLOGY 45: (ii 0-(i2 J, H17ti
l!'i!I. Fahmy N R, Selwyn AS, Patel D, ct al: Pulmonary vasomotor lone during general anesthesia and deliberate hyputcnsiun in man. ANESTtu:SIOLOGY 45:3-13, 197tl
160. Lappas DG, Geha D, FischerJ E: Filling pressures of the heart and pulmonary circulation of the patient with coronary artery disease alter large inu·,wcnous doses of morphine. ANESTHESIOLOGY 42:)53-)59, 1975
161. St,\rcnsun MB, Jacobsen E: Pulmonary hcmodynamics during induction of anesthesia. ANESTHESIOLOGY 4ti:24tl-25 J, 1977
lll2. St,\rcnscn MB: Pulmonary artery pressure measurements in surgical patients. Scand J Thorne Cardiuvasc Surg 9:2ti4-270, 1975
Hi3. Kaplan JA, Dunbar RW, Jones EL: Nitroglycerin infusion during coronary-artery surgery. ANESTHESIOLOGY 45: 14-21, 1976
Jti4. Hillis LD, Braunwuld E: Myocardial ischcmia. N Engl J Med 296:971-978, 1034-1041, 1093-1096, I !177
lll5. Attia RR, Murphy JD, Snider 1\1, ct al: Myocardial ischcmia due tu infrarcnal aortic cross-damping during aortic surgery in patients with severe coronary artery disease. Circulation 53:961-965, Hl76
lti6. Carroll RM, Laravuso RB, Schauhlc J F: Lcl'l ventricular function during aortic surgery. Arch Surg 111 :740-74,1, 1976
167. Munson ES, Paul WL, Perry JC, ct al: Early detection of venous air embolism using a Swan-Ganz catheter. ANt:sTHESIOLOGY 42:223-226, ) 975
168. Sink JD, Comer PB, James PM, et al: Evaluation of catheter placement in the treatment of venous air cmholism. Ann Surg 183:58-61, 1976
Obstetric Anesthesia
CLOSING VOLUME AND PREGNANCY New pulmonary function tests (e.g., flow-volume loops and closing volume), as well as standard pulmonary function tests, were performed on 19 healthy pregnant patients in the third trimester and after delivery. It was found that the flow characteristics manifested in the flow-volume loops and the closing volume remained unaltered during pregnancy. With regard to the standard pulmonary function tests, no statistically significant change was found except for a decrease in the expiratory reserve volume and in the functional residual capacity dming pregnancy. (/Jaldwiu GR, aud othe,:~: Nt'll' luug Ji111ctio11s aud prt'g11a11cy, Am J Obstl'I Gy11t'l'11! l2i:235-239, /9i7.)
ROLL-OVER TEST The supine pressor test was performed on 207 nulliparous young women between the twenty-eight and thirty-second weeks of gestation. The supine pressor test predicted pregnancy-induced hypertension in 78 per cent of those women in whom the condition subsequently developed. Ninety-six per cent of the women who failed to demonstrate a rise in diastolic pressure on position change remained normotensive throughout the remainder of the pregnancy. (Plwla11 JP, aucl otlwrs: ls the supine pressor It's/ ,111 mlequa/1' llll'tllls of' predicting acute hyper/1!11sio11 in pregnancy? A III J Ohs/I'/ Gy,wcol /28:173-176, 1977.)




















