
ARIC Manual 3 - NCBI
241
- -- ATHEROSCLEROSIS RBSK IN COMMUNITIES STUDY Manual 3 Surveillance Component Procedures The National Heart, Lung, and Blood Institute of the National Institutes of Health
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ARIC Manual 3 - NCBI
- --
ATHEROSCLEROSIS RBSK IN COMMUNITIES STUDY
Manual 3
Surveillance Component Procedures
The National Heart, Lung, and Blood Institute of the National Institutes of Health

ARIC Protocol
Manual 3
Surveillance component Procedures
. For copies, please contact:
ARIC Coordinating Center Department of Biostatistics
CB# 8030, Suite 203, NCNB Plaza The University of North Carolina
Chapel Hill, NC 27514
Version 2.0: February, 1991
ARIC PROTOCOL 3.Surveillance Component Procedures VERSION 2.0, 2/91
i
FOREWORD
This manual entitled, Surveillance Component Procedures, is one of a series of protocols and manuals of operation for the Atherosclerosis Risk in Communities (ARIC) Study. The complexity of the ARIC Study requires that a sizeable number of procedures be described, thus this rather extensive set of materials has been organized into the set of manuals listed below. Manual 1 provides the background, organization, and general objectives of the ARIC Study. Manuals 2 and 3 describe the operation of the Cohort and Surveillance Components of the study. Detailed Manuals of Operation for specific procedures, including reading centers and central laboratories, make up Manuals 4 through 11. Manual 12 on Quality Assurance contains a general description of the study's approach to quality assurance as well as the details for quality assurance for the different study procedures.
The version status of each manual is printed on the title sheet. The first edition of each manual is Version 1.0. Subsequent modifications of Version 1 (pages updated, pages added, or pages deleted) are indicated as Versions 1.1, 1.2, and so on, and are described in detail in the Revision Log located immediately after the title page. When revisions are substantial enough to require a new printing of the manual, the version number will be updated (e.g., Version 2.0) on the title page.
ARIC Study Protocols and Manuals of Operation
MANUAL TITLE 1 General Description and Study Management
2 Cohort Component Procedures
3 Surveillance Component Procedures
4 Pulmonary Function Assessment
5 Electrocardiography
6 Ultrasound Assessment
it: Ultrasound Scanning Ultrasound B-mode Image Reading Protocol
7 Blood Collection and Processing
8 Lipid and Lipoprotein Determinations
9 Hemostasis Determinations
10 Clinical Chemistry Determinations
11 Sitting Blood Pressure and Postural Changes in Blood Pressure and Heart Rate
12 Quality Assurance and Quality Control
ARIC PROTOCOL 3.Surveillance Component Procedures VERSION 2.0, 2/91

ii
Manual 3. Surveillance Component Procedures
TABLE OF CONTENTS
1. Introduction ..................................................
2. Identification of Events ......................................
2.1 Introduction ................................................. 2.2 Identification of Hospitalized MI ............................ 2.3 Identification of CHD Deaths .................................
3. Event Investigation ...........................................
3.1 Procedures for Fatal CHD ..................................... 3.2 Procedures for Hospitalized MI ............................... 3.3 Summary of CHD Event Investigations .......................... 3.4 Correction of Erroneous Event Investigation Procedures .......
4. Diagnostic Criteria ...........................................
4.1 Fatal Coronary Heart Disease (CHD) ........................... 4.2 Hospitalized Myocardial Infarction (MI) ......................
5. Event Determination ...........................................
6. Medical Care Assessment ......................................
7. Linkage of Multiple Events ....................................
8. Reliability and Validity of Community Surveillance Procedures.
8.1 Reliability .................................................. 8.2 Validity .....................................................
9. References ....................................................
1
2
2 3 7
10
10 14 15 16
17
17 18
27
29
30
31
31 32
33
10. Appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-l
ARIC PROTOCOL 3.Surveillance Component Procedures VERSION 2.0, 2/91

iii
TABLE OF CONTENTS (continued)
I ICD9 Codes for Identifying Surveillance Events 1. ICD9 Codes for Identifying CHD Deaths.....................A-1 2. ICD9 Codes for Identifying Hospitalized MI................A-2
II Forms and Instructions 1. Death Certificate Form .................................... A-3 2. Death Certificate Form Instructions.......................A- 9 3. Surveillance Event Eligibility Form.......................A-12 4. Surveillance Eligibility Form Instructions................A-16 5. Surveillance Event Investigation Summary Form.............A-2 0 6. Surveillance Event Investigation Summary Form InstructionsA- 7. Hospital Record Abstraction Form .......................... A-24 8. Hospital Record Abstraction Form Instructions.............A-4 6 9. Informant Interview Form .................................. A-80
10. Informant Interview Form Instructions.....................A-9 2 11. Physician Questionnaire ................................... A-99 12. Physician Questionnaire Instructions......................A-10 3 13. Coroner/Medical Examiner Form ............................. A-106 14. Coroner/Medical Examiner Form Instructions................A-115 15. Cohort Event Eligibility Form ............................. A-120 16. Cohort Event Eligibility Form Instructions................A-12 6 17. Cohort Event Investigation Summary Form...................A-13 1 18. Cohort Event Investigation Summary Form Instructions......A-13 3 19. Cohort Stroke Abstraction Form ............................ A-135 20. Stroke Form Instructions .................................. A-154
III Form Letters 1. Format 1:
2. Format 2:
3. Format 3:
4. Format 4: 5. Format 5: 6. Format 6:
7. Format 7: 8. Format 8: 9. Format 9:
10. Format 10:
Sample Letter to Informant: Known Telephone Number . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-193 Sample Letter to Informant: Unknown Telephone Number . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-194 Reply Postcard from Informant with Telephone Number . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-195 Letter to Neighbor re: Location of Informant...A-196 Reply Postcard on Location of Informant........A-197 Informant Release of Information Form - Nursing Home . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-198 Letter to Physician Signing Death Certificate..A-199 Letter to Attending Physician of Decedent......A-200 Informant Release of Information - Physician...A-201 Informant Release of Information - Out-of-Area Hospital . ..*................................... A-202
ARIC PROTOCOL 3,Surveillance Component Procedures VERSION 2.0, 2/91
1
1. INTRODUCTION
Through community surveillance, the ARIC study enumerates and validates cases (events) of hospitalized myocardial infarction (MI) and coronary heart disease (CHD) deaths occurring after January 1, 1987 in 35 through 74 year old male and female residents of the four ARIC study communities: Forsyth County, North Carolina; Jackson, Mississippi; suburbs of Minneapolis, Minnesota; and Washington County, Maryland.
This manual details the procedures for ARIC community surveillance. Section 2 describes the procedures by which potential events in the community are identified (i.e., death registries, hospital discharge indexes). Section 3 details procedures for collecting the additional information needed once an event has been identified. Diagnostic criteria are documented in Section 4, and review and classification procedures are described in Section 5. The procedures for obtaining information on certain indicators of medical care are described in Section 6. Procedures for linkage of multiple events are described in Section 7.
CHD events occurring among ARIC cohort participants are ascertained through cohort follow-up as well as through the routine community wide surveillance. Cohort follow-up provides a limited validation of routine surveillance. Methods for coordinating cohort and surveillance procedures are described in Section 8.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91

2
2. IDENTIFICATION OF EVENTS
2.1 Introduction
The basic features of the community surveillance design are summarized in Table 1. Events surveyed in each of the four communities include fatal CHD and hospitalized MI (see Appendix I), beginning January, 1987.
Table 1. ARIC Community Surveillance Eligibility Criteria
Criteria Eligibility
Age
Race
Place of residence
Date of discharge or death
ICD9 Codes for identification 250, 401, 402, 410-414, 427-429, of CHD death 440, 518.4, 798, 799
ICD9 Codes for identification of hospitalized MI
402, 410-414, 427, 428, 518.4
Between 35 and 74, inclusive
All races
Within the defined boundaries of the ARIC communities
January 1, 1987 - December 31, 1992
Events meeting the eligibility criteria given in Table 1 are investigated for conformity with ARIC surveillance diagnostic criteria. Identification of hospitalized events is limited to acute care hospitals in the catchment area (Section 2.2.3); no systematic attempt is made to obtain events from records of nursing homes, mental hospitals, private physicians, or hospitals out of the catchment area.
Hospitalized MIS are documented by ARIC field staff trained to identify ECG Q-waves using the Minnesota Code.
Out-of-hospital deaths (as defined in Section 3.1.2) are documented by means of informant interviews and family physician questionnaires. Coroner/medical examiner records are abstracted when available. Since Maryland laws prohibit the use of information found in death certificates as a means to contact relatives, validation of out-of- hospital deaths in Washington County is not carried out.
Deaths occurring in acute care hospitals are documented by abstracting the medical record, as with all nonfatal events.
ARIC! PROTOCOL 3. Surveillance Component Procediures VERSION 2.0, 5/91

3
The elements of the diagnostic criteria for the various events are abstracted onto standardized data forms. For hospitalized events, the occurrence of MI is determined when possible by computer analysis of the recorded diagnostic elements; for fatal events, cause of death is assigned by computer analysis or a Mortality and Morbidity Classification Committee (MMCC), according to criteria described in Section 4.
Quality control programs are carried out to assess reliability of abstracting medical records, both the reliability and validity of coding ECGs, and the reliability of MMCC procedures.
Two sources of identification of events are used: death certificates and hospital discharge indexes.
2.2 Identification of Hospitalized MI
2.2.1 Obtaining Access to Hospital Medical Records
A critical feature of surveillance is obtaining information from medical records. Without complete cooperation of hospitals, the usefulness of event rates in any community is limited. The following represents an approach for obtaining hospital cooperation which each Field Center adapts to suit the situation existing in its study community.
For the initial contact, a letter briefly describing the study is sent to the hospital administrator and the director of medical records. It is important to keep the director of medical records informed about the project and the progress of the research.
Following the initial letter, a detailed protocol is sent to each hospital administrator. Many hospitals have a medical ethics committee to review research protocols. Within two weeks of sending the protocol, the administrator and director of medical records are contacted to determine if there is difficulty in obtaining permission to review records.
Simultaneously with the submission of the protocol, the heads of cardiology are contacted. A face to face meeting with the cardiologists is important to enlist their cooperation. This may follow one of two formats. One is to arrange to meet individual cardiologists at their respective offices. The second consists of arranging a reception or dinner with the cardiologists in order to describe the study. The contact with the cardiologists is essential so that knowledge of the study is disseminated at each hospital. Moreover, if there is difficulty in obtaining permission to review records, the cardiologists can often assist in the review process.
It is also helpful to address the local medical records committees. Most require continuing education credits. A description of the epidemiologic research which provides the credits is beneficial to both the medical records librarians and the project.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
4
If there appears to be difficulty in obtaining permission, it is important to recontact the hospital administrators, arrange to meet with the administrators and house staff, as well as to offer to meet with the review committee. A critical feature is to emphasize the scientific importance and the non-threatening nature of the research. An additional point for the hospital administrator is to indicate that the research will not impede normal hospital function. It may be helpful for a senior investigator to arrange to meet with the director of medical records to describe the study. The director of medical records often is of considerable help in obtaining permission. These individuals are professionals and recognize the importance of employing medical records in research.
An additional approach which is often successful is to have faculty from the medical school contact the cardiologists. Faculty on the medical school staff who either work in the hospitals or have trained the physicians on the staff can often be very helpful for contact.
A critical reason for refusal is confidentiality of medical records. It is important to be able to respond to this issue. It may help to obtain clarification from the individual States if questions of confidentiality arise.
After permission is received, a senior investigator and the staff who do the abstracting may arrange to meet with the directors of medical records. At this time, the study should be reviewed in addition to describing the role of the medical record departments in the research. It is important to schedule time for the ARIC staff to review the records at periods when the record rooms are not busy. It is essential that the ARIC research staff control the record review.
It is sometimes necessary to compromise with the hospital review committees and house staff. Again, the major consideration is confidentiality. Some hospitals will not permit the abstraction of a patient's name. It is important to obtain the name because this is the surest method to reduce redundancy in the records. However, less optimal procedures are available. The first is to seek permission to code the name and record addresses, social security numbers, and birth dates. If these are available, the likelihood of redundancy can be reduced by sorting lists of individuals by birth dates or social security numbers.
It is important to keep the medical records directors, hospital administrators and cardiologists informed concerning the progress of the project. A periodic newsletter and reprints of publications from the project may help demonstrate the significance of the research and the lack of threat to the hospitals. This is also important because there is turnover in staff both for the researchers and the hospitals, thus the newsletters serve as a reminder to the continuing staff and an introduction to the newly hired staff.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91

5
2.2.2 Hospital Discharge Index
Eligible hospitalized MIS are identified from the discharge index of each hospital surveyed. Discharge indices are obtained directly from the hospital or from an indexing service such as the Commission on Professional and Hospital Activities (CPHA).
When a person is discharged from a hospital, the physician must indicate the major illness from which the patient suffers. Usually one such diagnosis accounted for the hospitalization. This is the primary discharge diagnosis. Other old or new diagnoses may be listed as secondary discharge diagnoses. Discharge diagnoses are coded by the hospital medical records personnel according to the International Classification of Diseases (ICD). Most hospitals subscribe to a service which takes these diagnostic codes and produces an index of discharges classified by code.
The ICD was originally constructed to provide comparable international data on causes of death. It is now extended by many countries for use in coding hospital discharge diagnoses. The extension of the ICD currently being used by hospitals is called ICD9-CM (Clinical Modification). The hospital or rCM1t modifications do not alter the basic three digit codes, but provide additional codes so that diagnoses may be classified with more detail. For instance, ICD9 uses the code 410 for acute MI: ICD9-CM adds a decimal point so that the location of the MI can be coded (e.g., an anterior wall MI is coded 410.1).
Using the discharge index for each hospital, hospitalized events are selected according to the following eligibility criteria.
1. m. ARIC examines cases only at ages 35 through 74 at time of discharge.
2. Place of Residence. Patients must live within the boundaries of the ARIC community. The discharge index may give only Zip Code, in which case a determination of residence eligibility may require checking the address in the hospital records. If a review of the medical record indicates the person was only visiting the area or had two residences, the address where the person lived at least six months of the year is considered the place of residence for ARIC purposes. People residing in a local jail at the time of hospitalization are counted.
3. Date. Time eligibility is determined from the date of discharge. Only cases discharged after January 1, 1987 are eligible.
4. ICD9-CM Code. Cases with primary or secondary diagnoses with ICDS-CM codes 402, 410-414, 427, 428 and 518.4 are selected for documentation of hospitalized MI.
The number of cases meeting these four eligibility criteria is reduced by applying various sampling fractions to different classes of ICD9-CM codes.
ARIC PROTOCOL 3. Gurveillance Component Procedures VERSION 2.0, 5/91

6
1.
2.
3.
4.
Code 410. 100% sample.
Code 411. 50% sample, when the record does not have a 410 code. The 50% sample is selected by choosing only the events with discharges occurring on even days of the month, i.e., days 2, 4, 6, etc.
Codes 412-414. 25% sample, when the record does not have a 410 or 411 code. The 25% sample is selected by choosing only the events with discharges occurring on days of the month divisible by 4, . I.e., days 4, 8, 12, 16, 20, 24 and 28.
Codes 402, 427, 428 and 518.4. 10% sample, when the record does not have a 410-414 code. The 10% sample is selected by choosing only the events with discharges occurring on days of the month divisible by 8, i.e, days 8, 16 and 24.
These sampling fractions are reassessed one year after community surveillance starts.
ICD codes listed on the hospital discharge index may not exactly correspond with those found in the corresponding hospital chart. Regardless, it is the codes listed on the discharge index which determine eligibility for selection and which are used to classify events.
2.2.3 MIS Occurring Outside the Study Community
Community residents with MI may be hospitalized out of the study area for the following reasons:
1. A major hospital catchment area for the region exists outside of the study area (e.g., tertiary care hospital referral centers).
2. Residents who work outside of the geographic area may be admitted to an out-of-area hospital if they have an MI at work.
3. A resident may have an event while in transit outside of the geographic area for recreation or social activities.
In order to select hospitals outside of the study area to include in surveillance, the Field Center first identifies those hospitals which are located in the surrounding areas. Second, the center determines by checking with local physicians, cardiologists, hospital administrators and others whether patients with acute MI are usually hospitalized locally prior to admission to a tertiary care facility outside the study area. Third, 1984 and 1985 death certificates for study area residents are reviewed. Surveillance is carried out in any hospital outside of the geographic area that contributed at least six eligible in-hospital MI deaths (ICD9-CM 410-414) in the 1984-1985 period. Major medical centers or tertiary referral facilities some distance from the study area are not included in surveillance unless there is evidence that patients with acute MI from the study area are directly admitted to such hospitals without treatment at a within-area
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
7
hospital. Selection of hospitals included in community surveillance is reassessed during the fourth year of the study.
Community residents hospitalized with acute MI while outside both the study area and the surrounding counties are not identified by routine surveillance. An estimate of the effect of this procedure is available from the surveillance for hospitalized events in cohort members.
2.2.4 Range of Facilities Covered in Surveillance
Hospitalized MI patients are identified by review of records only at acute care hospitals. Nursing homes, rehabilitation hospitals, long- term chronic disease hospitals, and psychiatric hospitals are excluded. A small number of MI patients hospitalized at these chronic care facilities for another disease, e.g., multiple sclerosis, peripheral vascular disease, diabetes, etc., may have an acute MI while in the chronic care facility and not be referred to an acute care facility or may die before referral. These individuals are lost to the surveillance system. Such an event is probably rare and would be difficult to identify from review of chronic care facility records.
Community surveillance does not identify nonfatal MI occurring outside of a hospital and for which the individual is not hospitalized (unrecognized MI).
2.3 Identification of CHD Deaths
2.3.1 Death Certificates
All deaths in the United States must be recorded on a death certificate which is filled out by a physician, medical examiner or coroner. The death certificate is a legally mandated, public document which is filed in the county of the decedent's residence. A copy is filed with the state. If a person dies away from his usual residence, a copy of the death certificate is (eventually) returned to the decedent's county of residence for filing and is also filed at the state health department. In each state, health department trained nosologists code the causes of death given on the death certificate according to the International Classification of Diseases (ICD). The 9th revision of the ICD (termed ICDS) is currently used.
Each of the four states containing the ARIC communities assigns the specific Wnderlying cause of death I1 from the nosologist's coding of the death certificate using the Automated Classification of Medical Entities (ACME) system. Computer files, which include the date of death, underlying cause, decedent's age and residence, are available. Each center obtains a monthly printout of potentially eligible cases based on the criteria listed below. The monthly printouts generally contain in-state deaths that occurred three to five months previously. In addition, all four centers annually obtain a final computer tape of eligible deaths to verify that ascertainment is complete and to provide numerators for rate calculations.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
8
Fatal events are selected according to the following eligibility criteria.
1. &g. ARIC examines deaths only at ages 35 to 74.
2. Place of Residence. The decedent must have lived within the boundaries of the ARIC community. The residence at death determines eligibility. However, if it is found in event investigation that the decedent was only visiting the area, or had two residences, the place where the person lived at least six months out of the year is considered the residence for ARIC purposes. Do not count anonymous "John Doe@@ deaths. But do count people residing in a local jail at the time of death.
3. Date. Only deaths occurring from January 1, 1987 through December 31, 1992 are eligible.
4. ICD9 Code. Deaths whose underlying cause is coded (using ICD9) 250, 401, 402, 410-414, 427-429, 440, 518.4, 798 and 799 are selected for documentation of MI or CHD.
Copies of death certificates for the potential fatal events identified on the monthly printouts are obtained from the respective State Departments of Health. Abstracters review each certificate to confirm the death meets age, residency, date, and ICD9 code criteria. ARIC cohort members are identified by comparison with the cohort clinic roster and other criteria outlined in Section 1.10 of Manual 2. The remaining fatal cases are reduced in number by applying various sampling fractions to different classes of ICD9 codes. These constitute the deaths to be investigated:
1. Codes 410-414 and 429.2. 100% sample.
2. Codes 250. 401. 402, 427-429 (extent 429.2). 440, 518.4, 798 and 799. 25% sample. For a 25% sample of cases, only deaths occurring on days of the month divisible by 4 are selected for further investigation.
A Surveillance Event Eligibility Form (Appendix II) is completed for each event to help with sample selection. An ID number is assigned to each event, a Death Certificate Form (DTH) (Appendix II) is completed (see Section 3.1), and the death certificate is filed locally.
2.3.2 CHD Deaths Occurring Outside the Study Community
For fatal hospitalized events, the address on the death certificate takes precedence over the address in the hospital record for determining eligibility.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
9
Deaths outside of the study area, but within the state, are included on State Health Department monthly printouts, but some delay between the death and the transfer of the certificate to the place of residence file is expected. If the death certificate file is reviewed for ARIC prior to receipt of out-of-area certificates, subsequent review is undertaken to identify in-transfer deaths.
Deaths that occurred in other states are relatively few in the ARIC study areas which do not closely border another state. The out-of- state deaths cannot be identified in a timely fashion but can be identified on the annual mortality computer tapes provided by the State Health Departments. Access to identifiers for out-of-state deaths is restricted. For these reasons, out-of-state deaths will only be enumerated from vital records and not investigated further.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91

10
3. EVENT INVESTIGATION
For hospitalized MI, event investigation entails review of the hospital record. Investigation of fatal CHD includes review of the death certificate and hospital record where available, and, for out- of-hospital deaths in Forsyth County, Jackson, and Minneapolis, physician questionnaires, interviews with next-of-kin and collection of other information. In Washington County, the medical examiner adds relevant questions to his routine inquiry but other out-of-hospital investigations are prohibited.
Procedures for the identification and investigation of hospitalized and fatal events in members of the ARIC cohort differ from community surveillance procedures at certain stages and are described in detail in Manual 2, Section 3. In the following paragraphs, general differences between surveillance and the investigation of cohort events are noted. References to specific procedures within Manual 2, Section 3 are identified where appropriate.
3.1 Procedures for Fatal CHD
The Death Certificate (DTH) Form and the Surveillance Event Eligibility (SEL) Form are completed for all eligible fatal events. A worksheet, the Surveillance Event Investigation Summary (SEI) Form, is used locally to monitor completion of investigation forms. One or more of the following data forms may be completed: Hospital Record Abstraction (HRA) Form, Stroke (STR) Form (for cohort members only), Informant Interview (IFI) Form, Physician Questionnaire (PHQ), and the Coroner/Medical Examiner Report (COR) Form. Autopsy reports for cohort members are copied. All forms and instructions are located in Appendix II.
For fatal events meeting ARIC eligibility criteria and sampling fractions, the Surveillance Event Eligibility form and the Death Certificate form are completed. Data from the Death Certificate form are entered into a computerized data base locally at each field center.
Some proportion of fatal events, either in-hospital or out-of- hospital, are coroner/medical examiner cases. This means that the county coroner or state medical examiner has performed an investigation of the circumstances of death in order to ascertain that the causes were natural. In this case, the coroner/medical examiner signs the death certificate. In general, the coroner/medical examiner takes cases of unexpected death where no physician was in attendance during the 24 hours prior to death. During his investigation, the coroner/medical examiner may or may not perform an autopsy. Any death where a legal question is likely to arise (e.g., after surgery, during an automobile accident, examiner case.
etc.) will probably be a coroner/medical If the death is certified by a coroner or medical
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91

11
examiner, the Coroner/Medical Examiner Report Form is completed, the data entered into the database at the field center, and later transferred to the Coordinating Center.
Medical Examiner and coroner reports are generally stored in their offices. The entirety of the documents generally require full review in order to complete the Coroner/Medical Examiner Report Form. Whatever can be retrieved from the records of these inquiries may be used to answer questions on the Coroner/Medical Examiner Form whether the document is called a report, an investigation, findings, or a summary.
Procedures for the investigation of fatal events in cohort members are described in Manual 2, Section 3.2.1. Briefly, a Cohort Eligibility Form and Death Certificate Form are completed for a fatal event occurring in a cohort member. A Coroner's Form is completed if the death is certified by a coroner/medical examiner, and the autopsy report copied if an autopsy is performed.
3.1.1 In-Hospital CHD Deaths
In-hospital deaths, which include deaths on the wards, in the ICU, CCU or operating room, may be identified by screening either the hospital discharges or the death certificates. Both the Hospital Record Abstraction Form (HRA, appendix A-II) and the Death Certificate Form are completed if the in-hospital death is eligible for study either as a hospitalized event (according to the discharge codes and sampling fractions specified in Section 2.2.2) or as a fatal event (according to the cause of death codes and sampling fractions specified in Section 2.3.1).
If the in-hospital death is initially identified from the death index, the hospital may occasionally lie outside the catchment area for the ARIC community. In this case, this fact is recorded on the Death Certificate Form and no attempt is made to obtain the hospital record.
Persons who upon record abstraction are found to have been admitted without vital signs are treated as out-of-hospital deaths (as defined in Section 3.1.2). Only the administrative data of the Hospital Record Abstraction Form are recorded in such cases. If the death is first identified from the death index and the death certificate indicates "dead on arrival", an attempt is made to find the hospital record to verify this information.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
If the hospital record indicates that the person was transferred within the study area directly from another acute care hospital, the record for the other hospitalization is found and abstracted onto
12
another Hospital Record Abstraction Form, provided the hospital discharge index contains an eligible ICD-9 discharge code regardless of day of discharge.
3.1.2 Out-of-Hospital CHD Deaths
CHD deaths occurring outside of regular acute care hospitals are categorized as 880ut-of-hospital CHD deaths". This includes deaths in nursing homes and other chronic care facilities. It also includes persons dead on arrival at acute care hospitals, dying in outpatient departments or emergency rooms, or admitted without vital signs. For purposes of defining out-of-hospital death, "no vital signs" means no pulse rate or no systolic blood pressure. A person admitted on a respirator who never had a pulse rate or a systolic blood pressure off the respirator is also considered an out-of-hospital death.
For out-of-hospital deaths in centers other than Washington County, information is sought from the decedent's family and physician(s) within 6 months after death. Prior to contacting the informant or the physician, it is ascertained whether the deceased was a member of the ARIC cohort. If the deceased was a cohort member, the cohort procedures for investigating deaths described in Manual 2, Section 3 are followed instead of the community surveillance procedures.
The family member is contacted for an interview, the physician is sent a questionnaire. Whenever possible, the informant is the spouse or another family member of the decedent. Also, the informant may be someone else who witnessed the death. Some death certificates contain the names of the spouse and a witness.
First an attempt is made to contact and interview the spouse or a first-degree relative (i.e., son, daughter, or sibling) of the decedent, or someone else who lived with the decedent. If another person witnessed the death, this person is interviewed as well. Using name and address information from the death certificate, an attempt is made to find the informant's telephone number in either the regular or the reverse (llcrisscrossll) telephone directory. If the telephone number is available, a Format 1 letter (Appendix III) is sent.
If a telephone number cannot be found, a Format 2 letter (Appendix III) is sent asking the informant to return a telephone number on an enclosed form in a self-addressed, stamped envelope (Format 3: Appendix III) to the Surveillance Supervisor at the Field Center. These letters include a request to the U.S. Post Office for address correction and are sent with both the interviewer and Field Center Principal Investigator's signatures.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, b/91

13
After enough time for the Format 1 letter to arrive or upon receipt of a reply form, the interview is conducted over the telephone, or if necessary, in person using the Informant Interview Form. If a Format 2 letter is sent and no reply is received in two weeks, another such letter is sent by registered mail. If no reply is received, a Format 4 letter (Appendix III) is sent to next-door neighbor(s) (identified through the reverse telephone directory) to request information on the whereabouts of the potential informants. A reply is requested on a self-addressed, stamped postcard (Format 5: Appendix III) to the Surveillance Supervisor at the Field Center. Format 2 and Format 4 letters are also sent when a telephone number is initially available, but attempts at telephone contacts with informants are unsuccessful. If no reply is received from the neighbors, no further effort is needed.
When the death is witnessed by someone other than a member of the decedent's family, both a family member and the witness are interviewed. In such a case, the information from both interviews are recorded on separate Informant Interview Forms. Up to three (the three best) Informant Interview Forms may be completed for a given event.
Information is sought from physicians by sending the Physician Questionnaire. One questionnaire is sent to the physician who signed the death certificate, if he/she is not the medical examiner. From the informant interview, an attempt is made to identify the decedent's usual physician and/or a physician who attended the decedent for heart disease during the four weeks prior to death. A questionnaire is sent to these physicians (if any, and if different from the one signing the death certificate). Sample cover letters are provided in Appendix III for each of these physician contacts (Formats 7 and 8, respectively). Up to two (the two best) Physician Questionnaires may be entered into the ARIC database for a given event.
If there is no response after four weeks of the initial mailing to a physician, a follow-up letter and another copy of the Physician Questionnaire are sent. If there is no response after eight weeks of the initial mailing, the physician is contacted by telephone. On occasion, prior to returning the Physician Questionnaire (or prior to answering questions over the telephone), the physician requests a release form signed by the informant, which can be modeled after the Release-of-Information Form for physicians (Format 9: or for nursing homes (Format 6:
Appendix III) Appendix III).
If the patient had no physician or no knowledgeable physician can be identified, and the patient's medical record or emergency room record is accessible, then it is permissible for an ARIC abstractor to complete the physician questionnaire using the record.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
14
If the fatal event was a coroner's or medical examiner's case, his/her report is abstracted onto the Coroner Form. The medical examiner/coroner may require a Release of Information Form. If the decedent died in a nursing home, nursing home personnel are asked to complete a Physician Questionnaire based on the nursing home record. Centers may offer to assist with abstraction if this would be helpful. The nursing home may require the family informant to provide a Release-of-Information Form (Format 6, Appendix III).
If information provided by the informants or physicians indicates that a person who died out-of-hospital was admitted to a catchment area hospitalized within 28 days prior to death for MI or heart surgery, an attempt is made to locate the hospital record. If the discharge diagnoses include an ARIC screening code, regardless of day of discharge, the chart is abstracted onto the Hospital Record Abstraction Form.
If neither an Informant Interview (IFI) nor a Physician Questionnaire (PHQ) form can be completed, then the Hospital Discharge Indices from eligible hospitals are checked for the period covering 28 days before death. If an ICD code eligible hospitalization is found, a HRA is abstracted, regardless of discharge day.
Procedures for the investigation of out-of-hospital deaths occurring in cohort members are described in Manual 2, Section 3.2.1.2. Procedures for contacting informants are similar to those described above, except that the letters refer to the decedent's participation in the ARIC Study (letters are in Manual 2, Appendix VII). A copy of the Release-of-Information forms signed by deceased accompany the Physician Questionnaire.
3.2 Procedures for Hospitalized MI
The Hospital Record Abstraction Form is used to abstract events meeting ARIC eligibility criteria for age, residence, date, hospital discharge code and sampling fraction (Section 2.2.2). If a patient was discharged alive without an ICD9 410 or 411 discharge code and with no ECGs taken and no cardiac enzymes measured, only the administrative information on the Hospital Record Abstraction Form is completed. Otherwise, the entire form is completed. There are a few cases in which the ICD9 code is recorded incorrectly, so that a code on the diagnostic index meets the ARIC criteria but none of the diagnoses recorded on the discharge summary of the medical record meet the study criteria. The HRA Form is still completed in such a case.
Prior to abstracting a record from a hospital for ARIC, information is collected on the normal ranges used for each of the cardiac enzymes abstracted. Many hospitals report use of more than one upper limit of normal for a particular enzyme, for example, when a different laboratory is used for determinations at night or on weekends.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, S/91

15
If an eligible hospital record indicates that the patient was transferred directly from another acute care hospital in the catchment area, or that the patient upon discharge is being transferred directly &g another acute care hospital in the catchment area, the record for the other hospitalization is found and abstracted if it has ARIC screening codes regardless of day of discharge.
Procedures for investigation of hospitalized events with a discharge diagnosis code for MI or stroke occurring in cohort members are described in Manual 2, Section 3.2.2. Selection codes are listed in Section 3.1.1.2. A Hospital Record Abstraction Form and/or Stroke Form may be used.
3.3 8ummary of CHD Event Investigations
The following scheme summarizes the forms completed for eligible surveillance events:
1. Out-of-hosnital CHD death, as defined in Section 3.1.2
a) Death Certificate Form, Surveillance Event Eligibility Form
b) Up to two Physician Questionnaires and three Informant Interview Forms
cl Coroner Form on all coroner/medical examiner's cases and Hospital Record Abstraction Form on cases admitted to a catchment area hospital in past 28 days with heart conditions meeting ARIC screening codes regardless of day of discharge.
2. *Hosnital CHD deaths, no vital sians in-hospital
a) Surveillance Event Eligibility Form
b) First part of Hospital Record Abstraction Form, then investigate as 1, above.
3. *Hospital CHD death. vital sians sometime in hosnital
a) Surveillance Event Eligibility Form, Death Certificate Form, Hospital Record Abstraction Form.
4. *Hosnitalized CHD case, discharaed alive
a) Surveillance Event Eligibility Form, Hospital Record Abstraction Form.
*If a patient also transferred to or from a catchment area hospital, complete the additional Hospital Record Abstraction forms.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
'16
3.4 Correction of Erroneous Event Investigation Procedures
A fatal or hospitalized CHD event may be identified by surveillance procedures (death certificates or hospital discharge indices) and investigated as a surveillance event, then discovered at a later time to have occurred in a cohort member. In the case of a hospitalized event, a second Hospital Record Abstraction Form is completed independently by a second abstractor (see Section 8.1). Twelve-lead ECGs have to be copied and sent to the Minnesota ECG Reading Center for coding. In addition, certain surveillance forms have to be replaced by cohort forms, certain items on other forms changed, and possibly additional forms appropriate for cohort members completed. Specifically, the Cohort Eligibility Form must replace the Surveillance Eligibility Form. Additional forms required for cohort members have to be indicated on the Death Certificate Form if the death occurred in an out-of-catchment area hospital. The Physician Questionnaire and Informant Interview Form remain unchanged.
If an eligible event has been investigated erroneously as a cohort event, the Cohort Eligibility Form must be deleted and replaced by the Surveillance Eligibility Form. If the event investigated was a stroke, the Stroke Form must be deleted.
ARIC PROTOCOL 3. Burveillance Component Procedures VERSION 2.0, 5/91
17
4. DIAGNOSTIC CRITERIA
4.1 Fatal Coronary Heart Disease (CHD)
4.1.1 Definite Fatal Myocardial Infarction (MI)
Must meet criteria 1. AND 2. below:
1. No known non-atherosclerotic or non-cardiac atherosclerotic process or event that was probably lethal.
2. Definite hospitalized MI within four weeks of death; use criteria in Section 4.2.2 for Definite Hospitalized MI.
4.1.2 Definite Fatal CHD
Must meet ALL of the following criteria:
1. Lack of sufficient evidence to diagnose Definite Fatal MI according to the criteria given in Section 4.1.1.
2. No known non-atherosclerotic or non-cardiac atherosclerotic process or event that was probably lethal.
3. Presence of one or both of the following findings:
a) A history of chest pain within 72 hours of death;
b) A history of ever having had chronic ischemic heart disease such as definite or possible MI, coronary insufficiency, or angina pectoris.
4.1.3 Possible Fatal CHD
Must meet ALL of the following criteria:
1. Lack of sufficient evidence to diagnose Definite Fatal MI or Definite Fatal CHD according to the criteria in Sections 4.1.1 and 4.1.2.
2. No known non-atherosclerotic or non-cardiac atherosclerotic process or event that was probably lethal.
3. Death certificate with consistent underlying cause, i.e., ICD9 codes: 410-414, 427.5, 429.2, and 799.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91

18
4.1.4 Non-CHD Death
All deaths that do not meet the above criteria for Definite Fatal MI, Definite Fatal CHD, or Possible Fatal CHD.
4.1.5 Chronology of Death
The time interval from onset of acute symptoms to time of death is recorded, where possible, for all CHD deaths.
4.1.6 Limitation of Activity
For out-of-hospital CHD deaths it is noted whether the decedent's activity was limited in the month before death because of sickness or illness.
4.2 Hospitalized Myocardial Infarction (MI)
4.2.1 Introduction
The aim of the ARIC Study is to establish a well standardized process for the identification of hospitalized coronary disease of an acute nature, allowing for valid inter-community and longitudinal comparisons. Mild and chronic manifestations of ischemic heart disease, such as angina pectoris, congestive heart failure, and arrhythmias are not identified as target diagnoses in community surveillance but are included in the screening process to aid in the identification of acute MI. So-called silent infarctions are excluded.
The criteria presented are based on two source documents: the findings of
19 h CCSP Pilot Study and the results of the Minnesota Heart Survey - , as well as other surveillance studies. The diagnostic criteria presented here approximate those contained in the above mentioned documents. The differences in diagnostic criteria are the lack of a duration requirement for cardiac pain, and the use of the more sensitive and specific CK-MH and LDH isoenzymes. The combinations of pain, ECG and enzyme categories required for each diagnosis below are approximately the same as those contained in the above-mentioned documents.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
19
It is recognized that aggressive treatment of early signs and symptoms of acute coronary events, such as coronary artery bypass graft or streptokinase infusion, may prevent the development of the full diagnostic syndrome. In such cases, it may be difficult to diagnose the event accurately. The use of such modalities are recorded and subject to data analysis, but not employed in the criteria for diagnosis.
4.2.2 Definite Hospitalized MI
Must meet one or more of the following criteria:
1. Evolving diagnostic ECG pattern (ED1 - ED7, defined below)
2. Diagnostic ECG pattern (Dl or D2) and abnormal enzymes (both defined below);
OR
3. Cardiac pain (defined below) and abnormal enzymes;
a) Evolving ST-T pattern (EVl through EX8)
OR
b) Equivocal ECG pattern (El through E4)
4.2.3 Probable Hospitalized MI
Must meet one or more of the following criteria in the absence of sufficient evidence for Definite Hospitalized MI:
1. Cardiac pain and abnormal enzymes
2. Cardiac pain and equivocal enzymes and
a) Evolving ST-T pattern
OR
b) Diagnostic ECG pattern
OR
3. a) Abnormal enzymes and
b) Evolving ST-T pattern
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91

20
4.2.4 Suspect hospitalized MI
Must meet one or more of the following criteria in the absence of sufficient evidence for Definite or Probable Hospitalized MI.
1.
2.
3.
4.
Abnormal enzymes
OR
Cardiac pain and incomplete enzymes and
a) Diagnostic ECG pattern
OR
b) Evolving ST-T pattern
OR
Cardiac pain and equivocal enzymes
OR
Equivocal enzymes and
a) Diagnostic ECG pattern
OR
b) Evolving ST-T pattern
OR
cl Equivocal ECG pattern
The Criteria for Definite Probable and Suspect Hospitalized MI are summarized in Table 2.
4.2.5. Definition of Cardiac Pain
Pain having both the following characteristics:
1. It occurs anywhere in the anterior chest, left arm or jaw.
AND
2. Absence of a definite non-cardiac cause of cardiac pain.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91

21
Table 2. Summary of ARIC Diagnostic Criteria for Hospitalized MI
Cardiac Pain ECG Findings Enzymes Diagnosis
Present Evolving Diagnostic ECG Pattern
Diagnostic ECG Pattern
Evolving ST-T Pattern
Equivocal
Absent, Uncodable, or Other
Not Present, Evolving Diagnostic Unknown or ECG Pattern Missing
Diagnostic ECG Pattern
Evolving ST-T Pattern
Equivocal ECG Pattern
Absent, Uncodable, or other
Abnormal Definite MI Equivocal Definite MI Incomplete Definite MI Normal Definite MI
Abnormal Equivocal Incomplete Normal
Definite MI Probable MI Suspect MI No MI
Abnormal Equivocal Incomplete Normal
Definite MI Probable MI Suspect MI No MI
Abnormal Equivocal Incomplete Normal
Definite MI Suspect MI No MI No MI
Abnormal Equivocal Incomplete Normal
Probable MI Suspect MI No MI No MI
Abnormal Equivocal Incomplete Normal
Definite MI Definite MI Definite MI Definite MI
Abnormal Equivocal Incomplete Normal
Definite MI Suspect MI No MI No MI
Abnormal Equivocal Incomplete Normal
Probable MI Suspect MI No MI No MI
Abnormal Equivocal Incomplete Normal
Suspect MI Suspect MI No MI No MI
4bnormal Equivocal Incomplete Normal
Suspect MI No MI No MI No MI
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91

22
4.2.6 Definitions of Electrocardiographic Criteria
The ECG series is assigned the highest category for which criteria are met, i.e., evolving diagnostic is greater than diagnostic is greater than evolving ST-T patterns are greater than equivocal is greater than other. The ECGs are coded using Minnesota Code (Manual 5, Electrocardiography, Appendix E).
4.2.6.1 Evolving Diagnostic Q Waves
An evolving Diagnostic Q Wave pattern is defined as an evolving pattern on serial ECGs of ECG changes within lead groups, i.e, anterior (VI - V5); lateral (I, aVL, V6) or inferior (II, III, aVF). Two or more ECG recordings during the hospitalization are needed for this classification.
4.2.6.2. Evolving Diagnostic ECG (Judged within lead group)
ED1 through ED7 cannot be assigned if a 7-l-l code is present. ED2 through ED7 cannot be assigned if a 7-2-l or 7-4 code is present.
EDl. No Q-code (no 1 code) in reference ECG followed by a record with a Diagnostic Q-code (Minn. code l-l-l through l-2-5 plus l-2-7), OR any code l-3-X in reference ECG followed by a record with any code 1-l-X.
ED2. An Equivocal Q-code [(Minn. code l-2-8 in the absence of 7-2-l or 7-4) or (any l-3 code)] and no major ST-segment depression in reference ECG followed by a record with a Diagnostic Q-code PLUS a major ST-segment depression (Minn. code 4-l-X or 4-2).
ED3. An Equivocal Q-code and no major T-wave inversion in reference ECG followed by a record with a Diagnostic Q-code PLUS a major T- wave inversion (Minn. code 5-l or 5-2).
ED4. An Equivocal Q-code and no ST-segment elevation in reference ECG followed by a record with a Diagnostic Q-code PLUS an ST segment elevation (Minn. code 9-2).
ED5. No Q-code and neither 4-l-X nor 4-2 in reference ECG followed by a record with an Equivocal Q-code PLUS 4-l-X or 4-2.
ED6. No Q-code and neither 5-l nor 5-2 in reference ECG followed by a record with an Equivocal Q-code PLUS a 5-l or 5-2.
ED7. No Q-code and no 9-2 in reference ECG followed by a record with an Equivocal Q-code PLUS a 9-2.
4.2.6.3 Evolving ST-T Pattern (Judged within lead group)
This diagnosis cannot be assigned if a 7-l-l or 7-2-l or 7-4 code is present.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91

23
Evl. Either 4-O (no I-code), 4-4 or 4-3 in reference ECG followed by a record with 4-2 or 4-l-2 or 4-l-l (confirmed by Significant Increase) OR, for hospital ECGs only, 4-2, 4-l-2 or 4-l-l in reference ECG followed by a record with 4-0, 4-4 or 4-3 (confirmed by Significant Decrease),
PLUS either no Q-code in both the reference ECG and the follow-up ECG or Q-code(s) present in reference ECG or follow-up ECG but no Significant Increase found.
EV2. Either 4-2 or 4-l-2 in reference ECG followed by a record with 4- l-l (confirmed by Significant Increase) OR, for hospital ECGs only, 4-l-l in reference ECG followed by a record with 4-2 or 4- 1-2 (confirmed by Significant Decrease),
PLUS either no Q-code in both the reference ECG and the follow-up ECG or Q-code(s) present in reference ECG or follow-up ECG but no Significant Increase found.
EV3. Either 5-0, 5-4 or 5-3 in reference ECG followed by a record with 5-2 or 5-l (confirmed by Significant Increase) OR, for hospital ECGs only, 5-2 or 5-l in reference ECG followed by a record with 5-0, 5-4 or 5-3 (confirmed by Significant Decrease),
PLUS either no Q-code in both the reference ECG and the follow-up ECG or Q-code(s) present in reference ECG or follow-up ECG but no Significant Increase found.
EV4. Code 5-2 in reference ECG followed by a record with 5-l (confirmed by Significant Increase) OR, for hospital ECGs only, 5-l in reference ECG followed by a record with 5-2 (confirmed by Significant Decrease),
PLUS either no Q-code in both the reference ECG and the follow-up ECG or Q-code(s) present in reference ECG or follow-up ECG but no Significant Increase found.
EV5. Code 9-O in reference ECG followed by a record with 9-2 (confirmed by Significant Increase) OR 9-2 in reference ECG followed by a record with 9-O (confirmed by Significant Decrease),
PLUS either no Q-code in both the reference ECG and the follow-up ECG or Q-code(s) present in reference ECG or follow-up ECG but no Significant Increase found.
EV6. Code 4-l in reference ECG followed by a record with 4-l (confirmed by Significant Increase) OR, for hospital ECGs only, 4-l in reference ECG followed by a record with 4-l (confirmed by Significant Decrease),
PLUS either no Q-code in both the reference ECG and the follow-up ECG or Q-code(s) present in reference ECG of follow-up ECG but no Significant Increase in Q-code found.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
24
EV7. Code 5-l-l in reference ECG followed by a record with 5-l-l (confirmed by Significant Increase) OR, for hospital ECGs only, 5-l-l in reference ECG followed by a record with 5-l-l (confirmed by Significant Decrease),
PLUS either no Q-code in both the reference ECG and the follow-up ECG or Q-code(s) present in reference ECG or follow-up ECG but no Significant Increase in Q-code found.
EV8. Code 5-l-2 in reference ECG followed by a record with 5-l-2 (confirmed by Significant Increase) OR, for hospital ECGs only, 5-l-2 in reference ECG followed by a record with 5-l-2 (confirmed by Significant Decrease),
PLUS either no Q-code in both the reference ECG and the follow-up ECG or Q-code(s) present in reference ECG or follow-up ECG but no Significant Increase in Q-code found.
4.2.6.4 Diagnostic ECG
Dl. (Diagnostic Q wave) An ECG record with any Diagnostic Q-code (Minn. code l-l-l through l-2-5 plus l-2-7).
D2. An ECG record with ST-segment elevation code 9-2 PLUS (T-wave inversion code 5-l or 5-2 in the absence of 7-2-l or 7-4).
4.2.6.5 Equivocal ECG
El. (Equivocal Q wave) An ECG record with an Equivocal Q-code [(Minn. code l-2-8 in the absence of 7-2-l or 7-4) or (any l-3 code)].
E2. An ECG record with ST-segment depression (code 4-l-X or 4-2 or 4- 3 in the absence of 7-2-l or 7-4).
E3. An ECG record with T-wave inversion (code 5-l or 5-2 or 5-3 in the absence of 7-2-l or 7-4).
E4. An ECG record with ST-segment elevation code 9-2.
4.2.6.6 Other ECG
01. Reference ECG coded 7-l-l. 02. Any ECG coded 7-l-l. 03. Normal ECG(s), defined as 1.0 in "clear I1 field of all ECGs. 04. Other findings including l-2-6.
4.2.6.7 Uncodable ECG
Ul. Technical errors coded 9-8-l by Minnesota Code.
4.2.6.8 Absent ECG
Al. No ECG available for coding.
4.2.6.9 Minnesota Coding Procedures
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5191

25
The following ECG tracings are identified:
1. The first codable ECG after admission; 2. The last codable ECG recorded before discharge; and 3. The last codable ECG recorded on day 3 (or the first ECG
thereafter) following admission or an in-hospital event.
Photocopies of the hospital ECGs are sent to the Minnesota Coding Center in Minneapolis for Minnesota Coding, using the Minnesota Coding for hospitalized ECGs shown in Appendix 0 of Manual 5. Each ECG is read one time blinded. Unlike for cohort, serial change rules are not applied. Minnesota Code criteria are in Appendix E of Manual 5.
4.2.7 Definitions of Cardiac Enzyme Criteria
All pertinent enzyme results (as defined below) recorded on days 1 through 4 after hospital admission or an in-hospital CHD event are abstracted. Information on non-ischemic cause for elevated enzymes is abstracted exclusively from the discharge summary on the medical chart.
4.2.7.1 Abnormal Cardiac Enzymes
Enzymes are classed as "abnormal" if any enzyme values recorded meet any of the following criteria:
1. a) CK-MB is "present" (if laboratory uses the criterion of
2.
3.
"present" or "absent" without reporting a more specific value) or CK-MB is twice the upper limits of normal (if the laboratory gives a normal range) a, if no normal range is given, the CK-MB (heart fraction) is greater than or equal to 10% of the total CK value,
AND
b) There is no known non-ischemic cause (cardiac surgery, severe muscle trauma, rhabdomyolysis) for the elevated enzyme value.
OR
a) The ratio LDHl : LDH2 > 1, m if LDH2 is missing LDHI is at least twice the upper limit of normal,
AND
b) There is no evidence of hemolytic disease.
OR
a) Total CK and LDH are both at least twice the upper limit of normal. (These increases do not have to occur on the same day. 1
AND
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
26
b) There is no known non-ischemic cause (surgery, severe muscle trauma, rhabdomyolysis) for the elevated enzyme value and no evidence of hemolytic disease.
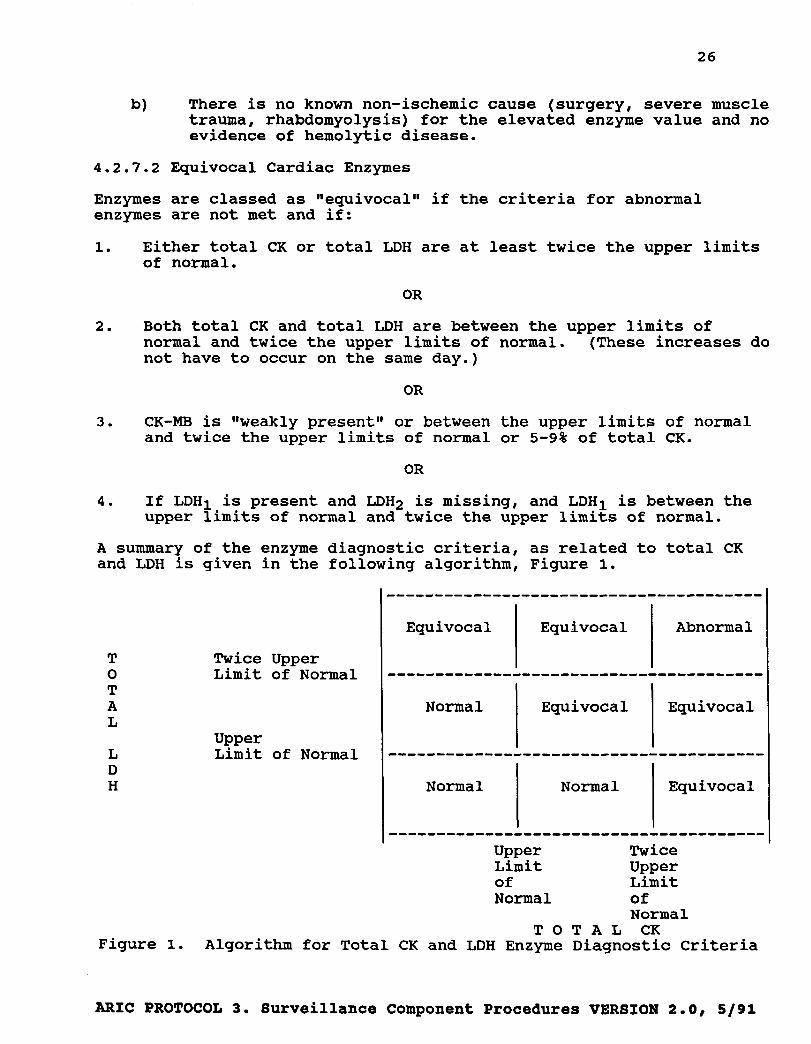
4.2.7.2 Equivocal Cardiac Enzymes
Enzymes are classed as "equivocal" if the criteria for abnormal enzymes are not met and if:
1.
2.
3.
4.
Either total CK or total LDH are at least twice the upper limits of normal.
OR
Both total CK and total LDH are between the upper limits of normal and twice the upper limits of normal. (These increases do not have to occur on the same day.)
OR
CK-MB is "weakly present" or between the upper limits of normal and twice the upper limits of normal or 5-9% of total CK.
OR
If LDHI is present and LDH2 is missing, and LDHI is between the upper limits of normal and twice the upper limits of normal.
A summary of the enzyme diagnostic criteria, as related to total CK and LDH is given in the following algorithm, Figure 1.
T 0 T A L
L D H
Twice Upper Limit of Normal
Upper Limit of Normal
---------------------------------------
Equivocal Equivocal Abnormal
---------------------------------------
Normal Equivocal Equivocal
---------------------------------------
Normal Normal Equivocal
I Upper Twice Limit Upper of Limit Normal of
Normal TOTAL CK
Figure 1. Algorithm for Total CK and LDH Enzyme Diagnostic Criteria
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, S/91
2ba
5. EVENT DETERMINATION
5.1 Hospitalized events are classified using a computer algorithm based on the criteria given in Section 4.2. The MMCC reviews the following hospitalized events for hospitalized MI diagnosis.
5.1.1. Those with a computer diagnosis of "Definite", "Probable" or "Suspect MIW if: a) there is evidence of chest pain of non-cardiac origin and/or b) spuriously elevated enzymes.
This type of case is first reviewed by one MMCC member to consider downgrading abnormal enzymes to "equivocalW or downgrading pain to "not present". After this consideration the computer diagnostic algorithm is run again to determine if further review is required as described in 5.1.2.
5.1.2. For hospitalized events linked to at least one other eligible within 28 day hospitalization admission, if: a) the computer diagnosis is "Definite MI" but discharge codes do not include 410 or 411. (Note: Computer "Definite MI” + 410 - 411 discharge codes lead to automatic classification of Definite MI.) b) the computer diagnosis is "No MI" and hospital discharge ICD9-CM codes include 410. (Note: Computer "No MI" + No 410 discharge code leads to automatic classification of "No MI".
This review, of linked hospitalizations, is done, when needed, by one MMCC member for hospitalized MI diagnosis, and is done prior to review, if needed, for death diagnosis.
5.2. In-hospital deaths are reviewed for death diagnosis by two MMCC reviewers, after final MI classification, then adjudicated by a third reviewer if there is no agreement between the two reviewers. The following cases, however, need no MMCC review.
5.2.1. Those with ICD-9 codes for underlying cause of death 410 - 414 or 427.5 or 429.2 or 799, and a linked hospitalization within 28 days with final diagnosis of "Definite MI". (Note: These cases are classified directly as "Definite Fatal MI" (Section 4.1.1).)
tC PROTOCOL 3. Surveillance Component Procedures VERSION 2.1, 8/91
5.2.2. Those with ICD-9 codes for underlying cause of death 410 - 414 or 427.5 or 429.2 or 799 for which the diagnosis of "Definite MIm could not be made according to ARIC criteria but who had pain of cardiac origin or a history of MI, angina pectoris or coronary insufficiency. (Note: These cases are classified directly as "Definite Fatal CHDW (Sections 4.1.2 and 4.1.3).)
5.2.3. Those with ICD-9 codes for underlying cause of death not including 410 - 414 or 427.5 or 429.2 or 799 for which the diagnosis of "Definite" MI could not be made according to ARIC Criteria and
1. No pain of cardiac origin and 2. No history of previous MI,.angina pectoris or
coronary insufficiency. (Note: These cases are classified directly as "Non-CHD death". (Section 4.1.4).)
This review for death diagnosis is done after final MI classification, by two MMCC reviewers, then adjudicated by a third reviewer if there is no agreement between the two reviewers.
5.3 Out-of-hospital deaths
5.3.1. All out-of-hospital deaths are reviewed by the MMCC for death diagnosis extent those with death certificate ICD-9 codes for underlying cause of death 410 - 414 or 427.5 or 429.2 or 799 and a catchment area hospital admission within 28 days with a final diagnosis of "Definite MI". (Note: These cases are classified as "Definite Fatal MI.")
This review for death diagnosis is done after final MI classification, in case there is an eligible linked hospital admission within 28 days of death, and is done by two MMCC reviewers, then adjudicated by a third reviewer if there is no agreement between the two reviewers.
5.3.2. "Definite" and WPossibleW CHD deaths are classified as to time from first symptoms to death.
5.4 Cohort Hospitalisations
All cohort eligible hospitalizations (fatal and non-fatal) as well as all cohort eligible out-of-hospital deaths are reviewed by the MMCC. For each event requiring an MMCC judgement, the process begins with two members independently reviewing the information, using both the narrative and the coded information in the data collection forms. A computer abstract of relevant coded information is used by the MMCC in reviewing each of these events. Relevant narrative information is reviewed from photocopies of the abstractor comments. If the two reviewers
rn mmnmnnnt. 9 a~run4llrnan rnmnnnnn+ PrnnrAraren VRRPTON 2-l. RI91

28
agree, further adjudication by the MMCC Committee is not required. If they disagree, the Coordinating Center informs them about which items disagree (without specifying the exact nature of the disagreement). If after re-review, the two reviewers still disagree, the MMCC chairman adjudicates, unless he was one of the original reviewers. In this case, one of two predetermined reviewers is assigned. Selection of the two reviewers for each event is made by the Coordinating Center by a randomized process. The Coordinating Center also assigns specific tasks to the reviewers for each case (diagnosis, chronology of death, cause of elevated enzymes, etc.).
5.5 Case Law
An important function of the MMCC is to maintain complete records of any clarifications of ARIC diagnostic criteria required to reach diagnostic decisions. such "case law'* is systematized for convenient reference purposes and, when appropriate, incorporated into the ARIC diagnostic protocol.
IC PROTOCOL 3. Surveillance Component Procedures VERSION 2.11 8/91

29
6. MEDICAL CARE AWBBSMENT
This section describes the assessment of medical care in community- wide surveillance. Medical care is also assessed in cohort members, as described in Manual 2, Section 4. Medical care elements which are recorded only in cohort members include the participant's access to and use of providers for routine and special care, use of all prescription and over-the-counter medications, records of all hospitalizations for all reasons, records of all cardiovascular procedures and all cardiovascular diagnoses received, and detailed information on hospitalizations for CHD and stroke.
Community surveillance for medical care includes information collected for out-of-hospital deaths, information abstracted from hospital records and information about the services provided in the community's acute care hospitals.
For out-of-hospital deaths, the Physician Questionnaire and Informant Interview Form allow collection of information about physician visits prior to the acute event, utilization of physician and emergency services during the acute event, history of hospital admission within one month prior to death, receipt of cardiopulmbnary resuscitation, delay in receiving definitive care, use of nitrates and digitalis shortly before death and history of coronary bypass surgery. The potential for cardiopulmonary resuscitation is assessed by the information on whether death was witnessed and the location of death.
Demographic information and much of the information collected on out-of-hospital deaths is also available in hospital abstracting. In addition, information is collected on transportation to the hospital, time of arrival, receipt of cardiopulmonary resuscitation, use of a number of new procedures and medications for treatment of the cardiovascular event (such as angioplasty and streptokinase infusion), and the use of diagnostic procedures (such as cardiac catheterization and echocardiography).
30
7. LINKAGE OF MULTIPLE EVENTS
Since many deaths are listed on both the hospital discharge index and the state death index, survey personnel must compare these lists carefully to avoid duplicating the investigation of in-hospital deaths. If an eligible in-hospital death is found first from death certificate lists, the case is flagged and it is linked with the hospital chart when that record is found. The linked forms are given the same event ID number. If an in-hospital death is found first using a hospital source, the hospital chart is abstracted, and the death certificate obtained as soon as possible. Again, only one event ID number is assigned to these forms. The procedures for identifying these as belonging to the same event will be established by the Coordinating Center.
If an eligible hospital record indicates that the patient was transferred directly from another acute care hospital, or that the patient upon discharge is being transferred directly &Q another acute care hospital, the record for the other hospitalization is abstracted onto another HRA Form, if it meets AFZIC screening codes regardless of discharge day. The two forms initially have different hospitalization I.D. numbers.
Over the duration of the ARIC surveillance, increasing numbers of community residents are hospitalized for cardiovascular conditions more than once. Others are hospitalized and subsequently die of CHD. Sufficient information for correct identification of these patients is collected, where hospitals permit, and matching procedures based on the identifiers which can be recorded must be developed.
On occasion, it is difficult to differentiate between two or more successive admissions for the same event and two or more different events in the same person. As it is often difficult to make this distinction on the basis of ECG, enzyme or pain characteristics, a simple rule is followed: a CHD death or a hospital admission for MI occurring within 28 days of a previous admission for MI is regarded as the same event, for purposes of calculating rates.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, S/91

31
8. RELIABILITY AND VALIDITY OF COMMUNITY SURVEILLANCE PROCEDURES
For cohort events, ascertainment must be as complete as possible and diagnoses as accurate as possible, in order to evaluate correctly the precursor status of each of the risk and medical care factors carefully measured at home interview, clinical examination and follow- up* Optimal cohort ascertainment and diagnoses also serve as a standard against which to compare the more routine ascertainment and diagnostic procedures used in community-wide surveillance.
Once data collection is complete for cohort events, a diagnosis is made both with and again without the additional information which is collected only for cohort members to compare the effect of the additional information.
For hospitalized events occurring among cohort members, diagnoses given by surveillance and cohort methods are compared directly using the same set of events in the same patients. For fatal events, cohort diagnoses in cohort members are compared with surveillance diagnoses in comparable non-cohort community residents. Additionally, for cohort decedents, diagnoses made on the basis of information available in surveillance are compared with diagnoses based on all the information available for cohort members.
8.1 Reliability
The extent to which cohort procedures can be used to confirm results of surveillance is limited, as described below, by the extent with which it is practical to undertake independent parallel investigations.
Hospital records are abstracted twice for cohort members whose hospital discharge codes are eligible for surveillance, once as a part of routine community surveillance and again as part of quality control, on the same schedule as reabstraction of Surveillance records. The determination that the patient is a cohort member is achieved both by routine checking of the names of surveillance patients against cohort member lists and by routine cohort follow-up. The abstraction of the hospital record for the cohort member is undertaken either by an abstractor supervisor or by a different abstractor from the one who abstracted the record for surveillance. Differences between abstracters on key items of information (1) lead to a third record abstraction for adjudication of these items, (2) are recorded for quality assurance documentation, and (3) are used in the continuing training of abstracters. Abstraction of hospital records for cohort and routine surveillance ECGs receive full Minnesota coding by the AHIC ECG Center.
Unlike hospital record abstraction, death investigations are not conducted in a fully independent manner. No interviews with family
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, S/91

32
informants or physician questionnaires are completed in surveillance until it is determined whether or not the decedent is a cohort member. If the decedent is a cohort participant, the special tracing information available for cohort members is used to establish contact with family members and physicians. The introduction to these informants includes reference to the permission which the decedent has given ARIC staff to undertake the investigation. If routine surveillance death investigation preceded use of the cohort approach, an early refusal or a reluctant level of cooperation might jeopardize an otherwise successful investigation.
Efficient methods for identifying surveillance residents who are cohort members and for appropriately scheduling the death investigations require direct assistance from the Coordinating Center to the Field Centers. These methods assure that where duplication of procedures is required for quality assurance, the duplication is appropriately blinded.
8.2 Validity
For cohort members, it is possible to validate information on selected variables obtained by community surveillance procedures, by using the more accurate information obtained by cohort procedures. An example of a variable for which the validity of surveillance approaches is assessed by using information available for cohort members is MI order (new vs. recurrent). Although community surveillance defines an MI as new when there is no mention in the medical chart of a past episode, additional information is available for cohort participants, including the clinic interview and a baseline ECG. Thus, the more accurate definitions of %ew" and 81recurrent11 available for the cohort are used as a "gold standard @I to determine sensitivity and specificity of surveillance procedures. Specifically, ECG findings at baseline are used to determine in cohort members to which extent a diagnostic Q wave, as classified in community surveillance, can be assumed to be either a Irnewll or an "oldB8 Q wave.
llEcologicV1 validation is also undertaken, by comparing event rates derived from community surveillance with those obtained from cohort follow-up. In addition to examining surveillance rates in population subgroups, the similarity of patterns of associations of rates with demographic variables between cohort and community surveillance is evaluated, using the former as the "gold standard".
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, S/91

33
9. REFERENCES
1. Gillum RF, S Fortmann, RJ Prineas, T Kottke. International Diagnostic Criteria for Myocardial Infarction and Acute Stroke. Prepared for the Committee on Criteria and Methods, Council on Epidemiology, American Heart Association. Am Heart J 108:150- 158, 1984.
2. World Health Organization. Proposal for the Multinational Monitoring of Trends and Determinations of Cardiovascular Disease and Provisional Protocol, October 1981.
3. CCSP Coordinating Center. Community Cardiovascular Surveillance Program: Final Report to the National Heart, Lung, and Blood Institute, June 1, 1984.
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, S/91

A-I
APPENDIX I.1
ICD9 Codes for the Identification of Fatal CHD
Code Title
Event: Coronarv Heart Disease
250 Diabetes Mellitus
401 Essential Hypertension
402 Hypertensive Heart Disease
410 Acute Myocardial Infarction
411 Other Acute and Subacute Ischemic Heart Disease
412 Old Myocardial Infarction
413 Angina Pectoris
414 Other Chronic Ischemic Heart Disease
427
428
429
440
518.4
798
799
Cardiac Dysrhythmias
Heart Failure
Ill-Defined Descriptions and Complications of Heart Disease
Atherosclerosis
Acute Edema of Lung
Sudden Death, Cause Unknown
Other Ill-Defined and Unknown Causes of Morbidity and Mortality
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91
A-2
APPENDIX I.2
Codes for the Identification of Hospitalized Myocardial Infarction
Code Title
Event: Mvocardial Infarction
402 Hypertensive Heart Disease
410 Acute Myocardial Infarction
411 Other Acute and Subacute Ischemic Heart Disease
412 Old Myocardial Infarction
413 Angina Pectoris
414 Other Chronic Ischemic Heart Disease
427 Cardiac Dysrhythmias
428 Heart Failure
518.4 Acute Edema of Lung, Unspecified
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 2.0, 5/91

- - 0.n.r. b92S-o2#Jl A-3
. 8x&l t-31-89 a
DEATH CERTIFiCATE l?ORl\
mmanI~mm (Dnup8g81of6)
1. Decedent:
8. lint #be: . . . . . Irlllllllll]
b. Middle m: . . . . . - I I I I Il.1 I I I I I
c. &St mmm: . . . . . . I I I I I I I I I I I I I I I I I I I I
2. DUtb hrtifiute lhmbu: . . . . I I I I I I I I I I I I I I I
.
c. sex: . . . . . . . . . . Blah n
?rala I
5. J&e cm rtlnxlt poup: . . . . . . . . . . mlit.8tbausi8n u
alack/~ n
AsimlPu$fic Eslmdu A
-IlIdidmatf~rlrrtrn I
uahwun/Wot bcordd U
i’ 1 I .f
. . .’
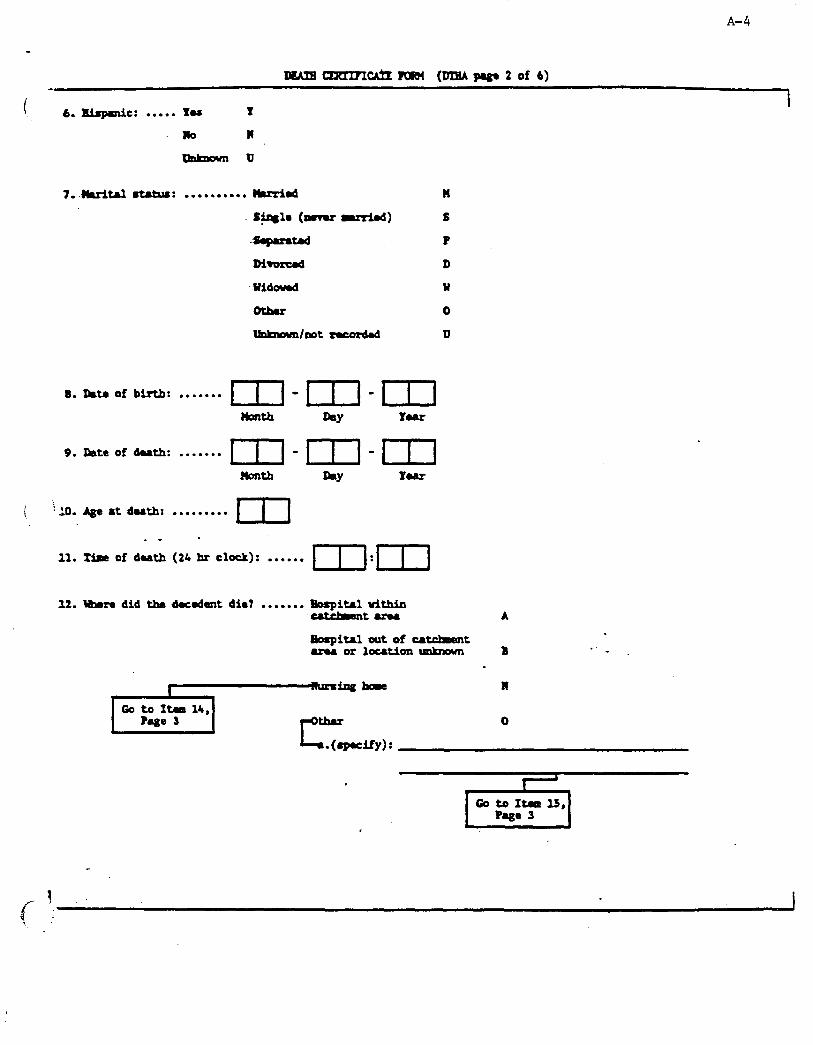
A-4
I. 6.
7.
8.
9.
I ‘i so.
11.
12.
lwAmcizxrrn~n]cbl (lrmpbga2of4)
I Bbgl8Oic: . . . . . xu 1
MO 11
uokmunu
B&i- mtams: . . . . . . . . . . mmid n
+w@ (0-u -1 S
-4-=- P
MIorcd D
~Yidaumd Y
0
tlObma/00t rwozdd U
Data of birth: ....... rr/-l - 171 . L]
Date of dutb: .......
Age at duth:
. -
Time of dath
Uhema did tba
bY Pur
. . . . . . . . . E
(21 hr clock): . . . . . . mIm
, I Gotoftmals,
Page 3 I

A-5
lb. amm rrd locatiar of bo8pitAl or ml%- h: . . . . . . . .
8. Nsu:
b. City:
c. sute:
15. ua8 this a ctomnu's or rdiul 8udnar'a cum? .*.... Yu Y
, 16. Corona or ?bdical &miner: . . . . . . . !
a. Nsm:
b. Addresr:
17. ha an ampry pufomedt . . . . . . . Yu Y . NO N .
1%. IeDs wde for m cats8 of death:
.
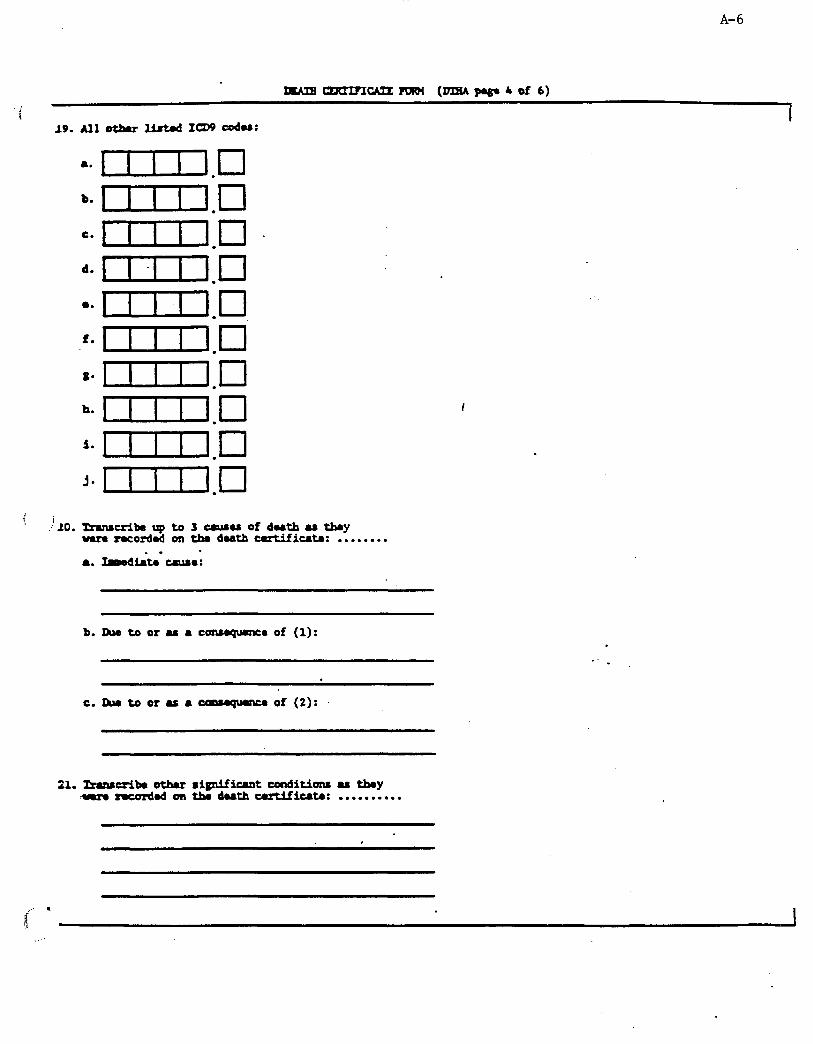
A-6
W-CAZZRRM (DlliA~4of 6)
: I 19.Allotbm.r usbd 14)9 codas:
a.
b.
c.
d.
0.
f.
t*
h.
i.
j*
i .L0.mnsuikupta3ula6uofdu+hufby
uarm mcordod on tha dutb certifiutn: . . . . . . . . . I
8. lmadirta we:
b. Ra to or u a c-e of (1):
C. Ru to or u a cm-qwnu of (2):
21. Imnsuiba othu rigdfiuat conditions u t&y :s mod on tha duth cutifiut.a: . . . . . . . . . .
SF - . I
;1 s J
..:

A-7
12. -1 bo~luls.. zpa I
for 1 : . . . . . . . . 5 daaun OI lur A
lbzrorlur B
ldBYOrlU8 C
1uwLorlwr D
l~thorlur t
?b~tbUllronth ?
c+thboun 01 oat ncordd IJ
23. XrLfoIuat: . . . . . . . .
a. Itam:
b. M~IUS:
26. Ralationsup of illfoIuzlt ta d-od: . . . . . spouar s f
w p&qLq~ ;
a. B8me:
b. Mdrasr:
26. crrtuying physician: . . . . . . .
&. lhmo: ,
b. Mdrur:
__-’
1 I .

A-8
27. mtm abmtnct cqdmtd: . . . . . . . a-m-m
Hmltb RY You
28.adoambu0fkbstmaercap1~~thiBfom . . . . . . . [ 1 1 1
-Baud l ololy onthe iaforrtion~tbumd inthis foxm, indiuta ulutddi+llau\ foxm am rnmdod:
(It-m 12-O or I) m (Itu l2-A or B rpd Itr U-&B, or C). ltms 23 8xxtior 25 eoqlotd (tantret nlativu fintuina possible).
(Itan 12-O or R) or (Ita 12-A or B mY Itr U-&B, or C). I- 23 ~/ot25~lotd(Lafonmtaotrlrvdywl~td above).
(Itma 12-O or 1() or (Itm 12-A or B rpd Ita U-A,B, or C). 1~26caqlotdcdthir~aot~wronuorrAiul~.
Itaull2-RrdIfrpu~lotb.
-1tml2 l A cd Ita 13 - 0, K, or F. (Sumaillmco only)
I-12 l Aor Bad I- l3 - D,E,erF. (Cohortonly)
(Itm 12-D or 1) Or (Itm l2=A or B d Ita U-A,B, or C). Itar116camplotd.
. Itm 17 cqhtad (cohort only)
.
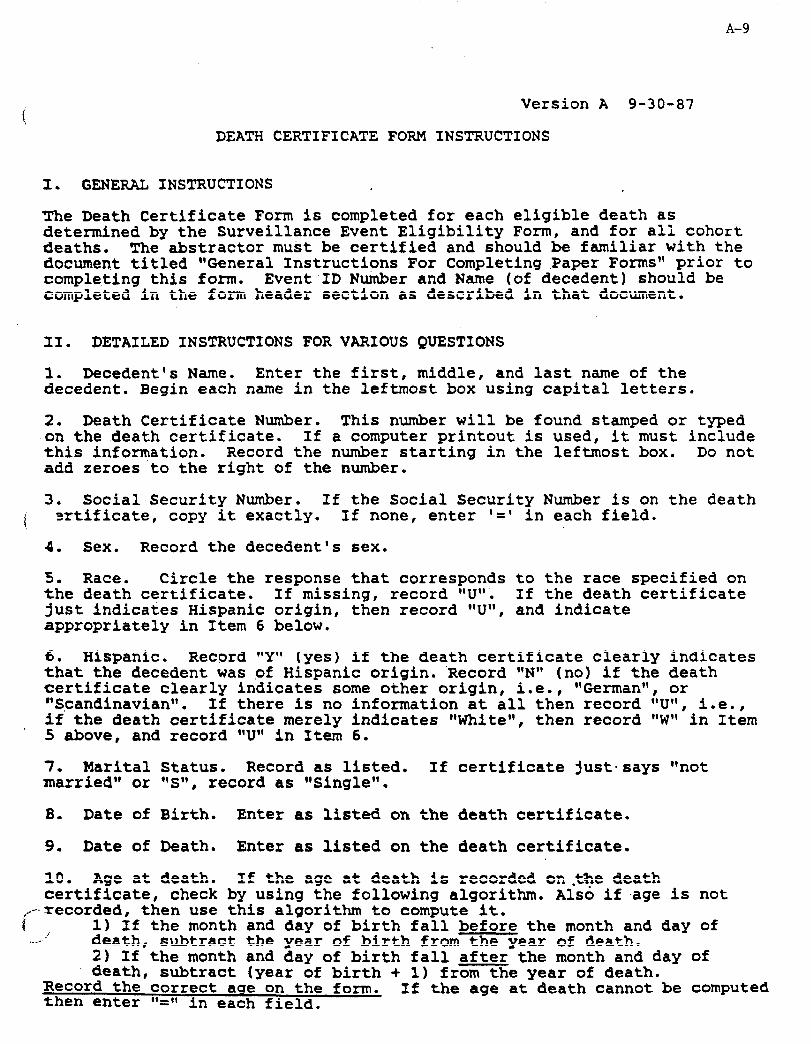
A-9
Version A g-30-87
DEATH CERTIFICATE FORM INSTRUCTIONS
3. GENERAL INSTRUCTIONS
The Death Certificate Form is completed for each eligible death as determined by the Surveillance Event Eligibility Form, and for all cohort deaths. The abstractor must be certified and should be familiar with the document titled "General Instructions For Completing Paper Forms" prior to completing this form. Event ID Number and Name (of decedent) should be completed in the form header section as described in that document.
31. DETAILED INSTRUCTIONS FOR VARIOUS QUESTIONS
1. Decedent's Name. Enter the first, middle, and last name of the decedent. Begin each name in the leftmost box using capital letters.
2. Death Certificate Number. This number will be found stamped or typed on the death certificate. If a computer printout is used, it must include this information. Record the number starting in the leftmost box. Do not add zeroes'to the right of the number.
3. Social Security Number. If the Social Security Number is on the death I srtificate, copy it exactly. If none, enter '=I in each field.
4. Sex. Record the decedent's sex.
5. Race. Circle the response that corresponds to the race specified on the death certificate. If missing, record llU'l. If the death certificate just indicates Hispanic origin, then record "Uqt, and indicate appropriately in Item 6 below.
6. Hispanic. Record "Ylr (yes) if the death certificate clearly indicates that the decedent was of Hispanic origin. 'Record l'N1' (no) if the death certificate clearly indicates some other origin, i.e., 'lGerman'l, or **Scandinaviantt. If there is no information at all then record *'U", i.e., if' the death certificate merely indicates "White", then record "W" in Item
. 5 above, and record "U" in Item 6.
1. Marital Status. Record as listed. If certificate just-says "not married" or "S" 8 record as "Single".
8. Date of Birth. Enter as listed on the death certificate.
9. Date of Death. Enter as listed on the death certificate.
10. Age at death. If the age at death is recorded on.the death certificate, check by using the following algorithm. Also if .age is not
/ --recorded, then use this algorithm to compute it. 1) If the month and day of birth fall before the month and day of death, subtract the year of birth from the year of death. 2) If the month and day of birth fall after-the month and day of death, subtract (year of birth + 1) from the year of death.
Record the correct aae-on the form. then enter '(=(I in each field.
If-the age at-death cannot be computed
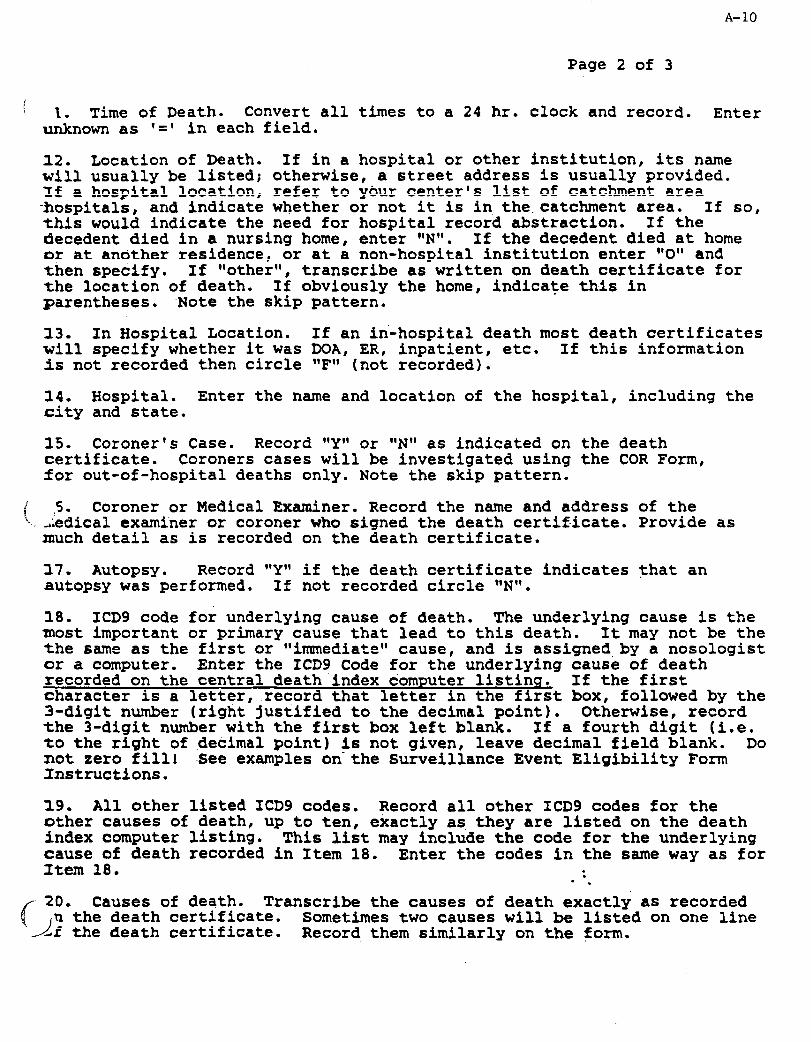
Page 2 of 3
A-10
! 1. Time of Death. Convert all times to a 24 hr. clock and record. Enter
unknown as I=' in each field.
12. Location of Death. If in a hospital or other institution, its name will usually be listed; otherwise, a street address is usually provided. If a hospital location, refer to your center's list of catchment area -hospitals, and indicate whether or not it is in, the.catchment area. If so, this would indicate the need for hospital record abstraction. If the decedent died in a nursing home, enter trN*l. If the decedent died at home or at another residence, or at a non-hospital institution enter q'O'Q and then specify. If *tother*t , transcribe as written on death certificate for the location of death. If obviously the home, indicate this in parentheses. 'Note the skip pattern.
13. In Hospital Location. If an in-hospital death most death certificates will specify whether it was DOA, ER, inpatient, etc. If this information 1s not recorded then circle *'F" (not recorded).
14. Hospital. Enter the name and location of the hospital, including the city and state.
15. Coroner's Case. Record "YrV or "N" as indicated on the death certificate. Coroners cases will be investigated using the COR Form, for out-of-hospital deaths only. Note the skip pattern.
i 1 S. Coroner or Medical Examiner. Record the name and address of the '.,iedical examiner or coroner who signed the death certif-icate. Provide as
much detail as is recorded on the death certificate.
17. Autopsy. Record r,YrQ if the death certificate indicates that an autopsy was performed. If not recorded circle g'NtV.
18. ICD9 code for underlying cause of death. The underlying cause is the most important or primary cause that lead to this death. It may not be the the same as the first or "immediateqV cause, and is assigned,by a nosologist or a computer. Enter the ICD9 Code for the underlying cause of death recorded on the central death'index computer listins. If the first character is a letter, record that letter in the first box, followed bv the 3-digit number (right-justified to the decimal point). Otherwise, record the 3-digit number with the first box left blank. If a fourth digit (i.e. to the right of .decimal point) is not given, leave decimal field blank. Do not zero fill! See examples on-the Surveillance Event Eligibility Form Instructions.
19. All other listed ICD9 codes. Record all other ICD9 codes for the other causes of death, up to ten, exactly as, they are listed on the death index computer listing. This list may include the code for the underlying cause of death recorded in Item 18. Enter the codes in the same way as for Item 18. :
l .
ac
20. Causes of death. Transcribe the causes of death exactly as recorded .n the death certificate.
-I- Sometimes two causes will be listed on one line
df the death certificate. Record them similarly on the $orm.
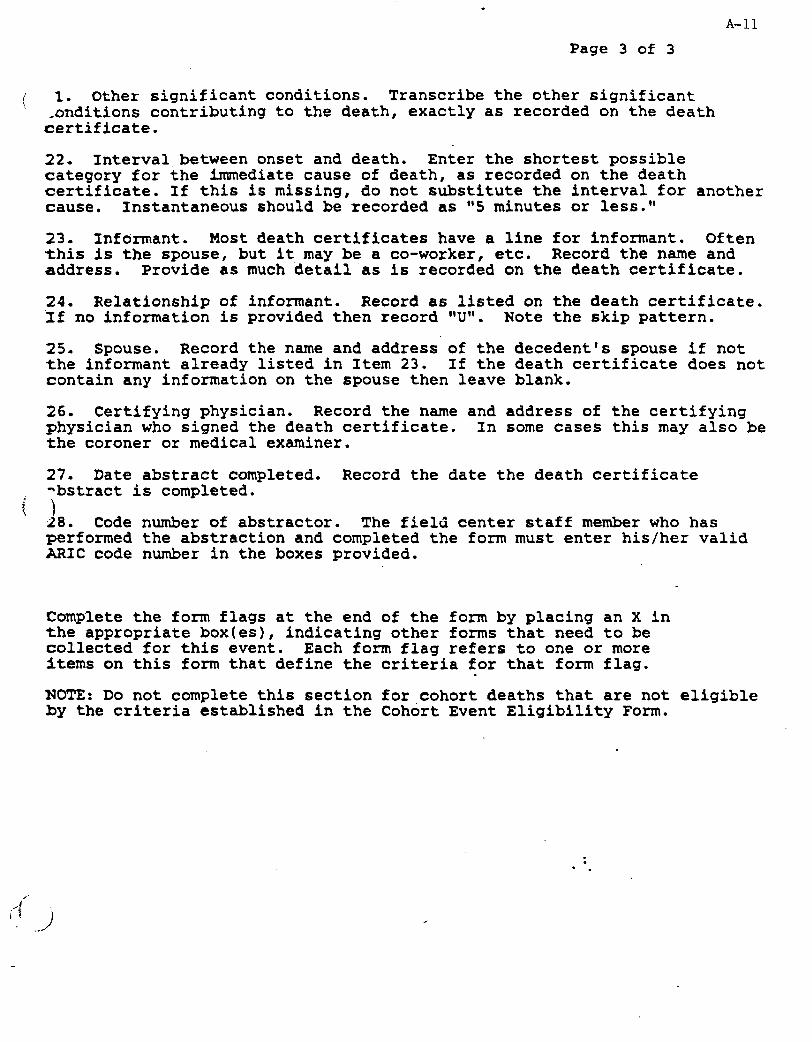
A-11 Page 3 of 3
! 1. Other significant conditions. Transcribe the other significant ' onditions contributing to the death, exactly as recorded on the death
certificate.
22. Interval between onset and death. Enter the shortest possible category for the immediate cause of death, as recorded on the death certificate. If this is missing, do not substitute the interval for another cause. Instantaneous should be recorded as "5 minutes or less."
23. Informant. Most death certificates have a line for informant. Often this is the spouse, but it may be a co-worker, etc. Record the name and address. Provide as much detail'as is recorded on the death certificate.
24. Relationship of informant. Record as listed on the death certificate. 'If no information is provided then record YJ1'. Note the skip pattern.
25. Spouse. Record the name and address of the decedent's spouse if not the informant already listed in Item 23. If the death certificate does not contain any information on the spouse then leave blank.
26. Certifying physician. Record the name and address of the certifying physician who signed the death certificate. In some cases this may also be the coroner or medical examiner.
27. Date abstract completed. Record the date the death certificate -bstract is completed. t
28. Code number of abstractor. The field center staff member who has performed the abstraction and completed the form must enter his/her valid ARIC code number in the boxes provided.
Complete the form flags at the end of the form by placing an X in the appropriate box(es), indicating other forms that need to be collected for this event. Each form flag refers to one or more items on this form that define the criteria for that form flag. . NOTE: Do not complete this section for cohort deaths that are not eligible by the criteria established in the Cohort Event Eligibility Form.
: - .
Z’ .J : a I ’ / ._

e ‘, .i SURVEILLANCE EVENT -‘ha ELXGIEILTTY FORM
.
I I I 1 F’ORH CXlDE: UII SEL VERSION: A 4/12/00
A-12
INSTRUCTIONS: This should be the first form completed for prospective Sumeillance events. For this fow only, the header information should be completed AF’IXR completing the rwinder of the form and ONLY for eligible events. entering ntnwrical respoties.
Refer to this form’s Q by Q instructions for informtim on For “multiple choice” and ‘8yes/no11 type questions, circle the
letter corresponding to the most appropriate response. If a letter is circled incorrectly, mark through it with an “X” and circle the correct response.
1
SURVEILLANCE EVENT ELIGIBILITY PORJI (SU page 1 of 4)
1. Name (First, Middle, Last):
i
2. Address of Individual:
IInclude street, city, county, state, zip]
3. Does the address fit within the Lounds of the MUC coxmnmity? . . . . . . . Yes Y
1, ’ No N
Gc, to Item 19,
t. Date of discharge or depth: . . . m-m-m
t4ont.h hY Year
I If I& bemeen 1/l/07 and 12131192, go to Item 19 on Page 4. .
S. Birthdate: . . . . . . . . . . . . . . . . . . . .
. . .&on* -d &Y Yesr
6. Age h discharge 01: death- . . . . . . . . . . . ..*............... m
.
If not between 35 and 7&, go to Item 19 on Page 4.
i . ..I /

. A-13
I
SURVEILLANCE EVENT ELIGIBILITY FmH (SM page 2 of 4)
7 Does the docuatent used to identify the event indicate that the individual died (either a death
i certificate/index or a hospital record indicating a death)? . . . . . . . . . . . Yes
No
8. Ir the individual a participant in the ARIC Cohort Study? . . . . . . . . . . . . . . Yes
No
9. Visit 1 date: . . . . . . . . . . . . . . . . . m-m-m
n0nt.h DAY Y0A.r
If item 9 is eiulier.than item 4, go to Item 19 on Page 4. Otherwise, contime with item 10.
c
10. Source used to identify event: . . . . . . . . . . . . . . . . . . . . OBath Iydex/Certificate
3. INFQRHUIOH FROM DEAlSi INDEX/CERTIFICATE
3.2. a. ICD code for underlving ususe
I I 1 1 I
b. Xr the code 410-414 or 429.27
of death:
.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Yes I
c. IA the code 250, 401, 402, 427-429 (not 429.2), , wI0;51.9.4, 798, or 7991 . . . . . . . . . . . . . . . . . Yes
No Go to Item 19,
d. Is t&e date of death (day of month) 4, 8, 12, 16,'20, 24, or 261 . . . . . Yes
-+,
D
H
-L
7-
,‘I . ..’

A-14
SlJRVEIIUNCEEVENTELIGIBILITYP0RJl (SELA page 3 of 4)
r 'WOWION FROn HOSPIIU. DISQURGE INDEX t i _ iospiull N8me:
: \
15. Hospital dir&urge diagnosis codes:
a* rl.03
be m.m
=.m.m
de a.m
ecm3.m
f. urn.1
s~uln.ul
h. umm
i-1.ul.
4nnm
k. n.m
1. m.m
D* lll.ccl
ncun.m
o~ma.m
p411zln.ul
14. fiospital Record Rumber:
I 16. a. IA & blo Code lirtadl . . . . . . . . . . . . . . . . . . Yes Y
b. Is A 411 code listed? . . . . . . . . . . . . . . . . . . Yes
No Go to Item 16d
c. Is the dAte of discharge (day of month) divisible W;~;%& q-e; .-; ;;; ig :;
Page 4
d. Is a 412-414 code listed? . . . . . . . . . . . . . . Yes
No
l . Is the Qte of dischA.rge (day of month) 4, 8, 12, 16, 20, 24, or 20? . . . . . . . . . . Yes
f. Is A 402, 427, 428, or 518.4 code listed? . . . . . . . . . . . . . . . . . Yes
No Got0 1taaJ19, .
Page 4
8. Is the date of discharge
.
Y
N
Y
w
Y
N
Y
N
Y
IN
Y
N

A-15
SURVEILLANCE EYMT ELIGIBILITY KM (SM pege 4 of 4)
I) 'JGIBILITY AND ID ASSI- I
i I fiecord Y, indicating that event is eligible. . . . . . . . . . . . Yes Y
I& Event Identification ?hmhex (assign here): I I I I I I] 1 After completing Iten 18, go to Item 20 1
19. Record N, indicating that @vent is not eligible. . . . . . . . No N
2. ADMINISTW~'EINFCRMUION
20. Oate of dAta collection: . . . . . . rT-1 - 1-J-l - 11
Month bY Y0AX
11. Code rmmber of person completing this form:........ I I 1
3ased solely on the information gathered in this form, indicate what additional forms are needed:
m
;7iiFa
Criteria based on th is form
Item 10 - H and Item 17 = Y
cl= Item7 - Y pd Item17 -Y
:a ~ It-7 -Y rrd It-8 = Y
ElQ;L Item 8 = Y ad Item 9 is earlier than Item I
1 .
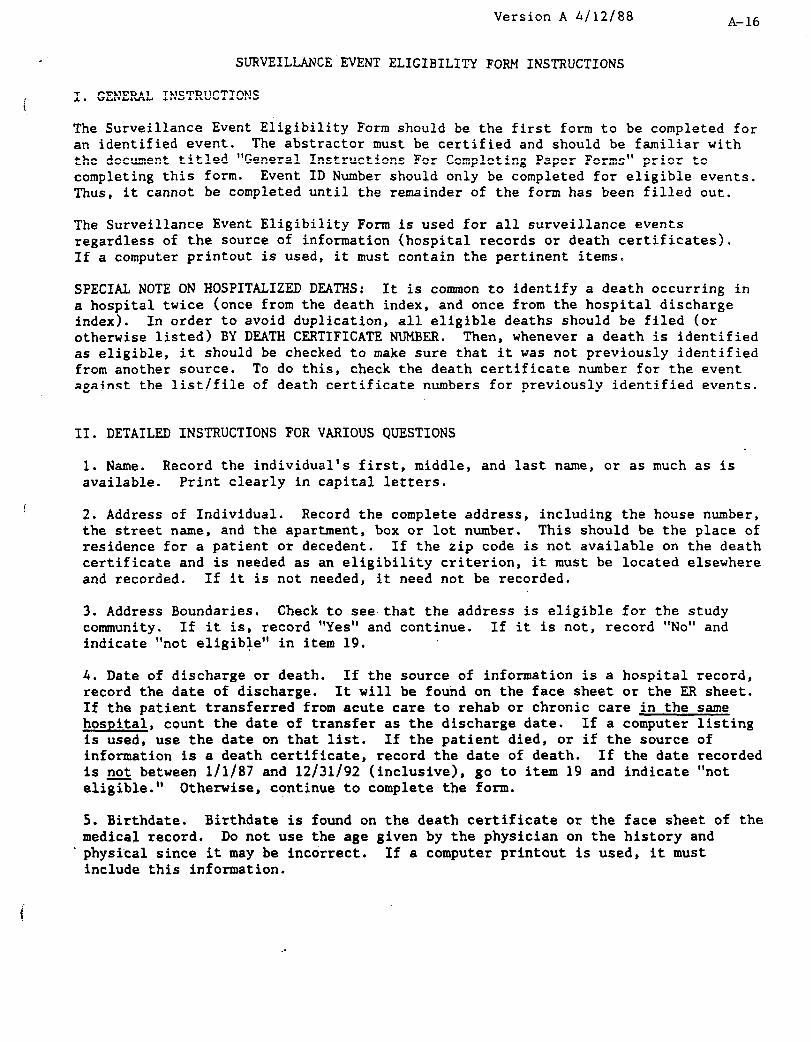
Version A h/12/88 A-16
SURVEILLANCE'EVENT ELIGIBILITY FORM INSTRUCTIONS
I. GENERAL INSTRUCTIONS
The Surveillance Event Eligibility Form should be the first form to be completed for an identified event. The abstractor must be certified and should be familiar with the document titled "General Instructions For Completing Paper Forms" prior to completing this form. Event ID Number should only be completed for eligible events. Thus, it cannot be completed until the remainder of the form has been filled out.
The Surveillance Event Eligibility Form is used for all surveillance events regardless of the source of information (hospital records or death certificates). If a computer printout is used, it must contain the pertinent items.
SPECIAL NOTE ON HOSPITALIZED DEATHS: It is common to identify a death occurring in a hospital twice (once from the death index, and once from the hospital discharge index). In order to avoid duplication, all eligible deaths should be filed (or otherwise listed) BY DEATH CERTIFICATE NUMBER. Then, whenever a death is identified as eligible, it should be checked to make sure that it was not previously identified from another source. To do this, check the death certificate number for the event against the list/file of death certificate numbers for previously identified events.
II. DETAILED INSTRUCTIONS FOR VARIOUS QUESTIONS
1. Name. Record the individual's first, middle, and last name, or as much as is available. Print clearly in capital letters.
2. Address of Individual. Record the complete address, including the house number, the street name, and the apartment, box or lot number. This should be the place of residence for a patient or decedent. If the zip code is not available on the death certificate and is needed as an eligibility criterion, it must be located elsewhere and recorded. If it is not needed, it need not be recorded.
3. Address Boundaries. Check to see that the address is eligible for the study community. If it is, record "Yes" and continue. If it is not, record "No" and indicate “not eligible" in item 19.
4. Date of discharge or death, If the source of information is a hospital record, record the date of discharge. It will be found on the face sheet or the ER sheet. If the patient transferred from acute care to rehab or chronic care in the same hospital, count the date of transfer as the discharge date. If a computer listing is used, use the date on that list. If the patient died, or if the source of information is a death certificate, record the date of death. If the date recorded is not between l/1/87 and 12/31/92 (inclusive), go to item 19 and indicate "not elizle." Otherwise, continue to complete the form.
5. Birthdate. Birthdate is found on the death certificate or the face sheet of the medical record. Do not use the age given by the physician on the history and
. physical since it may be incorrect. If a computer printout is used, it must include this information.
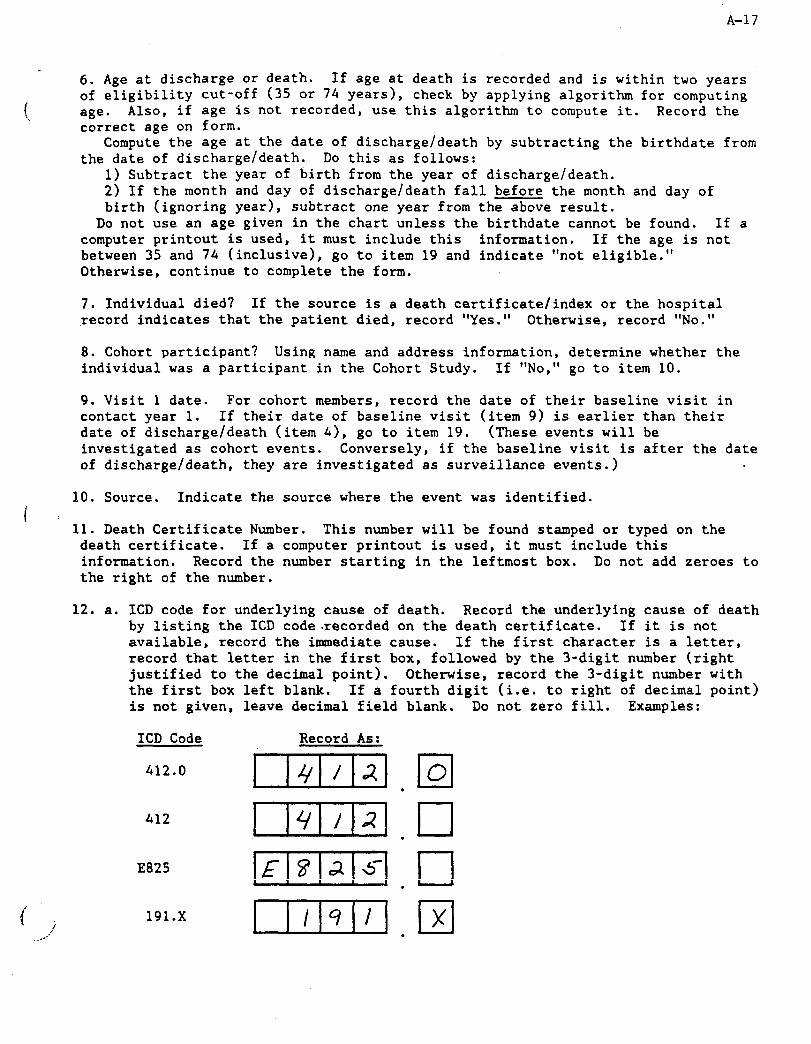
A-17
l.
6. Age at discharge or death. If age at death is recorded and is within two years of eligibility cut-off (35 or 74 years), check by applying algorithm for computing age. Also, if age is not recorded, use this algorithm to compute it. Record the correct age on form.
Compute the age at the date of discharge/death by subtracting the birthdate from the date of discharge/death. Do this as follows:
1) Subtract the year of birth from the year of discharge/death. 2) If the month and day of discharge/death fall before the month and day of birth (ignoring year) , subtract one year from the above result.
Do not use an age given in the chart unless the birthdate cannot be found. If a computer printout is used, it must include this information. If the age is not between 35 and 74 (inclusive), go to item 19 and indicate "not eligible." Otherwise, continue to complete the form.
7. Individual died? If the source is a death certificate/index or the hospital record indicates that the patient died, record "Yes." Otherwise, record "No."
8. Cohort participant ? Using name and address information, determine whether the individual was a participant in the Cohort Study. If "No,“ go to item 10.
9. Visit 1 date. For cohort members, record the date of their baseline visit in contact year 1. If their date of baseline visit (item 9) is earlier than their date of discharge/death (item 4), go to item 19. (These events will be investigated as cohort events. Conversely, if the baseline visit is after the date of discharge/death, they are investigated as surveillance events.)
10. Source. Indicate the source where the event was identified. ( i
11. Death Certificate Number. This number will be found stamped or typed on the death certificate. If a computer printout is used, it must include this information. Record the number starting in the leftmost box. Do not add zeroes to the right of the number.
12. a. ICD code for underlying cause of death. Record the underlying cause of death by listing the ICD code recorded on the death certificate. If it is not available, record the immediate cause. If the first character is a letter, record that letter in the first box, followed by the 3-digit number (right justified to the decimal point). Otherwise, record the 3-digit number with the first box left blank. If a fourth digit (i.e. to right of decimal point) is not given, leave decimal field blank. Do not zero fill. Examples:
ICD Code Record As:
412.0
412
E825
191.x
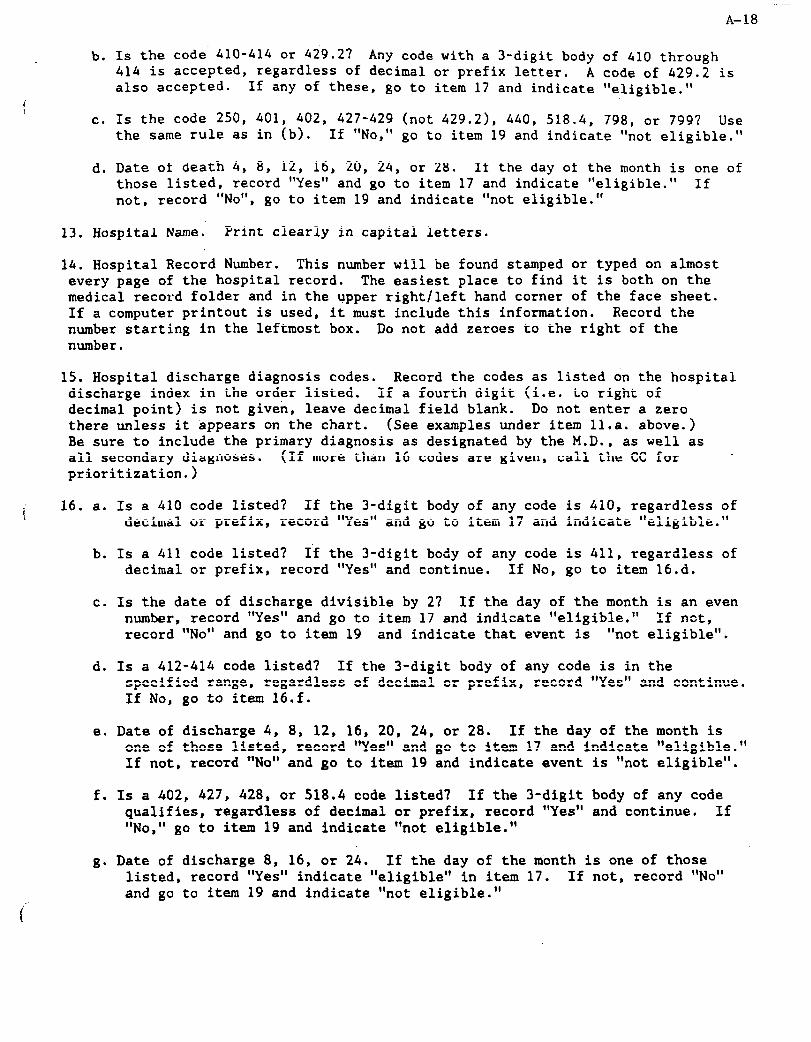
A-18
b. 1s the code 410-414 or 429.2? Any code with a 3-digit body of 410 through 414 is accepted, regardless of decimal or prefix letter, A code of 429.2 is also accepted. If any of these, go to item 17 and indicate 'eligible."
c. Is the code 250, 401, 402, 427-429 (not 429.21, 440, 518.4, 798, or 799? Use the same rule as in (b). If "No," go to item 19 and indicate "not eligible."
d. Date of death 4, 8, 12, 16, 20, 24, or 28. If the day of the month is one of those listed, record "Yes" and go to item 17 and indicate "eligible." If not, record "No", go to item 19 and indicate 'not eligible."
13. Hospital Name. Print clearly in capital letters.
14. Hospital Record Number. This number will be found stamped or typed on almost every page of the hospital record. The easiest place to find it is both on the medical record folder and in the upper right/left hand corner of the face sheet. If a computer printout is used, it must include this information. Record the number starting in the leftmost box. Do not add zeroes to the right of the number.
15. Hospital discharge diagnosis codes. Record the codes as listed on the hospital discharge index in the order listed. If a fourth digit (i.e. to right of decimal point) is not given, leave decimal field blank. Do not enter a zero there unless it appears on the chart. (See examples under item 1l.a. above.) Be sure to include the primary diagnosis as designated by the M.D., as well as all secondary diagnoses. (If more than 16 codes are given, call the CC for prioritization.)
i 16. a. Is a 410 code listed? If the 3-digit body of any code is 410, regardless of decimal or prefix, record 'Yes" and go to item 17 and indicate "eligible."
b. Is a 411 code listed? If the 3-digit body of any code is 411, regardless of decimal or prefix, record 'Yes" and continue. If No, go to item 16.d.
c. Is the date of discharge divisible by 2 ? If the day of the month.is an even number, record "Yes" and go to item 17 and indicate "eligible.' If not, record "No" and go to item 19 and indicate that event is "not eligible".
d. Is a 412-414 code listed? If the 3-digit body of any code is in the specified range, regardless of decimal or prefix, record 'Yes' and continue. If No, go to item 16.f.
e. Date of discharge 4, 8, 12, 16, 20, 24, or 28. If the day of the month is one of those listed, record "Yes" and go to item 17 and indicate "eligible." If not, record "No" and go to item 19 and indicate event is "not eligible".
f. Is a 402, 427, 428, or 518.4 code listed7 If the 3-digit body of any code qualifies, regardless of decimal or prefix, record 'Yes' and continue. If "No, " go to item 19 and indicate 'not eligible.'
g. Date of discharge 8, 16, or 24. If the day of the month is one of those listed, record "Yes" indicate "eligible" in item 17. If not, record "No" and go to item 19 and indicate 'not eligible.'

A-19
17. Eligible event. Any path leading to this item indicates that the event is eligible. Record "Yes," the only possible response.
lg. Event Identification Number. Assign the next available event ID number at this point. Record the number here and in the header. Afterward, skip to item 20.
19. Ineligible event. Any path leading to this item indicates that the event is not eligible. Record "No," the only possible response. Complete the remainder of this form, but no further action is necessary.
20. Date of data collection. Record the date on which the form was completed.
21. Code .number of person completing this form. The field center staff member who has performed the abstraction and completed the form must enter his/her valid ARIC code number in the boxes provided.
Complete the form flags at the end of the form by placing an X in the appropriate box(es), indicating other forms that need to be collected for this event. Each form flag refers to one or more items on this form that define the criteria for that form flag.
The SEL form should be kept on file at the field center for all eligible events.
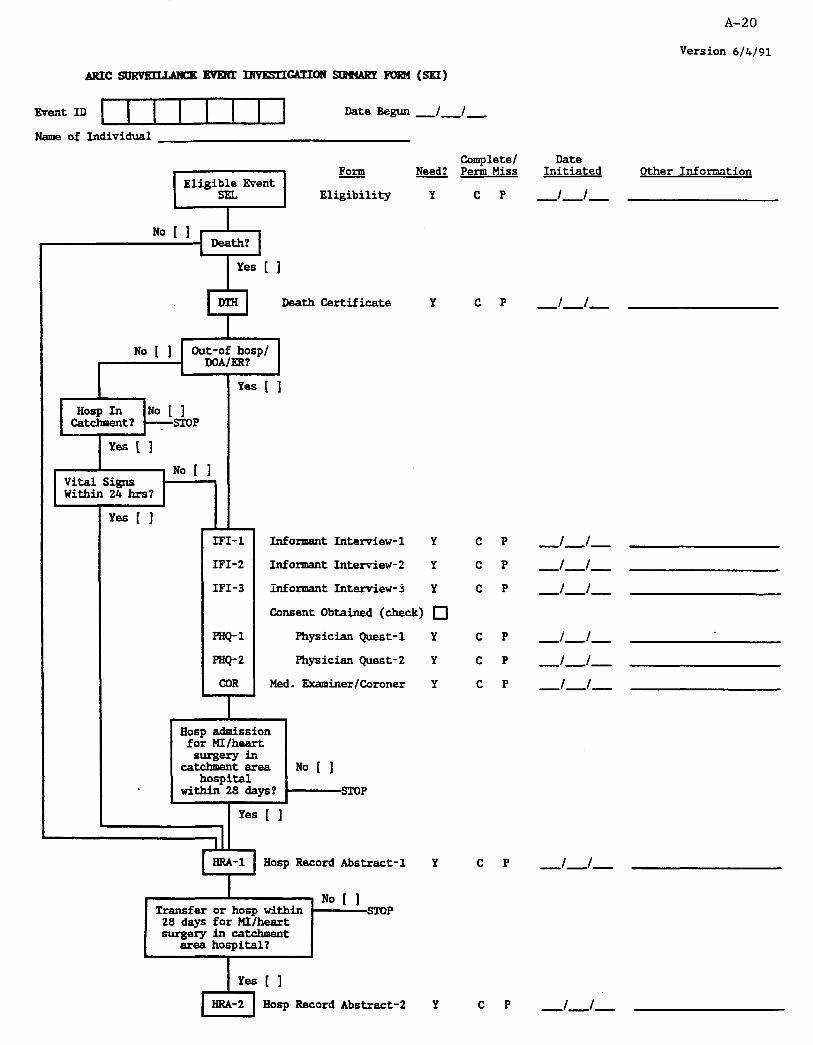
A-20
Version 6/k/91
Name of Individual
9 Death Certificate Y
Complete/ Perm Miss
c P
c P
Yes [ 1
hod CR? I
Yes [ 1
IFI-
IFI-
IFI-
PHQ-1
PHQ-2
Informant Interview-l Y
Informant Interview-2 Y
Informsnt Interview-3 Y
Consent Obtained (check) 0
Physician Quest-l Y
Physician Quest-2 Y
Med. Examiner/Coroner Y COR
I li;o"t ZhS
surgery~ catchment area No 1 1
hospital within28deys? STOP
Yes [ 1
Iiosp Record Abstract-l Y
I----NoI 1 Transfer or hosp within STOP
28 days for MI/heart surgery in catchment
area hospital?
c P
c P
c P
c P
c P
c P
c P
Date Initiated Other Information
-l-l-
-t-/-
-l-l-
-l--i-
-I-/-
-f-J- -i-l- -l-l-
-/-I-
Hasp Record Abstract-2 Y c P -l-f-
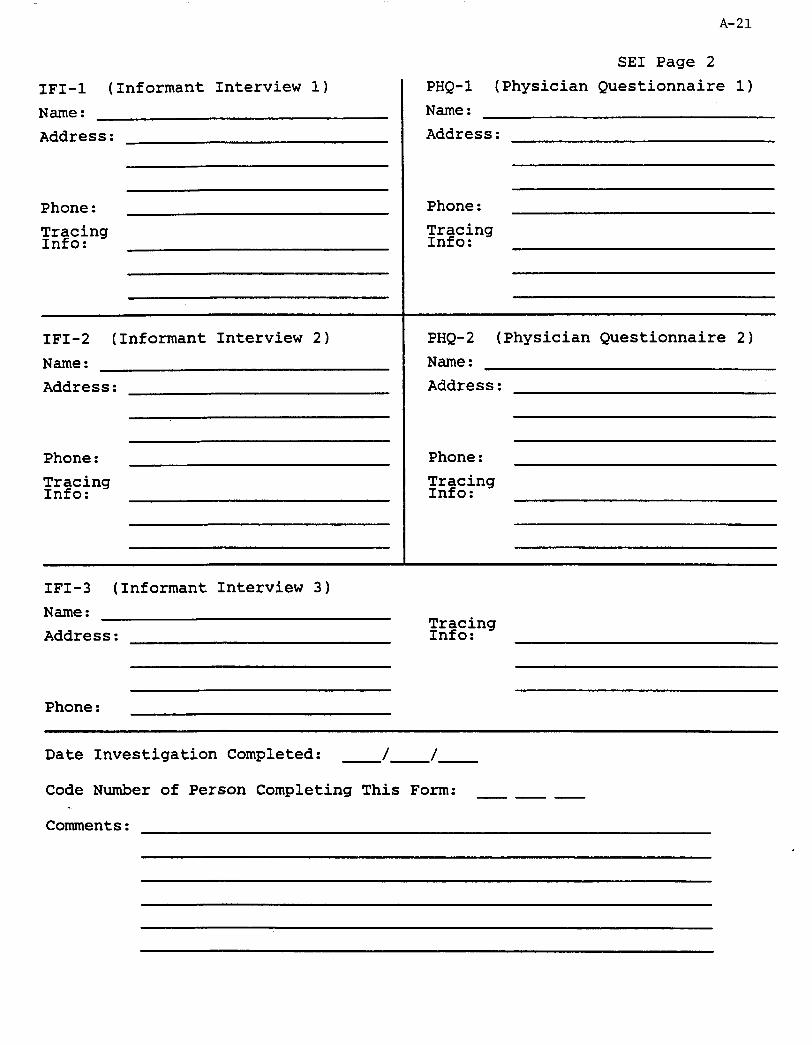
1~1-1 (Informant Interview 1) Name : Address:
Phone: Wlk~ing
:
IFI- (Informant Interview 2) Name : Address:
Phone:
Txing :
IFI- (Informant Interview 3) Name : Address:
Phone:
A-21
SE1 Page 2 PHQ-1 (Physician Questionnaire 1) Name : Address:
Phone: ?k&.ng
:
PHQ-2 (Physician Questionnaire 2) Name : Address:
Phone:
Txing :
W&ng :
Date Investigation Completed: -/-I-
Code Number of Person Completing This Form: --m
Comments:

A-22
SURVEILLANCEEVENT INVl3STIGATIONSUHHARYFORnINSTRUCTIONS
Version: A 06/04/91
I. GENERAL INSTRUCTIONS
The Surveillance Event Investigation Summary Form (SEI) is used to monitor the procedures of event investigation used in ARIC. It is intended to be used by the supervisor of Surveillance procedures at each field center. The SE1 Form should be completed according to information collected in other forms for a given eligible event. This information is summarized in the "form flags" at the end of each form, which indicate what additional forms should be collected for an event.
II. INSTRUCTIONS FOR FORM COMPLETION
The form is divided into four parts: procedure flowchart, form completion information for sources.
header information, information , and contacting
The header information at the top of page 1 should be completed as soon as an eligible event is identified by the Surveillance Event Eligibility Form (SIX). Complete the -event ID number as assigned on the SEL Form, and record the current date and the name of the individual whose event is under investigation.
The flowchart on the left side of page 1 depicts the procedures used in event investigation. "Yes" and "No" paths emerge from each decision box and should be checked to indicate which path to follow. The sources of information for these decisions are detailed in the next section, but they essentially repeat the rules defined by the form flags in each form. If the designated path passes through a box containing three-letter form codes, these forms should be collected. As many as three Informant
-Interview (IFI) Forms and two Physician Questionnaires (PHQ) may be required. It is possible that evidence acquired later in the process may conflict with evidence acquired earlier. In such cases, a path may have to be changed from the one which was previously defined. For example, a death is defined as "in-hospital" on the death certificate. However, when the hospital records are reviewed, in the Emergency Room (W).
it is shown that the person died The path is then changed to indicate
that the death is "out-of-hospital/D/RR."
The right-hand side of page 1 lists all the possible forms that could be scheduled for *completion for an event. Based on the path which is followed in the flowchart, certain forms should be designated as "Needed" by circling the "Y" in that column. When the effort to complete this needed form is begun, the date should be recorded in the "Date Initiated" column. (For the Physician Questionnaire, this should reflect the date it is first sent to the physician. If additional mailings are made, record the date in the "Other Information" column. Dates of mailings for the

Page 2 of 2 A-23
Informant Interview attempts should be kept in the "Record of Calls" section of that form.) As each needed form is completed, the "C" under "Completed/Permanently Missing" should be circled. If, after exhaustive effort, a needed fom cannot be completed, circle the "P" in this column. 'ALL FORMFLAGS MUST BE CAREFULLY REVIEWED IN COMBINATION WITH THESE PROCEDURES IN ORDER TO IDENTIFY EXACTLY WHICH FORMS SHOULD BE COLLECTED!
The second page of the SEI Form is used to record pertinent information for contacting of sources, such as names, addresses, and phone numbers. Space for additional comments is provided at the end. When the investigation is completed, i.e., all needed forms are designated either "completed" or "permanently missing," the date and code number are recorded at the end of the form.
The SE1 form should be kept on file at the field center for all eligible events.
III. SOURCES OF INFORMATION
The following list indicates what forms and item numbers to use in the process of defining the appropriate path on the SE1 Form:
Decision
Death?
Answer
Yes if: No if:
Out-of-hasp/
DOA/ER?
Yes if:
No if:
Hospital in catchment?
Vital Signs within 24 hrs?
Yes if: No if:
Hosp for MI/ Yes if: heart surgery in No if: catchment area hosp within 28 days?
Transfer or hosp within 28 days for MI/heart surgery in a catchment area hospital?
Source Form and Item, Response(s)
SEL 7 = Y SEL 7 = N
DTH 12 = N or 0 z DTH 13 = A, B, or c
DTH 12 = A and DTH 13 = D, E, or F OR DTH 12 -- B @ DTH 13 = D, E, or F
DTH12 =A DTH12 =B
HRA Form
IF1 ba = Y z IF1 6b = Y Otherwise
Transfer: HRA 13 = Y, ERA 13b completed and in a catchment area hospital
Hospitalization: BRA 19g=Y OR HRA 32=Y

A-.24
O.M.E. 0925-0281 exp. 7-31-92
HOSPITAL RECORD ATHEROSCLEROSIS RISK ’
1N COMMUNI7IE-S S’WOY ABSTRACTION FORM
FORM CODE: llll HRA VERSION: A. S/25/91
LASTNAME: I I I I I I I I I I I I INITIALS: 171
INSTRUCTIONS: The Hospital Record Abstraction Form is coqleted for each eligible hospitalized event as determined by the Surveillance Event Eligibility Form, and for all eligible Cohort hospitalizations as determined by the Cohort Eligibility Form. CPent ID, Name (or Soundex code) must be entered above. Refer to this form's Q by Q instructions for information on entering numerical responses. For multiple choice and "yes/no" questions, circle the letter corresponding to the most appropriate response. If a letter is circled incorrectly, mark through it with an IX' end circle the correct response.
Hospital Record Abstraction Form (HRAA Screen 1 of 39)
A. MEDICAL ABSTRACTION
1. a. Hospital code number: m [If code 96-99, name and location]:
b. Medical Record Number: II IIll IIll 1 II
2. Record the ICD9-CM diagnoses and procedure codes from the hospital discharge index (or Eligibility Form) if an index was used to select this case:
a.. ill.m
b. .=.a
c. II.1 d. unxn
e. llrl.m f. r-r.m
h.
. 1.
. J*
k.
1.
m.
n.
0.
Pa
9.
r.
6.
t.
U.
I.1 mm nmm I.1 =.m m.m rllll.m lllr1.m =.m 1171.1 mn:m 1-77.m . umm mn.m

A-25
Hospital Record Abstraction Form (HRhA Screen 2 of 39) ---
3. Abstracting for:
cohort......................... c
Sumeillance . . . . . . . . . . . . . . . . . . S
t. 3as the hospital chart for this event been located?
Yes..........Y
5
o........... N
Go to Item 97, Screen 38
3. If name not available, SOUNDEX:
6. Social Security/Medicare Number:
1IIHIHIIIH-l 7. Patient address:
City
8. sex:
County State Zip
Male . . . . . . . . . . . . . . . . . . . . . . . . . . M
Female . . . . . . . . . . . . . . . . . . . . . . . . F
Hospital Record Abstraction Form (HRM Screen 3 of 39)
9. Race or ethnic group:
Uhit&kucasian . . . . . . . . . . . . . . . W
Black/Negro . . . . . . . . . . . . . . . . . . . E
Asian/Pacific Islander . . . . . . . . A
American Indian/Native Alaskan . . . . . . . . . . . . . . . ...*... I
Other . . . . . . . . . . . . . . . . . . . . . . . . . 0
IJnlcnmn/not recorded . . . . . . . . . . U
lo. Birthdate:
IlHlHll llpD dd YY
11. a. Date of arrival at this hospital:
m dd YY
b. Arrival time at this hospital:
c. AM or PM AM . . . . . . . . . . . . A
PM . . . ...*..... P
12. Did an emergency medical service unit transport the patient to this hospital?
Yes . . . . . . . . . . . . Y
No . . . . . . . . . . . . . N
unknown........u

A-26
Hospital Record Abstraction Form (HRAA Screen 4 of 39) I
l3.a. Was the patient transferred from or to another
acute care hospital?
Yes...........Y
h No...........N
I- ~~ Go to Itam 14, Screen 4
.b. First transfer
Hospital Name
city
State
c. Date of admission to that hospital:
1 1 H 1 H I 1 am dd YY
d. Second transfer
Hospital name
City
State
e. Date of admission to that hospital:
1 1 H 1 H 1 I 1pm dd YY
14. gate of discharge (for nonfatal case) or death:
1 1 H 1 H 1 1 m dd YY
Hospital'Record Abstraction Form (HRAA Screen 5 of 39) a u. List the hospital discharge diagnosis and
procedure codes exactly as they appear on the front sheet of the medical record and/or on the discharge summary:
a
b.
C.
d.
8.
f. m
6*
h.
mom 1.1 r.m mn.m =.a rl.m m0.m =.a mum rl.m
k.
1.
m.
n.
0.
P*
90
r.
8.
t.
u.
u=lm mn.m rT171.m nmm mm3 nm.m mn.m mn.m tlnx= n.m m.m

A-27
Hospital Record Abstraction Form (HIM Screen 6 of 39)
r 1
16. Transcribe discharge diagnoses as they appear on front sheet of medical record and/or discharge SW.
1

A-28
Hospital Record Abstraction Form (HRAA Screen 7 of 39)
17. What was the disposition of the patient on discharge?
Daceased . . . . . . . . . . . . . . . . . . . . . . D
ischarged alive . . . . . . . . . . . . . . A
18. Was au autopsy performed?
Yes.. . . . . . . . .Y
No...........N
19.a. Was the patient either dead on arrival or did he/she die in the emergency room?
Yes..........Y
No
El
. . . . . . . . . . N
Co to Item lge. Screen 8
b. First recorded Systolic BP
If zero or not recorded, and patient died within 24 hrs., record 000 and go to Item 19e, Screen 8. If zero or not recorded and patient lived at least 24 hrs., enter 001.
Hospital Record Abstraction Form (HRAA Screen 8 of 39)
C. First recorded Diastolic BP
d. First recorded Pulse Rate
If pulse rate is greater than 0, go to item 22. If 0 or not recorded, and patient lived at leaat 24 hrs., enter 001 and go to item 22. If 0 or not recorded and patient died within 24 hrs., enter 000 and continue with item 19 e.
a. t&s there (an) acute episode(s) of pain or discomfortanyhere in the chest, left armor shoulder or jaw either just before death or within 72hours of death?
Yes..............Y
No...............N
. . . . . . . . . . U
f. Is there a history of myocardial infarction prior to onset of this event?
Yes..............Y
nknown..........U
I Go to Item 19h screen 9. I
e* Did a myocardial infarction occur within four weeks of this event?
Yes . . . . . . . . . . . ..Y
No...............N
unknom..........u
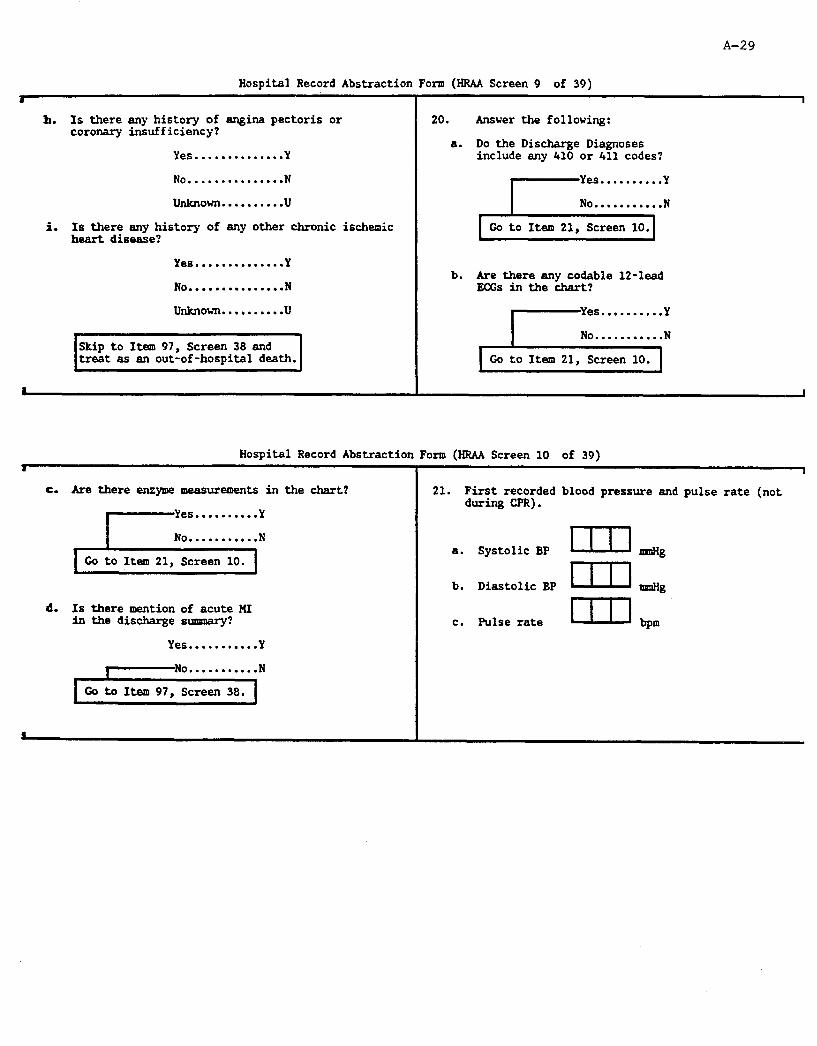
A-29
Hospital Record Abstraction Form (HRAA Screen 9 of 39)
h. Is there any history of angina pectoris or coronary insufficiency?
Yes..............Y
No...............N
Unknown..........U . L Is there any history of any other chronic ischeaic
heart disease?
Yes..............Y
No...............N
Unknovn..........U
Skip to Item 97, Screen 38 and treat as an out-of-hospital death.
8
20. Answer the following:
a. Do the Discharge Diagnoses include any 410 or 411 codes?
l-z:::::::::::
b. Are there any codable 12-lead EC& inthechart?
Hospital Record Abstraction Form (HRAA Screen 10 of 39)
c. &e there enzyme measurements in the &art?
) co !,,,~~~~~~:1,1:~:
d. Is there mention of acute MI in the discharge slrmn;w?
Yes...........Y
I
21. First recorded blood pressure and pulse rate (not during CPR).
a. Systolic BP I-111 mw3
b. Diastolic BP I mrJHa
c. Pulse rate
A-30
Hospital Record Abstraction Form (HRAA Screen 11 of 39)
I I
22. Narrative (Attach copy of d/c summary or abstract d/c summary. Include symptom onset, timing, hospital course, etc.)

Hospital Record Abstraction Form (RRM Screen 12 of 39) a
2S.a. Did acute cardiac symptoms begin prior to arrival at this hospital?
Yes . . . . . . . . . . . . . . . . . . . . . . . . . . .
A-31
I
b. Estimated time from onset of acute cardiac symptoms to arrival at this hospital.
<l hour . . . . . . . . . . . . . . . . . . . A
21 hour and <2 hours . . . . . . B
22 hours and <4 hours . . . . . C
24 hours and <6 hours . . . . . D
26 hours and Cl2 hours . . . . E
212 hours and C24 hours . . . F
11 day and <3 days . . . . . . . . G
23 days . . . . . . . . . . . . . . . . . . . H
Not recorded . . . . . . . . . . . . . . U
Go to Item 24b, Screen 13.
Hospital Record Abstraction Form (HRAA Screen 13 of 39) a
24-a. What was the primary diagnosis or mason for admission to this hospital?
Elective cardiac catheterization . . . . . . . . . A
Elective coronary bypass surgery . . . . . . . . . . . . . . . . . B
Other non-acute CHD evaluation . . . . . . . . . . . . . . C
Cancer . . . . . . . . . . . . . . . . . . . . D
Diabetes msllitus . . . . . . . . . E
stroke . . . . . . . . . . . . . . . . . . . . F
Chronic obstructive pulmonary disease . . . . . . . G
Peripheral vascular disease . . . . . . . . . . . . . . . . . Ii
Gallbladder disease . . . . . . . I
Other . . . . . . . . . . . . . . . . . . . . . 0
4
b. Was there mention of an acute CHD event with onset after arrival at this hospital?
Yes..........Y
I o........... N
Go to Item 25, Screen 14.
c. Date of in-hospital CHD event:
1 1 H 1 H 1 1 m dd YY
[NCTE: If Patient had both CUD et-ant present on admission (Item 23-Y) and after admission (Item 24b=Y), you must decide which event is most important (see Instructions). .Answer subsequent questions for the most important event.)
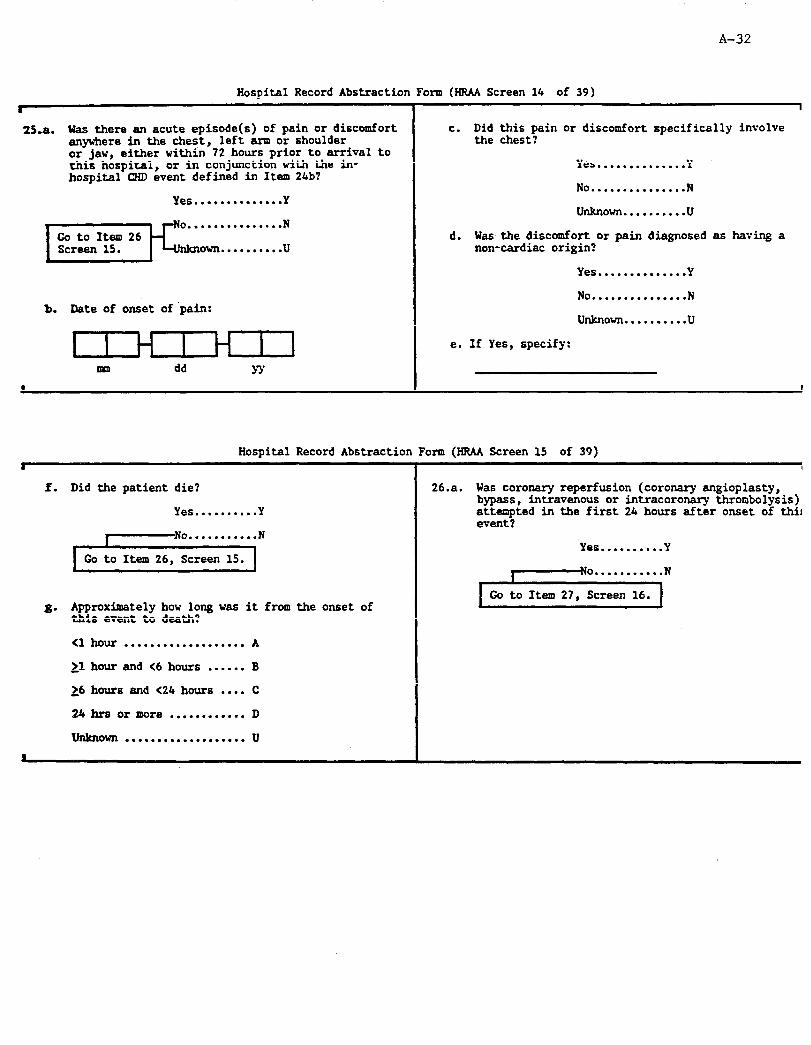
A-32
Hospital Record Abstraction Form (HR4A Screen 14 of 39) s
25-a. Was there an acute episode(s) of pain or discomfort anvwhere in the chest, left arm or shoulder or-jaw, either within-72 hours prior to arrival to this hospital, or in conjunction with the in- hospital CHD event defined in Item 24b?
Yes..............Y
);;;;:::::::::::
b. Date of onset of 'pain:
mm dd YY
c. Did this pain or discomfort specifically involve the chest?
Yes..............Y
No . . . . . . . . . . . . . . . N
unknown..........u
d. Was the discomfort or pain diagnosed as having a non-cardiac origin?
Yes . . . . . . . . . . . . . . Y
No...............N
unknown..........u
e. If Yes, specify:
Hospital Record Abstraction Fom (HRAA Screen 15 of 39) .
f. Did the patient die?
Yes..........Y
I No...........N
Go to Item 26, Screen 15.
g. Approximately how long was it from the onset of this event to death?
Cl hour . . . . . . . . . . . . . . . . . . . A
,1 hour and C6 hours . . . . . . B
26 hours and (24 hours . . . . C
24 hrs or more . . . . . . . . . . . . D
unknown . . . . . . . . . . . . . . . . . . . u
26.a. Was coronary reperfusion (coronary angioplasty, bypass, intravenous or intracoronary thrombolysis) attempted in the first 24 hours after onset of thi! event?
Yes..........Y
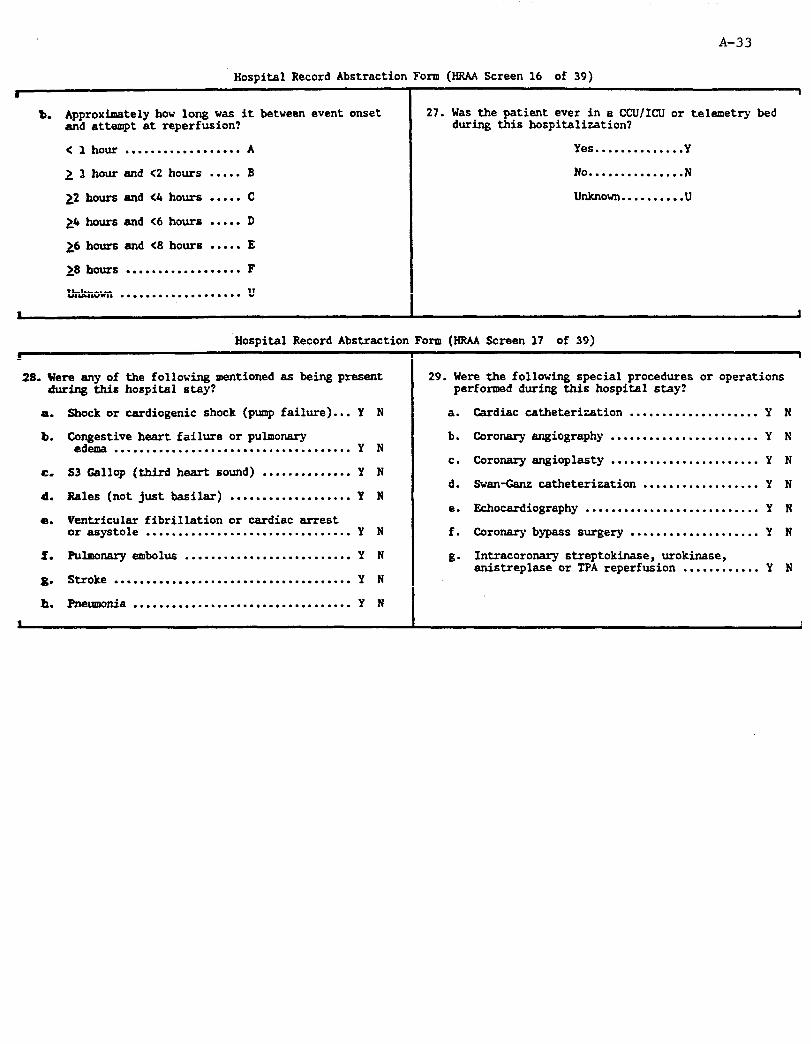
A-33
Hospital Record Abstraction Form (HJUA Screen 16 of 39)
8 1
b. Approximately how long was it between event onset 27. was the patient ever in a CCU/IClJ or telemetry bed and attempt at reperfusion? during this hospitalization?
< 1 hour . . . . . . . . . . . . . . . . . . A Yes . . . . . . . . . . . . . . Y
2 P hour and C2 hours . . . . . B No...............N
22 hours and <4 hours . . . . . C unknown..........u
24 hours and <6 hours . . . . . D
26 hours and (8 hours . . . . . E
18 hours . . . . . . . . . . . . . . . . . . F
unknown . . . . . . . . . . . . . . . . . . . u
Hospital Record Abstraction Form (HRAA Screen 17 of 39)
28. Were any of the following mentioned as being present during this hospital stay?
a.
b.
c.
d.
a.
f.
8.
h.
Shock or cardiogenic shock (pump failure) ... Y N
Co.gztive heart failure or pulmonary .... ...... ........ ... ................ Y N
S3 Callop (third heart sound) .............. Y N
Rales (not just basilar) ................... Y N
Ventricular fibrillation or cardiac errest or asystole ................................ Y N
Pulmonaryeslbolus .......................... Y N
Stroke ..................................... Y N
Pneumonia .................................. Y N
29. Were the following special procedures or operations performed during this hospital stay?
a.
b.
C.
d.
e.
f.
g-
Cardiac catheterization .................... Y N
Coronary angiography ....................... Y N
Coronary angioplasty ....................... Y N
Swan-Cans catheterization .................. Y N
Echocardiography ........................... Y N
Coronary bypass surgery .................... Y N
Intracoronary streptokinase, urokinase, anistreplase or TPA reperfusion ............ Y N
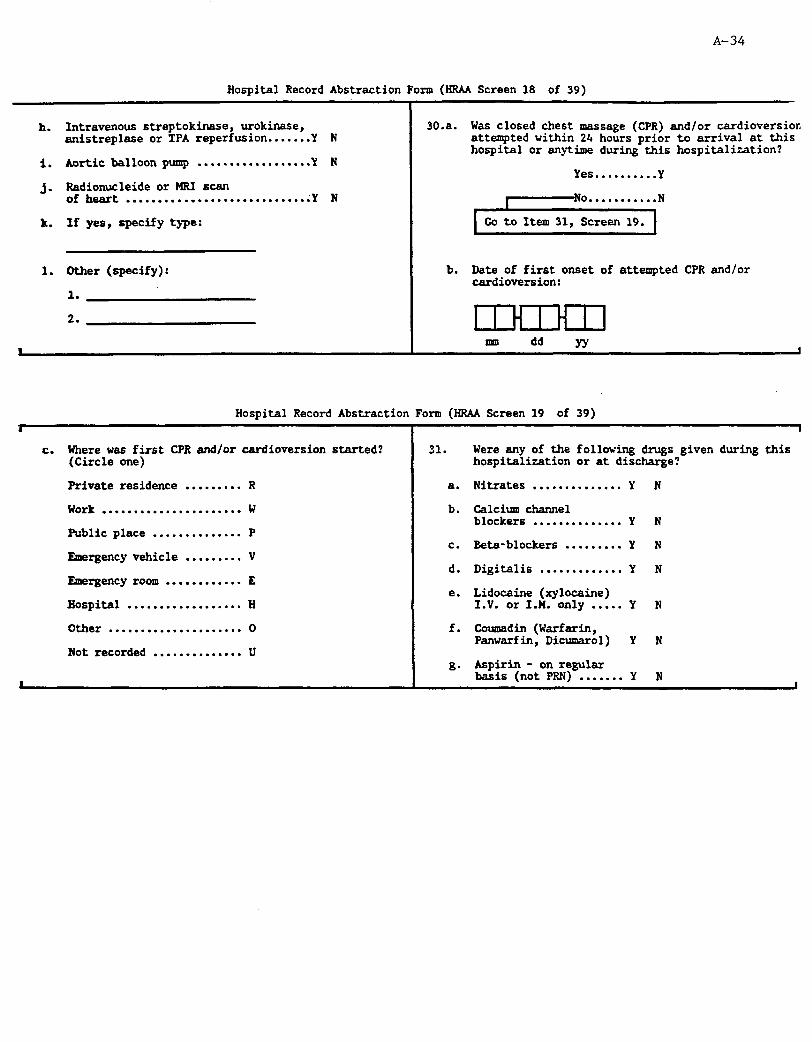
A-34
Hospital Record Abstraction Form (HRAA Screen 18 of 39)
h.
. 1.
j-
k.
1.
Intravenous streptokinase, urokinase, anistreplase or TPA reperfusion.......Y N
Aortic balloon pump . . . . . . . . . . . . . . . . ..Y N
Radionucleide or MRI scan ofheart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Y N
If yes, specify type:
Other (specify):
1.
2. I 1 H 1 H I I
I 30.a.
b.
Was closed chest massage (CPR) and/or cardioversior, attempted within 24 hours prior to arrival at this hospital or anytime during this hospitalization?
Yes..........Y
Date of first onset of attempted CPR and/or cardioversion:
mm dd YY I
Hospital Record Abstraction Form (RRAA Screen 19 of 39) .
I
I
c. Where was first CPR and/or cardioversion started? 31. Were any of the following drugs given during this (Circle one) hospitalization or at discharge?
a. Nitrates . . . . . . . . . . . . . . Y N Private residence ......... R
Work ...................... W b. Calcium channel blockers . . . . . . . . . . . . . . Y N
Public place .............. P c. Beta-blockers . . . . . . . . . Y N
Emergency vehicle ......... V d. Digitalis . . ..*.......* Y N
Rnergency room ............ E e. Lidocaine (xylocaine)
Hospital .................. H I.V. or 1-N. only . . . . . Y N
Other ..................... 0 f. Coumadin (Warfarin, Panwarfin, Dicmarol) Y N
Not recorded .............. U 80 Aspirin - on regular
....... Y N I
basis (not PRN) I

A-35
Hospital Record Abstraction Form (HRM Screen 20 of 39) t I
32. Is there a history of myocardial infarction prior 34.a. Is there a history of any other chronic ischemic to the onset of this event? heart disease?
Yes . . . . . ..*...... Y
No...............N
Yes..........Y
~-NO.. . . . . . . . . .N
unknown.. . . . . . . . .u
IIf U, also review previous discharge diagnoses. ]
33. Is there any history of angina pectoris or -coronary insufficiency?
Yes..............Y
Go to Item 35, Screen 21.
b. Specify:
No . . . . . . . . . . . . . . . N
Unknown. . . . . . . . . .U
a
Hospital Record Abstraction Form (HRM Screen 21 of 39) .
35. Is there a history of valmlar d5sease or cardiomyopathy?
Yes . . . . . . . . . . . . . . Y
No . . . . . . . . . . . . . . . N
36. Is there a history of coronary bypass surgery prior to this event?
Yes..............Y
No...............N
37. Is there a history of coronary angioplasty prior to this event?
Yes . . . . . . . . . . . . . . Y
No . . . . . . . . . . . . . . . N
I
38. Is there a history of hypertension (high blood pressure) prior to this event?
Yes..............Y
No...............N
Unknown. . . . . . . . . .U
39. Is there a history of stroke prior to this event?
Yes..............Y
Go to Item 41, Screen 22.
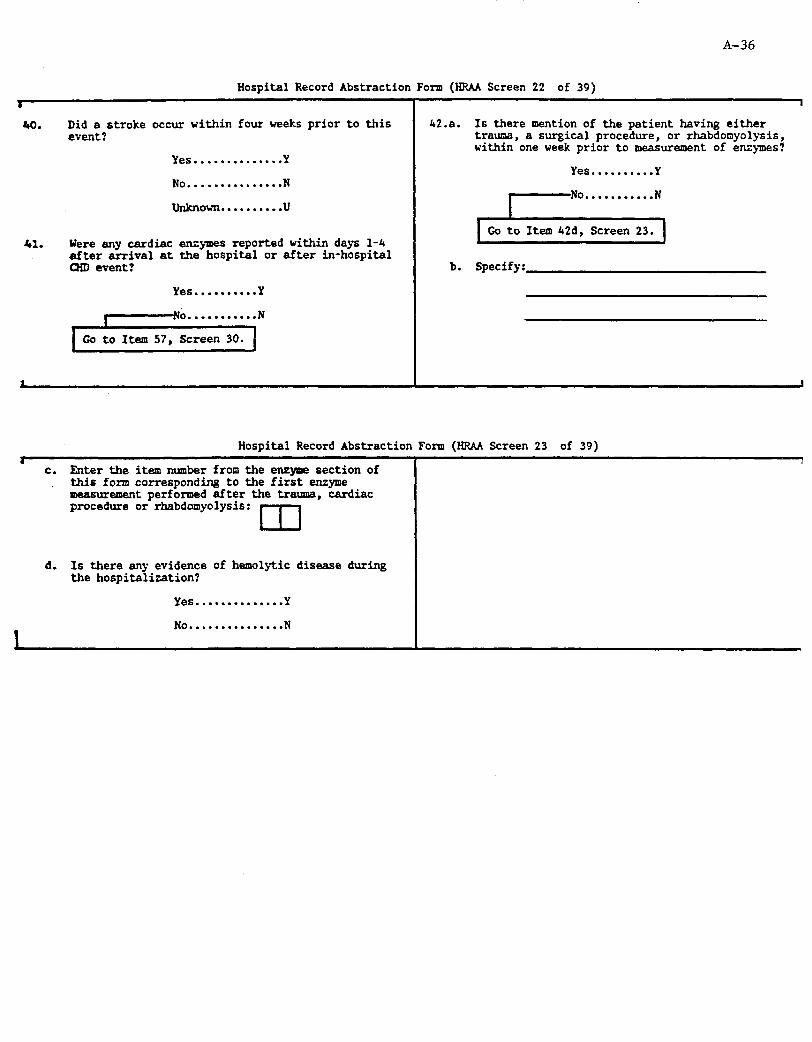
A-36
Hospital Record Abstraction Form (HRAA Screen 22 of 39) .
w). Did a stroke occur within four weeks prior to this event ?
Yes..............Y
No...............N
unknown.. . . . . . . . .u
41. Were any cardiac enzymes reported within days l-4 after arrival at the hospital or after in-hospital CXD event?
Yes..........Y
Go to Item 57, Screen 30.
42.a. Is there mention of the patient having either trauma, a surgical procedure, or rhabdomyolysis, within one week prior to measurement of enzymes?
Yes..........Y
b. Specify:
Hospital Record Abstraction Form (HRAA Screen 23 of 39) .
c. Enter the item number from the enzyme section of this form corresponding to the first enzyme measurement performed after the trauma, cardiac procedure or rhabdomyolysis: m
d. Is there any evidence of hemolytic disease during the hospitalization?
Yes . . . . . . . . . . . . . . Y
No . . . . . . . . . . . . . . . N

A-37
Hospital Record Abstraction Form (HRAA Screen 24 of 39)
1 1
B. EN7XMES
43. LAEORATORY STANDARDS
Ranee Set 1
Total CK (CPK) a* unn CK-MB (hrt frac) b.
Total LDH d.
LDHl e.
LDH2
LDHl/LDH2 1.
Ranee Set 2
Total CK (CPK) k.
CK-MB (M frac)
TotalLDH
LDHl
LDH2
LDHl/LDH2
1.
n.
0.
4.
S.
*Special Units:
CK-MB
Upper Limit of Normal
Specialw( Units
I I I I I 1.m f-n uIn.ul hcl
cIn.ul j- III Upper Limit Special* of Normal Units
I I I I I uul.m m. q I I I I I I.D P. cl
I.D r. lzl
m.m t. III
1 = (Negative/Positive) or (Absent/Present) or (N~~~sal/Abn~rs~al)
2 = (Negative/Weak Positive/Positive) or (Absent/Trace/Present) or (Normal/High Normal/Abnormal)
CK-MB, LDHl,LDH2
3 = Expressed as % of total enzyme .
4 = Exprassed as proportion (decimal units) of total enzyme
LDHl/LDH2
5 =%
6= Proportion (decimal)
1 7 = (Negative/Positive) or (LDHI. d. IDH2 / LDHl > LDH2)
I
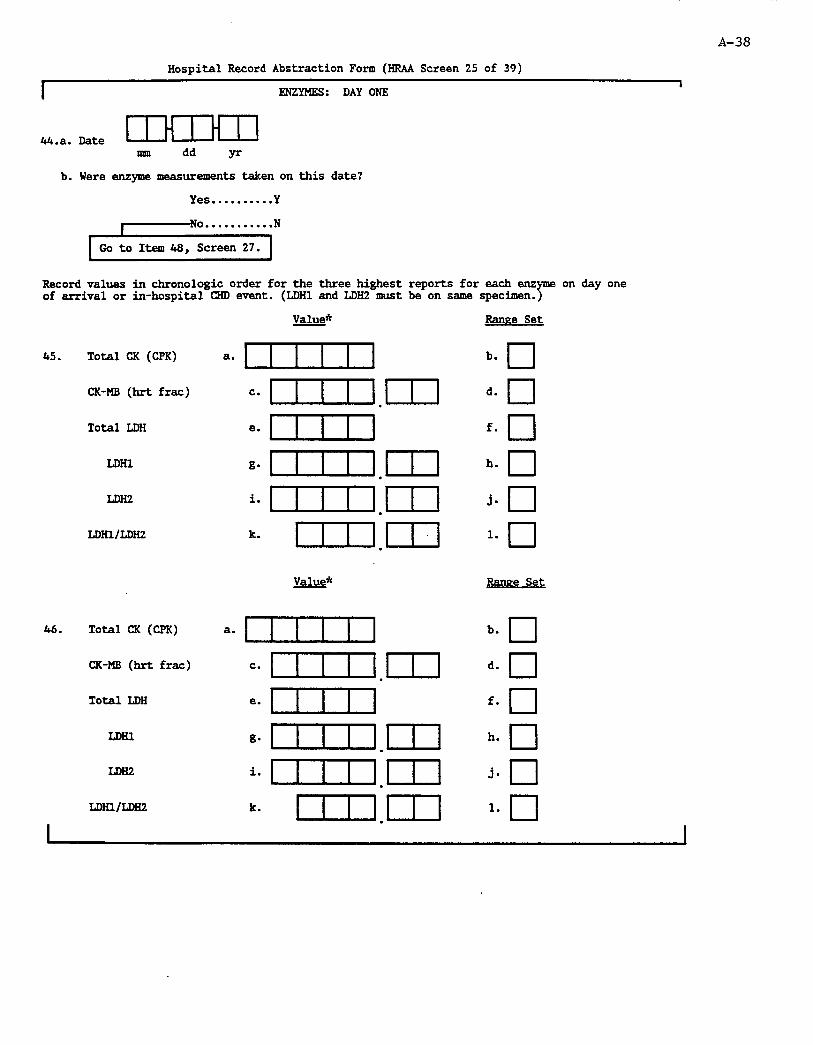
A-38
Hospital Record Abstraction Form (HRAA Screen 25 of 39)
I I ENZYMES: DAY ONE
44-a. Date IHIHI] mm dd yr
b. Were enzyme measurements taken on this date?
Yes.. . . . . . . . .Y
r-No. . . . . . . . . . .N
Go to Item 48, Screen 27.
Record values in chronologic order for the three highest reports for each enz me of arrival or in-hospital CHD event. (LDHl and LDH2 must be on same specimen. 2;
on day one
45. Total CK (CPK)
CK-MB (hrt frac)
Total LDH
LDHl
LDH2
LDHl/LDH2
46. TotalCK(CPK)
CK-MB (hrt frac)
Total LDH
LDHl
LDH2
mil/LDH2
Value*
a* 1
c*uln.ul
e* uul
g4zUn.ul
imuIn.ul
k- un.ul
Value*
e.
k.
Ranee Set
b. q d. q f. q h. q j- q 1.
cl
Ranee Set
b. cl
d. q f. q h. q j- q 1. q

A-39
I I
Hospita.Record Abstraction Form (HRAA Screen 26 of 39)
Value* Ranee Set
47. Total CK (CPK) b. q
I
CK-MB (hrt frac)
Total IDH LDIU
=- uIn.ul d- q *- urn f. q
LIni2 i* uIn.ul J- -I LDIu/LDH2 k- un.ul l* q
*Special Values:
M-Ma it
= Negative or absent or normal = Weak positive or weak present or trace or
high-normal or small C = Present or positive or abnormal or medium or large
LDHlILDH2 D = LDHl/LDH2 reported only as 1 upper limit or positive or LDHl > LDH2
E = LDHl/LDH2 reported only as < upper limit or negative
I or LDHl 5 LDH2
I

A-40
Hospital Record Abstraction Form (HRAA Screen 27 of 39)
ENZYl'fES: DAY TWO
4S.a. Date IHIHI] nm dd yr
b. Were enzyme measurements taken on this date?
Yes .......... Y
r-No. ......... .N
I--- Co to Item 51, Screen 28. I
Record values in chronologic order for the two highest reports for each enzyme on day two following arrival or in-hospital CHD event. (LDHl and LDH2 must be on same specimen.)
49. Total CK (CPK)
CK-MB (hrt frac)
Total LDH
LDHl
LDH2
LDHlmH2
50. Total CK (CPK)
CK-MB (hrt frac)
Total LDIi
LDHl
LDH2
LDHmDH2
*Special Values:
CK-MB
=*uIn.ul e. cun g”uln.ul 4IlIl.m km un.ul
a. I c~uln.ul e’ uln g*uIn.ul i*urn.ul k- cIn.ul
A = Negative or absent or normal B = Weak positive or weak present or trace or
high-normal or small
Ranee Set
b. cl
d. q f. q h.
cl
J* *El
1. q Ranee Set
b. q d. q
cl f.
h. q . J. q 1. q
C = Present or positive or abnormal or medium or large
LDli1/LDH2 D = LDHULDH2 reported only as 2 upper limit or positive or LDHl > L.DH2
E = LDHl/LDH2 reported only as C upper limit or negative
I or LDHl : LDH2
I

Hospital Record Abstraction Form (HRAA Screen 2% of 39) A-41
I i
ENZYMES: DAY THREE
51.a. Date IHlHll Imn dd yr b. Were enzyme measurements taken on this date?
Yes.. . . . . . . . .Y
1 0 . . . . . . . . . . . N
Go to Item 54, Screen 29.
Record values in chronologic order for the two highest reports for each enzyme on day three following arrival or in-hospital CHD event. (LDHl and LDH2 must be on same specimen.)
52. Total CK (CPK)
CK-MB (hrt frac)
Total LDH
LDHl
LDH2
LDHl/LDHZ
53. Total CK (CPK)
CK-MB (hrt frac)
Total LDH
LDHl/LDH2
*Special Values:
Value*
a* 111 c* iIIIa-1 e* uul g. lIII3n.m i* ~I.En L. un.m
Value*
e.
Iknee Set
b. q d. q f. q h. q j- q 1. q Ranee Set
b. q d. q f. q h. q j- q 1. q
CK-MB A * Negative or absent or normal B = Weak positive or weak present or trace or
high-normal or small C = Present or positive or abnormal or medim or large
LDIil/LDH2 D = LDHl/LDHZ reported only as 2 upper limit or positive or LDHl > LDH2
I
E = LDHl/LDH2 reported only as < upper limit or negative or LDHl < LDH2

A-42
I
Hospital Record Abstraction Foxm (BRAA Screen 29 of 39)
ENZYMES: DAY FCUR
54.a. Date IHIHI] mm dd yr
b. Were enzyme measurements taken on this date?
Yes..........Y
Record in chronologic order values for the two highest reports for each enzyme on day four following arrival or in-hospital CHD event. (LDHl and LDH2 must be on same specimen.)
55. Total CK (CPK)
CK-MB(hrtfrac)
Total LDH
LDHl
LDH2
LDHl/LDHZ
56. Total CK (CPK)
CK-MB (hrt
Total LDH
LDHl
LDH2
LDHl/LDH2
*Special Values:
CK-MB
LDHl/LDH2
frac)
a. I =* uIn.ul e- I gdzIzlIl.ul 4IInIl.ul lc* cln.m
a. CuIn =*uIn.ul e- uln g-uIn.ul i-uIn.ul k- cln.ul
Ranee Set
b. a
d. q f.
cl
h. q
Ranee Set
b. q d. q f. Cl h. q . J. q 1. q
A = Negative or absent or normal B = Weak positive or weak present or trace or
high-nonnal or small C = Present or positive or abnoxmal or medium or large D = I.DHl/LDHZ! reported only as 1 upper
limit or positive or LDHl > DDE2 E = LDHl/LDH2-reported only aa < upper limit or negative
or LDHl s LDH2

A-43
Hospital Record Abstraction Form (HRAA Screen 30 of 39)
I I E. EGG CODING
57. Were any 12 lead EGGS taken during this admission?
Yes..........Y
58. Are any of the EGGS codable:
Yes..........Y
FIRST GODAELEEGGAFTERARRIVALATIiOSPITAL(EGGF)
59. Date of ECGF: I 1 H 1 H 1 1 [Check calibration mark] m dd YY
70. Are there other codable EGGS?
Yes..........Y
I o........... N
Go to Itearl 94 Screen 38.
LAST CODABU EGG ON THIS ADMISSION (EGGL)
71. Date of EGGL: LIHIHIl
nml dd YY
82. Are there other codable EGGS taken on or after day 3 after admission, or on or after day 3 following an in-hospital event?
Yes..........Y
\-No.. . . . . . . . . . N
Find the last codable EGG on day 3 after admission, or on day 3 after an in-hospital event (EGGT). (If day 3 EGG is not available, use first available EGG thereafter.]
BiIRD DAY EGG (EGGT)
83. DateofEGGT:
I
I 1 H 1 H 1 1 mm dd YY I
A-44 -_
Hospital Record Abstraction Form (HRAA Screen 38 of 39)
I 94. Circle letter
Minnesota ECC for any Reading
ECG sent to Center for coding:
ECGF........Y N
I
ECGL........Y N
ECG'J!........Y N
D. ADMINISTRATIVE INFORMATION
97. UII Abstractor number:
98. Date abstract completed:
1 I H I H 1 1 ml dd YY 99. Method of data collection: Computer . . . ..C
Paper . . . . . . . . P I

A-45
Hospital Record Abstraction Form (HRAA Screen 39 of 39)
I I E. OTHER REQUIRED FORMS
SUINEILLARCECASE(Item 3 = S)
m
100. A D!CH
100. B m(s)
101. c IFI( mQ(s)
Criteria based on this fom
Item 17 = D
Item 13a = Y [If transfer was from/to study hospital, be sure to cross-check hospital discharge index to avoid duplication.]
Item 19a = Y or 19b = 0 or not recorded or Item 19d= 0 or not recorded. [Treat as out-of-hospital death]
COHORT CASE (Item 3 = C)
102. D
103. E
Criteria based on this form
Item 17 = D
ItevJl3a=Y (If transfer was from/to study hospital, be sure to cross-check hospital discharge index to avoid duplication.]
104. F
105. G
ADT Item 18 = Y
IFI( PHQ(s) Item 19a = Y or 19b = 0 or not recorded or Item 19d = 0 or not recorded [Treat as out-of-hospital death]
106. H STR Item 39 = Yes and Item 3 = C
107. I Copy ECGs Items 3 = Cand 58 = Y

A-46
INSTRUCTIONS FOR AB!XRACTING ARIC HOSPITAL RJEORU ABSTRACTION
General Instructions
1. The abstractor must be familiar with the ARIC Instructions for Completion of Paper forms.
2. Write legibly. Use black or blue erasable pens. Press hard when ~_
Version: A 05/28/91
FORM
filling in blanks with or circling numbers, letters, or X's. Pen will not photocopy if too light and will fade with time.
3. Several types of responses are used:
Fill in the blank.
Fill in the number, such as a date, time or medical record number.
To answer most questions you will have several choices, the simplest of all being Yes = Y, No = N, or Unknown = U. In that case, "Yes" or "No" will be marked only if there is no doubt due to information in the hospital record. If nothing is written down that definitely answers the question, 'U' should be circled. If the response categories are just Yes = Y or No = N, information not recorded is then marked as "No". In general, the following may be considered synonyms:
"Rule out" "Suggestive" "Equivocal" "suspicious" "Questionable" "Possible" "Uncertain" "Reportedly" "Could be" "Perhaps" "Low probability" "Might be" "May represent" "May be"
"Likely" "Apparent" "Consistent with" "Probable" "Definite" "Compatible with" "Highly suspicious" "Presumably" "Borderline" "Representing" "Minimal" "Thought to be"
4. Complete only the appropriate questions.
5. Be sure to follow correct skip patterns, i.e., follow form logic.
6. To record dates, fill in 2 digit numbers for month/day/year. Zero fill the left box for any single digit numbers (e.g., 03 for March and 06/08/45 for June 8, 1945). If part of the date is missing,

Page 2 A-47
record = for that part. For example, if the only information regarding date is June 1945, record 06/==/45.
7. To record times, use the 12-hour clock. If the time given in the chart is from the 24-hour clock, it should be converted to the 12-hour clock before being recorded. Explanation for conversion:
lAM= 01:oo am 12 NOON = 12:00 pm 2AM= 02:oo am 12 MIDNIGHT = 12:00 am
If an exact time cannot be recorded (i.e., is not given in the chart), the best estimate should be given. If a time cannot be clearly estimated, the following guidelines for estimating times may be used in conjunction with the admission time. Use these only as a last resort For no mention of the time of day, please see xii.
i) The middle of the night = 03:OO am ii> Early morning = 08:OO am
iii) Morning = 09:oo am iv) Late morning = 10:00 am v> Midday = 12 Noon = 12:00 pm
vi) Early afternoon = 02:OO pm vii) Afternoon or midafternoon = 03:OO pm
viii) Late afternoon = 04:OO pm ix) Early evening = 07:OO pm xl Evening = 09:OO pm
xi) Late evening = 10:00 pm xii) No mention of time of day = 12:00 Noon = 12:00 pm
8. To record other time frames, use the following guidelines:
Several days: 2 3 days Few days: 2 1 day and < 3 days Several hours: 14 hours and < 6 hours Few hours: 2 2 hours and < 4 hours
9. Whenever you have questions about the medical information recorded in the hospital record, consult with your surveillance director.
HEADER
Before going to the hospital, fill in event number as assigned on the CEL or SEL Form and patient name (if available).
1. a. Hospital Code Number. Using the hospital selection list prior to going to the hospital, enter the two digit code assigned to this hospital. (Appendix CC) If outside the study community , use the appropriate code (96-99) and write in name and address.
b. Medical Record Number. Before going to the hospital enter the record number from the selection list. Upon finding the
A-48 Page 3
chart, double check the record number. This number will be found stamped or typed on almost every page of the hospital record. The easiest place to find it is both on the medical record folder and in the upper right/left hand corner of the face sheet.
List the number from left to right. Enter only digits and letters; omit dashes and spaces. Do not add zeroes to the right of the number. If the number changes with each admission, use the appropriate number for the one (admission) being abstracted.
2. Discharge codes for selection. At the time this case is determined to be eligible, list the discharge and procedure codes from the hospital discharge index or the Eligibility Form. If the fourth digit, to the right of the decimal, is absent, leave it blank. Do not enter a zero there unless it appears in the index. If this caseas not identified using a discharge list (e.g., cohort annual follow-up), enter = in the first set of boxes.
3. Cohort/Surveillance. Check the cohort roster to determine if the case is a cohort member admitted after his/her baseline exam date. If so, record 'C'. If not in the cohort, or if the hospitalization occurred in a cohort member before his/her exam, indicate that the chart is for surveillance (S).
4. Lost Chart. Make every attempt to find the chart. If lost, indicate so, and follow skip.
5. SOUNDM. This is a phonetic spelling of the last name used when the hospital will not allow patient's name to be abstracted. Consult your SOUNDEX sheet (Appendix EE) for how to convert the name to SOUNDEX spelling.
6. Social Security/Medicare Number. If the SSN is in the chart, copy it exactly as given including the letter which may be at the end. If for some reason the entire SSN cannot be abstracted, then abstract the first, third, fifth, seventh and ninth digits, and record = in the remaining positions. If no SSN is available, fill all the blanks with - . (This number is extremely important. Check all available sheets for it and look at correspondence at the back of the chart.)
Medicare numbers are the same as Social Security Numbers, except that Medicare numbers are always followed by a letter. Letters A through E are used for various reasons.
7. Address. The patient's address which should include: the house number, the street name, and the apartment, box or lot number, names of the city, county and state. Zip code need only be recorded if it is used for determining address eligibility.
8. Sex. Indicate either male or female.
Page 4 A-49
9. Race or Ethnic Group. See Instructions for the Death Certificate Form on how to complete this. This category may be found on the face sheet of the chart. If not, review the entire chart, i.e., Admission, M.D.'s History, Admitting Nurse's Notes or Nurse's General Notes. If conflicting information is found, circle the "0" (other) category and write a note in the blank, specify. If the patient's race is one that falls outside the categories listed, for example, i f he is an Eastern Indian, circle "Other". The following definitions should be used for determining race/ethnicity:
. White/Caucasian. A person having origins in the original peoples of Europe, North Africa, or the Middle East.
Black/Negro. A person having origins in any of the black racial groups of Africa.
Asian or Pacific Islander. A person having origins in any of the original peoples of the Far East, Southeast Asia, the Indian subcontinent, or the Pacific Islands. This area includes, for example, China, India, Japan, Korea, the Philippine Islands, and Samoa.
American Indian or Alaskan Native. A person having origins in the original peoples of North America, who maintains cultural identification through tribal affiliation.
10. Birthdate. Birthdate is usually found on the face sheet of each medical record. Do not use the age given by the physician on the history and physical since it may be incorrect.
11. a - c. Date and Time of Arrival at Hospital. Note that the date and time of arrival at the hospital may be different from the time of admission. For example , a patient may first be taken to the emergency room (arrival at the hospital), but may not be admitted for several hours. In this case, record time of arrival at E.R. If the time of arrival at the hospital is not recorded explicitly in the chart, abstract the earliest time recorded in the chart (such as a time a procedure was ordered or time of the admitting history and physical examination).
12. Emergency Services. If an emergency medical service unit (ambulance, helicopter, etc., but not a private vehicle, taxi or on foot) transported the patient to the hospital, circle 'Yes". This information can be found on the ambulance or ER sheet, in the admitting notes , on the face sheet, etc. "Ambulatory" should be considered "No". If not specified, answer "U".
13. Transfer. If the patient was transferred to or from another acute care hospital, write the name of the hospital from which the patient was transferred, and the city and state in which it is located and the date of admission to that hospital. This information can be found on the face sheet of the chart and in admitting notes. (You may have to ask record room how this is
Page 5 A-50
coded if on the face sheet.) The purpose of this question is to identify recent hospitalization(s) of this patient, possibly to be reviewed at a later date. (For Surveillance cases, only hospitalization(s) in the catchment area will be reviewed. For Cohort cases, all hospitalizations are reviewed.) The hospitalizations should include multiple hospitalizations among different hospitals , or transfers from one hospital to another. If a patient went to one study hospital emergency room, and was not admitted, and then was sent to another study hospital and was admitted, this would not be a transfer from the first hospital (assuming that you are abstracting for the second hospital). The patient must have been admitted to the first hospital for a transfer to have taken place. A transfer to the rehabilitation unit of a hospital should generally be recorded as a "No", unless 1) it is a separate admission and 2)the chart appears to contain additional diagnostic information.
Note: In Washington County only, transfers to certain out-of-catchment area hospitals also need ERAS completed.
14. Date of Discharge (for nonfatal case) or Death. This information . will generally be found on the face sheet. If the patient died, then record the date of death. If transferred from acute care to rehabilitation or chronic care in the same hospital, count the date of transfer as the discharge date.
15. Discharge Diagnosis Codes. Fill in the discharge diagnoses and procedure codes as listed on the face sheet or discharge summary in the order listed. Use the most complete source. It is important that all diagnoses are coded. When a discrepancy exists between discharge codes and the code listed on the hospital index, the latter is used even if it represents a transcription error. If the fourth digit, to the right of the decimal, is absent, leave it blank. Do not enter a zero there unless it appears in the chart. Be sureto include all primary and secondary diagnoses as designated by the M.D. If ICD codes of the discharge diagnosis are not given on hospital charts and are only available from the diagnostic index, leave blank. Do not "mix and match" diagnoses and codes from different sources.
16. Discharge Diagnoses. Write in the diagnoses in the order in which they are listed on the face sheet. If not listed on the face sheet, use the discharge summary. (Procedures do not have to be written out here.) Attach ID number label where specified. .
17. Patient Disposition on Discharge. This information can be found in the discharge summary or on the face sheet. If the patient died in the E.R., this information can be found on the E.R. sheet. Some hospitals keep a separate log book for deaths.
18. Autopsy. If an autopsy is mentioned in the Death or Discharge Summary, circle "Yes". If not, circle "No".
Page 6 A-51
19. a. Dead on Arrival. If the patient died outside of the hospital but was brought in dead, he is considered dead on arrival (DOA). If the patient was brought to the RR alive but died in the emergency room, he is an HR death. If admitted to the ward, CCU, or ICU, answer "No".
If a m patient is DOA, an RR death, or hospitalized with no vital signs and dies within 24 hours of admission, s/he is treated as an out-of-hospital death. If s/he lived at least 24 hours in the hospital (or did not die), s/he is treated as an in-hospital event.
b-d. First Recorded Blood Pressure, Pulse. First attempt to obtain BP and pulse may be charted on the ambulance sheet, the RR sheet, the clinical graph or the nursing admission note. The pressure may be from sphygmomanometry or an arterial line. If both right and left arm blood pressures are given, take the one with the highest systolic pressure. If the systolic pressure is the same for both arms, record the highest diastolic value. If a BP or pulse range is
. given, take the highest value given. If the patient was admitted from a doctor's office, use the first BP recorded in the hospital. If the systolic BP or pulse was unobtainable and the patient died within 24 hours, enter three zeros (000). If the systolic blood pressure and/or pulse was unobtainable and the patient lived at least 24 hours, enter '001' for systolic BP or pulse to appropriately trigger skip patterns. If no BP or pulse is recorded, enter -.
e. For the event under consideration, was there acute pain anywhere in the chest, left arm or jaw, (this description may also have involved the back, shoulder, right arm or abdomen on one or both sides) mentioned anywhere in the hospital chart and present within 72 hours of arrival at this hospital, or at the onset of a CHD event beginning in this hospital? Included in this definition for pain are ischemic pain, angina, cardiac and substernal pain. "Chest tightness" "heaviness" or "discomfort" is equivalent to chest pain. Answer unknown if no history either way or no indication at all of timing. If the pain began in the RR but before admission, consider onsetas occurring out of hospital.
f. Previous history refers to a time preceding the onset of the event under consideration. For example , a transfer from another hospital should not be considered a "previous event". Historical questions generally refer to before 72 hours prior to admission or documented as long-standing by chest x-ray, echocardiogram, or other diagnostic test. Take information from the history of the resident, cardiologist, attending . physician, HR physician, or nursing notes, in that order. Also review face sheets of all previous admissions for previous MI. If this information states "previous silent

MI", "borderline heart attack", record the answer as "yes". An abnormal ECG alone, stating "old MI" cannot be used for positive previous history , unless the physician verifies it. Angiogram evidence cannot be taken as evidence unless explicitly verified by the physician. If conflicting information exists in the medical record, base your answer selection on the most reliable source. Statements such as: “No cardiac problems", "No adult illness", "Previously well", and "No previous history of heart disease" are sufficient to answer "No" to previous MI. If no indication either way, answer "Unknown".
8. If a previous myocardial infarction occurred within four weeks of the event under consideration, answer "Yes".
h. Angina. Examine the history for mention of previous angina pectoris or coronary insufficiency prior to this event (i.e., > 72 hours before admission). This would include mention of chronic chest pain, ischemic pain, and "history of chest pain". Chest pain specified as being "of unknown origin" does not qualify. Answer "Yes" if the history includes any mention of the patient taking nitroglycerin for chest pain or if the physician notes that the patient has "substernal pressure, pain, tightness, or burning distress precipitated by exercise or excitement, or both and is relieved by rest and/or nitroglycerin". Answer "No" if the history explicitly states that the patient has no history of any of the above. Answer U = unknown if none oFthe criteria for "Yes"/"No" responses apply.
. 1. History of other chronic ischemic heart disease, coronary
disease, etc. not specified as angina or MI. This includes CHF described as due to coronary disease or ASHD (Atherosclerotic Heart Disease). CHF due to hypertension or other reasons is "No". Arrhythmias are "No".
20. Discharge Statements. Examine the chart, i.e., the discharge summary, ECGs, laboratory reports, etc., and determine successively whether (A) through (D) are true or false. Item 20a may be answered from the discharge summary, face sheet, or hospital index , whichever is most complete. If not skipped out and 20d is answered “N” (i.e., this was a nonfatal event with no 410 and/or 411 ICDs, no 12-lead ECGs, and no enzymes), SKIP TO 97, AND DO NOT CONTINUE WITH THE FORM.
21. First Recorded Blood Pressure, Pulse. First attempt to obtain BP and pulse may be charted on the ambulance sheet. If the ambulance sheet is not available, take from the ER sheet, the clinical graph or the nursing admission note in that order. If more than one ambulance or ER is involved, use the first. The pressure may be from sphygmomanometry or an arterial line. If both right and left arm blood pressures are given, take the one with the highest systolic pressure. If the systolic pressure is the same for both arms, record the highest diastolic value. If a BP or pulse range
A-53 Page 8
22.
is given, take the highest value given. If the patient was admitted from a doctor's office, use the first BP recorded in the hospital. If the BP or pulse was unobtainable, enter three zeros (000). If no BP or pulse is recorded or BP is obtained by palpatation, enter ===. Note: If pulse or BP were absent and the patient died, this case is to be treated as an out-of-hospital death.
Narrative. Record the pertinent facts regarding the event, including onset, timing, and character of symptoms; presence or absence of chest pain; major diagnoses, procedures, and hospital course; vital status at discharge, etc. Attach ID number label where specified. (If convenient, you may attach a photocopy of the discharge summary instead. If discharge summary excludes history of present illness, then attach admission note too.) Attach ID number label to each photocopied page.
23. a. Acute Cardiac Symptoms. Check the admission history, etc., for mention of the beginning of acute cardiac symptoms which brought the patient to seek medical attention. Examples of cardiac or CHD symptoms are: chest pain, collapse, syncope, shortness of breath, gastrointestinal symptoms such as nausea, pain in the neck, left arm, and sternum and sudden death. Chest tightness, discomfort or heaviness is equivalent to chest pain. Marked fatigue and shortness of breath may be considered acute cardiac symptoms if the chart seems to indicate this. If the symptom includes one of these but is obviously noncardiac (e.g. chest pain from pneumonia, nausea from pancreatitis), answer "No".
Sometimes, as in cases with chronic angina, there may be no acute symptoms. If there were no acute symptoms, change in symptom quality or frequency (such as new unstable angina), or symptoms were only chronic, do not answer "Yes". The symptoms must have begun outside this hospital to answer "Yes" . There is no three day limit on the answer to this question, and it is not limited to chest pain. The symptoms must have begun outside this hospital to answer "Yes". For determining the location where symptoms occurred, count the ER as the hospital and the doctor's office as out-of-hospital. If this is a transfer from another hospital, acute symptoms before that hospitalization or in that hospital count as "Yes", because they occurred prior to arrival at this hospitalization.
b. Timing between onset and hospital arrival. Estimate the time to the best of your ability (refer to instructions for time expressions in General Instructions, item 7). If there were multiple new episodes of symptoms (e.g. chest pain), you must pick the likely onset which would be the first or most severe depending on the circumstances. In the case of someone with chronic angina, it is a change in the pain, prompting action, which usually marks the onset of an event. Stuttering and recurring pains should generally not be taken as separate
A-54
Page 9
events unless it is clear that they are such. Consult your surveillance director when in doubt.
24 a. Primary Diagnosis - Admission. If the patient had no pre-hospital cardiac symptoms (Item 23a), check the admit note or admission sheet diagnosis for the primary reason for admission. If a patient is admitted for elective angioplasty, consider this an "other non-acute CHD
1 evaluation" (C).
b. In-hospital CDD Event. Check the ER sheet, admit note, and history for reference to when the CHD event took place. CHD events in hospital of interest include new infarction or reinfarction (including a documented MI "extension"), but not procedures (such as CABG) or death. Also of note as an event is "primary chest pain" - acute chest pain happening for the first time during a hospitalization and prompting additional procedures. For example, if a patient was admitted electively and develops chest pain during the hospitalization, prompting procedures, this should be considered an event.
An answer of "No, After Arrival" to Item 23a does not mean that this question will automatically be answered "Yes". A patient could experience chest pain, shortness of breath, or other symptoms as a continuation of an event begun outside the hospital. Mere continuance of symptoms is not an in-hospital event ; nor is the occasional occurrence of a chronic angina1 pain. An event should be definitely identified on the medical record as new infarction, reinfarction, or fit the above definition of primary chest pain.
C. Date of In-hospital CHD Event. If more than one, pick the primary or most important , as described in the Note below.
[NOTE: A problem arises with subsequent questions if the patient had multiple CHD events before and/or during the same admission. (For example , multiple events would occur if a person was admitted for acute angina, recovered, but infarcted before discharge; or if a patient was admitted for an MI, then reinfarcted.) In the case of multiple events, the abstractor must decide which is primary or most important, based on severity, enzymes, physician notes, etc. In the case of angina followed by infarction, the most important would be the infarction. With a first infarction, then reinfarction or extension, the first infarction is considered primary. If two events seem equal, pick the first. When in doubt, consult your supervisor. Answer subsequent questions for the most important event. If a patient has acute symptoms which can be identified as an event and subsequently has a cardiac arrest, this should be treated as one event. In this case, the arrest is a complication of the first event. Likewise, after a myocardial infarction, additional episodes of pain which do not lead to a new MI are not to be considered new in-hospital events.

Page 10
Only new an separate infarctions, as determined by the physician, should be considered second events. For example, a person could have been admitted for an inferior myocardial infarction, and the day before discharge suffer a new anterior myocardial infarction. In summary, symptoms and signs that are complications or a continuation of a first MI should not be considered as a second event.]
25. a. Onset of Acute Pain. For the event under consideration, was there acute pain (tightness, heaviness, discomfort) anywhere in the chest, left arm or jaw, (this description may also have involved the back, shoulder, right arm or abdomen on one or both sides) mentioned anywhere in the hospital chart and present within 72 hours of arrival at this hospital, or at the onset of a CRD event beginning in this hospital? Included in this definition for pain are ischemic pain, angina, cardiac and substernal pain. If pain was chronic and/or no acute episode was evident, skip to Q. 26. Answer unknown if no history either way or no indication at all of timing. If the pain began in the RR but before admission, consider onset as occurring out of hospital.
NOTE: See Appendix DD for examples of how Items 23 and 25 should be answered for typical cases.
b. Date of Onset of Pain. If the pain is intermittent, then pick the most prominent pain in the last 72 hours. If intermittent and none seems more prominent, then give the date of the start of the first episode within 72 hours prior to arrival at the hospital or onset of the in-hospital event.
C. Chest location. Indicate specifically if pain involved the chest (yes) or did not (no). If not mentioned either way, answer "unknown".
d. Noncardiac pain. This question is asked to determine if the pain experienced satisfies the ARIC criteria for chest pain by establishing that there is no definite non-cardiac cause of chest pain. It refers to the final conclusion about a pain or discomfort, not the "rule-out" diagnosis. Only specific diagnoses of conditions or diseases made by an M.D. or D.O. to account for the pain in question should be recorded here. The pain may result from an old diagnosis, rather than a new one. Answer "Yes" if there is an explicit statement by a physician that the pain is definitely due to a non-cardiac cause. If yes , specify the diagnosis of what the pain was due to. Exampies could be: fractured ribs, costo- chrondritis, esophagitis , or an acute gallbladder attack. Pericarditis should be answered as 'yes" and specified. A charted impression 'R/O (rule out) fractured rib" should not be recorded as a "Yes" answer. The answer "No" is to be used when an explicit statement that the pain is definitely
A-55

Page 11 A-56
e.
f.
g*
26. a.
b.
cardiac. If neither a clear positive or negative statement is available, answer "U".
Specify as described above.
Death in Hospital. Look in discharge summary or on death record for whether or not the patient died in the hospital.
Timing of Death. Estimate time from onset of acute symptoms (defined in previous questions) and death.
Reperfusion refers to complete or partial restoration of coronary blood flow by coronary angioplasty, coronary art&y bypass graft (CABG), or thrombolysis using intracoronary or intravenous streptokinase, urokinase, anistreplase, or tissue plasminogen activator (TPA). Check procedure notes, EMS, ER notes, and medication lists. (See Appendix BB for drug information.) It must occur within 24 hours of onset of acute event (not necessarily the first symptom). Answer "Yes" even if reperfusion was unsuccessful. Note: The timing is not necessarily the same as that recorded by the physician.
Record time between event and onset of reperfusion attempt. To determine onset of CABG reperfusion, check anesthesia record for time patient place on bypass. IF PTCA, take first balloon inflation as the time of reperfusion attempt..
27. CCU/ICU. Check discharge summary or progress notes for any admissions or transfers to the CCU or ICU or a telemetry bed. Coronary care units (CCU) and intensive care units (ICU) are dedicated areas so assigned by the hospital administration. Notes designated as written while the patient was in one of these units is evidence of admission. Telemetry includes less intensive but continuous cardiac monitoring. In the case of a hospital that does not have either CCU or ICU or telemetry, mark the answer as "No" .
28. For this question, not recorded = "No". Record findings in this hospital. If a transfer, do not record findings at the previous hospital.
a. Shock. Cardiogenic shock (pump failure) is failure to maintain blood supply to the circulatory system and tissues because of inadequate cardiac output, i.e., faulty valves and/or faulty muscle action. A person in shock cannot maintain blood pressure or perfuse organs. The administration of Dopamine is a clue, but not definitive evidence that a patient had shock or pump failure. Look for the term "shock" or "pump failure". Answer "Yes" if shock occurred at home, at the ER or hospital or during the hospital stay.
b. Congestive Heart Failure or Pulmonary Edema. CRF is an inability to adequately maintain cardiac output, but not as
Page 12 A-57
C.
d.
e.
f.
g*
h.
severe as shock. Pulmonary edema is fluid in the lungs due to poor cardiac output. Check the physical exam, RR sheet, admission diagnosis and history, and x-rays. Definite or probable pulmonary edema, pulmonary congestion, or CRF noted on x-ray is considered "Yes". Slight, minimal or mild pulmonary congestion should be recorded as "No"; cardiac failure as "Yes".
S3 Gallop (third heart soundl. Also known as ventricular or sumnation gallop. This would be recorded in the physical exam notes or progress notes. gallop) as equivalent.
Do not consider S4 (atria1
Rales. This can be taken from physician's or nurse's notes. If the patient had rales (moist or widespread, not basilar alone), record this as a "Yes". Rales are also called "crackles". Rales are considered present if there are? "l/3 of the way.up" noted by a physician or noted by a nurse on a day when a physician does not comment on the pulmonary exam. A "few rales" or "scattered rales" is "No". Fine, diffuse, some or slight rales 2 l/3 up is "Yes".
Ventricular fibrillation. Chaotic contraction of heart resulting in cardiac arrest, sometimes reversible by electrical defibrillation. Documentation usually in progress notes, arrest record, or discharge summary.
Cardiac 'arrest. Cessation of effective heart pumping due to ventricular fibrillation or asystole. Would prompt cardiopulmonary resuscitation or death. Documentation would be found in progress notes, arrest record, or discharge summary.
Asystole. Complete cessation of heart beat, resulting in cardiac arrest. Documented usually in progress notes, arrest record, or discharge summary. Sinus pause is not asystole.
Pulmonary embolus. Blood clot to lung impairing oxygen exchange to blood would be documented in progress notes, discharge summary, lung scan, or pulmonary arteriogram.
Stroke. Synonyms are cerebrovascular accident (CVA), cerebral hemorrhage, cerebral infarction, cerebral thrombosis, subarachnoid hemorrhage. Documented in progress notes, discharge summary, or CT scan.
Pneumonia. Documented in progress notes, discharged summary, or chest x-ray. Synonym= pnenmonitis.
29. Special Procedures. Check the physician notes on procedures and the laboratory reports for the following procedures during the present hospital stay. (If a transfer, do not record procedures at the previous hospital unless a patient is transferred with a Swan Ganz catheter. Consider the Swan Ganz a monitoring
Page 13 A-58
procedure. Thus, although the catheter may have actually been inserted at the first hospital, if it remains in place for monitoring procedures, answer 29d "Yes".) Check for operations and procedures codes at the bottom of the face sheet. These codes may appear without a language description of the operations and procedures. If this is true, the codes will have to be translated in order to circle the appropriate procedures. If coronary angioplasty was attempted and completed, "yes" should be answered even if the procedure was not successful in reducing the lesion or increasing blood flow. If angioplasty was attempted, but for some reason the physician cannot get to the lesion because of some complication, then the answer is "No". For definitions and descriptions of each of the procedures and ICD procedure codes and the "other" category, please refer to Appendix AA.
30. a. Closed chest massage or cardiopulmonary resuscitation (CPR). This question has two aims: (a> to support or dispute diagnoses of definite myocardial infarction based on chart abstracts, and (b) to inquire after medical care delivery. CPR is defined as a basic emergency procedure for life support, consisting of artificial respiration and manual external cardiac massage. It is used in cases of cardiac ' arrest. Cardioversion is defined as the use of direct current counter shock through paddles to restore the heart's normal sinus rhythm during cardiac arrest. (Cardioversion may be used in treatment of atria1 fibrillation and arrhythmias, but such elective uses are to be considered “No”.) Refer to the EMS, RR, ICU/CCU, ward notes, CPR or cardiac arrest sheets. When there is precordial thump, the response should be "Yes". When cardioversion is part of CABG, the response should be "No".
b. Date of CPR/Cardioversion. List the date of the first emergency cardioversion or CPR attempt for this event.
C. Location. Indicate where first CPR and/or cardioversion was started.
31. Drugs used during hospitalization. Refer to Appendix BB for definitions of nitrates, calcium channel blockers, beta-blockers, digitalis preparations. Review the hospital medication record and discharge note to see if any of these were given during the hospital stay or at discharge. If a generic or trade name is listed, record as "Yes". If the medication is not listed, record as "No". Xylocaine (lidocaine) used as a local anesthetic is "No" for 31e.
32, History of Previous MI. Previous history refers to a time preceding the onset of the event under consideration. For example, a transfer from another hospital should not be considered a "previous event". Historical questions generally refer to before 72 hours prior to admission or documented as long-standing by chest x-ray , echocardiogram, or other diagnostic test. Take information from the history of the resident, cardiologist,
A-59
Page 14
attending physician, ER physician, or nursing notes, in that order. Also review face sheets of all previous admissions for previous MI. If this information states 'previous silent MI', "borderline heart attack", record the answer as "yes". An abnormal ECG alone, stating "old MI" cannot be used for positive previous history , unless the physician verifies it. Angiogram evidence cannot be taken as evidence unless exp,licitly verified by the physician. The question is answered "No" only if there is specific mention of no previous MI. If conflicting information exists in the medical record, base your answer selection on the most reliable source. Statements such as: "No cardiac problems", "No adult illness", "Previously well", and "No previous history of heart disease' are sufficient to answer "No' to previous MI. If no indication either way (an old MI is not mentioned, regardless of what is said about chest pain), answer "Unknown". "Essentially unremarkable history" should be answered as "unknown". An MI noted on the autopsy is recorded as "Yes".
33. Angina. Examine the history for mention of previous angina pectoris or coronary insufficiency prior to this event (i.e., > 72 hours before admission). This would include mention of chronic chest pain, ischemic pain, and 'history of chest pain". Chest pain specified as being 'of unknown origin' does not qualify. Answer "Yes" if the history includes any mention of the patient taking nitroglycerin for chest pain or if the physician notes that the patient has 'substernal pressure, pain, tightness, or burning distress precipitated by exercise or excitement, or both and is relieved by rest and/or nitroglycerin'. Answer “No” if the history explicitly states that the patient has no history of any of the above. Answer U = unknown if none of the criteria for "Yes"/"No" responses apply. "Angina equivalent" and "silent ischemic" are recorded as "Yes".
34. Chronic IHD. History of other chronic ischemic heart disease, coronary disease, etc. not specified as angina or MI. This includes CHP, cardiomyopathy, or arrhythmia described as due to coronary disease or ASHD (Atherosclerotic or Arteriosclerotic Heart Disease). If there is not mention of ASHD, coronary or ischemic disease, the answer is generally ‘No’. CHF due to hypertension or that is associated with an MI, only that is non-chronic or other reasons is "No". Arrhythmias are "No". ASCVD may be taken as "yes" unless the physician is obviously referring to ASCVD in other vascular beds (e.g. brain, leg). If
. in doubt, specify, and consult your Surveillance director.
35. History of valvular disease such as rheumatic heart disease, mitral valve prolapse , valvular stenosis or regurgitation? Review echocardiogram and cardiac catheterization reports, as well as the history. The new discovery of valvular disease by echo or angiogram can only be taken as "Yes" if confirmed as long-standing by the physician. Other valvular diseases include: Aortic Valve diseases or disorders, aortic valve incompetence, insufficiency, regurgitation, or stenosis, aortic valve failure; Mitral valve diseases, disorders, mitral valve incompetence, insufficiency,
Page 15 A-60
regurgitation and stenosis or mitral valve failure; or Pulmonary valve diseases, disorders, incompetence, insufficiency, regurgitation and stenosis; and Tricuspid valve diseases, disorders, incompetence, insufficiency, regurgitation, stenosis and failure. In addition, any mention of valvular endocarditis or the above mentioned in an autopsy warrants an answer of "Yes" to history of valvular disease. Not recorded, trace, trivial, or l+ regurgitation as seen on ECHO or catheterization is recorded as “No” .
History of cardiomyopathy. Types of cardiomyopathies include: Alcoholic cardiomyopathy, Amyloid cardiomyopathy, Beriberi cardiomyopathy, Congenital cardiomyopathy, Congestive cardiomyopathy, Constrictive cardiomyopathy, Endomyocardial fibrosis, Endomyocardial fibroelastosis, Familial cardiomyopathy, Hypertrophic cardiomyopathy, Idiopathic cardiomyopathy, Metabolic cardiomyopathy (Cardiac glycogenosis, Gouty tophi of the heart, and Mucopolysaccharidosis cardiomyopathy). Additional types of cardiomyopathies may be listed as: Nutritional, Obscure Cardiomyopathy of Africa (Becker's Disease), Obstructive, Postpartum, Secondary (Sarcoid or other), Tuberculous or Thyrotoxic cardiomyopathies. Not recorded is "No".
36, 37. Coronary bypass or angioplasty. Has the patient had previous coronary bypass surgery or coronary angioplasty (CABG) before this event (refer to Appendix AA for definitions)? CABG or angioplasty related to the acute event under consideration should be recorded under 26, not here. Not recorded is "No". An attempted PTCA that was unsuccessful is recorded as "No". Record a "Vinegerg" as "Yes".
38. Hypertension previous to this admission? If there is explicit mention of hypertension (high blood pressure) including labile hypertension as being present, answer "Yes". If hypertension history is explicitly recorded as negative, or "no known cardiac risk factors", answer "No". If no mention either way, record "U". Even if the patient is on a medication sometimes used for hypertension (e.g., beta-blocker), but hypertension is not mentioned, answer '9". "Borderline" or "mild" hypertensia = "Y".
39. History of stroke prior to this event.? Use the same guidelines for searching the chart as described in the previous MI question. Equivalents to stroke are CVA (cerebrovascular accident), cerebral embolus, intracranial, intracerebral or cerebral hemorrhage, subarachnoid hemorrhage, cerebral thrombosis, cerebral apoplexy, cerebral (artery) occlusion, cerebral infarction and lacunar infarction. Homonymous hemianopia (HH) or left field cut is recorded as "Unknown". "Denies chronic diseases" is recorded as "Unknown".
40. Stroke within four weeks prior to the event. Review history for recency of stroke.
41. Enzyme availability. The cardiac enzymes of interest are total creatinine kinase (CK or CPK) and its MB (myocardial band or
Page 16 A-61
heart) fraction, total lactate dehydrogenase (LDH or LD) and its LDHl and LDH2 fractions. Refer to laboratory reports. Do not use enzyme values recorded in progress notes unless some or all lab value reports are obviously missing. Were any cardiac enzymes reported within days 1 to 4 after arrival at this hospital or after the in-hospital CHD event. 7 You must first determine when the event occurred, then determine the appropriate enzymes to review.
42. a. Trauma. Locate laboratory values for enzyme values and note the date the enzymes were done. Look in the history, etc., for any mention of trauma (including any major surgery, CPR, CAHG, defibrillation - including that for atria1 fibrillation, crushing injury, extensive bruising, or electrical injury or injections) or rhabdomyolysis (disintegration of muscle) within one week prior to the measurement of enzymes. These major trauma factors are non-ischemic causes for elevated enzymes. IM injections do represent "trauma". The interest here is the penetration of the muscle and should be answered "Yes". A Swan Ganz insertion or Swan Ganz pacer is a "No" answer. Minor trauma such as scrapes, cuts, nicks, and psychological trauma call for an answer of "No". Dialysis, abdominal aortogram, dental surgery also should be answered as "No". Consider "nothing recorded" as "No".
Procedures. Did the patient have any cardiac surgical procedures during the week prior to the measurement of enzymes? These procedures include invasive (cutting) procedures only, such as cardiac cath, angioplasty, etc. Consider "nothing recorded" as “No”. Cardioversion is considered "Yes" .
b, c. If yes, specify the procedure, trauma, etc. Also indicate the item number from the enzyme section corresponding to the first enzyme measurements performed after trauma, cardiac procedure or rhabdomyolysis.
d. Hemolytic disease. Was there any evidence of hemolytic disease in the Discharge Summary (examples include: hemolytic anemia, disseminated intravascular coagulation, myelophthisic anemia , nonspherocytic anemia, etc.)? Treat "nothing recorded" as "No". Also, prenicious anemia, macrocytic anemia, normocytic anemia, hypochronic microcytic anemia, anemia due to chronic renal failure and microcytic anemia without hemolysis are all recorded as "No".

A-62 Page 17
43. Enzymes
Enzymes of interest are:
Total CK Synonyms: CK, CPK, Total CPK, creatine kinase, creatine phosphokinase, CKI
It has heart (MB), skeletal muscle (MM), and brain (BB) fractions. If MB, MM, and BB are given separately, add them to obtain total
CK.
CK-MB Synonyms: CPK-MB, CK-heart fraction
Total LDH Synonyms: Lactate dehydrogenase, LD
LDHl and LDH2
These are fractions of LDH
Synonym for LDHl = heat stable LDH. (There are three other fractions of LDH 3-5, which are not of interest.)
LDHl/LDH2 Their ratio. May not be given in some hospitals.
Enzyme Units
Enzyme units are variable from hospital to hospital. Some hospitals may use different normal ranges within their own laboratory or may even use normal ranges from another hospital. Possible units are:
Total CK Units/ml or I.U.
CK-MB Units/ml or I.U. Special units include: negative/positive, absent/present, normal/abnormal, negative/weak positive/positive, absent/weak present or trace/present, normal/high normal/abnormal, absent/small/moderate/large.
May also be reported as a percent or decimal proportion of total CK.
LDH Units/l or I.U.
LDHl, LDH2 Units/l or I.U. May also be reported as a percent or decimal proportion of total LDH.
LDHl/LDH2 Usually expressed as a percentage or decimal proportion. May be reported only as < or 2 1.0 or 0.8. May be reported as negative/positive or LDHl vs LDHZ, or not flipped/flipped.

Page 18 A-63
Refer to hospital charts or with the hospital lab for information concerning unusual formats.
Recording Procedure
The first step is to find the range sets in use for hospital days 1-4 and record the upper limit of enzymes pertinent to this patient in 443. Range Set 1 is the primary set, Set 2 is the alternate, if one. Only numbers should go in the upper limit field. If not numbers, leave the upper limit field blank and code special units. Code the special units as indicated on the form. (If there are two different units used for a single enzyme determination, select the most informative unit.)
Examples Upper {Normal Range Limit
CK-MB (O-10 IU) Ilijll~ll~ll~l qjlqjl l,ll,ll,1l,l*l,ll,l
CK-MB (Present/Absent) IIK,rr,rlTLII!I:I
LDHl (0-50X of total LDH) IpI~$~~~I~~~.~~~~~~
LDHl/LDH2 (0.0-1.0) ;$$i; Ii' qjlqjl ,1*1,11,1
Special Unit
-1 1-l
ill
131
$1
LDHl/LDH2 (< 100%)
When in doubt, consult the hospital lab.
Occasionally, there may be more than one method used by a hospital to measure a particular enzyme, e.g., a total LDH may be done as part of the admission battery, and also as part of the cardiac enzyme routine, with differing normal ranges with each test. List them as indicated and use the second range set. If enzymes are available in both units and percentages, units are preferred. Enzymes recorded for one item number should have been measured at the same time.
If the enzymes are drawn three times in a day and there is only room to record two sets, select the sets that have the highest CPK and highest LDH. Do not mix and match enzymes drawn at different times unless they are fairly close together (within 1 to 2 hours) and no cardiac procedure took place during that interval.
If an enzyme is not measured, leave the corresponding blocks blank, do not fill boxes with "=".
In cases where an enzyme (LDH, CPK) is reported both as a SMAC profile and as part of a specific isoenzyme battery, record the latter value for the total enzyme.
A-64 Page 19
Note: Whenever CK fractions (MB, MM, BB) are recorded in international units but not total CK, total CK should be calculated and recorded as the sum of MB + MM + BB. The upper range for total CK in this case is the sum of the upper ranges for MB + MM + BB.
44-56. Patient values.
Determine which enzymes are available for Days l-4. Day 1 is the first calendar day of admission to this hospital or of occurrence of in-hospital event. Day 2 is the next calendar day regardless of the time of the event. Days 3 and 4 are the succeeding calendar days. Use date of blood collection, if recorded on the lab report. If not recorded, use the date of arrival at or processing at the lab to determine Days l-4. If exact onset of event is unknown, use best estimate. (It is better to include enzymes on form than exclude if dates are questionable.)
Record values for each enzyme in chronological order. (The sequential acquisition number often stamped on the lab reports may be helpful in clarifying order.) If no time is listed, assume a time of 12:00 noon. If no enzymes were done on any of days l-4, indicate this and leave rest of the boxes blank.
Record values accurately, paying careful attention to units and decimal points for proportions and percents. LDHl and LDH2 must be reported on the same specimen ; otherwise the enzymes recorded in A, C (and E) need not be from the same specimen. If there is no value for a given enzyme, leave blank. Record LDHl/LDHZ only if it is already computed and recorded in chart. Do not compute from LDHl and LDH2 values. As indicated in the note in the instructions for the previous question, do calculate total CPK when all three fractions are given (MB, MM, BB).
When standard units, I.U., or percents are the enzyme units, and the value is given with decimal places, record it as it is. However , if the units are expressed as a decimal proportions (e.g., LDHl/LDH2 = 0.43), retain the decimal. A useful rule is that if the value is greater than one, you may round the decimal places to a whole unit. If less than one, keep the decimal places.
If a value is reported as a range (e.g., CPK = 20-30, or CPK < 30) record the higher value (i.e., 30). If a "special value" is used for CK-MB or LDHl/LDH2, fill in the corresponding letter (A through E) in the box immediately to the left of the decimal.
If a patient is discharged before day four, put "=" in the boxes for date of enzyme draw (Items 48a, Sla, 54a) for those dates following discharge.
57. If any 12-lead ECGs were taken during the admission and are available, record "Yes". (Do not count single-lead or 3-lead
A-65 Page 20
rhythm strips.) If no 12-lead ECGs were taken or none can be found, answer “No” and skip to end.
58. If at least one 12-lead ECG in the chart is codable, answer "Yes" . If no ECGs are codable, answer “No” and skip to end.
Reasons for uncodable are:
Three or more missing lead(s) (except aVR)
Muscle tremor artifact throughout record that produces possible false initial R's,
Other technical errors such as extreme lack of centering marked clipping which effect the Q-waves, or no calibration mark or calibration off by greater than + .5 mm.
When picking ECGs, do not take a l/2 standard ECG if full standard ECG taken at same time is available.
59. The "First ECG" (ECGF) is defined as the first codable ECG recorded after admission regardless of when the event occurred. Find and code that ECG for Q59-69. Do not chose an ECG if it is uncodable.
Record the date of the first ECG (ECGF) in Q59. If date is missing, enter "=".
DO NOT ANSWER QUESTIONS 60 - 69.
70. If there are other codable ECGs in the chart answer "Yes". If not, answer "No" and skip.
71. Enter the date of the last codable ECG taken during the admission in 471 and ignore 472 - 81.
For a one day admit, i f there are two ECGs done, use both ECGs, one for ECGF and the other for ECGL.
82. If the event began outside of hospital, day 3 is the third day after admission, regardless of time of day of admission. For example, for a patient admitted at 12:Ol a.m. on 8/25 day 3 is 8/27. Similarly, if admitted 11:59 p.m. on 8/25, day 3 is 8/27. If the event began in the hospital, day 3 is the third day after the event.
If there are codable ECGs (other than ECGL) taken on or after day 3, pick the last codable one on day three or the first available ECG thereafter that is codable be sure to enter the date into 483 and skip to Item 94.
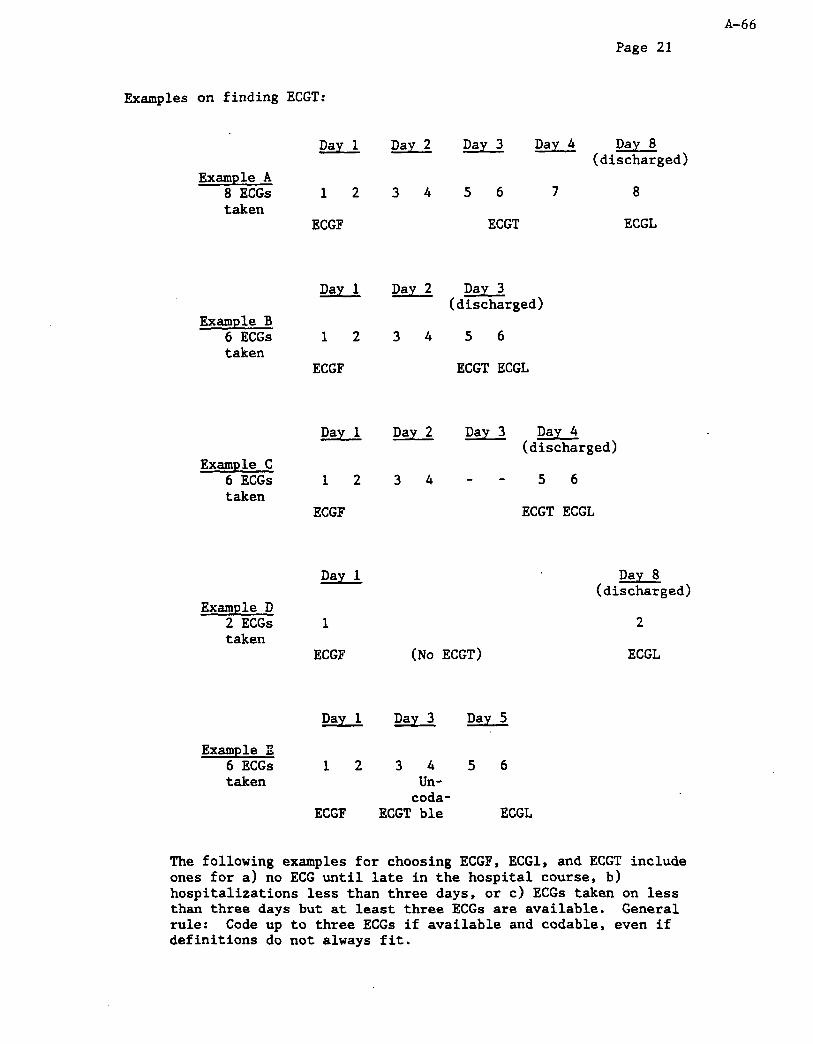
A-66 Page 21
Examples on finding ECGT:
Example A 8 ECGs taken
Example B 6 ECGs taken
Example C 6 ECGs taken
Example D 2 ECGs taken
Example E 6 ECGs taken
Day 1
12
ECGF
Day 1
12
ECGF
Day 1
12
ECGF
Day 1
1
ECGF
Day 1
12
ECGF
2 Day Day 3
34 56
ECGT
Day 4 Day 8 (discharged)
7 8
ECGL
2 Day Day 3 (discharged)
34 56
ECGT ECGL
Day 2 Day 3 Day 4 (discharged)
34 -- 56
ECGT ECGL
Day 8 (discharged)
2
(No ECGT) ECGL
Day 3 Day 5
34 56 Un-
coda- ECGT ble ECGL
The following examples for choosing ECGF, ECGl, and ECGT include ones for a) no ECG until late in the hospital course, b) hospitalizations less than three days, or c) ECGs taken on less than three days but at least three ECGs are available. General rule: Code up to three ECGs if available and codable, even if definitions do not always fit.

Example A 3 ECGs taken
Example B 4 ECGs taken
Day 1 . . . . .
None
1 Day
A-67 Page 22
. . . . Day 7 Day 9 Day 10 (discharged)
1 2 3
ECGF ECGT ECGL
Day 2 (discharged)
123 4
ECGF ECGT ECGL
94. Circle the letter(s) corresponding to the 12-lead ECG(s) that will be duplicated and sent to the Minnesota ECG Reading Center for coding. For example, a 11 three letters will be circled (F.L.T) if at least three ECGs in the chart were codable. Surveillance ECGs that need review should be handled locally by the field center.
Instructions for sending ECGs to Minneapolis ECG Reading Center for Coding
All ECGs are coded by the Minnesota ECG Reading Center. ECGs should be photocopied and the following protocol should be followed when sending ECGs to Minneapolis:
1. Staple together the pages belonging to each individual ECG, and label the first page clearly as follows:
a. Surveillance ID label b. "Cohort" or "Surveillance" as appropriate C. "ECGF" or "ECGL" or "ECGT" as appropriate d. Date of the ECG
2. If an ID has more than one photocopied ECG to be sent, place them in chronologic order and use a paper clip to bind these together.
3. Send them to the Minnesota ECG Reading Center in batches, each batch containing only cases of one type (i.e. Surveillance or Cohort), and accompanied by a shipping inventory (see Appendix GG) that lists in order of batch contents the Surveillance ID and the number of ECGs sent for that ID. Lots can be any size (the Reading Center prefers large ones), but you should send them at least monthly. A sample shipping inventory is attached for you to copy and use. The batch ID should be of the form ARcEnnnn, where "c" is replaced by the capital letter corresponding to your Field Center and "nnnn" is the sequential batch number, counting all batches you have sent to the Reading Center since the
Page 23 A-68
start of the project. Be sure to keep a copy of each completed batch inventory for your records. Note that the inventory form provides for exactly 100 IDS, so larger batches can be accommodated by simply inserting the appropriate leading digit(s) in the position ("Pas") columns.
97, Abstractor Number. This should be filled in, even when the chart proves to be ineligible. Double check that your code number has been written in on all the ineligibles since this is a common error. Include the date.
98. Date abstract completed.

Page 24 A-69
APPENDIX AA
26a. Cardiac Catheterization - invasive procedure usually performed by a cardiologist to visualize heart chambers and contraction. This procedure is usually accompanied by coronary angiography and is generally not performed at the bedside. Include right-sided, left-sided, and both-sided catheterization, but not Swan-Ganz ;;th$erization. (The ICD 9 Codes for cardiac cath include
. .
26b. Coronary Angiography - invasive radiologic procedure to visualize coronary arteries. It is always done with cardiac catheterization, so "cardiac catheterization" should also be checked "Yes" when coronary angiography was present. Occasionally, drugs such as streptokinase are given. References to coronary angiography may be found in radiology reports, chart notes, cardiologist, or consult notes, etc. (88.5) This category also includes Digital Subtraction Angiography - also for visualizing coronary arteries. This procedure is noninvasive (not done by catheterization) and involves radioisotopes (88.57).
26~. Coronary Angioplasty - dilation of coronaries via a balloon catheter or laser, sometimes done during an acute MI to reperfuse heart. (36.0)
26d. Swan-Ganz Catheterization - insertion of balloon tipped (Swan-Ganz) catheter at the bedside into the right side of the heart which can be used to monitor pulmonary arterial pressure continuously and pulmonary capillary wedge pressure and oxygen of mixed venous blood intermittently. Includes pacing Swan-Ganz. (89.64)
26e. Echocardiography - a noninvasive procedure, often abbreviated as "echo", used to visualize heart valves and chambers. Synonyms are: Ultrasound of the Heart; M-Mode and Pulsed Doppler Echocardiography. (88.72)
26f. Coronary Bypass Surgery - open-heart surgery in which a prosthesis or a section of blood vessel is grafted onto one of the coronary arteries and connected to the ascending aorta to bypass a narrowing or blockage in a coronary artery. The purpose of CABG is to improve blood supply to the heart, to reduce its workload and to relieve the pain of angina. (36.1)
26g.h. Streptokinase, urokinase, anistreplase or tissue plasminogen activator (TPA) coronary reperfusion (See Appendix BB). These are drugs given during the early stages of an MI to dissolve coronary thrombus or clots. The drugs may be administered intracoronary or in a peripheral intravenous solution. If given intracoronary , coronary angiography is almost always done, so item (b) should be marked. If given intravenously, answer (g) with "Yes", but do not mark (b). (99.29)

Page 25 A-70
26i. Aortic Balloon Pump - a mechanical procedure used in severe heart failure or shock or post surgery. Aortic balloon pumps are also called counterpulsation pumps, balloon counterpulsation pumps, intraaortic pumps, AVCO System 7, 10, Datascope System 80, IABP and Datscope, and Percor IABP. (37.6)
26j. Radionucleide Scan of Heart - a radioisotope procedure to a) visualize heart contractility and estimate ejection fraction, b) estimate infarct size, or c) gauge myocardial perfusion. Radioisotopes include thallium (T1201), technetium pyrophosphate (Tc99m). Procedures include "heart scan", MUGA (multigated equilibrium blood pool imaging), radionucleide angiography, ejection fraction radionucleide scan, thallium scan, infarct (MI) scan, magnetic resonance imaging (MRI) of the heart, positron imaging, etc. Digital subtraction angiography is "No" and is instead recorded under coronary angiography, above. These tests would be recorded in radiology or nuclear medicine reports or as procedure codes. (92.05)
261. Other procedures might include aortic aneurismectomy, cardiac transplant, CT scan of the heart, pacemaker insertion, insertion of an automatic defibrillator, pericardiocentesis, electrophysiology (EP) studies, etc.

A-71 Page 26
APPENDIX BB
31b. Calcium Channel Blockers
Generic
Diltiazem Nifedipine Verapamil Nicardipine Nimodipine
31a. Nitrates
Generic
Isosorbide Dinitrate Nitrates Nitrites Nitroglycerin Trinitroglycerine
31d. Digitalis
' Generic
Digitalis glycoside Digitoxin Digoxin
Trade
Adalat Calan Cardene Cardizem Isoptin Nimopt Procardia
Trade
Cardilate Deponit NTG Film Dilatrate Iso-Bid Isordil Isotrate Minitran Nitrobid Nitrocine Nitrodisc Nitrodur Nitrogard Nitroglyn Nitrol Nitrolin Nitrolingual Nitrong . Nitrospan Nitrostat Peritrate Sorbitrate Transderm Transdermal NTG Tridil
Trade
Cedilanid Crystodigin Lanoxicaps Lanoxin

31c. Beta-Blockers
Generic
Acebutolol Atenolol Carte0101 Esmolol Labetalol Metoprolol Nadolol Penbutolol Pindolol Propranolol Timolol
26a, Reperfusion ARents 29g.
Generic
Streptokinase Tissue Plasminogen
Activator (TPA) Urokinase Anistreplase
Trade
Blocadren Brevibloc Cartrol Corgard Corzide Inderal Inderide Levatol Lopressor Normozide Normodyne Sectral Tenoretoc Tenormin , Timolide Trandate Visken
Trade
Abbokinase Kabikinase Streptase Alteplase Activase Fhinase
Page 27 A-72
Page 28 A-73
31g. Aspirin (This is not all aspirin compounds, but the likely formulations used for heart conditions.)
Generic Trade
Aspirin ASA
Alka-Seltzer Anacin Arthritis Pain Formula A.S.A. Enseals Ascriptin Aspergum Baby Aspirin Bayer (Aspirin) Buffaprin Buffered Aspirin Bufferin Buffex Buffinol CAMA Arthritis Pain Reliever Easprin Ecotrin Empirin Excedrin Gelpirin Genprin Magnaprin Measurin Norwich St. Joseph Verin Wesprin Buffered ZORprin
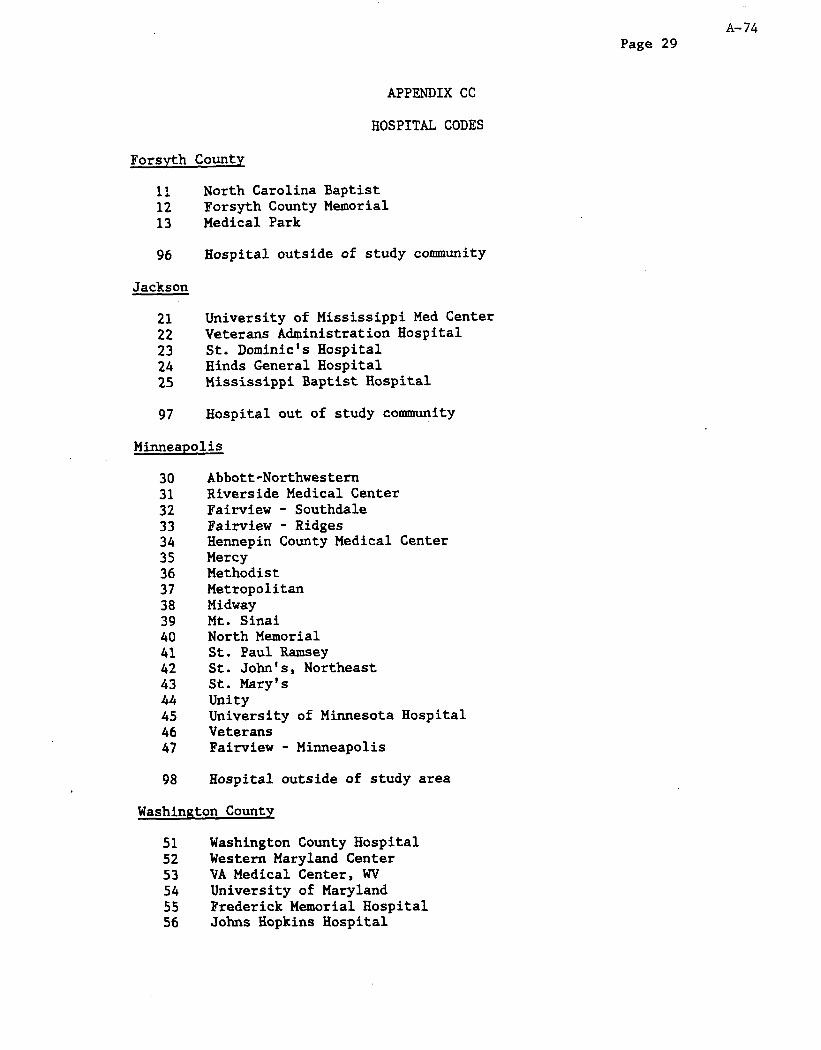
Page 29 A-74
Forsyth County
APPENDIX CC
HOSPITAL CODES
11 North Carolina Baptist 12 Forsyth County Memorial 13 Medical Park
96 Hospital outside of study community
Jackson
21 University of Mississippi Med Center 22 Veterans Administration Hospital 23 St. Dominic's Hospital 24 Hinds General Hospital 25 Mississippi Baptist Hospital
97 Hospital out of study community
Minneapolis
30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47
98
Abbott-Northwestern Riverside Medical Center Fairview - Southdale Fairview - Ridges Hennepin County Medical Center Mercy Methodist Metropolitan Midway Mt. Sinai North Memorial St. Paul Ramsey St. John's, Northeast St. Mary's Unity University of Minnesota Hospital Veterans Fair-view - Minneapolis
Hospital outside of study area
Washington County
51 Washington County Hospital 52 Western Maryland Center 53 VA Medical Center, WV 54 University of Maryland 55 Frederick Memorial Hospital 56 Johns Hopkins Hospital

A-75 Page 30
Washington County (cont.)
57 Washington Hospital Center 58 George Washington University 59 Georgetown University
99 Hospital outside of study community
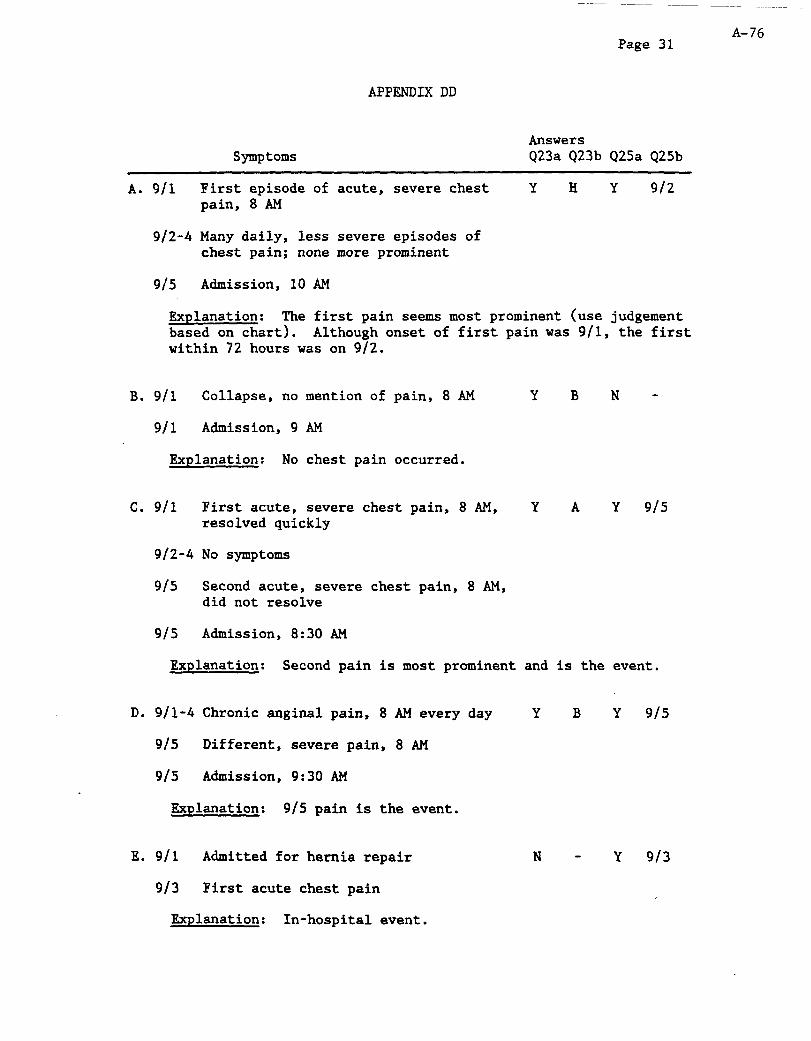
A-76 Page 31
APPENDIX DD
Symptoms Answers Q23a Q23b Q25a Q25b
A. 9/l First episode of acute, severe chest Y H Y 912 pain, 8 AM
9/2-4 Many daily, less severe episodes of chest pain; none more prominent
915 Admission, 10 AM
Explanation: The first pain seems most prominent (use judgement based on chart). Although onset of first pain was 9/l, the first within 72 hours was on 9/2.
B. 9/l Collapse, no mention of pain, 8 AM Y B N -
9/l Admission, 9 AM
Explanation: No chest pain occurred.
c. 9/l First acute, severe chest pain, 8 AM, Y A Y 9/s resolved quickly
9/2-4 No symptoms
g/5 Second acute, severe chest pain, 8 AM, did not resolve
915 Admission, 8:30 AM
Explanation: Second pain is most prominent and is the event.
D. 9/l-4 Chronic angina1 pain, 8 AM every day Y B Y 915
9/s Different, severe pain, 8 AM
9/s Admission, 9:30 AM
Explanation: 9/S pain is the event.
E. 9/l Admitted for hernia repair
913 First acute chest pain
Explanation: In-hospital event.
N - Y 9/3
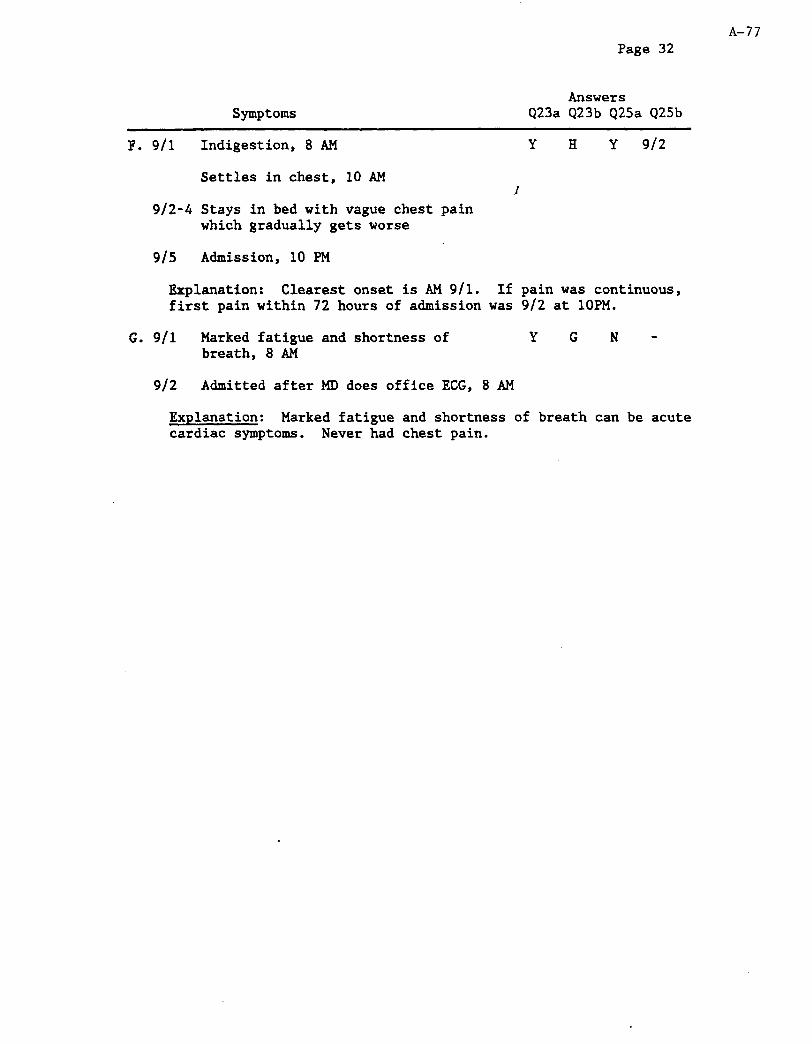
Page 32 A-77
Symptoms Answers
Q23a Q23b Q25a Q25b
F. 9/l Indigestion, 8 AM Y H Y 9/2
Settles in chest, 10 AM I
9/2-4 Stays in bed with vague chest pain which gradually gets worse
915 Admission, 10 PM
Explanation: Clearest onset is AM 9/l. If pain was continuous, first pain within 72 hours of admission was 9/2 at 1OPM.
G. 9/l Marked fatigue and shortness of Y G N - breath, 8 AM
9/2 Admitted after MD does office ECG, 8 AM
Explanation: Marked fatigue and shortness of breath can be acute cardiac symptoms. Never had chest pain.
A-78
Page 33
APPENDIX EE
souNDEx
Soundex is a system of converting names and addresses to a short abbreviation. It is used in ARIC abstracting when the hospital, for confidentiality reasons, will not let the patient name or address be abstracted verbatim. In that case it is often acceptable to record the Soundex code for the patient's name and address.
The following section is arranged in three parts. Part A discusses Soundex coding for surnames. Part B discusses Soundex coding for given names. Part C discusses coding for address.
(If needed, contact CSCC for SOUNDEX Instructions.)

Page 34 A-79
APPENDIX FF
ARIC SURVEILLANCE ECG SHIPPING INVENTORY
Batch: Date: Type of Case:
pas Surv.ID #ECG pas Surv.ID #ECG Pos Surv.ID #ECG Pos Surv.ID #ECG
01
02
03
04
05
06
07
08
09
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
I
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
00

A-80 O.M.B. 0925-0251 exp 7-31-92
ATHEROSCLEROSIS RISK IN COMMUNITIES SYUDY
INFORMANT INTERVIEW FORM
EVENT ID: -1 INFORMANTNuMBER: m m FORM CODE: VERSION: A 6/Q5/91
LASTNAME: I I I I I I I I I I I I INITIALS: m . INSTRDCTIONS:
The Informant Interview Form is completed for each informant for an out-of-hospital death as determined by the ARIC Event Investigation Summary. Event ID and Name must be entered above, as described in the document, "General Instructions For Completing Paper Forms*'. Informant Number should be determined from the Event Investigation Summary Form. For 9nultiple choice" and 8'yes/no" type questions, circle the letter corresponding to the most appropriate response. If a letter is circle incorrectly, mark through it with an 'X' and circle the correct response.
INFORMANT INTERVIEW TRACING INFORMATION
DECEDEM!
Address:
city state ixp Coae
Date of death: -'7Tr+T--
INFORMANT
Name :
Address:
cJ.ty s=:a= up Coae
Telephone: ( 1
Relationship to the deceased:

A-81
RECORD OF CALLS
Day of Week Date Time Notes Code* Int
;MTWRFS MM/DD/YY A
P
iMTWRFS MM/DD/W A
P
iMTWRFS MM/DD/W A
P
;MTWRFS MM/DD/YY A
P
;MTWRFS MM/DD/YY A
P
;MTWRFS MM/DD/YY A
P
SMTWRFS M?f/DD/YY A
P
SMTWRFS MM/DD/YY A
P
*msum CODES (CIRCLE THE FINAL SCREENING RESULT CODE)
1 Complete 2 Partially complete 3 Unknowledgable
4 Refusal 5 Informant away or 6 Language barrier can't be found
7 No one home 9 Other (specify in Notes)
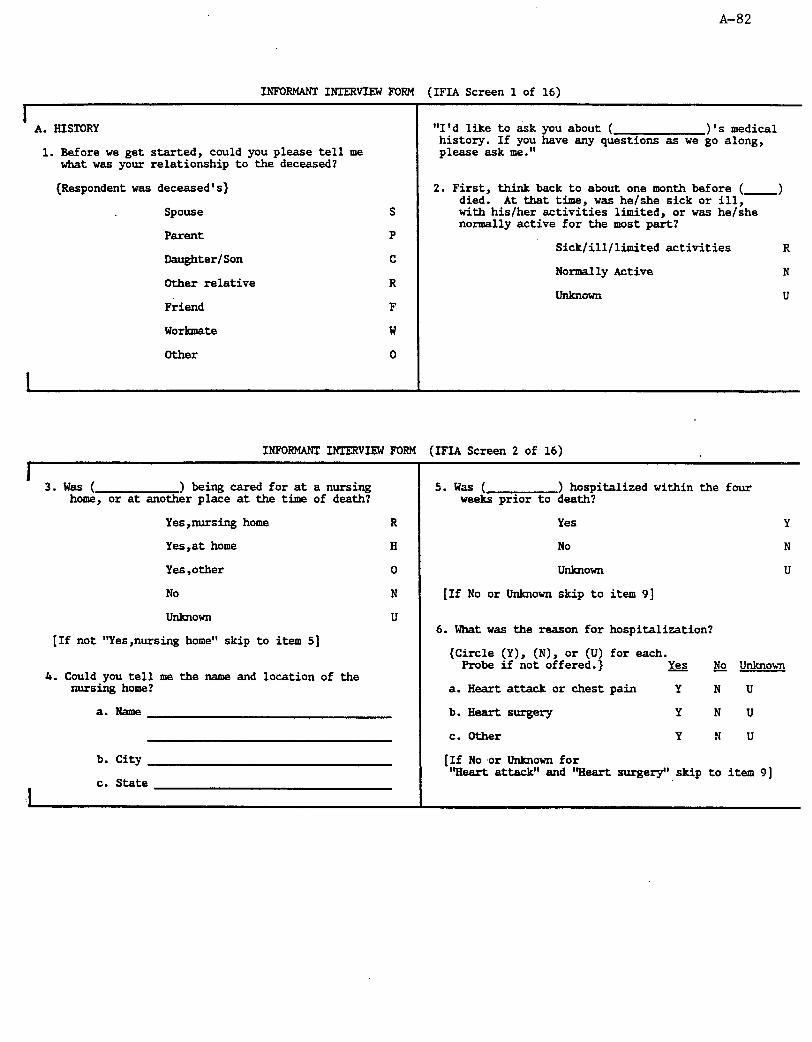
A-82
1NPoRMANT1RIERv1EWFoRM (IFIA Screen 1 of 16)
I A. HISTORY
1. Before we get started, could you please tell me what was your relationship to the deceased?
{Respondent was deceased's)
Spouse
parent
Daughter/Son
Other relative
Friend
Workmate
Other
"I'd like to ask you about ( )'s medical history. If you have any questions as we go along, please ask me."
2. First, think back to about one month before ( -1 died. At that time, was he/she sick or ill, with his/her activities limited, or was he/she normally active for the most part?
Sick/ill/limited activities R
Normally Active N
UdCllOWIl u
INFORMANT IRTERVIEW FORM (IFIA Screen 2 of 16)
3.was ( ) being cared for at a nursing home, or at another place at the time of death?
Yes,nursing home R
Yes,at home H
Yes ,other 0
No N
IhkllOWll U
[If not "Yes,nursing home" skip to item 51
4. Could you tell me the name and location of the nursinghome?
a. Name
b. City
c. State
5.wa.s ( ) hospitalized within the four weeks prior to death?
Yes Y
NO N
unknown U
[If No or Unknown skip to item 91
6. What was the reason for hospitalization?
(Circle (Y), (N), or (U) for each. Probe if not offered.) Yes & unhowl
a. Heart attack or chest pain Y N U
b.Iie.art surgery Y N U
c. Other Y N U
[If No .or Unknown for "Heart attack" and '%art surgery",skip to item 91
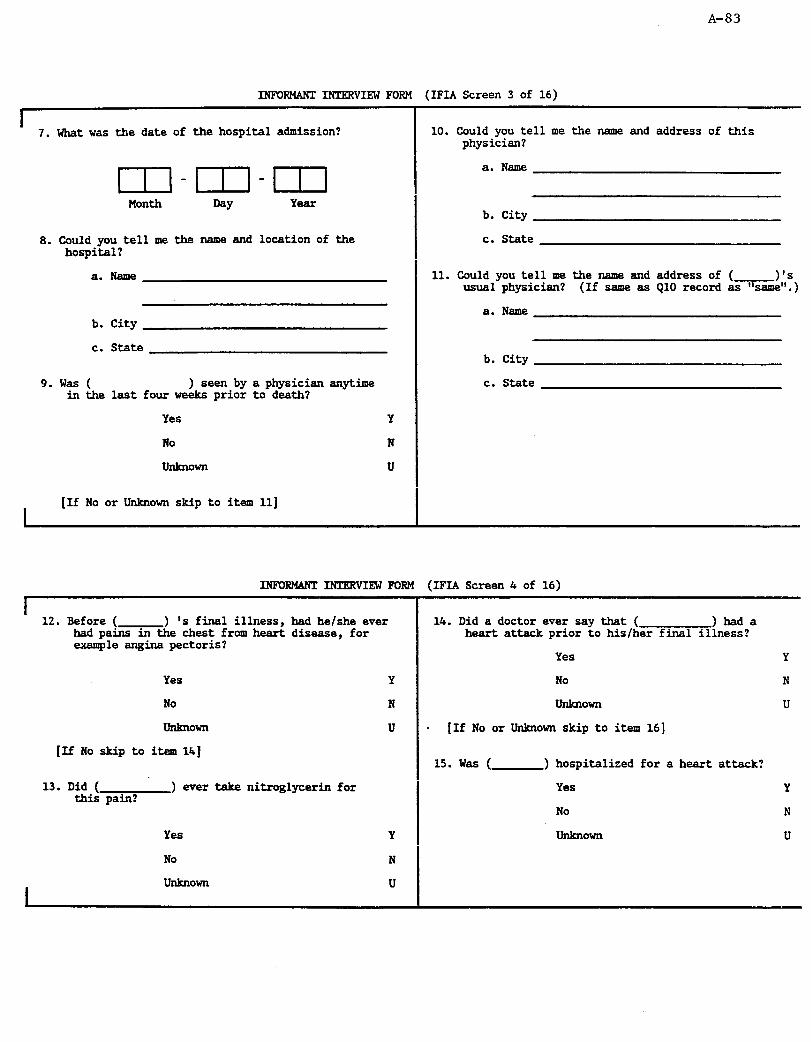
A-83
INFORMANT INTERVIEW FORM (IFIA Screen 3 of 16)
1 7. What was the date of the hospital admission?
m-m-m 8. Could you tell me the name and location of the
hospital?
a. Name
b. City
c. State
9. was ( ) seen by a physician anytime in the last four weeks prior to death?
Yes Y
No N
unknown U
I [If No or Unknown skip to item 11)
10. Could you tell me the name and address of this physician?
a. Name
b. City
c. State
11. Could you tell me the name and address of ( 1's usual physician? (If same as QlO record as %ame".)
a. Name
b. City
c. State
I
INFOglG4NT INIFXVIEW FORM (IFIA Screen 4 of 16)
I ' 12. Before ( > 's final illness, had he/she ever
had patime chest from heart disease, for example angina pectoris?
Yes
No
unknown
[If No skip to item Ih]
14. Did a doctor ever say that ( )had a heart attack prior to his/her final illness?
Yes Y
Y No N
N unknown u
U * [If No or Unknown skip to item 161
15. was ( ) hospitalized for a heart attack?
13.Did( ) ever take nitroglycerin for this pain?
Yes Y
No N I
Yes
No
unknown
unknown I
U
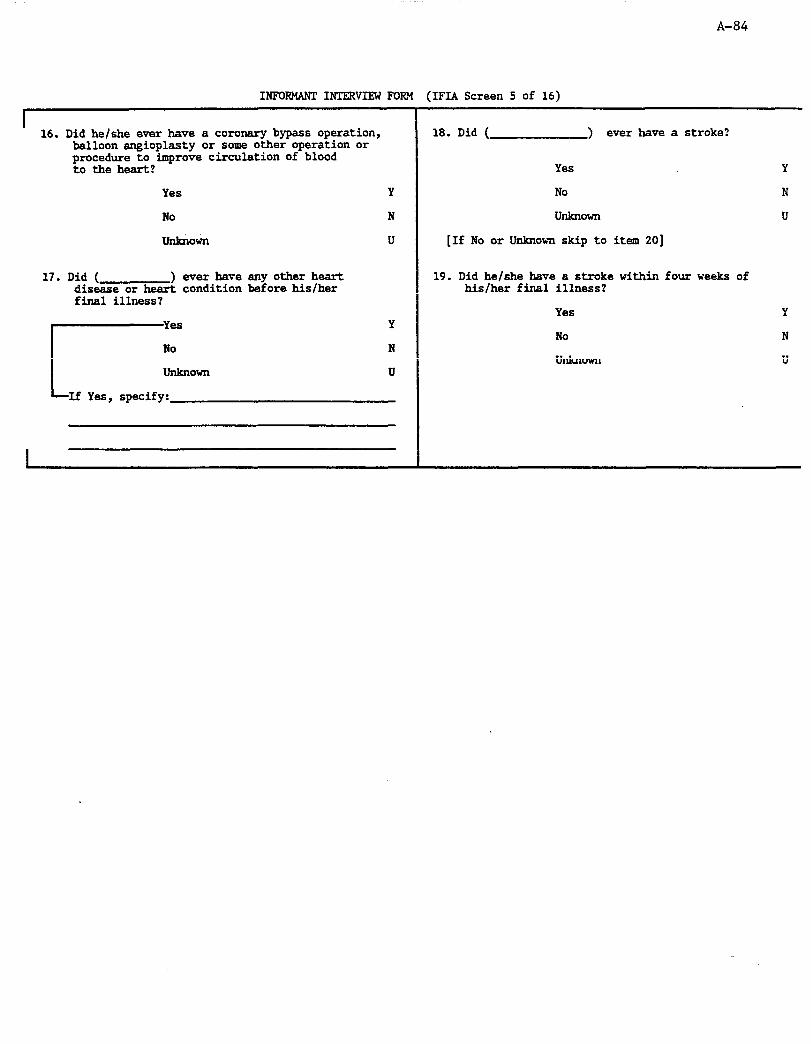
A-84
I
INFORMANT INTERVIEW FOR! (IFIA Screen 5 of 16)
I I
16. Did he/she ever have a coronary bypass operation, balloon angioplasty or some other operation or procedure to improve circulation of blood to theheart?
18. Did ( > ever have a stroke?
Yes
Yes
No
unknown
Y No
N
U I
[If No or Unknown skip to item 201
17. Did ( ) ever have any other heart disease or heart condition before his/her final illness?
Y
No
UllktlOWn
If Yes, specify:
N
U
19. Did he/she have a stroke within four weeks of his/her final illness?
No
unlcnown
I I

A-85
INFORMANT INTERVIEW FORM (IFIA Screen 6 of 16)
B.CIRCUMSTANCES SURROUNDINGDEAM Attach IWent ID Label Here
'Thenextfewquestions areconcernedwiththe circumstances surrounding(
20. Could you please tell me what you can of ( )'s general health, health on the day he/she died, and of the death itself?
)'s death."
Specify:
I

A-86
INFOEMANI INTERVIEW FORM (IFIA Screen 7 of 16)
1 Yll-ie next set of questions may go over some of what you have already told me. Although it may seem repetitious, I must ask these questions for consistency of information."
21. Were you present when (
Yes
No
[If Yes skip to item 251
) died?
Y
N
22. Did anyone see or hear (- ) when he/she died?
Yes Y
No N
unknown U
[If Yes skip to item 251
23. Was anyone close enough to hear ( he/she had called out?
) if
Yes Y
No N
unknown U
[If Yes skip to item 251
24. How long after ( ) was last knom to be alive was he/she found dead?
{Enter the shortest interval known to be true}
5 minutes or less A
1 hou? or less B
24 hours or less C
more than 24 hours D
unknown U
INFOEMABT INTERVIEW FORM (IFIA Screen 8 of 16)
I 25. Where was ( ) when he/she died?
Home (or other private residence) A
Work B
In a public building C
On abus or public transportation D
On the street E
In au automobile F
Inanursinghome G
In en emergency room H
Inanambulance I
In the hospital J
Other 0
UdCtlOWIl
I U
c. SYNPTOMS The next few questons are concerned with any symptoms
( ) may have had shortly before he/she died."
26. Did ( ) experience pain or discomfort in his/her chest,left arm or shoulder or jaw either just before death or within 3 days (72 hours) of death?
Yes
No
unknown
Y
N
U
[If No or Unknowa skip to item 301

A-87
I
INFOEMANI INTERVIEW FORM (IFIA Screen 9 of 16)
" The next set of questions deal specifically with 28. Did he/she take nitroglycerin because of this last the last episode of ( )'s pain or episode of pain or discomfort? discomfort. The last episode is defined as starting atthetime ( ) noticed discomfort that Yes Y caused him/her to stop or change what he/she was doing." No N
27. Did ( )'s last episode of pain or unknown U discomfort specifically involve the chest?
INFCEMANT INIEEVIEW FORM (IFIA Screen 10 of 16)
29. How long was it from the beginning of ( 1's last episode of pain or discomfort to the time he/she stopped breathing on his/her own?
(Circle the shortest internal known to be true}
5 minutes or less A
10 minutes or less B
lhour or less C
24 hours or less D
more than 24 hours E
IhkllOWIl U
30. Within 3 days of death or just before ( ) died, did any of the following symptoms begin for the first time?
{Circle (Y), (N), or (U) for each)
a. Shortness of breath
b. Dizziness
c. Palpitations (pounding in the chest)
d. Marked or increased fatigue, tiredness, or weakness
e.Headache
f. sweating
g. Paralysis
h. Loss of speech
i. Attack of indigestion or nausea or vomiting
rj- m= -If Other, specify
Yes
Y
Y
Y N U
Y
Y
& unknown
N U
N U
N U
N U
N U
N U
N U
N U
N U

A-88
INFCEMANI INTEEVIEW FORM (IFIA Screen 11 of 16)
I D.-CYMEDICALCAEE
*I The next few questions are concerned with emergency medical care ( ) may have received prior to or at the time of death. You may have already given this information in an answer to an earlier question. Since it is important to obtain information specifically on emergency medical care, I hope you don't mind if these questions seem repetitive."
I
31. Was a physician, ambulance, or other emergency medical team called?
Yes Y
No N
unknohTl U
[If No or Unknown skip to item 351
32. Was (the physician, ambulance, or EHS team) called because of symptoms ( he/she was already dead?
) was having or after
symptoms S
Already dead D
INFCEMANI INTERVIEW FORM (IFIA Screen 12 of 16)
I 33. Bow long was it from the time the last episode of
symptoms started to the time that medical assistance was called for?
{Circle the shortest interPa known to be true}
5 minutes or less A
10 minutes or less B
1 hour or less C
6 hours or less D
24 hours or less E
more than 24 hours F
unknown U
I
34. How long was it from the time that medical care was called to the time when it arrived?
{Circle the shortest interval known to be true}
5 minutes or less A
10 minutes or less B
1 hour or less C
6 hours or less D
24 hours or less E
more than 24 hours F
unknown U
Did not come X
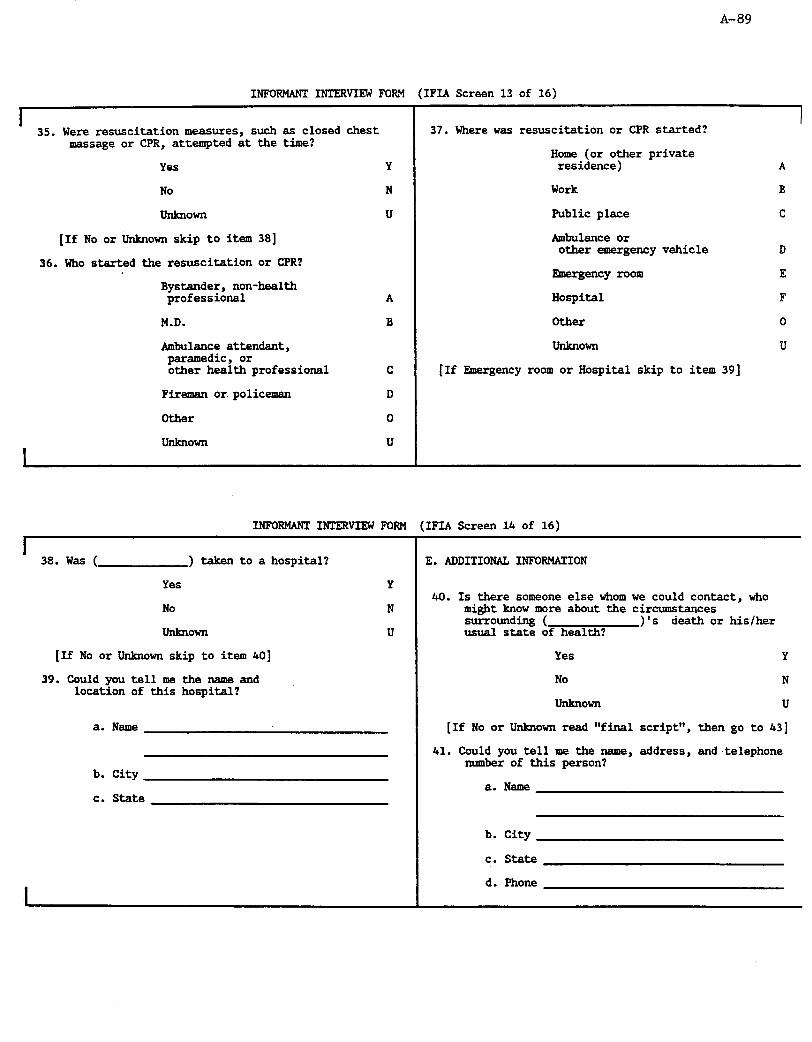
A-89
-_--- __._ - -_-__--. ---_.
(
a--. - _̂ - me\
1r‘l.A screen 13 or lb) INFUKHAN-1 IN-UKVIW P’UKH
1 35. Were resuscitation measures, such as closed chest
message or CPR, attempted at the time?
Yes Y
No N
hkIlOWll U
[If No or Unknown skip to item 381
36. Who started the resuscitation or CPR?
37. Where was resuscitation or CPR started?
Home (or other private residence) A
Work B
Public place c
Ambulance or other emergency vehicle D
Emergency room E
Hospital F
Other 0
unknown U
[If Emergency room or Hospital skip to item 391
Bystander, non-health professional A
M.D. B
Ambulance attendant, paramedic, or other health professional C
Fireman or policeman D
Other 0
unknown U
INFORMANT INTERVIEW FORM (IFIA Screen 14 of 16)
I 38. Was ( ) taken to a hospital?
Yes Y
No N
unknown U
[If No or Unknown skip to item 401
39. Could you tell me the name and location of this hospital?
a. Name
b. City
c. State
E. ADDITIONAL INFORMATION
40. Is there someone else whom we could contact, who might know more about the circumstances surrounding ( )'s death or his/her usual state of health?
Yes Y
No N
UXlkIlOWXl U
[If No or Unknown read "final script", then go to 431
41. Could you tell me the name, address, and ,telephone number of this person?
a. Name
b. City
c. state
d. Phone

A-90
I
INFORMANT INTERVIEW FORM (IFIA Screen 15 of 16)
42. How was he/she related to the deceased?
Spouse
Parent
Daughter/Son
Other relative
Friend
Workmate
Other
[Read "final script, then go to Item 431
F. RKLIARILITY
S {To be completed immediately after the interview}
P 43. Did the respondent frequently contradict himself/ herself or give information that he/she would have
C no way of knowing?
R Yes Y
F No N
W 44. Did the respondent seem to be reluctant to answer
0 questions and thus might not have given all the information the interviewer would wish to know?
No
I
INFORMANT INTERVIEW FORM (IFIA Screen 16 of 16)
I 45. On the basis of these questions, give your rating
of reliability of the int-iew.
Good G
Fair F
Poor P
46. Would you like to add other details concerning the quality of the intemiew?
L,,,.,:
Y
N
,
47. Informant agreed to provide consent to gather further information.
I
Yes Y
No N
Not applicable A
G. ADMINISTRATIVE INFORMATION
48. Date of data collection:
m-m-m Month MY YW
49. Method of data collection:
Computer
Paper Form
C
P
50. Code number of the person completing this form
I I I I
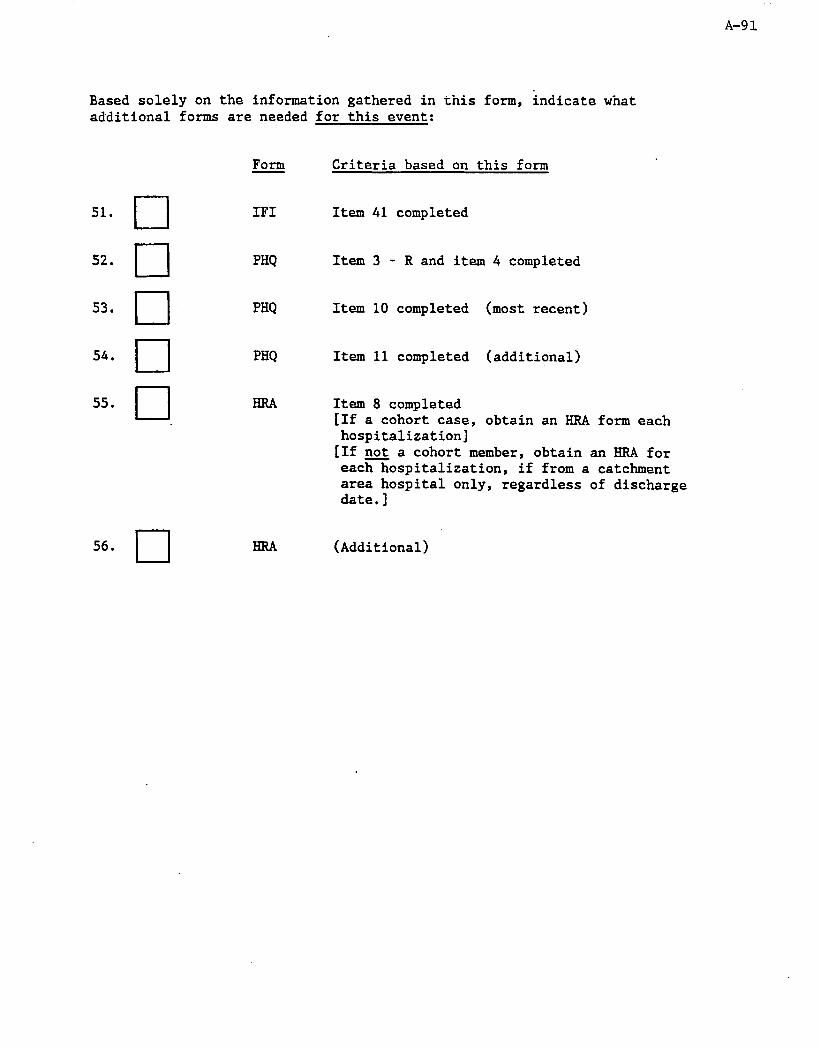
A-91
Based solely on the information gathered in this form, indicate what additional forms are needed for this event:
Form Criteria based on this form
51. cl
52. 0
53. q 54. cl
55. 0,
56. q
IF1 Item 41 completed
PHQ 1tem3 - R and item 4 completed
PHQ Item 10 completed (most recent)
PHQ Item 11 completed (additional)
Item 8 completed [If a cohort case, obtain an RRA form each hospitalization]
[If not a cohort member, obtain an HRA for each hospitalization, if from a catchment area hospital only, regardless of discharge date.]
(Additional)

Page 1
A-92
INIFORMANT INTERVIEW FORM INSTRUCTIONS
Version: A 6105191
I. (lxNKw& INsTRucTIoNs
The purpose of the informant interview is to obtain information about possible CHD events in order to classify cause of death. The interview with next-of-kin is potentially difficult because of the sensitive nature of a relative's death and the difficulty recalling or understanding the events related to the death. Even if the informant initially claims no knowledge, begin the form to see if the questions can be answered.
The interviewer should enter the information required on the first page before the contact is made with the informant, though some of the informant data made need to be filled after contact, such as relationship to the decedent. In some cases the informant may change after calling, as in the case where a spouse is to be contacted but the actual informant is a son or daughter. A record of calls should be maintained for the attempts at contacting the informant. The interviewer should put the date and time of each call, any explanatory notes, a result code for each call, and the interviewer's assigned code number. Eight attempts to contact an informant should be made over a two-week period. If no contact is made, repeat in a month.
The questionnaire is divided into six sections. Section A is concerned with the decedent's medical history, including previous hospitalizations. Section B addresses the events immediately surrounding the fatal event, and Section C is concerned with the symptoms the deceased experienced prior to the event. Section D addresses emergency medical care that may have been provided at the time of death, and Section E asks for information on other potential informants. Section F asks the interviewer about the reliablity of the information obtained during the interview.
Almost all questions have multiple choices for answers; however, if necessary the interviewer can write any additional information or comments that may be important to understanding the response in the margins next to the question (or use a Note log when done by computer). A few questions require the interviewer to write out descriptions of the death or the decedent's state of health as related by the informant. For these questions, the interviewer should write word-for-word (in short phrases, abbreviating) the response of the informant. For questions asking the informant to specify names , if more than one answer is given, write all responses.
when reading questions to the informant, the interviewer should fill in the blanks with the name of the decedent. For example, "I'd like to start by asking about 's medical history" should be read "I'd like to start by asking about Mr. Smith's medical history."
A-93 Page 2
The interviewer needs to know thoroughly the ARIC definition of death to complete the interview accurately. "Death" is defined as the point at which the decedent stops breathing on his/her own and never recovers. Thus, the onset of death for someone who is resuscitated or ventilated is the point at which he/she last breathes spontaneously. He/she may recover several times after resuscitation, but the last cessation of breathing is considered "death". Death is not the time "pronounced dead". If someone is "found dead", timing of death may be estimable if the time since last seen alive was short. However, if long, timing of death may be unknown.
The interviewer should be familiar with skip patterns and nature of each question. Several questions are similar, with only subtle differences. The interviewer must make the distinction clear to the informant. Such questions may sound repetitive and are easier if clarified.
If informant contradicts a previous answer, probe to clarify and correct if obviously wrong.
If informant says at the start of the interview that he/she does not know anything about the death, coax the informant to start the interview and try to complete. If the informant is obviously not helpful, gracefully end the interview.
Ask for next-of-kin record during the interview if appropriate but get written permission only if needed. Written release need not be witnessed. Attached is an example of a release form for written permission.
Finally, the interviewer is responsible for reviewing and editing the Informant Interview Form thoroughly following the interview. Review every question and the skip patterns carefully. Every question must be answered unless skip patterns indicate otherwise. The description of the events preceding the death (Q2) is extermely important for diagnostic purposes. Make sure that the description includes the timing of events and the symptoms experienced.
II. DRTAILED INSTRIKTIONS FORVARIOUS QUE!XtONS
A. HISTORY
1. This question asks for the relationship of the informant to the decedent. Make sure not to reverse this; for example, 'She was my mother" should be answered "daughter/son". "Other relative" includes aunt, uncle, cousin, in-law, and grandparent.
2. This question refers to any restriction from the decedent's usual day-to-day activities. It excludes the events at death.
A-94
Page 3
3. "Being cared for" refers to attendant medical care because of disability or sickness.
4. Fill in as much information as is known by informant. If the informant asks why this is needed, explain that it may be important to get additional information from the nursing home, with permission, to understand the cause of death.
5. Any hospitalization for any reason is "yes".
6. Read the list and mark appropriate answer(s). If "other" is marked, specify in informant's own words.
7. If decedent was hospitalized more than once or stayed in more 8. than one hospital , record the most recent on the form, then list
all dates, names, cities and states of other hospitalizations on a separate piece of paper. If exact days are unknown, fill in month and year. Missing values are indicated by "=" (equal sign) in appropriate field. Note: an HRA form will need to be completed for each hospitalization for "heart attack" or 'heart surgery" within 28 days of death, regardless of day of discharge. If a cohort case, obtain an BRA for each hospitalization. If not a cohort member, obtain an BRA for each hospitalization, if f= a catcbment area hospital, regardless of day of discharge. Each hospitalized event for "heart attack" or "heart surgery" occurring within 28 days of death and the death event should have different ID numbers.
9. Refers to any encounter with a physician for any reason in the month preceding death including final symptoms.
10. This should be the most recent. If more than one physician seen, provide names and addresses of most knowledgeable two.
11. Record name and address of decedent's 'usual" physician. If same as most recently seen (QlO), record 'same".
12. This question refers to chest pain from heart disease at any time before death. Angina or angina pectoris or a heart attack would be considered "yes" responses. Pain in the left arm or shoulder, jaw, or upper abdomen is considered equivalent to chest pain.
13. Refer to list of names for nitroglycerin if informant hesitates. Nitroglycerin is usually administered as a small tablet placed under the tongue but may be taken as a pill, an ointment, or as "skin patch".
14. Be aware that this refers to past history and does not include the fatal event under consideration (emphasize ever) and clarify to the interviewee, if required.
15. Synonyms for heart attack are "myocardial infarction", "MI", coronary occlusion.

Page 4 A-95
16.
17.
18.
19.
B.
20.
21.
22. 23.
24.
25.
Coronary bypass involves surgery bypassing the blocked coronary arteries with vessels removed from the arm or leg. "Balloon dilation" or "PTCA" are other terms for angioplasty. A cardiac catheterization, coronary angiography, or angiogram for diagnostic purposes without angioplasty should be answered "no".
If yes, specify the condition in the informant's own words. Hypertension does not qualify here as a heart disease or condition. Conditions recorded in this section should not be conditions directly related to or resulting from past MI recorded in 414. Probes may be needed.
A stroke is a brain hemorrhage or ischemia (blockage of blood flow) also known as cerebrovascular attack, cerebral hemorrhage, or blood clot on brain.
This includes the final, fatal event under consideration.
CIRCUMSTANCES SURROUNDiNG DEATH
Narrative: Write out as close to word-for-word as possible, using short phrases. Probe neutrally for symptoms, order and timing of events, medical care, etc. Record these important items verbatim; try to limit the narrative to the space provided. When describing the events surrounding the death itself, be sure to differentiate between the onset of the last symptoms, the death (recalling definition of death), and being "pronounced dead".
"Present" is defined as being within sight or sound of the deceased at the time of death; for example, Present: lying next to in bed, in next room and could be heard, left decedent alone momentarily. Not Present: in another room out of sight and sound, outsidext of sight and sound, left decedent alive and returned after 5 minutes, talked to on phone sometime right before.
These questions ask whether anyone was present at the time of the decedent's death (defined above). If the decedent died in his/her sleep with someone nearby; Question 22 should be answered "yes".
Mark the shortest interval known to be reliable. If the informant hesitates, read the intervals in order starting with the shortest.
This question refers to the place where the decedent died, as defined in the general instructions. Read the question, wait for a response , and mark appropriate answer. If the informant needs prompting, read the list. If the informant says "in the hospital" ask if he/she died in the emergency room. If yes, mark appropriate response.

Page 5
C. SYMPTOMS
26. We are primarily interested in acute symptoms, not chronic. Thus, if a person had been generally fatigued for a month and then had chest pain one hour before death, it is the chest pain that was the last episode. Similarly, if someone had a long history of angina but , not having acute pain, suddenly collapsed and stopped breathing, the onset of the final episode was the time of collapse. If the death occurred while sleeping or while someone was within hearing range of the decedent, the interval between onset and death is considered to be instantaneous. If the decedent was found dead (no one close enough to see or hear him/her), the onset may be unknown.
Onset of last episode is defined as being at that point in time when new symptoms cause a change in activity. If the symptom is chronic (e.g., longstanding exertional chest pain), there must be a change in severity or frequency. Symptoms might be stepwise (e.g., one chest pain, then a more severe one a hour later). In this case it is the first pain, if it was new and caused a change, that is the onset of the final episode. The final episode for someone who collapses, is revived, and collapses again began at the first collapse. Interviewers will have to probe and define onset specifically for each informant.
The difference between Q12 and 26 is the time period referred to. In 426, the time is specific: within 3 days of death. In 12, the decedent could have experienced pain at any time prior to death. If 426 is answered "no", skip to 430, as 427-29 refer to an episode of pain with 3 days of death.
The location of the pain or discomfort referred to in Q12 and 26 is specific. If the pain was experienced at sites other than the chest, left arm or shoulder or jaw), the answer should be "no". If the informant is unsure, but is leaning toward a "yes", then proceed as with a "yes".
If decedent was found dead, 426 must be answered either "yes" or "unknown". If the decedent was found dead, most of the answers will be "unknown". In this case, skip quickly through, verifying that the answers are unknown.
27. The option "yes" is checked if the pain occurred anywhere in chest within 3 days of death.
28. A list of names of "nitroglycerin" preparations is provided in the medication list and should be consulted if informant isn't sure or offers a brand name.
A-96
29. This is crucial question for timing of death. &e the definition provided above for death and onset of the final episode in order to clarify timing. Read the question, wait for response, and mark the shortest interval known to be true. If the informant hesitates, read the list and mark the appropriate
A-97
Page 6
response. The informant may have given a time interval when answering 426. If so, the interviewer may want to preface the question stating the time interval and asking for confirmation (e.g. "You mentioned that had chest pains two days before he died. Is that when the chest pain began?").
30. This question asks about any symptoms other than pain or discomfort in the chest. The timing of onset of these "other" symptoms is crucial. After each "yes" answer, sure the onset was within 2 days, and that the longstanding or "usual". Read the list slowly
. appropriate answers.
D. EMERGENCYMEDICAL CARE
probe to make condition was not and fill in the
31. This question refers to calling for help. If no one was called, skip to 435.
32. This question is to determine whether help was called for symptoms, or after informant knew decedent was already dead.
33. Read question, wait for response and mark the shortest interval known to be true. If informant hesitates, read the list. Timing is from the onset of the last episode. The following example would be coded E (24 hours or less): "decedent began having chest pain and nausea the night before, but ambulance was not called until the next morning."
34. Read the question, wait for response and mark appropriate answer. If the informant hesitates read the list and mark the shortest time known to be true. Be sure informant understands difference between 933 and Q34.
35. The informant may not be familiar with CPR or the procedure of closed chest massage. If this is the case, tell the informant that CPR is a procedure used to resuscitate (restore breathing or revive) persons who are experiencing heart attacks and have no pulse or breath. It usually involves mouth-to-mouth resuscitation with compression of the chest to circulate the blood.
36. 37.
Read the questions, wait for response, and mark appropriate answer. If informant hesitates, read the list and mark correct answer.
39. Fill in as much of the answer as is known.
Read the introductory statement. If an ambulance service (or other emergency medical service such as a fire department) was mentioned earlier, the interviewer may want to preface questions with a statement acknowledging that such information was given.
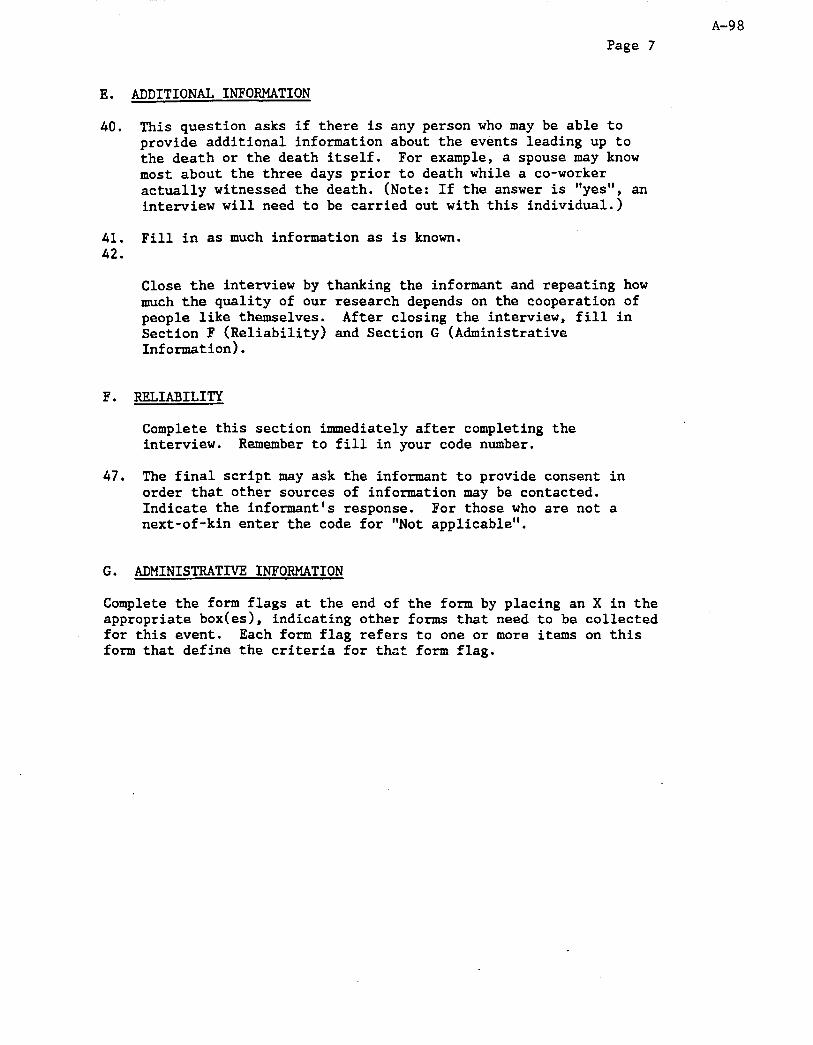
A-98 Page 7
E. ADDITIONAL INFORMATION
40. This question asks if there is any person who may be able to provide additional information about the events leading up to the death or the death itself. For example, a spouse may know most about the three days prior to death while a co-worker actually witnessed the death. (Note: If the answer is "yes", an interview will need to be carried out with this individual.)
41. Fill in as much information as is known. 42,
Close the interview by thanking the informant and repeating how much the quality of our research depends on the cooperation of people like themselves. After closing the interview, fill in Section F (Reliability) and Section G (Administrative Information).
F. RELIABILITY
Complete this section immediately after completing the interview. Remember to fill in your code number.
47. The final script may ask the informant to provide consent in order that other sources of information may be contacted. Indicate the informant's response. For those who are not a next-of-kin enter the code for "Not applicable".
G. ADMINISTRATIVE INFORMATION
Complete the form flags at the end of the form by placing an X in the appropriate boxces), indicating other forms that need to be collected for this event. Each form flag refers to one or more items on this form that define the criteria for that form flag.
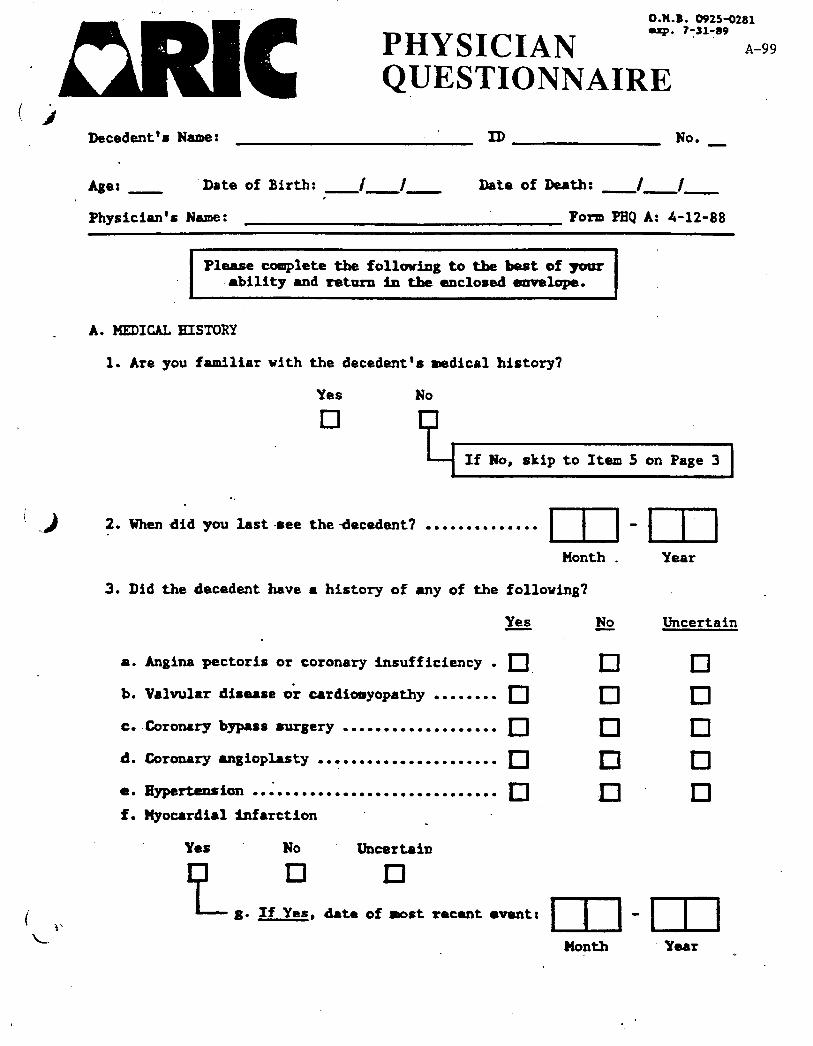
O.W.B. 0925-0281 mxp. 7;11?39
A-99 PHYSICIAN ESTIONNAIRE
Decedent's Name: ID No. -
Asa: - Date of Birth: I f Date of Death: -m- I / -- ,
Physician's Name: Form PHQ A: 4-12-88
Please complete the following to the best of ywr ability and return in the enclosed envelope.
A. HEDICAL HISTORY
1. Are you familiar with the decedent's medical history?
Yes
q No
If No, skip to Item 5 on Page 3
. .
2. When -did you last-ace the decedent? . . . . . . . . . . . . . . m Month .
3. Did the decedent have a history of any of the follouing?
P.
b.
C.
d.
e.
f.
Angina pectoris or coronary insufficiency . q Valvular disease 0; cardicnnyopathy . . . . . . . . q Coronary bypass surgery ................... q Coronary UlBiOphSty ...................... rJ
Eyp8l-ten8ion ............................... I Myocardial infarction _ .
No
I q El q El
-m Year
Uncertain
cl D 1 cl q
Yes No Uncert8in
e
D D
8. If Yes, date of most recent l mntz
Month Y88r
. .

Page 2 of 4 A-100
3: (cont'd) Did the decedent have a history of any of the following?
h. Other chronic irchemic heart disease
Yes Uncertain
D ;1” q i. Stroke (CVA)
Yeis No Uncertain
e
cl q j. If Yes, date of most recent event:
I-I-111 Month Year
k. Any non-cardiac condition that might have contributed to this death
Yes No Uncertain
e
cl q 1. If Yes, specify:
4. Was the decedent taking any of.the following medications within four veeks prior to death? _ l .i
Yes No Uncertain
a. Nitrates . . . . . . . . . . . . . . . . . . . q q cl‘ b. Calcium channel blockers . . . q D q C. Digitalis . . . . . . . . . . . . . . . . . . El q q d. Beta-blockers . . . . . . . . . . . . . . q q .n -8. Other cardiovascular drugs
Yes No Uncertain
q El f. If Yes,,specify:
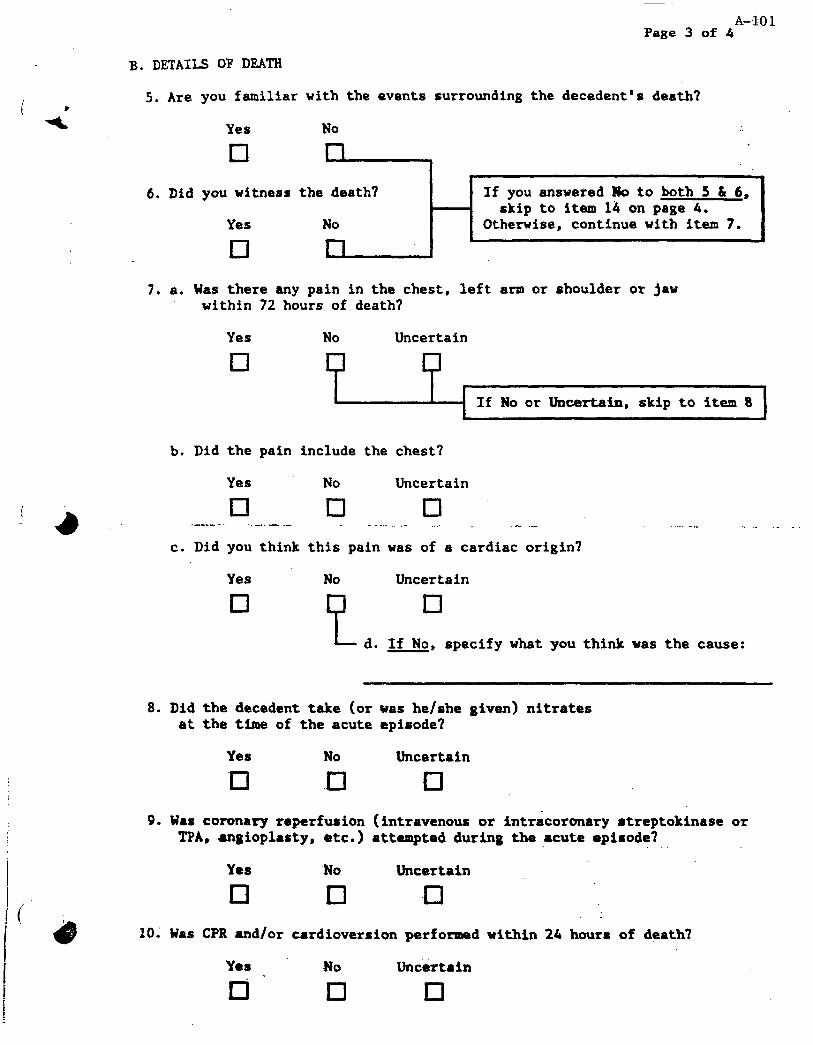
A-$01 Page 3 of 4
B. DETAILS OF DEATH
5. Are you familiar with the events surrounding the decedent’s death?
Yes
El
No
6. Did you witness the death?
Yes No
El
If you answeied No to both 5 S, 6, skip to item 14 on page 4.
Otherwise, continue with item 7.
7. a. Was there any pain in the chest, left arm or shoulder or jaw within 72 hours of death?
Yes
q No Uncertain
If No or Uncertain, skip to item 8
b. Did the pain include the chest?
Yes No Uncertain
q D u --... ..-. - - - . . .- ..- .- .- c. Did you think this pain was of a cardiac origin?
__ ., ._ _
Yes
q No Uncertain
1;1 q L d. If No, specify what you think was the cause:
8. Did the decedent take (or was he/she Riven) nitrates at the time of the acute episode?
Yes
cl
No
.a
Uncertain
cl
9. Was coronary reperfwion (intravenous or intracorcmary streptokinase or TM, angioplasty, etc.) attempted during the acute episode?
Yes No Uncertain
cl 0 -a
10; Was CPR and/or cardioversion perfomed within 24 hours of death?
Yes NO . El El
Uncertain
cl

--
Page 4 of 4
11. Please give time between onset of acute symptoms to death. (We are defining death as the point where spontaneous breathing ceased and the patient never recovered.)
A-102
D More than 3 days
0 2 - 3 days
q 1 day
cl At least 1 hour, i but less than 4 hours
q Less than 1 hour
El q Death instantaneous,
At least 12 hours, but less than 24 hours no symptoms
q At least 4 hours, but less than 12 hours cl UdCIiOWn
12. Would you classify the decedent's cause of death as due to CRD?
Yes , No Uncertain
El
e
q 13. If No, what do you believe to
be the cause of death?
Yes
.._-..
a. Pulmonary embolism . ..'. q b. Acute pulmonary edema . q .-. -._. .* ..-._ . c. Stroke . . . . . . . . . . . . . . . . u
d. Pneumonia . . . . . . . . . . . . . q e. Other
Yes No Uncertain
q cl f. Specify:
.
No
IJ El El El
C. SIGNATURE
14. Form completed by: Signature
15. Date: -rn-.m-m
Uncertain
.Month . Day Year
Thank you very much for your help. Please return this question- naire in the enclosed self-addressed eqvelope or aail it to: ARIC Central Receiving, Collabckative Studies Coordinating Center Suite 203 NCNB Plaza,137 B. Franklin Street,Chapel Hill NC 27514
I OFFICE USE ONLY: 16. Self- Interview _ E.R. records _ I

c A-103 Appendi% II (12) Version A 4-12-88
PHYSICIAN QUESTIONNAIRE INSTRUCTIONS
I. INTRODUCTION -
The PHQ is targeted for completson for each out-of-hospital death - (including DOA, RR death, or hospital death with no vital signs). UJ
to two PHQ forms may be needed:
1.
?*
One form should be completed by the certifying physician listed on the death certificate.
A second form is to be completed if.-there is another knowledgeable physician who cared for the decedent within four weeks of death. The name of such physicians could be obtained from one of several sources: informant interview,
* hospital or nursing home record , another PHQ, or coroner's report. (P ermissios.from next-of-kin may be required to contact this physician.-)
The Physician Questionnaire is used in nursing homes. In particular, if the patient was in a nursing home, completion by nursing home personnel should substitute for the second Physician Questionnaire.
II. PROCEDURE
Prior to the actual completion of the questionnaire, the "header" information should be completed at the field center. Write the event ID,number in the box at the top.- Also, indicate whether this is the first or second PHQ to be completed for this event by writing No. "1" or "2" in this box. Use no. 1 as described above for the certifying physician. Use no. 2 for as described above for another knowledgeable physician. Write in the patient's name, age, and dates of birth and death, as well as the physician's name.
The preferred method of obtaining the PHQ is by self-administration by the physician or his/her office staff. The PHQ is sent to the physician with a cover letter , as described in Manuals 2 and 3. Multiple contacts may be required to obtain the completed questionnaire. If the questionnaire is not returned within four weeks a second questionnaire is mailed. If there is no response within eight weeks, the PHQ is to be'completed by telephone.
‘-..
It is likely a telephone interview will be needed fog many physicians. The interviewer telephones the physician's office, and explains the call, for example:
"Hello, this is from the Atherosclerosis Risk in Communities Study, an epidemiologic research study of cardiovascular disease. Several weeks ago we mailed a brief questionnaire.to Dr. inquiring about the death of a patient, Mr./MS. , who died on / / . I am calling now to see if we could get the information by phone from Dr. :
or his/her nurg?. Is it possible'to talk to them now -a _ .- or would another time be better?"
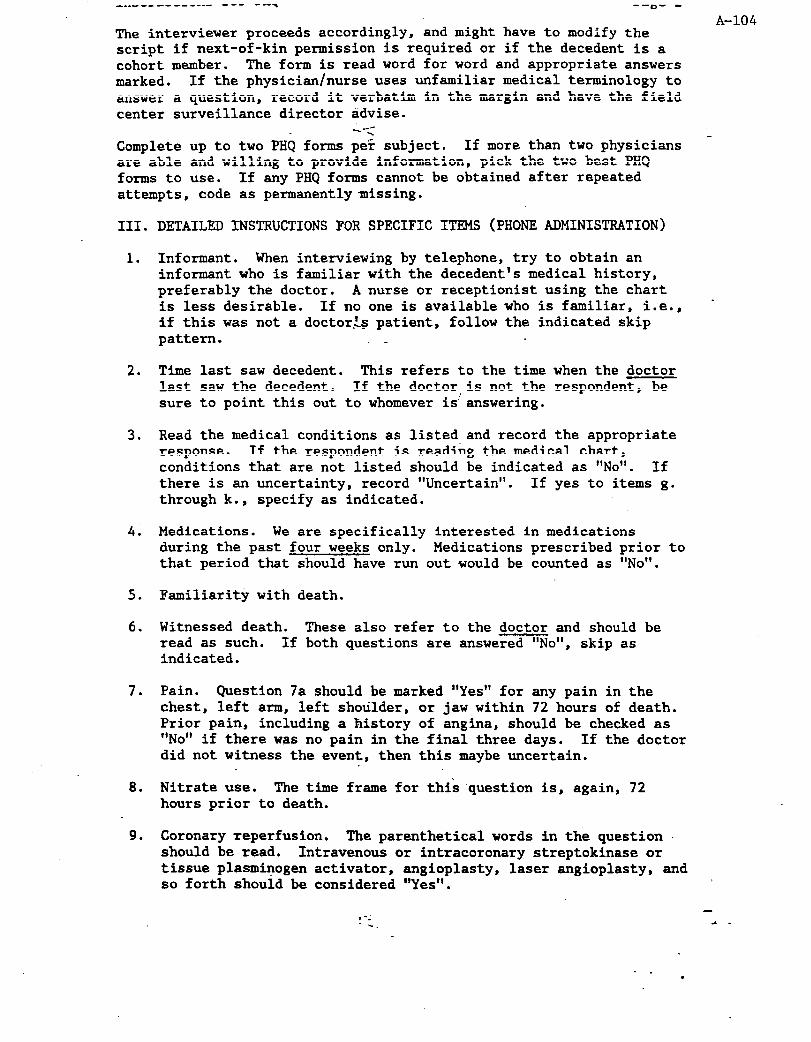
_..--- - ------ - --- ---T --m- -
A-104 The interviewer proceeds accordingly, and might have to modify the script if next-of-kin permission is required or if the decedent is a cohort member. The form is read word for word and appropriate answers marked. If the physician/nurse uses unfamiliar medical terminology to answer a question, record it verbatim in the margin and have the field center surveillance director advise.
N-c - Complete up to two PHQ forms per subject. If more than two physicians
are able and willing to provide information, pick the two best PHQ forms to use. If any PHQ forms cannot be obtained after repeated attempts, code as permanently missing.
III. DETAILED INSTRUCTIONS FOR SPECIFIC ITRMS (PHONE ADMINISTRATION)
1.
2.
3.
41
5.
6.
7.
8.
9.
Informant. When interviewing by telephone, try to obtain an informant who is familiar with the decedent's medical history, preferably the doctor. A nurse or receptionist using the chart is less desirable. If no one is available who is familiar, i.e., if this was not a doctor.Ls patient, follow the indicated skip pattern.
Time last saw decedent. This refers to the time when the doctor last saw the decedent. If the doctor,is not the respondent, be sure to point this out to whomever is! answering.
Read the medical conditions as listed and record the appropriate response. If the respondent is reading the medical chart, conditions that are not listed should be indicated as "No'. If there is an uncertainty, record "Uncertain". If yes to items g. through k., specify as indicated.
Medications. We are specifically interested in medications during the past four weeks only. Medications prescribed prior to that period that should have run out would be counted as ‘No’.
Familiarity with death.
Witnessed death. These also refer to the doctor and should be read as such. If both questions are answered "No", skip as indicated.
Pain. Question 7a should be marked "Yes" for any pain in the chest, left arm, left shoulder, or jaw within 72 hours of death. Prior pain, including a history of angina, should be checked as "No' if there was no pain in the final three days. If the doctor did not witness the event, then this maybe uncertain.
Nitrate use. The time frame for this question is, again, 72 hours prior to death.
Coronary reperfusion. The parenthetical words in the question should be read. Intravenous or intracoronary streptokinase or tissue plasminogen activator , angioplasty, laser angioplasty, and so forth should be considered "Yes".
-
.a - , -- -_
. . 0

Instructions for PHQ Pane -3 s io.
11.
12.
13.
14.
15.
16.
A-105 CPR/Cardioversion. Note that the time frame is the 24 hours prior to death.
Timing of death. Be certain to use the ARIC definition of death, . i.e., the point where spontaneous breathing ceased and the patient never recovered. ~ Record the time between the onset of acute symptoms and death-i? the most appropriate category.
Death due-to CHD.
Other cause of death. If the death is not due to CHD, ask Question 13. Wait for an answer and check the appropriate response. Then, if A-D were not mentioned, ask each of them individually. Check "Yes" or “No” or "Uncertain" as indicated. If "other", please specify.
If completed by phone interview, put the respondent's name in for Question 14 and the date of the interview. Write your code
.
number beside 414. L- -
Record the date of the interview.
Indicate whether the interview was interviewer-administered (Int) or self-administered (Self) by placing an "X" on the appropriate line.
-
.m -
. . .
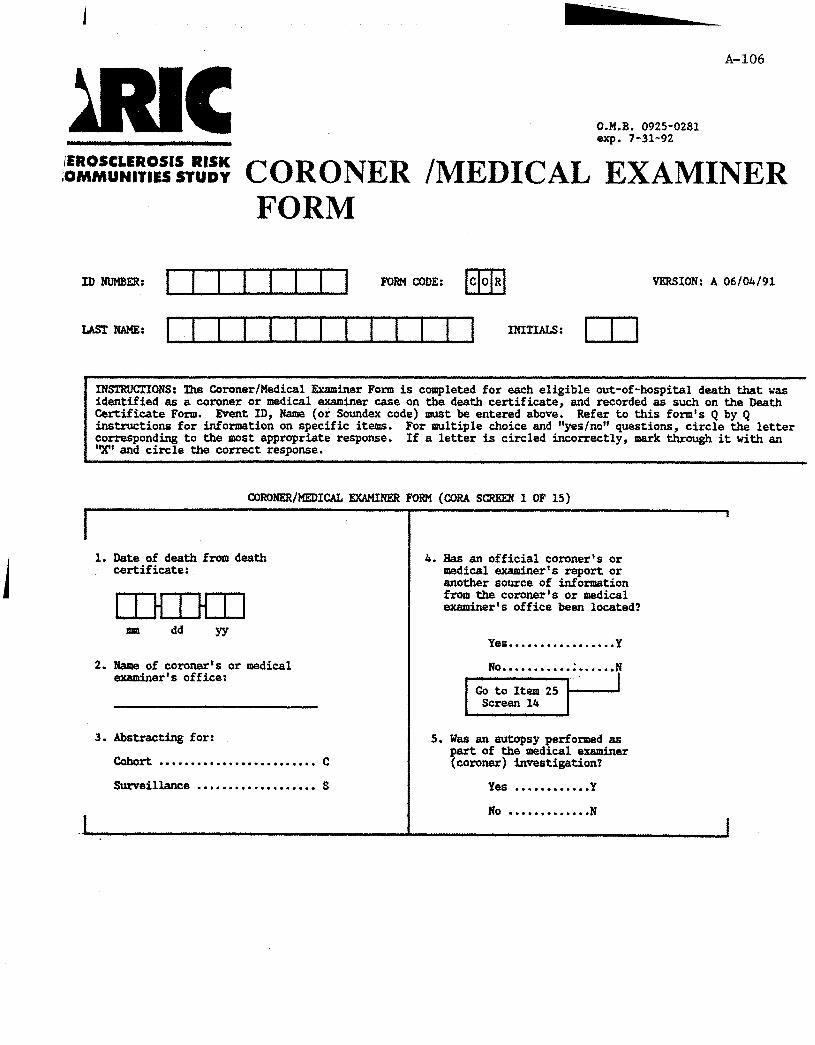
A-106
O.M.B. 0925-0281 exp. 7-31-92
~;%i:‘N:RI~‘:~%~ CORONER /MEDICAL EXAMINER FORM
IDNIJMBER: FORM CODE: UII COR
LASCNAME: lllIllllllI1 INITIALS: I
VERSION: A 06/04/91
INSTRUCTIONS: The Coroner/Medical Examiner Form is completed for each eligible out-of-hospital death that was identified as a coroner or medical examiner case on the death certificate, and recorded as such on the Death Certificate Form. Event ID, Name (or Soundex code) amst be entered above. instructions for information on specific items.
Refer to this form's Q by Q For multiple choice and "yes/no" questions, circle the letter
corresponding to the most appropriate response. 'X' end circle the correct remonse.
If a letter is circled incorrectly, mark through it with an
1. Date of death from death certificate:
t 1 H 1 H 11
2. Name of coroner's or medical examiner's office:
3. Abstracting for:
cohort . . . . . . . . . . . . . . . . . . . . . . . . . c
Surveillance ..+................ S
.
4. Has an official coroner's or medical exeminer's report or another source of information from the coroner's or medical examiner's office been located?
Yes.................Y
, ;i;i;;f"".*T
S.Wasanautopsyperformed as part of themedicaleuniner (coroner) investigation?
Yes . . . . . . . . . . ..Y
No . . . . . . . . . . . . .N ,

A-107
CORoNER/MEDIUL EXAMINER FORM (CORA SCREEN 2 OF 15)
6. Did the coroner’s report mention any of the following as contri- buting to or being present at death?
a. Recent myocardial infarction...............Y N
b. Coronary heart disease/ ischemic/atherosclerotic heart disease (other then MI)................ Y N
c. Hypertensive heart diseese..................Y N
d. Valvular heart disesse..................Y N
e. Other heart disease......Y N
f. Recent cerebral hemorrhage...............Y
g. Recent cerebral infarction...............Y
h. Recent cerebral embolus . . . . . . . . . . . . . . . . . . Y
i. Recent suberachnoid hemorrhage...............Y
j.Recentstroke,other or unspecified type......Y
aMx4ER/MEDICALExAUNKR FORM(CORA SCREEN 3 OF15)
7. a. Was any non-cardiac, non- stroke finding mentioned as contributing to death?
Yes . . . . . . . . . . ..Y
, ~r&-..&..$
b. kidney disease...........Y
c. Chronic respiratory disease..................Y
d. Psychiatric illness/
I depression...............Y
e. Alcohol or drug addiction................Y N
f. Epilepsy.................Y N
g. Liver disease............Y N
h. Other....................Y 7 1
. 1. Specify

A-108
CORONER/MEDICAL EXAMINER FORM (CORA SCREEN 4 OF 15)
I 8. List the final diagnoses:
I

A-109
CORONFR/KEDICALEXAMIRRRFORM(cORAScRGEN 5 OF15)
9. Pick one of the following:
Patient had acute symptoms Ccy.yf~edo;on;-==p 1
chenge in activity or to seeking medical care . . . . . . . . . ..A
Patient died suddenly end was known to have no acute symptoms . . . . . . . . . . . . . . . . . . . . . ..B
Patient was found dead with no documentation of symptoms . . . . . . . . . . . . . . . . . . . . C
Patient had symptoms but they were chronic (without change) or did not lead to a change in activity or seekingmedicalcare . . . . . . . . . . .
unknown . . . . . . . . . . . . . . . . . . . . . . ..u
cORONRR/MEDIcAL~ FORM (CORA SCREEN 6 OF 15)
I
10. Within 3 days of death or just before death, did any of the following symptoms begin for thefirstt&? -
a. Shortness of breath...Y
b. Dizziness.............Y
c. Palpitations..........Y
d. Marked or increased...Y fatigue, tiredness or weakness
e. Headache . . . . . . . . . . . . . . Y
I f. Swesting..............Y
I g. Paralysis.............Y N U
h. Loss of speech........Y N U
i. Attack of indi-.......Y N U gestion or nausea or vomiting
j. Other (specify).......Y N U I I
k. Specify:

A-110
CORORER/KEDICAL EXAMINER FOR?! (CORA SCREEN 7 OF 15)
I 11. a. Was there an acute episode(s) of
pain or discomfort anywhere in the chest, left arm or shoulder or jaw either just before death orwithin72hours of death?
Yes . . . . . . . . . . . . Y
. . . . . . . . . . . . . .
UlhOWll . . . . . . . . .
b. Did this pain or discomfort specifically involve the chest?
Yes . . . . . . . . . . . . Y
No ' . . . . . . . . . . . . . I
UdCllOWIl.........U
I
c. Did the patient take or was he/she given nitrates at the time of the acute episode?
Yes . . . . . . . . . . ..Y
No . . . . . . . . . . . ..N
unknown.........u
d. Was the discomfort or pain diagnosed as having a non-cardiac origin?
Yes . . . . . . . . . . . . Y
. ..*.........
unknown.........
,, ,
8. If YES, specify:
CQRONER/MEDICALE%AMIRERFORM(CORASCREER8 OF15)
I I I
12. Place of death (circle only one): In an automobile ............... F
Eome (or other private Innursinghome ................ G residence) . . . . . . . . . . . . . . . . . . . . A
In emergency room .............. H Work . . . . . . . . . . . . . . . . . . . . . . . . . . . B
In an ambulance ................ I In public building . . . . . . . . . . . . . C
In hospital .................... J On a bus or public trans- portation . . . . . . . . . . . . . . . . . . . . . D other .......................... 0
On the street . . . . . . . . . . . . . . . . . . E
1 I unknown ........................ u
1
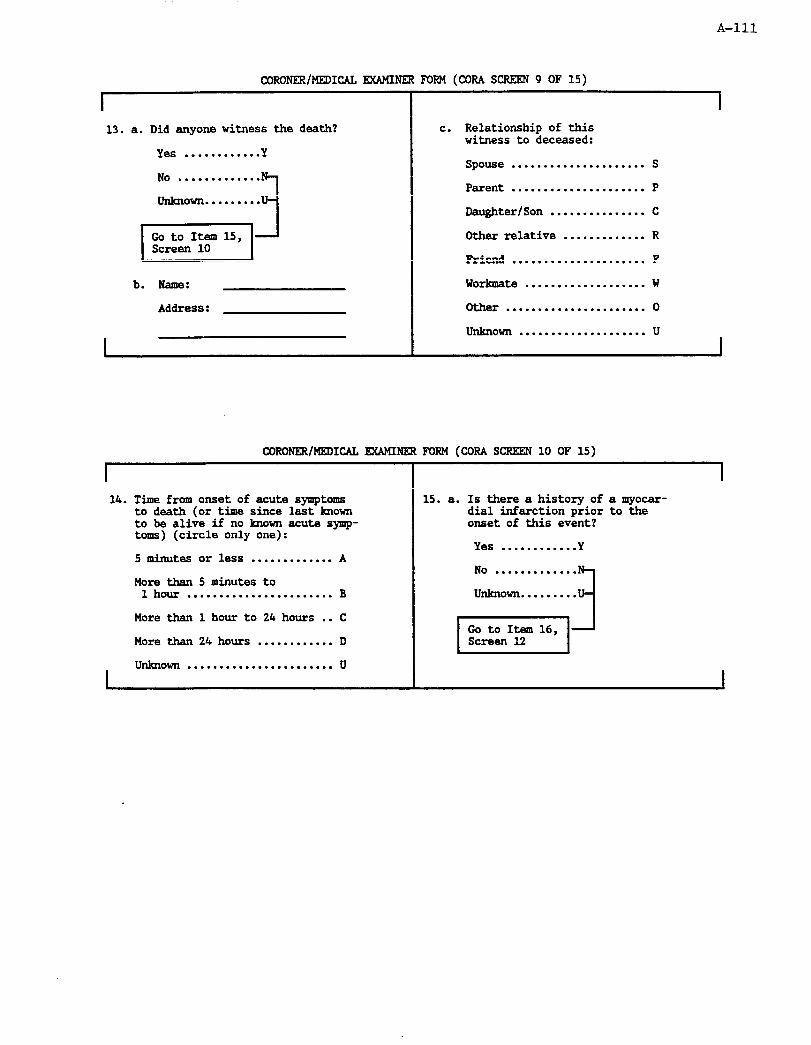
A-111
CORONEX/MEDICACFUMINFRFORM(CORASCREEN9 OF15)
13. a. Did anyone witness the death?
Yes . . . . . . . . . . . . Y
..*..........
UdUlOWn . . . . . . . . .
b. Rame:
Address:
I
c. Relationship of this witness to deceased:
Spouse . . . . . . . . . . . . . . . . . . . . . S
Parent . . . . . . . . . . . . . . . . . . . . . P
Daughter/Son . . . . . . . . . . . . . . . C
Cther relative . . . . . . . . . . . . . R
Friend . . . . . . . . . . . . . . . . . . . . . F
Worlanate . . . . . . . . . . . . . . . . . . . W
. . . . . . . . . . . . . . . . . . . . . . 0
unknown . . . . . . . . . . . . . . . . . . . . u
I
CORORRR/MEDICALEUMIRRRFORM(CORA SCRRERlO OF15)
I I
I
14. Time from onset of acute symptoms to death (or time since last known to be alive if no known acute synrp- toms) (circle only one):
5 minutes or less . . . . . . . . . . . . . A
More than 5 minutes to 1 hour . . . . . . . . . . . . . . . . . . . . . . . B
More than 1 hour to 24 hours . . C
More than 24 hours . . . . . . . . . . . . D
unknown . . . . . . . . . . . . . . . . . . . . . . . u I
15. a. Is there a history of a myocar- dial infarction prior to the onset of this event?
Yes . . . . . . . . . . ..Y
. . . . . . . . . . . . .
unknown.........

A-112
CORONER/MEDICAL EXAMINER FORM (CORA SCREEN 11 OF 15)
I I b. Did an MI occur within four
weeks prior to this event?
Yes . . . . . . . . . . . . Y
. . . . . . . . . . . . .
unknown. . . . . . . . .
c. Was the deceased hospitalized for the MI?
Yes . . . . . . . . . . ..Y
No . . . . . . . . . . . . .
unlcnown.........
d. Name of hospital: I
I
16. Is there any history of angina pectoris or coronary insuffi- ciency?
Yes . . . . . . . . . . ..Y
No . . . . . . . . . . . ..N
unknown.........u
17. Is there a history of any other chronic ischmic heart disease?
Yes . . . . . . . . . . ..Y
No . . . . . . . . . . . ..N
unlcnown.........u
I
I
18. Is there a history of valvular disease or cardiomyopathy?
Yes . . . . . . . . . . ..Y
No . . . . . . . . . . . ..N
unknown.........u
19. Is there a history of coronary bypass surgery prior to this event?
Yes . . . . . . . . . . ..Y
No . . . . . . . . . . . ..N
unknown.........u
I

A-113
CORONELR/MKDICAL EXAMINER FORM (CORA SCREEN 13 OF 15)
I
20. Is there a history of coronary angioplasty prior to this event?
Yes ,,,,........ Y
No . . . . . . . . . . . ..N
un&nown.. . . . . . . .u
21. a. Is there a history of stroke prior to this event?
Yes . . . . . . . . . . . . Y
. . . . . . . . . . . . .
b. Did a stroke occur within four weeks prior to this event?
Yes .,,......... Y
No . . . . . . . . . . . ..N
unknown.........u
22. Is there a history of hyper- tension (high blood pressure) prior to this event?
Yes . . . . . . . . . . ..Y
No . . . . . . . . . . . ..N
unknown.........u
CORONER/MEDICALEXMINER FORM (CORA SCREEN 14 OF 15)
I 23. Was the decedant Gking any of
the following medications as an outpatient within the four weeks prior to death?
a. Nitrates..............Y N U
b. Calcium channel blockers..............Y N U
c. Beta-blockers.........Y N U
d. Digitalis.............Y N U
I
24. Was this form completed by abstraction or by interview with the coroner?
Abstraction . . . . . . . . . . . . . . . ..A
Intemiew . . . . . . . . . . . . . . . . . ..I
25. Abstractor mmber: I I 1
26. Date abstract completed:
mm dd YY

A-114
CORONER/MEDICALEW4INERFORM(CORASCREEN15 OF15)
I I
Other required forms: (circle the letter corresponding to form(s) required)
Form Criteria baaed on this form
27. A. IFI Item 13a = Y and 13b completed.
28. B. IiiU Item 15c = Y and 15d completed. (If item 3 = S, 15d must also be a catchment area hospital.)
29. c. STR 1tem3 = C and Item 21b = Y.
30. D. AlJ'.C Item 3 = Cand Item 5 = Y.

A-115
Instructions for the
Coroner/Medical Examiner Form (COR) Version A a/W88
General Instructions
This form is completed for each eligible, out-of-hospital cohort or surveiilance event which was a medical examiner's (coroner's) case. The medical examiner's (coroner's) report may consist of an investigation, an autopsy, or both. If this is a cohort case and an autopsy was done, Form AUT must also be completed. The abstractor should be familiar with ARIC Instructions for Completion of Paper Forms and the instructions for the Hospital Record Abstraction Form and Informant Interview Form. Whenever you have difficulty interpreting the medical information in the medical examiner's (coroner's) report, consult with your surveillance director.
Header
Record the event ID number as assigned on the CEL or SEL form, the participant's last name and initials. Before going to the coroner/medical examiner office, complete items l-3.
1.
2.
3.
4.
5.
6.
7.
Date of Death: Transfer date from the death certificate or from the death printout.
Medical Examiner/Coroner's Office: Record the name of the office from the death certificate.
Cohort/Surveillance: Record C or S based on the SEL or CEL forms.
Report found? The report may be permanently lost. If so, indicate "no" and skip to Item 25. If "yes", complete the form.
Autopsy? Indicate whether an autopsy was done as part of the investigation. If an autopsy was done but not as part of the coroner's/medical examiner's investigation, record 'No".
Examiner's findings: Review the examiner's report and diagnoses completely for conditions contributing to or present at death. To answer "yes" these do not have to be listed among the final diagnoses, but need onFhave been present. "Recent' here generally means in the last month and may require your judgernent. If a condition (a-j) is specifically mentioned record as "yes". If definitely not present or not mentioned at all, record as "no'. If equivocal, consult your surveillance director. Synonyms for the conditions are provided in the instructions for the HRA and STR forms.
Non-cardiac, non-stroke cause: Answer this question as described for Item 6. If you are uncertain about a condition, record in "specify' space and check with Surveillance Director.
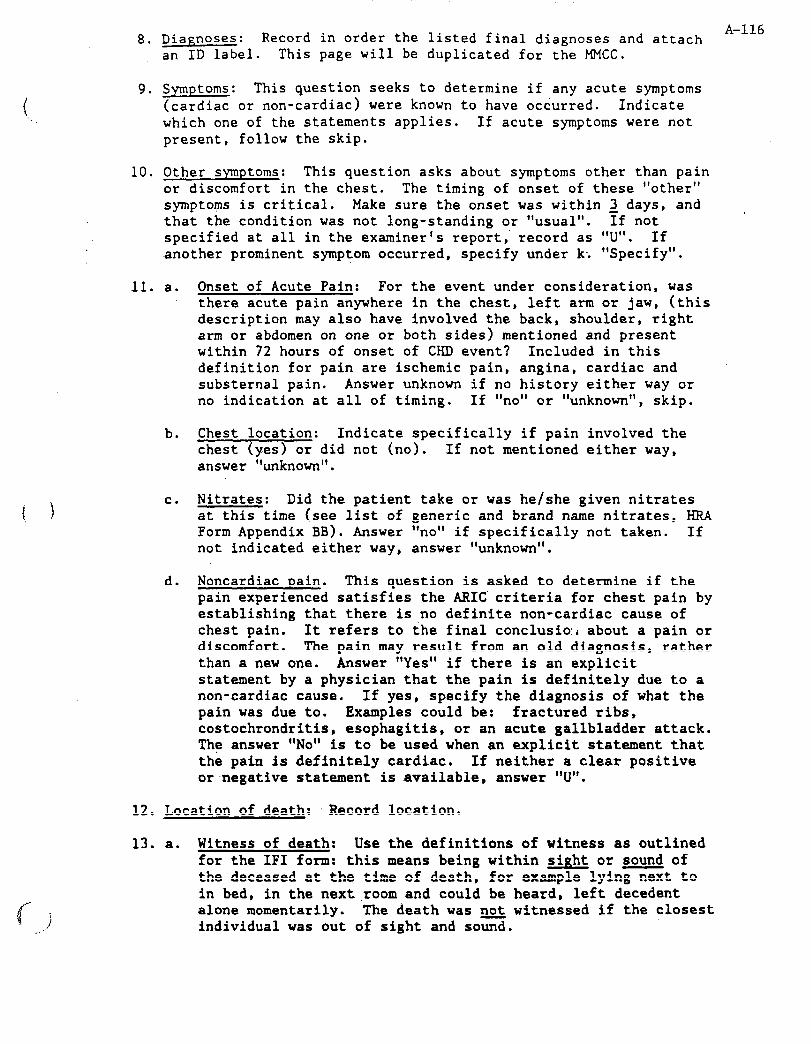
8. Diagnoses: Record in order the listed final diagnoses and attach A-116
an ID label. This page will be duplicated for the MMCC.
9. Symptoms: This question seeks to determine if any acute symptoms (cardiac or non-cardiac) were known to have occurred. Indicate which one of the statements applies. If acute symptoms were not present, follow the skip.
10. Other symptoms: This question asks about symptoms other than pain or discomfort in the chest. The timing of onset of these "other" symptoms is critical. Make sure the onset was within 2 days, and , that the condition was not long-standing or "usual". If not specified at all in the examiner's report; record as "U". If another prominent symptom occurred, specify under k; "Specify".
11. a. Onset of Acute Pain: For the event under consideration, was there acute pain anywhere in the chest, left arm or jaw, (this description may also have involved the back, shoulder, right arm or abdomen on one or both sides) mentioned and present within 72 hours of onset of CHD event? Included in this definition for pain are ischemic pain, angina, cardiac and substernal pain. Answer unknown if no history either way or no indication at all of timing. If "no" or "unknown", skip.
b. Chest location: Indicate specifically if pain involved the chest (yes) or did not (no). If not mentioned either way, answer "unknown".
c. Nitrates: Did the patient take or was he/she given nitrates at this time (see list of generic and brand name nitrates, KRA Form Appendix BB). Answer 'no' if specifically not taken. If not indicated either way, answer "unknown".
d. Noncardiac pain. This question is asked to determine if the pain experienced satisfies the ARIC criteria for chest pain by establishing that there is no definite non-cardiac cause of chest pain. It refers to the final conclusio:i about a pain or discomfort. The pain may result from an old diagnosis, rather than a new one. Answer "Yes" if there is an explicit statement by a physician that the pain is definitely due to a non-cardiac cause. If yes, specify the diagnosis of what the pain was due to. Examples could be: fractured ribs, costochrondritis, esophagitis, or an acute gallbladder attack. The answer "No" is to be used when an explicit statement that the pain is definitely cardiac. If neither a clear positive or negative statement is available, answer "U'.
12. Location of death: 'Record location.
13. a. Witness of death: Use the definitions of witness as outlined for the IF1 form: this means being within sight or sound of the deceased at the time of death, for example lying next to in bed, in the next room and could be heard, left decedent alone momentarily. The death was not witnessed if the closest individual was out of sight and so=.

.
A-117 b. Name and Address: Record the name and address of the witness.
c. Relationship: Circle the appropriate response.
14. Timing: Estimate time from acute symptom onset to death (IF1 definition) or if no known acute symptoms, time from last known to be alive until death. Make an estimate to fit the categories. If it cannot be determined, check "U". Acute symptom onset is defined as that point in time when new symptoms caused a change in activity. If the symptom is chronic, there must be a change in severity or frequency. Symptoms might be stepwise (e.g. one chest pain, then a more severe one an hour later). In this case it is the first pain, if it was new and caused a change, that is the onset of the episode. The final episode for someone who collapses, is revived and collapses again began at the first collapse.
Questions 15-23 refer to the patient's medical history before the onset of this event. Do not record the causes of death as 'Yes" here, since they are listed in Question 8.
15.
16.
17,
a. Previous MI: Previous history refers to a time preceding the onset of the event under consideration. If this information states "previous silent MI", "borderline heart attack", record the answer as "Yes". An "old MI" on autopsy can be used for positive previous history. A history of angina or chest pain. without documented MI should be recorded as ‘No”. Statements such as: "No cardiac problems", “No adult illness"i "Previously well", and "No previous history of heart disease" are sufficient to answer "No" to previous MI. If no indication either way, answer "Unknown".
b. MI within 4 weeks: Review recency of MI.
c. & d. Hospitalization: Circle the appropriate response and‘ record name if available.
Previous angina or coronary insufficiency: Examine the record for mention of previous angina pectoris or coronary insufficiency prior to this event (i.e., > 72 hours before admission). This would include mention of chronic chest pain, ischemic pain, and "history of chest pain". Chest pain specified as being "of unknown origin" does not qualify. Answer "Yes" if the history includes any mention of the-patient taking nitroglycerin for chest pain noted that the patient had "substernal pressure, pain, tightness, or burning distress precipitated by exercise or excitement, or both and is relieved by rest and/or nitroglycerin". Answer "No" if the history explicitly states that the patient has no history of any of the above. Answer U = unknown if none of the criteria for "Yes"/"No" responses apply.
Other .IHD: History of other chronic ischemic heart disease may include CHF described as due to coronary disease or ASHD (Atherosclerotic Heart Disease).
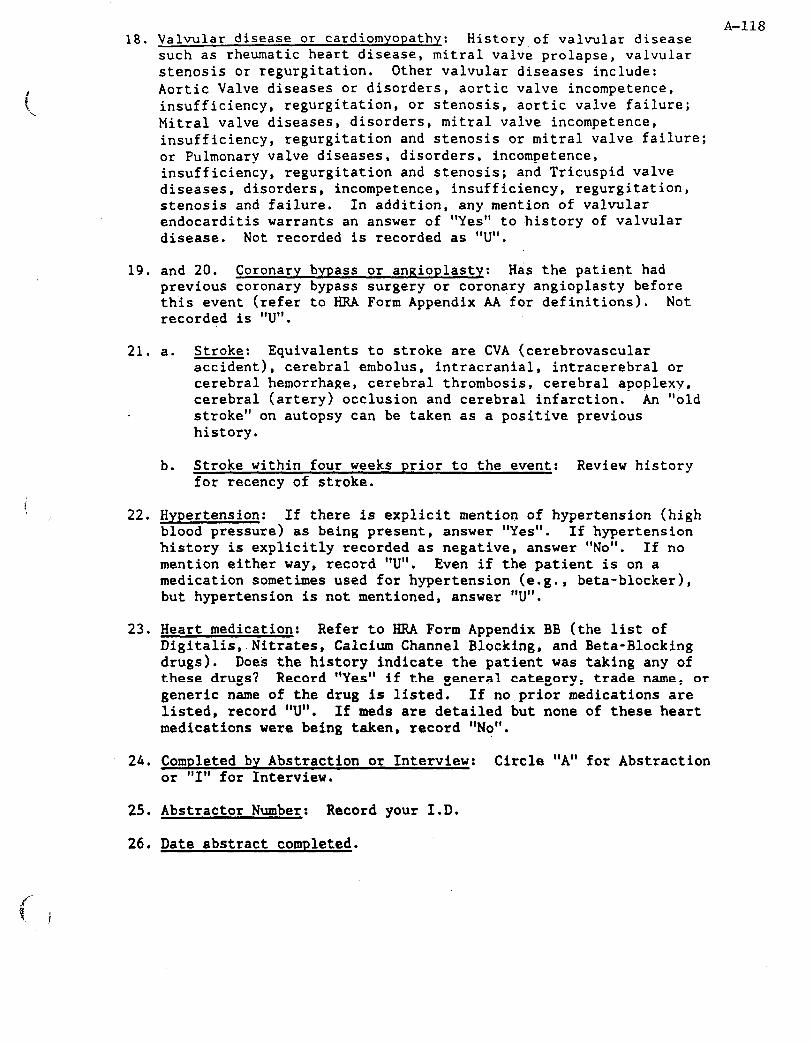
A-118 18. Valvular disease or cardiomyopathy: History.of valvular disease
such as rheumatic heart disease, mitral valve prolapse, valvular stenosis or regurgitation. Other valvular diseases include: Aortic Valve diseases or disorders, aortic valve incompetence, insufficiency, regurgitation, or stenosis, aortic valve failure; Mitral valve diseases, disorders , mitral valve incompetence, insufficiency, regurgitation and stenosis or mitral valve failure; or Pulmonary valve diseases, disorders, incompetence, insufficiency, regurgitation and stenosis; and Tricuspid valve diseases, disorders, incompetence, insufficiency, regurgitation, stenosis and failure. In addition, any mention of valvular endocarditis warrants an answer of "Yes" to .history of valvular disease. Not recorded is recorded as "U".
19. and 20. Coronary bypass or angioplasty: Has the patient had previous coronary bypass surgery or coronary angioplasty before this event (refer to HRA Form Appendix AA for definitions). Not recorded is "U".
21. a. Stroke: Equivalents to stroke are CVA (cerebrovascular
22
23
accident), cerebral embolus, intracranial, intracerebral or cerebral hemorrhage, cerebral thrombosis, cerebral apoplexy, cerebral (artery) occlusion and cerebral infarction. An "old stroke" on autopsy can be taken as a positive previous history.
b. Stroke within four weeks prior to the event: Review history for recency of stroke.
Hypertension: If there is explicit mention of hypertension (high blood pressure) as being present, answer "Yes". If hypertension history is explicitly recorded as negative, answer "No". If no mention either way, record "U". Even if the patient is on a medication sometimes used for hypertension (e.g., beta-blocker), but hypertension is not mentioned, answer "U".
Heart medication: Refer to HRA Form Appendix BB (the list of Digitalis,.Nitrates, Calcium Channel Blocking, and Beta-Blocking drugs). Does the history indicate the patient was taking any of these drugs? Record "Yes" if the general category, trade name, or generic name of the drug is listed. If no prior medications are listed , record "U" . If meds are detailed but none of these heart medications were being taken, record "No".
24. Completed by Abstraction or Interview: Circle "A" for Abstraction or "I" for Interview.
25. Abstractor Number: Record your I.D.
26. Date abstract completed.

27 - 30. Form flaRs
Be sure to complete. Circle the letter corresponding to the form(s) required. HRA and STR will be needed for cohort for any recent MI or stroke hospitalization and for surveillance if the .MI or stroke hospitalization occurred in a catchment area hospital.
A-119

A-120
COHORT.EVENT ELIGIBILITY FORM
VDZSIOi'i: B 8/19/88
IltmmxIoNs: llxir forr abaldba caPplated for l llCa&ortduths sndluapit~lizations, hcluding every ho8pitalimtion rmportod frm Annual ?ollaw-Up. krlgn An eYmlt ID IAmber before camplating thir fam, ms ~11 cohort events need an avunt ID mmbar rqardlasr of eligibility. Jtnfar to this fomP'6 Q by Q instructions for lnfoxmtion on antar- nrParica1 ruponsss. ~&~~;~le~ choice" and oybs/no 'I type questions, circle the lettar comasponding to the most
response. If a letter is circld incorrectly, mrk through it with an 'X' and c-&lb the co&t rwponse.
alinRT Evmr ELIGIBILITX Km (CELB pase 1 of 6)
r A. IDmrTFYm II@cmwIoN
1.LllstWrPe: I I I I I I I I I I I] Initials: 1 J 1 ‘!
PArticipAnt ID: IllIll]
3. Visit 1 date: . . . . . . . . . . . . . . . . . m-m-m )bnth Oau YeAr
4. Date of dirtbarge or death: . . . m-m-m mnth WY YW
If itm 3 ir pnf, 4Arlier tbn ita 4, go to Ita 16 on Page 5.
5. 8ource wed to idukFfY malt: . . . . . . ..I........... cohort &lmul Tollw-up
sum8illmcapmcuhru
6. xstuAw8nt8&th? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Y8S
m GotoItu8,
p-2 +
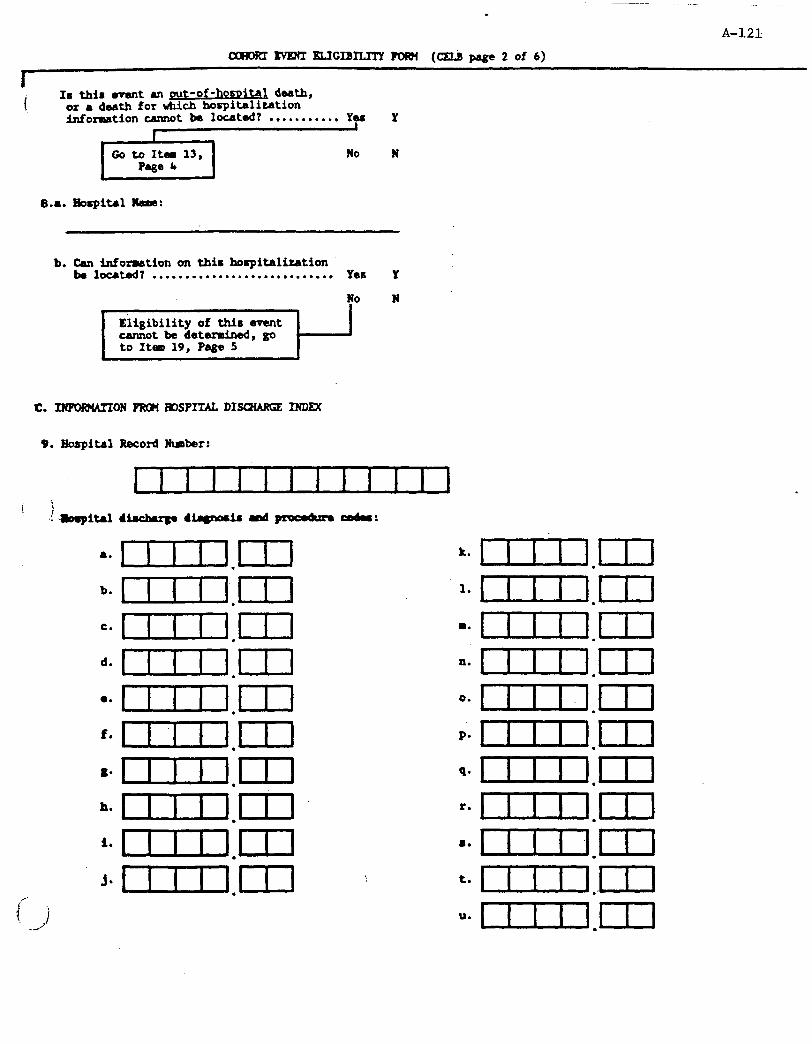
.
A-121
coFRKT)NEKI7D.ICIBILITYPOJ8l (CELBpageZof6)
I r Is this avant UI put-of-homitaa dmth,
or a death for tich hospitalkation
b. Can information on this hocpitalization be louted? . . . . . . . . . . . . . . . . . . . . . . . . . . . . Yes Y
p%Jip-1-r N
C. -ON PRan FIOSPITAL DI- INDm
9. &spit31 Record Nmber:
a-unJ.m b- umm
=nm.m
k r.m
l mn.m
f. mn.m
o* I.m hn 1mn.m
i- cm3.m Je n.m
i’
{
./ i
k. 1111.171
l*uln.m
4IlxIn.m
4zlIlIl.m
o*uIn.m
p.e tn.m
q*cnn.m
=*uul.m
‘* cun.m
te mn..m
“* lIl2n.m

A-l.22
I a. IS a 602, 410-414, 427, 420, or 518.4 bode listed7 . . . . . . . . Yea Y
No N
b. Is l 430-438 code lirt0d7 . . . . . . . . . . . . . . Yea Y
No N
c. Is l 35-39, 88.5, 250, 390-459, 745-747, 794.3, 798, or 799 code listed? . . . . . . . . . . . . . . Yes Y
No N
If fill of Items lU, llb, & llc are "No,"
I go to Itsa 12 on Page 4.
OUwwise, continue with Item lld. I
d. Ate any of the folloving mentioned or ruggested in the disckuge 8-7 . Yes Y
No N
- z&w Iu Unsfable angina QlD 16&6dC heart dir&se Atherorc lerotic besrt disease GsrdiAc arrest
Or durim this admission:
Coronary angiography orangioplasty csrdirrc cafhaterizdtion
iF!i!v~ CK-m Nitroglycerin
9. Are any of the following mantioned or suggested in the dirctuuge mnury? . Ye6 Y
No N
Cerebroyasculardimm~e Ccrebral btrhage Cerebral Matction Subaractmoid bmrrhaga Ckrobral rbolus Paralysis lrpharh Diplupia
Or: -bra1 angiography Carotid mdutuoctay CIrcm lkaro IWurr
,F
i /, i If gnv of Itms lla, llb, lld g lie is "Ye8,"
go to It4 15 on Page 5.
Othendse, continue with Itm 12. .
I
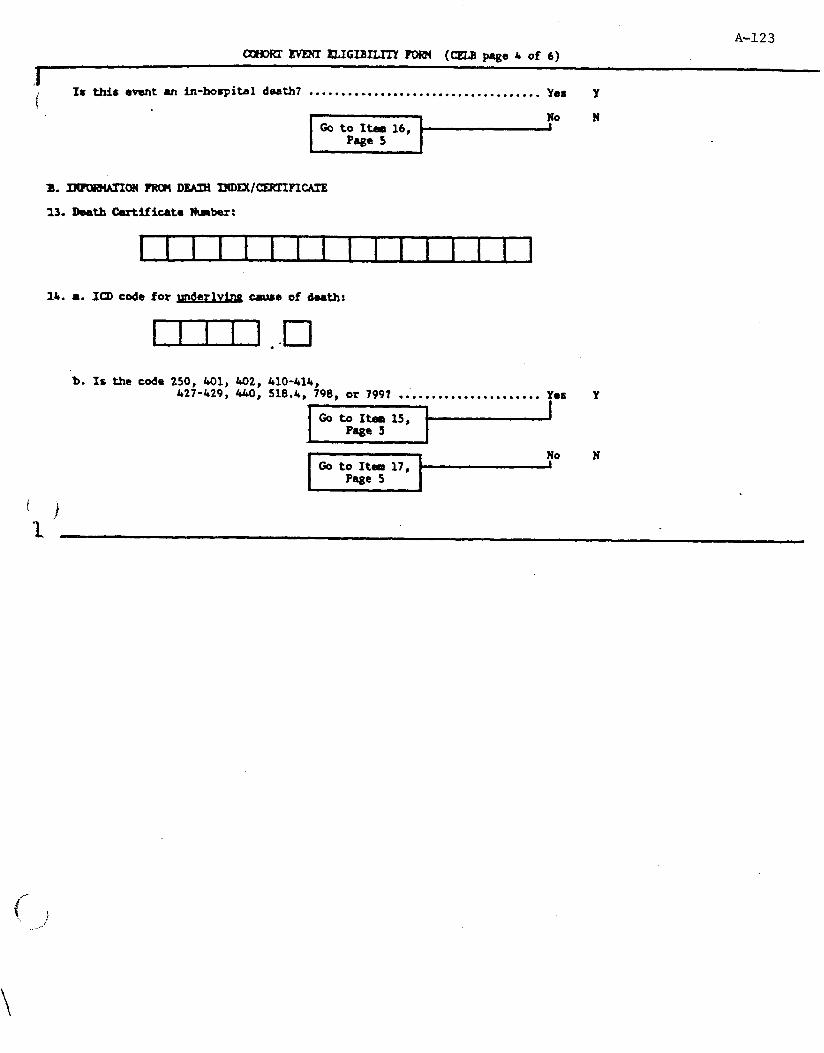
A-123
CXHO~E#XIELIGIBILITYpw(H (CELBpage 4 of 6)
.I i IS this eventan in-hospital death7 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Ye8 Y !
No N
14. 8. ICD code forynderly&g muse of denth:
b. Is the code 250, 401, 402, 410-414, 427-429, 440, 518.4, 798, or 7997 .i.................... Yes
Page 5
Y
* No N Gotoxtmll17, '
Page 5 4
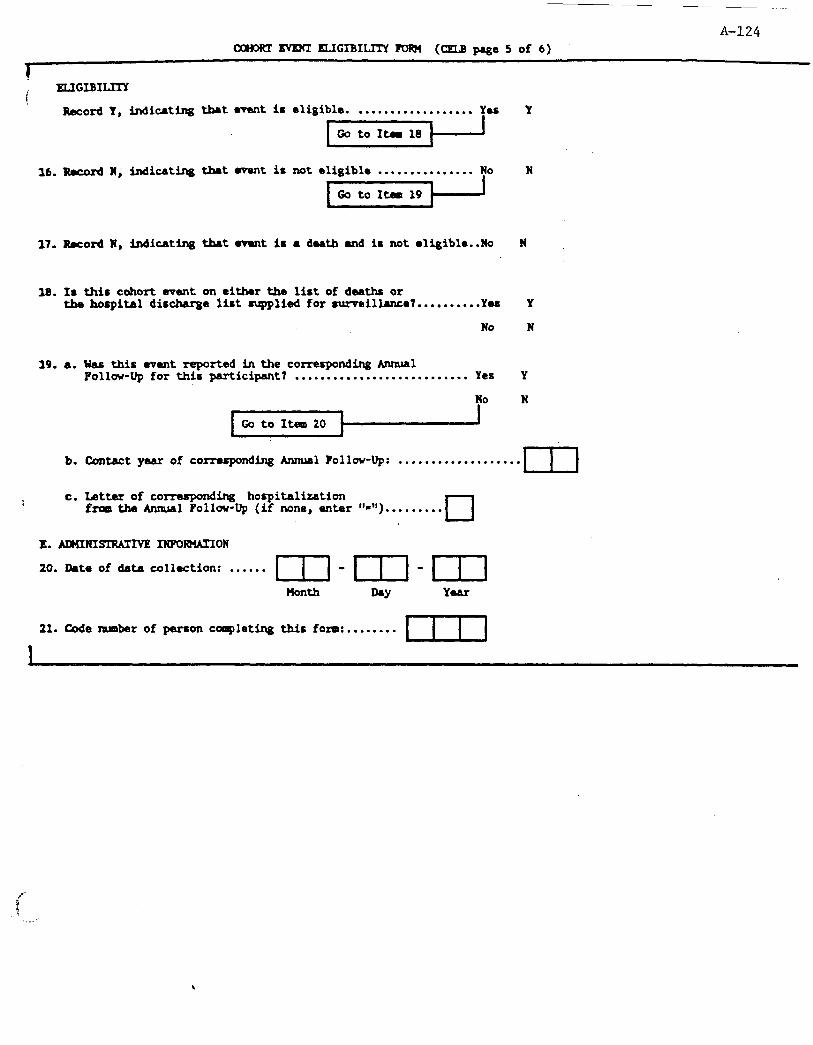
A-124
CXMXTWE3Il5.lGIBILITY?OFUl (CELBpagc5 of6)
1
! ELIGIBI-
&cord Y, indicting tbet event is eligible. . . . . . . . . . . . . . . . . . . Yes
16. Record N, indicating that event is not eligible . . . . . . . . . . . . . . . No
17. Word N, indicting that event is a dath and ir not eligible..Ua
18. Is this cohort went on either the list of deaths or the hospital discharge list mqplied for mawillarue7..........Ye6
19. a.
b.
C.
No
Was this event reported inthe correspondingAnma1 Follow-Up for this participant7 . . . . . . . . . . . . . . . . . . . . . . . . . . . Yes
No
Y
N
N
Y
N
Y
N
Cont8ctyM.r of corresponding &malPollov-up: . . . . . . . . . . . . . . . . . . . nzl
Letter of comwponding hospitalization from the Annual Pollow-Up (if none, enter "-").........
cl
E. AIUINISl?WIVE INKMATION
20. Date of data collection: . . . . . . 171 - 1-q - III
Uonth NY
21. C&e nmber of person cqleting this fom:........
I

WHORT ~ELIGIBILJTY FORM (CELBpage 6 of 6) A-125
1- I r -ad solely on the infowtim gtM in this fol¶, indicate what &ditiurml forms are zmeded
\ . . rlo corrupndirrg let-):
gritaria ba.seJd on this forpl
22-A AN Itam6.Y.
23-b mll 1-6'Y
21. c mu Item na - Y m It- lld - Y
25. D BRA ftg 12 = Y rad It- 14b - Y
26. E SXR It- llb = Y ar It- llt - Y
27. ? IFI It= 7,- Y (out-of-hospital) aml It- 15 - Y
28. G PHQ(r) ItEm 7 = Y (out-of-hospital) d Item 15 - Y
1
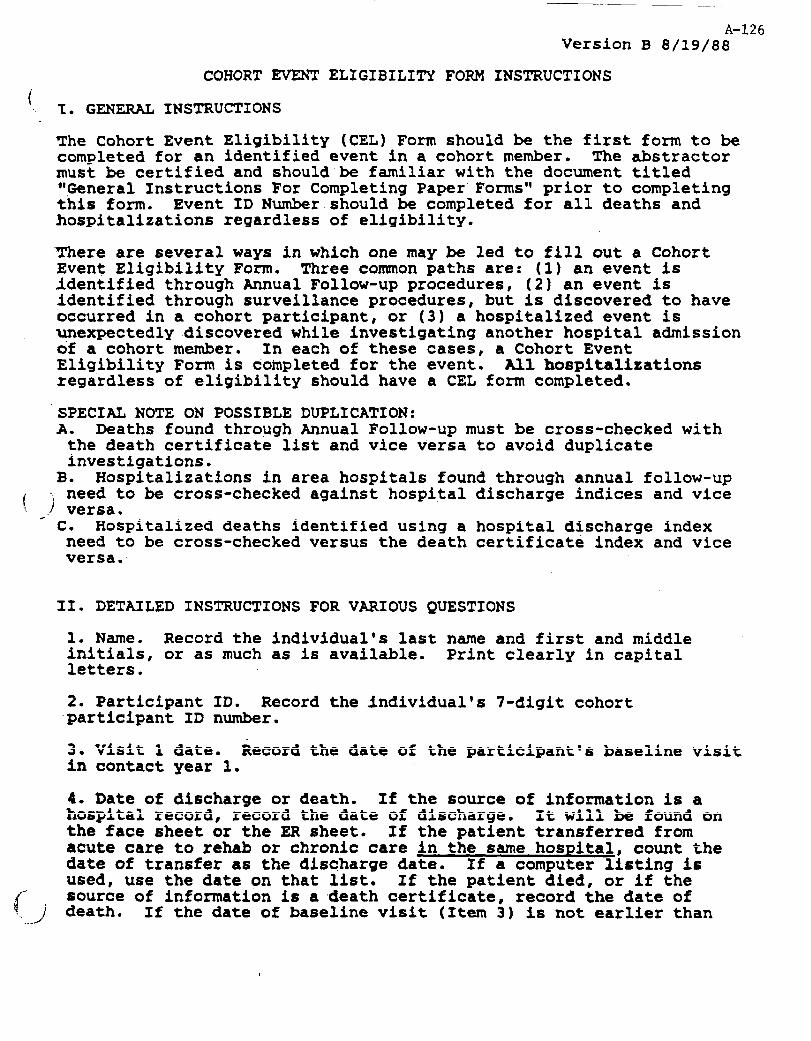
A-126 Version B 8/19/88
COHORT EVENT ELIGIBILITY FORM INSTRUCTIONS i . . 1. GENERAL INSTRUCTIONS
The Cohort Event Eligibility (CEL) Form should be the first form to be completed for an identified event in a cohort member. The abstractor must be certified and should be familiar with the document titled "General Instructions For Completing Paper Formsql prior to completing this form. Event ID Number should be completed for all deaths and hospitalizations regardless of eligibility.
There are several ways in which one may be led to fill out a Cohort Event Eligibility Form. Three common paths are: (1) an event is Identified through Annual Follow-up procedures, (2) an event is identified through surveillance procedures, but is discovered to have occurred in a cohort participant, or (3) a hospitalized event is unexpectedly discovered while investigating another hospital admission of a cohort member. In each of these cases, a Cohort Event Eligibility Form is completed for the event. All hospitalizations regardless of eligibility should have a CEL form completed.
SPECIAL NOTE ON POSSIBLE DUPLICATION: A. Deaths found through Annual Follow-up must be cross-checked with
the death certificate list and vice versa to avoid duplicate investigations.
B. Hospitalizations in area hospitals found through annual follow-up . need to be cross-checked against hospital discharge indices and vice
f j e. versa. c. Hospitalized deaths identified using a hospital discharge index need to be cross-checked versus the death certificate index and vice versa..
II. DETAILED INSTRUCTIONS FOR VARIOUS QUESTIONS
1, Name. Record the individual's last name and first and middle initials, or as much as is available. Print clearly in capital letters.
2. Participant ID. Record the .individual's 7-digit cohort participant ID number.
3. Visit 1 date. Record the date of the participant's baseline visit in contact year 1.
4. Date of discharge or death. If the source of information is a hospital record, record the date of discharge. It will be found on the face sheet or the ER sheet. If the Patient transferred from acute care to rehab or chronic care in the same hospital, count the date of transfer as the discharge date. If a computer lfstincr is used, use the date cn that list; If the patient died, or if the
ii' ..- .J
source of information is a .death certificate, record the date of death. If the date of baseline visit (Item 3) is not earlier than
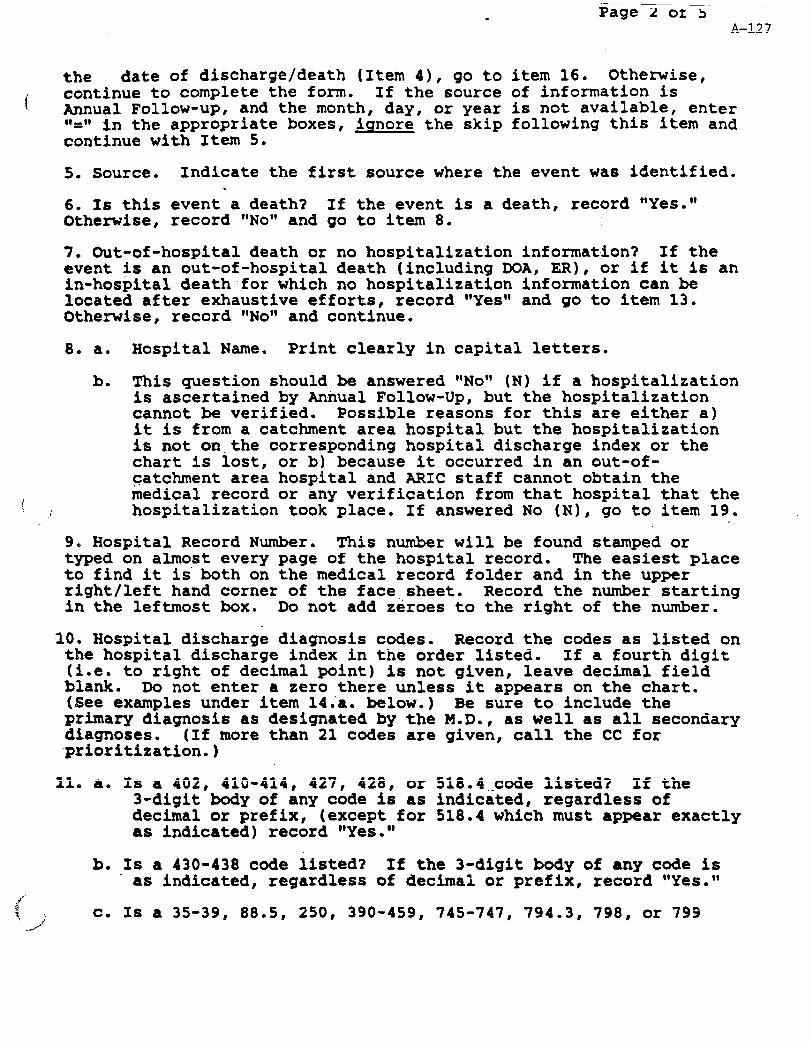
. Page Z or 5 A-127
the date of discharge/death (Item 4), go to item 16. Otherwise,
! continue to complete the form. If the source of information is Annual Follow-up, and the month, day, or year is not available, enter ‘)=*' in the appropriate boxes, iqnore the skip following this item and continue with Item 5.
5. Source. Indicate the first source where the event wa6 identified. .
6. Is this event a death? If the event is a death, record *lYes.wt Otherwioe, record "NON* and go to item 8.
7. Out-of-hospital death or no hospitalization information? If the event is an out-of-hospital death (including DOA, ER), or if it is an in-hospital death for which no hospitalization information can be located after exhaustive efforts, record VcYesrr and go to item 13. Otherwise, record *1N~91 and continue.
8. a. Hospital Name. Print clearly in capital letters.
b. This question should be answered wwNoww (N) if a hospitalization is ascertained by Annual Follow-Up, but the hospitalization cannot be verified. Possible reason6 for this are either a) it is from a catchment area hospital but the hospitalization is not on-the corresponding hospital discharge index or the chart is lost, or b) because it occurred in an out-of- catchment area hospital and ARIC staff cannot obtain the
[ medical record or any verification from that hospital that the .: hospitalization took place. If answered No (N), go to item 19.
9. Hospital Record Number. This number will be found stamped or typed on almost every page of the hospital record. The easiest place to find it is both on the medical record folder and in the upper right/left hand corner of the face sheet. Record the number starting in the leftmost box. Do not add zeroes to the right of the number.
10. Hospital discharge diagnosis codes. Record the code6 as listed on the hospital dibcharge index in the order li6ted. If a fourth digit (i.e. to right of decimal point) is not given, leave decimal field blank. Do not enter a zero there unless it appear6 on the chart. (See examples under item 14.'a. below.) Be sure to include the primary diagnosis a6 designated by the M.D., a6 well as all secondary diagnoses. (If more than 21 codes are given, call the CC for -prioritization.)
11, a. Is a 402, 410-414, 427, 428, or 518.4,-code listed? If the 3-digit body of any code is as indicated, regardless of decimal or prefix, (except for 518.4 which must appear exactly as indicated) record "Yes."
b. I6 a 430-438 code listed? If the 3-digit body of any code is ' as indicated, regardless of decimal or prefix, record 11Yes.11
r”. t
i c. I6 a 35-39, 88.5, 250, 390-459, 745-747, 794.3, 798, or 799
-J

Page 3 of 5 A-128
code listed? If the 3-digit body of any code is as indicated, regardless of decimal or prefix (except for 88.5 or 794.3 which must appear exactly as indicated), record wwYes.ww If not, record wwNow~. Review and carefully follow the applicable skip instruction in the box following this item.
d. Are any of the following mentioned in the discharge summary? Review the discharge summary for any of the CHD-related terms listed. Note that the first list of term6 must be considered wwacute,ww and the second list must pertain to this admission. If any one of the terms is found, record wYYes.w~
e. Are any of the following mentioned in the discharge summary? Review the discharge summary for any of the stroke-related terms listed. Note. that the first list of'terms must be considered wlacute,ww and the second list must pertain to this admission. If any one of the term6 is found, record wlYes."w Review and carefully follow the applicable skip instruction in the box following this item.
12, In-hospital death? If the event is an in-hospital death, record wwYesww and continue with item 13. Otherwise, record wlNoww and skip to item 16.
13. Death Certificate Number. This number will be found stamped or typed on the death certificate. If a computer printout is used, it
! : must include this information. Record the number starting in the leftmost box. Do not add zeroes to the right of the number.
14. a. ICD code for underlying cause of death. Record the underlying cause of death by listing the ICD code recorded on the death certificate. If it is not available, record the immediate cause. If the first character is a letter, record that letter in the first box, followed by the 3-digit number (right justified.to the decimal point). Otherwise, record the 3-digit number with the first box left blank. If a fourth digit (i.e. to right of decimal point) is not given, leave decimal field blank. Do not zero fill. Examples:
ICD Code
412.0
412
E825
191.x
Record As:
I.lal
lIzErm.cl
lIEEEEl.n

Page 4 of 5 A-129
(. b. Is the code 250, 401, 402, 410-414, 427-429, 440, 518.4, 798, or 7993 If the 3-digit body of any code is a6 indicated, regardless'of decimal or prefix (except for 518.4 which must appear exactly as indicated), record wwYesww. If not, record wwNoww and skip to item 17.
15. Eligible event. Any path leading to this item indicate6 that the event is.eligible. Record wwYesww, the only possible response and continue with item 18.
16. Ineligible event. Any path leading to this item indicate6 that the event-either occurred before visit one or is a non-fatal hospitalized event that is not eligible based on the discharge codes and discharge summaries. Record ONow~, the only possible response, and skip to item 19.
17. Ineligible death. Any path leading to this item indicate6 that the event is a death which is not eligible, but for which a DTH Form :must be obtained. Record qwN~ww continue with the next questlo;.
the only possible response, and
18. It is important to determine whether this cohort event would have been identified by the usual ARIC surveillance procedures. If this is a cohort death, check the death certificate list provided by the health department to determine whether the death appeared on the
i list. If this cohort event was a hospitalization, try to identify it : (based on any identifiers available and date) on the list provided by
that hospital. Be sure to check,all lists provided, even supplement6 at the end of the year. If the event can be found through surveillance~lists, indicate wwYeswt. If not, indicate wwN~ww.
19.a. To assure that all death6 and hospitalization6 which we discover through Annual Follow-Up are investigated, we need to link the CEL and Annual Follow-Up Forms. For each cohort event, determine whether the death or hospitalization was reported on the participantws Annual Follow-Up for the corresponding time period. To do this for deaths, simply double.check that each cohort death is indicated on both forms. For hospitalizations, the procedure is more complicated because participant report6 of dates and rea6onb for ho6pitalization on Annual Follow-Up may be inaccurate. Compare the name of the hospital, date of hospitalization, and discharge diagrioses as listed on the CEL Form with those on the Annual
.Follo~?-Up. ‘If the information matches exactly, answer 19.a. VwYe6w1. If these values do not match exactly, judgement6 will have to me made .&bout whether the hospitalizations are the same based on the following priorities: 1) hospital name, 2) date of hospitalization within plus or minus six months, and 3) the reason for hospitalization. The hospital name and date should match reasonable well. If the name of the hospital does not match, the participant should be recontacted to check this. If the ho6pitalization can be
(- confirmed within reason, answer 19.a. vwYes.wl If not, answer wwNoww and skip to item 20.


IFI- (Informant Interview 1) Name : Address:
Phone: W&.ng
:
IFI- (Informant Interview 2) Name : Address:
Phone: ?C;CEing
:
IFI- (Informant Interview 3) Name : Address:
Phone:
A-l.32 CEI Page 2
PHQ-1 (Physician Questionnaire 1) Name : Address:
Phone: W&ng
:
PHQ-2 (Physician Questionnaire 2) Name : Address:
Phone: T;&.ng
:
WZzing :
Date Investigation Completed: -/-I-
Code Number of Person Completing This Form: -m-
Comments:
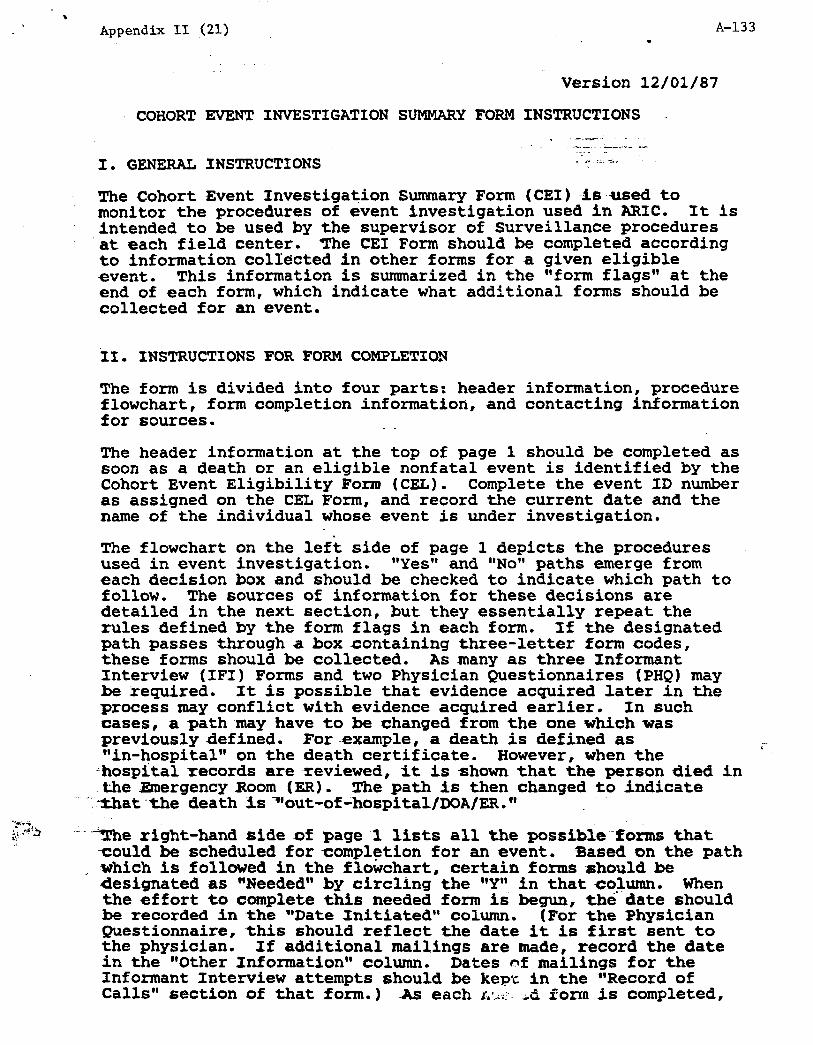
. Appendix II (21) A-133
.
Version 12/01/87
COHORT EVENT INVESTIGATION SUMMARY FORM INSTRUCTIONS . -.--.
.-._ - _..,_ -.
I. GENERAL INSTRUCTIONS r " ::. -k;
.. The Cohort ,Event Investigation Summary Form (CEI) is-used to monitor the procedures of event investigation used in ARIC. It is intended to be used by the supervisor of Surveillance procedures
'at each field center. The CEI Form should be completed according to information collected in other forms for a given eligible event. This information is summarized in the "form flags" at the end of each form, which indicate what additional forms should be collected for an event.
II. INSTRUCTIONS FOR FORM COMPLETION
The form is divided into four parts: header information, procedure flowchart, form completion information, and contacting information for sources. . .
The header information at the top of page 1 should be completed as soon as a death or an eligible nonfatal event is identified by the Cohort Event Eligibility Form (CEL). Complete the event ID number as assigned on the CEL Form, and record the current date and the name of the individual whose event is under investigation.
The flowchart on the lef't side of page 1 depicts the procedures used in event investigation. *tYesrr and otN~lV paths emerge from each decision box and should be checked to indicate which path to follow. The sources of information for these decisions are detailed in the next section, but they essentially repeat the rules defined by the form flags in each form. Sf the designated path passes through a-box containing three-letter form codes, these forms should be collected. As many as three Informant Interview (IFI) Forms and two Physician Questionnaires (PHQ) may be required. It is possible that evidence acquired later in the process may conflict with evidence acquired earlier. In such cases, a path .may have to be changed from the one which was previously defined. For-example, a death is defined as llin-hospitall' on the death certificate. However, when the
; Lhospi'talrecords arexeviewed, it is shown that the person died in the Emergency Room (ER). The path is then changed to indicate
-':-3hatthe death Is3'out-ofLhospitalfDOA/ER."
I
"The right-hand side of page.1 lists all the possible-ionns that *ould be scheduled for completion for an event. 3ased on the path which is followed in the flowchart, certain forms should be designated as *'Needed" by circling the trYr1 in that column. When the effort to complete this needed form iS begun, th6date should be recorded in the **Date Initiated" column. (For the Physician Questionnaire, this should reflect the date it is first sent to the physician. If additional mailings are made, record the date in the "Other Information*9 column. Dates nf mailings for the Informant Interview attempts should be kept in the "Record of Calls" section of that form.) As each T.:;~:.. ,d form is completed,
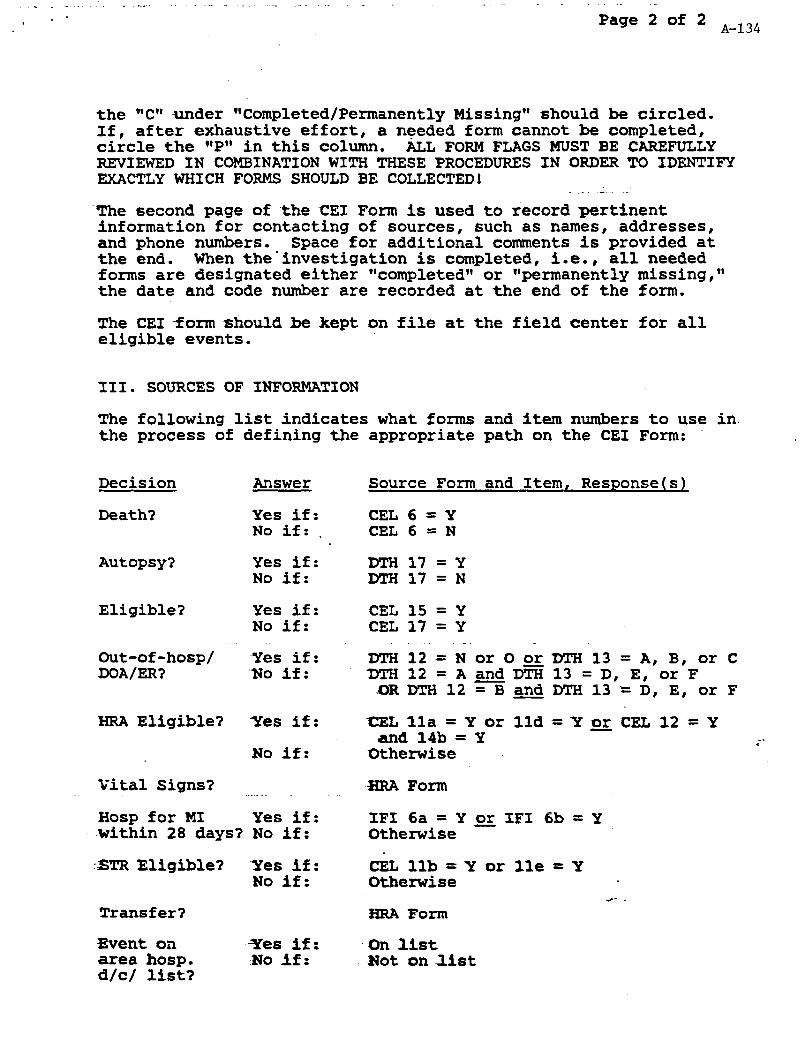
Page 2 of 2 A-134
the WCVi-under "Completed/Permanently Missing" should be circled. Sf, after exhaustive effort, a needed form cannot be completed, circle the *'PM in this column. ALL FORM FLAGS MUST BE CAREFULLY REVIEWED IN COMBINATION WITH THESE PROCEDURES IN ORDER TO IDENTIFY EXACTLY WHICH FORMS SHOULD BE COLLECTED!
'The second page of the CEI Form is used to record pertinent information for contacting of sources, such as names, addresses, and phone numbers. Space for additional comments is provided at the end. When the-investigation is completed, i.e., all needed forms are designated either "completedW or "permanently missing," the date and code number are recorded at the end of the form.
The CEI form should be kept on file at the field center for all eligible events.
III. SOURCES OF INFORMATION
The following list indicates what forms and item numbers to use in the process of defining the appropriate path on the CEI Form:
Decision
Death?
Autopsy?
Eligible?
Out-of-hasp/ DOA/ER?
MRA Eligible?
Vital Signs?
Hosp for MI
Answer
Yes if: No if: .
Yes if: No if:
Yes if: No if:
Yes if: 'NO if:
Yes if:
No if:
_ Yes if:
.within 28 days? No if:
5TR Eligible? Yes if: No if:
Transfer?
Event on Tes if: area hosp. No if: d/c/ list?
Source Form and Item, Response(s)
CEL 6 = Y CEL 6 = N
DTH17=Y DTH17=N
CEL 15 = Y CEL 17 = Y
liTi ii- -. = N or 0 or DTH 13 = A, B, or C DTH 12 = A and e 13 = 0, E, or F
OR DTH 12 =B and DTH 13 = D, E, or F
CEL lla = Y or lld = Y pi CEL 12 = Y and 14b = Y
Otherwise
SIRA Form
IF1 6a = Y or IF1 6b = Y Otherwise
CRL llb = Y or lie = Y Otherwise
d-- . HR?i Form
-On list -Not on list
-. <
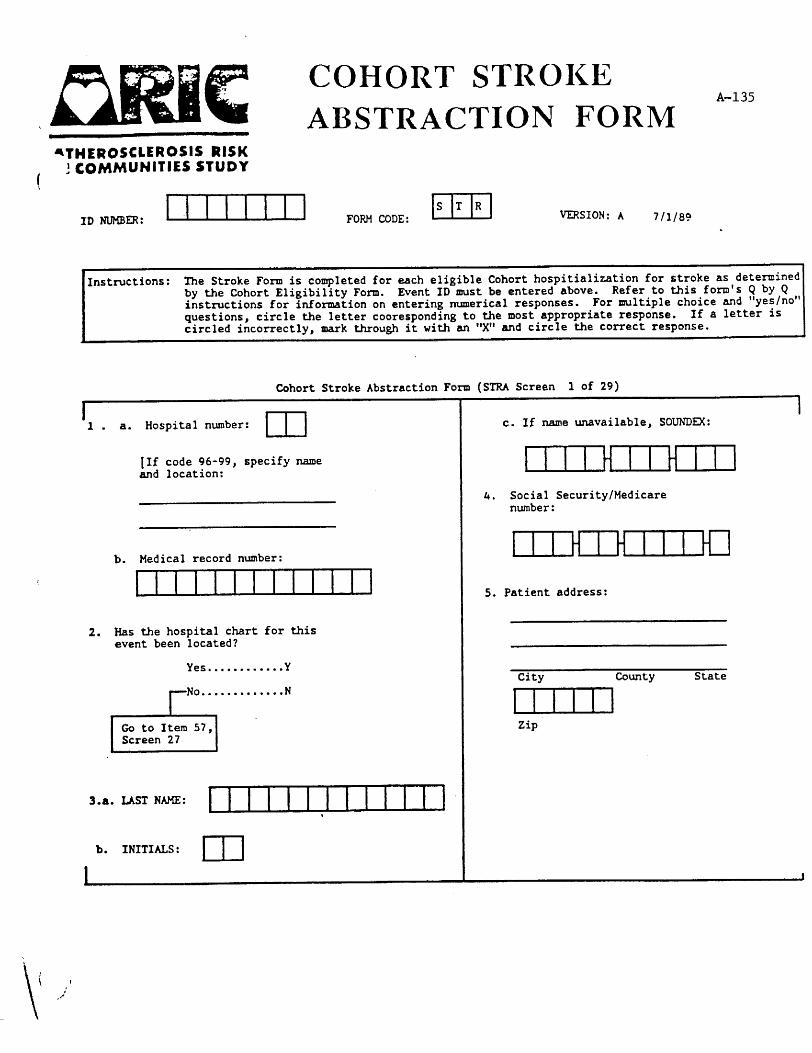
A-136
Cohort Stroke Abstraction Form (STRA Screen 2 of 29)
I 6. List all discharge diagnosis and
procedure codes exactly as they appear on the face sheet of the medical record and/or on the discharge s-.
a. mn.m ’ b. mn.m
c. mm
d. m.m
e. man
f. nl.m
‘g. rl.m
. h. m.m
i. mm
j. rr.m k. mar
I
1.
m.
n.
0.
P-
9*
r.
6.
t.
U.
I
umrn mam mn.m r.m mm mnm umjm nm.m mum mm

A-137
Cohort Stroke Abstraction Form (STRA Screen 3 of 29)
I I
7. Transcribe discharge diagnoses exactly as they appear on face sheet and/or on discharge asmary:
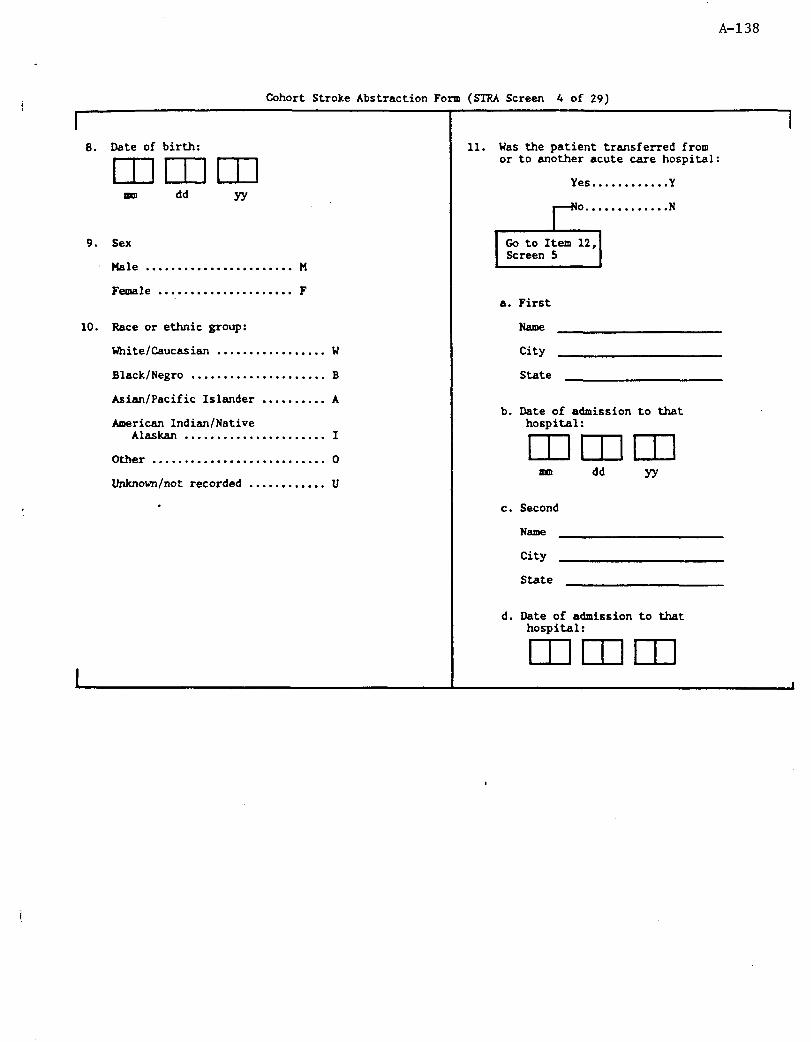
A-138
8. Date of birth: mmm m dd YY
Cohort Stroke Abstraction Form (!XRA Screen 4 of 29)
9. Sex
Hale . . . . . . . . . . . . . . . . . . . . . . . n
Fettle . . . . . . . . . . . . . . . . . . . . . F
10. Race or ethnic group:
Uhite/Cauca.sian ................. w
Black/Negro ..................... B
Asian/Pacific Islander .......... A
American Indian/Native Alaskan ...................... I
Other ........................... 0
Lhknovn/not recorded ............ u
I 11. Was the patient transferred from
or to another acute care hospital:
Yes............Y
a. First
City
State
b. Date of admission to that hospital: mmm
nul dd YY
c. Second
NS3lW
City
State
d. Date of admission to that hospital: mmm
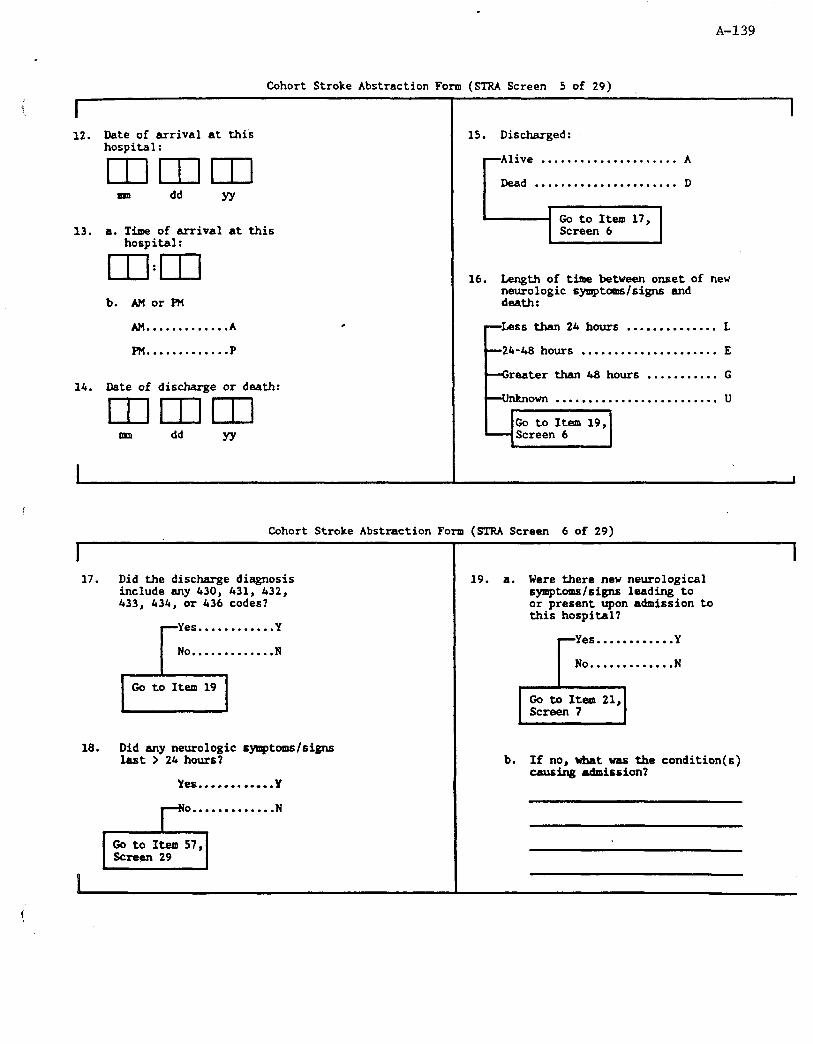
.
A-139
Cohort Stroke Abstraction Form (STFU Screen 5 of 29)
I 12. Date of arrival at this
hospital: Dmm m dd YY
13. a. Time of arrival at this hospital: mI:m
b. AMorFM
AM . . . . . . . . . . . . . A
PM . . . . . . . . . . . . . P
14. Date of discharge or death: mm-m mm dd YY
..................... A
...................... D
16. Length of time between onset of new
neurologic symptoms/signs and death:
. . . . . . . . . . . . . . L
. . . . . . . . . . . . . . . . . . . . . E
mater than 48 hours . . . . . . . . . . . G
. . . . . . . . . . . . . . . u
Cohort Stroke Abstraction Form (STRA Screen 6 of 29)
I 17. Did the discharge diagnosis
include any 430, 431, 432, 433, 434, or 436 codes?
Yes............Y
No.............N
18. Did any neurologic symptoms/signs last > 24hours?
Yes.... . . . . . ,..Y
o.............
r-5
N
Go to Item 57, Screen 29
I 19. a. Were there new neurological
symptoms/signs leading to or present upon admission to this hospital?
Yes............Y
No.............N
b. If no, what was the condition(s) musing admission?

A-140
f I
Cohort Stroke Abstraction Form (STRA Screen 7 of 29)
Did new neurological symptoms/signs develop during this hospitalization?
Yes . . . . . . . . . . . . Y
o............. N
unknown. . . . . . . .u
Date of onset of current neurological event: mmm
ml dd YY
Was the onset of the predominant neurologic symptom(s)/sign(s) either sudden or rapid?
Yes . . ..I....... Y
No . . . . . . . . . . . . . N
unknown. . . . . . . .u
I 23. History of previous stroke (also review
previous discharge diagnoses):
Yes............Y
24. UonthIyear of first stroke:
mm nm YY 25. Month/year of most recent stroke:
mm ml YY
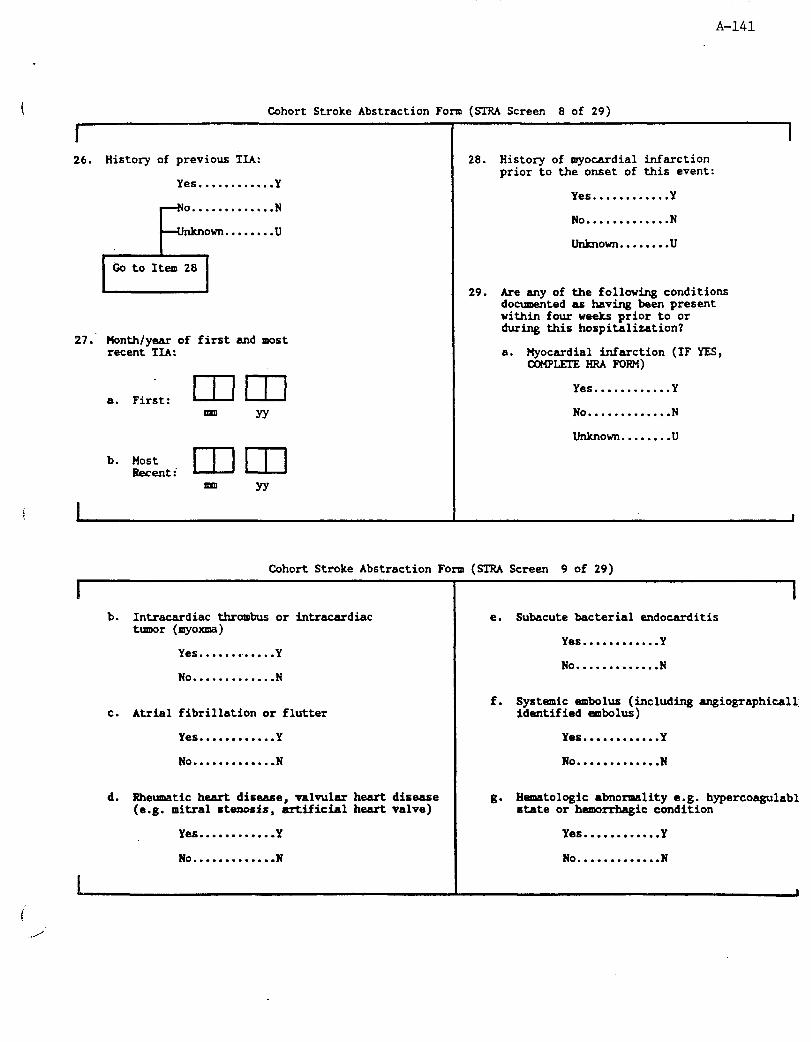
A-141
Cohort Stroke Abstraction Form (STRA Screen 8 of 29)
r 26. History of previous TIA:
Yes ............ Y
0 ............. N
nknown ....... .u
28.
29.
27: Month/year of first and most recent TIA:
. mm a. First: mm YY YY
History of myocardial infarction prior to the onset of this event:
Yes............Y
No . . . . . . . . . . . . . N
unlmown.. . . . . . .u
Are any of the following conditions documented as having been present within four weeks prior to or during this hospitalization?
a. Plyocardial infarction (IF YES, c0MPLEl-E HRA FORM)
Yes . . . . . . . . . . . . Y
No . . . . . . . . . . . . . N
unknown........u
Cohort Stroke Abstraction Form (STRA Screen 9 of 29)
I b. Intracardiac thrombus or intracardiac
tumor (myoxma)
Yes . . . . . . w . . . . . Y
No.............N
c. Atria1 fibrillation or flutter
Yes . . . . . . . . . . . . Y
No . . . . . . . . . . . . . N
d. Rheumatic heart disease, valvular heart disease (e.g. mitral stenosis, artificial heart valve)
I
Yes . . . . . . . . . . . . Y
No.............N
e. Subacute bacterial endocarditis
Yes............Y
No.............N
I
f. Systemic embolus (including angiographicall: identified embolus)
Yes . . . . . . . . . . . . Y
No.............N
B- Hematologic abnormality e.g. hypercoagulabl state or hemorrhagic condition
Yes . . . . . . . . . . . . Y
No.............N
I

A-142
Cohort Stroke Abstraction Form (SIRA Screen 10 of 29)
I h. Brain tumor (benign or malignant, primary
or metastatic)
Yes............Y
No.............N
i. Major head trauma, e.g., subdural hematoma, epidural henrat-, skull fracture
Yes............Y
No . . . . . . . . . . . . . N
j. Another nonstroke disease process which likely caused a focal neurologic deficit or coma
Yes............Y
No.............N
rc1
Go to Item 30
k. Specify:
I
I
30. Were any of the following performed or present in the week prior to the onset of acute neurologic symptoms?
a. Cardiac catherization
Yes............Y
No.............N
b. Open heart surgery
Yes............Y
No.............N
c. Cerebral angiography
Yes............Y
No.............N
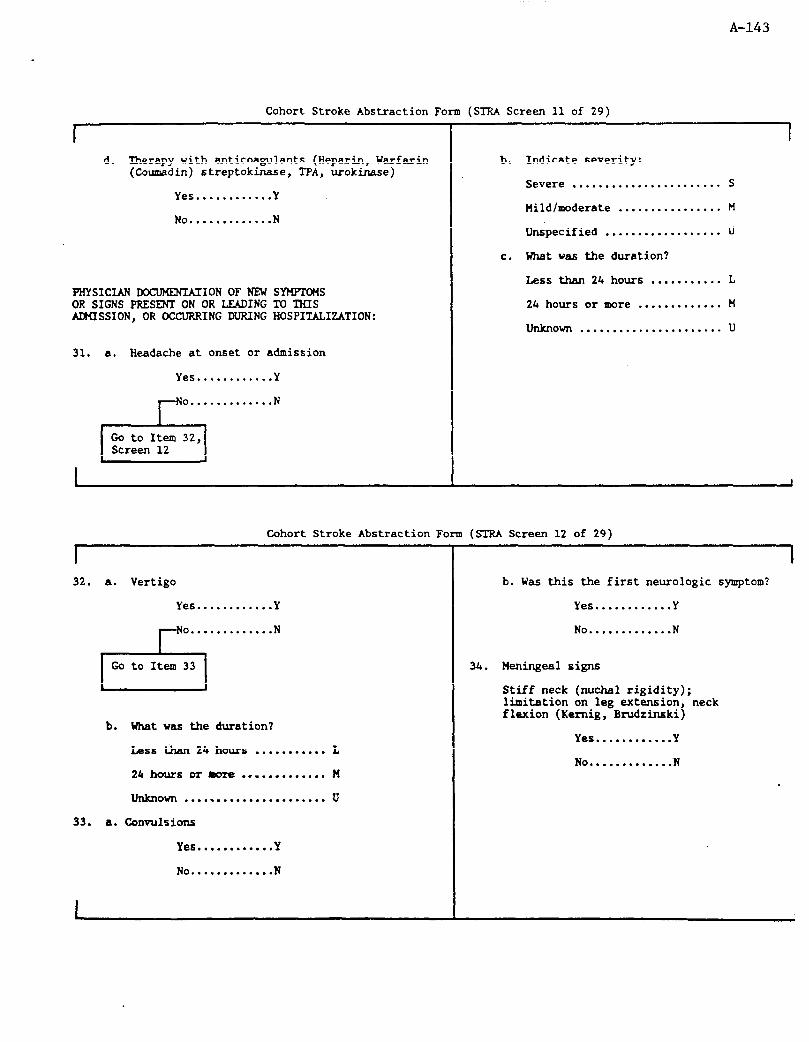
A-143
Cohort Stroke Abstraction Form (STRA Screen 11 of 29)
d. Therapy with anticoagulants (Heparin, Warfarin (Coumadin) streptokwe, TPA, urokinase)
Yes............Y
No . . . . . . . . . . . . . N
PHYSICIAN -ION OF NEW SYMFIOMS OR SIGNS PRESENT ON OR LEADING lY? THIS ADMISSION, OR OCCURRING DURING HOSPITALIZATION:
31. a. Headache at onset or admission
Yes .......... ..Y
0 ............. N
b.
C.
Indicate severity:
Severe ....................... S
Mild/moderate ................ M
Unspecified .................. U
What vas the duration?
Less than 24 hours ........... L
24 hours or more ............. H
unknown ...................... u
Cohort Stroke Abstraction Form (STRA Screen 12 of 29)
%
32. a. Vertigo
Yes............Y
. . . . . . . . . . . . . N
b. What was the duration?
Less than 24 hours . . . . . . . . . . . L
24 hours or boTe . . . . . . . . . . . . . H
unknown . . . . . . . . . . . . . . . . . . . . . . u
33. a. Convuulsions
Yes............Y
No . . . . . . . . . . . . . N
I
b. Was this the first neurologic symptom?
Yes............Y
No.............N
34. Heningealsigns
Stiff neck (mxhal rigidity); limitation on leg extension, neck flexion (Kernig, Bmdrinski)
Yes . . . . . . . . . . . . Y
No . . . . . . . . . . . . . N
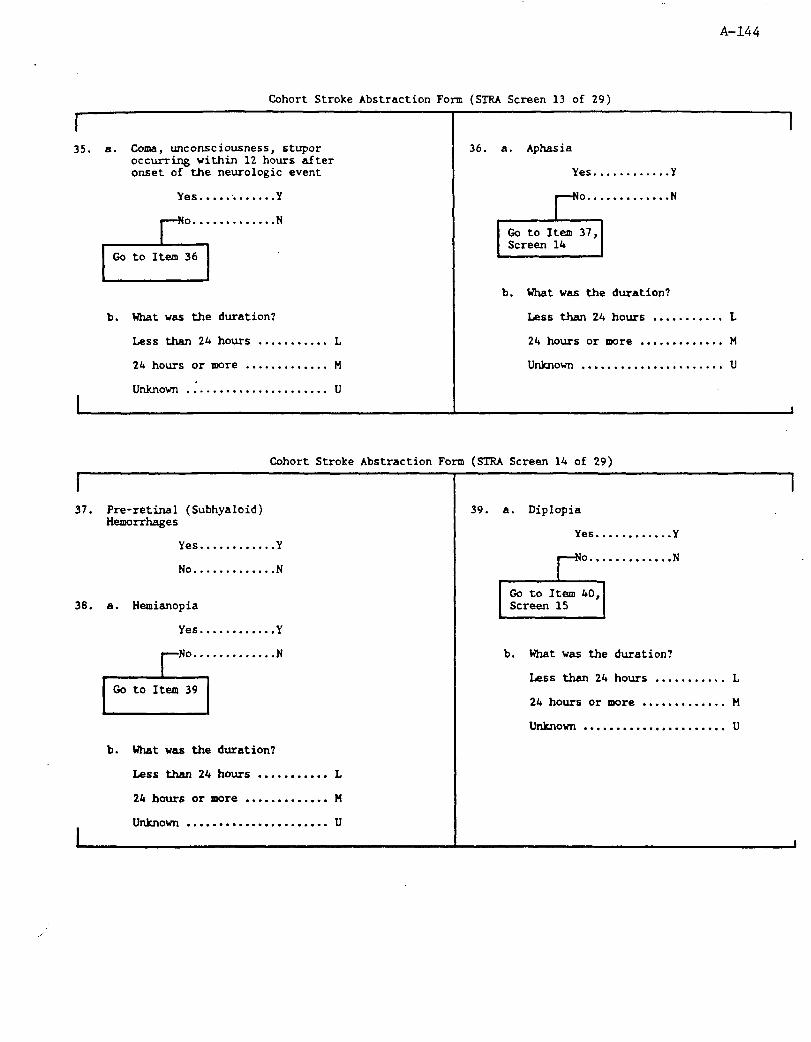
A-144
Cohort Stroke Abstraction Fo m (STRA Screen 13 of 29)
35. a. Coma, unconsciousness , stupor occurring within 12 hours after onset of the neurologic event
Yes............Y
36. a. Aphasia
Yes .,.......... Y
o............. N
I Go to Item 37, Screen 14 I
b. What was the duration?
b. What was the duration? Less than 24 hours . . . . . . . . . . . L
Less than 24 hours . . . . . . . . . . . L 24 hours or more . . . . . . . . . . . . . M
24 hours or awe . . . . . . . . . . . . . M unknown . . . . . . . . . . . . . . . . . . . . . . u
unknown .:.................... u I I I 1
Cohort Stroke Abstraction Form (STRA Screen 14 of 29)
I 37. Pre-retinal (Subhyaloid)
Hemorrhages
Yes............Y
No.............N
38. a. Hemianop ia
Yes . . . . . . . . . . . . Y
. . . . . . . . . . . . . N
b. What was the duration?
Less than 24 hours . . . . . . . . . . . L
24 hours or more . . . . . . . . . . . . . H
unknown . . . . . . . . . . . . . . . . . . . . . . U
I
1 39. a. Diplopia
Yes............Y
o............. N
b. What was the duration?
Less then 24 hours . . . . . . . . . . . L
24 hours or more . . . . . . . . . . . . . H
unknown . . . . . . . . . . . . . . . . . . . . . . u
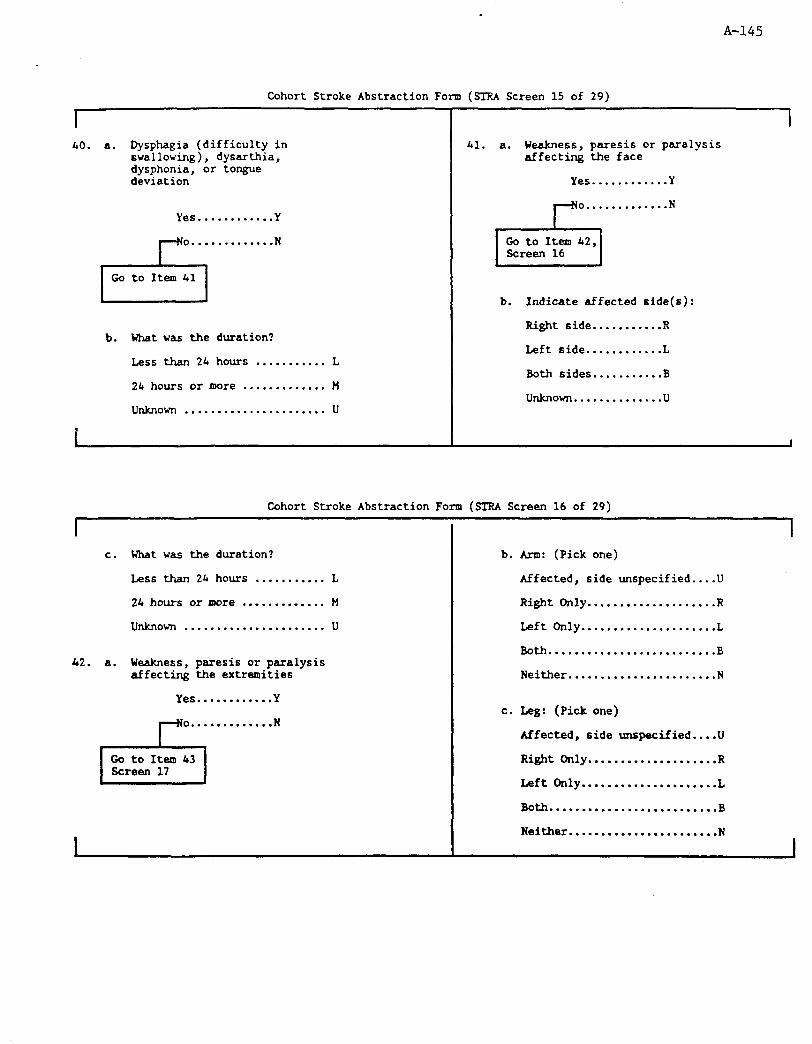
A-145
Cohort Stroke Abstraction Form (STRA Screen 15 of 29)
I 40. a. Dysphagia (difficulty in
swallowing), dysarthia, dysphonia, or tongue deviation
Yes............Y
0. . . . . . . . . . . . . N
b. What was the duration?
Less than 24 hours . . . . . . . . . . . L
24 hours or more . . . . . . . . . . . . . M
unknown . . . . . . . . ..*........... U
I 41. a. Weakness, paresis or paralysis
affecting the face
Yes............Y
b. Indicate affected side(s):
Right side ......... ..R
Left side .......... ..L
Both sides ......... ..B
unkrlown..............u
Cohort Stroke Abstraction Form (STRA Screen 16 of 29)
c. What was the duration?
Less than 24 hours . . . . . . . . . . . L
24 hours or more . . . . . . . ..I... M
unknown . . . . . . . . . . . . . . . . . . . . . . u
42. a. Weakness, paresis or paralysis affecting the extremities
Yes............Y
I Go to Item 43 Screen 17 ~ I
b. Arm: (Pick one)
Affected, side unspecified....U
Right Only....................R
Left only.....................L
Both . . . . . . . . . . . . . . . . . . . . . . . . . . B
Neither.......................N
c. Leg: (Pick one)
Affected, side unspecified....U
Right Only....................R
Left only . . . . . . . . . . . . . . . . . . . . . L
Both . . . . . . . . . . . . . . . . . . . . . . . . . . B
Neither.......................N
I
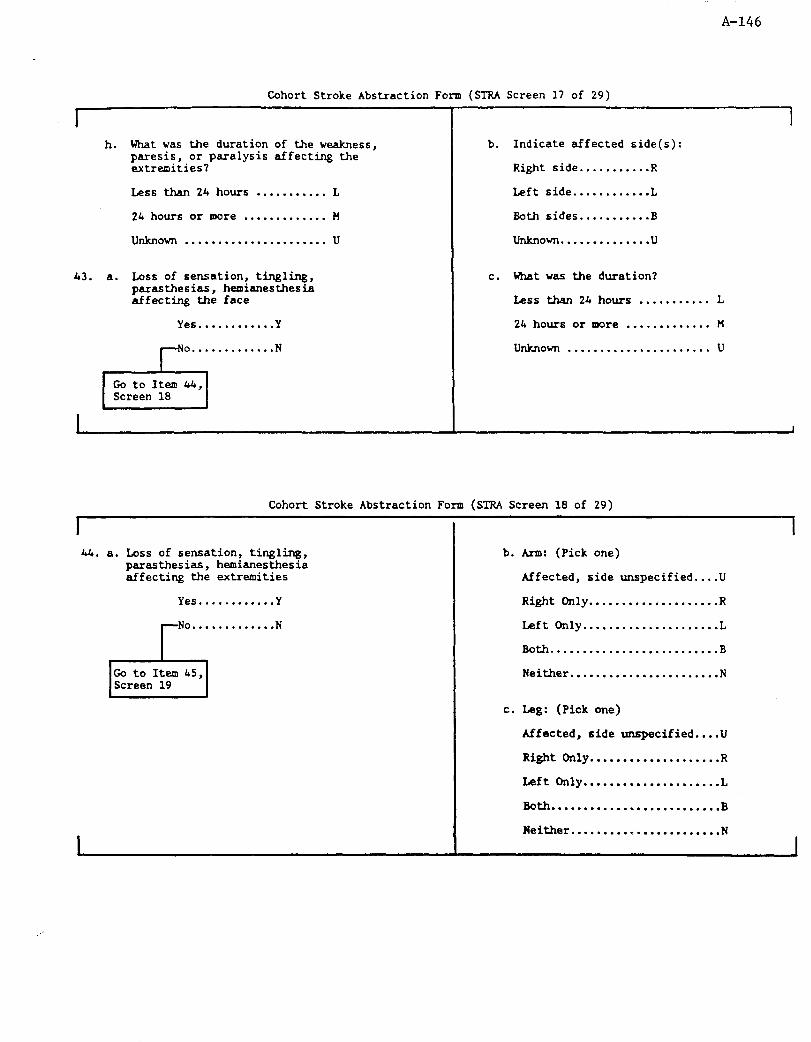
A-146
Cohort Stroke Abstraction Fom (STRA Screen 17 of 29)
h. What was the duration of the weakness, paresis, or paralysis affecting the extremities?
Less than 24 hours . . . . . . . . . . . L
24 hours or more . . . . . . . . . . . . . n
unknown . . . . . . . . . . . . . . . . . . . . . . U
43. a. Loss of sensation, tingling, parasthesias, hemianesthesia affecting the face
Yes . . . . . . . . . . . . Y
o............. N
b. Indicate affected side(s):
Right side ......... ..R
Left side .......... ..L
Both sides ......... ..B
unknown ............ ..u
c. What was the duration?
Less than 24 hours ........... L
24 hours or mre ............. H
unknown ...................... u
Cohort Stroke Abstraction Form (STRA Screen 18 of 29)
I
44. a. Loss of sensation, tingling, parasthesias, hemianesthesia affecting the wtremities
Yes............Y
No.............N
r-4 Go to Iteal 45, Screen 19
b. Arm: (Pick one)
Affected, side unspecified....U
Right Only....................R
Left only.....................L
Both . . . . . . . . . . . . . . . . . . . . . . . . . . B
Neither.......................N
I
c. Leg: (Pick one)
Mfected, side unspecified....U
Right Only....................R
Left only.....................L
Both . . . . . . . . . . . . . . . . . . . . . . . . . . B
Neither.......................N
I

A-147
Cohort Stroke Abstraction Form (STRA Screen 19 of 29)
I c. What was the total duration of the loss
of sensation, tingling, parasthesis, hemianesthesia affecting the extremeties?
Less than 24 hours . . . . . . . . . . . L
24 hours or more . . . . . . . . . . . . . H
unknown . . . . . . . . . . . . . . . . . . . . . . u
45. a. Gait disturbance
Yes............Y
o.............
ii
N
Go to Item 46
b. What was the duration?
Less than 24 hours . . . . . . . . . . . L
24 houx% or more . . . . . . . . . . . . . M
unknown . . . . . . . . . . . . . . . . . . . . . . u
I
46. Other neurologic symptom
Yes............Y
No.............N
[If yes, specify:
LABORA?ORYTESTSPERFORtEDpIIS ADMISSION
47. a. Was lumbar puncture performed?
Yes............Y

A-148
Cohort Stroke Abstraction Form (STRA Screen 20 of 29)
I Record for the first non- traumatic Lp after onset of symptoms or first LP if all traumitic.
b. Date: 171 m I dd YY
c. Traumatic?
Yes............Y
No . . . . . . . . . . . . . N
d. Appearance:
Clear fluid .................. c
Xanthochromic ................ X
Gross blood .................. B
unknown ...................... u
e. Microscopic RBCs (Tube 1):
Zero RBCs cu.m. . . . . . . . . . . . . . Z
l-999 RBC cu.m. . . . . . . . . . . . . . L
lOOO+ RBC cu.m. . . . . . . . . . . . . . G
unknown . . . . . . . . . . . . . . . . . . . . . . u
f. Microscopic RBCs (Tube 2):
No tube . . . . . . . . . . . . . . . . . . . . . . N
Zero RBCs cu.m. . . . . . . . . . . . . . Z
l-999 RBC cu.m. . . . . . . . . . . . . . L
lOOO+ RBC cu.m. . . . . . . . . . . . . . G
unknown . . . . . . . . . . . . . . . . . . . . . . u

A-149
Cohort Stroke Abstraction Form (STRA Screen 21 of 29)
l- g. Lumbar puncture diagnosis:
Normal Study............A
Exclusionary pathology..B
Unrelated pathology or traumatic tap...........C
Bloody (non-traumatic) or xanthocromic.........D
48. a. Was cerebral angiography performed?
Yes............Y
b. Date: m m m dd
I YY
c. Angiography diagnosis
Normal study ................ ..A
Exclusionary pathology ...... ..B
Unrelated pathology ......... ..C
Ruptured aneurysm ........... ..D
Avascular ws without evidence ruptured aneurysm/AV?4 ........ .E
d. Stenosis - Right internal carotid
Not studied ................. ..A
O-49% stenosis .............. ..B
50-79% stenosis ............. ..C
80-99% stenosis ............. ..D
100% (occlusion) ............ ..E
Cohort Stroke Abstraction Form (STRA Screen 22 of 29)
1
e. Stenosis - Left internal carotid
Not studied...................A
O-49% stenosis................B
SO-79% stenosis...............C
80-99% stenosis...............D
100% (occlusion)..............E
49. a. Was at least one CT wan per- formed during this hospitali- eation
Yes............Y
o............. N
I b. What was approximete time
between symptom onset and the first CT scan?
Less than 24 hours . . . . . . . . . . . A
24-48 hours . . . . . . . . . . . . . . . . . . B
Greater than 48 hours . . . . . . . . C
unlpl0Wl-l . . . . . . . . . . . . . . . . . . . . . . U
c. Date: mmm m dd. yy
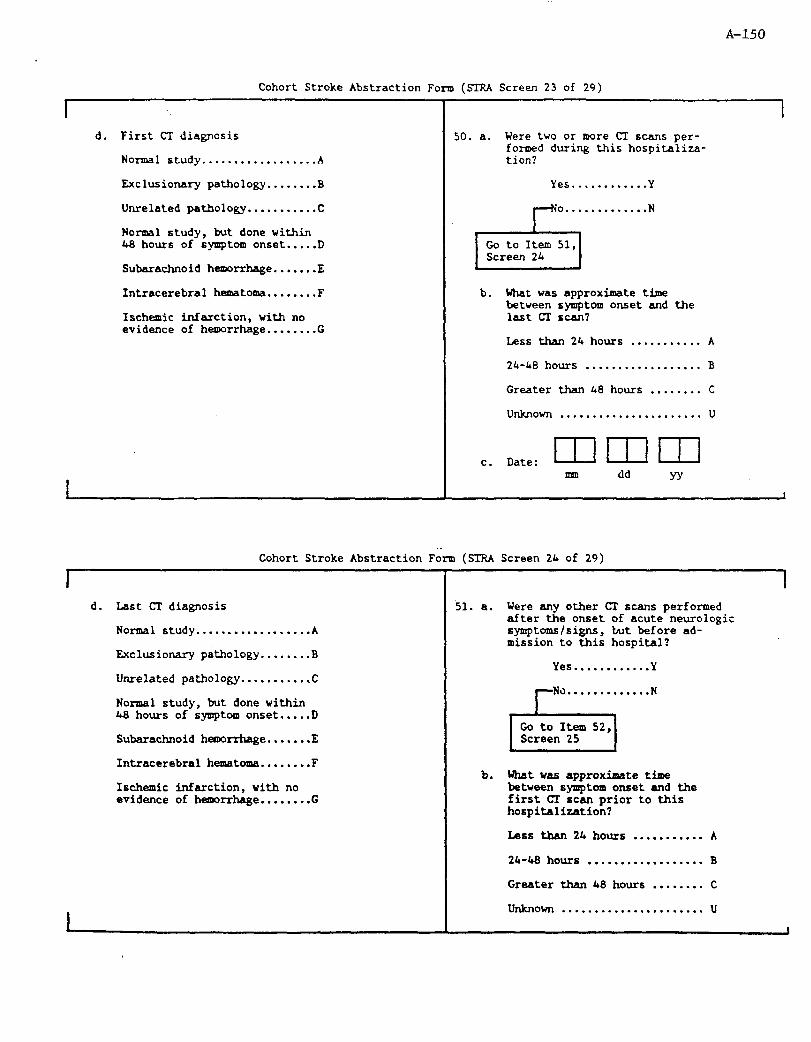
A-150
Cohort Stroke Abstraction Form (STRA Screen 23 of 29)
I d. First CT diagnosis
Normal rtudy..................A
Exclusionary pathology . . . . . . . . B
Unrelated pathology...........C
Normal study, but done within 48 hours of symptom onset.....D
Subarachnoid hemxrhage.......E
Intracerebral hematoma........F
Ischemic infarction, with no evidence of hemorrhage........G
50. a. Were two or more CI scans per- forroed during this hospitaliza- tion?
Yes . . . . . . . . . . . . Y
o............. N
Go to Item 51,
b. What was approximate time between symptom onset and the last CI scan?
Less than 24 hours . . . . . . . . . . . A
24-48 hours . . . . . . . . . . . . . . . . . . B
Greater than 48 hours . . . . . . . . C
unknown . . . . . . . . . . . . . . . . . . . . . . u
c. Date: mmm mm dd YY
Cohort Stroke Abstraction Form (SIRA Screen 24 of 29)
I d. Last CI diagnosis
Normal study..................A
Exclusionary pathology........B
Unrelated pathology . . . . . . . . . . . C
No-1 study, but done within 48 hours of symptom onset.....D
Subarachnoid hemorrhage.......E
Intracerebral hamatoma........F
~EChedC infarction, with no evidence of hemrrhage........G
I 51. a. Were any other CI suns performed
after the onset of acute neurologic symptoms/signs, but before ad- mission to this hospital?
Yes............Y
No.............N
b. What was approximate time between symptom onset and the first CI scan prior to this hospitalization?
Less tban 24 hours . . . . . . . . . . . A
24-48 hours . . . . . . . . . . . . . . . . . . B
Greater than 48 hours . . . . . . . . C
unknown . . . . . . . . . . . . . . . . . . . . . . u

A-151
Cohort Stroke Abstraction Form (SIRA Screen 25 of 29)
I
c. Date: mmm m dd YY
d. Re-admission CT diagnosis
Normal study . . . . . . . . . . . . . . . . . . A
Exclusionary pathology........B
Unrelated pathology...........C
Normal study, but done within 43 hours of symptom onset.....D
Subarachnoid heroorrhage.......E
Intracerebral hematoma........F
Ischamic infarction, with no evidence of hemorrhage........G
52. a. Was Magnetic Resonance Imaging (MRI) including the head performed?
Yes............Y
o............. N
b. What was approximate time between symptom onset and the KU? (If > 1 KRI, pick the most meaningful.)
Less than 24 hours . . . . . . . . . . . A
24-48 hours . . . . . . . . . . . . . . . . . . B
Greater than 4.8 hours . . . . . . . . C
unknown . . . . . . . . . . . . . . . . . . . . . . u
I
Cohort Stroke Abstraction Form (STFLA Screen 26 of 29)
I c. Date: mmm uml dd JY
d. EIRI diagnosis
Normal study..................A
Exclusionary pathology........B
Unrelated pathology...........C
Normal study, but done within 48 hours of symptom onset.....D
Subarachnoid hemorrhage.......E
Intracerebral heamtcma..,.....F
Sachemic infarction, with no
evidence of hemorrhage........G
I
53. a. Was B-Mode and/or Doppler Ultrasound on carotid(s) performed?
Yes............Y
o............. N
b. Date: m m m dd YY

A-152
Cohort Stroke Abstraction Form (STRA Screen 27 of 29)
1 c. Ultrasound diagnosis - Right
internal carotid
049% stenosis................A
SO-79% stenosis...............B
80-99% stenosis . . . . . . . . . . . . . . . C
100% (occlusion)..............D
*Hemdynamically significant lesion".....................E
Not studied...................F
d. Ultrasound diagnosis - Left internal carotid
O-49% stenosis................A
50-79% stenosis...............B
80-99% stenosis...............C
100% (occlusion)..............D
"hemodynamically significant lesion".....................E
Not studied...................F
I
I 54. a. Was a craniotomy performed (post
event)?
Yes . . . . . . . . . . . . Y
o............. N
b. Date: mmm m dd YY
Cohort Stroke Abstraction Form (STRA Screen 28 of 29)
I
c. Craniotomy diagnosis
No pathology ................ ..A
Exclusionary pathology ...... ..B
Unrelated pathology ......... ..C
Ruptured aneurysm ........... ..D
Intracerebral hemrrhage .... ..E
Infarction ................. ...?
55. a. Was an autopsy performed?
Yes .......... ..Y
No ........... ..N
I
I
Autopsy diagnosis
b.
C.
d.
e.
f.
Recent bleeding of saccular aneurysm.......................... Y N
Intracerebral hemorrhage..........Y N
Recent nonhemorrhagic infarction of brain...............Y N
Recent infarcted armed (bland or hemorrhagic)...................Y N
Source of emboli in a vessel or any organ, or an embolus in the brain......................Y N

A-15 3
I
Cohort Stroke Abstraction Form (STRA Screen 29 of 29)
I 1
56. 19) diagnosis impression
Definite SAH ................. ..A
Probable SAH ................. ..B
Definite IPH ................. ..C
Probable IPH ................. ..D
Definite TIB .................. ..E
Probable TIB ................. ..F
Definite EIB ................. ..G
Probable EIB ................. ..H
Possible stroke-undetermined I
I We ...........................
57. Abstractor Nmber: I I I
58. Date Abstracted: mmm mn dd YY
59.
.60.
61.
62.
ADDITIONAL FORMS
Form
A =Ns)
B DTH
c HRA
D AUT
Criteria based (Circle letter corresponding on this form to form required)
Item 11 = Y (If transfer was from/to study hospital, be sure to cross-check hospital discharge index to avoid duplication.)
Item 15 = D
Item 29a = Y
stem 55 = Y

ARIC
COHORT STROKE ABSTRACTION FORM (SIR)
INSTRUCTIONS
A-154
General Instructions for Field Center Abstracter/Surveillance Director:
1. Before going to the hospital to photocopy the medical record for this admission, record on the STR the Event ID number from the Cohort Eligibility Form, and complete Items la (hospital number) and 3 (name or Soundex).
2. Photocopy complete hospital record for the appropriate admission. Complete Items lb, 2, 4-15. Review records of previous admissions. If there is mention of TIA, stroke, or MI in a record of a previous hospitalization, or if there has been an admission for any reason - within the four weeks prior to the present admission, photocopy the record for the corresponding admission.
3, Complete Items 23 - 29a, and 55 based on review of both the record of the present admission and earlier records that have been copied.
4. Complete Items 59 - 62 (Additional Forms Needed), and note forms needed on Cohort Event Investigation Form (CEI) before sending this STR Form to the ARIC neurologist.
5. Send SIR Form and medical record(s) to Dr. Linda Goldman, University of Minnesota School of Public Health, Stadium Gate 27, 611 Beacon Street, S-E. Minneapolis, MN 55455, retaining a copy of the medical record in your files. Attach a cover memo instructing Dr. Goldman to return the completed STR Form to the Surveillance Director at your Field Center.
General Instructions for Neurologist Completing Stroke Form:
1. Items l-15 and several items concerning history will be completed by Surveillance staff at originating Field Center. Review the entire record carefully, and begin with Item 16. Item 29a will be completed at the Field Center; 29b-k must be completed by the neurologist.
2. The Abstractor should be familiar with the ARIC Instructions for Completion of Paper Forms.
3. Write legibly. Use black or blue erasable pens. Press hard when filling in blanks with or circling numbers, letters, or Xs. Pen will not photocopy if too light and will fade with time.
4. Several types of responses are used:
Fill in the blank.
Fill in the number, such as a date, time or medical record number.
To answer most questions you will have several choices, the simplest of all being Yes, No, Unknown or Undetermined. For this type of response, "Yes" or "NO" will be checked only if there is no doubt that the response is positive or negative based on information in the
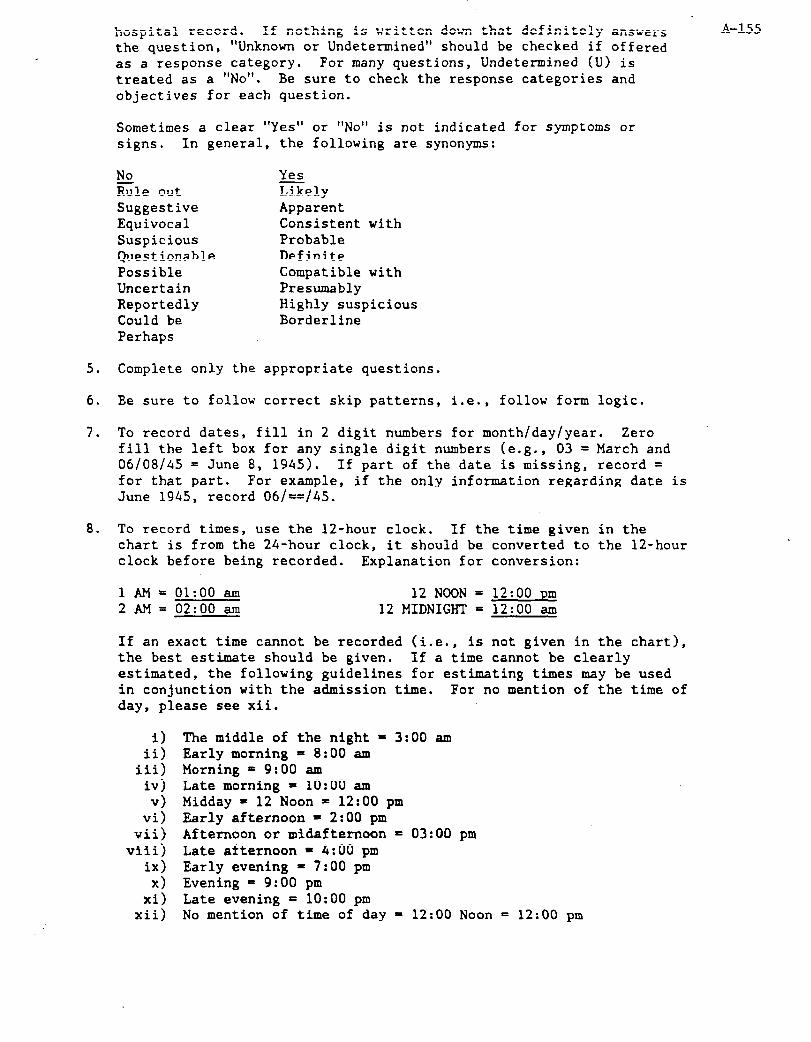
hospital record. If nothing is written down that definitely answers
the question, "Unknown or Undetermined" should be checked if offered as a response category. For many questions, Undetermined (U) is treated as a “NO”. Be sure to check the response categories and objectives for each question.
A-155
Sometimes a clear "Yes" or "No" is not indicated for symptoms or signs. In general, the following are synonyms:
No Yes Rule out Likely Suggestive Apparent Equivocal Consistent with Suspicious Probable Questionable Definite Possible Compatible with Uncertain Presumably Reportedly Highly suspicious Could be Borderline Perhaps
5. Complete only the appropriate questions.
6. Ee sure to follow correct skip patterns, i.e., follow form logic.
7, To record dates, fill in 2 digit numbers for month/day/year. Zero fill the left box for any single digit numbers (e.g., 03 = March and 06/08/45 = June 8, 1945). If part of the date is missing, record = for that part, For example, if the only information regarding date is June 1945, record 06/==/45.
8. To record times, use the 12-hour clock. If the time given in the chart is from the 24-hour clock, it should be converted to the 12-hour clock before being recorded. Explanation for conversion:
lAM= 01:oo am 2AM= 02:oo am
12 NOON = 12 MIDNIGHT =
If an exact time cannot be recorded (i.e., is not given in the chart), the best estimate should be given. If a time cannot be clearly estimated, the following guidelines for estimating times may be used in conjunction with the admission time. For no mention of the time of day, please see xii.
12:00 pm 12:oo am
i) The middle of the night = 3:00 am ii) Early morning = 8:00 am
iii) Morning = 9:00 am iv) Late morning = 10:00 am v) Midday = 12 Noon = 12:00 pm
vi) Early afternoon = 2:00 pm wii) Afternoon or midafternoon = 03:OO pm
viii) Late afternoon = 4:00 pm ix) Early evening = 7:00 pm x) Evening = 9:00 pm
xi) Late evening = 10:00 pm xii) No mention of time of day = 12:00 Noon = 12:00 pm
A-156 9. After completing the STR Form, return the form to the Surveillance
Director of the originating field center. Retain a copy of the STR
Form and the medical record in your files.
Instructions for Items 1 - 62
1.a. Hospital Number: Prior to going to the hospital, enter the code number assigned to the hospital for its identification. (Appendix 3) If outside the study community, use the appropriate code (96-99) and write in name and address.
b. Hospital Record Number: This number will be found stamped or typed on almost every page of the hospital record. The easiest place
3 -.
3.
4.
5.
6.
7.
a.
to-find it is both on the medical record folder and in the upper right/left hand corner of the face sheet. Double check this number with the record number on the label from the Field Center office.
List the number from left to right. Do not add zeroes to the right of the number. If the number changes with each admission, use the appropriate number for the one (admission) being abstracted.
Record "Yes" if chart has been obtained. Record "No" if record cannot be obtained.
Name and Soundex: If the hospital does not allow abstraction of names code last, first, middle name by Soundex code.
Social Security Number: Record Social Security Number or Medicare Number, being sure to add the last letter that may be associated. (See HRA Form instructions.) If the hospital does not allow full abstraction of Social Security Number, record every other digit, beginning with the first, and record = in the remaining positions.
Address: Record the patient's address. This should include: the house number, the street name, and the apartment, box or lot number. The last line is designated for the names of the city, county and state.
Discharge Diagnosis and Procedure Codes: Fill in the codes as listed on the face sheet, preferably, or discharge summary, as a second choice (up to 21 codes). Pick the source which is most complete. If digit(s) to the right of the decimal are missing from the ICD code, leave the box(es) blank on the form. Do not enter zero there unless it appears in the chart.
Transcribe discharge diagnoses as they appear on face sheet or discharge summary. Diagnosis listed should correspond with codes in Item 6. If not, ask field center to consult with medical records department.
Date of Birth: Birth date is usually found on the face sheet of each medical record. Do not use the age given by the physician on the history and physical since it may be incorrect.
9,lO. Sex and Race: Check either male or female. The following definitions should be used for determining race:
A-157
White (Caucasian). A person having origins in any of the original peoples of Europe, North Africa, or Middle East. Black (Negro). A person having origins in any of the black racial groups of Africa.

A-158
11.
Asian or Pacific Islander (A person having origins in any of the original peoples of the Far East, Southeast Asia, the Indian subcontinent, or the Pacific Islands. This area includes, for example, China, India, Japan, Korea, the Philippine Islands and Samoa; American Indian or Alaskan Native (A person having origins in the original peoples of North America, who maintains cultural identification through tribal affiliation).
Transfer from or to Another Hospital: If the patient was transferred from or to another acute care hospital, check "yes" and write the name of the hospital from or to which the patient was transferred, and the city and state that it is located in. Record the date of admission to the transfer hospital. If the patient was not transferred (i.e., admit note states patient first experienced symptoms at home, work, etc.), check "no". If no information is available regarding transfer, indicate this by checking unknown. This information can be found on the face sheet of the chart and in admitting notes.
The purpose of this question is to identify recent hospitalization(s) of this patient, possibly to be reviewed at a later date.
12. Date of Arrival at this Hospital Fill in the date the patient was admitted according to the guidelines specified in General Instructions.
13. Time of Arrival: If an exact time is not given in the chart, the best estimate should be given. See General Instructions for guidelines regarding recording times.
14. Date of Discharge (for nonfatal case) or Death This information will be found on the face sheet or on the RR sheet. If there is a discrepancy in time between the two, take the later time. If the patient died, then record the date and time of death.
15. Discharged: Indicate vital status.
16. Timing of Death: If dead, estimate or calculate the length of time between new symptom onset and death. Chronic symptoms should not be considered here.
17,18. The purpose of this question is to eliminate patients who did not have strokes, but who had focal neurologic deficits that were transient. If referred in Questions 17 or 18; proceed with abstraction. If you do not skip out of this question, it is unnecessary to complete the rest of this form. To answer Question 18, see description of neurologic symptoms below under question 19.
19.a. Neurolonic symptoms or signs on admission. Symptoms are complaints expressed by the patient or relayed by the patient's family or friends. Signs are physical exam findings observed by a physician.

A-159
Neurological symptoms include: weakness, paralysis, numbness, tingling, visual disturbance, speech abnormality, difficulty swallowing, difficulty chewing, difficulty hearing, dizziness, vertigo, gait difficulty, uncoordination, severe headache, seizures (convulsion), or decreased level of consciousness.
For our purpose, we are interested in new or acute findings (that is, not previously evaluated). Thus, for instance, a diabetic with long standing peripheral neuropathy who has had tingling in his feet for years would not have the same significance as someone who suddenly developed numbness in one leg.
If a patient is presenting for evaluation of neurologic symptoms that have not been previously evaluated and have occurred in the past two months, mark "Yes", even if the symptoms have resolved. If you are uncertain, describe in the summary (Item 18) and flag for field center physician review. If the patient had an old stroke with no new or recent symptoms, mark "No".
If in doubt about whether the finding is new, answer "Yes" and continue to 21.
b. If there are not new symptoms or signs present on admission or occurring in the recent past indicate the admission diagnosis.
20. New neu'rologic symptoms in hospital: The purpose of this question is to identify new symptoms that began in the hospital. Refer to neurological symptoms described above (019). If the patient did not have new neurologic symptoms when admitted, and did not develop them in the hospital, it is unnecessary to continue filling out this form.
21. When did the above new symptoms begin?
Fill in boxes with month, day, and year. Treat month, day, year as separate items, e.g., fill in year even if month and day are not given, enter = ,for the month and day. If the year is also missing, enter =. If there are multiple new symptoms, indicate the beginning of the first of the new symptoms.
22. Was the onset of symptoms sudden or rapid?
The following are examples of when to mark "Yes" response, and which description to specify. Mark "No" if symptoms were progressive in nature over a period longer than 24 hours. If symptoms occurred rapidly or suddenly, it should be pretty.obvious from the history that patient was doing something (i.e., drinking coffee) when he suddenly became symptomatic (dropped his cup and noticed he couldn't move his right hand). This would also include someone who awoke from sleep with a deficit. If a patient drops his cup of coffee and notices something wrong with his right hand which felt tingly and then over the next few minutes he realized he could no longer move it, mark
“Yes” . Another example would be someone who was walking and suddenly A-160 started limping and then fell down and couldn't move his leg compared to someone who suddenly became paralyzed. Stepwise progression is a little harder to document and may involve either stepwise worsening ("stuttering onset") of a simple symptom or several symptoms. This usually occurs over several hours to a day. For example, a patient may have a "funny sensation" on the right side of is body or feel dizzy prior to retiring in the evening. When awakening in the morning he may be weak and have some speech difficulty. Then a couple of hours later he may suddenly be a lot worse. If symptoms begin or progress over weeks to months, mark “No”. If onset is not described, mark "Unknown". If you are not sure, copy pertinent parts of patient history and flag for physician review.
23. Is there a history of previous stroke?
This refers to events preceding the present acute illness and hospitalization. Synonyms for "stroke" may include some of the following: cortical infarction, intracranial hemorrhage, cerebral thrombosis, cerebral artery occlusion, cerebral infarction, apoplexy, cerebrovascular accident (CVA), intracerebral hemorrhage. Answer "Yes" if one or more of the sources listed above makes explicit mention of previous "stroke" or states: a history of "probable stroke", a history "consistent with stroke", a diagnosis of "CVA vs. TIA", reversible ischemic neurological deficit, or partially reversible ischemic neurological deficit lasting > 24 hours. Answer "No" if absence of stroke is explicitly mentioned, if symptoms lasted less than 24 hours, if stroke was "possible" or "questionable" only, or if patient had "TIA" only with no documented residual findings. "No previous cerebrovascular disease" = no. (This means patient was normal within 24 hours after onset of symptoms and therefore did not have a stroke.) Answer "U", otherwise, or if the only information about old stroke is from a CT scan. This information is needed to distinguish first events from recurrent events in subsequent data analysis. (SEE APPENDIX 1 FOR ADDITIONAL CLARIFICATION.)
24,25. Date and Time: Enter month and year for first event and most recent. If there was only one previous event, complete Items 24 and 25 with the same date (i.e., the first and most recent event were the same). If specific dates are not given, use information available to calculate date. For instance, if stroke was "eight years ago" subtract eight from current year. If "month" is not available, fill in =. If dates not available, enter =.
26. Is there a history of previous TIA (Transient ischemic attack)?
This refers to events preceding this acute illness. If admitted for first TIA, answer "no". If TIA preceded current event, answer "yes". Synonyms for "TIA" may include: acute cerebrovascular insufficiency, spasm of cerebral arteries, insufficiency of basilar, carotid, or
27.
28.
29.
vertebral arteries, or neurological deficit lasting less than 24 hours. If TIA is not mentioned, only that symptoms lasted less than 24 hours, answer "Yes" to TIA, Amaurosis fugax (or transient monocular blindness) = TIA. (SEE APPENDIX 1)
Date and Time: Enter month and year for first event and most recent. If there was only one previous event, complete parts (a) and (b) with the same date (iie., the first and most recent event were the same). If specific dates are not given, use information available to calculate date. For instance, if stroke was "eight years ago" subtract eight from current year. If "month" is not available, fill in =. If date not available, enter =,
Is there a history of previous MI?
This information may be found in the history and physical exam done by the admitting physician or in the nurses admitting interview. This question refers to events that occurred prior to this hospitalization. Take information from the history of the resident or intern, if any, the attending physician, the cardiovascular consultant, the ER physician, nursing notes, or medical student, in that order. "History" refers to information from the patient and his family. Answer "Yes" or "No" only if mentioned, otherwise check “Undetermined". If information states silent MI, record that as a "Yes" to previous MI. An abnormal ECG, alone, stating "old MI" cannot be used as a source of history of previous cardiac disease. If conflicting information is recorded in two or more sources, choose the information from the most reliable source. If "No cardiac problems" or information indicates "No heart disease", “No history of cardiovascular disease", "No adult illness", "No medical history", or "Previously well", you may check "No" instead of "Undetermined". (SEE APPENDIX 1)
This question is designed to ascertain non-atherosclerotic etiologies (causes) for stroke or diseases that may mimic or present as stroke. Parts (a) through (f) specifically are an attempt to establish the presence of an "embolic source" - a mechanism where blood clots could form in the heart and travel through blood vessels to the brain, causing a specific type of stroke. To be documented the item must have been present within four weeks prior to or during this hospitalization.
a. Was there any evidence of MI?
A-161
To check "Yes" here there must be a history of severe chest pain, diagnostic or evolving ECG, or positive isoenzyme CPK-MB either four weeks before or during this admission. We need strong evidence of MI, chest pain, an evolving or diagnostic ECG, and/or positive enzymes. If there is an MI code, but not evidence of MI,

b.
C.
d.
e.
this can be checked "Unknown". Do not take admitting diagnosis of A-162
"R/O MI" alone, as we need more evidence.
Intracardiac Thrombus
This refers to a blood clot seen within the heart. It may also be called "intraventricular thrombus" (or clot) or "ventricular aneurysm with clot". Check to see if an echocardiogram, autopsy or cardiac CT was done. These should specify if intracardiac thrombus was present. Echocardiogram is the most frequently used clinical study to evaluate the heart for this problem. Rarely cardiac CT has been used for the same purpose. If an autopsy was performed, read the section that pertains specifically to the heart on gross examination. Coronary artery thrombosis or coronary thrombotic occlusion is not intracardiac thrombus.
Intracardiac tumor. Also called atria1 myxoma. Should be reported on echocardiogram, cardiac CT or autopsy if present (see above).
Atria1 fibrillation or flutter. This may also be called paroxysmal atria1 fibrillation. This does not include paroxysmal tachycardia, supraventricular tachycardia, sinus tachycardia, WT., or PAT. Check all ECGs interpretations for atria1 fibrillation or flutter. It may be abbreviated as A.F., A.fib or At.fib. If present on any ECG, check "Yes".
Atria1 fibrillation/flutter has important implications for stroke, regardless of the "timing" issue. Therefore, if any ECGs have atria1 fibrillation/flutter, answer "Yes", even if the atria1 fibrillation/flutter became apparent after the stroke occurred. The only exception to this would be if AF occurred as part of a terminal process, i.e., minutes before death in a patient who previously had no record of cardiac arrhythmias.
Valvular heart disease. Other descriptions include:
Rheumatic heart disease - abbreviated RHD, R.Ht. dis; this includes rheumatic valvular disease of mitral, aortic, tricuspid or pulmonary valves.
Mitral valve disease - Mitral Stenosis, MS, or calcified mitral valve
Artificial - artificial heart or prosthetic heart valve (i.e., Starr Edwards Valve, Bjork Shiley valve). Do not include porcine heart valves here.
Subacute bacterial endocarditis. This is an infection of the heart, abbreviated as SBE, which may predispose to emboli. The patient likely would be treated with IV antibiotics. This must be specifically diagnosed by a physician to answer 'Yes". If patient has acute bacterial endocarditis (abbreviated ABE) or maurantic endocarditis, a "Yes" response is also indicated.
A-163
f. Systemic Rmboli are emboli to the systemic arterial circulation, i.e., limbs, brain, kidney. They are to be distinguished from pulmonary emboli, which go to the pulmonary circulation, i.e., lungs only. A renal embolus or a femoral artery embolus is a systemic embolus. Although a cerebral embolus is technically a systemic embolus, we are looking for evidence to support the diagnosis of cerebral embolism (the presence of other systemic emboli). Therefore, if cerebral embolus is the only type of embolus mentioned, answer this question "no". The origin of a systemic emboli may be the heart. If a "paradoxical embolus" (a systemic embolus arising "paradoxically" from the systemic veins and travelling through a septal defect in the heart) is noted in the chart, check "Yes".
Also, check "Yes" if a blood clot is documented blocking a blood vessel by angiography. Read any non-cerebral or non-pulmonary angiograms for documentation of embolus. "Rule out or possible embolus" only should be coded as "No". "Consistent with" or "probable embolus" should be coded as "Yes".
8. Hematologic Abnormality
Hypercoagulable states include promyelocytic leukemia, polycythemic Vera, dysproteinemias, or other blood conditions specifically termed hypercoagulable or described as causing hyperviscosity by a physician.
Hemorrhagic conditions include blood diseases that lead to defects in clotting, such as thrombocytopenia, leukemia, aplastic anemia, liver disease, vitamin K deficiency and anticoagulation therapy.* Hemorrhagic conditions may also be side effects from the use of anticancer drugs which destroy the bone marrow. You may also see the term "hemorrhagic diathesis" which means a tendency to bleed.
*Although anticoagulant drugs such as Heparin and Coumadin may cause a hemorrhagic condition, these are asked about specifically in 430. If they are the only reason for hematologic abnormality, answer this question "No". All other conditions listed above would be recorded as "Yes".
h. Brain tumor. Synonyms include neoplasm of brain, glioma, meningioma, astrocytoma, oligodendroglioma, pituitary adenoma, metastasis to brain, neuroma or subarachnoid cyst. Answer "Yes" if any of these are mentioned as being present by physician or in CT report. "Rule out brain tumor' with no evidence should be coded as "No". "Probable" or "consistent with brain tumor" should be coded as "Yes".
i. Trauma is described as blunt trauma to the head with LOC (loss of consciousness), contusion (brain), or concussion. Check the admitting history for mention of trauma.
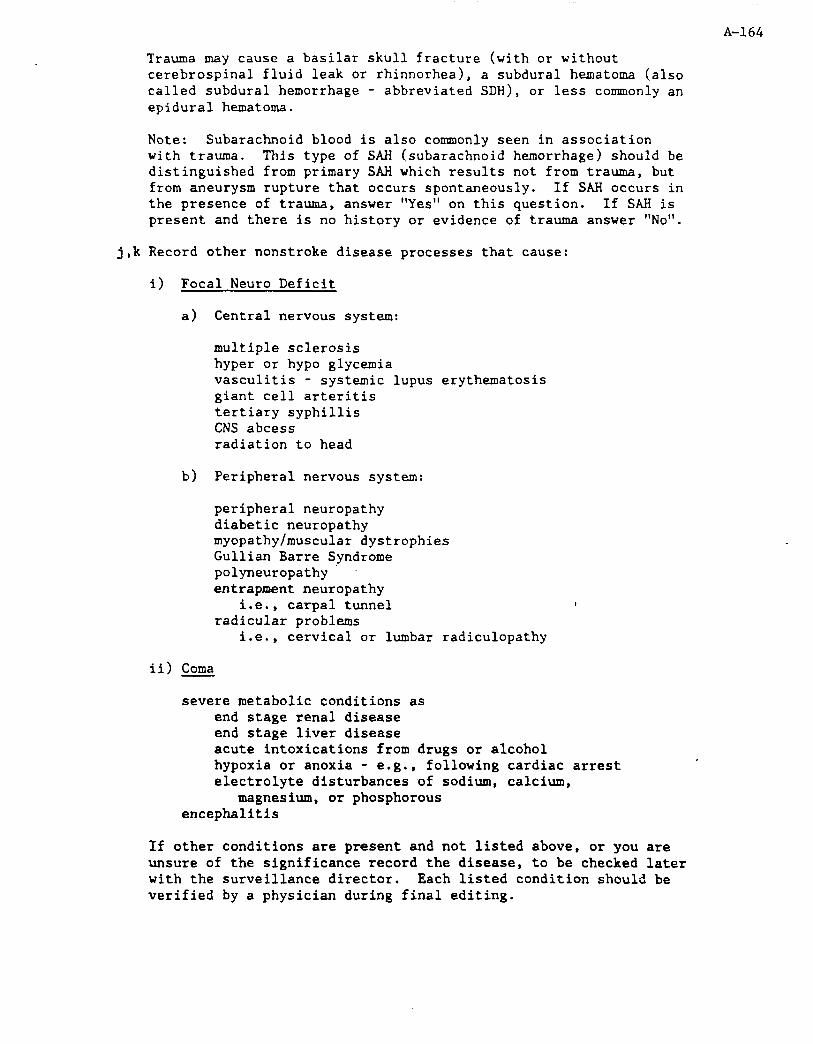
A-164
Trauma may cause a basilar skull fracture (with or without cerebrospinal fluid leak or rhinnorhea), a subdural hematoma (also called subdural hemorrhage - abbreviated SDH), or less commonly an epidural hematoma.
Note: Subarachnoid blood is also commonly seen in association with trauma. This type of SAH (subarachnoid hemorrhage) should be distinguished from primary SAH which results not from trauma, but from aneurysm rupture that occurs spontaneously. If SAH occurs in the presence of trauma, answer "Yes" on this question. If SAH is present and there is no history or evidence of trauma answer "No".
j,k Record other nonstroke disease processes that cause:
i) Focal Neuro Deficit
a) Central nervous system:
multiple sclerosis hyper or hypo glycemia vasculitis - systemic lupus erythematosis giant cell arteritis tertiary syphillis CNS abcess radiation to head
b) Peripheral nervous system:
peripheral neuropathy diabetic neuropathy myopathy/muscular dystrophies Gullian Barre Syndrome polyneuropathy entrapment neuropathy
i.e., carpal tunnel radicular problems . I.e., cervical or lumbar radiculopathy
ii) Coma
severe metabolic conditions as end stage renal disease end stage liver disease acute intoxications from drugs or alcohol hypoxia or anoxia - e.g., following cardiac arrest electrolyte disturbances .of sodium, calcium,
magnesium, or phosphorous encephalitis
If other conditions are present and not listed above, or you are unsure of the significance record the disease, to be checked later with the surveillance director. Each listed condition should be verified by a physician during final editing.

A-165
30. Procedures: The indicated procedures or treatments may lead to stroke. The first three procedures are invasive tests that could lead to clot formation or dislodgement of plaque, both of which may result in stroke. Answer "Yes" only if these procedures occurred prior to the neurologic event.
The same logic applies to treatment with anticoagulants such as Heparin, Warfarin, streptokinase, TPA (tissue plasminogen activator), or urokinase. These are anticoagulant medications which may lead to a hemorrhagic complication, such as cerebral (brain) hemorrhage. If anticoagulants are being used to treat something other than the acute neurologic syndrome that this form is evaluating, answer "Yes". If the patient presents with acute neurologic syndrome, and is placed on Heparin or Coumadin as treatment for this condition, answer "No". Synonyms and definitions of these medications are summarized below:
a. Cardiac catheterization. Catheter is placed in the heart chambers or coronary arteries for visualization. Also called coronary angiogram, coronary angiography.
b. Open heart surgery. Includes coronary artery bypass grafts (CAB or CABG), valve replacements or commisurotomy (mitral or aortic), repair of septal defect (ASD, patent foramen ovale).
c. Cerebral angiography. Also called cerebral angiogram, carotid angiography/angiogra, or 4 vessel angio. If only the carotids are visualized, this may be referred to as a 2 vessel angio. Also include vertebrobasilar angiograms.
d. Therapy with Heparin or Warfarin. This is "full dose" therapy, and does not include subcutaneous (SQ) Heparin.
31-46. The next series of questions is to determine the specific neurologic signs or symptoms of stroke. These symptoms may have occurred prior to hospitalization, and prompted the patient to seek medical care, or may have occurred while the patient was in the hospital for a different illness. If a symptom is present, additional questions may be asked regarding duration or affected body part. See each instruction below.
SEVERAL OF THE QUESTIONS, IF ANSWERED "YES", REQUIRE THAT ADDITIONAL INFORMATION MUST BE SPECIFIED. FOR MOST QUESTIONS, DISTINGUISH WHETHER THE DURATION OF SYMPTOMS FROM ONSET LASTED < 24 HOURS OR OVER 24 HOURS. IF THE PATIENT DIED, THE DURATION IS FROM ONSET TO DEATH. IF THE SAME SYMPTOM ~XME MORE sm (E.G., MARKED WEAKNESS PROGRESSING TO PGSIS), DO NOT JUDGE THE "WORSENING" TO BE A NEW SYMPTOM: DURATION STILL SHOULD BE FROM ONSET OF 0RIGlXA.L COMPLAINT. IF THE PATIENT'S SYMPTOMS RESOLVED, DURATION IS FROM ONSET UNTIL COMPLETE RESOLUTION. PARTIAL RESOLUTION SHOULD BE DISREGARDED FOR CALCULATING DURATION.
31. Headache. The occurrence headache should be described as part of the history. We are interested in headaches that are acute in onset or
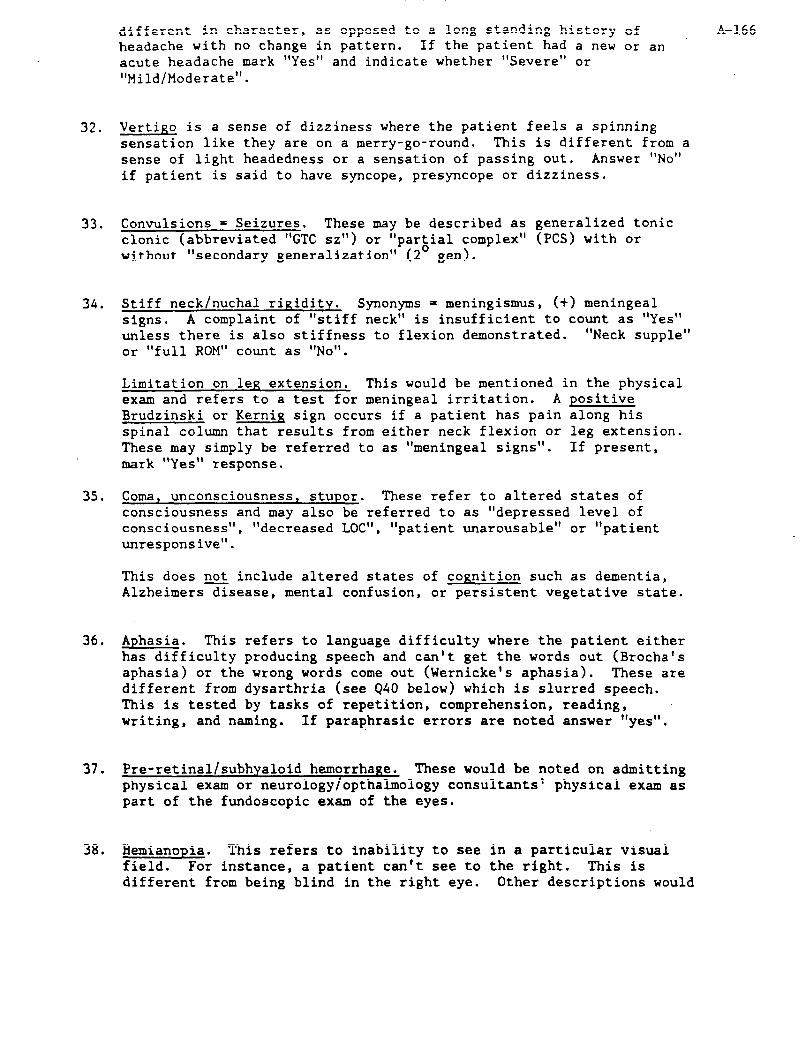
different in character, as opposed to a long standing history of headache with no change in pattern. If the patient had a new or an acute headache mark "Yes" and indicate whether "Severe" or "Mild/Moderate".
A-166
32. Vertigo is a sense of dizziness where the patient feels a spinning sensation like they are on a merry-go-round. This is different from a sense of light headedness or a sensation of passing out. Answer "NO" if patient is said to have syncope, presyncope or dizziness.
33. Convulsions = Seizures. These may be described as generalized tonic clonic (abbreviated "GTC sz") or "partial complex" (PCS) with or without "secondary generalization" (2' gen).
34. Stiff neck/nuchal rigidity. Synonyms = meningismus, (+) meningeal signs. A complaint of "stiff neck" is insufficient to count as "Yes" unless there is also stiffness to flexion demonstrated. "Neck supple" or "full ROM" count as "No".
Limitation on leg extension, This would be mentioned in the physical exam and refers to a test for meningeal irritation. A positive Brudzinski or Kerniq sign occurs if a patient has pain along his spinal column that results from either neck flexion or leg extension. These may simply be referred to as "meningeal signs". If present, mark "Yes" response.
35. Coma, unconsciousness, stupor. These refer to altered states of consciousness and may also be referred to as "depressed level of consciousness", "decreased LOCI', "patient unarousable" or "patient unresponsive".
This does not include altered states of cognition such as dementia, Alzheimersdisease, mental confusion, or persistent vegetative state.
36. Aphasia. This refers to language difficulty where the patient either has difficulty producing speech and can't get the words out (Brocha's aphasia) or the wrong words come out (Wernicke's aphasia). These are different from dysarthria (see 940 below) which is slurred speech. This is tested by tasks of repetition, comprehension, reading, writing, and naming. If paraphrasic errors are noted answer "yes",
37. Pre-retinal/subhyaloid hemorrhage. These would be noted on admitting physical exam or neurology/opthalmology consultants' physical exam as part of the fundoscopic exam of the eyes.
38. Hemianopia. This refers to inability to see in a particular visual field. For instance, a patient can't see to the right. This is different from being blind in the right eye. Other descriptions would
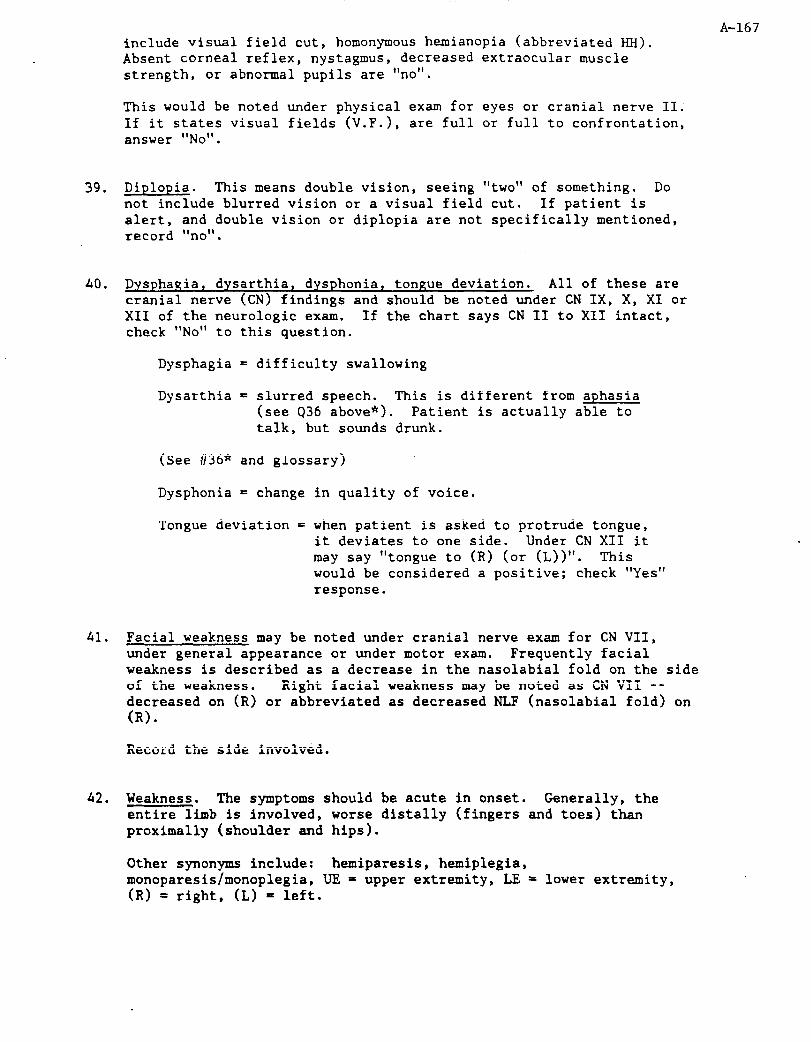
include visual field cut, homonymous hemianopia (abbreviated HH). Absent cornea1 reflex, nystagmus, decreased extraocular muscle strength, or abnormal pupils are "no".
This would be noted under physical exam for eyes or cranial nerve II. If it states visual fields (V.F.), are full or full to confrontation, answer "No".
39. Diplopia. This means double vision, seeing "two" not include blurred vision or a visual field cut.
of something. Do If patient is
ifically mentioned, alert, and double vision or diplopia are not spec record "no".
40. Dysphagia, dysarthia, dysphonia, tongue deviation. All of these are cranial nerve (CN) findings and should be noted under CN IX, X, XI or XII of the neurologic exam. If the chart says CN II to XII intact, check "No" to this question.
Dysphagia = difficulty swallowing
Dysarthia = slurred speech. This is different from aphasia (see 936 above*). Patient is actually able to talk, but sounds drunk.
(See #36* and glossary)
Dysphonia = change in quality of voice.
Tongue deviation = when patient is asked to protrude tongue, it deviates to one side. Under CN XII it may say "tongue to (R) (or (L))". This would be considered a positive; check "Yes" response.
41. Facial weakness may be noted under cranial nerve exam for CN VII, under general appearance or under motor exam. Frequently facial weakness is described as a decrease in the nasolabial fold on the side of the weakness. Right facial weakness may be noted as CN VII -- decreased on (R) or abbreviated as decreased NLF (nasolabial fold) on (RI.
Record the side involved.
42. Weakness. The symptoms should be acute in onset. Generally, the entire limb is involved, worse distally (fingers and toes) than proximally (shoulder and hips).
A-167
Other synonyms include: hemiparesis, haiplegia, monoparesis/monoplegia, UE = upper extremity, LE = lower extremity, (RI = right, (L) = left.

A-168
If there is weakness, paresis, or paralysis, record the affected limb and duration. "Arm" refers to any part of the extremity, including fingers or hand. Similarly "leg" includes any part of the lower extremity such as toes and/or foot.
Most grading systems for strength are on a scale of 0.5, where 5+ is normal. Asymmetric differences in extremity strength or anything < 5 is abnormal.
43. Fat ial numbness. May involve one whole side of face or just the cheek and chin. Perioral numbness means numbness.around the mouth and would be considered a positive response, unless there was evidence that the patient was hyperventilating.
Record the side affected.
44. Loss of sensation. This may be described as numbness, marked tingling, or abnormal sensation. We are interested in acute, not chronic, unchanged sensations. Generally, the entire limb is involved, worse distally (fingers and toes) than proximally (hips and shoulder).
Other synonyms include: hemianesthesia, parasthesias, analgesia.
UE= uPPer extremity, LE = lower extremity, (R) = right, (L) = left
If there is a sensation deficit, record the affected limb and duration. If intermittent, estimate the total duration of deficit.
45. Gait disturbance. Here we are looking primarily for ataxic or staggering gait. This would be described under cerebellar or coordination portion of neurologic exam. We are interested in acute changes that have occurred in gait, not chronic problems.
Answer "No" for patients with: Parkinson's Disease and shuffling gait, hemiparetic gait (but answer "Yes" for weakness), foot drop.
If not tested, check "No".
46. Other neurologic symptoms: apraxia, acalculia; agnosias - prosopagnosia, topograghnosia, finger agnosia; acalculia; agraphia; neglect syndrome; bulbar or pseudobular palsy; dysconjugate gaze; decerebratejdecorticate posturing; hyperreflexia, babinski absent cornea1 reflex.
The following would not be included: dizziness; blurred vision; pain syndromes; delirium;frontal release signs, confusion, dementia.

A-169 47. Lumbar puncture (L.P.) Also called "spinal tap", "spinal" or "tap".
Check physician progress notes for procedure note, as well as laboratory results, for first nontraumatic LP after onset of symptoms. Use results of first LP, if all traumatic. If a report is available, check "Yes"; if none, check "No". Record date.
If physician states LP was traumatic, check "Yes". Check the appropriate box for appearance and RBCs. If two tubes were sent for cell counts, please record results of both. Record the results of the first tube sent under Tube 1 (even if Tube 112 was actually sent first), and the results from the last tube sent under Tube 2. For example, frequently tubes 1 and 4 are sent for cell counts. Record this under Tube 1 and Tube 2, respectively. If only one tube was counted, record the results under Tube 1 regardless of what number the tube was. Note: These results apply to only one spinal tap. If more than one LP was performed, choose the first nontraumatic tap only.
478. Record L.P. diagnosis. Refer to Appendix 2.
48. Cerebral angiogram. Indicate if done. If this procedure was performed more than once, use the report you judge to be most pertinent for this case (i.e., the one most helpful to arrive at a diagnosis).
48~. Record angiography diagnosis. Refer to Appendix 2.
48d,e. Record maximum stenosis for right and left internal carotid.
49. and 50. CT Scan (first) and CT Scan (last). This would include ACTA,
49d,
51.
51d.
52.
EN, CT, CAT scans, but not brain scans of the nuclear imaging (radionuclide) type. Indicate if done. If so, mark appropriate time sequence on form to relate CT to onset of symptoms. Record whether contrast was used. If performed immediately "following cerebral angiography" then contrast
50d. Record first and last CT diagnosis. Refer to Appendix 2.
Prehospital CTs. There may be evidence of other CT(s) performed prior to this admission but after the onset of the neurologic event. The interpretation might be recorded in the physician's or consultant's progress notes, or a formal report of that CT may be in the chart. Frequently, outside CT Scans will be officially read by the radiologist at the second hospital and dictated as if it were done there, Identify this report by comparing the date of scan to the date of admission. If "Yes", complete Items b - d.
Record Pre-admission CT diagnosis. Refer to Appendix 2.
Magnetic Resonance Imaging. Again, if done, it is important to note the interval between symptom onset and MRI. If this procedure was performed more than once use the report you

judge to be most pertinent for this case (i.e., the one most helpful to arrive at a diagnosis).
52d. Record MRI diagnosis. Refer to Appendix 2.
53. B-Mode/Doppler. Also frequently referred to as "noninvasive studies" (of carotids). If done, indicate the test performed and copy report or attach copy in space provided. If this procedure was performed more than once, use the report you judge to be most pertinent for this case (i.e., the one most helpful to arrive at a diagnosis). Another term for B-mode is "real time" scan.
53c,d. Record Ultrasound diganosis for left and right internal carotid. Refer to Appendix 2.
54. Craniotomy. This is any operation performed by a neurosurgeon that involves opening the skull. This might be done to evacuate/remove a hematoma, clip an aneurysm, or relieve intracranial pressure, etc. If this procedure was performed more than once, use the report you judge to be most pertinent for this case (i.e., the one most helpful to arrive at a diagnosis).
54~. Record Craniotomy diagnosis.
55. Autopsy. May be referred to as "post-mortem exam" or "post". First check to see if patient died. If so, in Death Note (last progress note in chart), it should state if permission for autopsy was granted. If so, an Autopsy Form is needed.
SSb-f. Record Autopsy diagnosis.
56.
57.
58.
MD Diagnosis Impression: (see Appendix 5 or Manual 2, pages 107-113)
Abstractor Number: This is the code number assigned to you. It should be filled in each time a chart is abstracted, even one that is ineligible. Double check that your code number has been written in for all the ineligibles since this is a common error.
Date Abstracted: Fill in the date that the medical record was abstracted. Follow the procedure indicated in the General Instructions.
A-170
59-62. Record additional forms required by circling the capital letter corresponding to each form required.
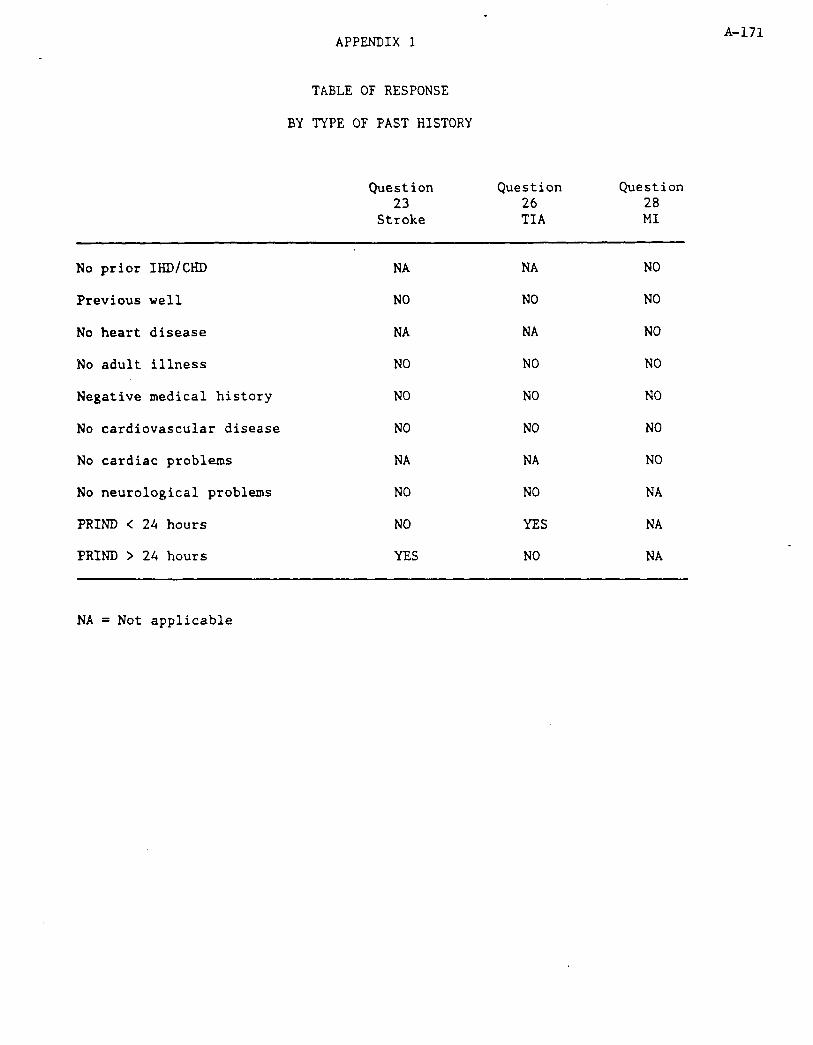
.
APPENDIX 1
TABLE OF RESPONSE
BY TYPE OF PAST HISTORY
Question Question 23 26
Stroke TIA
Question 28 MI
No prior IHD/CHD
Previous well
No heart disease
No adult illness
Negative medical history
No cardiovascular disease
No cardiac problems
No neurological problems
PRIND < 24 hours
PRIND > 24 hours
NA
NO
NA
NO
NO
NO
NA
NO
NO
YES
NA
NO
NA
NO
NO
NO
NA
NO
YES
NO
NO
NO
NO
NO
NO
NO
NO
NA
NA
NA
A-171
NA = Not applicable

A-172
APPENDIX 2
MD Instructions for Stroke Codes
Physician review is required for coding of procedures performed to assist in making the diagnosis of stroke and cerebral hemorrhage. You will record results of specific tests and diagnoses into the space provided on Questions 47-54. Review the available data and enter the appropriate diagnostic code in Items 47g, 48c, 49d, 50d, 51d, 52d, 53c-d, and 54~. A complete list of diagnostic definitions is attached. In addition, there are specific examples and instructions for each code on the following pages.
Some similarities exist for all procedure codes except autopsy. For instance, any "normal study" will be coded as A (except for a normal CT done within 24 hours of symptom onset). In addition, there will be two possible responses for "nonstroke" pathology for each procedure. The first will include "exclusionary findings". These refer to specific diagnoses, whose presence would eliminate a possible stroke case from analysis. These include disease processes such as CNS tumor, infection, vasculitis and head trauma which may mimic stroke by producing focal neurologic signs and symptoms. These exclusions are described on the last page of the stroke criteria and mentioned specifically under each procedure below. Exclusionary diagnoses are coded as B for all procedures. The second type of nonstroke pathology includes all other types of unrelated findings and should only be coded if none of the other categories apply. This category is called "unrelated pathology" and coded C for all procedures with the exception of autopsy.
L.P.
A Normal study. All of the following must be true, if the specified test was performed:
spinal fluid is clear and colorless
WBC < 10, at least 90X mononuclear unless traumatic, then expect 1 WBC:700 RBC
protein normal
glucose normal
RBC should be < 100; unless traumatic; then must decrease between 1st and last tube. Clotted blood indicates traumatic tap as well.
Other studies done, should be normal. This includes cultures, AFB, cryptoantigen, myelin basic protein, oligoclonal bands, protein electrophoresis.

B Exclusionary criteria include: A-173
infection - increased WBC without evidence of old hemorrhage; (+) cultures; (t) AFB, (t) VDRL, or (+) crypt0 antigen
Neoplasm - (+) cytology with or without increased protein
C Unrelated pathology includes:
traumatic tap - grossly bloody or pinked tinged fluid that clears by final tube. Associated with proportionate increased WBC (1:700 CBC) and increased protein
D Bloody, Nontraumatic; xanthochromia
Angiography
A Normal study - no abnormalities identified
B Exclusionary pathology
Neoplasm - may be described as tumor blush or displacement of vessels due to "avascular mass"
Vasculitis - including moya moya
Subdural hematoma
Ruptured AVM
C Unrelated pathology:
Unruptured aneurysm or AVM
Carotid artery stenosis/ulceration
Vertebrobasilar artery disease - including stenosis/tortuousity
D Aneurysm - this should be described in vicinity of recent hemorrhage or associated with clot.
E Avascular mass without evidence ruptured aneurysm/AVM
Stenosis: Fill in appropriate code for both right (10-14) and left (20-24) internal carotlds. If more than one lesion, select most stenotic plaque within internal carotid.

-
Computerized Tomography (CT)
A Normal study - must check timing to determine when study was done in relation to symptom onset. If 5 48 hours and normal, code 04.
B Exclusionary pathology includes
tumor; evidence of trauma such as fractured bones, coup and contrecoup injuries, soft tissue swelling over area of hematoma; subdural hematoma, epidural hematoms, and abcess or granuloma.
C Unrelated pathology or findings include
old stroke
generalized atrophy, encephomalacia
hydrocephalus
normal variants - cavum septum pellucidurn, calcification of falx/tentorim
D Normal study, but done within 48 hours of symptom onset.
E Subarachnoid hemorrhage - blood seen in Fissure of Sylvius, between the frontal lobes, in basal cisterns or within a ventricle with no associated intraparenchymal hematoma
F Intracerebral hematoma - blood clot within the brain parenchyma. Occasionally these occur within secondary rupture into the ventricle or subarachnoid space. "Hypertensive" or "spontaneous hemorrhage" would be included. Typical locations include basal ganglia, cerebellum, thalamus and pons.
G Ischemic infarction - these are described as areas of low density (attenuation) in a typical vascular distribution. There should be no evidence of hemorrhage or subarachnoid hemorrhage.
&- see CT. Also exclusionary pathology includes M.S. plaques.
A-174
U.S. - to follow
Craniotomy
A Normal
A-175
B Exclusionary pathology includes
tumor, subdural hematoma, epidural hematoma, trauma, abcess, AVM
C Unrelated pathology - includes incidental aneurysm/AVM
D Ruptured aneurysm - should describe evidence for recent bleed, or clot
E Intracerebral hematoma - if source is related to ruptured aneurysm, code 04,. If there is no apparent source and blood is primarily intraparenchymal, code 05.
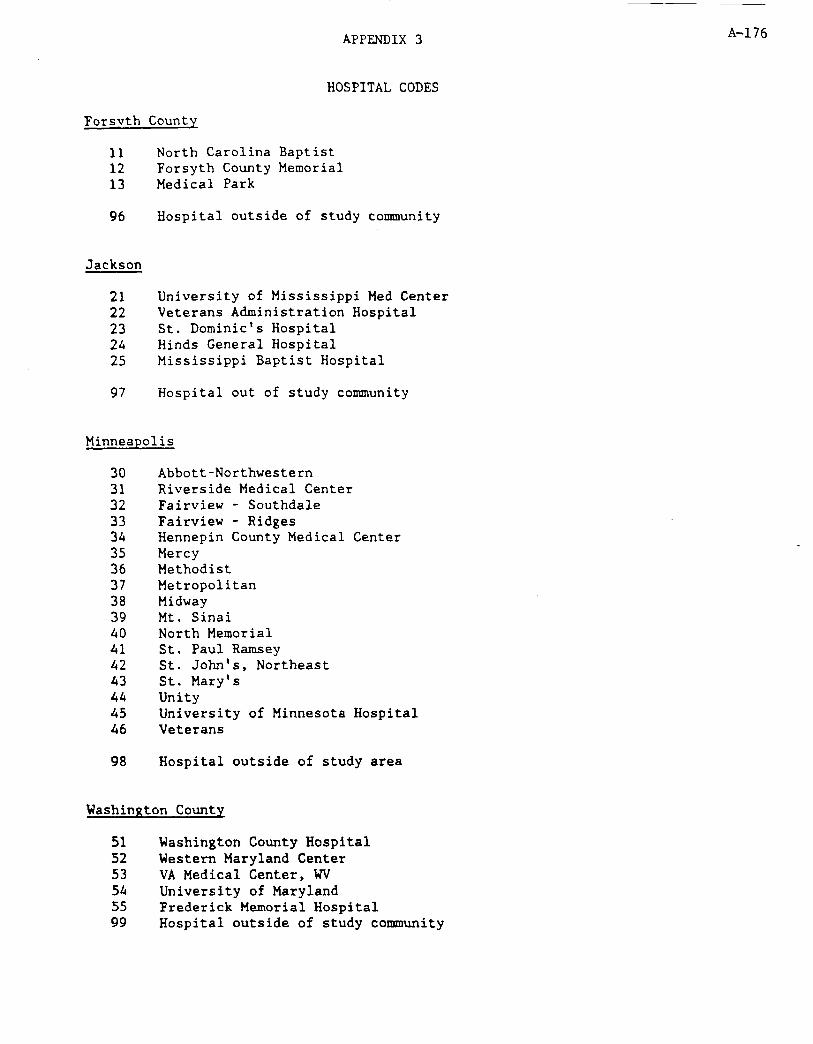
APPENDIX 3
HOSPITAL CODES
A-176
Forsvth County
11 North Carolina Baptist 12 Forsyth County Memorial 13 Medical Park
96 Hospital outside of study community
Jackson
21 University of Mississippi Med Center 22 Veterans Administration Hospital 23 St. Dominic's Hospital 24 Hinds General Hospital 25 Mississippi Baptist Hospital
97 Hospital out of study community
Minneapolis
30 Abbott-Northwestern 31 Riverside Medical Center 32 Fairview - Southdale 33 Fairview - Ridges 34 Hennepin County Medical Center 35 Mercy 36 Methodist 37 Metropolitan 38 Midway 39 Mt. Sinai 40 North Memorial 41 St. Paul Ramsey 42 St. John's, Northeast 43 St. Mary's 44 Unity 45 University of Minnesota Hospital 46 Veterans
98 Hospital outside of study area
Washinffton County
51 Washington County Hospital 52 Western Maryland Center 53 VA Medical Center, WV 54 University of Maryland 55 Frederick Memorial Hospital 99 Hospital outside of study community

APPENDIX 4
COMA
A-177
In general, the coma exam is very simple. Most neurologists will comment on five things:
1) Level of consciousness - (stupor, lethargy, coma: i.e., Item 35).
2) Pupillary position and reactivity -- (not on stroke form - can put under Item 46 "Other")
3) Extraocular response -- to either Doll's maneuver or ice water (not on stroke form may list under Item 46 as "Other")
4) Tone and posturing (list under Item 46)
5) Breathing pattern (List under Item 46)
Only one of these five points are considered in the stroke form.
What is more important when coma is present is how to interpret the other symptoms requested by the stroke form. As a general rule, a person in a coma in unable to experience symptoms. This includes headache, vertigo and double vision, etc. Most signs are unable to be elicited because of the comatose state. For instance, if someone is in a coma, he/she cannot talk. An examiner, (physician, etc.) therefore cannot assess whether or not a comatose patient is aphasic. Therefore, the correct response for aphasia during coma is unknown, which is recorded as "No."
On some occasions, focal signs are obvious -- even in coma. If a patient is spontaneously moving one side of his body, or withdraws to stimuli on one side but not the other; this asymmetry would constitute hemiparesis, or weakness on one side. On a Q by Q basis, the following principles apply when coma is present:
31) HA at onset - may be present prior to coma onset.
32) Vertigo - may be present prior to coma.
33) Seizures - these may occur at any time in association with CNS injury. Please note, however, that deceases LOC is normal following a seizure and is called a "postictal" state. If the "coma" under consideration refers only to the postictal state mark "No" under coma .
34) Meningeal Signs - these can be tested and determined despite the presence of coma. If present, mark "Yes".
36) Aphasia - in the setting of coma this cannot be assessed. Always
mark "no" unless there is evidence of aphasia prior to or following coma. In all other circumstances mark "No".
,’ .-

38) Hemianopia - cannot be tested if patient is comatose. In stupor A-178
or lethargy, if there is asymmetry in response to visual threat, mark "Yes".
39) Diplopia - it is common for semi-comatose p;atients to have "dysconjugate gaze". Do not consider this "yes" unless the patient, prior to or following coma, was able to complain of double vision.
40) Dysphagia/Dysarthria/Dysphonia - cannot test in coma. Ignore absent gag reflex when there is coma.
41) Weakness of face - Central VII may be mentioned and can be recorded. Otherwise mark."No" when there is coma.
42) Weakness of limbs - mark "Yes" in coma only if there is asymmetry in response to painful stimuli and spontaneous movements.
43) Facial sensation - probably not testable when there is coma unless specifically established by clinician.
44) Sensory loss of limbs - answer "Yes" in coma only if there is obvious asymmetry between sides. This may be difficult to distinguish from weakness. If the patient Brimaces to pain on one side and withdraws on that side, but has no response to pain on the other side (no withdraw1 and no grimaces) mark "Yes".
45) Gait - obviously cannot be tested in comatose patient - mark "No".

A-179
APPENDIX 5
3.3.2 Stroke
This section describes the ARIC diagnostic criteria used to define strokes. Stroke is broadly defined as a clinical syndrome consisting of a constellation of neurological findings, sudden or rapid in onset, which persist for more than 24 hours or lead to death. This definition excludes events whose neurologic findings are due to traumatic, metabolic, toxic, vasculitic, neoplastic, or infectious processes of the central nervous system. Based upon objective diagnostic or pathologic findings, strokes are subcategorized into five major categories: (1) Subarachnoid hemorrhage, (2) Brain hemorrhage, (3) Brain infarction, thrombotic, (4) Brain infarction, embolic, and (5) Stroke of undetermined type.
3.3.2.1 Definite Subarachnoid Hemorrhage (SK-i)
Evidence in the patient’s clinical record of sudden or rapid onset of neurologic symptoms lasting for more than 24 hours or leading to death, plus must meet the criteria specified under at least one of the four paragraphs below:
ARIC PROTOCOL 2. Cohort Component Procedures Version 2.0 l/88
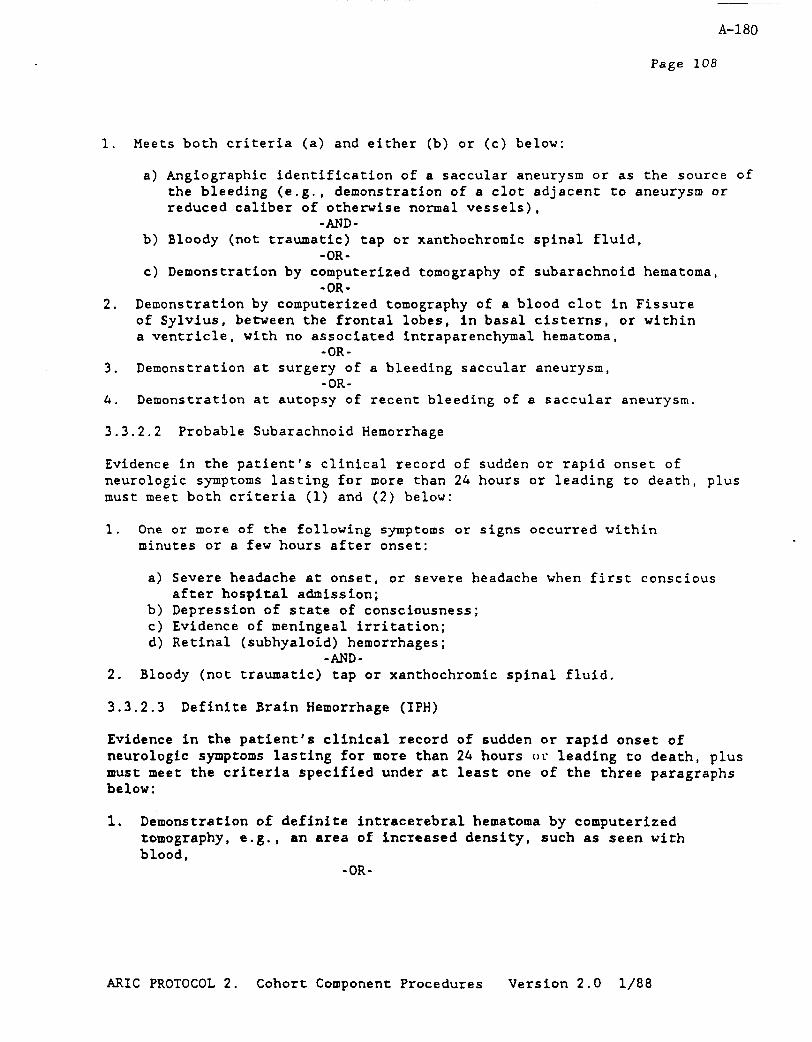
A-180
Page 108
Meets both criteria (a) and either (b) or (c) below:
of
. Demonstration by computerized tomography of a blood clot in Fissure of Sylvius, between the frontal lobes, in basal cisterns, or within a ventricle, with no associated intraparenchymal hematoma,
-OR- a. Demonstration at surgery of a bleeding saccular aneurysm,
-OR-
a) Angiographic identification of a saccular aneurysm or as the source the bleeding (e.g., demonstration of a clot adjacent to aneurysm or reduced caliber of otherwise normal vessels),
-AND- b) Bloody (not traumatic) tap or xanthochromic spinal fluid,
-OR- c) Demonstration by computerized tomography of subarachnoid hematoma,
-OR-
4. Demonstration at autopsy of recent bleeding of a saccular aneurysm.
3.3.2.2 Probable Subarachnoid Hemorrhage
Evidence in the patient's clinical record of sudden or rapid onset of neurologic symptoms lasting for more than 24 hours or leading to death, plus must meet both criteria (1) and (2) below:
1.
2.
One or more of the following symptoms or signs occurred within minutes or a few hours after onset:
a) Severe headache at onset, or severe headache when first conscious after hospital admission;
b) Depression of state of consciousness; c) Evidence of meningeal irritation; d) Retinal (subhyaloid) hemorrhages;
-AND- Bloody (not traumatic) tap or xanthochromic spinal fluid.
3.3.2.3 Definite Brain Hemorrhage (IPH)
Evidence in the patient's clinical record of sudden or rapid onset of neurologdc symptoms lasting for more than 24 hours oc leading to death, plus must meet the criteria specified under at least one of the three paragraphs below:
1. Demonstration of definite intracerebral hematoma by computerized tomography, e.g., an area of increased density, such as seen with blood,
-OR-
AIUC PROTOCOL 2. Cohort Component Procedures Version 2.0 l/88

A-181
Page 109
2. Demonstration at autopsy or surgery of intracerebral hemorrhage, -OR-
3. Evidence in the patient's clinical record that meet criteria (a), (b), (~1, and (d) below:
a) One major or two minor neurological signs or symptoms from the following list that lasted at least 24 hours or until the patient died:
o Hemiparesis involving two or more body parts o Unilateral numbness involving two or more body parts o Homonymous hemianopia o Aphasia
Hinor o Diplopia o Vertigo or gait disturbance o Dysarthia or dysphagia or dysphonia
-AND- b) Bloody (not traumatic tap) or xanthochromic spinal fluid,
-AND- c) Cerebral angiography demonstrates an avascular mass effect and
no evidence of aneurysm or arteriovenous malformation, -AND-
d) No computerized tomography was performed or the CT was technically inadequate.
3.3.2.4 Probable Brain Hemorrhage
Evidence in the patient's clinical record of sudden or rapid onset of neurologic symptoms lasting for more than 24 hours or leading to death, plus must meet all criteria (l), (2), (3) and (4) below:
1. One major ox two minor neurological signs or symptoms listed in Section 3.3.2.3, No. 3 above that lasted at least 24 hours or until the patient died,
-AND- 2. Decreased level of consciousness or coma that lasted at least 24
hours or until the patient died, -AND-
3. Bloody (not traumatic tap) or xanthochromic spinal fluid, -AND-
4. No computerized tomography was performed or the CT was technically inadequate.
3.3.2.5 Definite Brain Infarction, Thrombotic (TIB)
Evidence in the patient's clinical record of sudden or rapid onset of neurologic symptoms lasting for more than 24 hours or leading to death, plus must meet the criteria specified under at least one of the two paragraphs
ARIC PROTOCOL 2. Cohort Component Procedures Version 2.0 i/88

A-182
Page 110
below:
1. Demonstration at autopsy of nonhemorrhagic infarct in brain, -OR-
2. Evidence in the patient's clinical record that meet criteria (a), and (b) below:
a> One major or two minor neurological signs and symptoms that lasted at least 24 hours or until the patient died:
b)
3.3.2.6
o Hemiparesis involving two or more body parts o Unilateral numbness involving two or more body parts o Homonymous hemianopia o Aphasia
Binor o Diplopia o Vertigo or gait disturbance o Dysarthia or dysphagia or dysphonia
-AND- Computerized tomography shows an area of decreased density which may indicate edema or ischemia, with no evidence of hemorrhage, or "infarct" on CT report.
Probable Brain Infarction, Thrombotic
Evidence in the patient's clinical record of sudden or rapid onset of neurologic symptoms lasting for more than 24 hours or leading to death, plus must meet all criteria (l), (2), and (3) below:
1. One major or two minor neurological signs or symptoms listed in Section 3.3.2.5 (a) above that lasted at least 24 hours or until the patient died,
-AND- 2. Demonstration of negative or nonspecific findings and no evidence of
hemorrhage by computerized tomography performed in the first 48 hours after the onset of symptoms or signs,
-AND- 3. A spinal tap was either not done, or was a traumatic tap, or
yielded clear, colorless spinal fluid.
3.3.2.7 Definite Brain Infarction, Embolic (EIB)
Evidence in the patient's clinical record of sudden or rapid onset of neurologic symptoms lasting for more than 24 hours or leading to death, plus must meet the criteria specified under at least one of the two paragraphs below:
ARIC PROTOCOL 2. Cohort Component Procedures Version 2.0 l/88
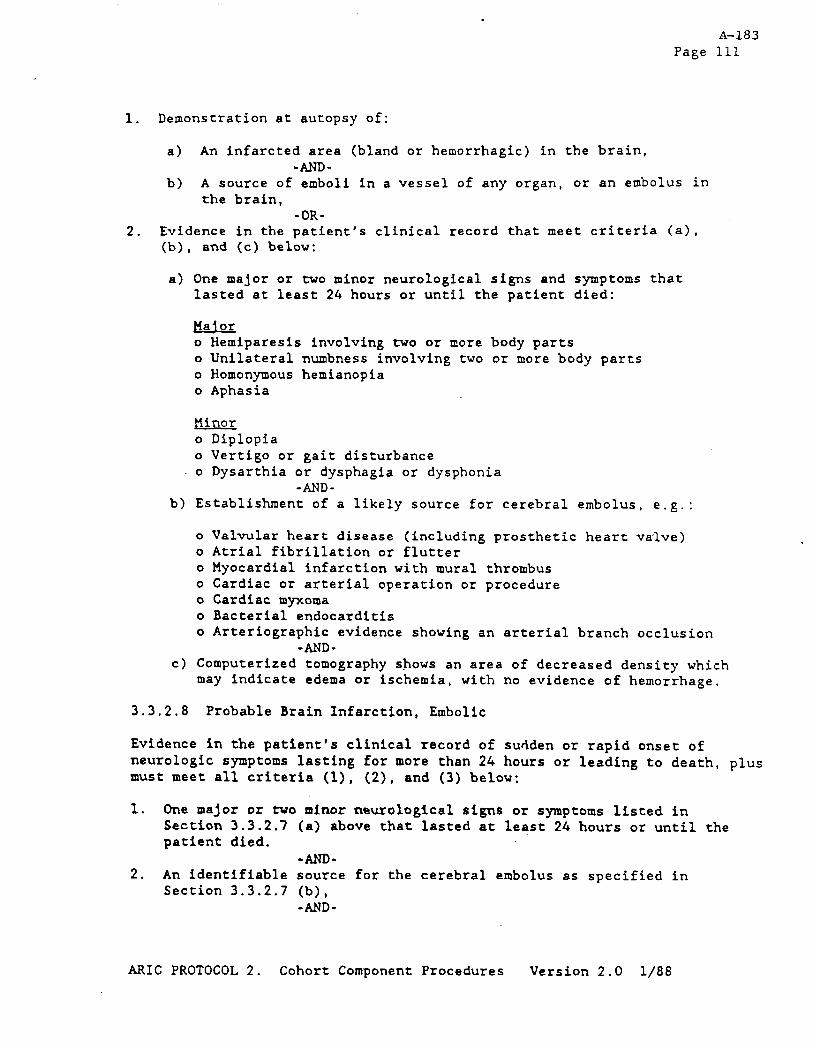
1. Demonstration at autopsy of:
A-183 Page 111
a> An infarcted area (bland or hemorrhagic) in the brain, -AND-
b) A source of emboli in a vessel of any organ, or an embolus in the brain,
-OR- 2. Evidence in the patient's clinical record that meet criteria (a),
(b), and (c) below:
a) One major or two minor neurological signs and symptoms that lasted at least 24 hours or until the patient died:
Pia! or o Hemiparesis involving two or more body parts o Unilateral numbness involving two or more body parts o Homonymous hemianopia o Aphasia
Hinor o Diplopia o Vertigo or gait disturbance o Dysarthia or dysphagia or dysphonia
-AND- b) Establishment of a likely source for cerebral embolus, e.g.:
Valvular heart disease (including prosthetic heart valve) Atria1 fibrillation or flutter Myocardial infarction with mural thrombus Cardiac or arterial operation or procedure Cardiac myxoma Bacterial endocarditis Arteriographic evidence showing an arterial branch occlusion
-AND- c) Computerized tomography shows an area of decreased density which
may indicate edema or ischemia, with no evidence of hemorrhage.
3.3.2.8 Probable Brain Infarction, Embolic
Evidence in the patient's clinical record of sudden or rapid onset of neurologic symptoms lasting for more than 24 hours or leading to death, plus must meet all criteria (l), (2), and (3) below;
1. One major or two minor neurological signs or symptoms listed in Section 3.3.2.7 (a) above that lasted at least 24 hours or until the patient died.
-AND- 2. An identifiable source for the cerebral embolus as specified in
Section 3.3.2.7 (b), -AND-
ARIC PROTOCOL 2. Cohort Component Procedures Version 2.0 l/88

A-184
Page 112
3. Demonstration of negative or nonspecific findings and no evidence of hemorrhage by computerized tomography performed in the first 48 hours after the onset of symptoms or signs,
3.3.2.9 Possible Stroke of Undetermined Type
Evidence in the patient's clinical record of sudden or rapid onset of at least one major or two minor signs and symptoms that lasted more than 24 hours or until the patient died:
o Hemiparesis involving two or more body parts o Unilateral numbness involving two or more body parts o Homonymous hemianopia o Aphasia
Binor o Diplopia o Vertigo or gait disturbance o Dysarthia or dysphagia or dysphonia o Severe headache at onset, or severe headache when first
conscious after hospital admission; o Depression of state of consciousness: o Evidence of meningeal irritation; o Retinal (subhyaloid) hemorrhages; o Palsy of the iii cranial nerve;
-AND-
Clinical history, signs, symptoms and findings from diagnostic tests and/or autopsy are not sufficient to meet the criteria for classifying the case as a "Definite" or "Probable" case of one of the four specific diagnostic categories of stroke.
3.3.2.10 Undocumented Fatal Stroke
Must meet the following criteria:
1. Does not meet criteria for definite, probable, or possible stroke noted above
-AND- 2. Underlying cause of death consistent with stroke (i.e. ICDA9:
430~438), but death occurred without hospitalization or hospital chart cannot be located.
3.3.2.11 Exclusionary Conditions for Diagnostic Criteria for Stroke
Cases are not considered a stroke if there is evidence in the patient's clinical record that the neurologic symptoms were the result of any of the following:
ARIC PROTOCOL 2. Cohort Component Procedures Version 2.0 l/88
1.
2.
3.
4.
5.
6.
7.
A-185
Page 113
Major head (brain) trauma; e.g., epidural hematoma, subdural hematoma, skull fracture
Neoplasm; e.g., primary or metastatic brain/CNS neoplasia (malignant or benign)
Coma due to metabolic disorders or disorders of fluid or electrolyte balance; .e.g., due to diabetes, hypoglycemia, epilepsy, hypovolemia, poisoning, drug overdose, uremia, or liver disease
Vasculitis involving the brain; e.g., SLE, radiation, etc.
Peripheral neuropathy
Hematologic abnormalities (considered exclusionary if present prior to event under consideration); e.g., DIG, thrombocytopenia, Heparin or Coumadin therapy
CNS infection: brain abcess, granulomas, meningitis, encephalitis, or any specific infection involving the brain or meninees.
ARIC PROTOCOL 2. Cohort Component Procedures Version 2.0 l/88

A-186
Page 114
Table 3. Stroke Diagnosis Summary for ARIC Cohort Study1
Specific Embolic CT Lumbar Category Symptoms Source Scan Angiogram Puncture Pathology
Subarachnoid Hemorrhaee iI "
Definite a. or b. or c.
Probable
Brain Hemorrhave
Definite a. w H or b. + or c. + s 0 + +
Probable 4-k 0 +
&rain Infarction. Thrombotic
Definite a. or b.
Probable
+ + e I + - N -
Brain Infarction. Embollc
Definite a. or b.
Probable
+ + + + I + + + N -
Stroke of Undetermined TvDe
Possible + +
Undocumented Fatal Stroke
Unconfirmed out-of-hospital stroke death (ICD9 430-38)
+ - present/positive - - absent 0 - either one must be present H - CT shows hemorrhage S - CT shows SAH I - CT shows infarction 0 - CT not helpful N - CT within 48 hours is negative
lAl1 strokes must have neurologic finding(s) lasting at least 24 hours or until death, and no nonvascular cause.
ARIC PROTOCOL 2. Cohort Component Procedures Version 2.0 l/88
GLOSSARY A&87
Acalculia: loss of ability to do math reckoning.
Adiadochokinesia: inability to perform rapidly alternating movements.
Agraphia: inability to write.
Alexia or Visual Aphasia: loss of ability to understand written word.
auditory: lack of comprehension of spoken word
argon or pharaphasia: words may be fluent but inappropriate
amnesic: loss of memory of special words with hesitant and fragmentary speech
nominal aphasia: (anemia, dysnomia) - loss of ability to name objects
semantic aphasia: loss of meaning of words
Amaurosis fugax: monocculer (one eye) transient blindness.
Analgesia: loss of pain sensation.
Aneurysm: saccular dilation of blood vessel. If it ruptures, it causes SAH.
Anisocoria: inequality of the diameter of pupils.
Anosmia: loss of smell.
Anoxia: lack of oxygen which can cause tissue damage if prolonged.
Aphasia: inability to express oneself properly through speech or loss of verbral comprehension
Apraxia: inability to perform certain movements without loss of motor power, sensation or coordination; loss of learned behavior, e.g., dressing (inability to dress oneself).
Astereognosis: loss of ability to recognize common objects by touching and handling them with eyes closed.
Atrophy: loss of tissue.
Autotopagnosia: inability to recognize one's self or part of one's self.
AVM: ateriovenous malformation - abnormal collection of blood vessels - prone to cause hemorrhages. If large, may exert mass effect.
Babinski reflex: on plantar stimulation large toe extends upward on involved side.
Bolt: peripheral monitor used to measure ICP,
Brudzinski: flexion of leg when neck is flexed. meningeal irritation,
Bruit: blowing sound heard with a stethescope in by turbulent blood flow. These may occur area of stenosis.
Bulbar palsy: involvement of brain stem.
Burr hole: hole drilled through skull.
CAD: coronary artery disease.
This is a sign of
blood vessel; caused over an aneurysm or
Carotid artery: arteries that supply front and middle portion of brain. These travel on either side of neck from clavicle bone to jaw.
Carotid endarterectomy: surgical removal of clot or atherosclerosis from carotid artery.
Clonus: spasm with rapidly alternating rigidity, relaxation. May be sustained (continuous) or unsustained.
Coma: decreased level of consciousness to the point of unresponsiveness to external environment, unable to be aroused.
Computerized tomography: "CAT Scan" or CT special radiographic procedure to visualize the brain.
Conjugate movement: describes normal appearance of how the eyes move together. Dysconjugate movement is seen in certain neurologic conditions or in a "lazy eye" where eyes don't move together.
Craniotomy: surgical procedure that involves entering the cranial cavity.
CSF : cerebrospinal fluid.
CVA: cerebrovascular accident (stroke).
Decerebrate: posturing response to stimuli with extension of upper and lower extremities frequently seen in coma.
Decorticate: posturing response to stimuli with flexion of upper extremities and extension of lower extremitiesa.
Diplopia: double vision.
A-188
Dizziness: sensation of unsteadiness with feeling of movement in head.
Dysarthria: difficult and defective speech due to impairment of the A-189 tongue or other muscles essential to speech causing slurred speech.
Dysconjugate gaze: see conjugate movement.
Dysesthesia: unpleasant cutaneous sensation (burn, tickle, etc.).
Dysphania: difficulty in swallowing.
Dysphonia: difficulty with phonation.
Edema: swelling.
Embolism: this is a blood clot that forms in one part of the body and travels in the blood stream to another part of the body. A thrombosis of an artery may break off of the "parent" vessel (i.e., carotid artery) and form an embolus that eventually lodges in a vessel of smaller size in an end organ (i.e., brain).
EOM: extraocular muscles or movement.
Fasiculations: irregular, inconstant, isolated contractions of fiber bundles within a muscle.
Flacid: describes muscle tone which is lax.
Frontal release signs: "primitive" reflexes that result from disinhibition of frontal lobe, includes snout, palmomental, suck, grasp reflexes.
Glabellar reflex: patient cannot refrain from blinking when tapped on forehead between their eyes.
Hemianousia: see homonymous hemianopsia (below).
Hemiparesis: weakness involving half of the body.
Hemiplegia: paralysis involving half of the body.
Herniation: a process which occurs when there is swelling or mass effect from other processes (tumor, brain hemorrhage) that leads to loss of brain function and death over several hours.
Hoffman sitzn: finger reflex - contraction of thumb and/or fingers when distant phalanx of middle finger (hand prone and relaxed) forcibly flexed by examiner.
Holme's sign: excessive flexion rebound after muscle extension pressure released.
Homonomous hemianopsia: impairment of half of the field of vision on the side of the lesion.
Homonymous hemianopsia: impairment of half of the field of vision of each eye on the side opposite the lesion.
Hy-palgesia: decreased pain, diminished sensitivity to pain.
Hypesthesia: decreased tactile sensation.
ICP: intracranial pressure.
ICP monitor: intracranial pressure monitor - may be a bolt or ventriculostomy.
pJ: ischemic heart disease.
Infarction: area of tissue (cell) death.
Ipsilateral: situation on or pertaining to same side.
lschemia: lack of blood flow.
Kemig: inability to straighten leg when hip is flexed. This is a sign of meningeal irritation.
Locked in: lesion in basis portis that causes patient to be quadrapaetic with intact cognition and eye movements only.
E: lumbar puncture (spinal tap)
MAE: moves all extremities.
Mass effect: results from inability of the cranial cavity (area inside of skull) to expand. Thus any mass such as blood (hematoma), tumor, or swelling, exerts a mass effect or pressure on the brain itself.
Meninges: membranes covering brain, consists of three layers.
dura: thick outer layer.
pia: intermost layer - wrapped around brain
arachnoid: middle membrane - vascular layer
Meningismus: patient exhibits signs of meningeal irritation such as stiff neck, Kernig or Brudzinski.
Myoclonus: clonic spasm of muscle or group of muscles.
Neglect syndrome: occurs in nondominant hemisphere events such as stroke. Affected patients will ignore their nondominant (usually left) side.
Nystams: oscillating or jering movements of the eyes.
A-190
Occlusion: refers to complete blockage of an artery or vein.

Oriented X3: oriented to person, time, place.
0x4: oriented to person, time, place; also includes situation.
Paraplegia: paralysis of legs and lower part of body - both in motion and sensation.
Paresthesia: unpleasant cutaneous sensation, i.e., numbness or tingling,
Parosmia: any disease or perversion of the sense of smell.
PERL: pupils
PERRL(d+C)A:
equal, react to light.
pupils equally round and reactive to light (direct and consensual) and to accomodation.
PM&R: physical medicine and rehab.
Post ictal: after an ictus or event, usually refers to period immediately following a seizure.
PRIND: partially reversible ischemic neurological deficit.
Proprioception: position sensation.
Ptosis: drooping of upper eyelid.
Quadriplegia: paralysis of all four limbs.
Reflexes:
Scale A
N = normal reaction 1+ = slightly hyperactive 2+ = markedly increased unsustained clonus 3+ = one that shows sustained clonus l- = reflex slightly decreased 2- = reflex markedly decreased 3- = reflex absent except on reinforcement 0 = reflex cannot be obtained at all
Scale B
2 3
4
1
gg: reversible ischemic neurologic deficit (symptoms last > 24 hours).
Romberg sign: patient unable to stand with feet placed close together and eyes closed.
SAH: subarachnoid hemorrhage, blood in space around the brain.
Scotoma : a blind or partially blind area in visual field.
A-191
Scotomata: optic nerve lesion producing impaired vision in one eye only.
m: subdural hematoma, blood clot outside of brain, but pressing against brain.
Seizure: convulsion; abnormal electrical activity of brain causing jerking A-192 movements, LOC.
Snout reflex: mouth puckers when chin tapped.
Spastic: muscles stiff, movements awkward (of the nature of or charac- terized by spasm).
Stenosis: narrowing of a blood vessel, frequently from atherosclerotic buildup.
Suck reflex: sucking occurs reflexively when something is placed in their mouth.
Syncope: faint, swoon.
Thrombosis: clot of blood that obstructs or blocks an artery or vein.
m: transient ischemic attack; fleeting focal.
Tinnitus: ringing sound in ear.
Todd's paralysis: focal weakness or paralysis following a seizure, usually lasting minutes to days, but resolving.
Tomography: see computerized tomography.
Trapezii: shoulder muscles.
Tremors: involuntary movements resulting in rhythmic movement of a joint.
Vasospasm: a complication of SAH where subarachnad blood irritates blood vessels causing them to constrict. As a result, blood flow is decreased, This can lead to ischemic infarction (strokes).
Vegetative: loss of all cognitive function. Patient appears alert and awake, but does not interact with environment.
Vertebrobasilar arteries: arteries in back of neck that supply brain stem and back of brain vessel.
Vertigo: abnormal sense of spinning-type movement.
Ventricles: fluid (CSF) filled cavities within the brain.
Ventriculostomy: catheter inserted into ventricles with the brain to relieve and or monitor ICP.
Xanthoromia: colored spinal fluid.
Appendix III (1) A-193
FORMAT. 1: SAMPLE LETER M INFORMANT: KNOWN TE'LEPBONE NUMBER
Dear :
I am writing on behalf of the National Heart, Lung, and Blood Institute's Atherosclerosis Risk in Comities study, a project of (name of institution) designed to tiasure the rates of heart disease in jname of state or area), to ask for your help. Your name is listed on the death certificate of (name1 who passed avay on (date). In a few days (name), a member of my staff, vi11 be calling to explain further about the project and seek your permission to ask a few medical questions. Of course, your participation is entirely voluntary.
The information ve need will be used for statistical purposes only, and vi11 remain strictly confidential. It will contribute to our efforts to better understand heart disease and prevent its occurrence in the future. Thank you very much in advance for your help in this important study.
Sincerely,
ARIC Principal Investigator (Name of Institution)
ARIC PROTOCOL 3. Surveillance Component Procedures. VERSION 1.0, 2/88

APPmDH III (2)
Dear ?
I am writing on behalf of the National Heart, Lung, and Blood Institute’s Atherosclerosis Risk in Cormunities study, a project of (name of institution) designed to measure the rates of heart disease in ( name of state or area , to ask for your help. Your name is listed on the death certificate of (name) who passed l vay on (date]. We would like to call you to explain more about the project and to ask a few medical questions, but have been unable to find your telephone number.
Could you take a few moments to fill out and mail the enclosed postcard? The information we will be calling about will be used for statistical purposes only, and vi11 remain strictly confidential. It will contribute to our efforts to better understand heart disease and prevent its occurrence in the future . Of course, your assistance in our research is entirely voluntary. Thank you very much in advance for your help in the important study.
. Sincerely,
ARIC Principal Investigator (Name of Institution)
(EXUXE POSTCARD,RETURNADDRESSEDANDSTAKPED. SEEPORMAT 3.)
A-194
ARK PROTOCOL 3. Surveillance Component Procedures. VERSION 1.0, 2/88
A-195
APPRmIx III (3)
PORHAT 3: REPLY POSTCARD FROM INFORMANT WITH TELEPHONE NUMBER
FORMS SHOULD BE RETURN-ADDRESSED TO LOCAL SURVEILLANCE CENTER AND STAMPED.
Dear (Name of Surveillance Supervisor):
I vi11 be able to help with your Atherosclerosis Risk in Ccnmunities study.
I do have a telephone number which is . The besttimesto ( ) reach me are or .
An alternative telephone number is: . Thebesttimesto ( ) reach me at this number are or .
I do not have a telephone number, but I agree to be interviewed in person, and will be calling your staff to set up a time and a place for the interview.
Sincerely,
Print Name of the Informant
.'")."X3L 3. Sxveillance Component Procedures. VERSION 1.0, 2/88

A-196
AlvRums III (4)
PORMAT4: SAM.PUlZlTER'l'O~NEIG'HBOR RE: LOCATION OF INFORMANT
Dem I
I am writing on behalf of the National Heart, Lung, and Blood Institute's Atherosclerosis Risk in Communities study, a project of lname of institution) designed to measure the rates of heart disease in (name of state or area), to ask for your help. As you may know, (na passed away on (date).
- As part of the study, ve are systematically attempting to contact a next-of-kin or another person who lived with the decedent, in order to obtain some medical information that vould help us to find out whether (name of decedent) died from a heart attack. Since ve have not been able to locate such a person and since you were (name of decedent)'s neighbor, we believe that you may he able to help us.
Could you take a few aoments to fill out and mail the enclosed postcard? The information we vish to obtain from a next-of-kin or another person who lived with (name of decedent) will be used for research purposes only, md will remain strictly confidential. It will contribute to our efforts to better understand heart disease and prevent its occurrence in the future. Of course, your assistance in our research is entirely voluntary.
If you have any questions, please feel free to call me collect at ( ) , or our local Surveillance Supervisor, (name) at
Thank you very much in advance for youxlp in
Sincerely,
ARIC Rincipal Investigator (Name of Field Center)
(ENCLOSE POSTCARD,RETURNADDRESSKDAND STAKPED. SEEPORMT 5.)
ARIC PROTOCOL 3. Surveillance Component Procedures VERSION 1.0

A-197
APPRUIH III (5)
FORMAT 5: REPLY FORM ON THE LOCATION OF INFORMANT
Dear (Name of Surveillance Supervisor):
The following individual(s) was (were) living with (name of the decedent) the time of his/her death:
at
Name Relationship to deceased Resent Address
Present Telephone Number
I do not have any information on persons who vere living with (name of the decedent) at the time of his/her death.
Sincerely,
(Print Name of Neighbor)
ARIC FWJTOCOL 3. S~rrnl.1l.a.n~~: Component Procedures. VERSION 1.0, 2/88

A-198
APPEND= III (6)
PORXAT 6:~ORMANTREZEASEOPINPORHATIONPORM:NURSINGB~
I hereby 8uthorite urd request to furnish to the Atherosclerosis Risk in Commun ities study the medical records on (Name of the decedent). These records will be reviewed only for research purposes and none of the information will be released to any individual other than the research team. Any costs for reproduction of records vi11 be covered by the study.
Date: Signed:
(Relationship to the Deceased)
Witness:
ARIC PROZDCOL 3. SurveiIlunm 3crmponent Procedures. I7ERSION 1.0, 2/88

APPmDIx III (7)
POFMAT 7: LETTER TO PEIYSICIAN SIGNING DEATH CERTIFICATE
lkar Doctor :
I am writing on behalf of the Atherosclerosis Risk in Comnunities study, an epidemiologic project of (Name of Institution) along with three other centers in the United States. The survey is assessing incidence of myocardial infarctions and coronary death in four comunities throughout the country. We need some information concerning (name of the decedent), whose death certificate you signed on ( Date ). The information is needed to supplement the death certificate in assigning 8 wuse of death. Could your nurse or you take a few moments to provide the ansvers to the questions on the enclosed form from your records?
This information will be used for stetistical purposes only, and will remain strictly confidential. If you have any questions, please feel free to call me collect at ( , or our local Surveillance ) Supervisor, (name) 8t( ) . Thank you very much in sdvance for your kind assistance and consideration of this request.
Sincerely,
ARIC Principal Investigator (Name of Field Center)
Enclosure: Physician Questionnaire
A-199
ARIC PROTWOL 3. Surveill8nce Component Rar&~re~. VERSION 1.0, 2/88

A-200
APmQ III (8)
FORMAT 8: LETTER TO ATTENDING PHYSICIAN OF DECEDENT
Dear Doctor :
I am writing on behalf of the Atherosclerosis Risk in Commrunities study, an epidemiologic project of (Name of Institution) along vith three other centers in the United States. The survey is assessing incidence of myocardial infarctions and coronary death in four comun ities throughout the country. We need 8ome information concerning (name of the decedent), who, 8ccording to the family, vas your patient. The information is needed to supplement the death certificate in assigning 8 muse of death. Could your nurse or you take 8 few moments to provide the answers to the questions on the enclosed form from your records?
This information will be used for statistical purposes only, and will remain strictly confidential. If you have any questions, please feel free to call me collect et ( , or our local Surveillance 1 Supervisor, (name) 8t( ) .Thank; you very much in edvance for your kind assistance and consideration of this request.
Sincerely,
ARIC Principal Investigator (Name of Field Center)
Enclosure: Physician Questionnaire
ARIC PROTOCOL 3. Surveillance Component Procedures. VERSION 1.0, 2/88

APPmmIx 111 (9)
FORMAT 9: INFORMANT RELEASE OF IN'FORMATION: PHYSICIAN
Physician:
The above named physician has my permission to release medical information to the Atherosclerosis Risk in Comunities study. This information will be used for stetistical purposes only, l d will reaain strictly confidential.
Decedent's name:
wy r&me:
Address:
Relationship to Decedent:
Date: Signed:
Relationship to Decedent
Witness :
A-201
ARIC PROTOCOL 3. Surveillance Component Procedures. VERSION 1.0, 2/88
A-202
APPmDJx III (10)
POIUUT 10: IMORMANT RELEASE OF INFORMATION: OUT-OF-AREA HOSPITAL
To: (Name of Hospital)
The above named hopsital has my permission to release medical information to the Atherosclerosis Risk in Comunities Study. This information will be used for statistical purposes only, and vi11 remain strictly confidential.
Decedent's Name
My Name:
Address:
Relationship to decedent:
Relationship to the Decedent:
Witness:
ARIC PROTOCOL 3. Surveillance Component Procedures. VERSION 1.0, 2/88




















